endothelium-dependent vasodilation of peripheral conduit arteries in patients with heart failure
TRANSCRIPT
Journal of Cardiac Failure Vol. 1 No. 1 1994
Endothelium-dependent Vasodilation of Peripheral Conduit Arteries in Patients With Heart Failure
ALAN J. BANK, MD,* THOMAS S. RECTOR, PhD,” LINDA K. TSCHUMPERLIN, RN,* MARK D. KRAEMER, MD,*
JANIS G. LETOURNEAU, MD,? SPENCER H. KUBO, MD, FACC”
Minneapolis, Minnesota
Abstract: Endothelium-dependent vasodilation of peripheral resistance vessels is abnormal in patients with heart failure, but there are little in vivo data on endothelium- dependent vasodilation of peripheral conduit vessels. This study assessed endothe- hum-dependent vasodilation of forearm conduit and resistance vessels in normal subjects and patients with heart failure. The effects of intraarterial endothelium- dependent and endothelium-independent vasodilators on both forearm conduit (bra- chial artery) and resistance vessels were assessed in 9 patients with New York Heart Association class II-III heart failure and 11 normal subjects of similar age. Brachial artery diameter was measured by two-dimensional, moderate-frequency (8 MHz) ultrasound, and forearm blood flow was measured by strain gauge plethysmography. The endothelium-dependent vasodilator, methacholine (0.3 and 1.5 kg/min), in- creased brachial artery diameter by 7.6 * I .3% and 12.2 + 1.5% in normal subjects as compared to 6.9 * 2.1% and 10.4 2 2.4% in patients with heart failure (P = NS, normal vs heart failure). The endothelium-independent vasodilator, nitroglycerin (0.15 kg), also produced similar increases in brachial artery diameter in the two groups (8.2 * 1.3% in normal subjects vs 11.1 * 1.4% in patients with heart failure, P = NS). In contrast, forearm blood flow responses to methacholine were signifi- cantly (P < .05) greater in normal subjects (4.1 2 0.5 and 9.2 ? 1.4 mL/min/lOO mL forearm volume) than in patients with heart failure (2.0 ? 0.8 and 5.1 +- 1.3 mL/ min/lOO mL forearm volume). Forearm blood flow responses to the endothelium- independent vasodilator, sodium nitroprusside, were similar between the two groups. This study suggests that endothelium-dependent and endothelium-independent vaso- dilation of the brachial artery is not impaired in patients with class II-III heart failure. This finding contrasts with abnormal endothelium-dependent vasodilation of forearm resistance vessels. These data suggest that there are regional differences in endothe- lial function in patients with heart failure. Key words: endothelium-derived relaxing factor, heart failure, conduit vessel, vasodilation.
From the Cardiovascular Division. Departments of *Medicine und iRudiology, University of Minnesota Medical School, Min- neapolis. Minnesota.
Supported in part by an American Heart Association Grant-in- Aid, an NIH-NHLBI Research Fellowship Award, and Program Project Grant POl-HL32427.
Presented in part at the Scientific Sessions of the American Heart Association, New Orleans, Louisiana, November 1992.
Reprint requests: Alan J. Bank, MD. Cardiovascular Division, Department of Medicine, University of Minnesota Medical School, Box 508 UMHC, 420 Delaware Street SE. Minneapolis, MN 55455.
The endothelium is an important modulator of vascular tone and reactivity.lm4 Previous studies in patients with heart failure have demonstrated abnor- mal peripheral resistance vessel dilation to the endo- thelium-dependent agents methacholine and acetyl- choline, but not to the direct smooth muscle vasodilator sodium nitroprusside.5-7 However, there are little in vivo data regarding endothelial modulation of peripheral conduit vessel tone and
35
36 Journal of Cardiac Failure Vol. 1 No. 1 October 1994
reactivity. Although conduit vessels do not regulate organ blood flow under basal conditions, they serve important functions, including buffering of pulsatile left ventricular outflow’ and vasodilation in re- sponse to increased flow. 9*1o Abnormal endothelial function could adversely affect the ability of conduit vessels to perform these functions in patients with heart failure.
This study was designed to assess endothelium- dependent and endothelium-independent vasodila- tion of a peripheral conduit vessel in patients with heart failure. Brachial artery diameter was mea- sured by two-dimensional (8.0 MHz) ultrasound, and changes in diameter in response to intraarterial vasodilators were compared in normal subjects and patients with heart failure.
Materials and Methods
Study Sample
The study sample consisted of 9 patients with New York Heart Association class II-III heart fail- ure and 11 normal subjects of similar age. Patients with heart failure were referred to the University of Minnesota for cardiac transplantation evaluation. Patients with diabetes mellitus, hypertension (> 160/ 90 mmHg), significant peripheral vascular disease, or recent myocardial infarction (~3 months) were excluded from the study. All patients had left ven- tricular systolic dysfunction as measured’ by radio- nuclide ventriculography and/or echocardiography. The etiology of heart failure was coronary artery disease in five and idiopathic dilated cardiomyopa- thy in four patients. Medications included diuretics (n = 9), digitalis (n = 7), angiotensin converting enzyme inhibitors (n = S), calcium blockers (n = 3), quinidine (n = 2), isosorbide dinitrate (n = I), and amiodarone (n = 1). None of the patients were taking nonsteroidal antiinflammatory agents, except one patient on aspirin. All medications were with- held for at least 12 hours. Digitalis, angiotensin con- verting enzyme inhibitors, and other vasodilators were withheld for at least 24-48 hours prior to the study. Normal subjects were recruited from news- paper advertisements. Subjects with hypertension, cardiovascular disease, or systemic medical prob- lems as determined by history, physical examina- tion, routine blood tests, and electrocardiogram were excluded. Normal subjects were not taking any medications. This study was approved by the Human Rights and Research Committee and all par- ticipants gave written informed consent. This inves- tigation conforms with the principles outlined in the Declaration of Helsinki.
