minting the glitter: - informa markets
TRANSCRIPT
MARKET ACCESSLESSONS FROM THE FRONT
SUPPLY CHAINTIME FOR TRACK & TRACE
MEDICAL INNOVATION’STOP 10 WINNERS
NO
VEM
BER
20
13
2014 P
ipelin
e R
eport
Mark
et A
ccess
Supply
Chain
M
edic
al In
novatio
n
VO
LU
ME
33
, NU
MB
ER
11
PHARM EXEC’S 2014 PIPELINE REPORT
Minting the Glitter:Are Blockbusters Back?
NOVEMBER 2013
WHERE BUSINESS MEETS POLICY
VOLUME 33, NUMBER 11
WWW.PHARMEXEC.COM
ES349144_PE1113_cv1.pgs 11.01.2013 17:23 ADV blackyellowmagentacyan

ES345529_PE1113_CV2_FP.pgs 10.26.2013 02:44 ADV blackyellowmagentacyan

Barbara recently joined the Firm’s /nternal /nvesƟgaƟons & White Collar
Defense Group, resident in Post & Schell’s Washington, D.C. Kĸce. She has
overseen or defended white collar government and internal invesƟgaƟons
from the vantage points of prosecutor, defense counsel and, most recently,
in-house counsel for major U.S. pharmacy retail and pharmaceuƟcal
manufacturing corporaƟons.
Contact:
(202) 661-6945 n [email protected]
Post & Schell Welcomes Barbara Rowland, Former Federal Prosecutor and
WharmaceuƟcal DanufacturinŐ and Retail WharmacLJ /nHouse ounsel
n Decades of naƟonal experience with corporate invesƟgaƟons
n Seasoned risk assessment
n Skillful advocacy in and out of the courtroom
n Insight into law enforcement decision-making
n Former Chief, Criminal Division,
U.S. AƩorney’s Kĸce, Eastern
District of Pennsylvania
n Former Deputy Chief, Civil
Division, U.S. AƩorney’s
Kĸce, direcƟng health
care fraud enforcement
within the Eastern District
of Pennsylvania, and Trial
AƩorney in U.S. Department
of :usƟce, Civil Fraud SecƟon
n Former U.S. Department of
:usƟce, dadž Division AƩorney,
Assistant U.S. AƩorney, and
author of the treaƟse, Criminal
Tax, Money Laundering, and
ĂŶŬ^ĞĐƌĞĐLJĐƚ>ŝƟŐĂƟŽŶ;E
^ervinŐ the pharmaceuƟcal &
medical device industries:
PharmaceuƟcal & Medical Device Industry
/nternal /nvesƟgaƟons & White Collar Defense
n Defend corporaƟons and
edžecuƟves in fraud and
abuse invesƟgaƟons ;oī-label
promoƟon, kickbacks, pharmacy
beneĮts management, cGDP,
FCPA, controlled substances
diversion, Sunshine Act,
excluded persons)
n Qui tam whistleblower defense
n “Conference room” advocacy to
preempt government intervenƟon
or charging
n Deep knowledge of self-
disclosure program
requirements and nuanced
analysis of when to self-disclose
Breadth & depth of experience:
&or more informaƟon contact:
Ronald H. Levine n PƌacƟce 'ƌoƵp haiƌ n Philadelphia n (215) 587-1071 n [email protected] www.postschell.com
ES345525_PE1113_003_FP.pgs 10.26.2013 02:44 ADV blackyellowmagentacyan
4
NOVEMBER 2013 www.PharmExec.comPHARMACEUTICAL EXECUTIVE
VP OF SALES & GROUP PUBLISHER TEL [732] 346.3018
Russ Pratt [email protected]
EDITOR-IN-CHIEF TEL [212] 951.6735
William Looney [email protected]
SENIOR MANAGING EDITOR TEL [732] 346.3022
Timothy Denman [email protected]
SENIOR EDITOR TEL [212] 951.6738
Benjamin Comer [email protected]
EUROPEAN & ONLINE EDITOR TEL 011 44 [208] 956.2660
Julian Upton [email protected]
ASSOCIATE EDITOR TEL [212] 951.6648
Clark Herman [email protected]
SPECIAL PROJECTS EDITOR TEL [212] 951.6742
Marylyn Donahue [email protected]
COMMUNITY MANAGER TEL [732] 346.3009
Hannah Becker [email protected]
ART DIRECTOR TEL [218] 740.6411
Steph Johnson-Bentz [email protected]
WASHINGTON CORRESPONDENT TEL [301] 656.4634
Jill Wechsler [email protected]
EDITORIAL OFFICES TEL [212] 951.6600
641 Lexington Avenue, 8th f oor FAX [212] 951.6604
New York, NY 10022 www.pharmexec.com
SALES MANAGER-EAST COAST TEL [732] 346.3054
Mike Moore [email protected]
SALES MANAGER–MIDWEST, SOUTHWEST, WEST COAST TEL [847] 283.0129
Bill Campbell [email protected]
SALES MANAGER–EUROPE, MIDDLE EAST, ASIA PACIFIC TEL 011 44 [124] 462.9318
Debbie Taylor-Higgins [email protected]
SENIOR PRODUCTION MANAGER TEL [218] 740.6371
Karen Lenzen [email protected]
AUDIENCE DEVELOPMENT MANAGER TEL [218] 740.7285
Kelly Kemper [email protected]
REPRINTS 877-652-5295 EXT. 121
Outside US, UK, direct dial: 281-419-5725. Ext. 121
CLASSIFIED SALES & RECRUITMENT TEL [440] 891.2793
Tod McCloskey [email protected]
DIRECT MAIL LISTS TEL [440] 891.2773
Tamara Phillips [email protected]
JOE LOGGIA, Chief Executive Off cer; TOM FLORIO, Chief Executive
Off cer Fashion Group, Executive Vice-President; TOM EHARDT,
Executive Vice-President, Chief Administrative Off cer & Chief
Financial Off cer; GEORGIANN DECENZO, Executive Vice-President;
CHRIS DEMOULIN, Executive Vice-President; RON WALL, Executive
Vice-President; REBECCA EVANGELOU, Executive Vice-President,
Business Systems; JULIE MOLLESTON, Executive Vice-President,
Human Resources; TRACY HARRIS, Sr Vice-President; FRANCIS HEID,
Vice-President, Media Operations; MICHAEL BERNSTEIN, Vice-President,
Legal; J VAUGHN, Vice-President, Electronic Information Technology
Murray L. Aitken
Senior Vice President,
Healthcare Insight,
IMS Health
Stan Bernard
President,
Bernard Associates
Frederic Boucheseiche
Chief Operating Off cer,
Focus Reports Ltd.
Joanna Breitstein
Director, Communications,
Global TB Alliance
Drew Bustos
Vice President, Global Communications,
Cegedim Relationship Management
Rich Daly
Founder,
Sage Path Partners
Rob Dhoble
CEO,
Adherent Health
Bill Drummy
CEO,
Heartbeat Ideas
James Forte
Vice President, Marketing,
Campbell Alliance
Fred Frank
Vice Chairman,
Burrill & Co.
Les Funtleyder
President,
Poliwogg Investment Advisors
Matt Gross
Director, Health and Life Sciences
Global Practice, SAS
Terry Hisey
Vice Chairman,
Nat’l Sector Leader, Life Sciences,
Deloitte
Michele Holcomb
Vice President Corporate Strategy,
Teva Pharmaceuticals
Bob Jansen
Principal Partner,
Zensights LLC
Kenneth Kaitin
Director & Professor,
Center for the Study of Drug Development,
Tufts University
Clifford Kalb
President,
C. Kalb & Associates
Daniel A. Kracov
Partner & Head,
FDA and Healthcare Practice,
Arnold & Porter
Bernard Lachappelle
President,
JBL Associates
Rajesh Nair
President,
Indegene
Daniel Pascheles
Vice President,
Global Business Intelligence,
Merck & Co.
Elys Roberts
President,
Ipsos Healthcare North America
Barbara Ryan
Managing Director, Strategic
Communications, FTI Consulting
Alexander Scott
Vice President, Business Development,
Eisai Corp. of North America
Michael Swanick
Global Practice Leader Pharmaceuticals
and Life Sciences, PwC
Mason Tenaglia
Managing Director,
The Amundsen Group
Peter Tollman
Senior Partner, Managing Director,
Boston Consulting Group
Al Topin
President,
Topin Associates
Bill Trombetta
Professor of
Pharmaceutical Marketing,
St. Joseph’s University Business School
David Verbraska
Vice President, Regulatory Policy,
Pf zer
Albert I. Wertheimer
Professor & Director,
Pharmaceutical Health Services Research,
Temple University
Ian Wilcox
Vice President,
Hay Group
Peter Young
President,
Young & Partners
Pharmaceutical Executive’s 2013 Editorial Advisory Board
is a distinguished group of thought leaders with expertise in
various facets of pharmaceutical research, business, and mar-
keting. EAB members suggest feature subjects relevant to the
industry, review article manuscripts, participate in and help
sponsor events, and answer questions from staff as they arise.
VOLUME 33, NUMBER 11
2011 Neal Award Winner for
“Best Commentary”
©2013 Advanstar Communications Inc. All rights reserved. No part of this publication
may be reproduced or transmitted in any form or by any means, electronic or mechani-
cal including by photocopy, recording, or information storage and retrieval without
permission in writing from the publisher. Authorization to photocopy items for internal/
educational or personal use, or the internal/educational or personal use of specif c
clients is granted by Advanstar Communications Inc. for libraries and other users
registered with the Copyright Clearance Center, 222 Rosewood Dr. Danvers, MA 01923,
978-750-8400 fax 978-646-8700 or visit http://www.copyright.com online. For uses
beyond those listed above, please direct your written request to Permission Dept. fax
440-756-5255 or email: [email protected].
Advanstar Communications Inc. provides certain customer contact data (such as
customers’ names, addresses, phone numbers, and e-mail addresses) to third parties
who wish to promote relevant products, services, and other opportunities that may
be of interest to you. If you do not want Advanstar Communications Inc. to make your
contact information available to third parties for marketing purposes, simply call toll-
free 866-529-2922 between the hours of 7:30 a.m. and 5 p.m. CST and a customer
service representative will assist you in removing your name from Advanstar’s lists.
Outside the U.S., please phone 218-740-6477.
PHARMACEUTICAL EXECUTIVE does not verify any claims or other information appear-
ing in any of the advertisements contained in the publication, and cannot take respon-
sibility for any losses or other damages incurred by readers in reliance of such content.
PHARMACEUTICAL EXECUTIVE welcomes unsolicited articles, manuscripts, photo-
graphs, illustrations, and other materials, but cannot be held responsible for their
safekeeping or return.
To subscribe, call toll-free 888-527-7008. Outside the U.S. call 218-740-6477.
ES349710_PE1113_004.pgs 11.04.2013 19:48 ADV blackyellowmagentacyan

At Quintiles, we call it Data-driven Trial Execution – a solution that expands on risk-based monitoring to improve patient safety and study quality while mitigating risk. We provide ongoing risk assessment, real-time data surveillance and a tailored dynamic monitoring strategy, to help you identify trends and take informed actions, faster. To optimize efficiency, we integrate study start-up, project management, clinical monitoring, and data management. The result: more predictable spend and execution outcomes, for maximum value.
Learn how Data-driven Trial Execution can help you deliver new levels of productivity and value. Call 1-866-267-4479 or visit quintiles.com/healthierDTE
Take the risk out of risk-based monitoring.
deeper insights,healthier results
Co
pyri
gh
t ©
20
13 Q
uin
tile
s.
ES345530_PE1113_005_FP.pgs 10.26.2013 02:44 ADV blackyellowmagentacyan
Contents6
NOVEMBER 2013 www.PharmExec.comPHARMACEUTICAL EXECUTIVE
Roundtable
Roundtable onMarket AccessWilliam Looney, Editor-in-Chief
Market Access is a window
on what matters in the real
world of soaring patient
expectations and crimped
budgets for innovation.
Pharm Exec convenes a
diverse panel of experts
to identify the key markers
of common ground: its
time, people, and money
against that greatest
intangible—hope.
26
Supply Chain
Scanning the FutureTimothy Denman,
Senior Managing Editor
In response to well-
publicized security threats,
regulatory authorities in
the United States and
Europe are moving toward
the enactment of new
legislation that will change
the way pharma products
are handled and shipped
throughout the supply chain.
36
Pharm Exec’s 2014 Pipeline ReportBen Comer, Senior Editor
Across a constellation of categories, bright
new drugs are moving into position. The
pharma model may have changed, but
companies are keeping their blockbusters.
16
NEWS & ANALYSIS
Washington Report
12 Transparency Troubles for PharmaJill Wechsler, Washington Correspondent
INSIGHTS
From the Editor
10 Payers: Late for the Party?William Looney, Editor-in-Chief
Back Page
66 Top Medical Innovations for 2014Ben Comer, Senior Editor
On The Cover: Tilton Widro
Country Report: Taiwan
42 Preparing for TakeoffFocus Reports, Sponsored Supplement
The past three years have been some of the most eventful in memory for Taiwan’s life sciences industry.
At this year’s Bio Taiwan exhibition, the annual conference that invites the international life sciences
community to the island, the excitement was palpable. Foreign companies turned out in record numbers
to a keynote address from President Ma Ying-Jeou, who acknowledged that Taiwan was a latecomer
to the sector, but nonetheless had the capability and will to compete. Buoyed by a successful wave of
f nancing, good product strategy, and increasing international penetration, the industry seems conf dent.
PHARMACEUTICAL EXECUTIVE VOLUME 33, NUMBER 11 (Print ISSN 0279-6570, Digital ISSN: 2150-735X) is published monthly by Advanstar Communications Inc., 131 W. First St., Duluth, MN 55802-2065. Subscription rates: $70 (1 year), $125 (2 years) in the United States and Possessions; $90 (1 year), $145 (2 years) in Canada and Mexico; $135 (1 year), $249 (2 years) in all other countries. Price includes air-expedited service. Single copies (prepaid only): $7 in the United States, $9 in all other countries. Back issues, if available, are $20 for the United States and Possessions, $25 for all other countries. Include $6.50 per order plus $2 per additional copy for US postage and handling. If shipping outside the United States, include an additional $10 per order plus $3 per additional copy. Periodicals postage paid at Duluth, MN 55806 and additional mailing off ces. POSTMASTER: Please send address changes to PHARMACEUTICAL EXECUTIVE, PO Box 6180, Duluth, MN 55806-6180. Canadian G.S.T. Number: r-12421 3133rt001, Publications mail agreements NO. 40612608. Return Undeliverable Canadian Addresses to: IMEX Global Solutions, P. O. Box 25542, London, ON N6C 6B2, Canada. Printed in the USA.
ES349564_PE1113_006.pgs 11.04.2013 16:26 ADV blackyellowmagentacyan
ES345548_PE1113_007_FP.pgs 10.26.2013 02:45 ADV blackyellowmagentacyan
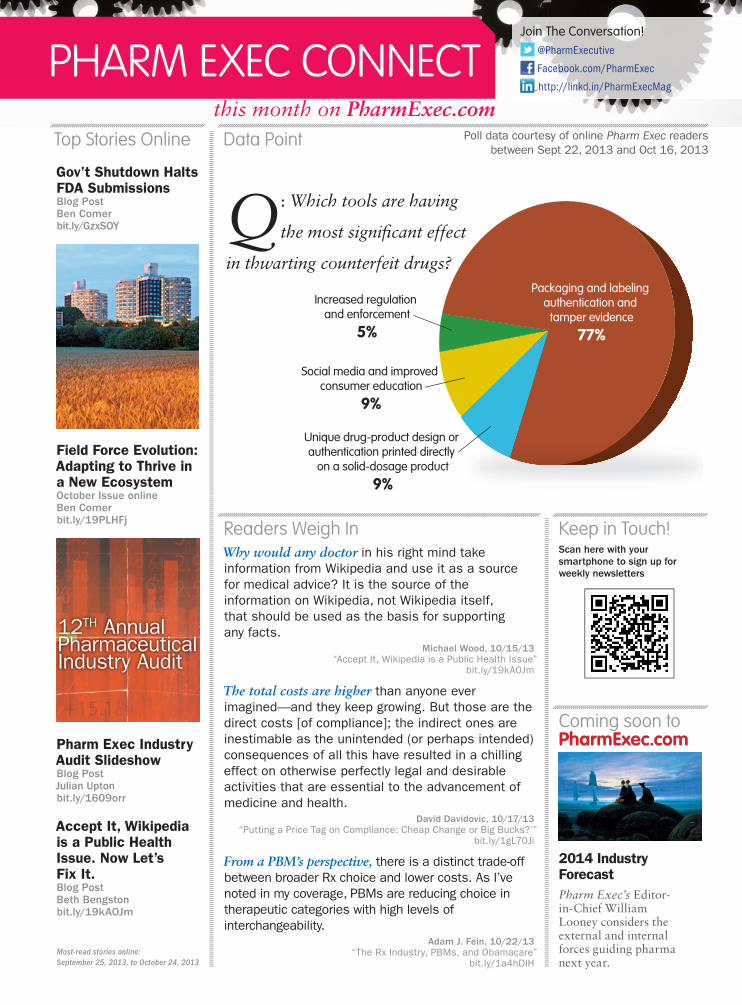
this month on PharmExec.com
Packaging and labeling authentication and
tamper evidence
77%
Social media and improved consumer education
9%
Increased regulation and enforcement
5%
Unique drug-product design or authentication printed directly
on a solid-dosage product
9%
Top Stories Online
Gov’t Shutdown Halts FDA SubmissionsBlog PostBen Comerbit.ly/GzxSOY
Field Force Evolution: Adapting to Thrive in a New Ecosystem October Issue onlineBen Comerbit.ly/19PLHFj
Pharm Exec Industry Audit SlideshowBlog PostJulian Uptonbit.ly/1609orr
Accept It, Wikipedia is a Public Health Issue. Now Let’s Fix It.Blog PostBeth Bengston bit.ly/19kAOJm
Readers Weigh InWhy would any doctor in his right mind take
information from Wikipedia and use it as a source
for medical advice? It is the source of the
information on Wikipedia, not Wikipedia itself,
that should be used as the basis for supporting
any facts.
Michael Wood, 10/15/13 “Accept It, Wikipedia is a Public Health Issue”
bit.ly/19kAOJm
The total costs are higher than anyone ever
imagined—and they keep growing. But those are the
direct costs [of compliance]; the indirect ones are
inestimable as the unintended (or perhaps intended)
consequences of all this have resulted in a chilling
effect on otherwise perfectly legal and desirable
activities that are essential to the advancement of
medicine and health.
David Davidovic, 10/17/13“Putting a Price Tag on Compliance: Cheap Change or Big Bucks?’”
bit.ly/1gL70Ji
From a PBM’s perspective, there is a distinct trade-off
between broader Rx choice and lower costs. As I’ve
noted in my coverage, PBMs are reducing choice in
therapeutic categories with high levels of
interchangeability.
Adam J. Fein, 10/22/13 “The Rx Industry, PBMs, and Obamacare”
bit.ly/1a4hDlH
Coming soon toPharmExec.com
2014 Industry Forecast
Pharm Exec’s Editor-in-Chief William Looney considers the external and internal forces guiding pharma next year.
Keep in Touch!Scan here with your
smartphone to sign up for
weekly newsletters
Data Point
Q: Which tools are having
the most signif cant effect
in thwarting counterfeit drugs?
Poll data courtesy of online Pharm Exec readers
between Sept 22, 2013 and Oct 16, 2013
12TH Annual Pharmaceutical Industry Audit
Join The Conversation!
@PharmExecutive
Facebook.com/PharmExec
http://linkd.in/PharmExecMag
Most-read stories online:
September 25, 2013, to October 24, 2013
ES349722_PE1113_008.pgs 11.04.2013 22:14 ADV blackyellowmagentacyan
91% adherence after 6 months.
$GECWUGYGHQEWUGFQPRGQRNGƂTUVAnxious patients faced with taking a new medication needed information and support. Overworked healthcare providers were limited on resources. That’s when Quintiles’ clinical educators reached out. Our highly specialized healthcare professionals helped patients and providers navigate a complex chronic condition and a novel treatment regimen. Making this personal connection led to some of the highest adherence rates in the industry.
Find out how our clinical educators can help you keep more patients on therapy. Call us today at 1-866-267-4479 or visit quintiles.com/healthieradherence.
better adherence,
healthier results
better adherence,
Co
pyr
ight
© 2
013 Q
uin
tile
s
ES345527_PE1113_009_FP.pgs 10.26.2013 02:44 ADV blackyellowmagentacyan

From the Editor10
NOVEMBER 2013 www.PharmExec.comPHARMACEUTICAL EXECUTIVE
Pharm ExEc’s two kEy FEaturEs this month illustrate the strategic contradiction facing today’s industry. On the one hand, our annual survey of R&D pipeline prospects reveals an open well of potential from the scientifc discoveries associated with the map-ping of the human genome. That was nearly a decade ago, and its legacy is now bearing fruit, in the form of a more precise targeting of trials and treatments that promise to save more lives, at lower cost. The larger meaning here is that the case for the blockbuster product—at least in clinical terms—is due for a revival.
But when we raise the other hand, we see a blank wall of indifference to this bounty. After a seven year hiatus, Pharm
Exec returns this month with a roundtable panel of experts to examine the state of market access in medicines—a state that our participants defne as one where that market is being managed to slow or even reduce access, particularly for new originator products that once were referenced as innovative. Now they are reference priced—of-ten against the oldest generic product in its class.
In most countries today, there is little or no premium allowed for innovation. Germany, the world’s fourth largest economy and surely one of the richest, is subjecting companies to a bewilder-ingly complex new drug beneft assessment pro-cess. In the case of life-saving oncology products, this requires delivering as primary endpoints evidence of progression free survival projected toward overall survival—a virtually impossible measurement for any new cancer product. Fail-ure to meet this hurdle risks a product being priced within fxed reference price classes, where older generics are the main comparator.
This is unfortunate because, as senior editor Ben Comer notes in the pipeline profle, all this new science carries a potentially large beneft on the cost side. It speeds up the development pro-cess. More precise molecular targeting enhances the selection criteria for clinical trials and thus provides more accuracy in test results. Companies are also faring better in focusing R&D spend-ing around areas of unmet medical need. For example, our survey tags a slow but steady resur-gence of Big Pharma interest in next-generation antibiotics to treat hospital borne infections that kill 23,000 people each year in the United States alone. Controlling antibiotic resistance with a single effective new drug could produce billions in savings on costly acute care services.
Hepatitis C is another silent consumer of healthcare dollars, with Gilead’s sofosbuvir emerg-ing as 2014’s biggest new launch. But payers are likely to sound a skeptical note given the potential cost exposures—this is a ticket punched at rare disease prices—as well as the fact that the drug’s constituency includes many from society’s mar-
ginalized elements, who are unfamiliar with the concept of the “empowered patient.” It will be in-teresting to see if the hype around sofosbuvir ends up confrming an unpleasant truth about even the best planned product launches: the pace of market uptake is today measured in years, not months.
Advances are also emerging to add value to patients, even in the most crowded therapeutic segments. Despite all the options that exist in the anti-hypertensive class, thousands of patients are still non-responsive to conventional treat-ment and face heart disease, kidney failure, and an early death. In yet another indication of how technology is building a stronger treatment con-vergence between drugs and devices, Medtronic has developed a new last-ditch invasive proce-dure called renal denervation that can reverse the decline. It underscores the point that, for sick patients, no treatment arsenal for their condition can ever be considered too big.
Of course, none of these advances matter if they don’t get the opportunity to prove their clinical value to patients. Our panel on market access offered a blunt assessment of the indus-try’s state of play with payers, contending that in most countries the drug assessment process is opaque and overtly politicized; that good evi-dence rarely, if ever, moves the needle on access or reimbursement decisions; and the invitation to dialogue early in the development cycle is not grounded in commitments that extend to the fnal stage of marketing authorization and reimbursement. Unfortunately, the process mo-tivates both sides to lower their tolerance for risk—even though the best clinical innovations require more up front risk, not less.
It is also apparent from the discussion that those who drive the market access function are often isolated from their company’s top decision-makers, many of whom have had virtually no exposure to the messy work that goes into ana-lyzing and understanding that “payer perspec-tive.” Ultimately, the market access function is all about education—and the need to enlighten extends not just to the payer, but to the “c suite” as well. Remember: It’s the balm of consensus that perfumes the pipeline.
Payers: Late for the Party?
william LooneyEditor-in-Chief
Follow Bill on Twitter:
@BillPharmExec
ES349565_PE1113_010.pgs 11.04.2013 16:26 ADV blackyellowmagentacyan

