minimally invasive genetic screen for gjb2 related deafness using dried blood spots
TRANSCRIPT
Minimally invasive genetic screen for GJB2 related deafness using driedblood spots§
Attila L. Nagy a,*, Robert Csaki b, Jozsef Klem c, Laszlo Rovo a, Ferenc Toth a, Gyula Talosi d,Jozsef Jori a, Kornel Kovacs c, Jozsef Geza Kiss a
a University of Szeged, Albert Szent-Gyorgyi Pharmaceutical and Medical Centre, Department of Oto-rhino-laryngology and Head and Neck Surgery, 6725,
Tisza Lajos krt. 111, Szeged, Hungaryb Alfa-Biosoft Ltd., 6720, Nador u. 10, Szeged, Hungaryc University of Szeged, Faculty of Sciences, Institute of Biotechnology, 6726, Kozep fasor 52, Szeged, Hungaryd University of Szeged, Albert Szent-Gyorgyi Pharmaceutical and Medical Centre, Department of Pediatrics, 6720, Koranyi fasor 14-15, Szeged, Hungary
International Journal of Pediatric Otorhinolaryngology 74 (2010) 75–81
A R T I C L E I N F O
Article history:
Received 28 May 2009
Received in revised form 18 October 2009
Accepted 21 October 2009
Available online 24 November 2009
Keywords:
Dried blood spot
Polymerase chain reaction
Whole blood
Nonsyndromic deafness
35delG
Screening
A B S T R A C T
Objective: Nonsyndromic hearing loss is one of the most abundant human sensory disorders, and can be
found in 1 out of 1000 newborns. In 60–70% of the cases this disorder is hereditary. The phenotype varies
from moderate hearing loss to almost complete deafness, often only revealed in late childhood.
Early detection of hearing related genetic variations in the first few weeks of life would allow planning
of the audiological and logopedical procedures to maintain the children’s normal audiological and
speech development, and if required a cochlear implantation can be planned in time.
We wanted to evaluate, whether the blood samples collected from neonates onto Guthrie cards (dried
blood spots, or DBS), and blood collected from people of various ages into blood collecting tubes is
equally usable for genetic testing. The quality of the samples on DBS’s for genetic tests after an extended
period of storage was evaluated. The methods for sample preparation and analysis were also evaluated.
Methods: Two DNA extraction methods were compared on the samples. We extracted DNA from whole
blood with the Versagene Blood Kit from Gentra, and from DBS’s with boiling. Allele-specific PCRs (AS-
PCR) were carried out on each sample. Samples were analyzed with AS-PCR and sequencing, for the
35delG mutation in the GJB2 (Cx26) gene. Freshly drawn and dried blood spot samples stored for several
years were used in the experiments.
Results: An AS-PCR method for detecting 35delG mutation on DNA extracted from Guthrie cards was
validated. Blood samples up to 10 years of storage were applicable in the screen. 84 patients were found
with 35delG mutations, both heterozygous (with no detected hearing related phenotypical
discrepancies), and homozygous (phenotipically with moderate to severe hearing loss) forms.
Conclusions: The dried blood spots on Guthrie cards require only three drops of blood to be collected
from children, which causes less stress than taking 3 ml of blood. The blood stored on Guthrie cards can
be used to store DNA samples for at least 10 years. Even under suboptimal storage conditions the
samples’ DNA remains intact for genetic testing. Compared to blood collection tubes Guthrie cards cost
less, are easier to transport and store.
� 2009 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
International Journal of Pediatric Otorhinolaryngology
journa l homepage: www.e lsev ier .com/ locate / i jpor l
1. Introduction
According to current knowledge physiological processes relatedto hearing are regulated by at least 100–150 genes. To date 146
§ The work described here was supported by the grant GVOP-3.1.1-2004-05-
0498/3.0.
* Corresponding author. Tel.: +36 62 54 58 50; fax: +36 62 54 58 48.
E-mail addresses: [email protected] (A.L. Nagy),
[email protected] (R. Csaki), [email protected] (L. Rovo),
[email protected] (F. Toth), [email protected] (J. Jori),
[email protected] (J.G. Kiss).
0165-5876/$ – see front matter � 2009 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.ijporl.2009.10.021
alleles of 42 genes have been identified (57 dominant, 77 recessive,8 X-linked, 1 Y-linked, 2 modifier, 1 auditory neuropathy) [1]. Thelarge number of genes and loci complicate the genetic analysis ofnonsydromic hearing losses. DFNB1 was the first identified locus;its autosomal recessive mutation causes nonsyndromic hearingloss [2]. Using co-segregation analysis, this locus was mapped to13q12-13 [3]. In 1994, Chaib et al. described the first dominantnonsyndromic hearing loss of genetic origin to 13q12-13 [4].Mutation in the coding region of Gap Junction protein Beta 2 (GJB2)– also called Connexin26 (Cx26) – was the first to be linked tononsyndromic hearing loss of genetic origin [5]. Connexin 26(Cx26) is a protein, which belongs to the family of connexins. In the

A.L. Nagy et al. / International Journal of Pediatric Otorhinolaryngology 74 (2010) 75–8176
cochlea [6,7] connexins facilitate the flux, and the recycling of K+
ions from the intracellular space to the endolympha [8]. The lengthof the functional, protein coding exon of GJB2 is 681 bp, and itcodes a 226 amino acid polypeptide. 35delG causes a frameshiftmutation, the deletion of one guanine residue in a stretch of sixguanines in the coding region of the gene at position 35, resultingin a nonsense mutation at the 13th codon. 35delG mutation of theGJB2 gene accounts for about 7–15% of nonsyndromic hearinglosses of genetic origin in the European population [9–11], andregarding this mutation, about 1–5% of the European population isa carrier [12].
