modification of atrioventricular node transmission properties by intraoperative neodymium-yag laser...
TRANSCRIPT

lACC Vol. 17, No.3 March I. 1991 :797-804
797
Modification of Atrioventricular Node Transmission Properties by Intraoperative Neodymium-Y AG Laser Photocoagulation in Dogs LASZLO LITTMANN, MD, FACC, ROBERT H. SVENSON, MD, FACC, ISTVAN TOMCSANYI, MD, CHRISTOPH HEHRLEIN, MD, JOHN J. GALLAGHER, MD, FACC,
SAROJA BHARATI, MD, FACC,* MAURICE LEV, MD, FACC,* ROBERT SPLINTER, MS, GEORGE P. TATSIS, MS, JAN R. TUNTELDER, BS
Charlotte, North Carolina and Palos Heights, Illinois
The purpose of this study was to test the feasibility of neodymiumyttrium-aluminum-garnet (Nd-YAG) laser photocoagulation of the atrioventricular (A V) node to control the ventricular rate during rapid atrial rhythms without creating A V block. In 12 dogs on normothermic cardiopulmonary bypass, short laser pulses were delivered to an area between the coronary sinus orifice and the site of the most proximally recorded His deflection until second degree A V block occurred at a paced atrial rate of 200 beats/min.
Long-term effects on A V node function were followed up for 3 months. Three animals developed chronic high grade A V block. In nine animals with preserved 1:1 conduction, the mean (±SEM) critical atrial cycle length resulting in AV node Wenckebach periodicity increased from 183 ± 6 to 261 ± 24 ms (+43%), the mean RR interval during induced atrial fibrillation increased from 248 ± 14 to 330 ± 27 ms (+32%) and the shortest RR interval
Atrial tachyarrhythmias may be refractory to pharmacologic therapy because of drug inefficacy, noncompliance or limiting side effects (1-4). A large body of experimental (5-7) and clinical (2,5,8-13) data suggest that chronic uncontrolled tachycardias lead to hemodynamic impairment, congestive heart failure and occasionally frank cardiomyopathy (14). Over the last 15 years, several surgical techniques have been devised to exclude the anatomic substrate of focal atrial tachycardias (15-19). The more common form of refractory supraventricular tachyarrhythmias associated with chronic atrial fibrillationlflutter can be treated by surgical dissection
From the Laser and Applied Technologies Laboratory. Heineman Medical Research Center and Carolinas Heart Institute. Charlotte. North Carolina and the 'Congenital Heart and Conduction System Center, Heart Institute for Children of Christ Hospital, Palos Heights. Illinois. This study was presented in part at the 62nd Annual Scientific Sessions of the American Heart Association, New Orleans, Louisiana. November 1989. This study was supported by a grant from the Heineman Medical Research Center of Charlotte, NC. Inc., Charlotte, North Carolina. Dr. Littmann is a visiting scientist at the Carolinas Heart Institute; parent institution: 3rd Department of Medicine, Semmelweis University Medical School. Budapest, Hungary.
Manuscript received May 23. 1990; revised manuscript received August 8. 1990, accepted September 5, 1990.
Address for reprints: Laszlo Littmann, MD. Laser and Applied Technologies Laboratory, Carolinas Heart Institute. P.O. Box 32861, Charlotte. North Carolina 28232.
©1991 by the American College of Cardiology
during atrial fibrillation increased from 215 ± 11 to 275 ± 20 ms (+28%). Laser effects were not reversed by isoproterenol infusion. Histologic examination of the irradiated area showed fibrotic changes in the A V node and fatty metamorphosis.
This study suggests that 1) graded Nd-YAG laser photocoagulation of the A V node region in dogs results in long-term modification of anterograde A V node transmission properties; 2) 1:1 conduction during sinus rhythm usually remains preserved, but ventricular rate during rapid atrial rhythms is chronically reduced; and 3) progression to high grade A V block occurs in a minority of animals. Laser modification of the A V node could become a form of nonpharmacologic heart rate control in patients with disabling atrial tachyarrhythmias.
() Am Coil CardioI1991;17:797-804)
or cryoablation of the atrioventricular (AV) node-His bundle and subsequent pacemaker implantation (20,21). More recently, a closed chest technique for electrical catheter ablation of the His bundle has been introduced (22,23). This procedure is also usually followed by complete A V block and thus necessitates implantation of a permanent pacemaker.
Experimental and clinical studies using surgical dissection (24,25), electrical shock ablation (26,27), cryosurgery (28-31), radiofrequency current (32-34) and transcatheter delivery of argon laser (35) have been performed by several investigators with the hope of finding a method that would modify the functional properties of the A V node without totally interrupting A V conduction. Encouraging experimental and clinical results have been reported (28,29) primarily with intraoperative cryoablation of peri-A V node tissue for control of A V node reentrant tachycardia. This technique, however, does not induce a long-term increase in AV node filtering properties and is therefore inadequate for limiting the ventricular rate during atrial tachycardias (28,29). On the basis of our favorable experience with intraoperative laser treatment of ventricular tachycardia (36,37) and experimental laser modification of sinus node function (38), neodymium-yttrium-aluminum-garnet (Nd-YAG) laser photocoag-
0735-1097/91/$3.50
798 LITTMANN ET AL. AV NODE MODIFICATION BY LASER
ulation of the A V node seemed to be a promising technique for delivering controlled damage to the A V node without insulting its structural integrity. The purpose of this experimental study was to test the feasibility of intraoperative Nd-Y AG laser photocoagulation of the A V node to chronically dampen the ventricular response rate to rapid atrial rhythms without creating A V block.
Methods Study animals. Sixteen healthy mongrel dogs of both
genders weighing 21 to 41 kg were included in the study. All animals underwent the same series of preoperative and postoperative testing. Group I included 12 dogs with intraoperative Nd-YAG laser photo ablation of the AV node. whereas 4 dogs (group 2) underwent a sham procedure. Dogs were followed up for 3 months after surgery. All interventions performed in this study conformed with the appropriate institutional guidelines and the Position of the American Heart Association on Research Animal Use adopted November 11, 1984.
