management of intracranial hypertension
TRANSCRIPT
Correspondence and Reprint requests : Dr Prof. Sunit Singhi,Head, Department of Pediatrics, Advanced Pediatric Centre,Chandigarh, 160012, India. Phone No. Office: 91-172-2755301and 5302; Residence: 91-172-2715619; Fax: 91172 2744401,2745078[Received March 17, 2009; Accepted March 17, 2009]
Symposium on Neurological Disorder–Advances in Management-II
Increased intracranial pressure (ICP) is a frequentlyencountered life threatening syndrome caused by avariety of neurologic and non neurological illnesses.About 20% of all admissions to our PICU are because ofraised ICP. If unchecked it may lead to catastrophicdeterioration and death. Appropriate and timelymanagement of raised ICP is possible with properunderstanding of pathphysiology, and varioustherapeutic modalities. We review here currentunderstanding and recent advances in management ofraised ICP. Most treatment modalities have evolvedfrom treating traumatic brain injury (TBI) and areapplied to treat raised ICP of other etiology.
PHYSIOLOGIC CONSIDERATIONS
Intracranial pressure: Normal values
The normal range for ICP varies with age. Values forchildren are not as well established as for adults.Normal values are less than 10 to 15mmHg for adultsand older children, 3 to 7 mm Hg for young children,and 1.5 to 6 mm Hg for term infants. ICP can be sub-
Management of Intracranial Hypertension
Sunit C Singhi and Lokesh Tiwari
Pediatric Emergency and Intensive Care Units, Department of Pediatrics, Advanced Pediatrics Centre, PostGraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India
ABSTRACT
Raised intracranial pressure (ICP) is a life threatening condition that is common to many neurological and non-neurologicalillnesses. Unless recognized and treated early it may cause secondary brain injury due to reduced cerebral perfusionpressure (CPP), and progress to brain herniation and death. Management of raised ICP includes care of airway, ventilationand oxygenation, adequate sedation and analgesia, neutral neck position, head end elevation by 200 -300, and short-termhyperventilation (to achieve PCO2 32- 35 mm Hg) and hyperosmolar therapy (mannitol or hypertonic saline) in criticallyraised ICP. Barbiturate coma, moderate hypothermia and surgical decompression may be helpful in refractory cases.Therapies aimed directly at keeping ICP <20 mmHg have resulted in improved survival and neurological outcome.Emerging evidence suggests that cerebral perfusion pressure targeted therapy may offer better outcome than ICP targetedtherapies. [Indian J Pediatr 2009; 76 (5) : 519-529] E-mail: [email protected]; [email protected]
Key words: Intracranial pressure; Children; Traumatic brain injury; Cerebral perfusion pressure; Hyperosmolar therapy.
atmospheric in newborns.1 Usually normal limits aretaken as 5 to 15 mm Hg. Current pediatric data supportan ICP >20 mm Hg as threshold to define intracranialhypertension requiring treatment. Sustained ICP valuesof greater than 40mm Hg indicate severe, life-threatening intracranial hypertension.2 There have beensome suggestions that lower threshold values foryounger children may be used, although there are nodata to support this.3 A surge in ICP normally occurswith activities such as suctioning, painful stimuli, andcoughing and does not warrant intervention unless itdoes not return to baseline within about 5 minutes. It isimportant to distinguish “normal” or expectedincreases in ICP vs intracranial hypertension becausethe latter requires immediate intervention.
CEREBRAL PRESSURE DYNAMICS
Monro-Kellie doctrine
Intracranial pressure is the sum total of pressure exertedby the brain, blood, and cerebrospinal fluid (CSF) in thenon-compliant cranial vault. The Monro-Kellie doctrinestates that sum of intracranial volume of brain (» 80%),blood (» 10%), and cerebrospinal fluid (» 10%) isconstant. An increase in any one of these componentsmust be offset by decrease in another to keep the totalvolume constant or else the ICP will increase. Inresponse to increase in intracranial volume initialcompensation occurs by displacement of CSF from theventricles and the cerebral subarachnoid space to
Indian Journal of Pediatrics, Volume 76—May, 2009 519

Sunit C Singhi and Lokesh Tiwari
520 Indian Journal of Pediatrics, Volume 76—May, 2009
spinal subarachnoid space (vertebral canal), decreasedproduction, and increased absorption of CSF. Infantsand children with open fontanels and sutures may beable to compensate better but will still be susceptible toacute increases in ICP.
Compliance
Compliance is an indicator of the brain’s tolerance toincreases in ICP. Each patient has varying degrees ofcompliance even with similar injuries. When thepatient’s compliance is exhausted, there is a dramaticincrease in the pressure/volume curve, leading to arapid elevation in ICP.
Cerebral blood flow
In an uninjured brain, cerebral blood flow (CBF) isregulated to supply the brain with adequate oxygenand substrates. Certain physiologic factors likehypercarbia, acidosis and hypoxemia causevasodilatation, leading to increased CBF. Seizureactivity and fever will increase cerebral metabolic rate andCBF. CBF in excess of tissue demand leads to hyperemiaand increased ICP. Methods to decrease the cerebralmetabolic rate, such as hypothermia and barbiturates,will decrease CBF and thus the ICP.
Cerebral perfusion pressure
Cerebral perfusion pressure (CPP) is the pressure atwhich brain is perfused. It is an important indicator ofcerebral blood flow. CPP provides an indirectmeasurement of adequacy of CBF. It is calculated bymeasuring the difference between the mean arterialpressure (MAP) and the ICP (MAP – ICP), where MAP= 1/3 systolic pressure plus 2/3 diastolic pressure. Areduction in CPP can occur from an increase in ICP, adecrease in blood pressure, or a combination of bothfactors. Normal CPP values for children are not clearlyestablished, but the values that are generally acceptedas the minimal pressure necessary to prevent ischemiaare: adults >70 mm Hg; children >50–60 mm Hg;infants/toddlers >40–50 mm Hg.4 CPP < 40 mm Hg is asignificant predictor of mortality in children with TBI.2
Autoregulation maintains a steady cerebral bloodflow (CBF) within a CPP range of 50-150 mmHg byvasoconstriction and vasodilatation of the cerebralvessels despite fluctuations in systemic blood pressure.Autoregulation is lost at CPP values less than 50 mmHg.Ability to pressure autoregulate may be impaired or losteven with a normal CPP, CBF can passively followchanges in CPP. Once autoregulation is lost, CBF andcerebral blood volume (CBV) become dependent onchanges in systemic blood pressure.
CAUSES OF RAISED ICP
An increase in intracranial pressure is commonly
caused by an increase in volume of brain (cerebraledema), blood (intracranial bleeding), space occupyinglesion, or CSF (hydrocephalous). These mechanismscould be operative singly or in various combinations.
Cerebral edema is the most important cause of raisedICP in non-traumatic brain injuries such as centralnervous system (CNS) infections, and systemic andmetabolic encephalopathies. It can be vasogenic,cytotoxic, or interstitial. Vasogenic cerebral edema isdue to injury to blood brain barrier and increasedcapillary permeability around the area of injury orinflammation particularly in CNS infections. It can belocal or diffuse and occurs around mass lesions andinflammatory processes (e.g., meningitis, encephalitis).Interstitial cerebral edema is due to an increase in thehydrostatic pressure of CSF and is often seen inpatients with obstructive hydrocephalus or excessiveCSF production. Cytotoxic cerebral edema (Cellularswelling) occurs following cerebral ischemia andhypoxia causing irreversible cell damage and death.Osmolar swelling may occur because of increased localosmolar load around necrotic foci caused by infarctionor contusion, and possibly because of increased cerebralblood volume (hyperemia) in CNS infections. Patientswith cerebral edema may have a combination of all 3mechanisms operating.
