prevalance of pulmonary hypertension in
TRANSCRIPT
PREVALANCE OF PULMONARY HYPERTENSION IN PATIENTS WITH
CREATININE CLEARANCE LESS THAN 30ML/MIN PER 1.73 METER
SQUARE ON DIALYSIS
Dissertation submitted to
The Tamil Nadu Dr. M.G.R Medical University, Chennai
In fulfilment of the requirements for the award of the degree of
Doctor of Medicine in General Medicine
Under the guidance of
Dr. R. Tolstoy M.D.,
DEPARTMENT OF GENERAL MEDICINE
PSG INSTITUTE OF MEDICAL SCIENCES & RESEARCH,
COIMBATORE
THE TAMILNADU DR. M.G.R MEDICAL UNIVERSITY,
CHENNAI, TAMILNADU
MAY 2018
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “PREVALANCE OF
PULMONARY HYPERTENSION IN PATIENTS WITH CREATININE
CLEARANCE LESS THAN 30ML/MIN PER 1.73 METER SQUARE ON
DIALYSIS ” is the bonafide original work of Dr .VIGNESH .S done under my direct
guidance and supervision in the Department of General Medicine, PSG Institute of
Medical Sciences and Research, Coimbatore in fulfilment of the regulations by The
Tamil Nadu Dr. MGR Medical University, Chennai for the degree of Doctor of Medicine
in General Medicine.
Signature of the guide
Dr. R. Tolstoy M.D,
Professor of Medicine,
Department of General Medicine,
PSG IMS&R, Coimbatore.
CERTIFICATE BY THE HOD AND DEAN OF THE INSTITUTION
This is to certify that the dissertation entitled, “PREVALANCE OF
PULMONARY HYPERTENSION IN PATIENTS WITH CREATININE
CLEARANCE LESS THAN 30ML/MIN PER 1.73 METER SQUARE ON
DIALYSIS” is the bonafide original research work of Dr. VIGNESH.S under the
guidance of Dr. R. Tolstoy M.D., Professor of Medicine, PSG IMS&R, Coimbatore in
partial fulfilment of the requirements for the degree of Doctor of Medicine in General
Medicine.
Seal and Signature of the HOD Seal and Signature the Dean
Dr. JAYACHANDRAN.K, M.D., Dr. RAMALINGAM.S, M.D.,
HOD, Professor of medicine, Dean
Department of General Medicine, PSG IMS&R, Coimbatore
PSG IMS&R, Coimbatore.
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “PREVALANCE OF
PULMONARY HYPERTENSION IN PATIENTS WITH CREATININE
CLEARANCE LESS THAN 30ML/MIN PER 1.73 METER SQUARE ON
DIALYSIS” is a bonafide and genuine research work carried out by me under the
guidance of Dr. R.Tolstoy M.D., Professor of Medicine, PSG IMS&R, Coimbatore. This
dissertation is submitted to The Tamil Nadu Dr. M.G.R Medical University in fulfilment
of the university regulations for the award of MD degree in General Medicine. This
dissertation has not been submitted for award of any other degree or diploma.
Signature of the Candidate
Dr. VIGNESH.S
CERTIFICATE – II
This is to certify that this dissertation work titled “PREVALANCE OF
PULMONARY HYPERTENSION IN PATIENTS WITH CREATININE
CLEARANCE LESS THAN 30ML/MIN PER 1.73 METER SQUARE ON
DIALYSIS” of the candidate VIGNESH.S with registration Number 201511506 for the
award of DOCTOR OF MEDICINE in the branch of GENERAL MEDICINE. I
personally verified the urkund.com website for the purpose of plagiarism Check. I found
that the uploaded thesis file contains from introduction to conclusion pages and result
shows 8% of plagiarism in the dissertation.
Guide & Supervisor sign with Seal.
ACKNOWLEDGEMENT
I would like to express my deep sense of gratitude to my respected guide and
teacher Dr. R. TOLSTOY M.D., Professor, Department of General Medicine for her
valuable advice and guidance. I am very much thankful for her constant inspiration and
timely suggestions without which this study would have not been completed.
I would also extend my gratitude to Dr.K.Jayachandran, Professor and Head of
Department, Department of General Medicine, for his constant encouragement and
structural support in carrying out this study.
I also thank Dr.Sujithkumar M.D, Dr.Murali M.D, Dr.Saravanan M.D,
Dr.Sujaya Menon, and Dr.L.S.Somasundaram M.D, Professors in Department of
General Medicine for their constant support and encouragement.
My heartful thanks to Dr.Anithkumar M.D, MRCP, Dr.DeneshNarasimham
M.D, Dr.Jagadeeshwaran, Associate Professors, Department of General Medicine for
their support and guidance.
My heartful thanks to Dr.Santhni, Dr.Zeya Ansari, Dr.Velammal,
Dr.Yoganathan Assistant professors, Department of general medicine for their support.
I also extend my sense of gratitude to all my colleague post graduates and my
friends for their constant help and cooperation during the study.

I also extend my thanks to all the staff of Department of General Medicine, for
their help in carrying out the study.
Last but not the least, I am very much thankful to the all the patients involved in
the study without which my study would not have been possible.
CONTENTS
1. INTRODUCTION 2
2. AIM AND OBJECTIVES 6
3. MATERIALS AND METHODS 8
4. REVIEW OF LITERATURE 11
5. RESULTS 57
6. DISCUSSION 82
7. CONCLUSION 85
8. BIBLIOGRAPHY
9. ANNEXURES
i. PROFORMA
ii. ABBREVIATIONS
iii. CONSENT FORM
iv. LIST OF FIGURES
v. LIST OF TABLES
vi. MASTER CHART

1
TITLE
PREVALANCE OF PULMONARY HYPERTENSION IN PATIENTS WITH
CREATININE CLEARANCE LESS THAN 30ML/MIN PER 1.73 METER
SQUARE ON DIALYSIS
2
INTRODUCTION
Inspire of having advancement in field which helps in diagnosing pulmonary
hypertension, it remains the disease that takes lot of time for diagnosis from the presence
of first symptom, many patients are diagnosed only in advanced stage of disease.1
Normal pressure in pulmonary artery is 25/10mmHg if the pulmonary artery pressure
exceeds 40/20mmhg or average pressure exceeds 25mmHg, then the pulmonary
hypertension is present. If the pressure in the pulmonary artery is persistently high then
the right ventricle of the heart, from which the pulmonary artery arises, will not be able to
pump properly and then the symptoms of right heart failure will occur2. Pulmonary artery
pressure is increased by many conditions and pulmonary hypertension was classified
accordingly. Prevalence of pulmonary artery hypertension of WHO class1 which is
caused mainly by connective tissue disorder, drug, and toxic agents is 15 cases/million
adult population3, 4
.Prevalence of idiopathic pulmonary artery hypertension
5.9cases/million adult population5, 6, 7, 8
.
Pulmonary hypertension due to systemic sclerosis is 7-12% 9, 10
Pulmonary hypertension due to portal hypertension is 2-16%11, 12
Pulmonary hypertension due to congenital heart disease is 30%13
Pulmonary hypertension in sleep apnea is 15-20%14
3
Up to 60%,70% of the patients with severe left ventricular systolic dysfunction, heart
failure with preserved ejection fraction may present with pulmonary hypertension
respectively. Almost all the patient’s mitral value diseases have pulmonary hypertension
and 65% of those with symptomatic aortic stenosis also will have pulmonary
hypertension15, 16, and 17
.
Chronic thrombo embolic pulmonary hypertension (CTEPH) prevalence was
3.2cases/million/year and incidents were 0.9cases/million/year. Severe pulmonary
hypertension is uncommon in this conditions, severe pulmonary hypertension is only
present in combined emphysema/fibrosis syndrome. A large survey that is conducted in
united states that registered information from all form of pulmonary hypertension from
1980-2002 documented that death rate in patients with pulmonary hypertension during
these time were stable and ranging from 5.2-5.4deaths/1,00,00018, 19, 20, 21
.
Chronic kidney disease (CKD) encompasses a spectrum of different pathophysiologic
processes associated with abnormal kidney function and a progressive decline in
glomerular filtration rate (GFR) 1
CKD is classified based on GFR category (G1-G5) and albuminuria category (A1-A3)
G1 – ≥ 90
G2 – 60-89
G3 – 45-54
G3b – 30-44
4
G4 – 15-29
G5 – < 15
A1 – <30mg/g, <3mg/mmol
A2 – 30-300mg/g, 3-30mg/mmol
A3 – >300mg/g, >30mg/mmol22
CKD is the global health burden with high economic cost to health system and is an
independent risk factor for coronary vascular disease. All stages of CKD are associated
with increased risk of cardio vascular premature mortality, morbidity and decreased
quality of life.
A symptomatic review and meta-analysis of observational study estimating CKD
prevalence in general population was conducted through literature searches in 8
databases. Assessed pooled data using a random effect model of 5842 potential articles,
100 studies of diverse quality were included comprising 6,908,440 patients.
CKD prevalence of stage 5 13.4% (11.7-15.1%) and stage 3.5 was 10.6% (9.2-12.2%).
Stage1 (eGFR>90 + ACR>30) prevalence was 3.5% (2.8-4.2%).
Stage2 (eGFR>60-89 +ACR>30) prevalence was 3.9% (2.7-5.3%).
Stage3 (eGFR 30-50) prevalence was 7.6% (6.4-8.9%).
Stage4 (eGFR 29-15) prevalence was 0.4% (0.3-0.5%).
Stage5 (eGFR <15) prevalence was 0.1% (0.1-0.1%) 23
.
5
Pulmonary artery hypertension in renal disease is an on-going research topic since it has
very limited data.
Prevalence of pulmonary hypertension ranges from 9-39% in stage5 CKD.
Prevalence of pulmonary hypertension in haemodialysis patients range from 18.8-68.8%
Prevalence was 0-4.2% in patients with peritoneal dialysis; no epidermological data are
available yet for early stages of CKD3.
Pulmonary hypertension has direct association with mortality in end stage renal disease.
ESRD increases cardio vascular disease & use of hospitalization in advanced centres.
Pulmonary hypertension in end stage renal disease is associated with the worst
outcomes24-33
.
Pulmonary hypertension should be prevented in patient with ESRD and it’s important
because even kidney transplantation may not reverse. The high risk of mortality
associated with established pulmonary hypertension3.
Finding prevalence of pulmonary hypertension in early stages of chronic kidney disease
is important because it has a large population and bears a very high burden of cardio
vascular mortality and morbidity24
.
6
AIMS AND OBJECTIVES
To find the prevalence of pulmonary hypertension in patients with glomerular
filtration rate less than 30ml/min per 1.73 meter square on dialysis in PSGIMSR
To find the significance of volume overload association with pulmonary
hypertension
To find the significance of mild left ventricular dysfunction association with
pulmonary hypertension
To find the significance of arterial venous fistula association with pulmonary
hypertension
To find the significance of duration of dialysis association
With pulmonary hypertension
To find the significance of left ventricular diastolic dysfunction association with
pulmonary hypertension
To find the significance of diabetic mellitus association with pulmonary
hypertension
To find the significance of systemic hypertension association with pulmonary
hypertension
To find the significance of anaemia association with pulmonary hypertension
To find the percentage of male and female in our study group and to find the
significance of their association with pulmonary hypertension
7
To find the distribution of the pulmonary hypertension among different age
groups
To find the significance of superimposed infection association with pulmonary
hypertension
To find the significance of creatinine clearance association with pulmonary
hypertension
8
MATERIALS AND METHODS
Type of study: hospital based prospective observational study
Duration of Study: One year (august 2016 – august 2017)
Sample size: 50
Study volunteers / participants are (specify population group & age group):
Patients with age more than 18 years of age whose creatinine clearance less than
30ml/min per 1.73 meter square on dialysis
Location: PSG Hospitals, PSGIMS&R, and Coimbatore.
Inclusion Criteria
Age>18years
Patients with GFR less than 30 ml/min per 1.73 meter square
Exclusion Criteria
Patients who has ejection fraction less than 45%
Patients who are known case of chronic lung disease
Patients who are known case of thrombo embolic disease
Patients who are known case of sarcoidosis
Patients who are known case of sickle cell disease
Patients who are known case of HIV
9
Patients who are known case of connective tissue disorder
Patients who are known case of sleep disordered breathing
Patients who are already diagnosed with portal hypertension
Patients who are known case of congenital heart disease
METHODOLOGY
The study is based on the prospective collection of patients aged more than 18 years who
fulfilled the inclusion criteria stated above with GFR less than 30 ml/min per 1.73 meter
square on dialysis, who were admitted in tertiary care centre (PSGIMSR) and found to
have pulmonary hypertension on echo during the study period of one year between
august 2016 to august 2017, are taken in to consideration for the study , where systemic
computer coding for registry is used. A Performa was made which included the detailed
history clinical examination requisite investigations available in the hospital. After taking
informed consent from the patient, history and risk factor attributed to pulmonary
hypertension in our study group are collected in detail. Investigations like complete
hemogram, routine urine analysis, blood sugar, serum electrolyte, serum creatinine, blood
urea, thyroid profile, liver function test, ultrasound abdomen and pelvis, retroviral
serology, hepatitis B and C serology, chest X-ray, echocardiogram, electrocardiogram
were done. GFR is calculated with the help of Cockcroft-gault formula. Diagnosis of
pulmonary hypertension is made with the help of echocardiogram (if RVSP more than
50). Finally the prevalence of pulmonary hypertension and the significance of risk factor
10
association with pulmonary hypertension is calculated, descriptive and statistical analysis
and interpretation of the data collected is done.
STATISTICAL TOOLS:
The data collected from the patients is tabulated using Microsoft Excel. The data
are reported as the mean +/- SD or the median, depending on their distribution. The
differences in quantitative variables between groups were assessed by means of the
unpaired t test. Comparison between groups was made by the non-parametric Mann-
Whitney test. ANOVA was used to assess the variables. The chi square test was used to
assess the difference in categorical variables between groups.
Descriptive analysis is done using chi square test and statistical analysis and
interpretation of the data collected is done by using SPSS version 20. p value of
<0.05 using two tailed test was taken as being of significance for all statistical tests. All
data were analysed with a statistical software package (SSPS version 16.0 for windows)
11
REVIEW OF LITERATURE
Pulmonary trunk gives origin to the pulmonary artery that brings deoxygenated blood
from the right ventricle just below vertebral level T4 pulmonary trunk bifurcates trachea
lies just in front of that left pulmonary artery is smaller than the right pulmonary artery.
Pulmonary artery passes through the mediastinum horizontally. pulmonary artery lies just
anterior to the right main bronchus and slightly inferior to the tracheal bifurcation after
entering the root of the lung pulmonary artery gives branch to the superior lobe of the
lung. Second branch originate from the main pulmonary artery after the main vessel
passes through the hilum of the lung. Superior lobe of the lung was applied by the second
branch of the main pulmonary artery then the main pulmonary artery supply the middle
and inferior lobes of the lung by dividing in to two branches just anterior to the
descending aorta left pulmonary artery will be present and it’s lies posterior to the
superior pulmonary vein and it gives of branches within the lung after passing through
the root and hilum34
.
The load on the right side of the heart is increased by constriction of pulmonary arteries.
Pulmonary blood flow is affected by various factors. There are lot of autonomic
innervation in the pulmonary vessels, and their sympathetic stimulation reduces
pulmonary blood flow. The vessels will also respond to several circulating molecules.
Different receptors have different effect on pulmonary smooth muscle. Pulmonary
vascular dilation is caused by number of circulating molecules but dilation occurs mainly
in response to release of nitric oxide (NO). Pulmonary blood flow is also influenced by
12
cardiac output and gravitational forces. Pulmonary arterial pressure increases in response
to exercise with no or minimal vasodilation. O2 saturation of the haemoglobin in the red
cells is not reduced while passing through the lung, that in turn increased the amount of
oxygen delivered to the systemic circulation. These leads to dilation of capillaries, so
previously non-functioning Capillaries will also become functional, so finally there will
be increase in blood flow to the pulmonary vessels. If an air way get obstructed
ventilation of alveoli will be reduced leading to hypoxia, this hypoxic state acts on the
vascular smooth muscle leading to vasoconstriction of the pulmonary vessels supplying
the particular area that gets obstructed and there will be shunting of blood away from the
hypoxic area. In obstructed area there will be accumulation of co2 that leads to fall in pH,
which causes vasoconstriction in the lungs (but in other parts of the body fall in pH
causes vasodilation). Conversely, if there is a reduction in flow to a part of the lung there
will be reduction in pco2 in that particular area which in turn leads to vasoconstriction of
the bronchi supplying it, shifting the ventilation away from that area. Systemic hypoxia
can also cause pulmonary arterial hypertension due to constriction of pulmonary
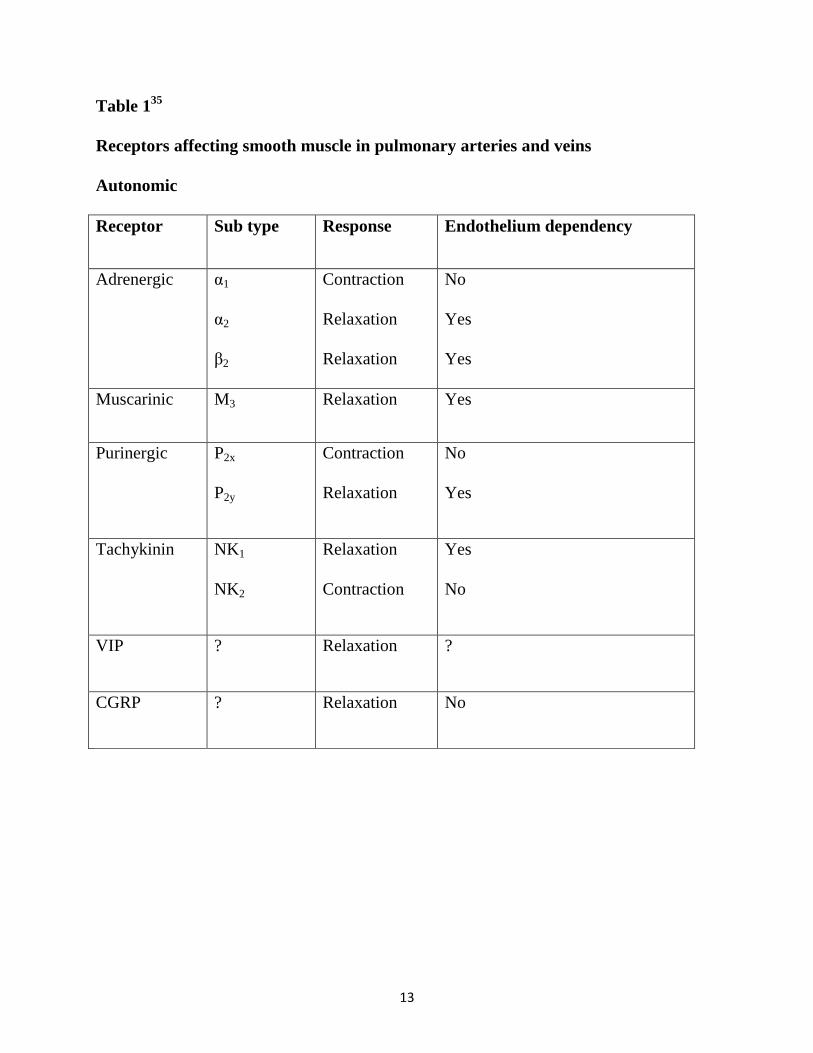
arterioles. Following are the autonomic and humoral agents that affect the receptors in the
pulmonary artery smooth muscles35
13
Table 135
Receptors affecting smooth muscle in pulmonary arteries and veins
Autonomic
Receptor Sub type Response Endothelium dependency
Adrenergic α1
α2
β2
Contraction
Relaxation
Relaxation
No
Yes
Yes
Muscarinic M3 Relaxation Yes
Purinergic P2x
P2y
Contraction
Relaxation
No
Yes
Tachykinin NK1
NK2
Relaxation
Contraction
Yes
No
VIP ? Relaxation ?
CGRP ? Relaxation No

14
Humoral
Receptor Sub type Response Endothelium
dependency
Adenosine A1
A2
Contraction
Relaxation
No
No
Angiotensin -2 AT1 Contraction No
ANP ANPA
ANPB
Relaxation
Relaxation
No
No
Bradykinin B1
B2
Relaxation
Relaxation
Yes
Yes
Endothelin ETA
ETB
Contraction
Relaxation
No
Yes
Histamine H1
H2
Relaxation
Relaxation
Yes
No
5-HT 5-HT1
5-HT1c
Contraction
Relaxation
No
Yes
Thromboyane TP Contraction No
Vasopressin V1 Relaxation Yes
15
DEFINITION
proper way measuring pulmonary artery pressure is by doing right heart catheterization
for the patient, pulmonary artery hypertension is defined as (PAPm) pulmonary artery
pressure more than or equal to 25mmHg at rest & the normal PAPm at rest should be
between 11 & 17. There is lack of data to define PH on exercise
pulmonary hypertension is hemodynamically classified into
pre capillary ,
post capillary,
isolated post capillary,
combined pre &post capillary
with the help of pulmonary artery pressure PAP, pulmonary artery wedge pressure
PAWP,pulmonary vascular resistance PVR, diastolic pressure gradient DPG.
16
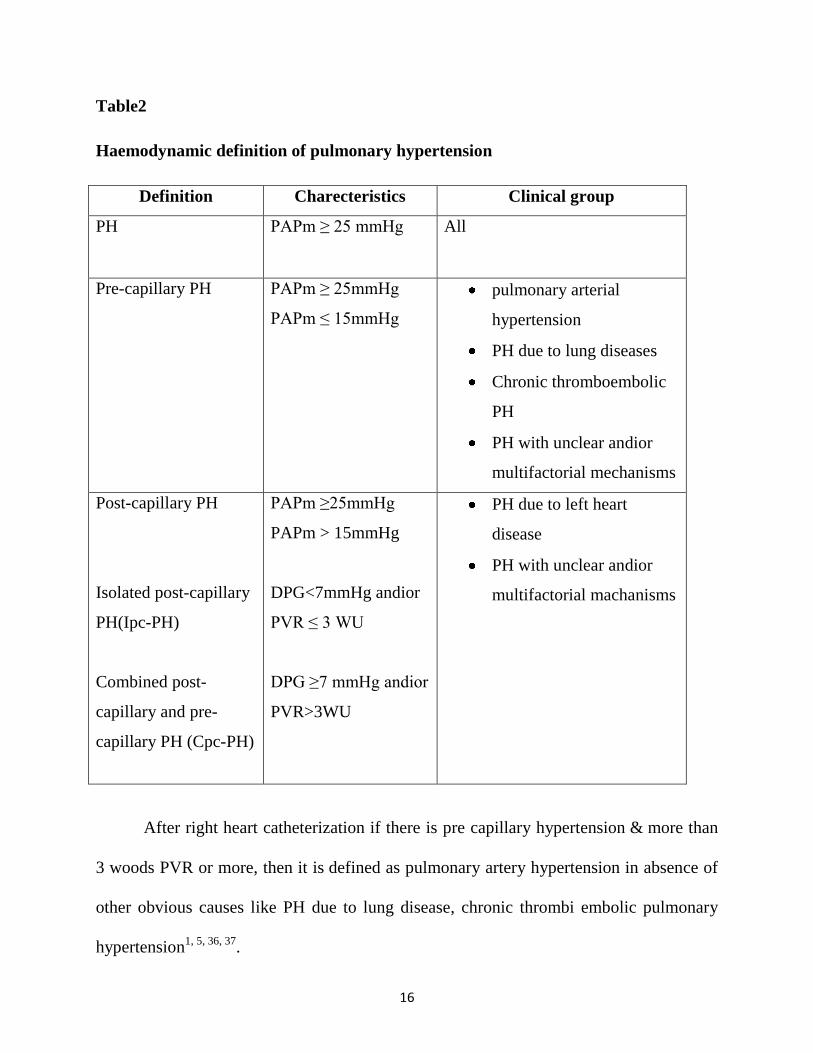
Table2
Haemodynamic definition of pulmonary hypertension
Definition Charecteristics Clinical group
PH PAPm ≥ 25 mmHg All
Pre-capillary PH PAPm ≥ 25mmHg
PAPm ≤ 15mmHg
pulmonary arterial
hypertension
PH due to lung diseases
Chronic thromboembolic
PH
PH with unclear andior
multifactorial mechanisms
Post-capillary PH
Isolated post-capillary
PH(Ipc-PH)
Combined post-
capillary and pre-
capillary PH (Cpc-PH)
PAPm ≥25mmHg
PAPm > 15mmHg
DPG<7mmHg andior
PVR ≤ 3 WU
DPG ≥7 mmHg andior
PVR>3WU
PH due to left heart
disease
PH with unclear andior
multifactorial machanisms
After right heart catheterization if there is pre capillary hypertension & more than
3 woods PVR or more, then it is defined as pulmonary artery hypertension in absence of
other obvious causes like PH due to lung disease, chronic thrombi embolic pulmonary
hypertension1, 5, 36, 37
.
17
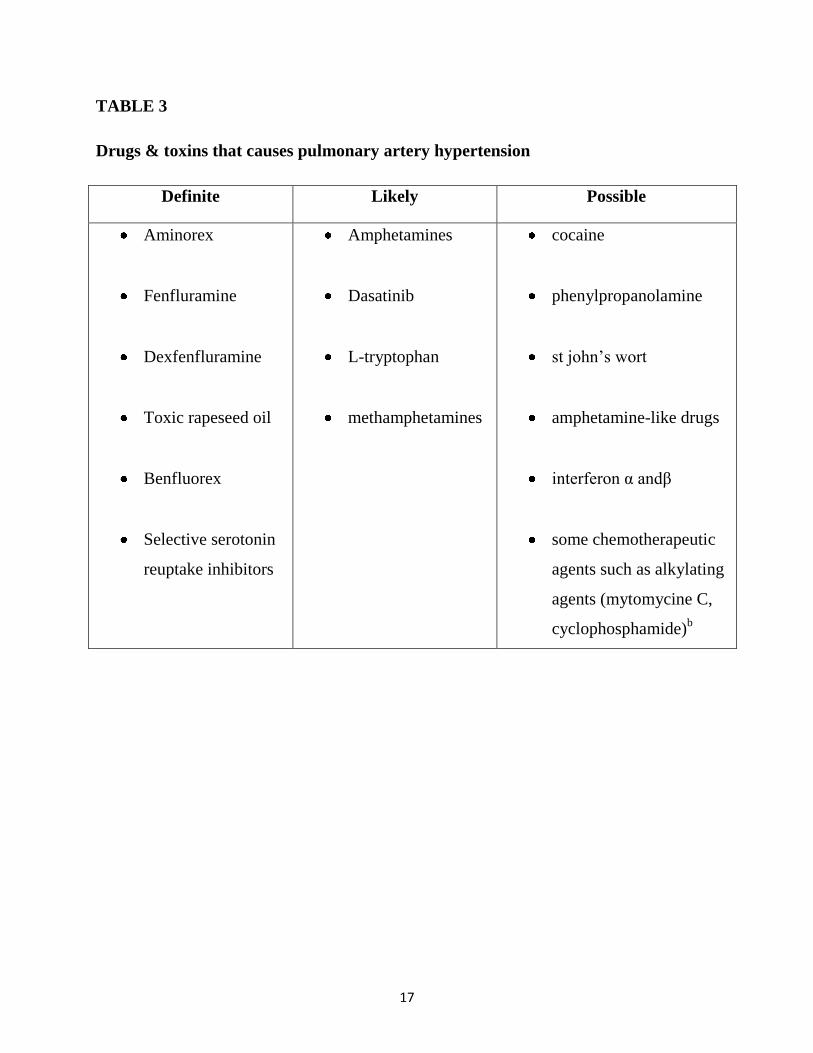
TABLE 3
Drugs & toxins that causes pulmonary artery hypertension
Definite Likely Possible
Aminorex
Fenfluramine
Dexfenfluramine
Toxic rapeseed oil
Benfluorex
Selective serotonin
reuptake inhibitors
Amphetamines
Dasatinib
L-tryptophan
methamphetamines
cocaine
phenylpropanolamine
st john’s wort
amphetamine-like drugs
interferon α andβ
some chemotherapeutic
agents such as alkylating
agents (mytomycine C,
cyclophosphamide)b
18
GENETICS
Heterogeneous BMPR2 mutation ,
mutation of genes coding for action receptor like kinase 1 & endoglin,
mutations in BMPR1B & SMAD9,
rarely mutations in genes coding for protein such as caveolin 1 & KCNK3 can be
the causative agent for group 1 PAH.
other possibilities that causes group 1 PAH includes recessive transmission from
consanguineous marriages, bi-allelic mutation in EIF2AK4.
