exclusive breastfeeding practices among women in the
TRANSCRIPT
SCHOOL OF PUBLIC HEALTH
COLLEGE OF HEALTH SCIENCES
UNIVERSITY OF GHANA
LEGON
EXCLUSIVE BREASTFEEDING PRACTICES AMONG WOMEN IN THE
FORMAL SECTOR OF THE GREATER ACCRA REGION AND IMPLICATIONS
FOR THE LACTATIONAL ROOM POLICY.
BY
JOAN ESE MORNY (10637263)
THIS DISSERTATION IS SUBMITTED TO THE UNIVERSITY OF GHANA
LEGON, IN PARTIAL FULFILLMENT OF THE REQUIREMENT FOR THE
AWARD OF MASTER OF PUBLIC HEALTH DEGREE
JULY, 2018
University of Ghana http://ugspace.ug.edu.gh
i
DECLARATION
I, Joan Ese Morny, do hereby declare that, apart from references made to the work done
in relation to this subject area which have been duly acknowledged, this work was
independently done by me under supervision. I further declare that this work has not
been submitted for the award of any degree in this University or elsewhere.
JOAN ESE MORNY
(STUDENT) SIGNATURE DATE
DR. PATRICIA AKWEONGO
(SUPERVISOR) SIGNATURE DATE
University of Ghana http://ugspace.ug.edu.gh
ii
ABSTRACT
BACKGROUND: In Ghana, even though the knowledge of the practice and benefits of
exclusive breast feeding amongst women is very high, only 52% of babies are breastfed
up to 6 months of life. In Ghana 49.52% of the work force are females, also 40.1% of
workers are within the formal sector. Better educated women participate more in the
formal sector and earn higher incomes. This study sought to examine exclusive
breastfeeding practices amongst women in the formal sector in the Greater Accra region
and the implication for the breastfeeding room policy in Ghana.
METHODS: The study was a cross sectional analytical study and it employed a
quantitative approach. The study was conducted at the Greater Accra Regional
Hospital, Police Hospital, Narh-Bita Hospital and Port Medical Centre. All consecutive
formal sector working mothers who reported to the immunization clinic of these
hospitals were recruited (359 mothers). They were interviewed using a structured
questionnaire. The data collection for the study covered a period of 4 weeks (June to
July 2018). The data was analysed using Stata 15.0, frequency tables and percentages
were used to describe the distribution of variables and cross tabulations with Chi-square
tests were also used to establish bivariate associations between exclusive breastfeeding
and independent variables. Logistic regression was then used to investigate if the
independent variables were jointly associated with the practice of exclusive
breastfeeding.
RESULTS: The results showed that 191(52.3%) of mothers in the formal sector
exclusively breastfeed their babies. The average number of months spent on practicing
exclusive breastfeeding was 5.2 months. The higher the income of the less likely a
woman was to exclusively breastfeed.
University of Ghana http://ugspace.ug.edu.gh
iii
Knowledge of EBF is high 111 (68%) among mothers working in the formal sector.
About 227 (93%) of formal sector working mothers had accurate knowledge of
exclusive breastfeeding but only 103 (45.4%) of them actually practiced exclusive
breastfeeding. Only mothers who received information about EBF from their partners
had the highest 60.6% EBF practice. Fifty three (14.8%) of mothers described their
workplace as very supportive for breastfeeding and out of that 29(54.7%) of them
practiced EBF.
CONCLUSION: Slightly over fifty percent of women in the formal sector practices
EBF. Despite the non-availability of organizational structures in place a breastfeeding
supportive workplace also increases the likelihood of a woman exclusively
breastfeeding her baby. Male involvement and partner support in EBF increases a
woman’s likelihood to practice EBF.
University of Ghana http://ugspace.ug.edu.gh

iv
DEDICATION
Dedicated to my dear mummy, Mrs Elizabeth Morny and to all hardworking women
trying to balance motherhood and career.
University of Ghana http://ugspace.ug.edu.gh
v
ACKNOWLEDGEMENT
I would like to thank my Lord and Saviour Jesus Christ for his overwhelming love
towards me. I would also like to thank my family and friends for their immense support.
To my supervisor, Dr Patricia Akweongo, thanks for your extraordinary patience. To
Mr. Tony Godi and Bernad Fiador I say a big thank you for the assistance. God bless
you.
University of Ghana http://ugspace.ug.edu.gh
vi
TABLE OF CONTENTS
DECLARATION ............................................................................................................ i
ABSTRACT ................................................................................................................... ii
DEDICATION .............................................................................................................. iv
ACKNOWLEDGEMENT ............................................................................................. v
LIST OF FIGURES ...................................................................................................... ix
LIST OF TABLES ......................................................................................................... x
LIST OF ABBREVIATIONS ....................................................................................... xi
DEFINITION OF TERMS .......................................................................................... xii
CHAPTER ONE ............................................................................................................ 1
INTRODUCTION ......................................................................................................... 1
1.1 Background .............................................................................................................. 1
1.2 Problem Statement ................................................................................................... 4
1.3 Justification of the Study ......................................................................................... 5
1.4 General Objective .................................................................................................... 6
1.5 Specific Objectives .................................................................................................. 6
1.6 Research Questions .................................................................................................. 6
1.7 Conceptual Framework ............................................................................................ 7
CHAPTER TWO ........................................................................................................... 9
LITERATURE REVIEW .............................................................................................. 9
2.1 Exclusive Breastfeeding........................................................................................... 9
2.2 The Health Belief Model ......................................................................................... 9
2.2.1 Theoretical Perspective of the study ................................................................... 10
2.3 Trends in Exclusive Breastfeeding Practices ........................................................ 11
2.4 Benefits of Exclusive Breastfeeding ...................................................................... 12
2.5 Determinants of Exclusive Breastfeeding .............................................................. 13
2.4.3 Behavioural Factors ............................................................................................ 16
2.6 Exclusive Breastfeeding among Women in the Formal Sector ............................. 17
2.7 The Breastfeeding Room Policy ............................................................................ 17
2.8 Benefits of the Breastfeeding Room ...................................................................... 18
2.9 Conclusion ............................................................................................................. 19
CHAPTER THREE ..................................................................................................... 20
METHODOLOGY ...................................................................................................... 20
University of Ghana http://ugspace.ug.edu.gh
vii
3.1 Introduction ............................................................................................................ 20
3.2 Study Design .......................................................................................................... 20
3.3 Study Sites ............................................................................................................. 20
3.4 Study Population .................................................................................................... 21
3.5 Sampling ................................................................................................................ 21
3.5.1 Sample Size Determination................................................................................. 21
3.6 Sampling Technique .............................................................................................. 22
3.7 Inclusion Criteria ................................................................................................... 23
3.8 Exclusion Criteria .................................................................................................. 24
3.9 Study Variables ...................................................................................................... 24
3.10 Data Collection Techniques and Tools ................................................................ 26
3.10.1 Pretesting........................................................................................................... 26
3.10.2 Quality Control ................................................................................................. 26
3.11 Data Analysis ....................................................................................................... 27
3.12 Ethical Consideration ........................................................................................... 27
3.13 Participant Consent .............................................................................................. 27
3.14 Privacy and Confidentiality ................................................................................. 28
3.15 Risk and Benefit ................................................................................................... 28
3.16 Permission for Study ............................................................................................ 28
3.17 Description of Subjects Involved In the Study .................................................... 28
3.18 Informed Consent Process ................................................................................... 28
3.19 Voluntary Consent/Withdrawal ........................................................................... 29
3.20 Data Storage and Usage ....................................................................................... 29
3.21 Compensation ...................................................................................................... 29
3.22 Proposal and Funding Information ...................................................................... 29
CHAPTER FOUR ........................................................................................................ 30
RESULTS .................................................................................................................... 30
4.1 Background Characteristics ................................................................................... 30
4.2 Mode of feeding ..................................................................................................... 33
4.3 Knowledge and Perception of Exclusive Breastfeeding ........................................ 33
4.4 Breastfeeding in the course of Work ..................................................................... 35
4.5 Organizational Support for Breastfeeding ............................................................. 39
4.6 Predictors of Exclusive Breastfeeding among formal sector working mothers ..... 41
CHAPTER FIVE ......................................................................................................... 45
University of Ghana http://ugspace.ug.edu.gh
viii
DISCUSSION .............................................................................................................. 45
CHAPTER SIX ............................................................................................................ 49
CONCLUSIONS AND RECOMMENDATIONS ...................................................... 49
REFERENCES ............................................................................................................ 51
APPENDIX .................................................................................................................. 57
CONSENT FORM ....................................................................................................... 57
University of Ghana http://ugspace.ug.edu.gh
ix
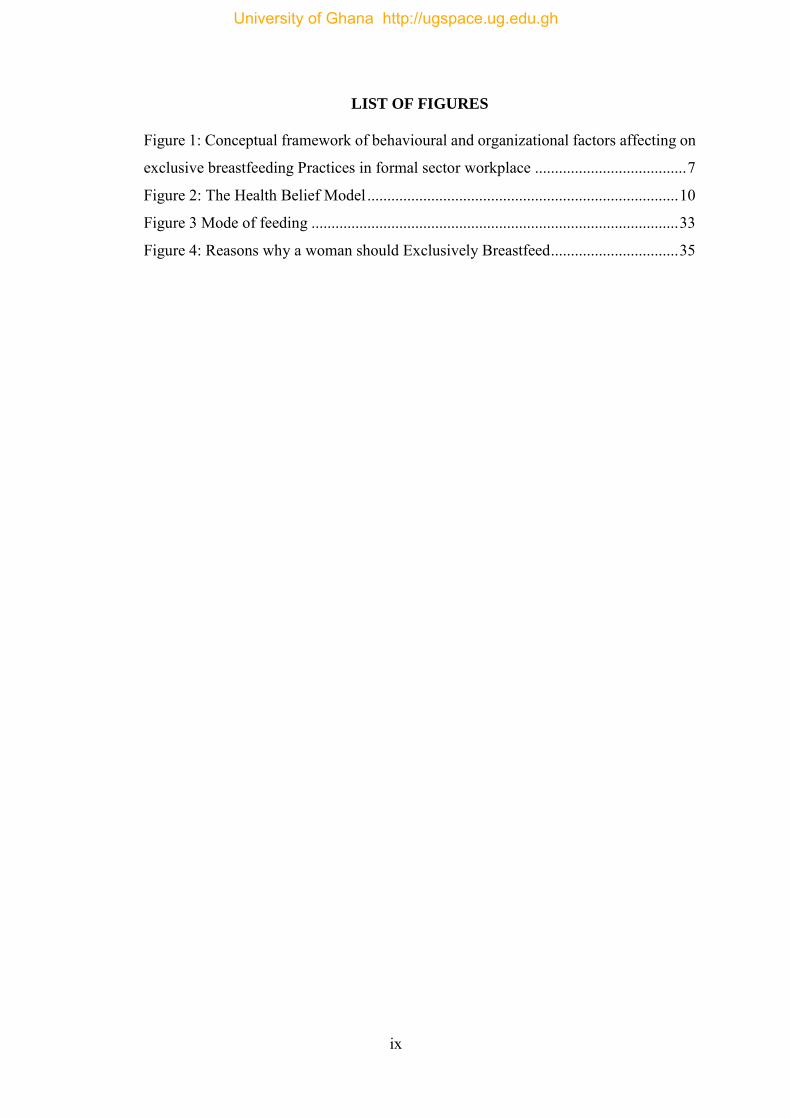
LIST OF FIGURES
Figure 1: Conceptual framework of behavioural and organizational factors affecting on
exclusive breastfeeding Practices in formal sector workplace ...................................... 7
Figure 2: The Health Belief Model .............................................................................. 10
Figure 3 Mode of feeding ............................................................................................ 33
Figure 4: Reasons why a woman should Exclusively Breastfeed ................................ 35
University of Ghana http://ugspace.ug.edu.gh
x
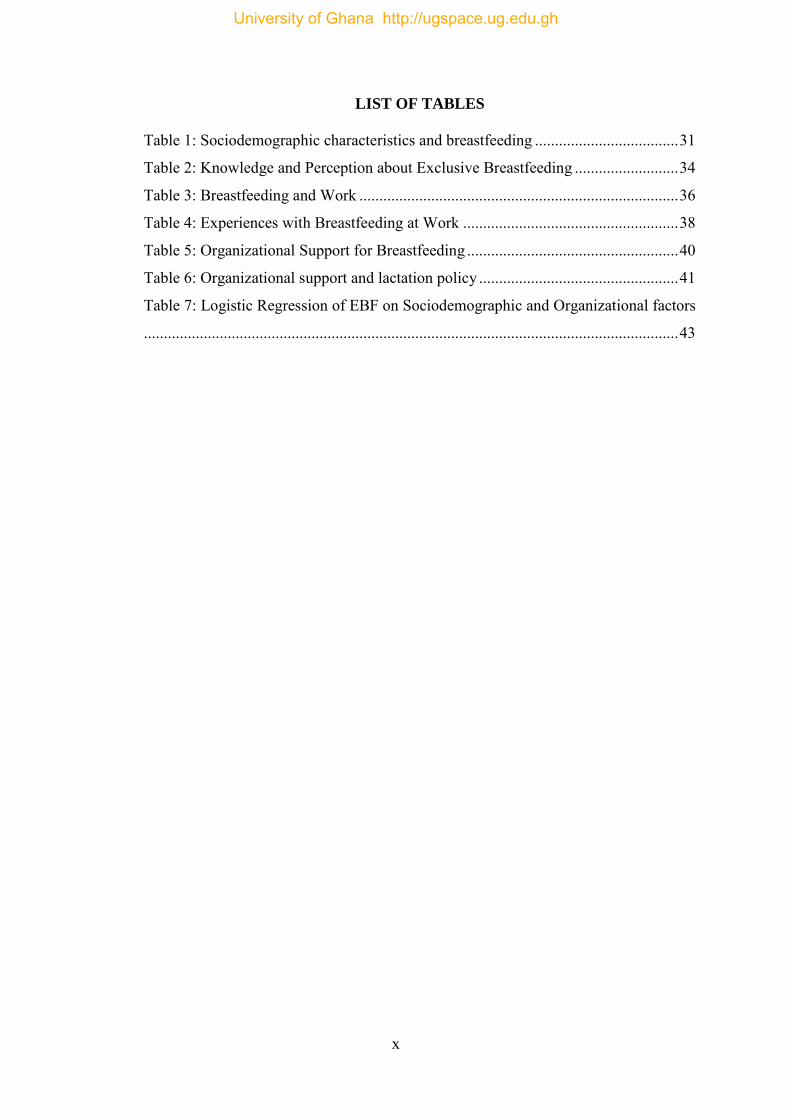
LIST OF TABLES
Table 1: Sociodemographic characteristics and breastfeeding .................................... 31
Table 2: Knowledge and Perception about Exclusive Breastfeeding .......................... 34
Table 3: Breastfeeding and Work ................................................................................ 36
Table 4: Experiences with Breastfeeding at Work ...................................................... 38
Table 5: Organizational Support for Breastfeeding ..................................................... 40
Table 6: Organizational support and lactation policy .................................................. 41
Table 7: Logistic Regression of EBF on Sociodemographic and Organizational factors
...................................................................................................................................... 43
University of Ghana http://ugspace.ug.edu.gh
xi
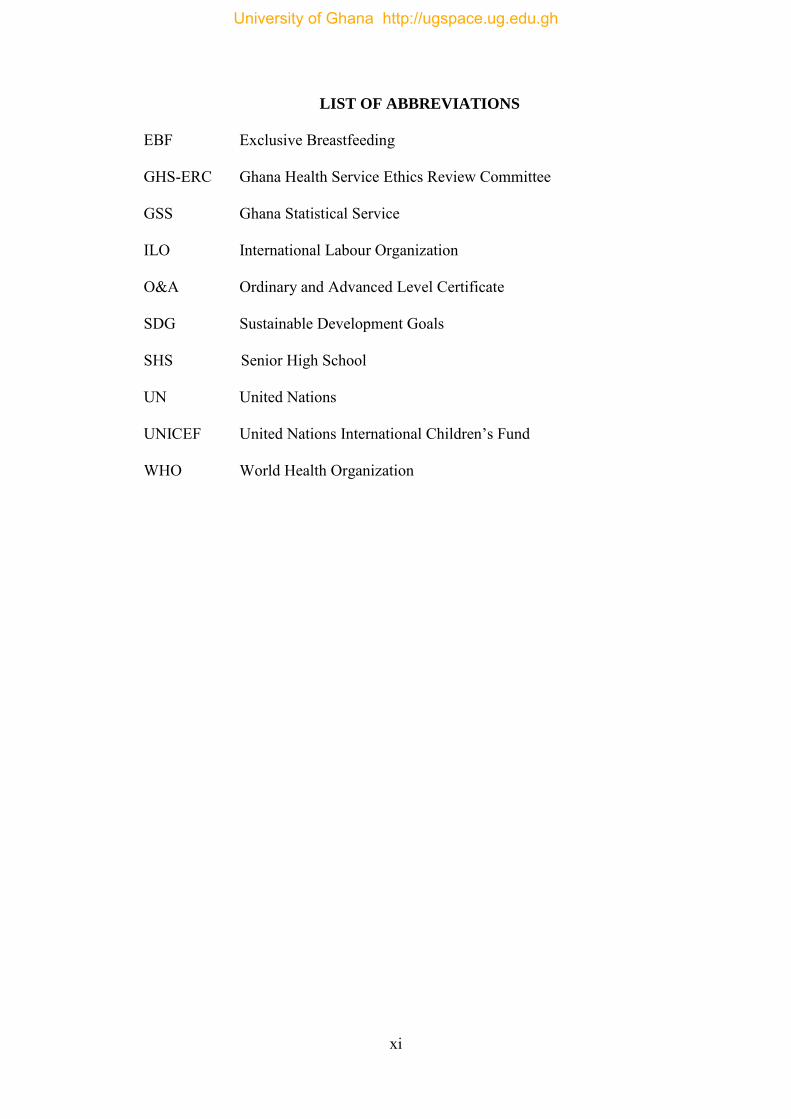
LIST OF ABBREVIATIONS
EBF Exclusive Breastfeeding
GHS-ERC Ghana Health Service Ethics Review Committee
GSS Ghana Statistical Service
ILO International Labour Organization
O&A Ordinary and Advanced Level Certificate
SDG Sustainable Development Goals
SHS Senior High School
UN United Nations
UNICEF United Nations International Children’s Fund
WHO World Health Organization
University of Ghana http://ugspace.ug.edu.gh

xii
DEFINITION OF TERMS
Formal sector worker: Formal sector worker is any worker whose job is within
usual hours (8am to 5 pm) who earn regular wages, and
are on a recognize income source, on which income
taxes is paid.
