long-term composite tissue allograft survival in a porcine model with cyclosporine/mycophenolate...
TRANSCRIPT

0041-1337/98/6612-1581$03.00/0TRANSPLANTATION Vol. 66, 1581–1587, No. 12, December 27, 1998Copyright © 1998 by Lippincott Williams & Wilkins Printed in U.S.A.
LONG-TERM COMPOSITE TISSUE ALLOGRAFT SURVIVAL IN APORCINE MODEL WITH CYCLOSPORINE/MYCOPHENOLATE
MOFETIL THERAPY1,2
E. TUNCAY USTUNER,3 MARTY ZDICHAVSKY,3 XIAOPING REN,3 JEAN EDELSTEIN,3
CLAUDIO MALDONADO,3 MOKUNDA RAY,4 ANTHONY W. JEVANS,5 WARREN C. BREIDENBACH,6
SCOTT A. GRUBER,7 JOHN H. BARKER,3,9 AND JON W. JONES8
Divisions of Plastic and Reconstructive, General, and Hand and Microsurgery, Department of Surgery, andthe Department of Pathology, University of Louisville School of Medicine, Louisville, Kentucky 40292;
the Department of Pathology, Jewish Hospital, Louisville, Kentucky 40202; andthe Division of Immunology and Organ Transplantation, Department of Surgery,
University of Texas at Houston Health Science Center, Houston, Texas 77030
Background. Low-dose cyclosporine (CsA)/mycophe-nolate mofetil (MMF) therapy has significantly re-duced the frequency of rejection and drug-inducedside effects in rat hindlimb allograft recipients. Withan eye toward direct clinical application, we devel-oped a large-animal extremity composite tissue allo-graft model to assess the antirejection efficacy andsystemic toxicity of combination CsA/MMF treatment.
Methods. Radial forelimb osteomyocutaneous flaptransplants were performed between size-matched,outbred pigs assigned to one of two groups: 5 controlpigs received no immunosuppression, and 10 pigs re-ceived a once-daily oral CsA/MMF/prednisone regi-men. Rejection was assessed by visual inspection offlap skin and correlated with serial histopathologicexamination of skin biopsies.
Results. In all control pigs, the flap was completelyrejected on day 7. Of the 10 pigs receiving treatment,one died from pneumonia and an another from ananesthetic complication on days 19 and 30, respec-tively, without signs of rejection. Two flaps were loston days 25 and 29 from severe rejection. Three pigswere free of rejection at the end of the 90-day fol-low-up period, and three had stable mild-to-moderaterejection at 90 days (P5 0.0007 vs. controls). Whiteblood cell and platelet counts, serum creatinine val-
ues, and liver function tests remained normal in allanimals receiving immunosuppressive therapy.
Conclusions. Our results, to our knowledge, demon-strate for the first time that rejection can be signifi-cantly delayed in a large-animal composite tissueallograft model including skin using only orally ad-ministered agents dosed according to clinically rele-vant strategies without significant drug-specificsystemic side effects.
Symbolized in the miracle of St. Cosmas and St. Damian,man’s dream of transplanting a limb from one person toanother may soon go from being a myth to becoming a pow-erful therapeutic tool in the hands of today’s reconstructivesurgeons. During the last 6 years, the first vascularizedallotransplants in humans using peripheral body parts, suchas the digital flexion system (1), femoral diaphysis (2), andknee joint (3), have been reported. These allografts did notinclude skin and muscle and were performed under cyclo-sporine (CsA*)-based maintenance immunosuppression, insome cases with concomitant antilymphocyte antibody induc-tion therapy.
Meanwhile, recent in vitro (4) and experimental (5–7) stud-ies have indicated that mycophenolate mofetil (MMF) hassignificant potential as a new immunosuppressive agent.Phase I and II clinical trials demonstrated the efficacy ofMMF in the treatment and prevention of kidney (8), heart(9), and liver (10) allograft rejection. Finally, phase III trialshave shown that MMF, when administered in combinationwith CsA, produces a clinically important reduction in thefrequency and severity of acute renal allograft rejection whencompared with azathioprine (11, 12).
The efficacy and toxicity of CsA/MMF combination therapyhas been examined in a rat hindlimb allograft model (13).The findings of this study demonstrated that subtherapeuticdoses of both agents could effectively prevent composite tis-sue allograft (CTA) rejection, while simultaneously reducingdrug-specific toxicity. On the basis of these findings, andrecognizing that antirejection therapy with minimal sys-temic morbidity is required if CTAs are to become a clinicalreality (14), we decided to test this combination therapy in alarge-animal extremity CTA model. This report presents our
1 Presented in abstract form at the 17th Annual Meeting of theAmerican Society of Transplant Physicians, May 9–13, 1998, Chi-cago, IL.
2 This work was supported by the Jewish Hospital Foundation ofLouisville, KY.
3 Division of Plastic and Reconstructive Surgery, Department ofSurgery, University of Louisville School of Medicine.
4 Department of Pathology, University of Louisville School of Med-icine.
5 Department of Pathology, Jewish Hospital, Louisville, KY.6 Division of Hand and Micro Surgery, Department of Surgery,
University of Louisville School of Medicine.7 Division of Immunology & Organ Transplantation, Department
of Surgery, University of Texas at Houston Health Science Center,Houston, TX.
8 Division of General Surgery, Department of Surgery, Universityof Louisville School of Medicine.
9 Address correspondence to: John H. Barker, MD, PhD, Divisionof Plastic and Reconstructive Surgery, University of LouisvilleSchool of Medicine, 320 MDR Building, 511 South Floyd Street,Louisville, KY 40292.
