neuroimaging of pediatric posterior fossa tumors including review of the literature
TRANSCRIPT
Review Article
Neuroimaging of Pediatric Posterior Fossa TumorsIncluding Review of the Literature
Andrea Poretti, MD,1,2 Avner Meoded, MD,1 and Thierry A.G.M. Huisman, MD1*
Conventional, anatomical MRI is an essential tool fordiagnosis and evaluation of location, quality, and extentof posterior fossa tumors, but offers limited informationregarding tumor grade and type. Advanced MRI techni-ques such as diffusion weighted imaging (DWI) and diffu-sion tensor imaging (DTI) may improve the specific diag-nosis of brain tumors in the posterior fossa in children.In this review the conventional neuroimaging findings, aswell as the DWI, and DTI characteristics of common pedi-atric posterior fossa tumors are discussed andsummarized.
Key Words: posterior fossa; brain tumors; children; mag-netic resonance imaging; diffusion weighted imaging; dif-fusion tensor imagingJ. Magn. Reson. Imaging 2011;000:000–000.VC 2011 Wiley-Liss, Inc.
BRAIN TUMORS ARE the most common solid neo-plasm in children. Their incidence varies between 1and 3 per 100,000 in different series (1). The locationdepends on the age. In infants there is a predomi-nance of supratentorial tumors, while in childrenolder than 4 years infratentorial tumors are more fre-quent. Overall, infratentorial tumors account for 45–60% of all brain tumors (2). Common posterior fossabrain tumors in children include juvenile pilocyticastrocytoma (JPA), medulloblastoma (MB), ependy-moma, and brainstem glioma. Less frequently,atypical rhabdoid/teratoid tumor (ATRT), hemangio-blastoma (HB), dermoids, schwannoma of the VIIIthcranial nerve, cerebellar gangliocytoma, meningioma,high grade glioma, and metastatic lesions are encoun-tered. Because these various tumors require very dif-ferent treatment approaches and have significantly
different natural histories and outcomes, an accurateand specific diagnosis is mandatory.
Conventional MRI is essential for diagnosis as wellas evaluation of location, quality, and extent of the tu-mor and involved brain tissues (gray matter versuswhite matter), but often offers limited informationregarding tumor grade and type. Additional, more spe-cific noninvasive diagnostic tests are needed. Recentstudies evaluated the role of diffusion weighted imag-ing (DWI) in differentiating grade and type of pediatricbrain tumors in the posterior fossa.
We aim to review the conventional neuroimagingfindings of pediatric posterior fossa tumors and dis-cuss the value of DWI and diffusion tensor imaging(DTI) in tumor characterization.
ASTROCYTOMA
Cerebellar astrocytomas are the most frequent poste-rior fossa tumors in children and account for approxi-mately 30–35% of the cases (3). They have a peakincidence between the age of 5–13 years and occurequally frequent in boys and girls. Approximately halfare purely midline tumors, but a lateral or hemi-spheric location is also seen. Cerebellar astrocytomasare usually sporadic, but association with neurofibro-matosis type 1, Turcot syndrome, PHACE(S) syn-drome, and Ollier’s disease has been reported.Because of the mostly slow growth, the children usu-ally present with a long history of waxing and waningsigns of increased intracranial pressure. Unilateral orasymmetric cerebellar signs can be present due to ahemispheric location or hemispheric extension of thetumor.
Cerebellar astrocytomas are mostly benign, low-grade, and slow growing (JPA, WHO 1, more than80%). Anaplastic, high-grade astrocytomas are rare(WHO III-IV, more common in older children) (4,5).
Juvenile pilocytic astrocytomas have an excellentprognosis with the 25 years survival rate being closeto 90% (6). The prognosis depends particularly on thecompleteness of resection and tumor characteristicssuch as location, gross structure, and size. Completeresection, hemispheric location, small size, and pres-ence of cysts are favorable prognostic factors (7).
The typical computer tomography (CT) imaging fea-tures are that of a large and predominantly cystic
1Division of Pediatric Radiology, Russell H. Morgan Department ofRadiology and Radiological Science, The Johns Hopkins UniversitySchool of Medicine, Baltimore, Maryland, USA.2Division of Pediatric Neurology, University Children’s Hospital ofZurich, Switzerland.
Contract grant sponsor: the Swiss National Science Foundation.
*Address reprint requests to: T.A.G.M.H., Division of Pediatric Radiol-ogy, Russell H. Morgan Department of Radiology and RadiologicalScience, The Johns Hopkins School of Medicine, Baltimore, MD.E-mail: [email protected]
Received February 4, 2011; Accepted June 23, 2011.
DOI 10.1002/jmri.22722View this article online at wileyonlinelibrary.com.
JOURNAL OF MAGNETIC RESONANCE IMAGING 000:000–000 (2011)
CME
VC 2011 Wiley-Liss, Inc. 1
mass arising from the vermis cerebelli or the cerebel-lar hemispheres. The solid part in JPA are almostalways hypodense, while high-grade gliomas may behyperdense on CT (8).
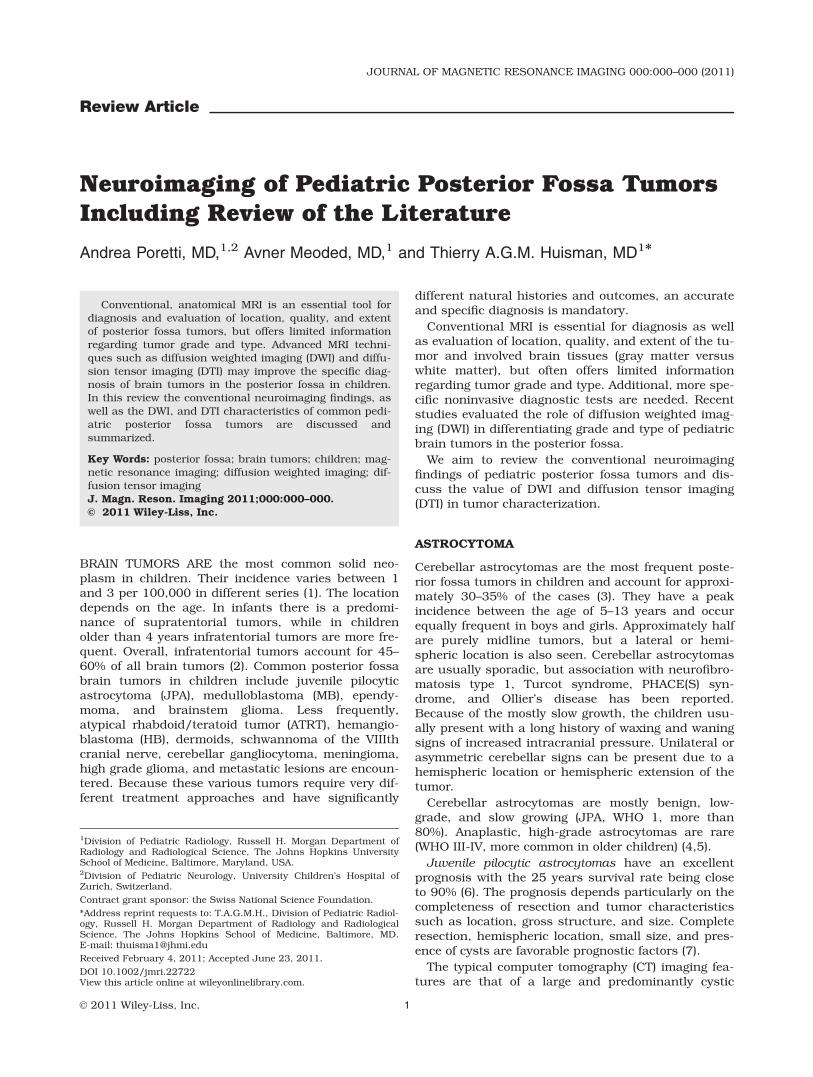
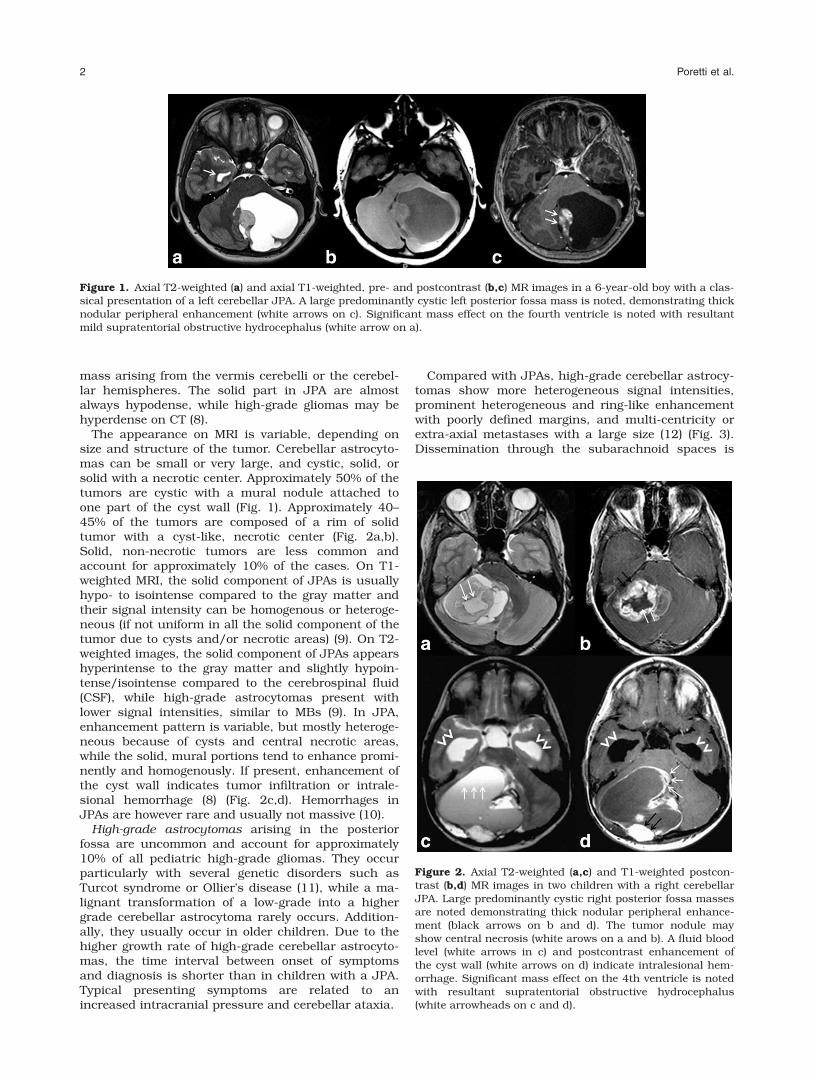
The appearance on MRI is variable, depending onsize and structure of the tumor. Cerebellar astrocyto-mas can be small or very large, and cystic, solid, orsolid with a necrotic center. Approximately 50% of thetumors are cystic with a mural nodule attached toone part of the cyst wall (Fig. 1). Approximately 40–45% of the tumors are composed of a rim of solidtumor with a cyst-like, necrotic center (Fig. 2a,b).Solid, non-necrotic tumors are less common andaccount for approximately 10% of the cases. On T1-weighted MRI, the solid component of JPAs is usuallyhypo- to isointense compared to the gray matter andtheir signal intensity can be homogenous or heteroge-neous (if not uniform in all the solid component of thetumor due to cysts and/or necrotic areas) (9). On T2-weighted images, the solid component of JPAs appearshyperintense to the gray matter and slightly hypoin-tense/isointense compared to the cerebrospinal fluid(CSF), while high-grade astrocytomas present withlower signal intensities, similar to MBs (9). In JPA,enhancement pattern is variable, but mostly heteroge-neous because of cysts and central necrotic areas,while the solid, mural portions tend to enhance promi-nently and homogenously. If present, enhancement ofthe cyst wall indicates tumor infiltration or intrale-sional hemorrhage (8) (Fig. 2c,d). Hemorrhages inJPAs are however rare and usually not massive (10).
High-grade astrocytomas arising in the posteriorfossa are uncommon and account for approximately10% of all pediatric high-grade gliomas. They occurparticularly with several genetic disorders such asTurcot syndrome or Ollier’s disease (11), while a ma-lignant transformation of a low-grade into a highergrade cerebellar astrocytoma rarely occurs. Addition-ally, they usually occur in older children. Due to thehigher growth rate of high-grade cerebellar astrocyto-mas, the time interval between onset of symptomsand diagnosis is shorter than in children with a JPA.Typical presenting symptoms are related to anincreased intracranial pressure and cerebellar ataxia.
