bilateral diffuse iris nodular nevi
TRANSCRIPT
Bilateral Diffuse Iris Nodular Nevi Clinical and Histopathologic Characterization
Benjamin H. Ticho, MD,I-2 Mordechai Rosner, MD,2 Marilyn B. Mets, MD/ Mark 0. M. Tso, MD2
Background: Diffuse nodular nevus of the iris is an uncommon condition that presents with multiple verrucous excrescences distributed diffusely on the iris surface.
Methods: The authors describe 30 patients with bilateral diffuse iris nodular nevi and report associations with bilateral congenital cataract, neurofibromatosis, oculodermal melanocytosis, congenital ptosis, morning glory anomaly, Axenfeld anomaly, or Peters anomaly.
Results: Iris nodules were uniform in size and distribution and were brown, as was the surrounding iris. Light and electron microscopy of iridectomy specimens from one patient showed elevated plaques composed of aggregates of plump, lightly pigmented nevoid cells interwoven with mature, densely pigmented spindle-shaped uveal melanocytes.
Conclusions: The authors report the largest clinical series and first ultrastructural description of bilateral diffuse iris nodular nevi, which represents a variant of neural crest development. No ocular complications could be attributed to the iris nodules, which should be differentiated from Lisch nodules and other pathologic iris lesions. Ophthalmology 1995;102:419-425
In 1912, both Coats' and Collins2 introduced the term iris melanosis to describe an uncommon condition char-
Originally received: October 14, 1993. Revision accepted: October 5, 1994. 1Department of Ophthalmology, The Children's Memorial Hospital, Chicago. 2 Ophthalmic Pathology Laboratory, Department of Ophthalmology and V1sual Sciences, University of Illinois at Chicago Eye and Ear Infirmary, Chicago. Presented in part as a poster at the American Academy of Ophthalmology Annual Meeting, Dallas, November 1992. Supported in part by core grant EY01792 from the National Eye Institute, Bethesda, Maryland: a grant from the Lions of Illinois Foundation, Hillside. Illinois: and an unrestricted research grant from Research to Prevent Blindness. Inc, New York, New York. Dr. Mark 0 . M. Tso is a Research to Prevent Blindness Senior Scientific Investigator. Reprint requests to Mark 0. M. Tso, MD, Department of Ophthalmology & Visual Sciences, University of Illinois at Chicago, UIC Eye Center. 1855 W. Taylor St. Rm L217, Chicago, IL 60612.
acterized by multiple verrucous excrescences distributed diffusely on the iris surface. Early reports'-4 described unilateral cases, often associated with hyperpigmentation of the uvea (ocular melanosis). In 1987, Traboulsi and Maumenee5 described a patient with bilateral nodules distributed diffusely in brown irides without associated conjunctival, episcleral, or choroidal hyperpigmentation. They called this condition bilateral iris melanosis. Joondeph and Goldberg6 described eight members of two Hispanic pedigrees with bilateral diffuse iris nodules. They argued that the term melanosis was inappropriate, because they did not observe abnormal iris or other uveal hyperpigmentation. Other terms used in the literature to describe this entity include dotted Swiss iris6 and iris mamilla/ions. 7·8 It has been suggested that the iris excrescences might be irregular thickening of the anterior iris surface tissue4 or aggregates of uveal melanocytes, as seen in ocular melanosis.6 Detailed histopathologic study of this condition has not been reported previously.
419
Ophthalmology Volume 102, Number 3, March 1995
We describe 30 patients with bilateral diffuse iris nodules associated with bilateral congenital cataracts, neurofibromatosis, oculodermal melanocytosis, congenital ptosis, morning glory anomaly, Axenfeld anomaly, or Peters anomaly. We also present light and electron microscopic findings of bilateral iridectomy specimens from one patient. Based on our clinical and pathologic observations, we propose the term diffuse iris nodular nevi to describe this entity.
Materials and Methods
In September 1991, a patient with bilateral cataracts and iris nodules (case 1) presented to the Ophthalmology Clinic at The Children's Memorial Hospital, Chicago. In the 18-month period after this initial presentation, we examined 29 additional patients with similar bilateral iris nodules, including five families with 15 affected members (Table 1 ). This series consists of 25 Hispanic patients, 3 African-American patients (cases 25, 26, and 30), and two Asian patients (cases 12 and 29). Affected children underwent a complete eye examination, including visual acuity determination, refraction, external examination, motility evaluation, slit-lamp examination, and dilated funduscopy. Available adult family members underwent slit-lamp examination.
Selected Case Reports
Case 1. A 4-year-old Hispanic girl presented after failing a school vision test. She had no other pertinent medical or ocular history. Best-corrected visual acuity (with -8.00 +2.00 X 90 correction) was 20/100 in both eyes. Nystagmus was not present. Results of slit-lamp examination showed numerous nodular, discrete excrescences distributed diffusely and symmetrically throughout both irides. These nodules were brown, as was the surrounding iris tissue. They were most prominent in the midperiphery but extended to the pupillary border (Fig I). Bilateral anterior and posterior subcapsular cataracts were noted. Results of dilated fundus examination were unremarkable, and there was no abnormal cutaneous, scleral, or choroidal pigmentation.