Surgical procedure. The dogs were anesthetized with intravenous sodium pentobarbital (30 mg/kg body weight) and ventilated by a volume-controlled respirator (Servo Ventilator, Siemens-Elema). A right thoracotomy was performed in the fourth or fifth intercostal space. The heart was suspended in a pericardial cradle. Quadripolar plaque electrodes for pacing and recording were sewn on the right atrial appendage and anterior surface of the right ventricle. After heparinization, the dogs were placed on normothermic car-
JACC Vol. 17, No.3 March 1, 1991:797-804
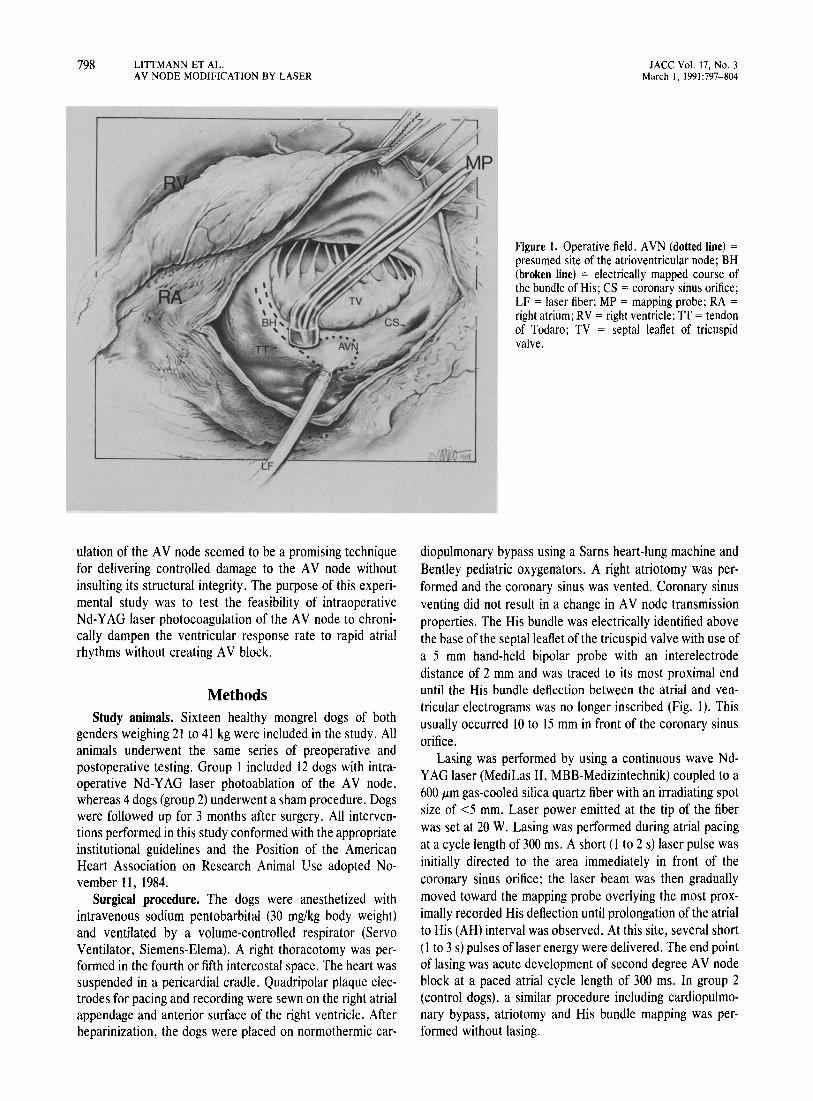
Figure 1. Operative field. A VN (dotted line) = presumed site of the atrioventricular node; BH (broken line) = electrically mapped course of the bundle of His; CS = coronary sinus orifice; LF = laser fiber; MP = mapping probe; RA = right atrium; RV = right ventricle; IT = tendon of Todaro; TV = septal leaflet of tricuspid valve.
diopulmonary bypass using a Sarns heart-lung machine and Bentley pediatric oxygenators. A right atriotomy was performed and the coronary sinus was vented. Coronary sinus venting did not result in a change in A V node transmission properties. The His bundle was electrically identified above the base of the septal leaflet of the tricuspid valve with use of a 5 mm hand-held bipolar probe with an interelectrode distance of 2 mm and was traced to its most proximal end until the His bundle deflection between the atrial and ventricular electrograms was no longer inscribed (Fig. 1). This usually occurred 10 to 15 mm in front of the coronary sinus orifice.
Lasing was performed by using a continuous wave NdY AG laser (MediLas II. MBB-Medizintechnik) coupled to a 600 J.Lm gas-cooled silica quartz fiber with an irradiating spot size of <5 mm. Laser power emitted at the tip of the fiber was set at 20 W. Lasing was performed during atrial pacing at a cycle length of 300 ms. A short (I to 2 s) laser pulse was initially directed to the area immediately in front of the coronary sinus orifice; the laser beam was then gradually moved toward the mapping probe overlying the most proximally recorded His deflection until prolongation of the atrial to His (AH) interval was observed. At this site, several short (l to 3 s) pulses of laser energy were delivered. The end point of lasing was acute development of second degree A V node block at a paced atrial cycle length of 300 ms. In group 2 (control dogs), a similar procedure including cardiopulmonary bypass, atriotomy and His bundle mapping was performed without lasing.
JACC Vol. 17, No.3 March I, 1991 :797-804
Electropharmacologic testing. Electrophysiologic and pharmacologic testing of anterograde A V node transmission properties was performed under sodium pentobarbital anesthesia before surgery and at I week, I month and 3 months after the laser procedure. Two 6F quadripolar electrode catheters with 6 mm interelectrode distances were introduced with the Seldinger technique through femoral veins and were advanced under fluoroscopic control to the high right atrium and His bundle area for pacing and recording local bipolar electrograms. Surface electrocardiographic (ECG) leads II and III and bipolar right atrial and His bundle electrograms were simultaneously displayed on a multichannel oscilloscope and recorded by an ink-jet recorder (Siemens Mingograf, Siemens-Elema AB) at paper speeds of 100 and 250 mmls. Band pass filters of 0.15 to 30 Hz and 50 to 1,000 Hz were used for the surface ECG and intracardiac bipolar electrograms, respectively. The AV node conduction intervals (AH intervals) were measured from the first sharp component of the low right atrial electrogram to the first sharp component of the His bundle electrogram in the His bundle lead.
