nonuniform changes in mri measurements of the thigh muscles after two hamstring strengthening...
TRANSCRIPT
TITLE
Non-uniform changes in MRI measurements of the thigh muscles following two hamstring strengthening exercises
Authors:
Jurdan Mendiguchia1, Mirian Aranzazu Garrues2, John Barry Cronin3,4, Bret Contreras3, Asier Los Arcos5, Nikos Malliaropoulos6, Nicola Maffulli7, Fernando Idoate8.
1. Zentrum rehab and performance Center.Department of Physical Therapy.Pamplona, Spain.
2. Public University of Navarre, Health Science Department .Graduate School for Health Sciences, Physical Therapy School, Tudela, Spain.
3. Sport Performance Research Institute New Zealand, AUT University, Auckland, New Zealand
4. School of Biomedical and Health Sciences, Edith Cowan University, Joondalup, Australia.
5. Club Atletico Osasuna.Pamplona. Spain.6. National Track & Field Centre, Sports Medicine Clinic of S.E.G.A.S., Thessaloniki,
Greece 7. The London School of Medicine and Dentistry Institute of Health Sciences
Education Centre for Sports and Exercise Medicine Mile End Hospital.8. Radiology Department, Clinica San Miguel, Pamplona, Spain
Corresponding Author:Jurdan Mendiguchia1
Zentrum rehab and performance CenterCalle B Nº 23Department of Physical TherapyPamplona, [email protected] 948229459
Licence for Publication
"The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd and its Licensees to permit this article (if accepted) to be published in BJSM editions and any other BMJPGL products to exploit all subsidiary rights, as set out in our licence(http://group.bmj.com/products/journals/instructions-for-authors/licence-forms/)."
1
123456789
101112131415161718192021222324252627
282930313233343536373839404142434445
1
Competing Interest
“ None to declare."
2
46
48495051
2
Abstract
This study investigated the effects of the eccentric leg curl (LC) and lunge (L) on the
biceps femoris (BF), semitendinosus (ST), semimembranosus (SM), adductor magnus
(AM) and gluteus maximus (GM). Each leg of eleven male professional soccer
players were randomly assigned to an eccentric leg curl (LC) or lunge (L) exercise
protocol (3 sets of 6 repetitions). Functional magnetic resonance imaging (fMRI) of the
subjects’ thighs were performed before and 48 hours after the intervention. Fifteen
axial scans of the thigh interspaced by a distance of 1 / 15 of the length of the right
femur (Lf) were obtained from the level of 1/15 Lf to 15/15 Lf . The fMRI data were
analyzed for signal intensity (SI) changes. While no significant changes were observed
in absolute short tau inversion recovery (STIR) values for the semimembranosus and
gluteus maximus, significant changes for the semitendinosus (~21-45%) from sections 4
to 10, adductor magnus (~2-13%) at section 4, and biceps femoris (~ -3 vs 8%) at
section 7 were noted. These two hamstring exercises did not result in a uniform
response (training stimulus) for the same muscles and regions. The ELC exercise was
better suited for loading all regions of the ST muscle, while the L exercise was more
effective for loading the proximal regions of biceps femoris and adductor magnus.
3
525354
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
3
Introduction
Acute hamstring injuries are the most prevalent muscle injuries reported in sport,
accounting for 6 to 37% of all injuries in Australian Rules football, rugby union,
football, basketball, cricket and track sprinters. [1-8] Appropriate training and
strengthening of the hamstring muscles for many sports is a fundamental focus of
prevention and rehabilitation. Although selective strengthening of the hamstring
muscles has been recommended as a key component in the management of hamstring
injury, [9-13] only limited literature exists to guide clinicians in designing effective
strengthening programs.
The architectures and innervation patterns of the various muscles in the posterior aspect
of the thigh (the biceps femoris muscle long head (BFl), the biceps femoris short head
(BFs), the semimembranosus (SM), and semitendinosus (ST)) differ [14-16], and each
muscle has unique inherent functions. If this were indeed the case, it would be of value
to strength and conditioning coaches as well as clinicians to understand which exercises
preferentially activate different muscle groups, so as programming is guided to better
effect.
Functional magnetic resonance imaging (fMRI) may be a sensitive method for
displaying the physiological changes that occur in muscles activated during exercise, as
it provides detailed anatomical analysis of associated soft tissues, which is lacking in
electromyography (EMG) experiments.[17-22] The short tau inversion recovery (STIR)
sequence is a T2-weighted sequence that suppresses signals from fat and displays
sensitivity in enhancing differences between the water content of tissues. [19-22].
Exercise produces changes in the distribution of water both intra- and inter-cellularly.
