mediterranean spotted fever in portugal
TRANSCRIPT

Ann. N.Y. Acad. Sci.
990: 285–294 (2003). ©2003 New York Academy of Sciences.
Mediterranean Spotted Fever in Portugal
Risk Factors for Fatal Outcome in 105 Hospitalized Patients
RITA DE SOUSA,
a
SÓNIA DÓRIA NÓBREGA,
b
FÁTIMA BACELLAR,
a
AND JORGE TORGAL
c
a
Centro de Estudos de Vectores e Doenças Infecciosas, Instituto Nacional de Saúde Dr. Ricardo Jorge, Águas de Moura, Portugal
b
Instituto Português de Oncologia de Francisco Gentil, Lisboa, Portugal
c
Departamento de Saúde Pública. Faculdade de Ciências Médicas de Lisboa, Lisboa, Portugal
A
BSTRACT
: Mediterranean spotted fever (MSF) is the most important tick–borne disease in Portugal. It is a notifiable disease and during 1989–2000 theannual incidence rate in Portugal was 9.8/10
5
inhabitants. Although recog-nized as a benign acute disease and treated mainly with ambulatory proce-dures, some cases are severe and fatalities have increased in the last few years.In 1997, MSF mortality became more evident in Beja, a Portuguese southerndistrict, with a case fatality rate of 32.3% in hospitalized patients. Analysis of55 variables regarding epidemiologic, clinical, laboratory, and therapeuticdata of fatal and nonfatal MSF cases were compared to identify risk factors in105 patients hospitalized in Beja District Hospital, between 1994 and 1998. Itwas statistically significant that the patients dying in 1997 were younger thanthose in other years. The risk of dying is statistically significant in those whopresented with diabetes, vomiting, dehydration, and uremia. The intervalbetween the onset of symptoms to administration of anti-rickettsial therapywas the same for all patients. Therapy delay, reported by some authors to beassociated with mortality of MSF, was not a risk factor in our study. Thepatients who died in 1997 died faster than those in other years. The variablesstudied could not explain the higher mortality rates observed in our study.Although one may speculate that the pathogenic strain of Israeli tick typhus,isolated in 1997, could be responsible for this increase of fatality rate, inheritedpatient factors might also be strongly associated with mortality.
K
EYWORDS
: Mediterranean spotted fever; Portugal; risk factors; mortalityrates
INTRODUCTION
Mediterranean Spotted Fever (MSF) is the notifiable tick-borne disease with thehighest incidence in Portugal. Although studies have indicated increased incidencesof MSF in Spain, France, Italy and Israel, during the last decade, Portugal still hasthe highest incidence rate compared to other Mediterranean countries.
1–4
Address for correspondence: Rita de Sousa, Centro de Estudos de Vectores e DoençasInfecciosas, Instituto Nacional de Saúde Dr. Ricardo Jorge, 2965 Águas de Moura, Portugal.

286 ANNALS NEW YORK ACADEMY OF SCIENCES
In Portugal, MSF is caused by two strains:
R. conorii
Malish and
Israeli ticktyphus
strain.
5
The disease is characterized as a vasculitis process with a picture ofthe classical triad: high fever (over 39
°
C), a typical rash,
2,3
and a single inoculationeschar at the site of a tick bite.
6–9
Recently, some authors reported that febrilepatients frequently lacked the eschar and rash, making it difficult for physicians torecognize the disease.
10–13
It is thus important for physicians to be aware of thisatypical form of the disease. Although, generally considered as a benign acute dis-ease, treatable mainly with ambulatory procedures, it is important to stress that in thelast five years a noticeable increase in the number of severe cases and fatalities inPortugal has been recorded.
3,12
This increase is most prominent in Beja, a southerndistrict of Portugal, in which a hospitalised case fatality rate of 32.3% was recordedin 1997. This rate is well above the hospitalized case fatality rates of 1.4–5.6% com-monly found in the literature.
2,12,14
In the present study MSF reported cases to official authorities during 1989 to2000 were analyzed in an attempt to determine epidemiologic picture of the diseasein Portugal
.
In addition, a retrospective study of 105 patients hospitalized with MSFat Beja District Hospital, during 1994–1998, was also presented in order to evaluateand compare epidemiologic, clinical and laboratory data of fatal and nonfatal MSFcases, in an attempt to identify the risk factors associated with the disease mortalityrate.
