health status in low-income countries: addressing health inequities in nigeria health status in...
TRANSCRIPT

HEALTH STATUS IN NIGERIA
Health status in low-income countries: Addressing
health inequities in Nigeria
Olanike Kehinde
Walden University
HEALTH STATUS IN NIGERIA
Health status in low-income countries: Addressing
health inequities in Nigeria
Sub-Saharan Africa is the poorest region of the world and it
bears the brunt of global health inequalities (Rispel, Palha de
Sousa, & Molomo, 2009). There are high levels of under-nutrition,
50% of maternal and child deaths, and a high burden of infectious
diseases (UNDP, 2008). A child born in Africa, may not live
beyond 47 years of age, has a high risk of being HIV positive at
birth, and is more likely to lose his/her mother at birth than in
any other region of the world (WHO, 2006). According to the World
Health Organization (2006), a child born in Africa is also likely
to be affected by drought, famine, floods, or civil war at least
once in his/her short life.
According to the Commission on Social Determinants of Health
(CSDH), there is a social gradient in health irrespective of the
country, and the lower the socioeconomic status (SES), the worse
the health of the people (WHO, 2008). These inequities are unfair
HEALTH STATUS IN NIGERIA
and must not be allowed to continue as the injustice contributes
to premature deaths; they must therefore be addressed by
governments at all levels and all stakeholders in health
including civil societies and communities. The social gradient in
health within countries, the poor health of the poor, and health
inequities amongst countries are as a result of unequal
distribution of power, income and resources globally and
nationally (WHO, 2008).
This paper will focus on health inequities in Nigeria, one
of the largest countries in Africa with a population of
177,155,754 (year 2014 estimates from The World Factbook 2014)
and a high level of inequalities and inequities in population
health. Current efforts being made to reduce health inequities
and the development of a health policy to address some inequities
will also be discussed.
Rationale for country selection
The rationale for selecting Nigeria by me for this project
is because of the poor health status of Nigeria on most health
HEALTH STATUS IN NIGERIA
indicators and a dearth of social policies targeting the social
determinants of health especially policies affecting early life
experiences.
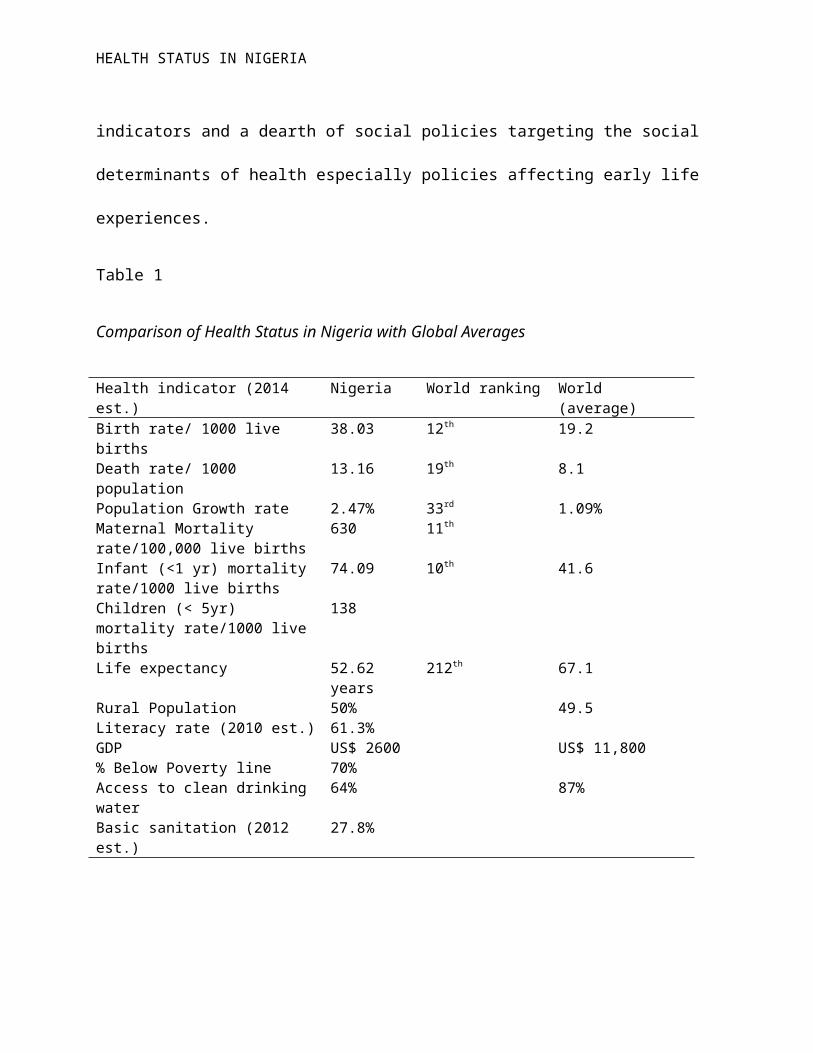
Table 1
Comparison of Health Status in Nigeria with Global Averages
Health indicator (2014 est.)