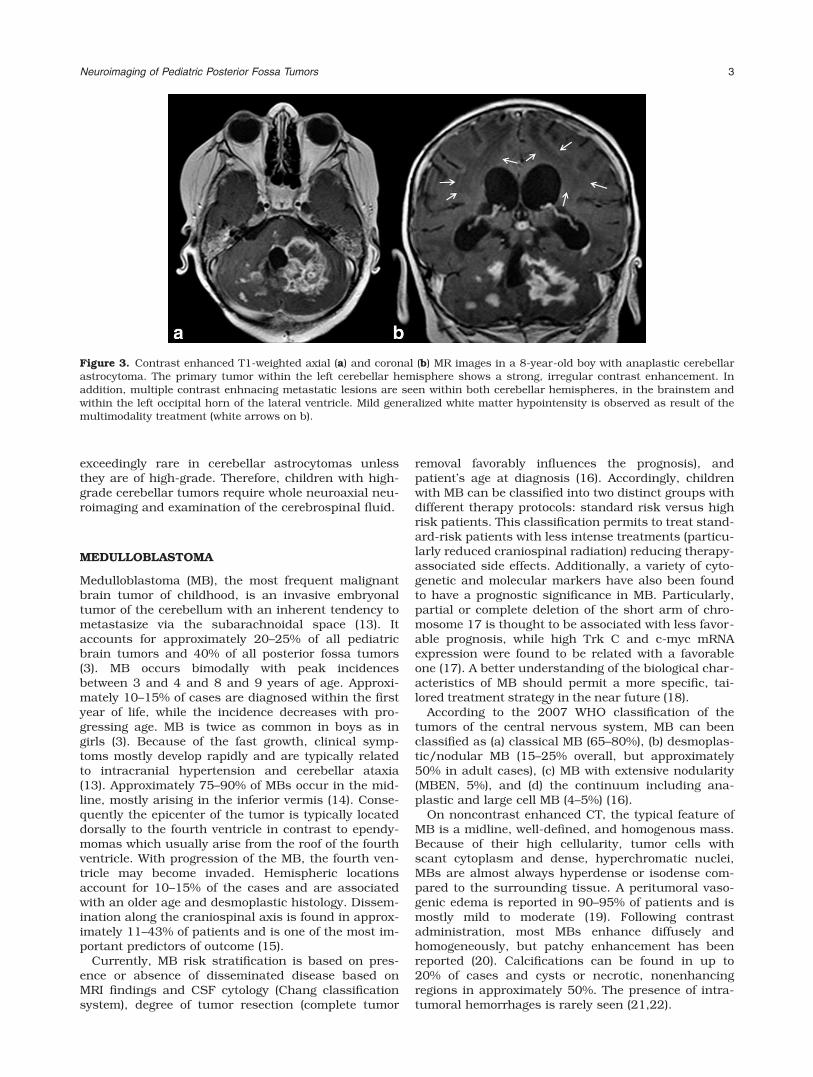
Compared with JPAs, high-grade cerebellar astrocy-tomas show more heterogeneous signal intensities,prominent heterogeneous and ring-like enhancementwith poorly defined margins, and multi-centricity orextra-axial metastases with a large size (12) (Fig. 3).Dissemination through the subarachnoid spaces is
Figure 1. Axial T2-weighted (a) and axial T1-weighted, pre- and postcontrast (b,c) MR images in a 6-year-old boy with a clas-sical presentation of a left cerebellar JPA. A large predominantly cystic left posterior fossa mass is noted, demonstrating thicknodular peripheral enhancement (white arrows on c). Significant mass effect on the fourth ventricle is noted with resultantmild supratentorial obstructive hydrocephalus (white arrow on a).
Figure 2. Axial T2-weighted (a,c) and T1-weighted postcon-trast (b,d) MR images in two children with a right cerebellarJPA. Large predominantly cystic right posterior fossa massesare noted demonstrating thick nodular peripheral enhance-ment (black arrows on b and d). The tumor nodule mayshow central necrosis (white arows on a and b). A fluid bloodlevel (white arrows in c) and postcontrast enhancement ofthe cyst wall (white arrows on d) indicate intralesional hem-orrhage. Significant mass effect on the 4th ventricle is notedwith resultant supratentorial obstructive hydrocephalus(white arrowheads on c and d).
2 Poretti et al.
exceedingly rare in cerebellar astrocytomas unlessthey are of high-grade. Therefore, children with high-grade cerebellar tumors require whole neuroaxial neu-roimaging and examination of the cerebrospinal fluid.
MEDULLOBLASTOMA
Medulloblastoma (MB), the most frequent malignantbrain tumor of childhood, is an invasive embryonaltumor of the cerebellum with an inherent tendency tometastasize via the subarachnoidal space (13). Itaccounts for approximately 20–25% of all pediatricbrain tumors and 40% of all posterior fossa tumors(3). MB occurs bimodally with peak incidencesbetween 3 and 4 and 8 and 9 years of age. Approxi-mately 10–15% of cases are diagnosed within the firstyear of life, while the incidence decreases with pro-gressing age. MB is twice as common in boys as ingirls (3). Because of the fast growth, clinical symp-toms mostly develop rapidly and are typically relatedto intracranial hypertension and cerebellar ataxia(13). Approximately 75–90% of MBs occur in the mid-line, mostly arising in the inferior vermis (14). Conse-quently the epicenter of the tumor is typically locateddorsally to the fourth ventricle in contrast to ependy-momas which usually arise from the roof of the fourthventricle. With progression of the MB, the fourth ven-tricle may become invaded. Hemispheric locationsaccount for 10–15% of the cases and are associatedwith an older age and desmoplastic histology. Dissem-ination along the craniospinal axis is found in approx-imately 11–43% of patients and is one of the most im-portant predictors of outcome (15).
Currently, MB risk stratification is based on pres-ence or absence of disseminated disease based onMRI findings and CSF cytology (Chang classificationsystem), degree of tumor resection (complete tumor
removal favorably influences the prognosis), andpatient’s age at diagnosis (16). Accordingly, childrenwith MB can be classified into two distinct groups withdifferent therapy protocols: standard risk versus highrisk patients. This classification permits to treat stand-ard-risk patients with less intense treatments (particu-larly reduced craniospinal radiation) reducing therapy-associated side effects. Additionally, a variety of cyto-genetic and molecular markers have also been foundto have a prognostic significance in MB. Particularly,partial or complete deletion of the short arm of chro-mosome 17 is thought to be associated with less favor-able prognosis, while high Trk C and c-myc mRNAexpression were found to be related with a favorableone (17). A better understanding of the biological char-acteristics of MB should permit a more specific, tai-lored treatment strategy in the near future (18).
According to the 2007 WHO classification of thetumors of the central nervous system, MB can beenclassified as (a) classical MB (65–80%), (b) desmoplas-tic/nodular MB (15–25% overall, but approximately50% in adult cases), (c) MB with extensive nodularity(MBEN, 5%), and (d) the continuum including ana-plastic and large cell MB (4–5%) (16).
On noncontrast enhanced CT, the typical feature ofMB is a midline, well-defined, and homogenous mass.Because of their high cellularity, tumor cells withscant cytoplasm and dense, hyperchromatic nuclei,MBs are almost always hyperdense or isodense com-pared to the surrounding tissue. A peritumoral vaso-genic edema is reported in 90–95% of patients and ismostly mild to moderate (19). Following contrastadministration, most MBs enhance diffusely andhomogeneously, but patchy enhancement has beenreported (20). Calcifications can be found in up to20% of cases and cysts or necrotic, nonenhancingregions in approximately 50%. The presence of intra-tumoral hemorrhages is rarely seen (21,22).
Figure 3. Contrast enhanced T1-weighted axial (a) and coronal (b) MR images in a 8-year-old boy with anaplastic cerebellarastrocytoma. The primary tumor within the left cerebellar hemisphere shows a strong, irregular contrast enhancement. Inaddition, multiple contrast enhnacing metastatic lesions are seen within both cerebellar hemispheres, in the brainstem andwithin the left occipital horn of the lateral ventricle. Mild generalized white matter hypointensity is observed as result of themultimodality treatment (white arrows on b).
Neuroimaging of Pediatric Posterior Fossa Tumors 3
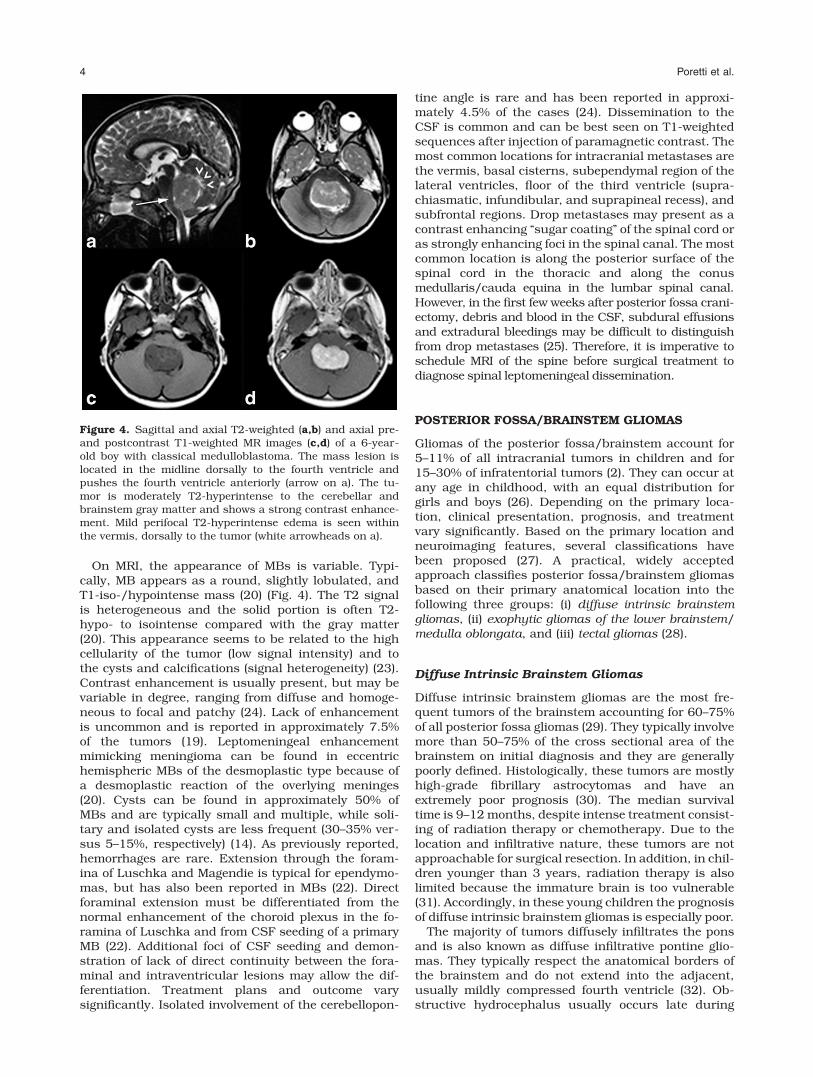
On MRI, the appearance of MBs is variable. Typi-cally, MB appears as a round, slightly lobulated, andT1-iso-/hypointense mass (20) (Fig. 4). The T2 signalis heterogeneous and the solid portion is often T2-hypo- to isointense compared with the gray matter(20). This appearance seems to be related to the highcellularity of the tumor (low signal intensity) and tothe cysts and calcifications (signal heterogeneity) (23).Contrast enhancement is usually present, but may bevariable in degree, ranging from diffuse and homoge-neous to focal and patchy (24). Lack of enhancementis uncommon and is reported in approximately 7.5%of the tumors (19). Leptomeningeal enhancementmimicking meningioma can be found in eccentrichemispheric MBs of the desmoplastic type because ofa desmoplastic reaction of the overlying meninges(20). Cysts can be found in approximately 50% ofMBs and are typically small and multiple, while soli-tary and isolated cysts are less frequent (30–35% ver-sus 5–15%, respectively) (14). As previously reported,hemorrhages are rare. Extension through the foram-ina of Luschka and Magendie is typical for ependymo-mas, but has also been reported in MBs (22). Directforaminal extension must be differentiated from thenormal enhancement of the choroid plexus in the fo-ramina of Luschka and from CSF seeding of a primaryMB (22). Additional foci of CSF seeding and demon-stration of lack of direct continuity between the fora-minal and intraventricular lesions may allow the dif-ferentiation. Treatment plans and outcome varysignificantly. Isolated involvement of the cerebellopon-
tine angle is rare and has been reported in approxi-mately 4.5% of the cases (24). Dissemination to theCSF is common and can be best seen on T1-weightedsequences after injection of paramagnetic contrast. Themost common locations for intracranial metastases arethe vermis, basal cisterns, subependymal region of thelateral ventricles, floor of the third ventricle (supra-chiasmatic, infundibular, and suprapineal recess), andsubfrontal regions. Drop metastases may present as acontrast enhancing ‘‘sugar coating’’ of the spinal cord oras strongly enhancing foci in the spinal canal. The mostcommon location is along the posterior surface of thespinal cord in the thoracic and along the conusmedullaris/cauda equina in the lumbar spinal canal.However, in the first few weeks after posterior fossa crani-ectomy, debris and blood in the CSF, subdural effusionsand extradural bleedings may be difficult to distinguishfrom drop metastases (25). Therefore, it is imperative toschedule MRI of the spine before surgical treatment todiagnose spinal leptomeningeal dissemination.