MATERIALS AND METHODS
Morbidity and mortality data of MSF cases reported between 1989 and 2000 wereobtained from official reports published by the Portuguese Ministry of Health’sDepartment of Epidemiology (DGS). Reported cases by private as well as publichealth physicians are categorized as “confirmed” or “probable” cases. A “confirmed”MSF case requires signs and symptoms compatible with the disease, and at least oneconfirmatory laboratory finding, whereas a “probable” MSF case is defined only onthe basis of clinical diagnosis.
15
Incidence rate was defined as the number of MSFcases officially reported during the specified period per 10
5
inhabitants. Mortalityrate was defined as the number of deaths reported during a specified period per 10
5
inhabitants. Hospitalized case fatality rate was defined as the number of deaths perthe total number of hospitalized MSF cases.
Data Collection
Epidemiologic, clinical and laboratory data on patients hospitalized at the BejaHospital for MSF during 1994–1998 were collected. Information pertaining to thefollowing intervals was also compiled: the onset of symptoms and first visit to a phy-sician; the first visit to a physician and initiation of effective therapy; and the onsetof symptoms to effective anti-rickettsial therapy. Definition of onset of symptomswas assumed as the first day of the observation of any of the following symptoms:fever, chills, rash, headache, or gastrointestinal upset.
Statistical Analysis
Exploratory data analysis was done by means of frequency distributions and cen-tral tendency measures. Differences were evaluated by Chi-square and Mann–
287SOUSA
et al.
: MEDITERRANEAN SPOTTED FEVER IN PORTUGAL
Whitney tests. Risk factors identification (odds ratio, OR) was obtained by univariatelogistic regression models adjusted by age in order to control the confounding effect.Stratified analysis by year of hospital admission (one group with 1997’s admissionsand other with 1994–1996 and 1998’s admissions) was also performed.
RESULTS
MSF Incidence and Mortality Data
During the period of January 1989 to December 2000, the Portuguese MSF inci-dence rate was 9.8/10
5
inhabitants. In this period, the incidence rate of MSF rangedbetween 6.6/10
5
inhabitants in 1994, to 14.5/10
5
inhabitants in 1991. The distribu-tion by age groups showed that the highest incidence rate (60.2/10
5
inhabitants) was
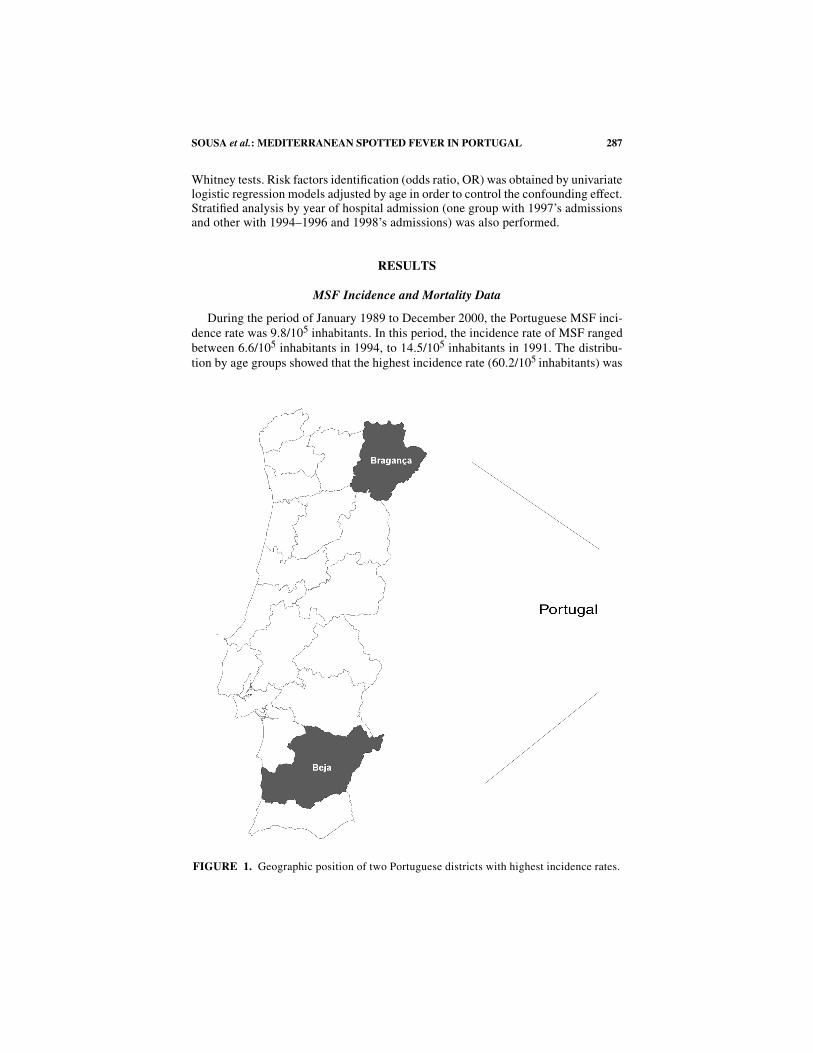
FIGURE 1. Geographic position of two Portuguese districts with highest incidence rates.
