effectiveness of planned teaching programme
TRANSCRIPT
A STUDY TO EVALUATE THE EFFECTIVENESS OF
PLANNED TEACHING PROGRAMME ON RENAL
CALCULI AND ITS MANAGEMENT AMONG
THE RENAL CALCULI PATIENTS
IN SELECTED HOSPITALS
IN MANGALORE TALUK.
by
CH. BABITA DEVI
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillment
Of the requirements for the degree of
Master of Science in Nursing
2005

In
Medical-Surgical Nursing
Under the guidance of
Prof. B A Yathi kumara Swamy Gowda
Department of Medical Surgical Nursing
Alva’s College Of Nursing
Moodbidri
2005
Rajiv Gandhi University of Health Sciences, Karnataka
DECLARATION BY THE CANDIDATE
ii
I hereby declare that this dissertation/thesis entitled “A Study to evaluate the
effectiveness of Planned Teaching Programme on Renal Calculi and its
management among the renal calculi patients in selected hospitals in Mangalore
taluk” is a bonafide and genuine research work carried out by me under the guidance
of Prof. B A Yathikumara Swamy Gowda, Principal and Head of the Department of
Medical-Surgical Nursing, Alva’s College of Nursing, Moodbidri.
Date: Signature of the Candidate
Place: Ch. Babita Devi
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “A study to evaluate the
effectiveness of Planned Teaching Programme on Renal Calculi and its
iii

management among the renal calculi patients in selected hospitals in Mangalore
taluk” is a bonafide research work done by Ms. Ch. Babita Devi in partial fulfillment
of the requirement for the degree of Master of Science in Nursing (Medical-Surgical
Nursing).
Date: Signature of the Guide
Place:
Prof. B A Yathikumara Swamy Gowda,
Head of the Department
Medical-Surgical Nursing,
Alva’s College of Nursing, Moodbidri.
ENDORSEMENT BY THE HOD, PRINCIPAL / HEAD OF THE
INSTITUTION
iv
This is to certify that the dissertation entitled “A study to evaluate the
effectiveness of Planned Teaching Programme on Renal Calculi and its
management among the renal calculi patients in selected hospitals in Mangalore
taluk” is a bonafide research work done by Ms. Ch. Babita Devi under the guidance of
Prof. B A Yathikumara Swamy Gowda, Principal and Head of the Department of
Medical-Surgical Nursing, Alva’s College of Nursing, Moodbidri.
Seal & Signature of the Seal & Signature of the
HOD Principal
Prof.. B A Yathikumara Prof. B A Yathikumara
Swamy Gowda Swamy Gowda
Date: Date:
Place: Place:
COPY RIGHT
v
Declaration by the Candidate
I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka
shall have the rights to preserve, use and disseminate this dissertation / thesis in print or
electronic format for academic / research purpose.
Date: Signature of the Candidate
Place: Ch. Babita Devi
© Rajiv Gandhi University of Health Sciences, Karnataka
ACKNOWLEDGEMENT
I acknowledge my love and gratitude to all those loving hearts that has helped me
throughout my endeavor.
I acknowledge with gratitude and devotion, The ALMIGHTY GOD for HIS abiding
grace, love, compassion and immense shower of blessings on me, which gave me the
strength and courage to overcome all the difficulties and completing the study.
vi
I express my sincere thanks to Dr. M. Mohan Alva, Chairman of Alva’s Education
Foundation for the opportunity given to me to under take this course in this esteemed
college.
The present study could never have been successfully completed without the expert
guidance of research supervisors.
I acknowledge my deep sense of gratitude to my research guide Prof. B.A,Yathi
Kumara Swamy Gowda, Principal of the college for his patience, valuable guidance,
direction and advice given for the completion of this study. I find myself lucky for
having been under his guidance.
I owe a deepest sense of gratitude to Prof. Alice Salins, Vice Principal of this college
for her intellectual enlightenment, valuable suggestions and sustained patience for the
successful completion of the study.
I express my sincere and whole-hearted gratitude to Assist. Prof. (Mrs) Baby S Nayak
for her expert and valuable guidance in every step of my work and scrutinized my
progress, inspiration, sustained patience, constant encouragement, suggestions and
support from the inception till the completion of this study. Her analytical approach
helped me in giving final shape to the report.
My heartfelt gratitude to Mrs. Priya Neetha Monis. Lecturer of this college who has
guided me and helped me whenever I approached her.
I have lot of happy moments to cherish with my classmate friends Simple M and Jaya
Mathew who have helped me and co-operated me throughout the course. Many thanks
and wishes to them.
My grateful acknowledge to all the experts who contributed their valuable time and
efforts towards validating the tools and contents of the PTP.
vii
My sincere gratitude to Dr. Krishna Mohan Prabhu, Managing Director of Prabhu
General Hospital, for granting permission to conduct pretesting and reliability of the
tool, Dr.Harish Nayak, Medical Superintendent of Alva’s Health Centre to conduct
pilot study and Dr. Prashanth Marla, Medical Director of A..J Hospital and Research
Centre to conduct main study.
My special thanks to all the participants who enthusiastically participated in the study
and for being very co-operative and also for adding light to my studies with their
heartfelt expression.
I extend my sincere gratitude to the non-teaching staff of this college for their
approachability.
I am thankful to the Dean and librarians of KMC, Manipal and librarians of Alva’s
Education Foundation for allowing me to use the library facilities.
I am indebted to my mother and father who have moulded me to lead so far with their
blessing and kindness and who has silently borne every trouble for my sake. To them I
owe my every success.
I am extremely grateful to my brothers and sisters for their understanding and
immense support for my studies
It is my privilege to acknowledge Dr. Geetchandra Singh who has supported in every
trouble, has given hands in times of need and has encouraged me to carry out my work
sincerely. Special thanks to him.
Lastly I am grateful to all of them who have directly or indirectly helped in completion
of this study.
Date: Signature of the Candidate
Place
Ch. Babita Devi
viii
LIST OF ABBREVIATIONS
Ca Calcium
GLV Green Leafy Vegetables
Ox Oxalate
P Phosphorus
PH4 Phosphate
PTP Planned Teaching Programme
RC Renal Calculi
UA Uric Acid
USG Ultrasonography
ix
ABSTRACT
Renal stone is a painful condition that affects 1 – 2% of the general
population.Kidney stones are aggregates of crystals mixed with a protein matrix that
cause obstruction of urine flow in the renal collecting system, ureters, or urethra and
result in severe pain, bleeding, or local erosion of kidney tissues 1 .
STATEMENT OF THE PROBLEM
A study to evaluate the effectiveness of Planned Teaching Programme on Renal
Calculi and its management among the renal calculi patients in selected hospitals in
Mangalore taluk.
OBJECTIVES OF THE STUDY
The objectives of the study are to :-
1) determine the pre test knowledge of the renal calculi patients regarding renal
calculi and its management.
2) plan and validate the planned teaching programme on renal calculi and its
management for the patients with renal calculi.
3) evaluate the effectiveness of planned teaching programme on renal calculi and
its management in terms of gain in knowledge in post test.
An evaluative approach with one group pre-test post-test design (pre-
experimental) was adopted in order to evaluate effectiveness of Planned teaching
programme on renal calculi and its management among renal calculi patients in a
x
selected hospital in Mangalore Taluk. The conceptual framework adopted for the study
was based on modified Rosen Stock’s Health Belief Model (1966).
The Content validity of the tool and Planned Teaching Programme was
established in consultation with thirteen experts in the field of medicine, nursing and
Food, Nutrition and Dietetic Department. Reliability of the tool was tested by split half
method (r=0.80)
Convenience sampling was used to select the sample for the study. Pilot study
was conducted to find out the feasibility of the study. Data collected from the sample
were analyzed by descriptive and inferential statistics. The final sample size was 48.
Results of the study
Majority of the sample belonged to age group 21 – 35 years (33.34%), male
(79.17%), having primary school education (27.08%), married (83.33%), doing
business (25%), having family income of Rs 1501 – 3000 (25%), Hindu
background (68.75%), Non-vegetarian (85.42%), had no history of previous
hospital admission (87.5%), no family history of renal calculi (91.67%), no habit of
smoking, chewing betal leaves and taking alcohol (68.75%) and had average
knowledge (89.58%).
There was a significant difference between pre-test and post-test knowledge scores
( t(47) =32.81, P<0.05; Tabled value = 2.02 ).
There was significant association between pre-test knowledge scores and age ( χ2(2)
= 17.28, p<0.05 ).
xi
There was no significant association between pre-test knowledge score and the
selected variables gender ( χ2(1) = 0.07, P>0.05 ), per capita income of the family (
χ2(1) = 0.89, P>0.05 )and dietary pattern ( χ2
(1) = 0.03, P>0.05 ).
The findings of the study show that the planned teaching programme was
effective in all the areas in improving the knowledge of the patients with renal calculi.
Keywords
Urinary system; renal calculi; renal calculi and its management; renal calculi patients;
urinary excretion; minerals; stone formation; food habits; occupational exposure.
xii
TABLE OF CONTENTS
1. Introduction 1 – 11
2. Objectives 12
3. Review of Literature 13 – 26
4. Methodology 27 – 38
5. Results 39 – 59
6. Discussion 60 – 61
7. Conclusion 62 – 67
8. Summary 68 – 73
9. Bibliography 74 – 79
10. Annexures 80 - 169
xiii
TABLES
Sl. No.
Tables Pages
1. Frequency and percentage distribution of patients with renal calculi on basis of demographic data.
41 – 43
2. Percentage of agreement by experts on areas of planned teaching programme in percentage and frequency.
49
3. Frequency and percentage distribution of pretest and posttest knowledge scores of patients with renal calculi.
50
4. Range, Mean, Median, Mean percentage and Standard deviation (SD) of pretest and posttest knowledge scores.
51
5. Area-Wise pretest and posttest knowledge scores on renal calculi and its management.
53
6. Mean, Mean deviation (MD), Standard deviation (SD), ‘t’ value between pretest and posttest knowledge scores of patients with renal calculi.
55
7. Area-Wise paired ‘t’ test showing the significant difference between pretest and posttest knowledge scores.
56
8. Association between pretest knowledge scores and selected demographic factors.
58
xiv
LIST OF FIGURES
Sl.
No.
Figures Pages
1. Conceptual framework on effectiveness of PTP based on modified
Rosenstock’s Health Belief Model (1966).
10
2. Pre experimental one group pre test post test design. 28
3. Schematic representation of research design. 28
4. Schematic representation of study plan. 29
5. Bar diagram showing the distribution of renal calculi patients
according to their age group.
46
6. Pie diagram showing the distribution of renal calculi patients
according to their sex.
47
7. Pie diagram showing the distribution of renal calculi patients
according to their dietary pattern.
48
8. Frequency polygon showing the mean and median of knowledge
scores of renal calculi patients in pretest and posttest scores on renal
calculi and its management.
52
xv

xvi
1
1. INTRODUCTION
Renal stone is a painful condition that affects 1 – 2% of the general
population. Kidney stones are aggregates of crystals mixed with a protein matrix that
cause obstruction of urine flow in the renal collecting system, ureters, or urethra and
result in severe pain, bleeding, or local erosion of kidney tissues 1 .
There are several types of kidney stone. The most common type of
kidney stone is composed of calcium oxalate and is caused by metabolic disorders that
are often treatable. In general, the crystallization of stone-forming salts owes to an
abnormal urinary composition that is either higher in crystallization promoters e.g.
calcium, oxalate, uric acid or lower in inhibitors e.g. citrate, glycosaminoglycans,
kidney proteins such as nephrocalcin, Tamm-Horsfall mucoprotein. Uropontin, or
both2.
The formation of the 4 basic chemical types of renal calculi is associated
with more than 20 underlying etiologies. Stone analysis, together with serum and 24-
hour urine metabolic evaluation, can identify an etiology in over 95% of patients.
Specific therapy can result in a remission rate of over 80% and can decrease the
individual recurrence rate by 90%. Emergency physicians, therefore, should stress the
importance of urologic follow-up, especially in patients with recurrent stones, solitary
kidneys, or previous kidney or stone surgery and in all children.
• Calcium stones (75%): Calcium oxalate, calcium phosphate, and calcium urate.
• Struvite (magnesium ammonium phosphate) stones (15%)
• Uric acid stones (6%): These are associated with urine pH less than 5.5, high
purine intake (eg, organ meats, legumes, fish, meat extracts, gravies), or
2
malignancy (ie, rapid cell turnover). Approximately 25% of patients with uric
acid stone have gout.
• Cystine stones (2%)3
The causes of renal calculi can be classified as follows
Metabolic abnormalities (a patient may show more than one)
* Supersaturation of urine with stone-forming salts
Hypercalciuria (>300 mg/24hr): 40-60% of cases
Hyperuricosuria (>750 mg/24hr): 20-35% of cases
Hyperoxaluria (>40 mg/24hr): 10-20% of cases
Cystinuria (>250 mg/L): 1-2% of cases
* Reduced inhibitors of stone formation
Hypocitraturia (<320 mg/day): 10-40% of cases
Hypomagnesuria
Abnormal nephrocalcin, or other glycoprotein defects (Tamm-
Horsfall protein, glycosaminoglycan, uropontin, crystal matrix
protein)
Infection with urease-producing organisms (mostly Proteus): 10-20% of
cases
Alterations in urinary pH
* pH<5.5 leads to uric acid stones
* pH>7.5 seen with struvite stones4
3
Calculus size and location are important determinants for the resultant
degree of disease. The most important factor for passage of a calculus though the
genitourinary tract is its size. The critical size for spontaneous passage is <5 mm.
Approximately 90% of stones that are less than 5 mm and located in the lower ureter
pass spontaneously within 4 weeks. 15% for stones between 5 and 8 mm. 95% of
stones larger than 8 mm become impacted along the genitourinary tract, generally
requiring lithotripsy or surgical removal. Intervention can usually be performed in the
outpatient setting5.
An increase in fluid intake is common advice for patients with renal
stones. A higher intake leads to increased urinary volume and, in turn, decreased in
concentration of stone formation components, which will presumably decrease rate of
stone formation. Alternatively, the increased urinary volume could decrease the
concentration of inhibitors of stone formation6.
NEED FOR THE STUDY
The formation of stones in the urinary tract is a common and important
problem that must be considered in daily urological practice. With a prevalence of
>10% and an expected recurrence rate of =50%, stone disease has an important effect
on the health care system. The condition affects 5-10% of the population in Europe and
North America. An even higher frequency has been reported from other parts of the
world and there are only a few geographical areas in which stone disease is rare e.g. in
Greenland and in the coastal areas of Japan7.
The annual incidence of stone formation in the industrialized world is
generally considered to be 1500-2000 cases per million. Over the past two or three
4
decades there has been a dramatic development in the techniques for stone removal.
Although the vast majority of stones pass spontaneously, open surgery for stone
removal was previously a very common urological procedure. Currently almost all
stones can be removed by non-or slightly invasive methods. Despite these
achievements the problem of recurrent stone formation remains and despite
considerable progress in this field, efforts to stop stone formation have so far been
insufficient. This raised the question of how much has been accomplished in the field
of further formation of renal calculi7.
Incidence/Prevalence in USA8
• 1-4/1000 annual incidence
• 5-12% lifetime incidence
• Higher incidence in the "stone belt" (southeastern USA)
• Recurrence rate - 50% in five years
• Predominant age: 20 -40 years
• Predominant sex: Male : Female (≈3:1), except for struvite (infection)
stones which are more common in females.
It has been estimated that 7 to 10 of every 1,000 hospital admissions are
due to renal calculi. In the U.S. the prevalence is 7% in men and 3% in women, and
70% of all ureteral calculi occur between the ages of 20 and 50 years5.
Low levels of urinary crystallization inhibitors were reported in
hypercalciuric, normocalciuric, and hyperuricosuric stone formers. In general, the level
of crystallization inhibitors in urine of stone-forming patients is low when compared
with individuals without stone formation9.
5
Citrate, a key component of the uric acid cycle, has received increasing
and renewed interest as an important inhibitor of stone formation. Citrate retards
crystallization by two means: It complexes calcium and reduces ionic calcium
concentration in urine, and it directly inhibits the crystallization of calcium oxalate and
calcium phosphate. In addition, nephrocalcin, an acidic glycoprotein, inhibits calcium
oxalate nucleation, growth, and aggregation. Tam-Horsfall protein also inhibits
aggregation, and uroprotein inhibits the growth of calcium oxalate crystals9.
Urinary oxalate is an important determinant of calcium-oxalate
supersaturation. Rather small increments in oxalate excretion markedly raise the
activity product of the ions contributing to stone formation by increasing the urinary
saturation of calcium oxalate. Dietary oxalate is responsible for only a minor fraction (≤
20%) of urinary oxalate. Endogenous oxalate production is a metabolic end product of
glycine and ascorbic acid metabolism. Hyperoxaluria (urinary levels > 40 mg/day) can
be either genetic or acquired. The genetic form, primary hyperoxaluria, is rare and can
be result from mutations in the gene for alanine: glyoxylate aminotransferase or in the
gene for glyoxalate reductase/D-glycerate dehydrogenase. Acquired hyperoxaluria is a
consequence of increased intestinal absorption of oxalate and is often found in patients
with malabsorption in the small bowel2.
Excessive urinary calcium excretion represents a major pathophysiologic
factor of kidney stones because many stone patients have idiopathic hypercalciuria, a
primary metabolic alteration. Hypercalciuria promotes calcium salt crystallization and
crystal growth. Theoretically, the risk of developing renal calcium stones increases as
urinary calcium excretion rises. The mechanism involved in hypercalciuria includes an