Study Preparation
Studies were performed in a temperature-con- trolled (22” 2 1’C) room in the morning. Subjects ate a light breakfast without caffeinated beverages on the morning of the study. An 18-gauge, 7.6 cm catheter was placed into the brachial artery of the nondominant arm using sterile technique and 1% li- docaine. The catheter was connected to a pressure transducer and an eight-channel recorder (Gould, TA 3200, Valley View, OH). Intraarterial infusions were administered using a mechanical syringe pump (Harvard Apparatus, South Natick, MA). Forearm blood flow was measured with a double strand mer- cury-in-Silastic strain gauge connected to an elec- tronically calibrated plethysmograph (Hokanson EC 5, DE Hokanson, Bellevue, WA), as previously described.““2 A pediatric blood pressure cuff was placed around the wrist and inflated to suprasystolic pressure to exclude hand circulation 30-60 seconds prior to measuring forearm blood flow. Five consec- utive flow measurements were averaged for each condition. Heart rate and contralateral arm blood pressure (cuff sphygmomanometer) were recorded before and during each infusion to assess the sys- temic effects of the interventions. Forearm volume (FAV) was measured by water displacement. Fore- arm vascular resistance was calculated as the ratio of mean arterial pressure to forearm blood flow.
Measurement of Brachial Artery Diameter
Brachial artery diameter was measured by two- dimensional, moderate-frequency (8.0 MHz) ultra- sound (Biosound 2000 II sa, Biosound, Indianapolis, IN). This device has been previously used in nonin- vasive studies of carotid artery atherosclerosis due to the high-quality images obtained.‘3,‘4 The 8 MHz frequency provides good tissue-blood interface res- olution, and a built-in water bath allows both offset of the ultrasound transducer from the vessel being imaged and improved focus of the ultrasound beam on superficial structures, such as the brachial artery. The transducer was held lightly on the skin overly- ing the brachial artery approximately 4 cm proximal to the antecubital area. The transducer was posi- tioned until a circular cross-section of the brachial artery was obtained. Any elliptic or noncircular im- ages were rejected. The brachial artery was distin- guished from venous structures based on (1) the presence of pulsations, (2) the lack of collapse with light pressure, and (3) the identification of the previ- ously placed catheter. The brachial artery image was recorded for 30 seconds on a standard videotape recorder. In approximately 15% of the individuals
Conduit Artery Vasodilation in Heart Failure l Bank et al. 37
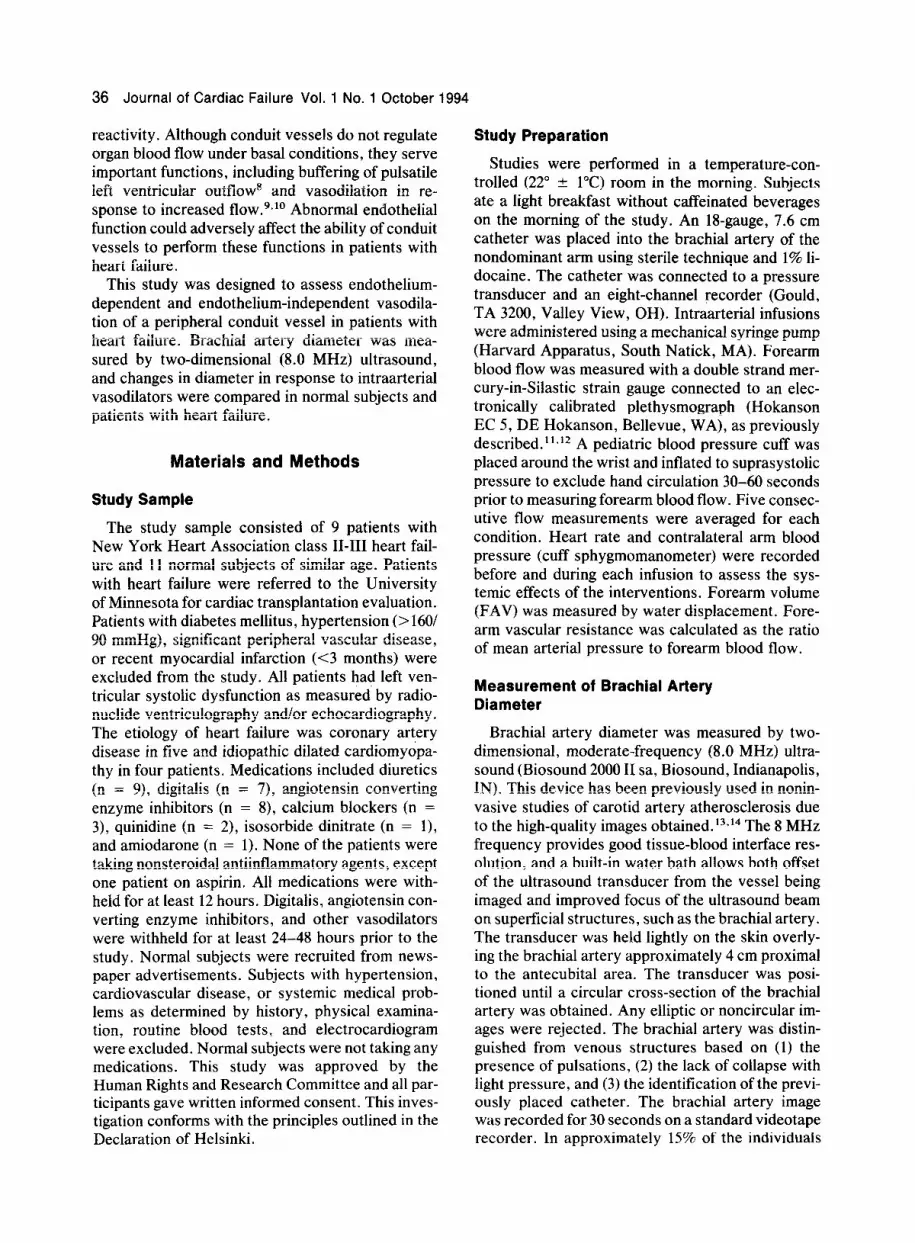
screened for this study, the image was of insufficient quality to accurately determine brachial artery di- ameter. Subjects with poor quality images on screening assessment were excluded prior to partici- pation in the study. Upon completion of the study, end-systolic frames were printed on paper for subse- quent measurement of brachial artery diameter. End-systole was defined as the largest arterial diam- eter for each cardiac cycle. Diameters were mea- sured in the axial plane, rather than in the lateral plane, because axial resolution is superior to lateral resolution (0.3 vs 0.7 mm, respectively according to manufacturers’ specifications). The lumen-wall bor- der was marked with a fine-point pencil, measured to the nearest 0.25 mm, and converted to actual length using a scale factor based on the ultrasound machine internal calipers. All diameters were mea- sured by a single individual who was blinded to the experimental condition during which the image was obtained. Eight frames were averaged for each con- dition. Examples of brachial artery ultrasound frames at baseline and during infusion of methacho- line (1.5 pg/min) are shown in Figure 1.