Nigeria World ranking World (average)
Birth rate/ 1000 live births
38.03 12th 19.2
Death rate/ 1000 population
13.16 19th 8.1
Population Growth rate 2.47% 33rd 1.09%Maternal Mortality rate/100,000 live births
630 11th
Infant (<1 yr) mortality rate/1000 live births
74.09 10th 41.6
Children (< 5yr) mortality rate/1000 live births
138
Life expectancy 52.62 years
212th 67.1
Rural Population 50% 49.5Literacy rate (2010 est.) 61.3%GDP US$ 2600 US$ 11,800% Below Poverty line 70%Access to clean drinking water
64% 87%
Basic sanitation (2012 est.)
27.8%
HEALTH STATUS IN NIGERIA
Table 1 above shows a comparison of health status in Nigeria with
global averages (statistics from The CIA - World Factbook 2014).
Nigeria has also not met the targets for the three nutrition
- related millennium development goals (MDGs) 1, 4, and 5. As at
2008, Nigeria recorded 25%, 33% and 26% reduction respectively in
underweight children, under-five mortality, and maternal
mortality. The expected targets for these indices by 2008 were
36%, 54%, and 54% respectively (Alles et. al., 2013). There is
gender disparity in education in favour of boys and girls in the
rural areas are half as likely to receive education as those in
urban areas (National population commission of Nigeria as cited
in Alles et. al.).
In Nigeria there is no universal access to health services.
Most people still pay for health care out of their pockets. The
health insurance scheme only works for government workers and
those in the organized private sector. There are inequities owing
to the high cost of medical care, uneven distribution of health
facilities, with the rural areas at a disadvantage (Alles et.
al., 2013).
HEALTH STATUS IN NIGERIA
A study by the Federal Ministry of Health (FMOH) in Nigeria
(cited in Alles et. al., 2013) indicated under-utilization of
ante natal care. Communicable diseases (topmost of which are
diarrhea, malaria, and pneumonia) are the major causes of child
mortality. These disease conditions contribute to malnutrition
which in turn predisposes to the same disease condition resulting
in a vicious cycle (Alles et. al., 2013).
Undernutrition in early life can affect brain development
and health of the individual in later life. The WHO recommends
exclusive breastfeeding in the first six months of life for
optimal growth, development and health. A study by Alles et. al.
(2013) showed that only 32% of children born in Nigeria are put
to the mother’s breast in the first hour of life. The study also
revealed that only 13% of babies are exclusively breastfed in the
first six months of life and 33% are given water in addition to
breast milk (Alles et. al., 2013).
Nigeria was also selected for this project because it is my
country and I intend to make a positive social change there as a
scholar practitioner and social change agent.
HEALTH STATUS IN NIGERIA
Social determinants of health in Nigeria
Social determinants of health (SDH) are those conditions
under which people are born, live, work and age that affect their
health outcomes (WHO, 2008). A person born and who lives in a
highbrow area of a city where public smoking is banned will
likely be healthier than one who resides in a slum where living
conditions are poor and there is no access to potable water.
Social determinants of health also refer to social, economic, and
political resources and structures that influence health outcomes
(Barnett and Casper as cited in Baker, Metzler, & Galea, 2005).
They include conditions as access to affordable healthy food,
potable water, safe housing, access to healthcare, supportive
social networks, and socioeconomic policies (Baker, Metzler, &
Galea, 2005; Gehlert et. al., 2008).
In Nigeria, the social determinants of health to be
addressed include universal access to health care, poverty and
equitable income distribution, decent and affordable housing,
safe environment, social exclusion and isolation, education,
gender disparity, crime rate, socioeconomic policies, and social
HEALTH STATUS IN NIGERIA
networks. These determinants influence inequalities and
inequities in health and so they must be addressed if population
health is to be improved in Nigeria (WHO, 2008).
Description of social determinants of health in Nigeria and the
need for addressing them
Access to healthcare: A study in Southeast Nigeria showed that a
large proportion of respondents (46.2%) considered public health
facilities to be inaccessible to the poor for reasons of cost and
insufficient number of facilities (Nnonyelu & Nwankwo, 2014).
According to The World Factbook 2014, there were 0.53beds /1000
Nigerians in 2004 and 0.4 physicians/1000 people in 2008 (Central
Intelligence Agency, 2014). There is disparity in access to
healthcare across regions in Nigeria. The rate of utilization of
healthcare facilities in Northern Nigeria in 2003 is 11% compared
to 60% in the South (Osazuwa - Peters, 2011).
