managing ict to solve the exploration-exploitation paradox in healthcare
TRANSCRIPT
1
Managing ICT to Solve the Exploration-Exploitation Paradox in Healthcare
Luca Gastaldi*, Mariano Corso Department of Management, Economics and Industrial Engineering Politecnico di Milano Via Lambruschini 4b, Building 26b — 20156 Milan (Italy)
* Corresponding author: [email protected]
Structured Abstract Purpose – Hospitals struggle to achieve and maintain a paradoxical balance between their exploratory and exploitatory activities in order to improve the quality of their services while
reducing their costs. Although Information and Communication Technology (ICT) can play a strategic role from this viewpoint, literature has only marginally analysed if and how ICT can be adopted—within and among hospitals—in order to manage the exploration-exploitation paradox and increase hospital performance. This paper addresses this gap. Design/methodology/approach – This study has an interpretative, inductive perspective, based on multiple and embedded case studies. 14 hospitals in North Italy have been con-sidered on the basis of the activities characterising, and the users involved in the adoption, the usage and the improvement of a set of different ICT-based solutions. The primary data source is 107 semi-structured interviews conducted over three years (from January 2009 to December 2011) with the C-levels and other knowledgeable informants of the hospitals. Originality/value – ICT can effectively solve the exploration-exploitation paradox and in-crease hospital performance through three complementary paths: (i) the digitalisation of the
assets utilised within hospitals; (ii) the ICT-based integration among healthcare stakeholders;
(iii) the disruption of clinical and administrative decision-making through the use of analytics.
The complementarity of the paths allows the construction of the dynamic capabilities neces-sary to continuously cope with the conflicting demands characterising the healthcare industry. Practical implications – The cross-analysis of the cases provides healthcare practitioners with useful information to prevent energies from dissipating during the management of ICT-driven innovation. More specifically the paper (i) proposes a prioritisation of the dif-ferent ICT-based paths to solve the exploration-exploitation paradox that allows for the evaluation of possible “next steps” that could prove beneficial, and (ii) provides potential elements that deserve particular attention. Keywords – Exploration; Exploitation; Paradox; ICT; Healthcare Paper type – Academic Research Paper

2
1 Introduction
Most hospitals are currently trying to reconfigure and innovate themselves in order to
continuously manage and progressively solve the conflict between quality improvement
and cost rationalisation (Angst et al., 2011). In fact, these two objectives have a contradic-
tory nature, and are tremendously difficult to attain simultaneously (Gastaldi et al.,
2012a). If a hospital focuses too much—as has proven to be the case historically (Chris-
tensen et al., 2009)—on the progress of the search for new and better treatment delivery
alternatives, there is the risk that its costs will soar (Christensen et al., 2009). On the other
hand, if too much pressure is placed on cutting costs, the quality of hospital services tends
to fall below acceptable levels (Connell and Young, 2007). Achieving and maintaining a
continuous balance between quality improvement and cost rationalisation is the main is-
sue tackled by hospital practitioners (IHO, 2011; Angst et al., 2011; Fichman et al., 2011).
This balance does not denote a mediocre split of bland compromise, but truly excel-
ling at both the competing demands (Atuahene-Gima, 2005). The difficulties in attaining
this double goal lie in the contradiction between the activities underlining the two objec-
tives (March, 1991; Levinthal and March, 1993). In fact:
• The improvement of the hospital quality is mainly a result of exploratory activi-
ties: it suffices to consider the field of infectious diseases—from Pasteur’s explo-
ration of germ theory to Fleming’s discovery of penicillin (Christensen et al., 2009);
• The rationalisation of the hospital cost is essentially achieved through exploitato-
ry investments: it suffices to consider the efforts to dematerialise a radiology de-
partment (Grunden, 2008) or a laboratory (Corso and Gastaldi, 2010).
Whereas exploration engages individuals and organisations in search, experimenta-
tion, and variation, exploitation enhances productivity and efficiency through choice, exe-
cution, and variance reduction (Lavie et al., 2010). These activities compete for the same
resources (Holmqvist, 2004) in an inertial environment (Søresen and Stuart, 2000) that
emphasises the tensions produced by a set of antecedents of exploratory rather than ex-
ploitatory behaviours (Lavie et al., 2010). The combined effect of these forces tends to
open up the gap between exploration and exploitation (Corso and Gastaldi, 2011), which
act as two opposing attractors between which an effective balance arises only if persis-
tent, on-going efforts are put in place. Complexity theory refers to this set of efforts as a
dissipative equilibrium (Brown and Eisehanrdt, 1998) while an increasing number of re-
searchers is focusing on how it is possible to unceasingly maintain this unstable “edge of
chaos” during time (e.g. Corso and Gastaldi, 2011; Martini et al., 2012; Jansen et al., 2012).

3
Starting from this perspective, it is interesting to consider not only the conflict between
quality improvement and cost rationalisation, but also the one present between the explorato-
ry and exploitatory activities underlying both these objectives. Studying the problem at this
double level seems promising because it provides a clue to explain how it is possible to com-
bine the diverging objectives to be reached. In fact, a system maintain a dissipative equilibri-
um between exploration and exploitation when it is able to positively combine (i) search, vari-
ation, risk-taking, experimentation, play, flexibility, discovery and innovation on the one
hand, with (ii) refinement, choice, production, efficiency, selection, implementation and exe-
cution on the other (March, 1991). The promising idea—diffused among academics (e.g.
Lavie et al., 2010) as well as practitioners (e.g. IHO, 2011)—is that this ambidextrous ca-
pability can lead to better performances because a paradoxical focus is maintained on
both current (exploitation) as well as future (exploration) processes of value generation—
going through positive reinforcing cycles that progressively solve the multiple and inter-
related tensions underlying the natural divergence present not only between exploratory
and exploitatory efforts (Lewis, 2000; Andriopoulos and Lewis, 2009), but also between
the related outcomes of quality improvement and cost reduction (Smith and Lewis, 2011).
Although this framework is still in a developmental phase (Martini et al., 2012), it can
be used to study the problems tackled by hospital practitioners. In fact, most of hospitals
strive to effectively manage the paradox characterising their exploratory and their exploi-
tatory activities in order to simultaneously cope with the contradictory yet interrelated ob-
jectives of quality improvement and cost rationalisation (Corso and Gastaldi, 2010). A
key notion that is progressively emerging as highly critical, from this viewpoint, is pro-
cess coordination, which refers to the efforts put in the continuous and real-time align-
ment (Brown and Eisenhardt, 1998) among the actors and the activities characterising
both intra- (Marks et al., 2001) and inter-organisational (Fjeldstad et al., 2012) processes.
Process coordination allows not only to have each agent updated on the changes affecting
the exploratory and exploitatory tasks under his or her responsibility, but also to encour-
age individuals to make widespread judgements about how to divide their time between
conflicting demands (Gibson and Birkinshaw, 2004). Increasingly scholars are recognis-
ing the importance of process coordination as a critical element to develop an effective
organisational ambidextrous capability (Brown and Eisenhardt, 1998; Gibson and Birkin-
shaw, 2004; Lavie et al., 2010; Martini et al., 2012). Moreover, most of the problems in
healthcare are actually related to the absence of coordination among the clinical and ad-
ministrative processes (Aarts et al., 2007)—especially the ones overcoming the organisa-
tional boundaries (Goes and Park, 1997; Angst et al., 2010).

4
From this perspective, Information and Communication Technology (ICT) can play a
strategic role. In hospital ICT has become indispensables, not only due to its increasing
pervasiveness (Fichman et al., 2011), but also to its ability to respond to the aforemen-
tioned sector challenges (Gastaldi et al., 2012a) as well as to process coordination issues
(Corso and Gastaldi, 2011). Under specific contextual conditions (Gastaldi et al., 2012a),
ICT leverages on knowledge assets (Sambamurthy and Subramani, 2005), nurtures inno-
vation (Tantiverdi, 2005), and offer opportunities to conciliate the capability to exploit the
current knowledge base with the capability to shift away from it in order to explore new
and better ways of delivering value (Joshi et al., 2010; Martini et al., 2012). Thus, ICT
has the potential to contribute to the strategies adopted within and among hospitals to in-
crease their performances—both in terms of quality improvement and cot rationalisa-
tion—by operating efficiently (exploit) and, at the same time, adapt continuously (explore).
If, on the one hand, there is currently somewhat a consensus not only about the value of
paradoxically balancing exploration and exploitation to achieve better organisational per-
formance (Lavie et al., 2010), but also about the role that ICT can play in moderating the out-
come of this balance by leveraging on process coordination (Joshi et al., 2010), on the other
hand, there is little agreement regarding if and how hospitals can actually use ICT as a lever to
manage the exploration-exploitation paradox in order to increase their quality while reducing
their costs. Literature, in fact, does not provide with a clear guidance, since previous contribu-
tions focused on subsets of the whole problem: (i) the balance between exploration and ex-
ploitation (Lavie et al., 2010); (ii) the dynamic process trough which the tensions between the-
se paradoxical activities are solved (Smith and Lewis, 2011); the multifaceted performance
implications of exploration and exploitation (Jansen et al., 2012); the impact of ICT on both
quality improvement and cost rationalisation (Gastaldi et al., 2012a); the importance of the
sequence of ICT-based solutions adoption (Angst et al., 2011). This paper aims to start con-
sidering all these issues by adopting a comprehensive perspective, which basically explores if
and how ICT can be adopted in order to successfully managing the exploration-exploitation
paradox, where «successfully managing the exploration-exploitation paradox» means a par-
adoxical balance able to improve hospitals quality while reducing their cost.
2 Research Method
This research is part of the activities of the ICT in Healthcare Observatory—a perma-
nent research initiative that, since 2007, has been addressing the topic of how the Italian
healthcare industry can strategically use ICT to tackle the main problems it is facing. Refer to

