fractionated stereotactic radiosurgery and preservation of hearing in patients with vestibular...
TRANSCRIPT
CLINICAL STUDIES
Fractionated Stereotactic Radiosurgery and Preservation ofHearing in Patients with Vestibular Schwannoma: A
Preliminary Report
Joseph C. Poen, M.D., Alexandra J. Golby, M.D.,Kenneth M. Forster, Ph.D., David P. Martin, M.D.,Daniel M. Chinn, M.D., Steven L. Hancock, M.D.,
John R. Adler, Jr., M.D.Departments of Radiation Oncology (JCP, KMF, DMC, SLH, JRA) and Neurosurgery
(AJG, DPM, JRA), Stanford University School of Medicine, Stanford, California
OBJECTIVE: Microsurgery and stereotactic radiosurgery (SRS) for vestibular schwannomas are associated with arelatively high incidence of sensorineural hearing loss. A prospective trial of fractionated SRS was undertaken inan attempt to preserve hearing and minimize incidental cranial nerve injury.
METHODS: Thirty-three patients with vestibular schwannomas were treated with 2100 cGy in three fractions duringa 24-hour period using conventional frame-based linear accelerator radiosurgery. The median tumor diameterwas 20 mm (range, 7–42 mm). Baseline and follow-up evaluations included audiometry and contrast-enhancedmagnetic resonance imaging. End points were tumor progression, preservation of serviceable hearing, andtreatment-related complications.
RESULTS: Thirty-one patients (32 tumors) were assessable for tumor progression and treatment-related complica-tions and 21 patients for preservation of serviceable hearing, with a median follow-up interval of 2 years (range,0.5–4.0 yr). Tumor regression or stabilization was documented in 30 patients (97%) and tumor progression in 1(3%). The patient with tumor progression remains asymptomatic and has not required surgical intervention. Fivepatients (16%) developed trigeminal nerve injury at a median of 6 months (range, 4–12 mo) after SRS; two ofthese patients had preexisting trigeminal neuropathy. One patient (3%) developed facial nerve injury (House-Brackmann Class 3) 7 months after SRS. Preservation of useful hearing (Gardner-Robertson Class 1–2) was 77%at 2 years. All patients with pretreatment Gardner-Robertson Class 1 to 2 hearing maintained serviceable (Class1–3) hearing as of their last follow-up examination.
CONCLUSION: Three-fraction SRS with a conventional stereotactic frame is feasible and well tolerated in thetreatment of acoustic neuroma. This study demonstrates a high rate of hearing preservation and few treatment-related complications among a relatively high-risk patient cohort (tumors >15 mm or neurofibromatosis Type 2).Longer follow-up will be required to assess the durability of tumor control. (Neurosurgery 45:1299–1307, 1999)
Key words: Acoustic neuroma, Fractionation, Hearing preservation, Radiosurgery, Vestibular schwannoma
Refinement of microsurgical techniques has substantiallyreduced the morbidity associated with surgical re-moval of vestibular schwannomas (VSs). The incidence
of significant facial nerve injury has declined to less than 10%in several modern series. Preservation of cochlear nerve func-tion continues to pose a significant challenge, however. In a1988 review of attempted hearing preservation using middlefossa or posterior fossa approaches, only 33% of patientsacross several surgical series maintained clinically useful
hearing (12). Although there have been improvements in thepast decade (38, 40), the overall rate of successful preservationof cochlear function remains 50% or lower and is particularlychallenging in patients with moderate- to large-size tumors(.10–15 mm). The inherent difficulty in separating theschwannoma capsule from the vestibulocochlear nerve with-out causing injury by vascular compromise or neuronal dis-ruption remains a significant obstacle to preservation of hear-ing with modern microsurgery.
1299Neurosurgery, Vol. 45, No. 6, December 1999

Stereotactic radiosurgery (SRS) is a noninvasive alternativeto conventional surgery that is applicable to small andmoderate-size (#3 cm) VSs. Pioneered by Leksell, this tech-nique was first used in the treatment of VS in 1969. Since itsintroduction, SRS has been used in more than 5000 patientswith VS worldwide (27), with reported follow-up periods aslong as 15 years (36). Although tumor control (90–95% at 5–10yr) (24) and trigeminal and facial nerve injury rates (10–20%)have been uniformly favorable (8, 31, 36, 37), SRS, like micro-surgery, continues to be associated with significant hearingloss. Most studies report preservation of useful hearing in lessthan 50% of treated patients (10, 18, 23, 24).
Efforts to improve the efficacy and safety of SRS havefocused primarily on increasing the precision of tumor local-ization and conformality of dose deposition to target tissues.Although SRS advances have been associated with reductionsin treatment-related morbidity (8), it remains improbablethat technical advances can achieve complete exclusion ofthe cochlear nerve from the high-dose target volume. Becausecochlear nerve injury remains a significant limitation of SRS,methods to exploit biological differences among the tumorand surrounding normal cranial nerves should be explored.
For decades, it has been axiomatic that fractionation oftherapeutic radiation (delivery of the total therapeutic dose inseveral smaller fractions during a period of time) enhancestumor susceptibility and allows for the recovery of normaltissues, thereby increasing tumor control and minimizing nor-mal tissue effects. Until recently, rigid fixation of the stereo-tactic localizing frame has largely precluded the considerationof fractionation in the stereotactic treatment of brain tumors.Recognition of the potential biological advantages of fraction-ated SRS prompted the development of removable or relocat-able stereotactic systems for fractionated SRS programs (13).However, changing from a rigid fixation system to a relocat-able frame results in some loss of precision. Furthermore,prolonged standard fractionation lacks the practicality of asingle outpatient procedure. In an effort to improve hearingpreservation for patients with VS, we designed a fractionatedSRS protocol to incorporate the physical advantages of rigidstereotactic localization, the practicality of a 1-day treatment,and the potential biological advantages of an abbreviatedfractionation schedule. Our goal has been to maintain a highrate of VS control while reducing incidental damage to thecochlear nerve and preserving serviceable hearing. This arti-cle summarizes our results 4 years after the initiation of thisprogram.
PATIENTS AND METHODS
Eligibility and patient characteristics
Between August 1994 and January 1998, 34 VSs in 33 pa-tients were treated with fractionated stereotactic radiosur-gery. Eligibility for this treatment protocol required radio-graphic evidence of a VS with documentation of tumorprogression or hearing deterioration within the previous 12months. Initially, all patients were required to have service-able hearing in the treated ear by objective (Class 1–3 on the
Gardner-Robertson [GR] scale) (12) or subjective criteria. Theeligibility was later expanded to include patients with signif-icant hearing deficits at baseline if there was preexisting tri-geminal or facial nerve dysfunction. These patients were in-cluded on the basis of the observation that fractionatedtreatment may also reduce injury to the trigeminal and facialnerves (43).