Peripheral iridectomy specimens were obtained at the time of bilateral uncomplicated lensectomy-anterior vitrectomy. Fragments from both iridectomy specimens were fixed in formalin, embedded in paraffin, stained with hematoxylin-eosin, and bleached with I% potassium permanganate. A portion of each iridectomy specimen was fixed in I% glutaraldehyde and 4% paraformaldehyde and processed for electron microscopic examination.
Postoperatively, the patient's best-corrected visual acuity was 20/30 in both eyes. Six family members underwent slit-lamp examination (Fig 2). The propositus' brother, mother, maternal aunt, and niece had variably prominent bilateral iris nodules.
Case 2. A 2-year-old Hispanic girl (case 7) had slate-gray periocular skin on the left side and scleral pigmentation characteristic of oculodermal melanocytosis since birth. There was
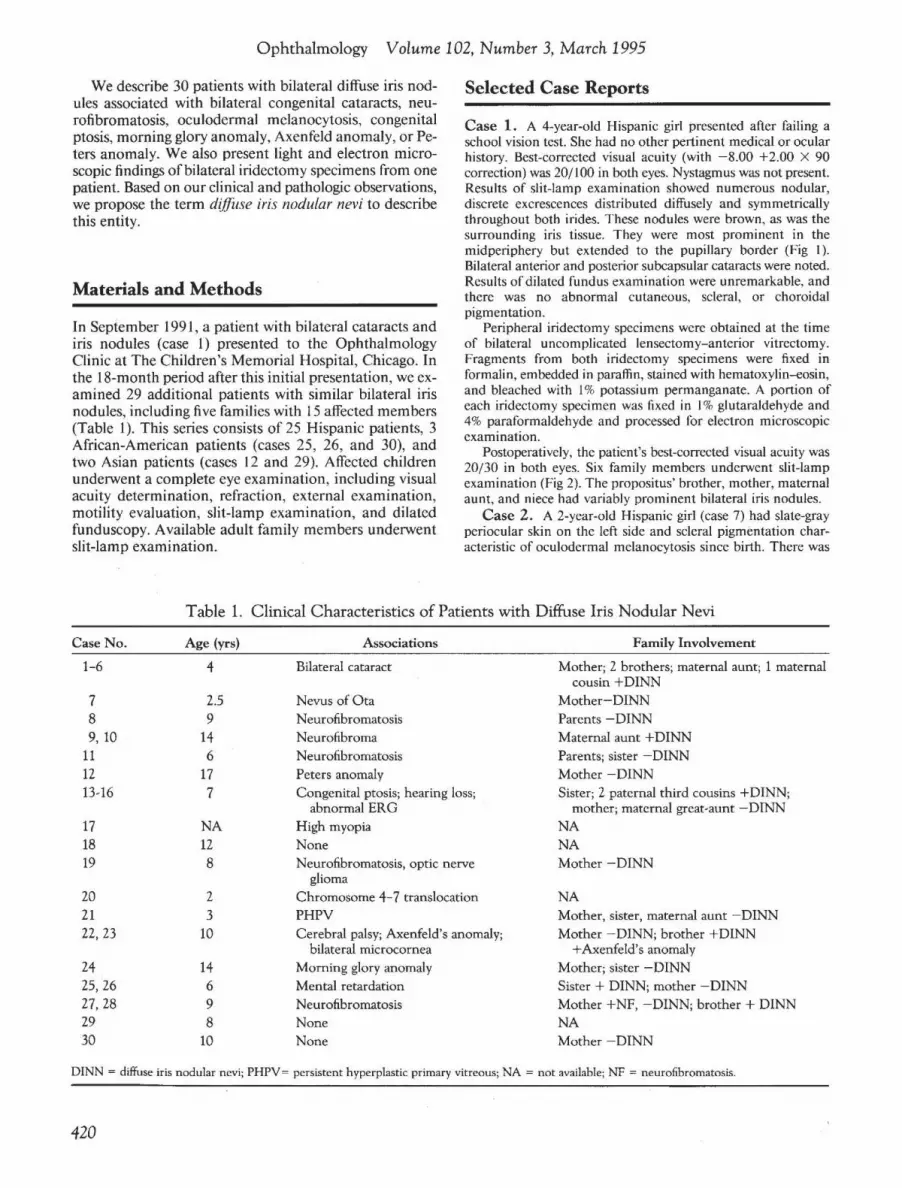
Table 1. Clinical Characteristics of Patients with Diffuse Iris Nodular Nevi
Case No.
