journal of health science 2014.7
TRANSCRIPT

Journal of Health
Science
Volume 2, Number 7, July 2014 (Serial Number 8)
David
David Publishing Company
www.davidpublishing.com
PublishingDavid

Publication Information Journal of Health Science is published monthly in hard copy (ISSN 2328-7136) by David Publishing Company located at 240 Nagle Avenue #15C, New York, NY 10034, USA. Aims and Scope Journal of Health Science, a monthly professional academic journal, covers all sorts of researches on Nutrition and Dietetics, Epidemiology and Public Health, Disaster Management, Physiology and Counseling, Health Psychology and Behavior, Health and Rehabilitation, Exercise and Nutrition Sciences, Nursing Practice and Health Care, Health Policies and Administrations, Health Informatics, Environmental and Occupational Health, Community Health, Public Health, Health Education and Research, as well as other issues related to Health Science. Editorial Board Members Bernhard Schlag (Germany), Masatsugu Tsuji (Japan), Panagiota Florou-Paneri (Greece), Khanferyan Roman (Russian), Subbiah Elango (India), Bruce C.M. Wang (USA), María del Carmen Solano Ruiz (Sweden), Viacheslav Kravtsov (Russia), Rajendra Prasad (India), Martinez Lanz Patricia (México), Marjan Malešič (The Republic of Slovenia), Beena Elizabeth Thomas (India), Metin Picakciefe (Turkey), Radostina Ivaylova Aleksandrova (Bangladesh), Jakir Hossain Bhuiyan Masud (Bangladesh), Kashef N. Zayed (Oman), Seyed Mohammad Jazayeri (Iran), Miguel Rego Costa Soares-Oliveira (Portugue), Mustafa Yildiz (Turkey), Trevor Cornelius Stuart Archer (Sweden). Editorial Office 240 Nagle Avenue #15C, New York, NY 10034, USA Tel: 1-323-984-7526, 323-410-1082; Fax: 1-323-984-7374, 323-908-0457 E-mail: [email protected], [email protected] Copyright©2014 by David Publishing Company and individual contributors. All rights reserved. David Publishing Company holds the exclusive copyright of all the contents of this journal. In accordance with the international convention, no part of this journal may be reproduced or transmitted by any media or publishing organs (including various websites) without the written permission of the copyright holder. Otherwise, any conduct would be considered as the violation of the copyright. The contents of this journal are available for any citation. However, all the citations should be clearly indicated with the title of this journal, serial number and the name of the author. Abstracted / Indexed in Database of EBSCO, Massachusetts, USA Universe Digital Library S/B, ProQuest Summon Serials Solutions, USA Google Scholar (scholar.google.com) American Federal Computer Library Center (OCLC), USA Universe Digital Library Sdn Bhd (UDLSB), Malaysia China National Knowledge Infrastructure (CNKI), China Subscription Information Price (per year): Print $520, Online $320, Print and Online $600. David Publishing Company 240 Nagle Avenue #15C, New York, NY 10034, USA Tel: 1-323-984-7526, 323-410-1082; Fax: 1-323-984-7374, 323-908-0457 E-mail: [email protected]
David Publishing Company
www.davidpublishing.com
DAVID PUBLISHING
D

Journal of Health Science
Volume 2, Number 7, July 2014 (Serial Number 8)
Contents Health Informatics
307 The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in
A549 Cell Line
Xiaobin Zeng, Hongbo Chen, Jun Tian, Yang Wang, Liao Cui and Xueyan Wang
318 Changes of Immunoreactivity Status in Patients with Osteosarcoma on the Background of
Chemotherapy
Djamilya Sh. Polatova, Margarita S. Gildieva and Khurshid G. Abdikarimov
325 From Awareness to Action Using the Survey Feedback Method
Ann Fridner, Birgit Pingel, Lise Tevik Løvseth, Marie Gustafsson Sendén and Karin Schenck-Gustafsson
Disaster Management
330 Nurse Documentation in Deteriorating Patients Prior to In-hospital Cardiac Arrest—A Pilot
Study in A Swedish University Hospital
Lars Aas, Maria Ouchterlony and Therese Djärv
338 Relation of Nausea and Vomiting in Acute Myocardial Infarction to Location of Infarct
Kooli Sami, Laamouri Noura, Raddaoui Abdelhafidh, El Heni Najla, Ghazali Hanene and Souissi Sami
340 Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker
Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in
Pre-migration Stage
Susiana Nugraha and Yuko Ohara-Hirano

Journal of Health Science 2 (2014) 307-317
The Effective Activation of Apoptosis by AO-95 from the
Aerial Part of Alpiniae officinarum in A549 Cell Line
Xiaobin Zeng1, 5, Hongbo Chen2, Jun Tian3, Yang Wang4, Liao Cui1 and Xueyan Wang5
1. Guangdong Key Laboratory for Research and Development of Natural Drugs, Department of Pharmacology, Guangdong Medical
College, Zhanjiang 524023, Guangdong, China
2. The Shenzhen Key Lab of Gene and Antibody Therapy, Graduate School at Shenzhen, Tsinghua University, Shenzhen 518055,
Guangdong, China
3. College of Life Science, Jiangsu Normal University, Xuzhou 221116, Jiangsu Province, China
4. Shenzhen Xinpeng Shengwu Gongcheng Co. LTD, Shenzhen 518055, Guangdong, China
5. Key Lab for New Drug Research of TCM and Shenzhen Branch, State R & D Centre for Viro-Biotech, Research Institute of
Tsinghua University in Shenzhen, Shenzhen 518057, Guangdong, China
Received: May 19, 2014 / Accepted: June 25, 2014 / Published: July 30, 2014. Abstract: The study was designed to examine the apoptosis inducing activity of the AO-95 from the aerial part of Alpiniae officinarum. The AO-95 treatment to three human lung cancer cell lines (A549, NCI-H460 and NCI-H23) resulted in a dose-dependent inhibition of cell growth. The authors selected A549 cell line as a test model system. The AO-95 induced apoptosis of A549 obviously, as shown by the results of cell cycle distribution analysis and cell apoptosis assay. Treatment of A549 with AO-95 markedly decreased the mitochondrial transmembrane potential (ΔΨm) suggesting AO-95-induced apoptosis may involve a mitochondrial-related pathway. Two compounds were isolated from AO-95 and their structures were identified as 3-phenylpropanal and 4-phenylbutan-2-one. Meanwhile, ten different components accounting for 98.38% of the total AO-95 composition were identified by gas chromatography-mass spectrometry. The major components were 3-phenylpropanal (33.09%) and 4-phenylbutan-2-one (51.16%). And these two compounds showed notable cytotoxic activity with IC50 values of 14.90-78.46 µg/mL. In summary, the AO-95, dominated by phenylpropanoid constituents, shows effective apoptosis inducing activity by mitochondrial-related pathway and may be developed as an agent against human lung cancer. Key words: Alpiniae officinarum, apoptosis, lung cancer, mitochondrial-related pathway.
1. Introduction
Alpiniae officinarum is a plant in the ginger family,
cultivated in Southeast Asia. It originated in China,
where its name ultimately derives. It can grow several
feet high, with long leaves and reddish-white flowers.
The rhizomes, known as galangal, are valued for their
spicy flavor and aromatic scent. These are used
throughout Asia in curries and perfumes, and were
previously used widely in Europe. They are also used
Corresponding author: Xiaobin Zeng, doctor, assistant
researcher, research field: Chinese medicine. E-mail: [email protected]. Jun Tian, doctor, lecturer, research field: Chinese medicine. E-mail: [email protected].
as a traditional Chinese medicine for their
anti-inflammatory, antioxidant, anti-proliferative,
anticancer, and antiemetic effects [1-5]. Previous
phytochemical studies on their rhizomes resulted in the
isolation of monoterpenes, diarylheptanoids, flavonoids
and phenylpropanoids [6-10]. However, to the best of
our knowledge, there has been remarkably little
research on the chemistry and bioactivity of the aerial
part of A. officinarum. The annual production of the
aerial part of A. officinarum now exceeds 1,000,000 t,
but the utilisation is still low. Every year, a large
number of the aerial parts of A. officinarum have been
thrown away as a waste from A. officinarum production.
DAVID PUBLISHING
D

The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
308
Lung cancer is one of the most common cancers with
annually increasing occurrence worldwide. Lung
cancer is the most common cause of cancer-related
death in men and women, and is responsible for 1.38
million deaths annually, as of 2008 [11]. Apoptosis is a
form of programmed cell death. It is also necessary for
the destruction of cells considered a threat such as cells
infected with viruses, cells with DNA damage, and
cancerous cells. During apoptosis, cellular contents are
not released and inflammation does not occur.
Impaired regulation of apoptosis leads to a variety of
diseases [12]. Cells undergoing apoptosis show
characteristic morphological and biochemical features.
These features include chromatin aggregation, nuclear
and cytoplasmic condensation, partition of cytoplasm
and nucleus into apoptotic bodies which contain
ribosomes, morphologically intact mitochondria and
nuclear material [13]. In vivo, these apoptotic bodies
are rapidly recognized and phagocytized by either
macrophages or adjacent epithelial cells. Due to this
efficient mechanism for the removal of apoptotic cells
in vivo no inflammatory response is elicited. In vitro,
the apoptotic bodies as well as the remaining cell
fragments ultimately swell and finally lyse. This
terminal phase of in vitro cell death has been termed
“secondary necrosis” [14]. Apoptosis inducer can
prevent tumor formation, and side effects are rare.
The aim of the present study was to investigate
components with the apoptosis inducing activity from
the aerial part of A. Officinarum, and the chemical
composition of AO-95 was also investigated.
2. Materials and Methods
2.1 Plant Materials
The aerial part of A. officinarum was collected in
Xuwen County, Guangdong province, China
(September 2012) and identified by Dr. Xiaobin Zeng
(Guangdong Key Laboratory for Research and
Development of Natural Drugs, Guangdong Medical
College, China). Voucher specimens (No. 120915)
were deposited at the herbarium of Guangdong Key
Laboratory for Research and Development of Natural
Drugs, Guangdong Medical College, China.
2.2 Chemicals and Reagents
Diaion D-101 macroporus resin was the product of
Xi’an Lanxiao Resin Corporation Ltd. (Xi’an, China).
RPMI-1640 medium, fetal bovine serum (FBS) and
trypsin-EDTA solution (1 ×) were obtained from
Hyclone (Logan, UT). Mitotracker green was
purchased from Invitrogen (Carlsbad, CA, USA).
Annexin-V/PI Apoptosis Detection Kit and JC-1 were
purchased from Beyotime Institute of Biotechnology
(Jiangsu, China), PI (Propidium iodide) was purchased
from Sigma (St. Louis, MO, USA). All other chemicals
were analytical or HPLC grade and obtained from
Shanghai Chemical Reagents Co., Ltd (Shanghai,
China).
2.3 Extraction and Fractionation of Plant Material
The herb (5.0 kg) was minced and extracted three
times with 95% ethanol. The solvent was removed
under vacuum to yield the crude extract (600 g). A
suspension of the extract in H2O was centrifuged and
then applied to a D-101 macroresin column (80 mm ×
1300 mm) and eluted with H2O (10 L), 10% ethanol
(10 L), 30% ethanol (10 L), 50% ethanol (10 L), 70%
ethanol (10 L), and 95% ethanol (10 L) successively.
Each eluent was concentrated and dried to yield 250.5
g, 110.0 g, 59.0 g, 130.0 g, 25.7 g, 12.6 g of dried
elutes, respectively. The 95% ethanol eluent (12.6 g)
was fractionated over a silica gel column (300 g, 70 ×
3 cm) by eluting with cyclohexane-ethyl acetate
(100:1, 5 L), (33:1, 4 L), (20:1, 5 L), (15:1, 5 L), (10:1,
3 L), (2:1, 4 L), (1:1, 5 L). This process yielded 10
fractions (AO-95-1-AO-95-10). AO-95-3 (1.35 g)
was separated on a silica gel column (50 g, 45 × 2 cm),
using cyclohexane-ethyl acetate (100:1, 1.5 L), (50:1,
3 L), (25:1, 1.5 L), (15:1, 1.2 L), (10:1, 1.3 L) to yield
compound 1 (368 mg). AO-95-6 (1.06 g) was further
purified by a silica gel column (30 g, 38 × 2 cm) and
eluted with cyclohexane-ethyl acetate (100:1, 1 L),