288 ANNALS NEW YORK ACADEMY OF SCIENCES
reported among children, being most noticeable in the 1–4 years group. In agegroups greater than 55 years, the incidence was between 8.6–9.1/10
5
inhabitants.Although
the disease was reported throughout the year, 88% of all cases reportedoccurred between June and September.
When the incidence rate was analyzed by districts, different national incidencepatterns were found. The two districts having the highest incidence rates were Bra-gança with 60.6/10
5
inhabitants and Beja with 48.5/10
5
inhabitants (see F
IGURE
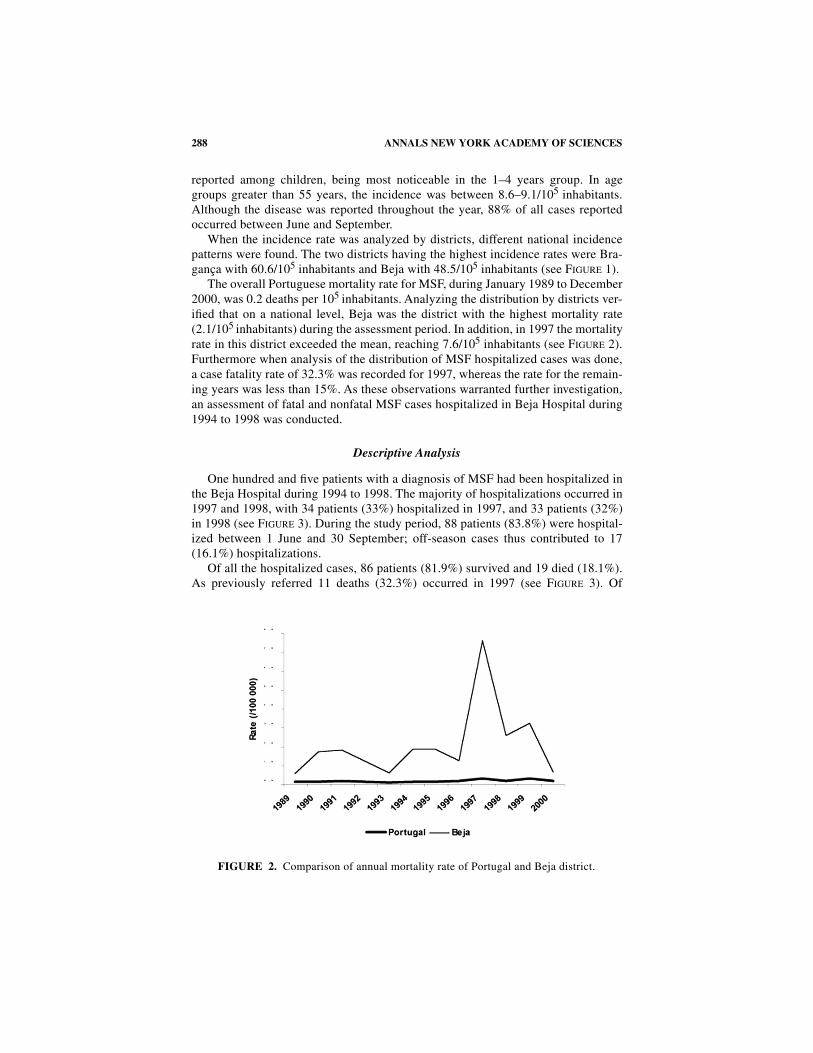
1).The overall Portuguese mortality rate for MSF, during January 1989 to December
2000, was 0.2 deaths per 10
5
inhabitants. Analyzing the distribution by districts ver-ified that on a national level, Beja was the district with the highest mortality rate(2.1/10
5
inhabitants) during the assessment period. In addition, in 1997 the mortalityrate in this district exceeded the mean, reaching 7.6/10
5
inhabitants (see F
IGURE
2).Furthermore when analysis of the distribution of MSF hospitalized cases was done,a case fatality rate of 32.3% was recorded for 1997, whereas the rate for the remain-ing years was less than 15%. As these observations warranted further investigation,an assessment of fatal and nonfatal MSF cases hospitalized in Beja Hospital during1994 to 1998 was conducted.