POSTERIOR FOSSA/BRAINSTEM GLIOMAS
Gliomas of the posterior fossa/brainstem account for5–11% of all intracranial tumors in children and for15–30% of infratentorial tumors (2). They can occur atany age in childhood, with an equal distribution forgirls and boys (26). Depending on the primary loca-tion, clinical presentation, prognosis, and treatmentvary significantly. Based on the primary location andneuroimaging features, several classifications havebeen proposed (27). A practical, widely acceptedapproach classifies posterior fossa/brainstem gliomasbased on their primary anatomical location into thefollowing three groups: (i) diffuse intrinsic brainstemgliomas, (ii) exophytic gliomas of the lower brainstem/medulla oblongata, and (iii) tectal gliomas (28).
Diffuse Intrinsic Brainstem Gliomas
Diffuse intrinsic brainstem gliomas are the most fre-quent tumors of the brainstem accounting for 60–75%of all posterior fossa gliomas (29). They typically involvemore than 50–75% of the cross sectional area of thebrainstem on initial diagnosis and they are generallypoorly defined. Histologically, these tumors are mostlyhigh-grade fibrillary astrocytomas and have anextremely poor prognosis (30). The median survivaltime is 9–12 months, despite intense treatment consist-ing of radiation therapy or chemotherapy. Due to thelocation and infiltrative nature, these tumors are notapproachable for surgical resection. In addition, in chil-dren younger than 3 years, radiation therapy is alsolimited because the immature brain is too vulnerable(31). Accordingly, in these young children the prognosisof diffuse intrinsic brainstem gliomas is especially poor.
The majority of tumors diffusely infiltrates the ponsand is also known as diffuse infiltrative pontine glio-mas. They typically respect the anatomical borders ofthe brainstem and do not extend into the adjacent,usually mildly compressed fourth ventricle (32). Ob-structive hydrocephalus usually occurs late during
Figure 4. Sagittal and axial T2-weighted (a,b) and axial pre-and postcontrast T1-weighted MR images (c,d) of a 6-year-old boy with classical medulloblastoma. The mass lesion islocated in the midline dorsally to the fourth ventricle andpushes the fourth ventricle anteriorly (arrow on a). The tu-mor is moderately T2-hyperintense to the cerebellar andbrainstem gray matter and shows a strong contrast enhance-ment. Mild perifocal T2-hyperintense edema is seen withinthe vermis, dorsally to the tumor (white arrowheads on a).
4 Poretti et al.

disease progression. Children with these tumors usu-ally present with a short history of neurological symp-toms (median 1 month), including cranial nerve palsies(especially VI and VII), pyramidal signs, and/or ataxia(33,34). Mood changes and irritability have also beenreported. The neuroimaging findings are consideredpathognomonic, and biopsy is rarely necessary (35).Diagnostic biopsy is only indicated in children with un-usual neuroimaging appearance or an atypical clinicalcourse. In these cases, imaging should guide biopsy tothe area of solid contrast enhancement, because theseareas are believed to represent tumor components withthe highest malignancy grade.
On CT imaging, diffuse pontine gliomas appear as ahypodense mass centered in an expanded pons withoccasionally a cystic component. They are T1-hypoin-tense and T2 heterogeneously hyperintense on MRI andare ill defined, reflecting their infiltrative nature (26) (Fig.5). They are usually larger than 2 cm in diameter at ini-tial diagnosis and tend to grow and extend superiorlyand inferiorly along the fiber tracts with progressiveenlargement of the brainstem. The fiber tracts are usu-ally respected for a long time period and may be seen asT2-hypointense bands within the T2-hyperintense tu-mor bulk (Fig. 5b). Anterior extension typically ‘‘embra-ces’’ the basilary artery, which remains patent in mostcases (Fig. 5a). Gadolinium enhancement can be vari-able, but mostly these tumors show no or only minimalcontrast enhancement (36). Contrast enhancement mayhowever progress over time. Increasing or newly appear-ing contrast enhancement may indicate tumor dediffer-entiation or response to radio-/chemotherapy (Fig. 5c).
Exophytic Gliomas of the LowerBrainstem/Medulla Oblongata
Exophytic gliomas of the lower brainstem/medullaoblongata arise from the dorsal surface of the lowerbrainstem or cervicomedullary junction (posterior exo-
phytic medullary tumors). Histologically, these tumorsare almost always low-grade gliomas and their prog-nosis is consequently more favorable. In addition,they are more approachable for surgical resectionbecause they tend to extent ‘‘exophytically’’ into thefourth ventricle or perimedullary cisterns rather thaninfiltrate the adjacent brainstem (26). Lateral and ven-tral growth is more characteristic for high-gradetumors (26).
Children mostly present with intractable vomiting(due to involvement of the area postrema). Young chil-dren may show a failure to thrive; while older childrenpresent with signs of increased intracranial pressuredue to obstruction of the fourth ventricle (37). In addi-tion, lower cranial nerve dysfunctions (mostly IX–XII)with swallowing and articulation failure, abducensnerve palsy due to hydrocephalus, and torticollis dueto herniation of the cerebellar tonsils may be noted.Pyramidal tract signs are unusual.
On CT, posterior exophytic medullary gliomas gen-erally appear as sharply demarcated iso- to hypo-dense mass lesions originating from the dorsal con-tour of the lower brainstem. After contrastadministration, most gliomas show a moderate–strongenhancement (37,38).
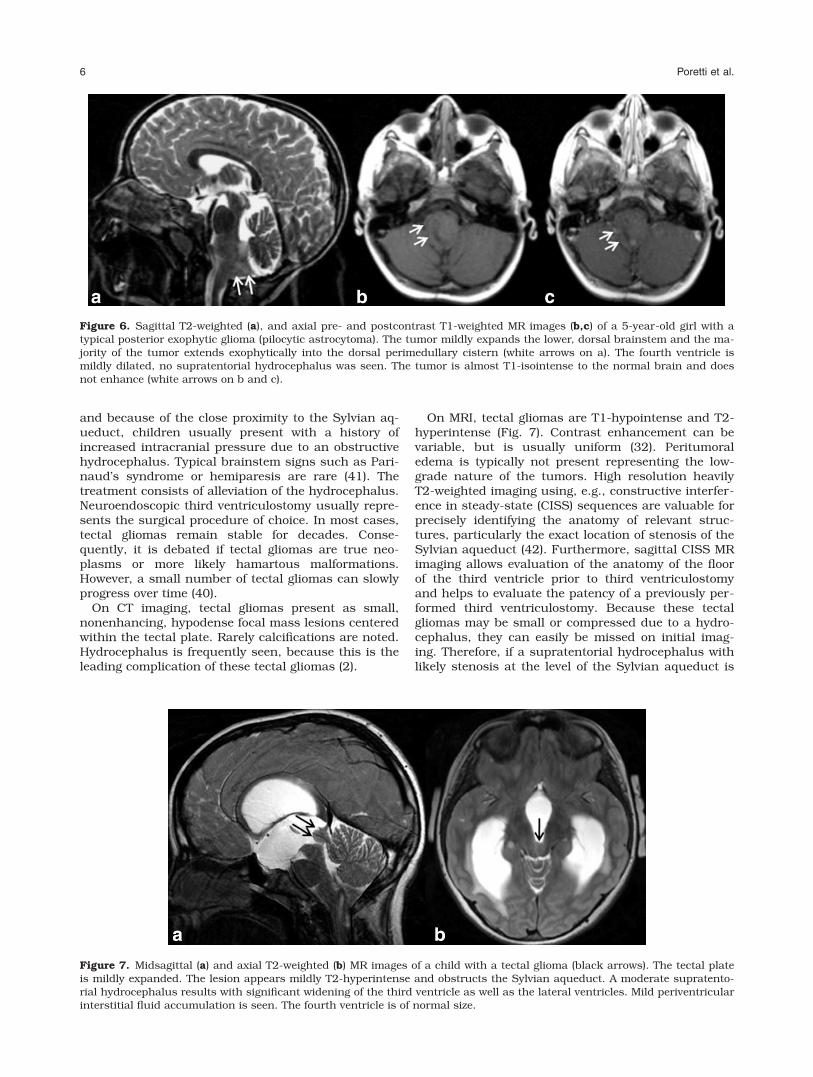
On MRI, the lesions are T1 hypointense and T2hyperintense (Fig. 6). Similar to CT, the tumor enhan-ces homo- or heterogeneously after intravenous con-trast injection (37). The typical exophytic growthmakes these tumors approachable for surgical resec-tion or tumor debulking. If total or near-total resec-tion is achieved, no other treatment is necessary andthe prognosis is excellent.
Tectal Gliomas
Tectal gliomas differ from the other posterior fossagliomas in nature, presentation, and clinical course(39,40). Tectal gliomas are centered to the tectal plate,
Figure 5. Axial T2 (a) and contrast enhanced T1-weighted (b) MR images of a 9-year-old boy with diffuse intrinsic brainstemglioma. The tumor diffusely infiltrates and expands the pons. The anterior exophytic component embraces the patent basilaryartery (white arrows). No significant contrast enhancement is seen. The fourth ventricle is located dorsally to the tumor, noobstructive hydrocephalus was seen. Sagittal contrast enhanced T1-weighted MR image (c) of another child with a diffuseintrinsic brainstem glioma. An area of strong contrast enhancement is seen in the dorsal component of the tumor most likelyrepresenting an area of higher grade malignancy (white arrows). The anterior exophytic component of the tumor embracesthe basilary artery (black arrows).
Neuroimaging of Pediatric Posterior Fossa Tumors 5
and because of the close proximity to the Sylvian aq-ueduct, children usually present with a history ofincreased intracranial pressure due to an obstructivehydrocephalus. Typical brainstem signs such as Pari-naud’s syndrome or hemiparesis are rare (41). Thetreatment consists of alleviation of the hydrocephalus.Neuroendoscopic third ventriculostomy usually repre-sents the surgical procedure of choice. In most cases,tectal gliomas remain stable for decades. Conse-quently, it is debated if tectal gliomas are true neo-plasms or more likely hamartous malformations.However, a small number of tectal gliomas can slowlyprogress over time (40).
On CT imaging, tectal gliomas present as small,nonenhancing, hypodense focal mass lesions centeredwithin the tectal plate. Rarely calcifications are noted.Hydrocephalus is frequently seen, because this is theleading complication of these tectal gliomas (2).
