health psychology proposal
TRANSCRIPT
MODULE TITLE: THE - 5PS511 - The Psychology of Health
MODULE LEADER: Evaggelia Nakopoulou
Research Proposal
The association between self efficacy, locus of control,
the demographic characteristics and major depression in
adopting physical activities among Coronary Heart Disease
patients, in Greece.
Digka Antonia
BSc (Hons) in Applied Psychology
1
Mediterranean College
23 February 2014
Thessaloniki
Introduction
Coronary heart disease (CDH) is defined as a significant
built up of plague, with calcium and cholesterol
deposits, specifically in the coronary arteries of the
heart (Ogden, 2004). It has been reported that more than
16 million Americans suffer from CDH and 500.000 people
lose their lives annually (Kivimäki, 2012). However,
studies have indicated that regular exercise makes the
heart work harder, therefore that means that with the
appropriate daily exercise someone can prevent from the
risk factors that are associated with CDH (Wankel, 1993).
In order to prevent death and heart attack among patients
who are diagnosed with CDH it is recommended necessarily
physical exercise 4-5 times per week for 30-60 minutes
(Wankel, 1993). However, it is difficult for someone who
suffers from CDH to change his/her lifestyle and adopt
daily exercise and new habits. Only the 30% of people who
suffer from CDH seem to comply and start exercise daily
(Finegold et al. 2012). Specifically, older patients tend
to not to follow the doctors instructions for adopting
physical exercise in their everyday life and it is more
2
possible for young patients to comply with the doctor’s
given advices (Stratton et al. 1994).
A factor associated with adoption of physical exercise is
locus of control. Locus of control is defined as
individual’s beliefs about how they control events in
their life that may affect them (Woolfe et al 2003). The
concept of locus of control is divided to external and
internal locus of control: External locus of control is
defined as the outcomes of a action that are associated
with the chance or with powerful others, while internal
locus of control is defined as the results of an action
that are associated with someone’s personal attitude-
behavior (Rotter, 1966). Also having higher levels of
locus of control is associated with reduced levels of
stress and anxiety, whereas lower levels of locus of
control may increase the possibility of anxiety even
depression (Flowers, 1994). Moreover the research has
indicated that the locus of control and the type of
personality (A or B or C) plays a significant role in
adopting physical exercise when someone suffers from CDH
(Carlson, 2007). Therefore is more possible for someone
who has higher levels of locus of control to adopt the
physical exercise in his/ her daily life even suffering
from CDH.
Self efficacy is defined as someone’s ability to succeed
in specific situations in his/her life (Omrod, 2006).
Also self efficacy is the main characteristic of
Bandura’s social cognitive theory that highlights the3
fact that social experience and observational learning
play an important role in the personality development
(Bandura, 1988; Luszczynska & Schwarzer, 2005).There is a
plethora of studies that confirm that self efficacy plays
a significant role in adopting physical activity. It has
been found that perceived self efficacy is a major
instigating force in forming intentions in order to adopt
daily physical exercise and to maintain the given
prescriptions for an extended time. (Dzewaltowski, Noble,
& Shaw, 1990; Feltz & Riessinger, 1990; Shaw,
Dzewaltowski, & McElroy, 1992). Also a study indicated
that patients, who were recovering from heart disease and
had high levels of self efficacy, were characterized from
overexertion during the programmed exercise (Schwarzer &
Renner, 2000). Also self efficacy has been characterized
as one of the most important factors in order to maintain
and have an effective physical exercise (Omrod, 2006).
In addition, a study has indicated that depression is
associated with treatment non adherence, not following
the doctor’s direction and not adopting new health
nutrition and physical exercise (Barefoot et al. 2000;
Blumenthal et al. 2000). The study explains that these
depressive patients with long term illness seem to have
given up on life (Yeung. 1996). Also physical exercise is
used as a treatment for depression, however the research
has shown that physical exercise can be an effective
treatment for depressive patients but often it is usually
4
characterized as an underused treatment for mild to
moderate depression (Veale et al. 1992).
Rationale
This study will highlight influence between self
efficacy, locus of control, demographic characteristics
and major depression in adopting physical exercise among
CHD patients. Previous literature has indicated that
people who suffer from CHD usually do not comply with
adopting physical exercise daily (Carlson, 2007).
Additionally there are studies that support that locus of
control and self efficacy can predict the adoption of
physical exercise among CHD patients (Ogden, 2006).
Moreover, through extensive investigation it was noted
that in the countries of Southern Europe there is limited
research on that subject. More specifically in Greece
there is limited published research on Coronary heart
disease in general. Taking into account all the previous
information, this study could be quite useful.
Aim
The aim this current study is to investigate the
association between self efficacy, locus of control, the
demographic characteristics and major depression with
adopting physical exercise by patients who suffer from
CHD in Greece.
Objectives
The purpose of this study is:
5
i. To research the relationship between locus of
control with adopting physical exercise among CDH
patients.
ii. To investigate the association between self efficacy
with adopting physical exercise among CDH patients.
iii. To research the effect of demographic
characteristics on adopting physical exercise among
CDH patients.
iv. To research the relationship between major
depression with adopting physical exercise among CDH
patients.
v. To research whether self efficacy, locus of control
and major depression can predict adoption of
physical exercise among CDH patients controlling for
demographic characteristics.
Methodology
Design
A mixed design will be used. A correlational design will
be used, in order to examine the interrelationship
between the predictors: self efficacy, locus of control,
the demographic characteristics, major depression and the
6
criterion variable: the adoption of physical activities.
