mo1429 intraductal aspiration: a promising new tissue sampling technique for diagnosis of suspected...
TRANSCRIPT
ORIGINAL ARTICLE: Clinical Endoscopy
Intraductal aspiration: a promising new tissue-sampling technique forthe diagnosis of suspected malignant biliary strictures
Gabriele Curcio, MD,1 Mario Traina, MD,1 Filippo Mocciaro, MD,1 Rosa Liotta, MD,2 Raffaella Gentile, MD,2
Ilaria Tarantino, MD,1 Luca Barresi, MD,1 Antonino Granata, MD,1 Fabio Tuzzolino, MS,3,5
Bruno Gridelli, MD4
Palermo, Italy
Background: Brushing is the most commonly used technique for biliary sampling at ERCP, despite its limitedsensitivity.
Objective: To evaluate intraductal aspiration (IDA) as a new combined endoscopic technique for cytodiagnosis,its cellular adequacy, diagnostic accuracy for cancer detection, feasibility, and safety.
Design: Prospective, observational study.
Setting: Single tertiary referral center.
Main Outcome Measurements: IDA cellular adequacy, diagnostic accuracy for cancer detection, feasibility,and safety.
Patients and Methods: From April 2009 to September 2010, 42 consecutive patients with suspected malignantbiliary stricture underwent ERCP, with tissue sampling obtained with IDA. IDA included performance of standardbrushing in all patients. After standard brushing, to perform IDA, we removed the brush from its catheter and usedthe tip of the catheter as a scraping device. The tip was scraped back and forth across the stricture at least 10 times.The catheter and a suction line were connected to a specimen trap to obtain intraductal aspiration of fluids andsamplings.
Results: Our cytopathologists found adequate cellular yield in 39 of the 42 IDA samples (92.8%) versus 15 of the 42brushing samples (35.7%) (P � .001). IDA showed a significantly higher sensitivity than brushing (89% vs 78% foradequate samples and 89% vs 37% for all samples) and provided significantly superior cellular adequacy (92.8% vs35.7%).
Limitations: Observational study, small number of patients.
Conclusions: IDA significantly improves brushing cellular adequacy and has high sensitivity for cancerdetection. It was also safe, simple, rapid, and applicable during routine diagnostic ERCP, with no additional costs.(Gastrointest Endosc 2012;75:798-804.)
cg
n
CtteU
RI
I
Biliary strictures are a common occurrence in clinicalpractice. Although many of these strictures are caused bymalignancies of the biliary tract, they may also have anonmalignant etiopathogenesis, such as inflammatory
Abbreviations: H&E, hematoxylin and eosin; IDA, intraductal aspira-tion; NPV, negative predictive value; PPV, positive predictive value; ROC,receiver-operating characteristic; ROSE, rapid on-site evaluation.
DISCLOSURE: The authors disclosed no financial relationships relevantto this publication.
Copyright © 2012 by the American Society for Gastrointestinal Endoscopy0016-5107/$36.00doi:10.1016/j.gie.2011.12.005
Received August 9, 2011. Accepted December 5, 2011. C
798 GASTROINTESTINAL ENDOSCOPY Volume 75, No. 4 : 2012
onditions, choledocholithiasis, chronic pancreatitis, sur-ical trauma, and ischemia.
Diagnostic tissue acquisition at ERCP may obviate theeed for further invasive testing, thus allowing for optimal
urrent affiliations: Departments of Endoscopy (1), Pathology (2), Informa-ion Technology (3), and Transplantation Surgery (4), Mediterranean Insti-ute for Transplantation and Advanced Specialized Therapies (IsMeTT), Pal-rmo, Italy, Department of Mathematics and Statistics (5), S. Vianelliniversity of Palermo, Palermo, Italy.
eprint requests: Gabriele Curcio, MD, Department of Gastroenterology,sMeTT, UPMC, Via Tricomi 1, Palermo 90100, Italy.
