thigh pain in primary total hip replacement: the effects of elastic moduli
TRANSCRIPT
Tpo1w
vM
taI(d
tM
The Journal of Arthroplasty Vol. 19 No. 7 Suppl. 2 2004
Thigh Pain in Primary Total Hip Arthroplasty
The Effects of Elastic Moduli
Carlos Lavernia, MD,* Michele D’Apuzzo, MD,* Victor Hernandez, MD,*and David Lee, PhD†
Abstract: Thigh pain after uncemented total hip arthroplasty (THA) remains acontroversial topic. Our objective was to assess the effect of material composition inthe development of thigh pain after primary THA. A cohort of 241 primary THAs wasfollowed for a minimum of 2 years. All patients received identically shaped taperedcementless femoral components; the first half received a Cr-Co-Mo implant and theother half an identical implant made of Ti-6Al-4V. There were no statisticallysignificant preoperative differences in the 2 component groups except that thepercentage of blacks in the Cr-Co-Mo group was larger than in the Ti-6Al-4V group(26% vs. 14%; P � .05). The overall 1- and 2-year incidence of thigh pain was 9.5%and 8.7%, respectively. Implant composition was unrelated to reported thigh pain 1and 2 years postoperatively. However, patients receiving larger versus smaller stemsirrespective of material composition were more likely to report thigh pain at year 1(relative risk � 4.68; 95% confidence interval � 1.41, 15.50). Thigh pain reported atyear 2 was also higher in patients with larger versus smaller implants; however, thisdifference was not statistically significant (RR � 1.73; 95% CI � 0.68, 4.43). Materialcomposition of this tapered stem design is unrelated to the incidence of thigh pain.Key words: thigh pain, cementless total hip arthroplasty, stem composition.© 2004 Elsevier Inc. All rights reserved.
bcmibstnbaabp
Lim
high pain is a recognized problem after cementlessrimary total hip arthroplasty (THA). The incidencef thigh pain reported in the literature ranges from.9–40.4% [1]. Factors that have been associatedith the occurrence of thigh pain after THA include
From the *Orthopaedic Institute at Mercy Hospital, and the †Uni-ersity of Miami School of Medicine, Department of Epidemiology,iami, FloridaBenefits or funds were received in partial or total support of
he research material described in this article. These benefitsnd/or support were received from Zimmer GmbH, Warsaw,ndiana; the Orthopeadic Research and Education FoundationOREF), Rosemont, Illinois; Arthritis Surgery & Research Foun-ation, Miami, Florida; and Mercy Foundation, Miami, Florida.
Reprint requests: Carlos J. Lavernia, MD, Orthopaedic Insti-ute at Mercy Hospital, 3659 South Miami Avenue, Suite 4008,
iami, Fl 33133.© 2004 Elsevier Inc. All rights reserved.0883-5403/04/1907-2003$30.00/0
mdoi:10.1016/j.arth.2004.06.023
10
one type, larger stem size, uncemented femoralomponents, straight femoral stem design, stematerial composition, femoral component instabil-
ty, and loosening [2–8]. After other causes haveeen ruled out (i.e., infection, stress fracture andpinal problem), the most accepted hypothesis forhigh pain in well-fixed cementless femoral compo-ents is a mismatch in flexural rigidity between theone and the stem [3,9]. The flexural rigidity (EI) ofstem is related to both stem morphometry as wells material composition. Both of these factors haveeen postulated as the primary etiology of thighain.The senior author (CJL) started using the Tri-
ock stem design (DePuy, Warsaw, IN) in 1997;nitially the implant was made of cobalt-chrome-
olybdenum (Cr-Co-Mo). In the year 2000 the
anufacturer introduced a new version of the same
s(TfOeoa
uppts2sCidJp1o
lwmuwptTscwml
mp(a((bdCancV
apldaatpttrewwCtsta
ctwb.TtbtpF(wfW11stP
oCwTgs(d
The Effects of Elastic Moduli • Lavernia et al. 11
tem made out of titanium-aluminum-vanadiumTi-6Al-4V). Our unit started to exclusively usei-6Al-4V implants at that time and we continue toollow patients receiving both types of implants.ur objective in the present study is to assess theffects of material composition in the developmentf thigh pain after primary cementless total hiprthroplasty in a tapered stem series.