* Abbreviations: CsA, cyclosporine; CTA, composite tissue allo-graft; MMF, mycophenolate mofetil.
1581
results using an oral CsA, MMF, and prednisone regimen ina porcine, brachial artery-based, radial forelimb osteomyocu-taneous flap allograft model developed specifically for thispurpose in our laboratory.
MATERIALS AND METHODS
Animals. Thirty age- (6–8 weeks old) and size- (15–24 kg)matched, outbred farm pigs were used in our study and cared for inaccordance with guidelines established by the Institutional AnimalCare and Use Committee of the University of Louisville School ofMedicine. Different farms for donors and recipients were requestedfrom the supplier. Animals were housed in separate cages in light-,temperature-, and airflow-controlled rooms and were fed standarddiets and water ad libitum. After an initial physical examination,baseline laboratory tests (complete blood count with differential,electrolytes, and liver function tests) were performed to assess theanimals’ general health. Pretransplant crossmatching was per-formed for each donor-recipient pair to avoid hyperacute rejection.
CTA model. Orthotopic allotransplantation of a right radial fore-limb osteomyocutaneous free flap was performed. The flap was de-signed according to the well-established concept of a radial forearmosteocutaneous free flap used clinically for reconstructing multitis-sue defects (15). Flaps were based on the brachial artery and cephalicvein and consisted of the flexor carpi radialis muscle, a segment ofthe median nerve including its branch to the transplanted muscle, asegment of the radial bone, and an island of overlying skin extendingfrom the craniomedial to the craniolateral aspect of the right fore-limb (Fig. 1).
Surgical procedure. To facilitate drug administration and bloodsampling both intra- and postoperatively, a central venous catheterwas placed into the left internal jugular vein and tunneled subcuta-neously to the midline on the dorsum of recipient pigs. Dissection ofthe donor flap and preparation of the recipient field were performedsimultaneously by two surgical teams. Corresponding flap vessels,nerves, and tendons were identified and marked in the donor andrecipient limbs. Ample nerve and vessel lengths were preserved toavoid tension on the anastomoses. Identical defects of correspondingstructures were created in the recipient limb to accommodate thedonor flap. After transfer, the donor radial bone segment was insetinto its recipient site adjacent to the ulnar bone and was fixed usingone 25- to 30-mm long stainless steel screw. After adjusting their
respective lengths, the brachial artery and the cephalic vein wereanastomosed proximally, and the median nerve was coapted bothproximally and distally with 8–0 and 9–0 nylon sutures, usingmicrosurgical techniques. No anticoagulants were administered. Thedonor flexor carpi radialis muscle was extended to its original lengthand sutured into the recipient site. After skin closure and wounddressing, a fiberglass cast was applied to the operated forelimb. Awindow was created in the cast to permit inspection and biopsy of thegraft until the cast was removed 3 weeks postoperatively. Donoranimals were euthanized after the operation while they were stillunder general anesthesia.
Experimental groups and immunosuppressive protocol. CTA re-cipients were randomly assigned to one of two groups: control (n55)and treatment (n510). The control group received no immunosup-pression, whereas the treatment group received once-daily oral CsA,MMF, and prednisone combination therapy. CsA (Sandimmune oralsolution, 100 mg/ml; Sandoz Pharmaceuticals Corporation, EastHanover, NJ) (40 mg/kg per day) was begun on the morning ofsurgery, with the dose subsequently adjusted to maintain 24-hourwhole-blood trough levels between 100 and 300 ng/ml by the enzyme-multiplied immunoassay-specific method (16). MMF (500 mg/day)was begun on the morning of surgery. Methylprednisolone (500 mg)was administered i.v. during the procedure just before flap transfer.Prednisone (2.0 mg/kg per day) was begun on the first postoperativeday and then tapered by 0.5 mg/kg per day every 3 days to amaintenance dose of 0.1 mg/kg per day. Animals in the treatmentgroup did not have access to food during the night to increase thelikelihood of their ingesting and absorbing the immunosuppressivedrugs, which were mixed with a small amount of food in the morning.Finally, drug doses were not adjusted based on the clinical progressof the animals.
Postoperative care. For infection prophylaxis, 30,000 units/kg ofprocaine penicillin G were administered intramuscularly to all re-cipient pigs for 10 days. Complete blood count with differential,electrolytes, and liver function tests were determined three timesduring the first week and then weekly. CsA trough levels of 24 hourswere obtained daily for the first 3 weeks, then three times per weekfor the next 3 weeks, and then weekly. All recipients were followedup for 3 months for the occurrence of acute rejection, graft loss, ordeath. Rejection was assessed clinically by daily visual inspection ofthe flap skin by two examiners. Skin biopsies were performed ondays 0, 2, 4, 7, 10, 14, 21, 30, 45, 60, and 90. Graft survival, definedas time to flap cyanosis and sloughing (indicating complete rejec-tion), animal death, or the end of the 3-month follow-up period wereconsidered study endpoints. A complete autopsy was performed in allcases.