f you would like to chat with an author of this article, you may contact Dr
urcio at [email protected].www.giejournal.org

esmd
dwsp(ocs
T(
fdCWtppaou
camut1fi
I
spr0Mgudvttitmtscucbts(s
Curcio et al Intraductal aspiration
intervention without delay.1 Adequacy of specimens isssential for tissue diagnosis, although several studieshowed that specimens obtained from a biliary strictureay lack adequate cellularity, resulting in a false-negativeiagnosis regardless of the technique used.2
Because no other single method has been found to besuperior, brushing remains the most commonly used tech-nique for biliary sampling at ERCP, despite its limitedsensitivity.3-6 The challenge in improving diagnosis of in-eterminate strictures is devising new and more effectiveays to target lesions and retrieve higher-quality cytology
pecimens. We evaluated the feasibility of intraductal as-iration (IDA) as a new combined endoscopic techniquebrushing plus scraping and aspiration) for cytodiagnosisf suspected malignant biliary strictures. We evaluated theellular adequacy of samples, diagnostic accuracy, and theafety of this new technique.
MATERIALS AND METHODS
PatientsFrom April 2009 to September 2010, after approval from
our internal review board, 42 consecutive adult patientswith suspected malignant biliary stricture and no previoushistological confirmation underwent ERCP at our institu-tion. Tissue samples were obtained with IDA in all pa-tients. The IDA technique included performance of stan-dard brushing, as specified in the following.
Patient characteristics are summarized in Table 1.wenty-eight male patients (66.7%) and 14 female patients33.3%) with a mean � standard deviation age of 61.9 �
18.6 years were enrolled. The majority of patients (95.2%)were symptomatic (eg, jaundice, abdominal pain, fever,pruritus).
Informed consent for ERCP, including acquisition of
TABLE 1. Patient characteristics at baseline
Characteristic Patients (N � 42)
Age � SD, y 61.9 � 18.6
Male sex, no. (%) 28 (66.7)
Symptomatic at presentation, no. (%) 40 (95.2)
Type of biliary stricture, no. (%)
Upper third 16 (38.1)
Intrahepatic 12 (28.6)
Middle third 8 (19)
Lower third 6 (14.3)
Stricture dilation performed beforesampling, no. (%)
5 (11.1)
SD, Standard deviation.
cytology specimens with IDA, was obtained in writing d
www.giejournal.org V
rom all patients. In all patients, routine diagnostic proce-ures included laboratory tests, abdominal US, abdominalT scan, and cholangio-magnetic resonance imaging.ith the patient under general anesthesia or deep seda-
ion, ERCP with tissue sampling was performed, with theatient continuously monitored by electrocardiography,ulse oximetry, and automatic recording of blood pressurend pulse. All patients were closely followed for any earlyr delayed complications related to the procedure andntil the final diagnosis.Patients with no finding of malignancy were also
losely followed with clinical observation, laboratory tests,nd imaging. Only patients with persistent suspicion ofalignancy, despite negative cytology findings for cancer,nderwent further cytopathological sampling at ERCP. Pa-ients with no finding of malignancy during a minimum of2 months of follow-up were considered negative for anal diagnosis of malignancy.
ntervention and techniqueERCP was performed with a standard videoduodeno-
cope (TFJ 160-VR; Olympus, Hamburg, Germany). Toerform IDA, bile duct strictures were identified underadiographic guidance and by using contrast fluid. A.035-inch guidewire (Jagwire; Boston Scientific, Natick,ass) was then advanced through the stricture. Over theuidewire, we did standard brushing of the stricture bysing the RX Wire-Guided Cytology Brush, 2.8 mm iniameter (Boston Scientific) (Fig. 1A). The brush was ad-anced from the catheter to a point proximal to the stric-ure, withdrawn slightly, and moved back and forth acrosshe stricture at least 10 times. The brush was then pullednto the tip of the catheter, still located immediately belowhe stricture, and the brush/catheter unit was finally re-oved, leaving the guidewire in place. We then pushed
he brush so that it protruded from the catheter and cut formearing. After that, we withdrew the stylet from theatheter, which we then used to perform the aspiration, bysing the tip as a scraping device (Fig. 1B). This modifiedatheter was advanced over the guidewire and movedack and forth, scraping across the stricture at least 10imes. During the IDA procedure, both the catheter and apecimen trap were connected to the central suction line0.6 Bar) to obtain intraductal aspiration of fluids andamples (Fig. 1C). After biliary sampling, a plastic stent for
Take-home Message
● Intraductal aspiration significantly improves brushingcellular adequacy and has a high sensitivity for cancerdetection. It is also safe, simple, rapid, and applicableduring routine diagnostic ERCP.