An Independent samples design will be used with gender,
education and occupation as independent variables and
adoption of physical exercise as the dependent variable.
Participants
For the study, 85 volunteer participants, where r=0,80
medium effect size Cohen (1988) aged from 35-80, who
suffer from CHD, will be needed. Also the quota sample
will be recruited from Cardiology departments at public
hospitals in the area of Thessaloniki, Greece, after the
specific approve from the responsible manager. Also, in
order to participate the participants should: i) be
diagnosed for coronary heart disease for at least 3
months ii) not suffer from mental disorders.
Materials
A demographics form will be used that contains
information about age, gender, education, occupation and
marital status. The depression questionnaire (Kroenke et
al. 2009) with 8 items, where a=0,86, and a 4 point
Likert scale was used: 0 for ‘’not at all’’ till 3 for ‘’
every day’’. The locus of control scale (Ferraro et al.,
1987) has 18 items: 6 items measure the internal locus of
control, 6 measure the powerful others locus of control
and other 6 items measure the chance of locus of control.
A 6 point Likert scale will be used: from 1 (strongly
disagree) to 6 (strongly agree), where a=0,67-0,77. The
physical activity scale (Lorig et al. 1996) has 6 items
7
and a 5 point Likert scale where 0 for ‘’none’’ and 4 for
‘’more than 3 hours’’ and a=0,56-0,72. The Self efficacy
scale (Schwarzwer & Renner, 2000), contains 5 items and a
4 point Likert scale where 1 is very ‘’uncertain’’ and 4
‘’very certain and a=0,88. Finally the Daily activities
scale (Lorig et al. 1996) has 4 items and a 5 point
Likert scale where 0 means ‘’not at all’’ and 4 ‘’almost
totally’’ and a=0,91 (see Appendix 1).The questionnaires
will be translated in Greek.
Procedure
After having the appropriate permission from the Health
Center in order to carry out the study the procedure will
start. The participants will get informed by leaflets in
the entrance of the hospitals. The procedure will take
place in the Health Center, in a comfortable environment
in a specific day and time. Firstly the appropriate
consent and briefing forms will be given to the
participants, in order to inform them about the
procedure. As the participants will agree with the terms
then they will start to fill in the demographics form and
questionnaires of Self efficacy and physical exercise,
Locus of control, Depression and Physical exercise in
order to complete them carefully in approximately 30
minutes. When the participants will complete all the
questionnaires they will be given a debriefing form (See
Appendix 2).
Ethical considerations
8
For the conduction of this research the responsible
manager of the Health Center must give the appropriate
permission. Also the participants who want to participate
to this study will be given a consent form and a brief
form to get informed extensively about the procedure of
the study and about their rights to confidentiality and
anonymity. It is also important to mention that the
participants are free to leave the procedure whenever
they want or to withdraw their answers in one week.
Statistical analysis
Using the SPSS 19 software the data from the
questionnaires will be screened and analyzed. Descriptive
statistics will be used to describe sample’s
characteristics and summarize data collected through
scales. Kolmogorov-Smirnov test will be used to examine
normal distribution of all scale scores. A series of
Pearson’s correlation tests will be conducted to test for
the relationship between self efficacy, major depression,
locus of control and adoption of physical exercise.
Moreover in order to estimate if self efficacy, major
depression, locus of control, the demographic
characteristics and are good predictors of adopting
physical exercise a multiple regression analysis and the
forced entry method will be used. Independent samples t-
test and one-way ANOVAs will be used to test the
influence of demographics on the adoption of physical
exercise.
9
Expected outcomes
Self efficacy, Locus of control, major depression,
demographic characteristics (age, gender, education
level, and occupation), and self-efficacy will influence
adoption of physical exercise among CHD patients. Also it
is expected it will be noted differences between younger
and older people in adopting physical exercise.
Implication of findings
This study aim is to investigate the relationship between
self efficacy, locus of control, demographic
characteristics, major depression and the adoption of
physical activities among CHD patients. Furthermore the
findings of this research may help Health psychologists,
physicians, counselors and even gymnasts who help people
with CHD and related health problems. So these experts
can help these people by choosing the appropriate
approach or therapy.
Also campaigns can be organized in order to inform the
citizens of every age about the positive outcomes of
physical exercise. Furthermore special seminars can be
conducted in Hospitals in order to inform further the
patients about the positive outcomes of physical exercise
and not only for CDH patients. Finally a psychologist can
create group with patients of CDH and try to guide and
motive them in order to adopt a healthier model of life
with daily physical exercise.
10
References
April, K. A., Dharani B., Peters K. "Impact of Locus of Control
Expectancy on Level of Well-Being". Review of European Studies 4
(2).
Bandura, A. (1988). Organizational Application of Social Cognitive
Theory. Australian Journal of Management, 13 (2), 275-302
Barefoot J.C., Brummett B.H., Helms M.J., Mark D.B.,
Siegler I.C., Williams R.B. (2000). Depressive symptoms and
survival of patients with coronary artery disease. Psychosom Med.
62,790–795.
Blumenthal J.A., Lett H.S., Babyak M.A., (2000). Depression
as a risk factor for mortality after coronary artery bypass
surgery. Lancet. 362,604–609
Bhatia C. & Sujata K. (2010). Biomaterials for clinical applications.
Springer: New York
Buchner DM. Physical activity. In: Goldman L, Shafer AI,
eds. Cecil Medicine. 24th ed. Philadelphia, Pa: Saunders
Elsevier; 2011:chap 15.
