fetal brain mri texture analysis identifies different microstructural patterns in adequate and small...
TRANSCRIPT

Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Fetal Diagn Ther 2013;33:122–129 DOI: 10.1159/000346566
Fetal Brain MRI Texture Analysis Identifies Different Microstructural Patterns in Adequate and Small for Gestational Age Fetuses at Term
M. Sanz-Cortés a F. Figueras a E. Bonet-Carne b N. Padilla a V. Tenorio a
N. Bargalló c I. Amat-Roldan b Eduard Gratacós a
a Maternal-Fetal Medicine Department, ICGON, Hospital Clínic, Universitat de Barcelona, Fetal and Perinatal Medicine Research Group, Institut d’Investigacions Biomediques August Pi i Sunyer (IDIBAPS), and Centro de Investigación Biomédica en Red de Enfermedades Raras (CIBERER), b Transmural Biotech SL, and c Department of Radiology Hospital Clinic, Centre de Diagnostic per la Imatge, Hospital Clínic, Barcelona , Spain
Introduction
An estimated 1 in 10 children suffer from neurodevel-opmental problems, most of which are considered to be of prenatal origin [1, 2] . Intrauterine growth restriction (IUGR) has long been considered among the main causes of neurodevelopmental problems. IUGR affects 5–8% of all pregnancies [3] and is a major contributor to perina-tal mortality and morbidity. Most instances of IUGR are secondary to placental insufficiency [4] which causes a prolonged disturbance in fetal oxygen and nutrient sup-ply and subsequently a deleterious effect on brain devel-opment [5] . An increasing amount of evidence has shown a strong association of IUGR with long-term neu-rological morbidity [6–10] and brain macro- and micro-structure differences [11–15] . Neurodevelopmental im-pairment is not exclusive of severe IUGR but it also oc-curs in late-onset forms, often referred to as small for gestational age (SGA) [16–19] . For a long time consid-ered a benign condition [20] , it is increasingly accepted that the diagnostic label of SGA is largely composed by late forms of true IUGR. SGA fetuses are associated with signs of brain redistribution [16, 21–24] and poorer peri-natal outcome [21, 24–28] . In addition, neonates and in-fants born SGA have an impaired neurodevelopment, as
Key Words
Fetal MRI · Intrauterine growth restriction · Small for gestational age · Texture analysis
Abstract
Objectives: We tested the hypothesis whether a texture analysis (TA) algorithm applied to MRI brain images identi-fied different patterns in small for gestational age (SGA) fe-tuses as compared with adequate for gestational age (AGA). Study Design: MRI was performed on 83 SGA and 70 AGA at 37 weeks’ GA. Texture features were quantified in the frontal lobe, basal ganglia, mesencephalon, cerebellum and cingu-lum. A classification algorithm based on discriminative models was used to correlate texture features with clinical diagnosis. Results: Region of interest delineation in all areas was achieved in 61 SGA (12 vasodilated) and 52 AGA; this was the sample for TA feature extraction which allowed clas-sifying SGA from AGA with accuracies ranging from 90.9 to 98.9% in SGA versus AGA comparison and from 93.6 to 100% in vasodilated SGA versus AGA comparison. Conclu-
sions: This study demonstrates that TA can detect brain dif-ferences in SGA fetuses. This supports the existence of brain microstructural changes in SGA fetuses.
Copyright © 2013 S. Karger AG, Basel
Received: July 4, 2012 Accepted after revision: December 11, 2012 Published online: February 6, 2013
Magdalena Sanz-Cortés Maternal-Fetal Medicine Department Hospital Clínic – Maternitat Sabino de Arana, 1, ES–08028 Barcelona (Spain) E-Mail msanz1 @ clinic.ub.es
© 2013 S. Karger AG, Basel1015–3837/13/0332–0122$38.00/0
Accessible online at:www.karger.com/fdt
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
9/16
/201
3 1:
37:5
3 P
M

Fetal Brain MRI Texture Analysis in SGA Fetuses
Fetal Diagn Ther 2013;33:122–129 123
shown by poorer results in neurobehavioral [18, 23, 24] and neurodevelopmental tests [17–19] . Furthermore, preliminary MRI data suggest abnormal brain metabo-lism and microstructure in SGA fetuses [29] . Consider-ing that the majority of SGA children are born near term, the impact of SGA in the risk of neurodevelopmental dis-abilities in children can hardly be overestimated. This stresses the need to improve the understanding of the processes underlying brain reorganization in SGA fetus-es and to develop biomarkers to detect brain changes at an individual level.
In this study we evaluated the hypothesis that quanti-tative imaging techniques could detect cerebral differenc-es in SGA fetuses. These techniques attempt to extract quantitative information from images by the detection of subtle differences induced by tissue changes. Among var-ious potential approaches, texture analysis (TA) has emerged as a promising technique [30] . Generally speak-ing, textures are complex visual patterns defined by the multiple features that characterize the visual properties of an image [30] . TA is based on the extraction and later analysis of features in a digital image. This allows to nu-merically describe its properties and compare it with oth-ers in a way that largely outperforms subjective compari-son. TA-based methods have been demonstrated to dif-ferentiate healthy from pathological tissues [30–34] . We have reported our experience using a TA software that was initially applied on ultrasound images showing the ability to predict white matter damage in subclinical stag-es on preterm neonatal brain scans with a high accuracy [35] . In addition, the software has demonstrated a strong correlation between fetal lung ultrasound texture features and gestational age (GA) [36] . We hypothesized that TA could also be used to detect different patterns in fetal brain MR images. If confirmed, this evidence would sup-port the existence of brain microstructural differences in late-onset IUGR. In addition, it might open new lines of research for the development of quantitative imaging methods to improve the detection of abnormal brain de-velopment in late-onset IUGR and possibly other fetal conditions.
