mr imaging of the brachial plexus: current imaging sequences, normal findings, and findings in a...
TRANSCRIPT

MR Imaging of the Brachial Plexus: Current Imaging Sequences, Normal Findings, and
Findings in a Spectrum of Focal Lesions with MR-Pathologic Correlation
Jayant R. Kichari, MD, Shahid M. Hussain, MD, PhD, Jan C. Den Hollander, MD, and Gabriel P. Krestin, MD, PhD
Currently in many centers, magnetic resonance (MR) imag- ing is the technique of choice for the assessment of brachial plexopathies. The anatomy of the brachial plexus is com- plex, and is surrounded by other anatomic structures, making artifact-free imaging quite challenging. With the faster breathing-independent and breath-hold MR imaging sequences, brachial plexopathies can be assessed with more confidence. Over a 2-year period, 20 patients under- went MR imaging of the brachial plexus at our department. MR imaging was based on a comprehensive protocol, including T,-weighted gradient echo, T,-weighted single- shot fast spin-echo, and gadolinium-enhanced T, -weighted gradient echo with fat suppression. Nine of the 20 patients had proved diagnoses at pathology, and included schwan- noma (n = 2), ganglioneuroblastoma (n = l), hemangioma (n = l), metastatic breast cancer (n = 2), Pancoast tumor (n = l), and metastatic lung cancer (n = 2). Most of the lesions had presenting symptoms, such as pain, swelling, pares- thesia, and arm weakness. At MR imaging, the location and characteristics of the lesions on different types of T,-weighted and T,-weighted sequences were described with pathologic correlation.
The brachial plexus is a complex network of nerves that provide sensory and motor innervation to the upper extremity. Abnormalities of the brachial plexus are common, and their clinical management needs a clear understanding of their relationship to the brachial plexus.’ For clinical evaluation of the brachial plexus in patients with suspected or known
From the Department of Radiology and Pathology, Erasmus University Medical Center, Rotterdam, The Netherlands Reprint requests: Shahid M. Hussain, MD: PhD, Department of Radiology, Erasmus University Medical Center, Dr. Molewaterplein 40, 3015 GD Rotterdam, The Netherlands. Curr Probl Diagn Radio1 2003;32:000. 0 2003 Mosby, Inc. All rights reserved. 0363-0188/2003/$35.00 + 0 doi: 10.1067/mdr.2003.12007
nontraumatic brachial plexopathy, magnetic reso- nance (MR) imaging is the modality of choice, because it has multiplanar capabilities and excellent soft tissue contrast that is superior to computer tomography (CT) and sonograph.2 Artifact-free im- aging of the brachial plexus may be challenging because the brachial plexus is comprised of vascular and nervous structures that are surrounded by a large amount fatty tissue, bony structures, neck and thoracic vessels, muscles, and lungs. In our experi- ence, all of these structures may be a source of artifacts on MR images, particularly if relatively older slower sequences are used.
During the last 2 years, 20 patients underwent MR imaging for assessment of the brachial plexus at our institution. To illustrate various causes of bra- chial plexopathy at MR imaging, we only included patients with pathologically proven diagnoses of focal lesions in the area of brachial plexus. The patients (n = 9) were comprised of four males and five females. The diagnoses were of primary lesions, including schwannoma (n = 2), ganglioneuroblas- toma (n = l), and hemangioma (n = l), and secondary lesions, such as metastases from breast carcinoma (n = 2), metastases from lung cancer (n = 2), and a Pancoast tumor (n = 1). These abnor- malities may present with variable and often over- lapping clinical signs and symptoms (Table 1).
This article will illustrate the MR-pathologic corre- lation of various disease entities that affected the brachial plexus in our patients. Specific topics dis- cussed include normal anatomy of the brachial plexus, MR imaging techniques, schwannoma, neuroblas- toma, cavernous hemangioma, metastatic breast can- cer, Pancoast tumor, and metastatic lung cancer.
