newborn care in maridi
TRANSCRIPT

MOTHER’S KNOWLEDGE, ATTITUDES AND PRACTICES (KAPs) ON
THE CARE OF NEWBORN IN MARIDI PAYAM, MARIDI COUNTY,
WESTERN EQUATORIA STATE,
SOUTH SUDAN
By Oyet Charles Okech
(2014)
Title page
i
ii
CERTIFICATION STATEMENT AND DECLARATION
Certification StatementI the undersigned, certify that this dissertation is the work of
the candidate carried out during his studies under my direct
supervision. I have read and hereby recommend for examination,
the dissertation entitled “Mothers’ Knowledge, Attitudes and Practices
(KAPs) on the Care of Newborn, Maridi Payam, Maridi County,”
……………………………………
Manana David
Date…../………../2014
DeclarationI Oyet Charles Okech declare that this dissertation is my own
work and it has never been presented to any other institution for
similar or any other award.
…………………………………
Oyet Charles Okech
Date………/…………./2014
iii
ACKNOWLEDGEMENTFirst of all I am grateful to Almighty God for his abundant
grace, blessings and unconditional love that enabled me to carry
out this study.
In addition my special thanks go to the following;
Mr. Vundru Dominic, head of research department, for his
guidance in research methodology
The Principal- Mr Patrick Taban, and Mrs. Ayakaka Margaret-
Head of midwifery department, for their expert guidance,
suggestions, encouragement, and support, and help rendered
to me throughout this study
My Supervisor- Mr. David Manana, for his guidance, support
and supervision during this study
My study respondents for their wholehearted participation in
the study, without them my study would be an incomplete one.
Finally I extend my sincere thanks to everyone who helped me
directly or indirectly in the successful completion of this
study.
May God Bless You All!
Oyet Charles Okech
iv
v
DEDICATIONThis work is dedicated to my mother, Ayaa Olga Dario and Dad
Okech Michael Okot, in appreciation for their efforts and the
tough times they went through in raising me.
vi
Table of ContentsTitle page.....................................................iCERTIFICATION STATEMENT AND DECLARATION.......................iiACKNOWLEDGEMENT..............................................iiiDEDICATION....................................................iv
List of tables.......................................viList of figures.....................................viiList of Acronyms...................................viiiDefinition of Terms & Concepts.......................ixABSTRACT.......................................................xCHAPTER ONE: INTRODUCTION......................................1
1.3 Justification.....................................21.6 Background to the Study Area.....................3CHAPTER TWO: LITERATURE REVIEW.................................4
2.1 Knowledge on the care of the newborn..............42.2 Attitudes/believes on the care of the newborn.....52.3 Mother’s Practices on the care of the newborn.....6CHAPTER THREE: METHODOLOGY....................................12
3.1 Introduction.....................................123.6 Data Analysis Method.............................13CHAPTER FOUR: RESULTS........................................14CHAPTER FIVE: DISCUSSION.....................................25CHAPTER SIX: CONCLUSION AND RECOMMENDATIONS...................30
6.1 Conclusion.......................................306.2 Recommendations..................................30REFERENCES....................................................31
vii

APPENDICES....................................................37APPENDICESNDIX I: INTRODUCTORY LATTER.........................37APPENDIX II: CONSENT FORM.....................................38APPENDIX III: QUESTIONNAIRE...................................39APPENDIX IV: MAP OF MARIDI COUNTY.............................44
List of tablesTable 1: Showing Maridi Payam Bomas with Total Population......3Table 4.1: Participants by Marital status.....................15Table 4.2: Respondent by Parity...............................15Table 4.3: Respondent by Age group............................15Table 4.4: Complications immediately after birth..............17Table 4.5: Place of care when the baby sick...................17Table 4.6: Preferred Place of delivery........................18Table 4.7: Assistance during Delivery.........................19Table 4.8: Status of Instrument Used to cut the cord..........20Table 4.9: Materials Used To Tie the Cord.....................20Table 4.10: Time of Initiating Breastfeeding..................21Table 4.11: Cleaning Of Breasts before Feeding................22Table 4.12: Daily Breastfeeding Practices.....................22Table 4.13: Immunizing the Newborn after Delivery.............23
viii
List of figures
Figure 4.1: Respondent by Education level.....................14Figure 4.2: Respondent by Religion............................14Figure 4.3: Awareness of the need to attend ANC clinic........16Figure 4.4: ANC Attendance among respondents..................16Figure 4.5: Number of ANC clinic visits per respondent........17Figure 4.6: Complications babies had at birth.................17Figure 4.7: Knowledge of symptoms of newborn illness..........18Figure 3.8: The Place Respondents would recommend others to deliver from..................................................19Figure 3.9: Showing instruments used to cut the cord..........20Figure 4.10: Material Applied On the Cord Stump...............21Figure 4.11: Giving Other Feeds after Birth...................22Figure 4.12: Time of initiating the first bath................23Figure 4.13: Measures taken to protect Baby from falling sick. 24
ix
List of Acronyms
ANNW; Africa Newborn Network
C/S; Caesarean Section
CHD; Community Health Department
CHD; County Health Department
ENC; Essential Newborn Care
FGD; Focuses Group Discursion
HBPs; Health Belief and Practices
KAPs; Knowledge Attitude and Practices
KMC; Kangaroo Mother Care
KMC; Kangaroo Mother Care Method
MNCH; Maternal, Newborn, and Child health
MoH; Ministry of Health
NHT; National Health Training Institute
PHC; Primary Health Care
STC; Save the Children
SVD; Spontaneous Vaginal Delivery
TBA; Traditional Birth Attainder
V/E; Vacuum Extraction
VDCs; Village Development committees
WHO; World Health Organizatio
x
Definition of Terms & Concepts
Mother: in this study are refers to any female parent or guardian
of children.
Caretaker: In this study are refers to nay one who are looking
after the newborn if the mother is dead of absent.
Knowledge: the facts, information, understanding that a person
has acquired through experience or education. (Soanes, 2007)
Attitude: is a way of thinking about something or behaving
towards something (Brooker, 2006)
Practice: the actual doing of something; action as contrasted
with ideas. (Soanes, 2007)
Exclusive breast-feeding: refers to giving the infant only breast
milk; no other liquid solids, except vitamin or mineral drops and
medicines up to 6 months.
Population: Is defined as group of individuals that share one or
more characteristics from which data can be gathered and analyzed
(Nieswiadomy, 2008).
Bomas: refers to a village within the payam.
Payam: refers to the sub-county
Newborn: In this study newborn refers to an individual from birth
to four weeks (28days) of age.
Newborn care: In this study this refers to care of the baby from
birth to four weeks of age.
xi
Assessment: In this study assessment refers to the critical
analysis and evaluation or judgment of status about mother/
caretaker.
Midwife: is a health care provider who is trained in the care of
pregnant women and young infants.
Traditional birth attendant: -traditional women with ability to
deliver pregnant women.
xii
ABSTRACT
A study on the care of the newborn in Maridi payam was carried
out in Maridi in July 2014 with the objective assessing Mother’s
knowledge, attitudes and practices on the care of the newborn in
the community.
It was be cross sectional explorative study that involved both
quantitative and qualitative data. Cluster and convenience
sampling techniques were used. Data was collected using
interviewer questionnaires and was analyzed manually.
The main findings of this study were that; the majority mothers
in Maridi payam had adequate and relevant knowledge in the care
of the new born in the community. The majority of mothers in the
payam generally had a positive attitude towards newborn care
services available at Maridi Hospital and other health facilities
in the payam despite the fact that the majority of them continued
to deliver from their homes.
It was then concluded that though most of the respondents in this
study had satisfactory knowledge and positive attitudes towards
the recommended newborn care, they generally lacked the practical
application especially in; hospital deliveries, improper cord
care and immunization.xiii
It was then recommended that all pregnant women in Maridi payam
encouraged to attend at least 4 ANC visits and to deliver from
Hospital. The State Minister of Health should organise training
for all TBAs in Maridi payam and beyond since more mothers in
this payam delivered at home than hospital. All women of
childbearing age should be educated more on proper neonatal care
including; proper cord are, prevention of neonatal hypothermia,
early initiation of breastfeeding, exclusive breastfeeding on
demand at least 8 times a day and general hygiene. All newborns
in Maridi payam should be vaccinated with BCG as early as
possible after birth and with OPV0 within the first 14 days.
Finally all health workers should include men in the campaigns to
promote proper care of the new born as substantial house hold
heads in Maridi payam.
xiv
CHAPTER ONE: INTRODUCTION
1.1 Background informationChild rearing practices depend on the traditional beliefs and
practices. Healthy beliefs and practices lead to a healthy child
upbringing. According to Save the Children (2004) the newborn
child is extremely vulnerable unless it receives appropriate
basic care, also called essential newborn care. When normal
babies do not receive this essential care, they quickly fall sick
and too often they die. For premature or low birth weight babies,
the danger is even greater.
Approximately four million global neonatal deaths that occur
annually, out of which 98% occur in developing countries. Most of
the newborns die at home under the cared of their mothers,
relatives and or traditional birth attendants. In Nepal, for
instance approximately 90% of birth occurs at home. In 2005, the
infant mortality rate in Nepal was 64 per 1000 live and the
neonatal mortality rate was 39 per 1000 live births. In addition
to the direct causes of death, many newborns die because of their
mother’s poor health or because of lack of access to essential
care. Sometimes the family may live hours away from a referral
facility or there may not be a skilled provider in their
community (Save the children, 2004).
In sub-Sahara Africa each year at least 1.16 million babies born.
This region has highest risk of newborn death and the slow
1
progress in reducing mortality and morbidity. More than two
thirds of these babies could be saved with lower cost, low skill
action, most of which are already in policy but do not reach the
poor (ANNW, 2009).
The greatest obstacle to quality Maternal, Newborn, and Child
Health (MNCH) in South Sudan is a lack of skilled MNCH care
providers, culture and mother knowledge on newborn care. The
infant and child mortality rates are estimated at 102 and 235
deaths per 1,000 live births, respectively. Meanwhile, more than
one in four children under the age of five is malnourished and
only approximately 10% of children are fully vaccinated. (Brett
et al, 2011)
This study therefore explored the knowledge, attitudes and
practices that influence the care of the newborn among
mothers/caretakers in Maridi community.
2
1.2 Statement of the Problem
The fact that only a few Mothers deliver from Maridi hospital
means that the majority deliver from their homes often with the
help of unskilled birth attendants. These newborns are often
subjected to unhygienic delivery practices arising from
traditional beliefs and taboos that put their survival at risk in
Maridi payam and Maridi County in general.
1.3 JustificationIt was anticipated that this study would identify the gaps in the
knowledge, attitude and practices on the care of the newborn and
recommend ways of bridging the identified gaps to improve
neonatal survival in Maridi Payam.
1.4 Research Question
What cultural beliefs and practices influence the care of newborn
in Maridi payam?
1.5 Study Objectives
1.5.1 Broad objective
This study sought to identify the household practices that
influence newborn care and survival in Maridi County
1.5.2 Specific objectives were;
1) To assess the Mothers’ knowledge on the care of the newborn
2) To assess the Mothers’ attitudes and beliefs towards the care
of the newborn.
3
3) To assess the Mothers’ practices in the care of the new born.
4
1.6 Background to the Study AreaMaridi payam is one of the six payams in Maridi County of Western
Equatorial State of South Sudan. This Payam subdivided in to 5
Bomas with an estimated population of 49,454 people. Maridi payam
is a peri-urban area inhabited by several ethnics groups of which
the Zande are the majority. Other tribes include; Moru, Avokaya
and Baka. Their cultural beliefs and practices on the care of the
newborn differ according to their ethnicity.
