panchayats in implementing nrhm: an experience in assam
TRANSCRIPT

Panchayats in Implementing NRHM: An Experience
in Assam
Abstract: Panchayats, though not like the Panchayati Raj Institutions of these days, but are the age-
old institutions working at the village level. These Panchayats work as decentralised institutions to
bring socio-economic and political development to the people. These developmental activities
include health security, sanitation and population stabilisation etc. When we talk about health and
Panchayats, we must look at the policies like National Health Policy, 2000 and National Health
Policy, 2001 etc. which indicate and ensure the role of PRIs as a responsible agency to provide
decentralised health services. The 73rd
Constitutional Amendment, which has strengthened the PRIs
and drawn clear areas of their jurisdiction, authority and funds also indicates Panchayats’ role in
providing health services.
The UPA government, to improve and uplift the condition of health services in rural India started a
comprehensive national campaigning and launched a programme called National Rural Health
Mission (NRHM) on 12th
April, 2005. NRHM has taken up myriad of action plans and goals those
include increasing public expenditure to health, reducing regional imbalance in health
infrastructure, pooling resources, integration of organizational structures, optimization of health
manpower, decentralization and district management of health programmes, community
participation etc. These goals also reflect the Millennium Developmental Goals (MDGs).
This paper starts on the above narrated ground and basically tries to focus on the roles and
responsibilities of the PRIs in implementing National Rural Health Mission in Assam. Empirical
data collection and scientific observation methods are used while articulating the research findings.
Keywords: PRIs, NRHM, MDGs, UPA, Assam.
Pankaj Bora
Assistant Professor, Bahona College
Merrychaya Patiri
Research Scholar, Gauhati University
Bitapi Bora
Assistant Teacher, Bahona Boys
ISSN 2319-9725
April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1067
1. Introduction:
Panchayats are one of the oldest decentralized democratic institutions working at the village
level in India to bring socio-economic and political development to the people. Panchayats
give power to the rural people. Through Panchayats people can participate in decision making
and policy implementation at village level. Panchayati Raj Institutions (PRIs) are considered
as vehicle for promoting development through popular participation (Misra, 2013). These
developmental activities include health security, sanitation and population stabilization etc.
When we talk about health and Panchayats, we must look at the policies like National Health
Policy (2000) and National Health Policy (2001), National Health Policy (2002), etc. which
indicate and ensure the role of PRIs as a responsible agency to provide decentralised health
services. The National Health Policy (2002) highlights the need for devolving programmes
and funds in the health sector through different levels of the Panchayati Raj Institutions
(Sekher, 2003). The 73rd
Amendment to the Constitution of India, which has strengthened the
PRIs and drawn clear areas of their jurisdiction, authority and funds also indicates
Panchayats’ role in providing health services.
The Government of India, to improve and uplift the condition of health services in rural
India, started a comprehensive national campaigning and launched a programme called
National Rural Health Mission (NRHM) on 12th
April, 2005. NRHM has taken up myriad of
action plans and goals those include increasing public expenditure to health, reducing
regional imbalance in health infrastructure, pooling resources, integration of organizational
structures, optimization of health manpower, decentralization and district management of
health programmes, community participation etc. These goals also reflect the Millennium
Developmental Goals (MDGs). So, these goals have global standards too.
This paper starts on the above narrated ground and basically tries to focus on the roles and
responsibilities of the PRIs in implementing National Rural Health Mission in Assam.
Empirical data collection and scientific observation methods are used while articulating the
research findings.
2. Objectives of the research:
The paper has both empirical objective and theoretical objective. Theoretically, it wants to
investigate the role of Panchayati Raj Institutions in uplifting health conditions and ensuring
health security. It also wants to know how PRIs as decentralized institutions work in
implementing NRHM. On the other hand, empirically it aims to find out how far good
April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1068
governance and decentralized administration has contributed towards making the health
service more effective. To be more precise we can point out the objectives of the research
like:
i. Theoretical Objective: To see the relationship between health security and
decentralized governance.
ii. Empirical objectives:
a. To know how far PRIs are responsible towards implementing NRHM and
improving health security.
b. To trace the progress in NRHM in Assam.
c. To find out whether the PRIs are actually working towards making the health
sector healthy.
3. Methodology:
In this research paper, both primary and secondary sources for data collection have been
used. Secondary data are mainly official reports, articles from journals, book etc. The
research paper extensively depends on policy documents and statistical input drawn from
these government official reports and articles.
