healing occurs in most patients that receive endoscopic stents for anastomotic leakage; dislocation...
TRANSCRIPT

btptowettr
4ieTetttte
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:202–210
ENDOSCOPY CORNER
Healing Occurs in Most Patients That Receive Endoscopic Stents forAnastomotic Leakage; Dislocation Remains a Problem
MARCUS FEITH,* SONJA GILLEN,* TIBOR SCHUSTER,‡ JÖRG THEISEN,* HELMUT FRIESS,* and RALF GERTLER*
*Department of Surgery, ‡Institute of Medical Statistics and Epidemiology, Klinikum Rechts der Isar, Technische Universität München, Munich, Germany
t
rmeopas
BACKGROUND & AIMS: There is controversy about theest way to treat esophageal anastomotic leakage. We evaluatedhe effects of treatment with self-expanding metal stents inatients with esophageal anastomotic leakage after esophagec-omy or gastrectomy for cancer. METHODS: We investigatedutcomes and procedure-related complications of 115 patientsho received endoscopic stents for anastomotic leakage after
sophagectomy or gastrectomy at a university hospital from 2004o 2009. We also performed a systematic literature review on stentherapy and compared outcomes with that of other treatmentegimens for esophageal anastomotic leakage. RESULTS:
Among the 115 patients who received stents, the in-hospitalmortality rate was 9% and complete anastomotic healing wasachieved in 70% (95% confidence interval [CI], 64%–76%). Stentdislocation occurred in 53% of the patients (95% CI, 43%–62%), inall patients with esophagocolonostomy, in 61% with esophagoje-junostomy, and in 49% with esophagogastrostomy. Three percentof patients (95% CI, 1%–5%) needed laparotomy to remove dislo-cated stents. Elective endoscopic stent removal was performed in80% of the patients after a median of 54 days (range 17–427 d);12% of these patients developed symptomatic anastomotic stric-tures after stent removal. CONCLUSIONS: Anastomosescompletely heal in 70% of patients that receive endoscopicstents for anastomotic leakage after esophagectomy or gas-trectomy. Stent therapy should be used in the management ofpatients with adequately perfused esophageal anastomoticleakage. However, stent dislocation remains a common prob-lem after surgery.
Keywords: Esophageal Cancer; Gastric Cancer; Cancer Therapy;Cancer Surgery.
Anastomotic leakage after gastroesophageal resection for can-cer is reported to occur with an incidence between 2% and
0% and to be responsible for about 50% of postoperative mortal-ty.1–4 The most efficient treatment of anastomotic leakage aftersophagectomy or gastrectomy, however, remains controversial.he spectrum of established therapeutic options range from reop-ration with discontinuity resection, diversion, or re-anastomosiso conservative treatment with perianastomotic drainage, paren-eral nutrition, naso-intestinal decompression, and broad-spec-rum antibiotics. Both surgical and conservative treatment op-ions, however, are associated with high mortality rates andxtensively long intensive care unit and hospital stays.1–8 In the
search for optimized management, the endoscopic placement ofstents has been introduced in the management of anastomoticleakages in the past decade. Although the permanent endoscopic
placement of self-expanding metal stents has long been establishedin the palliative treatment of esophagotracheal fistula and malig-nant obstruction in the upper gastrointestinal tract,9,10 the re-moval of stents after temporary therapeutic use has not beenreasonably possible until the emergence of completely coveredstents. First reports on the use of covered stents in the manage-ment of postoperative esophageal anastomotic leakages are prom-ising, however, they are limited to very small case series in heter-ogeneous patient cohorts.11–20 Moreover, complications of stentherapy for anastomotic leakage are mentioned rather anecdotally.
The aim of this observational study was to describe our expe-ience in the use of covered self-expanding stents in the manage-
ent of anastomotic leakage after resection for carcinoma of thesophagus or esophagogastric junction. We analyzed the outcomef stent therapy and report on stent-related complications. We alsoerformed a literature review on stent therapy for esophagealnastomotic leakage and compared stent therapy with other con-ervative and surgical treatment regimens.
Patients and MethodsStudy CohortBetween 2003 and 2009, there were 1296 patients who
underwent esophagectomy or trans-hiatally extended gastrectomyfor carcinomas of the esophagus or esophagogastric junction inthe Department of Surgery at the Klinikum Rechts der Isar, Tech-nische Universität München, as a national referral center for thesetumor entities. In 115 patients (9%; 95% confidence interval [CI],7.4%–10.5%), a fully covered self-expanding metal stent was placedendoscopically as the first treatment option for postoperativeanastomotic leakage. These 115 patients comprise the study co-hort of this report. The median age was 61 years (range, 22–88 y).Thirty-eight patients (33%) had squamous cell carcinomas of theesophagus and 77 patients (67%) had adenocarcinomas of theesophagus or esophagogastric junction. Surgery was performedafter neoadjuvant chemotherapy or chemoradiotherapy in 89 pa-tients (77%). Stent therapy was performed in 28 patients (24%)after trans-hiatally extended gastrectomy with Roux-en-Y esoph-agojejunostomy, in 84 patients (73%) after esophagectomy andgastric tube pull-up, and in 3 patients (3%) after esophagectomyand colonic interposition (Table 1). All 115 leakages were locateddirectly at the anastomosis of the remaining esophagus to thepulled-up jejunum (n � 28), the pulled-up gastric tube (n � 84),or the interposed colon (n � 3).