88 Curr Probl Diagn Radiol, March/April 2003
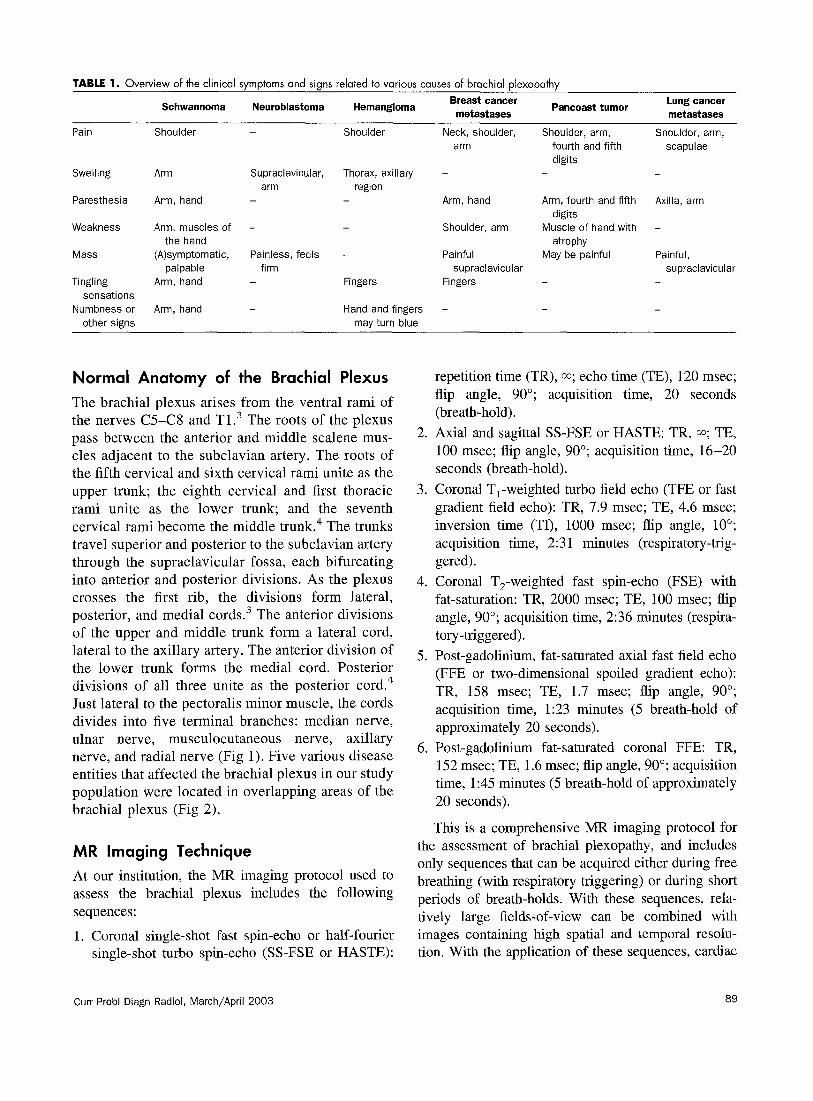
TABLE 1. Overview of the clinical symptoms and signs related to various causes of brachial plexopathy
Schwannoma Neuroblastoma Hemangioma Breast cancer
metastases Pancoast tumor
Lung cancer metastases
Pain Shoulder Shoulder Neck, shoulder, Shoulder, arm, Shoulder, arm, arm fourth and fifth scapulae
digits Swelling Arm Supraclavicular, Thorax, axillary - -
arm region Paresthesia Arm, hand Arm, hand Arm, fourth and fifth Axilla, arm
digits Weakness Arm, muscles of - Shoulder, arm Muscle of hand with -
the hand atrophy Mass (A)symptomatic, Painless, feels - Painful May be painful Painful,
palpable firm supraclavicular supraclavicular Tingling Arm, hand Fingers Fingers
sensations Numbness or Arm, hand Hand and fingers -
other signs may turn blue
Normal Anatomy of the Brachial Plexus
The brachial plexus arises from the ventral rami of the nerves C5-C8 and T1.3 The roots of the plexus pass between the anterior and middle scalene mus- cles adjacent to the subclavian artery. The roots of the fifth cervical and sixth cervical rami unite as the upper trunk; the eighth cervical and first thoracic rami unite as the lower trunk; and the seventh cervical rami become the middle trunk.4 The trunks travel superior and posterior to the subclavian artery through the supraclavicular fossa, each bifurcating into anterior and posterior divisions. As the plexus crosses the first rib, the divisions form lateral, posterior, and medial cords.3 The anterior divisions of the upper and middle trunk form a lateral cord, lateral to the axillary artery. The anterior division of the lower trunk forms the medial cord. Posterior divisions of all three unite as the posterior cord.4 Just lateral to the pectoralis minor muscle, the cords divides into five terminal branches: median nerve, ulnar nerve, musculocutaneous nerve, axillary nerve, and radial nerve (Fig 1). Five various disease entities that affected the brachial plexus in our study population were located in overlapping areas of the brachial plexus (Fig 2).
MR Imaging Technique
At our institution, the MR imaging protocol used to assess the brachial plexus includes the following sequences:
1. Coronal single-shot fast spin-echo or half-fourier single-shot turbo spin-echo (SS-FSE or HASTE):
Curr Probl Diagn Radiol, March/April 2003
2.
3.
4.
5.
6.
repetition time (TR), 00; echo time (TE), 120 msec; flip angle, 90”; acquisition time, 20 seconds (breath-hold). Axial and sagittal SS-FSE or HASTE: TR, ~0; TE, 100 msec; flip angle, 90”; acquisition time, 16-20 seconds (breath-hold). Coronal T,-weighted turbo field echo (TFE or fast gradient field echo): TR, 7.9 msec; TE, 4.6 msec; inversion time (TI), 1000 msec; flip angle, 10”; acquisition time, 2:3 1 minutes (respiratory-trig- gered). Coronal T,-weighted fast spin-echo (FSE) with fat-saturation: TR, 2000 msec; TE, 100 msec; flip angle, 90”; acquisition time, 2:36 minutes (respira- tory-triggered). Post-gadolinium, fat-saturated axial fast field echo (FFE or two-dimensional spoiled gradient echo): TR, 158 msec; TE, 1.7 msec; flip angle, 90”; acquisition time, 1:23 minutes (5 breath-hold of approximately 20 seconds). Post-gadolinium fat-saturated coronal FFE: TR, 152 msec; TE, 1.6 msec; flip angle, 90”; acquisition time, 1:45 minutes (5 breath-hold of approximately 20 seconds).
This is a comprehensive MR imaging protocol for the assessment of brachial plexopathy, and includes only sequences that can be acquired either during free breathing (with respiratory triggering) or during short periods of breath-holds. With these sequences, rela- tively large fields-of-view can be combined with images containing high spatial and temporal resolu- tion. With the application of these sequences, cardiac
89
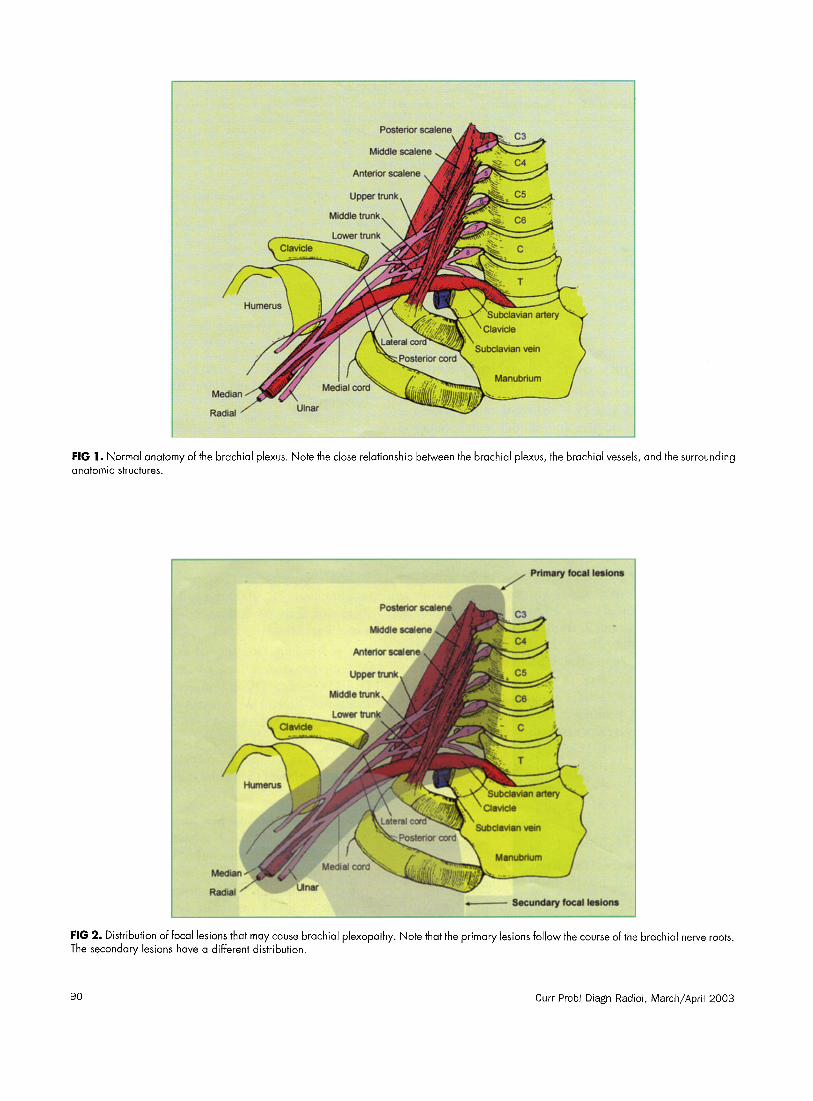
FIG 1. Normal anatomy of the brachial plexus. Note the close relationship between the brachial plexus, the brachial vessels, and the surrounding anatomic structures.
