one-stage bilateral open reduction through a medial approach in developmental dysplasia of the hip
TRANSCRIPT

VOL. 91-B, No. 1, JANUARY 2009 113
One-stage bilateral open reduction through a medial approach in developmental dysplasia of the hip
M. M. Zamzam, K. I. Khoshhal, A. A. Abak, K. A. Bakarman, A. M. M. AlSiddiky, K. O. AlZain, M. K. Kremli
From King Khalid University Hospital, Riyadh, Saudi Arabia
M. M. Zamzam, MD, MSc, Associate Professor, Consultant Orthopaedic Surgeon
A. A. Abak, Arab Board Orthopaedic Specialization (ABOS), Consultant Orthopaedic Surgeon
K. A. Bakarman, ABOS, Assistant Professor, Consultant Orthopaedic Surgeon
A. M. M. AlSiddiky, Saudi Specialisation Certificate in Orthopaedics (SSC)-Ortho, Assistant Professor, Consultant Orthopaedic Surgeon
K. O. AlZain, SSC-Ortho, Consultant Orthopaedic Surgeon
M. K. Kremli, FRCS(Glas), Professor, Consultant Orthopaedic SurgeonDepartment of OrthopaedicsCollege of Medicine and King Khalid University Hospital, P. O. Box 7805, Riyadh 11472, Saudi Arabia.
K. I. Khosshal, FRCS(Ed), Assistant Professor, Consultant Orthopaedic SurgeonKing Fahad Medical City, Surgical Department, PO Box 59046, Riyadh 11525, Saudi Arabia.
Correspondence should be sent to Professor M. M. Zamzam; e-mail: [email protected]
©2009 British Editorial Society of Bone and Joint Surgerydoi:10.1302/0301-620X.91B1.21429 $2.00
J Bone Joint Surg [Br] 2009;91-B:113-18.Received 19 June 2008; Accepted 25 September 2008
The outcome of one-stage bilateral open reduction through a medial approach for the treatment of developmental dysplasia of the hip in children under 18 months was studied in 23 children, 18 girls and five boys. Their mean age at operation was 10.1 months (6 to 17) and the mean follow-up was 5.4 years (3 to 8).
Acceptable clinical and radiological results were achieved in 44 (95.7%) and 43 (93.5%) of 46 hips, respectively. Excellent results were significantly evident in patients younger than 12 months, those who did not require acetabuloplasty, those whose ossific nucleus had appeared, and in those who did not develop avascular necrosis.
One-stage bilateral medial open reduction avoids the need for separate procedures on the hips and has the advantages of accelerated management and shorter immobilisation and rehabilitation than staged operations.
Most dislocations of the hip in childrenunder 18 months of age with developmentaldysplasia of the hip (DDH) can be success-fully treated by harness, splintage or closedreduction and a spica cast. However, somehips which are irreducible or unstablerequire open reduction. The aim of any pro-cedure is to achieve a comfortable reductionand a low rate of avascular necrosis(AVN).1,2 The choice of operative approachfor open reduction is between the traditionalanterior iliofemoral route and the recentlyrevived medial approach. Each offers advan-tages and disadvantages. Supporters of themedial approach describe it as simple andsafe, with minimal soft-tissue dissection andblood loss. The scar is cosmetically accept-able, and, both hips can be operated on at thesame occasion.3-5
Ludloff first described the medial approachto the congenitally dislocated hip in 1913,6 andmodifications of his technique were describedby Ferguson in 19737 and by Weinstein andPonseti in 1979.5,8,9 The various medialapproaches are criticised for the associated riskof AVN due to accidental injury of the medialcircumflex artery, but the relationship betweenthis injury and AVN is uncertain.4,10,11 Thelower age limit for a medial approach is sixmonths, and initially, the upper age limit wastwo years. However, this was reduced to18 months as it was felt that an anteriorapproach would be more suitable for older
patients so as to deal with superior obstaclesand allow the possibility of acetabuloplasty.3,8
The feasibility of one-stage bilateral openreduction through a medial approach in thetreatment of DDH has been mentioned in mostprevious series,2,4,5,11,12 but no study thereofhas so far been reported. We have reviewed ourexperience with this technique.