11
Carlson, N.R., et al. (2007). Psychology: The Science of
Behaviour - 4th Canadian ed .. Toronto, ON: Pearson
Education Canada.
Craft, L. L., & Landers, D. M. (1998). The effect of
exercise on clinical depression and depression resulting
from mental illness: A meta-analysis. Journal of Sport
and Exercise Psychology, 20, 339-357.
Cohen, J. (1988). Statistical power analysis for the behavioral
sciences. Psychology Press: New York.
Dzewaltowski, D. A., Noble, J. M., & Shaw, J. M. (1990).
Physical activity
participation: Social cognitive theory versus the theories of reasoned action
and planned behavior. Journal of Sport & Exercise Psychology,
12, 388-405.
Exercise and Physical Activity: Your Everyday Guide from
the National Institute on Aging Page. Updated Feb 2013.
Accessed May 6, 2013.
Feltz, D. L., & Riessinger, C. A. (1990). Effects of in vivo
emotive imagery and
performance feedback on self-efficacy and muscular endurance. Journal
of Sport & Exercise Psychology, 12, 132-143.
Flowers, B.J. (1994). Perceived control, illness status, stress, and
adjustment to cardiac illness. The Journal of Psychology, 128 (5),
567-57612
Finegold J.A., Asaria P., Francis D.P. (2012). "Mortality
from ischaemic heart disease by country, region, and age: Statistics from
World Health Organisation and United Nations". International journal
of cardiology 168 (2): 934-45.
Herbert M. & Lefcourt L. (1992). Locus of Control: Current Trends in
Thory and Research. Psychology Press: London.
Kroenke K., Strine T.W., Spritzer R.L., Williams J.B.,
Berry J.T, Mokdad A.H. (2009). The PHQ-8 as a measure of
current depression in the general population. J Affect
Disord.114(1-3),163-73.
Kivimäki M., Nyberg S.T., Batty G.D. (2012). "Job strain as a
risk factor for coronary heart disease: a collaborative meta-analysis of
individual participant data". Lancet. 380 (9852), 1491–1497.
Luszczynska, A., & Schwarzer, R. (2005). Social cognitive
theory. In M. Conner & P. Norman (Eds.), Predicting health
behaviour (2nd ed. Rev., Pp. 127-169).
Ogden, J. (2004). Health Psychology, a textbook (3rd edition). Open
University Press: USA.
Ormrod, J. E. (2006). Educational psychology: Developing learners
(5th ed.). NJ: Pearson / Merrill Prentice Hall: Upper Saddle
River.
Stratton J.R., Levy W.C., Cerqueira M.D., Schwartz R.S.,
Abrass I.B. (1994). Cardiovascular responses to exercise. Effects of
13
aging and exercise training in healthy men. US National Library of
Medicine National Institutes of Health 89 (4), 1648-1655.
Rotter, J. B. (1966). Generalized expectancies for
internal versus external control of reinforcement:
Psychological Monographs: General & Applied 80 (1) 1966,
1-28.
Shaw, J. M., Dzewaltowski, D. A., & McElroy, M. (1992).
Self-efficacy and causal attributions as mediators of perceptions of
psychological momentum. Journal of Sport & Exercise
Psychology, 14, 134-147. Schwarzer, R., & Renner, B. (2000). Social-cognitive
predictors of health behavior:Action self-efficacy and
coping self-efficacy, Health-Psychology, 19, 487-495.
Veale, D., Le Fevre, K., Pantelis, C, de Souza, V., Mann,
A., & Sargeant, A. (1992). Aerobic exercise in the
adjunctive treatment of depression: A randomized
controlled trial. Journal of the Royal Society of
Medicine,85 , 531-544.
Wallston, K., Wallston, B., & DeVellis, R. (1978).
Development of the multidimensional health locus of control (MHLC) scales.
Health Education Monographs, 6, 160-170.
Woolfe R., Dryden W., Strawbridge S. (2003). Handbook of
Counseling Psychology 2nd edition. Sage Pyblications: London.
14
Wankel, L. M. (1993). The importance of enjoyment to adherence and
psychological benefits from physical activity. International Journal
of Sport Psychology, 24, 151-169.
Yeung, R. R. (1996). The acute effects of exercise on
mood state. Journal of Psychosomatic Research, 40, 123-
141.
Appendix 1
DEMOGRAPHICS
Α1. Gender Male [ ] Female [ ]
Α2. Age……………
Α3. Marital status
Married [ ] Single [ ] In a relationship [ ]
Divorced /Widowed [ ]
Α4. Educational level
Primary [ ] ΑΕΙ – ΤΕΙ
[ ]
Secondary [ ] Postgraduate
studies [ ]
Technical school/IEK [ ]
15
Α5. Occupation
Public Employee [ ] Private Employee [ ]
Self-employed [ ] Student [ ] Housekeeping [ ]
Retired [ ] Unemployed [ ]
Α5. Background information:
How long do you suffer from coronary heart disease? [ ]
Questionnaire 1
Multidimensional Health Locus of Control (Wallston,
Wallston, & DeVellis ,1978)
Each item below is a belief statement about your medical
condition with which you may agree or disagree.
