efficiency of the normal human diaphragm with hyperinflation
TRANSCRIPT

doi: 10.1152/japplphysiol.01165.200499:1402-1411, 2005. First published 16 June 2005;J Appl Physiol
Kevin E. Finucane, Janine A. Panizza and Bhajan SinghhyperinflationEfficiency of the normal human diaphragm with
You might find this additional info useful...
67 articles, 55 of which you can access for free at: This article citeshttp://jap.physiology.org/content/99/4/1402.full#ref-list-1
3 other HighWire-hosted articles: This article has been cited by http://jap.physiology.org/content/99/4/1402#cited-by
including high resolution figures, can be found at: Updated information and serviceshttp://jap.physiology.org/content/99/4/1402.full
can be found at: Journal of Applied Physiology about Additional material and informationhttp://www.the-aps.org/publications/jappl
This information is current as of June 2, 2013.
http://www.the-aps.org/. © 2005 the American Physiological Society. ISSN: 8750-7587, ESSN: 1522-1601. Visit our website at year (monthly) by the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyrightphysiology, especially those papers emphasizing adaptive and integrative mechanisms. It is published 12 times a
publishes original papers that deal with diverse area of research in appliedJournal of Applied Physiology
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from

Efficiency of the normal human diaphragm with hyperinflation
Kevin E. Finucane,1,2 Janine A. Panizza,1,2 and Bhajan Singh1,2,3
1Department of Pulmonary Physiology, Sir Charles Gairdner Hospital, 2WestAustralian Sleep Disorders Research Institute, QEII Medical Centre, and 3Departmentof Physiology, University of Western Australia, Nedlands, Western Australia, Australia
Submitted 15 October 2004; accepted in final form 10 June 2005
Finucane, Kevin E., Janine A. Panizza, and Bhajan Singh.Efficiency of the normal human diaphragm with hyperinflation. J ApplPhysiol 99: 1402–1411, 2005. First published June 16, 2005;doi:10.1152/japplphysiol.01165.2004.—We evaluated an index of di-aphragm efficiency (Effdi), diaphragm power output (Wdi) relative toelectrical activation, in five healthy adults during tidal breathing atusual end-expiratory lung volume (EELV) and diaphragm length(Ldi ee) and at shorter Ldi ee during hyperinflation with expiratorypositive airway pressure (EPAP). Measurements were repeated withan inspiratory threshold (7.5 cmH2O) plus resistive (6.5cmH2O � l�1 �s) load. Wdi was the product of mean inspiratory trans-diaphragmatic pressure (�Pdimean), diaphragm volume displacementmeasured fluoroscopically, and 1/inspiratory duration (TI�1). Dia-phragm activation, measured with esophageal electrodes, was quan-tified by computing root-mean-square values (RMSdi). With EPAP, 1)EELV increased [mean r2 � 0.91 (SD 0.01)]; 2) in four subjects, Ldi ee
decreased [mean r2 � 0.85 (SD 0.07)] and mean Effdi decreased 34%per 10% decrease in Ldi ee (P � 0.001); and 3) in one subject, gastricpressure at EELV increased two- to threefold, Ldi ee was unchanged orincreased, and Effdi increased at two of four levels of EPAP (P �0.006, ANOVA). Inspiratory loading increased Wdi (P � 0.003) andRMSdi (P � 0.004) with no change in Effdi (P � 0.63) or itsrelationship with Ldi ee. Effdi was more accurate in defining changes inLdi ee [(true positives � true negatives)/total � 0.78 (SD 0.13)] than�Pdimean �RMSdi
�1, RMSdi, or �Pdimean �TI (all �0.7, P � 0.05,without load). Thus Effdi was principally a function of Ldi ee indepen-dent of inspiratory loading, behavior consistent with muscle force-length-velocity properties. We conclude that Effdi, measured duringtidal breathing and in the absence of expiratory muscle activity atEELV, is a valid and accurate measure of diaphragm contractilefunction.
in vivo diaphragm length; power output; electromyogram activity;diaphragm contractile function and efficiency; fluoroscopy
THE CONTRACTILE FUNCTION OF striated muscle segments, includ-ing the diaphragm, is characterized by the instantaneous rela-tionships between force, length, and velocity of shortening (4,19). The power output of a muscle is the product of forcedeveloped and velocity of shortening. The efficiency of amuscle determines the power output achieved for a given rateof oxygen consumption (VO2) and further defines the contrac-tile function of muscle (69). In humans, the diaphragm ac-counts for a substantial fraction of inspiratory work (44, 45);however, its efficiency is unknown. Measurement of dia-phragm efficiency (Effdi) could be more useful in recognizingand quantifying contractile dysfunction of the diaphragm thanmeasurements of strength or electromechanical effectivenessmeasured, respectively, by maximum transdiaphragmatic pres-sure (Pdi; Pdimax) and the ratio of Pdi to the amount of
electrical activity of the diaphragm (3, 31, 53). This hypothesisis suggested by the mechanical behavior of muscle in vitro.First, the mechanical output of a muscle during shortening isdefined by its power output and cannot be predicted frommaximum force alone (32). Second, during shortening, thepower output of a muscle is determined by muscle length andlevel of activation, decreasing approximately linearly with bothlength and activation (4, 11, 16, 19, 33). Third, muscle effi-ciency relates power output to the energy consumed, includingcosts of activation and cross-bridge cycling (62, 69).
Assessment of the efficiency of the intact human diaphragm(Effdi) requires breath-by-breath measurement of the inspira-tory power output and VO2 of the diaphragm (VO2 di) and,because efficiency and power output relative to activation varywith muscle length (4, 11, 19, 33, 62), measurement of dia-phragm length at end expiration (Ldi ee). Power output can beestimated as the product of the average change during inspi-ration of Pdi (�Pdimean) and the rate of volume displaced bythe diaphragm (�Vdi �TI�1, where �Vdi is the volume dis-placed by the diaphragm and TI is inspiratory duration). �Vdihas been estimated from motion of the chest wall (2, 17, 44),change in the length of the diaphragm apposed to the rib cagemeasured with ultrasound (30), and from analysis of radio-graphic images of diaphragm motion (58, 59). A fluoroscopicmethod, developed and validated by us (59), allows breath-by-breath measurement of �Vdi and of Ldi ee, enabling the effectof diaphragm length on Effdi to be examined. VO2 di cannot bemeasured in intact humans. However, studies in dogs (50) andlambs (61) have shown a linear relationship between VO2 di andthe amount of diaphragm electrical activity. Beck et al. (7–10)and Sinderby et al. (54, 56, 57) have developed and validatedmethods for accurately quantifying the amount of diaphragmelectrical activity using multiple electrodes positioned in theesophagus to span the crural diaphragm. This method controlsfor diaphragm position (8, 10, 57) and signal contamination(54, 56); electrical activity is quantified by the root meansquare of the electromyogram (EMG) signals (RMSdi) and isan accurate index of global diaphragm activation (7, 60). Wepropose that the inspiratory power output of the diaphragmrelative to the amount of electrical activity is an index of Effdi
Effdi � �Pdimean � �Vdi � TI�1 � RMSdi
�1 (1)
Interpretation of the proposed measurement of Effdi is compli-cated by the uncertain relationship between electrical activa-tion and VO2 of the human diaphragm in vivo and by datashowing that the distribution of tension within (13), and acti-vation of, the diaphragm (14, 22, 26) are inhomogeneous. In
Address for reprint requests and other correspondence: K. E. Finucane, Dept. ofPulmonary Physiology, Sir Charles Gairdner Hospital, Hospital Ave., Nedlands,Western Australia 6009, Australia (E-mail: [email protected]).
The costs of publication of this article were defrayed in part by the paymentof page charges. The article must therefore be hereby marked “advertisement”in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
J Appl Physiol 99: 1402–1411, 2005.First published June 16, 2005; doi:10.1152/japplphysiol.01165.2004.
