survival in schistosomiasis-associated pulmonary arterial hypertension
TRANSCRIPT
Pdscnpm
g
FSClhHAtP
2
Journal of the American College of Cardiology Vol. 56, No. 9, 2010© 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00P
Schistosomiasis Heart Disease
Survival in Schistosomiasis-Associated PulmonaryArterial Hypertension
Caio Julio Cesar dos Santos Fernandes, MD, PHD,* Carlos Vianna Poyares Jardim, MD, PHD,*Andre Hovnanian, MD,* Susana Hoette, MD,*† Bruno Arantes Dias, MD,* Silvia Souza, MD, PHD,*Marc Humbert, MD, PHD,† Rogerio Souza, MD, PHD*†
São Paulo, Brazil; and Clamart, France
Objectives The objective of this study was to evaluate the natural history of untreated schistosomiasis-associated pulmo-nary arterial hypertension (Sch-PAH) patients as compared to idiopathic pulmonary arterial hypertension (IPAH)with respect to hemodynamics recorded at presentation and 36 months survival.
Background Schistossomiasis (Sch) is one of the most prevalent chronic infectious diseases in the world. Nevertheless dataregarding one of its most severe clinical complications, pulmonary arterial hypertension (PAH), is scarce.
Methods We retrospectively analyzed case notes of all consecutive patients diagnosed of Sch-PAH and IPAH referred tothe Heart Institute in São Paulo, Brazil, between 2004 and 2008. None of the Sch-PAH received PAH specifictreatment whereas all IPAH patients did.
Results Sch-PH patients (n � 54) had less severe pulmonary hypertension as evidenced by lower levels of pulmonaryvascular resistance (11.3 � 11.3 W vs. 16.7 � 10.6 W; p � 0.002) and mean pulmonary artery pressure (56.7� 18.7 mm Hg vs. 64.6 � 17.4 mm Hg; p � 0.01) and higher cardiac output (4.62 � 1.5 l/min vs. 3.87 � 1.5l/min; p � 0.009) at presentation than IPAH patients (n � 95). None of the Sch-PAH patients demonstrated apositive response to acute vasodilator testing, whereas 16.2% of IPAH patients did (p � 0.015). Survival rates at1, 2, and 3 years were 95.1%, 95.1%, and 85.9% and 95%, 86%, and 82%, for Sch-PAH and IPAH, respectively(p � 0.49). Both groups had a higher survival rate when compared to IPAH survival as estimated by the NIHequation (71%, 61%, and 52%, respectively).
Conclusions Sch-PAH has a more benign clinical course than IPAH despite a lack of demonstrable acute vasoreactivity athemodynamic evaluation. (J Am Coll Cardiol 2010;56:715–20) © 2010 by the American College of CardiologyFoundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2010.03.065
iittract
toSsienCT
ulmonary arterial hypertension (PAH) is a life-threateningisease that may occur either in idiopathic form or in theetting of different associated medical conditions. PAH isharacterized by a marked and sustained elevation of pulmo-ary vascular resistance (PVR), leading to an increase inulmonary artery pressure, right ventricular failure, and ulti-ately death (1).Considerable advances in our understanding of the patho-
enesis and therapeutic approaches of PAH have been gained
rom the *Pulmonary Department, Heart Institute, University of São Paulo Medicalchool, São Paulo, Brazil; and the †Hôpital Antoine Béclère, Université Paris-Sud,lamart, France. Drs. dos Santos Fernandes, Jardim, and Hovnanian has received
ecture fees from Actelion and Pfizer. Drs. Hoette and Silvia Souza report that theyave no relationships to disclose. Dr. Dias has received lecture fees from Actelion. Dr.umbert is an investigator and a member of the scientific advisory board withctelion, Bayer Schering, GlaxoSmithKline, Novartis, Pfizer, and United Therapeu-
ics. Dr. Rogerio Souza has received consultancy and/or lecture fees from Actelion,fizer, and GlaxoSmithKline.
iManuscript received October 9, 2009; revised manuscript received February 8,
010, accepted March 9, 2010.
n recent years, based mainly on studies involving patients withdiopathic pulmonary arterial hypertension (IPAH) or connec-ive tissue diseases associated with PAH (2,3). Nevertheless,here is an increasing awareness of the burden posed by PAHesulting from other causes, such as sickle cell disease, HIV,nd schistosomiasis. As a result, studies addressing the clini-opathologic characteristics and outcomes of patients withhese forms of the disease are beginning to emerge (4,5).