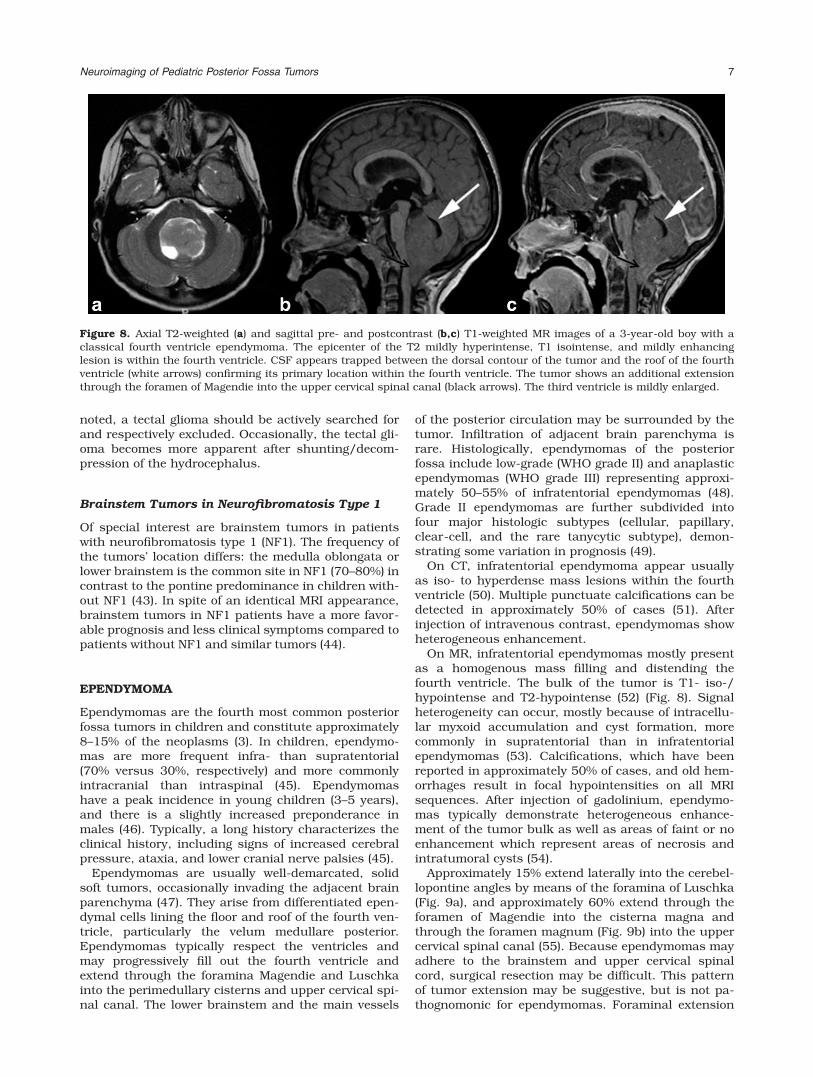
On MRI, tectal gliomas are T1-hypointense and T2-hyperintense (Fig. 7). Contrast enhancement can bevariable, but is usually uniform (32). Peritumoraledema is typically not present representing the low-grade nature of the tumors. High resolution heavilyT2-weighted imaging using, e.g., constructive interfer-ence in steady-state (CISS) sequences are valuable forprecisely identifying the anatomy of relevant struc-tures, particularly the exact location of stenosis of theSylvian aqueduct (42). Furthermore, sagittal CISS MRimaging allows evaluation of the anatomy of the floorof the third ventricle prior to third ventriculostomyand helps to evaluate the patency of a previously per-formed third ventriculostomy. Because these tectalgliomas may be small or compressed due to a hydro-cephalus, they can easily be missed on initial imag-ing. Therefore, if a supratentorial hydrocephalus withlikely stenosis at the level of the Sylvian aqueduct is
Figure 6. Sagittal T2-weighted (a), and axial pre- and postcontrast T1-weighted MR images (b,c) of a 5-year-old girl with atypical posterior exophytic glioma (pilocytic astrocytoma). The tumor mildly expands the lower, dorsal brainstem and the ma-jority of the tumor extends exophytically into the dorsal perimedullary cistern (white arrows on a). The fourth ventricle ismildly dilated, no supratentorial hydrocephalus was seen. The tumor is almost T1-isointense to the normal brain and doesnot enhance (white arrows on b and c).
Figure 7. Midsagittal (a) and axial T2-weighted (b) MR images of a child with a tectal glioma (black arrows). The tectal plateis mildly expanded. The lesion appears mildly T2-hyperintense and obstructs the Sylvian aqueduct. A moderate supratento-rial hydrocephalus results with significant widening of the third ventricle as well as the lateral ventricles. Mild periventricularinterstitial fluid accumulation is seen. The fourth ventricle is of normal size.
6 Poretti et al.
noted, a tectal glioma should be actively searched forand respectively excluded. Occasionally, the tectal gli-oma becomes more apparent after shunting/decom-pression of the hydrocephalus.
Brainstem Tumors in Neurofibromatosis Type 1
Of special interest are brainstem tumors in patientswith neurofibromatosis type 1 (NF1). The frequency ofthe tumors’ location differs: the medulla oblongata orlower brainstem is the common site in NF1 (70–80%) incontrast to the pontine predominance in children with-out NF1 (43). In spite of an identical MRI appearance,brainstem tumors in NF1 patients have a more favor-able prognosis and less clinical symptoms compared topatients without NF1 and similar tumors (44).
EPENDYMOMA
Ependymomas are the fourth most common posteriorfossa tumors in children and constitute approximately8–15% of the neoplasms (3). In children, ependymo-mas are more frequent infra- than supratentorial(70% versus 30%, respectively) and more commonlyintracranial than intraspinal (45). Ependymomashave a peak incidence in young children (3–5 years),and there is a slightly increased preponderance inmales (46). Typically, a long history characterizes theclinical history, including signs of increased cerebralpressure, ataxia, and lower cranial nerve palsies (45).
Ependymomas are usually well-demarcated, solidsoft tumors, occasionally invading the adjacent brainparenchyma (47). They arise from differentiated epen-dymal cells lining the floor and roof of the fourth ven-tricle, particularly the velum medullare posterior.Ependymomas typically respect the ventricles andmay progressively fill out the fourth ventricle andextend through the foramina Magendie and Luschkainto the perimedullary cisterns and upper cervical spi-nal canal. The lower brainstem and the main vessels
of the posterior circulation may be surrounded by thetumor. Infiltration of adjacent brain parenchyma israre. Histologically, ependymomas of the posteriorfossa include low-grade (WHO grade II) and anaplasticependymomas (WHO grade III) representing approxi-mately 50–55% of infratentorial ependymomas (48).Grade II ependymomas are further subdivided intofour major histologic subtypes (cellular, papillary,clear-cell, and the rare tanycytic subtype), demon-strating some variation in prognosis (49).
On CT, infratentorial ependymoma appear usuallyas iso- to hyperdense mass lesions within the fourthventricle (50). Multiple punctuate calcifications can bedetected in approximately 50% of cases (51). Afterinjection of intravenous contrast, ependymomas showheterogeneous enhancement.
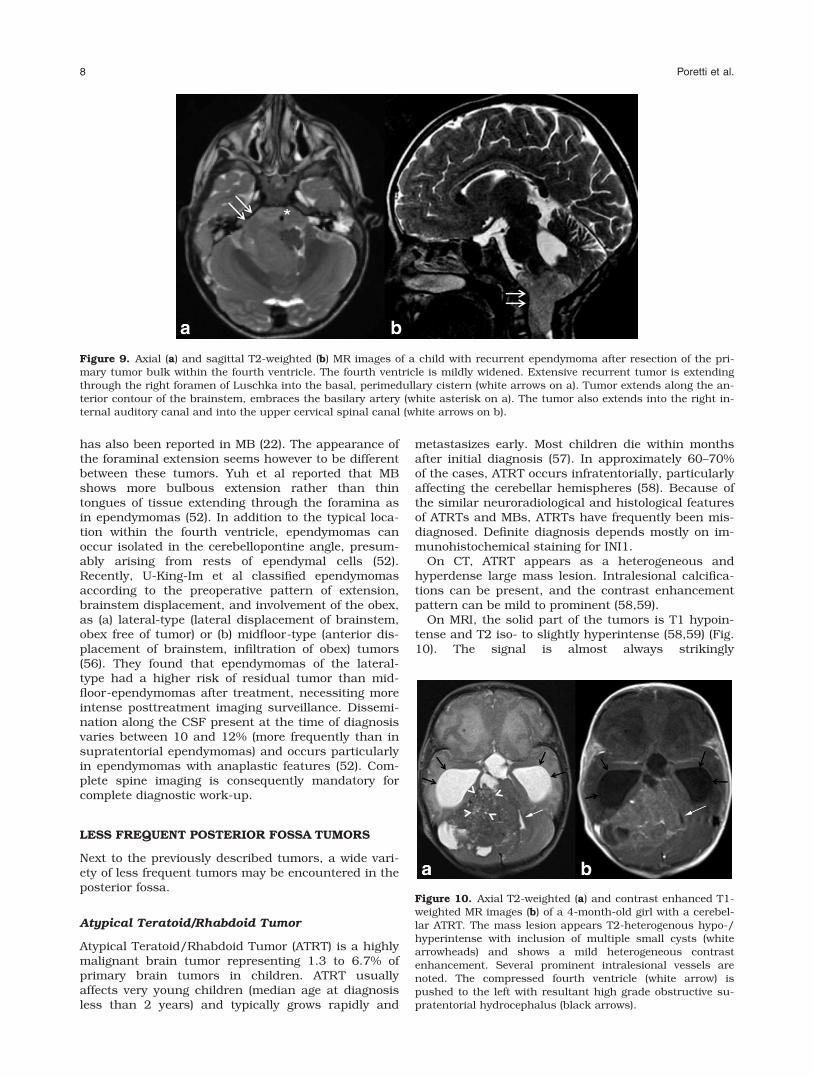
On MR, infratentorial ependymomas mostly presentas a homogenous mass filling and distending thefourth ventricle. The bulk of the tumor is T1- iso-/hypointense and T2-hypointense (52) (Fig. 8). Signalheterogeneity can occur, mostly because of intracellu-lar myxoid accumulation and cyst formation, morecommonly in supratentorial than in infratentorialependymomas (53). Calcifications, which have beenreported in approximately 50% of cases, and old hem-orrhages result in focal hypointensities on all MRIsequences. After injection of gadolinium, ependymo-mas typically demonstrate heterogeneous enhance-ment of the tumor bulk as well as areas of faint or noenhancement which represent areas of necrosis andintratumoral cysts (54).
Approximately 15% extend laterally into the cerebel-lopontine angles by means of the foramina of Luschka(Fig. 9a), and approximately 60% extend through theforamen of Magendie into the cisterna magna andthrough the foramen magnum (Fig. 9b) into the uppercervical spinal canal (55). Because ependymomas mayadhere to the brainstem and upper cervical spinalcord, surgical resection may be difficult. This patternof tumor extension may be suggestive, but is not pa-thognomonic for ependymomas. Foraminal extension
Figure 8. Axial T2-weighted (a) and sagittal pre- and postcontrast (b,c) T1-weighted MR images of a 3-year-old boy with aclassical fourth ventricle ependymoma. The epicenter of the T2 mildly hyperintense, T1 isointense, and mildly enhancinglesion is within the fourth ventricle. CSF appears trapped between the dorsal contour of the tumor and the roof of the fourthventricle (white arrows) confirming its primary location within the fourth ventricle. The tumor shows an additional extensionthrough the foramen of Magendie into the upper cervical spinal canal (black arrows). The third ventricle is mildly enlarged.
Neuroimaging of Pediatric Posterior Fossa Tumors 7
has also been reported in MB (22). The appearance ofthe foraminal extension seems however to be differentbetween these tumors. Yuh et al reported that MBshows more bulbous extension rather than thintongues of tissue extending through the foramina asin ependymomas (52). In addition to the typical loca-tion within the fourth ventricle, ependymomas canoccur isolated in the cerebellopontine angle, presum-ably arising from rests of ependymal cells (52).Recently, U-King-Im et al classified ependymomasaccording to the preoperative pattern of extension,brainstem displacement, and involvement of the obex,as (a) lateral-type (lateral displacement of brainstem,obex free of tumor) or (b) midfloor-type (anterior dis-placement of brainstem, infiltration of obex) tumors(56). They found that ependymomas of the lateral-type had a higher risk of residual tumor than mid-floor-ependymomas after treatment, necessiting moreintense posttreatment imaging surveillance. Dissemi-nation along the CSF present at the time of diagnosisvaries between 10 and 12% (more frequently than insupratentorial ependymomas) and occurs particularlyin ependymomas with anaplastic features (52). Com-plete spine imaging is consequently mandatory forcomplete diagnostic work-up.
LESS FREQUENT POSTERIOR FOSSA TUMORS
Next to the previously described tumors, a wide vari-ety of less frequent tumors may be encountered in theposterior fossa.
Atypical Teratoid/Rhabdoid Tumor
Atypical Teratoid/Rhabdoid Tumor (ATRT) is a highlymalignant brain tumor representing 1.3 to 6.7% ofprimary brain tumors in children. ATRT usuallyaffects very young children (median age at diagnosisless than 2 years) and typically grows rapidly and
metastasizes early. Most children die within monthsafter initial diagnosis (57). In approximately 60–70%of the cases, ATRT occurs infratentorially, particularlyaffecting the cerebellar hemispheres (58). Because ofthe similar neuroradiological and histological featuresof ATRTs and MBs, ATRTs have frequently been mis-diagnosed. Definite diagnosis depends mostly on im-munohistochemical staining for INI1.
On CT, ATRT appears as a heterogeneous andhyperdense large mass lesion. Intralesional calcifica-tions can be present, and the contrast enhancementpattern can be mild to prominent (58,59).
