current management of postoperative complications and benign biliary strictures
TRANSCRIPT
Gastrointest Endoscopy Clin N Am
13 (2003) 635–648
Current management of postoperative
complications and benign biliary strictures
Guido Costamagna, MD, FACG*,Saumil K. Shah, MD, DNB, DM, DNB, Andrea Tringali, MD
Digestive Endoscopy Unit, Department of Surgery, Catholic University, Largo A. Gemelli 8,
Rome 00168, Italy
Postoperative bile duct injuries may occur after any kind of surgical
procedure involving the biliary tract. Such injuries, however, are most frequent
following cholecystectomy and biliary anastomosis (eg, after liver transplan-
tation). Although laparoscopic cholecystectomy (LC) results in a shorter hos-
pital stay, faster recovery, lower overall morbidity, and a better abdominal
cosmetic outcome, the rate of bile duct injuries is two to six times higher than
with open cholecystectomy (OC) [1,2]. At least one third of these injuries are
not related to inexperience but reflect fundamental errors in the technique of
LC [3]. Compared with OC, biliary injuries sustained during LC present earlier,
are often associated with persistent bile leaks, and are usually high injuries (ie,
injuries usually located at the common hepatic duct or at the hilum) (Fig. 1A)
[4]. Unfortunately, biliary injury is seldom recognized during surgery; symp-
toms appear most often in the early postoperative course or months or years
after surgery.
Biliary complications are also a common cause of morbidity following or-
thotopic liver transplantation (OLT). Biliary complication after OLT occurs in one
of every six patients, usually within the first 3 months after transplantation.
Although bile duct leaks and strictures are the most common complications,
sphincter of Oddi dysfunction, hemobilia, and biliary obstruction from stones,
sludge, or casts have also been described [5]. Leaks usually present much earlier
than obstructive pathologies.
1052-5157/03/$ – see front matter D 2003 Elsevier Inc. All rights reserved.
doi:10.1016/S1052-5157(03)00103-X
* Corresponding author.
E-mail address: [email protected] (G. Costamagna).
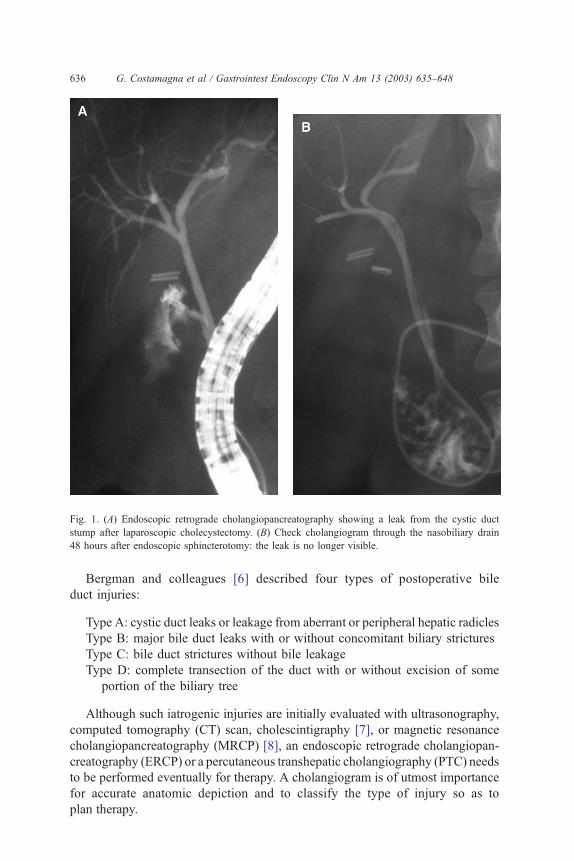
Fig. 1. (A) Endoscopic retrograde cholangiopancreatography showing a leak from the cystic duct
stump after laparoscopic cholecystectomy. (B) Check cholangiogram through the nasobiliary drain
48 hours after endoscopic sphincterotomy: the leak is no longer visible.
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648636
Bergman and colleagues [6] described four types of postoperative bile
duct injuries:
Type A: cystic duct leaks or leakage from aberrant or peripheral hepatic radicles
Type B: major bile duct leaks with or without concomitant biliary strictures
Type C: bile duct strictures without bile leakage
Type D: complete transection of the duct with or without excision of some
portion of the biliary tree
Although such iatrogenic injuries are initially evaluated with ultrasonography,
computed tomography (CT) scan, cholescintigraphy [7], or magnetic resonance
cholangiopancreatography (MRCP) [8], an endoscopic retrograde cholangiopan-
creatography (ERCP) or a percutaneous transhepatic cholangiography (PTC) needs
to be performed eventually for therapy. A cholangiogram is of utmost importance
for accurate anatomic depiction and to classify the type of injury so as to
plan therapy.
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648 637
Surgery has been the mainstay of therapy for such iatrogenic biliary injuries.
Surgery, however, is associated with considerable morbidity and mortality [9,10].