Since the 1950’s [13] and 1960’s [14] national neonatalscreening programs begun to operate in the advanced countries;they mostly perform screening for metabolic diseases [15,16].These programs generated an enormous amount of dried bloodspots (DBS) on so called Guthrie cards. These cards have theadvantage of easy transportation, and their storage conditions aremuch cheaper than any other way of storing blood samples. Thequestion arises whether they can be used as a basis of geneticscreening, and if yes, to what extent.
As national hearing screening programs gain more and moreattention, and financial funds, they become more and more‘‘sample-hungry’’. If these cards could be utilized to give properresults, they could serve as a complementary tool to the existingauditory and genetic screening methods. These blood spots areavailable for most of the newborns in those countries, and eachindividual can be tested in their absence. The procedure is also lesstraumatic to children.
2. Materials and methods
All participants involved in the trials were informed accordingto the University’s Ethical Committee’s Guidelines, and all havesigned a written consent. Double blind tests were performed on thespot blood samples taken for the routine, population widemetabolic screening tests of neonates. The samples were takenon Guthrie cards at the 3rd-4th life day of newborns at anyneonatal ward where the neonates were cared in the eastern partof Hungary and sent via conventional mail. The test cards werestored at room air at the Department of Paediatrics, University ofSzeged. The Guthrie cards were selected as follows: 48 pieces fromthe years 1996, and 1997, and further 96 pieces from the years1999, 2000, 2001, 2004, 2005, respectively. The total number ofDBS’s was n = 576, as these were selected randomly, we could usethem as a ‘‘generic population sample’’.
The other population we examined consists of 318 of patients.These patients were Cochlear Implant (CI) users, their relatives, CIcandidates, their relatives, and a few individual patients from theENT Clinic. CI users and CI candidates were selected based on twocriteria. They were selected if there was a family history of hearinglosses, and there were no organic abnormalities (anatomicalvariations, or developmental problems) or other diseases that areknown to cause hearing loss or deafness in the patient’s history. Incase of the CI users (n = 20 + 32 = 52) and CI candidates (n = 56) theaverage hearing threshold level was bellow 70 dB and speech
Table 1The primers used in this work and their sequences.
Primer name Sequence
ICF CCC ACC TTC CCC TCT CTC CAG GCA AAT GG
ICR GGG CCT CAG TCC CAA CAT GGC TAA GAG G
GJC AGT GAT CGT AGC ACA CGT TCT TGC A
GJW GCA CGC TGC AGA CGA TCC TGG GGA G
GJM CAC GCT GCA GAC GAT CCT GGG GAT
DF2F TCT CCC TGT TCT GTC CTA GC
DF2R TTT CCC AAG GCC TCT TCC AC
recognition performance was under 25%. We excluded thosepatients and CI users whose patient history contained some form ofdisease that can cause deafness, or who suffered a head trauma, orhead injury, that can account for their hearing problems. The CIusers’ and CI candidates’ family members (n = 163) have variouslevels of hearing loss, from no hearing loss at all to severe tomoderate levels. There were some individuals who wanted toparticipate in our study with various levels but with unknownorigin of hearing loss (n = 47). 20 CI users (out of n = 52) wereindividuals with no screened relatives. Our group of controlpersons consisted of people with hearing threshold levels at 5 dB orbetter on both ears (n = 20) and no family history of hearing losses.
2.1. Preparation of DNA extracts from DBS for AS-PCR
4 mm diameter pieces from the bloodspot test cards werepunched out and put into PCR tubes along with 200 ml 1� PCRbuffer (Eppendorf HotMaster taq). The DNA was extracted from theDBS by 20 min of incubation at 96 8C in a thermalcycler. Thesamples were then centrifuged at 16 000 � g for 2 min. Thesupernatant was then transferred into a sterile microcentrifugetube, and stored at 4 8C until utilization [17,18].
2.2. Preparation of DNA from venous blood for AS-PCR
We collected 3 ml blood from patients having Cochlear Implant,their relatives, and CI candidates. Blood anti-coagulant was EDTA.Genomic DNA (gDNA) was purified from 400 ml of blood usingVersagene Blood Kit (Gentra) according to the manufacturerinstructions. The concentration of the DNA was measured withspectrophotometer and was calculated by the adsorption at 260and 360 nm.
2.3. Polymerase chain reactions
DNA integrity test reactions were carried out using HotMasterTaq DNA Polymerase (Eppendorf). 30 ml final volume of thereaction mix contained 3 ml (10�) HotMasterTaq buffer (Eppen-dorf), 2.5 ml, dNTP (2.5 mM), 0.5–0.5 ml (15 pM) DF2F-DF2Rprimer pair (Table 1); 1 U HotMasterTaq (Eppendorf); 6 ml gDNStemplate and 16.5 ml water.