Descriptive Analysis
One hundred and five patients with a diagnosis of MSF had been hospitalized inthe Beja Hospital during 1994 to 1998. The majority of hospitalizations occurred in1997 and 1998, with 34 patients (33%) hospitalized in 1997, and 33 patients (32%)in 1998 (see F
IGURE
3). During the study period, 88 patients (83.8%) were hospital-ized between 1 June and 30 September; off-season cases thus contributed to 17(16.1%) hospitalizations.
Of all the hospitalized cases, 86 patients (81.9%) survived and 19 died (18.1%).As previously referred 11 deaths (32.3%) occurred in 1997 (see F
IGURE
3). Of
FIGURE 2. Comparison of annual mortality rate of Portugal and Beja district.

289SOUSA
et al.
: MEDITERRANEAN SPOTTED FEVER IN PORTUGAL
the 105 patients, 54 (51.4%) were males and 51 (48.6%) were females. The ages ofsurviving patients ranged from 1 to 89 years, whereas the ages of patients who diedranged from 53 to 89 years.
Risk Factor Analysis
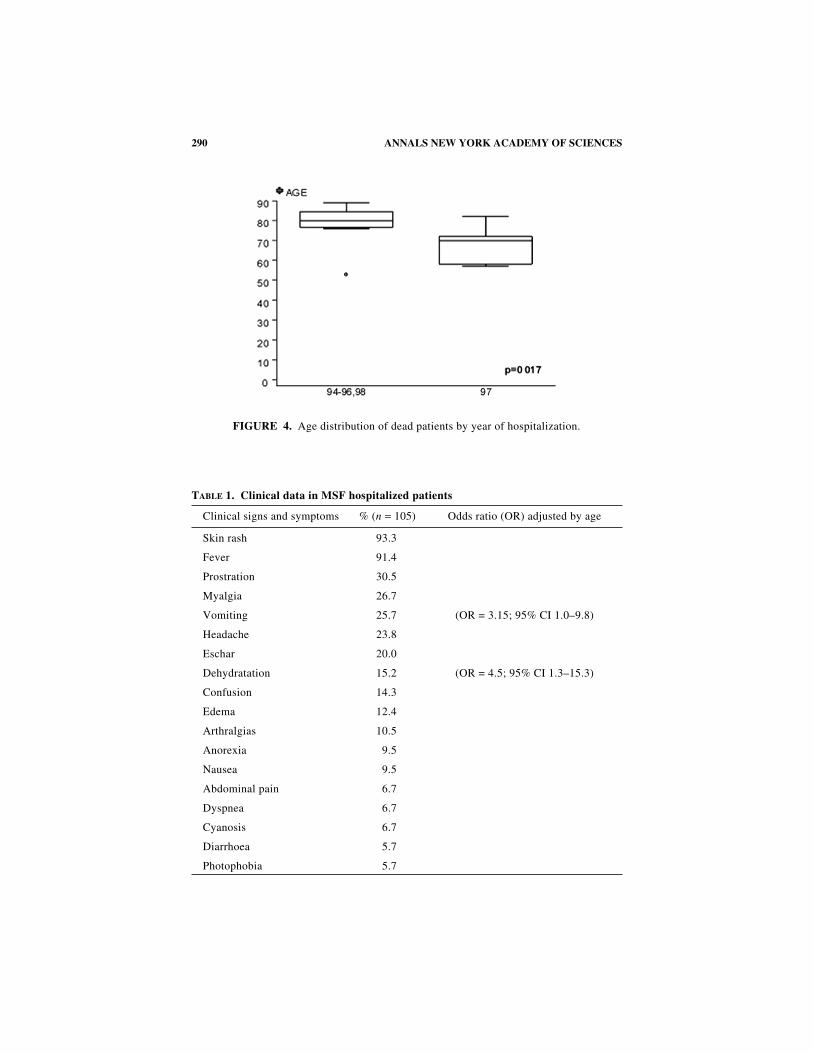
There were no statistically significant differences in the risk of dying by gender.Significant differences (
P
=
0.017) were found in the ages of patients who died in1997 and age of patients who had died in other years (1994–1996, 1998) (seeF
IGURE
4). The patients who died in 1997 were younger than those in other years(Median
97
=
70 years; Median
94-96, 98
=
80 years).MSF clinical and laboratory parameters analyzed are listed in T
ABLES
1, 2, and 3by percent of those exposed to the risk factor and the OR, if is statistically signifi-cant. In all patients hospitalized, rash was the most common (93.3%) clinical signreported followed by fever (91.4%). Eschar was reported in only 20% of patients.Diabetes was the most reported (19%) concomitant disease. Of all clinical variablesstudied (T
ABLE
1), the risk of death was statistically significant for patients withdiabetes (OR, 4.83; 95% CI, 1.53–15.18); vomiting (OR, 3.15; 95% CI, 1.01–9.80)and dehydration (OR, 4.53; 95% CI, 1.34–15.31).