8750-7587/05 $8.00 Copyright © 2005 the American Physiological Society http://www. jap.org1402
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from
addition, factors other than the contractile properties of musclemay affect the efficiency of the intact diaphragm. Principalamong these are the geometry and mechanical advantage of thediaphragm and the interaction between the diaphragm andother respiratory muscles. Diaphragm mechanical advantagedecreases with hyperinflation (68) tending to decrease poweroutput relative to VO2. Contraction of abdominal musclesduring expiration and their relaxation during inspiration canincrease diaphragm power output (Wdi) during subsequentinspiration (2, 45) and could increase efficiency.
The purpose of this study was to examine the validity andutility of the proposed measurement of Effdi by comparing, inhealthy subjects, measurements obtained during tidal breathingat usual end-expiratory lung volume (EELV) with those ob-tained at shorter diaphragm lengths during hyperinflation. Wehypothesized that any decrease in Ldi ee with hyperinflationwould be associated with a linear decrease in Effdi, consistentwith the force-length-velocity properties of muscle. Becausethe electrical activity of the intact, human gastrocnemius mus-cle increases proportionately with load at a given velocity ofshortening (11), we hypothesized further that measured Effdi
would be independent of an inspiratory load, which did notdecrease the rate of �Vdi.
METHODS
Five healthy, nonsmoking men were studied. Subjects gave written,informed consent. The Committee for Human Rights, University ofWestern Australia, approved the study.
Measurements
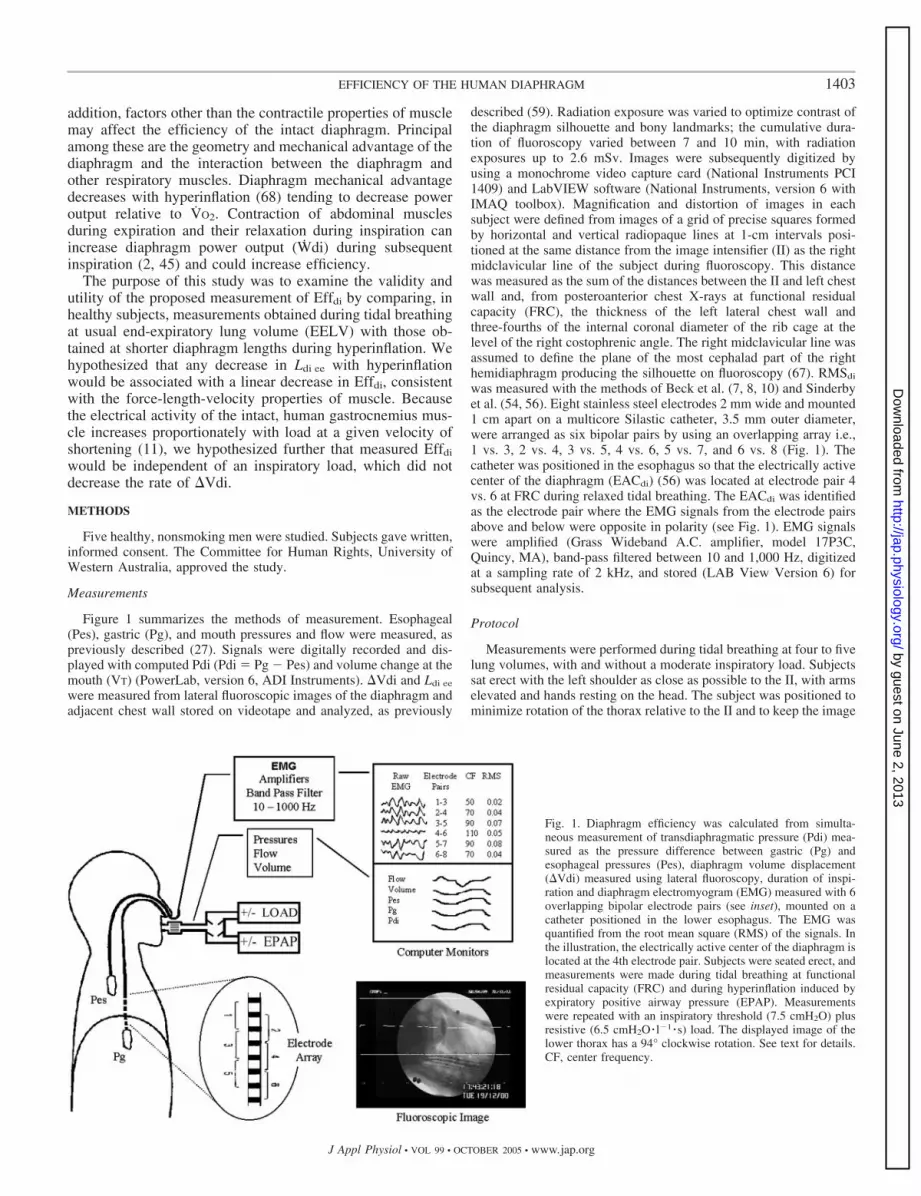
Figure 1 summarizes the methods of measurement. Esophageal(Pes), gastric (Pg), and mouth pressures and flow were measured, aspreviously described (27). Signals were digitally recorded and dis-played with computed Pdi (Pdi � Pg � Pes) and volume change at themouth (VT) (PowerLab, version 6, ADI Instruments). �Vdi and Ldi ee
were measured from lateral fluoroscopic images of the diaphragm andadjacent chest wall stored on videotape and analyzed, as previously
described (59). Radiation exposure was varied to optimize contrast ofthe diaphragm silhouette and bony landmarks; the cumulative dura-tion of fluoroscopy varied between 7 and 10 min, with radiationexposures up to 2.6 mSv. Images were subsequently digitized byusing a monochrome video capture card (National Instruments PCI1409) and LabVIEW software (National Instruments, version 6 withIMAQ toolbox). Magnification and distortion of images in eachsubject were defined from images of a grid of precise squares formedby horizontal and vertical radiopaque lines at 1-cm intervals posi-tioned at the same distance from the image intensifier (II) as the rightmidclavicular line of the subject during fluoroscopy. This distancewas measured as the sum of the distances between the II and left chestwall and, from posteroanterior chest X-rays at functional residualcapacity (FRC), the thickness of the left lateral chest wall andthree-fourths of the internal coronal diameter of the rib cage at thelevel of the right costophrenic angle. The right midclavicular line wasassumed to define the plane of the most cephalad part of the righthemidiaphragm producing the silhouette on fluoroscopy (67). RMSdi
was measured with the methods of Beck et al. (7, 8, 10) and Sinderbyet al. (54, 56). Eight stainless steel electrodes 2 mm wide and mounted1 cm apart on a multicore Silastic catheter, 3.5 mm outer diameter,were arranged as six bipolar pairs by using an overlapping array i.e.,1 vs. 3, 2 vs. 4, 3 vs. 5, 4 vs. 6, 5 vs. 7, and 6 vs. 8 (Fig. 1). Thecatheter was positioned in the esophagus so that the electrically activecenter of the diaphragm (EACdi) (56) was located at electrode pair 4vs. 6 at FRC during relaxed tidal breathing. The EACdi was identifiedas the electrode pair where the EMG signals from the electrode pairsabove and below were opposite in polarity (see Fig. 1). EMG signalswere amplified (Grass Wideband A.C. amplifier, model 17P3C,Quincy, MA), band-pass filtered between 10 and 1,000 Hz, digitizedat a sampling rate of 2 kHz, and stored (LAB View Version 6) forsubsequent analysis.