1=STRONGLY DISAGREE (SD) 4=SLIGHTLY AGREE (A)
16
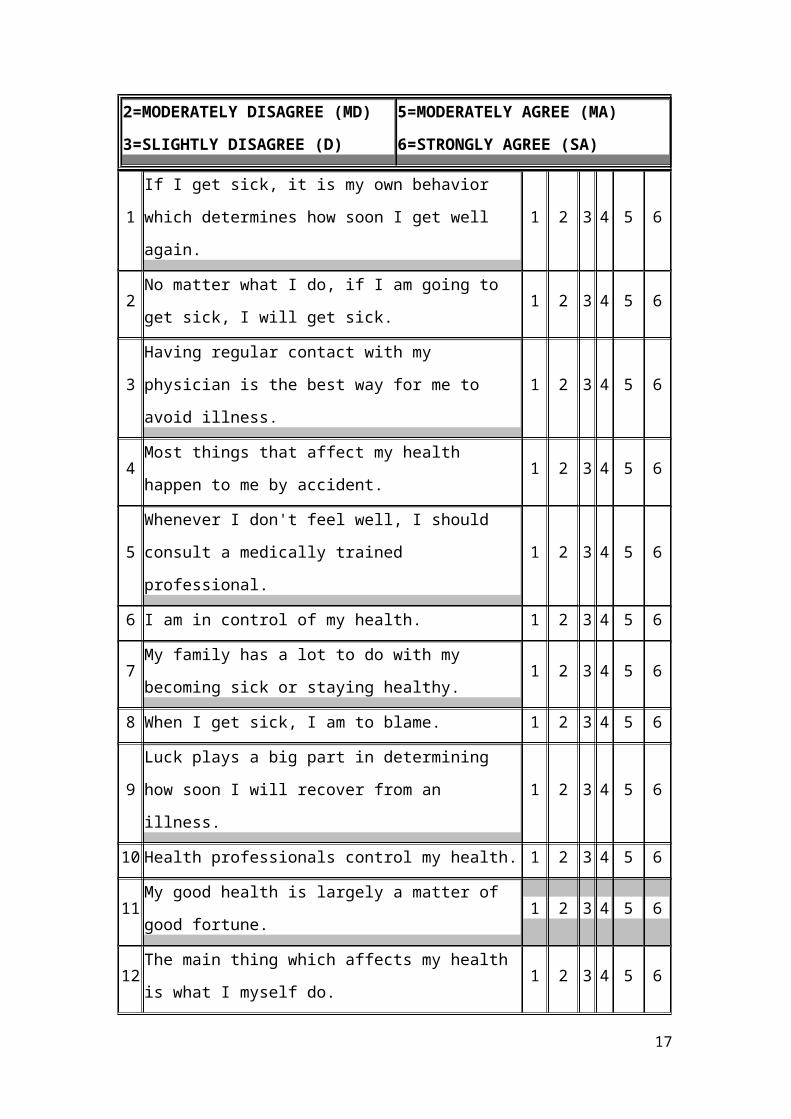
2=MODERATELY DISAGREE (MD)
3=SLIGHTLY DISAGREE (D)
5=MODERATELY AGREE (MA)
6=STRONGLY AGREE (SA)
1
If I get sick, it is my own behavior
which determines how soon I get well
again.
1 2 3 4 5 6
2No matter what I do, if I am going to
get sick, I will get sick.1 2 3 4 5 6
3
Having regular contact with my
physician is the best way for me to
avoid illness.
1 2 3 4 5 6
4Most things that affect my health
happen to me by accident.1 2 3 4 5 6
5
Whenever I don't feel well, I should
consult a medically trained
professional.
1 2 3 4 5 6
6 I am in control of my health. 1 2 3 4 5 6
7My family has a lot to do with my
becoming sick or staying healthy.1 2 3 4 5 6
8 When I get sick, I am to blame. 1 2 3 4 5 6
9
Luck plays a big part in determining
how soon I will recover from an
illness.
1 2 3 4 5 6
10 Health professionals control my health. 1 2 3 4 5 6
11My good health is largely a matter of
good fortune.1 2 3 4 5 6
12The main thing which affects my health
is what I myself do.1 2 3 4 5 6
17
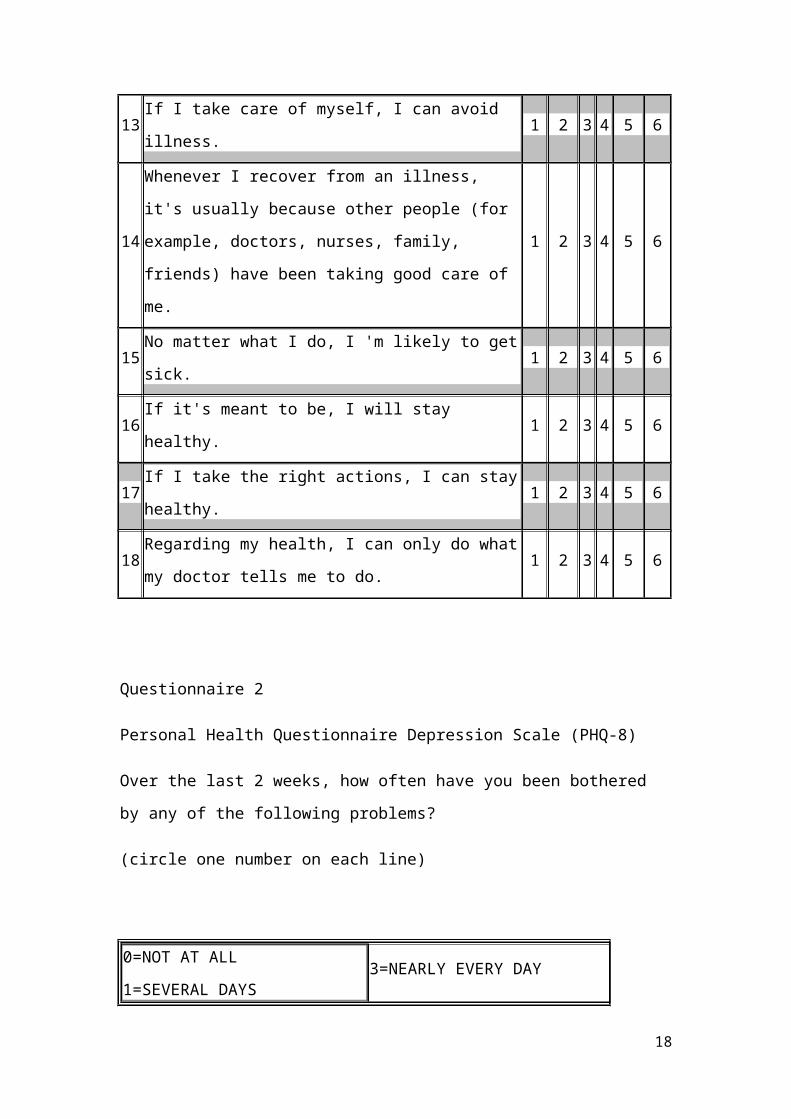
13If I take care of myself, I can avoid
illness.1 2 3 4 5 6
14
Whenever I recover from an illness,
it's usually because other people (for
example, doctors, nurses, family,
friends) have been taking good care of
me.