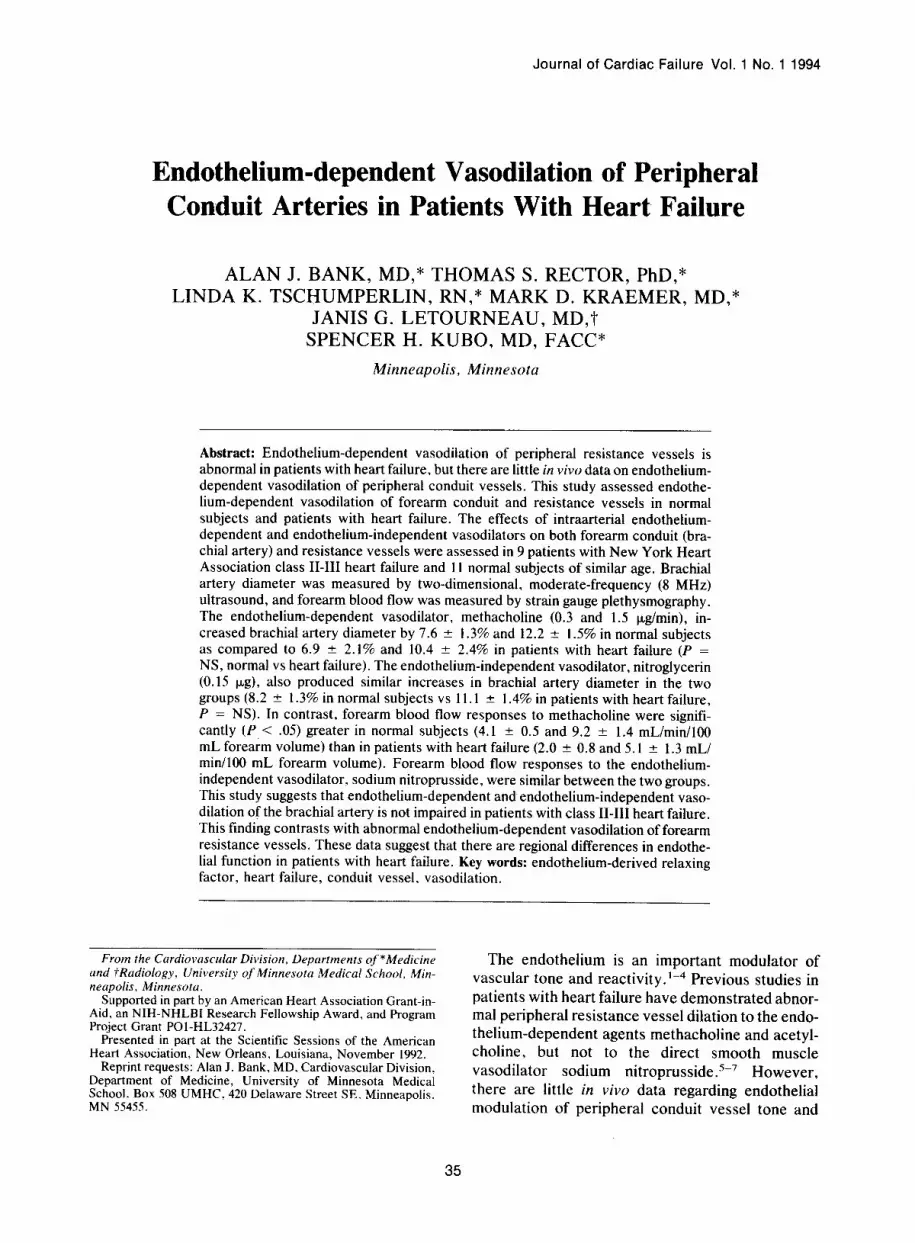
Reproducibility studies (Fig. 2) were performed in 28 normal subjects and 15 patients with heart fail- ure and included measurements of brachial artery diameter performed 10 minutes apart. Between mea- surements, the transducer was removed from its original position and repositioned on the forearm prior to the second measurement. The mean differ- ence between two measurements was 0.002 & 0.002 cm (P = NS), which is approximately 0.5% of the brachial artery diameter. The difference between di- ameter measurements of the arterial image by two different individuals averaged 0.008 + 0.003 cm,
0.30 0.30 0.40 0.50 0.60
DIAMETER 1 (cm)
Fig. 2. Reproducibility of brachial artery diameter ultra- sound measurements in 43 individuals. The mean differ- ence between the two measurements was 0.002 ? 0.002 cm V’ = NS). Data were randomly distributed near the line of identity.
