ers-all-documents-combined.pdf - shared health
TRANSCRIPT
1
Contents (alphanumeric)
TABLE OF CONTENTS (ALPHANUMERIC)
Version date: 2022-05-19 Publication date: 2022-06-01
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
NOTE: Except where otherwise indicated, there has been only minor reformatting: each care map & protocol will now list only the most recent changes within the document. Tracking of historical changes will now be listed in Section X.
A POLICIES & PROCEDURES
A01 Overview of Clinical Care
A02 Physician Orders, Clinical Support & OLMS
A05 Treatment / Transport Refusals
A06 EMS/PT Scope of Work
A09 Medical Procedures During COVID Revised
B DESTINATION
B01 Standard Destination
B02 Redirection Advisory
B03 Destination When the Closest ED is in Winnipeg
B04.1 Trauma Bypass for IERHA & SHSS Geographic Areas
B04.2 Trauma Bypass for PMH Geographic Area
B04.3 Trauma Bypass for NRHA Geographic Area
C RESUSCITATION
C01 Basic Resuscitation
C02 Advanced Resuscitation
C04 EZ-IO Insertion
C05 Unstable Bradycardia
C06 Unstable Tachycardia
C07 Shock
2
Contents (alphanumeric)
C08AB Left Ventricular Assist Device
C09AB Implanted Cardiovertor Defibrillator
C11 Airway Obstruction During COVID
C12 Managing Hypoxemia during COVID
D MATERNAL & NEWBORN CARE
D01 Newborn Care & Resuscitation
D02 Prehospital Delivery
D03.1 Prolapsed Cord
D03.2 Breech Presentation
D03.3 Multiple Gestations
D03.4 Shoulder Dystocia
D04 Maternal Hemorrhage
D05 Preeclampsia & Eclampsia
D07 Positioning the Pregnant Patient During Transport
E MEDICAL CONDITIONS
E02AB Agitation
E03 Anaphylaxis
E04A Acute Coronary Syndrome & STEMI
E06 Dyspnea & Respiratory Distress
E10 Hypoglycemia
E13A Hyperkalemia - adult
E13B Hyperkalemia - adolescent
E14 Seizures
E15A Acute Stroke
E20 Alcohol & Benzodiazepine Withdrawal
E25AB Methamphetamine Psychosis
3
Contents (alphanumeric)
E30A Palliative Care in the Home (IERHA)
F TRAUMA & ENVIRONMENTAL CONDITIONS
F01 Major Trauma New
F01A Exsanguinating External Hemorrhage - adult Contents moved into new F01
F01B Exsanguinating External Hemorrhage - adolescent Contents moved into new F01
F01C Exsanguinating External Hemorrhage - child Contents moved into new F01
F02A Traumatic Hemorrhage & Shock - adult Contents moved into new F01
F02B Traumatic Hemorrhage & Shock - adolescent Contents moved into new F01
F02C Traumatic Hemorrhage & Shock - child Contents moved into new F01
F03 Burns Revised
F04 Spinal Motion Restriction Revised
F05.3 Eye Trauma Revised & renumbered
F06.1 Long Bone Fracture Contents moved into new F01
F07 Amputations & Lacerations Contents moved into new F01
F08 Pelvic Trauma Contents moved into new F01
F09 Thoracic Trauma Contents moved into new F01
F10 Abdominal Trauma Contents moved into new F01
G PATIENT TRANSPORT
G01 Established Medication Infusions
G02 Scheduled Medications
G03 Adult Transport Team Primary Work Scope New
H REFERENCES
H01 Pediatric Vital Signs
H02 Left Ventricular Assist Device
H03.1 Patient Care Map Format
H03.2 Medication Protocol Format
4
Contents (alphanumeric)
H06 Mass Casualty Triage
H07 Differentiating Scopes of Practice & Work
H08 Stillbirth in the Prehospital Environment
H09 National Early Warning Score - 2
M MEDICATIONS
M01 Adenosine
M02.1 Acetaminophen
M02.2 Ibuprofen
M03.1 Morphine
M03.2 Fentanyl
M04.1 Dimenhydrinate
M04.2 Metoclopramide
M04.3 Ondansetron
M05.1 Epinephrine for anaphylaxis
M05.2 Epinephrine for cardiac arrest
M05.4 Epinephrine for croup
M06.1 Glucose
M06.2 Dextrose
M06.3 Glucagon
M07.1 Midazolam
M07.5 Lorazepam
M09 Furosemide
M10 Hyperkalemia Therapy
M11 Naloxone
M12 Tetracaine
M13 Hydrocortisone
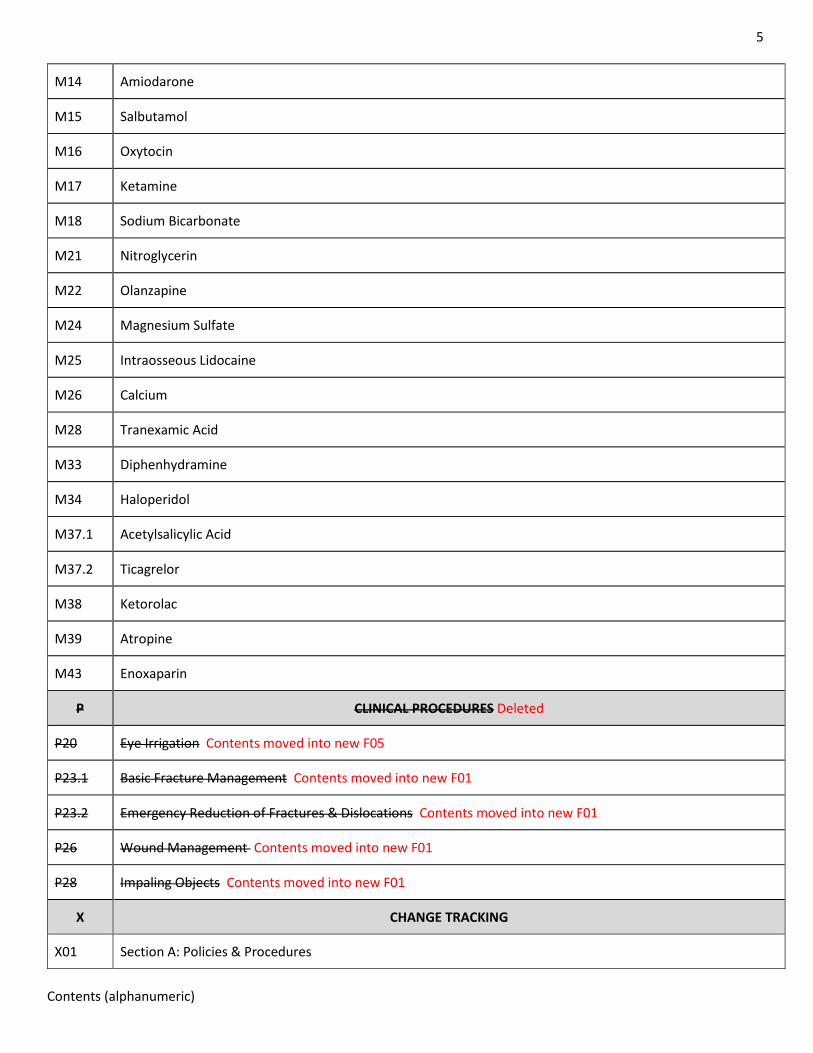
5
Contents (alphanumeric)
M14 Amiodarone
M15 Salbutamol
M16 Oxytocin
M17 Ketamine
M18 Sodium Bicarbonate
M21 Nitroglycerin
M22 Olanzapine
M24 Magnesium Sulfate
M25 Intraosseous Lidocaine
M26 Calcium
M28 Tranexamic Acid
M33 Diphenhydramine
M34 Haloperidol
M37.1 Acetylsalicylic Acid
M37.2 Ticagrelor
M38 Ketorolac
M39 Atropine
M43 Enoxaparin
P CLINICAL PROCEDURES Deleted
P20 Eye Irrigation Contents moved into new F05
P23.1 Basic Fracture Management Contents moved into new F01
P23.2 Emergency Reduction of Fractures & Dislocations Contents moved into new F01
P26 Wound Management Contents moved into new F01
P28 Impaling Objects Contents moved into new F01
X CHANGE TRACKING
X01 Section A: Policies & Procedures
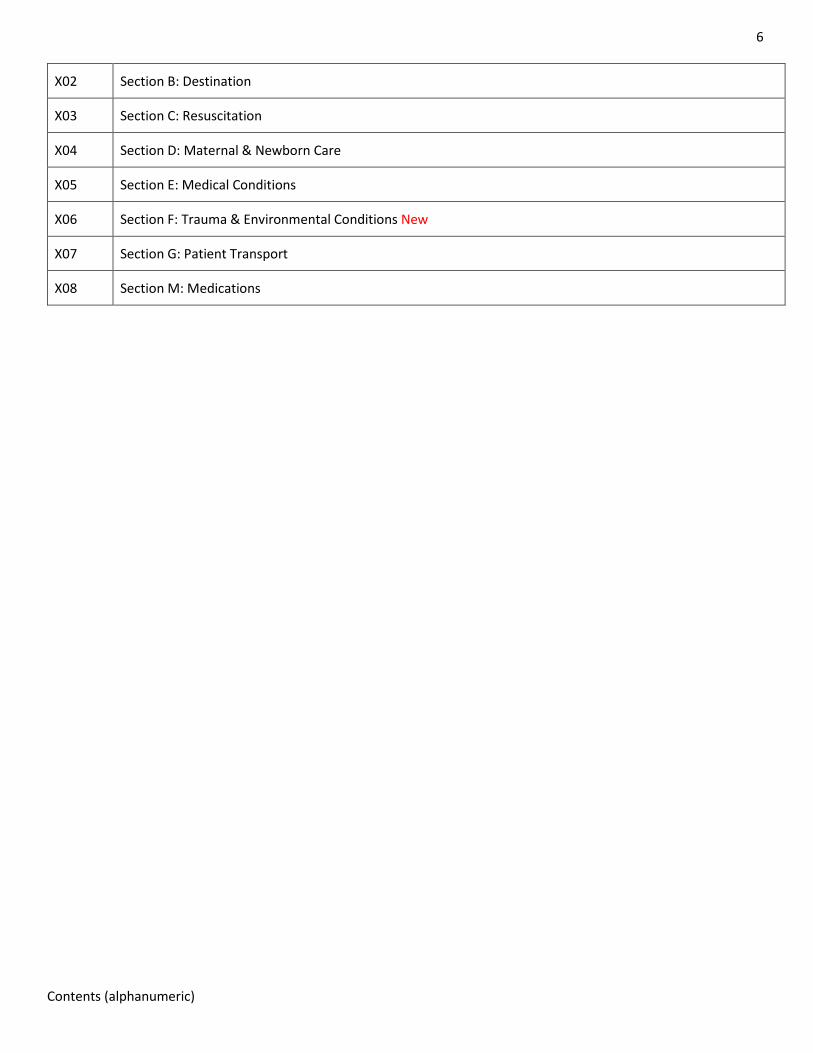
6
Contents (alphanumeric)
X02 Section B: Destination
X03 Section C: Resuscitation
X04 Section D: Maternal & Newborn Care
X05 Section E: Medical Conditions
X06 Section F: Trauma & Environmental Conditions New
X07 Section G: Patient Transport
X08 Section M: Medications
1
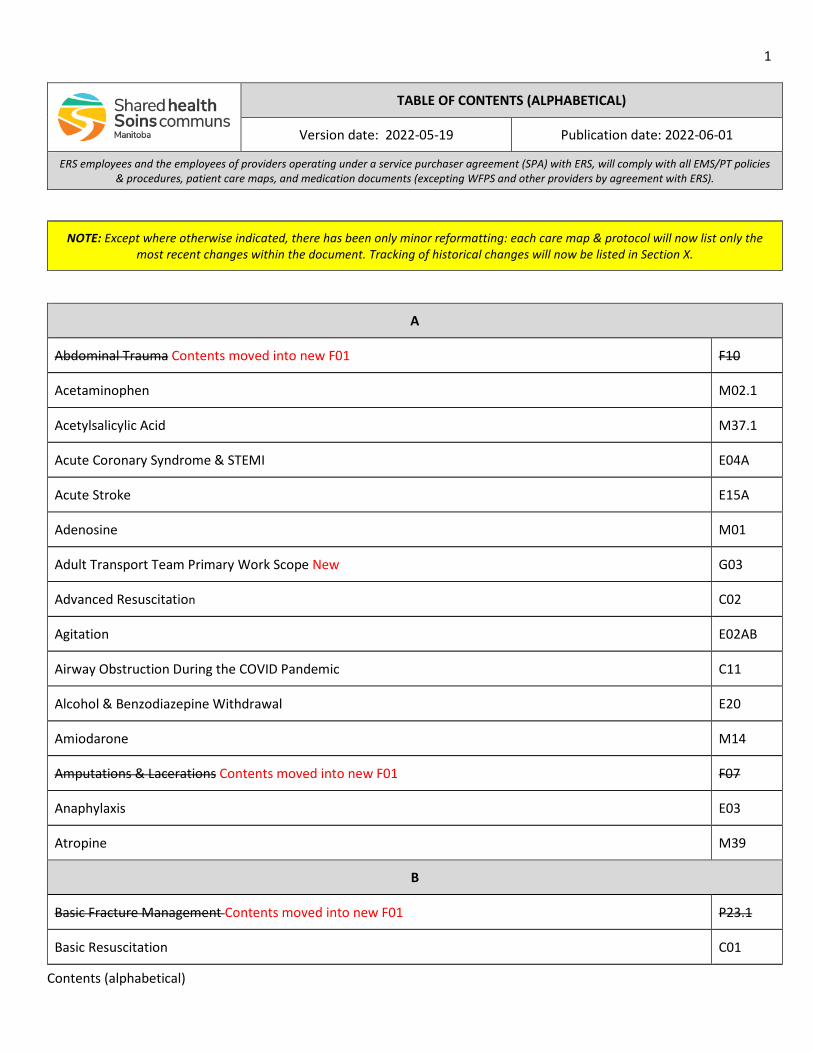
Contents (alphabetical)
TABLE OF CONTENTS (ALPHABETICAL)
Version date: 2022-05-19 Publication date: 2022-06-01
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
NOTE: Except where otherwise indicated, there has been only minor reformatting: each care map & protocol will now list only the most recent changes within the document. Tracking of historical changes will now be listed in Section X.
A
Abdominal Trauma Contents moved into new F01 F10
Acetaminophen M02.1
Acetylsalicylic Acid M37.1
Acute Coronary Syndrome & STEMI E04A
Acute Stroke E15A
Adenosine M01
Adult Transport Team Primary Work Scope New G03
Advanced Resuscitation C02
Agitation E02AB
Airway Obstruction During the COVID Pandemic C11
Alcohol & Benzodiazepine Withdrawal E20
Amiodarone M14
Amputations & Lacerations Contents moved into new F01 F07
Anaphylaxis E03
Atropine M39
B
Basic Fracture Management Contents moved into new F01 P23.1
Basic Resuscitation C01
2
Contents (alphabetical)
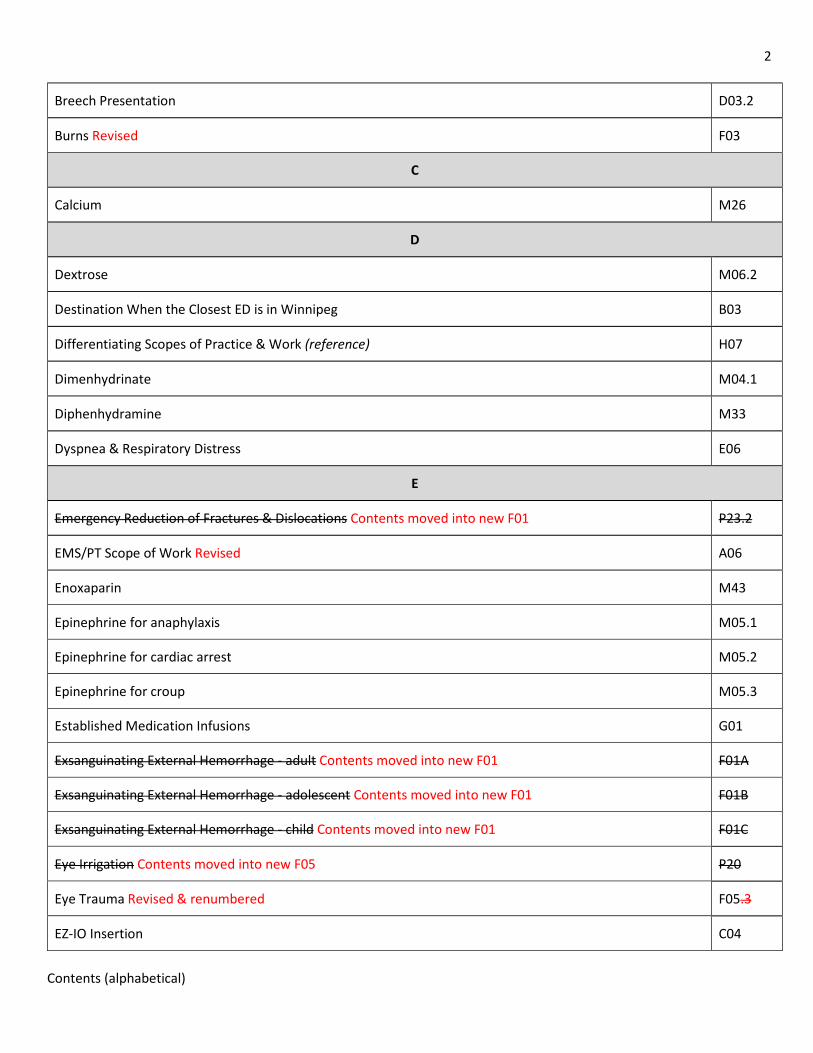
Breech Presentation D03.2
Burns Revised F03
C
Calcium M26
D
Dextrose M06.2
Destination When the Closest ED is in Winnipeg B03
Differentiating Scopes of Practice & Work (reference) H07
Dimenhydrinate M04.1
Diphenhydramine M33
Dyspnea & Respiratory Distress E06
E
Emergency Reduction of Fractures & Dislocations Contents moved into new F01 P23.2
EMS/PT Scope of Work Revised A06
Enoxaparin M43
Epinephrine for anaphylaxis M05.1
Epinephrine for cardiac arrest M05.2
Epinephrine for croup M05.3
Established Medication Infusions G01
Exsanguinating External Hemorrhage - adult Contents moved into new F01 F01A
Exsanguinating External Hemorrhage - adolescent Contents moved into new F01 F01B
Exsanguinating External Hemorrhage - child Contents moved into new F01 F01C
Eye Irrigation Contents moved into new F05 P20
Eye Trauma Revised & renumbered F05.3
EZ-IO Insertion C04
3
Contents (alphabetical)
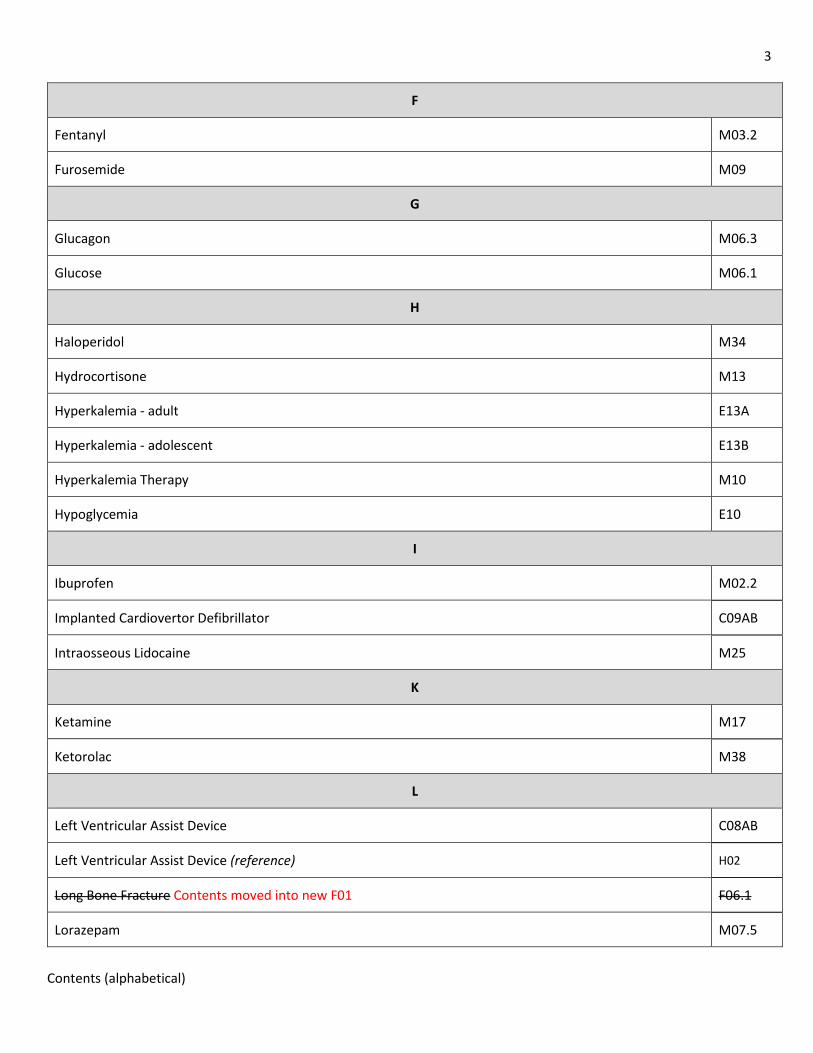
F
Fentanyl M03.2
Furosemide M09
G
Glucagon M06.3
Glucose M06.1
H
Haloperidol M34
Hydrocortisone M13
Hyperkalemia - adult E13A
Hyperkalemia - adolescent E13B
Hyperkalemia Therapy M10
Hypoglycemia E10
I
Ibuprofen M02.2
Implanted Cardiovertor Defibrillator C09AB
Intraosseous Lidocaine M25
K
Ketamine M17
Ketorolac M38
L
Left Ventricular Assist Device C08AB
Left Ventricular Assist Device (reference) H02
Long Bone Fracture Contents moved into new F01 F06.1
Lorazepam M07.5
4
Contents (alphabetical)
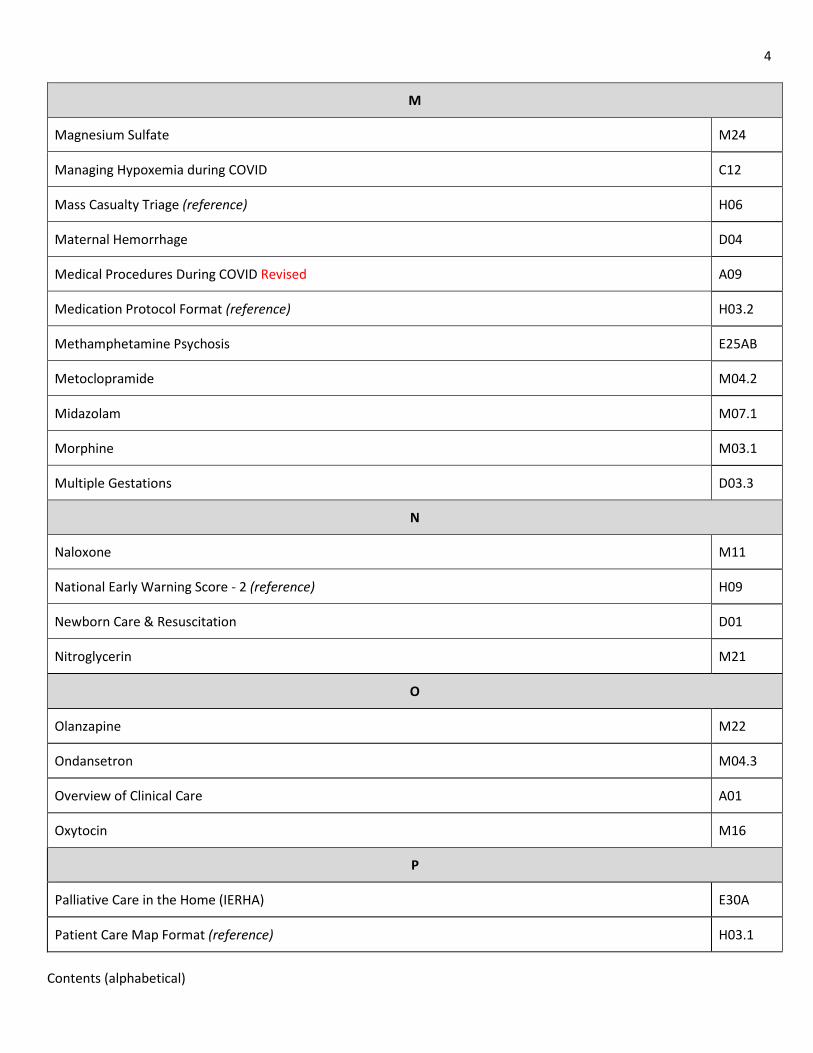
M
Magnesium Sulfate M24
Managing Hypoxemia during COVID C12
Mass Casualty Triage (reference) H06
Maternal Hemorrhage D04
Medical Procedures During COVID Revised A09
Medication Protocol Format (reference) H03.2
Methamphetamine Psychosis E25AB
Metoclopramide M04.2
Midazolam M07.1
Morphine M03.1
Multiple Gestations D03.3
N
Naloxone M11
National Early Warning Score - 2 (reference) H09
Newborn Care & Resuscitation D01
Nitroglycerin M21
O
Olanzapine M22
Ondansetron M04.3
Overview of Clinical Care A01
Oxytocin M16
P
Palliative Care in the Home (IERHA) E30A
Patient Care Map Format (reference) H03.1
5
Contents (alphabetical)
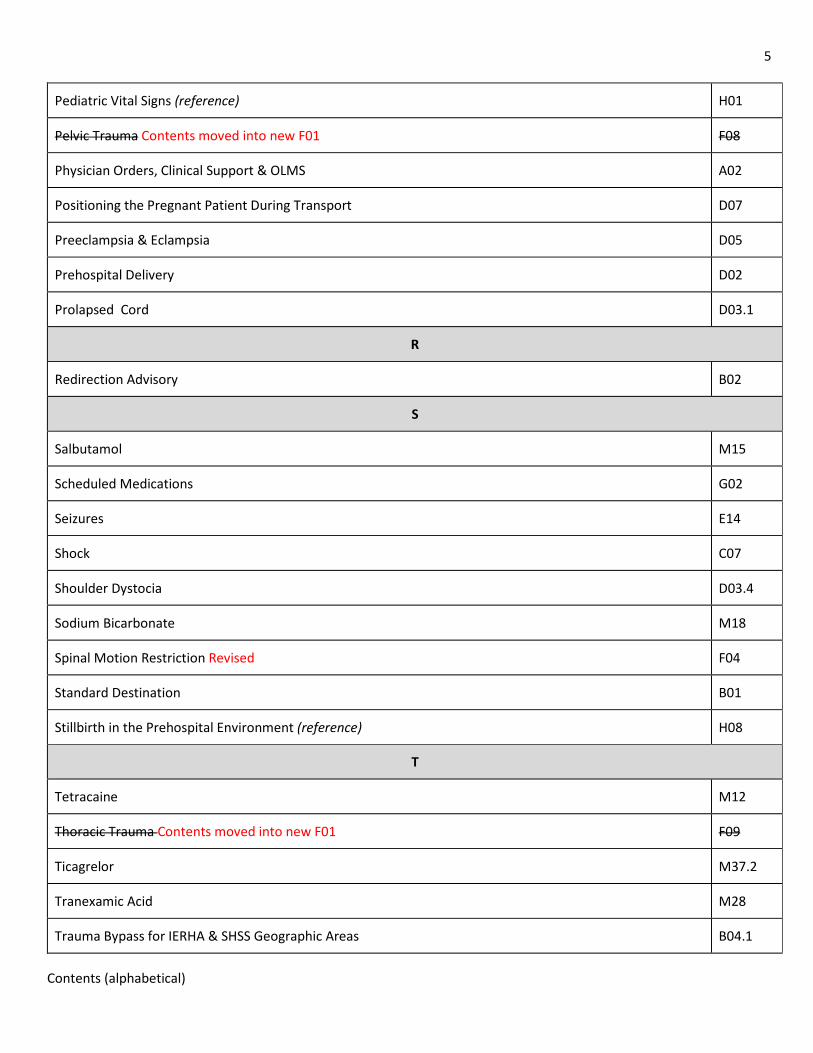
Pediatric Vital Signs (reference) H01
Pelvic Trauma Contents moved into new F01 F08
Physician Orders, Clinical Support & OLMS A02
Positioning the Pregnant Patient During Transport D07
Preeclampsia & Eclampsia D05
Prehospital Delivery D02
Prolapsed Cord D03.1
R
Redirection Advisory B02
S
Salbutamol M15
Scheduled Medications G02
Seizures E14
Shock C07
Shoulder Dystocia D03.4
Sodium Bicarbonate M18
Spinal Motion Restriction Revised F04
Standard Destination B01
Stillbirth in the Prehospital Environment (reference) H08
T
Tetracaine M12
Thoracic Trauma Contents moved into new F01 F09
Ticagrelor M37.2
Tranexamic Acid M28
Trauma Bypass for IERHA & SHSS Geographic Areas B04.1
6
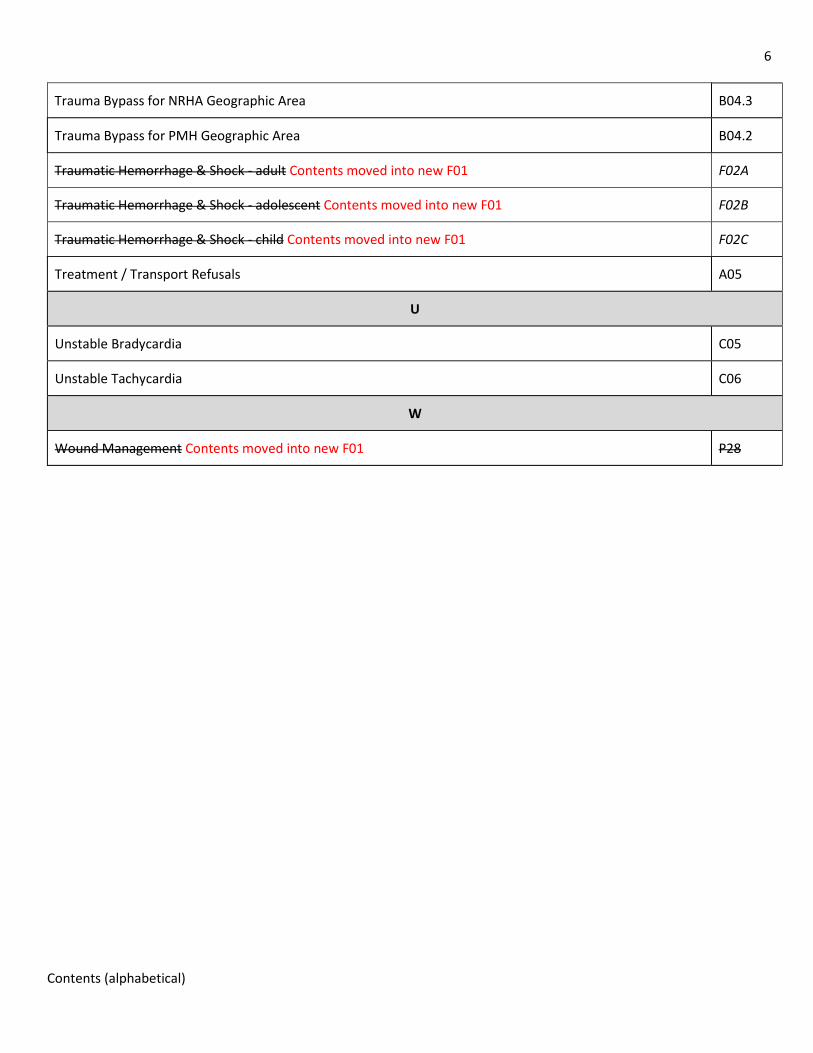
Contents (alphabetical)
Trauma Bypass for NRHA Geographic Area B04.3
Trauma Bypass for PMH Geographic Area B04.2
Traumatic Hemorrhage & Shock - adult Contents moved into new F01 F02A
Traumatic Hemorrhage & Shock - adolescent Contents moved into new F01 F02B
Traumatic Hemorrhage & Shock - child Contents moved into new F01 F02C
Treatment / Transport Refusals A05
U
Unstable Bradycardia C05
Unstable Tachycardia C06
W
Wound Management Contents moved into new F01 P28
1
A01 - CLINICAL CARE
A01 – OVERVIEW OF CLINICAL CARE
POLICIES & PROCEDURES
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-14 Effective Date: 2022-03-23 (0700 hrs)
SECTION A - DEFINITIONS
For the purposes of all EMS/PT policies, procedures, patient care maps and medication documents, the following definitions shall apply.
1. PARAMEDIC: All emergency medical responders (EMR) and paramedics employed by ERS, as well as those employed by any service provider operating under an SPA with ERS, with the exception of Winnipeg Fire Paramedic Service (or other SPA provider by agreement with ERS).
2. RESERVED ACT: A medical function that can only be performed by health professionals. With the establishment of the College of Paramedics of Manitoba (CPMB) in 2020, paramedics became a self-regulating profession and are lawfully allowed to perform certain reserved acts by virtue of being a registrant of the College.
3. SCOPE OF PRACTICE : The set of reserved acts that a paramedic is lawfully able to perform and is determined by the paramedic’s subregistration with the College (also referred to as practice scope, or professional scope). It is established by regulation and can only be changed by legislation. Paramedics may not perform a reserved act that is not allowed by the CPMB, even with a physician’s order, and could face disciplinary action by the College for doing so.
4. SCOPE OF WORK: The set of medical functions (reserved acts) that a paramedic is allowed to perform when working for EMS/PT or one of its SPA providers (also referred to as work scope). It cannot exceed a paramedic’s professional scope, even with a physician’s order (refer also to H07 - DIFFERENTIATING PRACTICE & WORK SCOPE).
The patient care maps and medication standing order identify the scope of work for EMS/PT, and are grouped as follows (refer also to A06 - EMS/PT SCOPE OF WORK):
a. BASIC WORK SCOPE: The set of medical functions that may be performed by individuals employed at the EMR or basic provider level , and registered with the CPMB at the emergency medical responder (EMR) level.
b. PRIMARY WORK SCOPE: The set of medical functions that may be performed by individuals employed at the PCP or primary provider level, and registered with the CPMB at the primary care paramedic (PCP) level, at minimum.
c. INTERMEDIATE WORK SCOPE: The set of medical functions that may be performed by individuals employed at the ICP or intermediate provider level, and registered with the CPMB at the primary care paramedic with the notation “intermediate care” level, at minimum.
5. PATIENT CARE MAP: A protocol outlining how a clinical condition or patient care situation is to be managed, when all indications are met, and no contraindications are present (also referred to as a care map). All EMS/PT care maps are intended to comply with the CPMB scopes of practice.
6. MEDICATION DOCUMENT: A protocol outlining how a medication or therapy is to be administered, including the indications, contraindications, dose, route, and frequency (also referred to as med documents). All EMS/PT med documents are intended to comply with the CPMB scopes of practice.
2
A01 - CLINICAL CARE
a. STANDING ORDER: A physician’s order to administer a medication or therapy that can be applied in all circumstances, where the indications are met and there are no contraindication, and does not require consultation with a physician.
b. INTERIM ORDER: A temporary physician’s order to administer a medication or therapy that applies to a unique patient, in a unique set of clinical circumstances, during this particular encounter only. This requires real-time consultation with a physician.
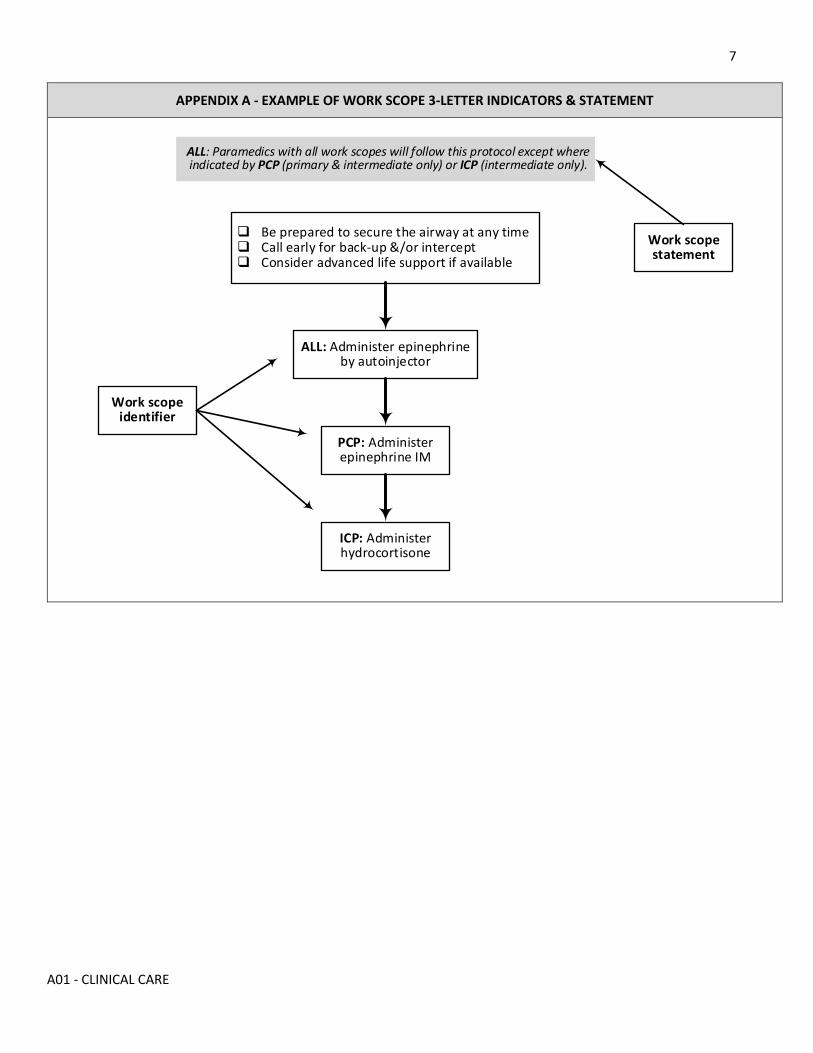
7. WORK SCOPE INDICATOR: Within each care map or medication document, paramedics with different work scopes will be authorized to perform different medical functions. This will be indicated by the following three letter indicators, and an italicized scope of work statement at the top or bottom of each flow chart (appendix A).
As used here, the abbreviations PCP and ICP refer to the EMS/PT work scope, and not specifically the CPMB subregistration level (eg. an individual registered with the CPMB at the PCP-IC level, may be employed with the primary work scope).
a. ICP: This medical function may be performed by paramedics with the intermediate work scope only.
b. PCP: This medical function may be performed by paramedics with the primary and intermediate work scopes only.
c. ALL: This medical function may be performed by paramedics with the basic, primary, and intermediate work scopes only. When all steps in a care map apply to all paramedics, there may be no work scope indicator.
8. AGE COHORTS: Different care maps and medication orders may apply to patients of different age. These cohorts are standardized as follows, and may be indicated by a suffix in the map’s alphanumeric indicator (eg. E04A - ACS & STEMI. When a care map applies to patients of all ages, or a clinical condition (rather than an age cohort) the suffix will be deleted (eg. D02 - PREHOSPITAL DELIVERY).
a. ADULT (A): seventeen (17) years and older)
b. ADOLESCENT (B): - ten (10) up to seventeen (17) years
c. CHILD (C): one (1) up to ten (10) years
d. INFANT (D): 72 hours up to twelve (12) months
e. NEWBORN (E): birth up to seventy-two (72) hours post-partum
9. KNOWN OR SUSPECTED: A clinical condition shall be known to be present if based on all currently available information a paramedic should reasonably conclude that the condition is present. A clinical condition shall be suspected to be present if based on all currently available information a paramedic reasonably concludes that the condition is more likely than not the cause of a patient’s presentation.
10. CONSIDER: Paramedics will consider performing an action by analyzing all currently available information to determine if that action may be more likely than not to benefit the patient given the clinical circumstances.
11. CLOSEST ED: An emergency department (ED) or health care facility will be considered closest if it has the shortest estimated transport time from the patient’s current location, regardless of Service Delivery Organization (SDO) boundaries or the Provincial border. When two facilities have similar transport times, the closest will be considered that which has the shortest estimated transport distance.
12. HEALTH CARE PROXY: An individual who has been appointed to make medical decisions for a patient if the patient is unable to do so (also referred to as a proxy, or representative). This may be indicated in a written document such as a living will or health care directive. In the absence of appropriate documentation, a paramedic may follow the directions of an individual who indicates that they have been designated as the proxy if they reasonably believe the individual to be truthful.
3
A01 - CLINICAL CARE
13. SUBSITUTE DECISION MAKER: In the absence of a proxy, the following hierarchy of individuals who may act as a on behalf of the patient: a. Spouse or common-law partner b. Parent with primary care and control c. Parent with legal access d. Child e. Sibling f. Other first degree relative
SECTION B - GENERAL
1. All patient care must be provided in accordance with the standards of practice established by the College of Paramedics of Manitoba (CPMB), and the policies and procedures (patient care maps, destination policies, medication & procedure documents, standard operating procedures) established by EMS/PT.
2. The EMS/PT medication documents constitute the standing orders that authorize paramedics to administer a medication or therapy where a physician order is required.
3. In a unique clinical situation that is not addressed by the current protocols, an EMS/PT physician or ERS-affiliated physician may provide an interim order temporarily allowing a paramedic to administer a medication or therapy. It may exceed the paramedic’s usual scope of work (ie. exceed a currently published medication document) but cannot exceed the CPMB scope of practice. CPMB registrants are responsible to know and maintain their scope of practice, regardless of a physician or paramedic order (refer also to A02 - PHYSICIAN ORDERS, CLINICAL SUPPORT & OLMS).
4. Paramedics will operate in good faith and provide care in accordance with the patient’s best interests and will work collaboratively with other health care providers in the shared care model.
5. Informed consent from the patient or their proxy is required for any significant intervention. Consent may be obtained verbally unless specified otherwise. In critical circumstances where consent cannot be obtained, the principle of implied consent will apply. Paramedics must abide by a valid health care directive (refer also to A05 - TREATMENT / TRANSPORT REFUSALS) .
SECTION C - ASSESSMENT
1. Paramedics must always utilize personal protective equipment (PPE) and follow appropriate body substance isolation (BSI) procedures; they must comply with all EMS/PT protocols and procedures for infection prevention control and post exposure care.
2. An initial scene assessment must be conducted, including an evaluation of safety, the need for additional EMS resources, and the need for assistance from other agencies or services (e.g., law enforcement). If additional resources are known or suspected to be required, paramedics should request these as soon as possible.
3. A primary clinical assessment must be conducted efficiently and systematically on every patient. Steps may be performed sequentially or concurrently, depending upon the patient’s condition and on-scene resources. Paramedics should repeat the primary assessment whenever there is a significant change in the patient’s condition.
4. For victims of major trauma, a rapid trauma survey including a screen for life-threatening injuries should precede the secondary assessment.
4
A01 - CLINICAL CARE
5. If an immediate life-threatening condition is identified or suspected, appropriate life-saving interventions must be promptly initiated before continuing the assessment. With sufficient resources on the scene, further assessment may be performed concurrently with life-saving procedures. In the event that a life-threatening condition is also time-sensitive (e.g., major trauma), certain interventions (eg. vascular access) should be initiated during transport.
6. After immediate life-threatening conditions are managed, paramedics will conduct a secondary clinical assessment that includes an appropriate history, collateral information, details of the incident, and a relevant physical examination. The examination may be generalized or focused as indicated by the patient’s condition or complaint(s).
7. Unless otherwise specified, at least one core set of vital signs including heart rate, respiratory rate, blood pressure and oxygen saturation must be performed for every patient, unless precluded by resuscitative or other life-saving measures. Temperature, Glasgow coma scale (GCS) and blood glucose measurements will be obtained as required. Vital signs must be repeated at appropriate intervals.
8. Appropriate monitoring and interventions will be performed as dictated by the patient’s complaint(s) or condition.
9. If a life-threatening or time-sensitive condition is not identified or suspected, further assessment can be initiated or performed on-scene or during transport as appropriate.
SECTION D - MANAGEMENT
1. Paramedics must consider the patient’s complaint(s), clinical condition, transport duration and potential for deterioration during transport when deciding to perform a medical function in the field. Medical functions that are more appropriately performed in a health care facility should be deferred, where safe and appropriate.
2. If a paramedic initiates or establishes a medical function (e.g., traction splinting, vascular access), they remain responsible for ongoing management until care is transferred to another appropriate health care provider or the intervention is discontinued.
3. Management of subjective symptoms (e.g., pain, nausea) should be carried out using pharmacologic and, where appropriate, non-pharmacologic measures (e.g., splinting of injuries) in accordance with the paramedic’s clinical judgment as to the cause and the patient’s stability. The patient’s subjective report as to the severity of a symptom (e.g., pain severity scale) must be used to inform management decisions.
4. Unstable patients should not receive anything by mouth (NPO), except for essential medications.
SECTION E - SUPPORT
1. Paramedics should contact the on-call superintendent / supervisor (OCS) for assistance with operational issues and problem solving, or where directed to do so by a specific care map.
2. Paramedics may contact the Medical Transportation Coordination Centre (MTCC) for assistance in determining the closest appropriate facility, or for information about hospital status.
5
A01 - CLINICAL CARE
SECTION F - TRANSPORT
1. The timing and urgency of transport, and the complexity and frequency of monitoring during transport, will be based on the patient’s condition or complaint(s). For time sensitive situations (e.g., acute stroke) paramedics should consider strategies (e.g., air intercept) that will expedite arrival at the destination.
2. Paramedics will transport as per the published destination and bypass protocols (section B).
Paramedics may contact the on-line medical support (OLMS) physician or on-call superintendent / supervisor (OCS) for assistance with destination decision making within the established protocols.
Paramedics may not contact OLMS or OCS to over-ride a destination protocol (eg. transporting a stable trauma patient who does not meet established indicators for bypass to an alternate destination to avoid a secondary interfacility transfer).
3. If it is known or reasonably anticipated that a medical function beyond the paramedic’s practice scope may be required during an interfacility transport (IFT), paramedics should request that an appropriate health care provider (HCP) who can perform the function (e.g., newborn resuscitation when transporting a patient in active labor) accompany the patient.
4. Non-clinical issues such as road and weather conditions that can impact patient, provider and public safety will be at the discretion of the vehicle operator.
5. Paramedics must transport at safe vehicular speeds and comply with all aspects of the Highway Traffic Act. All patients must be appropriately positioned, and all occupants must be appropriately secured prior to transport. Minors should be transported in the company of a parent or legal guardian.
6. Paramedics will transport as per established destination protocols. The on-line medical support (OLMS) physician or on-call superintendent / supervisor (OCS) may be contacted for assistance regarding destination decision making.
7. Mechanical devices (eg. Autopulse) may be used to provide chest compressions during transport.
SECTION G - DOCUMENTATION & TRANSFER OF CARE
1. Except for mass casualty situations, paramedics will only transfer the ongoing care of the patient to an appropriate HCP whose scope of work allows them to assume the transfer of care.
2. Paramedics must document in a legible fashion all relevant clinical information on the patient care record. Accepted medical terminology should be used and abbreviations should be avoided.
3. The transfer of care from SHM-ERS to facility personnel occurs with triage by a registered nurse and the assignment of a CTAS score.
4. Paramedics will cooperate with facility staff to ensure safe and appropriate off-loading.
5. Paramedics will provide an appropriate report to a receiving HCP and will ensure that EMS is not immediately required or further assistance or emergent IFT.
6
A01 - CLINICAL CARE
LINKS
A02 - PHYSICIAN ORDERS, CLINICAL SUPPORT & OLMS A05 - TREATMENT / TRANSPORT REFUSAL A06 - EMS/PT SCOPES OF WORK H07 - DIFFERENTIATING SCOPES OF PRACTICE & WORK
APPROVED BY
Medical Director, EMS & Patient Transport Associate Medical Director, EMS & Patient Transport
VERSION CHANGES (refer to X01 for change tracking)
• Minor reformatting
7
A01 - CLINICAL CARE
APPENDIX A - EXAMPLE OF WORK SCOPE 3-LETTER INDICATORS & STATEMENT
Be prepared to secure the airway at any time Call early for back-up &/or intercept Consider advanced life support if available
ALL: Administer epinephrine by autoinjector
PCP: Administer epinephrine IM
ICP: Administer hydrocortisone
Work scope identifier
Work scope statement
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only) or ICP (intermediate only).
1
A02 –Orders & Clinical Support
A02 - PHYSICIAN ORDERS, CLINICAL SUPPORT & OLMS
POLICIES & PROCEDURES
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-14 Effective Date: 2022-03-23 (0700 hrs)
SECTION A - PHYSICIAN ORDERS
1. Where a physician order is required, an EMS/PT medication document is a standing order from the EMS/PT medical director(s) and associate medical director(s) that authorizes the administration of that medication.
2. In a clinical situation that is not addressed by a current medication document, an EMS/PT physician 3 or ERS-affiliated physician 4 may provide a temporary or interim order that authorize the administration of a medication, limited to that particular patient and situation.
3. EMS/PT physicians: a. The on-line medical support (OLMS) physicians. b. The ERS Chief Medical Officer. c. The EMS/PT Medical Director or Associate Medical Director. d. The Winnipeg Fire Paramedic Service (WFPS) Medical Director or Associate Medical Director.
4. ERS-affiliated physicians: a. The referring or receiving physician for a patient on an interfacility transfer (IFT). b. The Shock Trauma Air Rescue Society (STARS) or Lifeflight transport physician (TP). c. The Code-STEMI physician or interventional cardiologist (“cath-lab” doctor) for suspected STEMI only. d. The stroke neurologist providing consultation to a stroke centre or telehealth stroke site for suspected acute
stroke only. e. The Left Ventricular Assist Device (LVAD) cardiologist for LVAD patients only.
5. While the following individuals may be able to provide expertise and some clinical assistance to paramedics, they cannot provide physician orders or delegate reserved acts.
a. The LVAD Coordinator b. The Shared Health ERS clinical service lead c. The EMS/PT on-call superintendent or supervisor
6. Paramedics may only carry out an interim order providing that all of the following conditions are satisfied. a. The order must comply with the paramedic’s College of paramedics of Manitoba (CPMB) scope of practice. b. The paramedic must be competent to carry out the order, including managing potential adverse occurrences. c. The paramedic does not believe that the order to be inaccurate, incorrect, or inappropriate to the particular
patient and situation.
7. For clinical care that may or will be required during patient transport, and is not already covered by an EMS/PT care map or medication document, a physician order must be obtained in writing, accompany the patient, and remain attached to the patient care record (PCR).
8. For unanticipated critical or time-sensitive care that is required during patient transport, a verbal order from a physician can be accepted. The order must be received directly from the physician, and must be appropriately documented in the PCR, including the name and role of the individual who gave the order (eg. J Smith, OLMS).
2
A02 –Orders & Clinical Support
SECTION B - PHYSICIAN ON SCENE
1. When encountering an individual on scene who identifies as a physician, EMS/PT paramedics may only carry out a medical order providing that all of the following conditions are met: a. They can confirm that the individual holds a current valid license from the College of Physicians and Surgeons of
Manitoba (CPSM). b. The order must comply with the paramedic’s CPMB scope of practice. c. The paramedic must be competent to carry out the order, including managing potential adverse occurrences. d. The paramedic does not believe that the order to be inaccurate, incorrect, or inappropriate to the particular
patient and situation.
2. If a physician on scene performs a reserved act that is beyond the scope of practice of a paramedic (e.g., endotracheal intubation) the physician must accompany the patient to the destination.
SECTION C - CLINICAL SUPPORT
1. Paramedics may contact the OLMS physician at any time for assistance with clinical issues and destination decision support. The OLMS physician is contacted through the Medical Transportation Coordination Centre (MTCC). In high risk situations (eg. obstetrical emergencies) contact should be made as early as possible.
2. Paramedics must contact the OLMS physician if the patient’s condition and the clinical requirements are not met by a current care map or medication document.
3. Paramedics must contact the OLMS physician when directed in the following specific care maps. a. C01 - Basic Resuscitation b. D01- Basic Newborn Resuscitation
4. When directed in the specific care map listed below, paramedics must contact the ERS-affiliated physician or clinical coordinator. If unable to reach the designated individual, paramedics must contact the OLMS physician. a. B04.x - Trauma Bypass - STARS transport physician b. E04A - ST Elevation Myocardial Infarction (Code-STEMI) - Code STEMI Physician c. E15A - Acute Stroke - HSC Stroke Neurologist d. C08A - Left Ventricular Assist Device (LVAD) - LVAD Coordinator (or LVAD cardiologist if the coordinator cannot
be reached)
5. Interfacility Transfer:
During an IFT paramedics should first attempt to contact the referring physician for medical support. The referring physician may advise paramedics to contact the receiving physician or OLMS as appropriate. If unable to reach the referring or receiving physician, paramedics should contact the OLMS physician for assistance. The referring physician should be updated as soon as possible thereafter.
3
A02 –Orders & Clinical Support
SECTION D - ON LINE MEDICAL SUPPORT (OLMS)
1. Online medical support (OLMS) is provided on a rotating basis by one of the Shared Health ERS medical directors or associate medical directors.
2. OLMS can be obtained by contacting the Medical Transportation Coordination Centre (MTCC) Paramedic Line at 1-800-689-2166. In areas of the Province where cellular service is poor or lacking, paramedics should contact MTCC by radio.
3. When consulting the OLMS physician, provide the following information to assist with clinical decision-making: • Your name and CPMB subregistration (EMR, PCP, PCP-IC, ACP) or your ERS scope of work (basic, primary,
intermediate, advanced) if different from your CPMB subregistration. • Your current location, including whether you are on scene or transporting from the scene. • The patient’s name and age, and the patient’s gender if relevant (eg. lower abdominal pain in a young
female) • A brief and focused description of the situation. • Any relevant scene information (eg. MVC with two occupants dead on scene). • Any relevant background information (eg. major trauma patient on “blood thinners”) • The values of all vital signs, including the blood glucose and Glasgow coma score if relevant. • Your clinical assessment of the patient. • A focused clinical question. • The location of, and transport time to, the closest ED and/or the closest designated site if relevant (eg.
laboring patient with an obstetrical facility 60 minutes away, but an open ED 10 minutes away). • Any barriers to prompt, safe transport (eg. white-out weather conditions).
APPROVED BY
Medical Director, EMS/PT Associate Medical Director, EMS/PT
VERSION CHANGES (refer to X01 for change tracking)
• Minor reformatting
1
A05 - REFUSAL
A05 - TREATMENT & TRANSPORT REFUSAL
POLICIES & PROCEDURES
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-14 Effective date: 2022-03-23 (0700 hrs)
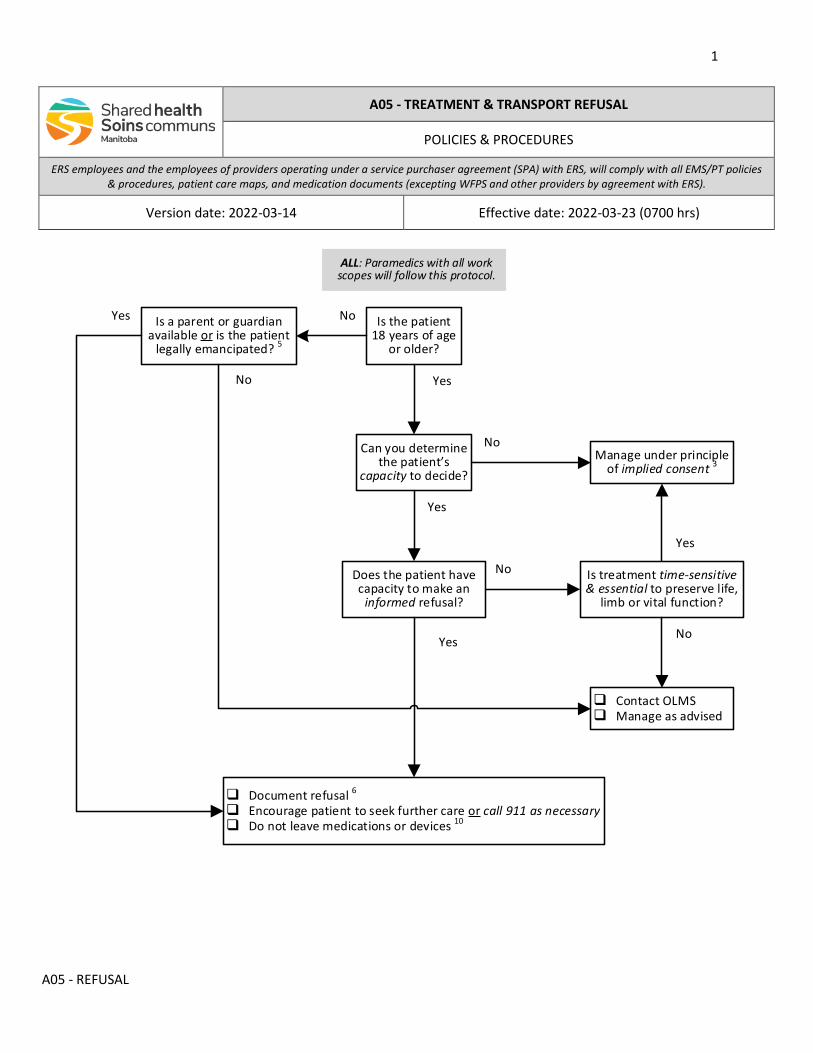
YesNo
Is the patient 18 years of age
or older?
Is a parent or guardian available or is the patient
legally emancipated? 5
Contact OLMS Manage as advised
Does the patient have capacity to make an
informed refusal?
Manage under principle of implied consent 3
Can you determine the patient’s
capacity to decide?
Is treatment time-sensitive & essential to preserve life,
limb or vital function?
No
No
Yes
Yes
Document refusal 6
Encourage patient to seek further care or call 911 as necessary Do not leave medications or devices 10
Yes
No
NoYes
ALL: Paramedics with all work scopes will follow this protocol.
2
A05 - REFUSAL
NOTES (refer to appendix B for detailed definitions)
1. Transport all patients from primary response calls, except when: a. The patient has the capacity to make an informed decision and refuses transport. b. The patient is incapacitated, but their health care proxy makes an informed decision to refuse transport. c. There is an EMS/PT treat and release protocol that allows for treatment without transport (table A). d. A qualified health care provider makes a request for a “facility-assist” only and maintains responsibility. 8
2. Patients have the right to make their own decisions about their health care, including the right to refuse treatment and / or transport, under all of the following conditions. a. They are the age of majority (18 years in Manitoba). 5
b. They are presented with all information relevant to their decision (ie. their decision is informed). c. They have the ability to understand all information relevant to their decision (ie. they have capacity).
3. If a patient is unable to give consent, the common law principle of implied consent can be relied upon if the situation is critical and time is of the essence, there is no substitute decision maker readily available, and paramedics have no knowledge of the existence of a health care directive.
4. Paramedics must always act in good faith and in the best interests of the patient, without regard to personal convenience or gain. Consent or refusal must not be obtained by omission, deception, or coercion.
5. Determining that an individual meets the test of a mature minor may not be possible with the limitations of prehospital care. For this reason, if a patient under the age of 18 years is refusing treatment or transport, paramedics should make reasonable efforts to contact the parent or legal guardian. If unable to reach a parent or legal guardian paramedics must contact the on-line medical support (OLMS) physician.
Similarly, if unable to confirm that a patient is a legally emancipated minor, paramedics must contact the on-line medical support (OLMS) physician.
6. Transport refusals are a high-risk situation. Complete documentation is essential. Even if a patient or their proxy signs a “release”, it may not hold up to legal scrutiny if the decision was not informed, was obtained by coercion or deception, or the patient did not have the capacity to make the decision.
7. Additional informed consent should be obtained for any medical intervention with significant risk (eg. procedural sedation). Verbal consent is acceptable, unless specified otherwise in a patient care map.
8. In the event of a response to a personal care home for a “facility-assist” paramedics must independently assess the patient and determine that there is no other clinical indication (eg. injury or illness) to transport, and a qualified health care provider at the facility will assume ongoing responsibility for the patient. In the event of a request for a “lift-assist” from a private citizen in their home, the patient must be advised to be that they should be transported to a health care facility for a medical assessment.
9. If requested to provide “medical clearance” so by law enforcement or any other agency, paramedics must advise that the patient should be transported to a health care facility for a medical assessment. While law enforcement has the authority to take an individual into custody and maintain custody of an individual, they cannot provide consent or refusal on behalf of a patient.
10. Leaving medication(s) or device(s) with a patient is considered “dispensing” under the Regulated Health Professions Act (RHPA) and not within the College of Paramedics of Manitoba (CPMB) professional scopes of practice.
3
A05 - REFUSAL
LINKS
• Not applicable
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X01 for change tracking)
• Minor reformatting
APPENDIX A: CURRENT ERS TREAT & RELEASE CARE MAPS
• None currently
4
A05 - REFUSAL
APPENDIX B: DEFINITIONS
For the purposes of this policy / procedure, the following definitions will apply.
CAPACITY: Although the terms are often used interchangeably, competence is a legal determination made by the Courts, while capacity is a medical term used by health care providers. Competence usually refers to the longer term (eg. dementia) while capacity may change over a few hours (eg. intoxication, concussion).
While capacity and competence (or the lack thereof) often go hand in hand, an individual deemed to be incompetent to handle their own financial affairs may still have the capacity to make their own health care decisions. In Manitoba, every adult person is presumed in general to be competent to give or refuse consent to medical treatment. Despite this presumption of competence, health care providers are required to ensure that a patient has the mental capacity to make that specific decision at that specific moment.
Determining decision-making capacity can present challenges. To be considered to have the capacity to make an informed decision, an individual must meet all the following conditions.
• They must be the age of majority (or legally emancipated if a minor). • They cannot be known to be under the influence of a substance that alters cognitive function and decision-
making ability (eg. alcohol, illicit drugs). • They must demonstrate that they understand and can retain all aspects of the discussion about their
circumstances. • They must demonstrate that they have appropriate judgment and insight.
INFORMED DECISION: For a health care decision to be informed, a discussion about the risks, benefits, and alternatives must take place. The information must be presented in plain language and the health care provider must ensure that it is understood.
HEALTH CARE DIRECTIVE: A health care directive allows an individual to express their wishes about the amount and type of health care they want to receive if they become unable to speak for themselves. It also allows for the appointment of another person (proxy) to make decisions on their behalf. It is often referred to as an advance health care directive (AHCD). Although specific forms are widely available, a directive does not have to be a formal document. It can be any written document which is signed and dated by the patient. The wishes expressed in an AHCD are legally binding on health care professionals.
Paramedics are not obliged (but should make reasonable efforts) to seek out or ask about a directive, or to determine its veracity. For example, individuals may often have a written AHCD included in their emergency response information kit (ERIK). If it is in plain view, paramedics would be expected to review it as soon as possible.
PROXY: An individual may be identified as a patient’s health care proxy or substitute decision-maker by a written health care directive (HCD) completed by the patient. In the absence of an AHCD, a competent patient may verbally designate an individual as their health care proxy.
In the absence of a previously designated proxy, a competent adult may act as a substitute proxy, according to the following legally established hierarchy.
1. Spouse or partner 2. Parent with primary care and control 3. Parent with legal access
5
A05 - REFUSAL
4. Child 5. Sibling 6. Other first degree relative
If a person is not able to make their own decisions about health care, the Courts may designate an individual to be their health care proxy. This is most commonly a close family member. If the patient has no family, the Courts may place them under the guardianship of a Public Trustee.
Note that power-of-attorney over financial or legal affairs does not by itself grant decision-making authority over health care matters.
EMANCIPATED MINOR: Some individuals between 16 and 18 years of age may be deemed by the Courts to be emancipated. This means that they are legally free from the control of a parent or legal guardian, and their parents or legal guardians are free from responsibility for them. Emancipated minors can legally consent or refuse medical treatment. However, they cannot act as a substitute proxy for another individual.
MATURE MINOR: The principle of the mature minor allows that some individuals under 18 years of age may have sufficient maturity and intellectual understanding to make their own health care decisions, including the right to refuse medical treatment.
The test of a maturity for a minor is not simply based of chronological age. It depends on the overall maturity of the individual. And it is unique to the situation: a 16 year old may be able to receive birth control without parental consent but may not be able to refuse a lifesaving amputation.
This can be a difficult determination to make, even with the benefit of time and familiarity with the patient.
HEALTH CARE DIRECTIVE: A health care directive allows a patient to express their wishes about the amount and type of health care they want to receive in the event
1
A06 - WORK SCOPE
A06 - EMS/PT SCOPE OF WORK
POLICIES & PROCEDURES
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-07 Effective date: 2022-04-27 (0700 hrs)
PREAMBLE
The College of Paramedics of Manitoba (CPMB) General Regulation defines the scope of practice for members by identifying the reserved acts that a registrant may (and may not) perform. For some of these reserved acts, the CPMB requires approved additional training. Shared Health ERS may also require testing and additional training for the confirmation and maintenance of competency.
This document defines the scope of work for Provincial EMS/PT paramedics providing ground ambulance services. It lists the medical functions (medications and procedures) that paramedics who are employed by Shared Health ERS, or one of its SPA providers, are authorized to perform in the course of their duties. The CPMB requires that a registrant comply with the scope of work established by the employer.
The scope of work may be less than the scope of practice. However, the scope of work cannot exceed the scope of practice, except with a written or verbal delegation from a physician or other appropriate CPMB member.
The EMS/PT medication documents are standing orders that authorize paramedics to administer certain medications under specific conditions. In exceptional circumstances a physician may provide an additional order or orders that will apply only to that particular patient and encounter.
EMS/PT paramedics may only accept an order or a delegation from an EMS/PT physician or ERS-affiliated physician.
A paramedic may only perform a reserved act if they are legally permitted and competent to do so and are satisfied on reasonable grounds that and it is safe and appropriate. CPMB members are responsible to know their respective scopes of practice and work, and to ensure their competency.
For further information, refer to A02 - PHYSICIAN ORDERS, CLINICAL SUPPORT & OLMS and the following CPMB references.
https://collegeparamb.ca/wp-content/uploads/2020/11/General-Regulation.pdf
https://collegeparamb.ca/wp-content/uploads/2020/11/Additional-Training-.pdf
https://collegeparamb.ca/wp-content/uploads/2020/12/Scope-of-Practice-final-1.pdf
2
A06 - WORK SCOPE
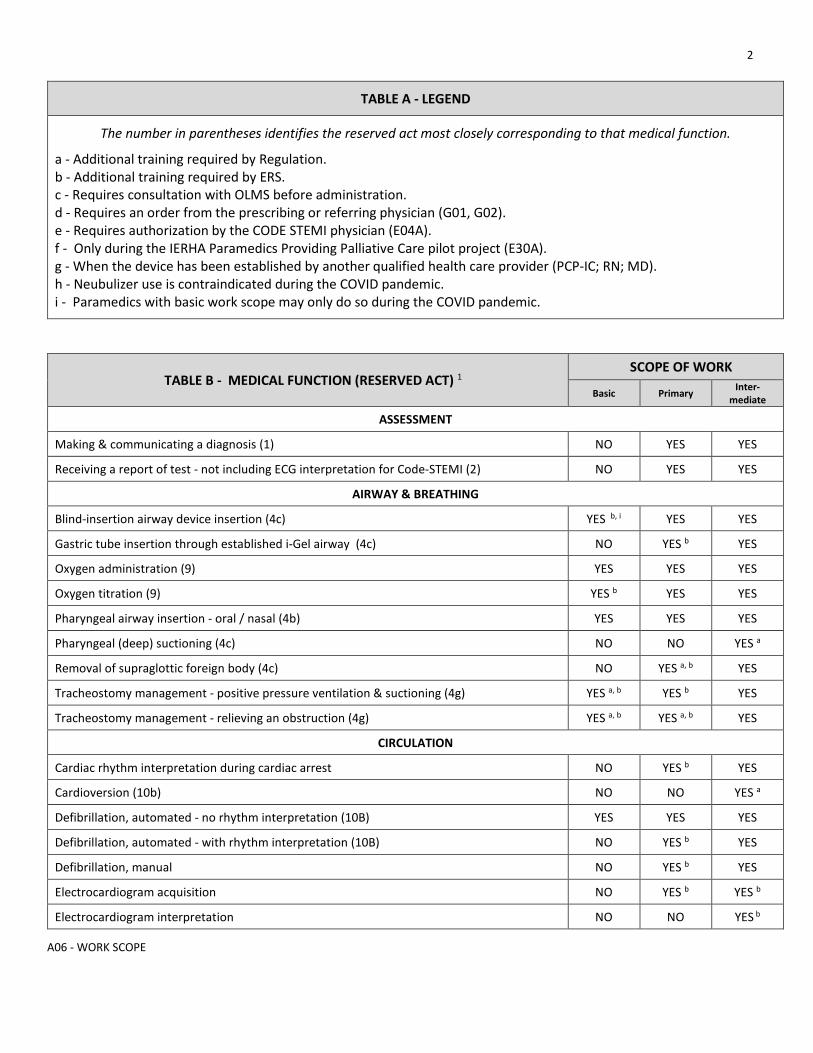
TABLE A - LEGEND
The number in parentheses identifies the reserved act most closely corresponding to that medical function.
a - Additional training required by Regulation. b - Additional training required by ERS. c - Requires consultation with OLMS before administration. d - Requires an order from the prescribing or referring physician (G01, G02). e - Requires authorization by the CODE STEMI physician (E04A). f - Only during the IERHA Paramedics Providing Palliative Care pilot project (E30A). g - When the device has been established by another qualified health care provider (PCP-IC; RN; MD). h - Neubulizer use is contraindicated during the COVID pandemic. i - Paramedics with basic work scope may only do so during the COVID pandemic.
TABLE B - MEDICAL FUNCTION (RESERVED ACT) 1 SCOPE OF WORK
Basic Primary Inter-mediate
ASSESSMENT
Making & communicating a diagnosis (1) NO YES YES
Receiving a report of test - not including ECG interpretation for Code-STEMI (2) NO YES YES
AIRWAY & BREATHING
Blind-insertion airway device insertion (4c) YES b, i YES YES
Gastric tube insertion through established i-Gel airway (4c) NO YES b YES
Oxygen administration (9) YES YES YES
Oxygen titration (9) YES b YES YES
Pharyngeal airway insertion - oral / nasal (4b) YES YES YES
Pharyngeal (deep) suctioning (4c) NO NO YES a
Removal of supraglottic foreign body (4c) NO YES a, b YES
Tracheostomy management - positive pressure ventilation & suctioning (4g) YES a, b YES b YES
Tracheostomy management - relieving an obstruction (4g) YES a, b YES a, b YES
CIRCULATION
Cardiac rhythm interpretation during cardiac arrest NO YES b YES
Cardioversion (10b) NO NO YES a
Defibrillation, automated - no rhythm interpretation (10B) YES YES YES
Defibrillation, automated - with rhythm interpretation (10B) NO YES b YES
Defibrillation, manual NO YES b YES
Electrocardiogram acquisition NO YES b YES b
Electrocardiogram interpretation NO NO YES b
3
A06 - WORK SCOPE
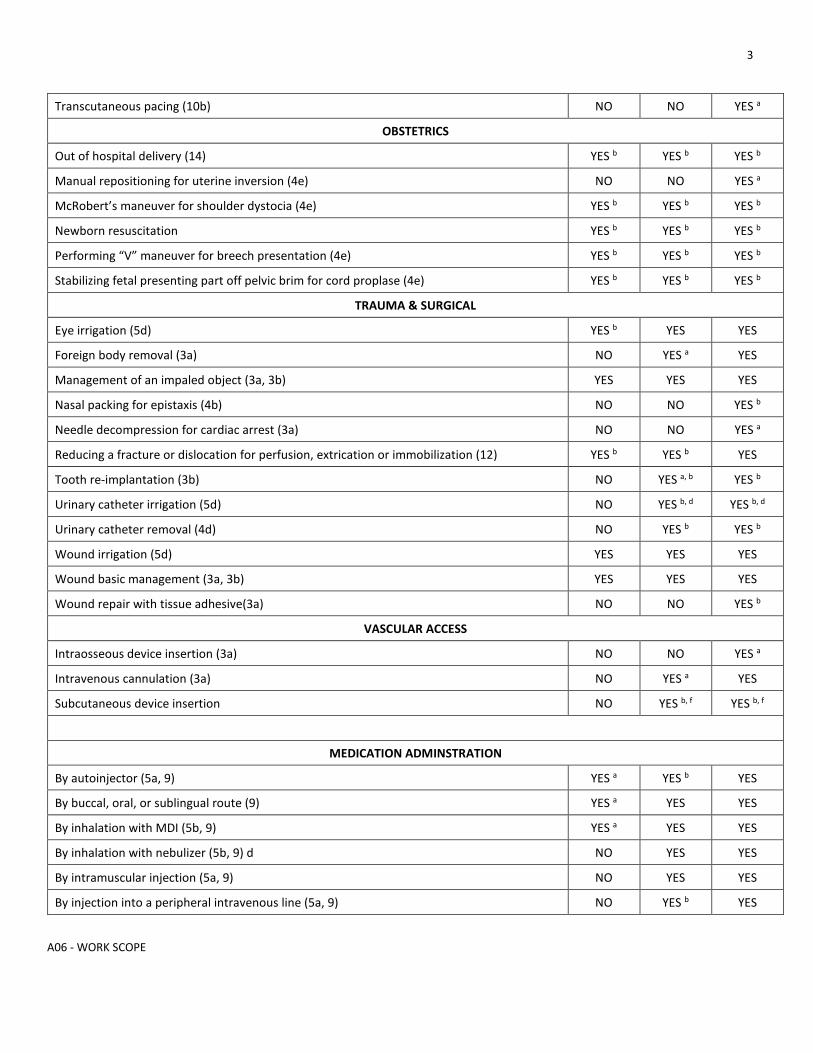
Transcutaneous pacing (10b) NO NO YES a
OBSTETRICS
Out of hospital delivery (14) YES b YES b YES b
Manual repositioning for uterine inversion (4e) NO NO YES a
McRobert’s maneuver for shoulder dystocia (4e) YES b YES b YES b
Newborn resuscitation YES b YES b YES b
Performing “V” maneuver for breech presentation (4e) YES b YES b YES b
Stabilizing fetal presenting part off pelvic brim for cord proplase (4e) YES b YES b YES b
TRAUMA & SURGICAL
Eye irrigation (5d) YES b YES YES
Foreign body removal (3a) NO YES a YES
Management of an impaled object (3a, 3b) YES YES YES
Nasal packing for epistaxis (4b) NO NO YES b
Needle decompression for cardiac arrest (3a) NO NO YES a
Reducing a fracture or dislocation for perfusion, extrication or immobilization (12) YES b YES b YES
Tooth re-implantation (3b) NO YES a, b YES b
Urinary catheter irrigation (5d) NO YES b, d YES b, d
Urinary catheter removal (4d) NO YES b YES b
Wound irrigation (5d) YES YES YES
Wound basic management (3a, 3b) YES YES YES
Wound repair with tissue adhesive(3a) NO NO YES b
VASCULAR ACCESS
Intraosseous device insertion (3a) NO NO YES a
Intravenous cannulation (3a) NO YES a YES
Subcutaneous device insertion NO YES b, f YES b, f
MEDICATION ADMINSTRATION
By autoinjector (5a, 9) YES a YES b YES
By buccal, oral, or sublingual route (9) YES a YES YES
By inhalation with MDI (5b, 9) YES a YES YES
By inhalation with nebulizer (5b, 9) d NO YES YES
By intramuscular injection (5a, 9) NO YES YES
By injection into a peripheral intravenous line (5a, 9) NO YES b YES
4
A06 - WORK SCOPE
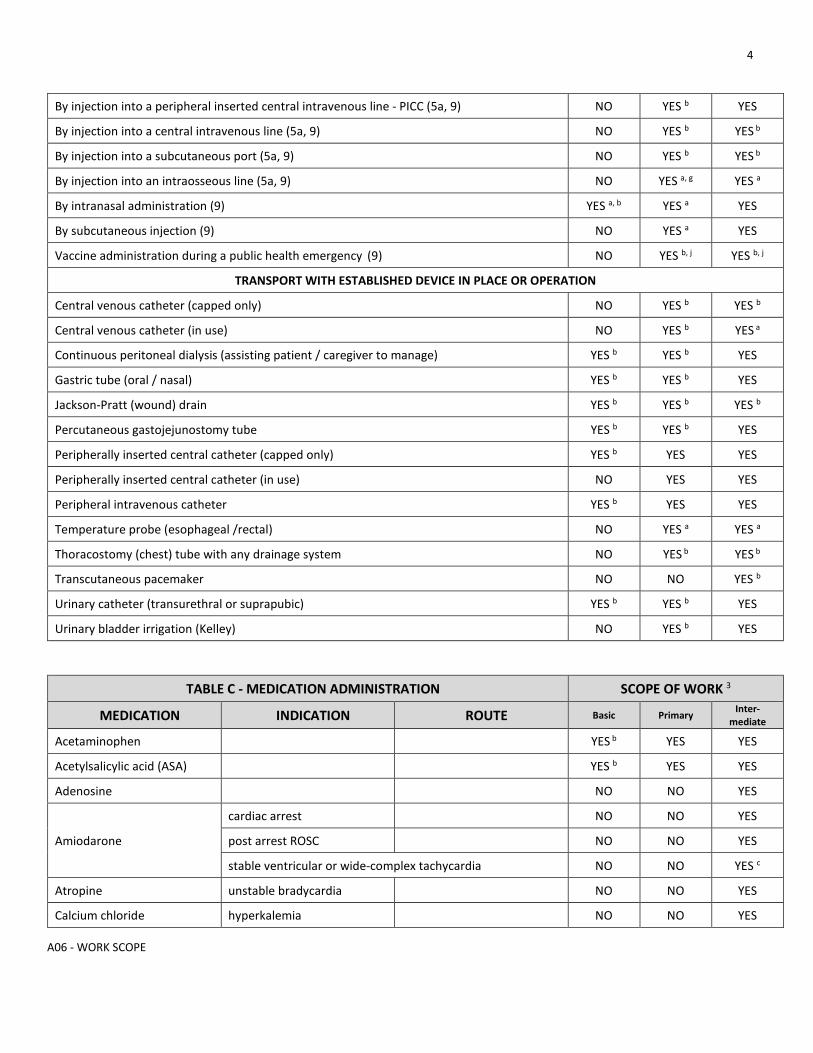
By injection into a peripheral inserted central intravenous line - PICC (5a, 9) NO YES b YES
By injection into a central intravenous line (5a, 9) NO YES b YES b
By injection into a subcutaneous port (5a, 9) NO YES b YES b
By injection into an intraosseous line (5a, 9) NO YES a, g YES a
By intranasal administration (9) YES a, b YES a YES
By subcutaneous injection (9) NO YES a YES
Vaccine administration during a public health emergency (9) NO YES b, j YES b, j
TRANSPORT WITH ESTABLISHED DEVICE IN PLACE OR OPERATION
Central venous catheter (capped only) NO YES b YES b
Central venous catheter (in use) NO YES b YES a
Continuous peritoneal dialysis (assisting patient / caregiver to manage) YES b YES b YES
Gastric tube (oral / nasal) YES b YES b YES
Jackson-Pratt (wound) drain YES b YES b YES b
Percutaneous gastojejunostomy tube YES b YES b YES
Peripherally inserted central catheter (capped only) YES b YES YES
Peripherally inserted central catheter (in use) NO YES YES
Peripheral intravenous catheter YES b YES YES
Temperature probe (esophageal /rectal) NO YES a YES a
Thoracostomy (chest) tube with any drainage system NO YES b YES b
Transcutaneous pacemaker NO NO YES b
Urinary catheter (transurethral or suprapubic) YES b YES b YES
Urinary bladder irrigation (Kelley) NO YES b YES
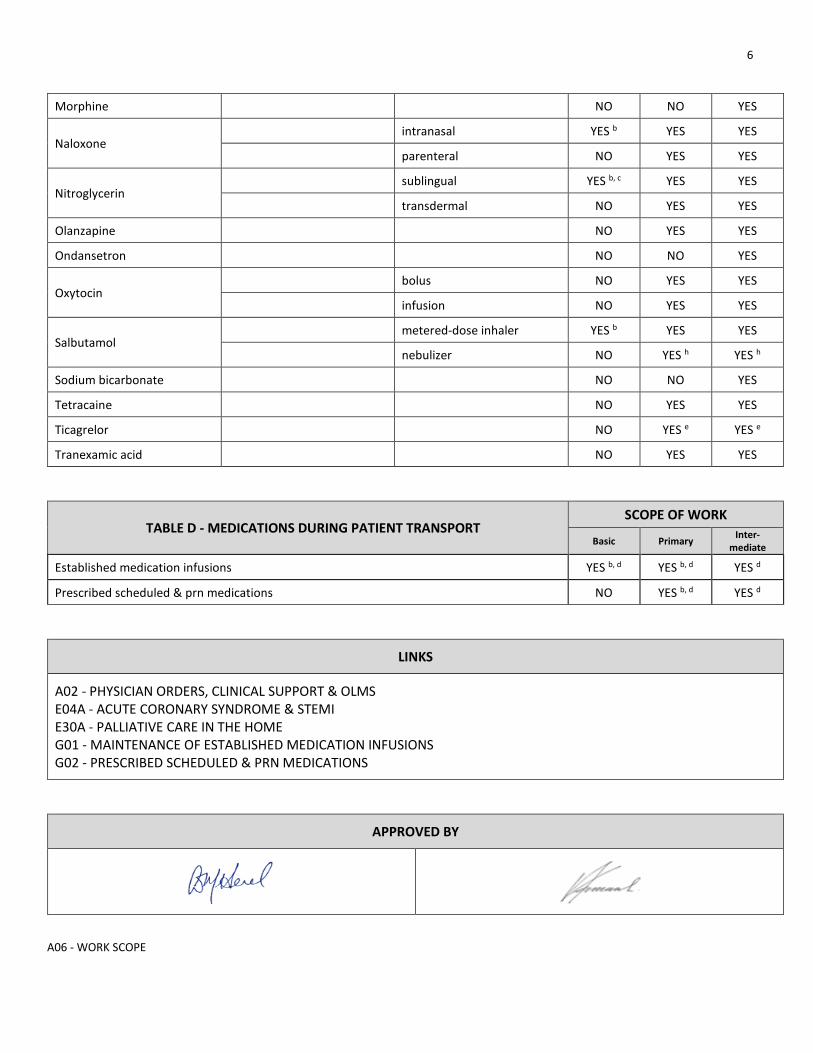
TABLE C - MEDICATION ADMINISTRATION SCOPE OF WORK 3
MEDICATION INDICATION ROUTE Basic Primary Inter-mediate
Acetaminophen YES b YES YES
Acetylsalicylic acid (ASA) YES b YES YES
Adenosine NO NO YES
Amiodarone
cardiac arrest NO NO YES
post arrest ROSC NO NO YES
stable ventricular or wide-complex tachycardia NO NO YES c
Atropine unstable bradycardia NO NO YES
Calcium chloride hyperkalemia NO NO YES
5
A06 - WORK SCOPE
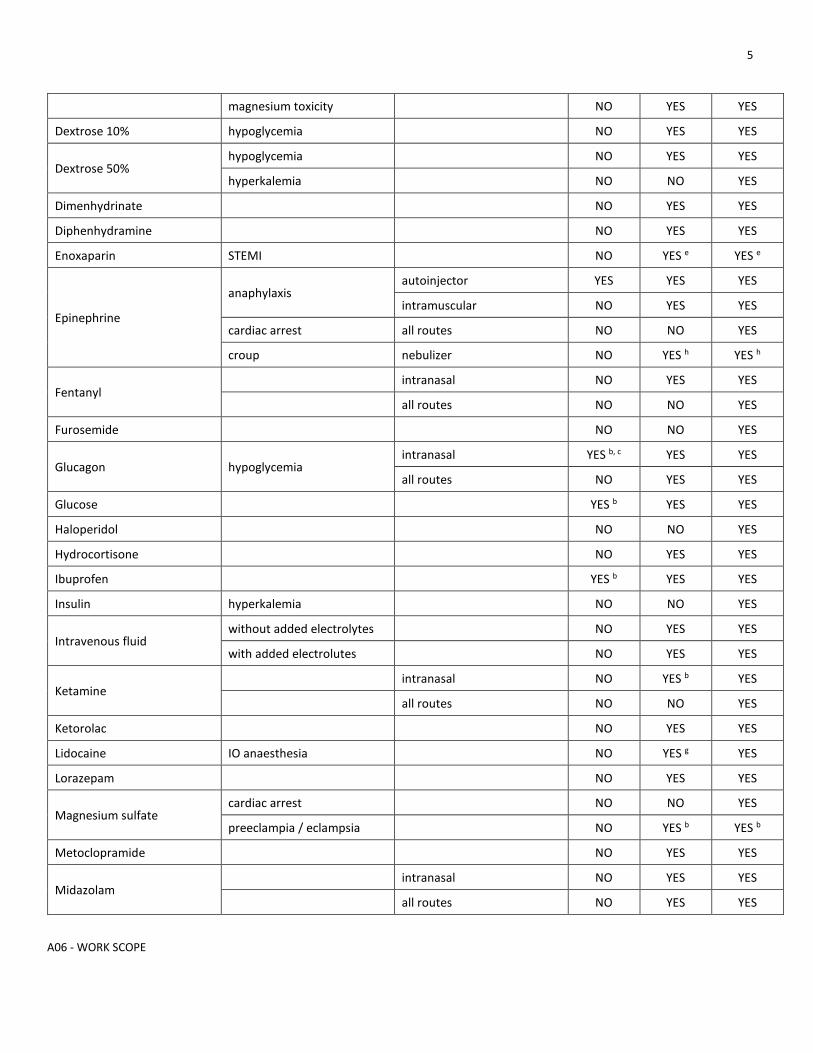
magnesium toxicity NO YES YES
Dextrose 10% hypoglycemia NO YES YES
Dextrose 50% hypoglycemia NO YES YES
hyperkalemia NO NO YES
Dimenhydrinate NO YES YES
Diphenhydramine NO YES YES
Enoxaparin STEMI NO YES e YES e
Epinephrine
anaphylaxis autoinjector YES YES YES
intramuscular NO YES YES
cardiac arrest all routes NO NO YES
croup nebulizer NO YES h YES h
Fentanyl intranasal NO YES YES
all routes NO NO YES
Furosemide NO NO YES
Glucagon hypoglycemia intranasal YES b, c YES YES
all routes NO YES YES
Glucose YES b YES YES
Haloperidol NO NO YES
Hydrocortisone NO YES YES
Ibuprofen YES b YES YES
Insulin hyperkalemia NO NO YES
Intravenous fluid without added electrolytes NO YES YES
with added electrolutes NO YES YES
Ketamine intranasal NO YES b YES
all routes NO NO YES
Ketorolac NO YES YES
Lidocaine IO anaesthesia NO YES g YES
Lorazepam NO YES YES
Magnesium sulfate cardiac arrest NO NO YES
preeclampia / eclampsia NO YES b YES b
Metoclopramide NO YES YES
Midazolam intranasal NO YES YES
all routes NO YES YES
6
A06 - WORK SCOPE
Morphine NO NO YES
Naloxone intranasal YES b YES YES
parenteral NO YES YES
Nitroglycerin sublingual YES b, c YES YES
transdermal NO YES YES
Olanzapine NO YES YES
Ondansetron NO NO YES
Oxytocin bolus NO YES YES
infusion NO YES YES
Salbutamol metered-dose inhaler YES b YES YES
nebulizer NO YES h YES h
Sodium bicarbonate NO NO YES
Tetracaine NO YES YES
Ticagrelor NO YES e YES e
Tranexamic acid NO YES YES
TABLE D - MEDICATIONS DURING PATIENT TRANSPORT SCOPE OF WORK
Basic Primary Inter-mediate
Established medication infusions YES b, d YES b, d YES d
Prescribed scheduled & prn medications NO YES b, d YES d
LINKS
A02 - PHYSICIAN ORDERS, CLINICAL SUPPORT & OLMS E04A - ACUTE CORONARY SYNDROME & STEMI E30A - PALLIATIVE CARE IN THE HOME G01 - MAINTENANCE OF ESTABLISHED MEDICATION INFUSIONS G02 - PRESCRIBED SCHEDULED & PRN MEDICATIONS
APPROVED BY

7
A06 - WORK SCOPE
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X01 for change tracking)
• Revised preamble language more closely aligned with CPMB regulations • “By injection into a subcutaneous port” at primary & intermediate scope added • Nitroglycerin and IN glucagon require OLMS consultation at basic scope added • Amiodarone for post arrest (ROSC) and stable VT or WCT at intermediate scope added • Transport with established running central line at primary scope added • “Injection into central line” revised (“during critical situation” removed) • Hydromorphone removed and replaced by new table D for all medications during patient transport
1
A09 - COVID / PROCEDURES
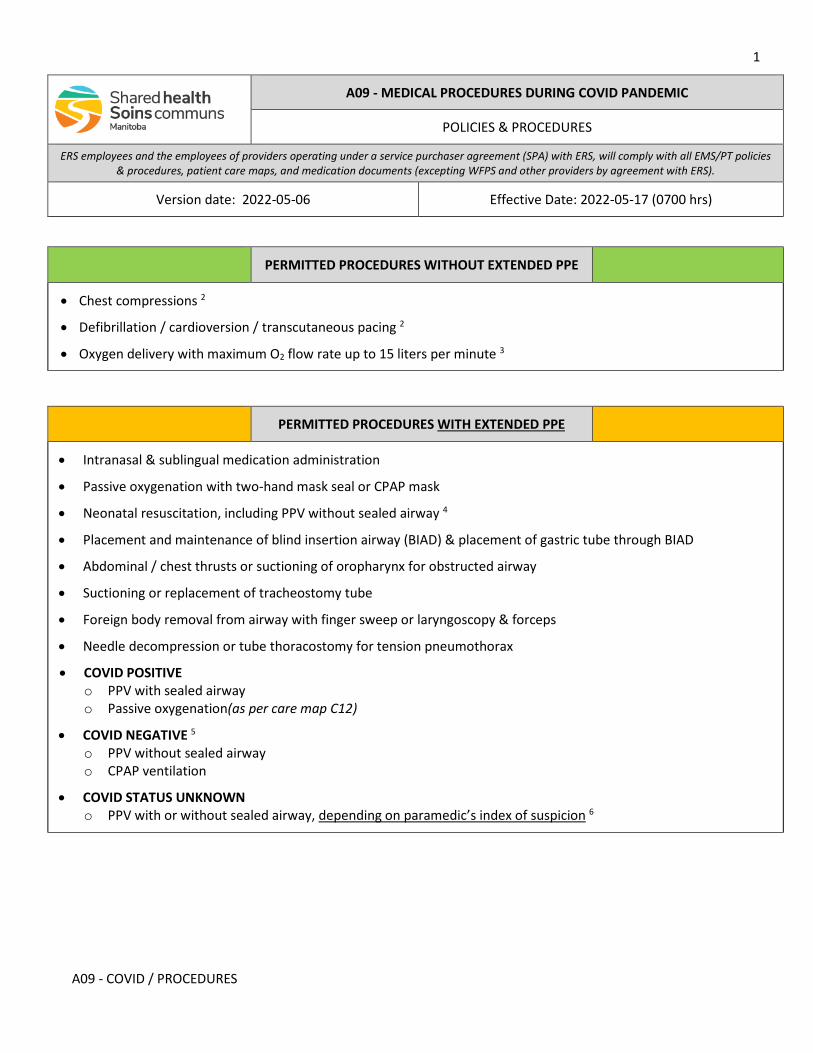
A09 - MEDICAL PROCEDURES DURING COVID PANDEMIC
POLICIES & PROCEDURES
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-05-06 Effective Date: 2022-05-17 (0700 hrs)
PERMITTED PROCEDURES WITHOUT EXTENDED PPE
• Chest compressions 2
• Defibrillation / cardioversion / transcutaneous pacing 2
• Oxygen delivery with maximum O2 flow rate up to 15 liters per minute 3
PERMITTED PROCEDURES WITH EXTENDED PPE
• Intranasal & sublingual medication administration
• Passive oxygenation with two-hand mask seal or CPAP mask
• Neonatal resuscitation, including PPV without sealed airway 4
• Placement and maintenance of blind insertion airway (BIAD) & placement of gastric tube through BIAD
• Abdominal / chest thrusts or suctioning of oropharynx for obstructed airway
• Suctioning or replacement of tracheostomy tube
• Foreign body removal from airway with finger sweep or laryngoscopy & forceps
• Needle decompression or tube thoracostomy for tension pneumothorax
• COVID POSITIVE o PPV with sealed airway o Passive oxygenation(as per care map C12)
• COVID NEGATIVE 5 o PPV without sealed airway o CPAP ventilation
• COVID STATUS UNKNOWN o PPV with or without sealed airway, depending on paramedic’s index of suspicion 6
2
A09 - COVID / PROCEDURES
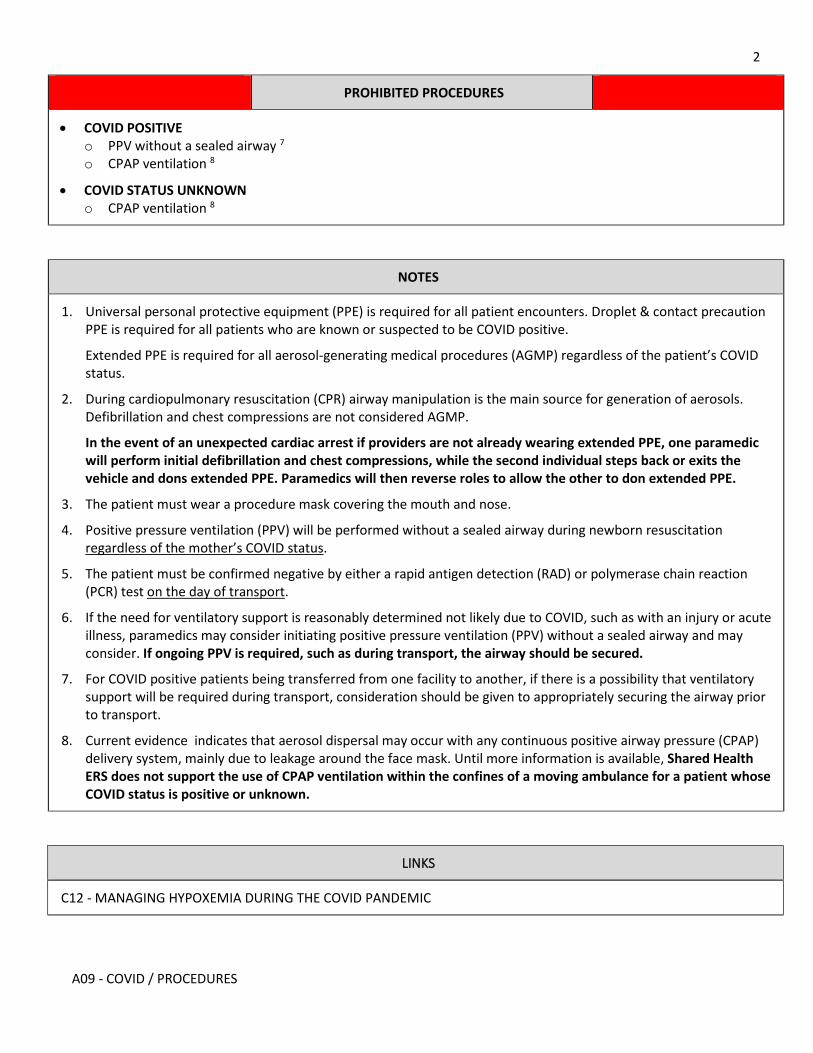
PROHIBITED PROCEDURES
• COVID POSITIVE o PPV without a sealed airway 7 o CPAP ventilation 8
• COVID STATUS UNKNOWN o CPAP ventilation 8
NOTES
1. Universal personal protective equipment (PPE) is required for all patient encounters. Droplet & contact precaution PPE is required for all patients who are known or suspected to be COVID positive.
Extended PPE is required for all aerosol-generating medical procedures (AGMP) regardless of the patient’s COVID status.
2. During cardiopulmonary resuscitation (CPR) airway manipulation is the main source for generation of aerosols. Defibrillation and chest compressions are not considered AGMP.
In the event of an unexpected cardiac arrest if providers are not already wearing extended PPE, one paramedic will perform initial defibrillation and chest compressions, while the second individual steps back or exits the vehicle and dons extended PPE. Paramedics will then reverse roles to allow the other to don extended PPE.
3. The patient must wear a procedure mask covering the mouth and nose.
4. Positive pressure ventilation (PPV) will be performed without a sealed airway during newborn resuscitation regardless of the mother’s COVID status.
5. The patient must be confirmed negative by either a rapid antigen detection (RAD) or polymerase chain reaction (PCR) test on the day of transport.
6. If the need for ventilatory support is reasonably determined not likely due to COVID, such as with an injury or acute illness, paramedics may consider initiating positive pressure ventilation (PPV) without a sealed airway and may consider. If ongoing PPV is required, such as during transport, the airway should be secured.
7. For COVID positive patients being transferred from one facility to another, if there is a possibility that ventilatory support will be required during transport, consideration should be given to appropriately securing the airway prior to transport.
8. Current evidence indicates that aerosol dispersal may occur with any continuous positive airway pressure (CPAP) delivery system, mainly due to leakage around the face mask. Until more information is available, Shared Health ERS does not support the use of CPAP ventilation within the confines of a moving ambulance for a patient whose COVID status is positive or unknown.