The primary etiology could be intracranial orextracranial (Table 1). When primary cause ofincreased ICP is intracranial, normalization of ICPdepends on rapidly addressing the underlying braindisorder. Intracranial hypertension due to anextracranial or systemic process is often remediable.Increased ICP can also occur after a neurosurgicalprocedure.
TABLE 1. Causes of Intracranial Hypertension
Intracranial (primary)• CNS infections – meningitis, encephalitis, brain abscess,
cerebral malaria, neurocysticercosis,• Trauma (epidural and subdural hematoma, cerebral
contusions and edema)• Brain tumor• Intracranial bleed – intracerebral and intraventricular
hemorrhage• Others – ischemic stroke, hydrocephalous, idiopathic or
benign intracranial hypertension.• Status epilepticus.
Extracranial (secondary)• Hypoxic Ischemic Injury - airway obstruction, hypoven-
tilation, shock.• Metabolic – hyperpyrexia, hepatic failure, lead intoxication.• Drug (e.g., tetracycline, rofecoxib)• Others – hypertensive encephalopathy
Postoperative• Mass lesion (hematoma)• Cerebral edema• Increased cerebral blood volume (vasodilation)• CSF obstruction.

Management of Intracranial Hypertension
Indian Journal of Pediatrics, Volume 76—May, 2009 521
Following traumatic brain injury (TBI), intracranialhypertension is multifactorial:
• Trauma induced epidural or subdural hematomas,hemorrhagic contusions, and depressed skullfractures
• Cerebral edema (most important cause afterhematomas).5
• Hyperemia due to loss of autoregulation• Hypoventilation leading to hypercarbia and
consequently cerebral vasodilation• Hydrocephalus resulting from obstruction of the
CSF pathways or its absorption• Increased intrathoracic or intra-abdominal pressure
as a result of mechanical ventilation, posturing,agitation, or Valsalva maneuvers.
A secondary increase in the ICP is often observed 3to 10 days after the trauma, mainly as a result of adelayed formation of epidural or acute subduralhematoma, or traumatic hemorrhagic contusions withsurrounding edema, sometimes requiring evacuation.Other potential causes of delayed increases in ICP arecerebral vasospasm,6 hypoventilation, andhyponatremia.
INTRACRANIAL PRESSURE MONITORING
Acute raised ICP is an important cause of secondarybrain injury hence at–risk patients should have closemonitoring of systemic parameters, includingtemperature, heart rate, blood pressure,electrocardiogram, blood glucose, ventilation,oxygenation, and fluid intake and output. They shouldbe on continuous monitoring with pulse oximetry andcapnography to avoid unrecognized hypoxemia andhypoventilation or hyperventilation. A central venouscatheter should be placed to evaluate volume status,and a Foley catheter for accurate urine output. Patientswith suspected intracranial hypertension should havemonitoring of ICP. Monitoring of cerebral oxygenextraction with jugular bulb oximetry is desirable, ifavailable.
Indications
Clinical symptoms of increased ICP, such as headache,nausea, and vomiting, are impossible to elicit incomatose patients. Papilledema, though a reliable signof intracranial hypertension, is uncommon after acuteevents, even in patients with documented elevated ICP.On the other hand, signs such as pupillary dilation anddecerebrate posturing can occur in the absence ofintracranial hypertension. CT scan signs of brainswelling, such as midline shift and compressed basalcisterns, are predictive of increased ICP, but intracranialhypertension can sometimes occur without thosefindings.7
Monitoring of ICP is an invasive technique and hassome associated risks. The aim of monitoring isprevention of cerebral ischemia and secondary braininjury. For a favorable risk-to-benefit ratio, therefore, ICPmonitoring is indicated only in selected at-riskpatients.8 These include patients with Glasgow ComaScale of 8 or less and patients with TBI who have anabnormal admission head CT scan.9 Patients who areable to follow commands have a low risk for developingraised ICP and can be followed with serial neurologicexaminations. Patients with a Glasgow Coma Scalescore greater than 8 also might be considered for ICPmonitoring if they require a treatment that mightincrease ICP, such as positive end-expiratory pressure(PEEP). Other, less common indications includepatients with multiple systemic injuries with alteredlevel of consciousness and subsequent to removal of anintracranial mass (e.g., hematoma, tumor). ICPmonitoring also must be considered in nontraumaticconditions in which an intracranial mass lesion ispresent (e.g., cerebral infarction) and has a likelihood ofexpansion leading to intracranial hypertension andclinical deterioration. The duration of monitoring isuntil ICP has been normal for 24 to 48 hours without aneed for therapy to reduce ICP. Although ICPmonitoring has never been subjected to randomizedcontrolled studies to evaluate its effectiveness, its usehas been associated with decreased morbidity andmortality, and improved outcome in patients with TBI,intracerebral hemorrhages, and CNS infections.8,10-12 ICPmonitoring is crucial to identify rapidly increasingpressure and to institute appropriate therapy to preventcerebral herniation and preserve cerebral perfusion. It isalso necessary to monitor ICP in order to calculate theCPP.
Sites for ICP monitoring
The most common sites used for ICP monitoring areintraventricular and intra-parenchymal. Intraventicularcatheter remained the preferred device for monitoringICP and the standard against which all newer monitorsare compared.13 These days the use of intraventricularcatheter placement, preferably with an implantablemicro-transducer (fiberoptic or strain-gauge)14 allowssimultaneous monitoring of ICP and management ofincreased ICP by CSF drainage.The advantages of theventriculostomy are its relatively low cost, the option touse it for therapeutic CSF drainage, and its ability torecalibrate to minimize errors owing to measurementdrift. Disadvantages are difficulties with insertion intocompressed or displaced ventricles, risk of infection,inaccuracies of the pressure measurements because ofobstruction of the fluid column, and the need tomaintain the transducer at a fixed reference pointrelative to the patient’s head. The system should bechecked for proper functioning at least every 2 to 4hours, and any time there is a change in the ICP,
Sunit C Singhi and Lokesh Tiwari
522 Indian Journal of Pediatrics, Volume 76—May, 2009
neurologic examination, and CSF output. This checkshould include assessing for the presence of anadequate waveform, which should have respiratoryvariations and transmitted pulse pressure. When theventricle cannot be cannulated, intraparenchymal sitecan be used. Other alternatives for monitoring ICPinclude subdural, subarachnoid, and epidural catheterplacement using microsensor transducer and fiberoptictransducer tipped catheters. The main advantages ofmicro-transducers are the ease of insertion, especially inpatients with compressed ventricles. However, none ofthe micro-transducer- tipped catheters can berecalibrated after they are inserted into the skull. Theyalso exhibit measurement drift over time15 and must bereplaced if monitoring is in excess of several days.