1-6
7 8 9, 10
11 12 13-16
17 18 19
20 21 22, 23
24 25, 26 27, 28 29 30
Age (yrs)
4
2.5 9
14 6
17 7
NA 12 8
2 3
10
14 6 9 8
10
Associations
Bilateral cataract
Nevus ofOta Neurofibromatosis Neurofibroma Neurofibromatosis Peters anomaly Congenital ptosis; hearing loss;
abnormal ERG High myopia None Neurofibromatosis, optic nerve
glioma Chromosome 4-7 translocation PHPV Cerebral palsy; Axenfeld's anomaly;
bilateral microcornea Morning glory anomaly Mental retardation Neurofibromatosis None None
Family Involvement
Mother; 2 brothers; maternal aunt; 1 maternal cousin +DINN
Mother-DINN Parents -DINN Maternal aunt +DINN Parents; sister -DINN Mother -DINN Sister; 2 paternal third cousins +DINN;
mother; maternal great-aunt -DINN NA NA Mother - DINN
NA Mother, sister, maternal aunt -DINN Mother -DINN; brother +DINN
+Axenfeld's anomaly Mother; sister -DINN Sister + DINN; mother -DINN Mother +NF, -DINN; brother+ DINN NA Mother -DINN
DINN = diffuse iris nodular nevi; PHPV= persistent hyperplastic primary vitreous; NA =not available; NF =neurofibromatosis.
420
Ticho et al · Diffuse Nodular Nevi
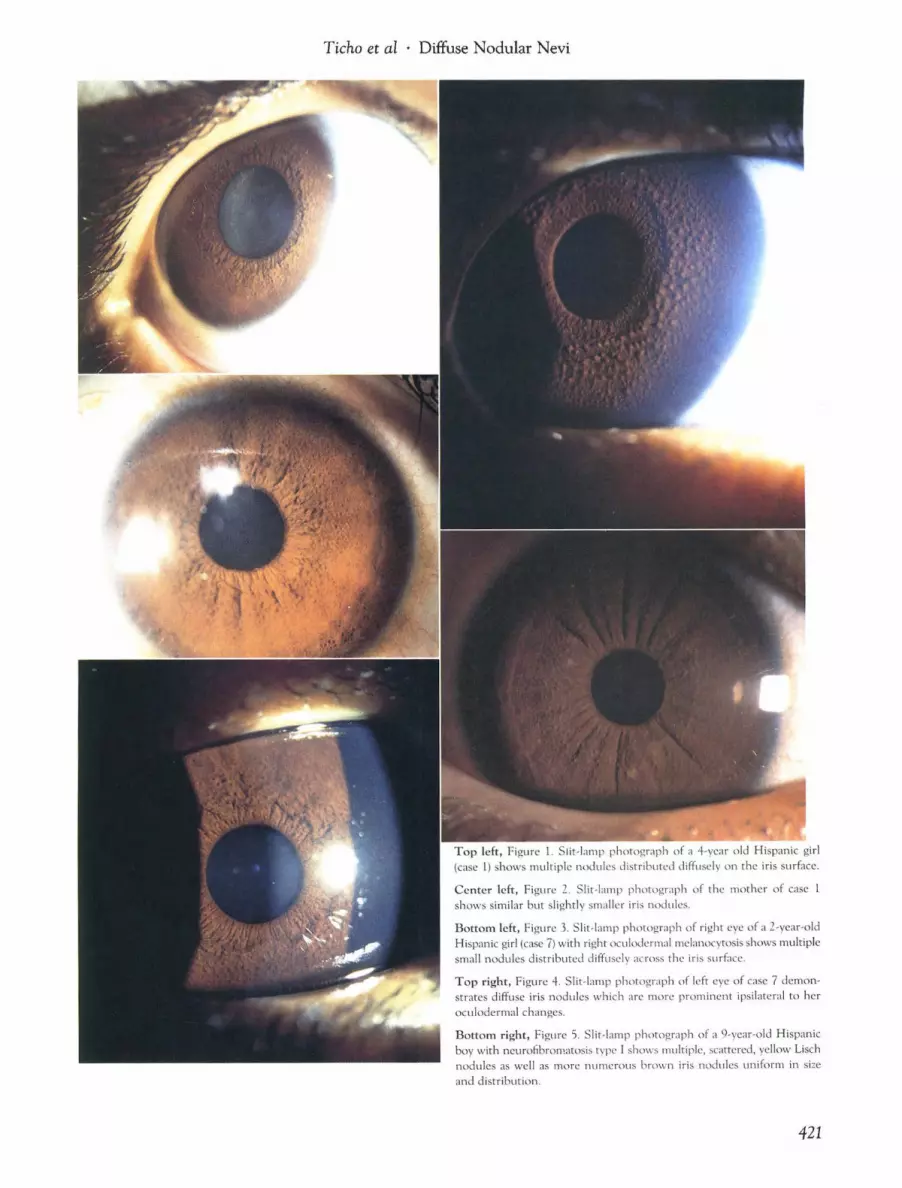
Top left, Figure 1. Slit-lamp photograph of a 4-year old Hispanic girl (case 1) shows multiple nodules distributed diffusely on the iris surface.