Methods
The initial study group consisted of 241 consec-tive patients each of which underwent cementlessrimary total hip replacement using the Tri-Lockrosthesis (DePuy, Warsaw, IN). This design is ariple-tapered, straight, collarless, proximally coatedtem that comes in 11 sizes ranging from 6.3 cm to2.5 cm. All study patients received identicallyhaped components; the first half received a Cr-o-Mo implant and the other half an identical
mplant made of Ti-6Al-4V. All procedures wereone consecutively between November 1997 andune 2001 by the senior author. The average age ofatients was 59.7 years (range, 18–93). There were41 women and 100 men; 114 operated hips weren the left side and 127 on the right side.Perioperative antibiotics were used for prophy-
axis, as was a standard protocol of postoperativearfarin for thromboembolism prophylaxis. Theodified direct lateral approach of Hardinge wassed in all procedures. The femoral componentsere inserted with a press-fit technique, based onreoperative templating and intraoperative subjec-ive determination of axial and rotational stability.he acetabular component was press-fitted, andupplemental fixation screws were used on allases. A gas-plasma-sterilized Polyethylene lineras used in all cases. Full weight-bearing was per-itted among all patients as tolerated the day fol-
owing surgery.Patients were followed prospectively for a mini-um of 2 years. Preoperative assessment was
erformed using a 10-point visual analog scaleVAS) with a pain drawing, the Western Ontariond McMaster University Osteoarthritis IndexWOMAC) [10] and the quality of well being indexQWB) [11]. Preoperative assessment of femoralone quality was made using the Spotorno’s in-ex [12] and the Dorr assessment (type A, B, or) [13]. Postoperative x-rays assessed alignmentnd fit of both the femoral and acetabular compo-ents on an anteroposterior radiograph. Postsurgi-al radiological and clinical information using the
AS and a pain drawing measure was gathered at 1 ind 2 years. For the pain drawing analyses, allatients were asked to shade an area over theocation of their pain on an anterior and posteriorrawing of both lower extremities. They were thensked to rate their lower extremity pain on thenalog scale from none (0) to severe (10). We usedhe definition of Barrack et al. [14] in which thighain was present only if a pain drawing showed thathe shaded area was on the anterior view and belowhe inguinal area. The shaded area over the poste-ior thigh or gluteal region alone was not consid-red thigh pain, nor was pain that radiated all theay to the toes. Chi-square and Student’s t-testere used to compare group differences (SPSS,hicago, IL). A P value � .05 was considered sta-
