pathogenesis of chagas disease cardiomyopathy
TRANSCRIPT
World J Clin Infect Dis 2012 June 25; 2(3): 39-53ISSN 2220-3176 (online)
© 2012 Baishideng. All rights reserved.
Online Submissions: http://www.wjgnet.com/[email protected]:10.5495/wjcid.v2.i3.39
World Journal ofClinical Infectious DiseasesW J C I D
Pathogenesis of Chagas disease cardiomyopathy
Priscila Camillo Teixeira, Amanda Farrage Frade, Luciana Gabriel Nogueira, Jorge Kalil, Christophe Chevillard, Edecio Cunha-Neto
Priscila Camillo Teixeira, Amanda Farrage Frade, Luciana Gabriel Nogueira, Jorge Kalil, Edecio Cunha-Neto, Labora-tory of Immunology, Heart Institute (Incor), School of Medicine, University of São Paulo, 05403-001 São Paulo, BrazilPriscila Camillo Teixeira, Amanda Farrage Frade, Luciana Gabriel Nogueira, Jorge Kalil, Edecio Cunha-Neto, Institute for Investigation in Immunology (III), INCT, 05403-001 São Paulo, BrazilJorge Kalil, Edecio Cunha-Neto, Division of Clinical Immunol-ogy and Allergy, School of Medicine, University of São Paulo, 05403-001 São Paulo, BrazilChristophe Chevillard, INSERM, UMR 906, 13385 Marseille, FranceChristophe Chevillard, Aix-Marseille University, UMR 906, 13385 Marseille, FranceAuthor contributions: All authors had an equal contribution. Chevillard C and Cunha-Neto E prepared the framework of the article; Teixeira PC, Frade AF, Nogueira LG prepared the multi-ple drafts; Kalil J, Chevillard C and Cunha-Neto E improved the quality of the draft.Supported by the Institut National de la Santé et de la Recherche Médicale; the Aix-Marseille University (Direction des Relations Internationales); USP-COFECUB program; the ARCUS II PACA Brésil program; CNPq (Brazilian National Research Council); and FAPESP (São Paulo State Research Funding Agency-Brazil); a São Paulo State Research Funding Agency - FAPESP fellowship to Teixeira PC, Nogueira LG and Frade AF; Brazilian Council for Sci-entific and Technological Development - CNPq productivity awards to Cunha-Neto ECorrespondence to: Dr. Christophe Chevillard, PhD, INSERM, U906, Genetics and Immunology of Infectious Diseases, Labora-tory of Parasitology-Mycology, School of Medicine, Marseilles, 27, Bd Jean, Moulin 13385 Marseilles Cedex 5, France. [email protected]: +33-491-324453 Fax: +33-491-796063Received: November 18, 2011 Revised: May 7, 2012Accepted: June 4, 2012Published online: June 25, 2012
AbstractChagas disease, or American trypanosomiasis, is a parasitic infection caused by the flagellate protozoan
Trypanosoma cruzi. Chagas disease is mainly affect-ing rural populations in Mexico and Central and South America. The World Health Organization estimates that 300 000 new cases of Chagas disease occur every year and approximately 20 000 deaths are attribut-able to Chagas. However, this organisation classified Chagas disease as a neglected tropical disease. The economic burden of this disease is significant. In many Latin American countries, the direct and indirect costs, including the cost of health care in dollars and loss of productivity, attributable to Chagas disease ranges from $40 million to in excess of $800 million per nation per annum. So, it remains a contemporary public health concern. In chronic phase, mortality is primarily due to the rhythm disturbances and congestive heart failure that result from the chronic inflammatory cardiomyopa-thy (CCC) due to the persistence presence of parasites in the heart tissue. Mechanisms underlying differential progression to CCC are still incompletely understood. In the last decades immunological proteomic genetic approaches lead to significant results which help to disperse the veil covering the knowledge of the patho-genic process. Here, we reported these significant pro-gresses.
© 2012 Baishideng. All rights reserved.
Key words: Chagas; Pathogenesis; Cardiomyopathy; Susceptibility; Parasitic
Peer reviewers: Dr. Roberto Zenteno-Cuevas, Public Health Institute, Luis Catelazo Ayala S/N, Col. Industrial Animas, Jalapa 91190, Mexico; Dr. Joseph U Igietseme, Natl Ctr for Emerging and Infectious Diseases, Centers for Disease Control and Prevention, 1600 Clifton Road, Mailstop G-36, Atlanta, GA 30333, United States
Teixeira PC, Frade AF, Nogueira LG, Kalil J, Chevillard C, Cunha-Neto E. Pathogenesis of Chagas disease cardiomyopa-thy. World J Clin Infect Dis 2012; 2(3): 39-53 Available from: URL: http://www.wjgnet.com/2220-3176/full/v2/i3/39.htm DOI:
REVIEW
39 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com

Teixeira PC et al . Chagas disease
so-called indeterminate form, or develop denervation and dilation of esophagus and colon[11]. The underlying causes for the differential progression of chronic T. cruzi infection are still unknown, but building evidence sug-gests a role for genetic host factors.
CCC is an inflammatory cardiomyopathy that can be accompanied by heart electric conduction defects, ar-rhythmias and thromboembolism[7]. Approximately 1/3 of individuals with cardiac disorders eventually develop life-threatening heart disease, such as severe dilated car-diomyopathy or arrhythmias. These patients may develop congestive heart failure, responsible for the high number of hospitalizations and significant mortality (52% in five years)[12]. Several studies suggest that heart failure due to CCC may have a worse prognosis with 50% shorter survival when compared to other cardiomyopathies of different etiologies such as ischemic cardiomyopathy and idiopathic dilated cardiomyopathy[12-14]. Significantly, a key difference between CCC and such cardiomyopathies is inflammation/myocarditis, present in greater intensity among CCC patients. In the absence of specific treat-ment, therapy for CCC is only supportive. In patients with refractory heart failure, the only available treatment is heart transplantation, while severe arrhythmia patients need pacemakers or implantable defibrillators.
The major histopathological feature attending dilated cardiomyopathy in CCC is the presence of a diffuse myocarditis, with intense cardiomyocyte damage and hypertrophy, and significant fibrosis, in the presence of very scarce T. cruzi forms[15,16]. Replacement by reparative fibrosis may be the main cause of pathologic ventricular remodeling[10,17,18]. Our group showed a significant cor-relation between myocarditis and ventricular dilation (manuscript in preparation) as well as fibrosis[19] in the Syrian hamster model of CCC. Since it is known that T. cruzi establishes a lifelong, low-grade infection, the pos-sibility that chronic myocardial inflammation and tissue damage in CCC are a consequence of recognition of parasite antigen on target tissue must be entertained[20,21]. A direct role for heart parasitism has been proposed after the identification of T. cruzi antigen and DNA in CCC hearts by immunohistochemical and PCR techniques[15,22]. In addition, T. cruzi-specific CD8+ T cells have been iso-lated from endomyocardial biopsies of a CCC patient[23], providing evidence for the recruitment and expansion of T. cruzi-specific T cells in the myocardium. In experimen-tal T. cruzi infection, a higher inoculum or parasite load has been associated to more aggressive chronic heart inflammation or disease[19,24]. However, the scarcity of T. cruzi in inflammatory lesions of CCC led early investiga-tors to suggest that tissue damage had an autoimmune nature. However, regardless of the triggering antigen, the bulk of the evidence indicates the inflammatory infiltrate is a significant effector of heart tissue damage. In this paper, we will review the immunologic, transcriptomic/proteomic, and genetics studies of the pathogenesis of Chagas disease.
40 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
http://dx.doi.org/10.5495/wjcid.v2.i3.39
INTRODUCTIONChagas disease (American trypanosomiasis) caused by the protozoan Trypanosoma cruzi (T. cruzi) and transmitted by the reduviid bug (called “barbeiro” or “chupança” in Brazil) was discovered in 1909 by the Brazilian physician Carlos Chagas. Unfortunately, Chagas disease remains a neglected disease, with no vaccines available so far and only very few anti-parasitic drugs proven efficient for treating the acute phase of the disease.
CLINICAL AND EPIDEMIOLOGICAL ASPECTS OF CHAGAS DISEASEMillions of people that were infected decades ago are still in need of appropriate treatment, since available anti-parasitic drugs are toxic and have not shown yet a reliable effect on progression to symptomatic disease[1]. These millions of patients require the attention of the scien-tific community. Despite many vector control programs, Chagas disease is still a significant cause of morbidity and mortality in many countries of South and Central Amer-ica, where it is estimated that 10 million people may be infected[2]. An important feature of this disease is the car-diac involvement in the chronic phase, the main cause of morbidity and mortality in about 10%-40% of individu-als chronically infected with T. cruzi[3,4]. As a result, much research has been directed to its pathogenesis. Since the bulk of evidence indicates the inflammatory infiltrate is a significant effector of heart tissue damage. This review aims to summarize the major recent advances in the understanding of the immunopathogenesis of Chagas disease cardiomyopathy. Recent reviews on alternative pathogenic mechanisms can be seen in[5,6].
Clinical and experimental studies have shown the natural history of Chagas disease can be divided into acute and chronic phases. The acute phase can last from 4 to 12 wk and is characterized by easily detectable blood and tissue parasitism and acute myocarditis of variable intensity of severity[7]. About 10% of those infected in-dividuals may show clinical manifestations that may vary from a flu-like disease to lethal fulminant myocarditis or infectious shock[8,9]. A strong innate and adaptive immune response partially controls T. cruzi-blood and tissue para-sitism, and chronic, low-grade parasitism is established. After the acute phase, a long period, which can range from five years to three decades and last throughout the life of the individual, where the clinical manifestations remain missing – the so-called “indeterminate” clinical form (IND)[10]. After this asymptomatic period up to 30% of infected individuals develop chronic Chagas dis-ease cardiomyopathy (CCC) while the remaining infected individuals may continue asymptomatic for life, in the

41 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
where T and B cells recognize parasite antigens that share structurally similar epitopes in host antigens, generat-ing crossreactive autoimmune responses (Table 1); and polyclonal activation leading to autoantibody production. Autoimmune and T. cruzi-specific responses secondary to parasite persistence are not incompatible or mutually exclusive in Chagas disease, and a combination of these types of immune responses could be involved in the es-tablishment of heart tissue lesions.
IMMUNOPATHOGENESIS OF CCCChagas cardiomyopathy is essentially a myocarditis. The inflammatory process, although more intense in the acute phase, is clinically silent but incessant in patients with the indeterminate and chronic phases of the disease[15].
Immunological dynamics of the acute phase of T. cruzi infectionData from animal models show that inflammatory cyto-kines play a central role in acute T. cruzi infection (Table 2). Shortly after the acute infection starts, T. cruzi com-ponents - including its DNA and membrane glycoconju-gates - trigger innate immunity via Toll-like receptors 2, 4 and 9 in macrophages and dendritic cells[37]. Upon activa-tion, such cells secrete proinflammatory cytokines and chemokines, express costimulatory receptors, and increase endocytosis and intracellular killing of parasites through release of reactive oxygen and nitrogen species. Proin-flammatory cytokines, such as interleukin (IL)-1, IL-6, IL-12, IL-18, IL-27 and tumor necrosis factor (TNF)-α are promptly released, and further activate other inflam-matory cells[6,38]. Macrophages and dendritic cells that have endocytosed the parasite subsequently elicit a strong T cell and antibody response against T. cruzi. Interferon-γ (IFN-γ)-producing T. cruzi-specific T cells are thus gener-ated[6], that migrate together with other blood leukocytes to sites of T. cruzi-induced inflammation in response to chemokines such as CCL2, CCL3, CCL4, CCL5, and CXCL10, participating in the immune response against the parasite[39]. These inflammatory T cells and antibody responses lead to control - but not complete elimination - of tissue and blood parasitism. On the other hand, the blockade of CCR5 with Met-RANTES significantly de-creased the intensity of cardiac inflammatory infiltrate, suggesting that lymphocyte migration to the myocardium in acute infection is dependent of CCR5 ligands[40]. A re-cent study has shown that Beagle dogs at the acute phase of T. cruzi infection presented higher mRNA expression of CCL1 and CXCL9 than uninfected animals[41]. Some studies have evaluated the role of chemokines in experi-mental T. cruzi infection in rat. Holtzman rats immunized with a CCL4-encoding DNA vaccine had enhanced heart inflammation but unchanged heart parasite load when infected with T. cruzi, suggesting that CCL4 could be re-cruiting regulatory cells to the infected tissue and, hence, regulating the intensity of the inflammatory response to the infection[42]. On the other hand, the vaccination
AUTOIMMUNITYCCC is one of the few examples of post-infectious auto-immunity in humans, where infectious episodes with an established pathogen clearly triggers antigenic mimicry with host self-antigens, in association to target organ immune damage. CCC heart lesions are consistent with inflammation: a T cell/macrophage-rich myocarditis, fibrosis and heart fiber damage, in the presence of very scarce T. cruzi forms. Several studies have shown that T. cruzi DNA is found in myocardial tissue of essentially all CCC and IND cases[25,26]; the finding of T. cruzi DNA in hearts of IND patients argues against the hypothesis that local parasite presence is the trigger to myocardial inflam-mation in CCC. The discrepancy between the parasitism and inflammation suggested that tissue-damaging T cells were of autoimmune nature, possibly elicited by cross-reactive immune responses with T. cruzi parasite[6].