The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
309
(25:1, 0.8 L), (15:1, 1 L), (10:1, 1.2 L), (5:1, 1.5 L) to
obtain compound 2 (550 mg).
2.4 Analysis the Chemical Component of AO-95
The chemical composition of the AO-95 was
analyzed using GC/MS. The AO-95 (10 μg) was
dissolved in cyclohexane (1 mL) and 1 μL of the
solution was injected into a GC/MS (QP-2010
Shimadzu Co., Kyoto, Japan). The capillary column
was HP-Innowax (length = 30 m, i.d = 0.25 mm,
thickness = 0.25 μM). Helium was used as the carrier
gas at a flow rate of 1 mL/min. The column inlet
pressure was 55.8 kPa. The GC column oven
temperature was increased from 50 to 280 °C at a rate
of 10 °C/min, with a final hold time of 10 min. Injector
and detector temperatures were maintained at 280 °C.
EI mode was at 70 eV, while mass spectra were
recorded in the 30-450 amu range and ion
source-temperature was 200 °C. The AO-95
components were identified by comparison of their
mass spectra with those in the NIST08s GC/MS library
and those in the literature [15].
2.5 Cell Culture
Human lung cancer cell lines (A549, NCI-H460 and
NCI-H23) were obtained from the American Type
Culture Collection and cultured in RPMI 1640 medium
containing 10% FBS, 100 U/mL penicillin and 100
μg/mL streptomycin. Cells were cultured at 37 °C in a
humidified 5% CO2 incubator. The extract (AO), the
0% ethanol elute (AO-0), the 10% ethanol elute
(AO-10), the 30% ethanol elute (AO-30), the 50%
ethanol elute (AO-50), the 70% ethanol elute (AO-70),
the 95% ethanol elute (AO-95), 4-phenylbutan-2-one,
3-phenylpropanal and cisplatin were dissolved in
dimethyl sulfoxide (DMSO) (final DMSO concentration
≤ 0.5%). In all experiments, the cells in RPMI 1640
medium plus DMSO only were used as the control.
2.6 Cell Viability Assay
Cells were seeded in a 96-well plate at a density of 5
× 103 cells/well. The total volume was adjusted to 200
μL with growth medium. At 24 h after the seeding, the
cells were exposed to AO, AO-0, AO-10, AO-30,
AO-50, AO-70, AO-95, 4-phenylbutan-2-one,
3-phenylpropanal and cisplatin. Cell viability was
examined after 24, 48 or 72 h using a standard MTT
method [16]. Drug effect was expressed as percentage
relative to the controls.
2.7 DNA Cell Cycle Analysis
A549 cells were seeded at a density of 1 × 105
cells/well in a six-well plate. 24 h after the seeding, the
cells were treated with AO-95 (0-50 μg/mL) for 48 h at
37 °C. Cells were fixed overnight with 95% ethanol at
-20 °C and stained with PI solution (100 μg/mL). Cell
cycle distribution analysis [17] was performed using a
flow cytometer (Beckman-Coulter, Inc., Indianapolis,
IN).
2.8 Cell Apoptosis Assay
Apoptotic cells were detected by flow cytometry
with Annexin V-FITC/PI dual staining [18]. After
AO-95 treatment, the cells were harvested by
trypsinization, rinsed twice with PBS, and suspended
in 500 µL of binding buffer. The suspended cells were
incubated for 15 min at 4 °C with 5 µL Annexin
V-FITC solution, and incubated for another 5 min at
4 °C after adding 10 µL of PI solution. Flow cytometric
analysis of apoptotic cells was performed with a flow
cytometer (Beckman-Coulter, Inc., Indianapolis, IN).
The emitted green fluorescence of annexin V (FL1) and
red fluorescence of PI (FL2) were detected by a flow
cytometer. For each sample, 10,000 events were
recorded. The amount of early apoptosis, late apoptosis,
and necrosis was determined as the percentage of
annexin-V+/PI-; annexin-V+/PI+; and annexin-V-/PI+
cells, respectively.
2.9 Detection of Mitochondrial Membrane Potential (ΔΨm)
JC-1 easily penetrates cells and healthy
mitochondria. A green fluorescent JC-1 probe exists as
a monomer at low membrane potentials. However, at
The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
310
higher potentials, JC-1 forms red-fluorescent
“J-aggregates”. The ratio of red/green JC-1
fluorescence is dependent only on the mitochondrial
membrane potential [19]. Briefly, after treatment, the
cells were incubated at 37 °C for 1 h with 5 mg/L JC-1
(Beyotime Biotech, Nantong, China), then washed
twice with PBS and placed in fresh medium without
serum. Lastly, images were viewed and scanned by
flow cytometry (Beckman-Coulter, Inc., Indianapolis,
IN) at 490 excitation and 530 emissions for green, and
at 540 excitation and 590 emissions for red. The ratios
of red/green fluorescent densities were calculated.
2.10 Statistical Analysis
All data were expressed as mean ± SD. from at least
three independent experiments, each performed in
quintuplicate.
3. Results and Analysis
3.1 Chemical Composition of AO-95
Comparing their GC-MS and NMR data with the
literature, the compounds isolated from AO-95 were
identified as 3-phenylpropanal (1) [15] and
4-phenylbutan-2-one (2) [15].
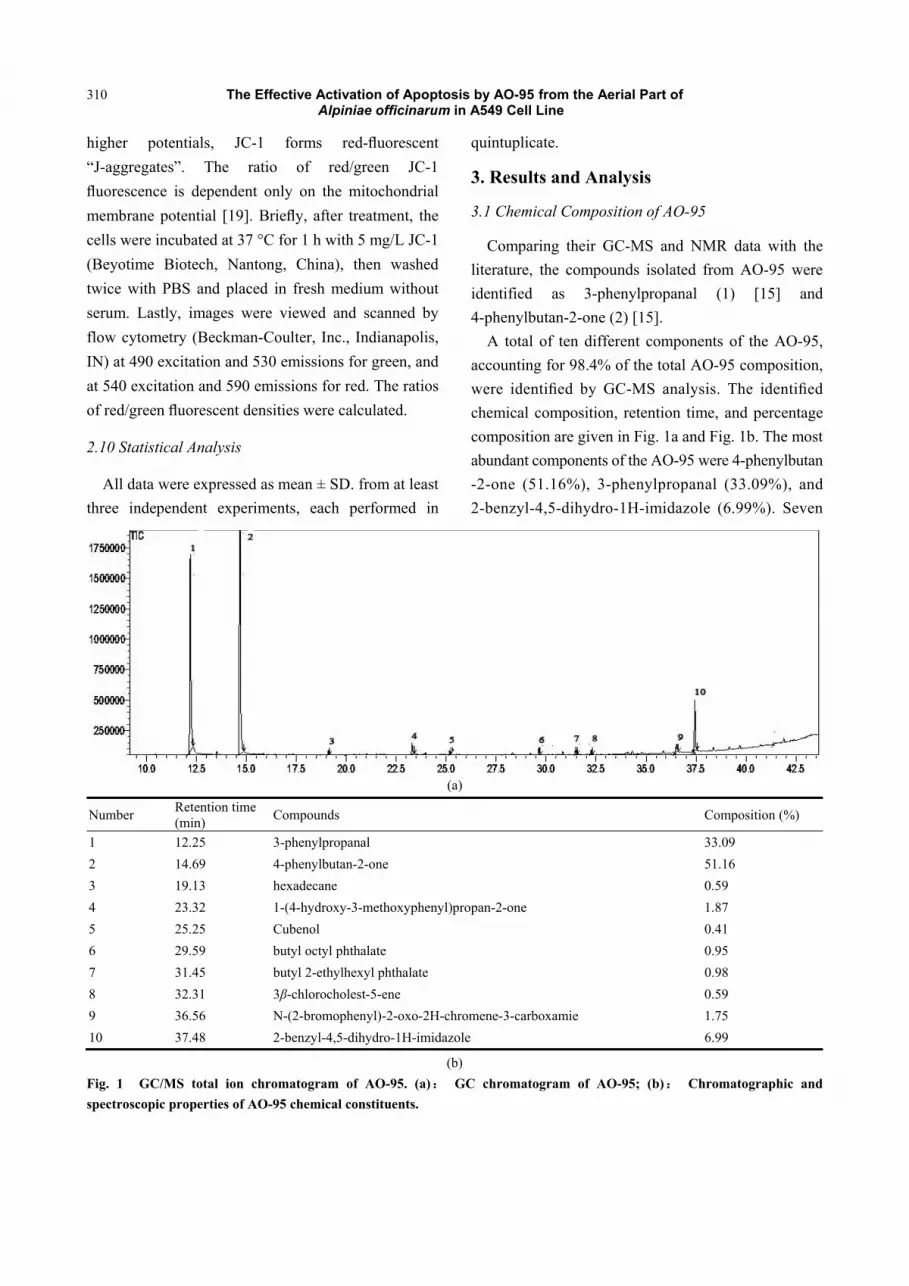
A total of ten different components of the AO-95,
accounting for 98.4% of the total AO-95 composition,
were identified by GC-MS analysis. The identified
chemical composition, retention time, and percentage
composition are given in Fig. 1a and Fig. 1b. The most
abundant components of the AO-95 were 4-phenylbutan
-2-one (51.16%), 3-phenylpropanal (33.09%), and
2-benzyl-4,5-dihydro-1H-imidazole (6.99%). Seven
(a)
Number Retention time (min)
Compounds Composition (%)
1 12.25 3-phenylpropanal 33.09
2 14.69 4-phenylbutan-2-one 51.16
3 19.13 hexadecane 0.59
4 23.32 1-(4-hydroxy-3-methoxyphenyl)propan-2-one 1.87
5 25.25 Cubenol 0.41
6 29.59 butyl octyl phthalate 0.95
7 31.45 butyl 2-ethylhexyl phthalate 0.98
8 32.31 3β-chlorocholest-5-ene 0.59
9 36.56 N-(2-bromophenyl)-2-oxo-2H-chromene-3-carboxamie 1.75
10 37.48 2-benzyl-4,5-dihydro-1H-imidazole 6.99
(b)
Fig. 1 GC/MS total ion chromatogram of AO-95. (a): GC chromatogram of AO-95; (b): Chromatographic and
spectroscopic properties of AO-95 chemical constituents.
The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
311
other components such as hexadecane (0.59%),
1-(4-hydroxy-3-methoxyphenyl) propan-2-one
(1.87%), Cubenol (0.41%), butyl octyl phthalate
(0.95%), butyl 2-ethylhexyl phthalate (0.98%),
3β-chlorocholest-5-ene (0.59%), and
N-(2-bromophenyl)-2-oxo-2H-chromene-3-carboxami
e (1.75%) were in less amounts. However, oxygenated
sesquiterpenes, sesquiterpene hydrocarbons, and others
were also found as trace or minor components.
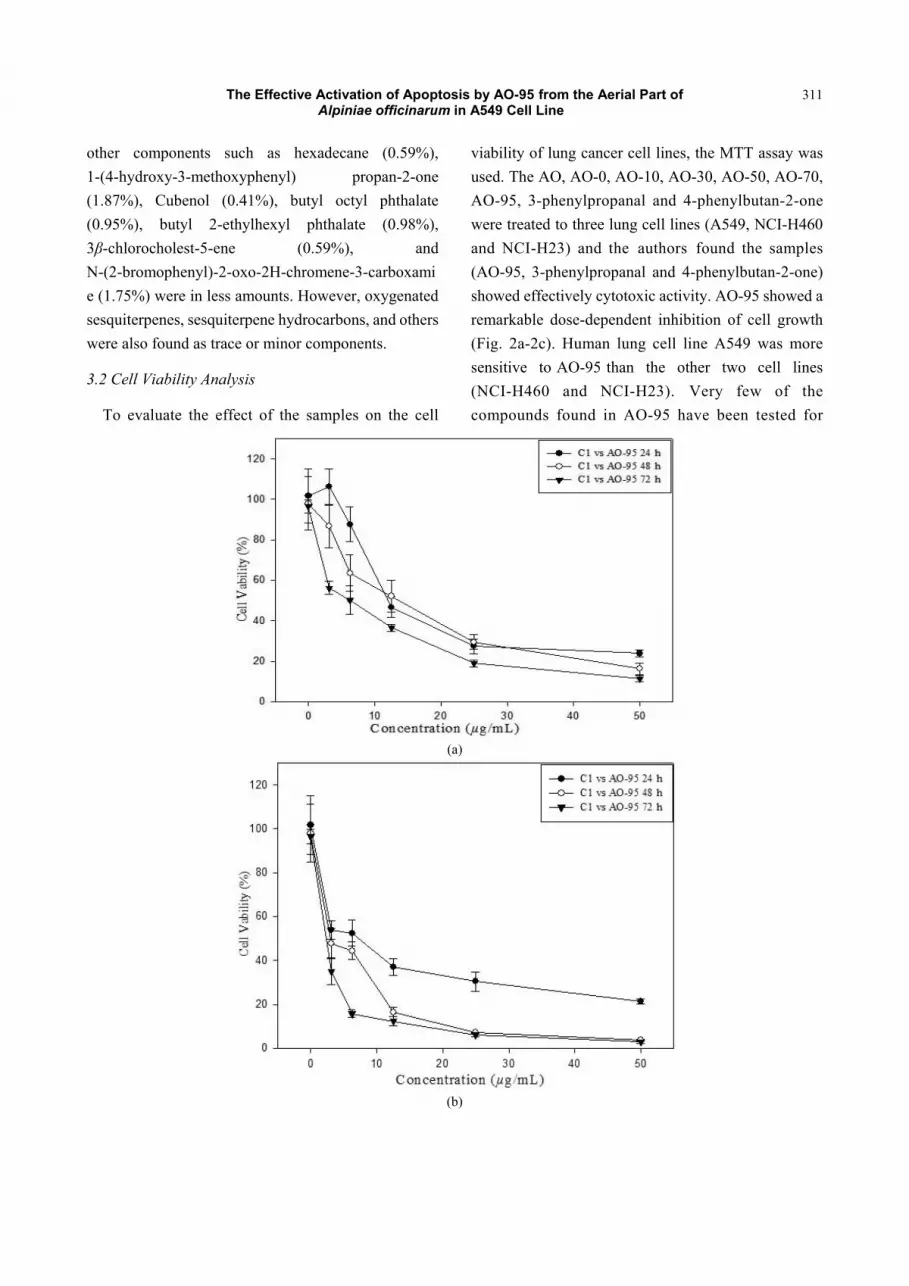
3.2 Cell Viability Analysis
To evaluate the effect of the samples on the cell
viability of lung cancer cell lines, the MTT assay was
used. The AO, AO-0, AO-10, AO-30, AO-50, AO-70,
AO-95, 3-phenylpropanal and 4-phenylbutan-2-one
were treated to three lung cell lines (A549, NCI-H460
and NCI-H23) and the authors found the samples
(AO-95, 3-phenylpropanal and 4-phenylbutan-2-one)
showed effectively cytotoxic activity. AO-95 showed a
remarkable dose-dependent inhibition of cell growth
(Fig. 2a-2c). Human lung cell line A549 was more
sensitive to AO-95 than the other two cell lines
(NCI-H460 and NCI-H23). Very few of the
compounds found in AO-95 have been tested for
(a)
(b)
The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
312
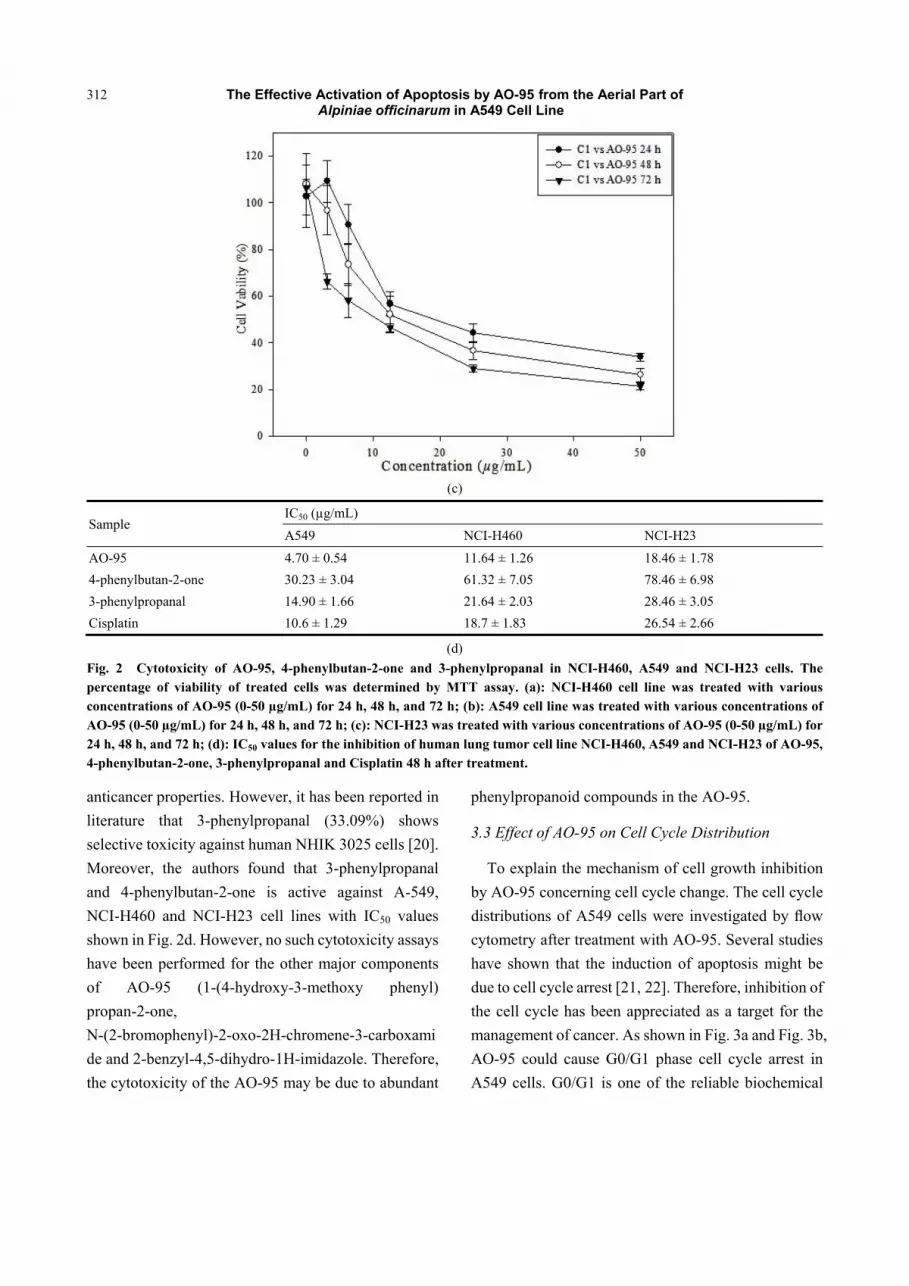
(c)
Sample IC50 (µg/mL)
A549 NCI-H460 NCI-H23
AO-95 4.70 ± 0.54 11.64 ± 1.26 18.46 ± 1.78
4-phenylbutan-2-one 30.23 ± 3.04 61.32 ± 7.05 78.46 ± 6.98
3-phenylpropanal 14.90 ± 1.66 21.64 ± 2.03 28.46 ± 3.05
Cisplatin 10.6 ± 1.29 18.7 ± 1.83 26.54 ± 2.66
(d)
Fig. 2 Cytotoxicity of AO-95, 4-phenylbutan-2-one and 3-phenylpropanal in NCI-H460, A549 and NCI-H23 cells. The percentage of viability of treated cells was determined by MTT assay. (a): NCI-H460 cell line was treated with various concentrations of AO-95 (0-50 µg/mL) for 24 h, 48 h, and 72 h; (b): A549 cell line was treated with various concentrations of AO-95 (0-50 µg/mL) for 24 h, 48 h, and 72 h; (c): NCI-H23 was treated with various concentrations of AO-95 (0-50 µg/mL) for 24 h, 48 h, and 72 h; (d): IC50 values for the inhibition of human lung tumor cell line NCI-H460, A549 and NCI-H23 of AO-95, 4-phenylbutan-2-one, 3-phenylpropanal and Cisplatin 48 h after treatment.
anticancer properties. However, it has been reported in
literature that 3-phenylpropanal (33.09%) shows
selective toxicity against human NHIK 3025 cells [20].
Moreover, the authors found that 3-phenylpropanal
and 4-phenylbutan-2-one is active against A-549,
NCI-H460 and NCI-H23 cell lines with IC50 values
shown in Fig. 2d. However, no such cytotoxicity assays
have been performed for the other major components
of AO-95 (1-(4-hydroxy-3-methoxy phenyl)
propan-2-one,
N-(2-bromophenyl)-2-oxo-2H-chromene-3-carboxami
de and 2-benzyl-4,5-dihydro-1H-imidazole. Therefore,
the cytotoxicity of the AO-95 may be due to abundant
phenylpropanoid compounds in the AO-95.
3.3 Effect of AO-95 on Cell Cycle Distribution
To explain the mechanism of cell growth inhibition
by AO-95 concerning cell cycle change. The cell cycle
distributions of A549 cells were investigated by flow
cytometry after treatment with AO-95. Several studies
have shown that the induction of apoptosis might be
due to cell cycle arrest [21, 22]. Therefore, inhibition of
the cell cycle has been appreciated as a target for the
management of cancer. As shown in Fig. 3a and Fig. 3b,
AO-95 could cause G0/G1 phase cell cycle arrest in
A549 cells. G0/G1 is one of the reliable biochemical
The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
313
AO-95 (0 µg/mL) AO-95 (3.125 µg/mL) AO-95 (6.25 µg/mL)
AO-95 (12.5 µg/mL) AO-95 (25 µg/mL) AO-95 (50 µg/mL)
(a)
Cell cycle Percentage (%)
0.5% DMSO
50 (µg/mL)
25 (µg/mL)
12.5 (µg/mL)
6.25 (µg/mL)
3.125 (µg/mL)
Apoptosis 0 9.507 0 0 0 1.976
Go/G1 55.871 64.323 62.753 61.218 55.037 54.685
s 35.575 24.534 32.548 32.703 32.962 34.963
G2/M 8.554 11.143 4.699 6.079 12.001 10.352
(b)
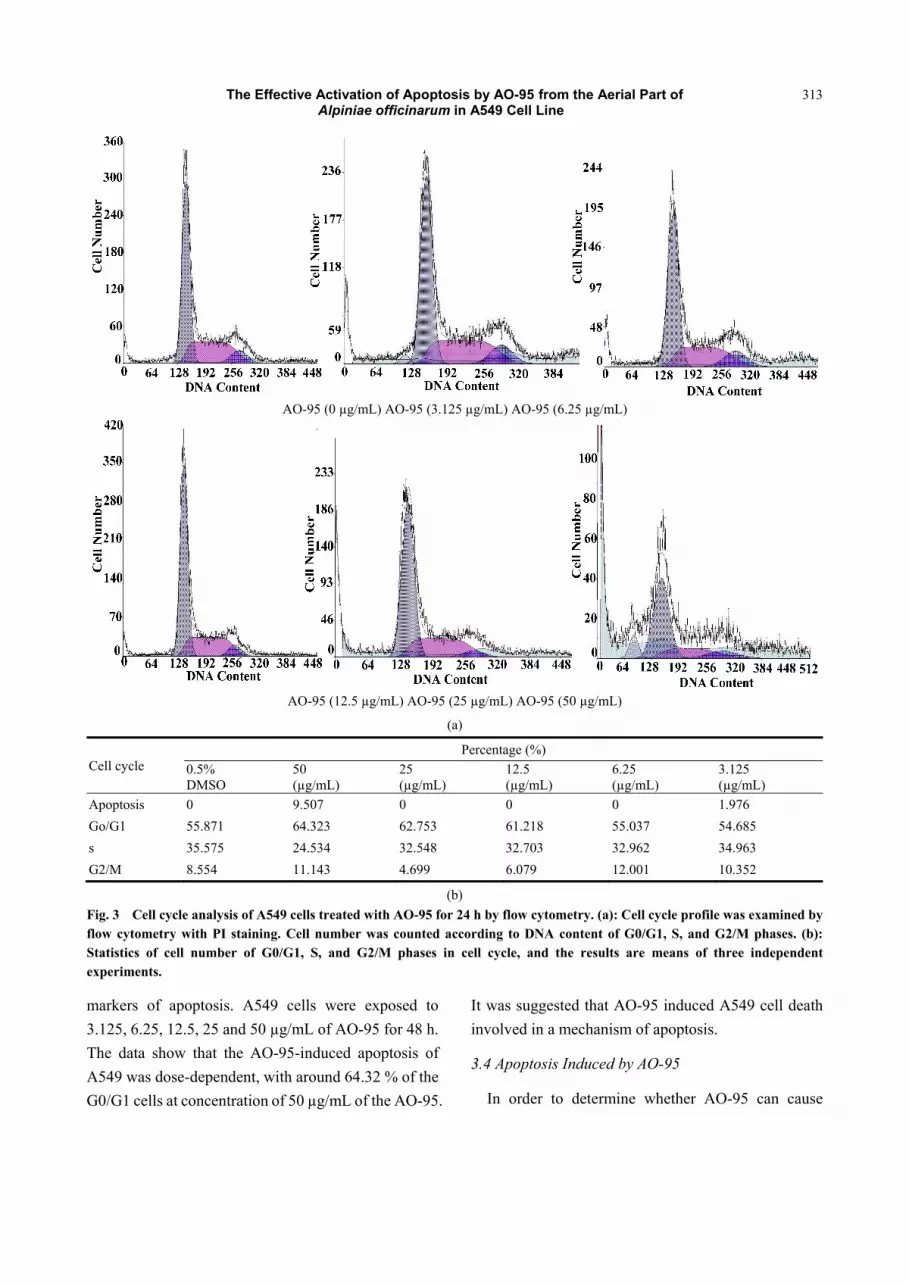
Fig. 3 Cell cycle analysis of A549 cells treated with AO-95 for 24 h by flow cytometry. (a): Cell cycle profile was examined by flow cytometry with PI staining. Cell number was counted according to DNA content of G0/G1, S, and G2/M phases. (b): Statistics of cell number of G0/G1, S, and G2/M phases in cell cycle, and the results are means of three independent experiments.
markers of apoptosis. A549 cells were exposed to
3.125, 6.25, 12.5, 25 and 50 µg/mL of AO-95 for 48 h.
The data show that the AO-95-induced apoptosis of
A549 was dose-dependent, with around 64.32 % of the
G0/G1 cells at concentration of 50 µg/mL of the AO-95.
It was suggested that AO-95 induced A549 cell death
involved in a mechanism of apoptosis.
3.4 Apoptosis Induced by AO-95
In order to determine whether AO-95 can cause
The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
314
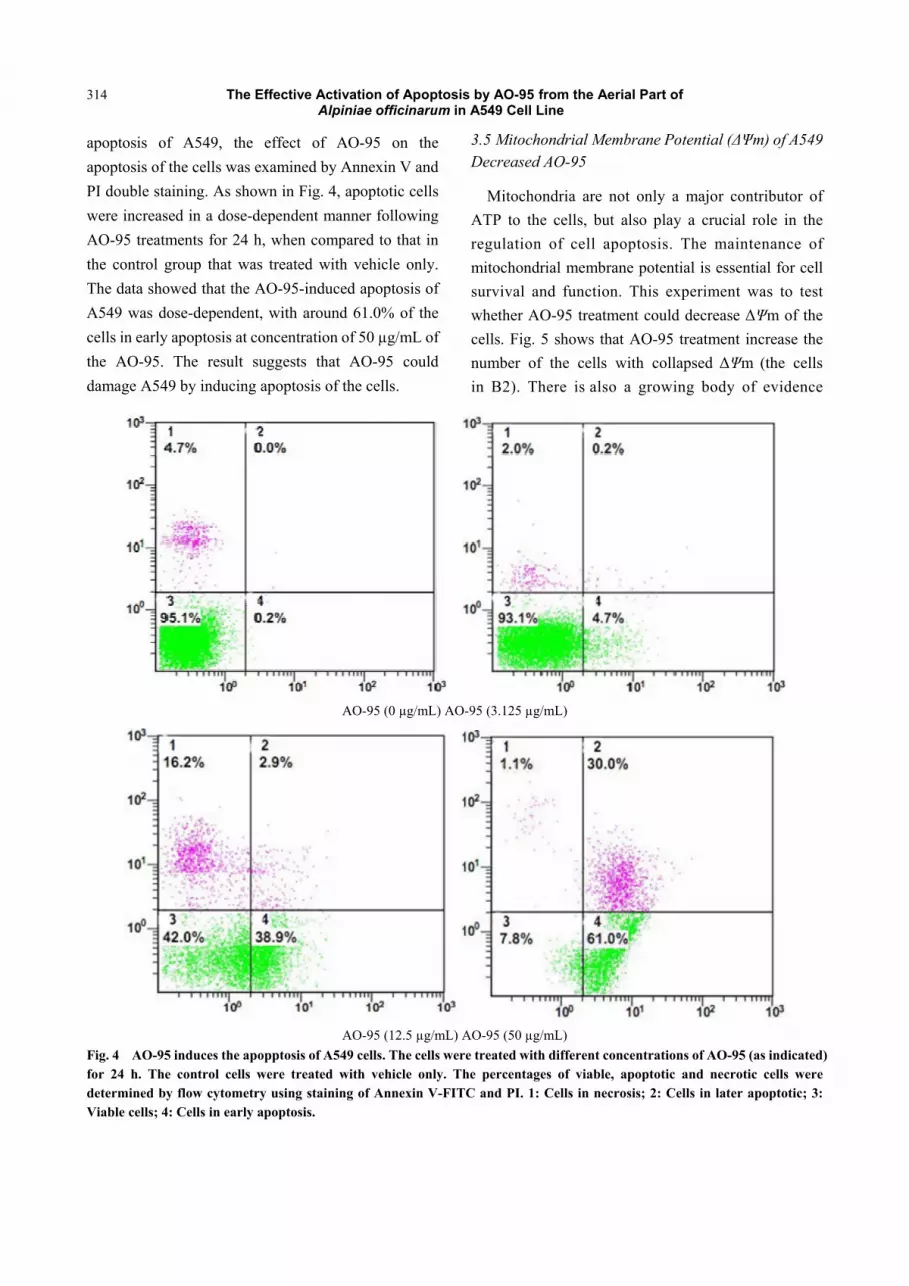
apoptosis of A549, the effect of AO-95 on the
apoptosis of the cells was examined by Annexin V and
PI double staining. As shown in Fig. 4, apoptotic cells
were increased in a dose-dependent manner following
AO-95 treatments for 24 h, when compared to that in
the control group that was treated with vehicle only.
The data showed that the AO-95-induced apoptosis of
A549 was dose-dependent, with around 61.0% of the
cells in early apoptosis at concentration of 50 µg/mL of
the AO-95. The result suggests that AO-95 could
damage A549 by inducing apoptosis of the cells.
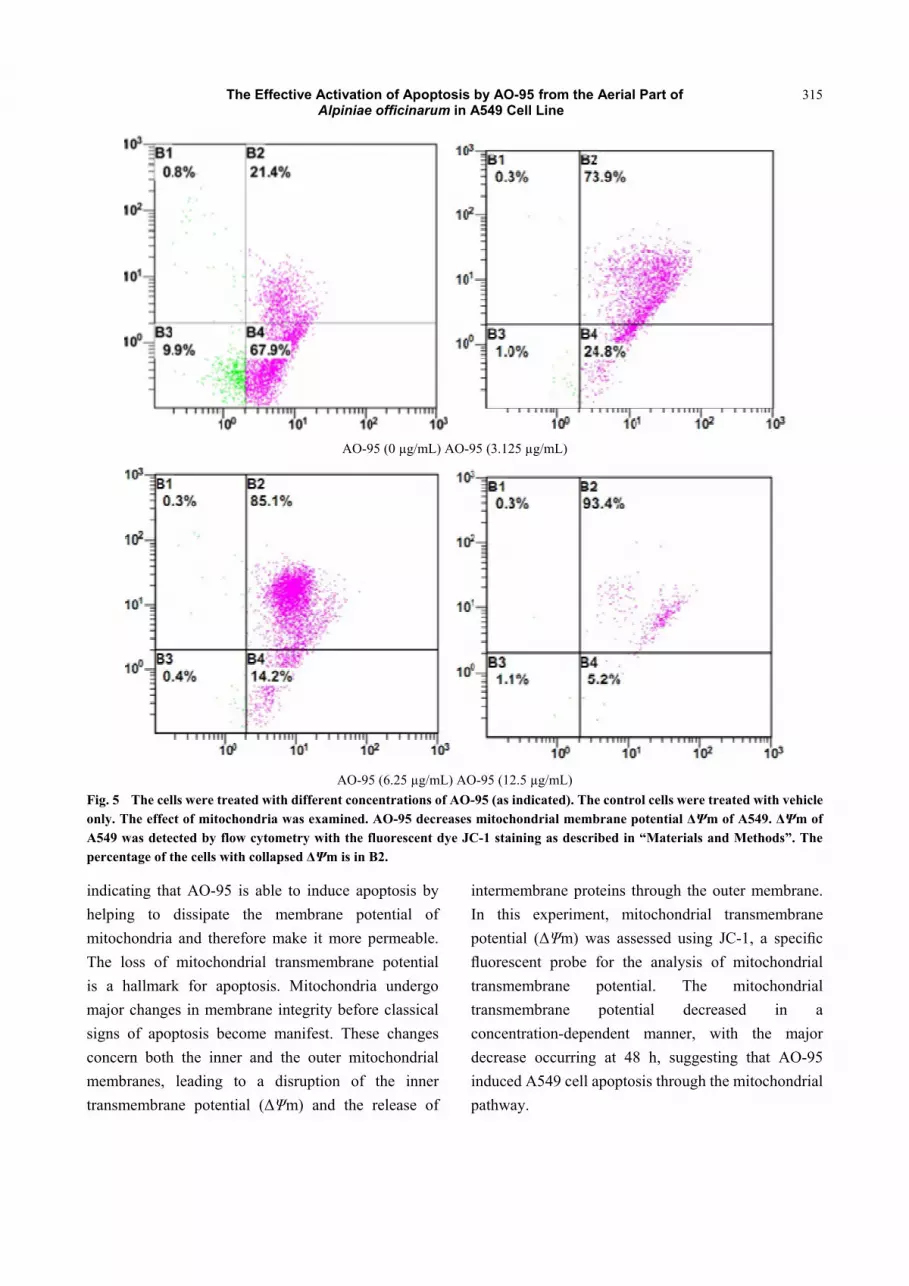
3.5 Mitochondrial Membrane Potential (ΔΨm) of A549 Decreased AO-95
Mitochondria are not only a major contributor of
ATP to the cells, but also play a crucial role in the
regulation of cell apoptosis. The maintenance of
mitochondrial membrane potential is essential for cell
survival and function. This experiment was to test
whether AO-95 treatment could decrease ΔΨm of the
cells. Fig. 5 shows that AO-95 treatment increase the
number of the cells with collapsed ΔΨm (the cells
in B2). There is also a growing body of evidence
AO-95 (0 µg/mL) AO-95 (3.125 µg/mL)
AO-95 (12.5 µg/mL) AO-95 (50 µg/mL)
Fig. 4 AO-95 induces the apopptosis of A549 cells. The cells were treated with different concentrations of AO-95 (as indicated) for 24 h. The control cells were treated with vehicle only. The percentages of viable, apoptotic and necrotic cells were determined by flow cytometry using staining of Annexin V-FITC and PI. 1: Cells in necrosis; 2: Cells in later apoptotic; 3: Viable cells; 4: Cells in early apoptosis.
The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
315
AO-95 (0 µg/mL) AO-95 (3.125 µg/mL)
AO-95 (6.25 µg/mL) AO-95 (12.5 µg/mL)
Fig. 5 The cells were treated with different concentrations of AO-95 (as indicated). The control cells were treated with vehicle only. The effect of mitochondria was examined. AO-95 decreases mitochondrial membrane potential ΔΨm of A549. ΔΨm of A549 was detected by flow cytometry with the fluorescent dye JC-1 staining as described in “Materials and Methods”. The percentage of the cells with collapsed ΔΨm is in B2.
indicating that AO-95 is able to induce apoptosis by
helping to dissipate the membrane potential of
mitochondria and therefore make it more permeable.
The loss of mitochondrial transmembrane potential
is a hallmark for apoptosis. Mitochondria undergo
major changes in membrane integrity before classical
signs of apoptosis become manifest. These changes
concern both the inner and the outer mitochondrial
membranes, leading to a disruption of the inner
transmembrane potential (ΔΨm) and the release of
intermembrane proteins through the outer membrane.
In this experiment, mitochondrial transmembrane
potential (ΔΨm) was assessed using JC-1, a specific
fluorescent probe for the analysis of mitochondrial
transmembrane potential. The mitochondrial
transmembrane potential decreased in a
concentration-dependent manner, with the major
decrease occurring at 48 h, suggesting that AO-95
induced A549 cell apoptosis through the mitochondrial
pathway.
The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
316
4. Conclusions
In the present study, the AO-95 could effectively
inhibit tumor growth in vitro. The results also indicate
that AO-95-induced apoptosis of A549 cells may
involve a mitochondrial-related pathway. Furthermore,
other pathways regulating apoptosis should be further
investigated. Also, AO-95 from the aerial part of A.
officinarum contains high phenylpropanoids (including
4-phenylbutan-2-one and 3-phenylpropanal).
Therefore, consumption of the aerial part of A.
officinarum may be an effective strategy for cancer
protection.
Acknowledgements
This research was partly supported by the Start Fund
of Guangdong Medical College (XB1302), National
Natural Science Foundation of China (31301585),
Science & Technology Innovation Fund of Guangdong
Medical College (STIF 201104), and Shenzhen basic
research project (JCYJ20120616142424467).
References
[1] Kiuchi, F., Shibuya, M., and Sankawa, U. 1982.
“Inhibitors of Prostaglandin Biosynthesis from Ginger.”
Chem. Pharm. Bull 30: 754-757.
[2] Shen, J., Zhang, H. Y., Xu, B., and Pan, J. X. 1998. “The
Antioxidative Constituents of Rhizomes of Alpinia
Offocinarum.” Nat. Prod. Res. Dev. 10: 33-36.
[3] Ali, M. S., Tezuka, Y., Banskota, A. H., and Kadota, S.
2001. “Blepharocalyxins C-E, Three New Dimeric
Diarylheptanoids, and Related Compounds from the Seeds
of Alpinia Blepharocalyx.” J. Nat. Prod. 64: 491-496.
[4] Heo, M. Y., Sohn, S. J., and Au, W. W. 2001.
“Anti-genotoxicity of Galangin as a Cancer
Chemopreventive Agent Candidate.” Mut. Res. 488:
135-150.
[5] Zhu, M., Lew, K. T., and Leung, P. 2002. “Protective
Effects of Plant Formula on Ethanol-Induced Gastric
Lesions in Rats.” Phytother. Res. 16: 276-280.
[6] Lu, W., and Jiang, L. H. 2006. “Chemical Constituents
and Pharmacological Activities of Alpinia Offcinarum
Hance.” Chin. Pharm 15: 19-21.
[7] Zhao, L., Qu, W., Fu, J. Q., and Liang, J. Y. 2010. “A New
Diarylheptanoid from the Rhizomes of Alpinia
Officinarum.” Chin. J. Nat. Med. 8: 241-243.
[8] An, N., Zhang, H. W., Xu, L. Z., Yang, S. L., and Zou, Z.
M. 2010. “New Diarylheptanoids from the Rhizome of
Alpinia officinarum Hance.” Food. Chem 119: 513-517.
[9] Liu, D., Qu, W., Zhao, L., and Liang, J. Y. 2012. “A Novel
Dimeric Diaryheptanoid from the Rhizomes of Alpinia
officinarum.” Chin. Chem. Lett 23: 189-192.
[10] Xu, S. M., Huang, X. J., Wang, Y., and Ye, W. C. 2012.
“A New Cadinane Sesequiterpene from the Rhizomes of
Alpinia officinarum.” Chin. J. Nat. Med. 10: 374-377.
[11] Ferlay, J., Shin, H. R., Bray, F., Forman, D., Mathers, C.,
and Parkin, D. M. 2010. “Estimates of Worldwide Burden
of Cancer in 2008: GLOBOCAN 2008.” Inter. J. Canc.
127: 2893-2917.
[12] He, X. J., Wang, Y. H., Hu, H., and Zhang, Z. X. 2012. “In
Vitro and In Vivo Antimammary Tumor Activities and
Mechanisms of the Apple Total Triterpenoids.” J. Agric.
Food Chem. 60: 9430-9436.
[13] Mancini, M., Anderson, B. O., Caldwell, E., Sedghinasab,
M., Paty, P. B., and Hockenbery, D. M. 1997.
“Mitochondrial Proliferation and Paradoxical Membrane
Depolarization During Terminal Differentiation and
Apoptosis in a Human Colon Carcinoma Cell Line.” J.
Cell. Biol. 138: 449-469.
[14] Eastman, A. 1993. “Apoptosis: A Product of Programmed
and Unprogrammed Cell Death.” Toxicol. Appl. Pharm.
121: 160-164.
[15] Adams, R. P. 2001. Identification of Essential Oils
Components by Gas Chromatography/Mass Spectroscopy.
Carol Stream, IL, USA: Allured Publishing Corporation.
[16] He, X. J., and Liu, R. H. 2007. “Triterpenoids Isolated
From Apple Peels Maybe Responsible for Their
Anticancer Activity.” J. Agric. Food. Chem. 55:
4366-4370.
[17] Yun, J. M., Afaq, F., Khan, N., and Mukhtar, H. 2009.
“Delphinidin, an Anthocyanidin in Pigmented Fruits and
Vegetables, Induces Apoptosis and Cell Cycle Arrest in
Human Colon Cancer Hct116 Cells.” Mol. Carcinog 48:
260-270.
[18] Chen, N. Y., Lai, H. H., Hsu, T. H., Lin, F. Y., Chen, J. Z.,
and Lo, H. C. 2008. “Induction of Apoptosis in Human
Lung Carcinoma A549 Epithelial Cells with an Ethanol
Extract of Tremella Mesenterica.” Biosci. Biotechnol.
Biochem. 72: 1283-1289.
[19] Reers, M., Smith, T. W., and Chen, L. B. 1991.
“J-aggregate Formation of a Carbocyanine as a
Quantitative Fluorescent Indicator of Membrane
Potential.” Biochem 30: 4480-4486.