The study evaluated whether TA applied to brain MR images could detect different patterns in a group of 83 SGA as compared with 70 term normally grown controls. We further explored whether differences were more pro-nounced when SGA cases with overt brain vasodilation, as a group supposed to represent a more advanced stage in the fetal adaptation to placental insufficiency, were se-lected.
Material and Methods
Study Cohort This study is part of a larger prospective research program on
IUGR involving fetal, and short- and long-term postnatal fol-low-up. The specific protocol of this study was approved by the institutional ethics committee (Institutional Review Board 2008/4422) and all participants gave written informed consent. A prospective cohort of 83 consecutive singleton pregnancies with the diagnosis of SGA was included. SGA was defined by an estimated fetal weight and confirmed birth weight below the 10th centile according to local standards [37] and normal um-bilical artery (UA) pulsatility index (PI) (below the 95th centile) [38] . A control group of 70 consecutive pregnancies with ade-quate for gestational age (AGA) fetuses with a confirmed birth weight above the 10th centile, was selected among normal preg-nancies and followed up at our institution after accepting to par-ticipate in the study. Cases with congenital malformations, chro-mosomal abnormalities, perinatal infections, chronic maternal pathology and non-cephalic presentations were considered non-eligible for this study.
Clinical and Ultrasound Data Prenatal (middle cerebral artery (MCA) PI and UA PI) and
neonatal data were prospectively recorded. GA was corrected from fetal crown-rump length in the first trimester [39] . Prenatal Doppler ultrasound examinations were performed (Siemens So-noline Antares; 6-2 MHz linear-curved-array transducer) within 1 week from MRI scan. Spectral Doppler parameters [38] were obtained from fetal UA and MCA in all participants. A MCA PI below the 5th centile was considered as a sign of fetal brain vaso-dilation [40] .
Fetal MRI Acquisition All cases were scanned at 37 weeks of gestation in a Tim Trio
3. 0 T scanner (Siemens, Germany) without sedation. A body coil with 8 elements was wrapped around the mother’s abdomen. Rou-tine fetal imaging required from 15 to 30 min. Fetal neuroimaging consisted of single-shot, fast-spin echo T2-weighted sequences (repetition time (TR) 990 ms, echo time (TE) 137 ms, slice thick-ness 3.5 mm, field of view 260 mm, voxel size 1.4 × 1.4 × 3.5 mm, in plane resolution 192, flip angle 1.80°, acquisition time 24 s) ac-quired in the three orthogonal planes. If the quality of the images was suboptimal, sequences were repeated.
Structural MR images were reviewed for the presence of ana-tomical abnormalities by an experienced neuroradiologist blinded to group membership.
Delineation of Regions of Interest in MR Images A custom-made graphical user interface (GUI) tool on MAT-
LAB R2007b (version 7.5. 0.342; MATLAB; The MathWorks, Inc., Natick, Mass., USA) was used to manually delineate all ten regions of interest (ROIs). Before delineation, all images were checked for artifacts. If the anatomic area to be delineated showed a suboptimal quality it was discarded and thus not delineated. Suboptimal qual-ity was mainly due to motion artifacts that caused blurry or not clearly visualized anatomical boundaries. If present, they were ex-cluded and therefore not delineated. Delineations were performed by two experienced operators in neuroanatomy blinded to group membership.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
9/16
/201
3 1:
37:5
3 P
M
Sanz-Cortés et al.
Fetal Diagn Ther 2013;33:122–129124
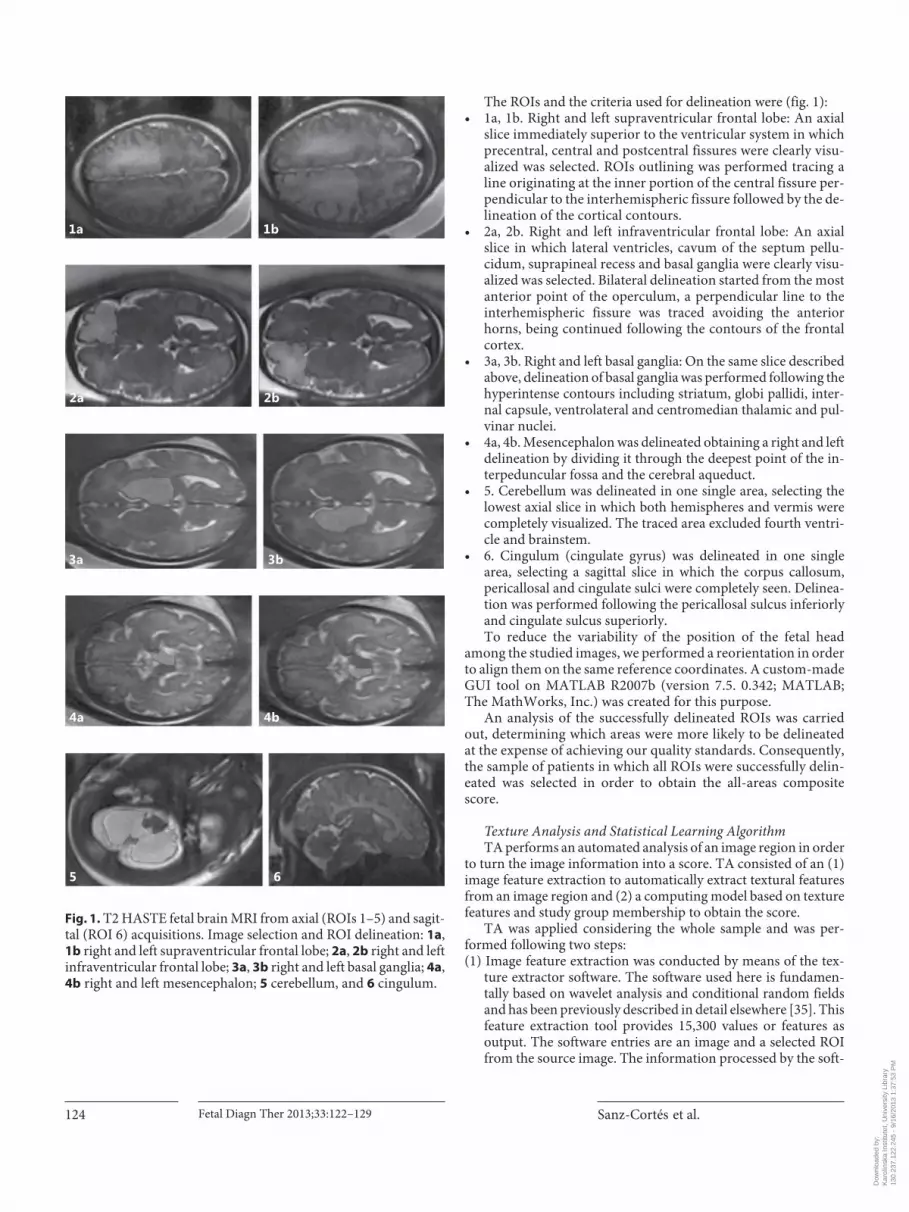
The ROIs and the criteria used for delineation were ( fig. 1 ): • 1a, 1b. Right and left supraventricular frontal lobe: An axial
slice immediately superior to the ventricular system in which precentral, central and postcentral fissures were clearly visu-alized was selected. ROIs outlining was performed tracing a line originating at the inner portion of the central fissure per-pendicular to the interhemispheric fissure followed by the de-lineation of the cortical contours.
