mitral valve reconstruction versus replacement for degenerative or ischemic mitral regurgitation
TRANSCRIPT

Mitral Valve Reconstruction Versus Replacementfor Degenerative or Ischemic Mitral RegurgitationCary W. Akins, MD, Alan D. Hilgenberg, MD, Mortimer J. Buckley, MD,Gus J. Vlahakes, MD, David F. Torchiana, MD, Willard M. Daggett, MD, andW. Gerald Austen, MDCardiac Surgical Unit, Massachusetts General Hospital, Boston, Massachusetts
Between January 1985 and June 1992, 263 consecutivepatients had mitral valve reconstruction (133 patients) orreplacement (130 patients) for degenerative or ischemicmitral regurgitation. The two groups were similar in sex,age, prior infarctions or cardiac operations, hypertension,angina, and functional class. Both groups were similar inmean ejection fraction, pulmonary artery pressure, cardiac index, and incidence of coronary artery disease.More reconstruction than replacement patients had ischemic etiology (22 [16%) versus 12 [9%)i P = not significant), and fewer reconstruction patients had rupturedanterior leaflet chordae (9 [7%) versus 39 [30%)i P < 0.01).More reconstruction than replacement patients had concomitant cardiac procedures (67 [50%) versus 59 [45%)ip = not significant). Hospital death occurred in 4 reconstruction patients (3%) and 15 (12%) replacement patients(p < 0.01). Median postoperative stay was shorter in
For many cardiac surgeons mitral valve reconstructionrather than replacement has become the procedure of
choice for nonrheumatic mitral valve regurgitation. Although the safety and efficacy of mitral valve reconstructive techniques have been established [1-3], several reports[4, 5) have noted a higher valve repair failure rate whenreconstruction is performed for mitral regurgitation ofrheumatic etiology. In North America the most commoncauses of mitral regurgitation are degenerative and ischemic disease [6). Numerous series [7-17] have comparedmitral valve reconstruction to mitral valve replacement,but in most of these studies the operative procedures wereeither not performed concurrently or were performed fordifferent valvular pathologies.
Thus, the current study was undertaken to compare theoperative and late results of mitral valve reconstructionand mitral valve replacement performed concurrently inone institution in the United States for mitral regurgitationof degenerative or ischemic origin. Because surgeons inour hospital have different philosophies concerning therelative merits of mitral valve reconstruction versus mitral
Presented at the Thirtieth Annual Meeting of The Society of ThoracicSurgeons, New Orleans, LA, Jan 31-Feb 2, 1994.
Address reprint requests to Dr Akins, Department of Surgery, Massachusetts General Hospital, White 503, Boston, MA 02114.
© 1994 by The Society of Thoracic Surgeons
reconstruction patients (10 versus 12 days; p = 0.02). Latevalve-related death occurred in 3 reconstruction patients(2%) and 8 (6%) replacement patients (p = 0.08). Six-yearactuarial freedom from thromboembolism was 92% forthe reconstruction group and 85% for the replacementgroup (p = 0.12). Freedom from all valve-related morbidity and mortality was 85% for the reconstruction patientsand 73% for the replacement patients ip = 0.03). Significant multivariate predictors of hospital death were age,mitral valve replacement, functional class, congestiveheart failure, no posterior chordal rupture, and nonelective operation. Mitral valve reconstruction, when technically feasible, is the procedure of choice for degenerativeor ischemic mitral regurgitation because of significantlylower hospital mortality and late valve-related events.
(Ann Thome Surg 1994;58:668 -76)
valve replacement, the two operations were performedduring the same time period on similar patients.
Material and Methods
A computerized registry of all patients having cardiacsurgical procedures at Massachusetts General Hospitalwas used to identify patients undergoing either mitralvalve reconstruction or mitral valve replacement for isolated mitral regurgitation at the Massachusetts GeneralHospital between January 1985 and June 1992. The recordsof those patients were then retrospectively reviewed bytrained research personnel. Specific attention was directedat the operative and pathologic descriptions of the mitralvalve; only those patients with valves that could be definedas being regurgitant on the basis of a degenerative orischemic etiology were included in the study. Two hundred sixty-three consecutive patients were found to havehad either mitral valve reconstruction (133 patients) ormitral valve replacement (130 patients) for degenerative orischemic mitral regurgitation. Specifically included were67 patients (50.4%) who had reconstruction and 59 patients(45.4%) who had replacement with other major simultaneous cardiac surgical procedures.
The hospital records of the study patients were thenreviewed to determine demographic information, clinical
0003-4975/94/$7.00

Ann Thorne Surg1994;58:668-76
AK1NS ET ALMITRAL REPAIR VERSUS REPLACEMENT
669
and catheterization findings, operative characteristics, andresults of the procedure.
Perioperative myocardial infarction was defined as either new Q waves, elevation of the myocardial fraction ofcreatine kinase in association with persistent ST segmentchanges or new conduction abnormalities, or pathologicfindings at autopsy. Urgent operations were defined asoperative procedures performed in patients whose accelerated symptoms prompted urgent hospital admission forevaluation and who were judged to be too unstable todischarge before operative intervention. True emergencyoperations were defined as operations performed on patients rushed to the first available operating room from thecatheterization laboratory or medical intensive care unitbecause of sudden, profound cardiovascular instability.
Operative TechniqueAll patients had mitral valve replacement or reconstructionperformed during some form of hyperkalemic cardioplegicarrest with aortic cross-clamping. Most concomitant cardiac procedures also were performed during cardioplegicarrest, although some patients in each group with concomitant coronary artery bypass grafting had that portion ofthe operation performed during hypothermic ventricularfibrillation without aortic occlusion. All patients in bothgroups were managed by the same anesthesia and perfusion staffs and were cared for by the same resident physician and nursing staffs.
The choice of mitral valve reconstruction versus replacement was left entirely to the patient's surgeon. The firstmitral valve reconstruction performed in our hospital bythe Carpentier technique was in April 1985. From that dateto the end of the study interval, for the surgeons involvedin this study who contributed at least 20 patients to thereview, the incidence of mitral valve reconstruction rangedfrom 6.2% to 95.6% of an individual surgeon's experience.Generally, patients with severe disease of both mitralleaflets or ruptured chordae to the anterior leaflet were lesslikely to receive a mitral valve reconstructive procedure.Of the 130 patients having mitral valve replacement, 3(2.3%) underwent an initial attempt at valvular reconstruction.
Mitral valve replacement was accomplished in the 130patients usually after total excision of the valvular apparatus, although 26 patients (20.0%), most in the latter yearsof the study, had preservation of at least some portion ofthe native mitral valve, usually the posterior leaflet. Valvular prostheses inserted included 29 bioprosthetic valves(22.3%) (all Carpentier-Edwards porcine valves) and 101mechanical valves (77.7%) (80 St. Jude Medical, 12 StarrEdwards model 6120, 6 Bjork-Shiley standard, and 3Medtronic-Hall). Postoperatively all valve replacement patients were routinely anticoagulated indefinitely.