Schistosomiasis is an infectious disease caused by parasiticrematode worms that is strongly linked to poverty and lackf basic sanitation (6). The 3 main pathogenic species arechistosoma mansoni, Schistosoma haematobium, and Schisto-oma japonicum, each of which has a characteristic geograph-cal distribution (7,8). Because of migratory practices, how-ver, schistosomiasis prevalence is also increasing inonendemic regions. According to the Center for Diseaseontrol and Prevalence and the International Society ofravel Medicine database—GeoSentinel—schistosomiasis
s also one of the 10 leading causes of morbidity among
goepstcdaaasue
M
Paii
(awipaHpapie
osaiwmppwuFuea6rvormlTtotiPtNrrScsb
ttddaroasSStibtas
t
716 Fernandes et al. JACC Vol. 56, No. 9, 2010Survival in Schistosomiasis Pulmonary Hypertension August 24, 2010:715–20
travelers (9), highlighting theimportance of the disease also indeveloped countries.
Pulmonary hypertension repre-sents one of the most severe com-plications of chronic schistosomia-sis (7). Recently, the results of ascreening program for pulmonaryhypertension identified a 4.6%prevalence of PAH among pa-tients diagnosed with hepato-splenic Schistosomiasis mansoni (5).When this prevalence rate is con-sidered in the context of the highprevalence of the infection globally(8), schistosomiasis may representthe most common cause of PAHworldwide; moreover, a clear bur-den of PAH may be revealed inthis context (10). The importanceof schistosomiasis in the setting ofpulmonary hypertension is even
reater in certain regions. Indeed, it is estimated that up to 30%f all pulmonary hypertension patients followed up at refer-nce centers in Brazil have schistosomiasis-associatedulmonary hypertension (11). Despite that, data relating tochistosomiasis-associated PAH (Sch-PAH) are scarce inhe literature. Hitherto, most published reports have fo-used on the clinical and echocardiographic features of theisease. Unlike IPAH, in which hemodynamics, survival,nd clinical response have been well defined (12,13), there islack of information available relating to the presentation
nd natural history of Sch-PAH. The objective of thistudy, therefore, was to evaluate the outcomes of a cohort ofntreated Sch-PAH patients followed up at a PAH refer-nce center in Brazil.
ethods
atient population. All patients diagnosed with Sch-PAHnd IPAH between January 2004 and June 2008 werencluded in this study. The study was approved by ournstitutional review board and ethics committee.
PAH was defined by a mean pulmonary artery pressuremPAP) of more than 25 mm Hg, with a normal pulmonaryrtery occlusion pressure (PAOP �15 mm Hg). Patientsere classified as having IPAH when PAH was diagnosed
n the absence of chronic thromboembolic pulmonary hy-ertension; associated significant left heart or lung disease;nd PAH associated with other known conditions, includingIV infection, portal hypertension, congenital systemic-to-
ulmonary shunts, connective tissue diseases, and exposure toppetite suppressants. Inclusion criteria for Sch-PAH was theresence of PAH associated with liver ultrasonographic find-ngs highly suggestive of Manson’s schistosomiasis (left lobe
Abbreviationsand Acronyms
IPAH � idiopathicpulmonary arterialhypertension
mPAP � mean pulmonaryartery pressure
PAH � pulmonary arterialhypertension
PAOP � pulmonary arteryocclusion pressure
PH � pulmonaryhypertension
PVR � pulmonary vascularresistance
Sch-PAH �
schistosomiasis-associatedpulmonary arterialhypertension
6MWT � length innonencouraged 6-min walktest
nlargement, periportal fibrosis, or both [14]) and at least one c
f the following features: 1) exposure to endemic region forchistosomiasis; 2) previous treatment for schistosomiasis;nd 3) presence of Schistosoma mansoni eggs in stool exam-nation or rectal biopsy. All patients included in the studyere referred to our center by primary or secondary careedical facilities for evaluation of dyspnea, of elevated
ulmonary artery pressures as estimated by echocardiogra-hy, or both. In most cases, the diagnosis of schistosomiasisas established at our center after specific investigation andsing the aforementioned criteria.unctional and hemodynamic evaluations. Baseline eval-ation included demographics, medical history, physicalxamination, New York Heart Association functional classssessment, routine laboratory testing, a nonencouraged-min walk test (6MWT) as previously described (15), andight heart catheterization using standard techniques. Acuteasodilator responsiveness was evaluated using inhaled nitricxide for 10 min, as previously described (16). A positiveesponse to acute vasodilator testing was defined as a fall inPAP of 10 mm Hg or more to a value of 40 mm Hg or
ess with a normal or increased cardiac output (17).reatment of pulmonary hypertension. All patients were
reated with conventional supportive therapies, includingral anticoagulation in the absence of any contraindica-ion (e.g., high risk of gastrointestinal bleeding), diuret-cs, and oxygen as needed. IPAH patients receivedAH-specific therapy based on guideline recommenda-
ions (18) and drug availability in our center. Patients inew York Heart Association functional class III or IV
eceived first-line therapy with either an endothelin-eceptor antagonist or phosphodiesterase type 5 inhibitor.ome patients in New York Heart Association functionallass IV who had progressive disease and worsening ofymptoms received combination therapy with agents fromoth classes of drug.Sch-PAH patients did not receive any PAH-specific
herapy as a routine because, in our country, specific PAHreatments are authorized only for IPAH, connective tissueisease related PAH, and PAH related to congenital heartisease. Two patients received off-label specific PAH ther-py after 2 and 7 months of follow-up because of progressiveight heart failure. These patients were censored at the timef treatment initiation. All Sch-PAH patients receiveddequate antiparasitic treatment before enrollment in thetudy.tatistical analysis. Analysis was performed using thePSS version 10 (SPSS, Inc., Chicago, Illinios). All con-inuous variables are expressed as mean � SD and categor-cal data are presented as proportions. For comparison of theaseline characteristics between IPAH and Sch-PAH pa-ients, an unpaired t test or chi-square test was used, asppropriate. A p value �0.05 was considered statisticallyignificant.