5
Corso and Gastaldi (2011) for a description of the overall participative, evolutionary, longitu-
dinal and multi-methodological framework characterising the research of the Observatory.
In order to cope with the issues raised by this paper, an interpretative, inductive per-
spective (Eisenhardt, 1989a), based on multiple case studies (Eisenhardt, 1989b) has been
considered appropriated. The interpretative, inductive perspective is useful because the
work aims to better understand the complex dynamics underlying effective exploration-
exploitation paradox in healthcare—retaining «the holistic and meaningful characteristics
of real-life events» (Yin, 2003). The interrelatedness of exploratory and exploitatory ac-
tivities (Andriopoulos and Lewis, 2009), their link to intra- and inter-organisational pro-
cesses (Smith and Lewis, 2011), the pervasiveness of ICT-based solutions (Stegwee and
Spill, 2001), and the blurred socio-technical nature of the contexts in which ICT is not on-
ly used but also evaluated (Goh et al., 2011), make quantitative methods mostly ineffec-
tive in accomplishing this task. Only the intimate connection with empirical reality per-
mits the development of a testable, relevant and actionable knowledge (Eisenhardt, 1989a;
Feldman and Orlikowski, 2011). The paper relies on multiple cases because they tend to yield
to more generalizable, robust results than single cases (Eisenhardt and Graebner, 2007).
After the selection of the main research method, the authors focused on the definitions of
the constructs to be used. In fact, an a priori specification of the constructs used in the study
helps in defining the unit of analysis to approach, and the kind of data to gather (Eisenhardt,
1989a). The definitions of exploratory and exploitatory activities are a specialisation within
the healthcare context of the definitions provided by March (1991) in his seminal work:
• Exploratory activities: activities that explore new and better alternatives to deliv-
er administrative and clinical services in order to change existing routines;
• Exploitatory activities: activities that refine and extend the existing competences,
simplifying the use of existing routines in the administrative and clinical domains.
Both the definitions are based not only on literature analysis, but also on the sugges-
tions—provided through social agreement (Coghlan and Shani, 2008)—of a group of
more than 60 practitioners that have also defined—together with the authors and other re-
searchers working in the Observatory—not only a taxonomy of the ICT-based solutions
that a hospital can adopt (which define the boundaries of the research), but also their clas-
sification in four main areas (which supported the cross-interpretation of the findings).
Table 4 reports the different solutions emerged from this collaborative effort.
According to Yin (2003), a major step in designing and conducting a case-based re-
search is defining the unit of analysis. Starting from the aim of the paper, the focus on the

6
ICT introduction process as a first unit of analysis was chosen. By «ICT introduction pro-
cess» this paper means the set of activities and users involved in the adoption, the usage
and the improvement of one of the ICT-based solutions listed in Table 4. In fact, if one
wants to study how ICT can successfully manage the exploration-exploitation paradox, the
analysis of how ICT-based solutions have been adopted, used and improved, provides a privi-
leged viewpoint to understand the support delivered to the exploratory and exploitatory activ-
ities of the hospital. The focus on the ICT introduction process facilitates the application of the
comparison of the otherwise incomparable ICT-based solutions in Table 4. Moreover, a pro-
cess-perspective such as the one chosen is broad enough to not need revising during data col-
lection—one of the problems associated with the selection of the unit of analysis (Yin, 2003).
In order to improve the likelihood of rich, accurate theory (Martin and Eisenhardt, 2010)
the authors considered the hospital as a second unit of analysis, and the regional healthcare
system around the hospital as a third unit of analysis. The selection of an embedded unit of
analysis was made to: (i) better measure the performances of the exploratory and exploitatory
activities impacted by the ICT introduction process, (ii) diminish the probabilities to conduct
the research at an abstract level (Yin, 2003), and (iii) tackle the expected shift in the orienta-
tion of some cases from the organisational to the regional level. Literature provides famous
examples of the usage of several embedded units of analysis within the same study to focus a
case inquiry (e.g. Martin and Eisenhardt, 2010). The whole Italian healthcare industry has
been considered as the context in which to perform the cases. In fact, Yin (2003) suggests to
taking into account the contextual conditions in relation to the case—considering that the
boundaries between the case and the context are not always sharp.
Central to building theory from case studies is replication logic (Eisenhardt, 1989a),
which is «each case serves as a distinct experiment that stands on its own as an analytic
unit» (Eisenhardt and Graebner, 2007). Like a series of related laboratory experiments,
multiple cases are discrete experiments that serve as replications, contrasts, and exten-
sions to the emerging theory (Yin, 2003). The choice of relying on multiple cases in-
volves their selection. Considering that the purpose of this research is not to test a theory,
but to develop it, a focus has been put on the ICT introduction processes of 14 hospitals in
Lombardy—a region in the north of Italy. A unique regional healthcare system provides
the same boundary conditions for all the cases, while the specific selection of Lombardy
is related to the simplicity in achieving the data on the cases (due to their proximity of the
hospitals to the School of Management of Polytechnic University of Milan, which have
all its facilities in Lombardy) and to the importance given to ICT topics within the relative
regional healthcare system (as explained in Gastaldi et al., 2012a or Lo Scalzo et al., 2009).

7
Hospital* Typology** Employees Ownership H1 AO 3,608 Public H2 AO 2,320 Public H3 ASL 1,286 Public H4 ASL 3,256 Public H5 IRCCS 304 Private H6 IRCCS 783 Private H7 IRCCS 606 Public H8 AO 4,129 Public H9 AO 3,814 Public H10 ASL 805 Public H11 IRCCS 1,446 Public H12 IRCCS 641 Private H13 IRCCS 1,495 Private H14 IRCCS 3,826 Private
* Pseudonyms are used to protect the anonymity of the hospitals and their members ** AO (in Italian: Azienda Ospedaliera): public hospital providing patient treatment by specialised staff and equipment as quasi-independent public agency; ASL (in Italian: Azienda Sanitaria Locale): geographically-based hospital responsible for assessing needs and providing comprehensive care to the population of a defined territory; IRCCS (in Italian: Istituto di Ricerca e Cura a Carattere Scientifico): hospital with competences in research and treatment of important diseases; see Lo Scalzo et al. (2009)
Table 1 – Theoretical sample used in the multiple, embedded case study
As suggested by the literature (e.g. Martin and Eisenhardt, 2010; Bingham and Eisen-
hardt, 2011), the authors relied on several data sources: face-to-face interviews, phone
conversations, follow-up emails, and archival data such as internal documents, press re-
leases, websites, and news articles. In order to maximise the benefits from these sources
of evidence, and better deal with the construct validity and reliability issues, two of the
three principle suggested by Yin (2003) have been followed: the triangulation of data
sources (Jick, 1979; Anand et al., 2007), and their organisation in an electronic and navi-
gable case study database (Miles and Huberman, 1994; Darke et al., 1998; Yin, 2003).
The primary data source was 107 semi-structured interviews conducted over three years
(form January 2009 to December 2011) with the Chief Information Officers (CIOs), at least
one of the other C-levels—Chief Executive Officers (CEOs), Chief Financial Officers
(CFOs), Chief Medical Officers (CMOs)—, and, through a snowball technique (Patton,
2002), other knowledgeable informants involved in the ICT-driven innovation process such
as nurses and physicians. Within each firm, authors continued recruiting informants until ad-
ditional interviews failed to dispute existing, or reveal new, categories or relationships—that
is, until theoretical saturation (Strauss and Corbin, 1990) was achieved. The interviews have
been designed on a common protocol that evolved systematically during the research. A
key advantage of the study is its three waves of data collection (Ozcan and Eisenhardt,
2009). As Glaser and Strauss (1967) recommend, the study began with general research
aims. In the first wave of data collection a focus has been put on the different solutions

8
present inside the hospitals, and the ones that would be developed in the near future (start-
ing before the end of 2012). The main information achieved are synthesised is summa-
rised in Table 3. In the second and in the third waves of interviews the authors focused of
the introduction process of some of the solutions under development in Table 3, and—as
data collection and analysis unfolded—the interviews became increasingly focused (An-
driopoulos and Lewis, 2009) on the activities and the users involved in the adoption, the us-
age and the improvement of these specific solutions. The different unit of analysis allowed to
focus on the performances achieved and the exploratory and exploitatory activities supported.
Potential informant bias has been addressed in several ways. First, the interviews col-
lected both real-time and retrospective longitudinal data in several waves over three years.
According to Ozcan and Eisenhardt (2009) these kinds of data collection are ideal be-
cause retrospective data enable efficient collection of more observations (thus enabling
better grounding), while real-time data mitigate retrospective bias (Leonard-Barton,
1990). Second, anonymity has been promised to companies and informants. According to
Eisenhardt (1989a; 1989b) this decision encourages candour. Third, the interviews have been
complemented with wide-ranging archival and observational data, as suggested by Bingham
and Eisenhardt (2011). Fourth, open-ended questioning has been used to give the informants
wide scope to relate the concept as they chose. According to Koriat and Goldsmith (2000) this
helps in addressing potential informant bias. Fifth, informants not only from multiple levels of
hierarchy, but also with different perspectives have been considered during the interviews. If
one considers that these informants were also highly interested in the solution under exam, the
accuracy of the interpretations increases (Ozcan and Eisenhardt, 2009). Finally, interview
techniques like courtroom questioning, event tracking, and nondirective questioning (Martin
and Eisenhardt, 2010) have been used to yield accurate information (Huber and Power, 1985).
Following recommendations for multiple case theory building (Eisenhardt and Grae-
bner, 2007), within- and cross-case analyses have been performed with no a priori hy-
potheses. The corresponding author began by building individual write-ups that triangulat-
ed all of the data—emphasizing themes that were supported by different data collection meth-
ods and confirmed by several informants (Jick, 1979). The other author integrated the first
draft with his comments, and highlighted missing details that have been successively filed
with calls and emails (Ozcan and Eisenhardt, 2009). Once the write-ups were consolidated,
each author red them to form an independent view (Yin, 2003) and develop primary concepts
and rough theoretical explanations (Bingham and Eisenhardt, 2011). Finally, a cross-case
analysis has been done—using replication logic across the cases—to probe for alternative
theoretical relationships and constructs that might fit the data better than the initial emergent

9
theory (Eisenhardt, 1989b). Tables and other cell designs have been used to compare several
possible constructs at once (Miles and Huberman, 1994). Moreover, numerous case pairings
have been employed to highlight similarities and differences among cases—separating and
combining comparisons of the sets of hospitals (Martin and Eisenhardt, 2010). From the
emerging constructs and themes, tentative relationships between constructs were formed.
Then these initial relationships were refined via replication logic—frequently revising
each case to compare and verify occurrence of specific construct, relationships, and logics
(Ozcan and Eisenhardt, 2009). Once the cross-case analysis was underway, the authors
cycled among the emergent theory, case data, and literature to refine further the emerging
construct definitions, abstraction levels, construct measures, and theoretical relationships
(Gilbert, 2005). The cycles continued until a strong match between the cases and the
emergent theory was achieved (Ozcan and Eisenhardt, 2009). To converge on a parsimo-
nious set of constructs, the authors focused only on the most robust findings (Andriopou-
los and Lewis, 2009).
3 Findings
An issue of case-based research is presenting the evidence from which the theory of inter-
est was inducted. According to Eisenhardt and Graebner (2007), the challenge is to stay within
spatial constraints while also conveying both the emergent theory (that is the research objec-
tive) as well as the rich empirical evidence supporting it. The best way to address this chal-
lenge is to develop a theory by distinct propositions in such a way that each is supported by
empirical evidence. Thus, the overarching organising frame of this paragraph is the theory,
and each part of the theory is demonstrated by evidence from at least some of the cases. But
since it is generally not realistic to support every theoretical proposition with every case, the
use of extensive tables that summarize the related case evidence is central to signalling the
depth and detail of empirical grounding (Eisenhardt, 1989a). In other words, the use of sum-
mary tables that summarize the case evidence complements the selective story descriptions of
the text and further emphasises the rigor and depth of the empirical grounding of the theory.
The analysis of the cases shows the presence of three complementary ICT-based paths
that foster and maintain a successful balance between exploratory and exploitatory activities:
• The digitalisation of the assets utilised within hospitals (1–2 in Figure 1);
• The ICT-based integration among healthcare stakeholders (2–3–5 in Figure 1);
• The disruption of clinical and administrative decision-making through the use of
analytics (2–4–5 in Figure 1).