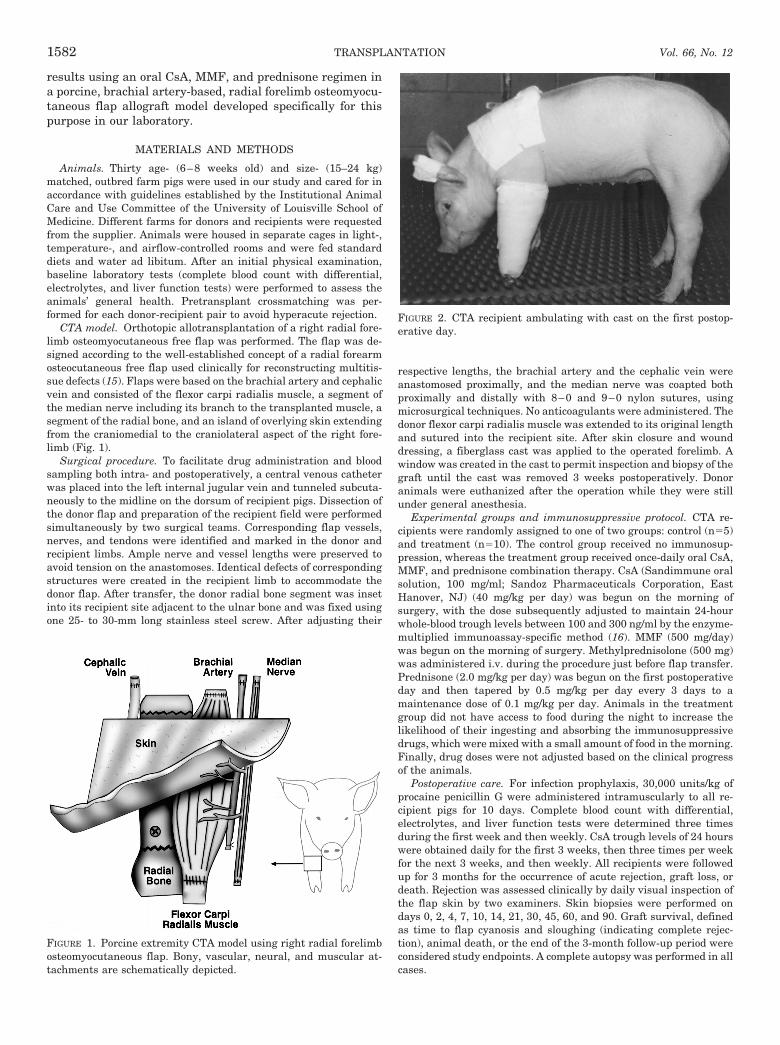
FIGURE 2. CTA recipient ambulating with cast on the first postop-erative day.
FIGURE 1. Porcine extremity CTA model using right radial forelimbosteomyocutaneous flap. Bony, vascular, neural, and muscular at-tachments are schematically depicted.
TRANSPLANTATION1582 Vol. 66, No. 12
Histopathology. Skin biopsies were initially fixed in 10% bufferedformaldehyde and then transferred to and stored in 70% ethyl alco-hol. For analysis, the tissue sections were stained with hematoxylinand eosin. On the basis of the type and severity of serial histopatho-logic changes occurring in control skin, an acute rejection gradingschema was established for the treatment group (see Results).
Data analysis. Control and treatment group graft survival timeswere compared using the Mann-Whitney U test. A values of P,0.05was regarded as statistically significant.
RESULTS
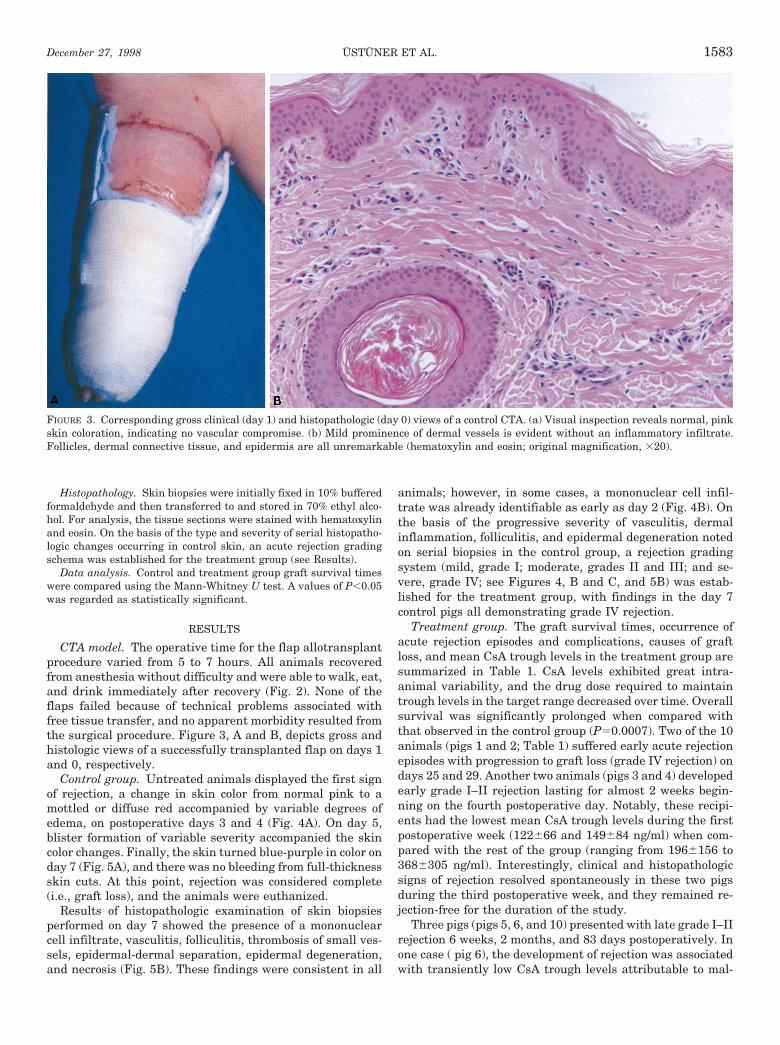
CTA model. The operative time for the flap allotransplantprocedure varied from 5 to 7 hours. All animals recoveredfrom anesthesia without difficulty and were able to walk, eat,and drink immediately after recovery (Fig. 2). None of theflaps failed because of technical problems associated withfree tissue transfer, and no apparent morbidity resulted fromthe surgical procedure. Figure 3, A and B, depicts gross andhistologic views of a successfully transplanted flap on days 1and 0, respectively.