The study group consisted of 21 men and 12 women. Themedian age was 50 years (range, 22–88 yr). Ten patients werediagnosed with neurofibromatosis Type 2 (NF2); eight ofthese patients were deaf in the contralateral ear as a conse-quence of prior surgical resection (n 5 6), SRS (n 5 1), ortumor progression (n 5 1). Pretreatment audiograms wereavailable for 31 treated ears: 23 were scored as GR Class 1 to3; 3 patients had Class 4 (detectable) hearing; and 5 patientshad Class 5 (not detectable) hearing. Twenty-seven tumorswere previously untreated, and seven tumors were recurrentand progressive after previous surgical resection.
Tumor dimensions were determined before treatment andat follow-up on gadolinium-enhanced T1-weighted thin-slice(2–5 mm) magnetic resonance imaging (MRI) of the internalauditory canals. The enhancing lesion was measured along itsmaximal intracanalicular-cerebellopontine angle length. Theother dimensions were obtained along the corresponding per-pendicular in the axial plane and the maximal height in thecoronal plane. The median maximal tumor diameter in thisseries was 20 mm (range, 7–42 mm). Four tumors were clas-sified as small (#15 mm), 27 were moderate in size (16–30mm), and three were large (.30 mm).
Radiosurgical technique
Patient immobilization and tumor localization were accom-plished with rigid cranial fixation using a Brown-Roberts-Wells stereotactic frame (Radionics, Burlington, MA). Imag-ing for localization and treatment planning was carried outwith 1-mm contrast-enhanced computed tomography or MRIthrough the internal auditory canals and cerebellopontineangle. Treatment planning software was developed at Stan-ford University. One to four isocenters were used to providea conformal dose distribution at the periphery of the contrast-enhancing lesion. The typical treatment plan consisted of twoisocenters, the larger centered on the cerebellopontine anglecomponent and the smaller on the intracanalicular compo-nent. The standard treatment arc arrangement has been de-scribed previously (1); it consisted of four noncoplanar arcsper isocenter with individual arc modifications to improvetumor/dose conformality and reduce incidental irradiation ofadjacent critical structures. The planned total dose was 2100cGy via 4-MV or 6-MV linear accelerator photons prescribedto the periphery of the contrast-enhancing lesion. The dosewas administered in three equal fractions of 700 cGy during a24-hour period. Frame placement, imaging, and treatmentplanning were performed in the afternoon on Day 0, with thefirst fraction administered early that evening. With theBrown-Roberts-Wells frame in place, the patient was admit-ted to the ambulatory treatment unit for an overnight stay.Most patients required mild analgesics and sedation for sleep.
1300 Poen et al.
Neurosurgery, Vol. 45, No. 6, December 1999

The second fraction was administered early the next morningand the third and final fraction in the late afternoon, approx-imately 24 hours after the first fraction. Immediately after thethird treatment, the stereotactic frame was removed and pa-tients were discharged home. Resumption of normal activitywas permitted on Day 2.
Patient follow-up
Clinical assessment for neurological injury was performedat 6-month intervals for the first 2 years and annually there-after. Audiometric and radiographic follow-up was obtainedat 6 months, 1 year, and annually thereafter. Trigeminal nerveinjury was scored for any paresthesia or anesthesia within thetrigeminal distribution. Facial nerve injury was scored accord-ing to House-Brackmann criteria (19). Standard audiometricassessments were used to measure pure tone average (PTA),speech reception threshold, and speech discrimination forclassification according to the system described by Gardnerand Robertson (12). Tumor measurements from thin-sectionMRI were performed pre- and posttreatment by a single ex-aminer (JCP). Tumor progression was defined as at least a3-mm increase in any one of the three tumor dimensions.Tumor regression was defined as at least a 3-mm decrease inany one dimension, with either stabilization or decrease in theother dimensions. Tumor stabilization was defined as changeless than 3 mm in all three dimensions when compared withpretreatment tumor measurements.
Statistical methods
Univariate analysis was applied to examine the effects ofpatient age, presence of NF2, presence of preexisting neurop-athy, prior conventional surgery, tumor size, computed to-mography versus MRI treatment planning, number of treat-ment isocenters, and dose heterogeneity (as measured by theratio of the prescribed dose to the maximal dose) on treatment-related complications and preservation of hearing. Actuarialcurves were constructed using the methods of Kaplan and Meier(22). Actuarial rates were compared using the log-rank test.Statistical significance was defined as P # 0.05.
RESULTS
Protocol compliance and follow-up
The treatment protocol was modified twice during the ini-tial phase so that two of the first three patients received dosesof 2550 cGy and 1950 cGy. All other patients received 2100cGy. Thirty-one of 33 patients received three fractions, with aminimum interfraction interval of 8 hours (mean interfractioninterval, 12 h). In one patient, the prescribed dose of 2100 cGywas delivered in two fractions because of a technical error indose calculation discovered at the completion of the firstfraction. One patient experienced severe claustrophobia-likesymptoms attributable to the stereotactic frame and was giventhe third and final treatment 5 hours after the second fraction.No patient was lost to follow-up. There were two deaths: onepatient died from complications of multiple sclerosis, and asecond patient, with advanced NF2, died from postoperative
complications after surgical resection of a 5-cm contralateralVS. The minimum, median, and maximum clinical follow-upintervals for the 31 surviving patients are 0.5, 2, and 4 years,respectively.
