modeling the posture of a cerebral palsy patient with hamstring syndrome after surgical correction...
TRANSCRIPT
ISSN 0027-1330, Moscow University Mechanics Bulletin, 2010, Vol. 65, No. 2, pp. 25–30. c© Allerton Press, Inc., 2010.Original Russian Text c© P.A. Kruchinin, O.V. Nikitina, 2010, published in Vestnik Moskovskogo Universiteta, Matematika.Mekhanika, 2010, Vol. 65, No. 2, pp. 18–23.
Modeling the Posture of a Cerebral Palsy Patientwith Hamstring Syndrome after Surgical Correction
by the Zhuravlev ProcedureP.A. Kruchinin and O. V. Nikitina
Moscow State University, Faculty of Mechanics and Mathematics,Leninskie Gory, Moscow, 119899, Russia
Received July 2, 2007; in final form, December 24, 2009
Abstract—Cerebral palsy patients with hamstring syndrome are characterized by an increased tensionin the posterior two-joint muscles of the thigh. The upright posture of such patients takes the Z-shapedform. The operations according to the procedure proposed by Eggers and the tendon plastic operationsproposed by Zhuravlev help the limbs to straighten. In this paper a mathematical model of the patientposture after a Zhuravlev operation is proposed. The numerical results obtained show that a patientunderwent such an operation can maintain a relatively upright posture even with an increased tonusof the rectus muscle of the thigh. This is impossible for a patient after an Eggers operation.
DOI: 10.3103/S0027133010020019
In this paper we model the posture of an infantile cerebral palsy patient. This is a disease of the centralnervous system during which the motion control is limited in skeleton joints. The patients with hamstringsyndrome are characterized by an increased tension (hypertonus) in the posterior two-joint muscles of thethigh (hamstring) [1]. In particular, such a disease results in the following: a patient is not able to maintainthe upright posture; instead, the patient posture takes the Z-shaped form because of triple flexion in thejoints of the lower limbs.
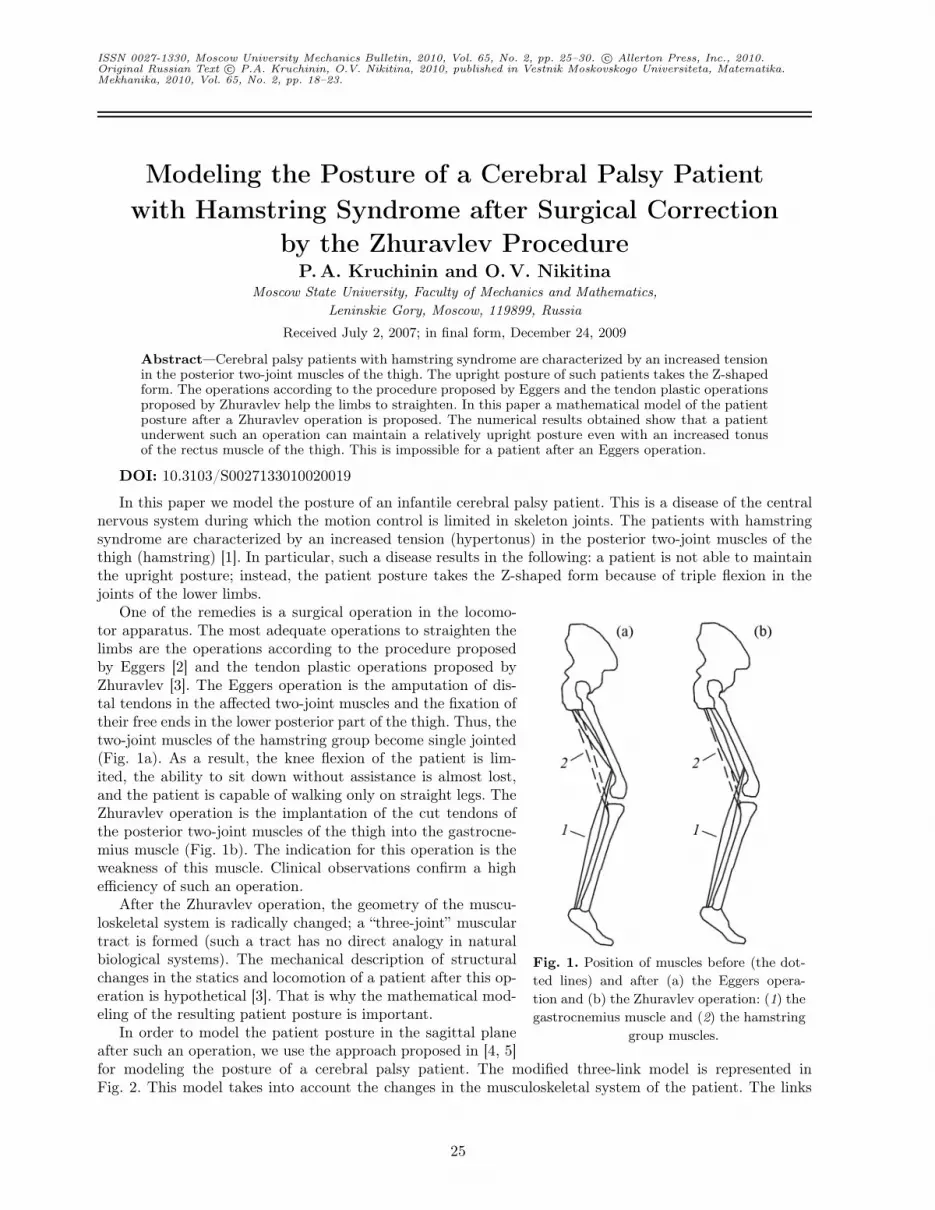
Fig. 1. Position of muscles before (the dot-ted lines) and after (a) the Eggers opera-tion and (b) the Zhuravlev operation: (1) thegastrocnemius muscle and (2) the hamstring