The STIR sequence has previously shown to be valuable in the investigation of signal
intensity (SI) changes in muscles after exercise. [19-22]
4
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
4
MRI has also been used to assess muscle damage following intensive exercise. [23,24]
The T2 value increased following eccentric exercise [18,25-30], and was positively
correlated with plasma creatine kinase (CK) activity, reflecting exercise-induced muscle
damage.[18,23,26,31] Furthermore, previous studies have investigated the intermuscle
differences and intramuscle regional differences of the T2 value between proximal and
distal regions of the muscles of interest. [18,29,32] For example, Kubota et al. [18]
reported that although all hamstring muscles and regions displayed a T2 increase
immediately following eccentric knee-flexion exercise (prone leg-curl machine), the
relationship between the changes of the plasma CK activity and the T2 value of the ST
was not statistically significant until the second day following exercise , which may be
indicative of severe localised muscle damage. These findings have interesting
implications in terms of the time course and effects of different exercises on the
hamstrings.
Some exercises are used to prevent hamstring injuries in elite athletes, [9,11-13]
but fMRI to our knowledge, has not been used to date to investigate muscle damage and
intermuscle and intramuscle regional differences in STIR values. This study assessed SI
changes in the upper thigh muscles using fMRI at 48 hours following a lunge and
eccentric leg curl exercises.
5
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
5
Materials and Methods
Subjects
Eleven male professional soccer players participated in this study. Participants were
excluded if they had an injury to their legs or back in the preceding 12 months or if they
were unsuitable for fMRI because of foreign metal bodies, electronic implants or
claustrophobia. Before the start of the investigation, each participant’s height, weight,
age, regular exercise program and any previous injuries to the legs were recorded (see
Table 1). Subjects were instructed to avoid strength training activities
for the lower legs and not to use icing or anti-inflammatory
medication for the week preceding and the week of the experiment.
Our institutional Ethics Committee approved the study and all participants gave
informed consent to participate in the study.
Insert Table 1 about here
GENERAL INITIAL CHARACTERISTICS
n MEAN SDHEIGHT(m) 11 1.80 0.05
WEIGHT(kg) 11 74.6 4.5
AGE(years) 11 22.1 1.8
Table 1: Initial characteristics of subjects.
Procedures
The left and right legs of the subjects were randomly assigned to an eccentric leg curl
(LC) or lunge (L) exercise protocol. The protocol involved 3 sets of 6 repetitions
with at least a two-minute rest between sets. Following the
6
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128129
130
131
132
133
134
6
completion of the exercise protocol for one leg (e.g LC), a two
minutes rest was taken before starting the second exercise (e.g. L) for
the other leg.
Exercise Protocol
For the L exercise, subjects were instructed to step forward a predetermined distance
marked on the floor whilst the trunk remained upright. The length of the step was
standardized for each subject and was equal to the distance from the greater trochanter
to the floor as measured with the subject standing. This normalized distance was chosen
based on pilot testing, in which a comfortable L step length was determined. Subjects
were asked to lower their trunk by flexing their lead and trailing knees simultaneously
to a point where the trail knee was approximately 2 to 3 cm short of contacting the
ground. The lunge was completed when the subjects returned to the starting position.
For the ELC exercise, subjects performed eccentric hamstring curls (Prone Leg Curl
Technogym, Italy) at 120% of their one repetition maximum (1RM). The ELC 1RM
was quantified via a typical incremental load to failure protocol. Once the subject could
not complete two concentric leg curls at the set load this was determined as their 1RM
to which a 20% load, which resulted in the 120% 1RM eccentric load. Subjects were
instructed to lower the weight from a knee-flexed position (100°) to a knee-extended
position (0°) in 3 seconds, maintaining a constant lowering velocity. The subjects kept
their ankle plantar flexed to reduce the contribution of the gastrocnemius muscle.
Subjects were verbally encouraged to exert maximal force at the starting position and to
resist maximally against the knee-extending action throughout the range of motion. The
weight was raised after each eccentric repetition by an examiner, thereby rendering the
exercise an eccentric-only task for the subject.
Imaging Technique
7
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
7
MR imaging was performed using a 1 T whole body imager (Magnetom Impact Expert;
Siemens-Erlangen, Germany), with the subjects supine with their knee extended
immediately before and 48 hours after the exercise. Once the subject was positioned
inside the magnet, the thighs of both legs were kept parallel to the MRI table and the
feet were strapped together to prevent rotation. The length of the right femur (Lf), taken
as the distance from the intercondylar notch of the femur to the superior boundary of the
femoral head, was measured in the coronal plane.
Subsequently, 15 axial scans of the thigh interspaced by a distance of 1 / 15 Lf were
obtained from the level of 1/15 Lf to 15/15 Lf . Every image obtained was labelled at its
location (i.e. slice 4 being closer to the coxofemoral joint and slice 12 closer to the
knee). Great care was taken to reproduce the same individual Lf each time by using the
appropriate anatomical landmarks [33] For the final calculation of the signal intensity
of each muscle, slices 4 / 15 – 12 / 15 were used for all muscles examined; the two
cranial slices (closer to the hip) and the three distal slices (closer to the knee) were
discarded given the presence of image artifacts. Then fast STIR MR axial images
[repetition time (TR) = 5,300 ms, echo time (TE) = 60ms, inversion time (TI) 115 ms,
flip angle (FA): 180] were collected using a 256 x 256 image matrix, with a 350 mm
field of view and 10-mm slice thickness using a body coil.