1 2 3 4 5 6
15No matter what I do, I 'm likely to get
sick.1 2 3 4 5 6
16If it's meant to be, I will stay
healthy.1 2 3 4 5 6
17If I take the right actions, I can stay
healthy.1 2 3 4 5 6
18Regarding my health, I can only do what
my doctor tells me to do.1 2 3 4 5 6
Questionnaire 2
Personal Health Questionnaire Depression Scale (PHQ-8)
Over the last 2 weeks, how often have you been bothered
by any of the following problems?
(circle one number on each line)
0=NOT AT ALL
1=SEVERAL DAYS 3=NEARLY EVERY DAY
18
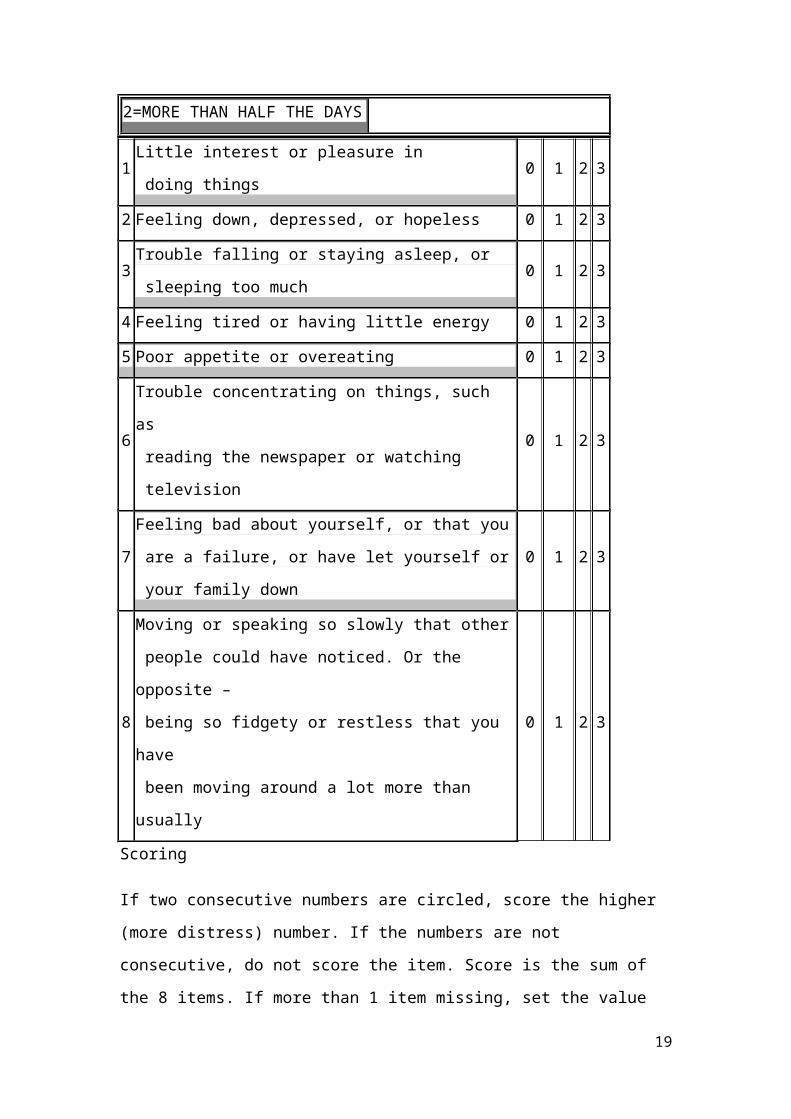
2=MORE THAN HALF THE DAYS
1Little interest or pleasure in
doing things0 1 2 3
2 Feeling down, depressed, or hopeless 0 1 2 3
3Trouble falling or staying asleep, or
sleeping too much0 1 2 3
4 Feeling tired or having little energy 0 1 2 3
5 Poor appetite or overeating 0 1 2 3
6
Trouble concentrating on things, such
as
reading the newspaper or watching
television
0 1 2 3
7
Feeling bad about yourself, or that you
are a failure, or have let yourself or
your family down
0 1 2 3
8
Moving or speaking so slowly that other
people could have noticed. Or the
opposite –
being so fidgety or restless that you
have
been moving around a lot more than
usually
0 1 2 3
Scoring
If two consecutive numbers are circled, score the higher
(more distress) number. If the numbers are not
consecutive, do not score the item. Score is the sum of
the 8 items. If more than 1 item missing, set the value
19
of the scale to missing. A score of 10 or greater is
considered major depress
http://patienteducation.stanford.edu/research/phq.pdf
Questionnaire 3
Physical Activities
During the past week, even if it was not a typical week
for you, how much total time (for the entire week) did
you spend on each of the following? (Please circle one
number for each question.)