PCR program was as follows: 96 8C 2 min, for 35 cycles (96 8C30 s–61 8C 30 s–68 8C 35 s), and after these 35 cycles 96 8C for5 min. Negative control experiment was also done with paper discsoriginating from the ‘‘blood-free’’ parts of the Guthrie papers. PCRfragments were analyzed by agarose gel electrophoresis on 1.5%agarose gel (AbGen) with 1X TBE buffer. The internal control usedin all the AS-PCR experiments were the primer pair ICF and ICR.They amplificate a part of the serine proteinase inhibitor gene(Table 1).
AS-PCR reactions: 30 ml final volume of the reaction mixcontained: 3 ml (10�) HotMasterTaq buffer (Eppendorf), 2.5 ml,dNTP (2.5 mM), 0.5–0.5 ml primers GJC-GJW pair for wild alleledetection and GJC-GJM for 35delG mutant allele detection(Table 1). (15 pM), 0.4–0.4 ml (15 pM) internal control primer
Description
G Internal control (serine proteinase inhibitor gene)
TG Internal control (serine proteinase inhibitor gene)
Common reverse primer for GJB2
Primer for 35delG Wild allele detection
Primer for 35delG mutant allele detection
GJB2 exon and flanking region for sequencing
GJB2 exon and flanking region for sequencing
A.L. Nagy et al. / International Journal of Pediatric Otorhinolaryngology 74 (2010) 75–81 77
pair (ICF-ICR); 1 U HotMasterTaq (Eppendorf); 6 ml gDNS templateand 16.5 ml water.
The PCR program was as follows: first denaturation step at 95 8Cfor 5 min, then 35 cycles at 96 8C 30 s, at 65 8C 35 s, and at 68 8C38 s, and as the last step, 10 min incubation time at 68 8C. PCRfragments were analyzed by agarose gel electrophoresis on 1.5%agarose gel (AbGen) with 1X TBE buffer.
2.4. DNA Sequencing and sequence analysis
PCR fragments were generated as described in section 2.3. PCRproducts were desalted on Microcon columns (Millipore). Thepurified PCR products were eluted in 30 ml of water. The DNAsequences were determined by automated sequencing at Macro-gen Inc. (Korea) on both strands. The sequences were aligned to thewild-type reference sequence by the CLUSTALW program [19].
3. Results
We have tested randomly selected cards dated from 1996 to2006. 576 (6 � 96) dried blood spot (DBS) samples, and 318 DNAsamples, that were extracted from EDTA coagulated blood wereanalyzed with AS-PCR during our test period, totaling a number of894 samples.
3.1. Sample preparation, PCR validation
First we evaluated the influence of the DNA source on PCR basedgenetic screens. Two types of DNA sources were tested: EDTAanticoagulated blood samples and blood spots on Guthrie cards.200 ml of DNA solution were obtained from one tube of EDTA
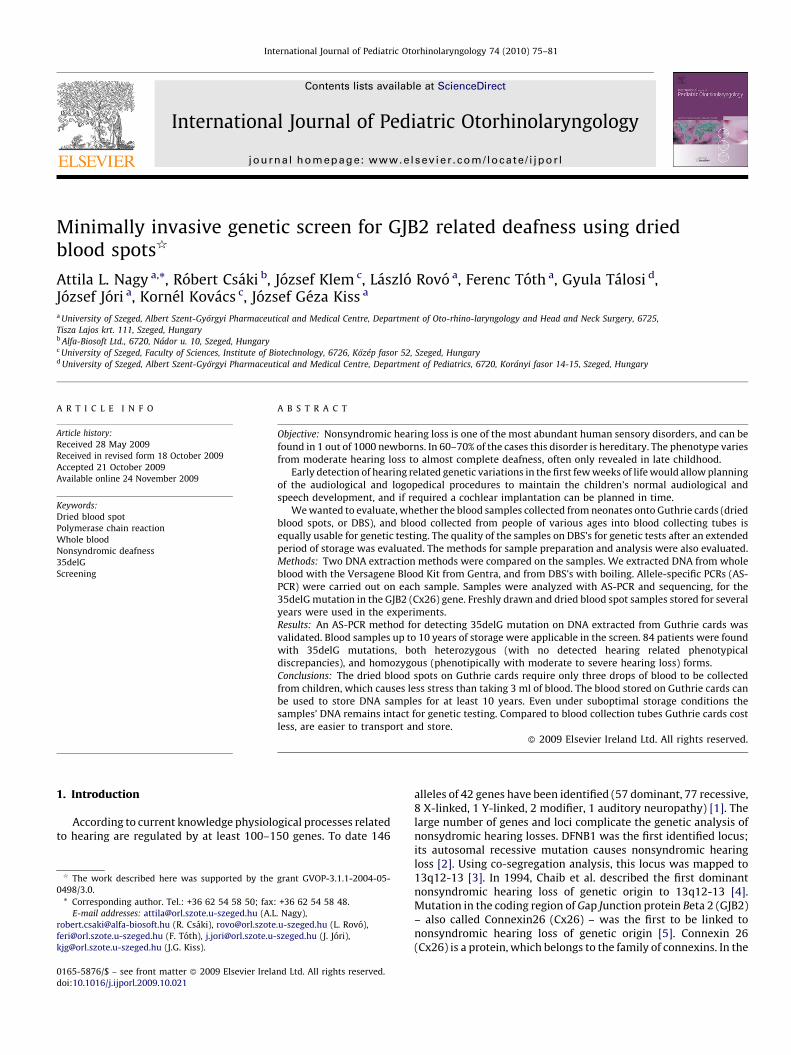
Fig. 1. (a) DNA dilution test. DNA was isolated from Dried Blood Spots from 1996 to 2005
runs resulted in a 809 bp fragment. Every sample was diluted by 50� (1); 5� (2); and 1�DNA size marker was labeled with M. Even the 50� diluted sample gave good results from
EDTA anticoagulated blood and GJB2’s coding exon was amplified with the GJB2F and GJB2
5000�. Up to 100� dilution the PCR reactions gave acceptable results, but at and above 50
GJB2R primers on a gel electrophoresis picture. As can be seen on the image, no aspecifi
samples we sent later for sequencing. (d) A few examples of other regions we examined
1,2,36: GJB2; 3,4: 12SrRNA; 5,6,7: COCH; 8: GJA1; 9,10: GJB3; 31,32,33,34: MYO6; 3
experiments, their sizes are in the range 135–420 bp.
