evaluating the feasibility and effect of using a hospital-wide coordinated approach to introduce...
TRANSCRIPT

Original Article
From the *Edith Cowan University;†Curtin Health Innovation Institute,
Curtin University of Technology;‡Sir
Charles Gairdner Hospital; §St. John
of God Hospital Subiaco, Perth,
Western Australia, Australia.
Address correspondence to Anne M.
Williams, PhD, RN, Associate
Professor, School of Nursing,
Midwifery and Postgraduate
Medicine, Edith Cowan University,
270 Joondalup Drive, Joondalup,
Western Australia 6027, Australia.
E-mail: [email protected]
Received October 27, 2009;
Revised August 11, 2010;
Accepted August 11, 2010.
1524-9042/$36.00
� 2012 by the American Society for
Pain Management Nursing
doi:10.1016/j.pmn.2010.08.001
Evaluating the Feasibilityand Effect of Using aHospital-Wide CoordinatedApproach to IntroduceEvidence-Based Changesfor Pain Management
--- Anne M. Williams, RN, PhD,*,†,‡
Christine Toye, RN, PhD,*,†,‡
Kathleen Deas, RN, PGrad Nurs,†
Denise Fairclough, RN, BN,‡
Kathryn Curro, RN, Grad Cert Pain Mgt,§
and Lynn Oldham, RN, PhD†
- ABSTRACT:This action research project explored the feasibility and effect of
implementing a hospital-wide coordinated approach to improve the
management of pain. The project used a previously developed
model to introduce three evidence-based changes in pain manage-
ment. Part of this model included the introduction of 30 pain re-
source nurses (PRNs) to act as clinical champions for pain at a local
level. Both quantitative and qualitative measures were used to assess
the feasibility and effect of the changes introduced. Quantitative
data were gathered through a hospital-wide document review and
assessment of the knowledge and attitude of the PRNs at two time
points: time 1 before the introduction of the PRNs and time 2 near
completion of the project (11 months later). A statistically signifi-
cant improvement in the documentation of pain scores on admis-
sion and each nursing shift was apparent. However, no difference
was found in the percentage of patients who had been prescribed
opioids for regular pain relief that had also been prescribed and
dispensed a laxative/aperient. Neither were any statistically signifi-
cant decreases in patient pain scores observed. An assessment of the
knowledge and attitudes of the PRNs showed an improvement from
time 1 to time 2 that was statistically significant. The qualitative data
revealed that despite the barriers encountered, the role was satis-
fying for the PRNs and valued by other hospital staff. Overall, the
results revealed that the new model of change incorporating PRNs
was a useful and effective method for introducing and sustaining
evidence-based organizational change.
� 2012 by the American Society for Pain Management Nursing
Pain Management Nursing, Vol 13, No 4 (December), 2012: pp 202-214

203Introducing Pain Management Changes
Extensive research regarding the assessment and man-
agement of pain has advanced our knowledge of effec-
tive pain management, and guidelines to improve the
management of pain have been developed by the
Agency for Health Care Policy and Research (USA),
the British College of Surgeons (U.K.), and the National
Health and Medical Research Council (Australia) (Yateset al., 2002). Within Australia, detailed management
strategies for pain in residential aged care facilities
have also been developed by the Australian Pain
Society (2005). However, despite the introduction of
these guidelines, the effective management of pain re-
mains a problem (Ardery, Herr, Hannon, & Titler, 2003;
Bucknall, Manias, & Botti, 2001; Carlson, 2008). The
reasons for poor management of pain at this timeseem to arise from difficulties in using the results of
research in clinical practice rather than from a lack
of knowledge on effective methods of pain relief
(Ellis et al., 2007; Idell, Grant & Kirk, 2007).
PILOT WORK
In a previous project (Williams et al., 2006), a new
model of research utilization for health care, which
could be used for multiple practices to improve the
quality of patient care, was developed. The action re-
search method was used to pilot a protocol directed
at improving pain assessment and management in
four acute care hospital wards. Changes were intro-
duced and then monitored using qualitative interviewswith 19 members of staff and audits of the documenta-
tion of 468 patients. The strategies found to promote
change in the project ward areas were: a planned, co-
ordinated educational program focusing on three
changes in pain assessment and management (deliv-
ered using a variety of methods); regular monitoring
of the changes introduced, with pathways established
for communication and feedback at all stages of theproject between the project team and all members of
the ward team; the use of reminders and prompts;
and the need for a clinical champion to sustain the
changes.
The model that was developed in this previous
project successfully changed three of the usual prac-
tices for pain assessment and management in each of
the studywards. A key feature of this subsequentmodelwas the use of award-based clinical champion. The role
of clinical champion in the previous project evolved
with the presence of a research nurse who became a fa-
miliar face on the project ward and was regularly con-
sulted by ward nurses in the management of pain
problems being experienced by patients. The research
nurse was responsible for providing feedback on pain
management through the audit results, initiating and
renewing documentation for pain assessment, provid-
ing resources for pain management, and acting as a re-
minder for staff. However, spot audits carried out on
the study wards 3 months after the completion of the
project showed a decrease in compliance with the
changes introduced. Sustainability of change without
the presence of a clinical champion was suggested tobe difficult to achieve.
In the current environment of accountability for
the delivery of quality care and health care budgets,
nurses are obliged to base practice on the best evi-
dence available. Formulating the link between re-
search and clinical practice requires ‘‘champions of
change.’’ For example, it has been suggested that
nurses with academic and experiential preparation be-yond the standard nursing education could be advo-
cates for improved professional practice (DeBourgh,
2001).
PAIN RESOURCE NURSES
A number of hospitals around the world have reportedthe use of ‘‘resource’’ or ‘‘link’’ nurses for pain manage-
ment. These nurses can be regarded as being clinical
champions for pain at an individual ward or clinical
area level. The implementation of pain resource nurses
(PRNs) was first described at the City of Hope Medical
Center in California (Ferrell, Grant, Ritchey, Ropchan,
& Rivera,1993). Since then, several studies evaluating
the role of the PRN have been conducted in the UnitedStates and Canada (Holley, McMillan, Hagan, Palacios, &
Rosenberg, 2005; Krystal, Carr, Gavaghan, Porterfield,
& Turner, 1997; McMillan, Tittle, Hagan, & Small,
2005; McCleary, Ellis, & Rowley, 2004; Paice, Barnard,
Creamer, & Omerod, 2006). Only one program was
identified in Australia, in Melbourne (Saward, Aranda,
Flemming, Pate, Williams, & Eichner, 2005). All of the
programs identified were for adult settings, exceptone (McCleary et al., 2004),which was for the pediatric
setting. The duration of training programs for PRNs has
varied between sites. The longest program was 40
hours (Ferrell et al., 1993), but most of the other pro-
grams carried out the initial training over 1-2 days
(Krystal et al., 1997; McCleary et al., 2004; McMillan
et al., 2005; Paice et al., 2006).