Recent experience with endotherapy has been encouraging [11–17]. Percutaneous
transhepatic techniques are usually reserved for failed endoscopic procedures.
For purposes of the present discussion, postoperative bile duct injuries have
been arranged in two groups: bile leaks and bile duct strictures.
Postoperative bile leaks
The reported incidence of biliary leaks following OC is 0.5% or less and
following LC is 1.1% [18]. Rates of intraoperative complication and conversion
to open surgery were greater among patients who developed leaks [19]. Bile leak
into the peritoneal cavity or externally through a drain positioned at surgery may
have multiple origins according to the type of surgery performed. The following
are the major causes of occurrence of leak:
� Cholecystectomy (open or laparoscopic)
1. Cystic duct stump leak caused by misplacement or displacement of clips
or ligature, a tear in the remnant proximal to the clip, or a necrotic duct
remnant that fails to close because of an ongoing necroinflamma-
tory response
2. Common bile duct (CBD) injury with subsequent leakage following er-
rant clip placement, inadvertent electrocautery or laser burn, excessive
traction on the cystic duct, or inadvertent transection
3. Injury of a sectorial, segmental, or subsegmental duct in the setting of an
anatomic variation of the main biliary confluence
4. Leakage from the gallbladder bed caused by transection of cystohepatic
ducts of Luschka
� Surgery involving the CBD1. Injury to the CBD or to a major branch at the main confluence
2. Leakage from the choledochotomy
3. Leakage from a duct-to-duct anastomosis (as in liver transplantation)
4. Leakage from a biliodigestive anastomosis
� Hepatic surgery1. Injury to the CBD or to a major branch at the main confluence
2. Leakage from a ligated or clipped hepatic radicle
3. Leakage from intrahepatic bile ducts at the hepatic surface after liver
resection
4. Leakage from intrahepatic bile ducts at the hepatic surface after peri-
cystectomy for hydatid cyst
5. Leakage from intrahepatic bile ducts after surgery for hepatic trauma
A high index of suspicion allows early treatment. Patients with postoperative
bile leaks occurring from either open or laparoscopic surgery have a similar
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648638
presentation. Patients may present with malaise, nausea, vomiting, fever, ileus,
jaundice, abdominal pain, or right shoulder pain. Presence of bilious ascites or a
palpable biloma is extremely unusual [18]. Abnormalities in the hepatic profile
are noted, and the white blood cell count may be elevated.
Once the diagnosis of bile leak is established (evidence of external fistula,
radionuclide hepatobiliary scan documenting a leak, or the presence of a biloma at
ultrasound or CT examination), a confirmatory cholangiography is mandatory and
is best accomplished by ERCP [1,12,18,20]. Apart from providing precise
anatomic diagnosis, it allows therapy. PTC or MRCP should be reserved for
patients in whom ERCP fails technically or fails to show the intrahepatic biliary
anatomy because of proximal ductal disruption [18]. For interpretation purposes,
especially in the case of complex hilar lesions, ERCP is best performed with the
patient in the supine position. Doing so allows changing of the patient’s position
obliquely and thus substantially helps in identifying the anatomy of themain biliary
confluence and of the segmental intrahepatic ducts.
Apart from complete transection of the CBD (type D lesion), which is generally
an indication for reconstructive surgery (typically by Roux-en-Y hepaticojeju-
nostomy), an endoscopic therapeutic approach may be envisaged. Endotherapy
has been highly successful in the treatment of postoperative bile leaks [11–13,
15,17,21–24]. Binmoeller and colleagues [11] reviewed 77 cases of endoscopic
therapy reported before 1991 and found technical success in 95% and healing of
the leak in 82% of patients. Elimination of the transpapillary pressure gradient,
thus equalizing the bile duct and duodenal pressures and allowing flow of bile into
the duodenum [12], results in healing within 2 to 8 days [15]. The transpapillary
pressure gradient can be equalized by endoscopic sphincterotomy (ES) alone
[15,17], ES and stent [17] or nasobiliary drain (NBD) placement [25], and stent
[21,26] or NBD insertion alone [27] without preliminary ES (Fig. 1B). All
methods seem to be equally effective in facilitating the closure of the biliary leak
within a few days [6,11,12,21], and the endoscopic approach of choice remains
controversial. The authors’ experience over 13 years in 105 patients with
postoperative biliary leaks has also been excellent. They performed ES plus
NBD placement in 70 patients (68%), ES plus stent placement in 21 patients
(20.4%), and ES alone in 12 patients (11.6%). They achieved a success rate of
98% and had a complication rate of 2% without any mortality. They prefer to place
a NBD because serial cholangiograms can be performed, and a repeat endoscopic
procedure is avoided. If a stent is to be placed, a stent of 10 F or larger is preferred
to avoid early clogging. Endoscopic sphincterotomy followed by stone extraction
should be preferred when dealing with associated residual CBD stones (29% of
cases in the authors’ experience).