To collect primary data, the research has followed the non-participatory observation method.
The primary data collected from the field study conducted as a part of the field survey for the
ICSSR sponsored major research project titled “Implementing NRHM in Assam: A study on
the convergence among Institutions, Infrastructure and Practices” under the guidance of
project director Dr. Akhil Ranjan Dutta.
Theoretical support: The focal point of this research moves round the concepts like
decentralized administration, role of state, social security, and health security etc. The
objectives reflect that all these areas are the core areas of this research. Based on the concepts
and research questions, the research has concentrated in two meta-narratives and tried to find
out a clubbed approach to interrogate the objectives and justify the findings. The research
looks the notion of Health Security as a part of Social Security and hence used the
perspective of Social Security to support the research. As it is a research investigating the role
played by PRIs, we are justifying our articulations on the basis of theory of decentralized
administration. Clubbing both the approaches in one approach, we have experimented the
April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1069
finding on the basis of the presumption that providing Social security and health security is
basic responsibility of a welfare state and they must ensure it in collaboration with
decentralized institution like PRIs.
4. Conceptual background of Panchayati Raj in India:
Democratic decentralization is a procedure to provide opportunity to strengthen the
democratic governance. The notion, democratic decentralization has dominated the
development discourses in contemporary period. It emerged as a popular policy in many
Asian, African and Latin American countries since the 1960s. The idea behind democratic
decentralization is that people will become the end as well as the means of development. It
rejects the idea of a highly centralized State and replaces it with the concept of distribution of
power to people at large. Here, people occupy the centre-stage of the development process.
India has also adopted the policy of democratic decentralization and introduced the
Panchayati Raj System and other decentralized mechanisms. They act as an institution of self
governance and people’s participation in rural areas of India (Bhattacharya(Mukhopadhyay),
2011, p. 344).
The Constitution of India, in Part IX, deals with Panchayat System and Municipalities
(Sarmah, Gogoi, & Bora, 2011, p. 13). The Constitution envisages a three-tiered system of
Panchayats. These are: The Village Panchayats at village level, The District Panchayats at the
district level, and The Intermediate Panchayat which stands between the Village Panchayats
and District Panchayats. The constitution says that all the seats in a Panchayats shall be filled
by persons chosen by direct election from territorial constituencies in the Panchayat areas
(Basu, 2011, p. 283). The 73rd
Amendment Act, 1992 of the Constitution came into force in
1993 introduced the Part IX from Article 243-243-O and Eleventh Schedule to the
Constitution. This amendment empowered the Panchayats with power in 29 subjects
(Bhattacharya(Mukhopadhyay), 2011, p. 249). Among the 29 subjects, health and sanitation
is also a significant one. This includes providing health services, regulation of hospitals,
primary health centers and dispensaries. Based on this amendment several policy initiatives
were taken, making the Panchayats core. In Assam too Panchayats carry out its role in
proving health security.
April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1070
5. Status of the PRI framework in Assam:
The Government of Assam enacted the Assam Panchayat Raj Act, 1994 incorporating almost
all the features of the 73rd Constitutional Amendment Act, 1992. The terms of Panchayat in
the state expired in October 1997. The state government had put off the Panchayat elections
several times citing different reasons. The elections of the Panchayat bodies were held in
2001 (year not sure) and December 2007 and since then the PRI bodies are active in the State.
The PRIs have been actively involved with developmental process at all the levels including
in the planning, implementation and monitoring of the activities envisaged under Sarbha
Siksha Abhiyan, Public Health Engineering, Total Sanitation Campaign, and National Rural
Health Mission etc.