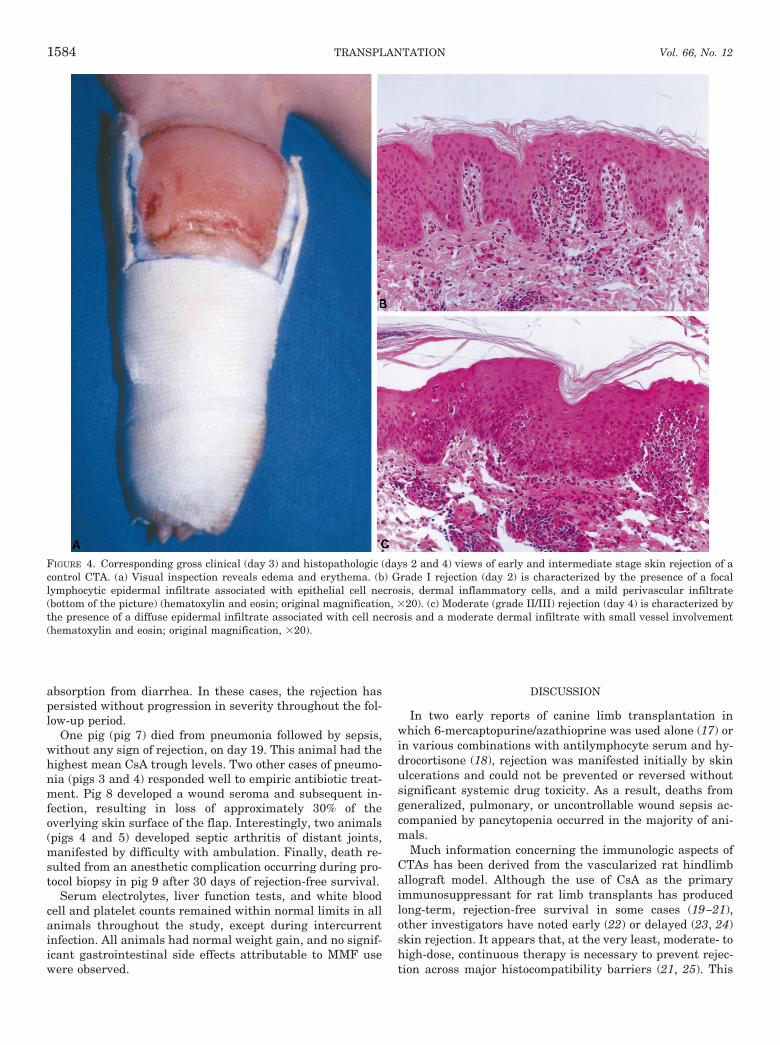
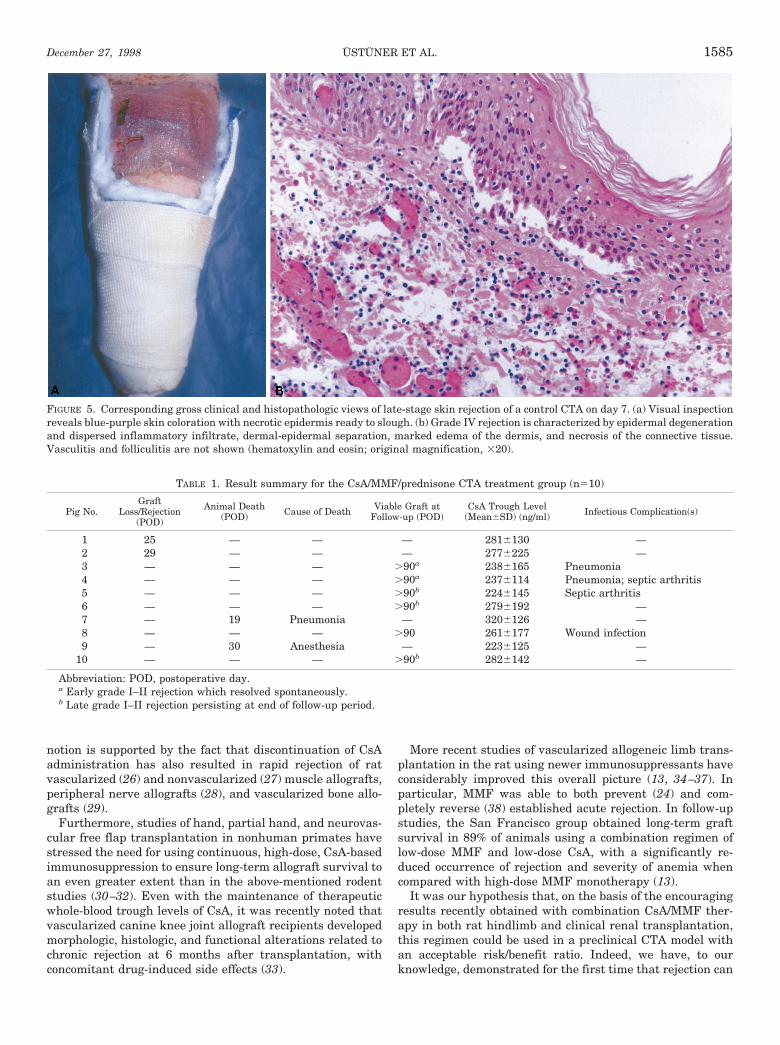
Control group. Untreated animals displayed the first signof rejection, a change in skin color from normal pink to amottled or diffuse red accompanied by variable degrees ofedema, on postoperative days 3 and 4 (Fig. 4A). On day 5,blister formation of variable severity accompanied the skincolor changes. Finally, the skin turned blue-purple in color onday 7 (Fig. 5A), and there was no bleeding from full-thicknessskin cuts. At this point, rejection was considered complete(i.e., graft loss), and the animals were euthanized.