The Effective Activation of Apoptosis by AO-95 from the Aerial Part of Alpiniae officinarum in A549 Cell Line
317
[20] Dornish, J. M., Pettersen, E. O., and Oftebro, R. 1989.
“Modifying Effect of Cinnamaldehyde and
Cinnamaldehyde Derivatives on Cell Inactivation and
Cellular Uptake of Cis-Diamminedichloroplatinum (П) in
Human NHIK 3025 Cells.” Canc. Res. 49: 3917-3921.
[21] Hartwell, L. H., and Kastan, M. B. 1994. “Cell Cycle
Control and Cancer.” Sci. 266: 1821-1828.
[22] Vermeulen, K., Berneman, Z. N., and Van Bockstaele, D.
R. 2003. “Cell Cycle and Apoptosis.” Cell. Prolif. 36:
165-175.
Journal of Health Science 2 (2014) 318-324
Changes of Immunoreactivity Status in Patients with
Osteosarcoma on the Background of Chemotherapy
Djamilya Sh. Polatova, Margarita S. Gildieva and Khurshid G. Abdikarimov Republican Oncology Research Center of the Ministry of Health of Uzbekistan, Tashkent, 100179, Uzbekistan Received: May 05, 2014 / Accepted: July 23, 2014 / Published: July 30, 2014. Abstract: Background: To study the features of cellular and humoral parameters of immune system in patients with osteosarcoma before and after chemotherapy. Methods: Clinical, laboratory, instrumental, immunological (immunofluorescence method, immunoassay analysis). Presented approved chemotherapy protocol for patients with osteosarcoma. Results: In all patients with osteosarcoma identified cell immunodeficiency and activation of humoral immunity factors before chemotherapy and significant increase of IgA and circulating immune complexes after chemotherapy. Conclusions: Imbalance in the immune system can serve as diagnostic and prognostic criterion of the disease on the background of chemotherapy. Key words: Cellular immunity, humoral immunity, osteosarcoma, immunoglobulins lymphocytes.
1. Introduction
Osteosarcoma-one of the most aggressive malignant
human tumors occurs mainly in adolescents, and
usually affects bones that form knee joint, and is
characterized by early hematogenous dissemination
[1-6]. Today one of the most promising directions of
modern oncology is to study the role of immune system
in the pathogenesis of malignant tumors. Over the last
20 years period of studying the role of immunology in
carcinogenesis obtained data supporting the role of
immune system in anticancer protection of organism,
there are studies on mechanisms leading to the
destruction of tumor cells and mechanisms of
phenomenon of immunological tolerance of tumor
cells [6, 7-11]. Thus, according to the literature, the
immune system of the body is essential in the
pathogenesis of malignant tumors, including
osteosarcoma [4, 5]. Nowadays, malignant bone
tumors present complicated and insufficient explored
problem. This is explained by rarity of their origin,
Corresponding author: Djamilya Sh. Polatova, Ph.D.,
research fields: skin, soft tissue, bone oncology. E-mail: [email protected].
biological features of this group of tumors and
connected with their pattern of clinical course,
approaches to diagnostics and therapy. It is known, that
bone malignant tumors are heterogeneous group of
nosological form of tumors. Mainly they were
presented by sarcomas with aggressive course, inclined
to early hematogenous metastasis and frequent
recurrence. In recent years, modern medicine has
achieved significant progress in the combined
treatment of bone tumors. At the same time, in spite of
dilation the complex treatment possibilities of applying
the new generation of chemotherapy remain unsolved
problem. Probably in most cases, it is associated with
the initial state of the immune system and tumor cell
resistance to drugs. It should be noted that, works on
the treatment of osteosarcomas are rare in the country
as well as abroad [2, 4, 11-15].
The purpose of research was to investigate the
characteristics of cellular and humoral immune system
parameters in patients with osteosarcoma before and
after chemotherapy.
2. Materials and Methods
The authors examined 42 patients with histological
DAVID PUBLISHING
D

Changes of Immunoreactivity Status in Patients with Osteosarcoma on the Background of Chemotherapy
319
verified osteosarcoma who were treated at the National
Cancer Center of Uzbekistan. Male patients
predominated, they were 28, and female patients are 14.
Average age of patients was 19.5 ± 0.6 years. In
majority of patients tumor was located on bones,
forming knee joint (77%). For the accurate definition
of prevalence of tumor process there was used
radiography or CT of thoracic organs and skeletal
scintigraphy. In National Cancer Center of Uzbekistan
there were confirmed different protocols of
preoperative chemotherapy up to 4 cycles by CAP
regimen (Cyclophosphamide 400-600 mg/m2,
Doxorubicin 50-60 mg/m2 and Cisplatin 100-120
mg/m2 intravenously during one day) or Doxorubicin
30 mg/m2 in 1-3 d, and also to the protocol inserted 72
hourly intra-arterial infusion of Doxorubicin 90 mg/m2
and Cisplatin 100-120 mg/m2 during the next 6 h.
Besides, according to the protocol patients were
inserted 72 hourly intra-arterial infusions of
Doxorubicin 90 mg/m2 and Cisplatin 100-120 mg/m2
during the next 6 h. Then local radiotherapy of total
focal dose (TFD) 36-40 Gy was performed. The next
stage was surgical removal of tumor-patients were
conducted organ conservative plastic-reconstructive
operations with replacement of defect with
endoprosthesis. There were provided from 6 to 9 cycles
of adjuvant chemotherapy after operation. At disease
progression patients underwent chemotherapy with
Iphosphamide 3 g/m2 in combination with Etoposide
150 mg/m2 during 3 d. Patient’s selection was carried
out according the tumor stage, spread, morphology and
age of examined patients.
Immunological investigations included study of
cellular and humoral parameter of patients’ immune
system with osteosarcoma before treatment and after
conduction of the first cycle of chemotherapy.
Immunological investigations were performed at the
Immunological Institute in the laboratory of
Immunocytokines. Determination of cellular immunity
(CD3+, CD4+, CD8+, CD16+, CD20+), and also
identification of activated markers of lymphocytes
(CD25+, CD38+ and CD95+) was carried out with
using of monoclonal antibodies with counting by
fluorescent microscope [16]. Humoral group of
immunity was assessed by definition of main serum of
immunoglobulins IgG, IgA and IgM in the serum of
peripheral blood with IFA method. Circulating
Immune Complexes (CIC) various measures defined
with spectrophotometer method [16]. Results of the
study were subjected to statistical analysis using the
Student-Fisher’s test, the data processed on PC using
soft Statistica-6. For clarity of obtained results all the
studied parameters of immune system were transferred
to percentage with respect to 100% for the norm.
3. Results and Discussion
Content of leukocytes insignificantly increased
before treatment in patients with osteosarcoma in
comparison control group. It should be noted that
reliable difference was observed in the group of
patients after the first cycle of chemotherapy with the
data of control group. General contents of leucocytes
was decreased up to 51% by attitude to 100% of control
group in the patients group with osteosacoma, that
conformed to 3275.8 ± 236.5 kL/mkL, at that time as
this index was equal to 6500 ± 295.0 kL/mkL (P < 0.05)
in control group (Diagram 1). It is known that leading
importance in antitumor protection of organism is
belonged to the cellular group of immunity, where the
T-lymphocytes play the key role. The authors also
analyzed the data by condition of lymphocytes of
peripheral blood. Investigation showed that authentic
repression of general number of lymphocytes was not
detected in patients with osteosarcoma before
treatment. As it can be seen from the table, percentage
of lymphocytes before chemotherapy compiled 91%.
Whereas after the first cycle of chemotherapy is
observed authentic increase of general number of
lymphocytes by compare with the data of control group
and groups of before treatment, which compiled 120%
regarding to control. So, comparative and absolute
content of lymphocytes were reliably increased after the
Changes of Immunoreactivity Status in Patients with Osteosarcoma on the Background of Chemotherapy
320
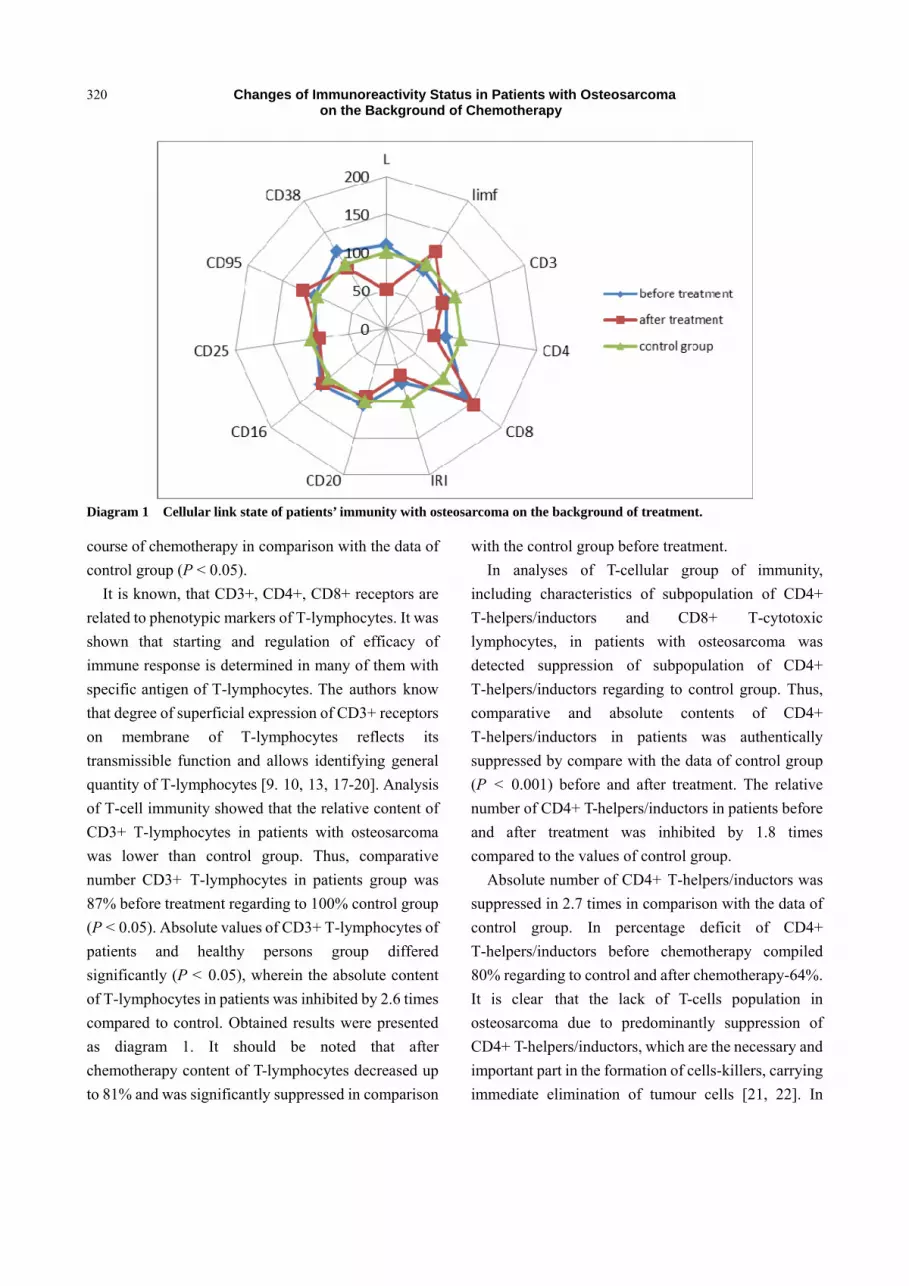
Diagram 1 Cellular link state of patients’ immunity with osteosarcoma on the background of treatment.
course of chemotherapy in comparison with the data of
control group (P < 0.05).
It is known, that CD3+, CD4+, CD8+ receptors are
related to phenotypic markers of T-lymphocytes. It was
shown that starting and regulation of efficacy of
immune response is determined in many of them with
specific antigen of T-lymphocytes. The authors know
that degree of superficial expression of CD3+ receptors
on membrane of T-lymphocytes reflects its
transmissible function and allows identifying general
quantity of T-lymphocytes [9. 10, 13, 17-20]. Analysis
of T-cell immunity showed that the relative content of
CD3+ T-lymphocytes in patients with osteosarcoma
was lower than control group. Thus, comparative
number CD3+ Т-lymphocytes in patients group was
87% before treatment regarding to 100% control group
(P < 0.05). Absolute values of CD3+ T-lymphocytes of
patients and healthy persons group differed
significantly (P < 0.05), wherein the absolute content
of T-lymphocytes in patients was inhibited by 2.6 times
compared to control. Obtained results were presented
as diagram 1. It should be noted that after
chemotherapy content of T-lymphocytes decreased up
to 81% and was significantly suppressed in comparison
with the control group before treatment.
In analyses of T-cellular group of immunity,
including characteristics of subpopulation of CD4+
Т-helpers/inductors and CD8+ Т-cytotoxic
lymphocytes, in patients with osteosarcoma was
detected suppression of subpopulation of CD4+
Т-helpers/inductors regarding to control group. Thus,
comparative and absolute contents of CD4+
Т-helpers/inductors in patients was authentically
suppressed by compare with the data of control group
(P < 0.001) before and after treatment. The relative
number of CD4+ T-helpers/inductors in patients before
and after treatment was inhibited by 1.8 times
compared to the values of control group.
Absolute number of CD4+ Т-helpers/inductors was
suppressed in 2.7 times in comparison with the data of
control group. In percentage deficit of CD4+
Т-helpers/inductors before chemotherapy compiled
80% regarding to control and after chemotherapy-64%.
It is clear that the lack of T-cells population in
osteosarcoma due to predominantly suppression of
CD4+ T-helpers/inductors, which are the necessary and
important part in the formation of cells-killers, carrying
immediate elimination of tumour cells [21, 22]. In