The MRI data were evaluated for SI of each hamstring muscle (BF, ST and SM),
adductor magnus (AM) and gluteus maximus (GM). The MR images were transferred to
a personal computer in the Digital Imaging and Communications in Medicine (DICOM)
format and analysed using image manipulation and analysis software (OSIRIX,
University Hospital of Geneva, Switzerland). Individual baseline SI readings, analysed
with a standardized radius of interest (ROI), were established with the preliminary scan
for each participant. The ROI was placed in the same position within the muscle for
8
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
8
each measurement, avoiding blood vessels and bone, which may have affected the
analysis of the intensity changes. The SI was measured in a circular region of interest
(ROI, 10-30 mm2) within each muscle assessed before and after exercise and a
percentage difference was calculated. The same technician (FIS) performed the MR
imaging scan and the SI measures.
Statistical Analysis
The STIR absolute values were reported as mean ± SD. Given the differences between
exercises utilized in this study, the principal comparison of interest was the within
exercise pre-post changes in absolute values of STIR of the muscles (BF, SM, ST, AM
and GM) for all the different sections (3, 4, 5, 6, 7, 8, 9, 10,11 and 12). To disentangle
the main effects a two factor (time x section) repeated measures ANOVA with post hoc
contrasts was used to determine significant differences between sections. Paired t-tests
were used to determine significant pre-post exercise changes in L and ELC and for the
relative change between the ELC and L exercises. Statistical significance was set at p <
0.05.
9
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
9
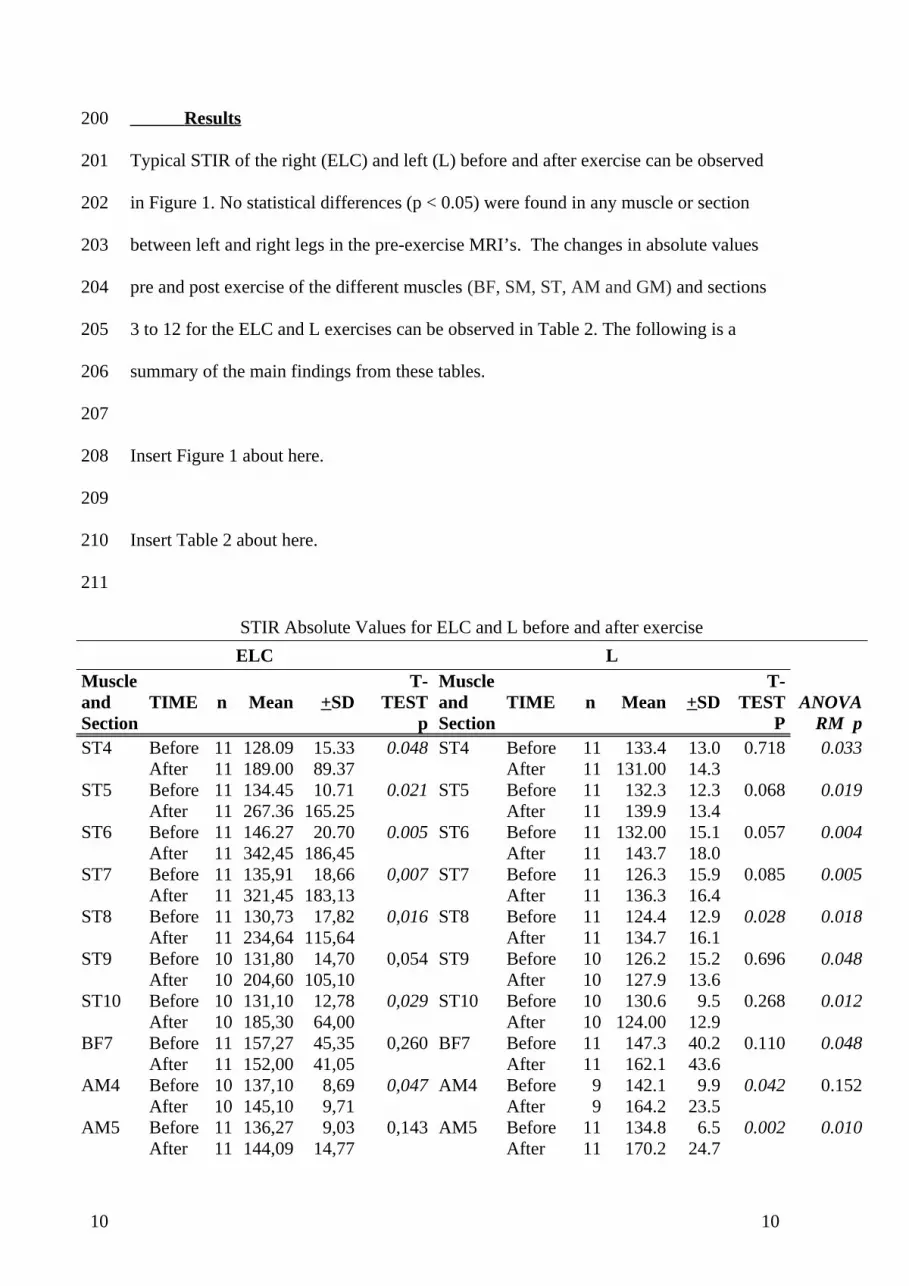
Results
Typical STIR of the right (ELC) and left (L) before and after exercise can be observed
in Figure 1. No statistical differences (p < 0.05) were found in any muscle or section
between left and right legs in the pre-exercise MRI’s. The changes in absolute values
pre and post exercise of the different muscles (BF, SM, ST, AM and GM) and sections
3 to 12 for the ELC and L exercises can be observed in Table 2. The following is a
summary of the main findings from these tables.