There is no association of genetic mutation with group 2 &group 4 pulmonary
hypertension.
Among group 3,gene polymorphism is associated with severity of pulmonary
hypertension in COPD38-42
.
19
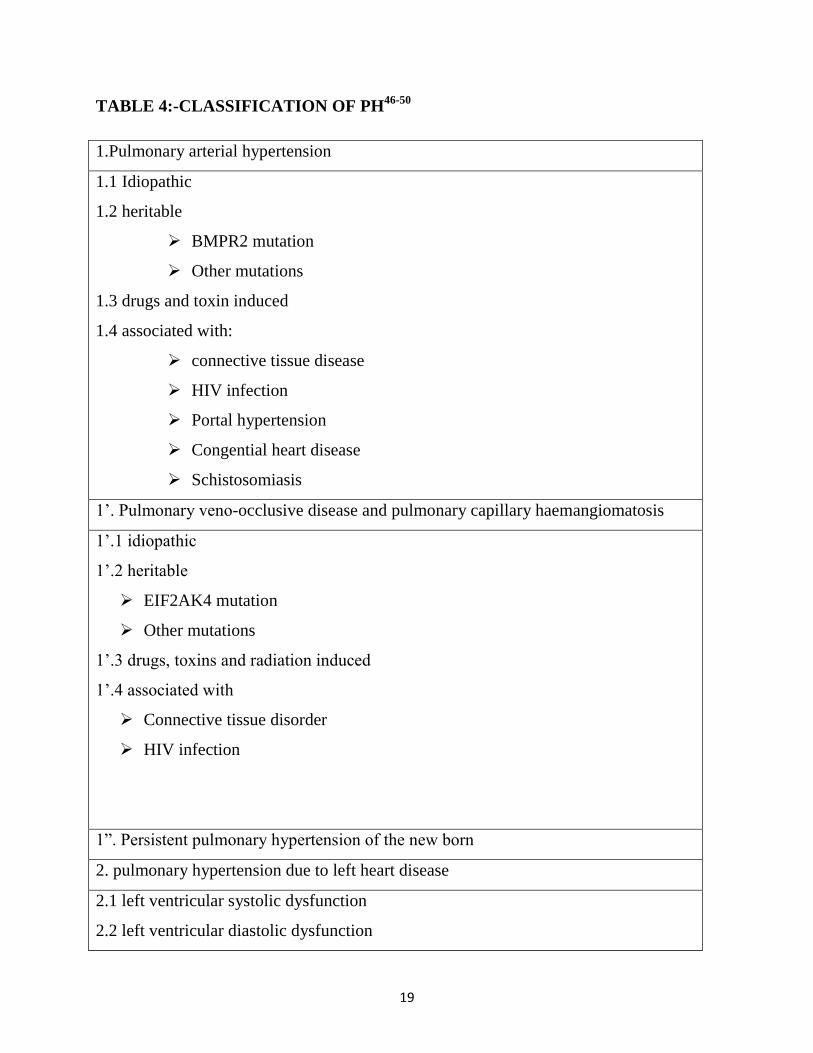
TABLE 4:-CLASSIFICATION OF PH46-50
1.Pulmonary arterial hypertension
1.1 Idiopathic
1.2 heritable
BMPR2 mutation
Other mutations
1.3 drugs and toxin induced
1.4 associated with:
connective tissue disease
HIV infection
Portal hypertension
Congential heart disease
Schistosomiasis
1’. Pulmonary veno-occlusive disease and pulmonary capillary haemangiomatosis
1’.1 idiopathic
1’.2 heritable
EIF2AK4 mutation
Other mutations
1’.3 drugs, toxins and radiation induced
1’.4 associated with
Connective tissue disorder
HIV infection
1”. Persistent pulmonary hypertension of the new born
2. pulmonary hypertension due to left heart disease
2.1 left ventricular systolic dysfunction
2.2 left ventricular diastolic dysfunction
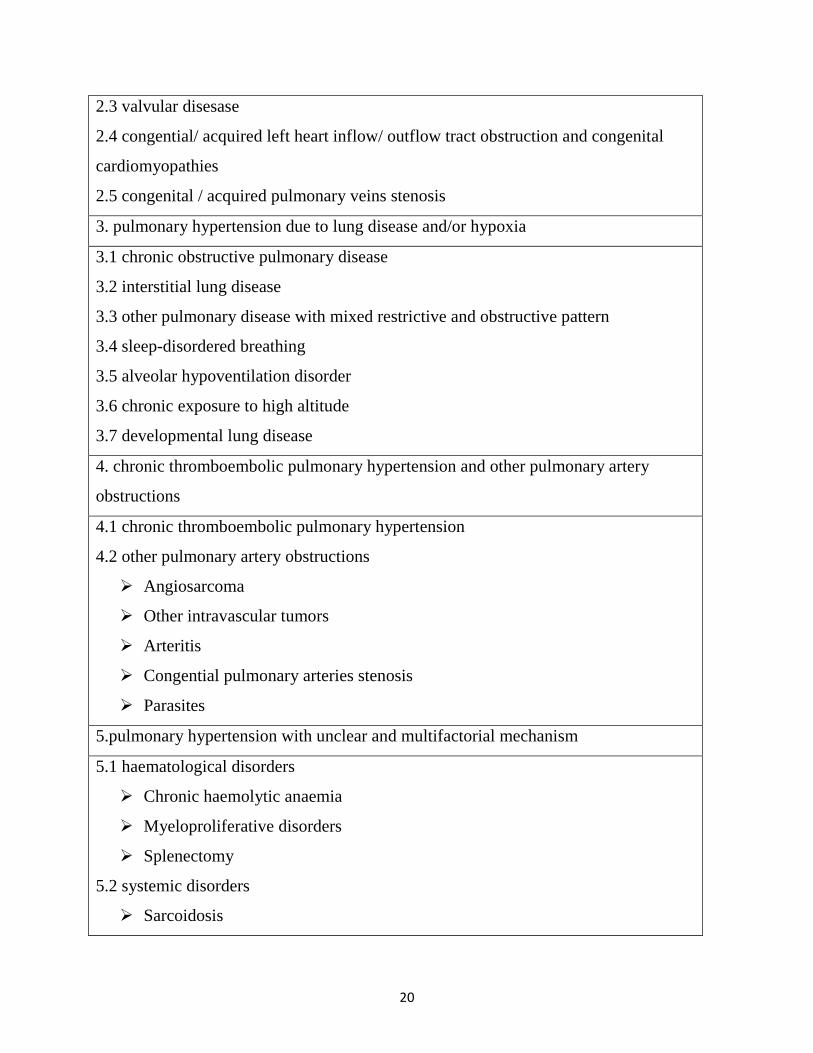
20
2.3 valvular disesase
2.4 congential/ acquired left heart inflow/ outflow tract obstruction and congenital
cardiomyopathies
2.5 congenital / acquired pulmonary veins stenosis
3. pulmonary hypertension due to lung disease and/or hypoxia
3.1 chronic obstructive pulmonary disease
3.2 interstitial lung disease
3.3 other pulmonary disease with mixed restrictive and obstructive pattern
3.4 sleep-disordered breathing
3.5 alveolar hypoventilation disorder
3.6 chronic exposure to high altitude
3.7 developmental lung disease
4. chronic thromboembolic pulmonary hypertension and other pulmonary artery
obstructions
4.1 chronic thromboembolic pulmonary hypertension
4.2 other pulmonary artery obstructions
Angiosarcoma
Other intravascular tumors
Arteritis
Congential pulmonary arteries stenosis
Parasites
5.pulmonary hypertension with unclear and multifactorial mechanism
5.1 haematological disorders
Chronic haemolytic anaemia
Myeloproliferative disorders
Splenectomy
5.2 systemic disorders
Sarcoidosis
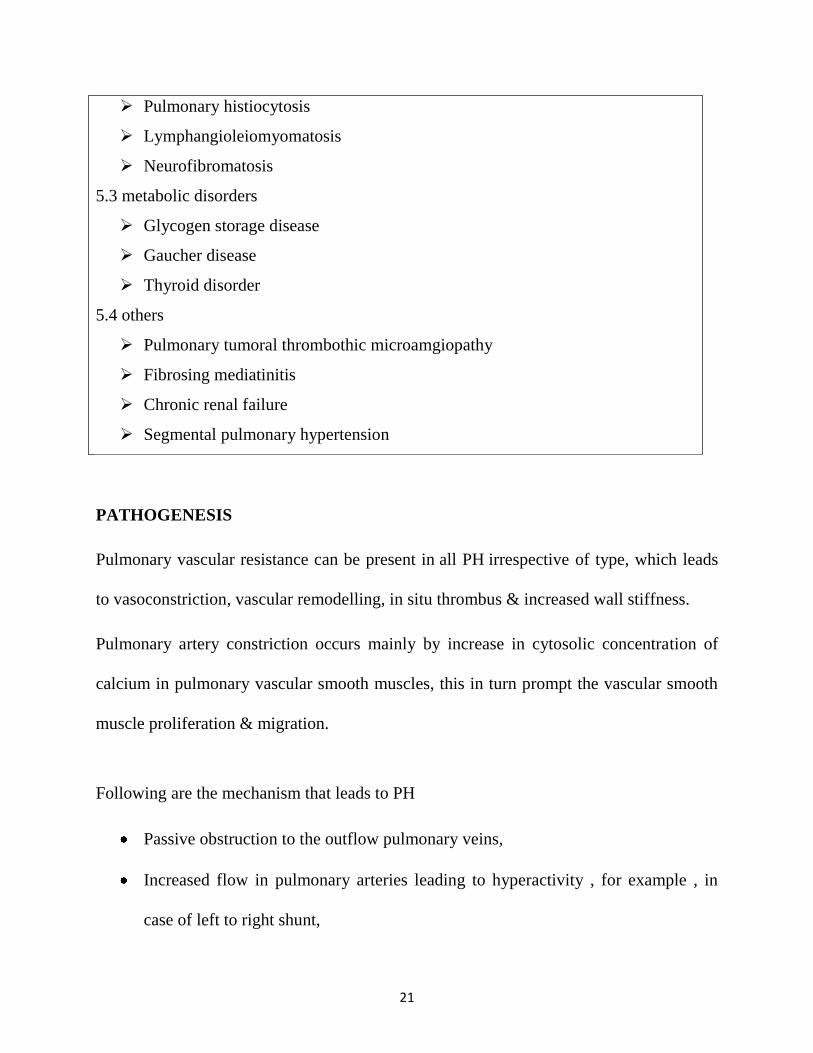
21
Pulmonary histiocytosis
Lymphangioleiomyomatosis
Neurofibromatosis
5.3 metabolic disorders
Glycogen storage disease
Gaucher disease
Thyroid disorder
5.4 others
Pulmonary tumoral thrombothic microamgiopathy
Fibrosing mediatinitis
Chronic renal failure
Segmental pulmonary hypertension
PATHOGENESIS
Pulmonary vascular resistance can be present in all PH irrespective of type, which leads
to vasoconstriction, vascular remodelling, in situ thrombus & increased wall stiffness.
Pulmonary artery constriction occurs mainly by increase in cytosolic concentration of
calcium in pulmonary vascular smooth muscles, this in turn prompt the vascular smooth
muscle proliferation & migration.
Following are the mechanism that leads to PH
Passive obstruction to the outflow pulmonary veins,
Increased flow in pulmonary arteries leading to hyperactivity , for example , in
case of left to right shunt,
22
damage to pulmonary vascular bed due to parenchymal disease,
hypoxia induced vasoconstriction,
Different groups of pulmonary hypertension has different pathological features , in case
of pulmonary artery hypertension distal arteries of diameter less than 500 mm in diameter
are more commonly involved.
Adventitialthickening,
intimal proliferative & fibrotic changes,
moderate perivascular inflammatory infiltrates,
complex lesions,
medial hypertrophy and
thrombotic lesions are the main pathological findings.
Pulmonary veins are involved only in case of pulmonary vent occlusive disease. Septal&
preseptal veins are mainly involved. Following are the main pathological findings in case
of venoocclussive disease
occlusive fibrotic lesions,
venous muscularization,
patchy capillary proliferation,
pulmonary edema,
occult alveolar haemorrhage,
23
inflammatory infiltrations &
lymphatic dilation with lymph node enlargement.
In this condition distal pulmonary arteries are involved due to medial hypertrophy,
intimal fibrosis, & uncommon complex lesions.
Pathological findings in left sided heart disease induced pulmonary hypertension include
enlarged & thickened pulmonary veins,
pulmonary capillary dilation,
interstitial edema,
alveolar haemorrhage and lymphatic vessels
& lymph node enlargement.
Medial hypertrophy & intimal fibrosis are the reason behind pulmonary artery
involvement.Pulmonary hypertension due to lung disease causes medial hypertrophy &
intimal obstructive proliferation of distal pulmonary arteries. There will be damage to
vascular bed around the involved parenchyma.
Thrombi that are formed from chronic thrombi embolic pulmonary hypertension will
firmly clinch to medial layer of pulmonary artery causing partial or complete occlusion,
collateral will originate from other systemic circulation
Group 5 PH has lot of causes hence pathogenesis also variable43-45
.

24
Diagram1
Features of plexogenic pulmonary arteriopathy are shown in this diagram1
25
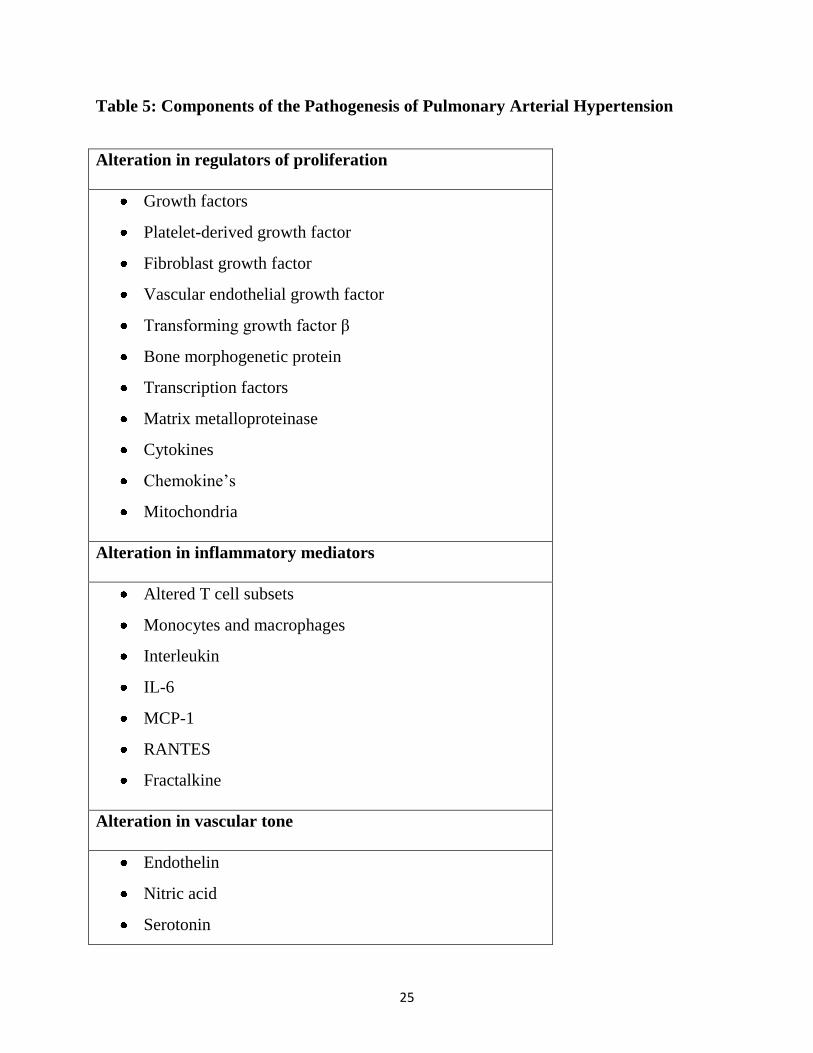
Table 5: Components of the Pathogenesis of Pulmonary Arterial Hypertension
Alteration in regulators of proliferation
Growth factors
Platelet-derived growth factor
Fibroblast growth factor
Vascular endothelial growth factor
Transforming growth factor β
Bone morphogenetic protein
Transcription factors
Matrix metalloproteinase
Cytokines
Chemokine’s
Mitochondria
Alteration in inflammatory mediators
Altered T cell subsets
Monocytes and macrophages
Interleukin
IL-6
MCP-1
RANTES
Fractalkine
Alteration in vascular tone
Endothelin
Nitric acid
Serotonin
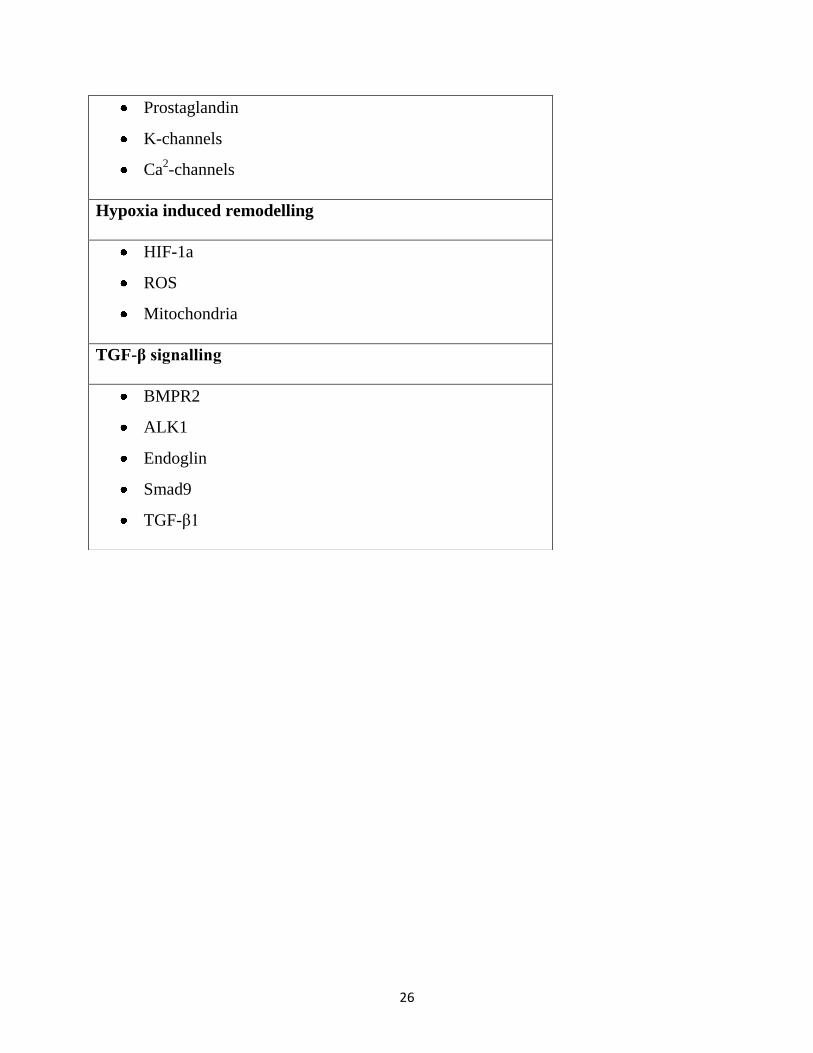
26
Prostaglandin
K-channels
Ca2-channels
Hypoxia induced remodelling
HIF-1a
ROS
Mitochondria
TGF-β signalling
BMPR2
ALK1
Endoglin
Smad9
TGF-β1
27
CLINICAL MANIFESTATIONS
Dyspnea is the most common symptom of PH; this is nonspecific because it can be
caused by variety of other conditions like
acute coronary syndrome,
bronchial asthma, and
other cardiac diseases.
other symptoms that are presenting PH includes
edema,
chest pain,
pre syncope,
Frank syncope
But these complaints have direct association with severity of the disease.
Dry cough can also occur in case of PH. fatigue can also occur in PH.
In some cases leg swelling, abdominal distension, are the main symptoms, these
symptoms occurs only if there is advanced disease with right heart failure.
Mechanical complication of ph. produces some symptoms those includes
haemoptysis,
hoarseness of voice,
wheeze,
angina,
28
haemoptysis occurs secondary to obstruction rupture of hypertrophied artery,
left laryngeal nerve compression by dilated pulmonary artery causes hoarseness of
voice,
compression to large airway causes wheeze,
compression of left main pulmonary artery causes myocardial ischemia,
signs & symptoms of cardiac tamponade occurs in case of rupture of pulmonary
artery.
Signs of right heart failure like elevated JVP, pedal edema & ascites will be there
in case of right heart failure.
Pulmonary stenosis murmur, tricuspid regurgitation murmur can be heard there
will be loud second heart sound especially p2 component. Parasternal heave may be
present.Clubbing cyanosis, sclerodactyly, Raynaud’s phenomenon, splenomegaly, palmar
erythema, icterus, and ascites may be present143,5
.