Changes of Immunoreactivity Status in Patients with Osteosarcoma on the Background of Chemotherapy
321
examining group of patient with osteosarcoma was
observed considerably increased expression of CD8+
in comparison with control group (P < 0.001) before
and after conducting of chemotherapy. Thus, relative
number of CD8+ Т-cytotoxic lymphocytes was
increased in 1.8 times before treatment but in the group
in 2.4 after chemotherapy in compare with control
group correspondingly. It is known that cytotoxic
CD8+ Т-lymphocytes play the important role in
pathogeneses of oncological diseases [23-25]. It was
established that the main function of cytotoxic
lymphocytes is their sharing in ensuring of antitumor
protection, which shows taken results [21, 25]. This
implies that correlation of CD4+/CD8+ (IRI) were
significantly differed from the data of control group
with significant suppression in the group of patients
before and after conducting of chemotherapy.
Individual amplitude of importance of IRI in patients
with osteosarcoma fluctuated from 0.4 to 1.14, but in
most part of patients IRI was lower than 1.0. In
percentage terms, it is obviously, that in the patients
before chemotherapy IRI was suppressed to 75%, but
in the group of after chemotherapy-64% regarding the
control group. Clearly, reducing the IRI observed due
to the suppression of the relative number of CD4+
T-lymphocytes and increase of relative content of
CD8+ T-lymphocytes. Consequently, in osteosarcoma
it is detected Т-cellular immune deficit, which was
connected with disbalance of the main immune
regulator subpopulation of Т-lymphocytes (CD4+
Т-helpers/inductors and CD8+ Т-cytotoxic
lymphocytes). It is known that CD16+ is membrane
low-affinity IgG-receptor of third type. At the stage of
activation of killer cells appear additional cofactors, in
presence of natural killers comes into cytolysis.
Apparently, in oncological process, in particularly in
osteosarcoma immunological surveillance at all stages
of development and functioning of the cells are
disturbed. Thus, analysis showed the presence of
significant changes were not detected in the group of
patients with control group before and after the
chemotherapy. It should be noted, that insignificant
increase the number of CD16+ is observed in the group
of patients in comparison with the data of control
before and after the treatment, although reliable
differences were not detected. By the data, some
energy is observed by killer cells concerning to
malignant cells (Diagram 1).
Also the authors studied activation markers of
peripheral blood lymphocytes in patients with
osteosarcoma. These markers began to be studied
relatively recently, so in the literature highlight a few
papers devoted to the study of their functional activity,
particularly in malignant processes, and this due to
their study in the research. Analysis of activated
markers of lymphocytes allows to study the processes
of activation, proliferations, differentiation and
apoptosis of immune competent cells [22, 24, 25].
Expression of CD25+, CD95+ and CD38+ were
studied from lymphocytes activation markers. It is
known, that receptor CD25+ presented with -chain,
which is expressed on activated Т-lymphocytes. In
activation of Т-lymphocytes, cytokine interleukin-2
plays the important role in development, maturation
and regulation of immune response, which supports the
proliferation of activated Т-lymphocytes and
B-lymphocytes [1]. Analysis of CD25+ expression on
lymphocytes did not detect the presence of authentic
differences between investigated groups. Thus,
expression of CD25+ in patients was differed in 1.2
times from the value of control group (Diagram. 1).
Expression of CD95+ on activated lymphocytes was
authentically increased in patients with osteosarcoma
after chemotherapy by compare with control group
correspondingly (P < 0.05), the contents of CD95+
before and after chemotherapy was increased to 103%
and 120%, correspondingly in comparison with control
group. It is obviously, that it was connected with the
process of apoptosis in immune competent cells, that is
explained appearing the immune deficit state.
Expression of CD38+ in lymphocytes of patients group
before and after chemotherapy composed 120% and
Changes of Immunoreactivity Status in Patients with Osteosarcoma on the Background of Chemotherapy
322
94%, correspondingly. It is known, that CD38+ is
precursor of Т- and В-lymphocytes [22, 25].
Humoral group of immunity was studied by
expression of markers CD20+ and B-lymphocytes and
by serum concentration of the main classes of
immunoglobulin IgA, IgG и IgM. Received data
showed that expression of CD20+ was insignificant
suppressed in the group of patients with osteosarcoma
after performing the first cycle of chemotherapy. The
authors detected, that the contents of CD20+ compiled
105% and 94%, correspondingly in comparison with
the control group before and after chemotherapy.
Immunoglobulins play an important intermediary
function in the cascade development of the immune
response and partially can condition the effectiveness
of final, effector responses of cellular immunity on the
inactivation and elimination of mutant cells [8, 10, 20].
It is known, that circulating antibody is one of their
effector factors of immunity, rendering antispecific
protection [24, 25]. Studying the concentration of
serum immunoglobulin allowed detecting disbalance
in the contents of main immunoglobulin after the
chemotherapy. The authors detected the reliable
increasing of IgА and prevalence of IgМ after
conducting chemotherapy. Content of IgА compiled
106% and 154%, in the group of patients before and
after chemotherapy, correspondingly in compare with
control group. IgМ level had not reliable differences in
control group before chemotherapy but after
chemotherapy its contents compiled 110% regarding
the control group.
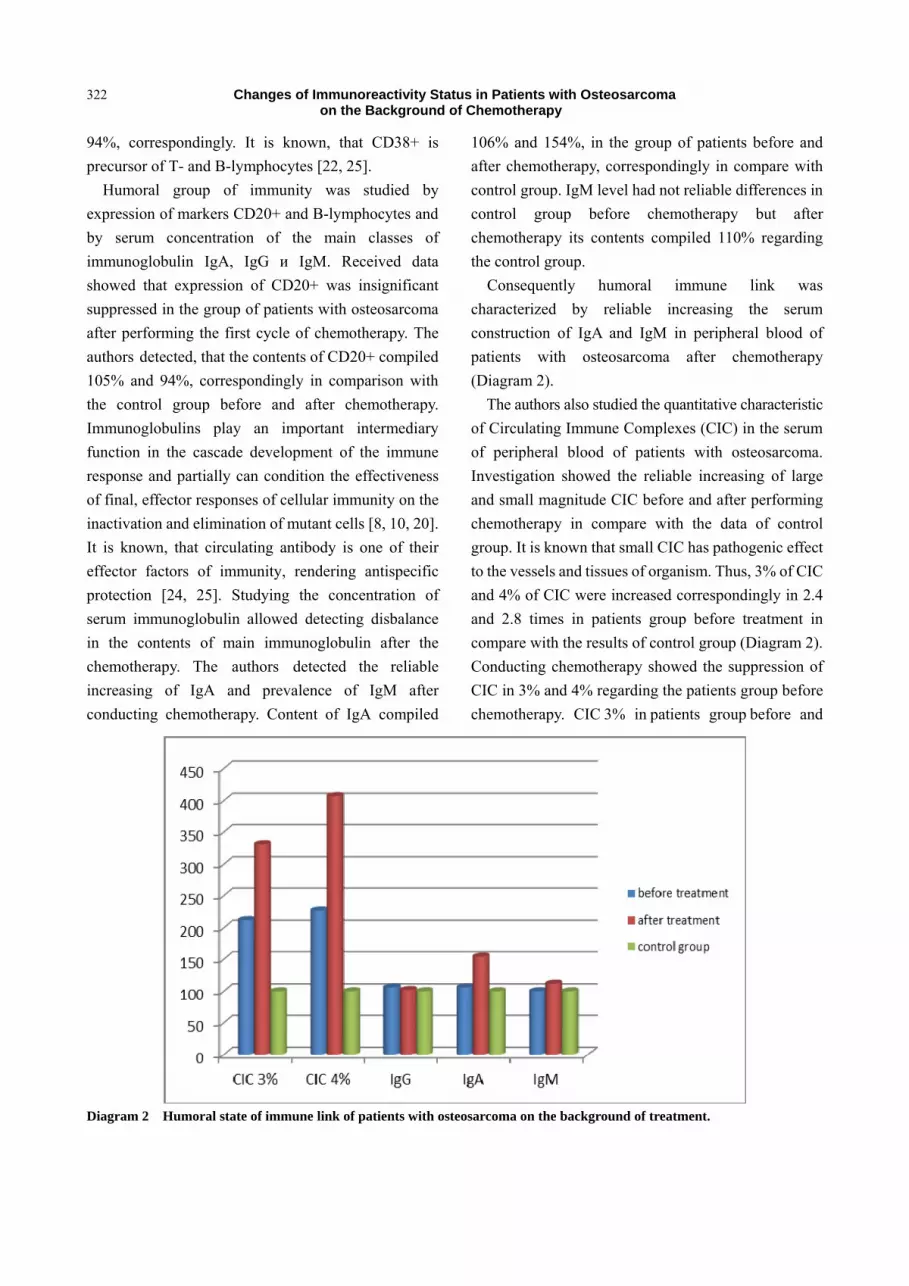
Consequently humoral immune link was
characterized by reliable increasing the serum
construction of IgA and IgМ in peripheral blood of
patients with osteosarcoma after chemotherapy
(Diagram 2).
The authors also studied the quantitative characteristic
of Circulating Immune Complexes (CIC) in the serum
of peripheral blood of patients with osteosarcoma.
Investigation showed the reliable increasing of large
and small magnitude CIC before and after performing
chemotherapy in compare with the data of control
group. It is known that small CIC has pathogenic effect
to the vessels and tissues of organism. Thus, 3% of CIC
and 4% of CIC were increased correspondingly in 2.4
and 2.8 times in patients group before treatment in
compare with the results of control group (Diagram 2).
Conducting chemotherapy showed the suppression of
CIC in 3% and 4% regarding the patients group before
chemotherapy. CIC 3% in patients group before and
Diagram 2 Humoral state of immune link of patients with osteosarcoma on the background of treatment.
Changes of Immunoreactivity Status in Patients with Osteosarcoma on the Background of Chemotherapy
323
after chemotherapy made up 212% and 331%,
according to relatively control group. But CIC 4%
made up 227% and 407%, correspondingly.
Consequently the authors detected activation of
humoral immune link (immunoglobulin A and
circulating immune complexes) independently from
performing chemotherapy, the greatest activation was
observed in patients group after conducting
chemotherapy.
4. Findings
(1) In patients with osteosarcoma was detected
T-cellular immune deficit, which is appeared by deficit
of CD4+ Т-helpers/inductors on the background of
increased number of CD8+ Т-lymphocytes.
(2) In the result of disbalance of subpopulation
T-lymphocytes it is marked significant decrease of
immune regulator index, which is the index of
inadequacy of immune response.
(3) Detected disbalance of humoral immune link
was intensified significant increase of immunoglobulin
A before the conducting of chemotherapy and CIC after
chemotherapy.
(4) From the side of activated markers are observed
suppression of functional activation of lymphocytes
after chemotherapy, except CD95+ marker of apoptosis,
which is increased and appeared forming of cellular
immune deficit after chemotherapy.
5. Conclusions
So, the authors have analyzed cellular and humoral
parameters of immune reactivity of patients with
osteosarcoma before and after chemotherapy. There has
been detected disbalance in the state of cellular and
humoral component of immunity before the starting of
chemotherapy in investigation. Increase the humoral
factors activity, in particularly immunoglobulin-A and
circulating immune complexes of great and small
magnitude was observed after conducting of
chemotherapy, practically in all patients with
osteosarcoma. Received data characterizes the
immunoreactivity state of patients with osteosarcoma
before and after treatment and can serve as diagnostic
and prognostic criteria of this disease on the
background of chemotherapy.
References
[1] Solovyev, Yu. N. 1993. “Bone Tumors.” In Pathologic
Anatomic Diagnostics of Human Tumor Guideline in 2
Books under Red, edited by Kraevskiy, N. A. Medicine.
[2] Trapeznikov, N. N., Erenina, L. A., Kutateladze, T. O.,
and co-authors, 1984. “Survival and Prognoses in the
Condition of Adjuvant Chemotherapy in Patients with
Osteogenic Sarcoma.” Questions of Oncology 30 (7):
33-40.
[3] Trapeznikov, N. N., Dolgushin, B. I., and Ishankhodjaev,
U. U. 1993. “Intraarterial Infusion and the Level of Blood
Circulation of Tumor in Osteogenic Sarcoma.” Reporter
ОSC RАМS 1: 40-42.
[4] Trapeznikov, N. N., Solovyev, Yu. N., and Yeremina, L.
A. 1993. “Progress in the Treatment of Osteogenic
Sarcoma.” Reporter ОSC RАМS 1: 3-9.
[5] Trapeznikov, N. N., Aliev, М .D., and Solovyev, Yu. N.
2001. “Osteosarcoma of Extremities Treatment During
The Century (Semi-Centennial Experience).” Reporter
RАМS 9: 46-49.
[6] Seshkovskiy, M. S. 1978. Primary Malignant Tumor of
Bones (Clinical-Rengeno-Morphological Investigation).
Moscow: Diss. M.D.
[7] Anichkov, N. M. 2005. “Pathogenesis of Cachexia in
Malignant Tumors.” Archive of pathology 67 (5): 51-56.
[8] Bogatirev, V. N. 1991. Value of Quantitative Methods of
Investigation (Morphometry, Flow Cytometry,
Microdencytometry) in Clinical Oncocytology. Moscow:
Dissert. Doct. Med. Sciences.
[9] Kadagidze, Z. G. 1994. “Subpopulation of Lymphocytes
in Malignant Growth.” Questions on Oncology 30 (1):
28-29.
[10] Ketlinskiy, S. A. 2002. “The Role of T-helpers Types 1
and 2 in Regulation Cellular and Humoral Immunity.”
Immunology 23 (2): 77-79.
[11] Trapeznikov, N. N., Erenina, L. A., and Kondratyev, V. G.
1981. “Combined Methods of Osteogenic Sarcoma
Treatment: Past Experience and Perspectives for The
Future.” Reporter АМS USSR 7: 65-69.
[12] Moisenko, V. M. 2002. “Pecularities Monoclonal
Antibodies in the Treatment of Malignant Tumors.”
Practical Oncology 3 (4): 253-261.
[13] Sinyukov, P. A. 1993. Up to Date Approaches to
Chemotherapy of Osteogenic Sarcoma, Abstract Dis.
M.D., Moscow.

Changes of Immunoreactivity Status in Patients with Osteosarcoma on the Background of Chemotherapy
324
[14] Abe, S., Higaki, S., Ogawa, К. 1997. “Long Term Intensive Chemotherapy For Osteosarcoma Around The Knee–Can We Minimize the Surgical Margins and Preserve the Joint?” In Proceedings of. ISOLS meeting, New York, 179-180.
[15] Ayala, A. G., Ro Jy, and Raymond, A. K. 1996. “Chemotherapy Induced Tumor Necrosis in Conventional Osteosarcoma of Bone: An Important Prognostic Factor.” In Proceedings of 2 Osteosarcoma Research Conference, Bologna, 91.
[16] Zalyalieva, M. V., and Prokhorova, P. S. 2001. Determination methods of subpopulation of lymphocytes. №1 DP 20000774 D/P МКП 6601 №33/48 26.02.2001.
[17] Afonina, G. B., and Bordonos, V. G. 1990. “Change of Membranes Structures and Function of Lymphocytes and Neutrophilic Granulocytes in Norm and Pathology.” Immunology and Allergology 24: 103-105.
[18] Ilina, N. I., Latisheva, T. B., Pinegin, B. V., and Setdikova, N. Kh. 2000. “Secondary Immune Deficiency Syndrome (Protocols of Diagnostics and Treatment).” Immunology 5: 8-9.
[19] Imelbaeva, E. A., Khayrulina, R. M., Medvedev, Y. A., Aznabaeva, L. F., and Gilmanov, A. J. 2004. “Methodical Indications to the Lessons in Immunology and Serology:
Educational-methodical Manual for Specialists in Clinical Laboratory Diagnostics.” Ufa: BSMU.
[20] Pinegin, B. V., and Khaitov, R. M. 1997. “Immundiagnostics of Disease, Connected with Immune Disorders.” Hemotology and Transfusiology 42 (2): 40-44.
[21] Cheredeyev, A. N., Gorlina, N. K., and Kozlov, I. G. 1999. “CD-markers in Practice of Clinical-Diagnostic Laboratory.” Clinical Laboratory of Diagnostics 6: 25-31.
[22] Chukhlovin, A. B. 1999. “Increase the Apoptosis of Leucocytes in Peripheral Blood Due to the Development of Leucopenia after Intensive Chemotherapy.” Questions of Oncology 45 (4): 384-387.
[23] Solovyev, Yu .A. 2000. “Cytokin Production in Patients VID in Dynamics of Immunocorrelating Therapy.” Allergology and Immunology 1 (2): 34.
[24] Filchenkov, A. A., Stepanov, Y. M., Lipkin, V. M., and Kushlinskiy, N. E. 2002. “Participation of Systems FAS/FAS-ligand in Regulation of Homeostases and Functioning of Immune System Cells.” Allergology and Immunology 3 (1): 24-35.
[25] Freidlin, I. S., Kuznetsova, S. A. 1999. Immune Complexes and Cytokines, Medical Immunology 1 (1-2): 27-36.

Journal of Health Science 2 (2014) 325-329
From Awareness to Action Using the Survey Feedback
Method
Ann Fridner1, 2, Birgit Pingel1, Lise Tevik Løvseth3, Marie Gustafsson Sendén1, 2 and Karin Schenck-Gustafsson2
1. Department of Psychology, Centre of Gender Medicine, Karolinska Institutet, Stockholm University, Stockholm, SE-10691,
Sweden
2. Centre of Gender Medicine, Karolinska Institutet, and Cardiac Unit, Department of Medicine, Karolinska University Hospital,
Stockholm, SE-10691, Sweden
3. Department of Research and Development Trondheim, St. Olavs University Hospital, Norway
Received: June 17, 2014 / Accepted: July 18, 2014 / Published: July 30, 2014. Abstract: Reports from European university hospitals show an increase in work-related mental strain. Four European university hospitals started a comprehensive research program called Health and Organisation among University hospitals Physicians in Europe—the HOUPE Study in the year 2003. Based on the results from the HOUPE study, the authors conducted an intervention project together with HR-consultants at one of the participating hospitals. A collected cross-sectional survey in 2005 among permanently employed academic physicians (N = 1800, response rate 60%) at Karolinska University Hospital in Sweden. Results from the study were used in survey feedback seminars (N = 250). This method is a way of systematic collection of data to process and give feedback to the organisation’s members in order to initiate organisational change. By providing results based on the total sample, on each division, and unpublished data from each clinic the authors aimed to improve physicians’ health and work satisfaction and thereby enhance the health of the physicians. Feedback seminars can arouse many emotions and might make people defensive. The role of resistance in the process of change is a paradox in that resistance slows down change. However, without resistance there will be no change at all. The authors conducted 20 feedback seminars of three hours duration where results were discussed relating mainly to the psychosocial work environment, psychological distress, and career paths, i.e., job demands, control at work, social interactions, leadership, commitment to the organisation, harassment at work, burnout, depression and suicide ideation. Altogether, 250 physicians participated in these meetings. To achieve acceptance for organisational change, data about relevant conditions in the organisation have to be processed in a systematic way in collaboration with all those who will benefit from changes, in concrete work units as divisions and clinics. Key words: Work interventions, HR-consultants, physician health.
I. Introduction
Reports from European university hospitals show an
increase in work-related mental strain, and increased
turnover rates among university hospitals physicians [1,
2]. Physicians face a heavy burden of work stressors,
whose contribution to psychological distress is
increasingly [3]. Physicians are at risk of burnout,
depression, and suicide [4, 5]. Physicians who are
mentally distressed are more likely to report making
Corresponding author: Ann Fridner, Ph.D., associated
professor, research fields: public health, work and organizational psychology, clinical psychology, gender medicine. E-mail: [email protected].
recent medical errors, to score lower in assessments
measuring empathy, to plan to retire early, and to have
higher job dissatisfaction, which have been associated
with reduced patient satisfaction [6-8]. Physicians seek
help to a lesser degree and later in the course of disease
than do other groups, and they appear to be especially
reluctant to seek help for mental health problems due to
concerns about confidentiality [9, 10].
Academic medicine is responsible for several
important tasks associated with improving the health of
the public, such as education, patient care, and clinical
research. Recent research has shown an increased
attrition from positions in academic medicine [11]. In
DAVID PUBLISHING
D