Intracranial pressure waveforms
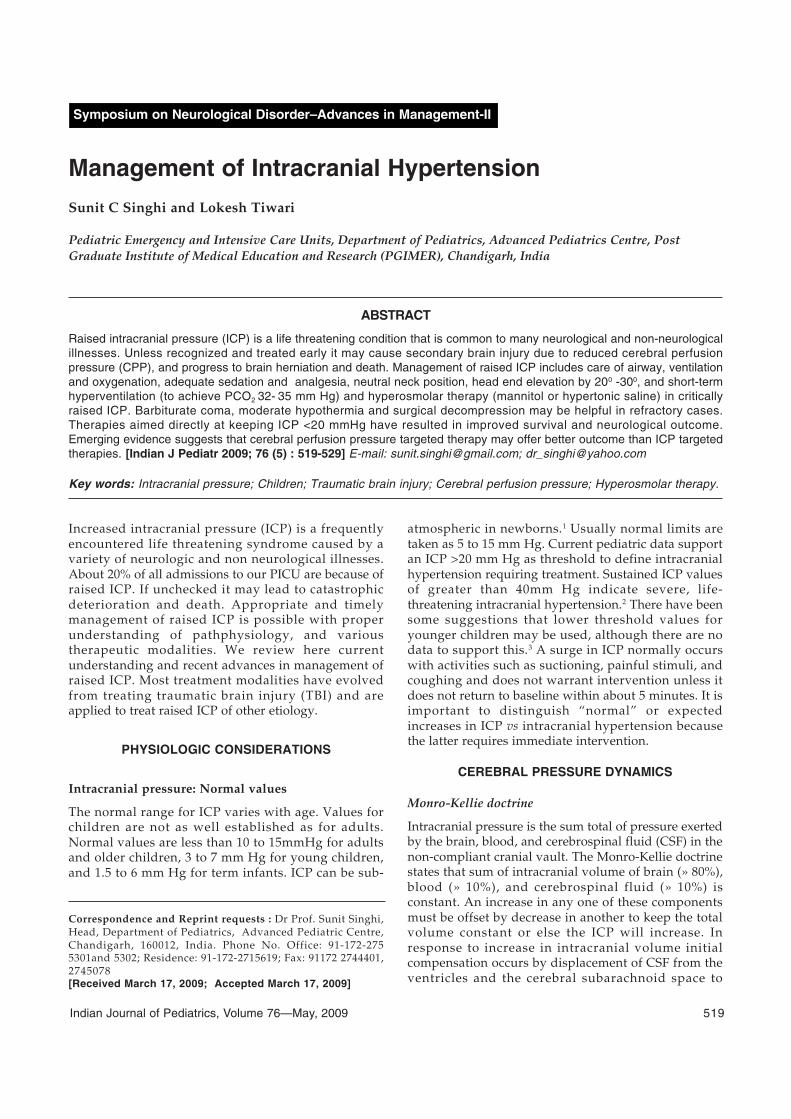
The normal ICP waveform contains three phases (Fig.1A)
• P1 (percussion wave) represents arterial pulsations.• P2 (rebound wave) reflects intracranial compliance.• P3 (dichrotic wave) represents venous pulsations.
waveform, but high amplitude. C waves may besuperimposed on plateau waves.16
Complications of ICP monitoring(13)
The most common complication of ventricular catheterplacement is infection (incidence of 5% to 14%);colonization of the device is more common than clinicalinfection.17 There was a nonlinear increase of riskduring 10 to 12 days, after which the risk diminished.17
Use of antibiotic-coated ventricular catheters has beenshown to reduce the risk of infection from 9.4% to1.3%.18 Other complications of ventricular catheters arehemorrhage (incidence 1.4%), malfunction, obstruction,and malposition.
MANAGEMENT OF INCREASED ICP
In patient with raised ICP in addition to treatment ofprimary cause-whether intracranial or extracranial, themain focus of treatment is to prevent and minimizesecondary injury. Secondary brain injury refers to theprocesses that occur within hours to days after theprimary injury that can be prevented or minimized—such as cerebral ischemia, cerebral edema, andneurochemical alterations including excitatoryneurotransmitters, the formation of free radicals, andincreased levels of intracellular calcium andpotassium.19 Factors that are known to worsensecondary injury are hypoxia and hypotension.20 Theneurological devastation caused by the secondaryinjury is often worse than the underlying primarydisorder. Most of the current treatment recommen-dations are based on consensus and clinicalexperience. Few specific treatment options have beensubjected to randomized trials.
Since there are limited outcome studies to supportthe current management of children with increased ICPfrom etiologies other than TBI it is the knowledgegained from treating TBI that is often applied to treatraised ICP of other etiologies also.
Goals of therapy
• Maintain ICP less than 20 to 25 mm Hg.• Maintain adequate CPP usually greater than 60 mm
Hg, by maintaining adequate MAP.• Avoid factors that aggravate or precipitate elevated
ICP.
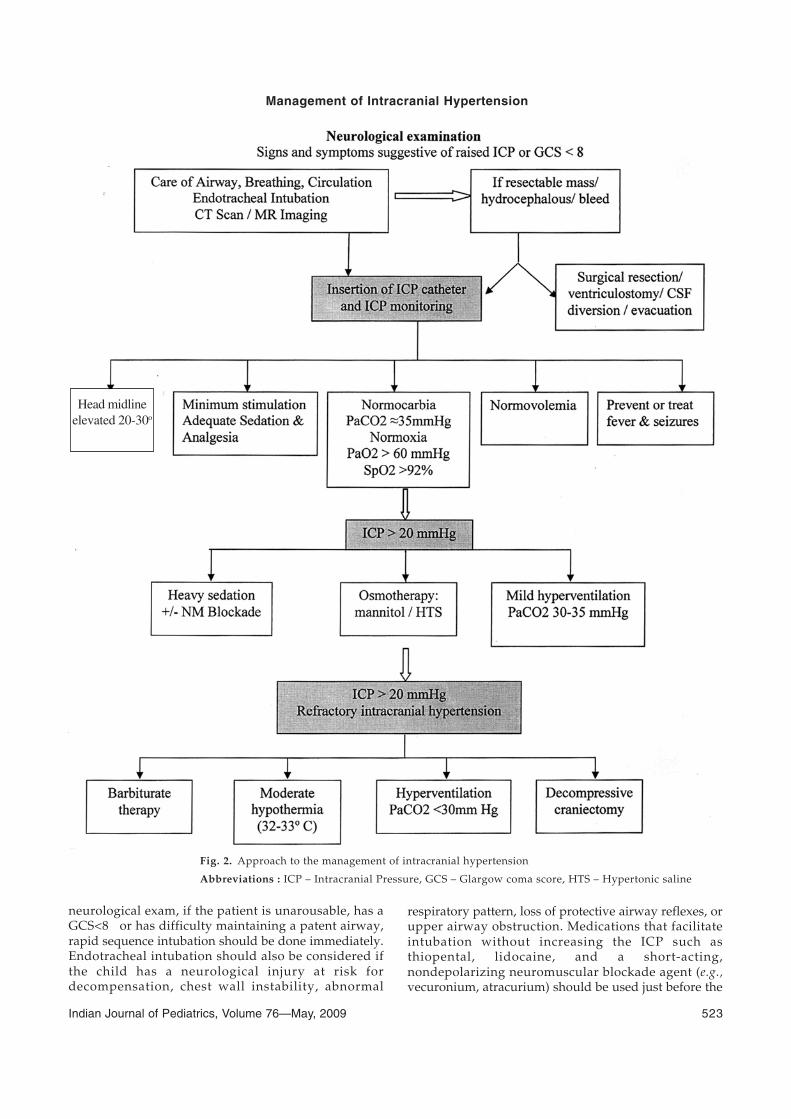
An overall approach to the management ofintracranial hypertension is presented in fig. 2.