Results of histopathologic examination of skin biopsiesperformed on day 7 showed the presence of a mononuclearcell infiltrate, vasculitis, folliculitis, thrombosis of small ves-sels, epidermal-dermal separation, epidermal degeneration,and necrosis (Fig. 5B). These findings were consistent in all
animals; however, in some cases, a mononuclear cell infil-trate was already identifiable as early as day 2 (Fig. 4B). Onthe basis of the progressive severity of vasculitis, dermalinflammation, folliculitis, and epidermal degeneration notedon serial biopsies in the control group, a rejection gradingsystem (mild, grade I; moderate, grades II and III; and se-vere, grade IV; see Figures 4, B and C, and 5B) was estab-lished for the treatment group, with findings in the day 7control pigs all demonstrating grade IV rejection.
Treatment group. The graft survival times, occurrence ofacute rejection episodes and complications, causes of graftloss, and mean CsA trough levels in the treatment group aresummarized in Table 1. CsA levels exhibited great intra-animal variability, and the drug dose required to maintaintrough levels in the target range decreased over time. Overallsurvival was significantly prolonged when compared withthat observed in the control group (P50.0007). Two of the 10animals (pigs 1 and 2; Table 1) suffered early acute rejectionepisodes with progression to graft loss (grade IV rejection) ondays 25 and 29. Another two animals (pigs 3 and 4) developedearly grade I–II rejection lasting for almost 2 weeks begin-ning on the fourth postoperative day. Notably, these recipi-ents had the lowest mean CsA trough levels during the firstpostoperative week (122666 and 149684 ng/ml) when com-pared with the rest of the group (ranging from 1966156 to3686305 ng/ml). Interestingly, clinical and histopathologicsigns of rejection resolved spontaneously in these two pigsduring the third postoperative week, and they remained re-jection-free for the duration of the study.
Three pigs (pigs 5, 6, and 10) presented with late grade I–IIrejection 6 weeks, 2 months, and 83 days postoperatively. Inone case ( pig 6), the development of rejection was associatedwith transiently low CsA trough levels attributable to mal-
FIGURE 3. Corresponding gross clinical (day 1) and histopathologic (day 0) views of a control CTA. (a) Visual inspection reveals normal, pinkskin coloration, indicating no vascular compromise. (b) Mild prominence of dermal vessels is evident without an inflammatory infiltrate.Follicles, dermal connective tissue, and epidermis are all unremarkable (hematoxylin and eosin; original magnification, 320).
USTUNER ET AL.December 27, 1998 1583
absorption from diarrhea. In these cases, the rejection haspersisted without progression in severity throughout the fol-low-up period.
One pig (pig 7) died from pneumonia followed by sepsis,without any sign of rejection, on day 19. This animal had thehighest mean CsA trough levels. Two other cases of pneumo-nia (pigs 3 and 4) responded well to empiric antibiotic treat-ment. Pig 8 developed a wound seroma and subsequent in-fection, resulting in loss of approximately 30% of theoverlying skin surface of the flap. Interestingly, two animals(pigs 4 and 5) developed septic arthritis of distant joints,manifested by difficulty with ambulation. Finally, death re-sulted from an anesthetic complication occurring during pro-tocol biopsy in pig 9 after 30 days of rejection-free survival.
Serum electrolytes, liver function tests, and white bloodcell and platelet counts remained within normal limits in allanimals throughout the study, except during intercurrentinfection. All animals had normal weight gain, and no signif-icant gastrointestinal side effects attributable to MMF usewere observed.
DISCUSSION
In two early reports of canine limb transplantation inwhich 6-mercaptopurine/azathioprine was used alone (17) orin various combinations with antilymphocyte serum and hy-drocortisone (18), rejection was manifested initially by skinulcerations and could not be prevented or reversed withoutsignificant systemic drug toxicity. As a result, deaths fromgeneralized, pulmonary, or uncontrollable wound sepsis ac-companied by pancytopenia occurred in the majority of ani-mals.
Much information concerning the immunologic aspects ofCTAs has been derived from the vascularized rat hindlimballograft model. Although the use of CsA as the primaryimmunosuppressant for rat limb transplants has producedlong-term, rejection-free survival in some cases (19–21),other investigators have noted early (22) or delayed (23, 24)skin rejection. It appears that, at the very least, moderate- tohigh-dose, continuous therapy is necessary to prevent rejec-tion across major histocompatibility barriers (21, 25). This
FIGURE 4. Corresponding gross clinical (day 3) and histopathologic (days 2 and 4) views of early and intermediate stage skin rejection of acontrol CTA. (a) Visual inspection reveals edema and erythema. (b) Grade I rejection (day 2) is characterized by the presence of a focallymphocytic epidermal infiltrate associated with epithelial cell necrosis, dermal inflammatory cells, and a mild perivascular infiltrate(bottom of the picture) (hematoxylin and eosin; original magnification, 320). (c) Moderate (grade II/III) rejection (day 4) is characterized bythe presence of a diffuse epidermal infiltrate associated with cell necrosis and a moderate dermal infiltrate with small vessel involvement(hematoxylin and eosin; original magnification, 320).