istically significant. Relative risks (RR) and corre-ponding 95% confidence intervals (CI) were usedo estimate the association between implant char-cteristics and risk of thigh pain.
Results
As can be seen in Table 1, there were no statisti-ally significant presurgical differences among pa-ients receiving Cr-Co-Mo versus Ti-6Al-4V stemsith the exception of the higher percentage oflacks in the Cr-Co-Mo group (26% vs. 14%; P �05). Six patients died and 3 were revised (6 withi-6Al-4V and 3 with Cr-Co-Mo stems), 1 for infec-ion and the other for failure of both componentsefore the 1 year follow-up. One patient with aitanium stem had a periprosthetic fracture. Theseatients were not included in subsequent analyses.ollow-up information was not available for 197.8%) patients (10 who received Cr-Co-Mo and 9ho received Ti-6Al-4V implants). Patients lost to
ollow-up had significantly higher preoperativeOMAC pain scores relative to patients with
-and/or 2-year follow-up information (mean �5.5 vs. 13.1; t � 2.25, P � .05). Baseline QWBcores were also significantly lower in patients losto follow-up (mean � 0.48 vs. 0.52; t � �2.2,� .05).There were also no significant differences in pre-
perative bone quality in patients receiving Cr-o-Mo versus Ti-6Al-4V stems, the majority ofhich were judged to have type A bone (Table 2).he I Moment of Inertia was identical in bothroups (2.75); Spotorno Index scores were alsoimilar in the Cr-Co-Mo and Ti-6Al-4V groups2.95 vs. 2.87). There was no statistically significantifference in the distribution of stem size implanted
n the 2 patient groups.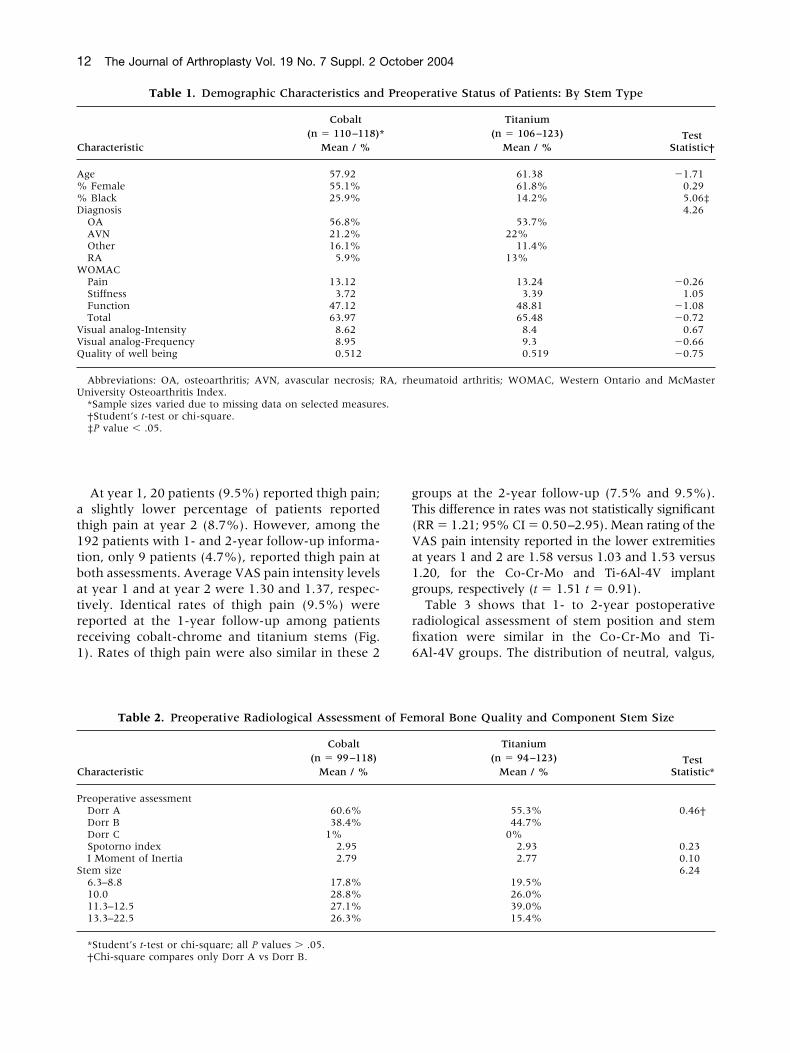
at1tbatrr1
gT(Va1g
rfi6
C
A%%D
W
VVQ
U
C
P
S
12 The Journal of Arthroplasty Vol. 19 No. 7 Suppl. 2 October 2004
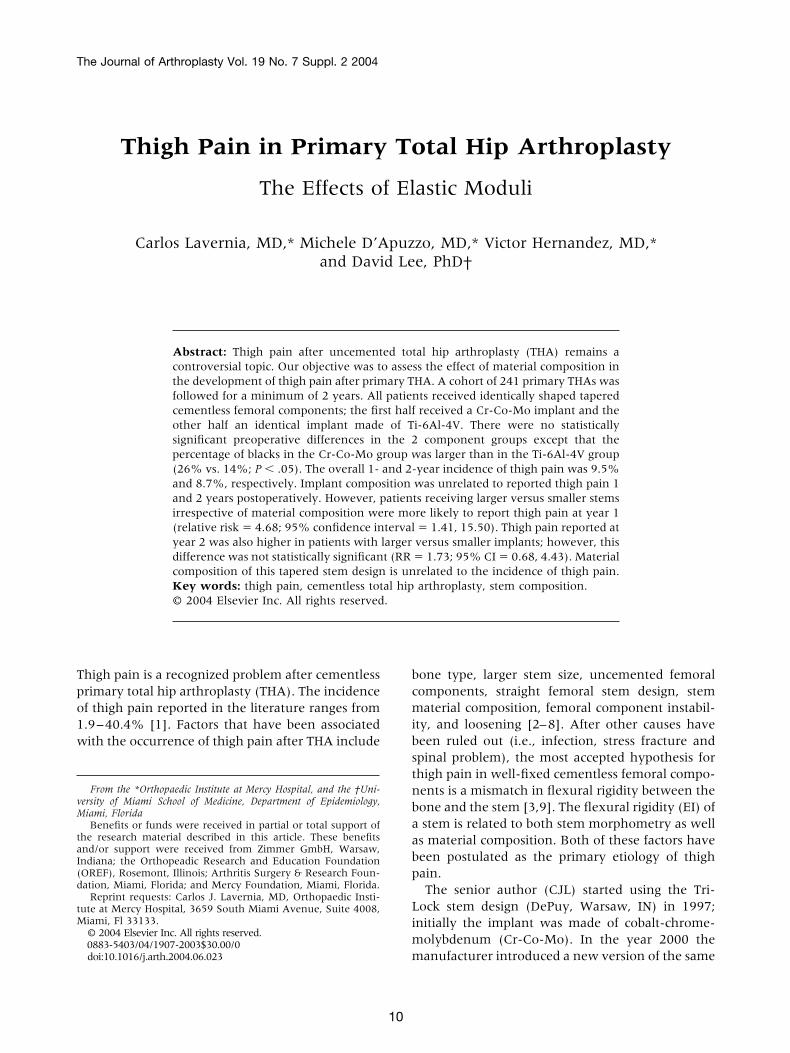
At year 1, 20 patients (9.5%) reported thigh pain;slightly lower percentage of patients reported
high pain at year 2 (8.7%). However, among the92 patients with 1- and 2-year follow-up informa-ion, only 9 patients (4.7%), reported thigh pain atoth assessments. Average VAS pain intensity levelst year 1 and at year 2 were 1.30 and 1.37, respec-ively. Identical rates of thigh pain (9.5%) wereeported at the 1-year follow-up among patientseceiving cobalt-chrome and titanium stems (Fig.). Rates of thigh pain were also similar in these 2
Table 1. Demographic Characteristics and
haracteristic
Cobalt(n � 110–118)*
Mean / %
ge 57.92Female 55.1%Black 25.9%
iagnosisOA 56.8%AVN 21.2%Other 16.1%RA 5.9%OMACPain 13.12Stiffness 3.72Function 47.12Total 63.97
isual analog-Intensity 8.62isual analog-Frequency 8.95uality of well being 0.512
Abbreviations: OA, osteoarthritis; AVN, avascular necrosis; Rniversity Osteoarthritis Index.*Sample sizes varied due to missing data on selected measure†Student’s t-test or chi-square.‡P value � .05.