Right atrial pacing was performed by cycle lengths decrementing in 10 ms steps until second degree A V node block developed; this cycle length was called the "Wenckebach cycle length." The A V node refractory period measurements were performed by programmed right atrial stimulation at paced cycle lengths of 350 and 300 ms. Atrial fibrillation was induced by atrial burst pacing. The mean RR interval during induced atrial fibrillation was determined from 10 consecutive ventricular cycles or, in cases of shorter runs of nonsustained atrial fibrillation, from the longest run of the arrhythmia. The shortest ventricular cycle was also measured. Conduction interval measurements, Wenckebach cycle length determinations and analyses of mean and shortest RR intervals during induced atrial fibrillation were repeated during intravenous infusion of isoproterenol (4 JLgl min) and propranolol (0.5 mglkg 15 min later). Conduction interval and refractory period measurements were performed at 250 mmls paper speed and were accurate to 2 ms. Measurements of mean and shortest ventricular cycles during induced atrial fibrillation were performed at 100 mmls and were accurate to 5 ms.
Histology. The heart was removed and morphologic studies were performed at 3 months after the laser procedure. Eight hearts from group I dogs were examined. A block containing the approaches to the AV node, the AV node, the penetrating part of the His bundle, the branching part of the His bundle and the beginning of the bundle branches up to the level of the moderator band was taken and serially sectioned. Every 20th section was retained and stained alternately with hematoxylin-eosin and Weigert-van Gieson stains. In this manner, a mean of 517 sections were examined from each heart.
Statistical methods. Data were expressed as mean values ± SEM. Student's paired t test was used to compare preoperative and postoperative measurements of A V node
LITTMANN ET AL. AV NODE MODIFICATION BY LASER
BASELINE
A
1It"""'---'i.-"'~ 5t 5t
LPC at 10 sec
B CL=300
III ~v~ __ J\,,-~)~~ RA RA
I I I ' RAA r-!r---I~I~-,~-~r----~-AH = 120 170 230 280 330 - 75 140
799
BH ~''----'''''';--'i'----v-'--J--~--Ij AHV AHV A HVA HVA HAV AHV AHV A HV
...m...
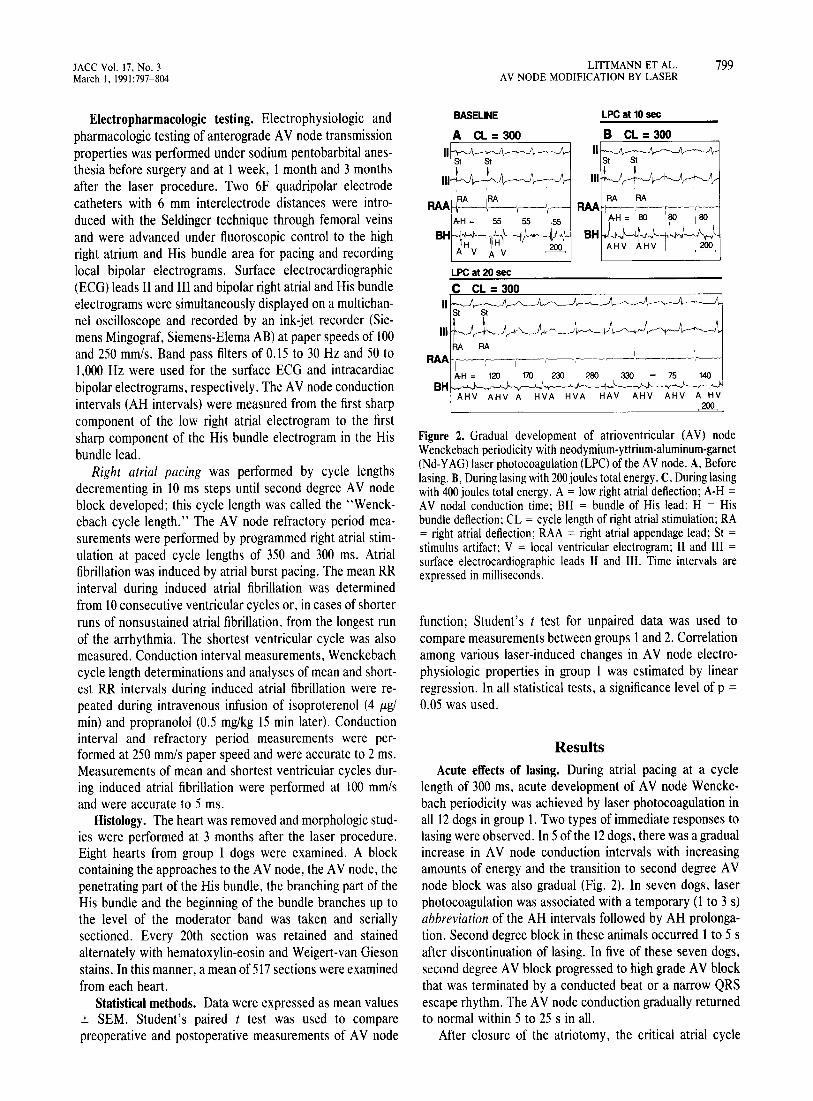
Figure 2. Gradual development of atrioventricular (A V) node Wenckebach periodicity with neodymium-yttrium-aluminum-garnet (Nd-Y AG) laser photocoagulation (LPC) of the A V node. A, Before lasing. B, During lasing with 200 joules total energy. C, During lasing with 400 joules total energy. A = low right atrial deflection; A-H = AV nodal conduction time; BH = bundle of His lead; H = His bundle deflection; CL = cycle length of right atrial stimulation; RA = right atrial deflection; RAA = right atrial appendage lead; St = stimulus artifact; V = local ventricular electrogram; II and III = surface electrocardiographic leads II and III. Time intervals are expressed in milliseconds.
function; Student's t test for unpaired data was used to compare measurements between groups 1 and 2. Correlation among various laser-induced changes in A V node electrophysiologic properties in group 1 was estimated by linear regression. In all statistical tests, a significance level of p =
0.05 was used.