Patients and MethodsBetween 1999 and 2004, 23 patients (18 girls,five boys) with bilateral DDH were treated byone-stage open reduction of both hips througha medial approach. Children with neuro-muscular or teratological dislocation, previousAVN or who had undergone a two-stagebilateral open reduction were excluded. Themedial approach was used in patients under18 months of age who had failed treatmentwith a Pavlik harness (Fillauer LLC, Chatta-nooga, Tennessee) or a closed reduction. Pre-liminary traction was not used in any case.
All patients had bilateral arthrographyunder general anaesthesia prior to surgery todefine the obstacles to reduction and toattempt closed reduction for patients who pre-sented after the age of six months who had noprevious treatment. Both hips were cleanedand draped. The details of the operation havebeen described previously,9 but some operativesteps deserve mention. The adductor longuswas divided routinely at its origin. Attempts topreserve the branch of the medial femoral

114 M. M. ZAMZAM, K. I. KHOSHHAL, A. A. ABAK, K. A. BAKARMAN, A. M. M. ALSIDDIKY, K. O. ALZAIN, M. K. KREMLI
THE JOURNAL OF BONE AND JOINT SURGERY
circumflex artery crossing the anteromedial capsule of thehip joint failed frequently (32 hips), and the artery was thencoagulated following its accidental injury. The ligamentumteres was totally excised and the transverse acetabular liga-ment incised routinely. The acetabular limbus was not dis-turbed, regardless of its type.
The femoral head was then reduced gently into the trueacetabulum and its position checked by image intensifier(Fig. 1). The capsule was left open and the adductor fascia,subcutaneous tissues and skin closed without drainage. Thesame procedure was repeated on the other side. Keepingboth hips reduced, a bilateral spica cast was applied withthe hips flexed to 90° and abducted to 40°. A radiograph inthe operating theatre confirmed reduction. All patientswere discharged on the first or second post-operative day.The cast was removed six to eight weeks later under generalanaesthesia and the stability was tested. Once this was con-firmed, a bilateral cylinder cast with an abduction bar, abroomstick cast, was applied for nine to 12 weeks, fol-lowed by an abduction splint at night. The children wereallowed unrestricted activities after removal of the cast, andformal physiotherapy was not needed.
The children were followed up every three months forone year, every six months for two years, and then annually.At each follow-up a radiograph of the pelvis was taken, inthe standing position for those walking, to assess acetabu-lar development by measuring the acetabular index (AI),the concentricity of the reduction and for signs of AVN.Acetabular development was considered satisfactory whenthe AI was below 24°.13 Acetabuloplasty was indicated forchildren over 18 months of age if there was lateralisation ofthe femoral head with disruption of Shenton’s line on thestanding anteroposterior view.
AVN of the femoral head was graded according to theclassification of Kalamchi and MacEwen.14 At the most
recent follow-up, all hips were evaluated clinically and radio-logically. The appearance of the scar, the presence of painand tenderness, the range of movement, any limb-length dis-crepancy and the Trendelenburg sign were evaluated.15 Clin-ical assessment was according to Berkeley et al16 excellent, apainless stable hip without a limp or positive Trendelenburgsign, with more than 15° of internal rotation and otherwisenormal motion; good, a painless stable hip with a slight limpor decreased motion and a negative Trendelenburg sign; fair,a positive Trendelenburg sign, minimum pain and moderatestiffness; and poor, significant pain. Severin’s criteria15 wereused to assess the radiological outcome. Acceptable resultswere those in Severin groups I and II and the unacceptableresults were in groups III, IV, V or VI.12
Statistical analysis of the data was by SPSS version 12(SPSS Inc., Chicago, Illinois). For crude analysis of indepen-dent groups of data the chi-squared and Fisher’s exact testwere used with p < 0.05 considered significant andp < 0.001 highly significant.