Insert Figure 1 about here.
Insert Table 2 about here.
STIR Absolute Values for ELC and L before and after exerciseELC L
ANOVA RM p
Muscle and Section
TIME n Mean +SDT-
TESTp
Muscle and Section
TIME n Mean +SDT-
TEST P
ST4 Before 11 128.09 15.33 0.048 ST4 Before 11 133.4 13.0 0.718 0.033After 11 189.00 89.37 After 11 131.00 14.3
ST5 Before 11 134.45 10.71 0.021 ST5 Before 11 132.3 12.3 0.068 0.019After 11 267.36 165.25 After 11 139.9 13.4
ST6 Before 11 146.27 20.70 0.005 ST6 Before 11 132.00 15.1 0.057 0.004After 11 342,45 186,45 After 11 143.7 18.0
ST7 Before 11 135,91 18,66 0,007 ST7 Before 11 126.3 15.9 0.085 0.005After 11 321,45 183,13 After 11 136.3 16.4
ST8 Before 11 130,73 17,82 0,016 ST8 Before 11 124.4 12.9 0.028 0.018After 11 234,64 115,64 After 11 134.7 16.1
ST9 Before 10 131,80 14,70 0,054 ST9 Before 10 126.2 15.2 0.696 0.048After 10 204,60 105,10 After 10 127.9 13.6
ST10 Before 10 131,10 12,78 0,029 ST10 Before 10 130.6 9.5 0.268 0.012After 10 185,30 64,00 After 10 124.00 12.9
BF7 Before 11 157,27 45,35 0,260 BF7 Before 11 147.3 40.2 0.110 0.048After 11 152,00 41,05 After 11 162.1 43.6
AM4 Before 10 137,10 8,69 0,047 AM4 Before 9 142.1 9.9 0.042 0.152After 10 145,10 9,71 After 9 164.2 23.5
AM5 Before 11 136,27 9,03 0,143 AM5 Before 11 134.8 6.5 0.002 0.010After 11 144,09 14,77 After 11 170.2 24.7
10
200
201
202
203
204
205
206
207
208
209
210
211
10
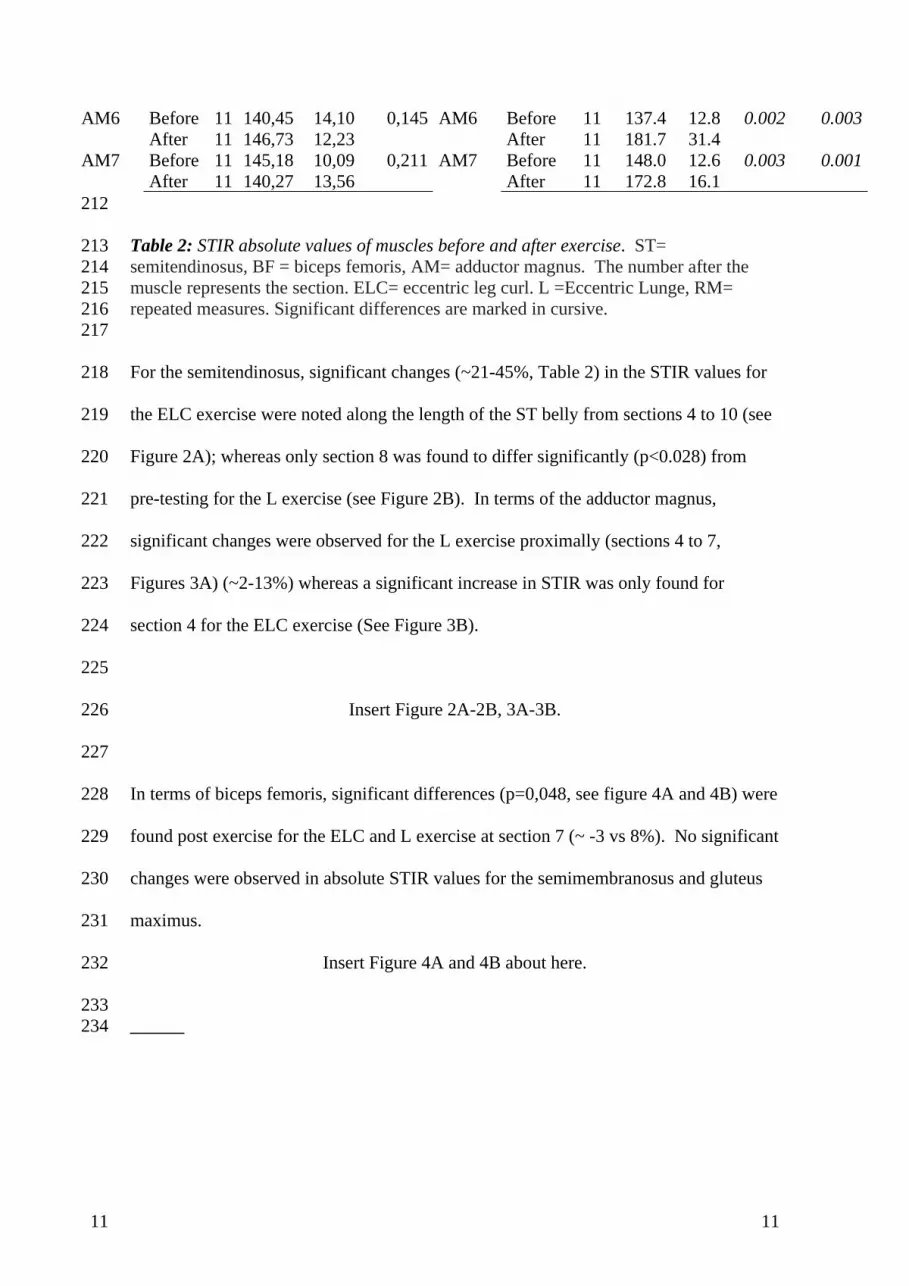
AM6 Before 11 140,45 14,10 0,145 AM6 Before 11 137.4 12.8 0.002 0.003After 11 146,73 12,23 After 11 181.7 31.4
AM7 Before 11 145,18 10,09 0,211 AM7 Before 11 148.0 12.6 0.003 0.001After 11 140,27 13,56 After 11 172.8 16.1
Table 2: STIR absolute values of muscles before and after exercise. ST= semitendinosus, BF = biceps femoris, AM= adductor magnus. The number after the muscle represents the section. ELC= eccentric leg curl. L =Eccentric Lunge, RM= repeated measures. Significant differences are marked in cursive.
For the semitendinosus, significant changes (~21-45%, Table 2) in the STIR values for
the ELC exercise were noted along the length of the ST belly from sections 4 to 10 (see