rainage was placed in each patient.
olume 75, No. 4 : 2012 GASTROINTESTINAL ENDOSCOPY 799

S
adc
S
bpwgclcsdn
R
ptr
flmb(ts5s
d
s
Intraductal aspiration Curcio et al
Cytopathological examinationThe cellular material adhering to the brush was directly
smeared, wet-fixed, and stained with rapid hematoxylinand eosin (H&E), allowing the cytopathologist to do arapid on-site evaluation (ROSE) and assess adequacy. Thebrush was subsequently stored in 50% ethanol and pro-cessed in our pathology laboratory to collect the remain-ing material by cytospin.
IDA fluid was stored in 50% ethanol. A drop of IDAfluid was directly smeared, wet-fixed, and stained withrapid H&E to perform ROSE. ROSE allowed interpretationof samples as adequate or inadequate based on the cellu-lar yield for both sets, ensuring at least 1 interpretablespecimen with brushing and/or IDA for each patient.
Smears of cell pellets were done for both sets of sam-ples, and cytospin preparations were done for both sets,when necessary, and stained with both the Papanicolaoumethod and H&E. When an adequate sample was avail-able, a cell block was done, and sections were stainedwith H&E and, occasionally, also with special or immuno-histochemical stains to typify the cells. Both brushing andIDA samples were jointly interpreted by our 2 cyto-pathologists, both experienced in GI cytopathology. Spec-imens were reported as inadequate or unsatisfactory whenacellular/hypocellular, or when showing poor fixation orcrush artifacts, excessive blood, necrosis, or debris thatobscured cellular details. Adequate specimens were re-ported as normal, atypical considered reactive, highlyatypical suspicious for cancer, and malignant. Specimensreported as benign or atypical considered reactive werecombined as negative for cancer, and the highly atypicalsuspicious for cancer and malignant categories were com-bined as positive for cancer.7,8
A cytopathological diagnosis of highly atypical sus-picious for cancer, together with imaging studies com-patible with a malignancy, was considered sufficientevidence of malignancy for consequent surgical or med-
Figure 1. Standard brushing catheter (A) before and (B) after removingpecimen trap.
ical treatment. o
800 GASTROINTESTINAL ENDOSCOPY Volume 75, No. 4 : 2012
tudy endpointsThe study endpoints were to evaluate IDA for cellular
dequacy of the samples, diagnostic accuracy for canceretection, feasibility, and safety. All of the results wereompared with those of standard brushing alone.
tatistical analysisAll collected data were recorded in an electronic data-
ase. Data were analyzed by using the SPSS 15 softwareackage (SPSS Inc, Chicago, Ill). Continuous variablesere summarized as means � standard deviation. Cate-orical variables were summarized as frequency and per-entage. Significant difference was calculated for the cel-ular adequacy by using a �2 test. Difference wasonsidered significant at a P value of �.05. Sensitivity,pecificity, positive predictive value (PPV), negative pre-ictive value (NPV), and overall accuracy of both tech-iques were calculated.
ESULTS
From April 2009 to September 2010, 42 consecutiveatients presenting with suspected malignant biliary stric-ure and no previous histological confirmation were en-olled and prospectively followed until final diagnosis.