• Increasing payor restrictions
• Barriers to speed to therapy
• Growing affordability concerns
• Educating patients on the clinical
of medication adherence
Omnicare SCG can help solve the
following challenges:
Set up your complimentary
Brand Workshop today!
We’ll assess your market challenges and develop
customized patient solutions to meet your unique
needs.
Join us for a collaborative workshop!
www.omnicarescg.com877-901-3711 [email protected]
ES345515_PE1113_011_FP.pgs 10.26.2013 02:43 ADV blackyellowmagentacyan
1212
PHARMACEUTICAL EXECUTIVE
Washington Report
It seems like open season on
the pharmaceutical industry.
Academics and consumer
activists charge pharma com-
panies with hiding clinical trial
information on medical product
safety, fueling the campaign to
expand public access to conf-
dential research information.
The federal government’s “Sun-
shine” program for disclosing
fnancial ties between industry
and physicians refects a lengthy
campaign to curb marketing
tactics perceived to boost inap-
propriate prescribing.
Media reports regularly at-
tack high drug prices, both for
life-saving specialty drugs and
for widely used treatments such
as asthma inhalers. And recent
disclosures raise questions about
too-close ties between pharma
companies and Food and Drug
Administration offcials.
The well-known industry re-
sponse to these and other charg-
es is that prescription drugs
account for only 10 percent of
US spending on healthcare and
that appropriate drug use saves
money by keeping people out of
hospitals and operating rooms.
Developing new drugs, more-
over, is enormously expensive
and risky, warranting strong
patent protection and a healthy
return on investment.
Such arguments, sadly, fail to
generate public confdence in the
biomedical research enterprise.
Public surveys give pharma com-
panies poor ratings, citing high
prices, low integrity, and failure
to disclose unfavorable safety
information. There’s a clamor
for valid data on drug effective-
ness and comparative prices, and
high hopes that health reform
initiatives will make such infor-
mation more transparent.
Data disclosure
One clear sign of the times is
the success of the campaign for
broader access to proprietary
clinical data. The conversation
already has shifted from data
“disclosure” to data “sharing,” as
sponsors seek strategies to retain
some control over proprietary
information in the face of the Eu-
ropean Medicines Agency (EMA)
proposal to release patient-level
clinical reports submitted in
regulatory dossiers beginning
January 2014. FDA is weighing
comments on its June 2013 query
about making available masked
and de-identifed data submitted
in applications. And an Institute
of Medicine committee began
deliberations last month on “Re-
sponsible Sharing of Clinical
Trial Data,” with the intent of
issuing guiding principles and a
framework for such initiatives.
An interim report is due in Janu-
ary, and a fnal report in De-
cember 2014 that will assess the
benefts and risks of data sharing
and opportunities for responsible
disclosure.
Pharma companies in the
United States and Europe are
pressing hard to modify or post-
pone the EMA data release plan
so that third-party programs and
voluntary initiatives will gain
time to demonstrate that they
can enhance data transparency
while protecting patients and the
research enterprise. There is gen-
eral agreement that clinical data
sharing can be benefcial in im-
proving the effciency of clinical
trials, validating regulatory deci-
sions, and increasing public con-
fdence in clinical research. But
sponsors are leery about who
controls access to data, the pur-
poses of disclosure, and the ad-
equacy of safeguards to protect
all parties.
A related fear is that releasing
full regulatory dossiers could
expose proprietary formulation
and manufacturing data and
information on product devel-
opment and future indications.
And public access to clinical
data could undermine product
exclusivity in countries such as
Australia, Brazil, China, and
Korea that link exclusivity to
data confdentiality, explained
Pfzer senior vice president Jus-
tin McCarthy at a Pharmaceuti-
cal Research and Manufacturers
Transparency Troubles for PharmaHigh prices, murky fnancial relations, and a reluctance to
disclose clinical data undermine public trust in industry and
the research enterprise.
Jill Wechsler is Pharm Exec’s Washington correspondent. She can be reached at
Public surveys give pharma companies poor ratings, citing high prices, low integrity, and failure to disclose unfavorable safety information.
ES347246_PE1113_012.pgs 10.30.2013 18:45 ADV blackyellowmagentacyan
13
NOVEMBER 2013 www.PharmExec.com
Washington Report
of America (PhRMA) briefng in
October. He warned that if the
EMA proceeds with its plan for
full release of regulatory submis-
sions, companies may rethink
their development and registra-
tion strategies, possibly by de-
laying submissions for approval
in Europe or limiting confden-
tial commercial information in
dossiers.
To head off the EMA pro-
posal, sponsors are rolling out
voluntary data sharing initia-
tives, as outlined in a “prin-
ciples” document issued in July
by PhRMA and the European
Federation of Pharmaceutical
Industries and Associations
(EFPIA). Companies are form-
ing independent scientifc re-
view boards to evaluate outside
data requests and procedures
to protect patient privacy. But
there’s a lot of skepticism about
how comprehensive and impar-
tial these programs will be.
Paying for access
Data sharing is integral to mul-
tiple FDA-industry partnerships
formed to evaluate and validate
innovative research methods to
accelerate testing of new drugs
and medical products. Yet such
initiatives frequently draw fre as
opportunities for industry to in-
fuence regulatory decision-mak-
ing. FDA’s increased reliance on
user fees, as well as its interest in
accelerating the development and
approval of breakthrough drugs,
prompt critics to question the ob-
jectivity and completeness of the
agency’s evaluation of new, risky
medicines.
FDA is examining whether
its policies for managing public-
private partnerships are suff-
ciently transparent and ethical
following a report that industry
“paid to play” in collaborative
efforts to improve the develop-
ment and testing of new opioids
and other pain medications. A
headlined article in the Wash-
ington Post (Oct. 10, 2013)
claimed that to participate,
pharma companies had to pay
a $25,000 sponsor fee to the
meeting organizers. Although
the cited activities are based on
10-year-old e-mail communica-
tions and have been superseded
by other FDA initiatives and
policies, Congress may investi-
gate the case, partly in light of
strong public concerns about
the marketing and distribution
of illegal opioids.
Trust critical
Low credibility with the pub-
lic and the medical community
makes it diffcult for pharma
companies to make their case on
these thorny policy issues. The
current level of trust in industry-
funded research and study re-
sults “is extremely low,” observe
Lisa Egbuonu-David, director
of ROI-Squared, and Tanisha
Carino, senior vice president at
Avalere Health, in a commen-
tary published by Health Affairs
in September. This “trust co-
nundrum,” they note, makes it
more challenging for sponsors
to produce credible evidence of
the value of new drugs. And such
evidence is key to justifying cov-
erage by payers and pharmacy
beneft managers, particularly for
costly but critical specialty drugs.
The authors emphasize that
it is important to restore trust
in industry-sponsored research
and to develop innovative mod-
els for obtaining evidence of
real-world effectiveness, in a
world with increased transpar-
ency in the cost of hospital pro-
cedures, medical care, and out-
of-pocket spending on medical
products that makes consumers
more conscious of perceived ex-
cessive charges for medical care.
Pharmaceutical companies need
to conduct real-world studies on
products and be able to discuss
results with key decision-mak-
ers. A comprehensive, consistent
approach to measuring the clini-
cal value of medical products
is central to a framework that
encourages industry funding of
scientifcally valid research for
all stakeholders.
Debating Tax DeductionsThe overhaul of the US corporate tax structure is still a top priority
for the business community, which seeks to lower the current 37
percent rate to enhance the global competitiveness of US compa-
nies. However, there continues to be debate over how low to go.
The Coalition for Healthcare Communications and the Advertising
Coalition fear that pushing corporate taxes down to the low 20s
will lead to curbs on tax deductions for advertising and promo-
tion. All marketing costs now are deductible, but proposals have
surfaced over the years to limit the break for consumer advertis-
ing, particularly expenditures on prescription drug ads. Without
the deduction, marketing costs increase by the tax rate, i.e., by 20
or 30 percent, explains CHC director John Kamp. Some pharma
companies are staying neutral on the issue, though, saving their
ammunition for policies favorable to intellectual property protec-
tion and tax treatment of foreign revenues.
ES347244_PE1113_013.pgs 10.30.2013 18:45 ADV blackyellowmagentacyan

SPECIAL SPONSORED SECTION
Front Center&Aligning Distribution Strategies with New Reimbursement and Market Landscapes
As the Affordable Care Act contin-
ues to unfold, bringing 27 million
new patients into the healthcare
system, the reimbursement landscape is
rapidly shifting. In addition, the specialty
market, particularly oncology, is under-
going a series of important changes.
To understand how new and criti-
cally important trends impact the com-
mercial success of specialty pharma-
ceuticals, McKesson Specialty Health
conducted a workshop during CBI’s
Bio/Pharmaceutical Retail Strategy
Summit on September 19, 2013.
McKesson Specialty Health’s work-
shop, entitled “Navigate the Reimburse-
ment Landscape and Align your Distri-
bution Strategies,” focused on the state
of the specialty pharmaceutical industry
for the next fve years, and the need to
create fexible distribution strategies to
take advantage of changing trends in re-
imbursement and the overall market.
The site of delivery of oncology care
has undergone many changes over the
past few years with many practices join-
ing large networks or hospital groups,
largely driven by changes in reimburse-
ment and legislation. This is happening
at a time when oncology is experiencing
other important transformations such as
the growth of targeted therapies requir-
ing biomarker testing, the rise of oral on-
colytics, the introduction of biosimilars
and cancer vaccines, and the growing
treatment choices and complexity in any
given cancer type.
Pharmaceutical and biotech compa-
nies need to be familiar with these chang-
es while creating novel distribution strat-
egies to enable the delivery of the right
product through the right channel at the
right time and at the right price.
An Eye To The Future
Kicking off the workshop was a review
of the results from a survey distributed to
the registered attendees prior to the work-
shop. The survey asked the respondents
what they thought the specialty market
would look like by 2018. Most believed
it would be “slightly different,” according
to presenter Anne Hoang, senior man-
ager of Corporate Strategy & Business at
McKesson. CBI respondents believed spe-
cialty pharmacies and patients will gain
infuence on driving brand volume. Con-
sequently, respondents expected a shift in
brand spend with more dollars allocated
to supporting and interacting with pa-
tients and pharmacists. Payers were also
expected to see an increase in spend.
“As we see a blurring of the lines be-
tween healthcare stakeholders, we often
ask our manufacturer customers: are
you doing enough to explore collabora-
tion with payers and employers?” Hoang
asked. “With the complexity of pay-
ments, many are starting to implement
risk sharing schemes; if you are not at
least experimenting today, it will be dif-
fcult to start that process in a few years.”
The specialty market’s future includes
familiar challenges of high operating
costs as well as the complexity of its
therapies. And now there’s the Afford-
able Care Act, changes in regulations
that include sequestration and 340(b),
as well as the rise of precision medicine
and changing reimbursement incentives -
all of which will have a direct effect on
where, how and by whom products are
acquired and used. When asked about
their current and expected shifts in dis-
tribution strategies, the survey respon-
dents expected a shift towards exclusive,
limited and direct distribution.
There is good news on the commer-
cial side for the specialty market: the
market is projected to grow from $92 bil-
lion in 2013 to $140 billion in 2017, said
Heather Morel, vice president and gener-
al manager, Informatics, Access & Safe-
ty Services, McKesson Specialty Health,
and second presenter at the workshop. By
2017, specialty will account for 40 to 45
percent of the total pharma market (in $
sales), and oncology alone will account
for 30 percent of the specialty market.
Within the oncology market, oral
products’ share of the market is expect-
ed to nearly double, from 22 percent in
2013, to 43 percent in 2018.
“While an important portion of the
market will be occupied by orals, there
is still going to be a signifcant portion
of the market that will be buy-and-bill,”
Morel predicted. “That will still require
getting product to the physician’s offce
so it can be administered.”
The Changing Face of Practice
Changes within the oncology sites of
care began years ago. “Over the past fve
years, many community oncology clin-
ics closed their doors, merged or joined
a network or hospital program,” said
Devon Dickey, vice president, Business
Development, Supply Chain Services,
McKesson Specialty Health, and the
third workshop presenter. Those changes
were largely driven by economic pres-
sures on practices facing increasing costs
ES347253_PE1113_014.pgs 10.30.2013 18:45 ADV blackcyan

SPECIAL SPONSORED SECTION
and decreasing reimbursement, as well
as economic incentives such as 340(b)
favoring hospitals.
As pharmaceutical and biotech com-
panies adapt their strategies to shifting
sites of care, they must also think ahead
and anticipate future changes. In a re-
port released in August 2013, the Moran
Company found that costs of outpatient
cancer care were 47% higher for Medi-
care benefciaries in the hospital outpa-
tient setting compared to those treated
in community practices. In light of such
results, pharmaceutical executives must
ask themselves if the current trend to-
wards patient care in a hospital outpa-
tient setting is sustainable. They must
also anticipate future trends.
The rise of oral oncolytics greatly
impacts community oncology practices
in several ways. While some practices
dispense oral medications, others rely
on pharmacy channels. Depending on
the way practices provide their patients
with access to oral therapies, methods of
compliance and monitoring may vary.
Practices must work in tandem with
other stakeholders such as pharmacists
and support services to educate, monitor
and help patients adhere to their treat-
ment, which often includes several medi-
cations. Practices, like pharmaceutical
and biotech companies, must adapt to
varying distribution channels and fnd
ways to ensure appropriate therapy and
provide compliance support to patients.
In addition, the rise of targeted
cancer therapies and immunotherapies
selected based on a patient’s genetics,
is expected to account for more than
60 percent of cancer therapeutics sales
by 2017 [Data Monitor, 2010]. More
than half of all cancer treatments in
early stage development rely on bio-
markers for patient selection. The use
of biomarkers may allow physicians to
predict a likely or unlikely response to
a specifc treatment in a matter of days,
rather than having to wait months.
As hopeful as that sounds, the future
of biomarkers and molecular testing is
cloudy. Little agreement exists on which
biomarkers are important, or what test-
ing methodologies are most effective –
both of which leave payers skeptical.
“If payers can’t identify what they
are paying for, it is much more diffcult
to get it paid,” Morel said. “McKes-
son Specialty Health is taking an ac-
tive hand in developing reimbursement
codes and working to codify which
molecular tests are being run. We are
developing standards around the kinds
of tests that should be done, such as
standard molecular panels around co-
lon, breast and other tumors. Payers
are more likely to pay once shown that
molecular testing is being used appro-
priately and productively.”
Fundamental changes to the health-
care landscape
The Affordable Care Act and its infux
of new patients into the healthcare sys-
tem, along with government-sponsored
plans and exchanges, add more stake-
holders and important infuencers to
the mix. Market consolidation means
fewer payers with a wider reach. How-
ever, with the advent of lower cost
health plans and the exchanges, the
burden of payment is on the patients,
which is likely to have large complica-
tions for expensive specialty care drugs.
According to an analysis by McKes-
son Specialty Health, sequestration is
costing the typical oncology practice
$30,000 per month in revenue. Most
of the loss is concentrated in 15 oncol-
ogy drugs. Providers are still providing
these drugs, but they are feeling the
fnancial pressure as well as increased
competition from hospitals, advantaged
through the benefts of drug acquisition
savings from participation in the 340(b)
program.
“Pharmaceutical companies need
real-time and actionable data on
reimbursement,” Morel said. “You must
have the ability to adjust strategies. The
reimbursement landscape shifts. While
it is diffcult to be nimble, deeply un-
derstanding what is happening to your
product and how it is fowing in the
marketplace real-time is essential.”
Adjusting Distribution Strategies
“Pharmaceutical and Biotech compa-
nies should consider a variety of factors
when evaluating distribution strate-
gies,” Dickey said. Four trends have
evolved over the past fve years: regu-
latory implications include the impact
of ACA, government policy decisions,
drug approvals and potential restric-
tions such as REMS. Changes in site
of care (hospital vs. clinic) also have a
direct impact on distribution channel
decisions. Payer decisions on reimburse-
ment affect utilization and distribution,
as does the evolution of patient popu-
lations as orphan launches turn into
products with multiple indications.
“As the population ages and survival
rates improve, cancer is becoming a
chronic disease that requires long term
treatment,” she said. “Physician pay-
ments for cancer care have decreased
14.5 percent in the past six years while
hospital payments have risen by 19.5
percent. The question is, are these pay-
ment advantages and changes in site of
care sustainable? So when you’re look-
ing at your distribution strategy—what
you thought fve years ago may no lon-
ger be viable. You need to look at what
is going on today and, more important-
ly, anticipate the next fve years and the
impact of the market changes on your
product and disease state”.
Dickey summarized by saying that
one needs to be smart in the present
to be proftable in the future. “Decide
where a product should and is likely to
be distributed in the future and then de-
sign your distribution channel with that
fexibility in mind.”
brought
to you by
ES347254_PE1113_015.pgs 10.30.2013 18:45 ADV blackmagentacyan
16
PHARMACEUTICAL EXECUTIVE
Pipeline Report
2014 PIPELINE REPORT:
The Sprintto ValueT
his year’s pipeline report is a little different from reports in previous years
in that it takes a closer look at fewerer categories -- the ones where the
biggest things are happening: cancer, heart failure, obesity and diabetes,
and hepatitis C, in addition to novel antibiotics, not a goldmine by any stretch,
but an absolutely critical need. The last category, Outsiders, Sleepers, and Early
Stagers, describes products that don’t f t neatly into this year’s setup, but are
nevertheless worthy of mention. In October, a study in Nature Reviews Drug Dis-
covery took pharma analysts to task for getting the numbers wrong—a lot—but
we’ve endeavored to corroborate the forecasts, both bullish and bearish, and are
conf dent that this year’s report spotlights real value, for patients and bottom-
lines. The pharma business model might have changed, but a lot of companies
have managed to hold on to their blockbusters.
Image: Tilton Widro
Genome-guided tumor diagnostics
and treatments with the power to
manipulate a patient’s immune response
have the potential to impact cancer
outcomes in dramatic fashion. At the
Cleveland Clinic’s recent Medical
Innovations Summit (see Pharm Exec’s
Back Page this month), Eric Klein, chair
at the Clinic’s Glickman Urological &
Kidney Institute, championed the work
of companies like Genomic Health
Inc.—and its recently CLIA-approved
OncoType Dx prostate cancer assay—as
critical to the future of cancer research
and drug development. The genotype of
a tumor may prove to be more useful
than the genotype of the patient in
which it resides. If identifying a “driver
mutation” in metastatic cancers turns
out to work in practice, it won’t matter
where a tumor originated in the body.
Consequently, “drug development will
be more rapid as a result,” says Klein.
Designing clinical trials around a
specif c tumor mutation instead of a
patient’s cancer type probably won’t
start happening next year. In the short-
er term, immunotherapies have main-
tained their buzz among researchers,
with a spotlight on the role of Pro-
Cancer: Multiple Targets
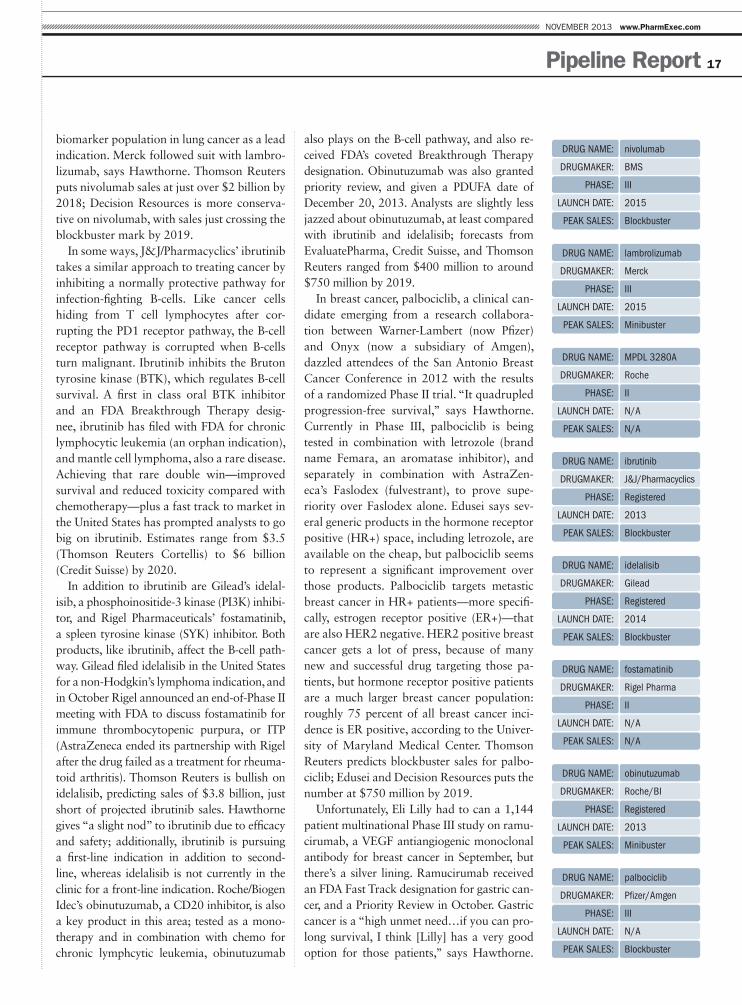
grammed Death-1 (PD1) as a way to
cut off one important safe harbor for
cancer cells looking to protect them-
selves from warring T cells. In addition
to Bristol-Myers Squibb’s nivolumab—
which received FDA Fast Track desig-
nations in malignant melanoma, renal
cell carcinoma and non-small cell lung
cancer last April, Stephanie Hawthorne,
director, clinical, and scientif c assess-
ment at Kantar Health, points to Mer-
ck’s lambrolizumab and Roche’s MPDL
3280A as key players in the PD1 game.
Compared with nivolumab, Roche’s
MPDL 3280A (which targets the PD1
ligand—PD-L1—as opposed to the re-
ceptor) may have a better safety prof le,
while Merck’s lambrolizumab may beat
nivolumab on eff cacy, although it’s too
early for excessive conf dence on that
prediction, says Hawthorne.
Lambrolizumab also received FDA’s
Breakthrough Therapy designation last
April, and clinical trials are initially fo-
cused on melanoma and non-small cell
lung cancer. Nivolumab is targeting
melanoma and lung cancer, with the ad-
dition of renal cell carcinoma in Phase
III. Merck announced plans to study
lambrolizumab in other haematolgical
malignancies, and has early trials run-
ning in triple negative breast cancer,
colorectal cancer, bladder cancer, and
other solid tumor cancers. Thompson
Reuters’ Cortellis database puts sales of
lambrolizumab at roughly $845 million
by 2018; Decision Resources’ Efua Edu-
sei made a similar prediction, around
$800 million by 2019. “Merck would
def nitely have a better commercial op-
portunity if Yervoy wasn’t already on
the market,” notes Edusea, adding that
nivolumab could eventually restrict sales
of lambrolizumab. With Zalboraf also
looming large in the melanoma space,
the initial label, launch date, and time-
line for additional indications on both
drugs could open or block the entrance
to blockbuster fame and revenues.
Roche is taking a different approach by
shifting melanoma to the backburner;
instead, MPDL 3280A is targeting the
By Ben Comer, Senior Editor
ES349928_PE1113_016.pgs 11.05.2013 00:01 ADV blackyellowmagentacyan
17
NOVEMBER 2013 www.PharmExec.com
Pipeline Report
biomarker population in lung cancer as a lead
indication. Merck followed suit with lambro-
lizumab, says Hawthorne. Thomson Reuters
puts nivolumab sales at just over $2 billion by
2018; Decision Resources is more conserva-
tive on nivolumab, with sales just crossing the
blockbuster mark by 2019.
In some ways, J&J/Pharmacyclics’ ibrutinib
takes a similar approach to treating cancer by
inhibiting a normally protective pathway for
infection-fghting B-cells. Like cancer cells
hiding from T cell lymphocytes after cor-
rupting the PD1 receptor pathway, the B-cell
receptor pathway is corrupted when B-cells
turn malignant. Ibrutinib inhibits the Bruton
tyrosine kinase (BTK), which regulates B-cell
survival. A frst in class oral BTK inhibitor
and an FDA Breakthrough Therapy desig-
nee, ibrutinib has fled with FDA for chronic
lymphocytic leukemia (an orphan indication),
and mantle cell lymphoma, also a rare disease.
Achieving that rare double win—improved
survival and reduced toxicity compared with
chemotherapy—plus a fast track to market in
the United States has prompted analysts to go
big on ibrutinib. Estimates range from $3.5
(Thomson Reuters Cortellis) to $6 billion
(Credit Suisse) by 2020.
In addition to ibrutinib are Gilead’s idelal-
isib, a phosphoinositide-3 kinase (PI3K) inhibi-
tor, and Rigel Pharmaceuticals’ fostamatinib,
a spleen tyrosine kinase (SYK) inhibitor. Both
products, like ibrutinib, affect the B-cell path-
way. Gilead fled idelalisib in the United States
for a non-Hodgkin’s lymphoma indication, and
in October Rigel announced an end-of-Phase II
meeting with FDA to discuss fostamatinib for
immune thrombocytopenic purpura, or ITP
(AstraZeneca ended its partnership with Rigel
after the drug failed as a treatment for rheuma-
toid arthritis). Thomson Reuters is bullish on
idelalisib, predicting sales of $3.8 billion, just
short of projected ibrutinib sales. Hawthorne
gives “a slight nod” to ibrutinib due to effcacy
and safety; additionally, ibrutinib is pursuing
a frst-line indication in addition to second-
line, whereas idelalisib is not currently in the
clinic for a front-line indication. Roche/Biogen
Idec’s obinutuzumab, a CD20 inhibitor, is also
a key product in this area; tested as a mono-
therapy and in combination with chemo for
chronic lymphcytic leukemia, obinutuzumab
also plays on the B-cell pathway, and also re-
ceived FDA’s coveted Breakthrough Therapy
designation. Obinutuzumab was also granted
priority review, and given a PDUFA date of
December 20, 2013. Analysts are slightly less
jazzed about obinutuzumab, at least compared
with ibrutinib and idelalisib; forecasts from
EvaluatePharma, Credit Suisse, and Thomson
Reuters ranged from $400 million to around
$750 million by 2019.
In breast cancer, palbociclib, a clinical can-
didate emerging from a research collabora-
tion between Warner-Lambert (now Pfzer)
and Onyx (now a subsidiary of Amgen),
dazzled attendees of the San Antonio Breast
Cancer Conference in 2012 with the results
of a randomized Phase II trial. “It quadrupled
progression-free survival,” says Hawthorne.
Currently in Phase III, palbociclib is being
tested in combination with letrozole (brand
name Femara, an aromatase inhibitor), and
separately in combination with AstraZen-
eca’s Faslodex (fulvestrant), to prove supe-
riority over Faslodex alone. Edusei says sev-
eral generic products in the hormone receptor
positive (HR+) space, including letrozole, are
available on the cheap, but palbociclib seems
to represent a signifcant improvement over
those products. Palbociclib targets metastic
breast cancer in HR+ patients—more specif-
cally, estrogen receptor positive (ER+)—that
are also HER2 negative. HER2 positive breast
cancer gets a lot of press, because of many
new and successful drug targeting those pa-
tients, but hormone receptor positive patients
are a much larger breast cancer population:
roughly 75 percent of all breast cancer inci-
dence is ER positive, according to the Univer-
sity of Maryland Medical Center. Thomson
Reuters predicts blockbuster sales for palbo-
ciclib; Edusei and Decision Resources puts the
number at $750 million by 2019.
Unfortunately, Eli Lilly had to can a 1,144
patient multinational Phase III study on ramu-
cirumab, a VEGF antiangiogenic monoclonal
antibody for breast cancer in September, but
there’s a silver lining. Ramucirumab received
an FDA Fast Track designation for gastric can-
cer, and a Priority Review in October. Gastric
cancer is a “high unmet need…if you can pro-
long survival, I think [Lilly] has a very good
option for those patients,” says Hawthorne.
Drug Name: nivolumab
Drugmaker: BmS
PhaSe: III
LauNch Date: 2015
Peak SaLeS: Blockbuster
Drug Name: lambrolizumab
Drugmaker: merck
PhaSe: III
LauNch Date: 2015
Peak SaLeS: minibuster
Drug Name: mPDL 3280a
Drugmaker: roche
PhaSe: II
LauNch Date: N/a
Peak SaLeS: N/a
Drug Name: ibrutinib
Drugmaker: J&J/Pharmacyclics
PhaSe: registered
LauNch Date: 2013
Peak SaLeS: Blockbuster
Drug Name: idelalisib
Drugmaker: gilead
PhaSe: registered
LauNch Date: 2014
Peak SaLeS: Blockbuster
Drug Name: fostamatinib
Drugmaker: rigel Pharma
PhaSe: II
LauNch Date: N/a
Peak SaLeS: N/a
Drug Name: obinutuzumab
Drugmaker: roche/BI
PhaSe: registered
LauNch Date: 2013
Peak SaLeS: minibuster
Drug Name: palbociclib
Drugmaker: Pfzer/amgen
PhaSe: III
LauNch Date: N/a
Peak SaLeS: Blockbuster
ES349940_PE1113_017.pgs 11.05.2013 00:01 ADV blackyellowmagentacyan