group muscles.
One of the remedies is a surgical operation in the locomo-tor apparatus. The most adequate operations to straighten thelimbs are the operations according to the procedure proposedby Eggers [2] and the tendon plastic operations proposed byZhuravlev [3]. The Eggers operation is the amputation of dis-tal tendons in the affected two-joint muscles and the fixation oftheir free ends in the lower posterior part of the thigh. Thus, thetwo-joint muscles of the hamstring group become single jointed(Fig. 1a). As a result, the knee flexion of the patient is lim-ited, the ability to sit down without assistance is almost lost,and the patient is capable of walking only on straight legs. TheZhuravlev operation is the implantation of the cut tendons ofthe posterior two-joint muscles of the thigh into the gastrocne-mius muscle (Fig. 1b). The indication for this operation is theweakness of this muscle. Clinical observations confirm a highefficiency of such an operation.
After the Zhuravlev operation, the geometry of the muscu-loskeletal system is radically changed; a “three-joint” musculartract is formed (such a tract has no direct analogy in naturalbiological systems). The mechanical description of structuralchanges in the statics and locomotion of a patient after this op-eration is hypothetical [3]. That is why the mathematical mod-eling of the resulting patient posture is important.
In order to model the patient posture in the sagittal planeafter such an operation, we use the approach proposed in [4, 5]for modeling the posture of a cerebral palsy patient. The modified three-link model is represented inFig. 2. This model takes into account the changes in the musculoskeletal system of the patient. The links
25
26 KRUCHININ, NIKITINA
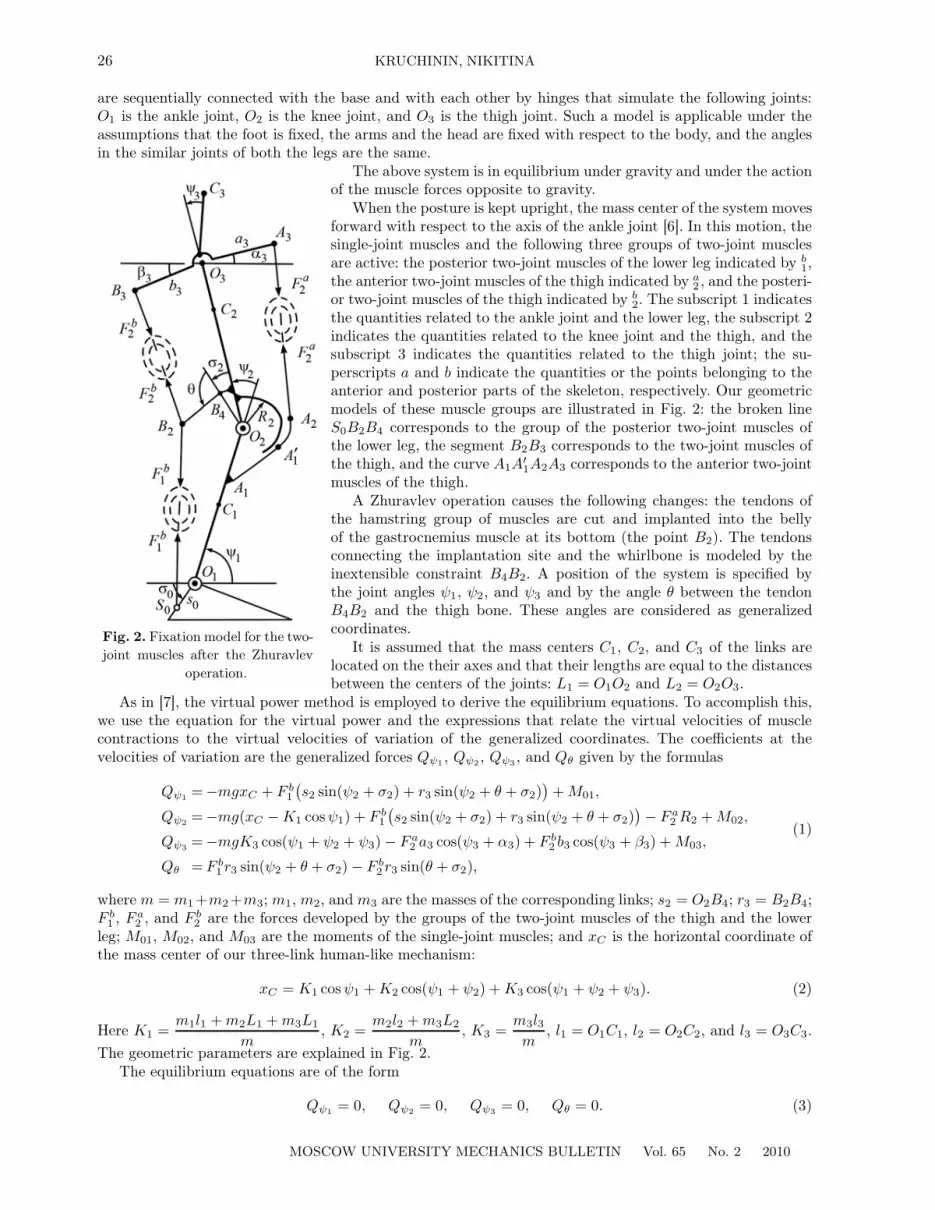
are sequentially connected with the base and with each other by hinges that simulate the following joints:O1 is the ankle joint, O2 is the knee joint, and O3 is the thigh joint. Such a model is applicable under theassumptions that the foot is fixed, the arms and the head are fixed with respect to the body, and the anglesin the similar joints of both the legs are the same.