Table 1: Showing Maridi Payam Bomas with Total Population
S/
No
Bomas Population
1. Maridi town 19,186
2. Mabirindi 6,519
3. Mboroko 8,567
4. Modobow 5,096
5. Nagbaka 10,086
Total 49,454
5

6
CHAPTER TWO: LITERATURE REVIEW
2.0 IntroductionIn this chapter the researcher reviewed publications and studies
on the care of the newborn in line with the study objectives. It
is divided into three study themes of knowledge, attitudes and
practices that influence the care of the newborn.
2.1 Knowledge on the care of the newbornNewborn care aims at ensuring that the baby is made comfortable,
is able to feed and facilities are available to help parents with
the attachment process. It is also important to ensure that the
baby is protected from airway obstruction, hypothermia, injuries,
and infections (Myles, 2003). Hygiene and aseptic conditions
may be unknown or very difficult to achieve in many poor
communities. People may not be aware of the environmental dangers
of infection and may not make much effort in combating them, this
pervasive acceptance of unhygienic conditions may extend to cord
care, drying and wrapping of the newborn etc (Parlato et al.,
2004).
According to BBC Media Action’s South Sudan (2012), found that
the majority of women who were or had been pregnant did know that
they should attend some form of antenatal care (ANC) more than
once. However, they were not clear about what ANC really
entailed. Many felt that having a TBA check the position of a
baby in the last months of pregnancy was adequate and were not
7
aware of any specific number of times that they should attend
ANC. Many women felt that they were unable to plan regular ANC
check-ups due to responsibilities at home and a lack of money.
According Tarimo (2000) & Chibwana et al, (2009) mothers and
caregivers in Tanzania and Malawi did not have inadequate
knowledge regarding the causes and treatment of conditions such
as sepsis and malaria. However they had knowledge of danger signs
such as fever in infants. In another study conducted in a rural
community in northern India to assess household knowledge that
can affect neonatal health among 200 caregivers, it was reported
that caregivers identified illness among neonates in the form of
continuous crying (Awasthi et al., 2008).
Panul & Deadihic, (2007) defined a healthy newborn as one born at
term (between 38 to 42 weeks of gestation), and cries immediately
after birth. The period from birth to 28 days of life was
referred to as neonatal period and the infant in this period is
termed as neonate or newborn. The morbidity and mortality rate in
newborn are high and hence the need for optimal for improved
survival.
According to Padiyath et al, (2010) the study done in India found
that older and educated women with higher social economic status
were significantly associated with higher knowledge scores for
right neonatal care practices. In another study to assess the
mothers' knowledge and practices of basic newborn care given at
home in Obstetric University Hospital in Tanta City revealed that
8
mothers' knowledge and practices were within good and
satisfactory in most of the studied items related to newborn care
giving at home except breast feeding Helmy, & Bahgat (1998).
A study conducted among postnatal mothers in southern India
revealed that the knowledge of mothers was inadequate in areas of
umbilical cord care (35%), thermal carea (76%) and vaccine
preventable diseases. However 19% of them still practiced oil
instillation into nostrils of newborns and 61% of them
administered gripe water to their babies (Asif et al, 2010).
2.2 Attitudes/believes on the care of the newbornIn Malawi Demographic and Health Survey it was reported that many
prevailing cultural and social norms and practices were known to
be barriers to improving survival and health of newborns in
Malawi concerning newborn care (Malawi National Statistics
Office, 2004).
An epidemiological study was carried out in Yaounde, Cameroon,
revealed that 98% of mothers breastfed their children. However 2%
of mothers who did not breast-feed their children because of the
belief that milk flow was not enough or the infant’s refusal to
suckle as the main reason (Pascale, et al., 2007).
A study conducted to determine behavior’s related to immediate
care of newborn in Kailali district, Nepal showed that most
people were unaware of importance of immediate care of newborn
and many unsafe behaviors did exist based on deep-seated
traditional beliefs (Gurong, 2008).
9
Another study in Nepal reported that newborn babies were
considered dirty as they came out of their mother’s womb, hence
almost all newborn babies were bathed within the first hour of
birth. The same study revealed that colostrum was regarded as
dirty milk in some communities, and as a result babies were fed
with cow or goat milk immediately after birth for the popular
belief that it will make the baby become more intelligent (Yadav,
2007).
According to results of study which conducted on traditional
beliefs as influencing factors on breast-feeding performance in
Turkey it found that more than 30% of the mothers believed that
colostrum should not be given to the newborn, and others believed
that breast milk could harm their babies, (HIzel et al., 2006).
Another study by Ergenekon-ozelci (2006) showed that the mothers
generally had a positive attitude towards breast-feeding. However
colostrum was usually perceived negatively. No woman was found to
feed her infant exclusively by breast-feeding.
According to Hake-Brooks & Anderson (2008) mothers' perception of
the skin-to-skin contact in the kangaroo-carrying position had
improved with the majority of them practicing it more competently
and confidently than mothers whose babies were under conventional
incubator care. Most mothers were happy because they felt that
the kangaroo method was safe, and did not separate them from
their infants.
10
A study on mother’s attitudes towards immunization in Western
Nigeria revealed that almost 97.6% mothers who attended antenatal
clinic thought their child should be immunized. However 8.2% of
the respondents believed that immunization caused fever while 5%
believed it causes deformity while others believed that local
herbs were good substitutes for immunization (Adeyinka, 2008).
Another study conducted in Aweil East and North counties in
northern Bahr-el-Ghazal region to determine attitude toward
immunization revealed that most mothers had good knowledge and
attitudes towards immunization and said it protected against
diseases such as polio and measles. However two mothers did not
like immunizations, especially the polio vaccine, because
complained that it made children sick. One mother said that the
child’s father was against immunization because it was against
their culture (Cyprian et al, 2011).
2.3 Mother’s Practices on the care of the newbornA survey was carried out in the immunization clinics of Pokhara
city of western Nepal revealed that 90% of deliveries took place
at home. However information about reasons for delivering at home
and newborn care practices in urban areas of Nepal is lacking
(Sachdev, 2006).
There are marked variations in patterns of newborn care and
interventions. Knowledge on what is needed for optimal newborn
care is lacking in many cases. Modern hospital practices as well
11
as traditional practices neglect the basic needs of newborns,
these basic needs include: warmth, cleanliness, breast milk,
safety and vigilance. Other interventions such as: thermal
protection, breast-feeding, eye care (to reduce blindness), have
essential preventive effects (WHO, 2006).
The World Health Organization (WHO, 1996) recommends the
following essential newborn care interventions:
Clean childbirth and cord care in order to prevent infection
Thermal protection in order to prevent and manage newborn
hypo/hyperthermia
Early and exclusive breastfeeding which should be started
within 1 hour after child birth
Initiation of breathing and resuscitation to facilitate
early asphyxia identification and management
Eye care for the prevention and management of ophthalmia
neonatorum
Immunization: at birth with Bacilli Calmette-Guerin (BCG)
vaccine, Oral Poliovirus vaccine (OPV) and Hepatitis B virus
(HBV) vaccine
Identification and management of the sick newborn
Care for the preterm and/or low birth weight newborn
The study focused specifically on practices such as clean
child birth, Early and exclusive
breastfeeding, immunization of BCG and OPV, recognition and
management of the sick newborn
12
There should be clean cord care procedures which are crucial in
infection prevention. The
Umbilical cord should be cut with a clean (sterilized) blade and
tied with clean (sterilized)
Materials, and no substances should be put on the cord stump
(WHO, 1996).
Sometimes blades of grass, bark fibres, reeds or fine roots are
used to cut the cord. This is Harmful because these materials
often harbour tetanus spores from the soil and thus increase the
risk of neonatal tetanus. Materials such as threads, strips of
cloth and strings are used to tie the cord (Woodruff et al.,
1984).
The cord stump remains the major means of entry for infections
after birth. Principles of clean cord stump care stipulate
keeping the cord dry and clean and nothing is applied anything on
it, neither at home nor in the health facility. The stump will
dry and mummify if exposed to air without any dressing, binding
or bandages. It will remain clean if it is protected with clean
clothes and is kept from urine and soiling. No antiseptics are
needed for cleaning. If soiled, the cord can be washed with clean
water and dried with clean cotton or gauze. Local practices of
putting various substances on the cord stump - whether in health
facilities or homes - should be carefully examined and
13
discouraged if found harmful and substituted with acceptable ones
(WHO, 2006).
If the umbilical stump becomes red, drains pus with the redness
extending to the skin around it, the baby stops suckling well, is
sleepy, does not wake up or is having difficulty breathing, this
may be a sign of serious infection. The mother or caretaker
should seek help from a health facility. The baby must be
referred immediately to the hospital for proper treatment (WHO,
2006).
In the Sylhet District of Bangladesh, among the substances that
were applied on the cord stump, after cord cutting; turmeric was
the most common. Umbilical stump care revolved around bathing,
skin massage with mustard oil and heat massage on the umbilical
stump.
Mothers were the principal provider for skin and cord care during
the neonatal period. Unhygienic cord care practices are prevalent
in the study area. (Alam et al., 2008).
According to NSO, UNICEF& MIC (2006 & 2008) in Malawi most
newborns and mothers do not receive postnatal care (PNC) services
from skilled health care providers during the critical first few
days after delivery. The result also established that only four
percent of newborns received post natal care the first week after
delivery. Community based study conducted in Sudan indicated that
14
54.2% of mothers initiated breastfeeding after one hour from
delivery and 39.7% of them initiated breastfeeding during from
two hours to 24 hours and only 6.0% of the mothers initiated
breastfeeding after one day (Haroun, 2008).
Mriso et at (2008) in their study on understanding home based
neonatal care practices in rural Tanzania reported that the
majority of detrimental practices to newborns during the neonatal
period included delay in providing warmth after delivery and
bathing newborns soon after birth.
A study by Mesko et al (2003) found that major obstacles to
accessing newborn care were “the need to wait and watch” and
preference to treat illness within the community. Similar
findings were also found in India where traditional medicines
were used for treatment of neonatal conditions such as bulging
fontanelle, chest in-drawing and rapid breathing (Ogunlesi &
Oufowora, 2010).
According to Zulfia et al., (2009) the material used for cutting
cord in urban slums included; a new blade in 59.9% of the cases
but by traditional objects such as the edge of a broken cup in
40.3% of the cases. In addition the results showed that 50% of
the home deliveries were attended by Trained Birth Attendants and
40% were attended by untrained birth attendants.
Culturally, most African communities practice mixed feeding
instead of exclusive breastfeeding. In most circumstances,
15
primary health practitioners advised mothers according to formal
guidelines without being adequately aware of the mothers’
preferences, skills and home circumstances (Bland et al., 2002).
A study conducted among the rural poor in western Uttar Pradesh,
to identify factors influencing
newborn care showed that nearly all newborns were left wet and
naked on the floor until the placenta was delivered and bathed
immediately after birth. Very few birth attendants
washed their hands with soap before assisting the delivery. It
also revealed that they used new blade dipped in hot water to cut
the cord but used unsterilized cord ligature (Sethi et al.,
2005).
Early contact (immediately after birth) between the mother and
the baby, according to the WHO (1999), has a beneficial effect on
breast-feeding. Early suckling provides the baby with colostrum
that offers protection from infection, gives important nutrients,
and has a beneficial effect on maternal uterine contractions.
Khadduri et al. (2007), state that most women breastfed their
babies, but initiation within 1 hour of birth and colostrum
feeding were not common.
The baby's skin and gastrointestinal tract are colonized with the
mother's microorganisms, against which she has antibodies in her
breast milk. Important factors in establishing and maintaining
breast-feeding after birth include:
• giving the first feed within one hour of birth,
16
• correct positioning that enables good
• attachment of the baby,
• frequent feeds,
• no prelacteal feeds or other supplements, and
• Psychosocial support for breast-feeding mothers.