Figure 2A); whereas only section 8 was found to differ significantly (p<0.028) from
pre-testing for the L exercise (see Figure 2B). In terms of the adductor magnus,
significant changes were observed for the L exercise proximally (sections 4 to 7,
Figures 3A) (~2-13%) whereas a significant increase in STIR was only found for
section 4 for the ELC exercise (See Figure 3B).
Insert Figure 2A-2B, 3A-3B.
In terms of biceps femoris, significant differences (p=0,048, see figure 4A and 4B) were
found post exercise for the ELC and L exercise at section 7 (~ -3 vs 8%). No significant
changes were observed in absolute STIR values for the semimembranosus and gluteus
maximus.
Insert Figure 4A and 4B about here.
11
212
213214215216217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233234
11
Discussion
This study measured whether the hamstring muscles responded in a uniform manner to
two different exercises, as quantified by the absolute changes in the STIR values of
fMRI. It has been assumed previously that during hamstring strengthening exercises,
individual hamstring muscles are activated in a similar manner. However, this is not the
case, as we observed that each hamstring muscle responded differently during the L and
ECL exercises respectively. The mechanics of the exercises used in this investigation
differ in many ways: 1) the ELC is an open kinetic chain exercise with differences in
hip flexion and tibial rotation [34,35] compared to the L which is a closed kinetic chain
exercise;[36,37] 2) the ELC is principally a monoarticular exercise, whereas the L is
biarticular; 3) as a result, the moments around the joints as well as the
length-tension/torque angle relationship of individual muscles will differ; 4) there is no
concentric component in the ELC which is not the case for the L; and, 5) the ELC is
supramaximally loaded at 120% 1RM which is not the case for the L. Given these
differences, it is difficult to ascertain whether a given exercise is ‘superior’ to the other,
and we shall focus on the site specific activation of each exercise and how each exercise
may be used for the conditioning of the hamstring muscle group.