Fig. 2. Fixation model for the two-joint muscles after the Zhuravlev
operation.
The above system is in equilibrium under gravity and under the actionof the muscle forces opposite to gravity.
When the posture is kept upright, the mass center of the system movesforward with respect to the axis of the ankle joint [6]. In this motion, thesingle-joint muscles and the following three groups of two-joint musclesare active: the posterior two-joint muscles of the lower leg indicated by b
1,the anterior two-joint muscles of the thigh indicated by a
2 , and the posteri-or two-joint muscles of the thigh indicated by b
2. The subscript 1 indicatesthe quantities related to the ankle joint and the lower leg, the subscript 2indicates the quantities related to the knee joint and the thigh, and thesubscript 3 indicates the quantities related to the thigh joint; the su-perscripts a and b indicate the quantities or the points belonging to theanterior and posterior parts of the skeleton, respectively. Our geometricmodels of these muscle groups are illustrated in Fig. 2: the broken lineS0B2B4 corresponds to the group of the posterior two-joint muscles ofthe lower leg, the segment B2B3 corresponds to the two-joint muscles ofthe thigh, and the curve A1A
′1A2A3 corresponds to the anterior two-joint
muscles of the thigh.A Zhuravlev operation causes the following changes: the tendons of
the hamstring group of muscles are cut and implanted into the bellyof the gastrocnemius muscle at its bottom (the point B2). The tendonsconnecting the implantation site and the whirlbone is modeled by theinextensible constraint B4B2. A position of the system is specified bythe joint angles ψ1, ψ2, and ψ3 and by the angle θ between the tendonB4B2 and the thigh bone. These angles are considered as generalizedcoordinates.
It is assumed that the mass centers C1, C2, and C3 of the links arelocated on the their axes and that their lengths are equal to the distancesbetween the centers of the joints: L1 = O1O2 and L2 = O2O3.