Mitral valve reconstruction was generally performedaccording to the techniques advocated by Carpentier. All133 reconstruction patients had insertion of a CarpentierEdwards ring, some with intentional deformation of the
anterior leaflet prongs. Additional reconstructive techniques included partial resection of one or both leaflets in81 patients (60.9%), some form of chordal shortening in 31patients (23.3%), posterior to anterior leaflet transpositionin 4 patients (3.0%), and a pericardiaI leaflet patch in 1patient (0.8%). Most reconstruction patients were anticoagulated postoperatively for 2 to 3 months, at which time theanticoagulation was stopped if the patient was in sinusrhythm and did not have another prosthetic heart valve orother medical condition that required warfarin anticoagulation.
Follow-upFollow-up clinical information about survival and subsequent valve-related events was obtained through directcommunication with the patients by trained research personnel. If subsequent hospitalization, death, or valverelated events had occurred, the patient's physician orappropriate hospital record department was contacted todocument the events and hospitalizations. All follow-upinformation was organized to conform with the publishedguidelines for reporting morbidity and mortality aftercardiac valvular operations [18].
Of the 263 patients in the study, 244 survived hospitalization, of whom 2 were completely lost to follow-up and2 had only partial follow-up. Thus, follow-up was 98%complete and was recorded as of September 30, 1992. Meanfollow-up for the 129 surviving valve reconstruction patients was 32.3 months; total follow-up was 345 patientyears. Mean follow-up for the 115 surviving valve replacement patients was 45.2 months; total follow-up was 430patient-years.
Statistical AnalysisDifferences in the demographic, clinical, angiographic, andpathology information between the two groups weretested for statistical significance by unpaired t tests in thecase of continuous, ie, interval, variables. The CaMPAREprogram in the RS/l statistical software package [19] wasused for this purpose in conjunction with the RS/l TESTNORMAL program to find variables needing mathematical transformation to achieve approximate Gaussian errordistributions before testing.
In the case of categorical variables, the RS/l CHISQUARE program was used to discover differences infrequencies between the two groups. In cases where anyexpected cell frequency fell to less than 5, the RS/l FISHERexact test was used.
To describe the long-term results and compare thoseresults between the two groups, in accordance with theguidelines, actuarial curves for mortality and late complications were obtained by the life-table method. The significance of differences between the two groups was determined by means of the Mantel-Cox test in the BMDPprogram PIL [20]. For completeness, late events were alsoreported using linearized rates. Patients who also had anaortic valvular prosthesis were censored from the reviewafter hospital discharge so that events possibly attributableto the aortic valve would not confound the assessment.
Significant univariate and multivariate predictors of
670 AKINS ET ALMITRAL REPAIR VERSUS REPLACEMENT
Ann Thorac Surg1994;58:668-76
~ Replacement
Year
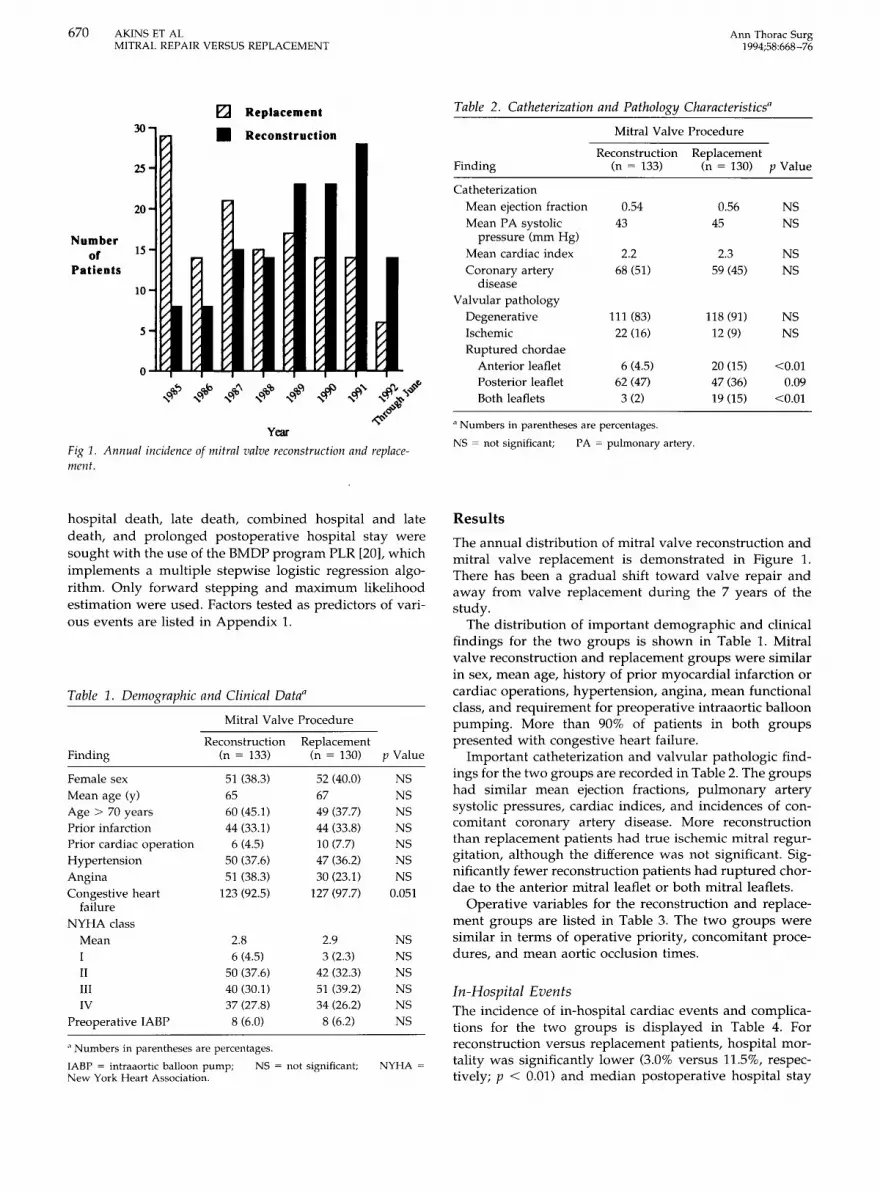
Fig 1. Annual incidence of mitral valve reconstruction and replacement.