Middle scaiene
+------ Secundary focal lesions -I 1--- __l____l__-- -1--..-- I -.--- _~ -__1_-- _ --..---^- I ---. ---._- _-.___I._.~.-I-__“._I
FIG 2. Distribution of focal lesions that may cause brachial plexopathy. Note that the primary lesions follow the course of the brachial nerve roots. The secondary lesions have a different distribution.
90 Curr Probl Diagn Radiol, March/April 2003

triggering or gating for patients with suspected abnor- mality in the area of brachial plexus is not necessary.
Schwannoma
Schwannomas are benign tumors of the nervous sys- tem originating in the neural sheath (Schwann’s cell).6’7 Most commonly, schwannomas occur as sol- itary encapsulated subcutaneous tumors in otherwise normal individuals. More rarely, they are multiple or arise from other points along the peripheral nervous system, including cranial nerves, spinal roots, the brachial and lumbasacral plexus, or major peripheral nerves .6,7
Schwannomas of the brachial plexus have a broad spectrum of clinical features, including asymptomatic or painful palpable mass located in the supraclavicular fossa or neck, shoulder pain, arm weakness, weakness of the intrinsic muscle of the hand, swelling of the arm, and paresthesia or hypesthesia of the arm or hand (Table 1). A palpable mass in the neck usually means that the schwannoma is located in the roots of the brachial plexus. Involvement of the fourth and fifth digits is a sign that the schwannoma is probably located in the medial cord of the brachial plexus. Typically, for a T,-nerve root tumor, there is pain and paresthesia on percussion of the supraclavicular fossa.‘-lo
At MR imaging, schwannomas are visible as well- delineated masses with low signal intensity (SI) on T,-weighted images, very high SI on T,-weighted images, and strong peripheral enhancement on post- contrast images. At pathology, schwannomas classi- cally contain areas of densely packed spindle cells, known as Antoni A tissue, intermixed with looser,
FIG 3. Schwannoma in a 72-year-old female. A, Coronal T,-weighted turbo field echo image shows a small hypointense tumor at the level of the left brachial plexus that is difficult to distinguish from the brachial vessels (arrow). Note the lack of artifacts and clear delineation of the mediastinum
and the lung parenchyma (curved arrow). Compare this finding to the next two images. 6, Coronal Tz-weighted fast spin-echo image with fat-saturation shows the tumor as a bright oval-shaped lesion (arrow). Note that the ghost artifacts, caused by the heart and large mediastinal
vessels, project over both lungs. C, A coronal and D, axial contrast-enhanced T,-weighted spoiled gradient echo images with fat suppression
shows a homogenous enhancement of the lesion (arrow). The lesion is well-circumscribed on these images. E, F, Photomicrograph (original magnification, x200, x400; hematoxylin-eosin [H-E] stain) shows fascicles of spindle cells next to somewhat less cellular areas (Antoni A and Antoni B pattern).
myxoid regions (Antoni B tissue) (Fig 3). In the denser areas, cell nuclei may form orderly pallisades (Vero- cay bodies).’ ’ The treatment for schwannoma of the brachial plexus is resection of the tumor.6’12
Neuroblastoma
Neuroblastoma is the most common extracranial solid tumor in infancy.13 Neuroblastoma accounts for 8.2% of all cancers diagnosed in children less than 15 years of age and 15% of all cancers in children less than 5 years of age.13 Neuroblastoma arises from the sympa- thetic nervous system, which is derived from primitive neural crest cells.i4
Because neuroblastoma may originate anywhere along the peripheral sympathetic nervous system, there are many manifestations of the disease. Thus, the symptoms may be nonspecific.‘3,14 Lymph nodes, bone, bone marrow, and liver are common sites of neuroblastoma metastases. Pulmonary, renal, subcuta- neous, and brain metastatic lesions are relatively less common. l4 Neuroblastomas involving the brachial plexus give rise to supraclaviculary swelling, extend- ing to the stemocleidomastoideus and thorax (Table 1). Occasionally, there is swelling of the arm or displacement of the trachea, which may cause stridor.
At MR imaging, neuroblastomas are visible as low SI on T,-weighted images, high SI on T,-weighted images, and show a homogeneous enhancement on gadolinium-enhanced images. At pathology, the pre- sumptive stem cell of the neural crest, the sympa- thogon, differentiates into sympathoblast, and into ganglioneurobastoma and ganglioneuroma (Fig 4). l5 Ganglioneuroblastoma is composed of predominantly ganglioneuromatous component (>50%) and a small
FIG 4. Ganglioneuroblastoma in 3-year-old male. A, Axial T,-weighted turbo field echo image shows a small well-defined hypointense tumor at the level of the left brachial plexus (arrow). 6, Axial T,-weighted fast spin-echo image with fat suppression at a slightly higher anatomic level shows
the tumor as a bright lesion that is slightly larger in size (arrow). Note the ghost artifacts (curved arrow). C, Axial contrast-enhanced T,-weighted spoiled gradient echo image with fat suppression shows a homogenous enhancement of the lesion (arrow). Note the ghost artifacts (curvedarrow).
D, A similar MR image at a higher anatomic level than the previous image shows the tumor extending into the left foramen (curved arrow) indicating the neurogenic origin of the lesion. E, F, Photomicrograph [original magnification, x200, x400; H-E stain) shows neuroblasts and larger cells
(arrow) with ganglionic differentiation in a fibrillary stroma consistent with ganglioneuroblastoma.