Tumor control
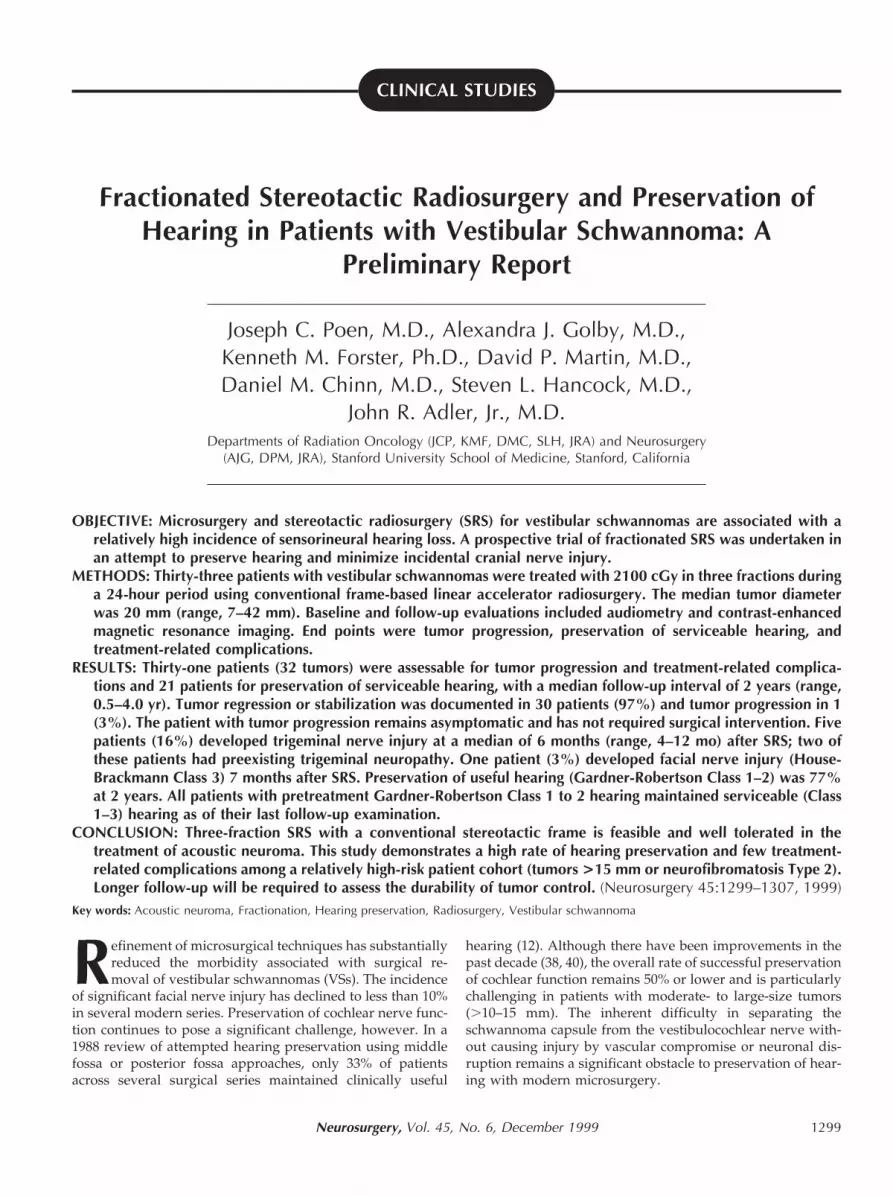
Radiographic follow-up was available for all surviving pa-tients (32 tumors) (Fig. 1). Twenty-two (85%) of 26 tumors hada significant loss of central contrast enhancement on the pa-tients’ 6-month follow-up MRI scans. Tumor regression wasdocumented in 11 patients (34%), tumor stabilization in 20(63%), and tumor progression in 1 (3%). The actuarial proba-bility of freedom from tumor progression at 2 years was 93%(Fig. 2). In the one patient with tumor progression, growth ofan NF2-associated VS was observed 1.8 years after SRS. Thispatient was assessed frequently during the next 2 years, dur-ing which time no further growth occurred and subsequenttumor regression was observed. During this continued obser-vation period, the patient remained asymptomatic and didnot require surgical intervention.
Trigeminal and facial nerve injury
Five patients (16%) developed trigeminal nerve injury at amedian of 6 months (range, 4–12 mo) after SRS. Three of thesepatients had no preexisting trigeminal symptoms. One patientexperienced worsening of a preexisting trigeminal dysesthesia.One patient with preexisting trigeminal neuralgia experienced asevere case of ipsilateral herpes zoster 3 months after SRS anddeveloped anesthesia of the affected trigeminal branches. One
FIGURE 1. Axial contrast-enhanced magnetic resonanceimages of left acousticneuroma. A, pretreatmentscan demonstrating contrast-enhancing tumor in thecerebellopontine angle. B,comparable image obtained 6months posttreatmentshowing characteristicdecreased central contrast
enhancement. C, image obtained 18 months posttreatmentshowing a decrease in the tumor size and recovery of somecontrast enhancement.
Fractionated Stereotactic Radiosurgery in Vestibular Schwannoma 1301
Neurosurgery, Vol. 45, No. 6, December 1999
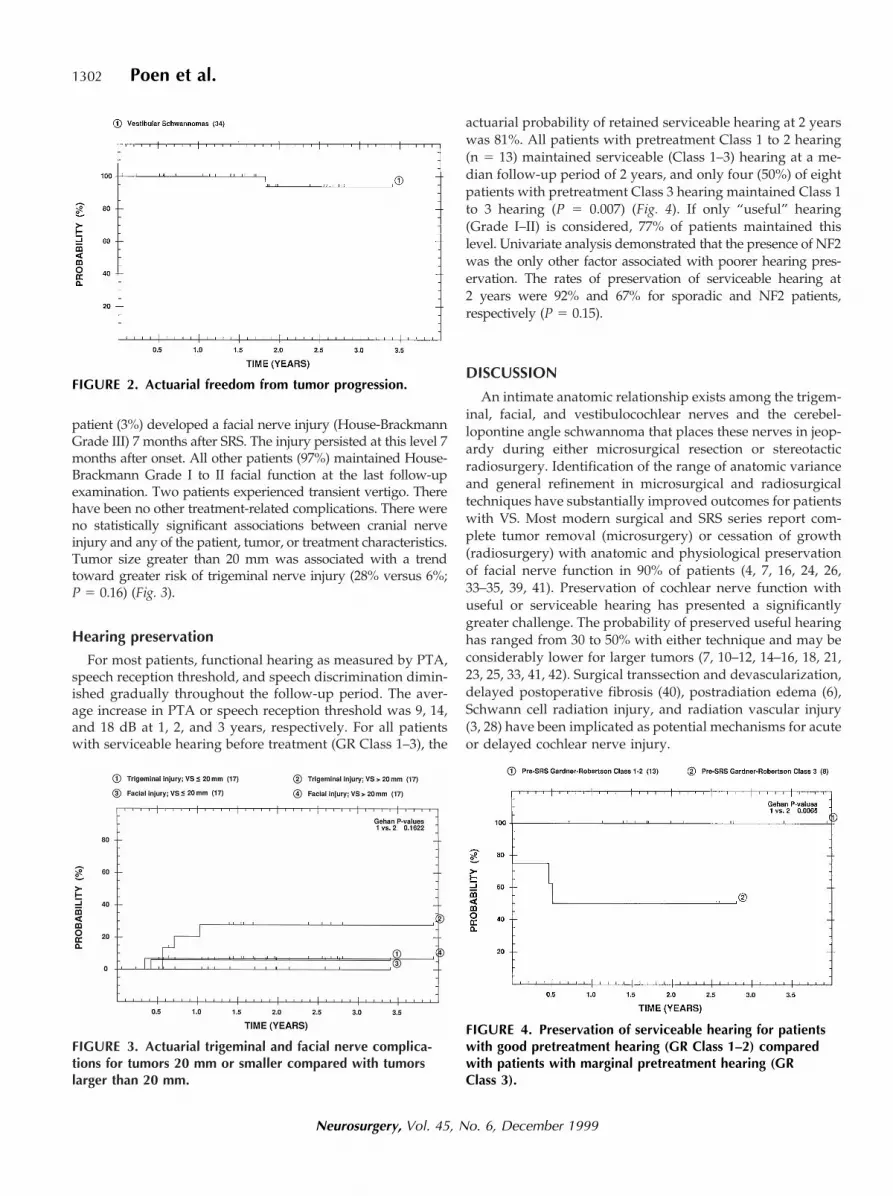
patient (3%) developed a facial nerve injury (House-BrackmannGrade III) 7 months after SRS. The injury persisted at this level 7months after onset. All other patients (97%) maintained House-Brackmann Grade I to II facial function at the last follow-upexamination. Two patients experienced transient vertigo. Therehave been no other treatment-related complications. There wereno statistically significant associations between cranial nerveinjury and any of the patient, tumor, or treatment characteristics.Tumor size greater than 20 mm was associated with a trendtoward greater risk of trigeminal nerve injury (28% versus 6%;P 5 0.16) (Fig. 3).