30
25
20
Numberor 15
Patients
10
5
0
[j • Reconstruction
V
~r;- ~
~/
/ ~ ~- ~~~
~ ~ ~ ~~
~~ ~ ~ ~ ~ ~
~~ ~ ~
~~
~ 7
~ ~ ~ ~~ ~ ~ ~/ / /
Table 2. Catheterization and Pathology Characteristics"
Mitral Valve Procedure
Reconstruction ReplacementFinding (n = 133) (n = 130) P Value
CatheterizationMean ejection fraction 0.54 0.56 NSMean PA systolic 43 45 NS
pressure (mm Hg)Mean cardiac index 2.2 2.3 NSCoronary artery 68 (51) 59 (45) NS
diseaseValvular pathology
Degenerative 111 (83) 118 (91) NSIschemic 22 (16) 12 (9) NSRuptured chordae
Anterior leaflet 6 (4.5) 20 (15) <0.01Posterior leaflet 62 (47) 47(36) 0.09Both leaflets 3 (2) 19 (15) <0.01
a Numbers in parentheses are percentages.NS ~ not significant; PA = pulmonary artery.
hospital death, late death, combined hospital and latedeath, and prolonged postoperative hospital stay weresought with the use of the BMDP program PLR [20], whichimplements a multiple stepwise logistic regression algorithm. Only forward stepping and maximum likelihoodestimation were used. Factors tested as predictors of various events are listed in Appendix 1.
Table 1. Demographic and Clinical Data"
Mitral Valve Procedure
Reconstruction ReplacementFinding (n = 133) (n = 130) P Value
Female sex 51 (38.3) 52 (40.0) NSMean age (y) 65 67 NSAge > 70 years 60 (45.1) 49 (37.7) NSPrior infarction 44 (33.1) 44 (33.8) NSPrior cardiac operation 6 (4.5) 10 (7.7) NSHypertension 50 (37.6) 47 (36.2) NSAngina 51 (38.3) 30 (23.1) NSCongestive heart 123 (92.5) 127(97.7) 0.051
failureNYHA class
Mean 2.8 2.9 NSI 6 (4.5) 3 (2.3) NSII 50 (37.6) 42 (32.3) NSIII 40 (30.1) 51 (39.2) NSIV 37 (27.8) 34 (26.2) NS
Preoperative IABP 8 (6.0) 8 (6.2) NS
,1 Numbers in parentheses are percentages.
IABP = intraaorlic balloon pump; NS = not significant; NYHA ~
New York HeartAssociation.
Results
The annual distribution of mitral valve reconstruction andmitral valve replacement is demonstrated in Figure 1.There has been a gradual shift toward valve repair andaway from valve replacement during the 7 years of thestudy.
The distribution of important demographic and clinicalfindings for the two groups is shown in Table 1. Mitralvalve reconstruction and replacement groups were similarin sex, mean age, history of prior myocardial infarction orcardiac operations, hypertension, angina, mean functionalclass, and requirement for preoperative intraaortic balloonpumping. More than 90% of patients in both groupspresented with congestive heart failure.
Important catheterization and valvular pathologic findings for the two groups are recorded in Table 2. The groupshad similar mean ejection fractions, pulmonary arterysystolic pressures, cardiac indices, and incidences of concomitant coronary artery disease. More reconstructionthan replacement patients had true ischemic mitral regurgitation, although the difference was not significant. Significantly fewer reconstruction patients had ruptured chordae to the anterior mitral leaflet or both mitral leaflets.
Operative variables for the reconstruction and replacement groups are listed in Table 3. The two groups weresimilar in terms of operative priority, concomitant procedures, and mean aortic occlusion times.
In-Hospital EventsThe incidence of in-hospital cardiac events and complications for the two groups is displayed in Table 4. Forreconstruction versus replacement patients, hospital mortality was significantly lower (3.0% versus 11.5%, respectively; p < 0.01) and median postoperative hospital stay
Ann Thorac Surg1994;58:668-76
AKINS ET ALMITRAL REPAIR VERSUS REPLACEMENT
671
Table 3. Operative Characteristics:"
Mitral Valve Procedure
Table 5. Six-Year Actuarial Event-Free Complication andEvent Rates"
a Numbers in parentheses are percentages. h None of these differencesreached significance. C Miscellaneous means combined other valve procedures and coronary artery bypass grafting or other cardiac procedures.d This includes only those patients whose only procedure performed duringthe cross-clamp interval was the mitral valve operation, ie, 71 patients withisolated mitral valve replacement, 2 patients with mitral valve replacementand coronary artery bypass grafting that was performed during hypothermic ventricular fibrillation without aortic occlusion, 66 patients with isolated mitral valve reconstruction, and 32 patients with mitral valve reconstruction and coronary artery bypass grafting that was performed duringhypothermic ventricular fibrillation without aortic occlusion.
lABP = intraaortic balloon pump.
Finding
Operative priorityElective
Urgent
Emergency
Concomitant procedures
Coronary artery grafting
Other valve
Miscellaneous"IABP
Mean cross-clamp time(min)"
Reconstruction(n = 133)
116 (87)16 (12)
1(1)
56 (42)
4 (3)
7(5)
4 (3)
52.5
Replacement(n = 130)
106 (82)22 (17)
2 (2)
43 (33)
10 (8)
6 (5)
5 (4)
51.7
Mitral Valve Procedure
Reconstruction ReplacementFinding (n = 133) (n = 130) P Value
Late death 78 ± 7 79 ± 6 NS
Structural 96 ± 2 100 NSdeterioration
N onstructural 100 96 ± 3 NSdysfunction
Thromboembolism 92 ± 4 85 ± 5 0.12
Thrombosis 100 100 NS
Anticoagulant- 96 ± 2 97 ± 1 NSrelated bleeding
Endocarditis 96 ± 2 96 ± 2 NS
Reoperation 96 ± 2 98 ± 3 NS
Valve-related death 96 ± 2 90 ± 4 0.12
Valve-related death 85 ± 4 73 ± 5 0.03and morbidity
Total mortality 75 ± 7 70 ± 6 NS
a Data are shown as percentages.
NS ~ not significant.
was significantly shorter (10 versus 12 days, respectively;p = 0.02). More reconstruction patients compared to replacement patients suffered perioperative infarctions,whereas fewer reconstruction patients had postoperativerenal failure, both differences that did not quite attainstatistical significance.