6
increase in the filtered calcium load and/or a decrease in the efficiency of tubular
reabsorption of calcium2.
The role of dietary sodium in the pathogenesis of hypercalciuria is
based on the close relationship between renal tubular calcium and sodium handling.
Reabsorption of calcium parallels the renal reabsorption of sodium in the proximal
tubule and Loop of Henle. High sodium intake may also influence renal reabsorption of
calcium in the distal tubule both directly or indirectly through its effects on parathyroid
hormone levels9.
The role of protein intake in calcium stone formation has been
investigated by several groups. The ingestion of a diet rich in animal protein (meat,
fish, poultry, eggs, and dairy products) increases the risk for calcium nephrolithiasis.
Conversely, the disorder is less common in populations who consume protein primarily
from plant sources. Protein feeding can lead to an increase in glomerular filtration rate,
an increase in serum ulfilterable calcium concentration, or both9.
The researcher takes interest in this study as she had come across a large
number of renal calculi in and out patients during her clinical postings so that she can
impart knowledge for such patients regarding the disease and make them aware to
prevent the recurrence of the disease.
STATEMENT OF THE PROBLEM
A study to evaluate the effectiveness of Planned Teaching Programme on
Renal Calculi and its management among the renal calculi patients in selected
hospitals in Mangalore taluk.
7
PURPOSE OF THE STUDY
The purpose of the study is to plan and validate the planned teaching
programme on renal calculi and its management for the patients who are suffering from
renal calculi that will help them to gain in their knowledge regarding renal calculi and
its management
OPERATIONAL DEFINITIONS
Effectiveness
It refers to the extent to which the planned teaching programme has achieved the
desired result in terms of patients’ gain in knowledge as evidence by higher mean post
test knowledge score than the mean pre test knowledge score.
Patients with renal calculi
It refers to patients who are clinically diagnosed to have renal calculi and are attending
the selected hospital for the treatment.
Planned Teaching Programme
It refers to the teaching given to the patients who are suffering from renal calculi on
renal calculi and its management using pamphlets, charts, and flash cards.
Management of renal calculi
It refers to the over all management of patients with renal calculi in respect of drugs,
diets and fluids.

8
Knowledge
It refers to correct response of the patients with renal calculi to knowledge items on
dietary modification and fluid therapy of renal calculi, expressed in terms of knowledge
score, which is graded arbitrarily as good, average and poor.
Variables
These are the selected factors, which are presumed to influence the subjects,
knowledge. The factors are age, gender, per capita income of the family and dietary
pattern.
ASSUMPTIONS
The study assumes that
the patients who are admitted to the hospital with the diagnosis of renal calculi
will have some knowledge regarding renal calculi, gained through mass media,
friends, relatives and other sources.
the patients who are attending the planned teaching programme will be able to
follow the instructions in their daily life.
Renal calculi are prone to get recurrence.
Health teaching can impart knowledge regarding renal calculi which make them
aware of their disease.
Creating health awareness will help in prevention of recurrence of renal calculi.
HYPOTHESES
H1 : The mean post test knowledge score of the patients with renal calculi on renal
calculi and its management will be significantly higher than the mean pre-test
knowledge scores, as measured by a structured knowledge questionnaire.
9
H2 : There will be significant association between the pre test knowledge scores
and the selected variables.
All the hypotheses will be tested at the 0.05 Levels of significance.
CONCEPTUAL FRAMEWORK
Conceptualization refers to the process of refining general or abstract ideas,
which are formulated by generalizing from particular manifestations of certain
behaviors or characteristics. These abstracts are referred to as concepts9.
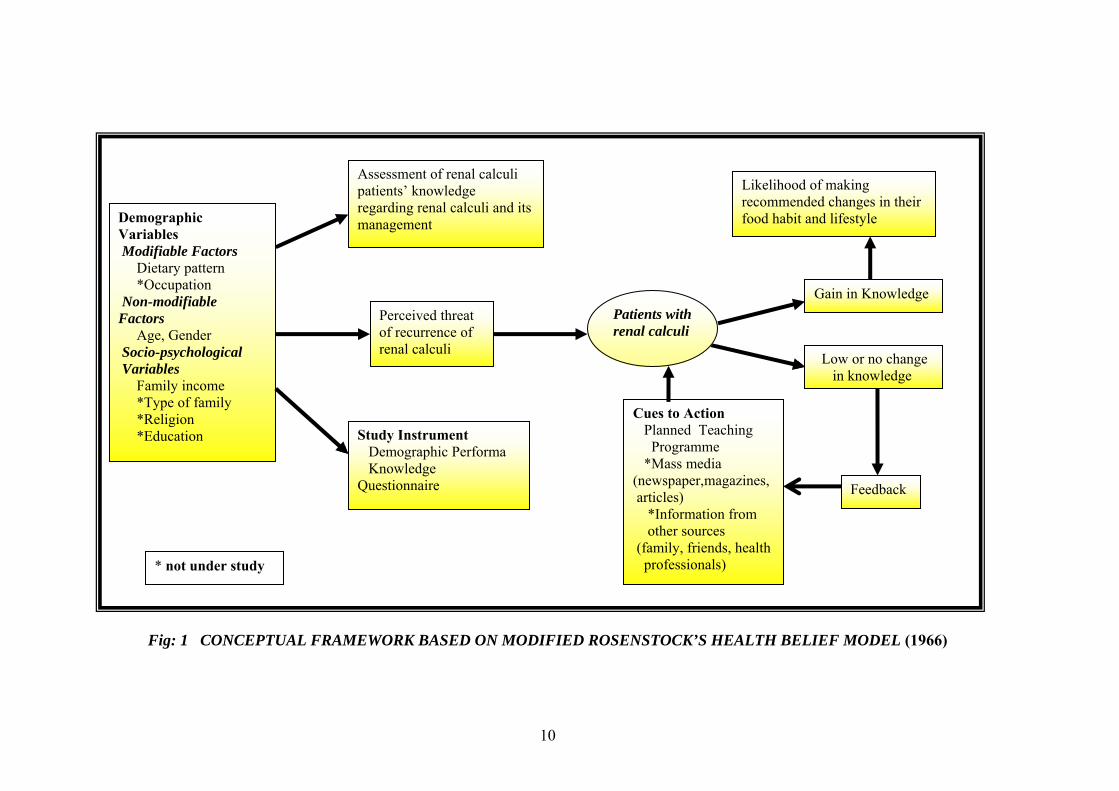
The framework of the present study, as shown in figure 1, is adopted
from Rosenstock’s Health Belief Model. This model stresses the importance of
learner’s motivation in seeking preventive health behaviour.
In the present study, there are certain demographic variables, which will
lead to development of renal calculi. There are also certain modifiable and non
modifiable risk factors, which cause renal calculi. These risk factors are known or little
known to the normal patients. A planned teaching programme can be conducted, which
will be helpful for them in sustaining knowledge and apply it in their daily life. Other
cues are mass media, information from other sources such as family, friends, health
professionals will have beneficiary effects for the individuals to take necessary actions.
If this programme is effective, there can be gain in knowledge of the
participants and there is a likelihood of making recommended changes in their food
habit and lifestyle and this can be measured by knowledge questionnaire. If there is no
change in knowledge, there is no change in practice. Hence feedback can be obtained
and repeated awareness programmes may be conducted.
10
Fig: 1 CONCEPTUAL FRAMEWORK BASED ON MODIFIED ROSENSTOCK’S HEALTH BELIEF MODEL (1966)
Assessment of renal calculi patients’ knowledge regarding renal calculi and its management
Perceived threat of recurrence of renal calculi
Study Instrument Demographic Performa Knowledge Questionnaire
Cues to Action Planned Teaching Programme *Mass media (newspaper,magazines, articles) *Information from other sources (family, friends, health professionals)
Gain in Knowledge
Low or no change in knowledge
Feedback
Likelihood of making recommended changes in their food habit and lifestyle Demographic
Variables Modifiable Factors Dietary pattern *Occupation Non-modifiable Factors Age, Gender Socio-psychological Variables Family income *Type of family *Religion *Education
* not under study
Patients with renal calculi
11
DELIMITATIONS
The study is delimited to patients with renal calculi:
admitted in the hospitals
know to read and write Kannada or Hindi or English
willing to participate
SCOPE OF THE STUDY
1) The findings of the study would reveal the existing knowledge of the renal calculi
patients regarding renal calculi and its management.
2) Nurse educators, public health nurses and student nurses can utilize this
information in providing health education to the patients with renal calculi to
prevent the recurrence of renal calculi.
SUMMARY
This chapter dealt with the introduction, need for the study, statement of the problem,
objectives, operational definitions, assumptions, hypotheses, conceptual framework,
delimitations and scope of the study.
12
2. OBJECTIVES
The objectives of the study are to :
1) determine the pre test knowledge of the renal calculi patients regarding renal
calculi and its management.
2) plan and validate the planned teaching programme on renal calculi and its
management for the patients with renal calculi.
3) evaluate the effectiveness of planned teaching programme on renal calculi and
its management in terms of gain in knowledge in post test.
13
3. REVIEW OF LITERATURE
Literature review refers to the activities involved in searching for information
on a topic and developing a comprehensive picture of the state of knowledge in that
topic10.
An extensive review of literature relevant to the research study topic is
done to gain information and insight to build the foundation of the study. The literature
reviewed for the present study is organized and presented under the following headings.
Epidemiology and Socio Economical aspects of Renal Calculi
Urine and Serum Composition of Renal Calculi
Biochemical Evaluation of Renal Calculi
Risk Factors in Renal Calculi
Epidemiology and Socio Economical aspects of Renal Calculi
The following series of studies give empirical evidence of the etiology, risk
factors and factors influencing the type of calculi formed in different environment and
setting.
14
An epidemiological study was conducted on the occurrence of
urolithiasis in the 19th century population in Asia. For this study 250 quotations from 54
countries concerning 340,000 urinary stone were collected. The analogy was
demonstrated for age distributed, stone location, male-female ratio, and stone
composition. The distribution of urolithiasis is an underdeveloped country population is
defined by highest frequency in children, (>40%) bladder stone, 20% female patients,
40& calcium oxalate stone,(>30%) uric acid stone. Typical for a population in a
developed country the characteristic of urolithiasis are : highest frequency among adult,
(<10%) bladder stones, (>25%) female patients, (>60%) calcium oxalate stone, (<20%)
uric acid stone11.
The results of the above study showed that the distribution of calcium
oxalate stone in a low socioeconomical level population is less than that of high
socioeconomical status. The high protein is related with occurrence of uric acid stone.
On conclusion he said that increasing socioeconomical level was accompanied by the
following distribution of urolithiasis, decrease in bladder stone, decrease in phosphate
stone, decrease in uric acid stone, increase in female patients and increase in calcium
stone.
An exploratory study was conducted on epidemiological determinations
of urolithiasis in Germany. The study samples were 271 males and 160 females and the
age limits were 20-30 for males 30-40 for females. There was evidence of urolithiasis
in patients of 15.91% of the patients and in grandparents of 3.1% of patients. For
23.64% of patients, infection of the urinary system was determined and for 19.62%
hypertension. The gastrointestinal disturbances were found in 18.28% of the patients.
Salaried employees (24.41%), house wives, and manual workers formed the largest
15
group of samples (23.08%), as opposed to the public servants 10.9%, school children,
apprentices and students were 8.75%, pensioners 5.85%, and self employed 2.91%12.
A study conducted on epidemiology of urolithiasis in terms of seasonal
variation, occupation and lifestyle in Kuwait shows that a postal questionnaires were
sent out to 5,476 men (>18 yrs) selected at random from the electoral roll. Since all the
questions were not returned, a further random sample of 200 men was chosen from the
group and who did not reply to the questionnaire were interviewed by telephone. The
findings showed that twice the number of renal colic seemed to occur during the summer
months. Patients with a family history of urolithiasis were more likely to get a recurrence
than those without. A large population of stone patients was of sedentary occupation,
and there was a high incidence of urolithiasis seen among sailors than any other
people13.
A study reviewed the urolithiasis from the standpoint of analytical
epidemiology, which examined a statistical association between a given disease and a
hypothesized factor with an aim of interfering its causality. Factors included
epidemiologically for the stone formation included age, sex, occupation, social class,
season of the year, the climate, dietary and the fluid intake and the genetic
predisposition. Since some of the factors were interlinked they were broadly classified
into 5 categories and epidemiologically looked over. The environmental factors were
looked as more important than the genetic predisposition. A hot sunny climate was
considered to be influencing stone formation through inducing dehydration. With
increased perspiration increased solute consideration and decreased urine volume,
coupled with inadequate liquid intake and possibly through the exposure to the ultra
16
violet radiation, which eventually resulted in an increased vitamin D production. This
resulted in the excretion of calcium oxalate through urine. Excessive intake of coffee,
tea and alcoholic beverages seemingly increases the risk of calcium stone formation.
An increased level of animal protein and sugar intake and a decreased ingestion of
dietary fiber and green leafy vegetables were linked with the higher probability of
formation of renal stone14.
A study was conducted on Hyperoxaluria in patients with recurrent
calcium oxalate calculi: dietary and other risk factors. The aim of the study was to
identify recurrent stone formers with mild hyperoxaluria and to classify them further by
assessing their response to a low oxalaye diet. In addition, the prevalence of other risk
factors for stone formation in this group of patients was investigated. A total of 207
consecutive patients with recurrent renal calculi were screened and 40 (19%) were
found to have mild hyperoxaluria. Of these, 18(45%) responded to dietary oxalate
restriction by normalizing their urinary oxalate. The remaining 22 patients were
classified as having idiopathic hyperoxaluria and were subdivided into those in whom
urinary oxalate excretion was consistently elevated in all specimens measured and
those in whom the elevation was intermittent in nature. Dietary oxalate restriction had a
partially beneficial effect in lowering oxalate excretion in the patients with persistent
hyperoxaluria. No difference in urinary excretion was found after dietary restriction in
the patients with intermittent hyperoxaluria. Other risk factors, including dietary,
absorptive and renal hypercalciuria and hypo citraturia, were documented, the
prevalence of which (65%) was not significantly different from that (62.5%) found in
40 age- and sex-matched calcium stone formers without hyperoxaluria. The prevalence
17
of hyperuricosuria was significantly greater in patients with hyperoxaluria when
compared with stone controls15.
An exploratory survey study was conducted on prevalence of the
nephrolithiasis and its relation to the environmental risk factors including the nutrition,
a correlation had been demonstrated between activity of the renal stone disease and
excessive protein intake and the low fiber diet, and the cause and effect relationship had
been suggested between the prevalence of the disease and low urine volume due to
under hydration. Indeed too much meat and drinking alcohol even in a little amount
could cause the disease. Defective intestinal absorption of citrate and the modifications
in the protein substances, which inhibited the urinary crystallization, had also been
observed16.
An exploratory study was conducted to identify the epidemiology of
renal calculi and nutrition worldwide. In the prevalence and incidence it was found that
the majority of the patients with urolithiais were men and the prevalence was more
found in the industrialized countries (>10,000 patients). For identification of the
nutritional intake, 100 healthy subjects were fed two different standard diets, one being
a mixed diet and the other a ovo-lacto vegetarian diet, both the diet consisted of equal
amount of energy and fluid. The result showed that the consumption of the ovo-lacto
vegetarian diet resulted in a statistically significant increase in oxalate excretion (by
30% as compared to the mixed diet). The intake of vegetarian diet resulted in a
statistically significant 20.4% decrease in urinary calcium formation. The result of the
study also showed that a well balanced nutrition with consecutive high intake of fluid
leads to a significant decrease in the risk of urinary stone formation. The stone formers
18
showed no significant difference in magnesium and citrate excretion. The magnesium
excretion was <50mg/24hr. in 53.9% in both stone formers and normal subjects. The
citrate excretion was with in the normal range in all the persons. Sodium excretion was
very low in stone formers as compared to normal patients. The result suggests that
hyperuricosuria and hyperoxaluria with concomitant lower magnesium and sodium
excretion could be important determinants in the causation of the urinary calcium
disease, and the hyper calciuria appears to play a comparatively minor role in this17.
A study was conducted on Urine volume: stone risk factor and
preventive measure. Using the data available in literature and partly unpublished
personal research, they examine the role of urine volume as a stone risk factor, its
impact on calcium crystallization mechanisms and its real importance as means of
prevention. The most important findings of the study are (1) a low urine volume must
be considered as a real factor, both as regards the onset of renal calculi and stone
relapses; (2) an increase in urine volume induced by a high water intake produces
favorable effects on the crystallization of calcium oxalate and does not reduce the
activity of natural inhibitors; (3) a sufficiently high intake of water and probably other
fluids such as coffee, tea, beer and wine has a preventive effect on nephrolithiasis and
its recurrence, and (4) the role of fruit juice is still to be defined the study concluded
that a high intake of fluids, especially water, is still the most powerful and certainly the
most economical meansof prevention of nephrolithiasis, and it is often not used to
advantage by stone formers18.
Urine and Serum Composition of Renal Calculi
19
Renal calculi are generally composed of varieties of chemical
substances, bound together in intricate chemical bondage. This section of the reviewed
literature presents information about each type of renal calculi and the sources of those
chemicals, which contribute the formation of renal calculi.
An exploratory study was conducted on composition of the calcium
oxalate stone. The purpose of the study was to compare the urine composition in the
stone formers and the normal subjects, and thereby providing a bio-chemical basis for
selective prophylactic treatment in calcium oxalate stone formers. For the study 483
male and 226 female calcium stone formers and 100 normal male and 40 normal female
were selected and their urine was collected on an out-patient basis with normal dietary
and drinking habits. 24 hrs urine compositions was analyzed with respect to calcium,
oxalate, magnesium, citrate, urate and the inhibition of calcium oxalate crystal growth
rate. In the result of the study stone formers had an increased excretion rate of both
calcium and oxalate, where as magnesium and the urates did not separate stone formers
from that of the normal subjects. A large number of both male and female had a low
citrate excretion. The inhibition of calcium oxalate crystal growth was lower in males
but not in female patients. As a conclusion he said that by means of the analytical
programme of this design, it was possible to evaluate the stone formers from a
biochemical point of view19.
A study was conducted to determine the relevance of urinary citrate
measurement in management of patients with idiopathic calcium urolithiasis. They
selected a group of 83 normal persons and 120 patients with idiopathic calcium
urolithiasis (ICU), in an ambulatory setting age 20 – 70 yrs with uninfected urine,
20
normal renal function, and on no medication that might interfere with the citrate
excretion. In the result of the study it was seen that there was a significant co relation of
urinary citrate excretion with age in normal persons (9p<0.001) and no significant
correlation of urinary citrate excretion and age among patients with renal calculi.
Hypocitraturia (29.2%) was demonstrated in stone formers. In 15 of those 22 patients
one normal urinary citrate measurement was obtained, among them three patients had
both hypercalciuria and hypocitraturia. 24 of 35 hupocitraturia patients had a proven
intact urinary acidification mechanism. In their study they could not find any
relationship between the 24 hr urinary excretion of citrate and the severity of the stone
disease, or the frequency of the stone growth or new stone formation in the patients at
their follow up. The design of the study was comparative descriptive20.
The study was done on the effect of the calcium restricted diet of
urolithiasis patients on risk of kidney stone and the osteopenia. For the study 25
patients were randomly selected from 6 hospitals to form the experimental group. This
group had calcium restriction to 500 mg/day, oxalate rich foods are discouraged and
normalization of the animal protein and sodium was done for 1 month. In the result of
the urinary calcium excretion did not decrease significantly. The calcium restricted diet,
which was low in calcium, animal protein and the table salt due to omission of the dairy
products; it might have been beneficial for absorptive calciuria type II patients without
enhancing the risk of osteopaenia21.
Bio chemical Evaluation of Renal Calculi