Abbreviations used in this paper: CI, confidence interval; CT, com-puted tomography.
© 2011 by the AGA Institute1542-3565/$36.00
doi:10.1016/j.cgh.2010.12.010
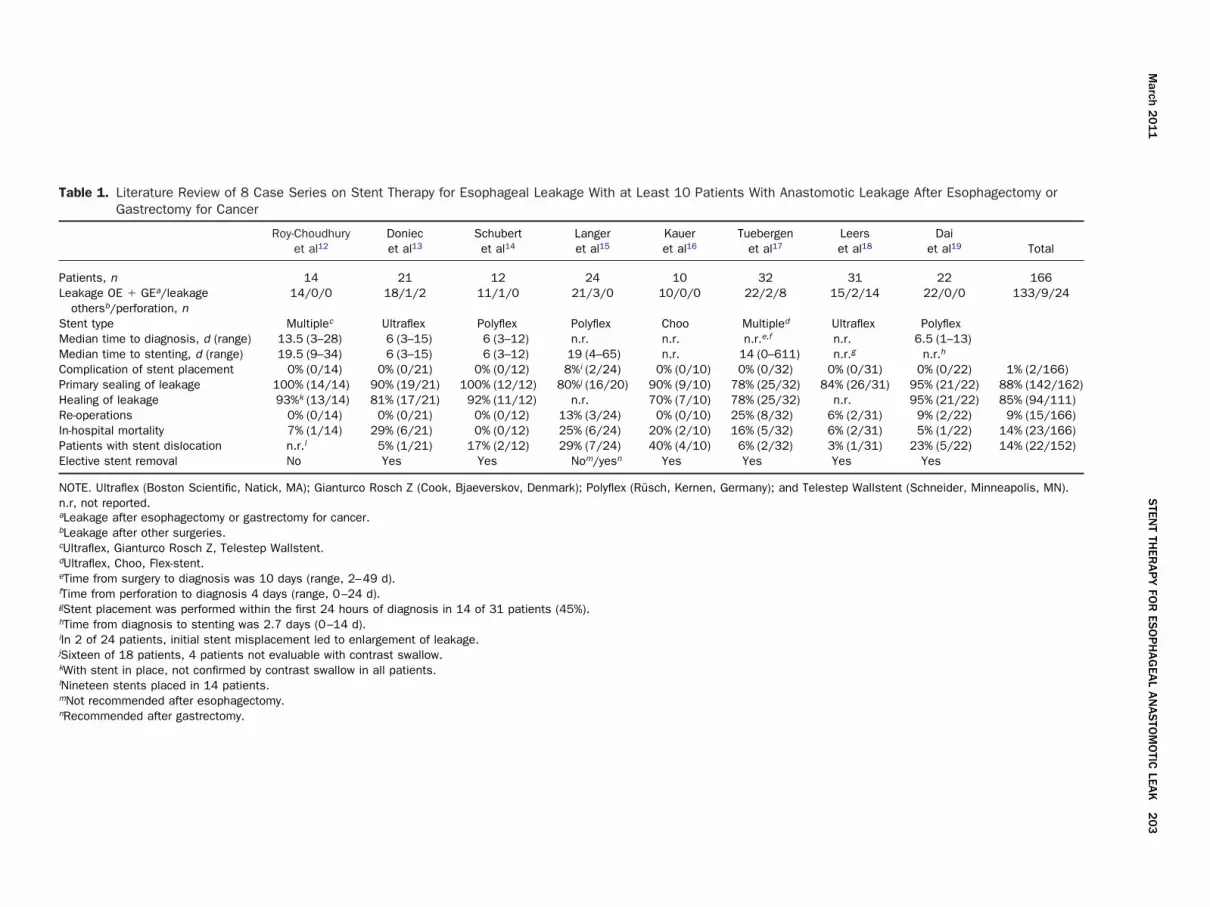
Table 1. Literature Review of 8 Case Series on Stent Therapy for Esophageal Leakage With at Least 10 Patients With Anastomotic Leakage After Esophagectomy orGastrectomy for Cancer
Roy-Choudhuryet al12
Doniecet al13
Schubertet al14
Langeret al15
Kaueret al16
Tuebergenet al17
Leerset al18
Daiet al19 Total
Patients, n 14 21 12 24 10 32 31 22 166Leakage OE � GEa/leakage
othersb/perforation, n14/0/0 18/1/2 11/1/0 21/3/0 10/0/0 22/2/8 15/2/14 22/0/0 133/9/24
Stent type Multiplec Ultraflex Polyflex Polyflex Choo Multipled Ultraflex PolyflexMedian time to diagnosis, d (range) 13.5 (3–28) 6 (3–15) 6 (3–12) n.r. n.r. n.r.e,f n.r. 6.5 (1–13)Median time to stenting, d (range) 19.5 (9–34) 6 (3–15) 6 (3–12) 19 (4–65) n.r. 14 (0–611) n.r.g n.r.h
Complication of stent placement 0% (0/14) 0% (0/21) 0% (0/12) 8%i (2/24) 0% (0/10) 0% (0/32) 0% (0/31) 0% (0/22) 1% (2/166)Primary sealing of leakage 100% (14/14) 90% (19/21) 100% (12/12) 80%j (16/20) 90% (9/10) 78% (25/32) 84% (26/31) 95% (21/22) 88% (142/162)Healing of leakage 93%k (13/14) 81% (17/21) 92% (11/12) n.r. 70% (7/10) 78% (25/32) n.r. 95% (21/22) 85% (94/111)Re-operations 0% (0/14) 0% (0/21) 0% (0/12) 13% (3/24) 0% (0/10) 25% (8/32) 6% (2/31) 9% (2/22) 9% (15/166)In-hospital mortality 7% (1/14) 29% (6/21) 0% (0/12) 25% (6/24) 20% (2/10) 16% (5/32) 6% (2/31) 5% (1/22) 14% (23/166)Patients with stent dislocation n.r.l 5% (1/21) 17% (2/12) 29% (7/24) 40% (4/10) 6% (2/32) 3% (1/31) 23% (5/22) 14% (22/152)Elective stent removal No Yes Yes Nom/yesn Yes Yes Yes Yes
NOTE. Ultraflex (Boston Scientific, Natick, MA); Gianturco Rosch Z (Cook, Bjaeverskov, Denmark); Polyflex (Rüsch, Kernen, Germany); and Telestep Wallstent (Schneider, Minneapolis, MN).n.r, not reported.aLeakage after esophagectomy or gastrectomy for cancer.bLeakage after other surgeries.cUltraflex, Gianturco Rosch Z, Telestep Wallstent.dUltraflex, Choo, Flex-stent.eTime from surgery to diagnosis was 10 days (range, 2–49 d).fTime from perforation to diagnosis 4 days (range, 0–24 d).gStent placement was performed within the first 24 hours of diagnosis in 14 of 31 patients (45%).hTime from diagnosis to stenting was 2.7 days (0–14 d).iIn 2 of 24 patients, initial stent misplacement led to enlargement of leakage.jSixteen of 18 patients, 4 patients not evaluable with contrast swallow.kWith stent in place, not confirmed by contrast swallow in all patients.lNineteen stents placed in 14 patients.mNot recommended after esophagectomy.nRecommended after gastrectomy.