On MRI, the solid part of the tumors is T1 hypoin-tense and T2 iso- to slightly hyperintense (58,59) (Fig.10). The signal is almost always strikingly
Figure 9. Axial (a) and sagittal T2-weighted (b) MR images of a child with recurrent ependymoma after resection of the pri-mary tumor bulk within the fourth ventricle. The fourth ventricle is mildly widened. Extensive recurrent tumor is extendingthrough the right foramen of Luschka into the basal, perimedullary cistern (white arrows on a). Tumor extends along the an-terior contour of the brainstem, embraces the basilary artery (white asterisk on a). The tumor also extends into the right in-ternal auditory canal and into the upper cervical spinal canal (white arrows on b).
Figure 10. Axial T2-weighted (a) and contrast enhanced T1-weighted MR images (b) of a 4-month-old girl with a cerebel-lar ATRT. The mass lesion appears T2-heterogenous hypo-/hyperintense with inclusion of multiple small cysts (whitearrowheads) and shows a mild heterogeneous contrastenhancement. Several prominent intralesional vessels arenoted. The compressed fourth ventricle (white arrow) ispushed to the left with resultant high grade obstructive su-pratentorial hydrocephalus (black arrows).
8 Poretti et al.
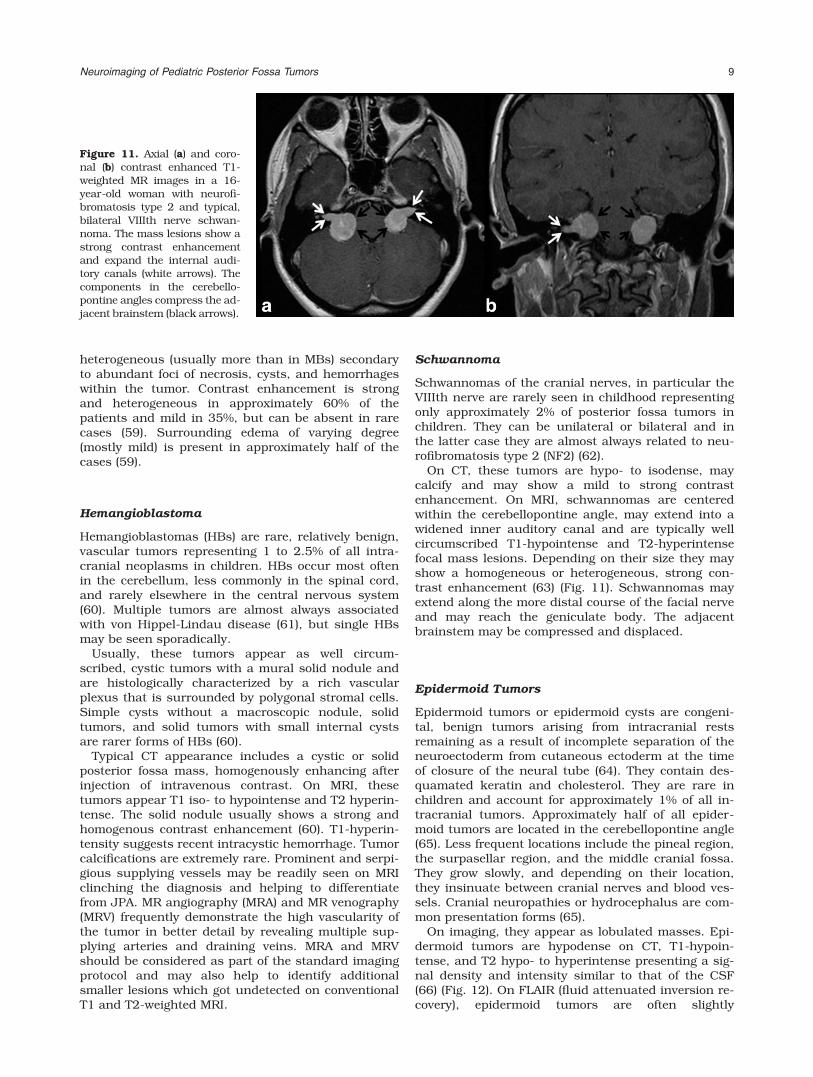
heterogeneous (usually more than in MBs) secondaryto abundant foci of necrosis, cysts, and hemorrhageswithin the tumor. Contrast enhancement is strongand heterogeneous in approximately 60% of thepatients and mild in 35%, but can be absent in rarecases (59). Surrounding edema of varying degree(mostly mild) is present in approximately half of thecases (59).
Hemangioblastoma
Hemangioblastomas (HBs) are rare, relatively benign,vascular tumors representing 1 to 2.5% of all intra-cranial neoplasms in children. HBs occur most oftenin the cerebellum, less commonly in the spinal cord,and rarely elsewhere in the central nervous system(60). Multiple tumors are almost always associatedwith von Hippel-Lindau disease (61), but single HBsmay be seen sporadically.
Usually, these tumors appear as well circum-scribed, cystic tumors with a mural solid nodule andare histologically characterized by a rich vascularplexus that is surrounded by polygonal stromal cells.Simple cysts without a macroscopic nodule, solidtumors, and solid tumors with small internal cystsare rarer forms of HBs (60).
Typical CT appearance includes a cystic or solidposterior fossa mass, homogenously enhancing afterinjection of intravenous contrast. On MRI, thesetumors appear T1 iso- to hypointense and T2 hyperin-tense. The solid nodule usually shows a strong andhomogenous contrast enhancement (60). T1-hyperin-tensity suggests recent intracystic hemorrhage. Tumorcalcifications are extremely rare. Prominent and serpi-gious supplying vessels may be readily seen on MRIclinching the diagnosis and helping to differentiatefrom JPA. MR angiography (MRA) and MR venography(MRV) frequently demonstrate the high vascularity ofthe tumor in better detail by revealing multiple sup-plying arteries and draining veins. MRA and MRVshould be considered as part of the standard imagingprotocol and may also help to identify additionalsmaller lesions which got undetected on conventionalT1 and T2-weighted MRI.
Schwannoma
Schwannomas of the cranial nerves, in particular theVIIIth nerve are rarely seen in childhood representingonly approximately 2% of posterior fossa tumors inchildren. They can be unilateral or bilateral and inthe latter case they are almost always related to neu-rofibromatosis type 2 (NF2) (62).
On CT, these tumors are hypo- to isodense, maycalcify and may show a mild to strong contrastenhancement. On MRI, schwannomas are centeredwithin the cerebellopontine angle, may extend into awidened inner auditory canal and are typically wellcircumscribed T1-hypointense and T2-hyperintensefocal mass lesions. Depending on their size they mayshow a homogeneous or heterogeneous, strong con-trast enhancement (63) (Fig. 11). Schwannomas mayextend along the more distal course of the facial nerveand may reach the geniculate body. The adjacentbrainstem may be compressed and displaced.
Epidermoid Tumors
Epidermoid tumors or epidermoid cysts are congeni-tal, benign tumors arising from intracranial restsremaining as a result of incomplete separation of theneuroectoderm from cutaneous ectoderm at the timeof closure of the neural tube (64). They contain des-quamated keratin and cholesterol. They are rare inchildren and account for approximately 1% of all in-tracranial tumors. Approximately half of all epider-moid tumors are located in the cerebellopontine angle(65). Less frequent locations include the pineal region,the surpasellar region, and the middle cranial fossa.They grow slowly, and depending on their location,they insinuate between cranial nerves and blood ves-sels. Cranial neuropathies or hydrocephalus are com-mon presentation forms (65).
On imaging, they appear as lobulated masses. Epi-dermoid tumors are hypodense on CT, T1-hypoin-tense, and T2 hypo- to hyperintense presenting a sig-nal density and intensity similar to that of the CSF(66) (Fig. 12). On FLAIR (fluid attenuated inversion re-covery), epidermoid tumors are often slightly
Figure 11. Axial (a) and coro-nal (b) contrast enhanced T1-weighted MR images in a 16-year-old woman with neurofi-bromatosis type 2 and typical,bilateral VIIIth nerve schwan-noma. The mass lesions show astrong contrast enhancementand expand the internal audi-tory canals (white arrows). Thecomponents in the cerebello-pontine angles compress the ad-jacent brainstem (black arrows).
Neuroimaging of Pediatric Posterior Fossa Tumors 9
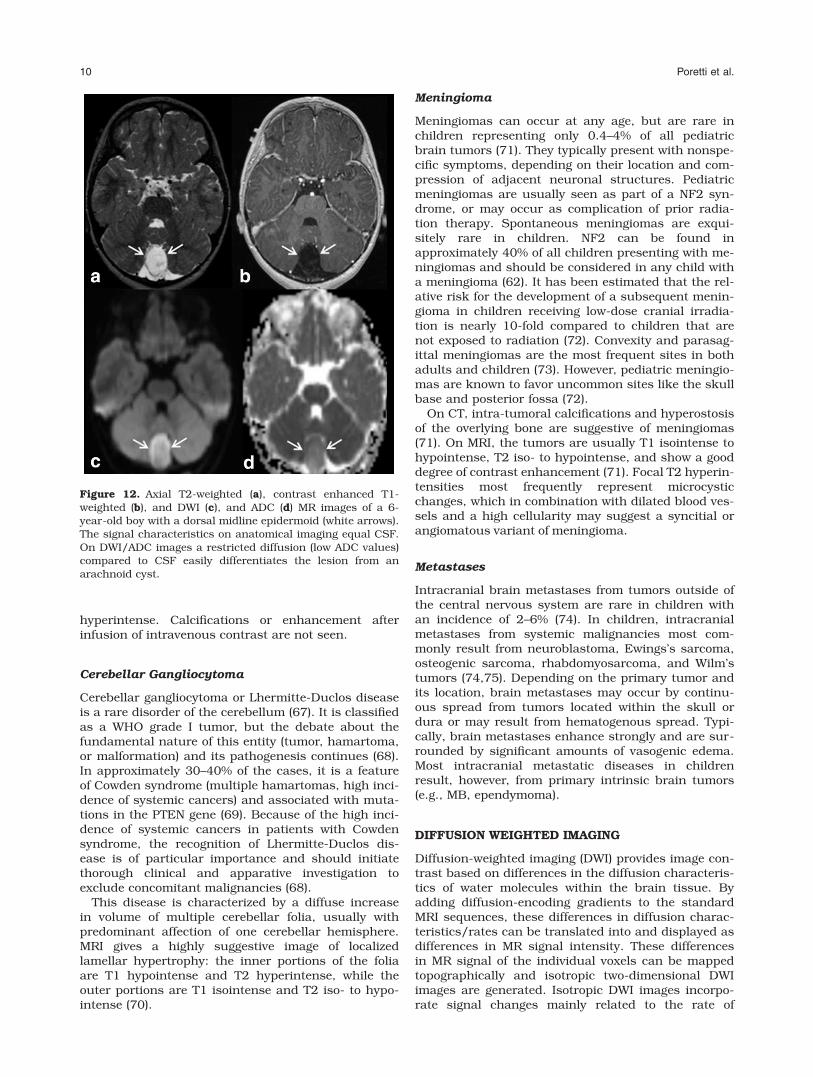
hyperintense. Calcifications or enhancement afterinfusion of intravenous contrast are not seen.
Cerebellar Gangliocytoma
Cerebellar gangliocytoma or Lhermitte-Duclos diseaseis a rare disorder of the cerebellum (67). It is classifiedas a WHO grade I tumor, but the debate about thefundamental nature of this entity (tumor, hamartoma,or malformation) and its pathogenesis continues (68).In approximately 30–40% of the cases, it is a featureof Cowden syndrome (multiple hamartomas, high inci-dence of systemic cancers) and associated with muta-tions in the PTEN gene (69). Because of the high inci-dence of systemic cancers in patients with Cowdensyndrome, the recognition of Lhermitte-Duclos dis-ease is of particular importance and should initiatethorough clinical and apparative investigation toexclude concomitant malignancies (68).
This disease is characterized by a diffuse increasein volume of multiple cerebellar folia, usually withpredominant affection of one cerebellar hemisphere.MRI gives a highly suggestive image of localizedlamellar hypertrophy: the inner portions of the foliaare T1 hypointense and T2 hyperintense, while theouter portions are T1 isointense and T2 iso- to hypo-intense (70).
Meningioma
Meningiomas can occur at any age, but are rare inchildren representing only 0.4–4% of all pediatricbrain tumors (71). They typically present with nonspe-cific symptoms, depending on their location and com-pression of adjacent neuronal structures. Pediatricmeningiomas are usually seen as part of a NF2 syn-drome, or may occur as complication of prior radia-tion therapy. Spontaneous meningiomas are exqui-sitely rare in children. NF2 can be found inapproximately 40% of all children presenting with me-ningiomas and should be considered in any child witha meningioma (62). It has been estimated that the rel-ative risk for the development of a subsequent menin-gioma in children receiving low-dose cranial irradia-tion is nearly 10-fold compared to children that arenot exposed to radiation (72). Convexity and parasag-ittal meningiomas are the most frequent sites in bothadults and children (73). However, pediatric meningio-mas are known to favor uncommon sites like the skullbase and posterior fossa (72).