For the survival analysis, the first hemodynamic evalua-ion was considered to be the date of diagnosis, and the
utoff date was June 2008. All-cause mortality was used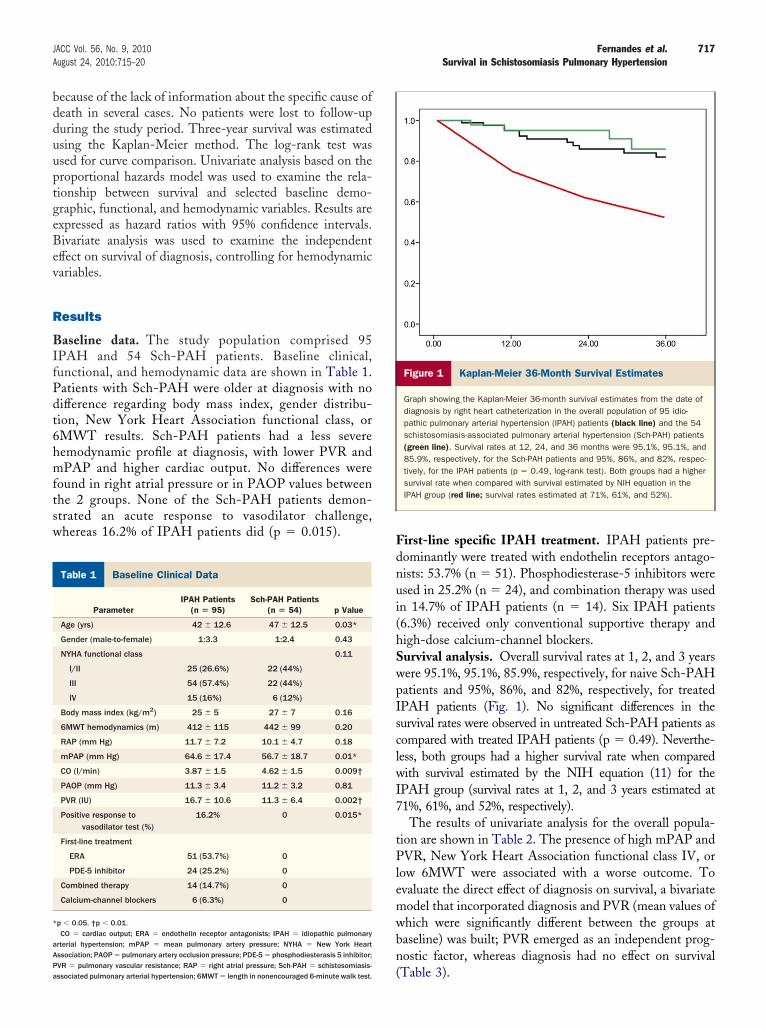
bdduuptgeBev
R
BIfPdt6hmftsw
Fdnui(hSwpIsclwI7
tPlemwbn
B
*
aAPa
717JACC Vol. 56, No. 9, 2010 Fernandes et al.August 24, 2010:715–20 Survival in Schistosomiasis Pulmonary Hypertension
ecause of the lack of information about the specific cause ofeath in several cases. No patients were lost to follow-upuring the study period. Three-year survival was estimatedsing the Kaplan-Meier method. The log-rank test wassed for curve comparison. Univariate analysis based on theroportional hazards model was used to examine the rela-ionship between survival and selected baseline demo-raphic, functional, and hemodynamic variables. Results arexpressed as hazard ratios with 95% confidence intervals.ivariate analysis was used to examine the independentffect on survival of diagnosis, controlling for hemodynamicariables.