29
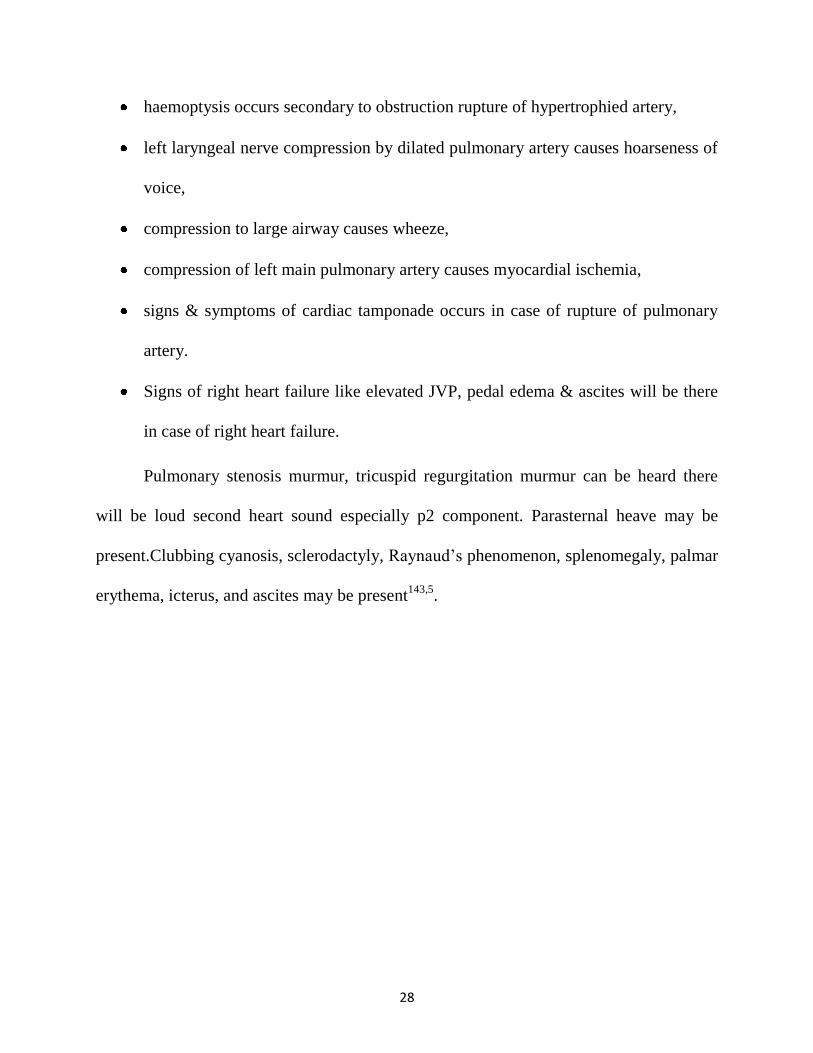
Table 6: Physical sign that suggest a possible underlying cause or associations of
pulmonary hypertension
Sign Implication
Central cyanosis Abnormal ventilation-perfusion ratio,
intrapulmonary shunt, hypoxemia,
pulmonary-to-systemic shunt
Clubbing CHD, pulmonary venopathy
Cardiac auscultatory findings, including
systolic murmurs, diastolic murmurs,
opening snap, and gallop
Congenital or acquired heart or valvular
disease
Rales, dullness, or decreased breath sounds Pulmonary congestion, effusion or both
Fine rales, accessory muscle use,
wheezing, protracted expiration,
productive cough
Pulmonary parenchymal disease
Obesity, kyphoscoliosis, enlarged tonsils Possible substrate for disordered
ventilation
Sclerodactyly, arthritis, telangiectasia,
Raynaud phenomenon, rash
Connective tissue disorder
Peripheral venous insufficiency or
obstruction
Possible venous thrombosis
Venous stasis ulcers Possible SCD
Pulmonary vascular bruits Chronic thromboembolic PH
Splenomegaly, spider angiomas, palmar
erythema, icterus, caput medusa, ascites
Portal hypertension
30
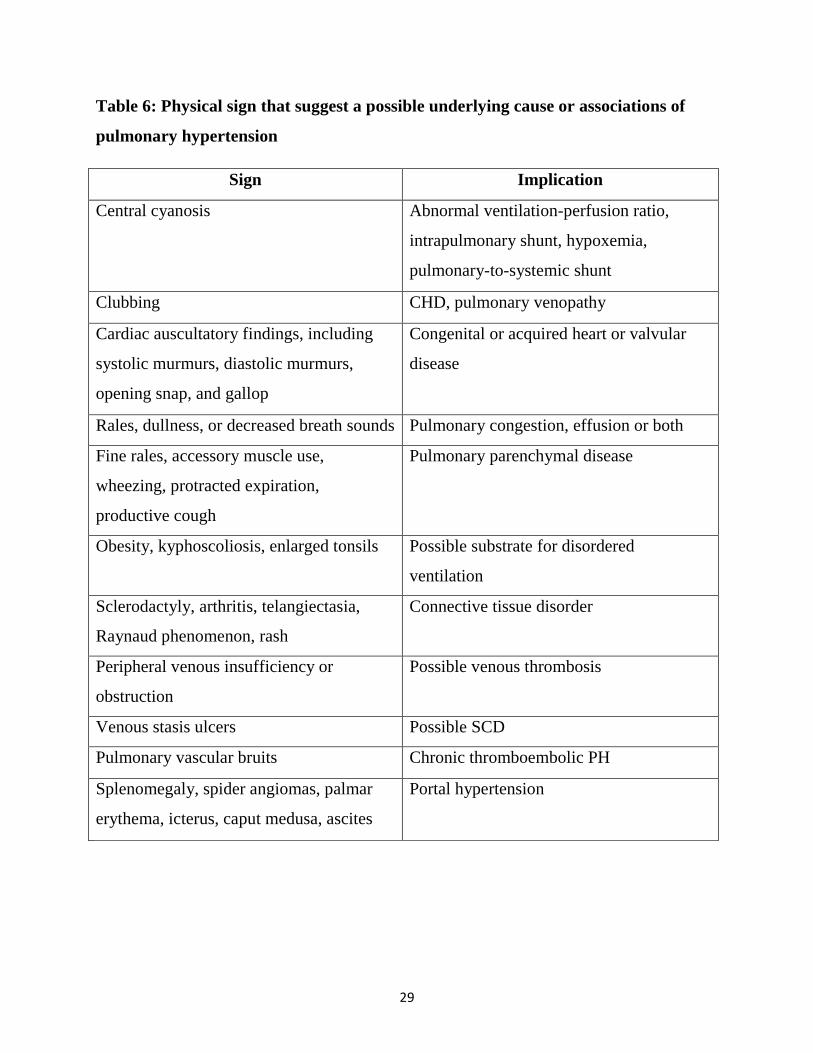
Table 6: Physical sign that reflect severity of pulmonary hypertension
Sign Implication
Accentuated pulmonary
component of s2 (audible at the
apex in>90%)
High pulmonary pressure increase the
force of pulmonic valve closure
Early systolic click Sudden interruption of opening of the
pulmonary valve in to high pressure
artery
Midsystolic ejection murmur Turbulent transvalvular pulmonary
outflow
Left parasternal lift High right ventricular pressure and
hypertrophy present
Right ventricular s4(in 38%) High right ventricular pressure and
hypertrophy present
Increased jugular a wave Poor right ventricular compliance
31
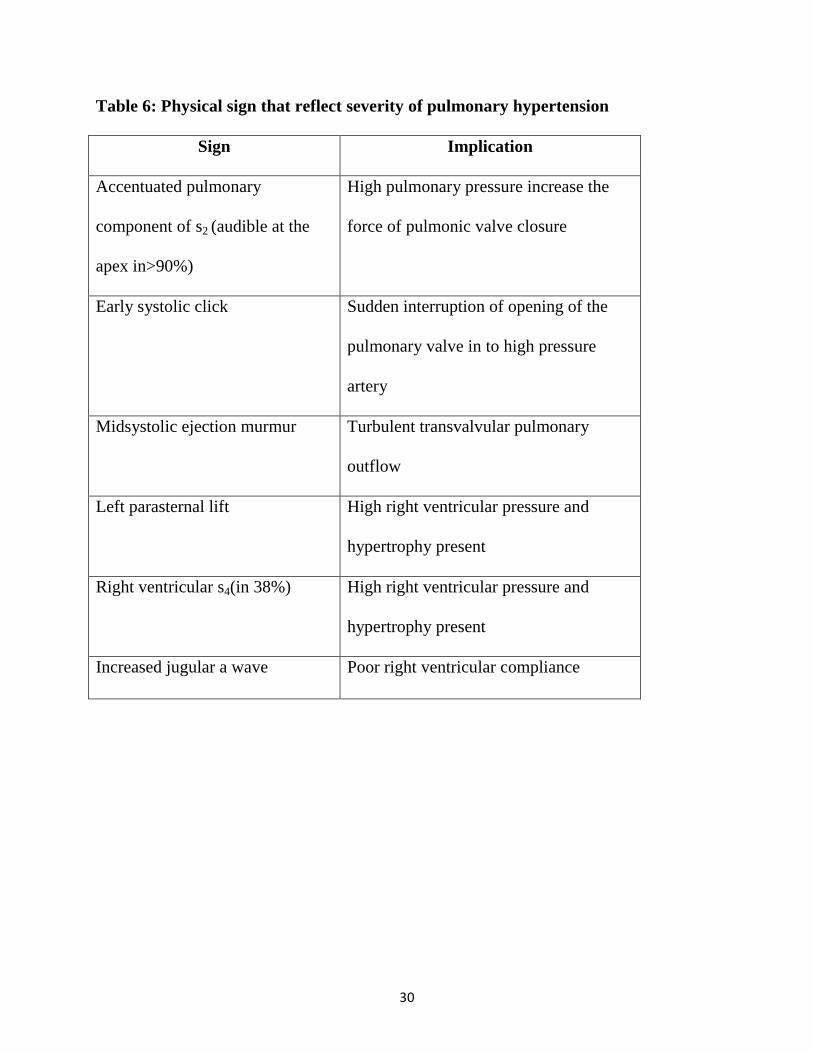
Physical signs that suggest moderate to severe pulmonary hypertension
Moderate to severe PH
Sign Implication
Holosystolic murmur that increase with inspiration Tricuspid regurgitation
Increased jugular v waves
Pulsatile liver
Diastolic murmur Pulmonary regurgitation
Hepatojugular reflux High central venous pressure
32
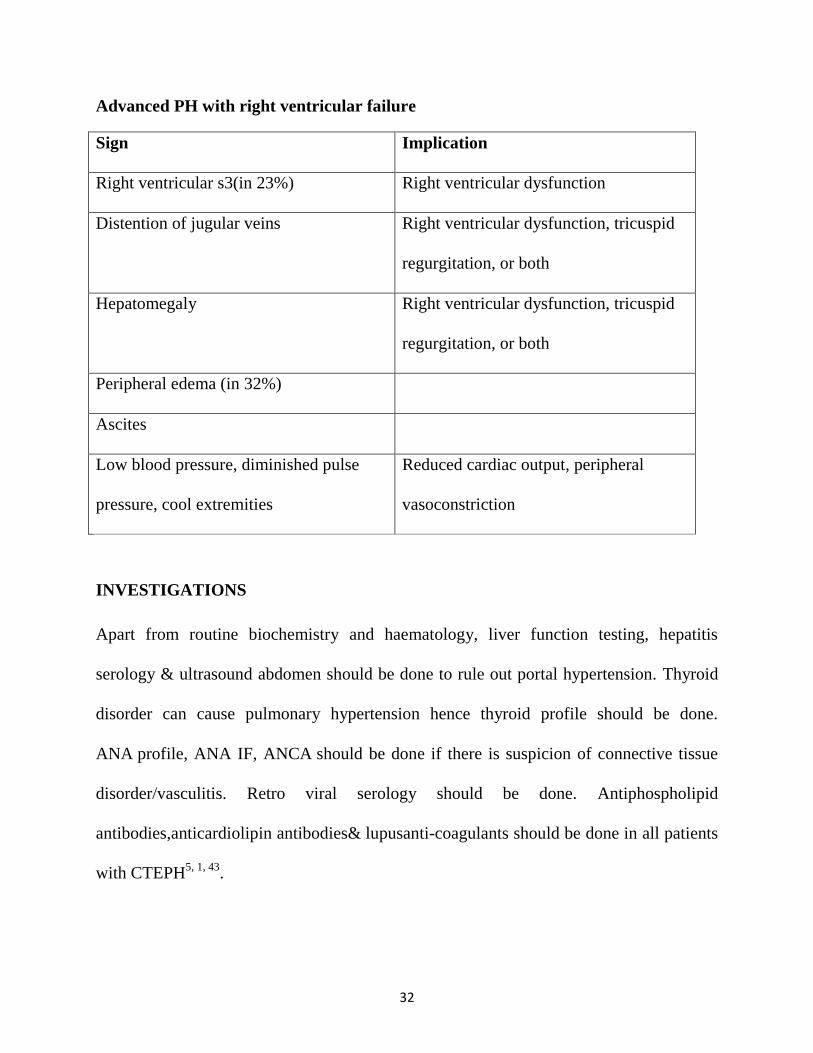
Advanced PH with right ventricular failure
Sign Implication
Right ventricular s3(in 23%) Right ventricular dysfunction
Distention of jugular veins Right ventricular dysfunction, tricuspid
regurgitation, or both
Hepatomegaly Right ventricular dysfunction, tricuspid
regurgitation, or both
Peripheral edema (in 32%)
Ascites
Low blood pressure, diminished pulse
pressure, cool extremities
Reduced cardiac output, peripheral
vasoconstriction
INVESTIGATIONS
Apart from routine biochemistry and haematology, liver function testing, hepatitis
serology & ultrasound abdomen should be done to rule out portal hypertension. Thyroid
disorder can cause pulmonary hypertension hence thyroid profile should be done.
ANA profile, ANA IF, ANCA should be done if there is suspicion of connective tissue
disorder/vasculitis. Retro viral serology should be done. Antiphospholipid
antibodies,anticardiolipin antibodies& lupusanti-coagulants should be done in all patients
with CTEPH5, 1, 43
.
33
ECG finding that are present in patients with pulmonary hypertension are
P pulmonale,
right axis deviation,
RV hypertrophy, RV strain,
right bundle branch block,
QTc prolongation.
Right ventricular strain pattern has more sensitivity & specificity compared to right
ventricular hypertrophy.in advanced pulmonary hypertension,supraventricular
tachyarrhythmia can occur especially when the patient has the disease for more than 5
years1, 43, 51-54
.
There may be no change in chest X-ray in PH patients, but findings that can be present
includes
pruning that is loss of peripheral blood vessels due to dilation of main pulmonary
artery .
Right atrium & ventricular hypertrophy is present mainly if there is right heart
failure. Pulmonary artery vein ratio helps in differentiating arterial from venous
pulmonary hypertension.
Signs of obstructive airway disease may be present, plural effusion may be present
in few patients1, 43, 55, 56
.

34
Lung volume will be reduced in patient with pulmonary hypertension & has association
with disease stage. Lung diffusion capacity for carbon monoxide will be low in many
patients with PH, but it can be normal. Abnormally low DLCO is associated with poor
outcome.PVOD, PAH associated with connective tissue disorder usually has low
DCLO.COPD has low DLCO, increased residual volume & irreversible airway
obstruction. Decrease in lung volume & DCLO indicate interstitial lung disease1, 43, 57-63
.
Ventilation/perfusion lung scan should be performed in all patients with PH who were
suspected to have chronic thrombi embolism. V/Q scan has a sensitivity & specificity of
90-100% & 94-100% respectively in ruling out CTEPH.
Findings that has high specificity in finding out pulmonary hypertension includes
pulmonary artery diameter of more than 29mm
Pulmonary to ascending aorta diameter ratio more than or equal to 1.0.
A segmental artery: bronchus ratio >1 : 1 in three or four lobes has been reported
to have high specificity for PH
CT will also find the evidence that support PH, it can also find out features of the
condition that leads to pulmonary hypertension like congenital defects in
heart,oesophageal dilation in systemic sclerosis.
High resolution CT helps in identifying interstitial lung disease & emphysema since it
shows clear picture of lung parenchyma. Pulmonary capillary haemangiomatosis is
35
suspected with diffuse bilateral thickening of the interlobular septa and the presence of
small, centrilobular, poorly circumscribed nodular opacities
Contrast angiography can be helpful in diagnosing & finding out surgical accessibility of
CTEPH. Traditional angiography can find out the patients who benefit from pulmonary
endarterectomy.
Both traditional & contrast angiography can also be helpful in finding vasculitis&
pulmonary arteriovenous malformations1, 43, 68-78
.
Contrast MRI cannot exclude PAH, it helps in measuring stroke volume,cardiac output,
pulmonary artery distensibility79-86
.
36
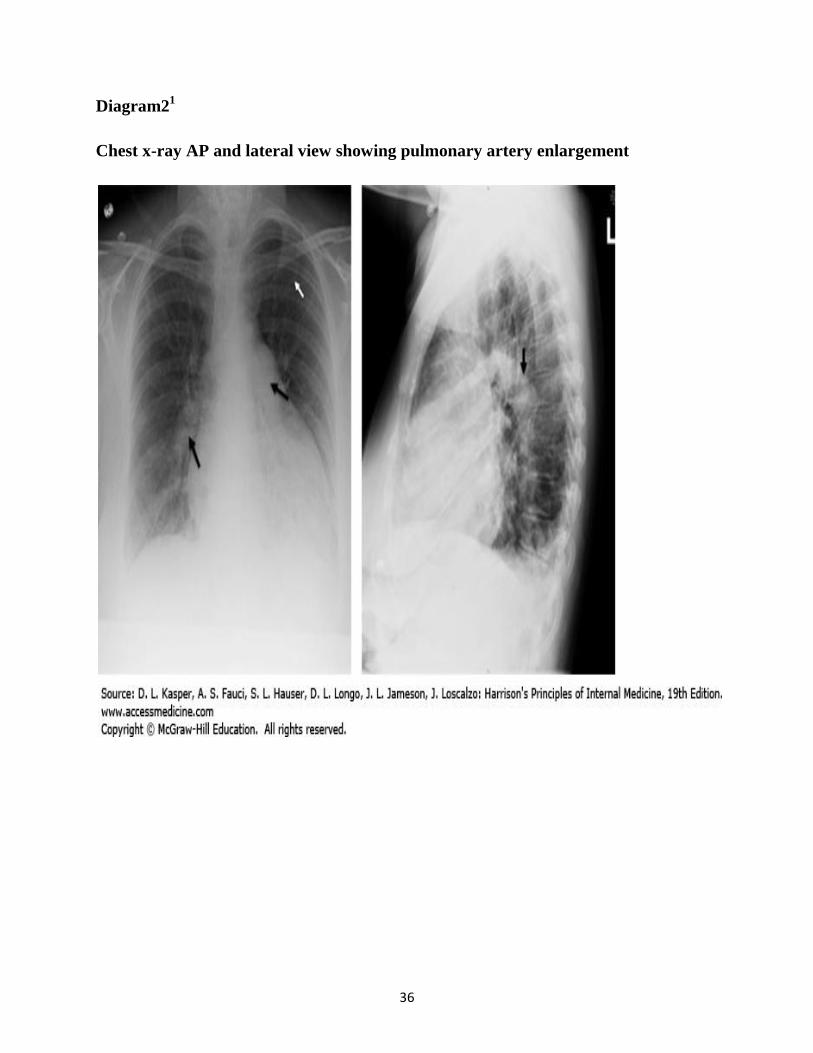
Diagram21
Chest x-ray AP and lateral view showing pulmonary artery enlargement
37
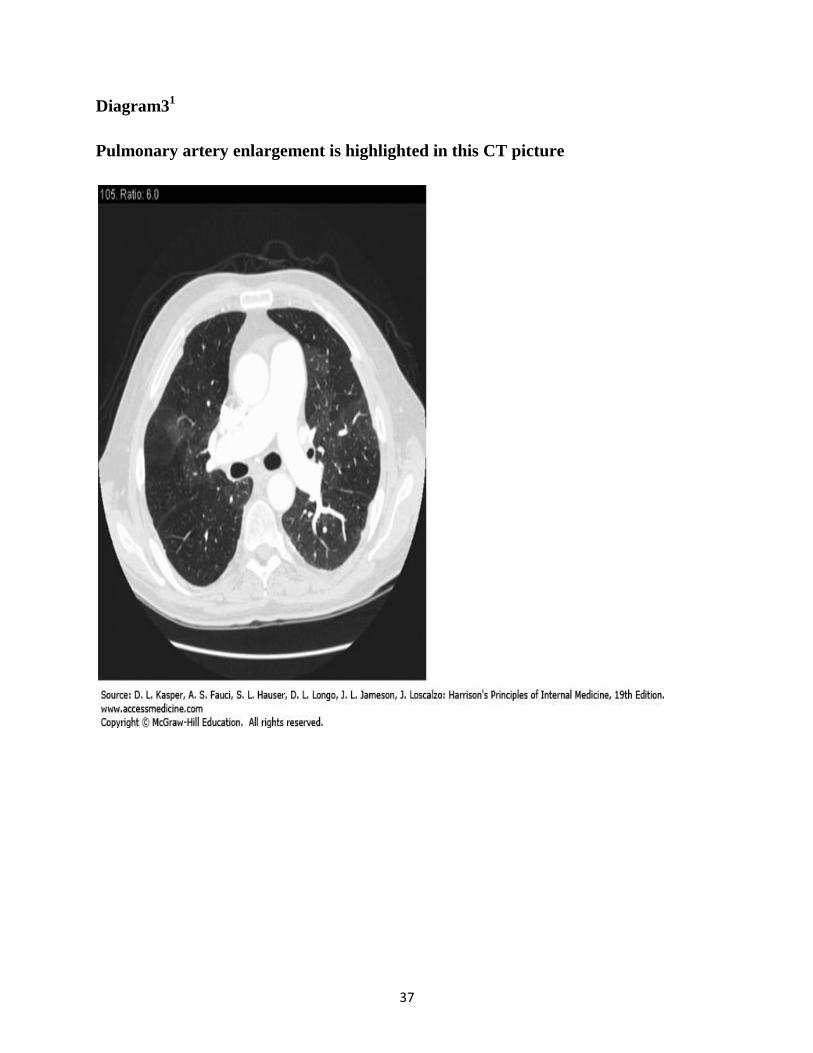
Diagram31
Pulmonary artery enlargement is highlighted in this CT picture
38
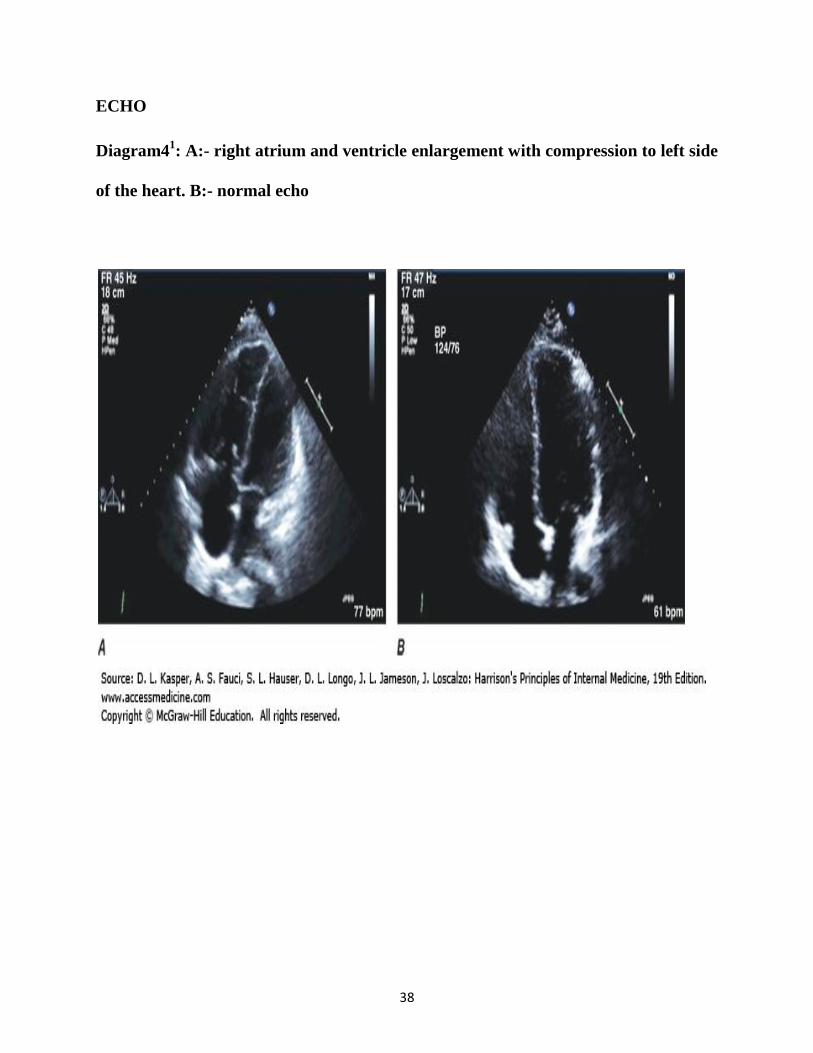
ECHO
Diagram41: A:- right atrium and ventricle enlargement with compression to left side
of the heart. B:- normal echo
39
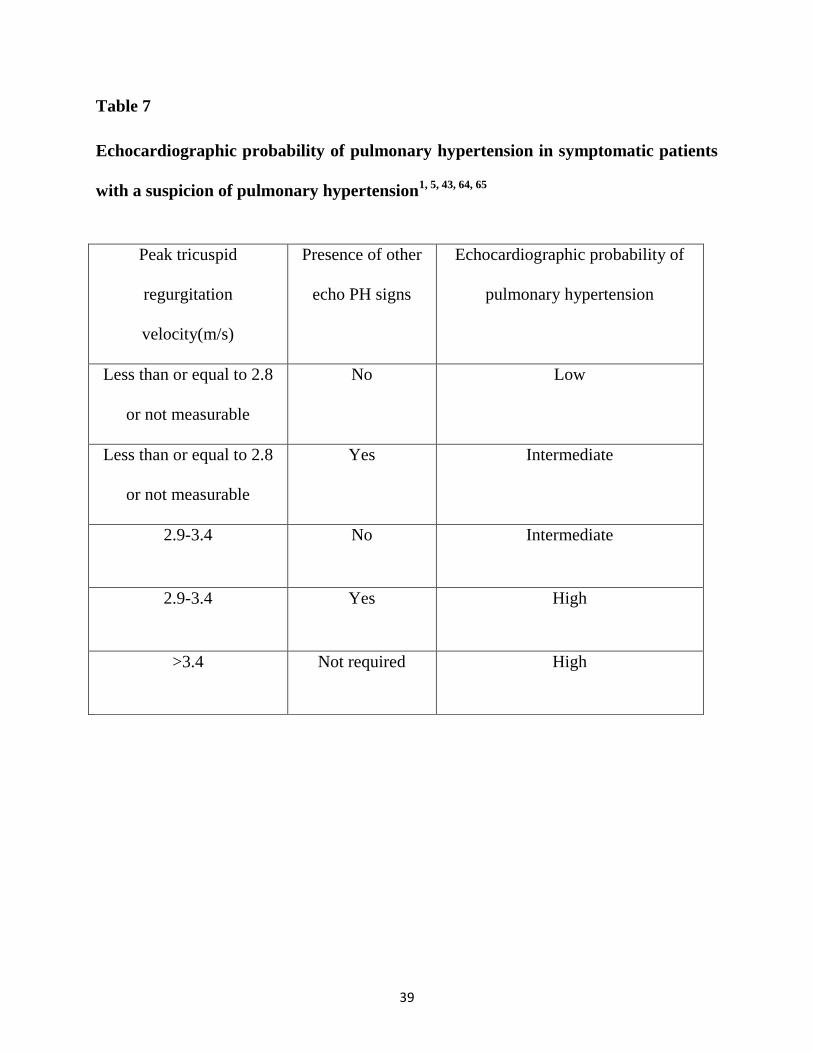
Table 7
Echocardiographic probability of pulmonary hypertension in symptomatic patients
with a suspicion of pulmonary hypertension1, 5, 43, 64, 65
Peak tricuspid
regurgitation
velocity(m/s)
Presence of other
echo PH signs
Echocardiographic probability of
pulmonary hypertension
Less than or equal to 2.8
or not measurable
No Low
Less than or equal to 2.8
or not measurable
Yes Intermediate
2.9-3.4 No Intermediate
2.9-3.4 Yes High
>3.4 Not required High

40
Table 8
Echocardiographic signs suggesting pulmonary hypertension used to assess the
probability of pulmonary hypertension in addition to tricuspid regurgitation
velocity measurement in table61, 5, 43, 64, and 65
A: the ventricles B: pulmonary artery C: inferior vena cava and
right atrium
Right ventricle/left ventricle
basal diameter ratio >1.0
Right ventricular
outflow Doppler
acceleration time
<105msec and/or
midsystolic notching
Inferior cava diameter >21
mm with decreased
inspiration collapse (<50%
with a sniff or <20% with
quiet inspiration)
Flattening of the
interventricular septum (left
ventricular eccentricity index
>1.1 in systole and/or
diastole
Early diastolic
pulmonary regurgitation
velocity >2.2m/sec
Right atrial area (end-
systole) >18 cm2
PA diameter > 25mm
41
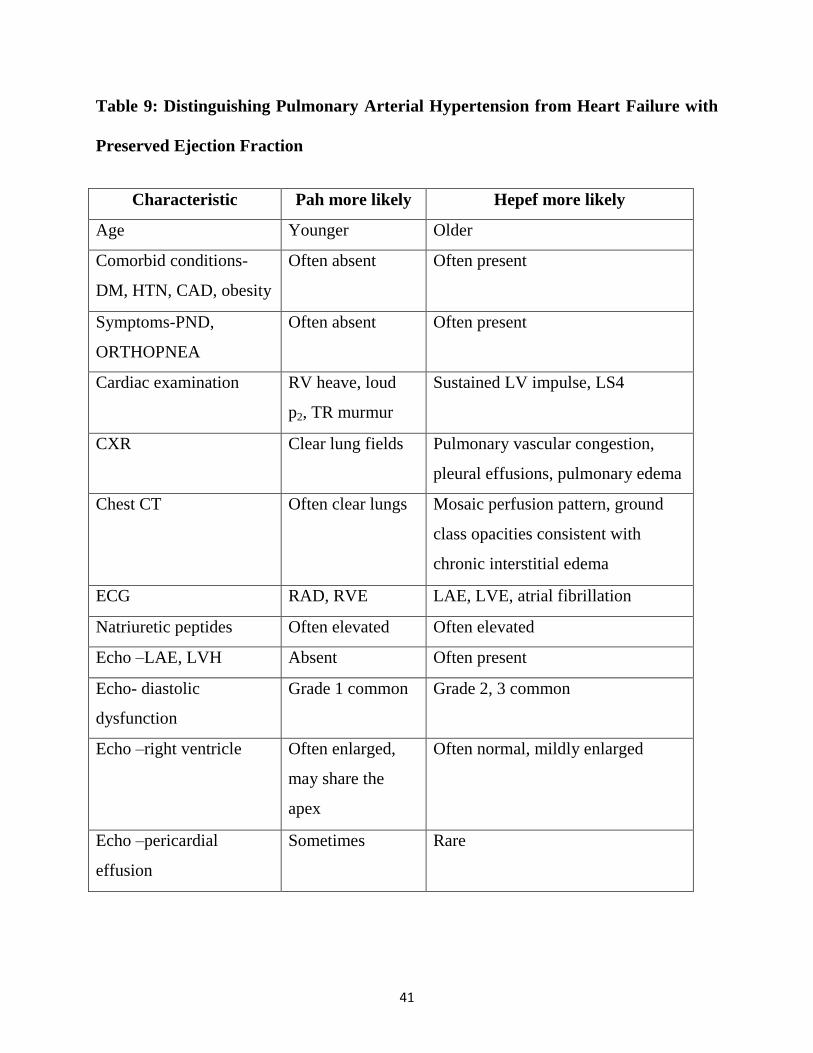
Table 9: Distinguishing Pulmonary Arterial Hypertension from Heart Failure with
Preserved Ejection Fraction
Characteristic Pah more likely Hepef more likely
Age Younger Older
Comorbid conditions-
DM, HTN, CAD, obesity
Often absent Often present
Symptoms-PND,
ORTHOPNEA
Often absent Often present
Cardiac examination RV heave, loud
p2, TR murmur
Sustained LV impulse, LS4
CXR Clear lung fields Pulmonary vascular congestion,
pleural effusions, pulmonary edema
Chest CT Often clear lungs Mosaic perfusion pattern, ground
class opacities consistent with
chronic interstitial edema
ECG RAD, RVE LAE, LVE, atrial fibrillation
Natriuretic peptides Often elevated Often elevated
Echo –LAE, LVH Absent Often present
Echo- diastolic
dysfunction
Grade 1 common Grade 2, 3 common
Echo –right ventricle Often enlarged,
may share the
apex
Often normal, mildly enlarged
Echo –pericardial
effusion
Sometimes Rare

42
Recommendation for right heart catheterization in pulmonary hypertension
RHC is recommended to confirm the diagnosis of pulmonary arterial hypertension
(group 1) and to support treatment decisions
In a patient with PH , it is recommended to perform RHC in expert centres as it
technically demanding and may be associated with serious complications
RHC should be considered in pulmonary arterial hypertension(group 1) to access
the treatment effect of drugs
RHC is recommended in the patients with congenital cardiac shunts to support
decisions on correction
RHC is recommended in patients with PH due to left heart disease(group 2) or
lung disease (group 3) if organ transplantation is considered
When measurement of PAWB is unreliable, left heart catheterization should be
considered to measure LVEDP
RHC may be considered in patients with suspected PH and left heart disease or
lung disease to assist in the differential diagnosis and support treatment decisions
RHC is indicated in patients with CTEPH (group 4) to confirm the diagnosis and
support treatment decisions1, 5, 43, 87
.