Each of these options has limitations, however. Endoscopic sphincterotomy is
associated with inherent immediate and long-term complications, stenting neces-
sitates a repeat procedure and can become clogged or can migrate, whereas a
NBD necessitates continued hospitalization, is uncomfortable for the patient, and
could be accidentally displaced. Recently, Marks and colleagues [28] docu-
mented significantly lower CBD pressures within 24 hours after injection of
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648 639
botulinum toxin (Botox, 100 units) into the sphincter of Oddi; the lower pressures
persisted for 14 days. The authors have suggested its use for the treatment of
bile leaks.
For type B lesions, despite absence of a stricture, the authors prefer to insert at
least one 10-F or 11.5-F stent to bypass the site of injury and to re-establish a
good bilioduodenal flow. The secondary intent of stent placement is to prevent
the development of stricture at the site of the injured bile duct wall. For long
ductal rents, others have also preferred to place long stents across the leak site
[12,18]. Therapeutic success may be obtained in 71% to 79% of cases in this
setting [6,29,30]. Biliary stents have also been successfully used to reestablish the
continuity of disrupted sectorial or segmental branches at the level of the main
hepatic confluence [31] and for leaks from accessory bile ducts [18,32].
Percutaneous drainage of localized bile collections can be a useful adjunctive
therapy when the size or duration of the leak has produced significant intra-
abdominal fluid collection [6,12].
In conclusion, postoperative bile leaks are often amenable to endoscopic man-
agement with high success rates and minimal complications. Endoscopic sphinc-
terotomy with or without placement of drains or stents according to the site and
extent of injury in an individual patient must be considered as the first-line
treatment in all cases of postoperative bile leaks with very few exceptions. Botox
injection in the sphincter of Oddi seems interesting and requires further evaluation.
Postoperative bile duct strictures
Postoperative bile duct strictures occur in 0.2% to 0.5% of patients following
cholecystectomy and are often the result of direct surgical trauma from partial or
complete transection by clipping or ligation of the bile duct. Occasionally, the
stricture is caused by an ischemic insult of the biliary wall secondary to dissection
or thermal injury [14].
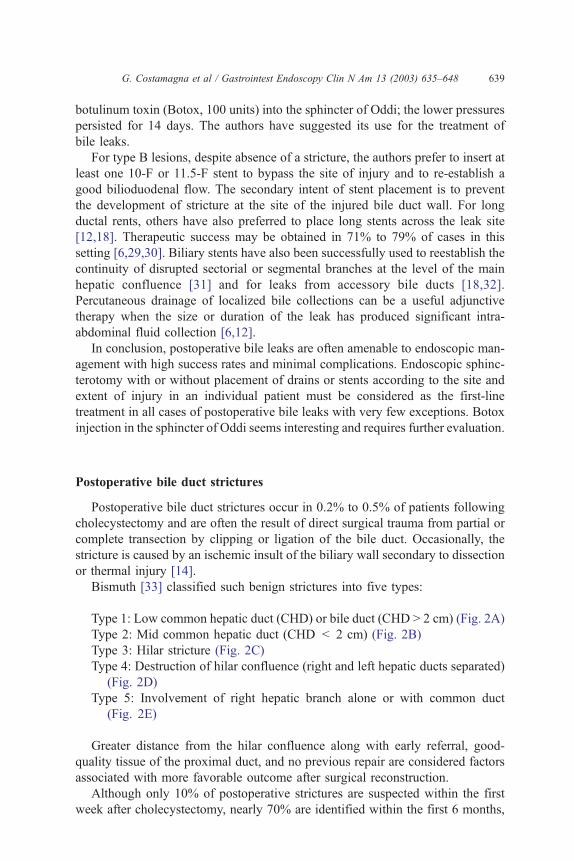
Bismuth [33] classified such benign strictures into five types:
Type 1: Low common hepatic duct (CHD) or bile duct (CHD > 2 cm) (Fig. 2A)
Type 2: Mid common hepatic duct (CHD < 2 cm) (Fig. 2B)
Type 3: Hilar stricture (Fig. 2C)
Type 4: Destruction of hilar confluence (right and left hepatic ducts separated)
(Fig. 2D)
Type 5: Involvement of right hepatic branch alone or with common duct
(Fig. 2E)
Greater distance from the hilar confluence along with early referral, good-
quality tissue of the proximal duct, and no previous repair are considered factors
associated with more favorable outcome after surgical reconstruction.