10
High
Low
Hig
h
Low
Exploitation
Exp
lora
tion
Radical innovation
Incremental innovation
Disruptive innovation
Efficiency stimulus
Decision support
experim.
Scale up
Internal process
Integration
EPI2
Asset integration
EPI1
1
4
3
5
2
Figure 1 – Using ICT to successfully manage the exploration-exploitation paradox
3.1 First Path: Asset Digitalisation
Coherently with the literature (e.g. Fichman et al., 2011; Aron et al., 2011; Ozdemir et
al., 2011), all the hospitals listed in Table 1 agreed on the fact that the first ICT invest-
ments have to be accomplished in the macro area of digitalisation. With the exception of
the tools supporting service management and delivery (DI1 in Table 3)—not strictly nec-
essary, and particularly useful only when a hospital has complex and/or big facilities—,
all the other ICT-based solutions that have been grouped under the digitalisation area, in
Table 4, are not only almost mandatory, but also a prerequisite of any other further ICT intro-
duction process. Using informants’ words: «It’s really difficult to capture the benefits of ICT-
driven innovations such as Electronic Medical Record or analytics without a preliminary set
of investments in infrastructure and digitalisation. Without a digital backbone, today a hospi-
tal is simply unavailable to generate value» (CEO of H2). The CIO of H13 agreed on this point,
and emphasised that «It’s impossible to develop an EMR if you have not first invested in the
digitalisation of healthcare data. […] I don’t want to focus on the roof without a basement…».
The cross-analysis of the cases provided interesting evidences supporting these
quotes. With a reference to Table 3, it is interesting to note that:
• 11 hospitals out of 14 had already developed a solution guaranteeing the security
of their data (ID2) before the start of 2009;

11
• 10 hospitals out of 14 have (i) either already developed a solution to virtualise their assets (DI3) before the start of 2009, (ii) or started a process of development of this kind of solution by the end of 2011;
• 12 hospitals out of 14 have already developed a set of solutions to dematerialise most
of their clinical documents (DI4) before the start of 2009; the remaining 2 hospitals
have started a process to dematerialise their clinical documents before the end of
2011, and have recognised the mistake of not having started the process earlier;
• 8 hospitals out of 14 have already developed solutions to dematerialise most of their administrative documents (DI5) before the start of 2009, 3 hospitals have started a process to dematerialise their clinical documents before the end of 2011, and 2 planned to start it by the end of 2012.
Obviously these numbers are neither representative of the entire Italian healthcare sys-
tem nor free of biases. However, the convergence of the opinions of practitioners and the
findings are significant enough to deserve further analyses. In order to accomplish these
analyses, the processes relative to the introduction of four different ICT-based solutions in
the digitalisation area have been compared. For each ICT introduction process, Table 5,
Table 6, Table 7 and Table 8, in the electronic companion presented in the Appendix sec-
tion of this paper, summarise: (i) the hospital in which it has been accomplished, (ii) the
ICT-based solution that has been studied in this hospital, (iii) the stimuli that have led to
the decision of investing in this solution, (iv) the problems faced during its adoption, (v)
the impacts produced on exploration, exploitation and on the performances of the hospi-
tal, (vi) the approaches utilised to balance the exploratory and the exploitatory activities
related to (or enabled by) the ICT-based solution, (vii) the challenges and the issues faced
during its usage and/or improvement, (viii) the next steps to be accomplished according to
the informants interviewed, and (ix) some of their quotes that are representative of the el-
ements depicted in the tables. To complement the analysis, it is useful to refer to Table 3
for an overview of the other ICT-based solutions that were already present inside the hos-
pitals when they decided to start the introduction processes presented in the tables.
As it is possible to see in Table 5, Table 6, Table 7 and Table 8, in all the cases the initial ob-
jectives of the investments in digitalisation were related to the willingness to better exploit the
resources in the hands of the hospital, and achieve efficiency—mainly in terms of cost and
time savings or managerial simplification. These tendencies find a confirmation in the other
cases accomplished outside the Lombard context by the Observatory. For example, a
healthcare CIO in the North of Italy told the authors that: «Most of hospitals start with the de-
materialisation of radiology and laboratory for the tons of savings it is possible to achieve».

12
A common element emerging from the cases is that it is better to focus on the digitali-
sation of one hospital unit at a time, not only to achieve in short time lags tangible results
to be shown to both the strategic board as well as to the users, but also to avoid the «over-
complications associated with the development of pervasive ICT-based solutions—at least
in the initial digitalisation stages and/or in the case of low ICT budgets available» (CIO
of H5). Moreover, the rest of the hospital can continue along its paths to solve the contrasts
present between the exploration and the exploitation of other hospital assets—making the
ambidextrous balance of exploratory and exploitatory activities comprehensively more
easily achieved. These evidences bring an initial contribution to both literature and practice.
If the importance of healthcare digitalisations is increasingly emphasised (Finchman et al.,
2011), as far as the authors know there are no indications regarding where to start the digitali-
sation of hospital assets. From this viewpoint, it is possible to state the following proposition:
P1A: The first effective ICT investments within a hospital support exploitatory-
based digitalisation paths—performed one hospital unit at a time—with the aim of
achieving efficiency in the management of hospital assets.
According to the informants, the digitalisation in the clinical domain is typically preferred
to the digitalisation in the administrative domain. In the opinion of the chief radiologist in H2,
the reasons «are mainly related to the higher value associated with clinical digitalisation». In
fact, most of the assets that can be digitalised within a hospital have a clinical nature. Inform-
ants not only confirmed this point, but also underlined that clinical digitalisation provides
more opportunities to both explore and exploit. In the words of the CMO of H4: «clinical data
provides more opportunities to both revise the existing paths through which the service of our
organisation is delivered to our patients, as well as to change and improve these paths. Ad-
ministrative processes are simply not such as pervasive as clinical processes in a hospital».
Moreover, as described by the informants of the cases, a digitalisation in the clinical area pro-
duces stronger positive impacts on the performances of the hospital—both the performances
directly perceived by the physicians (H2) and the patients (H7) as well as the ones not directly
perceived by most of the stakeholders (H5). Thus, the following proposition is proposed:
P1B: Clinical digitalisation is more likely to yield better results in effectively man-
aging the exploration-exploitation paradox than administrative digitalisation.
To provide some further consideration, it is possible to suggest radiology and labora-
tory as the first hospital units to digitalise. As indicated by the CIO of H7: «radiology and
laboratory are document-intensive departments, mostly detached by the core services of-
fered by their hospital, with technology-friendly physicians, and many efficiency needs».

13
According to the two propositions introduced, a generic hospital aiming to successfully
use ICT to cope exploration and exploitation can start to follow—preferably in clinical do-
main—the initial part of the path from 1 to 2 in Figure 1. If 12 of the 14 cases started with this
path, the analysis of the cases depicted in Table 5, Table 6, Table 7 and Table 8 allowed em-
phasising another interesting element. After the appropriation of the main benefits associated
with the initial digitalisation investments, the ICT-based solutions introduced have permitted
the exploration of radical new and better ways of providing healthcare services thanks to the
integration of the radiologic devices in H2, the queue management systems in H4, the software
virtualised in H5, and the laboratory devices in H7. For example, H2 started the digitalisation of
its radiology department mainly to reduce the usage of radiological films, save storage space
and rationalise the other resources used in this hospital unit. However, after a specific level of
exploitation of the benefits associated to the digital management of these assets, other oppor-
tunities have emerged. For instance, the integration of computed tomography with magnetic
resonance imaging has allowed radical new and better ways of providing diagnoses.
Thus, an initial ICT investment supporting pure exploitatory activities and efficiency
objectives has opened up exploration possibilities that, once seized, have allowed not only
to ambidextrously balance exploratory and exploitatory activities (the final part of the
path from 1 to 2 in Figure 1), but also to increase their overall performance—both in
terms quality improvement and cost rationalisation (see Table 5, Table 6, Table 7 and Table
8). In other terms, focusing on producing, finding, analysing and sharing information through
digital media (Freeman, 2007), the ICT-based solutions used to digitalise hospital assets pro-
gressively manifested their potential of successfully balancing exploration and exploitation.
Again, the cases seem to suggest that the greater the detachment from the rest of the
hospital of the unit in which asset digitalisation is accomplished, the smoother and the
more successful the ICT-driven balance between exploration and exploitation. Most of
the problems encountered during the adoption, usage and improvement of (i) the electron-
ic queue management systems in H4 and (ii) the virtualisation realised in H5 can be traced
back to the pervasiveness of these ICT-based solutions and the number of processes (as-
sets, activities, users) affected by the relative digitalisation. The discussions with the in-
formants explained these evidences mostly in terms of «protection of the unit» (CIOs of H2,
H4 and H5). In the initial digitalisation stage, the more the unit is protected, the more successful
the contribution provided by asset digitalisation. This summary suggests that:
P1C: The ICT-based integration among the assets within a hospital unit realised
through a digitalisation process positively affects the capability of the unit to success-fully manage the exploration-exploitation paradox—especially if the unit is protected.