Exclusive breastfeeding: Feeding baby with only breast milk and not food and
water for up to 6 months of life
Lactation Room: A private room in an institution where a nursing mother
can pump breast milk or nurse her baby. Also known as
the Breastfeeding room
University of Ghana http://ugspace.ug.edu.gh
1
CHAPTER ONE
INTRODUCTION
1.1 Background
Prior to the industrial revolution which spanned from the 18th to 20th century, the sole
role of a woman was defined by her household roles, that is to raise children and keep
the home. The industrial revolution required that more and more women were
incorporated into the labour force which allowed them to receive wages and which gave
them little time for household roles which included breastfeeding their babies
(Pinchbeck, 1930; Revolution, Clark, Hutchins, & George, 1991). This period
coincided with the era of the proliferation of breast milk substitutes as it seemed the
most convenient way of feeding an infant (Wolf, 2001). Also, researchers of that era
positioned infant formula as a better alternative to human breast milk (Stevens, Patrick,
& Pickler, 2009). This was corroborated by breast milk substitute key industry players
who through the adoption of effective promotional strategies managed to get a large
segment of the working population especially those in the formal sector to adapt to the
infant formula(Stevens et al., 2009).
Previously it was a status symbol in Ghana and worldwide to feed babies with infant
formula hence most young couples including those who were in the informal sector
resorted to the use of various brands of breast milk substitutes.
However, after some recorded adverse effects of breast milk substitutes on the health
of babies such as summertime milk spoilage where there was milk spoilage due to the
heat and inappropriate preservation of cow milk deeper research into human breast milk
was conducted, which resulted in a paradigm shift to human breast milk as the optimum
source of infant nutrition. In the 1970s breastfeeding support movements were formed
University of Ghana http://ugspace.ug.edu.gh
2
and the association between infant formula and diseases such as diarrhoea, diabetes
and allergy was established(Castilho & Filho, 2010). In the year 1990, the Innocenti
Declaration on the protecting, promotion and supporting of breastfeeding was made
(WHO & UNICEF, 1990). Over the last two decades, there has been a growing attention
in the endorsement of exclusive breastfeeding as the recommended feeding practice for
newly born babies(Castilho & Filho, 2010) This, to a great extent, has been encouraged
by increasing scientific research, discoveries and substantiation on the significance of
exclusive breastfeeding in reducing infant morbidity and mortality.
More than 100 years after the industrial revolution more women today find themselves
in the formal sector where they rub shoulders with their male counterparts despite the
need to still combine this with their traditional role as home keepers and nurturers of
children. In this highly competitive global marketing environment, employers have
become very sensitive to the returns on their investments hence time spent by an
individual employee in carrying out a task and the revenue generated through the act
has become very important(Saks, 2015). This situation has a heavy toll on breastfeeding
mothers who are faced with the decision as to the safest, most convenient, healthy and
sustainable ways of providing nutrition to their infants. Maternity leave periods are
short with the average period in Ghana being 12 weeks or 3 months according to the
Ghana labour act and a survey done by ILO as there is the need to resume full time
work (Centres & Agencies, 2003; ILO, n.d.).
Finding solution to the gaps created during the absence of the mothers whilst at work
has generated a lot of advocacy and debate as to how to find innovative ways of
providing human breastmilk while the nursing mother is at work. In recent times
University of Ghana http://ugspace.ug.edu.gh
3
governments and international bodies have encouraged workplace breastfeeding
support through policies and interventions.(Government, Government, & Government,
2010; Lyell, 2012; National Breastfeeding Policy And Action Plan, 2015)
The International Labour Organization (ILO) in partnership with the World Health
Organization (WHO) came out with conventions to ensure breastfeeding in nursing
mothers as a way of encouraging high breastfeeding rates amongst women in labour
organisations especially in the formal sector worldwide. These conventions and
recommendations are embodied in the ILO convention number 183 and
recommendation 191. ILO Recommendation convention number 183 and
recommendation 191 emphasize that nursing facilities are to be provided at the
workplace with one or more breastfeeding breaks to enable the mother express breast
milk for continual breastfeeding. Convention number 183 article 10 states that “the
period during which nursing breaks or the reduction of daily hours of work are allowed,
their number, the duration of nursing breaks and the procedures for the reduction of
daily hours of work shall be determined by national law and practice.”(ILO, 2017). This
gives room for the nation to design its own national breastfeeding policy as well as
workplace breastfeeding policy.
The global breastfeeding initiative which was an initiative set up by WHO and
UNICEF set up the Global Breastfeeding Scorecard, as a bench mark for the evaluation
of breastfeeding practices worldwide (UNICEF, 2017). The scorecard number 3 was
based on the availability of paid maternity leave as well as a workplace breastfeeding
policy (WHO, 2017). The ILO, WHO and UNICEF have come together to put down
laid down procedures for breastfeeding amongst working mothers globally. This was
University of Ghana http://ugspace.ug.edu.gh
4
done to ensure that mothers who had to return to work during the course of the exclusive
breastfeeding period could do so despite the need to return to work (UNICEF, 2017).
In Ghana the median breastfeeding period is 3 months which coincides with the period
when most mothers have to return to work (Aryeetey & Goh, 2013).
1.2 Problem Statement
According to the 2017 WHO report no single country globally has been able to reach
the estimated WHO breastfeeding rates of 90% (Mogre, Dery, & Gaa, 2016; UNICEF,
2017). The Global Breastfeeding Initiative Scorecard, which is a joint collective by
WHO and UNICEF indicated that globally the rate of exclusive breastfeeding for
infants for up to six months is 40%. Out of 194 countries they assessed that only 23 of
them have at least 60% rate of exclusive breast feeding among babies less than six
months. The Collective has established a target to increase the rate of exclusive
breastfeeding to at least 60% by 2030 (UNICEF, 2017).
Even though exclusive breastfeeding rates in Africa is high, West Africa records one of
the lowest breastfeeding rates in the world (Sokol, Aquago, & Clark, 2007). West
Africa also has the highest rates of childhood malnutrition in the world and
breastfeeding is one major factor to end malnutrition globally (Sokol et al., 2007). In
West Africa, there is inappropriate use of breast milk substitutes due to the literate level
of the population. Infants are left home with house helps and grandparents who at times
have challenges handling these breast milk substitutes.(Sokol et al., 2007). Breast milk
substitutes are used by most women in the formal sector as there is a need to return to
work as soon as possible. Breast milk substitutes have however been found to expose
University of Ghana http://ugspace.ug.edu.gh
5
children to diarrhoeal, pneumococcal, diabetes and allergic conditions later in life and
as such should not be encouraged.
In Ghana even though the knowledge of the practice and benefits of exclusive breast
feeding amongst women is very high, only 52% of babies are breastfed up to 6 months
of life.(UNICEF, 2016). For most women in the formal sector the return to work ends
the period of exclusive breastfeeding or breastfeeding in its entirety (Aryeetey & Goh,
2013) which means measures have to be taken to ensure the sustainability and practice
of exclusive breastfeeding amongst women in the formal sector. In the 2015 to the
World Bank in 2017, 49.52% of the work force in Ghana are females, also 40.1% of
workers in Ghana are within the formal sector (Ghana Statistical Service, 2015). Better
educated women participate more in the formal sector and earn higher incomes (World
Bank, 2017). However studies have shown that educated and wealthier women tend to
less likely breastfeed their babies (Shifraw et al., 2015; Tewabe et al., 2017). Despite
educational programmes and advocacy efforts by health and governmental bodies and
women advocacy groups, exclusive breastfeeding among working mothers is still poor.
This study seeks to investigate the practice of exclusive breastfeeding among formal
working mothers and possible implication for the lactational room policy.
1.3 Justification of the Study
In Ghana the median breastfeeding period is 3 months which coincides with the period
when most mothers working in the formal sector have to return to work (Aryeetey &
Goh, 2013). This suggests a need to look at breastfeeding in the workplace and the
workplace support by employers to ensure that Ghana reaches its 90% breastfeeding
University of Ghana http://ugspace.ug.edu.gh
6
rate. This research examines exclusive breastfeeding practices among women in the
formal sector in Ghana, the workplace support and its implication for the full
implementation of the breastfeeding policy. The findings may highlight the factors
affecting mothers in the formal sectors decision to exclusively feed the child which may
in turn affect the full implementation of the lactation room policy in Ghana to enable
the country conform to international policies and set goals.
1.4 General Objective
To examine the practice of exclusive breastfeeding amongst women in the formal sector
and its implication for the Lactation Room Policy
1.5 Specific Objectives
1. To determine the proportion of formal female workers who exclusively breastfeed
2. To determine the knowledge and perception of working mothers on exclusive
breastfeeding.
3. To examine factors that influence exclusive breastfeeding amongst women in the
formal sector.
1.6 Research Questions
1. What proportion of formal female workers exclusively breastfeed their babies?
2. What is the level of knowledge of Exclusive breastfeeding amongst mothers in the
formal sector.
3. What are the factors that promote exclusive breastfeeding practices in formal sector
workplace?
University of Ghana http://ugspace.ug.edu.gh
7
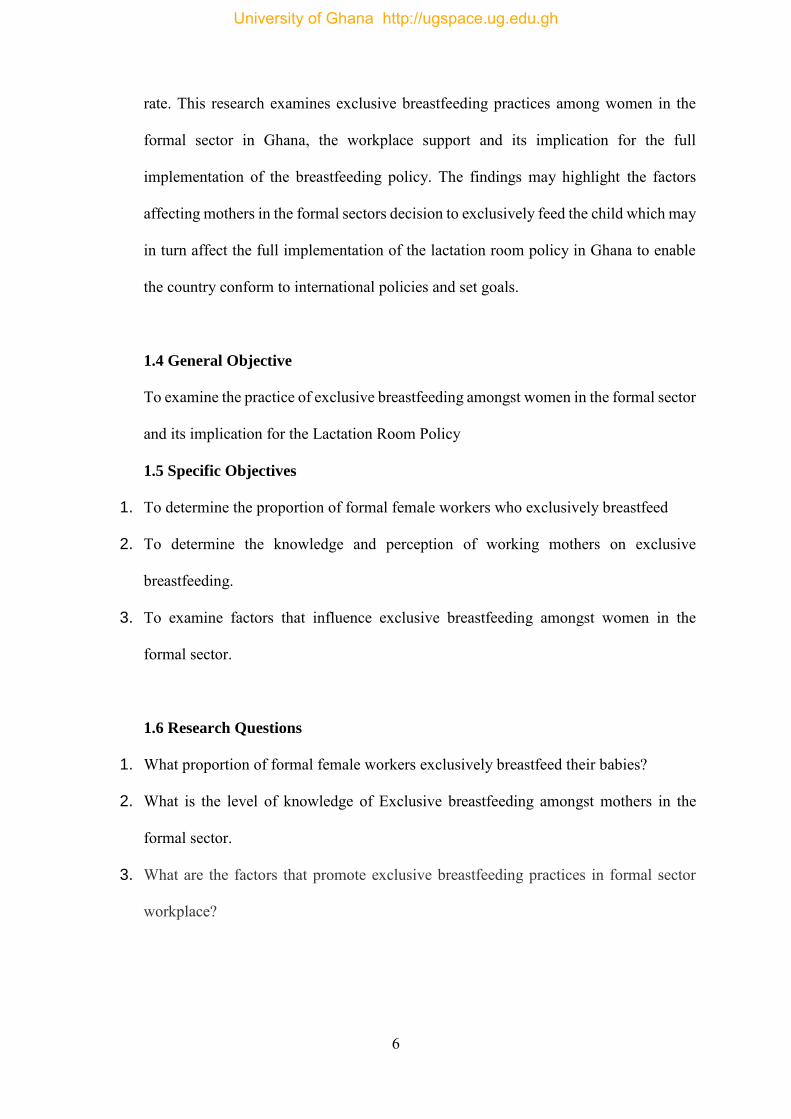
1.7 Conceptual Framework
This conceptual framework as drawn in with underpinnings of the health belief model
gives an overview of the factors that affect the practice of Exclusive breastfeeding in
mothers in the formal sector in Ghana. From the diagram, socio-demographic factors
(Age, Marital status, Educational level, Profession, Income, Working sector),
Organizational factors such as Working hours per day, Availability of lactation Rooms,
Number of breaks for Milk expression, Availability of lactation room policy and
behavioural factors (Knowledge of the of Exclusive, Breastfeeding (EBF), Sources of
Socio-demographic
factors
Age Marital status Educational background Current profession Level of income Working sector Number of children
Organizational factors
Working hours per day Availability of lactation rooms Number of breaks for Milk expression Availability of lactation room policy
Behavioural factors
Knowledge of Exclusive Breastfeeding (EBF) Sources of knowledge Knowledge of benefits of EBF Perception about EBF
Exclusive Breastfeeding
Figure 1: Conceptual framework of behavioural and organizational factors
affecting on exclusive breastfeeding Practices in formal sector workplace
University of Ghana http://ugspace.ug.edu.gh
8
knowledge, Knowledge of benefits of EBF) independently can affect the practice of
Exclusive breastfeeding. Although these factors individually influence EBF, there is
some interaction between socio-demographic factors, organizational factors and
behavioural factors. Older women may likely breastfeed their babies exclusively. On
the other hand, older women may have more responsibilities at work and that could
reduce the effect of age on EBF. Marital status, Educational level may influence the
organization they work for, amount of time spent at work and whether or not they enjoy
breaks at the workplace. Educational level, age and profession may influence one’s
knowledge and perception on breastfeeding. Increase in educational status may lead to
an increase in knowledge on exclusive breastfeeding Also the organization one works
for can influence the income level. Individuals’ knowledge on benefits of breastfeeding
and their perceptions on EBF may influence the need for formal sectors workers to
make use of lactation Breaks, lactation rooms at work place. With the availability of a
lactation room and lactation room policy, the mother may positive perception about
EBF and could increase her likelihood of practicing exclusive breastfeeding.
University of Ghana http://ugspace.ug.edu.gh
9
CHAPTER TWO
LITERATURE REVIEW
2.1 Exclusive Breastfeeding
According to WHO "Exclusive breastfeeding" is the practice of giving only breastmilk
including milk expressed or from a wet nurse and no other food or drink, not even water,
for 6 months of life, but allows the infant to receive ORS, drops and syrups (vitamins,
minerals and medicines (WHO, 2015).
Breastfeeding is the best way of providing healthy, natural and ideal food for the
growing infant. It provides all the nutrients and a balanced diet for a baby’s needs for
the first six months of life.
It also provides more than half of the babies nutritional needs for from 6months going
on and one third of the babies nutritional needs during the second year of life (WHO,
2017).
To enable mothers to establish and sustain exclusive breastfeeding for 6 months, WHO
and UNICEF recommend: “Initiation of breastfeeding within the first hour of life; the
infant only receives breast milk without any additional food or drink, not even water;
breastfeeding on demand – that is as often as the child wants, day and night and no use
of bottles, teats or pacifiers (WHO, 2017)”.
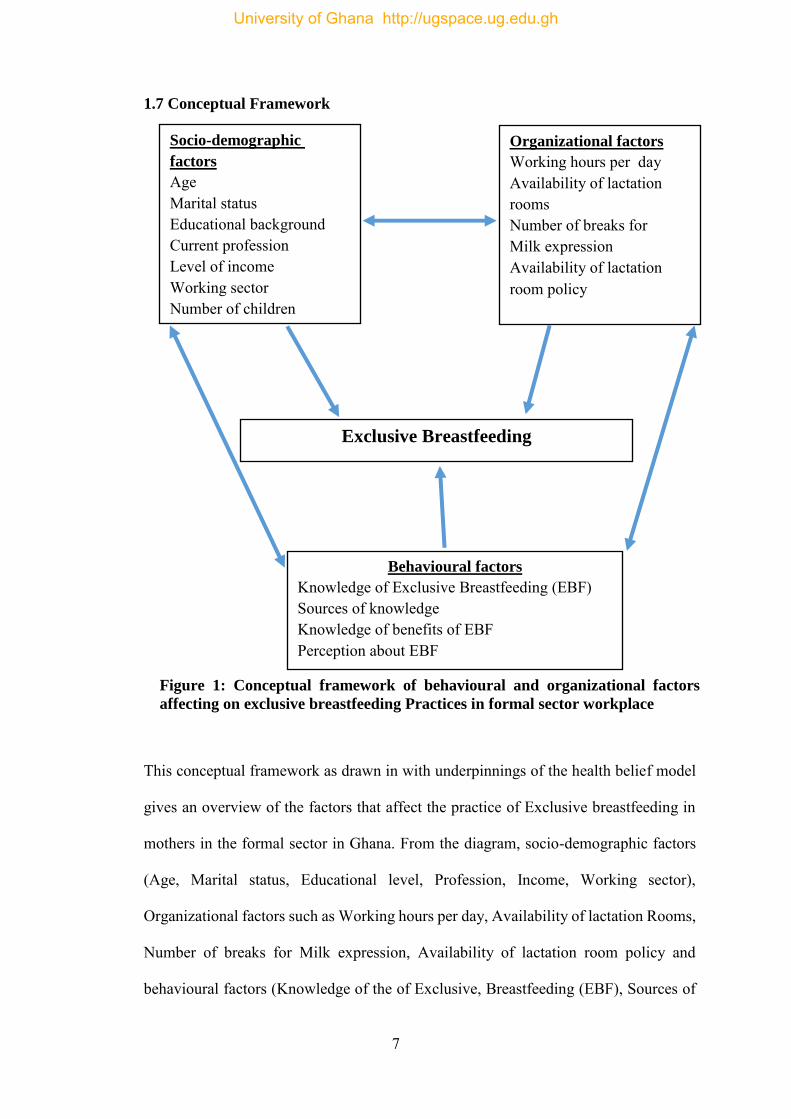
2.2 The Health Belief Model
The Health Belief Model is used to inform behaviour change interventions and assess
behaviour change. Originally, the Health Belief Model had four constructs: perceived
University of Ghana http://ugspace.ug.edu.gh
10
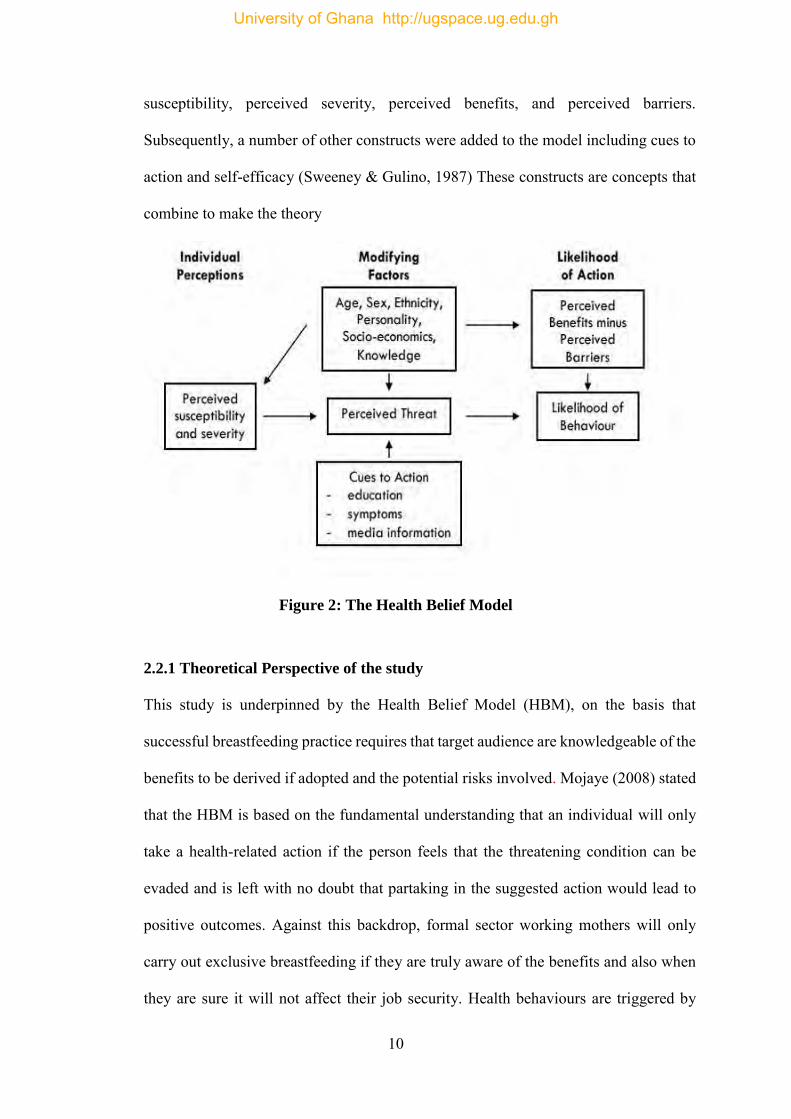
susceptibility, perceived severity, perceived benefits, and perceived barriers.