Curr Probl Diagn Radiol, March/April 2003 91
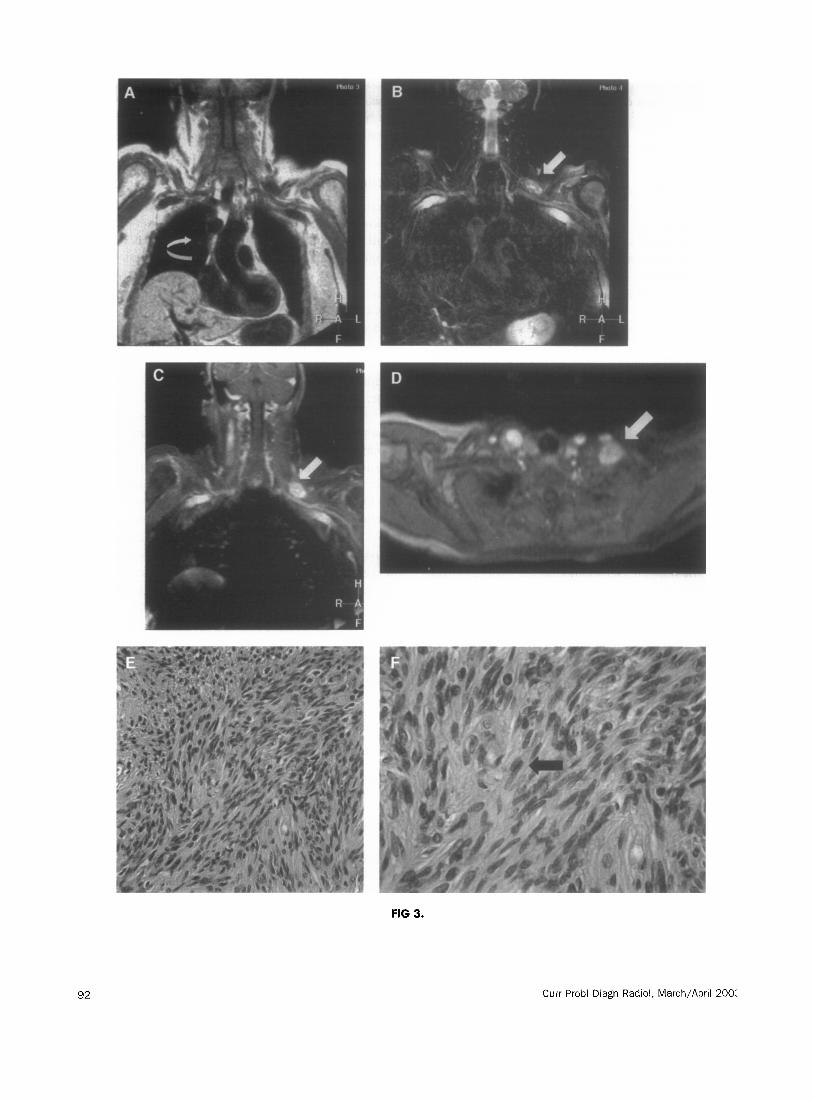
FIG 3.
Curr Probl Diagn Radiol, March/April 200:
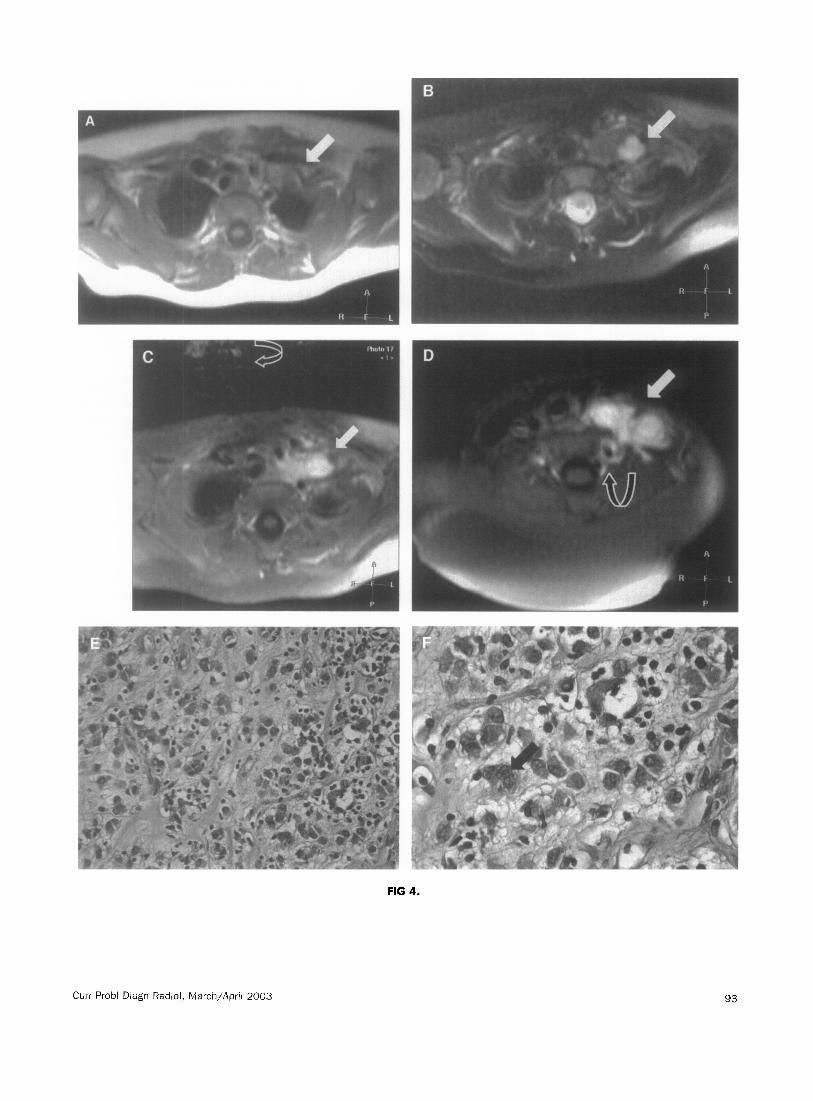
FIG 4.
Curr Probl Diagn Radiol, March/April 2003 93

neuroblastomatous component.i6 Total surgical exci- sion, when possible, remains the initial treatment of choice for localized neuroblastoma. Radiation therapy and chemotherapy play a role in the treatment of the patient with disseminated disease. l4
fingers. Symptoms vary in intensity and are not con- tinuously present (Table 1).