• 2a, 2b. Right and left infraventricular frontal lobe: An axial slice in which lateral ventricles, cavum of the septum pellu-cidum, suprapineal recess and basal ganglia were clearly visu-alized was selected. Bilateral delineation started from the most anterior point of the operculum, a perpendicular line to the interhemispheric fissure was traced avoiding the anterior horns, being continued following the contours of the frontal cortex.
• 3a, 3b. Right and left basal ganglia: On the same slice described above, delineation of basal ganglia was performed following the hyperintense contours including striatum, globi pallidi, inter-nal capsule, ventrolateral and centromedian thalamic and pul-vinar nuclei.
• 4a, 4b. Mesencephalon was delineated obtaining a right and left delineation by dividing it through the deepest point of the in-terpeduncular fossa and the cerebral aqueduct.
• 5. Cerebellum was delineated in one single area, selecting the lowest axial slice in which both hemispheres and vermis were completely visualized. The traced area excluded fourth ventri-cle and brainstem.
• 6. Cingulum (cingulate gyrus) was delineated in one single area, selecting a sagittal slice in which the corpus callosum, pericallosal and cingulate sulci were completely seen. Delinea-tion was performed following the pericallosal sulcus inferiorly and cingulate sulcus superiorly. To reduce the variability of the position of the fetal head
among the studied images, we performed a reorientation in order to align them on the same reference coordinates. A custom-made GUI tool on MATLAB R2007b (version 7.5. 0.342; MATLAB; The MathWorks, Inc.) was created for this purpose.
An analysis of the successfully delineated ROIs was carried out, determining which areas were more likely to be delineated at the expense of achieving our quality standards. Consequently, the sample of patients in which all ROIs were successfully delin-eated was selected in order to obtain the all-areas composite score.
Texture Analysis and Statistical Learning Algorithm TA performs an automated analysis of an image region in order
to turn the image information into a score. TA consisted of an (1) image feature extraction to automatically extract textural features from an image region and (2) a computing model based on texture features and study group membership to obtain the score.
TA was applied considering the whole sample and was per-formed following two steps: (1) Image feature extraction was conducted by means of the tex-
ture extractor software. The software used here is fundamen-tally based on wavelet analysis and conditional random fields and has been previously described in detail elsewhere [35] . This feature extraction tool provides 15,300 values or features as output. The software entries are an image and a selected ROI from the source image. The information processed by the soft-
1a 1b
2a 2b
3a 3b
4a 4b
5 6
Fig. 1. T2 HASTE fetal brain MRI from axial (ROIs 1–5) and sagit-tal (ROI 6) acquisitions. Image selection and ROI delineation: 1a , 1b right and left supraventricular frontal lobe; 2a , 2b right and left infraventricular frontal lobe; 3a , 3b right and left basal ganglia; 4a , 4b right and left mesencephalon; 5 cerebellum, and 6 cingulum.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
9/16
/201
3 1:
37:5
3 P
M

Fetal Brain MRI Texture Analysis in SGA Fetuses
Fetal Diagn Ther 2013;33:122–129 125
ware is only that contained within the ROI, in this manner the output only contains texture-related information from the de-sired image region. Textural features were obtained from each delineation independently due to feature extraction performed using only one ROI as input each time.
(2) The classification problem was approached with a total of 22 discriminative models that were computed and evaluated after independently studying the relationship between eleven fea-ture sets (one feature set for each of the ten ROIs and also from the combination of all the delineated ROIs) and two different dichotomic groups defined according to clinical criteria and detailed in the study cohort subsection (SGA against AGA and vasodilated SGA against AGA). Thus, each individual had 22 scores which enabled to estimate the importance of each ROI and the membership to each clinical group independently. Each discriminative model was computed on the whole sample
according to the following procedure: (1) a feature weighting step based on a leave-one-out scheme that combined principal compo-nent analysis that explained 95% of variability and discriminative analysis based on MANOVA to obtain the mean and variance weight of each feature, μ(i) and σ 2 (i) ; (2) a feature selection step that kept only those features that fulfilled log [μ(i)/σ 2 (i)] >20; (3) an individual score computed according to the formula score = ∑ω(i)· feature(i), and (4) a final fitting of data ( score against clini-cal group) on a logistic regression to optimize threshold criterion and maximize accuracy of classification.