Airway, Breathing, and Circulation
The initial management of the child with suspectedincreased ICP includes assessment of airway, brea-thing, and circulation. Even prior to a thorough
Fig. 1A. Normal ICP wave forms
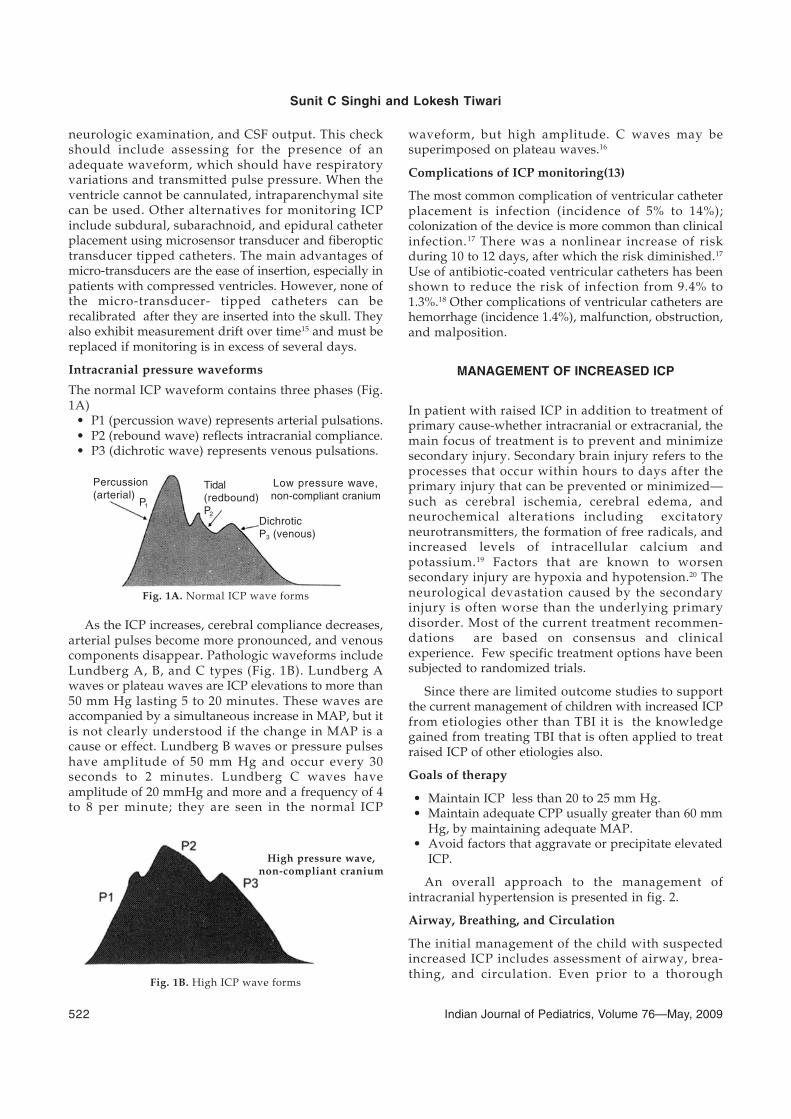
As the ICP increases, cerebral compliance decreases,arterial pulses become more pronounced, and venouscomponents disappear. Pathologic waveforms includeLundberg A, B, and C types (Fig. 1B). Lundberg Awaves or plateau waves are ICP elevations to more than50 mm Hg lasting 5 to 20 minutes. These waves areaccompanied by a simultaneous increase in MAP, but itis not clearly understood if the change in MAP is acause or effect. Lundberg B waves or pressure pulseshave amplitude of 50 mm Hg and occur every 30seconds to 2 minutes. Lundberg C waves haveamplitude of 20 mmHg and more and a frequency of 4to 8 per minute; they are seen in the normal ICP
High pressure wave,non-compliant cranium
Fig. 1B. High ICP wave forms
Low pressure wave,non-compliant cranium
DichroticP3 (venous)
Tidal(redbound)P2
Percussion(arterial)
P1
Management of Intracranial Hypertension
Indian Journal of Pediatrics, Volume 76—May, 2009 523
Fig. 2. Approach to the management of intracranial hypertension
Abbreviations : ICP – Intracranial Pressure, GCS – Glargow coma score, HTS – Hypertonic saline
Head midlineelevated 20-30o
neurological exam, if the patient is unarousable, has aGCS<8 or has difficulty maintaining a patent airway,rapid sequence intubation should be done immediately.Endotracheal intubation should also be considered ifthe child has a neurological injury at risk fordecompensation, chest wall instability, abnormal
respiratory pattern, loss of protective airway reflexes, orupper airway obstruction. Medications that facilitateintubation without increasing the ICP such asthiopental, lidocaine, and a short-acting,nondepolarizing neuromuscular blockade agent (e.g.,vecuronium, atracurium) should be used just before the

Sunit C Singhi and Lokesh Tiwari
524 Indian Journal of Pediatrics, Volume 76—May, 2009
procedure. Adequate oxygenation is necessary toprevent sequelae of secondary insults and should bemaintained with a PaO2 > 60 mm Hg, an oxygensaturation > 92%, and physiologic positive endexpiratory pressure (PEEP) of 5 cm H2O. Blood pressuremust be maintained at levels appropriate for age orrestored to ensure adequate CPP and prevent furtherischemia. Fluid boluses should be given to thehypotensive neurologically injured child in the sameway as any other child presenting in shock.Vasopressor support is initiated if the child remainshypotensive despite appropriate fluid resuscitation.
General measures
Prevention or treatment of factors that may aggravate orprecipitate intracranial hypertension should beundertaken. Specific factors that may aggravateintracranial hypertension include obstruction of venousreturn (head position, agitation), respiratory problems(airway obstruction, hypoxia, hypercapnia), fever,severe hypertension, hyponatremia, anemia, andseizures.
Head elevation and position
Elevation of the head-end of the bed and keeping thehead in a neutral position are standard recommen-dations to minimize resistance to venous outflow andpromote displacement of CSF from the intracranialcompartment to the spinal compartment. Elevation ofthe head up to 30o reduces ICP and increases CPP, butdoes not change brain tissue oxygenation.21 Thereduction in ICP resulting from 15o to 30o of headelevation is probably advantageous and safe for mostpatients. The child must be euvolemic prior to placingin this position to avoid orthostatic hypotension. Whenhead elevation is used, the pressure transducers forblood pressure and ICP must be zeroed at the same level(at the level of the foramen of Monro) to assess CPPaccurately.
Management of Respiratory failure
Comatose patients often have respiratory dysfunctionrequiring mechanical ventilation, pneumonia andpulmonary insufficiency, or periodic episodes ofhypoventilation. Resultant hypoxia and hypercapniacan increase ICP dramatically, and mechanicalventilation can alter cerebral hemodynamics. Controlledventilation may be needed for optimal managementand to maintain normal carbon dioxide . Duringmechanical ventilation high PEEP can increase ICP byimpeding venous return and increasing cerebral venouspressure, and by decreasing blood pressure leading to areflex increase of cerebral blood volume. The effects ofPEEP on ICP also depend on lung compliance; minimaleffect is seen when lung compliance is low.22
Sedation and analgesia
Children with acute brain injury, especially those whoare mechanically ventilated, should be appropriatelysedated and given adequate analgesia to prevent painand anxiety, both of which increase the cerebralmetabolic rate and ICP. There are no randomizedcontrolled studies comparing sedation methods inchildren with acute neurological injury. In general,benzodiazepines have no effect on ICP, whereas theopiates have been reported to increase ICP in adultpatients with TBI.23 One consideration in the choice ofsedative should be to minimize effects on bloodpressure because most available agents can decreaseblood pressure. Hypovolemia predisposes tohypotensive side effects and should therefore becorrected before administering sedatives. Selection of ashorter acting agent (midazolam) may have theadvantage of allowing brief interruption of sedation toexamine neurologic status. Propofol is not approved forsedation in PICU as its safety is not established by USFDA and UK committee on safety of Medicine.