Direct experimental evidence of autoimmunity in CCC and experimental models has been documented over the last 25 years and is reviewed by Marin-Neto et al[5]. Cross-reactive autoantibodies and T cells against several distinct host-T. cruzi antigenic pairs were described along the last decades (Table 1). In murine models of T. cruzi infection, our group[27] and others[28,29] have shown that cardiac myosin, the major heart protein, is an important target cardiac self-antigen. Cardiac myosin heavy chain is recognized by CD4+ T cells from T. cruzi-infected mice[27], and tolerance induction with cardiac myosin-rich heart ex-tracts was shown to ameliorate ameliorate T. cruzi-induced chronic cardiac inflammation and fibrosis[30]. We have shown that CCC patients display serum IgG anti-cardiac myosin heavy chain autoantibodies that cross-reactively recognize T. cruzi membrane protein B13[31]. Furthermore, CD4+ T cell clones infiltrating hearts from CCC patients also cross-reactively recognize cardiac myosin and B13 protein[30,32]. We have also found restricted heterogeneity of T cell receptor (TCR) variable regions in CCC heart tissue, which is in line with an antigen-driven, possibly autoimmune response[33]. Moreover, in vitro priming with B13 or its synthetic peptides leads to the recovery of car-diac myosin cross-reactive T cell clones[34,35]. We identified one such T cell clone that cross reactively recognized one epitope in B13 protein and twelve distinct low homology peptides in cardiac myosin, indicative of a very degener-ate TCR recognition pattern[34]. Molecular modeling of B13 and cardiac myosin epitopes identified shared TCR-exposed residues which could potentially explain the low-homology crossreactivity[36].
The existence of degenerate intramolecular recogni-tion, with multiple low-homology, cross-reactive epitopes in a single autoantigenic protein may have implications in increasing the magnitude of the autoimmune response in CCC and other autoimmune diseases. Several mecha-nisms have been suggested to play a role in the triggering of autoimmunity after T. cruzi infection. Antigen expo-sure secondary to tissue damage, followed by sensitiza-tion in an appropriate inflammatory environment (i.e., bystander activation); antigenic or molecular mimicry,
Teixeira PC et al . Chagas disease
42 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
with CCL3 and CCL5 increased heart parasitism and decreased local IFN-γ production, but did not influence the intensity of inflammation suggesting the chemokines are relevant for the control of parasitism, and may play a differential role in inflammatory cell recruitment during acute T. cruzi infection in rats[43].
On the other hand, some cytokines are associated with susceptibility to T. cruzi infection, as IL-10 and TGF-β[44-46]. Recent data show that IL-17 controls the resistance to T. cruzi infection in mice, with increased levels resulting in enhancement of myocarditis, prema-ture mortality and decreased parasite load in the heart. Neutralization of IL-17 neutralization resulted in in-creased production of IL-12, IFN-γ and TNF-α and enhanced specific type 1 chemokine and chemokine receptors expression[47]. In experimental T. cruzi infec-tion, CD4+CD25+GITR+Foxp3+ T cells migrate to the heart of T. cruzi infected mice, and the treatment with anti-GITR enhanced the myocarditis, with increased mi-gration of CD4+, CD8+, and CCR5+ leukocytes, TNF-α production, tissue parasitism leading to increased mortal-ity, suggesting that GITR+Foxp3+ regulatory T cells may control the heart inflammation, parasite replication, and
host resistance in the acute phase of infection[48].The Syrian hamster model of T. cruzi infection repro-
duces the range of different outcomes of human Chagas disease[19,49]. During acute T. cruzi infection, hamsters displaying high cardiac parasitism also showed increased expression of TNF-α, IFN-γ, IL-10, and CCL3 mRNA, as well as acute phase signs such as weight loss, vomiting and diarrhea, while animals showing low cardiac parasit-ism displayed a modest increase in cytokine/chemokine mRNA and no acute phase signs, suggesting that cardiac parasitism was apparently related to the increased expres-sion of cytokines and chemokines[6].
Few immunological studies have been performed with acutely infected patients. Acutely infected children have shown increased expression inflammatory cytokines, such as circulating IL-6 and TNF-α[50] and have also displayed increased production of IFN-γ by mononuclear cells[51].
Cytokines and chemokines in the chronic phase of T. cruzi infectionInflammatory cytokines are produced along the chronic phase of Chagas disease (Table 2). Increased levels of plasma TNF-α and peripheral blood mononuclear cell-
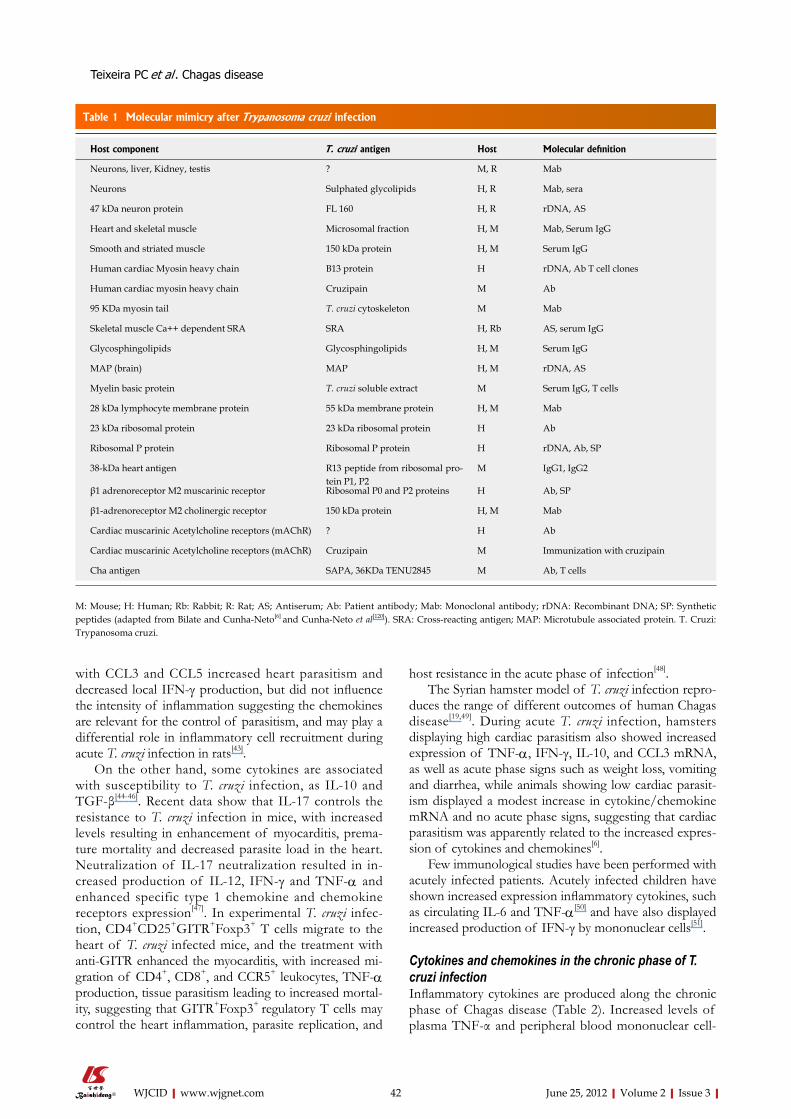
Table 1 Molecular mimicry after Trypanosoma cruzi infection
Host component T. cruzi antigen Host Molecular definition
Neurons, liver, Kidney, testis ? M, R Mab
Neurons Sulphated glycolipids H, R Mab, sera
47 kDa neuron protein FL 160 H, R rDNA, AS
Heart and skeletal muscle Microsomal fraction H, M Mab, Serum IgG
Smooth and striated muscle 150 kDa protein H, M Serum IgG
Human cardiac Myosin heavy chain B13 protein H rDNA, Ab T cell clones
Human cardiac myosin heavy chain Cruzipain M Ab
95 KDa myosin tail T. cruzi cytoskeleton M Mab
Skeletal muscle Ca++ dependent SRA SRA H, Rb AS, serum IgG
Glycosphingolipids Glycosphingolipids H, M Serum IgG
MAP (brain) MAP H, M rDNA, AS
Myelin basic protein T. cruzi soluble extract M Serum IgG, T cells
28 kDa lymphocyte membrane protein 55 kDa membrane protein H, M Mab
23 kDa ribosomal protein 23 kDa ribosomal protein H Ab
Ribosomal P protein Ribosomal P protein H rDNA, Ab, SP
38-kDa heart antigen R13 peptide from ribosomal pro-tein P1, P2
M IgG1, IgG2
β1 adrenoreceptor M2 muscarinic receptor Ribosomal P0 and P2 proteins H Ab, SP
β1-adrenoreceptor M2 cholinergic receptor 150 kDa protein H, M Mab
Cardiac muscarinic Acetylcholine receptors (mAChR) ? H Ab
Cardiac muscarinic Acetylcholine receptors (mAChR) Cruzipain M Immunization with cruzipain
Cha antigen SAPA, 36KDa TENU2845 M Ab, T cells
M: Mouse; H: Human; Rb: Rabbit; R: Rat; AS; Antiserum; Ab: Patient antibody; Mab: Monoclonal antibody; rDNA: Recombinant DNA; SP: Synthetic peptides (adapted from Bilate and Cunha-Neto[6] and Cunha-Neto et al[120]). SRA: Cross-reacting antigen; MAP: Microtubule associated protein. T. Cruzi: Trypanosoma cruzi.
Teixeira PC et al . Chagas disease
43 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
produced IFN-γ are detected even in infected individuals in the indeterminate form of the Chagas’ disease[52-54], probably in response to parasite persistence. The subsets of patients that develop Chagas cardiomyopathy display an array of immunological alterations consistent with an exacerbated Th1 immune response. CCC patients display increased circulating levels of TNF-α and CCL2 compared to individuals in the indeterminate form of the Chagas disease, or those with electrocardiogram (ECG) abnormalities alone but no ventricular dysfunc-tion[52,55]. Additionally, CCC patients show an increased number of the IFN-γ -producing CCR5+ CXCR3+ CD4+ and CD8+ T cells in the peripheral blood, with reduced numbers of IL-10-producing and CD4+CD25+FOXP3+ regulatory T cells[54,56,57] as compared to patients in the indeterminate form of Chagas disease. Recent stud-ies also have shown that FOXP3+ cells are significantly more abundant in myocardial sections from IND than in CCC patients or non-infected individuals, suggesting that regulatory T cells are less abundant in CCC than IND hearts[58]. Given the reduced levels of peripheral blood CD4+CD25+FOXP3+ regulatory T cells among CCC patients, this could indicate such cells may play a role in the control of the myocardial inflammatory process among chronic Chagas disease patients.