A number of measures were used in these studiesto evaluate the impact of the PRN role. Positive out-
comes such as higher patient satisfaction scores, lower
pain scores, an increase in pain documentation, and an
increase in staff discussions with patients about pain
were reported by Paice et al. (2006). An increase in
the knowledge and improved attitudes of PRNs toward
pain was reported by MacMillan et al. (2005). Saward
et al. (2005) reported an increase in pain referrals,

204 Williams et al.
documentation of pain, pain relief, and use of pain
tools and pain flow charts.
Overall, the PRNs described being empowered by
the initial education program, subsequent experience
in their role, and ability to practice as confident and
credible professionals (Ferrell et al., 1993; Holley
et al., 2005). However, frustrations were alsodescribed and attributed to the slow rate of change
in practice in individual ward areas and maintaining
momentum to motivate others (McCleary et al.,
2004). PRNs at some sites also reported experiencing
problems. For example, self-doubt in their relation-
ships with coworkers and physicians has been de-
scribed by several authors (Ferrell et al., 1993; Holley
et al., 2005; McCleary et al., 2004). The PRNs in onestudy felt that these barriers diminished as their role
became established and accepted by colleagues
(Holley et al., 2005).
A designated program director and the allocation
of sufficient time to perform the role is an essential
component for the success of the PRN program. Con-
tinued support through meetings, ongoing education
and additional pain management resources is also im-portant (McCleary et al., 2004; Paice et al., 2006).
Senesac (2004) observed that nurses who were in-
volved in bedside care experienced difficulties attend-
ing meetings and that a supportive environment was
essential to enable bedside nurses to actively partici-
pate in change.
The use of resource nurses or ‘‘link nurses’’ has
also been evaluated in other specialist health fields,such as diabetes, gastroenterology, and infection con-
trol (Ching & Seto, 1990; Cooper, 2004; Couch,
Sheffield, Gerthoffer, Ries, & Hollander, 2003; Perry-
Woodford & Whayman, 2005; Shepherd, Hattersley,
& Ellard, 2005). Link nurse programs are designed
to train specialist nurses to maintain patient-centerd
support services through the provision of evidenced-
based education programs and to support and educatenurses in the clinical environment (Cooper, 2004;
Perry-Woodford & Whayman, 2005; Shepherd et al.,
2005). Outcomes for patients, such as improved
clinical care, increased disease-specific assessments,
and an increase in clinical investigations and surveil-
lance have been reported (Ching & Seto, 1990;
Couch et al., 2003; Shepherd et al., 2005). There is
a growing body of evidence that supports nurseinterventions as a way to improve clinical care
(Couch et al., 2003). However, a supportive infrastruc-
ture or framework, with clear strategic guidelines for
practice and role performance, is essential to ensure
the success of this type of nursing intervention
(DeBourgh, 2001).
METHOD
AimThe aim of this project was to explore the feasibility
and effect of implementing a hospital-wide coordi-
nated approach to improve the management of pain.
This included the introduction of PRNs. Two acute
care hospitals in Western Australia participated in
this study, one public, Sir Charles Gairdner Hospital
(SCGH), and one private, St. John of God Hospital Sub-
iaco (SJOGHS).The project focused on three evidence-based indi-
cators of change in pain management. Two of these in-
dicators concerned the assessment of pain. It has been
suggested that pain assessment is a central feature in
the selection of appropriate pain management thera-
pies (Michaels, Hubbartt, Carroll, & Hudson-Barr,
2007). These indicators had been used previously in pi-
lot work, and the present project built on the work al-ready undertaken. The indicators targeted in this
project were:
The percentage of patients with a documented pain
score on admission.The percentage of patients with a documented painscore each nursing shift.
The percentage of patients who had been prescribedopioids for regular pain relief that had also been pre-scribed and dispensed a laxative/aperient.
DesignAction research, utilizing both quantitative and quali-
tative methods, was used in this feasibility study
which ran from June 2007 until June 2008. The pri-mary purpose of an action research design is to solve
problems and to make a difference to a specific situa-
tion. Strategies can be developed to address the iden-
tified problem. Action research is a method that
recognizes the impact of change on those directly in-
volved. It allows these individuals to participate in the
change process, thus reducing the negative feelings
that are often associated with the experience ofchange (Stringer, 1999).
Different phases are used in the action research
design. In this project the phases of planning, prepar-
ing for change, implementing change, and evaluating
change were used. A further phase of adjusting change
followed these phases, but it could not be incorpo-
rated into the actual project due to time constraints.
PlanningA team of nurse specialists for pain from the two hos-
pitals and nurse researchers from two universities

205Introducing Pain Management Changes
met regularly to plan the project and develop the edu-
cational resources. This team was supported and con-
tributed to by the Pain Management Committee at Sir
Charles Gairdner Hospital as well as the executive
nursing staff from both hospitals.
Planning involved the content and format of the
educational workshops for the PRNs as well as themonthly support group meetings. A Pain resource file
and a self-directed learning package were developed
to be given to each PRN for their ward area. These doc-
uments included strategies for staff to use when they
encountered patients unable to give a numeric pain
score, such as those unable to speak English, as well
as patients who had dementia or were confused. Post-
ers reminding staff to change practice in the targetedareas were also developed for distribution.
Preparing for ChangeAn expression of interest for the PRN role was sent out
at each hospital, and applicants were individually se-
lected at a ward level. The selection criteria were Reg-
istered Nurse with an interest in pain management,
working a minimum of 3 days per week, and at least
6 months experience in current area. A commitment
of 12 months was required.
Across two hospitals, 30 PRNs were introduced.There were 27 female and 3 male PRNs. Sixteen
were located at the private hospital and 14 at the pub-
lic hospital. Twenty-two of the nurses worked full-time
and eight worked part-time.
All prospective PRNs attended two 1-day educa-
tional workshops, which were scheduled aweek apart.
At the completion of the workshops each nurse was
presented with a badge that said ‘‘Pain Resource Nurse’’by the Director of Nursing (or their representative) of
each hospital.
Implementing ChangeThe PRNs started in their new roles after the comple-
tion of the educational workshops. Monthly support
group meetings for the PRNs, which incorporated an
educational component, were held at each hospital
throughout the project. These were organized and fa-
cilitated by the clinical nurse consultants for pain.
PRNs were allocated segments of time to attend the
support group meetings and attend to their PRN role.The PRNs promoted change in ward areas, focus-
ing specifically on the three evidence-based indicators
of change identified for use in the project. Each PRN
chose one indicator in particular to focus on and car-
ried out regular audits in their ward area to monitor
the initiation of any improvements.