anticoagulated blood and 200 ml DNA solution from one 4 mmdiameter piece of the bloodspot test cards.
The amount and the integrity of the purified DNA samples wastested by PCR with the primers DF1F and DF2F which amplify partsof GJB2’s coding exon. The length of the PCR products was 420 and324 bp. They covered the whole exon. The experiments wereperformed with 6 ml of genomic DNA (gDNA) template. Thesamples were analyzed by gel electrophoresis. 1�, 5�, 50�dilutions were made from blood spots and tested by PCR. The200 ml gDNA solution when diluted 50 times is still acceptable forPCR testing, and that volume (10 000 ml) is sufficient theoreticallyfor more than a thousand PCR reactions per purified sample, or4 mm paper disc (Fig. 1a). As a negative control we used a blood-free paper disc from a Guthrie card. As Fig. 1 shows, even the DNAextracted from a 12 years old blood spot gave good result. Therewere no experiments that produced no results, this means that wewere able to screen for 35delG with AS-PCR on all 576 DBS samples.The image shows randomly selected samples from our tests. As wecan see on the image there are no smaller sized fragments indetectable quantity bellow our AS-PCR product on the gel.
The gDNA solution prepared from whole blood could be dilutedby 100� and it still gave acceptable results (Fig. 1b). When dilutedfurther (500�, 1000�, 5000�), the PCR experiments did not givereliable results.
The longest PCR product we have worked with is the 809 bplong product of the primers GJB2F and GJB2R (Table 1). We usedthis PCR product to validate the AS-PCR experiments by sequenceanalysis. As can be seen on (Fig. 1c) there were no aspecific PCRproducts in these PCR experiments.
We were able to reliably detect the 35delG mutation on allgDNA samples from both DNA sources.
and GJB2’s coding exon was amplified with the GJB2F and GJB2R primers. The PCR
(3). As a negative control we used a blood-free paper disc from a Guthrie card. The
a 12 years old blood spot. (b) DNA dilution test. DNA was isolated from peripheral
R primers. The gDNA solution was diluted by 1�, 5�, 10�, 50�, 100�, 500�, 1000�,
0� the PCR product’s quantity noticeably drop. (c) The PCR product of the GJB2F and
c fragments were produced during the PCR run. These examples were amongst the