On CT, intra-tumoral calcifications and hyperostosisof the overlying bone are suggestive of meningiomas(71). On MRI, the tumors are usually T1 isointense tohypointense, T2 iso- to hypointense, and show a gooddegree of contrast enhancement (71). Focal T2 hyperin-tensities most frequently represent microcysticchanges, which in combination with dilated blood ves-sels and a high cellularity may suggest a syncitial orangiomatous variant of meningioma.
Metastases
Intracranial brain metastases from tumors outside ofthe central nervous system are rare in children withan incidence of 2–6% (74). In children, intracranialmetastases from systemic malignancies most com-monly result from neuroblastoma, Ewings’s sarcoma,osteogenic sarcoma, rhabdomyosarcoma, and Wilm’stumors (74,75). Depending on the primary tumor andits location, brain metastases may occur by continu-ous spread from tumors located within the skull ordura or may result from hematogenous spread. Typi-cally, brain metastases enhance strongly and are sur-rounded by significant amounts of vasogenic edema.Most intracranial metastatic diseases in childrenresult, however, from primary intrinsic brain tumors(e.g., MB, ependymoma).
DIFFUSION WEIGHTED IMAGING
Diffusion-weighted imaging (DWI) provides image con-trast based on differences in the diffusion characteris-tics of water molecules within the brain tissue. Byadding diffusion-encoding gradients to the standardMRI sequences, these differences in diffusion charac-teristics/rates can be translated into and displayed asdifferences in MR signal intensity. These differencesin MR signal of the individual voxels can be mappedtopographically and isotropic two-dimensional DWIimages are generated. Isotropic DWI images incorpo-rate signal changes mainly related to the rate of
Figure 12. Axial T2-weighted (a), contrast enhanced T1-weighted (b), and DWI (c), and ADC (d) MR images of a 6-year-old boy with a dorsal midline epidermoid (white arrows).The signal characteristics on anatomical imaging equal CSF.On DWI/ADC images a restricted diffusion (low ADC values)compared to CSF easily differentiates the lesion from anarachnoid cyst.
10 Poretti et al.

diffusion; however, DWI maps also incorporate signalchanges related to blood flow and T2-relaxation phe-nomena. By calculating the so-called apparent diffu-sion coefficient (ADC) maps, these additional compo-nents are cancelled out, consequently the ADC mapsshow the spatial distribution of diffusion within thebrain.
Diffusion of water molecules within tissue is deter-mined by a variety of factors. Especially, the micro-structure in which the studied diffusion happensdetermines the overall diffusion of water molecules(76). Accordingly, diffusion is restricted (high intensityon DWI, low ADC values) in densely packed cerebraltumors with high cellularity, small extracellularspace, and high nuclear-to-cytoplasmatic ratio. High-grade tumors are typically characterized by higher cel-lularity and larger nuclear area than low-gradetumors (47,77). Restricted diffusion has been demon-strated in high-grade brain tumors with high cellular-ity (78,79). Several studies have suggested that analy-sis of the ADC values may allow to characterize andgrade brain tumors noninvasively (78,79). This infor-mation can be particularly important when histologi-cal verification is lacking or difficult to acquire due tothe location of the tumor (e.g., within the brainstem).However, the literature is controversial concerning thevalue of the ADC-analysis for grading tumors becauseadditional studies have demonstrated a considerableoverlap between ADC values in high- and low-gradetumors (80,81).
Until recently, only four studies assessed the valueof DWI in differentiating brain tumors of the posteriorfossa in children (Fig. 13). Rumboldt et al retrospec-
tively reviewed ADC values of enhancing solid tumorcomponents in 32 children with cerebellar tumors(82). They reported that ADC values were significantlyhigher in JPA than in ependymomas and MBs, andthat the ADC values of ependymomas are significantlyhigher than of MBs. They found, however, a signifi-cant overlap between ADC values measured in JPAand ependymomas. ATRT and MBs had similar ADCvalues. They concluded that a 100% specific ADC cut-off values for JPA (>1.4 � 103 mm2/s) and MBs (>0.9� 103 mm2/s) could be found. Schneider et al retro-spectively studied 17 children with untreated poste-rior fossa tumors (83). They concluded that the ADCvalues were significantly lower in MBs than in allother tumors. Differentiation between the three otherposterior fossa tumors (JPA, ependymoma, brainstemglioma) by ADC analysis alone was however not possi-ble. Jaremko et al retrospectively evaluated MRimages, including ADC maps, in 40 children with pos-terior fossa tumors (84). They confirmed that diffusionrestriction is rare in low-grade tumors and common inhigh-grade tumors. They also found overlaps of themeasured ADC values for the different posterior fossatumors. The overlap in ADC values between differenttumor types was explained not only by technical fac-tors, but also by true histologic variability. Gauvain etal studied five posterior fossa tumors (78). They founda good correlation between ADC ratio (Tumor ADC:Normal brain ADC) and tumor classification. In addi-tion the absolute ADC values and tumor cellularity/total nuclear area also correlated well. In conclusion,these studies show that the assessment of ADC valuesof cerebellar tumors in children may distinguish
Figure 13. Axial DWI (a) and ADC (b) images of a patient with a right cerebellar JPA with a central necrosis. The cyst andcentral necrosis show a high degree of diffusion (DWI-hypointense, high ADC values, asterisks on a and b) while the solidnodule shows mildly increased ADC compared to the normal cerebellar tissue (white arrows on b). Axial DWI (c) and ADC (d)images of a patient with a desmoplastic medulloblastoma. The tumor demonstrates restricted diffusion (DWI-hyperintense,low ADC values) compared with the normal tissue (arrows on c and d). The intratumoral foci of high degree of diffusion (DWI-hypointense, high ADC values, asterisks on c and d) may represent area of necrosis.
Neuroimaging of Pediatric Posterior Fossa Tumors 11

tumor types and histologic grades. Overlap in ADCbetween tumor types, however, has been reported.This limits prediction of the tumor grade in individualcases.
Studying the perilesional brain tissue, it appearedthat perilesional ADC values are higher in high-gradesupratentorial tumors compared to low-grade tumors(85). This can be explained by the more aggressivereaction of the surrounding brain tissue for high-grade tumors. ADC values can be significantly higherwithin the necrotic part of high-grade tumors, or mayseem reduced in calcified regions. Therefore, ADC val-ues should be assessed in the solid part of the tumorsin which no frank areas of necroses, calcification orhemorrhage are noted.
In patients treated for supratentorial high-gradegliomas, Zeng et al. showed that ADC ratios (ADC ofcontrast-enhancing lesion versus matching normalappearing brain in the contralateral hemisphere) weresignificantly higher in regions with radiation injurycompared to areas of recurrent tumor (1.69 60.08versus 1.42 60.10, P < 0.001) (86). These findingsmay help to differentiate between recurrent gliomaand radiation injury (86). In support of a correlationbetween ADC values and response to treatment, Che-nevert et al showed that the ADC values increase dur-ing chemotherapy. The ADC increase most likelyresults from a reduction of tumor cellularity andincreasing extracellular space. They also showed thatthe ADC values again decrease back to baseline withtumor recurrence (87). If validated in larger studies,analysis of ADC values during therapy could have thepotential to serve as a valuable biomarker for moni-toring therapeutic efficacy of brain tumor treatment.
DWI is also an effective way to identify small epider-moids in the basal cistern and helps to differentiatebetween epidermoids and arachnoid cysts (88). Bothlesions present the same T1 and T2 signal intensitiesand may be difficult to differentiate. On DWI, epider-moid tumors are hyperintense (restricted diffusion)due to their content of cholesterol, whereas arachnoidcysts are hypointense, demonstrating high diffusivity(88) (Fig. 14c,d). The ADC values of epidermoidtumors are low (restricted diffusion) with similar char-acteristics of a solid tumor, whereas the ADC values
of arachnoid cysts are high, similar to those of CSF,facilitating differentiation (89).
DIFFUSION TENSOR IMAGING
Not only the magnitude of diffusion (ADC value), butalso the direction and three-dimensional shape of dif-fusion in space differs between brain structures (90).For example, the diffusion in the fiber tracts is pre-dominant along the direction parallel to the long axisof fiber tracts while limited in the direction perpendic-ular to the main axis of the fiber tracts (anisotropicdiffusion). Diffusion in water or within the cerebrospi-nal fluid is however equal in all directions (isotropicdiffusion). The three-dimensional shape of diffusioncan be studied by measuring the full tensor of the dif-fusion, known as diffusion tensor imaging (DTI). InDTI, maps of the spatial distribution and magnitudeof the anisotropic component of diffusion are gener-ated. In addition to the trace of diffusion (DWI) andADC maps, fractional anisotropy (FA) maps can becalculated. In these FA maps the signal intensity isrelated to the degree of anisotropic diffusion. FA val-ues range between 0 and 1; an FA value of 0 indicatescomplete isotropic diffusion while an FA value of 1indicates absolute anisotropic diffusion. In addition,the principal direction of diffusion can be displayedas a vector for each voxel and can be color coded.With powerful postprocessing software programs,those voxels that have a similar degree and directionof anisotropic diffusion, the course of fiber tracts canbe reconstructed and displayed (tractography). Evalu-ation of the FA values and reconstruction of fibertracts allow to study the degree of deviation, infiltra-tion, or interruption of fiber tracts by tumors. In addi-tion, the quantitative analysis of the FA values oftumors may give valuable information.
Low FA values have been correlated with high-gradetumors (91,92). Additionally, DTI may be able to moreaccurately differentiate between infiltrative tumor,vasogenic edema, and normal brain tissue than con-ventional MRI (93). Particularly, DTI can show therelation of a tumor to nearby fiber tracts (94,95).Assuming that the chief cause of anisotropy is related
Figure 14. Axial FA map (a) of a patient with an ependymoma. The area with high FA (white arrows) on the left side of the tu-mor represents the displaced brainstem and cerebellar white matter tracts by the tumor. Axial FA map (b) of a patient withdiffuse intrinsic brainstem glioma after partial resection (on the right side). FA appears to be decreased between the brain-stem white matter tracts representing infiltration by the tumor.
12 Poretti et al.
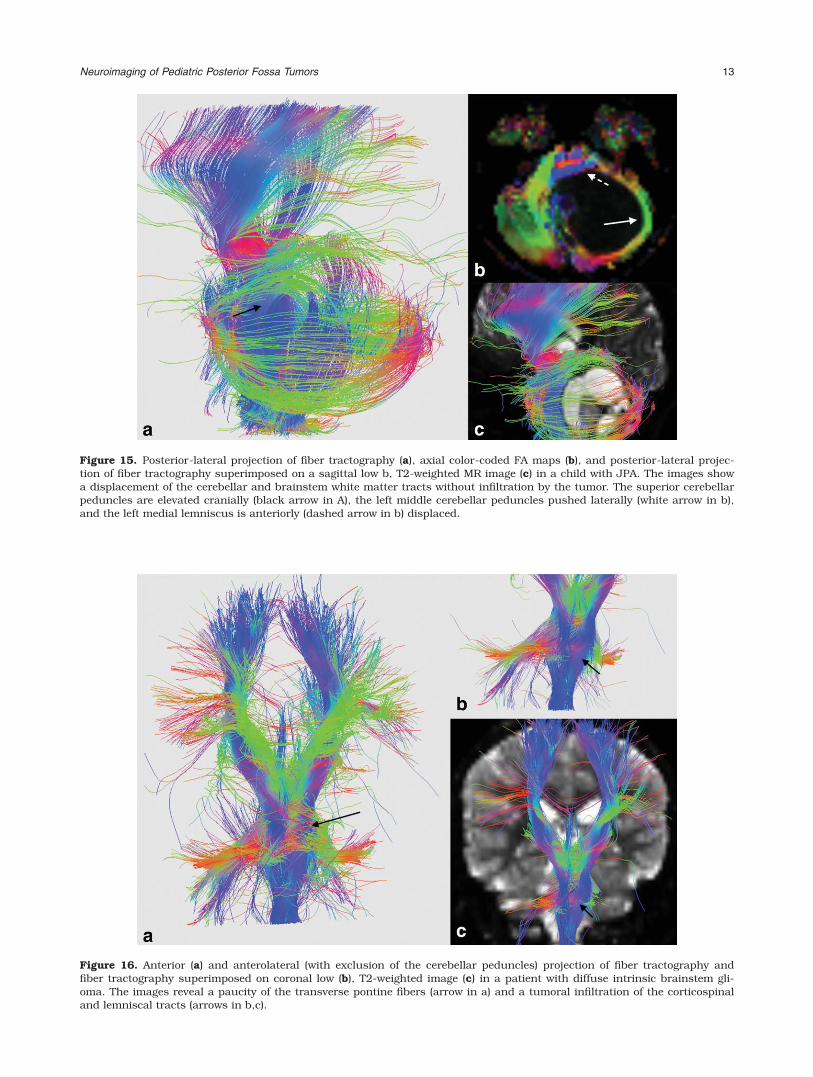
Figure 15. Posterior-lateral projection of fiber tractography (a), axial color-coded FA maps (b), and posterior-lateral projec-tion of fiber tractography superimposed on a sagittal low b, T2-weighted MR image (c) in a child with JPA. The images showa displacement of the cerebellar and brainstem white matter tracts without infiltration by the tumor. The superior cerebellarpeduncles are elevated cranially (black arrow in A), the left middle cerebellar peduncles pushed laterally (white arrow in b),and the left medial lemniscus is anteriorly (dashed arrow in b) displaced.