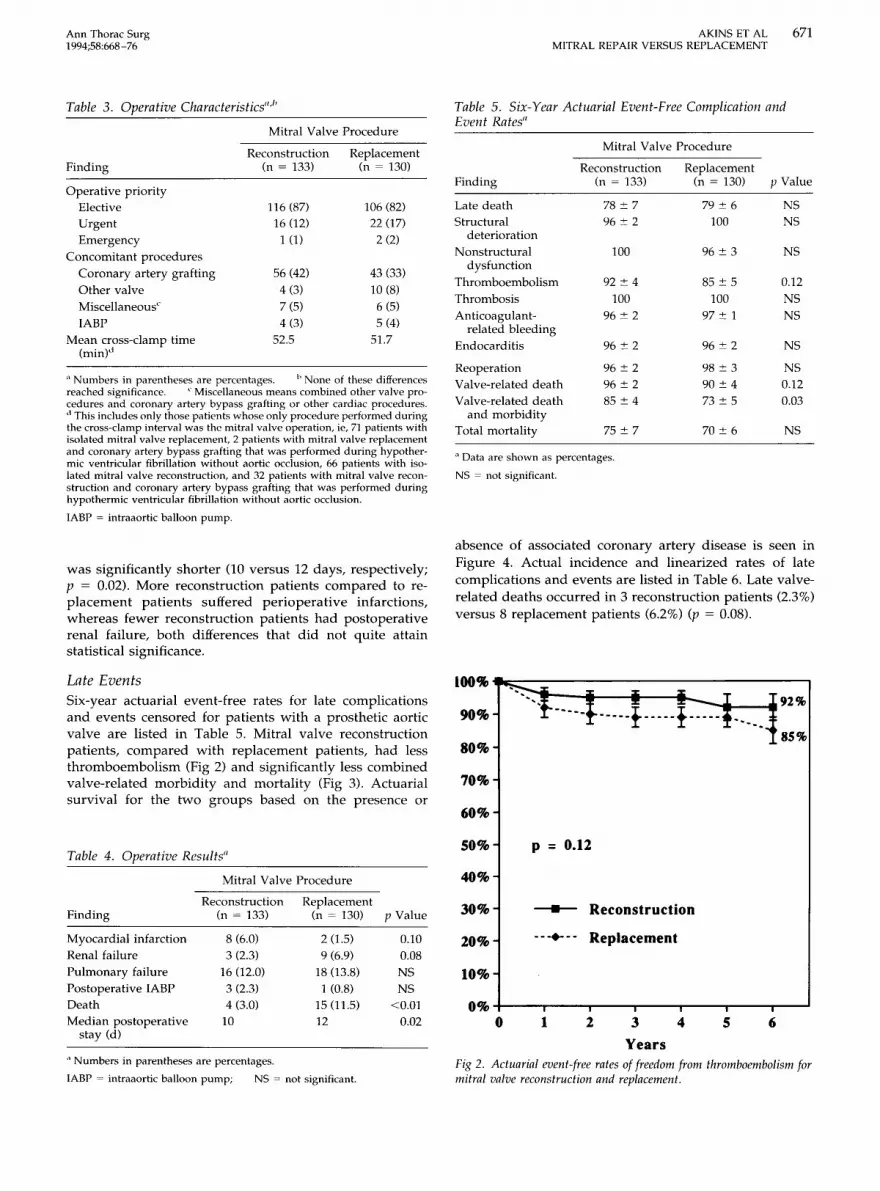
absence of associated coronary artery disease is seen inFigure 4. Actual incidence and linearized rates of latecomplications and events are listed in Table 6. Late valverelated deaths occurred in 3 reconstruction patients (2.3%)versus 8 replacement patients (6.2%) (p = 0.08).
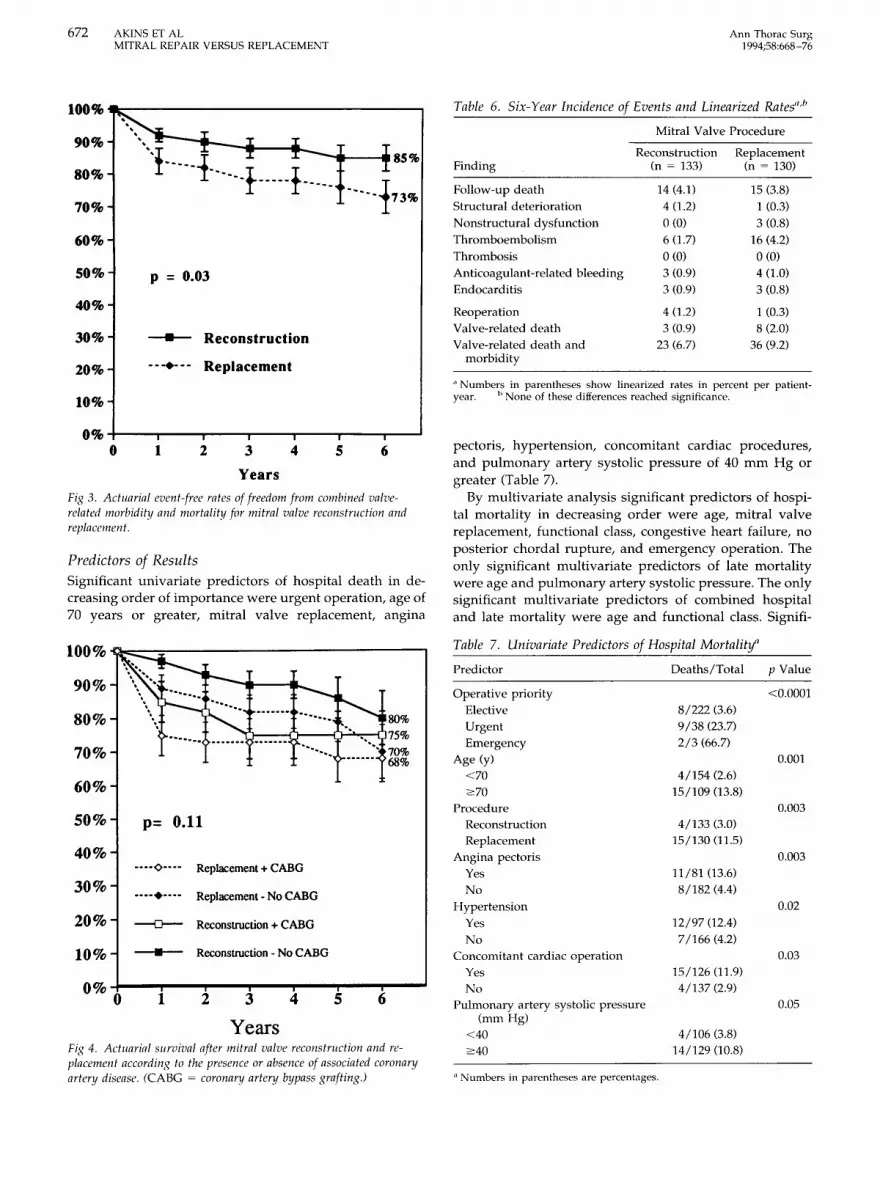
lOO% ...::-----------------,Late EventsSix-year actuarial event-free rates for late complicationsand events censored for patients with a prosthetic aorticvalve are listed in Table 5. Mitral valve reconstructionpatients, compared with replacement patients, had lessthromboembolism (Fig 2) and significantly less combinedvalve-related morbidity and mortality (Fig 3). Actuarialsurvival for the two groups based on the presence or
90%
80%
70%
60%
~=--.--_t""-1_--.....-.. 92%--.