18
PHARMACEUTICAL EXECUTIVE
Pipeline Report
Interestingly, ramucirumab targets the VEGF
receptor, whereas Avastin targets the ligand.
Avastin failed in Phase III trials for gastric can-
cer, which raises the question: is there a true
mechanistic difference in targeting the recep-
tor versus the ligand? If so, “these angiogenics
will start to separate themselves in terms of
where they might be active,” says Hawthorne.
Sanof/Regeneron haven’t announced plans
to test Zaltrap in gastric cancer, but Clinical-
Trial.gov shows a Phase II study of Zaltrap for
esophagogastric cancer, a malignancy in the
throat as opposed to the stomach. Gastric can-
cer incidence in Japan has risen sharply in re-
cent years; Decision Resources says the global
gastric cancer market will reach $2.3 billion
by 2021, with 44 percent of those revenues
coming from Japan. Thomson Reuters pegs
ramucirumab sales at $725 million by 2018,
Leerking Swann says $1.3 billion by 2020.
Drug Name: ramucirumab
Drugmaker: eli Lilly
PhaSe: registered
LauNch Date: 2014
Peak SaLeS: Blockbuster
Patients entering emergency rooms in the
United States are more likely to be there
as a result of acute heart failure than for any
other reason. In the last 25 years, heart failure
incidence has increased by about 175 percent,
and what’s worse is that drug development
in this high need area has been abysmal,
says Martin Sullivan, executive medical
director of cardiovascular medicine at INC
Research, and a board certifed internist and
cardiologist. Heart failure has been an “arena
of therapeutic futility…there have been
probably 20 candidate compounds tested
over the last 15 years, and we’re zero for 20
on these compounds,” says Sullivan.
That could change with Novartis’s serelaxin,
a peptide hormone currently under review in
the United States and Europe. FDA granted Fast
Track status in 2009, and Breakthrough Ther-
apy status last summer; Sullivan says serelaxin
could be a “home run” for heart failure. Citing
the RELAX-AHF Phase III data, Sullivan says
serelaxin “had a reduction in dyspnea, a small
improvement in [hospital] length of stay, and
most importantly, a signifcant reduction in re-
hospitalizations and death in 90 days.” Serelax-
in is a recombinant form of human relaxin-2, a
naturally occurring hormone; pregnant women
release relaxin during labor, which causes liga-
ments to relax and become more fexible to
facilitate childbirth. Using a hormonal treat-
ment like serelaxin for heart failure is interest-
ing because “it has so many different effects on
so many different pathways,” says Sullivan. “It
effects infammation, fbrosis, cell cyclin, it’s a
vasodilator, it does all kinds of things.”
It could also make Novartis the proud
parents of a new blockbuster for acute heart
failure. Thomson Reuters predicts sales of
roughly $1.2 billion by 2019, and serelaxin
could receive European approval by this year’s
end. Seamus Fernandez, managing director of
major and specialty pharmaceuticals at Leer-
ink Swann, wrote in a recent analyst note that
serelaxin’s Breakthrough Therapy status did
not confer an expedited FDA review of the
drug, according to Novartis management, but
the company expects a US approval in late
2014. Leerink Swann is predicting $1.3 bil-
lion in sales for serelaxin by 2020.
Sullivan also points to Acorda Thera-
peutics GGF2 candidate—a naturally oc-
curring neuregulin or growth factor—and
the results of an early stage trial, which im-
proved some patients’ ejection fraction by
nine percent. Ejection fraction is a measure
of how effectively the heart pumps blood.
Like serelaxin, GGF2 is a peptide prod-
uct with multifaceted effects in the body,
including “cell cyclin, cell death, CNS ef-
fects…and it effects cell programming a
little bit, potentially in vivo,” says Sullivan.
After a 24-hour infusion, patients given
a higher dosage of GGF2 showed a heart
function improvement at 28 days and 90
days. Acorda said it has discussed a new
trial protocol with FDA for 2013, presum-
ably a Phase II study, but ClinicalTrials.gov
shows only a small Phase Ib double-blind
study testing a single GGF2 infusion for
safety and tolerability. This product may
be further off, but Sullivan says if the data
holds through Phase III, “that would be a
major advance in heart failure.”
Incidentally, the Chinese company Zensun
is also testing a neuregulin drug candidate
Heart Failure: Possible Success
Drug Name: serelaxin
Drugmaker: Novartis
PhaSe: III
LauNch Date: 2014
Peak SaLeS: Blockbuster
Drug Name: ggF2
Drugmaker: acorda
PhaSe: Ib
LauNch Date: N/a
Peak SaLeS: N/a
Drug Name: Neucardin
Drugmaker: Zensun
PhaSe: II
LauNch Date: N/a
Peak SaLeS: N/a
ES349935_PE1113_018.pgs 11.05.2013 00:01 ADV blackyellowmagentacyan
19
NOVEMBER 2013 www.PharmExec.com
Pipeline Report
called Neucardin for chronic
heart failure. A Phase II trial has
been completed in the United
States, and drug has been fled
already in China. The company
is currently enrolling a Phase III
trials in the United States, but
Phase II data was less impres-
sive than Acorda’s. However, a
Zensun press release states that
678 people with chronic heart
failure have been given Neucar-
din, and Phase II data demon-
strated a “three to fve percent
placebo corrected improvement
in left ventricular ejection frac-
tion.” SciClone Pharmaceuticals
will market Neucardin in China,
in a deal worth upwards of $30
million if Zensun meets its regu-
latory milestones. Forecasting
for GGf2 and Neucardin is too
Device AlertIn hypertension, Sullivan says companies are tweaking the pharmacology of existing drugs, but
there isn’t a real gamechanger on the horizon. However, a minimally invasive procedure called renal
denervation “is the real breakthrough,” says Sullivan. Medtronic Vascular is currently enrolling a
580-patient Phase III trial to test its catheter-based renal denervation system for patients. That
trial, called SYMPLICITY HTN-4, is one of several the company is conducting, including a compre-
hensive observational trial with a read-out scheduled for next October. Medtronic introduced its frst
renal denervation Simplicity catheter in 2010, but the renal denervation system is currently only
available for investigation use in the United States. However, Medtronic announced in March that
FDA and CMS would conduct a parallel review to determine approval and to make a national cover-
age determination for Medicare patients. At the end of October, Medtronic presented three-year
results from its Symplicity HTN-2 trial; the data indicated an average blood pressure reduction of
-33/-14 mm from baseline, and an overall response rate of 85 percent.
Sullivan says physicians have “dozens of patients in their practices that are literally on fve drugs,
and they walk into the offce with a blood pressure of 180/100…and those patients do terrible, they
go into renal failure, stroke, and heart failure.” Clinical trials using renal denervation in these patients
“all look really good,” says Sullivan. “A drop in systolic blood pressure by 30mm is a big advance.”
Other companies, including St. Jude Medical and Boston Scientifc are also working on renal denerva-
tion for hypertension, but Medtronic currently leads the category. A Transparency Market Research
report predicts that the renal denervation market will grow to $1.9 billion by 2021, up from $88.5 mil-
lion in 2012. Medtronic’s share of the market in 2012 was a whopping 85%, according to the report.
$UH\RXORRNLQJIRUDQHIIHFWLYHZD\WRSUHVHQW\RXUSURGXFWVWRNH\GHFLVLRQPDNHUVLQWKHSD\RUPDUNHW"73*1DWLRQDO3D\RU5RXQGWDEOHLVDRQHRIDNLQGRSSRUWXQLW\WKDWSURYLGHV
$FFHVVWR0HGLFDO'LUHFWRUVDQG 3KDUPDF\'LUHFWRUV
)HHGEDFNRQSURGXFWSRVLWLRQLQJ DQGPDUNHWVWUDWHJLHVIRUWKH SD\RUPDUNHW
,QWHUDFWLYH(GXFDWLRQDO3URJUDPV ZKHUHGHFLVLRQPDNHUVPHHW
73*1DWLRQDO3D\RU5RXQGWDEOHRIIHUVXQLTXHDFFHVVWKURXJK
2QHGD\5RXQGWDEOH3URJUDPV
9LUWXDO5RXQGWDEOH3URJUDPV
0DUNHW5HVHDUFK
&XVWRPL]HG3URJUDPV
,VQ·WLWWLPH\RXKDGDVHDWDWWKHWDEOH"
&RQWDFW-LP6PHHGLQJ DWRUZZZWSJQSUWFRP
Get Your Seat at the Table!
“We saw 30 qualifi ed customer leads in one day and obtained quality market feedback on our products.”
Scan withSmartphone
Watch ourSuccess Story
ES349932_PE1113_019.pgs 11.05.2013 00:01 ADV blackyellowmagentacyan
20
PHARMACEUTICAL EXECUTIVE
20
PHARMACEUTICAL EXECUTIVE NOVEMBER 2013 www.PharmExec.com
Pipeline Report
speculative at this point to be meaningful, but
if any drug candidate shows it can improve
symptoms and survival in heart failure pa-
tients, the dollars will almost assuredly follow.
Last year’s pipeline covered the PCSK9
inhibitors—notably Amgen (AMG 145)
and Sanof/Regeneron’s (alirocumab) candi-
dates, both of which have important Phase
III data read-outs in 2014—but there isn’t
much new to report since last year aside
from forecasts on both drugs getting reined
in. Leerink Swann now estimates that AMG
145 won’t quite reach blockbuster status
by 2020, and Thomson Reuters scaled back
alirocumab to just under $500 million by
2019. Credit Suisse still thinks AMG 145
will reach blockbuster status by 2020, and
puts alirocumab’s sales at $865 million in
2020. During its 3Q earnings report in late
October, Pfzer announced a “major” Phase
III program for its PCSK9 inhibitor, called
bococizumab, according to an analyst note
from Fernandez at Leerink Swann. Three is
a crowd, so Pfzer tossing its hat into the
PCSK9 ring can’t be good news for Amgen
and Sanof/Regeneron.
Obesity and Diabetes: Two Birds One Stone
There’s still a lot to be said for the American
Dream (assuming it hasn’t succumbed to
heart failure), but the American Diet is not
worthy of admiration. “Other countries are
starting to live like us…and die like us,” said
Dean Ornish, president of the Preventative
Medicine Research institute, during the
Cleveland Clinic’s recent conference on
obesity and diabetes. “Weight loss can
reverse heart disease, prostate cancer, Type 2
diabetes” and other conditions, he said.
FDA has already approved two new obe-
sity drugs—Arena/Eisai’s Belviq, and Vivus’s
Qsymia—the frst FDA approvals for the
condition in over 15 years, but given the
size and extent of the health problem, not
to mention the cost, better treatments and
devices are needed. Future therapies will
attempt to target the “microbiome” or gut
fora, to change the way that food is synthe-
sized in the gastrointestinal tract. Anthony
Viscogliosi, principal at Viscogliosi Brothers,
a New York-based VC/private equity frm,
said he wants to invest in “meds that inhibit
fat syntheses…that can change the microbi-
ome to turn sugar and fat into water.”
Next-gen probiotics and nutraceuti-
cals could potentially impact the microbi-
ome—scientists have developed a trimethyl-
amine N-oxide (TMAO) assay that detects
TMAO—a microbial byproduct of intestinal
bacteria—in the blood, that is associated
with a 2.5-fold increase in stroke and heart
attack. But the microbial genome, or micro-
biome, contains about 3.3 million genes.
Compared with what we still don’t know
about the human genome, and its 23,000
genes, an active therapy for a specifc micro-
biome target probably won’t emerge in the
next couple of years. However, Steve Nissen,
the Cleveland Clinic’s department chair of
cardiovascular medicine, told conference-
goers that the TMAO biomarket “could take
off in 2014…and drugs will follow.”
In the shorter term, Orexigen Therapeu-
tics may be the most promising and lucra-
tive late-stage oral medication for the treat-
ment of obesity. In January, FDA asked for
additional cardiovascular outcomes data
and proposed a resubmission procedure for
Orexigen’s Contrave, a naltrexone/bupro-
pion combination pill, and the company ex-
pects to resubmit to FDA by the end of this
year. Orexigen appears to have faired better
in Europe; EMA has accepted its submission
under the centralized procedure, and Orexi-
gen expects approval in the second half of
2014. Despite a similar effcacy in compari-
son with Belviq and Qsymia, naltrexone/
bupropion is still getting blockbuster nods.
Thompson Reuters projects roughly $1.1 bil-
lion by 2019, and Credit Suisse corroborates
that approximation, putting 2020 sales at
$1.1 billion. Credit Suisse predicts very simi-
lar sales for both Belviq and Qysimia, which
suggests the level of need in the market, or
opportunities for the products to differenti-
ate from one another, or both.
Novo Nordisk is preparing to fle a 3-mg
version of its GLP-1 liraglutide (aka Victoza)
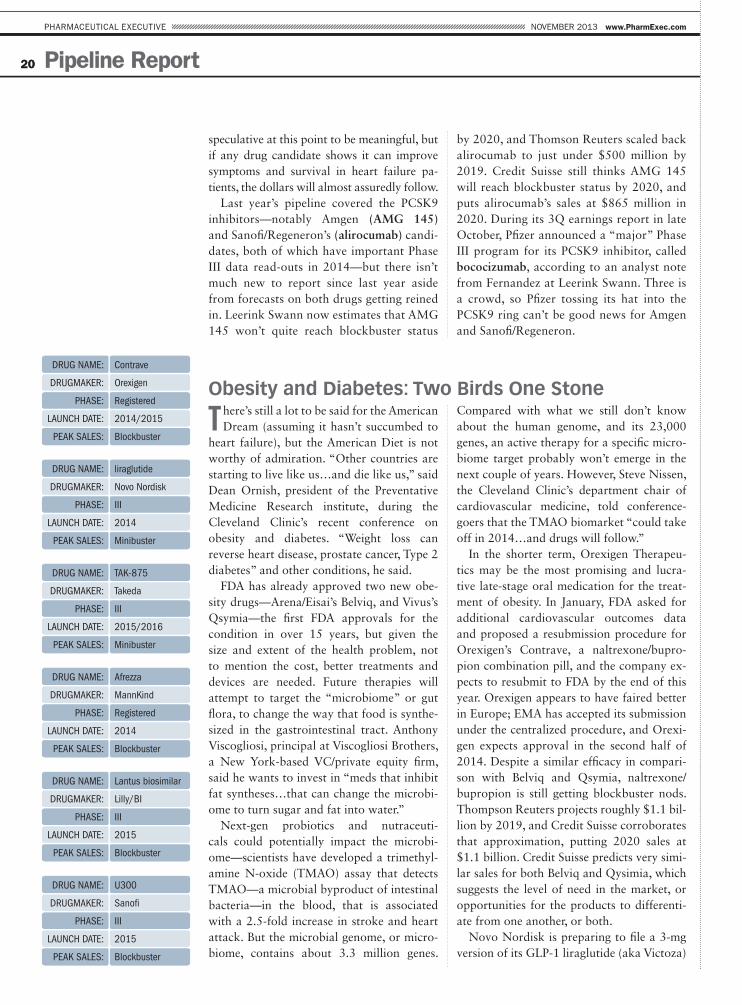
Drug Name: contrave
Drugmaker: Orexigen
PhaSe: registered
LauNch Date: 2014/2015
Peak SaLeS: Blockbuster
Drug Name: liraglutide
Drugmaker: Novo Nordisk
PhaSe: III
LauNch Date: 2014
Peak SaLeS: minibuster
Drug Name: tak-875
Drugmaker: takeda
PhaSe: III
LauNch Date: 2015/2016
Peak SaLeS: minibuster
Drug Name: afrezza
Drugmaker: mannkind
PhaSe: registered
LauNch Date: 2014
Peak SaLeS: Blockbuster
Drug Name: Lantus biosimilar
Drugmaker: Lilly/BI
PhaSe: III
LauNch Date: 2015
Peak SaLeS: Blockbuster
Drug Name: u300
Drugmaker: Sanof
PhaSe: III
LauNch Date: 2015
Peak SaLeS: Blockbuster
ES349930_PE1113_020.pgs 11.05.2013 00:01 ADV blackyellowmagentacyan

The Industry Channel Where Business Meets Policy
1. 2013 Industry Audit: Presentation by Bill
Looney, Editor Director,
Pharmaceutical
Executive, on key
trends identifi ed
from the analysis and
thoughts on the winner,
supplemented by an
interview with relevant
company executive.
2. Highlights of PE editorial RTs on
market access issues
and alternative R&D
fi nancing.
3. Conclusions from the 2013 Drug Pipeline review by Ben
Comer, Senior Editor,
Pharmaceutical
Executive.
4. Regulatory reform in China interview with
Ken Kaitin of Tufts
Center, by Bill Looney.
NEW PLATFORM. NEW CONTENT. NEW LAUNCH.
What makes PharmExec TV so exciting? You won’t see this on YouTube. PharmExec TV is exclusive to you. It’s positioned to provide essential content to assist with everyday work. We guarantee PharmExec TV:
To be serial programming
To have frequent content refreshment
To have editorially driven content
To have relevant content including market updates, breaking news, interviews, special features
PharmExec TVPROGRAMMING
HIGHLIGHTS
A NEW DIGITAL
OPPORTUNITY from
Pharmaceutical Executive editorial staff presents their
latest content in a brand new industry breaking format
ES345526_PE1113_021_FP.pgs 10.26.2013 02:44 ADV blackyellowmagentacyan

22
PHARMACEUTICAL EXECUTIVE
Pipeline Report
for an obesity indication in the United
States, and has entered Phase III trials in
over 20 countries for that indication. In
the United States, Novo will fle by the
end of this year, and expects to get an
approval in 2014. The company may try
to best the new raft of obesity treatments
by maximizing the label; in June, Novo
completed a Phase III trial studying
obese patients with sleep apnea. Clinical
studies indicate that liraglutide at 3 mg
could bring down body weight by an av-
erage of eight percent, a slight improve-
ment on Belviq and Qysmia, but liraglu-
tide is an injectable, not a pill, and it’s
expected to be costly. Gideon Heap, an
analyst with Decision Resources, says he
likes liraglutide in obesity for the follow-
ing reasons: “In theory, [liraglutide] will
avoid any of the CNS side effects that
trouble a lot of physicians in obesity, and
Novo also has some good trial designs
going,” says Heap. “They are develop-
ing it with a Phase II trial that attempts
to show prevention of the onset of Type
2 diabetes. If that gets a positive out-
come, I think it would represent a strong
bargaining chip for getting better reim-
bursement [over Belviq and Qsymia].”
Credit Suisse forecasts have liraglutide’s
obesity indication adding another $500
million a year to the increasingly lucra-
tive Victoza franchise, by 2019. Decision
Resources predicts roughly $800 million
by 2019, with a launch late next year.
Since 1997, there have been 10 new
classes of diabetes drugs, and yet, many
patients still aren’t able to keep their glyce-
mic levels under control. Takeda hopes to
bring an 11th class of drug to market with
its TAK-875 compound, a GPR40 ago-
nist. Currently in Phase III testing, TAK-
875 is going head-to-head against Janu-
via, and could potentially launch in 2015
or 2016, according to Heap. TAK-875 “is
causing a bit of excitement because it’s
showing good effcacy while maintaining
a high level of safety, of a kind you would
see with the DPP4 inhibitors,” says Heap.
“It’s as effcacious as sulfonylurea, but in
Phase II showed low rates of hypoglyce-
mia, and crucially, it doesn’t appear to in-
duce any kind of weight gain.”
Al Mann hopes to bring a new drug
delivery device to market; this time he’s
more hopeful than ever. In September,
Mann personally assured Pharm Exec
that Afrezza, a product that needs little
introduction, will receive its long-await-
ed FDA approval in April—if it isn’t ap-
proved somewhere else frst. Analysts
seem to agree that MannKind’s inhal-
able insulin will indeed get approved,
but a lingering question remains: will
patients want to use it? “There aren’t a
lot of patients out there demanding an
inhalable insulin,” says Heap. “Possibly,
the developers of these [inhalation] de-
vices are a bit carried away with how
important they think that is.” After com-
pleting two 24-week Phase III trials with
its next-gen Dreamboat inhaler device,
MannKind resubmitted with FDA in
October. Thomson Reuters is predict-
ing over $2 billion in sales, but Kiran
Meekings, a consultant at the Thomson
Reuters Life Sciences team, isn’t so sure.
She worries about the potential for ad-
verse pulmonary effects over the long
term. MannKind’s clinical work has at-
tempted to mitigate concerns about lung
function associated with chronic use
of an inhaled insulin, and Mann says
Afrezza “is not in the lungs very long,
we go quickly through the membrane
into the blood, with no accumulation.”
Meekings says MannKind’s pulmonary
safety study results “weren’t necessarily
cause for concern…but it’s something
that needs to be monitored.”
Finally, Eli Lilly and Boehringer Ingel-
heim are attempting to bring a biosimi-
lar insulin—the oldest biologic drug—
to market. The European Medicines
Agency (EMA) accepted the companies’
long-acting insulin glargine biosimilar
submission in July, and the product is
in Phase III in the United States. Insulin
glargine, also known as Lantus, is Sano-
f’s top seller, with over $6 billion in sales
last year. Credit Suisse is bullish on the
biosimilar version, with predicted sales
topping $1.2 billion by 2019, not bad
for a copycat. Thomson Reuters is more
conservative, with a forecast of $415
million in annual sales for the biosimilar
by 2019. Sanof, for its part, is rushing
forward on U300, a reformulated insu-
lin glargine; the company said during
a 3Q conference call that it would fle
in the United States and Europe during
the frst half of 2014. That product’s
new attributes, according to Sanof, are
fewer incidences of hypoglycemia, and
a smaller volume of subcutaneous injec-
tion compared with Lantus. Incidentally,
Lantus loses patent protection in 2015.
Novo Nordisk, the biggest seller of in-
sulins worldwide, hopes to wrest back
marketshare from Sanof, but prob-
ably won’t get Tresiba approved in the
United States before 2016, at the earliest.
Thomson Reuters estimates the new and
improved version of Lantus will earn
$1.1 billion by 2019, a fraction of Lan-
tus’s current annual sales.
Device AlertOn the device front, GI Dynamics’ EndoBarrier, an intestinal liner that doesn’t require
surgery to implant, is currently being tested in a 500-patient pivotal Phase III study in
the United States. “The product works more like a drug, but it’s technically a device,”
says Stuart Randle, CEO at GI Dynamics. Already commercially available in the United
Kingdom, Germany, Australia, Israel, Chile, and elsewhere, the EndoBarrier has shown “a
reduction in HbA1c levels [the key measure of glycemic control in diabetes], a signif-
cant reduction in weight, but also statistically signifcant reductions in blood pressure,
cholesterol, triglycerides, and other cardiovascular markers,” says Randle. The total cost
of the device and procedure, on average, is $10,000. Randle says the typical EndoBar-
rier patient is on one or two diabetes drugs, is obese, and is moving toward or is already
on insulin therapy. The Phase III study will read out in the frst half of 2016, and Randle
anticipates an FDA Premarket Approval (PMA) and US commercial launch in 2017.
ES349926_PE1113_022.pgs 11.05.2013 00:00 ADV blackyellowmagentacyan

23
NOVEMBER 2013 www.PharmExec.com
Pipeline Report
Hepatitis C: Banking on Sofosbuvir
Ben Weintraub, senior principal and
director of research at inThought, a
division of Symphony Health Solutions, calls
his $3 to $4 billion sales estimate on Gilead’s
sofosbuvir—a nucleoside analog polymerase
inhibitor targeting all six HCV genotypes—
conservative. “The question is not whether
sofosbuvir is going to be the biggest drug for
hepatitis C ever, or the biggest drug launch
ever…I think everyone agrees that it’s going
to be both of those things,” says Weintraub.
“The question is whether it’s going to be the
biggest drug ever.”
Weintraub says he’s seen estimates as high
as $15 billion, but the reason for his conser-
vatism is the misguided assumption that the
population of hepatitis C patients receiving
treatment will rise from a current level of
10 percent, to as much as 90 percent once
interferon, and it’s horrid side effects, are
taken out of the picture. Weintraub thinks
the percentage of HCV patients receiving
treatment will only increase to around 20
percent. The price of therapy is one access-
limiting element, but more importantly,
says Weintraub, is the fact that a substantial
portion of the HCV population won’t all of
sudden come in to the clinic for sofosbuvir,
or any other HCV drug. “If you’re an IV
drug user, if you’re homeless and you have
HCV, getting treated for it is not your pri-
mary concern,” says Weintraub. “Your de-
pression, your alcoholism, your drug abuse,
your 12 other diseases, those are the things
that doctors might be more worried about
taking care of frst.”
Several analysts including Weintraub
say sofosbuvir will receive FDA approval
by the end of this year. Sofosbuvir will be
prescribed in combination, but Weintraub
says it’s likely to be priced per regimen,
not per drug, at “whatever the market will
bear, $70,000 for sofosbuvir, riboviron and
a protease inhibitor, whatever that winds
up being.”
Raghuram Selvaraju, managing director
and head of healthcare equity research at
Aegis Capital Corp., says Enanta/AbbVie’s
ABT-450 combo is “every bit as good as
sofosbuvir,” but isn’t getting as much press
because the combination regimen will likely
be three or four drugs, instead of potentially
two with sofosbuvir. Selvaraju says both so-
fosbuvir and ABT-450 “are very, very good
at treating genotype-1 treatment naïve pa-
tients”—the largest HCV genotype glob-
ally, and the hardest to treat—“but they are
much less good at treating null responders.”
After the initial fanfare surrounding sofos-
buvir’s “marquee drug launch,” Selvaraju
says the quad ABT-450 regimen “is going to
show better activity against null responders
with genotype 1 than the sofosbuvir two-
drug regimen.” Phase III data from two
ABT-450 studies are scheduled to read out
this quarter, but the product isn’t expected
to launch until 2015. However, FDA gave
ABT-450 Breakthrough Therapy status in
May, which doesn’t automatically confer
an expedited approval, but could possibly
tip approval into 2014. On a recent AbbVie
earnings call, CEO Rick Gonzalez told in-
vestors that ABT-450’s interferon-free stud-
ies are “coming in April 2014.” Scott Brun,
AbbVie’s head of drug development, dis-
missed an analyst questions about “pill bur-
den” associated with the ABT-450 regimen,
mentioned above by Selvaraju. “Sustained
virologic response is king, and we’re in the
high 90 percent range,” said Brun.
Hepatitis C is heating up as these drugs
and others compounds get closer to mar-
ket, but the key late-stage players haven’t
changed. Recently approved in Japan,
J&J’s simeprevir is expected to be ap-
proved in the United States by this year’s
end, and BMS’s daclatasvir picked up
FDA’s Breakthrough Therapy designation
in April. For more information on these
products and others in HCV, see Pharm
Exec’s 2013 Pipeline Report. Weintraub
describes J&J’s simeprevir as an Incivek/
Victrelis follow-on drug, and says with
AbbVie and BMS both launching in late
2014 or 2015, “Gilead looks like it will
have a least a year” without meaningful
competition. But there’s a caveat: the ini-
tial sofosbuvir approval includes interfer-
on; the all-oral HCV combo everyone is
waiting for won’t get approved until 2014.
Drug Name: sofosbuvir
Drugmaker: gilead
PhaSe: registered
LauNch Date: 2013
Peak SaLeS: Blockbuster
Drug Name: aBt-450
Drugmaker: abbVie
PhaSe: III
LauNch Date: 2015
Peak SaLeS: Blockbuster
ES349938_PE1113_023.pgs 11.05.2013 00:01 ADV blackyellowmagentacyan
24
PHARMACEUTICAL EXECUTIVE
Pipeline Report
Drug Name: tedizolid
Drugmaker: cubist
PhaSe: registered
LauNch Date: 2014
Peak SaLeS: minibuster
Drug Name: cXa-201
Drugmaker: cubist
PhaSe: III
LauNch Date: 2015
Peak SaLeS: minibuster
Drug Name: solithromycin
Drugmaker: cempra
PhaSe: III
LauNch Date: 2015
Peak SaLeS: minibuster
Novel Antibiotics: HHS Begs for New Treatments
Most large pharmaceutical companies
haven’t rushed to develop new superbug-
swatting antibiotics or anti-infectives, despite
a dire need for such products. That’s because
historically, antibiotic R&D programs are
often long and expensive, without much of
a fnancial upside on the other end; prices
have been pushed down by generics, and
the course of therapy is short. The pricing
problem could change; in September, the
CDC announced that some 23,000 people in
the United States die from antibiotic-resistant
bacteria each year, and at least 2 million are
infected. “There’s a very direct correlation
between superbugs and incredibly high
hospital costs and mortality, says Thong Le,
managing director of WRF Capital, the VC
arm of the Washington Research Foundation.
“A lot of the antibiotics we’re using today
have been around for 50 years.”
Last year’s Generating Antibiotic Incen-
tives Now (GAIN) Act, ratifed as a provi-
sion PDUFA V, is designed to push drug mak-
ers back into the antibiotic and anti-infective
space. Thanks to the GAIN Act, incentives
for companies willing to take up the task of
novel antibiotic development include auto-
matic eligibility for Fast Track status and Pri-
ority Review, which shortens the FDA review
period to six months. Once approved, the
antibiotic would be granted an additional
fve years of market exclusivity.
It’s not clear whether that’s a strong
enough kick to make Big Pharma roll. Last
spring, HHS’s Biomedical Advanced Re-
search and Development Authority an-
nounced a deal with GlaxoSmithKline to
provide up to $200 million over fve years to
develop new antibacterial products. Similar
government-fnanced deals with Big Pharma
have been struck in Europe. Meanwhile, a
few smaller biotech frms are focusing on
the antibiotic-resistant and infectious disease
space, and several new products could go to
bat against the superbugs next year.
Raghuram Selvaraju at Aegis Capital Corp.
says Cubist, with its dual acquisitions of Trius
Therapeutics and Optimer Pharmaceuticals in
2013, has positioned itself “in the vanguard
of anti-infective drug development.” Fast
Tracked via the GAIN Act, Trius’s tedizolid
phosphate, a second-geneartion oxazolidi-
none antibacterial agent was fled with FDA
in October for the treatment of acute bacte-
rial skin and skin structure infections, and
is also being tested for the treatment of seri-
ous Gram-positive infections, including those
caused by methicillin-resistant staphylococ-
cus aureus (MRSA). The drug will compete
against Pfzer’s Zyvox, with a couple of added
benefts, like easier administration and dos-
ing, and slightly fewer side effects. Credit Su-
isse has modest estimates for tedizolid, $200
million by 2020. A second Cubist product,
CXA-201, in Phase III for complicated intra-
abdominal infections and complicated uri-
nary tract infections, is expected to fle at the
end of this year, assuming the Phase III data is
strong. Selvaraju thinks CXA-201 will launch
in early 2015, and earn $700 million by 2022.
That product will face off against meropen-
em, a broad-spectrum beta lactam antibiotic
to which bacteria is growing resistant.
The best targets for infectious disease, from
a fnancial perspective, are community-ac-
quired pneumonia and complicated skin and
skin structure infections (CSSSI), says Selvara-
ju. “We like CSSSI because the clinical trial de-
sign is pretty straight forward, compared with
a lot of other indications,” says Selvaraju. “We
like community-acquired pneumonia lung in-
fections because there are comparatively fewer
solutions for that currently available.”
Selvaraju says Cempra’s solithromycin,
a Phase III product targeting community-
acquired pneumonia, shows promise. In
September, Cempra reported in vivo data
showing that solithromycin is active against
a broad range of pathogens, including four
of FDA’s Qualifed Infectious Disease Patho-
gens under the GAIN Act.
For the moment, pharma doesn’t seem to
be answering Janet Woodcock’s increasingly
frantic calls for new novel antibiotics. Many
small companies, including Cellceutix, Du-
rata, Anacor, and others are moving through
clinical trials and targeting serious bacterial
infections, but more work is needed to better
understand the complex biology of the su-
perbugs, and to take them down.
ES349927_PE1113_024.pgs 11.05.2013 00:00 ADV blackyellowmagentacyan