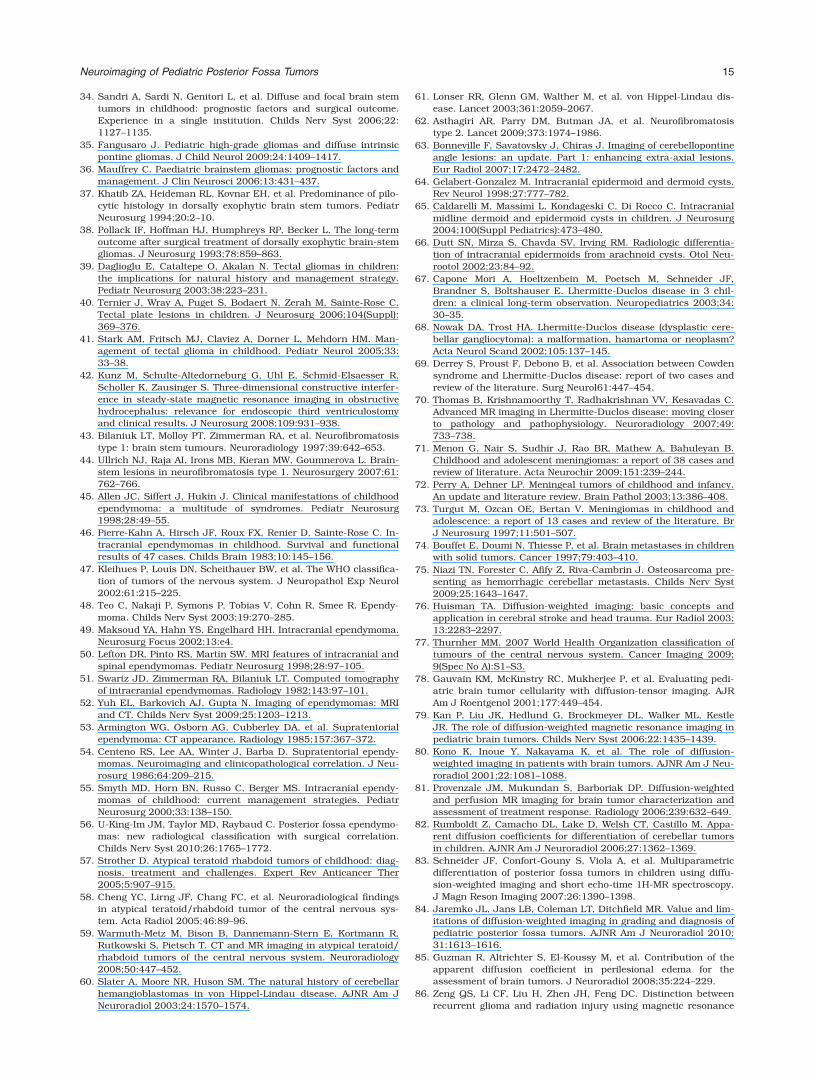
Figure 16. Anterior (a) and anterolateral (with exclusion of the cerebellar peduncles) projection of fiber tractography andfiber tractography superimposed on coronal low (b), T2-weighted image (c) in a patient with diffuse intrinsic brainstem gli-oma. The images reveal a paucity of the transverse pontine fibers (arrow in a) and a tumoral infiltration of the corticospinaland lemniscal tracts (arrows in b,c).
Neuroimaging of Pediatric Posterior Fossa Tumors 13

to the white matter bundles, white matter tract’sinvolvement by a tumor can be distinguished betweendisplaced (maintained normal degree of anisotropyrelative to the contralateral tract in the correspondinglocation but in an abnormal location/orientation,Figs. 14a and 15), invaded (slightly reduced degree ofanisotropy without displacement of white matterarchitecture but remains identifiable on color codedFA maps), infiltrated (reduced anisotropy but remainsidentifiable on color-coded FA maps, Figs. 14b and16), disrupted (marked reduced anisotropy andunidentifiable tracts on color coded FA maps), andedematous (maintained normal anisotropy and nor-mally orientation but located in an area of abnormalT2-weighted signal intensity) (96).
Differentiation between displacement and invasionof the white matter tracts by the tumors can be ofessential importance in the presurgical tumor stratifi-cation. In low-grade gliomas, deviation, withoutdestruction or invasion of the surrounding white mat-ter fibers has been reported (91,97) (Fig. 14). Addi-tionally, visualization of the relation between tumorand adjacent fiber tracts is helpful in both the neuro-surgical planning and the postoperative assessmentof brainstem lesions (94,95). Preservation of the integ-rity of white matter tracts during surgery seems tocorrelate with better postoperative neurological/func-tional outcome (98).
CONCLUSION
The role of conventional neuroimaging in the diagno-sis of pediatric brain tumors of the posterior fossa isessential regarding localization, characterization, andextension pattern of posterior fossa tumors. Althoughthere are several differences between the most fre-quent posterior fossa tumors, a reliable prediction oftumor histology or grade by neuroimaging is not yetpossible. Newer MRI techniques such as DWI and DTIprovide additional, presurgically important informa-tion, especially about the relation between tumor andadjacent fiber tracts. Despite the fact that trends havebeen reported in predicting histology and tumor gradebased upon ADC analysis, it remains currently impos-sible to predict tumor grade by MRI alone. Futuredevelopments including molecular imaging may giveimportant specific information about tumor histologyand grade.
REFERENCES
1. Baldwin RT, Preston-Martin S. Epidemiology of brain tumors inchildhood-a review. Toxicol Appl Pharmacol 2004;1992:118–131.
2. Pollack IF. Brain tumors in children. N Engl J Med 1994;331:1500–1507.
3. Davis FG, McCarthy BJ. Epidemiology of brain tumors. CurrOpin Neurol 2000;13:635–640.
4. Bristot R, Raco A, Vangelista T, Delfini R. Malignant cerebellarastrocytomas in childhood. Experience with four cases. ChildsNerv Syst 1998;14:532–536.
5. Viano JC, Herrera EJ, Suarez JC. Cerebellar astrocytomas: a 24-year experience. Childs Nerv Syst 2001;17:607–610.
6. Naidich TP, Zimmerman RA. Primary brain tumors in children.Semin Roentgenol 1984;19:100–114.
7. Villarejo F, de Diego JM, de la Riva AG. Prognosis of cerebellarastrocytomas in children. Childs Nerv Syst 2008;24:203–210.
8. Lee YY, Van Tassel P, Bruner JM, Moser RP, Share JC. Juvenilepilocytic astrocytomas: CT and MR characteristics. AJR Am JRoentgenol 1989;152:1263–1270.
9. Arai K, Sato N, Aoki J, et al. MR signal of the solid portion of pilo-cytic astrocytoma on T2-weighted images: is it useful for differen-tiation from medulloblastoma? Neuroradiology 2006;48:233–237.
10. Lee CS, Huh JS, Sim KB, Kim YW. Cerebellar pilocytic astrocy-toma presenting with intratumor bleeding, subarachnoid hemor-rhage, and subdural hematoma. Childs Nerv Syst 2009;25:125–128.
11. Walid MS, Troup EC. Cerebellar anaplastic astrocytoma in ateenager with Ollier Disease. J Neurooncol 2008;89:59–62.
12. Kasliwal MK, Gupta DK, Mahapatra AK, Sharma MC. Multicen-tric cerebellopontine angle glioblastoma multiforme. PediatrNeurosurg 2008;44:224–228.
13. Dhall G. Medulloblastoma. J Child Neurol 2009;24:1418–1430.
14. Tortori-Donati P, Fondelli MP, Rossi A, et al. Medulloblastomain children: CT and MRI findings. Neuroradiology 1996;38:352–359.
15. Koral K, Gargan L, Bowers DC, et al. Imaging characteristics ofatypical teratoid-rhabdoid tumor in children compared withmedulloblastoma. AJR Am J Roentgenol 2008;190:809–814.
16. Polkinghorn WR, Tarbell NJ. Medulloblastoma: tumorigenesis,current clinical paradigm, and efforts to improve risk stratifica-tion. Nat Clin Pract Oncol 2007;4:295–304.
17. Rutkowski S, von Bueren A, von Hoff K, et al. Prognostic rele-vance of clinical and biological risk factors in childhood medullo-blastoma: results of patients treated in the prospectivemulticenter trial HIT’91. Clin Cancer Res 2007;13:2651–2657.
18. Pizer BL, Clifford SC. The potential impact of tumour biology onimproved clinical practice for medulloblastoma: progress towardsbiologically driven clinical trials. Br J Neurosurg 2009;23:364–375.
19. Nelson M, Diebler C, Forbes WS. Paediatric medulloblastoma:atypical CT features at presentation in the SIOP II trial. Neurora-diology 1991;33:140–142.
20. Koeller KK, Rushing EJ. From the archives of the AFIP: medullo-blastoma: a comprehensive review with radiologic-pathologic cor-relation. Radiographics 2003;23:1613–1637.
21. Kyrnetskiy EE, Kun LE, Boop FA, Sanford RA, Khan RB. Types,causes, and outcome of intracranial hemorrhage in children withcancer. J Neurosurg 2005;102(Suppl):31–35.
22. Eran A, Ozturk A, Aygun N, Izbudak I. Medulloblastoma: atypicalCT and MRI findings in children. Pediatr Radiol 2010;40:1254–1262.
23. Meyers SP, Kemp SS, Tarr RW. MR imaging features of medullo-blastomas. AJR Am J Roentgenol 1992;158:859–865.
24. Kumar R, Achari G, Banerjee D, Chhabra DK. Uncommon pre-sentation of medulloblastoma. Childs Nerv Syst 2001;17:538–542.
25. Shaw DW, Weinberger E, Brewer DK, Geyer JR, Berger MS,Blaser SI. Spinal subdural enhancement after suboccipital crani-ectomy. AJNR Am J Neuroradiol 1996;17:1373–1377.
26. Jallo GI, Biser-Rohrbaugh A, Freed D. Brainstem gliomas. ChildsNerv Syst 2004;20:143–153.
27. Recinos PF, Sciubba DM, Jallo GI. Brainstem tumors: where arewe today? Pediatr Neurosurg 2007;43:192–201.
28. Donaldson SS, Laningham F, Fisher PG. Advances toward anunderstanding of brainstem gliomas. J Clin Oncol 2006;24:1266–1272.
29. Epstein F, Wisoff JH. Intrinsic brainstem tumors in childhood:surgical indications. J Neurooncol 1988;6:309–317.
30. Frazier JL, Lee J, Thomale UW, Noggle JC, Cohen KJ, Jallo GI.Treatment of diffuse intrinsic brainstem gliomas: failedapproaches and future strategies. J Neurosurger Pediatr 2009;3:259–269.
31. Mulhern RK, Hancock J, Fairclough D, Kun L. Neuropsychologi-cal status of children treated for brain tumors: a critical reviewand integrative analysis. Med Pediatr Oncol 1992;20:181–191.
32. Epstein FJ, Farmer JP. Brain-stem glioma growth patterns.J Neurosurg 1993;78:408–412.
33. Hargrave D, Bartels U, Bouffet E. Diffuse brainstem glioma inchildren: critical review of clinical trials. Lancet Oncol 2006;7:241–248.
14 Poretti et al.
34. Sandri A, Sardi N, Genitori L, et al. Diffuse and focal brain stemtumors in childhood: prognostic factors and surgical outcome.Experience in a single institution. Childs Nerv Syst 2006;22:1127–1135.