21
Health assessment is an integral part of health care. The following
research studies present information about the number of bio chemical evaluation to be
done for early identification of recurrence and early management.
A study was conducted on the metabolic evaluation of patients with
recurrent nephrolithiasis. In this study he said that the primary goal of a metabolic
diagnostic evaluation was to identify as efficiently and economically as possible. The
particular physiological and environmental defects present in a given patient with
nephrolithiasis to enabled rational therapy of the stone disease. A multi channel blood
screen as well as voided urinary specimens for urine analysis was necessary for all the
patients with recurrent episodes of renal stones as well as for the patients with only one
incident of renal stone formation. It has been suggested that the excretion of various
stone forming substances might be impaired in the presence of urinary tract obstruction
by a renal or ureteral calculus. In addition one might expect similar alteration of urinary
function to exist after various techniques of stone removal. Therefore it is advisable to
postpone a complete diagnostic evaluation for one month after removal of the ureteral
obstruction or infection or after undergoing a stone removal procedure. This delay
allowed recovery of normal renal function as well as reinstitution of regular dietary
habits22.
A study was conducted to determine the number of times the bio
chemical evaluation has to be done after stone surgery and or its excretion through
urinary passage. A total of 16 women and 13 men aged 15 – 75 yrs were selected over a
6 months period on out patients’ basis, for the study. Urine (24 hrs) and blood
specimens were obtained while the patients were on their customary diet. Biochemical
22
evaluations were done two times for 29 out patients with calcium stone disease, the first
time within one month after surgical extraction or excretion of stones and the second
time after two months23.
The data for constituents other than urinary calcium were generally in
agreement for the two trials, and there were no significant difference when the results
were compared statistically (Student’s t-test) Classification of the etiologic basis for the
stone disease was the same after both tests in 27 patients. In the other two patients the
diagnosis was changed from renal to absorptive hypercalciuria. Both of these patients
had creatinine clearance rates less than 60% of normal during the first test. One also
had multiple residual stone during both the evaluations, and the second had an urinary
tract infection during the first test that resolved with a normal creatinine clearance by
the second test period. As conclusion they had emphasized that almost all patients
could be evaluated and placed in the management programme within a few weeks after
the surgery. If the work up could be done earlier, it would allow to initiate medical
management earlier and most important, improve patients’ compliance.
Risk Factors in Renal Calculi
There are many factors which are responsible for the formation of renal calculi. The
following research studies describe about some of the risk factors which may cause the
formation or the recurrence of renal calculi.
A study was conducted on drinking water quality and urolithiasis. The
case reports analysed for 1240 surgeries done over 35 years in the Bitola Yugoslavia.
23
Of the 1240 operations in that area 496 (60%) were done on kidneys, 228 (18.40%) on
ureters 462(37.25%) on bladder and 54 (4.35%) on urethra. The highest percentages of
surgeries were on kidney, and the renal stone numbered 58.40%. The investigation
showed that the right side was more affected than the left side and the male to female
ratio was 1:1.07 which was practically equal. They came in to a conclusion that the
mineral content of the drinking water had an influence on the etiology of the etiology of
the calcium oxalate urolithiasis, and it confirmed the hypothesis about soft drinking
water poor in calcium and magnesium and the high incidence and prevalence of
urolithiasis24.
An experimental study was conducted on effect of protein intake record
and dietary history in renal stone patients. For this study 20 renal stone patients and 20
patients for control group where selected and asked to make a 1 week retrospective
dietary recall and a prospective 4 days dietary record. The control people were selected
by the renal stone patients on the basis of equality in age, sex, occupation and social
conditions, but without a history of renal stone. Two 24 hr urine collection were made
for measurement of potential risk factors. The result showed that 4 days record of
dietary intake of protein, sodium, potassium and phosphate were positively correlated
to the urinary excretion of nitrogen, sodium, potassium and phosphate respectively.
Whereas dietary recall was not correlated to the urinary output. There was no difference
between stone formers and control group in the dietary intake of protein, purine,
carbohydrates, fat, calcium, phosphate, potassium or iron according to the record. The
control group had a 50% higher consumption of vitamin C and 15% higher fiber intake
than the stone formers. Stone formers seemed to consume 45% more alcohol than the
controls. Despite a tendency to lower calcium intake, stone formers had a higher
24
amount of urinary calcium (p<0.005), as well as sodium, phosphate and urate, than the
controls. As a conclusion they emphasized that the diet registration seems to be more
accurate than the diet recall. No major differences in diets of stone formers and controls
could be found except regarding the alcohol and fiber intake25.
A study was conducted on Hyperoxaluria in patients with recurrent
calcium oxalate calculi: dietary and other risk factors. The aim of the study was to
identify recurrent stone formers with mild hyperoxaluria and to classify them further by
assessing their response to a low oxalate diet. In addition, the prevalence of other risk
factors for stone formation in this group of patients was investigated. A total of 207
consecutive patients with recurrent renal calculi were screened and 40 (19%) were
found to have mild hyperoxaluria. Of these, 18 (45%) responded to dietary oxalate
restriction by normalizing their urinary oxalate, the remaining 22 patients were
classified as having idiopathic hyperoxaluria and were subdivided into those in whom
urinary oxalate excretion was consistently elevated in all specimens measured and
those in whom the elevation was intermittent in nature. Dietary oxalate restriction had a
partially beneficial effect in lowering oxalate excretion in the patients with persistent
hyperoxaluria. No difference in urinary oxalate excretion was found after dietary
restriction in the patients with intermittent persistent hyperoxaluria. Other risk factors,
including dietary, absorptive and renal hypercalciuria and hypocitraturia, were
documented, the prevalence of which (65%) was not significantly different from that
(62.5%) found in 40 age- and sex-matched calcium stone formers without
hyperoxaluria. The prevalence of hyperuricosuria was significantly greater in patients
with hyperoxaluria when compared with stone controls26.
25
A study was conducted on High Excretion of Uric acid combined with
high excretion of Calcium Links Kidney Stone Disease to familial hypertension
revealed that 34% of the patients with the combined abnormalities of hyperuricosuria
and hypercalciuria had a positive family history of hypertension, defined as 2 or more
first degree relatives with treated hypertension, that are significantly higher than in
patients with either “pure” hyperuricosuria (15%, P<0.02), “pure” hypercalciuria (8%,
P<0.001), or patients with “other” abnormality (10%, P<0.001). the adjusted result for
positive family history of hypertension in the “combined” abnormality group compared
to the control Kidney Stone Disease patients group was 5.6 (2.39 – 13.30). The
prevalence of hypertension in siblings of patients with the combined abnormality (13%)
was significantly higher than in siblings of patients either “pure” hyperuricosuria (3%,
P<0.001), “pure” hypercalciuria (1%, P<0.001), or siblings of control patients with
“other” abnormality(4%, P<0.001). the adjusted result for hypertension in siblings of a
patient with “combined” abnormality compared to a control Kidney Stone Disease
patient was 3.4 (1.97 – 5.91). patients in the “combined” abnor,ality group were also
characterized by significantly elevated urinary sodium, phosphorus, citrate and
potassium excretions27.
A study was conducted on Effect of Ascorbic Acid and consumption on
Urinary stone Risk factor. In the study a total of 12 normal subjects and 12 CaOx stone
formers underwent 2, 6-day phase of study while maintained on a controlled metabolic
diet. In each phase subjects ingested 1 gm Ascorbic Acid or an identical appearing
placebo twice daily. On the last 2 days of each phase 2, 24- hour urine collections were
analyzed for pH and stone risk factors, and blood specimens were submitted for serum
chemistry studies. The study concluded ingestion of 2 gm Ascorbic Acid results in no

26
change in urinary pH but a moderate though statistically significant increase in urinary
oxalate in normal subjects (20%) and stone formers (33%). Stone formers respond no
differently to Ascorbic Acid than normal subjects28.
SUMMARY
This chapter dealt with related literature for the study under the following headings
such as Epidemiology and Socio Economical aspects of Renal Calculi, Urine and
Serum Composition of Renal Calculi, Biochemical Evaluation of Renal Calculi and
Risk Factors in Renal Calculi
27
4. METHODOLOGY
Methodology of the research indicates the general pattern for organizing
the procedure for empirical study together with the method of obtaining valid and
reliable data for problem under investigation.
The methodology adapted for the study including research approach,
research design, setting of the study, population, sample technique, development and
description of the instruments for data collected, development of teaching programme,
procedure for data collection and plan for data analysis.
RESEARCH APPROACH
In order to achieve the objectives of the study en Evaluative Approach
was found to be appropriate and selected for the study.
RESEARCH DESIGN
The research design is the overall plan for obtaining answers to the
questions being studied and for handling some of the difficulties encountered during the
research process29.