IDA was successful for all strictures, with no need forurther attempts because of clogging of catheter/suctionine system, possibly because of the back and forth move-ent of the catheter during IDA. Regarding the site of theiliary strictures, 16 (38.1%) were in the upper third, 1228.6%) were intrahepatic, 8 (19%) were in the middlehird, and 6 (14.3%) in the lower third. Because of theeverity of the stricture, balloon dilation was performed in
patients (11.1%) with biliary stricture before tissueampling.
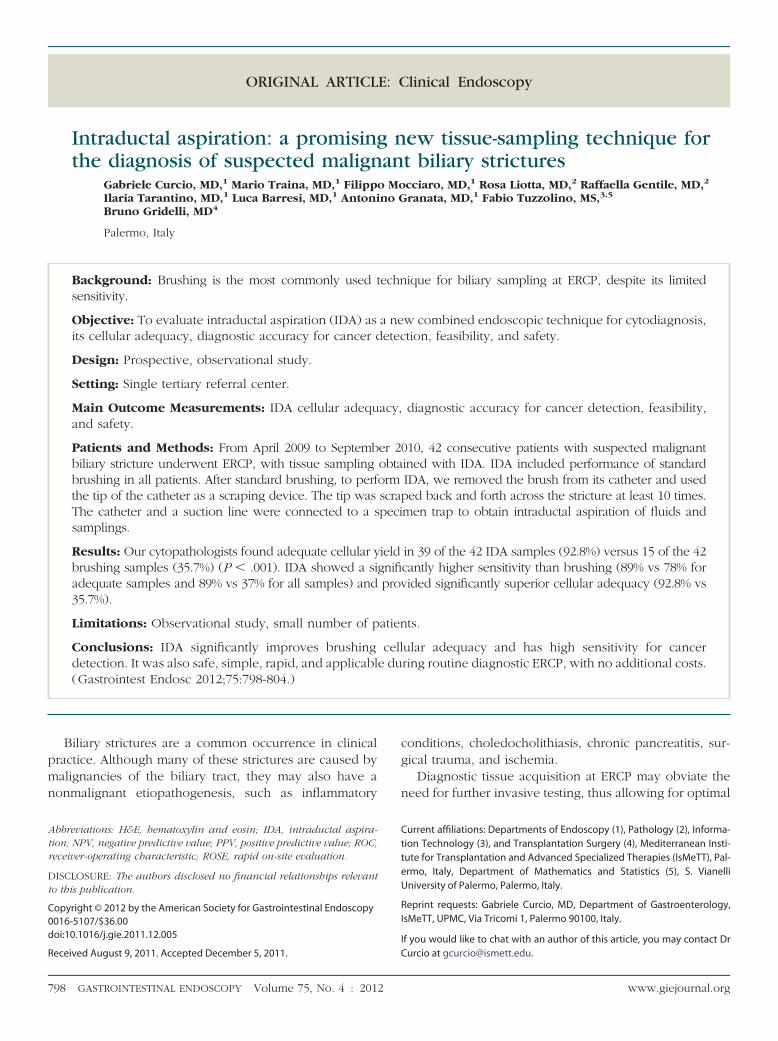
Our cytopathologists found adequate cellular yield foriagnosis in 39 of the 42 IDA samples (92.8%). Seventeen
rush. C, Intraductal aspiration catheter and suction line connected to a
the bf these were judged positive for cancer, with 12 malig-
www.giejournal.org
p1(pboe
aoatAcsa8N
oogoiw((bw
oaba3
saac
ibcI
S
t
D
wq
gptatwttAh6
otboc5v
eotbgtut
Curcio et al Intraductal aspiration
nant (71%) and 5 highly atypical suspicious (29%). In 3patients, the IDA sample had inadequate cellular yield,although the yield was adequate in the brushing sample.
A final diagnosis of malignant stricture was made in 19patients (45.2%). The final diagnoses in all patients areshown in Table 2. The mean follow-up for considering aatient negative for a final diagnosis of malignancy was of6.6 � 4.2 months. In 5 patients negative for malignancy3 with primary sclerosing cholangitis and 2 with chronicancreatitis), ERCP with biliary sampling was repeatedecause there was a high suspicion of malignancy. Nonef these patients were found positive for malignancy at thend of follow-up.