43
Recommendations for vasoreactivity testing
Vasoreactivity testing is indicated only in expert centres
Vasoreactivity testing is recommended in patients with IPAH, HPAH and PAH
associated with drugs use to detect patients who can be treated with high doses of
a CCB.
A positive response to the vasoreactivity testing is defined as a reduction of mean
PAP≥ 10mmHg to reach an absolute value of mean PAP ≤ 40mmHg with an
increased or unchanged cardiac output.
Nitric oxide is recommended for performing vasoreactivity testing.
Intravenous epoprostenol is recommended for performing vasoreactivity testing as
an alternative.
Adenosine should be considered for performing vasoreactivity testing as an
alternative.
Inhaled iloprost may be considered or performing vasoreativity testing as an
alternative.
The use of oral or intravenous CCBs in acute vasoreativity testing is not
recommended
Vasoreactivity testing to detect patients who can be safely treated with high doses
of a CCB is not recommended in patients with PAH other than IPAH,HPAH and
44
PAH associated with drugs use and is not recommended in PH groups 2,3,4 and 51,
5, 43.
TREATMENT
Recommendation for general measures
It is recommended that PAH patients avoid pregnancy.
Immunization of PAH patients against influenza and pneumococcal infection is
recommended
Psychosocial support is recommended in PAH patients
Supervised exercise training should be considered in physically deconditioned
PAH patients under medical therapy .
In-flight o2 administration should be considered for patients in WHO-FC3 AND 4
and those with arterial blood o2 pressure consistently <8kpa(60mmHg)
In elective surgery, epidural rather than general anaesthesia should be performed
whenever possible
Exercise physical activities that leads to distressing symptoms is not recommended
in PAH patients5.
45
Recommendation for supportive therapy
Diuretic treatment is recommended in PAH patients with signs of RV failure and
fluid retention.
Continuous long term o2 therapy is recommended in PAH patients when arterial
blood o2 pressure is consistently <8kpa(60mmhg)d.
Oral anticoagulant treatment may be considered in patients wih IPAH, HPAH and
PAH due to the use of anorexigens.
Correction of anaemia and iron status may be considered in PAH patients.
The use of angiotensin-converting enzyme inhibitors, angiotensin-2 receptor
antagonists, beta-blockers and ivabradine is not recommended in patients with
PAH unless required by co-morbidities( i.e. high blood pressure, coronary artery
disease or left heart failure)
46
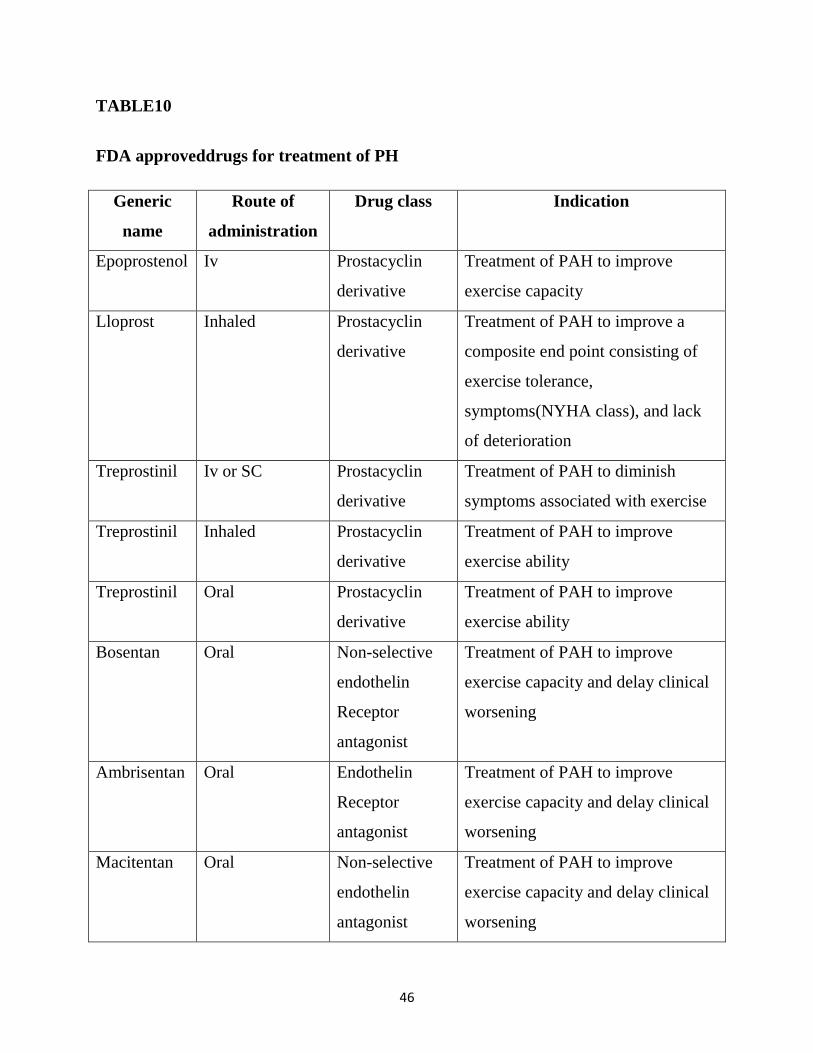
TABLE10
FDA approveddrugs for treatment of PH
Generic
name
Route of
administration
Drug class Indication
Epoprostenol Iv Prostacyclin
derivative
Treatment of PAH to improve
exercise capacity
Lloprost Inhaled Prostacyclin
derivative
Treatment of PAH to improve a
composite end point consisting of
exercise tolerance,
symptoms(NYHA class), and lack
of deterioration
Treprostinil Iv or SC Prostacyclin
derivative
Treatment of PAH to diminish
symptoms associated with exercise
Treprostinil Inhaled Prostacyclin
derivative
Treatment of PAH to improve
exercise ability
Treprostinil Oral Prostacyclin
derivative
Treatment of PAH to improve
exercise ability
Bosentan Oral Non-selective
endothelin
Receptor
antagonist
Treatment of PAH to improve
exercise capacity and delay clinical
worsening
Ambrisentan Oral Endothelin
Receptor
antagonist
Treatment of PAH to improve
exercise capacity and delay clinical
worsening
Macitentan Oral Non-selective
endothelin
antagonist
Treatment of PAH to improve
exercise capacity and delay clinical
worsening
47
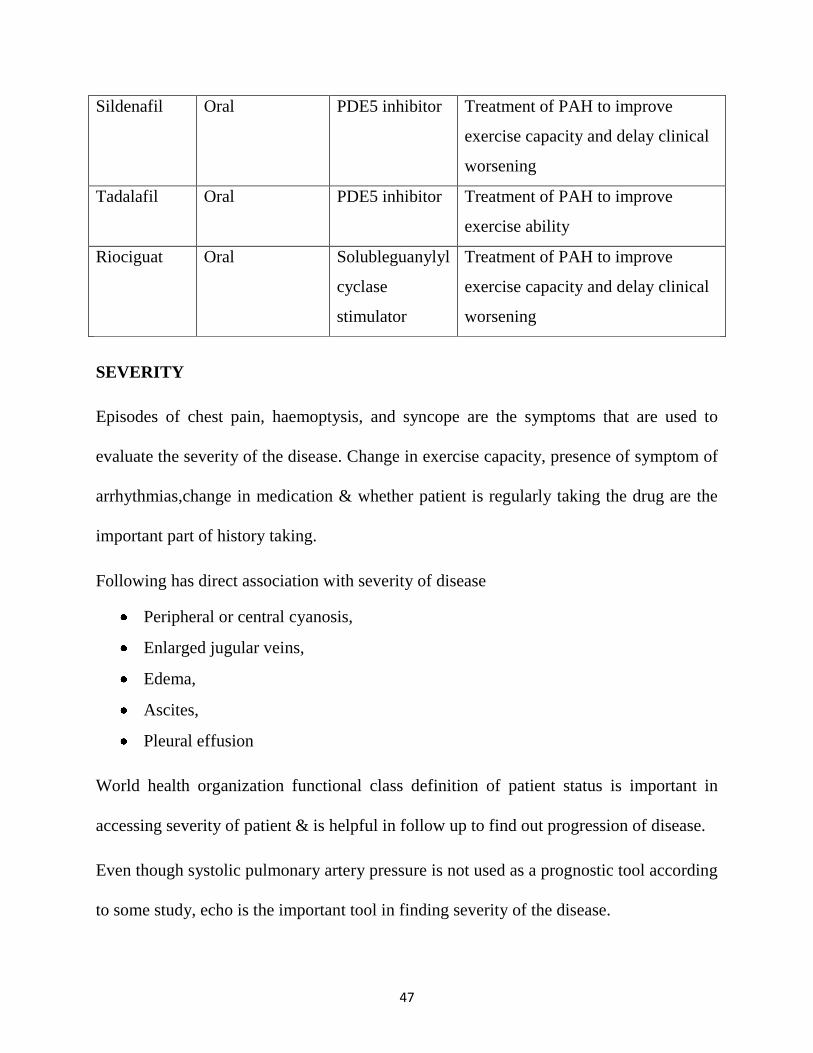
Sildenafil Oral PDE5 inhibitor Treatment of PAH to improve
exercise capacity and delay clinical
worsening
Tadalafil Oral PDE5 inhibitor Treatment of PAH to improve
exercise ability
Riociguat Oral Solubleguanylyl
cyclase
stimulator
Treatment of PAH to improve
exercise capacity and delay clinical
worsening
SEVERITY
Episodes of chest pain, haemoptysis, and syncope are the symptoms that are used to
evaluate the severity of the disease. Change in exercise capacity, presence of symptom of
arrhythmias,change in medication & whether patient is regularly taking the drug are the
important part of history taking.
Following has direct association with severity of disease
Peripheral or central cyanosis,
Enlarged jugular veins,
Edema,
Ascites,
Pleural effusion
World health organization functional class definition of patient status is important in
accessing severity of patient & is helpful in follow up to find out progression of disease.
Even though systolic pulmonary artery pressure is not used as a prognostic tool according
to some study, echo is the important tool in finding severity of the disease.
48
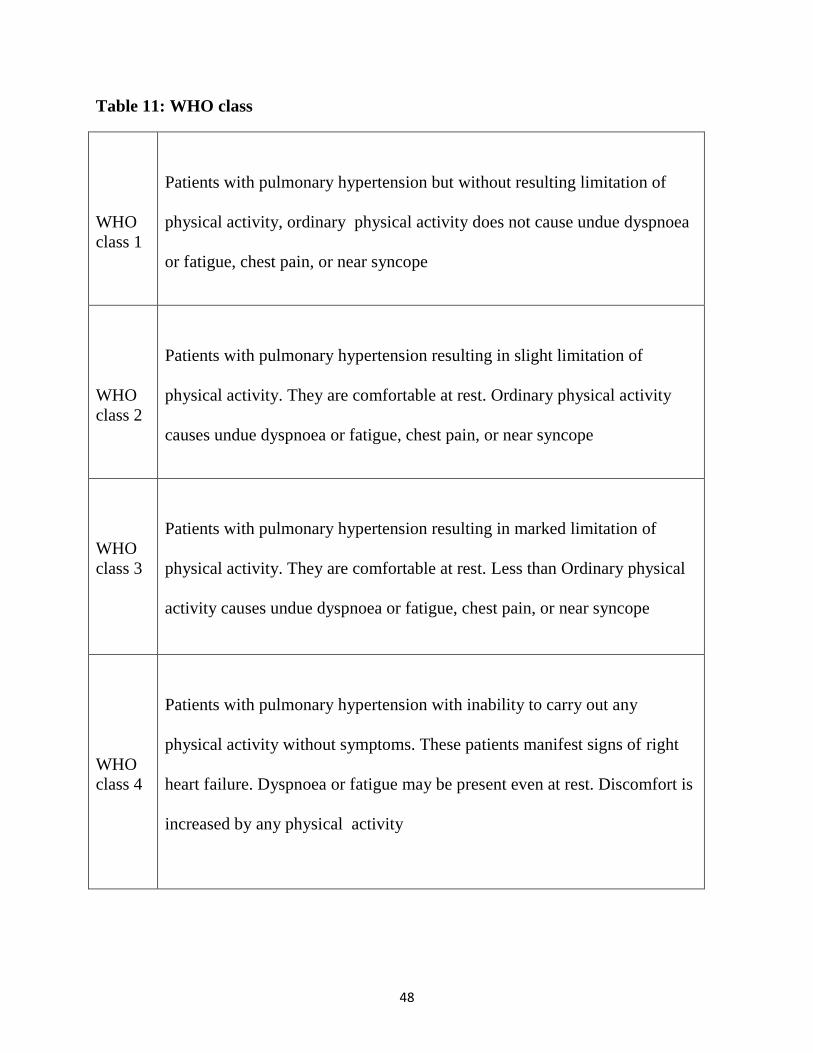
Table 11: WHO class
WHO
class 1
Patients with pulmonary hypertension but without resulting limitation of
physical activity, ordinary physical activity does not cause undue dyspnoea
or fatigue, chest pain, or near syncope
WHO
class 2
Patients with pulmonary hypertension resulting in slight limitation of
physical activity. They are comfortable at rest. Ordinary physical activity
causes undue dyspnoea or fatigue, chest pain, or near syncope
WHO
class 3
Patients with pulmonary hypertension resulting in marked limitation of
physical activity. They are comfortable at rest. Less than Ordinary physical
activity causes undue dyspnoea or fatigue, chest pain, or near syncope
WHO
class 4
Patients with pulmonary hypertension with inability to carry out any
physical activity without symptoms. These patients manifest signs of right
heart failure. Dyspnoea or fatigue may be present even at rest. Discomfort is
increased by any physical activity
49
Echo finds out
chamber size,
RA,
RV area,
magnitude of tricuspid regurgitation,
LV eccentricity index &
RV contractility
but CMR is more exact in finding RV morphology & function. Follow-up CMR can be
used.
Right heart catheterization also gives prognostic information about the patient both
during admission & during follow up. the indicator that gives prognostic information
during right heart catheterization are
RA pressure,
cardiac index &
mixed venous oxygen saturation.
6 minutes walking test is the most commonly used test to find exercise capacity of the
patient.
50
6MWT is influenced by following
sex,
age,
height,
weight,
co-morbidities,
need for O2,
learning curve and
motivation
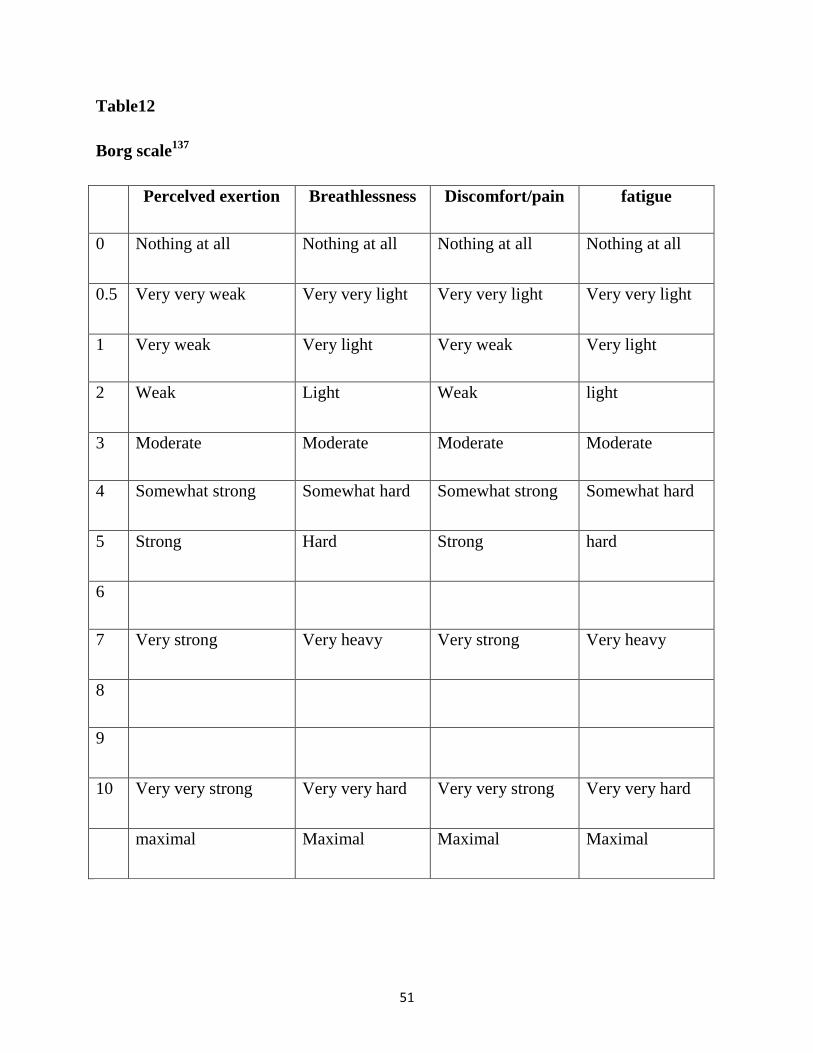
Borg score is useful in evaluating effort level at the end of test. Peripheral oxygen &
heart rate should also be measured to improve the prognostic relevance
One way to gauge how hard you are exercising is to use the Borg Scale of Perceived
Exertion. The Borg Scale takes into account your fitness level: It matches how hard
you feel you are working with numbers from 6 to 20; thus, it is a “relative” scale. The
scale starts with “no feeling of exertion,” which rates a 6, and ends with “very, very
hard,” which rates a 20. Moderate activities register 11 to 14 on the Borg scale (“fairly
light” to “somewhat hard”), while vigorous activities usually rate a 15 or higher (“hard”
to “very, very hard”).
51
Table12
Borg scale137
Percelved exertion Breathlessness Discomfort/pain fatigue
0 Nothing at all Nothing at all Nothing at all Nothing at all
0.5 Very very weak Very very light Very very light Very very light
1 Very weak Very light Very weak Very light
2 Weak Light Weak light
3 Moderate Moderate Moderate Moderate
4 Somewhat strong Somewhat hard Somewhat strong Somewhat hard
5 Strong Hard Strong hard
6
7 Very strong Very heavy Very strong Very heavy
8
9
10 Very very strong Very very hard Very very strong Very very hard
maximal Maximal Maximal Maximal
52
Cardiopulmonary testing can add more information to 6MWT diagnostically &
prognostically. It gives information on
exercise capacity,
exchange,
ventilator efficacy
And cardiac function during exercise.
Following are the typical findings that are present in patients with pulmonary artery
hypertension
a low end-tidal partial pressure of carbon dioxide (pCO2),
high ventilator equivalents for carbon dioxide (VE/VCO2),
low oxygen pulse (VO2/HR) &
Low peak oxygen uptake (peak VO2).
List of markers that have association with pulmonary artery hypertension are
Markers of vascular dysfunction includes asymmetric dimethylarginine (ADMA),
endothelin-1, angiopoeitins, von Willebrand factor132-137
,
Markers of inflammation includes C-reactive protein, interleukin 6, chemokines126-
129,
Markers of myocardial stress includes atrial natriuretic peptide, brain natriuretic
peptide (BNP)/NT-proBNP, troponins138, 139, 130-132
.
Markers of low CO and/or tissue hypoxia included pCO2, uric acid, growth
differentiation factor 15 (GDF15), osteopontin59, 134-136
53
Markers of secondary organ damage (creatinine, bilirubin)138, 131
.
Even though there are lot of markers for PH, there is no specific marker. The most
commonly used marker that have direct association with myocardial dysfunction are
BNP & NT-pro BNP. Hence it can be used as a prognostic marker during admission &
during follow up in patients with PH. it can be elevated in other heart diseases also. NT-
pro BNP is more reliable compared with BNP when it comes to prognosis.
54
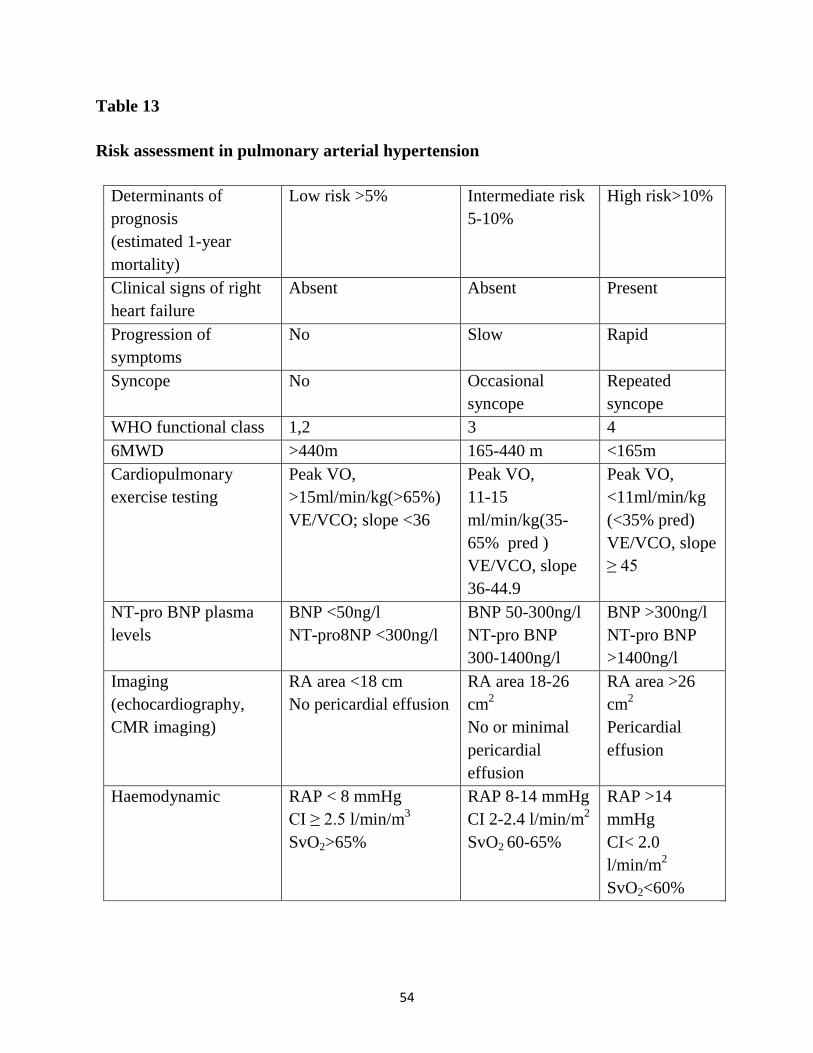
Table 13
Risk assessment in pulmonary arterial hypertension
Determinants of
prognosis
(estimated 1-year
mortality)
Low risk >5% Intermediate risk
5-10%
High risk>10%
Clinical signs of right
heart failure
Absent Absent Present
Progression of
symptoms
No Slow Rapid
Syncope No Occasional
syncope
Repeated
syncope
WHO functional class 1,2 3 4
6MWD >440m 165-440 m <165m
Cardiopulmonary
exercise testing
Peak VO,
>15ml/min/kg(>65%)
VE/VCO; slope <36
Peak VO,
11-15
ml/min/kg(35-
65% pred )
VE/VCO, slope
36-44.9
Peak VO,
<11ml/min/kg
(<35% pred)
VE/VCO, slope
≥ 45
NT-pro BNP plasma
levels
BNP <50ng/l
NT-pro8NP <300ng/l
BNP 50-300ng/l
NT-pro BNP
300-1400ng/l
BNP >300ng/l
NT-pro BNP
>1400ng/l
Imaging
(echocardiography,
CMR imaging)
RA area <18 cm
No pericardial effusion
RA area 18-26
cm2
No or minimal
pericardial
effusion
RA area >26
cm2
Pericardial
effusion
Haemodynamic RAP < 8 mmHg
CI ≥ 2.5 l/min/m3
SvO2>65%
RAP 8-14 mmHg
CI 2-2.4 l/min/m2
SvO2 60-65%
RAP >14
mmHg
CI< 2.0
l/min/m2
SvO2<60%
55
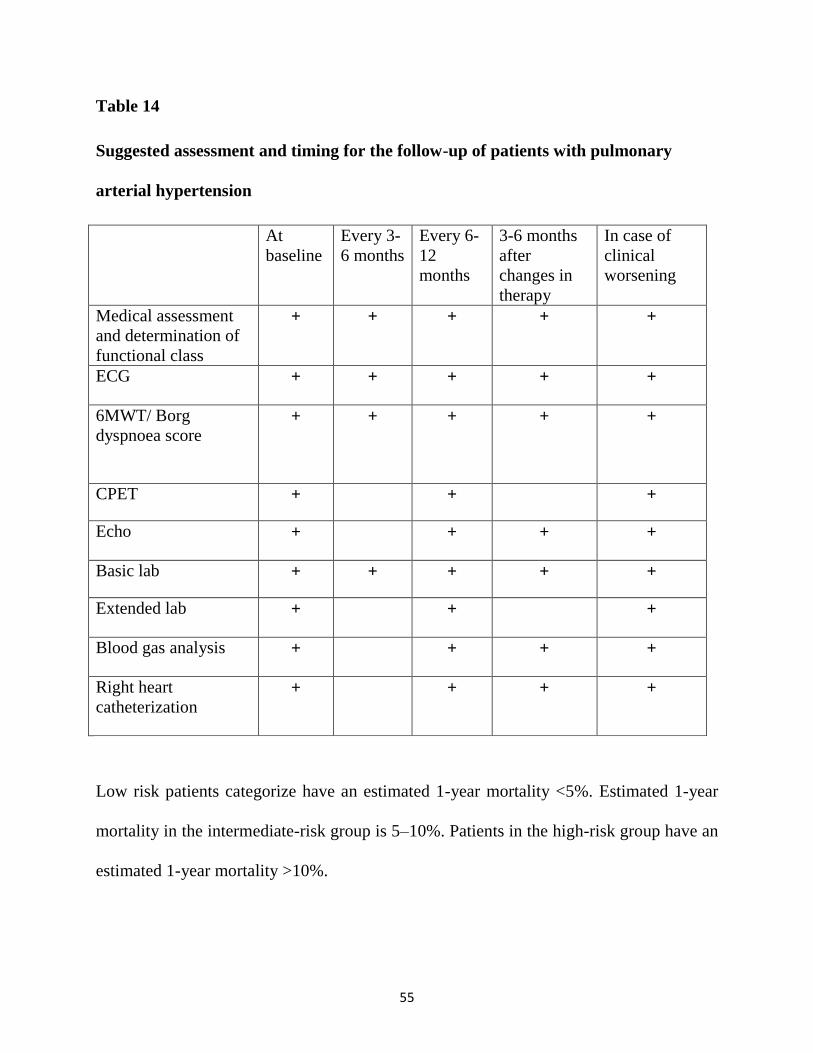
Table 14
Suggested assessment and timing for the follow-up of patients with pulmonary
arterial hypertension
At
baseline
Every 3-
6 months
Every 6-
12
months
3-6 months
after
changes in
therapy
In case of
clinical
worsening
Medical assessment
and determination of
functional class
+ + + + +
ECG + + + + +
6MWT/ Borg
dyspnoea score + + + + +
CPET + + +
Echo + + + +
Basic lab + + + + +
Extended lab + + +
Blood gas analysis + + + +
Right heart
catheterization + + + +
Low risk patients categorize have an estimated 1-year mortality <5%. Estimated 1-year
mortality in the intermediate-risk group is 5–10%. Patients in the high-risk group have an
estimated 1-year mortality >10%.