6. Conceptual background of Health Security and NRHM in India:
National Rural Health Mission (NRHM) 2005-12 is one of the ambitious projects of the
United Progressive Alliance Government pursued at a very crucial juncture in India’s
development trajectory. National Rural Health Mission (2005-2012) MISSION
DOCUMENT, the Government of India's document on NRHM, in its preamble highlights the
vision of the mission. To quote the document “Recognizing the importance of Health in the
process of economic and social development and improving the quality of life of our citizens,
the Government of India has resolved to launch the National Rural Health Mission to carry
out necessary architectural correction in the basic health care delivery system. The Mission
adopts a synergistic approach by relating health to determinants of good health viz. segments
of nutrition, sanitation, hygiene and safe drinking water. It also aims at mainstreaming the
Indian systems of medicine to facilitate health care. The Plan of Action includes increasing
public expenditure on health, reducing regional imbalance in health infrastructure, pooling
resources, integration of organizational structures, optimization of health manpower,
decentralization and district management of health programmes, community participation and
ownership of assets, induction of management and financial personnel into district health
system, and operationalizing community health centers into functional hospitals meeting
Indian Public Health Standards in each Block of the Country. The goals of NRHM are
reflection of Millennium Development Goals (MDGs) especially reduction of child mortality,
improve Maternal Health and combat HIV/AIDS, Malaria and TB. (Development Goals,
States of India Report, 2010)
April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1071
The Goal of the Mission is to improve the availability of and access to quality health care by
people, especially for those residing in rural areas, the poor, women and children. The
document, with 16 sub-headings, expresses the present condition of health, vision of the
mission, strategies, plan of action, institutional mechanism, technical support, role of state
government, PRI and NGOs, focus on NE states, importance of AYUSH, fundings, targets,
outcome and monitoring and evolution of the action taken to meet the target. Here, the
document says that status of current public health is not satisfactory. In Government annual
budget, Public health expenditure has declined from 1.3% of GDP in 1990 to 0.9% of GDP in
1999. There are many other evidences of poor health standard in India which is explained by
the document. The document also states the vision of the mission where it categories 18
states, including states from NE, as high focus states with special attention. It expresses the
above mentioned goal as prime objective with definite time programmes which will be
aquired with some well designed strategies and plan of action where the state governments,
Panchyats and NGOs will play a positive role. The document has included the financial
matters, institutional mechanism and technical support and it gives emphasis to AYUSH. It
has also pointed out some statistical targets to be achieved by the mission on time. The
Mission has some monitoring and evaluation committees in three tier level- Block, Panchayat
and District, for well functioning of the mission and to bring health security. It basically
stresses on role of the Panchayats.
As the Mission empowers, the Panchayati Raj Institutions has to look at many areas in
implementing National Rural Health Mission. The Mission Document puts down that-
i. The respective states will indicate their MoUs the commitment for devolution of
funds, functionaries and programmes for health to their PRIs.
ii. In the institutional set up, at the district level, a District Health Mission (DHM) will
be set up that to be led by Zila Parishad. The DHM will control, guide and manage all
public health institutions in the district level like Sub-Centres, PHCs and CHCs.
iii. ASHA is the one of the main stakeholders of NRHM. ASHA would be selected by
and be accountable to the village Panchayat.
iv. In the village level, in the Panchayat a Village Health Committee would be organised
and this committee would be liable to prepare the Village Health Plan and promote
intersectoral integration.
v. For well functioning of the sub-centres there will be an Untied Fund for local action
of Rs. 10,000 per annum. This Fund will be deposited in a joint account of the ANM
April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1072
and Head of the Panchayat i.e. Sarpanch and operated by the ANM, in consultation
with the Village Health Committee.
vi. In hospital management, Rogi Kalyan Samitis are held up and in such committee’s
involvement in PRI is the key factor.
vii. Training will be provided to the members of PRIs.
viii. Making available health related databases to all stakeholders including Panchayats at
all levels.