LINKS
C12 - MANAGING HYPOXEMIA DURING THE COVID PANDEMIC
3
A09 - COVID / PROCEDURES
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X01 for change tracking)
• PPV without sealing the airway can be considered in appropriate cases • Clarification that CPAP is not recommended with positive or unknown COVID status • Addition of sublingual medication administration & BiPAP to permitted procedures • Link to new C12 (removal of reference to E23)
1
B01 DESTINATION
B01 - STANDARD DESTINATION
All ages DESTINATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-17 Effective Date: 2022-05-17 (0700 hrs)
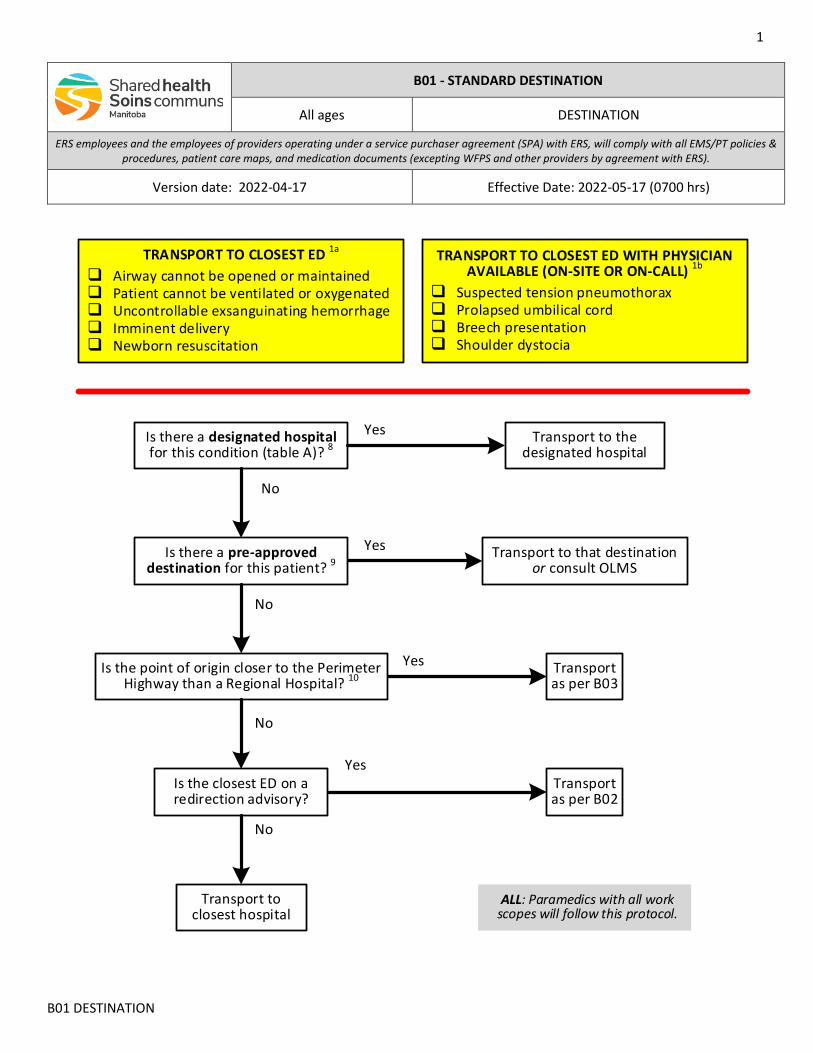
Is there a designated hospital for this condition (table A)? 8
Transport to closest hospital
ALL: Paramedics with all work scopes will follow this protocol.
TRANSPORT TO CLOSEST ED 1a
Airway cannot be opened or maintained Patient cannot be ventilated or oxygenated Uncontrollable exsanguinating hemorrhage Imminent delivery Newborn resuscitation
TRANSPORT TO CLOSEST ED WITH PHYSICIAN AVAILABLE (ON-SITE OR ON-CALL) 1b
Suspected tension pneumothorax Prolapsed umbilical cord Breech presentation Shoulder dystocia
No
Transport to the designated hospital
Is there a pre-approved destination for this patient? 9
Transport to that destination or consult OLMS
Is the point of origin closer to the Perimeter Highway than a Regional Hospital? 10
Transport as per B03
Is the closest ED on a redirection advisory?
Transport as per B02
No
Yes
No
Yes
No
Yes
Yes

2
B01 DESTINATION
INDICATIONS
• All primary response calls
CONTRAINDICATIONS
• Not applicable
NOTES
1. PARAMEDICS CAN OVER-RIDE A REDIRECTION ADVISORY FOR THESE CRITICAL, TIME-SENSITIVE CONDITIONS.
Survival is measured in minutes. If these cannot be resolved with the personnel, equipment, and expertise available on scene, emergency transport to a higher level of care (or at least a better resourced environment) may be the best of limited options.
Contact the online medical support (OLMS) physician as soon as possible if there is no local physician available or if the transport duration is expected to exceed the estimated survival time of the patient without appropriate intervention.
a. For these conditions transport to the closest emergency department (ED) regardless of physician availability. The benefits of additional “hands”, a stable treatment platform, and reliable communications outweigh the disadvantage of no physician.
b. These conditions require medical procedures beyond many paramedics’ scopes of practice or usual experience. Some of these may be within the scope of practice and capability of local nursing staff. In exceptional circumstances delegation from an ERS-associated physician to a paramedic competent to perform the procedure may be justified and life saving.
2. For the purposes of this policy & procedure, an emergency department (ED) will be considered closest if it has the shortest estimated transport time from the patient’s current location.
When two destinations have similar transport times, paramedics will transport to that which has the shortest estimated transport distance.
When two destinations have similar transport times or distances, a patient known or suspected to require a subsequent urgent interfacility transfer (IFT) will be transported to the ED closest to the most likely referral centre.
Estimated transport times must be based on safe vehicular speed. Non-clinical issues affecting patient, provider, and public safety such as road and weather conditions will be at the discretion of the vehicle operator.
3. Medical Transportation Coordination Centre (MTCC) personnel can advise paramedics regarding the location and status of the closest hospital.
4. Paramedics will ensure the appropriate pre-arrival notification of staff at the receiving hospital and provide updates as necessary. This is especially important with one of the critical, time-sensitive conditions as it may enable local staff to pre-alert the physician to be on-site prior to patient arrival.
5. Paramedics may consult the on-line medical support (OLMS) physician at any time for destination decision and/or clinical support.
6. Except for designated hospitals and pre-approved destinations paramedics will transport all primary response patients to the closest ED regardless of the Provincial border or regional health authority (RHA) boundary. 9, 10
3
B01 DESTINATION
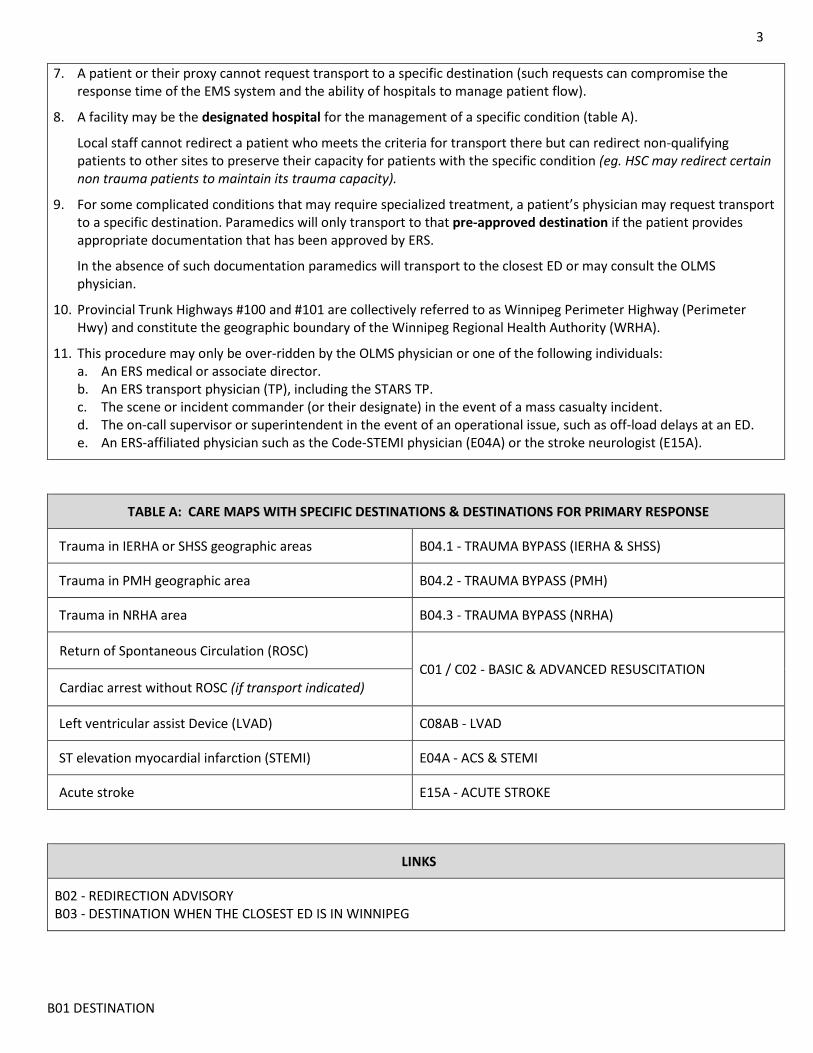
7. A patient or their proxy cannot request transport to a specific destination (such requests can compromise the response time of the EMS system and the ability of hospitals to manage patient flow).
8. A facility may be the designated hospital for the management of a specific condition (table A).
Local staff cannot redirect a patient who meets the criteria for transport there but can redirect non-qualifying patients to other sites to preserve their capacity for patients with the specific condition (eg. HSC may redirect certain non trauma patients to maintain its trauma capacity).
9. For some complicated conditions that may require specialized treatment, a patient’s physician may request transport to a specific destination. Paramedics will only transport to that pre-approved destination if the patient provides appropriate documentation that has been approved by ERS.
In the absence of such documentation paramedics will transport to the closest ED or may consult the OLMS physician.
10. Provincial Trunk Highways #100 and #101 are collectively referred to as Winnipeg Perimeter Highway (Perimeter Hwy) and constitute the geographic boundary of the Winnipeg Regional Health Authority (WRHA).
11. This procedure may only be over-ridden by the OLMS physician or one of the following individuals: a. An ERS medical or associate director. b. An ERS transport physician (TP), including the STARS TP. c. The scene or incident commander (or their designate) in the event of a mass casualty incident. d. The on-call supervisor or superintendent in the event of an operational issue, such as off-load delays at an ED. e. An ERS-affiliated physician such as the Code-STEMI physician (E04A) or the stroke neurologist (E15A).
TABLE A: CARE MAPS WITH SPECIFIC DESTINATIONS & DESTINATIONS FOR PRIMARY RESPONSE
Trauma in IERHA or SHSS geographic areas B04.1 - TRAUMA BYPASS (IERHA & SHSS)
Trauma in PMH geographic area B04.2 - TRAUMA BYPASS (PMH)
Trauma in NRHA area B04.3 - TRAUMA BYPASS (NRHA)
Return of Spontaneous Circulation (ROSC) C01 / C02 - BASIC & ADVANCED RESUSCITATION
Cardiac arrest without ROSC (if transport indicated)
Left ventricular assist Device (LVAD) C08AB - LVAD
ST elevation myocardial infarction (STEMI) E04A - ACS & STEMI
Acute stroke E15A - ACUTE STROKE
LINKS
B02 - REDIRECTION ADVISORY B03 - DESTINATION WHEN THE CLOSEST ED IS IN WINNIPEG
4
B01 DESTINATION
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X02 for change tracking)
• Renumbered from A04.1 and moved to section B • Reformatted (replacement of coloured boxes with scope of work statement & 3 letter indicators) • Revised flow chart for ease of use & expanded notes for greater clarity • Paramedics will contact OLMS (not OCS) for destination decision support (item #3) • Clarification that patient / proxy cannot request specific destination (item #5) • Clarification about which critical situations go to with or without a physician present (item #8) • Clarification that a designated site may redirect patients who do not meet criteria for designated site (item #9) • New table A for designated hospitals (reduced list of links) • Reminder to transport to Wpg hospital when closest to Perimeter
1
B02 - REDIRECTION ADVISORY
B02 - REDIRECTION ADVISORY
All ages DESTINATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-16 Effective Date: TBD (0700 hrs)
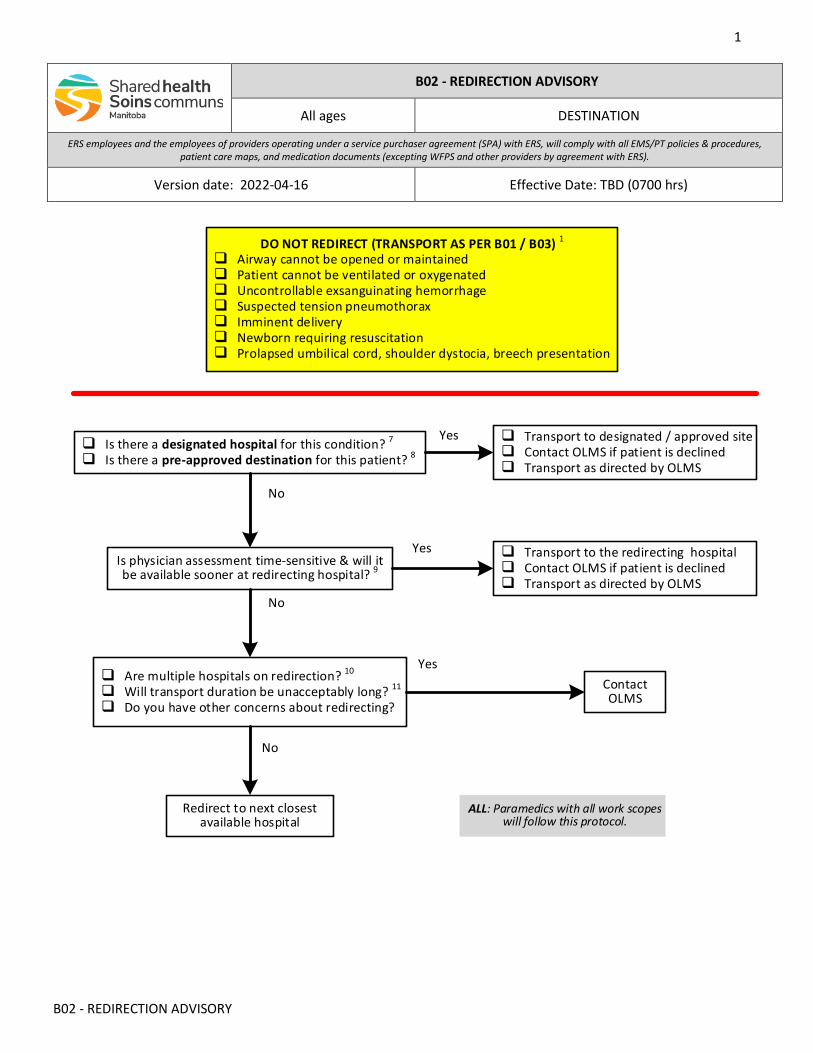
Yes
No
ALL: Paramedics with all work scopes will follow this protocol.
Is physician assessment time-sensitive & will it be available sooner at redirecting hospital? 9
Transport to the redirecting hospital Contact OLMS if patient is declined Transport as directed by OLMS
Are multiple hospitals on redirection? 10
Will transport duration be unacceptably long? 11
Do you have other concerns about redirecting?
Contact OLMS
Redirect to next closest available hospital
No
No
DO NOT REDIRECT (TRANSPORT AS PER B01 / B03) 1
Airway cannot be opened or maintained Patient cannot be ventilated or oxygenated Uncontrollable exsanguinating hemorrhage Suspected tension pneumothorax Imminent delivery Newborn requiring resuscitation Prolapsed umbilical cord, shoulder dystocia, breech presentation
Yes
Is there a designated hospital for this condition? 7
Is there a pre-approved destination for this patient? 8
Transport to designated / approved site Contact OLMS if patient is declined Transport as directed by OLMS
Yes
2
B02 - REDIRECTION ADVISORY
INDICATIONS
• The Medical Transportation Coordination Centre (MTCC) advises that the closest site, hospital, or emergency department (ED) has requested a redirection advisory
CONTRAINDICATIONS
• Not applicable
NOTES
1. PARAMEDICS CAN OVER-RIDE A REDIRECTION ADVISORY FOR THESE CRITICAL, TIME-SENSITIVE CONDITIONS.
Survival is measured in minutes. If these cannot be resolved with the personnel, equipment, and expertise available on scene, emergency transport to a higher level of care (or at least a better resourced environment) may be the best of limited options.
2. For the purposes of this policy & procedure, an emergency department (ED) will be considered next closest if it has the shortest estimated transport time from the patient’s current location.
When two destinations have similar transport times, paramedics will transport to that which has the shortest estimated transport distance.
When two destinations have similar transport times or distances, a patient known or suspected to require a subsequent urgent interfacility transfer (IFT) will be transported to the ED closest to the most likely referral centre.
Estimated transport times must be based on safe vehicular speed. Non-clinical issues affecting patient, provider, and public safety such as road and weather conditions will be at the discretion of the vehicle operator.
3. In the event of a reduction in services at a hospital, local or Regional staff may request a diversion, or redirection, of ambulances. ERS may issue a redirection advisory.
Paramedics will only comply with a redirection advisory that has been communicated to them by Medical Transportation Coordination Centre (MTCC) personnel.
MTCC staff can advise paramedics regarding the location and status of the next closest hospital(s).
4. Paramedics may consult the on-line medical support (OLMS) physician at any time for destination decision and/or clinical support.
5. Paramedics will ensure the appropriate pre-arrival notification of staff at the receiving hospital and provide updates as necessary. This is especially important with one of the critical, time-sensitive conditions as it may enable local staff to pre-alert the physician to be on-site prior to patient arrival.
If over-riding a redirection advisory, paramedics should indicate the reason for the over-ride if requested.
6. When redirecting, the patient and/or their representative must be informed of the redirection and the reason for it (eg. no physician at the redirecting site).
7. A facility may be the designated hospital for the management of a specific condition. They cannot redirect a patient who meets the criteria for transport there but can redirect non-qualifying patients to other sites to preserve their capacity for patients with the specific condition (eg. HSC may redirect certain non trauma patients to maintain its trauma capacity).
3
B02 - REDIRECTION ADVISORY
8. Some patients with complicated conditions may have a pre-approved destination for their care. Depending upon their chief complaint and condition, redirection may or may not be appropriate.
9. If a site is on a redirection due to the temporary absence of the physician (eg. accompanying a patient on transport) but the physician is expected to return sooner than the transport time to the next available ED, the OLMS physician may direct paramedics to over-ride the redirection advisory and transport the patient to the redirecting ED. Paramedics may be directed to remain with the patient until the physician returns.
10. If multiple adjacent sites are simultaneously on redirection, the OLMS physician may direct paramedics to transport to a site that has a physician available, even if that site is on a redirection for other reasons.
11. If the transport duration to another hospital will be unacceptably long and potentially impact the patient’s safety or the response capabilities of the EMS system, the OLMS physician may advise paramedics to transport to the redirecting site.
LINKS
B01 - STANDARD DESTINATION B03 - DESTINATION WHEN THE CLOSEST ED IS IN WINNIPEG
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X02 for change tracking)
• Renumbered from A04.2 and moved to section B • Reformatted (replacement of coloured boxes with scope of work statement & 3 letter indicators) • Revised flow chart for ease of use & expanded notes for greater clarity • Increased role of OLMS in managing redirections • Patient must be informed of redirection but consent not required • Clarification that redirection advisory might be over-ruled in some specific situations • Removal of table C
1
B03 - DESTINATION / WINNIPEG
B03 - DESTINATION WHEN THE CLOSEST ED IS IN WINNIPEG
All ages DESTINATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-16 Effective Date: 2022-05-17 (0700 hrs)
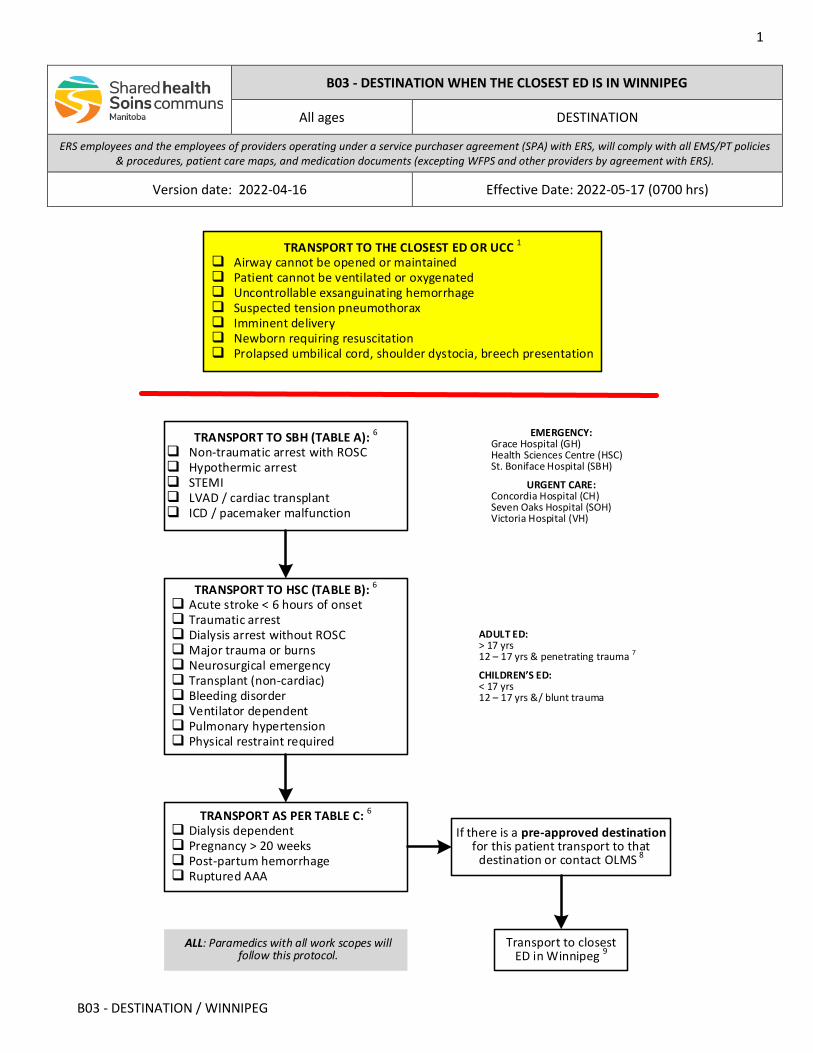
TRANSPORT TO SBH (TABLE A): 6
Non-traumatic arrest with ROSC Hypothermic arrest STEMI LVAD / cardiac transplant ICD / pacemaker malfunction
TRANSPORT TO HSC (TABLE B): 6
Acute stroke < 6 hours of onset Traumatic arrest Dialysis arrest without ROSC Major trauma or burns Neurosurgical emergency Transplant (non-cardiac) Bleeding disorder Ventilator dependent Pulmonary hypertension Physical restraint required
TRANSPORT AS PER TABLE C: 6
Dialysis dependent Pregnancy > 20 weeks Post-partum hemorrhage Ruptured AAA
ADULT ED:> 17 yrs12 – 17 yrs & penetrating trauma 7
CHILDREN’S ED:< 17 yrs12 – 17 yrs &/ blunt trauma
Transport to closest ED in Winnipeg 9
ALL: Paramedics with all work scopes will follow this protocol.
If there is a pre-approved destination for this patient transport to that
destination or contact OLMS 8
EMERGENCY:Grace Hospital (GH)Health Sciences Centre (HSC)St. Boniface Hospital (SBH)
URGENT CARE: Concordia Hospital (CH)Seven Oaks Hospital (SOH)Victoria Hospital (VH)
TRANSPORT TO THE CLOSEST ED OR UCC 1
Airway cannot be opened or maintained Patient cannot be ventilated or oxygenated Uncontrollable exsanguinating hemorrhage Suspected tension pneumothorax Imminent delivery Newborn requiring resuscitation Prolapsed umbilical cord, shoulder dystocia, breech presentation
2
B03 - DESTINATION / WINNIPEG
INDICATIONS
• All patients whose point of origin is closer to the Perimeter Highway than any other regional facility 10
CONTRAINDICATIONS
• Not applicable
NOTES
1. Winnipeg urgent care centres (UCC) have appropriate personnel and equipment for the initial stabilization of patients with these critical, time-sensitive conditions.
2. For the purposes of this protocol, an emergency department (ED) or UCC will be considered closest if it has the shortest estimated transport time from the patient’s current location.
When two destinations have similar transport times, paramedics will transport to that which has the shortest estimated transport distance.
3. Medical Transportation Coordination Centre (MTCC) personnel can advise paramedics regarding the status of the closest hospital.
4. Paramedics may consult the on-line medical support (OLMS) physician at any time for destination decision and/or clinical support.
5. Paramedics will ensure appropriate pre-arrival notification of staff at the receiving hospital and provide updates as necessary.
6. A patient with a condition listed in tables A, B, or C cannot be redirected away from the hospital designated for that condition.
Local staff may redirect patients without a condition listed in tables A, B, or C to other sites to preserve their capacity to receive patients with the listed conditions (eg. HSC may redirect certain non trauma patients to maintain its trauma capacity).
7. Patients 12 up to 17 years of age with penetrating trauma can only be rerouted to Children’s ED at the direction of trauma team leader, HSC emergency physician, or OLMS physician.
8. For some complicated conditions that may require specialized treatment, a patient’s physician may request transport to a specific destination. Paramedics will only transport to that pre-approved destination if the patient provides appropriate documentation that has been approved by ERS.
In the absence of such documentation paramedics will transport to the closest ED or may consult the OLMS physician.
9. Provincial EMS/PT will not routinely transport primary response patients to an UCC but may be directed by the on-call supervisor (OCS) to transport stable patients there to manage patient volumes and off-load times at the emergency departments.
10. Provincial Trunk Highways #100 and #101 are collectively referred to as Winnipeg Perimeter Highway (Perimeter Hwy) and constitute the geographic boundary of the Winnipeg Regional Health Authority (WRHA).
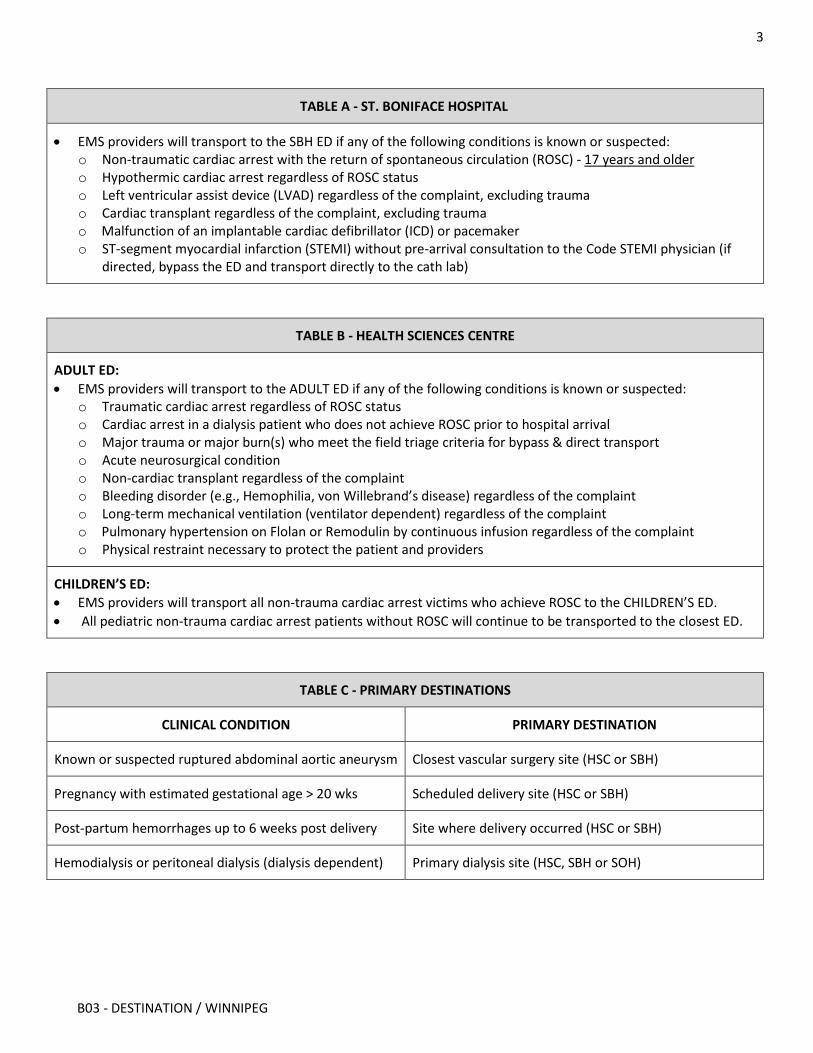
3
B03 - DESTINATION / WINNIPEG
TABLE A - ST. BONIFACE HOSPITAL
• EMS providers will transport to the SBH ED if any of the following conditions is known or suspected: o Non-traumatic cardiac arrest with the return of spontaneous circulation (ROSC) - 17 years and older o Hypothermic cardiac arrest regardless of ROSC status o Left ventricular assist device (LVAD) regardless of the complaint, excluding trauma o Cardiac transplant regardless of the complaint, excluding trauma o Malfunction of an implantable cardiac defibrillator (ICD) or pacemaker o ST-segment myocardial infarction (STEMI) without pre-arrival consultation to the Code STEMI physician (if
directed, bypass the ED and transport directly to the cath lab)
TABLE B - HEALTH SCIENCES CENTRE
ADULT ED: • EMS providers will transport to the ADULT ED if any of the following conditions is known or suspected:
o Traumatic cardiac arrest regardless of ROSC status o Cardiac arrest in a dialysis patient who does not achieve ROSC prior to hospital arrival o Major trauma or major burn(s) who meet the field triage criteria for bypass & direct transport o Acute neurosurgical condition o Non-cardiac transplant regardless of the complaint o Bleeding disorder (e.g., Hemophilia, von Willebrand’s disease) regardless of the complaint o Long-term mechanical ventilation (ventilator dependent) regardless of the complaint o Pulmonary hypertension on Flolan or Remodulin by continuous infusion regardless of the complaint o Physical restraint necessary to protect the patient and providers
CHILDREN’S ED: • EMS providers will transport all non-trauma cardiac arrest victims who achieve ROSC to the CHILDREN’S ED. • All pediatric non-trauma cardiac arrest patients without ROSC will continue to be transported to the closest ED.
TABLE C - PRIMARY DESTINATIONS
CLINICAL CONDITION PRIMARY DESTINATION
Known or suspected ruptured abdominal aortic aneurysm Closest vascular surgery site (HSC or SBH)
Pregnancy with estimated gestational age > 20 wks Scheduled delivery site (HSC or SBH)
Post-partum hemorrhages up to 6 weeks post delivery Site where delivery occurred (HSC or SBH)
Hemodialysis or peritoneal dialysis (dialysis dependent) Primary dialysis site (HSC, SBH or SOH)
4
B03 - DESTINATION / WINNIPEG
LINKS
B01 - STANDARD DESTINASTION FOR PRIMARY RESPONSE B02 - REDIRECTION ADVISORY
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X02 for change tracking)
• Renumbered from A08.1 & moved to section B • Reformatted (replacement of coloured boxes with scope of work statement & 3-letter indicator) • Revised flow chart for ease of use & revised notes for greater clarity • Removal of SBH as stroke centre
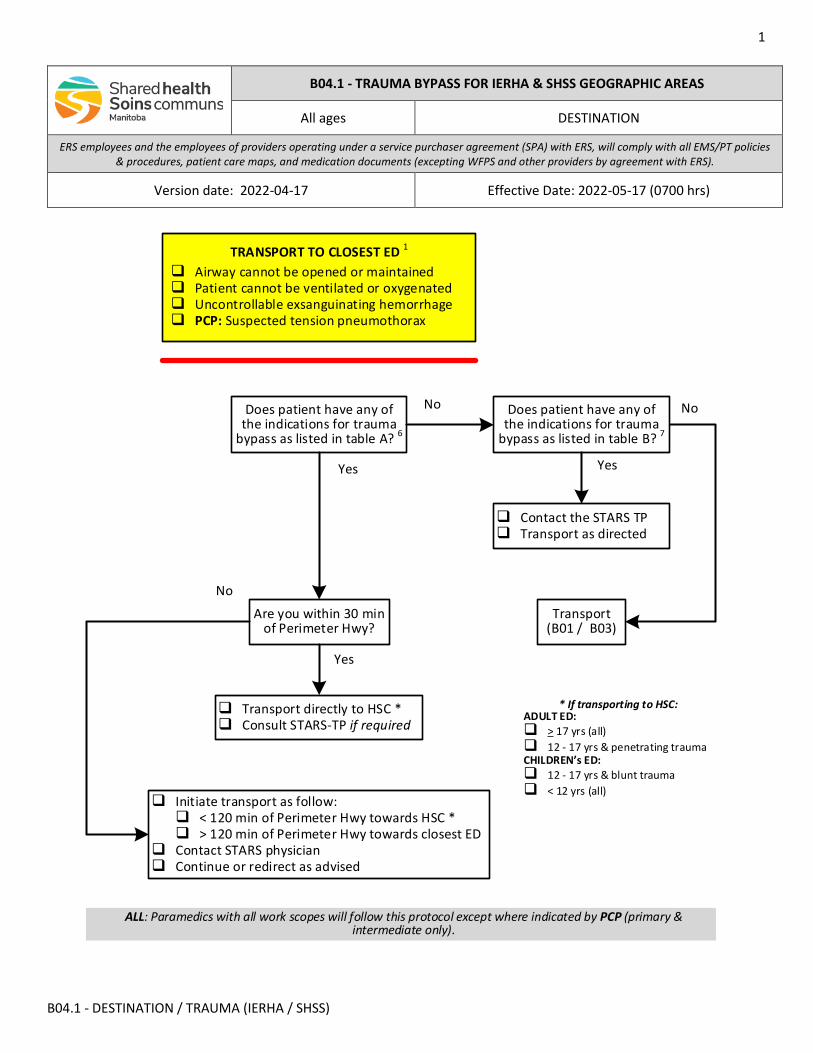
1
B04.1 - DESTINATION / TRAUMA (IERHA / SHSS)
Yes
Does patient have any of the indications for trauma
bypass as listed in table A? 6
Transport directly to HSC * Consult STARS-TP if required
Are you within 30 min of Perimeter Hwy?
No
Yes
Does patient have any of the indications for trauma
bypass as listed in table B? 7
Yes
No
No
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only).
Initiate transport as follow: < 120 min of Perimeter Hwy towards HSC * > 120 min of Perimeter Hwy towards closest ED
Contact STARS physician Continue or redirect as advised
Contact the STARS TP Transport as directed
Transport (B01 / B03)
* If transporting to HSC:ADULT ED: > 17 yrs (all) 12 - 17 yrs & penetrating traumaCHILDREN’s ED: 12 - 17 yrs & blunt trauma < 12 yrs (all)
TRANSPORT TO CLOSEST ED 1
Airway cannot be opened or maintained Patient cannot be ventilated or oxygenated Uncontrollable exsanguinating hemorrhage PCP: Suspected tension pneumothorax
B04.1 - TRAUMA BYPASS FOR IERHA & SHSS GEOGRAPHIC AREAS
All ages DESTINATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-17 Effective Date: 2022-05-17 (0700 hrs)
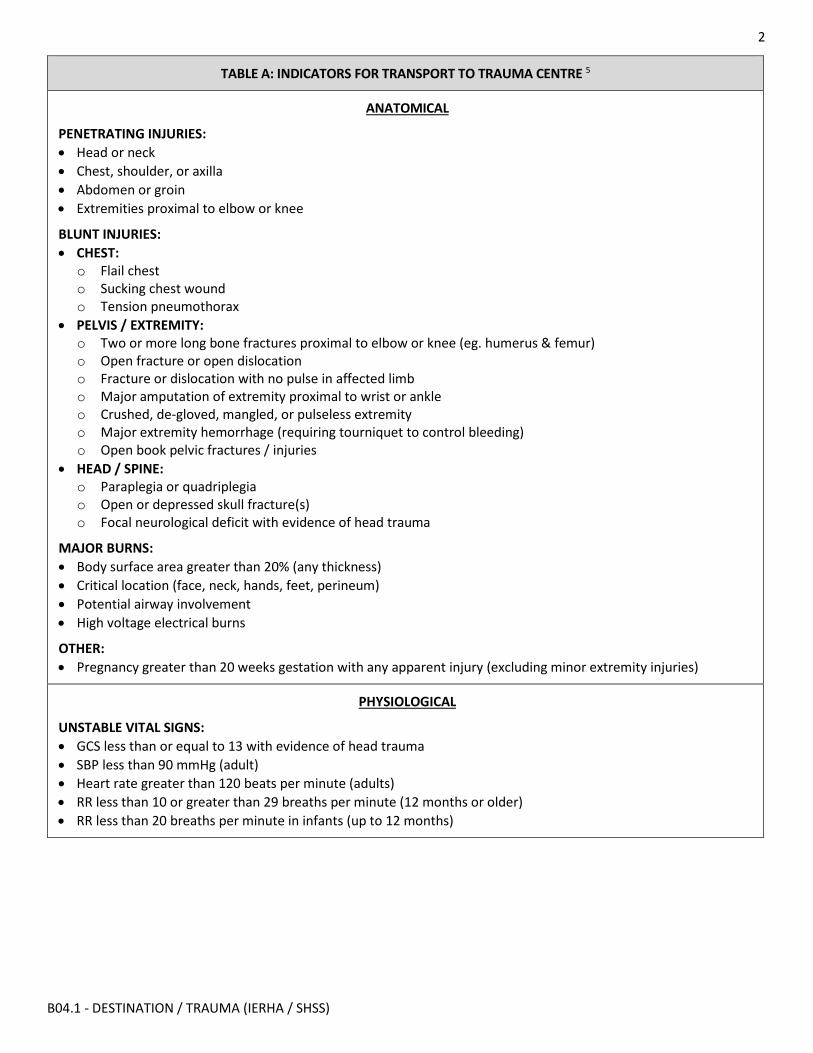
2
B04.1 - DESTINATION / TRAUMA (IERHA / SHSS)
TABLE A: INDICATORS FOR TRANSPORT TO TRAUMA CENTRE 5
ANATOMICAL
PENETRATING INJURIES: • Head or neck • Chest, shoulder, or axilla • Abdomen or groin • Extremities proximal to elbow or knee
BLUNT INJURIES: • CHEST:
o Flail chest o Sucking chest wound o Tension pneumothorax
• PELVIS / EXTREMITY: o Two or more long bone fractures proximal to elbow or knee (eg. humerus & femur) o Open fracture or open dislocation o Fracture or dislocation with no pulse in affected limb o Major amputation of extremity proximal to wrist or ankle o Crushed, de-gloved, mangled, or pulseless extremity o Major extremity hemorrhage (requiring tourniquet to control bleeding) o Open book pelvic fractures / injuries
• HEAD / SPINE: o Paraplegia or quadriplegia o Open or depressed skull fracture(s) o Focal neurological deficit with evidence of head trauma
MAJOR BURNS: • Body surface area greater than 20% (any thickness) • Critical location (face, neck, hands, feet, perineum) • Potential airway involvement • High voltage electrical burns
OTHER: • Pregnancy greater than 20 weeks gestation with any apparent injury (excluding minor extremity injuries)
PHYSIOLOGICAL
UNSTABLE VITAL SIGNS: • GCS less than or equal to 13 with evidence of head trauma • SBP less than 90 mmHg (adult) • Heart rate greater than 120 beats per minute (adults) • RR less than 10 or greater than 29 breaths per minute (12 months or older) • RR less than 20 breaths per minute in infants (up to 12 months)
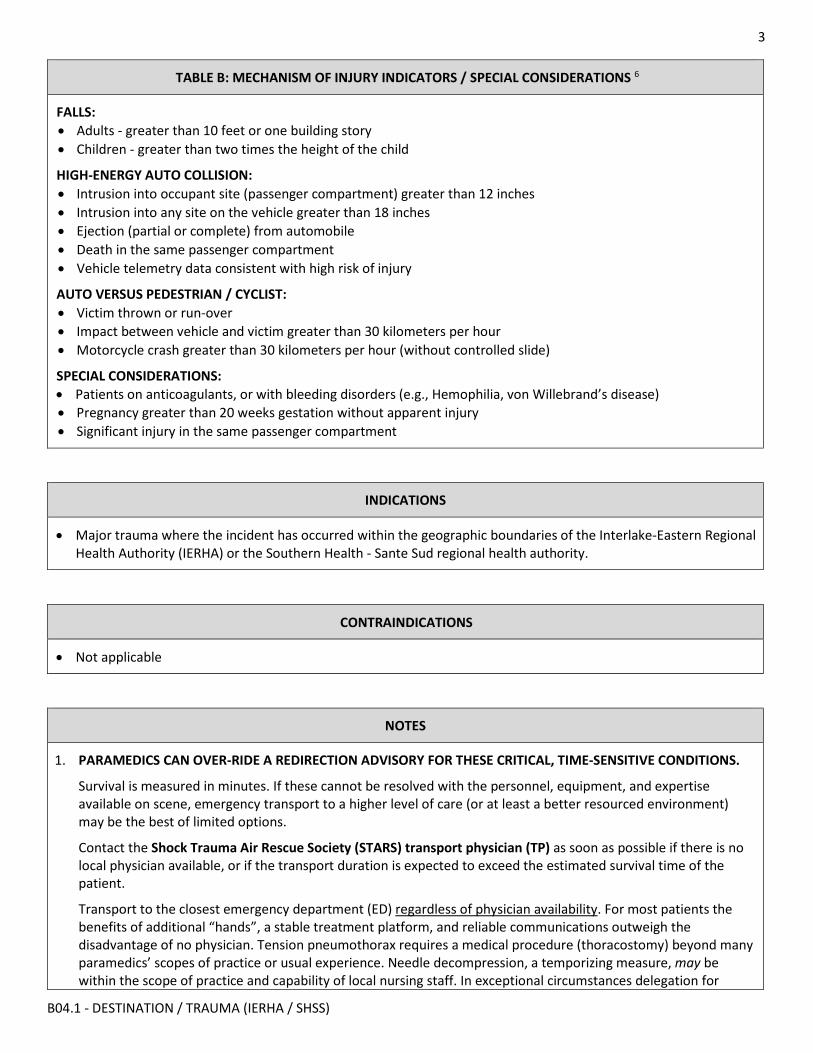
3
B04.1 - DESTINATION / TRAUMA (IERHA / SHSS)
TABLE B: MECHANISM OF INJURY INDICATORS / SPECIAL CONSIDERATIONS 6
FALLS: • Adults - greater than 10 feet or one building story • Children - greater than two times the height of the child
HIGH-ENERGY AUTO COLLISION: • Intrusion into occupant site (passenger compartment) greater than 12 inches • Intrusion into any site on the vehicle greater than 18 inches • Ejection (partial or complete) from automobile • Death in the same passenger compartment • Vehicle telemetry data consistent with high risk of injury
AUTO VERSUS PEDESTRIAN / CYCLIST: • Victim thrown or run-over • Impact between vehicle and victim greater than 30 kilometers per hour • Motorcycle crash greater than 30 kilometers per hour (without controlled slide)
SPECIAL CONSIDERATIONS: • Patients on anticoagulants, or with bleeding disorders (e.g., Hemophilia, von Willebrand’s disease) • Pregnancy greater than 20 weeks gestation without apparent injury • Significant injury in the same passenger compartment
INDICATIONS
• Major trauma where the incident has occurred within the geographic boundaries of the Interlake-Eastern Regional Health Authority (IERHA) or the Southern Health - Sante Sud regional health authority.
CONTRAINDICATIONS
• Not applicable
NOTES
1. PARAMEDICS CAN OVER-RIDE A REDIRECTION ADVISORY FOR THESE CRITICAL, TIME-SENSITIVE CONDITIONS.
Survival is measured in minutes. If these cannot be resolved with the personnel, equipment, and expertise available on scene, emergency transport to a higher level of care (or at least a better resourced environment) may be the best of limited options.
Contact the Shock Trauma Air Rescue Society (STARS) transport physician (TP) as soon as possible if there is no local physician available, or if the transport duration is expected to exceed the estimated survival time of the patient.
Transport to the closest emergency department (ED) regardless of physician availability. For most patients the benefits of additional “hands”, a stable treatment platform, and reliable communications outweigh the disadvantage of no physician. Tension pneumothorax requires a medical procedure (thoracostomy) beyond many paramedics’ scopes of practice or usual experience. Needle decompression, a temporizing measure, may be within the scope of practice and capability of local nursing staff. In exceptional circumstances delegation for
4
B04.1 - DESTINATION / TRAUMA (IERHA / SHSS)
LINKS
B01 - Standard Destination B03 - Destination When Closest ED is in Winnipeg
needle decompression from an ERS-associated physician to a paramedic competent to perform the procedure may be justified and life saving.
2. For the purposes of this policy & procedure, an emergency department (ED) will be considered closest if it has the shortest estimated transport time from the patient’s current location.
When two destinations have similar transport times, paramedics will transport to that which has the shortest estimated transport distance.
When two destinations have similar transport times or distances, a patient known or suspected to require a subsequent urgent interfacility transfer (IFT) will be transported to the ED closest to the most likely referral centre.
Estimated transport times must be based on safe vehicular speed. Non-clinical issues affecting patient, provider, and public safety such as road and weather conditions will be at the discretion of the vehicle operator.
3. Medical Transportation Coordination Centre (MTCC) personnel can advise paramedics regarding the location and status of the closest hospital.
4. Paramedics will ensure the appropriate pre-arrival notification of staff at the receiving hospital and provide updates as necessary. This is especially important with one of the critical, time-sensitive conditions as it may enable local staff to pre-alert the physician to be on-site prior to patient arrival.
5. For patients who meet any of the bypass indicators in tables A or B, the STARS-TP will assist paramedics by providing destination decision support; clinical guidance & interim physician orders; trauma team pre-alert; and may facilitate communication with the trauma team leader or receiving emergency physician. Even if you are within 30 minutes of the Perimeter Highway and proceeding directly to HSC, contact the STARS-TP if clinical assistance is required.
Contact the STARS-TP regardless of scene location within the province, even if the incident location is beyond the helicopter’s range. Additionally, paramedics will contact the TP even if the helicopter has already been launched (auto launched) and is en route, is not available due to weather or another mission, has been stood down, or is otherwise not be required.
Do not contact the STARS TP if the patient does not meet any of the bypass indicators in tables A or B. Transport as per the appropriate destination procedure (B01 or B03). Refer to B02 if the closest ED is under a redirection advisory.
6. TABLE A: Patients with any of the anatomical indicators require rapid transport to a dedicated trauma centre for management of these injuries. Patients with any of the physiological indicators require prompt transport to a dedicated trauma centre for assessment. Initiate emergency transport and contact the STARS-TP as soon as possible.
7. TABLE B: Patient with high-risk mechanisms of injury or special considerations may require transport to a dedicated trauma centre for assessment. Paramedics may be directed to transport these patients the closest ED for medical assessment before any decision is made to proceed to the trauma centre. Paramedics will contact the STARS-TP and transport as advised.
5
B04.1 - DESTINATION / TRAUMA (IERHA / SHSS)
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X02 for change tracking)
• Corrections to links section • Revised flow chart for ease of use • Increased note details for clarification
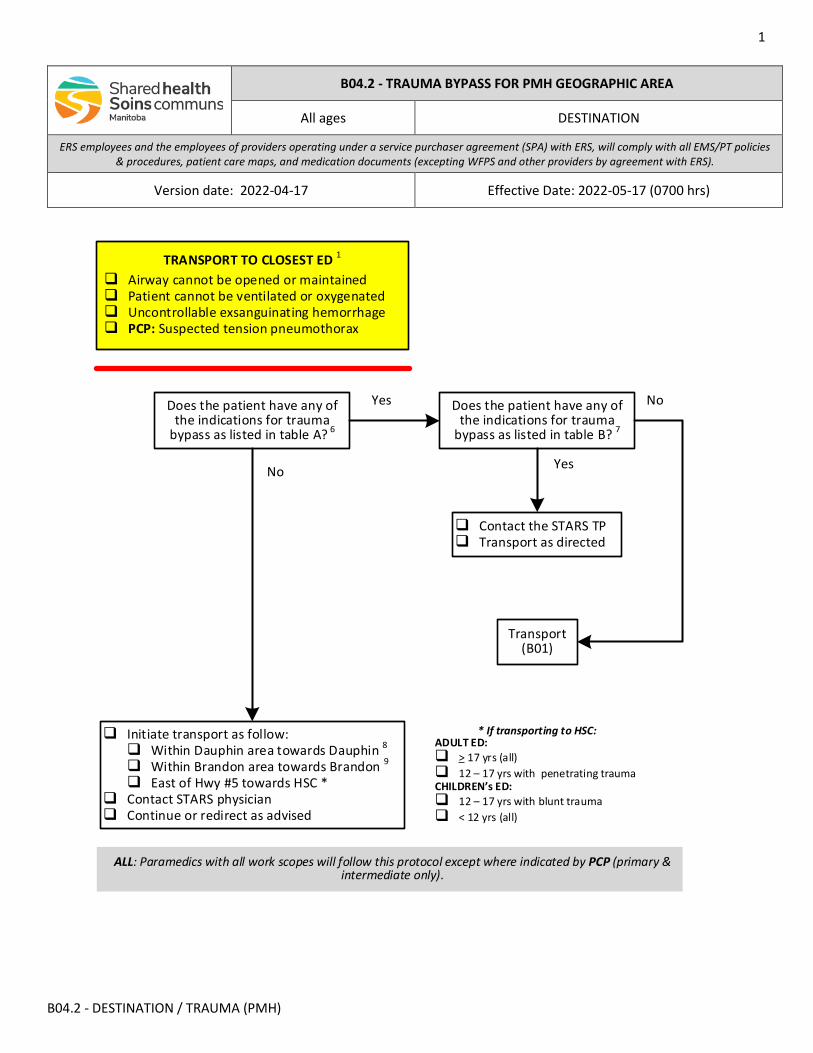
1
B04.2 - DESTINATION / TRAUMA (PMH)
Yes
Does the patient have any of the indications for trauma
bypass as listed in table A? 6
Does the patient have any of the indications for trauma
bypass as listed in table B? 7
Contact the STARS TP Transport as directed
No
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only).
Initiate transport as follow: Within Dauphin area towards Dauphin 8
Within Brandon area towards Brandon 9
East of Hwy #5 towards HSC * Contact STARS physician Continue or redirect as advised
* If transporting to HSC:ADULT ED: > 17 yrs (all) 12 – 17 yrs with penetrating traumaCHILDREN’s ED: 12 – 17 yrs with blunt trauma < 12 yrs (all)
Yes
No
Transport (B01)
TRANSPORT TO CLOSEST ED 1
Airway cannot be opened or maintained Patient cannot be ventilated or oxygenated Uncontrollable exsanguinating hemorrhage PCP: Suspected tension pneumothorax
B04.2 - TRAUMA BYPASS FOR PMH GEOGRAPHIC AREA
All ages DESTINATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-17 Effective Date: 2022-05-17 (0700 hrs)
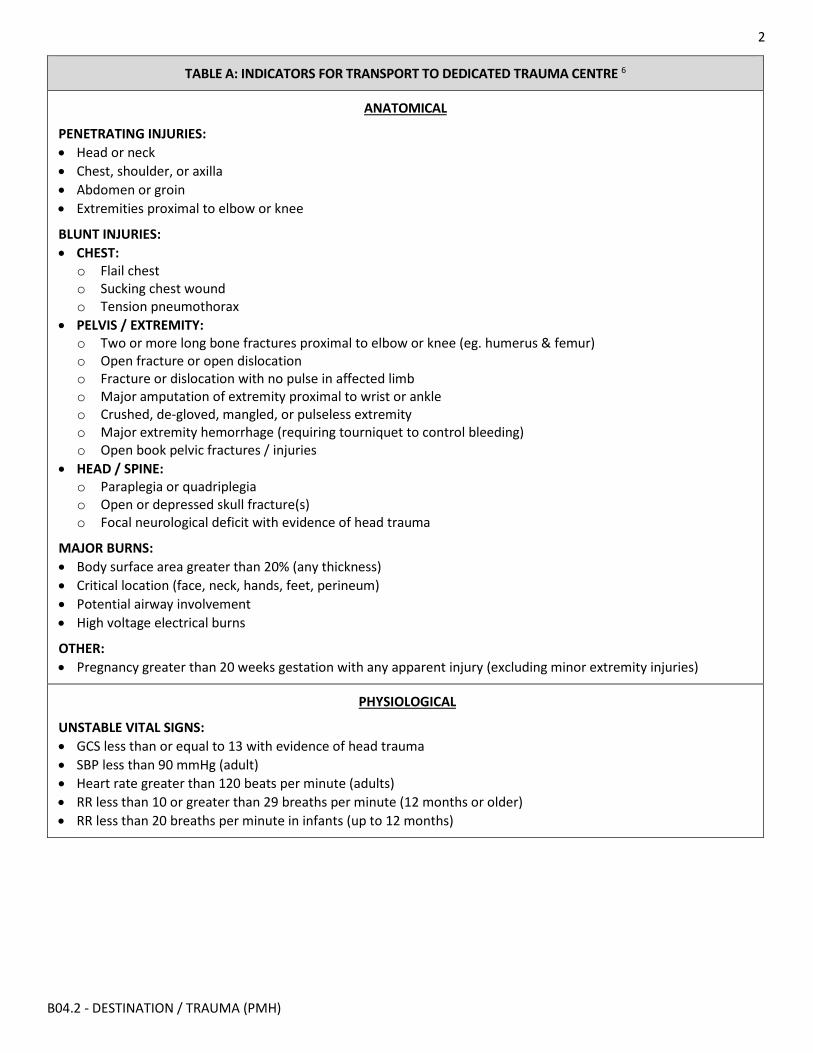
2
B04.2 - DESTINATION / TRAUMA (PMH)
TABLE A: INDICATORS FOR TRANSPORT TO DEDICATED TRAUMA CENTRE 6
ANATOMICAL
PENETRATING INJURIES: • Head or neck • Chest, shoulder, or axilla • Abdomen or groin • Extremities proximal to elbow or knee
BLUNT INJURIES: • CHEST:
o Flail chest o Sucking chest wound o Tension pneumothorax
• PELVIS / EXTREMITY: o Two or more long bone fractures proximal to elbow or knee (eg. humerus & femur) o Open fracture or open dislocation o Fracture or dislocation with no pulse in affected limb o Major amputation of extremity proximal to wrist or ankle o Crushed, de-gloved, mangled, or pulseless extremity o Major extremity hemorrhage (requiring tourniquet to control bleeding) o Open book pelvic fractures / injuries
• HEAD / SPINE: o Paraplegia or quadriplegia o Open or depressed skull fracture(s) o Focal neurological deficit with evidence of head trauma
MAJOR BURNS: • Body surface area greater than 20% (any thickness) • Critical location (face, neck, hands, feet, perineum) • Potential airway involvement • High voltage electrical burns
OTHER: • Pregnancy greater than 20 weeks gestation with any apparent injury (excluding minor extremity injuries)
PHYSIOLOGICAL
UNSTABLE VITAL SIGNS: • GCS less than or equal to 13 with evidence of head trauma • SBP less than 90 mmHg (adult) • Heart rate greater than 120 beats per minute (adults) • RR less than 10 or greater than 29 breaths per minute (12 months or older) • RR less than 20 breaths per minute in infants (up to 12 months)
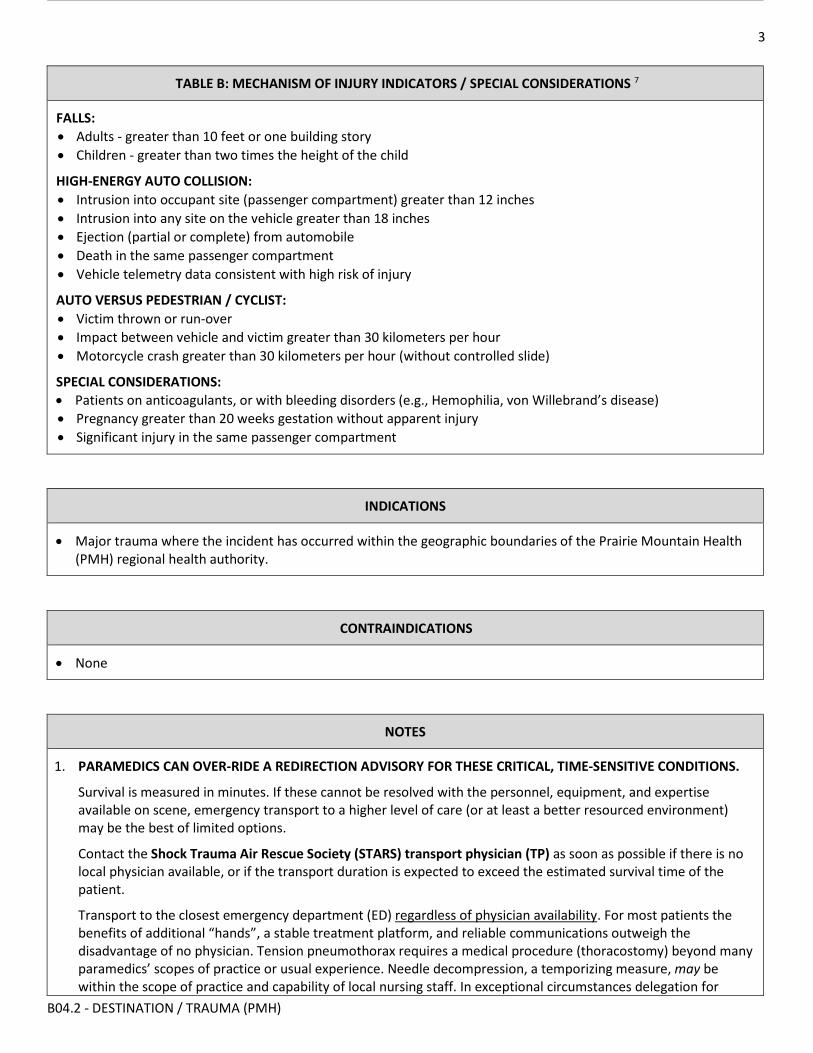
3
B04.2 - DESTINATION / TRAUMA (PMH)
TABLE B: MECHANISM OF INJURY INDICATORS / SPECIAL CONSIDERATIONS 7
FALLS: • Adults - greater than 10 feet or one building story • Children - greater than two times the height of the child
HIGH-ENERGY AUTO COLLISION: • Intrusion into occupant site (passenger compartment) greater than 12 inches • Intrusion into any site on the vehicle greater than 18 inches • Ejection (partial or complete) from automobile • Death in the same passenger compartment • Vehicle telemetry data consistent with high risk of injury
AUTO VERSUS PEDESTRIAN / CYCLIST: • Victim thrown or run-over • Impact between vehicle and victim greater than 30 kilometers per hour • Motorcycle crash greater than 30 kilometers per hour (without controlled slide)
SPECIAL CONSIDERATIONS: • Patients on anticoagulants, or with bleeding disorders (e.g., Hemophilia, von Willebrand’s disease) • Pregnancy greater than 20 weeks gestation without apparent injury • Significant injury in the same passenger compartment
INDICATIONS
• Major trauma where the incident has occurred within the geographic boundaries of the Prairie Mountain Health (PMH) regional health authority.
CONTRAINDICATIONS
• None
NOTES
1. PARAMEDICS CAN OVER-RIDE A REDIRECTION ADVISORY FOR THESE CRITICAL, TIME-SENSITIVE CONDITIONS.
Survival is measured in minutes. If these cannot be resolved with the personnel, equipment, and expertise available on scene, emergency transport to a higher level of care (or at least a better resourced environment) may be the best of limited options.
Contact the Shock Trauma Air Rescue Society (STARS) transport physician (TP) as soon as possible if there is no local physician available, or if the transport duration is expected to exceed the estimated survival time of the patient.
Transport to the closest emergency department (ED) regardless of physician availability. For most patients the benefits of additional “hands”, a stable treatment platform, and reliable communications outweigh the disadvantage of no physician. Tension pneumothorax requires a medical procedure (thoracostomy) beyond many paramedics’ scopes of practice or usual experience. Needle decompression, a temporizing measure, may be within the scope of practice and capability of local nursing staff. In exceptional circumstances delegation for
4
B04.2 - DESTINATION / TRAUMA (PMH)
needle decompression from an ERS-associated physician to a paramedic competent to perform the procedure may be justified and life saving.
2. For the purposes of this policy & procedure, an emergency department (ED) will be considered closest if it has the shortest estimated transport time from the patient’s current location.
When two destinations have similar transport times, paramedics will transport to that which has the shortest estimated transport distance.
When two destinations have similar transport times or distances, a patient known or suspected to require a subsequent urgent interfacility transfer (IFT) will be transported to the ED closest to the most likely referral centre.
Estimated transport times must be based on safe vehicular speed. Non-clinical issues affecting patient, provider, and public safety such as road and weather conditions will be at the discretion of the vehicle operator.
3. Medical Transportation Coordination Centre (MTCC) personnel can advise paramedics regarding the location and status of the closest hospital.
4. Paramedics will ensure the appropriate pre-arrival notification of staff at the receiving hospital and provide updates as necessary. This is especially important with one of the critical, time-sensitive conditions as it may enable local staff to pre-alert the physician to be on-site prior to patient arrival.
5. For patients who meet any of the bypass indicators in tables A or B, the STARS-TP will assist paramedics by providing destination decision support; clinical guidance & interim physician orders; trauma team pre-alert; and may facilitate communication with the trauma team leader or receiving emergency physician. Even if you are within 30 minutes of the Perimeter Highway and proceeding directly to HSC, contact the STARS-TP if clinical assistance is required.
Contact the STARS-TP regardless of scene location within the province, even if the incident location is beyond the helicopter’s range. Additionally, paramedics will contact the TP even if the helicopter has already been launched (auto launched) and is en route, is not available due to weather or another mission, has been stood down, or is otherwise not be required.
Do not contact the STARS TP if the patient does not meet any of the bypass indicators in tables A or B. Transport as per the appropriate destination procedure (B01 or B03). Refer to B02 if the closest ED is under a redirection advisory.
6. TABLE A: Patients with any of the anatomical indicators require rapid transport to a dedicated trauma centre for management of these injuries. Patients with any of the physiological indicators require prompt transport to a dedicated trauma centre for assessment. Initiate emergency transport and contact the STARS-TP as soon as possible.
7. TABLE B: Patient with high-risk mechanisms of injury or special considerations may require transport to a dedicated trauma centre for assessment. Paramedics may be directed to transport these patients the closest ED for medical assessment before any decision is made to proceed to the trauma centre. Paramedics will contact the STARS-TP and transport as advised.
8. The north / south divide between the Dauphin and Brandon catchment areas follows a course north of Russell along the southern boundary of Riding Mountain National, and south of McReary. Note that within the southern parts of Riding Mountain National Park (eg. Clear Lake) road and weather conditions may require transport south to Brandon (appendix A).
EXAMPLE: McCreary and Inglis fall within the Dauphin catchment area.
9. The east / west divide between the Brandon and Winnipeg catchment areas is just to the east of Provincial Highway #5 (appendix A).
EXAMPLE: Russell, Riding Mountain and Neepawa, fall within the Brandon catchment area.
5
B04.2 - DESTINATION / TRAUMA (PMH)
LINKS
B01 - Standard Destination
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X02 for change tracking)
• Corrections to links section • Revised flow chart for ease of use • Increased note details for clarification
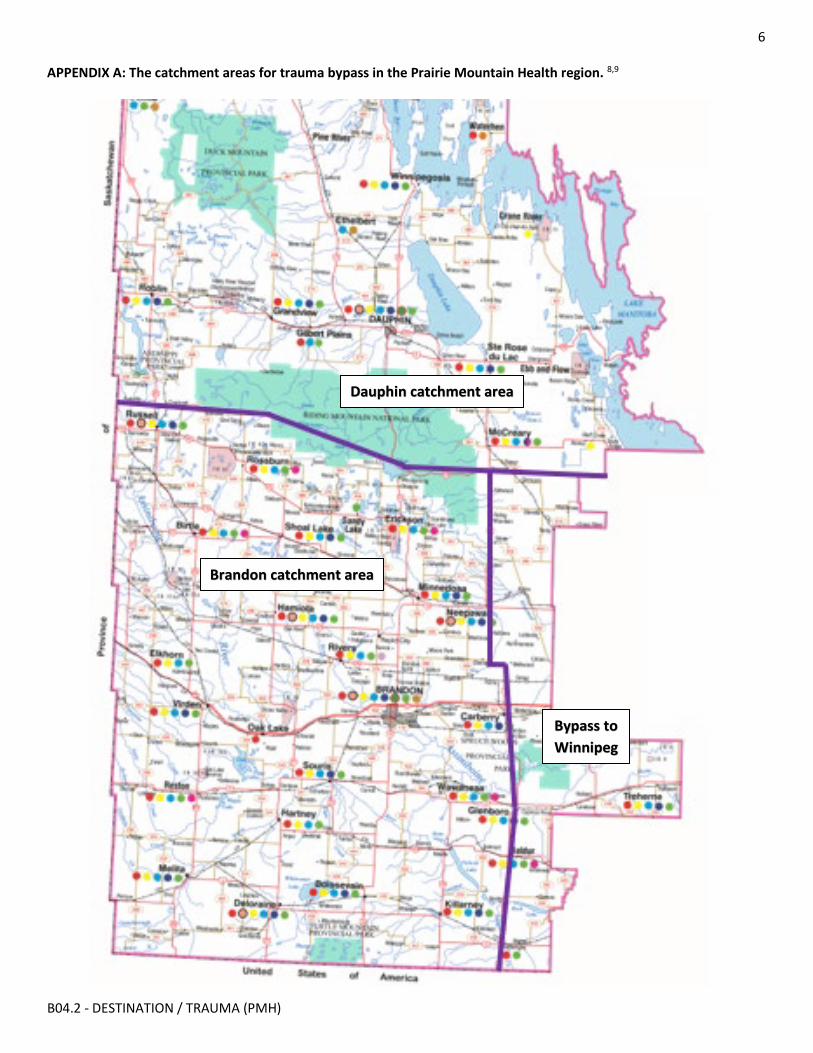
6
B04.2 - DESTINATION / TRAUMA (PMH)
APPENDIX A: The catchment areas for trauma bypass in the Prairie Mountain Health region. 8,9
Dauphin catchment area
Brandon catchment area
Bypass to Winnipeg
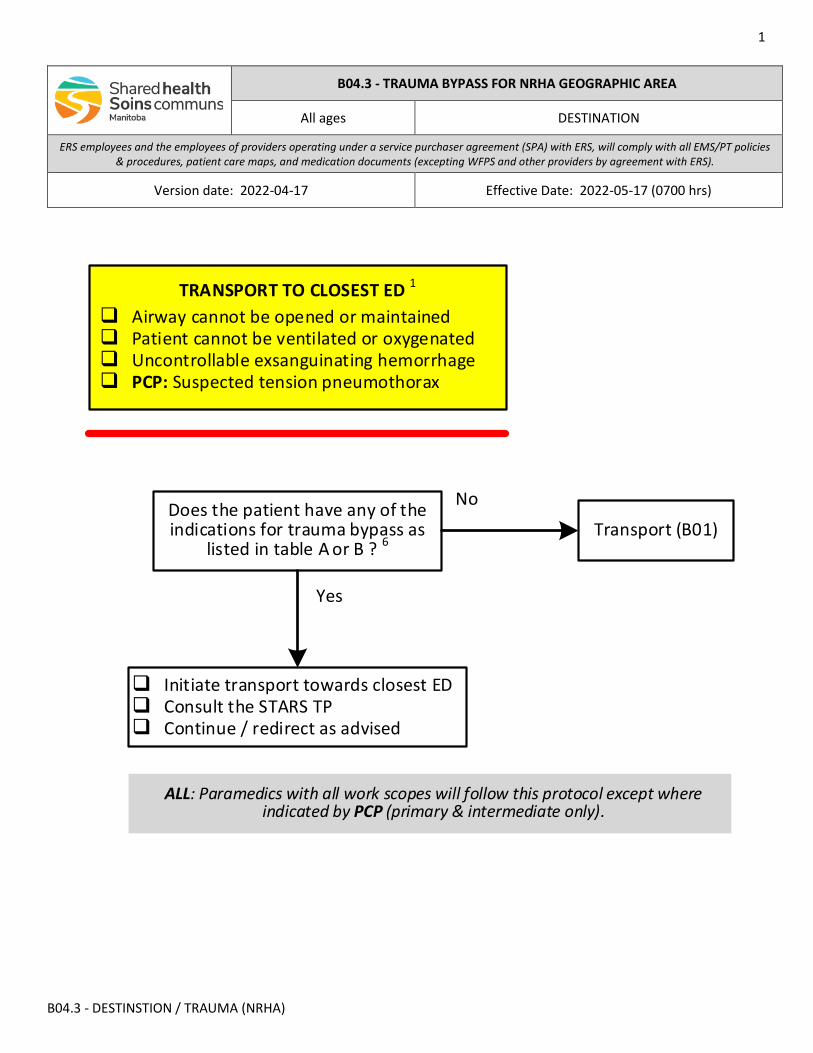
1
B04.3 - DESTINSTION / TRAUMA (NRHA)
Does the patient have any of the indications for trauma bypass as
listed in table A or B ? 6
Initiate transport towards closest ED Consult the STARS TP Continue / redirect as advised
Yes
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only).
No
Transport (B01)
TRANSPORT TO CLOSEST ED 1
Airway cannot be opened or maintained Patient cannot be ventilated or oxygenated Uncontrollable exsanguinating hemorrhage PCP: Suspected tension pneumothorax
B04.3 - TRAUMA BYPASS FOR NRHA GEOGRAPHIC AREA
All ages DESTINATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-17 Effective Date: 2022-05-17 (0700 hrs)
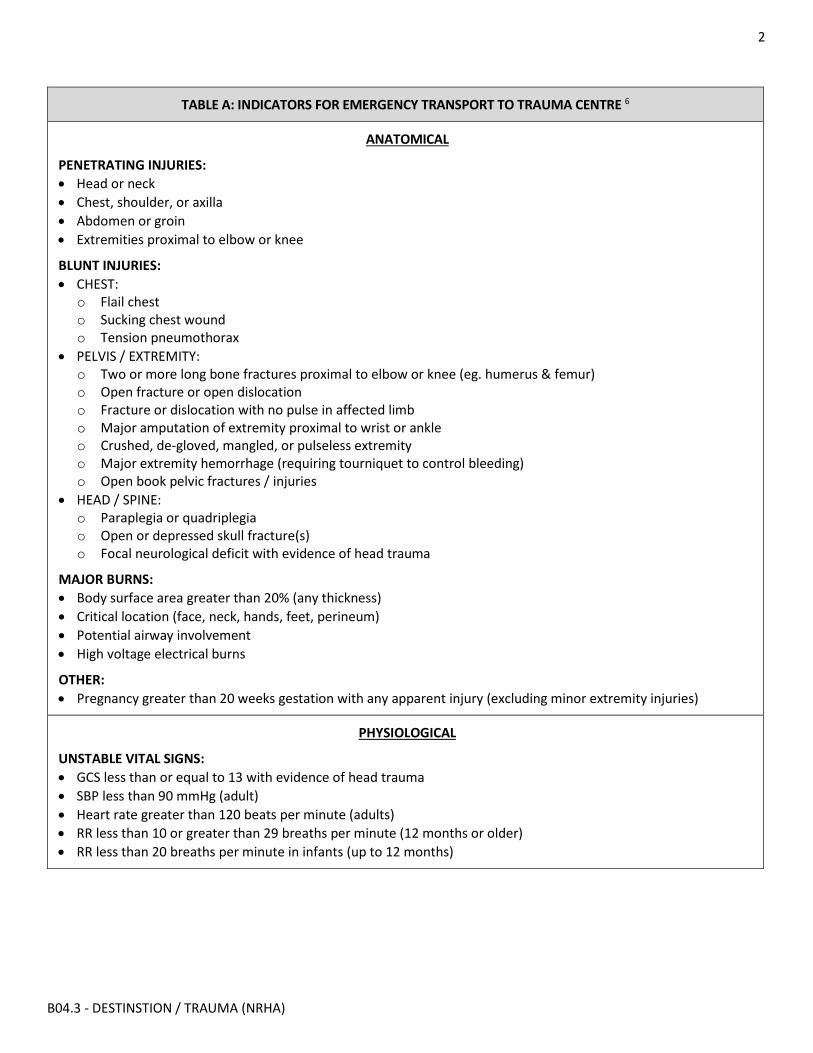
2
B04.3 - DESTINSTION / TRAUMA (NRHA)
TABLE A: INDICATORS FOR EMERGENCY TRANSPORT TO TRAUMA CENTRE 6
ANATOMICAL
PENETRATING INJURIES: • Head or neck • Chest, shoulder, or axilla • Abdomen or groin • Extremities proximal to elbow or knee
BLUNT INJURIES: • CHEST:
o Flail chest o Sucking chest wound o Tension pneumothorax
• PELVIS / EXTREMITY: o Two or more long bone fractures proximal to elbow or knee (eg. humerus & femur) o Open fracture or open dislocation o Fracture or dislocation with no pulse in affected limb o Major amputation of extremity proximal to wrist or ankle o Crushed, de-gloved, mangled, or pulseless extremity o Major extremity hemorrhage (requiring tourniquet to control bleeding) o Open book pelvic fractures / injuries
• HEAD / SPINE: o Paraplegia or quadriplegia o Open or depressed skull fracture(s) o Focal neurological deficit with evidence of head trauma
MAJOR BURNS: • Body surface area greater than 20% (any thickness) • Critical location (face, neck, hands, feet, perineum) • Potential airway involvement • High voltage electrical burns
OTHER: • Pregnancy greater than 20 weeks gestation with any apparent injury (excluding minor extremity injuries)
PHYSIOLOGICAL
UNSTABLE VITAL SIGNS: • GCS less than or equal to 13 with evidence of head trauma • SBP less than 90 mmHg (adult) • Heart rate greater than 120 beats per minute (adults) • RR less than 10 or greater than 29 breaths per minute (12 months or older) • RR less than 20 breaths per minute in infants (up to 12 months)
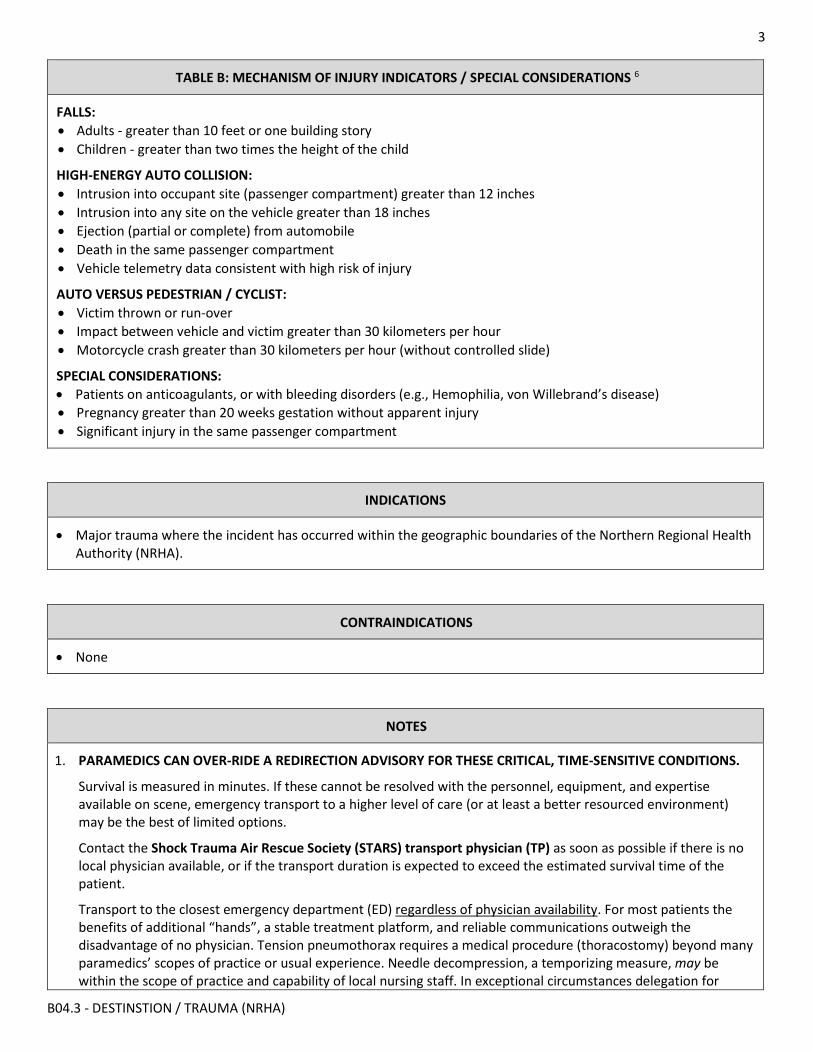
3
B04.3 - DESTINSTION / TRAUMA (NRHA)
TABLE B: MECHANISM OF INJURY INDICATORS / SPECIAL CONSIDERATIONS 6
FALLS: • Adults - greater than 10 feet or one building story • Children - greater than two times the height of the child
HIGH-ENERGY AUTO COLLISION: • Intrusion into occupant site (passenger compartment) greater than 12 inches • Intrusion into any site on the vehicle greater than 18 inches • Ejection (partial or complete) from automobile • Death in the same passenger compartment • Vehicle telemetry data consistent with high risk of injury
AUTO VERSUS PEDESTRIAN / CYCLIST: • Victim thrown or run-over • Impact between vehicle and victim greater than 30 kilometers per hour • Motorcycle crash greater than 30 kilometers per hour (without controlled slide)
SPECIAL CONSIDERATIONS: • Patients on anticoagulants, or with bleeding disorders (e.g., Hemophilia, von Willebrand’s disease) • Pregnancy greater than 20 weeks gestation without apparent injury • Significant injury in the same passenger compartment
INDICATIONS
• Major trauma where the incident has occurred within the geographic boundaries of the Northern Regional Health Authority (NRHA).
CONTRAINDICATIONS
• None
NOTES
1. PARAMEDICS CAN OVER-RIDE A REDIRECTION ADVISORY FOR THESE CRITICAL, TIME-SENSITIVE CONDITIONS.
Survival is measured in minutes. If these cannot be resolved with the personnel, equipment, and expertise available on scene, emergency transport to a higher level of care (or at least a better resourced environment) may be the best of limited options.
Contact the Shock Trauma Air Rescue Society (STARS) transport physician (TP) as soon as possible if there is no local physician available, or if the transport duration is expected to exceed the estimated survival time of the patient.
Transport to the closest emergency department (ED) regardless of physician availability. For most patients the benefits of additional “hands”, a stable treatment platform, and reliable communications outweigh the disadvantage of no physician. Tension pneumothorax requires a medical procedure (thoracostomy) beyond many paramedics’ scopes of practice or usual experience. Needle decompression, a temporizing measure, may be within the scope of practice and capability of local nursing staff. In exceptional circumstances delegation for
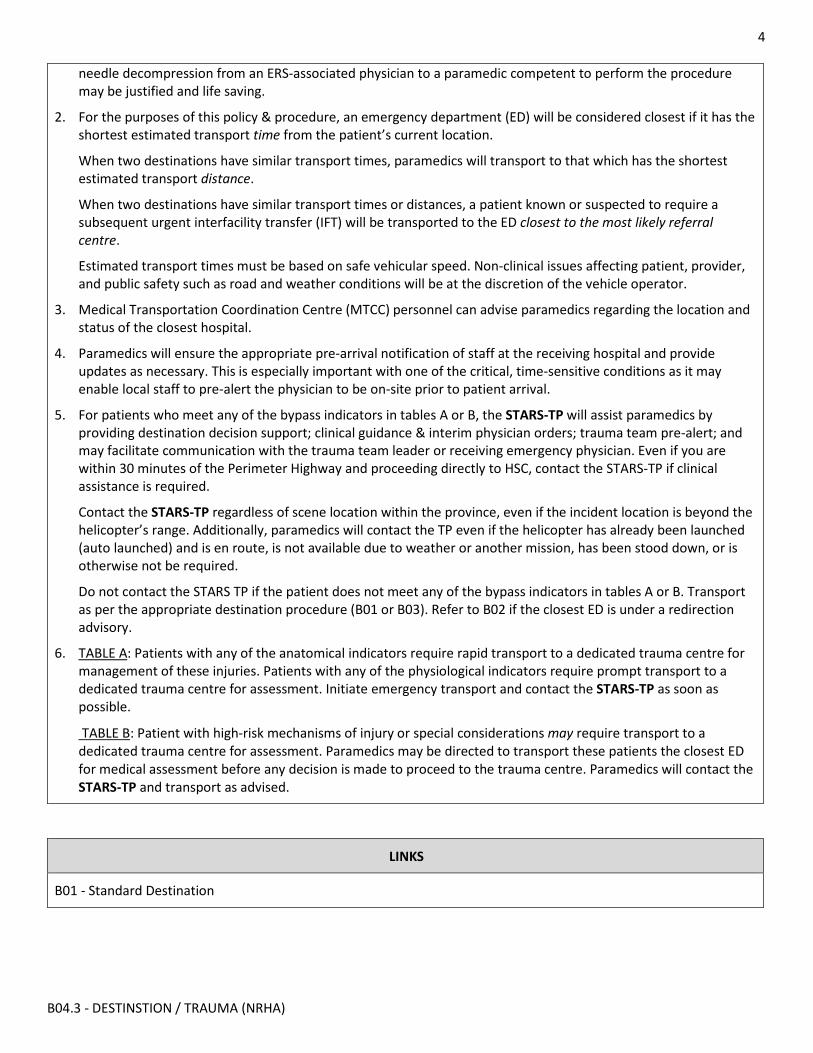
4
B04.3 - DESTINSTION / TRAUMA (NRHA)
needle decompression from an ERS-associated physician to a paramedic competent to perform the procedure may be justified and life saving.
2. For the purposes of this policy & procedure, an emergency department (ED) will be considered closest if it has the shortest estimated transport time from the patient’s current location.
When two destinations have similar transport times, paramedics will transport to that which has the shortest estimated transport distance.
When two destinations have similar transport times or distances, a patient known or suspected to require a subsequent urgent interfacility transfer (IFT) will be transported to the ED closest to the most likely referral centre.
Estimated transport times must be based on safe vehicular speed. Non-clinical issues affecting patient, provider, and public safety such as road and weather conditions will be at the discretion of the vehicle operator.
3. Medical Transportation Coordination Centre (MTCC) personnel can advise paramedics regarding the location and status of the closest hospital.
4. Paramedics will ensure the appropriate pre-arrival notification of staff at the receiving hospital and provide updates as necessary. This is especially important with one of the critical, time-sensitive conditions as it may enable local staff to pre-alert the physician to be on-site prior to patient arrival.
5. For patients who meet any of the bypass indicators in tables A or B, the STARS-TP will assist paramedics by providing destination decision support; clinical guidance & interim physician orders; trauma team pre-alert; and may facilitate communication with the trauma team leader or receiving emergency physician. Even if you are within 30 minutes of the Perimeter Highway and proceeding directly to HSC, contact the STARS-TP if clinical assistance is required.
Contact the STARS-TP regardless of scene location within the province, even if the incident location is beyond the helicopter’s range. Additionally, paramedics will contact the TP even if the helicopter has already been launched (auto launched) and is en route, is not available due to weather or another mission, has been stood down, or is otherwise not be required.
Do not contact the STARS TP if the patient does not meet any of the bypass indicators in tables A or B. Transport as per the appropriate destination procedure (B01 or B03). Refer to B02 if the closest ED is under a redirection advisory.
6. TABLE A: Patients with any of the anatomical indicators require rapid transport to a dedicated trauma centre for management of these injuries. Patients with any of the physiological indicators require prompt transport to a dedicated trauma centre for assessment. Initiate emergency transport and contact the STARS-TP as soon as possible.
TABLE B: Patient with high-risk mechanisms of injury or special considerations may require transport to a dedicated trauma centre for assessment. Paramedics may be directed to transport these patients the closest ED for medical assessment before any decision is made to proceed to the trauma centre. Paramedics will contact the STARS-TP and transport as advised.
LINKS
B01 - Standard Destination
5
B04.3 - DESTINSTION / TRAUMA (NRHA)
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X02 for change tracking)
• Corrections to links section • Revised flow chart for ease of use • Increased note details for clarification
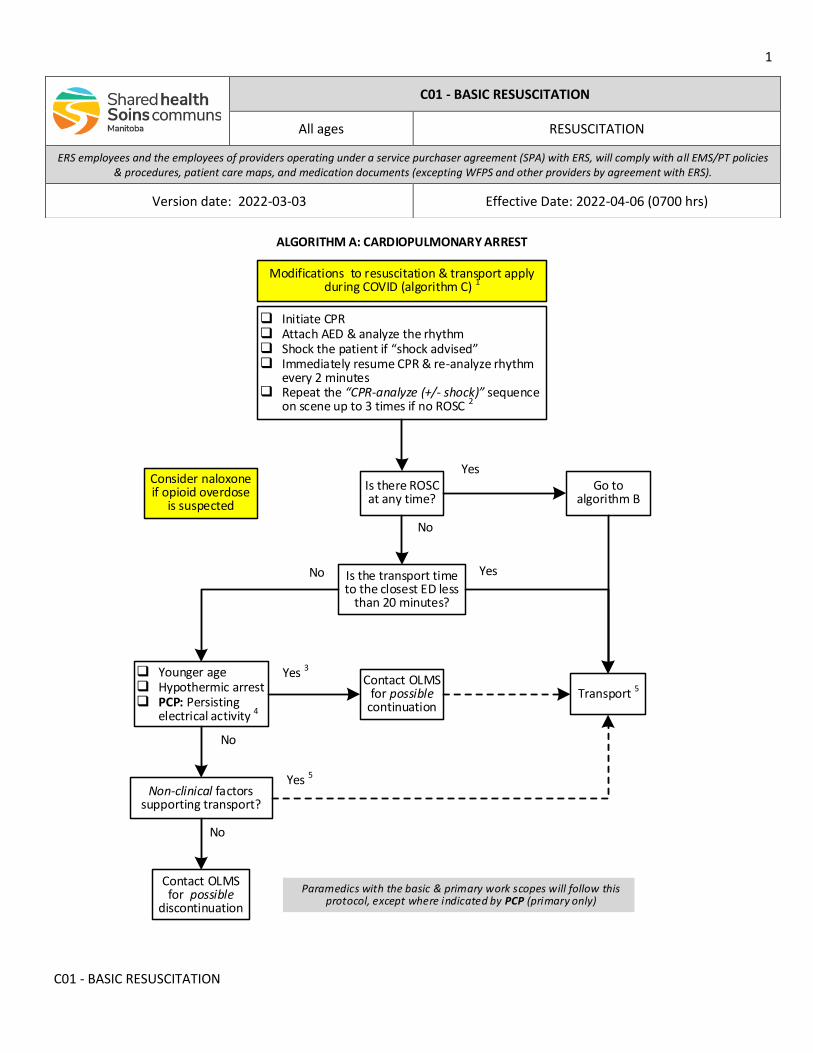
1
C01 - BASIC RESUSCITATION
Go to algorithm B
No
q Initiate CPRq Attach AED & analyze the rhythmq Shock the patient if shock advised q Immediately resume CPR & re-analyze rhythm
every 2 minutesq Repeat the CPR-analyze (+/- shock) sequence
on scene up to 3 times if no ROSC 2
Is there ROSC at any time?
Is the transport time to the closest ED less
than 20 minutes?
Yes
No
Contact OLMS for possible
discontinuation
No
Non-clinical factors supporting transport?
Modifications to resuscitation & transport apply during COVID (algorithm C) 1
ALGORITHM A: CARDIOPULMONARY ARREST
Paramedics with the basic & primary work scopes will follow this protocol, except where indicated by PCP (primary only)
Transport 5
Consider naloxone if opioid overdose
is suspected
q Younger ageq Hypothermic arrestq PCP: Persisting
electrical activity 4
Yes 5
No
Contact OLMS for possible
continuation
Yes 3
Yes
C01 - BASIC RESUSCITATION
All ages RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-03 Effective Date: 2022-04-06 (0700 hrs)
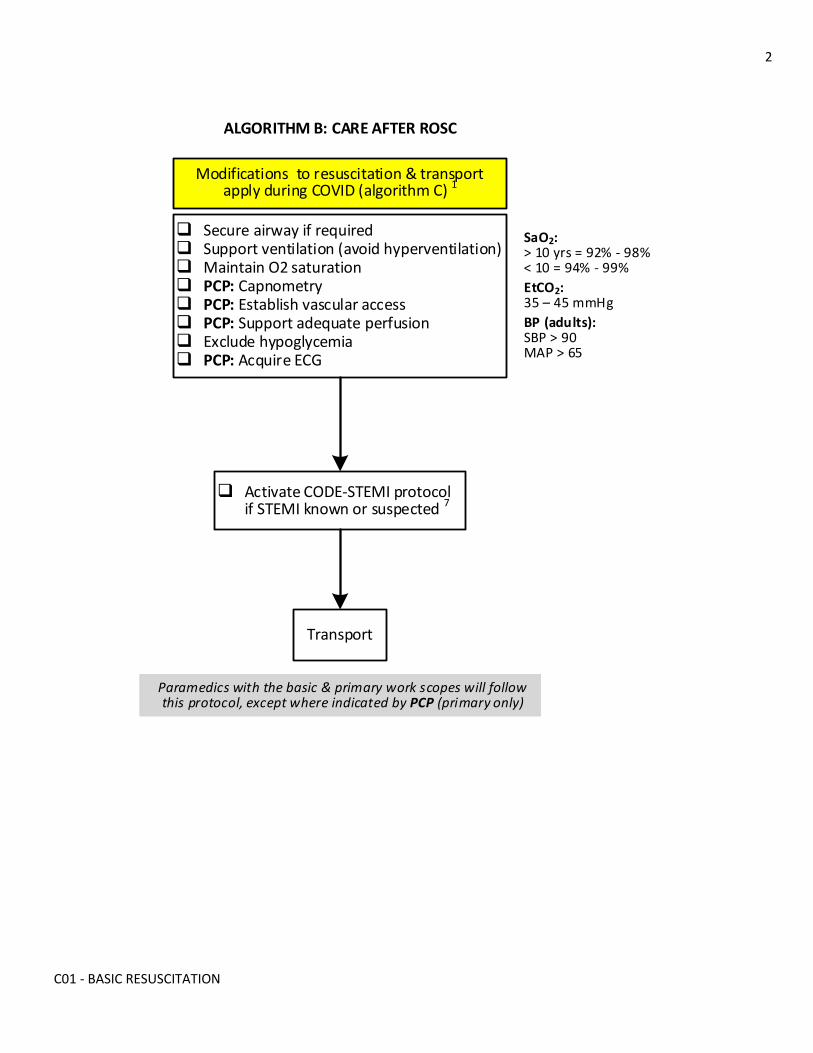
2
C01 - BASIC RESUSCITATION
ALGORITHM B: CARE AFTER ROSC
q Secure airway if requiredq Support ventilation (avoid hyperventilation)q Maintain O2 saturationq PCP: Capnometryq PCP: Establish vascular accessq PCP: Support adequate perfusionq Exclude hypoglycemiaq PCP: Acquire ECG
q Activate CODE-STEMI protocol if STEMI known or suspected 7
Transport
Modifications to resuscitation & transport apply during COVID (algorithm C) 1
Paramedics with the basic & primary work scopes will follow this protocol, except where indicated by PCP (primary only)
SaO2:> 10 yrs = 92% - 98%< 10 = 94% - 99%
EtCO2: – mmHg
BP (adults):SBP > 90MAP > 65
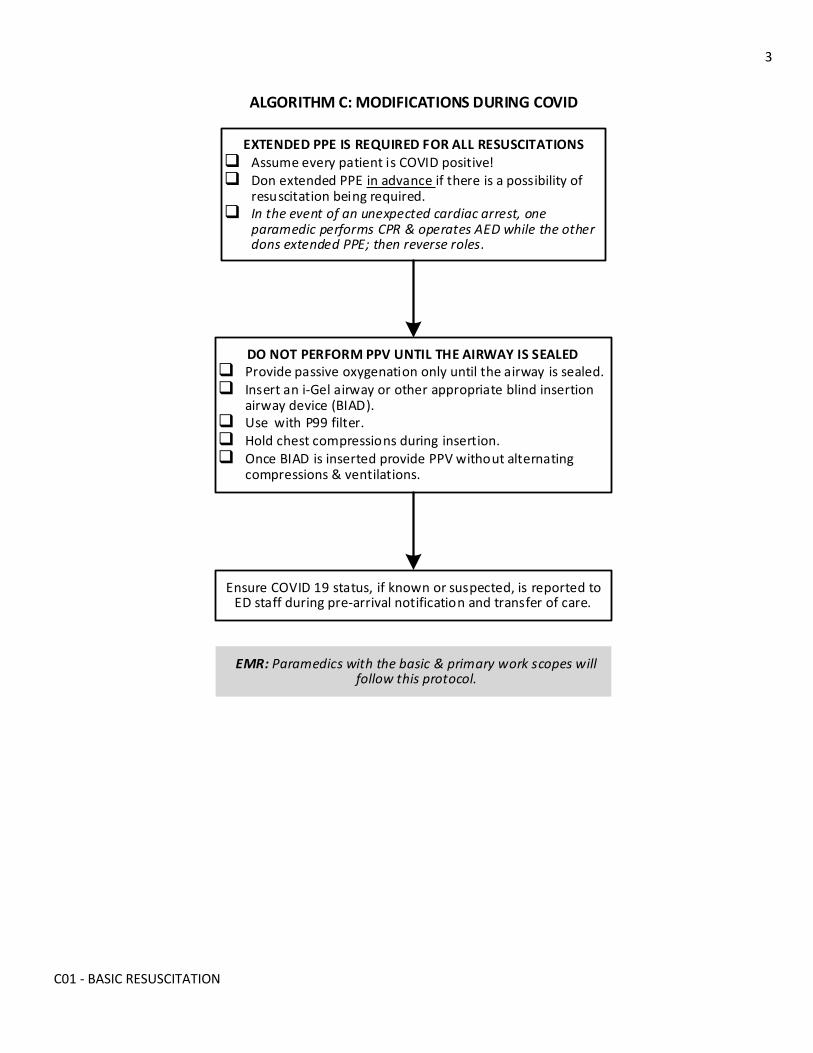
3
C01 - BASIC RESUSCITATION
ALGORITHM C: MODIFICATIONS DURING COVID
EXTENDED PPE IS REQUIRED FOR ALL RESUSCITATIONSq Assume every patient is COVID positive!q Don extended PPE in advance if there is a possibility of
resuscitation being required.q In the event of an unexpected cardiac arrest, one
paramedic performs CPR & operates AED while the other dons extended PPE; then reverse roles.
DO NOT PERFORM PPV UNTIL THE AIRWAY IS SEALEDq Provide passive oxygenation only until the airway is sealed.q Insert an i-Gel airway or other appropriate blind insertion
airway device (BIAD).q Use with P99 filter.q Hold chest compressions during insertion.q Once BIAD is inserted provide PPV without alternating
compressions & ventilations.
Ensure COVID 19 status, if known or suspected, is reported to ED staff during pre-arrival notification and transfer of care.
EMR: Paramedics with the basic & primary work scopes will follow this protocol.
4
C01 - BASIC RESUSCITATION
INDICATIONS
• Cardiac arrest from any cause
CONTRAINDICATIONS
• Obvious signs of death 9
• Confirmation of a valid health care directive prohibiting resuscitation from cardiac arrest
NOTES
1. During the COVID pandemic (algorithm C):
Airway manipulation is the main source for aerosol generation during cardiac resuscitation (chest compressions and defibrillation are not considered aerosol-generating medical procedures). Extended personal protective equipment (PPE) is required. All paramedics, including emergency medical responders (EMR) will insert a blind insertion airway device (BIAD) before initiating positive pressure ventilation (PPV). This is a temporary exemption from the College of Paramedics of Manitoba (CPMB) to the EMR scope of practice during the pandemic only.
2. If high-quality CPR and three shocks on the scene do not lead to a return of spontaneous circulation (ROSC), it is unlikely that further shocks will be effective without the prompt initiation of other advanced interventions.
3. Clinical factors such as younger age, hypothermia causing the arrest, or persisting electrical activity (PEA, VF, VT) indicate an increased chance of survival, and may support extended resuscitation efforts during a short duration transport.
Emergency transport exposes paramedics and the public to some risk. In these circumstances, transporting without ROSC should be carefully considered on a case-by-case basis. Paramedics must consult with the on-line medical support (OLMS) physician before discontinuing resuscitation.
4. Extended resuscitative efforts in patients with severe hypothermia (core body temperature below 28 degrees Celsius) has been associated with survival. Torso freezing is incompatible with life, and predicts no possibility of survival.
5. In certain non-clinical circumstances and even with little probability of survival, transporting to a health care facility and deferring the decision about discontinuation to a health care provider with additional training and experience may be in the best interest of the patient’s family and providers (e.g., pediatric cardiac arrest, distraught family).
6. If performing CPR during transporting, continue unless no longer possible due to fatigue or safety concerns. Do not interrupt CPR to repeat pulse or rhythm checks. Mechanical devices such as the “Autopulse” may be used to provide chest compressions.
7. If transporting to St. Boniface Hospital (SBH) post arrest, proceed directly to the emergency department (ED) for stabilization, unless advised otherwise. Be prepared to reroute to the cath lab if advised by the Code-STEMI physician or on-line medical support (OLMS) physician.
5
C01 - BASIC RESUSCITATION
8. For patients less than 8 years of age or 25 kilograms weight use pediatric pads. If pediatric pads are not available, use adult pads but ensure separation by at least 2.5 cm (consider antero-posterior placement). When using an AED in a patient with an implanted cardioverter-defibrillator (ICD) or pacemaker, place the electrodes at least 8 centimeters (3 inches) away from the pulse generator.