ResultsDetails of the patients are shown in Table I. Their mean age atdiagnosis was 6.2 months (1 day to 14 months) and the meanage at operation was 10.1 months (6 to 17). A total of 16patients (69.6%) were under 12 months of age at operationand seven (30.4%) were older. The mean age at final follow-up was 6.6 years (4 to 10). The mean duration of follow-upwas 5.4 years (3 to 8). A Pavlik harness had been used in tenchildren (43.5%), closed reduction followed by hip spica ineight (34.8%), and five (21.7%) had no previous treatment.In this group, the trial of closed reduction that was performedimmediately before open reduction had failed.
The ossific nucleus was present on the pre-operativeradiograph in 29 hips (63%) and absent in 17 (37%). Theoperations were performed by a senior paediatric
Fig. 1b
a) Bilateral arthrogram prior to surgery showing severe hour-glass constriction preventing closed reduction, and b) the reduction is checked by animage intensifier.
Fig. 1a
ONE-STAGE BILATERAL OPEN REDUCTION THROUGH A MEDIAL APPROACH IN DEVELOPMENTAL DYSPLASIA OF THE HIP 115
VOL. 91-B, No. 1, JANUARY 2009
orthopaedic surgeon in 17 patients (73.9%) and by asupervised specialist in six (26.1%). The mean blood losswas 34 ml (20 to 40) and blood transfusion was notneeded. The mean operating time, including applicationof the cast, for all patients was 137 minutes (112 to 185).It was 130 minutes (112 to 160) for senior surgeons and156 minutes (132 to 185) for supervised specialists. Themean period of post-operative immobilisation in a hipspica was 7.4 weeks (SD 0.7) and 10.5 weeks (SD 0.9) in abroomstick cast. Acetabuloplasty or a Salter