Brachial Plexopathy Caused by Cavernous Hemangioma
Hemangiomas are vascular neoplasms that appear anywhere in the body. Approximately 75% are present at birth, and approximately 60% occur in the head and neck area.17 The majority of hemangiomas in the infancy disappear spontaneously.i7 These lesions may be composed primarily of masses of cavernous (cav- ernous hemangioma) or capillary-like channels (cap- illary hemangioma) filled with either blood or lymph.17 Cavernous hemangiomas may arise in blood vessels or in lymphatics. Cavernous hemangiomas often occur on the skin and mucosal surfaces of the body, but may also arise in viscera, particularly in the liver, spleen, pancreas, and, rarely, the brain.18 In infants, cavernous hemangiomas sometimes constitute large lesions of the skin of the face or scalp, the so-called port wine stains or birthmarks.i8 Cavernous hemangiomas are generally red-blue, compressible, spongy lesions that are 2 to 3 cm in diameter, sharply defined at their margins, and composed of large cavernous spaces filled with blood; they have partially thrombosed channels.18 When picked up in internal organs by CT or MR imaging scans, they must be differentiated from more ominous lesions. Those in the brain are most threatening, because they may cause pressure symptoms or rupture. l8
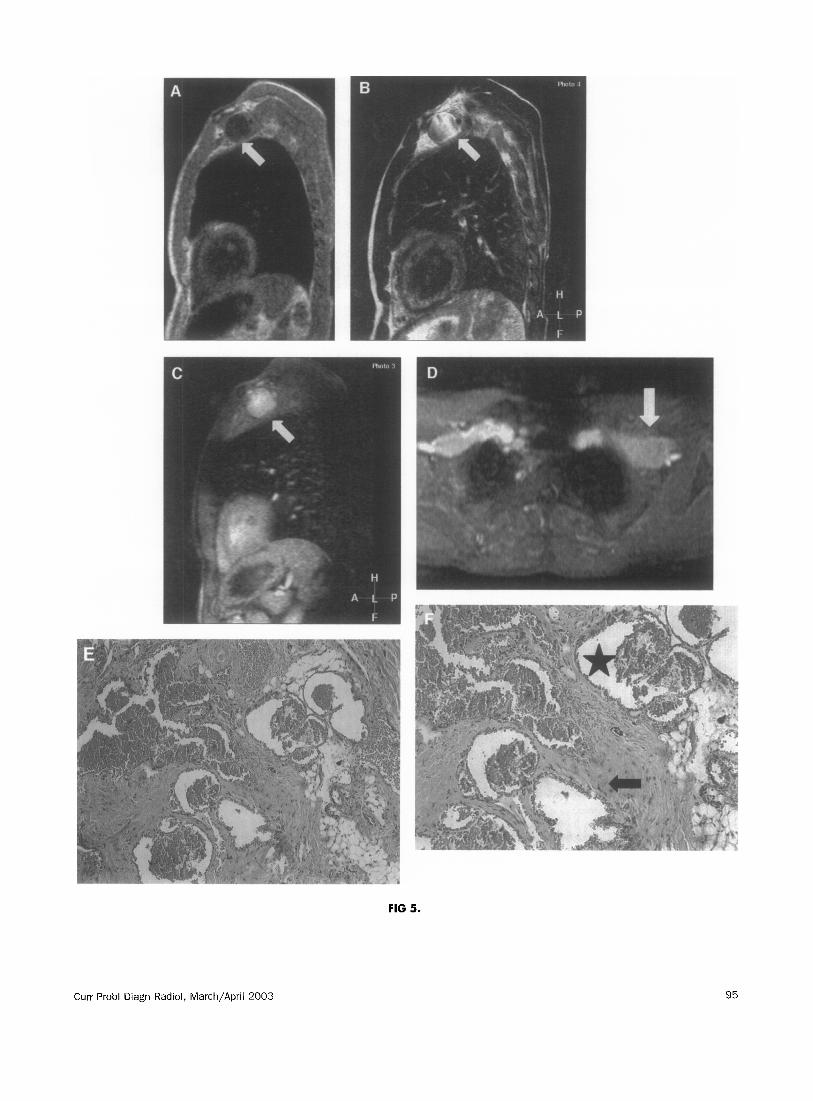
At MR imaging, the hemangiomas in the area of the brachial plexus appear as sharply marginated, very high signal intensity structures, and may show periph- eral nodular enhancement in the early phases of dynamic gadolinium-enhanced images. Hemangiomas often show sustained homogeneous enhancement on delayed gadolinium-enhanced images. At pathology, the lesions are composed of large cavernous spaces filled with blood and partially thrombosed channels (Fig 5). The lesions do not metastasize, and simple excision will often be curative.17
Brachial Plexopathy due to Metastatic Breast Cancer
Breast cancer is currently the second most common type of malignancy and by far most common cancer in women, with an incidence of 10.4%.19 Breast cancer can be either invase or noninvasive. Invasive carcino- mas are categorized into different histological types, including ductal and lobular.” Spread of invasive breast carcinoma occurs through lymphatic and hema- togenous channels. The axillary and internal mam- mary nodes are often affected after dissemination. More distant metastases occur in the lungs, skeleton, liver, and pituitary.20 The brachial plexus can also be affected by breast cancer metastases. Clinically, pa- tients may present with the following symptoms: pain (neck, shoulder, or arm), painful supraclavicular mass, muscle weakness (shoulder or arm), paresthesia (arm or hand), or a tingling sensation in the fingers (Table 1).
Hemangiomas in the shoulder or back area can At MR imaging, metastases or recurrent disease compromise the functions of the brachial plexus. in the area of the brachial plexus have a nonspecific Symptoms described by patients include feelings of appearance. Both metastases and recurrent disease pressure in the shoulder accompanied by pain and can present with low SI on T,-weighted images and swelling of the thorax and axillary region in which the relatively high SI on T,-weighted images. Recurrent skin may turn blue. Pain becomes worse when the breast carcinomas may be difficult to distinguish swelling increases and when the skin turns blue. The from fibrosis. Dynamic gadolinium-enhanced MR hands and fingers may sometimes become numb and imaging may facilitate in detection and character- blue. There may be also a tingling sensation in the ization of pathologic lymph nodes and in the dis-
FIG 5. Hemangioma in a 41.year-old male. A, Sagittal T,-weighted turbo field echo image shows a hypointense tumor with sharp margins at the level of the left brachial plexus (arrow). B, Sagittal T,-weighted fast spin-echo image shows a predominantly bright lesion (arrow). C, Sagittal and
D, axial T,-weighted spoiled gradient echo images with fat suppression show a homogenous enhancement of the lesion (arrow). E, F, Photomicrograph (original magnification x40, x60; H-E stain) shows blood filled vascular spaces (*) lined by flattened epithelial cells within a
fibrous-fatty stroma (urrow).
94 Curr Probl Diagn Radiol, March/April 2003
Curr Probl Diagn Radiol, March/April 2003
FIG 5.