Fever
Fever increases metabolic rate by 10% to 13% per degreeCelsius and is a potent vasodilator. Fever-induceddilation of cerebral vessels can increase CBF and mayincrease ICP. In patients at risk of intracranialhypertension, fever should be controlled withantipyretics and hydrotherapy. Etiology of fever mustbe sought and treated appropriately. A significantrelationship has been seen between fever and a poorneurologic outcome in head injury patients.24
Hypertension
Elevated blood pressure is seen commonly in patientswith raised ICP. Characteristically systolic bloodpressure increase is greater than diastolic increase. It isunwise to reduce elevated blood pressure associatedwith untreated raised ICP, especially in patients withintracranial mass lesion, because the high bloodpressure maintains cerebral perfusion. In the absenceof an intracranial mass lesion, the decision to treatelevated blood pressure has to be individualized. Whenautoregulation is impaired, which is common after TBI,systemic hypertension may increase CBF and ICP, mayexacerbate cerebral edema and increase the risk ofpostoperative intracranial hemorrhage. Systemichypertension may resolve with sedation. If the decisionis made to treat systemic hypertension, vasodilatingdrugs, such as nitroprusside, nitroglycerin, andnifedipine, should be avoided; these increase ICP,which may be deleterious to the marginally perfusedinjured brain. Sympathomimetic-blocking antihyper-tensive drugs, such as beta-blocking drugs (labetalol,esmolol) or central acting alfa-receptor agonists(clonidine), are preferred because they reduce blood

Management of Intracranial Hypertension
Indian Journal of Pediatrics, Volume 76—May, 2009 525
pressure without affecting the ICP. Agents with a shorthalf-life have an advantage when the blood pressure islabile.
Treatment of anemia
Patients with severe anemia have been reported topresent with symptoms of increased ICP and signs ofpapilledema, which resolve with treatment of theanemia.25 The mechanism is thought to be related to themarked increase in CBF that is required to maintaincerebral oxygen delivery when anemia is severe.Although anemia has not been clearly shown toexacerbate ICP after TBI, a common practice is tomaintain hemoglobin concentration around 10 g/dL. Alarge randomized trial of critically ill patients showedbetter outcome with a more restrictive transfusionthreshold of 7 g/dL.26. The issue of optimal hemoglobinconcentration in patients with raised ICP needs furtherstudy.
Prevention of seizures
Seizures occur commonly in association with raisedICP irrespective of etiology, be it meningitis,encephalitis or severe head injury. Seizures increasecerebral metabolic rate and lead to a dramatic rise inICP, but there is no clear relationship between theoccurrence of early seizures and a worse neurologicoutcome. In patients with severe TBI as well as in thosewith nontraumatic coma, seizures may be subclinicaland can be detected only with continuouselectroencephalographic monitoring. Prophylacticanti-seizure therapy may be considered for preventionof early posttraumatic seizures (PTS) in children at highrisk of seizure following TBI. However, prophylacticuse of anti-seizure therapy is not recommended forchildren for prevention of late post-traumatic seizure.27
If a late PTS occurs, the patient should be managed inaccordance with standard approaches to patients withnew-onset seizures.27
MEASURES FOR REFRACTORY INTRACRANIALHYPERTENSION
For patients with sustained ICP elevations of greaterthan 20 to 25 mm Hg, additional measures are neededto control the ICP.
Hyperosmolar therapy
Mannitol is the most commonly used hyperosmolaragent for the treatment of intracranial hypertension.28
More recently, hypertonic saline has also been used. Afew studies have compared the relative effectiveness ofthese two hyperosmotic agents, but more work isneeded.
Intravenous bolus administration of mannitol lowersthe ICP in 1 to 5 minutes with a peak effect at 20 to 60minutes. The effect of mannitol on ICP lasts 1.5 to 6hours, depending on the clinical condition.29 Mannitolis usually given as a bolus of 0.25 to 0.5g/kg; whenurgent reduction of ICP is needed, an initial dose of 1 g/kg may be given. Two prospective clinical trials inadults, one in patients with subdural hematoma andthe other in patients with herniation secondary todiffuse brain swelling, have suggested that a higherdose of mannitol (1.4 g/kg) may give significantly betterresults than a lower dose in these extremely criticalsituations.30 When long-term reduction of ICP isneeded, 0.25 to 0.5 g/kg can be repeated every 2 to 6hours. Attention should be paid to replacing fluid thatis lost because of mannitol-induced diuresis, or elseintravascular volume depletion would result.
Mannitol has rheologic and osmotic effects.31
Infusion of mannitol increases serum osmolarity, whichdraws edema fluid from cerebral parenchyma. Thisprocess takes 15 to 30 minutes until gradients areestablished. Immediately after infusion of mannitol,therefore there is an expansion of plasma volume and areduction in hematocrit and in blood viscosity, whichmay increase CBF and oxygen delivery to the brain.31 Inpatients with intact pressure autoregulation, infusionof mannitol induces cerebral vasoconstriction, whichmaintains constant CBF and causes a considerabledecrease in ICP. In patients with absent pressureautoregulation, infusion of mannitol increases CBF,and hence the decrease in ICP is less pronounced.
Mannitol opens the blood-brain barrier, and maycross it. Mannitol that has crossed the blood-brainbarrier may draw fluid into the central nervous system,which can aggravate vasogenic edema. For this reason,when it is time to stop mannitol, it should be tapered toprevent ICP rebound.31 For optimal effect of mannitol,serum osmolality should be between 300-320 mOsm.Keeping osmolality less than 320 mOsm also helps toprevent complications such as hypovolemia,hyperosmolarity, and renal failure. The adverse effectsof mannitol are more likely when it is present in thecirculation for extended periods, such as in slow orcontinuous infusions or with repeated administrationof high doses.
Hypertonic saline administration appears to be apromising therapy for control of cerebral edema. Givenin concentrations ranging from 3% to 23.4%, it createsan osmotic force to draw water from the interstitialspace of the brain parenchyma into the intravascularcompartment in the presence of an intact blood-brainbarrier, reducing intracranial volume and ICP. In somestudies in adults, hypertonic saline has been moreeffective in reducing ICP in TBI than mannitol.32
However, variations in hypertonic solution prepara-

Sunit C Singhi and Lokesh Tiwari
526 Indian Journal of Pediatrics, Volume 76—May, 2009
tions and dosing regimens, difference in inclusion andexclusion criteria, and small numbers of patients makethese studies difficult to compare. Hypertonic saline issaid to have advantage over mannitol in hypovolemicand hypotensive patients as it augments intravascularvolume and may increase blood pressure in addition todecreasing ICP. However, use of hypertonic saline asprehospital bolus to hypotensive patients with severeTBI was not associated with improved neurologicoutcomes.33
Adverse effects of hypertonic saline administrationinclude hematologic and electrolyte abnormalities, suchas bleeding secondary to decreased platelet aggregationand prolonged coagulation, hypokalemia, andhyperchloremic acidosis. Available data show onlylevel II evidence supporting the use of continuousinfusion of 3% saline for treatment of elevated ICP inpediatric TBI.34 An effective minimum dose on asliding scale (0.1 – 1.0 ml/kg/hour) to keep ICP <20mm/kg should be used.28 Infusion can be continued ifserum osmolality is below 360 mOsm/L.