March
20
11
STEN
TTH
ERA
PY
FOR
ESO
PH
AG
EAL
AN
AS
TOM
OTIC
LEAK
20
3

204 FEITH ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 9, No. 3
Diagnosis and Management of AnastomoticLeakageOur diagnostic and therapeutic management of esoph-
ageal anastomotic leakage is outlined in Figure 1. Anastomotichealing was monitored primarily by clinical means. Only in caseof clinical suspicion of anastomotic leakage did the patient
Figure 1. Diagnostic and therapeutic managem
undergo flexible upper endoscopy. If endoscopy revealed a com-plete ischemia or necrosis of the anastomosed jejunum, gastricconduit, or interposed colon, the patient immediately under-went re-operation with discontinuity resection of the primaryreconstruction. Stent therapy was performed only in patientswith adequate perfusion of the anastomotic region.
ent of esophageal anastomotic leakage.

hoo s
March 2011 STENT THERAPY FOR ESOPHAGEAL ANASTOMOTIC LEAK 205
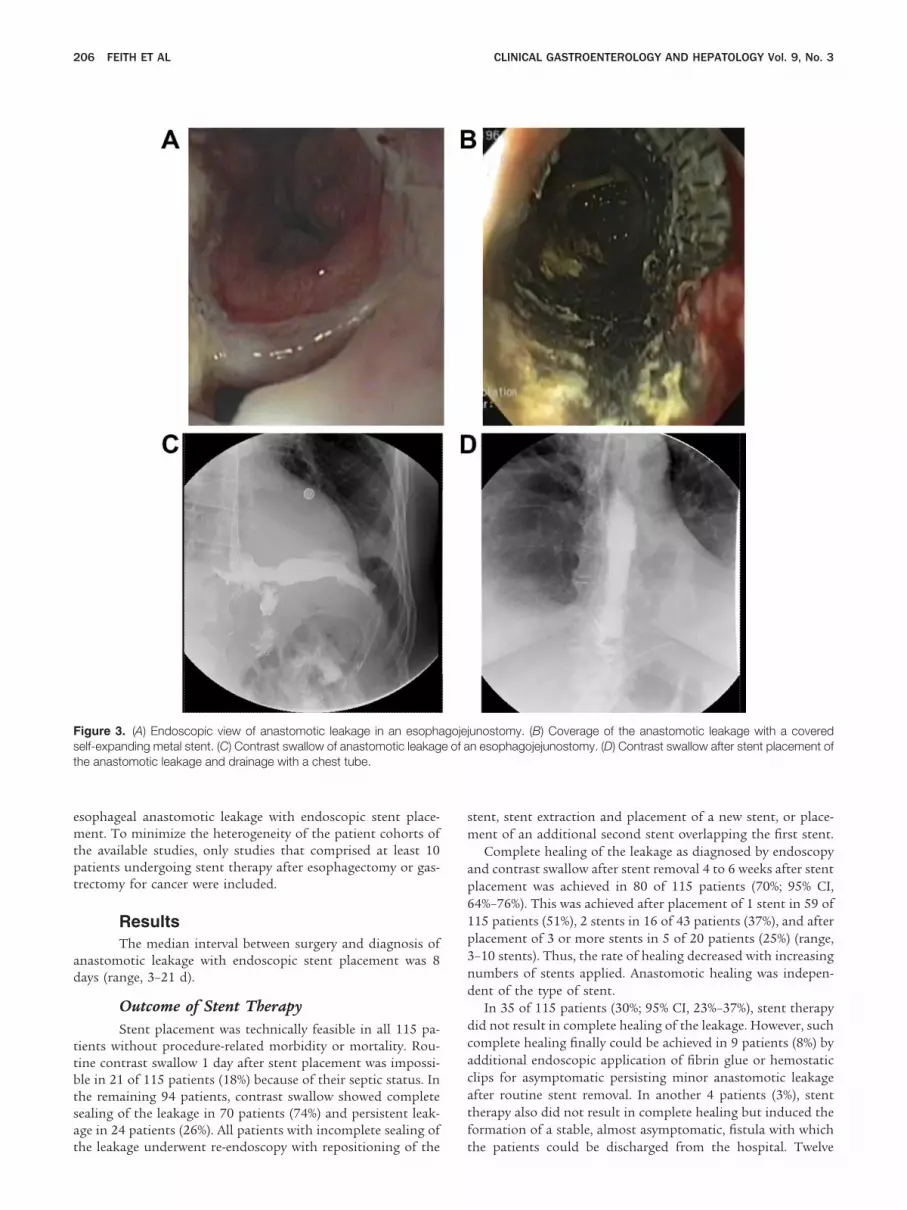
For stent therapy, 1 of 2 types of fully covered self-expandingmetal stents was placed by an experienced interventional en-doscopist: a Choo stent (diameter shaft, 18 mm; diameterproximal throat, 24 mm; M.I. Tech, Seoul, Korea) (Figure 2A) in109 patients or, since 2006, a Niti-S stent (diameter shaft, 20mm; diameter proximal throat, 28 mm; Taewoong Medical,Seoul, Korea) (Figure 2B) in 6 patients. The design of bothstents includes a retrieval lasso at both ends for removal andadjustment of the stent. For endoscopic stent placement, allpatients received intravenous sedation with midazolam 2 to 10mg combined with diisopropylphenol 20 to 200 mg. No patientrequired general anesthesia with intubation for the endoscopicprocedure. After the leakage was identified endoscopically andmarked by a radiopaque marker, the stent was placed tran-sorally with a guidewire. Per our normal routine, the stent waschecked by contrast swallow 1 day later to allow for completeexpansion of the stent. If complete sealing of the leakage wasachieved, enteral feeding was started orally with soft food instable patients or through enteral probes in intensive carepatients (Figure 3).
Endoscopic stent therapy was always accompanied by assess-ment of the perianastomotic region by computed tomography(CT) scan. If the intraoperatively placed drain had been re-moved already, or if the CT scan revealed inadequate drainageof the perianastomotic region by the intraoperatively placeddrain, additional chest tubes or pigtail drains were insertedunder CT guidance to completely drain all visible fluid collec-tions in all patients. Concomitantly, all patients also receivedbroad-spectrum antibiotic therapy.