As in [7], the virtual power method is employed to derive the equilibrium equations. To accomplish this,we use the equation for the virtual power and the expressions that relate the virtual velocities of musclecontractions to the virtual velocities of variation of the generalized coordinates. The coefficients at thevelocities of variation are the generalized forces Qψ1 , Qψ2 , Qψ3 , and Qθ given by the formulas
Qψ1 =−mgxC + F b1
(s2 sin(ψ2 + σ2) + r3 sin(ψ2 + θ + σ2)
)+ M01,
Qψ2 =−mg(xC − K1 cosψ1) + F b1
(s2 sin(ψ2 + σ2) + r3 sin(ψ2 + θ + σ2)
)− F a
2 R2 + M02,
Qψ3 =−mgK3 cos(ψ1 + ψ2 + ψ3) − F a2 a3 cos(ψ3 + α3) + F b
2 b3 cos(ψ3 + β3) + M03,
Qθ = F b1 r3 sin(ψ2 + θ + σ2) − F b
2 r3 sin(θ + σ2),
(1)
where m = m1+m2+m3; m1, m2, and m3 are the masses of the corresponding links; s2 = O2B4; r3 = B2B4;F b
1 , F a2 , and F b
2 are the forces developed by the groups of the two-joint muscles of the thigh and the lowerleg; M01, M02, and M03 are the moments of the single-joint muscles; and xC is the horizontal coordinate ofthe mass center of our three-link human-like mechanism:
xC = K1 cosψ1 + K2 cos(ψ1 + ψ2) + K3 cos(ψ1 + ψ2 + ψ3). (2)
Here K1 =m1l1 + m2L1 + m3L1
m, K2 =
m2l2 + m3L2
m, K3 =
m3l3m
, l1 = O1C1, l2 = O2C2, and l3 = O3C3.The geometric parameters are explained in Fig. 2.
The equilibrium equations are of the form
Qψ1 = 0, Qψ2 = 0, Qψ3 = 0, Qθ = 0. (3)
MOSCOW UNIVERSITY MECHANICS BULLETIN Vol. 65 No. 2 2010

MODELING THE POSTURE OF A CEREBRAL PALSY PATIENT 27
For the forces F a2 and F b
2 , we adopt the Fel’dman λ-model [8]. According to this model, the static forcesdeveloped by the muscles are specified by the current muscle length l and by the control parameter λ thatcorresponds to the stretch reflex threshold of the central nervous system:
F k2 (lk2 , λk
2) =
{0, lk2 < λk
2 ;
Kk2 (lk2 − λk
2), lk2 ≥ λk2 .
(4)
Here k = a, b and Kk2 is the positive coefficient expressed in units of stiffness and specified by the muscle
innervation level via the stretch reflex feedback.In general, the dependence of F k
2 on lk2 is nonlinear; however, the parameters of this dependence are knowninaccurately. In our further discussion, hence, we consider only the linear approximation. Note that lk2 is themuscle length together with the tendon end. The dependence of lk2 on the angles of the skeleton multilinksystem can be found by solving the geometric problem, as is done in [7]. The lengths la2 and lb2 of the two-jointmuscles are related to these angles by the formulas
la2 = la2(ψ2, ψ3) =(L2
2 + a23 + 2L2a3 sin(ψ3 + α3) − R2
2
)1/2 + R2(ψ2 − γa
23 + π),
lb2 = lb2(ψ3, θ) =(L2
2 + s22 + b2
3 + r23 + 2r3s2 cos θ − 2r3L2 cos(σ2 + θ)
+ 2r3b3 sin(ψ3 + β3 − σ2 − θ) − 2L2s2 cosσ2
+ 2s2b3 sin(ψ3 + β3 − σ2) − 2b3L2 sin(ψ3 + β3))1
/2,
(5)
whereγa23 = arccos
R2√L2
2 + a23 + 2L2a3 sin(ψ3 + α3)
+ arctana3 cos(ψ3 + α3)
L2 + a3 sin(ψ3 + α3).