Center left, Figure 2. Slit-lamp photograph of the mother of case 1 shows similar but slightly smaller iris nodules.
Bottom left, Figure 3. Slit-lamp photograph of right eye of a 2-year-old Hispanic girl (case 7) with right oculodermal melanocytosis shows multiple small nodules distributed diffusely across the iris surface.
Top right, Figure 4. Slit-lamp photograph of left eye of case 7 demonstrates diffuse iris nodules which are more prominent ipsilateral to her oculodermal changes.
Bottom right, Figure 5. Slit· lamp photograph of a 9-year-old Hispanic boy with neurofibromatosis type I shows multiple, scattered, yellow Lisch nodules as well as more numerous brown iris nodules uniform in size and distribution.
421

Ophthalmology Volume 102, Number 3, March 1995
no other pertinent medical, ocular, or family history. Fixation was central, steady, and maintained in both eyes. Multiple nodular excrescences were noted in both irides and were especially prominent in the midperipheral iris. The nodules were more numerous and slightly larger on the left iris (Figs 3 and 4). Slight iris heterochromia was noted. Results of dilated fundus examination showed no melanosis oculi or choroidal nevi in either eye. Results of slit-lamp examination of her mother disclosed no iris nodules.
Case 3. A 9-year-old Hispanic boy (case 8) had received a diagnosis of neurofibromatosis type I at 2 years of age due to multiple cafe-au-lait spots noted since birth, with axillary and inguinal freckling. Results of neurologic examination were unremarkable, but a magnetic resonance imaging scan showed a glioma of the right optic nerve without intracranial extension. Visual acuity was 20/25 in the right eye and 20/30 in the left. Pupils reacted equally to light and without afferent defect. Color vision testing was unremarkable in both eyes. Results of slitlamp examination showed multiple fleshy Lisch nodules and more numerous discrete nodules diffusely distributed in both irides (Fig 5). These brown iris nodules matched the color of the surrounding iris tissue and easily were distinguished from the yellow Lisch nodules. Results ofdilated fundus examination showed no choroidal nevi and normal-appearing optic nerve heads. Goldmann applanation tonometry yielded pressures of 14 mmHg in both eyes. Cycloplegic refraction showed 2.50 diopters of hyperopia in both eyes.
Results
All affected patients had bilateral discrete nodules distributed diffusely on the iris surface. The nodules were relatively uniform in size and distribution, extending from the iris root to the pupillary border; in some patients, they were more prominent in the midperipheral portion of the iris. In all patients, the nodules were uniformly brown, as was the surrounding iris. Two patients had asymmetric diffuse iris nodular nevi, with more prominent nodules in the eye with unilateral oculodermal melanocytosis (case 7) and morning glory anomaly (case 24). Pupillary reaction was normal in all patients with diffuse iris nodular nevi. In the affected pedigrees, we noted some variability in size of the iris nodules among family members. Only subtle differences in nodule size, distribution, and number were seen with increasing age. There was no known consanguinity in affected pedigrees. An autosomal dominant pattern was evident in two affected pedigrees. Conditions associated with the nevi in this series included neurofibromatosis ( 4 patients), isolated neurofibroma (I patient), oculodermal melanocytosis (I patient), bilateral congenital cataracts (I patient), congenital ptosis with decreased hearing and subnormal scotopic and photopic electroretinographic responses ( 1 patient), morning glory anomaly ( 1 patient), Axenfeld anomaly with bilateral microcornea ( 1 patient), Peters anomaly ( 1 patient), high myopia ( 1 patient), persistent hyperplastic primary vitreous (I patient), and q 4 to 7 chromosomal translocation ( 1 patient).
Histopathologic Findings The biopsy specimens consisted of portions of heavily pigmented iris tissue. Pigmented uveal melanocytes lined
the anterior surface of the iris, occasionally aggregating in plaques (Figs 6a and 6c). These uveal melanocytes had spindle-shaped nuclei and rare nucleoli (Fig 6d), intermingled with plumper nevoid melanocytes with oval nuclei (Fig 6d). As seen on electron microscopy, the spindleshaped cells were heavily loaded with mature melanin granules and contained few cytoplasmic organelles. Some of the plump cells had an infolded nuclear membrane (Fig 6e), relatively more abundant cytoplasm, fewer melanin granules, scattered mitochondria, and bundles ofcytoplasmic filaments. Melanosomes in both the spindleshaped and plump melanocytes varied in size from 0.1 to 0.6 ~min the long axis. Most of the melanosomes were mature and heavily melanized. Occasional melanin granules had rodlike structures and were not fully melanized (Fig 6f). Rarely, larger spheroidal pigment granules (approximately I ~m in diameter) were seen within phagosomes in the iris stroma (Figs 6g and 6h). However, no typical giant melanosomes were found in the sections examined.