TRANSPLANTATION1584 Vol. 66, No. 12
notion is supported by the fact that discontinuation of CsAadministration has also resulted in rapid rejection of ratvascularized (26) and nonvascularized (27) muscle allografts,peripheral nerve allografts (28), and vascularized bone allo-grafts (29).
Furthermore, studies of hand, partial hand, and neurovas-cular free flap transplantation in nonhuman primates havestressed the need for using continuous, high-dose, CsA-basedimmunosuppression to ensure long-term allograft survival toan even greater extent than in the above-mentioned rodentstudies (30–32). Even with the maintenance of therapeuticwhole-blood trough levels of CsA, it was recently noted thatvascularized canine knee joint allograft recipients developedmorphologic, histologic, and functional alterations related tochronic rejection at 6 months after transplantation, withconcomitant drug-induced side effects (33).
More recent studies of vascularized allogeneic limb trans-plantation in the rat using newer immunosuppressants haveconsiderably improved this overall picture (13, 34–37). Inparticular, MMF was able to both prevent (24) and com-pletely reverse (38) established acute rejection. In follow-upstudies, the San Francisco group obtained long-term graftsurvival in 89% of animals using a combination regimen oflow-dose MMF and low-dose CsA, with a significantly re-duced occurrence of rejection and severity of anemia whencompared with high-dose MMF monotherapy (13).
It was our hypothesis that, on the basis of the encouragingresults recently obtained with combination CsA/MMF ther-apy in both rat hindlimb and clinical renal transplantation,this regimen could be used in a preclinical CTA model withan acceptable risk/benefit ratio. Indeed, we have, to ourknowledge, demonstrated for the first time that rejection can
FIGURE 5. Corresponding gross clinical and histopathologic views of late-stage skin rejection of a control CTA on day 7. (a) Visual inspectionreveals blue-purple skin coloration with necrotic epidermis ready to slough. (b) Grade IV rejection is characterized by epidermal degenerationand dispersed inflammatory infiltrate, dermal-epidermal separation, marked edema of the dermis, and necrosis of the connective tissue.Vasculitis and folliculitis are not shown (hematoxylin and eosin; original magnification, 320).
TABLE 1. Result summary for the CsA/MMF/prednisone CTA treatment group (n510)
Pig No.Graft
Loss/Rejection(POD)
Animal Death(POD) Cause of Death Viable Graft at
Follow-up (POD)CsA Trough Level
(Mean6SD) (ng/ml) Infectious Complication(s)
1 25 — — — 2816130 —2 29 — — — 2776225 —3 — — — .90a 2386165 Pneumonia4 — — — .90a 2376114 Pneumonia; septic arthritis5 — — — .90b 2246145 Septic arthritis6 — — — .90b 2796192 —7 — 19 Pneumonia — 3206126 —8 — — — .90 2616177 Wound infection9 — 30 Anesthesia — 2236125 —
10 — — — .90b 2826142 —
Abbreviation: POD, postoperative day.a Early grade I–II rejection which resolved spontaneously.b Late grade I–II rejection persisting at end of follow-up period.
USTUNER ET AL.December 27, 1998 1585

be significantly delayed in a large-animal CTA model includ-ing skin using only orally administered agents dosed accord-ing to clinically relevant strategies without the developmentof drug-specific systemic side effects. Antilymphocyte anti-body induction therapy was not administered, and acuterejection episodes were not specifically treated. Despite ourdecision not to alter immunosuppressive drug doses on thebasis of the clinical course of the animals, only one pig, whichhad the highest mean CsA levels, was lost to the generalizedeffects of immunosuppression, and two grafts were lost fromrejection. When evaluating the infectious complications, thedifficulty of maintaining sterility in the pigs and multiplesurgical procedures that required general anesthesia needalso to be taken into consideration.
The large-animal model developed specifically for our CTAstudies proved exceedingly useful in that it contained all ofthe tissues of the limb except cartilage, was technically fea-sible, easily permitted the gross and histopathologic assess-ment of acute rejection, and lacked the surgical morbidity ofa whole-limb transplant. The wide intra-animal variabilityobserved in CsA trough levels might have been amelioratedwith use of the Neoral formulation of CsA. Finally, the 90-day follow-up period used for the study did not fully allow fordetermination of the rate of occurrence of chronic rejectionand malignancy in our model.
The favorable results obtained in this study represent afoundational step in the design of effective antirejection drugregimens for composite tissue transplantation in man andsuggest that the drug-specific and general adverse conse-quences of systemic immunosuppression may be sufficientlyreduced to permit more widespread clinical application of theprocedure. Furthermore, plans for future studies in our ex-tremity CTA model include not only studying the efficacy andtoxicity of tacrolimus-based systemic immunosuppressivetherapy (34, 35), but also examining the usefulness of pump-based, local intra-arterial infusion of CsA or tacrolimusagainst a background of low-dose oral MMF and prednisonetreatment as a means of establishing a more selective pres-ence of these agents in limb tissues and further improvingthe therapeutic index (14).
REFERENCES
1. Guimberteau JC, Baudet J, Panconi B, Boileau R, Potaux L.Human allotransplant of a digital flexion system vascularizedon the ulnar pedicle: a preliminary report and 1-year follow-upof two cases. Plast Reconstr Surg 1992; 89: 1135.