esults
aseline data. The study population comprised 95PAH and 54 Sch-PAH patients. Baseline clinical,unctional, and hemodynamic data are shown in Table 1.atients with Sch-PAH were older at diagnosis with noifference regarding body mass index, gender distribu-ion, New York Heart Association functional class, orMWT results. Sch-PAH patients had a less severeemodynamic profile at diagnosis, with lower PVR andPAP and higher cardiac output. No differences were
ound in right atrial pressure or in PAOP values betweenhe 2 groups. None of the Sch-PAH patients demon-trated an acute response to vasodilator challenge,hereas 16.2% of IPAH patients did (p � 0.015).
aseline Clinical DataTable 1 Baseline Clinical Data
ParameterIPAH Patients
(n � 95)Sch-PAH Patients
(n � 54) p Value
Age (yrs) 42 � 12.6 47 � 12.5 0.03*
Gender (male-to-female) 1:3.3 1:2.4 0.43
NYHA functional class 0.11
I/II 25 (26.6%) 22 (44%)
III 54 (57.4%) 22 (44%)
IV 15 (16%) 6 (12%)
Body mass index (kg/m2) 25 � 5 27 � 7 0.16
6MWT hemodynamics (m) 412 � 115 442 � 99 0.20
RAP (mm Hg) 11.7 � 7.2 10.1 � 4.7 0.18
mPAP (mm Hg) 64.6 � 17.4 56.7 � 18.7 0.01*
CO (l/min) 3.87 � 1.5 4.62 � 1.5 0.009†
PAOP (mm Hg) 11.3 � 3.4 11.2 � 3.2 0.81
PVR (IU) 16.7 � 10.6 11.3 � 6.4 0.002†
Positive response tovasodilator test (%)
16.2% 0 0.015*
First-line treatment
ERA 51 (53.7%) 0
PDE-5 inhibitor 24 (25.2%) 0
Combined therapy 14 (14.7%) 0
Calcium-channel blockers 6 (6.3%) 0
p � 0.05. †p � 0.01.CO � cardiac output; ERA � endothelin receptor antagonists; IPAH � idiopathic pulmonary
rterial hypertension; mPAP � mean pulmonary artery pressure; NYHA � New York Heartssociation; PAOP � pulmonary artery occlusion pressure; PDE-5 � phosphodiesterasis 5 inhibitor;
(VR � pulmonary vascular resistance; RAP � right atrial pressure; Sch-PAH � schistosomiasis-ssociated pulmonary arterial hypertension; 6MWT � length in nonencouraged 6-minute walk test.
irst-line specific IPAH treatment. IPAH patients pre-ominantly were treated with endothelin receptors antago-ists: 53.7% (n � 51). Phosphodiesterase-5 inhibitors weresed in 25.2% (n � 24), and combination therapy was usedn 14.7% of IPAH patients (n � 14). Six IPAH patients6.3%) received only conventional supportive therapy andigh-dose calcium-channel blockers.urvival analysis. Overall survival rates at 1, 2, and 3 yearsere 95.1%, 95.1%, 85.9%, respectively, for naive Sch-PAHatients and 95%, 86%, and 82%, respectively, for treatedPAH patients (Fig. 1). No significant differences in theurvival rates were observed in untreated Sch-PAH patients asompared with treated IPAH patients (p � 0.49). Neverthe-ess, both groups had a higher survival rate when comparedith survival estimated by the NIH equation (11) for the
PAH group (survival rates at 1, 2, and 3 years estimated at1%, 61%, and 52%, respectively).
The results of univariate analysis for the overall popula-ion are shown in Table 2. The presence of high mPAP andVR, New York Heart Association functional class IV, or
ow 6MWT were associated with a worse outcome. Tovaluate the direct effect of diagnosis on survival, a bivariateodel that incorporated diagnosis and PVR (mean values ofhich were significantly different between the groups ataseline) was built; PVR emerged as an independent prog-ostic factor, whereas diagnosis had no effect on survival
Figure 1 Kaplan-Meier 36-Month Survival Estimates
Graph showing the Kaplan-Meier 36-month survival estimates from the date ofdiagnosis by right heart catheterization in the overall population of 95 idio-pathic pulmonary arterial hypertension (IPAH) patients (black line) and the 54schistosomiasis-associated pulmonary arterial hypertension (Sch-PAH) patients(green line). Survival rates at 12, 24, and 36 months were 95.1%, 95.1%, and85.9%, respectively, for the Sch-PAH patients and 95%, 86%, and 82%, respec-tively, for the IPAH patients (p � 0.49, log-rank test). Both groups had a highersurvival rate when compared with survival estimated by NIH equation in theIPAH group (red line; survival rates estimated at 71%, 61%, and 52%).