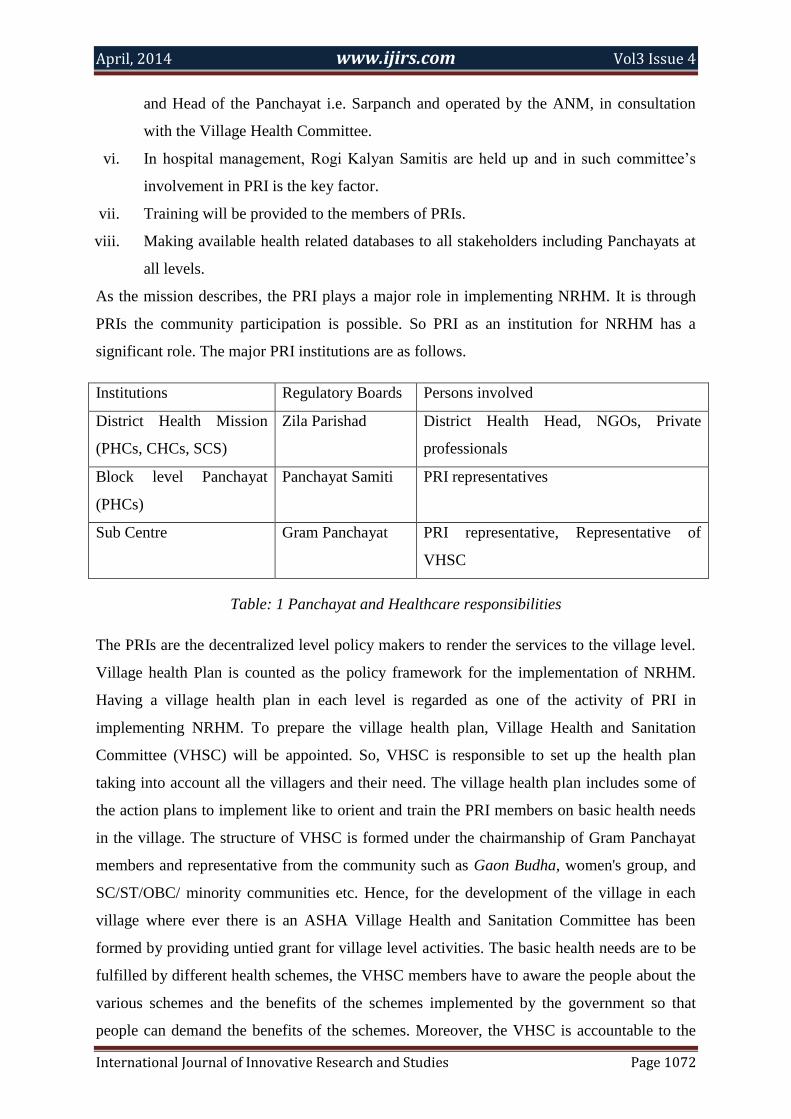
As the mission describes, the PRI plays a major role in implementing NRHM. It is through
PRIs the community participation is possible. So PRI as an institution for NRHM has a
significant role. The major PRI institutions are as follows.
Institutions Regulatory Boards Persons involved
District Health Mission
(PHCs, CHCs, SCS)
Zila Parishad District Health Head, NGOs, Private
professionals
Block level Panchayat
(PHCs)
Panchayat Samiti PRI representatives
Sub Centre Gram Panchayat PRI representative, Representative of
VHSC
Table: 1 Panchayat and Healthcare responsibilities
The PRIs are the decentralized level policy makers to render the services to the village level.
Village health Plan is counted as the policy framework for the implementation of NRHM.
Having a village health plan in each level is regarded as one of the activity of PRI in
implementing NRHM. To prepare the village health plan, Village Health and Sanitation
Committee (VHSC) will be appointed. So, VHSC is responsible to set up the health plan
taking into account all the villagers and their need. The village health plan includes some of
the action plans to implement like to orient and train the PRI members on basic health needs
in the village. The structure of VHSC is formed under the chairmanship of Gram Panchayat
members and representative from the community such as Gaon Budha, women's group, and
SC/ST/OBC/ minority communities etc. Hence, for the development of the village in each
village where ever there is an ASHA Village Health and Sanitation Committee has been
formed by providing untied grant for village level activities. The basic health needs are to be
fulfilled by different health schemes, the VHSC members have to aware the people about the
various schemes and the benefits of the schemes implemented by the government so that
people can demand the benefits of the schemes. Moreover, the VHSC is accountable to the
April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1073
overall village health plan. In theory, the VHSC will try to mitigate the health and nutrition
related problems of the community by organizing Village Health and Nutrition Day (VHND)
twice in a week. But, how far these theoretical arrangements have taken the actual color is a
matter of academic debate and for that we need to look at reports and other available sources.
7. Report from the secondary reports:
As far as the implementation of NRHM is concerned, certain reports are there to review the
institutionalization, infrastructure and convergence of the different institutions. According to
the Assam report, 2009; 26,816 VHSCs has been constituted & 24,085 Joint Accounts have
been operationalised. Rogi Kalyan Samities are operational at 22 DH, 103 CHCs & 844
PHCs. All districts have started developing their own IDHAP.
Common Review Mission (CRM) was conducted by the State wise Review Team for Assam
undertook the visit to Assam during a scheduled time frame from the year of 2007 onwards.
These CRM reports had examined the institutions, infrastructures of NRHM for the period
from 2007 to 2011.
The first Common Review Mission conducted in 2007 revealed that Village Health and
Sanitation Committee had not been set up at the village level as the Panchayat election was
not held. In the findings of second Common Review Mission, regarding the PRI involvement,
State has reported that 20,309 VHSCs are constituted and fund released to them. But in the
report, it is mentioned though VHSCs have been constituted, but the members have lack of
capacity building. In many cases, these members were not properly guided about their
responsibilities.