14
3.2 Second Path: Process Integration
According to the informants of three out of the four cases analysed in §3.1, the natural
«next step» (see Table 5, Table 6 and Table 7) to be accomplished after having digitalised
most of the units of a hospital is to develop an Electronic Medical Record (EMR). In all
14 cases, the practitioners explained this choice with the willingness of benefiting from
the integration—realised through ICT investments—among the processes of the whole
hospital. After having seen the benefits of asset integration within a generic hospital unit,
the basic idea is trying also to achieve these benefits at an organisational level as well—
through the integration of the different hospital units. In the words of a CEO of H1:
«We’re simply doing what we have done within each department. But on a bigger scale.
Information has to be available everywhere if you want to truly achieve the relative benefits».
As suggested by Table 4, the integration among the units of a hospital can be realised in
both the clinical as well as the administrative domains. If the clinical integration is almost
completely accomplished through the investments in an EMR (II3), administrative integra-
tion is realised mostly with administrative and human resource management systems (respec-
tively II1 and II2). In order to better understand which kind of value a hospital extracts by the
accomplishment of these integrations, the processes relative to the introduction of four differ-
ent ICT-based solutions in the «internal integration» area have been compared. Three cases
(H1, H9 and H14) focused on the process to adopt, use and improve an EMR, while one case
(H6) studied the introduction of an administrative management system. Table 9, Table 10, Ta-
ble 11 and Table 12, in the electronic companion, summarise the main findings achieved, and
have the same structure of the tables already proposed (to simplify cross-case comparison).
Interestingly, in all four cases, the stimuli that led to invest in the integration of intra-
organisational processes have the same nature, which can be traced back to improving the
effectiveness of the processes, reducing their comprehensive inefficiencies, and effective-
ly responding to an external pressure. The relative importance of these objectives is de-
fined in each case by the boundary conditions surrounding the ICT introduction process,
and is reflected in its nature. In H1, H9 and H14 the introduction of an EMR allowed to: (i)
improve the overall hospital capabilities to explore and exploit, (ii) better balance exploration
and exploitation at different levels (mainly hospital unit and whole hospital), and (iii) achieve
good performances in terms of both quality improvement as well as cost rationalisation. On
the other side, H6 encountered many problems in producing an impact over these dimensions.
These problems cannot be linked to the typology of the processes that H6 decided to inte-
grate. As already highlighted, clinical processes are more diffuse and important than adminis-
trative processes within a hospital, and if all the informants underlined the higher value asso-

15
ciated to the integration of the former in comparison to the latter, they have also emphasised
the higher difficulties in accomplishing the integration of clinical processes due both to their
pervasiveness as well as to their centrality in the creation of value for the hospital. Theoretical-
ly, thus, an integration realised among administrative processes should tackle fewer prob-
lems, and proceed smoothly. As a matter of fact, almost all the hospitals that have accom-
plished administrative integration in Table 3, invested in this area to collect what informants
have called «quick wins» between large waves of clinical integration. In the words of the CFO
of H14: «The benefits of an EMR are undoubtedly present. However it’s highly difficult to
measure them, because they’re diluted throughout the entire hospital. Moreover we are talk-
ing about complex projects—spanning multiple fiscal years. Sometimes it’s better to focus on
administrative processes. They won’t save lives, but their automation provides “quick wins”».
The CIO of the same hospital synthesised the issue in these terms: «Realising administrative
integration is like catching a goldfish. Realising clinical integration is like catching a whale».
According to the cases, the real element able to explain the different performances of
the ICT introduction processes is the level of digitalisation previously accomplished by
the hospitals. H1, H9 and H14 had good percentages (higher than 40%) of clinical docu-
mentation already dematerialised when they started the implementation of their EMR. H6
ran into many difficulties in trying to integrate administrative processes because the latter
were not adequately digitalised before, and the positive effect of asset integration within
hospital units was not explored yet. In fact, Table 3 shows that H6 planned to dematerial-
ise its administrative documents by the end of 2012, while Table 10 highlights the process
it went through which it has been though to solve the problems raised during the introduc-
tion of the ICT-based solution. Overall, it is possible to summarise the following propositions:
P2A: The ICT-based integration among hospital’s processes positively affects the ca-
pability of a hospital to successfully manage the exploration-exploitation paradox;
P2B: The level of digitalisation accomplished within hospital units moderates the
capability of ICT to successfully manage the exploration-exploitation paradox.
The contributions that these propositions provide to the literature and to practice are
synthesised in Figure 1. Although both academics and practitioners recognise the poten-
tial of ICT-based process integration in increasing organisational performances, there was
no clear evidence either to support such a contribution or to indicate the possibility to
achieve a synergistic, paradoxical balance of exploration and exploitation. The cases in
Table 9, Table 10, Table 11 and Table 12 provide these evidences. After the digitalisation
of hospital assets—within the different hospital units—it is possible to achieve further

16
synergistic combinations of exploratory and exploitatory activities that lead to better per-
formances using ICT in order to integrate the processes of the different hospital units.
There are multiple paths that allow switching from 2 to 3, and multiple combinations of
exploration and exploitation—both realised through radical and incremental innovations.
Figure 1 simply emphasises that, rather than a whole standalone project, it is more common to
proceed with a combination of exploratory and exploitatory investments. Moreover, the fig-
ure suggests the necessity to perform more studies on the topic to understand the pros and cons
of each path. In this spirit, Gastaldi et al. (2012b) propose three alternative paths to introduce
an EMR within a hospital and successfully manage the exploration-exploitation paradox.
Among the next steps to be accomplished after the introduction of an EMR, the in-
formants of H1, H9 and H14 considered to extend the underlying integration process out-
side their hospital as well (see Table 9, Table 11 and Table 12). Literature on ICT-driven
innovation management in healthcare (for a review, see Agarwal et al., 2010) mainly discuss-
es this topic in terms of Electronic Health Record (EHR) development. Basically, an EHR is
an EMR “shared” among healthcare providers. According to the literature, this ICT-based so-
lution has «the potential to fundamentally transform almost every aspect of health services»
(Agarwal et al., 2010), and to dramatically increase the performances of healthcare systems
(e.g. Bisbal and Berry, 2011). As a matter of fact, despite all the emphasis put by the academ-
ics on EHR, the cross-analysis of the 14 case studies performed in Lombardy showed another
typology of complementary, ICT-based path to better integrate healthcare stakeholders. With
a reference to Table 3, it is interesting to note that only four hospitals have fully integrated
their data warehouses to the regional EHR before the start of 2009 (EI3). The cross-analysis of
the cases showed not only that these hospitals were the ones with higher ICT maturity, but also
that—during the integration with the regional EHR—almost all these hospitals were focusing
also on introducing the other ICT-based solutions listed in “external integration” area.
If one considers that Lombardy is one of the most advanced regions in terms of EHR de-
velopment (Lo Scalzo et al., 2009), there are two complementary typologies of external inte-
gration paths that a hospital can follow in order to move from 3 to 5, and, thus, further suc-
cessfully manage the exploration-exploitation paradox (Figure 1). The first one (EI1) is driven
by the regional council, and is based on the development of an EHR. In this case the hospital
has to proactively answer the integration requests of the region—making its EMR interopera-
ble with the other EMRs, and/or following the guidelines released by the regional council on
EMR development (Locatelli et al., 2012). The second one (EI2) is characterised by the efforts
made by the hospital in directly connecting itself to its patients and to primary care physicians.
In order to understand if these two typologies of paths allow hospitals to successfully manage

17
the exploration-exploitation paradox, the processes accomplished to introduce three different
ICT-based solutions in the external integration area have been compared. Table 13, Table 14
and Table 15 summarise the findings achieved in the cross-case analysis.
During the introduction of an EMR, H3 also decided to better connect it to the region-
al EHR. As it is possible to see in Table 13, the relative ICT-driven innovation process is
highly similar to the one accomplished by H1, and ended in improved quality and lower
costs. According to the informants, however, these are only a small part of the potential
benefits that it is possible to achieve. In the words of the CIO of H3: «This is only the tip of the
iceberg. The integration with the EHR will bring tons of opportunities not only to further sim-
plify things, but also to discover new services to be offered to our patients». As a matter of fact,
despite the tremendous potential, in order to be effective the EHR requires years of explorato-
ry and exploitatory investments by both all the hospitals in a region as well as its council.
If H3 achieved better results in successfully managing the exploration-exploitation para-
dox through integration with the Lombard EHR, H10 and H12 seem to have made a step further
by following the path EI2. It is important to note that, before the start of 2009, both two hospi-
tals had already not only digitalised and internally integrated most of their processes, but also
connected their EMR to the regional EHR (Table 3). According to the informants, however:
«The benefits of the integration of the internal processes soon reach their potential, and the
Lombard EHR is not developed enough to further improve our services» (CIO of H10); «The
EHR will be an incredible tool once completed, [but] we need to offer better services to our
patients now. We simply cannot afford to go at a snail’s pace». (CEO of H12). As a conse-
quence, H10 engaged in the development of a telemedicine service (EI2) for a specific, prob-
lematic typology of patients suffering from chronic obstructive respiratory disease, while H12
developed a new channel to offer its services to its patients—through an application for latest-
generation smartphones (EI1). In both the cases, the stimuli that led to invest in these ICT-
based solutions had a dual nature (improving quality while reducing costs), and ICT has been
used according to a logic similar to the one adopted during the digitalisation phase (§3.1):
• An initial ICT-driven investment has been accomplished in one direction (explo-ration for H10, exploitation for H12) which soon manifested opportunities in the other direction as well (exploitation for H10, exploration for H12);
• By taking advantage of these opportunities, the hospital paradoxically balanced the two conflicting activities, and increased its quality while rationalising its costs.
It is useful to close this paragraph with some comprehensive considerations on the dif-
ferent integration paths studied within it. The paths from 2 to 5, in Figure 1, contribute
to successfully balance the exploitation-exploration paradox with the benefits achieved