Although only 10% of postoperative strictures are suspected within the first
week after cholecystectomy, nearly 70% are identified within the first 6 months,
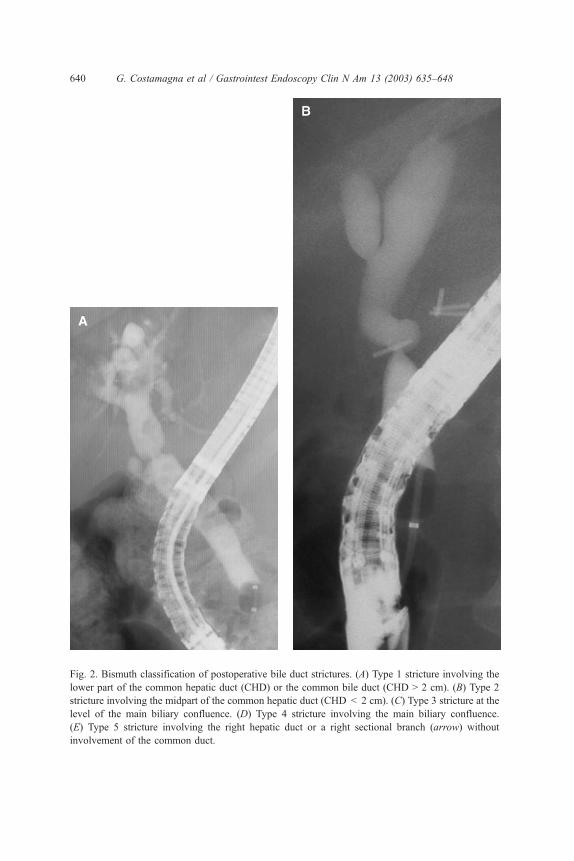
Fig. 2. Bismuth classification of postoperative bile duct strictures. (A) Type 1 stricture involving the
lower part of the common hepatic duct (CHD) or the common bile duct (CHD > 2 cm). (B) Type 2
stricture involving the midpart of the common hepatic duct (CHD < 2 cm). (C) Type 3 stricture at the
level of the main biliary confluence. (D) Type 4 stricture involving the main biliary confluence.
(E) Type 5 stricture involving the right hepatic duct or a right sectional branch (arrow) without
involvement of the common duct.
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648640
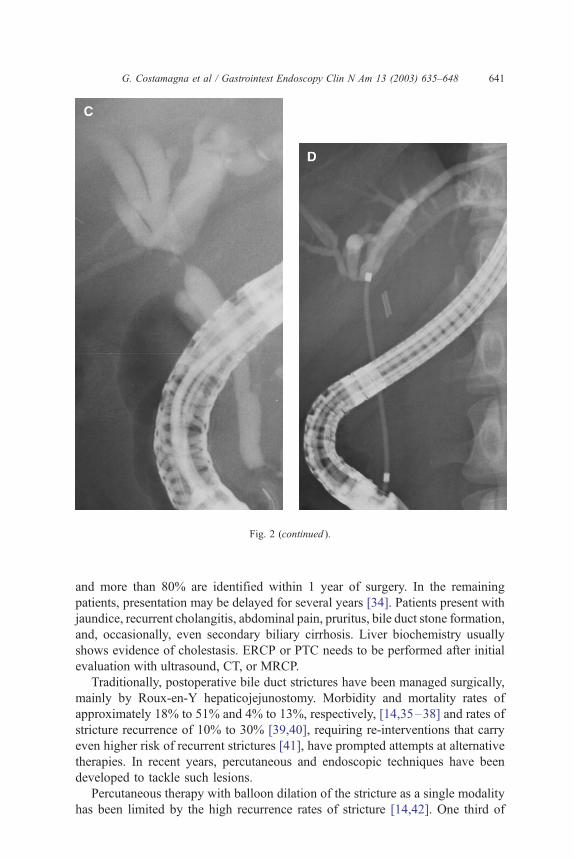
Fig. 2 (continued ).
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648 641
and more than 80% are identified within 1 year of surgery. In the remaining
patients, presentation may be delayed for several years [34]. Patients present with
jaundice, recurrent cholangitis, abdominal pain, pruritus, bile duct stone formation,
and, occasionally, even secondary biliary cirrhosis. Liver biochemistry usually
shows evidence of cholestasis. ERCP or PTC needs to be performed after initial
evaluation with ultrasound, CT, or MRCP.
Traditionally, postoperative bile duct strictures have been managed surgically,
mainly by Roux-en-Y hepaticojejunostomy. Morbidity and mortality rates of
approximately 18% to 51% and 4% to 13%, respectively, [14,35–38] and rates of
stricture recurrence of 10% to 30% [39,40], requiring re-interventions that carry
even higher risk of recurrent strictures [41], have prompted attempts at alternative
therapies. In recent years, percutaneous and endoscopic techniques have been
developed to tackle such lesions.
Percutaneous therapy with balloon dilation of the stricture as a single modality
has been limited by the high recurrence rates of stricture [14,42]. One third of
Fig. 2 (continued ).
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648642
patients experienced complications, and recurrent stenoses were noted in about
one fourth [43,44]. Reports from the John Hopkins Hospital documented a
success rate as low as 55% with significant hemobilia in 20% of patients [45].