osteotomyfor residual acetabular dysplasia was performed in 15 hips(32.6%). The mean age at acetabuloplasty was 40 months(35 to 48), the frequency of which was significantlyhigher in those who had absent ossific nuclei at openreduction (p = 0.028) and highly significant in those aged12 months or older at open reduction (p < 0.001).
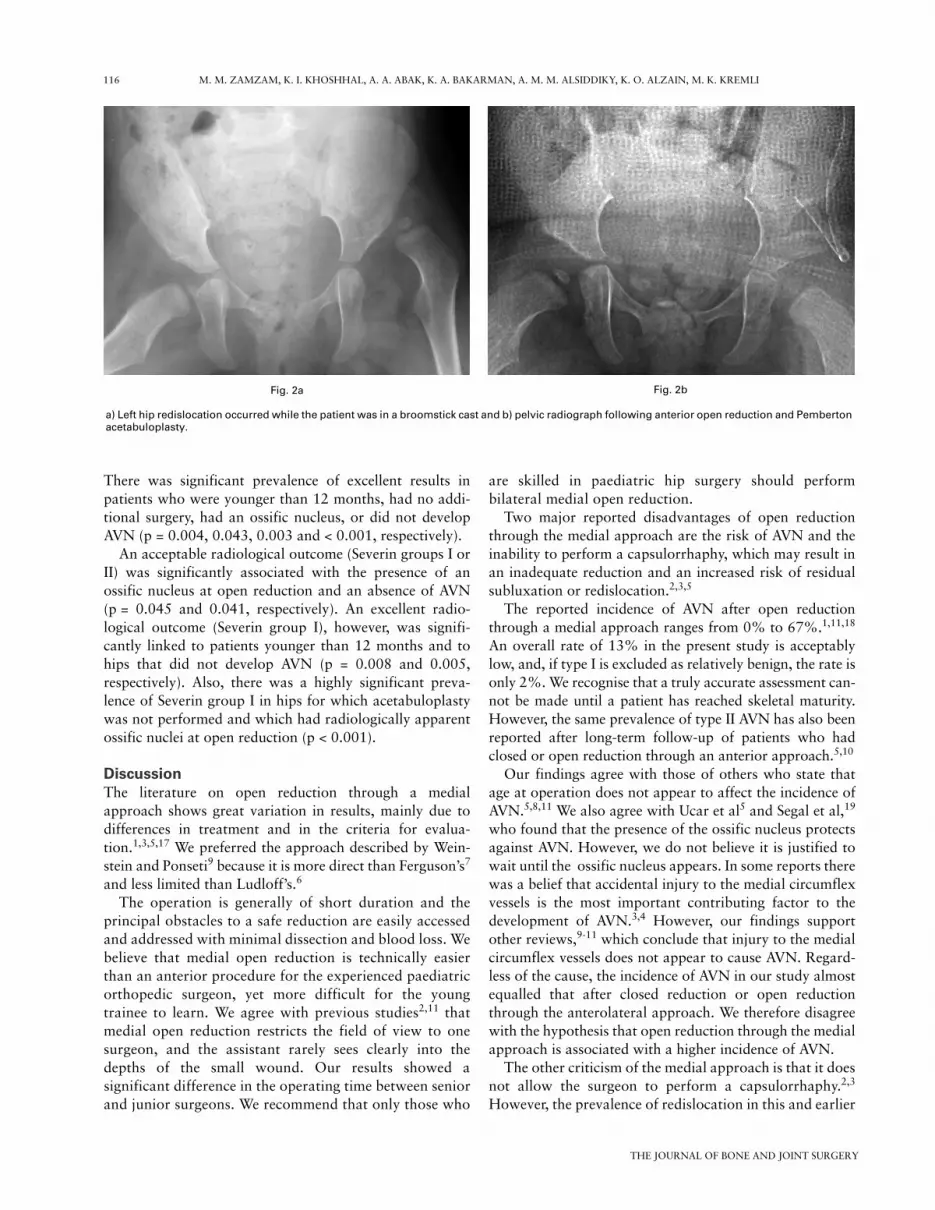
Bilateral superficial wound infections in one patientwere treated by wound care and antibiotics. This patientdeveloped grade I AVN in the right hip. Another patientredislocated the left hip while in the broomstick cast and
was treated by open reduction through the anteriorapproach (Fig. 2). Although her final assessment showedexcellent clinical and radiological results bilaterally, weconsidered her left hip to be fair clinically, with a positiveTrendelenburg test before the second open reduction, andSeverin type VI radiologically. Six hips (13%) in fivepatients developed AVN. Five were grade I and one wasgrade IV. Active treatment for AVN was needed in twopatients (Table I). Gender, age at open reduction,previous treatment, the need for additional surgery andthe experience of the surgeon did not significantlyaffect the development of AVN (p = 0.208, 0.097, 0.61,0.351 and 0.083, respectively), but an absent ossificnucleus at the time of open reduction had a significantassociation (p = 0.02).
At final follow-up the scar was almost invisible in allpatients. The clinical and radiological assessments areshown in Table I. Absence of AVN was the only factor tohave a significant relationship (p = 0.014) with an accept-able clinical outcome with an excellent and good result.