Babies have a wide range of behaviors following spontaneous
delivery and are not all ready to feed at the same time. A
skilled person can help to facilitate the process by ensuring
correct positioning and attachment. A healthy baby has no need
for large volumes of fluid any earlier than they become available
physiologically from the mother's breast. There is no evidence to
support the practice of providing supplementary feeds of water,
glucose or formula. Traditional prelacteal feeds should be
strongly discouraged although harmless rituals may be allowed so
long as they do not delay breast-feeding. Every birth attendant
should also know the importance of unrestricted feeding and the
ways to support breast-feeding mothers. Mothers should be
instructed about the need for an adequate diet to sustain
lactation. They should be helped and encouraged if they have
difficulties breast-feeding (WHO, 1996).
Another study conducted in Haryana, India revealed that 75
percent of newborns were given prelacteal feeds of honey, tea and
diluted milk, and babies are often not breastfed during the first
3 days. They were often given sweetened water; this presumes that
17
colostrum was discarded (Bhandari et al., 2003). In contrast Li
Salami., (2006) reported that 82% of the mothers in Edo State,
Nigeria practiced breastfeeding, 66% supplemented with corn gruel
and glucose water, and 14% used herbal brew. Only 20% practiced
exclusive breastfeeding.
A survey conducted in Aweil East and North counties in northern
Bahr-el-Ghazal region showed that most mothers (94%) breastfed
their babies within one hour of birth and 6% gave cow milk
immediately after birth. 82% of them breastfed on demand
especially during daylight, and 69% breastfed 2-3 times at night
(Cyprian, 2005)
The preterm infants on KMC have been found to have reduced rates
of severe morbidity compared to those on conventional care. Low
birth weight infants on Kangaroo Mother Method (KMM) had a
significantly lower rate of morbidity than the control group
(Sachdev, 2006& Sloan, 1994).
A study conducted on the impact of newborn bathing on the
prevalence of neonatal hypothermia in Uganda revealed that
bathing newborn babies shortly after birth increased the risk of
hypothermia. On the other hand the use of warm water and skin-to-
skin care for thermal protection of the newborn reduced the risk
of hypothermia (BergstrAqm et al., 2005).
18
The WHO (1996) stipulates that BCG should be given as soon after
birth as possible in all populations at high risk of tuberculosis
infection, and a single dose of OPV should be given at birth or
two weeks after birth (this is recommended to increase early
protection). Hepatitis B vaccine (HBV) should be integrated into
national immunization programmes in all countries by 1997. Where
perinatal infections are common it is important to administer the
first dose as soon as possible after birth.
Newborns are more likely to survive if delivery is clean, that is
if actions are taken to help prevent infection. Ensuring a clean
delivery implies:
• That all those attending to the mother and newborn wash
their hands with soap and water before during and after
delivery.
• The perineal area of the vagina is washed before each
examination and before delivery, and no foreign material is
introduced into the vagina (the examiner’s hand only when
necessary).
• Delivery surface is clean, or at a minimum, birth doesn’t
occur on the bare floor.
(Parlato et al., 2004).
According to the WHO (1996), many newborn problems can be
prevented by the interventions described above. However, when a
disease occurs, many deaths can be avoided if the signs are
recognized early and the newborn managed effectively.
19

20
CHAPTER THREE: METHODOLOGY3.1 Introduction
This Chapter presents the description of the methodological
approach that was used in collecting and analyzing the data. The
following sub-topics are covered in this chapter: research
design, target population, sampling methods Data collection
instruments (tools), and data collection procedures and data
analysis methods.
3.1 Study Design
This was a cross-sectional explorative study that employed both
quantitative and qualitative study approaches
3.2 Sampling Procedures
The sampling method used was cluster and convenience sampling
technique. The 5 bomas in Maridi payam formed 5 clusters from
which 10 mothers or caretakers of newborns per cluster were drawn
by convenience sampling to make a total of 50 mothers.
3.3 Study Population
The study population was 50 mothers and caretakers of newborn
babies in Maridi payam.
3.4 Data Collection Tools
21
A structured interview questionnaire was used to collect data
from respondents. Each questionnaire consisted of 2 main parts
namely;
Part A: That was used to assess the demographic data (age,
educational status, occupation, family income, religion, type of
family birth history, birth weight, area of residence).
Part B: That was used to assess the knowledge, attitudes and
practices of newborn care among mothers and caretakers in Maridi
payam.
3.5 Data Collection Methods
Data collection was by face to face interview guided by the
questionnaire.
3.6 Data Analysis Method
Both quantitative and qualitative data were analyzed manually.
3.7 Pretesting Methodology
A pre-test was carried out in a one boma out of the five in
Maridi payam before the actual study.
3.8 Quality Control
All filled questionnaires were checked daily for completeness and
consistency of the responses to eliminate possible errors.
3.9 Ethical Considerations
22
Relevant permissions and approval was sought from NHTI and Maridi
county authorities before the study. Every participant [mothers]
was briefed about the study in order to gain her informed consent
to participate.
3.10 Dissemination of the Study Findings
The findings of the study will be submitted to the Head of
Midwifery Department of NHTI for marking after which copies will
be disseminated to the Maridi County Health department (CHD) and
Maridi hospital.
23
CHAPTER FOUR: RESULTS
Introduction This chapter presents the finding of this study as detailed below
according to the study objective. In this 50 mothers were interviewed
about their knowledge attitudes and practices on the care of the
newborn in Maridi Payam.
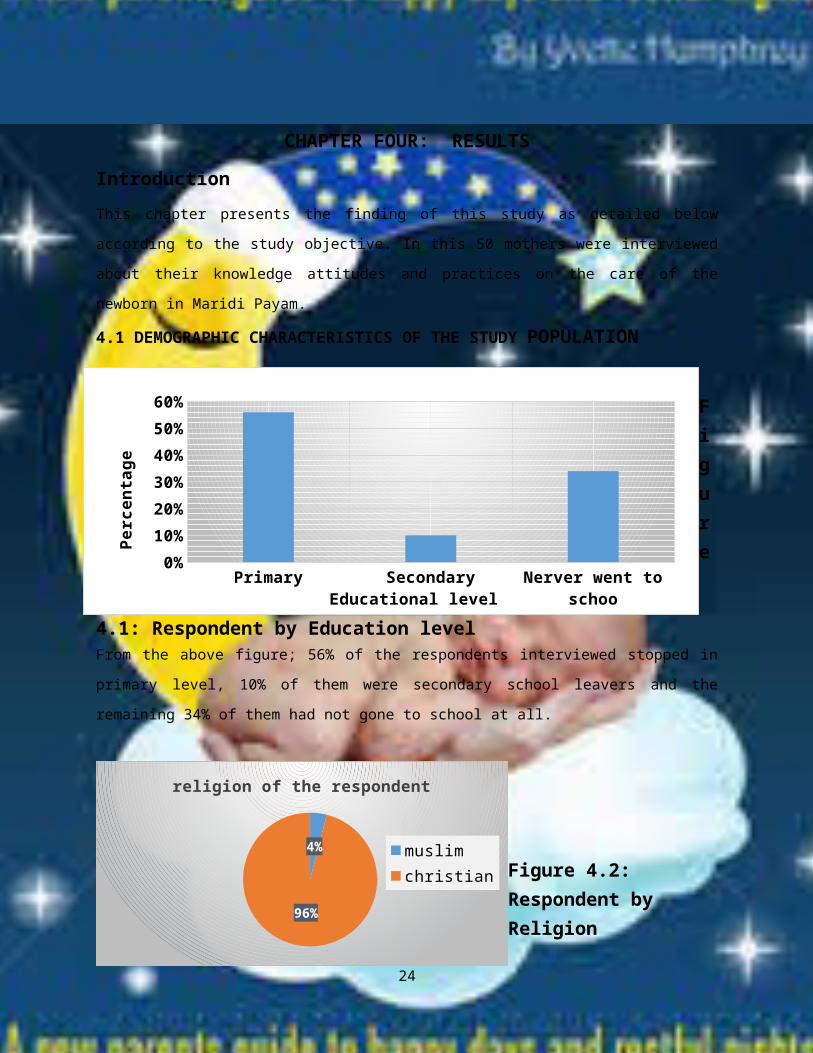
4.1 DEMOGRAPHIC CHARACTERISTICS OF THE STUDY POPULATION
Figure
4.1: Respondent by Education levelFrom the above figure; 56% of the respondents interviewed stopped in
primary level, 10% of them were secondary school leavers and the
remaining 34% of them had not gone to school at all.
Figure 4.2: Respondent by Religion
24
Primary Secondary Nerver went to schoo
0%10%20%30%40%50%60%
Educational level
Perc
enta
ge
4%
96%
religion of the respondent
muslimchristian
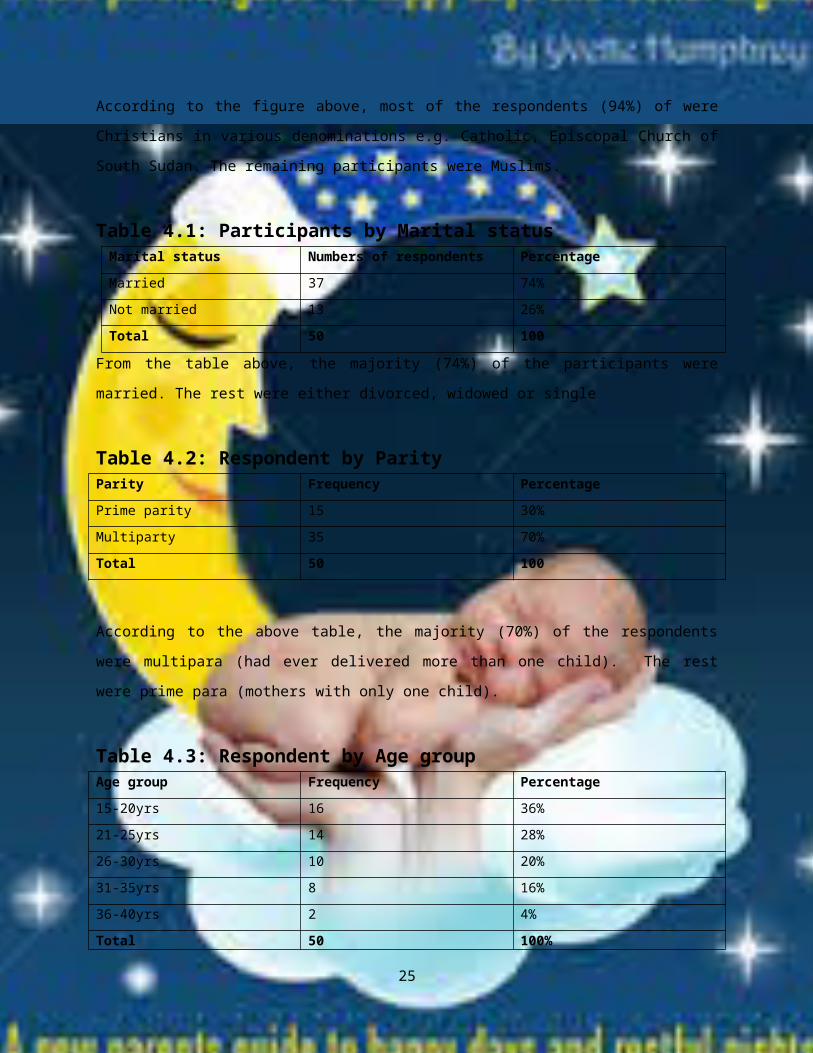
According to the figure above, most of the respondents (94%) of were
Christians in various denominations e.g. Catholic, Episcopal Church of
South Sudan. The remaining participants were Muslims.
Table 4.1: Participants by Marital status Marital status Numbers of respondents PercentageMarried 37 74%Not married 13 26%Total 50 100
From the table above, the majority (74%) of the participants were
married. The rest were either divorced, widowed or single
Table 4.2: Respondent by Parity Parity Frequency PercentagePrime parity 15 30%Multiparty 35 70%Total 50 100
According to the above table, the majority (70%) of the respondents
were multipara (had ever delivered more than one child). The rest
were prime para (mothers with only one child).