Education: The literacy level of the Nigerian population aged 15
and above who can read and write is 72.1% for males and 50.45%
for females (The World Factbook, 2014; 2010 estimates). The
HEALTH STATUS IN NIGERIA
higher the level of education of a people, the more likely they
are to seek treatment and the better their health is likely to be
(Nnonyelu & Nwankwo, 2014).
Poverty and Income distribution: 70% of Nigerians live below the
poverty line of less than $1 a day (Table 1). There is income
distribution inequality in Nigeria with high rural/urban
disparity (Bakare, 2012). The measure of income inequality – Gini
index for Nigeria in 2010 was 43 (World Bank data, 2015). The
greater the income inequality in a country, the worse off the
health of the people is and this cuts across all socioeconomic
strata. Poor nations are also worse affected (Weir, 2013).
Gender disparity: Women are being discriminated against right
from childhood and so they are more likely to be poor, uneducated
and without political power than men (WHO, 2005). Discrimination
will likely affect the health status of women negatively and so
it must be addressed. For instance, because women lack control
over their sexual activities, they become vulnerable to STIs and
HIV/AIDS (WHO, 2005).
HEALTH STATUS IN NIGERIA
Decent and affordable housing: a large proportion of Nigerians
still live in squalid accommodation and 65% live in rural areas
(WHO, 2005).
Safe environment: only 64% of Nigerians have access to clean
drinking water and 27.8% have access to basic sanitation services
(Table 1).
Crime rate: The overall crime rate in Nigeria was given as 31% in
2012 with 75% of the population claiming they were fearful of
being victims of criminal activities (Cleen Foundation, 2012).
Security has to be improved upon in Nigeria so that crime rate
can be reduced, people can feel safer, and their emotional and
physical health can be improved.
Socioeconomic policies: In Nigeria there is a dearth of policies
that affect early life development, income redistribution, safe
and comfortable housing and that encourage increasing physical
activity. These need to be addressed in order to reduce
inequities so as to improve the health status of the population.
HEALTH STATUS IN NIGERIA
Social exclusion and isolation: Rapid urbanization is related to
inequality and exclusion in Nigeria. The increasing numbers of
slum dwellers in Nigerian cities like Lagos suffer social
exclusion from access to resources and opportunities offered by
the city (Fotso et. al., 2010). For instance, social exclusion
through denial of education is common in slums as a result of
poverty. The rich may feel isolated in their homes as a result of
fear of being attacked by criminals.
Improvement in access to healthcare and other SDH will help
to reduce morbidity and mortality amongst Nigerians and thus
improve life expectancy. Education is a major factor influencing
health (WHO, 2005). The probability of children born to
illiterate mothers is two times higher than for those born to
educated women; Illiteracy is directly related to poverty,
malnutrition, ill health and high infant and child mortality
(WHO, 2005). Therefore addressing inequities in education will
help to improve the quality of life of Nigerians and thus life
expectancy and other health outcomes.
HEALTH STATUS IN NIGERIA
An understanding and assessment of the extent of the
influence of social determinants on health will help the
government of Nigeria and policy makers to formulate and
implement appropriate social policies that will help to reduce
inequities in health, engender the health of the people and thus
improve health status of the Nigerian populace. There is the need
to formulate policies that will improve the welfare of the poor
and create access to education as illiteracy is associated with
many of the determinants of health.
Issues in health literacy and cultural awareness in Nigeria
Cultural issues and poor health literacy contribute to poor
health status in Nigeria. Gender inequality is an aspect of
culture that affects health status in Nigeria. A study by
Nnonyelu & Nwankwo (2014), showed that some women in Southeast
Nigeria needed to obtain permission from the male family head
before they can access healthcare. In some other parts of the
country, women need to be given money by their husbands to be
able to access medical services. These point to the need to
HEALTH STATUS IN NIGERIA
empower females in order to improve population health status in
Nigeria.
At least 80% of rural dwellers go to traditional healers for
healthcare in Nigeria and they believe that there are spiritual
causes for illnesses (Yahya, 2007). For instance, among some
people in Zaria, Northern Nigeria, polio is believed to be caused
by an evil spirit who drinks the blood of his victims, and causes
paralysis or even death (Renne, 2006). The health practitioner
needs to understand the cultural beliefs of the people in order
to communicate health information effectively so as to influence
health outcomes. Cultural beliefs affect the uptake of
immunization in some parts of Nigeria. The belief in Northern
Nigeria that the polio vaccine was introduced in 2003 to reduce
the population led to massive boycott of the immunization
programme. This led to fresh outbreaks of polio that has hindered
eradication of polio out of Nigeria till date (Osazuwa - Peters,
2011). A study in Southeast Nigeria also found that 46.3% of the
subjects believed that herbalists can cure diabetes (Nwankwo,
Nandy, & Nwankwo, 2010).