Table 2. Preoperative Radiological Assessment
haracteristic
Cobalt(n � 99–118)
Mean / %
reoperative assessmentDorr A 60.6%Dorr B 38.4%Dorr C 1%Spotorno index 2.95I Moment of Inertia 2.79
tem size6.3–8.8 17.8%10.0 28.8%11.3–12.5 27.1%13.3–22.5 26.3%
*Student’s t-test or chi-square; all P values � .05.
†Chi-square compares only Dorr A vs Dorr B.roups at the 2-year follow-up (7.5% and 9.5%).his difference in rates was not statistically significantRR � 1.21; 95% CI � 0.50–2.95). Mean rating of theAS pain intensity reported in the lower extremitiest years 1 and 2 are 1.58 versus 1.03 and 1.53 versus.20, for the Co-Cr-Mo and Ti-6Al-4V implantroups, respectively (t � 1.51 t � 0.91).Table 3 shows that 1- to 2-year postoperative
adiological assessment of stem position and stemxation were similar in the Co-Cr-Mo and Ti-Al-4V groups. The distribution of neutral, valgus,
perative Status of Patients: By Stem Type
Titanium
TestStatistic†
(n � 106–123)Mean / %
61.38 �1.7161.8% 0.2914.2% 5.06‡
4.2653.7%
22%11.4%
13%
13.24 �0.263.39 1.05
48.81 �1.0865.48 �0.728.4 0.679.3 �0.660.519 �0.75
eumatoid arthritis; WOMAC, Western Ontario and McMaster
moral Bone Quality and Component Stem Size
Titanium
TestStatistic*
(n � 94–123)Mean / %
55.3% 0.46†44.7%
0%2.93 0.232.77 0.10
6.2419.5%26.0%39.0%15.4%
Preo
A, rh
s.