Table I. Patient data
Case Number Gender Primary treatment
Age at operation (mths) Complications Additional operation AVN*
Clinicalassessment†
Radiological assessment‡
1 F Closed reduction and hip spica
10 E, E I, I
2 F Pavlik harness 8 Valgus femoralosteotomy§
Right (IV) F, G III, II
3 F None 12 Left Pemberton G, E II, I 4 F Closed reduction and
hip spica15 Bilateral Salter G, G II, II
5 M None 13 Left Dega E, E I, II 6 F Closed reduction and
hip spica11 Left (I) E, G I, II
7 F Closed reduction and hip spica
16 Bilaterate Pemberton E, G I, I
8 F Pavlik harness 8 Left redislocation Left anterior open reduction + left Pemberton
Bilateral (I) E, F I, VI
9 M None 7 E, E I, I10 M Pavlik harness 6 E, E I, I11 F None 17 Bilateral Salter G, G III, II12 F Pavlik harness 7 E, E I, I13 F Closed reduction and
hip spica11 E, E I, I
14 F Pavlik harness 7 Infection Right (I) G, E II, I15 F Pavlik harness 7 E, E I, I16 F Closed reduction and
hip spica14 Bilateral Pemberton G, E II, II
17 F Closed reduction and hip spica
9 Right Pemberton E, E II, I
18 M Pavlik harness 8 E, G I, I19 F None 11 Left Salter§ Left (I) E, G I, II20 F Pavlik harness 6 E, E I, I21 M Closed reduction and
hip spica14 Bilateral Pemberton G, G II, II
22 F Pavlik harness 10 Right Pemberton E, E II, I23 F Pavlik harness 6 E E I, I
* AVN, avascular necrosis of the femoral head† according to Berkeley et al;16 E, excellent; F, fair; G, good‡ according to Severin15
§ Additional surgery needed for treating AVN
116 M. M. ZAMZAM, K. I. KHOSHHAL, A. A. ABAK, K. A. BAKARMAN, A. M. M. ALSIDDIKY, K. O. ALZAIN, M. K. KREMLI
THE JOURNAL OF BONE AND JOINT SURGERY
There was significant prevalence of excellent results inpatients who were younger than 12 months, had no addi-tional surgery, had an ossific nucleus, or did not developAVN (p = 0.004, 0.043, 0.003 and < 0.001, respectively).
An acceptable radiological outcome (Severin groups I orII) was significantly associated with the presence of anossific nucleus at open reduction and an absence of AVN(p = 0.045 and 0.041, respectively). An excellent radio-logical outcome (Severin group I), however, was signifi-cantly linked to patients younger than 12 months and tohips that did not develop AVN (p = 0.008 and 0.005,respectively). Also, there was a highly significant preva-lence of Severin group I in hips for which acetabuloplastywas not performed and which had radiologically apparentossific nuclei at open reduction (p < 0.001).
DiscussionThe literature on open reduction through a medialapproach shows great variation in results, mainly due todifferences in treatment and in the criteria for evalua-tion.1,3,5,17 We preferred the approach described by Wein-stein and Ponseti9 because it is more direct than Ferguson’s7
and less limited than Ludloff’s.6
The operation is generally of short duration and theprincipal obstacles to a safe reduction are easily accessedand addressed with minimal dissection and blood loss. Webelieve that medial open reduction is technically easierthan an anterior procedure for the experienced paediatricorthopedic surgeon, yet more difficult for the youngtrainee to learn. We agree with previous studies2,11 thatmedial open reduction restricts the field of view to onesurgeon, and the assistant rarely sees clearly into thedepths of the small wound. Our results showed asignificant difference in the operating time between seniorand junior surgeons. We recommend that only those who
are skilled in paediatric hip surgery should performbilateral medial open reduction.
Two major reported disadvantages of open reductionthrough the medial approach are the risk of AVN and theinability to perform a capsulorrhaphy, which may result inan inadequate reduction and an increased risk of residualsubluxation or redislocation.2,3,5
The reported incidence of AVN after open reductionthrough a medial approach ranges from 0% to 67%.1,11,18
An overall rate of 13% in the present study is acceptablylow, and, if type I is excluded as relatively benign, the rate isonly 2%. We recognise that a truly accurate assessment can-not be made until a patient has reached skeletal maturity.However, the same prevalence of type II AVN has also beenreported after long-term follow-up of patients who hadclosed or open reduction through an anterior approach.5,10
Our findings agree with those of others who state thatage at operation does not appear to affect the incidence ofAVN.5,8,11 We also agree with Ucar et al5 and Segal et al,19
who found that the presence of the ossific nucleus protectsagainst AVN. However, we do not believe it is justified towait until the ossific nucleus appears. In some reports therewas a belief that accidental injury to the medial circumflexvessels is the most important contributing factor to thedevelopment of AVN.3,4 However, our findings supportother reviews,9-11 which conclude that injury to the medialcircumflex vessels does not appear to cause AVN. Regard-less of the cause, the incidence of AVN in our study almostequalled that after closed reduction or open reductionthrough the anterolateral approach. We therefore disagreewith the hypothesis that open reduction through the medialapproach is associated with a higher incidence of AVN.