Patients that died in 1997 took longer to have their first physician visit after theironset of symptoms (Median
97
=
4 days; Median
94–96,98
=
2 days;
P
=
0.044). How-ever, when we analyzed the interval between the onset of symptoms to administra-tion of anti-rickettsial therapy no differences were found by year of hospitalizationand by discharge status (dead or alive). This is because the patients that died in yearsother than 1997 did not receive anti-rickettsial therapy during their first physicianvisit. In fact, the records showed that all patients had the same interval (4–5 days)from onset of symptoms to administration of anti-rickettsial therapy.
The median length of hospitalization for patients that survived was seven days in1997 and six days in the other years. A statistically significant difference by year of
FIGURE 3. Hospitalized patients in Beja Distrital Hospital during 1994–1998.
290 ANNALS NEW YORK ACADEMY OF SCIENCES
FIGURE 4. Age distribution of dead patients by year of hospitalization.
T
ABLE
1. Clinical data in MSF hospitalized patients
Clinical signs and symptoms % (
n
=
105) Odds ratio (OR) adjusted by age
Skin rash 93.3
Fever 91.4
Prostration 30.5
Myalgia 26.7
Vomiting 25.7 (OR = 3.15; 95% CI 1.0–9.8)
Headache 23.8
Eschar 20.0
Dehydratation 15.2 (OR = 4.5; 95% CI 1.3–15.3)
Confusion 14.3
Edema 12.4
Arthralgias 10.5
Anorexia 9.5
Nausea 9.5
Abdominal pain 6.7
Dyspnea 6.7
Cyanosis 6.7
Diarrhoea 5.7
Photophobia 5.7
291SOUSA
et al.
: MEDITERRANEAN SPOTTED FEVER IN PORTUGAL
hospitalization was found in those who died (Median
97
=
2 days; Median
94–96,98
=
6.5 days;
P
=
0.005). Following hospitalization, deaths in 1997 seemed to be moresudden.
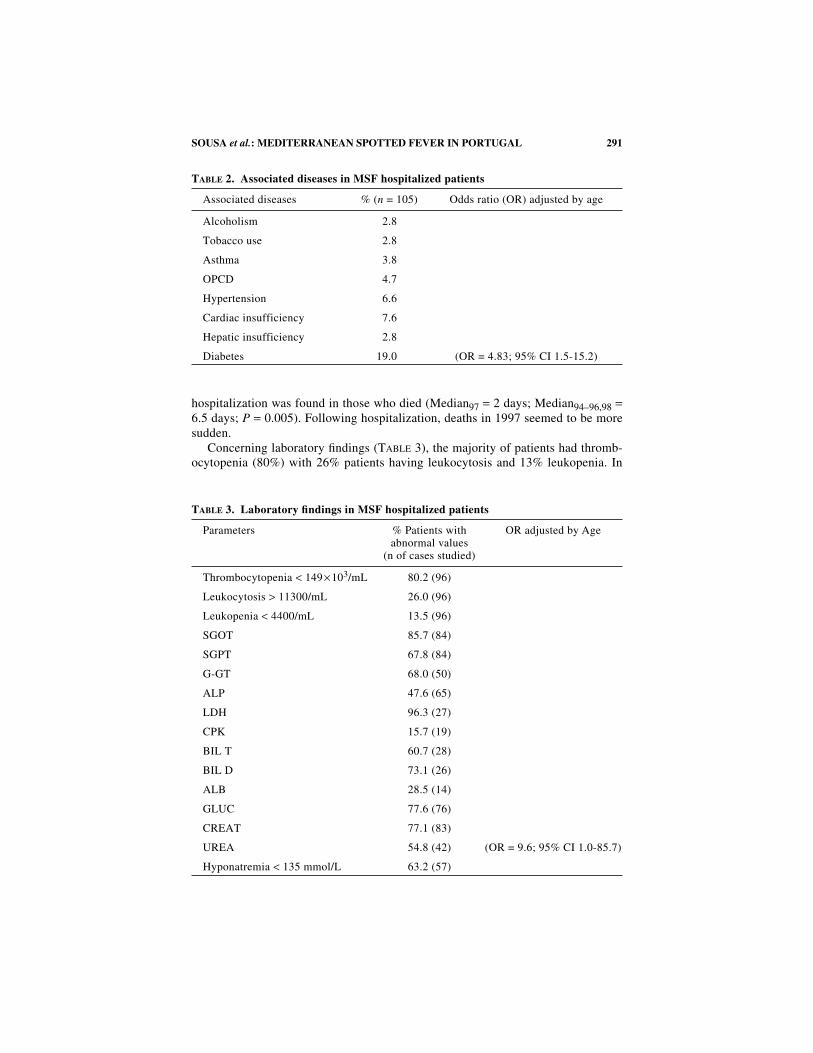
Concerning laboratory findings (T
ABLE
3), the majority of patients had thromb-ocytopenia (80%) with 26% patients having leukocytosis and 13% leukopenia. In
T
ABLE
2. Associated diseases in MSF hospitalized patients
Associated diseases % (
n
= 105) Odds ratio (OR) adjusted by age
Alcoholism 2.8
Tobacco use 2.8
Asthma 3.8
OPCD 4.7
Hypertension 6.6
Cardiac insufficiency 7.6
Hepatic insufficiency 2.8
Diabetes 19.0 (OR = 4.83; 95% CI 1.5-15.2)
T
ABLE
3. Laboratory findings in MSF hospitalized patients
Parameters % Patients with abnormal values
(n of cases studied)
OR adjusted by Age
Thrombocytopenia
<
149
×
10
3
/mL 80.2 (96)
Leukocytosis
>
11300/mL 26.0 (96)
Leukopenia
<
4400/mL 13.5 (96)
SGOT 85.7 (84)
SGPT 67.8 (84)
G-GT 68.0 (50)
ALP 47.6 (65)