56
Treatment goal in all patients with PH is achieving low risk status. once they achieve low
risk status the patient will have good exercise capacity, good quality of life, good RV
function and a low mortality risk88-131
57
RESULTS
In this prospective observational study conducted in PSGIMSR during the period of
august 2016 to august 2017 we included total of 50 patients who were admitted in
medical, nephrology ward and intensive care unit fulfilling inclusion criteria and in
whom echo was done during the admission. Prevalence of PH in patients with GFR less
than 30 is 22 percentage.
58
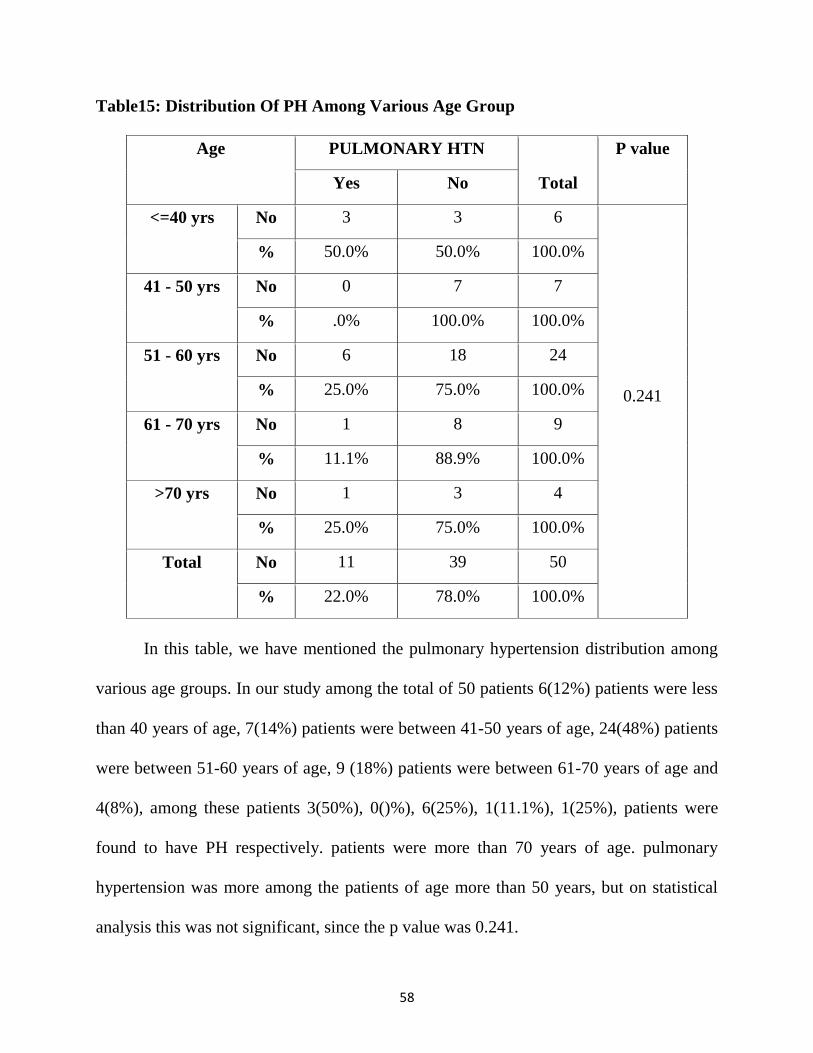
Table15: Distribution Of PH Among Various Age Group
Age PULMONARY HTN
Total
P value
Yes No
<=40 yrs No 3 3 6
0.241
% 50.0% 50.0% 100.0%
41 - 50 yrs No 0 7 7
% .0% 100.0% 100.0%
51 - 60 yrs No 6 18 24
% 25.0% 75.0% 100.0%
61 - 70 yrs No 1 8 9
% 11.1% 88.9% 100.0%
>70 yrs No 1 3 4
% 25.0% 75.0% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
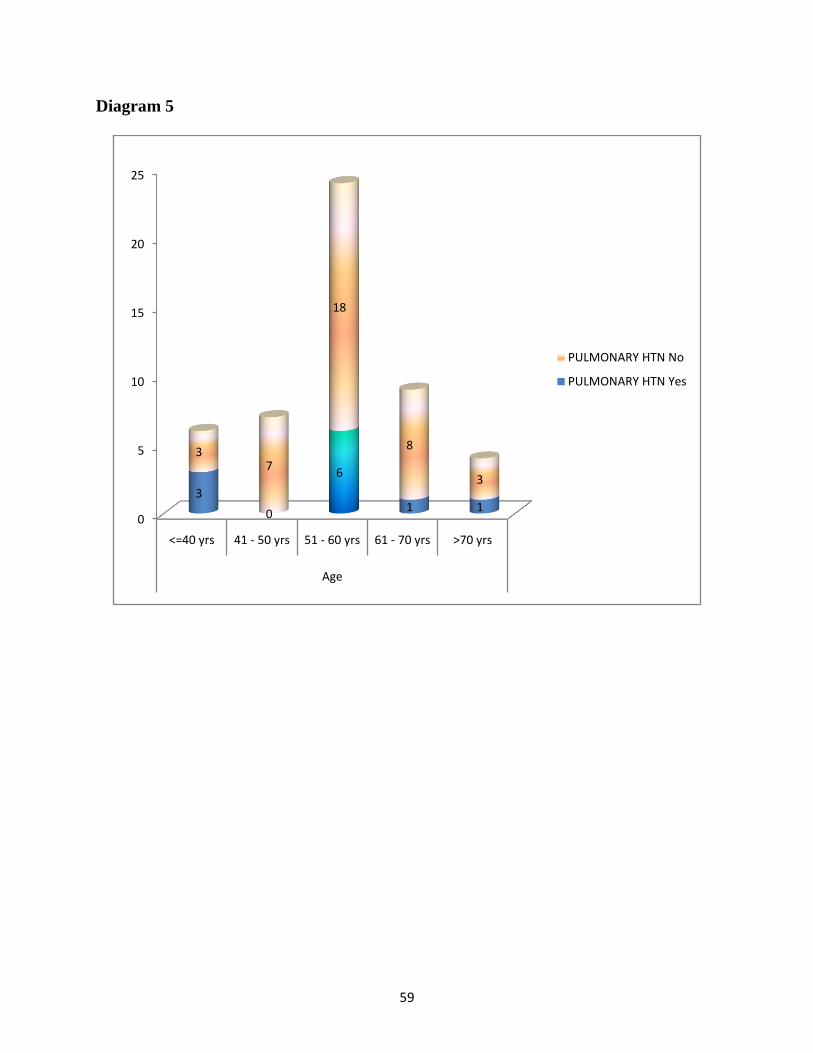
In this table, we have mentioned the pulmonary hypertension distribution among
various age groups. In our study among the total of 50 patients 6(12%) patients were less
than 40 years of age, 7(14%) patients were between 41-50 years of age, 24(48%) patients
were between 51-60 years of age, 9 (18%) patients were between 61-70 years of age and
4(8%), among these patients 3(50%), 0()%), 6(25%), 1(11.1%), 1(25%), patients were
found to have PH respectively. patients were more than 70 years of age. pulmonary
hypertension was more among the patients of age more than 50 years, but on statistical
analysis this was not significant, since the p value was 0.241.
59
Diagram 5
0
5
10
15
20
25
<=40 yrs 41 - 50 yrs 51 - 60 yrs 61 - 70 yrs >70 yrs
Age
3
0
6
1 1
37
18
8
3
PULMONARY HTN No
PULMONARY HTN Yes
60
Table16: Association of Sex and Pulmonary Hypertension
SEX PULMONARY HTN
Total
P value
Yes No
Male No 5 23 28
0.503
% 17.9% 82.1% 100.0%
Female No 6 16 22
% 27.3% 72.7% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table the compared the PH distribution among male and female population,
in which total of 28(56%) male and 22 (44%) female were there . Among males 5(17.9%)
patients are found to have pulmonary hypertension and among females 6 (27.3%) patients
had pulmonary hypertension. There were no significant association of pulmonary
hypertension among male and female, since the p value was 0.503.
61
Diagram 6
0 5 10 15 20 25 30
Male
Female
SEX
5
6
23
16
PULMONARY HTN Yes
PULMONARY HTN No
62
Table17: Association of DM and Pulmonary hypertension
DM PULMONARY HTN
Total
P value
Yes No
Yes No 7 24 31
0.595
% 22.6% 77.4% 100.0%
No No 4 15 19
% 21.1% 78.9% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table we analysed significance of association of diabetic mellitus with
pulmonary hypertension. In total of 50 patients, 31(62%) patients were found to have
DM, and among them 7(22.6%) patients were found to have PH. P value was 0.595,
hence there was no significance of DM association with PH.
63
Diagram 7
0 10 20 30 40
Yes
No
DM
7
4
24
15
PULMONARY HTN Yes
PULMONARY HTN No
64
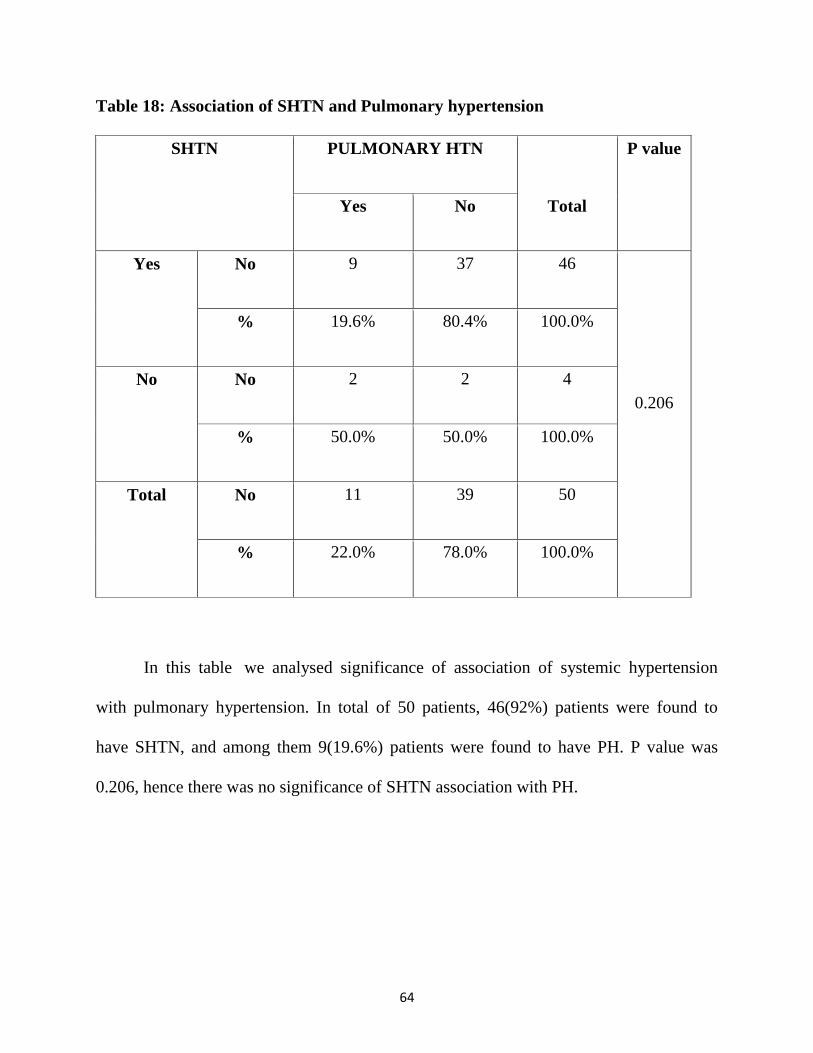
Table 18: Association of SHTN and Pulmonary hypertension
SHTN PULMONARY HTN
Total
P value
Yes No
Yes No 9 37 46
0.206
% 19.6% 80.4% 100.0%
No No 2 2 4
% 50.0% 50.0% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table we analysed significance of association of systemic hypertension
with pulmonary hypertension. In total of 50 patients, 46(92%) patients were found to
have SHTN, and among them 9(19.6%) patients were found to have PH. P value was
0.206, hence there was no significance of SHTN association with PH.
65
Diagram 8
0 10 20 30 40 50
Yes
No
SHTN
9
2
37
2
PULMONARY HTN Yes
PULMONARY HTN No
66
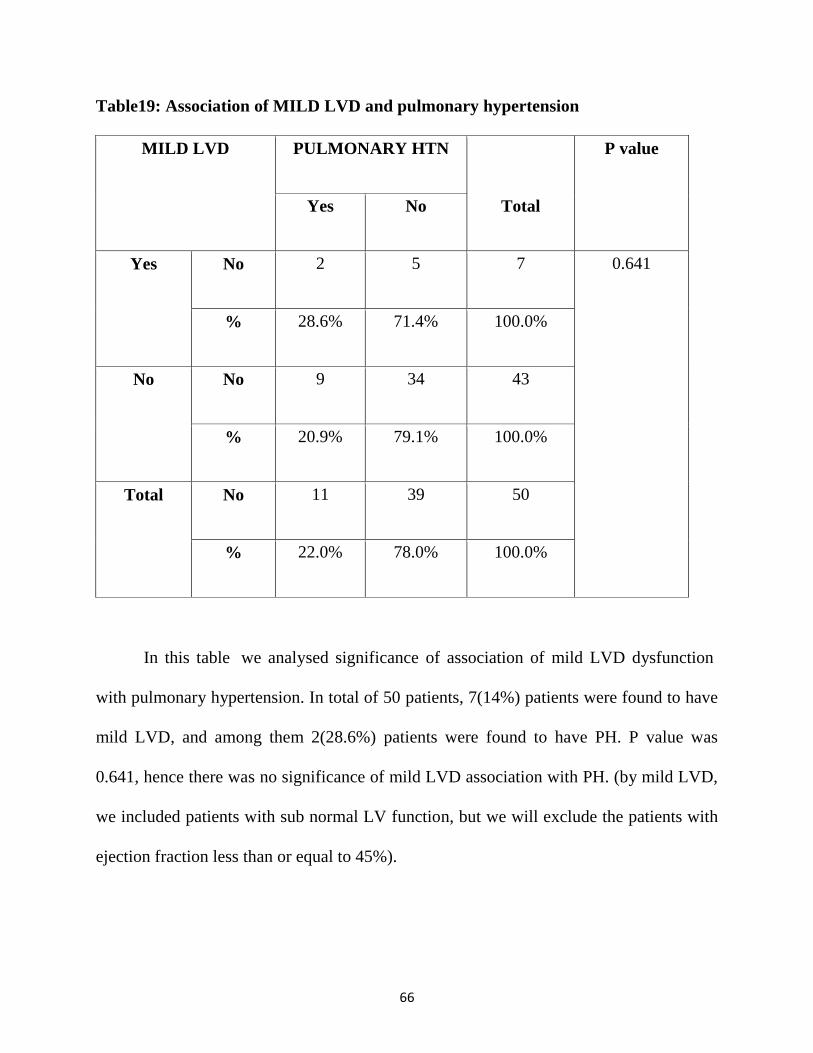
Table19: Association of MILD LVD and pulmonary hypertension
MILD LVD PULMONARY HTN
Total
P value
Yes No
Yes No 2 5 7 0.641
% 28.6% 71.4% 100.0%
No No 9 34 43
% 20.9% 79.1% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table we analysed significance of association of mild LVD dysfunction
with pulmonary hypertension. In total of 50 patients, 7(14%) patients were found to have
mild LVD, and among them 2(28.6%) patients were found to have PH. P value was
0.641, hence there was no significance of mild LVD association with PH. (by mild LVD,
we included patients with sub normal LV function, but we will exclude the patients with
ejection fraction less than or equal to 45%).
67
Diagram 9
0
5
10
15
20
25
30
35
40
45
Yes No
MILD LVD
2
95
34
PULMONARY HTN No
PULMONARY HTN Yes
68
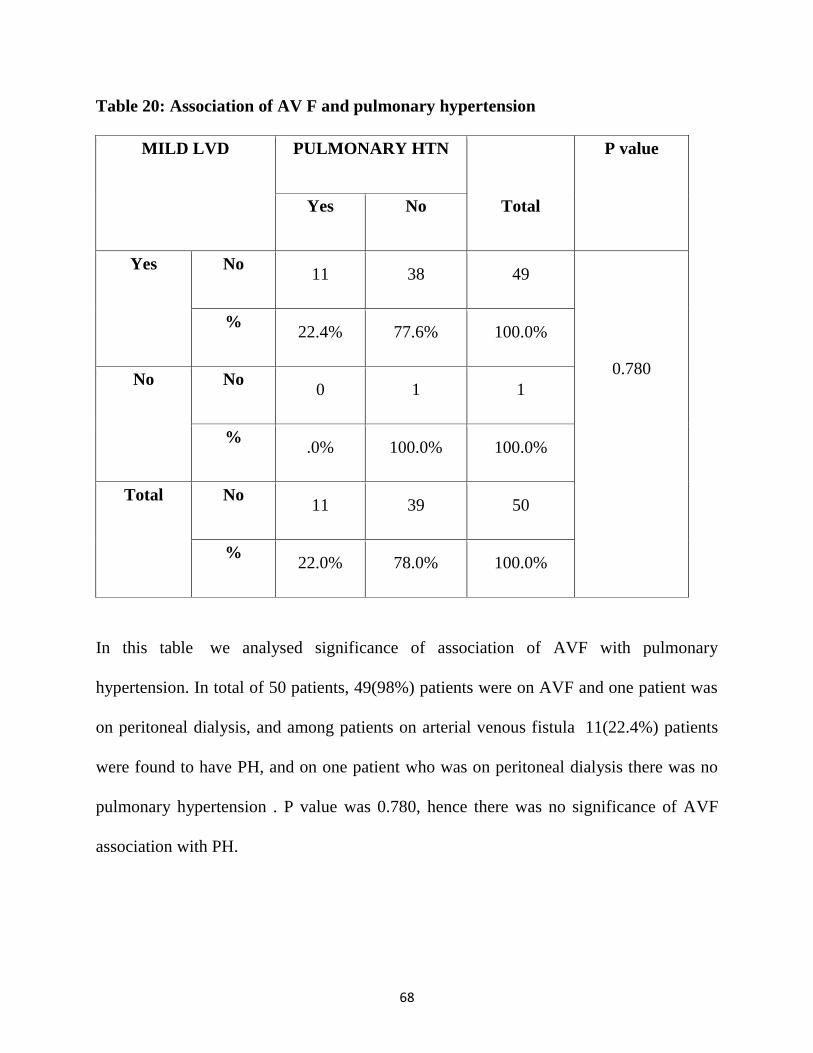
Table 20: Association of AV F and pulmonary hypertension
MILD LVD PULMONARY HTN
Total
P value
Yes No
Yes No 11 38 49
0.780
% 22.4% 77.6% 100.0%
No No 0 1 1
% .0% 100.0% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table we analysed significance of association of AVF with pulmonary
hypertension. In total of 50 patients, 49(98%) patients were on AVF and one patient was
on peritoneal dialysis, and among patients on arterial venous fistula 11(22.4%) patients
were found to have PH, and on one patient who was on peritoneal dialysis there was no
pulmonary hypertension . P value was 0.780, hence there was no significance of AVF
association with PH.
69
Diagram 10
0
5
10
15
20
25
30
35
40
Yes No
AV F
0
1114
25
PULMONARY HTN No
PULMONARY HTN Yes
70
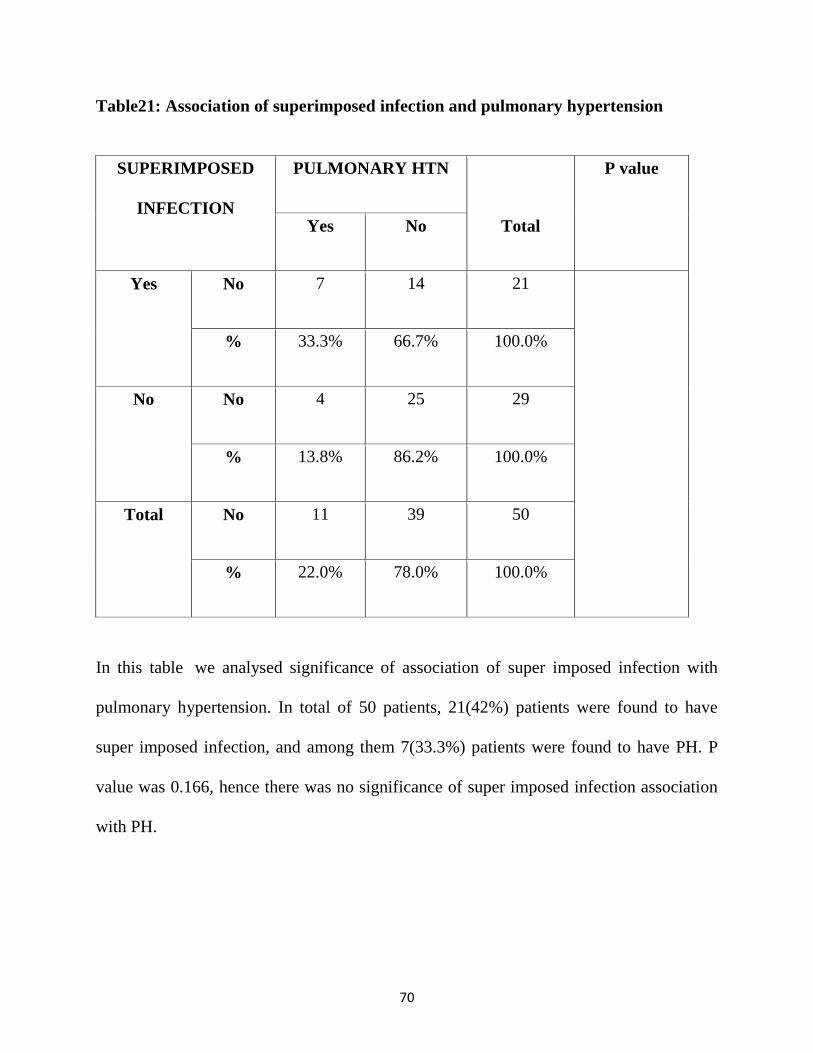
Table21: Association of superimposed infection and pulmonary hypertension
SUPERIMPOSED
INFECTION
PULMONARY HTN
Total
P value
Yes No
Yes No 7 14 21
% 33.3% 66.7% 100.0%
No No 4 25 29
% 13.8% 86.2% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table we analysed significance of association of super imposed infection with
pulmonary hypertension. In total of 50 patients, 21(42%) patients were found to have
super imposed infection, and among them 7(33.3%) patients were found to have PH. P
value was 0.166, hence there was no significance of super imposed infection association
with PH.
71
Diagram 11
0 5 10 15 20 25 30
Yes
No
SUP
ERIM
PO
SED
INFE
CTI
ON
7
4
14
25
PULMONARY HTN Yes
PULMONARY HTN No
72
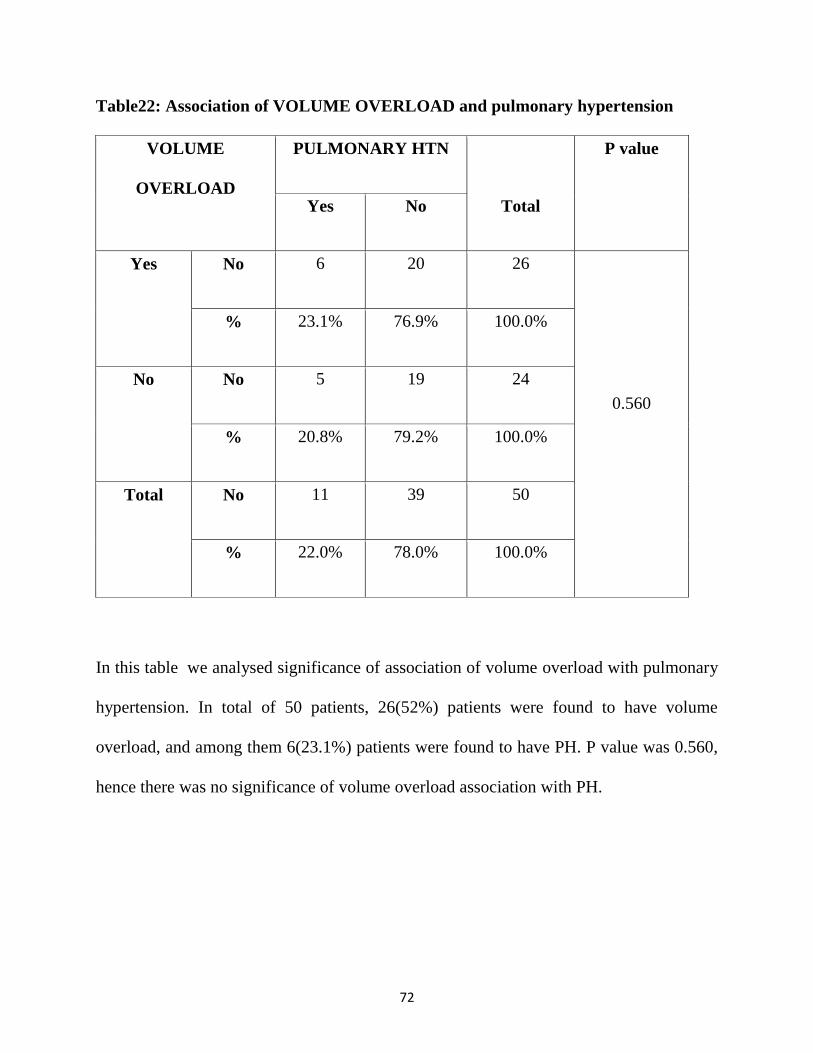
Table22: Association of VOLUME OVERLOAD and pulmonary hypertension
VOLUME
OVERLOAD
PULMONARY HTN
Total
P value
Yes No
Yes No 6 20 26
0.560
% 23.1% 76.9% 100.0%
No No 5 19 24
% 20.8% 79.2% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table we analysed significance of association of volume overload with pulmonary
hypertension. In total of 50 patients, 26(52%) patients were found to have volume
overload, and among them 6(23.1%) patients were found to have PH. P value was 0.560,
hence there was no significance of volume overload association with PH.