2. Hofmann GO, Kirschner MH, Buhren V, Land W. Allogenicvascularized transplantation of a human femoral diaphysisunder cyclosporin A immunosuppression. Transpl Int 1995; 8:418.
3. Hofmann GO, Kirschner MH, Wagner FD, Land W, Buhren V.Allogeneic vascularized grafting of a human knee joint withpostoperative immunosuppression. Arch Orthop Trauma Surg1997; 116: 125.
4. Eugui EM, Almquist SJ, Muller CD, Allison AC. Lymphocyte-selective cytostatic and immunosuppressive effects of myco-phenolic acid in vitro: role of deoxyguanosine nucleotide deple-tion. Scand J Immunol 1991; 33: 161.
5. Morris RE, Hoyt EG, Murphy MP, Eugui EM, Allison AC. My-cophenolic acid morpholinoethylester (RS-61443) is a new im-munosuppressant that prevents and halts heart allograft re-jection by selective inhibition of T- and B-cell purine synthesis.Transplant Proc 1990; 22: 1659.
6. Morris RE, Wang J, Blum JR, et al. Immunosuppressive effectsof morpholinoethyl ester of mycophenolic acid (RS-61443) inrat and nonhuman primate recipients of heart allografts.Transplant Proc 1991; 23(2 suppl 2): 19.
7. Platz KP, Bechstein WO, Eckhoff DE, Suzuki Y, Sollinger HW.RS-61443 reverses acute allograft rejection in dogs. Surgery1991; 110: 736.
8. Sollinger HW, Deierhoi MH, Belzer FO, Diethelm AG, KauffmanRS. RS-61443: a phase I clinical trial and pilot rescue study.Transplantation 1992; 53: 428.
9. Ensley RD, Bristow MR, Olsen SL, et al. The use of mycopheno-late mofetil (RS-61443) in human heart transplant recipients.Transplantation 1993; 56: 75.
10. Klintmalm GB, Ascher NL, Busuttil RW, et al. RS-61443 fortreatment-resistant human liver rejection. Transplant Proc1993; 25: 697.
11. Sollinger HW for the U.S. Renal Transplant MycophenolateMofetil Study Group. Mycophenolate mofetil for the preventionof acute rejection in primary cadaveric renal allograft recipi-ents. Transplantation 1995; 60: 225.
12. The Tricontinental Mycophenolate Mofetil Renal Transplanta-tion Study Group. A blinded, randomized clinical trial of my-cophenolate mofetil for the prevention of acute rejection incadaveric renal transplantation. Transplantation 1996; 61:1029.
13. Benhaim P, Anthony JP, Ferreira L, Borsanyi J-P, Mathes SJ.Use of combination of low-dose cyclosporine and RS-61443 in arat hindlimb model of composite tissue allotransplantation.Transplantation 1996; 61: 527.
14. Shirbacheh MV, Jones JW, Breidenbach WC, McCabe S, GruberSA. The case for local immunosuppression in composite tissueallotransplantation. Transplant Proc 1998; 30: 2739.
15. Strauch B, Yu H-L, Chen Z-W, Liebling R. Radial forearm osteo-cutaneous flap. In: Strauch B, et al., eds. Atlas of microvascu-lar surgery, anatomy and operative approaches. New York:Thieme, 1993: 63.
16. Beresini MH, Davalian D, Alexander S, et al. Evaluation ofEMIT cyclosporine assay for use with whole blood. Clin Chem1993; 39: 2235.
17. Goldwyn RM, Beach PM, Feldman D, Wilson RE. Canine limbhomotransplantation. Plast Reconstr Surg 1966; 37: 184.
18. Lance EM, Inglis AE, Figarola F, Veith FJ. Transplantation ofthe canine hind limb. J Bone Joint Surg Am 1971; 53A: 1137.
19. Black KS, Hewitt CW, Fraser LA, et al. Composite tissue (limb)allografts in rats. II. Indefinite survival using low-dose cyclo-sporine. Transplantation 1985; 39: 365.
20. Black KS, Hewitt CW, Hwang JS, Borger RW, Achauer BM.Dose response of cyclosporine-treated composite tissue allo-grafts in a strong histoincompatible rat model. TransplantProc 1988; 20 (suppl 2): 266.
21. Fritz WD, Swartz WM, Rose S, Futrell JW, Klein E. Limb allo-grafts in rats immunosuppressed with cyclosporine A. AnnSurg 1984; 199; 211.
22. Press BH, Sibley RK, Shons AR. Limb allotransplantation in therat: extended survival and return of nerve function with con-tinuous cyclosporin/prednisone immunosuppression. AnnPlast Surg 1986; 16: 313.
23. Hotokebuchi T, Arai K, Takagishi K, Arita C, Sugioka Y,Kaibara N. Limb allografts in rats immunosuppressed withcyclosporine: as a whole-joint allograft. Plast Reconstr Surg1989; 83: 1027.
24. Benhaim P, Anthony JP, Lin LY-T, McCalmont TH, Mathes SJ.A long-term study of allogeneic rat hindlimb transplants im-munosuppressed with RS-61443. Transplantation 1993; 56:911.
25. Hewitt CW, Black KS, Fraser LA, et al. Composite tissue (limb)allografts in rats. I. Dose-dependent increase in survival withcyclosporine. Transplantation 1985; 39: 360.
TRANSPLANTATION1586 Vol. 66, No. 12
26. Tan CM, Yaremchuk MJ, Randolph MA, Lee WPA, Burdick J,Weiland AJ. Vascularized muscle allografts and the role ofcyclosporine. Plast Reconstr Surg 1991; 87: 412.