HEALTH STATUS IN NIGERIA
Health literacy may be defined as the ability of an
individual to acquire, communicate, process and understand health
information with which informed decisions about health can be
made to achieve positive health outcomes (CDC, 2011). WHO (2015)
also defined health literacy as “the cognitive and social skills
which determine the motivation and ability of individuals to gain
access to, understand and use information in ways which promote
and maintain good health.” Poor health literacy contributes to
health inequities in Nigeria and improvements in health literacy
will help to reduce inequities (Onotai, 2008). A study in
Southeast Nigeria found that 96.3% of respondents lacked basic
knowledge of diabetes management (Nwankwo, Nandy, & Nwankwo,
2010).
My findings show that there has not been a lot of documented
evidence on the effect of health literacy and culture on health
inequities in Nigeria. There is the need for more studies to be
conducted on these aspects with a view to reducing inequities and
improving health outcomes.

HEALTH STATUS IN NIGERIA
Relationship between health inequality/inequities and life
expectancy for the Nigerian
Population
According to Wilkinson and Pickett (2010), inequalities
affect the health status of a population. The level of literacy
also affects health- seeking behaviors and health. High level of
illiteracy in Southeast Nigeria was found to contribute to low
life expectancy (Nnonyelu & Nwankwo, 2014). Equality in a society
also affects health outcomes. People that have the same level of
education, income, or social class are healthier in a more equal
society than in a society with higher level of inequality
(Wilkinson & Pickett, 2010). This implies that the quality of
life is higher in countries where there is a higher level of
equality. Greater equality affects the lower class more
positively than those who are in a higher economic class
(Wilkinson & Pickett, 2010).
Inequities lead to increased healthcare costs (Dankwa-Mullan
et. al., 2010). Gehlert et. al. (2008), stated that upstream
HEALTH STATUS IN NIGERIA
determinants of health (as socioeconomic status) influence and
regulate events at the cellular level to cause disease and thus
can affect life expectancy.
The Nigerian health policy does not focus directly on early
life experiences, and so the level of morbidity and mortality
increases and this impacts life expectancy negatively. For
instance, a pregnant woman in Nigeria prior to year 2000 was
entitled to six weeks maternity leave before and after delivery
(Federal Republic of Nigeria Laws, 1990). This meant that she
only had six weeks to bond with the baby before resuming work
unlike the woman who is self employed or who does not work at all
who can spend up to six months with the baby after delivery.
Policies that affect families early in life have been found to
produce health benefits throughout life (Laureate Education,
2011). In Sweden for instance, a woman is entitled to compulsory
maternity leave lasting 12 months which gives ample time to bond
with the baby (Laureate Education, 2011).
The disparities in access to education between genders and
in access to drinking water and sanitation between the rural and
HEALTH STATUS IN NIGERIA
urban areas contribute to health inequities which must be
addressed in order to improve life expectancy. The literacy
levels are 72.1% for males and 50.4% for females (Central
Intelligence Agency, 2014). In some cultures in Nigeria, the
female child is not educated and she is instead married off at an
early age. Only 49.1% of rural dwellers have access to clean
drinking water in Nigeria compared to 78.8% of urban dwellers
while 24.7% and 30.8% of rural and urban dwellers respectively
have access to basic sanitation services (Central Intelligence
Agency, 2014). These disparities contribute to disadvantages in
health for the female child and rural dwellers. There is no
support for the elderly in government policies and so they are
more prone to ill health and this will affect the health status
of the population negatively.
Low socioeconomic status of the rural dwellers and urban
slum dwellers in Nigeria also contribute to the low life
expectancy in Nigeria (Oyesola & Kadiri, 2010). Poor access to
healthcare for disadvantaged groups in Nigeria also contributes
to low life expectancy. In order to improve the life expectancy
HEALTH STATUS IN NIGERIA
of Nigerians, the governments at all levels must aim at reducing
inequities by addressing issues of poverty, living and working
conditions, universal access to healthcare irrespective of
location, and the physical environment.
Two current efforts in Nigeria aimed at reducing health
inequities
In addressing health inequities, the World Health
Organization [WHO] (2008), through the Commission on social
determinants of health advocates three levels of action:
Improve daily conditions in which people are born, grow,
live, and age.
Tackle the inequitable distribution of power, money, and
resources locally, nationally and globally.
Measure the problem, evaluate action, expand the knowledge
base, train appropriate workforce, and raise public
awareness about the social determinants of health.