Table 4.3: Respondent by Age group Age group Frequency Percentage15-20yrs 16 36%21-25yrs 14 28%26-30yrs 10 20%31-35yrs 8 16%36-40yrs 2 4%Total 50 100%
25

From the above table, the age group with highest fertility rate was
15-20years-just because this age group had more mothers participating
in this study. The age group with the least number of children was 36-
40 years
4.2 MOTHER’S KNOWLEDGE ON THE CARE OF THE NEWBORN
Figure 4.3: Awareness of the need to attend ANC clinicAccording to the figure above, the majority (94%) of the mothers were
aware of the importance of attending ANC checkup. However 6% of them
were not aware at all.
26
88
12%
Awareness of the need to attent ANC clinic
YesNo
Yes96%
No4%
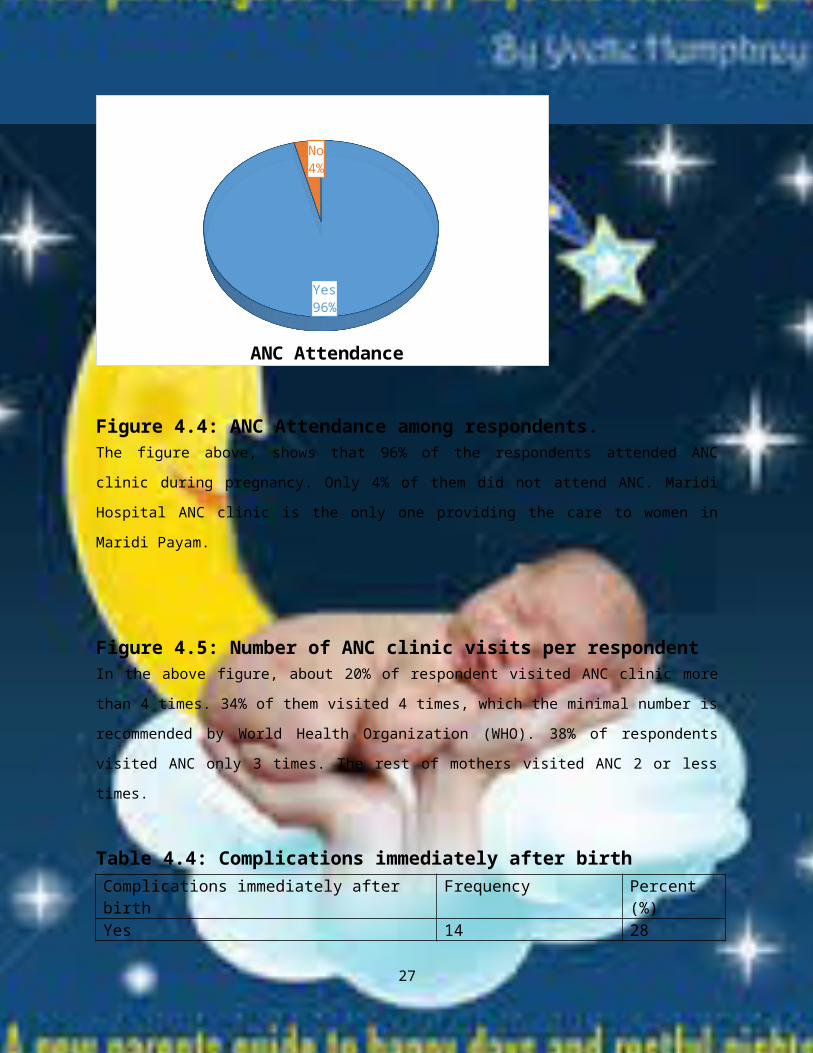
ANC Attendance
Figure 4.4: ANC Attendance among respondents.The figure above, shows that 96% of the respondents attended ANC
clinic during pregnancy. Only 4% of them did not attend ANC. Maridi
Hospital ANC clinic is the only one providing the care to women in
Maridi Payam.
Figure 4.5: Number of ANC clinic visits per respondentIn the above figure, about 20% of respondent visited ANC clinic more
than 4 times. 34% of them visited 4 times, which the minimal number is
recommended by World Health Organization (WHO). 38% of respondents
visited ANC only 3 times. The rest of mothers visited ANC 2 or less
times.
Table 4.4: Complications immediately after birth Complications immediately after birth
Frequency Percent (%)
Yes 14 28
27
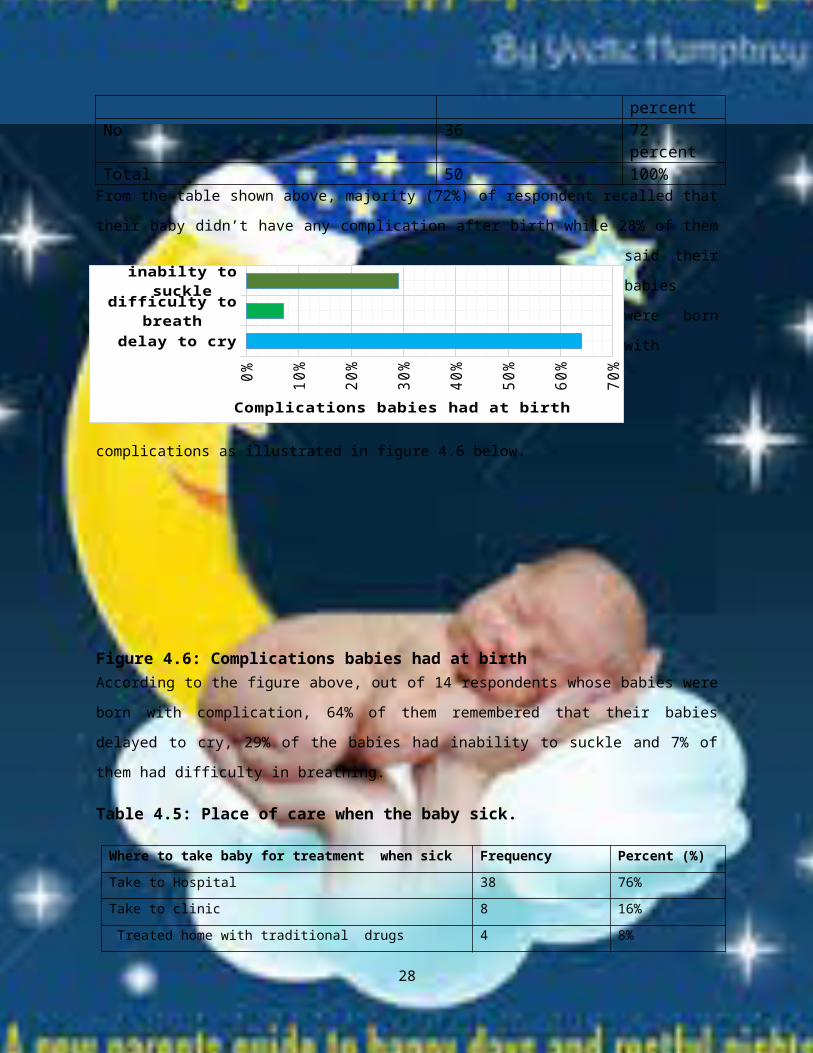
percentNo 36 72
percentTotal 50 100%From the table shown above, majority (72%) of respondent recalled that
their baby didn’t have any complication after birth while 28% of them
said their
babies
were born
with
complications as illustrated in figure 4.6 below.
Figure 4.6: Complications babies had at birth According to the figure above, out of 14 respondents whose babies were
born with complication, 64% of them remembered that their babies
delayed to cry, 29% of the babies had inability to suckle and 7% of
them had difficulty in breathing.
Table 4.5: Place of care when the baby sick.
Where to take baby for treatment when sick Frequency Percent (%)Take to Hospital 38 76%Take to clinic 8 16% Treated home with traditional drugs 4 8%
28
delay to cry
difficulty to breath
inabilty to suckle
0% 10%
20%
30%
40%
50%
60%
70%
Complications babies had at birth
Total 50 100%
According to the table above, majority (76%) of participants reported
that sought medical care in Maridi Hospital whenever their children
fell sick. 16% of them took their sick children to clinics or bought
drugs and treated at home. However, 8% of them used traditional
remedies if the condition was not severe.
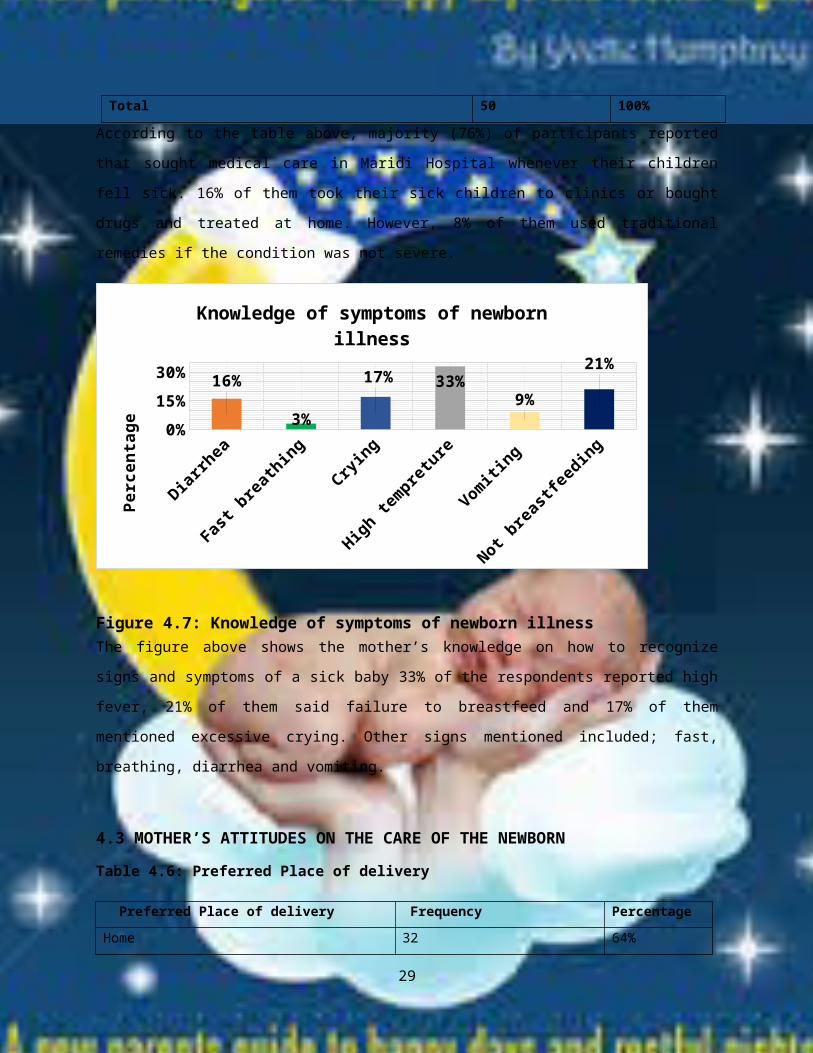
Diarrhea
Fast breathing
Crying
High tempreture
Vomiting
Not breastfeeding
0%15%30% 16%
3%
17% 33%9%
21%
Knowledge of symptoms of newborn illness
Perc
enta
ge
Figure 4.7: Knowledge of symptoms of newborn illnessThe figure above shows the mother’s knowledge on how to recognize
signs and symptoms of a sick baby 33% of the respondents reported high
fever, 21% of them said failure to breastfeed and 17% of them
mentioned excessive crying. Other signs mentioned included; fast,
breathing, diarrhea and vomiting.