Results Acute effects of lasing. During atrial pacing at a cycle
length of 300 ms, acute development of AV node Wenckebach periodicity was achieved by laser photocoagulation in all 12 dogs in group 1. Two types of immediate responses to lasing were observed. In 5 of the 12 dogs, there was a gradual increase in A V node conduction intervals with increasing amounts of energy and the transition to second degree A V node block was also gradual (Fig. 2). In seven dogs, laser photocoagulation was associated with a temporary (1 to 3 s) abbreviation of the AH intervals followed by AH prolongation. Second degree block in these animals occurred 1 to 5 s after discontinuation of lasing. In five of these seven dogs, second degree A V block progressed to high grade A V block that was terminated by a conducted beat or a narrow QRS escape rhythm. The A V node conduction gradually returned to normal within 5 to 25 s in all.
After closure of the atriotomy, the critical atrial cycle
800 LITTMANN ET AL. AV NODE MODIFICATION BY LASER
length resulting in AV node Wenckebach periodicity was again determined. This "immediate" postlasing Wenckebach cycle length measured 305 ± 17 ms (range 200 to 460), 71% longer than the preoperative Wenckebach cycle length that measured 178 ± 6 ms (p < 0.001). Lasing time (9 to 360 s) and the amount of total laser energy delivered varied to a great extent in individual experiments. This was due to the fact that observation of the acute effects of photocoagulation on AH intervals was one factor used to localize the A V node. This way, the total amount of laser energy delivered did not reflect the energy applied to the A V node region itself.
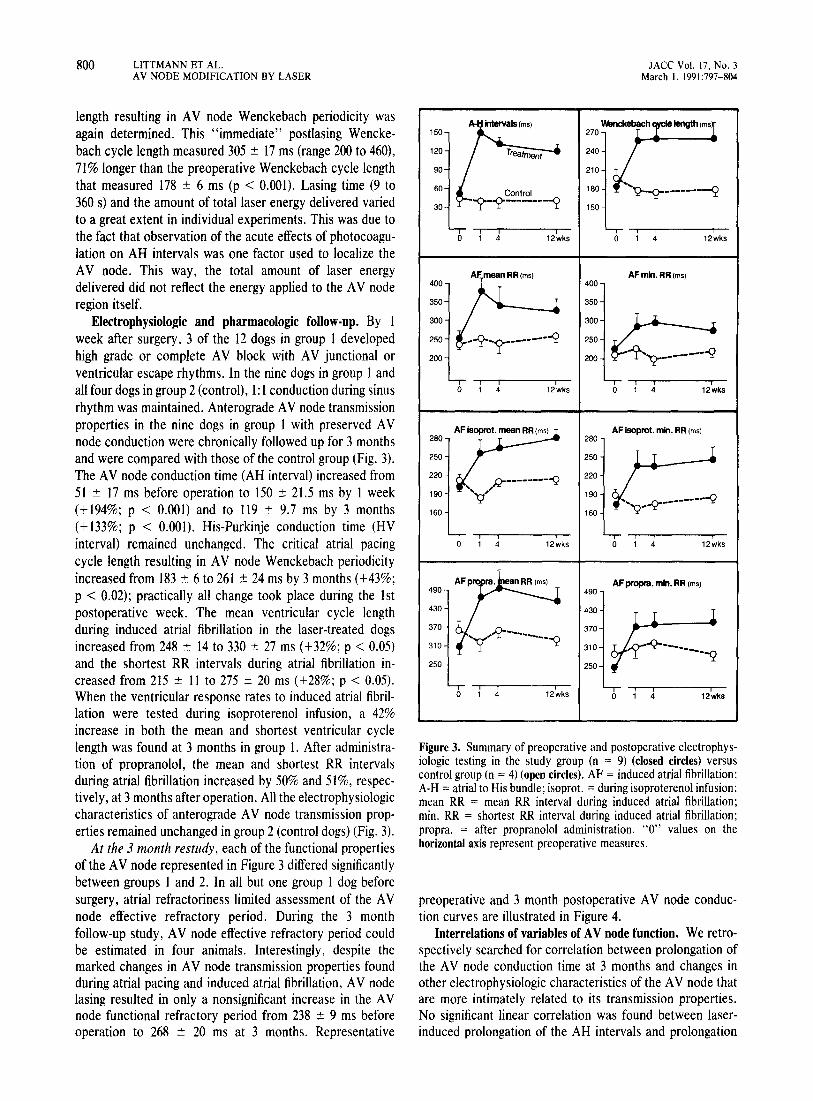
Electrophysiologic and pharmacologic follow-up. By 1 week after surgery, 3 of the 12 dogs in group 1 developed high grade or complete A V block with A V junctional or ventricular escape rhythms. In the nine dogs in group 1 and all four dogs in group 2 (control), 1: 1 conduction during sinus rhythm was maintained. Anterograde A V node transmission properties in the nine dogs in group 1 with preserved A V node conduction were chronically followed up for 3 months and were compared with those of the control group (Fig. 3). The A V node conduction time (AH interval) increased from 51 ± 17 ms before operation to 150 ± 21.5 ms by 1 week (+ 194%; p < 0.001) and to 119 ± 9.7 ms by 3 months (+ 133%; p < 0.001). His-Purkinje conduction time (HV interval) remained unchanged. The critical atrial pacing cycle length resulting in A V node Wenckebach periodicity increased from 183 ± 6 to 261 ± 24 ms by 3 months (+43%; p < 0.02); practically all change took place during the 1st postoperative week. The mean ventricular cycle length during induced atrial fibrillation in the laser-treated dogs increased from 248 ± 14 to 330 ± 27 ms (+ 32%; p < 0.05) and the shortest RR intervals during atrial fibrillation increased from 215 ± 11 to 275 ± 20 ms (+28%; p < 0.05). When the ventricular response rates to induced atrial fibrillation were tested during isoproterenol infusion, a 42% increase in both the mean and shortest ventricular cycle length was found at 3 months in group 1. After administration of propranolol, the mean and shortest RR intervals during atrial fibrillation increased by 50% and 51 %, respectively, at 3 months after operation. All the electrophysiologic characteristics of anterograde A V node transmission properties remained unchanged in group 2 (control dogs) (Fig. 3).