9. OBVIOUS SIGNS DEATH: Death can be reliably concluded by finding evidence of a significant time lapse from the cessation of circulation, or the recognition of injuries incompatible with survival.
• Evidence of significant time lapse: o Dependent lividity o Rigor mortis o Generalized tissue decomposition o Putrefaction o Torso freezing (chest cannot be compressed) 4
• Injuries incompatible with life: o Decapitation o Incineration o Transection of the thorax or abdomen o Substantial destruction of vital organs (heart, lungs, brain) o Separation of vital organs from the body
LINKS
• None
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to H08.3 for change tracking)
• Reformatting & revisions
• Replacement of coloured boxes with work scope statement & identifiers
• Information from C03 (care after ROSC), C10 (modifications during COVID) and H04 (signs of obvious death) now included
• Improved flow chart
• Reminders to consider naloxone & hypothermia
• Inclusion of promising clinical factors & requirement to contact OLMS for possible short duration transport
• Removal of requirement to notify OLMS before transporting non-ROSC COVID patients
• QRG for target VS added to ROSC flow chart
6
C01 - BASIC RESUSCITATION
• Alignment with current HSF ACLS & PALS cardiac arrest algorithms
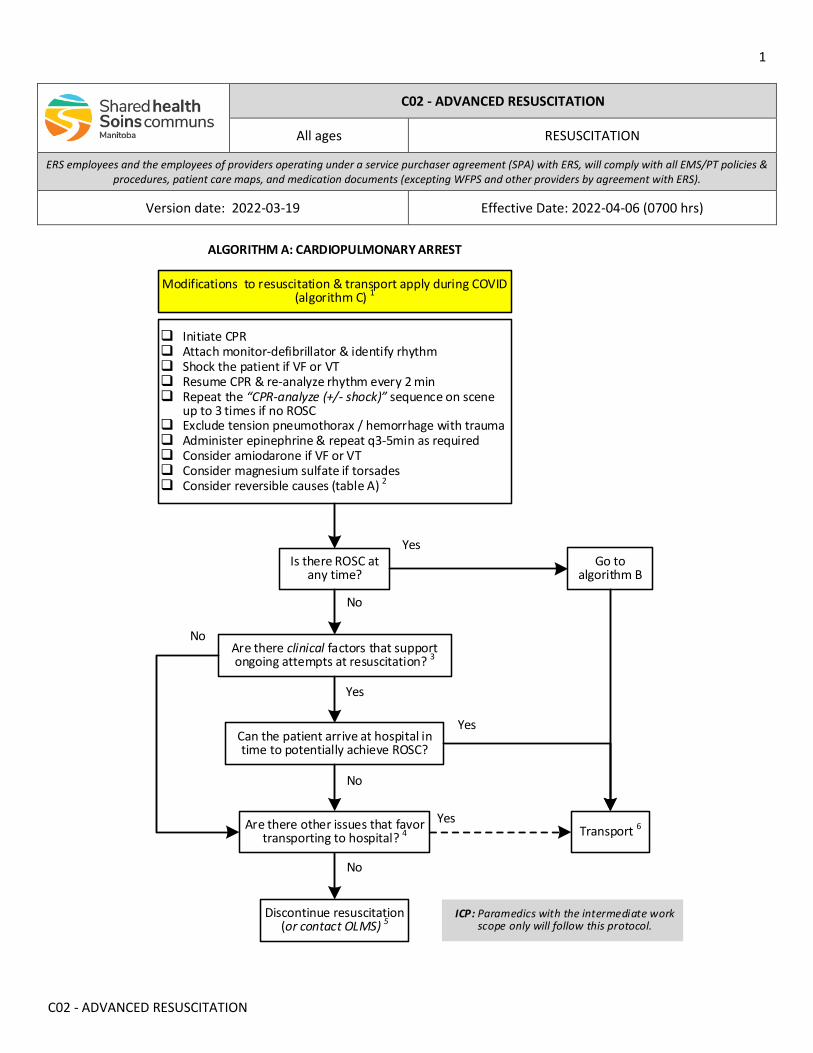
1
C02 - ADVANCED RESUSCITATION
C02 - ADVANCED RESUSCITATION
All ages RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-19 Effective Date: 2022-04-06 (0700 hrs)
Yes
Is there ROSC at any time?
Initiate CPR Attach monitor-defibrillator & identify rhythm Shock the patient if VF or VT Resume CPR & re-analyze rhythm every 2 min Repeat the “CPR-analyze (+/- shock)” sequence on scene
up to 3 times if no ROSC Exclude tension pneumothorax / hemorrhage with trauma Administer epinephrine & repeat q3-5min as required Consider amiodarone if VF or VT Consider magnesium sulfate if torsades Consider reversible causes (table A) 2
Yes
No
No
Are there clinical factors that support ongoing attempts at resuscitation? 3
Go to algorithm B
Yes
No
Are there other issues that favor transporting to hospital? 4
Discontinue resuscitation (or contact OLMS) 5
Can the patient arrive at hospital in time to potentially achieve ROSC?
No
Yes
ALGORITHM A: CARDIOPULMONARY ARREST
Transport 6
ICP: Paramedics with the intermediate work scope only will follow this protocol.
Modifications to resuscitation & transport apply during COVID (algorithm C) 1
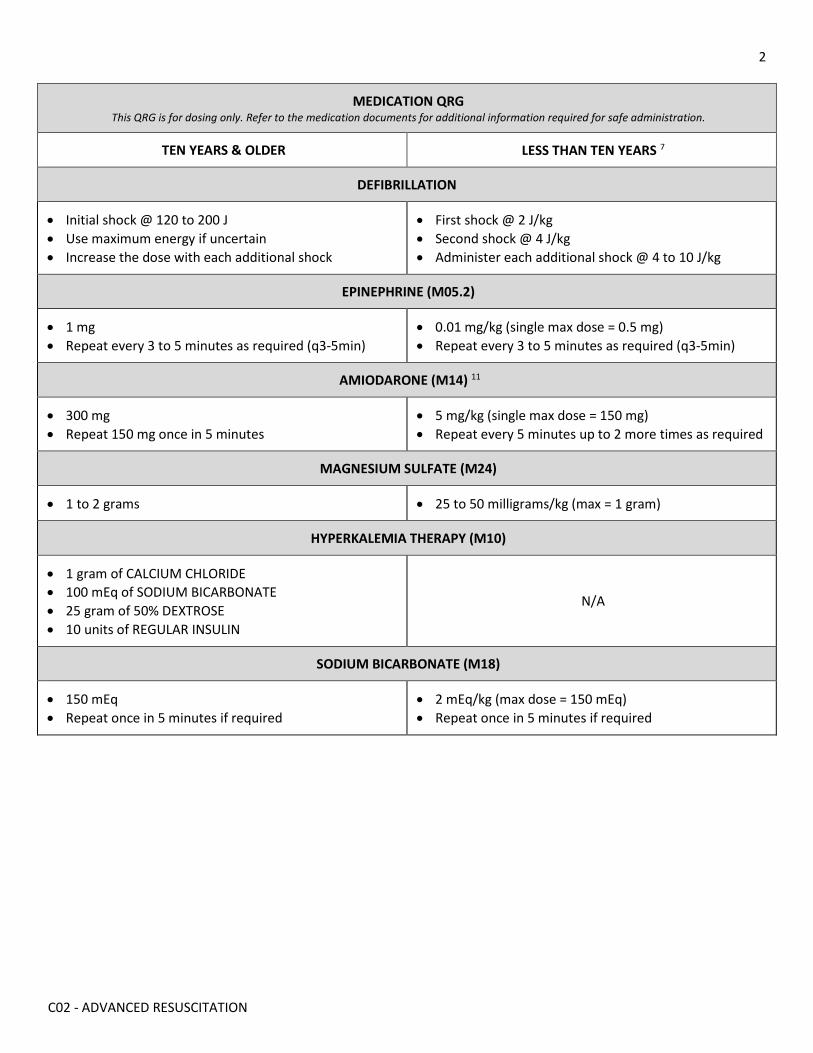
2
C02 - ADVANCED RESUSCITATION
MEDICATION QRG This QRG is for dosing only. Refer to the medication documents for additional information required for safe administration.
TEN YEARS & OLDER LESS THAN TEN YEARS 7
DEFIBRILLATION
• Initial shock @ 120 to 200 J • Use maximum energy if uncertain • Increase the dose with each additional shock
• First shock @ 2 J/kg • Second shock @ 4 J/kg • Administer each additional shock @ 4 to 10 J/kg
EPINEPHRINE (M05.2)
• 1 mg • Repeat every 3 to 5 minutes as required (q3-5min)
• 0.01 mg/kg (single max dose = 0.5 mg) • Repeat every 3 to 5 minutes as required (q3-5min)
AMIODARONE (M14) 11
• 300 mg • Repeat 150 mg once in 5 minutes
• 5 mg/kg (single max dose = 150 mg) • Repeat every 5 minutes up to 2 more times as required
MAGNESIUM SULFATE (M24)
• 1 to 2 grams • 25 to 50 milligrams/kg (max = 1 gram)
HYPERKALEMIA THERAPY (M10)
• 1 gram of CALCIUM CHLORIDE • 100 mEq of SODIUM BICARBONATE • 25 gram of 50% DEXTROSE • 10 units of REGULAR INSULIN
N/A
SODIUM BICARBONATE (M18)
• 150 mEq • Repeat once in 5 minutes if required
• 2 mEq/kg (max dose = 150 mEq) • Repeat once in 5 minutes if required
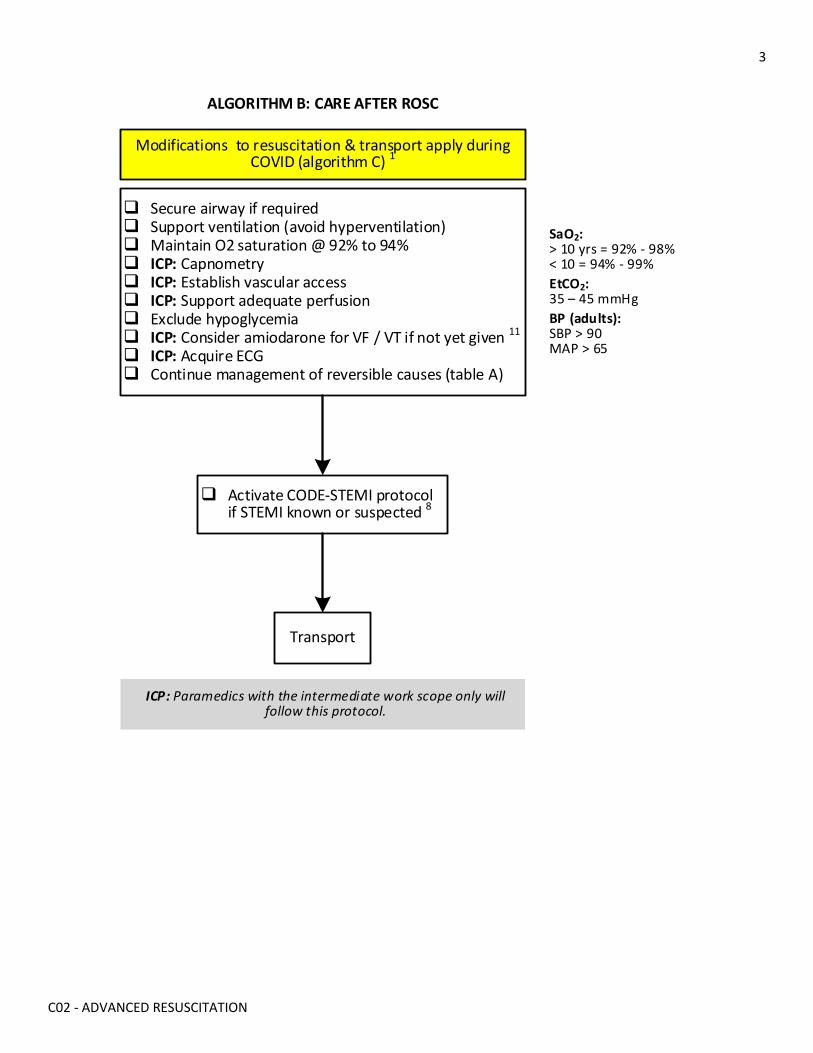
3
C02 - ADVANCED RESUSCITATION
ALGORITHM B: CARE AFTER ROSC
Secure airway if required Support ventilation (avoid hyperventilation) Maintain O2 saturation @ 92% to 94% ICP: Capnometry ICP: Establish vascular access ICP: Support adequate perfusion Exclude hypoglycemia ICP: Consider amiodarone for VF / VT if not yet given 11
ICP: Acquire ECG Continue management of reversible causes (table A)
Activate CODE-STEMI protocol if STEMI known or suspected 8
Transport
ICP: Paramedics with the intermediate work scope only will follow this protocol.
Modifications to resuscitation & transport apply during COVID (algorithm C) 1
SaO2:> 10 yrs = 92% - 98%< 10 = 94% - 99%EtCO2: 35 – 45 mmHgBP (adults):SBP > 90MAP > 65
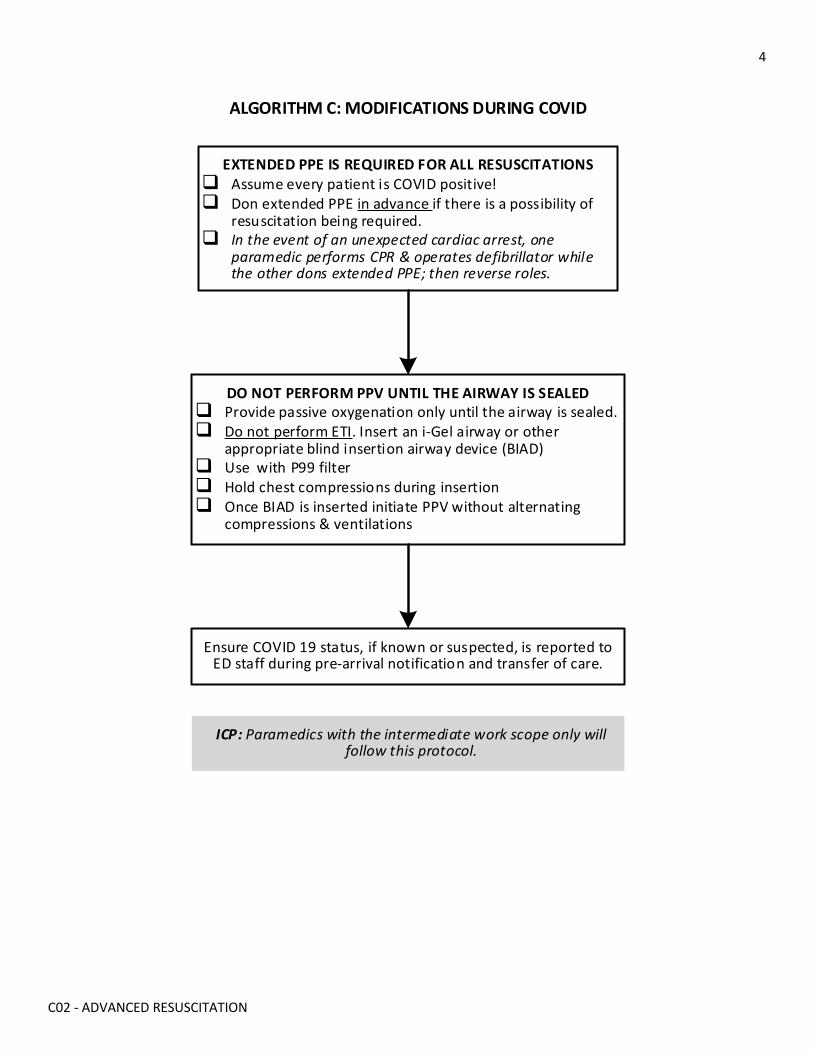
4
C02 - ADVANCED RESUSCITATION
ALGORITHM C: MODIFICATIONS DURING COVID
EXTENDED PPE IS REQUIRED FOR ALL RESUSCITATIONS Assume every patient is COVID positive! Don extended PPE in advance if there is a possibility of
resuscitation being required. In the event of an unexpected cardiac arrest, one
paramedic performs CPR & operates defibrillator while the other dons extended PPE; then reverse roles.
DO NOT PERFORM PPV UNTIL THE AIRWAY IS SEALED Provide passive oxygenation only until the airway is sealed. Do not perform ETI. Insert an i-Gel airway or other
appropriate blind insertion airway device (BIAD) Use with P99 filter Hold chest compressions during insertion Once BIAD is inserted initiate PPV without alternating
compressions & ventilations
Ensure COVID 19 status, if known or suspected, is reported to ED staff during pre-arrival notification and transfer of care.
ICP: Paramedics with the intermediate work scope only will follow this protocol.
5
C02 - ADVANCED RESUSCITATION
INDICATIONS
• Cardiac arrest from any cause
CONTRAINDICATIONS
• Obvious signs of death 9 • Confirmation of a valid health care directive prohibiting resuscitation from cardiac arrest
NOTES
1. During the COVID pandemic (algorithm C):
Airway manipulation is the main source for aerosol generation during cardiac resuscitation (chest compressions and defibrillation are not considered aerosol-generating medical procedures). Extended personal protective equipment (PPE) is required. Endotracheal intubation (ETI) is contraindicated. All paramedics will insert a blind insertion airway device (BIAD) before initiating positive pressure ventilation (PPV).
2. Some reversible causes of cardiac arrest often present initially with electrical activity (PEA) but will rapidly progress to asystole if uncorrected. Ventricular tachycardia (VT) or ventricular fibrillation (VF) due to a reversible cause such as hyperkalemia or a tricyclic antidepressant (TCA) overdose (table A) may not respond to defibrillation until the underlying cause is addressed. Prompt identification and correction of the cause while maintaining high-quality cardiopulmonary resuscitation (CPR) is the priority.
3. Factors that may support prolonged resuscitation attempts and emergency transport include the following. If in doubt, consult with the on-line medical support (OLMS) physician. • Younger age • Hypothermic arrest • Reversible cause with treatment available at a health care facility and short transport duration • Persistent electrical activity • Persistent EtCO2 levels greater than 10 mmHg
4. In certain circumstances (e.g., pediatric arrest, distraught family) and even with little probability of survival, transporting and deferring the decision about discontinuing resuscitation to a health care provider with additional training and experience may be in the best interest of the patient’s family and providers.
5. While some factors may support prolonging resuscitation efforts while transporting, emergency transport does expose paramedics and the public to some risk. Transport without ROSC should be carefully considered on a case-by-case basis. If in doubt, contact the OLMS physician for decision support.
6. If performing CPR while transporting, continue CPR unless no longer possible due to fatigue or safety concerns. Do not interrupt CPR to repeat pulse or rhythm checks. Mechanical devices such as the “Autopulse” may be used to provide chest compressions.
7. If the patient’s age is unknown, use visible signs of puberty as the differentiating feature for adolescent and child dosing.
8. If transporting to St. Boniface Hospital (SBH) post arrest, proceed directly to the emergency department (ED) for stabilization, unless advised otherwise. Be prepared to reroute to the cath lab if advised by the Code-STEMI physician or on-line medical support (OLMS) physician.
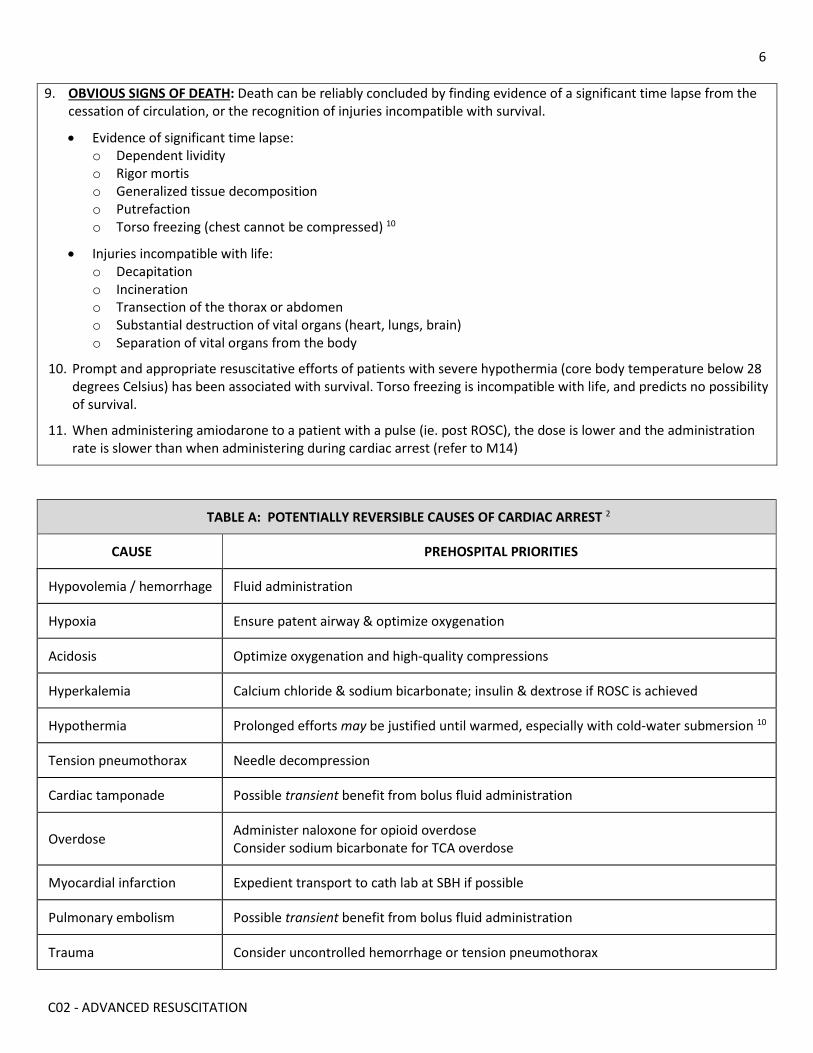
6
C02 - ADVANCED RESUSCITATION
9. OBVIOUS SIGNS OF DEATH: Death can be reliably concluded by finding evidence of a significant time lapse from the cessation of circulation, or the recognition of injuries incompatible with survival.
• Evidence of significant time lapse: o Dependent lividity o Rigor mortis o Generalized tissue decomposition o Putrefaction o Torso freezing (chest cannot be compressed) 10
• Injuries incompatible with life: o Decapitation o Incineration o Transection of the thorax or abdomen o Substantial destruction of vital organs (heart, lungs, brain) o Separation of vital organs from the body
10. Prompt and appropriate resuscitative efforts of patients with severe hypothermia (core body temperature below 28 degrees Celsius) has been associated with survival. Torso freezing is incompatible with life, and predicts no possibility of survival.
11. When administering amiodarone to a patient with a pulse (ie. post ROSC), the dose is lower and the administration rate is slower than when administering during cardiac arrest (refer to M14)
TABLE A: POTENTIALLY REVERSIBLE CAUSES OF CARDIAC ARREST 2
CAUSE PREHOSPITAL PRIORITIES
Hypovolemia / hemorrhage Fluid administration
Hypoxia Ensure patent airway & optimize oxygenation
Acidosis Optimize oxygenation and high-quality compressions
Hyperkalemia Calcium chloride & sodium bicarbonate; insulin & dextrose if ROSC is achieved
Hypothermia Prolonged efforts may be justified until warmed, especially with cold-water submersion 10
Tension pneumothorax Needle decompression
Cardiac tamponade Possible transient benefit from bolus fluid administration
Overdose Administer naloxone for opioid overdose Consider sodium bicarbonate for TCA overdose
Myocardial infarction Expedient transport to cath lab at SBH if possible
Pulmonary embolism Possible transient benefit from bolus fluid administration
Trauma Consider uncontrolled hemorrhage or tension pneumothorax
7
C02 - ADVANCED RESUSCITATION
LINKS
M05.2 - EPINEPHRINE FOR CARDIAC ARREST M10 - HYPERKALEMIA THERAPY M14 - AMIODARONE M18 - SODIUM BICARBONATE M24 - MAGNESIUM SULFATE
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X03 for change tracking)
• Reformatting & revisions • Replacement of coloured boxes with work scope statement & identifiers • Information from C03 (care after ROSC), C10 (modifications during COVID) and H04 (signs of obvious death) now
included • Simplified flow chart • QRG for target VS added to ROSC flow chart • Alignment with current HSF ACLS & PALS cardiac arrest algorithms
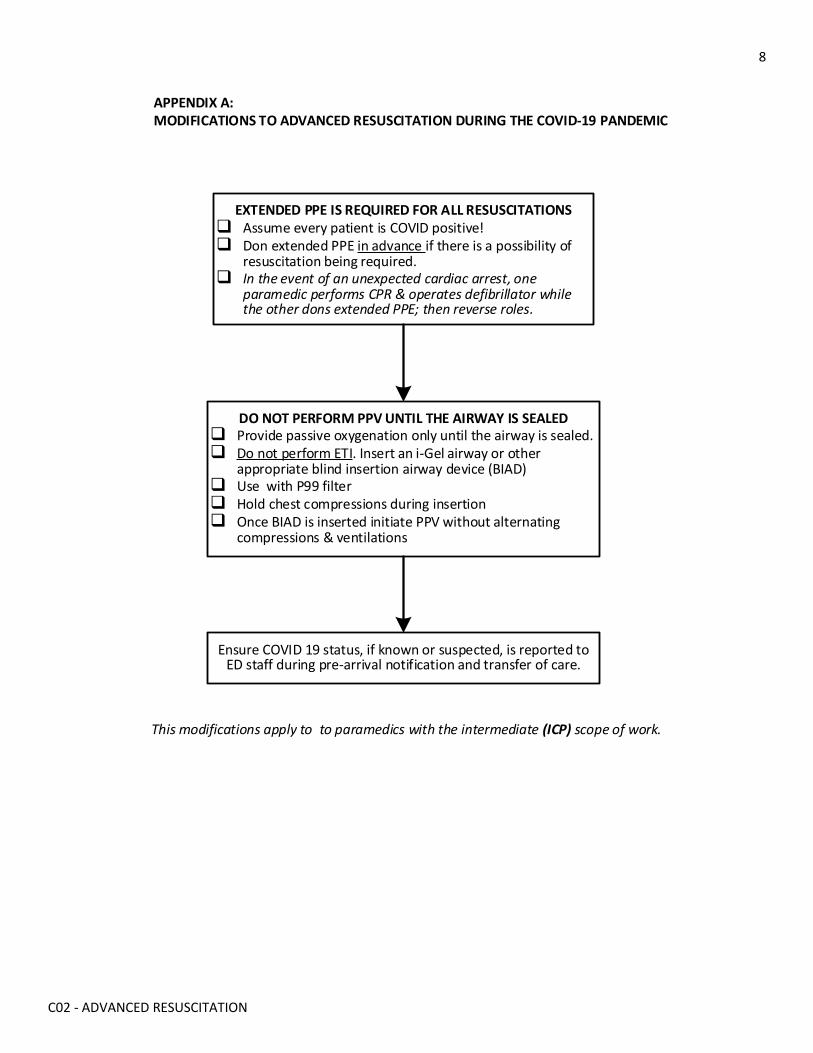
8
C02 - ADVANCED RESUSCITATION
APPENDIX A: MODIFICATIONS TO ADVANCED RESUSCITATION DURING THE COVID-19 PANDEMIC
EXTENDED PPE IS REQUIRED FOR ALL RESUSCITATIONS Assume every patient is COVID positive! Don extended PPE in advance if there is a possibility of
resuscitation being required. In the event of an unexpected cardiac arrest, one
paramedic performs CPR & operates defibrillator while the other dons extended PPE; then reverse roles.
DO NOT PERFORM PPV UNTIL THE AIRWAY IS SEALED Provide passive oxygenation only until the airway is sealed. Do not perform ETI. Insert an i-Gel airway or other
appropriate blind insertion airway device (BIAD) Use with P99 filter Hold chest compressions during insertion Once BIAD is inserted initiate PPV without alternating
compressions & ventilations
This modifications apply to to paramedics with the intermediate (ICP) scope of work.
Ensure COVID 19 status, if known or suspected, is reported to ED staff during pre-arrival notification and transfer of care.
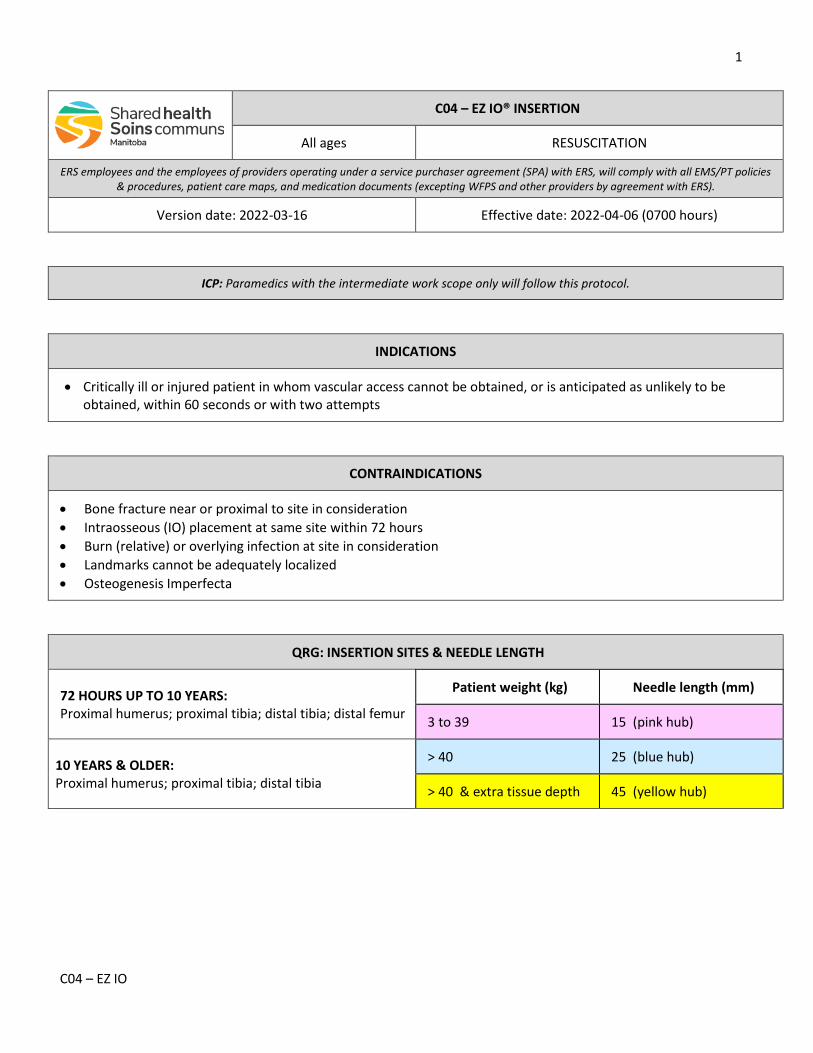
1
C04 – EZ IO
C04 – EZ IO® INSERTION
All ages RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-16 Effective date: 2022-04-06 (0700 hours)
ICP: Paramedics with the intermediate work scope only will follow this protocol.
INDICATIONS
• Critically ill or injured patient in whom vascular access cannot be obtained, or is anticipated as unlikely to be obtained, within 60 seconds or with two attempts
CONTRAINDICATIONS
• Bone fracture near or proximal to site in consideration • Intraosseous (IO) placement at same site within 72 hours • Burn (relative) or overlying infection at site in consideration • Landmarks cannot be adequately localized • Osteogenesis Imperfecta
QRG: INSERTION SITES & NEEDLE LENGTH
72 HOURS UP TO 10 YEARS: Proximal humerus; proximal tibia; distal tibia; distal femur
Patient weight (kg) Needle length (mm)
3 to 39 15 (pink hub)
10 YEARS & OLDER: Proximal humerus; proximal tibia; distal tibia
> 40 25 (blue hub)
> 40 & extra tissue depth 45 (yellow hub)
2
C04 – EZ IO
NOTES
1. Except for medications that are required to save life, limb, or vital function, intraosseous (IO) access should not be established solely to administer medication.
2. Any medication in the ERS formulary that can be administered by the intravenous (IV) route can be given through an IO device.
3. Select the best insertion site and appropriate needle length based on the patient’s weight and anatomy (QRG).
4. Position and stabilize the limb.
5. Using strict sterile technique to prepare the insertion site.
6. Pierce the skin and insert the needle into tissue. Confirm that the 5 mm mark is visible above the skin. If the mark is not visible, use the next larger needle length.
7. Using minimal pressure, drill the needle into bone.
8. Once inserted, stabilize the hub, and remove the driver.
9. Aspirate using a sterile syringe. Return of bone marrow confirms correct intramedullary needle tip placement, while the absence of marrow does not rule out correct placement.
10. Flush with the age-appropriate volume of sterile saline and watch for evidence of fluid extravasation. • Adults & adolescents - 5 to 10 ml • Infants & children - 2 to 5 ml
11. If fluid extravasation occurs, do not use this site but leave the device secured in place.
12. Apply the IO stabilizer and attached a primed extension set. Immobilize the limb for humerus and femur insertions.
13. Assess the site every 15 minutes to ensure the device remains secure and there are no signs of extravasation.
14. If the fluid flow subsequently slows or stops, repeat irrigation with sterile saline as noted in #10 above. If the device does not irrigate properly or there appears to be fluid extravasation, discontinue use but leave the device secured in place.
15. Serious injury, including compartment syndrome, may occur due to extravasation of fluid or medications into the surrounding tissues because of incorrect placement (either too deep or not deep enough). Secondary extravasation may result from increased intramedullary pressure from a high rate of infusion or due to a large infused volume.
16. INTRAOSSEOUS LIDOCAINE: In a conscious patient, consider the instillation of preservative-free 10 mg/ml (1%) or 20 mg/ml (2%) lidocaine to provide analgesia from the discomfort of infusion. • Infuse lidocaine into the device over 60 seconds • Allow to dwell for 120 seconds • Flush with 2.5 to 10 ml of sterile saline 10 • If pain relief is not adequate within 5 minutes, repeat with half dose • Repeat every 45 minutes as required
10 YEARS & OLDER: 50 mg
UP TO 10 YEARS: 0.1 mg/kg (single maximum dose = 50 mg)
Cumulative maximum dose: 3 mg/kg per hour
3
C04 – EZ IO
LINKS
M25 - INTRAOSSEOUS LIDOCAINE
APPROVED BY
Medical Director – Provincial EMS/PT Associate Medical Director – Provincial EMS/PT
VERSION CHANGES (refer to X03 for change tracking)
• Renumbered from P08 & reformatted • Inclusion of IO lidocaine dose from M25
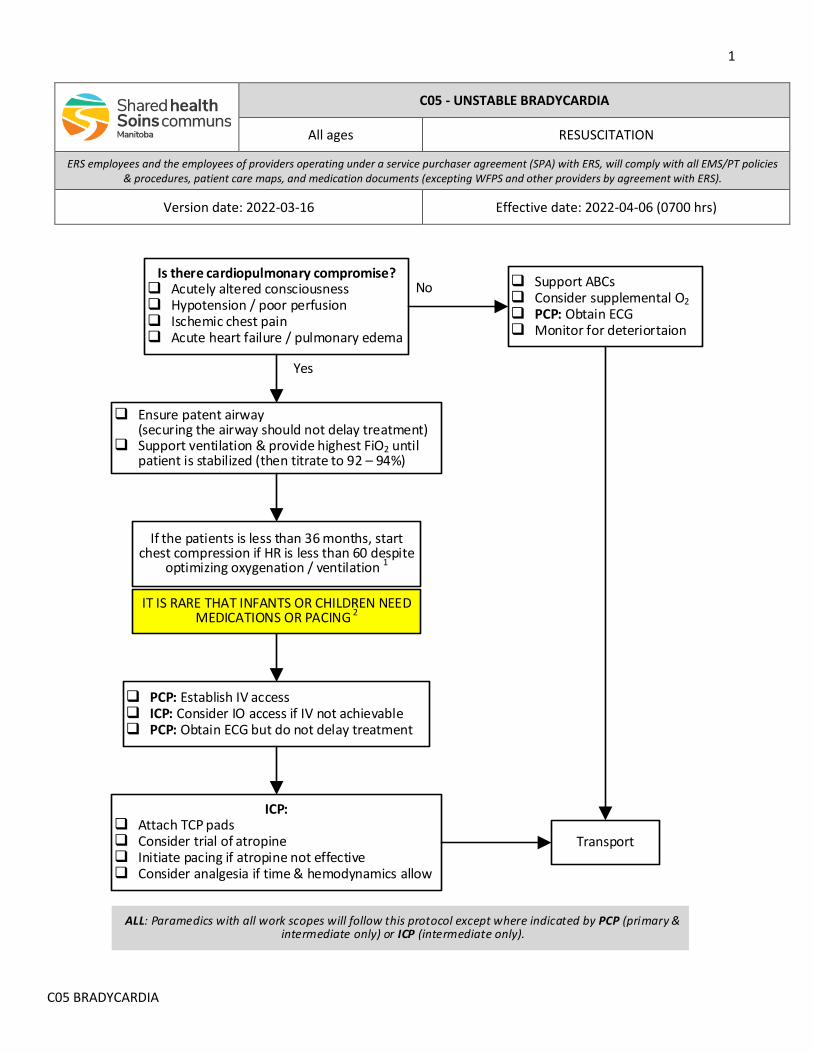
1
C05 BRADYCARDIA
C05 - UNSTABLE BRADYCARDIA
All ages RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-16 Effective date: 2022-04-06 (0700 hrs)
Is there cardiopulmonary compromise? Acutely altered consciousness Hypotension / poor perfusion Ischemic chest pain Acute heart failure / pulmonary edema
PCP: Establish IV access ICP: Consider IO access if IV not achievable PCP: Obtain ECG but do not delay treatment
Yes
No
ICP: Attach TCP pads Consider trial of atropine Initiate pacing if atropine not effective Consider analgesia if time & hemodynamics allow
Support ABCs Consider supplemental O2 PCP: Obtain ECG Monitor for deteriortaion
Ensure patent airway(securing the airway should not delay treatment)
Support ventilation & provide highest FiO2 until patient is stabilized (then titrate to 92 – 94%)
If the patients is less than 36 months, start chest compression if HR is less than 60 despite
optimizing oxygenation / ventilation 1
IT IS RARE THAT INFANTS OR CHILDREN NEED MEDICATIONS OR PACING 2
Transport
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only) or ICP (intermediate only).
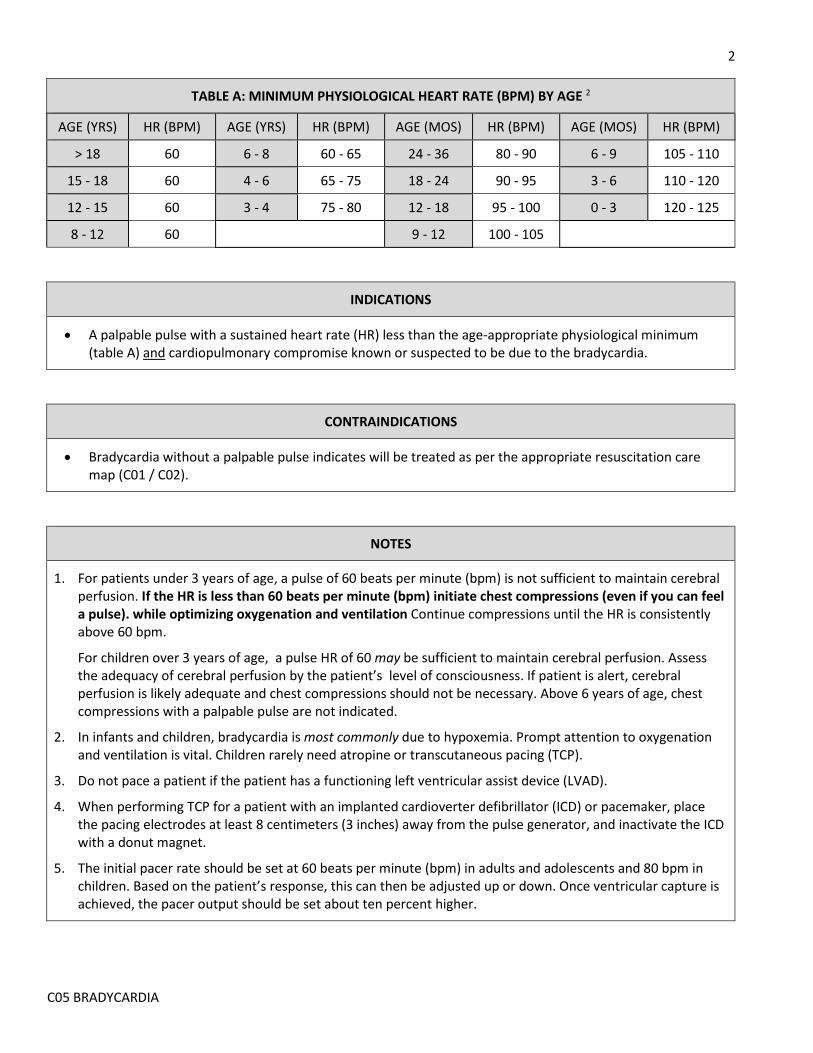
2
C05 BRADYCARDIA
TABLE A: MINIMUM PHYSIOLOGICAL HEART RATE (BPM) BY AGE 2
AGE (YRS) HR (BPM) AGE (YRS) HR (BPM) AGE (MOS) HR (BPM) AGE (MOS) HR (BPM)
> 18 60 6 - 8 60 - 65 24 - 36 80 - 90 6 - 9 105 - 110
15 - 18 60 4 - 6 65 - 75 18 - 24 90 - 95 3 - 6 110 - 120
12 - 15 60 3 - 4 75 - 80 12 - 18 95 - 100 0 - 3 120 - 125
8 - 12 60 9 - 12 100 - 105
INDICATIONS
• A palpable pulse with a sustained heart rate (HR) less than the age-appropriate physiological minimum (table A) and cardiopulmonary compromise known or suspected to be due to the bradycardia.
CONTRAINDICATIONS
• Bradycardia without a palpable pulse indicates will be treated as per the appropriate resuscitation care map (C01 / C02).
NOTES
1. For patients under 3 years of age, a pulse of 60 beats per minute (bpm) is not sufficient to maintain cerebral perfusion. If the HR is less than 60 beats per minute (bpm) initiate chest compressions (even if you can feel a pulse). while optimizing oxygenation and ventilation Continue compressions until the HR is consistently above 60 bpm.
For children over 3 years of age, a pulse HR of 60 may be sufficient to maintain cerebral perfusion. Assess the adequacy of cerebral perfusion by the patient’s level of consciousness. If patient is alert, cerebral perfusion is likely adequate and chest compressions should not be necessary. Above 6 years of age, chest compressions with a palpable pulse are not indicated.
2. In infants and children, bradycardia is most commonly due to hypoxemia. Prompt attention to oxygenation and ventilation is vital. Children rarely need atropine or transcutaneous pacing (TCP).
3. Do not pace a patient if the patient has a functioning left ventricular assist device (LVAD).
4. When performing TCP for a patient with an implanted cardioverter defibrillator (ICD) or pacemaker, place the pacing electrodes at least 8 centimeters (3 inches) away from the pulse generator, and inactivate the ICD with a donut magnet.
5. The initial pacer rate should be set at 60 beats per minute (bpm) in adults and adolescents and 80 bpm in children. Based on the patient’s response, this can then be adjusted up or down. Once ventricular capture is achieved, the pacer output should be set about ten percent higher.
3
C05 BRADYCARDIA
LINKS
C01 - BASIC RESUSCITATION C02 - ADVANCED RESUSCITATION M39 - ATROPINE
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X03 for change tracking)
• Reformatted • Replacement of colored boxes with scope of work “legend” • Simplified flow chart • More consistent with current HSFC bradycardia adult & pediatric algorithms • Further clarification as to when to initiate CPR in children
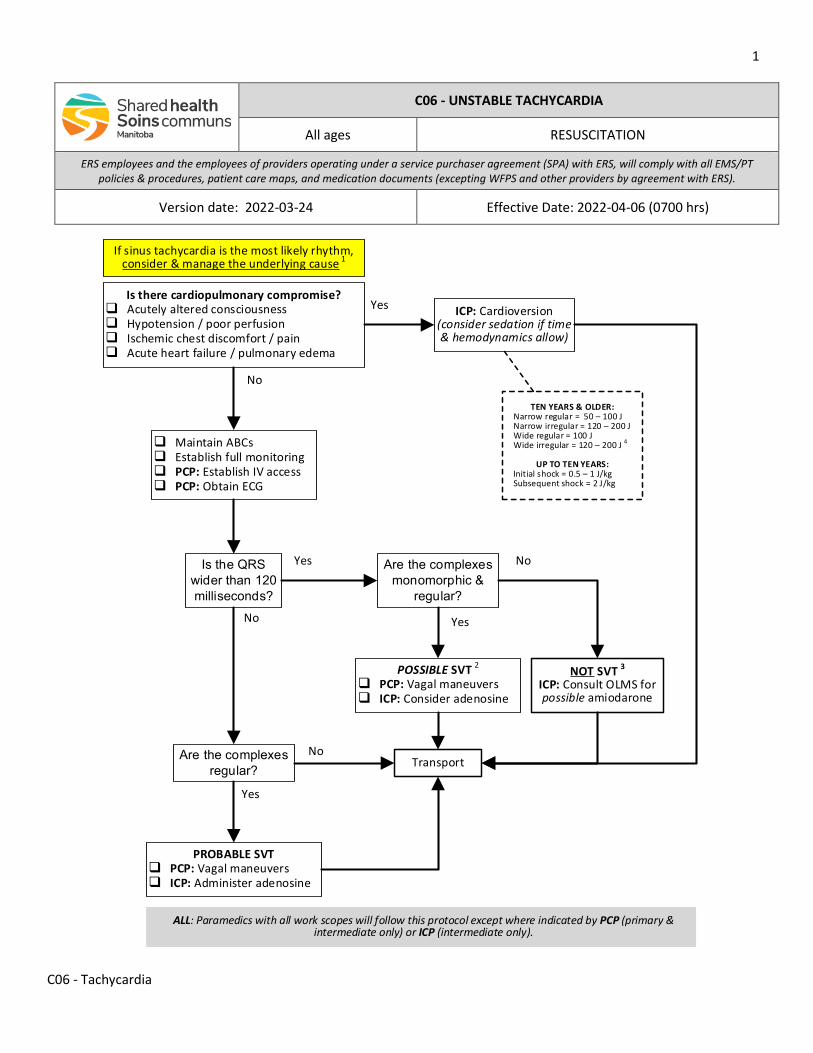
1
C06 - Tachycardia
C06 - UNSTABLE TACHYCARDIA
All ages RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-24 Effective Date: 2022-04-06 (0700 hrs)
No
Is there cardiopulmonary compromise? Acutely altered consciousness Hypotension / poor perfusion Ischemic chest discomfort / pain Acute heart failure / pulmonary edema
Yes
ICP: Cardioversion (consider sedation if time & hemodynamics allow)
Maintain ABCs Establish full monitoring PCP: Establish IV access PCP: Obtain ECG
If sinus tachycardia is the most likely rhythm, consider & manage the underlying cause 1
Yes
No
No
Yes
TEN YEARS & OLDER:Narrow regular = 50 – 100 JNarrow irregular = 120 – 200 JWide regular = 100 JWide irregular = 120 – 200 J 4
UP TO TEN YEARS:Initial shock = 0.5 – 1 J/kgSubsequent shock = 2 J/kg
Is the QRS wider than 120 milliseconds?
Are the complexes regular?
PROBABLE SVT PCP: Vagal maneuvers ICP: Administer adenosine
Are the complexes monomorphic &
regular?
POSSIBLE SVT 2
PCP: Vagal maneuvers ICP: Consider adenosine
No Yes
Transport
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only) or ICP (intermediate only).
NOT SVT 3ICP: Consult OLMS for possible amiodarone
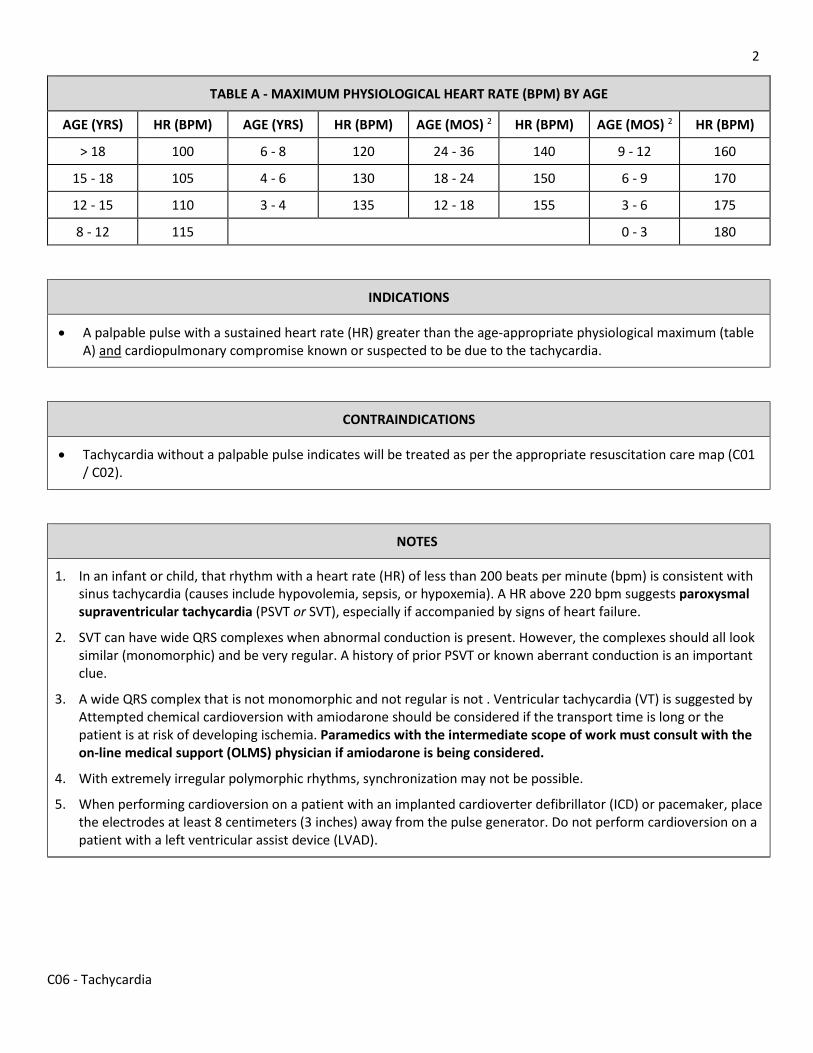
2
C06 - Tachycardia
TABLE A - MAXIMUM PHYSIOLOGICAL HEART RATE (BPM) BY AGE
AGE (YRS) HR (BPM) AGE (YRS) HR (BPM) AGE (MOS) 2 HR (BPM) AGE (MOS) 2 HR (BPM)
> 18 100 6 - 8 120 24 - 36 140 9 - 12 160
15 - 18 105 4 - 6 130 18 - 24 150 6 - 9 170
12 - 15 110 3 - 4 135 12 - 18 155 3 - 6 175
8 - 12 115 0 - 3 180
INDICATIONS
• A palpable pulse with a sustained heart rate (HR) greater than the age-appropriate physiological maximum (table A) and cardiopulmonary compromise known or suspected to be due to the tachycardia.
CONTRAINDICATIONS
• Tachycardia without a palpable pulse indicates will be treated as per the appropriate resuscitation care map (C01 / C02).
NOTES
1. In an infant or child, that rhythm with a heart rate (HR) of less than 200 beats per minute (bpm) is consistent with sinus tachycardia (causes include hypovolemia, sepsis, or hypoxemia). A HR above 220 bpm suggests paroxysmal supraventricular tachycardia (PSVT or SVT), especially if accompanied by signs of heart failure.
2. SVT can have wide QRS complexes when abnormal conduction is present. However, the complexes should all look similar (monomorphic) and be very regular. A history of prior PSVT or known aberrant conduction is an important clue.
3. A wide QRS complex that is not monomorphic and not regular is not . Ventricular tachycardia (VT) is suggested by Attempted chemical cardioversion with amiodarone should be considered if the transport time is long or the patient is at risk of developing ischemia. Paramedics with the intermediate scope of work must consult with the on-line medical support (OLMS) physician if amiodarone is being considered.
4. With extremely irregular polymorphic rhythms, synchronization may not be possible.
5. When performing cardioversion on a patient with an implanted cardioverter defibrillator (ICD) or pacemaker, place the electrodes at least 8 centimeters (3 inches) away from the pulse generator. Do not perform cardioversion on a patient with a left ventricular assist device (LVAD).
3
C06 - Tachycardia
LINKS
C01 - BASIC RESUSCITATION C02 - ADVANCED RESUSCITATION M01 - ADENOSINE M14 - AMIODARONE
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X03 for change tracking)
• Replacement of colored boxes with scope of work “legend” • Simplified flow chart • More consistent with current ACLS & PALS tachycardia algorithms • Reformatted
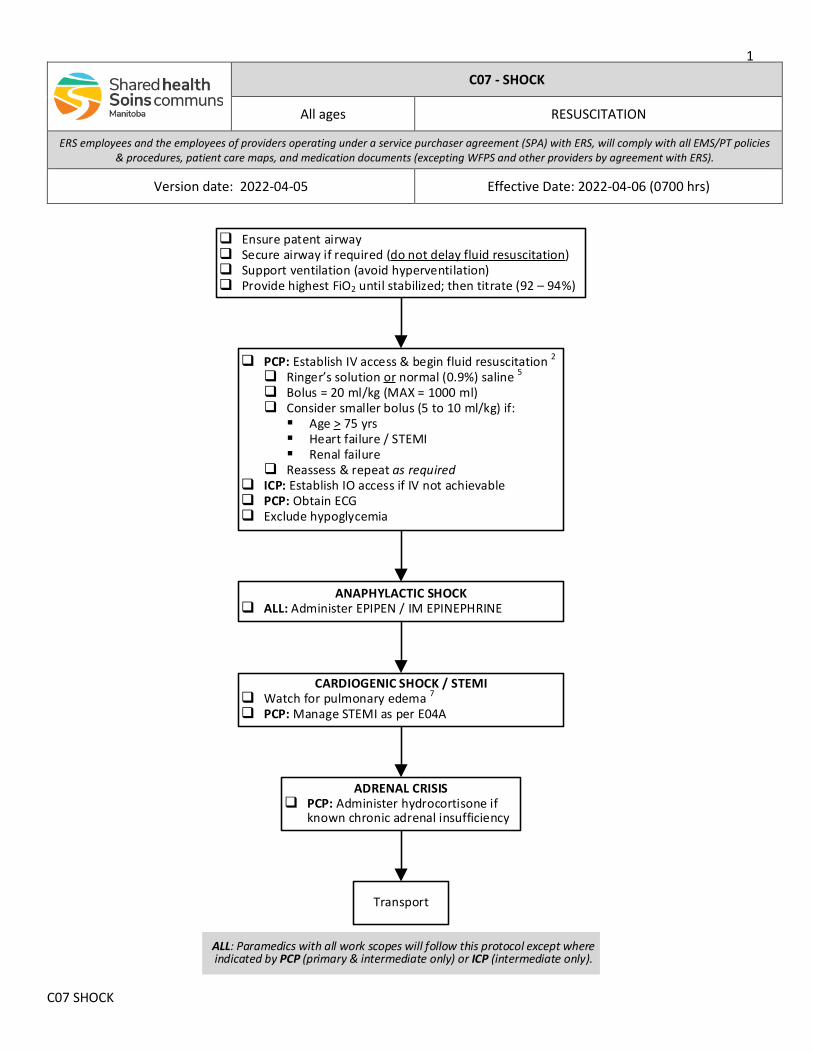
1
C07 SHOCK
ANAPHYLACTIC SHOCK ALL: Administer EPIPEN / IM EPINEPHRINE
Ensure patent airway Secure airway if required (do not delay fluid resuscitation) Support ventilation (avoid hyperventilation) Provide highest FiO2 until stabilized; then titrate (92 – 94%)
PCP: Establish IV access & begin fluid resuscitation 2
Ringer’s solution or normal (0.9%) saline 5
Bolus = 20 ml/kg (MAX = 1000 ml) Consider smaller bolus (5 to 10 ml/kg) if: Age > 75 yrs Heart failure / STEMI Renal failure
Reassess & repeat as required ICP: Establish IO access if IV not achievable PCP: Obtain ECG Exclude hypoglycemia
CARDIOGENIC SHOCK / STEMI Watch for pulmonary edema 7
PCP: Manage STEMI as per E04A
ADRENAL CRISIS PCP: Administer hydrocortisone if
known chronic adrenal insufficiency
Transport
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only) or ICP (intermediate only).
C07 - SHOCK
All ages RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-05 Effective Date: 2022-04-06 (0700 hrs)
2
C07 SHOCK
INDICATIONS
• Known or suspected shock that is not due to major trauma
CONTRAINDICATIONS
• Not applicable
NOTES
1. Circulatory shock is defined as a state of inadequate tissue perfusion. Although hypotension may be present, no specific blood pressure (BP) value defines shock. Shock may be present with a normal BP. Multiple factors (eg. age, fitness, medications) may impact the vital signs and complicate the presentation of shock.
2. The specific cause of shock can sometimes be difficult to determine in the prehospital setting, and multiple causes may sometimes be present (eg. myocardial dysfunction in septic shock). This is referred to as undifferentiated shock. Nonetheless, with a few exceptions, IV fluid administration is still an important early step in the management of most causes of shock.
3. The common categories and causes of shock that is not due to trauma include: o Hypovolemia (eg. vomiting, diarrhea, decreased oral intake, polyuria) o Hemorrhage o Sepsis / infection o Cardiogenic (eg. myocardial infarction, arrhythmia, acute valve dysfunction) o Obstructive (eg. tension pneumothorax, pericarditis) o Anaphylaxis o Adrenal insufficiency (adrenal crisis) o Neurogenic
4. Hemorrhagic shock can be due to major trauma or nontraumatic causes (eg. gastrointestinal bleed, severe epistaxis, tumor erosion). For the management of hemorrhagic shock due to major trauma, refer to F01 - MAJOR TRAUMA.
5. Either normal (0.9%) saline or lactated Ringer’s solution are both acceptable in prehospital care in all age groups. Emerging evidence suggest that lactated Ringer’s solution may improve various outcome parameters in most types of shock.
6. While there is limited research into the benefit of permissive hypotension in nontraumatic hemorrhagic shock, aggressive crystalloid administration is known to create coagulopathy and hypothermia (impairing clotting), and increases mortality. Consider smaller fluid boluses (5 ml/kg up to a maximum of 500 ml) targeted to an age-appropriate lower target systolic BP to maintain adequate blood flow to keep the heart and brain adequately perfused.
7. With cardiogenic shock, the conditions that cause poor cardiac output may also cause backup of fluid into the lungs. If the lungs are clear, use smaller volumes and continuously reassess to avoid pulmonary edema. Do not administer IV fluid in pulmonary edema, regardless of the presence of poor perfusion. The prehospital managment of cardiogenic shock can be extremely difficult. Paramedics may consult the on-line medical support (OLMS) physician at any time for clinical support,
3
C07 SHOCK
LINKS
E03 - ANAPHYLAXIS E04A - ACUTE CORONARY SYNDROME & STEMI M13 - HYDROCORTISONE
APPROVED BY
MEDICAL DIRECTOR - PROVINCIAL EMS/PT ASSOCIATE MEDICAL DIRECTOR - PROVINCIAL EMS/PT
VERSION CHANGES (refer to X03 for change tracking)
• Revised, reformatted & retitled (Hypotension & Shock) • Replacement of coloured boxes with scope of work statement and legend • Inclusion of specific management directions for anaphylactic, adrenal & cardiogenic shock • Emphasis on evidence of hypoperfusion rather than BP
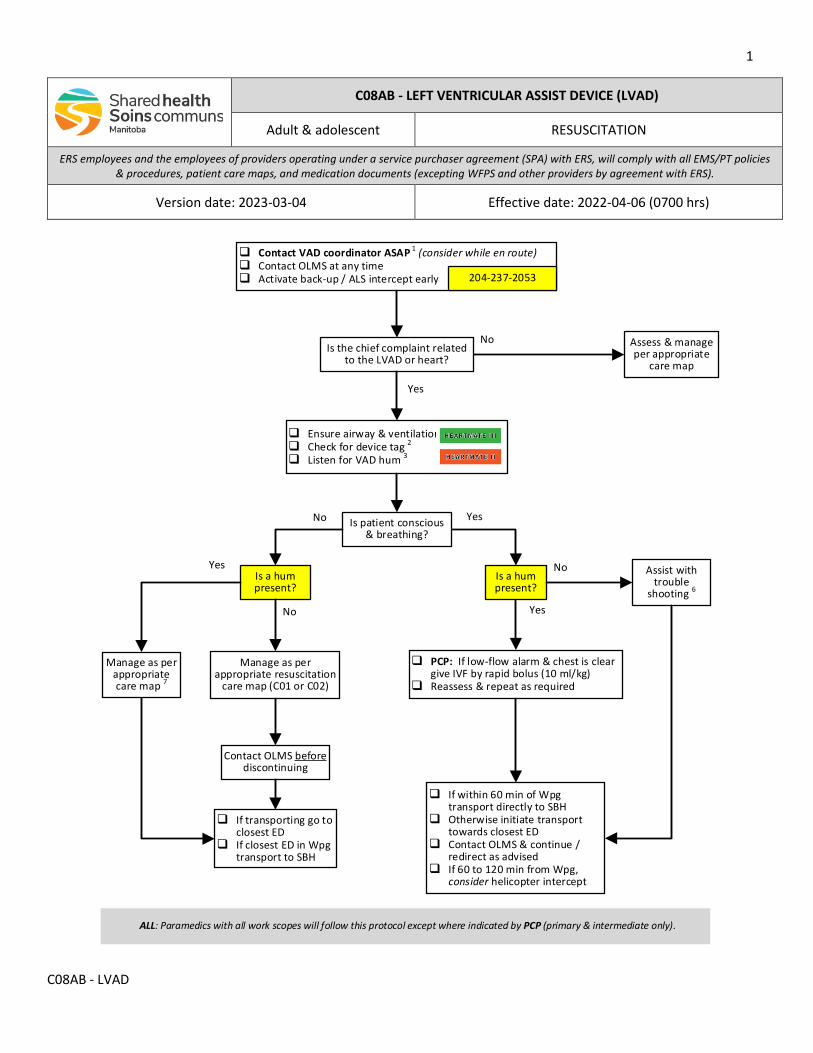
1
C08AB - LVAD
Contact VAD coordinator ASAP 1 (consider while en route) Contact OLMS at any time Activate back-up / ALS intercept early
Manage as per appropriate resuscitation
care map (C01 or C02)
Is a hum present?
PCP: If low-flow alarm & chest is clear give IVF by rapid bolus (10 ml/kg)
Reassess & repeat as required
No
Yes
204-237-2053
Ensure airway & ventilation Check for device tag 2
Listen for VAD hum 3
Is patient conscious & breathing?
No
If within 60 min of Wpg transport directly to SBH
Otherwise initiate transport towards closest ED
Contact OLMS & continue / redirect as advised
If 60 to 120 min from Wpg, consider helicopter intercept
Assess & manage per appropriate
care map
If transporting go to closest ED
If closest ED in Wpg transport to SBH
Assist with trouble
shooting 6
No Yes
Is the chief complaint related to the LVAD or heart?
Is a hum present?
Manage as per appropriate care map 7
Yes
No
Yes
Contact OLMS before discontinuing
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only).
C08AB - LEFT VENTRICULAR ASSIST DEVICE (LVAD)
Adult & adolescent RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2023-03-04 Effective date: 2022-04-06 (0700 hrs)
2
C08AB - LVAD
INDICATIONS
• All patients with a left ventricular assist device (VAD) regardless of the chief complaint.
CONTRAINDICATIONS
• Not applicable
NOTES
1. The St. Boniface Hospital (SBH) VAD Coordinator must be contacted through the SBH paging operator for all device-related issues and for all VAD patients, even if the issue is not associated with their VAD (204-237-2053). If unable to reach the VAD Coordinator, contact the on-line medical support (OLMS) physician.
2. The SBH Cardiac Sciences Program currently uses the Abbot Heartmate III (green tag) ventricular assist device. Paramedics may occasionally encounter a patient with an older Heartmate II (orange tag) unit. Technical device-related problems are rare. Patients and their caregivers are well-trained in VAD management and trouble-shooting, and will likely have contacted the VAD Coordinator or on call physician before calling 9-1-1.
3. A “humming” or “whirling” sound (heard best in the precordium) indicates that the pump is functioning. If the device is not pumping, the patient may rapidly go into acute heart failure or cardiogenic shock.
4. Both Heartmate devices have continuous flow pumps so you may not be able to palpate a pulse, or measure the blood pressure (BP) with a manual cuff. Use a non-invasive BP machine to monitor the mean arterial pressure (MAP). A MAP of 70 to 90 mmHg is adequate for most patients. It may be difficult to differentiate an extremely low perfusion from a true cardiac arrest with pulseless electrical activity (PEA). If in doubt, manage as per the appropriate resuscitation care map.
5. A low pulse oximetry reading may reflect inadequate peripheral perfusion, rather than hypoxemia. However, a normal pulse oximetry waveform is likely to be accurate.
6. Assist the patient or caregiver with device trouble-shooting and management (refer to appendix A). Trouble shooting includes the following steps: a. Checking & securing all connections to the controller. b. Replacing the batteries one at a time or connecting to the power base unit. Never remove both batteries at
the same time as this may cause the pump to stop. c. Changing the controller. Paramedics will only change the controller under the direction of the patient, their
caregiver or the VAD coordinator.
7. Major clinical conditions affecting LVAD patients include bleeding, sepsis and stroke.
8. Chest compressions can be done if necessary. Patients can be defibrillated or paced while attached to the device. All resuscitation drugs can be administered if indicated. The pump will not affect electrocardiogram acquisition or continuous cardiac monitoring.
9. Ensure that all VAD equipment and the patient’s caregiver, if available, accompany the patient, and provide appropriate pre-arrival notification of receiving emergency department (ED) personnel.
3
C08AB - LVAD
LINKS
C01 - BASIC RESUSCITATION C02 - ADVANCED RESUSCITATION
APPROVED BY
Medical Director – Provincial EMS/PT Associate Medical Director – Provincial EMS/PT
VERSION CHANGES (refer to X03 for change tracking)
• Reformatted • Addition of scope of work statement & legend (removal of colored boxes) • Reviewed with Cardiac Sciences Program clinical leadership

4
C08AB - LVAD
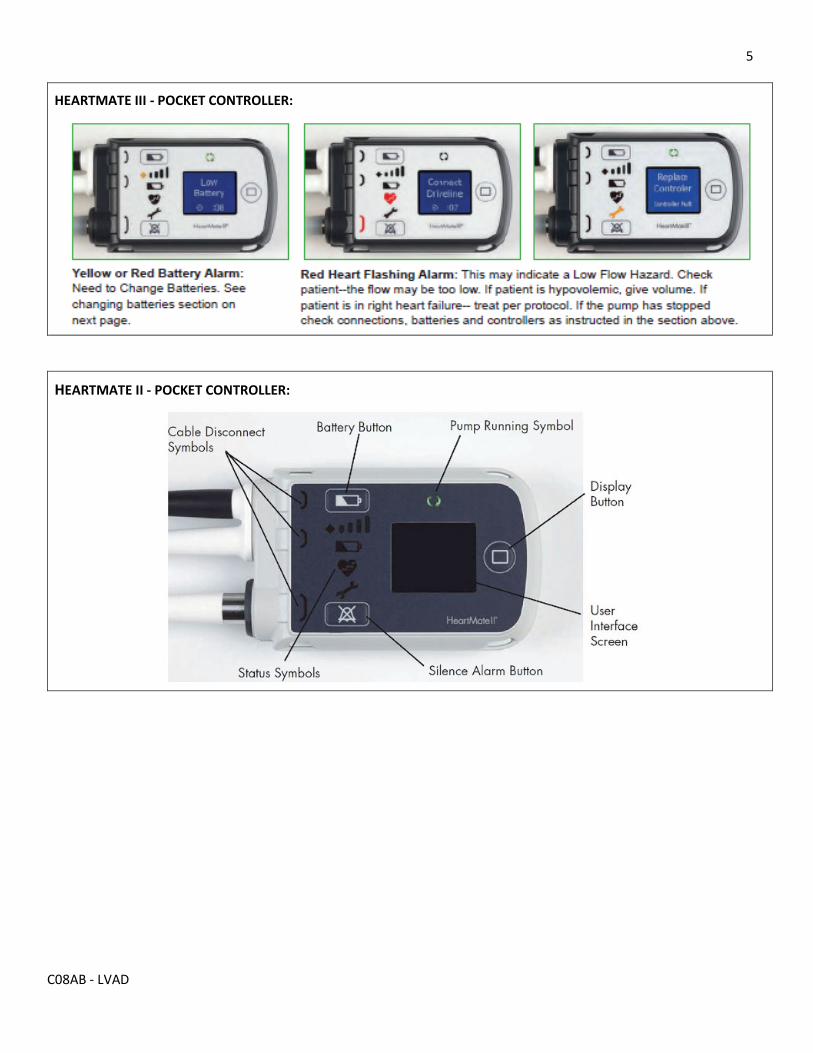
5
C08AB - LVAD
HEARTMATE III - POCKET CONTROLLER:
HEARTMATE II - POCKET CONTROLLER:

6
C08AB - LVAD
NOTE: At December 2020, the SBH Cardiac Science Program no longer supplies patients with the external peripheral controller (EPC) for the Heartmate II device.
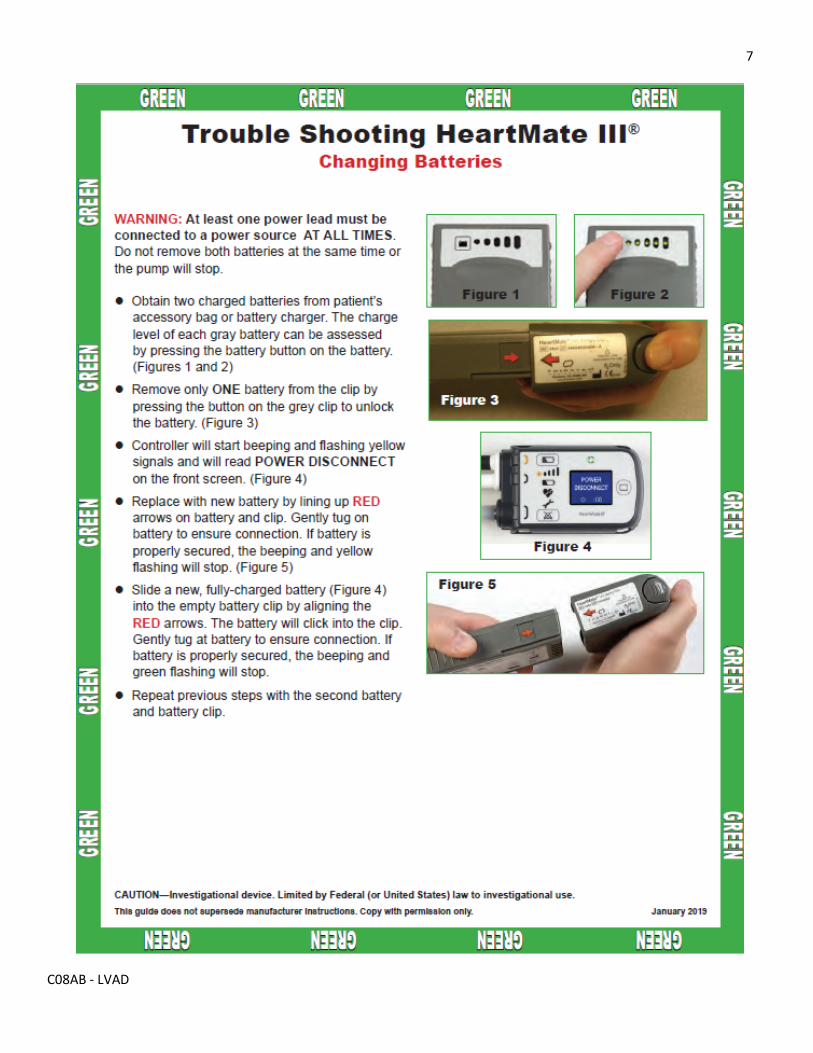
7
C08AB - LVAD
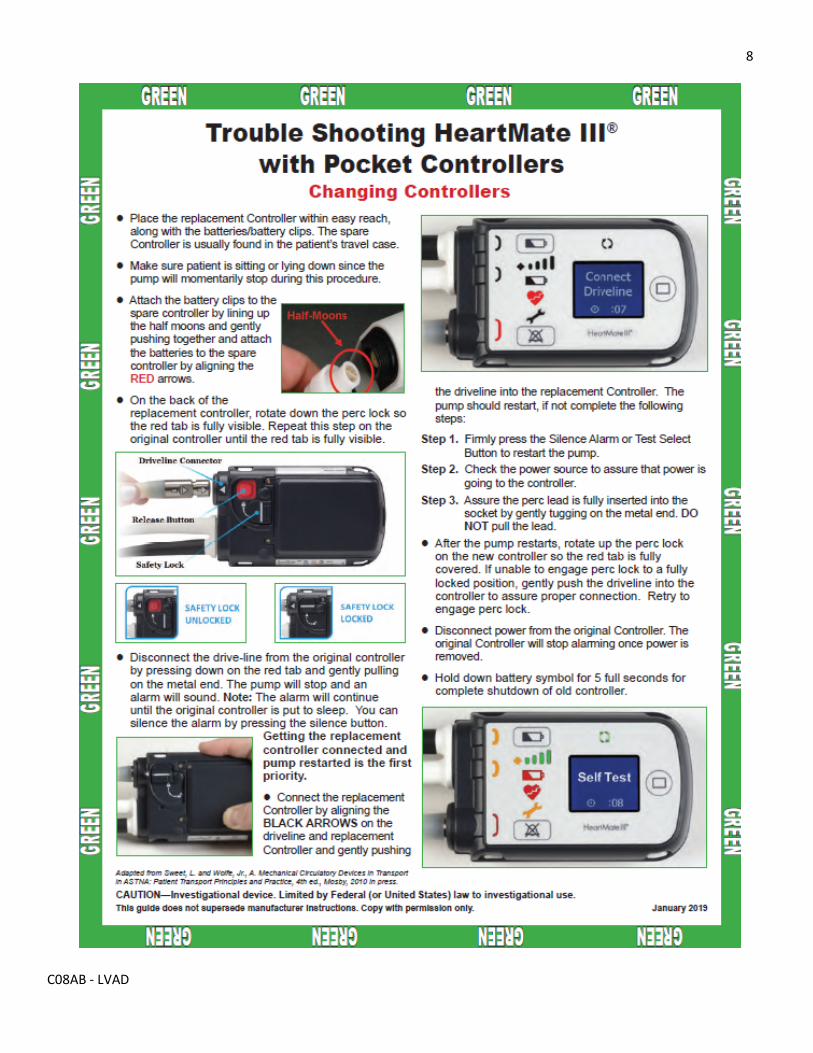
8
C08AB - LVAD
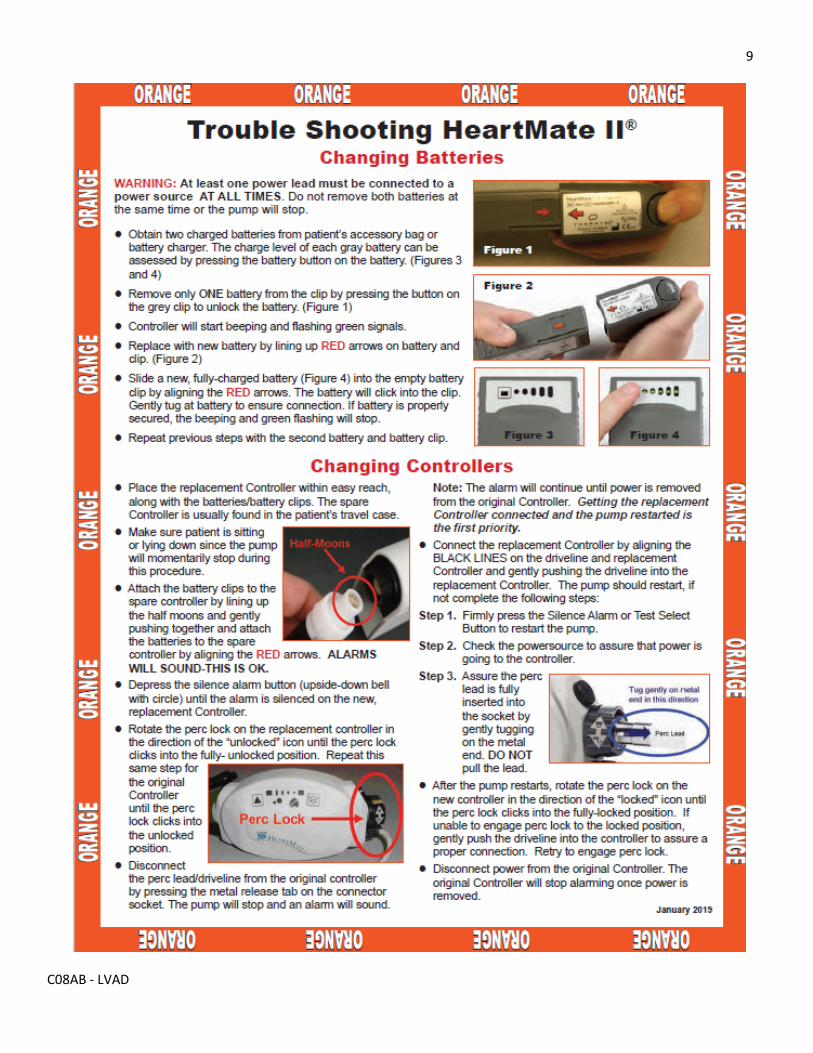
9
C08AB - LVAD
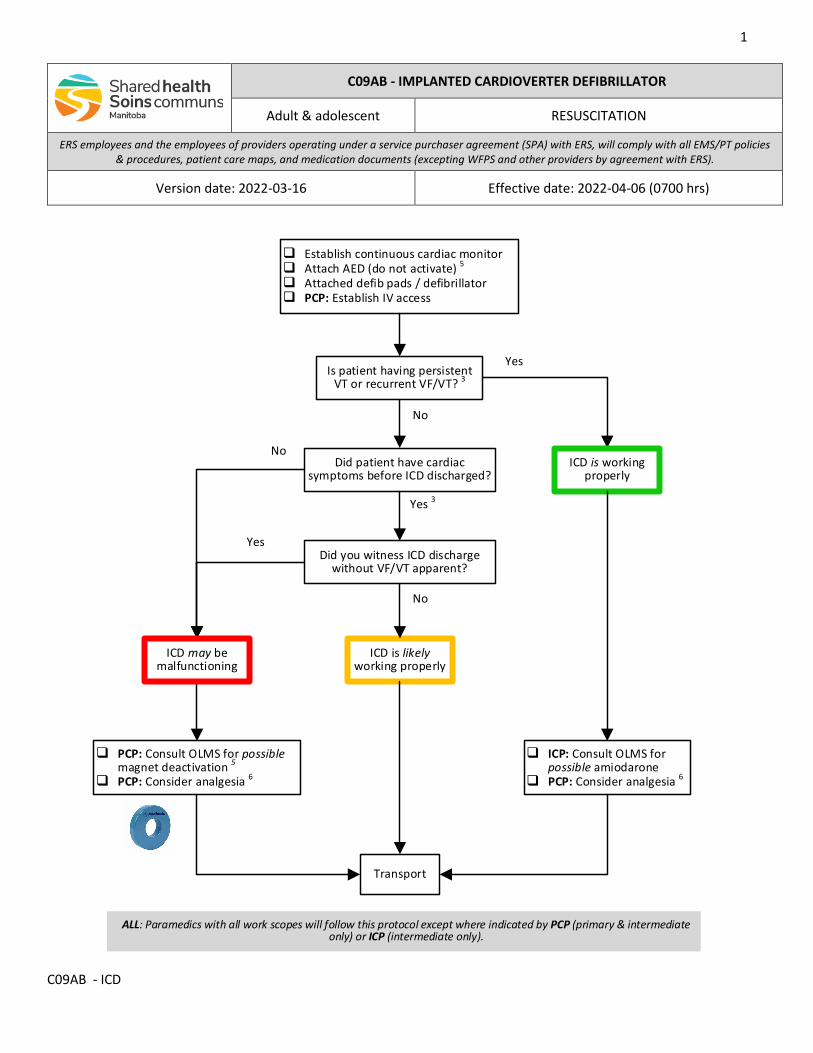
1
C09AB - ICD
C09AB - IMPLANTED CARDIOVERTER DEFIBRILLATOR
Adult & adolescent RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-16 Effective date: 2022-04-06 (0700 hrs)
Establish continuous cardiac monitor Attach AED (do not activate) 5
Attached defib pads / defibrillator PCP: Establish IV access
No
Yes 3
Is patient having persistent VT or recurrent VF/VT? 3
ICD is likely working properly
Did patient have cardiac symptoms before ICD discharged?
NoICD is working
properly
ICP: Consult OLMS for possible amiodarone
PCP: Consider analgesia 6
Yes
Did you witness ICD discharge without VF/VT apparent?
No
PCP: Consult OLMS for possible magnet deactivation 5
PCP: Consider analgesia 6
Yes
ICD may be malfunctioning
Transport
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only) or ICP (intermediate only).
2
C09AB - ICD
QRG: AMIODARONE (M14)
TEN YEARS & OLDER: • 150 mg IV over ten minutes • Repeat 150 mg once in ten minutes if required
This QRG is for dosing only. Refer to the medication document for
additional information required for safe administration.
INDICATIONS
• Any patient with implanted cardioverter defibrillator (ICD) who reports that it has discharged
CONTRAINDICATIONS
• Not applicable
NOTES
1. ICD malfunction is uncommon. If a patient reports that their ICD has discharged, paramedics should assume that a life-threatening dysrhythmia activated the ICD until proven otherwise. All patients should have continuous cardiac monitoring, and paramedics should be prepared for external defibrillation if necessary.
2. Proper ICD assessment requires interrogation of the ICD with specific expertise and special equipment only available in hospital.
3. The presence of ventricular tachycardia (VT) or ventricular fibrillation (VF) indicates that the ICD is discharging appropriately. DO NOT INACTIVATE THE ICD.
4. The acute onset of cardiac symptoms, including palpitations, fainting or lightheadedness, chest pain, or diaphoresis before the ICD shocked the patient, suggest that the shock was terminating VT and is working appropriately. DO NOT INACTIVATE.
5. Except during cardiac arrest, paramedics must consult the on-line medical support (OLMS) physician before attempting magnet inactivation.
Application of a donut magnet over top of an ICD temporarily suppresses the device’s arrhythmia monitoring and shocking functions, but the pacing function will continue to work. When a device’s arrhythmia functions are deactivated, it may emit a constant tone or intermittent beep depending upon the device manufacturer.
Removing the magnet will allow the ICD to resume its arrhythmia monitoring and suppression functions.
6. ICD shocks are painful and can be very distressing to the patient. Paramedics should consider administration of opioid analgesia, with adjunctive sedation as required.
3
C09AB - ICD
CARDIAC ARREST
7. Chest compressions can be safely delivered during ICD shock delivery.
8. When applying AED pads on a patient with an ICD place the electrodes at least 8 centimeters (3 inches) away from the pulse generator.
9. If performing transcutaneous pacing (TCP) inactivate the ICD with a donut magnet.
10. In the event of a cardiac arrest, the ICD will promptly deliver a pre-programmed cycle of multiple shocks over about 30 to 60 seconds.
Visible muscle contractions indicate that the unit is working and delivering its shocks. If present, paramedics should allow the cycle to complete before attempting external shocks.
If the ICD has exhausted all of its shocks (no more visible muscle contractions) and has failed to terminate the arrhythmia, paramedics should continue to provide external shocks using an automated or manual defibrillator. DO NOT INACTIVATE THE ICD.
LINKS
M14 - AMIODARONE
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X03 for change tracking)
• Reformatted & retitled • Addition of scope of work statement & legend (removal of colored boxes) • Removal of pacemaker from indications • Revised flowchart & notes to clarify management • Addition of amiodarone dosing for VT with a pulse for quick reference
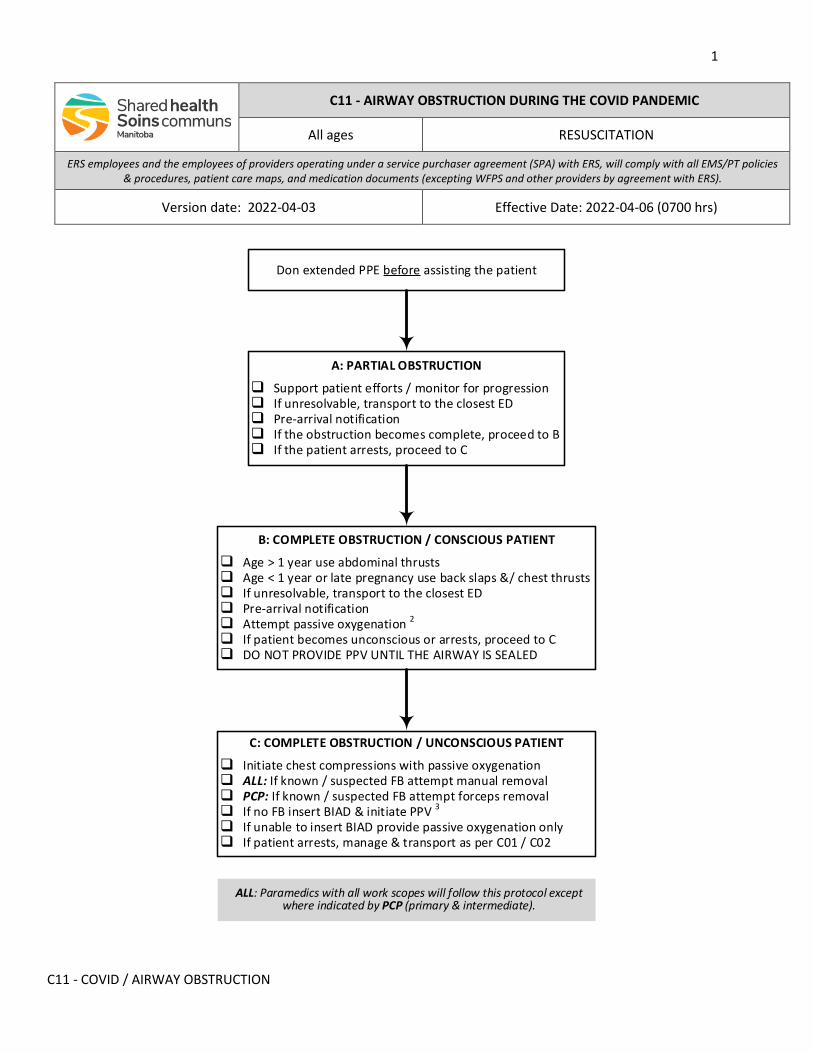
1
C11 - COVID / AIRWAY OBSTRUCTION
C11 - AIRWAY OBSTRUCTION DURING THE COVID PANDEMIC
All ages RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-03 Effective Date: 2022-04-06 (0700 hrs)
A: PARTIAL OBSTRUCTION
Support patient efforts / monitor for progression If unresolvable, transport to the closest ED Pre-arrival notification If the obstruction becomes complete, proceed to B If the patient arrests, proceed to C
B: COMPLETE OBSTRUCTION / CONSCIOUS PATIENT
Age > 1 year use abdominal thrusts Age < 1 year or late pregnancy use back slaps &/ chest thrusts If unresolvable, transport to the closest ED Pre-arrival notification Attempt passive oxygenation 2
If patient becomes unconscious or arrests, proceed to C DO NOT PROVIDE PPV UNTIL THE AIRWAY IS SEALED
Don extended PPE before assisting the patient
C: COMPLETE OBSTRUCTION / UNCONSCIOUS PATIENT
Initiate chest compressions with passive oxygenation ALL: If known / suspected FB attempt manual removal PCP: If known / suspected FB attempt forceps removal If no FB insert BIAD & initiate PPV 3
If unable to insert BIAD provide passive oxygenation only If patient arrests, manage & transport as per C01 / C02
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate).
2
C11 - COVID / AIRWAY OBSTRUCTION
INDICATIONS
• Airway obstruction during the COVID pandemic
CONTRAINDICATIONS
• Not applicable
NOTES
1. A choking and combative patient is at high risk for the ongoing generation of potentially infectious aerosols. Relief of the obstruction will be life-saving and lower the risk to providers (A09).
2. Passive oxygenation is provided using a self-inflating ventilation bag and mask (BVM) with oxygen delivered at a flow rate of 15 liters per minute. The system can be kept closed by using a two-hand mask seal. DO NOT SQUEEZE THE BAG.
3. If there is no foreign body (FB), providers at all levels will attempt placements of a blind insertion airway device (BIAD) before attempting positive pressure ventilation (PPV).
LINKS
A09 - MEDICAL PROCEDURES DURING COVID-19 PANDEMIC C01 - BASIC RESUSCITATION C02 - ADVANCED RESUSCITATION
APPROVED BY
Medical Director - EMS/PT Associate Medical Director - EMS/PT
VERSION CHANGES (refer to X03 for change tracking)
• Removal of colored boxes and addition of scope of work statement & legend • Clarification that providers with basic work scope cannot do forceps removal • Reformatted
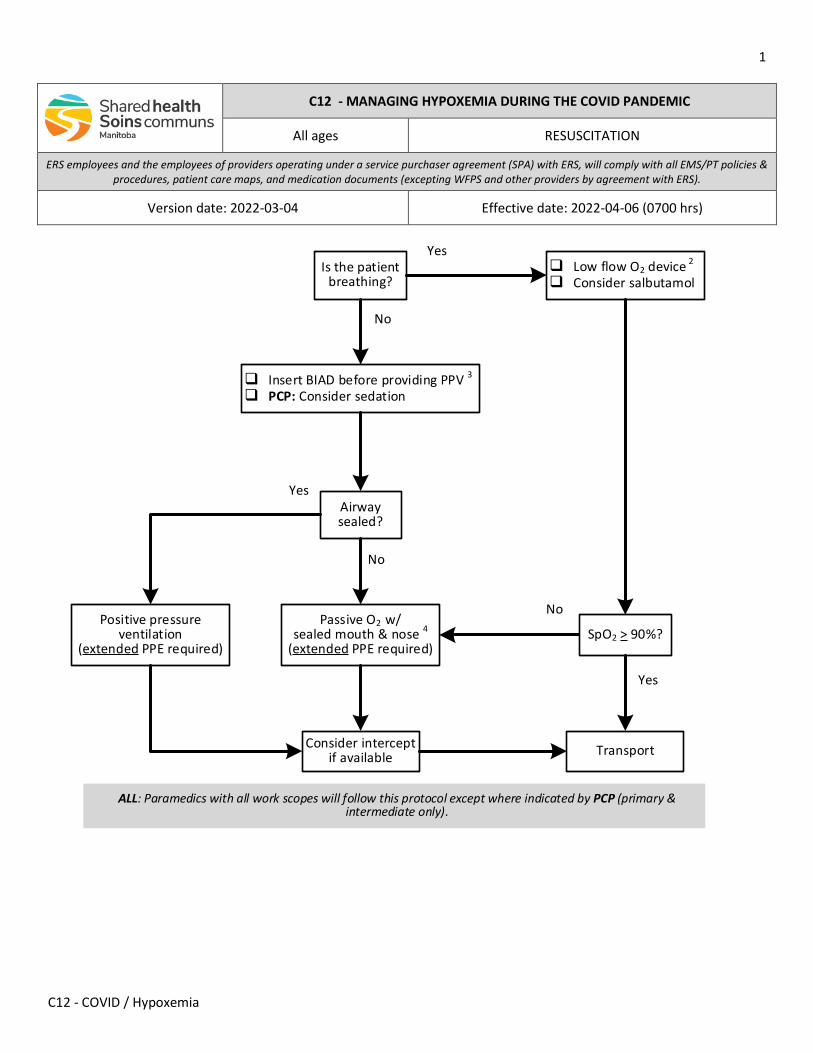
1
C12 - COVID / Hypoxemia
C12 - MANAGING HYPOXEMIA DURING THE COVID PANDEMIC
All ages RESUSCITATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-04 Effective date: 2022-04-06 (0700 hrs)
Insert BIAD before providing PPV 3
PCP: Consider sedation
Yes
No
Is the patient breathing?
Low flow O2 device 2
Consider salbutamol
Airway sealed?
Passive O2 w/sealed mouth & nose 4
(extended PPE required)
Positive pressure ventilation
(extended PPE required)
Transport
SpO2 > 90%?
Yes
No
Yes
Consider intercept if available
No
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only).
2
C12 - COVID / Hypoxemia
INDICATION
• Dyspnea respiratory distress, or respiratory failure (SpO2 < 90%) during the COVID pandemic
CONTRAINDICATION
• Newborns do not require a sealed airway for positive pressure ventilation (PPV) during neonatal resuscitation 3
NOTES
1. Assume every patient may be COVID positive.
a. Appendix A lists the symptoms and signs suspicious for COVID infection, which includes shortness of breath or difficulty breathing. A patient may be infected but asymptomatic.
b. All paramedics should wear contact & droplet personal protective equipment (PPE) if the patient is known or suspected to have COVID, regardless of the chief complaint.
c. If there is any possibility of aerosol generating medical procedure (AGMP) being required (refer to A09 - MEDICAL PROCEDURES DURING COVID PANDEMIC), paramedics should don extended PPE in advance.
d. Keep a distance of two meters (six feet) between the patient and family / friends / bystanders. All individuals not directly involved with the patient should be instructed to step well back. All individuals who cannot leave the immediate area should don procedure mask.
2. Low flow oxygen (O2) devices that are not considered AGMP include the following:
a. Nasal prongs (maximum flow 6 lpm)
b. Simple face mask (maximum flow 10 lpm)
c. Non-rebreather mask (maximum flow 15 lpm)
d. Oxymask (maximum flow 15 lpm)
3. This does not include positive pressure ventilation (PPV) during newborn resuscitation.
4. Passive oxygenation is provided using a self-inflating ventilation bag and mask (VBM) with oxygen delivered at a flow rate of 15 lpm (figure 1). The system is kept closed by using a two-hand mask seal, or by attaching the bag-valve device to a well-fitted CPAP facemask (figure A). DO NOT SQUEEZE THE BAG.