. The numbers represent specific regions (data not shown) of the following genes:
7,38,39: GJB6; and 40: POU3F4. As these fragments were optimized for dHPLC
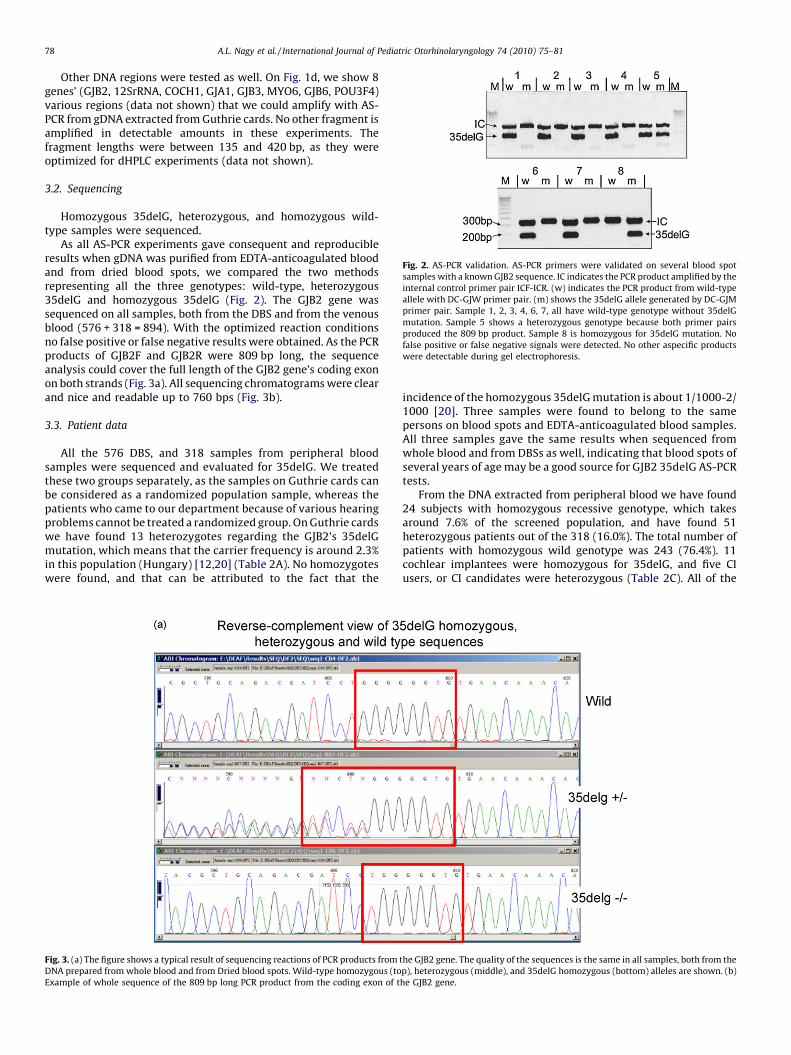
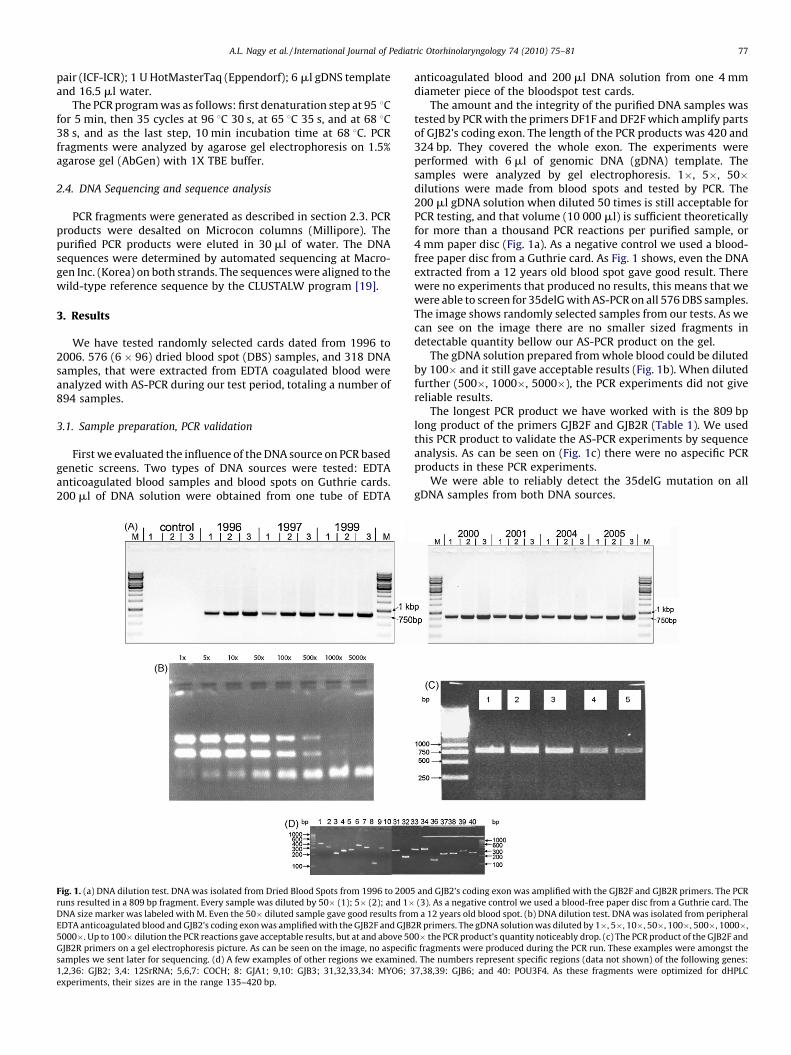
Fig. 2. AS-PCR validation. AS-PCR primers were validated on several blood spot
samples with a known GJB2 sequence. IC indicates the PCR product amplified by the
internal control primer pair ICF-ICR. (w) indicates the PCR product from wild-type
allele with DC-GJW primer pair. (m) shows the 35delG allele generated by DC-GJM
primer pair. Sample 1, 2, 3, 4, 6, 7, all have wild-type genotype without 35delG
mutation. Sample 5 shows a heterozygous genotype because both primer pairs
produced the 809 bp product. Sample 8 is homozygous for 35delG mutation. No
false positive or false negative signals were detected. No other aspecific products
were detectable during gel electrophoresis.
A.L. Nagy et al. / International Journal of Pediatric Otorhinolaryngology 74 (2010) 75–8178
Other DNA regions were tested as well. On Fig. 1d, we show 8genes’ (GJB2, 12SrRNA, COCH1, GJA1, GJB3, MYO6, GJB6, POU3F4)various regions (data not shown) that we could amplify with AS-PCR from gDNA extracted from Guthrie cards. No other fragment isamplified in detectable amounts in these experiments. Thefragment lengths were between 135 and 420 bp, as they wereoptimized for dHPLC experiments (data not shown).
3.2. Sequencing
Homozygous 35delG, heterozygous, and homozygous wild-type samples were sequenced.
As all AS-PCR experiments gave consequent and reproducibleresults when gDNA was purified from EDTA-anticoagulated bloodand from dried blood spots, we compared the two methodsrepresenting all the three genotypes: wild-type, heterozygous35delG and homozygous 35delG (Fig. 2). The GJB2 gene wassequenced on all samples, both from the DBS and from the venousblood (576 + 318 = 894). With the optimized reaction conditionsno false positive or false negative results were obtained. As the PCRproducts of GJB2F and GJB2R were 809 bp long, the sequenceanalysis could cover the full length of the GJB2 gene’s coding exonon both strands (Fig. 3a). All sequencing chromatograms were clearand nice and readable up to 760 bps (Fig. 3b).