28
The research design adopted for the present study was one group pre test
post testing. This design was adopted to assess the knowledge gain on renal calculi and
its management of patients with renal calculi following the administration of planned
teaching programme.
One group pre test post test design
Fig: 2 Schematic representation of the research design
01 : Pre test
X : Intervention (Planned teaching programme)
02 : Post test
Day 1 - Pre test
Day 1 - Intervention
Day 4 - Post test
Structured questionnaire to
assess the knowledge
Planned teaching
programme
Same as Day1 except the
intervention i.e. Planned
teaching programme
01 02 x
29
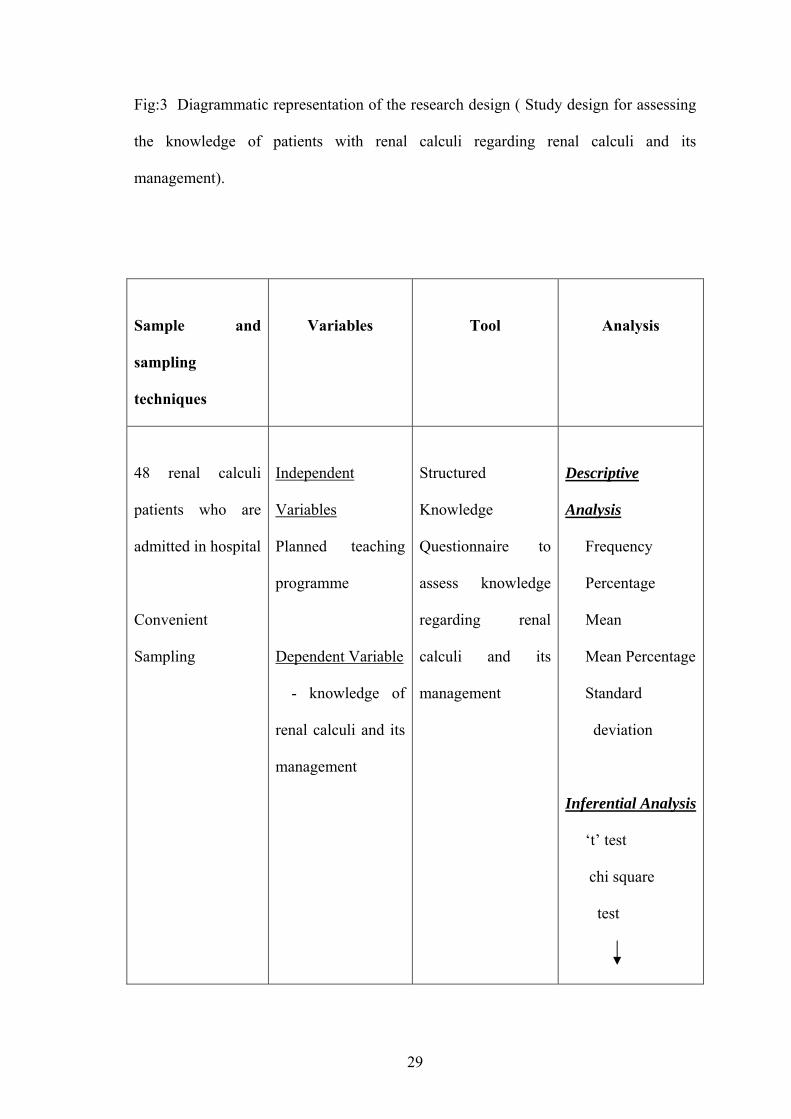
Fig:3 Diagrammatic representation of the research design ( Study design for assessing
the knowledge of patients with renal calculi regarding renal calculi and its
management).
Sample and
sampling
techniques
Variables
Tool
Analysis
48 renal calculi
patients who are
admitted in hospital
Convenient
Sampling
Independent
Variables
Planned teaching
programme
Dependent Variable
- knowledge of
renal calculi and its
management
Structured
Knowledge
Questionnaire to
assess knowledge
regarding renal
calculi and its
management
Descriptive
Analysis
Frequency
Percentage
Mean
Mean Percentage
Standard
deviation
Inferential Analysis
‘t’ test
chi square
test
30
Interpretation of
data
Fig: 4 Schematic representation of the study design
VARIABLES
Variables are qualities, properties or characteristics of person, things or
situation that change or vary30.
Independent Variable: Planned Teaching Programme
Dependent Variables: Knowledge about renal calculi and its management.
RESEARCH SETTING
The physical location and conditions in which data collection takes place
in a study31.
The study was conducted in A.J Hospital and Research Centre,
Mangalore in Karnataka State. The hospital has a urology department where all the
invasive and non invasive procedures are carry out. An average of 15 to 20 patients
with renal calculi is usually attending the urology OPD weekly. A free urology camp
for 45 days was conducted at the time of data collection.
POPULATION
31
The population is all elements (individuals, objects, or substances) that
meet certain criteria for inclusion in a study32.
In the present study, population consists of 48 patients who were
diagnosed to have renal calculi, admitted in A.J Hospital and Research Centre at the
time of data collected.
SAMPLE
A sample is a subset of the population that is selected for a particular
study, and the members of a sample are the subject30.
The sample of the study was the patients who were diagnosed to have
renal calculi and admitted in hospital.
SAMPLING TECHNIQUES
Sampling is a process of selecting subjects who are representative of the
population being studied30.
Convenience sampling, also called accidental sampling uses participants
who are easily accessible to the research and who meet the criteria o the study33.
Convenience sampling technique was adopted for this study. For the
study a convenient sample of 60 subjects was drawn from the study population on the
basis of criteria. There was a sample mortality of 12 patients with renal calculi for the
post test. Therefore the final sample consisted of 48 patients.

32
SAMPLE CRITERIA
Inclusive Criteria: Patients with renal calculi
who are admitted in the hospital
who know to read and write Kannada or English
who are willing to participate
who are above 20 years of age
Exclusive Criteria: Patients
from medical and paramedical profession
with past history of renal calculi
DATA COLLECTION INSTRUMENT
Structured Knowledge Questionnaire about renal calculi and its
management was used to assess the knowledge of patient with renal calculi.
DEVELOPMENT OF THE TOOL
Data collection tools are the procedures or instruments used by the
researchers to observe or measure the key variables in the research problem34. The
present study aimed to evaluate the effect of planned teaching programme on renal
calculi and its management. So structured knowledge questionnaire was developed as
the tool to collect data.

33
PREPARATION OF BLUE PRINT
A blue print was prepared with the objectives keeping in mind. It
depicted the distribution of items according to knowledge, comprehension and
application. The domains were anatomy and physiology of urinary system, causes,
clinical manifestations, management and prevention of recurrence of urinary stone.
TESTING OF THE INSTURMENT
CONTENT VALIDITY OF THE TOOL
Content Validity concerns the degree to which an instrument has an
appropriate sample of items for the construct being measured.
The Structured Knowledge Questionnaire, along with objectives and
blueprint was submitted to thirteen experts, five from the field of Nursing, three from
Consultant Urologists, two from surgeons, two from General Medicine Physicians and
one from the field of Food, Nutrition and Dietetic Department. There were 35 items in
the tool. There were 100% agreement for 30 items, and 84.62% of the four items were
given suggestion to reframe the stem. One item (80.2%) had suggested to delete
because it was beyond the level of understanding of the lay people. As this was found
relevant and meaningful, the necessary modification was made and the total number of
item was reduced to 34. The tool was translated in kannada and translated back to
English.
PRETESTING OF THE TOOL
34
Pretesting is the process of measuring effectiveness of an instrument.
The purpose is to reveal the problem relating to answering, completing and returning
the instrument and to point out weakness in the administration, organization and
distribution of the instrument35.
For the pretesting, modified version of the tool in English, Kannada was
carried out in Prabhu Hospital, Moodbidri. Ten patients who met the criteria were
selected. The respondents found the language of the questionnaire simple and
understandable. The average time taken to complete the tool was 15 to 22 minutes and
was acceptable to the subjects.
RELIABILITY OF THE TOOL
Reliability of an instrument is concerned with how consistently the
measurement technique measures the concept of interest30.
For reliability, the tool was administered to 20 renal calculi patients who
fulfilled the sampling criteria. Respondents did not find any difficulty in understand
and answering the questions.
The reliability coefficient of the tool was calculated using split half
method by Spearman’s Brown Formula. The reliability of the tool was found to be 0.84
which was statistically significant. This indicates that the tool was reliable.
DESCRIPTION OF THE FINAL TOOL
Structured Knowledge Questionnaire was used to assess the knowledge
of renal calculi patients regarding renal calculi and its management.
35
There were two tools used for the study, which are follows.
TOOL 1: Background Variables, which included 16 items such as name, age,
sex, address, hospital number, educational background, marital
status, occupational status, per capita income in rupees, religion,
food habits, information regarding the medical help taken before,
number of hospital admission before, formation of having similar
disease in their family and sources of their health information
regarding their disease condition.
TOOL 2: consists of 34 close ended questions to assess the knowledge of
renal calculi patients regarding renal calculi and its management.
The maximum score of each item was 1 and the minimum score was 0
and the total score was 34. The score was categorized on arbitrary basis as follows.
0 – 11 = Poor
12 – 23 = Average
24 – 34 = Good
PLANNED TEACHING PROGRAMME
Teaching programme is a guide for the teacher because it helps to cover the
topics comprehensively with proper sequence of points and without missing anything36.
The steps to prepare the teaching plan are
1. framing the outline of the teaching plan
2. framing the outline of the content
36
3. deciding methods of instruction and audio-visual aids
4. evaluation of the teaching plan
1. Framing the outline of the teaching plan
The outline on the basis of the teaching plan was framed. This includes
setting of the general and the specific objectives, specifying the place,
learners, duration of the session.
2. Framing the outline of the content
The content of the teaching plan included topics on renal calculi and its
management. It was explained under various heading such as anatomy and
physiology of urinary system, causes of urinary stone, clinical features of
urinary stone, management of urinary stone and prevention of recurrence of
urinary stone.
3. Deciding methods of instruction and audio-visual aids
The methods of instruction adopted was lecture cum discussion, visual aids
like charts, pamphlets on renal calculi and its management, booklets were
also given to each subject.
4. Evaluation of the teaching plan
Evaluation of the teaching plan was done by content validity, which was
ascertained by consulting experts in the fields of nursing, medicine and
Food, Nutrition and Dietatic Department. Details of the content validity is
enclosed in page no. 32.
37
PILOT STUDY
A pilot study is a small preliminary investigation, which has the same
general character on the main study35.
The pilot study was carried out at Alva’s Health Centre, Moodbidri
from 12th – 25th November, 2004. Written permission was obtained from the authority
before conducting the pilot study. Based on the predetermined criteria set by the
investigator through convenient sampling, pilot study was conducted on ten renal
calculi patients after taking written content from them. The subjects were informed
about the purpose of the study and requested to complete the questionnaire.
After obtaining data from renal calculi patients related to renal calculi,
planned teaching was given to them. Visual aids were used to facilitate understanding.
The time spent for teaching was 50 – 60 minutes. Pamphlets on renal calculi and its
management were distributed to the subjects. On 4th day of the planned teaching, post
test was given by administering the same pretest questionnaire. Statistical analysis of
the pilot study reveals that there was significant difference between pretest knowledge
and posttest knowledge of renal calculi patients on renal calculi and its management.
Time taken for pretest was 15 – 22 minutes and for posttest were 13 – 20 minutes.
DATA COLLECTION PROCEDURE
The final data collection was done from A.J Hospital and Research Centre,
Mangalore. Formal written permission was obtained from the Medical Director of the
hospital.
38
The data was collected from 60 renal calculi patients who were admitted in the
hospital and met the study criteria. Subjects were asked to participate in the study after
self-introduction by the investigator. The patients were informed the purpose of the
study and the consent was taken from them. Pre test was administered to each patient
on various day followed by teaching programme. Charts, pamphlets and booklet were
used to facilitate understanding of the teaching. The teaching was carried out in their
ward of the patients and the duration of the teaching was 50 – 60 minutes.
The method of instruction adopted was lecture cum discussion. After the
teaching session, patients were asked about the doubt and clarified them.
Post test was conducted using the same questionnaire on the fourth day of
teaching. There were twelve subjects mortality and the final sample was forty eight.
PLAN FOR DATA ANALYSIS
The investigator planned to analyze data by using both descriptive and
inferential statistics.
SUMMARY
This chapter dealt with the research approach, research design, setting of the
study, population, sample, sampling technique, development of the tool, method of data
collection, development of lesson, evaluation of the effectiveness of planned teaching
programme, plan for analysis of data and presentation.
39
5. RESULTS
This part deals with analysis and interpretation of data collected from 48
renal calculi patients to find out the effectiveness of Planned Teaching Programme and
association with selected demographic variables.
Master data sheet was prepared and the data was analyzed based on the
objectives and hypothesis, using descriptive and inferential statistics.
OBJECTIVES OF THE STUDY
1. To determine the pre test knowledge of the renal calculi patients regarding renal
calculi and its management.
2. To plan and validate the planned teaching programme on renal calculi and its
management for the patients with renal calculi.
3. To evaluate the effectiveness of planned teaching programme on renal calculi
and its management in terms of gain in knowledge in post test.
HYPOTHESES
The following hypotheses will be tested at 0.05 level of significance.
H1: The mean post test knowledge score of the patients with renal calculi on renal
calculi and its management will be significantly higher than the mean pre-test
knowledge scores, as measured by a structured knowledge questionnaire.