18
from higher levels of integration within the healthcare system—first inside a hospital,
then outside it (among both the providers and the users of healthcare services). The cases
depicted in this paragraph have shown that the integration accomplished with ICT-based
solutions progressively brings higher levels of flexibility and coordination to the overall
healthcare system—allowing each hospital to synergistically balance exploration and ex-
ploitation at different levels, and, thus, produce better performances during service deliv-
ery. Referring to the external integration, the following propositions can be proposed:
P2C: The ICT-based integration of the inter-organisational processes among healthcare stakeholders positively affects the capability of a healthcare system to successfully manage the exploration-exploitation paradox;
P2D: The ICT-based integration with the patients of a hospital tends to successfully manage the exploration-exploitation paradox in less time than the ICT-based inte-gration among the hospitals in a region.
3.3 Third Path: Active Support to Decision-making
If in the short or medium term the integration achieved with ICT allows to progres-
sively manage the exploration-exploitation paradox, the 14 cases in Lombardy show that,
in the long term, healthcare stakeholders (and especially hospitals) need to further explore,
exploit, improve and make affordable their services. The informants state that this is the only
way to maintain a successful paradoxical balance between exploration and exploitation. In
their words: «OK. Now we have an EMR. Can we sleep soundly? The answer is: No. The next
year we have planned to develop a set of digital services for our patients, and a governance
dashboard for our management. The year after we’ll have heaps of things to do… The real
problem (but also the real fun) is that you never see an end to such processes» (CIO of H14).
From this perspective, the recent (Christensen et al., 2009) examination of the
healthcare industry through the lenses of the disruptive innovation framework can be very
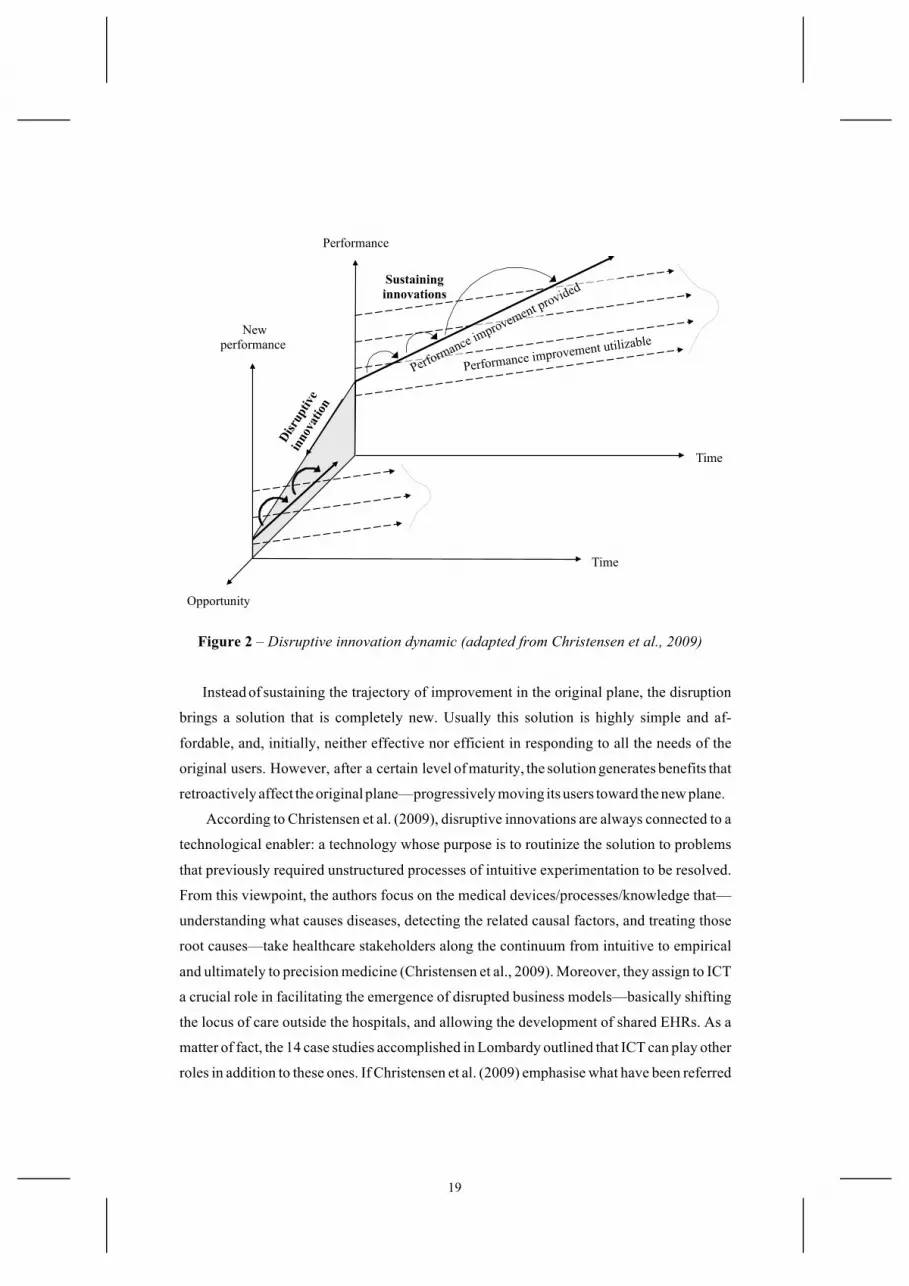
useful. The dynamic associated with disruptive innovations is related to the performance
of a solution over time. The initial solution, in the back plane of Figure 2, is typically
complicated and expensive. The solid line denotes the pace of improvements provided by
organisations to their users. Meanwhile, the dashed lines depict the rate of performance
improvement that users are able to utilise (there are multiple dashed lines to represent the
different tiers of users: from the most demanding ones to who is satisfied with very little).
The innovations driving the company up the trajectory of performance improvements are
called sustaining innovations. Some of these improvements are dramatic breakthroughs,
while others are incremental. Occasionally, however, a disruptive innovation emerges.
19
Performance improvement utilizable
Performance
Time
Time
New performance
Opportunity
Sustaining innovations
Figure 2 – Disruptive innovation dynamic (adapted from Christensen et al., 2009)
Instead of sustaining the trajectory of improvement in the original plane, the disruption
brings a solution that is completely new. Usually this solution is highly simple and af-
fordable, and, initially, neither effective nor efficient in responding to all the needs of the
original users. However, after a certain level of maturity, the solution generates benefits that
retroactively affect the original plane—progressively moving its users toward the new plane.
According to Christensen et al. (2009), disruptive innovations are always connected to a
technological enabler: a technology whose purpose is to routinize the solution to problems
that previously required unstructured processes of intuitive experimentation to be resolved.
From this viewpoint, the authors focus on the medical devices/processes/knowledge that—
understanding what causes diseases, detecting the related causal factors, and treating those
root causes—take healthcare stakeholders along the continuum from intuitive to empirical
and ultimately to precision medicine (Christensen et al., 2009). Moreover, they assign to ICT
a crucial role in facilitating the emergence of disrupted business models—basically shifting
the locus of care outside the hospitals, and allowing the development of shared EHRs. As a
matter of fact, the 14 case studies accomplished in Lombardy outlined that ICT can play other
roles in addition to these ones. If Christensen et al. (2009) emphasise what have been referred

20
to as «external integration paths» in Figure 1, there are not only the other preliminary paths
described in §3.1 and §3.2 to consider, but also a new path that progressively moves the hospi-
tals towards precision medicine. According to the informants, all the ICT-based solutions de-
scribed above combine sustaining and disrupting effects in both their exploratory and exploi-
tatory investments—«automating significant parts of hospital processes, and bringing com-
pletely new services that permanently change the way healthcare is provided» (CEO of H10).
However, ICT-driven innovations achieve their true disruptive potential when they deliver an
active support to decision-making (Vercellis, 2009). Analytics produce exactly this kind of
truly disruptive outcome and, according to informants, configure themselves as drivers to
manage the exploration-exploitation paradox in the long term. In the words of a CIO of a pri-
vate hospital in South-Italy: «Today the main focus of ICT is on connecting things, activities,
users, processes, etc. Today this is how, basically, healthcare systems effectively combine
costs and quality. In the long run the focus will be another. In ten years—maybe less—
everything will be hyper-connected… like Internet. Of course in that moment we’ll continue to
connect things, but the main emphasis of ICT will be on smartly using the data to improve our
decisions and, thus, both our capabilities and our performances. Actually we’re already
working with analytics in order to be ready for the future. The future, in my view, is there».
Davenport and Harris (2006) define analytics as an «extensive use of data, statistical and
quantitative analysis, explanatory and predictive models, and fact-based management to drive
decisions and actions». The field of analytics has improved significantly over the past years
(Kohavi et al., 2002), and has promising applications in the healthcare domain (Vercellis,
2009). However, there are any empirical evidence on the link between this kind of ICT-based
solution and the capability of hospitals of both disrupting their service as well as successfully
managing the exploration-exploitation paradox. In order to start an analysis in these fields, the
processes accomplished to introduce three different ICT-based solutions in the area of analyt-
ics have been compared: a clinical governance tool to better diagnose pneumonia (AN2 in H8),
a computerised drug management system (AN1 in H11), and a governance dashboard to sup-
port administrative decisions (AN3 in H13). Table 16, Table 17 and Table 18, in the electronic
companion, summarise the main findings achieved in the cross-analysis of the cases.
In all three cases, the very first stimulus leading to the investments in analytics was re-
lated to the desire of informants to explore new ways of extracting value from the administra-
tive and clinical data previously digitalised. As it is possible to see in Table 3, H8, H11 and H13
are hospitals with a high ICT maturity—especially in document digitalisation. As clearly not-
ed by the CEO of H8: «We’ve tons of unused clinical data. I don’t believe that we have digital-
ised them only to accomplish our EMR. We can make use of them to improve our decisions».