LDH 96.3 (27)
CPK 15.7 (19)
BIL T 60.7 (28)
BIL D 73.1 (26)
ALB 28.5 (14)
GLUC 77.6 (76)
CREAT 77.1 (83)
UREA 54.8 (42) (OR = 9.6; 95% CI 1.0-85.7)
Hyponatremia
<
135 mmol/L 63.2 (57)

292 ANNALS NEW YORK ACADEMY OF SCIENCES
general, all patients presented abnormal renal and hepatic functions. Hyponatremiawas observed in 63.2% of the 52 clinical charts that were studied. The risk factoranalysis identified only uremia as a statistically significant factor associated withMSF death (OR, 9.6; 95% CI, 1.08–85.68).
Most patients (75%) were treated with tetracycline. Quinolones was used in 10%of the cases, Chloramphenicol in 3%, and cotrimoxasol only in 2%. The risk factoranalysis identified cotrimoxazol as a statistically significant factor (OR, 1.1; 95% CI,1.0–1.2;
P
=
0.017) associated with MSF death in patients hospitalized in 1994 to1996 and in 1998.
Only five patients had serological confirmation.
DISCUSSION
MSF is an important disease in Portugal. Its incidence rate of 9.8/10
5
inhabitantsis high when compared with available data of other endemic countries such as Israel.During 1972-1981 Israel reported the highest MSF incidence rate (6.2/10
5
inhabit-ants), but this rate has decreased over the years to 0.9/10
5
inhabitants in 1994 andsubsequent years.
4
Although in Portugal around 1000 MSF cases are reported peryear, these values are underestimated and some authors refers that there are seventimes more cases than those reported.
3
Different patterns of incidence found in the Portuguese districts could be due tothe different rates of MSF case reporting, or alternatively related to vector dynamics.The various climatic conditions found throughout Portugal are known to influencethe activity and seasonal dynamics of ticks.
16,17
The Beja district is a subregion ofthe Alentejo, a region in Portugal with climatic conditions very favorable for
Rhipi-cephalus sanguineus,
the principal vector involved in MSF.
17
In this region, this tickcan have more than two life-cycles per year.
17
Analysis of the notified MSF casesrevealed that Bragança had the highest incidence rate, but it had only a few MSF-related deaths reported. Comparisons between Bragança and Beja MSF reporteddeaths revealed no clear explanation why the death rate in the former district is lower.
In the last years of the assessment period (1997–2000), an increase in the numberof MSF hospitalizations in Beja and in others districts of Portugal was observed aswell as a more severe clinical picture.