HEALTH STATUS IN NIGERIA
The Nigerian government through its poverty alleviation
programmes – SURE-P and NEEDS; and the National programme on
immunization (NPI) aim to tackle health inequities in the
population. In tackling MDG 1, the Federal Government of
Nigeria initiated the National Economic Empowerment and
Development Strategy (NEEDS). It is aimed at reducing poverty
by empowering people through job creation through the National
Directorate of Employment (NDE) and the National Poverty
Eradication Program (NAPEP). It also aims to create an
enabling environment for investment and local entrepreneurship
(Rispel, de Souza & Molomo). Through NAPEP many young people
in Nigeria have benefited from training and job creation
opportunities.
The Subsidy Reinvestment and Empowerment Programme (SURE-P)
is designed alleviate poverty through provision of critical
infrastructure and safety net projects. It aims to provide
necessary infrastructure and human resource empowerment
projects such programs as improvement in maternal and child
health programmes, public works, employment schemes, mass
HEALTH STATUS IN NIGERIA
transit programs, vocational training and skills acquisition
schemes (Federal Republic of Nigeria, 2013). The programme has
achieved some success. Within two years it has been able to
reduce the maternal mortality rate by 26% and reduce neonatal
mortality by 22% (Federal Republic of Nigeria, 2013).
The National Program on Immunization (NPI) was renamed in
1997 and it has a mandate to protect children from vaccine
preventable diseases through the provision of vaccines,
devices and technical support (National Primary Healthcare
Development Agency [NPHCDA] (2013). Since inception in 1979,
the vaccination coverage has reached above 80% (NPHCDA, 2013).
This initiative targets MDG 4 and it has a slogan, “to save
one million lives”. The under – 5 mortality rate has gone down
from 191/1000live births in 1990 to 94 in 2012 even though
this is still short of the 2015 target of 63.7/1000 live
births ((Federal Republic of Nigeria, 2013b).
To reduce health inequalities the Nigerian government must
continue to design social policies and effectively implement
them; address identified constraints; monitor and evaluate the
HEALTH STATUS IN NIGERIA
implementation policies; and ensure community participation by
providing enabling environments (Rispel, de Souza & Molomo).
Developing an acceptable health policy for Nigeria
According to Lee, Buse, & Fustukian (2002), health policies
aim to provide frameworks for filling gaps in the health field.
An appropriate health policy must take into consideration the
health problems of the population, equity, and interventions that
are culturally appropriate and affordable (Alem & Gureje as cited
in Kehinde, 2014b). The Nigerian health system focuses on
improving access to care, addressing issues of health manpower
and healthcare financing and costs, in addition to related social
issues (Federal Ministry of Health, 2004). It does not explicitly
focus on the life course approach to health even though it has
policies on reproductive and child health.
An acceptable health policy must be culturally relevant and
must involve community engagement in its formulation. It must
cater to the perceived needs of the population (Gregory, Hartz-
Karp, & Watson, (2008). Since the cultures of people influence
HEALTH STATUS IN NIGERIA
their beliefs in disease causation and health-seeking behaviors,
the culture of the people must be taken into consideration when
formulating health policies for them to be acceptable (Horton, &
Dickinson, 2011). A process for monitoring and evaluation must
also be built into health policy formulation (Rispel, Palha de
Sousa, & Molomo, 2009).
For instance, to develop a policy on childhood nutrition
with Nigerian local foods , the following steps will be followed:
Situation analysis: This involves identifying the need and
purpose for the policy. MDG 1 talks about eradicating extreme
hunger and poverty. Nigeria only achieved a 25% reduction in
underweight children in 2008; 33% reduction in under-5 mortality
rate, and 26% reduction in maternal mortality rate in 2008. The
targets were 36%, 54%, and 54% reduction in those indicators
respectively (Alles et. al., 2013). The need for healthy
nutrition in children and women in the reproductive age bracket
must be highlighted and met. The policy working group must
research into the traditional healthy foods across the nation and
identify how they can be prepared in a healthy way for children
HEALTH STATUS IN NIGERIA
and pregnant women. The goals and objectives are to be stated
including to promote eating of healthy foods such as soya beans
that are locally available to promote the health of the citizens
and reduce malnutrition. Other policy options will be debated
before finalizing the document.
Community engagement: community and opinion leaders, mothers,
grandmothers, fathers, carers, religious leaders, community
health workers, members of the community and other stakeholders
will be engaged through town hall meetings and focus group
discussions to get their input as well as to inform, educate and
communicate the issues at stake to them. They must be carried
along at each step to ensure acceptance of the policy and a
commitment to make it work (CDC, 2014).
Policy adoption and enactment: key policy actors and stakeholders
will agree on the final document and pass it on for enactment
into the national health policy. There will be massive
sensitization of the public about the policy. The framework will
include on healthy eatin habits, basic sanitation, and health
promotion activities. The community health workers will work hand
HEALTH STATUS IN NIGERIA
in hand with mothers and other carers, and schools and the need
for referral to appropriate health facilities when necessary in
severe cases of malnutrition will be emphasized in the policy.