Protocol
Measurements were performed during tidal breathing at four to fivelung volumes, with and without a moderate inspiratory load. Subjectssat erect with the left shoulder as close as possible to the II, with armselevated and hands resting on the head. The subject was positioned tominimize rotation of the thorax relative to the II and to keep the image
Fig. 1. Diaphragm efficiency was calculated from simulta-neous measurement of transdiaphragmatic pressure (Pdi) mea-sured as the pressure difference between gastric (Pg) andesophageal pressures (Pes), diaphragm volume displacement(�Vdi) measured using lateral fluoroscopy, duration of inspi-ration and diaphragm electromyogram (EMG) measured with 6overlapping bipolar electrode pairs (see inset), mounted on acatheter positioned in the lower esophagus. The EMG wasquantified from the root mean square (RMS) of the signals. Inthe illustration, the electrically active center of the diaphragm islocated at the 4th electrode pair. Subjects were seated erect, andmeasurements were made during tidal breathing at functionalresidual capacity (FRC) and during hyperinflation induced byexpiratory positive airway pressure (EPAP). Measurementswere repeated with an inspiratory threshold (7.5 cmH2O) plusresistive (6.5 cmH2O � l�1 � s) load. The displayed image of thelower thorax has a 94° clockwise rotation. See text for details.CF, center frequency.
1403EFFICIENCY OF THE HUMAN DIAPHRAGM
J Appl Physiol • VOL 99 • OCTOBER 2005 • www.jap.org
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from

of the dome of the diaphragm and adjacent chest wall within thefluoroscopic field over the volume range FRC to total lung capacity(TLC). Subjects breathed through a pneumotachograph and low-resistance two-way valve. The expiratory port was either open toatmosphere or connected to a positive airway pressure unit (BiPAP S,Respironics). The inspiratory port was either open to atmosphere orconnected to an inspiratory threshold valve (7.5 cmH2O) in series witha resistance (6.5 cmH2O � l�1 �s). Expiratory positive airway pressure(EPAP) levels were adjusted between measurements to achieve pre-determined levels of hyperinflation approximating 25, 50, and 75% ofthe inspiratory capacity (IC) at FRC. Measurements with fluoroscopywere made during five tidal breaths and an inspiration to TLC initiatedfrom end expiration. Conditions of measurement were randomized.Before each measurement, EMG signals were reviewed to ensure thatthe EACdi was at the fourth electrode pair. During measurement,subjects were encouraged to relax during expiration; no other instruc-tions were given regarding pattern of breathing. Where the level ofhyperinflation achieved differed substantially from the target levels orthe data appeared unsatisfactory, the measurements were repeated.Subjects had one to three fully instrumented studies before fluoros-copy to familiarize them with the protocol, define the levels of EPAPrequired to achieve targeted hyperinflation, and establish the range ofmovement, with hyperinflation, of the EACdi in relation to electrodepairs.
Data Analysis
For each breath, the TI was measured from the onset of inspiratoryflow or of a sustained decrease in Pes to the onset of expiratory flow.The end-expiratory and inspiratory changes (�) of Pg, Pes, and Pdiwere measured, and �Pdimean and diaphragm pressure-time productper breath (�Pdimean �TI) were computed, taking Pdi at end expiration(Pdiee) as baseline. EELV during EPAP was obtained by subtractingmeasured IC from the vital capacity (VC) and expressed as a percent-age of VC. The fluoroscopic images were digitized, and �Vdi andLdi ee of each breath were measured by using the methods describedpreviously (58, 59) and an interactive analysis program written inMATLAB (version 6.1.0.450). The first to fifth tidal breath andsubsequent inspiration to TLC of each condition of measurement wereidentified, and the images at end expiration and end inspiration of eachbreath were superimposed. Any mismatching between these imageswas corrected by using as landmarks adjacent vertebral bodies and theimages of two ball bearings adherent to the posterior chest wall in themidline at the level of the 10th thoracic vertebra. One image wasshifted relative to the other until cross-correlation of these markersapproximated 1. The images of the dome of the right hemidiaphragmat end expiration and end inspiration, the posterior chest wall, and theanterior border of the spinal column swept by the diaphragm weresegmented interactively by using a mouse-controlled cursor to iden-tify multiple points along each of these structures. The anterior andposterior insertions of the diaphragm at end expiration and endinspiration, identified from bony landmarks adjacent to the costo-phrenic angles at TLC (15), were defined as single points. Each pointof the segmented images was corrected for distortion and magnifica-tion, applying data obtained from the grid of precise squares. The gridimage showed rotational, pin cushion radial, and decentering distor-tions, which were corrected by using a look-up table comprising thecoordinates of all cross points on the grid (52). After correcting fordistortion and magnification, the average error per calibration pointwas 4.3%. Each point used to outline the diaphragm, spine, and chestwall was converted to its correct position in space using the look-uptable, the four closest calibration points, and a least squares minimi-zation technique (37). The points defining each structure were fittedwith lines using polynomial expressions. The square of the averageerror of these fitted lines was typically 0.2 to 1 mm2. �Vdi of eachinspiration and the lengths of the right hemidiaphragm in the sagittalplane at end expiration and end inspiration were computed from the
segmented, reconstructed images by using the methods and equationsdescribed previously (59). The EMG signals of each inspiration wereanalyzed in the time and frequency domains, as previously described(60), by using the methods of Sinderby et al. (54, 56). Briefly, thedigitized EMG signals of each breath were displayed, and a 300- to500-ms segment, including the maximum amplitude EMG, but avoid-ing any period containing an ECG complex, was selected for analysis.Power spectra were evaluated for signal quality, accepting only thosedata that met the criteria for uncontaminated signals (54). The EACdi
was defined by cross-correlation analysis of the signals from alternateelectrode pairs, and the RMSdi value was obtained by subtracting thesignals above and below the electrical center of the diaphragm (56).This analysis yielded a single value of RMSdi and of center frequencyfor each tidal inspiration. RMSdi was also measured during eachinspiration to TLC, and the maximum value (RMSdi max) was thehighest value obtained during any inspiration to TLC. RMSdi valueswere corrected for changes in power spectrum, as may occur withmuscle fatigue, using the diaphragm center frequency of each breathand the method of Beck et al. (7). Wdi (�Pdimean ��Vdi �TI�1) andEffdi of each breath were calculated.
Statistical Analysis
All variables were normalized by dividing the computed variablesof each breath by the mean value of that variable at FRC in eachsubject. RMSdi was also normalized by expressing it as a percentageof the highest value obtained during inspirations to TLC(RMSdi %max). Linear regression was used to examine the relation-ships between 1) EPAP and EELV; 2) normalized Ldi ee and EELV; 3)normalized Ldi ee and normalized Effdi and its components; and 4)normalized Pg at end expiration (Pgee) and normalized Effdi. Multiplelinear regression analysis with stepwise elimination was used todetermine the relationships between the normalized dependent vari-ables �Vdi and Effdi and the normalized independent variables Ldi ee,Pgee, Pdiee, TI, and VT �TI�1. One-way ANOVA was used to compareEffdi with and without EPAP. The effect of inspiratory loading on themeasured and computed variables and on the relationships betweenEffdi and the independent variables Ldi ee, Pgee, Pdiee, TI, and VT �TI�1
was examined with paired t-tests and multiple regression analysis,respectively. The relative utility of the different measures of dia-phragm function, i.e., efficiency, effectiveness, activation, and thepressure-time product, were examined by comparing the degree ofassociation of each with normalized Ldi ee using Pearson’s correlationcoefficients and by calculating their accuracy in detecting a change innormalized Ldi ee with hyperinflation. The accuracy of each variablewas calculated for each subject separately, as the number of truepositives plus true negatives divided by the total number of datapoints. The accuracy of each variable for the group was taken as themean of the individual values. All results were analyzed by usingSigmaStat statistical software (version 2, SPSS, Chicago, IL) and arereported as means and standard deviations (SD), unless otherwisestated. Significance was defined as P � 0.05.
RESULTS
Mean age, body mass index, height, VC, and IC of thesubjects were 52 yr (SD 10), 26 kg/m2 (SD 1), 1.78 m (SD0.05), 4.9 liters (SD 0.5), and 3.1 liters (SD 0.4), respectively.