27. Gulati AK, Zalewski AA. Muscle allograft survival after cyclo-sporin A immunosuppression. Exp Neurol 1982; 77: 378.
28. Yu LT, England J, Hickey WF, et al. Survival and function ofperipheral nerve allografts after cessation of long-term cyclo-sporin immunosuppression in rats. Transplant Proc 1989; 21:3178.
29. Paskert JP, Yaremchuk MJ, Randolph MA, Weiland AJ. The roleof cyclosporin in prolonging survival in vascularized bone al-lografts. Plast Reconstr Surg 1987; 80: 240.
30. Stark GB, Swartz WM, Narayanan K, Møller AR. Hand trans-plantation in baboons. Transplant Proc 1987; 19: 3968.
31. Skanes SE, Samulak DD, Daniel RK. Tissue transplantation forreconstructive surgery. Transplant Proc 1986; 18: 898.
32. Stevens HP, Hovius SE, Heeney JL, et al. Immunologic aspectsand complications of composite tissue allografting for upperextremity reconstruction: a study in the rhesus monkey.Transplant Proc 1991; 23: 623.
33. Rosso R, Schafer D, Fricker R, et al. Functional and morpholog-ical outcome of knee joint transplantation in dogs depends on
control of rejection. Transplantation 1997; 63: 1723.34. Fealy MJ, Umansky WS, Bickel KD, Nino JJ, Morris RE, Press
BHJ. Efficacy of rapamycin and FK 506 in prolonging rat hindlimb allograft survival. Ann Surg 1994; 219: 88.
35. Fealy MJ, Most D, Huie P, et al. Association of down-regulationof cytokine activity with rat hind limb allograft survival.Transplantation 1995; 59: 1475.
36. Yeh L-S, Gregory CR, Griffey SM, Lecouteur RA, Morris RE.Effects of leflunomide and cyclosporine on myocutaneous allo-graft survival in the rat. Transplantation 1996; 62: 861.
37. Yeh L-S, Gregory CR, Griffey SM, Lecouter RA, Hou S-M, MorrisRE. Combination leflunomide and cyclosporine prevents rejec-tion of functional whole limb allografts in the rat. Transplan-tation 1997; 64: 919.
38. van den Helder TB, Benhaim P, Anthony JP, McCalmont TH,Mathes SJ. Efficacy of RS-61443 in reversing acute rejection ina rat model of hindlimb allotransplantation. Transplantation1994; 57: 427.
Received 27 May 1998.Accepted 5 August 1998.
0041-1337/98/6612-1587$03.00/0TRANSPLANTATION Vol. 66, 1587–1596, No. 12, December 27, 1998Copyright © 1998 by Lippincott Williams & Wilkins Printed in U.S.A.
SYSTEMIC ADMINISTRATION OF ANTI-INTERLEUKIN-10ANTIBODY PROLONGS ORGAN ALLOGRAFT SURVIVAL IN
NORMAL AND PRESENSITIZED RECIPIENTS1,2
WEI LI,3 FUMIN FU,3 LINA LU,3 SATWANT K. NARULA,4 JOHN J. FUNG,3
ANGUS W. THOMSON,3,5 AND SHIGUANG QIAN3,6
Thomas E. Starzl Transplantation Institute and Departments of Surgery and of Molecular Genetics and Biochemistry,University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania 15213, and Department of Immunology,
Schering Plough Research Institute, Kenilworth, New Jersey 07033
Background. Systemic administration of cellular in-terleukin (IL)-10 at a dose of 100 mg/day for 1 weekafter transplantation accelerates mouse cardiac allo-graft rejection across MHC barriers. This effect is as-sociated with enhancement of donor-specific cytotoxicT lymphocyte and alloantibody (alloAb) titers. To fur-
ther evaluate the in vivo role of IL-10, we tested theinfluence of a neutralizing anti-IL-10 monoclonal an-tibody (mAb) in both normal and donor (skin) presen-sitized mouse organ allograft recipients.
Methods. Heart or liver transplants were performedfrom B10 (H2b) donors to C3H (H2k) recipients. Anti-IL-10 mAb (SXC.I) was administered intravenously ina single injection or repeated once daily injections.Cytotoxic activity of graft-infiltrating cells was deter-mined by 51Cr-release assay. Circulating alloAb levelswere quantified by complement-dependent cytotoxic-ity and flow cytometry.
Results. Survival of vascularized B10 cardiac allo-grafts in normal recipients was prolonged signifi-cantly in the mAb-treated groups. A single injection of1 mg of anti-IL-10 mAb immediately after heart trans-plantation gave a similar graft median survival time torepeated injections of lower dose mAb (0.5 mg/day for6 days after transplantation) (Ig isotype control 11days; single mAb injection 18 days; multiple injection20 days). In presensitized recipients, anti-IL-10 mAbfrom days 0 to 6 significantly prolonged survival of
1 Presented at the 17th Annual Meeting of the American Society ofTransplantation Physicians, May 9–13, 1998.
2 The work was supported by National Institutes of Health grantsDK29961 and DK49745 and by a grant from the Schering PloughResearch Institute.
3 Thomas E. Starzl Transplantation Institute and Department ofSurgery, University of Pittsburgh.
4 Department of Immunology, Schering Plough Research Insti-tute.
5 Department of Molecular Genetics and Biochemistry, Universityof Pittsburgh.
6 Address correspondence to: Shiguang Qian, MD, Thomas E.Starzl Transplantation Institute, E1540 Biomedical Science Tower,University of Pittsburgh Medical Center, 200 Lothrop Street, Pitts-burgh, PA 15213. E-mail: [email protected].
LI ET AL.December 27, 1998 1587