IDA showed a sensitivity for cancer detection of 89%nd a specificity of 100%, with a PPV of 100% and an NPVf 91%. Overall accuracy of IDA was 95% (Table 3). Welso did an intention-based diagnosis analysis, includinghose samples judged inadequate by the cytopathologists.ssuming that all inadequate samples can never provide aorrect final diagnosis, we assigned all those samples aensitivity, specificity, and accuracy of 0. On this secondnalysis, IDA showed a sensitivity for cancer detection of9%, and a specificity of 87%, with a PPV of 85% and anPV of 91%. Overall accuracy of IDA was 88% (Table 4).To be thorough, we calculated the same diagnostic
utcome for the standard brushing alone, which remainsur standard of care for tissue sampling. Our cytopatholo-ists found adequate cellular yield for diagnosis in only 15f the 42 brushing samples (35.7%) obtained with brush-ng alone. Seven of these were judged positive for cancer,ith 4 malignant (57%) and 3 highly atypical suspicious
43%). The adequacy was significantly lower than for IDA92.8%, P � .001). The sensitivity for cancer detection withrushing alone was 78% and the specificity was 100%,
TABLE 2. Final diagnoses in 42 patients with malignantbiliary stricture
No. (%)
Malignant, 19 patients
Cholangiocarcinoma 14 (74)
Metastases* 3 (16)
Gallbladder cancer 1 (5)
Intraductal papillary mucinous tumor 1 (5)
Benign, 23 patients
Primary sclerosing cholangitis 8 (35)
Postoperative biliary stricture 7 (30)
Chronic pancreatitis 5 (22)
Infective 3 (13)
*Primary tumors were colon (n � 2) and stomach (n � 1) cancer.
ith a PPV of 100% and an NPV of 75%. Overall accuracy s
www.giejournal.org V
f brushing was 87%. On the second analysis, consideringll patients, regardless of adequacy, the sensitivity ofrushing alone was 37% and the specificity was 26%, withPPV of 29% and an NPV of 33%. Overall accuracy was
1% (Table 4).Comparing the results only for patients with adequate
amples, the difference in sensitivity between brushinglone and IDA was not statistically significant (P � .4753),s calculated with receiver-operating characteristic (ROC)urves (brushing ROC area 0.8889, IDA ROC area 0.9474).
On second analysis, regardless of adequacy and includ-ng all patients, the difference in sensitivity betweenrushing and IDA was statistically significant (P � .001), asalculated with ROC curves (brushing ROC area 0.3146,DA ROC area 0.8822).
afetyNo adverse events related to IDA were recorded during
he entire follow-up.
ISCUSSION
Our results revealed that this new combined technique,hich we call IDA, significantly improved cellular ade-uacy, showing a high sensitivity for cancer detection.Tissue collection during ERCP is widely used for distin-
uishing between benign and malignant strictures and forroviding a definitive diagnosis that can be used for es-ablishing therapeutic strategies. However, tissue samplingt ERCP has always been challenging. Biliary brushing ishe most frequently used technique. It can be performedithout technical difficulty for most biliary strictures de-
ected at ERCP, although it has limited cytological sensi-ivity, which is often blamed on its low cellular yield.lthough this technique has a specificity of nearly 100%, itas only modest cancer sensitivity, ranging from 18% to0% in most published series.4-6
Tissue samples for histological investigation can be alsobtained from biliary strictures by using forceps. Thisechnique is more challenging and time-consuming thanrushing and is less widely used, but it provides a samplef subepithelial stroma. The popular combination of brushytology and forceps biopsy has a sensitivity ranging from2.0% to 70.4%, which is slightly higher than either indi-idual approach.9,10
A number of other sampling techniques have beenvaluated, with no evidence of an ideal technique in termsf sensitivity, specificity, cost-effectiveness, and safety. In-raductal bile aspiration cytology,2 stricture dilation beforerushing,11 the use of a basket after dilation,12 the use of auidewire to scrape the stricture,13 a new technique ofissue specimen preparation (Smash protocol),14 and these of different brush lengths and stiffness5 are reported inhe literature.