25
NOVEMBER 2013 www.PharmExec.com
Pipeline Report
Drug Name: amr 011
Drugmaker: NeoStem
PhaSe: II
LauNch Date: N/a
Peak SaLeS: N/a
Drug Name: secukinumab
Drugmaker: Novartis
PhaSe: III
LauNch Date: 2014
Peak SaLeS: Blockbuster
Drug Name: OrmD 0801
Drugmaker: Oramed
PhaSe: II
LauNch Date: N/a
Peak SaLeS: N/a
Drug Name: suvorexant
Drugmaker: merck
PhaSe: registered
LauNch Date: 2015
Peak SaLeS: Blockbuster
Drug Name: Sativex
Drugmaker: gW Pharma
PhaSe: III
LauNch Date: 2016
Peak SaLeS: minibuster
Drug Name: sebelipase alpha
Drugmaker: Synageva
PhaSe: III
LauNch Date: 2015
Peak SaLeS: minibuster
Outsiders, Sleepers, and Early Stagers
Like last year, some of the products uncovered
during the research phase of this year’s
pipeline report weren’t easily shoehorned
into the categories presented, for one reason
or another. Here are few category outsiders,
sleepers—defned as potential big sellers people
aren’t talking about—and early stage drugs
that look solid, but haven’t gotten far enough
in the clinic to prompt blockbuster whispers.
» Amorcyte’s (acquired by NeoStem in 2011)
AMR 001 drug candidate, an early-stager,
is a bone marrow-derived stem cell product
in development for the emergency treat-
ment of severe heart attack. The company
is assessing CD34-positive autologous stem
cells (autologous means the stem cells come
from the same patient they’re used to treat)
that would potentially improve health out-
comes following a severe heart attach. Re-
sults from the Phase II trial are expected
during the frst half of next year. Martin
Sullivan at INC Research says next-gen cell
therapies like AMR 001 represent the next
generation of better cell therapies, a promis-
ing development
» Novartis’s secukinumab is an Isle 17 mono-
clonal antibody for the treatment of psoria-
sis. A sleeper because psoriasis is often in the
shadow of rheumatoid arthritis, at least from
a biologic drug perspective, secukinumab
could wake up investors with blockbuster
sales as soon as 2018, according to several
forecasts. In Phase III trials, Novartis had to
toss out the psoriasis area and severity index
(PASI) 75 scale, because everyone in the trial
passed the 75 percent mark, says Ben Wein-
traub, at inThought.
» Even as an early-stager, Oramed Pharma-
ceuticals’ ORMD 0801 is ahead of the big
diabetes shops in the race to oral insulin for
diabetes. Oramed is pursuing a Type 2 in-
dication frst, for patients who don’t want
to transition to injected insulin, but the
company has also launched a trial study-
ing ORMD 0801 in Type 1 insulin depen-
dent patients. Raghuram Selvaraju, at Aegis
Capital Corp., says if ORMD 0801 fnds
its way to market in the next four or fve
years, “it would blow [MannKind’s] Afrez-
za away.” Liquid (and Afrezza’s powedered)
insulin must be kept refrigerated; an oral
version, particularly without the need to
keep it cold, could be huge in markets with
access issues.
» Merck’s suvorexant, a hypnotic and out-
sider, has been fled in the United States and
Japan for the treatment of insomnia. But
FDA denied the application last summer in
a Complete Response Letter, over worries
that the dosage was too large. Merck plans
to resubmit in the frst half of 2014; FDA
did not require additional trials. The con-
sensus among analysts prior to the CRL was
blockbuster sales, by 2019. Given the rela-
tively short hold up in resubmitting, Merck
may still get a sweet dream or two out of
suvorexant.
» GW Pharmaceuticals’ sleeper product Sa-
tivex is probably the frst drug derived from
raw cannabis to cross the FDA’s desk at
least since marijuana was slapped with a
schedule 1 classifcation in 1970. Schedule
1 drugs are considered to have “no currently
accepted medical use.” Sativex is approved
in 22 countries, but in the United States,
Phase III trials for a cancer pain indication
will conclude next year, with an NDA to fol-
low in early 2015, according to GW Pharma
CEO Justin Gover. Credit Suisse puts sales
at roughly half a billion by 2020.
» Synageva Biopharma’s sebelipase alfa is
an outsider in Phase III for the treatment
of Wolman disease, a rare lisosomal stor-
age disorder in which patients are unable
to break down certain lipids. Most infants
with the disease don’t survive more than a
year, and adults with the disease have prob-
lems with swelling of the abdomen, liver
enlargement and serious, life-threatening
digestive problems. Sebelipase alfa would
become the frst approved treatment for
Wolman disease, and FDA has granted Or-
phan Drug, Fast Track and Breakthrough
Therapies status. Given the pricing environ-
ment for orphan drugs, Synageva Biophar-
ma could be rewarded handsomely.
Ben Comer is Pharm Exec’s Senior Editor. He can be reached at [email protected].
Forecasting data in Pharm Exec’s 2014 Pipeline Report relies in part on Springer’s Adis R&D
Insight database, Thomson Reuters Cortellis, Credit Suisse, and Evaluate Pharma data. We very
much appreciate the use of these resources.
ES349936_PE1113_025.pgs 11.05.2013 00:01 ADV blackyellowmagentacyan

26
PHARMACEUTICAL EXECUTIVE
Roundtable
Roundtable on
Market Access Market Access is a window on what matters in the real world of soaring
patient expectations and crimped payer budgets for innovation. Pharm Exec
convenes a diverse panel of experts to identify the key markers of common
ground: its time, people, and money against that greatest intangible—hope.
William Looney, Pharm Exec: The biopharmaceutical indus-
try confronts a strategic dilemma: just as the genomics revolu-
tion is yielding a rich harvest of biologically-based medicines
that promise to raise the standard of treatment for patients, its
ability to price these medicines at will is eroding. In response,
the drug majors are redef ning the traditional one-to-one rela-
tionship to payers through messaging with appeal to a broader
set of stakeholders as well as detailed evidence to document
the medicine’s clinical and economic value. The industry calls
the new strategy “market access”—is it working, how is the
function likely to evolve over the next few years, and what are
the key considerations for companies?
Kevin Barnett, Promidian Consulting: My f rm has com-
pleted a new study that provides insight around this ques-
tion. Extensive surveys and interviews were conducted with
more than 50 leaders from managed care, employers, Med-
icaid, other institutions, as well as the biopharma industry.
Our focus was on elucidating how market access dynamics
will evolve over the next f ve years and def ning implications
for biopharma companies. We found that there is a very high
expectation of change, in 12 relevant areas ranging from the
role of biomarkers, IT and comparative effectiveness stan-
dards to formulary design, management, and contracting.
Interestingly, payers and manufacturers were aligned on the
By William Looney, Editor-in-Chief
ES349580_PE1113_026.pgs 11.04.2013 16:41 ADV blackyellowmagentacyan
27
NOVEMBER 2013 www.PharmExec.com
Roundtable
future direction and import of most of
these issues. The notable exceptions
were in the management of specialty
drugs, where payers expect increased
scrutiny, and on the role of compara-
tive effectiveness, where payers are
more bullish than manufacturers in
thinking that use of this particular tool
will increasingly drive pricing and ac-
cess decisions.
With specifc reference to the 12
“change drivers” we identifed, the
growth of personalized medicine
through biomarkers and compan-
ion diagnostics scored the highest
in terms of the expected degree of
change over the next three to fve
years. Both groups understand that
this is a positive trend because all
these tools have a common objective:
to improve outcomes and avoid inap-
propriate utilization by getting the
right medicine to the right patient at
the right time. This is the essence of
“managed” care, one where the pa-
tient is the chief benefciary.
Right behind this as a change
driver is IT and how it will shape pre-
scribing patterns, particularly as in-
centives for EHR and other integrat-
ed systems are implemented, at the
practice level. IT is a key enabler of
the third highest degree of expected
change, which is the role of emerging
models of care like the ACO, where
the “episode of care” approach de-
pends on having information systems
that can talk seamlessly to each other.
We spoke with managed care frms
and other payers about whether these
new models would succeed in sav-
ing money while improving quality.
The consensus is the jury is still out,
largely because earlier efforts to in-
tegrate care failed to take root; these
are in many ways a pilot effort. Ulti-
mately, ACOs may prove an interim
step in what is likely to be a lengthy
journey toward a common delivery
platform—one that binds patients,
providers, and payers around a more
effcient approach to treatment.
Beneft design issues came next as a
change driver. Clearly, the structures
by which patients access care are in
fux. There is a great deal of explo-
ration underway—focused on coin-
surance, deductibles, and preferred/
non-preferred tiering of formulary
access—to fnd the right balance be-
tween quality of outcomes and con-
tainment of costs. One issue from
our discussions is how the insurance
beneft offered under the Affordable
Care Act’s insurance exchanges will
infuence private insurance plans. The
exchanges are likely to offer drug ben-
efts less robust than what is currently
offered on the private commercial
side—will we see a spillover of that
trend to the private market? That’s an
important question for both manufac-
turers and payers.
Next on the list of expected changes
is the management of specialty drugs.
Most of the drugs being approved by
the FDA are specialty, and Express
Scripts forecasts that only fve years
from now this category will account
for half of total drug prescription ex-
penditures, up from 25 percent today.
The price tag for these therapies is a
major pain point for payers, of which
manufacturers are all too aware.
Progress and pitfalls
Looney: Does the study identify the
therapeutic areas most likely to set the
agenda on market access over the next
three years?
Barnett: Yes. We asked managed
care decision-makers to identify the
disease areas they would prioritize in
managing drug utilization and expen-
ditures during this period. Oncology
came out on top, followed by rheuma-
tology, diabetes, respiratory, orphan
diseases, neurology, and obesity. The
common link here is the impact that
actions by both manufacturers and
payers can have on addressing un-
met medical need. Targeted therapies
for cancer that address the etiology
of the tumor is a clear example, and
their novelty in raising the likelihood
that the medicine will end up in the
patients most suited for it suggests
access can be secured at a premium
price—a win for manufacturers. In
diabetes, the number of new patients
with all the co-morbidities of this
disease continues to expand the mar-
ket. Economically, it’s a huge burden
for payers and there is strong interest
in any medication that will help low-
er the overall cost of treatment. We
found too that the science of diabetes
looks promising, with new classes of
drugs coming on stream that attack
the disorder in different ways. There
is a big potential innovation premium
here for industry.
Obesity scored the greatest in-
crease in interest as a priority therapy
over the forecast period. Some of the
same co-morbidity factors driving
diabetes are at work here. The pipe-
line for new products with fewer side
List of ParticipantsKevin Barnett, Executive Vice-President and Managing Director, Promidian Consulting
Brendan Bertsch, Senior Director, Pricing. Contracts and Trade, Optimer Pharmaceuticals
Kara Clinton, Senior Director, Oncology Managed Markets, Eli Lilly & Co.
Michael McLellan, Head, Market Access, Oncology Business Unit, Pfzer Inc.
Joshua Parks, Senior Director, Pricing and Strategy, Bausch & Lomb, a Valeant Company
Sanjay Shah, Executive Vice-President, Optimal Strategix Group
Sanjiv Sharma, Vice-President, Commercial Operations, Duchesnay USA
Jim Smeeding, Executive Director, National Association of Specialty Pharmacy
Richard Stefanacci, MD, Associate Professor Health Policy, University of the Sciences,
and Chief Medical Offcer, The Access Group.
ES349582_PE1113_027.pgs 11.04.2013 16:41 ADV blackyellowmagentacyan

28
PHARMACEUTICAL EXECUTIVE
Roundtable
effects looks promising. And payers
appear willing to reimburse obesity
treatments because of the impact on
population wellness, which translates
to lower health costs.
Looney: The biopharma business
is uniquely affected by public policy
and legislation. Can we identify from
the study the key challenges coming
on the regulatory front?
Barnett: Executives on the man-
aged care side are very focused on
the implementation of the Affordable
Care Act. Uncertainty is the prevail-
ing sentiment. It remains to be seen
if this complex law is a growth op-
portunity. Will expansion of the
Medicaid-eligible population as well
as the individual insurance exchang-
es create a windfall of new customers
whose healthcare needs can be met at
reasonable cost, through a balance of
young and healthy against an older
demographic with serious health
risks? Another issue is coverage rules
for drugs, including formulary man-
agement and related design questions,
which are impacted in turn by rules
on whether manufacturers can offer
co-pay offset and coupon incentives
directly to patients in the exchanges.
The study also looked at the pros-
pects for biosimilars. A bare majority
of respondents from the managed care/
payer side believe biosimilars will be-
come widely available to US patients in
the next three years; there is a stron-
ger consensus that, if this happens, we
will see downward pricing pressure on
drugs that lead to meaningful savings
for payers. Realistically, however, most
payers contend that discounts of at
least 30 percent against the originator
brand will be required to deliver any
real savings.
Finally, the managed care group
struck a distinctive note on compara-
tive effectiveness rules. Surprisingly,
most aren’t currently employing this
evidence tool to shape decisions on
formulary coverage. Interviewees
said they are waiting for relevant
government agencies like CMS to
take action; many point to internal
resource constraints as the culprit in
their failure to making it a priority.
Structural transitions ahead
Jim Smeeding, National Association
of Specialty Pharmacy: Did the study
conf rm the trend toward a blurring
of the roles played by payers and pro-
viders in the healthcare system?
Barnett: Yes. The ACO model
with its focus on episode of care as
an alternative to traditional fee-for-
service is viewed as here to stay. If
payers want to reduce costs, it re-
quires that they embrace the concept
of active medical management; it’s
no longer f nancially viable to act as
a passive third-party.
Closed information loops
Sanjay Shah, Optimal Strategix Group:
There is some way to go before we
have truly integrated care in the United
States. This is because actions by all
parties—providers, payers, and manu-
facturers—remain driven by disjointed
f nancial incentives and misalignment
on assumed risk that are hard to re-
verse. Europe is further ahead, having
embraced payment schemes that are
built around performance and out-
comes, expressed via the accumulation
of evidence of comparative effective-
ness (which differs from eff cacy estab-
lished in well-controlled clinical trials)
through post-approval observational
studies, in the real world setting. It is
possible that policy pressures in the ex-
pensive, high- prof le specialty biologics
segment might accelerate a similar tran-
sition here.
Barnett: Payers we interviewed
will be demanding progressively
higher substantiation of clinical ef-
fectiveness for these biologics. They
admit, however, that creating work-
able criteria to demonstrate value—
criteria that are mutually acceptable
to payers and manufacturers—is still
a work in progress. Support is strong
on a conceptual level but the goal
now is to move from that to some-
thing that you can actually measure.
If by uniformity you mean the United
States will evolve toward a single fed-
eral standard of cost effectiveness, I
suspect this idea will be f ercely re-
sisted, not just on methodological
grounds but because of the politics.
Kara Clinton, Eli Lilly & Co.: There
is substantial discussion on how to
manage and reduce costs in healthcare.
Information and data will continue to
be critical as we examine disease and
treatment costs holistically. Pharma-
ceutical prices are relatively transpar-
ent and have been a major focus of re-
ducing costs. However, drugs are often
not the major driver of the expense of
treating a patient. To reduce healthcare
costs, stakeholders should start with
accurately measuring and comparing
all costs with improved transparency
and data. It is also important to cap-
ture cost offsets and savings in differ-
ent treatment options. What does it
cost to treat an individual throughout
Actions by all parties—providers, payers, and manufacturers—remain driven by disjointed f nancial incentives and misalignment on assumed risk that are hard to reverse.—Sanjay Shah, Optimal Strategix Group
ES349583_PE1113_028.pgs 11.04.2013 16:41 ADV blackyellowmagentacyan

29
NOVEMBER 2013 www.PharmExec.com
Roundtable
the full course of a disease? This is the
key principle in aligning market access
with treatment outcomes, in an afford-
able way.
Joshua Parks, Valeant: The situa-
tion in Europe today suggests it may
be naïve to assume that better infor-
mation combined with the right clini-
cal prof le will result in patient access
to a new drug. The patient popula-
tion is increasingly diverse, so it fol-
lows that there is an equally diverse
range of opinion on what constitutes
improvement in the standard of care.
All the industry’s computer models
will have little inf uence on that deter-
mination, which most often ends up
being, “we just can’t pay for it.” This
is the direction European countries
are taking, and it will be interesting
to see where that leaves the European-
based industry three to f ve years from
now. Precedent shows that there will
be less innovation and slower uptake
of newer drugs.
Looney: Don’t we need to start
with an agreed definition among
payers and manufacturers about
what the concept of “effectiveness”
really means? Does it apply to clini-
cal standards only or does it incor-
porate cost?
Smeeding: It carries a very broad
scope. Some of the larger provider
and managed care organizations
have evolved their own internal def -
nitions. Efforts by the networked
academic organizations like ISPOR
have also brought the various inter-
ests together, which is critical as the
mechanics of effectiveness evalua-
tions must make sense to the insur-
ance providers f rst, because they are
the ones who pay the bill. But drug
makers will confront price resistance,
regardless of the degree of consen-
sus on standards. It’s always been a
contest of wills to wrest a good price
from a payer, and I don’t expect that
to change very much.
Sanjiv Sharma, Duchesnay USA:
Each provider wants to design their
own cost effectiveness model because
everyone in the business claims their
covered patient base is unique. The
practical implication is a drug manu-
facturer is forced to do endless varia-
tions of the same thing to accommo-
date this pretense.
Brendan Bertsch, Optimer Phar-
maceuticals: In the United States, no
standard for effectiveness can include
a frank assessment of cost. Only
clinical applications are permissible;
anything beyond that entails endorse-
ment of rationed care, symbolized by
the “death panels” that are supposed
to be implicit in the Obamacare leg-
islation. European precedents don’t
travel well here.
Michael McLellan, Pf zer: Crite-
ria for effectiveness in Europe seems
to focus predominantly on cost, so
much that one might suspect that in
some countries, the institutionalized
process known as health technology
assessment [HTA] is more of a politi-
cal tool masquerading as an objective
evidentiary standard. It provides an
opportunity for payers to tactically
create negative assessments prior to
negotiating a reimbursement price.
The lack of objective and scientif c
benef t assessments becomes clear
when a manufacturer can submit
the same dossier of evidence for the
same drug to HTA authorities in a
number of countries and get a very
different conclusion in each one. It
would be unfortunate if these assess-
ments amounted to no more than a
clever way to manage a f xed budget
for medicines, instead of identifying
true innovations that benef t patients.
The situation could only change
if the agency doing the benefit as-
sessment was not so closely tied to
the payer negotiating reimburse-
ment. There are efforts underway to
create a pan-European assessment
process on relative effectiveness.
Opinions differ, but my view is that
this is unlikely to improve the cur-
rent problem of HTA bias and lack
of objectivity, in a way that rewards
drugs addressing unmet medical
needs. That’s because all reimburse-
ment negotiations are inherently po-
litical; payers in countries control-
ling access to new drugs are unlikely
to relinquish direct control over the
HTA process. The group coordinat-
ing the pan-European HTA assess-
ment pilot, the European Network
for Health Technology Assessment
[EUnetHTA], consists of representa-
tives of the national HTA agencies.
You can’t expect them to support
any significant changes to the sta-
tus quo in their home countries, as
it would adversely impact their pre-
rogatives as the gatekeepers on pa-
tient access.
In the United States, no standard for effectiveness can include a frank assessment of cost. Only clinical applications are permissible; anything beyond that entails endorsement of rationed care, symbolized by the “death panels” that are supposed to be implicit in the Obamacare legislation.
—Brendan Bertsch, Optimer Pharmaceuticals
ES349581_PE1113_029.pgs 11.04.2013 16:41 ADV blackyellowmagentacyan

3030 Roundtable
PHARMACEUTICAL EXECUTIVE
Sharma: Throughout my career,
I’ve been closely involved in negotia-
tions on clinical and cost effective-
ness standards, in Canada as well
as the United States. My experience
leads me to conclude that the only
way industry can avoid making this
process a narrow budgetary and f -
nancial calculation is to engage the
patient. Putting forward an articulate
patient perspective is unsettling to
the payer—which actually conf rms
we are doing the right thing. Patient
involvement tilts the discussion away
from a focus that is exclusively about
the cost of therapy.
What do payers want?
Richard Stefanacci, University of
the Sciences and the Access Group:
Through my work as chief medical of-
f cer for a number of Medicare Advan-
tage plans as well as membership on
a national P&T committee, I can say
there are only two things that drive
payers on market access. The f rst is re-
turn on investment—not just what do
we get by listing your drug, but, more
important, how soon? No longer do
payers want to be told about savings
over a 10-year time span. Their fall-
back position is to eschew any imme-
diate decision on coverage, in favor of
“watchful waiting.” If manufacturers
want to avoid this outcome, being able
to make that case for ROI is critical.
The second driver for payers is regula-
tion. If we are told we must cover a
drug, we do it. Academic judgments
about cost effectiveness have little, if
any, impact on the decision.
I am intrigued that in the survey,
respondents from both the manufac-
turer and managed care side seemed
to downplay the role of the patient.
In this new healthcare environment,
manufacturers must position value
from the point of view of the patient,
not just the provider. As patients will
be forced to bear more of the cost
burden, their adherence will be based
more on how they perceive value.
Smeeding: As costs for drugs
mount, particularly for life-threat-
ening conditions like cancer, patient
access programs will become a criti-
cal ethical issue. There are a lot of
uninsured and under-insured people
where the pressure will be intense to
get them on therapy. Such programs
are predominantly company-spon-
sored but I predict we will see more
government involvement in how these
programs work, and for whom.
Parks: Europe is already there.
In contrast to the United States, na-
tional authorities have to reconcile
two conf icting commitments: f rst,
to offer the broadest access possible
to all citizens, and, second, to con-
tain costs within a f xed annual bud-
get. Their response offers a precedent
for the United States: It requires some
people—those with more assets—to
pay a bigger portion of their health
costs out-of-pocket. Overall insur-
ance cover is important, but patient
share of costs is going to be right up
there too.
Stefanacci: The trade-off for pa-
tients from the Affordable Care Act
is lower plan premiums through gov-
ernment programs like the Health
Insurance Marketplace plans and
Medicaid, partly as a result from re-
stricted access to providers and cer-
tain types of care, including drugs as
well as higher patient cost sharing.
Clinton: Payers are interested in
data on how biopharma technologies
improve outcomes for a def ned popu-
lation relative to the current treatment
standard. In oncology, with rapidly
changing treatment standards, this
can be a signif cant practical challenge
for companies. Traditional Phase III
trials have protocols and standards
that are approved by regulators years
in advance of the trial completion. By
the time results come, the standards
can evolve and the relevance of the
data can be challenged. There are ef-
forts with regulators to address this
issue, but it is a current risk that bio-
pharma must take as a given in the de-
velopment process.
McLellan: Payers need to provide
industry a feasible way to develop
the evidence they are asking us for,
so that it is not a constantly moving
target. Right now they are not doing
this. The non-binding consultations
we have with them do not allow us to
agree on what will constitute a data
package to ensure access for drugs that
have a meaningful benef t, including
what should be the right comparator.
This is going to discourage future in-
novation. I submit that it is in the payer
interest to play this game, and it starts
with a fair playing f eld to help us work
through the payers’ fear of the budget
impact of true innovation, in areas of
Criteria for effectiveness in Europe seems to focus predominantly on cost, so much that one might suspect that in some countries, the institutionalized process known as health technology assessment is more of a political tool masquerading as an objective evidentiary standard.
—Michael McLellan, Pf zer
ES349593_PE1113_030.pgs 11.04.2013 16:42 ADV blackyellowmagentacyan