Policy implementation will take place and the Nigerian citizens
will be made to know that there is a policy on eating traditional
healthy foods especially for children to aid their development.
The need to cultivate more of such foods will be emphasized.
Monitoring and Evaluation: processes will be built into the
policy to assess and monitor its impact on the health outcomes.
Ways for revising the policy as appropriate based on impact will
be sought. The impact will also be communicated to government and
the people to build up evidence in favour of the policy or
otherwise.
Further insights from learning resources
Solutions to population health issues must be both upstream
and systemic (Ontario Prevention Clearinghouse [OPC], 2006).
Upstream interventions focus on the root causes of problems
relating to socioeconomic and environmental factors while
HEALTH STATUS IN NIGERIA
systemic involve policy formulation to address the problems (OPC,
2006). The socioeconomic factors are more than behavioral factors
and access to healthcare; they include living and working
conditions, social networks, poverty and the physical environment
(OPC, 2006).
Early child development affects both cognitive and affective
domains later in life. It influences their subsequent risks of
developing obesity, heart disease, diabetes, malnutrition, mental
health problems and criminality (WHO, 2008). It is said that,
“inequalities in health occur as a result of inequalities in the
society” (United Nations International Children's Emergency Fund
[UNICEF], 2010). Healthcare may only be able to mitigate the
effect of morbidities that develop later in life not cure them
and it is also expensive where available (Kehinde, 2014a).
According to a study by Shonkoff, Boyce, & McEwen, 2009, the risk
of coronary heart disease was found to be four times more in low
birth weight individuals (weighing less than 2.5kg) than those
with birth weights above 4kg; and61% of those who suffered
emotional disturbance in childhood developed depression later in
HEALTH STATUS IN NIGERIA
life compared to 18% for those who did not experience emotional
abuse. The society must therefore put in place conditions that
will enhance early childhood experiences and thus promote
population health. For instance, inequalities in poverty and
access to prenatal care must be addressed (WHO, 2008). In order
to promote population health there must be equitable distribution
of health care facilities and schools, equitable access to
education, conditions of work and leisure, and living
environments (WHO, 2008).
According to Stegeman et. al. (2010), health inequality is
a matter of life and death. Therefore, there must be successful
advocacy by the health sector for governments and others to
tackle inequities. Effective leadership at the societal,
organizational, and individual levels is necessary in tackling
health disparities (Koh & Nowinsky, 2010). To reduce mortality
rates in the 21st century involves partnership and long-term
commitment between the fields of public health and medicine.
A population centered approach of vulnerable groups is best
for tackling inequities (Stegeman et. al., 2010). Responsible
HEALTH STATUS IN NIGERIA
leadership must promote a sense of togetherness so that people
can focus on the common good and not just on personal well-being
(Koh & Nowinsky, 2010). The pathway for eliminating disparities
in health also involves improving daily living conditions,
addressing the distribution of power, money, and resources for
greater equity, and an assessment and evaluation of the problem
and taking necessary action (WHO, 2008).
Conclusion
Solutions to tackle health inequities must be both practical
and sustainable (Baker, Metzler, & Galea, 2005). Governments of
low-income countries as Nigeria must exercise political will and
strong commitment towards improving the health of their
populations. This can be done through the formulation of
appropriate social policies and laws that will help to reduce
inequities, redistribute income and provide conditions for a more
equitable society. All these will bring about an improvement in
population health. The process of policy formulation and
implementation must have built into it processes for community
engagement, as well as monitoring and evaluation to assess the
HEALTH STATUS IN NIGERIA
impact of outcomes. The issue of tackling inequalities and
population health is not for the government or health sector
alone, it requires a collaborative and multisectoral approach
involving governments at all levels, the private sector, NGOs,
religious organizations, communities, individuals, researchers,
public health practitioners, healthcare professionals,
environmentalists, transport, housing, and education sectors, as
well as other stakeholders in health.
References
Alles, M., Eussen, S., Ake-Tano, O., Diouf, S., Tanya, A.,
Lakati, A., & ... Mauras, C. (2013). Situational analysis
and expert evaluation of the nutrition and health status of
infants and young children in five countries in sub-Saharan
Africa. Food and Nutrition Bulletin, 34(3), 287-298. Retrieved
February 3, 2015 from http// waldenulibrary.org
HEALTH STATUS IN NIGERIA
Bakare, A. S. (2012). Measuring the income inequality in
Nigeria: the Lorenz curve and Gini co-efficient approach.
American Journal of Economics, 2(1), 47-52.
doi:10.5923/j.economics.20120201.06
Baker, E. A., Metzler, M. M., & Galea, S. (2005). Addressing
Social Determinants of Health Inequities: Learning From
Doing. American Journal of Public Health, 95(4), 553–555.
doi:10.2105/AJPH.2005.061812
Centers for Disease Prevention and Control (2011). Learn about
health literacy. Retrieved December 16, 2014 from
http://www.cdc.gov/healthliteracy/learn/index.html
Centers for Disease Prevention and Control (2014). CDC policy
process. Retrieved February 7, 2015 from http://www.cdc.gov
Central Intelligence Agency. (2014). The World Factbook. Nigeria.