Three study days were allocated to each PRN. Two
days were for the introductory educational workshops,
and 1 day was allocated to spend some time with their
choice of two of the pain teams (i.e., palliative,
chronic, or acute). Half a day was to be allocated to
each team. In addition to this, each PRN was allocated
2.5 hours per month on a designated day to attend to
some of their responsibilities. It was an expectation
that each PRN would:
Be a preceptor in pain management for new staff.Be a positive role model for pain assessment and man-agement.
Be available as a resource for the multidisciplinaryteam.Attend $75% of monthly PRN meetings.
Facilitate pain education sessions in ward area as re-quired or at the direction of the pain management com-mittee.Carry out bimonthly audits on one of the selected indi-
cators for pain management being used in the project.Regularly update the pain resource file.Directly contact the pain management committee if re-
sources or support relating to pain assessment or man-agement were required.Identify opportunities for improving pain management
in their own ward area and communicate this to thepain management committee.
Evaluating ChangeQuantitative data. To evaluate the impact of the
introduction of a coordinated approach to pain man-
agement, a hospital-wide document review and assess-ment of the knowledge and attitudes of the PRNs was
carried out at two time points. Time 1 was before the
introduction of the PRNs (June 2007), and time 2 was
near the completion of the project (May 2008). Data
were analyzed using the Statistical Package for the So-
cial Sciences (SPSS) version 15. Descriptive statistics
were produced including means, frequencies, and per-
centages. Significant differences in results from thechanges introduced were also tested by chi-square
analysis, t test, and Mann-Whitney test.
Document Review. An audit tool had been developedand used in the pilot work for this project. Minor mod-
ifications were made to this tool after extensive use in
the previous pilot program, and it was used to audit
the documentation at both hospitals in the present
project. Supporting information for auditors was devel-oped for use in this project. This supporting informa-
tion included exclusion criteria for the use of laxatives
and a list of possiblemedications that could be classified
as opioids or as laxatives. Auditors received a briefing
before commencing and worked in teams in each
ward area. Auditors were instructed to carry out
a spot check pain score (on rest and movement) on pa-
tients who were available and able to respond.

206 Williams et al.
Knowledge and Attitudes. The knowledge and atti-
tude of the PRNs before beginning the program and at
the completion of the program, were measured using
Ferrell and McCaffery’s ‘‘Knowledge and Attitudes Sur-vey Regarding Pain’’ (http://prc.coh.org). This instru-
ment was developed in 1987 and has been used
extensively worldwide to measure knowledge and atti-
tudes of pain in different settings. A recent revision of
the tool was tested on 800 subjects. The test-retest reli-
ability was established at 0.80,with internal consistency,
Cronbach alpha coefficient, of 0.70. Permission to use
this instrument was obtained from its first author.Some minor modifications were made to the ques-
tionnaire to make it suitable for the Australian context.
This included changing the names of some medica-
tions which in Australia were either not used routinely
or known under a different name. The following ques-
tions were altered: 9, 18, 24, 27, 29, 32, 33, 37B, and
38B (Table 1). No questions were removed, to enable
comparisons with other populations.Qualitative Data. Qualitative data were collected
from a number of sources. Content analysis was used
to identify major themes and categories which high-
lighted any problems or difficulties relating to the
changes that were implemented.
Ethical ConsiderationsEthical approval for this project was obtained from
each of the hospitals involved as well as Curtin Univer-
sity of Technology. There were three types of partici-pant in the project. First, the PRNs; second, a small
number of hospital staff who worked with the PRNs,
who were interviewed; and third, hospitalized patients
at each hospital.
PRNs were recruited after the distribution of an
expression of interest. Applicants were informed that
the role would be part of a research project and that
by participating in the role they also agreed to partici-pation in both qualitative and quantitative evaluation
of the role for the duration of the project. A consent
form was signed when the role commenced.
The hospital staff recruited for interview were di-
rectly approached by the project manager. The intent
and nature of the project was described, and a consent
form was signed if the person was willing to
participate.Hospitalized patients in all of the areas of the hos-
pital to which PRNs were to be assigned had the poten-
tial to participate in this project. An audit of patient
documentation and a spot check of numeric pain
scores were carried out before any changes were intro-
duced and 1 year after the introduction of changes.
The original intention of the project was to inform
each patient of the study and ask them to sign a consent
form if they were willing to participate. However, the
Scientific Review Committee at SCGH expressed con-
cern that some patients would be excluded from the
project because they were too unwell to give their con-
sent. It was possible that these patients may have been
the ones experiencing most pain. Because this part of
the project only involved a document review and spot-check pain score, it was assessed as being low risk, and
approval was given to omit the signed consent. How-
ever, wherever possible the auditors informed patients
about the project and elicited a verbal consent. Ethical
approval was given by each committee for use of this
approach.
RESULTS
Quantitative DataDocumentation Audit. The documentation was
audited in 20 ward areas across both hospitals at the
beginning and the end of the project to observe
whether the introduction of the PRN role had enabled
improvements in the specified indicators to occur.These areas maintained a PRN throughout the year.