Hearing preservation
For most patients, functional hearing as measured by PTA,speech reception threshold, and speech discrimination dimin-ished gradually throughout the follow-up period. The aver-age increase in PTA or speech reception threshold was 9, 14,and 18 dB at 1, 2, and 3 years, respectively. For all patientswith serviceable hearing before treatment (GR Class 1–3), the
actuarial probability of retained serviceable hearing at 2 yearswas 81%. All patients with pretreatment Class 1 to 2 hearing(n 5 13) maintained serviceable (Class 1–3) hearing at a me-dian follow-up period of 2 years, and only four (50%) of eightpatients with pretreatment Class 3 hearing maintained Class 1to 3 hearing (P 5 0.007) (Fig. 4). If only “useful” hearing(Grade I–II) is considered, 77% of patients maintained thislevel. Univariate analysis demonstrated that the presence of NF2was the only other factor associated with poorer hearing pres-ervation. The rates of preservation of serviceable hearing at2 years were 92% and 67% for sporadic and NF2 patients,respectively (P 5 0.15).
DISCUSSION
An intimate anatomic relationship exists among the trigem-inal, facial, and vestibulocochlear nerves and the cerebel-lopontine angle schwannoma that places these nerves in jeop-ardy during either microsurgical resection or stereotacticradiosurgery. Identification of the range of anatomic varianceand general refinement in microsurgical and radiosurgicaltechniques have substantially improved outcomes for patientswith VS. Most modern surgical and SRS series report com-plete tumor removal (microsurgery) or cessation of growth(radiosurgery) with anatomic and physiological preservationof facial nerve function in 90% of patients (4, 7, 16, 24, 26,33–35, 39, 41). Preservation of cochlear nerve function withuseful or serviceable hearing has presented a significantlygreater challenge. The probability of preserved useful hearinghas ranged from 30 to 50% with either technique and may beconsiderably lower for larger tumors (7, 10–12, 14–16, 18, 21,23, 25, 33, 41, 42). Surgical transsection and devascularization,delayed postoperative fibrosis (40), postradiation edema (6),Schwann cell radiation injury, and radiation vascular injury(3, 28) have been implicated as potential mechanisms for acuteor delayed cochlear nerve injury.
FIGURE 2. Actuarial freedom from tumor progression.
FIGURE 3. Actuarial trigeminal and facial nerve complica-tions for tumors 20 mm or smaller compared with tumorslarger than 20 mm.
FIGURE 4. Preservation of serviceable hearing for patientswith good pretreatment hearing (GR Class 1–2) comparedwith patients with marginal pretreatment hearing (GRClass 3).
1302 Poen et al.
Neurosurgery, Vol. 45, No. 6, December 1999

Rationale for fractionated SRS
The efficacy of SRS in the treatment of intracranial tumorsultimately depends on the inherent sensitivity of the tumorrelative to the tolerance of adjacent neural structures. It is wellestablished in conventional radiation therapy that both tumorsensitivity and normal tissue tolerance can be improved withfractionated treatment. Fundamental radiobiological princi-ples predict that fractionated radiotherapy (the delivery of thetotal radiation dose in several smaller increments over a pe-riod of time) allows for preferential repair of sublethal dam-age in normal tissues, reoxygenation of hypoxic tumor cells,and redistribution of surviving tumor cells into a more radi-osensitive cell cycle phase. The summation of these effectscauses a separation of the tissue injury thresholds of normaland neoplastic tissues, thereby enhancing the therapeutic in-dex. Although there are no experimental studies specificallydesigned to assess the biological effects of fractionated SRS inhuman VS, preclinical and clinical data exist to support thehypothesis of reduced neural injury with fractionation of theradiation dose. The optic chiasm is the classic example, inwhich injury may be observed after a single-fraction radio-surgery dose of 1000 cGy, although 5000 cGy administeredduring a 5-week interval with conventional fractionation iswell tolerated (20).
The optimal fractionation schedule in SRS for VS is notknown, and few useful clinical data exist. In vitro studies withhuman tissue cell lines suggest that repair of sublethal radia-tion damage occurs relatively rapidly, with a half-time of 30minutes (5). In vivo studies of the rat spinal cord support aslower mechanism for repair, with a half-time of approxi-mately 4 hours (2). Using the more conservative half-timeestimate of 4 hours, one can predict that 80 to 90% of sublethalinjury recovery occurs during interfraction intervals of 10 to14 hours. This estimate provided the rationale for the frac-tionation schedule used in our protocol. In developing ourtreatment strategy, we sought to preserve the accuracy of arigid fixation system and the practicality of a brief treatmentregimen. We designed a schedule consisting of three fractionsof 700 cGy, administered during a 24-hour period, allowinginterfraction intervals of 10 and 14 hours. By restricting thefractionation to three doses, the use of multiple isocenters toachieve dose conformality remained practical within the timeconstraints of a nondedicated medical linear accelerator. Thetotal dose of 2100 cGy was estimated to be biologically equiv-alent to a conventional fraction dose of 4700 to 6300 cGy(linear quadratic formula assuming an a/b of 1–2) or a single-fraction SRS dose of 1400 to 1500 cGy (5).
Tumor control and complications
Preliminary results from this series compare favorably withthose of single-fraction SRS. Our 2-year tumor control (93%)and trigeminal nerve injury (16%) rates are similar to thoseobserved at 4 years by the University of Pittsburgh (97% and23%, respectively) (9) and by the University of Florida (100%and 19%, respectively) (30). The most recently published re-sults imply both durability of tumor control (98%) and stabil-ity of trigeminal nerve function at 5 to 10 years of follow-up
(24). We have observed only one patient (3%) with facialnerve injury (House-Brackmann Grade III) of 31 assessablepatients, a slightly lower rate of injury than observed at theUniversity of Pittsburgh (17%) and the University of Florida(16%).
Hearing preservation
Comparisons of hearing preservation rates among pub-lished clinical series are more difficult because of a variety ofdefinitions for “useful” and “serviceable” hearing and differ-ences in referral patterns across institutions. At the Universityof Pittsburgh, serviceable hearing (defined there as a pretreat-ment GR Class 1–2) was present before treatment in 63 of 273patients receiving single-fraction SRS. Three years after radio-surgery, 30 (48%) of 63 patients maintained serviceable hear-ing (8). In contrast, nearly all patients referred to the Univer-sity of Florida had no useful hearing in the affected ear beforeSRS, and routine audiometric assessments were not per-formed (31). The present series is unique in that a largepercentage of patients (30%) had NF2 and eight of thesepatients had no hearing in the contralateral ear. In our expe-rience, patients with contralateral deafness consider any mea-sure of preserved hearing useful and generally have service-able hearing with PTAs (or speech reception thresholds)greater than 50 dB (GR Class 3). For these reasons, we haveavoided the term “useful” hearing and have designated GRClass 1 to 3 as “serviceable” to recognize a range of hearingusefulness within the Class 3 designation. All patients withgood (Class 1–2) pretreatment hearing who were treated onthis protocol maintained GR Class 1 to 3 hearing. In contrast,only 50% of patients in this study with Class 3 hearing pre-treatment maintained serviceable hearing (one patient im-proved to Class 2, and three maintained Class 3), and 50% hadno measurable hearing within 1 year of SRS. This suggests anadvantage with early intervention. The preservation rates ofserviceable hearing at 2 years were 92% and 67% for sporadicand NF2 patients, respectively. Given the inherent difficultyof surgically separating the embedded VIIIth cranial nervefrom the tumors associated with NF2 (17, 29), hearing pres-ervation in two-thirds of patients with NF2, most of whomwere deaf in the contralateral ear, may be the most significantpotential advantage of fractionated SRS.