Other studies have evaluated directed tissue biopsy
amples obtained with miniature cholangioscopic biopsyolume 75, No. 4 : 2012 GASTROINTESTINAL ENDOSCOPY 801

lbhew
bci
spc2asiiaTR
c
iteitbp
esbpeis
eawssddph
tlqab
, n � 2
e, n �
Intraductal aspiration Curcio et al
forceps15 or with a single-operator peroral cholangiopan-creatoscopy system known as Spyglass.16 Advanced cyto-ogical techniques for detecting malignancy in pancreato-iliary brushing specimens, including fluorescence in situybridization and digital image analysis, have also beenvaluated and have shown a higher sensitivity comparedith routine cytology.17 Recently, p53 immunocytochem-
ical staining as an adjunct in conventional cytology hasappeared useful in improving the sensitivity of brush cy-tology in malignant strictures.18
Data from several studies showed that combining tech-niques in the same ERCP session to obtain tissue samplesfrom biliary strictures enhances cancer detection. How-ever, multimodal sampling is more time-consuming andmore difficult technically compared with the use of asingle technique.6 Our aim was to develop a new com-ined sampling technique to improve cellular yield andancer detection, one that is rapid and easy to perform andncurs no added costs.
In our 42 patients, IDA provided a significantly higherensitivity than brushing (89% vs 78% for adequate sam-les and 89% vs 37% for all samples), providing a signifi-antly superior cellular adequacy (92.8% vs 35.7%) (Fig.). Cellular adequacy was evaluated on site for brushingnd IDA. In only 3 patients (7.2%) did ROSE find IDAamples inadequate, although for those 3 patients, brush-ng samples proved adequate. We did not repeat samplingn these cases because the brushing sample was adequatend because we wanted to avoid the risk of complications.he remaining 39 IDA samples (92.8%) were adequate atOSE.Although the sensitivity of standard brushing was ac-
TABLE 3. Sensitivity of brushing and IDA calculated for adequa
Cellular adequacy,no. (%)
Sensitivity, %(95% CI)
Spec(9
IDA* 39 (92.8) 89 (65-98) 100
Brushing† 15 (35.7) 78 (40-96) 100
IDA, Intraductal aspiration; CI, confidence interval; NPV, negative predictive va*True positive, n � 17; false positive, n � 0; true negative, n � 20; false negati†True positive, n � 7; false positive, n � 0; true negative, n � 6; false negative
TABLE 4. Sensitivity of brushing and IDA calculated for all sam
Cellular adequacy,no. (%)
Sensitivity, %(95% CI)
Spec(9
IDA* 39 (92.8) 89 (65-98) 87
Brushing† 15 (35.7) 37 (17-61) 26
IDA, Intraductal aspiration; CI, confidence interval; NPV, negative predictive va*True positive, n � 17; false positive, n � 3; true negative, n � 20; false negati†True positive, n � 7; false positive, n � 17; true negative, n � 6; false negativ
eptable, the cellular adequacy of the samples was unsat- b
802 GASTROINTESTINAL ENDOSCOPY Volume 75, No. 4 : 2012
sfactory, with a limited overall cancer detection rate, at-ributable to the low number of interpretable specimens,videnced by a sensitivity of 37% when calculated with anntention-based diagnosis analysis. In our opinion, it is ofhe utmost clinical importance to have the greatest possi-le number of interpretable samples, with the highestossible sensitivity, as we found with IDA.A number of factors that influence tissue sampling ad-
quacy have been identified, including proximally locatedtrictures, tight strictures that might not be fully traversedy the guidewire, sharp angulation in the distal duct thatrevents the passage of biopsy forceps or brush, the pres-nce of firm desmoplastic tumors, and the presence ofntraductal debris and blood that might contaminate thepecimen, particularly the brushings for cytology.19
A tissue sampling technique for use at ERCP shouldnsure the retrieval of good-quality cytology specimensnd, ideally, have a high sensitivity for cancer detection,ith absolute specificity. To be widely used, the technique
hould also be simple, safe, rapid, and relatively inexpen-ive.2 The development of a high-yield ERCP intraproce-ural tissue-sampling technique could also help avoid aelay in tissue diagnosis, obviate the need for additionalrocedures, permit appropriate stent selection, and reduceealth care costs.14
It could be hypothesized that the low cellular yield andhe unsatisfactory sensitivity of standard brushing are re-ated to the brushing itself, which may dislodge an ade-uate number of cells, but fail to collect them. IDA is anttempt to enhance standard brushing diagnostic powery aspirating fluids and samples previously dislodged by
mples
y, %I) NPV, % (95% CI) PPV, % (95% CI)
Accuracy,%
00) 91 (69-98) 100 (77-100) 95
00) 75 (36-96) 100 (56-100) 87
V, positive predictive value.2.