0=NONE
1=LESS THAN 30 MIN.
3=1-3 HOURS PER WEEK
4=MORE THAN 3 HOURS A WEEK
20
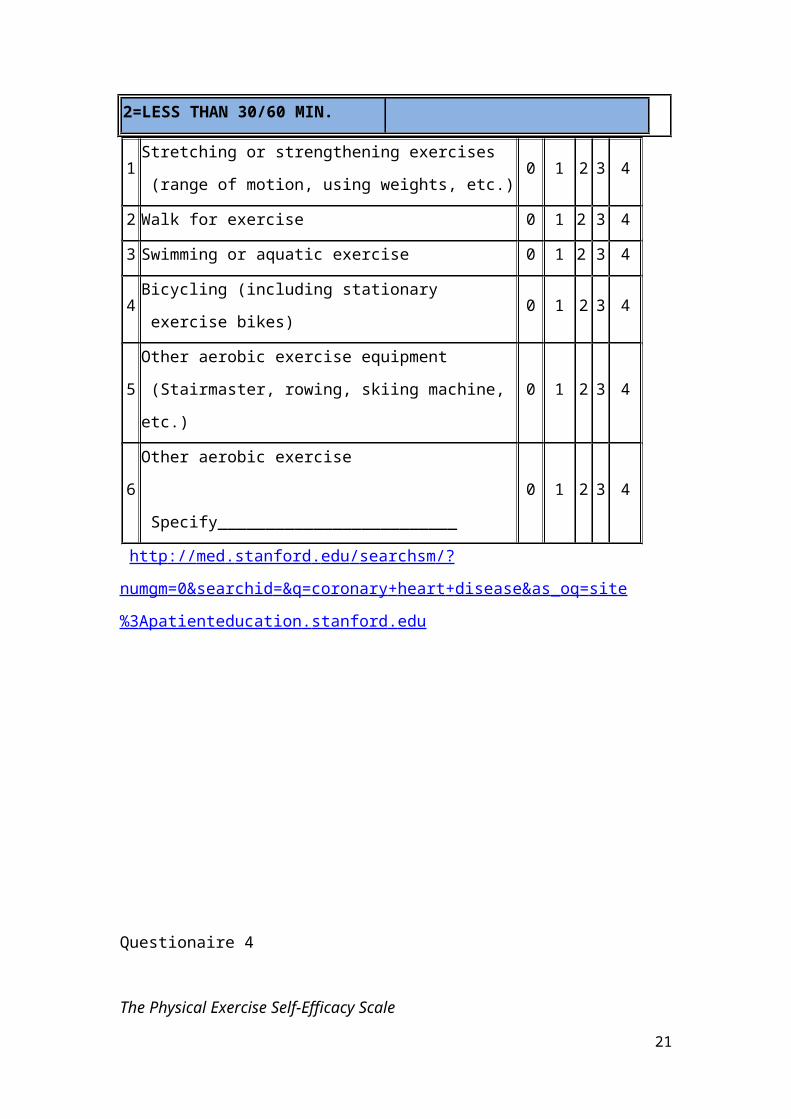
2=LESS THAN 30/60 MIN.
1Stretching or strengthening exercises
(range of motion, using weights, etc.)0 1 2 3 4
2 Walk for exercise 0 1 2 3 4
3 Swimming or aquatic exercise 0 1 2 3 4
4Bicycling (including stationary
exercise bikes)0 1 2 3 4
5
Other aerobic exercise equipment
(Stairmaster, rowing, skiing machine,
etc.)
0 1 2 3 4
6
Other aerobic exercise
Specify_________________________
0 1 2 3 4
http :// med . stanford . edu / searchsm /?