The cutoff with higher accuracy ((True positives + True nega-tives)/Total number of individuals) was chosen to dichotomize the score as positive and negative, as a measure to evaluate the ability of the TA (texture extractor plus discriminative model) to discrim-inate whether each subject pertained to the SGA versus AGA or vasodilated SGA versus AGA group comparison.
Additionally, to verify that the features contained relevant infor-mation, a validation of the extracted image texture features was per-formed for each ROI independently using the same procedure. Half of the sample (half of the population) was used to select the most relevant features. The relevant features were sorted for importance order and the first two were selected for the next step. A classification tree was then computed with the rest of the samples. We selected only two features to feed the classification tree to avoid overfitting.
Statistical Analysis of Clinical and Demographic Data Student’s t test for independent samples and Pearson’s χ 2 or
Fisher’s exact tests were used to compare quantitative and qualita-tive clinical data respectively as shown in table 1 . The results were considered to be significant at a Bonferroni-adjusted p value <0.05. All statistical calculations were done using SPSS statistical soft-ware, version 17.0 (SPSS for Windows; SPSS, Inc., Chicago, Ill., USA).
Results
Clinical Features in the Study Population A total of 153 fetuses, 83 SGA and 70 controls, were
evaluated. Ultrasound and MRI data were obtained from all patients included in the study. Doppler evaluation de-tected 16 (19.3%) SGA fetuses that showed brain vasodi-lation. No signs of intracranial pathology were found in any of the fetal MR images.
Table 1 describes the demographic and clinical data of the study groups. There was a significantly higher rate of
Table 1. Maternal and neonatal clinical characteristics of the study group (mean ± SD or percentage, as appropriate)
SGA (n = 83) VD SGA (n = 16) AGA (n = 70) p* p**
Maternal age (years) 31.8±5.3 32.8±5.1 32.4±4.4 <0.49 <0.39Body mass index 22.2±4.0 21.4±3.5 22.5±4.9 <0.67 <0.43Primiparity 75.9 75.0 64.3 <0.12 <0.41Non-Caucasian ethnicity 26.5 25.0 34.3 <0.29 <0.47Smoker 28.9 31.3 12.9 <0.02 <0.07GA at ultrasound (weeks) 37.3±0.8 37.2±0.92 37.1±1.1 <0.28 <0.71GA at MRI (weeks) 37.4±0.8 37.3±0.92 37.5±0.9 <0.62 <0.36GA at birth, weeks 38.4±1.0 38.4±1.3 39.7±1.2 <0.001 <0.001Cesarean section 36.1 56.3 21.4 <0.04 <0.005Birth weight (g) 2,377±272 2,317±319 3,219±360 <0.001 <0.0001Weight centile 3.5±2.8 2.9±3.0 40.7±24.4 <0.001 <0.001Male/female 1.37 3.0 2.04 <0.23 <0.54Neonatal acidosisa 10.4 18.8 8.1 <0.64 <0.21Apgar score <7 at 5 min 2.4 6.3 0 <0.19 <0.03Length of neonatal ICU stay (days) 0.19 0.31 0 <0.07 <0.33
Student’s t test for independent samples, Pearson’s χ2 or Fisher’s exact test as appropriate.* Comparison between all SGA vs. AGA. ** Comparison between vasodilated SGA (VD SGA) vs. AGA.a Umbilical artery pH <7.15 and base excess >12 mEq/l.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
9/16
/201
3 1:
37:5
3 P
M

Sanz-Cortés et al.
Fetal Diagn Ther 2013;33:122–129126
smoking during pregnancy in the SGA group. As expect-ed, SGA fetuses were delivered earlier and more frequent-ly by cesarean section than controls.
Delineation of ROIs in MR Images The quality of the MRI acquisitions allowed successful
delineation of the intended ROIs in most cases ( table 2 ) with lower performance in the cingulum. In order to cre-ate the all-areas composite score, 113 fetuses (61 cases (12 vasodilated) and 52 controls) showed an image quality that met our study standards in all their ROIs.
Due to the different sample sizes for each ROI, it was convened to select a constant sample size for all regions; therefore this subsample of 113 fetuses was selected to perform our discriminative study of fetal brain TA for all ROIs as well, and another subsample of 64 to discriminate vasodilated SGA vs. controls.
Texture Analysis and Statistical Learning Algorithm After applying the texture extractor software, a set of
15,300 descriptors was obtained for each brain area. Ma-chine learning analysis was then applied to the set of de-scriptors as described in Material and Methods to re-duce dimensionality and explore the existence of com-binations of descriptors that were useful to identify differential patterns between cases and controls, being able to successfully identify such set of descriptors for all ROIs. A regression model was then created and the abil-ity of the mathematical model to discriminate between study groups (SGA and AGA fetuses) was obtained.
Feature validation experiments obtained an average error not superior than 20% for each ROI (accuracy ≥ 80%). All ROIs presented very high accuracies being in all areas above 90% ( table 3 ). All-areas composite score seemed to present a slightly higher accuracy (98.9%) than each ROI independently. The same results were re-produced with a slightly higher overall accuracy when only vasodilated SGA were compared with AGA ( ta-ble 4 ), showing an overall accuracy above 93%, being particularly good in the frontal areas studied.