The exacerbated Th1 response observed in the pe-ripheral blood of CCC patients is reflected on the nature of the inflammatory infiltrate found in their heart tis-sue[59]. Mononuclear cells infiltrating CCC heart tissue ex-press IFN-γ, TNF-α, IL-6, with lower levels of IL-2, IL-4
and IL-10[54,60,61]. The survival cytokines IL-7 and IL-15 also show increased expression in CCC heart tissue, and may be the underlying reason for the predominance of CD8+ T cells, which express increased levels of IL-15Rα and γc chain receptor[62]. Real-time quantitative PCR anal-ysis in human CCC myocardium showed that the gene expression levels of IFN-γ-inducible chemokines CCL2, CXCL10 and CXCL9, as well as the chemokine receptors CCR2 and CXCR3, were selectively upregulated[59]. Cor-roborating these data, we were able to detect mononucle-ar cells that express CXCR3, CCR5, CXCL9 and CCL5 in the myocardium of CCC patients using confocal im-munofluorescence assays. We also observed abundantly increased mRNA expression of the CCR5 and CXCR3 as well as several of their chemokine ligands in the myo-cardium CCC patients. The intensity of the myocardial infiltrate correlated with chemokine mRNA expression. Significantly, a recent study of chemokine expression in the heart of chronically T. cruzi-infected Beagle dogs with the cardiac form also observed increased mRNA expres-sion of CXCR3, CCL4 and CCL5 as compared to those in the indeterminate form[41]. The increased expression of chemokines and their receptors in CCC heart tissue are in line with the increased amounts of CD4+ and CD8+ T cells expressing CXCR3/CCR5 and co-expressing IFN-γ/TNF-α observed in peripheral blood from CCC patients, as compared to T. cruzi-seropositive IND indi-viduals[63]. Taken together, these findings suggests that the recruitment of inflammatory cells to the CCC myo-cardium, a key pathogenetic event, may indeed be driven
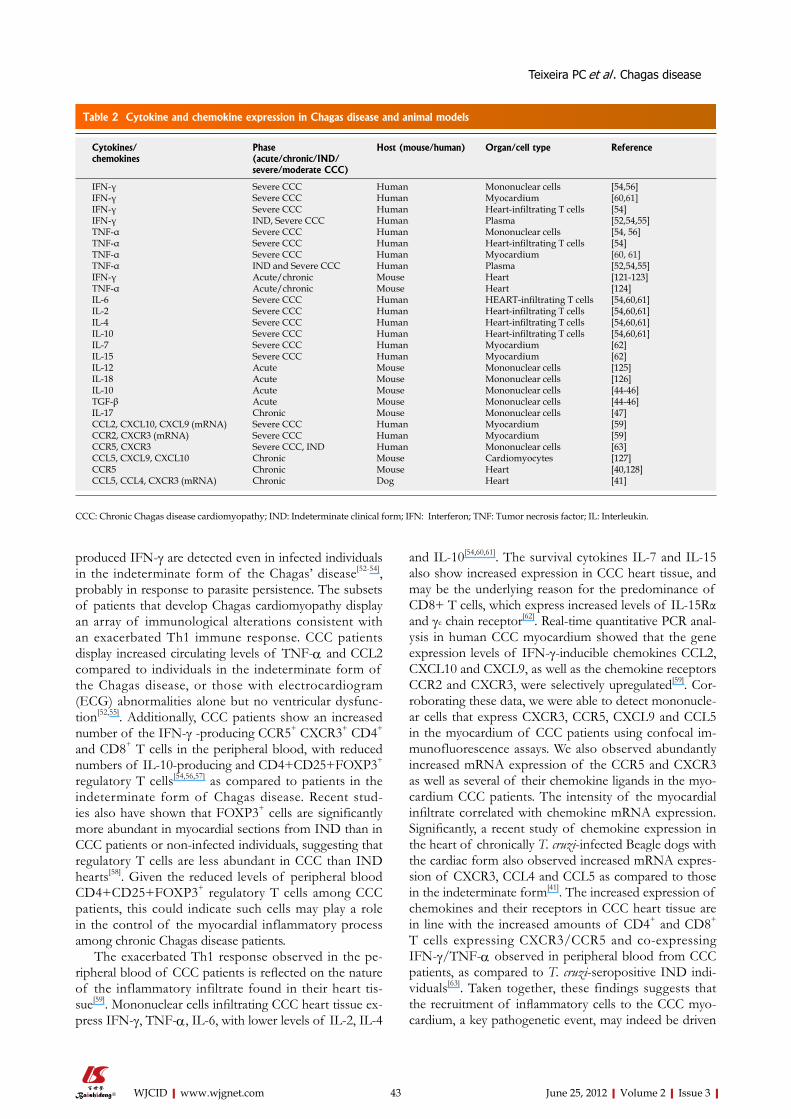
Table 2 Cytokine and chemokine expression in Chagas disease and animal models
Cytokines/chemokines
Phase (acute/chronic/IND/severe/moderate CCC)
Host (mouse/human) Organ/cell type Reference
IFN-γ Severe CCC Human Mononuclear cells [54,56]IFN-γ Severe CCC Human Myocardium [60,61]IFN-γ Severe CCC Human Heart-infiltrating T cells [54]IFN-γ IND, Severe CCC Human Plasma [52,54,55]TNF-α Severe CCC Human Mononuclear cells [54, 56]TNF-α Severe CCC Human Heart-infiltrating T cells [54]TNF-α Severe CCC Human Myocardium [60, 61]TNF-α IND and Severe CCC Human Plasma [52,54,55]IFN-γ Acute/chronic Mouse Heart [121-123]TNF-α Acute/chronic Mouse Heart [124]IL-6 Severe CCC Human HEART-infiltrating T cells [54,60,61]IL-2 Severe CCC Human Heart-infiltrating T cells [54,60,61]IL-4 Severe CCC Human Heart-infiltrating T cells [54,60,61]IL-10 Severe CCC Human Heart-infiltrating T cells [54,60,61]IL-7 Severe CCC Human Myocardium [62]IL-15 Severe CCC Human Myocardium [62]IL-12 Acute Mouse Mononuclear cells [125]IL-18 Acute Mouse Mononuclear cells [126]IL-10 Acute Mouse Mononuclear cells [44-46]TGF-β Acute Mouse Mononuclear cells [44-46]IL-17 Chronic Mouse Mononuclear cells [47]CCL2, CXCL10, CXCL9 (mRNA) Severe CCC Human Myocardium [59]CCR2, CXCR3 (mRNA) Severe CCC Human Myocardium [59]CCR5, CXCR3 Severe CCC, IND Human Mononuclear cells [63]CCL5, CXCL9, CXCL10 Chronic Mouse Cardiomyocytes [127]CCR5 Chronic Mouse Heart [40,128]CCL5, CCL4, CXCR3 (mRNA) Chronic Dog Heart [41]
CCC: Chronic Chagas disease cardiomyopathy; IND: Indeterminate clinical form; IFN: Interferon; TNF: Tumor necrosis factor; IL: Interleukin.
Teixeira PC et al . Chagas disease

44 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
by CC and CXC chemokines.Given the major role of Th1/inflammatory infiltrate
in CCC heart, we tried to dampen the inflammatory re-sponse in an attempt to reduce the heart damage. Using the hamster model of dilated cardiomyopathy of human CCC, it was observed that TNF-α blockade at the chronic phase (7 mo post infection) with the soluble receptor Etanercept paradoxically worsened cardiac function[64] in the absence of increased parasitism, direct drug toxicity or increased myocarditis. These results suggest a benefi-cial role for residual TNF-α signaling in Chagas disease cardiomyopathy, also suggesting that TNF-α antagonism in the chronic phase of the T. cruzi infection worsens ex-perimental cardiomyopathy – playing a cautionary note on cytokine-blocking intervention in human Chagas disease.
Non-immunological pathogenic effects of cytokines and chemokines in CCCOur group and others found significant evidence of non-inflammatory cytokine and chemokine effects on cardio-myocytes and other myocardial cell types, in addition to the inflammatory effects of cytokines and chemokines. Immunohistochemical analysis of cardiac biopsies in CCC patients showed phosphorylated Smad2, a compo-nent of the TGF-β signaling pathway, as well as fibronec-tin, a marker of fibrosis[65], suggesting that TGF-β could play a role in the induction of fibrosis in cardiac tissue of patients with CCC.
Significant IFN-γ signaling was observed in the myo-cardium of CCC patients, including genes that are not ordinarily expressed by inflammatory cells. In vitro experi-ments have shown that IFN-γ- alone or in combination with CCL2 - may induce deep changes in the cardiomyo-cyte gene expression program, including induction of atrial natriuretic factor and of the hypertrophic gene ex-pression program[59]. IL-18 and the CCR7 ligand CCL21, upregulated in CCC myocardium, induce cardiomyocyte hypertrophy and molecules involved in the fibrotic pro-cess[66,67]. We can thus hypothesize that, apart from the direct inflammatory damage, non-immunological effects of several mediators locally produced in the myocardium, like IFN-γ, TNF-α, IL-18, CCL2 and CCL21, may play a significant pathogenic role in CCC, by modulating gene and protein expression of cardiomyocytes and fibrocytes in pathways essential to the development of CCC, like hypertrophy and fibrosis. T cell migration to the myocar-dium, and non-immunological effects of chemokines and other mediators are thus prime candidates for interven-tion in Chagas disease. Understanding the importance of these pathways in the pathogenesis may be instrumen-tal for the development of more adequate therapy for chronic Chagas disease cardiomyopathy.
LARGE-SCALE GENE AND PROTEIN EXPRESSION PROFILING IN CCCIn recent years, new-generation high-throughput technol-ogies, including next-generation sequencing technology
and mass spectrometry methods, have been widely ap-plied in solving biological problems, especially in human diseases field. These data driven and large-scale research model enable the multi-level study of human diseases from the perspectives of genomics (the quantitative study of genes, regulatory and non-coding sequences), tran-scriptomics (RNA and gene expression) and proteomics (protein expression) levels. This type of investigation typically yield data that identify pathways involved in the pathogenesis of particular diseases. In addition, results of this type may provide novel targets for chemotherapy.
Several studies have applied global gene expression analysis with DNA microarrays in tissue derived from in-fected animals or in myocardial tissue from CCC patients to gain insight into the molecular events associated with Chagas disease. Cunha-Neto et al[59] analyzed the gene expression profiling of CCC myocardial tissues of CCC, idiopathic dilated cardiomyopathy (DCM) and heart do-nor by a 10 368 element cDNA microarray. The cardiac hypertrophy signature was shown to be up-regulated in both CCC and DCM heart tissue. Moreover, lipid metab-olism and mitochondrial oxidative phosphorylation genes were selectively up-regulated in myocardial tissue of the tested CCC patients. Immune response- related genes and IFN-γ-induced genes were prominently up-regulated only in CCC patients[59].
Several studies evaluating large-scale gene expression using animal models infected with T. cruzi have also been conducted. In a study, C57Bl/6 mice chronically infected with the Colombian strain of T. cruzi (8 mo post-infec-tion) showed a number of genes up-regulated in the myo-cardium that probably play a role in modulating inflam-mation and fibrosis. Pathways of genes significantly up-regulated in infected hearts prominently include immune response and related terms (e.g. inflammatory response, intracellular signaling cascade, and chemokine and cyto-kine receptor activity). In addition, up-regulated pathways include phosphate transport, cell proliferation, and actin binding (e.g. Arp2/3 protein complex and actin filament organization, cytoskeleton, and membrane ruffling). Path-ways containing an overrepresentation of down-regulated genes included mitochondrion, enzymatic activity of sev-eral types, and tyrosine kinase signaling[68]. Garg et al[69], in a time course experiment (up to 100 d post-infection), showed an up-regulation of genes associated with inflam-mation and IFN-γ-induced immune response; expression of extracellular matrix proteins and repressed structural and contractile genes, such as troponins, suggestive of ac-tive reparative and remodeling reactions following injury to the myocardium; and a depression of genes encoding mitochondrial oxidative phosphorylation complexes I and IV in T. cruzi-infected murine hearts. Mukherjee et al[70], using a single time point (100 d post-infection), reported that the heart from infected C57BL/6 mice showed symptoms of chronic inflammation, vasculitis, fibrosis and an up-regulation of atrial natriuretic peptide precur-sor, a strong indicator of cardiac pathogenesis[71]. In this study, it was found that the extracellular matrix genes, es-
Teixeira PC et al . Chagas disease

45 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
pecially those associated with fibrosis, were up-regulated in the chronic disease model, similar to that observed at day 37 post-infection[69]. These changes in structural components could possibly be initiated in response to myocardial injuries by invading and replicating parasites, and it is suggestive of active reparative and remodeling reactions. Moreover, Mukherjee et al[72] examined tran-scriptome changes in CD-1 mice infected with the Brazil strain of T. cruzi through the various stages of the disease (30, 60, 90, 120, 150 and 180 d post-infection). Several key genes belonging to important biological processes and pathways were found to be deregulated, including inflammatory mediators, growth factors, cell cycle, apop-totic and cytoskeletal genes.