Subsequently, a number of other constructs were added to the model including cues to
action and self-efficacy (Sweeney & Gulino, 1987) These constructs are concepts that
combine to make the theory
Figure 2: The Health Belief Model
2.2.1 Theoretical Perspective of the study
This study is underpinned by the Health Belief Model (HBM), on the basis that
successful breastfeeding practice requires that target audience are knowledgeable of the
benefits to be derived if adopted and the potential risks involved. Mojaye (2008) stated
that the HBM is based on the fundamental understanding that an individual will only
take a health-related action if the person feels that the threatening condition can be
evaded and is left with no doubt that partaking in the suggested action would lead to
positive outcomes. Against this backdrop, formal sector working mothers will only
carry out exclusive breastfeeding if they are truly aware of the benefits and also when
they are sure it will not affect their job security. Health behaviours are triggered by
University of Ghana http://ugspace.ug.edu.gh
11
one’s desire to prevent illness (perceived susceptibility) or to live in a state of wellness.
The assumption is that, understanding the advantages of exclusive breastfeeding
(perceived benefits) and having a clear knowledge of the dangers of not exclusively
breastfeeding the child (perceived severity), mothers’ confidence will be activated to
overcome the challenges and that can improve the practice of exclusively breastfeeding
their babies. Providing information improves knowledge which affects perception and
this promotes acceptance (Ogwezzy-Ndisika, 2012). Sensitization and education of
mothers on the advantages of exclusive breastfeeding; and provision of adequate
information on how to deal with the challenges of breastfeeding in the workplace will
help mothers adopt the desired behaviour. Certain factors such as working hours, non-
availability of lactation room at work place, no/inadequate break time at work as
perceived by the individual may serve as barriers to the desired behaviour (perceived
barriers). For example, a mother might not breast-feed the baby for fear of the breast-
milk not being adequate for the infant due to hours spent at the work place and not
breastfeeding. External factors also influence the desired behaviour, serving as cues to
action. For exclusive breastfeeding, information from health professionals, radio and
television as well as support and encouragement from partner and other relatives may
influence mother to exclusively breastfeed their babies (Ogwezzy-ndisika, 2016)
2.3 Trends in Exclusive Breastfeeding Practices
In the United States, a national survey found that only 16.8% of infants had been
exclusively breastfed for six months(Jones & Kogan, 2011). Dop &Benbouzid (1999)
reported a mean rate of 24% of infants exclusively breastfed at the age of 4months after
they combined data from Lebanon (7%), Yemen (15%), Pakistan (16%), Jordan (32%),
and Iran (48%). In a study by Ong et al in Singapore 20% of working mothers
exclusively breastfed for up to 6 months of life(Ong, Yap, Li, & Choo, 2018)
University of Ghana http://ugspace.ug.edu.gh
12
In Ethiopia, a study conducted to assess factors associated with exclusive breastfeeding
practices in Debre Berhan District by Asfaw, Argaw, & Kefene, (2015) reported a
prevalence 68.6 % mothers who exclusively breastfed their babies. In another study in
Ethiopia, 188 (74%) of the children were fed breast milk exclusively for the first 6
months of life (Gizaw, Woldu, & Bitew, 2017).
In Ghana, periodic national surveys report the practice of exclusive breastfeeding (EBF)
in the general population to be over 50 %. However a study conducted by Dun-Dery &
Laar, (2016) among 389 professional working mothers revealed a low rate of EBF at
six months of 10.3%.
2.4 Benefits of Exclusive Breastfeeding
Breast milk promotes healthy growth and development of infants as it promotes sensory
and cognitive development (Kramer et al., 2008; León-Cava, Ross, Lutter, & Martin,
2002). It protects and reduces the risk of certain infectious diseases such as otitis media,
diarrhoeal diseases, pneumonias or lower respiratory tract infections and meningitis as
well as chronic disease such as asthma and diabetes(Allen & Hector, 2005; Bachrach,
Schwarz, & Bachrach, 2003). Breastfed infants have a lower risks of developing atopic
diseases such as asthma(Greer, Sicherer, & Burks, 2008). Breastfed infants have a
reduced risk of sudden death syndrome, Hodgkin’s lymphoma and leukaemia (Allen &
Hector, 2005).
University of Ghana http://ugspace.ug.edu.gh
13
Breast milk does this by building the babies immune system thereby helping to fight
against diseases. Breast feeding promotes gastrointestinal development. Breast fed
infants have a lower risk of obesity compared to formula fed infant.
Breastfeeding delays ovulation which has benefits such as lactation amenorrhoea and
the prevention of certain diseases such as breast, ovarian and endometrial
cancers(WHO, 2002). Breast feeding also promotes the bond between the mother and
the baby. Breastfeeding, especially immediately after delivery helps in the involution
of the uterus and helps to prevent postpartum haemorrhage(Negishi et al., 1999). In the
long term breastfeeding helps to shed off the excessive weight gained by most women
during pregnancy which is a desirable effect in most cases.
Socioeconomic benefits of exclusive breastfeeding includes the fact it is freely
produced by the body so the mother would not have to spend money on baby formula
which is quite expensive (UNICEF, 2003). The child is healthier and less prone to
sicknesses thereby reducing the cost of drugs and hospitalization. According to
UNICEF in 2003, breastmilk substitutes are diluted in an excessive amount of water or
if the water is impure leaves the child susceptible to growth deficiency or illness.
2.5 Determinants of Exclusive Breastfeeding
2.5.1 Socio-demographic factors associated with EBF
Age
Gizaw, Woldu, & Bitew, (2017) conducted community based cross-sectional study to
assess EBF of children aged between 6 and 24 months during the first 6 months of life
and reported that exclusive breastfeeding was significantly associated with mothers
aged above 35 years. Age was also reported to be statistically associated with EBF in
University of Ghana http://ugspace.ug.edu.gh
14
another study conducted to assess factors associated with exclusive breastfeeding
practices in Debre Berhan District, Central Ethiopia. The odds of mothers aged 25 to
35 years to practice EBF was found to be nearly 9 times more than mothers whose ages
were less than 25 years (Asfaw et al., 2015).
Marital status
Adugna, Tadele, Reta, & Berhan, (2017) in a study to assess prevalence and
determinants of EBF practice among infants less than six months age in Hawassa city,
Ethiopia reported that married mothers practiced EBF more likely than single mothers.
Educational status
Some studies have found positive significant association between maternal educational
status and exclusive breastfeeding. They reported increased odds of EBF among
mothers with higher education(Dashti, Scott, Edwards, & Al-sughayer, 2010; Dorgham
& Hafez, 2018). Other studies have reported that mothers with lower educational status
have had significantly higher odds of EBF (Amin, 2014; Batal, Boulghourjian,
Abdallah, & Afifi, 2006; Radwan, 2013). Some other studies assessed association
between educational status of the mothers and EBF but found no association(Adugna
et al., 2017; Al-Kohji, Said,& Selim, 2012; Gizaw et al., 2017; Shifraw, Worku, &
Berhane, 2015; Tewabe et al., 2017)
Income
A facility based cross-sectional study with internal comparison was conducted among
mothers attending immunization sessions in all public health centres in Addis Ababa,
Ethiopia, This study revealed that mothers with lower monthly income were more
likely to exclusively breastfeed than their counterparts who earned more(Shifraw et al.,
2015). Another study which was a community-based cross-sectional study was
conducted among local health extension workers of each Kebele with total of 423
University of Ghana http://ugspace.ug.edu.gh
15
mothers also indicated that low income mothers had significantly three times the odds
of breastfeeding their children compared those who earned more(Tewabe et al., 2017).
Number of children
Three different studies in Egypt (Mohamed, El, & Labib, 2016), Lebanon, (Batal et al.,
2006)and Saudi Arabia(Amin, 2014) have found significant association between
number of children born by mothers and EBF. Two of these studies reported significant
reduction in odds of exclusive breastfeeding among multiparous women(Amin, 2014;
Mohamed et al., 2016). Batal M, Boulghourjian, Abdallah, & Afifi, (2006) reported
that increased number of children significantly increased the odds of EBF.
2.5.2 Organizational factors associated with EBF
Work hours
It is a known fact that about 98% of mothers initiate Breast feeding within the first
hours of life but at 6 months the number of mothers still exclusively breastfeeding
drops significantly as low as 2.8% in a Kinshasa study(Babakazo, Donnen, Akilimali,
Ali, & Okitolonda, 2015). This goes to show that very few women in Sub-Saharan
Africa exclusively breast feed for up to 6 months even though the initiation rate is high.
One reason for discontinuing breastfeeding was due to the problems encountered during
the first days after childbirth i.e. problems with lack of breast milk production, improper
positioning of mother and baby, the frustration that the baby couldn’t be fed enough.
This could explain the high rate of exclusive breastfeeding discontinuation during the
first month of life. Another factor in discontinuation of exclusive breastfeeding during
the fourth month was probably due to the resumption of income-generating activities
(Babakazo et al., 2015). As such postnatal breastfeeding support in a form of workplace
support is needed to aid mothers to surmount breastfeeding challenges
University of Ghana http://ugspace.ug.edu.gh
16
The contribution of the mother’s employment on exclusive breastfeeding depends on
the job flexibility. It has been noted that full- time workers stop breastfeeding earlier
than unemployed mothers. However, it is good to note that the exclusive breastfeeding
practice of self-employed mothers did not vary significantly from unemployed mothers
(Babakazo et al., 2015).
2.4.3 Behavioural Factors
Knowledge and Practice of Exclusive Breast Feeding
In a study by Tadele et al. carried out in Ethiopia, up to 93.6% of mothers had
knowledge on what exclusive breast feeding was and 59.3% thought breast milk alone
was enough for the child for up to 6 months of life even though 89.5% did practice
exclusive breastfeeding for up to 6 months of life mostly due to recommendations and
enforcement by health workers (Tadele, Habta, Akmel, & Deges, 2016).
In a study by Nkrumah done in the Effutu Municipal of Ghana it showed that
breastfeeding initiation is high and women in the informal sector are 8 times more
likely to practice exclusive breastfeeding than their counterparts in the formal
sector(Nkrumah, 2017).
A prospective study conducted in Kinshasa, Democratic Republic of the Congo to
determine factors that significantly predict discontinuing exclusive breast feeding
revealed that mothers with low level of breastfeeding knowledge had 52% increase
in their hazard of discontinuing breastfeeding compared to mothers with high level of
knowledge on breastfeeding (Babakazo et al., 2015)
University of Ghana http://ugspace.ug.edu.gh
17
Other studies in Egypt, Saudi Arabia, and North East of Iran have found associations
between mothers knowledge on breastfeeding and EBF (Alzaheb, 2017; El Shafei &
Labib JR, 2014; Vafaee , Khabazkhoob, Moradi,& Najafpoor ,2010).
2.6 Exclusive Breastfeeding among Women in the Formal Sector
In a study by Dun-Dery et al., it was noted that awareness of exclusive breastfeeding
(EBF) amongst mothers in the formal sector is universal about 99% with the actual
practice of EBF as low as 10.3% (Dun-Dery & Laar, 2016). This same study indicated
that lack of commitment, limited workplace support and the unavailability of work
place breastfeeding facilities, lack of breastfeeding breaks as some of the barriers to the
continual practice of exclusive breastfeeding among professional working mothers
(Dun-Dery & Laar, 2016).
2.7 The Breastfeeding Room Policy
The exclusive breastfeeding room policy stems from the International Labour
Organization to support working mothers have concessions at work when they are
breastfeeding. In the ILO Convention number 183 article 10: “A woman shall be
provided with the right to one or more daily breaks or a daily reduction of hours of
work to breastfeed her child”.
Secondly, “the period during which nursing breaks or the reduction of daily hours of
work are allowed, their number, the duration of nursing breaks and the procedures for
the reduction of daily hours of work shall be determined by national law and practice.
These breaks or the reduction of daily hours of work shall be counted as working time
and remunerated accordingly” (ILO, 2017).
University of Ghana http://ugspace.ug.edu.gh
18
Where practicable and with the agreement of the employer and the woman concerned,
it should be possible to combine the time allotted for daily nursing breaks to allow a
reduction of hours of work at the beginning or at the end of the working day.”
ILO Recommendation, 2000 (No. 191) Paragraph 8 (ILO, 2017)
“Where practicable, provision should be made for the establishment of facilities for
nursing under adequate hygienic conditions at or near the workplace.”
ILO Recommendation, 2000 (No. 191) Paragraph 9 (ILO, 2017)
The Ghana Labour Act 651 entitles a breastfeeding mother of at least one hour during
her normal working period to nurse her baby. The one hour is within her normal
working period and should be fully paid for (Centres & Agencies, 2003).
A study done by Aryeetey and Goh showed that the median age in Ghana for
breastfeeding for working mothers is 3 months and that the proportion of exclusively
breastfed (EBF) infants declines rapidly after 3 months (Aryeetey & Goh, 2013). This
decline in EBF coincides with the period most mothers return to work. As such there is
a need for the implementation of the breastfeeding room policy as most maternity leave
end before the stipulated time for exclusive breastfeeding which is 6 months as such
policies have to be put in place to ensure continual exclusive breastfeeding of the baby
even whilst the mother is at work.
2.8 Benefits of the Breastfeeding Room
A study done at the Los Angeles Department of Power and Water, which provides a
comprehensive breastfeeding programme to support workers, including on-site
lactation rooms and flexible scheduling showed that a few years after the programme
University of Ghana http://ugspace.ug.edu.gh
19
was introduced, health-care claims were 35 per cent lower, 33 per cent of new mothers
returned to work sooner than anticipated, absenteeism rates were 27 per cent lower
among both men and women, and 67 per cent of all employees said they planned to stay
with the company in the long run (“Breastfeeding in the workplace: Good for the
mother, child, business and society,” n.d.).
2.9 Conclusion
In summary, prevalence of exclusive breastfeeding have varied across different
geographical locations of the world. Particularly, among formal sector workers, these
have been influenced by several factors ranging from those that have to do with the
individual (socio-demographic, perceptions and knowledge) to organisational/
workplace factors. The ILO has put in place measures to increase the prevalence of
EBF amongst women in the formal sector with the passing of the maternity protection
convention of which the implementation of lactation rooms at workplaces is required.
The study was guided by this literature and underpinned by the health belief model.
University of Ghana http://ugspace.ug.edu.gh
20
CHAPTER THREE
METHODOLOGY
3.1 Introduction
This chapter discusses the research design, target and study population, sampling
technique and calculation of sample size, types and sources of data, research instrument,
administering of research instrument, data handling and ethical considerations.
3.2 Study Design
The study was an analytical cross-sectional study by design and employed quantitative
methods to give an insight into Exclusive Breastfeeding practices among women in the
formal sector and the implication for the lactational room policy. The study was carried
out on nursing mothers who presented to the immunization clinic of some selected
hospitals in the Greater Accra region.
3.3 Study Sites
The Greater Accra Region is the regional and administrative capital of Ghana and
contains the main and largest metropolitan areas i.e. Accra and Tema which are the
countries major industrial and administrative areas, The region is the smallest of the 10
administrative regions with a land surface area of 3,245 square kilometres which is 1.4
per cent of the total land area of Ghana. It is also the second most populated region,
after the Ashanti Region, with a population of 4,010,054 in 2010, accounting for 15.4
per cent of Ghana’s total population.
University of Ghana http://ugspace.ug.edu.gh
21
The administrative areas within the region are as follows: Accra Metropolitan Area
(AMA) Accra, Tema Municipal Area Tema, Ga East District, Ga West District,
Dangme West District, Dodowa and Dangme East District, Ada-Foah. Since the region
is the centre of Ghana’s politico administrative and industrial hub, the region has a
higher concentration of professional and technical workers (10.8%) compared to the
national figure of 6.5 percent (GOVERNMENT OF GHANA OFFICE PORTAL, n.d.).
The study locations were in the two major industrial and commercial areas in the region
namely; Tema and Accra. The study was done in 2 public Hospitals and 2 private
hospitals with the public ones being Ghana Police Hospital, The Greater Accra
Regional Hospital, and the private ones being Port Clinic Tema and Narh Bita Hospital.
The above named private hospitals were chosen on the basis that the serve a large
population of professional or formal workers based on the fact that both have contracts
to treat and serve the staff of a number of companies in the Tema district.
3.4 Study Population
The study population was all nursing mothers who attended postnatal clinic in the above
mentioned hospitals and who work in the formal sector.
3.5 Sampling
3.5.1 Sample Size Determination
In a similar study in Ghana by Dun-Dery and Laar , 69% of professional working
breastfeeding mothers did not receive work place breastfeeding support (Dun-Dery &
University of Ghana http://ugspace.ug.edu.gh
22
Laar, 2016). Using 69% as the sample proportion, the sample size of this current study
was computed using Cochran’s formula (1965) as follows: Where
n= Sample size
z = Confidence interval at 95% which is 1.96
p = estimated proportion of the outcome of interest
d = Maximum error allowed
For the purposes of the study, the following assumptions were made in calculating the
sample size:
95% confidence level (standard value 1.96), and
Maximum margin of error of 5%
Substituting into the formula, the sample size was computed as follows:
n = (z2pq)/d2
Thus, sample size n = 1.96² × 0.69 (1-0.69)
0.05²
n = 329 approximately 330
A 10% non-response rate will be applied. The total sample will therefore be 365.