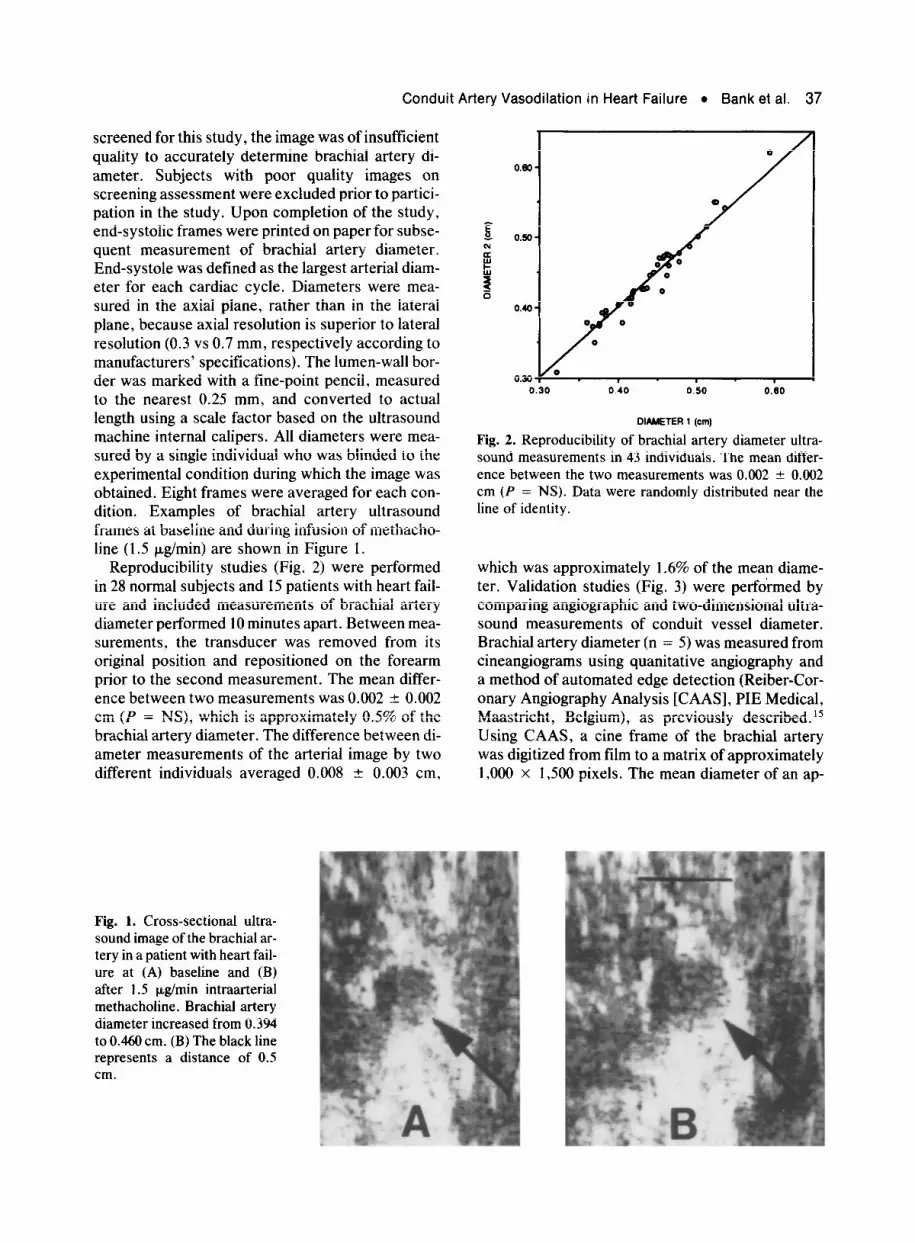
which was approximately 1.6% of the mean diame- ter. Validation studies (Fig. 3) were performed by comparing angiographic and two-dimensional ultra- sound measurements of conduit vessel diameter. Brachial artery diameter (n = 5) was measured from cineangiograms using quanitative angiography and a method of automated edge detection (Reiber-Cor- onary Angiography Analysis [CAAS], PIE Medical, Maastricht, Belgium), as previously described.15 Using CAAS, a tine frame of the brachial artery was digitized from film to a matrix of approximately 1,000 x 1,500 pixels. The mean diameter of an ap-
Fig. 1. Cross-sectional ultra- sound image of the brachial ar- tery in a patient with heart fail- ure at (A) baseline and (B) after 1.5 p,g/min intraarterial methacholine. Brachial artery diameter increased from 0.394 to 0.460 cm. (B) The black line represents a distance of 0.5 cm.
38 Journal of Cardiac Failure ‘Vol. 1 No. 1 October 1994
O.O-
0.6 -
0.7-
0.0 -
0.5-
0.4 -
0.3 Y 1 1 I 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 1.1
ANGlDGRAPHlC DIAMETER (an)
Fig. 3. Comparison of brachial artery (n = 5) and femoral artery (n = 8) diameter measured by ultrasound and angi- ography. The mean difference between measurements using the two techniques was 0.015 ? 0.012 cm (P = NS). Data were randomly distributed near the line of identity.
proximately 10 mm long segment whose midportion corresponded with the location of ultrasound mea- surement of diameter was determined using an auto- mated algorithm and computer smoothing. Common femoral artery diameter (n = 8) was measured using calipers from cut-film angiograms, since cineangio- grams were not performed on these patients. The common femoral artery was imaged with ultrasound at a point just below the inguinal ligament (which was used as a landmark for determining the place where angiographic diameter measurement was made). For both brachial and femoral measure- ments, angiographic catheter (7 or 8 F) diameter was also measured and used as a scale factor to correct for magnification. The mean difference between an- giographic and ultrasound conduit vessel diameter measurements was 0.015 ? 0.012 cm (P = NS).
Experimental Protocol
After the catheter was placed, the patients rested for 30 minutes and then blood samples were ob- tained for assay of plasma norepinephrine. Baseline forearm blood flow and brachial artery diameter were measured on two occasions, separated by 10 minutes. The catheter tip was several centimeters proximal to the site of the brachial artery diameter measurement, as demonstrated by ultrasound. Five percent dextrose in water was administered as a control measure. Methacholine (Provocholine, Roche Laboratories, Hutley, NJ) was administered intraarterially at 0.3 and 1.5 pg/min to assess endo-
thelium-dependent vasodilation. Nitrovasodilators were given to assess endothelium-independent re- sponses, since both methacholine (through release of endothelium-derived relaxing factor) and nitrates produce vasodilation predominantly via stimulation of soluble guanylate cyclase in vascular smooth muscle cells.16 Sodium nitroprusside (Elkins-Sinn, St. Davids, PA) was administered at 5 and 10 pg/ min to assess resistance vessel endothelium-inde- pendent vasodilation. Sodium nitroprusside was given after the brachial artery catheter had been re- positioned several centimeters distal to the site of diameter measurement, since preliminary studies showed prolonged effects of this drug on brachial artery diameter and this drug was used only to as- sess resistance vessel endothelium-independent di- lation. Nitroglycerin (DuPont Pharmaceutical, Wil- ington, DE) was given intraarterially as a bolus infusion of 0.15 p,g to assess endothelium-indepen- dent vasodilation of the brachial artery. Brachial ar- tery response to nitroglycerin was measured ap- proximately 30 seconds after administration. Nitroglycerin was administered last due to its pro- longed vasodilatory effect on conduit arteries. These two nitrovasodilators were used, since pre- liminary studies demonstrated that nitroglycerin had a greater effect on conduit vessels, whereas nitro- prusside had a greater effect on resistance vessels. Continuous infusions were administered for 1.5 min- utes at 1 mL/min before measuring the first diameter and then forearm blood flow because preliminary studies showed steady-state responses by this time. The transducer was kept in the same position for each drug infusion and the corresponding baseline. The transducer was removed between drug infu- sions and repositioned prior to the next baseline measurements at a location previously marked on the arm. All participants received infusions in as- cending doses in the following order: 5% dextrose in water, methacholine, sodium nitroprusside, and nitroglycerin.