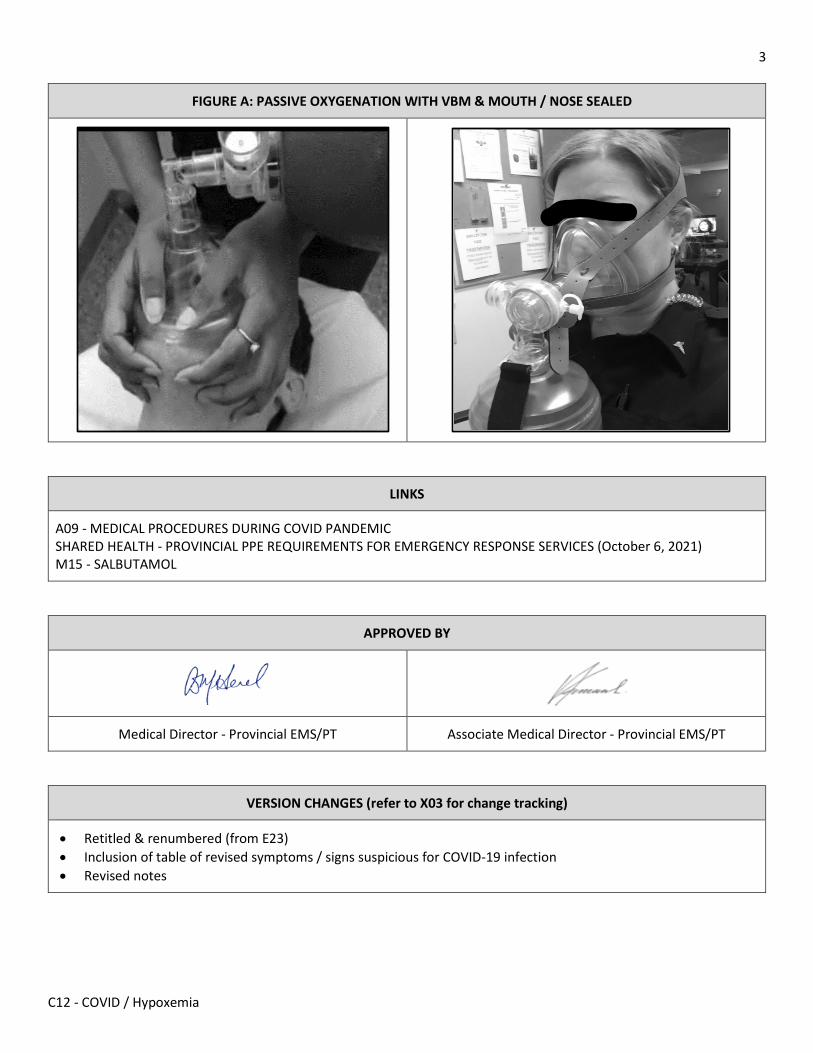
3
C12 - COVID / Hypoxemia
FIGURE A: PASSIVE OXYGENATION WITH VBM & MOUTH / NOSE SEALED
LINKS
A09 - MEDICAL PROCEDURES DURING COVID PANDEMIC SHARED HEALTH - PROVINCIAL PPE REQUIREMENTS FOR EMERGENCY RESPONSE SERVICES (October 6, 2021) M15 - SALBUTAMOL
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X03 for change tracking)
• Retitled & renumbered (from E23) • Inclusion of table of revised symptoms / signs suspicious for COVID-19 infection • Revised notes

4
C12 - COVID / Hypoxemia
APPENDIX A: SYMPTOMS & SIGNS SUSPCIOUS FOR COVID INFECTION
• Fever / chills • Cough (or increased severity of chronic cough) • Shortness of breath / difficulty breathing • Hypoxemia / hypoxemia (not due to trauma) • Sore throat / hoarse voice (not due to trauma) • Runny nose • Headache • Muscle aches (not due to trauma or exercise) • Loss of smell / taste • Conjunctivitis • Nausea / Loss of appetite • Poor feeding in infants • Diarrhea / vomiting for more than 24 hours • Fatigue • Skin rash of unknown cause
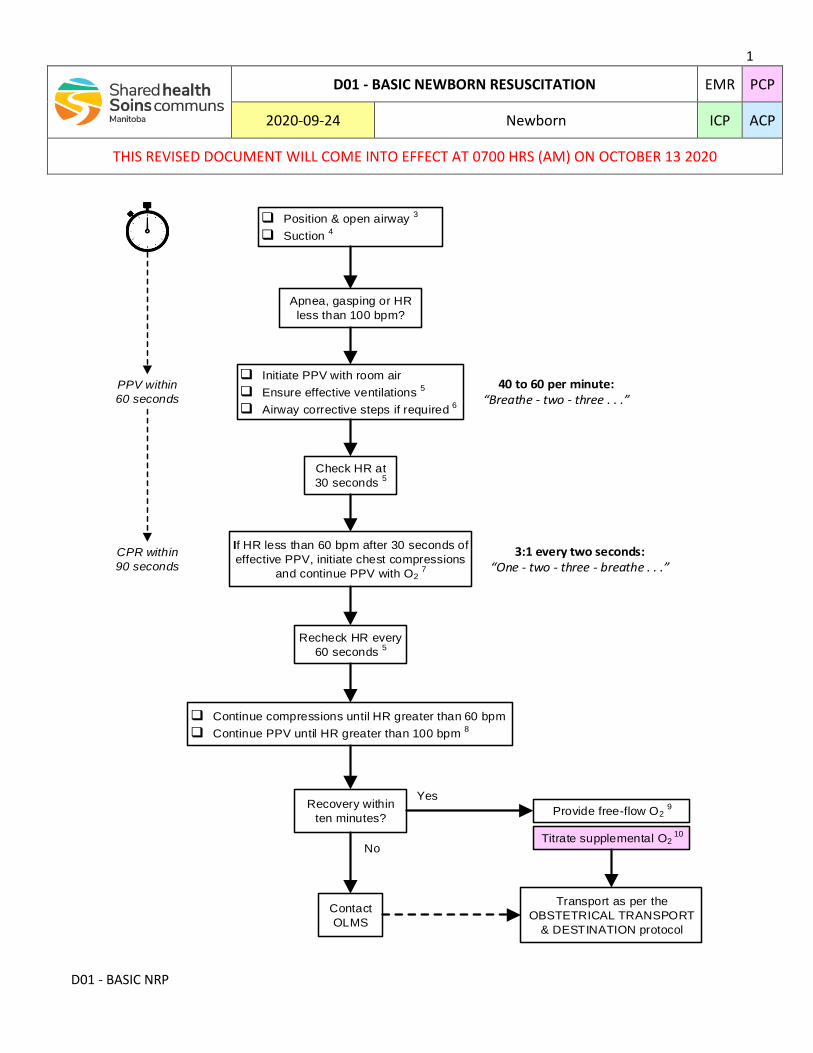
1
D01 - BASIC NRP
D01 - BASIC NEWBORN RESUSCITATION EMR PCP
2020-09-24 Newborn ICP ACP
THIS REVISED DOCUMENT WILL COME INTO EFFECT AT 0700 HRS (AM) ON OCTOBER 13 2020
q Initiate PPV with room air
q Ensure effective ventilations 5
q Airway corrective steps if required 6
Transport as per the
OBSTETRICAL TRANSPORT
& DESTINATION protocol
PPV within
60 seconds
Provide free-flow O2 9
Titrate supplemental O2 10
Yes
No
q Position & open airway 3
q Suction 4
Check HR at
30 seconds 5
If HR less than 60 bpm after 30 seconds of
effective PPV, initiate chest compressions
and continue PPV with O2 7
CPR within
90 seconds
Recovery within
ten minutes?
Contact
OLMS
40 to 60 per minute: Breathe - two - three . . .
3:1 every two seconds: One - two - three - breathe . . .
q Continue compressions until HR greater than 60 bpm
q Continue PPV until HR greater than 100 bpm 8
Apnea, gasping or HR
less than 100 bpm?
Recheck HR every
60 seconds 5
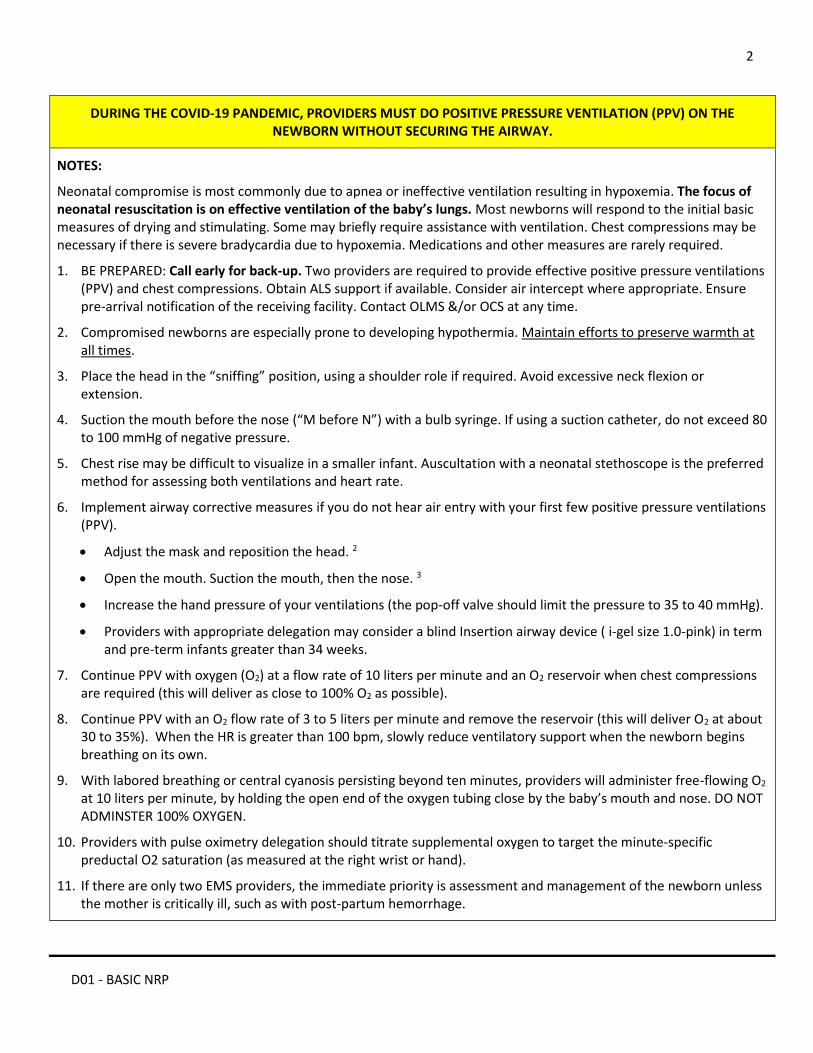
2
D01 - BASIC NRP
DURING THE COVID-19 PANDEMIC, PROVIDERS MUST DO POSITIVE PRESSURE VENTILATION (PPV) ON THE NEWBORN WITHOUT SECURING THE AIRWAY.
NOTES:
Neonatal compromise is most commonly due to apnea or ineffective ventilation resulting in hypoxemia. The focus of neonatal resuscitation is on effective ventilation of the baby’s lungs. Most newborns will respond to the initial basic measures of drying and stimulating. Some may briefly require assistance with ventilation. Chest compressions may be necessary if there is severe bradycardia due to hypoxemia. Medications and other measures are rarely required.
1. BE PREPARED: Call early for back-up. Two providers are required to provide effective positive pressure ventilations (PPV) and chest compressions. Obtain ALS support if available. Consider air intercept where appropriate. Ensure pre-arrival notification of the receiving facility. Contact OLMS &/or OCS at any time.
2. Compromised newborns are especially prone to developing hypothermia. Maintain efforts to preserve warmth at all times.
3. Place the head in the “sniffing” position, using a shoulder role if required. Avoid excessive neck flexion or extension.
4. Suction the mouth before the nose (“M before N”) with a bulb syringe. If using a suction catheter, do not exceed 80 to 100 mmHg of negative pressure.
5. Chest rise may be difficult to visualize in a smaller infant. Auscultation with a neonatal stethoscope is the preferred method for assessing both ventilations and heart rate.
6. Implement airway corrective measures if you do not hear air entry with your first few positive pressure ventilations (PPV).
Adjust the mask and reposition the head. 2
Open the mouth. Suction the mouth, then the nose. 3
Increase the hand pressure of your ventilations (the pop-off valve should limit the pressure to 35 to 40 mmHg).
Providers with appropriate delegation may consider a blind Insertion airway device ( i-gel size 1.0-pink) in term and pre-term infants greater than 34 weeks.
7. Continue PPV with oxygen (O2) at a flow rate of 10 liters per minute and an O2 reservoir when chest compressions are required (this will deliver as close to 100% O2 as possible).
8. Continue PPV with an O2 flow rate of 3 to 5 liters per minute and remove the reservoir (this will deliver O2 at about 30 to 35%). When the HR is greater than 100 bpm, slowly reduce ventilatory support when the newborn begins breathing on its own.
9. With labored breathing or central cyanosis persisting beyond ten minutes, providers will administer free-flowing O2 at 10 liters per minute, by holding the open end of the oxygen tubing close by the baby’s mouth and nose. DO NOT ADMINSTER 100% OXYGEN.
10. Providers with pulse oximetry delegation should titrate supplemental oxygen to target the minute-specific preductal O2 saturation (as measured at the right wrist or hand).
11. If there are only two EMS providers, the immediate priority is assessment and management of the newborn unless the mother is critically ill, such as with post-partum hemorrhage.
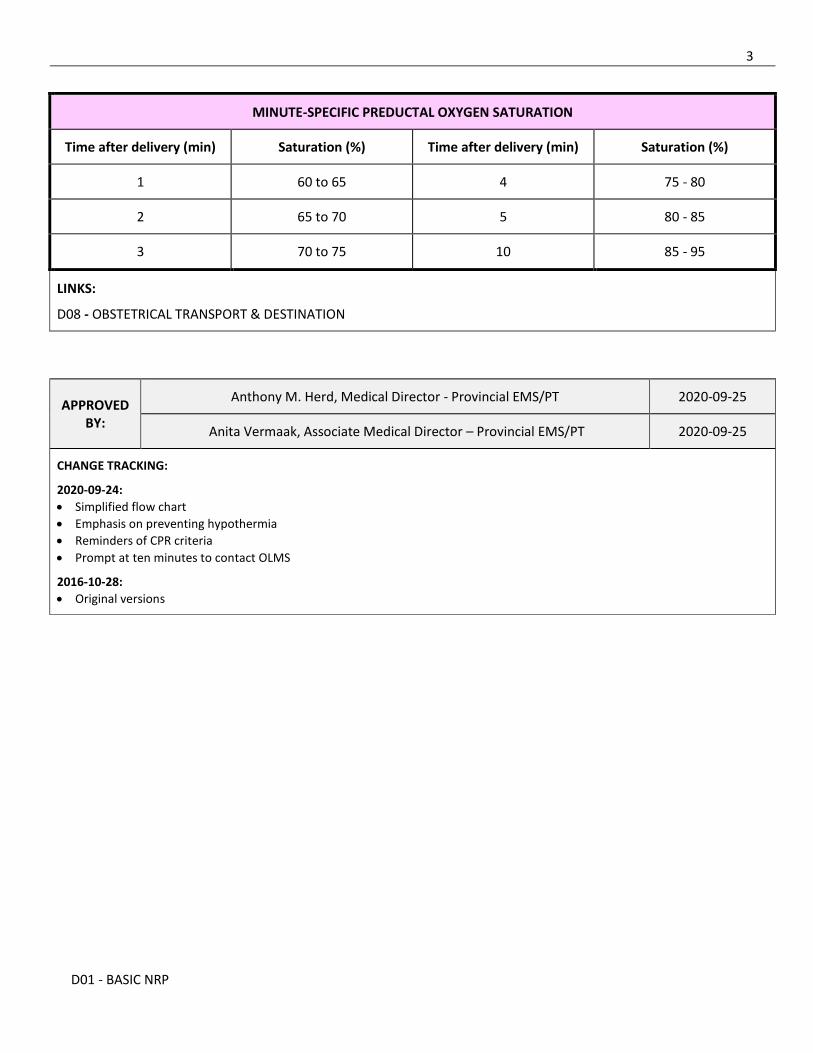
3
D01 - BASIC NRP
MINUTE-SPECIFIC PREDUCTAL OXYGEN SATURATION
Time after delivery (min) Saturation (%) Time after delivery (min) Saturation (%)
1 60 to 65 4 75 - 80
2 65 to 70 5 80 - 85
3 70 to 75 10 85 - 95
LINKS:
D08 - OBSTETRICAL TRANSPORT & DESTINATION
APPROVED BY:
Anthony M. Herd, Medical Director - Provincial EMS/PT 2020-09-25
Anita Vermaak, Associate Medical Director – Provincial EMS/PT 2020-09-25
CHANGE TRACKING:
2020-09-24:
Simplified flow chart
Emphasis on preventing hypothermia
Reminders of CPR criteria
Prompt at ten minutes to contact OLMS
2016-10-28:
Original versions
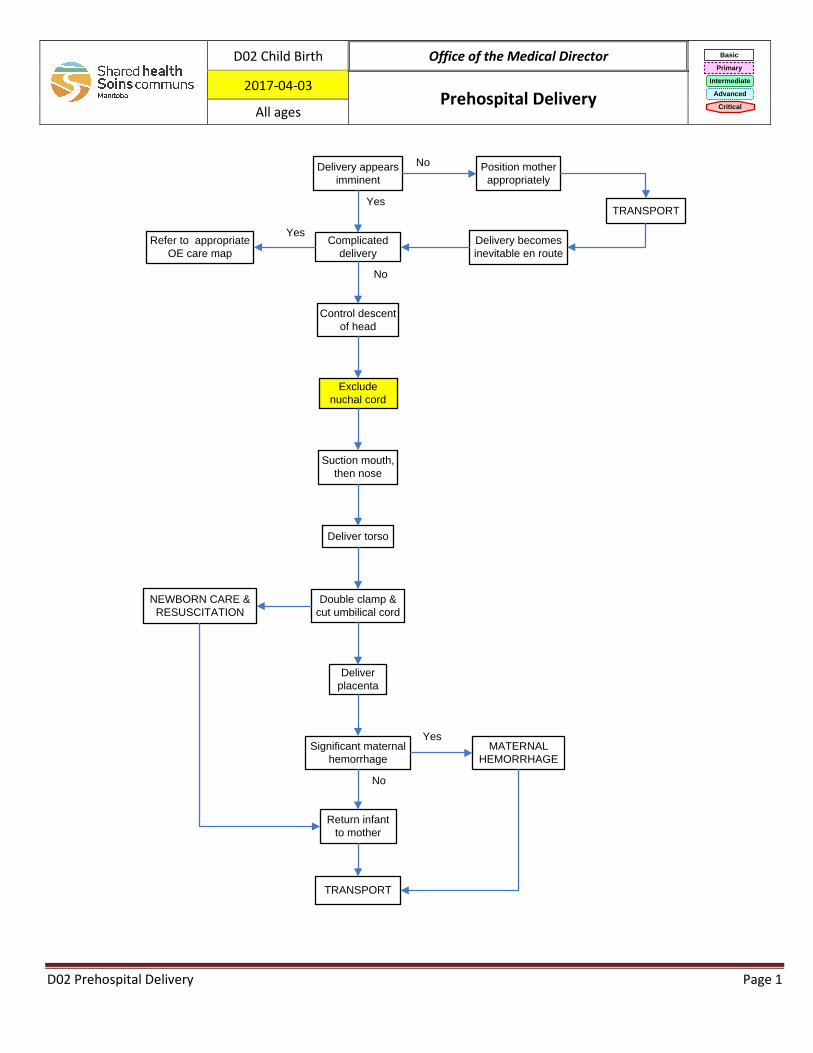
Yes
NoDelivery appears
imminent
TRANSPORT
Control descent
of head
Yes
No
Double clamp &
cut umbilical cord
NEWBORN CARE &
RESUSCITATION
Complicated
delivery
Significant maternal
hemorrhage
MATERNAL
HEMORRHAGE
Refer to appropriate
OE care map
Deliver
placenta
No
Position mother
appropriately
Exclude
nuchal cord
Suction mouth,
then nose
Deliver torso
Return infant
to mother
Yes
Delivery becomes
inevitable en route
TRANSPORT
D02 Child Birth Office of the Medical Director Basic
Primary
Intermediate
Advanced
Critical
2017-04-03 Prehospital Delivery
All ages
D02 Prehospital Delivery Page 1
INDICATIONS:
• All patients in labour
CONTRAINDICATIONS:
• None
NOTES: All reasonable efforts should be made to ensure in-hospital delivery.
• Initiate contact early for additional resources. Consider OLMS at any time. • Delivery is imminent (likely to occur within several minutes) when contractions are less than 2 minutes apart.
Multiple clinical and non-clinical factors must be considered in deciding upon transport versus delivery on scene including transport time to next level of care, road and weather conditions, and time to available backup.
• Delivery is inevitable if the perineum is bulging, the head is crowning or the patient complains of an urge to “push”, “bear down”, or “have a bowel movement”. In these circumstances, EMS providers must prepare to deliver the baby. The vehicle operator must stop the ambulance and assist with delivery.
• For complicated delivery refer to the following OBSTETRICAL EMERGENCIES care maps: o D03.1 Prolapsed Umbilical Cord o D03.2 Breech Presentation o D03.3 Multiple Gestations o D03.4 Shoulder Dystocia
• Unwind the cord from around the baby’s neck and gently lift the cord over its head. • If unable to remove the cord, suction out the mouth then nose (this will stimulate breathing), double-clamp
and cut the cord, then deliver the baby as quickly as possible. • Suction the baby’s mouth and then nose (“M” before “N”) prior to the torso delivering if possible. • After returning infant to mother, keep warm and encourage breast feeding.
ABBREVIATIONS:
• OE – obstetrical emergencies • OLMS – on line medical support
D02 Prehospital Delivery Page 2
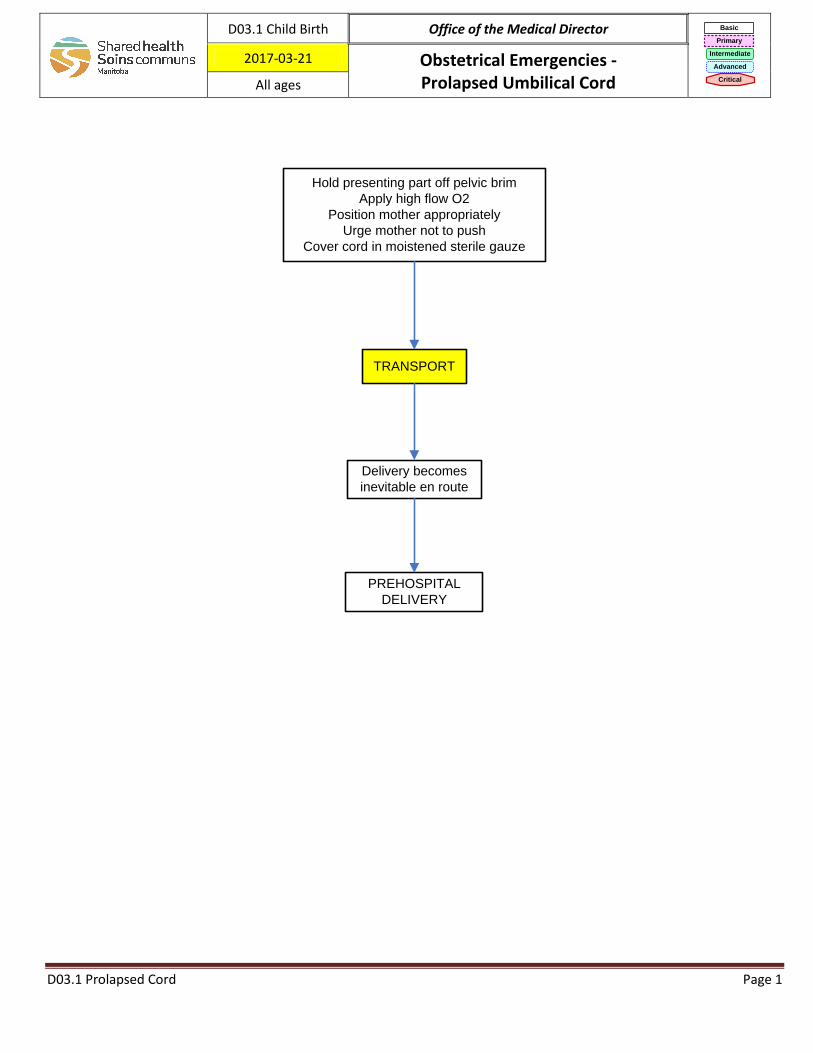
Hold presenting part off pelvic brim
Apply high flow O2
Position mother appropriately
Urge mother not to push
Cover cord in moistened sterile gauze
TRANSPORT
Delivery becomes
inevitable en route
PREHOSPITAL
DELIVERY
D03.1 Child Birth Office of the Medical Director Basic
Primary
Intermediate
Advanced
Critical
2017-03-21 Obstetrical Emergencies - Prolapsed Umbilical Cord All ages
D03.1 Prolapsed Cord Page 1
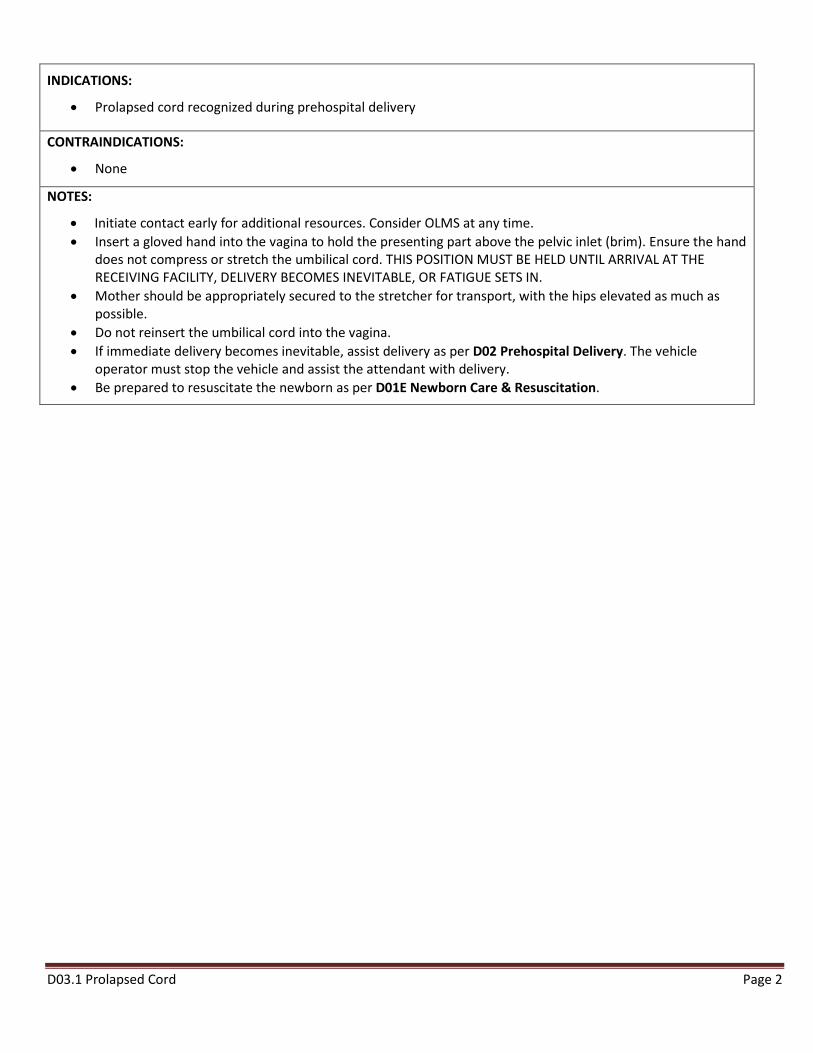
INDICATIONS:
• Prolapsed cord recognized during prehospital delivery
CONTRAINDICATIONS:
• None
NOTES:
• Initiate contact early for additional resources. Consider OLMS at any time. • Insert a gloved hand into the vagina to hold the presenting part above the pelvic inlet (brim). Ensure the hand
does not compress or stretch the umbilical cord. THIS POSITION MUST BE HELD UNTIL ARRIVAL AT THE RECEIVING FACILITY, DELIVERY BECOMES INEVITABLE, OR FATIGUE SETS IN.
• Mother should be appropriately secured to the stretcher for transport, with the hips elevated as much as possible.
• Do not reinsert the umbilical cord into the vagina. • If immediate delivery becomes inevitable, assist delivery as per D02 Prehospital Delivery. The vehicle
operator must stop the vehicle and assist the attendant with delivery. • Be prepared to resuscitate the newborn as per D01E Newborn Care & Resuscitation.
D03.1 Prolapsed Cord Page 2
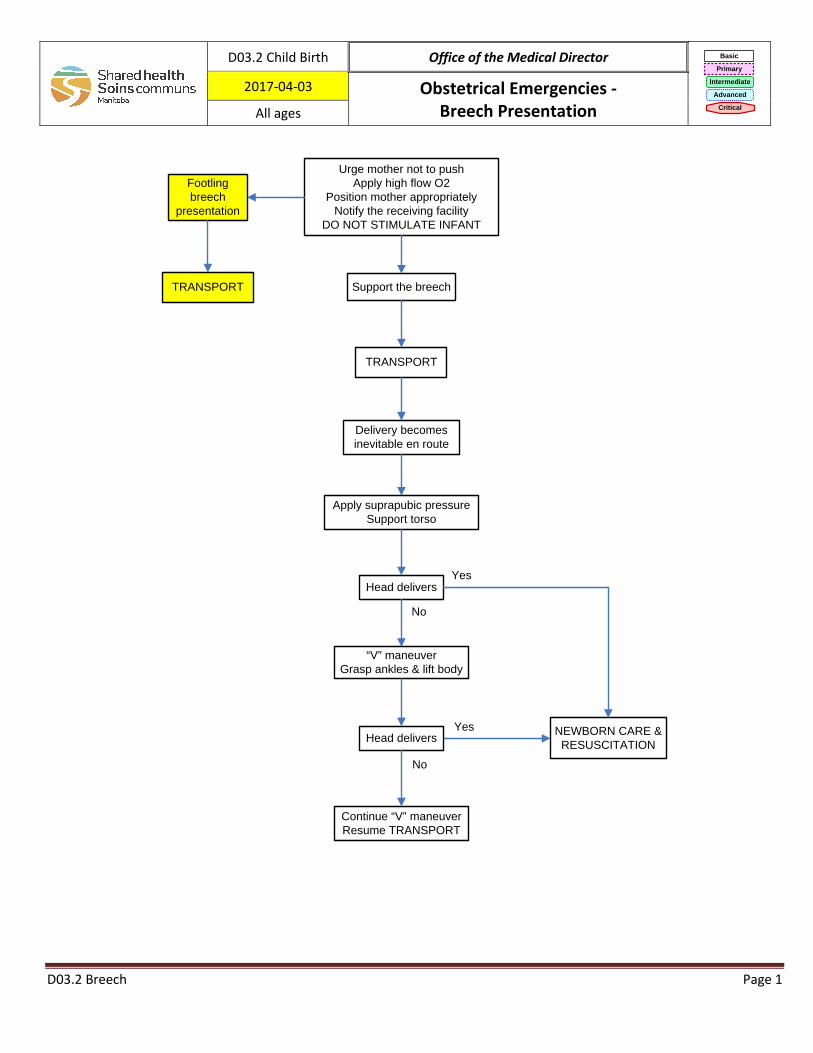
Support the breech
NEWBORN CARE &
RESUSCITATION
Footling
breech
presentation
Head delivers
Continue “V” maneuver
Resume TRANSPORT
No
Yes
Urge mother not to push
Apply high flow O2
Position mother appropriately
Notify the receiving facility
DO NOT STIMULATE INFANT
TRANSPORT
Delivery becomes
inevitable en route
Yes
No
TRANSPORT
Head delivers
“V” maneuver
Grasp ankles & lift body
Apply suprapubic pressure
Support torso
D03.2 Child Birth Office of the Medical Director Basic
Primary
Intermediate
Advanced
Critical
2017-04-03 Obstetrical Emergencies - Breech Presentation All ages
D03.2 Breech Page 1
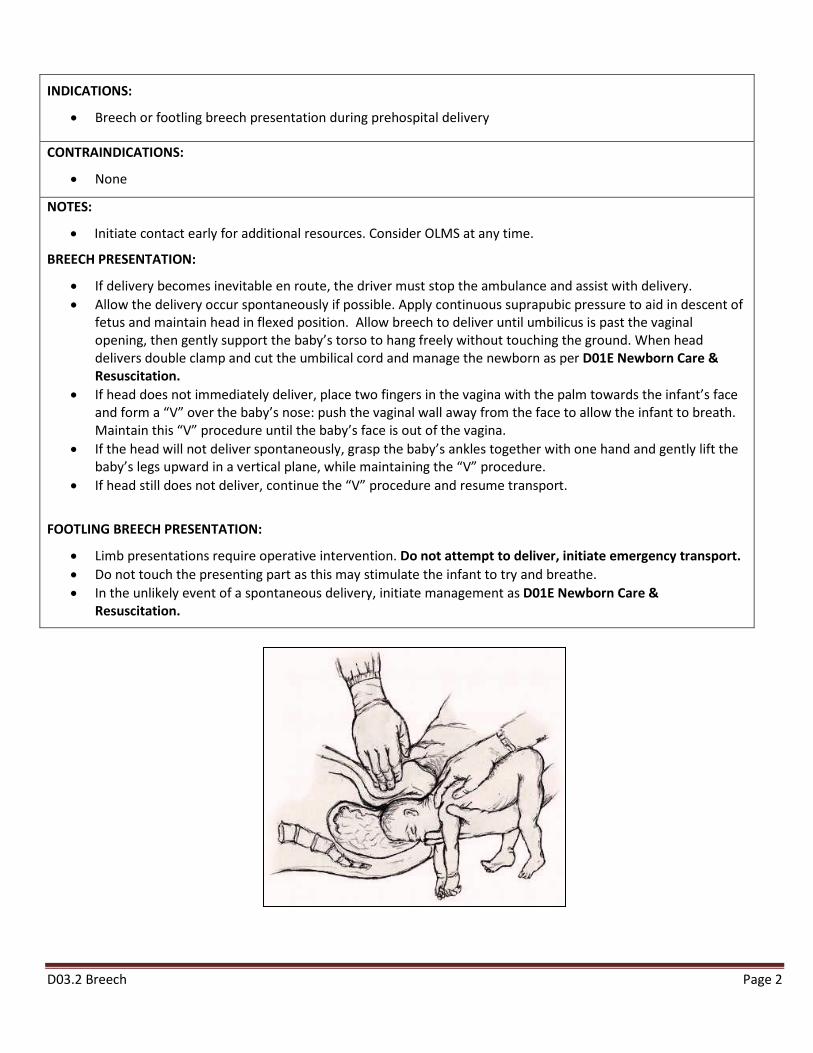
INDICATIONS:
• Breech or footling breech presentation during prehospital delivery
CONTRAINDICATIONS:
• None
NOTES:
• Initiate contact early for additional resources. Consider OLMS at any time.
BREECH PRESENTATION:
• If delivery becomes inevitable en route, the driver must stop the ambulance and assist with delivery. • Allow the delivery occur spontaneously if possible. Apply continuous suprapubic pressure to aid in descent of
fetus and maintain head in flexed position. Allow breech to deliver until umbilicus is past the vaginal opening, then gently support the baby’s torso to hang freely without touching the ground. When head delivers double clamp and cut the umbilical cord and manage the newborn as per D01E Newborn Care & Resuscitation.
• If head does not immediately deliver, place two fingers in the vagina with the palm towards the infant’s face and form a “V” over the baby’s nose: push the vaginal wall away from the face to allow the infant to breath. Maintain this “V” procedure until the baby’s face is out of the vagina.
• If the head will not deliver spontaneously, grasp the baby’s ankles together with one hand and gently lift the baby’s legs upward in a vertical plane, while maintaining the “V” procedure.
• If head still does not deliver, continue the “V” procedure and resume transport.
FOOTLING BREECH PRESENTATION:
• Limb presentations require operative intervention. Do not attempt to deliver, initiate emergency transport. • Do not touch the presenting part as this may stimulate the infant to try and breathe. • In the unlikely event of a spontaneous delivery, initiate management as D01E Newborn Care &
Resuscitation.
D03.2 Breech Page 2
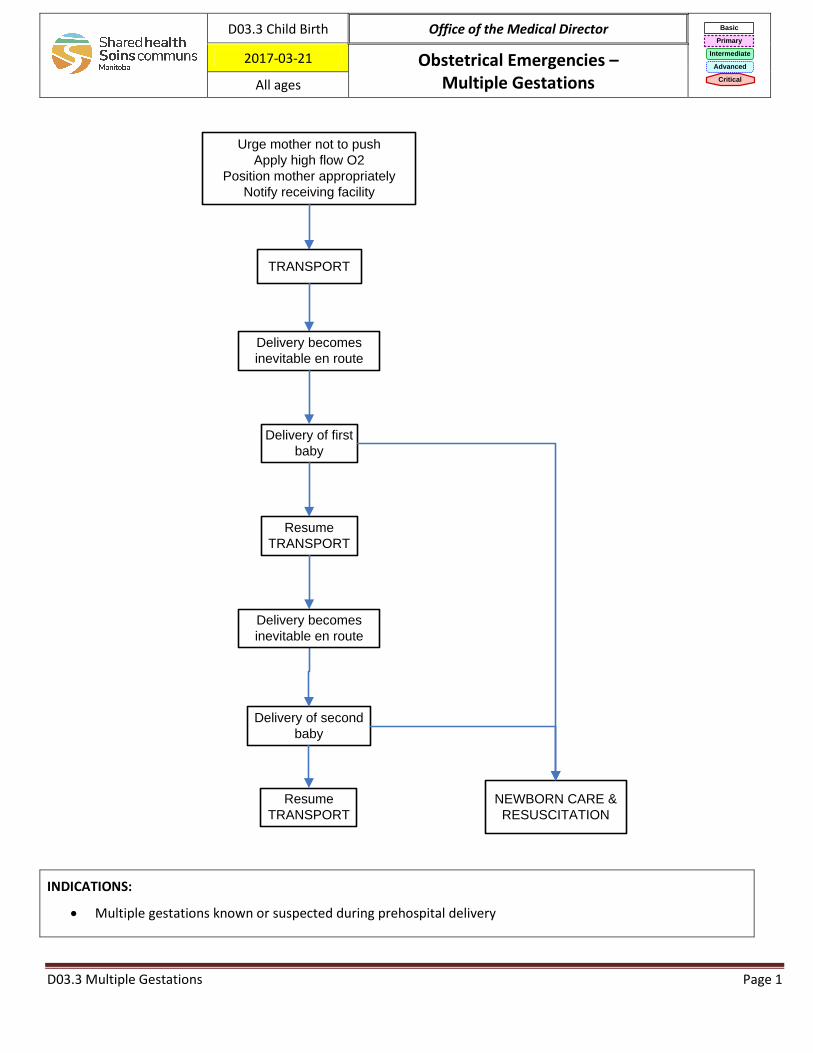
Urge mother not to push
Apply high flow O2
Position mother appropriately
Notify receiving facility
TRANSPORT
Delivery of first
baby
NEWBORN CARE &
RESUSCITATION
Resume
TRANSPORT
Delivery of second
baby
Resume
TRANSPORT
Delivery becomes
inevitable en route
Delivery becomes
inevitable en route
D03.3 Child Birth Office of the Medical Director Basic
Primary
Intermediate
Advanced
Critical
2017-03-21 Obstetrical Emergencies – Multiple Gestations All ages
INDICATIONS:
• Multiple gestations known or suspected during prehospital delivery
D03.3 Multiple Gestations Page 1
CONTRAINDICATIONS:
• Oxytocin is contraindicated until all babies have delivered
NOTES:
• Initiate contact early for additional resources. Consider OLMS at any time. • If delivery becomes inevitable en route, the vehicle operator must stop the ambulance, remove securements
from the mother and assist the attendant with delivery. Manage delivery of the first baby as per D02 Prehospital Delivery.
• There may be some time after delivery of the first baby to allow for emergency transport (A04 Transport) to resume. Multiple clinical and non-clinical factors must be considered in deciding upon transport versus delivery of the second baby on scene including transport time to next level of care, road and weather conditions, and time to available backup. However, all efforts should be made to ensure in-hospital delivery of the second baby.
• If delivery of the second baby becomes inevitable en route, the vehicle operator must stop the ambulance, remove securements from the mother and assist the attendant with delivery. Manage delivery of the second baby as per D02 Prehospital Delivery.
• After delivery of the second baby, the driver may be required to continue to assist the attendant with three patients. The decision about resuming transport versus staying on scene and awaiting back-up will depend mainly on the transport time to receiving facility versus the time to available backup. All efforts should be made to transport to the receiving facility as efficiently and safely as possible.
D03.3 Multiple Gestations Page 2
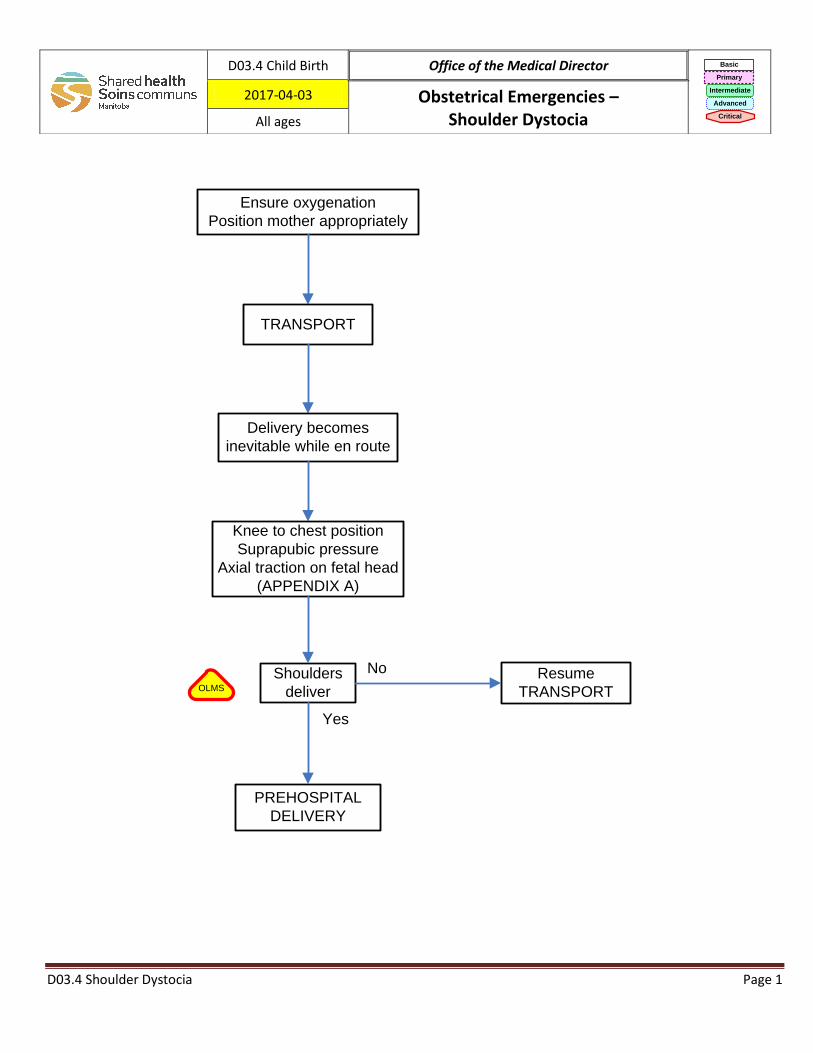
D03.4 Shoulder Dystocia Page 1
Shoulders
deliver
Ensure oxygenation
Position mother appropriately
TRANSPORT
Delivery becomes
inevitable while en route
Knee to chest position
Suprapubic pressure
Axial traction on fetal head
(APPENDIX A)
PREHOSPITAL
DELIVERY
Yes
Resume
TRANSPORT
NoOLMS
D03.4 Child Birth Office of the Medical Director Basic
Primary
Intermediate
Advanced
Critical
2017-04-03 Obstetrical Emergencies – Shoulder Dystocia All ages
D03.4 Shoulder Dystocia Page 2
INDICATIONS:
Failure of shoulders to deliver during prehospital delivery
CONTRAINDICATIONS:
None
NOTES:
Initiate contact early for additional resources. Consider OLMS at any time.
REMINDER: Often the shoulders are not truly impeded but will deliver with the next contraction.
If delivery becomes inevitable while en route, all providers must initiate consult with OLMS physician.
Two providers will be required for delivery(appendix A): o PROVIDER #1:
o Assist the mother in assuming a knees-to-chest position o Apply firm suprapubic pressure
o PROVIDER #2: o Apply axial traction on the fetal head during contractions
Wood’s maneuver (appendix B) should only be attempted by providers with appropriate delegation after consultation with OLMS.
ABBREVIATIONS:
OLMS – on line medical support
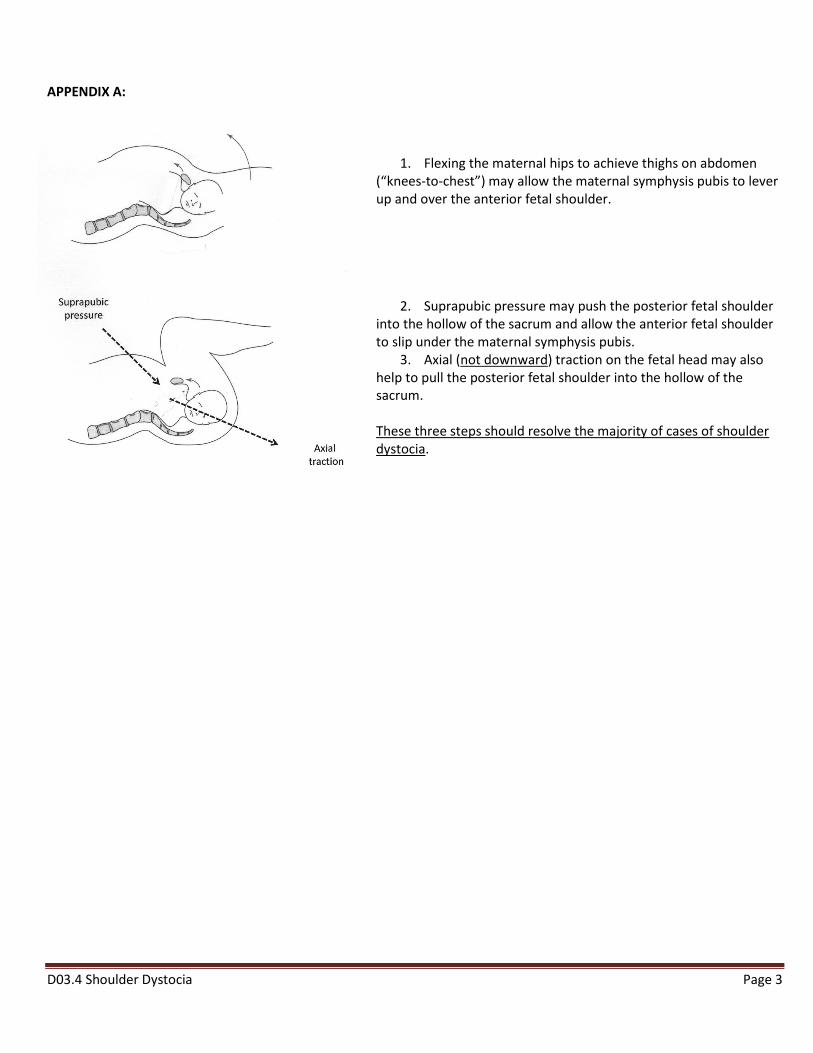
D03.4 Shoulder Dystocia Page 3
APPENDIX A:
1. Flexing the maternal hips to achieve thighs on abdomen (“knees-to-chest”) may allow the maternal symphysis pubis to lever up and over the anterior fetal shoulder.
2. Suprapubic pressure may push the posterior fetal shoulder into the hollow of the sacrum and allow the anterior fetal shoulder to slip under the maternal symphysis pubis.
3. Axial (not downward) traction on the fetal head may also help to pull the posterior fetal shoulder into the hollow of the sacrum. These three steps should resolve the majority of cases of shoulder dystocia.
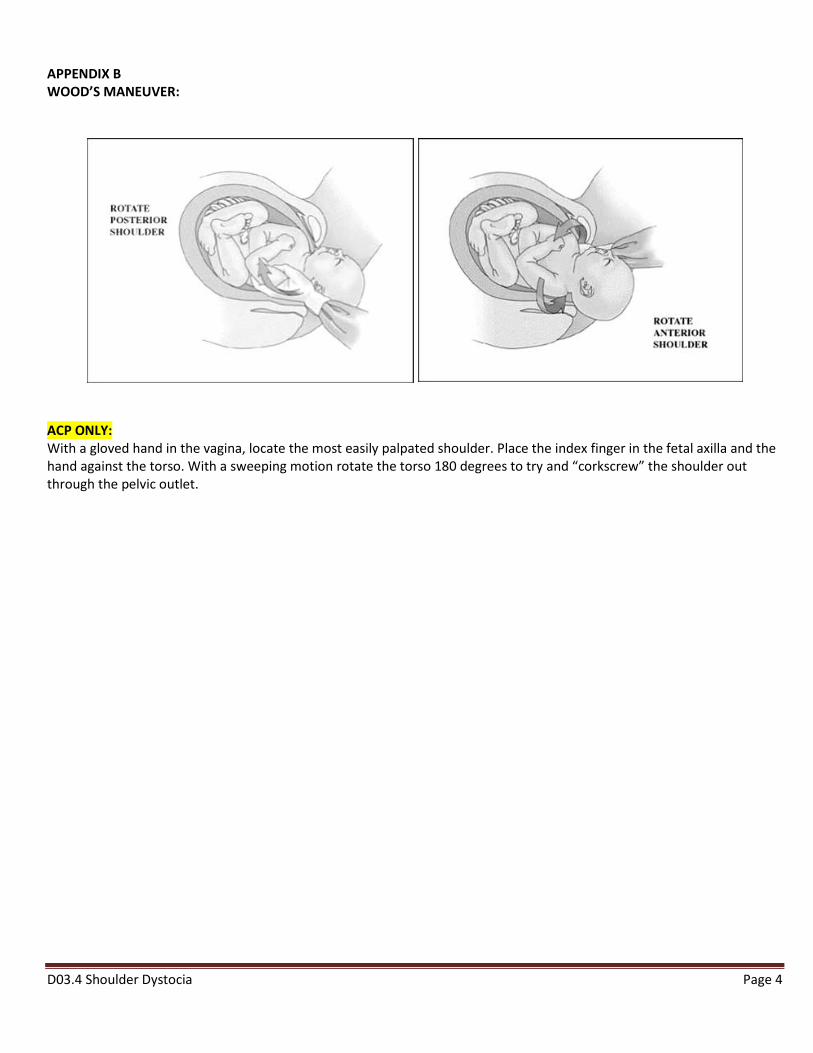
D03.4 Shoulder Dystocia Page 4
APPENDIX B WOOD’S MANEUVER:
ACP ONLY: With a gloved hand in the vagina, locate the most easily palpated shoulder. Place the index finger in the fetal axilla and the hand against the torso. With a sweeping motion rotate the torso 180 degrees to try and “corkscrew” the shoulder out through the pelvic outlet.
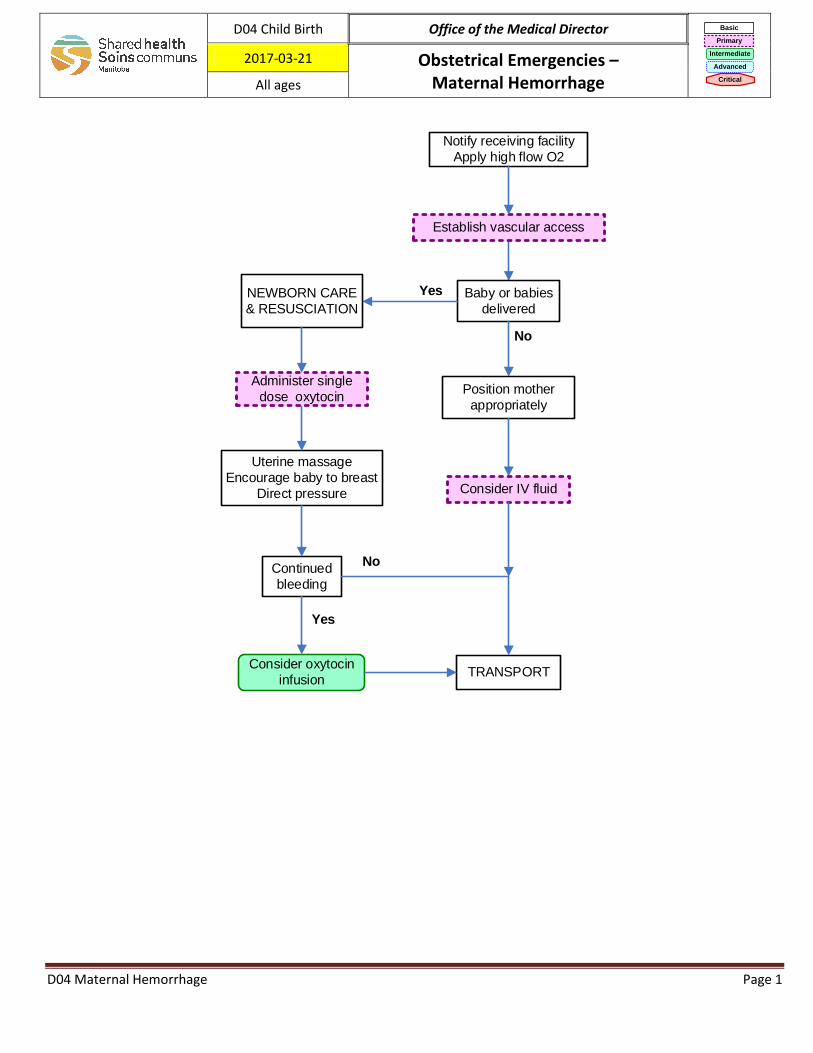
Notify receiving facility
Apply high flow O2
Baby or babies
delivered
Yes
No
Uterine massage
Encourage baby to breast
Direct pressure
Administer single
dose oxytocin
TRANSPORTConsider oxytocin
infusion
Continued
bleeding
No
Establish vascular access
Position mother
appropriately
Yes
Consider IV fluid
NEWBORN CARE
& RESUSCIATION
D04 Child Birth Office of the Medical Director Basic
Primary
Intermediate
Advanced
Critical
2017-03-21 Obstetrical Emergencies – Maternal Hemorrhage All ages
D04 Maternal Hemorrhage Page 1
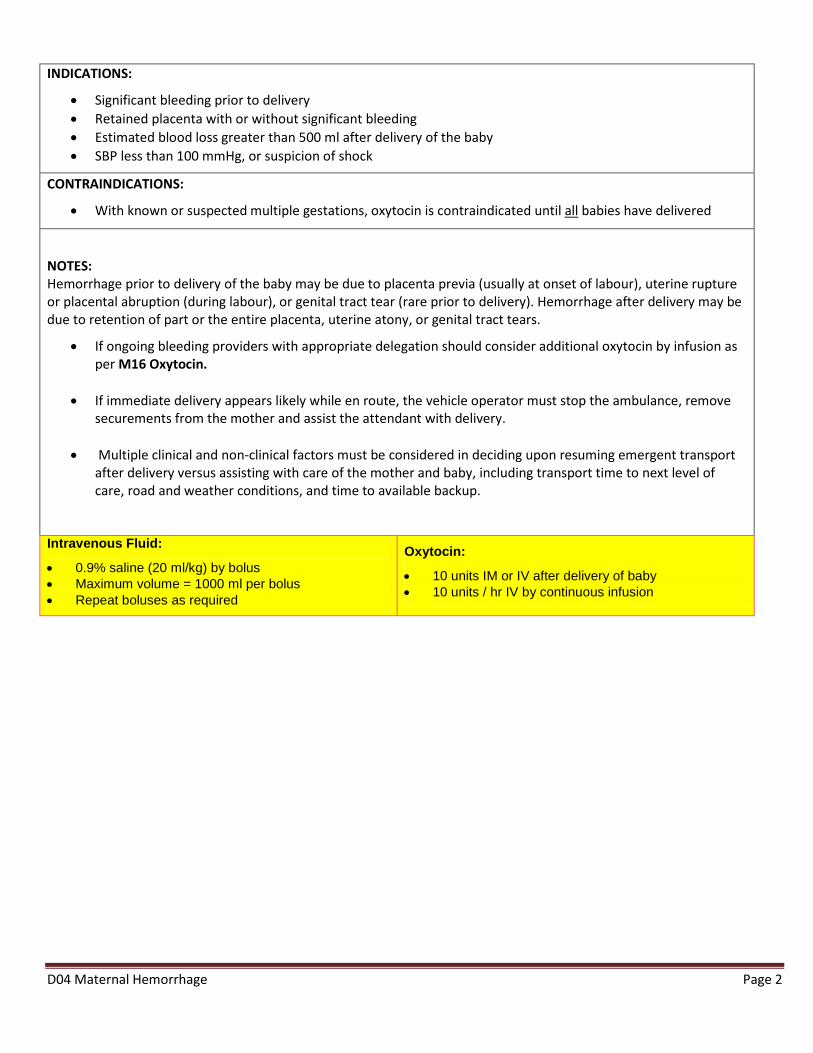
INDICATIONS:
• Significant bleeding prior to delivery • Retained placenta with or without significant bleeding • Estimated blood loss greater than 500 ml after delivery of the baby • SBP less than 100 mmHg, or suspicion of shock
CONTRAINDICATIONS:
• With known or suspected multiple gestations, oxytocin is contraindicated until all babies have delivered
NOTES: Hemorrhage prior to delivery of the baby may be due to placenta previa (usually at onset of labour), uterine rupture or placental abruption (during labour), or genital tract tear (rare prior to delivery). Hemorrhage after delivery may be due to retention of part or the entire placenta, uterine atony, or genital tract tears.
• If ongoing bleeding providers with appropriate delegation should consider additional oxytocin by infusion as per M16 Oxytocin.
• If immediate delivery appears likely while en route, the vehicle operator must stop the ambulance, remove securements from the mother and assist the attendant with delivery.
• Multiple clinical and non-clinical factors must be considered in deciding upon resuming emergent transport after delivery versus assisting with care of the mother and baby, including transport time to next level of care, road and weather conditions, and time to available backup.
Intravenous Fluid:
• 0.9% saline (20 ml/kg) by bolus
• Maximum volume = 1000 ml per bolus
• Repeat boluses as required
Oxytocin:
• 10 units IM or IV after delivery of baby
• 10 units / hr IV by continuous infusion
D04 Maternal Hemorrhage Page 2
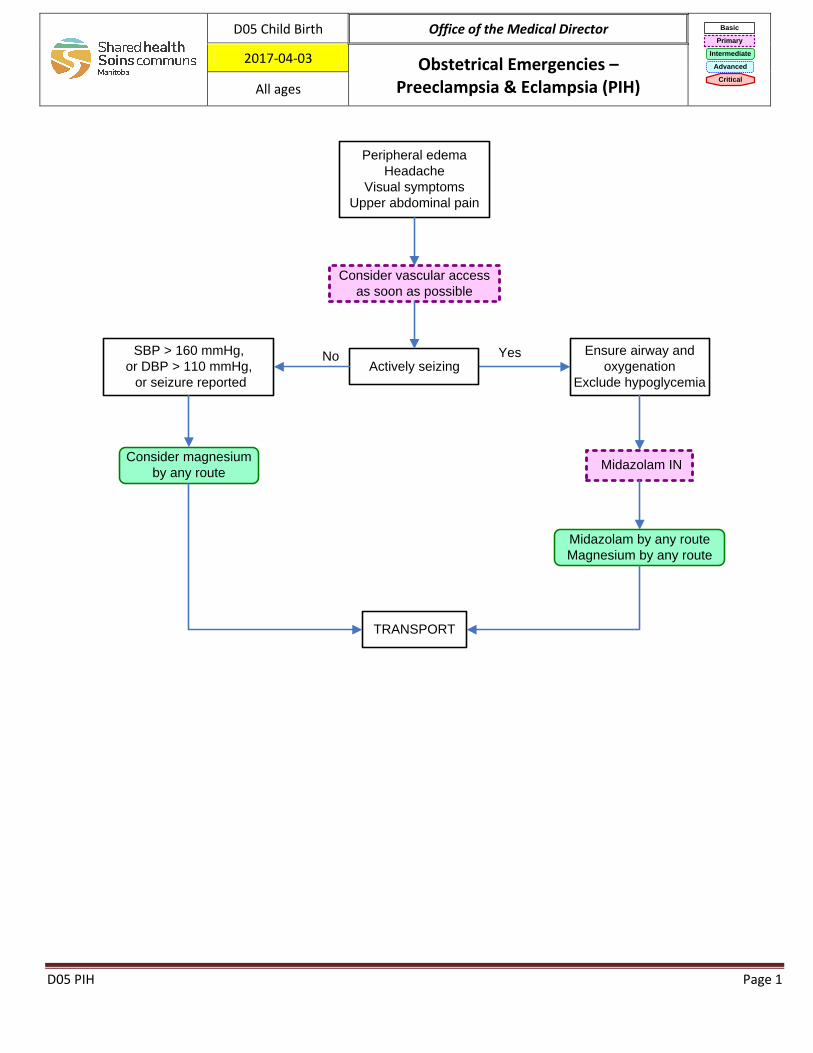
Peripheral edema
Headache
Visual symptoms
Upper abdominal pain
SBP > 160 mmHg,
or DBP > 110 mmHg,
or seizure reported
No YesActively seizing
Midazolam IN
Midazolam by any route
Magnesium by any route
TRANSPORT
Consider magnesium
by any route
Consider vascular access
as soon as possible
Ensure airway and
oxygenation
Exclude hypoglycemia
D05 Child Birth Office of the Medical Director Basic
Primary
Intermediate
Advanced
Critical
2017-04-03 Obstetrical Emergencies – Preeclampsia & Eclampsia (PIH) All ages
D05 PIH Page 1
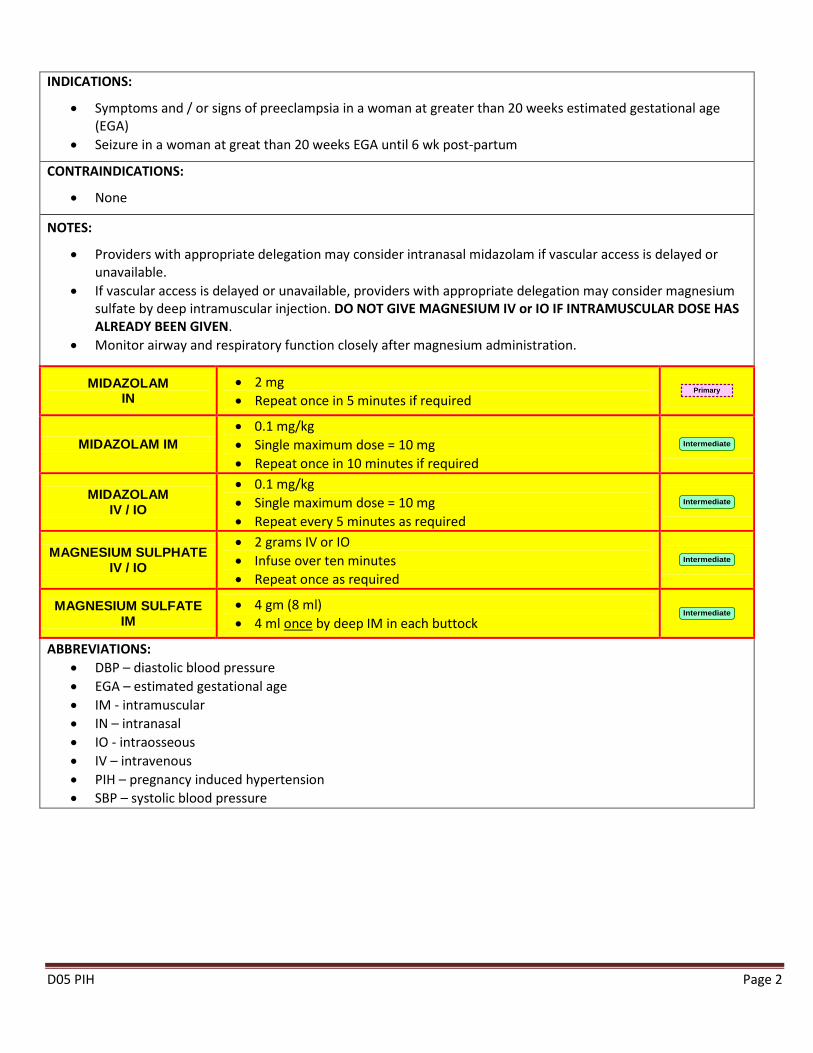
INDICATIONS:
• Symptoms and / or signs of preeclampsia in a woman at greater than 20 weeks estimated gestational age (EGA)
• Seizure in a woman at great than 20 weeks EGA until 6 wk post-partum
CONTRAINDICATIONS:
• None
NOTES:
• Providers with appropriate delegation may consider intranasal midazolam if vascular access is delayed or unavailable.
• If vascular access is delayed or unavailable, providers with appropriate delegation may consider magnesium sulfate by deep intramuscular injection. DO NOT GIVE MAGNESIUM IV or IO IF INTRAMUSCULAR DOSE HAS ALREADY BEEN GIVEN.
• Monitor airway and respiratory function closely after magnesium administration.
MIDAZOLAM IN
• 2 mg • Repeat once in 5 minutes if required
Primary
MIDAZOLAM IM
• 0.1 mg/kg • Single maximum dose = 10 mg • Repeat once in 10 minutes if required
Intermediate
MIDAZOLAM IV / IO
• 0.1 mg/kg • Single maximum dose = 10 mg • Repeat every 5 minutes as required
Intermediate
MAGNESIUM SULPHATE IV / IO
• 2 grams IV or IO • Infuse over ten minutes • Repeat once as required
Intermediate
MAGNESIUM SULFATE IM
• 4 gm (8 ml) • 4 ml once by deep IM in each buttock
Intermediate
ABBREVIATIONS: • DBP – diastolic blood pressure • EGA – estimated gestational age • IM - intramuscular • IN – intranasal • IO - intraosseous • IV – intravenous • PIH – pregnancy induced hypertension • SBP – systolic blood pressure
D05 PIH Page 2
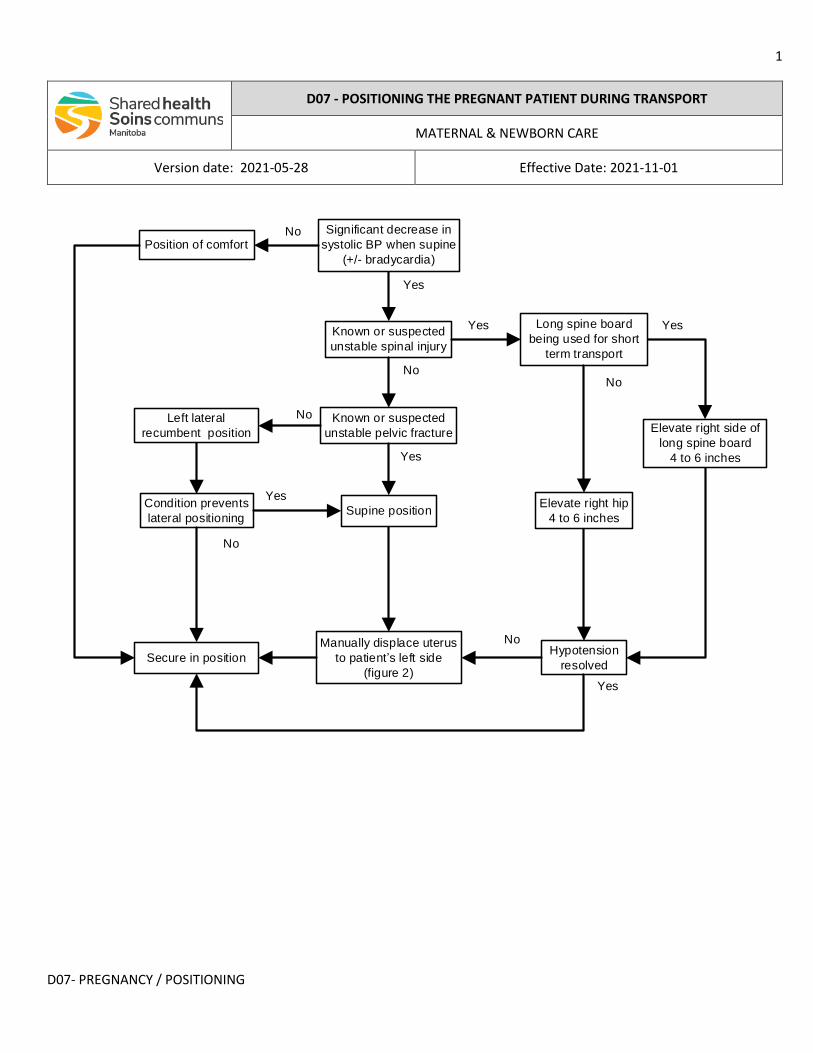
1
D07- PREGNANCY / POSITIONING
Yes
NoNo
No
Yes
Elevate right side of
long spine board
4 to 6 inches
Manually displace uterus
to patient s left side
(figure 2)Yes
Yes
No
Significant decrease in
systolic BP when supine
(+/- bradycardia)
Position of comfort
Known or suspected
unstable spinal injury
Long spine board
being used for short
term transport
Elevate right hip
4 to 6 inches
Known or suspected
unstable pelvic fracture
Supine position
Hypotension
resolvedSecure in position
No
Condition prevents
lateral positioning
Yes
Yes
No
Left lateral
recumbent position
D07 - POSITIONING THE PREGNANT PATIENT DURING TRANSPORT
MATERNAL & NEWBORN CARE
Version date: 2021-05-28 Effective Date: 2021-11-01
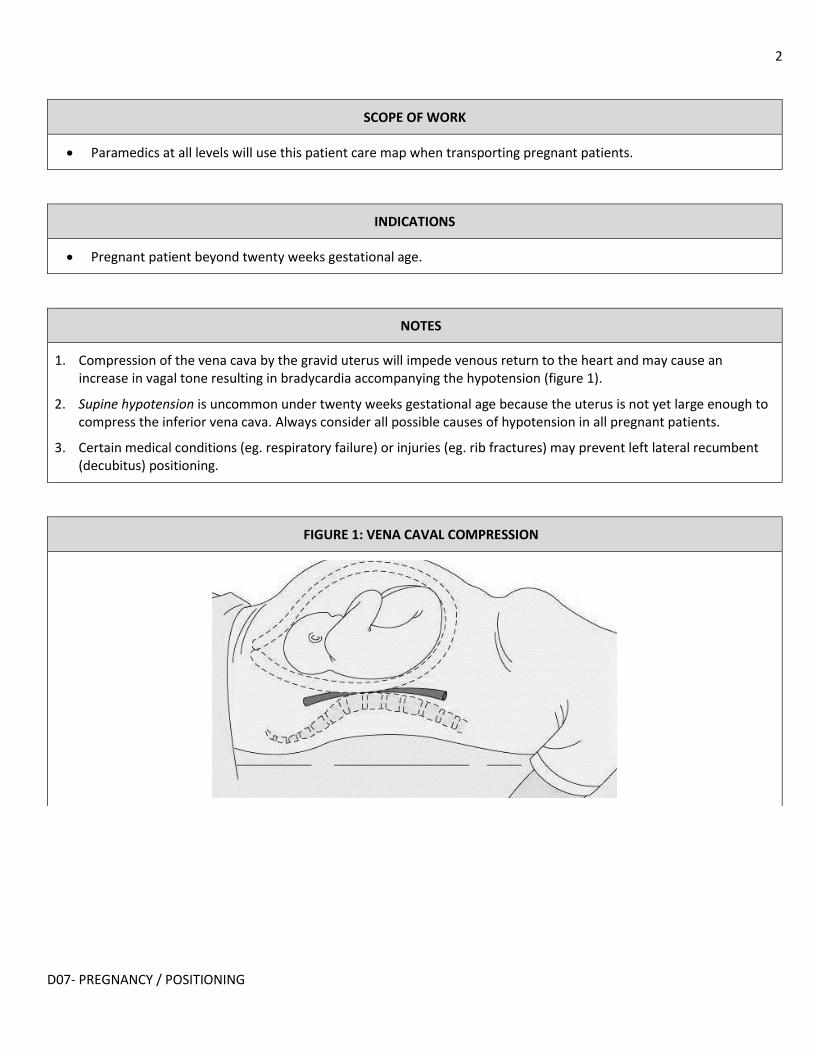
2
D07- PREGNANCY / POSITIONING
SCOPE OF WORK
• Paramedics at all levels will use this patient care map when transporting pregnant patients.
INDICATIONS
• Pregnant patient beyond twenty weeks gestational age.
NOTES
1. Compression of the vena cava by the gravid uterus will impede venous return to the heart and may cause an increase in vagal tone resulting in bradycardia accompanying the hypotension (figure 1).
2. Supine hypotension is uncommon under twenty weeks gestational age because the uterus is not yet large enough to compress the inferior vena cava. Always consider all possible causes of hypotension in all pregnant patients.
3. Certain medical conditions (eg. respiratory failure) or injuries (eg. rib fractures) may prevent left lateral recumbent (decubitus) positioning.
FIGURE 1: VENA CAVAL COMPRESSION
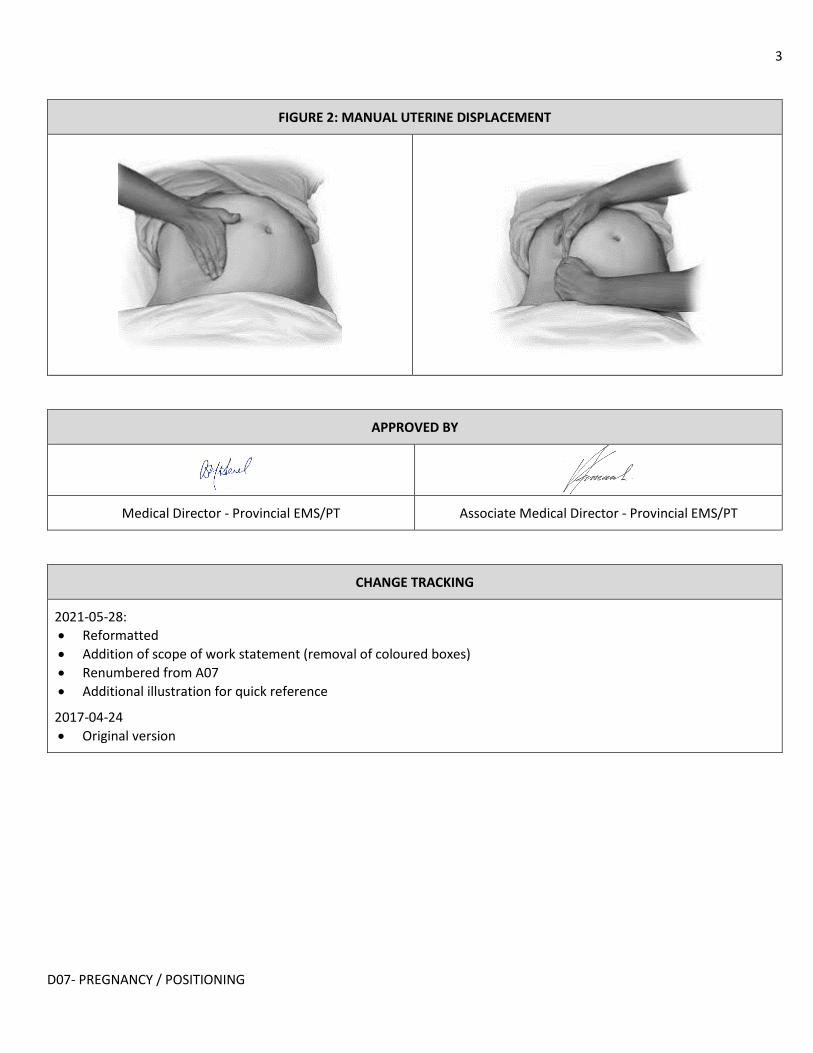
3
D07- PREGNANCY / POSITIONING
FIGURE 2: MANUAL UTERINE DISPLACEMENT
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
CHANGE TRACKING
2021-05-28:
• Reformatted
• Addition of scope of work statement (removal of coloured boxes)
• Renumbered from A07
• Additional illustration for quick reference
2017-04-24
• Original version
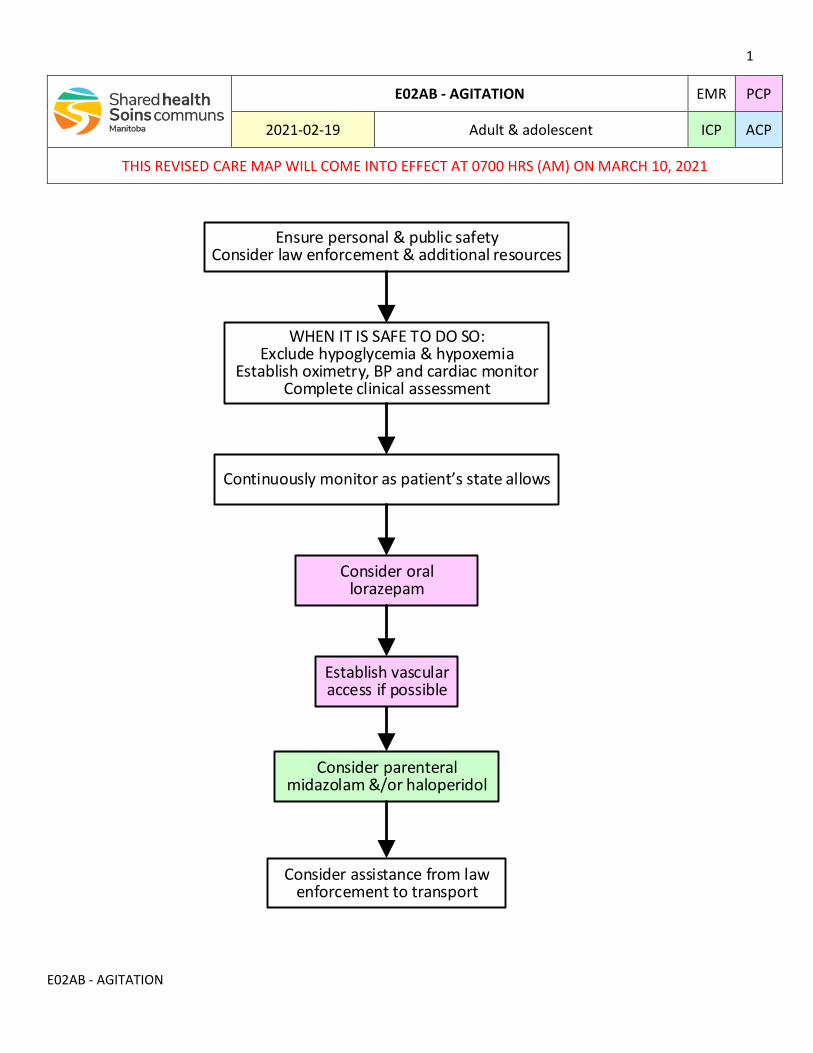
1
E02AB - AGITATION
E02AB - AGITATION EMR PCP
2021-02-19 Adult & adolescent ICP ACP
THIS REVISED CARE MAP WILL COME INTO EFFECT AT 0700 HRS (AM) ON MARCH 10, 2021
Ensure personal & public safetyConsider law enforcement & additional resources
WHEN IT IS SAFE TO DO SO:Exclude hypoglycemia & hypoxemia
Establish oximetry, BP and cardiac monitorComplete clinical assessment
Continuously monitor as patient s state allows
Consider oral lorazepam
Establish vascular access if possible
Consider parenteral midazolam &/or haloperidol
Consider assistance from law enforcement to transport
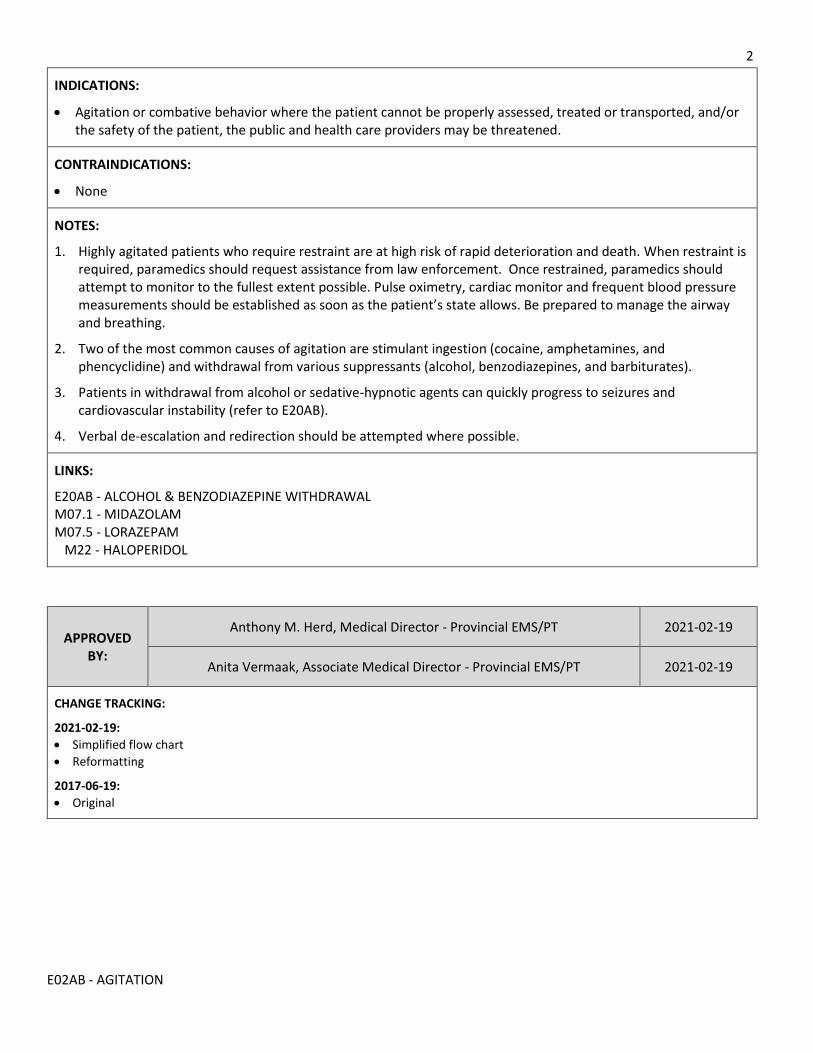
2
E02AB - AGITATION
INDICATIONS:
Agitation or combative behavior where the patient cannot be properly assessed, treated or transported, and/or the safety of the patient, the public and health care providers may be threatened.
CONTRAINDICATIONS:
None
NOTES:
1. Highly agitated patients who require restraint are at high risk of rapid deterioration and death. When restraint is required, paramedics should request assistance from law enforcement. Once restrained, paramedics should attempt to monitor to the fullest extent possible. Pulse oximetry, cardiac monitor and frequent blood pressure measurements should be established as soon as the patient’s state allows. Be prepared to manage the airway and breathing.
2. Two of the most common causes of agitation are stimulant ingestion (cocaine, amphetamines, and phencyclidine) and withdrawal from various suppressants (alcohol, benzodiazepines, and barbiturates).
3. Patients in withdrawal from alcohol or sedative-hypnotic agents can quickly progress to seizures and cardiovascular instability (refer to E20AB).
4. Verbal de-escalation and redirection should be attempted where possible.
LINKS:
E20AB - ALCOHOL & BENZODIAZEPINE WITHDRAWAL M07.1 - MIDAZOLAM M07.5 - LORAZEPAM M22 - HALOPERIDOL
APPROVED BY:
Anthony M. Herd, Medical Director - Provincial EMS/PT 2021-02-19
Anita Vermaak, Associate Medical Director - Provincial EMS/PT 2021-02-19
CHANGE TRACKING:
2021-02-19:
Simplified flow chart
Reformatting
2017-06-19:
Original
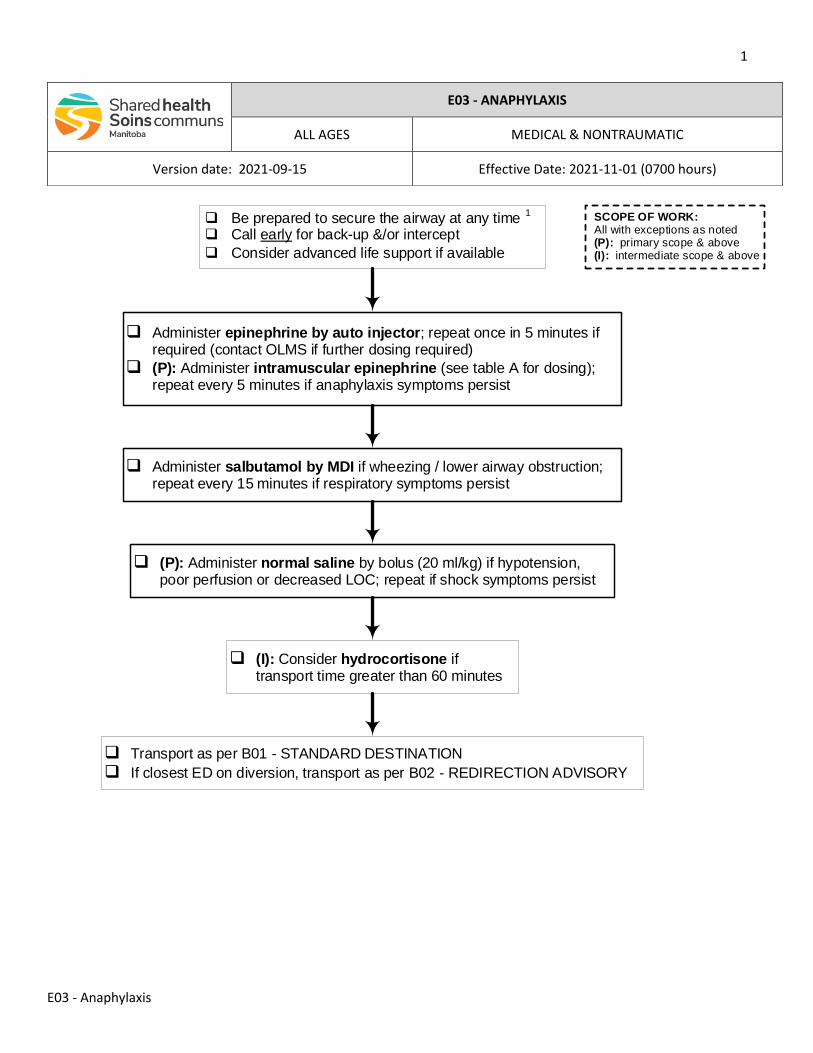
1
E03 - Anaphylaxis
q (I): Consider hydrocortisone if transport time greater than 60 minutes
q Transport as per B01 - STANDARD DESTINATION
q If closest ED on diversion, transport as per B02 - REDIRECTION ADVISORY
q Be prepared to secure the airway at any time 1
q Call early for back-up &/or intercept
q Consider advanced life support if available
q Administer epinephrine by auto injector; repeat once in 5 minutes if required (contact OLMS if further dosing required)
q (P): Administer intramuscular epinephrine (see table A for dosing); repeat every 5 minutes if anaphylaxis symptoms persist
q Administer salbutamol by MDI if wheezing / lower airway obstruction; repeat every 15 minutes if respiratory symptoms persist
q (P): Administer normal saline by bolus (20 ml/kg) if hypotension, poor perfusion or decreased LOC; repeat if shock symptoms persist
SCOPE OF WORK: All with exceptions as noted(P): primary scope & above(I): intermediate scope & above
E03 - ANAPHYLAXIS
ALL AGES MEDICAL & NONTRAUMATIC
Version date: 2021-09-15 Effective Date: 2021-11-01 (0700 hours)
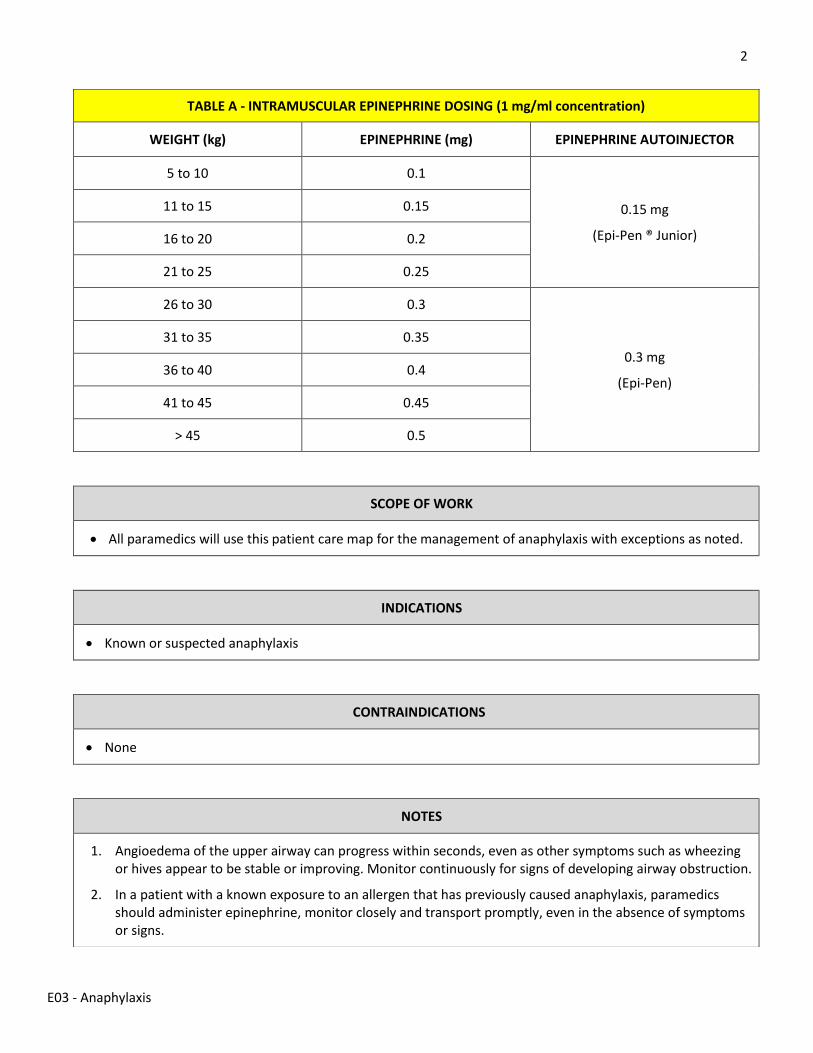
2
E03 - Anaphylaxis
TABLE A - INTRAMUSCULAR EPINEPHRINE DOSING (1 mg/ml concentration)
WEIGHT (kg) EPINEPHRINE (mg) EPINEPHRINE AUTOINJECTOR
5 to 10 0.1
0.15 mg
(Epi-Pen ® Junior)
11 to 15 0.15
16 to 20 0.2
21 to 25 0.25
26 to 30 0.3
0.3 mg
(Epi-Pen)
31 to 35 0.35
36 to 40 0.4
41 to 45 0.45
> 45 0.5
SCOPE OF WORK
• All paramedics will use this patient care map for the management of anaphylaxis with exceptions as noted.
INDICATIONS
• Known or suspected anaphylaxis
CONTRAINDICATIONS
• None
NOTES
1. Angioedema of the upper airway can progress within seconds, even as other symptoms such as wheezing or hives appear to be stable or improving. Monitor continuously for signs of developing airway obstruction.
2. In a patient with a known exposure to an allergen that has previously caused anaphylaxis, paramedics should administer epinephrine, monitor closely and transport promptly, even in the absence of symptoms or signs.
3
E03 - Anaphylaxis
LINKS
M05.1 - EPINEPHRINE FOR ANAPHYLAXIS M13.2 - HYDROCORTISONE M15 - SALBUTAMOL
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
CHANGE TRACKING
2021-09-15:
• Revised & reformatted
• Revised indications
• Addition of scope of work statement & legend (removal of coloured boxes)
• Simplified flow chart o Glucagon removed as rarely required in initial prehospital management o Nebulized epinephrine removed as inferior to parenteral administration o Removal of IV dosing until pumps are universally available
2021-02-04
• Revised hydrocortisone dosing
• Refractory anaphylaxis transport time increased to 60 minutes
2021-01-13:
• Simplified linear flow chart & reformatting
• Modified indications and clarification of management around exposure to known allergen
• Modified to align with new guidelines (e.g., Canadian Pediatric Society)
• Addition of weight based dosing for IM epinephrine
• Removal of antihistamines which may mask signs of worsening of anaphylaxis and biphasic reactions
• Switch to hydrocortisone to simplify Shared Health ERS formulary
• Inclusion of anaphylaxis as additional reason for redirection advisory over-ride
2017-06-06:
• Original version
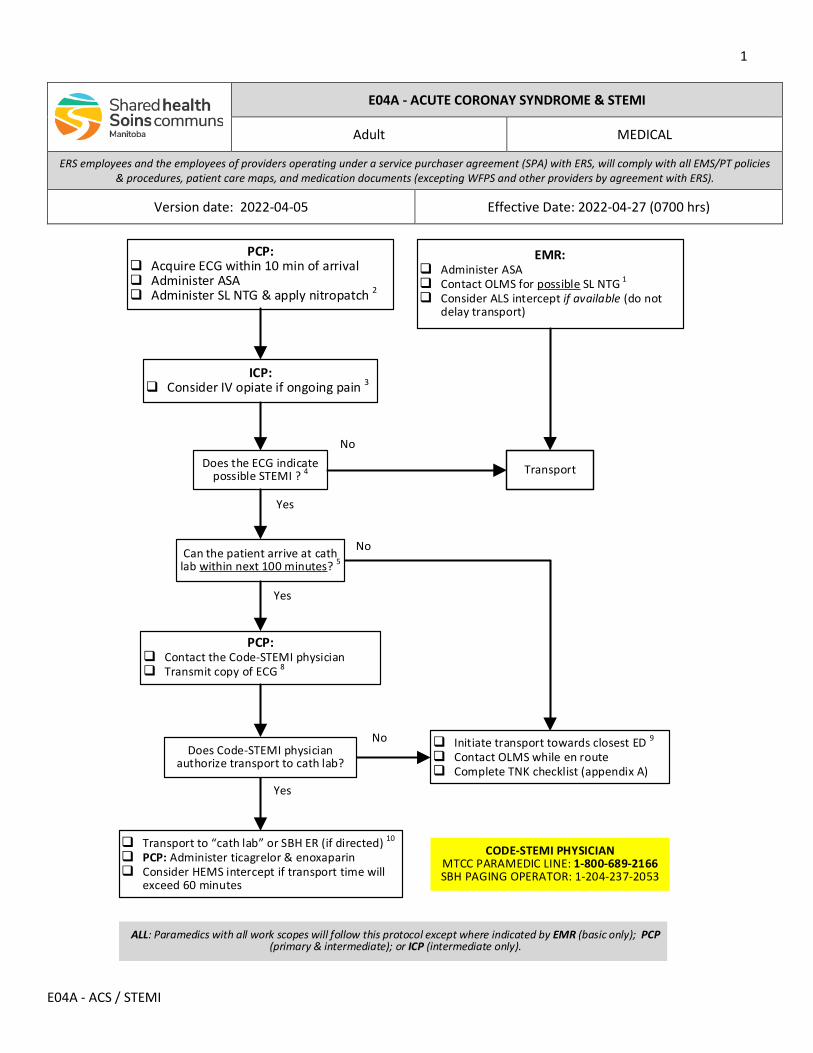
1
E04A - ACS / STEMI
No
PCP: Acquire ECG within 10 min of arrival Administer ASA Administer SL NTG & apply nitropatch 2
Yes
Initiate transport towards closest ED 9
Contact OLMS while en route Complete TNK checklist (appendix A)
Can the patient arrive at cath lab within next 100 minutes? 5
PCP: Contact the Code-STEMI physician Transmit copy of ECG 8
Does Code-STEMI physician authorize transport to cath lab?
Transport to “cath lab” or SBH ER (if directed) 10
PCP: Administer ticagrelor & enoxaparin Consider HEMS intercept if transport time will
exceed 60 minutes
Does the ECG indicate possible STEMI ? 4
No
Yes
Yes
No
CODE-STEMI PHYSICIANMTCC PARAMEDIC LINE: 1-800-689-2166 SBH PAGING OPERATOR: 1-204-237-2053
Transport
ALL: Paramedics with all work scopes will follow this protocol except where indicated by EMR (basic only); PCP (primary & intermediate); or ICP (intermediate only).
EMR: Administer ASA Contact OLMS for possible SL NTG 1
Consider ALS intercept if available (do not delay transport)
ICP: Consider IV opiate if ongoing pain 3
E04A - ACUTE CORONAY SYNDROME & STEMI
Adult MEDICAL
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-05 Effective Date: 2022-04-27 (0700 hrs)
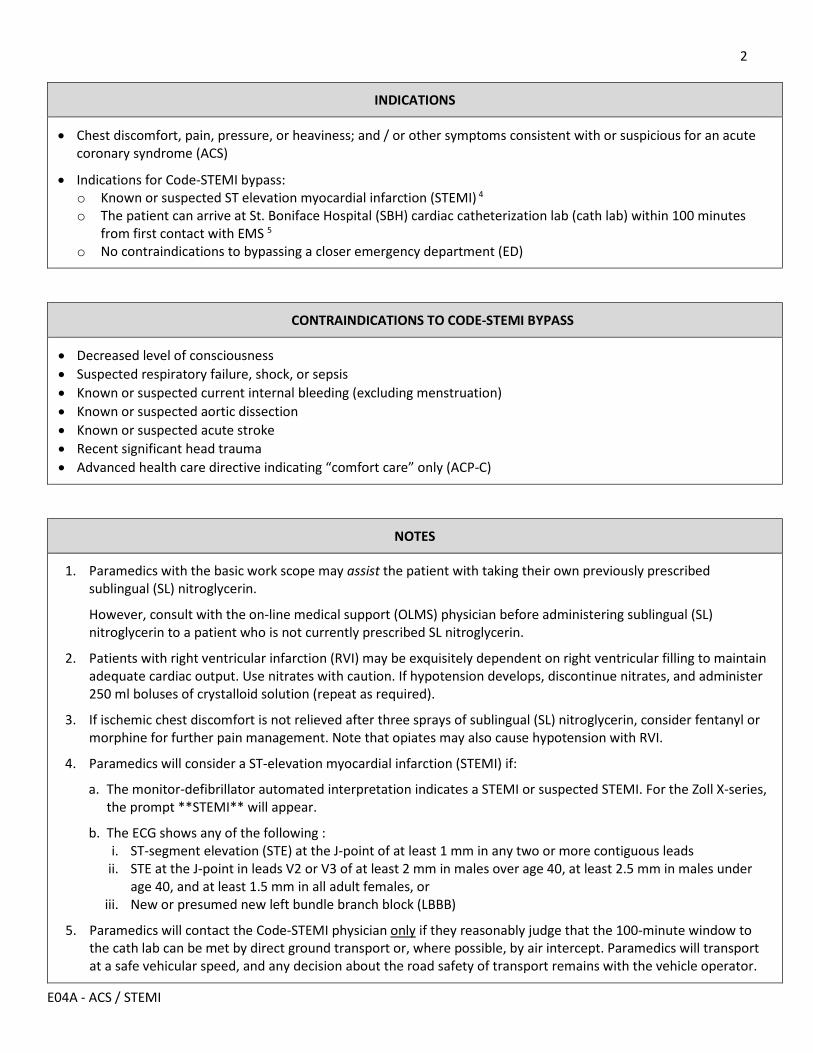
2
E04A - ACS / STEMI
INDICATIONS
• Chest discomfort, pain, pressure, or heaviness; and / or other symptoms consistent with or suspicious for an acute coronary syndrome (ACS)
• Indications for Code-STEMI bypass: o Known or suspected ST elevation myocardial infarction (STEMI) 4 o The patient can arrive at St. Boniface Hospital (SBH) cardiac catheterization lab (cath lab) within 100 minutes
from first contact with EMS 5 o No contraindications to bypassing a closer emergency department (ED)
CONTRAINDICATIONS TO CODE-STEMI BYPASS
• Decreased level of consciousness • Suspected respiratory failure, shock, or sepsis • Known or suspected current internal bleeding (excluding menstruation) • Known or suspected aortic dissection • Known or suspected acute stroke • Recent significant head trauma • Advanced health care directive indicating “comfort care” only (ACP-C)
NOTES
1. Paramedics with the basic work scope may assist the patient with taking their own previously prescribed sublingual (SL) nitroglycerin.
However, consult with the on-line medical support (OLMS) physician before administering sublingual (SL) nitroglycerin to a patient who is not currently prescribed SL nitroglycerin.
2. Patients with right ventricular infarction (RVI) may be exquisitely dependent on right ventricular filling to maintain adequate cardiac output. Use nitrates with caution. If hypotension develops, discontinue nitrates, and administer 250 ml boluses of crystalloid solution (repeat as required).
3. If ischemic chest discomfort is not relieved after three sprays of sublingual (SL) nitroglycerin, consider fentanyl or morphine for further pain management. Note that opiates may also cause hypotension with RVI.