of Fe
aghgsC
ctalytdtp2c36i
(d92sd1davt
cwrpHl
F1d
C
S
S
F1
The Effects of Elastic Moduli • Lavernia et al. 13
nd varus stem positions were similar in the 2roups. The presence of spot welds was slightlyigher in the Co-Cr-Mo versus Ti-6Al-4V patientroups (76% vs. 68%); this difference was nottatistically significant. One patient in the Co-r-Mo group had evidence of a Pedestal.Given the lack of association between material
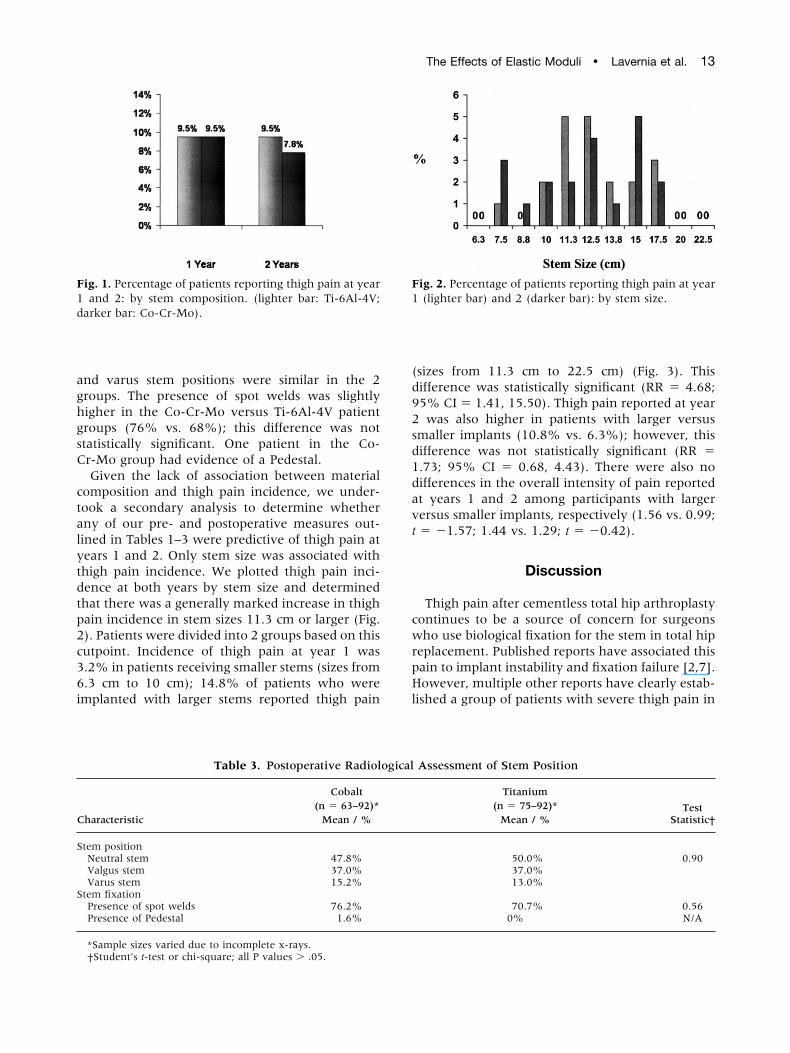
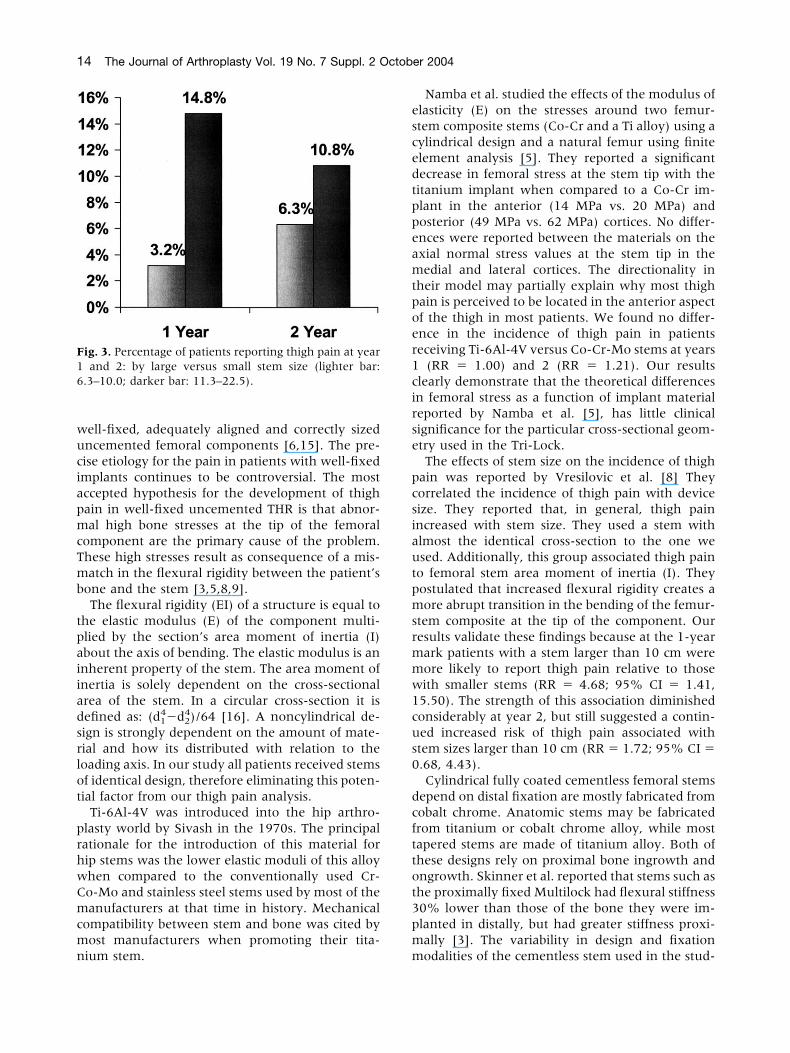
omposition and thigh pain incidence, we under-ook a secondary analysis to determine whetherny of our pre- and postoperative measures out-ined in Tables 1–3 were predictive of thigh pain atears 1 and 2. Only stem size was associated withhigh pain incidence. We plotted thigh pain inci-ence at both years by stem size and determinedhat there was a generally marked increase in thighain incidence in stem sizes 11.3 cm or larger (Fig.). Patients were divided into 2 groups based on thisutpoint. Incidence of thigh pain at year 1 was.2% in patients receiving smaller stems (sizes from.3 cm to 10 cm); 14.8% of patients who weremplanted with larger stems reported thigh pain
ig. 1. Percentage of patients reporting thigh pain at yearand 2: by stem composition. (lighter bar: Ti-6Al-4V;
arker bar: Co-Cr-Mo).