Endoscopic treatment of postoperative bile duct stricture is often preferred
over percutaneous techniques, because it avoids the need for liver puncture and
because access to nondilated intrahepatic ducts is easier. Also, the endoscopic
approach is more comfortable for the patient and is safer in the presence of
cirrhosis, ascites, or coagulopathy.
All patients with postoperative bile duct strictures are amenable to a trial of
endoscopic management except those with complete transection or ligation of
the bile duct (Fig. 3). The advantage with endotherapy is that, if it fails, surgery
is still feasible, whereas hepaticojejunostomy makes future endotherapy difficult
if not impossible. The major disadvantage of endotherapy is the need for mul-
tiple procedures. Strictures at or above the main hepatic confluence are often
more challenging than strictures below the hepatic confluence. Endotherapy in-
volves temporary placement of plastic stents with or without preliminary hydro-
static balloon dilation. Balloon dilation is usually performed to a size 1- to 2-mm
larger than the downstream bile duct diameter. In most published experiences,
one or two 10- to 12-F stents were placed, with scheduled exchanges every 3 to
4 months for up to 1 year [14,46–48]. Successful stricture dilation has been
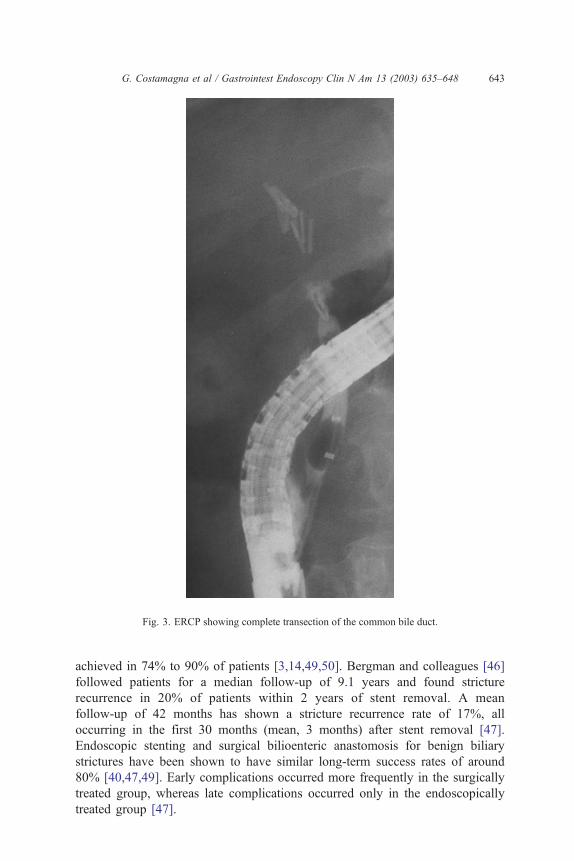
Fig. 3. ERCP showing complete transection of the common bile duct.
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648 643
achieved in 74% to 90% of patients [3,14,49,50]. Bergman and colleagues [46]
followed patients for a median follow-up of 9.1 years and found stricture
recurrence in 20% of patients within 2 years of stent removal. A mean
follow-up of 42 months has shown a stricture recurrence rate of 17%, all
occurring in the first 30 months (mean, 3 months) after stent removal [47].
Endoscopic stenting and surgical bilioenteric anastomosis for benign biliary
strictures have been shown to have similar long-term success rates of around
80% [40,47,49]. Early complications occurred more frequently in the surgically
treated group, whereas late complications occurred only in the endoscopically
treated group [47].
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648644
Stricture at the choledochocholedochostomy anastomotic site is a major cause
of morbidity following OLT. Encouraging results have also been obtained
following endoscopic balloon dilatation or stent placement in patients with
anastomotic biliary strictures after OLT [21,22]. In 63% of patients, a single or
repeat balloon dilatation (8–11.5 mm) alone was sufficient [16]. Repeated
treatment was required more frequently for benign strictures complicating OLT
than for other surgical procedures [47].