73
DIAGRAM 12
0 5 10 15 20 25 30
Yes
No
VO
LUM
E O
VER
LOA
D
6
5
20
19
PULMONARY HTN Yes
PULMONARY HTN No
74
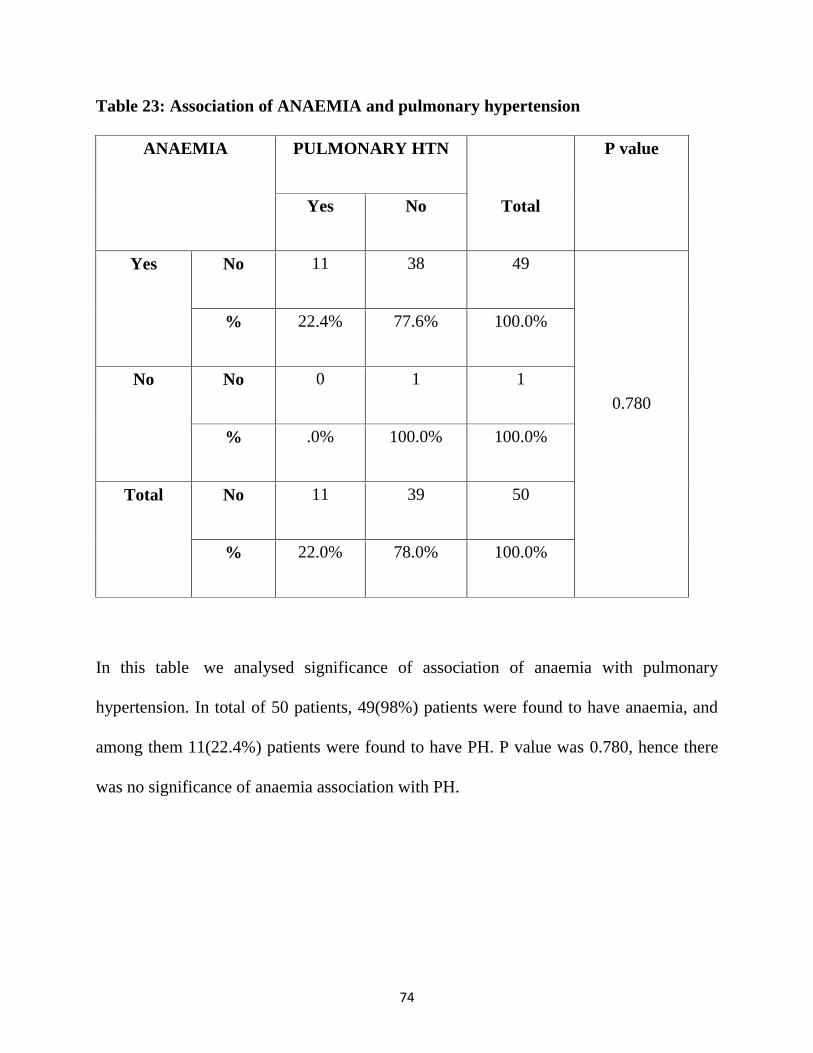
Table 23: Association of ANAEMIA and pulmonary hypertension
ANAEMIA PULMONARY HTN
Total
P value
Yes No
Yes No 11 38 49
0.780
% 22.4% 77.6% 100.0%
No No 0 1 1
% .0% 100.0% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table we analysed significance of association of anaemia with pulmonary
hypertension. In total of 50 patients, 49(98%) patients were found to have anaemia, and
among them 11(22.4%) patients were found to have PH. P value was 0.780, hence there
was no significance of anaemia association with PH.
75
Diagram 13
0
5
10
15
20
25
30
35
40
45
50
Yes No
ANAEMIA
11
0
38
1
PULMONARY HTN No
PULMONARY HTN Yes
76
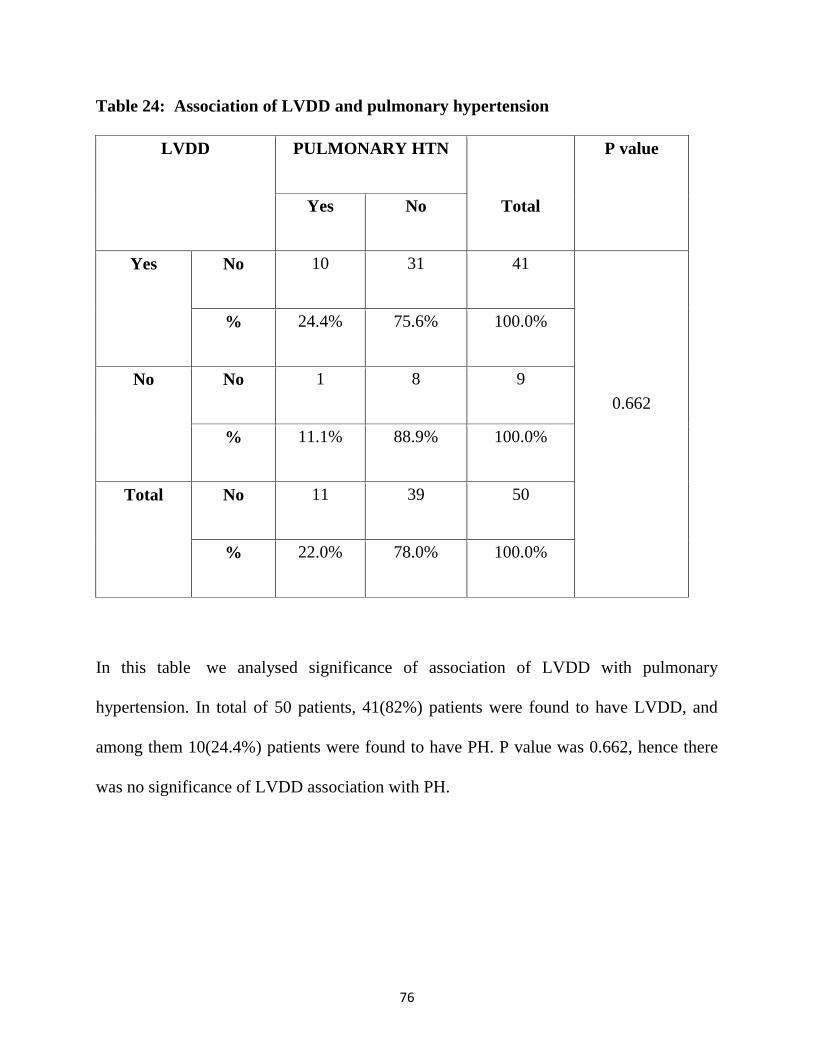
Table 24: Association of LVDD and pulmonary hypertension
LVDD PULMONARY HTN
Total
P value
Yes No
Yes No 10 31 41
0.662
% 24.4% 75.6% 100.0%
No No 1 8 9
% 11.1% 88.9% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table we analysed significance of association of LVDD with pulmonary
hypertension. In total of 50 patients, 41(82%) patients were found to have LVDD, and
among them 10(24.4%) patients were found to have PH. P value was 0.662, hence there
was no significance of LVDD association with PH.

77
Diagram 14
0 10 20 30 40 50
Yes
No
LVD
D
10
1
31
8
PULMONARY HTN Yes
PULMONARY HTN No
78
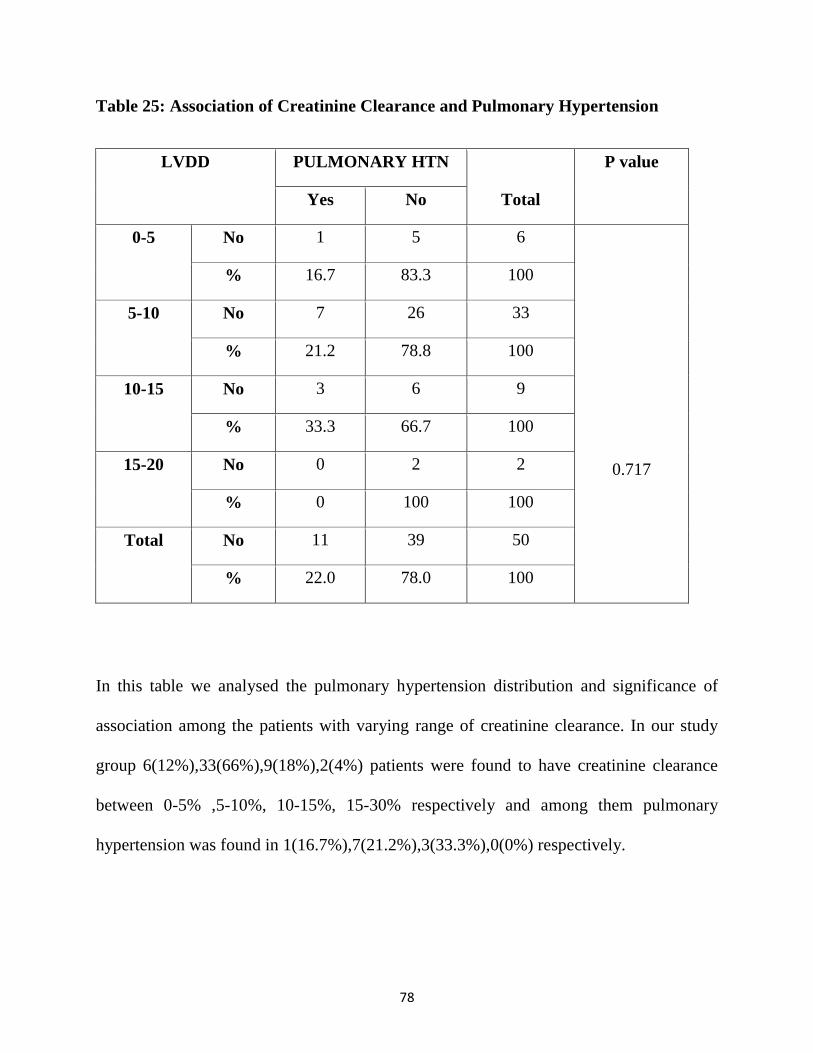
Table 25: Association of Creatinine Clearance and Pulmonary Hypertension
LVDD PULMONARY HTN
Total
P value
Yes No
0-5 No 1 5 6
0.717
% 16.7 83.3 100
5-10 No 7 26 33
% 21.2 78.8 100
10-15 No 3 6 9
% 33.3 66.7 100
15-20 No 0 2 2
% 0 100 100
Total No 11 39 50
% 22.0 78.0 100
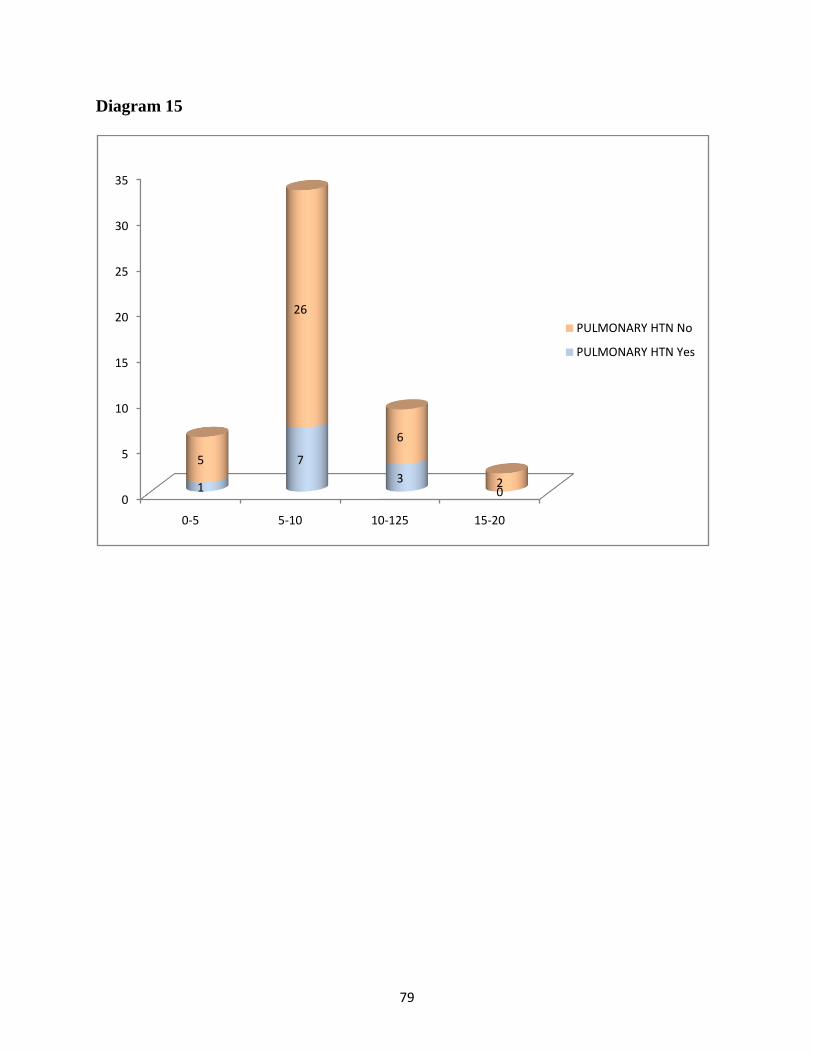
In this table we analysed the pulmonary hypertension distribution and significance of
association among the patients with varying range of creatinine clearance. In our study
group 6(12%),33(66%),9(18%),2(4%) patients were found to have creatinine clearance
between 0-5% ,5-10%, 10-15%, 15-30% respectively and among them pulmonary
hypertension was found in 1(16.7%),7(21.2%),3(33.3%),0(0%) respectively.
79
Diagram 15
0
5
10
15
20
25
30
35
0-5 5-10 10-125 15-20
1
7
30
5
26
6
2
PULMONARY HTN No
PULMONARY HTN Yes
80
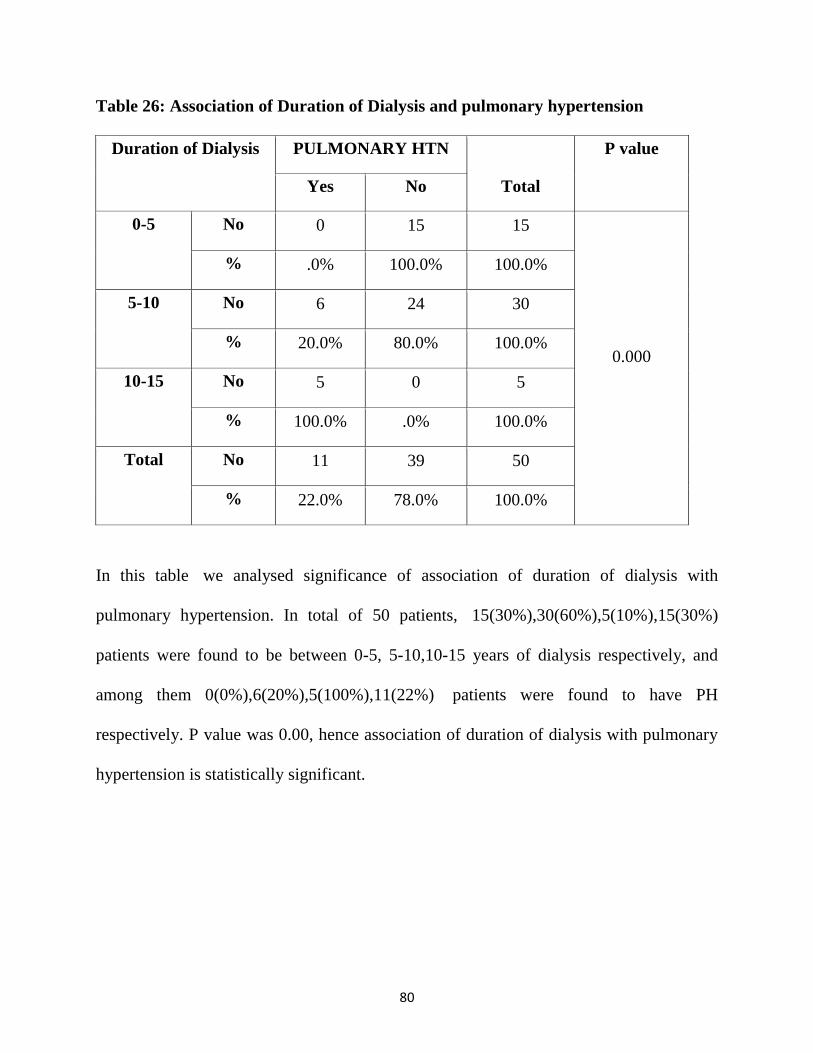
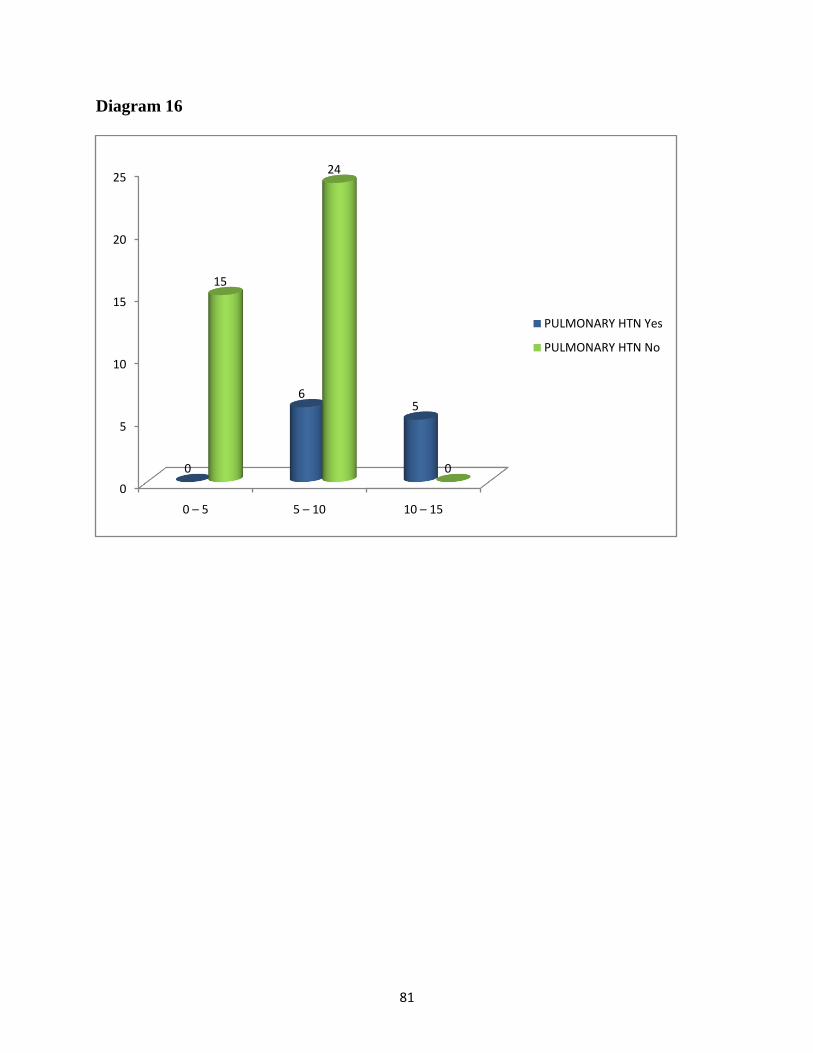
Table 26: Association of Duration of Dialysis and pulmonary hypertension
Duration of Dialysis PULMONARY HTN
Total
P value
Yes No
0-5 No 0 15 15
0.000
% .0% 100.0% 100.0%
5-10 No 6 24 30
% 20.0% 80.0% 100.0%
10-15 No 5 0 5
% 100.0% .0% 100.0%
Total No 11 39 50
% 22.0% 78.0% 100.0%
In this table we analysed significance of association of duration of dialysis with
pulmonary hypertension. In total of 50 patients, 15(30%),30(60%),5(10%),15(30%)
patients were found to be between 0-5, 5-10,10-15 years of dialysis respectively, and
among them 0(0%),6(20%),5(100%),11(22%) patients were found to have PH
respectively. P value was 0.00, hence association of duration of dialysis with pulmonary
hypertension is statistically significant.
81
Diagram 16
0
5
10
15
20
25
0 – 5 5 – 10 10 – 15
0
65
15
24
0
PULMONARY HTN Yes
PULMONARY HTN No
82
DISCUSSION
There is no availability of epidemiological data in many developing countries including
India, but in India most common causes PH are due to rheumatic heart disease,
obstructive airway disease & congenital heart disease unlike western countries where
idiopathic pulmonary artery hypertension & PH due to right heart disease are common.
Exposure of dialysis membrane to blood leads to activation of neutrophil which is
associated with sequestration of neutrophils in the lungs, these phenomenon’s if present
is usually present with worsening of lung disease in HD patients, it is more common if
cellulose membranes are used142-146.
presence of connective tissue disease,
super imposed infection,
hematological &
liver diseases
Can cause pulmonary hypertension in patients with CKD.
These conditions cause PH mainly by affecting micro vascular tone in lungs. Endothelial
dysfunction has association with pulmonary hypertension in patients with CKD on HD.
main mechanism behind that includes imbalance between vasoconstrictors &
vasodilators. High endothelia 1 & low nitric oxide levels affects Vascular tone leading to
PH147, 148, 149, 142
.
83
Low nitric oxide levels in patients on HD confirms the mechanism26, Sleep disorder
breathing is important risk factor of CKD irrespective of patient on HD or not150, 151
.
According to various studies PH is highly prevalent in CKD & associated with adverse
outcomes 3
it is more common in dialysis dependent kidney disease140
in one study
prevalence of patient on HD was21.8 percent,in another study prevalence of HD on
haemodialysis was 56 percent various study used various echo parameters & cut off
values to include patients under pulmonary hypertension group3.
In one study right heart catheterization was used as criteria to diagnose pulmonary
hypertension, among them 13 percent were found to have pulmonary hypertension on
dialysis group & 6 percent among non-dialysis group27
This study demonstrated a high prevalence of pulmonary hypertension among patients
with CKD on and without dialysis. The prevalence was highest among patients with
ESRD receiving long-term haemodialysis (41.53%) than those on per- itoneal dialysis
especially in patients with older age, longer duration of dialysis treatment, higher AV
fistula flow, cardiac output, serum creatinine; lower haemoglobin, haematocrit, ser- um
bicarbonate values, and EF% which all positively corre- lated with PAP and may be
involved in the pathogenesis of pulmonary hypertension141
.
In one study echo was used to diagnose pulmonary hypertension & in that study
prevalence of pulmonary hypertension in ESRD was17-56 percent28-33
.
84
compared to previous studies our study population has a prevalence of 22percent.
compared with previous studies risk factors like age ,sex ,diabetes, systemic
hypertension, mild LVD, AVF, superimposed infection, volume overload, anaemia,
LVDD are not associated with pulmonary hypertension in our study.& longer the
duration of dialysis higher the possibility of presence of pulmonary hypertension.
Following are the limitations in our study, ideal way to diagnose pulmonary hypertension
is through right heart catheterization but we are using only echo, in exclusion criteria we
are excluding the patient only if they are already diagnosed with the disease but we are
not excluding by doing specific investigation for the disease.
Presence of PH in CKD carries a high cardiovascular risk, also there are large population
of people from early stages of CKD,and hence screening of PH on early stages of CKD is
very important in finding out real burden of PH in CKD 24
.
Prevention of PH in patients with CKD is very important because once if PH developed
in patients with CKD, even kidney transplantation may not reverse the mortality
associated with established PH3.
85
CONCLUSION
Prevalence of pulmonary hypertension in our study is 22 percentage. The risk factors like
age, sex, diabetes, systemic hypertension, mild LVD, AVF, superimposed infection,
volume overload, anaemia, LVDD has no influence on PH in our study. Only association
that we have in our study population in patients with PH is longer duration of dialysis.
BIBLIOGRAPHY
1. Dennis Kasper; Anthony Fauci; Stephen Hauser; Dan Longo; J Jameson.
Pulmonary hypertension. Dennis L. Kasper, MD, Stephen L. Hauser, MD, J. Larry
Jameson, MD, PhD, Anthony S. Fauci, MD, Dan L. Longo, MD, Joseph Loscalzo,
Ph. D. (eds). Harrison's Principles of Internal Medicine, 19 th ed. : ; 2015. pp.
1655-1660.
2. Thoracicorg. [Online]. Available from: https://www.thoracic.org/patients/patient-
resources/breathing-in-america/resources/chapter-17-pulmonary-hypertension.pdf
3. R.EDavide Bolignano, MD, Stefania Rastelli, MD, Rajiv Agarwal, MD, Danilo
Fliser, MD, Ziad Massy, MD, Alberto Ortiz, MD, Andrzej Wiecek, MD, Alberto
Martinez-Castelao, MD, Adrian Covic, MD, David Goldsmith, MD, Gultekin
Suleymanlar, MD, Bengt Lindholm, MD, Gianfranco Parati, MD, Rosa Sicari,
MD, Luna Gargani, MD, Francesca Mallamaci, MD,Gerard London, MD, and
Carmine Zoccali, MD,. Pulmonary Hypertension in CKD. AMERICAN
JOURNAL OF KIDNEY DISEASE 2013; 61(4): 612-622.
4. Simonneau, G., Robbins, I.M., Beghetti, M. et al. Updated clinical classification of
pulmonary hypertension. J Am Coll Cardiol. 2009; 54: S43–S54
5. Nazzareno Galiè Marc Humbert Jean-Luc Vachiery Simon Gibbs Irene Lang
Adam Torbicki Gérald Simonneau Andrew Peacock Anton Vonk Noordegraaf
Maurice Beghetti Ardeschir Ghofrani Miguel Angel Gomez Sanchez Georg
Hansmann Walter Klepetko Patrizio Lancellotti Marco Matucci Theresa
McDonagh Luc A. Pierard Pedro T. Trindade Maurizio Zompatori Marius Hoeper
Authors/Task Force Members Document Reviewers: Victor Aboyans , Antonio
Vaz Carneiro , Stephan Achenbach , Stefan Agewall , Yannick Allanored ,
Riccardo Asteggiano , Luigi Paolo Badano , Joan Albert Barberà a , Hélène
Bouvaist , Héctor Bueno , Robert A. Byrne , Scipione Carerj , Graça Castro , Çetin
Erol , Volkmar Falk , Christian Funck-Brentano , Matthias Gorenflob , John
Grantonc , Bernard Iung , David G. Kiely , Paulus Kirchhof , Barbro Kjellstrom ,
Ulf Landmesser , John Lekakis , Christos Lionis , Gregory Y. H. Lip , Sty. 2015
ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension:
The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension
of the European Society of Cardiology and the European Respiratory Society :
Endorsed by: Association for European Paediatric and Congenital Cardiology ,
International Society for Heart and Lung Transplantation . European society of
cardiology 2015; 37(1):
6. Humbert MSitbon OChaouat ABertocchi MHabib GGressin VYaici
AWeitzenblum ECordier JFChabot FDromer CPison CReynaud-Gaubert
MHaloun ALaurent MHachulla ESimonneau G. Pulmonary arterial hypertension
in France: results from a national registry. Am J Respir Crit Care Med
2006;173:1023–1030.
7. Peacock AJMurphy NFMcMurray JJVCaballero LStewart S. An epidemiological
study of pulmonary arterial hypertension. Eur Respir J 2007;30:104–109.
8. McGoon MDBenza RLEscribano-Subias PJiang XMiller DPPeacock AJPepke-
Zaba JPulido TRich SRosenkranz SSuissa SHumbert M. Pulmonary arterial
hypertension: epidemiology and registries. J Am Coll Cardiol
2013;62(Suppl):D51–D59.
9. Hachulla E, Gressin V, Guillevin L, et al. Early detection of pulmonary arterial
hypertension in systemic sclerosis: a French nationwide prospective multicenter
study. Arthritis Rheum. 2005;52:3792-3800.
10. Mukerjee D, St George D, Coleiro B, et al. Prevalence and outcome in systemic
sclerosis associated pulmonary arterial hyper- tension: application of a registry
approach. Ann Rheum Dis. 2003;62:1088-1093.2. Badesch DB, Champion HC,
Sanchez MA, et al. Diagnosis and assessment of pulmonary arterial hypertension.
J Am Coll Cardiol. 2009;54(1 suppl):S55-S66.
11. Badesch DB, Champion HC, Sanchez MA, et al. Diagnosis and assessment of
pulmonary arterial hypertension. J Am Coll Cardiol. 2009;54(1 suppl):S55-S66.
12. Krowka MJ, Swanson KL, Frantz RP, McGoon MD, Wiesner RH.
Portopulmonary hypertension: results from a 10-year screening algorithm.
Hepatology. 2006;44:1502-1510.
13. Friedman WF. Proceedings of National Heart, Lung, and Blood Institute Pediatric
Cardiology Workshop: pulmonary hyper- tension. Pediatr Res. 1986;20:8-11.