4.3 MOTHER’S ATTITUDES ON THE CARE OF THE NEWBORN
Table 4.6: Preferred Place of delivery
Preferred Place of delivery Frequency PercentageHome 32 64%
29
Hospital 18 36%Total 50 100%
From the table above, it is clear that majority (64%) of participants
preferred to deliver from home while 36% of them delivered from the
hospital. Their reasons for preferring to deliver at home included;
Presence of the TBA with in the community
Abrupt onset of labour,
Long distance from home to hospital
Demand for money by Midwives demand at Maridi hospital maternity.
Those who preferred to deliver from Hospital gave the following
reasons;
Getting medication
Better management of prolonged labor
Better management of bleeding during labour
Management of complications like the baby’s failure to breath at
birth
Cleaner delivery environment in hospital.
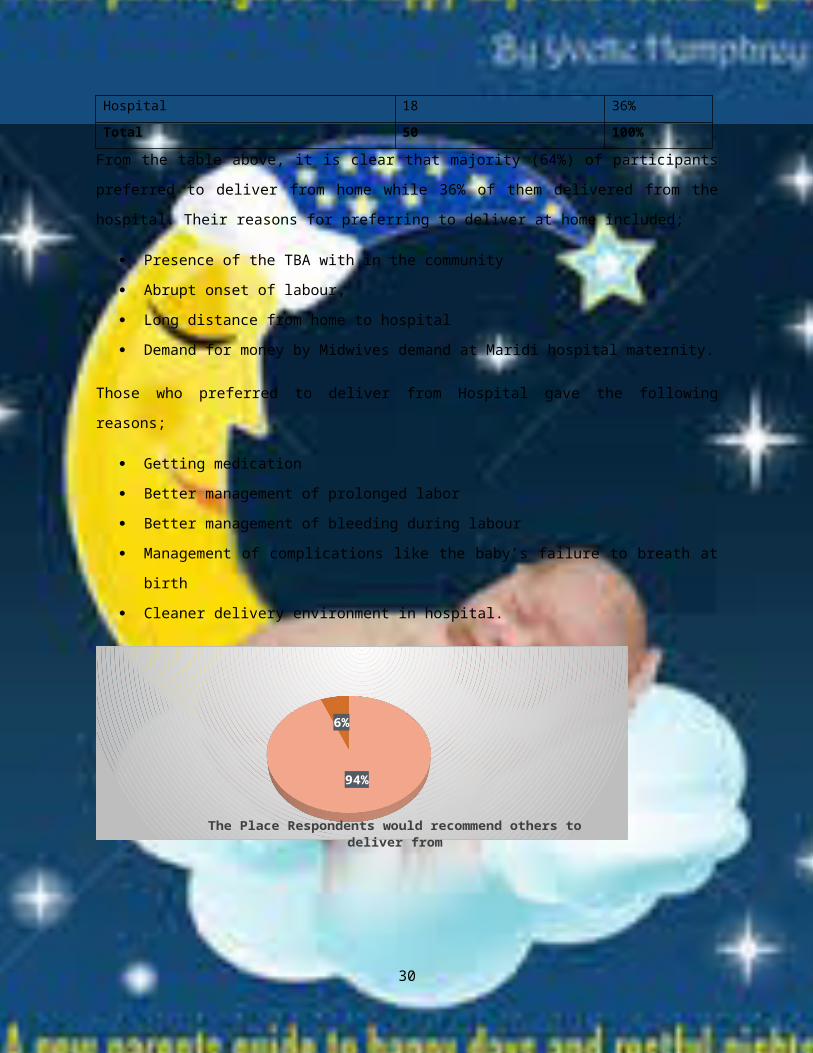
94%
6%
The Place Respondents would recommend others to deliver from
30
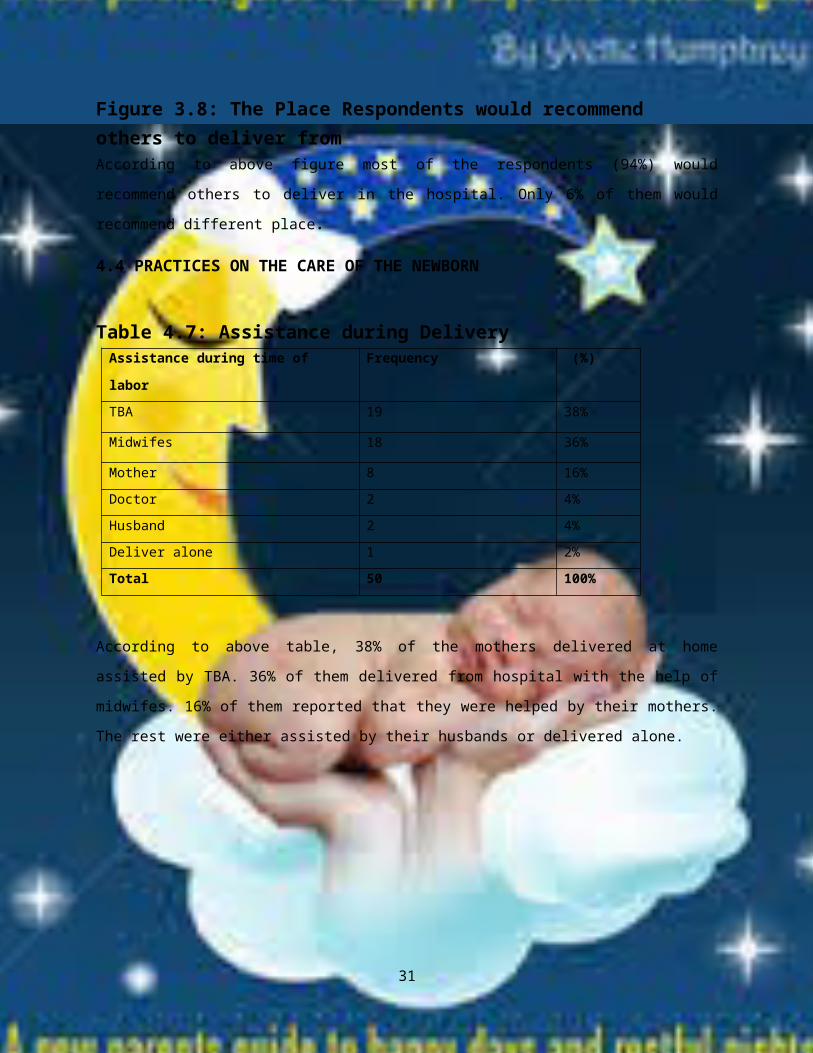
Figure 3.8: The Place Respondents would recommend others to deliver fromAccording to above figure most of the respondents (94%) would
recommend others to deliver in the hospital. Only 6% of them would
recommend different place.
4.4 PRACTICES ON THE CARE OF THE NEWBORN
Table 4.7: Assistance during DeliveryAssistance during time of
labor
Frequency (%)
TBA 19 38%
Midwifes 18 36%
Mother 8 16%Doctor 2 4%Husband 2 4%Deliver alone 1 2%Total 50 100%
According to above table, 38% of the mothers delivered at home
assisted by TBA. 36% of them delivered from hospital with the help of
midwifes. 16% of them reported that they were helped by their mothers.
The rest were either assisted by their husbands or delivered alone.
31
Scissor
32%
Razorblade 60%
Others 8%
Intrument used to cut the cord
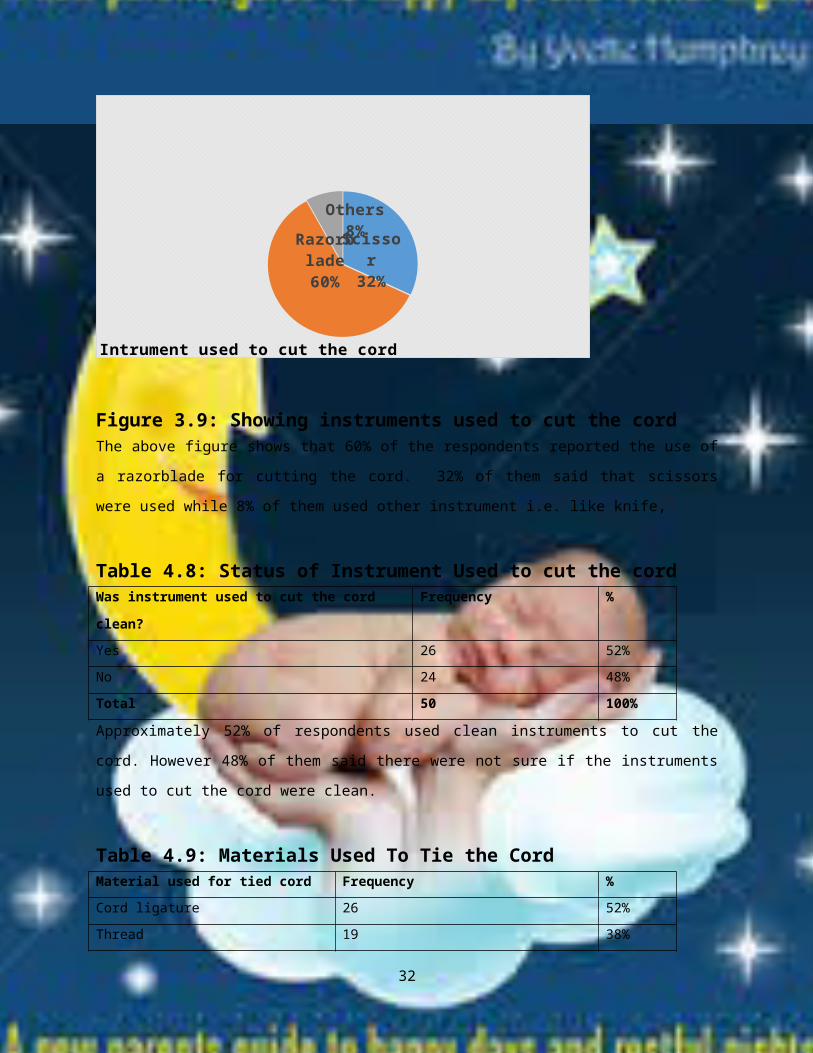
Figure 3.9: Showing instruments used to cut the cordThe above figure shows that 60% of the respondents reported the use of
a razorblade for cutting the cord. 32% of them said that scissors
were used while 8% of them used other instrument i.e. like knife,
Table 4.8: Status of Instrument Used to cut the cordWas instrument used to cut the cord
clean?
Frequency %
Yes 26 52%No 24 48%Total 50 100%
Approximately 52% of respondents used clean instruments to cut the
cord. However 48% of them said there were not sure if the instruments
used to cut the cord were clean.
Table 4.9: Materials Used To Tie the CordMaterial used for tied cord Frequency %Cord ligature 26 52%Thread 19 38%
32
Cloths 5 10%Total 50 100%
From the table above, 52% of the mothers said cord ligature was used
for tying the cord. 38% of them used threads for tying the cord and
the rest used cloths.