.
y, %I) NPV, % (95% CI) PPV, % (95% CI)
Accuracy,%
6) 91 (69-98) 85 (61-96) 88
9) 33 (14-59) 29 (13-51) 31
V, positive predictive value.2.
12.
te sa
ificit5% C
(80-1
(52-1
lue; PPve, n �
ples
ificit5% C
(65-9
(11-4
lue; PPve, n �
rushing. Furthermore, aspiration and scraping through
www.giejournal.org

asc
R
N(
Curcio et al Intraductal aspiration
the stricture probably allowed for more adequate samplesalso by exposing subepithelial malignant tissue.
In addition, the IDA procedure appeared to be safe,with no evidence of adverse events. It was also simple,rapid, and applicable during routine diagnostic ERCP, byusing the same brushing catheter, with no additional costs.
To ensure the standard of care for all patients, standardbrushing was performed before intraductal aspiration. As aresult, this study does not provide sufficient informationfor establishing whether IDA, done by scraping the stric-ture and aspirating fluids without previous brushing,would have achieved the same important results.
In summary, our results were very promising, showingthat IDA significantly improves brushing cellular adequacyand has a high sensitivity for cancer detection. Random-ized, controlled trials are needed to evaluate the potential
Figure 2. A, Intraductal aspiration (IDA) sample composed of diagnostepithelium, and normal GI tract contamination (cell block section, H&Erepresenting moderately differentiated components of adenocarcinomafragments with glandular differentiation and single atypical cells in a muc
eoplastic cells with enlarged and pleomorphic nuclei. A few cells havehigh power).
advantages of this new technique, comparing IDA (with
www.giejournal.org V
nd without brushing before scraping and aspiration) withtandard brushing, which remains the actual standard ofare for diagnostic tissue acquisition.
EFERENCES
1. NIH state-of-the-science statement on endoscopic retrograde cholan-giopancreatography (ERCP) for diagnosis and therapy. NIH ConsensState Sci Statements 2002;19:1-26.
2. De Bellis M, Sherman S, Fogel EL, et al. Tissue sampling at ERCP in sus-pected malignant biliary strictures (part 1). Gastrointest Endosc 2002;56:552-61.
3. Eisen GM, Dominitz JA, Faigel DO, et al. An annotated algorithmic ap-proach to malignant biliary obstruction. Gastrointest Endosc 2001;53:849-52.
4. Nguyen K, Sing JT Jr. Review of endoscopic techniques in the diagnosisand management of cholangiocarcinoma. World J Gastroenterol 2008;
gments of malignant epithelium, as well as non-neoplastic ductal typelow power). B, Detail of A. Atypical back-to-back glandular formationspower). C, IDA sample composed of several atypical epithelial tissue
s background (cell block section, H$E stain, low power). D, Detail of C.lumnar shape; others have lost their polarity and show disorganization
ic frastain,(highinoua co
14:2995-9.
olume 75, No. 4 : 2012 GASTROINTESTINAL ENDOSCOPY 803

1
1
1
1
1
1
1
1
Intraductal aspiration Curcio et al
5. Fogel EL, deBellis M, McHenry L, et al. Effectiveness of a new long cytol-ogy brush in the evaluation of malignant biliary obstruction: a prospec-tive study. Gastrointest Endosc 2006;63:71-7.