Heavy sedation and paralysis
Routine paralysis of patients with severe raised ICP isnot indicated; however, intracranial hypertensioncaused by agitation, posturing, or coughing can beprevented by deep sedation and nondepolarizingmuscle relaxants that do not alter cerebrovascularresistance.35,36 A commonly used regimen is morphineand lorazepam for analgesia/sedation and cisatra-curium or vecuronium as a muscle relaxant, with thedose titrated by twitch response to stimulation. Thedisadvantage of this therapy is that the neurologicexamination cannot be monitored closely. The sedativesand muscle relaxants can be interrupted once a day,usually before morning rounds, to allow neurologicassessments. Since the use of neuromuscular block willeliminate motor activity associated with seizures, butnot brain epileptiform activity, children at high risk forseizures should have continuous electroencepha-lograph (EEG) monitoring.36
Hyperventilation
Hyperventilation decreases PaCO2, which inducesconstriction of cerebral arteries; the resulting reductionin cerebral blood volume decreases ICP.37,38 Acutehyperventilation decreases global CBF. Sometimes thisreduction in flow could be sufficient to induce ischemiain injured brain.39,40 Hyperventilation has limited use inthe management of intracranial hypertension, becauseits effect on ICP is time limited. The vasoconstrictiveeffect on cerebral arterioles lasts only 11 to 20 hoursbecause the pH of the CSF rapidly equilibrates to thenew PaCO2 level. As the CSF pH equilibrates, thecerebral arterioles redilate, possibly to a larger caliberthan at baseline, and a possible rebound phase of
increased ICP.38 The precise relationship betweenhyperventilation and outcome has not been studied inchildren with raised ICP of any etiology. Based oncurrent evidence, following suggestions can be made:
• Prophylactic hyperventilation should be avoided.• Mild hyperventilation (PaCO2 30–35 mm Hg) may
be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy.
• Aggressive hyperventilation (PaCO2 <30 mm Hg)titrated to clinical effect may be considered as asecond tier option in the setting of refractoryhypertension and for brief periods in cases ofcerebral herniation or acute neurologicdeterioration.37
Barbiturate coma
Small studies of high-dose barbiturate therapy suggestthat barbiturates are effective in lowering ICP in selectedcases of refractory intracranial hypertension in childrenwith severe head injury. However, studies on the effectof barbiturate therapy for uncontrolled ICP have notevaluated neurologic outcome.41 Thiopental is given ina loading dose of 5mg/kg over 30 minutes,(monitor forhypotension) followed by infusion of 1-5 mg/kg houruntil the electroencephalogram shows a burstsuppression pattern. The mechanism of ICP reductionby barbiturates is unclear. It probably reflects a coupledreduction in CBF and cerebral metabolic rate with animmediate effect on ICP.42 Complications of barbituratecoma include hypotension, hypokalemia, respiratorydepression, infections, and hepatic and renaldysfunction. Hypotension caused by barbiturate shouldbe treated first with volume replacement and then withdopamine, if necessary. Dopamine infusion increasescerebral metabolic requirements and may partiallyoffset the beneficial effects of barbiturates on cerebralmetabolic rate. There is no evidence to support use ofbarbiturates for the prophylactic neuroprotective effectsor prevention of the development of intracranialhypertension in children with severe TBI.43
Induced Hypothermia
A phase II trial to test safety and efficacy of hypothermiain children with TBI did not show a beneficial effect onneurologic outcome, however, a reduction in ICP wasevident during the hypothermia treatment.44 There wereno significant differences between the hypothermia andno-hypothermia patients with respect to complicationsviz. arrhythmia, coagulopathy or infection. However,the early hypothermia group had a trend toward betterneurological outcome at 3 and 6 months.44 A recentlycompleted multicentre trial by Hypothermia PediatricHead injury Trial investigators, Canadian Critical CareGroups that included 225 children, found a detrimental

Management of Intracranial Hypertension
Indian Journal of Pediatrics, Volume 76—May, 2009 527
trend with hypothermia.45 Currently therefore, routineinduction of hypothermia is not indicated. However,hypothermia may be an effective adjunctive treatmentfor increased ICP refractory to other medicalmanagement.
Corticosteroids
Steroids are commonly used for primary andmetastastic brain tumors, to decrease the vasogeniccerebral edema. Focal neurologic signs and decreasedmental status secondary to surrounding edematypically begin to improve within hours.46 IncreasedICP, when present, decreases over the following 2 to 5days, in some cases to normal. The most commonlyused regimen is intravenous dexamethasone, 4 mgevery 6 hours. For other neurosurgical disorders, suchas TBI or spontaneous intracerebral hemorrhage inadults, corticosteroids are not useful. Use ofmethylprednisolone for 48 hours in CRASH trialresulted in a significant increase in the risk of deathfrom 22.3% to 25.7% (relative risk 1.15, 95% confidenceinterval 1.07–1.24).47 This trial confirmed previousstudies and guidelines that routine administration ofsteroids is not indicated for patients with TBI.
Resection of mass lesions
Intracranial masses producing elevated ICP should beremoved when possible. Acute epidural and subduralhematomas are hyperacute surgical emergencies. Brainabscess must be drained, and pneumocephalus must beevacuated if it is under sufficient tension to increaseICP. Surgical management of spontaneous intracerebralbleeding is controversial.48
Cerebrospinal fluid drainage
CSF drainage lowers ICP immediately by reducingintracranial volume and more long-term by allowingedema fluid to drain into the ventricular system.Drainage of even a small volume of CSF can lower ICPsignificantly, especially when intracranial complianceis reduced by injury. If the brain is diffusely swollen, theventricles may collapse, this modality then has limitedutility. CSF drainage is generally done intermittentlywhenever ICP spikes above a threshold—such as 20mmHg, but can also be done continuously usinggravity, often to a level set at 5-10 cm above the center ofthe head. In a recent two-center study, in pediatric TBI,continuous CSF drainage was associated with higherCSF volume drainage and lower ICP, as compared tointermittent drainage.49
Decompressive craniectomy
This involves surgical removal of part of the calvaria tocreate a window in the cranial vault, which allows forherniation of swollen brain through the bone windowto relieve pressure. Decompressive craniectomy has
been used to treat uncontrolled intracranialhypertension of various origins, including cerebralinfarction, trauma, subarachnoid hemorrhage, andspontaneous hemorrhage.50 Patient selection, timing ofoperation, type of surgery, and severity of clinical andradiologic brain injury are factors that determine theoutcome of this procedure. A small randomized clinicaltrial in 27 children with TBI found a reduced risk ratiofor death and vegetative status, or severe disability 6 to12 months after injury.51 Ruf et al52 and Figaji et al53
collectively reported no mortality and favorableoutcome in 7 of the 11 pediatric cases where very earlyapplication of either unilateral or bilateraldecompression was used. In a retrospective study of 23children (mean admission GCS score of 4.6) whounderwent decompressive craniectomy if ICP remainedabove 20mm Hg, even after medical management, 16 ofthe 23 patients survived and 13 of the 16 had afavorable outcome.54 Reported complications ofdecompressive craniectomy include hydrocephalus,hemorrhagic swelling ipsilateral to the craniectomy site,and subdural hygroma.