Table 3. Postoperative Radiol
haracteristic
Cobalt(n � 63–92)*
Mean / %
tem positionNeutral stem 47.8%Valgus stem 37.0%Varus stem 15.2%
tem fixationPresence of spot welds 76.2%Presence of Pedestal 1.6%
*Sample sizes varied due to incomplete x-rays.
†Student’s t-test or chi-square; all P values � .05.sizes from 11.3 cm to 22.5 cm) (Fig. 3). Thisifference was statistically significant (RR � 4.68;5% CI � 1.41, 15.50). Thigh pain reported at yearwas also higher in patients with larger versus
maller implants (10.8% vs. 6.3%); however, thisifference was not statistically significant (RR �.73; 95% CI � 0.68, 4.43). There were also noifferences in the overall intensity of pain reportedt years 1 and 2 among participants with largerersus smaller implants, respectively (1.56 vs. 0.99;� �1.57; 1.44 vs. 1.29; t � �0.42).
Discussion
Thigh pain after cementless total hip arthroplastyontinues to be a source of concern for surgeonsho use biological fixation for the stem in total hip
eplacement. Published reports have associated thisain to implant instability and fixation failure [2,7].owever, multiple other reports have clearly estab-
ished a group of patients with severe thigh pain in
Assessment of Stem Position
Titanium
TestStatistic†
(n � 75–92)*Mean / %
50.0% 0.9037.0%13.0%
70.7% 0.560% N/A
ig. 2. Percentage of patients reporting thigh pain at year(lighter bar) and 2 (darker bar): by stem size.
ogical
wuciapmcTmb
tpaiiadsrlot
prhwCmcmn
escedtppeamtpoer1cirse
pcsiautpmsrmmw1cus0
dcfttot3pm
F16
14 The Journal of Arthroplasty Vol. 19 No. 7 Suppl. 2 October 2004
ell-fixed, adequately aligned and correctly sizedncemented femoral components [6,15]. The pre-ise etiology for the pain in patients with well-fixedmplants continues to be controversial. The mostccepted hypothesis for the development of thighain in well-fixed uncemented THR is that abnor-al high bone stresses at the tip of the femoral
omponent are the primary cause of the problem.hese high stresses result as consequence of a mis-atch in the flexural rigidity between the patient’s
one and the stem [3,5,8,9].The flexural rigidity (EI) of a structure is equal to
he elastic modulus (E) of the component multi-lied by the section’s area moment of inertia (I)bout the axis of bending. The elastic modulus is annherent property of the stem. The area moment ofnertia is solely dependent on the cross-sectionalrea of the stem. In a circular cross-section it isefined as: (d1
4�d24)/64 [16]. A noncylindrical de-
ign is strongly dependent on the amount of mate-ial and how its distributed with relation to theoading axis. In our study all patients received stemsf identical design, therefore eliminating this poten-ial factor from our thigh pain analysis.
Ti-6Al-4V was introduced into the hip arthro-lasty world by Sivash in the 1970s. The principalationale for the introduction of this material forip stems was the lower elastic moduli of this alloyhen compared to the conventionally used Cr-o-Mo and stainless steel stems used by most of theanufacturers at that time in history. Mechanical
ompatibility between stem and bone was cited byost manufacturers when promoting their tita-
ig. 3. Percentage of patients reporting thigh pain at yearand 2: by large versus small stem size (lighter bar:
.3–10.0; darker bar: 11.3–22.5).