95
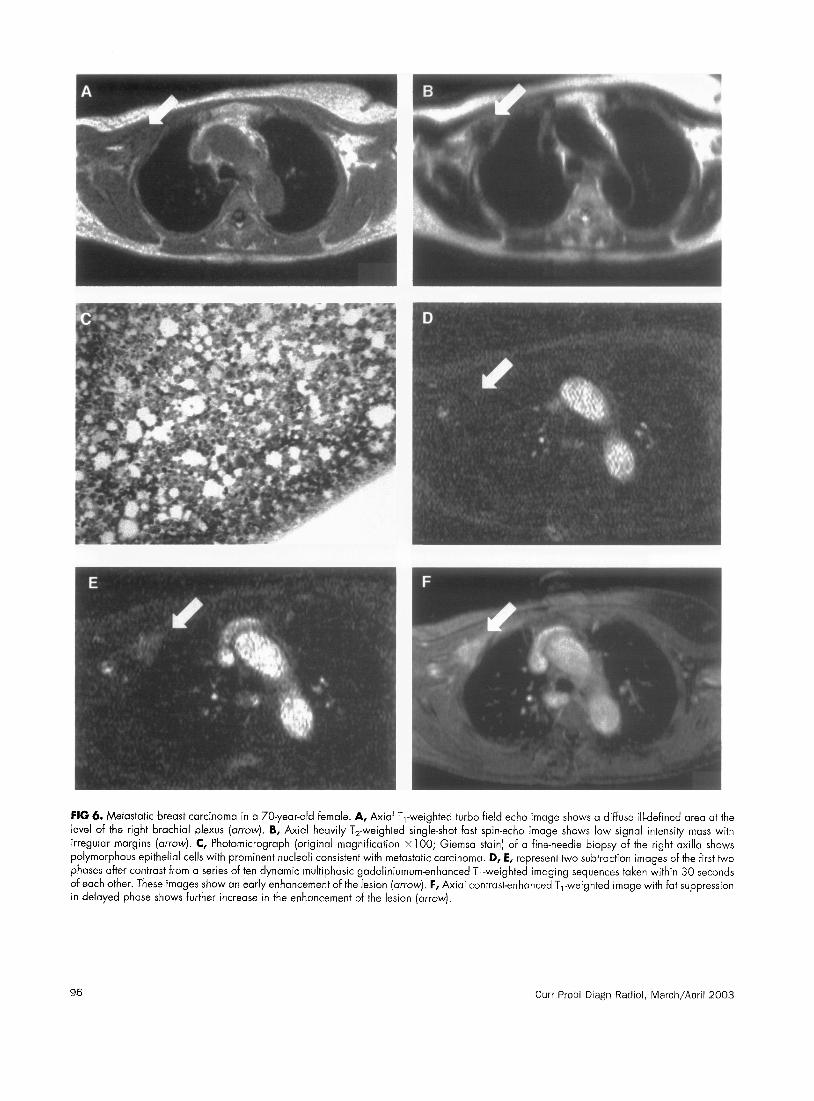
FIG 6. Metastatic breast carcinoma in a 70-year-old female. A, Axial T,-weighted turbo field echo image shows a diffuse ill-defined area at the
level of the right brachial plexus (arrow]. 6, Axial heavily T,-weighted single-shot fast spin-echo image shows low signal intensity mass with irregular margins (arrow). C, Photomicrograph (original magnification x 100; Giemsa stain] of a fine-needle biopsy of the right axilla shows
polymorphous epithelial cells with prominent nucleoli consistent with metastatic carcinoma. D, E, represent two subtraction images of the first two phases after contrast from a series of ten dynamic multiphasic gadoliniumum-enhanced T,-weighted imaging sequences taken within 30 seconds of each other. These images show an early enhancement of the lesion (arrow]. F, Axial contrast-enhanced T,-weighted image with fat suppression
in delayed phase shows further increase in the enhancement of the lesion (arrow).
96 Curr Probl Diagn Radiol, March/April 2003

tinction between recurrent disease and fibrosis.2’ Pathologic lymph nodes and recurrent disease often show early enhancement during dynamic MR imag- ing (Fig 6).21 Treatment of patients with plexopathy may include lymph node dissection and palliation, including chemotherapy and radiotherapy, in cases of recurrent disease.
Pancoast Tumor (Superior Sulcus Tumor)
Pancoast tumor is an uncommon lung cancer arising at the level of the superior pulmonary sulcus and limited to the upper apical segment but with direct spread to the para-apical structures causing Pancoast’s syn- drome.22 Pancoast’s syndrome is a constellation of characteristic symptoms and signs that includes shoul- der and arm pain along the distribution of the eighth cervical nerve trunk and first and second thoracic nerve trunks.23 Horner’s syndrome and weakness and atrophy of the muscles of the hand are also present. Radiographic evidence of destruction of the first tho- racic rib or vertebral body could also be part of Horner’s syndrome.“2 Other causes of Pancoast’s syn- drome include other primary thoracic neoplasms, me- tastases, infection, neurogenic tumors, and pulmonary amyloid nodules.23 The most common initial symptom is shoulder pain, which is produced by neoplastic involvement of the brachial plexus, parietal pleura, endothoracic fascia, vertebral bodies, and first, second, and third ribs.23 Pain can radiate up to the head and neck or down to the medial aspect of the scapula, axillary anterior part of the chest, or ipsilateral arm,
often along the distribution of the ulnar nerve. Hom- er’s syndrome, which consists of ipsilateral ptosis, miosis, and anhidrosis, is caused by invasion of the paravertebral sympathetic chain and the inferior cer- vical (stellate) ganglion.23
Weakness and atrophy of the intrinsic muscles of the hand are not uncommon, along with pain and paresthesia of the medial aspect of the arm, forearm, and the fourth and fifth digits, caused by extension of the tumor to C8 and Tl nerve roots (Table 1).23
MR imaging findings may include asymmetry of the apical regions, an apical mass, and bone destruc- tion. The multiplanar nature of MR imaging provides better assessment of invasion through subpleural fat and pleura, involvement of the subclavian artery and brachial plexus. MR imaging appearance of the tumors in the superior sulcus is nonspecific, and needs biopsy for definite diagnosis (Fig 7). At pathology, findings vary depending of the nature of the tumor. Preopera- tive radiotherapy followed by extended surgical resec- tion is the most common treatment.22-25
Brachial Plexopathy Caused by Metastatic Lung Cancer
Lung cancer is currently the most common type of malignancy with an incidence of 12.3%.19 According to the International Classification of Diseases for Oncology (ICD-0), lung cancer can be classified as either invasive or in situ lung cancer.26 The four major histologic types of invasive lung cancer include squa- mous cell (or epidermoid) carcinoma, small cell (oat
FIG 7. Pancoast tumor in a 73-year-old female. A, Coronal T,-weighted turbo field echo image shows retraction of the brachial plexus on the left side (straight arrow). A large tumor with the mediastinal lymph adenopathy is clearly visible due to the lack of artifacts [curved arrow]. B, T,-weighted fast spin-echo image with fat saturation shows again the asymm’etric brachial plexus (straight arrow) and the tumor (curved arrow].
Because of the close vicinity to the lungs and the large field-of-view, the fat saturation was suboptimal in this particular case. C, Axial heavily T,-weighted single-shot fast spin-echo image shows the tumor (straight arrow) as a hypointense lesion. Because of the sub-second acquisition time,
the artifacts are minimized. D, Sagittal gadolinium-enhanced T,-weighted image on the normal side shows the normal putmonary vessels and normal brachial plexus area [curved arrow). E, Sagittal gadolinium-enhanced T,-weighted image on the affected side shows the tumor (straight
arrow) invading the brachial plexus area (curvedarrow). F, Photomicrograph (original magnification x400; H-E stain) shows the tumorwith highly polymorphous epithelial cells with prominent nucleoli and intercellular bridges. Several mitoses are evident. Keratin praduction was evident in other
areas of the lesion (not shown). The findings were consistent with bronchogenic squamous cell carcinoma.