numgm =0& searchid =& q = coronary + heart + disease & as _ oq = site
%3 Apatienteducation . stanford . edu
Questionaire 4
The Physical Exercise Self-Efficacy Scale
21
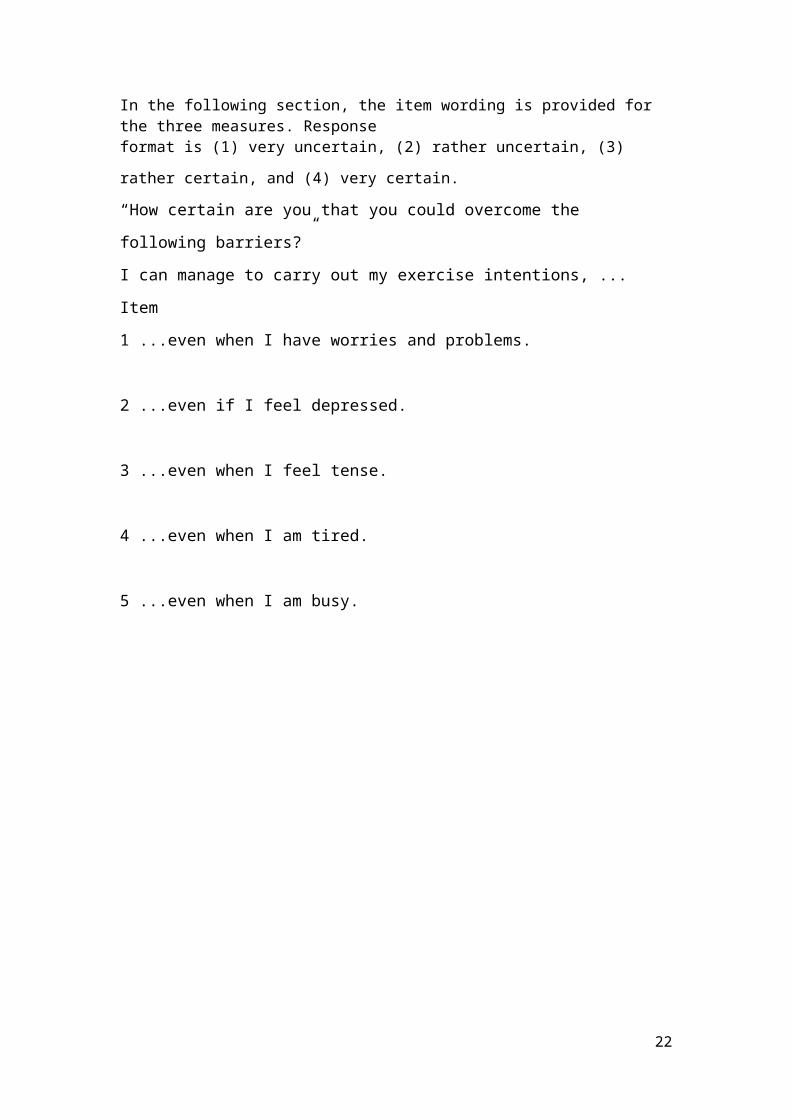
In the following section, the item wording is provided for the three measures. Responseformat is (1) very uncertain, (2) rather uncertain, (3)
rather certain, and (4) very certain.
“How certain are you that you could overcome the
following barriers?”
I can manage to carry out my exercise intentions, ...
Item
1 ...even when I have worries and problems.
2 ...even if I feel depressed.
3 ...even when I feel tense.
4 ...even when I am tired.
5 ...even when I am busy.
22
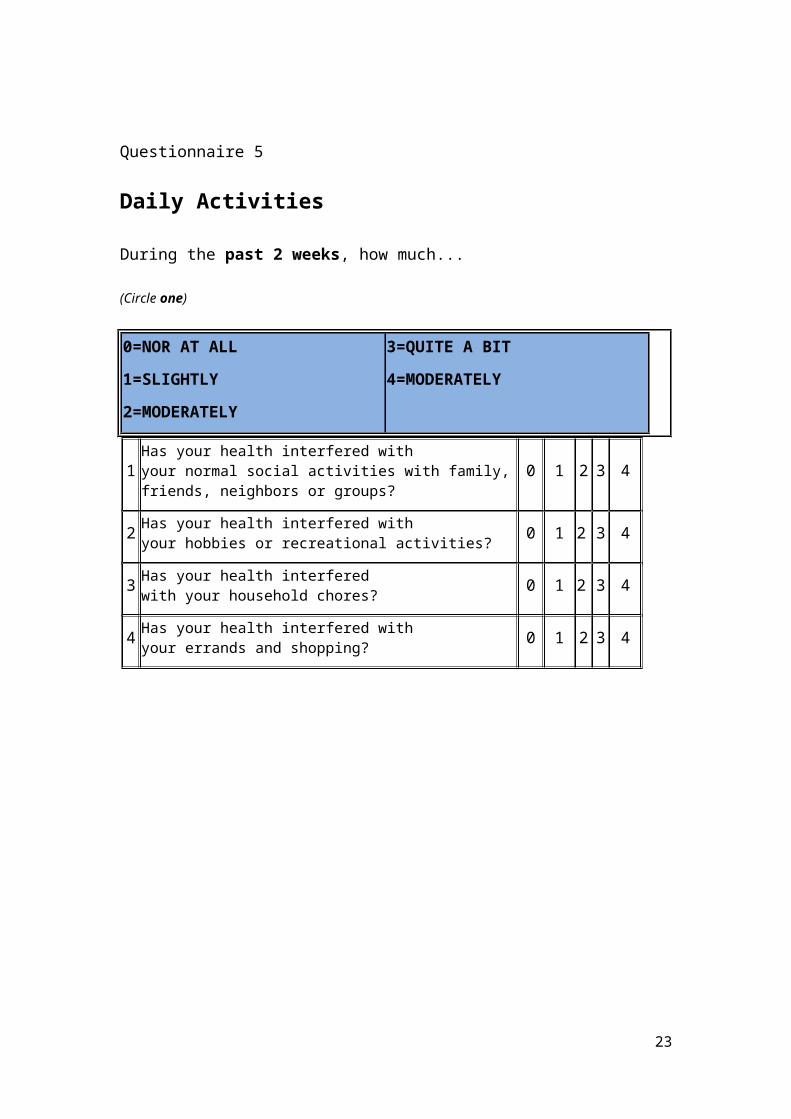
Questionnaire 5
Daily Activities
During the past 2 weeks, how much...