Although these studies provided important insights into the molecular events associated with the pathogen-esis of CCC at the organ level, the response of cardio-myocytes themselves to infection at different time points could provide further details. Goldenberg et al[73] em-ployed microarrays (7624 annotated unigenes) to examine infected cardiac myocyte cultures 48 h post-infection. Major categories of affected genes included those in-volved in immune response (e.g. CXCL12 was down-regulated, while CXCL16, CCL7, CXCL1 AND CXCL16 were up-regulated), extracellular matrix and cell adhesion. These findings on infected cardiac myocytes in culture re-veal that alterations in cardiac gene expression described in Chagas disease are the consequence of both direct infection of the myocytes themselves as well as resulting from the presence of other cell types in the myocardium and systemic effects of the infection.
Since proteins are the ultimate biological determi-nants of disease phenotype, studies have used proteomic analysis to get a better understanding of pathophysiologi-cal mechanisms of diseases, including cardiomyopathies, and to find new biomarkers for diagnosis and progno-sis[74-77]. Several studies mapping the proteins expressed by the parasite T. cruzi were performed[78-86]; however, few studies have examined the proteins in cardiac tis-sue infected by the parasite. In one study, the protein expression profile in the human CCC myocardium were analyzed by two-dimensional electrophoresis and mass spectrometry[87]. Authors identified 246 proteins in the CCC myocardium samples, corresponding to 112 distinct proteins. Along with structural/contractile and metabo-lism/energy metabolism proteins, proteins involved in apoptosis (e.g. caspase 8, caspase 2), immune system (T cell receptor beta chain, granzyme A, HLA class I) and stress processes (including several oxidative stress pro-teins) were identified. The identification of active caspase isoforms and oxidative stress proteins may indicate the occurrence of active apoptosis and significant oxidative stress in CCC myocardium. Differential protein expres-sion analysis between CCC and DCM cardiac samples identified significantly reduced expression of proteins involved in the generation of cytoplasmic ATP, such as creatine kinase M (Teixeira et al[88] unpublished observa-tions), suggesting the myocardium of CCC patients may
be under energy deprivation. T. cruzi–infected outbred hamsters reproduce the range of different outcomes of Chagas disease noted in humans[19]. While in the acute phase of infection, 50% of animals displayed weight loss and signs of acute-phase infection (APS) (e.g., lethargy, vomiting, and diarrhea). Proteomic analysis of these ani-mals showed that T. cruzi infection and the presence of APS were associated to distinct myocardial expression of contractile, stress response, and metabolism proteins. The study has shown the up-regulation of selective forms of the structural/contractile proteins (ACTC), muscle-specific intermediate filament (DES), proteins involved in cardiac myofibril assembly (MLC2), and proteins involved in actin cytoskeleton regulation (MYL3) in animals with APS but not in animals without APS, this may be associ-ated with the greater cardiac parasitism observed among infected animals with APS. Moreover, the increased expression of stress response proteins, such as CRYAB, HSPA5, and HSPA9, in infected animals, compared with uninfected controls, might be associated with a stress re-sponse triggered by T. cruzi infection[89].
The discovery of biomarkers associated with a particular disease or disease stage could also give valu-able insights into the basic biology of the host–parasite interface. Technologies such as surface-enhanced laser desorption/ionization time-of-flight (SELDI-TOF) mass spectrometry can be applied to discover biomark-ers associated with parasitic diseases. Such biomarkers can represent host proteins, fragments of host proteins or parasite proteins that appear in body fluids or tissues following infection. Individual biomarkers or biomarker patterns/signatures not only have diagnostic utility (e.g. in active disease, prognosis, tests of cure) but can also provide unique insights into the mechanisms underlying host responses and pathogenesis[90]. SELDI-TOF analysis identified several host protein fragments found almost exclusively in sera from subjects with Chagas Disease[90]. These include both N- and C-terminal fragments of hu-man apolipoprotein A-I, a C-terminal (desArg) trunca-tion of C3a anaphylatoxin, and an N-terminal fragment of fibronectin. In a western blot format, the anti-sera directed against the truncated form of human fibronec-tin were found to be both sensitive and specific for the diagnosis of latent Chagas disease, indicating the antigens were biomarkers[90]. Such protein biomarkers not only can reveal new targets for therapies and vaccines but could also suggest new diagnostic tests.
In conclusion, the results of these types of studies may yield data identifying pathways involved in the patho-genesis of particular diseases. In addition, results of this type may provide novel targets for chemotherapy or diag-nosis for Chagas disease. Considering the role of proteins and genes that were found differentially expressed in the cited studies, we can hypothesize that cytokine-induced modulation of cardiomyocyte gene/protein expression may be a novel disease mechanism in CCC, in addition to direct inflammatory damage, that in turn, could contrib-ute to the severe outcome commonly observed among
Teixeira PC et al . Chagas disease

46 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
CCC patients.
SEVERAL GENE POLYMORPHISMS WERE ASSOCIATED TO AN HIGHEST RISK FOR CCCThe first report suggesting that host genetic factors may be involved in disease susceptibility to CCC progression was done by Zicker et al[91]. Indeed, a case-control study was conducted in a population survey in Goiânia, Brazil, including 247 cases of Chagas’ heart disease, 345 asymp-tomatic seropositive subjects and 529 seronegative sub-jects. Increasing age and male sex were consistently and significantly related to an increased risk of electrocardio-graphic abnormalities. No association was found between length of residence in an endemic area, physical activity, and electrocardiographic abnormalities. A clear signifi-cant concordance of clinical types with sharing the same household has been described. Comparing seronegative to seropositive subjects, it was shown that males were at greater risk of any electrocardiographic alteration and left anterior hemiblock compared to females. An increasing risk of ventricular premature beats with age was clearer for seropositive than for seronegative subjects. Subjects with history of heart disease were at an increased risk of electrocardiographic abnormalities. These findings sug-gest a possible geographical clustering or a familial aggre-gation of cases of Chagas’ heart disease. Several genetic studies have been performed, so far, in order to identify genetic factors that control human susceptibility to severe diseases. All these studies were based on case control studies. These approaches have leaded to significant re-sults that were partially confirmed in independent studies. We will summarize all these studies.
Regarding the Major Histocompatibility Complex (MHC) genes, several studies show contradictory results that vary with the population studied. Fernandez-Mestre et al[92] demonstrate the first evidence of association between Chagas disease and HLA genetic susceptibil-ity when analysed HLA class II alleles in a sample of 67 serologically positive individuals with and without cardiomyopathy and compare with 156 healthy controls of similar ethnic origin. The comparison of DRB1 and DQB1 allele frequencies among the patients and control subjects showed a decreased frequency of DRB1*14 and DQB1*0303 in the patients, suggesting independent pro-tective effects to the chronic infection in that population. Allele frequencies comparison between patients with and without cardiomyopathy showed a higher frequency of DRB1*01, DRB1*08 and DQB1*0501 and a decreased frequency of DRB1*1501 in the patients with arrhythmia and congestive heart failure[92]. These results suggest that HLA Class II genes may be associated with the develop-ment of a chronic infection and with heart damage in Chagas’ disease.
Later on, Layrisse et al[93] have shown, on the same population, a strong association of HLA class I gene to
cardiac damage. HLAC*03 allele showed increased fre-quencies among patients with cardiac damage compared to asymptomatic subjects.
At the same time, Deghaide et al[94] have characterised a Brazilian population including 176 patients presenting with pure cardiomyopathy with heart failure (n = 60), car-diomyopathy without heart failure (n = 18), pure diges-tive tract manifestations (n = 25), cardiac plus digestive disease (n = 40), and asymptomatic patients with positive serology for chronic T. cruzi infection (n = 33) and non infected individuals (n = 448). Serologic HLA class II analysis showed that HLA-DQ1 conferred susceptibility to, while HLA-DQ7 antigen conferred protection against the development of the disease in the total group of patients. Oligonucleotide typing has shown that HLA-DQB1*06 alleles were underrepresented in the total group and in the subgroups presenting with pure diges-tive or cardiac disease, conferring closely similar relative risks and preventive fractions. Asymptomatic patients showed a significant increase of HLA-DQB1*0302 spe-cificity[94].
These data were confirmed at study in a Venezuelan population by Colorado et al[95] that studied 35 asympto-matic cases and 72 symptomatic cases. The asymptomatic population (33.68%) consisted of apparently healthy individuals having normal, borderline, or abnormal ECG, without cardiomegaly. The symptomatic population was divided in 2 distinct groups, group B (33.68%) included patients with either arrhythmia-related symptoms, five or more extrasystoles per minute, or embolic episodes as first symptom; and group C (32.63%) by patients with overt congestive heart failure[95]. Most had severe cardi-omegaly and arrhythmias. Statistical analysis confirmed the significant increment of the DRB1*01 DQB1*0501 haplotype (P = 0.03). The DPB1*0401 allele frequency is also significantly increased in patients with heart disease (groups B + C) (P = 0.009, OR = 6.0) while DPB1*0101 frequency is higher among the asymptomatic group (P = 0.04, OR = 0.32) compared with individuals of group C. The DPB1*0401 allele in homozygous form or in combi-nation with allele DPB1*2301 or 3901, was found present more often in patients of groups B and C. Thus, the combination of two of these three alleles, sharing spe-cific sequence motifs in positions 8, 9, 76, and 84-87 con-fers a relative risk of 6.55 to develop cardiomyopathy in seropositive patients (P = 0.041). Furthermore, 32% of the cardiomyopathics have either DRB1*01 DQB1*0501 and/or DPB1*0401/*0401, 0401/*2301, or* 0401/*3901 compared with 9% of the seropositive asymptomatics (P = 0.006, OR = 5.0).
Rodriguez-Perez et al[96] have studied 54 Mexican patients (27 asymptomatic subjects and 27 patients with chronic cardiomyopathy) and 169 healthy individuals. The whole group of patients showed increased frequencies of TNFA-308A allele when compared to healthy controls (P = 0.008, OR = 3.03). Similar results were obtained when CCC patients were compared to asymptomatic individu-als (P = 0.0002) or healthy controls (P = 4 × 10−7, OR =
Teixeira PC et al . Chagas disease

47 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
7.02). Similar results were obtained when they took into account the AG genotype[96].
Similarly, Campelo et al[97] have conducted on evalu-ation of genetic susceptibility to chronic disease in rela-tionship of five microsatellite polymorphisms in a series of Brazilian Chagasic patients stratified according to the clinical form of disease presentation, i.e., cardiac, diges-tive, digestive plus cardiac, or indeterminate form. A total of 162 chronic patients including 54 patients with cardio-myopathy with heart failure, 17 patients with cardiomy-opathy without heart failure, 25 patients with pure diges-tive manifestations, 33 patients with digestive plus cardiac manifestations in 33 patients and 33 other patients char-acterized by indeterminate form. An additional group of 221 negative serology subjects was also included. After patient stratification according to the clinical form, the frequencies of several TNF microsatellite alleles were significantly increased in each clinical group. The relative risks associated with the susceptibility alleles ranged from 1.674 (P = 0.04) (TNFa2 in digestive plus cardiac form) to 10.21 (P = 0.010) (TNFd7 in digestive plus cardiac form), indicating that the individuals who possess these susceptibility alleles have almost 2 to 10 times higher risk of developing a given form of chronic disease if infect-ed. On the other hand, some other alleles are associated to protection[97]. Exact tests done haplotype frequencies revealed significant differences when patients were con-sidered as a whole or stratified according to the clinical variant were compared to controls. All these results sug-gest that this chromosomal region is associated with sus-ceptibility to or resistance against CCC forms.
Several other investigations were done by other groups to determine the role of the TNF gene in the human susceptibility to the Chagas disease chronic forms. Drigo et al[98] have analyzed the allele distribution of the TNFA microsatellite and TNFA-308 promoter polymorphisms in 166 CCC patients compared to 80 asymptomatic individuals employed as control group. The comparisons of TNFA microsatellite and TNFA-308 promoter allele frequencies between the two groups do not lead to detection of statistical difference. This lack of association was also found in a Peruvian population in-cluding 85 serologically positive chagasic individuals and in 87 healthy controls[99].