Hyperinflation Without Load
Volumes and pressures. EELV increased with EPAP in allsubjects [mean r2 � 0.91 (SD 0.01)] (Fig. 2). Relative to FRC,Pgee and �Pes increased with EPAP in all subjects (Fig. 3).Pgee was greatest in subject 5, increasing two- to threefold atthree of four levels of EPAP. Inspiratory �Pg with EPAP wasvariable; relative to FRC, �Pg changed little in three subjects,decreased in subject 2, and increased twofold in subject 5.
1404 EFFICIENCY OF THE HUMAN DIAPHRAGM
J Appl Physiol • VOL 99 • OCTOBER 2005 • www.jap.org
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from

Diaphragm length and volume change. At FRC, mean Ldi ee
was 27.0 cm (SD 2.5) (Table 1). Relative to its length at FRC,Ldi ee decreased with hyperinflation in four subjects [mean r2 �0.85 (SD 0.07)] and did not change in subject 5, despite a 28%increase in EELV (Fig. 4). Fractional shortening of the dia-phragm between FRC and TLC was 0.28 (SD 0.1). �Vdirelative to VT was 55% (SD 14) at FRC and tended to decreasewith Ldi ee, being 35% (SD 12) (n � 4) at the shortest Ldi ee
achieved (P � 0.06). Multiple regression analysis showed that�Vdi was positively correlated with Ldi ee (P � 0.001) and TI
(P � 0.02) and not correlated with Pdiee (P � 0.46) or Pgee
(P � 0.14). Where the diaphragm shortened with EPAP (n �4), �Vdi was positively correlated with Ldi ee (P � 0.003) andTI (P � 0.001) and negatively correlated with Pgee (P �0.006).
EMG. At each condition of measurement, there was at leastone and usually two electrode pairs distal to the EACdi. MeanRMSdi %max was 15.9% (SD 3.0) at FRC and 66.5% (SD 6.2)at the shortest Ldi ee (P � 0.001) (Table 1). Where Ldi ee
decreased with hyperinflation, RMSdi %max increased (r2 �0.44, P � 0.001).
Efficiency. A total of 126 tidal breaths and 28 inspirations toTLC, distributed between 25 separate conditions of measure-ment among the five subjects, were imaged. Eighteen breathscould not be analyzed because of loss or distortion of radio-graphic images (10 breaths), Pes artifact (4 breaths), and/orEMG signal quality (5 breaths). A minimum of three tidalbreaths and the inspiration to TLC could be analyzed for eachcondition of measurement in all subjects. Absolute values ofEffdi and its components at FRC and maximum hyperinflationfor all subjects are summarized in Table 1. The relationshipsbetween normalized Ldi ee and normalized �Pdimean,�Vdi �TI�1, RMSdi, and Effdi are shown for subject 3 in Fig. 5.In the four subjects in whom Ldi ee decreased with hyperinfla-tion, diaphragm shortening was associated with an increase inRMSdi (P � 0.001), a decrease in Effdi (P � 0.001), and nochange in Wdi and �Vdi �TI�1. In subject 5, where Ldi ee
changed �10% with hyperinflation, there was no significantchange in �Pdimean, �Vdi �TI�1, RMSdi, or Effdi with Ldi ee.The relationship between normalized Ldi ee and normalizedEffdi for all breaths in all subjects is shown in Fig. 6. In subject5, Effdi was highly variable and greater than that at FRC at twoof four levels of EPAP, i.e., 6 (P � 0.006) and 13 cmH2O (P �0.003, ANOVA) (Fig. 6). Multiple regression analysis (n � 5)showed that normalized Effdi was highly correlated with Ldi ee
(P � 0.001) and not correlated with Pdiee (P � 0.204) or Pgee
(P � 0.193). Where Ldi ee decreased with hyperinflation (n �4), normalized Effdi was positively correlated with Ldi ee (P �0.001) and Pdiee (P � 0.01) and negatively correlated with Pgee
(P � 0.002); the latter accounted for �5% of the varianceof Effdi.
Hyperinflation with Load
There were 20 conditions of measurement where all datawere obtained with and without inspiratory loading, includingthree to four levels of EPAP in each subject. Consideringpaired data at each level of EPAP, loading was associated withan increase in �Pdimean (P � 0.001), Wdi (P � 0.003), andRMSdi (P � 0.004). Load had no effect on Ldi ee (Fig. 4B),EELV, �Vdi �TI�1, Pgee, Pdiee, or Effdi (Fig. 7B). The relation-ships between normalized Ldi ee and Effdi with and without loadare compared in Fig. 7. There was no difference in the slope or
Fig. 3. Effect of EPAP on end-expiratory Pes (Pesee), peakinspiratory Pes (Pespeak), end-expiratory Pg (Pgee), andpeak inspiratory Pg (Pgpeak) during tidal breathing in eachsubject. Data are means (SD) for each condition of mea-surement.
Fig. 2. Shown are end-expiratory lung volume (EELV) as percent vitalcapacity (%VC) at rest, EPAP � 0, and each level of EPAP in each subject(n � 5). The regression line is the mean slope and intercept of the individualregressions.
1405EFFICIENCY OF THE HUMAN DIAPHRAGM
J Appl Physiol • VOL 99 • OCTOBER 2005 • www.jap.org
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from

intercept of the mean regression for all subjects or for the foursubjects in whom Ldi ee decreased with hyperinflation. Multipleregression analysis in the four subjects in whom Effdi de-creased with Ldi ee showed that Effdi was highly correlated withLdi ee (P � 0.001), positively correlated with Pdiee (P � 0.037),and not correlated with Pgee (P � 0.27).
Comparison of measures of diaphragm function. See Table2. Normalized Ldi ee was more highly correlated with normal-ized Effdi than with other measures of diaphragm function,independent of inspiratory loading. Effdi more accurately re-flected changes in Ldi ee than other measures of diaphragmfunction; however, with inspiratory loading, the differenceswere not significant due to an increased variance of themeasurements.
DISCUSSION
In this study, diaphragm shortening, induced by hyperinfla-tion, and inspiratory loading were used to evaluate a novel, invivo measure of diaphragm function, the ratio of inspiratorypower output to neural activation. This index of Effdi wasprincipally a function of diaphragm length and was indepen-dent of a modest inspiratory load. These findings are consistentwith the in vitro force-length-velocity and power output-neuralactivation behavior of muscle (4, 11, 19) and suggest that themeasurement reflects the contractile properties of the dia-phragm.
Critique of Methods and Assumptions
The efficiency of respiratory muscles is usually measured byrelating power output to the rate of respiratory muscle VO2 (18,21, 43, 48). VO2 di is not measurable in intact humans but islikely to be linearly related to the amount of electrical activityof the diaphragm, independent of diaphragm length. First, inhumans, during submaximal rates of positive (miometric)
work, electrical activity and VO2 of the quadriceps muscle arelinearly related (12). Second, in dogs (50) and lambs (61),diaphragm electrical activity increased linearly with VO2 di
over an approximately sixfold increase in VO2 di. Third, therelationship between VO2 and maximum isometric tension ofvascular smooth muscle is independent of muscle length (47).Fourth, the VO2 associated with isotonic contraction of theintact dog gastrocnemius muscle performing maximal work fora short duration is a function of the number of nerve impulsesdelivered to the muscle (28). Finally, the diaphragm obtains itsenergy by oxidative metabolism over a wide range of workoutputs (5, 34, 41, 49, 51).
The amount of diaphragm electrical activity during eachinspiration was quantified by using the methods of Beck et al.(7–10) and Sinderby et al. (54, 56, 57). These studies are thebasis of several assumptions that are central to our analysis ofEffdi. Namely, that the RMSdi of the crural diaphragm mea-sured with these methods 1) accurately reflects activation of theentire diaphragm (7); 2) is linearly related to diaphragm acti-vation (7); 3) is not subject to artifact related to changes of lungvolume (7) or chest wall configuration (9); and 4) minimizesartifact related to changes in the muscle to electrode distance(8, 10).