At the 3 month restudy, each of the functional properties of the A V node represented in Figure 3 differed significantly between groups 1 and 2. In all but one group 1 dog before surgery, atrial refractoriness limited assessment of the A V node effective refractory period. During the 3 month follow-up study, A V node effective refractory period could be estimated in four animals. Interestingly, despite the marked changes in A V node transmission properties found during atrial pacing and induced atrial fibrillation, A V node lasing resulted in only a nonsignificant increase in the A V node functional refractory period from 238 ± 9 ms before operation to 268 ± 20 ms at 3 months. Representative
JACe Vol. 17, No.3 March 1, 1991:797-804
Figure 3. Summary of preoperative and postoperative electrophysiologic testing in the study group (n = 9) (closed circles) versus control group (n = 4) (open circles). AF = induced atrial fibrillation; A-H = atrial to His bundle; isoprot. = during isoproterenol infusion; mean RR = mean RR interval during induced atrial fibrillation; min. RR = shortest RR interval during induced atrial fibrillation; propra. = after propranolol administration. "0" values on the horizontal axis represent preoperative measures.
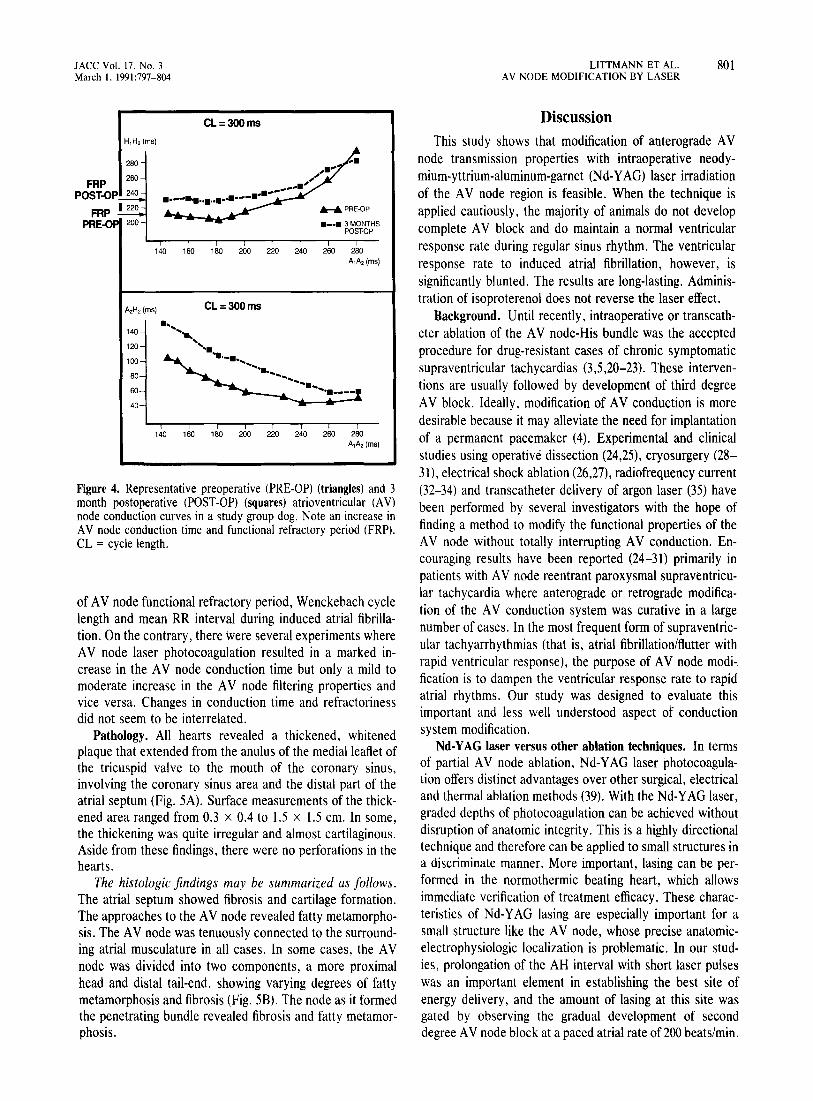
preoperative and 3 month postoperative A V node conduction curves are illustrated in Figure 4.
Interrelations of variables of AV node function. We retrospectively searched for correlation between prolongation of the A V node conduction time at 3 months and changes in other electrophysiologic characteristics of the A V node that are more intimately related to its transmission properties. No significant linear correlation was found between laserinduced prolongation of the AH intervals and prolongation
lACC Vol. 17, No.3 March 1, 1991:797-804
H,H,(ms)
280
FRP 260
CL=300ms
POST-OP 240
FRP 1220 .-~~ ....... -.-.. -~-.'
PRE-O 200
... --......
;; ~ ... ;
........ PRE-OP
• __ • 3 MONTHS POST-OP
140 160 180 200 220 240 260 280
A,H, (ms)
140
120
100
80
60
40
A,A,(ms)
CL=300ms
140 160 180 200 220 240 260 280 A,A,(ms)
Figure 4. Representative preoperative (PRE-OP) (triangles) and 3 month postoperative (POST-OP) (squares) atrioventricular (A V) node conduction curves in a study group dog. Note an increase in A V node conduction time and functional refractory period (FRP). CL = cycle length.
of A V node functional refractory period, Wenckebach cycle length and mean RR interval during induced atrial fibrillation. On the contrary, there were several experiments where A V node laser photocoagulation resulted in a marked increase in the A V node conduction time but only a mild to moderate increase in the A V node filtering properties and vice versa. Changes in conduction time and refractoriness did not seem to be interrelated.