Table 3).

D
TSImfbtt
wtweaf4jcsrudpn1Pr(tP
oiteomcd
AvcintcsSaualtto
fncoopvP
nthciipnpcstsiase
ttr
Uo
*
Bo
718 Fernandes et al. JACC Vol. 56, No. 9, 2010Survival in Schistosomiasis Pulmonary Hypertension August 24, 2010:715–20
iscussion
he present study analyzed the outcomes of a cohort ofch-PAH patients compared with those of a cohort ofPAH patients treated with locally available specific treat-ents. Our results showed that Sch-PAH has a more
avorable hemodynamic profile at diagnosis and a moreenign clinical course, even in the absence of specific PAHreatment. To the best of our knowledge, this is the firstime that such an observation has been reported.
Sch-PAH may be one of the main causes of PAH in theorld. Although the World Health Organization estimates
hat there are approximately 200,000 patients worldwideith IPAH (19), the United Nations Children’s Fund
stimates that 8.5 million people have Schistosoma mansoni-ssociated hepatosplenic disease (6). Extrapolating the datarom a recent prevalence study (5), there may be as many as25,000 patients with Sch-PAH worldwide, the vast ma-
ority of whom are in developing countries. However, mostases remain undiagnosed. Why patients with Sch-PAHeem to have a more benign clinical course (3-year mortalityate of 14.1%) compared with other forms of PAH isnclear. Infection with schistosomiasis is considered en-emic in Brazil, and the ratio of Sch-PAH to IPAHatients attending our service (which is a national pulmo-ary hypertension reference center) is approximately 0.57 to. Thus, Sch-PAH accounts for a greater proportion of totalAH cases at our center when compared with recently
eported estimates in other national or regional registries20,21). This fact clearly underscores the need to developreatment policies for rare diseases based on unique regionalAH profiles (10).Diagnosis of schistosomiasis is based on the identification
f the parasites’ eggs in stool examination or rectal biopsy inndividuals at risk of infection based on geographical loca-ion. Nevertheless, the absence of viable eggs does notxclude the diagnosis. Abdominal ultrasonographic findingsf left lobe of liver enlargement or periportal fibrosis alsoay suggest the diagnosis of schistosomiasis in patients
oming from endemic areas. However, the disease can
nivariate Cox Proportional-Hazards Analysisf Selected Baseline VariablesTable 2 Univariate Cox Proportional-Hazards Analysisof Selected Baseline Variables
Hazard Ratio (95% CI) p Value
Age (yrs) 0.962 (0.922–1.004) 0.075
Diagnosis (Sch-PAH vs. IPAH) 0.676 (0.218–2.099) 0.498
NYHA functional class 0.117
III 3.363 (0.737–15.355)
IV 6.312 (1.153–34.554)
6MWT (m) 0.991 (0.986–0.997) 0.001*
mPAP (mm Hg) 1.048 (1.018–1.079) 0.002*
CO (l/min) 0.835 (0.546–1.275) 0.403
PVR (IU) 1.081 (1.035–1.129) 0.001*
p � 0.01.CI � confidence interval; PVR � pulmonary vascular resistance; other abbreviations as in Table 1.
evelop even in the absence of manifest liver involvement.*
s a result, distinguishing Sch-PAH from IPAH in indi-iduals from regions in which schistosomiasis is endemican be challenging if there is no evidence of hepatosplenicnvolvement. Furthermore, lung biopsy is neither sensitiveor specific enough to establish the diagnosis (22). Thus,he presence of hepatosplenic alterations is a marker ofhronic disease that raises the association between schisto-omiasis and the presence of pulmonary hypertension.erology testing (by means of the enzyme-linked immuno-dsorbent assay technique) also is useful to identify individ-als with prior exposure to different forms of schistosomi-sis. However, the usefulness of this approach may beimited to assessment of patients from nonendemic areas ofhe disease, because massive population exposure to schis-osomiasis lowers its value as a marker of disease in regionsf high prevalence.Our results revealed a nonsignificant trend for better
unctional and exercise capacity and less severe hemody-amic compromise at diagnosis for Sch-PAH patients asompared with IPAH patients. However, the low numberf events in the Sch-PAH group did not allow the analysisf functional class and 6MWT as prognostic markers in thisopulation. Thus, these surrogate markers remain to bealidated before they can be used as end points in Sch-AH, as is the case in IPAH (23).Since the first case series description of invasively diag-
osed pulmonary hypertension (PH) associated with schis-osomiasis nearly 50 years ago (24), considerable advancesave been made in the understanding of the hemodynamicharacteristics of this unique patient population, as reflectedn the recently updated PH clinical classification (25). It isnteresting to note that a preserved cardiac output atresentation is typical, even in the presence of high pulmo-ary pressure levels (24). Lack of data regarding PAOPrevented the differentiation between precapillary and post-apillary PH in both early (24,26) and more recent (27)tudies. Nonetheless, postcapillary PH is clearly an impor-ant cause of PH in schistosomiasis, as demonstrated by atudy by Vargas et al. (28). These observations highlight themportance of invasive hemodynamic measurements forccurate diagnosis (29) of Sch-PAH. Indeed, in the currenttudy, only patients with normal PAOP were included tonsure a homogeneous group of Sch-PAH patients.