Diarrhea
Fast breathing
Crying
High tempreture
0% 5% 10% 15% 20% 25% 30% 35%
Material Applied On the Cord Stump
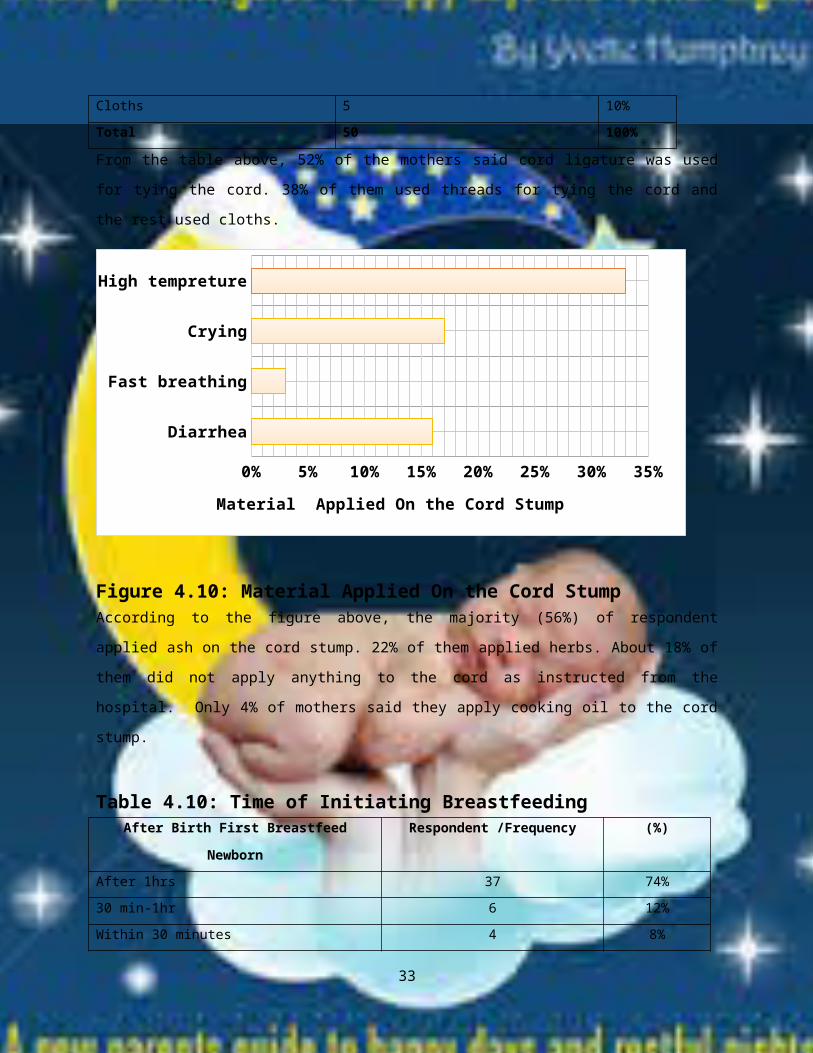
Figure 4.10: Material Applied On the Cord Stump According to the figure above, the majority (56%) of respondent
applied ash on the cord stump. 22% of them applied herbs. About 18% of
them did not apply anything to the cord as instructed from the
hospital. Only 4% of mothers said they apply cooking oil to the cord
stump.
Table 4.10: Time of Initiating Breastfeeding After Birth First Breastfeed
Newborn
Respondent /Frequency (%)
After 1hrs 37 74%30 min-1hr 6 12%Within 30 minutes 4 8%
33
Immediately 3 6%Total 50 100%
From the table above: majority (74%) of the respondents reported that
they initiated breastfeeding after 1 hour of birth. While only 6% of
them initiated breastfeeding immediately after delivery and the rest
said they started breastfeeding between 30 minutes to 1 hour.
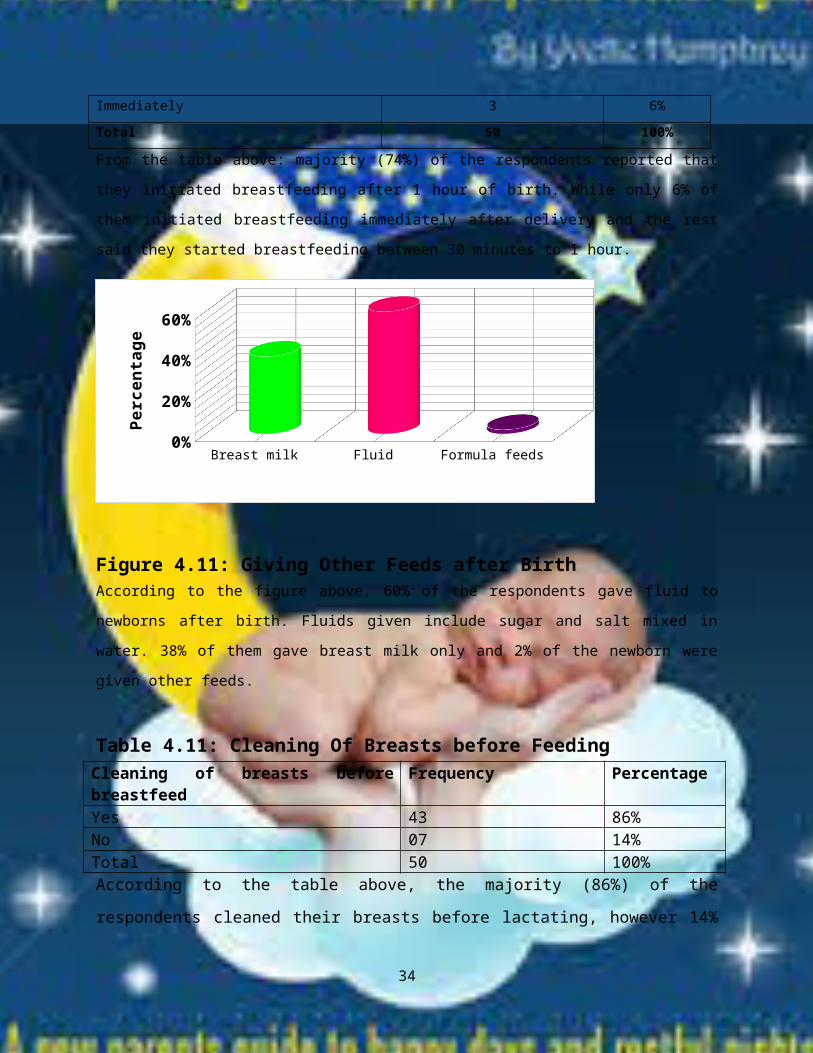
Figure 4.11: Giving Other Feeds after BirthAccording to the figure above, 60% of the respondents gave fluid to
newborns after birth. Fluids given include sugar and salt mixed in
water. 38% of them gave breast milk only and 2% of the newborn were
given other feeds.
Table 4.11: Cleaning Of Breasts before FeedingCleaning of breasts beforebreastfeed
Frequency Percentage
Yes 43 86%No 07 14%Total 50 100%According to the table above, the majority (86%) of the
respondents cleaned their breasts before lactating, however 14%
34
Breast milk Fluid Formula feeds0%
20%
40%
60%
Perc
enta
ge

did not clean their breasts before breastfeeding. Out of those
who cleaned breasts before breastfeeding, 65% used wash their
breast with water first before breastfeeding. 35% of them only
clean their breasts with baby towel or cloth before
breastfeeding.
Table 4.12: Daily Breastfeeding PracticesNumber of timesmothers breastfednewborns in a day
Frequency %
On demand 8 timesand above
45 90%
Less than 8 times in24hrs
8 8%
Other (specify) 1 2%Total 50 100%From the table above, majority (90%) of the participants said they
breastfeed their babies on demand at least 8 times a day. However the
rest breastfed less than 8 times a day.
Figure 4.12: Time of initiating the first bath
35
Immdiately after b...
After 24hrs Within 2...0%
10%20%30%40%50%60%
perc
enta
ge

From the figure above, 52% of the respondents had their babies bathed
after 24 hours. 38% of them had their babies bathed immediately after
delivering and 10% of them delayed the bathing but was done within 24
hours of birth.
Table 4.13: Immunizing the Newborn after Delivery Was your baby immunized immediately after
birth
Frequency Percentage
Yes 6 12%No 44 88%Total 50 100%
According to the table above, the majority (88%) of the mothers said
their babies were not immunized with BCG and OPV0 either on the day of
delivery nor within two weeks after delivery. However 12% of them said
their babies were vaccinated before discharge from hospital. Most of
mothers whose babies were not immunize within 2 weeks had delivered at
home and they had to wait till after 6 weeks for DPT1 and OPV1. Some of
them said they delivered in hospital but when vaccines were out of
stock and therefore their babies could not be immunized.
Hygiene Net Good nutrition
Providing warm
Don't knows
0%
10%
20%
30%
40%
50%
Measures taken to protect Baby from falling sick
Perc
enta
ge
36
Figure 4.13: Measures taken to protect Baby from falling sickMajority (42%) of the respondents said they protected babies from
becoming ill by practicing good hygiene. 50% of them said sleeping
under mosquito net, good nutrition, keeping the newborn warm prevented
illness. The rest did not know what to do to protect babies from
becoming sick.
37
CHAPTER FIVE: DISCUSSION5.0 INTRODUCTION
This chapter discusses the findings of this study as detailed
below based on the study objectives. It discusses the study
findings and their significance especially in relation to what
has already been published. It is divided into three main
sections i.e. mother’s knowledge, attitudes and practices on the
care of the newborn in Maridi payam.
5.1 MOTHER’S KNOWLEDGE ON THE CARE OF THE NEWBORN
Results of this study have shown that the majority (94%) of the
mothers were aware of the importance of attending ANC checkup.
This finding is similar to what was reported by BBC Media
Action’s South Sudan (2012), who established that the majority of
women in their study knew that they should attend some form of
antenatal care (ANC) more than once. This study also established
that only about 20% of respondent visited ANC clinic more than 4
times and 34% of them visited 4 times. These findings revealed
that mothers in Maridi payam were more informed about the need
and frequency of attending ANC clinic than what was reported by
BBC Media Action (2012)
The majority (72%) of respondents in this study reported that
their babies didn’t have any complication after birth while 28%
of them said their babies were born with complications.
38
Complications reported included delay to cry, inability to suckle
and difficulty in breathing.
Most respondents (76%) in this study sought medical care from
Maridi Hospital whenever their children fell sick while 16% of
them took their sick children to clinics or bought drugs and
treated at home. This is better health services seeking behavior
than what was reported by Tarimo (2000) and Chibwama et al.
(2009). The good health services seeking behavior seem to have
been enhance by their good knowledge of the symptoms of childhood
illness such as high fever reported by 33% of the respondents,
failure to breastfeed by 21% of them and excessive crying by 17%
of them. Other signs mentioned included; fast breathing, diarrhea
and vomiting. This findings were similar to those reported by
Awasthi et al, (2008), Tarimo (2000) and Chibwana et al, (2009).
It was then concluded that the majority mothers in Maridi payam
had adequate and relevant knowledge in the care of the new born
in the community. This included knowledge of the need for and the
frequency of attending ANC, knowledge about the complications of
childbirth as well as symptoms and signs of illness in the
newborn.
5.2 MOTHER’S ATTITUDES ON THE CARE OF THE NEWBORN
This study found out that the majority (64%) of the respondents
preferred to deliver from home but assisted by an untrained birth
attendant. Their reasons for preferring to deliver at home
included; presence of the TBA with in the community, abrupt onset
39
of labour, long distance from home to hospital, and demand for
money by Midwives demand at Maridi hospital maternity. However
36% of them had given birth from the hospital. Those who
preferred to deliver from Hospital gave the following reasons;
getting medication, better management of prolonged labor, better
management of bleeding during labour, management of complications
like the baby’s failure to breath at birth and a cleaner delivery
environment in hospital. This findings however were better that
what was found in western Nepal where 90% of the deliveries took
place at home (Sachdev, 2006). Unlike in Malawi, cultural and
social norms and practices do not appear to be barriers to
improving survival and health of newborns in Maridi payam (Malawi
National Statistics Office, 2004).
It was also established that most of the respondents (94%) would
recommend others to deliver in the hospital. Only 6% of them
would recommend different place. This finding reflects a positive
attitude to hospital delivery despite that the majority of the
mothers still deliver from their homes
It was then concluded that the majority of mothers in Maridi
payam generally had a positive attitude towards newborn care
services available at Maridi Hospital and other health facilities
in the payam despite the fact that the majority of them continue
to deliver from their homes.
5.3 MOTHERS’ PRACTICES ON THE CARE OF THE NEWBORN
40
Place of delivery and Birth attendant
This study revealed that the majority (60%) of the mothers
delivered from home than in hospital to the ratio of almost 2:1.
Out of those who delivered from home 38% were assisted by TBAs,
16% of them were assisted by their mothers. The rest were either
assisted by their husbands or delivered alone. This finding is
better than what was established by (Sachdev, 2006), where 90 %
the deliveries took place at home in western Nepal.