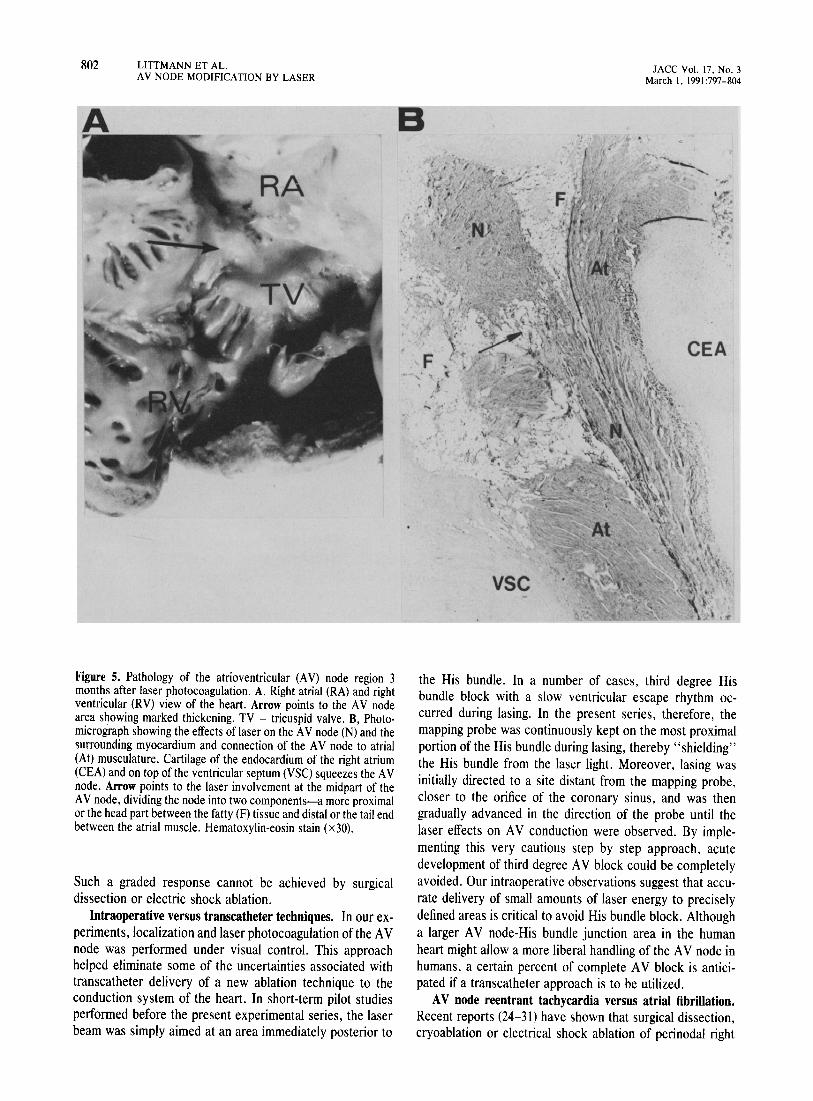
Pathology. All hearts revealed a thickened, whitened plaque that extended from the anulus of the medialleaftet of the tricuspid valve to the mouth of the coronary sinus, involving the coronary sinus area and the distal part of the atrial septum (Fig. 5A). Surface measurements of the thickened area ranged from OJ x 0.4 to 1.5 x 1.5 cm. In some, the thickening was quite irregular and almost cartilaginous. Aside from these findings, there were no perforations in the hearts.
The histologic findings may be summarized as follows. The atrial septum showed fibrosis and cartilage formation. The approaches to the A V node revealed fatty metamorphosis. The A V node was tenuously connected to the surrounding atrial musculature in all cases. In some cases, the AV node was divided into two components, a more proximal head and distal tail-end, showing varying degrees of fatty metamorphosis and fibrosis (Fig. 5B). The node as it formed the penetrating bundle revealed fibrosis and fatty metamorphosis.
LITTMANN ET AL. 801 AV NODE MODIFICATION BY LASER
Discussion This study shows that modification of anterograde A V
node transmission properties with intraoperative neodymium-yttrium-aluminum-garnet (Nd-YAG) laser irradiation of the A V node region is feasible. When the technique is applied cautiously, the majority of animals do not develop complete A V block and do maintain a normal ventricular response rate during regular sinus rhythm. The ventricular response rate to induced atrial fibrillation, however, is significantly blunted. The results are long-lasting. Administration of isoproterenol does not reverse the laser effect.
Background. Until recently, intraoperative or transcatheter ablation of the AV node-His bundle was the accepted procedure for drug-resistant cases of chronic symptomatic supraventricular tachycardias (3,5,20-23). These interventions are usually followed by development of third degree AV block. Ideally, modification of AV conduction is more desirable because it may alleviate the need for implantation of a permanent pacemaker (4). Experimental and clinical studies using operative dissection (24,25), cryosurgery (28-31), electrical shock ablation (26,27), radiofrequency current (32-34) and transcatheter delivery of argon laser (35) have been performed by several investigators with the hope of finding a method to modify the functional properties of the A V node without totally interrupting A V conduction. Encouraging results have been reported (24-31) primarily in patients with A V node reentrant paroxysmal supraventricular tachycardia where anterograde or retrograde modification of the A V conduction system was curative in a large number of cases. In the most frequent form of supraventricular tachyarrhythmias (that is, atrial fibrillation/flutter with rapid ventricular response), the purpose of AV node modification is to dampen the ventricular response rate to rapid atrial rhythms. Our study was designed to evaluate this important and less well understood aspect of conduction system modification.
Nd-YAG laser versus other ablation techniques. In terms of partial AV node ablation, Nd-YAG laser photocoagulation offers distinct advantages over other surgical, electrical and thermal ablation methods (39). With the Nd-YAG laser, graded depths of photocoagulation can be achieved without disruption of anatomic integrity. This is a highly directional technique and therefore can be applied to small structures in a discriminate manner. More important, lasing can be performed in the normothermic beating heart, which allows immediate verification of treatment efficacy. These characteristics of Nd-Y AG lasing are especially important for a small structure like the A V node, whose precise anatomicelectrophysiologic localization is problematic. In our studies, prolongation of the AH interval with short laser pulses was an important element in establishing the best site of energy delivery, and the amount of lasing at this site was gated by observing the gradual development of second degree A V node block at a paced atrial rate of 200 beats/min.
802 LITIMANN ET AL. A V NODE MODIFICATION BY LASER
A
Figure 5. Pathology of the atrioventricular (A V) node region 3 months after laser photocoagulation. A, Right atrial (RA) and right ventricular (RV) view of the heart. Arrow points to the AV node area showing marked thickening. TV = tricuspid valve. B, Photomicrograph showing the effects of laser on the A V node (N) and the surrounding myocardium and connection of the A V node to atrial (At) musculature. Cartilage of the endocardium of the right atrium (CEA) and on top of the ventricular septum (VSC) squeezes the A V node. Arrow points to the laser involvement at the midpart of the A V node, dividing the node into two components-a more proximal or the head part between the fatty (F) tissue and distal or the tail end between the atrial muscle. Hematoxylin-eosin stain (x30).
Such a graded response cannot be achieved by surgical dissection or electric shock ablation.
Intraoperative versus transcatheter techniques. In our experiments, localization and laser photocoagulation of the AV node was performed under visual control. This approach helped eliminate some of the uncertainties associated with transcatheter delivery of a new ablation technique to the conduction system of the heart. In short-term pilot studies performed before the present experimental series, the laser beam was simply aimed at an area immediately posterior to
B
.....