So, these three studies lead to conflicting results. Ac-cording to these three previous studies we performed a meta-analysis on the TNFA-308 polymorphism that leads to significant association (Table 3 and 4). The fact that significant association was also detected into meta analy-sis is indicating that this chromosomal region is involved into the genetic control of human susceptibility to CCC forms. These discrepancies between the three studies may be due either to modest clinical group size or to differing genetic backgrounds. According to this hypothesis into Mexican population the TNFA-308 polymorphism may be in strong disequilibrium with the functional variant. This local linkage disequilibrium map may be different from one population to the other one. As soon as, this
linkage disequilibrium decreases the association with the TNFA-308 polymorphism may be lost.
Even though Drigo et al[100] didn’t confirm the previ-ous association, they studied putative correlation between this polymorphism and differential survival of severe CCC patients. On an independent population done in Brazil, including 42 patients with severe ventricular dys-function (left ventricular ejection fraction ≤ 40%), Drigo et al[100] have shown that patients (16) positive for TNFA-308A allele display a significantly shorter survival time compared to those (26) carrying other allele. The median survival times were 2.9 (positive patients) and 8 mo (neg-ative patients) (P = 0.020, hazard ratio = 2.28).
A Colombian study was based on 130 patients with cardiomyopathy and 130 asymptomatic subjects on IL1B genes[101]. A significant difference was detected for the IL1B+5810GA polymorphism. The IL1B+5810GG genotype frequency was higher in the CCC patient group than in the asymptomatic group (P = 0.03, OR = 2.64)[101]. Differences in the distribution of the allele frequencies confirmed the association. A haplotype covering the IL1A, IL1B and IL1RN genes was also associated to pro-tection. Putative association for the IL1 antagonist gene (IL1RN) was described on a Mexican population[102]. This study included 86 individuals seropositive for T. cruzi (58 CCC patients and 28 asymptomatics), 50 seronegative in-dividuals with idiopathic dilated cardiomyopathy and 109 healthy individuals. An increased IL-1RN.4CC genotype frequency was detected when T. cruzi-infected infected patients were compared to idiopathic dilated cardiomyop-athy patients (P = 0.028, OR = 11.46). A similar increase was also detected between CCC patients and controls (P = 0.011, OR = 3.6)[102].
In Brazil, a study on the IL10 gene was performed. One hundred fifty-five patients in the chronic phase of the disease were enrolled in this study as well as 43 indi-viduals without Chagas disease[103]. The IL10-1082G/A polymorphism, which correlates with lower expression of IL-10, was associated with the development of Cha-gas disease cardiomyopathy. Comparison of genotype distribution, between the indeterminate group and CCC patients, showed an association (P < 0.01, OR = 1.6)[103]. The frequency of the IL10-1082A allele (associated with lower expression of IL-10) was higher in the severe pa-tient group than in the indeterminate group (P < 0.01, OR = 0.84)[103]. An independent study suggests that an epistasis between MHC and IL-10 is associated to sus-ceptibility/resistance to Chagas’ disease[104].
A study performed on Colombian population on IL12B gene has detected an association with the poly-morphism IL12B+1188A/C located in the 3’UTR region of this gene[105]. Two hundred seronegative individuals and 260 serologically positive patients (130 with Chagas cardiomyopathy and 130 asymptomatic) were enrolled. The IL12B+1188CC genotype was significantly increased among cardiomyopathic patients as compared to asymp-tomatic individuals (P = 0.005, OR = 3.39). In addition, the authors observed that the IL12B+1188C allele was
Teixeira PC et al . Chagas disease

48 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
present at significantly higher frequency in CCC patients (P = 0.008, OR = 1.69) than in asymptomatic ones[105]. However, this polymorphism failed to discriminate the seropositive patients from the control individuals[105].
Ramasawmy et al[106] performed an analysis of the following TLR1, TLR2, TLR4, TLR5, TLR9, and MAL/TIRAP genes, on a Brazilian cohort. One hundred and sixty-nine patients with cardiomyopathy and 76 asympto-matic individuals were investigated. Comparison of the asymptomatic and CCC groups with respect to genotype distribution for each SNP showed a statistically signifi-cant difference only for the MAL/TIRAPS180L vari-ant[106]. Indeed, the frequency of homozygosity for the MAL/TIRAP180S allele was significantly higher among patients with CCC than among asymptomatic patients (P = 0.0004, OR = 3.1), whereas while the percentage of subjects homozygous for the MAL/TIRAP180L allele was similar in both groups. The percentage of subjects heterozygous for MAL/TIRAPS180L among patients with CCC was significantly different from the percent-age found on asymptomatic patients (P = 0.0004, OR = 3.1)[106].
The same authors have also four other candidate genes. Ramasawmy et al[107] assessed CCL2-2518A/G variants in 245 Brazilian individuals, all of whom were in-fected with T. cruzi. One hundred sixty-nine patients had CCC, and 76 were asymptomatic. Genotype distributions were different between the CCC group and the asymp-tomatic group (p=0.009)[107]. When the frequency of genotypes possessing at least 1 CCL2-2518A allele was compared with the genotype CCL2-2518A GG between CCC and asymptomatic groups, the observed difference reached statistical significance (P = 0.004, OR = 3.4)[107]. Thus, The A allele seems to confer susceptibility to CCC (P = 0.001, OR = 1.9).
Ramasawmy et al[108] have also focused their efforts on UAP56 genes which encodes BAT1 protein. For the polymorphism UAP56-22G/C, a significant difference in frequency between the CCC patients (154) and the asymptomatic patients (76) was revealed at the genotype level (P = 0.004, OR = 4.7). The UAP56-22C allele seems to confer susceptibility to CCC.
Lymphotoxin-α protein (encodes by LTA gene) is a proinflammatory cytokine which also induces adhesion molecules and cytokines from vascular endothelial cells and vascular smooth-muscle cells, which may contribute to the inflammation process. The putative involvement of this gene has been also investigated by Ramasawmy et al[109]. The LTA+80C/C genotype was significantly more
common in patients with CCC (169) than asymptomatic patients (76) (P = 0.006, OR = 3.1)[109]. A significant difference in the frequencies of alleles LTA+80A and LTA+80C between patients with CCC and asympto-matic patients (P = 0.007, OR = 1.7) was also observed were compared. Similar results were obtained with the polymorphism LTA+252A/G. The LTA+252G allele was associated with susceptibility to CCC (P = 0.006, OR = 1.7)[109]. Authors performed also an haplotype analysis based on these two polymorphisms. The LTA+80C-LTA+252G haplotype was associated with susceptibility to CCC (P = 0.018), whereas, LTA+80A-LTA+252A haplotype was more common in the asymptomatic pa-tients (P = 0.009), suggesting that it provides protection against CCC[109].
Finally this group has looked at the IKBL gene which encodes an inhibitor of NF-κB. Ramasawmy et al[110] provide evidence that two variants (IKBL-62A/T and IKBL-262A/G) in the promoter region of the IKBL gene are associated to susceptibility to develop CCC. In-deed, Genotype distributions for both IKBL-62A/T and IKBL-262A/G differed between the CCC patients and asymptomatic subjects (P = 0.025 and P = 0.03, respec-tively)[110]. Subjects homozygous for the IKBL-62A allele, had three-fold risk of developing CCC compared with those carrying the IKBL-62TT genotype (P = 0.0095, OR = 2.9). Similar trend was observed for the IKBL-262A homozygotes (P = 0.005, OR = 2.7). An haplotype analy-sis led to the identification of a susceptibility haplotype (IKBL-262A IKBL-62A) more frequent in CCC patients (P = 0.0014, OR = 2.1)[110].
As mentioned before, Cunha-Neto et al[59] characterized gene expression profiles of human Chagas’ cardiomyopa-thy and dilated cardiomyopathy to identify selective disease pathways. Among these altered genes we may notice the CCR5 gene[59]. Putative implication of the CCR5 gene in the development of chronic disease was investigated on 85 seropositive and 87 seronegative Peruvian individu-als[111]. No differences in the distribution of CCR5-59029 promoter genotype or phenotype frequencies between chagasic patients and controls. The authors observed that the CCR5-59029A/G genotype was significantly increased in asymptomatic compare to cardiomyopathic patients (P = 0.02, OR = 0.33)[111]. In addition, the presence of the CCR5-59029G allele was also increased in asymptomat-ics when compared with cardiomyopathics (P = 0.02, OR = 0.35)[111]. The authors suggest that the CCR5-59029 promoter polymorphism may be involved in a differential susceptibility to chagasic cardiomyopathy. An independent
Table 3 Case control studies done on the TNFA-308 polymorphism
Study name CasesNo. of chr carryingthe TNFA-308T2 allele
CasesTotal No. of chromosome
ControlsNo. of chr carryingthe TNFA-308T2 allele
ControlsTotal No. ofchromosome
Rodriguez-Perez et al[96] 13 108 14 324Drigo et al[98] 37 332 16 160Beraun et al[99] 5 66 4 104
Teixeira PC et al . Chagas disease

49 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
study, performed in Venezuela, indicates that this polymor-phism is also associated to Chagas disease. However, the associated genotype was not the same one[112].
Torres et al[113] performed two independent studies on 240 chagasic patients and 199 controls from Colom-bia; and 74 chagasic patients and 85 controls from Peru. For the polymorphism, MIF-173G/C, a statistically sig-nificant difference was detected between patients and controls in the Colombian cohort (P = 0.006, OR = 1.6). Similar association was found in the Peruvian cohort (P = 0.003, OR = 2.4). A meta-analysis of the Colombian and Peruvian cohorts has demonstrated that the MIF-173C allele confers a risk effect in Chagas patients Moreover, a dose effect for the susceptibility allele was observed (P = 0.004)[113].
All these positive association studies support the idea that host genetic factors may be involved in disease susceptibility to CCC progression. It identified main genes and pathways involved into the control of this sus-ceptibility. However these studies were conducted on a limited number of SNPs. So, the real functional variants are probably not identified. Moreover, some studies lead to unreplicated results that will need to be confirmed. Lacks of association were also reported for TLR2[114], TLR4[114], PTPN22[115], angiotensin-converting enzyme[116], NRAMP1[117], NOS2[118], IL4[119] and IL4R (weak associa-tion[119]) genes. These lacks of association may be due to the limited number of tested SNPs and to the cohort size which remained relatively limited. It is now essential to set up a whole genome genetic study using new technolo-gies on large study populations characterized by an acute phenotype. The identification of susceptibility genes and functional variants will be useful to understand the pathogenic process, for diagnosis and theranostic.
Even if twenty thousand deaths attributable to Chagas disease occur annually, it is still considered as a neglected disease. However, it remains a contemporary public health concern, even more so because of the threat of its re-emergence in some endemic areas where it was thought to have been controlled and emergence in non-endemic ar-eas. Unfortunately, the mechanisms underlying differential progression to CCC are still incompletely understood.
Chagas disease is not a single disease, but rather a conundrum of several clinical syndromes triggered by T. cruzi infection in a group of susceptible individuals. Ex-pression of clinical syndromes can be non-overlapping. It is therefore not surprising that several different systems of molecular mimicry, and genetic susceptibility factors
have been identified. T cell migration to the myocardium and ensuing inflammation, non-immunological effects of cytokines and chemokines in the myocardium, and genetic components are clearly key events. It is likely that the progression to overt inflammatory dilated car-diomyopathy may result from the combined effect and inadequate counter regulation of expression of relevant genes such as those mentioned above. It is possible to speculate that the combined effect of several gene poly-morphisms, together non-inflammatory events such as differential myocardial resilience to damage, could gener-ate the observed distinct disease forms, progression rates, and gender differences. It is likely that the persistence of a parasite which induces strong innate immunity and proinflammatory cytokines may continuously boost the production of potentially pathogenic Th1 T cells cross-reactively recognizing T. cruzi and heart-specific epitopes. Such Th1 T cells may migrate to heart tissue in response to locally expressed CXCR3 ligand chemokines. Once they reach myocardial tissue, cross-reactive T cells could be activated by cardiac antigen even in the absence of T. cruzi antigens. This would elicit local production of Th1 cytokines. Local production of Th1 cytokines could exert their pathophysiological role by causing direct inflam-matory damage, as well as modulating cardiac cell gene expression. Functional agonistic autoantibodies directed against adrenergic or cholinergic receptors may play a role in heart conduction disorders and arrhythmias. Ge-netic polymorphisms of immune response genes may affect recognition, migration and effector characteristics of autoreactive T cells and autoantibodies. Finally, it must be stressed that autoimmune and T. cruzi-specific innate or adaptative responses are not incompatible or mutually exclusive, and it is likely that a combination of both is involved in the pathogenesis of CCC.