19
While no direct factors inducing deaths in1997 were found, it is anticipated that this could be related to the presence of the newpathogenic strain, Israeli tick typhus, isolated in 1997 for the first time in Portugal.
5
This strain was previously only known to be present in Israel.
20
Data from officialauthorities indicates that more severe and fatal cases are occurring in younger peoplesince 1997; however, the reason for this trend is unclear to us.
The retrospective study presented here identified diabetes, vomiting, dehydration,and uremia as risk factors for death among MSF hospitalized patients. These findingsare largely consistent with risk factors identified individually or in combination withother epidemiologic and clinical characteristics in studies of MSF.
6–9,21–23
The factthat we did not find significant differences with other concomitant diseases such asalcoholism, tobacco use, cardiac and renal insufficiency, is probable due to a lack ofsample representativeness. Glucose–6-phosphate-dehydrogenase enzyme deficiencyhas been related to be a predisposing factor for severe course of MSF, however, as this

293SOUSA
et al.
: MEDITERRANEAN SPOTTED FEVER IN PORTUGAL
variable was only mentioned in one patient’s record, it was not possible to analyze itin the present investigation.
24–26
In our study all the patients were classified as prob-able cases owing to the lack of laboratory confirmation. No general differences werefound between clinical signs and symptoms in alive and dead patients. This could bedue to the fact that only hospitalized patients were involved in this study and that allhospitalized patients, independent of outcome, are generally considered severe. Wealso did not find an association between delayed initiation of adequate and effectivetherapy and fatal outcome. Although therapeutics delay was reported in some studiesto be a risk factor for fatal outcome,
27,28
here all patients received anti-rickettsial ther-apy within similar time periods. Physicians in Beja district are well aware of the atyp-ical signs and symptoms of MSF and so are not hesitant in the prompt initiation oftherapy in these cases.
Results showed that in 1997, MSF patients died more suddenly than in otheryears, and mainly with fulminant courses. Compared to other time intervals studied,it seems that the signs and symptoms were not so exuberant in other years, but ratherthat the disease progression seems to be more aggressive after it had been detected.This is in spite of the fact that all patient groups studied had effective anti-rickettsialtherapy within the same time period.
Treatment with cotrimozaxol was in fact associated with deaths that occurred inothers years previous to 1997. Since some reports have referred that this drug is nota good choice and could in fact enhance the gravity of the disease, medical doctorshave no longer been using this drug.
29,30
In this retrospective study, no isolation ofthe pathogenic agent was mentioned, thus no associations between the epidemiolog-ic, clinical, and laboratory findings and the features of the isolated strain could beevaluated. Further research is thus required in order to fill this gap in data. A pro-spective study comparing all these parameters is suggested. Results from such astudy should help to clarify whether the clinical observations found here are effec-tively due to differences in virulence between these two strains of
Rickettsia conorii
complex or if they are simply related to genetic characteristics of the patients.
REFERENCES
1. MUMCUOGLU, K.Y., A. KEYSARY & L. GILEAD. 2002. Mediterranean spotted fever inIsrael: a tick-borne Disease. Isr. Med. Assoc. J. 4: 44–49.
2. WALKER, D.H. et al. 1987. The Pathology of Fatal Mediterranean Spotted Fever. Am.J. Clin. Pathol. 87:669–672.
3. SOUSA, R. 2002. Sobre a Realidade Epidemiológica da Febre Escaro-nodular. MSc.Thesis, Universidade Nova de Lisboa, Lisboa.
4. AHARONOWITZ, G. et al. 1999. Epidemiological characteristics of spotted fever inIsrael over 26 years. Clin. Infect. Dis. 29:1321–1322.
5. BACELLAR, F.C. et al. 1999. Israeli spotted fever Rickettsia (Rickettsia conorii com-plex) associated with humam diseses in Portugal. Emerg. Infect. Dis. 5(6): 835–836.
6. RAOULT, D. et al. 1986. Mediterranean spotted fever: clinical, laboratory, and epidemi-ological features of 199 cases. Am. J. Trop. Med. Hyg. 35: 845–850.
7. RAOULT, D. et al. 1986. Incidence, clinical observations and risk factors in the severeform of mediterranean spotted fever among patients admitted to hospital inMarseilles 1983–1984. J. Infect. Dis. 12: 111–116.
8. FONT-CREUS, B. et al. 1985. Mediterranean spotted fever. A cooperative study of 227cases. Rev. Infect. Dis. 7: 635–642.