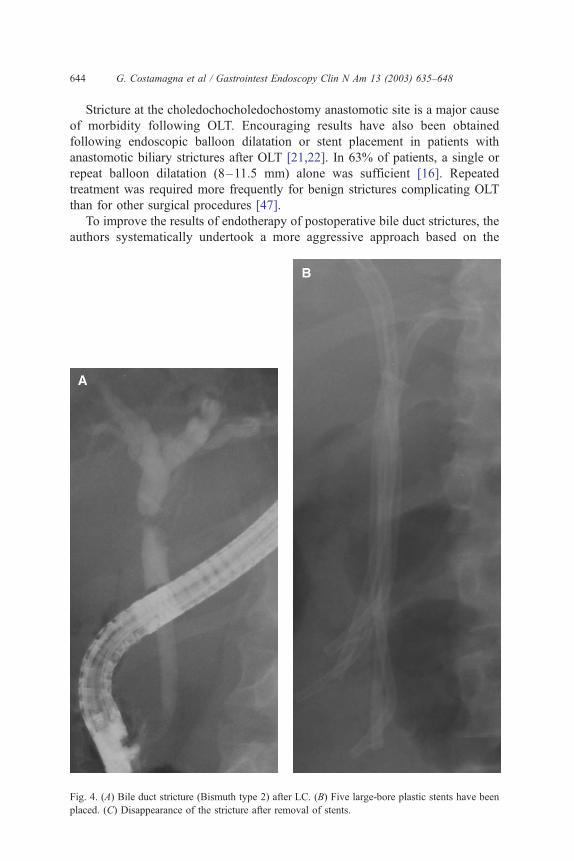
To improve the results of endotherapy of postoperative bile duct strictures, the
authors systematically undertook a more aggressive approach based on the
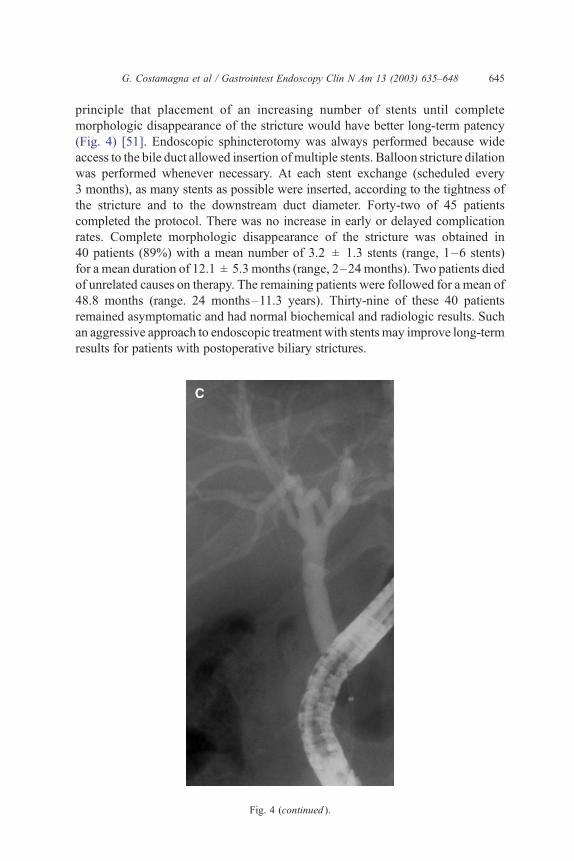
Fig. 4. (A) Bile duct stricture (Bismuth type 2) after LC. (B) Five large-bore plastic stents have been
placed. (C) Disappearance of the stricture after removal of stents.
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648 645
principle that placement of an increasing number of stents until complete
morphologic disappearance of the stricture would have better long-term patency
(Fig. 4) [51]. Endoscopic sphincterotomy was always performed because wide
access to the bile duct allowed insertion ofmultiple stents. Balloon stricture dilation
was performed whenever necessary. At each stent exchange (scheduled every
3 months), as many stents as possible were inserted, according to the tightness of
the stricture and to the downstream duct diameter. Forty-two of 45 patients
completed the protocol. There was no increase in early or delayed complication
rates. Complete morphologic disappearance of the stricture was obtained in
40 patients (89%) with a mean number of 3.2 ± 1.3 stents (range, 1–6 stents)
for a mean duration of 12.1 ± 5.3 months (range, 2–24 months). Two patients died
of unrelated causes on therapy. The remaining patients were followed for a mean of
48.8 months (range. 24 months–11.3 years). Thirty-nine of these 40 patients
remained asymptomatic and had normal biochemical and radiologic results. Such
an aggressive approach to endoscopic treatment with stents may improve long-term
results for patients with postoperative biliary strictures.
Fig. 4 (continued ).
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648646
Long-term results with the use of metallic stents for such strictures have been
disappointing because patency is usually short term, and most stents eventually
obstruct [49,52].
The use of self-expanding metal stents is also not recommended. An
experimental study on pigs [53] showed inflammation, fibrosis, and intramural
abscess after removal of nitinol stents. The authors conclude that endoscopic
removal of self-expandable metal stents is not yet demonstrably reliable and safe.
Other endoscopic devices for the treatment of postoperative biliary strictures
are expected in the future. The development of bioabsorbable stents, removable
large-bore stents, or a stent that may be coated with steroids or chemotherapeutic
agents (such as coronary stents) could offer new possibilities for treatment.
In conclusion, an endoscopic attempt at management of postoperative bile
duct strictures should be undertaken as a first-line treatment in most instances. An
aggressive approach placing multiple stents improves results. Surgical recon-
struction should be considered for complete transection of the bile duct or when
endotherapy fails or stricture recurs.
References
[1] Deziel DJ, Millikan KW, Economou SG, et al. Complications of laparoscopic cholecystectomy:
a national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J Surg 1992;165:L9–14.
[2] MacFadyen Jr BV, Vecchio R, Ricardo AE, et al. Bile duct injury after laparoscopic cholecys-
tectomy. The United States experience. Surg Endosc 1998;12:315–21.