In contrast to our decision to define serviceable hearingas Grades 1 to 3, prior studies have defined useful hearing asonly Grades 1 to 2. For comparison, 10 (77%) of 13 patients inour study maintained this level of hearing. This comparesfavorably with recent published results. The University ofPittsburgh group demonstrated an increase in preservation ofClass 1 and 2 hearing of 40 to 56% after dose reduction andimplementation of magnetic resonance targeting (8). Anotherstudy did not include sufficient numbers of patients in thelower-dose group to assess improvement in hearing preser-vation, which was 39% overall (Class 1–2) (32). As with frac-tionation, the long-term effect of dose reduction on tumorcontrol is unknown.
Another method for assessing cochlear nerve injury usingpurely objective criteria is the measurement of PTA or speech
Fractionated Stereotactic Radiosurgery in Vestibular Schwannoma 1303
Neurosurgery, Vol. 45, No. 6, December 1999
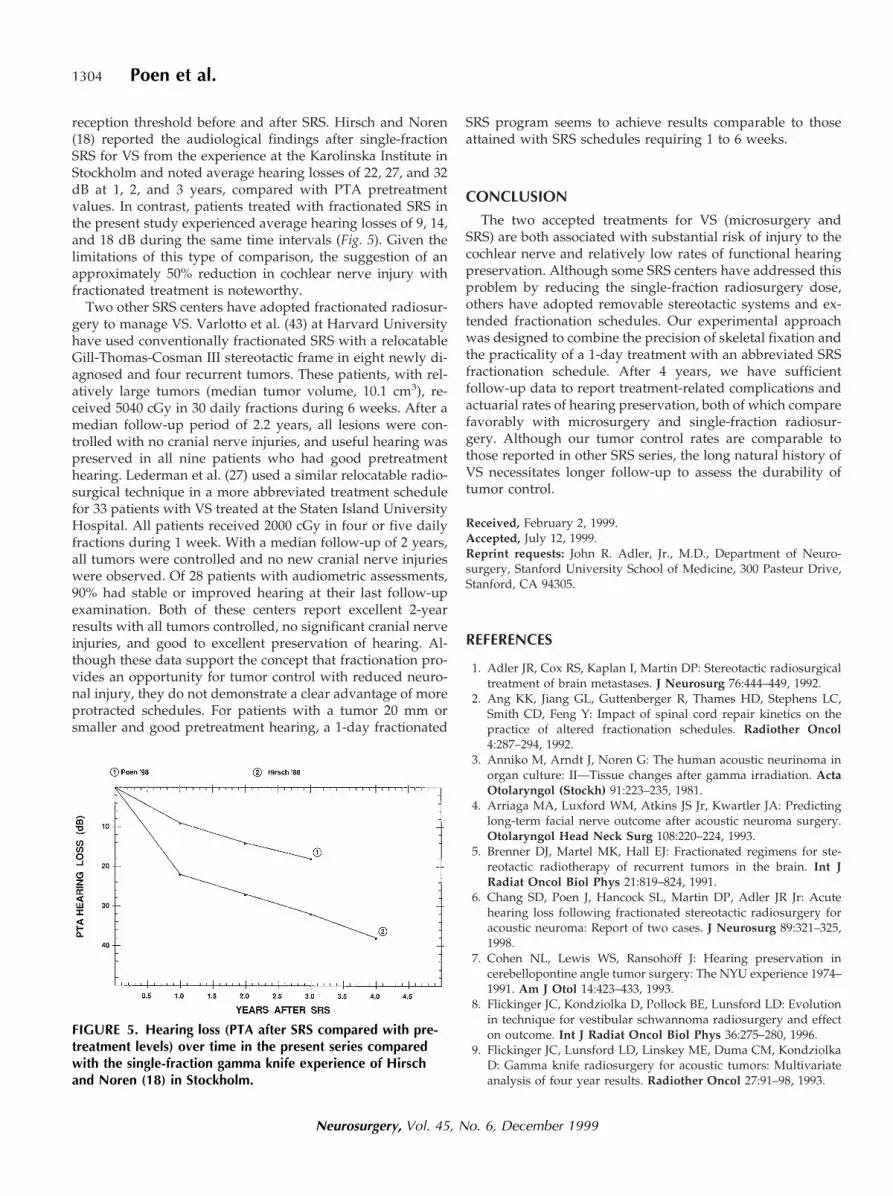
reception threshold before and after SRS. Hirsch and Noren(18) reported the audiological findings after single-fractionSRS for VS from the experience at the Karolinska Institute inStockholm and noted average hearing losses of 22, 27, and 32dB at 1, 2, and 3 years, compared with PTA pretreatmentvalues. In contrast, patients treated with fractionated SRS inthe present study experienced average hearing losses of 9, 14,and 18 dB during the same time intervals (Fig. 5). Given thelimitations of this type of comparison, the suggestion of anapproximately 50% reduction in cochlear nerve injury withfractionated treatment is noteworthy.
Two other SRS centers have adopted fractionated radiosur-gery to manage VS. Varlotto et al. (43) at Harvard Universityhave used conventionally fractionated SRS with a relocatableGill-Thomas-Cosman III stereotactic frame in eight newly di-agnosed and four recurrent tumors. These patients, with rel-atively large tumors (median tumor volume, 10.1 cm3), re-ceived 5040 cGy in 30 daily fractions during 6 weeks. After amedian follow-up period of 2.2 years, all lesions were con-trolled with no cranial nerve injuries, and useful hearing waspreserved in all nine patients who had good pretreatmenthearing. Lederman et al. (27) used a similar relocatable radio-surgical technique in a more abbreviated treatment schedulefor 33 patients with VS treated at the Staten Island UniversityHospital. All patients received 2000 cGy in four or five dailyfractions during 1 week. With a median follow-up of 2 years,all tumors were controlled and no new cranial nerve injurieswere observed. Of 28 patients with audiometric assessments,90% had stable or improved hearing at their last follow-upexamination. Both of these centers report excellent 2-yearresults with all tumors controlled, no significant cranial nerveinjuries, and good to excellent preservation of hearing. Al-though these data support the concept that fractionation pro-vides an opportunity for tumor control with reduced neuro-nal injury, they do not demonstrate a clear advantage of moreprotracted schedules. For patients with a tumor 20 mm orsmaller and good pretreatment hearing, a 1-day fractionated
SRS program seems to achieve results comparable to thoseattained with SRS schedules requiring 1 to 6 weeks.