From Awareness to Action Using the Survey Feedback Method
326
2003, four university hospitals started a comprehensive
research program called Health and Organisation
among University hospitals Physicians Europe—The
HOUPE study. This project aims to provide a
systematic investigation of how research activity, work
conditions, gender equality, and career advancement,
affect the health and wellbeing of physicians. Based on
the results from the HOUPE study the authors
conducted an intervention project with academic
physicians at Karolinska University Hospital in
Sweden. By presenting data from different
organisational levels within one hospital, the authors
aimed to ameliorate working conditions and thereby
enhance the health of physicians. When data are seen as
objective and specific, new social facts about one’s
own organisational situation become a more significant
force for change than general principles about human
behaviour used in psychology theory. For participants,
the more meaningful, relevant and understandable the
material is, the greater the likelihood of change [12].
Past literature on survey feedback often deals with
how to change opinions and attitudes of individuals in
different organisations in a top-down fashion. The
employee is expected to experience the organisation
and the working environment in a new way [13], and
thereby be able to create and implement changes in the
workplace. The current project primarily used a
bottom-up design in which the authors obtained a
record of the physicians’ experiences of their work
environment and their suggestions for changes as
outcome. The study was interactive and the researchers
sought knowledge together with those concerned.
Assessment of wellbeing using valid instruments
creates a common language that can help physicians
and their organisation to address well-being issues.
2. Case Description
The authors used a cross-sectional survey among
academic physicians permanently employed at a
governmental university hospital in Sweden (N = 1800,
response rate 60 %). Assessment instruments:
Physician Career Path Questionnaire, General Health
Questionnaire-12, Mini Oldenburg Burnout Inventory,
Question About Suicidal Ideation and Attempted
Suicide, and selected scales from the Questionnaire
about Psychological and Social Factors at Work
[14-18]. All scales are presented in Fridner, et al. [4, 5,
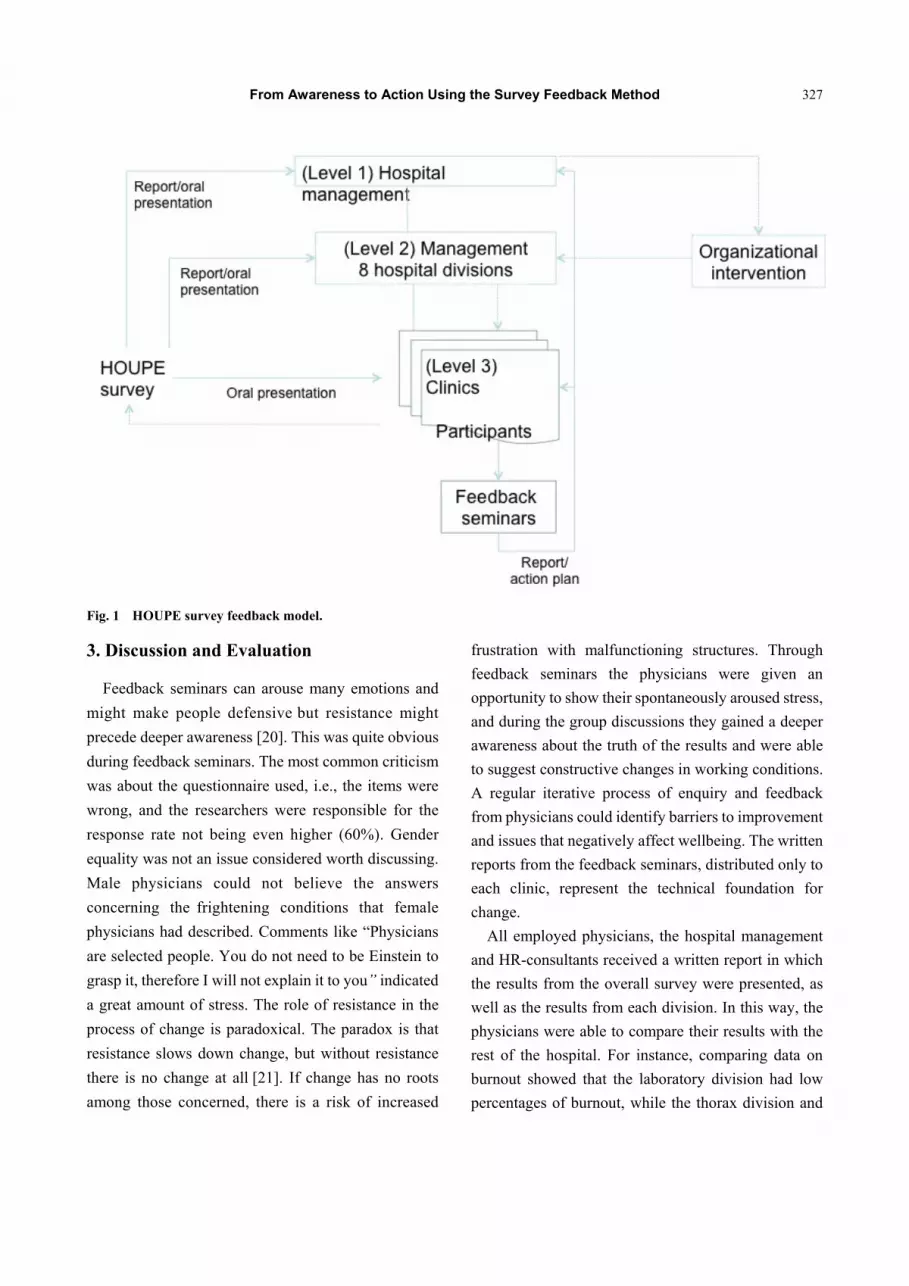
9]. The results of the survey were presented (Fig. 1)
during meetings with: the management of the hospital
(level 1), management of eight divisions (level 2), the
local medical association, and the HR departments
(level 1 and 2). Written reports were distributed to
levels one and two [19]. The third level included clinics
with at least 50 physicians before data were presented.
If fewer physicians were working in the clinic, clinics
were merged. Clinical data were only presented during
the feedback meetings.
The survey feedback method means making a
systematic collection of data, which is then processed
and fed back to the organisation’s members. A
distinction is made between a top-down and a
bottom-up method. In the project, the authors used both
top-down and bottom-up methods, i.e., the authors
started by giving back compiled data to the
management of the hospital, management of the eight
divisions, the local physician’s association and the
central HR-department. Then physicians working in all
clinics were invited to participate in a survey feedback
seminar with the aim of suggesting changes in their
own work places as well as in the organisation.
Seminar proceedings were as follows:
Introduction by the head of clinic and
HR-consultant
Presentation of results (researcher)
Group discussions
- How the physicians think and feel regarding the
responses they have studied today.
- What are the physicians good at, and what can
they do better?
All groups presented their discussions
A researcher from HOUPE documented the
seminars and wrote a report on each
From Awareness to Action Using the Survey Feedback Method
327
Fig. 1 HOUPE survey feedback model.
3. Discussion and Evaluation
Feedback seminars can arouse many emotions and
might make people defensive but resistance might
precede deeper awareness [20]. This was quite obvious
during feedback seminars. The most common criticism
was about the questionnaire used, i.e., the items were
wrong, and the researchers were responsible for the
response rate not being even higher (60%). Gender
equality was not an issue considered worth discussing.
Male physicians could not believe the answers
concerning the frightening conditions that female
physicians had described. Comments like “Physicians
are selected people. You do not need to be Einstein to
grasp it, therefore I will not explain it to you” indicated
a great amount of stress. The role of resistance in the
process of change is paradoxical. The paradox is that
resistance slows down change, but without resistance
there is no change at all [21]. If change has no roots
among those concerned, there is a risk of increased
frustration with malfunctioning structures. Through
feedback seminars the physicians were given an
opportunity to show their spontaneously aroused stress,
and during the group discussions they gained a deeper
awareness about the truth of the results and were able
to suggest constructive changes in working conditions.
A regular iterative process of enquiry and feedback
from physicians could identify barriers to improvement
and issues that negatively affect wellbeing. The written
reports from the feedback seminars, distributed only to
each clinic, represent the technical foundation for
change.
All employed physicians, the hospital management
and HR-consultants received a written report in which
the results from the overall survey were presented, as
well as the results from each division. In this way, the
physicians were able to compare their results with the
rest of the hospital. For instance, comparing data on
burnout showed that the laboratory division had low
percentages of burnout, while the thorax division and
From Awareness to Action Using the Survey Feedback Method
328
oncology division had higher rates. In all, 250
physicians participated in a three-hour survey feedback
seminar.
The HOUPE project manager, the head of clinic, and
the HR-consultant were responsible for the feedback
process at each clinic. Feedback meetings were held to
discuss results related mainly to the psychosocial work
environment, psychological distress and career paths,
i.e., job demands, control at work, social interactions,
leadership, commitment to the organization,
harassment at work, burnout, depression and suicide
ideation. Out of 27 invited clinics/merged clinics, 20
were participating in feedback meetings at the hospital.
It was recommended that feedback seminars should
lead to a written action plan specifying concrete
specific activities, which should be integrated in the
different clinics’ action plans. An action plan with
concrete activities enhances the improvements regarding
factors in the work organisation [22]. Researchers
documented the seminars and wrote written reports for
each of them. A composite report presented the
feedback processes during all meetings [23].
What this paper adds
It demonstrates how the feedback process is original
by:
(1) Showing the resistance, anger and stress about
the survey results.
(2) Addressing results in a constructive way.
(3) Showing that written reports and informative
meetings with HR-consultants, head of clinics and
research team together with the physicians provide a
basis for joint efforts towards change.
4. Funding
AF: Vinnova (Dnr 2002-01943, 2005-00749,
2008-02262) and KSG: Centre of Gender Medicine,
Karolinska Institutet and Erica Lederhausen foundation.
5. Competing Interests
There is no competing interest for any of the
authors (neither financial nor other).
6. Authors’ contribution
AF designed the study. AF, KSG and LTL were
responsible for data collection and are guarantors of the
study. AF and LTL prepared the data sets. AF, BP and
MGS reviewed the literature. AF and BP conducted the
interventions, and wrote the drafts of the manuscripts.
All authors read and approved the final manuscript.
Acknowledgement
The authors are grateful to the physicians who
participated in this study. The authors thank the entire
HOUPE Study Research Group.
References
[1] Misra-Hebert, A. D., Kay, R., and Stoller, J. K. 2004. “A Review of Physician Turnover: Rates, Causes, and Consequences.” Am J Med Qual 19: 56-66.
[2] Wallace, J. E., Lemaire, J. B., and Ghali, W. A. 2009. “Physician Wellness: A Missing Quality Indicator.” Lancet 374: 1714-1721.
[3] Tyssen, R. 2007. “Health Problems and the Use of Health Services among Physicians: A Review Article with Particular Emphasis on Norwegian Studies. [Review].” Ind Health 45: 599-610.
[4] Fridner, A., Belkic, K., Marini, M., Minucci, D., Pavan, L., and Schenck-Gustafsson, K. 2009. “Survey on Recent Suicidal Ideation among Female University Hospital Physicians in Sweden and Italy (The Houpe Study): Associations with Work Stressors.” Gender Medicine 6: 314-328.
[5] Fridner, A., Belkic, K., Minucci, D., Marini, M., Putoto, G., Simonato, P., and Schenck-Gustafsson, K. 2011. “Work Environment and Recent Suicidal Thoughts among Male University Hospital Physicians in Europe (HOUPE) Study.” Gender Medicine 8: 269-279.
[6] Taylor, C., Graham, J., Potts, H., Candy, J., Richards, M., and Ramirez, A. 2007. “Impact of Hospital Consultants´Poor Mental Health on Patient Care.” BMJ 190: 268-269.
[7] Leiter, M. P., Frank, E., and Marheson, T. J. 2009. “Demands, Values, and Burnout. Relevance for Physicians.” Can Fam Physician 55:1224-5.e1-6.
[8] Orton, P., Orton, C., and Gray, D. P. 2012. “Depersonalised Doctors: a Cross-Sectional Study of 564 doctors, 760 Consultations and 1876 Patient Reports in Uk General Practice.” BMJ Open 2: e000274.
[9] Fridner, A., Belkić, K., Marini, M., Gustafsson Sendén, M., and Schenck-Gustafsson, K. 2012. “Why Don´t
From Awareness to Action Using the Survey Feedback Method
329
Physicians Seek Needed Professional Help for Mental Distress?” Swiss Med Wkly 142: w13626.
[10] Løvseth, L. T., Aasland, O. G., Fridner, A., Schenck-Gustafsson, K., Jónsdóttir, L. S., Einarsdóttir, T., Marini, M., Minucci, M., Pavan, L., Götestam, K. G., and Linaker, O. M. 2013. “Psychosocial Work Factors as Moderators of Confidentiality as a Barrier to Seeking Social Support. A Cross-Sectional Study of University Hospital Physicians in Four European Cities [the HOUPE Study].” Work 09/2013; doi:10.3233/WOR-131725.
[11] Pololi, L., Krupat, E., and Brennan. R. 2012. “Why Are A Quarter of Faculty Considering Leaving Academic Medicine? A Study of Their Perceptions of Institutional Culture And Intenion to Leave at 26 Representative U.S. Medical schools.” Academic Medicine 87: 858-869.
[12] Mann, C., F. 1961 Studying and Creating Change. In the planning of change, edited by Bennis, W. G., Benne, K. D., and Chin. R. New York: Holt, Rinehart, and Winston.
[13] Elo, A-L., Leppänen, A., and Sillanpä, P. 1998. “Applicability of Survey Feedback for an Occupational Health Method in Stress Management.” Occupational Medicine 48: 181-188.
[14] Fridner, A. 2004. “Career Paths and Career Patterns among Physicians with a Ph.D.” Ph.D. thesis, Uppsala University, Department of Psychology.
[15] Goldberg, D., and Williams, P. 1991. A user’s Guide to the General Health Questionnaire. London: Nfer-Nelson.
[16] Demerouti, E., Bakker, A. B., Vardakou, I., and Kantas, A. 2003. “The Convergent Validity of Two Burnout
Instruments: A Multitrait-Multimethod Analysis.” Eur J Psychol Assess 19: 12-23.
[17] Meehan, P. J., Lamb, J. A., and Saltzman, L. E. 1992. “O’Carroll PW. Attempted Suicide among Young Adults: Progress Toward a Meaningful Estimate of Prevalence.” Am J Psychiatry 149: 41-44.
[18] Lindström, K. 2002. User’s Guide for the QPS Nordic General Nordic Questionnaire for Psychological and Social Factors at Work. Copenhagen, Denmark: Nordic Council of Ministers.
[19] Fridner, A., Pingel, B., and Hansen, N. 2006. Läkares hälsa och arbetsvillkor vid Karolinska Universitetssjukhuset (Physicians’ Health and Working Conditions at Karolinska University Hospital). Stockholm: Karolinska University Hospital.
[20] Peiro, J., Gonzalez-Roma, V., and Canero, J. 1999. “Survey Feedback as a Tool for Changing Managerial Culture: Focusing on Users Interpretations—A Case Study.” European Journal of Work and Organizational Psychology 8: 537-550.
[21] Arhenfelt, B. 2001. Förändring som tillstånd [Changes as a state]. Lund: Studentlitteratur.
[22] Björklund, C., Grahn, A., Jensen, I., and Bergström, G. 2007. “Does Survey Feedback Enhance the Psychological Work Environment and Decrease Sick Leave?” European Journal of Work and Organizational Psychology 16: 76-93.
[23] Pingel, B., Schenck-Gustafsson, K., and Fridner, A. 2009. On Gender Inequality among Physicians—the HOUPE Study. Stockholm: Stockholm City Council.
Journal of Health Science 2 (2014) 330-337
Nurse Documentation in Deteriorating Patients Prior to
In-hospital Cardiac Arrest—A Pilot Study in A Swedish
University Hospital
Lars Aas1, Maria Ouchterlony1 and Therese Djärv1, 2
1. Department of Emergency Medicine, Karolinska University Hospital, Solna, Stockholm, SE-171 76, Sweden
2. Department of Medicine in Solna, Karolinska Institutet, Stockholm, Sweden
Received: May 23, 2014 / Accepted: July 25, 2014 / Published: July 30, 2014. Abstract: Presence of abnormal vital signs prior to IHCA and consequently higher mortality has been found in numerous studies. It is unknown whether abnormal vital signs are acted upon or not and how this affects the outcome of the IHCA. Aim: Compare differences in journal notes regarding abnormal vital signs or worry by nurses up until 24 h between survivors and non-survivors after an in-hospital cardiac arrest (IHCA). Design: Pragmatic retrospective case-control study in a Swedish university hospital. Methods: All IHCA during 2007-2011 was reviewed (n = 720). Out of them, 20 (3%) fulfilled the inclusion criteria; survived 30 d, had their IHCA at a general ward, were aged > 18 years and had documented abnormal vital signs or nurse worries. Out of the non-survivors, two controls were after matching for age, sex and number of diseases randomly drawn for each case. Pearson's chi test was used to assess significance on the level of 0.05 in differences between survivors and non-survivors. Results: Of 20 survivors with preceding abnormal vital signs prior to IHCA, 15 patients (75%) had documented worries or action taken by a nurse compared to 23 patients (58%) among non-survivors (p-value: 0.258). Conclusion: The journal documentation 24 h prior to a IHCA was fairly equal in numbers between patients surviving at least 30 d afterwards compared to those not surviving, but the content of the journal notes had a slightly higher, but not statistical significant, frequency of worry or action taken by attending nurses in survivors. Keywords: In-hospital cardiac arrest, abnormal vital signs, nurse management, survival rate.
1. Introduction
Observations are a key factor when working with ill
patients at a hospital and a cornerstone in a nursing job
[1]. Unexpected patient deterioration is a normal
clinical problem at a hospital and nurses are
continuously exposed to problems such as time
pressure, not enough time spent with the patient, the
level of their clinical experience, less autonomous
manner of working, being able to communicate with
correct medical language to convey the seriousness of
the situation, proper documentation and recognizing a
worry or an issue that needs to be dealt with straight
Corresponding author: Lars Aas, master, research fileds:
nursing science, emergency medicine. E-mail: [email protected].
away [2-5]. It has been shown that with early
identification and timely patient management, patient
outcomes can be improved [5] but during an 8 h shift a
single nurse can face up to 50 significant clinical
judgments in a medical admissions unit in where
abnormal vital signs might only be one [6]. However,
since it has been found that patients expressing
abnormal vital signs have higher mortality it is
important with high nurse awareness despite many
difficult clinical judgments [7, 8]. By detecting these
abnormal vital signs timely treatment can be
administered leading to less organ dysfunction and
therefore a reduced risk of in-hospital cardiac arrest
(IHCA) [9]. One systematic approach aiming to reduce
adverse events is through the identification of early
DAVID PUBLISHING
D

Nurse Documentation in Deteriorating Patients Prior to In-hospital Cardiac Arrest —A pilot Study in A Swedish University Hospital
331
warning signals (EWS) [10, 11]. The basis of the EWS
is the constant monitoring of patients’ basic vital signs
such as respiratory rate, pulse, blood pressure and
conscious level [5, 12]. If the patient triggers any of
these EWS, appropriate actions must be taken by the
nurse and the nurse needs to decide whether an
appropriate nursing action is suitable or if more
advanced medical support is needed since these EWS
often precede cardiac arrest or death [6, 12]. In order to
increase patient safety and early identification of
deteriorating patients, effective observation and
documentation of concern regarding patients and
abnormal vital signs can be done with a standard
structure in journal entries [13, 14]. Even if it is known
that nurses tend to lack documentation in deteriorating
patients and that patients demonstrate abnormal vital
signs many hours prior to IHCA [6, 11, 15], it remains
unknown, whether these abnormal vital signs were
acted upon, i.e., noted and given appropriate attention
within the regular clinic work among all other tasks
performed simultaneously, and if this is related to the
survival of an IHCA.
2. Materials and Methods
2.1 Aim
To compare differences in journal notes regarding
abnormal vital signs or worry by nurses up until 24 h
between 30-days survivors and non-survivors after an
in-hospital cardiac arrest.
2.2 Design
The study design was a pragmatic retrospective
case-control study in a university hospital. The data
source used was the national cardiac arrest register
(NCAR) in Sweden as previously described in detail by
[16].
2.3 Setting
The Karolinska University Hospital (Karolinska) is
one of Europe’s biggest university hospitals. In its
region, Karolinska is especially responsible for
providing highly specialized medical care and serves as
the trauma referral center of its area. Karolinska has
about 1680 hospital beds, about 109 000 care instances
are produced every year and the hospital receives more
than 162 000 acute visits per year [17].
2.4 Participants
All IHCA at Karolinska reported to the NCAR
during 2007-2011 were reviewed (n = 720). The case
definitions (inclusion criteria’s) were age above 18
years, IHCA, survival ≥ 30 d, general ward as place of
IHCA (medical-, surgical-, geriatric-, oncology-,
neurological-, orthopedic-, ear-nose-throat-, infection-,
gynecology-, rheumatic wards and radiology
department) and one or more in journal text
documented abnormal vital sign(s) by the attending
nurse in charge according to local medical emergency
team (MET) criteria as advocated by Bell et al.[17]
(Table 1). The time frame of 30 d was chosen as
previous study done by Bell et al. [17] showed that
patients with abnormal vital signs had almost a ten-fold
increased mortality rate during the first 30 d. Exclusion
criteria’s were patients with normal or missing
information on vital signs, designated “do not attempt
Table 1 Local Medical Emergency Team criteria at Karolinska University Hospital as developed by Bell et al. (2005).
The Medical Emergency Team criteria
Acute change in respiratory rate to < 8 or > 30 breaths/min
Acute change in pulse oximetry saturation to < 90%
Acute change in heart rate to < 40 or > 130/min (beats/min)
Acute change in systolic blood pressure to < 90 mm/Hg
Acute change in conscious state
Staff member is worried about the patient.

Nurse Documentation in Deteriorating Patients Prior to In-hospital Cardiac Arrest —A pilot Study in A Swedish University Hospital
332
resuscitation”, patients < 18 years and patients at the
various intensive care units, emergency room and
surgical theaters since these patients per definition
often had abnormal vital signs and medical teams were
working on these patients continuously. Also, a nurse
often only had one or very few patients to attend during
the shift and thus was not representative for the nurses
working at general wards.
Of all 720 patients experiencing IHCA during
2007-2011, only 20 (3%) patients met the inclusion
criteria and were identified as cases. For each case, two
controls were matched regarding sex, age group (< 30
years, 30-64 years, 65-80 years, > 80 years) and
number of diseases documented in the medical record
when admitted to the hospital (none, one, at least two).
When matching cases with controls, if there were more
than two possible controls, the control closest in age
was chosen. An acute change in consciousness was not
found in any journal notes made by the attending nurse
24 h prior to IHCA and thusly not presented any further
in this study.
2.5. Data Collection and Classification
All survivors and non-survivors were identified
through NCAR and data were drawn from the ordinary
medical record by the personal security numbers. All
medical records were reviewed by a study specific
protocol developed by experienced clinicians on the
basis of Harrisson [18] protocol and local MET
criterion (Table 1). The protocol gathered data such as
sex, age, medical history (yes or no regarding the
following conditions; cardiovascular disease, diabetes
mellitus, lung disease, kidney disease, joint disease,
psychiatric illness, cancer and other, number of
diseases at point of admission and vital signs (yes or no
according to local MET criterion, normal or missing
vital signs as illustrated in Table 1: respiratory rate,
pulse oximetry saturation, heart rate and systolic blood
pressure) in journal notes. All journal notes were
printed, given a unique number and anonymized
regarding survival status so reviewers were unaware of
dealing with a case or a control while gathering data
from the journal files to the database.
After gathering all data, medical history as grouped
into three categories (none, one, at least two) and
categorization of the vital signs and documented
actions taken according to journal notes by the nurse
was made into five categories. 1) Not noted meant that
no abnormal vital signs or nurse worry regarding
deterioration of the patient were noted in the text of the
journal notes, but numbers mentioning abnormal vital
signs was found somewhere in the journal. 2) Noted,
not acted meant that abnormal vital signs or nurse
worry for the patient was noted but no action was taken
according to the journal notes. 3) Noted, unclear acted
meant that the journal notes did not provide a clear
answer to whether action was taken in regards to the
abnormal vital signs. 4) Noted, acted upon meant that
abnormal vital signs or nurse worry for the
deteriorating patient were noted and some form of
action was taken, i.e., nursing action including
notifying the doctor in charge. Results will be
presented in these categories but since it might be of
clinical interest to know which vital sign stood out as
missed, even if numbers will be small and test for
statistical significance will not be done, data will be
presented in hypothesis generating purposes for future
studies. All matters where confusion regarding how to
classify journal notes occurred was discussed until
consensus and doubled checked for accuracy by two
independent researchers.
2.6. Ethical Consideration
The study was reviewed by the regional ethics
committee in Stockholm, Sweden.
2.7. Data Analysis
Descriptive statistics were used for survivors and
non-survivors (median and range for age, length of stay,
time of journal note prior to IHCA and number of
journal notes and frequency for gender, number of
diseases at time of admission, time of IHCA, journal
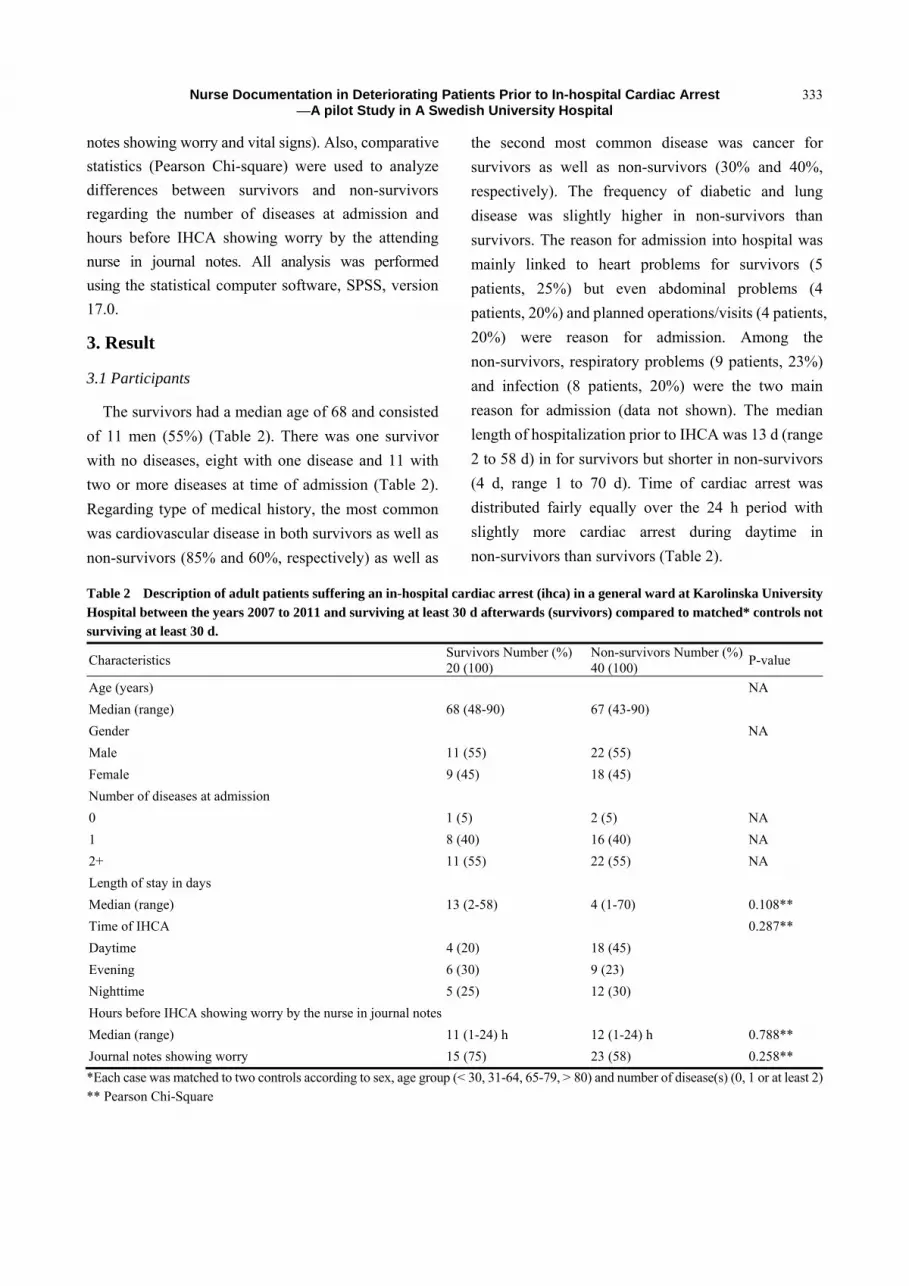
Nurse Documentation in Deteriorating Patients Prior to In-hospital Cardiac Arrest —A pilot Study in A Swedish University Hospital
333
notes showing worry and vital signs). Also, comparative
statistics (Pearson Chi-square) were used to analyze
differences between survivors and non-survivors
regarding the number of diseases at admission and
hours before IHCA showing worry by the attending
nurse in journal notes. All analysis was performed
using the statistical computer software, SPSS, version
17.0.
3. Result
3.1 Participants
The survivors had a median age of 68 and consisted
of 11 men (55%) (Table 2). There was one survivor
with no diseases, eight with one disease and 11 with
two or more diseases at time of admission (Table 2).
Regarding type of medical history, the most common
was cardiovascular disease in both survivors as well as
non-survivors (85% and 60%, respectively) as well as
the second most common disease was cancer for
survivors as well as non-survivors (30% and 40%,
respectively). The frequency of diabetic and lung
disease was slightly higher in non-survivors than
survivors. The reason for admission into hospital was
mainly linked to heart problems for survivors (5
patients, 25%) but even abdominal problems (4
patients, 20%) and planned operations/visits (4 patients,
20%) were reason for admission. Among the
non-survivors, respiratory problems (9 patients, 23%)
and infection (8 patients, 20%) were the two main
reason for admission (data not shown). The median
length of hospitalization prior to IHCA was 13 d (range
2 to 58 d) in for survivors but shorter in non-survivors
(4 d, range 1 to 70 d). Time of cardiac arrest was
distributed fairly equally over the 24 h period with
slightly more cardiac arrest during daytime in
non-survivors than survivors (Table 2). Table 2 Description of adult patients suffering an in-hospital cardiac arrest (ihca) in a general ward at Karolinska University Hospital between the years 2007 to 2011 and surviving at least 30 d afterwards (survivors) compared to matched* controls not surviving at least 30 d.
Characteristics Survivors Number (%) 20 (100)
Non-survivors Number (%) 40 (100)
P-value
Age (years) NA
Median (range) 68 (48-90) 67 (43-90)
Gender NA
Male 11 (55) 22 (55)
Female 9 (45) 18 (45)
Number of diseases at admission
0 1 (5) 2 (5) NA
1 8 (40) 16 (40) NA
2+ 11 (55) 22 (55) NA
Length of stay in days
Median (range) 13 (2-58) 4 (1-70) 0.108**
Time of IHCA 0.287**
Daytime 4 (20) 18 (45)
Evening 6 (30) 9 (23)
Nighttime 5 (25) 12 (30)
Hours before IHCA showing worry by the nurse in journal notes
Median (range) 11 (1-24) h 12 (1-24) h 0.788**
Journal notes showing worry 15 (75) 23 (58) 0.258**
*Each case was matched to two controls according to sex, age group (< 30, 31-64, 65-79, > 80) and number of disease(s) (0, 1 or at least 2) ** Pearson Chi-Square
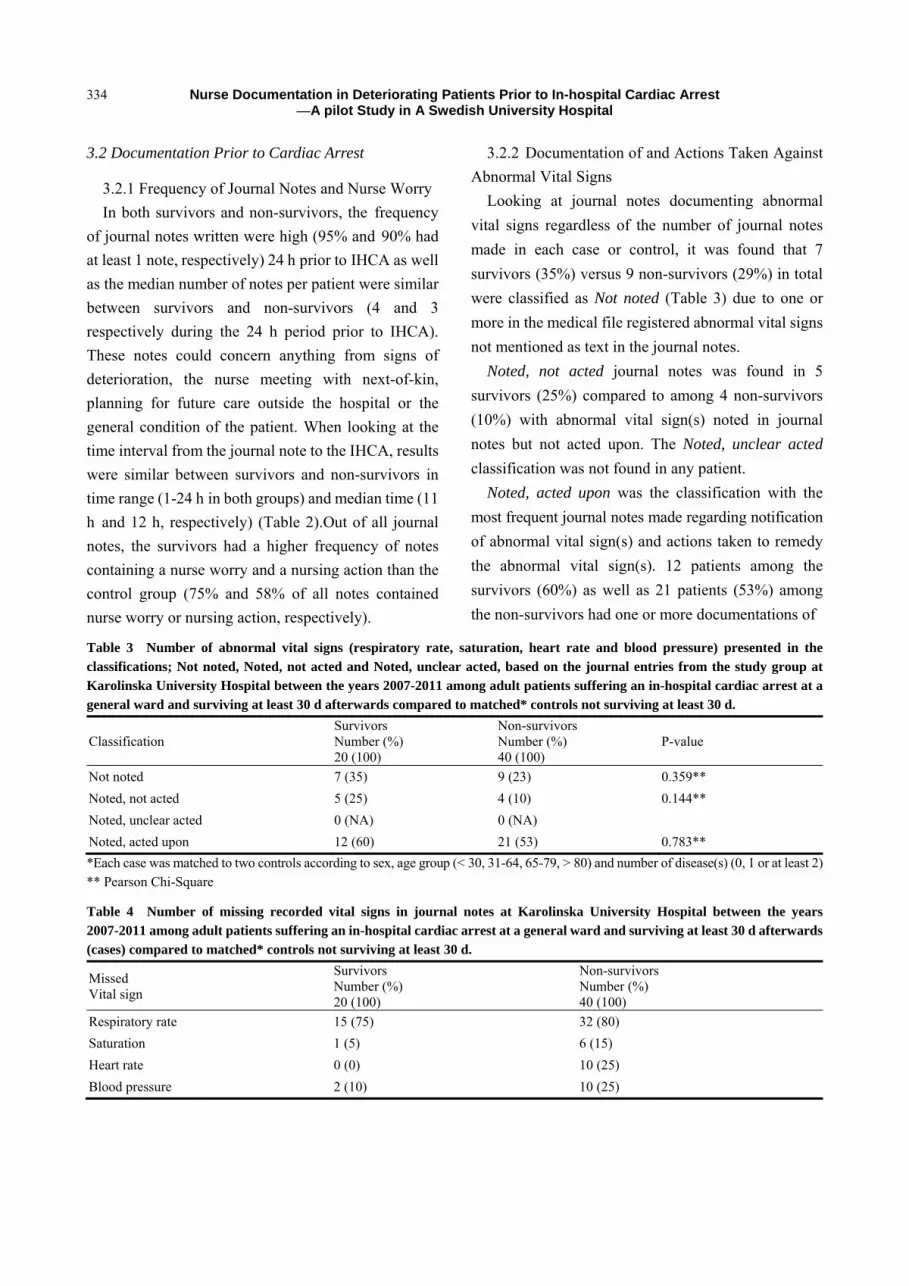
Nurse Documentation in Deteriorating Patients Prior to In-hospital Cardiac Arrest —A pilot Study in A Swedish University Hospital
334
3.2 Documentation Prior to Cardiac Arrest
3.2.1 Frequency of Journal Notes and Nurse Worry
In both survivors and non-survivors, the frequency
of journal notes written were high (95% and 90% had
at least 1 note, respectively) 24 h prior to IHCA as well
as the median number of notes per patient were similar
between survivors and non-survivors (4 and 3
respectively during the 24 h period prior to IHCA).
These notes could concern anything from signs of
deterioration, the nurse meeting with next-of-kin,
planning for future care outside the hospital or the
general condition of the patient. When looking at the
time interval from the journal note to the IHCA, results
were similar between survivors and non-survivors in
time range (1-24 h in both groups) and median time (11
h and 12 h, respectively) (Table 2).Out of all journal
notes, the survivors had a higher frequency of notes
containing a nurse worry and a nursing action than the
control group (75% and 58% of all notes contained
nurse worry or nursing action, respectively).
3.2.2 Documentation of and Actions Taken Against
Abnormal Vital Signs
Looking at journal notes documenting abnormal
vital signs regardless of the number of journal notes
made in each case or control, it was found that 7
survivors (35%) versus 9 non-survivors (29%) in total
were classified as Not noted (Table 3) due to one or
more in the medical file registered abnormal vital signs
not mentioned as text in the journal notes.
Noted, not acted journal notes was found in 5
survivors (25%) compared to among 4 non-survivors
(10%) with abnormal vital sign(s) noted in journal
notes but not acted upon. The Noted, unclear acted
classification was not found in any patient.
Noted, acted upon was the classification with the
most frequent journal notes made regarding notification
of abnormal vital sign(s) and actions taken to remedy
the abnormal vital sign(s). 12 patients among the
survivors (60%) as well as 21 patients (53%) among
the non-survivors had one or more documentations of
Table 3 Number of abnormal vital signs (respiratory rate, saturation, heart rate and blood pressure) presented in the classifications; Not noted, Noted, not acted and Noted, unclear acted, based on the journal entries from the study group at Karolinska University Hospital between the years 2007-2011 among adult patients suffering an in-hospital cardiac arrest at a general ward and surviving at least 30 d afterwards compared to matched* controls not surviving at least 30 d.
Classification Survivors Number (%) 20 (100)
Non-survivors Number (%) 40 (100)
P-value
Not noted 7 (35) 9 (23) 0.359**
Noted, not acted 5 (25) 4 (10) 0.144**
Noted, unclear acted 0 (NA) 0 (NA)
Noted, acted upon 12 (60) 21 (53) 0.783**
*Each case was matched to two controls according to sex, age group (< 30, 31-64, 65-79, > 80) and number of disease(s) (0, 1 or at least 2) ** Pearson Chi-Square
Table 4 Number of missing recorded vital signs in journal notes at Karolinska University Hospital between the years 2007-2011 among adult patients suffering an in-hospital cardiac arrest at a general ward and surviving at least 30 d afterwards (cases) compared to matched* controls not surviving at least 30 d.
Missed Vital sign
Survivors Number (%) 20 (100)
Non-survivors Number (%) 40 (100)
Respiratory rate 15 (75) 32 (80)
Saturation 1 (5) 6 (15)
Heart rate 0 (0) 10 (25)
Blood pressure 2 (10) 10 (25)