Eleven of these areas were at SCGH and nine were at
SJOGHS. At time 1, the total number of patients
audited on the PRN wards was 400 (221 at SCGH
[55.2%] and 179 at SJOGHS [44.8%]). At time 2, the to-
tal number of patients audited on the PRN wards was
437 (220 at SCGH [50.3%] and 217 at SJOGHS
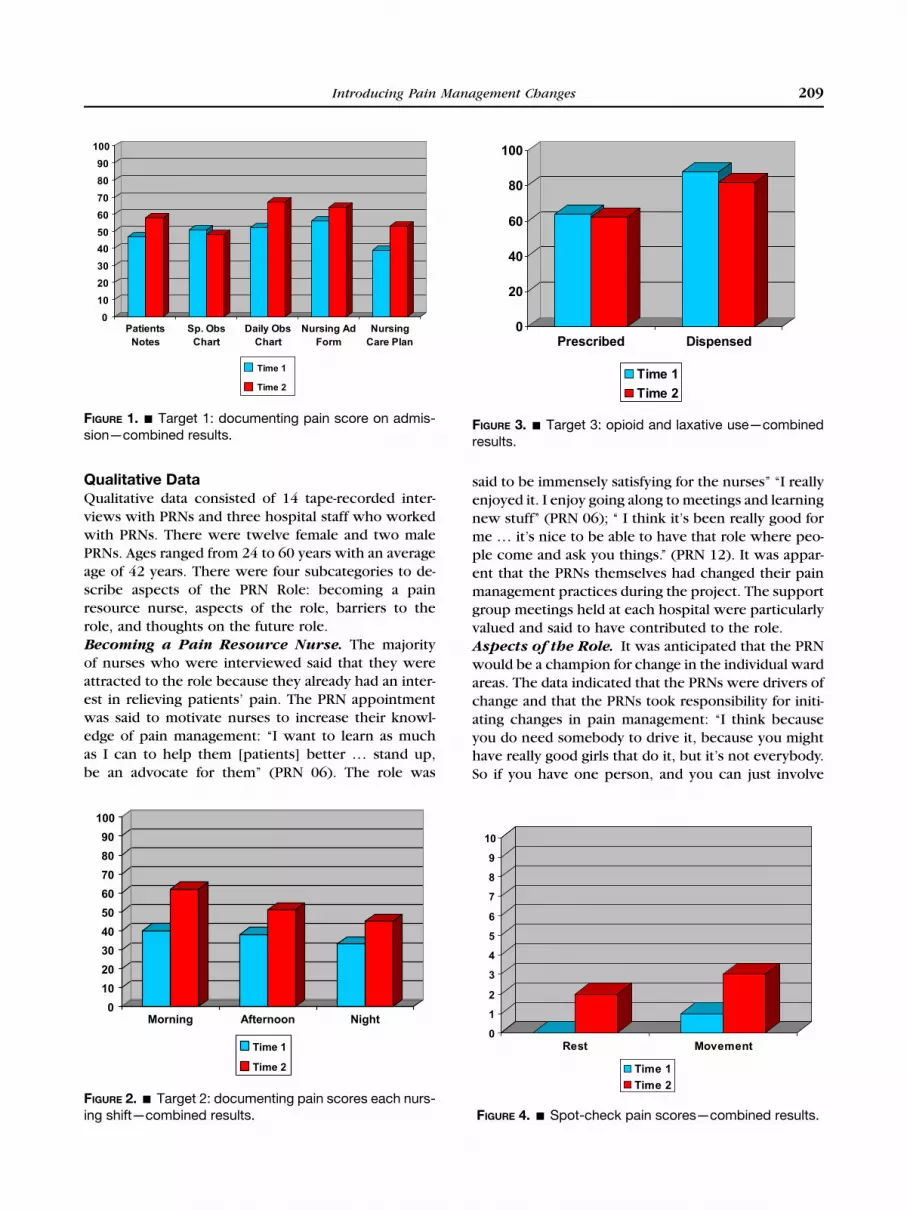
[49.7%]).Target 1: The Percentage of Patients with
a Documented Pain Score on Admission. For thecombined data, statistically significant differences
were evident between time 1 and time 2 for the Daily
Observational Chart (c2 ¼ 6.038; p ¼ .014) and Nurs-
ing Care Plans (c2 ¼ 5.11; p ¼ .024) (see Figure 1).
There were no significant differences for Patient Notes,
Special Observation Chart, and Nursing AdmissionForms. However, additional analysis identifying the
documentation of a pain score in any of the patient
documents was also statistically significant (c2 ¼35.187; p < .001). These findings indicated that there
had been an improvement in the percentage of pa-
tients with a documented pain score on admission.
Target 2: The Percentage of Patients withaDocumented Pain Score eachNursing Shift. Forthe combined data, statistically significant differences
were evident between time 1 and time 2 for the Morn-
ing Shift (c2 ¼ 35.146; p < .001), the Afternoon Shift
(c2 ¼ 11.717; p < .001), and the Night Shift (c2 ¼10.700; p < .001) (Fig. 2). These findings indicated
that there had been an improvement in the percentage
of patients with a documented pain score on each
nursing shift.
TABLE 1.
Changes Made to Ferrell and McCaffery’s ‘‘Knowledge and Attitudes Survey Regarding Pain’’
Original Questions Project Revisions for Australian Context
9. Research shows that promethazine(Phenergan) and hydroxyzine (Vistaril) arereliable potentiators of opioid analgesics.
9. Research shows that promethazine(Phenergan) is a reliable potentiator ofopioid analgesics.
18. Vicodin (hydrocodone 5 mg þacetaminophen 500 mg) PO isapproximately equal to 5-10 mg morphinePO.
18. Oxycodone 5mgPO is approximately equalto 7.5 mg morphine PO.
24. Which of the following analgesicmedications is considered to be the drugof choice for the treatment of prolongedmoderate to severe pain for cancerpatients?a. codeineb. morphinec. meperidined. tramadol
24. Which of the following analgesicmedications is considered to be the drugof choice for the treatment of prolongedmoderate to severe pain for cancerpatients?a. codeineb. morphinec. pethidined. tramadol
27. A patient was receiving morphine 200 mg/hintravenously. Today he has been receiving250 mg/h intravenously. The likelihood ofthe patient developing clinically significantrespiratory depression in the absence ofnew comorbidity is:a. <1%b. 1-10%c. 11-20%d. 21-40%e. >41%
27. A patient with persistent cancer pain hasbeen receiving daily opioid analgesics for2 months. Yesterday the patient wasreceiving morphine 50 mg/h intravenously.Today he has been receiving 65 mg/hintravenously. The likelihood of the patientdeveloping clinically significant respiratorydepression in the absence of newcomorbidity is:a. <1%b. 1-10%c. 11-20%d. 21-40%e. >41%
29. Which of the following is useful for treatmentof cancer pain?a. ibuprofen (Motrin)b. hydromorphone (Dilaudid)c. gabapentin (Neurontin)d. all of the above
29. Which of the following is useful for treatmentof cancer pain?a. ibuprofen (Nurofen)b. hydromorphone (Dilaudid)c. gabapentin (Neurontin)d. all of the above
32. Narcotic/opioid addiction is defined asa chronic neurobiologic disease,characterized by behaviors that include oneor more of the following: impaired controlover drug use, compulsive use, continueduse despite harm, and craving. Using thisdefinition in patients without a history ofdrug abuse, how likely is it that opioidaddiction will occur as a result of treatingpain with opioid analgesics?<1% 5% 25% 50% 75% 100%
32. Opioid addiction is defined as chronicneurobiologic disease, characterised bybehaviours that include one or more of thefollowing: impaired control over drug use,compulsive use, continued use despiteharm and craving. Using this definition inpatients without a history of drug abuse,how likely is it that opioid addiction willoccur as a result of treating pain with opioidanalgesics?<1% 5% 25% 50% 75% 100%
33. How likely is it that patients who developpain already have an alcohol and drugabuse problem?<1% 5%-15% 25%-50% 75%-100%
33. Approximately 5%-20% of the Australianpopulation are known to have an alcoholand drug abuse problem. How likely is it thatpatients who present with pain also have analcohol and drug abuse problem?<1% 5%-15% 25%-50% 75%-100%
(Continued )
207Introducing Pain Management Changes

TABLE 1.Continued
Original Questions Project Revisions for Australian Context
37B. Your assessment, above, is made 2 hoursafter he received morphine 2 mg IV.Half-hourly pain ratings following theinjection ranged from 6 to 8, and he had noclinically significant respiratorydepression, sedation, or other untowardside effects. He has identified 2/10 as anacceptable level of pain relief. Hisphysician’s order for analgesia is‘‘morphine IV 1-3mg q1h PRN pain relief.’’Check the action you will take at this time.1. Administer no morphine at this time.2. Administer morphine 1 mg IV now.3. Administer morphine 2 mg IV now.4. Administer morphine 3 mg IV now.