31
NOVEMBER 2013 www.PharmExec.com
Roundtable
unmet medical need, because these in-
novations do not always carry a cost
saving or cost offset.
Innovation—the moving target
Shah: The cost challenge is com-
pounded by the lack of consensus
on how to decide which innovation
creates value. Not every player in
healthcare shares our view of what
we would characterize as innovative. I
recall inviting a senior executive from
Humana to participate in a payer ad-
visory board for a J&J compound we
were developing for diabetes. He not-
ed that, at his company, innovation
was rarely described as coming from
a bottle. Instead, innovation came in
a Nike shoe box, because it motivated
employees with diabetes to exercise.
McLellan: It is commonly assumed
that it is up to the payer to defne inno-
vation. Not true: their frst responsi-
bility is to allocate a fxed budget. You
cannot pay for things with money you
do not have. The concern is how pay-
ers are managing the process. It is not
a coincidence that virtually every pre-
liminary beneft assessment of oncol-
ogy products by NICE in the United
Kingdom is negative, regardless of the
clinical data presented or the patient
access scheme we present upfront.
Another new trend I fnd alarming is
the separation of the beneft assess-
ment [the value] and reimbursement
negotiations [the price] in countries
like Germany. This puts manufactur-
ers in a diffcult position and allows
the payer to gain the higher ground,
stating “we think your product falls
short...so let’s now talk about price.”
In the new payer environment, pro-
viding the clinical data that payers
are asking for, such as showing clini-
cal superiority in a head-to-head tri-
al, or developing molecularly targeted
drugs that identify for treatment only
those patients most likely to respond,
isn’t producing the expected response.
This is because the payer is so focused
on cost relative to any clinical value. I
have heard it said that the only thing
a payer dislikes more than a product
without good data is a product with
good data. Understanding this per-
ception is a frst step in defning what
motivates payers in a price controlled
market. Their beneft assessments
seem to stray from the consensus in
the medical community and any re-
quest by companies for even a small
price premium over comparator prod-
ucts—based on data demonstrating
signifcant statistical superiority over
those comparators—will likely lead
to prolonged negotiations. This chal-
lenge is further compounded when
the comparators are generics. In some
cases, payers are now settling limits
on how much they will pay, per pa-
tient, per year. To remedy this, there
is going to have to be some give on
both sides, but unless society is satis-
fed with only having the treatments
of today, more alignment must be
made on the incentives to advance
medicines ability to improve popula-
tion health.
Parks: Industry still has some le-
verage in that we can decide where we
choose to launch—or not launch. As
some of the emerging markets become
bigger over the next fve to 10 years,
there will be more options to pursue
a launch strategy beyond the budget-
constrained countries. I believe the
biggest threat is the erosion of support
for so-called incremental innovations.
These are the products with clinical
attributes that are quite meaningful
to patients and whose success has al-
ways fueled the next round of frst-in-
class breakthroughs. These products
are in wide disfavor now, with some
companies reconsidering plans to ad-
vance next generation therapies.
Managing many parts
Looney: Market access is still a rela-
tively new function within Big Phar-
ma. What are the key elements of a
What’s Next for Market Access?
Promidian’s Future of Market Access study reviews how market access issues are likely
to evolve over the next three to fve years, with a particular focus on defning the implica-
tions for biopharma companies. The study includes two components: primary research
with managed market executives and market access KOLs (including those from MCOs,
PBMs, Medicaid, employers, and ACOs); and primary research with executives from lead-
ing biopharma companies.
Key areas of focus in the study are:
• Where the most change is expected in managed care/market access over the next
three to fve years.
• Degree to which and how the US Affordable Care Act will affect business.
• Top business priorities for managed care.
• Therapeutic categories that represent the highest priorities for payers, currently
and over the next three years.
• The biggest market access-related changes and priorities for biopharma.
• Expectations on what will happen with biosimilars and comparative effectiveness
research.
• Which biopharma companies are most effective in dealing with payers, and what
differentiates these companies.
• Opportunities and requirements for biopharma companies to positively differentiate
themselves in the way they interact and conduct business with payers.
• Assessment of how perceptions and expectation of payers and manufacturers
compare across the questions included in the study.
For more information, contact Kevin Barnett at [email protected]
ES349592_PE1113_031.pgs 11.04.2013 16:42 ADV blackyellowmagentacyan

32
PHARMACEUTICAL EXECUTIVE
Roundtable
successful market access program,
from both a strategic and operational
perspective?
Parks: By def nition, market access
is a cross-functional activity. It re-
quires pooled expertise from clinical
development, commercial affairs, and
professional relations, among other
functions. Most important, it must
carry forward a global perspective
that incorporates a detailed aware-
ness of conditions in individual target
countries. What really distinguishes a
successful program is the capacity to
communicate and engage with stake-
holders who can build out messages
that promote the value of the product.
The point is to create a groundswell of
support for a new product, ensuring
that key players like the patient com-
munity are aware of its benef ts and
how it can help them.
Stefanacci: Market access is not
a project that should be launched at
the 11th hour. Everyone knows that,
but still most companies come to
the table too late. It is amazing as a
payer representative to see companies
visit us for the f rst time when they
are well into the Phase III trial pro-
cess. At that point, it is too late for
our viewpoint to have much impact
on the value proposition. We wonder
why we are being consulted.
Barnett: Our work indicates a key
differentiating factor for successful
companies is that senior management
truly “gets it.” They have a strong
understanding of payers and market
access. These executives ensure the
realities of payer and market access
dynamics are ref ected in commercial
processes and the way their compa-
nies conduct business with payers. It
all has to tie together from a clinical
and marketing perspective, leading
ultimately to a strong value message
that differentiates the product and
justif es the price point.
It’s a race car: but who’s driving?
McLellan: Market access is not really
a function; it’s a goal. We all know
the goal must be def ned early on in
the process. The challenge is that even
when the goal is agreed, the incentives
of the internal players are often very
different. Clinical development peo-
ple are vital, yet their organizational
mandate is to maximize the number
of molecules that make it to registra-
tion. It is hard to get them to think
beyond that marker of success. The
elusive target here is integration of the
market access strategy. Yet you will
f nd many companies are still working
within a model of over-specialization
around small parts of the process. It
is like designing a race car, where one
expert pushes the accelerator, another
applies the brakes, and still another
turns the steering wheel. This race car
is unlikely to reach its goal anytime
soon and more likely will crash into a
wall. Expertise in pricing, reimburse-
ment, outcomes research, real-world
data, and other relevant functions
sit on the same team, with the same
reporting lines and priorities. Pf zer
is now working toward such an inte-
grated model.
Clinton: This approach can have a
damaging effect because it leaves the
impression that the essential objec-
tive in market access—a strong value
proposition and access of technology
to patients who need it—are some
other function’s problem. In reality,
every part of the development and
commercial process should be asking
the question: What is the value of this
drug to patients who have the disease
and how can we improve on that?
Shah: I would call market access
both a business function and an en-
terprise capability platform, span-
ning many activities. The objective
is to ensure that as an enterprise we
create value during the entire product
lifecycle, starting with early phase
drug development, and compete
across the full continuum of health-
care, not just the pharmaceutical
benef t in isolation. The value propo-
sition is going to fail if it is conf ned
only to the pharmacy benef t “silo.”
Sharma: Every market access lead-
er should have two major strengths.
The first is the ability to think like
a lawyer on the bench—you must
know the rules, inside and out, and
methodically define what the op-
tions are. The second is putting all
the disconnected strands of activity
together into a set of arguments that
will deliver results, and be commu-
nicated in a way that stakeholders
can understand. Another aspect of
this role is how important it can be
to avoid the conventional wisdom.
The best practitioners in this field
are those with the ability to think
outside the box—because in market
access, there is no box.
Success seeds from the top
Bertsch: People who do market access
tend to be mid-level executives. There
is much less expertise and awareness
the further up you go in the chain of
command. The absence of people with
As some of the emerging markets become bigger over the next f ve to 10 years, there will be more options to pursue a launch strategy beyond the budget-constrained countries.
—Joshua Parks, Bausch & Lomb
ES349596_PE1113_032.pgs 11.04.2013 16:42 ADV blackyellowmagentacyan

33
NOVEMBER 2013 www.PharmExec.com
Roundtable
real clout can make it harder to com-
pel others to collaborate.
Looney: What options exist to ad-
dress these challenges? Might open-
ing your doors to payers raise the
level of engagement internally?
McLellan: In the United States,
we can talk with the payers and have
a fairly open exchange of views, in-
cluding with people at the top of the
decision chain. Outside the United
States, this kind of dialogue is diff -
cult, often for cultural reasons. The
only way to really understand the
payer environment is to sit across
the negotiation table with payers in
a price control country. It is unfortu-
nate that few in the organization will
ever get that chance.
Shah: Successful market access
programs make a commitment to
cross-organization pollination of
talent to codify the market access
mindset throughout (e.g., through
rotational assignments for promising
staff in related areas). For example,
managers who are designated “fast
track” for advancement must include
a stint on market access work in their
career development and progression
plan. Obviously, this will take time
for us to see a CEO with day-to-day
exposure to payers in his resume.
Contact with payers has not been re-
warded among those who follow the
traditional routes to the “c suite.”
Looney: What about the patient
perspective? Is it f rmly embedded
in the market access mindset of your
companies?
Stefanacci: Some of the larger pa-
tient advocacy groups are increas-
ingly active partners of the industry
in early- and mid-stage drug devel-
opment. These groups are actually
funding some of this work, so as a re-
sult patients are signaling their value
proposition right at the very start.
This assures their voice in the treat-
ment development process.
McLellan: We say that the work we
do must benef t the patient. Neverthe-
less, patients factor too infrequently
into a decision to reimburse a new
drug. Patients—and their families—
have a clear stake in our efforts to
develop new treatments. They want
to see and understand our data. If the
data shows an advance in the standard
of care, patient groups are likely to be-
come a factor in the payer decision to
budget for a new drug or to speak out
when a benef t assessment decision
lacks a strong medical rationale.
Sharma: To achieve that objec-
tive, industry has to move beyond the
intellectual level and engage on the
basis of a direct, emotional connec-
tion with the patient. This is a tactic
that industry handles relatively well
on the promotional side. But we are
less proactive in making that real-
world connection to the patient when
it comes to negotiating a price or a
position on the formulary.
Def ning the best in Market Access
Looney: Can we come to a consen-
sus on what factors are likely to de-
termine success in an era that we all
agree is going to pose more challenges
to market access?
Parks: One issue facing the indus-
try is the gap between patients with
drug coverage and those without it.
There is a real ethical divide. Some
patients will get the cutting edge
therapies that can cure or extend life;
others may not and suffer the conse-
quences. What if society no longer
supports the incremental innovations
required to fund the next generation
of breakthroughs? We can say that
industry’s task is simply to develop
medicines that pay for research and
deliver returns to shareholders. But
some very powerful forces in society
don’t see it this way. Resolving this is
going to require some diff cult con-
versations. One cannot be conf dent
that the politicians will step up to
lead in building a new consensus on
P&R. What I fear more is the “kick
the can down the road” mindset that
gives industry little clarity in manag-
ing all this uncertainty.
Shah: We must press for a better
def nition of what constitutes value in
pharmaceuticals. The dialogue must
shift from cost to value. If a product
shows it has value, then intrinsically
the cost is aligned with the def nition
of benef ts and outcomes desired,
which is what value is. A good start
toward moving the debate away from
being exclusively about cost is con-
testing the idea that an incremental
advance has no value. Drugs carry a
high variability in the individual re-
sponse, which shows how important
having a choice of therapy is when a
clinician treats a patient.
Clinton: The days of approach-
ing market access and cost cutting
with an “Us vs. Them” philosophy
are numbered. We need to focus the
discussion on how to help the pa-
tient with his disease instead of a
Every market access leader should have two major strengths. The f rst is the ability to think like a lawyer on the bench. The second is putting all the disconnected strands of activity together into a set of arguments that will deliver results.
—Sanjiv Sharma, Duchesnay USA
ES349597_PE1113_033.pgs 11.04.2013 16:42 ADV blackyellowmagentacyan

34
PHARMACEUTICAL EXECUTIVE
Roundtable
limited focus on what happens when
he receives our drug. If we can think
through the entire disease from di-
agnosis through resolution, we can
identify other, creative ways to opti-
mize outcomes and control costs.
Bertsch: There is a contradiction
at the heart of market access that
poses more diff culty in the years
ahead. While everyone lauds the idea
of closer partnerships with payers,
no one wants to assume any risk in
that relationship. Contracting deals
are a good example. Payers demand
a payback when outcome goals are
not achieved, while manufacturers
fret that performance metrics are
unrealistic because the data on their
product is f awed or unavailable. So
both sides hesitate because there is
too much risk.
Shah: Data is ref ective of a frag-
mented delivery system. It cannot
demonstrate cross-sector impacts be-
cause the process by which that data
is generated, managed, and accessed
is siloed. Our greatest contribution to
value, which is how the drugs budget
impacts the cost of healthcare over-
all, is virtually impossible to prove
with the data we can compile today.
Smeeding: This is a bit of an ex-
aggeration. I have been fortunate to
work with a specialized employer
database whose model is integrated
across the full range of health ser-
vices and encompasses a relatively
stable survey population tracked over
a long period of time. We have been
able to draw out some very interest-
ing data that links pharmaceutical
access to health outcomes.
Clinton: My challenge is whether
our market access capabilities are
able to address the complexity of the
new insurance models that are part
of health reform. The industry is well
prepared to assist patients without
insurance through direct patient as-
sistance programs. There is less guid-
ance for us on how to assist people
who are under-insured, with minimal
coverage but are not indigent. Under
the new reform law, I suspect we
will see large numbers of people who
opt for less than adequate coverage,
with high deductibles and co-pays
for drugs. We will face an interesting
situation—more insured people who
will be seeking sources to help pay
for their medicines.
Coupons conf ict
Looney: A source of tension between
payers and manufacturers today is
the latter’s use of co-pay offsets and
discount coupons to maintain brand
loyalty and discourage patients from
switching to the lower cost gener-
ics mandated by provider formulary
programs. How is this debate likely
to shake out, particularly as the pool
of insured patients grows with imple-
mentation of the individual mandate
under the Affordable Care Act?
Stefanacci: The consensus among
payers—including the Center for
Medicare and Medicaid Services
[CMS], where I served as Health
Policy Scholar—is that these offsets
have a distortive effect on the effort
to manage drug utilization. It contra-
venes the spirit of the Medicare Part
D drug benef t, where the so-called
“doughnut hole” was introduced
to ensure patients are motivated to
choose the lowest-cost generic option
to avoid full liability for the cost of
higher priced branded medications.
Payers prefer that companies support
patient assistance programs [PAP]
that don’t circumvent their utiliza-
tion management protocols.
Smeeding: Co-pay offsets and dis-
count cards exist because of the tier-
ing of formulary access. Manufactur-
ers want to defend brand share and
argue that these incentives reduce
costs to patients and thus promote
better adherence and fewer hospi-
tal stays. Payers say in return they
have made very careful assessments
that some products are preferred to
others; on eff ciency grounds, their
covered population should adhere to
that judgment and not be inf uenced
by outsiders with a vested interest in
promoting an alternative. Both par-
ties are defensive and are reluctant to
put their case directly to the public.
And a growing volume of data indi-
cates that co-pays in general are a
disincentive to adherence, can lead to
poor health choices, and thus don’t
make much sense economically.
Stefanacci: This presents a tough
balancing act for payers. They real-
ize that patients are primarily driven
into plans by the premium; in fact,
rich benef ts typically attract high
utilizers. So one balancing act is be-
tween premiums and benef ts. Anoth-
er is between patient out-of-pocket
charges and outcomes. While high
The days of approaching market access and cost cutting with an
“Us vs. Them” philosophy are numbered. We need to focus the discussion on how to help the patient with his disease instead of a limited focus on what happens when he receives our drug.
—Kara Clinton, Eli Lilly & Co.
ES349594_PE1113_034.pgs 11.04.2013 16:42 ADV blackyellowmagentacyan

35
NOVEMBER 2013 www.PharmExec.com
Roundtable
out-of-pocket reduces a plan’s Rx ex-
penses, it could actually cost a plan
in poorer health outcomes, tipping
the balance. We will see how plans
fare in accommodating these con-
f icting forces.
Finding common ground
Looney: Can you identify areas where
payers are making constructive con-
tributions to the dialogue that all
sides seem to want?
Smeeding: We are seeing increased
alignment of incentives between
manufacturers and payers, result-
ing in coordinated management of
pharmacy benef ts. And adherence is
f nally being taken seriously by both
parties, with much productive work
taking place in the neglected special-
ty segment. Data is being shared for
use in specif c applications linked to
outcomes. For example, there is ex-
citing work underway in Medicare
on medication therapy management
where reimbursement will be based
on star ratings covering how well you
are following patients after treatment
and avoiding adverse events linked to
the inappropriate use of drugs. This
is encouraging the development of
patient registries, where payers and
drug f rms can both contribute to the
generation of real-world data that
leads to savings system-wide.
Clinton: United Healthcare and
Aetna are conducting numerous pi-
lot experiments with the industry
focused on oncology medicines. They
do not put price at the center of the
discussion but instead consider how
to eliminate inappropriate f nancial
barriers to positive patient outcomes.
Parks: Data is not always pris-
tine. There is a difference between
the careful, well-controlled popula-
tion of a clinical trial monitored by
regulators and the observational data
taken from clinical settings and pa-
tient registries. Once a drug gets used
in the real world, the “confounders”
on data rise exponentially. These are
diff cult to scrub to obtain a clean
result. We’d like more support from
payers and regulators in f nding ways
to reconcile the confounders and get
at least some semblance of a pure
data set—one that is useful for deci-
sion-making.
Looney: Any f nal comments
about the pace of change affecting
market access?
Stefanacci: The US healthcare
system is facing a revolutionary
shift away from employer-based
insurance. We will see movement
toward the new Health Insurance
Marketplace [HIM] exchanges, led
by a gradual mass exodus from em-
ployer-sponsored plans. The Obama
Administration has actually given a
boost to this trend by delaying the
penalty on employers for not provid-
ing coverage. The other shift is in
care delivery, specifically where phy-
sicians like myself practice. This is
different than the physician hospital
organization model of the 1990s that
failed, forcing physicians back into
private practice. Physicians today
are accepting these new care models
as they tend to be more comfortable
with being salaried, committed to
normal work hours, and handing
the administrative burdens over to
someone else. This new “organized
customer” is here to stay. With the
shift of physicians toward these new
care delivery models, treatment de-
cisions will be decided not by phy-
sician “pull through” but instead in
the “c suites” of these new provider
groups. Decisions on drugs are no
longer in the hands of the physician.
Access determinations will be made
at a much higher level, based on the
delivery of outcomes that these new
provider groups are being held ac-
countable for.
Parks: Information is equally
transformative. Apple recently un-
veiled a new digital product it calls
Life Tracker that is primarily de-
signed for athletes interested in eval-
uating their training progress. But
imagine how payers could use this
technology to follow the routine life-
styles of their insured populations
and make coverage and treatment as-
sessments around that data. Whoever
can f nd commercially advantageous
uses from this rising tide of informa-
tion technology will get to the top of
the market f rst. Just think of what
this data retrieval could mean for
managing Type 2 diabetes.
William Looney is Pharma Exec’s Editor-
in-Chief. He can be reached at wlooney@
advanstar.com
Author’s Note: Statements attributed to
participants in this roundtable do not necessarily
represent the off cial views or positions of their
aff liated companies.
We are seeing increased alignment of incentives between manufacturers and payers, resulting in coordinated management of pharmacy benef ts. Adherence is f nally being taken seriously by both parties, with much productive work taking place in the neglected specialty segment.
—Jim Smeeding, National Association of Specialty Pharmacy
ES349595_PE1113_035.pgs 11.04.2013 16:42 ADV blackyellowmagentacyan

36
PHARMACEUTICAL EXECUTIVE
36
PHARMACEUTICAL EXECUTIVE NOVEMBER 2013 www.PharmExec.com
Supply Chain
Scanning the Future In response to some high-profle
thefts and product counterfeits that
have occurred over that past few years,
governments around the world have
turned their attention to securing the
supply chain through regulation fo-
cused on product serialization.
Currently, during manufacture
every batch of pharmaceuticals is as-
signed a lot number. Each container
of product produced in that batch has
the same lot, or serial, number. This al-
lows the manufacturer some ability to
track its product as it moves through
the supply chain to its fnal stop at
the pharmacists’ bench. Product is be-
ing followed, but it is being tracked
with a wide net. If there is a problem
with the lot from theft, tampering, or
counterfeiting the entire lot must be re-
called—there is no way to differentiate
individual containers produced in the
same lot.
“The issue with pharmaceuti-
cal cargo is not so much the impact
of the product itself that is stolen [or
Getty Images/fotostorm
In response to well-publicized security threats, regulatory
authorities in the United States and Europe are moving
toward the enactment of new legislation that will change
the way pharma products are handled and shipped
throughout the supply chain.
The state of the pharmaceutical
supply chain can be summed up
in three words: serialization is
coming. The era of “track and trace” is
upon us. Although it is unclear at this
moment what level of tracking will ul-
timately be required, companies need
to be prepared for regulations that will
alter the way pharmaceuticals are pack-
aged and shipped. New laws will raise
your risk profle—particularly in ensur-
ing product safety.
The changes are occurring as the
act of manufacture itself has become a
strategic global priority for Big Phar-
ma. Unlike a decade or two ago when
much of the production was handled
in-house, pharma is relying more on
contract vendor manufacturing to keep
pharmacy shelves full. As more and
more of the R&D and manufacturing
functions are outsourced, the impor-
tance of a safe and secure supply chain
becomes ever more prevalent.
By Timothy Denman, Senior Managing Editor
ES347278_PE1113_036.pgs 10.30.2013 19:32 ADV blackyellowmagentacyan
Presented by
Sponsored by
ON-DEMAND WEBINAR
Register free at www.pharmexec.com/provider_engagement
EVENT OVERVIEW:Oncology continues to evolve towards a promising, but increas-ingly intricate future. Physicians face rapidly changing technology and legislations, more complex treatment decisions, as well as reim-bursement and time pressure. All of these factors have created a shift in physician needs, impacting their relations with the pharma-ceutical-biotech industry. During this presentation, we will examine how industry trends are impacting the way Pharmaceutical and Biotech companies interact with physicians, and how to implement strategies to optimize
engagement with providers.
Specifcally, we will discuss:
n Key industry trends impacting oncology providers
n How to implement strategies that foster strong relationships with providers
n New approaches to deliver relevant and timely information to providers
PRESENTERS
Debra Patt, MD
Medical Director of Healthcare Informatics,
McKesson Specialty Health,
practicing physician at Texas Oncology
afliated with The US Oncology Network
Sandy Smith, RN, MSN, AOCN
Senior Director of Clinical Education Services,
McKesson Specialty Health
MODERATOR
Julian Upton
Senior Editor,
Pharmaceutical Executive
For questions, contact Sara Barschdorf at [email protected]
Key Learning Objectives:
n Understand key trends in oncology impacting physicians
n Review physicians’ preferences when engaging with the Industry
n Examine strategies that drive sales force efectiveness
n Discuss ways to foster long-term relationships with physicians and other providers
n Learn how to develop a multi-pronged approach to maximize your time with providers
Integrated Strategies for
Oncology Provider Engagement
Who Should Attend:
Professionals from
pharmaceutical
companies who
are interested in
learning more about
best practices when
engaging with
providers
ES346840_PE1113_037_FP.pgs 10.30.2013 01:43 ADV blackyellowmagentacyan

38
PHARMACEUTICAL EXECUTIVE
Supply Chain
counterfeited],” says Don Hsieh, di-
rector of commercial and industrial
marketing at Tyco Integrated Secu-
rity. “The products are made in lots.
If that particular lot has to be recalled
the cost will be in multiples of the
original loss.”
Under the upcoming regulations,
product will need to be traceable at
the unit level. Giving each unit it own
serial number will allow individual
packages to be tracked up and down
the supply chain, allowing for great-
er security and lessening large-scale
recalls.
The United States and Europe have
fallen behind Turkey, Italy, Chile, and
even India and China in the area of
regulatory requirements for track and
trace and are in the process of playing
catch up. Although each entity is pro-
posing different levels of traceability,
one thing remains constant: increased
regulations are on the way.
Legislation: a closer look
United States. The idea of unit seri-
alization is not new—the California
Board of Pharmacy has been working
on a bill that will require an electron-
ic pedigree at the unit level for over
a decade. Under the legislation that
is scheduled to go live on January 1,
2015, every change of ownership of an
individual unit as it passes through the
supply chain needs to be recorded and
available for inspection at the pharma-
cy level. At least 50 percent of a com-
pany’s product that is sold in the state
will need to comply with the new leg-
islation by the start of 2015, with the
remainder on January 1, 2016.
As the California initiative gets
closer to implementation, the federal
government is working on legislation
simultaneously that would supersede
the California law. The House and
Senate approved a draft version of the
Drug Quality and Security Act in late
September. Should the proposed leg-
islation be enacted (www.govtrack.us
gives it a 42 percent chance of being
signed into law), it would supplant any
and all state legislation on track and
trace and ePedigree.
Despite the uncertainty surround-
ing which legislation will ultimately
become the standard, industry is fo-
cused on the January 2015 deadline
for implementation and the California
ePedigree legislation, as it is likely to
come on line frst.
“I would say that nearly half of the
frms that we have polled have already
started their pilot testing,” Jamie
Hintlian, principal, Americas at EY,
told Pharm Exec. “It is a very tight
pack. No one is out front in the sense
that they have 100 percent of their
lines and products serialized. I think
most are going to come close to hitting
the 50 percent mark by January 2015,
but there are concerns. Concerns
about how much do you invest versus
hedge because maybe there will be a
federal law that trumps California.
While many would like to wait and
see, they are not ready to play chicken
with the state of California, the 12th
largest economy in the world.”
The proposed legislation gaining
traction in Congress does not go as far
as the California initiative, at least at
the start. The main points of the pro-
posed bill, H.R. 3204, include:
» Four years after enactment, manu-
facturers need to serialize each
package of product distributed
within the United States.
» At the start of 2015 for manufac-
turers and July 2015 for dispens-
ers—as product changes owner-
ship, companies need to provide
or receive transaction information,
history, and statements in a single
document (paper or electronic).
Four years from enactment, all in-
formation needs to be exchanged
electronically.
» Ten years after enactment transac-
tion information needs to be ex-
changed in an electronic matter at
the unit level starting at the point of
manufacture.
The glaring difference between the
California and Federal proposals is the
timeline required for full serialization
at the unit level. California calls for
unit serialization on January 1, 2015,
while the Federal legislation requires
the same four years after the Drug
Quality and Security Act takes effect.
The differences are forcing industry to
decide whether to pull for a particular
piece of legislation. But which one?
“To some degree, industry’s prefer-
ence for one piece of legislation over
the other will depend on where or-
ganizations are on the readiness con-
tinuum,” Hintlian says. “It appears
based on the recent September agree-
ment between the House and Senate,
the federal direction may be closer to
California’s direction, as it requires se-
rialization at the package level. In this
case, organizations that have made
progress with their California com-
pliance programs will likely continue
with their programs, although some
may alter their timelines for deploy-
ment based on how the federal direc-
tion is fnalized.”
European Union. Like their US
counterparts, EU lawmakers are in the
midst of hammering out some form of
serialization legislation. The Direc-
tive 2011/62/EU the European Parlia-
ment issued in June of 2011 gives EU
member states until 2016 to enact se-
rialization legislation. Just like in the
United States the exact legislation is
unclear—with each of the 28 Member
States being charged with creating its
own legislation things are bound to
get increasingly complicated.
Unlike the proposed US legislation,
the likely EU laws will focus on the au-
thentication of the product at the time
of dispensing, instead of the individual
movement of the product through the
entire supply chain. When a pharma-
cist scans a blister pack (the most com-
mon form of dispensing in Europe) at
the counter, the product’s serial num-
ber would be run through a database
to check if that particular number was
ES347279_PE1113_038.pgs 10.30.2013 19:32 ADV blackyellowmagentacyan