CONCLUSION
The two accepted treatments for VS (microsurgery andSRS) are both associated with substantial risk of injury to thecochlear nerve and relatively low rates of functional hearingpreservation. Although some SRS centers have addressed thisproblem by reducing the single-fraction radiosurgery dose,others have adopted removable stereotactic systems and ex-tended fractionation schedules. Our experimental approachwas designed to combine the precision of skeletal fixation andthe practicality of a 1-day treatment with an abbreviated SRSfractionation schedule. After 4 years, we have sufficientfollow-up data to report treatment-related complications andactuarial rates of hearing preservation, both of which comparefavorably with microsurgery and single-fraction radiosur-gery. Although our tumor control rates are comparable tothose reported in other SRS series, the long natural history ofVS necessitates longer follow-up to assess the durability oftumor control.
Received, February 2, 1999.Accepted, July 12, 1999.Reprint requests: John R. Adler, Jr., M.D., Department of Neuro-surgery, Stanford University School of Medicine, 300 Pasteur Drive,Stanford, CA 94305.
REFERENCES
1. Adler JR, Cox RS, Kaplan I, Martin DP: Stereotactic radiosurgicaltreatment of brain metastases. J Neurosurg 76:444–449, 1992.
2. Ang KK, Jiang GL, Guttenberger R, Thames HD, Stephens LC,Smith CD, Feng Y: Impact of spinal cord repair kinetics on thepractice of altered fractionation schedules. Radiother Oncol4:287–294, 1992.
3. Anniko M, Arndt J, Noren G: The human acoustic neurinoma inorgan culture: II—Tissue changes after gamma irradiation. ActaOtolaryngol (Stockh) 91:223–235, 1981.
4. Arriaga MA, Luxford WM, Atkins JS Jr, Kwartler JA: Predictinglong-term facial nerve outcome after acoustic neuroma surgery.Otolaryngol Head Neck Surg 108:220–224, 1993.
5. Brenner DJ, Martel MK, Hall EJ: Fractionated regimens for ste-reotactic radiotherapy of recurrent tumors in the brain. Int JRadiat Oncol Biol Phys 21:819–824, 1991.
6. Chang SD, Poen J, Hancock SL, Martin DP, Adler JR Jr: Acutehearing loss following fractionated stereotactic radiosurgery foracoustic neuroma: Report of two cases. J Neurosurg 89:321–325,1998.
7. Cohen NL, Lewis WS, Ransohoff J: Hearing preservation incerebellopontine angle tumor surgery: The NYU experience 1974–1991. Am J Otol 14:423–433, 1993.
8. Flickinger JC, Kondziolka D, Pollock BE, Lunsford LD: Evolutionin technique for vestibular schwannoma radiosurgery and effecton outcome. Int J Radiat Oncol Biol Phys 36:275–280, 1996.
9. Flickinger JC, Lunsford LD, Linskey ME, Duma CM, KondziolkaD: Gamma knife radiosurgery for acoustic tumors: Multivariateanalysis of four year results. Radiother Oncol 27:91–98, 1993.
FIGURE 5. Hearing loss (PTA after SRS compared with pre-treatment levels) over time in the present series comparedwith the single-fraction gamma knife experience of Hirschand Noren (18) in Stockholm.
1304 Poen et al.
Neurosurgery, Vol. 45, No. 6, December 1999

10. Foote RL, Coffey RJ, Swanson JW, Harner SG, Beatty CW, KlineRW, Stevens LN, Hu TC: Stereotactic radiosurgery using thegamma knife for acoustic neuromas. Int J Radiat Oncol Biol Phys32:1153–1160, 1995.
11. Frerebeau P, Benezech J, Uziel A, Coubes P, Segnarbieux F,Malonga M: Hearing preservation after acoustic neurinoma op-eration. Neurosurgery 21:197–200, 1987.
12. Gardner G, Robertson JH: Hearing preservation in unilateralacoustic neuroma surgery. Ann Otol Rhinol Laryngol 97:55–66,1988.
13. Gill SS, Thomas DG, Warrington AP, Brada M: Relocatable framefor stereotactic external beam radiotherapy. Int J Radiat OncolBiol Phys 20:599–603, 1991.
14. Glasscock ME III, Hays JW, Minor LB, Haynes DS, Carrasco VN:Preservation of hearing in surgery for acoustic neuromas.J Neurosurg 78:864–870, 1993.
15. Goel A, Sekhar LN, Langheinrich W, Kamerer D, Hirsch B: Latecourse of preserved hearing and tinnitus after acoustic neurilem-oma surgery. J Neurosurg 77:685–689, 1992.
16. Gormley WB, Sekhar LN, Wright DC, Kamerer D, Schessel D:Acoustic neuromas: Results of current surgical management.Neurosurgery 41:50–60, 1997.
17. Hamada Y, Iwaki T, Fukui M, Tateishi J: A comparative study ofembedded nerve tissue in six NF2-associated schwannomas and17 nonassociated NF2 schwannomas. Surg Neurol 48:395–400,1997.
18. Hirsch A, Noren G: Audiological findings after stereotactic radio-surgery in acoustic neurinomas. Acta Otolaryngol (Stockh) 106:244–251, 1988.
19. House JW, Brackmann DE: Facial nerve grading system.Otolaryngol Head Neck Surg 93:146–147, 1985.
20. Jiang GL, Tucker SL, Guttenberger R, Peters LJ, Morrison WH,Garden AS, Ha CS, Ang KK: Radiation-induced injury to thevisual pathway. Radiother Oncol 30:17–25, 1994.
21. Kane NM, Kazanas S, Maw AR, Coakham HB, Torrens MJ,Morgan MH, Stranjalis G, Butler SR: Functional outcome in pa-tients after excision of extracanalicular acoustic neuromas usingthe suboccipital approach. Ann R Coll Surg Engl 77:210–216,1995.
22. Kaplan EL, Meier P: Nonparametric estimation from incompleteobservations. J Am Stat Assoc 53:457–481, 1958.
23. Kobayashi T, Tanaka T, Kida Y: The early effects of gamma knifeon 40 cases of acoustic neurinoma. Acta Neurochir Suppl (Wien)62:93–97, 1994.
24. Kondziolka D, Lunsford LD, McLaughlin MR, Flickinger JC:Long-term outcomes after radiosurgery for acoustic neuromas.N Engl J Med 339:1426–1433, 1998.
25. Koos WT, Matula C, Levy D, Kitz K: Microsurgery versus radio-surgery in the treatment of small acoustic neurinomas. ActaNeurochir (Wien) 63:73–80, 1995.
26. Lalwani AK, Butt FY, Jackler RK, Pitts LH, Yingling CD: Facialnerve outcome after acoustic neuroma surgery: A study from theera of cranial nerve monitoring. Otolaryngol Head Neck Surg111:561–570, 1994.