21
Recognising the necessity of years of exploratory and exploitatory investments in order to
achieve sound performance, all the three CIOs of the analysed hospitals were following—at a
different pace—similar ICT introduction processes to implement analytics. These processes
are characterised by four elements. The first is an initial verticalisation (Kohavi et al., 2002) in
a pilot unit and/or in a functional area in order to (i) protect the development of the solution, (ii)
facilitate the definition of the desired achievements and their measurement, and (iii) develop a
solid base to be later extended to the rest of the hospital. The second is the involvement of clin-
ical (H8 and H11) and administrative (H13) decision makers in the ICT introduction process—
not only to achieve a clear viewpoint regarding the requirements of the specific niche selected
to pilot the solution, but also to compress the time needed for the overall cycle of collecting,
analysing, acting and systematising the clinical and/or the administrative data. The third ele-
ment is a progressive refinement and improvement of the ICT-based solution. The idea is to
make it more effective in supporting the decisions—exploiting different data sources, adopt-
ing more accurate algorithm and/or procedures, routinizing the decisions, and making the us-
er able to take them without an external help. Finally, the last element is an extension to the rest
of the hospital, which is performed through a set of exploratory and exploitatory innova-
tions—both of a radical as well as an incremental in nature—spanning multiple years.
The path through which analytics contribute in successfully managing the explora-
tion-exploitation paradox is depicted in Figure 1. Obviously there are many other alterna-
tive paths, and the one showed emphasises only the tendencies emerged by the cross-
analysis of the Lombard cases. Further research is necessary to understand how analytics
contribute both to the disruption of healthcare as well to the successful balance of explor-
atory and exploitatory activities. This paper proposes a preliminary set of evidences on
the topics. As already anticipated, the hospitals start to explore the benefits of analytics
only after significant percentages of digitalization accomplished (thus, at approximately
point 2 in Figure 1). Exactly as happened in the digitalisation and in the process integra-
tion paths, the informants underlined that the potential of analytics is stronger in the clini-
cal domain than in the administrative domain. It suffices to note that H13—which has in-
vested in an ICT-based solution supporting administrative decision-making—planned to
also support clinical decisions because, according to the CEO: «the real value is there»
(see Table 18 for further evidences). The solutions are realised in (more or less) protected
niches, in which the ICT-based support to decision-making is progressively tested, and
the disrupted way of performing the activities explored (the path from 2 to 4). Initially
(and coherently with the disruption innovation framework), these experimentations tend
to negatively affect both the exploitatory capability of the niche as well as its efficiency.

22
According to the informants, the reasons explaining these results are related to the fact
that—differently from the solutions in §3.1 and §3.2—the disadvantages associated with the
experimentations are not covered by the benefits generated by the analytics, which initially
tend to produce only potential valuable scenarios of disrupted activities that have to be tested
and progressively refined before being utilisable. The test and the refinement phases require a
set of exploratory and exploitatory innovations (the path from 4 to 5) to be accomplished. As
already emphasised in the description of the paths from 2 to 3 and from 3 to 5, the path
from 4 to 5 depicted in Figure 1 aims simply to remind that the introduction of analytics is
characterised by multiple combinations of exploratory and exploitatory innovation—both of
an incremental as well as a radical nature. As it is possible to see in Table 16, Table 17 and Ta-
ble 18, H8, H11 and H13 adopted different combinations to balance exploration and exploita-
tion. If further research is necessary to analyse the different paths to move from 4 to 5, with
the respective pros and cons, the common element to the analytics introduction processes is
the progressive improvement of: (i) the capabilities to explore and exploit manifested by the
hospital; (ii) the performance achieved thanks to ICT usage—both in terms of quality and
cost. Overall, two propositions are proposed to synthesise the considerations made:
P3A: The introduction of analytics to support decision-making positively affects the
capability of a hospital to successfully manage the exploration-exploitation paradox;
P3B: The analytics supporting clinical decision-making are more likely to yield bet-
ter results in managing the exploration-exploitation paradox than the analytics
supporting administrative decision-making.
4 Conclusions
Comprehensively, the propositions emerged in the previous paragraph underline the
presence of a link between ICT investments and a successful management of the explorato-
ry and exploitatory activities accomplished by the different healthcare stakeholders—with
an emphasis on hospitals. In fact, only the administrative management system introduced
by H6 worsened the performances of the hospital, and—according to the informants—the
main reason explaining these results is related to an ineffective ICT usage, i.e. starting the
integration of administrative units, that were not adequately digitalised yet. In all the other
cases, the adoption, the usage and the progressive improvement of the ICT-based solu-
tions were effectively managed by the hospitals, and ended in both an improvement in
their quality as well as a rationalisation of their costs. Informants clearly linked the im-
provement of the performances to the introduction of the ICT-based solutions.
23
Id Area Proposition
P1 Digitalisation
A. The first effective ICT investments within a hospital support exploitatory- based digitalisation paths—performed one hospital unit at a time—with the aim of achieving efficiency in the management of hospital assets
B. Clinical digitalisation is more likely to yield better results in effectively managing the exploration-exploitation paradox than admin. digitalisation
C. The ICT-based integration among the assets within a hospital unit realised through a digitalisation process positively affects the capability of the unit to successfully manage the exploration-exploitation paradox—especially if the unit is protected
P2 Process integration
A. The ICT-based integration among hospital’s processes positively affects the capability of a hospital to successfully manage the exploration- exploitation paradox
B. The level of digitalisation accomplished within hospital units moderates the capability of ICT to successfully manage exploration-exploitation paradox
C. The ICT-based integration of the inter-organisational processes among healthcare stakeholders positively affects the capability of a healthcare system to successfully manage the exploration-exploitation paradox
D. The ICT-based integration with the patients of a hospital tends to successfully manage the exploration-exploitation paradox in less time than the ICT-based integration among the hospitals in a region
P3 Active decision- support
A. The introduction of analytics to support decision-making positively affects the capability of a hospital to successfully manage the exploration-exploitation paradox
B. The analytics supporting clinical decision-making are more likely to yield better results in managing the exploration-exploitation paradox than the analytics supporting administrative decision-making
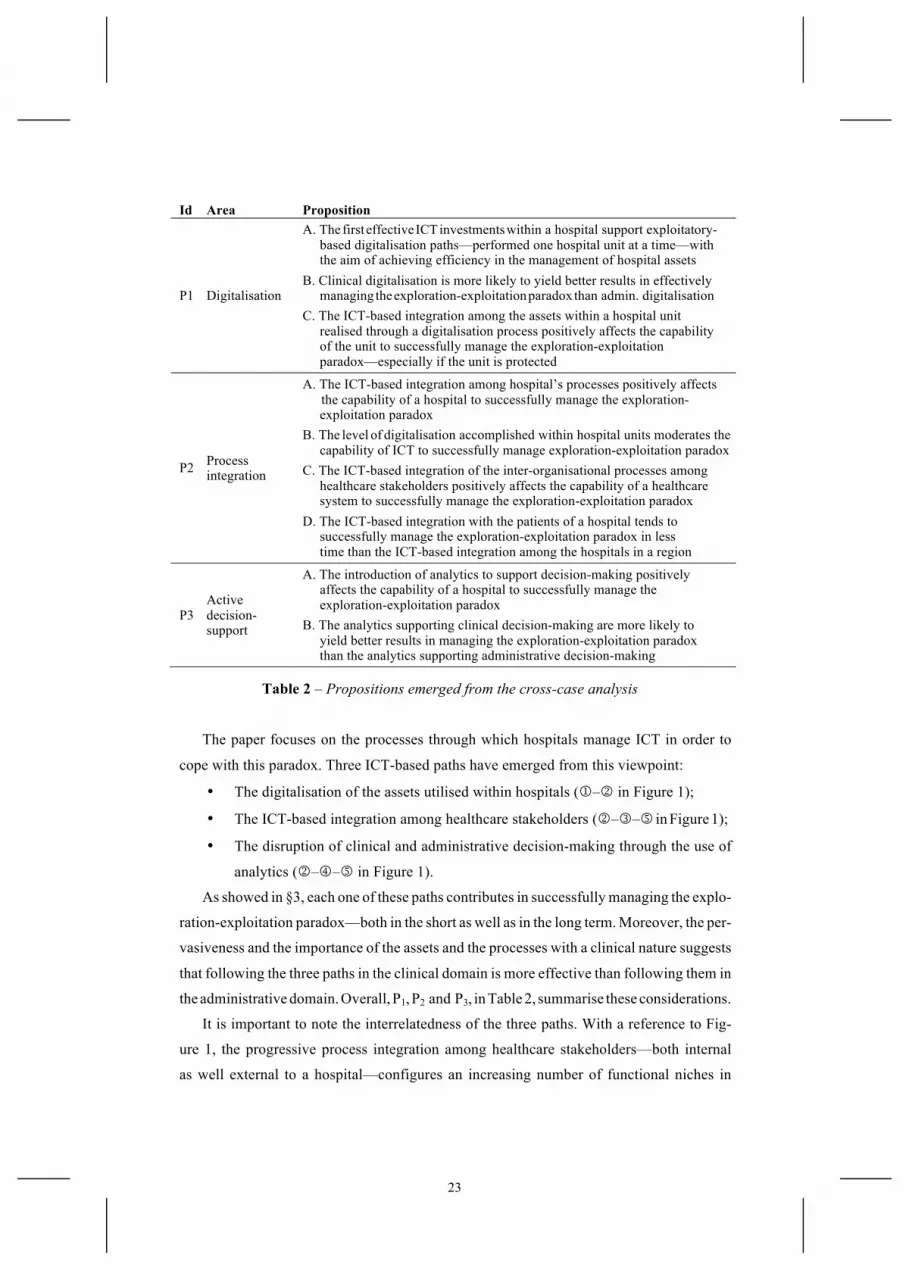
Table 2 – Propositions emerged from the cross-case analysis
The paper focuses on the processes through which hospitals manage ICT in order to
cope with this paradox. Three ICT-based paths have emerged from this viewpoint:
• The digitalisation of the assets utilised within hospitals (1–2 in Figure 1);
• The ICT-based integration among healthcare stakeholders (2–3–5 in Figure 1);
• The disruption of clinical and administrative decision-making through the use of
analytics (2–4–5 in Figure 1).
As showed in §3, each one of these paths contributes in successfully managing the explo-
ration-exploitation paradox—both in the short as well as in the long term. Moreover, the per-
vasiveness and the importance of the assets and the processes with a clinical nature suggests
that following the three paths in the clinical domain is more effective than following them in
the administrative domain. Overall, P1, P2 and P3, in Table 2, summarise these considerations.
It is important to note the interrelatedness of the three paths. With a reference to Fig-
ure 1, the progressive process integration among healthcare stakeholders—both internal
as well external to a hospital—configures an increasing number of functional niches in