The RMS of the crural diaphragm may not accurately defineactivation of the entire diaphragm because regional activationand shortening of the diaphragm during breathing are notuniform (13, 22, 26, 64, 68). Furthermore, RMSdi is not linearwith activation, being proportional to the square root of thenumber and firing frequency of motor units (7), thus tending tounderestimate higher levels of activation. Studies in both dogsand humans suggest that regional activation within individualrespiratory muscles is directly proportional to regional me-chanical advantage (23, 25, 39, 40). In the dog, diaphragmmechanical advantage and blood flow are inhomogeneous but
Table 1. Diaphragm efficiency and its components at FRC and maximum hyperinflation
Subject 1 Subject 2 Subject 3 Subject 4 Subjects 1–4 Subject 5
Ldi ee, cm@FRC 27.1 (0.2) 29.2 (0.6) 28.3 (0.9) 22.7 (0.2) 27.0 (2.5) 27.9 (0.6)@Maximum EELV 18.8 (0.4) 22.3 (1.1) 22.0 (0.2) 19.5 (0.5) 21.0 (1.6)† 28.5 (0.7)
�Pdimean, cmH2O@FRC 10.3 (1.2) 5.2 (0.6) 6.4 (0.3) 11.3 (1.5) 8.3 (3.0) 7.5 (0.6)@Maximum EELV 14.6 (1.6) 7.0 (0.9) 18.8 (2.8) 16.9 (2.9) 14.3 (5.1)* 24.8 (1.3)†
�Vdi, liter@FRC 0.26 (0.04) 0.79 (0.09) 0.58 (0.03) 0.49 (0.04) 0.53 (0.22) 0.35 (0.07)@Maximum EELV 0.19 (0.02) 0.35 (0.09) 0.73 (0.75) 0.15 (0.04) 0.36 (0.26) 0.43 (0.07)
�Vdi/TI, l/s@FRC 0.21 (0.0) 0.47 (0.06) 0.39 (0.09) 0.21 (0.03) 0.32 (0.13) 0.24 (0.04)@Maximum EELV 0.23 (0.03) 0.17 (0.05) 0.41 (0.20) 0.15 (0.04) 0.24 (0.12) 0.30 (0.06)
Power, W@FRC 0.21 (0.04) 0.24 (0.05) 0.17 (0.01) 0.21 (0.02) 0.24 (0.03) 0.18 (0.03)@Maximum EELV 0.32 (0.07) 0.12 (0.04) 0.72 (0.1) 0.30 (0.12) 0.37 (0.26) 0.95 (0.26)†
RMSdi%max
@FRC 15.8 (3.7) 17.0 (3.3) 11.0 (2.0) 15.5 (0.9) 15.9 (3.0) 19.8 (3.2)@Maximum EELV 67.0 (4.5) 63.0 (6.6) 61.0 (25.8) 75.0 (8.4) 66.5 (6.2)† 50.5 (7.1)†
Effdi, au@FRC 4.72 (1.4) 1.6 (0.3) 10.4 (1.1) 4.24 (0.5) 5.48 (3.5) 2.35 (0.4)@Maximum EELV 1.55 (0.3) 0.4 (0.15) 7.75 (1.6) 1.3 (0.6) 2.1 (2.03)† 4.80 (1.2)‡
Values are means (SD). Ldi ee, diaphragm length at end expiration; FRC, functional residual capacity; EELV, end-expiratory lung volume; �Pdimean, meaninspiratory transdiaphragmatic pressure; �Vdi, volume displaced by diaphragm motion; �Vdi/TI, mean inspiratory flow rate from diaphragm, where TI isinspiratory duration; Power, diaphragm power output; RMSdi%max, electrical activity of the diaphragm as a percent maximum; Effdi, diaphragm efficiency; au,arbitrary units. Significant difference from FRC: *P � 0.01, ‡P � 0.009, †P�0.001 (paired t-test).
1406 EFFICIENCY OF THE HUMAN DIAPHRAGM
J Appl Physiol • VOL 99 • OCTOBER 2005 • www.jap.org
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from

highly and positively correlated: they differ little betweenadjacent costal and crural regions, and, with exercise, theregional distribution of blood flow does not change (35). Thesefindings suggest a direct relationship between crural and globaldiaphragm EMG that is independent of the level of activation.In humans, the RMS of the crural diaphragm is linearly relatedto a measure of global activation of the diaphragm, the ratio ofPdi to Pdimax, up to 75% of Pdimax independent of diaphragmlength (7). We have shown that, with hypercapnia in healthysubjects, RMSdi increases linearly with end-tidal PCO2 up to atleast 60% RMSdi max, suggesting a linear relationship betweenneural drive to the diaphragm and the RMS of the cruraldiaphragm (60). Thus available evidence suggests that theRMS of the crural diaphragm is linearly related to activation ofthe entire diaphragm, up to �75% maximum. In the presentstudy, all measurements without load and the majority withload were within the range at which RMSdi and global dia-phragm activation are linearly related (7, 60). RMSdi exceeded75% of RMSdi max during inspiratory loading at the highest
level of EPAP in two subjects, potentially underestimatingactivation and overestimating efficiency. However, in keepingwith results at lower levels of EPAP and diaphragm activation,Effdi of these measurements was not different from thosewithout load.
Hyperinflation with EPAP causes an inspiratory thresholdload that would have contributed to an increase of RMSdi withhyperinflation, independent of diaphragm shortening. How-ever, we found that a moderate inspiratory threshold plusresistive load was associated with approximately proportionalchanges in Wdi and RMSdi and was not associated with achange in Effdi or in the relationship between efficiency anddiaphragm length. This result is in keeping with the in vivorelationships between force, velocity of shortening, andamount of muscle electrical activity of human gastrocnemiuswhere, at a given muscle length and velocity of shortening, theamount of electrical activity increased proportionately withload (11). In healthy subjects breathing against resistive loads,respiratory efficiency is constant over a wide range of poweroutputs (21), and, in dogs, Effdi is constant with progressiveresistive loading (48). Taken together, these results suggestthat, in the intact human diaphragm, inspiratory loading asso-ciated with the levels of EPAP used in this study was notresponsible for the decrease in measured Effdi with diaphragmshortening.
�Vdi was derived as previously described (58, 59); inaccu-racy associated with the computer-assisted method of imageanalysis was small (see METHODS) and did not add significantlyto the errors of measurement of Ldi or �Vdi. Mean �Vdi �VT�1
at FRC and fractional shortening of the diaphragm betweenFRC and TLC were not different from those in the 10 healthysubjects reported previously (59). Measured �Vdi does notinclude the contribution to inspired lung volume resulting fromthe action of the costal diaphragm in expanding and elevatingthe rib cage. Although this component of �Vdi is believed tobe small (36, 66), any effect would tend to diminish withhyperinflation so that consequent underestimates of efficiencywould be greatest at FRC, thereby reducing the change in Effdi
with decreasing Ldi ee. In our study, RMSdi %max during tidalbreathing at FRC was 1.9 times greater than that reported forhealthy subjects by Sinderby et al. (53). This difference isattributable to a lower respiratory rate and larger (1.8 times) VT
in our subjects relative to those of Sinderby et al.
Implications
In our study, the decrease in Effdi with hyperinflation wasdue principally to a decrease in diaphragm length and wasindependent of modest inspiratory loading. These findings areconsistent with the interdependence of force, velocity of short-ening, length, and electrical activity of muscle (4, 11, 19) andsuggest that measured Effdi reflects the contractile properties ofdiaphragm muscle. Additionally, the results suggest that otherfactors can affect in vivo measurements of Effdi. First, activityof expiratory muscles at end expiration, as in subject 5, canincrease Effdi. To the extent that Wdi at a given level ofactivation and muscle length is approximately constant andindependent of load (11), only passive recoil of the diaphragmwould act to increase efficiency. However, this contributioncould be modulated by the degree of relaxation of abdominalmuscles during inspiration, perhaps explaining the variable
Fig. 4. A: effect of pulmonary hyperinflation, without inspiratory loading, ondiaphragm length at end expiration (Ldi ee) normalized for diaphragm length atFRC. EELV is expressed as %VC. Data are means (SD) at each condition ofmeasurement. The regression line is the mean slope and intercept of theindividual regressions in the 4 subjects where the diaphragm shortened withhyperinflation [mean r2 � 0.85 (0.07)]. B: Bland and Altman comparison ofthe mean Ldi ee at each level of EPAP (0–14 cmH2O) in the 5 subjects. Thesolid line is the mean difference between load (L) and no load (NL) (P � 0.67),and the dashed lines are limits of the 95% confidence intervals.