CPP targeted protocols
The conventional approach in management of raisedICP aims at reducing ICP below 20 mmHg. Emergingevidence however favours CPP targeted therapywherein the paradigm is shifting to target optimumCPP. It is believed that a certain minimum CPP isneeded to maintain adequate supply of O2 and essentialnutrients to brain. What should this minimum be andwhether this minimum should be adjusted according toa child’s age remains unclear. A review of availablestudies in pediatric TBI suggests that a CPP between 40-65 mmHg represents an optimum threshold; a CPP <40mmHg is associated with high risk of death.55
In a prospective observational study at Chandigarh,in children 3 months – 12 years old with raisedintracranial pressure caused by central nervous systeminfection, we were able to achieve a CPP greater than 50mm Hg in first 24 hours mainly by increasing the bloodpressure, and after 24 hours by using measures toreduce ICP. All 4 patients with mean CPP less than 50mm Hg died. In contrast, only 3 of 16 patients withmean cerebral perfusion pressure more than 50 mm Hgdied.56
CONCLUSION
Effective treatment of intracranial hypertensioninvolves meticulous avoidance of factors thatprecipitate or aggravate increased ICP. When ICPbecomes elevated, it is important to rule out surgicallytreatable lesions. Medical management of increased ICPshould include sedation, and osmotherapy with either

Sunit C Singhi and Lokesh Tiwari
528 Indian Journal of Pediatrics, Volume 76—May, 2009
mannitol or hypertonic saline and controlled short termhyperventilation if needed. For intracranialhypertension refractory to initial medical management,barbiturate coma, hypothermia, or decompressivecraniectomy should be considered. Steroids have a verylimited role and are not indicated routinely inintracranial hypertension resulting from TBI. Studieswith rather large sample size are needed to evaluatevarious established doctrine and therapies—to improvethe current standard of care. Few recent outcomestudies suggest that optimum values of CPP in childrenlie between 50-65 mm Hg, depending of their age.Pediatric Intensivity Level of Therapy (PILOT) scalemay be a useful tool to monitor intensity of treatmentused for ICP control and optimize the therapies.57
REFERENCES
1. Welch K. The intracranial pressure in infants. J Neurosurg1980;52:693-699.
2. Downward C, Hulka F, Mullins R et al. Relationship ofcerebral perfusion pressure and survival in pediatric brain-injured patients. J Trauma 2000;49: 654-659.
3. Adelson PD, Bratton SL, Carney NA et al. Guidelines for theacute medical management of severe traumatic brain injuryin infants, children, and adolescents: Chapter 6. Thresholdfor treatment of intracranial hypertension. Pediatr Crit CareMed 2003; 4: S25–S27.
4. Mazzola CA, Adelson PD. Critical care management ofhead trauma in children. Crit Care Med 2002; 30: S393–S401.
5. Marmarou A, Fatouros PP, Barzo P et al. Contribution ofedema and cerebral blood volume to traumatic brainswelling in head-injured patients. J Neurosurg 2000;93: 183–193.
6. Taneda M, Kataoka K, Akai F et al. Traumaticsubarachnoid hemorrhage as a predictable indicator ofdelayed ischemic symptoms. J Neurosurg 1996; 84: 762–768.
7. Kishore PR, LipperMH, Becker DP et al. Significance of CTin head injury: correlation with intracranial pressure. AJRAm J Roentgenol 1981; 137: 829–833.
8. Adelson PD, Bratton SL, Carney NA et al. Guidelines for theacute medical management of severe traumatic brain injuryin infants, children, and adolescents: Chapter 5. Indicationsfor intracranial pressure monitoring in pediatric patientswith severe traumatic brain injury. Pediatr Crit Care Med2003; 4: S19-S24.
9. O’Sullivan MG, Statham PF, Jones PA et al. Role ofintracranial pressure monitoring in severely head-injuredpatients without signs of intracranial hypertension on initialcomputerized tomography. J Neurosurg 1994; 80: 46–50.
10. Valentin A, Lan T, Karnik R, Ammerer HP, Ploder J, SlanyJ. Intracranial pressure monitoring and case mix-adjustedmortality in intracranial hemorrhage. Crit Care Med 2003; 31:1539–1542.
11. Lindvall P, Ahlm C, Ericsson M, Gothefors L, Naredi S,Koskinen LD. Reducing intracranial pressure may increasesurvival among patients with bacterial meningitis. Clin InfectDis 2004; 38: 384–390.
12. Rebaud R, Berthie JC, Hartemann E, Floret D. Intracranialpressure in childhood central nervous system infections.Intensive Care Med 1988; 14 : 522–525.
13. Adelson PD, Bratton SL, Carney NA et al. Guidelines for theacute medical management of severe traumatic brain injury
in infants, children, and adolescents: Chapter 7. Intracranialpressure monitoring technology. Pediatr Crit Care Med 2003;4: S28–S30.
14. Gopinath SP, Robertson CS, Contant CF et al. Clinicalevaluation of a miniature strain-gauge transducer formonitoring intracranial pressure. Neurosurgery 1995; 36:1137-1140.
15. Czosnyka M, Czosnyka Z, Pickard JD. Laboratory testingof three intracranial pressure microtransducers: technicalreport. Neurosurgery 1996; 38 : 219–224.
16. Lundberg N, Troupp H, Lorin H. Continuous recording ofthe ventricular fluid pressure in patients with severe acutetraumatic brain damage. A preliminary report. J Neurosurg1965; 22 : 581–90.
17. Mayhall CG, Archer NH, Lamb VA et al. Ventriculostomy-related infections: a prospective epidemiologic study. NEngl J Med 1984; 310 : 553–559.
18. Zabramski JM, Whiting D, Darouiche RO et al. Efficacy ofantimicrobial-impregnated external ventricular draincatheters: a prospective, randomized, controlled trial. JNeurosurg 2003; 98 : 725–730.
19. Roth P, Farls K. Pathophysiology of traumatic brain injury.Crit Care Nurs Q 2000; 23 : 14–25.
20. Pigula FA, Wald SL, Shackford SR, Vane DW. The effectof hypotension and hypoxia on children with severe headinjuries. J Pediatric Surg 1993; 28 : 310-316.
21. Ng I, Lim J, Wong HB. Effects of head posture on cerebralhemodynamics: its influences on intracranial pressure,cerebral perfusion pressure, and cerebral oxygenation.Neurosurgery 2004; 54 : 593–597.
22. Caricato A, Conti G, Della CF et al. Effects of PEEP on theintracranial system of patients with head injury andsubarachnoid hemorrhage: the role of respiratory systemcompliance. J Trauma 2005; 58 : 571–576.
23. Albanese J, Viviand X, Potie F et al. Sufentanil, fentanyl, andalfentanil in head trauma patients: a study on cerebralhemodynamics. Crit Care Med 1999; 27 : 407–411.
24. Jones PA, Andrews PJD, Midgley S et al. Measuring theburden of secondary insults in head-injured patients duringintensive care. J Neurosurg Anesth 1994; 6 : 4–14.