24
which it is possible to effectively follow the 2–4–5 path. In fact, the higher the integration,
the greater the opportunities to use data to create, use and refine the statistical models through
which analytics support the administrative and the clinical decisions. These niches produce
not only disrupted healthcare services and a paradoxical balance of exploratory and exploita-
tory activities, but also a greater amount of data to be integrated with the 2–3–5 path. Thus,
the two macro-paths tend to feed each other. According to the informants, this complementa-
rity allows the construction of the dynamic capabilities necessary to paradoxically balance
exploration and exploitation. In the words of the CIO of H13: «The more you connect, the more
digital data you can exploit to support decisions. The more you use digital data to support de-
cisions, the more you need to connect the underlying resources producing these digital data.
It’s a sort of virtuous cycle than never ends». If further research is necessary to test if this quote
is reliable or not, it is clear that, without a preliminary digitalisation (the 1–2 path), none of
the benefits of process integration and decision-making support can be realised.
The results at this stage are still preliminary, and need to be further refined. However, the
work represents a good starting point to frame potential research that could be interesting to
perform in the future. The main problem of the findings achieved by this thesis concern their
generalizability. The focus on a specific lever (ICT), on a specific industry (healthcare) and on
a specific context (Lombardy), combined with the extensive use of interpretative studies risk
to produce «very idiosyncratic phenomena» (Eisenhardt, 1989b)—not easily generalizable to
other context, industries and levers. There are three further developments already planned to
fill this gap. First, it would be extremely useful to combine the interpretative methodology
used in this paper with a more quantitative-oriented set of vertical researches that could for-
mally test in specific subfields the effectiveness of the proposed contributions in all their de-
tails. The second is a progressive extension of the research context to other healthcare systems
in order to test the effectiveness of the models and the propositions emerged during the empir-
ical analysis in other healthcare systems, and see how the considerations achieved by this
thesis change according to the different contingent contexts of analysis tackled. Finally, it
would be useful to the test the model in different industries facing pressing necessities to
balance exploration and exploitation. A promising sector seams the banking one.
The second main limitation is related to the operationalisation of the constructs. A
successful management of the exploration-exploitation paradox necessitates of multidi-
mensional concepts able to discern between exploratory and exploitatory efforts. Howev-
er, the empirical analysis has showed that is not so simple to completely separate these forces.
Each operationalisation has its pros and cons to be taken into account, and there are many bi-
ases affecting the results and their interpretation. The further developments that have been

25
planned, from this viewpoint, are mainly related to the usage of variables that are not only in-
dependent by informants’ perceptions, but also able to precisely measure the level of explora-
tion and exploitation accomplished within and among hospitals, the performances achieved
through their ambidextrous balance, and the impact that ICT plays over the achieved results.
The third main limitation of this work concerns the locus of innovation. The technol-
ogy base of the healthcare industry is both complex and expanding, and the sources of
expertise are widely dispersed. According to Powel et al. (1996), in these contexts the lo-
cus of innovation is found in the network, rather than in individual hospitals. Following
their perspective, many healthcare stakeholders have been only marginally considered by
this study: the regions, the ICT providers, the physicians working in primary care, and the
patients—just to name the main ones. ICT-based solutions are developed, maintained and in-
novated by a complex ecology of multiple agents that share knowledge and resources in often
previously unknown interaction paths (Anderson, 1999). If, as a result of this complex pro-
cess, ICT-based solutions emerge almost unpredictably over considerable time periods—as
various agents in the ecology interact with and react to the actions of others—their governance
is naturally characterized by a shared and multilevel nature (Dougherty and Dunne, 2011),
which this thesis has not explored in detail. In order to fill this gap further research develop-
ments will place greater effort in understanding how ICT fosters the necessary collaboration
among many diverse hospitals over long and uncertain time periods, while, at the same time,
continuing to respond to the hospital’s necessities of successfully exploring and exploiting.
References
Aarts, J., Ash, J.S. and Berg M. (2007) “Extending the Understanding of Computerized Physician Order Entry: Implications for Professional Collaboration, Workflow and Quality of Care”, In-ternational Journal of Medical Informatics, Vol. 76, No. 1, pp. 4–13.
Adler, P.S., Benner, M., Brunner, D.J., Macduffie, J.P., Osono, E., Staats, B.R., Takeuchi, H., Tushman, M.L. and Winter, S.G. (2009) “Perspectives on the Productivity Dilemma”, Journal of Operations Management, Vol. 27, No. 2, pp. 99–113.
Anderson, P. (1999) “Complexity Theory and Org. Science”, Org. Science, Vol. 10, No. 3, pp. 216–232. Andriopoulos, C. and Lewis, M.W. (2009) “Exploration-Exploitation Tensions and Organizational
Ambidexterity”, Organization Science, Vol. 56, No. 8, pp. 1219–1241. Angst, C.M., Agarwal, R., Sambamurthy, V. and Kelly, K. (2010) “Social Contagion and Infor-
mation Technology Definition Diffusion: The Adoption of Electronic Medical Records in U.S. Hospitals”, Management Science, Vol. 56, No. 8, pp. 1219–1241.
Angst, C.M., Devaraj, S., Queenan, C. and Greenwood, B. (2011) “Performance Effects Related to the Sequence of Integration of Health Tech.”, Production & OM, Vol. 4, No. 2, pp. 204–218.
Atuahene-Gima, K. (2005) “Resolving the Capability-Rigidity Paradox in New Product Innova-tion”, Journal of Marketing, Vol. 69, No. 4, pp. 61–83.
Bingham, C.B. and Eisenhardt, K.M. (2011) “Rational Heuristics: The ‘Simple Rules’ that Strate-gist Learn from Process Experience”, Strategic Management J., Vol. 32, No. 13, pp. 1437–1464.

26
Bisbal, J. and Berry, D. (2011) “An Analysis Framework for EHR Systems: Interoperation and Col-laboration in Shared Healthcare”, Methods of Information Medicine, Vol. 50, No. 2, pp. 180–189.
Brown, S.L. and Eisenhardt, K.M. (1998) Competing on the Edge: Strategy as Structured Chaos, Harvard Business School Press, Boston (MA).
Christensen, C.M., Grossman, J.H. and Hwang, J. (2009) The Innovator’s Prescription: A Disrup-tive Solution for Health Care, McGraw–Hill, New York (NY).
Coghlan, D. and Shani, A.B. (Rami) (2008) Collaborative Management Research Through Com-munities of Inquiry, in: Shani, A.B. (Rami), Mohrman, S.A., Pasmore, W.A., Stymne B. and Adler, N. (Eds.) Handbook of Collaborative Management Research, Sage, Thousand Oaks (CA).
Connell, N.A.D. and Young, T.P. (2007) “Evaluating Healthcare Information Systems through an “Enterprise” Perspective”, Information and Management, Vol. 44, No. 4, pp. 433–440.
Corso, M. and Gastaldi, L. (2010) “Managing ICT-driven Innovations to Overcome the Exploita-tion-Exploration Trade-off: A Multiple and Collaborative Research Methodology in the Italian Health Care Industry”, 11th Int. CINet Conference, Zürich (CH), Sep. 5–7, pp. 274–289.
Corso, M. and Gastaldi, L. (2011) “Toward a Relevant, Reflective and Rigorous Methodology Able to Study Continuous Innovation at Affordable Resource-consumption Levels”, 12th Interna-tional CINet Conference, Århus (DK), Sep. 11–13, pp. 230–254.
Davenport, T.H. and Harris, J.G. (2006) “Competing on Analytics: The New Science of Winning”, Harvard Business School Press, Boston (MA).
Dougherty, D. and Dunne, D.D. (2011) “Organizing Ecologies of Complex Innovation”, Organiza-tion Science, Vol. 22, No. 5, pp. 1214–1223.
Eisenhardt, K.M. (1989a) “Building Theory from Case Study Research”, Academy of Management Review, Vol. 14, No. 4, pp. 532–549.
Eisenhardt, K.M. (1989b) “Making Fast Strategic Decisions in High-velocity Environments”, Academy of Management Journal, Vol. 32, No. 3, pp. 543–576.
Eisenhardt, K.M., Furr, N.R. and Bingham, C.B. (2010) “Microfoundations of Performance: Bal-ancing Efficiency and Flexibility in Dynamic Environments”, Organization Science, Vol. 21, No. 6, pp. 1263–1273.
Eisenhardt, K.M. and Graebner, M.E. (2007) “Theory Building from Cases: Opportunities and Challenges”, Academy of Management Journal, Vol. 50, No. 1, pp. 25–32.
Feldman, M.S. and Orlikowski, W.J. (2011) “Theorizing Practice and Practicing Theory”, Organi-zation Science, Vol. 22, No. 5, pp. 1240–1253.
Fichman, R., Kohli, R. and Krishnan, R. (2011) “Editorial Review—The Role of Information Sys-tems in Healthcare: Current Research and Future Trends”, Information Systems Research, Vol. 22, No. 3, pp. 419–428.
Fjeldstad, Ø.D., Snow, C.S., Miles, R.E. and Lettl, C. (2012) “The Architecture of Collaboration”, Strategic Management Journal, Vol. 33, No. 6, pp. 734–750.
Freeman, F. (2007) The ICT Paradigm, in: Mansell, R., Avgerou, C., Quah, D. and Silverstone, R. (Eds.) The Oxford Handbook of ICTs, Oxford University Press, Oxford (UK).
Gastaldi, L., Corso, M. and Balocco, R. (2012) “Is ICT and Effective Lever to Paradoxically Bal-ance Quality Improvement and Cost Rationalisation in Health Care?”, 13th International CINet Conference, Rome (Italy), Sep. 16–18, pp. 1–24.
Gastaldi, L., Lettieri, E., Corso, M. and Masella, C. (2012) “Managing ICT to Combine Exploration and Exploitation in Health Care: Emerging Strategies for EMR Development”, 13th Interna-tional CINet Conference, Rome (Italy), Sep. 16–18, pp. 1–20.
Gibson, C.B. and Birkinshaw, J. (2004) “The Antecedents, Consequences, and Mediating Role of Organizational Ambidexterity”, Academy of Management Journal, Vol. 47, No. 2, pp. 209–226.
Gilbert, C.G. (2005) “Unbundling the Structure of Inertia: Resource versus Rigidity”, Academy of Management Journal, Vol. 48, No. 5, pp. 741–763.
Glaser, B.G. and Strauss, A.L. (1967) The Discovery of Grounded Theory: Strategies for Qualita-tive Research, Aldine, Chicago (IL).