1407EFFICIENCY OF THE HUMAN DIAPHRAGM
J Appl Physiol • VOL 99 • OCTOBER 2005 • www.jap.org
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from

increase in Effdi in subject 5. Second, a decrease in diaphragmmechanical advantage is suggested by the small decrease inEffdi with Pgee in the four subjects in whom Ldi ee decreasedwith hyperinflation and Pgee increased. Passive hyperinflationincreases Pg and decreases the mechanical advantage of thediaphragm in dogs (68). A decreased mechanical advantagewould be expected to decrease Effdi because, at a givendiaphragm length, mechanical advantage determines poweroutput relative to diaphragm oxygen uptake (35). Third, theefficiency of muscle in vitro decreases at low and high veloc-ities of shortening (32). In our study, mean diaphragm flow ratechanged little with hyperinflation (Table 1) or loading and wasnot systematically related to Effdi. Thus, in our study, flow-related changes in Effdi were not observed. Expiratory muscleactivity at end expiration is not a usual response to continuouspositive airway pressure in supine humans (65) but is usual
with exercise (1), hypercapnia (65), inspiratory loading (42),and chronic obstructive pulmonary disease (COPD) (46). Itsoccurrence has the potential to increase Effdi relative to dia-phragm length and confound interpretation of the measurementbecause, in this event, Effdi reflects both the contractile prop-erties of the diaphragm and the work performed on the dia-phragm by expiratory muscles. In these circumstances, a mea-surement of Effdi, which principally reflects contractile func-tion relative to diaphragm length, could be obtained byincremental measurement during a continuous inspiration fromrelaxed FRC to near TLC.
The results are qualitatively in accord with previous humanstudies showing a reduced efficiency of respiratory muscleswith increasing lung volume (20, 43). Previous in vitro studiesshow a substantial, although variable, effect of muscle lengthon the efficiency or maximum power output of striated musclesegments during cyclical activation (4, 33, 38, 62). The effi-ciency of frog and maximum power of rat ventricular muscleand of fast and slow skeletal muscles of mice decreasedlinearly by 54, 56, 39, and 32% of maximum, respectively, per10% decrease in muscle length below 90% of the length atmaximum isometric force. In our study, efficiency decreasedby �34% for each 10% decrease in diaphragm length. Thesimilar effects of muscle shortening on efficiency or maximumpower output in vitro and in the intact human diaphragmsupport the concept that diaphragm inspiratory power outputrelative to neural activation is an index of the efficiency of thediaphragm.
In emphysema with hyperinflation, we found that Ldi ee atFRC was �25% less than in healthy controls (58). The datafrom the present study (Fig. 6) suggest that a 25% decrease inLdi ee would, in the absence of remodeling of the diaphragm(63), be associated with an �80% decrease in Effdi and requirean approximately fourfold increase in activation to maintainWdi at normal levels (Table 2). This finding is in generalaccord with previous results in subjects with COPD in whom
Fig. 5. Results in subject 3 without inspira-tory loading. Relationships between Ldi ee
and mean inspiratory Pdi (�Pdimean; A),mean inspiratory flow rate from the dia-phragm (�Vdi �TI�1, where TI is inspiratoryduration; B), electrical activity of the dia-phragm (RMSdi; C), and diaphragm effi-ciency (Effdi; D) for each tidal breath. Alldata are normalized to the mean value ofeach variable at FRC. Linear regressionsand their coefficients of determination (r2)and P values are displayed.
Fig. 6. Relationship between normalized Effdi and normalized Ldi ee for eachbreath in all subjects without load. Subject 5 is represented by open squares.The regression line is the mean regression and intercept of the individualregressions in the 5 subjects.
1408 EFFICIENCY OF THE HUMAN DIAPHRAGM
J Appl Physiol • VOL 99 • OCTOBER 2005 • www.jap.org
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from

RMSdi %max during quiet breathing was approximately fivetimes that in healthy subjects (53). In COPD, during quietbreathing (24, 53) and progressive exercise (55), diaphragmelectrical activity is markedly increased, implying either de-creased Effdi, or increased respiratory loads, or both. However,without measurement of the rate of �Vdi and power output, theEffdi in COPD remains undefined.
Effdi was more closely correlated with diaphragm length andmore accurate in defining changes of Ldi ee than diaphragmeffectiveness (�Pdimean �RMSdi
�1). Although the differenceswere small and not significant with inspiratory loading (Table2), the results imply that assessment of diaphragm contractilefunction is incomplete without considering both the pressuredeveloped by the diaphragm and its rate of �Vdi. This con-clusion differs from that of Beck et al. (6), who showed nodecrease in �Pdimean �RMSdi
�1 with increasing inspiratoryflows up to 1.4 l/s, suggesting no measurable effect of dia-phragm velocity of shortening. However, the need to considerthe rate of volume displacement is emphasized by the dia-phragm pressure-velocity behavior during progressive exercisein healthy subjects (2). In this latter study, �Pdi increased lessthan twofold, whereas estimated velocity of diaphragm short-ening increased more than sixfold between rest and exercise to70% maximum workload. In this case, diaphragm effectivenesswould underestimate efficiency by a factor of 6. Similarly,measured efficiency was more accurate than RMSdi %max and�Pdimean �TI in defining changes in Ldi ee, implying that indexesof diaphragm activation (24, 53) or of VO2 di (29) provide a lesscomplete assessment of diaphragm function than one whichconsiders both power output and neural activation.
Measurement of Effdi should allow an estimate of the max-imum power output and reserve capacity of the diaphragm inindividuals. For example, in the four subjects in whom Ldi ee
decreased with hyperinflation, mean RMSdi %max was 67% (SD6) at the shortest Ldi ee achieved without inspiratory loading.Assuming that efficiency does not change with power out-put, this finding implies a maximum power output reserve ofthe diaphragm of �33% at diaphragm lengths commonlyfound in COPD.
In conclusion, the results of this study suggest that the poweroutput of the diaphragm relative to the amount of electricalactivity during tidal inspirations reflects the efficiency and
Fig. 7. A: normalized Effdi relative to normalized Ldi ee for each breath without(solid symbols) and with (open symbols) inspiratory loading. Subject 5 isrepresented by squares. The regression lines are the means of the individualregressions in the 5 subjects without (dashed line) and with (solid line)inspiratory loading. The mean slopes and intercepts were not different (P �0.61 and 0.42, respectively). B: Bland and Altman comparison of the meanEffdi (arbitrary units, au) at each level of EPAP (0–14 cmH2O) in the 5subjects. The solid line is the mean difference between L and NL (P � 0.63),and the dashed lines are limits of the 95% confidence interval.