CONCLUSIONLarge-scale gene and protein profiling in CCC are prom-ising new avenues of research that may identify additional important disease pathways. Identification of the mecha-nisms involved into the host-pathogen interactions at the establishment and chronic phases of the disease will lead to a better understanding of the immunological and path-ological processes and facilitate the development of new drugs. It will also allow an earlier detection of susceptible subjects who will require stronger medical survey in order to avoid the development of severe cardiomyopathy. It
Table 4 Meta-analysis on the TNFA-308 polymorphism
Study name Statistics for each study
P value Odds ratio Lower limit Upper limit
Rodriguez-Perez et al[96] 0.006 3.03 1.376 6.671Drigo et al[98] 0.701 1.129 0.608 2.097Beraun et al[99] 0.299 2.049 0.530 7.927Meta analysis(fixed effect)
0.025 1.687 1.067 2.668
Teixeira PC et al . Chagas disease
50 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
will be also benefit for the understanding of the common mechanisms to the other dilated cardiomyopathies.
REFERENCES1 Teixeira AR, Cunha Neto E, Rizzo LV, Silva R. Trypanocidal
nitroarene treatment of experimental Trypanosoma cruzi in-fection does not prevent progression of chronic-phase heart lesions in rabbits. J Infect Dis 1990; 162: 1420
2 Schofield CJ, Jannin J, Salvatella R. The future of Chagas disease control. Trends Parasitol 2006; 22: 583-588
3 DIAS E, LARANJA FS, MIRANDA A, NOBREGA G. Cha-gas’ disease; a clinical, epidemiologic, and pathologic study. Circulation 1956; 14: 1035-1060
4 Dias JC. [Epidemiological surveillance of Chagas disease]. Cad Saude Publica 2000; 16 Suppl 2: 43-59
5 Marin-Neto JA, Cunha-Neto E, Maciel BC, Simões MV. Pathogenesis of chronic Chagas heart disease. Circulation 2007; 115: 1109-1123
6 Bilate AM, Cunha-Neto E. Chagas disease cardiomyopathy: current concepts of an old disease. Rev Inst Med Trop Sao Paulo 2008; 50: 67-74
7 Rassi A, Rassi A, Little WC. Chagas’ heart disease. Clin Car-diol 2000; 23: 883-889
8 Parada H, Carrasco HA, Añez N, Fuenmayor C, Inglessis I. Cardiac involvement is a constant finding in acute Chagas’ disease: a clinical, parasitological and histopathological study. Int J Cardiol 1997; 60: 49-54
9 Andrade ZA. Mechanisms of myocardial damage in Try-panosoma cruzi infection. Ciba Found Symp 1983; 99: 214-233
10 Macêdo V, Prata A, da Silva GR, Castilho E. [Prevalence of electrocardiographic changes in Chagas’ disease patients (preliminary information about the National Electrocardio-graphic survey]. Arq Bras Cardiol 1982; 38: 261-264
11 Andrade ZA. Pathogenesis of Chagas’ disease. Res Immunol 1991; 142: 126-129
12 Mady C, Cardoso RH, Barretto AC, da Luz PL, Bellotti G, Pi-leggi F. Survival and predictors of survival in patients with congestive heart failure due to Chagas’ cardiomyopathy. Circulation 1994; 90: 3098-3102
13 Bocchi EA. [Update on indications and results of the surgical treatment of heart failure]. Arq Bras Cardiol 1994; 63: 523-530
14 Bestetti RB, Muccillo G. Clinical course of Chagas’ heart disease: a comparison with dilated cardiomyopathy. Int J Cardiol 1997; 60: 187-193
15 Higuchi Mde L, Gutierrez PS, Aiello VD, Palomino S, Bocchi E, Kalil J, Bellotti G, Pileggi F. Immunohistochemical char-acterization of infiltrating cells in human chronic chagasic myocarditis: comparison with myocardial rejection process. Virchows Arch A Pathol Anat Histopathol 1993; 423: 157-160
16 Higuchi ML, De Morais CF, Pereira Barreto AC, Lopes EA, Stolf N, Bellotti G, Pileggi F. The role of active myocarditis in the development of heart failure in chronic Chagas’ disease: a study based on endomyocardial biopsies. Clin Cardiol 1987; 10: 665-670
17 Rossi MA. The pattern of myocardial fibrosis in chronic Chagas’ heart disease. Int J Cardiol 1991; 30: 335-340
18 Higuchi ML, Fukasawa S, De Brito T, Parzianello LC, Bellot-ti G, Ramires JA. Different microcirculatory and interstitial matrix patterns in idiopathic dilated cardiomyopathy and Chagas’ disease: a three dimensional confocal microscopy study. Heart 1999; 82: 279-285
19 Bilate AM, Salemi VM, Ramires FJ, de Brito T, Silva AM, Umezawa ES, Mady C, Kalil J, Cunha-Neto E. The Syrian hamster as a model for the dilated cardiomyopathy of Cha-gas’ disease: a quantitative echocardiographical and histo-pathological analysis. Microbes Infect 2003; 5: 1116-1124
20 Higuchi MD, Ries MM, Aiello VD, Benvenuti LA, Gutierrez PS, Bellotti G, Pileggi F. Association of an increase in CD8+
T cells with the presence of Trypanosoma cruzi antigens in chronic, human, chagasic myocarditis. Am J Trop Med Hyg 1997; 56: 485-489
21 Kalil J, Cunha-Neto E. Autoimmunity in chagas disease cardiomyopathy: Fulfilling the criteria at last? Parasitol Today 1996; 12: 396-399
22 Jones EM, Colley DG, Tostes S, Lopes ER, Vnencak-Jones CL, McCurley TL. Amplification of a Trypanosoma cruzi DNA sequence from inflammatory lesions in human cha-gasic cardiomyopathy. Am J Trop Med Hyg 1993; 48: 348-357
23 Fonseca SG, Moins-Teisserenc H, Clave E, Ianni B, Nunes VL, Mady C, Iwai LK, Sette A, Sidney J, Marin ML, Goldberg AC, Guilherme L, Charron D, Toubert A, Kalil J, Cunha-Neto E. Identification of multiple HLA-A*0201-restricted cruzipain and FL-160 CD8+ epitopes recognized by T cells from chronically Trypanosoma cruzi-infected patients. Mi-crobes Infect 2005; 7: 688-697
24 Marinho CR, D’Império Lima MR, Grisotto MG, Alvarez JM. Influence of acute-phase parasite load on pathology, parasit-ism, and activation of the immune system at the late chronic phase of Chagas’ disease. Infect Immun 1999; 67: 308-318
25 Carrasco HA, Guerrero L, Parada H, Molina C, Vegas E, Chuecos R. Ventricular arrhythmias and left ventricular myocardial function in chronic chagasic patients. Int J Cardiol 1990; 28: 35-41
26 Olivares-Villagómez D, McCurley TL, Vnencak-Jones CL, Correa-Oliveira R, Colley DG, Carter CE. Polymerase chain reaction amplification of three different Trypanosoma cruzi DNA sequences from human chagasic cardiac tissue. Am J Trop Med Hyg 1998; 59: 563-570
27 Rizzo LV, Cunha-Neto E, Teixeira AR. Autoimmunity in Chagas’ disease: specific inhibition of reactivity of CD4+ T cells against myosin in mice chronically infected with Try-panosoma cruzi. Infect Immun 1989; 57: 2640-2644
28 Tibbetts RS, McCormick TS, Rowland EC, Miller SD, Eng-man DM. Cardiac antigen-specific autoantibody production is associated with cardiomyopathy in Trypanosoma cruzi-infected mice. J Immunol 1994; 152: 1493-1499
29 Leon JS, Godsel LM, Wang K, Engman DM. Cardiac myosin autoimmunity in acute Chagas’ heart disease. Infect Immun 2001; 69: 5643-5649
30 Pontes-de-Carvalho L, Santana CC, Soares MB, Oliveira GG, Cunha-Neto E, Ribeiro-dos-Santos R. Experimental chronic Chagas’ disease myocarditis is an autoimmune disease pre-ventable by induction of immunological tolerance to myo-cardial antigens. J Autoimmun 2002; 18: 131-138
31 Cunha-Neto E, Kalil J. Autoimmunity in Chagas’ heart dis-ease. Sao Paulo Med J 1995; 113: 757-766
32 Cunha-Neto E, Kalil J. Heart-infiltrating and peripheral T cells in the pathogenesis of human Chagas’ disease cardio-myopathy. Autoimmunity 2001; 34: 187-192
33 Cunha-Neto E, Moliterno R, Coelho V, Guilherme L, Bocchi E, Higuchi Mde L, Stolf N, Pileggi F, Steinman L, Kalil J. Re-stricted heterogeneity of T cell receptor variable alpha chain transcripts in hearts of Chagas’ disease cardiomyopathy pa-tients. Parasite Immunol 1994; 16: 171-179
34 Cunha-Neto E, Coelho V, Guilherme L, Fiorelli A, Stolf N, Kalil J. Autoimmunity in Chagas’ disease. Identification of cardiac myosin-B13 Trypanosoma cruzi protein crossreactive T cell clones in heart lesions of a chronic Chagas’ cardiomy-opathy patient. J Clin Invest 1996; 98: 1709-1712
35 Abel LC, Kalil J, Cunha Neto E. Molecular mimicry between cardiac myosin and Trypanosoma cruzi antigen B13: identi-fication of a B13-driven human T cell clone that recognizes cardiac myosin. Braz J Med Biol Res 1997; 30: 1305-1308
36 Abel LC, Iwai LK, Viviani W, Bilate AM, Faé KC, Ferreira RC, Goldberg AC, Juliano L, Juliano MA, Ianni B, Mady C, Gruber A, Hammer J, Sinigaglia F, Kalil J, Cunha-Neto E. T cell epitope characterization in tandemly repetitive Trypano-soma cruzi B13 protein. Microbes Infect 2005; 7: 1184-1195
Teixeira PC et al . Chagas disease
51 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
37 Bafica A, Santiago HC, Goldszmid R, Ropert C, Gazzinelli RT, Sher A. Cutting edge: TLR9 and TLR2 signaling together account for MyD88-dependent control of parasitemia in Try-panosoma cruzi infection. J Immunol 2006; 177: 3515-3519
38 Michailowsky V, Celes MR, Marino AP, Silva AA, Vieira LQ, Rossi MA, Gazzinelli RT, Lannes-Vieira J, Silva JS. In-tercellular adhesion molecule 1 deficiency leads to impaired recruitment of T lymphocytes and enhanced host suscepti-bility to infection with Trypanosoma cruzi. J Immunol 2004; 173: 463-470
39 Teixeira MM, Gazzinelli RT, Silva JS. Chemokines, inflam-mation and Trypanosoma cruzi infection. Trends Parasitol 2002; 18: 262-265
40 Marino AP, da Silva A, dos Santos P, Pinto LM, Gazzinelli RT, Teixeira MM, Lannes-Vieira J. Regulated on activation, normal T cell expressed and secreted (RANTES) antagonist (Met-RANTES) controls the early phase of Trypanosoma cruzi-elicited myocarditis. Circulation 2004; 110: 1443-1449
41 Guedes PM, Veloso VM, Talvani A, Diniz LF, Caldas IS, Do-Valle-Matta MA, Santiago-Silva J, Chiari E, Galvão LM, Silva JS, Bahia MT. Increased type 1 chemokine expression in ex-perimental Chagas disease correlates with cardiac pathology in beagle dogs. Vet Immunol Immunopathol 2010; 138: 106-113
42 Roffê E, Souza AL, Caetano BC, Machado PP, Barcelos LS, Russo RC, Santiago HC, Souza DG, Pinho V, Tanowitz HB, Camargos ER, Bruña-Romero O, Teixeira MM. A DNA vac-cine encoding CCL4/MIP-1beta enhances myocarditis in experimental Trypanosoma cruzi infection in rats. Microbes Infect 2006; 8: 2745-2755