In the case of a clinically uneventful postinterventionalcourse, no intermediate controls were performed; in fact, thestent was removed endoscopically 4 to 6 weeks later. Again,
Figure 2. (A) Example of a used, fully covered C
stent removal was performed under intravenous sedation with
midazolam and diisopropylphenol using a single-channel en-doscope. With a forceps, the proximal retrieval lasso wasgrasped and the stent was pulled out. Complete healing of theleakage was assessed by endoscopy, and a post–stent-extractioncontrast swallow. In patients with residual leakage after routinestent removal, a new stent was placed or an alternative endo-scopic therapy such as application of fibrin glue or hemostaticclips was used. In the case of clinical signs of persistent leakagein the postinterventional course, repeated endoscopies, contrastswallows, or CT scans were performed immediately on-demandand further interventions were performed as necessary.
MethodsClinical data of patients with esophageal and gastric
cancer were entered prospectively in our gastroesophageal da-tabase. Assuming that all stents were positioned correctly atinitial stent placement, any kind of incorrect stent position inthe further course was defined as stent dislocation. Becausestent dislocations were encountered at different time points, wedistinguished early, intermediate, and late dislocations. Incom-plete sealing of the leakage at routine contrast swallow 1 dayafter stent placement was assumed to be caused by (minor)stent dislocation and was classified as early dislocation. Inter-mediate stent dislocations occurred after routine postinterven-tional contrast swallow and before complete healing of theleakage. Early and intermediate stent dislocations with persis-tent leakage required re-endoscopy with stent repositioning orstent removal with placement of a new stent. Late stent dislo-cations occurred after complete healing of the leakage and thusrequired no re-stenting.
We analyzed our clinical database and the medical files of115 consecutive patients with stent therapy. In addition, we
tent. (B) Example of a fully covered Niti-S Stent.
performed a systematic literature review on the management of
206 FEITH ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 9, No. 3
esophageal anastomotic leakage with endoscopic stent place-ment. To minimize the heterogeneity of the patient cohorts ofthe available studies, only studies that comprised at least 10patients undergoing stent therapy after esophagectomy or gas-trectomy for cancer were included.