4. Paramedics will consider a ST-elevation myocardial infarction (STEMI) if:
a. The monitor-defibrillator automated interpretation indicates a STEMI or suspected STEMI. For the Zoll X-series, the prompt **STEMI** will appear.
b. The ECG shows any of the following : i. ST-segment elevation (STE) at the J-point of at least 1 mm in any two or more contiguous leads
ii. STE at the J-point in leads V2 or V3 of at least 2 mm in males over age 40, at least 2.5 mm in males under age 40, and at least 1.5 mm in all adult females, or
iii. New or presumed new left bundle branch block (LBBB)
5. Paramedics will contact the Code-STEMI physician only if they reasonably judge that the 100-minute window to the cath lab can be met by direct ground transport or, where possible, by air intercept. Paramedics will transport at a safe vehicular speed, and any decision about the road safety of transport remains with the vehicle operator.
3
E04A - ACS / STEMI
6. Paramedics will contact the Medical Transportation Coordination Center (MTCC) paramedic line for the name of the “Code-STEMI physician” and contact that physician directly with the number provided.
If unable to contact the Code-STEMI physician, paramedics will contact the SBH paging operator and request to speak to the “on-call interventional cardiologist for a code-25 outside call”.
If unable to reach either of these individuals, paramedics will contact the MTCC dispatcher and ask to speak to the on-line medical support (OLMS) physician.
7. Communication with the physicians should include the patient’s name, age, and gender; current symptoms; time of symptom onset; relevant medical history, medications, and allergies; current vital signs and relevant physical findings.
8. When transmitting an ECG by text or e-mail, the Personal Health Information Act (PHIA) requires you to obscure or cover the patient’s identifying data.
9. Some patients beyond the 100-minute concentric may benefit from transport to an ED capable of providing emergent fibrinolytic therapy, followed by prompt transfer to the cath lab for subsequent percutaneous coronary intervention (PCI).
Initiate transport towards the closest ED and contact the OLMS physician while en route. If time allows, paramedics will perform the TNK checklist (appendix A) while en route to the ED. Unless otherwise advised, paramedics will remain with the patient pending a decision about emergent secondary interfacility transfer.
10. If the patient is stable on arrival at SBH, paramedics will transport directly to the cath lab, unless otherwise advised. If the patient is unstable on arrival at SBH, paramedics will go first to the SBH ED.
If the patient deteriorates en route to Winnipeg, paramedics will redirect to the ED that has the shortest estimated transport time from the patient’s current location. Always ensure appropriate pre-arrival notification of ED staff.
LINKS
M03.1 - MORPHINE M03.2 - FENTANYL M21 - NITROGLYCERIN M37.1 - ASA M37.2 - TICAGRELOR M43 - ENOXAPARIN
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
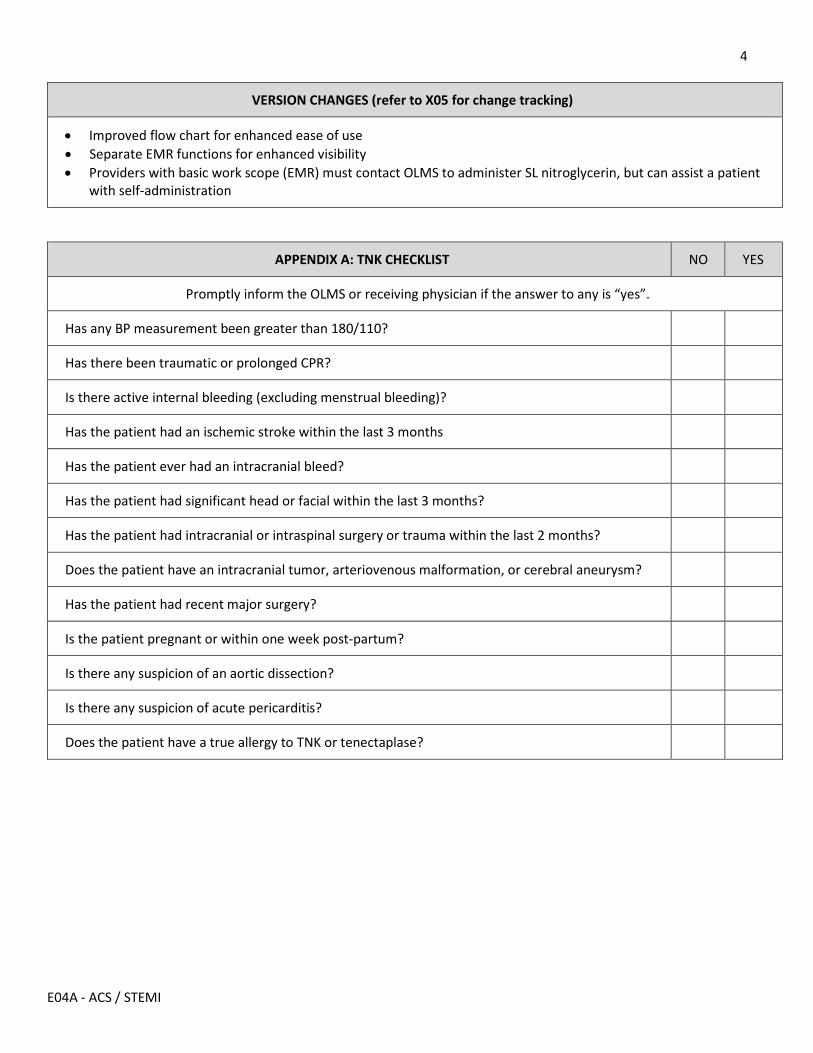
4
E04A - ACS / STEMI
VERSION CHANGES (refer to X05 for change tracking)
• Improved flow chart for enhanced ease of use • Separate EMR functions for enhanced visibility • Providers with basic work scope (EMR) must contact OLMS to administer SL nitroglycerin, but can assist a patient
with self-administration
APPENDIX A: TNK CHECKLIST NO YES
Promptly inform the OLMS or receiving physician if the answer to any is “yes”.
Has any BP measurement been greater than 180/110?
Has there been traumatic or prolonged CPR?
Is there active internal bleeding (excluding menstrual bleeding)?
Has the patient had an ischemic stroke within the last 3 months
Has the patient ever had an intracranial bleed?
Has the patient had significant head or facial within the last 3 months?
Has the patient had intracranial or intraspinal surgery or trauma within the last 2 months?
Does the patient have an intracranial tumor, arteriovenous malformation, or cerebral aneurysm?
Has the patient had recent major surgery?
Is the patient pregnant or within one week post-partum?
Is there any suspicion of an aortic dissection?
Is there any suspicion of acute pericarditis?
Does the patient have a true allergy to TNK or tenectaplase?
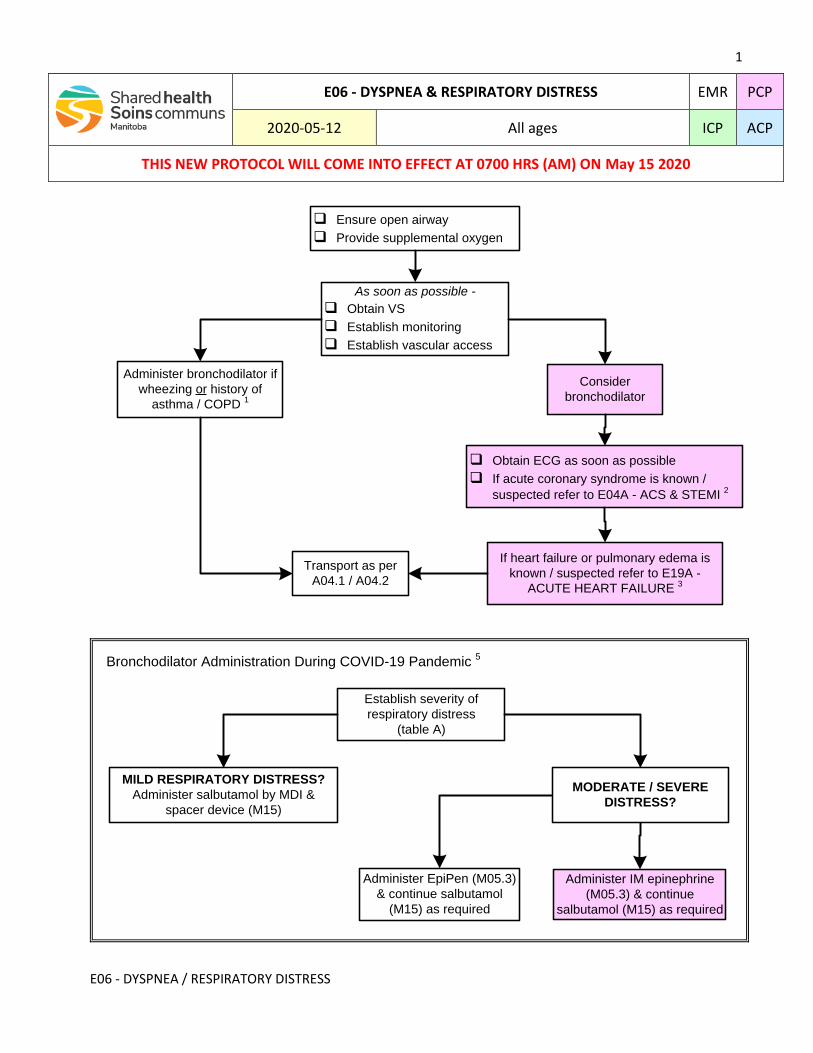
1
E06 - DYSPNEA / RESPIRATORY DISTRESS
q Ensure open airway
q Provide supplemental oxygen
Transport as per
A04.1 / A04.2
q Obtain ECG as soon as possible
q If acute coronary syndrome is known /
suspected refer to E04A - ACS & STEMI 2
If heart failure or pulmonary edema is
known / suspected refer to E19A -
ACUTE HEART FAILURE 3
Administer bronchodilator if
wheezing or history of
asthma / COPD 1
As soon as possible -
q Obtain VS
q Establish monitoring
q Establish vascular access
Consider
bronchodilator
Establish severity of
respiratory distress
(table A)
MILD RESPIRATORY DISTRESS?
Administer salbutamol by MDI &
spacer device (M15)
MODERATE / SEVERE
DISTRESS?
Administer EpiPen (M05.3)
& continue salbutamol
(M15) as required
Administer IM epinephrine
(M05.3) & continue
salbutamol (M15) as required
Bronchodilator Administration During COVID-19 Pandemic 5
E06 - DYSPNEA & RESPIRATORY DISTRESS EMR PCP
2020-05-12 All ages ICP ACP
THIS NEW PROTOCOL WILL COME INTO EFFECT AT 0700 HRS (AM) ON May 15 2020
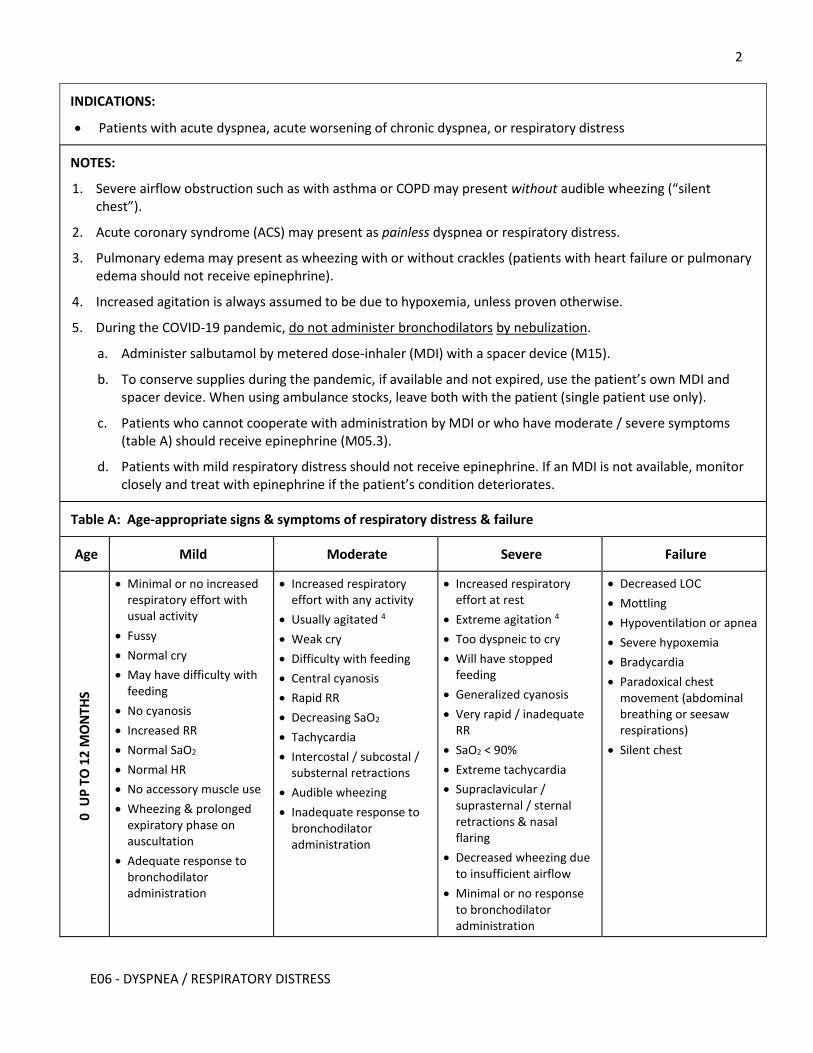
2
E06 - DYSPNEA / RESPIRATORY DISTRESS
INDICATIONS:
Patients with acute dyspnea, acute worsening of chronic dyspnea, or respiratory distress
NOTES:
1. Severe airflow obstruction such as with asthma or COPD may present without audible wheezing (“silent chest”).
2. Acute coronary syndrome (ACS) may present as painless dyspnea or respiratory distress.
3. Pulmonary edema may present as wheezing with or without crackles (patients with heart failure or pulmonary edema should not receive epinephrine).
4. Increased agitation is always assumed to be due to hypoxemia, unless proven otherwise.
5. During the COVID-19 pandemic, do not administer bronchodilators by nebulization.
a. Administer salbutamol by metered dose-inhaler (MDI) with a spacer device (M15).
b. To conserve supplies during the pandemic, if available and not expired, use the patient’s own MDI and spacer device. When using ambulance stocks, leave both with the patient (single patient use only).
c. Patients who cannot cooperate with administration by MDI or who have moderate / severe symptoms (table A) should receive epinephrine (M05.3).
d. Patients with mild respiratory distress should not receive epinephrine. If an MDI is not available, monitor closely and treat with epinephrine if the patient’s condition deteriorates.
Table A: Age-appropriate signs & symptoms of respiratory distress & failure
Age Mild Moderate Severe Failure
0 U
P T
O 1
2 M
ON
THS
Minimal or no increased respiratory effort with usual activity
Fussy
Normal cry
May have difficulty with feeding
No cyanosis
Increased RR
Normal SaO2
Normal HR
No accessory muscle use
Wheezing & prolonged expiratory phase on auscultation
Adequate response to bronchodilator administration
Increased respiratory effort with any activity
Usually agitated 4
Weak cry
Difficulty with feeding
Central cyanosis
Rapid RR
Decreasing SaO2
Tachycardia
Intercostal / subcostal / substernal retractions
Audible wheezing
Inadequate response to bronchodilator administration
Increased respiratory effort at rest
Extreme agitation 4
Too dyspneic to cry
Will have stopped feeding
Generalized cyanosis
Very rapid / inadequate RR
SaO2 < 90%
Extreme tachycardia
Supraclavicular / suprasternal / sternal retractions & nasal flaring
Decreased wheezing due to insufficient airflow
Minimal or no response to bronchodilator administration
Decreased LOC
Mottling
Hypoventilation or apnea
Severe hypoxemia
Bradycardia
Paradoxical chest movement (abdominal breathing or seesaw respirations)
Silent chest
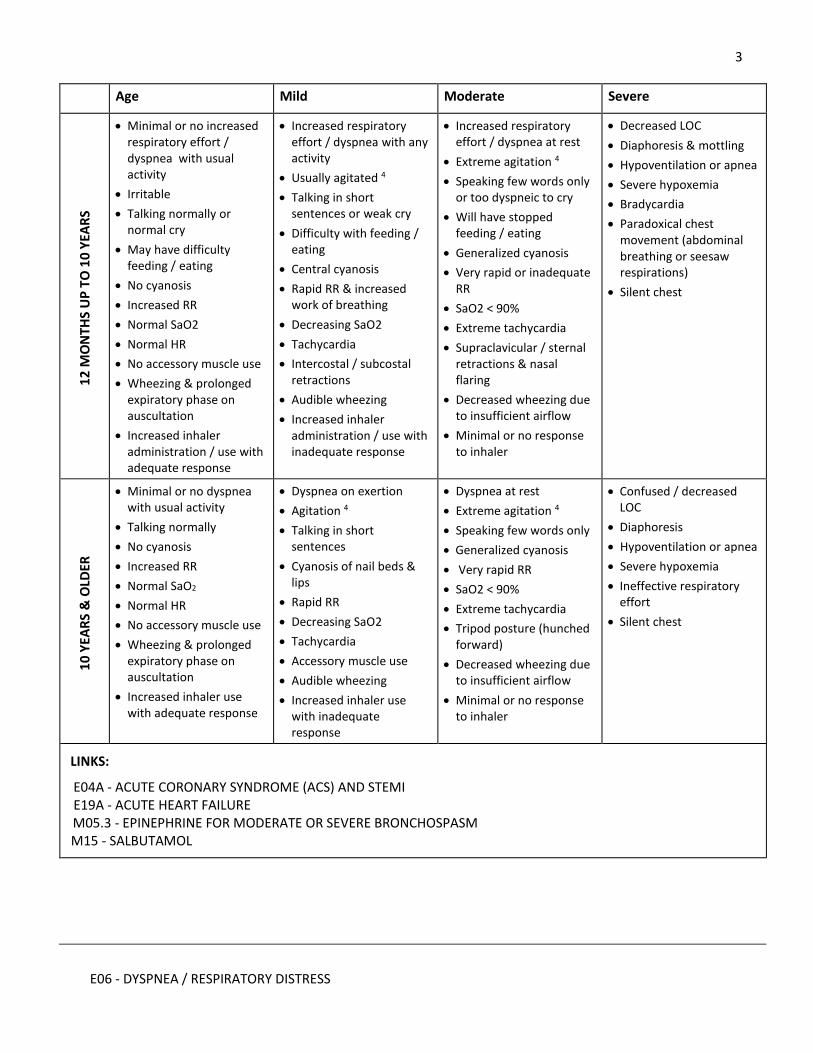
3
E06 - DYSPNEA / RESPIRATORY DISTRESS
Age Mild Moderate Severe 1
2 M
ON
THS
UP
TO
10
YEA
RS
Minimal or no increased respiratory effort / dyspnea with usual activity
Irritable
Talking normally or normal cry
May have difficulty feeding / eating
No cyanosis
Increased RR
Normal SaO2
Normal HR
No accessory muscle use
Wheezing & prolonged expiratory phase on auscultation
Increased inhaler administration / use with adequate response
Increased respiratory effort / dyspnea with any activity
Usually agitated 4
Talking in short sentences or weak cry
Difficulty with feeding / eating
Central cyanosis
Rapid RR & increased work of breathing
Decreasing SaO2
Tachycardia
Intercostal / subcostal retractions
Audible wheezing
Increased inhaler administration / use with inadequate response
Increased respiratory effort / dyspnea at rest
Extreme agitation 4
Speaking few words only or too dyspneic to cry
Will have stopped feeding / eating
Generalized cyanosis
Very rapid or inadequate RR
SaO2 < 90%
Extreme tachycardia
Supraclavicular / sternal retractions & nasal flaring
Decreased wheezing due to insufficient airflow
Minimal or no response to inhaler
Decreased LOC
Diaphoresis & mottling
Hypoventilation or apnea
Severe hypoxemia
Bradycardia
Paradoxical chest movement (abdominal breathing or seesaw respirations)
Silent chest
10
YEA
RS
& O
LDER
Minimal or no dyspnea with usual activity
Talking normally
No cyanosis
Increased RR
Normal SaO2
Normal HR
No accessory muscle use
Wheezing & prolonged expiratory phase on auscultation
Increased inhaler use with adequate response
Dyspnea on exertion
Agitation 4
Talking in short sentences
Cyanosis of nail beds & lips
Rapid RR
Decreasing SaO2
Tachycardia
Accessory muscle use
Audible wheezing
Increased inhaler use with inadequate response
Dyspnea at rest
Extreme agitation 4
Speaking few words only
Generalized cyanosis
Very rapid RR
SaO2 < 90%
Extreme tachycardia
Tripod posture (hunched forward)
Decreased wheezing due to insufficient airflow
Minimal or no response to inhaler
Confused / decreased LOC
Diaphoresis
Hypoventilation or apnea
Severe hypoxemia
Ineffective respiratory effort
Silent chest
LINKS:
E04A - ACUTE CORONARY SYNDROME (ACS) AND STEMI E19A - ACUTE HEART FAILURE M05.3 - EPINEPHRINE FOR MODERATE OR SEVERE BRONCHOSPASM M15 - SALBUTAMOL
4
E06 - DYSPNEA / RESPIRATORY DISTRESS
APPROVED BY:
Anthony M. Herd, Medical Director - Provincial EMS/PT 2020-05-12
Anita Vermaak, Associate Medical Director – Provincial EMS/PT 2020-05-12
CHANGE TRACKING:
2020-05-12:
Consolidation of previous documents E06A; E06B; E06C; and E06D into single care map
Incorporation of additional information from COVID-19 care map E22
Revised table A
Simplified flow chart
2017-05-15:
Original versions
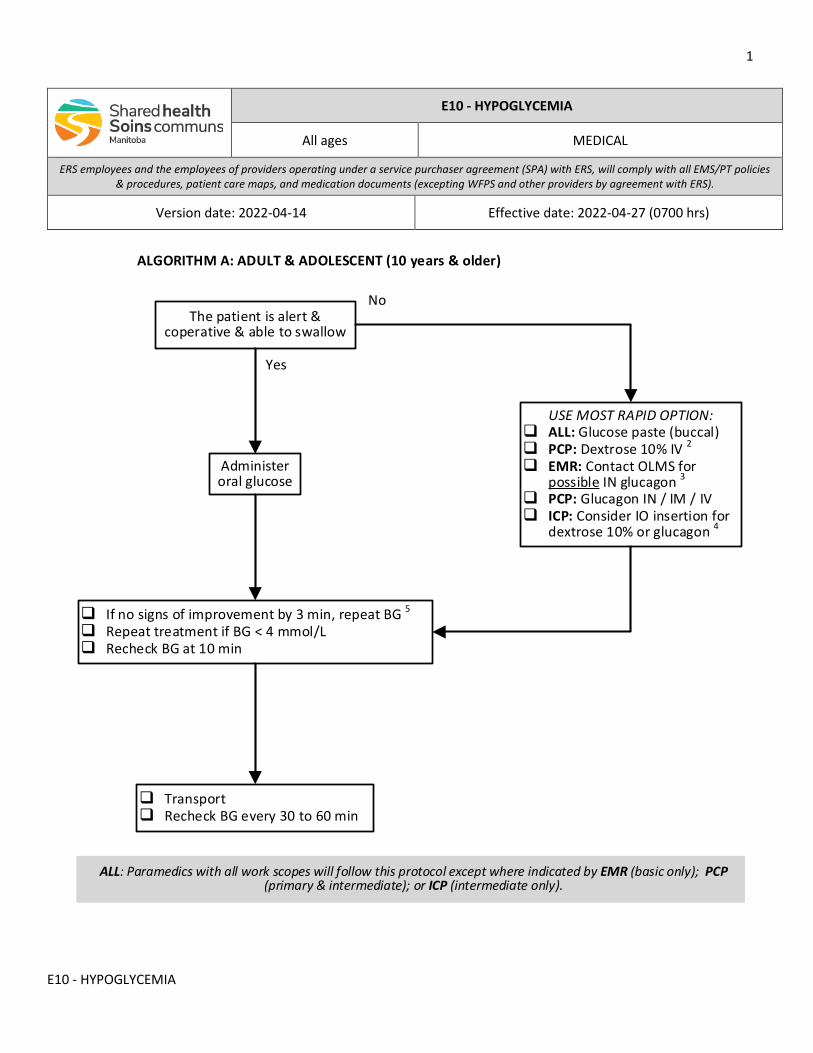
1
E10 - HYPOGLYCEMIA
The patient is alert & coperative & able to swallow
Yes
No
USE MOST RAPID OPTION: ALL: Glucose paste (buccal) PCP: Dextrose 10% IV 2
EMR: Contact OLMS for possible IN glucagon 3
PCP: Glucagon IN / IM / IV ICP: Consider IO insertion for
dextrose 10% or glucagon 4
Administer oral glucose
If no signs of improvement by 3 min, repeat BG 5
Repeat treatment if BG < 4 mmol/L Recheck BG at 10 min
Transport Recheck BG every 30 to 60 min
ALL: Paramedics with all work scopes will follow this protocol except where indicated by EMR (basic only); PCP (primary & intermediate); or ICP (intermediate only).
ALGORITHM A: ADULT & ADOLESCENT (10 years & older)
E10 - HYPOGLYCEMIA
All ages MEDICAL
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-14 Effective date: 2022-04-27 (0700 hrs)
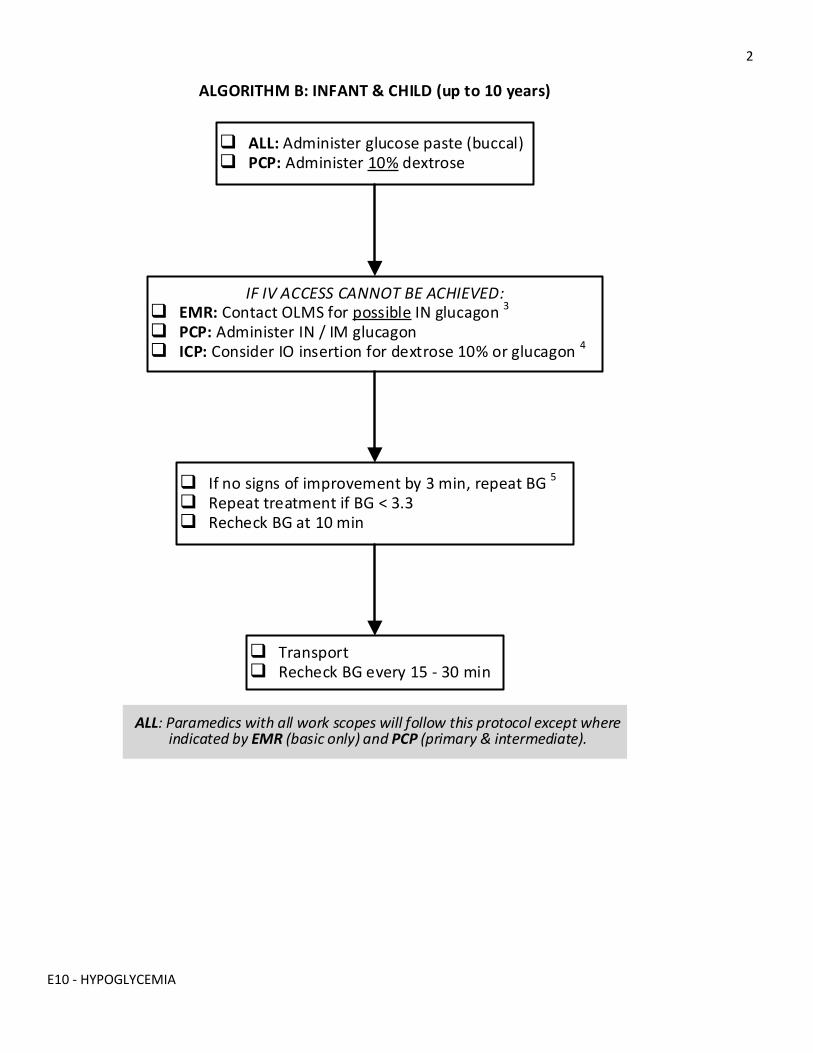
2
E10 - HYPOGLYCEMIA
ALL: Administer glucose paste (buccal) PCP: Administer 10% dextrose
If no signs of improvement by 3 min, repeat BG 5
Repeat treatment if BG < 3.3 Recheck BG at 10 min
IF IV ACCESS CANNOT BE ACHIEVED: EMR: Contact OLMS for possible IN glucagon 3
PCP: Administer IN / IM glucagon ICP: Consider IO insertion for dextrose 10% or glucagon 4
Transport Recheck BG every 15 - 30 min
ALL: Paramedics with all work scopes will follow this protocol except where indicated by EMR (basic only) and PCP (primary & intermediate).
ALGORITHM B: INFANT & CHILD (up to 10 years)
3
E10 - HYPOGLYCEMIA
INDICATIONS
• Confirmed hypoglycemia as indicated by a point-of-care blood glucose (BG) of: o Adult & adolescent (10 years & older) = 4.0 mmol/L or less o Child & infant (up to 10 years of age) = 3.3 mmol/L or less
• Suspected hypoglycemia when BG measurement is not readily available 1
CONTRAINDICATIONS
• Not applicable
NOTES
1. Due to the development of autonomic neuropathy with longstanding diabetes, some patients may no longer exhibit the neurogenic “warning symptoms” of hypoglycemia, and directly proceed to lethargy, confusion, decreased level of consciousness or seizures.
Symptoms in infants & preverbal children are frequently nonspecific and include irritability, lethargy, poor feeding, cyanosis and tremor or jitteriness. Commonly infants may not manifest any signs until they present with a hypoglycemic seizure.
2. When limited volume is required, use 50% dextrose in adults and adolescents only. DO NOT USE 25% OR 50% DEXTROSE IN INFANTS OR CHILDREN.
3. Paramedics with the basic scope of work must contact the on-line medical support (OLMS) physician before administering intranasal glucagon.
4. If no other treatment option is available, paramedics with the intermediate scope of work may establish an intraosseous (IO) device for correction of hypoglycemia.
5. After a prolonged period of hypoglycemia, a patient may require some time to return to their baseline cognitive level. However, there should be a prompt increase in their level of consciousness after administration of glucose or dextrose. If there are no signs of improvement by 3 minutes, repeat BG measurement. If BG measurement is not promptly available, repeat treatment.
6. Hypoglycemia in children may be an indication of sepsis or fasting. Evidence of starvation should raise the suspicion for child neglect or abuse.
LINKS
M06.1 – GLUCOSE M06.2 - DEXTROSE M06.3 – GLUCAGON
4
E10 - HYPOGLYCEMIA
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X05 for change tracking)
• Reformatted (replacement of coloured boxes with scope of work statement & icons) • Revised title & content
o Consolidation of adult, adolescent, and childcare maps into one document o Separate flow charts for adult / adolescent and child / infant o Revised BG lower limit for diagnosing infant & child hypoglycemia o Improved flow chart for enhanced ease of use o Use of 10% dextrose in adults & adolescents when volume is a concern
• Providers with basic work scope (EMR) must contact OLMS to administer IN glucagon
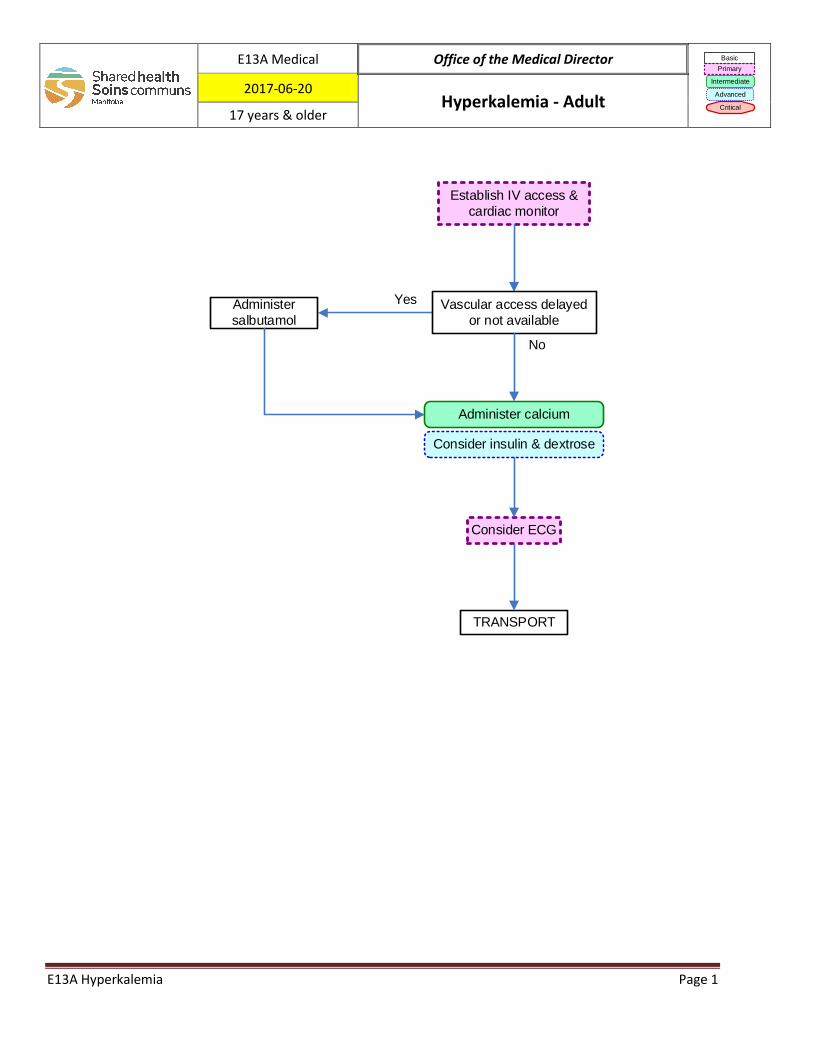
Establish IV access &
cardiac monitor
TRANSPORT
Administer
salbutamol
Administer calcium
Vascular access delayed
or not available
Consider ECG
Yes
No
Consider insulin & dextrose
E13A Medical Office of the Medical Director Basic
Primary
Intermediate
Advanced
Critical
2017-06-20 Hyperkalemia - Adult
17 years & older
E13A Hyperkalemia Page 1
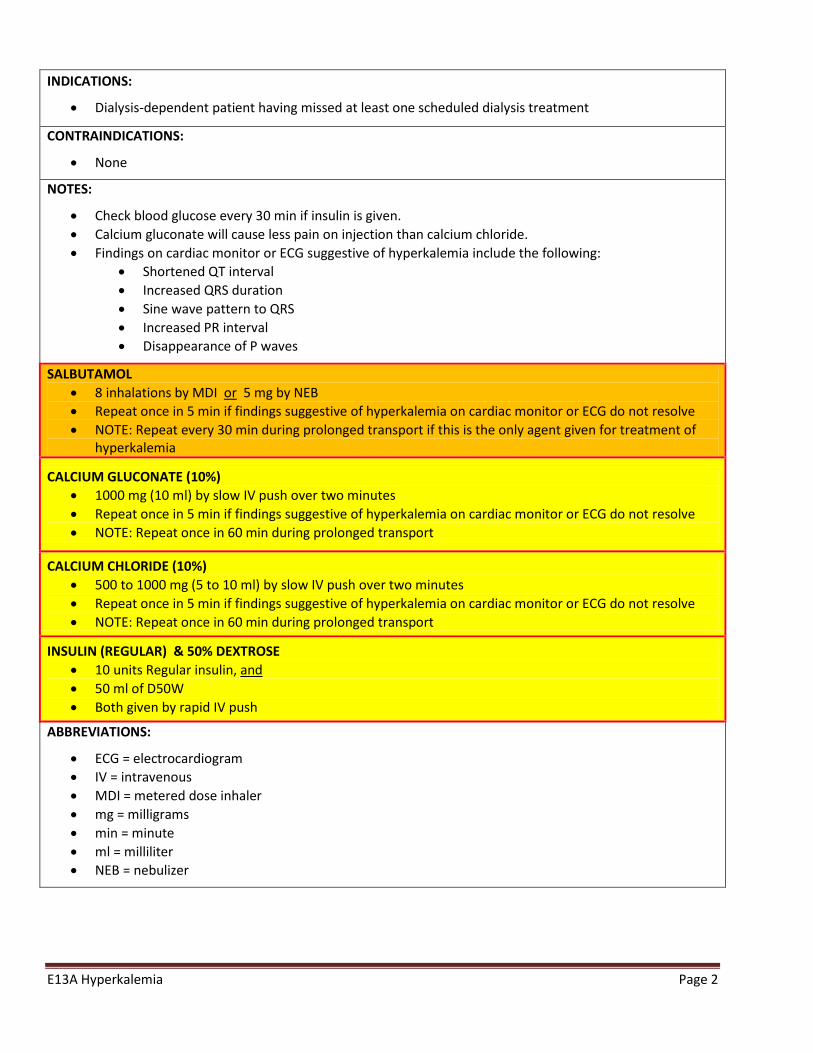
INDICATIONS:
• Dialysis-dependent patient having missed at least one scheduled dialysis treatment
CONTRAINDICATIONS:
• None
NOTES:
• Check blood glucose every 30 min if insulin is given. • Calcium gluconate will cause less pain on injection than calcium chloride. • Findings on cardiac monitor or ECG suggestive of hyperkalemia include the following:
• Shortened QT interval • Increased QRS duration • Sine wave pattern to QRS • Increased PR interval • Disappearance of P waves
SALBUTAMOL • 8 inhalations by MDI or 5 mg by NEB • Repeat once in 5 min if findings suggestive of hyperkalemia on cardiac monitor or ECG do not resolve • NOTE: Repeat every 30 min during prolonged transport if this is the only agent given for treatment of
hyperkalemia
CALCIUM GLUCONATE (10%) • 1000 mg (10 ml) by slow IV push over two minutes • Repeat once in 5 min if findings suggestive of hyperkalemia on cardiac monitor or ECG do not resolve • NOTE: Repeat once in 60 min during prolonged transport
CALCIUM CHLORIDE (10%) • 500 to 1000 mg (5 to 10 ml) by slow IV push over two minutes • Repeat once in 5 min if findings suggestive of hyperkalemia on cardiac monitor or ECG do not resolve • NOTE: Repeat once in 60 min during prolonged transport
INSULIN (REGULAR) & 50% DEXTROSE • 10 units Regular insulin, and • 50 ml of D50W • Both given by rapid IV push
ABBREVIATIONS:
• ECG = electrocardiogram • IV = intravenous • MDI = metered dose inhaler • mg = milligrams • min = minute • ml = milliliter • NEB = nebulizer
E13A Hyperkalemia Page 2
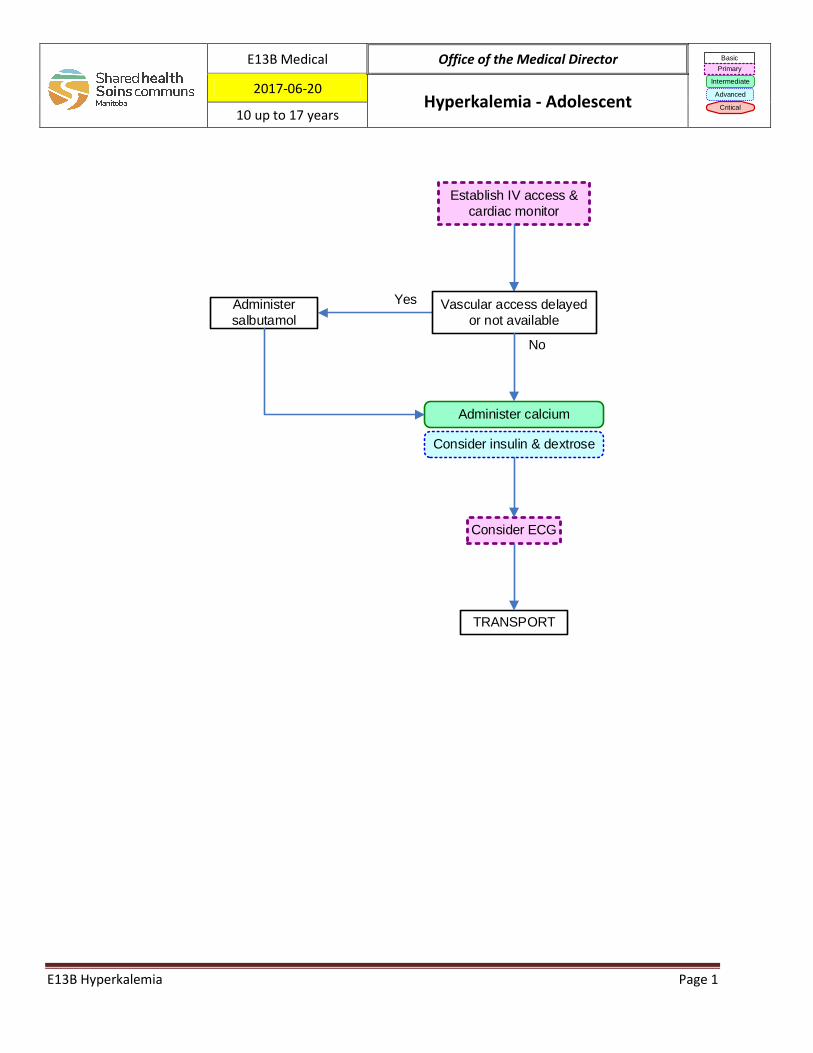
Establish IV access &
cardiac monitor
TRANSPORT
Administer
salbutamol
Administer calcium
Vascular access delayed
or not available
Consider ECG
Yes
No
Consider insulin & dextrose
E13B Medical Office of the Medical Director Basic
Primary
Intermediate
Advanced
Critical
2017-06-20 Hyperkalemia - Adolescent
10 up to 17 years
E13B Hyperkalemia Page 1
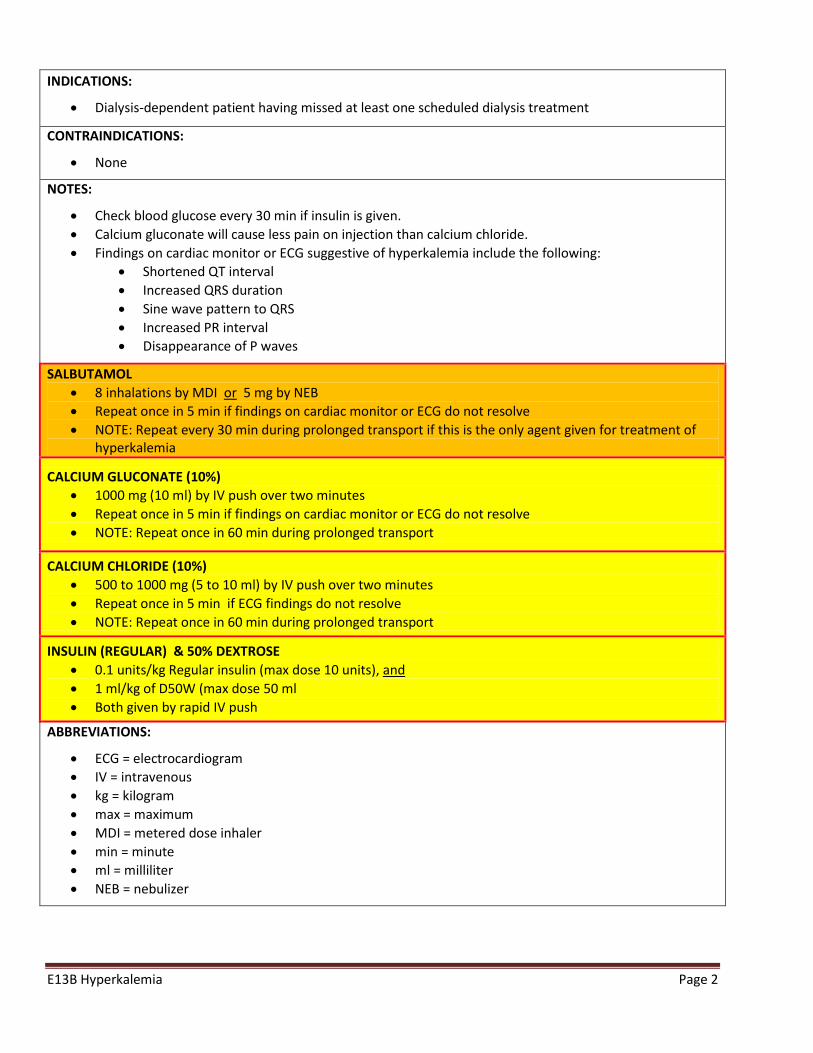
INDICATIONS:
• Dialysis-dependent patient having missed at least one scheduled dialysis treatment
CONTRAINDICATIONS:
• None
NOTES:
• Check blood glucose every 30 min if insulin is given. • Calcium gluconate will cause less pain on injection than calcium chloride. • Findings on cardiac monitor or ECG suggestive of hyperkalemia include the following:
• Shortened QT interval • Increased QRS duration • Sine wave pattern to QRS • Increased PR interval • Disappearance of P waves
SALBUTAMOL • 8 inhalations by MDI or 5 mg by NEB • Repeat once in 5 min if findings on cardiac monitor or ECG do not resolve • NOTE: Repeat every 30 min during prolonged transport if this is the only agent given for treatment of
hyperkalemia
CALCIUM GLUCONATE (10%) • 1000 mg (10 ml) by IV push over two minutes • Repeat once in 5 min if findings on cardiac monitor or ECG do not resolve • NOTE: Repeat once in 60 min during prolonged transport
CALCIUM CHLORIDE (10%) • 500 to 1000 mg (5 to 10 ml) by IV push over two minutes • Repeat once in 5 min if ECG findings do not resolve • NOTE: Repeat once in 60 min during prolonged transport
INSULIN (REGULAR) & 50% DEXTROSE • 0.1 units/kg Regular insulin (max dose 10 units), and • 1 ml/kg of D50W (max dose 50 ml • Both given by rapid IV push
ABBREVIATIONS:
• ECG = electrocardiogram • IV = intravenous • kg = kilogram • max = maximum • MDI = metered dose inhaler • min = minute • ml = milliliter • NEB = nebulizer
E13B Hyperkalemia Page 2
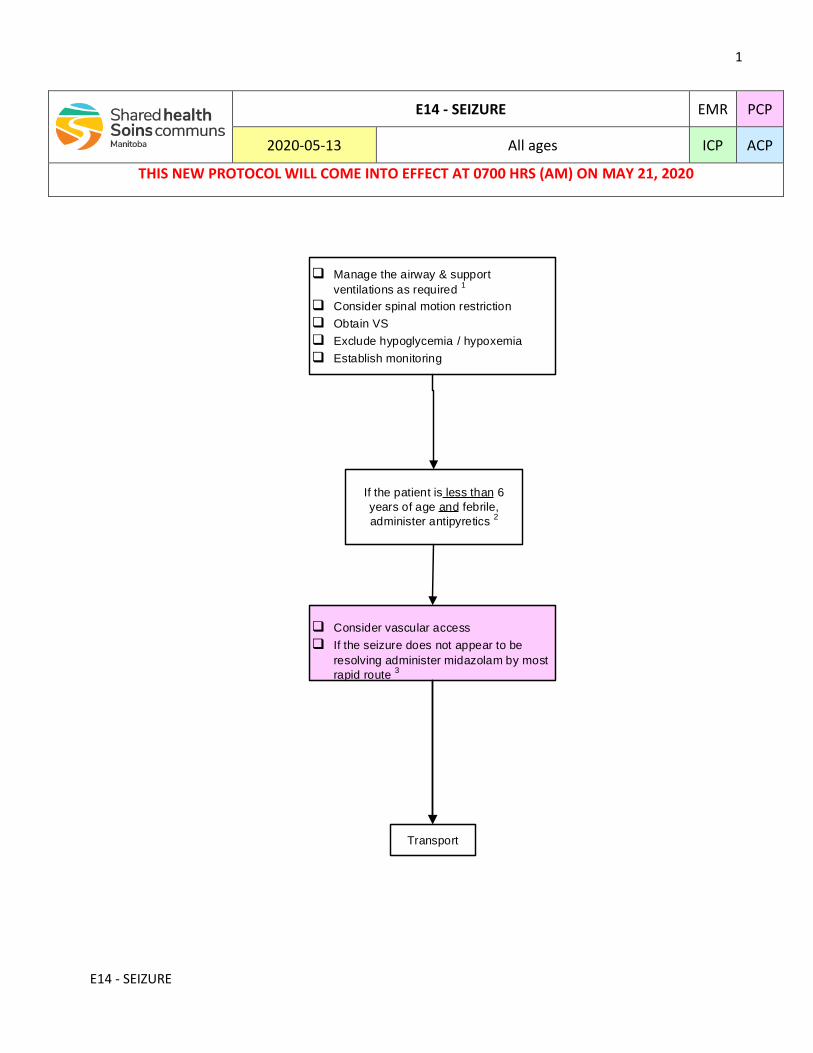
1
E14 - SEIZURE
q Manage the airway & support
ventilations as required 1
q Consider spinal motion restriction
q Obtain VS
q Exclude hypoglycemia / hypoxemia
q Establish monitoring
q Consider vascular access
q If the seizure does not appear to be
resolving administer midazolam by most
rapid route 3
Transport
If the patient is less than 6
years of age and febrile,
administer antipyretics 2
E14 - SEIZURE EMR PCP
2020-05-13 All ages ICP ACP
THIS NEW PROTOCOL WILL COME INTO EFFECT AT 0700 HRS (AM) ON MAY 21, 2020
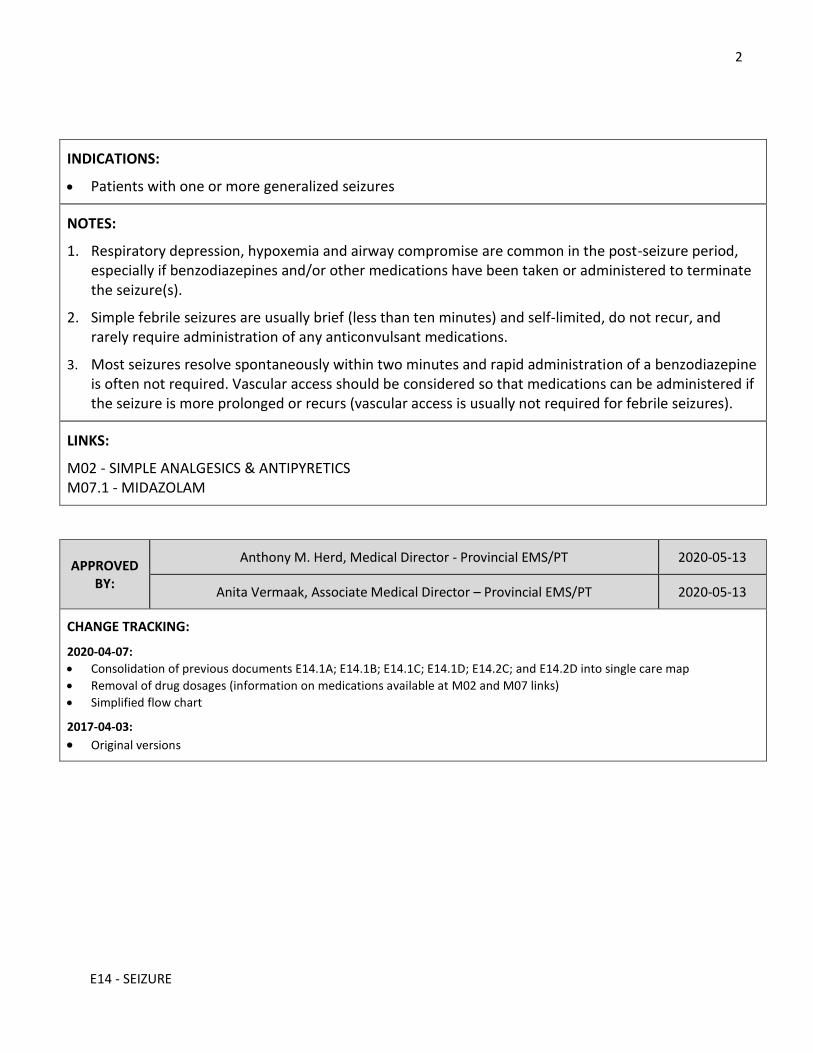
2
E14 - SEIZURE
INDICATIONS:
Patients with one or more generalized seizures
NOTES:
1. Respiratory depression, hypoxemia and airway compromise are common in the post-seizure period, especially if benzodiazepines and/or other medications have been taken or administered to terminate the seizure(s).
2. Simple febrile seizures are usually brief (less than ten minutes) and self-limited, do not recur, and rarely require administration of any anticonvulsant medications.
3. Most seizures resolve spontaneously within two minutes and rapid administration of a benzodiazepine is often not required. Vascular access should be considered so that medications can be administered if the seizure is more prolonged or recurs (vascular access is usually not required for febrile seizures).
LINKS:
M02 - SIMPLE ANALGESICS & ANTIPYRETICS M07.1 - MIDAZOLAM
APPROVED BY:
Anthony M. Herd, Medical Director - Provincial EMS/PT 2020-05-13
Anita Vermaak, Associate Medical Director – Provincial EMS/PT 2020-05-13
CHANGE TRACKING:
2020-04-07:
Consolidation of previous documents E14.1A; E14.1B; E14.1C; E14.1D; E14.2C; and E14.2D into single care map
Removal of drug dosages (information on medications available at M02 and M07 links)
Simplified flow chart
2017-04-03:
Original versions
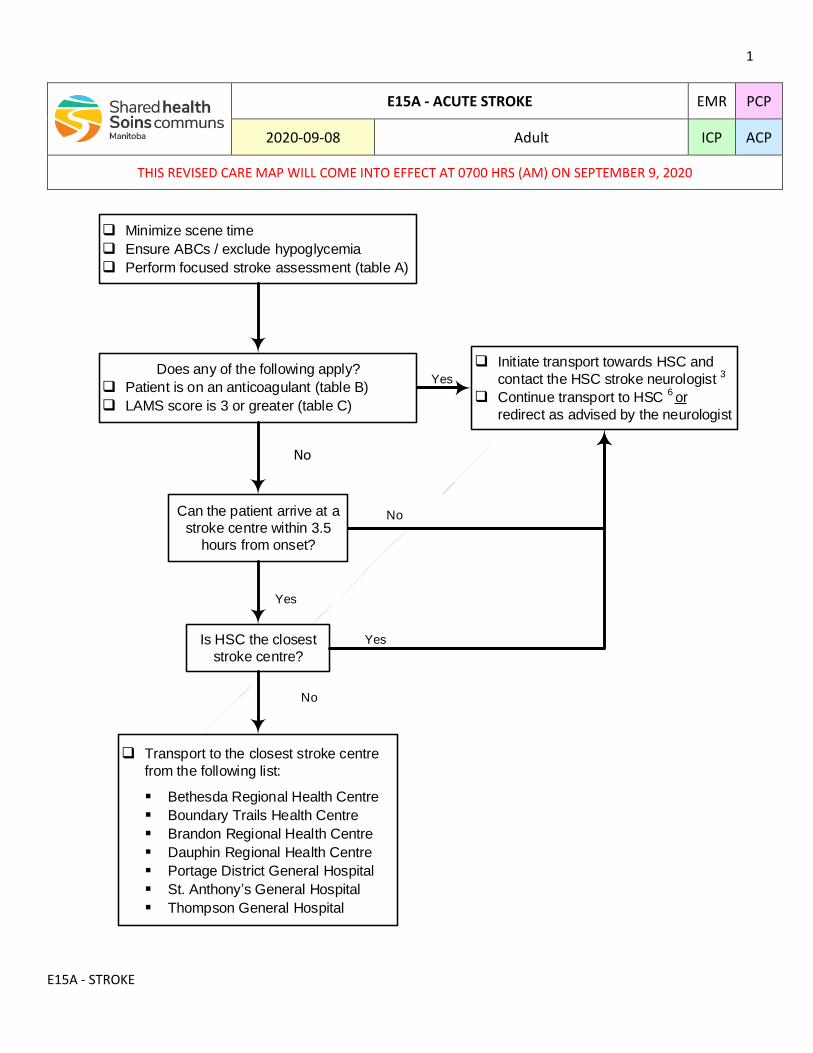
1
E15A - STROKE
E15A - ACUTE STROKE EMR PCP
2020-09-08 Adult ICP ACP
THIS REVISED CARE MAP WILL COME INTO EFFECT AT 0700 HRS (AM) ON SEPTEMBER 9, 2020
q Minimize scene time
q Ensure ABCs / exclude hypoglycemia
q Perform focused stroke assessment (table A)
Does any of the following apply?
q Patient is on an anticoagulant (table B)
q LAMS score is 3 or greater (table C)
q Initiate transport towards HSC and
contact the HSC stroke neurologist 3
q Continue transport to HSC 6 or
redirect as advised by the neurologist
Yes
Can the patient arrive at a
stroke centre within 3.5
hours from onset?
No
Yes
q Transport to the closest stroke centre
from the following list:
Bethesda Regional Health Centre
Boundary Trails Health Centre
Brandon Regional Health Centre
Dauphin Regional Health Centre
Portage District General Hospital
St. Anthony s General Hospital
Thompson General Hospital
Is HSC the closest
stroke centre?
Yes
No
No
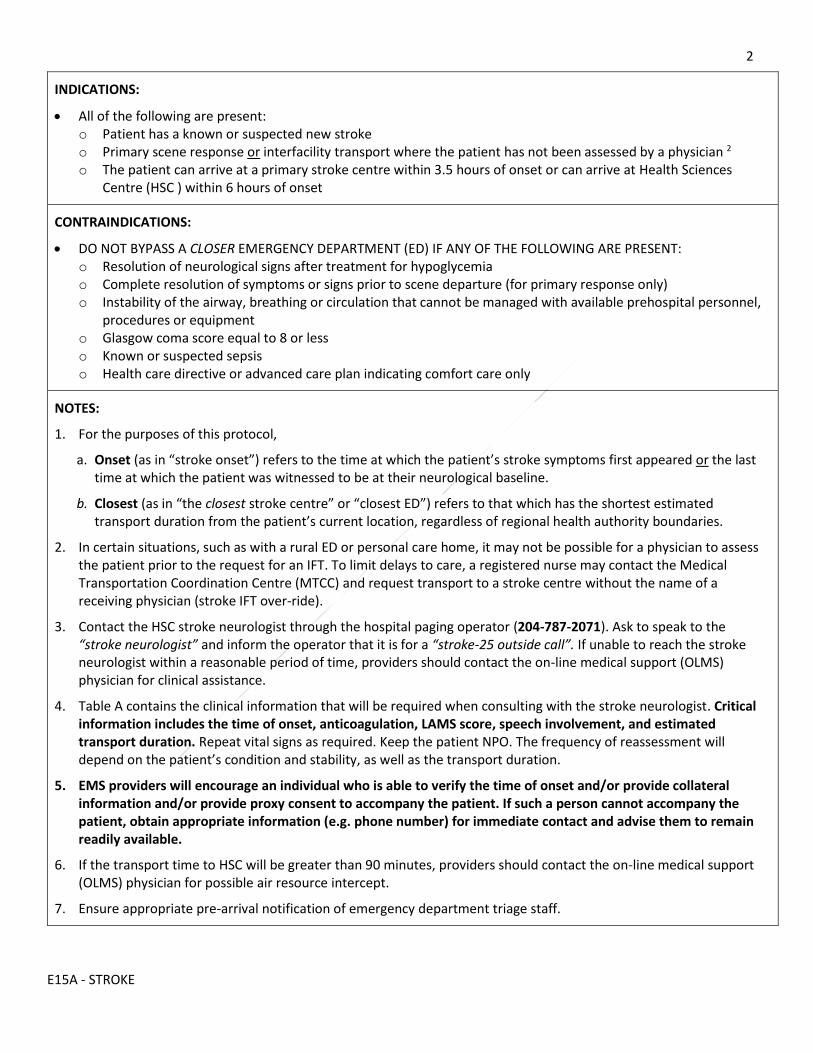
2
E15A - STROKE
INDICATIONS:
All of the following are present: o Patient has a known or suspected new stroke o Primary scene response or interfacility transport where the patient has not been assessed by a physician 2 o The patient can arrive at a primary stroke centre within 3.5 hours of onset or can arrive at Health Sciences
Centre (HSC ) within 6 hours of onset
CONTRAINDICATIONS:
DO NOT BYPASS A CLOSER EMERGENCY DEPARTMENT (ED) IF ANY OF THE FOLLOWING ARE PRESENT: o Resolution of neurological signs after treatment for hypoglycemia o Complete resolution of symptoms or signs prior to scene departure (for primary response only) o Instability of the airway, breathing or circulation that cannot be managed with available prehospital personnel,
procedures or equipment o Glasgow coma score equal to 8 or less o Known or suspected sepsis o Health care directive or advanced care plan indicating comfort care only
NOTES:
1. For the purposes of this protocol,
a. Onset (as in “stroke onset”) refers to the time at which the patient’s stroke symptoms first appeared or the last time at which the patient was witnessed to be at their neurological baseline.
b. Closest (as in “the closest stroke centre” or “closest ED”) refers to that which has the shortest estimated transport duration from the patient’s current location, regardless of regional health authority boundaries.
2. In certain situations, such as with a rural ED or personal care home, it may not be possible for a physician to assess the patient prior to the request for an IFT. To limit delays to care, a registered nurse may contact the Medical Transportation Coordination Centre (MTCC) and request transport to a stroke centre without the name of a receiving physician (stroke IFT over-ride).
3. Contact the HSC stroke neurologist through the hospital paging operator (204-787-2071). Ask to speak to the “stroke neurologist” and inform the operator that it is for a “stroke-25 outside call”. If unable to reach the stroke neurologist within a reasonable period of time, providers should contact the on-line medical support (OLMS) physician for clinical assistance.
4. Table A contains the clinical information that will be required when consulting with the stroke neurologist. Critical information includes the time of onset, anticoagulation, LAMS score, speech involvement, and estimated transport duration. Repeat vital signs as required. Keep the patient NPO. The frequency of reassessment will depend on the patient’s condition and stability, as well as the transport duration.
5. EMS providers will encourage an individual who is able to verify the time of onset and/or provide collateral information and/or provide proxy consent to accompany the patient. If such a person cannot accompany the patient, obtain appropriate information (e.g. phone number) for immediate contact and advise them to remain readily available.
6. If the transport time to HSC will be greater than 90 minutes, providers should contact the on-line medical support (OLMS) physician for possible air resource intercept.
7. Ensure appropriate pre-arrival notification of emergency department triage staff.
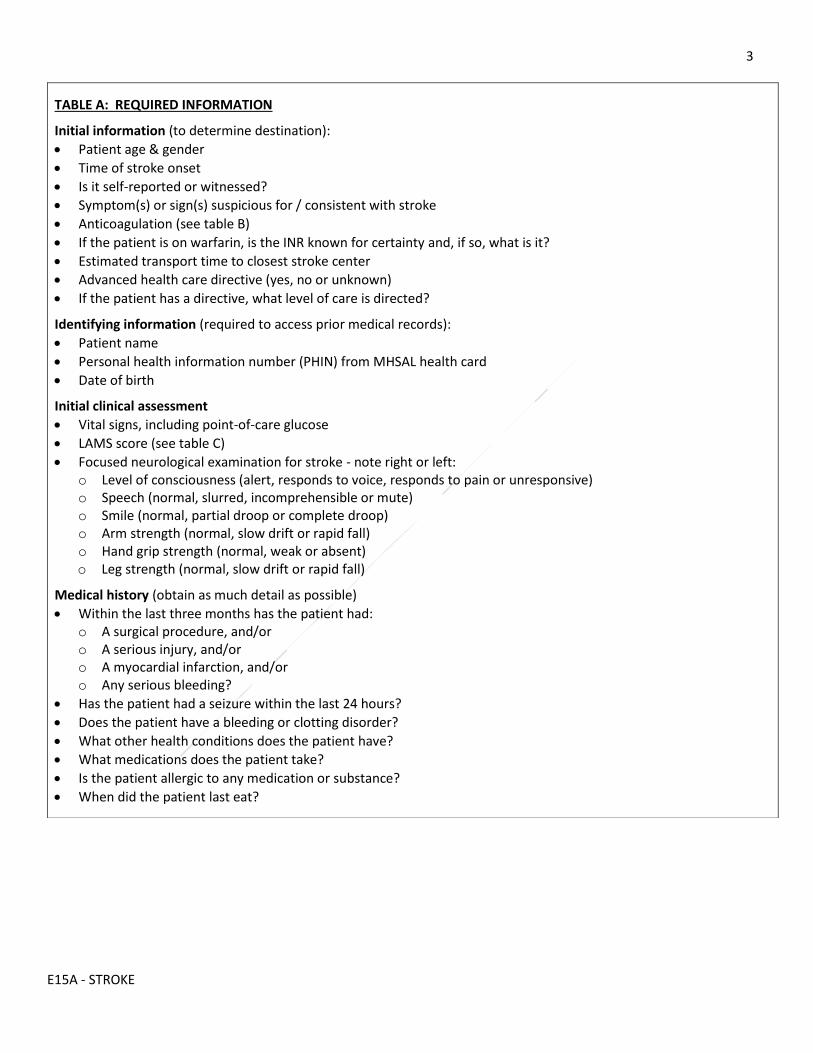
3
E15A - STROKE
TABLE A: REQUIRED INFORMATION
Initial information (to determine destination):
Patient age & gender
Time of stroke onset
Is it self-reported or witnessed?
Symptom(s) or sign(s) suspicious for / consistent with stroke
Anticoagulation (see table B)
If the patient is on warfarin, is the INR known for certainty and, if so, what is it?
Estimated transport time to closest stroke center
Advanced health care directive (yes, no or unknown)
If the patient has a directive, what level of care is directed?
Identifying information (required to access prior medical records):
Patient name
Personal health information number (PHIN) from MHSAL health card
Date of birth
Initial clinical assessment
Vital signs, including point-of-care glucose
LAMS score (see table C)
Focused neurological examination for stroke - note right or left: o Level of consciousness (alert, responds to voice, responds to pain or unresponsive) o Speech (normal, slurred, incomprehensible or mute) o Smile (normal, partial droop or complete droop) o Arm strength (normal, slow drift or rapid fall) o Hand grip strength (normal, weak or absent) o Leg strength (normal, slow drift or rapid fall)
Medical history (obtain as much detail as possible)
Within the last three months has the patient had: o A surgical procedure, and/or o A serious injury, and/or o A myocardial infarction, and/or o Any serious bleeding?
Has the patient had a seizure within the last 24 hours?
Does the patient have a bleeding or clotting disorder?
What other health conditions does the patient have?
What medications does the patient take?
Is the patient allergic to any medication or substance?
When did the patient last eat?
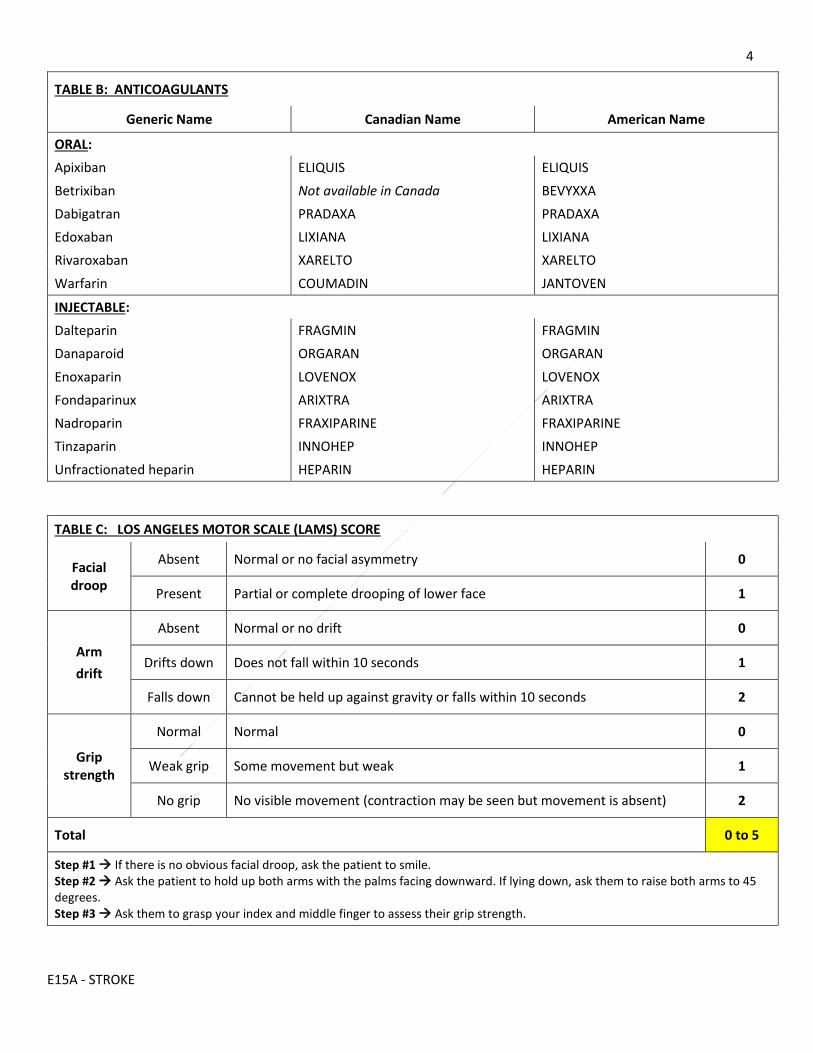
4
E15A - STROKE
TABLE B: ANTICOAGULANTS
Generic Name Canadian Name American Name
ORAL:
Apixiban ELIQUIS ELIQUIS
Betrixiban Not available in Canada BEVYXXA
Dabigatran PRADAXA PRADAXA
Edoxaban LIXIANA LIXIANA
Rivaroxaban XARELTO XARELTO
Warfarin COUMADIN JANTOVEN
INJECTABLE:
Dalteparin FRAGMIN FRAGMIN
Danaparoid ORGARAN ORGARAN
Enoxaparin LOVENOX LOVENOX
Fondaparinux ARIXTRA ARIXTRA
Nadroparin FRAXIPARINE FRAXIPARINE
Tinzaparin INNOHEP INNOHEP
Unfractionated heparin HEPARIN HEPARIN
TABLE C: LOS ANGELES MOTOR SCALE (LAMS) SCORE
Facial droop
Absent Normal or no facial asymmetry 0
Present Partial or complete drooping of lower face 1
Arm
drift
Absent Normal or no drift 0
Drifts down Does not fall within 10 seconds 1
Falls down Cannot be held up against gravity or falls within 10 seconds 2
Grip strength
Normal Normal 0
Weak grip Some movement but weak 1
No grip No visible movement (contraction may be seen but movement is absent) 2
Total 0 to 5
Step #1 If there is no obvious facial droop, ask the patient to smile. Step #2 Ask the patient to hold up both arms with the palms facing downward. If lying down, ask them to raise both arms to 45 degrees. Step #3 Ask them to grasp your index and middle finger to assess their grip strength.
5
E15A - STROKE
APPROVED BY: Anthony M Herd, Medical Director - EMS/PT 2020-09-08
Anita Vermaak, Associate Medical Director – EMS/PT 2020-09-08
CHANGE TRACKING:
2020-09-08:
Removal of speech impairment as an indication to contact the HSC stroke neurologist 2020-08-24:
SBH removed as stroke centre
Addition of speech impairment as an indication to contact the HSC stroke neurologist
Addition of 90-minute marker to consider air intercept
Formatting / simplified flow chart
2019-09-16:
Shared Health interim release
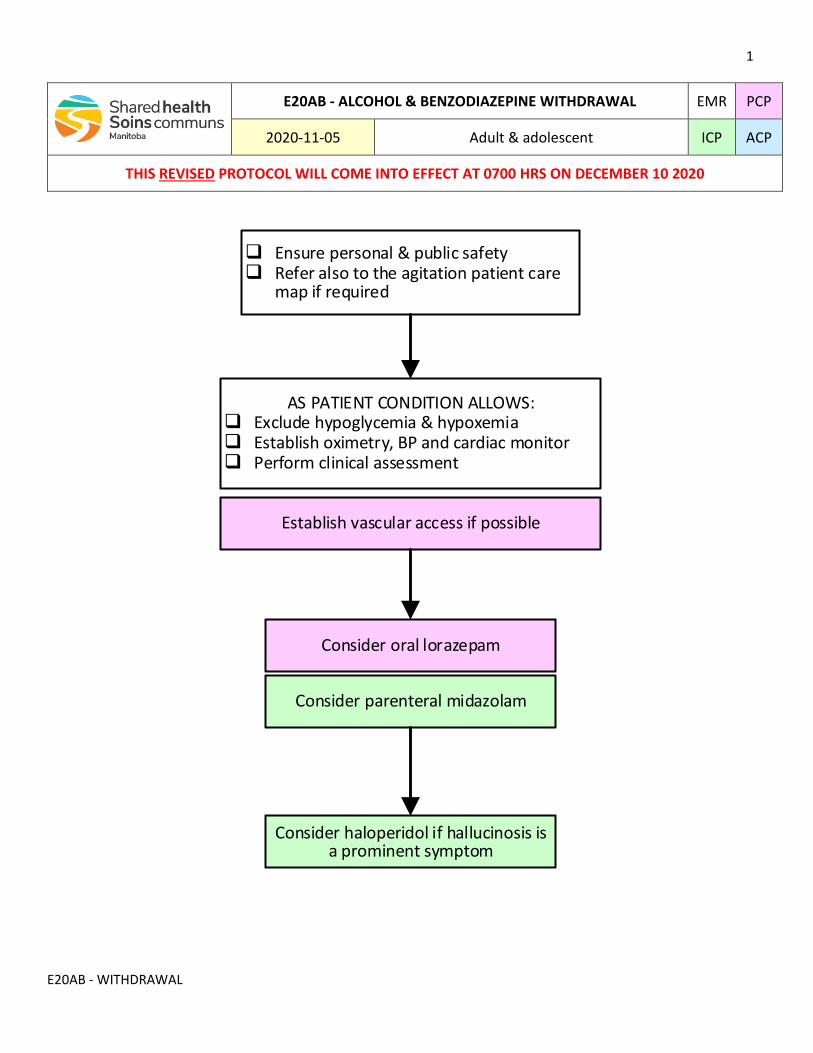
1
E20AB - WITHDRAWAL
E20AB - ALCOHOL & BENZODIAZEPINE WITHDRAWAL EMR PCP
2020-11-05 Adult & adolescent ICP ACP
THIS REVISED PROTOCOL WILL COME INTO EFFECT AT 0700 HRS ON DECEMBER 10 2020
q Ensure personal & public safetyq Refer also to the agitation patient care
map if required
AS PATIENT CONDITION ALLOWS:q Exclude hypoglycemia & hypoxemiaq Establish oximetry, BP and cardiac monitorq Perform clinical assessment
Consider oral lorazepam
Establish vascular access if possible
Consider parenteral midazolam
Consider haloperidol if hallucinosis is a prominent symptom
2
E20AB - WITHDRAWAL
INDICATIONS:
Known or suspected withdrawal from alcohol or benzodiazepine-type sedative-hypnotics
NOTES:
1. Patients who regularly consume large amounts of alcohol often have concomitant pathology. Always exclude hypoglycemia and hypoxemia.
2. Patients in withdrawal from alcohol or sedative-hypnotic agents can quickly progress to seizures and cardiovascular instability. Large doses of benzodiazepines may be required.
LINKS:
M07.1 - MIDAZOLAM M07.5 - LORAZEPAM M34 - HALOPERIDOL
APPROVED BY: Anthony M. Herd, Medical Director - Provincial EMS/PT 2020-11-26
Anita Vermaak, Associate Medical Director –EMS/PT 2020-11-27
CHANGE TRACKING:
2020-11-05:
Oral benzodiazepine changed to lorazepam
Revised indication
Simplified flow chart
Reformatting
Updated links
2017-06-19:
Original
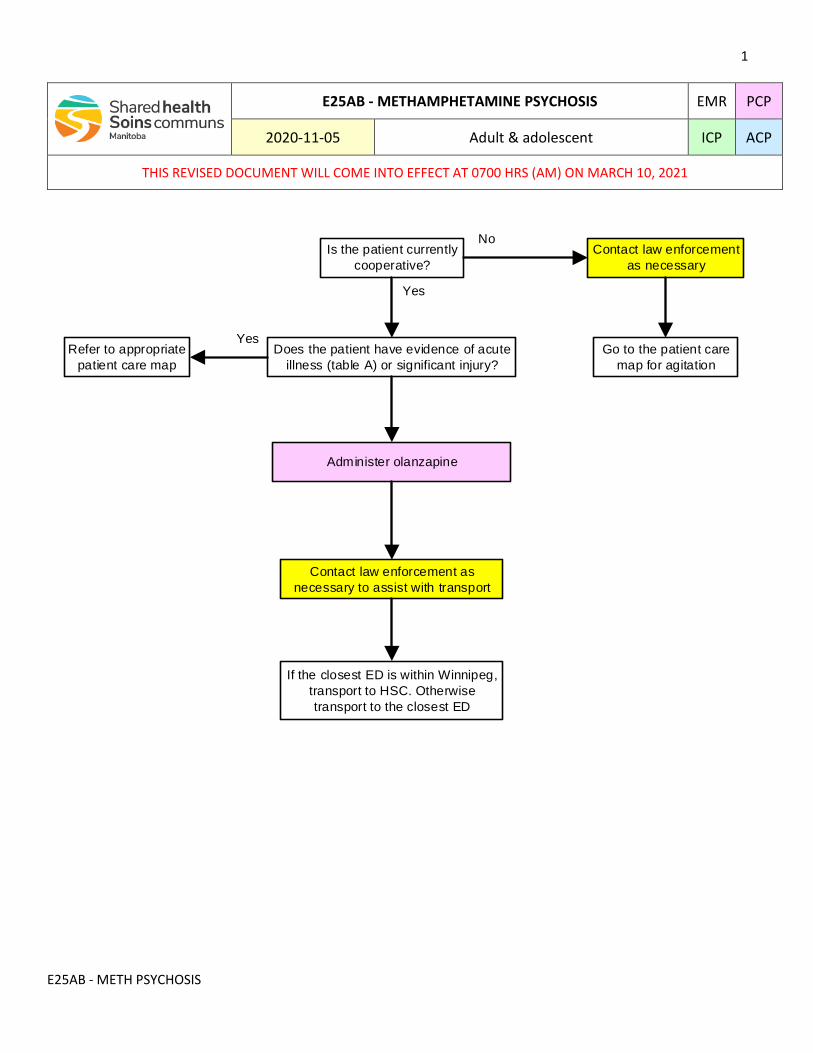
1
E25AB - METH PSYCHOSIS
E25AB - METHAMPHETAMINE PSYCHOSIS EMR PCP
2020-11-05 Adult & adolescent ICP ACP
THIS REVISED DOCUMENT WILL COME INTO EFFECT AT 0700 HRS (AM) ON MARCH 10, 2021
Is the patient currently
cooperative?
Does the patient have evidence of acute
illness (table A) or significant injury?
Administer olanzapine
If the closest ED is within Winnipeg,
transport to HSC. Otherwise
transport to the closest ED
Go to the patient care
map for agitation
Refer to appropriate
patient care map
Contact law enforcement as
necessary to assist with transport
Contact law enforcement
as necessary
Yes
No
Yes
2
E25AB - METH PSYCHOSIS
INDICATIONS:
Known or suspected amphetamine-type stimulant (eg. methamphetamine) psychosis.
CONTRAINDICATIONS:
Known or suspected acute illness or significant injury
NOTES:
1. Amphetamine-type stimulants can cause a psychosis in up to one-third of users. The predominant symptoms include paranoia, persecutory delusions and hallucinations. It can last for several days post-ingestion and can recur during periods of abstinence. In the case of methamphetamine, it may be accompanied by the rapid development of extreme paranoia, and violent behavior with enhanced physical strength.
2. Early administration of olanzapine may lessen the severity and duration of psychosis.
3. Findings of amphetamine-type stimulant ingestion include dilated pupils (mydriasis), sympathetic nervous system hyperactivity (fever, tachycardia and hypertension) and psychomotor agitation (including pacing and excessive talking).
4. The onset of psychosis is suggested by increased restlessness and agitation, disorientation, hallucinations (auditory, visual and/or tactile) and extreme paranoia.
5. After the onset of the psychosis medication administration may be difficult. Without coercion, EMS providers will encourage appropriate patients to voluntarily take olanzapine.
6. Patients who have taken amphetamine-type stimulants, especially methamphetamine, may deteriorate rapidly with the development of high fever, extremely high blood pressure and seizures. Olanzapine may cause significant hypotension.
7. If the patient has received prehospital olanzapine, document appropriately and ensure receiving emergency department have been notified.
Table A: Symptoms or signs suggesting acute illness and contraindicating olanzapine administration.
Chest / abdominal / back pain
Dyspnea
Headache / seizure / acute neurological deficit
Fever
LINKS:
E02AB - AGITATION M22 - OLANZEPINE
APPROVED BY: Anthony M. Herd, Medical Director – EMS/PT 2020-11-26
Anita Vermaak, Associate Medical Director –EMS/PT 2020-11-27
CHANGE TRACKING:
2020-11-05:
Retitled
Simplified flow chart
3
E25AB - METH PSYCHOSIS
Reformatting
2018-11-26:
Original version
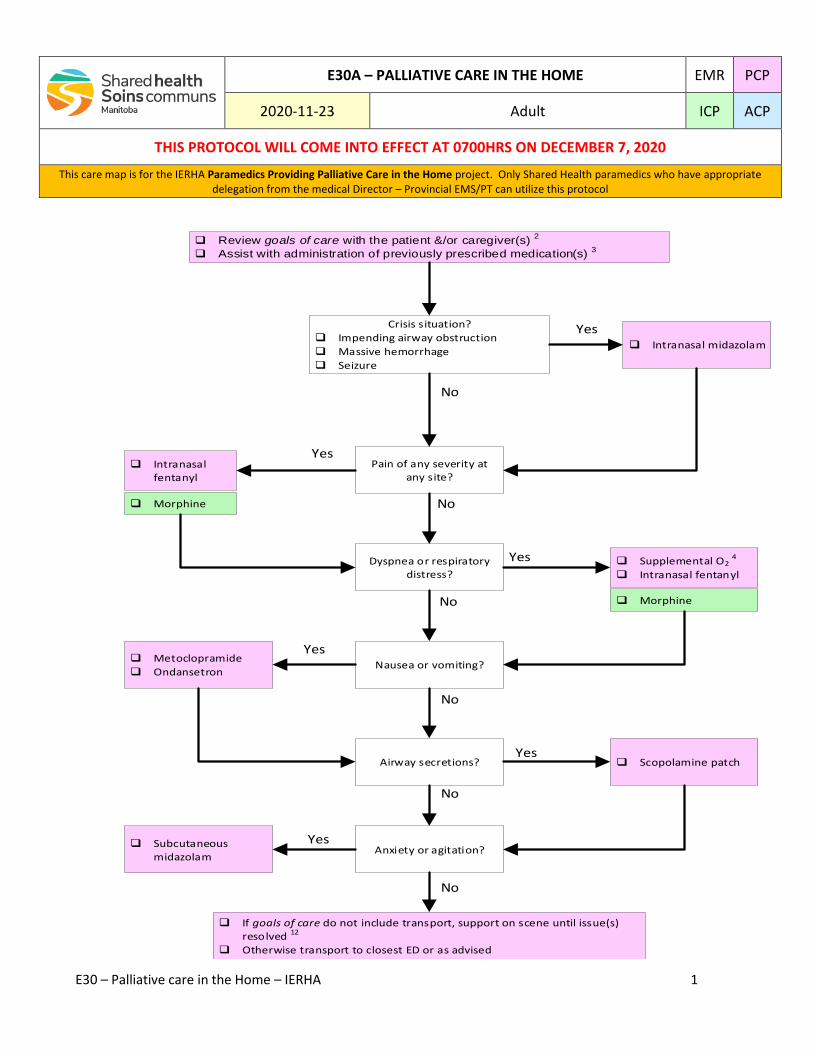
E30 – Palliative care in the Home – IERHA 1
E30A – PALLIATIVE CARE IN THE HOME EMR PCP
2020-11-23 Adult ICP ACP
THIS PROTOCOL WILL COME INTO EFFECT AT 0700HRS ON DECEMBER 7, 2020
This care map is for the IERHA Paramedics Providing Palliative Care in the Home project. Only Shared Health paramedics who have appropriate delegation from the medical Director – Provincial EMS/PT can utilize this protocol
q Review goals of care with the patient &/or caregiver(s) 2
q Assist with administration of previously prescribed medication(s) 3
Crisis situation?
q Impending airway obstruction
q Massive hemorrhage
q Seizure
Pain of any severity at any site?
Dyspnea or respiratory distress?
Nausea or vomiting?
Airway secretions?
Anxiety or agitation?
q If goals of care do not include transport, support on scene until issue(s) resolved 12
q Otherwise transport to closest ED or as advised
q Intranasal midazolam
q Intranasal fentanyl
q Morphine
q Supplemental O2 4
q Intranasal fentanyl
q Morphine
q Metoclopramide
q Ondansetron
q Subcutaneous midazolam
q Scopolamine patch
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
No
Yes
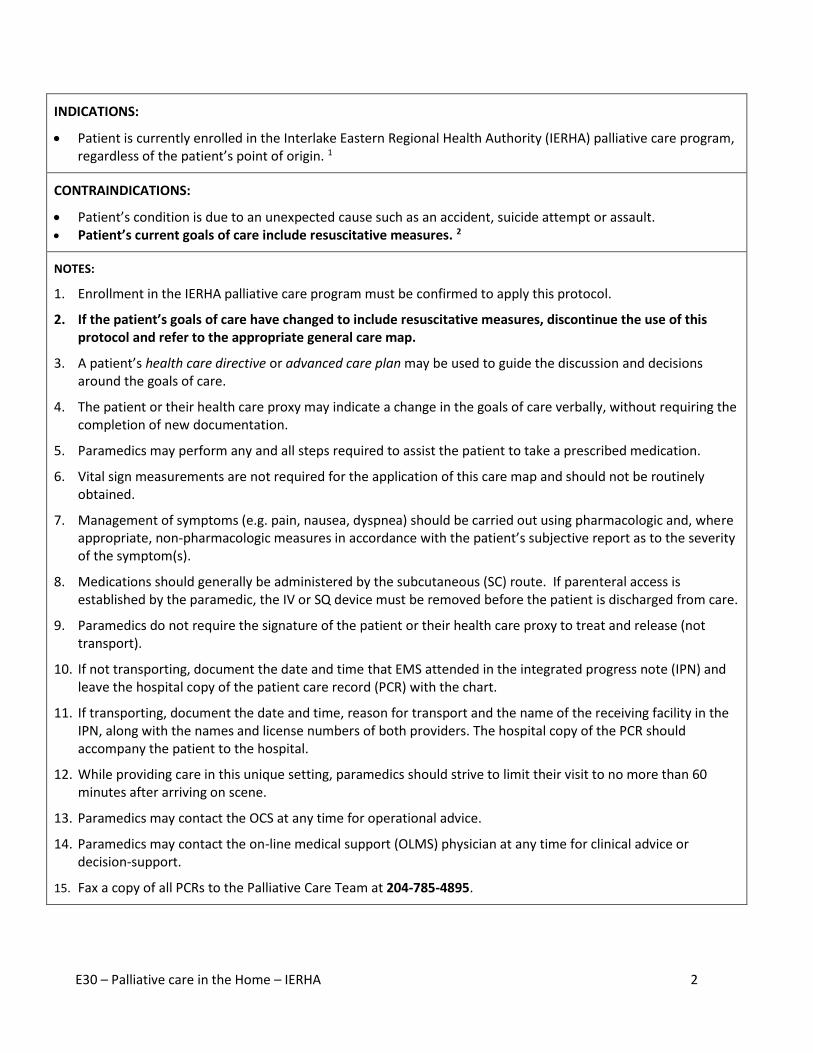
E30 – Palliative care in the Home – IERHA 2
INDICATIONS:
Patient is currently enrolled in the Interlake Eastern Regional Health Authority (IERHA) palliative care program,
regardless of the patient’s point of origin. 1
CONTRAINDICATIONS:
Patient’s condition is due to an unexpected cause such as an accident, suicide attempt or assault. Patient’s current goals of care include resuscitative measures. 2
NOTES:
1. Enrollment in the IERHA palliative care program must be confirmed to apply this protocol.
2. If the patient’s goals of care have changed to include resuscitative measures, discontinue the use of this protocol and refer to the appropriate general care map.
3. A patient’s health care directive or advanced care plan may be used to guide the discussion and decisions around the goals of care.
4. The patient or their health care proxy may indicate a change in the goals of care verbally, without requiring the completion of new documentation.
5. Paramedics may perform any and all steps required to assist the patient to take a prescribed medication.
6. Vital sign measurements are not required for the application of this care map and should not be routinely obtained.
7. Management of symptoms (e.g. pain, nausea, dyspnea) should be carried out using pharmacologic and, where appropriate, non-pharmacologic measures in accordance with the patient’s subjective report as to the severity of the symptom(s).
8. Medications should generally be administered by the subcutaneous (SC) route. If parenteral access is established by the paramedic, the IV or SQ device must be removed before the patient is discharged from care.
9. Paramedics do not require the signature of the patient or their health care proxy to treat and release (not transport).
10. If not transporting, document the date and time that EMS attended in the integrated progress note (IPN) and leave the hospital copy of the patient care record (PCR) with the chart.
11. If transporting, document the date and time, reason for transport and the name of the receiving facility in the IPN, along with the names and license numbers of both providers. The hospital copy of the PCR should accompany the patient to the hospital.
12. While providing care in this unique setting, paramedics should strive to limit their visit to no more than 60 minutes after arriving on scene.
13. Paramedics may contact the OCS at any time for operational advice.
14. Paramedics may contact the on-line medical support (OLMS) physician at any time for clinical advice or decision-support.
15. Fax a copy of all PCRs to the Palliative Care Team at 204-785-4895.
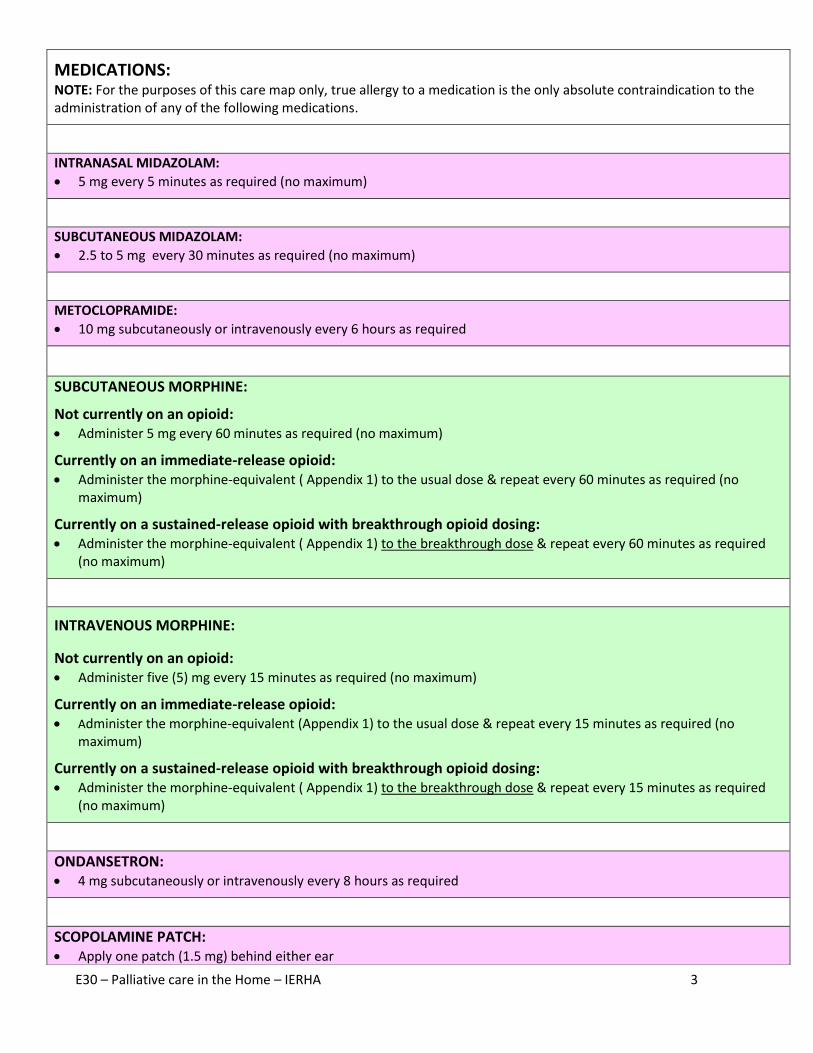
E30 – Palliative care in the Home – IERHA 3
MEDICATIONS: NOTE: For the purposes of this care map only, true allergy to a medication is the only absolute contraindication to the administration of any of the following medications.
INTRANASAL MIDAZOLAM:
5 mg every 5 minutes as required (no maximum)
SUBCUTANEOUS MIDAZOLAM:
2.5 to 5 mg every 30 minutes as required (no maximum)
METOCLOPRAMIDE:
10 mg subcutaneously or intravenously every 6 hours as required
SUBCUTANEOUS MORPHINE:
Not currently on an opioid: Administer 5 mg every 60 minutes as required (no maximum)
Currently on an immediate-release opioid: Administer the morphine-equivalent ( Appendix 1) to the usual dose & repeat every 60 minutes as required (no
maximum)
Currently on a sustained-release opioid with breakthrough opioid dosing: Administer the morphine-equivalent ( Appendix 1) to the breakthrough dose & repeat every 60 minutes as required
(no maximum)
INTRAVENOUS MORPHINE:
Not currently on an opioid: Administer five (5) mg every 15 minutes as required (no maximum)
Currently on an immediate-release opioid: Administer the morphine-equivalent (Appendix 1) to the usual dose & repeat every 15 minutes as required (no
maximum)
Currently on a sustained-release opioid with breakthrough opioid dosing: Administer the morphine-equivalent ( Appendix 1) to the breakthrough dose & repeat every 15 minutes as required
(no maximum)
ONDANSETRON: 4 mg subcutaneously or intravenously every 8 hours as required
SCOPOLAMINE PATCH: Apply one patch (1.5 mg) behind either ear
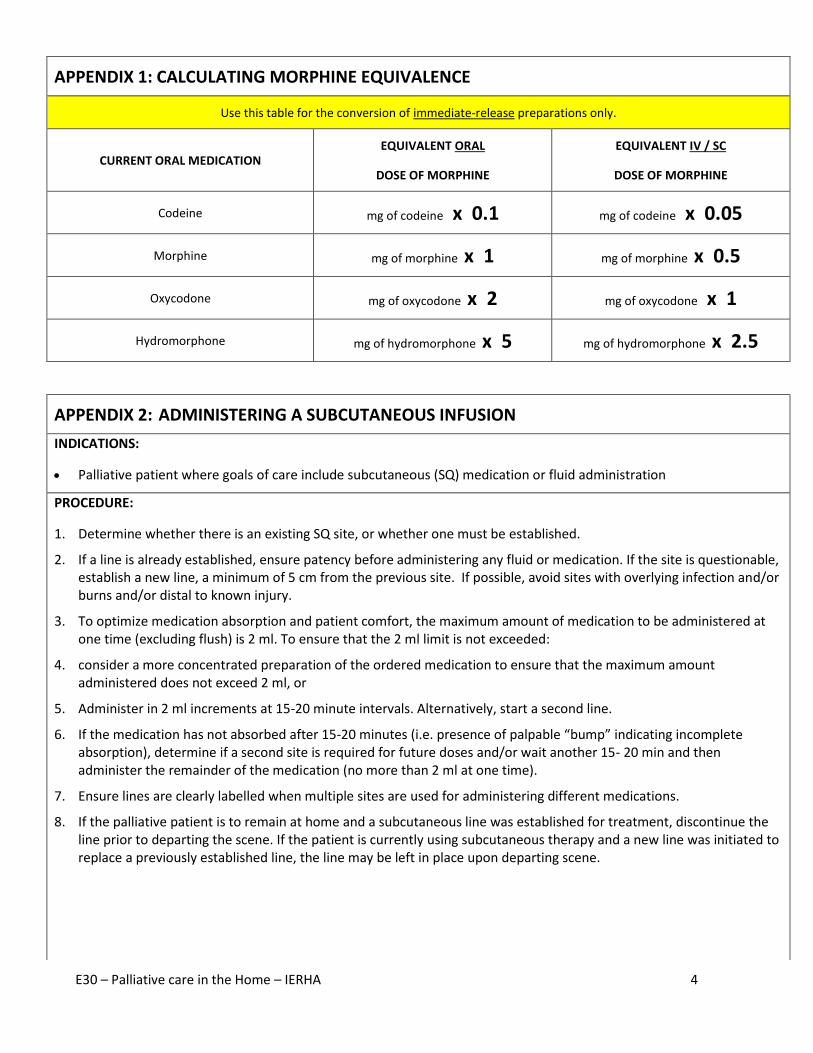
E30 – Palliative care in the Home – IERHA 4
APPENDIX 1: CALCULATING MORPHINE EQUIVALENCE
Use this table for the conversion of immediate-release preparations only.
CURRENT ORAL MEDICATION EQUIVALENT ORAL
DOSE OF MORPHINE
EQUIVALENT IV / SC
DOSE OF MORPHINE
Codeine mg of codeine x 0.1 mg of codeine x 0.05
Morphine mg of morphine x 1 mg of morphine x 0.5
Oxycodone mg of oxycodone x 2 mg of oxycodone x 1
Hydromorphone mg of hydromorphone x 5 mg of hydromorphone x 2.5
APPENDIX 2: ADMINISTERING A SUBCUTANEOUS INFUSION
INDICATIONS:
Palliative patient where goals of care include subcutaneous (SQ) medication or fluid administration
PROCEDURE:
1. Determine whether there is an existing SQ site, or whether one must be established.
2. If a line is already established, ensure patency before administering any fluid or medication. If the site is questionable, establish a new line, a minimum of 5 cm from the previous site. If possible, avoid sites with overlying infection and/or burns and/or distal to known injury.