85%
Table 4. Operative Results"50% p = 0.12
Mitral Valve Procedure 40%
65421
-- -... -- Replacement
----- Reconstruction
0% +---r--.......,--~--r--~--r----J
o
10%
20%
30%
3
YearsFig 2. Actuarial event-freerates of freedom from thromboembolism formitral valve reconstruction and replacement.
Reconstruction ReplacementFinding (n = 133) (n = 130) P Value
Myocardial infarction 8 (6.0) 2 (1.5) 0.10Renal failure 3 (2.3) 9 (6.9) 0.08Pulmonary failure 16 (12.0) 18 (13.8) NSPostoperative IABP 3 (2.3) 1 (0.8) NSDeath 4 (3.0) 15 (11.5) <0.01Median postoperative 10 12 0.02
stay (d)
a Numbers in parentheses are percentages.
IABP ~ intraaortic balloon pump; NS ~ not significant.
672 AKINS ET ALMITRAL REPAIR VERSUS REPLACEMENT
Ann Thorac Surg1994;58:668-76
100%~-----------------, TabLe 6. Six-Year Incidence of Events and Linearized Rates"·b
Mitral Valve Procedure90%
80%
70%
60%
50%
40%
30%
20%
....····t··. -Ir-,-----t-...,~--18S%
-- ------f---+---- -----1"'.
p = 0.03
---- Reconstruction
...•... Replacement
Finding
Follow-up deathStructural deteriorationNonstructural dysfunctionThromboembolismThrombosisAnticoagulant-related bleedingEndocarditis
ReoperationValve-related deathValve-related death and
morbidity
Reconstruction(n = 133)
14(4.1)4 (1.2)
0(0)60.7)0(0)
3 (0.9)3 (0.9)
4 (1.2)3 (0.9)
23 (6.7)
Replacement(n = 130)
15 (3.8)1 (0.3)3 (0.8)
16 (4.2)0(0)
4 (1.0)3 (0.8)
1 (0.3)8 (2.0)
36 (9.2)
10%a Numbers in parentheses show linearized rates in percent per patient-year. h None ot these differences reached significance.
Years
pectoris, hypertension, concomitant cardiac procedures,and pulmonary artery systolic pressure of 40 mm Hg orgreater (Table 7).
By multivariate analysis significant predictors of hospital mortality in decreasing order were age, mitral valvereplacement, functional class, congestive heart failure, noposterior chordal rupture, and emergency operation. Theonly significant multivariate predictors of late mortalitywere age and pulmonary artery systolic pressure. The onlysignificant multivariate predictors of combined hospitaland late mortality were age and functional class. Signifi-
65432I0% +---.-----r--~-"""'T"""----..--.___---l
o
Fig 3. Actuarial event-free rates of freedom from combined valverelated morbidity and mortality for mitral valve reconstruction andreplacement.
Predictors of ResultsSignificant univariate predictors of hospital death in decreasing order of importance were urgent operation, age of70 years or greater, mitral valve replacement, angina
Predictor Deaths/Total P Value
Operative priority <0.0001Elective 8/222 (3.6)Urgent 9/38 (23.7)
Emergency 2/3 (66.7)Age (y) 0.001
<70 4/154 (2.6)2:70 15/109 (13.8)
Procedure 0.003Reconstruction 4/133 (3.0)Replacement 15/13001.5)
Angina pectoris 0.003Yes 11/81 03.6)No 8/182 (4.4)
Hypertension 0.02
Yes 12/9702.4)
No 7/166 (4.2)Concomitant cardiac operation 0.03
Yes 15/12601.9)No 4/137 (2.9)
Pulmonary artery systolic pressure 0.05(mmHg)
<40 4/106 (3.8)2:40 14/12900.8)
a Numbers in parentheses are percentages.
TabLe 7. Univariate Predictors of Hospital Mortality"
65
80%'Yl1----o---o-..:.a..,,......075%
70%68%
234
Years
Reconstruction - No CABO
1
•
p= 0.11
_._...... Replacement- No CABO
---0-- Reconstruction + CABO
._--<>.... Replacement + CABO
10%
40%
20%
60%
70%
50%
30%
90%
80%
Fig 4. Actuarial survival after mitral valve reconstruction and replacement according to the presence or absence of associated coronaryartery disease. (CABG = coronaryartery bypass grafting.)
100% -0..:=----=--------------.

Ann Thorac Surg1994;58:668 -76
AKINS ET ALMITRAL REPAIR VERSUS REPLACEMENT
673
cant multivariate predictors of prolonged postoperativehospital stay were advanced age and presence of associated coronary artery disease.
Comment
Numerous studies [7-17] have compared mitral valvereconstruction with mitral valve replacement. Most ofthese studies have suffered from comparing operationsperformed during different time intervals [9, 16], operations for different pathologic conditions or causes of mitralvalve dysfunction [7, 10-17], or operations for rheumaticmitral valve disease [8, 11], an entity with a defined poorerlong-term prognosis after reconstruction [4, 5].
Our study, although retrospective, nonrandomized, andinvolving several surgeons, was directed at evaluatingmitral reconstruction and replacement performed concurrently in one institution for pure mitral valve regurgitationdue to a degenerative or ischemic cause. This was possiblebecause in our hospital there has been an importantdifference of opinion among the cardiac surgeons concerning the efficacy of mitral valve reconstruction. Thus similarpatients have undergone either of two different operativeapproaches to generally the same valvular pathology.
Our finding of improved hospital survival for mitralvalve reconstruction compared with replacement confirmsthat finding in numerous other studies [7-9, 11-14, 16, 17],although Oliveira and co-workers [10] and Cohn andassociates [15] could not document a difference. We believe, however, that our two patient groups are morecomparable than those in most other reports. In addition,by accounting for possible group differences with multivariate regression analysis, we found that having mitralvalve replacement rather than reconstruction is in itself asignificant predictor of hospital mortality.
Analysis of the subset of patients with ischemic mitralregurgitation reveals several interesting findings. Of the 62valve reconstruction patients who had concomitant coronary artery bypass grafting, only 21 (34%) had regurgitation judged to be of ischemic origin. Of the 48 replacementpatients with concomitant coronary artery bypass grafting,only 10 (21%) had ischemic regurgitation. Thus, for thetotal group with concomitant coronary artery bypass grafting, 72% of patients had degenerative mitral regurgitation.Therefore, studies that attribute mitral regurgitation toischemic causes just because of associated coronary arterydisease may inappropriately assess the origin of the regurgitation to be ischemic in the majority of patients. Of all 34patients with ischemic mitral regurgitation, 22 (65%) hadreconstruction rather than replacement.