Retrieved February 5, 2015 from https://www.cia.gov
Cleen foundation (2012). Summary of findings of 2012 national
crime and safety survey. Retrieved February 6, 2015 from
http://cleenfoundation.blogspot.com/
HEALTH STATUS IN NIGERIA
Dankwa-Mullan, I., Rhee, K. B., Williams, K., Sanchez, I., Sy,
F. S., Stinson, N., & Ruffin, J. (2010). The science of
eliminating health disparities: Summary and analysis of the
NIH summit recommendations. American Journal of Public
Health, 100(Suppl. 1), S12–S18. Retrieved February 6, 2015
from the Walden Library databases.
Federal Ministry of Health ( 2004). Revised National Health
Policy. Federal republic of Nigeria, Abuja. Retrieved
December 23, 2014 from
http://cheld.org/wp-content/uploads/2012/04/Nigeria-
Revised-National-Health-Policy-2004.pdf
Federal Republic of Nigeria (1990). Labour Act . Laws of the
Federation of Nigeria, chapter 198. Retrieved February 6, 2015
from http://www.nigeria-law.org/
Federal Republic of Nigeria (2013a). About SURE-P. The
Presidency, Federal Republic of Nigeria. Retrieved
February 6, 2015 from http://www.surepmch.org/
HEALTH STATUS IN NIGERIA
Federal Republic of Nigeria (2013b). Nigeria Millennium
Development Goals 2013 Report. Retrieved February 6, 2015
from http://www.ng.undp.org/
Fotso JC, Friel S, Khadr Z, Meresman S, Patil-Deshmukh A, Saenz
R, Salgado N (2010). Social Conditions and Urban Health Inequities.
Working Paper Global Research Network on Urban Health
Equity.
Gehlert, S., Sohmer, D., Sacks, T., Mininger, C., McClintock,
M., & Olopade, O. (2008). Targeting health disparities: a
model linking upstream determinants to downstream
interventions. Health Affairs (Project Hope), 27(2), 339-349.
doi:10.1377/hlthaff.27.2.339
Gregory, J., Hartz-Karp, J., & Watson, R. (2008). Using
deliberative techniques to engage the community in policy
development. Australia and New Zealand Health Policy, 5, 16.
doi:10.1186/1743-8462-5-16
Horton, K., & Dickinson, A. (2011). The role of culture and
diversity in the prevention of falls among older Chinese
HEALTH STATUS IN NIGERIA
people. Canadian Journal on Aging, 30(1), 57-66.
doi:10.1017/S0714980810000826
Kehinde O. (2014a, December 24). Re: Moving upstream to improve
population health down the road [Online discussion].
Retrieved from https://class.waldenu.edu
Kehinde O. (2014b, December 31). Re: Culture and Policy
Development [Online discussion]. Retrieved from
https://class.waldenu.edu
Koh, H. K., & Nowinski, J. M. (2010). Health equity and public
health leadership. American Journal Of Public Health, 100 Suppl 1S9-
S11. doi:10.2105/AJPH.2010.191379
Laureate Education (Producer). (2011). “Health Status in the
European Union.” Global health and issues in disease
prevention [Multimedia file]. Retrieved from
https://class.waldenu.edu
Lee, K., Buse, K. & Fustukian, S. (Eds.). (2002). Health policy
in a globalising world (pp 3-17). Cambridge, United
Kingdom: Cambridge University Press.
HEALTH STATUS IN NIGERIA
National Primary Healthcare Development Agency (2013). Nigerian
National Routine Immunization Strategic Plan(2013-2015).
Retrieved February 5, 2015 from
http://www.nationalplanningcycles.org/
Nnonyelu, N & Nwankwo, U. (2014). Social determinants of
differential access to health services across five states
of Southeast Nigeria. European Scientific Journal,
3(special),1857 – 7881. Retrieved February 5, 2015 from
http://eujournal.org/
Nwankwo, C., Nandy, B., & Nwankwo, B. O. (2010). Factors
influencing diabetes management outcome among patients
attending government health facilities in South East,
Nigeria. International Journal of Tropical Medicine,
5(2), 28- 36. doi:10.3923/ijtmed.2010.28.36
Onotai , L. O. (2008). A Review of the impact of the health
literacy status of patients on health outcomes. Nigerian
Health Journal, 8(3-4), 32 – 38. Retrieved February 6, 2015
from
www.ajol.info/index.php/nhj/article/download/90801/8023
HEALTH STATUS IN NIGERIA
Ontario Prevention Clearinghouse (2006). The Case for
Prevention: Moving Upstream to Improve Health for all
Ontarians, Ontario Prevention Clearinghouse, Toronto.