Our study is the first to confirm the lack of acute responseo vasodilator testing among Sch-PAH patients. In con-rast, 16.2% of IPAH patients demonstrated an acuteesponse to inhaled nitric oxide, which is comparable with
ivariate Proportional-Hazards Analysisf Selected Baseline VariablesTable 3 Bivariate Proportional-Hazards Analysisof Selected Baseline Variables
Hazard Ratio (95% CI) p Value
Diagnosis (Sch-PAH vs. IPAH) 1.160 (0.287–4.683) 0.835
PVR 1.083 (1.033–1.134) 0.001*
p � 0.01.Abbreviations as in Tables 1 and 2.

psflrttrtsnptmvach
uehitsdmtAtmtPfuItTPs(dtgs
ldpawtq
Sf
primhgptpph(aeSnsrdaPlittibb
C
WtnarestS
ATt
RnSB
R
719JACC Vol. 56, No. 9, 2010 Fernandes et al.August 24, 2010:715–20 Survival in Schistosomiasis Pulmonary Hypertension
reviously published data (17). Previous investigators havepeculated that Sch-PAH simply may represent anotherorm of portopulmonary hypertension without coexistentiver failure (30). Le Pavec et al. (31) recently reportedesults from a case-control study of portopulmonary hyper-ension and, similarly, did not identify any acute responderso acute vasodilator challenge. In that study, the survivalates observed among patients with portopulmonary hyper-ension without cirrhosis were similar to those found in ourtudy, strengthening the hypothesis that Sch-PAH andoncirrhotic portopulmonary hypertension may share someathophysiologic mechanisms. Several processes may con-ribute to the development of Sch-PAH, including theechanical impact Schistosoma eggs within the pulmonary
essels (32), inflammation within the lung vasculature (33),nd an increase in pulmonary blood flow that develops as aonsequence of arteriovenous shunts characteristic of portalypertension (34).Survival analysis did not show any difference between
ntreated Sch-PAH and treated IPAH populations. Nev-rtheless, there was a significant difference in baselineemodynamics between the 2 groups that could have
nfluenced the survival analysis significantly. To account forhe possible effect of baseline hemodynamics on Sch-PAHurvival, a bivariate model was built that incorporatediagnosis and PVR, because the later represents a compro-ise between the vascular pressure levels and cardiac func-
ion and was found to be significant by univariate analysis.multivariate model could not be constructed because of
he limited number of events in the cohort as a whole, whichay have driven to an overfitted model. The results from
he bivariate model suggested that the diagnosis of Sch-AH had no significant effect on survival, even accounting
or hemodynamics at baseline. Indeed, the survival ofntreated Sch-PAH patients was no different from that ofPAH patients receiving specific PAH therapy, suggestinghe former population had a more benign clinical course.he suggestion of an improved survival among our Sch-AH cohort is supported further when predicted IPAHurvival (as estimated by the NIH equation) is calculated12). The favorable results revealed in our study, however,o not preclude the need for studies that specifically addresshe impact of specific PAH therapy in Sch-PAH patients,iven the substantial 3-year 14.1% mortality rate we ob-erved in this group.
Our results have to be interpreted in the light of someimitations imposed by the study design. Recently reportedata regarding survival in IPAH in a large, multicenter,rospective cohort revealed a significantly lower survival ratet 3 years than was the case in our cohort (35). Our studyas performed in a single tertiary center, with a retrospec-
ive analysis of prevalent and incident cases. As a conse-uence, survival rates might have been overestimated.Evidence to support the use of specific PAH treatment for
ch-PAH patients remains scarce in the literature. Cases of
avorable responses with the use of sildenafil have been re-orted (36). However, there is a lack of compelling data fromandomized controlled trials in support of this strategy. Theres also lack of data regarding the effect of antiparasitic treat-
ent on pulmonary arteriopathy. In schistosomiasis-associatedepatosplenic disease, the effect of antiparasitic treatment isreatly variable, ranging from complete resolution of peri-ortal fibrosis to no response (37). Although antiparasiticreatment is not believed to have a significant effect over theulmonary circulation, at least one case report has beenublished showing significant improvement in pulmonaryemodynamics after treatment for Schistosoma haematobium38). Nevertheless, all of our Sch-PAH patients receiveddequate treatment for Schistosoma mansoni before studynrollment.tudy limitations. Our study has some limitations thateed to be acknowledged. The monocentric nature of thetudy and the fact that our center is located in a nonendemicegion of schistosomiasis infection may account for someegree of selection bias. However, we believe that our statuss one of the largest reference centers in Brazil for bothAH and schistosomiasis-related hepatosplenic disease
essens the potential impact of this limitation. The compar-son of Sch-PAH with IPAH is useful to understand betterhe respective clinical courses, because both groups simul-aneously were followed concomitantly. However, a histor-cal group of naïve IPAH patients would help to understandetter any differences in disease progression that may existetween IPAH and Sch-PAH.