3.6 Sampling Technique
The calculated sample size was divided into the selected facilities by using
proportionate to size sampling (PSS). Information on total number of mothers who
attended postnatal care at the selected facilities the previous year was sought from the
University of Ghana http://ugspace.ug.edu.gh
23
facilities. Also information on average daily attendance to the facilities’ immunization
centres was obtained from the various facilities. Average daily attendance was 70, 50,
45 and 30 for the Greater Accra Regional Hospital, Police Hospital, Narh-Bita Hospital,
Port Medical Centre respectively. This was used as basis for the PSS to arrive at
facility-specific sample sizes of 130, 94, 84, 56 for Greater Accra Regional Hospital,
Police Hospital, Narh-Bita Hospital, Port Medical Centre respectively. These facility-
specific samples were further divided by the 4 clinic days for data collection for each
facility to arrive at daily targets. On each day, all consecutive mothers who met the
inclusion criteria were recruited into the study until the daily targets were met. On
clinic days mothers typically queued up for services early in the morning. Just before
the clinic began, mothers present were approached with to find out whether or not they
were formal sector workers per the study definition of formal sector workers and the
other inclusion citeria. The study was explained to those who met the criteria, only
mothers who gave informed consent were recruited. This was done on one clinical day
per week until the quota for the facility was met. For the facilities that had more than
one clinical day per week, one of the days was randomly selected weekly. Participants
were recruited simultaneously in all four facilities to achieve the overall sample size of
365. However a total of 359 formal sector working mothers participated in the study.
3.7 Inclusion Criteria
All nursing mothers who attended the immunization clinic who were working in the
formal sector. Dun Dery and Laar in their study defined the formal sector as all jobs
with usual hours (8 am to 5 pm) who earn regular wages, and are on a recognized
University of Ghana http://ugspace.ug.edu.gh
24
income source, on which income taxes is paid (Dun-Dery & Laar, 2016). This was
established through interaction with the mothers.
3.8 Exclusion Criteria
Nursing mothers in the formal sector who attended the postnatal clinic but did not
consent to the interview. Mothers with twins or multiple babies as well as mothers with
babies with special needs were excluded because according to the Ghana Labour Act
these category of nursing mothers are entitled to up to 2 weeks extra on the stipulated
maternity leave or as per the medical practitioners assessment and discretion (Centres
& Agencies, 2003).
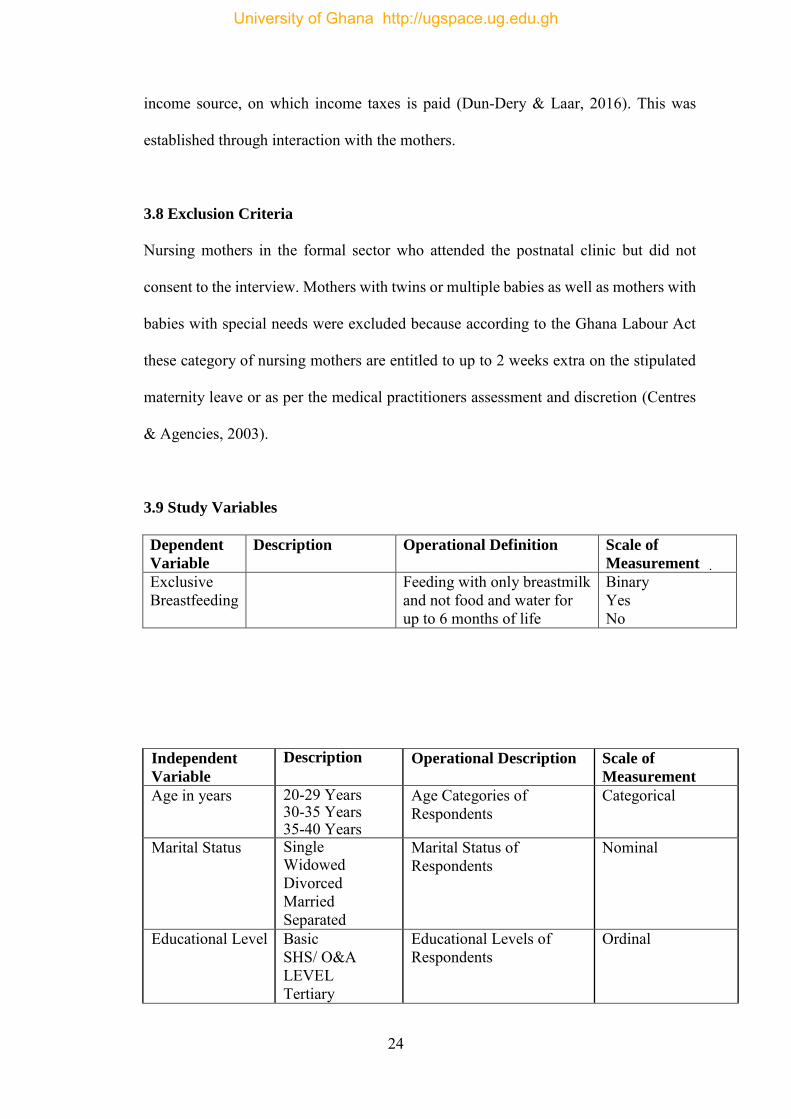
3.9 Study Variables
Dependent
Variable
Description Operational Definition Scale of
Measurement
Exclusive Breastfeeding
Feeding with only breastmilk and not food and water for up to 6 months of life
Binary Yes No
Independent
Variable
Description Operational Description Scale of
Measurement
Age in years 20-29 Years 30-35 Years 35-40 Years
Age Categories of Respondents
Categorical
Marital Status Single Widowed Divorced Married Separated
Marital Status of Respondents
Nominal
Educational Level Basic SHS/ O&A LEVEL Tertiary
Educational Levels of Respondents
Ordinal
University of Ghana http://ugspace.ug.edu.gh
25
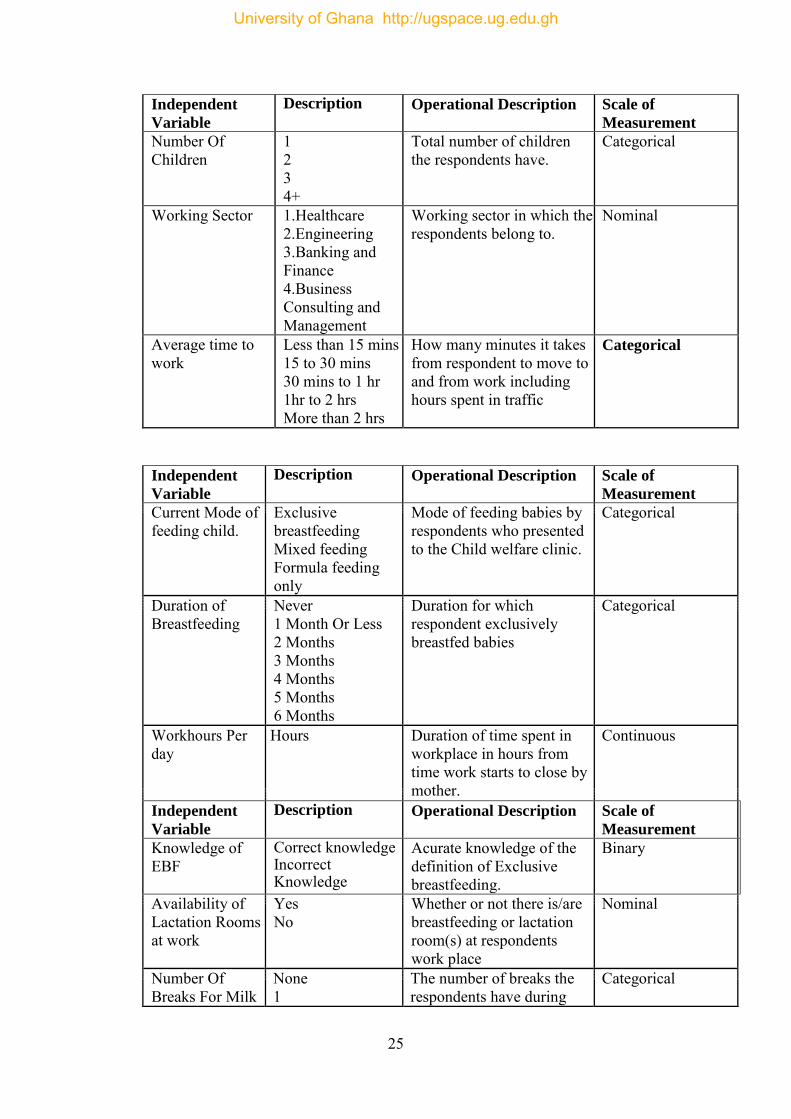
Independent
Variable
Description Operational Description Scale of
Measurement
Number Of Children
1 2 3 4+
Total number of children the respondents have.
Categorical
Working Sector 1.Healthcare 2.Engineering 3.Banking and Finance 4.Business Consulting and Management
Working sector in which the respondents belong to.
Nominal
Average time to work
Less than 15 mins 15 to 30 mins 30 mins to 1 hr 1hr to 2 hrs More than 2 hrs
How many minutes it takes from respondent to move to and from work including hours spent in traffic
Categorical
Independent
Variable
Description Operational Description Scale of
Measurement
Current Mode of feeding child.
Exclusive breastfeeding Mixed feeding Formula feeding only
Mode of feeding babies by respondents who presented to the Child welfare clinic.
Categorical
Duration of Breastfeeding
Never 1 Month Or Less 2 Months 3 Months 4 Months 5 Months 6 Months
Duration for which respondent exclusively breastfed babies
Categorical
Workhours Per day
Hours Duration of time spent in workplace in hours from time work starts to close by mother.
Continuous
Independent
Variable
Description Operational Description Scale of
Measurement
Knowledge of EBF
Correct knowledge Incorrect Knowledge
Acurate knowledge of the definition of Exclusive breastfeeding.
Binary
Availability of Lactation Rooms at work
Yes No
Whether or not there is/are breastfeeding or lactation room(s) at respondents work place
Nominal
Number Of Breaks For Milk
None 1
The number of breaks the respondents have during
Categorical
University of Ghana http://ugspace.ug.edu.gh
26
Expression during working hours excluding lunch breaks
2 or more working hours for milk expression
Number of minutes per breastfeeding break
15 min or less 15- 30 mins 30 mins or more
The duration of breaks for milk expression during working hours that respondents have at their workplace.
Categorical
3.10 Data Collection Techniques and Tools
Data was collected with the aid of a semi-structured questionnaire which was adapted
from CDC questionnaire on breastfeeding. The questionnaire was self-administered as
well as face to face interview depending on the literacy level of the mothers. Assistance
to filling the questionnaire was provided by the research assistants.
3.10.1 Pretesting
The developed questionnaire was pretested at the Tema General Hospital. This facility
was used because it shares similar characteristics with the hospitals to be used for the
research. Tema General Hospital is a Sub-Metropolitan hospital based in Tema which
also serves a wide range of patients in the formal sector due to its location in Tema. The
pretesting gave a fair idea on what needed to change on the questionnaire. The aim was
to test for validity and reliability of the instruments. Errors in the questionnaire were
corrected before the final data collection.
3.10.2 Quality Control
To ensure quality control, I trained the data collectors to understand the questions and
to ask the questions appropriately. All questionnaires submitted by data collectors were
University of Ghana http://ugspace.ug.edu.gh
27
previewed to ensure completeness and consistency of responses. The data was double
entered to ensure consistency and validity.
3.11 Data Analysis
Data were analysed using the Stata software version 15. Descriptive analysis was
employed that generated frequencies and percentages for categorical variables. Chi
square analysis and logistic regression was used in the study to compare the
independent variables with exclusive breastfeeding which was the dependent variable.
A significance level of 5% was used for all tests. Results have been presented in tables
and figures.
3.12 Ethical Consideration
Approval of the study was obtained from Ghana Health Service Ethics Review
Committee (GHS-ERC). Permission letters were sent to the various hospitals involved
in the study and granted before the study was carried out.
3.13 Participant Consent
Consent forms were issued out to every prospective participant for prior approval
before the study was carried out. Approval was in the form of thumb print or signatures
and with the background of women in the formal sector there was assumption that most
of them can read and write those unable understand the issues involved in the
questionnaire explanation was provided by the data collectors.
University of Ghana http://ugspace.ug.edu.gh
28
3.14 Privacy and Confidentiality
Respondent privacy was assured as the questionnaires did not require them to provide
their names, numbers were used. Also as part of the consent form they were assured of
privacy and also given the assurance that the information given is for academic
purposes only.
3.15 Risk and Benefit
The purpose of this study is to inform a policy on a breastfeeding room and as such the
risk element was minimal. The participants of the study were assured that they are only
adding to academic knowledge and also getting involved in a policy that when instituted
would benefit future generations and the country as a whole.
3.16 Permission for Study
Permission to conduct the study letters were sent to the Medical Directors of the above
named hospitals. This ensured the necessary support needed to make the study
successful.
3.17 Description of Subjects Involved In the Study
In this cost-effective study, data was collected from nursing mothers who presented to
the immunization clinic.
3.18 Informed Consent Process
Individual written consent was sought from all the nursing mothers who presented to
the immunization clinic and are in the formal sector health. The nature of the data
collection process as well as the reason for carrying out the research was explained to
University of Ghana http://ugspace.ug.edu.gh
29
the participants and written consent was signed before the start of the activity. Consent
forms were approved by the ethical review committee of the Ghana Health Service.
3.19 Voluntary Consent/Withdrawal
Participation in the study was voluntary and no coercion or inducement was applied to
get subjects to participate. Moreover, those who decided not to participate were given
the right to withdraw from the study at any point without justifying or explaining to the
researcher their reason for exit. Their withdrawal did not in any way attract any sanction
or their access to health care.
3.20 Data Storage and Usage
The data collection materials in the form of questionnaires had identifiers which were
anonymous codes. There were no personal identifiers to link subjects’ personal
information to the data. The answered questionnaires were collated with limited access
by only the principal investigator. Even though the study had minimal risk and data are
not sensitive in nature, no personal identifiers were included in the electronic database.
All data that was collected was strictly used for the purpose of this study and nothing
more. The original dataset is being kept by the principal investigator and will be
destroyed after 5 years.
3.21 Compensation
No payments was made to survey respondents.
3.22 Proposal and Funding Information
This project was self-funded by the researcher.
University of Ghana http://ugspace.ug.edu.gh
30
CHAPTER FOUR
RESULTS
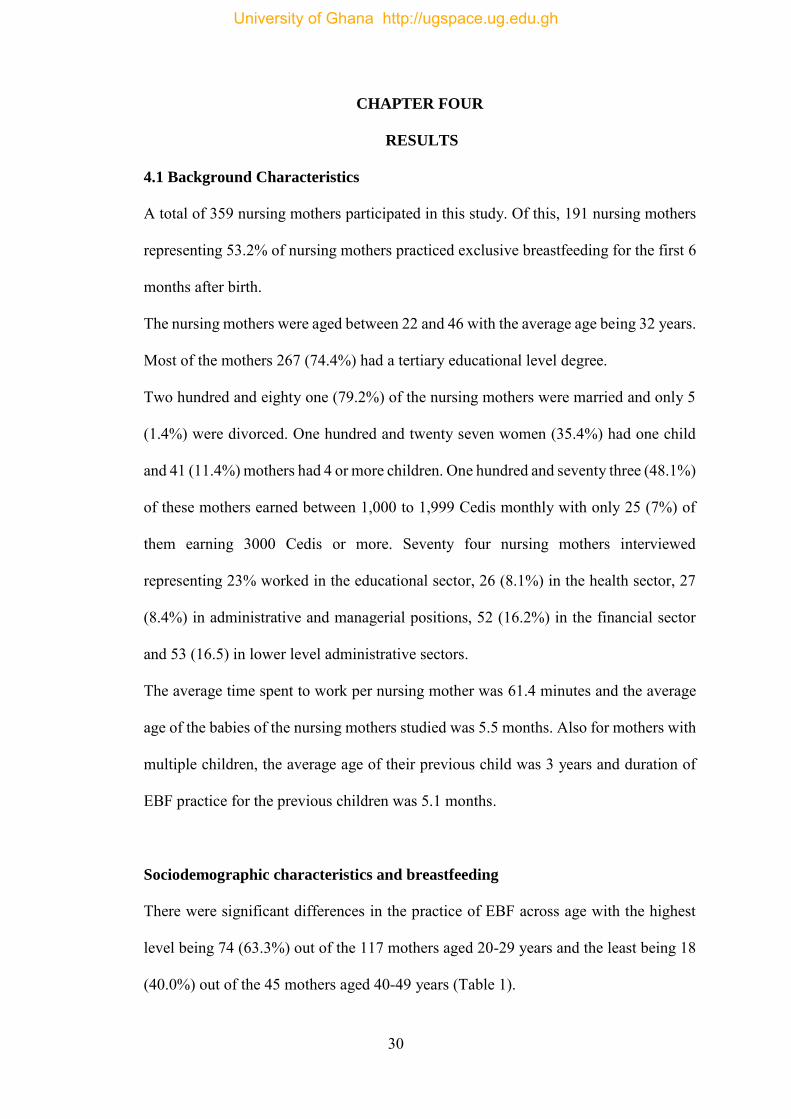
4.1 Background Characteristics
A total of 359 nursing mothers participated in this study. Of this, 191 nursing mothers
representing 53.2% of nursing mothers practiced exclusive breastfeeding for the first 6
months after birth.
The nursing mothers were aged between 22 and 46 with the average age being 32 years.
Most of the mothers 267 (74.4%) had a tertiary educational level degree.
Two hundred and eighty one (79.2%) of the nursing mothers were married and only 5
(1.4%) were divorced. One hundred and twenty seven women (35.4%) had one child
and 41 (11.4%) mothers had 4 or more children. One hundred and seventy three (48.1%)
of these mothers earned between 1,000 to 1,999 Cedis monthly with only 25 (7%) of
them earning 3000 Cedis or more. Seventy four nursing mothers interviewed
representing 23% worked in the educational sector, 26 (8.1%) in the health sector, 27
(8.4%) in administrative and managerial positions, 52 (16.2%) in the financial sector
and 53 (16.5) in lower level administrative sectors.
The average time spent to work per nursing mother was 61.4 minutes and the average
age of the babies of the nursing mothers studied was 5.5 months. Also for mothers with
multiple children, the average age of their previous child was 3 years and duration of
EBF practice for the previous children was 5.1 months.