With regards to the ST, it appears that the greatest changes in the MRI measurements
followed the ELC loading, in agreement with previous research. [18,38] The changes
in fMRI measurements of the ST may relate to its architectural characteristics as it has
the longest fascicle length and smallest physiological cross-sectional area (PSCA) of the
hamstring muscles [16], and it is a fusiform muscle compared with more pennate BF
and SM muscles. Muscles containing long fascicles produce forces over large length
ranges and at high shortening speeds, because they have a large number of
simultaneously contracting, serially arranged sarcomeres. [39] Such morphological
12
235236237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
12
properties of ST may be selectively used to perform eccentric knee flexion more
efficiently.
The region-specific activation within the proximal, middle and distal regions of the
same muscle found in this study were in contrast to the Kubota et al. [18] findings,
where significant differences between proximal and distal regions were detected. This
was explained by the fact that the ST is the only hamstring muscle that was
anatomically partitioned as defined by its architecture and innervation [16]. In addition,
this division into partitions was augmented by the presence of a tendinous inscription
with each partition receiving innervation from one muscle nerve, or from a primary
branch of the nerve [16]. The differences between ours and Kubota et al.’s findings [18]
could be attributed to methodological differences, as we divided the thigh into fifteen
regions while they only divided the thigh into three regions. Only in one instance did
one section (Section 8) of the ST show changes after the lunge exercise.
In the AM, significant changes (section 4,~12%; section 5, ~19%; section 6, ~22%; and
section 7, ~14%s) were observed for the L exercise proximally (sections 4 to 7), as
compared to section 4 ( 5%) for the ELC exercise. The greater evidence of
intramuscular changed of the AM during lunges may result from greater hip extension
moments when the hip is flexed. The large hip extension moment arm in addition to
adduction has been noted previously for this muscle. [40,41] The lesser involvement of
the AM during the ELC may be due to a fixed hip angle position (15º) during the
exercise.
No significant changes in fMRI were observed for the BF after ECL loading. In
contrast, significant absolute changes in STIR values were observed at one region
(Section 7) for the BF after L loading. As T2 values are more sensitive to eccentric
exercise [18,25-30] compared to concentric exercise[26] this study may support
13
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
13
previous findings where a very short and rapid period of eccentric hamstring contraction
during the forward lunge has been documented .[36,37] Hamstring length depends on
both knee and hip joint angles since the hamstrings are biarticular muslces. The angle of
the hip has more impact on the length of the biceps femoris than the angle of the knee,
[42,43] given the longer moment arm at the hip, and this relationship increases with
increasing knee angle. Hip flexion-extension exercise resulted in greater BF activation
as measured by MRI compared with a hip fixed exercise .[18,38] Given this
information and based on muscle mechanics and physiology, greater BF damage during
lunges may arise from larger internal hip extension moments when the hip is flexed.
It is difficult to ascertain which variables differ between exercises to produce site
specific activation differences. However, greater proximal activation (section 5, 23%;
section 6, 10%; section 7, 8%; and section 8, 7%) is present after the L exercise ( see
figure 3) while minimal or negative changes after ELC exercise (section 5, 11%; section
6, -3%; section 7, -3%; and section 8, -4%) are evident. It is possible that exercise
intensity accounts for the finding that only one region showed significant changes for
the BF. Exercise-induced changes in fMRI vary according to exercise intensity:
previous studies have reported greater SI changes after maximal loads compared to
lower loads. [19,21,22,44-46] To better define this load effect, more research is needed
investigating whether a loaded lunge produces greater changes across the proximal BF
in comparison to the bodyweight lunge.
This study used fMRI to assess the relative damage to lower leg muscles after two
different exercises. Different exercises can increase hamstring strength, [11,47] but
various hamstring exercises do not result in a uniform response, and therefore training
stimulus, for the same muscles and the same regions of the muscles. Because hamstring
strains affect different hamstring muscles, proper exercise selection is crucial to target
14
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
14

the desired muscle/s. When the goal of a therapeutic intervention is to specifically
strengthen the ST, AM, and/or BF, a progressive resistive training program that
incorporates ELC or L is indicated, as these exercises selectively and effectively
activate the aforementioned muscles. In conclusion, the present study demonstrates that
the ELC exercise is better suited for loading all regions of ST muscle and the L exercise
is more effective for loading the proximal regions of biceps femoris and adductor
magnus.
15
311
312
313
314
315
316
317
15
References
1. Garrett WE Jr.Muscle strain injuries. Am J Sports Med. 1996: 24(6 Suppl): S2-
8. Garrett WE Jr. Am J Sports Med. 1996;24(6 Suppl):S2-8.
2. Woods C, Hawkins RD, Maltby S, et al. The Football Association Medical
Research Programme: an audit of injuries in professional football--analysis of
hamstring injuries. Br J Sports Med. 2004: 38(1): 36-41.