onclusions
e conclude that Sch-PAH, which may represent one ofhe most prevalent forms of PAH, has a better hemody-amic profile at diagnosis and a more benign clinical courses compared with IPAH, even in the absence of acuteesponse at the vasodilator challenge during hemodynamicvaluation. Nevertheless, the 3-year mortality found in ourtudy population underscores the need for additional studieso establish formally the impact of specific PAH therapies inch-PAH patients.
cknowledgmenthe authors thank Dr. Dermot O’Callaghan for his assis-
ance in the review of the manuscript.
eprints requests and correspondence: Dr. Rogerio Souza, Pulmo-ary Department, Heart Institute, University of São Paulo Medicalchool, Av. Dr. Eneas de Carvalho Aguiar, 44, São Paulo 05403-000,razil. E-mail: [email protected].
EFERENCES
1. Rubin LJ. Primary pulmonary hypertension. N Engl J Med 1997;336:111–7.
2. Farber HW, Loscalzo J. Pulmonary arterial hypertension. N EnglJ Med 2004;351:1655–65.
3. Souza R, Jardim C. Trends in pulmonary arterial hypertension. EurRespir Rev 2009;18:6.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
720 Fernandes et al. JACC Vol. 56, No. 9, 2010Survival in Schistosomiasis Pulmonary Hypertension August 24, 2010:715–20
4. Michelakis ED, Wilkins MR, Rabinovitch M. Emerging concepts andtranslational priorities in pulmonary arterial hypertension. Circulation2008;118:1486–95.
5. Lapa M, Dias B, Jardim C, et al. Cardiopulmonary manifestations ofhepatosplenic schistosomiasis. Circulation 2009;119:1518–23.
6. World Health Organization. Schistosomiasis. Geneva: World HealthOrganization, 2007.
7. Souza R, Fernandes CJ, Jardim CV. Other causes of PAH (schistosomi-asis, porto-pulmonary hypertension and hemolysis-associated pulmonaryhypertension). Semin Respir Crit Care Med 2009;30:448–57.
8. Ross AG, Bartley PB, Sleigh AC, et al. Schistosomiasis. N Engl J Med2002;346:1212–20.
9. Freedman DO, Kozarsky PE, Weld LH, Cetron MS. GeoSentinel:the global emerging infections sentinel network of the InternationalSociety of Travel Medicine. J Travel Med 1999;6:94–8.
0. Humbert M, Khaltaev N, Bousquet J, Souza R. Pulmonary hyperten-sion: from an orphan disease to a public health problem. Chest2007;132:365–7.
1. Lapa MS, Ferreira EV, Jardim C, Martins Bdo C, Arakaki JS, SouzaR. [Clinical characteristics of pulmonary hypertension patients in tworeference centers in the city of Sao Paulo]. Rev Assoc Med Bras2006;52:139–43.
2. D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients withprimary pulmonary hypertension. Results from a national prospectiveregistry. Ann Intern Med 1991;115:343–9.
3. Barst RJ, Rubin LJ, McGoon MD, Caldwell EJ, Long WA, Levy PS.Survival in primary pulmonary hypertension with long-term continu-ous intravenous prostacyclin. Ann Intern Med 1994;121:409–15.
4. Hatz C, Jenkins JM, Ali QM, Abdel-Wahab MF, Cerri GG, TannerM. A review of the literature on the use of ultrasonography inschistosomiasis with special reference to its use in field studies. 2.Schistosoma mansoni. Acta Trop 1992;51:15–28.
5. Guyatt GH, Sullivan MJ, Thompson PJ, et al. The 6-minute walk: anew measure of exercise capacity in patients with chronic heart failure.Can Med Assoc J 1985;132:919–23.
6. Costa EL, Jardim C, Bogossian HB, Amato MB, Carvalho CR, SouzaR. Acute vasodilator test in pulmonary arterial hypertension: evalua-tion of two response criteria. Vascul Pharmacol 2005;43:143–7.