Sociodemographic characteristics and breastfeeding
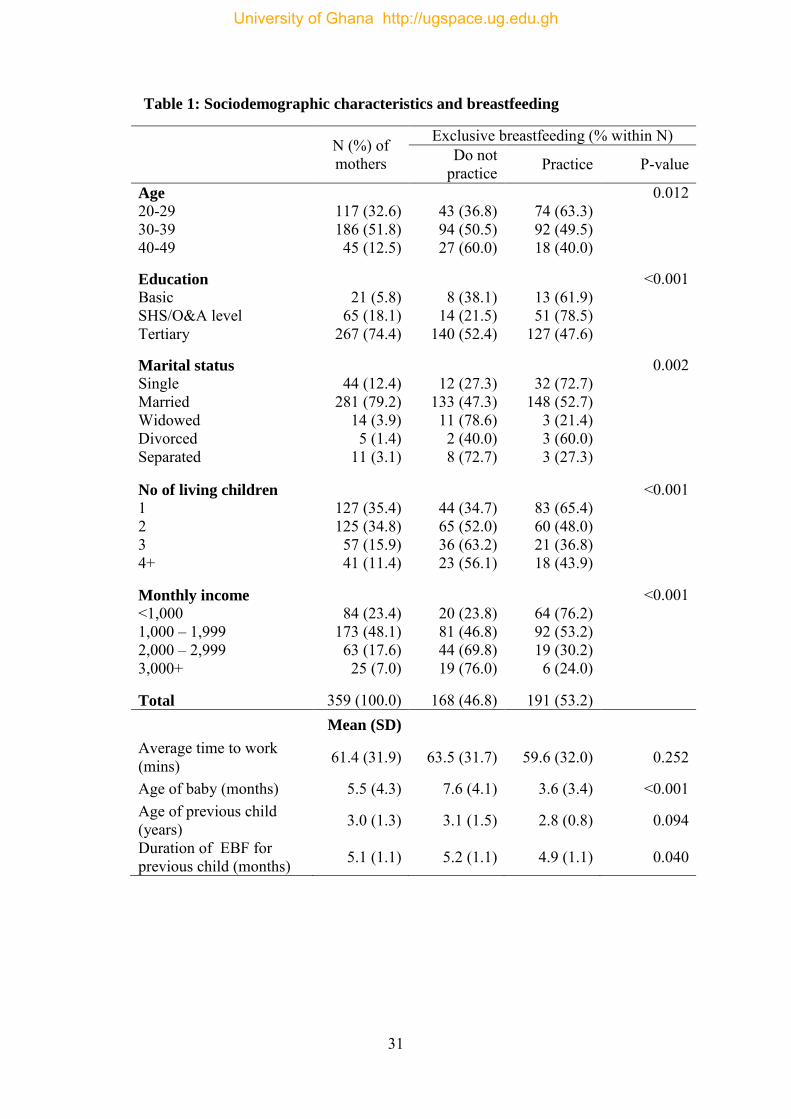
There were significant differences in the practice of EBF across age with the highest
level being 74 (63.3%) out of the 117 mothers aged 20-29 years and the least being 18
(40.0%) out of the 45 mothers aged 40-49 years (Table 1).
University of Ghana http://ugspace.ug.edu.gh
31
Table 1: Sociodemographic characteristics and breastfeeding
N (%) of mothers
Exclusive breastfeeding (% within N) Do not
practice Practice P-value
Age
20-29 30-39 40-49
117 (32.6) 186 (51.8) 45 (12.5)
43 (36.8) 94 (50.5) 27 (60.0)
74 (63.3) 92 (49.5) 18 (40.0)
0.012
Education
Basic SHS/O&A level Tertiary
21 (5.8)
65 (18.1) 267 (74.4)
8 (38.1)
14 (21.5) 140 (52.4)
13 (61.9) 51 (78.5)
127 (47.6)
<0.001
Marital status
Single Married Widowed Divorced Separated
44 (12.4)
281 (79.2) 14 (3.9) 5 (1.4)
11 (3.1)
12 (27.3)
133 (47.3) 11 (78.6) 2 (40.0) 8 (72.7)
32 (72.7)
148 (52.7) 3 (21.4) 3 (60.0) 3 (27.3)
0.002
No of living children
1 2 3 4+
127 (35.4) 125 (34.8) 57 (15.9) 41 (11.4)
44 (34.7) 65 (52.0) 36 (63.2) 23 (56.1)
83 (65.4) 60 (48.0) 21 (36.8) 18 (43.9)
<0.001
Monthly income
<1,000 1,000 – 1,999 2,000 – 2,999 3,000+
84 (23.4)
173 (48.1) 63 (17.6) 25 (7.0)
20 (23.8) 81 (46.8) 44 (69.8) 19 (76.0)
64 (76.2) 92 (53.2) 19 (30.2) 6 (24.0)
<0.001
Total 359 (100.0) 168 (46.8) 191 (53.2) Mean (SD)
Average time to work (mins) 61.4 (31.9) 63.5 (31.7) 59.6 (32.0) 0.252
Age of baby (months) 5.5 (4.3) 7.6 (4.1) 3.6 (3.4) <0.001 Age of previous child (years) 3.0 (1.3) 3.1 (1.5) 2.8 (0.8) 0.094
Duration of EBF for previous child (months) 5.1 (1.1) 5.2 (1.1) 4.9 (1.1) 0.040
University of Ghana http://ugspace.ug.edu.gh
32
Practice of EBF was significantly lowest among the women with tertiary education,
followed by those with basic education and highest among the women whose highest
education was SHS/O&A level as shown in Table 1. There was a significant association
marital status and educational level were significantly associated practice of EBF. Of
the 44 (12%) who were single 32 (72.7%) of were practicing EBF. Also amongst the
281 who
Mothers with only one child practiced EBF the most followed by mothers with 2
children, although those with four or more children did so more than those with three
with the differences being highly significant (p<0.001). The 84 women who earned less
than 1,000 Cedis practiced EBF the most with 64 (76.2%) of them doing so compared
with their counterparts who earned much higher.
There were no significant differences in terms of average commuting time to work
between women who practiced EBF (61.4 ± 31.9 minutes) and those who didn’t (63.5
± 31.7 minutes). There were significant differences with regards to the average age of
the babies of mothers who practised EBF and those who did not, with those doing so
having much lower ages. The average age of the previous child for mothers who
practiced EBF (3.1 ± 1.5 years) was also not too different from those who did not (2.8
± 0.8 years).
Mothers who practiced EBF for the current child surprisingly had done same for a
shorter period for their previous child compared to the mothers who did not practice
EBF for the current baby but this difference was not too strong (p=0.040).
University of Ghana http://ugspace.ug.edu.gh
33
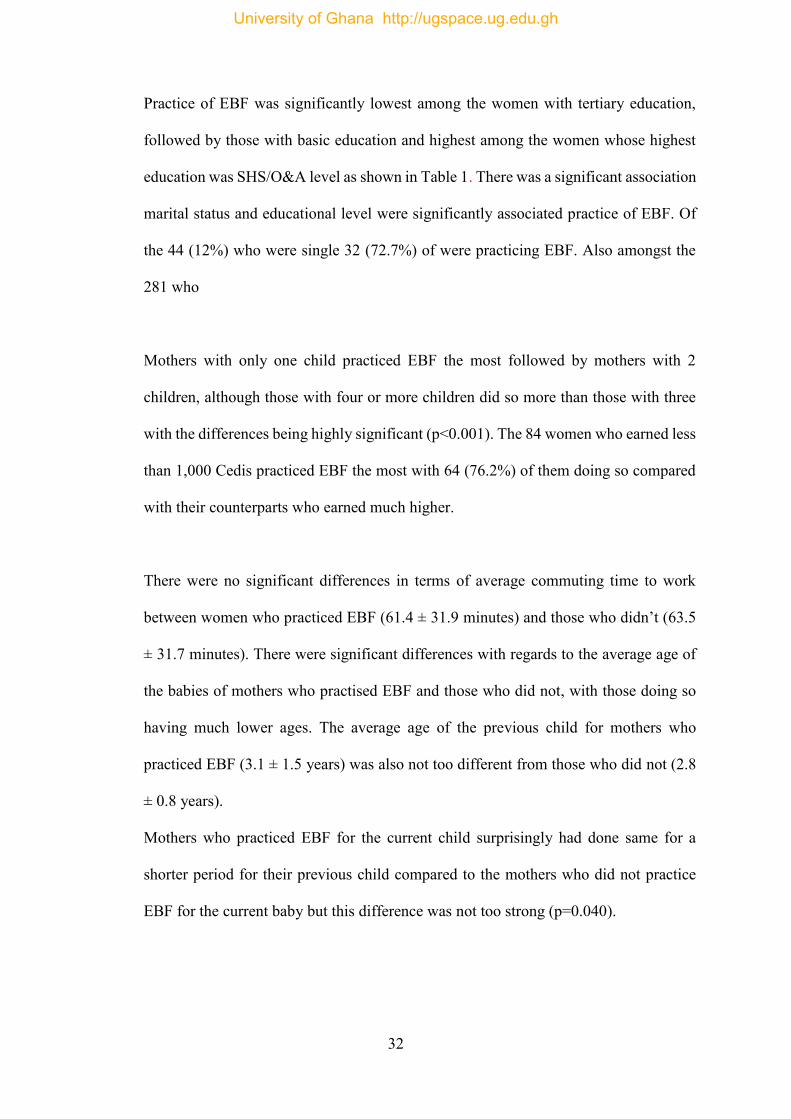
4.2 Mode of feeding
Most of the women practiced exclusive breastfeeding with 191 (53.2%) of them doing
so followed by baby formula only, infant formula only and other household foods only
as seen in Figure 3.
Figure 3 Mode of feeding
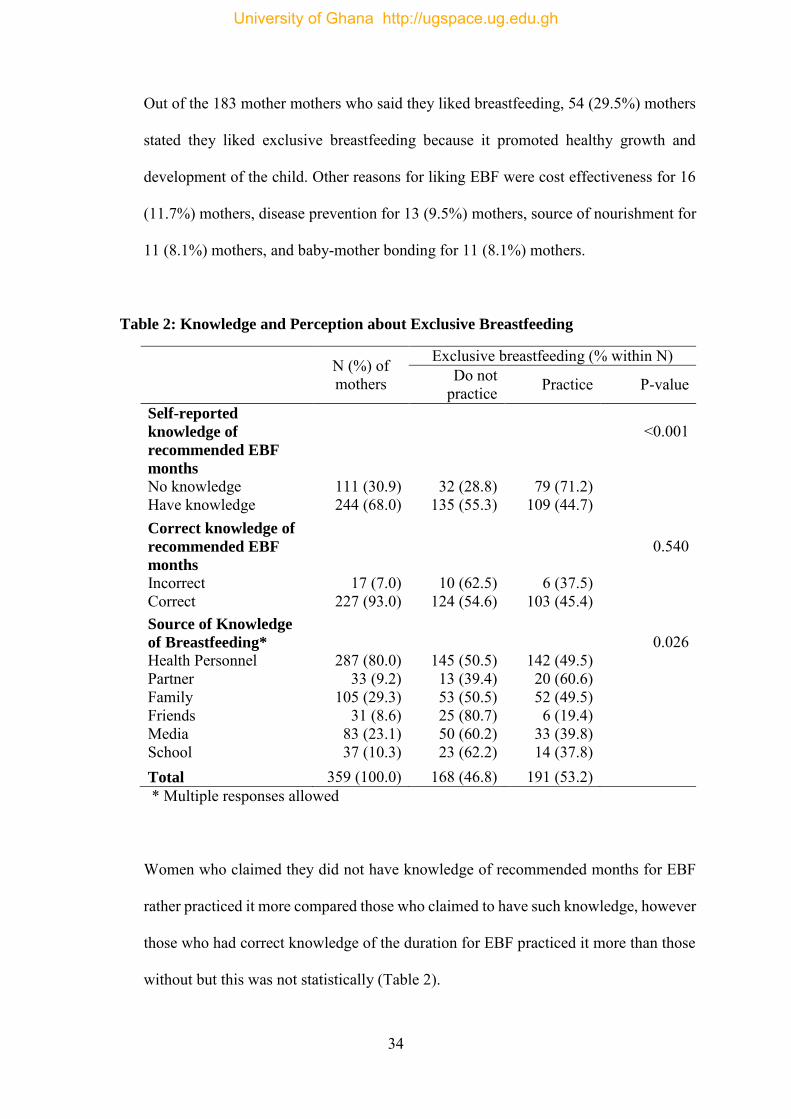
4.3 Knowledge and Perception of Exclusive Breastfeeding
Two hundred and forty four mothers (68%) said they had knowledge of the
recommended number of months for EBF whilst 227 (93.0%) out of those who said this
had accurate or correct knowledge of EBF. The majority of nursing mothers 287 (80%)
mentioned health personnel as their source of knowledge on EBF with the 31 mothers
(8.6%) receiving such information from friends as seen in out of 33 (9.2%) of mothers
who received information from partners, 20(60.6%) were practicing EBF (Table 2).
Eighty three mothers (90.2%) stated pain, discomfort and annoyance as the top most
reason why they did not like breastfeeding. Other reasons stated where the fact that
their babies could not suck well, 2 (2.2%) and that it was time consuming, 4 (4.4%).
53.2
6.410.0
3.1
0.0
10.0
20.0
30.0
40.0
50.0
60.0
Exclusivebreastfeeding
Infant formula only Baby food only Household foodonly
(%)
Mode of feeding
University of Ghana http://ugspace.ug.edu.gh
34
Out of the 183 mother mothers who said they liked breastfeeding, 54 (29.5%) mothers
stated they liked exclusive breastfeeding because it promoted healthy growth and
development of the child. Other reasons for liking EBF were cost effectiveness for 16
(11.7%) mothers, disease prevention for 13 (9.5%) mothers, source of nourishment for
11 (8.1%) mothers, and baby-mother bonding for 11 (8.1%) mothers.
Table 2: Knowledge and Perception about Exclusive Breastfeeding
N (%) of mothers
Exclusive breastfeeding (% within N) Do not
practice Practice P-value
Self-reported
knowledge of
recommended EBF
months
No knowledge Have knowledge
111 (30.9) 244 (68.0)
32 (28.8) 135 (55.3)
79 (71.2) 109 (44.7)
<0.001
Correct knowledge of
recommended EBF
months
Incorrect Correct
17 (7.0) 227 (93.0)
10 (62.5) 124 (54.6)
6 (37.5) 103 (45.4)
0.540
Source of Knowledge
of Breastfeeding*
Health Personnel Partner Family Friends Media School
287 (80.0) 33 (9.2)
105 (29.3) 31 (8.6)
83 (23.1) 37 (10.3)
145 (50.5) 13 (39.4) 53 (50.5) 25 (80.7) 50 (60.2) 23 (62.2)
142 (49.5) 20 (60.6) 52 (49.5) 6 (19.4)
33 (39.8) 14 (37.8)
0.026
Total 359 (100.0) 168 (46.8) 191 (53.2) * Multiple responses allowed
Women who claimed they did not have knowledge of recommended months for EBF
rather practiced it more compared those who claimed to have such knowledge, however
those who had correct knowledge of the duration for EBF practiced it more than those
without but this was not statistically (Table 2).
University of Ghana http://ugspace.ug.edu.gh
35
There were significant differences in the practice of EBF by the source of information
on the practice with the highest practice by mothers who received their breastfeeding
information from their partners and the least by those who got theirs from friends as
shown in Table 2.
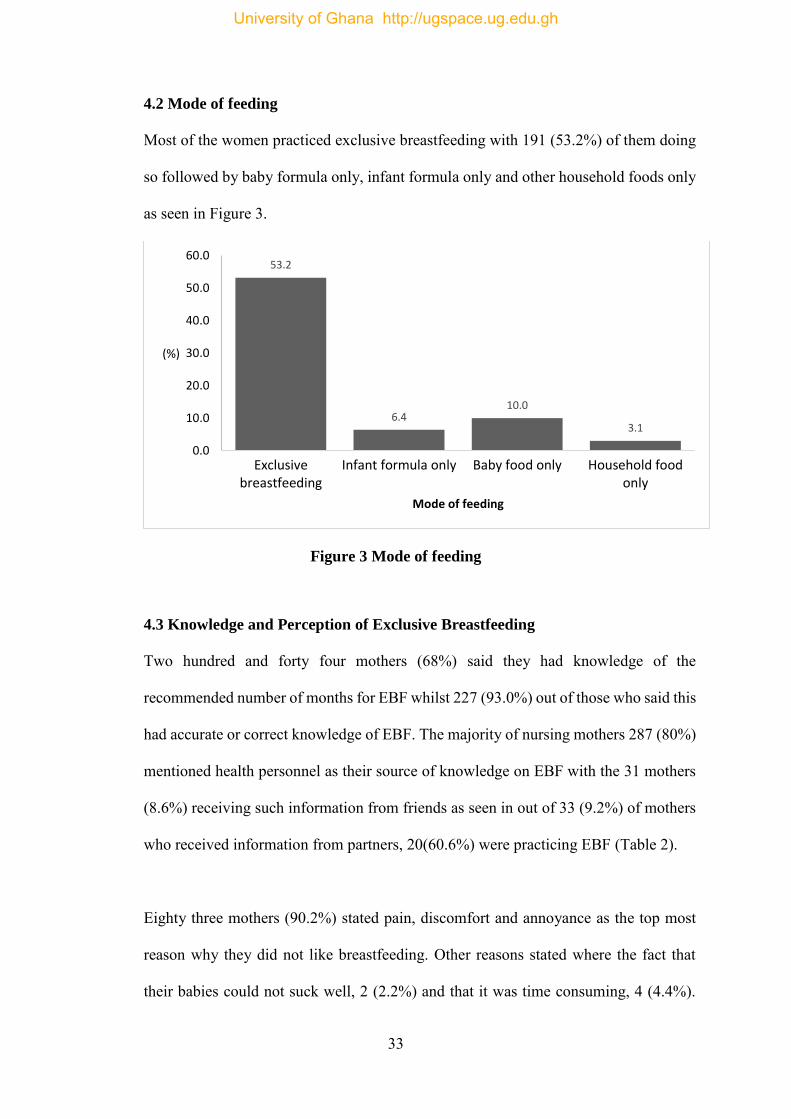
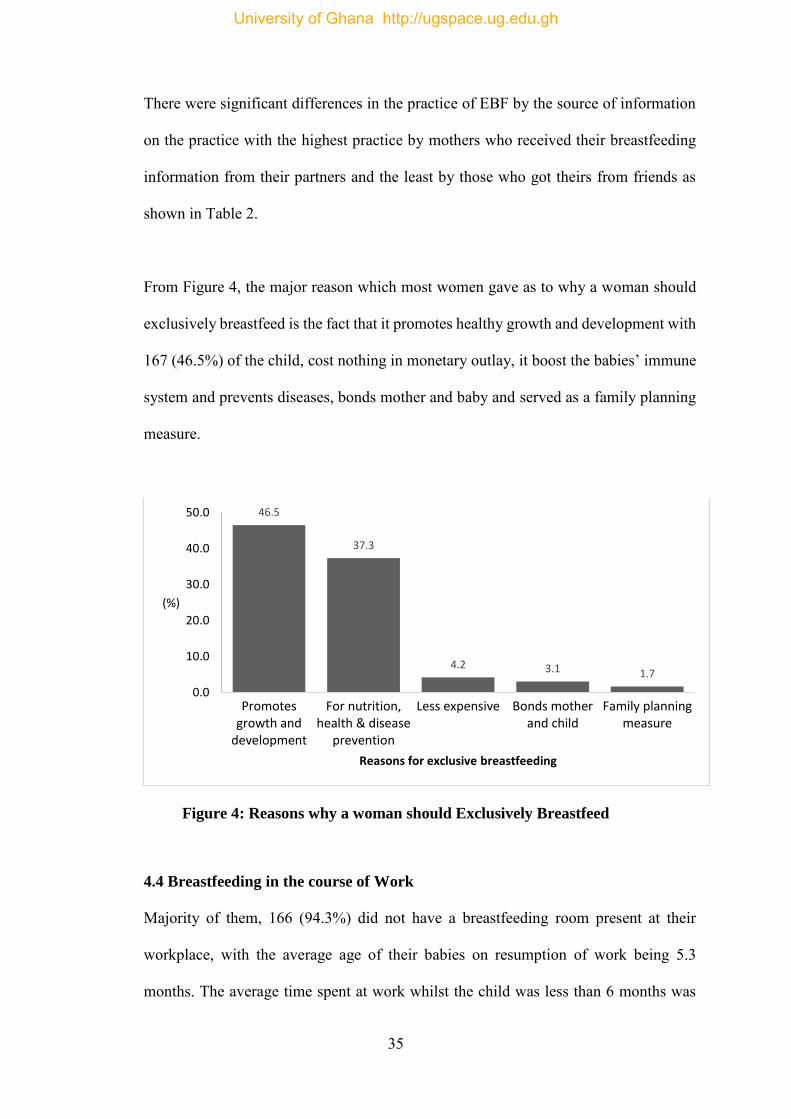
From Figure 4, the major reason which most women gave as to why a woman should
exclusively breastfeed is the fact that it promotes healthy growth and development with
167 (46.5%) of the child, cost nothing in monetary outlay, it boost the babies’ immune
system and prevents diseases, bonds mother and baby and served as a family planning
measure.