Retrieved January 7, 2014 from
http://en.healthnexus.ca/sites/en.healthnexus.ca/files/u4/c
aseforprevention.pdf
Osazuwa-Peters, N. (2011). Determinants of health disparities:
the perennial struggle against polio in Nigeria. International
Journal of Preventive Medicine, 2(3), 117-121. Retrieved February
6, 2015 from http://www.ncbi.nlm.nih.gov/
Oyesola, O. B., & Kadiri, T.S. (2010). Effects of Rural – Urban
Interaction on Socio-Economic Status of Rural Dwellers in
Oyo-State, Nigeria. African Journals Online, 6(2), 1 – 10.
Retrieved February 6, 2015 from http://www.ajol.info/
Renne, E. (2006). Perspectives on polio and immunization in
Northern Nigeria.Social Science & Medicine. 63(7):1857-1869.
HEALTH STATUS IN NIGERIA
Retrieved February 5, 2015 from
http://www.ncbi.nlm.nih.gov/
Rispel, L. C., Palha de Sousa, C. A. ., & Molomo, B. G. (2009).
Can Social Inclusion Policies Reduce Health Inequalities in
Sub-Saharan Africa?—A Rapid Policy Appraisal. Journal of Health,
Population, and Nutrition, 27(4), 492–504. Retrieved February 4,
2015 from http://www.ncbi.nlm.nih.gov/
Ruffin, J. (2010, April 2). The Science of Eliminating Health
Disparities: Embracing a New Paradigm. American Journal of Public
Health. pp. S8-S9. doi:10.2105/A]PH2010.191957.
Shonkoff, J. P., Boyce, W. T., & McEwen, B. S. (2009).
Neuroscience, molecular biology, and the childhood roots of
health disparities: Building a new framework for health
promotion and disease prevention. JAMA: The Journal of the
American Medical Association, 301(21), 2252–2259. Retrieved
December 21, 2014 from the Walden Library databases.
Stegeman, I., Costongs, C., Needle C., & DETERMINE Consortium.
(2010).The story of DETERMINE: Mobilising action for health equity in the EU
HEALTH STATUS IN NIGERIA
—Final report of the DETERMINE consortium. Brussels: EuroHealthNet.
Retrieved January 21, 2015 from
http://eurohealthnet.eu/sites/eurohealthnet.eu/files/public
ations/DETERMINE-Final-Publication-Story.pdf
United Nations Development Programme [UNDP] (2008). Human
development report 2007/2008: fighting climate change:
human solidarity in a divided world; p. 256. New York, NY:
United Nations Development Programme. Retrieved February 4,
2015 from
http://hdr.undp.org/sites/default/files/reports/268/hdr_200
72008_en_complete.pdf
United Nations International Children's Emergency Fund (UNICEF,
2010). Annual Report. Retrieved December 23, 2014 from
http://www.unicef.org/lac/UNICEF_Annual_Report_2010_EN_0527
11.pdf
Weir, K. (2013). Closing the health-wealth gap. American
Psychological Association,44(9), 36. Retrieved February 7, 2015
from http://www.apa.org/
HEALTH STATUS IN NIGERIA
WHO Commission on Social Determinants of Health. (2008). Closing
the Gap in a Generation: Health Equity Through Action on the Social
Determinants of Health: Commission on Social Determinants of Health Final
Report. World Health Organization(Ed.). World Health
Organization. Retrieved February 4, 2015 from
https://books.google.com.ng/books?
Wilkinson, R., & Pickett, K. (2010). The spirit level: Why greater equality
makes societies stronger. New York, NY: Bloomsbury Press.
The World Bank (2015). Gini index (World Bank estimate).
Retrieved February 5, 2015 from http://data.worldbank.org/
World Health Organization (2005). Social determinants of health-
Nigerian perspective. Retrieved February 4, 2015 from
http://www.who.int/
socialdeterminants/countryaction/NIGERIA %20Dr%20ADETUNJI
%20Labiran.pdf
World Health Organization (2006). The health of the people: the
African regional health report, p. 196. Geneva: Regional
Office for Africa, World Health Organization. Retrieved
February 4, 2015 from https://books.google.com.ng
HEALTH STATUS IN NIGERIA
World Health Organization (2015). Track 2: Health literacy
and health behaviour
7th Global Conference on Health Promotion: track themes.
Retrieved February 6, 2015 from
http://www.who.int/healthpromotion/
Yahya M. (2007). Polio vaccines - no thank you! Barriers to
polio eradication in Northern Nigeria. African Affairs, 106(423),
185–204. doi: 10.1093/afraf/adm016