Nurse Documentation in Deteriorating Patients Prior to In-hospital Cardiac Arrest —A pilot Study in A Swedish University Hospital
335
abnormal vital sign(s) in their journal notes.
4. Discussion
This pragmatic retrospective case-control study in a
university hospital demonstrated that journal
documentation 24 h prior to a IHCA was fairly equal in
numbers between patients surviving at least 30 d
afterwards compared to those not surviving, but the
content of the journal notes had a slightly higher, but
not statistical significant, frequency of worry or action
taken by attending nurses in survivors. The equal
frequency of journal notes in the 24 h interval prior to
IHCA might indicate a frequent contact with the patient
during. Respiratory rate was found to be missing in a
majority of journal notes whilst heart rate was noted in
all survivors. Weakness of the study include the small
numbers of cases identified, due to narrow selected
inclusion criteria to assess the hypothesis of a
difference in nurse documentation as a proxy for nurse
awareness prior to a IHCA in survivors compared to
non-survivors. Initially it was thought that the study,
with its 720 patients with IHCA, would give more than
20 cases. The researchers chose not to prolong the time
period to gather more cases since clinical practice and
awareness of vital signs likely have improved over the
years. Another limitation was the lack of possibility of
measuring what actions, worries or thoughts were not
noted in the journal notes. A prospective study could
remedy this, however the author believe there exists no
difference between case and control groups since it is
unknown for the attending nurse that the patient will
suffer IHCA within 24 h when the journal notes were
documented.
Strengthens of the study include the matched
case-control design, access to the NCAR, the range of
the study enveloped four years and included initially all
IHCA reported at the hospital. The pre-determined
protocol provided transferability along with audit
ability and data was as far as possible anonymized for
cases and controls which increased reliability. Another
strength is the use of established well-known objective
MET criteria as well as priori decided study protocol
based on Harrisson et al.´s study from 2005. The
finding of a median time of journal notes of 11 h prior
to IHCA in survivors might mask a deterioration of the
patients the hours closest to the IHCA since Hillman et
al. [15] found that the presence of antecedents prior to
IHCA were slightly higher 0-8 h prior to IHCA than
8-48 h prior to IHCA. Looking at the number of
patients with documented worry or action taken by the
nurse, the number varied from over two-thirds in the
survivors compared to just over half in the
non-survivors. The portion with notes is in line with
previous studies demonstrating notes in about half to
two thirds of the patients [15, 19, 20, 22]. On possible
reason for journal notes classified into the categories
not noted and noted, not acted might be due to
multitasking, in a study by Berg et al. [21],
multitasking information exchange was found in
almost half of the total number of observed activities.
This high number of activities made when multitasking
the very important activity, information exchange,
could be a reason result in easily get lost or forgotten
information. The lack of action taken noted in these
journal notes is something which should prompt a
reaction seeing that studies shows an increase in
abnormal vital signs prior to IHCA [7, 8, 15, 19, 22].
The findings of this study is of importance as it
shows that attending nurses often missed to note
respiratory rate in journal notes, if this would be
repeated in larger future studies, it could prompt efforts
to educate staff in the importance of discovering EWS
in regards to the missing respiratory rates and
documenting of general vital signs on a regular basis,
encouraging staff to keep acting on their worry. The
findings of this pilot study showed that the both
survivors as well as non-survivors had a high number
of journal notes in the 24 h interval prior IHCA.
Journal notes did not necessarily show abnormal vital
signs or nurse worry, but showed that the attending
nurse had contact with the patient frequently the last 24
h thus increasing patient safety and increasing the
Nurse Documentation in Deteriorating Patients Prior to In-hospital Cardiac Arrest —A pilot Study in A Swedish University Hospital
336
chances of detecting deterioration in vital signs of the
patient. This finding, of an equal frequent
documentation in both cases and controls together with
the high amount of notes containing information
regarding worry or vital signs might indicate high nurse
awareness.
In conclusion, this pragmatic case-control study has
demonstrated that nurse worry was more frequently,
not statistical significant, noted in journal notes prior to
an IHCA in 30 d survivors compared to non-survivors.
References
[1] Pinsky, M. R. 2007. “Hemodynamic Evaluation and
Monitoring in the ICU.” Chest 133: 1-17.
[2] Kenward, G., and Hodgetts, T. 2002. “Nurse Concern: A
Predictor of Patient Deterioration.” Nursing Times 98 (22):
38-39.
[3] Andrews, T., and Waterman, H. 2005. “Packaging: A
Grounded Theory of How to Report Physiological
Deterioration Effectively.” Journal of Advanced Nursing
52 (5): 473-481.
[4] Thompson, C., Bucknall, T., Estabrookes, C. A.,
Hutchinson, A., Fraser, K., de Vos, R., Binnecade, J.,
Barrat, G., and Saunders, J. 2007. “Nurses’ Critical Event
Risk Assessments: A Judgment Analysis.” Journal of
Clinical Nursing 18: 601-612.
[5] Endacott, R., Scholes, J., Cooper, S., McConnell-Henry,
T., Porter, J., Missen, K., Kinsman, L., and Champion, R.
2012. “Identifying Patient Deterioration: Using
Simulation and Reflective Interviewing to Examine
Decision Making Skills in a Rural Hospital.” International
Journal of Nursing Studies 29: 710-717.
[6] Cooper, S., McConnell-Henry, T., Cant, R., Porter, J.,
Missen, K., Kinsman, L., Endacott, R., and Scholes, J.
2011. “Managing Deteriorating Patients: Registered
Nurses´ Performance in A Simulated Setting.” The Open
Nursing Journal 5: 120-126.
[7] Lighthall, G. K., Markar, S., and Hsiung, R. 2009.
“Abnormal Vital Signs are Associated with An Increased
Risk for Critical Events in US Veteran Inpatients.”
Resuscitation 80: 1264-1269.
[8] Bleyer, A. J., Vidya, S., Russel, G. B., Jones, C. M., Sujata,
L., Daeihagh, P., and Hire, D. 2011. “Longitudinal
Analysis of One Million Vital Signs in Patients in An
Academic Medical Center.” Resuscitation 82: 1387-1392.
[9] Rivers, E., Nguyen, B., Havstad, S., Ressler, J., Muzzin,
A., Knoblich, B., Peterson, E., and Tomlanovich, M. 2007.
“Early Goal Directed Therapy in the Treatment of Severe
Sepsis and Septic Shock.” New England Journal of
Medicine 345: 1368-77.
[10] Hodgetts, T. J., Kenward, G., Vlackonikolis, I., Payne, S.,
Castle, N., Crouch, R., Ineson, N., and Shaikh, L. 2002.
“Incidence, Location and Reasons for Avoidable
In-hospital Cardiac Arrest in A District General Hospital.”
Resuscitation 54: 115-123.
[11] Furhman, L., Lippert, A., Perner, A., and Östergaard, D. 2008. Incidence, “Staff Awareness and Mortality of Patients at Risk on General Wards.” Resuscitation 7: 325-330.
[12] Hogan, J. 2006. “Why don’t Nurses Monitor Respiratory Rates of Patients?” British Journal of Nursing 15 (9): 489-492.
[13] Odell, M., Victor, C., and Oliver, D. 2009. “Nurses’ Role in Detecting Deterioration in Ward Patients: Systematic Literature Review.” Journal of Advanced Nursing 65 (10): 1992-2006.
[14] Stevenson, J. E., and Nilsson, G. 2012. “Nurses’ Perception of An Electronic Patient Record from A Patient Safety Perspective: A Qualitative Study. Journal of Advanced Nursing 68 (3): 667-676.
[15] Hillman, K. M., Bristow, P. J., Chey, T., Daffurn, K., Jacques, T., Norman, S. L., Bishop, G. F., and Simmons, G. 2002. “Duration of Life-threatening Antecedents Prior to Intensive Care Admission.” Intensive Care Medicine 28: 1629-1634.
[16] Källestedt, M. L., Berglund, A., Enlund, M., and Herlitz, J. 2012. ”In-hospital Cardiac Arrest Characteristics and Outcome after Defibrillator Implementation and Education: from 1 Single Hospital in Sweden.” American Journal of Emergency Medicine 30 (9): 1712-1718.
[17] Bell, M. B., Konrad, D., Granath, F., Ekbom, A., and Martling, C-R. 2006. “Prevalence and Sensitivity of MET-criteria in a Scandinavian University Hospital.” Resuscitation 70: 66-73.
[18] Harrisson, G. A., Jaques, T. C., Kilborn, G., and McLaws, M-L. 2005. “The Prevalence of Recordings of the Signs of Critical Conditions and Emergency Responses in Hospital Wards—the SOCCER Study.” Resuscitation 65: 149-157.
[19] Schein, R., Hazday, N., Pena, M., Ruben, B. H., and
Sprung, C. L. 1990. “Clinical Antecedents to In-hospital
Cardiopulmonary Arrest.” Critical care medicine 96 (6):
1388-1392.
[20] Stokke, T., and Kahlfoss, C. 1999. “Structure and Content
in Norwegian Nursing Care Documentation.”
Scandinavian Journal of Caring Sciences 13: 18-25.
[21] Berg, L. M., Ehrenberg, A., Florin, J., Östergren, J., and

Nurse Documentation in Deteriorating Patients Prior to In-hospital Cardiac Arrest —A pilot Study in A Swedish University Hospital
337
Göransson, K. E. 2012. ”An Observational Study of
Activities and Multitasking Performed by Clinicians in
Two Swedish Emergency Departments.” European
Journal of Medicine 19: 246-251.
[22] Franklin, C., and Mathew, J. 1994. “Developing Strategies
to Prevent In-hospital Cardiac Arrest: Analyzing
Responses of Physicians and Nurses in the Hours Before
the Event.” Critical Care Medicine 22 (2): 244-248.
Journal of Health Science 2 (2014) 338-339
Relation of Nausea and Vomiting in Acute Myocardial
Infarction to Location of Infarct
Kooli Sami, Laamouri Noura, Raddaoui Abdelhafidh, El Heni Najla, Ghazali Hanene and Souissi Sami
Emergency Department, Regional Hospital Ben Arous, Tunis, 1089, Tunisia
Received: May 23, 2014 / Accepted: July 23, 2014 / Published: July 30, 2014. Abstract: Nausea and vomiting occur frequently in patients with acute myocardial infarction (AMI). To determine whether the incidence of nausea and vomiting in patients with AMI varies with infarct location, the authors studied 80 patients who had been admitted to the hospital for ST-segment elevation AMI. Data were prospectively collected from patients with AMI and nausea or vomiting for one year. Patients were enrolled if the diagnosis of AMI with nausea or vomiting is retained. The infarct location (i.e., inferior vs. anterior) in the patients with STEMI was determined using the established World Health Organization electrocardiographic criteria. Of the 80 patients included, nausea was reported in 44 patients (55%) and vomiting in 36 patients (45%). The mean age was 58, 1 ± 11, 8 years old, and males comprised 62 patients (77.5%). Inferior AMI was present in 47 patients (58.8%) and anterior AMI in 33 patients (41.2%). The peak serum troponin I concentrations was significantly greater in those with anterior AMI than in those with inferior AMI respectively 0.52 ± 0.28 ng/mL and 0.50 ± 0.34 ng/mL. In conclusion, nausea and vomiting are common presenting symptoms in patients with either inferior or anterior wall AMI, but their frequency is unrelated to the infarct location. Key words: Acute myocardial infarction, location, nausea, vomiting.
1. Introduction
Nausea and vomiting are common presentation of
acute myocardial infarction (AMI). The
pathophysiology of this atypical presentation remains
uncertain. Few studies have reported that nausea and
vomiting as symptoms of AMI and its location [1, 2].
To try to determine the relation between this two
symptoms and the location of AMI, the authors
performed a cohort study of 80 patients admitted to the
emergency department of the hospital for AMI.
2. Methods
Data were prospectively collected from patients with
AMI and nausea or vomiting for one year: October
2010 to September 2011. Subjects were enrolled if the
diagnosis of AMI with nausea or vomiting is retained.
The infarct location (i.e., inferior vs. anterior) in the
patients with STEMI was determined using the
Corresponding author: Kooli Sami, doctor, research field:
practioner. E-mail: [email protected].
established World Health Organization
electrocardiographic criteria and was confirmed by an
experienced cardiologist. The anterolateral, lateral and
the anteroseptal infarcts were classified as anterior. The
inferoposterior and inferolateral infarcts were
classified as inferior.
Data were collected and treated using SPSS 18.0.
3. Results
Of the 80 patients with AMI, 47 (58%) were
diagnosed with inferior wall AMI and 33 (42%) with
anterior wall AMI. The baseline characteristics of the
patients with inferior and anterior wall AMI were
similar (Table 1). The peak serum Troponin I
concentration was significantly higher greater in
patients with anterior AMI than in those inferior AMI.
The vast majority of patients in each infarct group were
treated using thrombolytic agents 70 patients (87.5%)
with success in 62.4% of patients.
Nausea was reported at clinical presentation in 51%
of patients with inferior AMI and 60% of patients with
DAVID PUBLISHING
D
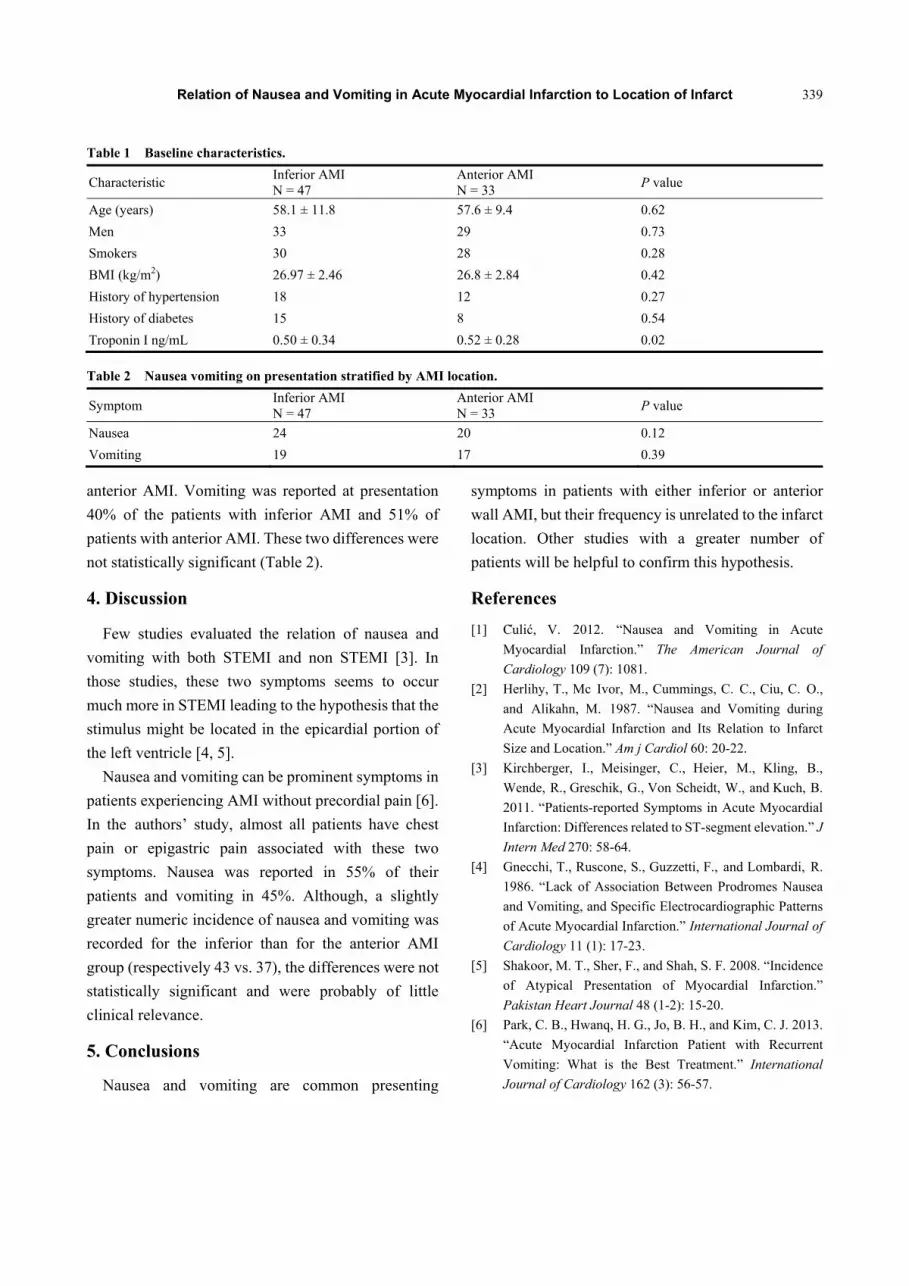
Relation of Nausea and Vomiting in Acute Myocardial Infarction to Location of Infarct
339
Table 1 Baseline characteristics.
Characteristic Inferior AMI N = 47
Anterior AMI N = 33
P value
Age (years) 58.1 ± 11.8 57.6 ± 9.4 0.62
Men 33 29 0.73
Smokers 30 28 0.28
BMI (kg/m2) 26.97 ± 2.46 26.8 ± 2.84 0.42
History of hypertension 18 12 0.27
History of diabetes 15 8 0.54
Troponin I ng/mL 0.50 ± 0.34 0.52 ± 0.28 0.02
Table 2 Nausea vomiting on presentation stratified by AMI location.
Symptom Inferior AMI N = 47
Anterior AMI N = 33
P value
Nausea 24 20 0.12
Vomiting 19 17 0.39
anterior AMI. Vomiting was reported at presentation
40% of the patients with inferior AMI and 51% of
patients with anterior AMI. These two differences were
not statistically significant (Table 2).
4. Discussion
Few studies evaluated the relation of nausea and
vomiting with both STEMI and non STEMI [3]. In
those studies, these two symptoms seems to occur
much more in STEMI leading to the hypothesis that the
stimulus might be located in the epicardial portion of
the left ventricle [4, 5].
Nausea and vomiting can be prominent symptoms in
patients experiencing AMI without precordial pain [6].
In the authors’ study, almost all patients have chest
pain or epigastric pain associated with these two
symptoms. Nausea was reported in 55% of their
patients and vomiting in 45%. Although, a slightly
greater numeric incidence of nausea and vomiting was
recorded for the inferior than for the anterior AMI
group (respectively 43 vs. 37), the differences were not
statistically significant and were probably of little
clinical relevance.
5. Conclusions
Nausea and vomiting are common presenting
symptoms in patients with either inferior or anterior
wall AMI, but their frequency is unrelated to the infarct
location. Other studies with a greater number of
patients will be helpful to confirm this hypothesis.
References
[1] C̆ulić, V. 2012. “Nausea and Vomiting in Acute
Myocardial Infarction.” The American Journal of
Cardiology 109 (7): 1081.
[2] Herlihy, T., Mc Ivor, M., Cummings, C. C., Ciu, C. O.,
and Alikahn, M. 1987. “Nausea and Vomiting during
Acute Myocardial Infarction and Its Relation to Infarct
Size and Location.” Am j Cardiol 60: 20-22.
[3] Kirchberger, I., Meisinger, C., Heier, M., Kling, B.,
Wende, R., Greschik, G., Von Scheidt, W., and Kuch, B.
2011. “Patients-reported Symptoms in Acute Myocardial
Infarction: Differences related to ST-segment elevation.” J
Intern Med 270: 58-64.
[4] Gnecchi, T., Ruscone, S., Guzzetti, F., and Lombardi, R.
1986. “Lack of Association Between Prodromes Nausea
and Vomiting, and Specific Electrocardiographic Patterns
of Acute Myocardial Infarction.” International Journal of
Cardiology 11 (1): 17-23.
[5] Shakoor, M. T., Sher, F., and Shah, S. F. 2008. “Incidence
of Atypical Presentation of Myocardial Infarction.”
Pakistan Heart Journal 48 (1-2): 15-20.
[6] Park, C. B., Hwanq, H. G., Jo, B. H., and Kim, C. J. 2013.
“Acute Myocardial Infarction Patient with Recurrent
Vomiting: What is the Best Treatment.” International
Journal of Cardiology 162 (3): 56-57.
Journal of Health Science 2 (2014) 340-352
Mental Health Predictor of the Sixth Batch Indonesian
Nurse and Certified Care Worker Candidates Migrate to
Japan under the Japan–Indonesia Economic
Partnership Agreement in Pre-migration Stage
Susiana Nugraha and Yuko Ohara-Hirano
Nagasaki University, Graduate School of Biomedical Science, 1-7-1 Sakamoto, Nagasaki, 852-8520, Japan
Received: May 12, 2014 / Accepted: June 23, 2014 / Published: July 30, 2014. Abstract: Under the JI-EPA (Japan-Indonesia Economic Partnership Agreement), approximately one thousand nurse and certified care worker candidates have been migrated to Japan since 2008. Migration has been known as a risk factor of mental well-being. Little is known about how the in pre-migration stage may affect the migrant’s mental health. The study examines the mental health predictor in pre-migration stage using cross sectional design. Gender, Age, EPA course, educational degree, working background, language proficiency, motivation for migration and knowledge about destination country selected as mental health predictor. The results showed
that the variable knowledge about living environment is the only independent variable which is correlate with GHQ in the model, =
-0.20, P < 0.05. The finding may assume that the knowledge as part of cognitive preparation plays important role in explaining the mental health of the EPA candidates in pre-migration stage. Key words: Nurse, certified care worker, pre-migration, mental health.
1. Introduction
International migration has been becoming a fact of
current modern life and increasing by the year. Boosted
by the forces of globalization, uneven development and
demographic changes, migration has become a
defining feature of economic, social and political life in
a mobile world [1]. People migrate to improve their
well-being, through economic expansion and social
opportunity [2]. Migration of the high skilled-worker
such as health certified care workers has been linked
with globalization and closely followed by general
trend in international migration. With an estimated
worldwide shortage of 4.3 million health care
professionals, international migration and recruitment
of health certified care worker from developing
Corresponding author: Yuko Ohara-Hirano, Ph.D.,
professor, research field: study on EPA nurse and care worker. E-mail: [email protected]/[email protected].
country to developed countries has become
pre-eminent issue in global health [3]. Nurse and
physicians have sought employment abroad for many
reasons, including high unemployment in the
health-care labor market in their home country [4]. On
the other side, there are a lot of shortage of professional
health certified care worker in some developed country
due to increasing the ageing population and technology
advancement in medical field. According to Kingma
(2008), nurse migration has become social
phenomenon which occurs in a context of increasing
global mobility and a growing competition for scarce
skills, including skills needed in the healthcare sector.
Japan is a developed country with the third world’s
highest longevity of life expectancy (84.19 years)
combined with low fertility rate (1.21/couple) [5], and
elderly population was more than 23.30% in 2011
census [6]. By 2035, predicted 33.40% of the total
DAVID PUBLISHING
D

Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
341
population, corresponding to one in three people, will
be elderly [7]. The increasing number of the elderly has
required several changes in policy and strategy such as
health system. Japan tried to reduce the demand for
medical services by improving social services for the
elderly and their families and providing long-term care
services [8]. Implementation of long term care
insurance encourages shifting the place for treating and
rehabilitating patients in chronic illness from hospital
to facilities for long term care, in care facilities, and
home visiting nursing. This program implementation
might also increase demand in care workforce such as
nurse and certified care worker to support the
operational of long term care facilities. The demand of
care worker personnel estimated in range 2,320,000 to
2,440,000 by the year of 2025 [9]. On the other hand,
the demand of nurse workforce also sharply have been
increasing, in line with the growing aged population,
revision of the standard ratio of nurses per patient for
quality care (from 1:10 to 1:7), the revision of medical
treatment fees, and the high turnover of nursing
personnel [10]. Although the number of nurse license
holders has been increasing, as Japanese Government
optimistically calculate [11] geographic imbalanced of
nurse workforce has been increasing. Hirano pointed
out that most of the nurse especially fresh graduate
nurses tend to work in highly-equipped hospital instead
of working in midsize or small hospital in rural area
[12]. Eventually, as shown in scenarios presented by
Fushimi and Kobayashi (2013) on the long term
perspectives of the demand of practice nursing
personnel, in 2025, the demand of the nurses are out of
supply.
Considering the above condition, in 2008, Japan
started to globalize their health human resources by
opening labor market for foreign nurses and certified
care worker under Economic Partnership Agreement
with some South East Asian countries including
Indonesia, Japan–JI-EPA (Indonesia Economic
Partnership Agreement) is a bilateral trade agreement
between Indonesia and Japan outlining certain term to
facilitate trade relation and favorable trading term. On
the other hand this agreement also contains a unique
chapter named “movement of the natural person”. This
program was developed to facilitate Indonesian health
care professional to work in Japan under prescribed
condition [13]. According to the agreement,
“movement of the natural person” under JI-EPA
contains two health care professions, namely, nurse
and certified care worker. To be qualified for EPA
nurse candidate, one have to be a qualified registered
nurse under the laws and regulation of Indonesia,
having obtained Diploma III (three years professional
education) from an academy of nursing in Indonesia or
having graduated from a faculty of nursing of
university in Indonesia, with total experience as nurse
for at least two years. Whereas for the certified care
worker candidates, ones should have graduated from a
faculty of nursing or obtained Diploma III from an
academy of nursing in Indonesia without any working
experience qualification [14]. Health care migration
under JI-EPA is the first system which involves
government to government cooperation. Unlike other
migration, the program under JI-EPA is a special case
in term of policy and system. This program governed
by a bilateral agreement and underpinned by the
intention to promote free trade [13].
Under the agreement, the nurse and certified care
workers arriving under EPA are designated as
“candidate” until they pass the national board
examination for registered nurse and certified care
worker [15] despite of that they formerly have already
been as registered nurses in their home country. Under
the program, the candidates are allowed to work as
trainee at medical institution and or long term care
facilities in Japan for a maximum of three years for the
nurses and maximum of four years for the certified care
worker candidates, while learning Japanese language
and preparing for national board examination. If they
pass national board examination within the duration,
they will be licensed as registered nurse or certified
care worker, and allowed to stay in Japan as long as

Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
342
they work as a nurse/certified care worker with three
years visa renewal, but if they fail in the examination,
they have to return to their home country [14]. National
board examination which is conducted in Japanese
language has been being noticed as a hurdle for the
candidates, as the low passing rate among foreign
examinees proved that condition [1].
Migration is the process of social change whereby an
individual moves from one cultural setting to another
for the purposes of settling down either permanently or
for a prolonged period. A basic underlying theme in the
existing literature linking migration and mental health
is that the disruptions of moving to a new environment
can negatively affect health, including mental
well-being and reducing the net benefit of the
migration [2, 16]. The migration process was
influenced by diverse psychological and social factors,
whose complex interaction affected well-being/health
[17]. The process of migration itself is not just a phase,
but a series of event, which are influenced by number
of factors prolonged period of time and these phases in
return are influenced by other factors at social and
individuals level [16]. Stillman et al. (2006) suggested
that to truly understand the effect of migration on
mental health, one must compare the mental health of
migrants to what their mental health would have been
had when they stayed in their home country. In the
context of migration, pre-departure phase can be
considered as the beginning of the migration process as
such affects the rest of migratory journey [18].
The preparation of migration undertakes their
acceptance by the new host community and the process
of migration itself are some of the macro-factors in the
origin of mental disorders [19]. The pre-migration
experiences, interpretations, and actions considerably
influenced immigration and establishing experiences.
Bughra, et al. (2011), identified the pre-migration
process that predispose individual to mental well-being
such as reason for migration, preparations, group or
singly migration, degree of control to the migration.
Socio-demographic background was also identified as
risk factor for mental health such as gender, age,
socioeconomic status, social support, and occupational
status [20].
Several studies related to the mental health of the
EPA nurse and certified care worker candidates have
been performed both qualitatively and quantitatively.
However, no studies that specifically examined mental
health condition in the pre-migration stage. Few of
them are qualitative studies conducted by Alam and
Wulansari, (2010), and Setyowati, et al. (2010), which
revealed numereus socio cultural issues faced by the
EPA candidates that may lead their job and cultural
stress in their working field namely communication
barrier, salary and rewards issues, being treated as
assistance nurse, feeling loneliness, different in
working culture, facing national board examination,
and lack of information provided during pre-departure
program. A quantitative study has been conducted by
Hirano (2012), to figure out the mental health status of
Indonesian EPA candidates leaving for Japan after the
Great East Japan Earthquake, revelaed that knowledge
about actual living and working condition in Japan is a
major indicator of the mental health of the candidates,
but not their worry concerning the earthquake.
Considering the research finding toward EPA
candidates, mental health predictor in pre-migration
stage and common mental health risk factors, this study
aimed to figure out the best model for mental health
predictors in determining mental health of the sixth
batch Indonesian EPA nurse and certified care worker
candidates in pre-migration stage.
2. Methods
2.1 Participants and Data Collection
The participants of this study were the sixth batch
Indonesian EPA nurses and certified care worker
candidates departed in 2013, with total of 156
candidates. The data collection was conducted in June
23th to 24th 2013. Before departure to Japan, the
candidates must finish 6 month Japanese language
training. The pre-departure orientation program

Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
343
conducted few days before the departure. The
questionnaires were distributed to all candidates who
attended the pre-departure orientation which was held
in June 22nd to 24th 2013, at Depok, West Java,
Indonesia, in cooperation with the National Agency for
Placement and Protection of Indonesian Migrant
Workers (BNP2TKI). A total 148 of the candidates
have agreed to participate in the baseline study and
signed the information consent, whilst another 8
candidates did not participate in the survey.
Seven pages of questionnaire were prepared for this
study; consist of socio-demographic status, motivation
to work in Japan, preparation for going to Japan,
self-reported social support, 12 items from the GHQ
(General Health Questionnaire) in Indonesian version,
degree of knowledge on information about Japan,
Indonesian version SCAS-R (Sociocultural Adaptation
Scale-Revision), and self-rated Japanese language
proficiency. All questions were conveyed in
Indonesian language. Using computer-based statistic
software SPSS 16, the descriptive statistics analysis
conducted for describing the demographic
characteristic of the participants. Person’s correlation
coefficient and independent sample t-test analysis are
conducted for bivariate analysis and multiple linear
regression models have been selected to figure out the
correlation between mental health and its predictors.
This research has been approved by the ethical
committee of Nagasaki University.
2.2 Term and Measurement
2.2.1 Mental Health
This study selects mental health as outcome variable.
Mental health is a vital component of people
well-being. The WHO (World Health Organization)
defines mental health as a state of well-being in which
the individual realizes his or her own abilities, can cope
with the normal stresses of life, can work productively
and fruitfully, and is able to make a contribution to his
or her community (WHO, 2007). The health and
mental well-being of migrant populations is influenced
by complex and interrelated factors. According to
Ornstein (2002), the social determinants of health,
which are the socio-economic conditions that influence
the health of individuals, communities and
jurisdictions, affect both physical health and mental
health. GHQ, a self-administered instrument designed
to identify nonpsychotic psychiatric disturbance in the
community, is selected to be dependent variable. The
GHQ-12 is a measure of current mental health, which is
focus on two major areas–the inability to carry out
normal function and appearance of new and distressing
experiences [21]. GHQ has been used worldwide with
versions available in a large number of languages
including Indonesian language. The GHQ-12 is used in
this research to identify the overarching mental health
condition and coded as 1-2-3-4.
2.2.2 Socio-demographic Data
The demographic data such as Age, Gender, Final
degree, Economic status, Working background, and
Occupation they classified under the EPA program
(nurse or certified care worker) have been selected as
control variables. Basic nursing educational background
in Indonesia, divided into two basic nursing educational
pathways, namely vocational nurse and professional
nurse. The three years nursing school also called D3 is
basic nursing educational for vocational nurse.
Professional education for nursing school conducted in
two phases, whereas the academic level performed in
four years and one year for professional level. The
economic status divided into two self-reported
economic condition, i.e., “Very difficult/Difficult to
survive” and “Not so difficult to survive”. Working
background in this study was defined as “Previous
working status before applying EPA program” which is
categorize into “Working” and “Not working”. This
study categorized EPA course in nurse course and
certified care worker course.
2.2.3 Motivation for Migration
To assess motivation for migration, 16 questions
about the reason for applying to work in Japan under
EPA program were asked, which was used in previous

Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
344
study (Hirano, 2010). From that list, 10 questions being
selected as the pull factor from the destination country
that motivated the candidates to migrate. Pull factor in
this study is defined as an attractiveness of Japan as the
destination country to encourage the candidate to
perform the migration. Ward, et al. (2001) proposed
that voluntary immigrant are pulled or attracted toward
new country in pursuit of personal familial, social,
financial and political goals and voluntarily choose to
resettle in a new country. Therefore pull factors in this
study include “I have some family/relatives who have
already lived in Japan”, “I wish to develop my
professional carrier”, “I can have chance to work in
Japan sooner than work in other country”, “I am
interested in Japanese culture such as Cartoon and
Comic”, “I wish to support my family economically”,
“I can earn a higher salary in Japan than in other
country”, “I wish to learn advanced Japanese technology
in nursing”, “I want to utilize my experience in Japan
for my future work at the hospital/elderly home in other
country”,” I want to marry Japanese partner” and “I am
not required to pay commission fees for overseas
placement”. Yes and No answers were provided and
being scored with 1 and 0.
2.2.4 Preparation for Migration
Three questions regarding with the preparation for
migration were asked with Yes and No answers as “I
contacted some of early batches of Indonesian
nurses/certified care worker who went to Japan”, “I
have started to collect information about Japanese
society and culture”, and “I have met my future
Japanese employer in Indonesia”.
2.2.5 Knowledge about Destination Country
To assess the degree of knowledge about destination
country, twenty questions were asked about Japan in
term of security, climate, working condition, the
amount of income to be earned, and how to get in touch
with Indonesian community, and etc. These questions
have been used in previous study by Hirano (2012),
with slight modification to adjust to the current
condition of the candidates.
To select the most appropriate indicators in term of
knowledge about destination country, factor analysis
using principal component analysis with Varimax
rotation in three step factor analysis was conducted.
Using confirmatory factor analysis and considering
the logic theory and previous study, the reliability and
validity of the factors and item in selected model were
assessed. The knowledge about destination country
into two factors was divided. The first factor was
labeled as “Knowledge about working condition”, and
contains of “Salary I can actually receive after
deducted with tax, insurance housing etc.”, “Kind of
nursing intervention that I can perform while I am
candidate”, “Job description of nurse/certified care
worker candidates in Japan”, and “Responsibility I
have to take/shoulder at my work place in Japan”. This
factor has been confirmed by reliability analysis with
Cronbach’s alpha = 0.70. The second factor was
labeled as Knowledge about living environment,
contains of “Security of the residential area Where I
will stay in Japan”, “whether I will welcomed by
Japanese people”, “Climate where I will stay in
Japan”, “experience of work and lives of EPA
program earlier batch from Indonesia”, and “Working
culture of Japanese such as their custom to work 2-3
hours longer than the written in the contract”. The
questions were confirmed by Cronbach’s alpha = 0.78.
2.2.6 Self-reported Japanese Language Proficiency
All of the candidates have had minimum 6 m
language training program prior the departure to Japan.
Self-reported language proficiency was used to
measure the candidate’s level of language proficiency
by providing multiple choice questions i.e. “How is
your Japanese language proficiency at this moment?”
The choices are “Advance”, “Intermediate”
“Elementary” and “Beginner”.
2.2.7 Social Support
In this study, social support is considered as the
factor that affects mental health. Moral support given
by family or relative to go to Japan is measured by
Likert scale “Very much”, “Much”, “Not so much”,

Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
345
and “Not at all”.
2.2.8 Socio-cultural Adaptation
Socio-cultural adaptation is defined in term of
behavioral skills, as an ability to “fit in” or effectively
interact with member of the host country [22]. To
assess the socio-cultural adaptation scale, Ward and
Kennedy (1996) revealed the SCAS (socio-cultural
adaptation scale). This scale measures the amount of
behavioral and cognitive difficulties experienced by
individual when adjusting to a new culture and society.
In this research, SCAS is used to assess the level of
socio-cultural adaptation especially in pre-migration
stage. Before asking the question, an introductory
statement is used i.e., “Living in a different culture
often involves learning new skills and behavior.
Thinking about living in Japan, please rate your
competence at each the following behaviors (from 1 =
Not at all competent; to 5 = Extremely competent)”.
The score shows the level of competency in adjusting
with socio-cultural different. This scale measures the
amount of behavioral and cognitive difficulties
experienced by the candidates when adjusting to the
new culture or society [23].
3. Results
3.1 Socio-demographic Characteristics
Table 1 shows the distribution of the socio
demographic status of the study participants. The
average age is 24.61 years, with age range 21-35 years
old with 63.5% female. Percentage number of certified
care worker candidates is 71.60% while nurse
candidates are only 28.40%. All of candidates hold
nursing educational background where 68.90% are
graduated from three years diploma of nursing school
and 31.10% are graduated from the bachelor of nursing.
The current economic condition of the candidates
shows that 1.40% of the candidates are in “very
difficult to survive” condition, 42.60% in “difficult but
able to survive” condition, and 56.00% in “not so
difficult to survive” condition. The previous working
status of the candidates, before applying EPA program,
shows that 60.80% of the candidates are being
employed and 38.5% are being unemployed.
Self-rated language proficiency was administered to
identify the level of language proficiency. The results
showed that 2% of the candidates rate themselves in
“Advance level” of language proficiency, 29.70% in
“Intermediate level”, 59.50% in “Elementary level”,
and 8.80% in “Basic level”.
3.2 Bivariate Analysis
The association between each predictor variables
with GHQ as outcome variable is estimated using
bivariate analysis. Independent sample t-test and
Pearson’s correlation has been conducted to find direct
correlation between each independent variable and
GHQ. The result from t-test analysis shows that there is
significant difference of GHQ score in term of
educational background (P < 0.05) the candidates who
graduated from three years diploma nursing school
tend to have healthier mental health compare with the
ones who graduated from bachelor nursing school. In
terms of working status when applying EPA program,
the candidates who were not worked tend to have
healthier mental health compare with those who were
worked (P < 0.05). There is no significant different in
Gender, EPA course, Economic status, Motivation for
migration, and Preparation for migration with GHQ.
Pearson’s correlation coefficient test shows that the
strongest correlation with GHQ-12 score are found in
knowledge about living environment in destination
country (r = -0.38, P < 0.01), followed by knowledge
about working condition (r = -0.32, P < 0.01), Age (r =
0.24, P < 0.01), Japanese language proficiency (r =
0.24, P < 0.05), Socio cultural adaptation (SCAS) (r =
-0.22, P < 0.05), Pull factor for migration (r = -0.21, P
< 0.05) and Moral support from family/relatives to go
to Japan (r = -0.19, P < 0.05).
3.3 Multivariate Analysis
The independent variables are selected and
evaluated by multiple linear regression analysis models
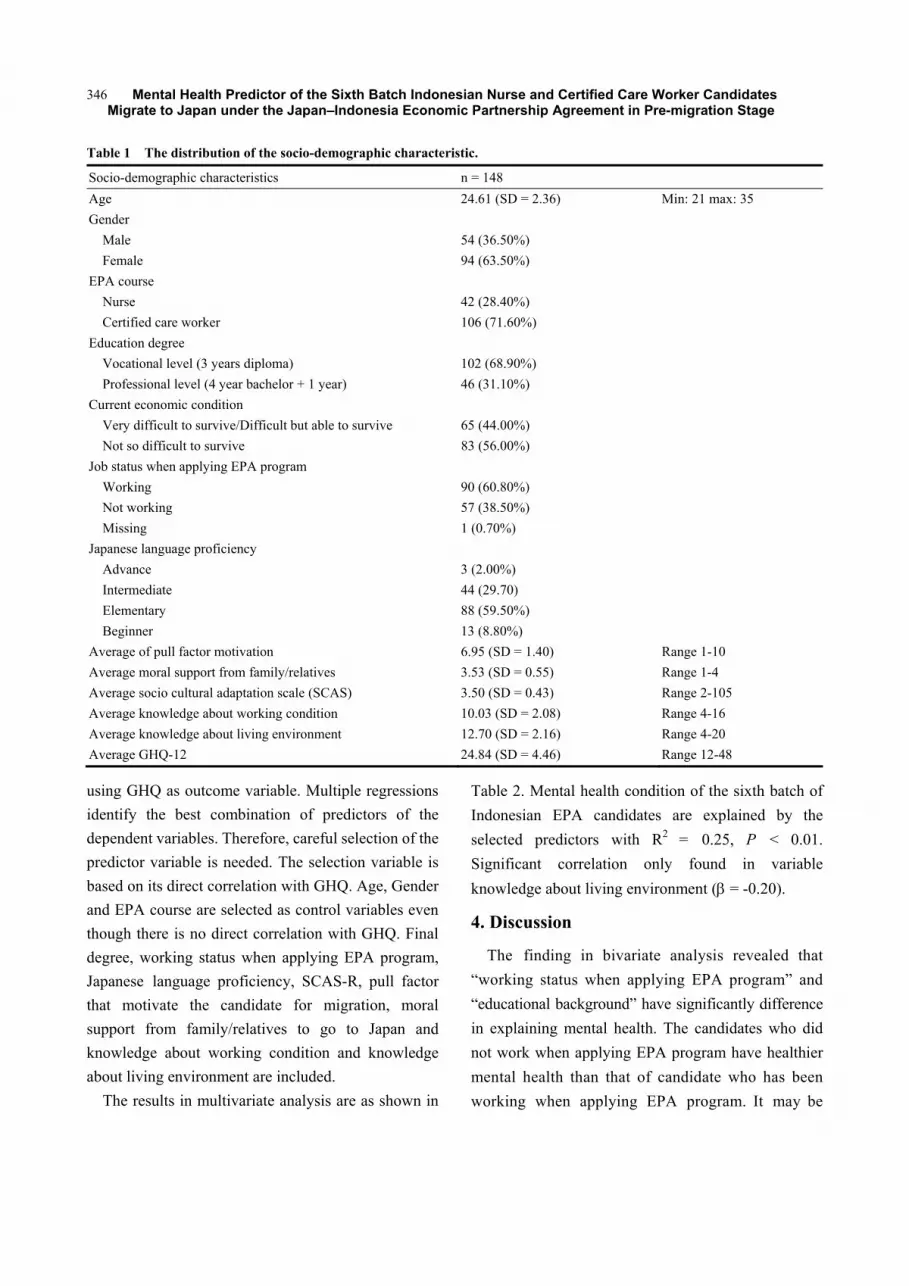
Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
346
Table 1 The distribution of the socio-demographic characteristic.
Socio-demographic characteristics n = 148
Age 24.61 (SD = 2.36) Min: 21 max: 35
Gender
Male 54 (36.50%)
Female 94 (63.50%)
EPA course
Nurse 42 (28.40%)
Certified care worker 106 (71.60%)
Education degree
Vocational level (3 years diploma) 102 (68.90%)
Professional level (4 year bachelor + 1 year) 46 (31.10%)
Current economic condition
Very difficult to survive/Difficult but able to survive 65 (44.00%)
Not so difficult to survive 83 (56.00%)
Job status when applying EPA program
Working 90 (60.80%)
Not working 57 (38.50%)
Missing 1 (0.70%)
Japanese language proficiency
Advance 3 (2.00%)
Intermediate 44 (29.70)
Elementary 88 (59.50%)
Beginner 13 (8.80%)
Average of pull factor motivation 6.95 (SD = 1.40) Range 1-10
Average moral support from family/relatives 3.53 (SD = 0.55) Range 1-4
Average socio cultural adaptation scale (SCAS) 3.50 (SD = 0.43) Range 2-105
Average knowledge about working condition 10.03 (SD = 2.08) Range 4-16
Average knowledge about living environment 12.70 (SD = 2.16) Range 4-20
Average GHQ-12 24.84 (SD = 4.46) Range 12-48
using GHQ as outcome variable. Multiple regressions
identify the best combination of predictors of the
dependent variables. Therefore, careful selection of the
predictor variable is needed. The selection variable is
based on its direct correlation with GHQ. Age, Gender
and EPA course are selected as control variables even
though there is no direct correlation with GHQ. Final
degree, working status when applying EPA program,
Japanese language proficiency, SCAS-R, pull factor
that motivate the candidate for migration, moral
support from family/relatives to go to Japan and
knowledge about working condition and knowledge
about living environment are included.
The results in multivariate analysis are as shown in
Table 2. Mental health condition of the sixth batch of
Indonesian EPA candidates are explained by the
selected predictors with R2 = 0.25, P < 0.01.
Significant correlation only found in variable
knowledge about living environment ( = -0.20).
4. Discussion
The finding in bivariate analysis revealed that
“working status when applying EPA program” and
“educational background” have significantly difference
in explaining mental health. The candidates who did
not work when applying EPA program have healthier
mental health than that of candidate who has been
working when applying EPA program. It may be

Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
347
Table 2 Multiple regression analysis results for pre-departure mental health.
Predictor variables Beta
Age 0.15
Gender 0.07
EPA course 0.01
Educational degree 0.03
Moral support from family/relatives to go to Japan -0.11
Socio cultural adaptation scale -0.09
Knowledge about working condition -0.15
Knowledge about living environment -0.20*
Job status when applying EPA program 0.01
Japanese language proficiency 0.08
Pull factor motivation 0.07
R square 0.25
Significant 0.00
F 4.04
Number of study participant 148
*: P < 0.05
assumed that the candidates who have been working as
registered nurse when applying EPA program, faced
difficult situation because they have to quit from their
stable job. Joining the EPA program put them on the
uncertain condition whether they will be passed the
national board examination to be a registered nurse in
Japan. On the other hand, the candidates who have not
been working when applying EPA program, tend to be
more enthusiastic because this program will give them
a new job and make them exited entering new working
environment. The candidates who graduate from 3
years diploma nursing school have healthier mental
health compare with the bachelor degree. This finding
might be assumed that to join with the EPA program,
regardless their basic nursing educational degree, the
candidate will start the same level of job in Japan. This
system is adjusted to the current existing system in
Japan, whereas the national board examination has
become the main factor in determining career path [24].
Regardless the final degree in Indonesia, as long as
hold the nursing license or certified care worker license,
they can start the same level of job in nursing or
certified care worker job. On the other hand, final
degree of nursing education has the very important
role in nursing carrier development in their home
country. According to Indonesian nursing standard of
competency, the authority and competency in
performing nursing practice is based on nursing
educational background [25]. Consequently, for the
three years diploma nursing graduate, to work as EPA
candidates could be a distinct “advantage” because
they obtain the same position with BSN (Bachelor of
Nursing).
Moral support from family and relatives,
significantly correlate with GHQ. Social support is
assumed to become critically important in the
pre-migration phase because in this phase the
candidates faced fairly unstable conditions, to leave
their family and friends. The candidates who have
better social support tend to have less stress facing
pre-migration stage. Research conducted by Ryan, et al.
(2006) suggested that adequate social support may
protect those who were poorly prepared for their
migration from being depressed. In line with the
reseach conducted by Chou (2009), that perceived
social support not only significantly related to
depressive symptom reversely but also moderating the
harmful effect of poor migration planning on
depressive symptomatology in post migration.
Compare with the one who have lesser support, the

Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
348
candidate who have better social support tend to be
mentally healthier, and they are sorrounded by the
people who support them to deal with such stressfull
event in pre-migration stage.
SCAS in pre migration stage measures the
competency level of expectation in socio cultural
adaptation after migration. The result of bivariate
analysis shows that SCAS significantly correlate with
GHQ. The candidates who have higher competency
expectation show healthier mental health.
Pre-migration socio cultural adaptation expectation
research conducted by Jasinskaja-Lahti and Yijala
(2011) revealed that the expected difficulties in
socio-cultural adapatation were directly related to
increase pre-acculturative stress. Acculturative define
as the psychological, somatic, and social difficulties
that may accompany acculturation processes, often
manifesting in anxiety, depression and other forms of
mental and physical maladaptation [26]. In other words
the competency level of sociocultural adaptation in
pre-migration stage will help the candidates dealing
with the stressful event before migration and help to
enhance their confidentiality in cultural adjustment in
the new society.
The bivariate analysis also proved that the language
proficiency significantly correlate with GHQ, whereas
the better proficiency shows healthier mental health.
Japanese language proficiency plays important role for
successful interaction with the host country’s
community. It has been noticed that Japanese language
becomes a hurdle for those who did not get accustomed
with Chinese character such as Indonesian. Mastering
Japanese language might improve and potentially
facilitate psycho-social adjustment to a host society.
Study conducted among Japanese Brazilian migrant,
found that with moderate fluency in Japanese to be
psychologically less distress [27]. Another study of
migration also cited that, communication competence
in the language of the host country language is
positively related with cultural adjustment [23, 28]. In
other words we can say in that, those who have higher
language proficiency in pre-migration stage tend to be
more confidence to migrate to Japan and keep healthier
mental health.
The study also found the significant correlation
between pull factors that motivated the candidate to
migrate to Japan. The candidates who were more
motivated by pull factors likely to have healthier
mental health. Pull factor defined as something
concerning the country to which a person migrates.
People will migrate generally because the new place
has “pull” factors that motivated their movement.
Study among Japanese Brazilian who migrate to Japan
showed that those who motivated by pull factors to
improve their quality of life in Japan, were better
equipped to tolerate with living condition in Japan [27].
Knipscheer, et al. (2000), on his study among Ghanaian
migrants in the Netherland showed that those who
motivated by pull factor in the host country were more
adapted to the host country. It may assume that the
candidate who more motivated by pull factor from the
host country tend to have better preparartion for
adjustment towards destination country.
The knowledge about destination country which
devided into knowledge about working condition and
living environment has stronger correlation with
mental health, compare with other variables.
Particularly, variable “Knowledge about living
environment” in Japan was also consistently correlates
with GHQ in multiple regression models. Whereas,
other predictor variables such as Age, Gender, EPA
course, moral support and knowledge about working
condition showed non-significant correlation with
GHQ, although the entire model have statistically
significant in explaining mental health of the sixth
batch Indonesian nurse and certified care worker
candidates in pre-migration stage. This study showed
that the knowledge about living environment become
substantial factor in determining mental health in
pre-migration stage. Bughra (2004), revealed that the
preparation for the act of migration is a significant
factor in the outcome on pre-migration stress.

Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
349
This finding also accordance with former research
conducted by Hirano (2012) toward the fourth batch
EPA candidates who depart to Japan few months after
the East Great Earthquake (2011). The result showed
that knowledge about the actual living and working
conditions in Japan is a major indicator of the mental
health of the Indonesian nurse and certified care worker
candidates, instead of their worry concerning the
earthquake. Previous study toward the first batch also
conducted by Setyowati, et al. (2010) identified that
one of the stress predictor among the EPA candidates is
lack of information about the condition of the
destination country such as working and living
condition provided during pre-departure program. This
study finding is consistent with previous studies,
although each study subject (EPA batch) was exposed
with information about Japan in different time range.
The sixth batch exposed with six month Japanese
language training prior to migration, whereas the fourth
batch with three months language training and the first
batch have no pre-departure language training program.
This finding may assume that although the candidates
have been exposed with pre-departure language
training program in different time range, the
knowledge about living environment still becoming
their concern to be aware. Another assumption is that
the disseminated knowledge in pre-departure program
is general knowledge about Japanese society and
environment when in the fact is that the candidates will
be assigned in various working place with different
living environment. Therefore, the knowledge about
living environment still becomes a concern for the
candidates prior to migration. Degree of knowledge
about the condition of in destination country shows the
level of cognitive preparedness for migration.
Successful preparation in term of knowledge
acquisition of the new societies may lessen
psychological maladjustment prior to migration [17].
Several limitation of the present study should be
addressed where this study is based on cross sectional
data. Consequently, any findings in mental health
predictor cannot show the causal sense. Longitudinal
data are needed to figure out the causal and temporal
relation between pre-migration and post-migration.
Any finding in this research should encourage further
investigation on examining how pre-migration factors
affected mental health of new migrant in post migration
stage. Some variables measured the self-reported of
current condition; therefore the results could not be
generalized for clinical mental health condition.
However, as being noticed that mental health
measurements are measured the perceived feeling, this
study contributes to resolving the predictors of
the mental health of EPA candidate in pre-migration
stage.
5. Conclusions
In this study, the concepts of mental health were
used overarching concept, not referring to any specific
type of illness or disorder. Pre-migration defined as an
early step of migration, whereas the potential migrant
such as EPA candidates may involve in pre-migratory
activities organized by the receiving society as well as
collecting information about destination country.
Knowledge about living environment such as security
of residential area, whether they will be welcomed by
Japanese people, climate in their residence in Japan,
experience of work and life of EPA earlier batch and
working culture of Japanese, such as their custom to
work 2-3 hour longer than the written in contract
become a very important factor in determining the
candidate’s mental health. In this study, the knowledge
about living environment refers the living environment
in the future assigned working place.
Health care worker migration under JI-EPA involves
government to government cooperation. Unlike other
migration, the migration program under JI-EPA is a
special case in term of policy and system, this program
governed by a bilateral agreement under the Economic
Partnership Agreement. Some pre-migration condition
may not emerge in this study as being revealed in other
voluntary migration. Data collecting instrument
Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
350
(questionnaire) modification might be necessary for
further study to find the most appropriate mental health
predictor in nurse and care worker migration EPA
program in pre-migration stage. However, this study
finding may become an input for both countries in
improvement for pre-departure preparation. These
finding suggests an improvement in knowledge
dissemination about the destination country.
Improvement in disseminating knowledge about
working condition and living environment, during
pre-departure orientation might become an effective
aid in dealing with pre-migration stress and assist the
candidates preparing the better adaptation with the new
living condition in destination country. Mental health
condition in pre-migration stage may affect the mental
health condition in post migration stage.
Acknowledgements
This article is part of “Study on mental health
condition of the 6th batch nurse and care worker
candidates’ under JI-EPA agreement, in pre and post
migration stage”.
This research was supported by the president's
discretionary fund of Nagasaki University, Japan
(Principal Investigator: Yuko Ohara-HIRANO).
References
[1] International Organization for Migration 2006. “Migration and Human Resouces for Health : From Awareness to Action.” Geneva: International Organization for Migration.
[2] Stillman, S., McKenzie, D., and Gibson, J. 2006. Migration and Mental Health: Evidence from Natural Experiement. Bureau for Research and Economic Analysis of Development.
[3] Taylor, A., Hwenda, L., Larsen, B., and Daulaire, N. 2011. “Stemming the Braindarin—A WHO Global Code of Practice on International Recruitent of Health Personnel.” The New England Journal of Medicine 365: 2348-2351.
[4] Bach, S. 2003. International Migration of Health Workers: Labor and Social Isues. Sectoral Activities Program
[5] WHO 2010. “World Life Expectancy.” Geneva: World
Health Organization. [6] Cabinet Office, Government of Japan. 2012. “Policies on
Cohesive Society, Cabinet Office, Government of Japan.” Accessed October 28, 2013. http://www8.cao.go.jp/kourei/whitepaper/w-2012/zenbun/s1_1_1_02.html.
[7] National Institute of Population and Social Security Research 2012. “Population Projections for Japan (January 2012): 2011 to 2060.” Tokyo: National Institute of Population and Social Security Research.
[8] Horlacher, D. E., and MacKellar, L. 2003. “Population Ageing in Japan: Policy Lessons for South East Asia.” Asia Pacific Development Journal 3: 97-122.
[9] Ministry of Health and Welfare 2012. “The Future Vision of the Integrated Reform of Social Security Service and Taxation.” Ministry of Health and Welfare.
[10] Matsuno, A. 2009. “Nurse Migration: The Asian Perspectives.” ILO Regional Office for Asia and the Pacific.
[11] MHLW 2014. “Ministry of Health Labour and Welfare, Japan.” Accessed May 5, 2014. http://www.mhlw.go.jp/file/05-Shingikai-11601000-Shokugyouanteikyoku-Soumuka/0000037613.pdf.
[12] Hirano-Ohara, Y. 2014. “Beyond the Myth of the JPEPA: Realities and Suggestion.” in Migration of Filiupino Nurses under the Japan-Philippine Economic Partnership Agreemnet—Trend and Challange, edited by Hirano-Ohara, Y., and Yonneno-Reyes, M. Manila: Nagasaki University.
[13] Ogawa, R. 2012. Globalization of Care and the Context of Reception of SouthEast Asian Care Worker in Japan. International Migration of South East Asian Care Worker to Japan under Economic Partnership Agreement.
[14] IJ-EPA Agreement. “Annex 10 referred to chapter 7-Specific Commitment for The Movement of Natural Person.” Accessed December 11, 2007. http://www.ditjenkpi.kemendag.go.id/website_kpi/Umum/IJEPA/Annex10(ID).pdf.
[15] Ohno, S. 2012. “South East Asian Nurses and Cregiving
Workers Transending the National Boundaries: An
Overview of Indonesian and Filipino Workers in Japan
and Abroad.” International Migration of South East Asian
Nurses and Care worker to Japan under Econonomic
Partnership Agreement: 541-569.
[16] Bughra, D. 2004. “Migration and Mental Health” Acta
Psychiatrica Scandinavica 109: 243-258.
[17] Burgelt, P. T., Morgan, M., and Pernice, R. 2008.
“Staying or Returning: Pre-Migration Influences on the
Migration Process of German Migrant in New Zaeland."
Journal of Community & Applied Social Psychology 18:
280-298.
[18] Gushulak, B., and MacPherson, D. 2011. “Health Aspect
Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
351
of the Pre-departure Phase of Migration.” PLoS Medicines
8 (5): 1-7.
[19] Bughra, D., Ghupta, S., Bhui, K., Craig, T., Nisha, D.,
INGLEBY, J., Kikbride J., and Moussaoui, D. 2011.
“WPA Guidance on Mental Health and Mental Health
Care in Migrants." Official Journal of The World
Psychiatry Association 10 (1): 2-10.
[20] Tinghog, P., Hemmingsson, T., and Lundberg, I. 2007.
“To What Extent May the Association Between Immigrant
Status and Mental Illness be Explained by Socioeconomic
Factor?” Soc Psychiatry sychiatr Epidemiol 42:
990-996.
[21] Goldberg, D., and William, P. 1988. “General Health
Questionnaire (GHQ-12)." Accessed February 12, 2014.
http://shop.gl-assessment.co.uk/home.php?cat=416.
[22] Ward, C., and Kennedy, A. 1994. “Acculturation Strategy
and Psychological Adjustment and Sociocultural
Competence During Cross-cultural Transition.”
International Journal of Psychology 18 (3): 329-343.
[23] Ward, C., and Kennedy, A. 1999. “The Measurement of
Socio-cultural Adaptation.” Intrenational Journal of
Intercultural Relation 23 (4): 659-657.
[24] Japan Nursing Association 2011. “Nursing in Japan.”
Shibuya-Tokyo: Departement of International Afair Japan
Nursing Association.
[25] Indonesian Health Profession Educational Quality 2012. Accessed March 24, 2014. http://hpeq.dikti.go.id/v2/images/Produk/18.3-Draf-STANDAR-KOMPETENSI-PERAWAT.pdf.
[26] Berry, J. 2006. “Stress Perspective on Acculturation.” In The Cambridge Handbook of Acculturation Psychology, edited by Sam, L. D., and Berry, W. J. Cambridge: Cambridge University Prss.
[27] Asakura, T., and Murata, A. K. 2006. “Demography, Immigration Background, Difficulties with Living in Japan and Psychological Distress Among Japanese Brazilians i Japan." Journal Immigration Health 8 (4): 325-328.
[28] Yang, R., Noels, K., and Saumure, K. 2006. “Multiple Routes to Cross-cultural Adaptation for International Students; Mapping the Path Between Self-construals, English Language Confidence and Adjustment.” International Journal of Intercultural Relation 30 (4): 487-505.
[29] Cabinet Secretariat. 2012. “The Future Vision of the Integrated Reform of social security service and taxation.” Accessed December 24, 2013. http://www.cas.go.jp/jp/ seisaku/syakaihosyou/seihu_yotou/kourou.pdf.
[30] Yagi, N., Mackey, T. K., Liang, B. A., and Gerlt, L. 2013. “Japan-Phiulipines Economic Partnesrhip Agreement (JPEPA)-Analysis of a Failed Nurse Migration Policy.” International Journal of Nursing Studies 51 (2): 243-250.
[31] World Health Organization 2010. “World Life Expectancy.” World Health Organization.
[32] Kingma, M. 2008. “Nurses on the Move: Historical Perspective and Current Issues.” JIN: The Online Journal of Issues in Nursing 13.
[33] Hirano-Ohara, Y. 2012. “The Mental Health Status of Indonesian Candidates Leaving for Japan under the Japan–Indonesia Economic Partnership Agreement: After the Great East Japan Earthquake.” International Journal of Japanese Sociology 21.
[34] Setyowati, Susanti, H., Yetti, K., Hirano Y., and Kawaguchi, Y. 2010. “Indonesian Nurse in Japan Who Face Job and Cultural Stress in Major Problems Faced by the Nurse Candidates Working in Japan Under IJ-EPA Agreement.” Bulletin of Kyushu University Asia Center 5.
[35] Alam, B., and Wulansari, S. A. 2010. “Creative Friction :Some preliminary Consideration on the Socio-cultural Issues Encountered by Indonesian Nurses in Japan.” Bulletin of Kyushu University 5: 183-193.
[36] Setyowati, Susanti, H., Yetti, K., Hirano, Y., and Kawaguchi, Y. 2010. “The Experience of Indonesian Nurses in Japan who Face the Job and Cultural Stress in Their Work: Qualitative study.” Bulletine of Kyushu University 5:109-209
[37] Zimet, G., Dahlem, N., Zimet, S., and Farley, G. 1988. “The multidimensional scale of perceived social support.” J. Pers Assess 52: 30-41.
[38] Chou, K.-L. 2009. “Pre-migration Planning and Depression among New Migrants to Hong Kong: The Moderationg Role of Social Support.” Journal of Affective Disorder 114: 85-93.
[39] Ryan, L., Leavey, G., Golden, A., Blizard, R., and King, M. 2006. “Depression in Irish Immigrant living in London: Case-control Study.” British Journal of Psychiatry 188: 560-566.
[40] Update, J. “Indonesia Today.” Accessed October 12,
2010. http://www.jakartaupdates.com/.
[41] Jasinskaja-Lahti and Yijala, A. 2011. “The Model of
Pre-acculturative Stress—A Pre-migration Study of
Potential Migrant from Rusia to Finland.” International
Journal of Intercultural Relations 35: 499-510.
[42] Ward, C., Furnham, A., and Bochner, S. 2001. The
Psychology of Culture Shock. Philadelphia: Routledge.
[43] Knipscheer, Jong, E., De, Klebber, R., and Lamptey, E.
2000. “Ghanaian Migrants in The Netherlands: General
Health, Acculturative Stress and Utilization of Mental
Health Care.” Journal of Community Psychology 28 (4):
459-476.
[44] Ministry of Health Labour and Welfare. “Ministry of
Health Labour and Welfare.” Accessed March 25, 2014.
www.mhlw.go.jp/file/04-Houdohapyou-10805000-Iseiky

Mental Health Predictor of the Sixth Batch Indonesian Nurse and Certified Care Worker Candidates Migrate to Japan under the Japan–Indonesia Economic Partnership Agreement in Pre-migration Stage
352
oku-Kangoka/0002.pdf.
[45] Ministry of Health, Labour and Welfare. “Dai 26 Kai Kaigofukushishi EPA ni Motodzuku Kokka Shiken no Kekka (The Breakdown of the 26th Care Worker National Examination Results).” Accessed March 27, 2014. Available: www.mhlw.go.jp.
[46] Fushimi and Kobayashi, M. 2013. “Chōki-teki Kango Shokuin Jukyū Mitōshi no Suikei (Estimation of the Long Term Manpower Demands and Supplies of Nursing Personnel).” Accessed May 12, 2014. http://www.mhlw.go.jp/stf2/shingi2/2r9852000000eydo-att/2r9852000000eyf5.pdf.