Hospital mortality was higher, though not significantly,in patients with ischemic versus degenerative regurgitation for combined replacement and reconstruction by univariate testing (14.7% versus 6.1%; P = 0.07). However, anischemic cause was not a significant multivariate predictorof hospital death. Our hospital mortality in ischemic patients of 13.6% for repair and 16.7% for replacementcompares with the results of Rankin and colleagues [21],who reported a mortality of 26% for repair and 53% forreplacement for ischemic mitral regurgitation, although 37
of their 55 patients required "acute operations" afterinfarction.
One finding of our review has received little attention inother studies but is of increasing interest to cardiac surgeons and third-party payers: mitral valve reconstructionis associated with a significantly shorter postoperativehospital stay than is mitral valve replacement. Part of thereason for this may be the lower rate of postoperative renaland pulmonary complications in reconstruction patients.Indeed, this may reflect the growing belief that for mostpatients with mitral regurgitation, valve reconstructionresults in better left ventricular function postoperativelythan does valve replacement [22].
In contrast to other surgeons [23] who advocate preservation of the native valve during replacement, we couldnot demonstrate a survival advantage for replacementpatients who had preservation of the native valve structure. Hospital death occurred in 5 (19.2%) of the 26replacement patients with some of their native valvepreserved compared with 10 (9.6%) of the 104 replacementpatients with no native valve preservation (p = 0.18). Latedeath occurred in another 4 patients with native valvepreservation; two of the deaths were valve related.
The 6-year freedom from thromboembolism of 92% inour reconstruction group, compared with 85% in ourreplacement group (p = 0.12), verifies reports from priorinvestigations in similar patients [16,24] and is somewhatbetter than the 82% at 8 years reported by David andcolleagues [25]. In contrast the most popular prosthesis, theSt. Jude valve, had a linearized thromboembolic rate of4.6% per patient-year compared with 1.7% per patient-yearfor mitral reconstruction. Added to this is the obviousadvantage for most mitral reconstruction patients: they donot require long-term anticoagulation. Conversely, in onlyrare instances will we stop anticoagulation in patients withprosthetic mitral valves, eg, porcine valves in patients withsinus rhythm, a small left atrium, and no thromboembolichistory for whom there is a major contraindication towarfarin anticoagulation.
Finally, the advantage of a significantly greater freedomfrom total valve-related morbidity and mortality for thereconstruction group versus the replacement group (85%versus 73%; p = 0.03) confirms the combined in-hospitaland late efficacy of mitral valve reconstruction versusreplacement.
One postoperative event that was not better in ourreconstruction group was the incidence of perioperativemyocardial infarction, 6.0% versus 1.5%, a difference thatwas not quite significant. A similar report of increasedinfarctions in reconstruction patients was presented byObarski and colleagues [26] from The Cleveland Clinic,who noted an incidence of either new Q waves or enzymeelevations with important electrocardiographic changes in5.4% of reconstruction patients versus 1.8% of replacementpatients. Obarski and colleagues attributed this in part toair embolization to the right coronary artery during salineflushing to test mitral valve competence after repair. Of theeight perioperative infarctions in our reconstruction patients, seven were in patients who had concomitant coronary artery bypass grafting. In addition both mitral valve

674 AKINS ET ALMITRAL REPAIR VERSUS REPLACEMENT
Ann Thorae Surg1994;58:668-76
replacement patients with perioperative infarctions died,as did 3 of the 8 mitral valve reconstruction patients whohad documented infarctions.
Reoperation was required in 5 reconstruction patientsversus 1 replacement patient. Of the reconstructive reoperations, three were due to late postoperative rupture ofpreviously unrepaired chordae at 2, 6, and 14 months. Thisproblem raises the question whether mitral valve reconstruction can alter stresses on intrinsically diseased valvesthat may result in late failure. The remaining reconstruction reoperations occurred at 5 months in a patient inwhom late endocarditis developed secondary to urinaryobstruction and at 11 months in a patient with persistentsevere heart failure who required transplantation afterreoperative aortic valve replacement, coronary artery bypass grafting, and mitral reconstruction. The only replacement patient requiring reoperation had repair of a paravalvular leak with coronary artery bypass grafting 5 yearspostoperatively.
Thus, our data, which strongly support attempts toreconstruct the mitral valve for degenerative or ischemicmitral regurgitation, beg the question of whether there arepatients for whom mitral valve reconstruction is not thepreferred operation. In our study severe disease of bothmitral leaflets or ruptured chordae to the anterior leaflet,although not predictors of hospital mortality, were pathologic features that caused our surgeons to more frequentlyperform mitral valve replacement because of concernabout the ability to achieve a good repair. This sentimentalso has been expressed by David and associates [25], whothink that patients with extensive myxomatous changesand prolapse of multiple areas of both leaflets may dobetter with mitral valve replacement because of the significant risk of reoperation in this group. We, however, havenot noted an important increase in reoperative risk in thepatients who underwent successful reconstruction for disease of the anterior leaflet or both leaflets.
A second patient cohort for whom mitral valve reconstruction may have questionable benefit is patients withsevere ischemic mitral regurgitation in association withprofoundly depressed left ventricular function. In a previous study from our institution Radford and co-workers[27] documented an increased hospital mortality rate of31% for mitral valve replacement for ischemic mitralregurgitation in patients with left ventricular ejection fractions less than 0.35. In addition even if patients in thatsubset did survive hospitalization, their longevity wassignificantly diminished, with an actuarial survival of only38% at 4 years. This experience led us to attempt mitralvalve reconstruction in several patients with ejection fractions less than 0.20 in association with coronary arterybypass grafting. Although we were able to demonstratecompetent mitral valves in these patients by transesophageal echocardiography in the operating room after cardiopulmonary bypass, significant recurrent mitral regurgitation developed in several of them within 6 months,presumably due to progressive ischemic changes withsubvalvular fibrosis and retraction. Thus, the choice inthese patients becomes weighing the significantly increased hospital mortality of mitral valve replacement
against the possibility of recurrent mitral regurgitationafter valve reconstruction.
The results of our review suggest that when mitral valvereconstruction can be successfully accomplished in patients with pure mitral valve regurgitation due to a degenerative or ischemic etiology, those patients have a lowerhospital mortality and shorter postoperative hospital staycompared to valve replacement patients. During followup, reconstruction patients have a decreased incidence ofthromboembolism and a significantly greater freedomfrom total valve-related morbidity and mortality thanreplacement patients. Mitral valve reconstruction is theprocedure of choice for patients with mitral regurgitationdue to a degenerative or ischemic etiology.