ium stem. m
Namba et al. studied the effects of the modulus oflasticity (E) on the stresses around two femur-tem composite stems (Co-Cr and a Ti alloy) using aylindrical design and a natural femur using finitelement analysis [5]. They reported a significantecrease in femoral stress at the stem tip with theitanium implant when compared to a Co-Cr im-lant in the anterior (14 MPa vs. 20 MPa) andosterior (49 MPa vs. 62 MPa) cortices. No differ-nces were reported between the materials on thexial normal stress values at the stem tip in theedial and lateral cortices. The directionality in
heir model may partially explain why most thighain is perceived to be located in the anterior aspectf the thigh in most patients. We found no differ-nce in the incidence of thigh pain in patientseceiving Ti-6Al-4V versus Co-Cr-Mo stems at years
(RR � 1.00) and 2 (RR � 1.21). Our resultslearly demonstrate that the theoretical differencesn femoral stress as a function of implant materialeported by Namba et al. [5], has little clinicalignificance for the particular cross-sectional geom-try used in the Tri-Lock.The effects of stem size on the incidence of thigh
ain was reported by Vresilovic et al. [8] Theyorrelated the incidence of thigh pain with deviceize. They reported that, in general, thigh painncreased with stem size. They used a stem withlmost the identical cross-section to the one wesed. Additionally, this group associated thigh paino femoral stem area moment of inertia (I). Theyostulated that increased flexural rigidity creates aore abrupt transition in the bending of the femur-
tem composite at the tip of the component. Ouresults validate these findings because at the 1-yearark patients with a stem larger than 10 cm wereore likely to report thigh pain relative to thoseith smaller stems (RR � 4.68; 95% CI � 1.41,5.50). The strength of this association diminishedonsiderably at year 2, but still suggested a contin-ed increased risk of thigh pain associated withtem sizes larger than 10 cm (RR � 1.72; 95% CI �.68, 4.43).Cylindrical fully coated cementless femoral stems
epend on distal fixation are mostly fabricated fromobalt chrome. Anatomic stems may be fabricatedrom titanium or cobalt chrome alloy, while mostapered stems are made of titanium alloy. Both ofhese designs rely on proximal bone ingrowth andngrowth. Skinner et al. reported that stems such ashe proximally fixed Multilock had flexural stiffness0% lower than those of the bone they were im-lanted in distally, but had greater stiffness proxi-ally [3]. The variability in design and fixation
odalities of the cementless stem used in the stud-
iseeswmaep
h(aWcpeitHsttf2edr
wstapitalaiaa
wnhlahpglpc
pfc
dtWf6iwftstp
1
The Effects of Elastic Moduli • Lavernia et al. 15
es published to date make it difficult to study thepecific interaction of design and modulus in thetiology of thigh pain. Comparing clinical differ-nces in the incidence of this problem with differenttems further confounds the issues. In our study weere able to eliminate fixation modality and areaoment of inertia as potentially confounding vari-
bles. Our data show that for this tapered design thelastic modulus of the stem has no effect on theresence and intensity of thigh pain.Some of the initial studies in uncemented total
ip replacement used the porous-coated anatomicPCA) stem (Howmedica, Rutherford, NJ) and thenatomic medullary locking (AML) stem (DePuy,arsaw, IN). These are cylindrical stems with large
ross-sectional areas (high moment of inertia) bothroximally and distally, as well as high modulus oflasticity Co-Cr-Mo. This partially explains the highncidence of thigh pain (12–27%) [1] reported inhese series. Anatomic Ti-6Al-4V designs like thearris-Galante Porous femoral stem (Zimmer, War-
aw, IN) were also associated with incidences ofhigh pain as high as 17% [17,18]. Furthermore, inhis particular design (HGP-I), the lack of circum-erential coating produced loosing rates of as high as5% [17] at 4–6 years. It is highly probable thatarly reports of thigh pain with this design occurredue to loose devices that could not be identifiedadiologically.
Multiple reports of uncemented femoral fixationith tapered stems have demonstrated excellent
urvival and minimal thigh pain. Designs such ashe Mallory-Head (Biomet, Warsaw, IN) [1,19,20]nd the Tri-Lock have yielded an incidence of thighain of 3% [21–24]. These stems depend on prox-mal fixation and have cross-sectional geometrieshat taper distally with a concomitant decrease inrea moment of inertia (I). Our results confirm theow incidence of thigh pain with a tapered stem andre similar to those previously reported. We had anncidence of thigh pain of 9.5% at year 1 and 8.7%t year 2; only 4.7% of patients reported thigh paint both the 1- and 2-year follow-up.Several study limitations should be noted. First,e have incomplete follow-up information onearly 8% of our cohort. These patients scoredigher on the WOMAC pain subscale and reported
ower quality of life relative to patients with avail-ble follow-up information. It should be noted,owever, that patients lost to follow-up were ap-roximately evenly divided across the 2 componentroups. It is therefore unlikely that incomplete fol-ow-up biased our central conclusion that thighain incidence is not associated with component
omposition. We also reported that there was no 1re- or post-operative radiological evidence of dif-erences in the 2 component groups, although thisomparison was limited by incomplete x-rays.To summarize, we used the same tapered stem
esign in all patients, with the elastic modulus ofhe stem being the only difference between cohorts.
e found no clinical or statistically significant dif-erence in patients with Co-Cr-Mo stems and Ti-Al-4V stems, in terms of presence of thigh pain orn the overall intensity of the pain among patientsho were followed for at least 2 years. Instead we
ound a positive association between thigh pain andhe larger stem sizes for both materials. Our datahows that the modulus of elasticity has no role inhe development of thigh pain with this tapered,roximally coated stem design.