VSC
JACC Vol. 17. NO. 3 March \, 1991 :797-804
CEA
the His bundle. In a number of cases, third degree His bundle block with a slow ventricular escape rhythm occurred during lasing. In the present series, therefore, the mapping probe was continuously kept on the most proximal portion of the His bundle during lasing, thereby "shielding" the His bundle from the laser light. Moreover, lasing was initially directed to a site distant from the mapping probe, closer to the orifice of the coronary sinus, and was then gradually advanced in the direction of the probe until the laser effects on A V conduction were observed. By implementing this very cautious step by step approach, acute development of third degree A V block could be completely avoided. Our intraoperative observations suggest that accurate delivery of small amounts of laser energy to precisely defined areas is critical to avoid His bundle block. Although a larger A V node-His bundle junction area in the human heart might allow a more liberal handling of the A V node in humans, a certain percent of complete A V block is anticipated if a transcatheter approach is to be utilized.
A V node reentrant tachycardia versus atrial fibrillation. Recent reports (24-31) have shown that surgical dissection, cryoablation or electrical shock ablation of peri nodal right

JACC Vol. 17. No.3 March I. 1991:797-804
atrial tissue will allow the control of tachycardia without disruption of A V conduction in patients with A V node reentrant tachycardia. The exact mechanism of tachycardia control in these cases is not well understood. Our study with intraoperative use of Nd-YAG laser photocoagulation was aimed at a different potential group of patients (namely, patients with chronic atrial fibrillation/flutter and uncontrolled ventricular response) (33). To this end, currently employed investigational A V node modification procedures have not been uniformly successful because some (40) resulted in a high incidence of chronic complete heart block, whereas others (41) caused a decrease rather than an increase in the A V node refractory period. Cryoablation of periatrioventricular node tissue successfully controlled A V node reentrant tachycardia but did not result in a reduced ventricular response rate to rapid atrial rhythms (28,29). In our experiments with laser photoablation, however, the filtering properties of the AV node were uniformly increased and only three of the experimental animals developed chronic high grade A V block.
Electrophysiologic-histologic correlations. In the eight lased hearts undergoing detailed histologic evaluation, varying degrees and occasionally severe pathologic changes were found, extending from the atrial septal approaches to the A V node down to the branching portion of the His bundle. Amazingly, 1: 1 conduction during sinus rhythm with normal His-Purkinje conduction was maintained in each of these cases, suggesting a considerable margin of safety within the entire A V conduction system. In those experiments showing a larger increase in the "filtering" properties of the AV node compared with AV node conduction time (long Wenckebach cycle lengths and long RR intervals during induced atrial fibrillation versus only a mild increase in the AH intervals), there was more pathologic involvement of the atrial septum and the approaches to the A V node and less involvement of the compact A V node. Conversely, whenever there was significant increase in the A V node conduction time, marked pathologic changes were found both at the approaches to the A V node and in the A V node itself. Accurate interpretation of these data requires more experiments with less extensive laser damage delivered to specific areas within the conduction system.
Conclusions. This study shows that 1) anatomically and electrophysiologically guided graded intraoperative NdY AG laser photocoagulation of the A V node results in a blunted response to rapid atrial rates; 2) in the majority of cases, 1: 1 conduction during normal sinus rhythm remains preserved; and 3) the effects are long-lasting. This intraoperative technique could replace surgical dissection or cryosurgical ablation of the His bundle in symptomatic patients with uncontrolled tachyarrhythmias undergoing surgery for atherosclerotic or rheumatic heart disease (20,21).
We acknowledge the expert assistance of Kathleen T. Seifert. Cathy Nichelson, Katherine D. Linder. Kathy Dezern. Mary Ellen Kurek, Debbi Nichols. Nancy Friesenhahn, Steve Carico and Keyna C. Winkler.
LITTMANN ET AL. 803 AV NODE MODIFICATION BY LASER
References I. Hurst JW, Paulk EA. Proctor HD, Schlant RC. Management of patients
with atrial fibrillation. Am J Med 1964;37:728-41. 2. Arbel ER, Cohen HC, Langendorf R. Glick G. Successful treatment of
drug-resistant atrial tachycardia and intractable congestive heart failure with permanent coupled atrial pacing. Am J CardioI1978;41:336-40.
3. Gallagher JJ, Selle JG. Svenson RH, et al. Surgical treatment of arrhythmias. Am J CardioI1988;61:27A-44A.
4. Scheinman M. Catheter and surgical treatment of cardiac arrhythmias. JAMA 1990;263:79-82.
5. McIntosh HD, Kong Y. Morris JJ. Hemodynamic effects of supraventricular arrhythmias. Am J Med 1964;37:712-27.
6. Coleman HN. Taylor RR. Pool PE, et aI. Congestive heart failure following chronic tachycardia. Am Heart J 1971 ;81 :790-8.
7. Damiano RJ, Tripp HF, Asano T, Small KW, Jones RH, Lowe JE. Left ventricular dysfunction and dilatation resulting from chronic supraventricular tachycardia. J Thorac Cardiovasc Surg 1978;94: 135-43.
8. Shachnow N, Spellman S. Rubin I. Persistent supraventricular tachycardia: case report with review of literature. Circulation 1954;10:232-6.
9. Brill IC, Rosenbaum EE. Flanery JR. Congestive failure due to auricular fibrillation in an otherwise normal heart: report of a case with twenty-five year follow-up. JAMA 1960;173:784-5.
10. Engel TR. Bush CA. Schaal SF. Tachycardia-aggravated heart disease. Ann Intern Med 1974;80:384-8.
11. Kugler 10. Baisch SD. Cheatham JP, et al. Improvement of left ventricular dysfunction after control of persistent tachycardia. J Pediatr 1984; 105:543-8.
12. Gillette PC. Smith RT. Garson A. et al. Chronic supraventricular tachycardia: a curable cause of congestive cardiomyopathy. JAMA 1985;253: 391-2.
13. Packer DL, Bardy GH. Worley SJ. et al. Tachycardia-induced cardiomyopathy: a reversible form of left ventricular dysfunction. Am J Cardiol 1986;57:563-70.