ResultsThe median interval between surgery and diagnosis of
anastomotic leakage with endoscopic stent placement was 8days (range, 3–21 d).
Outcome of Stent TherapyStent placement was technically feasible in all 115 pa-
tients without procedure-related morbidity or mortality. Rou-tine contrast swallow 1 day after stent placement was impossi-ble in 21 of 115 patients (18%) because of their septic status. Inthe remaining 94 patients, contrast swallow showed completesealing of the leakage in 70 patients (74%) and persistent leak-age in 24 patients (26%). All patients with incomplete sealing of
Figure 3. (A) Endoscopic view of anastomotic leakage in an esophaself-expanding metal stent. (C) Contrast swallow of anastomotic leakagthe anastomotic leakage and drainage with a chest tube.
the leakage underwent re-endoscopy with repositioning of the
stent, stent extraction and placement of a new stent, or place-ment of an additional second stent overlapping the first stent.
Complete healing of the leakage as diagnosed by endoscopyand contrast swallow after stent removal 4 to 6 weeks after stentplacement was achieved in 80 of 115 patients (70%; 95% CI,64%–76%). This was achieved after placement of 1 stent in 59 of115 patients (51%), 2 stents in 16 of 43 patients (37%), and afterplacement of 3 or more stents in 5 of 20 patients (25%) (range,3–10 stents). Thus, the rate of healing decreased with increasingnumbers of stents applied. Anastomotic healing was indepen-dent of the type of stent.
In 35 of 115 patients (30%; 95% CI, 23%–37%), stent therapydid not result in complete healing of the leakage. However, suchcomplete healing finally could be achieved in 9 patients (8%) byadditional endoscopic application of fibrin glue or hemostaticclips for asymptomatic persisting minor anastomotic leakageafter routine stent removal. In another 4 patients (3%), stenttherapy also did not result in complete healing but induced theformation of a stable, almost asymptomatic, fistula with which
unostomy. (B) Coverage of the anastomotic leakage with a coveredn esophagojejunostomy. (D) Contrast swallow after stent placement of
gojeje of a
the patients could be discharged from the hospital. Twelve

t
March 2011 STENT THERAPY FOR ESOPHAGEAL ANASTOMOTIC LEAK 207
patients (10%) with progressive septic symptoms during stenttherapy underwent reoperation, the anastomosis disconnected,and the primary reconstruction was removed. Only 2 of them(2%) underwent reconstruction secondarily with colonic inter-position after clinical stabilization. Of the remaining 10 pa-tients undergoing reoperation, 2 (2%) died in the postoperativecourse, 5 (4%) died of tumor progress after discharge from thehospital, and 3 (3%) are still alive but not in condition forfurther reconstructive surgery. Finally, another 8 patients (7%)who did not undergo reoperation died in the course of stenttherapy during their primary hospital stay with 5 of them (4%)showing perpetuating septic course, 2 of them (2%) dying ofacute cardiac failure, and 1 patient (1%) dying of fulminantpulmonary embolism resulting from a deep venous thrombosis.Overall, the in-hospital mortality rate was 9% (10 of 115 pa-tients).
Complications of Stent TherapyStent perforation was seen in 1 of 115 patients (1%). In
this case, the stent, which was correctly placed over a leakingesophagogastrostomy, perforated through the pulled-up gastrictube into the trachea. We performed immediate re-thoracotomywith resection of the gastric tube and closure of the trachealfistula using a muscle flap.
The most frequent complication of stent therapy was stentdislocation and occurred in 61 of 115 patients (53%), including41 of 84 patients (49%) with esophagogastrostomy, 17 of 28patients (61%) with esophagojejunostomy, and all 3 patients(100%) with esophagocolonostomy. Although 60 of 109 pa-tients (55%) who primarily were stented with a Choo stent hada stent dislocation, the rate of stent dislocation for the Niti-Sstent was 1 of 6 patients (17%). Early, intermediate, and latestent dislocations were encountered in 24, 28, and 17 of 115patients (21%, 24%, and 15%), respectively. Early and interme-diate stent dislocation with persistent leakage led to repeatedstent placements in 43 patients. Overall, 72 patients (63%)received 1 stent, 23 patients (20%) received 2 stents, 9 patients(8%) received 3 stents, and 11 patients (10%) received more than3 stents (range, 4 –10 stents). Patients with late stent dislocation
Figure 4. Abdominal radiograph showing a dislocated stent stuck athe Roux-en-Y anastomosis in a patient after gastrectomy.
presented in 3 different ways. First, in 6 of 115 patients (5%), the
stent dislocated completely, migrated asymptomatically th-rough the entire intestinum, and was harvested from the pa-tient’s excretion by chance. Second, the stent was not in place atroutine endoscopy 4 to 6 weeks after stent placement and wasnot detectable by other means such as radiographs in 7 of 115patients (6%). Thus, unrecognized complete intestinal passagemust have been assumed as well. Third, surgical interventionswere necessary in 4 of 115 patients (3%), all owing to late stentdislocations. In 3 of these patients, all stented for leakingesophagojejunostomy, the stent also was not detectable at rou-tine endoscopy 4 to 6 weeks after stent placement, but wasfound on abdominal radiographs in the small intestine notreachable by endoscopy. Because all 3 patients were completelyasymptomatic, we made no further effort to remove the stent atthat time and waited for completion of the intestinal passage.However, all 3 patients presented with acute abdomen 3months, 2 months, and 1 week later (Figure 4) and underwentemergency laparotomy. The stents were stuck at the Roux-en-Yanastomosis in 2 patients and at the ileocecal valve in 1 patient,causing intestinal perforations at these sites. We performedresection of the affected part of the intestine in all 3 patients(Figure 5). In the remaining patient undergoing surgical inter-vention, we performed prophylactic open gastrotomy to removea dislocated stent before the onset of symptoms because thisstent had asymptomatically migrated into the stomach butcould not be removed endoscopically because of a stricture ofthe esophagogastrostomy.