FIG 8. Metastatic lung carcinoma in a 4%year-old male. A, Coronal T,-weighted turbo field echo image shows a large hypointense tumor in the right superior sulcus with invasion and encasement of the structures of the brachial plexus (arrow). B, T,-weighted fast spin-echo image with fat
saturation shows the tumor as a bright lesion [arrow). Note the artifacts caused by the cardiovascular structures and the lack of fat suppression around the tumor, most likely because of the vicinity of the air in the lungs and outside of the patients. C, Coronal heavily T,-weighted single-shot fast spin-echo image shows the tumor (arrow) as a hypointense lesion. Because of the sub-second acquisition time, the artifacts are minimized. D,
A coronal and E, an axial T,-weighted gadolinium-enhanced spoiled gradient echo with fat suppression images show homogenous enhancement of the lesion (arrow). Note the encasement with extension of the tumor along the brachial plexus (curved arrow). F, Photomicrograph (original magnification, x 100; H-E stain) shows a central area with tumor comprised of polymorphous epithelial cells with intercellular bridges consistent
with a metastasis of squamous cell carcinoma.
Curr Probl Diagn Radiol, March/April 2003 97
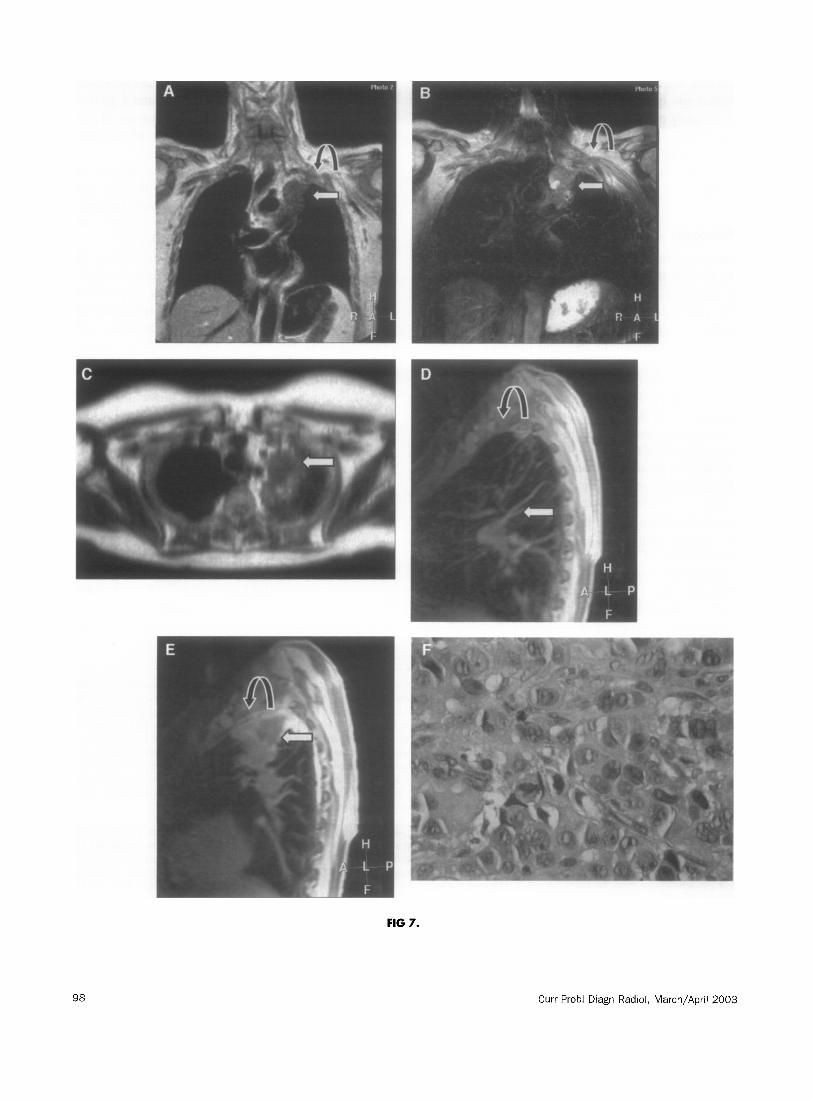
FIG 7.
Curr Probl Diagn Radiol, March/April 2003
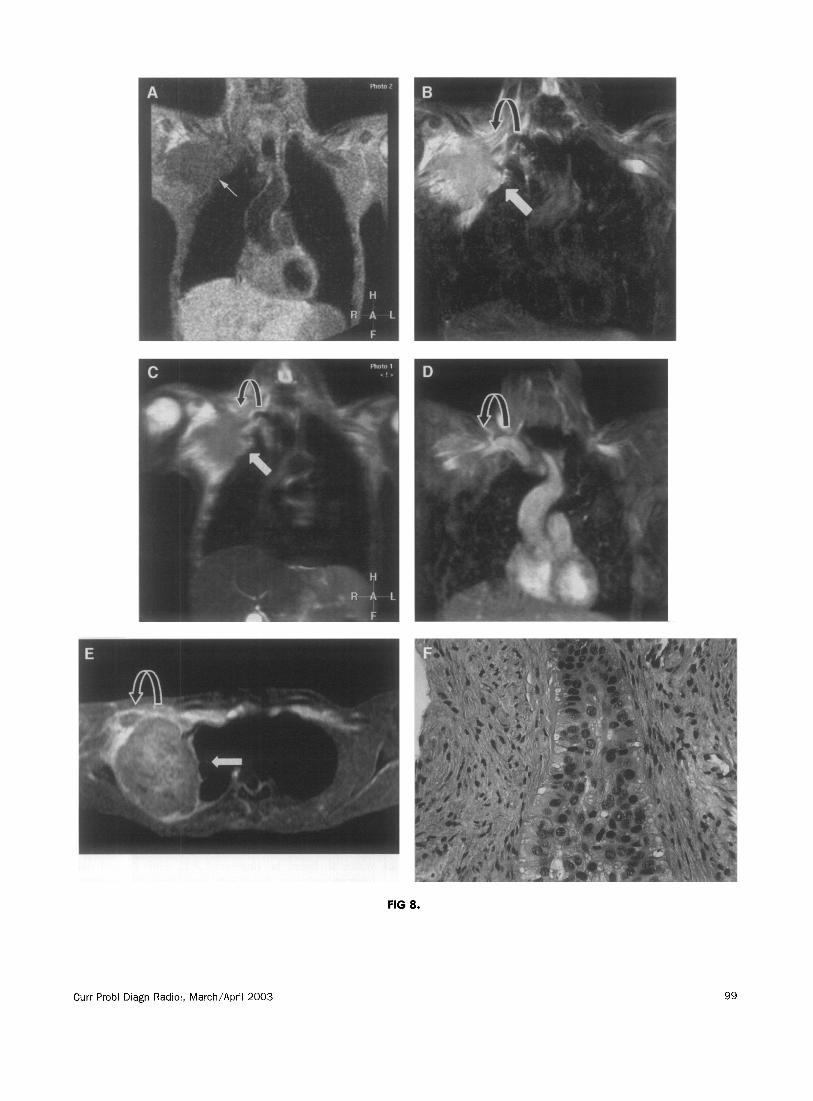
FIG 8.