We thank Barbara Akins, BSN, and Annetta Boisselle, BSN, forhelp in data acquisition and management and John Newell,Director of the Cardiac Computer Center, Massachusetts GeneralHospital, for assistance with statistical evaluations.
References
1. Carpentier A, Chauvaud S, Fabiani J-N, et al. Reconstructivesurgery of mitral valve incompetence: ten-year appraisal.J Thorac Cardiovasc Surg 1980;79:338-48.
2. Cosgrove DM, Chavez AM, Lytle BW, et al. Results of mitralvalve reconstruction. Circulation 1986;74(Suppl I);82-7.
3. Galloway AC, Colvin SB, Baumann FG, et al. Long-termresults of mitral valve reconstruction with Carpentier techniques in 148 patients with mitral insufficiency. Circulation1988;78(Suppl I):97-105.
4. Antunes MJ, Magalhaes MP, Colsen PR, et al. Valvuloplastyfor rheumatic mitral valve disease. J Thorac Cardiovasc Surg1987;94:44-56.
5. Duran CG, Revuelta JM, Gaite L, et al. Stability of mitralreconstructive surgery at 10-12 years for predominantly rheumatic valvular disease. Circulation 1988;78(Suppl I):91-6.
6. Olson LJ, Subramanian R, Ackermann DM, Orszulak TA,Edwards WD. Surgical pathology of the mitral valve: a studyof 712 cases spanning 21 years. Mayo Clin Proc 1987;62:22-34.
7. Kay JH, Zubiate P, Mendez M, Vanstrom N, Yokoyama T.Mitral valve repair for significant mitral insufficiency. AmHeart J 1978;96:253-62.
8. Duran CG, Pomar JL, Revuelta JM, et al. Consecutive operation for mitral insufficiency. Critical analysis supported bypostoperative hemodynamic studies in 72 patients. J ThoracCardiovasc Surg 1980;79:326-37.
9. Yacoub M, Halim M, Radley-Smith R, McKay R, Nijveld A,Towers M. Surgical treatment of mitral regurgitation causedby floppy valves: repair versus replacement. Circulation 1981;64(SuppllI):21O-6.
10. Oliveira DBG, Dawkins KD, Kay PH, et al. Chordal rupture. II.Comparison between repair and replacement. Br Heart J1983;50:318-24.
11. Perier P, Deloche A, Chauvaud S, et al. Comparative evaluation of mitral valve repairs and replacement with Starr, Bjorkand porcine valve prostheses. Circulation 1984;70(Suppl I):187-92.
12. Orszulak TA, Schaff HV, Danielson GK, et al. Mitral regurgitation due to ruptured chordae tendineae. Early and lateresults of valve repair. J Thorac Cardiovasc Surg 1985;89;491-8.
13. Angell WW, Oury JH, Shah P. A comparison of replacementand reconstruction in patients with mitral regurgitation.J Thorac Cardiovasc Surg 1987;93:665-74.

Ann Thorae Surg1994;58:668-76
AKINS ET ALMITRAL REPAIR VERSUS REPLACEMENT
675
14. Sand ME, Naftel DC, Blackstone EH, Kirklin JW. A comparison of repair and replacement for mitral valve incompetence.J Thorac Cardiovasc Surg 1987;94:208-19.
15. Cohn LH, Kowalker W, Bhatia S, et al. Comparative morbidityof mitral valve repair versus replacement for mitral regurgitation with and without coronary artery disease. Ann ThoracSurg 1988;45:284-90.
16. Galloway AC, Colvin SB, Baumann FG, et al. A comparison ofmitral valve reconstruction with mitral valve replacement:intermediate-term results. Ann Thorac Surg 1989;47:655-62.
17. Craver JM, Cohen C, Weintraub WS. Case-matched comparison of mitral valve replacement and repair. Ann Thorac Surg1990;49:964-9.
18. Edmunds LH [r, Clark RE, Cohn LH, Miller DC, Weisel RD.Guidelines for reporting morbidity and mortality after cardiacvalvular operations. Ann Thorac Surg 1988;46:257-9.
19. RS/l software, release 4.4. Cambridge, MA: BBN SoftwareProducts Corp, 1992.
20. Dixon WJ, Brown MB, Engleman L, [ennrich RI. BMDPstatistical software manual, release 7. 1992;2:1105-44.
21. Rankin JS, Feneley MP, Hickey MSJ, et al. A clinical comparison of mitral valve repair versus valve replacement in ischemic mitral regurgitation. J Thorac Cardiovasc Surg 1988;95:165-77.
22. Tischler MD, Cooper KA, Rowen M, LeWinter MM. Mitralvalve replacement versus mitral valve repair: a Doppler andquantitative stress echocardiographic study. Circulation 1994;89:132-7.
23. David TE, Uden DE, Strauss HD. The importance of the mitralvalve apparatus in left ventricular function after correction ofmitral regurgitation. Circulation 1983;68(SuppllI):76-82.
24. Iebara VA, Dervanian P, Acar C, et al. Mitral valve repairusing Carpentier techniques in patients more than 70 yearsold. Circulation 1992;86(SuppllI):53-9.
25. David TE, Armstrong S, Sun Z, Daniel L. Late results of mitralvalve repair for mitral regurgitation due to degenerativedisease. Ann Thorac Surg 1993;56:7-14.
26. Obarski TP, Loop FD, Cosgrove DM, Lytle BW, Stewart WJ.Frequency of acute myocardial infarction in valve repairsversus valve replacement for pure mitral regurgitation. Am JCardiol 1990;65:887-90.
27. Radford MJ, Johnson RA, Buckley MJ, Daggett WM, LeinbachRC, Gold HK. Survival following mital valve replacement formitral regurgitation due to coronary artery disease. Circulation 1979;60(Suppl 1):39-47.
DISCUSSION
DR BRADLEY S. ALLEN (Chicago, IL): I congratulate Dr Akinsand associates on a very extensive and elegant study. My questions concern chordal preservation. Although I believe repair isprobably superior to replacement in most cases, it has beendemonstrated there is a marked difference in outcome dependingon whether the chordal apparatus is preserved or excised.
Doctor Miller and his group from Stanford showed at thismeeting that preserving both the anterior and the posteriorchordal apparatus led to improved postoperative ventricularfunction. In addition, in a poster session, Dr David and co-workersdemonstrated improved survival when the chordal apparatus waspreserved in valve replacement. I believe their results showed 89%long-term survival when the chordal apparatus was preservedversus 76% when it was sacrificed.
In your follow-up of patients undergoing replacement with lowejection fraction (who you said had a higher mortality), did youexamine just those patients in whom you preserved the mitralannulus apparatus and chordal attachments? Did these patientshave outcomes comparable with those of patients undergoingrepair?