(Circle one)
0=NOR AT ALL
1=SLIGHTLY
2=MODERATELY
3=QUITE A BIT
4=MODERATELY
1Has your health interfered withyour normal social activities with family,friends, neighbors or groups?
0 1 2 3 4
2 Has your health interfered withyour hobbies or recreational activities? 0 1 2 3 4
3 Has your health interferedwith your household chores? 0 1 2 3 4
4 Has your health interfered withyour errands and shopping? 0 1 2 3 4
23
Appendix 2
To the manager of the Cardiology Department:
Dear sir or madam,
Within the Mediterranean College, a research is conducted
on dealing with longterm illnesses and how patients face
them and live with a longterm illness. More specifically,
the subject of my study is to investigate ‘’The
association between self efficacy, locus of control, the
demographic characteristics and major depression in
adopting physical activities among Coronary Heart Disease
patients, in Greece’’. Your participation in the
procedure in really important because in Greece there is
limited published research on Coronary heart disease in
general.
The patients who will want to participate to the
procedure will be given a briefing form and a consent
form, where they will get informed about the purpose of
the study, the procedure and their rights to
confidentiality and anonymity. The participants have the
ability to withdraw their answers in one week or leave
the procedure whenever they want. When the procedure
24
starts they will be given a demographics form, a self
efficacy questionnaire, a locus of control questionnaire,
a depression questionnaire and a physical exercise
questionnaire with a form about their daily activities in
order to complete.
The manager of the Cardiology Department has the right to
check the questionnaires!!
BRIEF FORM
The aim of this current study is to investigate the
association between self efficacy, locus of control, the
demographic characteristics (gender, age, education
level, and occupation) and major depression in adopting
physical activities among Coronary Heart Disease
patients, in Greece
WHAT YOU WILL BE REQUIRED TO DO
Before starting the survey’s procedure, please sign the
particular contract document. According to that, whenever
you feel the necessity to leave as the investigation is
25
in process you will have the right to do so. Your
participation in this research is regarded as of great
and vital importance for the required completion of the
present study.
The procedure includes the careful completion of two
questionnaires: the Locus of Control Scale, the physical
exercise and Self efficacy scale, the Demographics form,
the Depression scale and the Physical exercise scale.
After having finished with the above form and
questionnaires at your own time frame, you will be
dismissed.
ACCESS TO THE DATA Apart from researchers who are to
conduct this survey, only the leader researcher of the
present study will have the right to access the data once
permission has been granted by the administrator of every
Cardiology departments that have attended at public
hospitals in the area of Thessaloniki. The above are
clauses of the terms of confidentiality and anonymity and
are applied by recording only the demographic
characteristics of the participants of the survey.
INFORMATION ABOUT THE SURVEY’S RESULTS After the
completion of the study, you will be given one week in
order to withdraw your answers that were given in this
study, in case of regretting your participation. In one
month you will be informed about the results of this
study from the Cardiology departments at public hospitals
in the area of Thessaloniki.
26
Thank you for your special interest as well as your
valuable time.
CONSENT FORM
Investigating the association between self efficacy,
locus of control, the demographic characteristics
(gender, age, education level and occupation) and major
depression in adopting physical activities among Coronary
Heart Disease patients, in Greece.
I have already read and considered the Consent Form which
is given to me and to all the participants and it is
related with the above research for my acceptance to
participate in it. I am aware of the anonymity of the
data, as well as, researchers’ ultimate confidentiality.
Also, I have been explicitly informed that whenever I
would like to leave from this survey’s procedure, I have
the right to do it without misgivings and doubts.
PARTICIPANT
Full Name ………………………………………………………………….
Signature: …………………………………………………………………
Date: ……………………………………………………………………….
RESEARCHER
Full Name ………………………………………………………………….
Signature: …………………………………………………………………
27
Date: ………………………………………………………………………..
I would like to receive a briefing form with the research
results upon completion (if you choose ‘’ yes’’, please
put a tick: V):
------------------------------
DEBRIEF FORM
Thank you for participating in this study! The general
purpose of this research is to examine the association
between self efficacy, locus of control, the demographic
characteristics (gender, age, education level and
occupation) and major depression in adopting physical
activities among Coronary Heart Disease patients, in
Greece.
Coronary heart disease (CDH) is defined as a significant
built up of plague, with calcium and cholesterol
deposits, specifically in the coronary arteries of the
heart. Furthermore through coronary arteries oxygen and
blood are transferred in order to supply the heart.
However, due to malnutrition, negative habits (smoking,
drinking) and absence of daily exercise, the coronary
28
arteries tend to block and the ‘’delivery’’ blood and
oxygen is reduced. It is scientifically proven that
physical exercise not only can prevent CDH but also helps
patients to overcome this long term illness. Also the
majority of scientific evidence proves that self
efficacy, locus of control, the demographic
characteristics and major depression are significant
factors that play an important role in adopting physical
exercise among CHD patients.
The participants were given 4 different questionnaires
and demographics form in order to complete them
carefully. The questionnaires were: The physical exercise
and Self efficacy scale, the Locus of control scale, the
Depression scale and the Physical exercise scale. Data
was rated for processing and then for analysis to verify
whether or not the hypothesis that the above factors of
self efficacy, locus of control, the demographic
characteristics, major depression will be significant
contributors in adopting physical exercise among CHD
patients.
Thank you for your participation in this study. In this
study you participate anonymously and your data will be
used in complete privacy.
29