35. Fangusaro J. Pediatric high-grade gliomas and diffuse intrinsicpontine gliomas. J Child Neurol 2009;24:1409–1417.
36. Mauffrey C. Paediatric brainstem gliomas: prognostic factors andmanagement. J Clin Neurosci 2006;13:431–437.
37. Khatib ZA, Heideman RL, Kovnar EH, et al. Predominance of pilo-cytic histology in dorsally exophytic brain stem tumors. PediatrNeurosurg 1994;20:2–10.
38. Pollack IF, Hoffman HJ, Humphreys RP, Becker L. The long-termoutcome after surgical treatment of dorsally exophytic brain-stemgliomas. J Neurosurg 1993;78:859–863.
39. Daglioglu E, Cataltepe O, Akalan N. Tectal gliomas in children:the implications for natural history and management strategy.Pediatr Neurosurg 2003;38:223–231.
40. Ternier J, Wray A, Puget S, Bodaert N, Zerah M, Sainte-Rose C.Tectal plate lesions in children. J Neurosurg 2006;104(Suppl):369–376.
41. Stark AM, Fritsch MJ, Claviez A, Dorner L, Mehdorn HM. Man-agement of tectal glioma in childhood. Pediatr Neurol 2005;33:33–38.
42. Kunz M, Schulte-Altedorneburg G, Uhl E, Schmid-Elsaesser R,Scholler K, Zausinger S. Three-dimensional constructive interfer-ence in steady-state magnetic resonance imaging in obstructivehydrocephalus: relevance for endoscopic third ventriculostomyand clinical results. J Neurosurg 2008;109:931–938.
43. Bilaniuk LT, Molloy PT, Zimmerman RA, et al. Neurofibromatosistype 1: brain stem tumours. Neuroradiology 1997;39:642–653.
44. Ullrich NJ, Raja AI, Irons MB, Kieran MW, Goumnerova L. Brain-stem lesions in neurofibromatosis type 1. Neurosurgery 2007;61:762–766.
45. Allen JC, Siffert J, Hukin J. Clinical manifestations of childhoodependymoma: a multitude of syndromes. Pediatr Neurosurg1998;28:49–55.
46. Pierre-Kahn A, Hirsch JF, Roux FX, Renier D, Sainte-Rose C. In-tracranial ependymomas in childhood. Survival and functionalresults of 47 cases. Childs Brain 1983;10:145–156.
47. Kleihues P, Louis DN, Scheithauer BW, et al. The WHO classifica-tion of tumors of the nervous system. J Neuropathol Exp Neurol2002;61:215–225.
48. Teo C, Nakaji P, Symons P, Tobias V, Cohn R, Smee R. Ependy-moma. Childs Nerv Syst 2003;19:270–285.
49. Maksoud YA, Hahn YS, Engelhard HH. Intracranial ependymoma.Neurosurg Focus 2002;13:e4.
50. Lefton DR, Pinto RS, Martin SW. MRI features of intracranial andspinal ependymomas. Pediatr Neurosurg 1998;28:97–105.
51. Swartz JD, Zimmerman RA, Bilaniuk LT. Computed tomographyof intracranial ependymomas. Radiology 1982;143:97–101.
52. Yuh EL, Barkovich AJ, Gupta N. Imaging of ependymomas: MRIand CT. Childs Nerv Syst 2009;25:1203–1213.
53. Armington WG, Osborn AG, Cubberley DA, et al. Supratentorialependymoma: CT appearance. Radiology 1985;157:367–372.
54. Centeno RS, Lee AA, Winter J, Barba D. Supratentorial ependy-momas. Neuroimaging and clinicopathological correlation. J Neu-rosurg 1986;64:209–215.
55. Smyth MD, Horn BN, Russo C, Berger MS. Intracranial ependy-momas of childhood: current management strategies. PediatrNeurosurg 2000;33:138–150.
56. U-King-Im JM, Taylor MD, Raybaud C. Posterior fossa ependymo-mas: new radiological classification with surgical correlation.Childs Nerv Syst 2010;26:1765–1772.
57. Strother D. Atypical teratoid rhabdoid tumors of childhood: diag-nosis, treatment and challenges. Expert Rev Anticancer Ther2005;5:907–915.
58. Cheng YC, Lirng JF, Chang FC, et al. Neuroradiological findingsin atypical teratoid/rhabdoid tumor of the central nervous sys-tem. Acta Radiol 2005;46:89–96.
59. Warmuth-Metz M, Bison B, Dannemann-Stern E, Kortmann R,Rutkowski S, Pietsch T. CT and MR imaging in atypical teratoid/rhabdoid tumors of the central nervous system. Neuroradiology2008;50:447–452.
60. Slater A, Moore NR, Huson SM. The natural history of cerebellarhemangioblastomas in von Hippel-Lindau disease. AJNR Am JNeuroradiol 2003;24:1570–1574.
61. Lonser RR, Glenn GM, Walther M, et al. von Hippel-Lindau dis-ease. Lancet 2003;361:2059–2067.
62. Asthagiri AR, Parry DM, Butman JA, et al. Neurofibromatosistype 2. Lancet 2009;373:1974–1986.
63. Bonneville F, Savatovsky J, Chiras J. Imaging of cerebellopontineangle lesions: an update. Part 1: enhancing extra-axial lesions.Eur Radiol 2007;17:2472–2482.
64. Gelabert-Gonzalez M. Intracranial epidermoid and dermoid cysts.Rev Neurol 1998;27:777–782.
65. Caldarelli M, Massimi L, Kondageski C, Di Rocco C. Intracranialmidline dermoid and epidermoid cysts in children. J Neurosurg2004;100(Suppl Pediatrics):473–480.
66. Dutt SN, Mirza S, Chavda SV, Irving RM. Radiologic differentia-tion of intracranial epidermoids from arachnoid cysts. Otol Neu-rootol 2002;23:84–92.
67. Capone Mori A, Hoeltzenbein M, Poetsch M, Schneider JF,Brandner S, Boltshauser E. Lhermitte-Duclos disease in 3 chil-dren: a clinical long-term observation. Neuropediatrics 2003;34:30–35.
68. Nowak DA, Trost HA. Lhermitte-Duclos disease (dysplastic cere-bellar gangliocytoma): a malformation, hamartoma or neoplasm?Acta Neurol Scand 2002;105:137–145.
69. Derrey S, Proust F, Debono B, et al. Association between Cowdensyndrome and Lhermitte-Duclos disease: report of two cases andreview of the literature. Surg Neurol61:447–454.
70. Thomas B, Krishnamoorthy T, Radhakrishnan VV, Kesavadas C.Advanced MR imaging in Lhermitte-Duclos disease: moving closerto pathology and pathophysiology. Neuroradiology 2007;49:733–738.
71. Menon G, Nair S, Sudhir J, Rao BR, Mathew A, Bahuleyan B.Childhood and adolescent meningiomas: a report of 38 cases andreview of literature. Acta Neurochir 2009;151:239–244.
72. Perry A, Dehner LP. Meningeal tumors of childhood and infancy.An update and literature review. Brain Pathol 2003;13:386–408.
73. Turgut M, Ozcan OE, Bertan V. Meningiomas in childhood andadolescence: a report of 13 cases and review of the literature. BrJ Neurosurg 1997;11:501–507.
74. Bouffet E, Doumi N, Thiesse P, et al. Brain metastases in childrenwith solid tumors. Cancer 1997;79:403–410.
75. Niazi TN, Forester C, Afify Z, Riva-Cambrin J. Osteosarcoma pre-senting as hemorrhagic cerebellar metastasis. Childs Nerv Syst2009;25:1643–1647.
76. Huisman TA. Diffusion-weighted imaging: basic concepts andapplication in cerebral stroke and head trauma. Eur Radiol 2003;13:2283–2297.
77. Thurnher MM. 2007 World Health Organization classification oftumours of the central nervous system. Cancer Imaging 2009;9(Spec No A):S1–S3.
78. Gauvain KM, McKinstry RC, Mukherjee P, et al. Evaluating pedi-atric brain tumor cellularity with diffusion-tensor imaging. AJRAm J Roentgenol 2001;177:449–454.
79. Kan P, Liu JK, Hedlund G, Brockmeyer DL, Walker ML, KestleJR. The role of diffusion-weighted magnetic resonance imaging inpediatric brain tumors. Childs Nerv Syst 2006;22:1435–1439.
80. Kono K, Inoue Y, Nakayama K, et al. The role of diffusion-weighted imaging in patients with brain tumors. AJNR Am J Neu-roradiol 2001;22:1081–1088.
81. Provenzale JM, Mukundan S, Barboriak DP. Diffusion-weightedand perfusion MR imaging for brain tumor characterization andassessment of treatment response. Radiology 2006;239:632–649.
82. Rumboldt Z, Camacho DL, Lake D, Welsh CT, Castillo M. Appa-rent diffusion coefficients for differentiation of cerebellar tumorsin children. AJNR Am J Neuroradiol 2006;27:1362–1369.
83. Schneider JF, Confort-Gouny S, Viola A, et al. Multiparametricdifferentiation of posterior fossa tumors in children using diffu-sion-weighted imaging and short echo-time 1H-MR spectroscopy.J Magn Reson Imaging 2007;26:1390–1398.
84. Jaremko JL, Jans LB, Coleman LT, Ditchfield MR. Value and lim-itations of diffusion-weighted imaging in grading and diagnosis ofpediatric posterior fossa tumors. AJNR Am J Neuroradiol 2010;31:1613–1616.
85. Guzman R, Altrichter S, El-Koussy M, et al. Contribution of theapparent diffusion coefficient in perilesional edema for theassessment of brain tumors. J Neuroradiol 2008;35:224–229.
86. Zeng QS, Li CF, Liu H, Zhen JH, Feng DC. Distinction betweenrecurrent glioma and radiation injury using magnetic resonance
Neuroimaging of Pediatric Posterior Fossa Tumors 15

spectroscopy in combination with diffusion-weighted imaging. IntJ Radiat Oncol Biol Phys 2007;68:151–158.
87. Chenevert TL, McKeever PE, Ross BD. Monitoring earlyresponse of experimental brain tumors to therapy using diffu-sion magnetic resonance imaging. Clin Cancer Res 1997;3:1457–1466.
88. Tsuruda JS, Chew WM, Moseley ME, Norman D. Diffusion-weighted MR imaging of the brain: value of differentiatingbetween extraaxial cysts and epidermoid tumors. AJNR Am JNeuroradiol 1990;11:925–931.
89. Chen S, Ikawa F, Kurisu K, Arita K, Takaba J, Kanou Y. Quanti-tative MR evaluation of intracranial epidermoid tumors by fastfluid-attenuated inversion recovery imaging and echo-planar dif-fusion-weighted imaging. AJNR Am J Neuroradiol 2001;22:1089–1096.
90. Huisman TA, Tekes A. Advanced MR brain imaging. Why? PediatrRadiol 2008;38:S415–S432.
91. Price SJ, Burnet NG, Donovan T, et al. Diffusion tensor imagingof brain tumours at 3T: a potential tool for assessing white mat-ter tract invasion? Clin Radiol 2003;58:455–462.
92. Inoue T, Ogasawara K, Beppu T, Ogawa A, Kabasawa H. Diffu-sion tensor imaging for preoperative evaluation of tumor grade ingliomas. Clin Neurol Neurosurg 2005;107:174–180.
93. Cruz Junior LC, Sorensen AG. Diffusion tensor magnetic resonanceimaging of brain tumors. Neurosurg Clin N Am 2005;16:115–134.
94. Helton KJ, Phillips NS, Khan RB, et al. Diffusion tensor imagingof tract involvement in children with pontine tumors. AJNR Am JNeuroradiol 2006;27:786–793.
95. Helton KJ, Weeks JK, Phillips NS, et al. Diffusion tensor imagingof brainstem tumors: axonal degeneration of motor and sensorytracts. J Neurosurg 2008;1:270–276.
96. Witwer BP, Moftakhar R, Hasan KM, et al. Diffusion-tensor imag-ing of white matter tracts in patients with cerebral neoplasm.J Neurosurg 2002;97:568–575.
97. Goebell E, Paustenbach S, Vaeterlein O, et al. Low-grade andanaplastic gliomas: differences in architecture evaluated withdiffusion-tensor MR imaging. Radiology 2006;239:217–222.
98. Chen X, Weigel D, Ganslandt O, Buchfelder M, Nimsky C. Diffu-sion tensor imaging and white matter tractography in patientswith brainstem lesions. Acta Neurochir 2007;149:1117–1131.
16 Poretti et al.