37B. Your assessment, above, is made 2 hoursafter he received morphine 2 mg IV.Half-hourly pain ratings following theinjection ranged from 6 to 8, and he had noclinically significant respiratorydepression, sedation, or other untowardside effects. He has identified 2/10 as anacceptable level of pain relief. Hisphysician’s order for analgesia is‘‘morphine IV 1-3 mg hourly PRN painrelief’’. Tick the action you will take at thistime.1. Administer no morphine at this time2. Administer morphine 1 mg IV now3. Administer morphine 2 mg IV now4. Administer morphine 3 mg IV now
38B. Your assessment, above, is made 2 hoursafter he received morphine 2 mg IV.Half-hourly pain ratings following theinjection ranged from 6 to 8, and he had noclinically significant respiratorydepression, sedation, or other untowardside effects. He has identified 2/10 as anacceptable level of pain relief. Hisphysician’s order for analgesia is‘‘morphine IV 1-3mg q1h PRN pain relief.’’Check the action you will take at this time:1. Administer no morphine at this time.2. Administer morphine 1 mg IV now.3. Administer morphine 2 mg IV now.4. Administer morphine 3 mg IV now.
38B. Your assessment, above, is made twohours after he received morphine 2 mg IV.Half-hourly pain ratings following theinjection ranged from 6 to 8, and he had noclinically significant respiratorydepression, sedation, or other untowardside effects. He has identified 2/10 as anacceptable level of pain relief. Hisphysicians’ order for analgesia is‘‘morphine IV 1-3 mg hourly PRN painrelief’’. Tick the action you will take at thistime.1. Administer no morphine at this time2. Administer morphine 1 mg IV now3. Administer morphine 2 mg IV now4. Administer morphine 3 mg IV now
208 Williams et al.
Target 3: The Percentage of Patients who havebeen Prescribed Opioids for Regular Pain Reliefthat have also been Prescribed and Dispenseda Laxative. At both time 1 and time 2, similar propor-
tions of patients were prescribed opioids and laxatives
and similar proportions were prescribed opioids and
dispensed laxatives. No statistically significant im-
provement was evident between time 1 and time 2
(Fig. 3).
Spot-Check Pain Scores. To observe whether therewas any significant difference in the patients’ experi-
ence of pain at time 1 and time 2, a spot-check pain
score was performed at the time of the document audit
on those patients able to verbalize their pain at rest
(time 1: n ¼ 113; time 2: n ¼ 109) and on movement
(time 1: n ¼ 140; time 2: n ¼ 140). Median scores
were calculated. Of note, the greatest median score
was at time 2, and this was a comparatively lowscore of 3 on movement. No statistically significant
decrease in pain scores was observed between time
1 and time 2 (Fig. 4).
Knowledge and Attitudes of PRNs. The PRNs com-
pleted the Knowledge and Attitude questionnaire
(http://prc.coh.org) in June 2007, before attending
the educational workshop (time 1), and in May 2008,near the completion of the project (time 2). Five
PRNs left the project (moved away from the hospital
or to new jobs at the same hospital) before being
able to complete the questionnaire at time 2. There-
fore, data for both time periods was obtained for a sam-
ple of 25 PRNs. A paired-samples t test analysis was
performed for all of the data (combined) and for each
hospital. For the combined data, statistically significantdifferences were evident between time 1 and time 2.
At time 1, the mean score was 29.32 (SD 2.673, range
23-36). At time 2, the mean score had increased to
31.84 (SD 2.357, range 27-36; t ¼ �4.817; p < .000;
Fig. 5).
0
10
20
30
40
50
60
70
80
90
100
Patients
Notes
Sp. Obs
Chart
Daily Obs
Chart
Nursing Ad
Form
Nursing
Care Plan
Time 1
Time 2
FIGURE 1. - Target 1: documenting pain score on admis-sion—combined results.
0
20
40
60
80
100
Prescribed Dispensed
Time 1
Time 2
FIGURE 3. - Target 3: opioid and laxative use—combinedresults.
209Introducing Pain Management Changes
Qualitative DataQualitative data consisted of 14 tape-recorded inter-
views with PRNs and three hospital staff who worked
with PRNs. There were twelve female and two malePRNs. Ages ranged from 24 to 60 years with an average
age of 42 years. There were four subcategories to de-
scribe aspects of the PRN Role: becoming a pain
resource nurse, aspects of the role, barriers to the
role, and thoughts on the future role.
Becoming a Pain Resource Nurse. The majority
of nurses who were interviewed said that they were
attracted to the role because they already had an inter-est in relieving patients’ pain. The PRN appointment
was said to motivate nurses to increase their knowl-
edge of pain management: ‘‘I want to learn as much
as I can to help them [patients] better . stand up,
be an advocate for them’’ (PRN 06). The role was
0
10
20
30
40
50
60
70
80
90
100
Morning Afternoon Night
Time 1
Time 2
FIGURE 2. - Target 2: documenting pain scores each nurs-ing shift—combined results.
said to be immensely satisfying for the nurses’’ ‘‘I really
enjoyed it. I enjoy going along to meetings and learning
new stuff’’ (PRN 06); ‘‘ I think it’s been really good for
me . it’s nice to be able to have that role where peo-
ple come and ask you things.’’ (PRN 12). It was appar-
ent that the PRNs themselves had changed their pain
management practices during the project. The supportgroup meetings held at each hospital were particularly
valued and said to have contributed to the role.
Aspects of the Role. It was anticipated that the PRN
would be a champion for change in the individual ward
areas. The data indicated that the PRNs were drivers of
change and that the PRNs took responsibility for initi-
ating changes in pain management: ‘‘I think because
you do need somebody to drive it, because you mighthave really good girls that do it, but it’s not everybody.
So if you have one person, and you can just involve
0
1
2
3
4
5
6
7
8
9
10
Rest Movement
Time 1
Time 2
FIGURE 4. - Spot-check pain scores—combined results.

0
10
20
30
40
50
60
70
80
90
100
Total Percent
Time 1
Time 2
FIGURE 5. - Nurses’ knowledge and attitude survey—combined results (n ¼ 25).
210 Williams et al.
everybody and it all snowballs from there. But you do
need to have somebody that’s not in charge, but over-
seeing’’ (PRN 01).
Various techniques were described in the qualita-tive data as being used by the PRNs to drive the
changes targeted in the project. Most of the PRNs indi-
cated that they had educated others directly. Mostly
this had been done informally, directly to individual
nurses: ‘‘Sometimes, if I hear conversations I’ll butt in
and say . something or clarify something’’ (PRN 06);
‘‘as you work, just do it as you go and people learn
that a bit easier as well’’ (PRN 12); ‘‘nothing’s too for-mal, it’s just wherever you can squeeze a moment’’
(PRN 13). Providing feedback at ward meetings was an-
other method that was mentioned. One PRN said that
they had held a pain seminar in the ward.