3. To optimize medication absorption and patient comfort, the maximum amount of medication to be administered at one time (excluding flush) is 2 ml. To ensure that the 2 ml limit is not exceeded:
4. consider a more concentrated preparation of the ordered medication to ensure that the maximum amount administered does not exceed 2 ml, or
5. Administer in 2 ml increments at 15-20 minute intervals. Alternatively, start a second line.
6. If the medication has not absorbed after 15-20 minutes (i.e. presence of palpable “bump” indicating incomplete absorption), determine if a second site is required for future doses and/or wait another 15- 20 min and then administer the remainder of the medication (no more than 2 ml at one time).
7. Ensure lines are clearly labelled when multiple sites are used for administering different medications.
8. If the palliative patient is to remain at home and a subcutaneous line was established for treatment, discontinue the line prior to departing the scene. If the patient is currently using subcutaneous therapy and a new line was initiated to replace a previously established line, the line may be left in place upon departing scene.
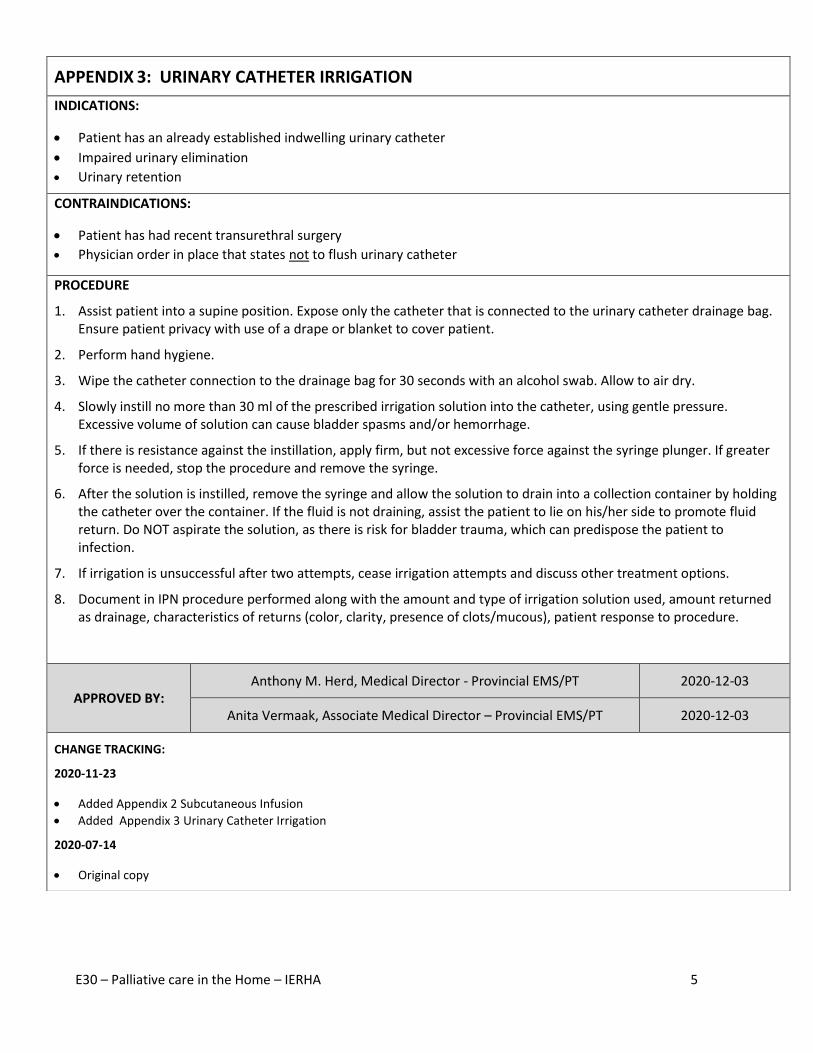
E30 – Palliative care in the Home – IERHA 5
APPENDIX 3: URINARY CATHETER IRRIGATION
INDICATIONS:
Patient has an already established indwelling urinary catheter
Impaired urinary elimination
Urinary retention
CONTRAINDICATIONS:
Patient has had recent transurethral surgery
Physician order in place that states not to flush urinary catheter
PROCEDURE
1. Assist patient into a supine position. Expose only the catheter that is connected to the urinary catheter drainage bag. Ensure patient privacy with use of a drape or blanket to cover patient.
2. Perform hand hygiene.
3. Wipe the catheter connection to the drainage bag for 30 seconds with an alcohol swab. Allow to air dry.
4. Slowly instill no more than 30 ml of the prescribed irrigation solution into the catheter, using gentle pressure. Excessive volume of solution can cause bladder spasms and/or hemorrhage.
5. If there is resistance against the instillation, apply firm, but not excessive force against the syringe plunger. If greater force is needed, stop the procedure and remove the syringe.
6. After the solution is instilled, remove the syringe and allow the solution to drain into a collection container by holding the catheter over the container. If the fluid is not draining, assist the patient to lie on his/her side to promote fluid return. Do NOT aspirate the solution, as there is risk for bladder trauma, which can predispose the patient to infection.
7. If irrigation is unsuccessful after two attempts, cease irrigation attempts and discuss other treatment options.
8. Document in IPN procedure performed along with the amount and type of irrigation solution used, amount returned as drainage, characteristics of returns (color, clarity, presence of clots/mucous), patient response to procedure.
APPROVED BY: Anthony M. Herd, Medical Director - Provincial EMS/PT 2020-12-03
Anita Vermaak, Associate Medical Director – Provincial EMS/PT 2020-12-03
CHANGE TRACKING:
2020-11-23
Added Appendix 2 Subcutaneous Infusion
Added Appendix 3 Urinary Catheter Irrigation
2020-07-14
Original copy
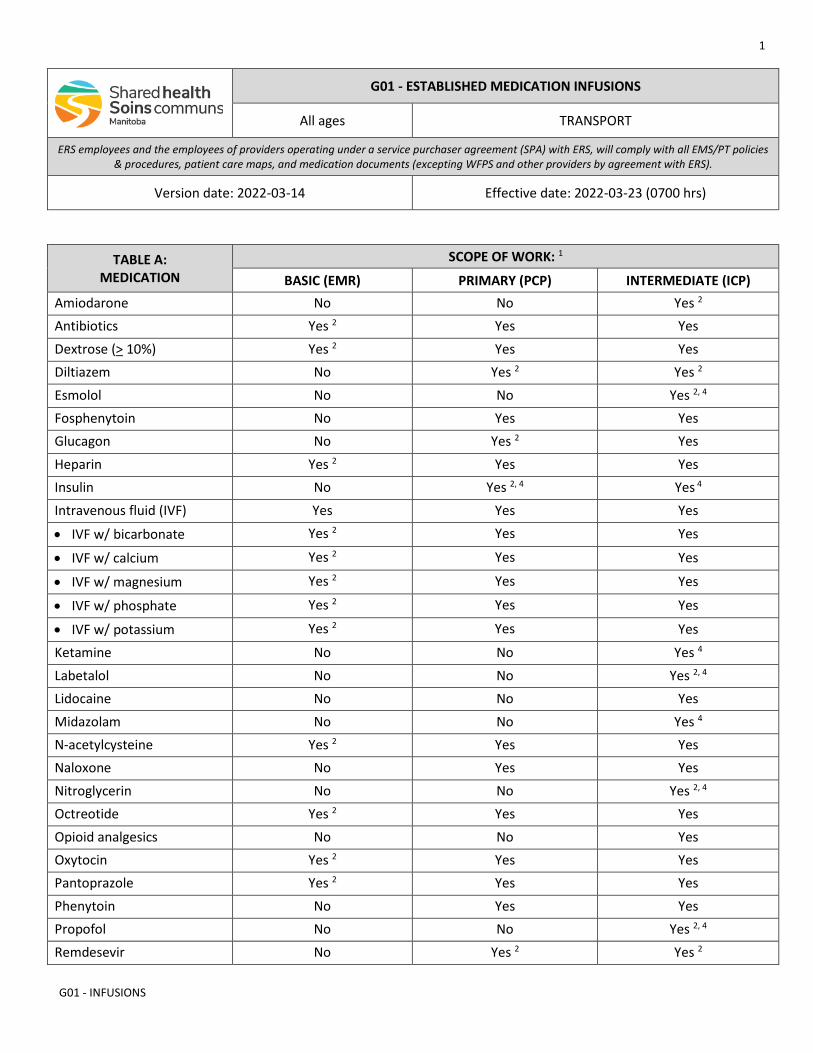
1
G01 - INFUSIONS
G01 - ESTABLISHED MEDICATION INFUSIONS
All ages TRANSPORT
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-14 Effective date: 2022-03-23 (0700 hrs)
TABLE A: MEDICATION
SCOPE OF WORK: 1
BASIC (EMR) PRIMARY (PCP) INTERMEDIATE (ICP) Amiodarone No No Yes 2 Antibiotics Yes 2 Yes Yes Dextrose (> 10%) Yes 2 Yes Yes Diltiazem No Yes 2 Yes 2 Esmolol No No Yes 2, 4 Fosphenytoin No Yes Yes Glucagon No Yes 2 Yes Heparin Yes 2 Yes Yes Insulin No Yes 2, 4 Yes 4 Intravenous fluid (IVF) Yes Yes Yes
• IVF w/ bicarbonate Yes 2 Yes Yes
• IVF w/ calcium Yes 2 Yes Yes
• IVF w/ magnesium Yes 2 Yes Yes
• IVF w/ phosphate Yes 2 Yes Yes
• IVF w/ potassium Yes 2 Yes Yes
Ketamine No No Yes 4 Labetalol No No Yes 2, 4 Lidocaine No No Yes Midazolam No No Yes 4 N-acetylcysteine Yes 2 Yes Yes Naloxone No Yes Yes Nitroglycerin No No Yes 2, 4 Octreotide Yes 2 Yes Yes Opioid analgesics No No Yes Oxytocin Yes 2 Yes Yes Pantoprazole Yes 2 Yes Yes Phenytoin No Yes Yes Propofol No No Yes 2, 4 Remdesevir No Yes 2 Yes 2
2
G01 - INFUSIONS
Tocilizumab No Yes 2 Yes 2
INDICATIONS
• Medication infusion(s) that is/are essential during the episode of care and have been initiated at the referring facility by a non-ERS health care provider (HCP) prior to transport.
CONTRAINDICATIONS
• Not applicable
NOTES
1. This document constitutes the standing order that enables the administration of the medications listed in table A. Additional medications may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02.1). Paramedics must always operate within their CPMB scope of practice. Table A defines the scopes of work for ERS paramedics and the paramedics employed by SPA providers.
2. Consult with the on-line medical support (OLMS) physician for these medications that are not within the usual ERS scopes of work or standard paramedic competencies.
3. A written order for the medication infusion from the ordering physician must accompany the patient and remain with the patient care record (PCR) after completion of the transfer. If telephone / radio orders are received during transport, these must be documented in the PCR, including the full name of the ordering physician.
4. For medications that may require titration, the written order must contain titration parameters.
5. A large volume infusion pump must be used for all infusions. Paramedics must also have sufficient knowledge of the specific infusion pump (including the ability to troubleshoot all alarms) to safely maintain the infusion.
6. Paramedics must ensure that they have sufficient quantities of medications to last the entire episode of care. If additional medication is required, it should be acquired from the sending facility.
7. Monitoring appropriate to the specific medication infusion and clinical case must be performed.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
3
G01 - INFUSIONS
VERSION CHANGES (refer to X07 for change tracking)
• Minor reformatting
1
G02 - SCHEDULED MEDICATIONS
G02 - SCHEDULED MEDICATIONS
All ages TRANSPORT
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-14 Effective date: 2022-03-23 (0700 hrs)
INDICATIONS
• Administration of scheduled oral 5 and parenteral 6 medications during interfacility transfer.
CONTRAINDICATIONS
• All contraindications must be addressed by the prescribing provider.
DOSING
• Dose, administration route, repeat dose and dosing interval will be established by the prescribing provider. 2
NOTES
1. Paramedics must always operate within their College of Paramedics of Manitoba (CPMB) scope of practice.
2. This document is not a standing order. A written order from the prescribing provider is required.
3. The written order constitutes a temporary increase in the EMS/PT scope of work for the duration of that patient encounter only.
4. Paramedics will not comply with an order that they know to be wrong, inaccurate, or illegible.
5. Parmedics with the basic (EMR), primary (PCP), & intermediate (ICP) work scopes may administer all scheduled oral medications.
6. Paramedics with the intermediate (ICP) work scope may initate and administer all scheduled parenteral medications.
7. The on-line medical support (OLMS) physician may be able to assist with interim order(s), if the prescribing provider cannot be reached.
2
G02 - SCHEDULED MEDICATIONS
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X07 for change tracking)
• Minor reformatting
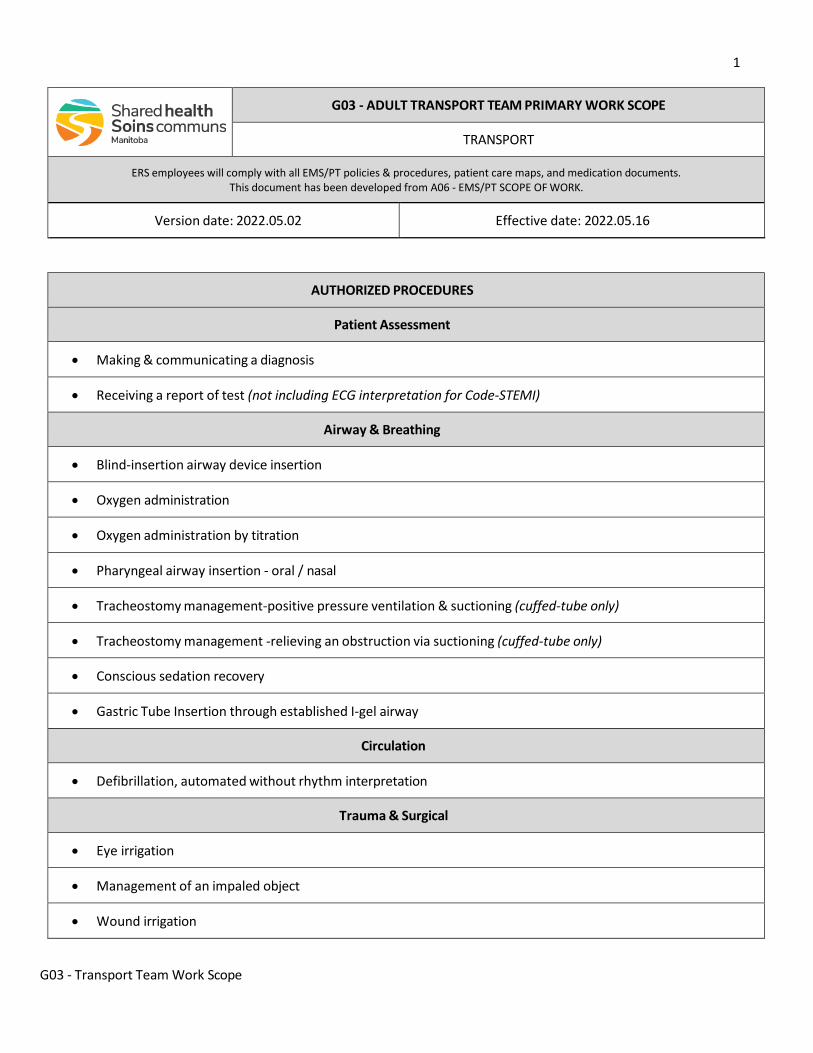
1
G03 - Transport Team Work Scope
G03 - ADULT TRANSPORT TEAM PRIMARY WORK SCOPE
TRANSPORT
ERS employees will comply with all EMS/PT policies & procedures, patient care maps, and medication documents. This document has been developed from A06 - EMS/PT SCOPE OF WORK.
Version date: 2022.05.02 Effective date: 2022.05.16
AUTHORIZED PROCEDURES
Patient Assessment
• Making & communicating a diagnosis
• Receiving a report of test (not including ECG interpretation for Code-STEMI)
Airway & Breathing
• Blind-insertion airway device insertion
• Oxygen administration
• Oxygen administration by titration
• Pharyngeal airway insertion - oral / nasal
• Tracheostomy management-positive pressure ventilation & suctioning (cuffed-tube only)
• Tracheostomy management -relieving an obstruction via suctioning (cuffed-tube only)
• Conscious sedation recovery
• Gastric Tube Insertion through established I-gel airway
Circulation
• Defibrillation, automated without rhythm interpretation
Trauma & Surgical
• Eye irrigation
• Management of an impaled object
• Wound irrigation
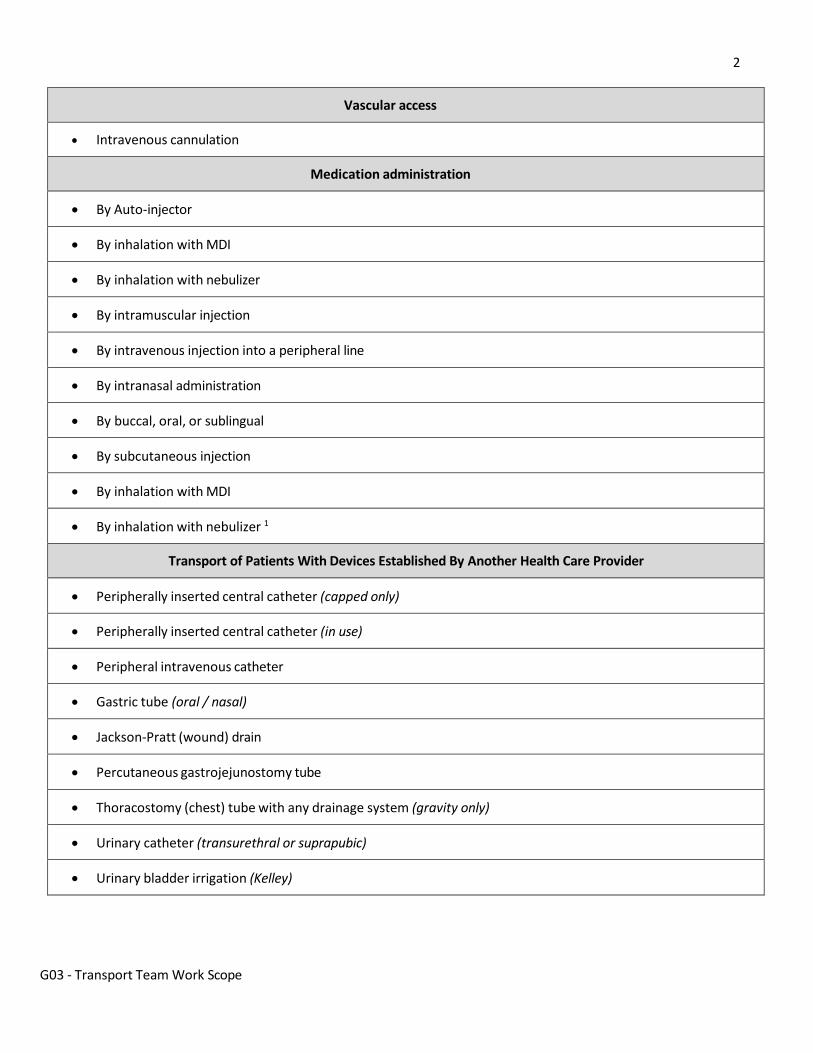
2
G03 - Transport Team Work Scope
Vascular access
• Intravenous cannulation
Medication administration
• By Auto-injector
• By inhalation with MDI
• By inhalation with nebulizer
• By intramuscular injection
• By intravenous injection into a peripheral line
• By intranasal administration
• By buccal, oral, or sublingual
• By subcutaneous injection
• By inhalation with MDI
• By inhalation with nebulizer 1
Transport of Patients With Devices Established By Another Health Care Provider
• Peripherally inserted central catheter (capped only)
• Peripherally inserted central catheter (in use)
• Peripheral intravenous catheter
• Gastric tube (oral / nasal)
• Jackson-Pratt (wound) drain
• Percutaneous gastrojejunostomy tube
• Thoracostomy (chest) tube with any drainage system (gravity only)
• Urinary catheter (transurethral or suprapubic)
• Urinary bladder irrigation (Kelley)
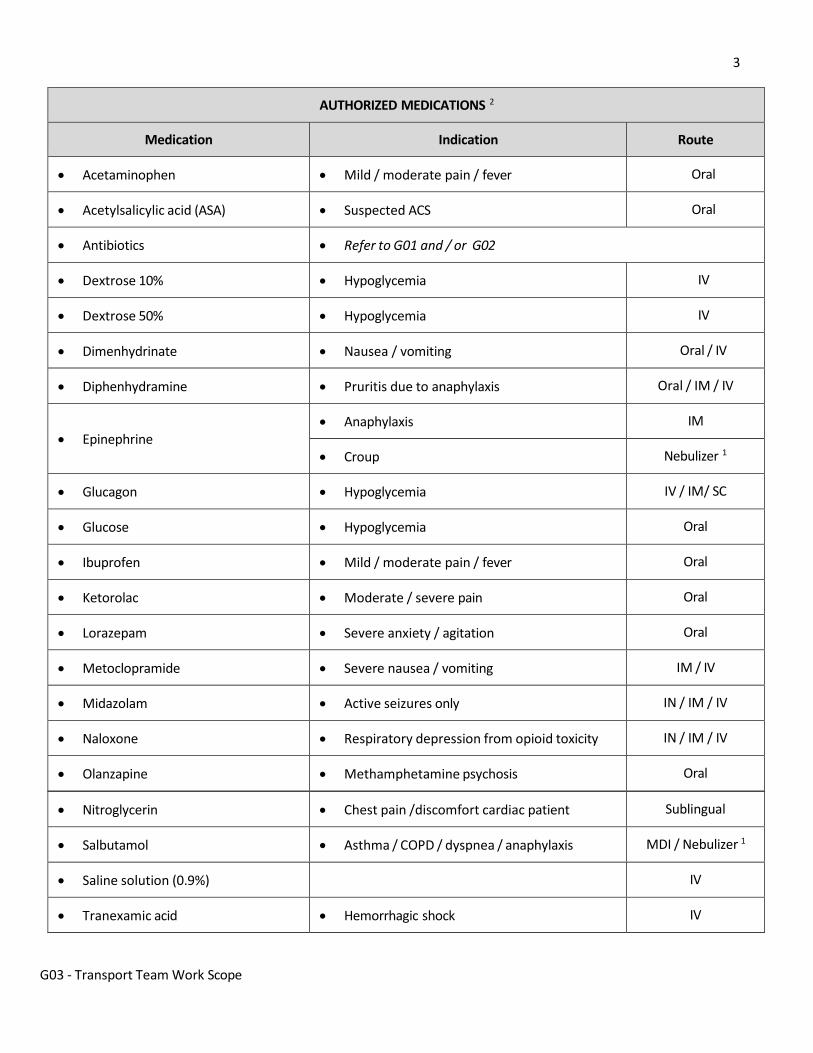
3
G03 - Transport Team Work Scope
AUTHORIZED MEDICATIONS 2
Medication Indication Route
• Acetaminophen • Mild / moderate pain / fever Oral
• Acetylsalicylic acid (ASA) • Suspected ACS Oral
• Antibiotics • Refer to G01 and / or G02
• Dextrose 10% • Hypoglycemia IV
• Dextrose 50% • Hypoglycemia IV
• Dimenhydrinate • Nausea / vomiting Oral / IV
• Diphenhydramine • Pruritis due to anaphylaxis Oral / IM / IV
• Epinephrine
• Anaphylaxis IM
• Croup Nebulizer 1
• Glucagon • Hypoglycemia IV / IM/ SC
• Glucose • Hypoglycemia Oral
• Ibuprofen • Mild / moderate pain / fever Oral
• Ketorolac • Moderate / severe pain Oral
• Lorazepam • Severe anxiety / agitation Oral
• Metoclopramide • Severe nausea / vomiting IM / IV
• Midazolam • Active seizures only IN / IM / IV
• Naloxone • Respiratory depression from opioid toxicity IN / IM / IV
• Olanzapine • Methamphetamine psychosis Oral
• Nitroglycerin • Chest pain /discomfort cardiac patient Sublingual
• Salbutamol • Asthma / COPD / dyspnea / anaphylaxis MDI / Nebulizer 1
• Saline solution (0.9%) IV
• Tranexamic acid • Hemorrhagic shock IV
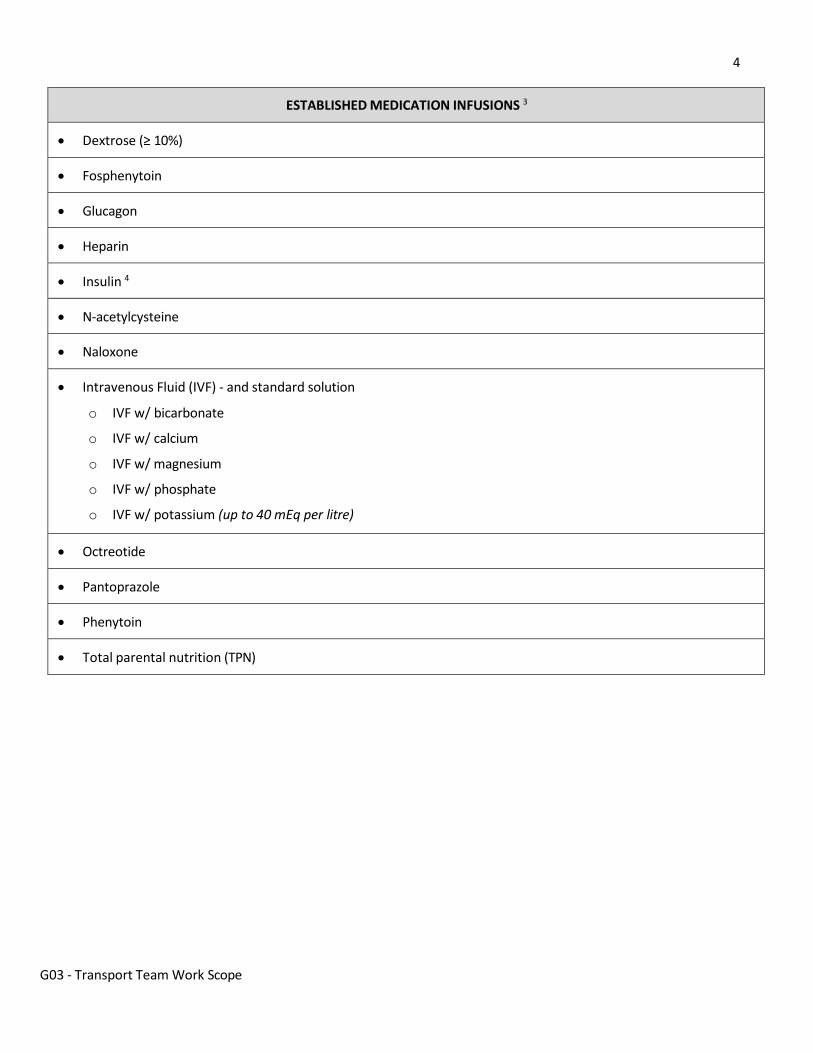
4
G03 - Transport Team Work Scope
ESTABLISHED MEDICATION INFUSIONS 3
• Dextrose (≥ 10%)
• Fosphenytoin
• Glucagon
• Heparin
• Insulin 4
• N-acetylcysteine
• Naloxone
• Intravenous Fluid (IVF) - and standard solution
o IVF w/ bicarbonate
o IVF w/ calcium
o IVF w/ magnesium
o IVF w/ phosphate
o IVF w/ potassium (up to 40 mEq per litre)
• Octreotide
• Pantoprazole
• Phenytoin
• Total parental nutrition (TPN)
5
G03 - Transport Team Work Scope
NOTES
1. Medication administration by nebulizer is contraindicated during the COVID pandemic (refer to A09).
2. In the event of unanticipated clinical situations during transport, paramedics will follow the Shared Health ERS medication protocols (M documents) which are standing orders that authorize the administration of these medications, and the pertinent patient care map.
3. Medication infusions established by another health care provider at the referring site are to be managed during transport as per Shared Health ERS transport care map G01. They require advance consultation with the referring prescriber or clinical service lead (CSL) and a written order from the prescriber.
4. If titration is required a written order outlining the titration parameters is required from the prescriber or designate.
5. Scheduled and PRN medications that are to be administered during patient transport should be administered as per G02. They require a written order from the prescriber. Consider advance consultation with the referring prescriber or CSL.
LINKS
• A09 - MEDICAL PROCEDURES DURING COVID • G01 - ESTABLISHED MEDICATION INFUSIONS • G02 - SCHEDULED MEDICATIONS
ESTABLISHED BY
Shared Health ERS Adult Transport Team
VERSION CHANGES (refer to X07 for change tracking)
• New document
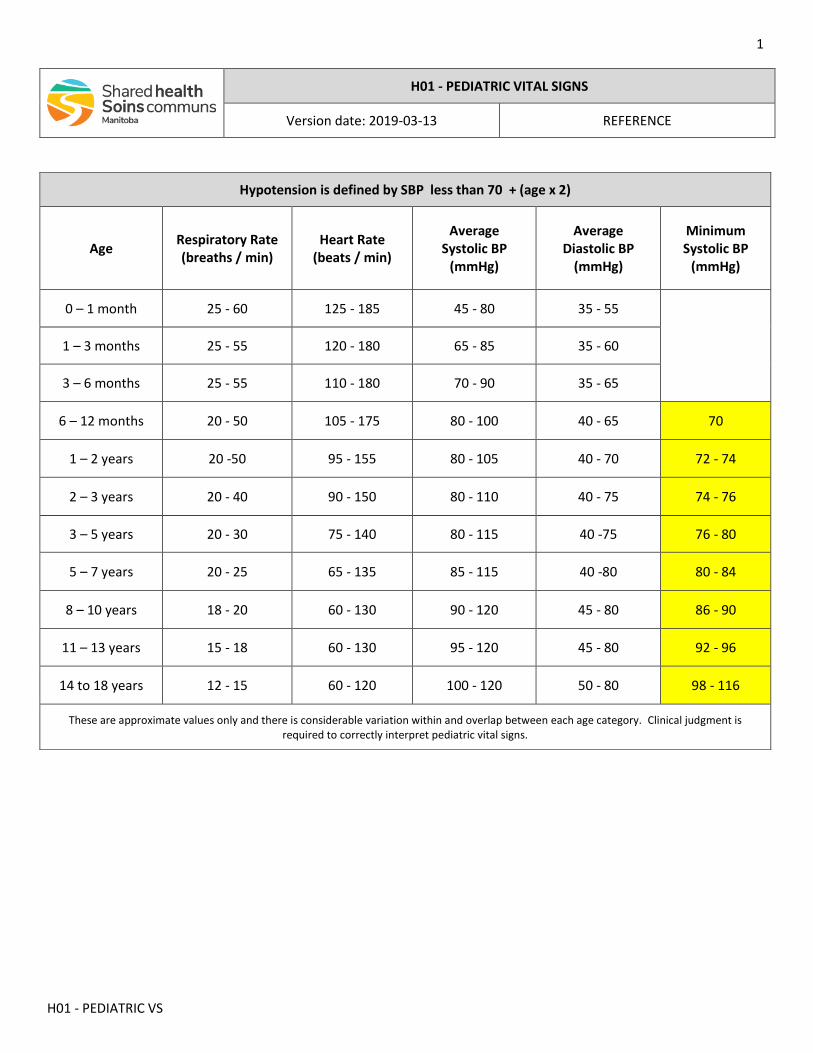
1
H01 - PEDIATRIC VS
H01 - PEDIATRIC VITAL SIGNS
Version date: 2019-03-13 REFERENCE
Hypotension is defined by SBP less than 70 + (age x 2)
Age
Respiratory Rate (breaths / min)
Heart Rate (beats / min)
Average Systolic BP
(mmHg)
Average Diastolic BP
(mmHg)
Minimum Systolic BP
(mmHg)
0 – 1 month 25 - 60 125 - 185 45 - 80 35 - 55
1 – 3 months 25 - 55 120 - 180 65 - 85 35 - 60
3 – 6 months 25 - 55 110 - 180 70 - 90 35 - 65
6 – 12 months 20 - 50 105 - 175 80 - 100 40 - 65 70
1 – 2 years 20 -50 95 - 155 80 - 105 40 - 70 72 - 74
2 – 3 years 20 - 40 90 - 150 80 - 110 40 - 75 74 - 76
3 – 5 years 20 - 30 75 - 140 80 - 115 40 -75 76 - 80
5 – 7 years 20 - 25 65 - 135 85 - 115 40 -80 80 - 84
8 – 10 years 18 - 20 60 - 130 90 - 120 45 - 80 86 - 90
11 – 13 years 15 - 18 60 - 130 95 - 120 45 - 80 92 - 96
14 to 18 years 12 - 15 60 - 120 100 - 120 50 - 80 98 - 116
These are approximate values only and there is considerable variation within and overlap between each age category. Clinical judgment is required to correctly interpret pediatric vital signs.
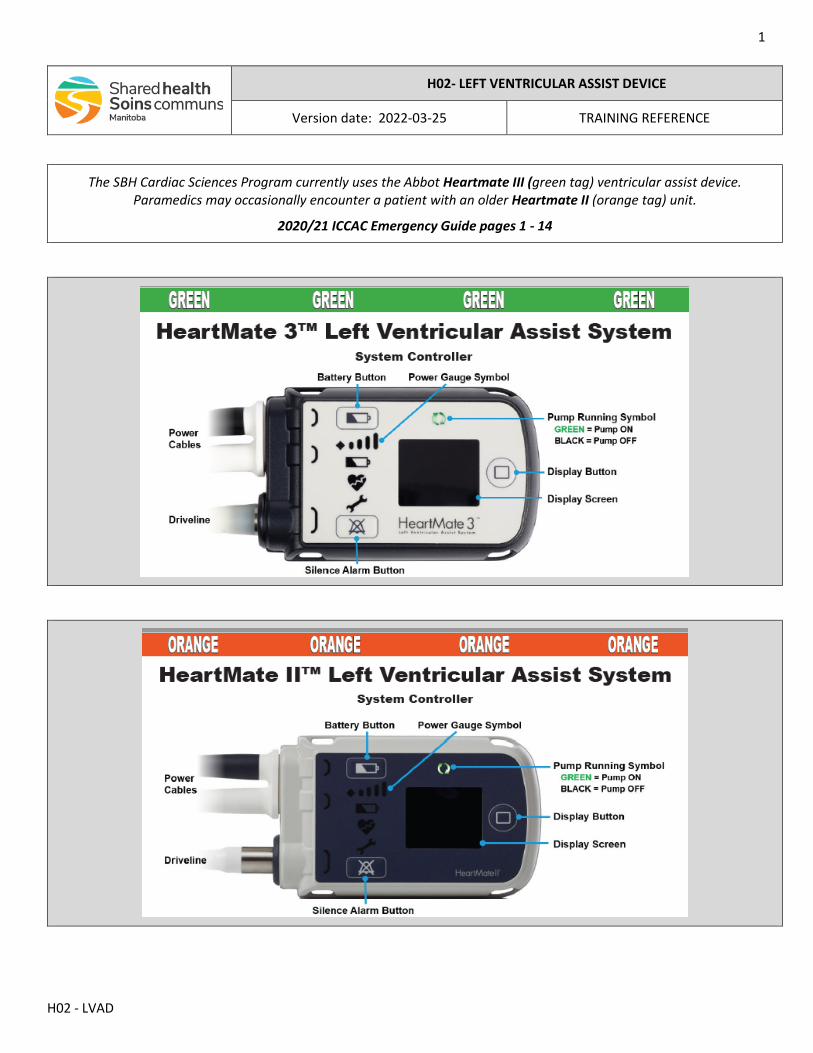
1
H02 - LVAD
H02- LEFT VENTRICULAR ASSIST DEVICE
Version date: 2022-03-25 TRAINING REFERENCE
The SBH Cardiac Sciences Program currently uses the Abbot Heartmate III (green tag) ventricular assist device. Paramedics may occasionally encounter a patient with an older Heartmate II (orange tag) unit.
2020/21 ICCAC Emergency Guide pages 1 - 14
This guide was created in 2008 by the innovation of VAD Coordinators from some of the largest and most successful VAD implantation hospitals in the United States. ICCAC has ensured that this document continues to be a current resource for not only emergency medical services but to all healthcare workers providing care to the mechanical circulatory support patient population. The purpose is to be a quick emergency guide and should not replace the manufacturers’ Instructions For Use as the primary source of information for each device listed in this guide.
2020-2021
Disclaimer:The information provided by International Consortium of Circulatory Assist Clinicians is for educational and convenience purposes only to illustrate concepts and considerations and may not cover or be complete for all situations. They are general resources to consider and adapt as you deem appropriate. International Consortium of Circulatory Assist Clinicians makes no claims, promises or guarantees about the appropriateness or completeness of the content, examples or information for any intended use. In addition, the information provided to you does not constitute legal, business or medical advice, and should not be relied on as such. You are solely responsible for understanding and complying with all applicable laws, rules and regulations associated with the subject matter of the information contained herein, including but not limited to laws, rules and regulations relating to marketing and business practices, medical practice and judgment, advertising, data privacy and security. Please also refer to the manufacturers’ prescribing information and instructions for use for the indications, contraindications, warnings, risks, and precautions associated with any medications and devices referenced in these materials. International Consortium of Circulatory Assist Clinicians recommends that you consult your legal and business advisors for guidance.
EMERGENCY GUIDE
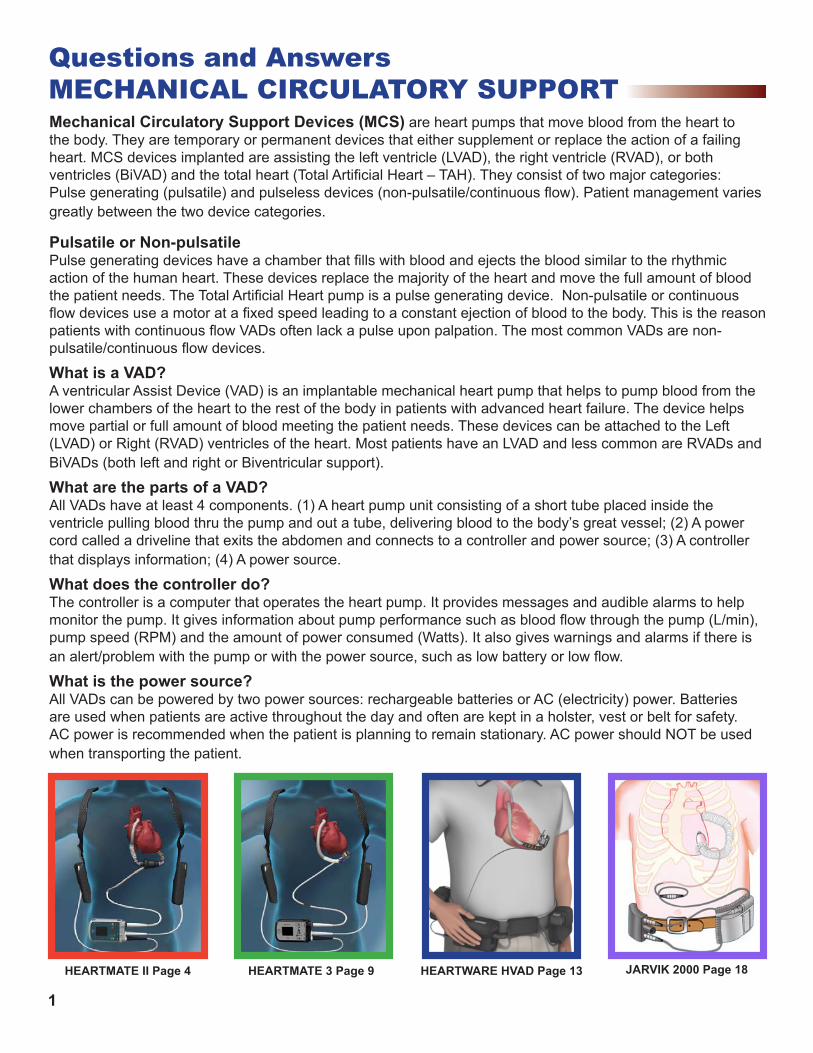
Mechanical Circulatory Support Devices (MCS) are heart pumps that move blood from the heart to the body. They are temporary or permanent devices that either supplement or replace the action of a failing heart. MCS devices implanted are assisting the left ventricle (LVAD), the right ventricle (RVAD), or both ventricles (BiVAD) and the total heart (Total Artificial Heart – TAH). They consist of two major categories: Pulse generating (pulsatile) and pulseless devices (non-pulsatile/continuous flow). Patient management varies greatly between the two device categories.
Pulsatile or Non-pulsatile Pulse generating devices have a chamber that fills with blood and ejects the blood similar to the rhythmic action of the human heart. These devices replace the majority of the heart and move the full amount of blood the patient needs. The Total Artificial Heart pump is a pulse generating device. Non-pulsatile or continuous flow devices use a motor at a fixed speed leading to a constant ejection of blood to the body. This is the reason patients with continuous flow VADs often lack a pulse upon palpation. The most common VADs are non-pulsatile/continuous flow devices.
What is a VAD?A ventricular Assist Device (VAD) is an implantable mechanical heart pump that helps to pump blood from the lower chambers of the heart to the rest of the body in patients with advanced heart failure. The device helps move partial or full amount of blood meeting the patient needs. These devices can be attached to the Left (LVAD) or Right (RVAD) ventricles of the heart. Most patients have an LVAD and less common are RVADs and BiVADs (both left and right or Biventricular support).
What are the parts of a VAD?All VADs have at least 4 components. (1) A heart pump unit consisting of a short tube placed inside the ventricle pulling blood thru the pump and out a tube, delivering blood to the body’s great vessel; (2) A power cord called a driveline that exits the abdomen and connects to a controller and power source; (3) A controller that displays information; (4) A power source.
What does the controller do?The controller is a computer that operates the heart pump. It provides messages and audible alarms to help monitor the pump. It gives information about pump performance such as blood flow through the pump (L/min), pump speed (RPM) and the amount of power consumed (Watts). It also gives warnings and alarms if there is an alert/problem with the pump or with the power source, such as low battery or low flow.
What is the power source?All VADs can be powered by two power sources: rechargeable batteries or AC (electricity) power. Batteries are used when patients are active throughout the day and often are kept in a holster, vest or belt for safety. AC power is recommended when the patient is planning to remain stationary. AC power should NOT be used when transporting the patient.
Questions and AnswersMECHANICAL CIRCULATORY SUPPORT
JARVIK 2000 Page 18HEARTMATE II Page 4 HEARTMATE 3 Page 9 HEARTWARE HVAD Page 13
1
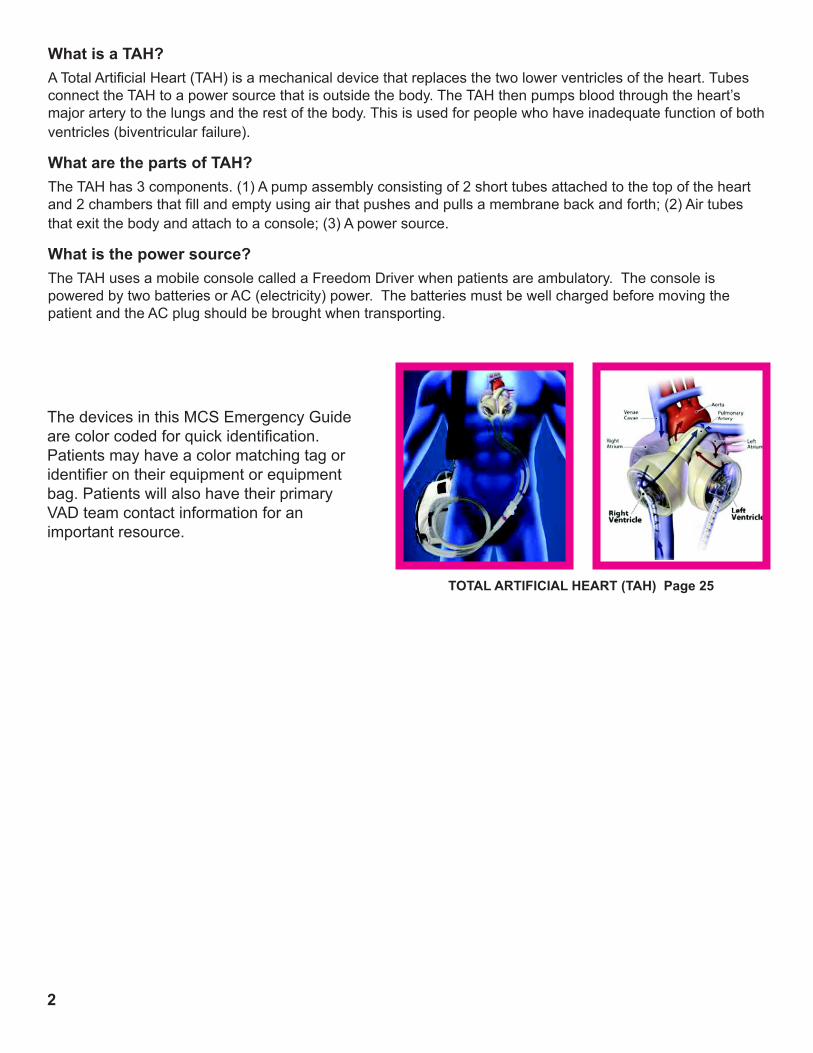
2
TOTAL ARTIFICIAL HEART (TAH) Page 25
The devices in this MCS Emergency Guide are color coded for quick identification. Patients may have a color matching tag or identifier on their equipment or equipment bag. Patients will also have their primary VAD team contact information for an important resource.
What is a TAH?A Total Artificial Heart (TAH) is a mechanical device that replaces the two lower ventricles of the heart. Tubes connect the TAH to a power source that is outside the body. The TAH then pumps blood through the heart’s major artery to the lungs and the rest of the body. This is used for people who have inadequate function of both ventricles (biventricular failure).
What are the parts of TAH?The TAH has 3 components. (1) A pump assembly consisting of 2 short tubes attached to the top of the heart and 2 chambers that fill and empty using air that pushes and pulls a membrane back and forth; (2) Air tubes that exit the body and attach to a console; (3) A power source.
What is the power source?The TAH uses a mobile console called a Freedom Driver when patients are ambulatory. The console is powered by two batteries or AC (electricity) power. The batteries must be well charged before moving the patient and the AC plug should be brought when transporting.
Patient Management For VADs
1. Treat the patient and follow your protocols. Do not focus only on the device. Most patients do not have a primary pump malfunction. Common MCS patient problems that arise are stroke, bleeding disorders (GI, nose bleeds), arrhythmias, dehydration and right heart failure.
2. Assess the patients airway and intervene per your protocol.
3. Auscultate heart sounds to determine if the device is functioning. If it is continuousflowdevice,youshouldheara“hummingsound”.
4. Assessvitalsigns.Non-pulsatileorcontinuousflowdevicesprovide continuousbloodflowfromthehearttotheaorta.Thiscontinuousflowresultsinanarrowarterialpulsepressure.Thismeansitmaybedifficultto obtain a pulse or blood pressure reading which may be a normal state foracontinuousflowdevicepatients.Toobtainabloodpressureanautomated cuff or doppler method can be used. If unable to obtain with automatedcuffusethemeanBPwithadoppler(firstsoundyouhear–MAP). Rely on other methods to assess perfusion e.g. mental status, skin color,capillaryrefill.Thedeviceflowshownonthecontrollerdisplayreflectsthepatient’scardiacoutput.
5. Start IV if indicated.
6. Assess the device for device information and alarms located on the controller display.
7. Interveneappropriatelybasedonthetypeofalarm.Seespecificdevice alarm guides on the pages that follow.
8. Refertothepatient’smedicationlist.Theyaretypically,butnotalways, on anticoagulation and antiplatelet therapy.
9. CalltheVADCenter’s24houremergencynumberonthepatient’scontact list, controller/equipment, or emergency bag for assistance in the management of the patient and transportation determination and location.
10. Bring all of the patients equipment. 11. Bring the significant other if possible to act as a expert on the device in the absence of consciousness in the patient.
3
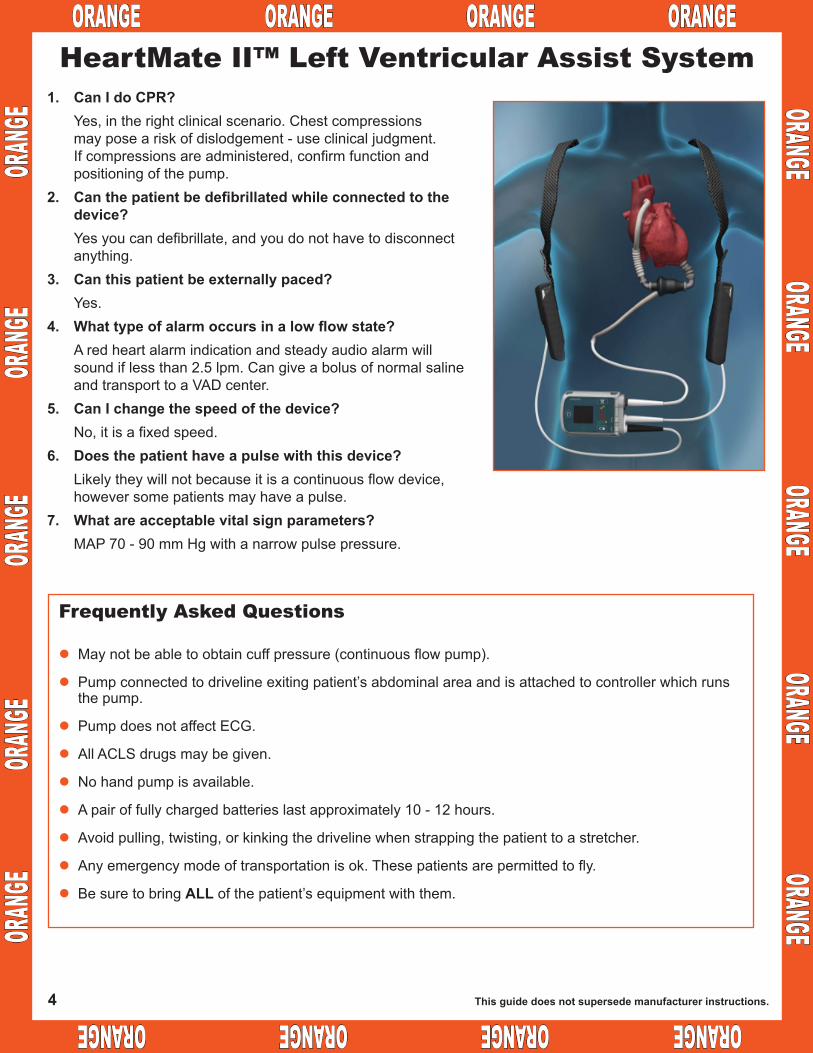
ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE
ORANGE ORANGE
ORANGE ORANGE
ORANGE
ORAN
GE
ORAN
GE
ORAN
GE
ORAN
GE
ORAN
GE
1. Can I do CPR? Yes, in the right clinical scenario. Chest compressions may pose a risk of dislodgement - use clinical judgment. Ifcompressionsareadministered,confirmfunctionand positioning of the pump.2. Canthepatientbedefibrillatedwhileconnectedtothe device? Yesyoucandefibrillate,andyoudonothavetodisconnect anything.3. Canthispatientbeexternallypaced? Yes.4. Whattypeofalarmoccursinalowflowstate? A red heart alarm indication and steady audio alarm will soundiflessthan2.5lpm.Cangiveabolusofnormalsaline and transport to a VAD center.5. CanIchangethespeedofthedevice? No,itisafixedspeed.6. Doesthepatienthaveapulsewiththisdevice? Likelytheywillnotbecauseitisacontinuousflowdevice, howeversomepatientsmayhaveapulse.7. Whatareacceptablevitalsignparameters? MAP 70 - 90 mm Hg with a narrow pulse pressure.
HeartMate II™ Left Ventricular Assist System
Frequently Asked Questions
lMaynotbeabletoobtaincuffpressure(continuousflowpump).
lPumpconnectedtodrivelineexitingpatient’sabdominalareaandisattachedtocontrollerwhichrunsthe pump.
lPump does not affect ECG.
lAllACLSdrugsmaybegiven.
lNohandpumpisavailable.
lApairoffullychargedbatterieslastapproximately10-12hours.
lAvoidpulling,twisting,orkinkingthedrivelinewhenstrappingthepatienttoastretcher.
lAnyemergencymodeoftransportationisok.Thesepatientsarepermittedtofly.
lBesuretobringALLofthepatient’sequipmentwiththem.
Thisguidedoesnotsupersedemanufacturerinstructions.4
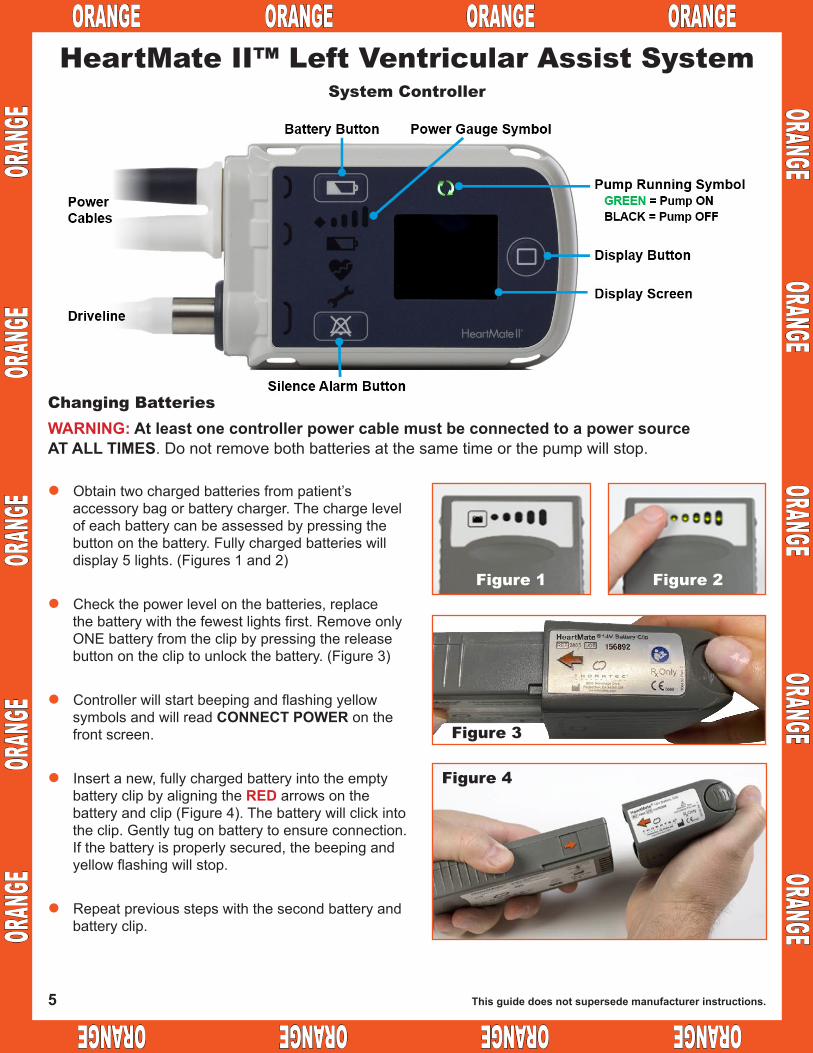
ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE
ORANGE ORANGE
ORANGE ORANGE
ORANGE
ORAN
GE
ORAN
GE
ORAN
GE
ORAN
GE
ORAN
GEHeartMate II™ Left Ventricular Assist System
l Obtaintwochargedbatteriesfrompatient’saccessorybagorbatterycharger.Thechargelevelofeachbatterycanbeassessedbypressingthebuttononthebattery.Fullychargedbatterieswilldisplay5lights.(Figures1and2)
l Checkthepowerlevelonthebatteries,replacethebatterywiththefewestlightsfirst.RemoveonlyONEbatteryfromtheclipbypressingthereleasebuttononthecliptounlockthebattery.(Figure3)
l ControllerwillstartbeepingandflashingyellowsymbolsandwillreadCONNECT POWER on the front screen.
l Insertanew,fullychargedbatteryintotheemptybatteryclipbyaligningtheRED arrows on the batteryandclip(Figure4).Thebatterywillclickintotheclip.Gentlytugonbatterytoensureconnection.Ifthebatteryisproperlysecured,thebeepingandyellowflashingwillstop.
l Repeatpreviousstepswiththesecondbatteryandbatteryclip.
System Controller
Changing BatteriesWARNING:AtleastonecontrollerpowercablemustbeconnectedtoapowersourceAT ALL TIMES.Donotremovebothbatteriesatthesametimeorthepumpwillstop.
Thisguidedoesnotsupersedemanufacturerinstructions.
Figure 3
Figure 4
Figure 2Figure 1
5
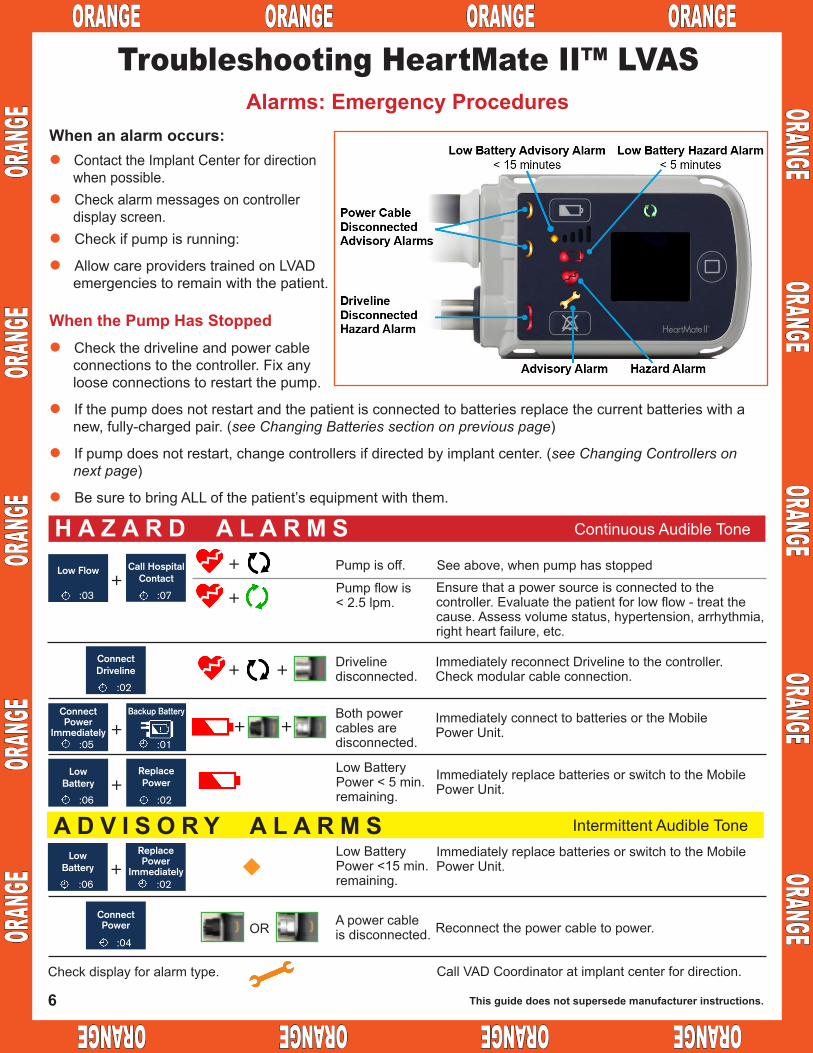
ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE
ORANGE ORANGE
ORANGE ORANGE
ORANGE
ORAN
GE
ORAN
GE
ORAN
GE
ORAN
GE
ORAN
GETroubleshooting HeartMate II™ LVAS
l Contact the Implant Center for direction whenpossible.
l Check alarm messages on controller display screen.
l Check if pump is running:
l AllowcareproviderstrainedonLVADemergencies to remain with the patient.
WhenthePumpHasStoppedl Checkthedrivelineandpowercable
connectionstothecontroller.Fixanyloose connections to restart the pump.
l Ifthepumpdoesnotrestartandthepatientisconnectedtobatteriesreplacethecurrentbatterieswithanew,fully-chargedpair.(see Changing Batteries section on previous page)
l Ifpumpdoesnotrestart,changecontrollersifdirectedbyimplantcenter.(see Changing Controllers on next page)
l BesuretobringALLofthepatient’sequipmentwiththem.
Alarms:EmergencyProceduresWhenanalarmoccurs:
Ensure that a power source is connected to the controller.Evaluatethepatientforlowflow-treatthecause.Assessvolumestatus,hypertension,arrhythmia,right heart failure, etc.
H A Z A R D A L A R M S ContinuousAudibleTone
Low Flow
:03
+
++
Call HospitalContact
:07
ConnectDriveline
:02
ConnectPower
Immediately:05
+Backup Battery
:01
ConnectPower
:04
LowBattery
:06+
ReplacePower
:02
LowBattery
:06+
ReplacePower
Immediately:02
+ +
Low Battery Power < 5 min. remaining.
A D V I S O R Y A L A R M S IntermittentAudibleTone
Both power cablesaredisconnected.
Drivelinedisconnected.
Pumpflowis< 2.5 lpm.
Pump is off. Seeabove,whenpumphasstopped
ImmediatelyreplacebatteriesorswitchtotheMobilePower Unit.
ImmediatelyconnecttobatteriesortheMobilePower Unit.
ImmediatelyreconnectDrivelinetothecontroller.Checkmodularcableconnection.
+ +
Apowercableis disconnected.
Low Battery Power<15min.remaining.
Reconnectthepowercabletopower.
ImmediatelyreplacebatteriesorswitchtotheMobilePower Unit.
Call VAD Coordinator at implant center for direction.Check display for alarm type.
OR
Thisguidedoesnotsupersedemanufacturerinstructions.6
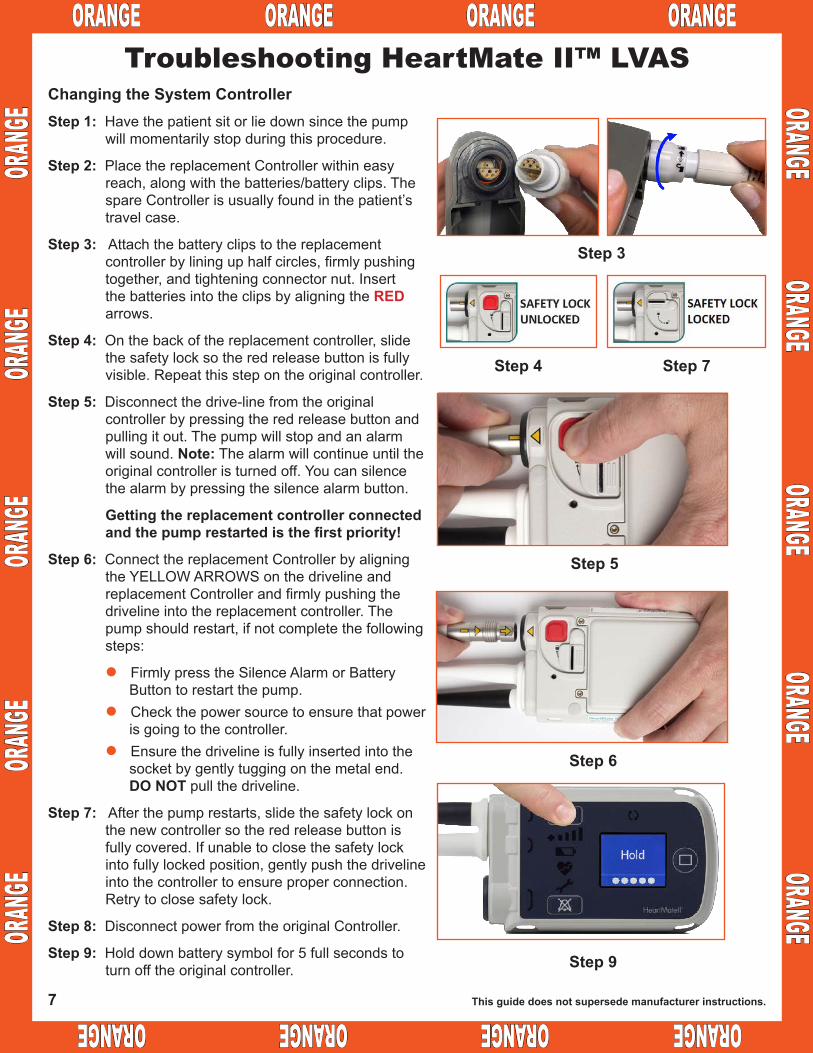
OR
ANGE
OR
ANGE
OR
ANGE
OR
ANGE
OR
ANGE
ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE
ORANGE ORANGE
ORANGE ORANGE
ORANGE
ChangingtheSystemControllerStep 1:Havethepatientsitorliedownsincethepump
will momentarily stop during this procedure.
Step 2: Place the replacement Controller within easy reach,alongwiththebatteries/batteryclips.ThespareControllerisusuallyfoundinthepatient’stravelcase.
Step 3:Attachthebatteryclipstothereplacementcontrollerbylininguphalfcircles,firmlypushingtogether, and tightening connector nut. Insert thebatteriesintotheclipsbyaligningtheRED arrows.
Step 4:Onthebackofthereplacementcontroller,slidethesafetylocksotheredreleasebuttonisfullyvisible.Repeatthisstepontheoriginalcontroller.
Step 5:Disconnectthedrive-linefromtheoriginalcontrollerbypressingtheredreleasebuttonandpulling it out. The pump will stop and an alarm will sound. Note: The alarm will continue until the original controller is turned off. You can silence thealarmbypressingthesilencealarmbutton.
Gettingthereplacementcontrollerconnectedandthepumprestartedisthefirstpriority!
Step 6:ConnectthereplacementControllerbyaligningtheYELLOWARROWSonthedrivelineandreplacementControllerandfirmlypushingthedrivelineintothereplacementcontroller.Thepump should restart, if not complete the following steps:
l FirmlypresstheSilenceAlarmorBatteryButton to restart the pump.
l Check the power source to ensure that power is going to the controller.
l Ensurethedrivelineisfullyinsertedintothesocketbygentlytuggingonthemetalend.DO NOTpullthedriveline.
Step 7: After the pump restarts, slide the safety lock on thenewcontrollersotheredreleasebuttonisfullycovered.Ifunabletoclosethesafetylockintofullylockedposition,gentlypushthedrivelineinto the controller to ensure proper connection. Retrytoclosesafetylock.
Step 8: Disconnect power from the original Controller.
Step 9: Holddownbatterysymbolfor5fullsecondstoturn off the original controller.
Troubleshooting HeartMate II™ LVAS
Step 3
Step 4 Step 7
Step 5
Step 6
Step 9
Thisguidedoesnotsupersedemanufacturerinstructions.7

ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE ORANGE
ORAN
GE
ORAN
GE
ORAN
GE
ORAN
GE
ORAN
GE
ORANGE ORANGE
ORANGE ORANGE
ORANGEHeartMate II™ Left Ventricular Assist SystemThefollowinginformationappliestotheoriginalcontrollerversioncalledExternalPeripheral
Controller(EPC).Somepatientshavethiscontroller.
2 MODES: ON, OFFOn: Driveline+Powersourceconnected.Off:Nodrivelineorpowersourceconnected.CELL MODULE BATTERYNobackupbattery.ThecellmodulebatterypowersanaudibletoneifEPCisremovedfrompowerwhilethedrivelineisconnected.ThecellmodulebatteryissuppliedSTERILE.EVENT LOGGEREPCdoesnotincludedate/timerecordsineventhistory.EPCcanstore120events.GREEN POWER SYMBOL
Green light only mead that the controllerisreceivingpower.
Listenoverthepumppocketforconfirmationthatthepumpisrunning.CONTROLLER BUTTONSAlarmSilenceButton: Displays thebatteryfuelgauge.Alsosilenceshazard alarms for 2 minutes and advisoryalarmsfor4hours.TestSelectButton:Activatesaselftestwhenheldfor3seconds.Note: EPC does not include a display buttonoruserinterfacescreen.TheDisplayModuleisusedtoviewpumpparameterandalarmevents.SELF TEST
Press and hold the Test Select Buttonfor3seconds.
Alarms: Emergency Procedures
YelloworRedBatteryAlarm:Need to Change Batteries. See changing batteriessectiononpage5.
RedHeartFlashingAlarm:This may indicateaLowFlowHazard.Checkpatient--theflowmaybetoolow.Ifpatientishypovolemic,givevolume.Ifpatient is in right heart failure-- treat per protocol. If the pump has stopped check connections,batteriesandcontrollersasinstructed on page 5.
Abatteryclipcanbeattached to the EPC controller byliningupthehalf moons and gently pushing. Batteries can beattachedtothebatteryclipbyaligningtheREDarrowsonthebatteryandclip.
DrivelineConnection: The PercLockmustbe“unlocked”inorderforthedrivelinetoberemovedinacontrollerexchange.ThePerclockremains in locked position oncethedrivelinehasbeenfully inserted.
ExternalPeripheralController(EPC):A percutaneous lock is located on the side of the controller.
Unlock Locked
ExternalPeripheralController(EPC)
LOW POWERYellowBatterySymbol: Displayedwhenonly15
minutesofexternalpowerisremaining.
RedBatterySymbol: Displayed when only 5 minutes
ofexternalpowerisremaining.POWER SAVER MODE: Enteredwhenthebatteryvoltagefallstoacriticallylowlevel.PumpSpeedisreducedto8000RPM.STARTINGTHEPUMP>8000 RPM: Pump starts automatically.<8000 RPM:StartpumpbypressingAlarm Silence Button or Test Select Button on EPC.SYSTEM MONITOR EVENT HISTORYSCREENPI Event:
SystemInformation:
COMPATIBILITYSystem Monitors I and II, Power Module,PowerBaseUnit(PBU),PowerModulePatientCable(12Voltand14Volt),14VoltLithium-ionBatteriesandBatteryClips,12VoltSLA and NiMH Batteries and Clips.ALARMSForareviewofalarmsandtheirmeanings, reference the HeartMate IIAlarmsforClinicians,Item103851.Note that EPC does not include Drivelinefaultdetection.
AlarmSilentButton BatteryAlarm
BatteryGauge
RedHeartAlarm CellModularAlarm TestSelectButtonPowerSymbol
8
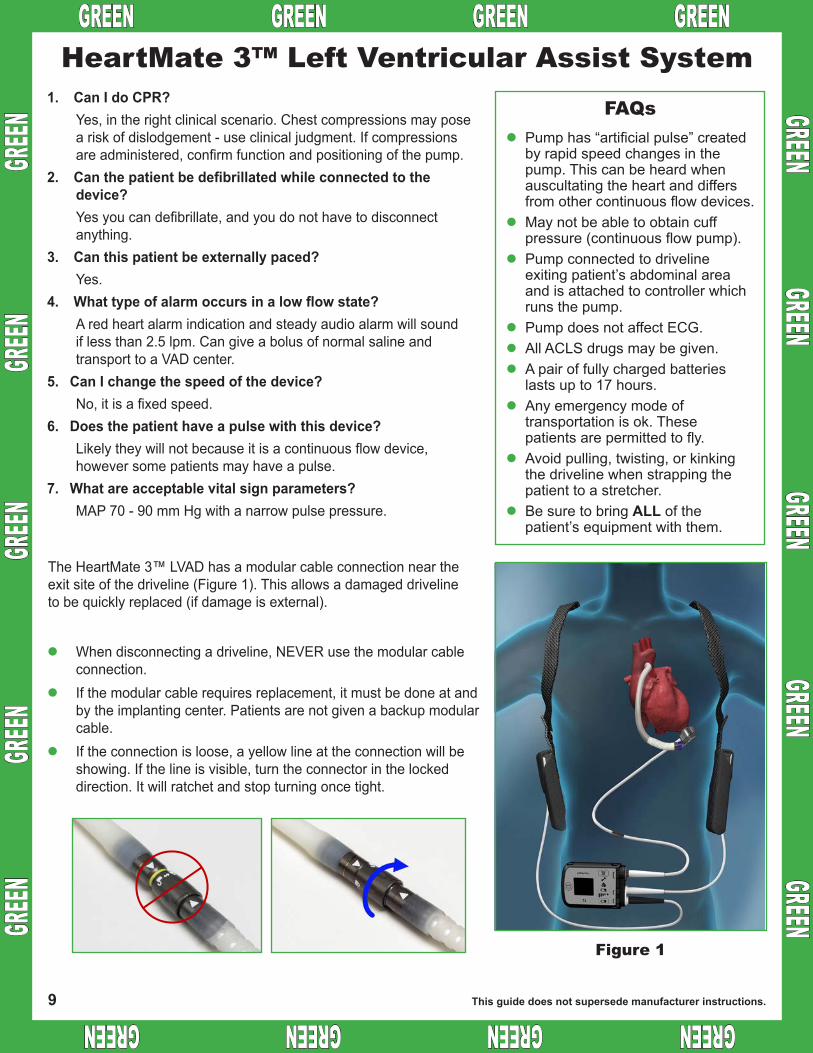
GREEN GREEN GREEN GREEN GREEN GREEN GREEN GREEN
GREEN GREEN
GREEN GREEN
GREEN
GREEN
GR
EEN
GREEN
GR
EEN
GREEN
1. Can I do CPR?Yes, in the right clinical scenario. Chest compressions may pose a risk of dislodgement - use clinical judgment. If compressions are administered, confirm function and positioning of the pump.
2. Canthepatientbedefibrillatedwhileconnectedtothedevice?Yes you can defibrillate, and you do not have to disconnect anything.
3. Canthispatientbeexternallypaced?Yes.
4. Whattypeofalarmoccursinalowflowstate?A red heart alarm indication and steady audio alarm will sound if less than 2.5 lpm. Can give a bolus of normal saline and transport to a VAD center.
5. CanIchangethespeedofthedevice?No, it is a fixed speed.
6. Doesthepatienthaveapulsewiththisdevice?Likely they will not because it is a continuous flow device, however some patients may have a pulse.
7. Whatareacceptablevitalsignparameters?MAP 70 - 90 mm Hg with a narrow pulse pressure.
HeartMate 3™ Left Ventricular Assist SystemFAQs
lPump has “artificial pulse” created by rapid speed changes in the pump. This can be heard when auscultating the heart and differs from other continuous flow devices.
lMay not be able to obtain cuff pressure (continuous flow pump).
lPump connected to driveline exiting patient’s abdominal area and is attached to controller which runs the pump.
lPump does not affect ECG. lAll ACLS drugs may be given. lA pair of fully charged batteries
lasts up to 17 hours.lAny emergency mode of
transportation is ok. These patients are permitted to fly.
lAvoid pulling, twisting, or kinking the driveline when strapping the patient to a stretcher.
lBe sure to bring ALL of the patient’s equipment with them.
Figure 1
Thisguidedoesnotsupersedemanufacturerinstructions.
The HeartMate 3™ LVAD has a modular cable connection near the exit site of the driveline (Figure 1). This allows a damaged driveline to be quickly replaced (if damage is external).
l When disconnecting a driveline, NEVER use the modular cable connection.
l If the modular cable requires replacement, it must be done at and by the implanting center. Patients are not given a backup modular cable.
l If the connection is loose, a yellow line at the connection will be showing. If the line is visible, turn the connector in the locked direction. It will ratchet and stop turning once tight.
9
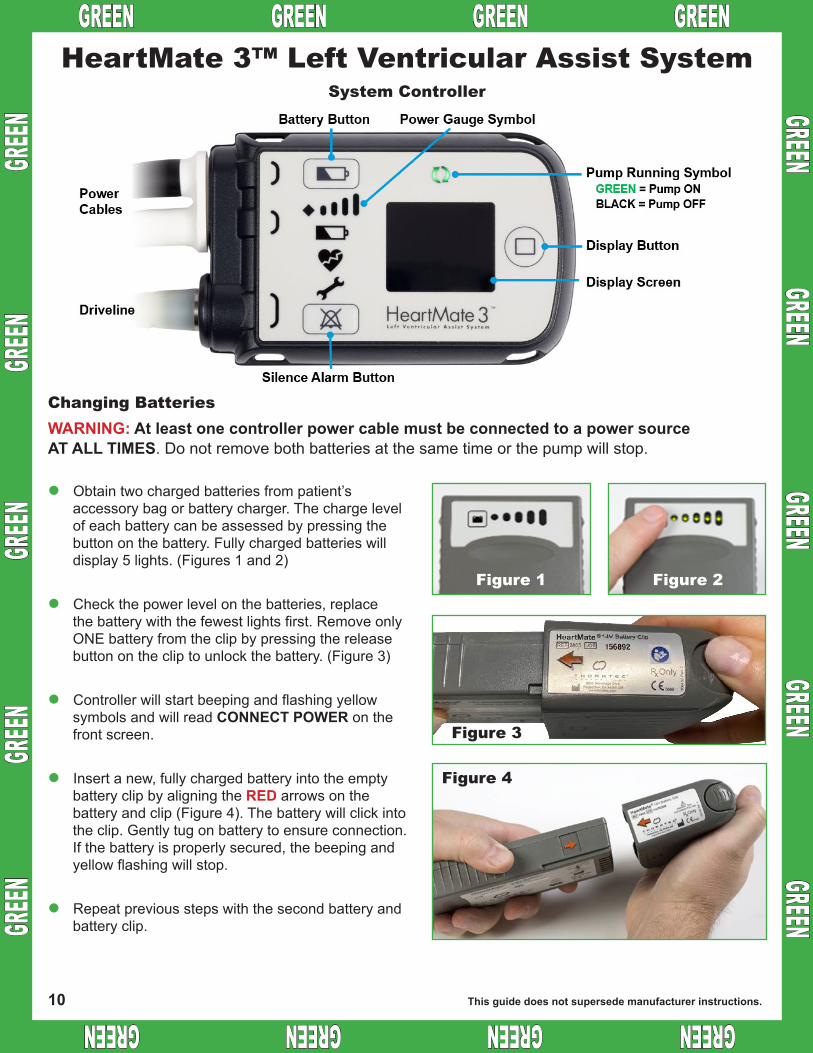
GREEN GREEN GREEN GREEN GREEN GREEN GREEN GREEN
GREEN GREEN
GREEN GREEN
GREEN
GREEN
GR
EEN
GREEN
GR
EEN
GREEN
HeartMate 3™ Left Ventricular Assist System
l Obtain two charged batteries from patient’s accessory bag or battery charger. The charge level of each battery can be assessed by pressing the button on the battery. Fully charged batteries will display 5 lights. (Figures 1 and 2)
l Check the power level on the batteries, replace the battery with the fewest lights first. Remove only ONE battery from the clip by pressing the release button on the clip to unlock the battery. (Figure 3)
l Controller will start beeping and flashing yellow symbols and will read CONNECT POWER on the front screen.
l Insert a new, fully charged battery into the empty battery clip by aligning the RED arrows on the battery and clip (Figure 4). The battery will click into the clip. Gently tug on battery to ensure connection. If the battery is properly secured, the beeping and yellow flashing will stop.
l Repeat previous steps with the second battery and battery clip.
System Controller
Changing BatteriesWARNING:AtleastonecontrollerpowercablemustbeconnectedtoapowersourceAT ALL TIMES. Do not remove both batteries at the same time or the pump will stop.
Thisguidedoesnotsupersedemanufacturerinstructions.
Figure 3
Figure 4
Figure 2Figure 1
10
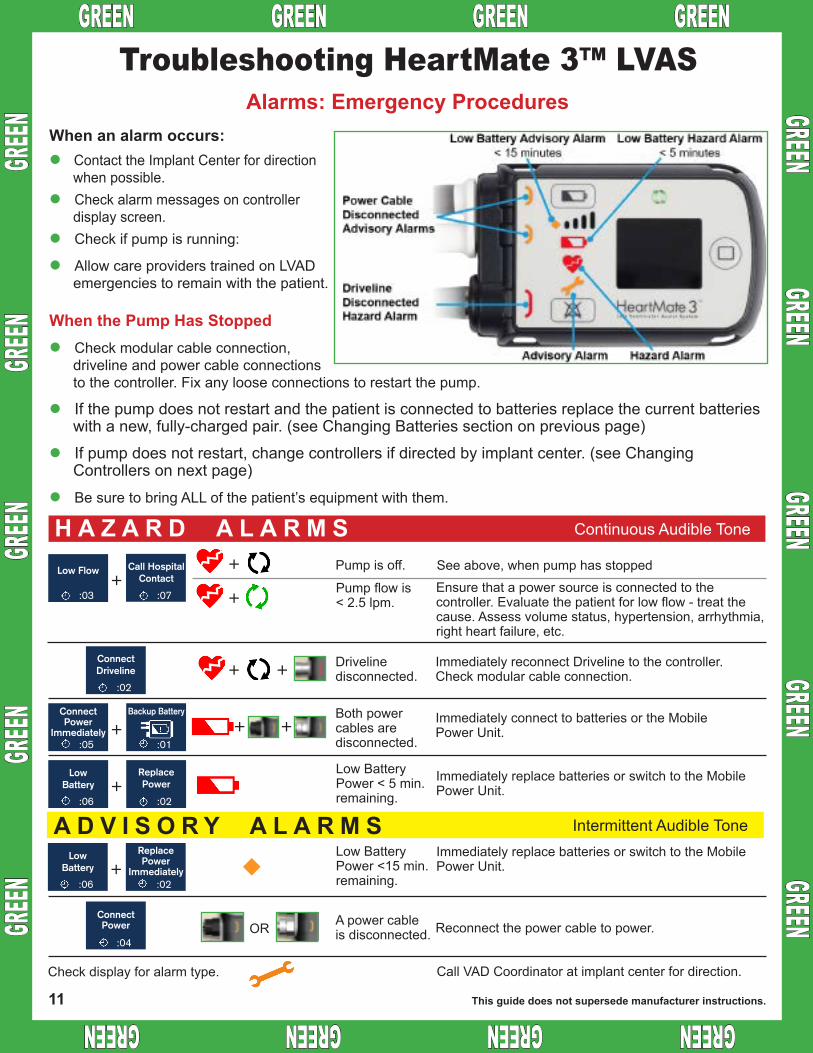
GREEN GREEN GREEN GREEN GREEN GREEN GREEN GREEN
GREEN GREEN
GREEN GREEN
GREEN
GREEN
GR
EEN
GREEN
GR
EEN
GREEN
Troubleshooting HeartMate 3™ LVAS
l Contact the Implant Center for direction when possible.
l Check alarm messages on controller display screen.
l Check if pump is running:
l Allow care providers trained on LVAD emergencies to remain with the patient.
WhenthePumpHasStoppedl Check modular cable connection,
driveline and power cable connections to the controller. Fix any loose connections to restart the pump.
l If the pump does not restart and the patient is connected to batteries replace the current batteries with a new, fully-charged pair. (see Changing Batteries section on previous page)
l If pump does not restart, change controllers if directed by implant center. (see Changing Controllers on next page)
l Be sure to bring ALL of the patient’s equipment with them.
Alarms:EmergencyProceduresWhenanalarmoccurs:
Ensure that a power source is connected to the controller. Evaluate the patient for low flow - treat the cause. Assess volume status, hypertension, arrhythmia, right heart failure, etc.
H A Z A R D A L A R M S Continuous Audible Tone
Low Flow
:03
+
++
Call HospitalContact
:07
ConnectDriveline
:02
ConnectPower
Immediately:05
+Backup Battery
:01
ConnectPower
:04
LowBattery
:06+
ReplacePower
:02
LowBattery
:06+
ReplacePower
Immediately:02
+ +
Low Battery Power < 5 min. remaining.
A D V I S O R Y A L A R M S Intermittent Audible Tone
Both power cables are disconnected.
Drivelinedisconnected.
Pump flow is < 2.5 lpm.
Pump is off. See above, when pump has stopped
Immediately replace batteries or switch to the Mobile Power Unit.
Immediately connect to batteries or the Mobile Power Unit.
Immediately reconnect Driveline to the controller. Check modular cable connection.
+ +
A power cable is disconnected.
Low Battery Power <15 min. remaining.
Reconnect the power cable to power.
Immediately replace batteries or switch to the Mobile Power Unit.
Call VAD Coordinator at implant center for direction.Check display for alarm type.
OR
Thisguidedoesnotsupersedemanufacturerinstructions.11
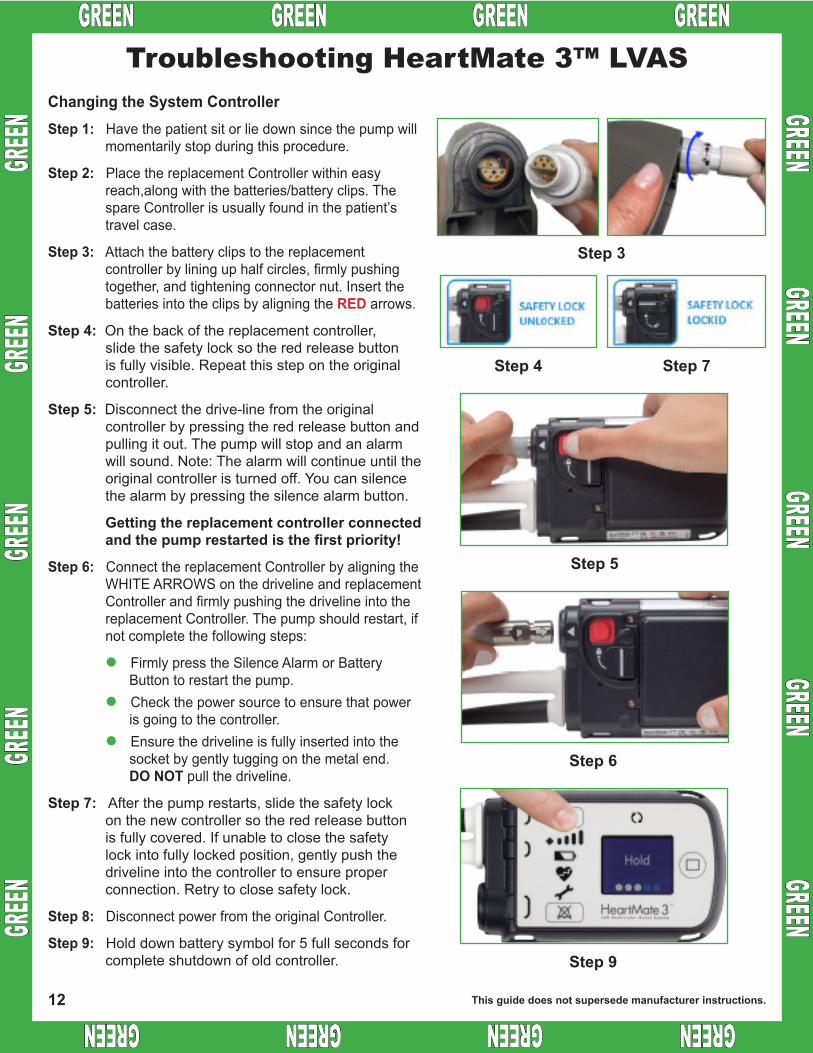
GR
EEN
GREEN
GR
EEN
GREEN
GR
EEN GREEN GREEN GREEN GREEN GREEN GREEN GREEN GREEN
GREEN GREEN
GREEN GREEN
GREEN
ChangingtheSystemControllerStep 1: Have the patient sit or lie down since the pump will
momentarily stop during this procedure.
Step 2: Place the replacement Controller within easy reach,along with the batteries/battery clips. The spare Controller is usually found in the patient’s travel case.
Step 3: Attach the battery clips to the replacement controller by lining up half circles, firmly pushing together, and tightening connector nut. Insert the batteries into the clips by aligning the RED arrows.
Step 4: On the back of the replacement controller, slide the safety lock so the red release button is fully visible. Repeat this step on the original controller.
Step 5: Disconnect the drive-line from the original controller by pressing the red release button and pulling it out. The pump will stop and an alarm will sound. Note: The alarm will continue until the original controller is turned off. You can silence the alarm by pressing the silence alarm button.
Gettingthereplacementcontrollerconnectedandthepumprestartedisthefirstpriority!
Step 6: Connect the replacement Controller by aligning the WHITE ARROWS on the driveline and replacement Controller and firmly pushing the driveline into the replacement Controller. The pump should restart, if not complete the following steps:
l Firmly press the Silence Alarm or Battery Button to restart the pump.
l Check the power source to ensure that power is going to the controller.
l Ensure the driveline is fully inserted into the socket by gently tugging on the metal end. DO NOT pull the driveline.
Step 7: After the pump restarts, slide the safety lock on the new controller so the red release button is fully covered. If unable to close the safety lock into fully locked position, gently push the driveline into the controller to ensure proper connection. Retry to close safety lock.
Step 8: Disconnect power from the original Controller.
Step 9: Hold down battery symbol for 5 full seconds for complete shutdown of old controller.
Troubleshooting HeartMate 3™ LVAS
Step 3
Step 4 Step 7
Step 5
Step 6
Step 9
Thisguidedoesnotsupersedemanufacturerinstructions.12
1
H03.1 - PCM FORMAT
H03.1 - PATIENT CARE MAP FORMAT
Version date: 2022-02-26 REFERENCE
NOTES
1. The patient care maps are listed by category (A00.1) and alphabetically (A00.2). Medication documents are listed by category (A00.3) and alphabetically (A00.4). The alphabetical listings (index) may have multiple terms referring to the same care map for ease of retrieval (eg. “basic resuscitation” or “resuscitation, basic” both refer to care map C01).
2. The header appears on page 1 only. The page number will appear at the top right corner of each page. The alpha- numeric identifier and a brief running title will be at the bottom left corner of each page.
3. The top right row of the header on the front page will contain the alphanumeric identifier and title of each document.
4. The left column of the second right row contains the age group if applicable. If no age group is specified, the document apples to all ages.
Different care maps and medication orders may apply to patients of different age. These cohorts are standardized as follows, and may be indicated by a suffix in the map’s alphanumeric indicator (eg. E04A - ACS & STEMI). When a care map applies to patients of all ages, or a clinical condition (rather than an age cohort) the suffix will be deleted (eg. D02 - PREHOSPITAL DELIVERY).
• ADULT (A): seventeen (17) years and older)
• ADOLESCENT (B): - ten (10) up to seventeen (17) years
• CHILD (C): one (1) up to ten (10) years
• INFANT (D): 72 hours up to twelve (12) months
• NEWBORN (E): birth up to seventy-two (72) hours post-partum
5. The right column of the second row contains the care map category. The care maps are grouped into the following categories:
• Section A - POLICIES & PROCEDURES
• Section B - DESTINATION
• Section C - RESUSCITATION
• Section D - MATERNAL & NEWBORN CARE
• Section E - MEDICAL CONDITIONS
• Section F - TRAUMA
• Section G - PATIENT TRANSPORT
• Section H - REFERENCES
6. The third row contains the compliance statement, which pertains to the employees working for the Provincial EMS/PT division of Shared Health ERS and providers operating under a service purchase agreement (SPA) with ERS to provide emergency medical services to EMS.
SPA provider may be exempted from some or all of the EMS/PT care maps, policies, procedures, and protocols by agreement with ERS. Winnipeg Fire Paramedic Service is not within the division of Provincial EMS/PT.
7. The version date is important for ensuring that the most up-to-date document is being used.
8. The documents will always come into effect at 0700 hrs on the effective date, unless otherwise specified.
2
H03.1 - PCM FORMAT
9. Each care map will have a work scope statement and the following work scope identifiers will replace the previous coloured boxes (example B):
• ALL: The overall document or a specific medical function applies to paramedics with all work scopes.
• EMR: The overall document or a specific medical function applies to paramedics with the basic and primary work scopes.
• PCP: The overall document or a specific medical function applies to paramedics with the primary and intermediate work scopes.
• ICP: The overall document or a specific medical function applies to paramedics with the intermediate work scope only.
10. Most patient care maps will have a flow chart that will help with a quick review of the approach to a clinical condition.
In each flow chart there may be superscript numbers that refer to specific items in the notes section (example C).
11. Where applicable, a care map may include a QUICK REFERENCE GUIDE (QRG) which may illustrate a key medication dose, age-adjusted vital signs, or other information that will be helpful at the point of care.
12. The NOTES section will include more detailed information that helps in the correct application of various steps in the care map. This section may also highlight pertinent information from the training materials for this care map.
13. The LINKS section will include other clinical documents related to the care map.
14. The CHANGES sections will include significant revisions to the current version of each care map. The tracking of historical changes will be listed in other EMS/PT documents.
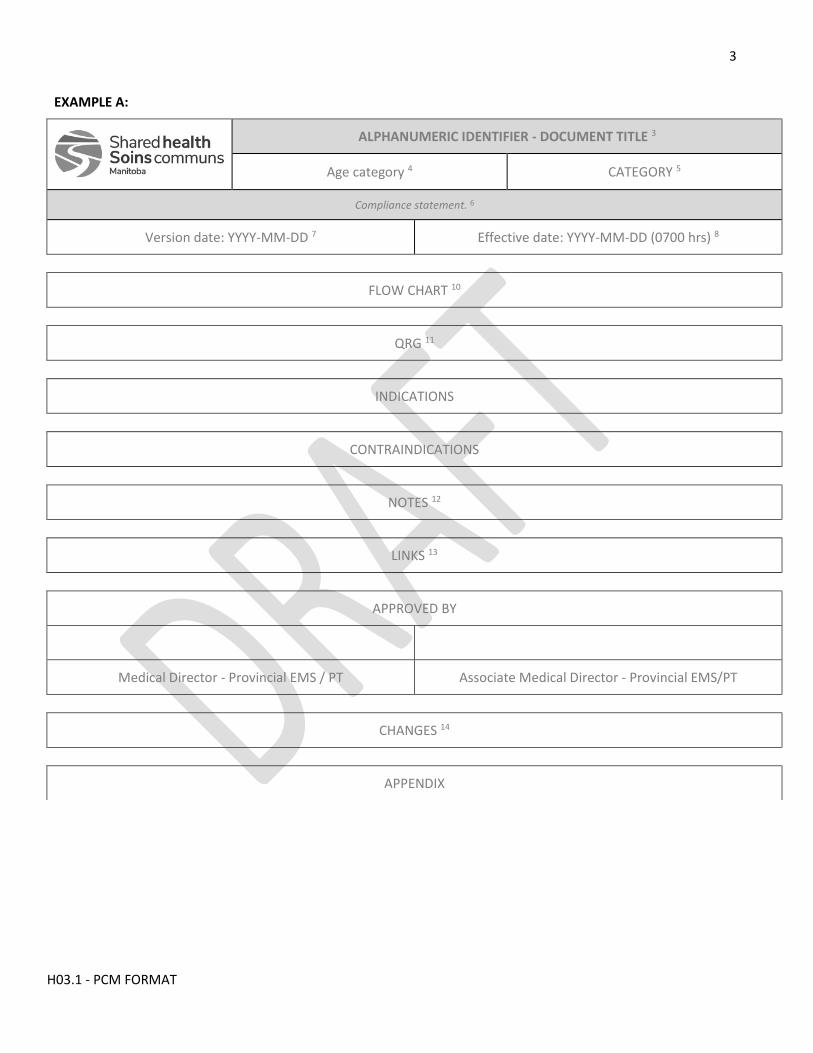
3
H03.1 - PCM FORMAT
EXAMPLE A:
ALPHANUMERIC IDENTIFIER - DOCUMENT TITLE 3
Age category 4 CATEGORY 5
Compliance statement. 6
Version date: YYYY-MM-DD 7 Effective date: YYYY-MM-DD (0700 hrs) 8
FLOW CHART 10
QRG 11
INDICATIONS
CONTRAINDICATIONS
NOTES 12
LINKS 13
APPROVED BY
Medical Director - Provincial EMS / PT Associate Medical Director - Provincial EMS/PT
CHANGES 14
APPENDIX
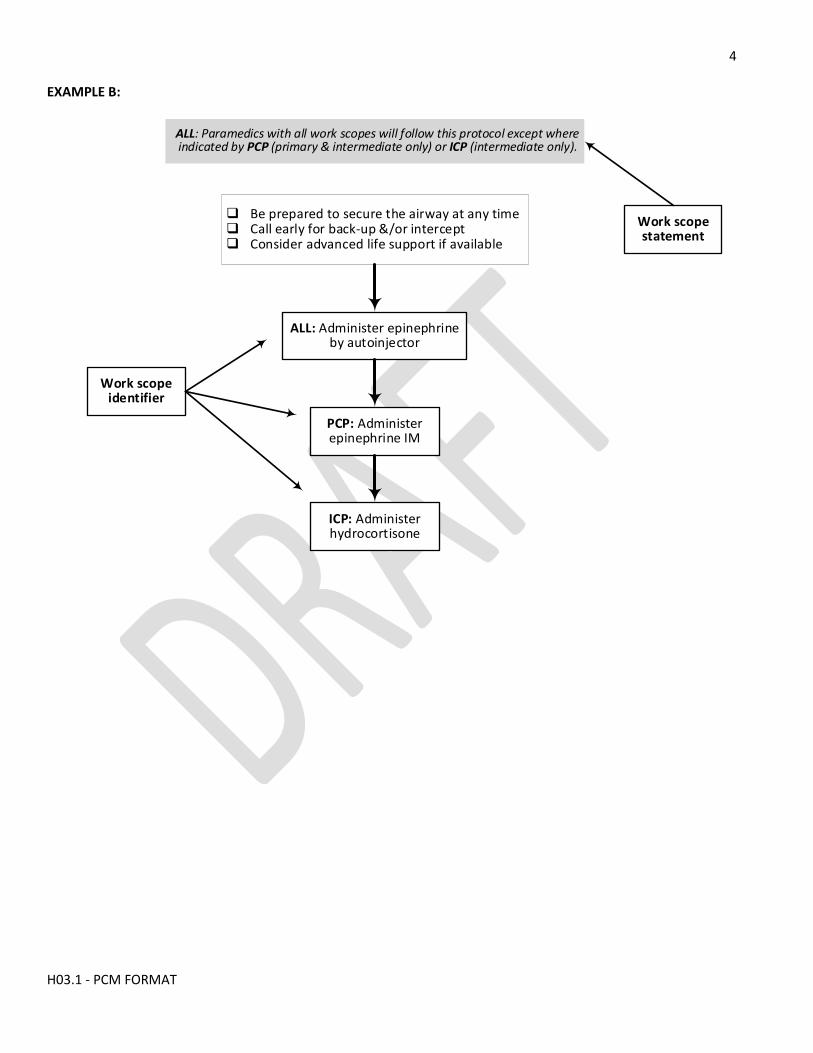
4
H03.1 - PCM FORMAT
EXAMPLE B:
q Be prepared to secure the airway at any timeq Call early for back-up &/or intercept q Consider advanced life support if available
ALL: Administer epinephrine by autoinjector
PCP: Administer epinephrine IM
ICP: Administer hydrocortisone
Work scope identifier
Work scope statement
ALL: Paramedics with all work scopes will follow this protocol except where indicated by PCP (primary & intermediate only) or ICP (intermediate only).