27. Lederman GS, Wertheim S, Lowry J, Rashid H, Silverman P, QianGX, Lombardi E, Wronski M, Arbit E: Acoustic neuromas treatedby fractionated stereotactic radiotherapy. Radiosurgery 2:25–30,1998.
28. Linskey ME, Martinez AJ, Kondziolka D, Flickinger JC, Maitz AH,Whiteside T, Lunsford LD: The radiobiology of human acousticschwannoma xenografts after stereotactic radiosurgery evaluatedin the subrenal capsule of athymic mice. J Neurosurg 78:645–653,1993.
29. Linthicum FH Jr, Brackmann DE: Bilateral acoustic tumors. ArchOtolaryngol Head Neck Surg 106:729–731, 1980.
30. Mendenhall WM, Friedman WA, Bova FJ: Linear accelerator-based stereotactic radiosurgery for acoustic schwannomas. Int JRadiat Oncol Biol Phys 28:803–810, 1994.
31. Mendenhall WM, Friedman WA, Buatti JM, Bova FJ: Prelimi-nary results of linear accelerator radiosurgery for acousticschwannomas. J Neurosurg 85:1013–1019, 1996.
32. Miller RC, Foote RL, Coffey RJ, Sargent DJ, Gorman DA,Schomberg PJ, Kline RW: Decrease in cranial nerve complicationsafter radiosurgery for acoustic neuromas: A prospective study ofdose and volume. Int J Radiat Oncol Biol Phys 43:305–311, 1999.
33. Nadol JB Jr, Chiong CM, Ojemann RG, McKenna MJ, Martuza RL,Montgomery WW, Levine RA, Ronner SF, Glynn RJ: Preservationof hearing and facial nerve function in resection of acoustic neu-roma. Laryngoscope 102:1153–1158, 1992.
34. Nissen AJ, Sikand A, Welsh JE, Curto FS, Gardi J: A multifactorialanalysis of facial nerve results in surgery for cerebellopontineangle tumors. Ear Nose Throat J 76:37–40, 1997.
35. Noren G, Arndt J, Hindmarsh T: Stereotactic radiosurgery incases of acoustic neurinoma: Further experiences. Neurosurgery13:12–22, 1983.
36. Noren G, Greitz D, Hirsch A, Lax I: Gamma knife surgery inacoustic tumours. Acta Neurochir Suppl (Wien) 58:104–107, 1993.
37. Ogunrinde OK, Lunsford LD, Flickinger JC, Kondziolka DS: Cra-nial nerve preservation after stereotactic radiosurgery for smallacoustic tumors. Arch Neurol 52:73–79, 1995.
38. Samii M, Matthies C: Management of 1000 vestibular schwan-nomas (acoustic neuromas): Hearing function in 1000 tumorresections. Neurosurgery 40:248–262, 1997.
39. Shelton C, Hitselberger WE: The treatment of small acoustic tu-mors: Now or later? Laryngoscope 101:925–928, 1991.
40. Shelton C, Hitselberger WE, House WF, Brackmann DE: Hearingpreservation after acoustic tumor removal: Long-term results.Laryngoscope 100:115–119, 1990.
41. Sterkers JM, Morrison GAJ, Sterkers O, El-Dine MM: Preservationof facial, cochlear, and other nerve functions in acoustic neuromatreatment. Otolaryngol Head Neck Surg 110:146–155, 1994.
42. Tatagiba M, Samii M, Matthies C, el Azm M, Schonmayr R: Thesignificance for postoperative hearing of preserving the labyrinthin acoustic neurinoma surgery. J Neurosurg 77:677–684, 1992.
43. Varlotto JM, Shrieve DC, Alexander E III, Kooy HM, Black PM,Loeffler JS: Fractionated stereotactic radiotherapy for the treat-ment of acoustic neuromas: Preliminary results. Int J RadiatOncol Biol Phys 36:141–145, 1996.
COMMENTS
The authors and several other groups are beginning tofractionate radiosurgical doses in an attempt to reduce cranialnerve complications. In doing so, they risk inferior tumorcontrol because fractionation will reduce the biological effecton the tumor as well as on the normal tissue. The authorsinvoke postirradiation cell cycle reassortment and reoxygen-ation as factors enhancing tumor cell kill with fractionation;however, even if these factors occur in schwannomas, whichis speculative, they are far weaker than the tumor-sparingeffect of postirradiation sublethal damage repair allowed bythe intervals between doses.
Preservation of hearing and facial nerve function as re-ported here may be slightly better than the University ofPittsburgh experience with single-fraction gamma knife treat-
Fractionated Stereotactic Radiosurgery in Vestibular Schwannoma 1305
Neurosurgery, Vol. 45, No. 6, December 1999

ment of acoustic tumors (1), but this series is smaller and hasa shorter follow-up period. It is reasonable to think thatfractionation will have a propitious effect on normal tissue,but critical information on comparable efficacy awaits furtherfollow-up.
Philip H. GutinNew York, New York
1. Kondziolka D, Lunsford LD, McLaughlin MR, Flickinger JC:Long-term outcomes after radiosurgery for acoustic neuromas.N Engl J Med 339:1426–1433, 1998.
Poen et al. report their initial 2-year experience in patientstreated with “fractionated radiosurgery.” In this particularinstance, I have less argument with the concept of fractionatedradiosurgery because the patient was treated during a 24-hour period. The authors used frame-based linear acceleratorradiosurgery, for which the frame remained attached to thepatient’s head during the delivery of three 700-cGy fractions.The authors compare their results with rather outdated liter-ature. During the last 5 years, dose reduction, magnetic res-onance imaging targeting techniques, and improved confor-mal plans (an average of 7–10 isocenters per patient usingsmall beam diameters) have significantly improved results atmany sites where gamma knife radiosurgery is performed. Itis estimated that in the year 2000, more than half of annuallydiagnosed acoustic neuroma patients will undergo radiosur-gery as the primary treatment modality. This statistic revealsthe significant impact of new technologies in the managementof a rare tumor. The authors have used this technique effec-tively, but the need for fractionation is inversely related to theconformality of the treatment plan. The less conformal thetreatment plan, the more fractions must be administered toreduce the dose to adjacent structures. Although the authorsquote the radiation therapy mantra on the reasons for frac-tionation (reoxygenation, repair, redistribution), there is sur-prisingly little fundamental radiobiological evidence to sup-port these concepts. A slow-growing benign brain tumor hasa cell cycle time not greatly different from cell cycle times inthe surrounding brain. In this case, the mechanism of radio-surgical action is the creation of inalterable DNA damage thatis not recognized until the cell attempts division, at whichpoint it probably becomes apoptotic. In addition, a secondaryvascular effect from radiosurgery results in an additionalcumulative benefit by obliteration of the intratumoral vascu-lature. This leads to hyalinization and fibrosis within thetumor.
This technique, as well as true radiosurgery, must be signifi-cantly differentiated from the use of relocatable stereotacticframes to achieve abbreviated treatment schedules in patientswith vestibular schwannomas. The results of fractionated radi-ation have yet to be reviewed in any significant way.