Table 2. Correlations between and accuracy of measures of diaphragm function with respect to diaphragmlength at various lung volumes
Measures ofDiaphragm Function Definition
Correlation Coefficients Accuracy
No Load Load No Load Load
0.64 0.64Efficiency Wdi/RMSdi P�0.001 P�0.001 0.78 (0.13) 0.89 (0.10)
0.61 0.58 0.69 (0.14) 0.64 (0.37)Effectiveness �Pdimean/RMSdi P�0.001 P�0.001 P � 0.029 P � 0.076
0.52 0.45 0.67 (0.20) 0.67 (0.35)Neural activation RMSdi%max P�0.001 P�0.001 P � 0.048 P � 0.145
0.10 0.42 0.45 (0.36) 0.61 (0.34)Pressure � time �Pdimean�TI P � 0.31 P�0.001 P � 0.025 P � 0.109
Pearson’s correlations are shown between measures of diaphragm function and Ldi ee for all subjects (n � 5). Wdi/RMSdi, inspiratory diaphragm poweroutput/amount of inspiratory diaphragm electromyogram (EMG); �Pdimean/RMSdi, mean transdiaphragmatic pressure/amount of inspiratory diaphragm EMG;RMSdi%max, amount of inspiratory diaphragm EMG normalized to the maximum value obtained during inspirations to total lung capacity; �Pdimean�TI, productof mean transdiaphragmatic pressure and inspiratory time. Measures of diaphragm function and Ldi ee were normalized by dividing the value obtained for eachbreath by the mean value at FRC in each subject. Accuracy of each measure of diaphragm function was calculated as the mean (SD) of the individual values.Under Accuracy, the P values define the significance of the difference from diaphragm efficiency (paired t-test).
1409EFFICIENCY OF THE HUMAN DIAPHRAGM
J Appl Physiol • VOL 99 • OCTOBER 2005 • www.jap.org
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from

contractile function of the human diaphragm. Expiratory mus-cle activity at end expiration can maintain diaphragm lengthnear that at FRC, despite hyperinflation, and increase effi-ciency. However, this effect was variable, indicating that theinteractions between activity of respiratory muscles, Ldi ee, andpassive recoil of the diaphragm require systematic evaluation.
ACKNOWLEDGMENTS
The authors thank Y. M. Lam and Kai Shen for developing, respectively,the EMG and �Vdi analysis software, Karen Wills for assistance with dataanalysis and preparation of the manuscript, Y. M. Lam and Satvinder Dhaliwalfor statistical advice, N. Hicks for performing fluoroscopy, and the Departmentof Radiology, Sir Charles Gairdner Hospital, for access to equipment andmaterials.
GRANTS
This study was supported by a grant from the Medical Research Fund ofWestern Australia and Sir Charles Gairdner Hospital Research Fund. B. Singhis the recipient of an Australian Lung Foundation/Boehringer IngelheimChronic Airflow Limitation Research Fellowship.
REFERENCES
1. Abraham KA, Feingold H, Fuller DD, Jenkins M, Mateika JH, andFregosi RF. Respiratory-related activation of human abdominal musclesduring exercise. J Physiol 541: 653–663, 2002.
2. Aliverti A, Cala SJ, Duranti R, Ferrigno G, Kenyon CM, Pedotti A,Scano G, Sliwinski P, Macklem PT, and Yan S. Human respiratorymuscle actions and control during exercise. J Appl Physiol 83: 1256–1269, 1997.
3. American Thoracic Society/European Respiratory Society. ATS/ERSstatement on respiratory muscle testing. Am J Respir Crit Care Med 166:518–624, 2002.
4. Bahler AS, Fales JT, and Zierler KL. The dynamic properties ofmammalian skeletal muscle. J Gen Physiol 51: 369–384, 1968.
5. Bazzy AR, Pang LM, Akabas SR, and Haddad GG. O2 metabolism ofthe sheep diaphragm during flow resistive loaded breathing. J Appl Physiol66: 2305–2311, 1989.
6. Beck J, Sinderby C, Lindstrom L, and Grassino A. Crural diaphragmactivation during dynamic contractions at various inspiratory flow rates.J Appl Physiol 85: 451–458, 1998.
7. Beck J, Sinderby C, Lindstrom L, and Grassino A. Effects of lungvolume on diaphragm EMG signal strength during voluntary contractions.J Appl Physiol 85: 1123–1134, 1998.
8. Beck J, Sinderby C, Lindstrom L, and Grassino A. Influence of bipolaresophageal electrode positioning on measurements of human crural dia-phragm electromyography. J Appl Physiol 81: 1434–1449, 1996.
9. Beck J, Sinderby C, Lindstrom L, and Grassino G. Diaphragm inter-ference pattern EMG and compound muscle action potentials: effects ofchest wall configuration. J Appl Physiol 82: 520–530, 1997.
10. Beck J, Sinderby C, Weinberg J, and Grassino A. Effects of muscle-to-electrode distance on the human diaphragm electromyogram. J ApplPhysiol 79: 975–985, 1995.
11. Bigland B and Lippold OC. The relation between force, velocity andintegrated electrical activity in human muscles. J Physiol 123: 214–224,1954.
12. Bigland-Ritchie B and Woods JJ. Integrated EMG and oxygen uptakeduring dynamic contractions of human muscles. J Appl Physiol 36:475–479, 1974.
13. Boriek AM, Rodarte JR, and Reid MB. Shape and tension distributionof the passive rat diaphragm. Am J Physiol Regul Integr Comp Physiol280: R33–R41, 2001.
14. Brancatisano A, Kelly SM, Tully A, Loring SH, and Engel LA.Postural changes in spontaneous and evoked regional diaphragmatic ac-tivity in dogs. J Appl Physiol 66: 1699–1705, 1989.
15. Braun NM, Arora NS, and Rochester DF. Force-length relationship ofthe normal human diaphragm. J Appl Physiol 53: 405–412, 1982.
16. Brooks SV, Faulkner JA, and McCubbrey DA. Power outputs of slowand fast skeletal muscles of mice. J Appl Physiol 68: 1282–1285, 1990.
17. Cala SJ, Kenyon CM, Ferrigno G, Carnevali P, Aliverti A, Pedotti A,Macklem PT, and Rochester DF. Chest wall and lung volume estimation
by optical reflectance motion analysis. J Appl Physiol 81: 2680–2689,1996.
18. Campbell EJM, Westlake EK, and Cherniack RM. The oxygen con-sumption and efficiency of the respiratory muscles of young male subjects.Clin Sci (Lond) 18: 55–64, 1959.
19. Coirault C, Riou B, Bard M, Suard I, and Lecarpentier Y. Contraction,relaxation, and economy of force generation in isolated human diaphragmmuscle. Am J Respir Crit Care Med 152: 1275–1283, 1995.
20. Collett PW and Engel LA. Influence of lung volume on oxygen cost ofresistive breathing. J Appl Physiol 61: 16–24, 1986.
21. Collett PW, Perry C, and Engel LA. Pressure-time product, flow, andoxygen cost of resistive breathing in humans. J Appl Physiol 58: 1263–1272, 1985.
22. Darian GB, DiMarco AF, Kelsen SG, Supinski GS, and Gottfried SB.Effects of progressive hypoxia on parasternal, costal, and crural diaphragmactivation. J Appl Physiol 66: 2579–2584, 1989.
23. De Troyer A, Gorman RB, and Gandevia SC. Distribution of inspira-tory drive to the external intercostal muscles in humans. J Physiol 546:943–954, 2003.
24. De Troyer A, Leeper JB, McKenzie DK, and Gandevia SC. Neuraldrive to the diaphragm in patients with severe COPD. Am J Respir CritCare Med 155: 1335–1340, 1997.
25. De Troyer A and Legrand A. Inhomogeneous activation of the paraster-nal intercostals during breathing. J Appl Physiol 79: 55–62, 1995.
26. Easton PA, Fitting JW, Arnoux R, Guerraty A, and Grassino AE.Costal and crural diaphragm function during CO2 rebreathing in awakedogs. J Appl Physiol 74: 1406–1418, 1993.
27. Eastwood PR, Hillman DR, and Finucane KE. Ventilatory responses toinspiratory threshold loading and role of muscle fatigue in task failure.J Appl Physiol 76: 185–195, 1994.
28. Fales JT, Heisey R, and Zierler KL. Dependency of oxygen consump-tion of skeletal muscle on number of stimuli during work in the dog. Am JPhysiol 198: 1333–1342, 1960.
29. Field S, Sanci S, and Grassino A. Respiratory muscle oxygen consump-tion estimated by the diaphragm pressure-time index. J Appl Physiol 57:44–51, 1984.