[3] Archer SB, Brown DW, Smith CD, et al. Bile duct injury during laparoscopic cholecystectomy:
results of a national survey. Ann Surg 2001;234:549–58.
[4] Chaudhary A, Manisegran M, Chandra A, et al. How do bile duct injuries sustained during
laparoscopic cholecystectomy differ from those during open cholecystectomy? J Laparoendosc
Adv Surg Tech A 2001;11:187–91.
[5] Tung BY, Kimmey MB. Biliary complications of orthotopic liver transplantation. Dig Dis 1999;
17:133–44.
[6] Bergman JJGHM, van den Brink GR, Rauws EAJ, et al. Treatment of bile duct lesions after
laparoscopic cholecystectomy. Gut 1996;38:141–7.
[7] Brugge WR, Rosenberg DJ, Alavi A. Diagnosis of postoperative bile leaks. Am J Gastroenterol
1994;89:2178–83.
[8] Khalid TR, Casillas VJ, Montalvo BM, et al. Using MR cholangiopancreatography to evaluate
iatrogenic bile duct injury. AJR 2001;177:1347–52.
[9] Martin JK, Van Heerden JA. Surgery of the liver, biliary tract and pancreas. Mayo Clin Proc
1980;55:333–7.
[10] Mcsherry CK, Glenn F. The incidence and causes of death following surgery for nonmalignant
biliary tract disease. Ann Surg 1980;191:271–5.
[11] Binmoeller KF, Katon RM, Shneidman R. Endoscopic management of postoperative biliary
leaks. Review of 77 cases and report of two cases with biloma formation. Am J Gastroenterol
1991;86:227–31.
[12] Bjorkman DJ, Carr-Locke DL, Lichtenstein DR, et al. Postsurgical bile leaks: endoscopic oblit-
eration of the transpapillary pressure gradient is enough. Am J Gastroenterol 1995;90:2128–33.
[13] Davids PHP, Rauws EAJ, Tytgat GNH, et al. Post-operative bile leakage: endoscopicmanagement.
Gut 1992;33:1118–22.
[14] Huibregtse K, Katon RM, Tytgat GNJ. Endoscopic treatment of postoperative biliary strictures.
Endoscopy 1986;18:133–7.
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648 647
[15] Liguory C, Vitale GC, Lefebre JF, et al. Endoscopic treatment of post-operative biliary fistulae.
Surgery 1991;100:779–84.
[16] Mahajani RV, Cotler SJ, Uzer MF. Efficacy of endoscopic management of anastomotic biliary
strictures after hepatic transplantation. Endoscopy 2000;32:943–9.
[17] Ponchon T, Gallez JF, Valette PJ, et al. Endoscopic treatment of biliary tract fistulas. Gastrointest
Endosc 1989;35:490–8.
[18] Mehta SN, Pavone E, Barkun JS, et al. A review of the management of post-cholecystectomy
biliary leaks during the laparoscopic era. Am J Gastroenterol 1997;92:1262–7.
[19] Barkun AN, Rezieg M, Mehta SN, et al. Postcholecystectomy biliary leaks in the laparoscopic
era: risk factors, presentation, and management. Gastrointest Endosc 1997;45:277–82.
[20] Mortensen J, Kruse A. Endoscopic management of postoperative bile leaks. Br J Surg 1992;79:
1339–41.
[21] Foutch PG, Harlan JR, Hoefer M. Endoscopic therapy for patients with a postoperative bile leak.
Gastrointest Endosc 1993;39:416–21.
[22] Pfau PR, Kochman ML, Lewis JD, et al. Endoscopic management of postoperative biliary
complications in orthotopic liver transplantation. Gastrointest Endosc 2000;52:55–63.
[23] Ryan ME, Geenen JE, Lehman GA, et al. Endoscopic intervention for biliary leaks after laparo-
scopic cholecystectomy: a multicenter review. Gastrointest Endosc 1998;47:261–6.
[24] Saab S, Martin P, Soliman GY, et al. Endoscopic management of biliary leaks after T-tube removal
in liver transplant recipients: nasobiliary drainage versus biliary stenting. Liver Transpl 2000;
6:627–32.
[25] Chow S, Bosco JJ, Heiss FW, et al. Successful treatment of post-cholecystectomy bile leaks
using nasobiliary tube drainage and sphincterotomy. Am J Gastroenterol 1997;92:1839–43.
[26] Marks JM, Ponsky JL, Shillingstad RB, et al. Biliary stenting is more effective than sphincter-
otomy in the resolution of biliary leaks. Surg Endosc 1998;12:327–30.
[27] Sugiyama M, Mori T, Atomi Y. Endoscopic nasobiliary drainage for treating bile leak after
laparoscopic cholecystectomy. Hepatogastroenterology 1999;46:762–5.