14. Kessler R, Chaouat A, Weitzenblum E, et al. Pulmonary hypertension in the
obstructive sleep apnoea syndrome: preva- lence, causes and therapeutic
consequences. Eur Respir J. 1996;9: 787.
15. Badesch BDChampion HCGomez-Sanchez MAHoeper MLoyd JManes
AMcGoon MNaeije ROlschewski HOudiz RTorbicki A. Diagnosis and
assessment of pulmonary arterial hypertension. J Am Coll Cardiol
2009;54(Suppl):S55–S56.
16. Oudiz RJ. Pulmonary hypertension associated with left-sided heart disease. Clin
Chest Med 2007;28:233–241.
17. Vahanian AAlfieri OAndreotti FAntunes MJBaron-Esquivias GBaumgartner
HBorger MACarrel TPDe Bonis MEvangelista AFalk VIung BLancellotti
PPierard LPrice SSchafers HJSchuler GStepinska JSwedberg KTakkenberg JVon
Oppell UOWindecker SZamorano JLZembala M. Guidelines on the management
of valvular heart disease (version 2012). Eur Heart J 2012;33:2451–2496.
18. Seeger WAdir YBarberà JAChampion HCoghlan JGCottin VDe Marco TGaliè
NGhio SGibbs SMartinez FJSemigran MJSimonneau GWells AUVachiéry JL.
Pulmonary hypertension in chronic lung diseases. J Am Coll Cardiol
2013;62(Suppl):D109–D116.
19. Hurdman JCondliffe RElliot CASwift ARajaram SDavies CHill CHamilton
NArmstrong IJBillings CPollard LWild JMLawrie ALawson RSabroe IKiely DG.
Pulmonary hypertension in COPD: results from the ASPIRE registry. Eur Respir
J 2013;41:1292–1301.
20. Cottin VNunes HBrillet PYDelaval PDevouassoux GTillie-Leblond IIsrael-Biet
DCourt-FortuneValeyre DCordier JF. Combined pulmonary fibrosis and
emphysema: a distinct underrecognised entity. Eur Respir J 2005;26:586–593.
21. Escribano-Subias PBlanco ILopez-Meseguer MLopez-Guarch CJRoman
AMorales PCastillo-Palma MJSegovia JGomez-Sanchez MABarbera JA. Survival
in pulmonary hypertension in Spain: insights from the Spanish registry. Eur Respir
J 2012;40:596–603.
22. Garabed Eknoyan, MD Norbert Lameire, MD. Clinical Practice Guideline Update
for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney
Disease–Mineral and Bone Disorder (CKD-MBD). JOURNAL OF THE
INTERNATIONAL SOCIETY OF NEPHROLOGY 2017; 7(1): .
23. Nathan R. Hill* Samuel T. Fatoba, Jason L. Oke, Jennifer A. Hirst, Christopher A.
O’Callaghan, Daniel S. Lasserson, and F. D. Richard Hobbs. Global Prevalence of
Chronic Kidney Disease – A Systematic Review and Meta-Analysis. PLOS
ONE 2016; 11(7): .
24. Mark J. Sarnak, Kari E. Roberts. Pulmonary Hypertension in CKD: Some
Answers, Yet More Questions. Journal Of American Society of Nephrology 2015;
27. .
25. Agarwal R: Prevalence, determinants and prognosis of pulmonary hypertension
among hemodialysis patients. Nephrol Dial Transplant 27: 3908–3914, 2012
26. Yigla M, Nakhoul F, Sabag A, Too N, Gorevich B, Abassi Z, Reisner SA:
Pulmonary hypertension in patients with end-stage renal disease. Chest 123:
1577–1582, 2003
27. Stefan Pabst, Christoph Hammerstingl, Felix Hundt, Thomas Gerhardt, Christian
Grohé, Georg Nickenig, Rainer Woitas,and Dirk Skowasch,. Pulmonary
Hypertension in Patients with Chronic Kidney Disease on Dialysis and without
Dialysis: Results of the PEPPER-Study. Plus One 2012; 7(4): .2. Yigla M,
Nakhoul F, Sabag A, Tov N, Gorevich B, et al. Pulmonary hypertension in
patients with end-stage renal disease. Chest. 2003;123:1577–1582.
28. Yigla M, Nakhoul F, Sabag A, Tov N, Gorevich B, et al. Pulmonary hypertension
in patients with end-stage renal disease. Chest. 2003;123:1577–1582]
29. Havlucu Y, Kursat S, Ekmekci C, Celik P, Serter S, et al. Pulmonary hypertension
in patients with chronic renal failure. Respiration. 2007;74:503–510.
30. Bozbas SS, Akcay S, Altin C, Bozbas H, Karacaglar E, et al. Pulmonary
hypertension in patients with end-stage renal disease undergoing renal
transplantation. Transplant Proc. 2009;41:2753–2756
31. Ramasubbu K, Deswal A, Herdejurgen C, Aguilar D, Frost AE. A prospective
echocardiographic evaluation of pulmonary hypertension in chronic hemodialysis
patients in the United States: prevalence and clinical significance. Int J Gen Med.
2010;3:279–286
32. Abdelwhab S, Elshinnawy S. Pulmonary hypertension in chronic renal failure
patients. Am J Nephrol. 2008;28:990–997.
33. Yigla M, Fruchter O, Aharonson D, Yanay N, Reisner SA, et al. Pulmonary
hypertension is an independent predictor of mortality in hemodialysis patients.
Kidney Int. 2009;75:969–975.
34. Richard Drake , A. Wayne Vogl PhD , Adam W. M. Mitchell. Gray's Anatomy for
Students, 3rd ed. : Churchill Livingstone; 2014.
35. Kim E. Barrett , Susan M. Barman , Scott Boitano , Heddwen L. Brooks. Ganong's
Review of Medical Physiology, 25th ed. : McGraw-Hill Education / Medical;
2015.
36. Hoeper MMBogaard HJCondliffe RFrantz RKhanna DKurzyna MLangleben
DManes ASatoh TTorres FWilkins MRBadesch DB. Definitions and diagnosis of
pulmonary hypertension. J Am Coll Cardiol 2013;62(Suppl):D42–D50.
37. Kovacs GBerghold AScheidl SOlschewski H. Pulmonary arterial pressure during
rest and exercise in healthy subjects A systematic review. Eur Respir J
2009;34:888–894.
38. Soubrier FChung WKMachado RGrunig EAldred MGeraci MLoyd JEElliott
CGTrembath RCNewman JHHumbert M. Genetics and genomics of pulmonary
arterial hypertension. J Am Coll Cardiol 2013;62(Suppl):D13–D21.
39. Ma LRoman-Campos DAustin EDEyries MSampson KSSoubrier FGermain
MTregouet DABorczuk ARosenzweig EBGirerd BMontani DHumbert MLoyd
JEKass RSChung WK. A novel channelopathy in pulmonary arterial
hypertension. N Engl J Med 2013;369:351–361.
40. Eyries MMontani DGirerd BPerret CLeroy ALonjou CChelghoum NCoulet
FBonnet DDorfmuller PFadel ESitbon OSimonneau GTregouet DAHumbert
MSoubrier F. EIF2AK4 mutations cause pulmonary veno-occlusive disease, a
recessive form of pulmonary hypertension. Nat Genet 2014;46:65–69.
41. Oudiz RJ. Pulmonary hypertension associated with left-sided heart disease. Clin
Chest Med 2007;28:233–241.
42. Eddahibi SChaouat AMorrell NFadel EFuhrman CBugnet ASDartevelle PHousset
BHamon MWeitzenblum EAdnot S. Polymorphism of the serotonin transporter
gene and pulmonary hypertension in chronic obstructive pulmonary
disease. Circulation 2003;108:1839–1844.
43. Mann . Pulmonary Hypertension. (ed). Braunwald's Heart Disease: A Textbook of
Cardiovascular Medicine, 10 th ed. : ; 2014. pp. 1682-1700.
44. Fraser . Pulmonary Hypertension. (ed). Fraser and Pare's Diagnosis of Diseases of
the Chest . : Elsevier Health Sciences - India; 2013. pp. 1879-1936.
45. Michael A. Grippi , Jack A. Elias , Jay A. Fishman , Allan I. Pack , Robert M.
Senior , Robert Kotloff. Pulmonary Arterial Hypertension. (ed). Fishman's
Pulmonary Diseases And Disorders, 5th ed. : Mc Graw Hill Education/Exclusively
distd . By Jaypee; 2015. pp. 1064-1091.
46. Simonneau GGaliè NRubin LJLangleben DSeeger WDomenighetti GGibbs
SLebrec DSpeich RBeghetti M. Clinical classification of pulmonary
hypertension. J Am Coll Cardiol 2004;43(Suppl 1):S5–S12.
47. Simonneau GGatzoulis MAAdatia ICelermajer DDenton CGhofrani AGomez
Sanchez MAKrishna Kumar RLandzberg MMachado RFOlschewski HRobbins
IMSouza R. Updated clinical classification of pulmonary hypertension. J Am Coll
Cardiol 2013;62:D34–D41.
48. Dhillon R. The management of neonatal pulmonary hypertension. Arch Dis Child
Fetal Neonatal Ed 2012;97:F223–F228.
49. Porta NFSteinhorn RH. Pulmonary vasodilator therapy in the NICU: inhaled nitric
oxide, sildenafil, and other pulmonary vasodilating agents. Clin Perinatol
2012;39:149–164.
50. Ivy DDAbman SHBarst RJBerger RMFBonnet DFleming TRHaworth SGRaj
JURosenzweig EBSchulze Neick ISteinhorn RHBeghetti M. Pediatric pulmonary
hypertension. J Am Coll Cardiol 2013;62:D117–D126.
51. Bonderman DWexberg PMartischnig AMHeinzl HLang MBSadushi RSkoro-Sajer
NLang IM. A noninvasive algorithm to exclude pre-capillary pulmonary
hypertension. Eur Respir J 2011;37:1096–1103.
52. Rich JDThenappan TFreed BPatel ARThisted RAChilders RArcher SL. QTc
prolongation is associated with impaired right ventricular function and predicts
mortality in pulmonary hypertension. Int J Cardiol 2013;167:669–676.
53. Sun PYJiang XGomberg-Maitland MZhao QHHe JYuan PZhang RJing ZC.
Prolonged QRS duration: a new predictor of adverse outcome in idiopathic
pulmonary arterial hypertension. Chest 2012;141:374–380.
54. Olsson KMNickel NPTongers JHoeper MM. Atrial flutter and fibrillation in
patients with pulmonary hypertension. Int J Cardiol 2013;167:2300–2305.
55. Rich SDantzker DRAyres SMBergofsky EHBrundage BHDetre KMFishman
APGoldring RMGroves BMKoerner SK. Primary pulmonary hypertension: a
national prospective study. Ann Intern Med 1987;107:216–223.
56. Milne EN. Forgotten gold in diagnosing pulmonary hypertension: the plain chest
radiograph. Radiographics 2012;32:1085–1087.
57. Trip PNossent EJde Man FSvan den Berk IABoonstra AGroepenhoff HLeter
EMWesterhof NGrunberg KBogaard HJVonk-Noordegraaf A. Severely reduced
diffusion capacity in idiopathic pulmonary arterial hypertension: patient
characteristics and treatment responses. Eur Respir J 2013;42:1575–1585.
58. Sun XGHansen JEOudiz RJWasserman K. Pulmonary function in primary
pulmonary hypertension. J Am Coll Cardiol 2003;41:1028–1035.
59. Hoeper MMPletz MWGolpon HWelte T. Prognostic value of blood gas analyses
in patients with idiopathic pulmonary arterial hypertension. Eur Respir J
2007;29:944–950.
60. Pellegrino RViegi GBrusasco VCrapo ROBurgos FCasaburi RCoates Avan der
Grinten CPGustafsson PHankinson JJensen RJohnson DCMacIntyre NMcKay
RMiller MRNavajas DPedersen OFWanger J. Interpretative strategies for lung
function tests. Eur Respir J 2005;26:948–968.
61. Holverda SBogaard HJGroepenhoff HPostmus PEBoonstra AVonk-Noordegraaf
A. Cardiopulmonary exercise test characteristics in patients with chronic
obstructive pulmonary disease and associated pulmonary
hypertension. Respiration 2008;76:160–167.
62. Jilwan FNEscourrou PGarcia GJaïs XHumbert MRoisman G. High occurrence of
hypoxemic sleep respiratory disorders in precapillary pulmonary hypertension and
mechanisms. Chest 2013;143:47–55.
63. Rafanan ALGolish JADinner DSHague LKArroliga AC. Nocturnal hypoxemia is
common in primary pulmonary hypertension. Chest 2001;120:894–899.
64. Rudski LGLai WWAfilalo JHua LHandschumacher MDChandrasekaran
KSolomon SDLouie EKSchiller NB. Guidelines for the echocardiographic
assessment of the right heart in adults: a report from the American Society of
Echocardiography endorsed by the European Association of Echocardiography, a
registered branch of the European Society of Cardiology, and the Canadian
Society of Echocardiography. J Am Soc Echocardiogr 2010;23:685–713.
65. Lang RMBadano LPMor-Avi VAfilalo JArmstrong AErnande LFlachskampf
FAFoster EGoldstein SAKuznetsova TLancellotti PMuraru DPicard
MHRietzschel ERRudski LSpencer KTTsang WVoigt JU. Recommendations for
cardiac chamber quantification by echocardiography in adults: an update from the
American Society of Echocardiography and the European Association of
Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2015;16:233–271.
66. Foale RNihoyannopoulos PMcKenna WKleinebenne ANadazdin ARowland
ESmith G. Echocardiographic measurement of the normal adult right ventricle. Br
Heart J 1986;56:33–44.
67. Hachulla EGressin VGuillevin LCarpentier PDiot ESibilia JKahan ACabane
JFrances CLaunay DMouthon LAllanore YKiet PTClerson Pde Groote PHumbert
M. Early detection of pulmonary arterial hypertension in systemic sclerosis: a
French nationwide prospective multicenter study. Arthritis Rheum 2005;52:3792–
3800.
68. Tunariu NGibbs SJRWin ZGin-Sing WGraham AGishen PAL-Nahhas A.
Ventilation-perfusion scintigraphy Is more sensitive than multidetector CTPA in
detecting chronic thromboembolic pulmonary disease as a treatable cause of
pulmonary hypertension. J Nucl Med 2007;48:680–684.
69. Meng JJZhang LJWang QFang WDai HJYan JWang TYao ZMHe JLi MMi
HZJiao JZheng YM. [A comparison of ventilation/perfusion single photon
emission CT and CT pulmonary angiography for diagnosis of pulmonary
embolism]. Zhonghua Jie He He Hu Xi Za Zhi 2013;36:177–181.
70. Rajaram SSwift AJTelfer AHurdman JMarshall HLorenz ECapener DDavies
CHill CElliot CCondliffe RWild JMKiely DG. 3D contrast-enhanced lung
perfusion MRI is an effective screening tool for chronic thromboembolic
pulmonary hypertension: results from the ASPIRE Registry. Thorax
2013;68:677–678.
71. Rajaram SSwift AJCondliffe RJohns CElliot CAHill CDavies CHurdman JSabroe
IWild JMKiely DG. CT features of pulmonary arterial hypertension and its major
subtypes: a systematic CT evaluation of 292 patients from the ASPIRE
Registry. Thorax 2015;70:382–387.
72. Shen YWan CTian PWu YLi XYang TAn JWang TChen LWen F. CT-base
pulmonary artery measurement in the detection of pulmonary hypertension: a
meta-analysis and systematic review. Medicine (Baltimore) 2014;93:e256.
73. Tan RTKuzo RGoodman LRSiegel RHaasler GBPresberg KW. Utility of CT scan
evaluation for predicting pulmonary hypertension in patients with parenchymal
lung disease. Chest 1998;113:1250–1256.
74. Resten AMaitre SHumbert MRabiller ASitbon OCapron FSimonneau GMusset D.
Pulmonary hypertension: CT of the chest in pulmonary venoocclusive disease. Am
J Roentgenol 2004;183:65–70.
75. Dartevelle PFadel EMussot SChapelier AHerve Pde Perrot MCerrina JLadurie
FLLehouerou DHumbert MSitbon OSimonneau G. Chronic thromboembolic
pulmonary hypertension. Eur Respir J 2004;23:637–648.
76. Reichelt AHoeper MMGalanski MKeberle M. Chronic thromboembolic
pulmonary hypertension: evaluation with 64-detector row CT versus digital
substraction angiography. Eur J Radiol 2008;71:49–54.
77. Fedullo PFAuger WRKerr KMRubin LJ. Chronic thromboembolic pulmonary
hypertension. N Engl J Med 2001;345:1465–1472.
78. Fukui SOgo TMorita YTsuji ATateishi EOzaki KSanda YFukuda TYasuda
SOgawa HNakanishi N. Right ventricular reverse remodelling after balloon
pulmonary angioplasty. Eur Respir J 2014;43:1394–1402.
79. Castaner EAlguersuari AAndreu MGallardo XSpinu CMata JM. Imaging findings
in pulmonary vasculitis. Semin Ultrasound CT MR 2012;33:567–579.
80. Nawaz ALitt HIStavropoulos SWCharagundla SRShlansky-Goldberg RDFreiman
DBChittams JPyeritz RETrerotola SO. Digital subtraction pulmonary
arteriography versus multidetector CT in the detection of pulmonary arteriovenous
malformations. J Vasc Interv Radiol 2008;19:1582–1588.
81. Peacock AJVonk Noordegraaf A. Cardiac magnetic resonance imaging in
pulmonary arterial hypertension. Eur Respir Rev 2013;22:526–534.
82. Swift AJRajaram SCondliffe RCapener DHurdman JElliot CAWild JMKiely DG.
Diagnostic accuracy of cardiovascular magnetic resonance imaging of right
ventricular morphology and function in the assessment of suspected pulmonary
hypertension results from the ASPIRE registry. J Cardiovasc Magn Reson
2012;14:40–50.
83. Swift AJRajaram SHurdman JHill CDavies CSproson TWMorton ACCapener
DElliot CCondliffe RWild JMKiely DG. Noninvasive estimation of PA pressure,
flow, and resistance with CMR imaging: derivation and prospective validation
study from the ASPIRE registry. JACC Cardiovasc Imaging 2013;6:1036–1047.
84. Ley SKauczor HUHeussel CPKramm TMayer EThelen MKreitner KF. Value of
contrast-enhanced MR angiography and helical CT angiography in chronic
thromboembolic pulmonary hypertension. Eur Radiol 2003;13:2365–2371.

85. van Wolferen SAMarcus JTBoonstra AMarques KMJBronzwaer
JGFSpreeuwenberg MDPostmus PEVonk-Noordegraaf A. Prognostic value of
right ventricular mass, volume, and function in idiopathic pulmonary arterial
hypertension. Eur Heart J 2007;28:1250–1257.
86. Peacock AJCrawley SMcLure LBlyth KVizza CDPoscia RFrancone MIacucci
IOlschewski HKovacs GVonkNoordegraaf AMarcus JTvan de Veerdonk
MCOosterveer FPT. Changes in right ventricular function measured by cardiac
magnetic resonance imaging in patients receiving pulmonary arterial
hypertension–targeted therapy: the EURO-MR Study. Circ Cardiovasc Imaging
2014;7:107–114.
87. Van de Veerdonk MCKind TMarcus JTMauritz GJHeymans MWBogaard
HJBoonstra AMarques KMWesterhof NVonk-Noordegraaf A. Progressive right
ventricular dysfunction in patients with pulmonary arterial hypertension
responding to therapy. J Am Coll Cardiol 2011;58:2511–2519.
88. Albrecht TBlomley MJCosgrove DOTaylor-Robinson SDJayaram VEckersley
RUrbank AButler-Barnes JPatel N. Non-invasive diagnosis of hepatic cirrhosis by
transit-time analysis of an ultrasound contrast agent. Lancet 1999;353:1579–1583.
89. Naeije R. Hepatopulmonary syndrome and portopulmonary hypertension. Swiss
Med Wkly 2003;133:163–169.
90. Hoeper MMLee SHVoswinckel RPalazzini MJaïs XMarinelli ABarst RJGhofrani
HAJing ZCOpitz CSeyfarth HJHalank MMcLaughlin VOudiz RJEwert RWilkens
HKluge SBremer HCBaroke ERubin LJ. Complications of right heart
catheterization procedures in patients with pulmonary hypertension in experienced
centers. J Am Coll Cardiol 2006;48:2546–2552.
91. Taichman DBMcGoon MDHarhay MOArcher-Chicko CSager JSMurugappan
MChakinali MMPalevsky HIGallop R. Wide variation in clinicians' assessment of
New York Heart Association/World Health Organization functional class in
patients with pulmonary arterial hypertension. Mayo Clin Proc 2009;84:586–592.
92. Sitbon OHumbert MNunes HParent FGarcia GHerve PRainisio MSimonneau G.
Long-term intravenous epoprostenol infusion in primary pulmonary hypertension:
prognostic factors and survival. J Am Coll Cardiol 2002;40:780–788.
93. Nickel NGolpon HGreer MKnudsen LOlsson KWesterkamp VWelte THoeper
MM. The prognostic impact of follow-up assessments in patients with idiopathic
pulmonary arterial hypertension. Eur Respir J 2012;39:589–596.
94. Barst RJChung LZamanian RTTurner MMcGoon MD. Functional class
improvement and 3-year survival outcomes in patients with pulmonary arterial
hypertension in the REVEAL Registry. Chest 2013;144:160–168.
95. Benza RLMiller DPGomberg-Maitland MFrantz RPForeman AJCoffey CSFrost
ABarst RJBadesch DBElliott CGLiou TGMcGoon MD. Predicting survival in
pulmonary arterial hypertension: insights from the Registry to Evaluate Early and
Long-Term Pulmonary Arterial Hypertension Disease Management
(REVEAL). Circulation 2010;122:164–172.
96. McLaughlin VVSitbon OBadesch DBBarst RJBlack CGaliè NRainisio
MSimonneau GRubin LJ. Survival with first-line bosentan in patients with
primary pulmonary hypertension. Eur Respir J 2005;25:244–249.
97. Sachdev AVillarraga HRFrantz RPMcGoon MDHsiao JFMaalouf JFAmmash
NMMcCully RBMiller FAPellikka PAOh JKKane GC. Right ventricular strain for
prediction of survival in patients with pulmonary arterial hypertension. Chest
2011;139:1299–1309.
98. Raymond RJHinderliter ALWillis PWRalph DCaldwell EJWilliams WEttinger
NAHill NSSummer WRde Boisblanc BSchwartz TKoch GClayton LMJobsis
MMCrow JWLong W. Echocardiographic predictors of adverse outcomes in
primary pulmonary hypertension. J Am Coll Cardiol 2002;39:1214–1219.
99. Bustamante-Labarta MPerrone SDe La Fuente RLStutzbach PDe La Hoz
RPTorino AFavaloro R. Right atrial size and tricuspid regurgitation severity
predict mortality or transplantation in primary pulmonary hypertension. J Am Soc
Echocardiogr 2002;15:1160–1164.
100. Forfia PRFisher MRMathai SCHousten-Harris THemnes ARBorlaug BAChamera
ECorretti MCChampion HCAbraham TPGirgis REHassoun PM. Tricuspid annular
displacement predicts survival in pulmonary hypertension. Am J Respir Crit Care
Med 2006;174:1034–1041.
101. Thenappan TShah SJRich STian LArcher SLGomberg-Maitland M. Survival in
pulmonary arterial hypertension: a reappraisal of the NIH risk stratification
equation. Eur Respir J 2010;35:1079–1087.
102. Wensel ROpitz CFAnker SDWinkler JHoffken GKleber FXSharma RHummel
MHetzer REwert R. Assessment of survival in patients with primary pulmonary
hypertension: importance of cardiopulmonary exercise testing. Circulation
2002;106:319–324.
103. McLaughlin VVShillington ARich S. Survival in primary pulmonary
hypertension: the impact of epoprostenol therapy. Circulation 2002;106:1477–
1482.
104. Fine NMChen LBastiansen PMFrantz RPPellikka PAOh JKKane GC. Outcome
prediction by quantitative right ventricular function assessment in 575 subjects
evaluated for pulmonary hypertension. Circ Cardiovasc Imaging 2013;6:711–721.
105. Shimada YJShiota MSiegel RJShiota T. Accuracy of right ventricular volumes
and function determined by three-dimensional echocardiography in comparison
with magnetic resonance imaging: a meta-analysis study. J Am Soc Echocardiogr
2010;23:943–953.
106. Smith BCDobson GDawson DCharalampopoulos AGrapsa JNihoyannopoulos P.
Three-dimensional speckle tracking of the right ventricle: toward optimal
quantification of right ventricular dysfunction in pulmonary hypertension. J Am
Coll Cardiol 2014;64:41–51.
107. Grunig ETiede HEnyimayew EOEhlken NSeyfarth HJBossone ED'Andrea
ANaeije ROlschewski HUlrich SNagel CHalank MFischer C. Assessment and
prognostic relevance of right ventricular contractile reserve in patients with severe
pulmonary hypertension. Circulation 2013;128:2005–2015.
108. Swift AJRajaram SMarshall HCondliffe RCapener DHill CDavies CHurdman
JElliot CAWild JMKiely DG. Black blood MRI has diagnostic and prognostic
value in the assessment of patients with pulmonary hypertension. Eur Radiol
2012;22:695–702.
109. Swift AJRajaram SCampbell MJHurdman JThomas SCapener DElliot CCondliffe
RWild JMKiely DG. Prognostic value of cardiovascular magnetic resonance
imaging measurements corrected for age and sex in idiopathic pulmonary arterial
hypertension. Circ Cardiovasc Imaging 2014;7:100–106.
110. Sitbon OMcLaughlin VVBadesch DBBarst RJBlack CGaliè NHumbert MRainisio
MRubin LJSimonneau G. Survival in patients with class III idiopathic pulmonary
arterial hypertension treated with first line oral bosentan compared with an
historical cohort of patients started on intravenous epoprostenol. Thorax
2005;60:1025–1030.
111. Rich JDArcher SLRich S. Noninvasive cardiac output measurements in patients
with pulmonary hypertension. Eur Respir J 2013;42:125–133.
112. Savarese GPaolillo SCostanzo PD'Amore CCecere MLosco TMusella FGargiulo
PMarciano CPerrone-Filardi P. Do changes of 6-minute walk distance predict
clinical events in patients with pulmonary arterial hypertension?: a meta-analysis
of 22 randomized trials. J Am Coll Cardiol 2012;60:1192–1201.
113. Gabler NBFrench BStrom BLPalevsky HITaichman DBKawut SMHalpern SD.
Validation of 6-minute walk distance as a surrogate end point in pulmonary
arterial hypertension trials. Circulation 2012;126:349–356.
114. Fritz JSBlair COudiz RJDufton COlschewski HDespain DGillies HKawut SM.
Baseline and follow-up 6-min walk distance and brain natriuretic peptide predict
2-year mortality in pulmonary arterial hypertension. Chest 2013;143:315–323.
115. Paciocco GMartinez FBossone EPielsticker EGillespie BRubenfire M. Oxygen
desaturation on the six-minute walk test and mortality in untreated primary
pulmonary hypertension. Eur Respir J 2001;17:647–652.
116. Provencher SChemla DHerve PSitbon OHumbert MSimonneau G. Heart rate
responses during the 6-minute walk test in pulmonary arterial hypertension. Eur
Respir J 2006;27:114–120.
117. Sun XGHansen JEOudiz RJWasserman K. Exercise pathophysiology in patients
with primary pulmonary hypertension. Circulation 2001;104:429–435.