Substituting (1), (4), and (5) into (3), we come to the system of three equations with the ten unknowns ψ1,ψ2, ψ3, θ, F b
1 , λa2 , λb
2, M01, M02, and M03. This system has an infinite number of solutions.In order to determine the posture of a patient, we supplement this system with the equations based on
the following assumptions resulting from a number of clinical observations [1, 6].1. In the upright position, a patient keeps the mass center over the foot, i.e., at a distance of xC 0 ≈ 3 cm
ahead of the ankle joint:xC = xC 0. (6)
2. The human organism minimizes a certain functional J :
J(F b1 , F a
2 , F b2 , M01, M02, M03) −→ min . (7)
This assumption supplements the formulation of our problem. Such a functional should characterizethe metabolic expenditures of the human organism; the choice of this functional is a difficult problem.When studying the biomechanical systems, several types of the functional are considered in [9]. The mostappropriate one is
J =(
M01
l01m01
)2
+(
M02
l02m02
)2
+(
M03
l03m03
)2
+(
F b1
mb1
)2
+(
F a2
ma2
)2
+(
F b2
mb2
)2
. (8)
This functional minimizes the sum of squared muscle forces reduced to unit mass. Here m01, m02, m03, mb1,
ma2 , and mb
2 are the muscle masses of the corresponding single-joint and two-joint muscles; the numericalvalues of these parameters are taken from [10]. In (10) the parameters l01 = s0 tan σ0, l02 = R2, andl03 = b3 cosβ3 stand for the characteristic arms of the forces developed by the single-joint muscles.
3. A patient keeps the upright position: ψ1 + ψ2 + ψ3 = π/2.Note that we should take into account the anatomical properties expressed by the following constraints:
λk2 min ≤ λk
2 ≤ λk2 max, lk2 min ≤ lk2 ≤ lk2 max, and 0 ≤ F k
n ≤ F kn max (here n = 1, 2 and k = a, b). The exact
values of these constraints are unknown. When analyzing the results obtained, however, we should keep inmind that the maximum force of the muscles does not exceed a ton and that the muscle lengthening andthe variation of λ are less than 10 cm.
Further we assume that the upright posture corresponds to the equilibrium position of the entire sys-tem; for the muscle groups under consideration, this position is specified by constant values of the controlparameter λ.
MOSCOW UNIVERSITY MECHANICS BULLETIN Vol. 65 No. 2 2010

28 KRUCHININ, NIKITINA
In the case of cerebral palsy, according to [11], the nervous system sends a pathological signal to themuscles; this signal causes a decrease of λk
2 . When modeling the patient posture, for the pathological statewe have λk
2 = lk(0)2 − �λk
2 , where lk(0)2 is the length of the generalized muscle for the anterior (posterior)
group of the two-joint muscles of the thigh in the upright posture of a healthy person (i.e., ψ1 = 90◦ andψ2 = ψ3 = 0), �λk
2 is the additive correction modeling an increased muscle tonus, and k = a, b. The clinicalobservations discussed in [3] show that, for patients, λb
2 is less than lb(0)2 by �λb
2 ≈ 4 cm.In order to solve our problem of determining the patient posture, thus, it is necessary to minimize
functional (7) with the constraints given by (1)–(6), i.e., by the functions of the nine variables ψ1, ψ2, ψ3, θ,F b
1 , λa2 , M01, M02, and M03. Our numerical study of the problem show a number of difficulties; we overcome
these difficulties by reducing the number of the unknowns.For the upright posture, from (2) and (6) we obtain ψ1 = ψ1(ψ3) and ψ2 = ψ2(ψ3) = π/2− ψ3 −ψ1(ψ3).
Substituting these equalities into (5), (4), (1), and (3), we come to the expressions for the forces F a2 and F b
2
and for the force moments M01, M02, and M03 as a functions of the angles ψ3 and θ, the parameter λa2
used to control the muscle forces of the two-joint muscles of the thigh, and the force F b1 developed by the
gastrocnemius muscle.The minimization problem is solved by one of the gradient methods in the framework of the MATLAB
system for the following parameters: m1 = 4.7 kg, m2 = 14.7 kg, m3 = 30.6 kg, L1 = O1O2 = 0.37 m,L2 = O2O3 = 0.40 m, l1 = O1C1 = 0.2 m, l2 = O2C2 = 0.22 m, l3 = O3C3 = 0.33 m, α3 = 45◦, β3 = 52◦,σ2 = 2◦30′, a3 = 5.2 cm, b3 = 5,2 cm, R2 = 5,5 cm, r2 = 4 cm, and s2 = 3cm. These parameters aremeasured in [10] on the basis of the anthropometric data corresponding approximately to a patient of 1.5 mon height and 50 kg in weight. The muscle stiffness is assumed to be the same for the muscle groups underconsideration: Ka
2 = Kb2 = K = 104 kg/s2.