5.3.1 Prevention and management of Neonatal Hypothermia
This study established that 52% of the respondents bathed their
newborns after 24 hours. 38% of them bathed their babies
immediately after birth. This immediate bathing of the newborns
carries with it a risk of neonatal hypothermia as reported by
BergstrAqm et al. (2005) and Mriso et al. (2008). There is
therefore need to teach about the need to delay bathing of
newborns as recommended by WHO (2006), Parlato et al. (2005) and
Mriso et al. (2008) in order to minimize the risk of neonatal
hypothermia. There is also need to promote the Kangaroo
Mothercare Method (KMM) in preventing and managing neonatal
hypothermia as recommended by Sachdev (2006), Sloan (1994) and
Hake-Brooks and Anderson (2008).
5.3.2 Cord Care
60% of the respondents in this study reported the use of a
razorblade for cutting the cord. 32% of them said that scissors
were used while 8% of them used other instruments e.g. knife.
41
Approximately 52% of respondents thought a clean instrument was
used to cut the umbilical cord. However 48% of them said there
were not sure if the instruments used to cut the cord were clean.
52% of the mothers said cord ligature was used for tying the
cord. 38% of them used threads for tying the cord and the rest
used pieces of cloths. The majority (56%) of respondent applied
ash on the cord stump. 22% of them applied herbs. 4% of mothers
said they applied cooking oil to the cord stump. Only 18% of
them did not apply anything to the cord as instructed from the
hospital. These findings were similar to what was reported by
Zulfia et al., (2009), Sethi et al. (2005) and Awasthi et al.
(2008). However principles of clean cord stump care recommend
keeping of the cord dry and clean and ensuring that nothing is
applied on it, either at home or in the health facility. To sum
clean cord care procedures are crucial in infection prevention in
the newborn (WHO, 1996).
5.3.3 Breastfeeding Practices
Findings of this study indicate that only 6% of the respondents
initiated breastfeeding immediately after delivery. 20% of them
initiated breast feeding between 30 and 60 minutes. However the
majority (74%) of them initiated breastfeeding after 1 hour of
birth. A good proportion (60%) of respondents gave fluid e.g.
sugar salt solution newborn as the first feed. This is slightly
better than what was reported by Haroun (2008) about initiation
of breastfeeding in Sudan where 54.2% of mothers initiated
42
breastfeeding after one hour from delivery and 39.7% of them
initiated breastfeeding between 2 and 24 hours. 38% of the
respondents gave breast milk as the first feed to their newborns
while 2% gave formula feed as the first feed. The reasons for
giving formula feed and sugar salt solution included;
insufficient or lack of breast milk. This is similar to what
Bhandari et al. (2003) found out in Haryana, India, where 75% of
newborns were given prelacteal feeds of honey, tea and diluted
milk. However early contact between the mother and the baby,
according to the WHO (1999), has a beneficial effect on breast-
feeding. For instance early suckling provides the baby with
colostrum that offers protection from infection, gives important
nutrients, and has a beneficial effect on maternal uterine
contractions. Important factors in establishing and maintaining
breast-feeding after birth include: giving the first feed within
one hour of birth, correct positioning that enables good,
attachment of the baby, frequent feeds, no prelacteal feeds or
other supplements, and psychosocial support for breast-feeding
mothers Khadduri et al. (2007). Mothers therefore should be
instructed about the need for an adequate diet to sustain
lactation. They should be helped and encouraged if they have
difficulties during breast-feeding (WHO, 1996).
This study also established that the most (86%) of the
respondents cleaned their breasts before lactating, however 14%
did not clean their breasts before breastfeeding. Out of those
43
who cleaned breasts before breastfeeding, 65% washed their breast
with water before breastfeeding. 35% of them only cleaned their
breasts using a baby towel or cloth before breastfeeding. In
addition this study found out that most 90%) of the respondents
breastfed their babies on demand at least 8 times a day, which is
the recommended practice. The rest (10%) of them breastfed less
than 8 times a day. This is similar to what was reported by in
Aweil East and North by Cyprian (2005).
5.3.4 Immunization status of the newborns in Maridi payam
The immunization status of children whose mothers were
interviewed was worrying as most of (88%) them reported that
babies were missed BCG and OPV0. Only 12% of them said their
babies were immunized with BCG and OPV0 before discharge from
hospital. Most of the newborns who missed the first vaccines were
delivered at home. Some of them reported that they delivered in
hospital but vaccines were out of stock the and therefore their
babies could not be immunized before discharge. Missing BCG and
OPV0 was also reported from Pokhara city of western Nepal where
90% of deliveries took place at home (Sachdev, 2006). In contrast
the WHO (1996) recommended that BCG be given as soon as possible
after birth in all populations, and a single dose of OPV should
be given at birth or within two weeks after birth. This calls for
more immunization campaigns targeting all babies who are
delivered at home while ensuring that all those born at the
health facilities receive BCG and OPV0 before they are
discharged.
44
5.3.3 Other measures of preventing neonatal illnesses.
Most respondents in this study new and practiced some preventive
measures against illness among the newborns. For instance 50% of
them slept under mosquito nets and kept the newborn warm as a way
of preventing illness. 42% of the respondents suggested that good
hygiene as a prevention measure against neonatal illness. The
rest did not know what to do to protect babies from becoming
sick. According to Parlato et al. (2004) newborns are more likely
to survive if delivery is clean, that is if actions are taken to
help prevent infection. Ensuring a clean delivery implies: clean
and gloved hands, clean perineal area and clean delivery surface
(Parlato et al., 2004). These infection prevention measures are
similar to what was recommended by recommended by (WHO, 1996 and
2006).
It was then concluded that though respondents in this study had
satisfactory knowledge and positive attitudes towards the
recommended newborn care, they generally lacked the practical
application especially in hospital deliveries, improper cord care
and immunization.
45
CHAPTER SIX: CONCLUSION AND RECOMMENDATIONS
6.1 Conclusion
It was then concluded that the majority mothers in Maridi payam
had adequate and relevant knowledge in the care of the new born
in the community. This included knowledge of the need for and the
frequency of attending ANC, knowledge about the complications of
childbirth as well as symptoms and signs of illness in the
newborn. The majority of mothers in the payam generally had a
positive attitude towards newborn care services available at
Maridi Hospital and other health facilities in the payam despite
the fact that the majority of them continued to deliver from
their homes. Finally, though respondents in this study had
satisfactory knowledge and positive attitudes towards the
recommended newborn care, they generally lacked the practical
application especially in; hospital deliveries, improper cord
care and immunization.
6.2 Recommendations
In view the above the following measures are the recommended way
forward;
The Midwives at Maridi Hospital should encourage all
pregnant women attending ANC at Maridi Hospital to deliver
from hospital for neonatal outcomes.
46
The recommended number of not less than four ANC visits per
pregnancy should be promoted though health education during
ANC visits and other gatherings by the midwife.
The State Minister of Health should organize training for
all TBAs in Maridi payam and beyond since more mothers in
this payam delivered at home than hospital.
All women of childbearing age should be educated more on
proper neonatal care including; proper cord are, prevention
of neonatal hypothermia, early initiation of breastfeeding,
exclusive breastfeeding on demand at least 8 times a day and
general hygiene by the health workers.
Health workers see all newborns in Maridi payam should be
vaccinated with BCG as early as possible after birth and
with OPV0 within the first 14 days.
All health workers should include men in the campaigns to
promote proper care of the new born as substantial house
hold heads in Maridi payam.
47
REFERENCESAdeyinka D., Oladimeji O., Adeyinka F., & Aimakhu C., 2008.
Uptake of Childhood Immunization Among Mothers Of Under-Five In
Southwestern Nigeria. The Internet Journal of Epidemiology. Volume 7 Number
2.
http://ispub.com/IJE/7/2/3255
Accessed on 1/06/2014
Awashi S., Verma T., Agarwal M., 2006. Danger signs of neonatal
illnesses perception of care givers and health workers amongst
mothers in India, Bull World Health Organization; 84(10):819-245.
Asif P., Mohamed B., Vishnu B., Ekambaram M., 2010. Knowledge
attitude and practice of neonatal care among postnatal mothers,
Current Pediatric Research; Vol. 14 Issue 2, p147.
http://connection.ebscohost.com/c/articles/74462996/knowledge-
attitiude-practice-neonatal- care-among-postnatal-mothers
Accessed on 31/05 /2014
BergstrAqm A., Byaruhanga R., Okong P., 2005. The impact of
newborn bathing on the prevalence of neonatal hypothermia in
Uganda: a randomized, controlled trial, Act Pediatric 2005 Oct; 94(10):
1462-7.
http://14.139.159.4:8080/jspui/bitstream/123456789/9166/1/Mamtha
%20kumari%20yadav%20OBG.pdf.
Accessed 1/06/2014
48
Brett D., Nelson M., Maya F., Melody J., Eckardt, Roy A.,
Margaret T., Genevieve P., Sarah B., El-BashirA., MPH, Emily K.,
Ghirmai E., Thomas F., Burke, 2011. Innovative package for
frontline maternal, newborn and child health workers in South
Sudan,
http://www.southsudanmedicaljournal.com/archive/november-2011/
innovative-package-for-frontline-maternal-newborn-and-child-
health-workers-in-south-sudan.htm
Accessed on 3/06/2014
Bhandari N., Bahl R., Mazumdar s., Martines J, Black R., Bhan M.,
2003. Effect of community- based promotion of exclusive
breastfeeding on diarrhoeal illness sand growth,: a cluster
randomized controlled trial. Lancet.
Bland R.M., Rollins N., Coutsoudis A., & Coovadia H., 2002.
Breastfeeding Practices in an Area of high HIV Prevalence in
rural South Africa. Act Pediatrics Scandinavia, 91, 704-711.
Brooker C., 2006. Churchill Livingstone’s dictionary of nursing.
(19th ed). UK: Elsevier.
Chibwana A., Mathanga D., Chinkhumba J., Campbell CH., 2009,
Social- Cultural predictors of health-seeking behavior for
febrile under five children in Mwanza – Neno district, “Malawi.
Malaria Journal; 8:219.
www.malariajournal.com/content/8//219
49
Accessed 5/06/2014
Cyprian O., 2011. Knowledge, attitudes and practices of
caretakers of malnourished children in Aweil East and North
counties, South Sudan
http://www.southsudanmedicaljournal.com/archive/february-2011/kno
wledge-attitudes-and-practises-of-caretakers-of-malnourished-
children-in-aweil-east-and-north-counties-south-sudan.html
Accessed 30/05/2014
Ergenekon-ozelci P., Elmaci N., Ertem M., Saka G., 2006.
Breastfeeding beliefs and practices among migrant mothers in
slums of Diyarbakir, Turkey. Eur J Public Health 2006 Apr; 16(2):143-
148.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3439284/
Accessed 20/04/2014
Gurong G., 2008. Practice on immediate care of new born in the
communities of Kalilali district Nepal. Med Coll J; 10(1):41-4.
www.rguhs.ac.in/cdc/onlinecdc/uploads/05_N006_31351.doc
Accessed 5/06/2014
Hake-Brooks S., Anderson G., 2008. Kangaroo care and breast
feeding of mother-preterm day 0-18 months: a randomized controlled
trail. Neonatal network, 27(3):151-9.