Calculations and Statistical Analyses
The reproducibility of repeated ultrasound mea- surements of brachial artery diameter and the com- parison to angiographic diameter measurements were assessed by paired t-tests. Baseline character- istics were compared using unpaired t-tests. Metha- choline, nitroprusside, and nitroglycerin responses were evaluated by analysis of variance with a re- peated measure (dose) and grouping factor (normal versus heart failure). P values 5 .05 were consid- ered significant. Values reported are mean + SEM except where specified.

Conduit Artery Vasodilation in Heart Failure l Bank et al. 39
Table 1. Baseline Characteristics
Normal (n = 11) Heart Failure (n = 9)
Age (years) Male/Female Forearm volume (mL) Forearm blood flow (mLlmini100 mL FAV) Mean arterial pressure (mmHg) Forearm vascular resistance (mmHg/mL/min/100 mL FAV) Brachial artery diameter (cm) Ejection fraction (%) Norepinephrine (pg/mL) Cholesterol (mg/dL)
41.5 k 5.3 (range, 21-66) 1110
1,145 k 31 2.93 k 0.38 86.4 ” 3.3 33.6 ” 4.1
0.442 + 0.021
287 2 26 192 2 13
45.2 + 3.0 (range, 29-56) 712
1.217 -+ 100 2.53 zk 0.33 79.0 t 6.0 38.6 -c 8.1
0.450 + 0.021 14 k 2
548 2 93* 206 t 23
* P < .05. FAV, forearm volume.
Results
Baseline Characteristics
Baseline characteristics of the two groups are shown in Table I. The mean ejection fraction in the patients with heart failure was 14 + 2%. There were no statistically significant differences between the groups for any of the baseline characteristics mea- sured, except for plasma norepinephrine concentra- tion, which was significantly higher (548 + 93 vs 287 + 26 pg/mL; P < .05) in the patients with heart failure.
Responses to Vasodilators
There was no significant change ( - 0.001 k 0.004 cm; 0.23%) in brachial artery diameter in response to intraarterial 5% dextrose in water-vehicle infu- sion. The percent changes in brachial artery diame- ter for both groups in response to intraarterial meth- acholine and nitroglycerin infusions are shown in Figure 4. All individuals, except one, exhibited dila- tion in response to methacholine. In the normal sub- jects, brachial artery diameter increased by a mean
Fig. 4. Percent change in bra- chial artery diameter in re- sponse to intraarterial metha- choline and nitroglycerin in 11 normal subjects and 9 patients with heart failure. There were no significant differences be- tween the groups in brachial artery response to either drug. MTC 1, methacholine 0.3 kg/ min; MTC 2, methacholine I .5 pg/min; NTG, nitroglycerin 0.15 pg.
of 7.6 + 1.3% and 12.2 +- 1.5% for the two doses of methacholine. The corresponding changes in bra- chial artery diameter in the patients with heart fail- ure were 6.9 +- 2.1% and 10.4 + 2.4%. There was no significant difference between the two groups re- garding the conduit vessel response when analyzed as either absolute or percent change in diameter. The brachial artery responses to nitroglycerin were also not significantly different between the groups, with diameter increasing by 8.2 + 1.3% in the nor- mal subjects and 11.1 + 1.4% in the patients with heart failure.
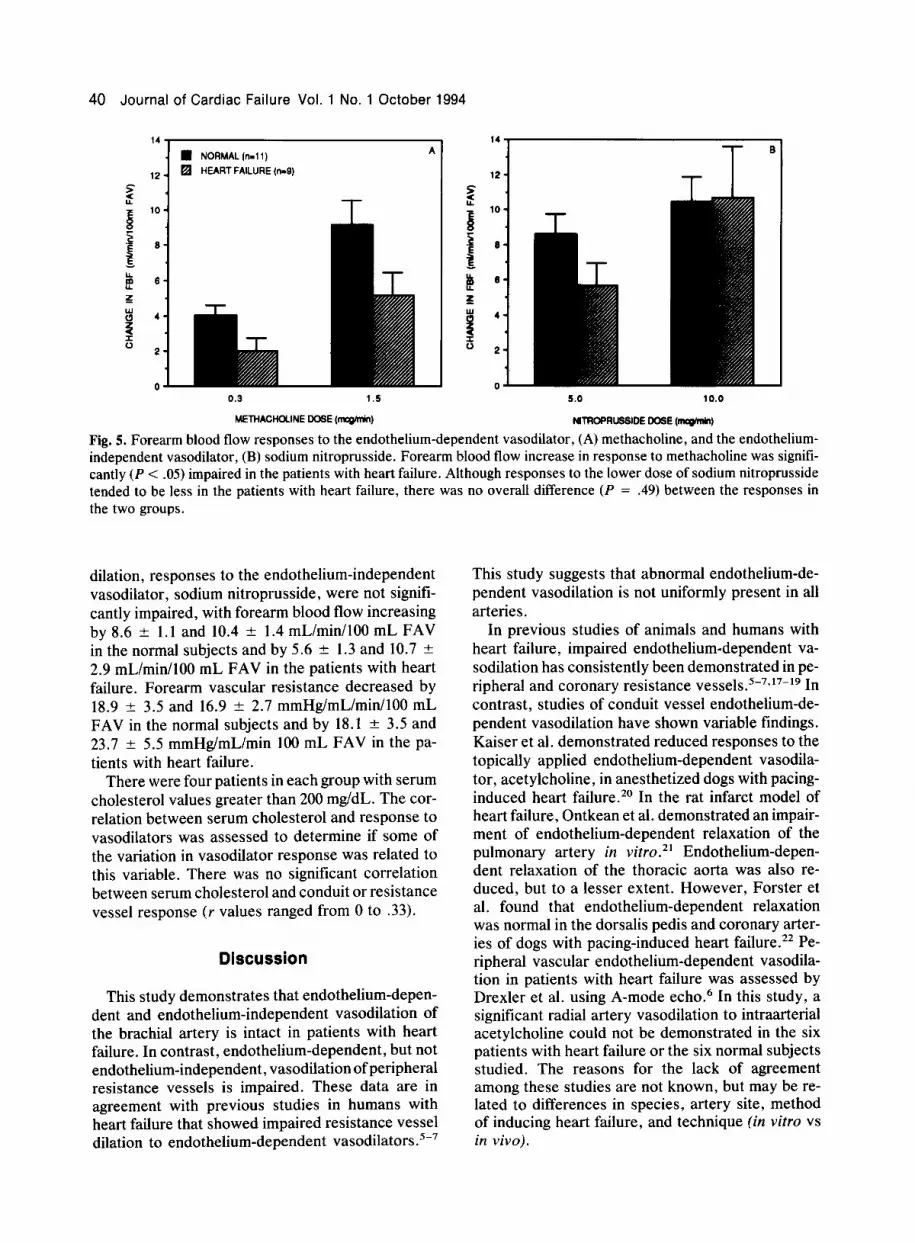
Responses of forearm resistance vessels are shown in Figure 5. Methacholine increased forearm blood flow by 4.1 + 0.5 and 9.2 + 1.4 mL/min/lOO mL FAV in the normal subjects and by 2.0 + 0.8 and 5.1 2 1.3 mL/min/lOO mL FAV in the patients with heart failure (P < .05 normal vs heart failure). Methacholine decreased forearm vascular resis- tance by 20.7 -+ 4.2 and 25.7 + 5.2 mmHg/mL/min/ 100 mL FAV in the normal subjects and by 9.5 + 3.6 and 19.7 t 4.1 mmHg/mL/min/lOO mL FAV in the patients with heart failure. In contrast to the impaired endothelium-dependent resistance vessel
12s
MART FAILURE A
40 Journal of Cardiac Failure Vol. 1 No. 1 October 1994
n NORMAL (n-l 1) A
q HEART FAILURE (n-9)
0.3 1.5
METHACHCLINE DOSE (mcqhbin)
5.0 10.0
NlTROPRlJWDE DOSE (mc@hM)
Fig. 5. Forearm blood flow responses to the endothelium-dependent vasodilator, (A) methacholine, and the endothelium- independent vasodilator, (B) sodium nitroprusside. Forearm blood flow increase in response to methacholine was signifi- cantly (P < .05) impaired in the patients with heart failure. Although responses to the lower dose of sodium nitroprusside tended to be less in the patients with heart failure, there was no overall difference (P = .49) between the responses in the two groups.