294 ANNALS NEW YORK ACADEMY OF SCIENCES
9. FONT-CREUS, B. et al. 1991. Fiebre botonosa mediterránea. Estudio de 246 casos. 96:121–125.
10. BROUQUI, P. et al. 1992. Spotless boutonneuse fever. Clin. Infect. Dis. 14: 114–116.11. LANCET (editorial). 1991. Bitten, hot, and mostly spotty. Lancet 337: 143–144.12. RAOULT, D. & V. ROUX. 1997. Rickettsiosis as paradigms of new or emerging infec-
tious diseases. Clin. Microbiol. Rev. 10(4): 694–719.13. GROSS, E.M. & P. YAGUPSKY. 1987. Israeli rickettsial spotted fever in children. A
review of 54 cases. Acta Trop. 44: 91–96.14. REGEV-YOCHAY, G., E. SEGAL & E. RUBINSTEIN. 2000. Glucose-6-phosphate dehydro-
genase deficiency: possible determinant for a fulminant course of Israeli spottedFever. Isr. Med. Assoc. J. 2: 781–782.
15. DGS-SERVIÇO DE INFORMAÇÃO DE SAÚDE. Doenças de Declaração Obrigatória 1989-1998. Ministério da Saúde, Direcção Geral da Saúde, Lisboa, Portugal.
16. Gilot, B. et al. 1990. Relationships between the Rhipicephalus sanguineus complexecology and Mediterranean Spotted Fever Epidemiology in France. Eur. J. Epidemiol.6(4): 357–362.
17. CAEIRO, V. 1992. As carraças em Portugal: seus hospedeiros domésticos e silvestres.Ciclos vitais, preferências de vegetação e de clima. Med. Vet. 28: 7–25.
18. CAEIRO, V. 1999. General review of tick species present in Portugal. Parassitologia(Rome) 41(Suppl.1): 11–15.
19. FRANÇA, A. et al. 2000. Fatal Mediterranean spotted fever in Portugal. Similaritieswith RMSF. Presented at International Conference on Emerging Infectious Diseases.Atlanta, Georgia, USA, July 16–19.
20. GOLDWASSER, R.A. et al. 1974. The Isolation of strains of rickettsiae of the spottedfever group in Israel and their differentiation from another members of the group byimmunofluorescence methods. Scand. J. Infect Dis. 6: 53–62.
21. RUIZ-BELTRAN, R. et al. 1985. Formas graves de fiebre exantemática mediterránea.Análisis prospectivo de 71 enfermos. An. Med. Interna. II: 365–368.
22. JUFRESA, J. et al. 1997. Study of 86 of Mediterranean boutonneuse fever hospitalizedat a university hospital. An. Med. Interna. 14(7): 325–327.
23. GRILLO-REINA, A. et al. 1982. Fiebre botonosa. Estudio de los factores pronósticos.Rev. Clin. Esp. 164: 387–390.
24. ROUSSEAU, M.C., P. BROUQUI & S. BOURGEADE. 1994. Fièvre boutonneuseméditerranéenne maligne chez un patient porteur d’un déficit partiel en glucose-6-phosphate-déshydrogénase. Rev. Méd. Interne. 15: 362–366.
25. RAOULT, D. et al 1986. Hemolysis with mediterranean spotted fever and glucose-6-phosphate-desidrogenase defficiency. Trans. Roy. Soc. Trop. Med. Hyg. 80: 961–962.
26. PIRAS, M.A. et al. 1983. Glucose 6-phosphate dehydrogenase deficiency in malepatients with mediterranean spotted fever in Sardinia. J. Infect. Dis. 147: 607–608.
27. HOLMAN, R.C. et al. 2001. Analysis of risk factors for Rocky Mountain spotted fever:evidence for superiority of tetracyclines for therapy. J. Infect. Dis. 184: 1437–1444.
28. KIRKLAND, B.K., W.E. WILKINSON & D.J. SEXTON. 1995. Therapeutic delay and mor-tality in cases of Rocky Mountain spotted fever. Clin. Infect. Dis. 20: 1118–1121.
29. MAURIN, M. & D. RAOULT. 1999. Antimicrobial therapy of rickettsial diseases. Pro-ceedings of Rickettsiae and Rickettsial Diseases at the Turn of the Third Millenium.D. Raoult & P. Brouqui. Elsevier.
30. RUIZ-BELTRAN, R. & J.L. HERRERO-HERRERO. 1992. Deleterious effect of trimetrhop-rim-sulfamethoxazol in Mediterranean spotted fever (letter). Antimicrob. AgentsChemother. 36: 1342–1344.