40
H2: There will be significant association between the pre test knowledge scores
and the selected variables.
ORGANIZATION OF THE STUDY FINDINGS
The data was presented under the following headings.
Section I : Sample Characteristics
Section II : Validation of Planned Teaching Programme
Section III : Evaluation of Planned Teaching Programme in terms of gain in
knowledge scores.
Section IV : Significance of difference between the mean pretest and posttest
knowledge scores.
Section V : Association between the pretest knowledge and selected demographic
variables.
Section I : Sample characteristics
This section deals with the characteristics of the patients with renal calculi in
terms of frequency and percentage.
41
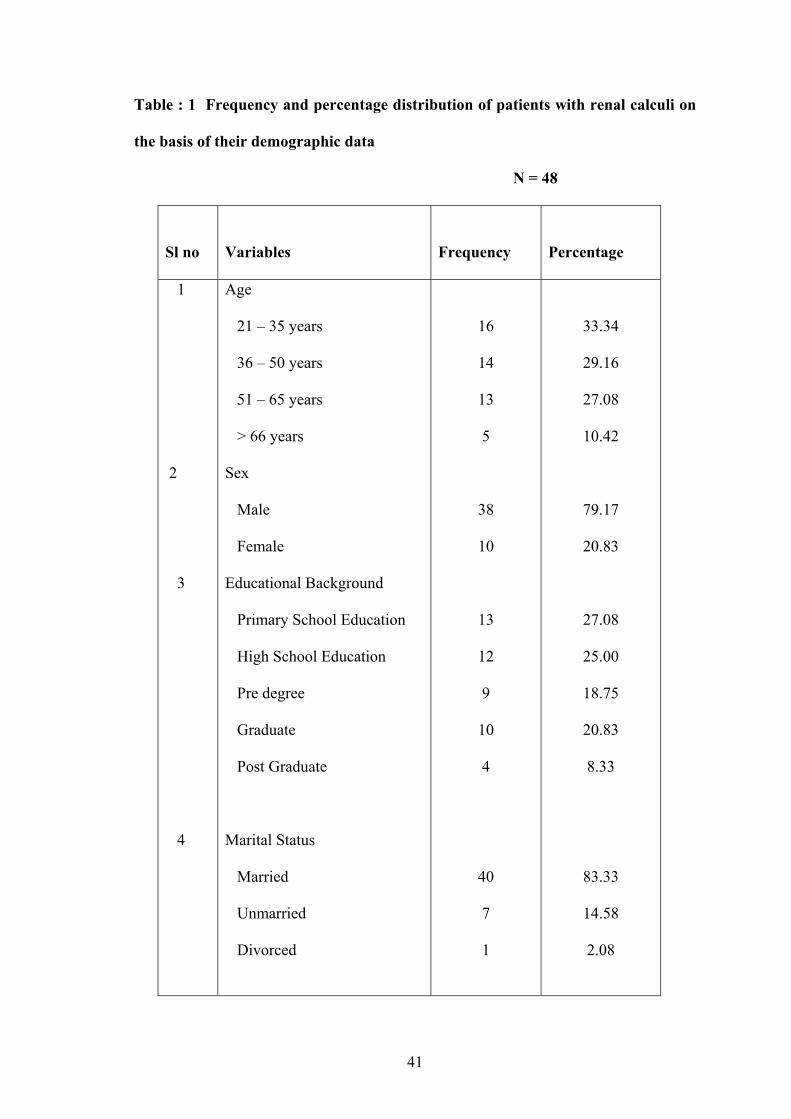
Table : 1 Frequency and percentage distribution of patients with renal calculi on
the basis of their demographic data
N = 48
Sl no
Variables
Frequency
Percentage
1
2
3
4
Age
21 – 35 years
36 – 50 years
51 – 65 years
> 66 years
Sex
Male
Female
Educational Background
Primary School Education
High School Education
Pre degree
Graduate
Post Graduate
Marital Status
Married
Unmarried
Divorced
16
14
13
5
38
10
13
12
9
10
4
40
7
1
33.34
29.16
27.08
10.42
79.17
20.83
27.08
25.00
18.75
20.83
8.33
83.33
14.58
2.08
42
5
6
7
8
Occupational Status
Coolie
Agriculture
Beedi Worker
House Wife
Business
Any other
Student
Teacher
Driver
Bank Employee
Government Employee
Per Capita Income in Rupees
1 – 1500
1501 – 3000
3001 – 4500
>4501
Religion
Hindu
Muslim
Christian
Dietary Pattern
Vegetarian
Non-vegetarian
3
9
1
5
12
5
4
2
3
4
7
16
12
13
33
9
6
7
41
6.25
18.75
2.08
10.42
25.00
10.42
8.33
4.17
6.25
8.33
14.58
33.34
25.00
27.08
68.75
18.75
12.5
14.58
85.42
43
9
10
11
12
13
Previous hospital Admission
Yes
No
Number of Previous Hospital Admission One time Two times Three times Any Family History of Renal
Calculi
Yes
No
Sources of health information
on the disease condition
Doctor
Relatives
Friends
Any other
Any following habit(s)
Smoking
Betal leaves chewing
Alcohol
None of the above
6
42
2
3
1
4
44
44
2
1
1
10
8
3
32
12.5
87.5
4.17
6.25
2.08
8.33
91.67
91.67
4.17
2.08
2.08
20.83
16.66
6.25
68.75

44
Data presented in Table 1 depict the distribution of sample according to
Age, Gender. Educational background, Marital status, Occupational status, Per capita
income in rupees, Religion, Dietary pattern, Previous hospital admission, Number of
hospital admission, Family history of renal calculi, Sources of health information and
Habit.
Age
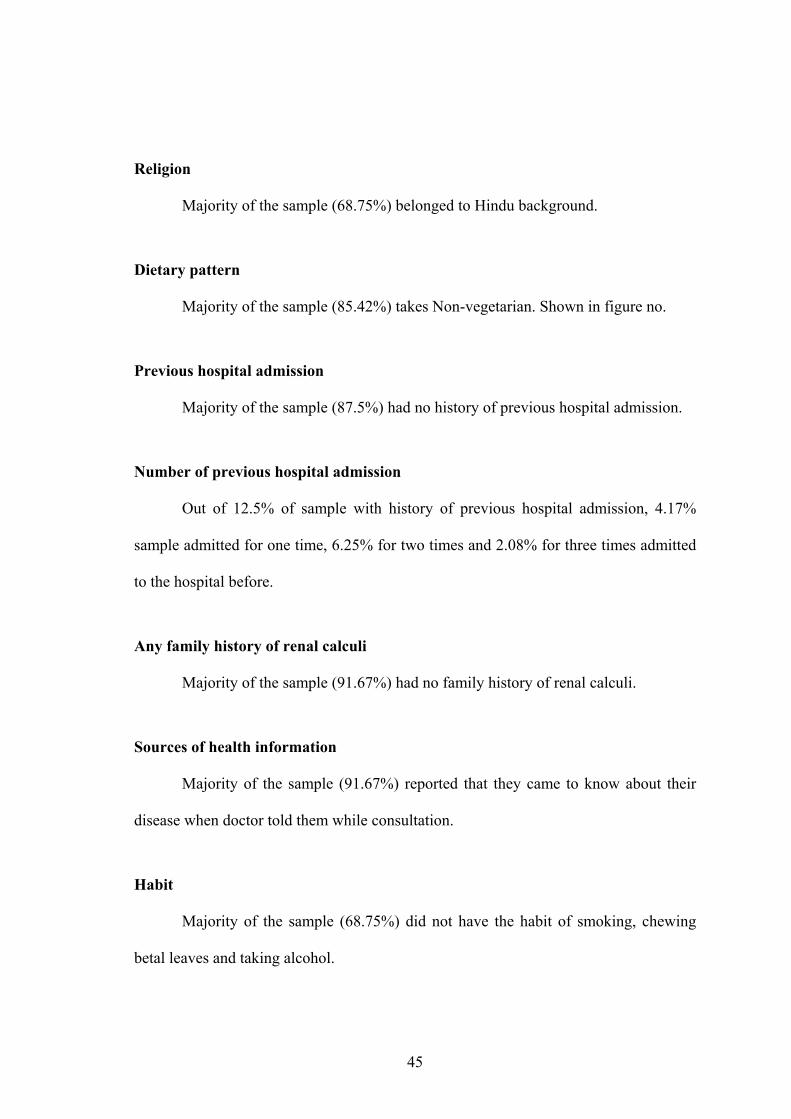
Majority of the sample ( 33.34%) belonged to age group 21 – 35 years.
Gender
Majority of the sample (79.17%) were male. Shown in figure no.
Educational background
Maximum number of the sample (27.08%) was having Primary School
Education.
Marital status
Majority of the sample (83.33%) were married.
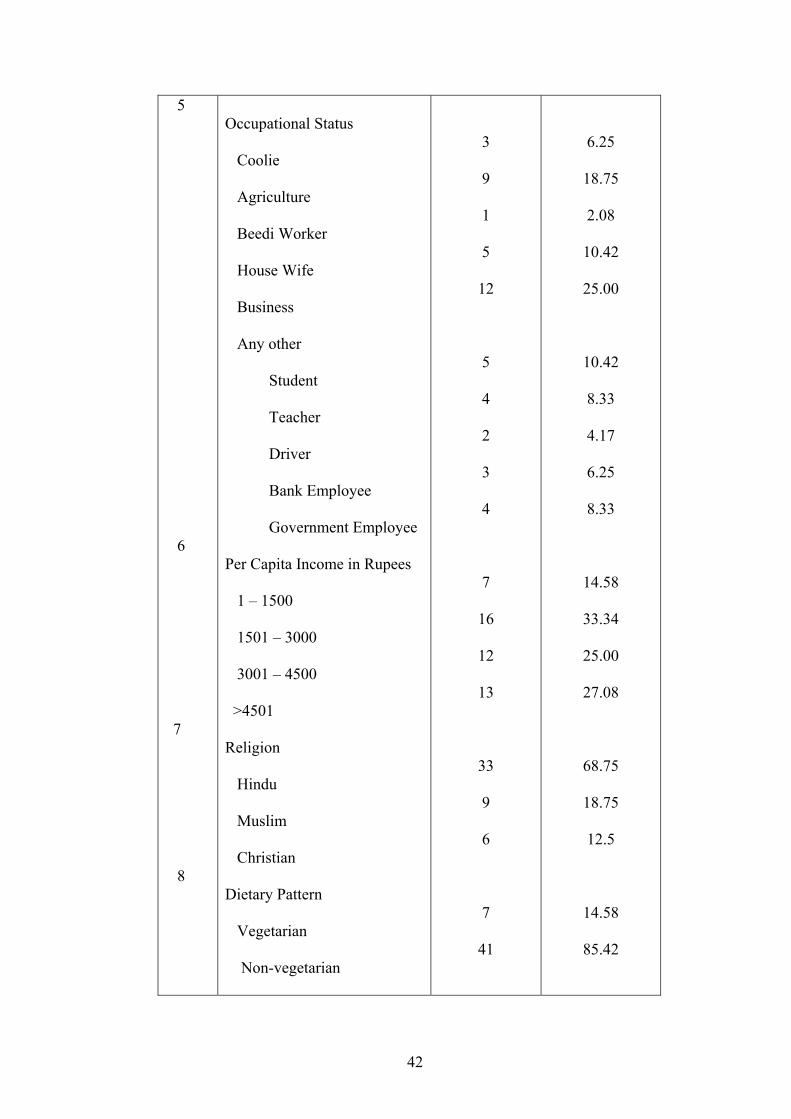
Occupational status
Majority of the sample (25%) were doing business.
Per capita income in rupees
Greater percentage of sample (25%) had family income of Rs 1501 – 3000.
45
Religion
Majority of the sample (68.75%) belonged to Hindu background.
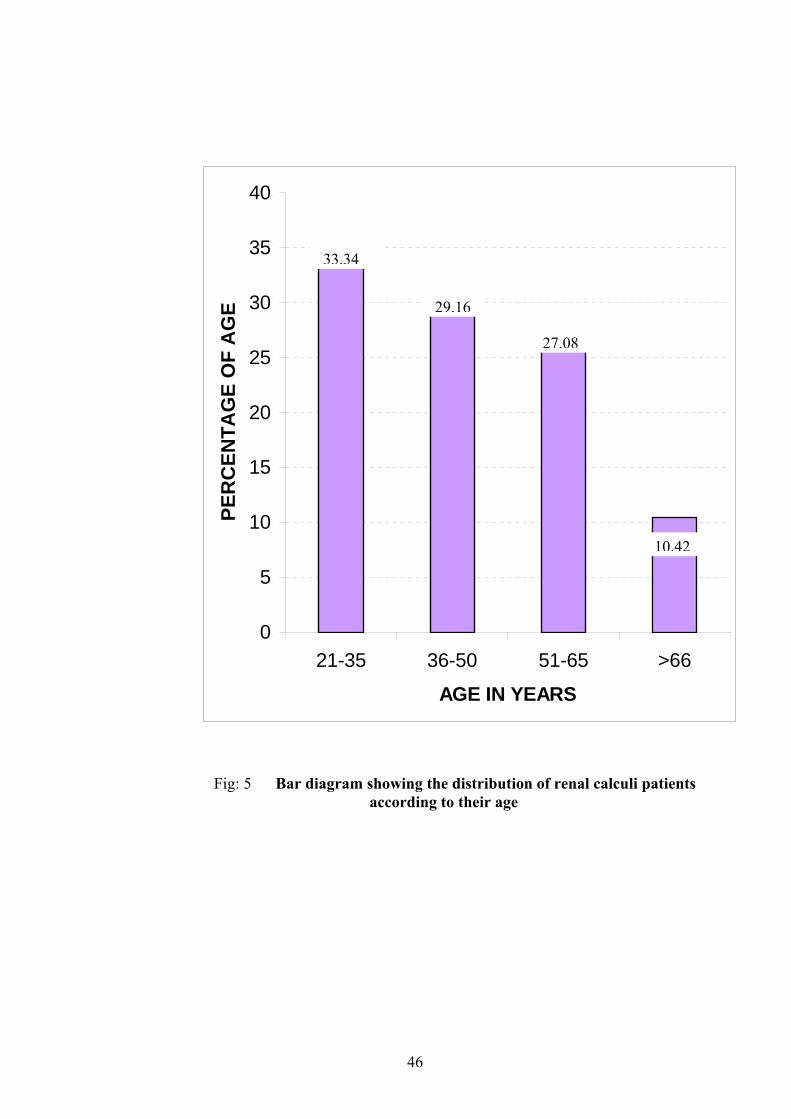
Dietary pattern
Majority of the sample (85.42%) takes Non-vegetarian. Shown in figure no.
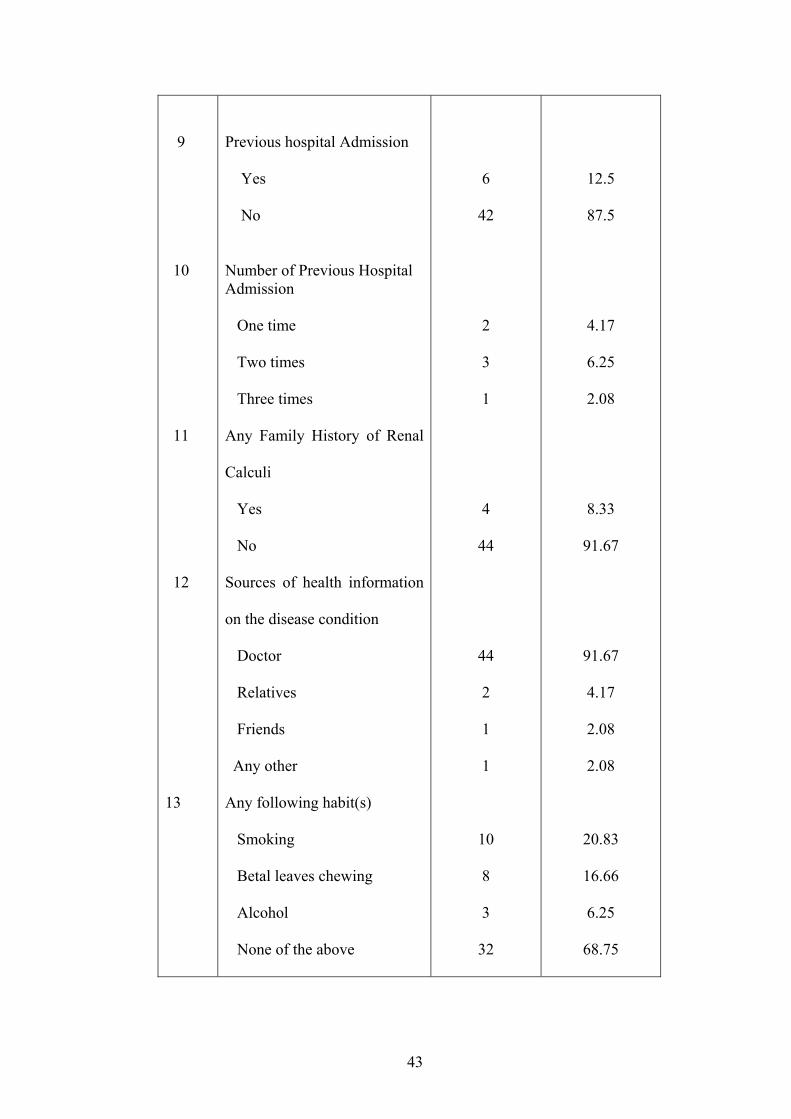
Previous hospital admission
Majority of the sample (87.5%) had no history of previous hospital admission.
Number of previous hospital admission
Out of 12.5% of sample with history of previous hospital admission, 4.17%
sample admitted for one time, 6.25% for two times and 2.08% for three times admitted
to the hospital before.
Any family history of renal calculi
Majority of the sample (91.67%) had no family history of renal calculi.
Sources of health information
Majority of the sample (91.67%) reported that they came to know about their
disease when doctor told them while consultation.
Habit
Majority of the sample (68.75%) did not have the habit of smoking, chewing
betal leaves and taking alcohol.
46
Fig: 5 Bar diagram showing the distribution of renal calculi patients according to their age
0
5
10
15
20
25
30
35
40
21-35 36-50 51-65 >66
AGE IN YEARS
PER
CEN
TAG
E O
F A
GE
10.42
27.08
29.16
33.34