3.3. Patient data
All the 576 DBS, and 318 samples from peripheral bloodsamples were sequenced and evaluated for 35delG. We treatedthese two groups separately, as the samples on Guthrie cards canbe considered as a randomized population sample, whereas thepatients who came to our department because of various hearingproblems cannot be treated a randomized group. On Guthrie cardswe have found 13 heterozygotes regarding the GJB2’s 35delGmutation, which means that the carrier frequency is around 2.3%in this population (Hungary) [12,20] (Table 2A). No homozygoteswere found, and that can be attributed to the fact that the
Fig. 3. (a) The figure shows a typical result of sequencing reactions of PCR products from
DNA prepared from whole blood and from Dried blood spots. Wild-type homozygous (to
Example of whole sequence of the 809 bp long PCR product from the coding exon of t
incidence of the homozygous 35delG mutation is about 1/1000-2/1000 [20]. Three samples were found to belong to the samepersons on blood spots and EDTA-anticoagulated blood samples.All three samples gave the same results when sequenced fromwhole blood and from DBSs as well, indicating that blood spots ofseveral years of age may be a good source for GJB2 35delG AS-PCRtests.
From the DNA extracted from peripheral blood we have found24 subjects with homozygous recessive genotype, which takesaround 7.6% of the screened population, and have found 51heterozygous patients out of the 318 (16.0%). The total number ofpatients with homozygous wild genotype was 243 (76.4%). 11cochlear implantees were homozygous for 35delG, and five CIusers, or CI candidates were heterozygous (Table 2C). All of the
the GJB2 gene. The quality of the sequences is the same in all samples, both from the
p), heterozygous (middle), and 35delG homozygous (bottom) alleles are shown. (b)
he GJB2 gene.

Fig. 3. (Continued ).
A.L. Nagy et al. / International Journal of Pediatric Otorhinolaryngology 74 (2010) 75–81 79
35delG homozygous recessives’ relatives (whom we couldinvestigate) were heterozygous. 36 of the implantees, and 78 ofall the implantees’ relatives were homozygous wild out of the totalof 318 patients.
Table 2The abundance of the 35delG mutation in the randomly selected population in
Hungary (A), in the selected population of our patients (B), and in the group of our CI
users who had hearing loss of unknown origin (C).
35delG +/� 35delG �/� No 35delG
allele
A
Total number of persons: 576 13 0 563
Percent: 100 2.3 0 97.7
B
Total number of persons: 318 51 24 243
Percent: 100 16.0 7.6 76.4
C
Investigated CI users: 52 5 11 36
Percent: 100 9.6 21.2 69.2
4. Discussion
Different blood storage methods were tested if they canproduce appropriate DNA samples for AS-PCR tests and forsequencing the GJB2 gene. DNA was obtained from EDTA-anticoagulated venous blood, and from dried blood spots. Wehave evaluated the possibility of the use of dried blood spots onGuthrie cards as a source of DNA for genetic testing after anextended period of storage under suboptimal conditions.
According to our experiments both DNA sources gavesatisfactory results. The usability of the PCR products from eithertemplate is equal when used in AS-PCR experiments, or insequencing. Previous works have shown that extracting DNA orRNA is possible from DBSs [17,18], but none have evaluated theeffect of storage conditions.
AS-PCR primers were validated on samples that contain the35delG mutation in the GJB2 gene’s coding exon. All the DBSsamples with the 35delG allele were sequenced and all sequencescertified the AS-PCR results. Whole GJB2 gene sequences ofsamples resulted in wild-type signals with AS-PCR proved that the

A.L. Nagy et al. / International Journal of Pediatric Otorhinolaryngology 74 (2010) 75–8180
AS-PCR experiments did not give false negative results. Our AS-PCRtest is suitable for large scale screening of dried blood spots as wellas for simple and cost-effective detection of selected – and notonly, or necessarily GJB2-related – point mutations on individualsor in family samples.
Carrier rates of mutations that cause nonsyndromic deafnessshow strong variation according to the literature. The frequency ofsome of these mutations is not even known, as they are onlyanalyzed on one or two families [21]. Some of these mutations areresearched in more detail, and we do know their carrier rates [21]According to some researchers the 35delG mutation is the singlemost responsible mutation for nonsyndromic hearing losses in theEuropean population [22]. Still, if not the single cause for most ofthe nonsydromic hearing losses, this is one of the leading causes forautosomal recessive nonsydromic hearing losses (ARNSLs) [21].Our findings indicate that in the Hungarian population the carrierfrequency of the 35delG mutation is around 2.3%, as we have found13 heterozygotes on Guthrie cards. We got similar results as Tothet al. showed in their work in a population in Northern Hungary[20]. It seems that geographic (and hence minor ethnic) differencesdo not play an important role in the distribution of the 35delGalleles in Hungary, because our randomized samples came mostlyfrom the Southern-, and South-Eastern parts of the country. Theincidence of the homozygous 35delG mutation is roughly 1/1000to 1/2000, the carrier rates are in the range of 1–3% [9,12,23] and,as expected, we found no 35delG homozygous patient in therandomized group.