Deep in the iris stroma, the melanocytes were mostly spindle-shaped and were arranged around the iris capillaries (Fig 6b). Morphologically, these melanocytes were comparable to the spindle-shaped uveal melanocytes found in the surface plaques. No nesting of the pigmented cells was seen within the iris stroma. No musculature or iris pigment epithelium and only occasional macrophages were seen in the sections examined.
Discussion
The 30 patients with bilateral diffuse iris nodular nevi could be categorized into two groups: familial and sporadic (occasionally asymmetric) associated with other disorders. Familial diffuse iris nodular nevi showed an autosomal dominant pattern of inheritance in two pedigrees. Family members with diffuse iris nodular nevi usually did not have associated ocular abnormalities. Disorders associated with nonfamilial diffuse iris nodular nevi included such putative neurocristopathies9 as neurofibromatosis, oculodermal melanocytosis, Peters anomaly, and Axenfeld anomaly. Histologically, the iris nodules in the iridectomy specimens (case I) were characterized by hyperpigmented, elevated plaques composed ofaggregates ofspindle-shaped uveal melanocytes, and plump nevoid cells.
The differential diagnosis of multiple iris nodules includes both benign and malignant disorders (Table 2). In particular, this condition should be distinguished from generalized ocular melanosis with or without associated dermatologic hyperpigmentation, iris nevus with surface plaque, Lisch nodules in neurofibromatosis type I, and Cogan-Reese (iris nevus) syndrome.
Traboulsi and Maumenee5 argued that iris melanosis may be a limited form of melanosis oculi. Diffuse iris nodular nevi may be differentiated from generalized ocular melanosis by its bilaterality, the nodules' diffuse distribution, and the absence of increased pigmentation of the iris, ciliary body, choroid, sclera, conjunctiva, or optic disc.4•10 Results of histopathologic examination
422
Ticho et al Diffuse Nodular Nevi
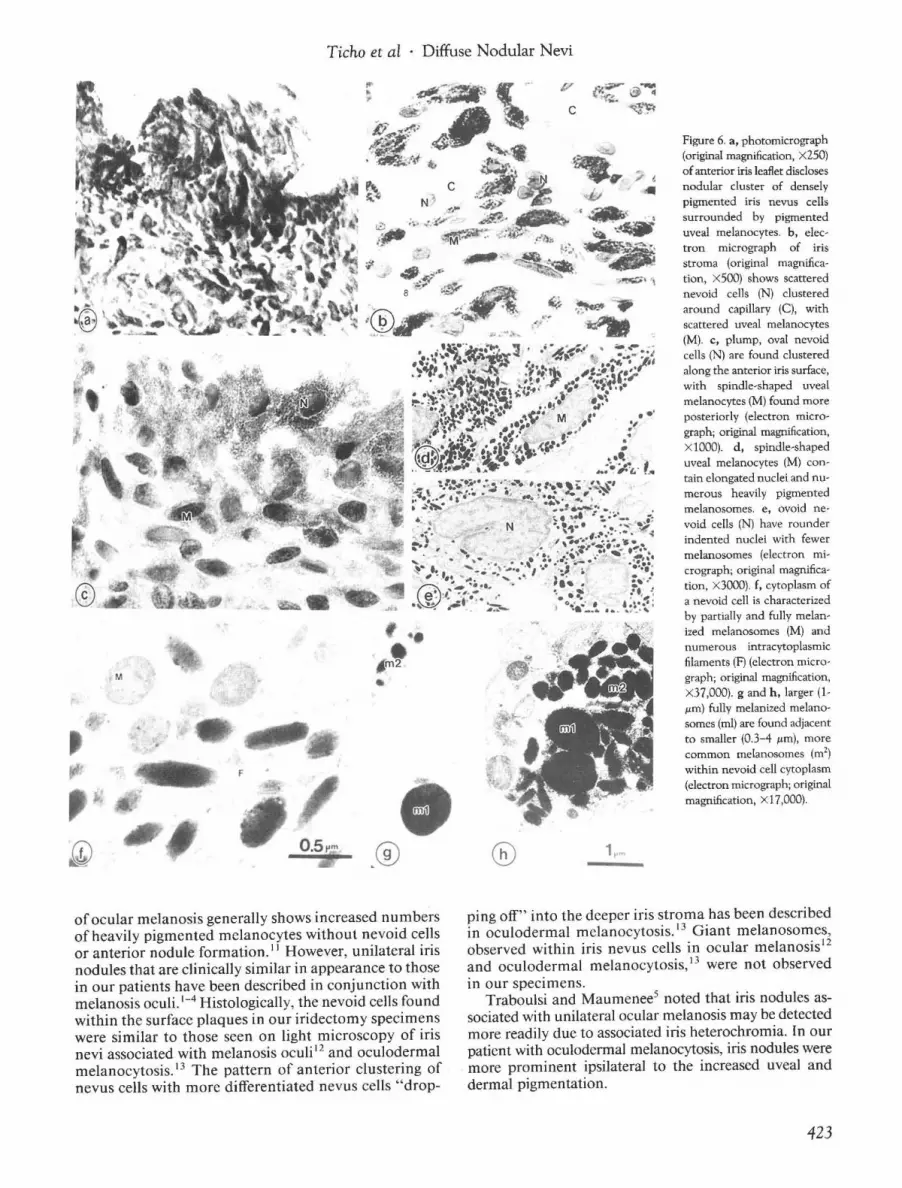
Figure 6. a, photomicrograph (original magnification, x 250) ofanterior iris leaflet discloses nodular cluster of densely pigmented iris nevus cells surrounded by pigmented uveal melanocytes. b, electron micrograph of iris stroma (original magnification, X500) shows scattered nevoid cells (N) clustered around capillary (C), with scattered uveal melanocytes (M). c, plump, oval nevoid celJs (N) are found clustered along the anterior iris surface, with spindle-shaped uveal melanocytes (M) found more posteriorly (electron micrograph; original magnification, XlOOO). d, spindle-shaped uveal melanocytes (M) contain elongated nuclei and numerous heavily pigmented me!anosomes. e, ovoid nevoid celJs (N) have rounder indented nuclei with fewer melanosomes (electron micrograph; original magnification, X3000). f, cytoplasm of a nevoid cell is characterized by partially and fuJly melanized melanosomes (M) and numerous intracytoplasmic filaments (F) (electron micrograph; original magnification, X37,000). g and h, larger (1!Lm) fully melanized melanosomes (ml) are found adjacent to smaller (0.3-4 !Lm), more common melanosomes (m2)