47
Fig: 6 Pie diagram showing distribution of renal calculi patients according to gender
FemaleMale
79.17%
20.83%
48
Fig:7 Pie diagram showing distribution of renal calculi patients according to their dietary pattern
VegetarianNon-vegetarian
85.42%
14.58%
49
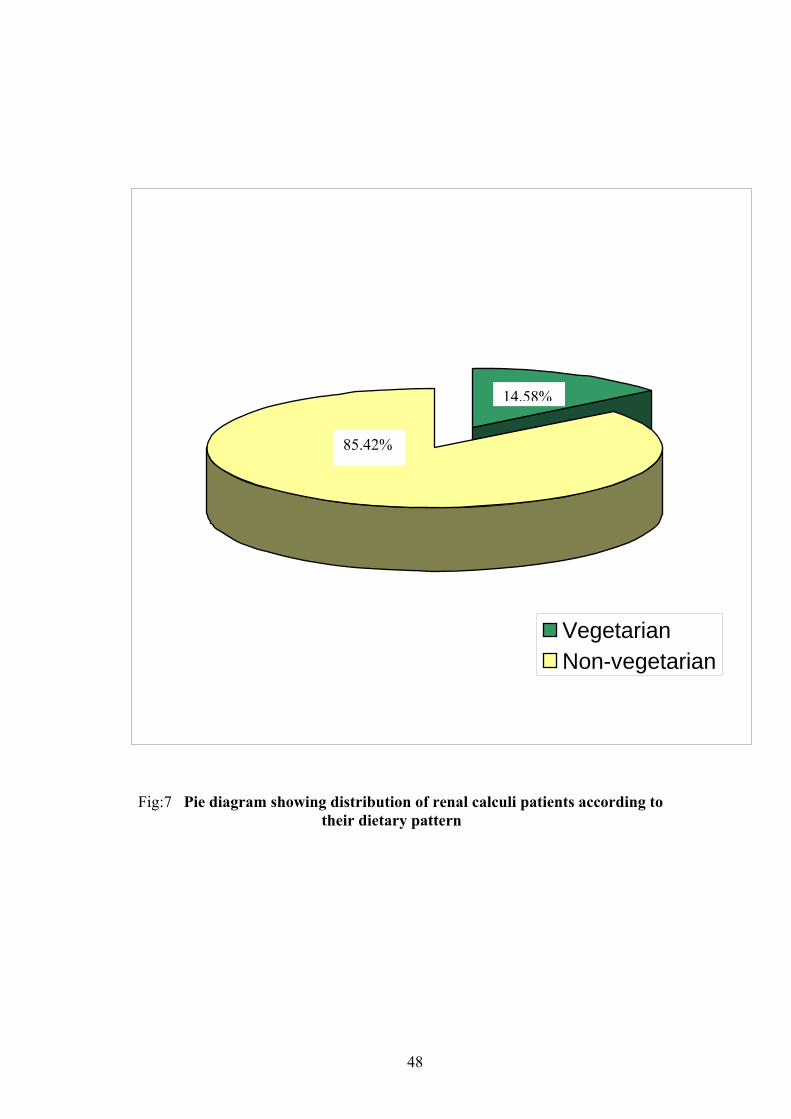
Section II Validation of Planned Teaching Programme
The Planned Teaching Programme on Renal Calculi and its Management
developed by the investigator was validated by thirteen experts. The percentage of
agreement and suggestions are given below.
Table 2: Percentage of agreement by experts on areas of planned teaching
programme in percentage and frequency
N = 48
Agree Disagree Sl
No
Area Frequency % Frequency %
Suggestion
Action
Taken
1 Objectives 13 100 ------ --- No
suggestion
No action
taken
2 Selection and
Organization
of Content
13 100 ------ --- Provides
adequate
information
No action
taken
3
Language
Used
13 100 ----- ---
No
suggestion
No action
taken
4 Feasibility 13 100 ----- --- Feasible No action
taken
5 Practicability 13 100 ----- --
-
No
suggestion
No action
taken
50
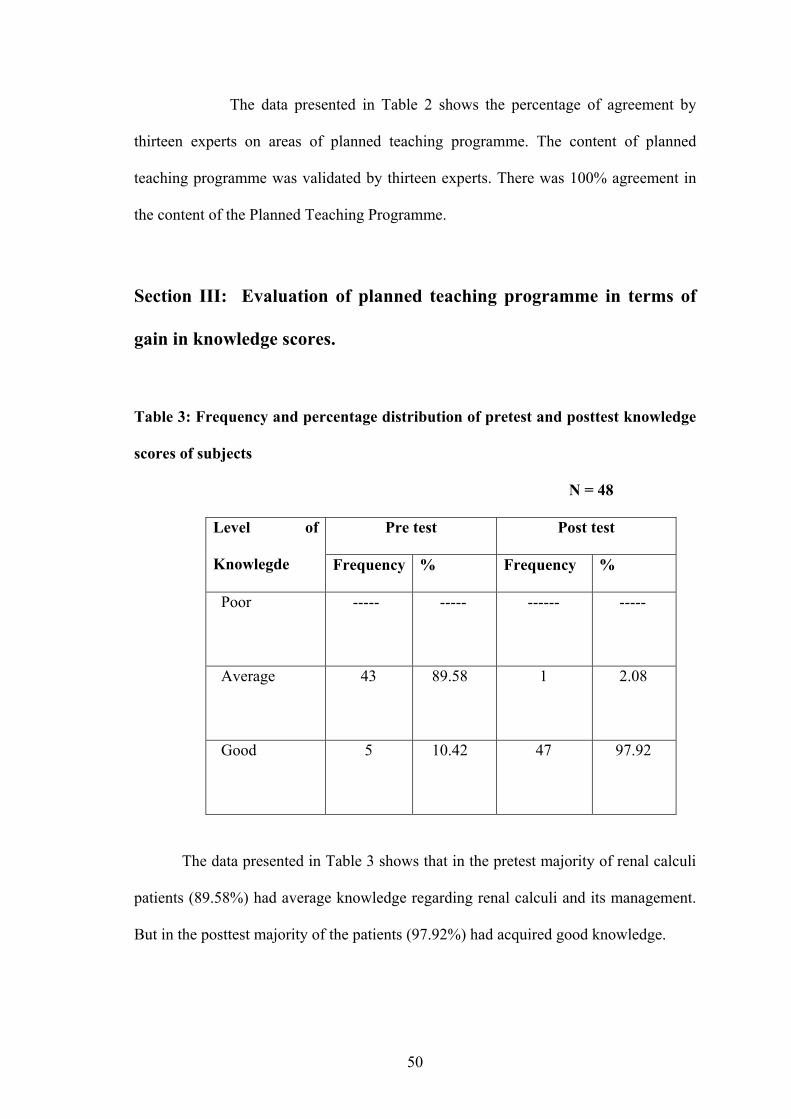
The data presented in Table 2 shows the percentage of agreement by
thirteen experts on areas of planned teaching programme. The content of planned
teaching programme was validated by thirteen experts. There was 100% agreement in
the content of the Planned Teaching Programme.
Section III: Evaluation of planned teaching programme in terms of
gain in knowledge scores.
Table 3: Frequency and percentage distribution of pretest and posttest knowledge
scores of subjects
N = 48
Pre test Post test Level of
Knowlegde Frequency % Frequency %
Poor ----- ----- ------ -----
Average 43 89.58 1 2.08
Good 5 10.42 47 97.92
The data presented in Table 3 shows that in the pretest majority of renal calculi
patients (89.58%) had average knowledge regarding renal calculi and its management.
But in the posttest majority of the patients (97.92%) had acquired good knowledge.
51
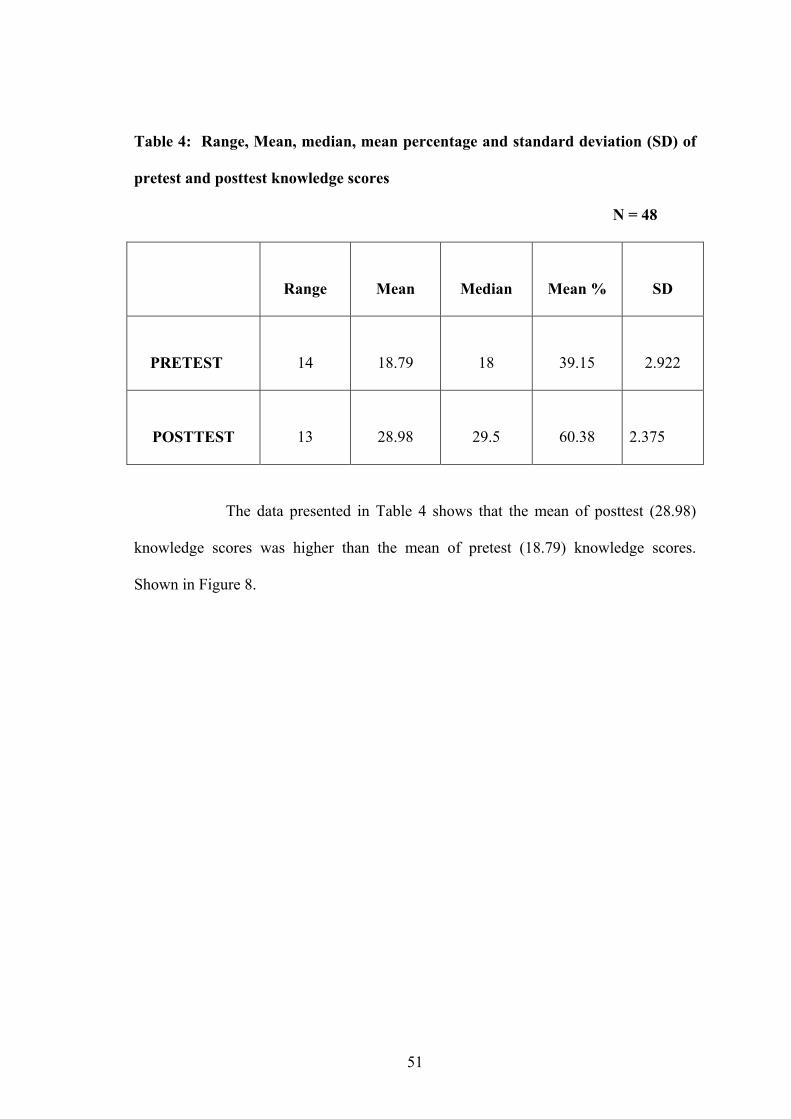
Table 4: Range, Mean, median, mean percentage and standard deviation (SD) of
pretest and posttest knowledge scores
N = 48
Range
Mean
Median
Mean %
SD
PRETEST
14
18.79
18
39.15
2.922
POSTTEST
13
28.98
29.5
60.38
2.375
The data presented in Table 4 shows that the mean of posttest (28.98)
knowledge scores was higher than the mean of pretest (18.79) knowledge scores.
Shown in Figure 8.