References
1. Brown T, Larson B, Shen F, Moskal J: Thigh painafter cementless total hip arthroplasty: evaluationand management. J Am Acad Orthop Surg 10:6,2002
2. Burkart B, Bourne R, Rorabeck C, Kirk P: Thigh painin cementless total hip arthroplasty: a comparison oftwo systems at 2 years’ follow up. Orthop Clin NorthAm 24:4, 1993
3. Skinner H, Curlin F: Decrease pain with lower flex-ural rigidity of uncemented femoral prostheses. Or-thopedics 13:11, 1990
4. Maloney W, Harris W: Comparison of a hybrid withan uncemented total hip replacement. J Bone JointSurg Am 72:9, 1990
5. Namba R, Keyak J, Kim A, Vu L, Skinner H: Cement-less implant composition and femoral stress: a finiteelement analysis. Clin Orthop 347:261, 1998
6. Barrack R, Jasty M, Bragdon C, et al: Thigh paindespite bone ingrowth into uncemented femoralstems. J Bone Joint Surg Am 74:4, 1992
7. Campbell A, Rorabeck C, Bourne R, et al: Thigh painafter cementless hip arthroplasty: annoyance or illomen? J Bone Joint Surg Am 74:1, 1992
8. Vresilovic E, Hozack W, Rothman R: Incidence ofthigh pain after uncemented total hip arthroplasty asa function of femoral stem size. J Arthroplasty 11:3,1996
9. Domb B, Hostin E, Mont M, Hungerford D: Corticalstrut grafting for enigmatic thigh pain following totalhip arthroplasty. Orthopedics 23:1, 2000
0. Bellamy N, Buchanan WW, Goldsmith CH, et al:Validation study of WOMAC: a health status instru-ment for measuring clinically important patient rel-evant outcomes to antirheumatic drug therapy inpatients with osteoarthritis of the hip or knee.J Rheumatol 15:1833, 1988
1. Kaplan RM, Bush JW: Health related quality of life
1
1
1
1
1
1
1
1
2
2
2
2
2
16 The Journal of Arthroplasty Vol. 19 No. 7 Suppl. 2 October 2004
measurement for evaluation research and policyanalysis. Health Psychol 1:61, 1982
2. Blaha J, Spotorno L, Romagnoli S: CLS press-fit totalhip arthroplasty. Tech Orthop 6:80, 1991
3. Cohen J, Bindeglass D, Dorr L: Total hip replacementusing the APR II system. Tech Orthop 6:40, 1991
4. Barrack RL, Paprosky W, Butler A, et al: Patients’perception of pain after total hip arthroplasty. J Ar-throplasty 15:5, 2000
5. Engh C, Bobyn J, Glassman A: Porous coated hipreplacement: the factors governing bone ingrowth,stress, shielding, and clinical results. J Bone JointSurg Am 69:45, 1987
6. Von Recum AHandbook of biomaterial evaluation-scientific, technical, and clinical testing of implantmaterials. New York, Macmillan, 1986
7. Cruz P, Garcia C: The Harris-Galante total hip arthro-plasty: a minimum 8 year follow up study. J Arthro-plasty 16:5, 2001
8. Petersilge W, D’Lima D, Walker R, Colwell C: Pro-spective study of 100 consecutive Harris-Galante po-rous total hip arthroplasties: 4 to 8 year follow-upstudy. J Arthroplasty 12:185, 1997
9. Bourne R, Rorabeck C, Patterson J, Guerin J: Tapered
titanium cementless total hip replacements: a 10 to13 year follow-up study. Clin Orthop 393:112, 2001
0. Mallory T, Head W, Lombardi A: Tapered design forthe cementless total hip arthroplasty femoral compo-nent. Clin Orthop 344:172, 1997
1. Teloken M, Bisset G, Hozack W, et al: Ten to fifteen-year follow-up after total hip arthroplasty with atapered cobalt-chromium femoral component (Tri-Lock) inserted without cement. J Bone Joint SurgAm 84:12, 2002
2. Burt C, Garvin K, Otterberg E, et al: A femoralcomponent inserted without cement in total hip ar-throplasty: a study of the Tri-Lock component withan average ten-year duration of follow-up. J BoneJoint Surg Am 80:7, 1998
3. Pellegrini V, Hughes S, Evarts C: A collarless cobalt-chrome femoral component in uncemented total hiparthroplasty: five- to eight-year follow-up. J. BoneJoint Surg Am 74:6, 1992
4. Burt C, Garvin K, Otterberg E, Jardon M: A femoralcomponent inserted without cement in total hip ar-throplasty: a study of the Tri-Lock component withan average ten-year duration of follow-up. J Joint
Bone Surg Am 80:7, 1998