25. Biousse V, Rucker JC, Vignal C et al. Anemia andpapilledema. AmJ Ophthalmol 2003; 135 : 437–446.
26. Lacroix J, Herbert PC, Hutchison JS et al. Transfusionstrategies for patients in pediatric intensive care units. NEngl J Med 2007; 356: 1609-1619.
27. Adelson PD, Bratton SL, Carney NA et al. Guidelines for theacute medical management of severe traumatic brain injuryin infants, children, and adolescents: Chapter 19. The role ofanti-seizure prophylaxis following severe pediatrictraumatic brain injury. Pediatr Crit Care Med 2003; 4: S72–S74.
28. Adelson PD, Bratton SL, Carney NA et al. Guidelines for theacute medical management of severe traumatic brain injuryin infants, children, and adolescents: Chapter 11. Use ofhyperosmolar therapy in the management of severepediatric traumatic brain injury. Pediatr Crit Care Med 2003;4: S40-S44.
29. Knapp JM. Hyperosmolar therapy in the treatment of severehead injury in children: mannitol and hypertonic saline.AACN Clin Issues 2005; 16 : 199–211.
30. Cruz J, Minoja G, Okuchi K et al. Successful use of the newhigh-dose mannitol treatment in patients with GlasgowComa Scale scores of 3 and bilateral abnormal pupillarywidening: a randomized trial. J Neurosurg 2004; 100 : 376–383.
31. Paczynski RP. Osmotherapy. Crit Care Clin 1997; 13 : 105-129.

Management of Intracranial Hypertension
Indian Journal of Pediatrics, Volume 76—May, 2009 529
32. Battison C, Andrews PJ, Graham C et al. Randomized,controlled trial on the effect of a 20% mannitol solution anda 7.5% saline/6% dextran solution on increased intracranialpressure after brain injury. Crit Care Med 2005; 33 : 196–202.
33. Cooper DJ, Myles PS, McDermott FT et al. Prehospitalhypertonic saline resuscitation of patients with hypotensionand severe traumatic brain injury: a randomized controlledtrial. JAMA 2004; 291 : 1350-1357.
34. Khanna S, Davis D, Peterson B et al. Use of hypertonicsaline in the treatment of severe refractory posttraumaticintracranial hypertension in pediatric traumatic brain injury.Crit Care Med 2000; 28 : 1144-1151.
35. SchrammWM,Papousek A, Michalek-Sauberer A et al. Thecerebral and cardiovascular effects of cisatracuriumandatracurium in neurosurgical patients. Anesth Analg 1998; 86:123-127.
36. Adelson PD, Bratton SL, Carney NA et al. Guidelines for theacute medical management of severe traumatic brain injuryin infants, children, and adolescents: Chapter 9. Use ofsedation and neuromuscular blockade in the treatment ofsevere pediatric traumatic brain injury. Pediatr Crit Care Med2003; 4: S34-S37.
37. Adelson PD, Bratton SL, Carney NA et al. Guidelines for theacute medical management of severe traumatic brain injuryin infants, children, and adolescents: Chapter 12. Use ofhyperventilation in the acute management of severepediatric traumatic brain injury. Pediatr Crit Care Med 2003;4: S45-48.
38. Stocchetti N, Maas AI, Chieregato A et al. Hyperventilationin head injury: a review. Chest 2005; 127 : 1812-1827.
39. Coles JP, Steiner LA, Johnston AJ et al. Does inducedhypertension reduce cerebral ischaemia within thetraumatized human brain? Brain 2004; 127 : 2479-2490.
40. Diringer MN, Videen TO, Yundt K et al. Regionalcerebrovascular and metabolic effects of hyperventilationafter severe traumatic brain injury. J Neurosurg 2002; 96 :103-108.
41. Bader MK, Arbour R, Palmer S. Refractory increasedintracranial pressure in severe traumatic brain injury:barbiturate coma and bispectral index monitoring. AACNClin Issues 2005; 16 : 526-541.
42. Nordstrom CH, Messeter K, Sundbarg G et al. Cerebralblood flow, vasoreactivity, and oxygen consumption duringbarbiturate therapy in severe traumatic brain lesions. JNeurosurg 1988; 68 : 424-431.
43. Adelson PD, Bratton SL, Carney NA et al. Guidelines for theacute medical management of severe traumatic brain injuryin infants, children, and adolescents: Chapter 13. The use ofbarbiturates in the control of intracranial hypertension in
severe pediatric traumatic brain injury. Pediatr Crit Care Med2003; 4 : S49-S51.
44. Adelson PD, Ragheb J, Kanev P et al. Phase II clinical trialof moderate hypothermia after severe traumatic braininjury in children. Neurosurgery 2005; 56 : 740-754.
45. Hutchison JS, Ward RE, Lacroix J et al. Hypothermiatherapy after traumatic brain injury in children. N Engl JMed 2008; 358 : 2447-2457.
46. Kaal EC, Vecht CJ. The management of brain edema inbrain tumors. Curr Opin Oncol 2004; 16 : 593-600.
47. Edwards P, Arango M, Balica L et al. Final results of MRCCRASH, a randomised placebo controlled trial ofintravenous corticosteroid in adults with head injuryoutcomes at 6 months. Lancet 2005; 365 : 1957-1959.
48. Marchuk G, Kaufmann AM. Spontaneous supratentorialintracerebral hemorrhage: the role of surgical management.Can J Neurol Sci 2005; 32(Suppl 2) : S22-S30.
49. Shore P, Thomas NJ, Clark RSB et al. Continuous vs.intermittent cerebrospinal fluid drainage after severetraumatic brain injury in children: effect on biochemicalmarkers. J Neurotrauma 2004; 21 : 1113-1122.
50. Cheung A, Telaghani CK, Wang J et al. Neurologicalrecovery after decompressive craniectomy for massiveischemic stroke. Neurocrit Care 2005; 3 : 216-223.
51. Taylor A, Butt W, Rosenfeld J et al. A randomized trial ofvery early decompressive craniectomy in children withtraumatic brain injury and sustained intracranialhypertension. Childs Nerv Syst 2001; 17 : 154-162.
52. Ruf B, Heckmann M, Schroth I et al. Early decompressivecraniectomy and duraplasty for refractory intracranialhypertension in children: results of a pilot study. Crit Care2003; 7: R133-R138.
53. Figaji AA, Fieggen AG, Peter JC. Early decompressivecraniotomy in children with severe traumatic brain injury.Childs Nerv Syst 2003; 19 : 666-673.
54. Jagannathan J, Okonkwo DO, Dumont AS et al. Outcomefollowing decompressive craniectomy in children withsevere traumatic brain injury: a 10-year single-centerexperience with long-term follow up. J Neurosurg 2007; 106:268-275.
55. Adleson PD, Bratton SL, Carney NA et al. Chapter 8Cerebral perfusion pressure. PCCM 2003; 4 : 531-533.
56. Shetty R, Singhi S, Singhi P Jayashree M Cerebral perfusionpressure—targeted approach in children with centralnervous system infections and raised intracranial pressure:is it feasible? Child Neurol 2008; 23 : 192-198.
57. Shore PM, Hard LL, Roy L et al. Reliability and validity ofthe Pediatric Intensity Level of Therapy (PILOT) scale; Ameasure of the use of intracranial pressure - directedtherapies. Crit Care Med 2006; 34 : 1981-1987.