Endoscopic Follow-Up EvaluationOf the 95 surviving patients who were stented and did
not undergo reoperation, 93 patients (98%) were followed up inour department for at least 3 months after initial surgery witha mean follow-up period of 17 months (range, 3–73 mo). En-doscopic stent removal was performed in 74 of 93 patients(80%) after a median of 54 days (range, 17– 427 d) after initialstent placement. In 5 of these patients (5%), the retrieval lassocould not be grasped as a result of tissue ingrowth. In thesecases, the proximal end of the stent itself was mobilizedendoscopically and directly grasped with a forceps to removethe stent. In 2 more patients (2%), the stent was not remov-able at all because of hyperplastic tissue overgrowth. Thewhereabouts of the stents in the remaining 17 patients al-ready have been exemplified earlier with surgical removal in
Figure 5. Resection specimen of a dislocated stent that got stuck and
caused intestinal perforation at the ileocecal valve.
at
m
cemlst
rFa6tasltt
t
aitmsdpoasp
oats
208 FEITH ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 9, No. 3
4 patients (4%) and asymptomatic complete intestinal pas-sage in 13 patients (14%). Eleven patients (12%) developedsymptomatic anastomotic strictures and all were treated en-doscopically by bougie dilations. Endoscopy revealed anas-tomotic stricture in another 24 patients (26%) who, however,were clinically asymptomatic. In these patients, we per-formed prophylactic bougie dilations.
Literature ReviewQuantitative analysis of our literature review with all
available studies on stent therapy that comprised 10 or morepatients with esophageal anastomotic leakage after esophagec-tomy or gastrectomy for cancer is shown in Table 1.
DiscussionThe concept of additional stent placement in the con-
servative management of esophageal anastomotic leakage afteresophagectomy or gastrectomy provides the advantage of im-mediate leak occlusion, which allows early oral feeding, avoidsfurther contamination of the mediastinum, and, finally, resultsin shorter hospital stays.12–19 However, stent placement alsoforces the need for adequate perianastomotic drainage becausestents not only stop further intestinal leakage to the extraint-estinal perianastomotic region but also prevent internal drain-age of any fluid collection in the mediastinum or pleural cavi-ties.
These issues have been emphasized repeatedly in severalreports, however, without finally rendering endoscopic stenttherapy the treatment of choice for anastomotic esophagealleakage.12–19 This is mainly owing to fundamental deficits of the
vailable studies, among them small case loads (all �32 pa-ients),12–19 different underlying diseases (malignant and be-
nign),14,15,17 heterogeneous causes of esophageal leaks (anasto-otic leakages and esophageal perforations),13–15,17,18 and
varying therapeutic regimens with different time intervals be-tween diagnosis and treatment (stent therapy as first treatmentoption, after ineffective other therapeutic means, or even aslast-choice procedure).15,17 In the present study, we only in-luded patients with esophageal anastomotic leakages aftersophagectomy or gastrectomy for cancer that primarily wereanaged with stent placement right after diagnosis of the
eakage. Our series of 115 patients is a large cohort. However,imilar to all other studies, ours also was not randomized andherefore lacked a control group.
Thus, comparison of stent therapy with other treatmentegimens can be made only by looking into published figures.or surgical revision and for conservative treatment withoutstent, in-hospital mortality rates are reported at 35% to
4%1– 4 and 19% to 46%,4,6 – 8,21,22 respectively. Compared withhese numbers, the in-hospital mortality in our series (9%)nd in other reports on stent therapy (0%–29%)12–19 is sub-tantially lower. With respect to healing of the esophagealeakage, numbers are given at 59%22 and 58%21 for conserva-ive treatment without a stent but at 70% to 95% with stentherapy.12–19 It must be mentioned, however, that compari-
sons of stent therapy with other treatment regimen foresophageal leakages are limited by the heterogeneous natureof the patient cohorts. Because there is common agreementin the literature that extensive ischemia of the conduit is not
an indication for stent therapy but necessitates immediate preoperation, these assumingly most severe cases consistentlyare excluded from the stent group and find themselves un-exceptionally in the surgical revision group. Apart from that,the criteria qualifying for stent therapy, if at all clearlydefined, differ considerably between studies. Although westented all adequately perfused anastomotic leakages irre-spective of size, some investigators restrict stent therapyto leakages affecting less than one third,15 less thanwo thirds,17 or less than 70% of the circumference,14 and
some also set a minimum size of the leakage for stenttherapy.12–14,16 We believe that the state of perfusion of the
nastomotic region is the paramount determinant for heal-ng, and that therefore endoscopy is the decisive diagnosticool and that all adequately perfused esophageal anasto-
otic leakages qualify for stent therapy. Nevertheless, theize of the leakage, the time from appearance of leakage toiagnosis and treatment, and the degree of mediastinal orleural infection are important parameters that influence theutcome of stent therapy. With these parameters in mind, itppears highly plausible that the most favorable outcomes oftent therapies have been reported for iatrogenic esophagealerforation.5,23 To mimic this ideal situation in the postop-
erative course, we strongly recommend immediate endoscopyon the slightest clinical suspicion of anastomotic leakageand stent placement without the least delay to keep extra-esophageal infection as minimal as possible.