Figure 4: Reasons why a woman should Exclusively Breastfeed
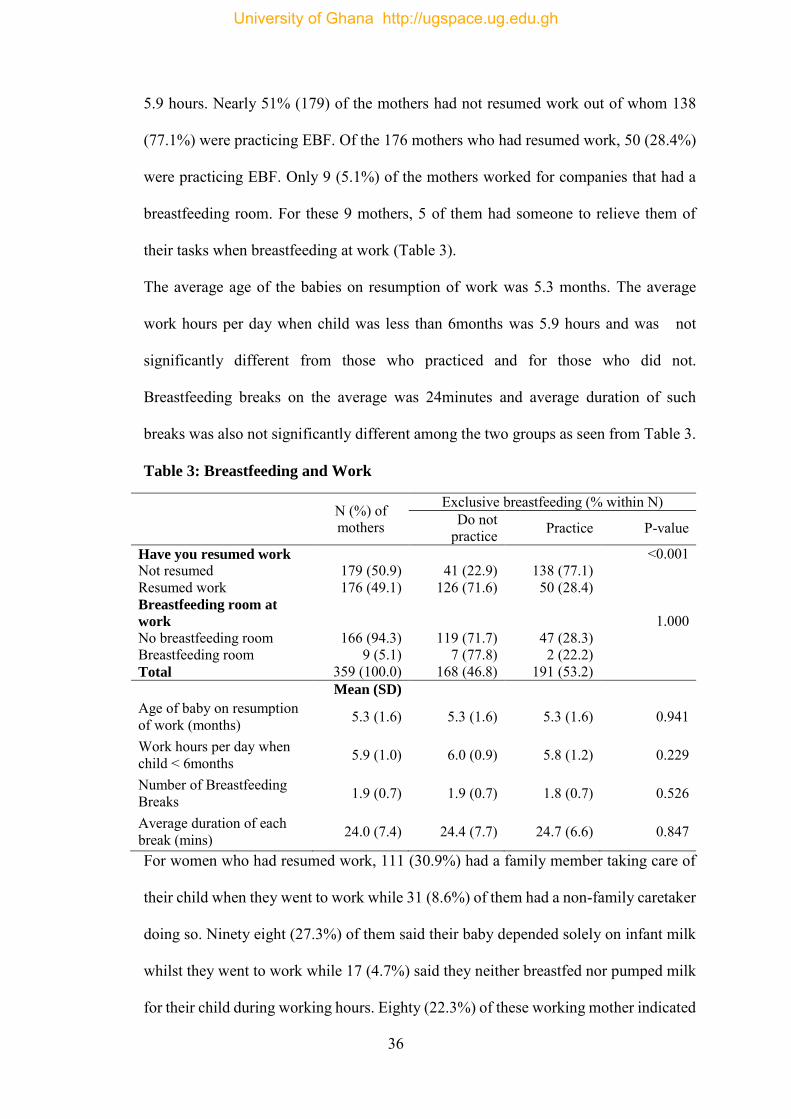
4.4 Breastfeeding in the course of Work
Majority of them, 166 (94.3%) did not have a breastfeeding room present at their
workplace, with the average age of their babies on resumption of work being 5.3
months. The average time spent at work whilst the child was less than 6 months was
46.5
37.3
4.2 3.1 1.7
0.0
10.0
20.0
30.0
40.0
50.0
Promotesgrowth and
development
For nutrition,health & disease
prevention
Less expensive Bonds motherand child
Family planningmeasure
(%)
Reasons for exclusive breastfeeding
University of Ghana http://ugspace.ug.edu.gh
36
5.9 hours. Nearly 51% (179) of the mothers had not resumed work out of whom 138
(77.1%) were practicing EBF. Of the 176 mothers who had resumed work, 50 (28.4%)
were practicing EBF. Only 9 (5.1%) of the mothers worked for companies that had a
breastfeeding room. For these 9 mothers, 5 of them had someone to relieve them of
their tasks when breastfeeding at work (Table 3).
The average age of the babies on resumption of work was 5.3 months. The average
work hours per day when child was less than 6months was 5.9 hours and was not
significantly different from those who practiced and for those who did not.
Breastfeeding breaks on the average was 24minutes and average duration of such
breaks was also not significantly different among the two groups as seen from Table 3.
Table 3: Breastfeeding and Work
N (%) of mothers
Exclusive breastfeeding (% within N) Do not
practice Practice P-value
Have you resumed work
Not resumed Resumed work
179 (50.9) 176 (49.1)
41 (22.9)
126 (71.6)
138 (77.1)
50 (28.4)
<0.001
Breastfeeding room at
work
No breastfeeding room Breastfeeding room
166 (94.3) 9 (5.1)
119 (71.7) 7 (77.8)
47 (28.3) 2 (22.2)
1.000
Total 359 (100.0) 168 (46.8) 191 (53.2) Mean (SD) Age of baby on resumption of work (months) 5.3 (1.6) 5.3 (1.6) 5.3 (1.6) 0.941
Work hours per day when child < 6months 5.9 (1.0) 6.0 (0.9) 5.8 (1.2) 0.229
Number of Breastfeeding Breaks 1.9 (0.7) 1.9 (0.7) 1.8 (0.7) 0.526
Average duration of each break (mins) 24.0 (7.4) 24.4 (7.7) 24.7 (6.6) 0.847
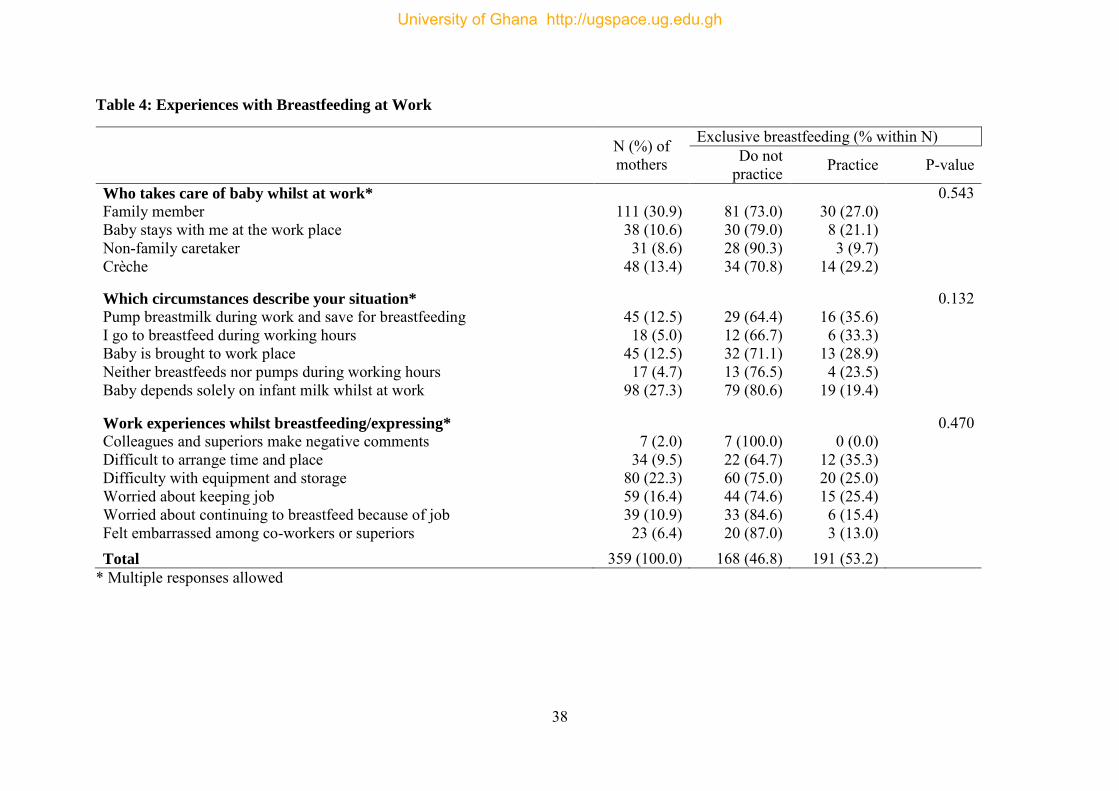
For women who had resumed work, 111 (30.9%) had a family member taking care of
their child when they went to work while 31 (8.6%) of them had a non-family caretaker
doing so. Ninety eight (27.3%) of them said their baby depended solely on infant milk
whilst they went to work while 17 (4.7%) said they neither breastfed nor pumped milk
for their child during working hours. Eighty (22.3%) of these working mother indicated
University of Ghana http://ugspace.ug.edu.gh
37
difficulties with equipment for expressing milk and its storage for their children while
at work and only 7 (2.0%) had experienced negative comments from their colleagues
and superiors regarding breastfeeding while at work.
Six of the women stated that work prevented exclusive breastfeeding, while four stated
that EBF slowed down productivity at their workplace.
Effect of work on breastfeeding choice in first 6 months
There were no significant differences (p=0.543) in the practice of EBF depending on
who took care of the babies while their mothers were at work as seen from Table 4.
EBF practice across lactation and other feeding circumstances of the children did not
also vary significantly. The mothers’ work experiences whilst breastfeeding/expressing
milk also did not significantly affect the practice of EBF as seen from Table 4.
University of Ghana http://ugspace.ug.edu.gh
38
Table 4: Experiences with Breastfeeding at Work
N (%) of mothers
Exclusive breastfeeding (% within N) Do not
practice Practice P-value
Who takes care of baby whilst at work*
Family member Baby stays with me at the work place Non-family caretaker Crèche
111 (30.9) 38 (10.6) 31 (8.6)
48 (13.4)
81 (73.0) 30 (79.0) 28 (90.3) 34 (70.8)
30 (27.0) 8 (21.1)
3 (9.7) 14 (29.2)
0.543
Which circumstances describe your situation*
Pump breastmilk during work and save for breastfeeding I go to breastfeed during working hours Baby is brought to work place Neither breastfeeds nor pumps during working hours Baby depends solely on infant milk whilst at work
45 (12.5) 18 (5.0)
45 (12.5) 17 (4.7)
98 (27.3)
29 (64.4) 12 (66.7) 32 (71.1) 13 (76.5) 79 (80.6)
16 (35.6) 6 (33.3)
13 (28.9) 4 (23.5)
19 (19.4)
0.132
Work experiences whilst breastfeeding/expressing*
Colleagues and superiors make negative comments Difficult to arrange time and place Difficulty with equipment and storage Worried about keeping job Worried about continuing to breastfeed because of job Felt embarrassed among co-workers or superiors
7 (2.0)
34 (9.5) 80 (22.3) 59 (16.4) 39 (10.9) 23 (6.4)
7 (100.0) 22 (64.7) 60 (75.0) 44 (74.6) 33 (84.6) 20 (87.0)
0 (0.0)
12 (35.3) 20 (25.0) 15 (25.4) 6 (15.4) 3 (13.0)
0.470
Total 359 (100.0) 168 (46.8) 191 (53.2) * Multiple responses allowed
University of Ghana http://ugspace.ug.edu.gh
39
4.5 Organizational Support for Breastfeeding
One hundred and fifty six (43.5%) of mothers said they had an organizational policy on
breastfeeding whilst 76 (21.2%) said they did not know if their workplace had such a
policy. Most of the mothers, 238 (66.3%) stated that their workplace offered work
schedule flexibility with 202 (56.3%) claiming their organizations allowed scheduled
breaks for nursing babies.
One hundred and eighty seven (52.1%) worked with institutions that allowed bringing
breastfed infants to work while 143 (39.8%) of mothers said their organization was
supportive for EBF and 93 (25.9%) claiming their organization was not supportive for
this.
EBF was significantly highest among women who worked for companies with a policy
on breastfeeding and lowest among those who worked for companies without such a
policy as seen from Table 5 although the details of such policies were not obtained for
analysis. It was also significantly higher among women whose work schedules were
flexible. Surprisingly, EBF was much lower for mothers who worked for organizations
that had scheduled breaks for nursing and significantly higher where women were not
allowed to bring their breastfed infants to work as seen from Table 5.
Ironically mothers who described their workplace as not supportive for EBF practiced it
the most compared to those who described their workplace as providing some level of
support with significant differences in the level of EBF across the various levels of
support as seen from the Table 5.
University of Ghana http://ugspace.ug.edu.gh
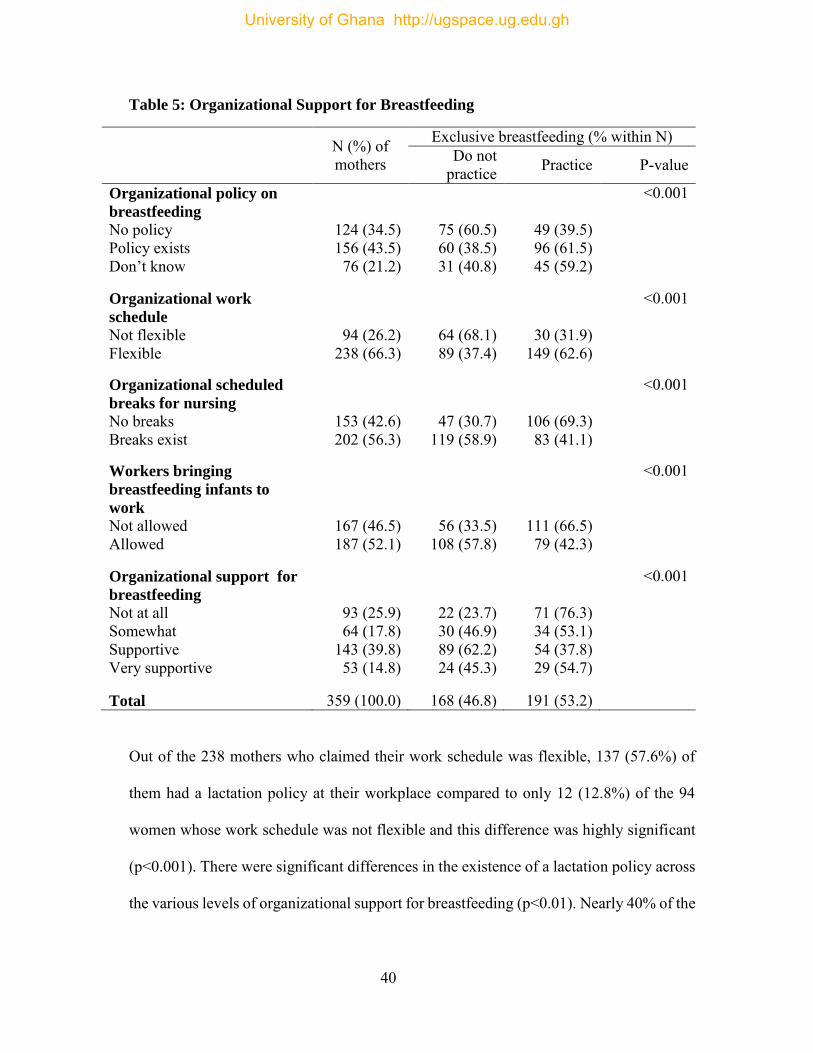
40
Table 5: Organizational Support for Breastfeeding
N (%) of mothers
Exclusive breastfeeding (% within N) Do not
practice Practice P-value
Organizational policy on
breastfeeding
No policy Policy exists Don’t know
124 (34.5) 156 (43.5)
76 (21.2)
75 (60.5) 60 (38.5) 31 (40.8)
49 (39.5) 96 (61.5) 45 (59.2)
<0.001
Organizational work
schedule
Not flexible Flexible
94 (26.2) 238 (66.3)
64 (68.1) 89 (37.4)
30 (31.9) 149 (62.6)
<0.001
Organizational scheduled
breaks for nursing
No breaks Breaks exist
153 (42.6) 202 (56.3)
47 (30.7) 119 (58.9)
106 (69.3) 83 (41.1)
<0.001
Workers bringing
breastfeeding infants to
work
Not allowed Allowed
167 (46.5) 187 (52.1)
56 (33.5) 108 (57.8)
111 (66.5) 79 (42.3)
<0.001
Organizational support for
breastfeeding
Not at all Somewhat Supportive Very supportive
93 (25.9) 64 (17.8)
143 (39.8) 53 (14.8)
22 (23.7) 30 (46.9) 89 (62.2) 24 (45.3)
71 (76.3) 34 (53.1) 54 (37.8) 29 (54.7)
<0.001
Total 359 (100.0) 168 (46.8) 191 (53.2)
Out of the 238 mothers who claimed their work schedule was flexible, 137 (57.6%) of
them had a lactation policy at their workplace compared to only 12 (12.8%) of the 94
women whose work schedule was not flexible and this difference was highly significant
(p<0.001). There were significant differences in the existence of a lactation policy across
the various levels of organizational support for breastfeeding (p<0.01). Nearly 40% of the
University of Ghana http://ugspace.ug.edu.gh
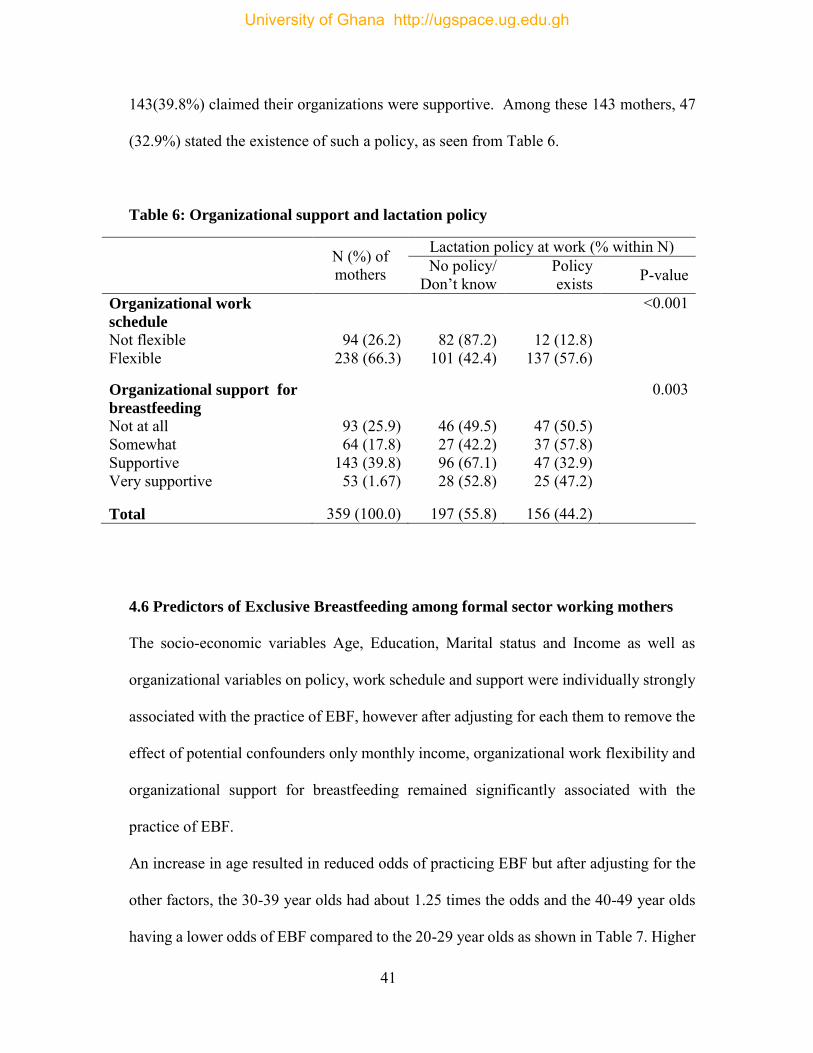
41
143(39.8%) claimed their organizations were supportive. Among these 143 mothers, 47
(32.9%) stated the existence of such a policy, as seen from Table 6.