The other criticism of the medial approach is that it doesnot allow the surgeon to perform a capsulorrhaphy.2,3
However, the prevalence of redislocation in this and earlier
Fig. 2b
a) Left hip redislocation occurred while the patient was in a broomstick cast and b) pelvic radiograph following anterior open reduction and Pembertonacetabuloplasty.
Fig. 2a

ONE-STAGE BILATERAL OPEN REDUCTION THROUGH A MEDIAL APPROACH IN DEVELOPMENTAL DYSPLASIA OF THE HIP 117
VOL. 91-B, No. 1, JANUARY 2009
studies9,17 compares favourably with other series studyingthe anterior approach.4 Although lateralisation of the fem-oral head was sometimes noticed after splintage was dis-continued, this did not seem to be a problem, as the hipswere stable at the first change of the cast. Furthermore, webelieve that such lateralisation is usually benign andrequires only a longer period of immobilisation to ensure aconcentric reduction and to stimulate acetabular develop-ment (Fig. 3). This situation is different in older childrenwith high dislocations because the medial approach cannotdeal with obstructions in the superior acetabulum, whichare usually present in ambulant children.8,10
We undertook additional pelvic surgery for residualacetabular dysplasia in 15 hips (32.6%). This figure isacceptable when compared with previous studies.4,5,13
Although pelvic osteotomy was indicated to protect areduced hip from subluxation or redislocation, the needfor acetabuloplasty is not related specifically to the medialapproach because the reduced hip is prone to residual dys-plasia after closed reduction or open reduction through theanterior approach. The need for acetabuloplasty in thisstudy is highly significant in children older than12 months. Therefore, as concurrent pelvic surgery cannotbe achieved through a medial approach, we do not per-form medial open reduction in children over 12 months ofage with severe acetabular dysplasia (acetabular index> 40 and/or acetabular cartilaginous angle > 24°).20 Wefeel that as such children are destined to have residualacetabular dysplasia, a combined open reduction and pel-vic osteotomy through the anterior approach is preferable.This could be carried out in patients approaching18 months of age or delayed for a few months in thoseaged 12 to 16 months.
The combined excellent and good outcomes in previousseries that advocated open reduction through the medialapproach ranged between 73% and 98%.5,10,11 Conversely,Koizumi et al12 found acceptable results in only 45.7%, andsuggested that open reduction through a medial approach isunsatisfactory in DDH. In our study, an acceptable clinical
outcome was obtained in 95.7% of hips, of which 65.2%had excellent results. An acceptable radiological outcomewas seen in 93.5% of the hips, of which 60.9% had excel-lent results. Our results are almost equal to those from pre-vious studies5,8,9,11 supporting medial open reduction,although they were mainly unilateral cases.
Open reduction using the approach described by Wein-stein and Ponseti9 is a safe and effective treatment for dis-locations in infants between 6 and 12 months of age withDDH. It requires minimum soft-tissue dissection, the iliacapophysis and abductor muscles are not disturbed, bloodloss is minimal and the scar is cosmetically acceptable. One-stage bilateral open reduction through a medial approachhas all the advantages of operating on one hip together witha shorter time for treatment and cast immobilisation,thereby accelerating rehabilitation and reducing disruptionto the family. We recommend that the bilateral operation bedone by a surgeon experienced in paediatric hip surgery.
No benefits in any form have been received or will be received from a commer-cial party related directly or indirectly to the subject of this article.
References1. Kalamchi A, Schmidt TL, MacEwen GD. Congenital dislocation of the hip: open
reduction by the medial approach. Clin Orthop 1982;169:127-32.
2. Konigsberg DE, Karol LA, Colby S, O’Brien S. Results of medial open reduction ofthe hip in infants with developmental dislocation of the hip. J Pediatr Orthop2003;23:1-9.
3. Baki C, Sener M, Aydin H, Yildiz M, Saruhan S. Single-stage open reductionthrough a medial approach and innominate osteotomy in developmental dysplasia ofthe hip. J Bone Joint Surg [Br] 2005;87-B:380-3.