Discussion
This study provides evidence that TA can extract re-producible quantitative image features from fetal brain MRIs that allow differentiating brain MR images of SGA and AGA fetuses. This data supports the existence of brain reorganization and microstructural changes in SGA fetuses, which might provide clues to better under-
Table 2. Successful ROI delineation in the sample expressed as ab-solute and relative (%) frequencies
SGA(n = 83)
VD SGA(n = 16)
AGA(n = 70)
All-areas composite score 61 (73.5) 12 (75) 52 (74.3)Supraventricular frontal right 78 (94) 14 (87.5) 63 (90)Supraventricular frontal left 78 (94) 14 (87.5) 63 (90)Infraventricular frontal lobe right 80 (96.4) 16 (100) 67 (95.7)Infraventricular frontal lobe left 80 (96.4) 16 (100) 68 (97.1)Basal ganglia right 80 (96.4) 16 (100) 68 (97.1)Basal ganglia left 80 (96.4) 16 (100) 67 (95.7)Mesencephalon right 80 (96.4) 15 (93.8) 68 (97.1)Mesencephalon left 80 (96.4) 15 (93.8) 68 (97.1)Cerebellum 78 (94) 16 (100) 68 (97.1)Cingulum 69 (83.1) 14 (87.5) 60 (85.7)
Table 3. Detection of group membership (all SGA vs. AGA) by fe-tal brain MRI TA expressed by their accuracy and p value after Bonferroni correction
Accuracy, % p
All-areas composite score 98.92 <0.001Supraventricular frontal right 90.16 <0.001Supraventricular frontal left 97.24 <0.001Infraventricular frontal lobe right 93.62 <0.001Infraventricular frontal lobe left 90.92 <0.001Basal ganglia right 95.46 <0.001Basal ganglia left 92.54 <0.001Mesencephalon right 97.08 <0.001Mesencephalon left 97.46 <0.001Cerebellum 94.7 <0.001Cingulum 91.3 <0.001
Table 4. Detection of group membership (vasodilated SGA vs. AGA) by fetal brain MRI TA expressed by their accuracy and p value after Bonferroni correction
Accuracy, % p
All-areas composite score 100 <0.001Supraventricular frontal right 100 <0.001Supraventricular frontal left 100 <0.001Infraventricular frontal lobe right 100 <0.001Infraventricular frontal lobe left 100 <0.001Basal ganglia right 96.76 <0.001Basal ganglia left 100 <0.001Mesencephalon right 96.76 <0.001Mesencephalon left 100 <0.001Cerebellum 93.62 <0.001Cingulum 95.14 <0.001
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
9/16
/201
3 1:
37:5
3 P
M

Fetal Brain MRI Texture Analysis in SGA Fetuses
Fetal Diagn Ther 2013;33:122–129 127
stand the neurodevelopmental abnormalities occurring in postnatal life.
Previous research on the evaluation of brain reorgani-zation has mostly been focused on early-onset IUGR. Sev-eral studies suggest the existence of a ‘brain remodeling’ in IUGR neonates, including smaller hippocampal vol-umes, [13] disrupted gyrification pattern, [15] decreased cortical gray matter volume [11, 14] and decreased fractal dimension [12] . Concerning SGA, in spite of abundant evidence suggesting abnormal neurodevelopment in this population [18–20, 22, 25, 41] there has been scarce proof about the existence of brain reorganization. The findings are in line with previous preliminary evidence suggesting the existence of brain alterations and microstructural changes in SGA fetuses [29] . The existence of MRI chang-es suggesting abnormal brain development has previous-ly been reported in fetuses and newborns with congenital heart disease [42–44] . The data provided in this and pre-vious studies support that suboptimal conditions in utero cause adaptive changes that could be detected by quanti-tative MRI techniques.
Given that the texture of different brain regions and structures is different, the objective of this work was to apply TA to specific and clinically relevant regions. Ex-perimental and human studies coincide in the regional-ization of vascular redistribution showing increased brain perfusion in frontal lobe, basal ganglia and cerebel-lum [45, 46] . The preferential involvement of the frontal lobe in fetal growth restriction has been reported by dif-ferent authors. There is a relative decrease in the frontal lobe volume in early growth-restricted fetuses, SGA neo-nates and 1-year-old IUGR infants shown by ultrasound [47, 48] and MRI studies [11] . In addition, long-term follow-up studies demonstrate that the neurodevelop-mental dysfunction in IUGR mainly involves general cognitive competence, suggesting a particular dysfunc-tion in the frontal lobe networking [19, 49] . Secondly, we selected basal ganglia due to its role as a relevant con-necting hub of the brain with strong links to the cerebral cortex, thalami and other brain areas [50] . Thirdly, the cerebellum was selected since it is implicated in motor learning, memory, cognition and behavior [51] . As a fourth area, mesencephalon contains relevant nuclei im-plied in motor and sensorial functions, which are altered in IUGR [41] . Finally, the cingulum was selected due to the known involvement of the limbic system and hippocampus in IUGR [13, 19, 49] . The analysis demon-strated strong correlations between TA and the diagnos-tic category for all analyzed areas. The fact that the cor-relation was stronger in vasodilated SGA is in line with
recent evidence suggesting that brain redistribution is associated to worse neurodevelopmental outcomes [22, 52, 53] .
The results of this study support that quantitative im-aging analysis of the fetal brain is feasible and deserves further research in order to assess its potential to improve clinical practice. Given the high prevalence of SGA and its impact in neurodevelopment, the development of bio-markers to detect brain changes at an individual level is a challenge for fetal medicine in the years to come. Early detection is a critical goal to trigger strategies such as de-livery planning, breast-feeding promotion and early edu-cational interventions, which have shown to improve the neurodevelopmental outcome in similar populations at risk [54–56] . The relevance of these results is determined by the potential detection of those SGA fetuses that may be at risk of an abnormal neurodevelopment, especially considering the relatively high prevalence of this condi-tion. TA is a promising technique to achieve the develop-ment of biomarkers in fetal medicine. This method has shown the ability to detect brain differences in subclinical conditions such as unapparent white matter damage in preterm neonates [35] or those with minor clinical reper-cussion [30, 33] .