According to the literature far more 35delG alleles are foundamongst CI users than in the normal population, but the geneticbackground of hearing loss does not seem to make any differencein the success of the later rehabilitation [24,25]. Speech develop-ment, however, can be normal, or close to normal, when the child isfitted with cochlear implant in the early ages. As a consequence,the procedure for the selection of a Cochlear implantation must becarried out in the very early years of life—ideally between 1.5–3years, or even earlier if possible [26]. In the cochlear implantedpopulation we found 8 patients with homozygous 35delGgenotype. Five cochlear implantees were heterozygous for 35delG.All of the 11 homozygous recessives’ relatives (whom we couldinvestigate) were heterozygous. 28 of the implantees, and 78 of allthe implantees’ relatives were homozygous wild out of the total of318 patients.
We have found three samples on blood spots in the randomizedgroup that belonged to our patients from whom we drew blood inEDTA-anticoagulated tubes. The samples were analyzed both withAS-PCR and sequencing, and these two methods showed the sameresults, not only on these three samples, but on all that wecompared using the two approaches. However, all six experiments(AS-PCR and sequencing on all three corresponding DBS andwhole-blood samples) showed the respective, matching results aswell. We acknowledge that carrying out more experiments fromthe same patients’ whole blood and DBS might have been moreconvincing, and this is one limitation of the present study. Mainlyfinancial reasons and partly organizational reasons played a criticalrole in this regard.
About 1/4th of our country belongs to our department and thattakes around 2 million people. According to statistics, there arearound 800–1000 people per 10 million inhabitants per year whomay need cochlear implantation, and the number of severe orprofound hearing losses is higher, around 1–2% in the Europeanpopulation. That takes about 100 000–200 000 subjects whoideally should be screened for the background of their hearinglosses, just based on the severity of their hearing loss, because thiscould help them to be a potential CI receiver. These are estimatesbased on our daily work, and our own experiences with patients.Others suggested somewhat lower numbers [27].
The costs of traveling this amount of people to hospitals, oruniversity hospitals, just to draw blood are enormous. With DBS’sthe costs can be cut down. Blood can be drawn by their physician,and blood transport do not need to take place in a controlledmanner, the temperature for transportation and the time it takes totransport the anticoagulated blood to the screening centers is of noconsideration anymore.
On the other hand if the need arises to carry out further genetictesting, the DNA we can get from a DBS is enough to carry outhundreds or even more than a thousand PCR experiments. In factvery little amount of gDNA solution is needed to carry out asuccessful PCR. Whole blood cannot be stored long until it noticeablydegrades, and the costs of storing the gDNA solution from peripheralblood (buying, or maintaining a refrigerator for example), and thelaboratory room consumed by the needed equipment cannot becompared to the storage demands of the dried blood spots. With themethods presented dried blood spots can be used not only test formetabolic diseases but to carry out genetic experiments as well.
As calculated by our lab we can get enough gDNA for a fewhundreds of PCR runs from about 2/3 of the money if working withDBS, than needed to do the same number of experiments withEDTA-anticoagulated whole blood, and this is only the financialcalculation regarding the acquisition and the maintenance of theequipment. We can add to this that the time consumed is evenlower, because to purify 96 samples one needs about an hour withthe previously described method from DBS, but almost a whole dayto purify it from whole blood even with a very good and productivekit. Significantly more work can be done in a given time-framewhen we use dried blood spots to extract gDNA. Purifying gDNAfrom DBS’s is more simple, requires less work and lab equipment,and the gDNA’s quality – based on the PCR experiments we made –is on par with the gDNA solution we got from the EDTA-anticoagulated blood. Beyond all these advantages, AS-PCR is acost effective, precise, and quick tool that can help us to screennewborns for specific alleles.
Acknowledgements
We would like to thank all our patients for accepting ourparticipating in our work, and Dr. Krisztina Boda for helping us torandomize the selection of samples in the DBS experiments. Wealso would like to thank to both Institutes of Hard of Hearing inSzeged and Kaposvar, for helping us to collect blood samples. Wewould also like to thank Barna Fodor PhD for carefully reading themanuscript and helping us with his advices.
References
[1] G. Van Camp, RJH Smith, Hereditary Hearing Loss Homepage. URL: http://webh01.ua.ac.be/hhh/January, 2009.
[2] P. Guilford, S. Ben Arab, S. Blanchard, J. Levilliers, J. Weissenbach, A. Belkahia, et al.,A non-syndrome form of neurosensory, recessive deafness maps to the pericen-tromeric region of chromosome 13q, Nat. Genet. 6 (1) (1994) 24–28.
[3] K.A. Brown, A.H. Janjua, G. Karbani, G. Parry, A. Noble, G. Crockford, et al., Linkagestudies of nonsyndromic recessive deafness (NSRD) in a family originating fromthe Mirpur region of Pakistan maps DFNB1 centromeric to D13S175, Hum. Mol.Genet. 5 (1) (1996) 169–173.
[4] H. Chaib, G. Lina-Granade, P. Guilford, H. Plauchu, J. Levilliers, A. Morgon, et al., Agene responsible for a dominant form of neurosensory nonsyndromic deafnessmaps to the NSRD1 recessive deafness gene interval, Hum. Mol. Genet. 3 (12)(1994) 2219–2222.
[5] D.P. Kelsell, J. Dunlop, H.P. Stevens, N.J. Lench, J.N. Liang, G. Parry, et al., Connexin26 mutations in hereditary nonsyndromic sensorineural deafness, Nature 387(6628) (1997) 80–83.