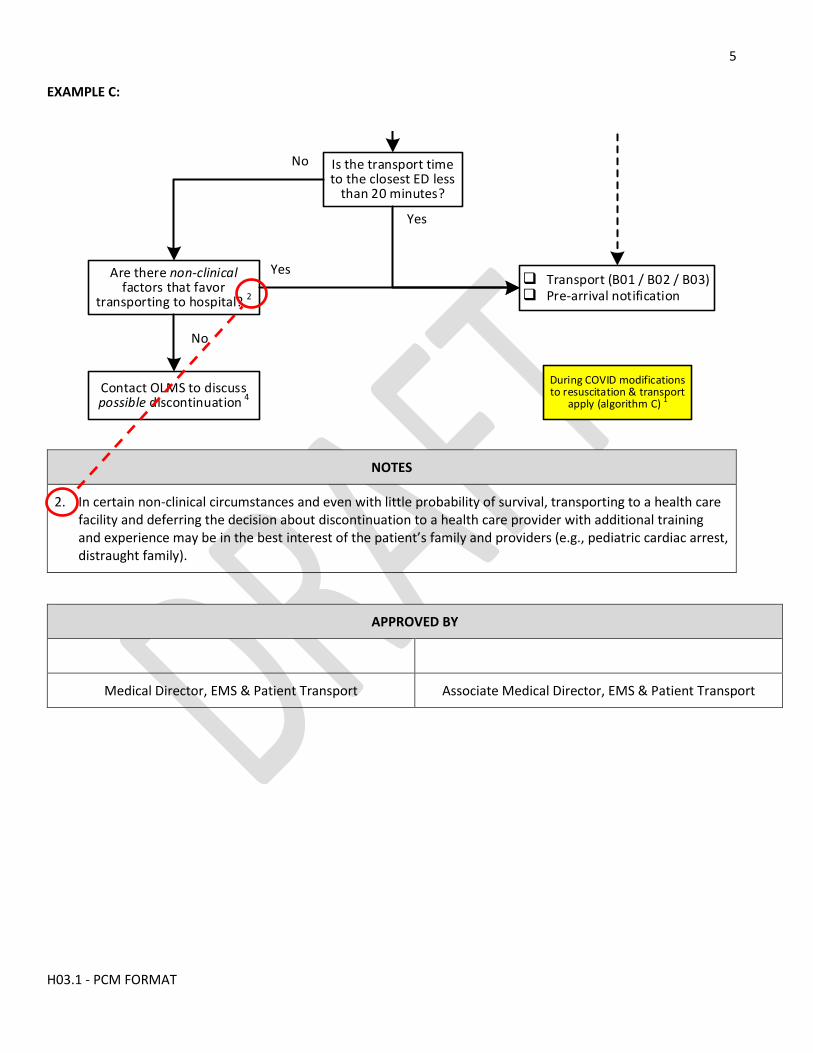
5
H03.1 - PCM FORMAT
EXAMPLE C:
Go to algorithm B
No
Yes
q Initiate CPRq Attach AED & analyze the rhythmq Shock the patient if shock advised q Immediately resume CPR & re-analyze
rhythm every 2 minutesq Repeat the CPR-analyze (+/- shock)
sequence on scene up to 3 times if no ROSC
Is there ROSC at any time?
Is the transport time to the closest ED less
than 20 minutes?
Yes
No
Contact OLMS to discuss possible discontinuation 4
No
Are there non-clinical factors that favor
transporting to hospital? 2
During COVID modifications to resuscitation & transport
apply (algorithm C) 1
Yesq Transport (B01 / B02 / B03)q Pre-arrival notification
ALGORITHM A: CARDIOPULMONARY ARREST
EMR: Paramedics with the basic & primary work scopes will follow this protocol.
NOTES
2. In certain non-clinical circumstances and even with little probability of survival, transporting to a health care facility and deferring the decision about discontinuation to a health care provider with additional training and experience may be in the best interest of the patient’s family and providers (e.g., pediatric cardiac arrest, distraught family).
APPROVED BY
Medical Director, EMS & Patient Transport Associate Medical Director, EMS & Patient Transport
1
H03.2 - MED FORMAT
H03.2 - MEDICATION PROTOCOL FORMAT
Version date: 2022-02-26 REFERENCE
NOTES (example A)
1. The medication documents are listed by category (A00.3) and alphabetically (A00.4).
2. The header appears on page 1 only. The page number will appear at the top right corner of each page. The alpha- numeric identifier and the medication generic name will be at the bottom left corner of each page.
3. The top right row of the header on the front page will contain the alphanumeric identifier and the generic name ofthe medication. If a medication is also commonly referred to by its proprietary name, that will also appear in italicsafter the generic name, such as with ketorolac which is more commonly known as Toradol (M12).
4. The alphanumeric indicator for all medications will begin with the letter “M”.
5. The left column of the second right row contains the age range to which the medication applies. If no age group isspecified, the document apples to all ages.
6. The right column of the second row indicates that this is from the medication documents section.
7. The third row contains the compliance statement, which pertains to the employees working for the ProvincialEMS/PT division of Shared Health ERS and providers operating under a service purchase agreement (SPA) with ERS toprovide emergency medical services to EMS.
SPA provider may be exempted from some or all of the EMS/PT care maps, policies, procedures, and protocols byagreement with ERS. Winnipeg Fire Paramedic Service is not within the division of Provincial EMS/PT.
8. The version date is important for ensuring that the most up-to-date document is being used.
9. The documents will always come into effect at 0700 hrs on the effective date, unless otherwise specified.
10. Each medication document will have a WORK SCOPE STATEMENT in a grey bar at the under the header.• ALL: The overall document or a specific medical function applies to paramedics with all work scopes.• EMR: The overall document or a specific medical function applies to paramedics with the basic and primary
work scopes.• PCP: The overall document or a specific medical function applies to paramedics with the primary and
intermediate work scopes.• ICP: The overall document or a specific medical function applies to paramedics with the intermediate work scope
only.
11. The INDICATIONS section includes those as they pertain only to EMS/PT protocols. It does not include everyindication for a medication as promoted by the manufacturer, or approved by Health Canada. Generally, EMS/PT willavoid the use of off-label indications unless there is a large body of credible supporting evidence.
EXAMPLE: The EMS/PT indications for magnesium (M24) include torsade des pointes and preeclampsia / eclampsia,but not severe asthma. Giving it to an asthmatic patient would exceed the paramedic’s scope of work for EMS/PT.
However, because magnesium is within the paramedic’s scope of practice, it could be given to an asthmatic patientwith an interim order from an ERS-affiliated physician (which word temporarily put it within the paramedic’s workscope).
2
H03.2 - MED FORMAT
12. Similarly, the CONTRAINDICATIONS section includes only those relevant to the EMS/PT scope of work. It does not include every contraindication.
13. The DOSING section will include the amount, route of administration, rate of administration (if applicable), repeat interval, and both the “single-dose maximum” and “cumulative-dose maximum” (if applicable).
14. The NOTES section will include more detailed information that helps in the correct and safe administration of the medication. This section may also highlight limited selected information from the training materials.
15. The LINKS section will include other the patient care maps for which this medication may be part of the therapy.
16. The CHANGES sections will include significant revisions to the current version of each document. The tracking of historical changes will be listed in other EMS/PT documents.

3
H03.2 - MED FORMAT
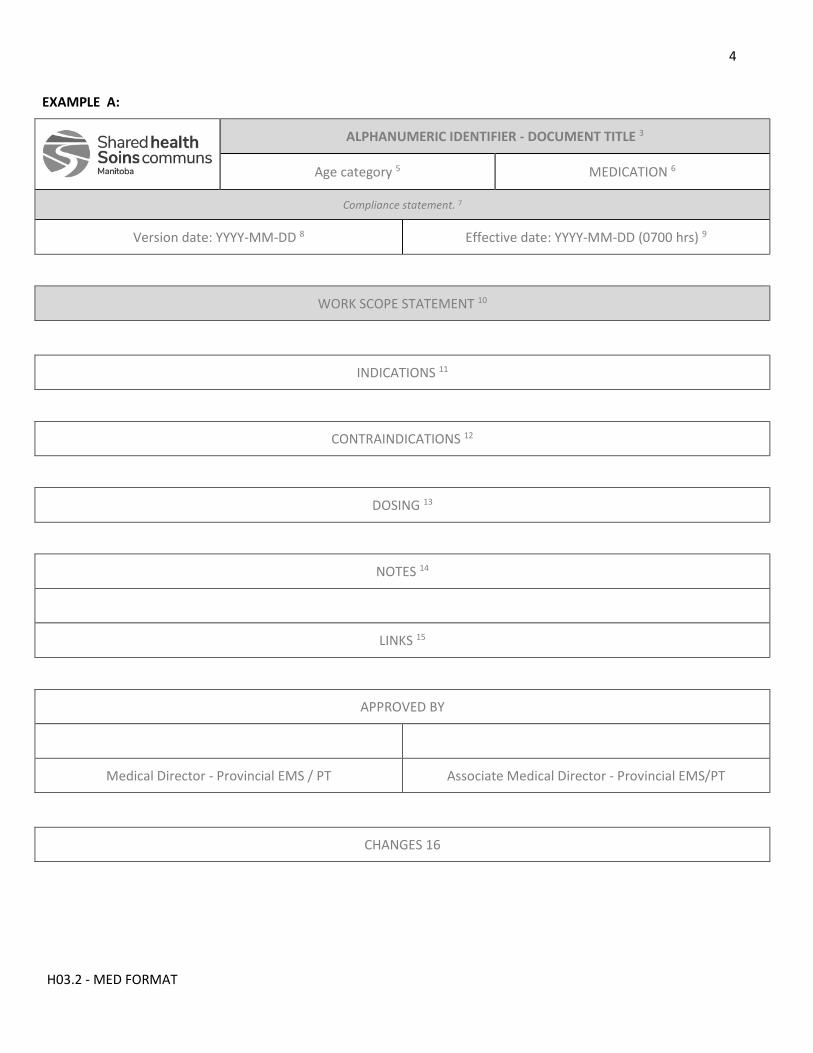
4
H03.2 - MED FORMAT
EXAMPLE A:
ALPHANUMERIC IDENTIFIER - DOCUMENT TITLE 3
Age category 5 MEDICATION 6
Compliance statement. 7
Version date: YYYY-MM-DD 8 Effective date: YYYY-MM-DD (0700 hrs) 9
WORK SCOPE STATEMENT 10
INDICATIONS 11
CONTRAINDICATIONS 12
DOSING 13
NOTES 14
LINKS 15
APPROVED BY
Medical Director - Provincial EMS / PT Associate Medical Director - Provincial EMS/PT
CHANGES 16
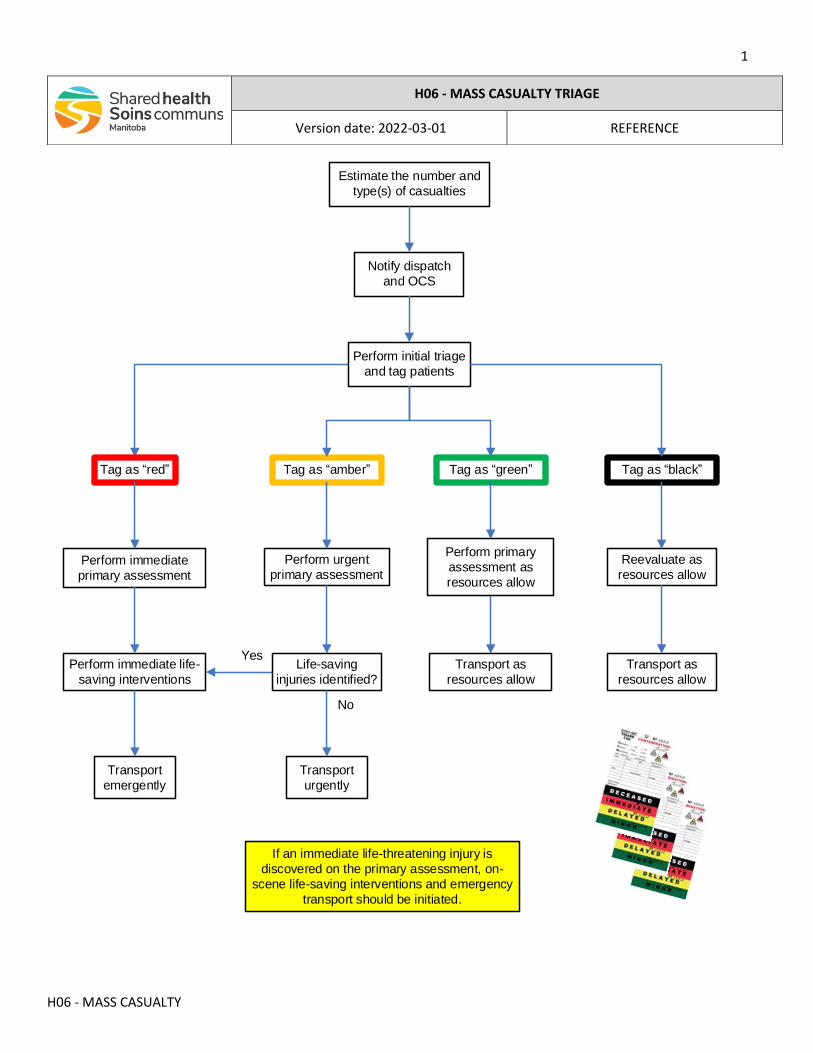
1
H06 - MASS CASUALTY
Estimate the number and
type(s) of casualties
Notify dispatch
and OCS
Perform immediate
primary assessment
Transport
emergently
Perform primary
assessment as
resources allow
Transport
urgently
Transport as
resources allow
Reevaluate as
resources allow
Perform initial triage
and tag patients
Perform urgent
primary assessment
Perform immediate life-
saving interventions
Tag as red Tag as amber
Tag as green Tag as black
Life-saving
injuries identified?
Transport as
resources allow
Yes
No
If an immediate life-threatening injury is
discovered on the primary assessment, on-
scene life-saving interventions and emergency
transport should be initiated.
H06 - MASS CASUALTY TRIAGE
Version date: 2022-03-01 REFERENCE
2
H06 - MASS CASUALTY
NOTES
• A mass casualty incident (MCI) is defined as any traumatic incident where the number and severity of casualties significantly exceeds the available personnel and resources currently on scene.
• Two triage tools (START and JUMPSTART) can be utilized to help the initial health care providers on the scene to rapidly sort through multiple casualties.
• The total number of casualties should be rapidly estimated and reassessed regularly, to ensure that no patients are missed.
• Perform an initial triage on all patients. Patients age ten years and older should be prioritized using the START triage algorithm (appendix A). Use the JumpSTART algorithm for patients under ten years of age or when a child’s age is unknown (appendix B). A triage tag should be attached to all patients to ensure that no patients are missed.
• RED: These patients are given the highest priority, and should have an immediate trauma primary assessment to rapidly exclude immediate life-threatening injuries (airway obstruction, hypoxemia, exsanguinating hemorrhage, tension pneumothorax). Providers with the appropriate delegations should treat immediate life-threatening injuries on scene. These patients require emergency transport to a facility capable of providing trauma care to survive.
• AMBER: These patients are of intermediate priority, and should have an urgent primary assessment. Immediately life-threatening injuries should be treated on-scene as with “red” patients. These patients will require prompt treatment of their injuries. The urgency of transport will depend on findings from the primary survey. If immediate life-threatening injuries are discovered, they should be upgraded to highest transport priority.
• GREEN: These patients are of lower priority. They should have a primary assessment as soon as possible after the “red” and “amber” patients have been cared for. The treatment of their injuries can often be safely deferred or delayed to allow care to higher priority patients. The timing of transport will depend on the findings from the primary survey and other transport priorities.
• BLACK: These patients are predicted not to survive. In a MCI, patients with a chance of recovery must be given a higher priority. The priority for transport is lowest and depends upon available resources.
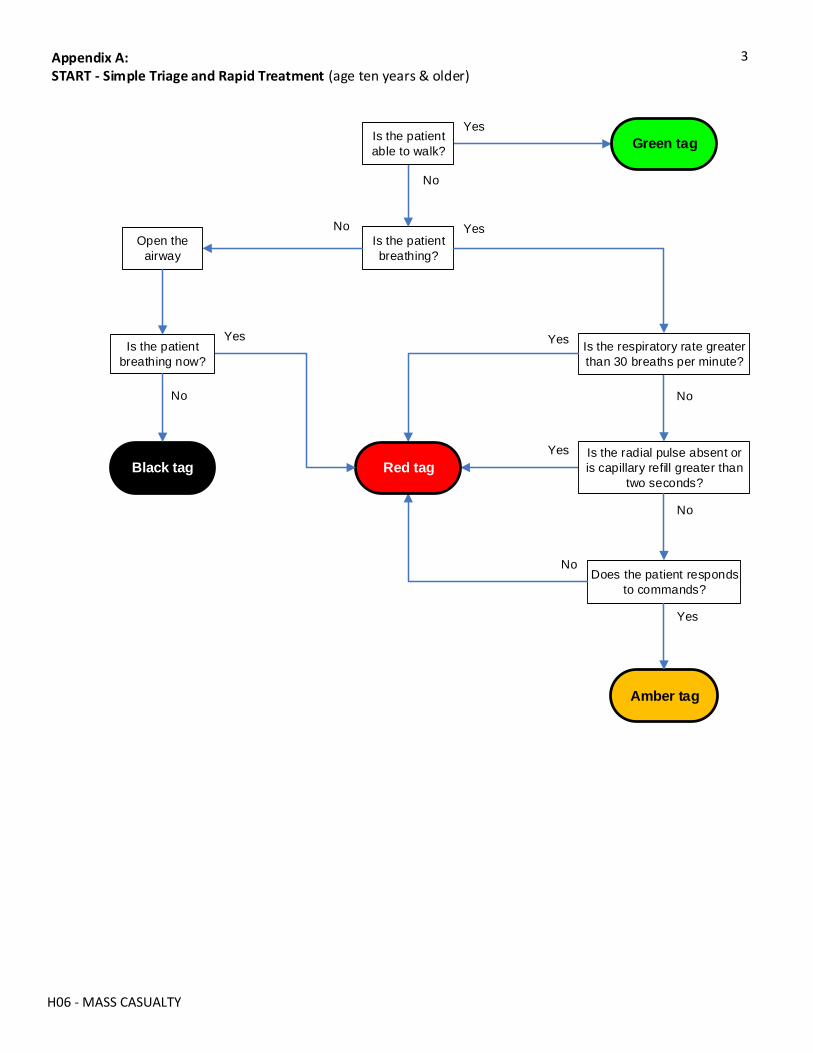
3
H06 - MASS CASUALTY
Is the patient
breathing?
Open the
airway
Is the respiratory rate greater
than 30 breaths per minute?
Amber tag
Green tag
Does the patient responds
to commands?
Yes
Is the radial pulse absent or
is capillary refill greater than
two seconds?
Black tag Red tag
No
Appendix A:START - Simple Triage and Rapid Treatment (age ten years & older)
Is the patient
able to walk?
Is the patient
breathing now?
No
No
Yes
Yes Yes
No
Yes
No
No
Yes
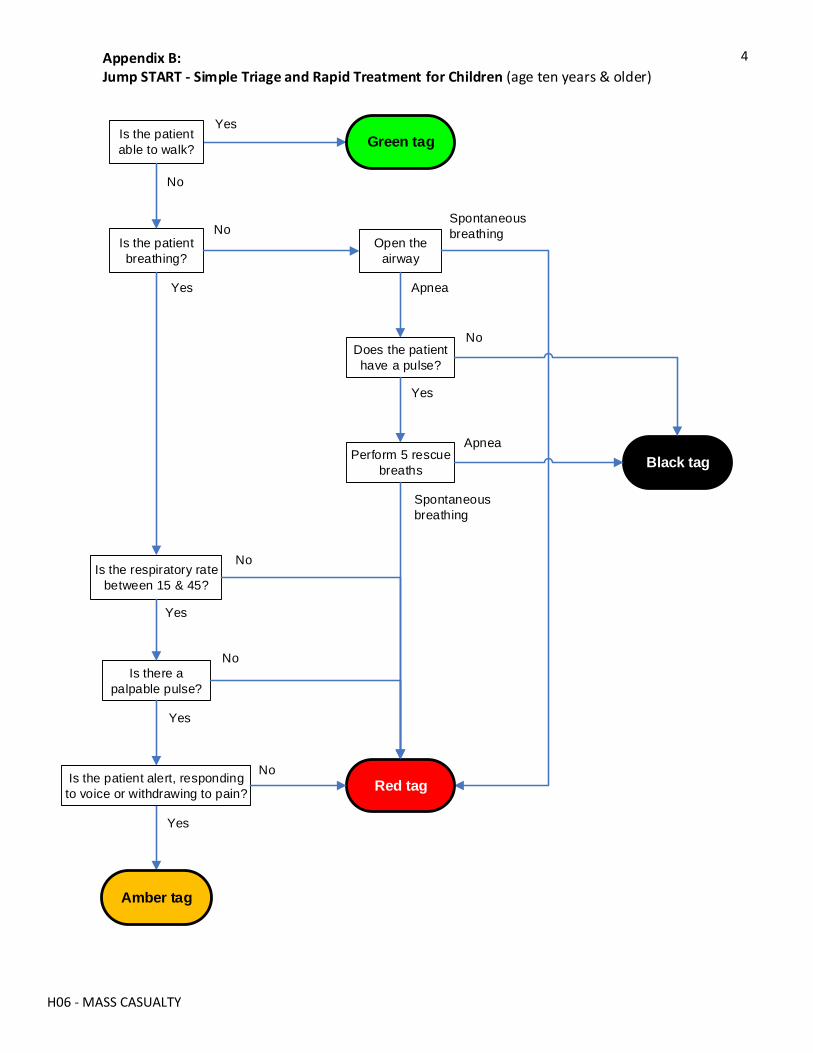
4
H06 - MASS CASUALTY
Is the patient
breathing?
Is the respiratory rate
between 15 & 45?
Green tag
Is there a
palpable pulse?
Appendix B:Jump START - Simple Triage and Rapid Treatment for Children (age ten years & older)
Is the patient
able to walk?
No
Yes
Yes
No
Open the
airway
Spontaneous
breathing
Does the patient
have a pulse?
Black tagPerform 5 rescue
breaths
Apnea
Apnea
Spontaneous
breathing
Is the patient alert, responding
to voice or withdrawing to pain?
Amber tag
Yes
No
No
Yes
Yes
No
Red tag
Yes
No
H07 - SCOPES
H07 - DIFFERENTIATING PRACTICE SCOPE & WORK SCOPE
Version date: 2021-11-05 REFERENCE
All paramedics are required to know their scope of practice and adhere to it at all times. A paramedic may not perform a medical function that exceeds their regulated scope of practice or their competency. A paramedic cannot
accept a physician’s order if it carrying out the order would exceed their scope of practice or their competency.
SCOPE OF PRACTICE
A paramedic’s scope of practice is the group of reserved acts that a paramedic is lawfully able to perform and is determined by the paramedic’s subregistration with the College of Paramedics of Manitoba (CPMB), or the College.
A reserved act is a medical function that can only legally be performed by health professionals, and is defined by the Regulated Health Professions Act (RHPA). With the establishment of the College of Paramedics of Manitoba (CPMB) in 2020, paramedicine became a self-regulated profession and members are permitted to perform certain of the reserved acts by virtue of being a registrant of the College.
The authority of the College to set scope of practice for paramedics is established by legislation, and only the College can regulate the paramedics’ scope of practice. Paramedics may not perform a reserved act that is not allowed by the College, even with a physician’s order, and could face disciplinary action from the College for doing so.
EXAMPLE: A primary care paramedic (PCP) who has been doing “observer” shifts in the local ER. The physician on-duty offers them a chance to suture a patient while he supervises. Can the paramedic do this because the physician says he can?
ANSWER: NO! As a PCP they cannot perform suturing, even under the direct supervision of a physician, because it is not within his scope of practice as a PCP.
SCOPE OF WORK
A paramedic’s scope of work is the set of medical functions that the employer allows a paramedic to perform when working for that employer.
The scope of work is established by the employer and may differ among different employers. It might be equivalent to or smaller than the paramedic’s regulated scope of practice, but it can never exceed a paramedic’s scope of practice. Exceeding the employer’s scope of work could lead to disciplinary action by the employer, and could potentially result in a complaint to the College.
The scope of work for the employees of Shared Health ERS and its affiliates is defined by the patient care maps, medication documents, clinical policies, and standard operating propcedures. In the event of any discrepancy between the Shared Health documents and the CPMB standards of practice, the latter takes precedence.
EXAMPLE: An advanced care paramedic (ACP) works for an EMS service whose policy is to use blind insertion airway devices (BIAD) for airway management. The ACP believes that it is unethical to insert a BIAD when they are very
H07 - SCOPES
competent at endotracheal intubation (ETI) and the College allows it. They are also concerned about their legal liability. Should they opt for ETI?
ANSWER: NO! Even though it is within their scope of practice and competenct, ETI is not within the work scope of the employer. If they transferred to a different EMS service that supported a broader scope of practice, they could do ETI as long as they could prove and maintain their competency. In terms of liability, if they were to cause patient harm they could be in greater legal jeopardy with the plaintiff, the employer, and the College.
COMPETENCY & SELF REGULATION
A paramedic will be viewed as competent to perform a medical function, based upon their education and training, how many times and how recently they have performed the function, as well as their personal aptitude and motivation. Competency can change over time. It may wane if one has not done a particular medical function in quite some time.
A paramedic is required by regulation to self monitor and self identify their competency, and must not perform any reserved act that exceeds their competency. A paramedic’s performance will be judged against that of their peers. If the profession has established a consensus about how often a medical function should be performed, that is the standard of care that a parmedic will be judged by. Hence, the term self-regulation.
EXAMPLE: Due to a variety of factors an ACP has not performed a single ETI in 12 months and no longer feels comfortable or competent to do so. Should they just keep quiet about this?
ANSWER: NO! The paramedic is ethically (and legally) required to identify that they need additional practice. If they were to inform their employer, arrangements could be made for them to spend a few days in the OR with an anaesthesiologist practicing ETI.
STANDING ORDERS
Depending on the subregistration with the College, a paramedic’s scope of practice will include the administration of medications. But, this requires an order from a prescribing provider, such as a physician. This is analgous to the practice scope of a registered nurse (RN).
The Shared Health ERS medication documents are standing orders by which a paramedic may give a medication. They are established in advance (hence, the term “standing”) and include the conditions under which a paramedic may administer a medication. These conditions include the indications and contraindications; dose, route and frequency; and the work scope of a paramedic who can administer the medication.
If something is not covered by a current standing order, a Shared Health physician may provide a temporary or interim order that deviates from the established orders, but allows the parmedic to tailor treatment to a specific patient or circumstance.
But, physicain orders, whether standing or temporary, do not allow a paramedic to exceed their scope of practice.
EXAMPLE: A protocol allows for only three doses of the medication to be administered during a transport of the usual duration. Due to bad weather conditions, the transport is taking twice as long as usual and the patient requires a fourth dose. Should the paramedic just go ahead and administer the fourth dose?
ANSWER: No!

H07 - SCOPES
They should contact the on-line medical support (OLMS) physician for an interim order. Of note, the service’s medical director should then revise the protocol to allow for such contingencies.
EXAMPLE: A EMR reads an article describing how to insert in intravenous (IV) line. The EMR responds to a primary response call and believes the patient would benefit from an IV line. Should they contact the OLMS physician to obtain an interim order for an IV line?
ANSWER: No! It is not within their scopes of practice or work, and probably exceeds their competency. If they do not self-identify to the OLMS physician that their scope of work does not allow for IV starts, they could face consequences from both the College and the employer.
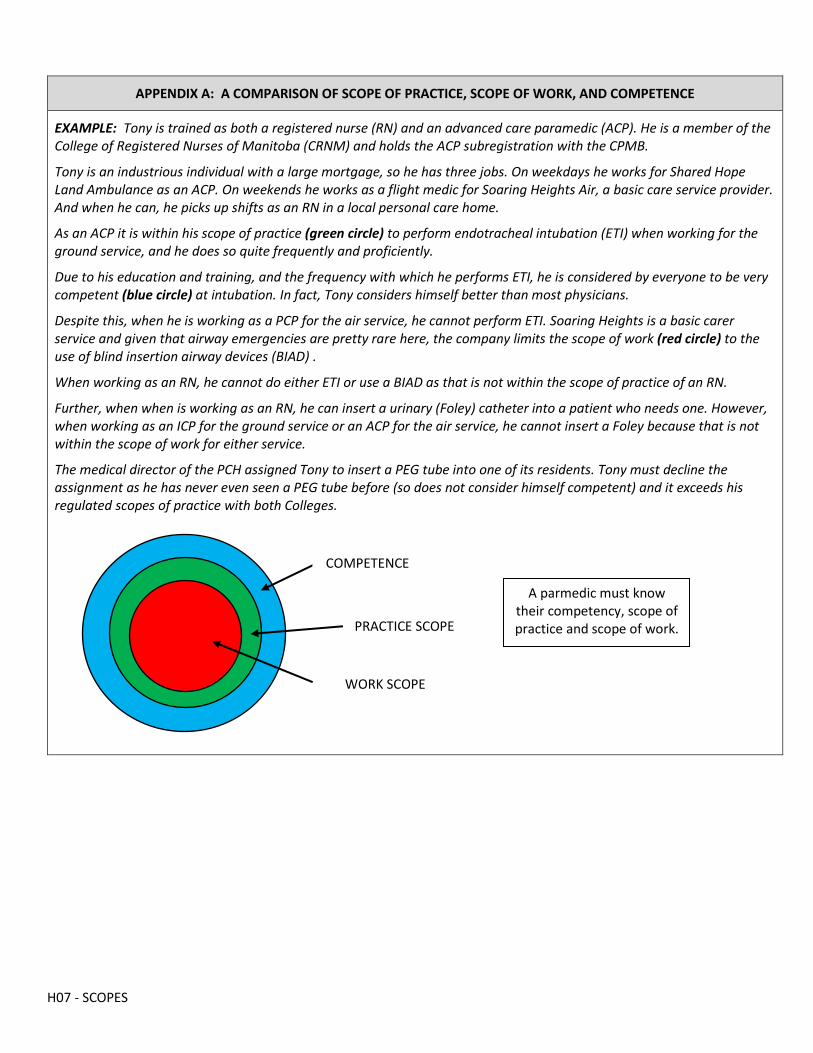
H07 - SCOPES
APPENDIX A: A COMPARISON OF SCOPE OF PRACTICE, SCOPE OF WORK, AND COMPETENCE
EXAMPLE: Tony is trained as both a registered nurse (RN) and an advanced care paramedic (ACP). He is a member of the College of Registered Nurses of Manitoba (CRNM) and holds the ACP subregistration with the CPMB.
Tony is an industrious individual with a large mortgage, so he has three jobs. On weekdays he works for Shared Hope Land Ambulance as an ACP. On weekends he works as a flight medic for Soaring Heights Air, a basic care service provider. And when he can, he picks up shifts as an RN in a local personal care home.
As an ACP it is within his scope of practice (green circle) to perform endotracheal intubation (ETI) when working for the ground service, and he does so quite frequently and proficiently.
Due to his education and training, and the frequency with which he performs ETI, he is considered by everyone to be very competent (blue circle) at intubation. In fact, Tony considers himself better than most physicians.
Despite this, when he is working as a PCP for the air service, he cannot perform ETI. Soaring Heights is a basic carer service and given that airway emergencies are pretty rare here, the company limits the scope of work (red circle) to the use of blind insertion airway devices (BIAD) .
When working as an RN, he cannot do either ETI or use a BIAD as that is not within the scope of practice of an RN.
Further, when when is working as an RN, he can insert a urinary (Foley) catheter into a patient who needs one. However, when working as an ICP for the ground service or an ACP for the air service, he cannot insert a Foley because that is not within the scope of work for either service.
The medical director of the PCH assigned Tony to insert a PEG tube into one of its residents. Tony must decline the assignment as he has never even seen a PEG tube before (so does not consider himself competent) and it exceeds his regulated scopes of practice with both Colleges.
COMPETENCE
PRACTICE SCOPE
WORK SCOPE
A parmedic must know their competency, scope of practice and scope of work.
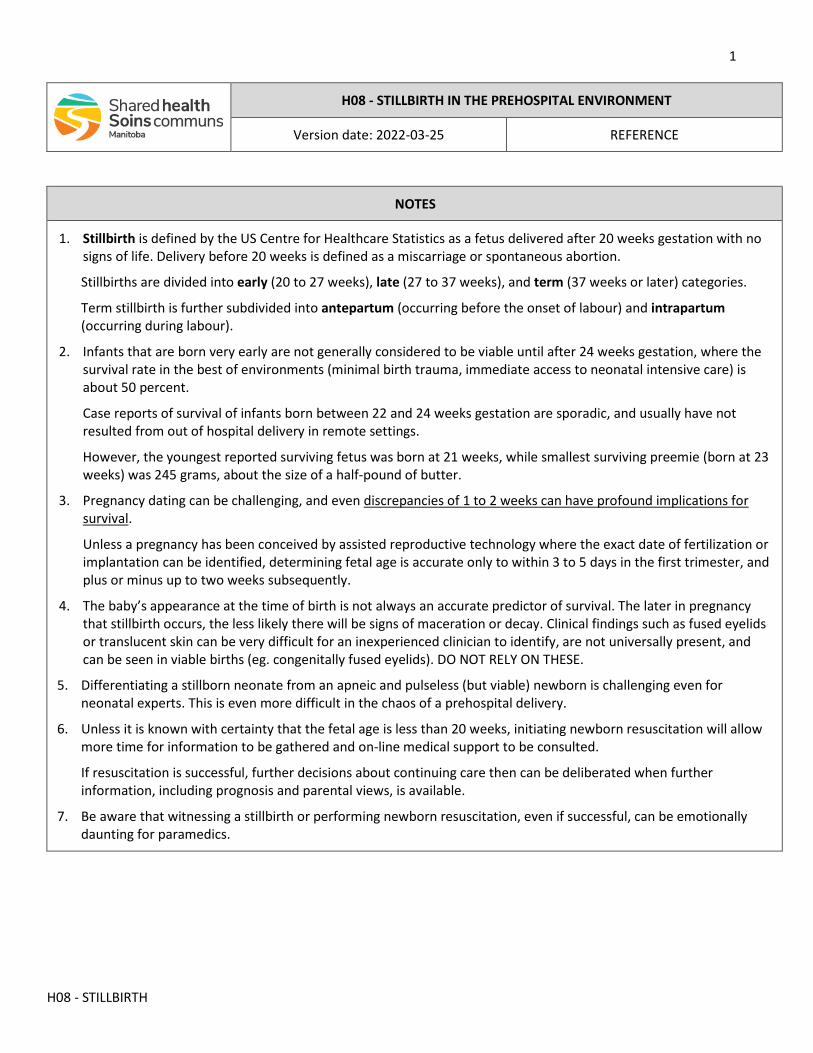
1
H08 - STILLBIRTH
H08 - STILLBIRTH IN THE PREHOSPITAL ENVIRONMENT
Version date: 2022-03-25 REFERENCE
NOTES
1. Stillbirth is defined by the US Centre for Healthcare Statistics as a fetus delivered after 20 weeks gestation with no signs of life. Delivery before 20 weeks is defined as a miscarriage or spontaneous abortion.
Stillbirths are divided into early (20 to 27 weeks), late (27 to 37 weeks), and term (37 weeks or later) categories.
Term stillbirth is further subdivided into antepartum (occurring before the onset of labour) and intrapartum (occurring during labour).
2. Infants that are born very early are not generally considered to be viable until after 24 weeks gestation, where the survival rate in the best of environments (minimal birth trauma, immediate access to neonatal intensive care) is about 50 percent.
Case reports of survival of infants born between 22 and 24 weeks gestation are sporadic, and usually have not resulted from out of hospital delivery in remote settings.
However, the youngest reported surviving fetus was born at 21 weeks, while smallest surviving preemie (born at 23 weeks) was 245 grams, about the size of a half-pound of butter.
3. Pregnancy dating can be challenging, and even discrepancies of 1 to 2 weeks can have profound implications for survival.
Unless a pregnancy has been conceived by assisted reproductive technology where the exact date of fertilization or implantation can be identified, determining fetal age is accurate only to within 3 to 5 days in the first trimester, and plus or minus up to two weeks subsequently.
4. The baby’s appearance at the time of birth is not always an accurate predictor of survival. The later in pregnancy that stillbirth occurs, the less likely there will be signs of maceration or decay. Clinical findings such as fused eyelids or translucent skin can be very difficult for an inexperienced clinician to identify, are not universally present, and can be seen in viable births (eg. congenitally fused eyelids). DO NOT RELY ON THESE.
5. Differentiating a stillborn neonate from an apneic and pulseless (but viable) newborn is challenging even for neonatal experts. This is even more difficult in the chaos of a prehospital delivery.
6. Unless it is known with certainty that the fetal age is less than 20 weeks, initiating newborn resuscitation will allow more time for information to be gathered and on-line medical support to be consulted.
If resuscitation is successful, further decisions about continuing care then can be deliberated when further information, including prognosis and parental views, is available.
7. Be aware that witnessing a stillbirth or performing newborn resuscitation, even if successful, can be emotionally daunting for paramedics.
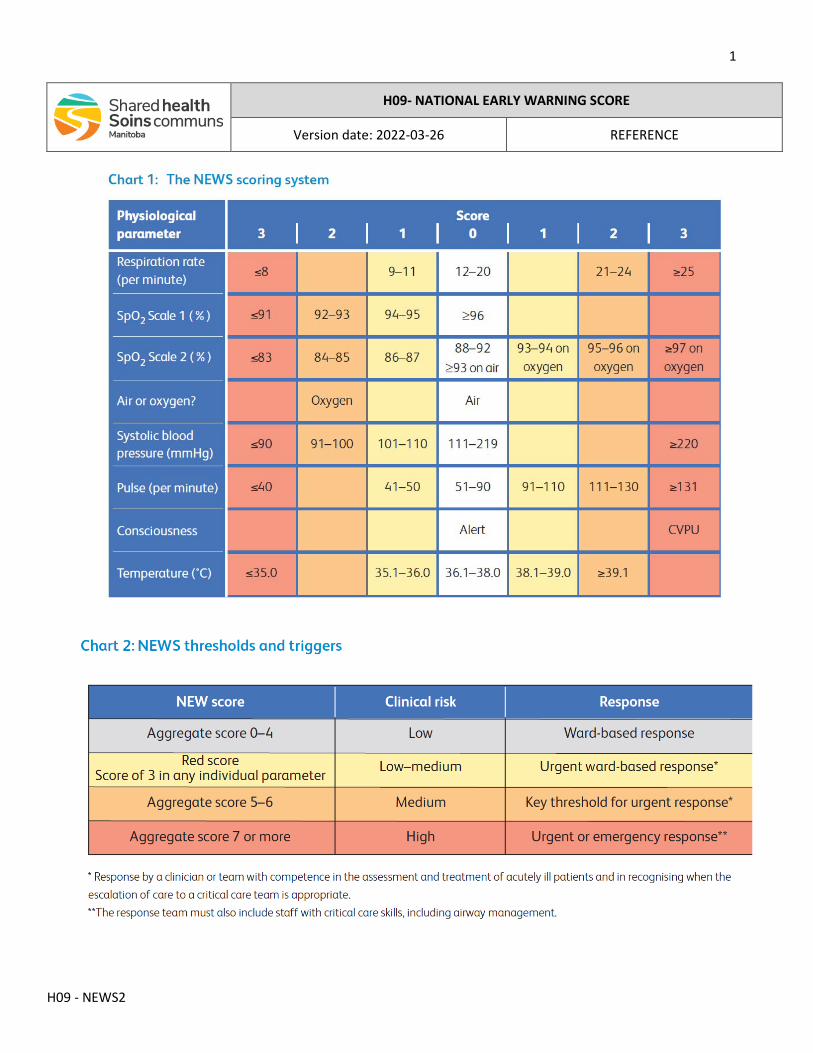
1
H09 - NEWS2
H09- NATIONAL EARLY WARNING SCORE
Version date: 2022-03-26 REFERENCE
1
M01 - ADENOSINE
M01 - ADENOSINE (ADENOCARD)
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-12 Effective date: 2022-03-16 (0700 hours)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
• Paroxysmal supraventricular tachycardia (PSVT) with stable hemodynamics • Regular narrow-complex tachycardia (NCT) suspected to be PSVT with stable hemodynamics • PSVT with known aberrant conduction and stable hemodynamics 2
CONTRAINDICATIONS
• Tachycardia (regardless of QRS duration) with unstable hemodynamics • Known or suspected ventricular tachycardia • Undifferentiated wide-complex tachycardia (WCT)
INTRAVENOUS / INTRAOSSEOUS DOSING
• 10 YEARS & OLDER: o First dose - 6 mg o Second dose - 12 mg
• 12 MONTHS UP TO 10 YEARS: o First dose - 0.1 mg/kg (single-dose maximum = 6 mg) o Second dose - 0.2 mg/kg (single-dose maximum = 12 mg)
• Administer by rapid push, followed with saline flush • Consider repeat dosing as required 5 • May be administered by IO route if already established for another indication
2
M01 - ADENOSINE
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Administer adenosine for paroxysmal supraventricular tachycardia (PSVT) with known aberrant conduction (QRS complexes greater than 120 milliseconds) and stable hemodynamics only if the QRS complexes are regular and monomorphic.
3. Patients should be forewarned about the subjective sensations (dyspnea, lightheadedness, nausea, sense of impending doom) that accompany the drug.
4. There should be evidence of successful central drug delivery such as bradycardia or asystole on the ECG monitor, and the patient may complain of the above-noted sensations.
5. If the tachycardia initially converts but then recurs, providers may consider repeated dosing. However, recurrence remains likely. Consider the transport duration and the patient’s ability to tolerate the tachycardia until additional assessment and other interventions can be initiated if arrhythmia recurs.
6. An ERS affiliated physician and/or designated paramedic may temporarily authorize the administration of this medication by a delegation. The receiving paramedic are responsible to know their CPMB scope of practice and may not exceed it. The receiving paramedic may only accept a delegation that is within their knowledge, experience and competency.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M02.1 - ACETAMINOPHEN
M02.1 - ACETAMINOPHEN (TYLENOL)
All ages MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-05-03 Effective date: 2022-05-04 (0700 hrs)
ALL: Paramedics with the all work scopes may administer this medication.
INDICATIONS
• Mild to moderate pain • Fever
CONTRAINDICATIONS
• True allergy to acetaminophen • Known or suspected liver failure
ORAL DOSING
• 12 YEARS & OLDER: o 325 to 650 mg (regular strength) or o 500 to 1000 mg (extra strength)
• 72 HOURS UP TO 12 YEARS: o 10 to 15 mg/kg o Single-dose maximum = 325 mg
• Repeat every 4 hours as required • Do not administer if surgery is anticipated within the next 4 hours
2
M02.1 - ACETAMINOPHEN
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Rectal dosing route removed
1
M02.2 - IBUPROFEN
M02.2 - IBUPROFEN (ADVIL, MOTRIN)
3 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-12 Effective date: 2022-03-16 (0700 hrs)
ALL: Paramedics with the all work scopes may administer this medication.
INDICATIONS
• Mild to moderate pain • Fever
CONTRAINDICATIONS
• True allergy to ibuprofen or aspirin (ASA) induced asthma or bronchospasm • Major trauma or other active bleeding • Pregnancy • End-stage renal failure
ORAL DOSING
• 12 YEARS & OLDER: o 400 to 800 mg
• 3 MONTHS UP TO 12 YEARS: o 10 mg/kg PO o Single-dose maximum = 400 mg
• Repeat every 6 hours as required • Do not administer if surgery is anticipated within the next 4 hours
2
M02.2 - IBUPROFEN
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M03.1 - MORPHINE
M03.1 - MORPHINE
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-12 Effective date: 2022-03-16 (0700 hrs)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
INTRAMUSCULAR: • Moderate to severe pain from an acute illness, injury, or an exacerbation of a chronic condition that is significant
enough to require analgesic to facilitate safe and comfortable patient transport
INTRAVENOUS / INTRAOSSEOUS: • Moderate to severe pain from an acute illness, injury, or an exacerbation of a chronic condition that is significant
enough to require analgesic to facilitate safe and comfortable patient transport • Dyspnea due to pulmonary edema
CONTRAINDICATIONS
• True allergy to morphine • Decreased level of consciousness or known / suspected significant head injury • Significant drug or alcohol intoxication • Uncorrected / uncorrectable hypotension or hypo-perfusion • Hypoventilation or respiratory failure
2
M03.1 - MORPHINE
INTRAMUSCULAR DOSING
• 10 YEARS & OLDER: 2 o 0.1 mg/kg o Single-dose maximum = 10 mg o Cumulative maximum = 20 mg per hour
• 12 MONTHS UP TO 10 YEARS: o 0.1 mg/kg o Single-dose maximum = 5 mg o Cumulative maximum = 10 mg per hour
• Repeat every 30 minutes as required • If known bleeding disorder or anticoagulation is present, use caution when administering by IM route
INTRAVENOUS / INTRAOSSEOUS
• 10 YEARS & OLDER: 3 o 0.1 mg/kg o Single-dose maximum = 10 mg o Cumulative maximum = 20 mg per hour
12 MONTHS UP TO 10 YEARS: o 0.1 mg/kg o Single maximum dose = 5 mg o Cumulative maximum = 10 mg per hour
• Administered by slow push over 60 seconds • Repeat every 15 minutes as required • May administer by IO route if IV access is not available and IO access has been established for another indication
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Patients who are compensating for hemodynamic compromise may develop hypotension after morphine administration. If hypotension develops, give IV fluid by rapid bolus and reassess before repeating opioid administration.
3. Morphine may have more pronounced effects on the central nervous, respiratory and cardiovascular systems in the elderly, especially if frail or compromised. Consider smaller doses and slower administration in patients greater than 75 years of age.
3
M03.1 - MORPHINE
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
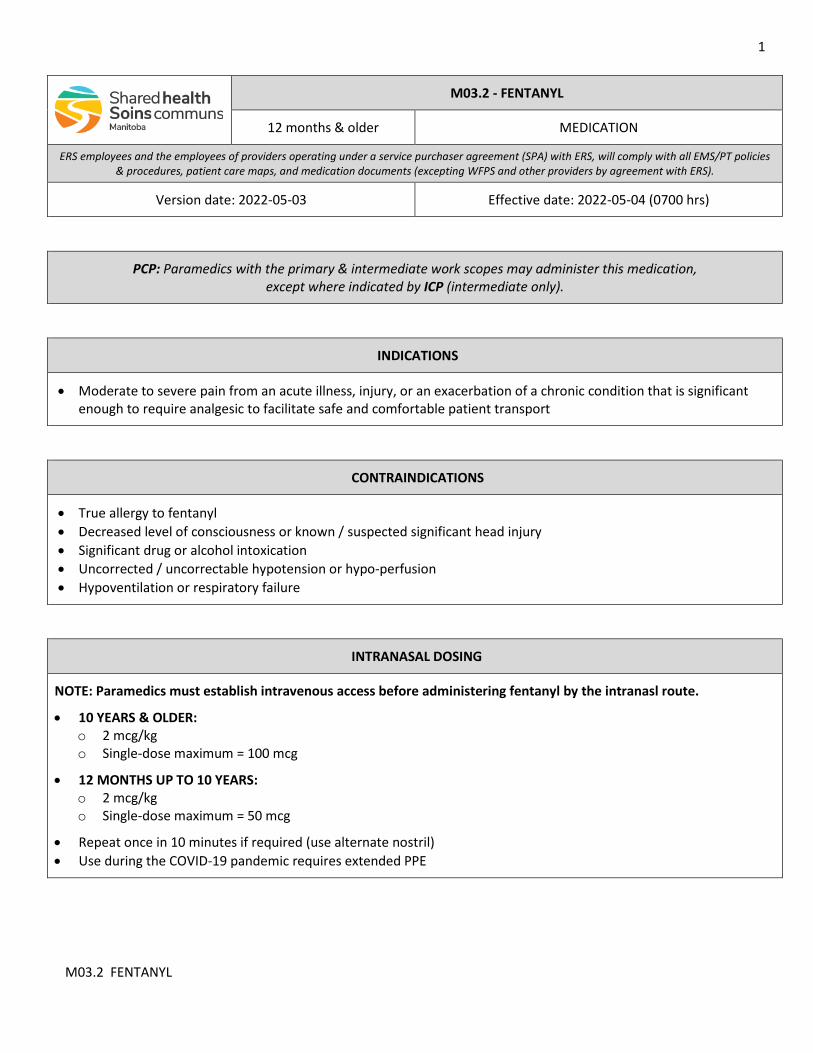
1
M03.2 FENTANYL
M03.2 - FENTANYL
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-05-03 Effective date: 2022-05-04 (0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication, except where indicated by ICP (intermediate only).
INDICATIONS
• Moderate to severe pain from an acute illness, injury, or an exacerbation of a chronic condition that is significant enough to require analgesic to facilitate safe and comfortable patient transport
CONTRAINDICATIONS
• True allergy to fentanyl • Decreased level of consciousness or known / suspected significant head injury • Significant drug or alcohol intoxication • Uncorrected / uncorrectable hypotension or hypo-perfusion • Hypoventilation or respiratory failure
INTRANASAL DOSING
NOTE: Paramedics must establish intravenous access before administering fentanyl by the intranasl route.
• 10 YEARS & OLDER: o 2 mcg/kg o Single-dose maximum = 100 mcg
• 12 MONTHS UP TO 10 YEARS: o 2 mcg/kg o Single-dose maximum = 50 mcg
• Repeat once in 10 minutes if required (use alternate nostril) • Use during the COVID-19 pandemic requires extended PPE
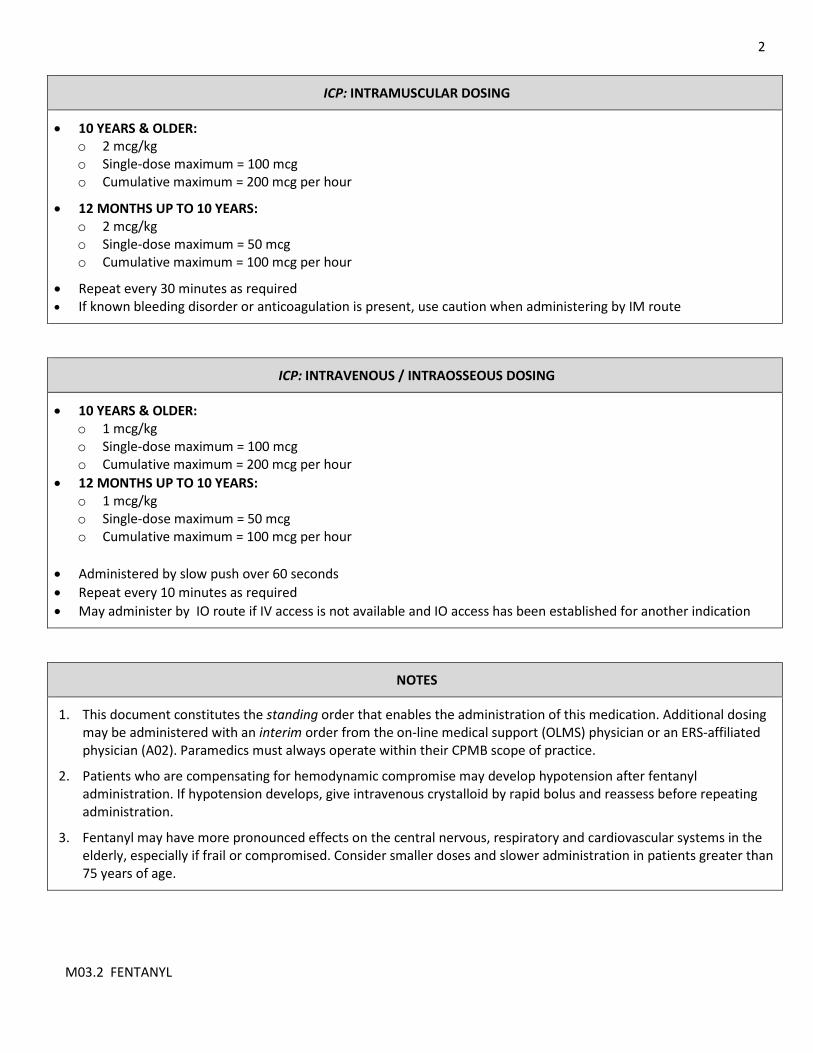
2
M03.2 FENTANYL
ICP: INTRAMUSCULAR DOSING
• 10 YEARS & OLDER: o 2 mcg/kg o Single-dose maximum = 100 mcg o Cumulative maximum = 200 mcg per hour
• 12 MONTHS UP TO 10 YEARS: o 2 mcg/kg o Single-dose maximum = 50 mcg o Cumulative maximum = 100 mcg per hour
• Repeat every 30 minutes as required • If known bleeding disorder or anticoagulation is present, use caution when administering by IM route
ICP: INTRAVENOUS / INTRAOSSEOUS DOSING
• 10 YEARS & OLDER: o 1 mcg/kg o Single-dose maximum = 100 mcg o Cumulative maximum = 200 mcg per hour
• 12 MONTHS UP TO 10 YEARS: o 1 mcg/kg o Single-dose maximum = 50 mcg o Cumulative maximum = 100 mcg per hour
• Administered by slow push over 60 seconds • Repeat every 10 minutes as required • May administer by IO route if IV access is not available and IO access has been established for another indication
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Patients who are compensating for hemodynamic compromise may develop hypotension after fentanyl administration. If hypotension develops, give intravenous crystalloid by rapid bolus and reassess before repeating administration.
3. Fentanyl may have more pronounced effects on the central nervous, respiratory and cardiovascular systems in the elderly, especially if frail or compromised. Consider smaller doses and slower administration in patients greater than 75 years of age.
3
M03.2 FENTANYL
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Mandatory IV access added
1
M04.1 - DIMENHYDRINATE
M04.1 – DIMENHYDRINATE (GRAVOL)
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Nausea and/or vomiting • Nausea and vomiting during pregnancy • Prevention of opioid-induced nausea or vomiting
CONTRAINDICATIONS
• True allergy to dimenhydrinate
INTRAMUSCULAR / INTRAVENOUS / INTRAOSSEOUS DOSING
• 17 YEARS & OLDER: o 50 mg
• 10 UP TO 17 YEARS: o 25 to 50 mg
• 12 MONTHS UP TO 10 YEARS: o 0.5 mg/kg o Single-dose maximum = 25 mg
• Repeat every 4 hours as required • If known bleeding disorder or anticoagulation is present, use caution when administering by IM route • May administer by IO route if IV access is not available and IO access has been established for another indication
2
M04.1 - DIMENHYDRINATE
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M04.2 - METOCLOPRAMIDE
M04.2 – METOCLOPRAMIDE (MAXERAN)
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Nausea and/or vomiting • Nausea and vomiting during pregnancy • Prevention of opioid-induced nausea or vomiting
CONTRAINDICATIONS
• True allergy to metoclopramide • Known or suspected bowel obstruction
INTRAMUSCULAR / INTRAVENOUS / INTRAOSSEOUS DOSING
• 17 YEARS & OLDER: o 10 mg
• 10 UP TO 17 YEARS: o 5 to 10 mg
• 12 MONTHS UP TO 10 YEARS: o 0.1 mg/kg o Single-dose maximum = 5 mg
• Repeat every 6 hours as required • If known bleeding disorder or anticoagulation is present, use caution when administering by IM route • May administer by IO route if IV access is not available and IO access has been established for another indication
2
M04.2 - METOCLOPRAMIDE
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
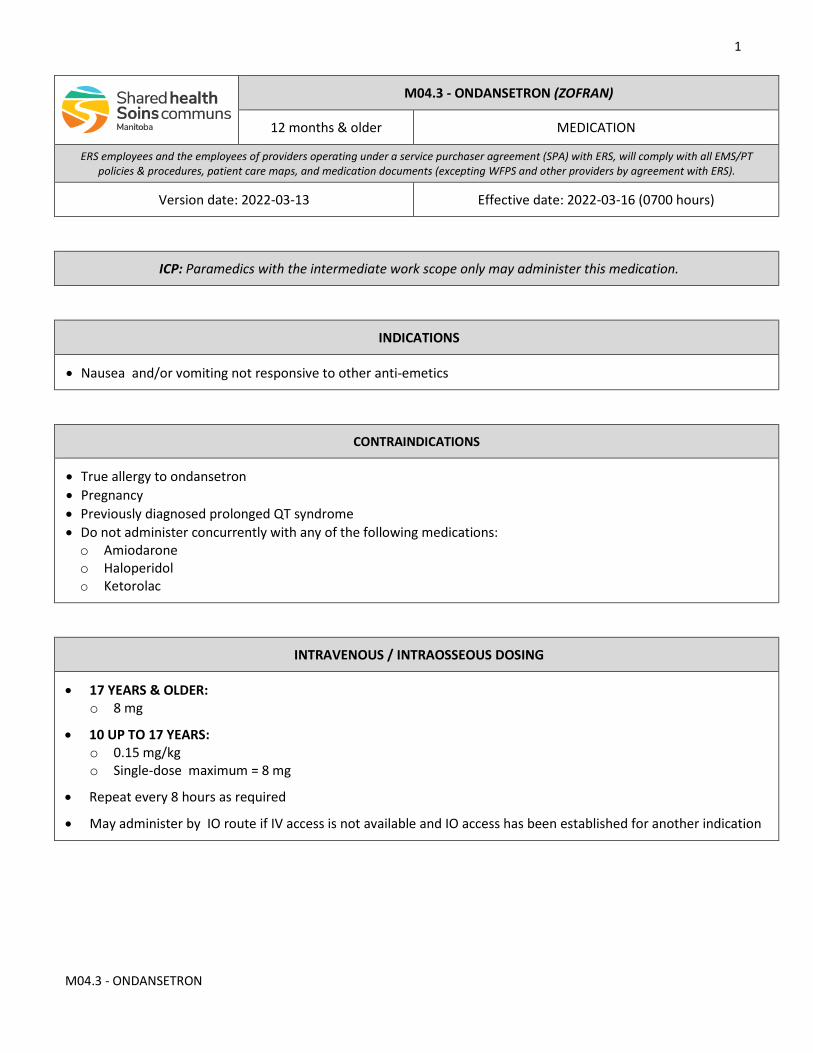
1
M04.3 - ONDANSETRON
M04.3 - ONDANSETRON (ZOFRAN)
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
• Nausea and/or vomiting not responsive to other anti-emetics
CONTRAINDICATIONS
• True allergy to ondansetron • Pregnancy • Previously diagnosed prolonged QT syndrome • Do not administer concurrently with any of the following medications: o Amiodarone o Haloperidol o Ketorolac
INTRAVENOUS / INTRAOSSEOUS DOSING
• 17 YEARS & OLDER: o 8 mg
• 10 UP TO 17 YEARS: o 0.15 mg/kg o Single-dose maximum = 8 mg
• Repeat every 8 hours as required
• May administer by IO route if IV access is not available and IO access has been established for another indication
2
M04.3 - ONDANSETRON
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional medications may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
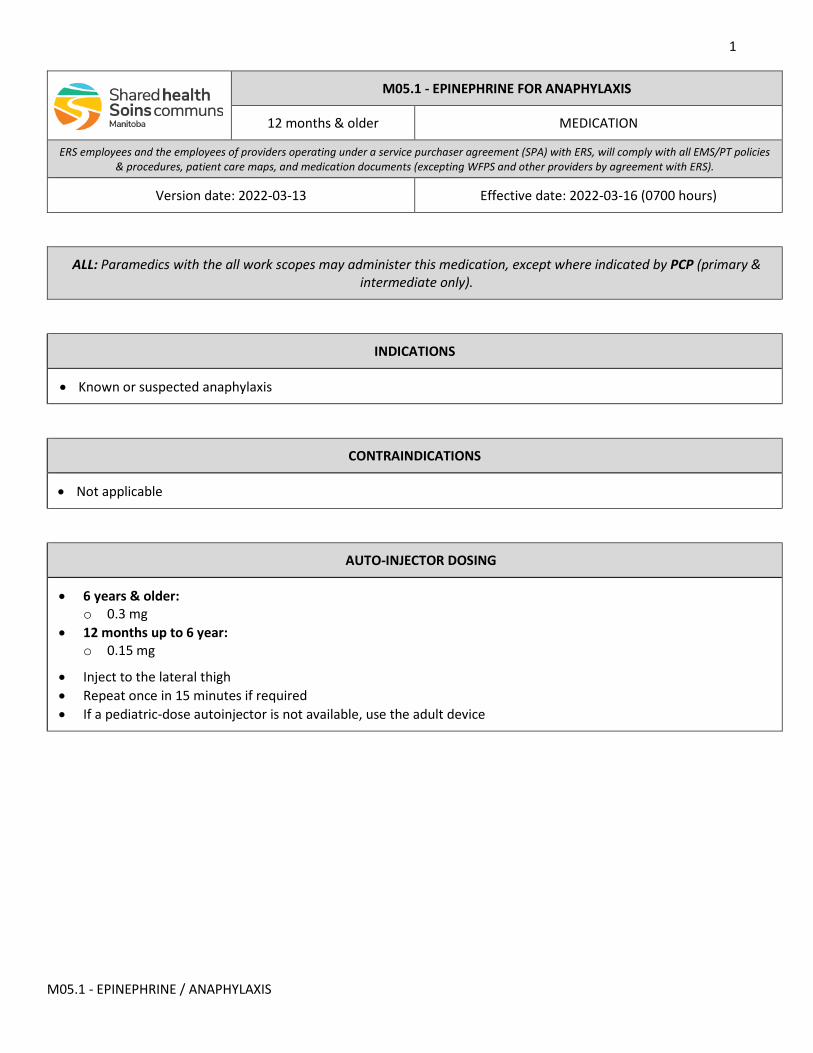
1
M05.1 - EPINEPHRINE / ANAPHYLAXIS
M05.1 - EPINEPHRINE FOR ANAPHYLAXIS
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
ALL: Paramedics with the all work scopes may administer this medication, except where indicated by PCP (primary & intermediate only).
INDICATIONS
• Known or suspected anaphylaxis
CONTRAINDICATIONS
• Not applicable
AUTO-INJECTOR DOSING
• 6 years & older: o 0.3 mg
• 12 months up to 6 year: o 0.15 mg
• Inject to the lateral thigh • Repeat once in 15 minutes if required • If a pediatric-dose autoinjector is not available, use the adult device
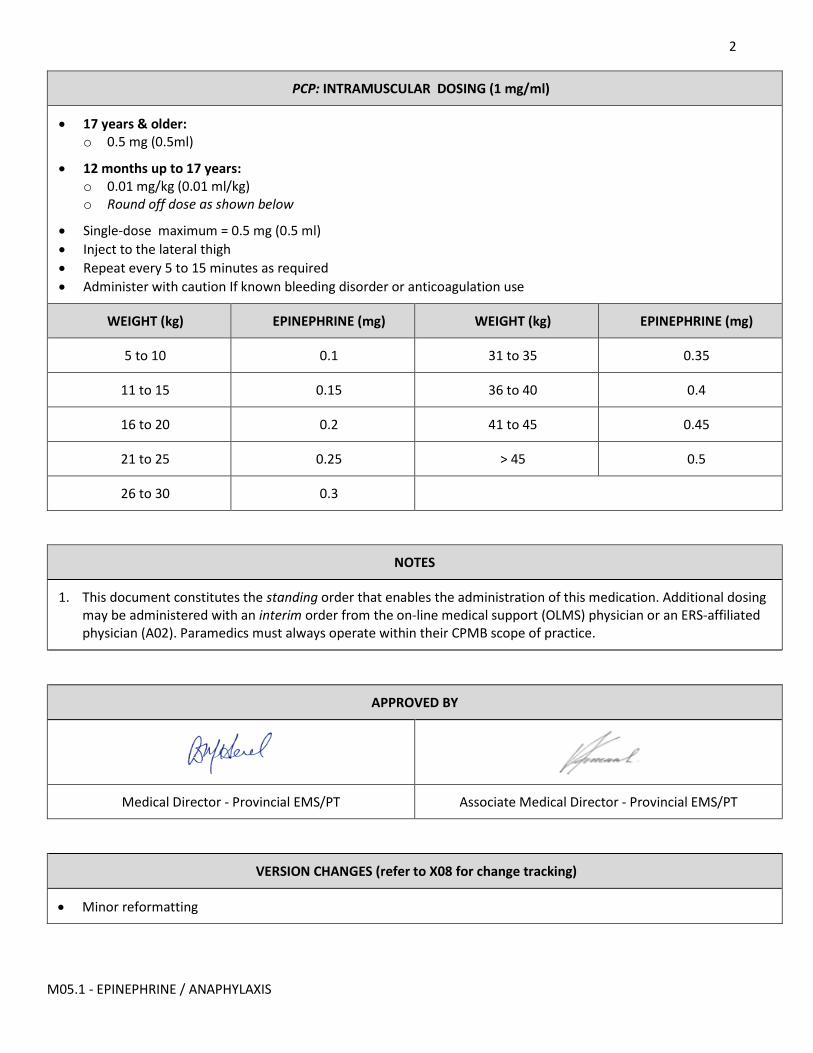
2
M05.1 - EPINEPHRINE / ANAPHYLAXIS
PCP: INTRAMUSCULAR DOSING (1 mg/ml)
• 17 years & older: o 0.5 mg (0.5ml)
• 12 months up to 17 years: o 0.01 mg/kg (0.01 ml/kg) o Round off dose as shown below
• Single-dose maximum = 0.5 mg (0.5 ml) • Inject to the lateral thigh • Repeat every 5 to 15 minutes as required • Administer with caution If known bleeding disorder or anticoagulation use
WEIGHT (kg) EPINEPHRINE (mg) WEIGHT (kg) EPINEPHRINE (mg)
5 to 10 0.1 31 to 35 0.35
11 to 15 0.15 36 to 40 0.4
16 to 20 0.2 41 to 45 0.45
21 to 25 0.25 > 45 0.5
26 to 30 0.3
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M05.2 - EPINEPHRINE / CARDIAC ARREST
M05.2 - EPINEPHRINE FOR CARDIAC ARREST
All ages MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
• Cardiac arrest from any cause
CONTRAINDICATIONS
• None
INTRAVENOUS / INTRAOSSEOUS DOSING
• 10 YEARS & OLDER: o 1 mg
• 72 HOURS UP TO 10 YEARS: o 0.01 mg/kg o Single-dose maximum = 0.5 mg
• Use the 0.1 mg/ml concentration • Administer by rapid push; follow with saline flush • Repeat every 3 to 5 minutes as required • IO administration should be be used in cardiac arrest when IV access is not available
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Alternative dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2
M05.2 - EPINEPHRINE / CARDIAC ARREST
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M05.4 - EPINEPHRINE / CROUP
zsxa
M05.4 - EPINEPHRINE FOR CROUP
1 month up to 5 years MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Moderate to severe croup
CONTRAINDICATIONS
• Stridor known or suspected to be due to epiglottitis, angioedema or a foreign body airway obstruction
NEBULIZER DOSING (1 mg/ml)
• 0.5 ml/kg over 15 minutes (max volume 5 ml) • Cumulative maximum = 3 doses • Repeat every 15 minutes as required • Do not administer by nebulizer during COVID pandemic
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Parents or caregivers can assist in administering epinephrine using the blow-by technique.
3. The effects of nebulized epinephrine will generally last about two to by three hours.
2
M05.4 - EPINEPHRINE / CROUP
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M06.1 - GLUCOSE
M06.1 - GLUCOSE
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
ALL: Paramedics with the all work scopes may administer this medication.
INDICATIONS
• Confirmed hypoglycemia • Suspected hypoglycemia in a known diabetic when a point-of-care blood glucose (POCG) measurement is not
available
CONTRAINDICATIONS
• Not applicable
ORAL / BUCCAL DOSING 2
• 17 YEARS & OLDER: o 25 to 50 gm
• 10 UP TO 17 YEARS: o 12.5 to 25 gm
• 12 MONTHS UP TO 10 YEARS: o 12.5 gm
• Repeat every 10 minutes as required • Cumulative maximum = 3 doses
2
M06.1 - GLUCOSE
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. If the patient is unable to chew or swallow, has a depressed level of consciousness , or is unable to protect the airway (and other options for correcting hypoglycemia are not promptly available) turn the patient on their side & apply glucose paste to the inside of the lower cheek. Be alert for potential aspiration.
3. The amount of glucose may differ by preparation or manufacturers. Prompt administration is often more important than the exact dosing. Consult the package directions for the exact dosing recommendations. If uncertain, assume the following: • A commonly available solution contains approximately 25 grams of glucose per 100 ml. • A commonly available gel contains approximately 30 grams of glucose per tube. • Commonly available tablets contain approximately 4 grams of glucose per tablet.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M06.2 - DEXTROSE
M06.2 - DEXTROSE
72 hours & older MEDICATION
Version date: 2022-04-14 Effective date: 2022-04-27 (0700 hours)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Confirmed hypoglycemia • Suspected hypoglycemia in a known diabetic when a point-of-care blood glucose (POCG) measurement is not
available
CONTRAINDICATIONS
• Not applicable
INTRAVENOUS / INTRAOSSEOUS DOSING 2
HIGH-ALERT MEDICATION: A two person check of the dosage is required in infants & young children.
• 10 YEARS & OLDER: o 5 ml/kg of 10% solution or 1 ml/kg of 50% soultion 2 o Single-dose maximum volume = 250 ml
• 72 HOURS UP TO 10 YEARS: o 5 ml/kg of 10% solution 3 o Single-dose maximum volume = 100 ml
• Infuse slowly in infants and young children • Repeat once in 5 minutes if required • IO access should be used if hypoglycemia cannot be corrected with glucose or glucagon and IV access is not
available
2
M06.2 - DEXTROSE
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. When limited volume is required, use 1 ml/kg of 50% solution in adults and adolescents.
3. Do not use 50% concentration in infants or children.
4. The standard dosing for intravenous dextrose is 0.5 grams per kilogram regardless of age. • 10% dextrose contains 0.1 gm glucose per ml • 50% dextrose contains 0.5 gm glucose per ml
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
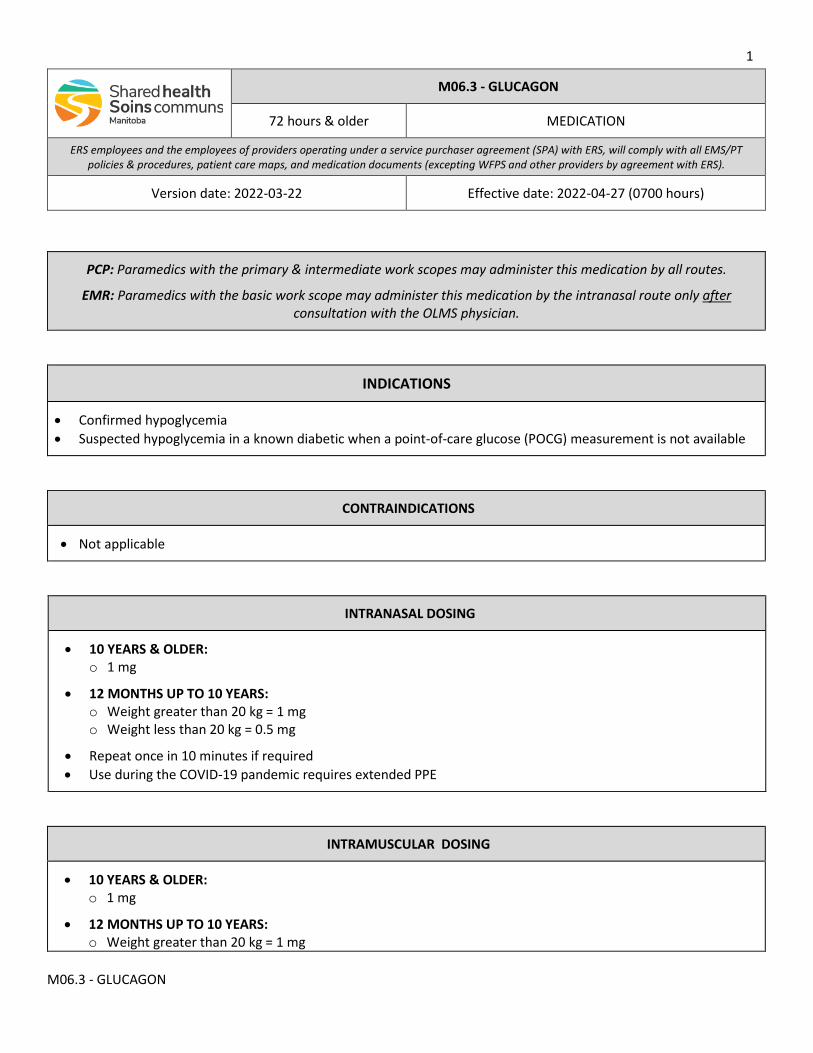
1
M06.3 - GLUCAGON
M06.3 - GLUCAGON
72 hours & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-22 Effective date: 2022-04-27 (0700 hours)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication by all routes.
EMR: Paramedics with the basic work scope may administer this medication by the intranasal route only after consultation with the OLMS physician.
INDICATIONS
• Confirmed hypoglycemia • Suspected hypoglycemia in a known diabetic when a point-of-care glucose (POCG) measurement is not available
CONTRAINDICATIONS
• Not applicable
INTRANASAL DOSING
• 10 YEARS & OLDER: o 1 mg
• 12 MONTHS UP TO 10 YEARS: o Weight greater than 20 kg = 1 mg o Weight less than 20 kg = 0.5 mg
• Repeat once in 10 minutes if required • Use during the COVID-19 pandemic requires extended PPE
INTRAMUSCULAR DOSING
• 10 YEARS & OLDER: o 1 mg
• 12 MONTHS UP TO 10 YEARS: o Weight greater than 20 kg = 1 mg
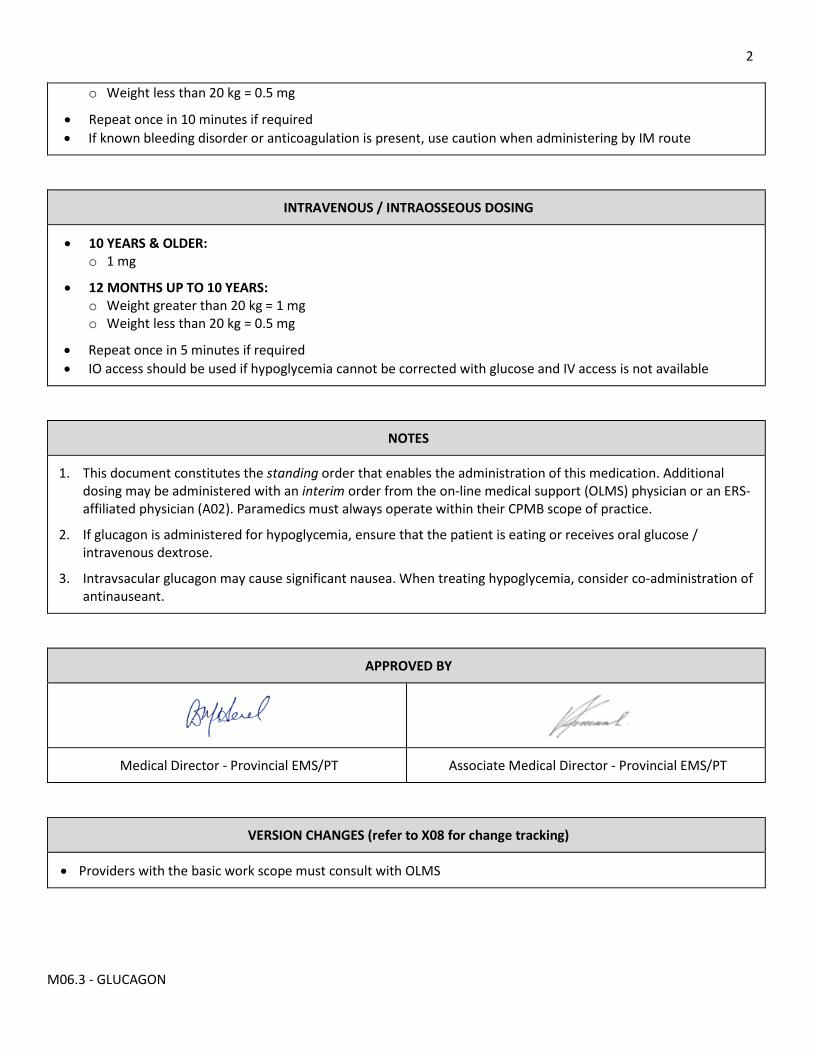
2
M06.3 - GLUCAGON
o Weight less than 20 kg = 0.5 mg
• Repeat once in 10 minutes if required • If known bleeding disorder or anticoagulation is present, use caution when administering by IM route
INTRAVENOUS / INTRAOSSEOUS DOSING
• 10 YEARS & OLDER: o 1 mg
• 12 MONTHS UP TO 10 YEARS: o Weight greater than 20 kg = 1 mg o Weight less than 20 kg = 0.5 mg
• Repeat once in 5 minutes if required • IO access should be used if hypoglycemia cannot be corrected with glucose and IV access is not available
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. If glucagon is administered for hypoglycemia, ensure that the patient is eating or receives oral glucose / intravenous dextrose.
3. Intravsacular glucagon may cause significant nausea. When treating hypoglycemia, consider co-administration of antinauseant.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Providers with the basic work scope must consult with OLMS
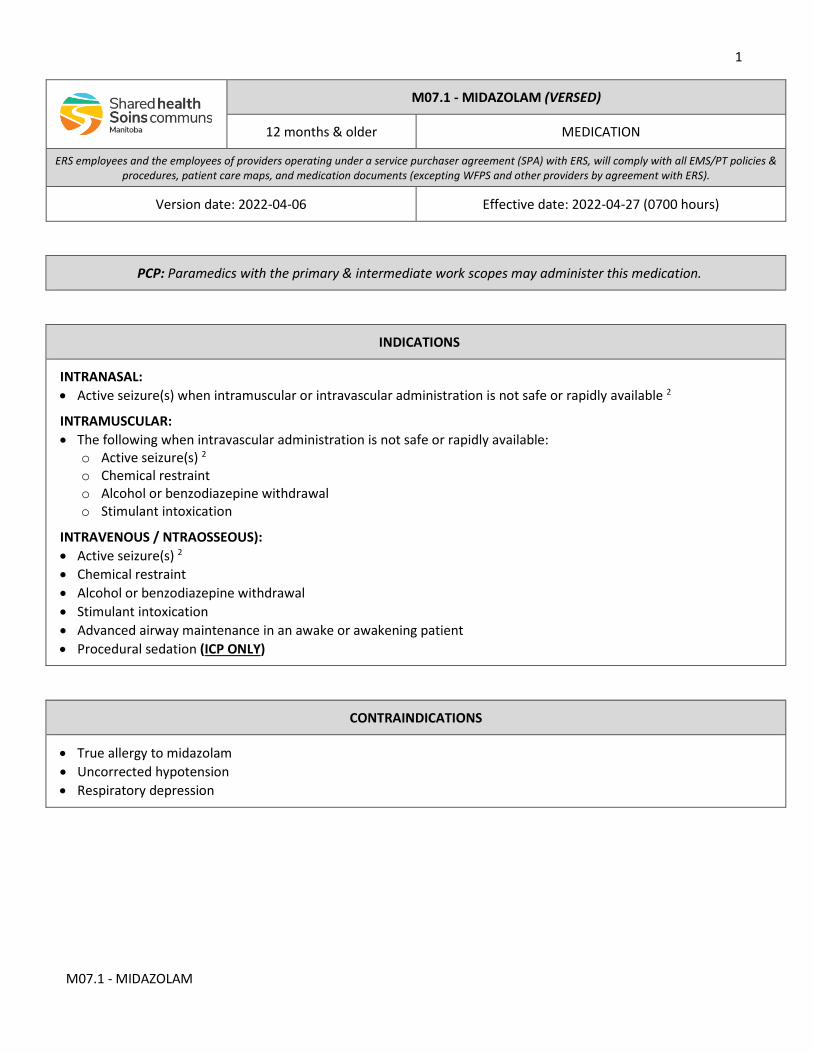
1
M07.1 - MIDAZOLAM
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
INTRANASAL: • Active seizure(s) when intramuscular or intravascular administration is not safe or rapidly available 2
INTRAMUSCULAR: • The following when intravascular administration is not safe or rapidly available:
o Active seizure(s) 2 o Chemical restraint o Alcohol or benzodiazepine withdrawal o Stimulant intoxication
INTRAVENOUS / NTRAOSSEOUS): • Active seizure(s) 2 • Chemical restraint • Alcohol or benzodiazepine withdrawal • Stimulant intoxication • Advanced airway maintenance in an awake or awakening patient • Procedural sedation (ICP ONLY)
CONTRAINDICATIONS
• True allergy to midazolam • Uncorrected hypotension • Respiratory depression
M07.1 - MIDAZOLAM (VERSED)
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-06 Effective date: 2022-04-27 (0700 hours)
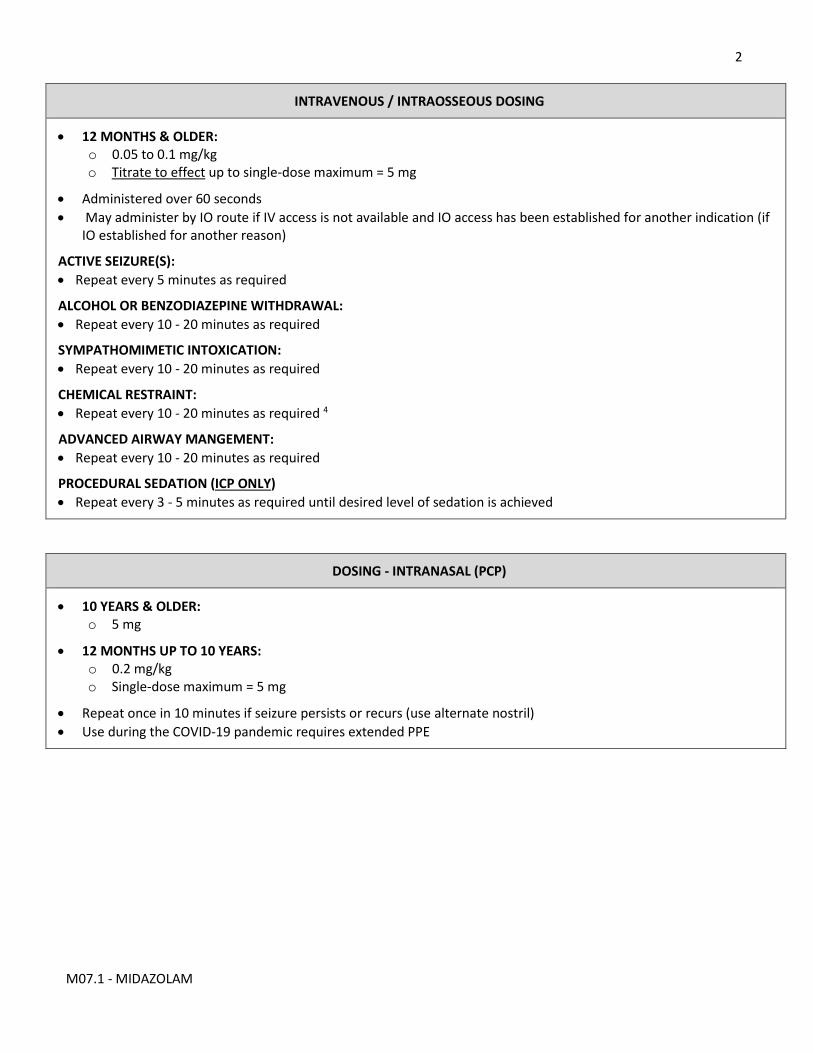
2
M07.1 - MIDAZOLAM
INTRAVENOUS / INTRAOSSEOUS DOSING
• 12 MONTHS & OLDER: o 0.05 to 0.1 mg/kg o Titrate to effect up to single-dose maximum = 5 mg
• Administered over 60 seconds • May administer by IO route if IV access is not available and IO access has been established for another indication (if
IO established for another reason)
ACTIVE SEIZURE(S): • Repeat every 5 minutes as required
ALCOHOL OR BENZODIAZEPINE WITHDRAWAL: • Repeat every 10 - 20 minutes as required
SYMPATHOMIMETIC INTOXICATION: • Repeat every 10 - 20 minutes as required
CHEMICAL RESTRAINT: • Repeat every 10 - 20 minutes as required 4
ADVANCED AIRWAY MANGEMENT: • Repeat every 10 - 20 minutes as required
PROCEDURAL SEDATION (ICP ONLY) • Repeat every 3 - 5 minutes as required until desired level of sedation is achieved
DOSING - INTRANASAL (PCP)
• 10 YEARS & OLDER: o 5 mg
• 12 MONTHS UP TO 10 YEARS: o 0.2 mg/kg o Single-dose maximum = 5 mg
• Repeat once in 10 minutes if seizure persists or recurs (use alternate nostril) • Use during the COVID-19 pandemic requires extended PPE
3
M07.1 - MIDAZOLAM
DOSING - INTRAMUSCULAR (PCP)
• 10 YEARS & OLDER: o 5 mg
• 12 MONTHS UP TO 10 YEARS: o 0.2 mg/kg o Single-dose maximum = 5 mg
• Administer by IM route with caution if known bleeding disorder or anticoagulated • Repeat every 30 minutes as required
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Respiratory depression and hypotension can occur after administration, especially in the post-seizure period. Continuously monitor respiratory and cardiac status. Providers must be prepared to manage the airway, support ventilations, and treat hypotension as required.
3. Benzodiazepines may have more pronounced respiratory and central nervous system effects in the elderly, especially if frail or compromised. Consider smaller doses and slower administration in patients greater than 75 years of age.
4. For chemical restraint consider second agent if patient requires more than 20 mg per hour
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Removal of CNS depression as a contraindication
1
M07.5 - LORAZEPAM
M07.5 - LORAZEPAM (ATIVAN)
10 years & older MEDICATION
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Severe anxiety or agitation that is interfering with, or may interfere with, the management and safe transport of the patient
CONTRAINDICATIONS
• True allergy to lorazepam • Uncorrected hypotension • Respiratory depression • Central nervous system (CNS) depression
ORAL / SUBLINGUAL DOSING
• 75 YEARS & OLDER: 2 o 1 mg & repeat once if required
• 17 UP TO 75 YEARS: o 2 mg & repeat once if required
• 10 UP TO 17 YEARS: o 1 mg & repeat once if required
2
M07.5 - LORAZEPAM
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Respiratory depression can occur even after oral administration. Frequently reassess CNS and respiratory status. Providers must be prepared to manage the airway and support ventilations as required.
3. Benzodiazepines may have more pronounced respiratory and central nervous system effects in the elderly, especially if frail or compromised.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M09- FUROSEMIDE
M09 - FUROSEMIDE (LASIX)
17 years & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
• Heart failure with evidence of fluid overload
CONTRAINDICATIONS
• True allergy to furosemide • Hypotension • Dehydration
INTRAVENOUS / INTRAOSSEOUS DOSING
• Currently on furosemide: o Equivalent to the patient’s usual total daily dose
• Not currently on furosemide o 0.25 mg/kg
• Not currently on furosemide with known renal insufficiency o 0.5 mg/kg
• Administer once by slow IV push over 90 seconds • May administer by IO route if IV access is not available and IO access established for another indication
2
M09- FUROSEMIDE
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
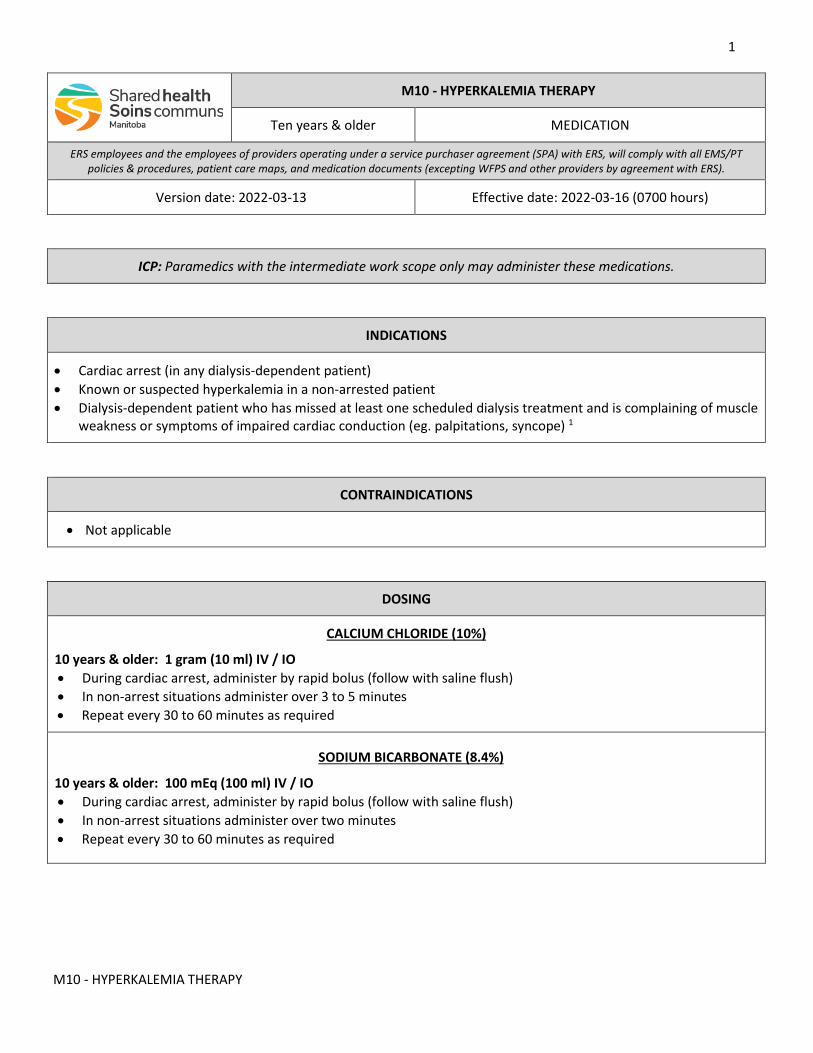
1
M10 - HYPERKALEMIA THERAPY
M10 - HYPERKALEMIA THERAPY
Ten years & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
ICP: Paramedics with the intermediate work scope only may administer these medications.
INDICATIONS
• Cardiac arrest (in any dialysis-dependent patient) • Known or suspected hyperkalemia in a non-arrested patient • Dialysis-dependent patient who has missed at least one scheduled dialysis treatment and is complaining of muscle
weakness or symptoms of impaired cardiac conduction (eg. palpitations, syncope) 1
CONTRAINDICATIONS
• Not applicable
DOSING
CALCIUM CHLORIDE (10%)
10 years & older: 1 gram (10 ml) IV / IO • During cardiac arrest, administer by rapid bolus (follow with saline flush) • In non-arrest situations administer over 3 to 5 minutes • Repeat every 30 to 60 minutes as required
SODIUM BICARBONATE (8.4%)
10 years & older: 100 mEq (100 ml) IV / IO • During cardiac arrest, administer by rapid bolus (follow with saline flush) • In non-arrest situations administer over two minutes • Repeat every 30 to 60 minutes as required
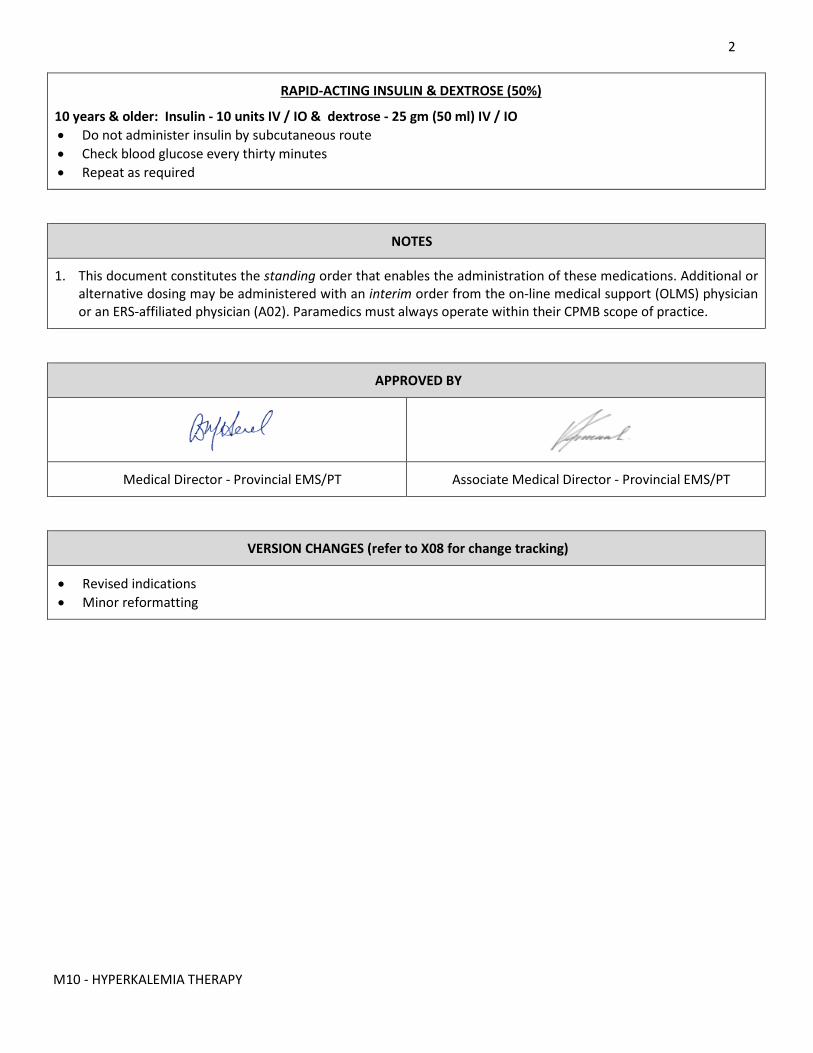
2
M10 - HYPERKALEMIA THERAPY
RAPID-ACTING INSULIN & DEXTROSE (50%)
10 years & older: Insulin - 10 units IV / IO & dextrose - 25 gm (50 ml) IV / IO • Do not administer insulin by subcutaneous route • Check blood glucose every thirty minutes • Repeat as required
NOTES
1. This document constitutes the standing order that enables the administration of these medications. Additional or alternative dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Revised indications • Minor reformatting
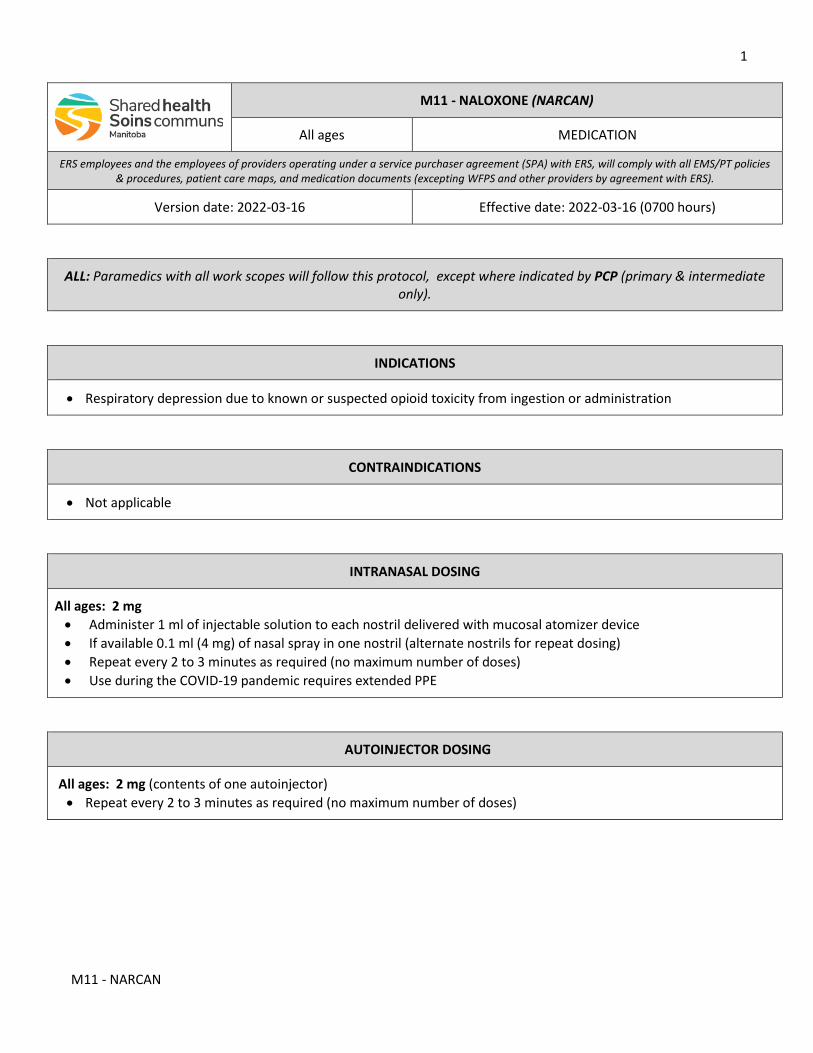
1
M11 - NARCAN
M11 - NALOXONE (NARCAN)
All ages MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-16 Effective date: 2022-03-16 (0700 hours)
ALL: Paramedics with all work scopes will follow this protocol, except where indicated by PCP (primary & intermediate only).