We grant that this study presents some limitations and merits some methodological comments. The algorithm developed to classify the study groups was validated on the same sample on which it was developed. In order to improve as much as possible the validity of the model, several strategies of leave-one-out validation were ap-plied. However, the study was essentially conceived to test the proof-of-concept that TA was capable of extracting meaningful information that correlated with each diag-nostic category. Furthermore, we acknowledge that the differentiation between AGA and SGA is artificial by def-inition and there will always be individual SGA cases that in reality do not suffer restriction, and the other way around. However, classifying fetuses as AGA or SGA un-questionably allows differentiating groups that on aver-age behave differently. If significant quantitative differ-ences would not exist, the quantitative analysis methods could not find them. Once the differences exist, the clas-sificatory works on a given number of subjects and it finds the combination of descriptors that differentiates the two samples. Additional research is required to evaluate the value of brain TA to predict neurodevelopmental out-comes in a prospective fashion. This research is now un-der way. In addition, we acknowledge that the use of quantitative analysis of fetal MRIs is still limited due to motion artifacts. However, TA can be applied in T2
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
9/16
/201
3 1:
37:5
3 P
M

Sanz-Cortés et al.
Fetal Diagn Ther 2013;33:122–129128
HASTE standard images, which can partially overcome the constraint of motion artifacts.
In summary, this study demonstrates that the evalua-tion of fetal brain MRI TA is feasible. The data demon-strate that quantitative imaging analysis identifies changes in fetal brain texture patterns of SGA fetuses, which may be missed by visual inspection. These results further sup-port the notion that SGA is associated with microstruc-tural brain changes that underlie later neurodevelopmen-tal problems. In addition, this study supports further re-search to establish the potential use of quantitative imaging techniques to develop potential imaging biomarkers of ab-normal neurodevelopment in late-onset IUGR fetuses.
Acknowledgements
This work was supported by grants from The Cerebra Founda-tion for the Brain Injured Child (Carmarthen, Wales/UK), the Thrasher Research Fund (Salt Lake City, Utah, USA), Fundacion Dexeus (Barcelona, Spain) and Banca Cívica de Caja Navarra (Proyecto TETD). M.S.C. was supported by Instituto de Salud Car-los III Rio Hortega (CM10/00222) Spain. N.P. was supported by Instituto de Salud Carlos III Sara Borrell (CD09/00263). The as-sistance of Jordi Luque is gratefully acknowledged. E.B.-C. and Transmural Biotech acknowledge ‘Comissionat per a Universitat i Recerca del Departament d’Innovació, Universitats i Empreses de la Generalitat de Catalunya’ for financial support.
References
1 Boyle CA, Boulet S, Schieve LA, Cohen RA, Blumberg SJ, Yeargin-Allsopp M, Visser S, Kogan MD: Trends in the prevalence of devel-opmental disabilities in US children, 1997–2008. Pediatrics 2011; 127: 1034–1042.
2 Rees S, Harding R, Walker D: The biological basis of injury and neuroprotection in the fe-tal and neonatal brain. Int J Dev Neurosci 2011; 29: 551–563.
3 Bernstein IM, Horbar JD, Badger GJ, Ohlsson A, Golan A: Morbidity and mortality among very-low-birth-weight neonates with intra-uterine growth restriction. The Vermont Ox-ford Network. Am J Obstet Gynecol 2000; 182: 198–206.
4 Lackman F, Capewell V, Gagnon R, Richard-son B: Fetal umbilical cord oxygen values and birth to placental weight ratio in relation to size at birth. Am J Obstet Gynecol 2001; 185: 674–682.
5 Mallard C, Loeliger M, Copolov D, Rees S: Re-duced number of neurons in the hippocam-pus and the cerebellum in the postnatal guin-ea-pig following intrauterine growth-restric-tion. Neuroscience 2000; 100: 327–333.
6 Low JA, Handley-Derry MH, Burke SO, Pe-ters RD, Pater EA, Killen HL, Derrick EJ: As-sociation of intrauterine fetal growth retarda-tion and learning deficits at age 9 to 11 years. Am J Obstet Gynecol 1992; 167: 1499–1505.
7 Low JA, Galbraith RS, Muir D, Killen H, Pater B, Karchmar J: Intrauterine growth retarda-tion: A study of long-term morbidity. Am J Obstet Gynecol 1982; 142: 670–677.
8 Regev RH, Lusky A, Dolfin T, Litmanovitz I, Arnon S, Reichman B: Excess mortality and morbidity among small-for-gestational-age premature infants: a population-based study. J Pediatr 2003; 143: 186–191.
9 Alkalay AL, Graham JM Jr, Pomerance JJ: Evaluation of neonates born with intrauterine growth retardation: review and practice guidelines. J Perinatol 1998; 18: 142–151.
10 Guellec I, Lapillonne A, Renolleau S, Charla-luk ML, Roze JC, Marret S, Vieux R, Monique K, Ancel PY: Neurologic outcomes at school age in very preterm infants born with severe or mild growth restriction. Pediatrics 2011; 127:e883–e891.
11 Padilla N, Falcon C, Sanz-Cortes M, Figueras F, Bargallo N, Crispi F, Eixarch E, Arranz A, Botet F, Gratacos E: Differential effects of in-trauterine growth restriction on brain struc-ture and development in preterm infants: a magnetic resonance imaging study. Brain Res 2011; 1382: 98–108.
12 Esteban FJ, Padilla N, Sanz-Cortes M, de Mi-ras JR, Bargallo N, Villoslada P, Gratacos E: Fractal-dimension analysis detects cerebral changes in preterm infants with and without intrauterine growth restriction. Neuroimage 2010;53: 1225–1232.
13 Lodygensky GA, Seghier ML, Warfield SK, Tolsa CB, Sizonenko S, Lazeyras F, Huppi PS: Intrauterine growth restriction affects the preterm infant’s hippocampus. Pediatr Res 2008; 63: 438–443.
14 Tolsa CB, Zimine S, Warfield SK, Freschi M, Sancho Rossignol A, Lazeyras F, Hanquinet S, Pfizenmaier M, Huppi PS: Early alteration of structural and functional brain development in premature infants born with intrauterine growth restriction. Pediatr Res 2004; 56: 132–138.