within nevoid celJ cytoplasm (electron micrograph; original magnification, Xl7,000).
ping off" into the deeper iris stroma has been describedofocular melanosis generally shows increased numbers of heavily pigmented melanocytes without nevoid cells in oculodermal melanocytosis. 13 Giant melanosomes, or anterior nodule formation . 11 However, unilateral iris observed within iris nevus cells in ocular melanosis 12
nodules that are clinically similar in appearance to those and oculodermal melanocytosis, 13 were not observed in our patients have been described in conjunction with in our specimens. melanosis oculi. 1-
4 Histologically, the nevoid cells found Traboulsi and Maumenee5 noted that iris nodules aswithin the surface plaques in our iridectomy specimens sociated with unilateral ocular melanosis may be detected were similar to those seen on light microscopy of iris more readily due to associated iris heterochromia. In our nevi associated with melanosis oculi 12 and oculodermal patient with oculodermal melanocytosis, iris nodules were melanocytosis. 13 The pattern of anterior clustering of more prominent ·ipsilateral to the increased uveal and nevus cells with more differentiated nevus cells "drop- dermal pigmentation.
423

Ophthalmology Volume 102, Number3, March 1995
Table 2. Differential Diagnosis of Multiple Iris Nodules
Nevus 1. Diffuse iris nodular nevi
Familial; bilateral Isolated; bilateral/unilateral Associated with ocular abnormalities (ptosis, congenital cataract, morning glory anomaly) Associated with other neurocristopathies (neurofibromatosis, oculodermal melanocytosis, Axenfelds anomaly, Peters anomaly)
2. Melanosis oculi3-s/occulodermal melanocytosis5•6
•14
3. Spindle A nevus13
Intrastromal spindle cell nevus Spindle cell nevus with surface plaque Balloon cell nevus30
4. Epithelioid cell nevus of iris31 •32
5. Familial aggressive nevi of iris in childhood33
6. Neurofibromatosis Lisch nodules16- 20
7. Brushfield spots
Melanoma 1. Malignant melanoma of iris13
Spindle cell melanoma Epithelioid cell melanoma Mixed spindle/epithelioid cell melanoma
2. Tapioca melanoma34
Inflammatory Nodules 1. Granulomas
Sarcoidosis (Bussaca, Koeppe nodules) Tuberculosis (tuberculoma) Syphilis (gumma) Lepromatous leprosy (leprotic pearls)
2. Nodular iritis
Developmental Anomalies 1. lridocorneal endothelial syndromes35•36
Cogan-Reese iris nevus syndrome21 - 27
Essential iris atrophy37
2. Anterior segment dysgenesis Axenfeld-Rieger anomaly, syndrome Peters anomaly
3. Floccculus of the iris
(Adapted from Shields MB, et al. Arch Ophrhalmol 1976;94:406-10. Copyright © 1976, American Medical Association.)
Diffuse iris nodular nevi differs from typical iris nevi by the nodules' excrescent configuration, diffuse distribution, and absence of excess pigmentation compared with the surrounding iris. While most iris nevi consist of stromal nests of nevoid cells, surface plaques14 occasionally are noted.