Indirect methods of informing others were also
said to have been used. These methods included using
a specific notice board and posters, as well as keeping
the pain resource file updated with relevant articles.However, a strong theme was a feeling from the
PRNs that they were not doing enough to promote
changes in pain management: ‘‘I wish I could have
done more’’ (PRN 05); ‘‘I probably could have done
more to promote the actual role itself’’ (PRN 03); ‘‘I
feel really guilty’’ (PRN 06).
There was evidence in these data that the PRN
role had become a resource for ward staff: ‘‘And peopleknow that I’m the Pain Resource Nurse and they do
come to me and ask what I think about something
and they ask my advice’’ (PRN 12). The PRN was
seen as a person who was accessible and easy to con-
tact for advice on pain management issues. The PRN
was also said to be a primary resource for nurses
who were new to a particular ward area, especially
new graduate nurses and nurses with less experience:‘‘And when the grads come to the ward . I showed
them [the Self-Directed Learning Package for Pain
Assessment and Management], and because you are
the Pain Resource Nurse they do listen to you more’’
(PRN 12).
Each of the PRNs had selected one of the three
pain management indicators being targeted in the pro-
ject to focus on and improve in their own area. PRNswere asked to monitor any changes in this indicator
by carrying out bimonthly audits. Data were given to
the research assistant, who produced colorful graphs
for the PRNs to display in their area. Previous projects
had indicated that these graphs provided an additional
reminder to staff about the changes in pain manage-
ment that were being promoted.
The majority of the nurses were able to carry outthese audits with assistance from the research assis-
tant. The number of audits varied between nurses.
The feedback sheet indicated that of the required six
audits, the least number completed was two and the
most was eight. Those nurses that talked about the
audits when they were interviewed described initial
difficulties that were easily overcome. Finding time to
do the auditing was an issue for some of the PRNs.One of the PRNs said that she had been able to do
the audits only by coming in after hours or by doing
them when on a nightshift.
Barriers to the Role. Finding enough time to carry
out the role of the PRN was a barrier encountered by
themajority of nurses in the project. Although 2.5 hours
per month had been allocated to the nurses to attend to
some of the aspects of their role, it was often impossibleto use this time. Extreme staffing shortages were expe-
rienced throughout theproject and thiswas said to have
made it very difficult for nurses to attend the support
group meetings and to do the bimonthly audits: ‘‘Time
is always the problem, especially with the short staffing
. I still haven’t made it to that many meetings, and
again it’s difficult to do audits’’ (PRN 05).
Some of the nurses suggested that they carried outaspects of the PRN role in their own time: ‘‘I mainly do
it in my own time or my days off when I get home .But I think everybody ends up doing that’’ (PRN 04).
The high turnover of staff in ward areas was seen as
a particular barrier to the PRNs in terms of educating
staff and changing pain management practices.
Thoughts on the Future Role. As an action research
project it was essential that feedback be obtained fromthe PRNs and from the staff working with the PRNs
regarding the future direction of the role. The plan
for the ongoing role was to offer it again to those
already working in the position. An interesting com-
ment from one of the PRNs suggested that it might
be better to have a new nurse each year to increase
the expertise in pain management across the nursing

211Introducing Pain Management Changes
population: ‘‘I think that it would be good to . keep
rotating this every year so somebody else gets the
chance of doing it, because it’s better the more people
that do it, the more people that can spread the word
really’’ (PRN, 12).
Several of the participants interviewed felt that
two PRNs in some areas would be beneficial. Increas-ing the time available for nurses to attend to aspects
of the PRN role was another suggestion. One nurse
suggested the allocation of time to work occasionally
as a PRN without a patient load.
A New Model of Introducing Change intoAcute-Care HospitalsThe model used to introduce evidence-based changes
into clinical practice in this project was developed
through previous work and was found to be an effec-
tive method of implementing change within the acute
care hospital setting. This model is illustrated in
Figure 6. The model used a layered approach to change
practice, in which change was initiated and coordi-
nated by a multidisciplinary pain management commit-tee. The committee was able to identify the three areas
of pain assessment and management that could be tar-
geted for improvement in the project. This committee
included a nurse researcher, which enabled the devel-
opment of the project using a collaborative partner-
ship with clinicians. In the present study, the pain
management committee at the public hospital was
able to coordinate and initiate change in its own hospi-tal, and this was also reflected at the private hospital.
At the time of the project, the nurse researcher on
the pain management committee was employed by
both organizations. This facilitated the adoption of
the project at each hospital.
The second layer of changing practice in this pro-
ject was composed of the nurse consultants for pain.
At the public hospital, there were three primary nurseconsultants: one designated for acute pain, one for
chronic pain, and one for palliative care. At the private
hospital, there were two primary nurse consultants
who dealt with both chronic and acute pain issues.
There was also a nurse consultant for palliative care.
These expert nurses were the leaders and supporters
of change. They developed the educational resources
for the project and provided support to the cliniciansin the ward areas. The educational resources were
a 2-day educational workshop for the newly appointed
PRNs, monthly support-group meetings, a self-directed
learning package, a pain resource file, and wall charts
and posters related to the project. A website was also
initiated at the public hospital.
The third layer of changing practice was the intro-
duction of PRNs. These nurses worked in various ward
areas of the hospital and were clinical champions for
change. They were found to:
Facilitate change by increasing their own personalknowledge and skills.Be drivers of change.
Be a resource for pain issues.Carry out regular audits on the indicators selected forchange in their area.Educate staff (especially novice staff).
Ensure that the educational resources developed by thenurse consultants were accessible to staff.
The final layer of changing practice was the healthcare staff who interacted directly with patients. These
were the agents of change who participated in the
change by increasing their personal knowledge and
skills and consistently changed their clinical practice
in response to the strategies used by the PRNs.
DISCUSSION
This action research project used a coordinated
approach to introduce evidence-based changes for painmanagement. The feasibility and effect of introducing
a new model of PRNs in conjunction with education
for staff were evaluated using both quantitative and qual-
itative methods. The qualitative data for this project re-
vealed that the newly introduced PRN role was
immensely satisfying to those in the role and valued by
those working in the wards. Previous qualitative work
on the PRN role has also found this to be the case(Holley et al., 2005). However, a number of barriers to
the role were identified. Time in particular was a factor
that strongly affected the PRN’s ability to fulfill his or
her role, and thishadbeen identified as a barrier in earlier
studies (McCleary et al., 2004; Paice et al., 2006).