INDICATIONS
• Respiratory depression due to known or suspected opioid toxicity from ingestion or administration
CONTRAINDICATIONS
• Not applicable
INTRANASAL DOSING
All ages: 2 mg • Administer 1 ml of injectable solution to each nostril delivered with mucosal atomizer device • If available 0.1 ml (4 mg) of nasal spray in one nostril (alternate nostrils for repeat dosing) • Repeat every 2 to 3 minutes as required (no maximum number of doses) • Use during the COVID-19 pandemic requires extended PPE
AUTOINJECTOR DOSING
All ages: 2 mg (contents of one autoinjector) • Repeat every 2 to 3 minutes as required (no maximum number of doses)
2
M11 - NARCAN
PCP: INTRAMUSCULAR DOSING
5 years & older: 0.4 to 2 mg
72 hours up to 5 years: 0.1 mg/kg
• Single-dose maximum = 2 mg • Repeat every 2 to 3 minutes as required (no maximum number of doses) • If known bleeding disorder or anticoagulation is present, use caution when administering by IM route
PCP: INTRAVENOUS / INTRAOSSEOUS DOSING 3
5 years & older: 0.1 to 2 mg
72 hours up to 5 years: 0.1 mg/kg
• Single-dose maximum = 2 mg • Repeat every 2 to 3 minutes as required (no maximum number of doses) • IO access should be used if opiate toxicity cannot be corrected with IN or IM dosing and IV access is not available
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. With known or suspected opioid toxicity, management of the airway and breathing takes priority over naloxone administration.
3. For patients who are chronic opiate / opioid users, paramedics may titrate naloxone to achieve adequate respirations without precipitating acute withdrawal.
4. Multiple doses at the higher end of the dosing range may be required for known or suspected high potency opioids (eg. fentanyl, carfentanil).
5. During prolonged transports, repeat dosing (every 20 to 60 minutes) may be required if the duration of action of the opioid exceeds that of naloxone.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
3
M11 - NARCAN
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M12 - TETRACAINE
M12 - TETRACAINE 0.5%
All ages MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Thermal or chemical eye injury • Corneal abrasion or foreign bodies
CONTRAINDICATIONS
• Known or suspected open globe injury • True allergy to benzocaine or procaine
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
TOPICAL DOSING
• Instill 1 to 2 drops to affected eye • Repeat every ten minutes as required
2
M12 - TETRACAINE
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Reintroduced
1
M13 - HYDROCORTISONE
M13 - HYDROCORTISONE
All ages MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
PCP: Paramedics with the primary and intermediate work scopes may administer this medication.
INDICATIONS
• Refractory anaphylaxis, or anaphylaxis with transport time greater than 60 minutes • Known or suspected acute adrenal insufficiency (adrenal crisis) with known chronic adrenal insufficiency
CONTRAINDICATIONS
• Not applicable
INTRAVENOUS / INTRAOSSEOUS DOSING
ANAPHYLAXIS • 5 mg/kg IV / IO once • Single-dose maximum = 400 mg
ADRENAL CRISIS • 2 mg/kg IV / IO once • Single-dose maximum = 100 mg
GENERAL INSTRIUCTIONS: • Infuse over two minutes • May administer by IO route if IV access is not available and IO access has been established for another indication
2
M13 - HYDROCORTISONE
NOTES:
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Patients with known adrenal insufficiency may have their own supply of prepared doses of hydrocortisone for emergencies, and this can be susbstituted when available.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting • Work scope expanded to include paramedics with primary work scope
1
M14 - AMIODARONE
M14 - AMIODARONE
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-15 Effective date: 2022-03-16 (0700 hours)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
• Cardiac arrest due to ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT) that has not responded to at least one shock, one cycle CPR, and one dose of epinephrine
• Return of spontaneous circulation (ROSC) after CPR and defibrillation when amiodarone has not yet been given.
CONTRAINDICATIONS
• Unstable tachycardia requires immediate DC cardioversion
INTRAVENOUS / INTRAOSSEOUS DOSING
HIGH-ALERT MEDICATION: Post-ROSC the dose is lower & adminstion is slower than during arrest.
CARDIAC ARREST:
• 10 YEARS & OLDER: o Initial dose = 300 mg IV / IO o May repeat 150 mg once in 5 minutes if required
• 12 MONTHS UP TO 10 YEARS: o Initial dose = 5 mg/kg IV / IO (single-dose maximum = 150 mg) o May repeat 5 mg/kg every 5 minutes up to two more times if required
• Administer by rapid push, follow with saline flush • IO administration should be be used in cardiac arrest when IV access is not available
POST ROSC (ADULT ONLY):
• 17 YEARS & OLDER o 150 mg over 10 minutes o Repeat 150 mg once in ten minutes if required
2
M14 - AMIODARONE
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting (removal of change tracking from care map) • Minor content change (removal of VT & WCT dosing; addition of post-ROSC dosing & high-alert statement)
1
M15 -SALBUTAMOL
M15 – SALBUTAMOL (VENTOLIN)
All ages MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
ALL: Paramedics with the all work scopes may administer this medication.
INDICATIONS
• Acute exacerbation of known asthma • Acute exacerbation of chronic obstructive pulmonary disease (COPD) • Dyspnea or respiratory distress where wheezing can be heard, or bronchospasm is otherwise suspected • Acute anaphylaxis, or severe allergic reaction with difficulty breathing or audible wheezing
CONTRAINDICATIONS
• Not applicable
METERED-DOSE INHALER (MDI) DOSING
• MILD SYMPTOMS: o 2 to 4 inhalations by MDI o Repeat every 15 minutes as required
• MODERATE / SEVERE SYMPTOMS: o 4 to 8 inhalations o Repeat as required
• ANAPHYLAXIS: o 8 inhalations o Repeat as required
• Always use a spacer device (e.g. AeroChamber) with the MDI • For moderate / severe symptoms or anaphylaxis there is no cumulative maximum
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2
M15 -SALBUTAMOL
2. Both the MDI and spacer device are for single patient use only.
3. When salbutamol is not available, Combivent Respimat® may be substituted with dosing based on the salbutamol content.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M16 - OXYTOCIN
M16 - OXYTOCIN (SYNTOCINON)
MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• All post-partum patients will receive an IV or IM bolus • Patients with ongoing significant blood loss after delivery should receive a continuous infusion in addition to the
bolus dose
CONTRAINDICATIONS
• Multiple gestations before all fetuses are delivered • Uterine inversion
DOSING
HIGH-ALERT MEDICATION: Continuous infusion requires a two-person check of the infusion rate.
• BOLUS: o 10 units IV / IM
• CONTINUOUS IV INFUSION: o 10 units per hour x 4 hours 2
• If known bleeding disorder or anticoagulation is present, use caution when administering by IM route • Adminsiter by slow IV push over 2 minutes (an infusion is required)
2
M16 - OXYTOCIN
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Mix 40 units of oxytocin in one liter of normal saline, and administer at 250 ml per hour by infusion pump.
3. If an infusion pump is not available, ensure 10 units/hour (250 ml/hr) with a macro-drip set at 42 drips per minute.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M17 - KETAMINE
M17 - KETAMINE
12 months & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication, except where indicated by ICP (intermediate only).
INDICATIONS
• Moderate to severe pain from an acute illness, injury, or the exacerbation of a chronic condition • Analgesia is required to safely extricate, immoblize and transport the patient • Alternative agents cannot be used or are ineffective
CONTRAINDICATIONS
• Uncorrectable severe hypoperfusion 2 • Risk of respiratory or CNS depression 3 • Known schizophrenia • Previous emergence reaction from ketamine • True allergy to ketamine
PCP: INTRANASAL DOSING
• 12 MONTHS & OLDER: o To achieve adequate initial analgesia, administer 0.5 to 1 mg/kg & repeat 0.25 to 0.5 mg/kg after 10 to 15
minutes, if necessary o To maintain adequate analgesia, administer 0.25 to 0.5 mg/kg every 30 minutes as required
• Use during the COVID-19 pandemic requires extended PPE
2
M17 - KETAMINE
ICP: INTRAMUSCULAR / INTRAVENOUS / INTRAOSSEOUS (DOSING)
• 12 months & older: o CUMULATIVE MAXIMUM = 1 mg/kg per hour 5 o Administer 0.5 mg/kg; if adequate analgesia is not achieved in 15 minutes, repeat 0.25 mg/kg once only o To maintain adequate analgesia for prolonged transport, administer 0.25 to 0.5 mg/kg every 30 minutes as
required • Administer by slow IV push over 90 seconds • If known bleeding disorder or anticoagulation is present, use caution when administering by IM route • May administer by IO route if IV access is not available and IO access has been established for another indication
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. In a hemodnamically compromised patient who is compensating, ketamine can cause hypotension and deterioration. Priority should be given to adequate resuscitation before administering analgesia.
3. Ketamine may enhance the effects of CNS depressants such as the opioid analgesics. Consider smaller dosing if given with or after opioids.
4. A consensus on the optimal dosing for acute pain relief is not available. Consider consulting the on-line edical support (OLMS) physician at any time.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M18 - BICARB
M18 - SODIUM BICARBONATE
72 hrs & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
• Cardiac arrest due to known or suspected tricyclic antidepressant (TCA) overdose • Known TCA overdose with malignant cardiac rhythm or unstable hemodynamics • For the treatment of hyperkalemia, refer to M10 - HYPERKALEMIA THERAPY
CONTRAINDICATIONS
• Not applicable
INTRAVENOUS / INTRAOSSEOUS DOSING
• 17 YEARS & OLDER: o 150 mEq (150 ml of 8.4% concentration)
• 10 UP TO 17 YEARS: o 2 mEq/kg (2 ml/kg of 8.4% concentration) o Single-dose maximum = 150 mEq
• 72 HOURS UP TO 10 YEARS: o 2 mEq/kg IV (4 ml/kg of 4.2% concentration)
• In cardiac arrest,administer by rapid push; follow with saline flush • In a conscious patient, infuse slowly over two minutes • IO administration should be be used in cardiac arrest when IV access is not available
2
M18 - BICARB
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Sodium bicarbonate is not compatible with calcium salts (flush intravenous tubing well between administration of calcium and bicarbonate).
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M21 - NITROGLYCERIN
M21 - NITROGLYCERIN
Adult MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-04-14 Effective date: 2022-04-27 (0700 hours)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication by all routes. EMR: Paramedics with the basic work scope must consult with the on-line medical support (OLMS) physician before
administering this medication, and may only administer it by the sublingual route.
INDICATIONS
• Chest pain or discomfort consistent with or suspicious for myocardial ischemia • Pulmonary edema
CONTRAINDICATIONS
• Hypotension (SBP less than 90 mmHg) 2
• Known right ventricular infarct (RVI) 3a
• Use of any of the following within the last 24 hours o VIAGRA (sildefanil) o CIALIS (tadalafil) o LEVITRA (vardenafil)
• Increased intracranial pressure
• Hypersensitivity to nitroglycerin
SUBLINGUAL DOSING (Paramedics with the basic work scope must consult with OLMS)
17 YEARS & OLDER: • 0.4 mg • Repeat every 5 minutes as required
2
M21 - NITROGLYCERIN
TRANSDERMAL DOSING
17 YEARS & OLDER: • 0.4 mg/hr
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Do not administer further doses (and remove topical nitroglycerin) if the SBP drops more than 30 mmHg below the pre-administration (baseline) value.
3. Use with caution if any of the following is known or suspected: a. Inferior myocardial infarction, with suspected right ventricular involvement b. Marked bradycardia (HR < 50) or tachycardia (HR > 120) c. Volume depletion d. Aortic or mitral stenosis e. Hypertrophic cardiomyopathy with LV outflow obstruction f. Constrictive pericarditis or pericardial tamponade
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Providers with the basic work scope must consult with OLMS • Clarification of contraindicating conditions versus “use with caution” conditions
1
M22 - OLANZAPINE
M22 - OLANZAPINE
12 years & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Known or suspected methamphetamine psychosis
CONTRAINDICATIONS
• Uncooperative patient • Hypotension • Seizure or acute neurological deficit • Chest pain or dyspnea suspicious for acute cardiac syndrome (ACS)
ORAL DOSING
• 12 YEARS & OLDER: o 10 mg ODT (oral disintegrating tablet) once
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Patients who have taken methamphetamine may rapidly develop extreme paranoia and demonstrate violent behavior with enhanced physical strength. After the onset of psychosis, forced medication administration may be difficult. Administration of olanzapine while the patient is cooperative may lessen the severity of psychotic symptoms.
3. Olanzapine is a chemical restraint and any regional policy should be followed when administering.
APPROVED BY
2
M22 - OLANZAPINE
Medical Director - Provincial EMS/PT Associate Medical Director – Provincial EM/SPT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M24 - MAGNESIUM
M24 - MAGNESIUM SULFATE
MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication, except where indicate by ICP (intermnediate only).
INDICATIONS
• Cardiac arrest due to torsades de pointes • Known or suspected preeclampsia / eclampsia
CONTRAINDICATIONS
• Myasthenia gravis (when treating preeclampsia / eclampsia)
PREECLAMPSIA / ECLAMPSIA DOSING
• SEIZURE PROPHYLAXIS IN PREECLAMPSIA: 2 o 4 grams over 15 minutes
• TREATMENT OF SEIZURE IF PATINT HAS NOT RECEIVED PROPHYLAXIS: o 4 grams over 10 minutes o Repeat 2 grams over 5 minutes up to twice more if seizure(s) persist or recur 3
• TREATMENT OF SEIZURE IF PATIENT HAS RECEIVED PROPHYLAXIS: o 2 grams over 5 minutes o Repeat 2 grams over 5 minutes once if seizure(s) persist or recur 3
• DO NOT ADMINISTER BY RAPID PUSH • May be administered by intravenous (IV) or intraosseous (IO) routes • 20% solution contains 0.2 gram per ml • Monitor frequently for signs of magnesium toxicity 4
2
M24 - MAGNESIUM
ICP: CARDIAC ARREST DOSING
• 17 YEARS & OLDER: o 1 to 2 grams once
• 12 MONTHS UP TO 17 YEARS: o 25 to 50 mg/kg once o Single-dose maximum = 2 gm
• May be administered by intravenous (IV) or intraosseous (IO) route • Administer by rapid push; follow with saline flush • 20% solution contains 0.2 gram per ml
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. In patients with preeclampsia without severe features, many clinicians no longer administer seizure prophylaxis, as the incidence of seizures is low, and magnesium sulfate administration is not without risk. Paramedics at the intermediate scope of work and above must carefully weigh the risks and benefits. Paramedics with the primary scope of work must consult with the on-line medical support (OLMS) physician before administering magnesium.
3. Magnesium doses in excess of 8 grams in an hour may result in magnesium toxicity. Before administration of additional magnesium sulfate consult the OLMS physician.
4. Loss of deep tendon reflexes is the first sign of magnesium toxicity. Other manifestations include slurred speech, decreased level of consciousness, decreased muscle tone, and hypoventilation. DO NOT GIVE IF DEEP TENDON REFLEXES ARE DEPRESSED OR RESPIRATORY RATE IS 12 OR LESS
5. Calcium gluconate or calcium chloride may be given to counteract magnesium toxicity. Before calcium administration consult the OLMS physician.
LINKS
C01 - ADVANCED RESUSCITATION D06 - PREECLAMPSIA & ECLAMPSIA M26 - CALCIUM
3
M24 - MAGNESIUM
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director – Provincial EMS/SPT
VERSION CHANGES (refer to X08 for change tracking)
• Revised dosing for preeclampsia & eclampsia • Additional information regarding magnesium toxicity & treatment • Minor reformatting
1
M25 – IO LIDOCAINE
M25 - INTRAOSSEOUS LIDOCAINE
72 hours & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
• Pain management from the ongoing infusion of medications or crystalloid solution into an intraosseous (IO) device in an awake or awakening patient
CONTRAINDICATIONS
• Evidence of extravasation
DWELL DOSING
• 10 YEARS & OLDER: o 50 mg o Repeat every 45 minutes as required
• 72 HOURS UP TO 10 YEARS: o 0.5 mg/kg o Single maxium dose = 50 mg
• Infuse lidocaine into the device over 120 seconds • Allow to dwell for 60 seconds • Flush with 2.5 to 10 ml of sterile saline • If pain relief is not adequate within 5 minutes, repeat with half dose • Repeat every 45 minutes as required • Cumulative maxiumum dose = 3 mg/kg per hour
2
M25 – IO LIDOCAINE
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Use preservative-free 1% (10 mg/ml) or 2% (20mg/ml) lidocaine.
3. Monitor closely for any signs of extravasation at or near the IO insertion site.
APPROVED BY
Medical Director – Provincial EMS/PT Associate Medical Director – Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting (removal of change tracking from care map) • Content change (infuse over 120 seconds instead of 60 seconds)
1
M26 - CALCIUM
M26 - CALCIUM
MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
PCP: Paramedics with the primary & intermediate work scopes only may administer this medication, except where indicated by ICP (intermediate only).
INDICATIONS
• Magnesium toxicity • For treatment of hyperkalemia, refer to M10 - HYPERKALEMIA THERAPY
CONTRAINDICATIONS
• None
MAGNESIUM TOXICITY DOSING
CALCIUM GLUCONATE: • 1500 to 3000 mg (15 to 30 ml)
CALCIUM CHLORIDE: • 500 to 1000 mg (5 to 10 ml)
• May be administered by intravenous (IV) or intraosseous (IO) route • DO NOT ADMINISTER BY RAPID PUSH (administer over 3 to 5 minutes)
ICP: HYPERKALEMIA DOSING
TEN YEARS & OLDER: • Calcium chloride 1 gram (10 ml) • May be administered by intravenous (IV) or intraosseous (IO) route • During cardiac arrest, administer by rapid bolus (followed by saline flush) • In non-arrest situations, administer over 3 to 5 minutes • 10% solution contains 0.1 gram calcium salt per ml
2
M26 - CALCIUM
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Calcium gluconate 10% contains 100 mg calcium salt per ml. Calcium chloride 10% contains 100 mg calcium salt per ml (the chloride salt contains 3 times as much elemental calcium as the gluconate)
3. Calcium chloride is more irritating during intravenous administration and more likely to cause tissue necrosis in extravasation.
LINKS
D06 - PREECLAMPSIA & ECLAMPSIA M10 - HYPERKALEMIA THERAPY M24 - MAGNESIUM SULFATE
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director – Provincial EMS/SPT
VERSION CHANGES (refer to X08 for change tracking)
• New document
1
M28 - TXA
M28 - TRANEXAMIC ACID (TXA)
All ages MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-25 Effective date: 2022-04-06 (0700 hours)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Major trauma and hemorrhage with or without signs of shock 2
CONTRAINDICATIONS
• True allergy to tranexamic acid
INTRAVENOUS / INTRAOSSEOUS DOSING 3
ALL AGES: • 1 gram over ten minutes once 4 • May administer by IO route if IV access is not available and IO access has been established for another indication
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. A normal blood pressure (BP) does not rule out significant hemorrhage. Vital signs may be normal with up to 15% loss of blood volume. Subtle signs like tachycardia or narrowed pulse pressure may indicate substantial blood loss. BP may be maintained until a loss of up to 40% of total blood volume
3. TXA may be administered with either Ringer’s or 0.9% saline solution.
4. Administration faster than 100 mg per minute may cause hypotension.
5. Although the use of TXA in traumatic hemorrhage is an off-labelindication, there is substantial evidence from the trauma literature supporting its use.
2
M28 - TXA
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Clarification of indications to allow administration without waiting for shock to develop
1
M33 - DIPHENHYDRAMINE
M33 - DIPHENHYDRAMINE (BENADRYL)
All ages MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Pruritis not due to anaphylaxis
CONTRAINDICATIONS
• Not applicable
INTRAMUSCULAR / INTRAVENOUS DOSING
• 10 YEARS & OLDER: o 25 to 50 mg once
• 12 MONTHS UP TO 10 YEARS: o 1 mg/kg once o Single dose maximum = 50 mg
• Administer IV by slow push over 90 seconds • Administer by IM route with caution if known bleeding disorder or anticoagulation use
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Do not use antihistamine as initial or sole therapy in anaphylaxis. They will not alleviate stridor, shortness of breath, GI symptoms, hypotension or shock. Antihistamines may mask signs or worsening anaphylaxis. Pruritis will resolve with epinephrine administration.
2
M33 - DIPHENHYDRAMINE
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Mionor reformatting
1
M34 - HALOPERIDOL
M34 - HALOPERIDOL (HALDOL)
10 years & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
• Acute agitation or combative behavior where the safety of the patient, health care providers and the public at large is or may be at risk
CONTRAINDICATIONS
• Known or suspected neuroleptic malignant syndrome • Known or suspected shock • Known or suspected prolonged QT or prolonged QT syndrome • Active seizures or suspected or known postictal delirium
INTRAMUSCULAR / INTRAVENOUS / INTRAOSSEOUS DOSING
• 75 YEARS & OLDER: o 2.5 to 5 mg once
• 17 UP TO 75YEARS: o 5 to 10 mg o Repeat once in 15 minutes if required
• 10 UP TO 17 YEARS o 2.5 to 5 mg o Repeat once in 15 minutes if required
• If known bleeding disorder or anticoagulation is present, use caution when administering by IM route • May administer by IO route if IV access is not available and IO access has been established for another indication
2
M34 - HALOPERIDOL
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Always treat correctable underlying causes of agitation or combative behavior, such as hypoglycemia or hypoxemia, before administering haloperidol.
3. Administration requires continuous monitoring of cardiorespiratory status.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M37.1 ASA
M37.1 - ACETYLSALICYLIC ACID (ASA)
Adult MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
ALL: Paramedics with all work scopes may administer this medication.
INDICATIONS
• Known or suspected acute coronary syndrome (ACS)
CONTRAINDICATIONS
• Active bleeding that cannot be controlled by basic measures or at a non-compressible site • True ASA allergy • Known ASA-induced asthma
ORAL DOSING
• 160 mg • Instruct patient to chew
NOTES:
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2
M37.1 ASA
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M37.2 - TICAGRELOR
M37.2 - TICAGRELOR (BRILINTA)
Adult MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 -(0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Known or suspected ST elevation myocardial infarction (STEMI) only when the patient is going directly to primary coronary intervention (PCI)
CONTRAINDICATIONS
• Patient may be candidate for fibrinolysis with TNK • Active bleeding that cannot be controlled by basic measures or at a non-compressible site • True allergy to ticagrelor
ORAL DOSING
• 180 mg once
NOTES
1. This document constitutes the standing order that enables the administration of this medication, after consultation with the CODE-STEMI physician and confirmation that the patient will be going for primary PCI. Alternative dosing may be administered with an interim order from the CODE-STEMI physician or on-line medical support (OLMS) physician (A02). Paramedics must always operate within their CPMB scope of practice.
2
M37.2 - TICAGRELOR
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M38 - KETOROLAC
M38- KETOROLAC (TORADOL)
2 years & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Moderate to severe pain from an acute illness, injury, or an exacerbation of a chronic condition that is significant enough to require analgesic to facilitate safe and comfortable patient transport
CONTRAINDICATIONS
• Known / suspected acute coronary syndrome (ACS) • Known / suspected intracranial injury or hemorrhage • True allergy to ketorolac • History of aspirin (ASA) induced asthma or bronchospasm • Pregnancy • Known renal failure
INTRAMUSCULAR / INTRAVENOUS (INTRAOSSEOUS) DOSING
• 17 YEARS & OLDER: o 30 mg once
• 2 UP TO 17 YEARS: o 0.5 mg/kg once
o Single maximum dose = 30 mg
• If known bleeding disorder or anticoagulation is present, use caution when administering by IM route • May administer by IO route if IV access is not available and IO access has been established for another indication
2
M38 - KETOROLAC
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
M39 - ATROPINE
M39 - ATROPINE
72 hrs & older MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hours)
ICP: Paramedics with the intermediate work scope only may administer this medication.
INDICATIONS
• All of the following: o A sustained heart rate less than the age-appropriate minimum o Signs of poor perfusion o The poor perfusion is known or suspected to be due to the bradycardia
CONTRAINDICATIONS
• True hypersensitivity to atropine
INTRAVENOUS (INTRAOSSEOUS) DOSING
• 17 YEARS & OLDER: o 0.5 - 1 mg o Use 1 mg for severe bradycardia (eg. hypotension/shock, altered mental status, acute heart failure) o Repeat every 3 to 5 minutes as required
• Cumulative maximum = 3 mg • 72 HOURS UP TO 17 YEARS:
o 0.02 mg/kg o Single-dose minimum = 0.1 mg o Single-dose maximum = 0.5 mg o Repeat once in 5 minutes
• Administer by rapid push; follow with saline flush • May administer by IO route if IV access is not available and IO access has been established for another indication
2
M39 - ATROPINE
NOTES
1. This document constitutes the standing order that enables the administration of this medication. Additional dosing may be administered with an interim order from the on-line medical support (OLMS) physician or an ERS-affiliated physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. Atropine may not be effective in type II second-degree or third-degree AV blocks. Be prepared to proceed to transcutaneous pacing (TCP).
3. Atropine is usually ineffective in heart transplant patients due to lack of cholinergic innervation, although reinnervation may occur over years. If required, atropine may be used cautiously but observe for paradoxical slowing of the heart rate and high-degree AV block.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
3
M39 - ATROPINE
1
M43 - ENOXAPARIN
M43 - ENOXAPARIN (LOVENOX)
Adult MEDICATION
ERS employees and the employees of providers operating under a service purchaser agreement (SPA) with ERS, will comply with all EMS/PT policies & procedures, patient care maps, and medication documents (excepting WFPS and other providers by agreement with ERS).
Version date: 2022-03-13 Effective date: 2022-03-16 (0700 hrs)
PCP: Paramedics with the primary & intermediate work scopes may administer this medication.
INDICATIONS
• Known or suspected ST elevation myocardial infarction (STEMI) only when the patient is going directly to primary coronary intervention (PCI)
CONTRAINDICATIONS
• Patient may be candidate for fibrinolysis with TNK • Known hypersensitivity to enoxaparin • Patient is known to be on an anticoagulant and has taken it that day • History of heparin-induced thrombocytopenia (HIT) within the past 100 days • Active bleeding that cannot be controlled by basic measures or at a non-compressible site
INTRAVENOUS / SUBCUTANEOUS DOSING: 2
AGE LESS THAN 75 YEARS: 3 • 0.5 milligrams per kilogram (maximum = 50 mg) IV, or • 1.0 milligrams per kilogram (maximum = 100 mg) SC
AGE GREATER THAN 75 YEARS: • 0.75 mg/kg (maximum = 75 mg) SC only
2
M43 - ENOXAPARIN
NOTES
1. This document constitutes the standing order that enables the administration of this medication, after consultation with the CODE-STEMI physician and confirmation that the patient will be going for primary PCI. Alternative dosing may be administered with an interim order from the CODE-STEMI physician or on-line medical support (OLMS) physician (A02). Paramedics must always operate within their CPMB scope of practice.
2. The dose should be rounded off to the nearest 10 mg
3. In patients under 75 years of age, SC enoxaparin is administered only if IV access cannot be obtained, or at the direction of the Code-STEMI physician.
APPROVED BY
Medical Director - Provincial EMS/PT Associate Medical Director - Provincial EMS/PT
VERSION CHANGES (refer to X08 for change tracking)
• Minor reformatting
1
X01 - SECTION A CHANGES
X01 - SECTION A CHANGE TRACKING (POLICIES & PROCEDURES)
Version date: 2022-05-09 Publication Date: 2022-06-01
A01 - OVERVIEW OF CLINICAL CARE
2022-03-14: • Minor reformatting (removal of change tracking from care map)
2022-01-05: • Addition of compliance statement • Temporary removal of advanced work scope • Definition of standing order (medication document) and interim order. • New work scope 3-letter indicators & statement (appendix A)
2021-06-01: • Clarification of standing orders and temporary delegations • Inclusion of section on scope of work • Reformatted
2021-01-29: • New note 2 added to Section B regarding medication administration
2021-01-08: • Consolidation and revision / reformatting of previous A01 and A02. • Alignment with College of Paramedics regulatory authority • Clarified definitions, standardized terminology, and age ranges • Adjustment to patient monitoring expectations
2017-05-04: • Original version
A02 - PHYSICIAN ORDERS, CLINICAL SUPPORT & OLMS
2022-03-14: • Minor reformatting (removal of change tracking from care map)
2021-12-12: • A02.1 and A02.2 combined • Scope of work section replaced by compliance statement in header • Affiliated physicians defined • STARS TP now provides support for all trauma bypass candidates
2021-06-01: • Clarification of standing orders and temporary delegations • Reformatted
2021-01-13: • New document
A05 - TREATMENT & TRANSPORT REFUSALS
2022-03-14:
2
X01 - SECTION A CHANGES
• Minor reformatting (removal of change tracking from care map)
2022-01-05: • New document
A06 - EMS/PT WORK SCOPE
2022-04-07: • Revised preamble language more closely aligned with CPMB regulations • “By injection into a subcutaneous port” at primary & intermediate scope added • Nitroglycerin and IN glucagon require OLMS consultation at basic scope added • Amiodarone for post arrest (ROSC) and stable VT or WCT at intermediate scope added • Transport with established running central line at primary scope added • “Injection into central line” revised (“during critical situation” removed) • Hydromorphone removed and replaced by new table D for all medications during patient transport
2022-03-14: • Removal of nitroglycerin from basic (EMR) work scope • Minor reformatting (removal of change tracking from care map)
2022-02-02: • TEMPORARY removal of advanced work scope and related medical functions to facilitate the urgently needed and
complex task of revising all the clinical document. • Specification of procedures for obstetrical emergencies & wound repair with tissue adhesive. • Expanded list of established devices that can be managed during patient transport. • Addition of IV fluid with & without added electrolytes • Addition of calcium chloride for magnesium toxicity • Addition of furosemide, haloperidol, and hydrocortisone at primary level • Removal of IM epinephrine for bronchospasm & glucagon for anaphylaxis due to lack of evidence of benefit • Removal of amiodarone for stable VT • Remdesivir & tocilizumab moved to established medication infusions (G01)
2021-11-17: • Addition of oral hydromorphone to PCP scope of work with an interim order • Addition of remdesivir and tocilizumab for COVID pandemic
2021-08-13: • Addition of gastric tube insertion through i-Gel airway • Correction of midazolam to PCP level
2021-06-01: • New document
A09 - MEDICAL PROCEDURES DURING COVID
2022-05-06: • PPV without sealing the airway can be considered in appropriate cases • Clarification that CPAP is not recommended with positive or unknown COVID status • Addition of sublingual medication administration & BiPAP to permitted procedures • Link to new C12 (removal of reference to E23)
2022-03-14: • Minor reformatting (removal of change tracking from care map)
2021-12-14:
3
X01 - SECTION A CHANGES
• Reformatting only; no content change
2021-10-02: • CPAP ventilation during IFT in a patient tested negative for COVID-19 that day is now allowed with extended PPE • Addition of scope of work statement
2021-05-12: • Intranasal medications now permitted procedure
2020-07-07:
• Clarification of situations requiring droplet & precaution PPE • Inclusion of oxygenation by NRB mask as permitted procedure • Clarification regarding newborn PPV
2020-05-05: • Regrouped & reordered for quick access • Reference to Shared Health policy on PPE definitions (removal of same) • Clarification based on consensus for defibrillation, chest compression and nitroglycerin administration
2020-04-13: • New document
1
X02 - SECTION B CHANGES
X02 - SECTION B CHANGE TRACKING (DESTINATION)
Version date: 2022-04-17 Publication Date: 2022-05-17
B01 - STANDARD DESTINATION FOR PRIMARY RESPONSE
2022-04-17: • Renumbered from A04.1 and moved to section B • Reformatted (replacement of coloured boxes with scope of work statement & 3 letter indicators) • Revised flow chart for ease of use & expanded notes for greater clarity • Paramedics will contact OLMS (not OCS) for destination decision support (item #3) • Clarification that patient / proxy cannot request specific destination (item #5) • Clarification about which critical situations go to with or without a physician present (item #8) • Clarification that a designated site may redirect patients who do not meet criteria for designated site (item #9) • New table A for designated hospitals (reduced list of links) • Reminder to transport to Wpg hospital when closest to Perimeter
2020-04-24: • Inclusion of flow chart for quick reference • Revised notes for clarification • Alignment with protocols that have specific destinations • Updated list of current destination protocols • Inclusion of some content from the previous A04 (note #6)
2018-10-16: • Original version
B02 - REDIRECTION ADVISORY
2022-04-16: • Renumbered from A04.2 and moved to section B • Reformatted (replacement of coloured boxes with scope of work statement & 3 letter indicators) • Revised flow chart for ease of use & expanded notes for greater clarity • Increased role of OLMS in managing redirections • Patient must be informed of redirection but consent not required • Clarification that redirection advisory might be over-ruled in some specific situations • Removal of table C
2020-04-28: • Simplified flow chart • Revised notes for clarification • Updated list of current destination protocols 2019-11-26: • Original version
2019-11-26: • Original version
B03 - DESTINATION WHEN THE CLOSEST ED IS IN WINNIPEG
2
X02 - SECTION B CHANGES
2022-04-16: • Renumbered from A08.1 & moved to section B • Reformatted (replacement of coloured boxes with scope of work statement & 3-letter indicator) • Revised flow chart for ease of use & revised notes for greater clarity • Removal of SBH as stroke centre
2020-04-13: • Clarification of destination for trauma victims by age • Alignment with COVID 19 protocols 4 A08.1 – DESTINATION ED-WINNIPEG • Reformatting
2019-09-25: • Original version
B04.1 - TRAUMA BYPASS FOR IERHA & SHSS
2022-04-17: • Corrections to links section • Revised flow chart for ease of use • Increased note details for clarification
2022-01-20: • Reformatted, renumbered (B04.1.1 B04.1) & retitled • Statement regarding compliance with ERS policies / procedures / care maps added to header • Work scope identifiers (ALL / PCP) replace coloured boxes & standardized to 3-letter abbreviations • Revised & simplified flow chart • Work scope statement has been moved to the top of flow chart • Revised notes
o Immediate life-threatening conditions have been clarified for those relevant to trauma o All calls for trauma bypass to go through STARS TP o Paramedics will not call TP or bypass closest ED for patient who do not meet trauma bypass indicators
2021-09-28: • Renumbered from F11 (section B will become repository for all destination policies) and reformatted • Applies only to incidents within the boundaries of IERHA and SHSS (B04.1.1); PMH (B04.1.2); and NRHA (B04.1.3) • Revised and simplified flow chart • Clarification of calling STARS or OLMS physician for clinical support • Revised table of field triage criteria includes HR > 120 (adults), focal neurological deficits, significant injury ion
pregnant patient and extremity hemorrhage (to align with Provincial Trauma Program and WFPS Trauma Triage protocol)
2021-06-16: • New
B04.2 - TRAUMA BYPASS FOR PMH
2022-04-17: • Corrections to links section • Revised flow chart for ease of use • Increased note details for clarification
2022-01-20:
3
X02 - SECTION B CHANGES
• Reformatted, renumbered (B04.1.2 B04.2) & retitled • Statement regarding compliance with ERS policies / procedures / care maps added to header • Work scope identifiers (ALL / PCP) replace coloured boxes & standardized to 3-letter abbreviations • Revised & simplified flow chart • Work scope statement has been moved to the top of flow chart • Revised notes
o Immediate life-threatening conditions have been clarified for those relevant to trauma o All calls for trauma bypass to go through STARS TP o Paramedics will not call TP or bypass closest ED for patient who do not meet trauma bypass indicators
2021-09-28: • Renumbered from F11 (section B will become repository for all destination policies) and reformatted • Applies only to incidents within the boundaries of PMH • Revised and simplified flow chart • Clarification of calling STARS or OLMS physician for clinical support • Definition of north-south and east-west divides • Revised table of field triage criteria includes HR > 120 (adults), focal neurological deficits, significant injury ion
pregnant patient and extremity hemorrhage (to align with Provincial Trauma Program and WFPS Trauma Triage protocol)
2021-06-16: • New
B04.3 - TRAUMA BYPASS FOR NRHA
2022-04-17: • Corrections to links section • Revised flow chart for ease of use • Increased note details for clarification
2022-01-20: • Reformatted, renumbered (B04.1.3 B04.3) & retitled • Statement regarding compliance with ERS policies / procedures / care maps added to header • Work scope identifiers (ALL / PCP) replace coloured boxes & standardized to 3-letter abbreviations • Revised & simplified flow chart • Work scope statement has been moved to the top of flow chart • Revised notes
o Immediate life-threatening conditions have been clarified for those relevant to trauma o All calls for trauma bypass to go through STARS TP o Paramedics will not call TP or bypass closest ED for patient who do not meet trauma bypass indicators
2021-09-28: • Renumbered from F11 (section B will become repository for all destination policies) and reformatted • Applies only to incidents within the boundaries of PMH • Revised and simplified flow chart • Clarification of calling STARS or OLMS physician for clinical support • Definition of north-south and east-west divides • Revised table of field triage criteria includes HR > 120 (adults), focal neurological deficits, significant injury ion
pregnant patient and extremity hemorrhage (to align with Provincial Trauma Program and WFPS Trauma Triage protocol)
2021-06-16:

4
X02 - SECTION B CHANGES
• New
1
X03 - SECTION C CHANGES
X03 - SECTION C CHANGE TRACKING (RESUSCITATION)
Version date: 2022-04-11 Publication Date: 2022-04-27
C01 - BASIC RESUSCITATION
2022-03-03: • Reformatting & revisions • Replacement of coloured boxes with work scope statement • Information from C03 (care after ROSC), C10 (modifications during COVID) and H04 (signs of obvious death) now
included • Reminders to consider naloxone & hypothermia • Inclusion of promising clinical factors & requirement to contact OLMS for possible short duration transport • Removal of requirement to notify OLMS before transporting non-ROSC COVID patients • QRG for target VS added to ROSC flow chart • Alignment with current HSF ACLS & PALS cardiac arrest algorithms
2021-01-13: • Reformatting & revisions (correction of pathway director)
2020-05-05: • Alignment with COVID 19 care maps • Simplified flow chart
2020-04-13: • Criteria to discontinue field resuscitation included (clinical procedure P13.3A has been deleted) • Critical transport duration reduced from 20 to 15 minutes • Alignment with COVID 19 care maps • Simplified flow chart
2017-06-12: • Original version
C02 - ADVANCED RESUSCITATION
2022-03-05: • Reformatting & revisions • Replacement of coloured boxes with work scope statement & identifiers • Information from C03 (care after ROSC), C10 (modifications during COVID) and H04 (signs of obvious death) now
included • Simplified flow chart • QRG for target VS added to ROSC flow chart • Alignment with current HSF ACLS & PALS cardiac arrest algorithms
2020-09-24: • Clarification of criteria to discontinue in the field
2020-05-05: • Alignment with COVID-19 care maps and A08 destination protocol • Incorporation of trauma arrest care map • Simplified flow charts
2017-03-23:
2
X03 - SECTION C CHANGES
• Original version
C04 – EZ IO® INSERTION
2022-03-16: • Renumbered from P08 & reformatted • Inclusion of IO lidocaine dose from M25
2021-10-25: • Removal of coloured boxes & replacement by scope of work statement • Statement regarding IV / IO meds added • Reformatted
2020-05-05: • Notes written specific to EZ-IO insertion
C05 - UNSTABLE BRADYCARDIA
2022-03-16: • Reformatted • Replacement of colored boxes with scope of work “legend” • Simplified flow chart • More consistent with current HSFC bradycardia adult & pediatric algorithms • Further clarification as to when to initiate CPR in children
2020-11-09: • Simplified flow chart • Addition of lower limit HR by age group • Removed SBP reference • Revised notes for clarification • Medication doses removed and Links added for Medication documents
2017-03-09: • Original version
C06 - UNSTABLE TACHYCARDIA
2022-04-11: • Correction of typos and further clarification in note #3
2022-03-22: • Replacement of colored boxes with scope of work “legend” • Simplified flow chart • More consistent with current ACLS & PALS tachycardia algorithms • Reformatted
2020-12-14: • Algorithm revised (“stable” removed)
2020-11-09: • Simplified flow chart • Addition of upper limit HR by age group • Removed SBP reference • Revised notes for clarification
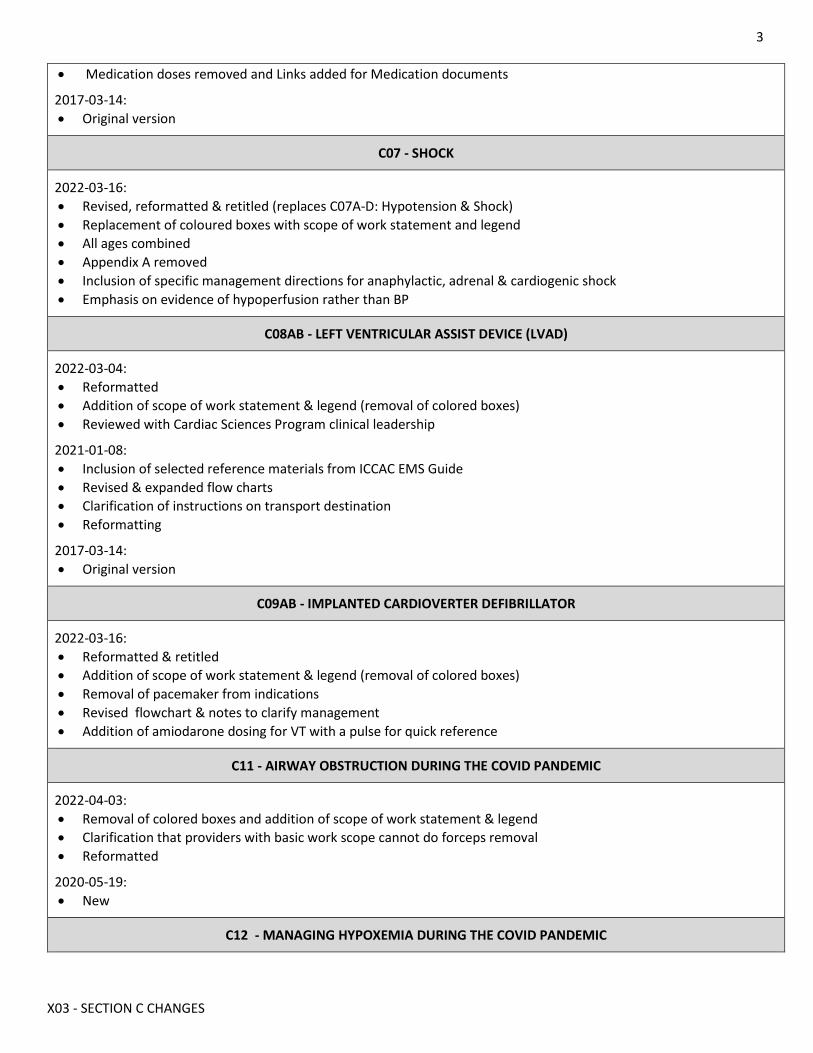
3
X03 - SECTION C CHANGES
• Medication doses removed and Links added for Medication documents
2017-03-14: • Original version
C07 - SHOCK
2022-03-16: • Revised, reformatted & retitled (replaces C07A-D: Hypotension & Shock) • Replacement of coloured boxes with scope of work statement and legend • All ages combined • Appendix A removed • Inclusion of specific management directions for anaphylactic, adrenal & cardiogenic shock • Emphasis on evidence of hypoperfusion rather than BP
C08AB - LEFT VENTRICULAR ASSIST DEVICE (LVAD)
2022-03-04: • Reformatted • Addition of scope of work statement & legend (removal of colored boxes) • Reviewed with Cardiac Sciences Program clinical leadership
2021-01-08: • Inclusion of selected reference materials from ICCAC EMS Guide • Revised & expanded flow charts • Clarification of instructions on transport destination • Reformatting
2017-03-14: • Original version
C09AB - IMPLANTED CARDIOVERTER DEFIBRILLATOR
2022-03-16: • Reformatted & retitled • Addition of scope of work statement & legend (removal of colored boxes) • Removal of pacemaker from indications • Revised flowchart & notes to clarify management • Addition of amiodarone dosing for VT with a pulse for quick reference
C11 - AIRWAY OBSTRUCTION DURING THE COVID PANDEMIC
2022-04-03: • Removal of colored boxes and addition of scope of work statement & legend • Clarification that providers with basic work scope cannot do forceps removal • Reformatted
2020-05-19: • New
C12 - MANAGING HYPOXEMIA DURING THE COVID PANDEMIC
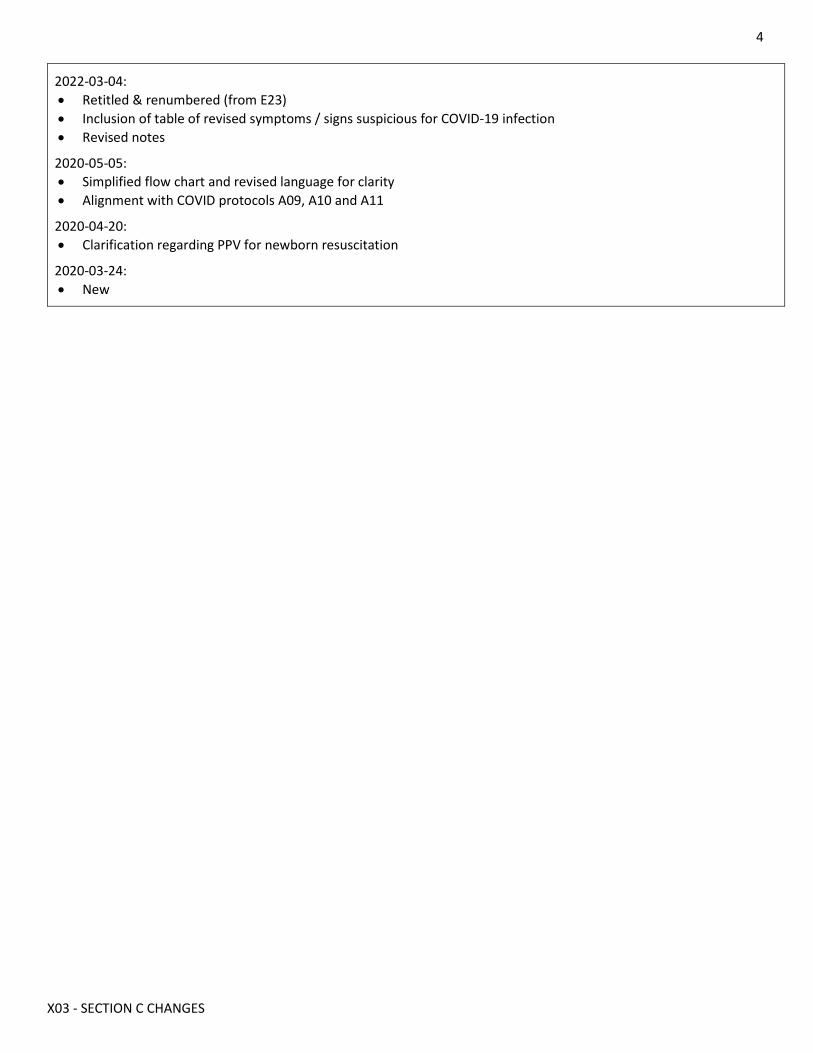
4
X03 - SECTION C CHANGES
2022-03-04: • Retitled & renumbered (from E23) • Inclusion of table of revised symptoms / signs suspicious for COVID-19 infection • Revised notes
2020-05-05: • Simplified flow chart and revised language for clarity • Alignment with COVID protocols A09, A10 and A11
2020-04-20: • Clarification regarding PPV for newborn resuscitation
2020-03-24: • New
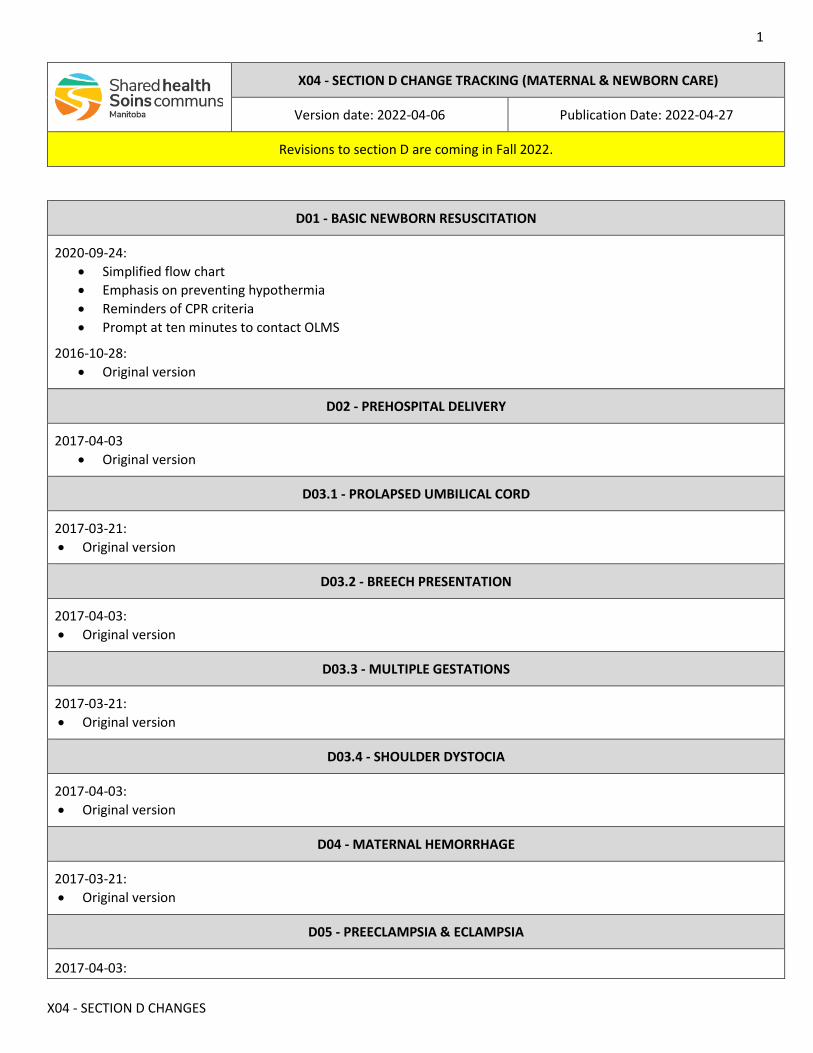
1
X04 - SECTION D CHANGES
X04 - SECTION D CHANGE TRACKING (MATERNAL & NEWBORN CARE)
Version date: 2022-04-06 Publication Date: 2022-04-27
Revisions to section D are coming in Fall 2022.
D01 - BASIC NEWBORN RESUSCITATION
2020-09-24: • Simplified flow chart • Emphasis on preventing hypothermia • Reminders of CPR criteria • Prompt at ten minutes to contact OLMS
2016-10-28: • Original version
D02 - PREHOSPITAL DELIVERY
2017-04-03 • Original version
D03.1 - PROLAPSED UMBILICAL CORD
2017-03-21: • Original version
D03.2 - BREECH PRESENTATION
2017-04-03: • Original version
D03.3 - MULTIPLE GESTATIONS
2017-03-21: • Original version
D03.4 - SHOULDER DYSTOCIA
2017-04-03: • Original version
D04 - MATERNAL HEMORRHAGE
2017-03-21: • Original version
D05 - PREECLAMPSIA & ECLAMPSIA
2017-04-03:
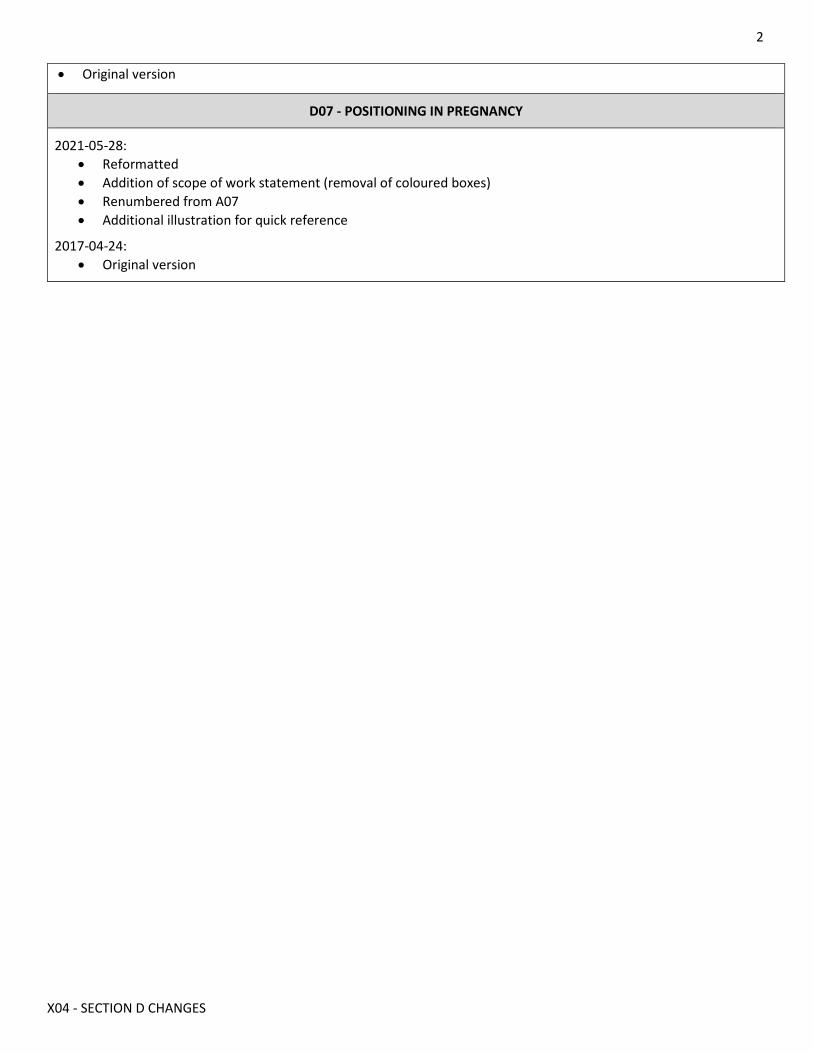
2
X04 - SECTION D CHANGES
• Original version
D07 - POSITIONING IN PREGNANCY
2021-05-28: • Reformatted • Addition of scope of work statement (removal of coloured boxes) • Renumbered from A07 • Additional illustration for quick reference
2017-04-24: • Original version
1
X05 - SECTION E CHANGES
X05 - SECTION E CHANGE TRACKING (MEDICAL CONDITIONS)
Version date: 2022-04-14 Publication Date: 2022-04-27
Further revisions to section E are coming in Fall 2022.
E02AB - AGITATION
2021-02-19: • Simplified flow chart • Reformatting
2017-06-19: • Original version
E03 - ANAPHYLAXIS
2021-09-15: • Revised & reformatted • Revised indications • Addition of scope of work statement & legend (removal of coloured boxes) • Simplified flow chart • Glucagon removed as rarely required in initial prehospital management • Nebulized epinephrine removed as inferior to parenteral administration • Removal of IV dosing until pumps are universally available
2021-02-04: • Revised hydrocortisone dosing • Refractory anaphylaxis transport time increased to 60 minutes
2021-01-13: • Simplified linear flow chart & reformatting • Modified indications and clarification of management around exposure to known allergen • Modified to align with new guidelines (e.g., Canadian Pediatric Society) • Addition of weight based dosing for IM epinephrine • Removal of antihistamines which may mask signs of worsening of anaphylaxis and biphasic reactions • Switch to hydrocortisone to simplify Shared Health ERS formulary • Inclusion of anaphylaxis as additional reason for redirection advisory over-ride
2017-06-06: • Original version
E04A - ACUTE CORONARY SYNDROME & STEMI
2022-04-05: • Improved flow chart for enhanced ease of use • Separate EMR functions for enhanced visibility • Providers with basic work scope (EMR) must contact OLMS to administer SL nitroglycerin, but can assist a patient
with self-administration
2021-05-25: • Addition of scope of work statement (removal of coloured boxes)
2
X05 - SECTION E CHANGES
• Addition of instruction to contact OLMS for STEMI patient who cannot reach SBH within 100 minutes • Addition of PHIA warning for transmitting of ECG • Addition of TNK checklist to streamline process for initiating fibrinolysis • Reformatted
2021-01-13: • Further clarification of process for consulting Code-STEMI physician and emphasis on 100 minute concentric • Clarification to Notes 11, 12 and 13
2020-04-08: • Switch in sequence of steps on flow chart to emphasize that transport to PCI is the priority with STEMI • Enoxaparin switched to PCP scope with physician order • Inclusion of LBBB as possible criterion for STEMI bypass • Instruction to enable providers to bypass the SBH ED if patient is unstable • Further information about managing RVI
2019-11-25: • Original versions from MHSAL / EMSB
E06 - DYSPNEA & RESPIRATORY DISTRESS
2020-05-12: • Consolidation of previous documents E06A; E06B; E06C; and E06D into single care map • Incorporation of additional information from COVID-19 care map E22 • Revised table A • Simplified flow chart
2017-05-15: • Original version
E10 - HYPOGLYCEMIA
2022-03-24: • Reformatted (replacement of coloured boxes with scope of work statement & icons) • Revised title & content
o Consolidation of adult, adolescent, and childcare maps into one document o Separate flow charts for adult / adolescent and child / infant o Revised BG lower limit for diagnosing infant & child hypoglycemia o Improved flow chart for enhanced ease of use o Use of 10% dextrose in adults & adolescents when volume is a concern
• Providers with basic work scope (EMR) must contact OLMS to administer IN glucagon
2012-06-13: • Original versions from MHSAL / EMSB
E10A - HYPOGLYCEMIA (Adult)
2022-04-20: • Deleted (combined into E10)
2017-06-13: • Original version
E10B - HYPOGLYCEMIA (Adolescent)
3
X05 - SECTION E CHANGES
2022-04-20: • Deleted (combined into E10)
2017-06-13: • Original version
E10C - HYPOGLYCEMIA (Child)
2022-04-20: • Deleted (combined into E10)
2017-06-13: • Original version
E13A - HYPERKALEMIA (Adult)
2017-06-20: • Original version
E13B - HYPERKALEMIA (Adolescent)
2017-06-20: • Original version
E14 - SEIZURE
2020-04-07: • Consolidation of previous documents E14.1A; E14.1B; E14.1C; E14.1D; E14.2C; and E14.2D into single care map • Removal of drug dosages (information on medications available at M02 and M07 links) • Simplified flow chart
2017-04-03: • Original version
E15A - ACUTE STROKE
2020-09-08: • Removal of speech impairment as an indication to contact the HSC stroke neurologist
2020-08-24: • SBH removed as stroke centre • Addition of speech impairment as an indication to contact the HSC stroke neurologist • Addition of 90-minute marker to consider air intercept • Formatting / simplified flow chart
2019-09-16: • Shared Health interim release
2017-03-26: • Original version
E20AB - ALCOHOL & BENZODIAZEPINE WITHDRAWAL
2020-11-05: • Oral benzodiazepine changed to lorazepam
4
X05 - SECTION E CHANGES
• Revised indication • Simplified flow chart • Reformatting • Updated links
2017-06-19: • Original version
E25AB - METHAMPHETAMINE PSYCHOSIS
2020-11-05: • Retitled • Simplified flow chart • Reformatting
2018-11-26: • Original version
E30A - PALLIATIVE CARE IN THE HOME
2020-11-23: • Added Appendix 2 Subcutaneous Infusion • Added Appendix 3 Urinary Catheter Irrigation
2020-07-14: • Original version
1
X06 - SECTION F CHANGES
X06 - SECTION F: TRAUMA
Version date: 2022-05-09 Publication date: 2022-06-01
F01 MAJOR TRAUMA
2022-04-08: • Replaces original TRAUMA ASSESSMENT patient care map (A02) • Incorporates information from multiple documents (F01, F02, F06.1, F07, F08, F09, F10; P23.1, P23.2, P26, and P28)
into one document
F01A/B/C- EXSANGUINATING EXTERNAL HEMORRHAGE
2022-06-01: • Deleted; contents moved into new major trauma overview (F01)
2017-04-04: • Original version
F02A/B/C - TRAUMATIC HEMORRHAGE & SHOCK
2022-06-01: • Deleted; contents moved into new major trauma overview (F01)
2017-04-04: • Original version
F03 BURNS
2022-04-07: • Replacement of colored boxes with scope of work statement and legend • Removal of some educational materials from notes section • Paramedics with primary work scope will consult OLMS for pain management • Reformatting
2017-04-06: • Original version
F04 - SPINAL MOTION RESTRICTION
2022-04-07:
• Replacement of colored boxes with scope of work statement and legend • Removal of some information from notes section and placement into flow chart • Reformatting
2017-04-04: • Original version
F05 - ISOLATED EYE INJURY
2022-04-07:
2
X06 - SECTION F CHANGES
• Revised flow chart & notes • Renumbered from F05.3) • Reformatted (replacement of coloured boxes with scope of work statement and identifiers) • Inclusion of information arounds eye irrigation (previously P20)
2017-06-20: • Original version
F06.1 - LONG BONE FRACTURES
2022-06-01: • Deleted; contents moved into new major trauma overview (F01)
2017-06-20: • Original version
F07 - AMPUTATIONS & LACERATIONS
2022-06-01: • Deleted; contents moved into new major trauma overview (F01)
2017-06-20: • Original version
F08 - PELVIC TRAUMA
2022-06-01: • Deleted; contents moved into new major trauma overview (F01)
2017-08-01: • Original version
F09 -THORACIC TRAUMA
2022-06-01: • Deleted; contents moved into new major trauma overview (F01)
2017-08-01: • Original version
F10 - ABDOMINAL TRAUMA
2022-06-01: • Deleted; contents moved into new major trauma overview (F01)
2017-08-01: • Original version
1
X07 - SECTION G CHANGES
X07- SECTION G: PATIENT TRANSPORT
Version date: 2022-05-19 Publication date: 2022-06-01
G01 - ESTABLISHED MEDICATION INFUSIONS
2022-03-14: • Minor reformatting (removal of change tracking from care map)
2022-01-04: • Renumbered from M08 • Reformatted (replacement of coloured boxes with scope of work statement • Statement regarding stranding & interim orders; need to consult OLMS: and need for written order
2021-11-17: • Renumbered from P08 • Revised & reformatted • Removal of colored boxes & replacement with scope of work statement • Clarification regarding standing and interim orders; need for written medication order; and need to consult OLMS
for certain medications and certain providers • Addition of amiodarone, ketamine, remdesivir and tocilizumab • Expanded list of authorized medications at basic and primary level of work scope
2017-06-27: • Original version
G02 - SCHEDULED MEDICATIONS
2022-03-14: • Minor reformatting (removal of change tracking from care map)
2022-01-06: • New
G03 - ADULT TRANSPORT TEAM PRIMARY WORK SCOPE
2022-05-02: • New
1
X08 - SECTION M CHANGES
X08 - SECTION M: MEDICATIONS
Version date: 2022-05-03 Publication date: 2022-05-04
M01 - ADENOSINE
2022-03-12: • Minor reformatting (removal of change tracking from care map)
2021-10-19: • Minor reformatting
2021-05-18: • Replacement of coloured boxes by scope of work statement & icons • New standing & interim order statements • Reformatting
2020-06-15 • Clarification of indications & contraindications • Reformatting
2017-03-20: • Original version
M02.1 - ACETAMINOPHEN
2022-05-03: • Rectal dosing route removed
2022-03-12: • Minor reformatting (removal of change tracking from care map)
2021-10-19: • Minor reformatting
2021-05-18: • Addition of scope of work and standing order statements • Revised age range for dosing & revised PR dosing • Reformatting
2020-06-16: • Replaces M02 • Contraindication added for liver failure • Removal of naproxen • Adolescent and adult weight based dosing removed • Reformatting
2018-02-03: • Original version
M02.2 - IBUPROFEN
2022-03-12:
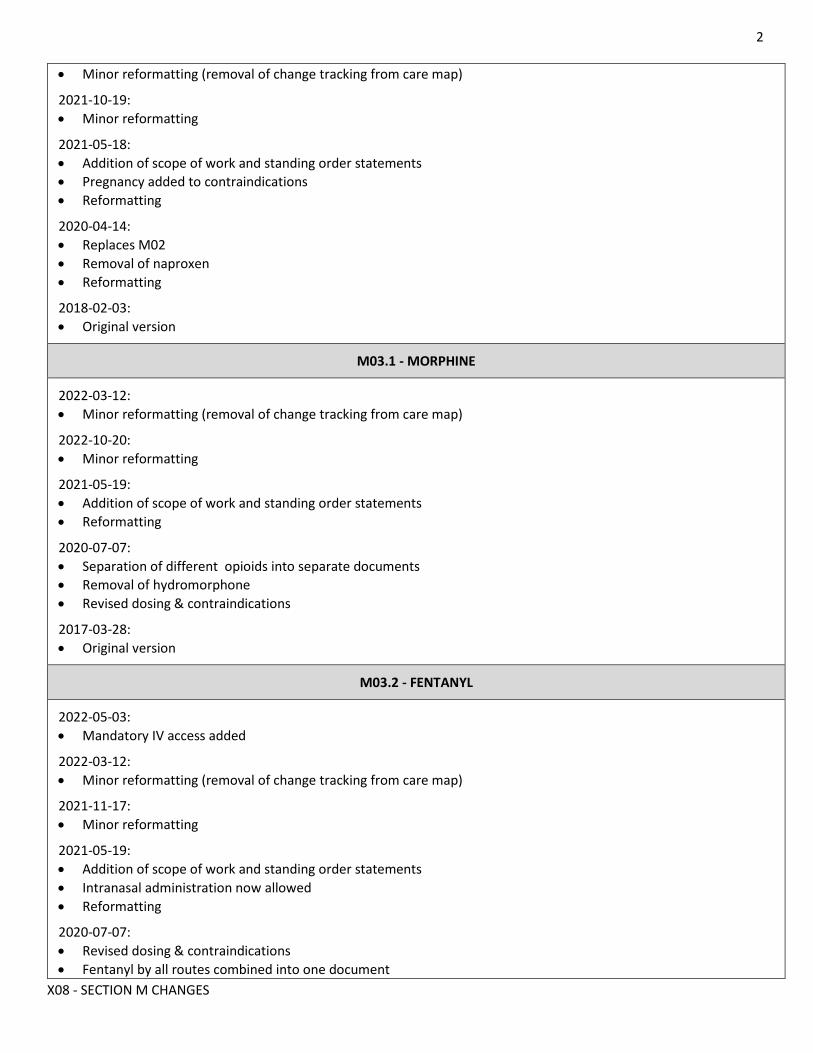
2
X08 - SECTION M CHANGES
• Minor reformatting (removal of change tracking from care map)
2021-10-19: • Minor reformatting
2021-05-18: • Addition of scope of work and standing order statements • Pregnancy added to contraindications • Reformatting
2020-04-14: • Replaces M02 • Removal of naproxen • Reformatting
2018-02-03: • Original version
M03.1 - MORPHINE
2022-03-12: • Minor reformatting (removal of change tracking from care map)
2022-10-20: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Reformatting
2020-07-07: • Separation of different opioids into separate documents • Removal of hydromorphone • Revised dosing & contraindications
2017-03-28: • Original version
M03.2 - FENTANYL
2022-05-03: • Mandatory IV access added
2022-03-12: • Minor reformatting (removal of change tracking from care map)
2021-11-17: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Intranasal administration now allowed • Reformatting
2020-07-07: • Revised dosing & contraindications • Fentanyl by all routes combined into one document
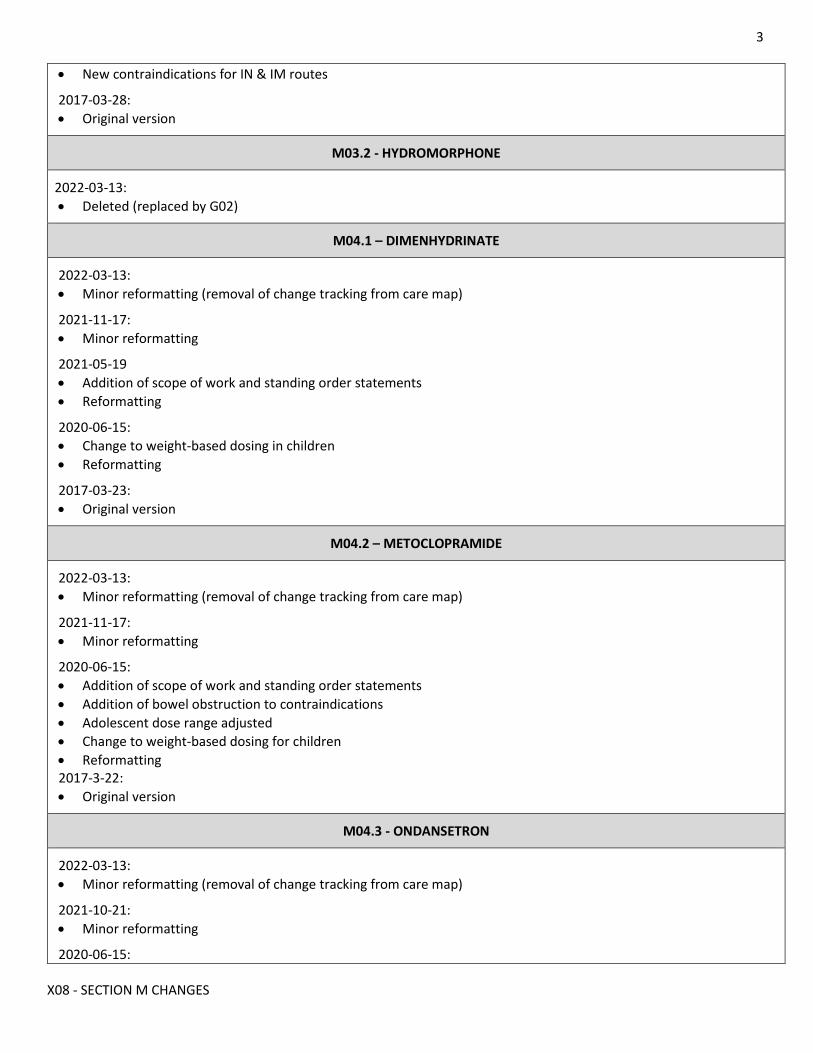
3
X08 - SECTION M CHANGES
• New contraindications for IN & IM routes
2017-03-28: • Original version
M03.2 - HYDROMORPHONE
2022-03-13: • Deleted (replaced by G02)
M04.1 – DIMENHYDRINATE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-11-17: • Minor reformatting
2021-05-19 • Addition of scope of work and standing order statements • Reformatting
2020-06-15: • Change to weight-based dosing in children • Reformatting
2017-03-23: • Original version
M04.2 – METOCLOPRAMIDE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-11-17: • Minor reformatting
2020-06-15: • Addition of scope of work and standing order statements • Addition of bowel obstruction to contraindications • Adolescent dose range adjusted • Change to weight-based dosing for children • Reformatting 2017-3-22: • Original version
M04.3 - ONDANSETRON
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-21: • Minor reformatting
2020-06-15:
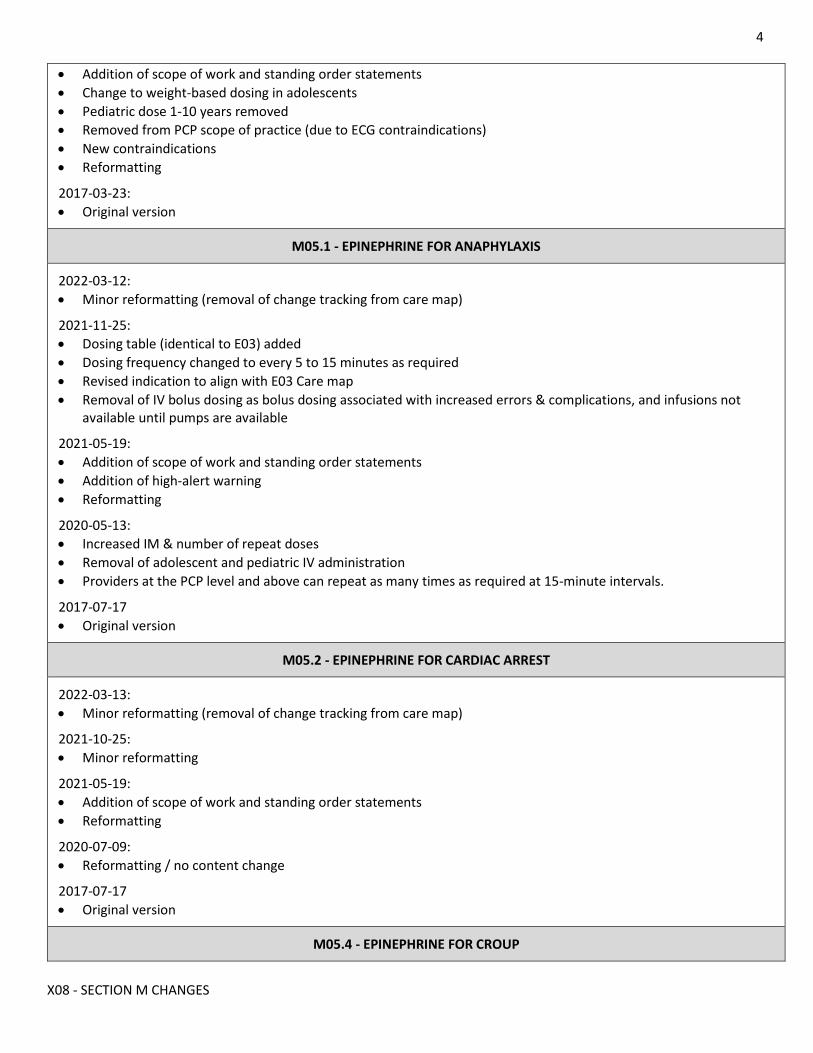
4
X08 - SECTION M CHANGES
• Addition of scope of work and standing order statements • Change to weight-based dosing in adolescents • Pediatric dose 1-10 years removed • Removed from PCP scope of practice (due to ECG contraindications) • New contraindications • Reformatting
2017-03-23: • Original version
M05.1 - EPINEPHRINE FOR ANAPHYLAXIS
2022-03-12: • Minor reformatting (removal of change tracking from care map)
2021-11-25: • Dosing table (identical to E03) added • Dosing frequency changed to every 5 to 15 minutes as required • Revised indication to align with E03 Care map • Removal of IV bolus dosing as bolus dosing associated with increased errors & complications, and infusions not
available until pumps are available
2021-05-19: • Addition of scope of work and standing order statements • Addition of high-alert warning • Reformatting
2020-05-13: • Increased IM & number of repeat doses • Removal of adolescent and pediatric IV administration • Providers at the PCP level and above can repeat as many times as required at 15-minute intervals.
2017-07-17 • Original version
M05.2 - EPINEPHRINE FOR CARDIAC ARREST
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-25: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Reformatting
2020-07-09: • Reformatting / no content change
2017-07-17 • Original version
M05.4 - EPINEPHRINE FOR CROUP
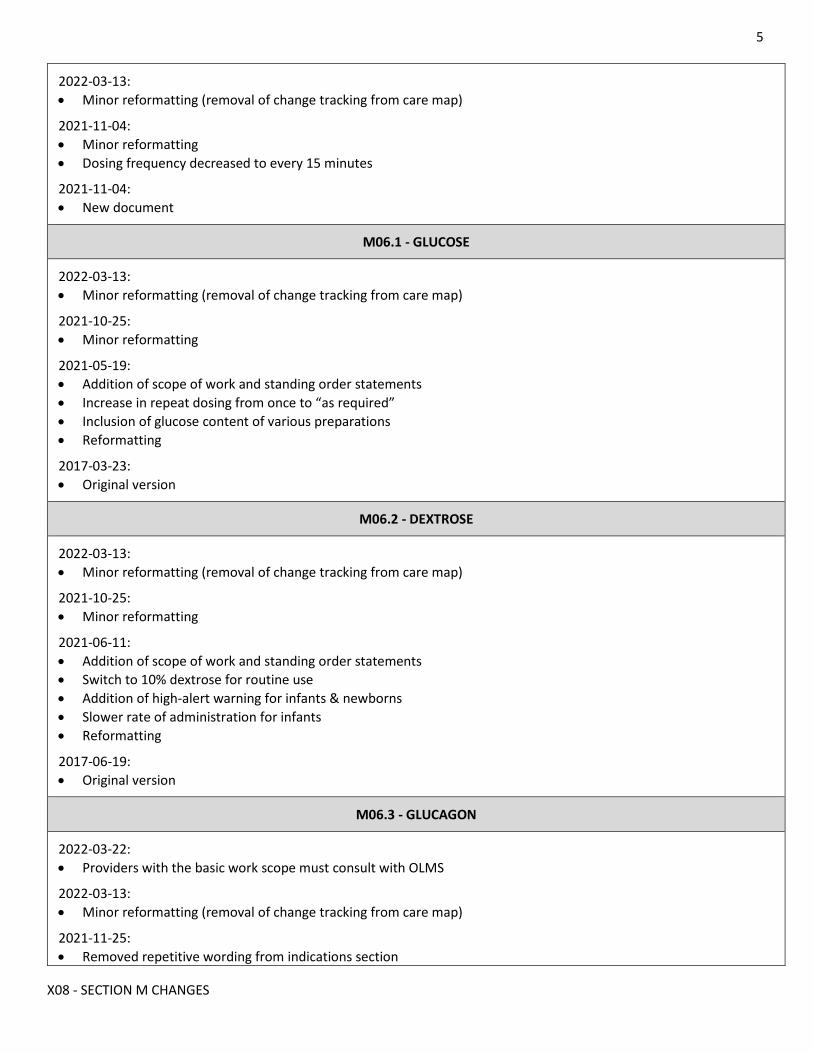
5
X08 - SECTION M CHANGES
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-11-04: • Minor reformatting • Dosing frequency decreased to every 15 minutes
2021-11-04: • New document
M06.1 - GLUCOSE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-25: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Increase in repeat dosing from once to “as required” • Inclusion of glucose content of various preparations • Reformatting
2017-03-23: • Original version
M06.2 - DEXTROSE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-25: • Minor reformatting
2021-06-11: • Addition of scope of work and standing order statements • Switch to 10% dextrose for routine use • Addition of high-alert warning for infants & newborns • Slower rate of administration for infants • Reformatting
2017-06-19: • Original version
M06.3 - GLUCAGON
2022-03-22: • Providers with the basic work scope must consult with OLMS
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-11-25: • Removed repetitive wording from indications section
6
X08 - SECTION M CHANGES
• Added missing title IV/IO to dosing section
2021-10-25: • Minor reformatting • Revised - refractory anaphylaxis removed as indication
2021-06-11: • Addition of scope of work and standing order statements • Clarification of dosing for refractory anaphylaxis • Intranasal administration now allowed • Reformatting
2021-02-19 • Indication of refractory anaphylaxis added
2020-04-15: • IM & IV administration now in scope for PCP • Caution regarding IM route added
2017-06-19: • Original version
M07.1 - MIDAZOLAM
2022-04-06: • Removal of CNS depression as a contraindication
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-11-05: • Minor reformatting • Clarification that IV dose is to be titrated to effect
2021-06-08: • Airway maintenance added at PCP level with consultation with OLMS • Correction of dosing at 10 years & older • Simplification of IV (IO) dosing
2021-05-19: • Addition of scope of work and standing order statements • Intranasal administration now allowed Clarification of choice of route for active seizures • More detail regarding titration of dosing for various indications • More detail regarding IO access for various indications • Dosing changes • Reformatting
2020-05-11: • Consolidation of previous documents M07.1; M07.2; and M07.3 into single protocol • Decreased dosing for intravenous administration • IM administration now in scope for PCP • IV & IO administration now in scope for PCP for specific indications
2017-06-19 • Original version
7
X08 - SECTION M CHANGES
M07.5 - LORAZEPAM
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-25: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Reformatting
2020-05-28: • Removal of parenteral routes of administration • Revised dosing • Reformatting
2017-06-19 • Original version
M09 - FUROSEMIDE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-25: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Reformatting
2020-08-20: • Revised dosing
2017-04-03: • Original version
M10 - HYPERKALEMIA THERAPY
2022-03-13: • Minor reformatting (removal of change tracking from care map) • Content change (revised indications)
2021-11-17: • Revised indications
2021-05-19 • Addition of scope of work and standing order statements • Increased administration frequency for insulin • Removal of salbutamol as nebulizers no longer in use • Reformatting
2020-04-12: • Removal of calcium gluconate from formulary • Consolidation of into one document
8
X08 - SECTION M CHANGES
• Simplification of dosing • Reformatting
2017-06-20: • Original versions (M10.1, M10.2, M10.3, M10.4)
M11 - NALOXONE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-25: • Addition of scope of work and standing / provisional order statements • Intranasal administration during COVID now allowed with extended PPE • Updated dosing information & dosing frequency to allow for titration • Reformatting
2020-05-25: • Correction for intranasal dose & IV administration also within PCP scope • All dosing simplified for ease of recall
2020-05-01 • IM administration now in scope for PCP
2017-06-27: • Original version
M12 - TETRACAINE
2022-03-13 • Reintroduced
M13 - HYDROCORTISONE
2022-03-13: • Minor reformatting (removal of change tracking from care map) • Work scope expanded to include paramedics with primary work scope
2021-10-25: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Reformatting
2021-02-04: • New (replaces Methylprednisolone)
M14 - AMIODARONE
2022-03-13: • Minor reformatting (removal of change tracking from care map) • Content change ( removal of VT & WCT dosing; addition of post-ROSC dosing & high-alert statement)
2021-11-08:
9
X08 - SECTION M CHANGES
• Addition of scope of work and standing order statements • Removal of infant dosing • Addition of dosing for VT and WCT • Renumbered from 14.1 Reformatting
2020-07-07: • Clarification of dosing
2017-03-23: • Original version
M15 – SALBUTAMOL
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-11-05: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Removal hyperkalemia as an indication as nebulizers no longer in use • Clarification / simplification of dosing • Reformatting
2020-11-05: • Anaphylaxis indication added • Removed Combivent nebulizer dosing • Added reference to M10 for hyperkalemia dosing
2020-05-12: • Addition of caution about nebulization during COVID-19 pandemic
2019-10-02: • Original version
M16 - OXYTOCIN
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-27: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Clarification of indication for continuous infusion • Addition of high-alert warning • Reformatting
2017-04-04: • Original version
M17 - KETAMINE
2021-11-10:
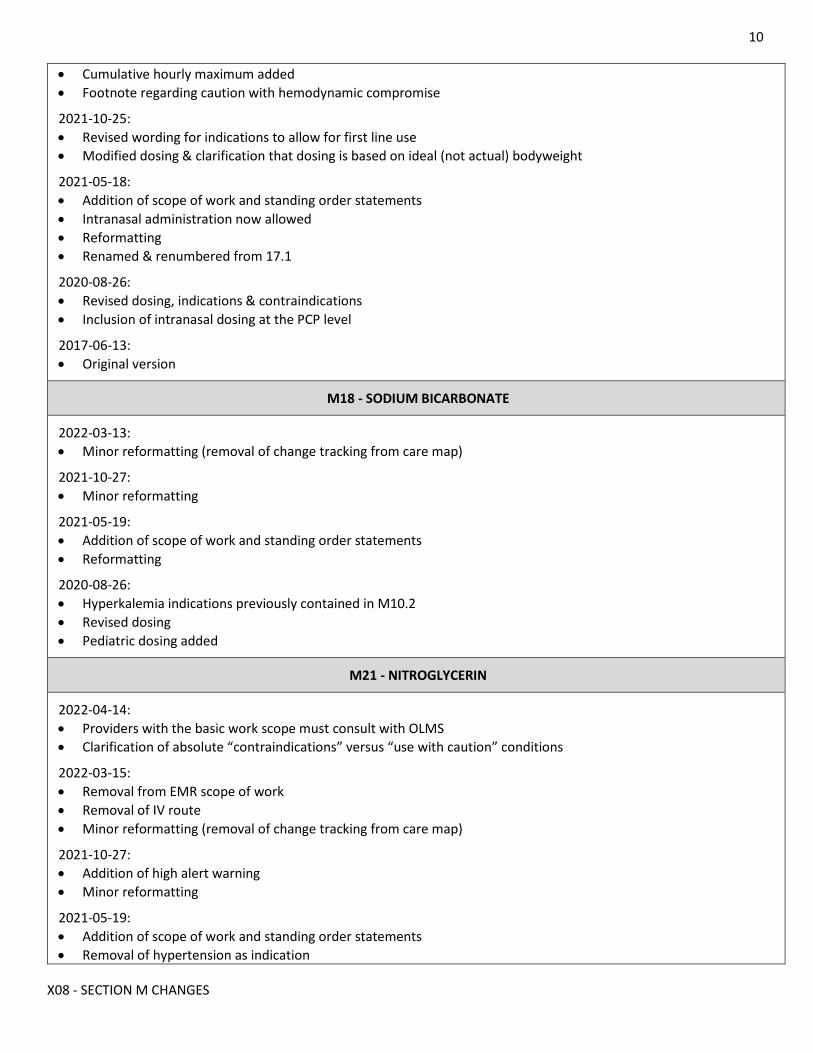
10
X08 - SECTION M CHANGES
• Cumulative hourly maximum added • Footnote regarding caution with hemodynamic compromise
2021-10-25: • Revised wording for indications to allow for first line use • Modified dosing & clarification that dosing is based on ideal (not actual) bodyweight
2021-05-18: • Addition of scope of work and standing order statements • Intranasal administration now allowed • Reformatting • Renamed & renumbered from 17.1
2020-08-26: • Revised dosing, indications & contraindications • Inclusion of intranasal dosing at the PCP level
2017-06-13: • Original version
M18 - SODIUM BICARBONATE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-27: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Reformatting
2020-08-26: • Hyperkalemia indications previously contained in M10.2 • Revised dosing • Pediatric dosing added
M21 - NITROGLYCERIN
2022-04-14: • Providers with the basic work scope must consult with OLMS • Clarification of absolute “contraindications” versus “use with caution” conditions
2022-03-15: • Removal from EMR scope of work • Removal of IV route • Minor reformatting (removal of change tracking from care map)
2021-10-27: • Addition of high alert warning • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Removal of hypertension as indication
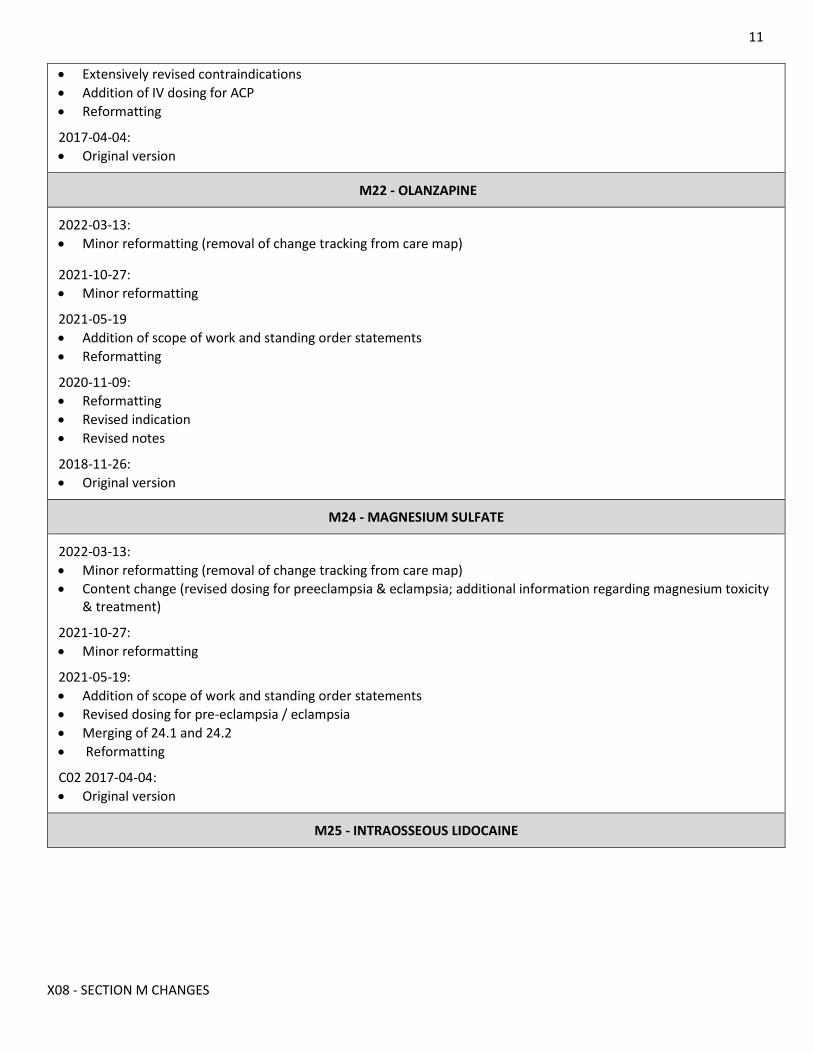
11
X08 - SECTION M CHANGES
• Extensively revised contraindications • Addition of IV dosing for ACP • Reformatting
2017-04-04: • Original version
M22 - OLANZAPINE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-27: • Minor reformatting
2021-05-19 • Addition of scope of work and standing order statements • Reformatting
2020-11-09: • Reformatting • Revised indication • Revised notes
2018-11-26: • Original version
M24 - MAGNESIUM SULFATE
2022-03-13: • Minor reformatting (removal of change tracking from care map) • Content change (revised dosing for preeclampsia & eclampsia; additional information regarding magnesium toxicity
& treatment)
2021-10-27: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Revised dosing for pre-eclampsia / eclampsia • Merging of 24.1 and 24.2 • Reformatting
C02 2017-04-04: • Original version
M25 - INTRAOSSEOUS LIDOCAINE
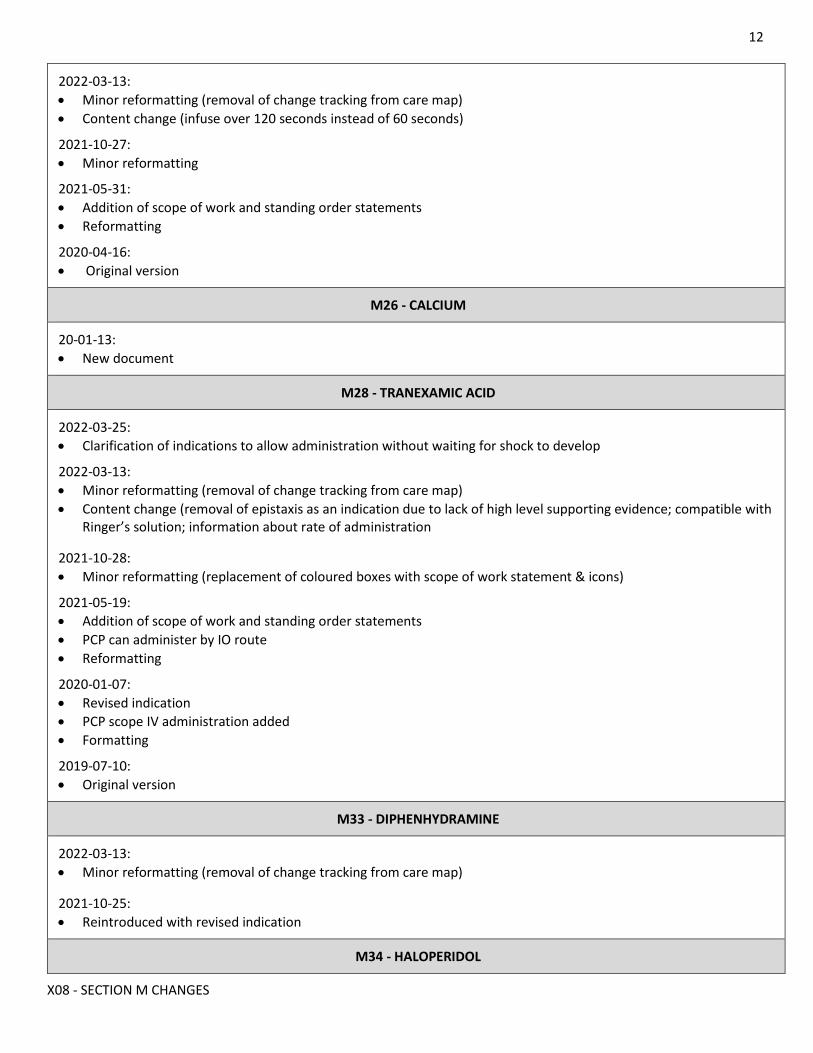
12
X08 - SECTION M CHANGES
2022-03-13: • Minor reformatting (removal of change tracking from care map) • Content change (infuse over 120 seconds instead of 60 seconds)
2021-10-27: • Minor reformatting
2021-05-31: • Addition of scope of work and standing order statements • Reformatting
2020-04-16: • Original version
M26 - CALCIUM
20-01-13: • New document
M28 - TRANEXAMIC ACID
2022-03-25: • Clarification of indications to allow administration without waiting for shock to develop
2022-03-13: • Minor reformatting (removal of change tracking from care map) • Content change (removal of epistaxis as an indication due to lack of high level supporting evidence; compatible with
Ringer’s solution; information about rate of administration
2021-10-28: • Minor reformatting (replacement of coloured boxes with scope of work statement & icons)
2021-05-19: • Addition of scope of work and standing order statements • PCP can administer by IO route • Reformatting
2020-01-07: • Revised indication • PCP scope IV administration added • Formatting
2019-07-10: • Original version
M33 - DIPHENHYDRAMINE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-25: • Reintroduced with revised indication
M34 - HALOPERIDOL
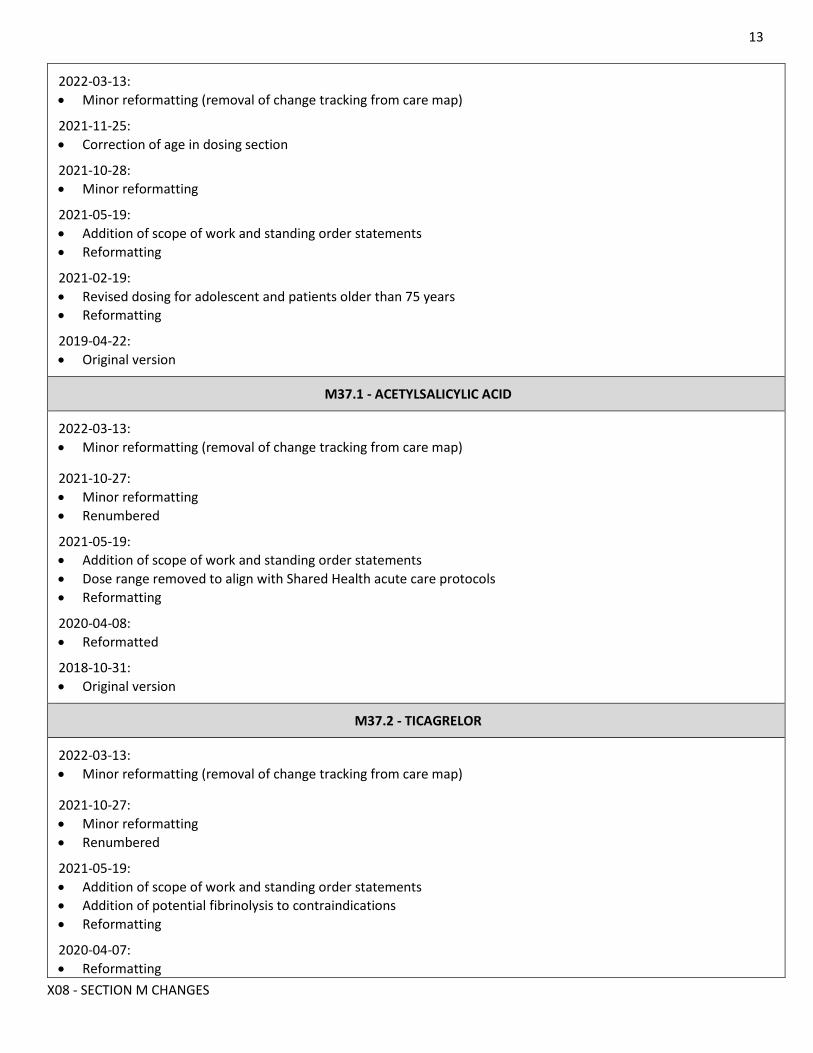
13
X08 - SECTION M CHANGES
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-11-25: • Correction of age in dosing section
2021-10-28: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Reformatting
2021-02-19: • Revised dosing for adolescent and patients older than 75 years • Reformatting
2019-04-22: • Original version
M37.1 - ACETYLSALICYLIC ACID
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-27: • Minor reformatting • Renumbered
2021-05-19: • Addition of scope of work and standing order statements • Dose range removed to align with Shared Health acute care protocols • Reformatting
2020-04-08: • Reformatted
2018-10-31: • Original version
M37.2 - TICAGRELOR
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-27: • Minor reformatting • Renumbered
2021-05-19: • Addition of scope of work and standing order statements • Addition of potential fibrinolysis to contraindications • Reformatting
2020-04-07: • Reformatting
14
X08 - SECTION M CHANGES
2018-10-31: • Original version
M38- KETOROLAC
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-28: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Pregnancy added as contraindication • IV dosing at PCP level added • Reformatting
2020-05-01: • Minimum age for child raised to 2 years & modification of dosing • IM administration now in scope for PCP • Additional contraindications
2017-04-04: • Original version
M39 - ATROPINE
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-05-19: • Addition of scope of work and standing order statements • Increased adult dosing range for severe bradycardias in adults • Hypersensitivity added as contraindication • Caution regarding patients with heart transplants and high grade blocks • Reformatting
2017-03-23: • Original version
M43 - ENOXAPARIN
2022-03-13: • Minor reformatting (removal of change tracking from care map)
2021-10-27: • Minor reformatting
2021-05-19: • Addition of scope of work and standing order statements • Addition of potential fibrinolysis to contraindications • Renumbered from 43.1 • Reformatting
2020-03-17:
15
X08 - SECTION M CHANGES
• Intravenous dosing included for patients less than 75 years of age
2018-10-31: • Original version