43 Roffê E, Oliveira F, Souza AL, Pinho V, Souza DG, Souza PR, Russo RC, Santiago HC, Romanha AJ, Tanowitz HB, Valenzuela JG, Teixeira MM. Role of CCL3/MIP-1alpha and CCL5/RANTES during acute Trypanosoma cruzi infection in rats. Microbes Infect 2010; 12: 669-676
44 Silva JS, Twardzik DR, Reed SG. Regulation of Trypano-soma cruzi infections in vitro and in vivo by transforming growth factor beta (TGF-beta). J Exp Med 1991; 174: 539-545
45 dos Santos RR, Rossi MA, Laus JL, Silva JS, Savino W, Men-gel J. Anti-CD4 abrogates rejection and reestablishes long-term tolerance to syngeneic newborn hearts grafted in mice chronically infected with Trypanosoma cruzi. J Exp Med 1992; 175: 29-39
46 Hölscher C, Mohrs M, Dai WJ, Köhler G, Ryffel B, Schaub GA, Mossmann H, Brombacher F. Tumor necrosis factor al-pha-mediated toxic shock in Trypanosoma cruzi-infected in-terleukin 10-deficient mice. Infect Immun 2000; 68: 4075-4083
47 da Matta Guedes PM, Gutierrez FR, Maia FL, Milanezi CM, Silva GK, Pavanelli WR, Silva JS. IL-17 produced during Trypanosoma cruzi infection plays a central role in regulat-ing parasite-induced myocarditis. PLoS Negl Trop Dis 2010; 4: e604
48 Mariano FS, Gutierrez FR, Pavanelli WR, Milanezi CM, Cavassani KA, Moreira AP, Ferreira BR, Cunha FQ, Cardoso CR, Silva JS. The involvement of CD4+CD25+ T cells in the acute phase of Trypanosoma cruzi infection. Microbes Infect 2008; 10: 825-833
49 Ramírez LE, Lages-Silva E, Soares Júnior JM, Chapadeiro E. The hamster (Mesocricetus auratus) as experimental model in Chagas’ disease: parasitological and histopathological studies in acute and chronic phases of Trypanosoma cruzi infection. Rev Soc Bras Med Trop 1994; 27: 163-169
50 Moretti E, Basso B, Cervetta L, Brigada A, Barbieri G. Pat-terns of cytokines and soluble cellular receptors in the sera of children with acute chagas’ disease. Clin Diagn Lab Immunol 2002; 9: 1324-1327
51 Samudio M, Montenegro-James S, de Cabral M, Martinez J, Rojas de Arias A, Woroniecky O, James MA. Differential expression of systemic cytokine profiles in Chagas’ disease is associated with endemicity of Trypanosoma cruzi infections. Acta Trop 1998; 69: 89-97
52 Ferreira RC, Ianni BM, Abel LC, Buck P, Mady C, Kalil J, Cunha-Neto E. Increased plasma levels of tumor necrosis factor-alpha in asymptomatic/”indeterminate” and Chagas disease cardiomyopathy patients. Mem Inst Oswaldo Cruz 2003; 98: 407-411
53 Talvani A, Rocha MO, Ribeiro AL, Correa-Oliveira R, Teixei-ra MM. Chemokine receptor expression on the surface of pe-ripheral blood mononuclear cells in Chagas disease. J Infect Dis 2004; 189: 214-220
54 Abel LC, Rizzo LV, Ianni B, Albuquerque F, Bacal F, Carrara D, Bocchi EA, Teixeira HC, Mady C, Kalil J, Cunha-Neto E. Chronic Chagas’ disease cardiomyopathy patients display an increased IFN-gamma response to Trypanosoma cruzi infection. J Autoimmun 2001; 17: 99-107
55 Talvani A, Rocha MO, Barcelos LS, Gomes YM, Ribeiro AL, Teixeira MM. Elevated concentrations of CCL2 and tumor necrosis factor-alpha in chagasic cardiomyopathy. Clin Infect Dis 2004; 38: 943-950
56 Gomes JA, Bahia-Oliveira LM, Rocha MO, Martins-Filho OA, Gazzinelli G, Correa-Oliveira R. Evidence that develop-ment of severe cardiomyopathy in human Chagas’ disease is due to a Th1-specific immune response. Infect Immun 2003; 71: 1185-1193
57 Araujo FF, Gomes JA, Rocha MO, Williams-Blangero S, Pin-heiro VM, Morato MJ, Correa-Oliveira R. Potential role of CD4+CD25HIGH regulatory T cells in morbidity in Chagas disease. Front Biosci 2007; 12: 2797-2806
58 da Silveira AB, de Araújo FF, Freitas MA, Gomes JA, Chaves AT, de Oliveira EC, Neto SG, Luquetti AO, da Cunha Souza G, Bernardino Júnior R, Fujiwara R, d’Avila Reis D, Correa-Oliveira R. Characterization of the presence and distribu-tion of Foxp3(+) cells in chagasic patients with and without megacolon. Hum Immunol 2009; 70: 65-67
59 Cunha-Neto E, Dzau VJ, Allen PD, Stamatiou D, Benve-nutti L, Higuchi ML, Koyama NS, Silva JS, Kalil J, Liew CC. Cardiac gene expression profiling provides evidence for cytokinopathy as a molecular mechanism in Chagas’ disease cardiomyopathy. Am J Pathol 2005; 167: 305-313
60 Reis DD, Jones EM, Tostes S, Lopes ER, Chapadeiro E, Gazzinelli G, Colley DG, McCurley TL. Expression of major histocompatibility complex antigens and adhesion molecules in hearts of patients with chronic Chagas’ disease. Am J Trop Med Hyg 1993; 49: 192-200
61 Reis MM, Higuchi Mde L, Benvenuti LA, Aiello VD, Gutier-rez PS, Bellotti G, Pileggi F. An in situ quantitative immu-nohistochemical study of cytokines and IL-2R+ in chronic human chagasic myocarditis: correlation with the presence of myocardial Trypanosoma cruzi antigens. Clin Immunol Im-munopathol 1997; 83: 165-172
62 Fonseca SG, Reis MM, Coelho V, Nogueira LG, Monteiro SM, Mairena EC, Bacal F, Bocchi E, Guilherme L, Zheng XX, Liew FY, Higuchi ML, Kalil J, Cunha-Neto E. Locally pro-duced survival cytokines IL-15 and IL-7 may be associated to the predominance of CD8+ T cells at heart lesions of human chronic Chagas disease cardiomyopathy. Scand J Immunol 2007; 66: 362-371
63 Gomes JA, Bahia-Oliveira LM, Rocha MO, Busek SC, Teixei-ra MM, Silva JS, Correa-Oliveira R. Type 1 chemokine recep-tor expression in Chagas’ disease correlates with morbidity in cardiac patients. Infect Immun 2005; 73: 7960-7966
64 Bilate AM, Salemi VM, Ramires FJ, de Brito T, Russo M, Fonseca SG, Faé KC, Martins DG, Silva AM, Mady C, Kalil J, Cunha-Neto E. TNF blockade aggravates experimental chronic Chagas disease cardiomyopathy. Microbes Infect 2007; 9: 1104-1113
65 Araújo-Jorge TC, Waghabi MC, Hasslocher-Moreno AM, Xavier SS, Higuchi Mde L, Keramidas M, Bailly S, Feige JJ. Implication of transforming growth factor-beta1 in Chagas disease myocardiopathy. J Infect Dis 2002; 186: 1823-1828
66 Riol-Blanco L, Sánchez-Sánchez N, Torres A, Tejedor A, Na-
Teixeira PC et al . Chagas disease
52 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
rumiya S, Corbí AL, Sánchez-Mateos P, Rodríguez-Fernán-dez JL. The chemokine receptor CCR7 activates in dendritic cells two signaling modules that independently regulate che-motaxis and migratory speed. J Immunol 2005; 174: 4070-4080
67 Liu R, Zhou C, Wang D, Ma W, Lin C, Wang Y, Liang X, Li J, Guo S, Wang Y, Zhang Y, Zhang S. Enhancement of DNA vaccine potency by sandwiching antigen-coding gene be-tween secondary lymphoid tissue chemokine (SLC) and IgG Fc fragment genes. Cancer Biol Ther 2006; 5: 427-434
68 Soares MB, de Lima RS, Rocha LL, Vasconcelos JF, Rogatto SR, dos Santos RR, Iacobas S, Goldenberg RC, Iacobas DA, Tanowitz HB, de Carvalho AC, Spray DC. Gene expression changes associated with myocarditis and fibrosis in hearts of mice with chronic chagasic cardiomyopathy. J Infect Dis 2010; 202: 416-426
69 Garg N, Popov VL, Papaconstantinou J. Profiling gene tran-scription reveals a deficiency of mitochondrial oxidative phosphorylation in Trypanosoma cruzi-infected murine hearts: implications in chagasic myocarditis development. Biochim Biophys Acta 2003; 1638: 106-120
70 Mukherjee S, Belbin TJ, Spray DC, Iacobas DA, Weiss LM, Kitsis RN, Wittner M, Jelicks LA, Scherer PE, Ding A, Tanowitz HB. Microarray analysis of changes in gene expres-sion in a murine model of chronic chagasic cardiomyopathy. Parasitol Res 2003; 91: 187-196
71 Vikstrom KL, Bohlmeyer T, Factor SM, Leinwand LA. Hy-pertrophy, pathology, and molecular markers of cardiac pathogenesis. Circ Res 1998; 82: 773-778
72 Mukherjee S, Nagajyothi F, Mukhopadhyay A, Machado FS, Belbin TJ, Campos de Carvalho A, Guan F, Albanese C, Jelicks LA, Lisanti MP, Silva JS, Spray DC, Weiss LM, Tanowitz HB. Alterations in myocardial gene expression associated with experimental Trypanosoma cruzi infection. Genomics 2008; 91: 423-432
73 Goldenberg RC, Iacobas DA, Iacobas S, Rocha LL, da Silva de Azevedo Fortes F, Vairo L, Nagajyothi F, Campos de Carvalho AC, Tanowitz HB, Spray DC. Transcriptomic al-terations in Trypanosoma cruzi-infected cardiac myocytes. Microbes Infect 2009; 11: 1140-1149
74 Arrell DK, Neverova I, Van Eyk JE. Cardiovascular pro-teomics: evolution and potential. Circ Res 2001; 88: 763-773
75 Ping P. Identification of novel signaling complexes by func-tional proteomics. Circ Res 2003; 93: 595-603
76 Agnetti G, Husberg C, Van Eyk JE. Divide and conquer: the application of organelle proteomics to heart failure. Circ Res 2011; 108: 512-526
77 Ping P, Chan DW, Srinivas P. Advancing cardiovascular bi-ology and medicine via proteomics: Opportunities and pres-ent challenges of cardiovascular proteomics. Circulation 2010; 121: 2326-2328
78 Marchini FK, de Godoy LM, Rampazzo RC, Pavoni DP, Probst CM, Gnad F, Mann M, Krieger MA. Profiling the Try-panosoma cruzi phosphoproteome. PLoS One 2011; 6: e25381
79 Kikuchi SA, Sodré CL, Kalume DE, Elias CG, Santos AL, de Nazaré Soeiro M, Meuser M, Chapeaurouge A, Perales J, Fernandes O. Proteomic analysis of two Trypanosoma cruzi zymodeme 3 strains. Exp Parasitol 2010; 126: 540-551
80 Alves LR, Avila AR, Correa A, Holetz FB, Mansur FC, Manque PA, de Menezes JP, Buck GA, Krieger MA, Golden-berg S. Proteomic analysis reveals the dynamic association of proteins with translated mRNAs in Trypanosoma cruzi. Gene 2010; 452: 72-78
81 Ayub MJ, Atwood J, Nuccio A, Tarleton R, Levin MJ. Pro-teomic analysis of the Trypanosoma cruzi ribosomal pro-teins. Biochem Biophys Res Commun 2009; 382: 30-34
82 Magalhães AD, Charneau S, Paba J, Guércio RA, Teixeira AR, Santana JM, Sousa MV, Ricart CA. Trypanosoma cruzi alkaline 2-DE: Optimization and application to comparative proteome analysis of flagellate life stages. Proteome Sci 2008; 6: 24
83 Atwood JA, Weatherly DB, Minning TA, Bundy B, Cavola C, Opperdoes FR, Orlando R, Tarleton RL. The Trypanosoma cruzi proteome. Science 2005; 309: 473-476