4. Mankey MG, Arntz GT, Staheli LT. Open reduction through a medial approach forcongenital dislocation of the hip: a critical review of the Ludloff approach in sixty-sixhips. J Bone Joint Surg [Am] 1993;75-A:1334-45.
5. Ucar DH, Isiklar ZU, Stanitski CL, Kandemir U, Tumer Y. Open reduction througha medial approach in developmental dislocation of the hip: a follow-up study to skel-etal maturity. J Pediatr Orthop 2004;24:493-500.
6. Ludloff K. The open reduction of the congenital hip dislocation by an anterior inci-sion. Am J Orthop Surg 1913;10:438-54.
7. Ferguson AB Jr. Primary open reduction of congenital dislocation of the hip using amedian adductor approach. J Bone Joint Surg [Am] 1973;55-A:671-89.
8. Kiely N, Younis U, Day JB, Meadows TM. The ferguson medial approach for openreduction of developmental dysplasia of the hip: a clinical and radiological review of49 hips. J Bone Joint Surg [Br] 2004;86-B:430-3.
Fig. 3b
a) Radiograph after bilateral medial open reduction showing bilateral residual acetabular dysplasia and slight lateralisation of the right femoral headand b) the lateralisation has disappeared and the acetabular dysplasia has improved two years later.
Fig. 3a

118 M. M. ZAMZAM, K. I. KHOSHHAL, A. A. ABAK, K. A. BAKARMAN, A. M. M. ALSIDDIKY, K. O. ALZAIN, M. K. KREMLI
THE JOURNAL OF BONE AND JOINT SURGERY
9. Weinstein SL, Ponseti IV. Congenital dislocation of the hip. J Bone Joint Surg [Am]1979;61-A:119-24.
10. Morcuende JA, Meyer MD, Dolan LA, Weinstein SL. Long-term outcome afteropen reduction through an anteromedial approach for congenital dislocation of thehip. J Bone Joint Surg [Am] 1997;79-A:810-17.
11. Tumer Y, Ward WT, Grudziak J. Medial open reduction in the treatment of devel-opmental dislocation of the hip. J Pediatr Orthop 1997;17:176-80.
12. Koizumi W, Moriya H, Tsuchiya K, et al. Ludloff’s medial approach for open reduc-tion of congenital dislocation of the hip: a 20-year follow-up. J Bone Joint Surg [Br]1996;78-B:924-9.
13. Lindstrom JR, Ponseti IV, Wenger DR. Acetabular development after reduction incongenital dislocation of the hip. J Bone Joint Surg [Am] 1979;61-A:112-18.
14. Kalamchi A, MacEwen GD. Avascular necrosis following treatment of congenital dis-location of the hip. J Bone Joint Surg [Am] 1980;62-A:876-88.
15. Severin E. Congenital dislocation of the hip: development of the joint after closed reduc-tion. J Bone Joint Surg [Am] 1950;32-A:507-18.
16. Berkeley ME, Dickson JH, Cain TE, Donovan MM. Surgical therapy for congenitaldislocation of the hip in patients who are twelve to thirty-six months old. J Bone Joint Surg[Am] 1984;66-A:412-20.
17. O’Hara JN, Bernard AA, Dwyer NS. Early results of medial approach open reduction incongenital dislocation of the hip: use before walking age. J Pediatr Orthop 1988;8:288-94.
18. Arac S, Bozhurt M, Kiter E, Günal I. Medial approach without opening the joint capsulefor developmental dislocation of the hip. J Orthop Sci 2003;8:522-5.
19. Segal LS, Boal DK, Borthwick L, et al. Avascular necrosis after treatment of DDH: theprotective influence of the ossific nucleus. J Pediatr Orthop 1999;19:177-84.
20. Zamzam MM, Kremli MK, Khoshhal KI, et al. Acetabular cartilaginous angle: a newmethod for predicting acetabular development in DDH in children between 2 to 18 monthsof age. J Pediatr Orthop 2008;28:518-23.