Table 6: Organizational support and lactation policy
N (%) of mothers
Lactation policy at work (% within N) No policy/
Don’t know Policy exists P-value
Organizational work
schedule
Not flexible Flexible
94 (26.2) 238 (66.3)
82 (87.2) 101 (42.4)
12 (12.8) 137 (57.6)
<0.001
Organizational support for
breastfeeding
Not at all Somewhat Supportive Very supportive
93 (25.9) 64 (17.8)
143 (39.8) 53 (1.67)
46 (49.5) 27 (42.2) 96 (67.1) 28 (52.8)
47 (50.5) 37 (57.8) 47 (32.9) 25 (47.2)
0.003
Total 359 (100.0) 197 (55.8) 156 (44.2)
4.6 Predictors of Exclusive Breastfeeding among formal sector working mothers
The socio-economic variables Age, Education, Marital status and Income as well as
organizational variables on policy, work schedule and support were individually strongly
associated with the practice of EBF, however after adjusting for each them to remove the
effect of potential confounders only monthly income, organizational work flexibility and
organizational support for breastfeeding remained significantly associated with the
practice of EBF.
An increase in age resulted in reduced odds of practicing EBF but after adjusting for the
other factors, the 30-39 year olds had about 1.25 times the odds and the 40-49 year olds
having a lower odds of EBF compared to the 20-29 year olds as shown in Table 7. Higher
University of Ghana http://ugspace.ug.edu.gh
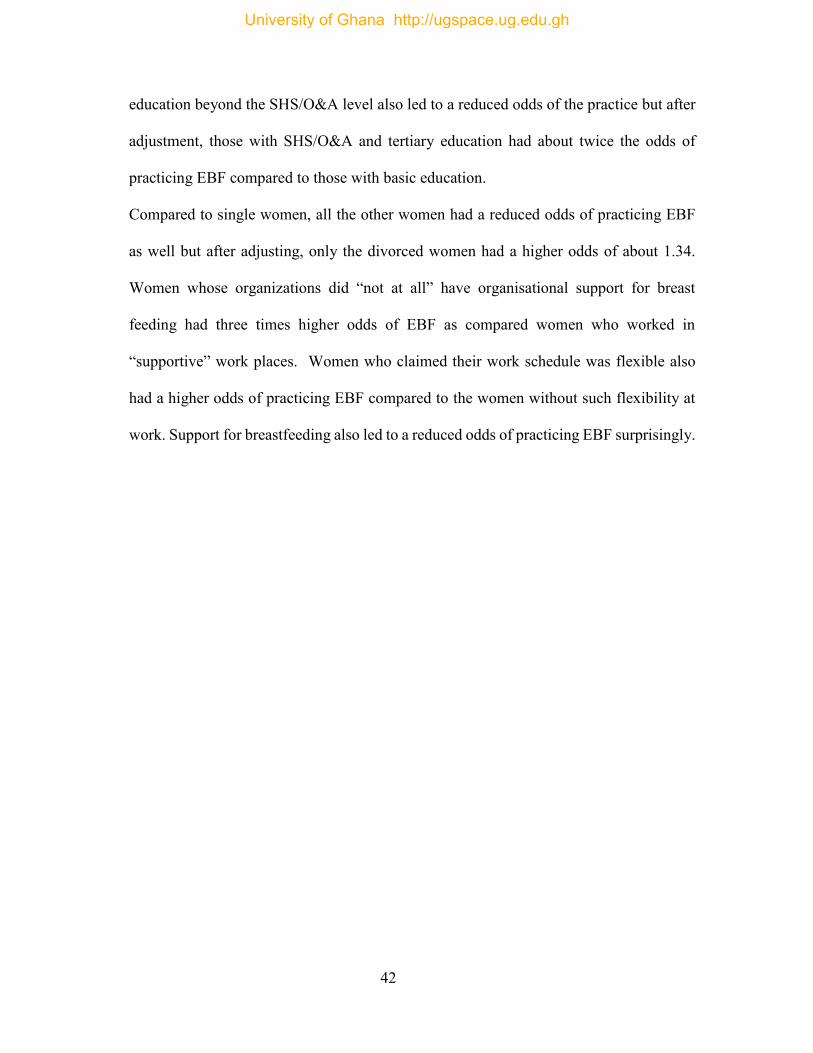
42
education beyond the SHS/O&A level also led to a reduced odds of the practice but after
adjustment, those with SHS/O&A and tertiary education had about twice the odds of
practicing EBF compared to those with basic education.
Compared to single women, all the other women had a reduced odds of practicing EBF
as well but after adjusting, only the divorced women had a higher odds of about 1.34.
Women whose organizations did “not at all” have organisational support for breast
feeding had three times higher odds of EBF as compared women who worked in
“supportive” work places. Women who claimed their work schedule was flexible also
had a higher odds of practicing EBF compared to the women without such flexibility at
work. Support for breastfeeding also led to a reduced odds of practicing EBF surprisingly.
University of Ghana http://ugspace.ug.edu.gh
43
Table 7: Logistic Regression of EBF on Sociodemographic and Organizational
factors
Unadjusted Adjusted OR (95% CI) P-value OR (95% CI) P-value Age (years)
20 – 29 30 – 39 40 – 49
Ref 0.57 (0.35, 0.91) 0.39 (0.19, 0.78)
0.011 Ref 1.25 (0.62, 2.52) 0.85 (0.30, 2.41)
0.605
Education
Basic SHS/O&A level Tertiary
Ref 2.24 (0.78, 6.48) 0.56 (0.22, 1.39)
<0.001 Ref 2.29 (0.53, 9.90) 2.10 (0.48, 9.18)
0.518
Marital status
Single Married Widowed Divorced Separated
Ref 0.47 (0.21, 0.84) 0.10 (0.02, 0.43) 0.56 (0.08, 3.79) 0.14 (0.03, 0.62)
0.003 Ref 0.62 (0.23, 1.66) 1* 1.34 (0.08, 21.62) 0.18 (0.03, 1.21)
0.329
Monthly income
<1,000 1,000 – 1,999 2,000 – 2,999 3,000+
Ref 0.35 (0.20, 0.64) 0.13 (0.06, 0.28) 0.10 (0.03, 0.28)
<0.001 Ref 0.32 (0.10, 0.99) 0.19 (0.05, 0.70) 0.08 (0.01, 0.44)
0.022
Organizational policy
on breastfeeding
No policy Policy exists Don’t know
Ref 2.45 (1.51, 3.97) 2.22 (1.24, 3.98)
0.001
Ref 1.39 (0.68, 2.85) 1.67 (0.72, 3.86)
0.454
Organizational work
schedule
Not flexible Flexible
Ref 3.57 (2.15, 5.93)
<0.001
Ref 2.81 (1.37, 5.76)
0.005
Organizational
support for
breastfeeding
Supportive Not at all Somewhat Very supportive
Ref 5.32 (2.96, 9.55) 1.87 (1.03, 3.39) 1.99 (1.05, 3.77)
<0.001
Ref 3.2 (1.50, 6.67) 1.68 (0.78, 3.59) 1.49 (0.67, 3.33)
0.044
*All mothers in category did not practice EBF for the adjusted model
University of Ghana http://ugspace.ug.edu.gh
44
Perceived benefits of Workplace lactation room
Some of the perceived benefits of a workplace lactation room stated by mothers was that
it enhanced productivity, prevent infections in children, and promoted EBF. One of the
mothers stated that “I know that having a place at my workplace to breastfeed my child
will give me piece of mind to work well and be productive”.
Another respondent stated that “ the presence of a place to breastfeed my child at work
will encourage me to breastfeed up to six months before introducing any food”.
University of Ghana http://ugspace.ug.edu.gh
45
CHAPTER FIVE
DISCUSSION
The aim of this study was to examine the Exclusive breastfeeding practices of women in
the formal sector and its implication on the workplace breastfeeding room policy.
In this study, 53.2% of the mothers in the study practiced Exclusive Breastfeeding and
this is consistent with the national exclusive breastfeeding rate of 52% in Ghana.
Similarly, Tewabe et al., (2017) reported a prevalence of 50.1% among formal sector
workers who were health extension officers. The comparability of the results may be in
design and characteristics of study participants as these studies included formal sector
workers. However this finding is in contrast with what was reported in other studies in
Ethiopia that found higher prevalence of 68.9% (Asfaw et al., 2015) and 74.0% (Gizaw
et al., 2017). Other studies in the USA have reported lower prevalence of EBF of 16.8%
In this study, monthly income, organizational work flexibility and organizational support
for breastfeeding were significantly associated with the practice of EBF.
An increase in age resulted in reduced odds of practicing EBF but after adjusting for the
other factors, the 30-39 year olds had about a 25% higher odds and the 40-49 year olds
having about 15% lower odds of EBF compared to the 20-29 year olds. These may be
perhaps the result of mothers aged 40-49 having previous children thereby decreasing
their likelihood of practicing EBF. Formal sector working mothers may have climbed the
career ladder and may have more responsibilities at the work side and thus decrease their
University of Ghana http://ugspace.ug.edu.gh
46
odds of EBF. These findings are in consistent with what was reported by Gizaw, Woldu,
& Bitew, (2017) who reported that that exclusive breastfeeding was significantly higher
among mothers aged above 35 years. However this findings overlap the findings of
Asfaw et al., (2015) which found significantly higher odds EBF practice among mothers
aged 25 to 35 years as compared to mothers whose ages were less than 25 years.
Higher education beyond the SHS/O&A level also led to a reduced odds of the practice
but after adjustment, those with SHS/O&A level and tertiary education had about twice
the odds of practicing EBF compared to those with basic education. This finding agrees
with some studies who found positive significant association between maternal
educational status and exclusive breastfeeding. They reported increased odds of EBF
among mothers with higher education (Dashti et al., 2010; Dorgham & Hafez, 2018).
However, some others found that mothers with lower educational status have had
significantly higher odds of EBF (Amin, 2014; Batal et al., 2006; Radwan, 2013). Some
other studies assessed association between educational status of the mothers and EBF but
found no association (Adugna et al., 2017; Al-Kohji, Said,& Selim, 2012; Gizaw et al.,
2017; Shifraw, Worku, & Berhane, 2015; Tewabe et al., 2017). The educational status of
formal sector working mothers was generally high and perhaps these highly educated
mothers were in a better position to comprehend the benefits of breast feeding and accept
the practice than the less educated mothers.
With high monthly income the numbers of mothers practicing EBF also decrease. The
lower the monthly income the more likely the mother was to practice EBF. This finding
University of Ghana http://ugspace.ug.edu.gh
47
is consistent with what was reported in other studies that mothers with lower monthly
income were more likely to exclusively breastfeed than their counterparts who earned
more (Shifraw et al., 2015;Tewabe et al., 2017). This is probably because those women
with lower income cannot afford breastmilk substitutes or infant formula and are left with
no choice than breastfeed their babies to save cost.
Compared to single women, all the other women had a reduced odds of practicing EBF
as well but after adjusting, only the divorced women had a higher odds of about 34%.
This increase in odds may be as a result of divorced women being more attached to their
babies. This finding is in sharp contrast to what Adugna, Tadele, Reta, & Berhan, (2017)
found in a study while assessing prevalence and determinants of EBF practice. They
reported that married mothers practiced EBF more likely than single mothers.
Women who reported their work schedule was flexible also had a higher odds of
practicing EBF compared to the women without such flexibility at work. Support for
breastfeeding also led to a reduced odds of practicing EBF surprisingly. Some work places
already have this flexibility for such mothers to be able to breastfeed. This finding may
create need for some more work places to allow such flexibility to be created for lactating
mothers to be able to enhance breastfeeding.
Knowledge of exclusive breastfeeding is high amongst women in the formal sector with
68% reporting the accurate number of months recommended for EBF, but 93% of them
accurately gave 6 months as the recommended number of months a mother should
University of Ghana http://ugspace.ug.edu.gh
48
exclusively breastfeed her baby. This finding is higher than a study done in Nigeria which
showed a 60% knowledge of the duration of EBF and 30 had accurate knowledge of the
recommended duration with 31% of them practicing Exclusive breastfeeding (Oche,
Umar, & Ahmed, 2011).
A study also done by Tadele et al in Ethiopia found that 93.6% of mothers had
knowledge of EBF (Tadele et al., 2016). Even though in this current study the knowledge
was high (93%) only 45.4% of women who had this correct knowledge of EBF actually
practiced it. This did not tally with a study done by Tadele et al in Ethiopia which found
that 89.5% practiced EBF.
Pain, discomfort, annoyance and time consuming were the major reasons why mothers
did not like EBF.
EBF was significantly highest among mothers who worked for companies with a policy
on breastfeeding and lowest among those who worked for companies without such a
policy although the details of such policies were not obtained for analysis. It was also
significantly higher among women whose work schedules were flexible. Surprisingly, it
was much lower for women who worked for organizations that had scheduled breaks for
nursing and significantly higher where women were not allowed to bring their breastfed
infants to work. Ironically mothers who described their workplace as not-at-all supportive
for EBF practiced it the most compared to those who described their workplace as
providing some level of support with significant differences in the level of EBF across
the various levels of support. The supportiveness of the work environment does not appear
to have an influence on EBF when the mother is very willing.
University of Ghana http://ugspace.ug.edu.gh
49
CHAPTER SIX
CONCLUSIONS AND RECOMMENDATIONS
This study sought to examine exclusive breastfeeding practices among women in the
formal sector and its implications for the lactation room policy. The study found that high
socioeconomic status such as high income and high educational status negatively impacts
a nursing mother in the formal sectors decision to practice exclusive breastfeeding. Those
with low income are more likely to practice EBF probably due to its cost effectiveness.
Although knowledge of EBF is high amongst mothers in the formal sector only half of
them actually practice it. Exclusive Breastfeeding rates are high when the source of
knowledge of exclusive breastfeeding is from the partner thus involving males in
breastfeeding offer support for mothers.
Exclusive breastfeeding rates drops drastically when a mother resumes work at an average
age of baby being 5.3 months which extends their stay at home beyond the stipulated 12
weeks or 3 month leave period, thus indicating that the maternity leave is short. Hence
making a policy of 6 months maternity leave will encourage women not to take days off
unofficially in addition to their annual and maternity leave. Half of the mothers who
resumed work fed babies solely on infant formula thus affecting the effectiveness of the
exclusive breastfeeding policy of 6 months.
Also women who have a workplace support are likely to practice Exclusive breastfeeding
as women who do not. This is because women with time have adapted ways of exclusively
University of Ghana http://ugspace.ug.edu.gh
50
breastfeeding their children. Even so more should be done in terms of organizational
support for breastfeeding women.
RECOMMENDATIONS
The Government of Ghana under the Ministry of Health, Ministry of Employment
and Labour Relations, Ministry of Gender, Children and Social protection should
come out with a National Breastfeeding Policy as well as a National Workplace
Breastfeeding policy
Further studies on male involvement in breast feeding support as well a partner
education to strengthen community action on exclusive breastfeeding should be
explored.
Ministry of Health, Ministry of Gender and Ministry of Employment and Labour
relations should extend the maternity leave period to 6 months to enable working
mothers fully practice exclusive breastfeeding.
University of Ghana http://ugspace.ug.edu.gh
51
REFERENCES
Adugna, B., Tadele, H., Reta, F., & Berhan, Y. (2017). Determinants of exclusive
breastfeeding in infants less than six months of age in, 4–11.
https://doi.org/10.1186/s13006-017-0137-6
Allen, J., & Hector, D. (2005). Benefits of breastfeeding. New South Wales Public Health
Bulletin, 16(4), 42. https://doi.org/10.1071/NB05011
Amin, T. T. (2014). Determinants of Initiation and Exclusivity of Breastfeeding, (October
2010). https://doi.org/10.1089/bfm.2010.0018
Aryeetey, R. N. O., & Goh, Y. E. (2013). Duration of Exclusive Breastfeeding and
Subsequent Child Feeding Adequacy. Ghana Medical Journal, 47(1), 24–29.