As a result, we obtain the following values of the joint angles: ψ1 = 85◦, ψ2 = 4◦, and ψ3 = 1◦; theseangles correspond to the upright posture. It is well known that, although the angles ψ2 and ψ3 decreasesignificantly, the patient posture keeps the Z-shape form. This can be explained by the fact that the patienthas an increased tonus in the anterior group of the two-joint muscles of the thigh. We model this tonus withthe aid of the following constraint imposed on the control parameter λa
2 :
λa2 < l
a(0)2 −�λa
2 . (9)
Here la(0)2 is the length of the corresponding muscle group of a healthy person in the upright posture with
the straight legs and �λa2 is the degree of affection. The weakness of the gastrocnemius muscle is modeled
by the following constraint imposed on its force:
F b1 ≤ F b
1 max. (10)
Our preliminary analysis of the problem shows that the above functionals reach their minima near theboundaries of inequalities (9) and (10). That is why we consider the simplified problem when F b
1 and λa2 are
fixed.Substituting the second equality of (5) into (4), we numerically solve the last equation of (3) with respect
to ψ3 and obtain the dependence of this angle on θ: ψ3 = ψ3(θ). Thus, the forces of the two-joint musclesand the moments of the single-joint muscles depend only on the variable θ.
Table 1 contains the values of the angles for the skeleton multilink system obtained by solving theminimization problem for functional (8) with �λb
2 = 4 cm and with various fixed values of �λa2 and F b
1 .The empty blocks of this table correspond to �λa
2 and F b1 for which there exist no joint angles satisfying (10)
for the above constraints.Our numerical results show that, after a Zhuravlev operation, a patient is able to keep a relatively
upright original posture even in the case of an increased tonus of the rectus muscle of the thigh whenthe gastrocnemius muscle is weakened. This muscle develops significant forces larger than 50 N, which isimpossible after an Eggers operation. This fact is confirmed by the clinical practice [12].