Curr Probl Diagn Radiol, March/April 2003 99

cell) carcinoma, adenocarcinoma, and large cell (large cell anaplastic) carcinoma.26 The brachial plexus can be involved as a result of metastases of a bronchial carcinoma to the plexus area.27 Lung cancer patients with involvement of the brachial plexus present with pain in the shoulder radiating to axillary region, arm, and scapula. In addition, paresthesia of the axilla and medial aspect of the arm may be present (Table 1). Cough may aggravate pain. A supraclaviculary mass without pain or paraesthesia may also be a mode of presentation.
At MR imaging, metastatic lung cancer is visible as low SI on T,-weighted images, high SI on T,- weighted images, and show enhancement on gadolin- ium-enhanced images. Multiplanar capability of MR imaging is able to show the extent of the entire lesion and involvement of anatomic structures of brachial plexus as well as mediastinum (Fig 8). Chemotherapy can be used as treatment for brachial plexopathy due to metastases of lung cancer.
2. Iyer RB, Fenstermacher MJ, Libshitz HI. MR imaging of the treated brachial plexus. AJR Am J Roentgen01 1996;167: 22.5-9.
3. Posniak HV, Olson MC, Dudiak CM, Wisniewski R, O’Malley C. MR imaging of the brachial plexus. AJR Am J Roentgen01 1993;161:373-9.
4. Berry MM, Bannister LH, Standring SM. Nervous system. In: Williams PL, Bannister LH, Berry MM, et al, editors. Gray’s anatomy,. 38th ed. Edinburgh, PA: Churchill Livingstone; 1995901-1397.
5. Van Es HW. MRI of the brachial plexus. Eur Radio1 2001; 11:325-36.
6. MacCollin M, Woodfin W, Kronn D, Short MP. Schwannomatosis: a clinical and pathologic study. Neurology 1996;46: 1072-9.
7. Purcell SM, Dixon SL. Schwannomatosis. An unusual variant of neurofibromatosis or a distinct clinical entity? Arch Der- matol 1989;125:390-3.
8. Gibson R, Bell MJ. Malignant schwannoma of the brachial plexus: a lesson in presentation. J Hand Surg 1991;16:113.
9. Inoue M, Kawana T, Matsumura H, Mori K, Yoshida T. Solitary benign schwannoma of the brachial plexus. Surg Neurol 1983;20:103-8.
10. Zbkeb P, Becker M. Schwannoma of the brachial plexus. Ann Otol Rhino1 Laryngol 1996;105:748-50.
11. Bums DK. The nervous system. In: Kumar V, Cotran RS,
Discussion and Conclusions Robbins SL, editors. Basic pathology,. 6th ed. Philadelphia: Saunders; 1997:713-44.
This article discusses and illustrates a number points. First, the anatomy of the brachial plexus is complex and is interrelated with other anatomic structures, such as lung parenchyma including large airways, large mediastinal and neck vessels, bones of the shoulder girdle, and muscles and fat sur- rounding the plexus area. Second, MR imaging is capable to visualize the anatomy of brachial plexus and the interrelated anatomic structures on rela- tively artifact-free images with a large field-of- view, and without the need for cardiac gating or triggering. Third, our article shows that a spectrum of primary and secondary focal lesions may involve the brachial plexus and cause brachial plexopathy. In addition, the clinical signs and symptoms of brachial plexopathy often overlap. Hence, MR im- aging can facilitate in better detection and charac- terization of the lesions. Finally, our article illus- trates a comprehensive but a simple approach for the assessment of the brachial plexus and its abnor- malities.
REFERENCES
12. Lusk MD, Kline DG, Garcia CA. Tumors of the brachial plexus. Neurosurgery 1987;21:439-53.
13. Young G, Toretsky JA, Campbell AB, Eskenazi AE. Recog- nition of common childhood malignancies, Am Fam Physician 2000;61:2144-54.
14. Angstman KB, Miser JS, Franz WB III. Neuroblastoma. Am Fam Physician 1990;41:238-44.
15. Pizzo PA, Horowitz ME, Poplack DG, Kun LE. Solid tumors of childhood. In: DeVita VT, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology,. 3rd ed. Philadelphia: Lippincott; 1989:1612-70.
16. Joshi VV, Cantor AB, Altshuler G, et al. Conventional versus modified morphologic criteria for ganglioneuroblastoma: a review of cases from the pediatric oncology group. Arch Path01 Lab Med 1996;120:859-65.
17. Chang AE, Rosenberg SA, Glatstein EJ, Antman KH. Sarco- mas of soft tissues. In: DeVita VT, Hellamn S, Rosenberg SA, editors. Cancer: principles and practice of oncology,. 3rd ed. Philadelphia: Lippincott; 1989: 1345-98.
18. Kumar V, Cotran RS, Robbins SL. Blood vessels. In: Kumar V, Cotran RS, Robbins SL, editors. Basic pathology,. 6th ed. Philadelphia: Saunders; 1997:281-307.
19. Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000. The global picture. Eur J Cancer 2001;37(Suppl 8):S4-S66.
20. Walker R. Breast. In: Underwood JCE, editor. General and systematic pathology,. 2nd ed. New York: Churchill Livingstone; 1996523-50.
1. Hayes CE, Tsuruda JS, Mathis CM, Maravilla KR, Kliot M, 21. Davis PL, McCarty KS Jr. Sensitivity of enhanced MRI for Filler AG. Brachial plexus: MR imaging with a dedicated the detection of breast cancer: new, multicentric, residual, phased array of surface coils. Radiology 1997;203:286-9. and recurrent. Eur Radio1 1997;7(Suppl 5):289-98.
100 Cur Probl Diagn Radiol, March/April 2003
22. Muscolino G, Valente M, Andreani S. Pancoast tumors: clinical assessment and long term results of combined radio- surgical treatment. Thorax 1997;52:284-6.
23. Arcasoy SM, Jett JR. Superior pulmonary sulcus tumors and Pancoast’s syndrome. N Engl J Med 1997;337:1370-6.
24. Okubo K, Wada H, Fukuse T, et al. Treatment of Pancoast tumor. Combined irradiation and radical resection. Thorac Cardiovasc Surgeon 199.5;43:284-6.
25. Van Gee1 AN, Jansen PP, Slingerland R, Seynaeve C. Multi- disciplinary treatment of patients with a Pancoast tumour. Ned Tijdschr Geneesk 1997;141:809-13.
26. Travis WD, Travis LB, Devesa SS. Lung cancer. Cancer 1995;75(Suppl):191-202.
27. Wittenberg KH, Adkins MC. MR imaging of nontraumatic brachial plexopathies: frequency and spectrum of findings. Radiographics 2000;20:1023-32.
Curr Probl Diagn Radiol, March/April 2003 101