dilation, responses to the endothelium-independent vasodilator, sodium nitroprusside, were not signifi- cantly impaired, with forearm blood flow increasing by 8.6 + 1.1 and 10.4 & 1.4 mL/min/lOO mL FAV in the normal subjects and by 5.6 t 1.3 and 10.7 -+ 2.9 mL/min/lOO mL FAV in the patients with heart failure. Forearm vascular resistance decreased by 18.9 + 3.5 and 16.9 & 2.7 mmHg/mL/min/lOO mL FAV in the normal subjects and by 18.1 ? 3.5 and 23.7 ? 5.5 mmHg/mL/min 100 mL FAV in the pa- tients with heart failure.
There were four patients in each group with serum cholesterol values greater than 200 mg/dL. The cor- relation between serum cholesterol and response to vasodilators was assessed to determine if some of the variation in vasodilator response was related to this variable. There was no significant correlation between serum cholesterol and conduit or resistance vessel response (r values ranged from 0 to .33).
Discussion
This study demonstrates that endothelium-depen- dent and endothelium-independent vasodilation of the brachial artery is intact in patients with heart failure. In contrast, endothelium-dependent, but not endothelium-independent, vasodilation of peripheral resistance vessels is impaired. These data are in agreement with previous studies in humans with heart failure that showed impaired resistance vessel dilation to endothelium-dependent vasodilators .5-7
This study suggests that abnormal endothelium-de- pendent vasodilation is not uniformly present in all arteries.
In previous studies of animals and humans with heart failure, impaired endothelium-dependent va- sodilation has consistently been demonstrated in pe- ripheral and coronary resistance vessels.5-7,17-19 In contrast, studies of conduit vessel endothelium-de- pendent vasodilation have shown variable findings. Kaiser et al. demonstrated reduced responses to the topically applied endothelium-dependent vasodila- tor, acetylcholine, in anesthetized dogs with pacing- induced heart failure. *O In the rat infarct model of heart failure, Ontkean et al. demonstrated an impair- ment of endothelium-dependent relaxation of the pulmonary artery in vitro.*’ Endothelium-depen- dent relaxation of the thoracic aorta was also re- duced, but to a lesser extent. However, Forster et al. found that endothelium-dependent relaxation was normal in the dorsalis pedis and coronary arter- ies of dogs with pacing-induced heart failure.** Pe- ripheral vascular endothelium-dependent vasodila- tion in patients with heart failure was assessed by Drexler et al. using A-mode echo.6 In this study, a significant radial artery vasodilation to intraarterial acetylcholine could not be demonstrated in the six patients with heart failure or the six normal subjects studied. The reasons for the lack of agreement among these studies are not known, but may be re- lated to differences in species, artery site, method of inducing heart failure, and technique (in vitro vs in vivo).

Conduit Artery Vasodilation in Heart Failure l Bank et al. 41
This study demonstrates a differential response of conduit and resistance vessels to endothelium- dependent, but not endothelium-independent, vaso- dilators in patients with heart failure. This finding contrasts with the results of studies in humans with atherosclerosis that demonstrate both impaired con- duit and resistance vessel endothelium-dependent vasodilation. 23-25 However, other investigators have shown size-dependent differences in the endo- thelial function of human blood vessels.26 For exam- ple, calcitonin gene-related peptide and vasoactive intestinal peptide produce endothelium-dependent relaxation in the conduit arteries, but endothelium- independent relaxation in the resistance vessels2’ Furthermore, in humans with hypertension, endo- thelium-dependent vasodilation of forearm resis- tance vessels is impaired,28*29 but flow-mediated vasodilation of the brachial artery (an endothelium- dependent response) is intact.30 Therefore, size-de- pendent differences in endothelium-dependent va- sodilation may be present in both hypertension and heart failure.