Iris nevi are presumed to be derived from neural crest cells. 12
· 13 Dryja and Albert 15 reported bilaterally equal iris
nevus pigmentation in a patient with iris heterochromia and unilateral congenital Horner syndrome, suggesting that iris nevoid cells may be embryologically distinct from iris stromal melanocytes. In a previously described patient with diffuse iris nodular nevi, 5 a unilateral black flat iris "freckle" was noted to be different in configuration and color from the iris nodules, which were of similar pigmentation as the surrounding iris tissue. The cells that form the nodules of these nevi are arguably developmentally distinct from those of typical iris freckles and nevi.
Four children (cases 8, II , 19, and 27) with diffuse iris nodular nevi had associated neurofibromatosis type I, including the presence oftypical Lisch nodules. One patient (case 9) with the condition also had an isolated cheek neurofibroma but did not have Lisch nodules and did not meet other diagnostic criteria for neurofibromatosis. The mother ofone patient (case 28) also had neurofibromatosis but did not have diffuse iris nodular nevi. The nodules of diffuse iris nodular nevi match the color of the surrounding brown iris tissue and can be distinguished readily from Lisch nodules, which are typically less pigmented, often yellow or tan, and more variable in size, height, and distribution. Lisch nodules usually have a characteristic fleshy or velvety texture and often have a glassy or translucent appearance. Histologically, iris nodules in both diffuse iris nodular nevi and neurofibromatosis are composed of spindle-shaped melanocytes with slender dendritic processes intermixed with plumper, round cells. 16 However, the iris nodules in neurofibromatosis have been described to be mainly intrastromal, whereas the prominent feature in diffuse iris nodular nevi is anterior superficial aggregates of melanocytes and nevoid cells. Furthermore, the melanocytes of iris nodules in neurofibromatosis 16
may be more metabolically active, with more immature melanosomes, mitochondria, cytoplasmic filaments, and polyribosome clusters, than melanocytes in diffuse iris nodular nevi, which rarely contain immature melanosomes and only a few mitochondria, scattered filaments, and other intracytoplasmic organelles. We believe that previous descriptions of ms hamartomas in neurofibromatosis 16
-20 may not always have distinguished
between the type oflesions we are describing in this report and true Lisch nodules.
On slit-lamp examination, the lesions seen in our patients resemble somewhat those seen in the Cogan-Reese iridocorneal endothelial dysgenesis (iris-nevus) syndrome. The iris nodules in Cogan-Reese syndrome21 are unilateral, however, and histologically quite distinct. 21
-27
In our patients, no ocular complications could be attributed to the iris nodules. Open-angle glaucoma and ocular hypertension have been associated with iris nodules in diffuse iris nodular nevi6 and diffuse iris nevus.27 Applanation tonometry (10 patients), gonioscopy (3 patients), and optic disc evaluation (19 patients) yielded normal findings in our patients.
When iris nevi are associated with diffuse uveal melanosis, as in melanosis oculi and oculodermal melanocytosis, there is potential for malignant transformation . Growth or enlargement has been suggested to indicate malignant transformation of iris nevi. We noted only
424
Ticho et al · Diffuse Nodular Nevi
subtle differences in nodule size, distribution, and number with increasing patient age.
Diffuse iris nodular nevi appear to be more common than previously reported. The autosomal dominant pattern of inheritance suggested a heritable variant of neural crest cell migration in familial cases. The nodules are not intrinsically harmful but should be differentiated from other iris lesions,28- 37 such as ocular melanosis and Lisch nodules. The frequency ofassociated ocular abnormalities in our series probably relates in part to the referral nature of our patient population. Further characterization of a possible association ofdiffuse iris nodular nevi with other neurocristopathies may be forthcoming with further study.
References
I. Coats G. Unilateral diffuse melanosis of the uvea, with small elevations on the surface of the iris. Trans Ophthalmol Soc UK 1912;32:165-71.
2. Collins ET. Unilateral melanosis of the uvea and sclera, with numerous small elevations on the surface of the iris. Trans Ophthalmol Soc UK 1912;32:171-3.
3. Duke-Elder S. Normal and abnormal development. In: Duke-ElderS, ed. System of Ophthalmology. Vol. III, pt. 2: Congenital Deformities. St. Louis: Mosby, 1964;794-8.
4. Friedenwald H, Friedenwald JS. Melanosis of lids, conjunctiva and sclera, with wartlike growths on the iris. Arch Ophthalmol 1925;54:51-4.
5. Traboulsi EI, Maumenee IH. Bilateral melanosis of the iris [letter]. Am J Ophthalmol 1987;103:115-16.
6. Joondeph BC, Goldberg MF. Familial iris melanosis-a misnomer? Br J Ophthalmol 1989;73:289-93.
7. Walton DS. Discussion, 354. Of: Lewis RA, Riccardi VM. von Recklinghausen neurofibromatosis. Incidence of iris hamartomata. Ophthalmology 1981 ;88:348-54.
8. Gilliam AC, Ragge NK, Perez MI, Bolognia JL. Phakomatosis pigmentovascularis type lib with iris mamillations. Arch Dermatol 1993; 129:340-2.
9. Bolande RP. The neurocristopathies. A unifying concept of disease arising in neural crest maldevelopment. Hum Pathol 1974;5:409-29.