39
NOVEMBER 2013 www.PharmExec.com
Supply Chain
fagged for any reason. If the product
was fagged the pharmacist would be
unable to dispense.
Biggest threats to the supply chain
Counterfeit pharmaceutical drugs are
becoming more and more prevalent
around the globe—as counterfeiters
become more sophisticated it becomes
increasingly diffcult to tell the differ-
ence between a counterfeit product
and the real McCoy, especially at frst
blush. While there will always be a
black market for prescription drugs,
the adoption of stricter tracking of
pharmaceuticals as they cycle through
the supply chain will make it tougher
for counterfeits to make their way into
the legitimate trade.
UPS’s 7th annual “Pain in the (Sup-
ply) Chain Survey” polled healthcare
executives across the globe on their
top business and logistics concerns.
According to the report, 48 percent of
those polled believed that counterfeiter
sophistication is growing faster than
countermeasures. In Asia, 76 percent
of those polled were concerned about
product security, signifcantly more
than their peers elsewhere.
“As more and more companies are
moving into the Asian, Latin Ameri-
can, and African markets, the length
of the supply chain and the handoffs
have increased,” William Hook, vice
president, global strategy, healthcare
logistics at UPS said. “Every time
the chain is increased you leave a
vulnerable point.”
As the supply chain lengthens in a
global marketplace, the possibility of
theft increases as well. While most
would agree that the supply chain in
the United States is relatively secure
from theft, the same cannot be said of
other areas of the globe.
“On a percentage basis, pharma-
ceutical theft in the supply chain is not
high,” Hsieh says. “What is interesting
is it is usually one of the higher value
products that are stolen. There was
a high of several million dollars per
theft incidence a couple years back.
Then many pharma companies put a
limit on the amount that can go out
in one shipment. Last year the average
pharmaceutical cargo theft was valued
at about half a million dollars.”
Be Proactive—and Think Small
In anticipation of serialization legis-
lation taking effect, pharmaceutical
companies need to review not only
their own internal practices, but also
those of their outsourcing partners. As
more and more work is outsourced the
possibility for mishandling of product
becomes greater and greater, and the
need for technology solutions for both
sides of the outsourcing relationship
becomes more evident.
“We are seeing OEMs who are
struggling with small contract manu-
facturers who don’t have systems that
can facilitate the sharing of product
information,” John Danese, senior
director, life sciences at Oracle says.
“I have spoken with some of our
OEMs who are preparing for the Cal-
ifornia ePedigree regulation and oth-
er global track and trace regulations.
They say some of their CMO’s idea
of an advanced data sharing mecha-
nism is a fax machine. Additional
electronic communication is needed
moving forward as these regulations
come online in order for these small
companies to be able to exchange the
necessary data.”
The global pharma supply chain
continues to grow with each passing
year. With every additional link in the
chain greater risk follows.
Timothy Denman is Pharm Exec’s Senior
Managing Editor. He can be reached at
E D U C A T I N G L E A D E R S F O R B U S I N E S S A N D S O C I E T Y
The Yale School of Management’s
MBA for Executives offers a focused
program of study created to prepare
the next generation of healthcare
leaders. Join entrepreneurs, health
practitioners, executives and others
from across healthcare sectors.
Develop critical leadership and
management skills through a
rigorous MBA curriculum with an
emphasis on the rising complexities
of an industry in transition.
Learn more at mbae.som.yale.edu
ES347381_PE1113_039.pgs 10.30.2013 20:04 ADV blackyellowmagentacyan

Special SponSored Section
In the 6th annual UPS Pain in the (Supply) Chain survey, UPS sees emerging evi-
dence of a coming shift in the healthcare supply chain.
Judging by the results of the latest Pain in the (Supply) Chain survey, while most healthcare companies continue to grapple with all-too-familiar pain points in their supply chains, some are reporting that the strategies they employed have brought about success.
Meanwhile, the increasing complexity of healthcare products, the burdens of the regulatory environment and the promise of emerging markets are combining to generate not only new challenges but also opportunities to rethink the supply chain.
This year’s expanded survey reveals that while healthcare companies have been successful to varying degrees in address-ing the industry’s most prevalent logistics challenges, the strategies that ensure bal-anced success are elusive .
New insights, however, show that those who have been most successful are increasingly leveraging logistics and dis-tribution partnerships for expertise and
support in areas such as new market ac-cess, supply chain optimization, regulatory compliance, IT, monitoring and interven-tion, and even shipment insurance. UPS sees the trend towards partnership gain-ing momentum as healthcare logistics ex-ecutives seek proven methods for optimiz-ing their intricate, elongated supply chains.
While many healthcare manufacturers rely primarily on their own initiative and resources to manage their supply chains, it is becoming increasingly apparent that the industry leaders reporting the most signif-cant and sustained supply chain improve-ments are leveraging global supply chain solution providers. This leaner model is less capital intensive, freeing up resources and allowing companies to focus on their core life sciences competencies.
New growth opportunities exist along-side an increasingly complex regulatory
and legislative environment.
Supply chain concernsRegulatory compliance, product security and cost management top the list of global supply chain concerns in 2013. For the frst time, product security jumped ahead of cost management to become the second top global supply chain pain point. (see chart above). The latest survey shows that
companies are focusing on technology adoption, increasing regulatory expertise and using partnerships with outside ex-perts to overcome compliance challenges. Despite other countries’ regulations, three-quarters of healthcare executives are still planning to tap new global markets within the next fve years.
Today, supply chains are longer and products are more high-value and com-plex, making product protection para-mount to success. As product protection challenges grow in intricacy, many logis-tics executives are insuring shipments with trusted partners and also investing in technology solutions. Top cost chal-lenges include shipping and labor, and more complex supply chains. Healthcare professionals then are focused on logistics and distribution partnerships, technology investment and supply chain optimization
as leading cost management strategies.
Future strategiesThe top three growth strategies for health-care executives over the next fve years are technology investment, global market expansion and increased use of new distri-bution channels — with signifcant jumps in the number of executives employing these strategies.
In the three leading supply chain con-cerns (regulatory compliance, product pro-tection and managing costs), two themes surface as supply chain best practices: accumulating or partnering for expertise, and using best-in-class technologies.
Logistics professionals are ensuring they have the supply chain and regula-tory profciency — whichever route they choose to conquer these challenges.
Order management and web ordering technology will continue to lead as the top IT investments, but healthcare logistics executives also plan to invest signifcantly more in temperature-sensitive, security-specifc, and e-pedigree and serialization technologies over the next fve years (see adjacent chart).
Clearly, within the constantly evolving marketplace of healthcare logistics, deci-sion makers are fnding ways to surmount emerging challenges. At UPS, our broad healthcare-optimized portfolio and unpar-alleled expertise ofer healthcare manu-facturers the opportunity to solve their logistics problems with a mix of fexible, customized solutions, in one place, from a single provider. Whatever the challenge, we have a solution. What’s more, we never forget: “It’s a Patient, not a Package. ”®
Preparing for Healthcare Supply Chain Transformation
thenewlogistics.ups.com/healthcare
ES349364_PE1113_040.pgs 11.01.2013 22:08 ADV blackyellowmagentacyan

Copyright ©2013 United Parcel Service of America, Inc.
HOW LOGISTICS FINDS HIDDEN
VALUE IN YOUR SUPPLY CHAIN.
network of healthcare distribution facilities. Coupled with our
flexible transportation network, UPS can help identify cost savings
throughout your supply chain.
LESS LOSS
Your products are developed for specific outcomes. If there’s a
compromise in quality, everyone loses. The patient’s health suffers,
your spoilage rates go up and your reputation can be tarnished.
At UPS, our experts work with you to understand your products
and offer a range of safeguard options to help shipments arrive
in optimal condition, reducing product
loss and improving your bottom line.
Knowing where to look is vital. Looking across your supply chain reinforces how enormously complex it can be to
manage for greater agility, find efficiencies and identify cost savings. When you collaborate with UPS, you can tap
into our expertise in healthcare logistics and utilize tools that can help better position your company for success.
ENGINEERED SUCCESS
The health of your supply chain has never been more important
or strategic. The ability to quickly respond to market demands,
target growth markets and ensure reliable supply is essential
for success. UPS can help you rethink and redesign your supply
chain to take advantage of new opportunities, investigate new
channels and improve outcomes.
FINDING EFFICIENCIES
Turning supply chain inefficiencies into opportunities takes
collaboration and innovation. You can reduce waste by using
only the space you need when you leverage UPS’s global
UPS has the expertise and experience to find hidden value in your supply chain.See how we did it for EndoChoice at ups.com/endochoice.
ES346841_PE1113_041_FP.pgs 10.30.2013 01:43 ADV blackyellowmagentacyan
ES349728_PE1113_042.pgs 11.04.2013 22:48 ADV blackyellowmagentacyan
Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S2
This sponsored supplement was produced by Focus Reports.
Project Director: Andrey MuntyanProject Coordinator: Emilie LaumondProject Assistants: Joan Abellan Ponce de Leon,
Stephen WagerProject Publisher: Julie AvenaGraphic Assistance: Omar Rahli
For exclusive interviews and more info, please log onto www.pharmaboardroom.comor write to [email protected]
The past three years have been some of the most event-
ful in memory for Taiwan’s life sciences industry. At
this year’s Bio Taiwan exhibition, the annual confer-
ence that invites the international life sciences com-
munity to the island, the excitement was palpable. Foreign
companies turned out in record numbers to a keynote ad-
dress from President Ma Ying-Jeou, who acknowledged
that Taiwan was a latecomer to the sector, but nonetheless
had the capability and will to compete. Buoyed by a suc-
cessful wave of fnancing, good product strategy, and in-
creasing international penetration, the industry seems
confdent.
Painting by Adele Chen
Preparing for TakeoffTAIWAN:TAIWAN:
ES349730_PE1113_043.pgs 11.04.2013 22:48 ADV blackyellowmagentacyan

taiwan report
Special SponSored Sectionpharmaboardroom.com
S3 FOCUS REPORTS noVeMBer 2013
Albert Liou, vice chairman of PAREXEL International,
thinks that now Taiwan needs leadership, and success stories.
He points to the drug development chain. “Taiwan has great
capabilities in each step along the chain,” he says. “But the
linkages are not as strong as they could be. Academically and
therapeutically, Taiwan is very capable in certain areas, like
liver disease. But in terms of drug development from discov-
ery to market, we are several years behind the West. We need
leadership that can unite the links in the chain. We need, as
well, our frst success stories to serve as motivation and as
development models.”
“We believe those frst stories are coming shortly,” Liou
says. As for leadership, many in Taiwan look to a man that has
emerged as a major connector in the country’s life sciences in-
dustry: Johnsee Lee, who chairs Taiwan’s Development Center
for Biotechnology (DCB) and the Taiwan Bio Industry Orga-
nization (TBIO).
When Lee took over his post at the DCB in 2010, he felt
that the institute focused too much on academic research:
“The wrong place for us,” he says. Many industry stakehold-
ers have pointed out that in the life sciences, Taiwan has too
long emphasized—“perhaps overemphasized,” says Lee—basic
research over commercialization, and that the DCB was do-
ing the same work as other national institutes like Academia
Sinica.
Lee quickly got to work positioning DCB as the “second
baton in the relay race,” a translational facilitator between
the lab and the shelf. As Taiwan implements a strategy that
its economic council calls Diversify-Innovate-Globalize
(DIG) to ease away from the country’s reliance on informa-
tion and communication technologies (ICT), commercializ-
ing new industries is the name of the game. Biotech is at the
top of a list of six strategic emerging sectors: the “key indus-
try” to watch in Taiwan today, says EY’s country managing
partner James Wang.
In his capacity as chairman of the TBIO, a unifying as-
sociation in Taiwan’s life science industry, Lee is responsible
not only for helping Taiwan’s drug development effort, but for
connecting the dots in a staggeringly diverse sector. In 2013,
Taiwan’s Ministry of Economic Affairs (MOEA) counted 1505
life sciences companies in this market of 23 million people.
Grouped under the heading “biotechnology”—the term that
we will use throughout this report—these companies may be
surprising in number for a small island nation, but they are
perhaps most impressive in variety. Taiwan has 450 companies
in the applied biotech segment, 350 companies in the pharma-
ceutical segment and 705 medical devices companies!
From left: Johnsee Lee, Chairman, Development Center for
Biotechnology; Albert Liou, Vice Chairman Asia Pacifc, Parexel;
James Wang, Country Managing Partner, EY
Bio Taiwan 2013 with President Ma Ying-Jeou
ES349727_PE1113_044.pgs 11.04.2013 22:48 ADV blackyellowmagentacyan

Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S4
Focus Reports frst met Medigen chairman
Stanley Chang in 2010. “Three years ago,” he
says, “we sat and spoke in the very same offce,
with the very same furniture. The difference is
that today, our company has grown almost 40
times in value.”
Medigen, whose early-stage liver cancer drug
PI-88 should “by all indicators” be the second
innovative drug to come out of Taiwan after Tai-
gen’s Nemonoxacin, went public on the GreTai
exchange in 2011 in an IPO that Chang calls highly suc-
cessful.
“In the past,” he says, “investors in Taiwan believed
that this sector was hopeless, and that drug development
was mission impossible. But we have championed the
idea that as long as the vision is correct, as long as the
strategy is correct, and as long as the market conditions
are correct, our goals are achievable!”
Chang believes that investor confdence was bolstered
by two factors: trial results, and market potential. PI-88
has now successfully moved to Phase III. Its
intended target, liver cancer, is a leading killer
in China, Taiwan, and Asia at large.
Medigen is participating in the pilot program
that is testing the waters for clinical collaboration
between Taiwan and China. Chang is excited: “In-
vestors saw two hurdles for our industry in the
past: approval in Taiwan, and approval in China.
In the next year or two, those two hurdles will for-
mally become one. There will be mutual recogni-
tion—saving huge amounts of time and money.”
Is his company overvalued? Chang says no. “Let’s con-
sider the typical case in the West: normally, when a bio-
tech company has several projects in its portfolio, its fron-
tier product is in Phase III, and its business fundamentals
are strong, its share price hovers around 10 USD. Hence,
our stock price is not over-infated—rather, companies
like Medigen were undervalued in the past. We are now
approaching the international standard. In fact, I believe
there is room for further growth.”
An IPO case study: Medigen
Stanley Chang,
CEO & Chairman,
Medigen
Biotechnology Corp
Medigen Biotechnology Corporation upholds the vision of “Innovations for a Better Life” focusing at the
developments of new therapies for liver diseases and cancers. Medigen has three major business units:
New Drug Development, Nucleic Acid Testing, and Cell-Based Vaccine Technology.
We believe that, through international collaborations and persistence in pursuing best innovations,
Medigen will become one of the premier biotechnology companies in Asia.
14F, Bldg F, Park St., Nangang District, Taipei City 115, Taiwan (R.O.C.) / Tel: 886-2-2653-5200 / Fax: 886-2-2785-6120
www.medigen.com.tw
ES349726_PE1113_045.pgs 11.04.2013 22:48 ADV blackyellowmagentacyan
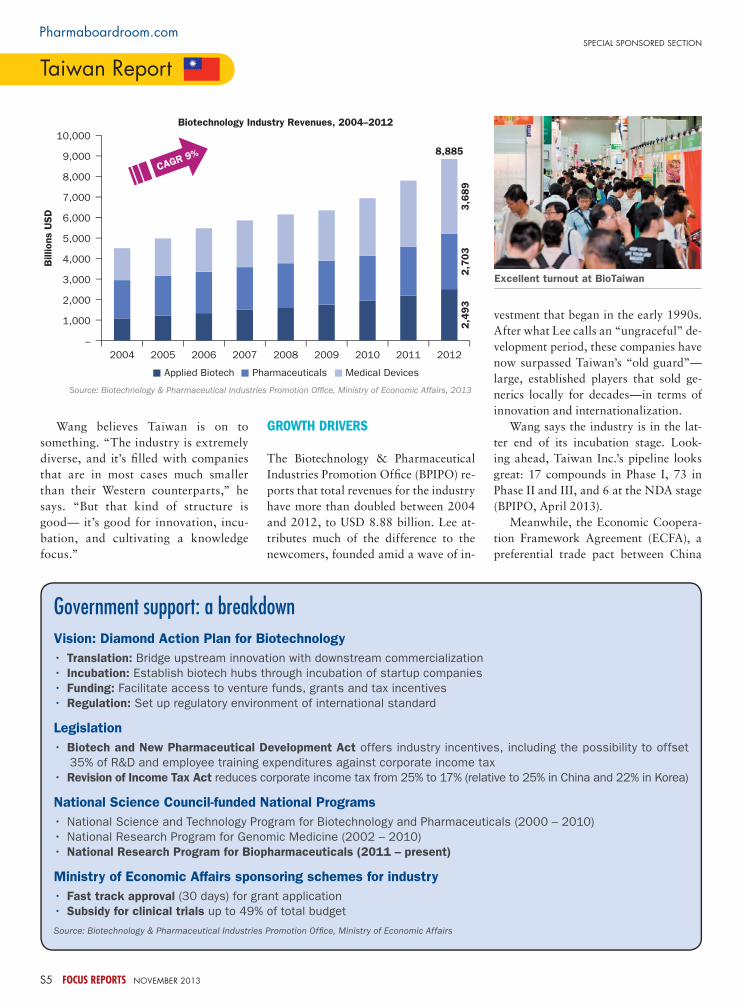
taiwan report
Special SponSored Sectionpharmaboardroom.com
S5 FOCUS REPORTS noVeMBer 2013
Wang believes Taiwan is on to
something. “The industry is extremely
diverse, and it’s flled with companies
that are in most cases much smaller
than their Western counterparts,” he
says. “But that kind of structure is
good— it’s good for innovation, incu-
bation, and cultivating a knowledge
focus.”
Growth drivers
The Biotechnology & Pharmaceutical
Industries Promotion Offce (BPIPO) re-
ports that total revenues for the industry
have more than doubled between 2004
and 2012, to USD 8.88 billion. Lee at-
tributes much of the difference to the
newcomers, founded amid a wave of in-
vestment that began in the early 1990s.
After what Lee calls an “ungraceful” de-
velopment period, these companies have
now surpassed Taiwan’s “old guard”—
large, established players that sold ge-
nerics locally for decades—in terms of
innovation and internationalization.
Wang says the industry is in the lat-
ter end of its incubation stage. Look-
ing ahead, Taiwan Inc.’s pipeline looks
great: 17 compounds in Phase I, 73 in
Phase II and III, and 6 at the NDA stage
(BPIPO, April 2013).
Meanwhile, the Economic Coopera-
tion Framework Agreement (ECFA), a
preferential trade pact between China
Biotechnology Industry Revenues, 2004–2012
Source: Biotechnology & Pharmaceutical Industries Promotion Office, Ministry of Economic Affairs, 2013
10,000
9,000
8,000
7,000
6,000
5,000
4,000
3,000
2,000
1,000
–
2004 2005 2006 2007 2008 2009 2010 2011 2012
8,885
3,6
89
2,7
03
Billions U
SD
Applied Biotech Pharmaceuticals Medical Devices
CAGR 9%
2,4
93
Vision: Diamond Action Plan for Biotechnology
• Translation: Bridge upstream innovation with downstream commercialization
• Incubation: Establish biotech hubs through incubation of startup companies
• Funding: Facilitate access to venture funds, grants and tax incentives
• Regulation: Set up regulatory environment of international standard
Legislation
• Biotech and New Pharmaceutical Development Act offers industry incentives, including the possibility to offset
35% of R&D and employee training expenditures against corporate income tax
• Revision of Income Tax Act reduces corporate income tax from 25% to 17% (relative to 25% in China and 22% in Korea)
National Science Council-funded National Programs
• National Science and Technology Program for Biotechnology and Pharmaceuticals (2000 – 2010)
• National Research Program for Genomic Medicine (2002 – 2010)
• National Research Program for Biopharmaceuticals (2011 – present)
Ministry of Economic Affairs sponsoring schemes for industry
• Fast track approval (30 days) for grant application
• Subsidy for clinical trials up to 49% of total budget
Source: Biotechnology & Pharmaceutical Industries Promotion Offce, Ministry of Economic Affairs
Government support: a breakdown
Excellent turnout at BioTaiwan
ES349757_PE1113_046.pgs 11.04.2013 22:50 ADV blackyellowmagentacyan

Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S6
Chang Yi Wang, chairperson & CSO of United
Biomedical Inc. (UBI) and UBI Asia, is working
on a functional cure for HIV and a vaccine for
Alzheimer’s.
Wang: At UBI Asia, we helped change the
ecosystem in Taiwan. From the outset, we in-
sisted on developing truly heavyweight products
in this country.
When we frst arrived here, the environment
was quite immature. Despite the fact that Tai-
wan was investing in biotech, there seemed
to be no cohesive planning. The market had money and
knew how to sell and make generics, but did not have
experience in transforming researchers’ ideas into new
commercial drugs.
I have not seen any true biopharma products come
out of Taiwan yet, despite the establishment of institu-
tions to bridge academia and industry. I believe this is
because the emphasis in the past was on technology
development, rather than products. Technology is impor-
tant, but the ecosystem needs a product focus
to elevate technology to the next stage. A plat-
form can deliver a thousand results, but which
results? Without a product, you cannot tie the
pieces of the puzzle together.
UBI’s fagship HIV receptor antibody was able
to act as that catalyst. We have built a very sol-
id drug development platform and team in this
country, and we have worked closely with agen-
cies like the Center for Drug Evaluation (CDE)
to obtain Phase I approval for drugs that are
frst-in-man. CDE had little experience in such matters:
in the past, Taiwan was a hub only for Phase IV trials, or
bioequivalence studies for generics. Nobody had looked
to Taiwan for frst-in-man research before us. Today, we
can bring a pipeline of drugs through Taiwan—some are
already in Phase II, and others will soon get there.
The next stage will be to scale up. We are preparing for
Phase III, and commercialization. The government contin-
ues to lag behind us, but we can help them to catch up.
Products make the platform
Chang Yi Wang,
Chairperson & CEO,
United Biomedical
Asia, Inc.
ES349746_PE1113_047.pgs 11.04.2013 22:49 ADV blackyellowmagentacyan

taiwan report
Special SponSored Sectionpharmaboardroom.com
S7 FOCUS REPORTS noVeMBer 2013
and Taiwan signed in 2010, has lowered trade barriers and
opened the door for broader collaboration with a country that
IMS estimates will become the world’s second largest pharma
market by 2015. “If Taiwanese companies develop a new mol-
ecule for a condition with high prevalence in Asia, why not
beneft a larger population?,” DCB’s Lee points out.
Investors smell an opportunity. “In the past,” Lee says,
“we were missing a crucial element of our ecosystem: fnanc-
ing. Now, because of the health of our capital market, venture
capitalists are quite willing to come on board because they see
an exit: sell the shares when companies foat their stock on
the public market. If Initial Public Offerings (IPOs) weren’t
so feasible in Taiwan at the moment, investors would be very
reluctant to participate in the long-term play that is biotech.”
eCFA: Just thAt—A FrAmework
Call it a promise. Taiwanese companies report that just be-
cause ECFA is in place doesn’t mean working with the jugger-
naut is straightforward.
Christopher Tsai, whose blood banking and genetic testing
company Bionet has successfully penetrated China, isn’t par-
ticularly bullish. When asked whether China is an easy market
for a neighbor with a shared heritage, Tsai offers mixed feel-
ings: “Is it easier for Taiwanese companies to do business
in China than it might be for companies with less cultural,
geographical, and political proximity? Absolutely. But that
doesn’t mean we have a free ticket. Penetrating China is still
very, very diffcult.”
For instance, three years after ECFA was put is in place,
pharmaceutical and med tech manufacturers in Taiwan still
need a separate license to sell their products in China, which is
not the case for Chinese healthcare products entering Taiwan.
As the chairman of the medical diagnostics company General
Biologics Corp, T.C. Lin, reports, “Today, it is not easy to get
licenses in China for our products, particularly with the furor
surrounding recent Big Pharma scandals in the country. The
Taiwan government is pushing for mutual recognition, and
producers on this side of the strait are eagerly anticipating a
change.” For those that rely heavily on the mainland, a China-
based manufacturing plant is often the best bet for now.
And yet, Taiwan has high hopes that this and other barriers
will come down one by one as ECFA gains steam. One particu-
lar focus area for cooperation is clinical research. The Taiwan
Food and Drug Administration (TFDA), which—crucially—is
by all accounts an excellent regulator, is working in concert
with the China Food & Drug Administration (CFDA) to pave
the way for what Taigen chair Ming-Chu Hsu calls a “faster,”
“lower cost” paradigm for reaching the Greater China market
with innovation.
Taigen, a drug development company that is at the New
Drug Application (NDA) stage with its diabetes-focused prod-
uct Nemonoxacin, is expected to release Taiwan’s frst innova-
tive drug capable of meeting the CFDA’s Category 1.1 New
Drug requirements. The company is participating in a clinical
trial pilot program with a handful of other late-stage peers.
Industry stakeholders hope the program will lead to broad
harmonization of protocols and mutual data recognition. The
“ultimate goal,” says Parexel’s Albert Liou, is that “any new
drug will be simultaneously approved in Taiwan and China.”
The typical model may look something like this: compa-
nies will conduct Phase I and Phase II trials in Taiwan, where
today the IP protection is more stringent, the clinical trial
From left: Christopher Tsai, CEO, Bionet Corp; T.C. Lin, Chairman
& President, General Biologicals Corporation; Ming-Chu Hsu,
Chairman and CEO, TaiGen Biotechnology
EY Life ScienceWe help drive your business performance
Bringing together a worldwide team of industry profes-sionals, we have over 5,000 industry professionals with deep experience in providing assurance, tax, transaction and advisory services.
Ernst & Young Taiwan
+886-2-2757-8888www.ey.com/taiwan
安永聯合會計師事務所
© 2
01
3 E
rnst
& Y
ou
ng
, Ta
iwan
All
Rig
hts
Rese
rve
d.
ES349739_PE1113_048.pgs 11.04.2013 22:49 ADV blackyellowmagentacyan
APIs for injectables
Complex molecules
Custom cGMP peptides
High potency & cytotoxic compounds
Special Capabilities
A Global Leading Provider of API ServicesScinoPharm delivers high-value solutions with speed and flexibility
through a full range of services from custom synthesis for early phase
pharmaceutical activities to brand companies as well as APIs for the
generic industry. The Company also provides a vertically integrated,
one-stop-shopping service for its API customers by expanding into the
field of oncological injectable formulations.
ht tp : / /www.sc inopharm.com
ES349767_PE1113_049.pgs 11.04.2013 22:51 ADV blackyellowmagentacyan
taiwan report
Special SponSored Sectionpharmaboardroom.com
S9 FOCUS REPORTS noVeMBer 2013
authorization process
is faster (two to three
months in Taiwan, ver-
sus 12 to 24 months
in China), the patient
protection system is
mature, and there are
a number of great hos-
pitals and researchers.
“Ideally,” says Liou,
“Chinese authorities
will accept this data,
and Phase III trials will
take place in Taiwan
and China, with an eye
toward simultaneous
NDA flings.”
Some remain skepti-
cal. Fang-Yue Lin, the
superintendent of Tai-
pei Veterans General
Hospital (TVGH), a
major clinical research
Ex-Genentech veterans Racho
Jordanov and Rose Lin co-found-
ed the drug development servic-
es startup JHL Biotech in 2012.
In their frst round of fnancing,
they raised more money than
the Genentech IPO!
Why headquarter this company in
Taiwan?
Firstly, Taiwan is in Asia—and
this region is where the growth is.
Within Asia, Taiwan has a num-
ber of advantages for us. First of
all, it has wonderful science and
a great entrepreneurial spirit.
They understand technology, and
they understand manufacturing.
Taiwan also respects intellectual
property, and has excellent sup-
port for clinical trials.
What gap can you fll in the market?
Most countries in this region have
the same issue: they cannot af-
ford Western drug prices, and while
they have the science and the
funds to make drugs themselves,
they lack technical understanding.
That is something we can provide
in both biosimilar and new drug
development.
What’s next for JHL?
Our dream has always been to cre-
ate what we call our ‘solar system’:
a technology center in Taiwan, with
manufacturing companies spread
around China and Southeast Asia.
We are already putting the largest
single-use biopharma factory in the
world in China—but we won’t stop
there.
The startup
Racho Jordanov,
President & CEO,
JHL Biotech
Rose Lin, General
Manager, JHL Biotech
ES349777_PE1113_050.pgs 11.04.2013 22:51 ADV blackyellowmagentacyan

Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S10
center in Taiwan, remarks, “It would re-
quire a lot of ‘advantage sharing’ for Chi-
na to accept clinical trial results obtained
in Taiwan—and in my personal opinion,
it will be very diffcult to persuade the
Chinese on this point.” Industry leaders
point to the fact that similar agreements
with Hong Kong have looked great on pa-
per but meant less in practice.
Liou is more optimistic. “I think the
model will work, and eventually, it will
work quite smoothly,” he says. He doesn’t
believe that Hong Kong is a fair compari-
son. After all, both men agree on one thing: as Lin puts it, Tai-
wan has a “very robust” indigenous pharmaceutical industry,
with “many new drugs” under development—“something that
differentiates this country from its neighbors.” Liou observes
that the government has a vested interest in seeing this indus-
try succeed, and will work hard to fnd a way to penetrate
Taiwan’s biggest potential market.
Moreover, although currently only local companies are
involved in the clinical pilot program with the mainland, it
is feasible that once the kinks are worked out, benefts will
extend to multinationals too. Lin, whose
hospital has a research cooperation
agreement with GSK, has a confdent
partner on his hands. GSK’s local general
manager, Thomas Willemsen, says, “Tai-
wan remains one of the best R&D loca-
tions in the Asia Pacifc region, despite its
relatively small market size. And in addi-
tion to being a good research platform,
Taiwan is also the perfect epidemiologi-
cal environment for proof of concept or
early phase trials for products destined
for the Chinese market.”
ECFA, as the name implies, is just that—a framework. It’s
up to the stakeholders to bring real cases through.
the enAbler
The buck doesn’t stop at R&D. In Taiwan, the saying goes
that from a strategic standpoint, the fastest route to Beijing
is through Taipei. Marietta Wu, who heads the Taiwan sub-
sidiary of US-based venture capital frm Burrill and Com-
pany, calls the country an “enabler.” An enabler for large
From left: Thomas Willemsen, Vice
President and General Manager, GSK;
Fang-Yue Lin, Superintendent, Taipei
Veterans General Hospital
Integrated ADC
Service
DrugLinker
Monoclonal Antibody
Small Molecule Synthesis
Process Development
Analytical Method
Development
Scaling Up
GMP Production
High Potency Drug from
Development to
Commercial Manufacturing
Cell Line Development
Process Development
Analytical Science and
Protein Characterization
GMP Manufacturing
Project Management
CMC
Development
Nonclinical
Material Supply
Clinical
Material Supply
Regulatory
Support
ES349754_PE1113_051.pgs 11.04.2013 22:50 ADV blackyellowmagentacyan
taiwan report
Special SponSored Sectionpharmaboardroom.com
S11 FOCUS REPORTS noVeMBer 2013
multinationals, but principally an enabler for the second tier:
small to mid-size biotechs.
“When these companies attempt to penetrate the Chinese
market, they inevitably face various hurdles,” says Wu. “Espe-
cially now that ECFA is in place, Taiwanese partners can serve
as a springboard. Taiwan understands Western business prac-
tices, can offer a strong talent pool to the industry, and also
has very strong IP protection and transparent governance—all
issues that Western companies care about deeply.”
One common approach for international companies, ac-
cording to Audrey Tseng, deputy chairman at PwC Taiwan is
to “undertake R&D in Taiwan and use China for market and
commercial purposes”.
For companies moving from East to West, it may be that the
fastest route to Washington is through Taipei as well. Wu men-
tions a China-based Burrill portfolio company that is looking
to establish an operation
in Taiwan. Why? Wu
explains, “As the com-
pany has grown and
established itself in the
Chinese market, it has
decided to try to reach
the US. They found
that Taiwan is a great
place to do clinical stud-
ies, and a great place to
bridge to the West.”
Taiwan is known for meeting international standards at a
time when China still lags behind. “A good partnership in Tai-
wan can enable a Chinese company to attain US FDA compli-
ance. FDA certifcation is a long process—having an already-
certifed Taiwanese partner can help them to climb that ladder
much faster,” Wu says. Where once Taiwan outsourced to
China for low-value manufacturing, China is increasingly out-
sourcing to Taiwan when it needs to climb up the value chain.
need Fuel? GAs up At the GretAi
“Perhaps the most profound change in the industry has been
the ascent of biotech companies pursuing an IPO,” says Au-
drey Tseng, deputy chairman at PwC Taiwan. “By pursuing
this capital raising path, many companies have reaped the
rewards. As a result of the sector’s development and
Taiwan’s unique stock trading environment, there has
been a conspicuous shift in investment capital from
the ICT sector and towards the biotech arena.”
ASLAN, a Singapore-based virtual drug develop-
ment company, took the decision to set up an offce in
Taipei. Its CEO Carl Firth says he and his team came
for the forward-thinking clinical environment—but
they don’t mind the fnancing options either.
Firth says, “Look at the number of venture funds
that exist in Taiwan. There may well be hundreds!
Many are now actively looking for a piece of the pie
in biotech. At the same time, we have the ‘Mom and
Pop’ investors sitting at home and thinking that they
want a bit of risk in their stock portfolio, and don’t
just want to buy into blue chips. A younger, up and
coming biotech company can look quite appealing. Fi-
nally, we have big corporates that have set up venture
funds. YFY—a paper conglomerate that set up YFY
Biotech Management Company—is a good example.
These funds have an appetite for risk that is quite
unique in Asia Pacifc.”
As the ICT sector has matured, investors are
looking for a new outlet. Lai-Shou Su, deputy ex-
ecutive secretary of the state-controlled National
Number of compounds that have reached Phase I: 17*
Number of compounds that have reached Phase II and III: 73*
Number of compounds that have reached NDA stage: 6*
Percentage of compounds applied for IND with U.S. FDA: 45%**
*Source: Biotechnology & Pharmaceutical Industries Promotion Offce, Ministry of
Economic Affairs, April 2013
**Source: Department of Industrial Information, Development Center for Biotechnol-
ogy, December 2012
Drug Development in Taiwan
Small molecules47%
Others1%
Biologics23%
Botanics32%
From left: Marietta Wu, Managing Director Taiwan, Burrill & Company; Audrey Tseng, Deputy Chairman,
PwC; Carl Firth, CEO, ASLAN Pharmaceuticals; Hong-Jen Chang, Chairman & CEO, YFY Biotech Management
Company; Lai-Shou Su, Deputy Executive Secretary, National Development Fund, Executive Yuan
ES349765_PE1113_052.pgs 11.04.2013 22:50 ADV blackyellowmagentacyan

Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S12
Development Fund (NDF), says
that the Ministry of Economic
Affairs recognized the waning
opportunities in Taiwan’s prize
industry, and looked toward in-
cubation. “For the past thirty
years, this country has been very
successful in semiconductors,”
he reports. “But increasingly,
the proft margins in this feld
are shrinking. Meanwhile, in the
year 2000, the human genome
was sequenced—and like many
other countries, Taiwan became
very excited about the future of
biotech. The sector was chosen
as an important driver in the
diversifcation of our economy
away from high tech.”
Refecting on his place in the
ecosystem, Su says, “the reason
the government created this
fund is to help build new indus-
tries from the ground up, when
there is not yet much guaran-
tee of success. In this way, the private sector can build conf-
dence.” The NDF must “set the fre—then others will join in
by throwing more kindling!”
Among the private sector, the fre is now raging. According
to the Market Post Observation System of the Taiwan Stock
Exchange, the market capitalization of listed and over-the-
counter (OTC) biotech companies in Taiwan has grown an
astounding 520% in the last four years alone, from USD 2.5
billion in January 2009 to USD 15.7 billion in March 2013.
Of course, biotech tends to be a much longer-term play than
high tech. Investors have had to taper their expectations. Be-
fore the mentality shifted, many of the early-mover companies
had to demonstrate steady revenues before they could get into
the larger rounds of fnancing. But increasingly, companies
are able to sell the dream: “Some time ago,” reports Lee-Chen
Liu, president and CEO of the startup EirGenix, “investors
in Taiwan would always ask if they could see a return within
two or three years. Now, they ask about the product, and the
potential. Now, they seem willing to wait.”
EirGenix recently bought DCB’s biopharmaceutical pilot
plant facility, with an eye toward providing contract development
and manufacturing services (CDMO) to the world. “Our experi-
ence was quite remarkable,” Liu says. “We raised USD 18 million
in just two months. Our investors include active pharmaceutical
ingredient (API) producer Formosa Laboratories—which owns
20 percent of the company—venture capital frms, and banks. I
have never seen a fundraising round go this fast in the US.”
Total number of listed and OTC biotech companies in 2012: 71 (up from 13 in 2011)
Total revenues of companies in 2012: USD 3.31 billion (up 27% from 2011)
Total market capitalization of companies in 2012: USD 13.86 billion
Total market capitalization of companies in April 2013: USD 15.7 billion
Market cap growth, January 2009 – April 2013: 520%
Source: Market Observation Post System, Taiwan Stock Exchange, April 2013
Biotechnology Industry Market Capitalization, 2007–2013
16.00
14.00
12.00
10.00
8.00
6.00
4.00
2.00
0.00
2007 2008 2009 2010 2011 2012
Billion U
SD
200
160
120
80
40
0
13.86
3.51
371.43
No. of com
panie
s
Total revenue
Total market value
No. of listed companies
71
3.31
ES349770_PE1113_053.pgs 11.04.2013 22:51 ADV blackyellowmagentacyan

taiwan report
Special SponSored Sectionpharmaboardroom.com
S13 FOCUS REPORTS noVeMBer 2013
When it is ready, EirGenix will have
a great option for going public: the Gre-
Tai Securities Market (GTSM). Built
with small and medium enterprises
(SMEs) in mind—helping Taiwan’s
economy to develop the “Taiwan way”
says GreTai chairman Sou-Shan Wu—
the multifunction GreTai offers both
listed and over-the-counter (OTC) trad-
ing, tailored for companies that are part
of emerging industries.
Biotech has taken over the exchange.
At the time of writing, the top three
stocks traded on GreTai’s ‘emerging,’ or
OTC, market, are Taigen, TWi Pharma,
and OBI; Mycenax is 6th: all pharma
companies. Meanwhile, the biotechnol-
ogy and healthcare index leads GTSM
listed stock categories, more than dou-
bling the numbers put up by the major-
ity of other sectors. In 2012, more bio-
techs went public in Taiwan—13—than
companies from any other industry.
bubble, bubble, toil And trouble
Are we looking at a bubble? Wu is frank:
we are. “I think more than 30
percent of the biotech compa-
nies trading on the GTSM are
overvalued,” he says. “The
GTSM has a higher average
turnover ratio, and higher av-
erage P/E ratio, than the ex-
changes you will fnd in places
like Shanghai, New York, To-
kyo, or even Seoul. The ratios
for biotech are higher still.
Based on the numbers, no one
can say this isn’t a bubble in the truest
sense of the word.”
Dr. Soo, managing director of the Su-
pra Integration and Incubation Center
(Si2C), is equally candid: “The environ-
ment is starting to overheat. The prob-
lem is that this shooting star might have
promoted a short-term investment strat-
egy which is antithetical to the interests
of the development of the industry. We
need to address this danger.”
“And yet,” Wu continues,
“we need that bubble to grow.
Moreover, I would say the
bubble is still under control.
Why? First, we have more NT
dollars circulating in Taiwan
today than in years past—for
better or worse, this is a result
of the low interest rates we
have today.
The second reason is this
dream is a good one. Look
at how many people there are in China
that need safe drugs.”
Still, investors would do well to ex-
ercise caution. Tsu-Der Lee, chairman
of Taipei Medical University, says of the
state of the public market, “In a hurri-
cane, even a turkey can fy!”
For now, some companies are opting
Soushan Wu,
Chairman, GreTai
Securities Market
TWi Pharmaceuticals, Inc.3F, No. 41, Lane 221, Kang Chien Rd., Nei Hu Dist.
Tel: 886-2-26573350Fax: [email protected]
Innovation, Integrity and Integration
TWi Pharmaceuticals, Inc., headquartered in Taipei, Taiwan, is a technology-based specialty pharmaceutical company focusing on the development and commercialization of high barrier generic prescription products and branded drugs.
ES349774_PE1113_054.pgs 11.04.2013 22:51 ADV blackyellowmagentacyan

Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S14
for a more traditional approach. TWi
Pharmaceuticals, a US-focused generics
company, presents itself to investors frst
and foremost as a business that cares
about the bottom line.
Calvin Chen, the company’s presi-
dent, reports, “We told our underwrit-
ers and analysts not to look at us as a
pharma company, but rather as a proft-
driven business, regardless of our sector.
Better to compare us to the IT industry!
In fact, IT companies’ proft margins
typically approach 20-30 percent, while
ours is closer to 60 or 70. We believe
that revenues, rather than story, should
drive up the valuation of a company.”
Chen has a few words of caution.
“The market is quite hot right now,” he
says, “and my background as a venture
capitalist makes me look at the situation
with a bit of concern. Certain Taiwanese
drug development companies have out-
licensed their compounds to US compa-
nies, and now their market cap is equal
or greater than that of their US partners.
“That seems very strange to me. In my
experience, unless a US biotech can sell
its own product—unless they have the
capabilities of a Celgene or an Amgen—
they cannot become very proftable. The
reason US investors recognize the value
of smaller biotechs is because the typical
expectation for these companies is that a
larger player will acquire them. For the
investor, it’s almost like buying an op-
tion. But I wonder about the biotechs
in Taiwan. What is the ultimate exit for
their investors? We haven’t seen any such
acquisitions in this country yet.
“Local investors may not be sophis-
ticated enough today. I wonder, when
reality hits, what their reaction will be.”
Perhaps the market and its investors
could use a bit more education, and a
bit more experience. Indeed, implant-
ing a new thought process is at the heart
of Si2C’s strategy. “It is critical that the
government, academic institutions and
investors reaffrm a stable, long-term in-
vestment approach and do not panic and
fee at the frst sign of diffculty,” says Dr
Soo. “Staying true to that approach will
insert confdence and faith and stability
in the system, and in the process, avert-
ing a psychologically driven run on the
exchange.”
FindinG A niChe
Hsing-Jien Kung, president of Taiwan’s
National Health Research Institutes,
believes that “instead of developing
along the same lines as the industry in
the US,” Taiwan should “look to po-
sition itself as a niche player, that can
offer innovative solutions to larger
countries.”
Rongjin Lin, chairman of TTY Bio-
pharm, perhaps the most pioneering and
internationally successful of Taiwan’s
‘old guard’ of generics companies, puts
it more succinctly. He tells his peers in
the industry, “Find a cost advantage, or
fnd a niche!”
From left: Lee-Cheng Liu, President & CEO, Eirgenix; C.Y. Cheng, President, Formosa
Laboratories; Whaijen Soo, Managing Director, SI²C; Tsu-Der Lee, Chairman, Board of
Trustees, Taipei Medical University
Onko-Sure® (DR-70 ELISA Assay) catches what CEA alone cannot. FDA approval for Colorectal Cancer Monitoring.
FOR A BETTER LIFE QUALITY
Uni Pharma Co., Ltd. ( Onko-Sure Asia Pacific Manufacturing and Distribution Headquarter )
8F, No. 43, Lane 115, Sec. 2, Chung Shan N. Road, Taipei, 104, Taiwan.
Tel: 886-2-2525-1480 Fax: 886-2-2525-1477
Email: [email protected] Contact Person: Freia Wei
ES349772_PE1113_055.pgs 11.04.2013 22:51 ADV blackyellowmagentacyan

taiwan report
Special SponSored Sectionpharmaboardroom.com
S15 FOCUS REPORTS noVeMBer 2013
Costs in Taiwan aren’t too bad, with
a corporate tax rate of 17 percent and la-
bor outlays that the industry reports are
stable relative to China’s more infation-
ary environment. But Taiwan’s generic
industry, populated by SMEs who in this
small, M&A-averse market may form
consortia but not mega-companies, lacks
the scale and vertical integration to play
the commodity game.
Taiwan has opted for a niche.
Charles Lin of US-focused generics
producer Lotus Pharmaceuticals reports, “We have focused
on so-called ‘multiple barrier’ products—products that are
diffcult to produce, and therefore represent signifcant bar-
riers to entry: formulation barriers, potency barriers, bio-
equivalence barriers, and so on. We have partnered with
strong local API producers like Formosa Laboratories,
which are also capable of operating on this level. Our strat-
egy is to avoid competition, rather than meet other compa-
nies head-on.”
Charles Lin hopes that this strategy
will be his entry ticket to the global mar-
ket—especially the US. He says that Lo-
tus doesn’t want to be a ‘local’ company
anymore. Like many of its peers, Lotus
sees diminishing returns from its tradi-
tional Taiwan-based business, and is con-
strained by the size of the market even on
good years. “Most of us are trying to go
global, but the problem is in the capabil-
ity. Only two or three local generics com-
panies, ourselves included, are actively
pursuing an international agenda,” says Lin.
Even when they reach the international stage with a high-
barrier product, the future may be uncertain. Rongjin Lin
believes, “After 2015, ‘diffcult’ generics will become ‘simple’
generics again! So even here, Taiwan has only a very small
window to compete.” Recently, TTY has jumped to develop-
ing patented drugs, following a progression that started with
medium-barrier generics in Taiwan, moved to high-barrier
generics internationally, and will culminate with incremental
From left: Calvin Chen, President, TWi
Pharmaceuticals; Rongjin Lin, Chairman,
TTY Biopharm
ES349763_PE1113_056.pgs 11.04.2013 22:50 ADV blackyellowmagentacyan
Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S16
innovation and then “truly” innovative
products by 2020—the “only way for us
to survive,” says TTY’s chairman.
Developing an innovative pipeline
while pursuing shorter-term gains is a
popular approach in Taiwan, especially
given the cultural proclivity for safer bets
that investors are only now shedding. For
instance, Taiwan Advance Biopharma-
ceutical Inc. (TABP), founded in 2000 as
the frst DCB spin-off, laid a foundation
with businesses like food testing. Today,
it is on its way to transforming into a bio-
pharmaceutical company.
Like its generics-focused peers, TABP takes a niche strategy.
Wen-Lung Su, Chairman, explains, “Our strategy is based on
collaboration rather than competition. Our development ef-
forts are currently focused on oncology, and today, the global
cancer drug market is worth tens of billions of USD. If all play-
ers in this feld adopted a competitive policy, then the current
market environment—wherein the large players make billions,
and the small players make very little—will never change. On
the other hand, if smaller companies shift their approach and
collaborate to expand the market, to the scale of hundreds
of billions of USD, then these partners can share the profts
from a new and larger pie.” True its strategy, TABP’s lead drug
Picture of National Health Research Institutes (NHRI) facilities
Hsing-Jien Kung,
President, National
Health Research
Institutes
ES349743_PE1113_057.pgs 11.04.2013 22:49 ADV blackyellowmagentacyan
taiwan report
Special SponSored Sectionpharmaboardroom.com
S17 FOCUS REPORTS noVeMBer 2013
candidate will look to complement, rather than compete with,
an Amgen oncology drug.
For many Taiwanese drug developers, the right niche is to
apply a unique technology platform to an acquire-and-develop
model, with an eye toward generating ‘me-better’ compounds
for Asia-prevalent diseases. Perhaps the most prominent cham-
pion of this approach is Taiwan Liposome Company (TLC),
which completed an IPO on the GreTai last year.
George Yeh, the company’s president, speaks of a ‘vacuum
area’: “TLC’s approach is based on creating value-added prod-
ucts. We do not look to develop frst-in-class or best-in-class
molecules. Instead, we innovate in areas like drug delivery. For
example: can our delivery system turn a daily dosage drug into
a weekly dosage drug?
“Such products typically will generate yearly global sales of
400-500 million USD, which I call the ‘vacuum area.’ At one
end of the vacuum you have the top twenty companies, which
are hunting for the next game changing, billion-plus block-
buster. At the other end you have small, localized generics
companies looking to enter the market quickly, with products
that can generate peak sales of 100-200* million USD. Due
to their lack of technical expertise, the small generics players
cannot enter the vacuum area; Big Pharma, on the other hand,
isn’t very interested in it. As such, this third, value-added ap-
proach comes in under the radar, and is perfectly tailored
for emerging markets—notably China—that are looking for
discounted innovation.”
Other companies are using their unique technologies to
establish a foundation in service provision that can help
fuel the development of their own drugs. This is the route
taken by EirGenix, as well as a Rongjin Lin’s TTY invested
company, Mycenax Biotech. Both have focused on the bio-
pharmaceutical space.
“CDMO service provides us not only revenue, but also new
opportunities,” explains Karen Wen, Mycenax’s president.
“We hope to make long-term relationships with our clients.
Later along the road, we hope that with some of them, we
can launch shared investment projects, and plan a long pipe-
line together”—particularly in an area like biosimilars, where
Taiwan hopes to establish a competitive edge. Mycenax’s
TuNEX, now in Phase III, should be Taiwan’s frst commer-
cialized biosimilar.
When the pipeline is ready, the typical strategy for Taiwan’s
biotechs is to market or co-market in Taiwan and China, and
out-license elsewhere. But some are bolder: TWi, for instance,
which will start with generics but has long-term plans for in-
novation, plans to use its IPO capital to buy into a sales and
marketing operation in the US.
In a market where many compa-
nies are still only selling a promise,
API producer ScinoPharm is selling
products—very successfully. Val-
ued at USD 1.76 billion as of July
2013, making it the largest biotech
company in Taiwan, ScinoPharm is
emerging as a leader on the global
stage. By the numbers:
Founded: 1997
Revenues: USD 154.8 million in
2012, relative to USD 133.87 mil-
lion in 2011
Sales by region: 50 percent in US and Canada, 20
percent in the EU, remainder in Asia Pacifc
Number of customers: Over 300, including names like
Teva and Sandoz
Facilities: Over 450 cubic meters of combined reactor
volume in Taiwan and China, with approval in place or
coming from US FDA, EMA, Japanese PMDA, and oth-
ers; 200 + GMP audits by customers in Taiwan
In 2011, 65% of the APIs exported from Taiwan were
made by ScinoPharm. The company is now leveraging
this core competency to move into areas like formula-
tion, and even drug marketing and eventually new drug
development. Why not rest on its laurels? Jo Shen,
president and CEO, says, “Why should we sit still? Why
should we not keep climbing? We have people that are
smart, energetic, and capable. And we have the cus-
tomers: perhaps our most valuable asset. Any product
that comes out of our door has a built-in audience of
300 of the best companies in the business.
“Look at 7-Eleven in Taiwan. There are more than
four or fve thousand of these stores throughout the
country. If you want to sell your candy in 7-Eleven, you
have to pay the company a substantial fee to reach
the shelf, because the minute your product is on that
shelf, poof! It fies off in huge numbers. We have the
distribution channels. What we need now is to create
more products. Of course, we need strong leadership
regarding the direction we take—time is the one thing
you can never get back.”
ScinoPharm: By the numbers
Jo Shen, President
& CEO, ScinoPharm
From left: Karen Wen, President, Mycenax Biotech Inc.; Wen Lung
Su, Chairman, Taiwan Advance Bio-Pharmaceutical Inc.; George Yeh,
President, Taiwan Liposome Company
ES349744_PE1113_058.pgs 11.04.2013 22:49 ADV blackyellowmagentacyan

Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S18
speCiAl look:
inside the loCAl mArket
According to IMS
data, the Taiwan
pharma market
experienced its
frst contraction in
20 years in 2012.
Growth in this
USD 4.5 billion
market was nega-
tive at 0.9 percent,
and the hospital
segment, which is particularly affected
by Taiwan’s reimbursement system, ex-
perienced a 2.3 percent decline.
Taiwan is a reimbursed market with
a single-payer framework covering 99.8
percent of the population. GDP spent on
healthcare, meanwhile, is only about 6.6
percent (Ministry of Health and Welfare
(MOHW)). For Chih-Ping Yang, presi-
dent of the International Research-Based
Pharmaceutical Manufacturers’ Asso-
ciation (IRPMA), the unifying body for
multinational pharma organizations in
Rongjin Lin, Chairman, TTY Biopharm: Absolutely not! A
number of companies in the market are, say, happy to have
fnally reached Phase II in their drug development effort.
So what? Out of every 10,000 compounds researched,
perhaps fve reach the market—and out of every ten prod-
ucts that successfully reach the market, perhaps two make
real money. But the public doesn’t always realize that. They
don’t think about whether certain products have the right
pharmaco-economics behind them or not. Phase II is a
long way from monetization.
During the IPO announcement for an invested compa-
ny of mine, Pharma Engine, someone asked me how he
should invest in the project. I told him he could never be
sure to win! Even a PHD holder cannot be sure. You have to
gamble. As for myself, why did I gamble on Pharma Engine?
Because it has the right leader, and the right team. Its data
is good. After that, I have to roll the dice.
Jen Chen, Chairman, Genovate: I currently see Taiwan
as a small tiger in the global pharmaceutical industry. This
is not because of the IPO opportunities here, but rather, the
potential to see a blockbuster developed here in the near
future. Big drugs are how a country becomes famous in the
pharmaceutical world, and gains access to the ‘country
club’ of big names, just has Belgium has done through the
success of UCB.
I haven’t yet seen a drug under development in Taiwan
that has the potential to give us access to the country
club, but some years from now, I think that will change.
C.Y.Cheng, Chairman, Formosa Laboratories: We are
not quite there yet. Our inherent weakness is that we are
small. We hope the industry and the government can work
together to make this island more modern, and more in-
ternational. We hope that Taiwan can do better in the edu-
cational system, which does not do enough to teach our
young people concrete industrial skills. We hope that we
can attract more foreign talent, and more foreign money.
It is also important that we fnd our identity, and we
should start with our political identity. We cannot depend
too much on China. If we talk about ‘Taiwan Inc.’, we frst
have to fgure out exactly what it is that we’re talking about.
Time to Celebrate for Taiwan Inc.?
Alex Ho, General
Manager, IMS
Value-chain capability building and sourcing of best possible technologies Funding mechanisms to support efficient R&D and tech transfer activities Connection and collaboration with China, Asia Pacific and global network New talents through training and recruiting Mission oriented bio park with “One-Stop Shop” ecosystems
2Si C as a promoter:We want to enter the business and value chain of the biotechnology industry
for Taiwan to be recognized as a regional leader and a global player.
Supra Integration and Incubation Center Si²C
Branding
Taiwan
Rm.245, Greenhouse Bldg, 128 Academia Road,
Sec.2, Nankang, Taipei 115, Taiwan, R.O.C
Tel: 886-2-27875209 Fax: 886-2-27875207
ES349737_PE1113_059.pgs 11.04.2013 22:48 ADV blackyellowmagentacyan

taiwan report
Special SponSored Sectionpharmaboardroom.com
S19 FOCUS REPORTS noVeMBer 2013
Top 20 list of Multinational companies
Ranking in 2012
ManufacturerSales Value
(US$ Million)
1 PFIZER 428.0
2 NOVARTIS 304.3
3 MERCK SHARP& DOHME 259.5
4 ROCHE 258.1
5 SANOFI 246.2
6 GLAXOSMITHKLINE 197.1
7 ASTRAZENECA 191.2
8 BAYER 131.3
9 LILLY 126.9
10 BRISTOL-M & SQUIBB 105.0
11 TAKEDA 84.1
12 ABBOTT 80.1
13 JANSSEN-CILAG 80.1
14 NOVO NORDISK 79.6
15 ASTELLAS PHARMA 73.7
16 BAXTER HEALTHCARE 68.4
17 BOEHRINGER ING 59.5
18 MERCK SERONO 59.1
19 DAIICHI SANKYO 49.4
20 OTSUKA 36.0
Source: IMS Audit 4Q 2012
Top 20 list of local companies
Ranking in 2012
ManufacturerSales Value
(US$ Million)
1 YUNG SHIN 99.6
2 C.C.P.C 91.3
3 TUNG YANG 89.3
4 STANDARD 62.7
5 SINTONG 46.2
6 ORIENT EUROPHARMA 39.2
7 SYNMOSA BIOPHARMA 30.5
8 SINPHAR 29.0
9 NANG KUANG 25.0
10 GENOVATE 22.8
11 KINGDOM 22.5
12 SWISS 22.3
13 WEIDAR 18.1
14 LOTUS PHARMA. 17.7
15 U CHU 17.7
16 EVEREST PHARM 16.8
17 PEI LI 16.0
18 PURZER 15.0
19 CENTER 13.9
20 PANION & BF LAB. 13.2
Source: IMS Audit 4Q 2012
Taiwan Advance Bio-Pharmaceutical Inc.12F., No.25, Ln. 169, Kangning St., Xizhi Dist.,
New Taipei City 221, Taiwan
TEL:886-2-2692-6222
FAX:886-2-2692-6229
Your best antibiotics testing kits providerYour best partner in new drug development
Our 28-year expertise has made us the biggest antibiotics testing kits provider in Taiwan, and with the most potential in pharmaceuticals. Choose us to be your antibiotics testing kits supplier and invest in the company with the most potential in new generation protein drug development.
ES349750_PE1113_060.pgs 11.04.2013 22:49 ADV blackyellowmagentacyan

Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S20
Taiwan, the math is simple: “Yes, our current system covers
over 99 percent of the population. But do we want hamburger,
or steak? Do we want patients with treatable diseases to go
without help because the state cannot afford their medicine?
Everybody wants steak, but the national health insurance
(NHI) system has barely enough money to offer our people
hamburger. We have to pay more for steak: it’s that simple.”
Dr. Yu-Ray Chen, chairman of the steering committee at
Chang Gung Memorial Hospital, echoes Yang’s sentiment.
“The population needs educating on this issue to understand
that quality services need to be f nanced. There is no such
thing as a free lunch. The system should not be exploited. In
Taiwan, despite a golden era of public healthiness, inpatient
and outpatient appointments are growing annually. It is the
politicians’ responsibility to educate the people and help them
to understand that healthcare resources are f nite and should
be used appropriately.”
The 2012 contraction of the market was the product of the
seventh biennial round of price cuts under a mechanism called
the Price-Volume Survey (PVS), introduced after the Bureau
From left: Maoting Shen, Director of the Pharmaceutical and
Medical Reviews, BNHI; Wen-ta Chiu, Ministry of Health and
Welfare; Yu-Ray Chen, Chairman of Steering Committee, Chang
Gung Memorial Hospital
Today, the Taiwanese market is
extremely diff cult. Prices are con-
stantly decreasing, more compa-
nies compete for market share
every year, and product life cycles
are becoming shorter. We have to
put our full efforts into every ac-
tion we take, every single day. –
Mark Lee, vice chairman of local
distributor Morris Enterprise
The perspective from:
Mark Lee, Vice
Chairman of the
Board, Morris
Enterprise
ES349752_PE1113_061.pgs 11.04.2013 22:50 ADV blackyellowmagentacyan
taiwan report
Special SponSored Sectionpharmaboardroom.com
S21 FOCUS REPORTS noVeMBer 2013
of National Health Insurance (BNHI) experienced its frst
defcit. Alex Ho, general manager of IMS Health Taiwan, says
that the bureau “tried everything it could to control spending.
One of their major tactics was to reduce drug prices—and they
have employed this tactic continually ever since.”
“Ideally,” says Ho, the impact of price cuts “would be offset
by the introduction of new products. However, getting products
to the market has been quite diffcult in Taiwan. The BNHI has
not only cut the prices of existing products, but also delayed
and heavily controlled the reimbursement of innovative drugs.”
On January 1, 2013, Taiwan’s Second Generation National
Health Insurance Act came into force: the frst major overhaul
of the system since it was introduced in 1995. According to
Taiwan’s minister of health and welfare, Wen-ta Chiu, one of
the aims of the reform was to “release some of the pressure the
system has put on pharmaceutical companies.”
Chiu says that he understands the diffculties these com-
panies have faced in this market in recent years. “It is for this
reason,” he says, “that as part of second generation NHI, we
have looked to increase premium payments. Medical expendi-
tures as a percentage of GDP will increase 0.2 or 0.3 percent
by the end of this year.”
Bringing more money into the system is something the in-
dustry has been clamoring for, but other reforms are a mixed
bag. For one, the newly formed Pharmaceutical Beneft and
Reimbursement Scheme (PBRS) committee, responsible for re-
imbursement decisions, has introduced patients into the deci-
sion-making process: something Ho expects will further delay
product launches. In 2013, the number of new drugs approved
in Taiwan may be as much as 50-70 percent less than 2012.
The PVS system will be replaced by a Drug Expenditure
Target (DET): a virtual budget given to the industry based on
a growth rate that is decided by the National Health Insurance
Committee. There will be no price cuts in 2013; in 2014, should
costs exceed the target, the market will experience another round
From left: Chih-Ping Yang, President, IRPMA; Heather Lin, COO,
IRPMA; Christian Macher, Country President, AstraZeneca
Lotus Pharmaceutical Co., Ltd.
No. 30, Chenggong 1st Rd., Nantou City, Nantou County 540, Taiwan (ROC)11F, No. 200 Sec.1, Fuxing S. Rd., Daan District, Taipei City 106, Taiwan (ROC)
Lotus Pharmaceutical Co., Ltd.
Global Generic Company dedicated to file 505b2 and hard entry generic areas including Cytotoxic, High Potency, Soft gel Cap. and Extended Release
A Taiwanese pharmaceutical company inspected by US FDA, EU EMA and
Japan PMDA
ES349748_PE1113_062.pgs 11.04.2013 22:49 ADV blackyellowmagentacyan
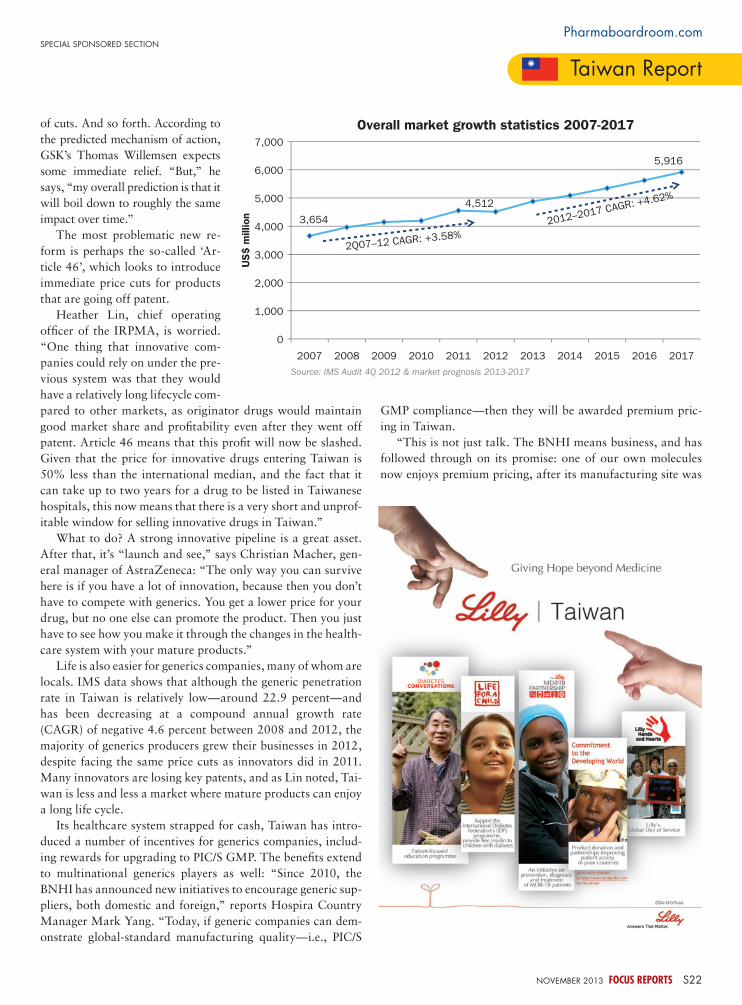
Special SponSored Section
taiwan report
pharmaboardroom.com
noVeMBer 2013 FOCUS REPORTS S22
of cuts. And so forth. According to
the predicted mechanism of action,
GSK’s Thomas Willemsen expects
some immediate relief. “But,” he
says, “my overall prediction is that it
will boil down to roughly the same
impact over time.”
The most problematic new re-
form is perhaps the so-called ‘Ar-
ticle 46’, which looks to introduce
immediate price cuts for products
that are going off patent.
Heather Lin, chief operating
offcer of the IRPMA, is worried.
“One thing that innovative com-
panies could rely on under the pre-
vious system was that they would
have a relatively long lifecycle com-
pared to other markets, as originator drugs would maintain
good market share and proftability even after they went off
patent. Article 46 means that this proft will now be slashed.
Given that the price for innovative drugs entering Taiwan is
50% less than the international median, and the fact that it
can take up to two years for a drug to be listed in Taiwanese
hospitals, this now means that there is a very short and unprof-
itable window for selling innovative drugs in Taiwan.”
What to do? A strong innovative pipeline is a great asset.
After that, it’s “launch and see,” says Christian Macher, gen-
eral manager of AstraZeneca: “The only way you can survive
here is if you have a lot of innovation, because then you don’t
have to compete with generics. You get a lower price for your
drug, but no one else can promote the product. Then you just
have to see how you make it through the changes in the health-
care system with your mature products.”
Life is also easier for generics companies, many of whom are
locals. IMS data shows that although the generic penetration
rate in Taiwan is relatively low—around 22.9 percent—and
has been decreasing at a compound annual growth rate
(CAGR) of negative 4.6 percent between 2008 and 2012, the
majority of generics producers grew their businesses in 2012,
despite facing the same price cuts as innovators did in 2011.
Many innovators are losing key patents, and as Lin noted, Tai-
wan is less and less a market where mature products can enjoy
a long life cycle.
Its healthcare system strapped for cash, Taiwan has intro-
duced a number of incentives for generics companies, includ-
ing rewards for upgrading to PIC/S GMP. The benefts extend
to multinational generics players as well: “Since 2010, the
BNHI has announced new initiatives to encourage generic sup-
pliers, both domestic and foreign,” reports Hospira Country
Manager Mark Yang. “Today, if generic companies can dem-
onstrate global-standard manufacturing quality—i.e., PIC/S
GMP compliance—then they will be awarded premium pric-
ing in Taiwan.
“This is not just talk. The BNHI means business, and has
followed through on its promise: one of our own molecules
now enjoys premium pricing, after its manufacturing site was
Overall market growth statistics 2007-2017
3,654
4,512
5,916
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
US$ m
illion
Source: IMS Audit 4Q 2012 & market prognosis 2013-2017
2Q07Ð12 CAGR: +3.58%
2012Ð2017 CAGR: +4.62%
ES349738_PE1113_063.pgs 11.04.2013 22:49 ADV blackyellowmagentacyan

taiwan report
Special SponSored Sectionpharmaboardroom.com
S23 FOCUS REPORTS noVeMBer 2013
granted PIQ/S GMP certifcation. Our team is currently pre-
paring the ground for further molecule launches that can take
advantage of these benefts.”
Yang also hedges his bets with a strong focus on medical
devices, and some business in the oft-neglected self-pay seg-
ment: “As a supplier in this marketplace, you have to manage
your reimbursement business very carefully. However, if at the
same time you can introduce the right products on the self-pay
side, you will fnd that you have a good combination: you will
mitigate the risks of the reimbursement market, where you will
face price cuts and heavy competition. If you have the portfolio
to play in the self-pay segment in Taiwan, you should.”
This is a call that is well heard by local distributor Uni-
Pharma. Terry Lin and Freia Wei, General Manager and Senior
Consultant, report, “Uni-Pharma was founded shortly after the
creation of the national health insurance (NHI) system—but
actually, the majority of our products are not reimbursed. Until
recently, it was the state’s policy to cut reimbursement prices
every two years! We decided to develop the self-pay market,
and our business has concentrated on this segment since 2005.
Less that ten percent of our products are reimbursed today.
“We also began to focus more on medical devices, because
we fnd that the entrance barriers are considerably lower. Med
tech currently accounts for nearly 90 percent of our revenues.”
Now, the company is looking to leverage its market knowl-
edge to diversify beyond distribution to the introduction of its
own branded line of diagnostics. With license in hand for a
cancer-detection device, Uni-Pharma has formed a partnership
to manufacture and market products for the regional market-
place and beyond: “We saw that there was a constraint on the
pharmaceutical industry, so we moved from pharma products
to medical devices and diagnostics. But we also want to build a
foundation for the long-term. The distribution business can be
diffcult to sustain: after all, the principal can always revoke the
product rights if they chose!”
From left: Freia Wei, Senior Consultant, Unipharma; Terri Lin,
General Manager, Unipharma; Mark Yang, Country Manager,
Hospira
Hospira is a global specialty pharmaceutical and medication delivery company driven by its vision of Advancing Wellness™. Bringing proven leadership and experience, Hospira provides solutions to help improve the productivity, safety and effectiveness of patient care.
18F, 333 Tun Hwa S. Road. Section 2, Taipei 106, TaiwanT +886 2 8176 8888
www.hospira.com.tw
advancing wellness
ES349760_PE1113_064.pgs 11.04.2013 22:50 ADV blackyellowmagentacyan
Time is risk. If time to market
is slowed then the cost for
a company is lost revenues,
profits, and ultimately lost
opportunities for patients.
The message is clear. To
compete and win, companies
must wrest more value from
every stage of a new product’s
tightly projected lifecycle.
To download go to
http://bit.ly/16YI8po or scan here:
PHARMACEUTICAL EXECUTIVE IS
PLEASED TO PRESENT AN EXCITING NEW
E-BOOK, LIFECYCLE SOLUTIONS:
POSITIONING
PHARMACEUTICALS
FOR COMMERCIAL
SUCCESS.
SPONSORED BY
TRIALCARD.
ES345516_PE1113_065_FP.pgs 10.26.2013 02:43 ADV blackyellowmagentacyan
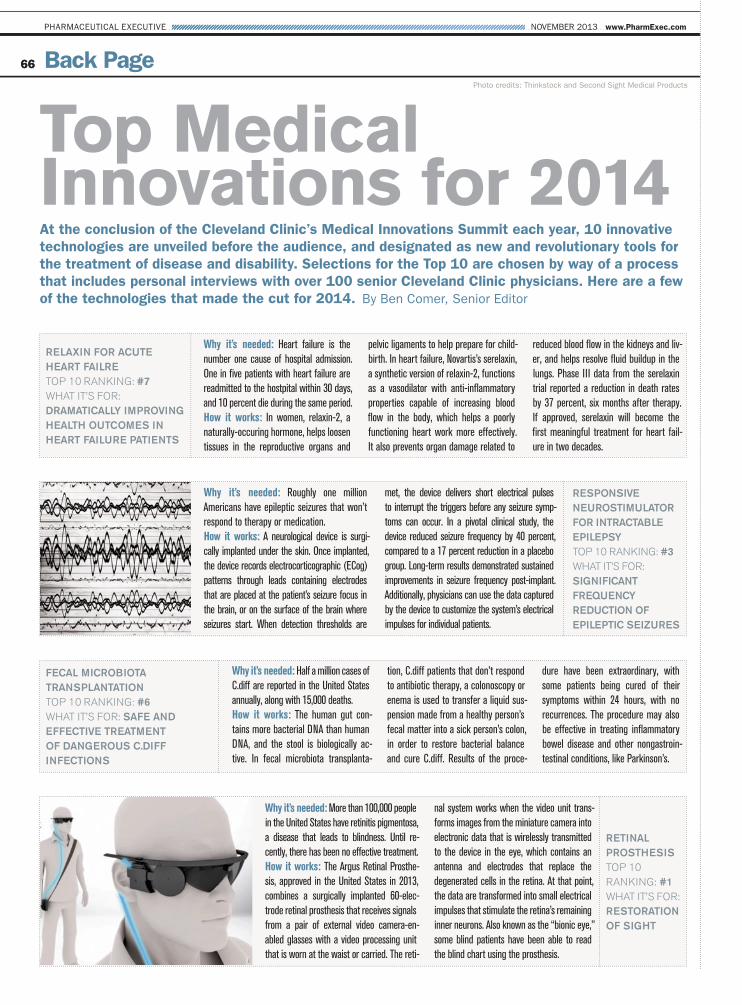
6666
NOVEMBER 2013 www.PharmExec.comPHARMACEUTICAL EXECUTIVE
Back Page
Top MedicalInnovations for 2014At the conclusion of the Cleveland Clinic’s Medical Innovations Summit each year, 10 innovative
technologies are unveiled before the audience, and designated as new and revolutionary tools for
the treatment of disease and disability. Selections for the Top 10 are chosen by way of a process
that includes personal interviews with over 100 senior Cleveland Clinic physicians. Here are a few
of the technologies that made the cut for 2014. By Ben Comer, Senior Editor
Photo credits: Thinkstock and Second Sight Medical Products
Relaxin foR acute
heaRt failRe
Top 10 Ranking: #7
WhaT iT’s foR:
DRamatically impRoving
health outcomes in
heaRt failuRe patients
Why it’s needed: Heart failure is the
number one cause of hospital admission.
One in five patients with heart failure are
readmitted to the hostpital within 30 days,
and 10 percent die during the same period.
How it works: In women, relaxin-2, a
naturally-occuring hormone, helps loosen
tissues in the reproductive organs and
pelvic ligaments to help prepare for child-
birth. In heart failure, Novartis’s serelaxin,
a synthetic version of relaxin-2, functions
as a vasodilator with anti-inflammatory
properties capable of increasing blood
flow in the body, which helps a poorly
functioning heart work more effectively.
It also prevents organ damage related to
reduced blood flow in the kidneys and liv-
er, and helps resolve fluid buildup in the
lungs. Phase III data from the serelaxin
trial reported a reduction in death rates
by 37 percent, six months after therapy.
If approved, serelaxin will become the
first meaningful treatment for heart fail-
ure in two decades.
Responsive
neuRostimulatoR
foR intRactable
epilepsy
Top 10 Ranking: #3
WhaT iT’s foR:
significant
fRequency
ReDuction of
epileptic seizuRes
Why it’s needed: Roughly one million
Americans have epileptic seizures that won’t
respond to therapy or medication.
How it works: A neurological device is surgi-
cally implanted under the skin. Once implanted,
the device records electrocorticographic (ECog)
patterns through leads containing electrodes
that are placed at the patient’s seizure focus in
the brain, or on the surface of the brain where
seizures start. When detection thresholds are
met, the device delivers short electrical pulses
to interrupt the triggers before any seizure symp-
toms can occur. In a pivotal clinical study, the
device reduced seizure frequency by 40 percent,
compared to a 17 percent reduction in a placebo
group. Long-term results demonstrated sustained
improvements in seizure frequency post-implant.
Additionally, physicians can use the data captured
by the device to customize the system’s electrical
impulses for individual patients.
fecal micRobiota
tRansplantation
Top 10 Ranking: #6
WhaT iT’s foR: safe anD
effective tReatment
of DangeRous c.Diff
infections
Why it’s needed: Half a million cases of
C.diff are reported in the United States
annually, along with 15,000 deaths.
How it works: The human gut con-
tains more bacterial DNA than human
DNA, and the stool is biologically ac-
tive. In fecal microbiota transplanta-
tion, C.diff patients that don’t respond
to antibiotic therapy, a colonoscopy or
enema is used to transfer a liquid sus-
pension made from a healthy person’s
fecal matter into a sick person’s colon,
in order to restore bacterial balance
and cure C.diff. Results of the proce-
dure have been extraordinary, with
some patients being cured of their
symptoms within 24 hours, with no
recurrences. The procedure may also
be effective in treating inflammatory
bowel disease and other nongastroin-
testinal conditions, like Parkinson’s.
Retinal
pRosthesis
Top 10
Ranking: #1
WhaT iT’s foR:
RestoRation
of sight
Why it’s needed: More than 100,000 people
in the United States have retinitis pigmentosa,
a disease that leads to blindness. Until re-
cently, there has been no effective treatment.
How it works: The Argus Retinal Prosthe-
sis, approved in the United States in 2013,
combines a surgically implanted 60-elec-
trode retinal prosthesis that receives signals
from a pair of external video camera-en-
abled glasses with a video processing unit
that is worn at the waist or carried. The reti-
nal system works when the video unit trans-
forms images from the miniature camera into
electronic data that is wirelessly transmitted
to the device in the eye, which contains an
antenna and electrodes that replace the
degenerated cells in the retina. At that point,
the data are transformed into small electrical
impulses that stimulate the retina’s remaining
inner neurons. Also known as the “bionic eye,”
some blind patients have been able to read
the blind chart using the prosthesis.
ES349408_PE1113_066.pgs 11.01.2013 23:16 ADV blackyellowmagentacyan
More 2013 IIHS Top Safety Picks than any other brand.1
IIHS
Longest lasting vehicles of any full-line automotive manufacturer.2
Polk
Best retained value of any full-line car manufacturer on the road today.3
IntelliChoice
More vehicles named in the Cars.com American-Made Index’s Top 10 than any other brand.4
Cars.com
Best Resale Value of all brands for 2013.5
Kelley Blue Book’s KBB.com
Time and again, the critics have spoken, and their message is always the same: For all your Fleet Vehicle
needs, you can’t beat a Toyota. Call 1-800-732-2798 or visit fleet.toyota.com for more information.
But it sure feels like it around here.
Praise like thisdoesn’t come aroundevery day.
Prototypes shown with options. Production models will vary. 1. For more details on 2013 Top Safety Pick Awards, see www.iihs.org. 2. Longevity based on Polk U.S.
Vehicles In Operation registration statistics MY 1987-2012 as of October 2012. Full-line manufacturer based on car, SUV, minivan, compact and full-size pickup.
3. 2013 IntelliChoice, www.IntelliChoice.com; Popular Brand. Based on 2013 model year study. 4. For more information about the 2013 American-Made Index, visit
Cars.com. 5. Vehicle’s projected resale value is specific to the 2013 model year. For more information, visit Kelley Blue Book’s KBB.com. Kelley Blue Book is a
registered trademark of Kelley Blue Book Co., Inc. ©2013 Toyota Motor Sales, U.S.A., Inc.
ES345528_PE1113_CV3_FP.pgs 10.26.2013 02:44 ADV blackyellowmagentacyan
inVentivHealth.com/WeCanHelp
At inVentiv Health there are no silos—only the seamless convergence
of Clinical, Commercial, and Consulting services delivered by 12,000
people working together around the globe.
Our clients say we solve problems no one else can, and turn to us
for outcomes that are strategic, cost-effective and fast.
How can we help you?
CONVERGENCE IN ACTION:
In today’s complex marketplace, companies must engage more healthcare
stakeholders than ever before to achieve desired results. inVentiv Health Selling
Solutions uses advanced analytics to target crucial stakeholder communities.
Then we deploy highly skilled sales teams, nurse educators and medical
science liaisons who speak their language. The result for clients: accelerated
commercial performance.
Transforming Promising Ideas into Commercial Reality
ES345523_PE1113_CV4_FP.pgs 10.26.2013 02:44 ADV blackyellowmagentacyan