Measurement of brachial artery diameter was ac- complished in this study by using two-dimensional (8.0 MHz) ultrasound. Similar techniques have been used to assess carotid artery atherosclerosis during natural history and intervention trials,‘3*14 and to measure brachial artery response to hyperemia and sublingual nitroglycerin. 31 We have demonstrated that this technique is both accurate and reproduci- ble. This technique also offers some advantages over existing methods of determining human con- duit vessel diameter. Angiography and intravascular ultrasound may provide higher resolution, but they are invasive. Calculation of the cross-sectional area and diameter using the quotient of forearm blood flow and Row velocity introduces the error of two different measurements to calculate conduit vessel diameter.32 Unlike bidimensional-pulsed Doppler velocimetry,33 our method allows direct visualiza- tion of brachial artery diameter for each heart beat. Resolution is comparable in both techniques, since the smallest sample volume that can be obtained by pulsed Doppler velocimetry is approximately 0.38 mm (approximately 9% of the normal brachial artery diameter) as compared to 0.30 maximal axial resolu- tion with the 8 MHz Biosound ultrasound trans- ducer.
There are, however, some limitations to this tech- nique . The accuracy and reproducibility depend highly on the image quality of the brachial artery. This technique requires careful attention to the angle created between the transducer and vessel, since a tangential view would overestimate brachial artery diameter. This problem was minimized by re-
jetting any cross-sectional images that appear non- circular.
In this study, no significant difference was found between patients with heart failure and normal sub- jects regarding brachial artery diameter response to methacholine. The averages of the responses to the two doses of methacholine were 9.9% in the normal subjects and 8.6% in the patients with heart failure. If the one heart failure patient who vasoconstricted in response to methacholine is excluded from analy- sis, the brachial artery responses to methacholine are equal at 9.9% in both groups. Based on the 95% confidence interval on the difference in response be- tween the two groups, the true heart failure response should be no more than 3.5% less than the normal response. The magnitude of this potential difference in conduit vessel endothelium-dependent vasodila- tion is less than that seen in other diseases associ- ated with abnormal large artery endothelial func- tion, such as atherosclerosis, where large arteries frequently fail to dilate or constrict in response to endothelium-dependent vasodilators .23-25
It is possible that atherosclerosis or hypercholes- terolemia affected the brachial artery responses. However, no patient had overt peripheral vascular disease, and there was no correlation between the conduit or resistance vessel response to methacho- line and serum cholesterol. It is possible that the drugs taken by the patients with heart failure could have altered the response to endothelium-dependent vasodilators. For example, cardiac glycosides im- pair endothelium-dependent vasodilation in some vascular beds,34,35 but not in others.36,37 Neverthe- less, studies in animals with heart failure (and on no medication) still show abnormal endothelium-de- pendent vasodilation of peripheral resistance ves- sels. ‘8-‘9 Alternatively, converting enzyme inhibitor therapy has been shown to improve endothelium- dependent vasodilation in spontaneously hyperten- sive rats,38.39 and in the forearm vasculature of nor- mal subjects4’ and patients with hypertension.4’ However, if these drugs altered endothelium-depen- dent vasodilation, the magnitude or time course of the effect would have to differ between the conduit and resistance vessels to produce the results ob- tained.
In conclusion, endothelium-dependent vasodila- tion of forearm resistance, but not conduit vessels, is impaired in patients with heart failure. A better understanding of the regional and size-dependent differences in endothelial function may help in the search for the underlying mechanism of arteriolar endothelial dysfunction in heart failure.
42 Journal of Cardiac Failure Vol. 1 No. 1 October 1994
Acknowledgments
The authors thank Andrea Dahl for assistance in preparing the manuscript, and Stephen M. Schwabacher, RVT, for assistance with ultrasound imaging of the brachial artery.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12
13.
14.
References
Furchgott RF, Zawadski JV: The obligatory role of endothelial cells in the relaxation of arterial smooth muscle by acetylcholine. Nature 1980;280:373-82 Vanhoutte PM: Endothelium and control of vascular function: state of the art lecture. Hypertension 1988; 12:797-806 Moncada S, Palmer RMJ, Higap EA: The discovery of nitric oxide as the endogenous nitrovasodilator. Hypertension 1988;12:365-72 Vane JR, Anggard EE, Botting RM: Regulatory func- tions of the vascular endothelium. N Engl J Med 1990; 323:27-36 Kubo SH, Rector TS, Bank AJ, Williams RE, Heifetz SM: Endothelium-dependent vasodilation is attenu- ated in patients with heart failure. Circulation 1991; 84: 1589-96 Drexler H. Hayoz D, Mtinzel T, Hornig B, Just H, Brunner H, Zelis R: Endothelial function in chronic heart failure. Am J Cardiol 1992;69:1596-601 Katz SD, Biasucci L, Sabba C, Strom JA, Jondeau G, Galvao M, Solmon S, Nikdic SD, Forman R, Le- Jemtel TH: Impaired endothelium-mediated vasodila- tion in the peripheral vasculature of patients with congestive heart failure. J Am Co11 Cardiol 1992;19: 918-25 O’Rourke MF: Vascular impendence and cardiac function. In O’Rourke MF: Arterial function in health and disease. Churchill Livingstone, New York, 1982, pp. 153-69 Pohl U, Holtz J, Busse R, Bassenge E: Crucial role of the endothelium in the vasodilator response to in- creased flow in vivo. Hypertension 1986;8:37-44 Rubanyi GM, Romero JC, Vanhoutte PM: Flow in- duced release of endothelium-derived relaxing factor. Am J Physiol 1986;250:H1145-9 Cody RJ, Muller FB, Kubo SH, Rutman H, Leonard D: Identification of the direct vasodilator effects of milrinone with an isolated limb preparation in patients with chronic congestive heart failure. Circulation 1986;73:124-9 Kubo SH, Rector TS, Heifetz SM, Cohn JN: Alpha* receptor mediated vasoconstriction in patients with congestive heart failure. Circulation 1989;80: 1660-7 Bond MG, Wilmoth SK, Enevold GL, Strickland HL: Detection and monitoring of asymptomatic athero- sclerosis in clinical trials. Am J Med 1989;86(suppl 4A):33-6 Malinow MR, Nieto FJ, Szklo M, Chambles SLE, Bond G: Carotid artery intimal-medial wall thickening