10. Zimmerman LE. Melanocytes, melanocytic nevi, and meIanocytomas. Invest Ophthalmol 1965;4: 11-41.
II. Green WR: Uveal tract. In: Spencer WH, ed. Vol III: Ophthalmic Pathology. Philadelphia: WB Saunders, 1986;1375-82.
12. Rennie IG, Bleehen SS. Melanosis oculi. An ultrastructural study of an affected iris. Arch Ophthalmol 1983; 10 I: 19126.
13. Jakobiec FA, Silbert G. Are most iris 'melanomas' really nevi? A clinicopathologic study of 189 lesions. Arch Ophthalmol 1981 ;99:2117-32.
14. Ticho BH, Tso MOM, Kishi S. Diffuse iris nevus in oculodermal melanocytosis: a light and electron microscopic study. J Pediatr Ophthalmol Strabismus 1989;26:244-50.
15. Dryja TP, Albert DM. Lack of adrenergic influence on the pigmentation of iris nevus cells. Arch Ophthalmol 1980;98: 1996.
16. Williamson TH, Garner A, Moore AT. Structure of Lisch nodules in neurofibromatosis type I. Ophthalmic Paediatr Genet 1991;12:11-7.
17. Perry HD, Font RL. Iris nodules in von Recklinghausen's neurofibromatosis. Electron microscopic confirmation of their melanocytic origin. Arch Ophthalmol 1982;100:163540.
18. Grant WM, Walton DS. Distinctive gonioscopic findings in glaucoma due to neurofibromatosis. Arch Ophthalmol 1968;79: 127-34.
19. Lewis RA, Riccardi VM. von Recklinghausen neurofibromatosis. Incidence of iris hamartomata. Ophthalmology 1981 ;88:348-54.
20. Wolter JR, Butler RG. Pigment spots of the iris and ectropion uveae: with glaucoma in neurofibromatosis. Am J Ophthalmol 1963;56:964-73.
21. Cogan DG, Reese AB. A syndrome of iris nodules, ectopic Descemet's membrane, and unilateral glaucoma. Doc Ophthalmol 1969;26:424-33.
22. Radius RL, Herschler J. Histopathology in the iris-nevus (Cogan-Reese) syndrome. Am J Ophthalmol 1980;89:7806.
23. Eagle RC Jr, Font RL, Yanoff M, Fine BS. The iris naevus (Cogan-Reese) syndrome: light and electron microscopic observations. Br J Ophthalmol 1980;64:446-52.
24. Daus W, Volcker HE, Steinbriick M, Rentsch F. Zur Klinik und Histopathologie des Cogan-Reese-Syndroms. Klin Monatsbl Augenheilkd 1990;197: 150-5.
25. Khalil MK, Finlayson MH. Electron microscopy in iris nevus syndrome. Can J Ophthalmol 1980; 15:44-8.
26. Inomata H, Sakai Y, Ishimoto S, Egashira J. Iris nevus (Cogan-Reese) syndrome-clinicopathological correlations [in Japanese]. Nippon Ganka Gakkai Zasshi 1990;94:80-8.
27. Nik NA, Hidayat A, Zimmerman LE, Fine BS. Diffuse iris nevus manifested by unilateral open angle glaucoma. Arch Ophthalmol 1981 ;99: 125-7.
28. Francois J. Heredity in Ophthalmology. St. Louis: CV Mosby, 1961 ;532.
29. Waardenburg PJ, Franceschetti A, Klein D. Genetics and Ophthalmology. Vol. I. Springfield: Charles C. Thomas, 1961;702.
30. Margo CE, Groden L. Balloon cell nevus of the iris [letter]. Am J Ophthalmol 1986;102:282-3.
31. J akobiec FA, Moorman L T, Jones IS. Benign epithelioid cell nevi ofthe iris. Arch Ophthalmol1979;97:917-21.
32. Shields JA, Karan DS, Perry HD, Donoso LA. Epithelioid cell nevus ofthe iris. Arch Ophthalmol 1985;103:235-7.
33. Paridaens D, Lyons CJ, McCartney A, Hungerford JL. Familial aggressive nevi of the iris in childhood. Arch Ophthalmol 1991;109:1552-4.
34. Vittone P, Traverso C, Zingirian M, Bertagno R. Tapioca melanoma of the iris: a contribution to the fine structure and its significance. Ophthalmologica 1983; 186:125-35.
35. Shields MB. Progressive essential iris atrophy, Chandler's syndrome, and the iris nevus (Cogan-Reese) syndrome: a spectrum of disease. Surv Ophthalmol 1979;24:3-20.
36. Sugar HS. The iris nevus and Cogan-Reese syndromes: separate entities? Ann Ophthalmol 1981; 13:405-7.
37. Shields MB, Campbell DG, Simmons RJ, Hutchinson BT. Iris nodules in essential iris atrophy. Arch Ophthalmol 1976;94:406-10.
425