Asfaw, M. M., Argaw, M. D., & Kefene, Z. K. (2015). Factors associated with exclusive
breastfeeding practices in Debre Berhan District , Central Ethiopia : a cross sectional
community based study. International Breastfeeding Journal, 1–9.
https://doi.org/10.1186/s13006-015-0049-2
Babakazo, P., Donnen, P., Akilimali, P., Ali, N. M. M., & Okitolonda, E. (2015). Predictors
of discontinuing exclusive breastfeeding before six months among mothers in Kinshasa:
a prospective study. International Breastfeeding Journal, 10(1), 19.
https://doi.org/10.1186/s13006-015-0044-7
Bachrach, V. R. G., Schwarz, E., & Bachrach, L. R. (2003). Breastfeeding and the Risk of
Hospitalization for Respiratory Disease in Infancy. Archives of Pediatrics & Adolescent
Medicine, 157(3), 237. https://doi.org/10.1001/archpedi.157.3.237
Batal, M., Boulghourjian, C., Abdallah, A., & Afifi, R. (2006). Breast-feeding and feeding
practices of infants in a developing country : A national survey in Lebanon Breast-
feeding and feeding practices of infants in a developing country : a national survey in
University of Ghana http://ugspace.ug.edu.gh
52
Lebanon, (June). https://doi.org/10.1079/PHN2006860
Breastfeeding in the workplace: Good for the mother, child, business and society. (n.d.).
Retrieved from http://www.ilo.org/global/about-the-
ilo/newsroom/news/WCMS_218710/lang--en/index.htm
Castilho, S. D., & Filho, A. de A. B. (2010). The history of infant nutrition. Jornal de
Pediatria, 86(3), 179–188. https://doi.org/10.2223/JPED.1984
Centres, P. E., & Agencies, P. E. (2003). Labour Act , 2003 PART II – PUBLIC
EMPLOYMENT CENTRES AND PRIVATE PART III – PROTECTION OF
EMPLOYMENT PART IV – GENERAL CONDITIONS OF EMPLOYMENT Sub-
Part II – Hours of work Sub-Part III – Rest periods PART V – Employment of persons
with disability PART VI, 1–58.
Dashti, M., Scott, J. A., Edwards, C. A., & Al-sughayer, M. (2010). Determinants of
breastfeeding initiation among mothers in Kuwait, 1–9.
Dorgham, L. S., & Hafez, S. (2018). Assessment of initiation of breastfeeding , prevalence
of exclusive breast feeding and their predictors in Taif , KSA, (January 2014).
Dun-Dery, E. J., & Laar, A. K. (2016). Exclusive breastfeeding among city-dwelling
professional working mothers in Ghana. International Breastfeeding Journal, 11(1), 23.
https://doi.org/10.1186/s13006-016-0083-8
Effective, P., & Care, P. (2002). Essential Newborn Care and Breastfeeding Training
modules Regional Office for Europe.
Gizaw, Z., Woldu, W., & Bitew, B. D. (2017). Exclusive breastfeeding status of children
aged between 6 and 24 months in the nomadic population of Hadaleala district , Afar
Region , northeast Ethiopia, 1–7. https://doi.org/10.1186/s13006-017-0129-6
GOVERNMENT OF GHANA OFFICE PORTAL, 2017. (n.d.). Greater Accra - Government
University of Ghana http://ugspace.ug.edu.gh
53
of Ghana. Retrieved December 5, 2017, from
http://www.ghana.gov.gh/index.php/about-ghana/regions/greater-accra
Government, Q., Government, T. Q., & Government, T. Q. (2010). Application : Effective
date : Policy :, 1–4.
Greer, F. R., Sicherer, S. H., & Burks, A. W. (2008). Effects of Early Nutritional
Interventions on the Development of Atopic Disease in Infants and Children: The Role
of Maternal Dietary Restriction, Breastfeeding, Timing of Introduction of
Complementary Foods, and Hydrolyzed Formulas. Pediatrics, 121(1), 183–191.
https://doi.org/10.1542/peds.2007-3022
ILO. (n.d.). Length of Maternity Leave.
ILO. (2017). Convention C003 - Maternity Protection Convention, 1919 (No. 3). Retrieved
November 12, 2017, from
http://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO:12100:P12100
_INSTRUMENT_ID:312148:NO
Jones, A. J. R., & Kogan, M. D. (2011). Factors Associated With Exclusive Breastfeeding in
the United States, (December). https://doi.org/10.1542/peds.2011-0841
Kramer, M. S., Aboud, F., Mironova, E., Vanilovich, I., Platt, R. W., Matush, L., … Stanley,
S. (2008). Breastfeeding and child cognitive development. Archives of Genetic
Psychiatry, 65(5), 578–584. https://doi.org/10.1111/j.1365-2214.2009.01070.x
León-Cava, N., Ross, J., Lutter, C., & Martin, L. (2002). Quantifying the benefits of
breastfeeding: a summary of the evidence. The Food and Nutrition Program (HPN) Pan
American Health Organization (PAHO), 177.
Lyell, G. J. (2012). WHA Global Nutrition Targets 2025 : Breastfeeding Policy Brief.
Mogre, V., Dery, M., & Gaa, P. K. (2016). Knowledge, attitudes and determinants of
University of Ghana http://ugspace.ug.edu.gh
54
exclusive breastfeeding practice among Ghanaian rural lactating mothers. International
Breastfeeding Journal, 11(1). https://doi.org/10.1186/s13006-016-0071-z
Mohamed, A., El, H., & Labib, J. R. (2016). Determinants of Exclusive Breastfeeding and
Introduction of Complementary Determinants of Exclusive Breastfeeding and
Introduction of Complementary foods in Rural Egyptian Communities, (July 2014).
https://doi.org/10.5539/gjhs.v6n4p236
National Breastfeeding Policy And Action Plan. (2015).
Negishi, H., Kishida, T., Yamada, H., Hirayama, E., Mikuni, M., & Fujimoto, S. (1999).
Changes in uterine size after vaginal delivery and cesarean section determined by
vaginal sonography in the puerperium. Archives of Gynaecology & Obstetrics, 263, 13–
16. https://doi.org/10.1007/s004040050253
Nkrumah, J. (2017). Maternal work and exclusive breastfeeding practice: A community
based cross-sectional study in Efutu Municipal, Ghana. International Breastfeeding
Journal, 12(1), 1–9. https://doi.org/10.1186/s13006-017-0100-6
Oche, M. O., Umar, A. S., & Ahmed, H. (2011). Knowledge and practice of exclusive
breastfeeding in Kware, Nigeria. African Health Sciences, 11(3), 518–523.
https://doi.org/10.4314/tjmr.v15i2.
Ogwezzy-ndisika, A. O. (2016). Application of the Health Belief Model to the Practice of
Exclusive Breastfeeding Application of the Health Belief Model to the Practice of
Exclusive Breastfeeding among Women in Lagos State , Nigeria, (March 2017).
Ong, G., Yap, M., Li, F. L., & Choo, T. B. (2018). Impact of working status on breastfeeding
in Singapore Evidence from the National Breastfeeding Survey 2001, 15(4), 424–430.
https://doi.org/10.1093/eurpub/cki030
Pinchbeck, I. (1930). Women Workers in the Industrial Revolution 1750-1850.
University of Ghana http://ugspace.ug.edu.gh
55
Radwan, H. (2013). Patterns and determinants of breastfeeding and complementary feeding
practices of Emirati Mothers in the United Arab Emirates.
Revolution, T. I., Clark, A., Hutchins, B. L., & George, D. (1991). Spring 1991 Recent
Findings of Research in Economic & Social History. Retrieved from
http://www.ehs.org.uk/dotAsset/03e09441-1fde-4aac-812a-79f18507fcc4.pdf
Saks, A. M. (2015). Antecedents and consequences of employee engagement, (June).
https://doi.org/10.1108/02683940610690169
Shifraw, T., Worku, A., & Berhane, Y. (2015). Factors associated exclusive breastfeeding
practices of urban women in Addis Ababa public health centers , Ethiopia : a cross
sectional study. International Breastfeeding Journal, 4–9.
https://doi.org/10.1186/s13006-015-0047-4
Sokol, E., Aquago, V., & Clark, D. (2007). Breastfeeding in West and Central Africa; 25
years of implementing the International Code of Marketing Breastmilk Substitutes.
UNICEF Regional Office for West and Central Africa, June 18, 2009. Retrieved from
http://www.unicef.org/wcaro/WCAR_Protecting_Breasfeeding_Code_of_Marketing_
En.pdf
Stevens, E. E., Patrick, T. E., & Pickler, R. (2009). A History of Infant Feeding. Journal of
Perinatal Education, 18(2), 32–39. https://doi.org/10.1624/105812409X426314
Tadele, N., Habta, F., Akmel, D., & Deges, E. (2016). Knowledge, attitude and practice
towards exclusive breastfeeding among lactating mothers in Mizan Aman town,
Southwestern Ethiopia: descriptive cross-sectional study. International Breastfeeding
Journal, 11(1), 3. https://doi.org/10.1186/s13006-016-0062-0
Tewabe, T., Mandesh, A., Gualu, T., Alem, G., Mekuria, G., & Zeleke, H. (2017). Exclusive
breastfeeding practice and associated factors among mothers in Motta town , East
University of Ghana http://ugspace.ug.edu.gh
56
Gojjam zone , Amhara Regional State , Ethiopia , 2015 : a cross-sectional study, 1–7.
https://doi.org/10.1186/s13006-017-0103-3
UNICEF. (2016). Delayed breastfeeding increases risk of newborn deaths by up to 80
percent. Retrieved from https://www.unicef.org/ghana/media_10519.html
UNICEF, W. (2017). Tracking Progress for Breastfeeding Policies and Programmes, 7.
WHO. (2015). WHO | The World Health Organization’s infant feeding recommendation.
Retrieved November 9, 2017, from
http://www.who.int/nutrition/topics/infantfeeding_recommendation/en/
WHO. (2017). WHO | Exclusive breastfeeding. Retrieved November 23, 2017, from
http://www.who.int/nutrition/topics/exclusive_breastfeeding/en/
WHO, & UNICEF. (1990). Innocenti Declaration, 2. Retrieved from
http://www.unicef.org/programme/breastfeeding/innocenti.htm
Wolf, J. H. (2001). Don’t kill your Baby.
University of Ghana http://ugspace.ug.edu.gh
57
APPENDIX
CONSENT FORM
RESPONDENT INFORMATION SHEET
General information
I, Dr. Joan Ese Morny, a student of Health Policy Planning and Management in the School of Public Health,
University of Ghana, Legon pursuing a Master of Public Health Degree Programme. I am here with my
research assistants to carry out a survey on mothers attending your postnatal clinic on the Topic: Exclusive
Breastfeeding Practices amongst women in the formal sector and its implication for the Breastfeeding Room
Policy. This is purely for academic purposes and forms part of the requirement for the award of Master of
Public Health Degree. I, the researcher has no conflict of interest in this study.
Confidentiality
No name will be recorded. Your name and identity are not needed in the study. However the information
you are going to provide will be coded and will be treated strictly confidential. You are assured of total
confidentiality to the information you will give. Apart from the researcher and supervisor of this research,
no one else will have access to information provided whether in part or whole. Data collected will be stored
under lock and key then destroyed after a minimum of three years as per research protocol.
Right to refuse
Participation in this study is voluntary. You are free to answer part or the entire questionnaire. You can
choose to withdraw from the study or stop the interview at any time you want. You can also choose not to
answer any question(s) you find uncomfortable about. Should you choose not to participate, it will not
affect you or your clinic in any way. However you are encouraged to participate fully in this study to help
in determining exclusive breastfeeding practices amongst women in the formal sector and its implication
for the breastfeeding room policy in Ghana and beyond.
If yes, please indicate any questions below
University of Ghana http://ugspace.ug.edu.gh
58
If you have any question(s) or further clarification concerning this study and/or the conduct of the researcher
and research assistants, please do not hesitate to contact the following; Dr. Joan Ese Morny, School of
Public Health, University of Ghana, Legon [email protected]/[email protected] Tel:0206739260;
Dr. Patricia Akweongo, School of Public Health, University of Ghana, Legon, [email protected] Tel:
0243138376 and; Mrs. Hannah Frimpong (Administrator), Ghana Health Service Ethical Review
Committee Secretariat, Accra. Tel: 0507041223/0243235225.
INFORMED CONSENT
I have read the information given above, and I understand. I have been given a chance to ask questions
concerning this study and questions have been answered to my satisfaction. I now voluntarily agree to
participate in this study knowing that I have the right to withdraw at any time without it affecting my current
or future use of health care services.
Signature/Thumb print: …………………………………………… Date: ………………………..
I, the undersigned, have explained this consent to the respondent in English and that she/he understands
the purpose of the study, procedures to be followed as well as the risks and benefits of the study. The
participant has fully agreed to participate in the study.
Signature of interviewer:……………………………………….… Date: …………………………
University of Ghana http://ugspace.ug.edu.gh
59
QUESTIONNAIRE
SECTION A: DEMOGRAPHIC CHARACTERISTICS
1. Age (years):
2. Educational Level:
[0] None [2] JHS/Middle School [4] Undergraduate [1] Primary [3] SHS/O’ & A’ Level [5] Graduate [6]Postgraduate Other:
3. Marital Status
[1] Single [3] Widowed [5] Separated [2] Married [4] Divorced [6] Co-habiting
4. Number of living children:
5. Level of monthly income in Ghana Cedis
[1] Less than 1,000 [3] 2,000 – 2,999 [5] 4,000 – 4,999 [2] 1,000 – 1,999 [4] 3,000 – 3,999 [6] 5,000+
6. Where do you work?
7. What is your job title/position?
8. Average time it takes you to move from work to home: hours, minutes
9. How old is your baby? years, months, weeks, days
10. How old is your youngest child before this baby? years, months
11. How long did you exclusively breastfeed the child before this baby? months, weeks, days
12. What do you currently feed your baby with ? (Tick all applicable) ***
[1] Breast milk [1] Infant formula [1] Baby food ****** Other:
University of Ghana http://ugspace.ug.edu.gh
60
SECTION B: KNOWLEDGE AND PERCEPTION ON EXCLUSIVE BREASTFEEDING
13. Do you have an idea about the recommended number of months to exclusively breastfeed
a baby?
[0] No [1] Yes, how many months? 14. Where did you obtain knowledge about breast feeding from? (Tick all applicable)
[1] Health personnel [1] Family [1] Partner [1] Friends [1] Media [1] School
Other:
15. In your opinion, which statement best describes the preference of the following people
about feeding your baby within the first 6 months? No
preference
[0]
Exclusive
breastfeeding
[1]
Formula
Feeding
[2]
Mixed
Feeding
[3]
Don’t
know
[4]
Family
Partner
Friends
Health personnel
16. Why do you think a mother should exclusively breastfeed her child?
17. What was your impression about the concept of breastfeeding in your first few
days/weeks/months of doing so? [1] Disliked very much [2] Disliked [3] Indifferent [4] Liked [5] Liked very
much
University of Ghana http://ugspace.ug.edu.gh
61
18. Give reasons for your answer:
SECTION C: BREASTFEEDING AND WORK
19. Have you resumed work? [0] No (go to Section D) [1] Yes (continue) 20. How old was your baby when you resumed work after maternity leave or how old would
the baby be when you are expected to resume work? (If you are not sure, give your best time estimate)
years, months, weeks, days 21. Does your company have a breastfeeding room? [0] No [1] Yes 22. If yes how does it operate 23. How does it affect your work, do you have a reliever whilst breastfeeding. [0] No
[1] Yes 24. What do you have in your workplace place breastfeeding room
25. How many hours per day do/did you usually work at your job during the time when your
child is/was less than 6 months? hours 26. Who takes care of your baby whilst at work? (Tick all applicable)
[1] My baby is cared for by a family member [1] I keep my baby with me at the work place [1] My baby is cared for by a non-family caretaker [1] My baby is cared for by a crèche [1] I house a house help who takes care of my baby
27. Which of the following circumstances describe your situation? (Tick all applicable)
[1] I pump breastmilk during my work day and save it for breastfeeding during my work day [1] I pump breastmilk during my working day and save it for my baby to drink later [1] I go to my baby and breastfeed him during working hours [1] My baby is brought to me to breastfeed at my work place [1] I breastfeed my baby during break time [1] I neither pump breastmilk nor breastfeed during my working hours [1] My baby depends solely on infant milk whilst I am at work [1] My baby depends on infant milk whilst I am at work and I continue with breastfeeding after work
28. Assuming you breastfeed or express breastmilk at work, have you had any of the following
experiences during of workplace breastfeeding? (Tick all applicable) [1] A co-worker made negative comments or complained to me about breastfeeding or expressing breastmilk
University of Ghana http://ugspace.ug.edu.gh
62
[1] My employer or my supervisor made negative comments or complained to me about time spent on breastfeeding or breastmilk expression. [1] It was hard for me to arrange break time for breastfeeding or pumping milk [1] It was hard for me to find a place to breastfeed or pump milk [1] It was hard for me to arrange a place to store pumped breast milk [1] It was hard for me to carry the equipment I needed to pump milk at work [1] I felt worried about keeping my job because of breastfeeding [1] I felt worried about continuing to breastfeed because of my job [1] I felt embarrassed among co-workers, my supervisor, or my employer because of breastfeeding
29. How many breaks do you get within work hours for breastfeeding or breastmilk expression
each work day? 30. What is the average duration of each break? minutes 31. Would you consider your workplace a breastfeeding friendly workplace? [0] No
[1] Yes
32. How does/did your work affect the choice of the mode of feeding your baby within the first
6 months?
SECTION D: ORGANIZATIONAL/WORKPLACE FACTORS
33. Does your organization have a policy outlining organizational support for breastfeeding
employees? [0] No [1] Yes [2] Don’t know 34. Does your organization offer work schedule flexibility? [0] No [1] Yes 35. Does your organization allow nursing mothers to schedule breaks and work patterns to
provide time to breastfeed their babies or to express or pump breastmilk during the workday? [0] No [1] Yes
36. Does your organization allow employees to routinely bring breastfeeding infants to work
with them? [0] No [1] Yes 37. In your opinion, how supportive of breastfeeding is your place of employment?
[0] Not at all [1] Somewhat [2] Supportive [3] Very supportive
University of Ghana http://ugspace.ug.edu.gh

63
SECTION E: PERCEIVED BENEFITS OF WORKPLACE BREASTFEEDING ROOM
How do you think the implementation of a breastfeeding room policy in your organization would
affect your breastfeeding behaviour?
University of Ghana http://ugspace.ug.edu.gh