[6] R. Rabionet, P. Gasparini, X. Estivill, Molecular genetics of hearing impairment dueto mutations in gap junction genes encoding beta connexins, Hum. Mutat. 16(September (3)) (2000) 190–202.
[7] H.B. Zhao, T. Kikuchi, A. Ngezahayo, T.W. White, Gap junctions and cochlearhomeostasis, J. Membr. Biol. 209 (February–March (2–3)) (2006) 177–186.
[8] K. Willecke, S. Kirchhoff, A. Plum, A. Temme, E. Thonnissen, T. Ott, Biologicalfunctions of connexin genes revealed by human genetic defects, dominant

A.L. Nagy et al. / International Journal of Pediatric Otorhinolaryngology 74 (2010) 75–81 81
negative approaches and targeted deletions in the mouse, Novartis Found Symp.219 (1999) 76–88 (discussion 88–96).
[9] A. Pampanos, J. Economides, V. Iliadou, P. Neou, P. Leotsakos, N. Voyiatzis, et al.,Prevalence of GJB2 mutations in prelingual deafness in the Greek population, Int.J. Pediatr. Otorhinolaryngol. 65 (September (2)) (2002) 101–108.
[10] M. Tekin, T. Duman, G. Bogoclu, A. Incesulu, E. Comak, I. Ilhan, et al., Spectrum ofGJB2 mutations in Turkey comprises both Caucasian and Oriental variants: rolesof parental consanguinity and assortative mating, Hum. Mutat. 21 (May (5))(2003) 552–553.
[11] Y.C. Wang, C.Y. Kung, M.C. Su, C.C. Su, H.M. Hsu, C.C. Tsai, et al., Mutations of Cx26gene (GJB2) for prelingual deafness in Taiwan, Eur. J. Hum. Genet. 10 (August (8))(2002) 495–498.
[12] A. Bors, H. Andrikovics, L. Kalmar, N. Erdei, S. Galambos, A. Losonczi, et al.,Frequencies of two common mutations (c.35delG and c.167delT) of the connexin26 gene in different populations of Hungary, Int. J. Mol. Med. 14 (December (6))(2004) 1105–1108.
[13] M. Downing, R. Pollitt, Newborn bloodspot screening in the UK—past, present andfuture, Ann. Clin. Biochem. 45 (January (Pt 1)) (2008) 11–17.
[14] B.L. Therrell, J. Adams, Newborn screening in North America, J. Inherit. Metab. Dis.30 (August (4)) (2007) 447–465.
[15] J.L. Dhondt, Neonatal screening: from the ‘Guthrie age’ to the ‘genetic age’, J.Inherit. Metab. Dis. 30 (August (4)) (2007) 418–422.
[16] G.D. Vladutiu, Third Robert Guthrie Memorial Lecture, Mol. Genet. Metab. 91(August (4)) (2007) 303–304.
[17] C. Carducci, L. Ellul, I. Antonozzi, A. Pontecorvi, DNA elution and amplification bypolymerase chain reaction from dried blood spots, Biotechniques 13 (November(5)) (1992) 735–737.
[18] Y. Matsubara, H. Ikeda, H. Endo, K. Narisawa, Dried blood spot on filter paper as asource of mRNA, Nucleic Acids Res. 20 (April (8)) (1992) 1998.
[19] http://www.ebi.ac.uk/Tools/clustalw2/index.html.[20] T. Toth, S. Kupka, B. Haack, K. Riemann, S. Braun, F. Fazakas, et al., GJB2 mutations
in patients with nonsyndromic hearing loss from Northeastern Hungary, Hum.Mutat. 23 (June (6)) (2004) 631–632.
[21] J. Finsterer, J. Fellinger, Nuclear and mitochondrial genes mutated in nonsyn-dromic impaired hearing, Int. J. Pediatr. Otorhinolaryngol. 69 (May 5) (2005) 621–647.
[22] E.S. Cohn, P.M. Kelley, Clinical phenotype and mutations in connexin 26 (DFNB1/GJB2), the most common cause of childhood hearing loss, Am. J. Med. Genet. 89(September (3)) (1999) 130–136.
[23] L.P. Gravina, M.E. Foncuberta, R.C. Estrada, C. Barreiro, L. Chertkoff, Carrierfrequency of the 35delG and A1555G deafness mutations in the Argentineanpopulation. Impact on the newborn hearing screening, Int. J. Pediatr. Otorhino-laryngol. 71 (April (4)) (2007) 639–643.
[24] L.R. Lustig, D. Lin, H. Venick, J. Larky, J. Yeagle, J. Chinnici, et al., GJB2 genemutations in cochlear implant recipients: prevalence and impact on outcome,Arch. Otolaryngol. Head Neck Surg. 130 (May (5)) (2004) 541–546.
[25] T.C. Fischer, J. Samanich, B.E. Morrow, J. Chobot-Rodd, A. Shanske, S.R. Parikh,Genetic evaluation of American minority pediatric cochlear implant recipients,Int. J. Pediatr. Otorhinolaryngol. 73 (February (2)) (2009) 195–203.
[26] L. Colletti, Long-term follow-up of infants (4-11 months) fitted with cochlearimplants, Acta Otolaryngol. (January) (2009) 1–6.
[27] A. Davis, H. Fortnum, G. O’Donoghue, Children who could benefit from a cochlearimplant: a European estimate of projected numbers, cost and relevant character-istics, Int. J. Pediatr. Otorhinolaryngol. 31 (March (2–3)) (1995) 221–233.