Nonclinical time had been allocated to the PRN in the
design of this project. However, in reality and amid
severe staffing shortages, it was impossible for someof the PRNs to use this allocated time to carry out
PRN activities. A number of the PRNs stated that they
had carried out aspects of their role in their own time.
Suggestions were provided for the future development
of the role. Finding more time for the role was seen as
important, as well as the consideration of appointing
two nurses in some areas to the role. Further
discussions on the appointment of two nurses by theproject team concluded that primary and associate
PRN roles could be trialed.
The quantitative data showed a statistically signifi-
cant difference in the knowledge and attitudes of the
PRNs from the beginning to the end of the project. An
increase in these scores has been reported in other pro-
jects with nurses assessed by the same instrument be-
fore and after an educational intervention (Idell,

NURSE CONSULTANTS
FOR PAIN
Leaders and Supporters
of Change
PAIN RESOURCE
NURSES
Clinical Champions
for Change
Identification of Indicators of Change in Pain Management:
• The percentage of patients with a documented pain score on admission
• The percentage of patients with a documented pain score each nursing shift
• The percentage of patients who have been prescribed opioids for regular pain relief that have also been prescribed an dispensed a laxative/aperient
Development of educational resources for implementation of selected indicators:
• Two day educational workshop for PRNs • Monthly support group meetings • Self-Directed Learning Package • Pain resource file • Wall charts and posters
Facilitating Change • Increasing personal knowledge and skills • Driving change • Being a resource • Auditing and providing feedback • Educating staff (especially novice staff) • Ensuring that wall charts, posters, self-
directed learning packages and pain resource file are accessible to staff
HEALTHCARE STAFF
Agents of Change
Participation in change
• Increasing personal knowledge and skills • Consistently changing practice in
response to direction from PRN
PAIN MANAGEMENT
COMMITTEE
Multidisciplinaryrepresentatives
Co-ordinators and Initiators of
Change
FIGURE 6. - Model of change management.
212 Williams et al.
Grant, & Kirk, 2007; Paice et al. 2006; Zhang, Hsu, Zou,
Li, Wang, & Huang, 2008). Interestingly, the meanscores for these Western Australia nurses were higher
at the start of the project than the baseline scores
obtained for other newly appointed PRN nurses
(Paice et al. 2006), general nurses (Zhang, Hsu, Zou,
Li, Wang, & Huang, 2008), and oncology nurses (Idell,
Grant, & Kirk, 2007). Compared with other studies
that have carried out a one-time assessment of pain atti-
tudes and knowledge, these Western Australian nursesalso scored higher than student nurses in the U.S.
(Plaisance & Logan, 2006) and emergency nurses in Tai-
wan (Tsai et al., 2007). However, similar scores to theseWestern Australian nurses were obtained by registered
nurses in Ireland (Matthews & Malcolm, 2007).
The quantitative evaluation of changes in the iden-
tified indicators found a statistically significant im-
provement in the documentation of pain scores on
admission and each nursing shift from the beginning
to the end of the project. Nurses had been document-
ing pain scores in the private hospital for several yearsbefore the start of the project, and the nursing

213Introducing Pain Management Changes
documentation included a specific area with a prompt
for pain assessment. At the public hospital, the prompt
for pain assessment had only recently been introduced
across the hospital at the start of the project. Changes
in the daily observation chart had been instigated after
the pilot work for this project. Improvements in the
practice of documenting pain scores were apparentin the combined results as well as at each individual
hospital. It should be noted that documentation was
evaluated only for patients who were able to report
pain. Further work is warranted on the assessment
strategies used for patients unable to report pain.
Other projects in Canada and the U.S. that have intro-
duced a similar model of PRNs have also demonstrated
improvements in the documentation of pain assess-ment (Ellis et al., 2007; Paice et al., 2006).
The results for the indicator relating to the ad-
ministration of laxatives when an opioid was used
on a regular basis did not indicate any obvious change
in practice. Although nursing staff are able to initiate
the first dose of a laxative, the prescription of further
doses is the responsibility of medical staff. The educa-
tion for this project focused predominately on nurs-ing staff; more focused initiatives for medical staff
would be needed to make significant changes to this
indicator.
A spot-check pain score was used when the
patient documentation was reviewed hospital-wide
before and after the project. This was an attempt to
measure a patient-related outcome of the implementa-
tion of change. The results for this did not demon-strate any particular pattern of decreased levels of
pain. This may in part, be due to a lack of sensitivity
in this measurement technique and the recording of
average low pain scores at both recording intervals.
Furthermore, numerous factors are likely to affect
the level of pain experienced by patients located in
the hospital at any particular time. On reflection,
this approach to measuring patient outcomes can beregarded as ineffective. Of note, the median pain
scores, even on movement, were not greater than 3/
10. This reflects comparatively low pain scores across
both hospitals.
The framework of this project was a model for
changing clinical practice in the acute-care hospital
setting. This model had recently been developed
through pilot work, and drew on the experience ofother hospitals where clinical champions have been
used to assist in the ongoing coordination of translating
and using research evidence to improve clinical prac-
tice. The model incorporated a number of strategies
found in the literature relating to the translation of re-
search into practice. It was envisaged at the start of this
project that this model of change management could
be used to facilitate evidence-based practice in other
aspects of health care apart from pain. The success
of this current project would warrant further explora-
tion and use of this model.
CONCLUSIONS
The feasibility and effect of using a coordinated ap-proach to improve the management of pain was
evaluated using both quantitative and qualitative
methods. The results revealed that the PRN role was
an acceptable and effective method of introducing
and sustaining changes in nursing care. However, fur-
ther initiatives would be required to influence the
practice of medical staff.
A number of educational resources were devel-oped for use in this project. These were assessed as
valuable items for supporting the selected pain man-
agement changes. The coordination of change using
a layered, directed approach was evaluated as a useful
method for introducing and sustaining evidence-based
change in clinical practice.
Recommendations
Continue the role of PRNs with regular support-groupmeetings.Increase the time available for PRNs to carry out the
activities related to their role.Consider the introduction of two PRNs in some clinicalareas: a primary and associate PRN.
Develop and introduce more focused initiatives regard-ing pain management for medical staff.Explore the assessment strategies used for patientsunable to report pain.
Further explore the use of thismodel of changemanage-ment as described in this project to facilitate evidence-based practice change in other aspects of health care.
Acknowledgments
The authors thank the Australian Research Council (project
no. LP0775460); Corporate Nursing, Sir Charles Gairdner
Hospital; the Nursing Division, St. John of God Hospital Sub-
iaco; staff at Sir Charles Gairdner Hospital: Ms. Lyn Hellier,
Ms. Jan Stiberc, Ms. Wendy Scott, Clinical Associate Professor
Roger Goucke, Professor Di Twigg, and Ms. Sue Davis; staff at
St. John of God Hospital Subiaco: Ms. Patricia Clarke, Ms.