15 Dubois J, Benders M, Borradori-Tolsa C, Ca-chia A, Lazeyras F, Ha-Vinh Leuchter R, Si-zonenko SV, Warfield SK, Mangin JF, Huppi PS: Primary cortical folding in the human newborn: an early marker of later functional development. Brain 2008; 131: 2028–2041.
16 Hershkovitz R, Kingdom JC, Geary M, Ro-deck CH: Fetal cerebral blood flow redistribu-tion in late gestation: identification of com-promise in small fetuses with normal umbili-cal artery Doppler. Ultrasound Obstet Gynecol 2000; 15: 209–212.
17 Figueras F, Eixarch E, Meler E, Iraola A, Figueras J, Puerto B, Gratacos E: Small-for-gestational-age fetuses with normal umbilical artery Doppler have suboptimal perinatal and neurodevelopmental outcome. Eur J Obstet Gynecol Reprod Biol 2008; 136: 34–38.
18 McCowan LM, Pryor J, Harding JE: Perinatal predictors of neurodevelopmental outcome in small-for-gestational-age children at 18 months of age. Am J Obstet Gynecol 2002; 186: 1069–1075.
19 Geva R, Eshel R, Leitner Y, Valevski AF, Harel S: Neuropsychological outcome of children with intrauterine growth restriction: a 9-year prospective study. Pediatrics 2006; 118: 91–100.
20 Soothill PW, Bobrow CS, Holmes R: Small for gestational age is not a diagnosis. Ultrasound Obstet Gynecol 1999; 13: 225–228.
21 Cruz-Martinez R, Figueras F, Hernandez- Andrade E, Oros D, Gratacos E: Fetal brain Doppler to predict cesarean delivery for non-reassuring fetal status in term small-for-ges-tational-age fetuses. Obstet Gynecol 2011; 117: 618–626.
22 Cruz-Martinez R, Figueras F, Oros D, Padilla N, Meler E, Hernandez-Andrade E, Gratacos E: Cerebral blood perfusion and neurobehav-ioral performance in full-term small-for-ges-tational-age fetuses. Am J Obstet Gynecol 2009; 201: 474.e1–474.e7.
23 Habek D, Salihagic A, Jugovic D, Herman R: Doppler cerebro-umbilical ratio and fetal bio-physical profile in the assessment of peripartal cardiotocography in growth-retarded fetuses. Fetal Diagn Ther 2007; 22: 452–456.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
9/16
/201
3 1:
37:5
3 P
M

Fetal Brain MRI Texture Analysis in SGA Fetuses
Fetal Diagn Ther 2013;33:122–129 129
24 Severi FM, Bocchi C, Visentin A, Falco P, Co-bellis L, Florio P, Zagonari S, Pilu G: Uterine and fetal cerebral Doppler predict the out-come of third-trimester small-for-gestation-al-age fetuses with normal umbilical artery Doppler. Ultrasound Obstet Gynecol 2002; 19: 225–228.
25 Doctor BA, O’Riordan MA, Kirchner HL, Shah D, Hack M: Perinatal correlates and neonatal outcomes of small for gestational age infants born at term gestation. Am J Obstet Gynecol 2001; 185: 652–659.
26 McCowan LM, Harding JE, Stewart AW: Um-bilical artery Doppler studies in small for ges-tational age babies reflect disease severity. BJOG 2000; 107: 916–925.
27 Padidela RN, Bhat V: Neurobehavioral as-sessment of appropriate for gestational and small for gestational age babies. Indian Pedi-atr 2003; 40: 1063–1068.
28 Figueras F, Eixarch E, Gratacos E, Gardosi J: Predictiveness of antenatal umbilical artery Doppler for adverse pregnancy outcome in small-for-gestational-age babies according to customised birthweight centiles: population-based study. BJOG 2008; 115: 590–594.
29 Sanz-Cortes M, Figueras F, Bargallo N, Padil-la N, Amat-Roldan I, Gratacos E: Abnormal brain microstructure and metabolism in small-for-gestational-age term fetuses with normal umbilical artery Doppler. Ultrasound Obstet Gynecol 2010; 36: 159–165.
30 Holli KK, Harrison L, Dastidar P, Waljas M, Liimatainen S, Luukkaala T, Ohman J, Soi-makallio S, Eskola H: Texture analysis of MR images of patients with mild traumatic brain injury. BMC Med Imaging 2010; 10: 8.
31 Holli K, Laaperi AL, Harrison L, Luukkaala T, Toivonen T, Ryymin P, Dastidar P, Soimakal-lio S, Eskola H: Characterization of breast cancer types by texture analysis of magnetic resonance images. Acad Radiol 2010; 17: 135–141.
32 Jirak D, Dezortova M, Taimr P, Hajek M: Tex-ture analysis of human liver. J Magn Reson Imaging 2002; 15: 68–74.
33 De Oliveira MS, Balthazar ML, D’Abreu A, Yasuda CL, Damasceno BP, Cendes F, Castel-lano G: MR imaging texture analysis of the corpus callosum and thalamus in amnestic mild cognitive impairment and mild Alz-heimer disease. AJNR Am J Neuroradiol 2011; 32: 60–66.
34 McLaren CE, Chen WP, Nie K, Su MY: Pre-diction of malignant breast lesions from MRI features: a comparison of artificial neural net-work and logistic regression techniques. Acad Radiol 2009; 16: 842–851.
35 Tenorio V, Bonet-Carne E, Botet F, Marques F, Amat-Roldan I, Gratacos E: Correlation be-tween a semiautomated method based on ul-trasound texture analysis and standard ultra-sound diagnosis using white matter damage in preterm neonates as a model. J Ultrasound Med 2011; 30: 1365–1377.