52
0123456789
10111213141516171819202122
14-16 16-18 18-20 20-22 22-24 24-26 26-28 28-30 30-32 32-34 34-36
KNOWLEDGE SCORES
FREQ
UEN
CY
18
18.79 28.98
29.9
PRETEST POSTTEST
12-1410-12
Fig: 8 Frequency polygon showing the mean and median of knowledge scores of
patients with renal calculi in pretest and posttest
----- Mean ----- Median
53
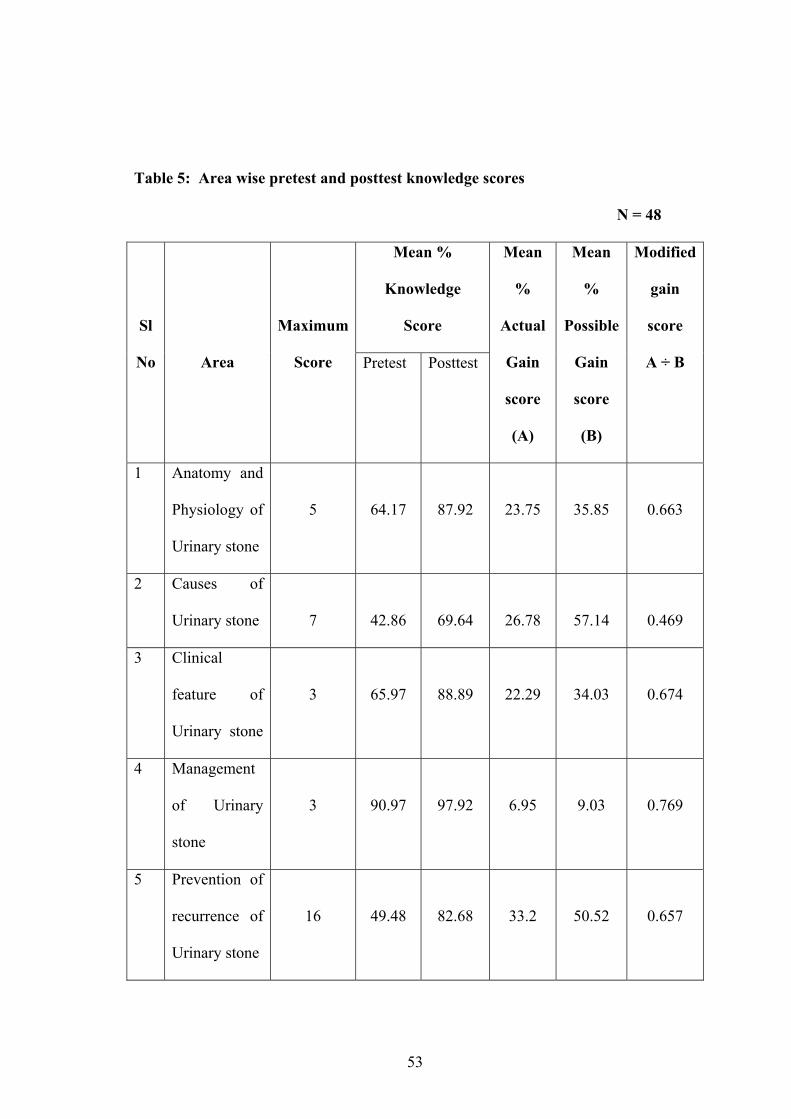
Table 5: Area wise pretest and posttest knowledge scores
N = 48
Mean %
Knowledge
Score
Sl
No
Area
Maximum
Score Pretest Posttest
Mean
%
Actual
Gain
score
(A)
Mean
%
Possible
Gain
score
(B)
Modified
gain
score
A ÷ B
1 Anatomy and
Physiology of
Urinary stone
5
64.17
87.92
23.75
35.85
0.663
2 Causes of
Urinary stone
7
42.86
69.64
26.78
57.14
0.469
3 Clinical
feature of
Urinary stone
3
65.97
88.89
22.29
34.03
0.674
4 Management
of Urinary
stone
3
90.97
97.92
6.95
9.03
0.769
5 Prevention of
recurrence of
Urinary stone
16
49.48
82.68
33.2
50.52
0.657
54
The data presented in Table 5 shows that maximum gain was in the
area of management of urinary stone (0.769), second highest in the area of clinical
feature of urinary stone (0.674), third highest in the area of anatomy and physiology of
urinary system (0.663), fourth highest in the area of prevention of recurrence of urinary
stone (0.657) and the last highest is in the area of causes of urinary stone (0.469) as
indicated by modified gain score. The data further indicate that the posttest mean
percentage knowledge score in all content areas were higher than the pretest mean
percentage knowledge scores. The maximum gain was in the area of management of
urinary stone (97.92%), followed by area of clinical feature of urinary stone (88.89%),
area of anatomy and physiology of urinary stone (87.92%), area of prevention of
recurrence of urinary stone (82.68%) and area of causes of urinary stone (69.64%).
Modified gain score is a ratio of the amount actually learnt to the
amount that could possibly have been learnt. The difference between the mean pretest
and posttest percentage score indicates the actual gain. The possible gain is obtained by
subtracting mean pretest percentage score from 100.
To calculate the modified gain scores the mean score on the pretest as
well as the posttest is calculated followed by dividing the actual gain with the possible
gain which indicates that the gain in knowledge relative to the possible gain. Modified
gain score was calculated to adjust the achievement variable for a effect which would
predict that areas having low pretest scores would demonstrate greater amount of gain
than areas having high pretest scores.
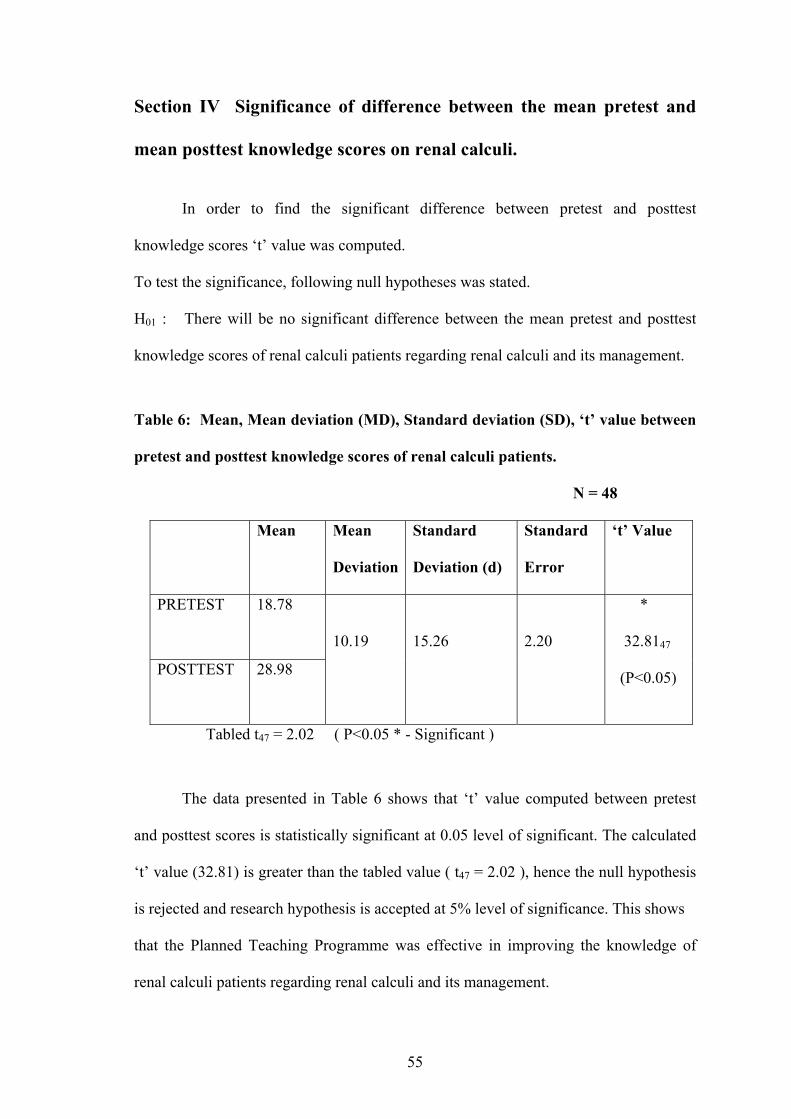
55
Section IV Significance of difference between the mean pretest and
mean posttest knowledge scores on renal calculi.
In order to find the significant difference between pretest and posttest
knowledge scores ‘t’ value was computed.
To test the significance, following null hypotheses was stated.
H01 : There will be no significant difference between the mean pretest and posttest
knowledge scores of renal calculi patients regarding renal calculi and its management.
Table 6: Mean, Mean deviation (MD), Standard deviation (SD), ‘t’ value between
pretest and posttest knowledge scores of renal calculi patients.
N = 48
Mean Mean
Deviation
Standard
Deviation (d)
Standard
Error
‘t’ Value
PRETEST
18.78
POSTTEST
28.98
10.19
15.26
2.20
*
32.8147
(P<0.05)
Tabled t47 = 2.02 ( P<0.05 * - Significant )
The data presented in Table 6 shows that ‘t’ value computed between pretest
and posttest scores is statistically significant at 0.05 level of significant. The calculated
‘t’ value (32.81) is greater than the tabled value ( t47 = 2.02 ), hence the null hypothesis
is rejected and research hypothesis is accepted at 5% level of significance. This shows
that the Planned Teaching Programme was effective in improving the knowledge of
renal calculi patients regarding renal calculi and its management.
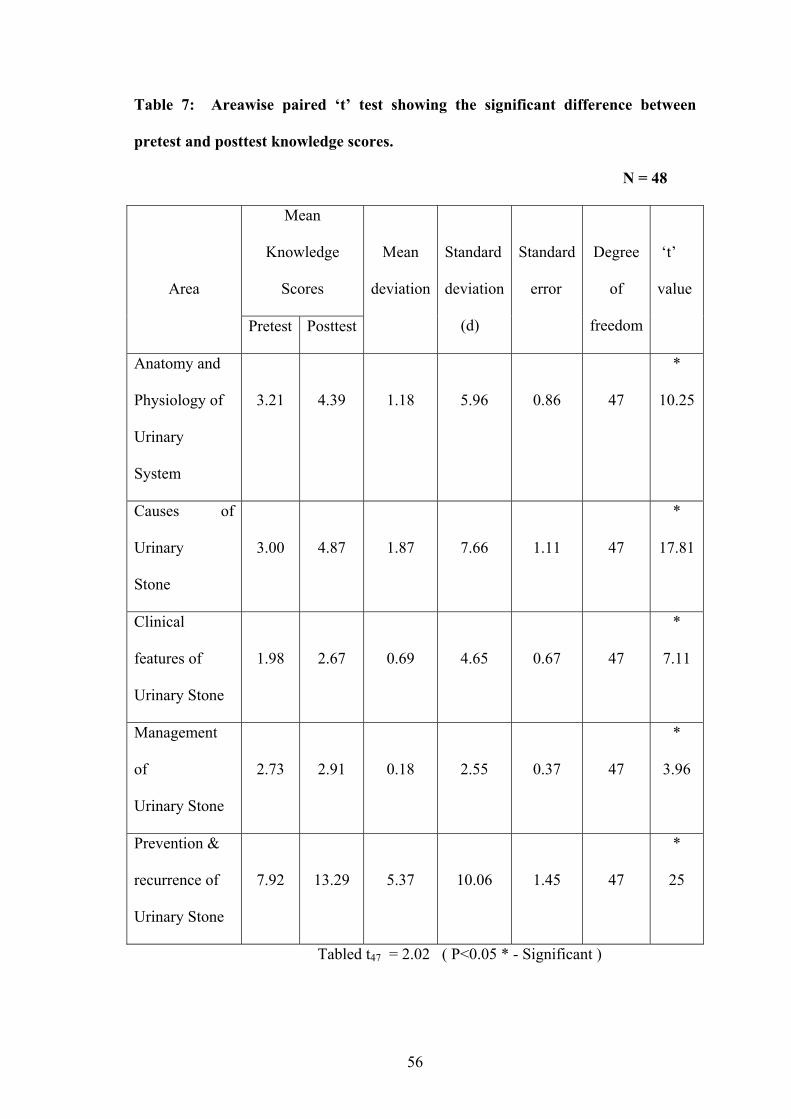
56
Table 7: Areawise paired ‘t’ test showing the significant difference between
pretest and posttest knowledge scores.
N = 48
Mean
Knowledge
Scores
Area
Pretest Posttest
Mean
deviation
Standard
deviation
(d)
Standard
error
Degree
of
freedom
‘t’
value
Anatomy and
Physiology of
Urinary
System
3.21
4.39
1.18
5.96
0.86
47
*
10.25
Causes of
Urinary
Stone
3.00
4.87
1.87
7.66
1.11
47
*
17.81
Clinical
features of
Urinary Stone
1.98
2.67
0.69
4.65
0.67
47
*
7.11
Management
of
Urinary Stone
2.73
2.91
0.18
2.55
0.37
47
*
3.96
Prevention &
recurrence of
Urinary Stone
7.92
13.29
5.37
10.06
1.45
47
*
25
Tabled t47 = 2.02 ( P<0.05 * - Significant )