7. Sitbon O, Humbert M, Jais X, et al. Long-term response to calciumchannel blockers in idiopathic pulmonary arterial hypertension. Cir-culation 2005;111:3105–11.
8. Galie N, Torbicki A, Barst R, et al. Guidelines on diagnosis andtreatment of pulmonary arterial hypertension. The Task Force onDiagnosis and Treatment of Pulmonary Arterial Hypertension of theEuropean Society of Cardiology. Eur Heart J 2004;25:2243–78.
9. Hatano S, Strasser T, editors. Primary pulmonary hypertension.Geneva: World Health Organization, 1975.
0. Jing ZC, Xu XQ, Han ZY, et al. Registry and survival study in chinesepatients with idiopathic and familial pulmonary arterial hypertension.Chest 2007;132:373–9.
1. Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hyper-tension in France: results from a national registry. Am J Respir CritCare Med 2006;173:1023–30.
2. Pozzan G, Souza R, Jardim C, et al. Histopathological features of
pulmonary vascular disease in chronic Schistosomia mansoni infection Kare not different from those in idiopathic pulmonary hypertension.Am J Respir Crit Care Med 2008;177:A443.
3. Snow JL, Kawut SM. Surrogate end points in pulmonary arterialhypertension: assessing the response to therapy. Clin Chest Med2007;28:75–89, viii.
4. de Cavalcanti IL, Tompson G, de Souza G, Barbosa FS. Pulmonaryhypertension in schistosomiasis. Br Heart J 1962;24:363–71.
5. Simonneau G, Robbins IM, Beghetti M, et al. Updated clinicalclassification of pulmonary hypertension. J Am Coll Cardiol 2009;54:S43–54.
6. Guimaraes AC. [Present state of knowledge of cardiopulmonaryinvolvement in schistosomiasis mansoni]. Arq Bras Cardiol 1982;38:301–9.
7. de Cleva R, Herman P, Pugliese V, et al. Prevalence of pulmonaryhypertension in patients with hepatosplenic Mansonic schistosomia-sis—prospective study. Hepatogastroenterology 2003;50:2028–30.
8. Vargas FS, Checchi H, Pereira Barreto AC, Bellotti G, Romeiro NetoM, Pileggi F. [Hemodynamic changes in schistosomiasis mansoni].Arq Bras Cardiol 1981;37:443–9.
9. Hoeper MM, Barbera JA, Channick RN, et al. Diagnosis, assessment,and treatment of non-pulmonary arterial hypertension pulmonaryhypertension. J Am Coll Cardiol 2009;54:S85–96.
0. Pereira GA Jr., Bestetti RB, Leite MP, et al. Portopulmonaryhypertension syndrome in schistosomiasis mansoni. Trans R Soc TropMed Hyg 2002;96:427–8.
1. Le Pavec J, Souza R, Herve P, et al. Portopulmonary hypertension:survival and prognostic factors. Am J Respir Crit Care Med 2008;178:637–43.
2. Shaw AP, Ghareeb A. The pathogenesis of pulmonary schistosomiasisin Egypt with special reference to Ayerza’s disease. J Pathol Bacteriol1938;46:401–24.
3. Chaves E. The pathology of the arterial pulmonary vasculature inmanson’s schistosomiasis. Dis Chest 1966;50:72–7.
4. Zhou YG, Yang Z, Li DJ. [The experimental study on pathologicalchanges of pulmonary tissues in portal hypertensive rabbits withschistosomal cirrhosis]. Zhonghua Wai Ke Za Zhi 2005;43:587–90.
5. Humbert M, Sitbon O, Chaouat A, et al. Survival in patients withidiopathic, familial and anorexigen-associated pulmonary arterial hy-pertension in the modern management era. Circulation 2010;122:156–63.
6. Loureiro R, Mendes A, Bandeira A, Cartaxo H, Sa D. Oral sildenafilimproves functional status and cardiopulmonary hemodynamic inpatients with severe pulmonary hypertension secondary to chronicpulmonary schistosomiais: a cardiac magnetic resonance study (abstr).Circulation 2004;110 Suppl III:572.
7. Richter J, Evolution of schistosomiasis-induced pathology after ther-apy and interruption of exposure to schistosomes: a review of ultra-sonographic studies. Acta Trop 2000;77:111–31.
8. Bouree P, Piveteau J, Gerbal JL, Halpen G. [Pulmonary arterialhypertension due to bilharziasis. Apropos of a case due to Schistosomahaematobium having been cured by praziquantel]. Bull Soc PatholExot 1990;83:66–71.
ey Words: schistosomiasis y pulmonary hypertension y survival.