118. Wensel RFrancis DPMeyer FJOpitz CFBruch LHalank MWinkler JSeyfarth
HJGlaser SBlumberg FObst ADandel MHetzer REwert R. Incremental prognostic
value of cardiopulmonary exercise testing and resting haemodynamics in
pulmonary arterial hypertension. Int J Cardiol 2013;167:1193–1198.
119. Blumberg FCArzt MLange TSchroll SPfeifer MWensel R. Impact of right
ventricular reserve on exercise capacity and survival in patients with pulmonary
hypertension. Eur J Heart Fail 2013;15:771–775.
120. Diller GPDimopoulos KOkonko DLi WBabu-Narayan SVBroberg CSJohansson
BBouzas BMullen MJPoole-Wilson PAFrancis DPGatzoulis MA. Exercise
intolerance in adult congenital heart disease: comparative severity, correlates, and
prognostic implication. Circulation 2005;112:828–835.
121. Arena RLavie CJMilani RVMyers JGuazzi M. Cardiopulmonary exercise testing
in patients with pulmonary arterial hypertension: an evidence-based review. J
Heart Lung Transplant 2010;29:159–173.
122. Pullamsetti SKiss LGhofrani HAVoswinckel RHaredza PKlepetko WAigner
CFink LMuyal JPWeissmann NGrimminger FSeeger WSchermuly RT. Increased
levels and reduced catabolism of asymmetric and symmetric dimethylarginines in
pulmonary hypertension. FASEB J 2005;19:1175–1177.
123. Kielstein JTBode-Boger SMHesse GMartens-Lobenhoffer JTakacs AFliser
DHoeper MM. Asymmetrical dimethylarginine in idiopathic pulmonary arterial
hypertension. Arterioscler Thromb Vasc Biol 2005;25:1414–1418.
124. Kielstein JTImpraim BSimmel SBode-Boger SMTsikas DFrolich JCHoeper
MMHaller HFliser D. Cardiovascular effects of systemic nitric oxide synthase
inhibition with asymmetrical dimethylarginine in humans. Circulation
2004;109:172–177.
125. Kawut SMHorn EMBerekashvili KKWidlitz ACRosenzweig EBBarst RJ. von
Willebrand factor independently predicts long-term survival in patients with
pulmonary arterial hypertension. Chest 2005;128:2355–2362.
126. Kumpers PNickel NLukasz AGolpon HWesterkamp VOlsson KMJonigk
DMaegel LBockmeyer CLDavid SHoeper MM. Circulating angiopoietins in
idiopathic pulmonary arterial hypertension. Eur Heart J 2010;31:2291–2300.
127. Rubens CEwert RHalank MWensel ROrzechowski HDSchultheiss HPHoeffken G.
Big endothelin-1 and endothelin-1 plasma levels are correlated with the severity of
primary pulmonary hypertension. Chest 2001;120:1562–1569.
128. Quarck RNawrot TMeyns BDelcroix M. C-reactive protein: a new predictor of
adverse outcome in pulmonary arterial hypertension. J Am Coll Cardiol
2009;53:1211–1218.
129. Balabanian KFoussat ADorfmuller PDurand-Gasselin ICapel FBouchet-Delbos
LPortier AMarfaing-Koka AKrzysiek RRimaniol ACSimonneau GEmilie
DHumbert M. CX(3)C chemokine fractalkine in pulmonary arterial
hypertension. Am J Respir Crit Care Med 2002;165:1419–1425.
130. Dorfmuller PZarka VDurand-Gasselin IMonti GBalabanian KGarcia GCapron
FCoulomb-Lhermine AMarfaing-Koka ASimonneau GEmilie DHumbert M.
Chemokine RANTES in severe pulmonary arterial hypertension. Am J Respir Crit
Care Med 2002;165:534–539.
131. Humbert MMonti GBrenot FSitbon OPortier AGrangeot-Keros LDuroux
PGalanaud PSimonneau GEmilie D. Increased interleukin-1 and interleukin-6
serum concentrations in severe primary pulmonary hypertension. Am J Respir Crit
Care Med 1995;151:1628–1631.
132. Nagaya NNishikimi TUematsu MSatoh TKyotani SSakamaki FKakishita
MFukushima KOkano YNakanishi NMiyatake KKangawa K. Plasma brain
natriuretic peptide as a prognostic indicator in patients with primary pulmonary
hypertension. Circulation 2000;102:865–870.
133. Leuchte HHEl NMTuerpe JCHartmann BBaumgartner RAVogeser MMuehling
OBehr J. N-terminal pro-brain natriuretic peptide and renal insufficiency as
predictors of mortality in pulmonary hypertension. Chest 2007;131:402–409.
134. Fijalkowska AKurzyna MTorbicki ASzewczyk GFlorczyk MPruszczyk
PSzturmowicz M. Serum N-terminal brain natriuretic peptide as a prognostic
parameter in patients with pulmonary hypertension. Chest 2006;129:1313–1321.
135. Torbicki AKurzyna MKuca PFijalkowska ASikora JFlorczyk MPruszczyk
PBurakowski JWawrzynska L. Detectable serum cardiac troponin T as a marker of
poor prognosis among patients with chronic precapillary pulmonary
hypertension. Circulation 2003;108:844–848.
136. Nickel NKempf TTapken HTongers JLaenger FLehmann UGolpon HOlsson
KWilkins MRGibbs JSHoeper MMWollert KC. Growth differentiation factor-15
in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med
2008;178:534–541.
137. Nagaya NUematsu MSatoh TKyotani SSakamaki FNakanishi NYamagishi
MKunieda TMiyatake K. Serum uric acid levels correlate with the severity and the
mortality of primary pulmonary hypertension. Am J Respir Crit Care Med
1999;160:487–492.

138. Lorenzen JMNickel NKramer RGolpon HWesterkamp VOlsson KMHaller
HHoeper MM. Osteopontin in patients with idiopathic pulmonary
hypertension. Chest 2011;139:1010–1017.
139. Medicine and Science in Sports and Exercise. 1982; 14:377-381.
140. Nickel NGolpon HGreer MKnudsen LOlsson KWesterkamp VWelte THoeper
MM. The prognostic impact of follow-up assessments in patients with idiopathic
pulmonary arterial hypertension. Eur Respir J 2012;39:589–596.
141. Fritz JSBlair COudiz RJDufton COlschewski HDespain DGillies HKawut SM.
Baseline and follow-up 6-min walk distance and brain natriuretic peptide predict
2-year mortality in pulmonary arterial hypertension. Chest 2013;143:315–323.
142. Magdy M. Emaraa ,g,*, Mohamad A. Habeb b, Alsayed Ahmed Alnahal c, Tarek
A. Elshazly d, Faisal O. Alatawi e, Amer S. Masoud f. Prevalance of pulmonary
hypertension in patients with chronic kidney disease on and without
dialysis. Egyptian Journal of chest diseases and tuberculosis 2013; 62(): .
143. Craddock PR, Fehr J, Dalmasso AP, Brigham KL, Jacob HS. Hemodialysis
leucopenia. J Clin Invest. 1977;59:879– 888.
144. Craddock PR, Fehr J, Brigham KL, Kronenberg RS, Jacob HS. Complement and
leukocyte-mediated pulmonary dysfunction in hemodialysis. N Engl J Med.
1977;296:769–774.
145. Yigla M, Abassi Z, Reisner SA, Nakhoul F. Pulmonary hypertension in
hemodialysis patients: an unrecognized threat. Semin Dial. 2006;19:353–357.
146. Kiykim AA, Horoz M, Ozcan T, Yildiz I, Sari S, Genctoy G. Pulmonary
hypertension in hemodialysis patients without arteriovenous fistula: the effect of
dialyzer composition. Ren Fail. 2010;32:1148–1152.
147. Giaid A. Nitric oxide and endothelin-1 in pulmonary hypertension. Chest.
1998;114:208S-212S.
148. Zoccali C. The endothelium as a target in renal diseases. J Nephrol.
2007;20(12):39–44.
149. Giaid A, Saleh D. Reduced expression of endothelial nitric oxide synthase in the
lungs of patients with pulmonary hypertension. N Engl J Med. 1995;333:214–
221.
150. Sakaguchi Y, Shoji T, Kawabata H, et al. High prevalence of obstructive sleep
apnea and its association with renal function among nondialysis chronic kidney
disease patients in Japan: a cross-sectional study. Clin J Am Soc Nephrol.
2011;6:995–1000.
151. Zoccali C, Mallamaci F, Tripepi G. Nocturnal hypoxemia predicts incident
cardiovascular complications in dialysis patients. J Am Soc Nephrol. 2002;3:729–
733.
PSG Institute of Medical Science and Research, Coimbatore
Institutional Human Ethics Committee
INFORMED CONSENT FORMAT FOR RESEARCH PROJECTS
(strike off items that are not applicable)
I / We (write name of the investigator(s) here), DR.S.VIGNESH, am / are carrying out a
study on the topic: Prevalence of pulmonary hypertension in patients with GFR less than
30 ml/min per 1.73 meter square on dialysis, as part of my / our research project being
carried out under the aegis of the Department of general medicine
(Applicable to students only):
My Research Guide: DR. R . TOLSTOY
The justification for this study:
There are many patients with end stage renal disease who present with dyspnea with no
obvious reason so it is important to look for pulmonary hypertension in these patients .
Risk factors for developing pulmonary hypertension in end stage renal disease includes
endothelial dysfunction, exposure to dialysis membrane, AV fistula, volume overload
status.
The objectives of this study are:
Primary Objective:
To find Prevalence of pulmonary hypertension in patients with e GFR less than 30
ml/min per 1.73 meter square on dialysis.
Sample size: 50
Study volunteers / participants are (specify population group & age group): patients
>18 year of age.
Location: PSGIMSR.
We request you to kindly cooperate with us in this study. We propose collect background
information and other relevant details related to this study. We will be carrying out:
Initial interview (specify approximate duration): 15minutes.
Data collected will be stored for a period of 1 years. We will / will not use the data as part
of another study.
Health education sessions:
Number of sessions: 1.
Approximate duration of each session: 15 minutes.
Clinical examination (Specify details and purpose): general examination
Blood sample collection: Specify quantity of blood being drawn: nil
Medication given, if any, duration, side effects, purpose, benefits: nil
Whether medication given is part of routine procedure: Yes / No (If not, state reasons for
giving this medication)
Whether alternatives are available for medication given: Yes / No (If not, state reasons
for giving this particular medication)

Final interview (specify approximate duration):15 minutes.
If photograph is taken, purpose: no
Benefits from this study:
If there is high prevalence of pulmonary hypertension in patients with end stage renal
disease on dialysis, we can make it a routine to screen for pulmonary hypertension in
these patients & it can be treated with appropriate medication to reduce symptoms of
pulmonary hypertension in these patients
Risks involved by participating in this study: nil
How the results will be used: for post graduate thesis purpose only
If you are uncomfortable in answering any of our questions during the course of the
interview / biological sample collection, you have the right to withdraw from the
interview / study at any time. You have the freedom to withdraw from the study at any
point of time. Kindly be assured that your refusal to participate or withdrawal at any
stage, if you so decide, will not result in any form of compromise or discrimination in the
services offered nor would it attract any penalty. You will continue to have access to the
regular services offered to a patient. You will NOT be paid any remuneration for the time
you spend with us for this interview / study. The information provided by you will be
kept in strict confidence. Under no circumstances shall we reveal the identity of the
respondent or their families to anyone. The information that we collect shall be used for
approved research purposes only. You will be informed about any significant new
findings - including adverse events, if any, – whether directly related to you or to other
participants of this study, developed during the course of this research which may relate
to your willingness to continue participation.
Consent: The above information regarding the study, has been read by me/ read to me,
and has been explained to me by the investigator/s. Having understood the same, I hereby
give my consent to them to interview me. I am affixing my signature / left thumb
impression to indicate my consent and willingness to participate in this study (i.e.,
willingly abide by the project requirements).
Signature / Left thumb impression of the Study Volunteer / Legal Representative:
Signature of the Interviewer with date: Witness:
Contact number of PI: 9791449144
Contact number of Ethics Committee Office: 0422 4345818
LIST OF FIGURES
Figure 1: Features of plexogenic pulmonary arteriopathy are shown in this diagram
Figure 2: Chest x-ray AP and lateral view showing pulmonary artery enlargement
Figure 3: Pulmonary artery enlargement is highlighted in this CT picture
Figure 4: Echo
Figure 5: Distribution Of PH Among Various Age Group
Figure 6: Association of SEX and Pulmonary hypertension
Figure 7: Association of DM and Pulmonary hypertension
Figure 8: Association of SHTN and Pulmonary hypertension
Figure 9: Association of MILD LVD and Pulmonary hypertension
Figure 10: Association of AV F and Pulmonary hypertension
Figure 11: Association of Superimposed Infection and Pulmonary hypertension
Figure 12: Association of Volume Overload and Pulmonary hypertension
Figure 13: Association of Anaemia and Pulmonary hypertension
Figure 14: Association of LVDD and Pulmonary hypertension
Figure 15: Association of Creatine Clearance and Pulmonary hypertension
Figure 16: Association of Duration of Dialysis and Pulmonary hypertension
LIST OF TABLES
Table 1: Receptors Affecting Smooth Muscle in Pulmonary Arteries and Vein
Table 2: Haemodynamic Definition of Pulmonary Hypertension
Table 3: Drugs & Toxins That Causes Pulmonary Artery Hypertension
Table 4: Classification of PH46-50
Table 5: Components of the Pathogenesis Of Pulmonary Arterial Hypertension
Table 6: Physical Sign That Suggest a Possible Underlying Cause or Associations of
Pulmonary Hypertension
Table 7: Echocardiographic Probability of Pulmonary Hypertension in Symptomatic
Patients with a Suspicion of Pulmonary Hypertension1, 5, 43, 64, 65
Table 8: Echocardiographic Signs Suggesting Pulmonary Hypertension Used To
Assess The Probability Of Pulmonary Hypertension In Addition To Tricuspid
Regurgitation Velocity Measurement In Table61, 5, 43, 64, And 65
Table 9: Distinguishing Pulmonary Arterial Hypertension from Heart Failure with
Preserved Ejection Fraction
Table 10: FDA Approved Drugs for Treatment of PH
Table 11: WHO Class
Table 12: Borg Scale137
Table 13: Risk Assessment in Pulmonary Arterial Hypertension
Table 14: Suggested Assessment and Timing for the Follow-Up of Patients with
Pulmonary Arterial Hypertension
Table 15: Distribution of PH among Various Age Groups
Table 16: Association of SEX and Pulmonary hypertension
Table 17: Association of DM and Pulmonary hypertension
Table 18: Association of SHTN and Pulmonary hypertension
Table 19: Association of MILD LVD and Pulmonary hypertension
Table 20: Association of AV F and Pulmonary hypertension
Table 21: Association of Superimposed Infection and Pulmonary hypertension
Table 22: Association of Volume Overload and Pulmonary hypertension
Table 23: Association of Anaemia and Pulmonary hypertension
Table 24: Association of LVDD and Pulmonary hypertension
Table 25: Association of Creatine Clearance and Pulmonary hypertension
Table 26: Association of Duration of Dialysis and Pulmonary hypertension
PROFOMA
1. IP NUMBER:
2. SEX:
3. AGE:
4. CHIEF COMPLAINTS:
5. SYMPTOMS & SIGNS:
6. PRESENCE OF SUPERIMPOSED INFECTION
7. PRESENCE OF VOLUME OVERLOAD STATE
8. COMORBID CONDITIONS:
9. GFR:
10. STAGING CKD:
11. TYPE OF DIALYSIS PATIENT IS ON:
12. SCREENING FOR PULMONARY HYPERTENSION:
13. PRESENCE OF LVDD
14. ASSESSING LV STATUS
15. DURATION OF DIALYSIS
ABBREVIATIONS
PH- Pulmonary Hypertension
PAH- Pulmonary Artery Hypertension
WHO- World Health Organization
CKD- Chronic Kidney Disease
CTEPH - Chronic Thrombi Embolic Pulmonary Hypertension
GFR - Glomerular Filtration Rate
ESRD - End Stage Renal Disease
PSGIMSR - Peelamedu Samanaidu Govindasamy Naidu Institute of Medical
Science & Research Centre
LVDD- Left Ventricular Diastolic Dysfunction
LVD- Left Ventricular Systolic Dysfunction
HIV-Human Immuno Deficiency Virus
SD- Standard Deviation
SSPS- Statistical Software Package
NO- Nitric Oxide
pH- Pouvoir Hydrogène
PCO2- Partial Pressure of Carbon Dioxide
PAP- Pulmonary Artery Pressure
PAPm-Mean Pulmonary Artery Pressure
PAPs- Pulmonary Artery Systolic Pressure
PAWP- Pulmonary Artery Wedge Pressure
PVR- Pulmonary Vascular Resistance
DPG- Diastolic Pulmonary Vascular Pressure Gradient
COPD- Chronic Obstructive Pulmonary Disease
JVP- Jugular Venous Pressure
P2- Second Pulmonary Component Of Second Heart Sound
ANA- Antinuclear Antibody
ANA IF- Antinuclear Antibody Immunofluorescence
ANCA- Anti-Neutrophil Cytoplasmic Antibody
RV- Right Ventricle
ECG- Electrocardiography
ECHO- Echocardiography
DLCO- Diffusing Capacity of Lung for Carbon Monoxide
PVOD- Peripheral Vascular Obstructive Disease
V/Q scan- Ventilation Perfusion Scan
CT- Computed Tomography
HRCT- High Resolution Computed Tomography
APview- Anterior Posterior View
RHC- Right Heart Catheterization
NYHA-New York Heart Association
PDE5- Phosphodiesterase
RA- Right Atrium
LV -Left Ventricle
CMR- Cardiac Magnetic Resonance Index
6MWT- 6 minutes walk test
NT pro BNP- N Terminal Pro Brain Natriuretic Peptide
HD- Haemodialysis
AVF- Arterio Venous Fistula
CO - Cardiac Output
DPG - diastolic pressure gradient (diastolic PAP – mean PAWP);
WU - Wood units.
BMPR2 - Bone Morphogenetic Protein Receptor, type 2;
EIF2AK4 - Eukaryotictranslation Initiation Factor 2 Alpha kinase 4;
BMPR2 - A type 2 receptor for bone morphogenetic proteins involved in the
control of vascular cell proliferation
KCNK3-The Potassium Channel Subfamily K Member 3
CAV1- Caveolin 1
LVEDP - Left Ventricular End-Diastolic Pressure; .
CCB - Calcium Channel Blocker
HPAH - Heritable Pulmonary Arterial Hypertension
IPAH - Idiopathic Pulmonary Arterial Hypertension
CTEPH - Chronic Thromboembolic Pulmonary Hypertension
CMR - Cardiac Magnetic Resonance
pred. - Predicted
RA -Right Atrium
RAP - Right Atrial Pressure;
SvO2 - Mixed Venous Oxygen Saturation
ALAT - Alanine Aminotransferase;
ASAT - Aspartate Aminotransferase;
BGA - Blood Gas Analysis;
BNP - Brain Natriuretic Peptide
CPET - Cardiopulmonary Exercise Testing
ERAs - Endothelin Receptor Antagonists
FC - Functional Class
INR - international normalized ratio;
Lab - laboratory assessment;
TSH - Thyroid Stimulating Hormone
WHO-FC - World Health Organization functional class.
HPAH - Heritable Pulmonary Arterial Hypertension
IPAH - Idiopathic Pulmonary Arterial Hypertension
RVSP – Right Ventricular Systolic Pressure
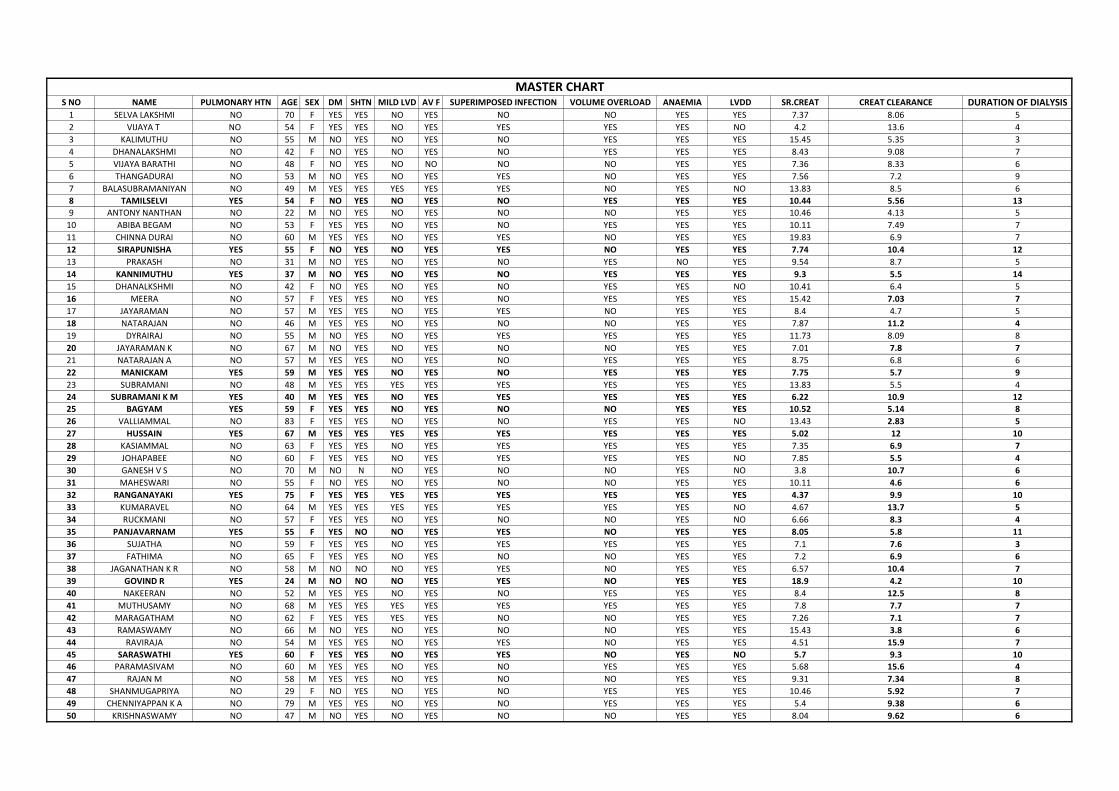
S NO NAME PULMONARY HTN AGE SEX DM SHTN MILD LVD AV F SUPERIMPOSED INFECTION VOLUME OVERLOAD ANAEMIA LVDD SR.CREAT CREAT CLEARANCE DURATION OF DIALYSIS1 SELVA LAKSHMI NO 70 F YES YES NO YES NO NO YES YES 7.37 8.06 5
2 VIJAYA T NO 54 F YES YES NO YES YES YES YES NO 4.2 13.6 4
3 KALIMUTHU NO 55 M NO YES NO YES NO YES YES YES 15.45 5.35 3
4 DHANALAKSHMI NO 42 F NO YES NO YES NO YES YES YES 8.43 9.08 7
5 VIJAYA BARATHI NO 48 F NO YES NO NO NO NO YES YES 7.36 8.33 6
6 THANGADURAI NO 53 M NO YES NO YES YES NO YES YES 7.56 7.2 9
7 BALASUBRAMANIYAN NO 49 M YES YES YES YES YES NO YES NO 13.83 8.5 6
8 TAMILSELVI YES 54 F NO YES NO YES NO YES YES YES 10.44 5.56 13
9 ANTONY NANTHAN NO 22 M NO YES NO YES NO NO YES YES 10.46 4.13 5
10 ABIBA BEGAM NO 53 F YES YES NO YES NO YES YES YES 10.11 7.49 7
11 CHINNA DURAI NO 60 M YES YES NO YES YES NO YES YES 19.83 6.9 7
12 SIRAPUNISHA YES 55 F NO YES NO YES YES NO YES YES 7.74 10.4 12
13 PRAKASH NO 31 M NO YES NO YES NO YES NO YES 9.54 8.7 5
14 KANNIMUTHU YES 37 M NO YES NO YES NO YES YES YES 9.3 5.5 14
15 DHANALKSHMI NO 42 F NO YES NO YES NO YES YES NO 10.41 6.4 5
16 MEERA NO 57 F YES YES NO YES NO YES YES YES 15.42 7.03 7
17 JAYARAMAN NO 57 M YES YES NO YES YES NO YES YES 8.4 4.7 5
18 NATARAJAN NO 46 M YES YES NO YES NO NO YES YES 7.87 11.2 4
19 DYRAIRAJ NO 55 M NO YES NO YES YES YES YES YES 11.73 8.09 8
20 JAYARAMAN K NO 67 M NO YES NO YES NO NO YES YES 7.01 7.8 7
21 NATARAJAN A NO 57 M YES YES NO YES NO YES YES YES 8.75 6.8 6
22 MANICKAM YES 59 M YES YES NO YES NO YES YES YES 7.75 5.7 9
23 SUBRAMANI NO 48 M YES YES YES YES YES YES YES YES 13.83 5.5 4
24 SUBRAMANI K M YES 40 M YES YES NO YES YES YES YES YES 6.22 10.9 12
25 BAGYAM YES 59 F YES YES NO YES NO NO YES YES 10.52 5.14 8
26 VALLIAMMAL NO 83 F YES YES NO YES NO YES YES NO 13.43 2.83 5
27 HUSSAIN YES 67 M YES YES YES YES YES YES YES YES 5.02 12 10
28 KASIAMMAL NO 63 F YES YES NO YES YES YES YES YES 7.35 6.9 7
29 JOHAPABEE NO 60 F YES YES NO YES YES YES YES NO 7.85 5.5 4
30 GANESH V S NO 70 M NO N NO YES NO NO YES NO 3.8 10.7 6
31 MAHESWARI NO 55 F NO YES NO YES NO NO YES YES 10.11 4.6 6
32 RANGANAYAKI YES 75 F YES YES YES YES YES YES YES YES 4.37 9.9 10
33 KUMARAVEL NO 64 M YES YES YES YES YES YES YES NO 4.67 13.7 5
34 RUCKMANI NO 57 F YES YES NO YES NO NO YES NO 6.66 8.3 4
35 PANJAVARNAM YES 55 F YES NO NO YES YES NO YES YES 8.05 5.8 11
36 SUJATHA NO 59 F YES YES NO YES YES YES YES YES 7.1 7.6 3
37 FATHIMA NO 65 F YES YES NO YES NO NO YES YES 7.2 6.9 6
38 JAGANATHAN K R NO 58 M NO NO NO YES YES NO YES YES 6.57 10.4 7
39 GOVIND R YES 24 M NO NO NO YES YES NO YES YES 18.9 4.2 10
40 NAKEERAN NO 52 M YES YES NO YES NO YES YES YES 8.4 12.5 8
41 MUTHUSAMY NO 68 M YES YES YES YES YES YES YES YES 7.8 7.7 7
42 MARAGATHAM NO 62 F YES YES YES YES NO NO YES YES 7.26 7.1 7
43 RAMASWAMY NO 66 M NO YES NO YES NO NO YES YES 15.43 3.8 6
44 RAVIRAJA NO 54 M YES YES NO YES YES NO YES YES 4.51 15.9 7
45 SARASWATHI YES 60 F YES YES NO YES YES NO YES NO 5.7 9.3 10
46 PARAMASIVAM NO 60 M YES YES NO YES NO YES YES YES 5.68 15.6 4
47 RAJAN M NO 58 M YES YES NO YES NO NO YES YES 9.31 7.34 8
48 SHANMUGAPRIYA NO 29 F NO YES NO YES NO YES YES YES 10.46 5.92 7
49 CHENNIYAPPAN K A NO 79 M YES YES NO YES NO YES YES YES 5.4 9.38 6
50 KRISHNASWAMY NO 47 M NO YES NO YES NO NO YES YES 8.04 9.62 6
MASTER CHART