L. Dade LunsfordPittsburgh, Pennsylvania
Poen et al. treated 31 patients with acoustic schwannomaswith a hypofractionated course (three fractions in 20 h) ofstereotactic radiosurgery. Three doses of 700 cGy were deliv-ered, for a total peripheral dose of 2100 cGy. With a medianfollow-up of 2 years, 97% tumor control was demonstrated.Five patients developed trigeminal nerve injury. One patientdeveloped a facial nerve injury. Preservation of serviceablehearing was 81% at 2 years.
As the authors point out, these are preliminary data. Onesuspects that tumor control and hearing preservation willdecline as median follow-up time increases. Nonetheless, theyhave carefully studied and reported a completely new frac-tionation protocol for acoustic schwannomas. This protocol ismuch more convenient than conventional fractionation (30fractions), but it may still take advantage of some of thenormal tissue-sparing effects that are lost in single-fractionradiosurgery.
The debate about fractionation versus single-fraction radio-surgery for acoustic schwannomas is unresolved. Unfortu-nately, the debate is clouded by reports of single-fractionresults using inaccurate radiation delivery, computed tomo-graphic dose planning only, poorly conformal dose planning,or doses that are now known to be too high. Along with theUniversity of Pittsburgh, our group thinks that single-fractiontreatment, delivered with magnetic resonance imaging, mod-ern highly conformal dose planning, and at lower doses(1000–1250 cGy) than originally recommended, is the bestchoice. Using this approach, we expect tumor control andhearing preservation rates similar to those reported by theauthors. In addition, the incidence of trigeminal neuropathy isexpected to be much lower.
William A. FriedmanGainesville, Florida
The number of reports on radiosurgical treatment of ves-tibular schwannomas by gamma knife or linear accelerator isincreasing. However, few note improved hearing preserva-tion as a major goal. In 31 of 32 patients, the authors reportstable tumor size at 6 months to 4 years after fractionatedradiosurgery. Of previously hearing patients, 81% retainedsome hearing at Gardner-Robertson Class 1 to 3. The authorspresent their new protocol of fractionated radiosurgery per-formed in three applications within 24 hours. These earlyresults seem comparable to those obtained using gamma knifesurgery for tumor control and cranial nerve morbidity.
The problem of cranial nerve morbidity deserves specialconsideration. Vestibular function is rarely reported or possi-bly receives little consideration in radiotherapy. Especially insmall tumors with a predominantly vestibular presentation,persistent recurrence of vestibular disturbances poses a prob-lem. The incidence of trigeminal nerve neuropathy is consid-erable in all radiosurgical reports to date (1, 2, 5), with veryrare exceptions (3), and it severely compromises life quality.Trigeminal disturbance before treatment is a completely dif-ferent matter in vestibular schwannomas, because nerve in-tegrity is not usually endangered by the microsurgical pro-cess. Rather, it is improved by decompression from the tumor
1306 Poen et al.
Neurosurgery, Vol. 45, No. 6, December 1999

with reversibility of symptoms. Trigeminal neuropathy afterapplication of radiosurgery is a serious lesion, and a cure isvirtually impossible. Its effects include postradiotherapeuticonset of burning, dysesthesia, and corneal problems that can-not be reliably treated surgically or medically. This is a seriousand highly underestimated morbidity.
Preservation of auditory function is reported at promisinglevels and rates. Still, as learned from previous experience,hearing stability is not obtained during the 1st or 2nd yearafter radiosurgery. Therefore, a judgment on the reliability ofhearing preservation and the stability of tumor control isimpossible for the treatment protocol presented.
Patients with neurofibromatosis Type 2 (NF2) pose a specialchallenge in making the right treatment decision at the righttime. In our series of 195 patients with NF2, hearing could bepreserved in 35% of operated ears. In a trial of hearing pres-ervation in the last hearing ear, subtotal tumor resection anddecompression of the internal auditory canal succeeded inpreserving hearing in 15 patients; tumor regrowth has beenmoderate and has not necessitated reoperation. None of thepatients so treated lost hearing during the follow-up period.Furthermore, preserved hearing has remained serviceable forperiods up to 12 years. In the case of a secondary hearing lossat tumor recurrence many years later, this concept fully pre-serves the option of placing an auditory brainstem implant.Therefore, this treatment program seems more suited to thedifficult situation of NF2 patients and avoids the possible riskof malignant tumor formation (4). Profound knowledge of thevariability in NF2 disease courses and individual patient his-tories is essential to patient selection for this mode oftreatment.
The authors’ attempts to develop a protocol focusing onfunction protection should be acknowledged. A radiosurgeryprotocol with fractionated treatment as an option for patientswho cannot undergo surgery, but who need tumor reduction,would be most welcome. Nonetheless, we must be aware thatthese and similar trials are currently performed in high num-
bers without the ability to foresee the long-term effects andpossible problems. Some patients who would have had arealistic chance for long-term definitive cure and functionalcranial nerve preservation by microsurgery will experience anincreasing hearing loss without any chance of surgical inter-ference. Some patients will need surgery at a later stage; thissurgery is more difficult and hazardous and bears a reducedchance for functional facial nerve preservation (statistically, 1of 3 patients). Clinically and scientifically, the most criticalpoint is the current lack of communication among specialists.The surgeons who will be confronted with these patients at alater stage are not consulted by the radiosurgeons at the timethe initial treatment decision is made. Teaching and handlingthis difficult surgery is not sufficiently discussed amongcolleagues.
Madjid SamiiCordula MatthiesHannover, Germany
1. Flickinger JC, Kondziolka D, Pollock BE, Lunsford LD: Evolutionin technique for vestibular schwannoma radiosurgery and effecton outcome. Int J Radiat Oncol Biol Phys 36:275–280, 1996.
2. Foote RL, Coffey RJ, Swanson JW, Harner SG, Beatty CW, KlineRW, Stevens LN, Hu TC: Stereotactic radiosurgery using thegamma knife for acoustic neuromas. Int J Radiat Oncol Biol Phys32:1153–1160, 1995.
3. Lederman G, Lowry J, Wertheim S, Fine M, Lombardi E, WronskiM, Arbit E: Acoustic neuroma: Potential benefits of fractionatedstereotactic radiosurgery. Stereotact Funct Neurosurg 69:175–182,1997.
4. Noren G: Long-term complications following gamma knife radio-surgery of vestibular schwannomas. Stereotact Funct Neurosurg70[Suppl 1]:65–73, 1998.
5. Pollock BE, Lunsford LD, Noren G: Vestibular schwannoma man-agement in the next century: A radiosurgical perspective. Neuro-surgery 43:475–483, 1998.
2000 Annual MeetingCongress of Neurological Surgeons
Henry B. Gonzalez Convention CenterSan Antonio, Texas
September 23 through September 28
Edward R. Laws, Jr., Honored Guest
Vincent C. Traynelis, Meeting ChairmanDouglas S. Kondziolka, Program Chairman
Thomas A. Kingman, Local Arrangements Chairman
Fractionated Stereotactic Radiosurgery in Vestibular Schwannoma 1307
Neurosurgery, Vol. 45, No. 6, December 1999