27
Goes, J.B. and Park, S.H. (1997) “Interorganizational Links and Innovation: The Case of Hospital Services”, Academy of Management Journal, Vol. 40, No. 3, pp. 673–696.
Goh, J.M., Gao, G. and Agarwal, R. (2011) “Evolving Work Routines: Adaptive Routinization of Infor-mation Technology in Healthcare”, Information Systems Research, Vol. 22, No. 3, pp. 565–585.
Grunden, N. (2008) The Pittsburgh Way to Efficient Healthcare: Improving Patient Care using Toyota Based Methods, Healthcare Performance Press, New York (NY).
Holmqvist, M. (2004) “Experiential Learning Processes of Exploitation and Exploration Within and Between Organizations: An Empirical Study of Product Development”, Organization Science, Vol. 15, No. 1, pp. 70–81.
Huber, G.P. and Power, D.J. (1985) “Retrospective Reports of Strategic-level Managers: Guidelines for Increasing their Accuracy”, Strategic Management Journal, Vol. 6, No. 2, pp. 171–180.
IHO, ICT in Healthcare Observatory (2011) ICT in Healthcare: Innovation in Search of an Author, School of Management of Politecnico di Milano, www.osservatori.net, pp. 1–150 (in Italian).
Jansen, J.J.P., Simsek, Z. and Cao, Q. (2012) “Ambidexterity and Performance in Multiunit Con-texts: Cross-level Moderating Effects of Structural and Resource Attributes”, Strategic Man-agement Journal, pp. 1–18.
Jick, T. D. (1979) “Mixing Qualitative and Quantitative Methods: Triangulation in Action”, Admin-istrative Science Quarterly, Vol. 24, No. 3, pp. 602–611.
Joshi, K.D., Chi, L., Datta, A. and Han, S. (2010) “Changing the Competitive Landscape: Continu-ous Innovation Through IT-enabled Knowledge Capabilities”, Information Systems Research, Vol. 22, No. 5, pp. 472–495.
Kohavi, R., Rothleder, N.J. and Simoudis, E. (2002) “Emerging Trends in Business Analytics”, Communication of the ACM, Vol. 45, No. 8, pp. 45–48.
Koriat, A. and Goldsmith, M. (2000) “Toward a Psychology of Memory Accuracy”, in: Fiske, S.T., Shcacter, D.L. and Zahn-Wexler, C. (Eds.) Annual Review of Psychology, BK, Palo Alto (CA).
Lavie, D., Stettner, U. and Tushman, M.L. (2010) “Exploration and Exploitation Within and Across Organizations”, Academy of Management Annals, Vol. 4, No. 1, pp. 109–153.
Leonard-Barton, D. (1990) “A Dual Methodology for Case Studies: Synergistic Use of a Longitudi-nal Single Site with Replicated Multiple Sites”, Organization Science, Vol. 1, No. 3, pp. 248–266.
Levinthal, D. and March, J.G. (1993) “The Myopia of Learning”, Strategic Management Journal, Vol. 14, No. S2, pp. 95–112.
Lewis, M.W. (2000) “Exploring Paradox: Toward a More Comprehensive Guide”, Academy of Management Review, Vol. 25, No. 4, pp. 760–776.
Locatelli, P., Restifo, N., Gastaldi, L. and Corso, M. (2012) “Health Care Information Systems”, in: Kal-loniatis, C. (Ed.) Innovative Information Systems Modelling and Techniques, InTech, pp. 71–96.
Lo Scalzo, A., Donatini, A., Orzella, L., Cicchetti, A. and Profili, S (2009) “Italy: Health System Review”, Health Systems in Transition, Vol. 11, No. 6, pp. 1–243.
March, J.G. (1991) “Exploration and Exploitation in Organizational Learning”, Organizational Sci-ence, Vol. 2, No. 1, pp. 71–87.
Marks, M.A., Mathieu, J.E. and Zaccaro, S.J. (2001) “A Temporally Based Framework and Taxon-omy of Team Processes”, Academy of Management Review, Vol. 26, No. 3, pp. 356–376.
Martin, J.A. and Eisenhardt, K.M. (2010) “Rewiring: Cross-business-unit Collaboration in Multi-business Organizations”, Academy of Management Journal, Vol. 53, No. 2, pp. 265–301.
Martini, A., Laugen, B.T., Gastaldi, L. and Corso, M. (2012) “Continuous Innovation: Towards a Paradoxical, Ambidextrous Combination of Exploration and Exploitation”, International Jour-nal of Technology Management.
Miles, M.B. and Huberman, A.M. (1994) Qualitative Data-analysis, Sage, Thousand Oaks (CA). Ozcan, P. and Eisenhardt, K.M. (2009) “Origin of Alliance Portfolios: Entrepreneurs, Network
Strategies, and Firm Performance”, Academy of Management Journal, Vol. 52, No. 2, pp. 246–279. Patton, M. (2002) Qualitative Research and Evaluation Methods (3rd
Ed.), Sage, Thousand Oaks (CA).

28
Pettigrew, A.M. (1990) “Longitudinal Field Research on Change”, Organization Science, Vol. 1, No. 3, pp. 267–292.
Powel, W.W., Koput, K.W. and Smith-Doerr, L. (1996) “Interorganizational Collaboration and the Locus of Innovation”, Administrative Science Quarterly, Vol. 41, No. 1, pp. 116–145.
Sambamurthy, V. and Subramani, M.R. (2005) “Special Issue on Information Technologies and Knowledge Management”, MIS Quarterly, Vol. 29, No. 1, pp. 1–7.
Smith, W.K. and Lewis, M.W. (2011) “Toward a Theory of Paradox: A Dynamic Equilibrium Model of Organizing”, Academy of Management Review, Vol. 36, No. 2, pp. 381–403.
Søresen, J.B. and Stuart, T.E. (2000) “Aging, Obsolescence, and Organisational Innovation”, Ad-ministrative Science Quarterly, Vol. 45, No. 1, pp. 81–112.
Strauss, A.L. and Corbin, J. (1990) Basics of Qualitative Research, Sage, Newbury Park (CA). Tantiverdi, H. (2005) “Information Technology Relatedness, Knowledge Management Capability,
and Performance of Multibusiness Firms”, MIS Quarterly, Vol. 29, No. 2, pp. 311–334. Van de Ven, A.H. (2007) Engaged Scholarship, Oxford University Press, New York (NY). Vercellis, C. (2009) Business Intelligence, Wiley, West Sussex (UK). Yin, R.K. (2003) Case Study Research: Design and Methods (3rd Ed.), Sage, Thousand Oaks (CA).
Appendix and Electronic Companion
This appendix contains the ICT-based solutions whose introduction process has been studied (Table 3) and their definitions (Table 4). Because of space constraint, most of the tables describing the evi-dences collected through the interviews are contained in an electronic companion that is available at the following link: http://j.mp/AiIG_eCompanion_2012.
Hospital* Digitalisation** Int. Integration** Ext. Integration** Analytics**
DI1 DI2 DI3 DI4 DI5 II1 II2 II3 EI1 EI2 EI3 AN1 AN2 AN3 H1 C C C F D[8] F H2 C D D[7] C C C F F F H3 C F C C D C D[9] H1 D[8] D C C C F C F H4 D D[7] C C F F H5 C C C F D[5] C C C
H6 D C D[8] F C F H7 C C C C D C D C C F C D[8] F H8 C C C C D[10] F F F H9 C D C C C C C C D[9] C F H10 C C C C C D C C F F C D[6] C H11 D C C C D D C C D[6] C F F H12 C C C D C C C C C F D[7] H13 C D C C C C D[9] F D F H14 C C C F D[8] F * C means «present at January 2009»; D means «under development in the period from January 2009 to December 2011»; F means «development starting before the end of 2012»; the ICT-based solutions with the squared parentheses are the one whose introduction process has been studied; the number within the parentheses indicates the interviews performed in the three years of the research ** The four overarching macro-areas of ICT-driven innovation have been defined by the authors of the paper through a deep analysis of the literature and a focus group with a multidisciplinary group of more than 66 healthcare practitioners among which: C-levels (CEOs, CFOs, CMOs and CIOs) of the principal Italian hospitals, national and international health technology suppliers, professionals from national and international healthcare associations, and healthcare experts; refer to Table 4 for their definitions
Table 3 – ICT-based solutions whose introduction process has been studied

29
Macro-area* Id Solution** Definition***
Digitalisation
ID1 Tools supporting service manag. and delivery
ICT-based solutions used in the admissions processes, in directing the user flows within the hospital, and in the communication that is oriented towards the users who are waiting for service delivery
ID2 ICT security ICT-based solutions guaranteeing the production of infor-mational data, preventing access of unauthorised individu-als and guaranteeing their access after catastrophic events
ID3 Virtualisation ICT-based solutions that create a virtual version of HW, operating systems, storage devices or network resources
ID4 Systems for the dematerialisation of clinical docs.
ICT-based solutions that allow to eliminate the paper-based or film-based documents that are used in a depart-ment, transforming them into electronic documents
ID5 Systems for the dematerialisation of admin. docs.
ICT-based solutions that allow to eliminate the paper-based documents used in the administrative offices of a HCO, transforming them into electronic documents
Internal Integration
II1 Administrative management systems
ICT-based solutions for the management of accounting, financial flows, logistics, etc.
II2 Human resources management systems
ICT-based solutions used for the management of all aspects tied to the hospital’s personnel (legal, economic, social, as well as attendances and absences, etc.)
II3 Electronic Medical Record
ICT-based solutions providing support to the computerised, uniform, updated and integrated management of personal, clinical data of a patient throughout the entire cycle of medical assistance given within the hospital
External Integration
EI1 Digital services to the patients
ICT-based solution to deliver services to the patients through digital channels; included in this category it is possible to find the communication services, those for patient access of clinical information, those supporting the use of healthcare resources, CRM services, and services to support the interaction among patients
EI2 Regional medicine and home assistance
ICT-based solutions that respond to the aims of creating integration between the hospital, the district services and family doctors operating within the region
EI3 Integration with the EHR
ICT-based solutions used to create integration with the platforms for Electronic Health Record, defined as the record format for healthcare data coming from various people in charge of treatment in the same territorial area
Analytics
AN1 Computerised drug management systems
ICT-based solutions to support drug prescription, preparation and administration
AN2 Clinical Governance tools
ICT-based solutions that support clinical decisions with the objective of improving the quality of services offered, and reaching/maintaining elevated healthcare standards (e.g. the systems to define diagnostic paths)
AN3 Governance dashboards
ICT-based solutions that support the governance and admin. decisions with the objective of improving the quality of the administrative processes (e.g. the business intelligence tools adopted to balance the peaks of demand)
* The four overarching macro-areas of ICT-driven innovation have been defined by the authors of the paper through a deep analysis of the literature and a focus group with a multidisciplinary group of more than 66 practitioners among which: C-levels (CEOs, CFOs, CMOs and CIOs) of the principal Italian hospitals, national and international health technology suppliers, professionals from health associations, and healthcare experts ** The solutions have been defined through a deep analysis of the literature and the focus group mentioned in note * ***
The definitions are based on literature analysis and on the suggestions by the practitioners mentioned in note *
Table 4 – ICT-based solutions adopted by a generic hospital