The outcome of stent therapy presented in this study andpublished elsewhere is convincing because the mainly technicalconcerns on temporary stent placement appear unwarranted.The available data show that stent placement was technicallyfeasible in virtually all patients without procedure-related mor-bidity or mortality and led to instant primary sealing of theleakage in 74% of our patients and in 88% (range, 78%–100%) ofthe patients in other studies.12–19 Moreover, elective stent re-moval proved to be endoscopically feasible in the vast majorityof patients and most investigators, including us, explicitly rec-ommend elective stent removal to avoid possible complicationsof permanent stenting such as penetration, dislocation, steno-sis, and reflux with aspiration.13,14,16 –19 Finally, all anastomoticstrictures after stent removal in our series and most otherreports could be handled endoscopically.13,15
Nevertheless, there can be no denying that a couple ofstent-specific problems may occur. The rate of patients withstent dislocation was remarkably high at 53% in our series.Interestingly, we saw stent dislocation in all patients withesophagocolonostomies. The numbers for esophagojejunos-tomies and esophagogastrostomies in our series were 61%and 49%, respectively. Langer et al15 had similar results foresophagocolonostomies (100%) and esophagogastrostomies(44%) but encountered stent dislocation in only 1 of 5 pa-tients with esophagojejunostomies (20%). It is important tomention that stent dislocation is observed more frequentlyin the therapy of anastomotic leakage than in the palliativetreatment of malignant stenosis in which rigid tumor steno-sis provides an outer force on the stent for a tight fit andreduced risk of dislocation.24 In this context, our observation
f less stent dislocations with the Niti-S stent also could bettributed to its larger diameter, possibly resulting in aighter fit to the esophageal wall. However, numbers are toomall to draw conclusions on stent sizes from our study. In
arallel, the different rates of stent dislocation encountered
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
March 2011 STENT THERAPY FOR ESOPHAGEAL ANASTOMOTIC LEAK 209
for the different types of anastomoses also might be causedby differences in the anatomic texture and motility of theanastomosed colon, stomach, and small intestine. Althoughall early and intermediate stent dislocations could be man-aged endoscopically, both complete intestinal passage andsurgical stent removals were seen only in late stent disloca-tions. This most likely is owing to early diagnosis in patientswith early or intermediate stent dislocation because theybecome symptomatic for persisting leakage before the stentvanishes out of endoscopic range. In these patients, evenrepeated endoscopic interventions appear worthwhile,15 al-beit the rate of healing decreased with the number of stentsapplied in our series. Stent dislocation with intestinal ob-struction and subsequent intestinal perforation, however, isa major complication requiring surgery. However, cases ofbowel perforation caused by stent migration rarely are re-ported in the literature but appear to be associated mostlywith small-bowel obstruction.25–27 We assume that the rate ofpatients requiring surgical intervention for removal of dis-located stents is still underestimated in the literature becausemost reports on stent dislocations are from nonsurgicalpatients. It appears plausible that the risk for stents to getstuck somewhere in the intestine is higher in patients whounderwent extended abdominal surgeries with altered intra-abdominal anatomy and, most likely, adhesions than innonoperated patients with a high chance of asymptomaticcomplete intestinal passage. Surgical revision clearly is re-quired in patients with intestinal perforation. However,based on our experience, we also suggest early surgical inter-vention in the case of endoscopically unreachable stent dis-location in patients undergoing surgery for upper gastroin-testinal carcinomas.
In summary, the available data clearly show the feasibilityof temporary stent placement and removal with low proce-dure-related morbidity and mortality and, because of thefavorable outcome of stent therapy compared with othertreatment regimens, suggest stent therapy as the treatmentof choice in the management of adequately perfused esoph-ageal anastomotic leakage. However, because stent disloca-tion remains a common problem in these postoperative pa-tients, the optimal type of stent, the best time for stentremoval, and useful additional endoscopic means for stentfixation have yet to be defined in these patients.25,26 On thisbasis, it can be concluded that an experienced interventionalendoscopist is indispensable for any surgical unit performingesophageal surgery.
References
1. Griffin SM, Lamb PJ, Dresner SM, et al. Diagnosis and manage-ment of mediastinal leak following radical oesophagectomy. Br JSurg 2001;88:1346–1351.
2. Urschel JD. Esophagogastrostomy anastomotic leaks compli-cating esophagectomy: a review. Am J Surg 1995;169:634–640.
3. Alanezi K, Urschel JD. Mortality secondary to esophageal anas-tomotic leak. Ann Thorac Cardiovasc Surg 2004;10:71–75.
4. Lang H, Piso P, Stukenborg C, et al. Management and resultsof proximal anastomotic leaks in a series of 1114 total gas-trectomies for gastric carcinoma. Eur J Surg Oncol 2000;26:168–171.