84 Paba J, Ricart CA, Fontes W, Santana JM, Teixeira AR, Mar-chese J, Williamson B, Hunt T, Karger BL, Sousa MV. Pro-teomic analysis of Trypanosoma cruzi developmental stages using isotope-coded affinity tag reagents. J Proteome Res 2004; 3: 517-524
85 Parodi-Talice A, Durán R, Arrambide N, Prieto V, Piñeyro MD, Pritsch O, Cayota A, Cerveñansky C, Robello C. Pro-teome analysis of the causative agent of Chagas disease: Try-panosoma cruzi. Int J Parasitol 2004; 34: 881-886
86 Paba J, Santana JM, Teixeira AR, Fontes W, Sousa MV, Ricart CA. Proteomic analysis of the human pathogen Trypano-soma cruzi. Proteomics 2004; 4: 1052-1059
87 Teixeira PC, Iwai LK, Kuramoto AC, Honorato R, Fiorelli A, Stolf N, Kalil J, Cunha-Neto E. Proteomic inventory of myo-cardial proteins from patients with chronic Chagas’ cardio-myopathy. Braz J Med Biol Res 2006; 39: 1549-1562
88 Teixeira PC, Santos RH, Fiorelli AI, Bilate AM, Benvenuti LA, Stolf NA, Kalil J, Cunha-Neto E. Selective decrease of components of the creatine kinase system and ATP synthase complex in chronic Chagas disease cardiomyopathy. PLoS Negl Trop Dis 2011; 5: e1205
89 Bilate AM, Teixeira PC, Ribeiro SP, Brito T, Silva AM, Russo M, Kalil J, Cunha-Neto E. Distinct outcomes of Trypanosoma cruzi infection in hamsters are related to myocardial para-sitism, cytokine/chemokine gene expression, and protein expression profile. J Infect Dis 2008; 198: 614-623
90 Ndao M, Rainczuk A, Rioux MC, Spithill TW, Ward BJ. Is SELDI-TOF a valid tool for diagnostic biomarkers? Trends Parasitol 2010; 26: 561-567
91 Zicker F, Smith PG, Netto JC, Oliveira RM, Zicker EM. Phys-ical activity, opportunity for reinfection, and sibling history of heart disease as risk factors for Chagas’ cardiopathy. Am J Trop Med Hyg 1990; 43: 498-505
92 Fernandez-Mestre MT, Layrisse Z, Montagnani S, Acquatel-la H, Catalioti F, Matos M, Balbas O, Makhatadze N, Domin-guez E, Herrera F, Madrigal A. Influence of the HLA class II polymorphism in chronic Chagas’ disease. Parasite Immunol 1998; 20: 197-203
93 Layrisse Z, Fernandez MT, Montagnani S, Matos M, Bal-bas O, Herrera F, Colorado IA, Catalioti F, Acquatella H. HLA-C(*)03 is a risk factor for cardiomyopathy in Chagas disease. Hum Immunol 2000; 61: 925-929
94 Deghaide NH, Dantas RO, Donadi EA. HLA class I and II profiles of patients presenting with Chagas’ disease. Dig Dis Sci 1998; 43: 246-252
95 Colorado IA, Acquatella H, Catalioti F, Fernandez MT, Lay-risse Z. HLA class II DRB1, DQB1, DPB1 polymorphism and cardiomyopathy due to Trypanosoma cruzi chronic infec-tion. Hum Immunol 2000; 61: 320-325
96 Rodríguez-Pérez JM, Cruz-Robles D, Hernández-Pacheco G, Pérez-Hernández N, Murguía LE, Granados J, Reyes PA, Vargas-Alarcón G. Tumor necrosis factor-alpha promoter polymorphism in Mexican patients with Chagas’ disease. Immunol Lett 2005; 98: 97-102
97 Campelo V, Dantas RO, Simões RT, Mendes-Junior CT, Sousa SM, Simões AL, Donadi EA. TNF microsatellite alleles in Brazilian Chagasic patients. Dig Dis Sci 2007; 52: 3334-3339
98 Drigo SA, Cunha-Neto E, Ianni B, Mady C, Faé KC, Buck P, Kalil J, Goldberg AC. Lack of association of tumor necrosis factor-alpha polymorphisms with Chagas disease in Brazil-ian patients. Immunol Lett 2007; 108: 109-111
99 Beraún Y, Nieto A, Collado MD, González A, Martín J. Poly-morphisms at tumor necrosis factor (TNF) loci are not asso-ciated with Chagas’ disease. Tissue Antigens 1998; 52: 81-83
100 Drigo SA, Cunha-Neto E, Ianni B, Cardoso MR, Braga PE, Faé KC, Nunes VL, Buck P, Mady C, Kalil J, Goldberg AC. TNF gene polymorphisms are associated with reduced sur-
Teixeira PC et al . Chagas disease
53 June 25, 2012|Volume 2|Issue 3|WJCID|www.wjgnet.com
vival in severe Chagas’ disease cardiomyopathy patients. Microbes Infect 2006; 8: 598-603
101 Flórez O, Zafra G, Morillo C, Martín J, González CI. Interleu-kin-1 gene cluster polymorphism in chagas disease in a Co-lombian case-control study. Hum Immunol 2006; 67: 741-748
102 Cruz-Robles D, Chávez-González JP, Cavazos-Quero MM, Pérez-Méndez O, Reyes PA, Vargas-Alarcón G. Association between IL-1B and IL-1RN gene polymorphisms and Cha-gas’ disease development susceptibility. Immunol Invest 2009; 38: 231-239
103 Costa GC, da Costa Rocha MO, Moreira PR, Menezes CA, Silva MR, Gollob KJ, Dutra WO. Functional IL-10 gene poly-morphism is associated with Chagas disease cardiomyopa-thy. J Infect Dis 2009; 199: 451-454
104 Moreno M, Silva EL, Ramírez LE, Palacio LG, Rivera D, Arcos-Burgos M. Chagas’ disease susceptibility/resistance: linkage disequilibrium analysis suggests epistasis between major histocompatibility complex and interleukin-10. Tissue Antigens 2004; 64: 18-24
105 Zafra G, Morillo C, Martín J, González A, González CI. Polymorphism in the 3’ UTR of the IL12B gene is associated with Chagas’ disease cardiomyopathy. Microbes Infect 2007; 9: 1049-1052
106 Ramasawmy R, Cunha-Neto E, Fae KC, Borba SC, Teix-eira PC, Ferreira SC, Goldberg AC, Ianni B, Mady C, Kalil J. Heterozygosity for the S180L variant of MAL/TIRAP, a gene expressing an adaptor protein in the Toll-like receptor pathway, is associated with lower risk of developing chronic Chagas cardiomyopathy. J Infect Dis 2009; 199: 1838-1845]
107 Ramasawmy R, Cunha-Neto E, Fae KC, Martello FG, Müller NG, Cavalcanti VL, Ianni B, Mady C, Kalil J, Goldberg AC. The monocyte chemoattractant protein-1 gene polymor-phism is associated with cardiomyopathy in human chagas disease. Clin Infect Dis 2006; 43: 305-311
108 Ramasawmy R, Cunha-Neto E, Faé KC, Müller NG, Cav-alcanti VL, Drigo SA, Ianni B, Mady C, Kalil J, Goldberg AC. BAT1, a putative anti-inflammatory gene, is associated with chronic Chagas cardiomyopathy. J Infect Dis 2006; 193: 1394-1399
109 Ramasawmy R, Fae KC, Cunha-Neto E, Müller NG, Caval-canti VL, Ferreira RC, Drigo SA, Ianni B, Mady C, Goldberg AC, Kalil J. Polymorphisms in the gene for lymphotoxin-alpha predispose to chronic Chagas cardiomyopathy. J Infect Dis 2007; 196: 1836-1843
110 Ramasawmy R, Faé KC, Cunha-Neto E, Borba SC, Ianni B, Mady C, Goldberg AC, Kalil J. Variants in the promoter region of IKBL/NFKBIL1 gene may mark susceptibility to the development of chronic Chagas’ cardiomyopathy among Trypanosoma cruzi-infected individuals. Mol Immunol 2008; 45: 283-288
111 Calzada JE, Nieto A, Beraún Y, Martín J. Chemokine recep-tor CCR5 polymorphisms and Chagas’ disease cardiomy-opathy. Tissue Antigens 2001; 58: 154-158
112 Fernández-Mestre MT, Montagnani S, Layrisse Z. Is the CCR5-59029-G/G genotype a protective factor for cardiomy-opathy in Chagas disease? Hum Immunol 2004; 65: 725-728
113 Torres OA, Calzada JE, Beraún Y, Morillo CA, González CI, González A, Martín J. Association of the macrophage migra-tion inhibitory factor -173G/C polymorphism with Chagas
disease. Hum Immunol 2009; 70: 543-546114 Zafra G, Flórez O, Morillo CA, Echeverría LE, Martín J, Gon-
zález CI. Polymorphisms of toll-like receptor 2 and 4 genes in Chagas disease. Mem Inst Oswaldo Cruz 2008; 103: 27-30
115 Robledo G, González CI, Morillo C, Martín J, González A. Association study of PTPN22 C1858T polymorphism in Try-panosoma cruzi infection. Tissue Antigens 2007; 69: 261-264
116 Pascuzzo-Lima C, Mendible JC, Bonfante-Cabarcas RA. Angiotensin-converting enzyme insertion/deletion gene polymorphism and progression of Chagas’ cardiomyopathy. Rev Esp Cardiol 2009; 62: 320-322
117 Calzada JE, Nieto A, López-Nevot MA, Martín J. Lack of as-sociation between NRAMP1 gene polymorphisms and Try-panosoma cruzi infection. Tissue Antigens 2001; 57: 353-357
118 Calzada JE, López-Nevot MA, Beraún Y, Martín J. No evi-dence for association of the inducible nitric oxide synthase promoter polymorphism with Trypanosoma cruzi infection. Tissue Antigens 2002; 59: 316-319
119 Flórez O, Martín J, González CI. Interleukin 4, interleukin 4 receptor-α and interleukin 10 gene polymorphisms in Cha-gas disease. Parasite Immunol 2011; 33: 506-511
120 Cunha-Neto E, Teixeira PC, Fonseca SG, Bilate AM, Kalil J. Myocardial gene and protein expression profiles after auto-immune injury in Chagas’ disease cardiomyopathy. Autoim-mun Rev 2011; 10: 163-165
121 Aliberti JC, Cardoso MA, Martins GA, Gazzinelli RT, Vieira LQ, Silva JS. Interleukin-12 mediates resistance to Trypano-soma cruzi in mice and is produced by murine macrophages in response to live trypomastigotes. Infect Immun 1996; 64: 1961-1967
122 Torrico F, Heremans H, Rivera MT, Van Marck E, Billiau A, Carlier Y. Endogenous IFN-gamma is required for resistance to acute Trypanosoma cruzi infection in mice. J Immunol 1991; 146: 3626-3632
123 Gazzinelli RT, Oswald IP, James SL, Sher A. IL-10 inhibits parasite killing and nitrogen oxide production by IFN-gam-ma-activated macrophages. J Immunol 1992; 148: 1792-1796
124 Muñoz-Fernández MA, Fernández MA, Fresno M. Activa-tion of human macrophages for the killing of intracellular Trypanosoma cruzi by TNF-alpha and IFN-gamma through a nitric oxide-dependent mechanism. Immunol Lett 1992; 33: 35-40
125 Graefe SE, Jacobs T, Gaworski I, Klauenberg U, Steeg C, Fleischer B. Interleukin-12 but not interleukin-18 is required for immunity to Trypanosoma cruzi in mice. Microbes Infect 2003; 5: 833-839
126 Müller U, Köhler G, Mossmann H, Schaub GA, Alber G, Di Santo JP, Brombacher F, Hölscher C. IL-12-independent IFN-gamma production by T cells in experimental Chagas’ disease is mediated by IL-18. J Immunol 2001; 167: 3346-3353
127 Machado FS, Martins GA, Aliberti JC, Mestriner FL, Cunha FQ, Silva JS. Trypanosoma cruzi-infected cardiomyocytes produce chemokines and cytokines that trigger potent nitric oxide-dependent trypanocidal activity. Circulation 2000; 102: 3003-3008
128 Machado FS, Koyama NS, Carregaro V, Ferreira BR, Mila-nezi CM, Teixeira MM, Rossi MA, Silva JS. CCR5 plays a critical role in the development of myocarditis and host pro-tection in mice infected with Trypanosoma cruzi. J Infect Dis 2005; 191: 627-636
S- Editor Wu X L- Editor A E- Editor Wu X
Teixeira PC et al . Chagas disease