Haroun H., Mahfouz M., Ibrahim B., 2008. Breast feeding
indicators in Sudan: A case study of Wad Medani town. Sudanese Journal of
public health; 3(2): 81C90Sudanese Journal of Public Health:; 3 (2)
50
Helmy F., Bahgat S., 1998. Newborn care giving by primipara and
multipara mothers at home in Tanta City . J Egypt Public Health Assoc.;
73(5-6):501-18. http://www.ncbi.nlm.nih.gov/pubmed/17217021
Accessed 1/06/2014
HIzel S., Ceyhum G., Tanzer F., Sanli C., 2006. Traditional
beliefs as forgotten influencing factors on breast-feeding
performance in Turkey. Saudi Med J; 27(4):511-518.
www.ncbi.nlm.nih.gov/pub med /16598330
Accessed20/03/2014
Li Salami., 2006. Factors influencing breastfeeding practices in
Edo state, Nigeria African Journal of Food, Agriculture, Nutrition and
Development search 2,o11,936 article,
http://www.oalib.com/paper/1333040#.U4raBt4dxdh
Accessed 1/06/2014
Mesko N., Osrin D., Tamang S., 2003. Care for perinatal illness
in rural Nepal”a descriptive study with cross sectional and
qualitative components. BMC International Health and Human Rights; 3:3.
www.midwiferyjour nal .com/article/S0266-6138(13)00081-8/references
Accessed on 20/ 05/ 2014
Mrisho M., Schellenberg A., Mushi A., Obrist B., Mshinda H.,
Tanner M., 2008. Understanding home-based neonatal care practice
in rural southern Tanzania. Trans. R. Soc. Trop. Med. Hyg. 2008;102:669-
678
51
http://www.ncbi.nlm.nih.gov/pubmed/18513769
Accessed 2/06/2014
Myles a text Book of Midwives, 2003. 14th Edition Elsevies
British library publication pp No:736-739
National Statistical Office (NSO), and ORC Macro 2005. Malawi
demographic and health survey 2004. Calverton, Maryland: NSO and
ORC Macro; www.mamaye.org/sites/default/.../mamaye-refsheet-
factsheet- malawi .doc .
Accessed 4/06/2014
National Statistical Office and UNICEF. Malawi Multiple Indicator
Cluster Survey 2006. Final Report. Lilongwe, Malawi: National
Statistical Office and UNICEF, (2008).
www.childinfo.org/files/MICS3_ Malawi _ Final Report _ 2006 _eng.pdf
Accessed 20/04/2014
Nieswiadomy, M. R. 2008. Foundations of Nursing Research (6 th.
Ed.). U.S.A: Pearson
Ogunlesi T., & Oufowora B., 2010. “Predictors of Mortality in
Neonatal Septicemia in an under source setting. Journal of the
National Medical Association;
102(10):915-.http://www.medcol.mw/commhealth/mph/dissertations/T
riza%20Kakhobwe%20Hara_MPH_Thesis_approved.pdf
Accessed 1/05/2014
52
Panul D, &Deadihic Nursing Jaypee Brothers Medical Publishers LTD
New Delhi, 2007. Pag 66
Parlato R., Darmstadt G., Tinker A., 2004. “Qualitative Research
to Improve Newborn Care Practices Saving Newborn Lives Tools for
Newborn Health. Washington DC
Pascale K., Laure N., Enyong O., 2007. Factors Associated with
Breast feeding as Well as the Nutritional Status of Infants (0-
12) Months: An Epidemiological Study in Yaounde, Cameroon .
Pakistan Journal of Nutrition, 6 (3): 259-263.
http://etd.aau.edu.et/dspace/bitstream/123456789/2360/1/104
Accessed 23/05/2014
Padiyath M., Bhat V., Ekambaram M., 2010. Knowledge, attitude and
practices of neonatal care among postnatal mothers. Cur Pediatric Res.;
14(2):147-152.
www. pediatricresearch .info/yahoo_site_admin/.../19.176181814.pdf
Accessed 5/2014
BBC Media action’s., 2012."Maternal and child health in South
Sudan
http://www.bbc.co.uk/mediaaction/publicationsandpress/
research_health_south_sudan_page.htl
Sachdev, H.P.S., 2006. Kangaroo Mother Care method to reduce
morbidity and mortality in low-birth-weight infants. The WHO
Reproductive Health
53
Save the Children 2004. Saving Newborn lives.
http://resourcecentre.savethechildren.se/sites/default/files/
documents/1945.pdf Accessed 21/04/2014
Sethi V., Kashyap S.,Agarwal S. 2005. Contextual factors
influencing newborn care Amongst rural poor in western Uttar
Pradesh Pakistan Journal of Nutrition. 4: 273-275
Shoaeib F., El-Barrawy M., 2005. Alcohol or traditional methods
versus natural drying for newborn’s cord care, J Egypt Public Health
Assoc.; 80(1- 2):169-201. www.biomedcentral.com/1471-2393/ 12 /50/
Accessed 13/04/2014
Sloan, N.L, et al. 1994. Kangaroo mother method: randomized
controlled trial of an alternative method of care for stabilized
low-birth weight infants. Lancet. Sep 17; 344(8925):782-5
Soanes C., 2007. Oxford English Mini Dictionary. 17th Edition,
United States: Oxford University.
Tarimo D., Lwihula G., Minjas J., Bygbjerg C.,2000. Mothers'
perceptions and knowledge on childhood malaria in the holoendemic
Kibaha district”, Tanzania: implications for malaria control and the IMCI
strategy. Trop Med Int Health. 2000; 5:179–84. www.bio med central.com/1472-
698X/6/7
Accessed on 14/05/2014
The Africa newborn network, 2009. Addressing critical knowledge
gap in newborn health”
54

http://www.healthynewbornnetwork.org/partner/africa-newborn-
network
Access on 22/04/2014
World Health Organization (WHO), 2006, Neonatal & Perinatal
Mortality; Country, Regional and Global Estimates.
World Health Organization (WHO), 1996, Perinatal mortality; a
listing of available information. FRH/MSM.96.7. Geneva.
Yadav S., 2007. Newborn care: traditional practices in Nepal,
Archive.student.bmj.com/issues/07/09/life/308.pdf,
Accessed 23rd March 2014
Zulfia K . , Saira M . , Najam K . , MohdA.A ., Abdul R ., 2009. Poor
Perinatal Care Practices in Urban Slums: Possible Role of Social
Mobilization Networks.Indian J Community Med. Apr 2009; 34(2): 102–107.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2781114/
Accessed 22/05/2014
55

APPENDICES
APPENDICESNDIX I: INTRODUCTORY LATTER
56
APPENDIX II: CONSENT FORM
I am Mr. Oyet Charles Okech is a third year student in NHTI-
Maridi, am doing Diploma in Midwifery. I pursue a study to assess
the knowledge, attitude and Practices of mothers on newborn care
at maridi payam. Although the study will not benefit you
directly, it will provide health professionals with information,
which may result in better care of newborn.
The study data will be kept secretly and your name will not be
included in this study so that your identity will not be revealed
during or after the study to anyone. All the study data
pertaining to you will be stored in a secure place of the
investigator and will not be shared with any person without your
permission.
Your participation in the study is voluntary and you are under no
force to participate. You have the right to refuse the study any
time you wish to do so and they will be no payment for it. I
kindly request you to pay attention to me for just 10 minute.
I have read/heard what was explained on the consent form and was
explained that the information provided by me would be kept
confidential and used only for the above mentioned study purpose.
I voluntarily consent to participate in the study.
57
Participant Signature /thumb………………………..
Date:………../…………./2014
I have explained the study to the above participant and sought
her understanding of the informed consent.
Researcher Signature…………………………… Date:………../…..
……../2014
58

APPENDIX III: QUESTIONNAIREINSTRUCTIONS:
This questionnaire contains some questions section about care ofnewborn. I kindly requesting you to listen to the questions asked
by the interviewer carefully and provide the necessary information
by giving appropriate response. The information collected from you
will be used only for the purpose of the study and kept in
confidential
Questionnaire on Mothers’ Knowledge, Attitudes and
Practices on Care of the Newborn
Section A. Demographic CharacteristicsQuestionnaire
NumberDate of
Interview
1. Age of RespondentAge
group
Cod
e
Tick
one15-20
yrs
1
21-
25yrs
2
26-
30yrs
3
31-
35yrs
4
36- 5
59
40yrs41-
45yrs
6
46-
50yrs
7
2. Address…………………………Boma 3.
Parity…………………………………
4. Youngest child’s age……………………… 5. Sex of
Baby…………………………..
6. Ethnicity/tribe…………………………….. 7. Respondent’s
Religion………………
8. Marital Status of the respondent…………… 9. Level
of Education…………………..
10. Occupation………………………………..
Chapter B. Mothers’ Knowledge on care of newborn11. Are you aware that you are supposed to attend ANC clinic?
Yes No
12. Did you attend ANC during pregnancy of your youngest child?
Yes No
13. If yes where…………………………………………...
60

14. How many times
15. What advice did you
receive from ANC clinic?Advice Code TickPersonal hygiene 1.Nutrition during
pregnancy
2.
Infant and child
nutrition
3.
Care of cord 4.Importance of hospital
Delivery
5.
Importance of
Immunization
6.
Importance of
Breastfeeding
7.
How to identify sign
of illness
8.
Advantage of ANC 9.Family planning 10.
16. Are you on any family planning method? Yes
No
61
No. of
Visits
Code Tick one
1 time 12 times 23 times 34 times 4Over 4times 5
17. If yes which
methods?......................................................
......................
18. Did your baby have any complication immediately after birth?
Yes No
19. If yes, what was baby suffering from?Difficulty in
Breathing
1
Jaundice 2Bleeding 3Inability to
suckle
4
Inability to
urinate
5
Delay to cry 6Other (specify) 7
20. What do you do when either you or your baby falls sick?
..............................................................
..............................................................
..............................................................
..............................................................
..............................................................
..............................................................
..............................................................
................
21. How do you know when baby is sick?Has diarrhea 1.High body temperature 2.
62
Fast breathing 3.Feels hot/cold 4.Sweating 5.Shivering 6.Vomiting 7.
Chapter C: Mother’s Attitudes on Care of Newborn22. Where did you deliver your last child
from? ........................................................
...........
23. Who attended to you during
delivery?.....................................................
....................................
24. Why did you choose to deliver at the above place?
……………………………………………………………………………………………………………………………………………………………………
………………………………..
25. What is your comment about the place where you delivered
from?
……………………………………………………………………………………………………………………………………………………………………
………………………………
26. Would you recommend other women to deliver from the same
place? ..........................
63

Chapter D, Practice on Newborn Care27. How did you deliver your last baby?
SVD 1C/S 2V/E 3Other
(specify)
4
28. What was used to cut the cord after
delivery? ....................................................
........
29. Was the above mentioned material clean? Yes
No
30. What material was used for tying a
cord? ........................................................
...........
31. What was applied on the cord
stump? .......................................................
..................
32. How was baby cleaned after delivery?
………………………………………………………………………………………..
33. What was used to wrap baby after
delivery? ....................................................
..........
64
34. Approximately how long after delivery did you first
breastfeed your baby?
35. What other feeds did you give to baby
immediately after delivery?Breast milk 1Fluid 2Formula feed 3Other(specifi
c)
4
36. Do you clean your breast before breastfeeding the baby? Yes
No
37. If yes, what do you use to clean your breast before
breastfeeding? ..............................
38. How often do you breastfeed baby in a day?
On demand 8times and
above
1
Less than 8times in
24hrs
2
Don’t breastfeed 3Other (specify) 4
39. When did you start bathing the baby after birth?
65
Immediately 1Within 30
minutes
2
30min-1hr 3After 1hrs 4Other
(specify)
5

Immediately after
birth
1
After 24hrs 2within 24hrs 3
40. What do you apply on the baby’s body after bathing?
………………………………………………………………………………………………
41. Was your baby immunized at birth? Yes
No
42. If no to Q41, why?
……………………………………………………………………………………………
43. What traditional method of treatment newborn illness do you
use?
44. What methods of preventing newborn
illness do you practice in this
community?
……………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………
Thank you for answering the questions
66
Procedure Tick
oneEnema 1Herbal 2Take
traditional
healer
3
APPENDIX IV: MAP OF MARIDI COUNTY
67