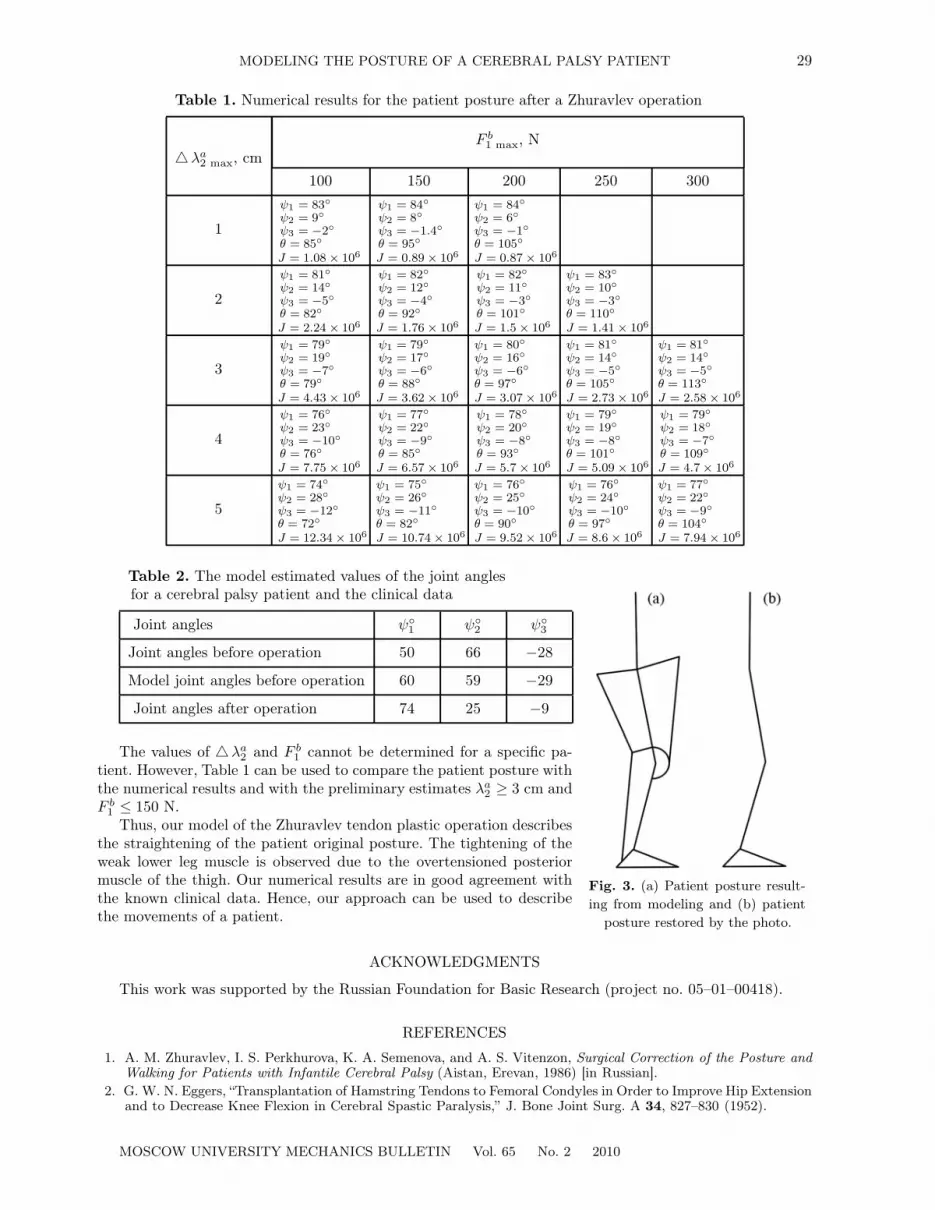
The first and third rows of Table 2 illustrate the values of the joint angles corresponding to the photoof a patient before [5] and after a Zhuravlev operation, respectively. The second row contains the values ofthe joint angles obtained by modeling the patient posture after the operation for �λb
2 = 4 cm. The posturekept after the operation is illustrated in Fig. 3.
MOSCOW UNIVERSITY MECHANICS BULLETIN Vol. 65 No. 2 2010
MODELING THE POSTURE OF A CEREBRAL PALSY PATIENT 29
Table 1. Numerical results for the patient posture after a Zhuravlev operation
F b1 max, N
�λa2 max, cm
100 150 200 250 300
1
ψ1 = 83◦
ψ2 = 9◦
ψ3 = −2◦
θ = 85◦
J = 1.08 × 106
ψ1 = 84◦
ψ2 = 8◦
ψ3 = −1.4◦
θ = 95◦
J = 0.89 × 106
ψ1 = 84◦
ψ2 = 6◦
ψ3 = −1◦
θ = 105◦
J = 0.87 × 106
2
ψ1 = 81◦
ψ2 = 14◦
ψ3 = −5◦
θ = 82◦
J = 2.24 × 106
ψ1 = 82◦
ψ2 = 12◦
ψ3 = −4◦
θ = 92◦
J = 1.76 × 106
ψ1 = 82◦
ψ2 = 11◦
ψ3 = −3◦
θ = 101◦
J = 1.5 × 106
ψ1 = 83◦
ψ2 = 10◦
ψ3 = −3◦
θ = 110◦
J = 1.41 × 106
3
ψ1 = 79◦
ψ2 = 19◦
ψ3 = −7◦
θ = 79◦
J = 4.43 × 106
ψ1 = 79◦
ψ2 = 17◦
ψ3 = −6◦
θ = 88◦
J = 3.62 × 106
ψ1 = 80◦
ψ2 = 16◦
ψ3 = −6◦
θ = 97◦
J = 3.07 × 106
ψ1 = 81◦
ψ2 = 14◦
ψ3 = −5◦
θ = 105◦
J = 2.73 × 106
ψ1 = 81◦
ψ2 = 14◦
ψ3 = −5◦
θ = 113◦
J = 2.58 × 106
4
ψ1 = 76◦
ψ2 = 23◦
ψ3 = −10◦
θ = 76◦
J = 7.75 × 106
ψ1 = 77◦
ψ2 = 22◦
ψ3 = −9◦
θ = 85◦
J = 6.57 × 106
ψ1 = 78◦
ψ2 = 20◦
ψ3 = −8◦
θ = 93◦
J = 5.7 × 106
ψ1 = 79◦
ψ2 = 19◦
ψ3 = −8◦
θ = 101◦
J = 5.09 × 106
ψ1 = 79◦
ψ2 = 18◦
ψ3 = −7◦
θ = 109◦
J = 4.7 × 106
5
ψ1 = 74◦
ψ2 = 28◦
ψ3 = −12◦
θ = 72◦
J = 12.34 × 106
ψ1 = 75◦
ψ2 = 26◦
ψ3 = −11◦
θ = 82◦
J = 10.74 × 106
ψ1 = 76◦
ψ2 = 25◦
ψ3 = −10◦
θ = 90◦
J = 9.52 × 106
ψ1 = 76◦
ψ2 = 24◦
ψ3 = −10◦
θ = 97◦
J = 8.6 × 106
ψ1 = 77◦
ψ2 = 22◦
ψ3 = −9◦
θ = 104◦
J = 7.94 × 106
Fig. 3. (a) Patient posture result-ing from modeling and (b) patient
posture restored by the photo.