Valerie Colgan, Ms. Sally Greenway, Ms. Jayne Playle, Adjunct
Associate Professor Chris Hanna, and Ms. Danielle Darragh;
the Sir Charles Gairdner Hospital Pain Management Commit-
tee; Ms. Jenny Lalor and Ms. Leanne Lester for statistical sup-
port; Ms. Melissa Berg, Ms. Jenny Clarke, Ms. Belinda
Cobcroft, Ms. Linda Coventry, Ms. Maree Gilbert, Ms. Sylvia
Heavens, Ms. Tracey Klonowski, Ms. Simone Lee, Ms.
Rebecca Osseiran-Moisson, Dr. Anna Petterson, Ms. Jannie
Piercy, Mr. Chris Rompotis, Ms. Jo Siffleet, Ms. Sue Slatyer,

214 Williams et al.
Ms. Louise Winton, and Ms. Mel Zilembo for data collection;
and the National Institute of Clinical Studies, Professor Linda
Kristjanson, and Mr. Gareth Griffiths for supporting the pilot
work.
REFERENCES
Ardery, G., Herr, K., Hannon, B. J., & Titler, M. G. (2003).Lack of opioid administration in older hip fracture patients.Geriatric Nursing, 24(6), 353–360.
Australian Pain Society (2005). Pain in residential aged
care facilities-management strategies. North Sydney, NewSouth Wales: APS. Retrieved from http://www.apsoc.org.au.
Bucknall, T., Manias, E., & Botti, M. (2001). Acute painmanagement: Implications of scientific evidence for nursingpractice in the postoperative context. International Jour-nal of Nursing Practice, 7, 266–273.
Carlson, C. (2008). Development and testing of four in-struments to assess prior conditions that influence nursesadoption of evidence-based pain management practices.Journal of Advanced Nursing, 64(6), 632–643.
Ching, T. Y., & Seto,W. H. (1990). Evaluating the efficacy ofthe infection control liaison nurse in the hospital. Journal ofAdvanced Nursing, 15(10), 1128–1131.
Cooper, T. (2004). Delivering an infection control linknurse programme: Improving practice. British Journal of
Infection Control, 5(6), 24–27.Couch, C., Sheffield, P., Gerthoffer, T., Ries, A., &
Hollander, P. (2003). Clinical outcomes in patients with type2 diabetesmanaged by a diabetes resource nurse in a primarycare practice. Baylor University Medical Center Proceed-
ings, 16(3), 336–340.DeBourgh, G. A. (2001). Champions for evidence-based
practice: A critical role for advanced practice nurses. Amer-
ican Association of Critical Care Nurses Clinical Issues,
12(4), 491–508.Ellis, J. A., McCleary, L., Blouin, R., Dube, K., Rowley, B.,
MacNeil, M., & Cooke, C. (2007). Implementing bestpractice pain management in a pediatric hospital. Journalfor Specialists in Pediatric Nursing, 12(4), 264–277.
Ferrell, B. R., Grant, M., Ritchey, K. J., Ropchan, R., &Rivera, L. M. (1993). The pain resource nurse training pro-gram: A unique approach to pain management. Journal ofPain and Symptom Management, 8(8), 549–556.
Holley, S., McMillan, S. C., Hagan, S. J., Palacios, P., &Rosenberg, D. (2005). Pain resource nurses: Believing thepatients, believing in themselves.Oncology Nursing Forum,
32(4), 843–848.Idell, C. S., Grant, M., & Kirk, C. (2007). Alignment of pain
reassessment practices and national comprehensive cancernetwork guidelines. Oncology Nursing Forum, 34(3),661–671.
Krystal, A., Carr, J., Gavaghn, K., Porterfield, P., &Turner, L. (1997). Implementing a hospital-wide painmanagement strategy. Canadian Journal of Nursing
Administration, 10(3), 74–89.Matthews, E., & Malcolm, C. (2007). Nurses knowledge
and attitudes in pain management practice. British Journal
of Nursing, 16(3), 174–179.
McCleary, L., Ellis, J. A., & Rowley, B. (2004). Evaluationof the pain resource nurse role: A resource for improvingpediatric pain management. Pain Management Nursing,
5(1), 29–36.McMillan, S. C., Tittle, M., Hagan, S. J., & Small, B. J. (2005).
Training pain resource nurses: Changes in their knowledgeand attitudes. Oncology Nursing Forum, 32(4), 835–842.Michaels, T. K., Hubbartt, E., Carroll, S. A., & Hudson-
Barr, D. (2007). Evaluating an educational approach to im-prove pain assessment in hospitalized patients. Journal ofNursing Care Quality, 22(3), 260–265.Paice, J. A., Barnard, C., Creamer, J., & Omerod, K. (2006).
Creating organizational change through the pain resourcenurse program. Journal on Quality and Patient Safety,
32(1), 24–31.Perry-Woodford, Z., & Whayman, K. (2005). Link-nurse
programme. Education in practice: A colorectal link-nurseprogramme. British Journal of Nursing, 14(6), 862–866.Plaisance, L., & Logan, C. (2006). Nursing student’s
knowledge and attitudes regarding pain. Pain Management
Nursing, 7(4), 167–175.Saward, D., Aranda, S., Flemming, J., Pate, K., Williams, P.,
& Eichner, C. (2005). Improving pain management:
Insights from a study using neer-peer facilitation. Paperpresented at the Partners in Pain, Sydney, Australia.Senesac, P.M. (2004). The Roy Adaptation Model: An
action research approach to the implementation of a pain
management organizational change project. Doctoraldissertation. Retrieved from http://search.epnet.com/login.aspx?direct=true&db=jlh&an=200509781Shepherd, M., Hattersley, A., & Ellard, S. (2005). Integra-
tion of the MODY link nurse project: 20-month evaluation.Journal of Diabetes Nursing, 9(12), 47–52.Stringer, E. T. (1999).Action research, (2nd ed.) California:
Sage Publications.Williams, A.M., Griffiths, G., Fairclough, D., Hellier, L.,
Oldham, L., Kristjanson, L., Goucke, R., & Slatyer, S. (2006).Using action research as a model of research utilisation to
improve pain assessmentandmanagement. Perth, WesternAustralia: WA Centre for Cancer and Palliative Care, EdithCowan University & Centre for Nursing Research, Sir CharlesGairdner Hospital.Yates, P. M., Edwards, H. E., Nash, R. E., Walsh, A. M.,
Fentiman, B. J., & Skerman, H. M., et al. (2002). Barriers toeffective cancer pain management: A survey of hospitalisedcancer patients in Australia. Journal of Pain and Symptom
Management, 23(5), 393–405.Zhang, C., Hsu, L., Zou, B., Li, J., Wang, H., & Huang, J.
(2008). Effects of a pain education program on nurses’ painknowledge, attitudes and pain assessment practices inChina. Journal of Pain and Symptom Management, 36(6),616–627.