14. Gallagher JJ. Tachycardia and cardiomyopathy: the chicken-egg dilemma revisited. J Am Coli Cardiol 1985;6: 1172-3.
15. Wyndham CRC, Arnsdorf MF. Levitsky S, et al. Successful surgical excision of focal paroxysmal atrial tachycardia: observations in vivo and in vitro. Circulation 1980;62:1365-72.
16. Josephson ME. Spear JF. Harken AH, Horowitz LN. Dorio RJ. Surgical excision of automatic atrial tachycardia: anatomic and electrophysiologic correlates. Am Heart J 1982;104: 1076-85.
17. Anderson KP. Stinson EB. Mason JW. Surgical exclusion of focal paroxysmal atrial tachycardia. Am J Cardiol 1982;49:869-74.
18. Giorgi LV. Hartzler GO. Hamaker WR. Incessant focal atrial tachycardia: a surgically remediable cause of cardiomyopathy. J Thorac Cardiovasc Surg 1984;87:466-73.
19. Lawrie GM. Lin H-T. Wyndham CRC, DeBakey ME. Surgical treatment of supraventricular arrhythmias: results in 67 patients. Ann Surg 1987; 205:700-11.
20. Harrison L. Gallagher JJ. Kasell J. et al. Cryosurgical ablation of the A-V node-His bundle: a new method for producing A-V block. Circulation 1977;55:463-70.
21. Sealy WC, Gallagher JJ, Kasell J. His bundle interruption for control of inappropriate ventricular responses to atrial arrhythmias. Ann Thorac Surg 1981;32:429-38.
22. Gallagher JJ. Svenson RH, Kasell JH. et al. Catheter technique for closed-chest ablation of the atrioventricular conduction system: a therapeutic alternative for the treatment of refractory supraventricular tachycardia. N Engl J Med 1982;306:194-200.
23. Scheinman MM. Morady F. Hess DS. Gonzalez R. Catheter-induced ablation of the atrioventricular junction to control refractory supraventricular arrhythmias. JAMA 1982;248:851-5.
24. Johnson DC, Nunn GR, Richards DA. Uther JB, Ross DL. Surgical therapy for supraventricular tachycardia. a potentially curable disorder. J Thorac Cardiovasc Surg 1987;93:913-8.
25. Gartman DM. Bardy GH, Williams AB, Ivey TD. Direct surgical treatment of atrioventricular node reentrant tachycardia. J Thorac Cardiovasc Surg 1989;98:63-72.
804 LITTMANN ET AL. A V NODE MODIFICATION BY LASER
26. Haissaguerre M, Warin JF, Lemetayer P, Saoudi N, Guillem JP, Blanchot P. Closed-chest ablation of retrograde conduction in patients with atrioventricular nodal reentrant tachycardia. N Engl J Med 1989;320:426-33.
27. Epstein LM, Scheinman MM, Langberg JJ, Chilson D, Goldberg HR, Griffin JC. Percutaneous catheter modification of the atrioventricular node: a potential cure for atrioventricular nodal reentrant tachycardia. Circulation 1989:80:757-68.
28. Holman WL, Ikeshita M. Lease JG, Ferguson TB, Lofland GK, Cox JL. Alteration of antegrade atrioventricular conduction by cryoablation of peri-atrioventricular nodal tissue: implications for the surgical treatment of atrioventricular nodal reentry tachycardia. J Thorac Cardiovasc Surg 1984;88:67-75.
29. Cox JL, Holman WL. Cain ME. Cryosurgical treatment of atrioventricular node reentrant tachycardia. Circulation 1987;76:1329-36.
30. Holman WL. Hackel DB, Lease JG, Ikeshita M. Cox JL. Cryosurgical ablation of atrioventricular nodal reentry: histologic localization of the proximal common pathway. Circulation 1988;77: 1356-62.
31. Wood DL, Hammill Sc. Porter CJ, et al. Cryosurgical modification of atrioventricular conduction for treatment of atrioventricular node reentrant tachycardia. Mayo Clin Proc 1988;63:988-92.
32. Lopez-Merino V, Sanchis J, Chorro FJ, et al. Induction of partial alterations in atrioventricular conduction in dogs by percutaneous emission of high-frequency currents. Am Heart J 1988;115:1214-21.
33. Kunze K-P. Geiger M, Schluter M. Kuck K-H. Katheter-induzierte Modulation der elektrischen Leitfahigkeit des Atrioventrikularknotens mittels Hochfrequenzstroms. Dtsch Med Wschr 1988:113: 1343-8.
JACC Vol. 17, No.3 March 1. 1991 :797-804
34. Huang SKS. Bharati S, Graham AR, Gorman G, Lev M. Chronic incomplete atrioventricular block induced by radiofrequency catheter ablation. Circulation 1989;80:951-61.
35. Narula OS. Boveja BK. Cohen DM. Narula JT. Tadan PP. Laser catheter-induced atrioventricular nodal delays and atrioventricular block in dogs: acute and chronic observations. J Am Coli Cardiol 1985;5:259-67.
36. Svenson RH, Gallagher JJ. Selle JG, Zimmern SH, Fedor JM, Robicsek F. Neodymium:YAG laser photocoagulation: a successful new mapguided technique fOf the intraoperative ablation of ventricular tachycardia. Circulation 1987;76:1319-28.
37. Svenson RH. Littmann L. Gallagher JJ. et al. Termination of ventricular tachycardia with epicardial laser photocoagulation: a clinical comparison with patients undergoing successful endocardial photocoagulation alone. J Am Coli Cardiol 1990;15: 163-70.
38. Littmann L. Svenson RH. Gallagher JJ. et al. Modification of sinus node function by epicardial laser irradiation in dogs. Circulation 1990;81:350-9.
39. Svenson RH. Littmann L, Splinter R, et al. Application of lasers for arrhythmia ablation. In: Zipes DP. Jalife J, eds. Cardiac Electrophysiology. From Cell to Bedside. Philadelphia: W.B. Saunders, 1990:986-97.
40. Budde T, Borggrefe M. Martinez-Rubio A. et al. Acute and long-term results of radiofrequency ablation of the A V conduction system (abstr). Circulation 1989:~0(suppl Il):II-44.
41. Wilensky RL. M es WM, Klein LS. Mohamed Y, King RD, Zipes DP. Effects of surger} for AV nodal reentry on AV nodal physiology (abstr). Circulation 1989;80(suppl 11):11-221.