Table 2. The model estimated values of the joint anglesfor a cerebral palsy patient and the clinical data
Joint angles ψ◦1 ψ◦
2 ψ◦3
Joint angles before operation 50 66 −28
Model joint angles before operation 60 59 −29
Joint angles after operation 74 25 −9
The values of �λa2 and F b
1 cannot be determined for a specific pa-tient. However, Table 1 can be used to compare the patient posture withthe numerical results and with the preliminary estimates λa
2 ≥ 3 cm andF b
1 ≤ 150 N.Thus, our model of the Zhuravlev tendon plastic operation describes
the straightening of the patient original posture. The tightening of theweak lower leg muscle is observed due to the overtensioned posteriormuscle of the thigh. Our numerical results are in good agreement withthe known clinical data. Hence, our approach can be used to describethe movements of a patient.
ACKNOWLEDGMENTS
This work was supported by the Russian Foundation for Basic Research (project no. 05–01–00418).
REFERENCES
1. A. M. Zhuravlev, I. S. Perkhurova, K. A. Semenova, and A. S. Vitenzon, Surgical Correction of the Posture andWalking for Patients with Infantile Cerebral Palsy (Aistan, Erevan, 1986) [in Russian].
2. G. W. N. Eggers, “Transplantation of Hamstring Tendons to Femoral Condyles in Order to Improve Hip Extensionand to Decrease Knee Flexion in Cerebral Spastic Paralysis,” J. Bone Joint Surg. A 34, 827–830 (1952).
MOSCOW UNIVERSITY MECHANICS BULLETIN Vol. 65 No. 2 2010

30 KRUCHININ, NIKITINA
3. A. M. Zhuravlev, “Surgical Correction of Hamstring Syndrome Complicated by the Weakness of the Lower LegTriceps for Patients with Infantile Cerebral Palsy,” Vestn. Traumatol. Orthopedics, No. 3, 40–43 (2006).
4. P. A. Kruchinin, “Mathematical Modeling of Posture Abnormality for Patients with Rectus Syndrome,” in Proc.First Int. Conf. on New Technologies in Medicine, St. Petersburg, 2004 (Int. Sci. Surg. Ass., St. Petersburg,2004), pp. 116–118.
5. I. V. Novozhilov and P. A. Kruchinin (Eds.), Mathematical Modeling of Human Movements in Norm and inPathology (Mosk. Gos. Univ., Moscow, 2005) [in Russian].
6. V. S. Gurfinkel, Ya. M. Kots, and M. L. Shik, Human Posture Regulation (Nauka, Moscow, 1965) [in Russian].7. I. A. Kopylov, P. A. Kruchinin, and I. V. Novozhilov, “On the Implementation of Motions According to N. A. Bern-
stein,” Izv. Ross. Akad. Nauk, Mekh. Tverd. Tela, No. 5, 39–49 (2003) [Mech. Solids 38 (5), 31–39 (2003)].8. A. G. Fel’dman, Central and Reflex Control Mechanisms (Nauka, Moscow, 1979) [in Russian].9. V. M. Zatsiorskii and B. I. Prilutskii, “Determining the Human Muscle Forces in a Given Motion,” in Contempo-
rary Problems in Biomechanics (Nauchn. Sov. Ross. Akad. Nauk, Nizhnii Novgorod, 1992), Issue 7, pp. 81–123.10. A. V. Voronov, Anatomical Structure and Biomechanical Characteristics of Muscles and Joints in Lower Extrem-
ities (Fizlult. Obraz. Nauka, Moscow, 2003) [in Russian].11. M. F. Levin, “Sensorimotor Deficits in Patients with Central Nervous System Lesion: Explanation Based on the
λ-Model of Motor Control,” Hum. Mov. Sci. 19, 107–137 (2000).12. A. M. Zharavlev, Surgical Correction of Posture and Walking for Patients with Infantile Cerebral Palsy, Doctoral
Dissertation in Medical Sciences (Central Inst. of Traumatology and Orthopedics, Moscow, 1999).
Translated by O. Arushanyan
MOSCOW UNIVERSITY MECHANICS BULLETIN Vol. 65 No. 2 2010