3. Orchard J, Seward H. Epidemiology of injuries in the Australian Football
League, seasons 1997-2000. Br J Sports Med. 2002: 36(1): 39-44.
4. Meeuwisse WH, Sellmer R, Hagel BE. Rates and risks of injury during
intercollegiate basketball. Am J Sports Med. 2003: 31(3): 379-85.
5. Croisier JL. Factors associated with recurrent hamstring injuries. Sports Med.
2004: 34(10): 681-95.
6. Brooks JH, Fuller CW, Kemp SP, et al. Epidemiology of injuries in English
professional rugby union: part 1 match injuries. Br J Sports Med. 2005: 39(10):
757-66.
7. Brooks JH, Fuller CW, Kemp SP, et al. Epidemiology of injuries in English
professional rugby union: part 2 training Injuries. Br J Sports Med. 2005:
39(10): 767-75.
8. Ekstrand J, Hägglund M, Waldén M.Epidemiology of Muscle Injuries in
Professional Football (Soccer). Am J Sports Med. Published online first:
February 18, 2011.
9. Askling C, Karlsson J, Thorstensson A. Hamstring injury occurrence in elite
soccer players after preseason strength training with eccentric overload. Scand J
Med Sci Sports. 2003;13(4):244-50.
16
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
16
10. Croisier JL, Ganteaume S, Binet J, Genty M, Ferret JM .Strength imbalances
and prevention of hamstring injury in professional soccer players: a prospective
study. Am J Sports Med. 2008; 36(8):1469-75.
11. Jönhagen S, Ackermann P, Saartok T.J. Forward lunge: a training study of
eccentric exercises of the lower limbs. Strength Cond Res. 2009;23(3):972-8.
12. Holcomb WR, Rubley MD, Lee HJ, Guadagnoli MA. Effect of hamstring-
emphasized resistance training on hamstring:quadriceps strength ratios. J
Strength Cond Res. 2007; 21(1):41-7.
13. Mjølsnes R, Arnason A, Østhagen T, Raastad T, Bahr R. A 10-week randomized
trial comparing eccentric vs. concentric hamstring strength training in well-
trained soccer players. Scand J Med Sci Sports. 2004 ;14(5):311-7.
14. Friederich JA, Brand RA .Muscle fiber architecture in the human lower limb. J
Biomech. 1990;23(1):91-5.
15. Wickiewicz TL, Roy RR, Powell PL, Edgerton VR. Muscle architecture of the
human lower limb. Clin Orthop Relat Res. 1983 ;(179):275-83.
16. Woodley SJ, Mercer SR. Hamstring muscles: architecture and innervation. Cells
Tissues Organs. 2005;179(3):125-41.
17. Kubota J, Ono T, Araki M, Tawara N, Torii S, Okuwaki T, Fukubayashi T.
Relationship between the MRI and EMG measurements. Int J Sports Med.
2009 ;30(7):533-7.
18. Kubota J, Ono T, Araki M, Torii S, Okuwaki T, Fukubayashi T Non-uniform
changes in magnetic resonance measurements of the semitendinosus muscle
following intensive eccentric exercise. Eur J Appl Physiol. 2007 ;101(6):713-20.
17
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
17
19. Horrigan JM, Shellock FG, Mink JH, Deutsch AL. Magnetic resonance imaging
evaluation of muscle usage associated with three exercises for rotator cuff
rehabilitation. Med Sci Sports Exerc. 1999;31(10):1361-6.
20. Takeda Y, Kashiwaguchi S, Endo K, Matsuura T, Sasa T. The most effective
exercise for strengthening the supraspinatus muscle: evaluation by magnetic
resonance imaging. Am J Sports Med. 2002;30(3):374-81.
21. Green RA, Wilson DJ. A pilot study using magnetic resonance imaging to
determine the pattern of muscle group recruitment by rowers with different
levels of experience. Skeletal Radiol. 2000;29(4):196-203.
22. Baczkowski K, Marks P, Silberstein M, Schneider-Kolsky ME. A new look into
kicking a football: an investigation of muscle activity using MRI. Australas
Radiol. 2006;50(4):324-9.
23. LeBlanc AD, Jaweed M, Evans H. Evaluation of muscle injury using magnetic
resonance imaging. Clin J Sport Med. 1993;3(1):26-30.
24. Chen YW, Hubal MJ, Hoffman EP, Thompson PD, Clarkson PM. Molecular
responses of human muscle to eccentric exercise. J Appl Physiol.
2003 ;95(6):2485-94.
25. Jayaraman RC, Reid RW, Foley JM, Prior BM, Dudley GA, Weingand KW,
Meyer RA. MRI evaluation of topical heat and static stretching as therapeutic
modalities for the treatment of eccentric exercise-induced muscle damage. Eur J
Appl Physiol. 2004;93(1-2):30-8.