The fourth Common Review Mission also revealed the disappointment in practicing of
implementation of NRHM, though the Panchayati Raj Institutions have been constituted, the
actual capacity building of these institutions have not been up to the mark.
But the fifth Common Review Mission has portrayed another picture of involvement of PRI
in NRHM. Under the NRHM, in each village a Village Health Sanitation (& Nutrition)
Committee (VHSNC) has been formed where the elected PRI members are the Chairman of
the committee and the ASHAs are the Member Secretary. 26,312 VHSNC have been formed
in Assam. The ASHAs are working in close co-ordination with the VHSNC members for
improving the health scenario of the village. Every year under NRHM, each VHSNC receives
Rs. 10,000/- which is used for providing safe drinking water, construction of sanitary toilets,
April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1074
arranging emergency referral transport and organizing Village Health & Nutrition Day.
Source: (5th
Common Review Mission, 8th
-15th
November, 2011, Assam).
All the VHSNC members have been trained under NRHM regarding their roles and
responsibilities in the years 2009-10 and 2010-11. In 2010-11 and 2011-12, on sample basis
Model Village Plans have been prepared in each Block PHC. So, we have seen a mixed
picture of NRHM and its relation with PRIs in these reports. To have a better insight of it we
need a closer observation.
8. Observation from the field survey:
The structured interview schedule was mainly targeted for the stakeholders of NRHM like,
the ASHAs, the ANMs, the BPMs and the health care seekers. As stated earlier, the
stakeholders like ASHAs and ANMs have to work with PRI officials. Their cooperation is in
workings of policy developments and implementation of these policies and then to see how
far these stakeholders are able to make the convergence among institutions, infrastructures
and practices. The observation with the field experience reveals that some of the ASHAs we
interviewed are not satisfied working with the PRI members as they are not really
cooperative. As per their knowledge, the Panchayat members are corrupted and are not
regular and honest in using the untied fund. Some of the BPMs who have been interviewed
are also said that PRI members and the officials from department are not so much
cooperative. PRI have to lead the Mission in three ways- planning, control and monitoring
health institutions and funds. But, the people in general are not aware of the involvement of
the PRI members in the implementation of NRHM. The patients from Sualkuchi PHCs are
not aware of Village Health and Sanitation Committee and Village Health and Nutrition Day.
This is also seen during the field visit to Silchar Medical College where very few people
know about Village Health and Sanitation Committee and Rogi Kalyan Samiti.
9. Conclusion:
Though the PRIs in Assam in particular and in India as a general have a large potentiality in
improving the health indicators in reality and create awareness among people about the health
schemes and other necessary concerns. But there are some constraints to the workings of the
PRIs like lack of accountability, domination of political party, absence of regular periodic

April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1075
elections etc. Along with that, PRIs are not in Sixth Scheduled areas like BTAD. Absence of
PRIs in these areas has resulted adversely in popularizing healthcare facilities in Assam.
April, 2014 www.ijirs.com Vol3 Issue 4
International Journal of Innovative Research and Studies Page 1076
References:
1. Basu, D. D. (2011). Introduction to the Constitution of India. New Delhi: LexisNexis
Butterworths Wadhwa Nagpur.
2. Bhattacharya (Mukhopadhyay), M. (2011). Democratic Decentralisation and
Panchayati Raj. In N. Chandhoke, & P. Priyadarshi, Contemporary India: Economy,
Society, Politics (pp. 344-357). New Delhi: Pearson.
3. (2010). Development Goals, States of India Report. Ministry of Statistics and
Programme.
4. Misra, S. N. (2013). Democracy, Development and Decentralisation: Rural
Development Through Institutional Intervention. Odisha Review, 126.
5. Sarmah, P., Gogoi, C. F., & Bora, P. (2011). Brief Understanding of Indian
Constitution. In P. Bora, & C. F. Gogoi, An Introduction To Indian Government and
Politics (pp. 1-18). Guwahati: K.M. Publishing.
6. Sekher, T. V. (2003). Sensitising Grass Roots Leadership on Health Issues:
Experiences of a Pilot TV Project. Economic and Political Weekly, 4873.
7. 5th Common Review Mission, 8th-15th November 2011, Assam; National Rural
Health Mission, Ministry of Health and Family Welfare, Government of India.