36 Cobo T, Bonet-Carne E, Martínez-Terrón M, Perez-Moreno A, Elías N, Luque J, Amat-Roldan I, Palacio M: Feasibility and reproduc-ibility of fetal lung texture analysis by auto-matic quantitative ultrasound analysis and correlation with gestational age. Fetal Diagn Ther 2012; 31: 230–236.
37 Santamaria R, Verdu ML, Martin C, Garcia G: Tablas españolas de peso neonatal segun edad gestacional. Badalona, Ed Artes Gráfi-cas Beatulo, 1998.
38 Arduini D, Rizzo G: Normal values of pulsa-tility index from fetal vessels: a cross-section-al study on 1,556 healthy fetuses. J Perinat Med 1990; 18: 165–172.
39 Robinson HP, Fleming JE: A critical evalua-tion of sonar ‘crown-rump length’ measure-ments. Br J Obstet Gynaecol 1975; 82: 702–710.
40 Baschat AA, Gembruch U: The cerebropla-cental Doppler ratio revisited. Ultrasound Obstet Gynecol 2003; 21: 124–127.
41 Figueras F, Oros D, Cruz-Martinez R, Padilla N, Hernandez-Andrade E, Botet F, Costas-Moragas C, Gratacos E: Neurobehavior in term, small-for-gestational-age infants with normal placental function. Pediatrics 2009; 124:e934–e941.
42 Limperopoulos C, Tworetzky W, McElhinney DB, Newburger JW, Brown DW, Robertson RL Jr, Guizard N, McGrath E, Geva J, Annese D, Dunbar-Masterson C, Trainor B, Laussen PC, du Plessis AJ: Brain volume and metabo-lism in fetuses with congenital heart disease: evaluation with quantitative magnetic reso-nance imaging and spectroscopy. Circulation 2010; 121: 26–33.
43 Berman JI, Hamrick SE, McQuillen PS, Stud-holme C, Xu D, Henry RG, Hornberger LK, Glenn OA: Diffusion-weighted imaging in fe-tuses with severe congenital heart defects. AJNR Am J Neuroradiol 2011; 32:E21–E22.
44 Miller SP, McQuillen PS, Hamrick S, Xu D, Glidden DV, Charlton N, Karl T, Azakie A, Ferriero DM, Barkovich AJ, Vigneron DB: Abnormal brain development in newborns with congenital heart disease. N Engl J Med 2007; 357: 1928–1938.
45 Hernandez-Andrade E, Figueroa-Diesel H, Jansson T, Rangel-Nava H, Gratacos E: Chang-es in regional fetal cerebral blood flow perfu-sion in relation to hemodynamic deterioration in severely growth-restricted fetuses. Ultra-sound Obstet Gynecol 2008; 32: 71–76.
46 Hilario E, Rey-Santano MC, Goni-de-Cerio F, Alvarez FJ, Gastiasoro E, Mielgo VE, Cabal-lero A, Valls-i-Soler A, Gomez-Urquijo S, Al-varez A: Cerebral blood flow and morpholog-ical changes after hypoxic-ischaemic injury in preterm lambs. Acta Paediatr 2005; 94: 903–911.
47 Benavides-Serralde A, Hernandez-Andrade E, Fernandez-Delgado J, Plasencia W, Scheier M, Crispi F, Figueras F, Nicolaides KH, Gratacos E: Three-dimensional sonographic calculation of the volume of intracranial structures in growth-restricted and appropri-ate-for-gestational age fetuses. Ultrasound Obstet Gynecol 2009; 33: 530–537.
48 Makhoul IR, Soudack M, Goldstein I, Smolkin T, Tamir A, Sujov P: Sonographic biometry of the frontal lobe in normal and growth-re-stricted neonates. Pediatr Res 2004; 55: 877–883.
49 Leitner Y, Fattal-Valevski A, Geva R, Eshel R, Toledano-Alhadef H, Rotstein M, Bassan H, Radianu B, Bitchonsky O, Jaffa AJ, Harel S: Neurodevelopmental outcome of children with intrauterine growth retardation: a longi-tudinal, 10-year prospective study. J Child Neurol 2007; 22: 580–587.
50 Stocco A, Lebiere C, Anderson JR: Condition-al routing of information to the cortex: a mod-el of the basal ganglia’s role in cognitive coor-dination. Psychol Rev 2010; 117: 541–574.
51 Baillieux H, De Smet HJ, Paquier PF, De Deyn PP, Marien P: Cerebellar neurocognition: in-sights into the bottom of the brain. Clin Neu-rol Neurosurg 2008; 110: 763–773.
52 Oros D, Figueras F, Cruz-Martinez R, Padil-la N, Meler E, Hernandez-Andrade E, Grata-cos E: Middle versus anterior cerebral artery Doppler for the prediction of perinatal out-come and neonatal neurobehavior in term small-for-gestational-age fetuses with nor-mal umbilical artery Doppler. Ultrasound Obstet Gynecol 2010;35: 456–461.
53 Eixarch E, Meler E, Iraola A, Illa M, Crispi F, Hernandez-Andrade E, Gratacos E, Figueras F: Neurodevelopmental outcome in 2-year-old infants who were small-for-gestational-age term fetuses with cerebral blood flow re-distribution. Ultrasound Obstet Gynecol 2008; 32: 894–899.
54 Isaacs EB, Fischl BR, Quinn BT, Chong WK, Gadian DG, Lucas A: Impact of breast milk on intelligence quotient, brain size, and white matter development. Pediatr Res 2010; 67: 357–362.
55 Vanderveen JA, Bassler D, Robertson CM, Kirpalani H: Early interventions involving parents to improve neurodevelopmental out-comes of premature infants: a meta-analysis. J Perinatol 2009; 29: 343–351.
56 Maulik PK, Darmstadt GL: Community-based interventions to optimize early child-hood development in low resource settings. J Perinatol 2009; 29: 531–542.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
9/16
/201
3 1:
37:5
3 P
M