5. DeMeester TR. Perforation of the esophagus. Ann Thorac Surg
1986;42:231–232. 26. Sauvanet A, Baltar J, Le Mee J, et al. Diagnosis and conservativemanagement of intrathoracic leakage after oesophagectomy. Br JSurg 1998;85:1446–1449.
7. Viste A, Eide GE, Søreide O. Stomach cancer: a prospective studyof anastomotic failure following total gastrectomy. Acta ChirScand 1987;153:303–306.
8. Griffin S, Desai J, Charlton M, et al. Factors influencing mortalityand morbidity following oesophageal resection. Eur J Cardiotho-rac Surg 1989;3:419–423.
9. Utidehaag MJ, Hooft JE, Veschuur EM, et al. A fully-coveredstent (Alimaxx-E) for the palliation of malignant dysphagia: aprospective follow-up study. Gastrointest Endosc 2009;70:1082–1089.
0. Brown TH, Nicholson DA, Irving MH, et al. Use of a self-expandingmetal stent for oesophagogastric fistulation. Br J Surg 1995;82:663–664.
1. Hünerbein M, Stroszczynski C, Moesta KT, et al. Treatment ofthoracic anastomotic leaks after esophagectomy with self-ex-panding plastic stents. Ann Surg 2003;240:801–807.
2. Roy-Choudhury SH, Nicholson AA, Wedgwood KR, et al. Symptom-atic malignant gastroesophageal anastomotic leak: managementwith covered metallic esophageal stents. AJR Am J Roentgenol2001;176:161–165.
3. Doniec JM, Schniewind B, Kahlke V, et al. Therapy of anasto-motic leaks by means of covered self-expanding metallicstents after esophagogastrectomy. Endoscopy 2003;35:652–658.
4. Schubert D, Scheidbach H, Kuhn R, et al. Endoscopic treatmentof thoracic esophageal anastomotic leaks by using silicone-cov-ered, self-expanding polyester stents. Gastrointest Endosc2005;61:891–896.
5. Langer FB, Wenzl E, Prager G, et al. Management of postopera-tive esophageal leaks with the Polyflex self-expanding coveredplastic stent. Ann Thorac Surg 2005;79:398–403.
6. Kauer WKH, Stein HJ, Dittler HJ, et al. Stent implantation as atreatment option in patients with thoracic anastomotic leaksafter esophagectomy. Surg Endosc 2007;22:50–53.
7. Tuebergen D, Rijcken E, Mennigen R, et al. Treatment of thoracicesophageal anastomotic leaks and esophageal perforations withendoluminal stents: efficacy and current limitations. J Gastroin-test Surg 2008;12:1168–1176.
8. Leers JM, Vivaldi C, Schäfer H, et al. Endoscopic therapy foresophageal perforation or anastomotic leak with a self-ex-pandable metallic stent. Surg Endosc 2009;23:2258–2262.
9. Dai YY, Gretschel S, Dudeck O, et al. Treatment of oesophagealanastomotic leaks by temporary stenting with self-expandingplastic stents. Br J Surg 2009;96:887–891.
0. Eloubeidi MA, Lope TL. Novel removable internally fully coveredself-expanding metal esophageal stent: feasibility, technique ofremoval, and tissue response in humans. Am J Gastroenterol2009;104:1374–1381.
1. Fan ST, Lau WY, Yip WC, et al. Healing of esophageal fistulasafter surgical treatment for carcinoma of the esophagus and theupper part of the stomach. Surg Gynecol Obstet 1988;166:307–310.
2. Tersløv-Jørgensen S, Pedersen H, Larsen V. Conservative treat-ment with total parenteral nutrition in patients with gastroesoph-ageal anastomotic leaks (anastomotic leaks conservativelytreated). Acta Chir Scand 1979;145:173–175.
3. Brinster CJ, Singhal S, Lee L, et al. Evolving options in themanagement of esophageal perforation. Ann Thorac Surg 2004;77:1475–1483.
4. Verschuur EM, Steyerberg EW, Kuipers EJ, et al. Effect of stentsize on complications and recurrent dysphagia in patients withesophageal or gastric cardia cancer. Gastrointest Endosc 2007;66:211–212.
5. Lowe AS, Beckett CG, Jowett S, et al. Self-expandable metal

210 FEITH ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 9, No. 3
stent placement for palliation of malignant gastroduodenal ob-struction: experience in a large, single, UK centre. Clin Radiol2007;62:738–744.
26. Diller R, Senninger N, Kautz G, et al. Stent migration necessi-tating surgical intervention. Surg Endosc 2003;17:1803–1807.
27. Stawowy M, Kruse A, Mortensen FV, et al. Endoscopic stentingfor malignant gastric outlet obstruction. Surg Laparosc Endosc
Percutan Tech 2007;17:5–9.Reprint requestsAddress requests for reprints to: Prof. Marcus Feith, MD, Chirurgis-
che Klinik und Poliklinik, Klinikum Rechts der Isar, Technische Univer-sität München, Ismaningerstr 22, 81675 Munich, Germany. e-mail:
[email protected]; fax: �49 89 4140 4870.
Conflicts of interest
The authors disclose no conflicts.