26. Larsen RG, Ringgaard S, Overgaard K. Localization and quantification of
muscle damage by magnetic resonance imaging following step exercise in young
women. Scand J Med Sci Sports. 2007;17(1):76-83.
18
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
18
27. Prior BM, Jayaraman RC, Reid RW, Cooper TG, Foley JM, Dudley GA, Meyer
RA. Biarticular and monoarticular muscle activation and injury in human
quadriceps muscle. Eur J Appl Physiol. 2001;85(1-2):185-90.
28. Yanagisawa O, Niitsu M, Takahashi H, Itai Y. Magnetic resonance imaging of
the rotator cuff muscles after baseball pitching. J Sports Med Phys Fitness.
2003 ;43(4):493-9.
29. Segal RL, Song AW. Nonuniform activity of human calf muscles during an
exercise task. Arch Phys Med Rehabil. 2005;86(10):2013-7.
30. Sesto ME, Radwin RG, Block WF, Best TM. Anatomical and mechanical
changes following repetitive eccentric exertions. Clin Biomech (Bristol, Avon).
2005 Jan;20(1):41-9.
31. Schwane JA, Buckley RT, Dipaolo DP, Atkinson MA, Shepherd JR. Plasma
creatine kinase responses of 18- to 30-yr-old African-American men to eccentric
exercise. Med Sci Sports Exerc. 2000;32(2):370-8.
32. Akima H, Takahashi H, Kuno SY, Katsuta S. Coactivation pattern in human
quadriceps during isokinetic knee-extension by muscle functional MRI. Eur J
Appl Physiol. 2004;91(1):7-14.
33. Häkkinen K, Pakarinen A, Kraemer WJ, Häkkinen A, Valkeinen H, Alen M.
Selective muscle hypertrophy, changes in EMG and force, and serum hormones
during strength training in older women. J Appl Physiol. 2001;91(2):569-80.
34. Kwak SD, Ahmad CS, Gardner TR, Grelsamer RP, Henry JH, Blankevoort L,
Ateshian GA, Mow VC. Hamstrings and iliotibial band forces affect knee kinematics
and contact pattern. J Orthop Res. 2000;18(1):101-8.
19
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
19
35. Mesfar W, Shirazi-Adl A. Knee joint biomechanics in open-kinetic-chain flexion
exercises. Clin Biomech (Bristol, Avon). 2008;23(4):477-82.
36. Pincivero DM, Aldworth C, Dickerson T, Petry C, Shultz T. Quadriceps-
hamstring EMG activity during functional, closed kinetic chain exercise to
fatigue Eur J Appl Physiol. 2000;81(6):504-9.
37. Jönhagen S, Halvorsen K, Benoit DL. Muscle activation and length changes during
two lunge exercises: implications for rehabilitation. Scand J Med Sci Sports.
2009;19(4):561-8.
38. Ono T, Okuwaki T, Fukubayashi T. Differences in activation patterns of knee flexor
muscles during concentric and eccentric exercises. Res Sports Med. 2010 ;18(3):188-
98
39. Blazevich AJ. Effects of physical training and detraining, immobilisation, growth and
aging on human fascicle geometry. Sports Med. 2006;36(12):1003-17. Review.
40. Neumann DA. Kinesiology of the hip: a focus on muscular actions. J Orthop Sports
Phys Ther. 2010;40(2):82-94.
41. Ward SR, Winters TM, Blemker SS. The architectural design of the gluteal muscle
group: implications for movement and rehabilitation. J Orthop Sports Phys Ther.
2010;40(2):95-102.
42. Visser JJ, Hoogkamer JE, Bobbert MF, Huijing PA. Length and moment arm of
human leg muscles as a function of knee and hip-joint angles. Eur J Appl Physiol
Occup Physiol. 1990;61(5-6):453-60.
20
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
20
43. Hawkins D, Hull ML. A method for determining lower extremity muscle-tendon
lengths during flexion/extension movements. J Biomech. 1990;23(5):487-94.
44. Shellock F, Fleckenstein J. Muscle physiology and pathophysiology: magnetic
resonance imaging evaluation. Semin Musculoskelet Radiol 2000; 4: 459–79.
45. Fleckenstein JC, Parkey R, Peshock R. Acute effects of exercise on MR imaging of
skeletal muscle in normal volunteers. AJR 1988;15: 231–87.
46. Adams GR, Duvoisin, MR, Dudley GA. Magnetic resonance imaging and
electromyography as indexes of muscle function. J Appl Physiol 1992; 73: 1578-83.
47. Potier TG, Alexander CM, Seynnes OR. Effects of eccentric strength training on
biceps femoris muscle architecture and knee joint range of movement. Eur J Appl
Physiol. 2009 Apr;105(6):939-44
21
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
21