Appendix 1. Factors Assessed as Predictors ofHospital Mortality, Late Mortality, and Length ofPostoperative Stay
Hospital Late PostoperativeFactor Mortality Mortality Stay
Sex X X XAge X X XAngina X X XCongestive heart failure X X XHypertension X X XNew York Heart X X X
Association classPrior myocardial infarction X 0 0Prior cardiac operation X 0 0Ejection fraction X X XPulmonary artery systolic X X X
pressureOperative priority X 0 0
ElectiveUrgentEmergency
Simultaneous operation X X XCoronary graftingValveOther
Valve pathology X X XDegenerativeIschemic
Ruptured chordae X 0 0Anterior leafletPosterior leafletBoth leaflets
Procedure X X XReconstructionReplacement
X = assessed; o ~ not assessed.
DR AKINS: It obviously is a point of great contention amongcardiac surgeons as to whether mitral valve reconstruction isequivalent to mitral valve replacement with preservation of thenative valve apparatus. We have not been able to document in ourstudy, albeit with relatively small numbers, a survival advantageover a longer period, nor could we document even an operativesurvival advantage for preservation of the native valve structure.
There are two issues that I would bring up as part of this. First,I know of several cases in the United States where insertion of alow-profile disc prosthesis with preservation of a portion of thenative valve structure was followed more than 6 months later byrupture of a portion of the chordae of those leaflets, and theruptured chordae impinged on the occluder of the mechanicalvalve.
Second, to me the concept of preserving the native valvemechanism is understandable with mitral reconstruction becausewe are talking about normal mitral valve function during systole.In systole there is creation of tension with basically a right anglebetween the leaflet, then the chordae to the papillary muscle. Ifyou are merely plastering the posterior leaflet to the back wall of

676 AKINS ET ALMITRAL REPAIR VERSUS REPLACEMENT
Ann Thorac Surg1994;58:668-76
the heart and inserting a mitral valve, I am not certain that youhave really gained a lot in terms of actually preserving systolic leftventricular function unless you are careful to gather up a portionof the posterior leaflet so that you are able to get tension on thevalve apparatus in systole.
One of the things we have looked at in terms of long-term leftventricular function is ejection fraction, and we know that thegeometry of the left ventricle changes when the native mitral valveapparatus is divided. It becomes more globular rather than conicalas the normal heart contracts, and it may be that part of thecomputer models used to generate ejection fractions, which arebased on the truncated cone, may confuse the issue as to howbadly ejection fraction truly is diminished.
DR PETER P. McKEOWN (Tampa, FL): I also compliment you ona very excellent paper that reinforces some of the other papers wehave heard about the advantages of repair or replacement. I havedifficulty at times deciding whether to do a replacement or repair,and I wonder if you could expand on that.
My colleagues and I have tried to use transesophageal echocardiography and break it down into a component analysis. Forinstance, in the ischemic patient, we look at how much is relatedto isolated ventricular dysfunction, annular dilatation, papillarymuscle rupture, or ischemic dysfunction. I think the crux of thematter is this: What can we do to try to make the decision aboutrepair or replacement, and can we do that prospectively before weactually enter the operating room?
DR AKINS: Your question is very well taken. We have usedtransesophageal echocardiography in the operating room andoften will request it preoperatively if there is a concern aboutrepair or replacement. The other factor with a great impact on thedecision is the surgeon's preference. In our study if we look at thepractice of the surgeons involved, the incidence of repair in theirpractices ranged from 96% to 6% of their patients, and yet theywere seeing similar distributions of pathology.
Part of it becomes a conscious commitment to believing thatreconstruction is better and therefore taking the time and effort toreconstruct a valve. I think, however, that if we try to usereconstruction for every patient, we will find that there may besome patients who would be better served with mitral valvereplacement.
DR McKEOWN: Is an anterior leaflet rupture necessarily acontraindication to reconstruction, or is it something that youwould definitely not repair in these patients?
DR AKINS: It is not a contraindication for me, but it is for someof our surgeons. I have reconstructed quite a number of valveswith anterior leaflet problems by either chordal transposition oractual resection of parts of the anterior leaflet if they are redundant and myxomatous. I know that Carpentier originally taughtthat you should not do anything to the anterior leaflet, but I havefound that in some patients with very floppy valves, you actuallycan take out parts of the anterior leaflet and get away with it.
DR McKEOWN: What about papillary muscle rupture?
DR AKINS: That is something we tend to replace more thanrepair.
DR BEN R. BARTON (Nashville, TN): I too enjoyed your papervery much. I have two questions concerning ischemic mitralregurgitation preoperatively, and I am sure others also have beenfaced with the dilemma of whether bypass alone would serve toimprove the regurgitation. Transesophageal echocardiographyafter induction of anesthesia often shows less mitral regurgitationthan you are led to believe exists at catheterization. I am curiousabout your criteria for deciding whether to replace or repair in theface of these findings. In your repairs for ischemic mitral regurgitation, are you more often just inserting a ring or doing a morein-depth reparative procedure?
DR AKINS: I will answer your second question first. In our seriesthere were more than 100 patients who had associated coronaryartery bypass grafting, but of those patients, 72% actually haddegenerative mitral regurgitation. Thus the presence of mitralregurgitation in association with coronary artery bypass graftingin our population actually has a higher chance of predictingdegenerative disease than truly ischemic disease.
Like you, we have been very interested in looking at thetransesophageal echocardiogram before operation. We have anexcellent anesthesia staff. What we do is look at the function of themitral valve as the patient goes to sleep, as we administernitroglycerin, and as we try to control heart function, perhaps byunloading the left ventricle. If we can document that regurgitationis falling to levels we consider acceptable, we often will just bypassthe coronary arteries. I think there is some rationale for doing that.
The majority of patients who have this operation are less than 70years of age and therefore would receive a mechanical prosthesis.The mechanical prostheses available today in the sizes we aretalking about have regurgitant fractions as high as 10% to 13%.Therefore, leaving a patient with trace or 1+ mitral regurgitationwith the native valve in place and without anticoagulation is, tome, probably as good as putting in a mechanical prosthesis, if youhave a successful revascularization.
DR I. EDWARD TURNER (Johannesburg, South Africa): There isanother reason for preserving the posterior leaflet, and that isprevention of left ventricular rupture. Could you please commenton that and how you decide whether to preserve the leaflet or not?
DR AKINS: There was a time in the history of our institutionwhen the leading identifiable cause of mortality in the hospitalafter mitral valve replacement with a porcine prosthesis wasrupture of the left ventricle. We somehow have been able toeliminate that problem, maybe in part by not putting manyporcine valves in the mitral position anymore. I think it is not asmuch of an issue for mechanical replacement of the mitral valve.It is still an issue if you are going to be replacing the mitralapparatus with a porcine prosthesis, and saving the posteriorleaflet may have an impact on that ability to avoid left ventricularrupture.