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
and plasma homocyst(e)ine in asymptomatic adults. The atherosclerosis risk in communities study. Circu- lation 1993;87: 1107-13 Reiber JH, Serruys PW, Kooijman CJ, Wijns W, Slager CJ, Gerbrands JJ, Schuubiers JCH, den Boer A, Hugenholtz PG: Assessment of short-, medium-, and long-term variations in arterial dimensions from computer-assisted quantitation of coronary cineangi- ograms. Circulation 1985;71:280-8 Griffith TM, Lewis MJ, Newby A, Henderson AH: Endothelium-derived relaxing factor. J Am Co11 Car- diol 1988;12:797-806 Treasure CB, Vita JA, Cox DA, Fish D, Gordon JB, Mudge GH, Colucci WS, St. John Sutton MG, Selwyn AP, Alexander RW, Ganz P: Endothelium-dependent dilation of the coronary microvasculature is impaired in dilated cardiomyopathy. Circulation 1990;81:772-9 Drexler H, Lu W: Endothelial dysfunction of hind- quarter resistance vessels in experimental heart fail- ure. Am J Physiol 1992;262:H1640-5 Kiuchi K, Sata N, Shannon RP, Vatner DE, Morgan K, Vatner SF: Depressed B-adrenergic receptor- and endothelium-mediated vasodilation in conscious dogs with heart failure. Circ Res 1993;73: 1013-23 Kaiser L, Spickard RC, Olivier NB: Heart failure de- presses endothelium-dependent responses in canine femoral artery. Am J Physiol 1989;256:H962-7 Ontkean M, Gay R, Greenberg B: Diminished endo- thelium-derived relaxing factor activity in an experi- mental model of chronic heart failure. Circ Res 1991; 69: 1088-96 Forster C, Main JS, Armstrong PW: Endothelium modulation of the effects of nitroglycerin on blood vessels from dogs with pacing-induced heart failure. Br J Pharmacol 1990;101:109-14 Ludmer PL, Selwyn AP, Shook TL, Wayne RR, Mudge GH, Alexander RW, Ganz P: Paradoxical vasoconstriction induced by acetylcholine in athero- sclerotic coronary arteries. N Engl J Med 1986:315: 1046-5 1 Zeiher AM, Drexler H, Wollschlager H, Just H: En- dothelial dysfunction of the coronary microvascula- ture is associated with impaired coronary blood flow regulation in patients with early atherosclerosis. Cir- culation 1991;84:1984-92 Liao JK, Bettmann MA, Sandor T, Tucker JI, Cole- man SM, Creager M: Differential impairment of vaso- dilator responsiveness of peripheral resistance and conduit vessels in humans with atherosclerosis. Circ Res 1991;68: 1027-34 Hughes AD, Thorn SA, Martin GN, Nielsen H, Hair WM, Schachter M, Sever PS: Size and site-dependent heterogeneity of human vascular responses in vitro. J Hypertension 1988;6:5173-5 Thorn S, Hughes A, Goldberg P, Martin G, Schacter M, Sever P: The action of CGRP and VIP as vasodila- tors in man in vivo and in vitro. Br J Clin Pharmacol 1987;24:139-44 Panza JA, Quiyyumi AA, Brush JE, Epstein SE: Ab- normal endothelium-dependent vascular relaxation in

Conduit Artery Vasodilation in Heart Failure l Bank et al. 43
29.
30.
31
32.
33.
34.
patients with essential hypertension. N Engl J Med 1990;323;22-7 Linder L, Kiowski W, Buhler FR, Luscher TF: Indi- rect evidence for release of endothelium-derived re- laxing factor in human forearm circulation in vivo:
blunted response in essential hypertension. Circula- tion 1990;8 1: 1762-7 Laurent S, Lacolley P, Brunei P, Laloux B, Pannier B, Safar M: Flow-dependent vasodilation of brachial artery in essential hypertension. Am J Physiol 1990: H1004-11 Celermajer D, Sorensen KE, Gooch VM, Spie- gelhauter DJ, Miller 01, Sullivan ID, Lloyd JK, Dean- field JE: Non-invasive detection of endothelial dys- function in children and adults at risk of
atherosclerosis. Lancet 1992;340: 111 l-5 Sinoway LI, Hendrickson C, Davidson WR, Prophet S, Zelis R: Characteristics of flow-mediated brachial artery vasodilation in human subjects. Circ Res 1989; 64:32-42 Safar ME, Perronneau PA, Levenson JA, Tot-Mou- kouo JA, Simon AC: Pulsed Doppler diameter, blood flow velocity and volumic flow of the brachial artery in essential hypertension. Circulation 1981:63: 393-400 Woolfson RG, Poston L: Effect of ouabain on endo- thelium-dependent relaxation of human resistance ar- teries. Hypertension 1991;17:619-25
35.
36.
37.
38.
39.
40.
41
De Mey JG, Vanhoutte PM: Interaction between Na,K exchanges and the direct inhibitory effect of acetylcholine on canine femoral arteries. Circ Res 1980;46:826-35 Chen G, Hashitani H, Suzuki H: Endothelium-depen- dent relaxation and hyperpolarization of canine coro- nary artery smooth muscles in relaxation to the elec- trogenic Na-K pump. Br J Pharmacol 1989;98:950-6 Suzuki H: The electrogenic Na-K pump does not con- tribute to endothelium-dependent hyperpolarization in the rabbit ear artery. Eur J Pharmacol 1988;156: 295-7 Clozel M, Kuhn H, Hefti F: Effects of angiotensin converting enzyme inhibitors and of hydralazine on endothelial function in hypertensive rats. Hyperten- sion 1990:16:532-40 Clozel M: Mechanism of action of angiotensin con- verting enzyme inhibitors on endothelial function in hypertension. Hypertension 1991:18(suppl II): 1X37-42 Nakamura M, Funakoshi T, Yoshida H, Arakawa N, Suzuki T, Hiramori K: Endothelium-dependent vaso- dilation is augmented by angiotensin converting en- zyme inhibitors in healthy volunteers. J Cardiovasc Pharmacol 1992;20:949-54 Hirooka Y, Imaizumi T, Masaki H, Ando S, Harada S, Momohara M, Takeshita A: Captopril improves impaired endothelium-dependent vasodilation in hy- pertensive patients. Hypertension 1992;20: 175-80