30. Gorman RB, McKenzie DK, Pride NB, Tolman JF, and Gandevia SC.Diaphragm length during tidal breathing in patients with chronic obstruc-tive pulmonary disease. Am J Respir Crit Care Med 166: 1461–1469,2002.
31. Grassino A, Goldman MD, Mead J, and Sears TA. Mechanics of thehuman diaphragm during voluntary contraction: statics. J Appl Physiol 44:829–839, 1978.
32. Hill AV. The heat of shortening and the dynamic constants of muscle.Proc R Soc London Ser B 126: 136–195, 1938.
33. James RS, Altringham JD, and Goldspink DF. The mechanical prop-erties of fast and slow skeletal muscles of the mouse in relation to theirlocomotary function. J Exp Biol 198: 491–502, 1995.
34. Jardim J, Farkas G, Prefaut D, Thomas D, Macklem PT, and RoussosC. The failing inspiratory muscles under normoxic and hypoxic condi-tions. Am Rev Respir Dis 124: 274–279, 1981.
35. Johnson RL Jr, Hsia CC, Takeda S, Wait JL, and Glenny RW.Efficient design of the diaphragm: distribution of blood flow relative tomechanical advantage. J Appl Physiol 93: 925–930, 2002.
36. Kenyon CM, Cala SJ, Yan S, Aliverti A, Scano G, Duranti R, PedottiA, and Macklem PT. Rib cage mechanics during quiet breathing andexercise in humans. J Appl Physiol 83: 1242–1255, 1997.
37. Lagarias JC, Reeds JA, Wright MH, and Wright PE. Convergenceproperties of the Nelder-Mead method in low dimensions. SIAM J Opti-mization 9: 112–147, 1998.
38. Layland J, Young IS, and Altringham JD. The length dependence ofwork production in rat papillary muscle in vitro. J Exp Biol 198: 2491–2499, 1995.
39. Legrand A, Brancatisano A, Decramer M, and De Troyer A. Rostro-caudal gradient of electrical activation in the parasternal intercostal mus-cles of the dog. J Physiol 495: 247–254, 1996.
40. Legrand A and De Troyer A. Spatial distribution of external and internalintercostal activity in dogs. J Physiol 518: 291–300, 1999.
41. Manohar M and Hassan AS. Diaphragmatic energetics during prolongedexhaustive exercise. Am Rev Respir Dis 144: 415–418, 1991.
42. Martin JG and De Troyer A. The behaviour of the abdominal musclesduring inspiratory mechanical loading. Respir Physiol 50: 63–73, 1982.
1410 EFFICIENCY OF THE HUMAN DIAPHRAGM
J Appl Physiol • VOL 99 • OCTOBER 2005 • www.jap.org
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from

43. McCool FD, Tzelepis GE, Leith DE, and Hoppin FG Jr. Oxygen costof breathing during fatiguing inspiratory resistive loads. J Appl Physiol 66:2045–2055, 1989.
44. Mead J and Loring SH. Analysis of volume displacement and lengthchanges of the diaphragm during breathing. J Appl Physiol 53: 750–755,1982.
45. Mead J, Loring SH, and Smith JC. Volume displacements of the chestwall and their mechanical significance. In: The Thorax (2nd ed.), edited byRoussos C. New York: Dekker, 1995, p. 565–586.
46. Ninane V, Rypens F, Yernault JC, and De Troyer A. Abdominalmuscle use during breathing in patients with chronic airflow obstruction.Am Rev Respir Dis 146: 16–21, 1992.
47. Paul RJ and Peterson JW. Relation between length, isometric force, andO2 consumption rate in vascular smooth muscle. Am J Physiol 228:915–922, 1975.
48. Reid MB and Johnson RLJ. Efficiency, maximal blood flow, and aerobicwork capacity of the canine diaphragm. J Appl Physiol 54: 763–772, 1983.
49. Robertson CHJ, Foster GH, and Johnson RLJ. The relationship ofrespiratory failure to the oxygen consumption of, lactic acid by, anddistribution of blood flow among respiratory muscles during increasinginspiratory resistance. J Clin Invest 59: 31–42, 1977.
50. Rochester DF and Bettini G. Diaphragmatic blood flow and energyexpenditure in the dog. Effects of inspiratory airflow resistance andhypercapnia. J Clin Invest 57: 661–672, 1976.
51. Rochester DF and Briscoe AM. Metabolism of the working diaphragm.Am Rev Respir Dis 119: 101–106, 1979.
52. Shen K. Interactive Computerised Functional Analysis of Lateral Fluo-roscopy Images to Quantify the Volume Displaced by Motion of theDiaphragm (Honours Thesis). Perth: University of Western Australia,2002.
53. Sinderby C, Beck J, Spahija J, Weinberg J, and Grassino A. Voluntaryactivation of the human diaphragm in health and disease. J Appl Physiol85: 2146–2158, 1998.
54. Sinderby C, Lindstrom L, and Grassino AE. Automatic assessment ofelectromyogram quality. J Appl Physiol 79: 1803–1815, 1995.
55. Sinderby C, Spahija J, Beck J, Kaminski D, Yan S, Comtois N, andSliwinski P. Diaphragm activation during exercise in chronic obstructivepulmonary disease. Am J Respir Crit Care Med 163: 1637–1641, 2001.
56. Sinderby CA, Beck JC, Lindstrom LH, and Grassino AE. Enhance-ment of signal quality in esophageal recordings of diaphragm EMG.J Appl Physiol 82: 1370–1377, 1997.
57. Sinderby CA, Comtois AS, Thomson RG, and Grassino AE. Influenceof the bipolar electrode transfer function on the electromyogram powerspectrum. Muscle Nerve 19: 290–301, 1996.
58. Singh B, Eastwood PR, and Finucane KE. Volume displaced by dia-phragm motion in emphysema. J Appl Physiol 91: 1913–1923, 2001.
59. Singh B, Panizza JA, and Finucane KE. Breath-by-breath measurementof the volume displaced by diaphragm motion. J Appl Physiol 94:1084–1091, 2003.
60. Singh B, Panizza JA, and Finucane KE. Diaphragm electromyogramroot mean square response to hypercapnoea and its intersubject andday-to-day variation. J Appl Physiol 98: 274–281, 2005.
61. Soust M, Walker AM, and Berger PJ. Diaphragm VO2, diaphragmEMG, pressure-time product and calculated ventilation in newborn lambsduring hypercapnic hyperpnoea. Respir Physiol 76: 107–117, 1989.
62. Syme DA. The efficiency of frog ventricular muscle. J Exp Biol 197:143–164, 1994.
63. Thomas AJ, Supinski GS, and Kelsen SG. Changes in chest wallstructure and elasticity in elastase-induced emphysema. J Appl Physiol 61:1821–1829, 1986.
64. Wakai Y, Leevers AM, and Road JD. Regional diaphragm shorteningmeasured by sonomicrometry. J Appl Physiol 77: 2791–2796, 1994.
65. Wakai Y, Welsh MM, Leevers AM, and Road JD. Expiratory muscleactivity in the awake and sleeping human during lung inflation andhypercapnia. J Appl Physiol 72: 881–887, 1992.
66. Ward ME, Ward JW, and Macklem PT. Analysis of human chest wallmotion using a two-compartment rib cage model. J Appl Physiol 72:1338–1347, 1992.
67. Whitelaw WA. Shape and size of the human diaphragm in vivo. J ApplPhysiol 62: 180–186, 1987.
68. Wilson TA, Boriek AM, and Rodarte JR. Mechanical advantage of thecanine diaphragm. J Appl Physiol 85: 2284–2290, 1998.
69. Woledge RC, Curtin NA, and Homsher E. Energetic aspects of musclecontraction. Monogr Physiol Soc 41: 1–357, 1985.
1411EFFICIENCY OF THE HUMAN DIAPHRAGM
J Appl Physiol • VOL 99 • OCTOBER 2005 • www.jap.org
by guest on June 2, 2013http://jap.physiology.org/
Dow
nloaded from