6. De Bellis M, Sherman S, Fogel EL, et al. Tissue sampling at ERCP in sus-pected malignant biliary strictures (part 2). Gastrointest Endosc 2002;56:720-30.
7. Guidelines of the Papanicolaou Society of Cytopathology for fine-needle aspiration procedure and reporting. The Papanicolaou Societyof Cytopathology Task Force on Standards of Practice. Diagn Cyto-pathol 1997;17:239-47.
8. Henke AC, Jensen CS, Cohen MB. Cytologic diagnosis of adenocarci-noma in biliary and pancreatic duct brushings. Adv Anat Pathol 2002;9:301-8.
9. Weber A, von Weyhern C, Fend F, et al. Endoscopic transpapillary brushcytology and forceps biopsy in patients with hilar cholangiocarcinoma.World J Gastroenterol 2008;14:1097-101.
10. Farrell RJ, Jain AK, Brandwein SL, et al. The combination of stricturedilation, endoscopic needle aspiration, and biliary brushings signifi-cantly improves diagnostic yield from malignant bile duct strictures.Gastrointest Endosc 2001;54:587-94.
11. De Bellis M, Fogel EL, Sherman S, et al. Influence of stricture dilation andrepeat brushing on the cancer detection rate of brush cytology in theevaluation of malignant biliary obstruction. Gastrointest Endosc 2003;
58:176-82.804 GASTROINTESTINAL ENDOSCOPY Volume 75, No. 4 : 2012
2. Dumonceau JM, Macias Gomez C, Casco C, et al. Grasp or brush forbiliary sampling at endoscopic retrograde cholangiography? A blindedrandomized controlled trial. Am J Gastroenterol 2008;103:333-40.
3. Uehara H, Tatsumi K, Masuda E, et al. Scraping cytology with a guidewirefor pancreatic-ductal strictures. Gastrointest Endosc 2009;70:52-9.
4. Wright ER, Bakis G, Srinivasan R, et al. Intraprocedural tissue diagnosisduring ERCP employing a new cytology preparation of forceps biopsy(smash protocol). Am J Gastroenterol 2011;106:294-9.
5. Shah RJ, Langer DA, Antillon MR, et al. Cholangioscopy and cholangio-scopic forceps biopsy in patients with indeterminate pancreaticobiliarypathology. Clin Gastroenterol Hepatol 2006;4:219-25.
6. Chen YK, Pleskow DK. SpyGlass single-operator peroral cholangiopan-creatoscopy system for the diagnosis and therapy of bile-duct disor-ders: a clinical feasibility study (with video). Gastrointest Endosc 2007;65:832-41.
7. Fritcher EG, Halling KC. Advanced cytologic approaches for the diagno-sis of pancreatobiliary cancer. Curr Opin Gastroenterol 2010;26:259-64.
8. Kim YS, Kim HG, Han J, et al. The significance of p53 and K-ras immuno-cytochemical staining in the diagnosis of malignant biliary obstructionby brush cytology during ERCP. Gut Liver 2010;4:219-25.
9. Papachristou GI, Smyrk TC, Baron TH. Endoscopic retrograde cholangio-pancreatography tissue sampling: when and how? Clin Gastroenterol
Hepatol 2007;5:783-90.Availability of Journal back issues
As a service to our subscribers, copies of back issues of GastrointestinalEndoscopy for the preceding 5 years are maintained and are available forpurchase from Elsevier until inventory is depleted. Please write to Elsevier Inc.,Subscription Customer Service, 3251 Riverport Lane, Maryland Heights, MO63043 or call 800-654-2452 or 314-447-8871 for information on availability ofparticular issues and prices.
www.giejournal.org