[28] Marks JM, Bower AL, Goormastic M, et al. A comparison of common bile duct pressures after
botulinum toxin injection into the sphincter of Oddi versus biliary stenting in a canine model.
Am J Surg 2001;181:60–4.
[29] Traverso LW, Kozarek RA, Ball TJ, et al. Endoscopic retrograde cholangiopancreatography after
laparoscopic cholecystectomy. Am J Surg 1993;165:581–6.
[30] Woods MS, Traverso LW, Kozarek RA, et al. Characteristics of biliary tract complications during
laparoscopic cholecystectomy: a multi-institutional study. Am J Surg 1994;167:27–33.
[31] Mutignani M, Shah SK, Tringali A, et al. Endoscopic therapy for biliary leaks from aberrant
right hepatic ducts severed during laparoscopic cholecystectomy. Gastrointest Endosc 2002;55:
932–6.
[32] Mergener K, Strobel JC, Suhocki P, et al. The role of ERCP in diagnosis and management of
accessory bile duct leaks after cholecystectomy. Gastrointest Endosc 1999;50:527–31.
[33] Bismuth H. Postoperative strictures of the bile duct. In: Blumgart LH, editor. The biliary tract.
Edinburgh: Churchill Livingstone; 1982. p. 209–18.
[34] Pitt HA, Miyamoto T, Parapatis SK, et al. Factors influencing outcome in patients with post-
operative biliary strictures. Am J Surg 1982;144:14–21.
[35] Bismuth H, Franco D, Corlette MB, et al. Long-term results of Roux-en-Y hepaticojejunostomy.
Surg Gynecol Obstet 1978;146:161–7.
[36] Bottger T, Junginger T. Long-term results after surgical treatment of iatrogenic injury of the bile
ducts. Eur J Surg 1991;157:477–80.
[37] Frattaroli FM, Reggio D, Guadalaxara A, et al. Benign biliary strictures: a review of 21 years of
experience. J Am Coll Surg 1996;183:506–13.
[38] Raute M, Podlech P, Jaschke W, et al. Management of bile duct injuries and strictures following
cholecystectomy. World J Surg 1993;17:553–62.
[39] Kozarek RA. Endoscopic techniques in management of biliary tract injuries. Surg Clin North Am
1994;74:883–93.
G. Costamagna et al / Gastrointest Endoscopy Clin N Am 13 (2003) 635–648648
[40] Tocchi A, Mazzoni G, Liotta G, et al. Management of benign biliary strictures: biliary enteric
anastomosis vs endoscopic stenting. Arch Surg 2000;135:153–7.
[41] Genest JF, Nanos E, Grundfest-Broniatowski S, et al. Benign biliary strictures: an analytic review
(1970 to 1984). Surgery 1986;99:409–13.
[42] Trambert JJ, Bron KM, Zajko AB, et al. Percutaneous transhepatic balloon dilatation of benign
biliary strictures. Am J Radiol 1987;149:945–8.
[43] Mueller PR, van Sonnenberg E, Ferrucci Jr JT, et al. Biliary stricture dilatation: multicenter
review of clinical management in 73 patients. Radiology 1986;160:17–22.
[44] Williams HJ, Bender CE, May GR. Benign postoperative biliary strictures: dilatation with
fluoroscopic guidance. Radiology 1987;163:629–34.
[45] Pitt HA, Kaufman SL, Coleman J, et al. Benign postoperative strictures: operate or dilate? Ann
Surg 1989;210:417–27.
[46] Bergman JJGHM, Burgemeister L, Bruno MJ, et al. Long-term follow-up after biliary stent
placement for postoperative bile duct stenosis. Gastrointest Endosc 2001;54:154–61.
[47] Davids PHP, Tanka AKF, Rauws EAJ, et al. Benign biliary strictures. Surgery or Endoscopy?
Ann Surg 1993;217:237–43.
[48] Geenen DJ, Geenen JE, Hogan WJ, et al. Endoscopic therapy for benign bile duct strictures.
Gastrointest Endosc 1989;35:367–71.
[49] Dumonceau J-M, Deviere J, Delhaye M, et al. Plastic and metal stents for postoperative benign
biliary strictures: the best and the worst. Gastrointest Endosc 1998;47:8–17.
[50] Smith MT, Sherman S, Lehman GA. Endoscopic management of benign strictures of the biliary
tree. Endoscopy 1995;27:253–66.
[51] Costamagna G, Pandolfi M, Mutignani M, et al. Long-term results of endoscopic management of
postoperative bile duct strictures with increasing number of stents. Gastrointest Endosc 2001;54:
162–8.
[52] Lopez RR, Cosenza CA, Lois J, et al. Long-term results of metallic stents for benign biliary
strictures. Arch Surg 2001;136:664–9.
[53] Van Os EC, Petersen BT, Batts KP. Spiral nitinol biliary stents in a porcine model: evaluation of
the potential for use in benign strictures. Endoscopy 1999;31:253–9.