57
The data presented in Table 7 shows that ‘t’ value computed between
pretest and posttest knowledge scores for each area is statistically significant ( t47 =
2.02, P<0.05 ). The maximum difference was in the area of prevention and recurrence
of urinary stone (20) followed by the area of Causes of urinary stone (17.81), Anatomy
and Physiology of urinary system (10.25), Clinical features (7.11) and Management of
urinary stone (3.96).
Section V: Association between pretest knowledge scores and
demographic variables – age, gender, per capita income of the family
and dietary pattern.
To test the association following hypothesis was stated and tested using chi-square.
H02 : There is no significant association between pretest knowledge scores and selected
demographic variables – age, gender, per capita income of the family and dietary
pattern.
Chi-square was computed in order to determine the significance of
association between Pretest Knowledge Scores with demographic variables – age,
gender, per capita income of the family and dietary pattern.
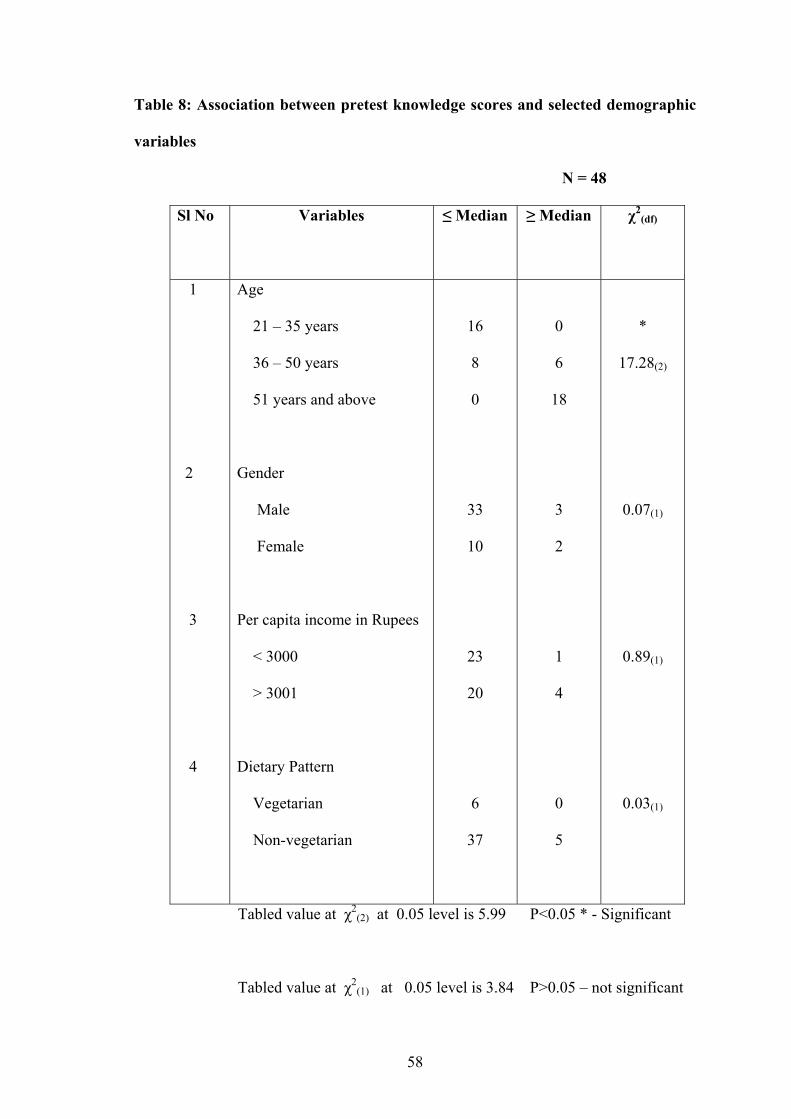
58
Table 8: Association between pretest knowledge scores and selected demographic
variables
N = 48
Sl No
Variables ≤ Median ≥ Median χ2(df)
1
2
3
4
Age
21 – 35 years
36 – 50 years
51 years and above
Gender
Male
Female
Per capita income in Rupees
< 3000
> 3001
Dietary Pattern
Vegetarian
Non-vegetarian
16
8
0
33
10
23
20
6
37
0
6
18
3
2
1
4
0
5
*
17.28(2)
0.07(1)
0.89(1)
0.03(1)
Tabled value at χ2(2) at 0.05 level is 5.99 P<0.05 * - Significant
Tabled value at χ2(1) at 0.05 level is 3.84 P>0.05 – not significant
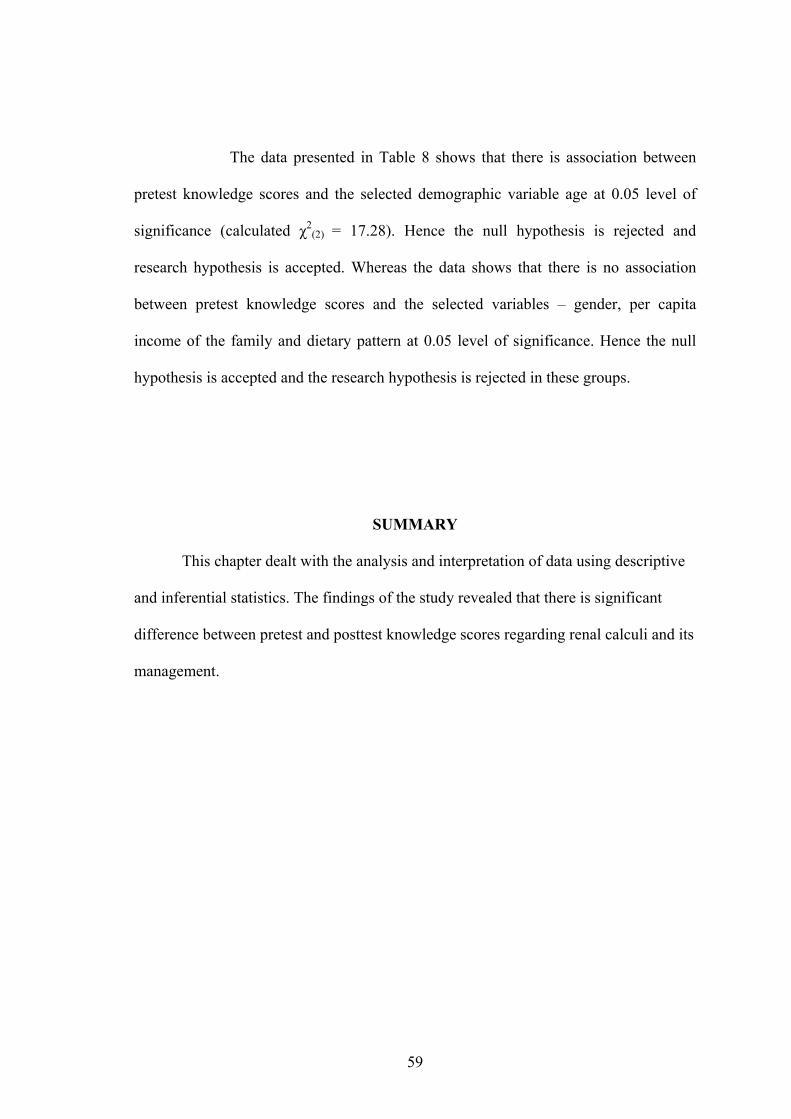
59
The data presented in Table 8 shows that there is association between
pretest knowledge scores and the selected demographic variable age at 0.05 level of
significance (calculated χ2(2) = 17.28). Hence the null hypothesis is rejected and
research hypothesis is accepted. Whereas the data shows that there is no association
between pretest knowledge scores and the selected variables – gender, per capita
income of the family and dietary pattern at 0.05 level of significance. Hence the null
hypothesis is accepted and the research hypothesis is rejected in these groups.
SUMMARY
This chapter dealt with the analysis and interpretation of data using descriptive
and inferential statistics. The findings of the study revealed that there is significant
difference between pretest and posttest knowledge scores regarding renal calculi and its
management.
60
6. DISCUSSION
The findings of the study had been discussed with reference to the
objectives and hypothesis stated in chapter I and in relation with the findings of other
studies.
Demographic Data
The findings of the study demonstrated that among all the respondents,
majority of them belonged to hindu, non-vegetarian, male within the age group of 21 –
35 years.
Knowledge of renal calculi patients regarding renal calculi and its management.
Findings of the study shows that in the pretest most of the renal calculi
patients (89.58%) had average knowledge regarding renal calculi and its management.
This indicates that less number of patients had adequate knowledge regarding renal
calculi and its management. The study conducted by Thankachan A (2004) on the
effectiveness of planned teaching programme on prevention of anemia among
adolescent girls revealed that 70% of the sample in experimental group had average
knowledge and majority of the sample in control group (73.33%) had poor knowledge
regarding prevention of anemia (n = 60, 30 each for experimental and control groups).
61
Comparison between Pretest and Posttest knowledge scores
The findings of the study revealed that there was a significant difference
between pretest and posttest knowledge scores. The pretest mean percentage
knowledge scores regarding renal; calculi and its management was found to be less
than the posttest mean percentage knowledge scores.
A study conducted on the effectiveness of planned teaching
programme about home care of patients with chronic renal failure on chronic renal
failure patients and their attendants, showed a significant improvement in knowledge
level of patients as well as their family members after the administration of a planned
teaching programme56.
Association of pretest knowledge with selected demographic variables
The findings of the study showed that there was significant association
between pretest knowledge and the patient’s age, whereas there was no association
between pretest knowledge level and the gender, per capita income of the family and
dietary pattern.
A study was conducted to evaluate a planned teaching programme on
prevention of recurrence of renal calculi in terms of knowledge, dietary practices, and
selected biochemical components in serum and urine of patients with renal calculi. The
study revealed that there was significant association between the knowledge and the
patient’s level of education and occupation whereas there was no association between
the knowledge level and the age, gender, religion and exposure to mass media57.
62
7. CONCLUSION
The following conclusions were made on the basis of the findings of the study.
Most of the sample (89.58%) had average knowledge regarding renal calculi
and its management in the pretest. The mean percentage posttest scores and the
modified gain scores in all areas were found to be high.
There was significant difference between the pretest and posttest knowledge
scores ( t(47) =32.81, P<0.05).
There was significant association between pre-test knowledge scores and age (
χ2(2) = 17.28, p<0.05), whereas there was no significant association between
pre-test knowledge score and the selected variables gender ( χ2(1) = 0.07,
P>0.05), per capita income of the family ( χ2(1) = 0.89, P>0.05; ) and dietary
pattern ( χ2(1) = 0.03, P>0.05).
NURSING IMPLICATIONS
Health is wealth is a saying and it is truth. It is the responsibility and right of
every individual to attain a state of health. A large number of diseases could be
prevented with little or no medical intervention if people were adequately informed
about the likely complications and encourage to take timely and necessary precautions.
The findings of the study have implications for nursing practice; nursing
education; and research; and nursing administration.
63
Nursing Practice
The present study has several implications for nursing practice. Planned
teaching programme on renal calculi and its management is a practical strategy to make
the patients aware of their disease and to reduce the recurrence of the disease and thus
reduce complications and also help them to take self-responsibility for their own health.
Health promotion is one of the major roles a nurse has to play; hence its
accountability has to be stressed. Patient education is a process of assisting people to
learn and incorporate health related behaviour into every day like. The educative role of
the nurse has to be emphasized. Educative teaching may motivate clients to practice
self care.
The patients suffering with renal calculi are under severe psychological
stress as well as depression because of their severe pain and their hospitalization.
Providing teaching programme helps them better in their adjustment psychologically by
instilling confidence in them to prevent the complications.
Health information can be imparted through various methods like
lecture, mass media, pamphlet, self instructional module etc. Any teaching strategy
which is simple, clear and attractive makes interested learners to follow the instructions
easily. Nurses have to impose themselves in all the areas of community health
practices, so as to help people in leading healthy lifestyle by preventing health
problems.
64
Nursing Education
The present study has got nursing implication in nursing education since
today’s nursing students are tomorrow’s staff nurses, educators, administrators and
supervisors. Nursing teachers should emphasize the importance of health education and
the methods of imparting education in an effective way during students learning period.
Students should get opportunities to give health education in an appropriate way during
their clinical practice.
In the present era of primary health care more emphasize is given for
developing self care abilities of the individuals. Nursing education should emphasize
more on preparing prospective nurses to impart health information and assist the
community in developing their self care potentials. This can be best done by equipping
the nursing curriculum with the knowledge regarding dissemination of health
information used in various methods of education technology. The planned teaching
programme prepared and examined by this study for its effectiveness in improving the
knowledge of patients with renal calculi about renal calculi and its management is the
proof by itself. As the effectiveness of this teaching plan is well established, this may
be used in patients as well as students’ learning.
Nursing research
There is a great scope for nurses to conduct research in this area to find
the effectiveness of various strategies to educate the patients, their care givers, and the
public at large. Research should be done on preparation on innovative method of
65
teaching, better practice of nursing care and development of good and effective
teaching material.
Research can also focus in specific area of renal calculi’s management
and on specific area of prevention of recurrence of renal calculi, preparation of booklet
on renal calculi and its management, survey to find the incidence of renal calculi and
related complications, self instructional module on renal calculi and its management,
survey to assist the psychosocial problems of patients with renal calculi. In fact, this
study has helped to open avenue to a new area for nursing research.
Nursing administration
Nurses as administrators should take great interest formulating short and
long term policies in an organization or institution. The patients who are visiting the
hospital should gain some kind of health information according to their needs.
The nurse administrators should take initiative in organizing in service
education programme for nurses and motivate nurses to participate in such activities.
Nursing administrators will serve as a resource person for other nurses, students, clients
and relatives. The nurse administrators should see that enough support is provided in
terms of manpower, money, and materials for disseminating health information.
Periodical educational sessions by health personals should be conducted. Health camps
can be conducted and referrals should be cared adequately. The study findings have
shown clearly that the responsibility of nurse administrators in organizing in service
education on such topics is of importance.

66
LIMITATIONS
The limitations recognized in the study are:
1. The study did not use control group. Hence, the result of the study must be
generalized with caution as there is threat internal validity due to history.
2. Incidental teaching by the nurses, doctors, and other health team members could not
be controlled in between pretest and posttest because of ethical reason.
3. The sample being convenient one limits generalization to larger population with
similar characteristic.
4. The time gap between pretest and posttest was only 4 days.
SUGGESTIONS
1. Patients with renal calculi are encourage for check up for every three to four months
to rule out recurrence of renal calculi and to seek medical help on time.
2. The booklet on renal calculi and its management can be distributed to the renal
calculi patients right at the time of diagnosis.
3. Health education programmes should be organized in hospital and institutional
settings.
67
RECOMMENDATIONS
On the basis of the findings of the study, it is recommended that
1. A similar study be replicated on a larger sample with a control group.
2. A similar study be replicated for patients with specific type of renal calculi.
3. A longitudinal follow up study be conducted after three months to determine the
effectiveness of this planned teaching programme on renal calculi and its
management, in terms of gain in knowledge and change in dietary practices of
patients with renal calculi.
4. A comparative study be done to find the effectiveness the teaching programme and
other teaching strategy like self instructional module on renal calculi and its
management, in bringing gain in knowledge and change in dietary practices of
patients with renal calculi.
5. A survey study can be conducted to find the incidence of renal calculi and related
complications.

68
8. SUMMARY
Renal calculi is a common disorder and a significant problem because of
incidence, recurrence and severe complications. Stone disease is a surgical as well as a
medical problem. Major progress has been made recently in understanding the
pathophysiological disturbances responsible for stone formation as well as in the
techniques of stone removal. The introduction of extra corporeal shock wave lithotripsy
has considerably reduced the need for surgery.
The annual incidence of stone formation in the industrialized world is
generally considered to be 1500 – 2000 cases per million. With a prevalence of >10%
and an expected recurrence rate of = 50% stone disease has an important effect on the
health care system.
Dietary and drug treatment of renal calculi depend mainly on the
mineral composition of renal stone. However, a high intake of fluids, especially water,
is still the most powerful and certainly the most economical means of prevention of
renal calculi.
Health care providers take important role, in providing renal calculi
patients with accurate and upto date information. Well conducted education campaigns
can indeed change knowledge, attitude and behaviour and thereby dietary pattern.
69
The objectives of the study were
4) to determine the pre test knowledge of the renal calculi patients regarding renal
calculi and its management.
5) to plan and validate the planned teaching programme on renal calculi and its
management for the patients with renal calculi.
3) to evaluate the effectiveness of planned teaching programme on renal calculi
and its management in terms of gain in knowledge in post test.
The study attempted to examine the following hypotheses which were tested at 0.05
level of significance.
H1: The mean post test knowledge score of the patients with renal calculi on renal
calculi and its management will be significantly higher than the mean pre-test
knowledge scores, as measured by a structured knowledge questionnaire.
H2: There will be significant association between the pre test knowledge scores
and the selected variables.
The study assumed that
the patients who are admitted to the hospital with the diagnosis of renal calculi
will have some knowledge regarding renal calculi, gained through mass media,
friends, relatives and other sources.
70
the patients who are attending the planned teaching programme will be able to
follow the instructions in their daily life.
Renal calculi are prone to get recurrence.
Health teaching can impart knowledge regarding renal calculi which make them
aware of their disease.
Creating health awareness will help in prevention of recurrence of renal calculi.
The conceptual framework adopted for the study was based on
modified Rosen Stock’s Health Belief Model. This model stressed the importance of
learner’s motivation in seeking preventive health behaviour.
The study design was Pre experimental one group pre test post-test
design. The population of the study was patients with renal calculi aged above 20 years.
Convenient sampling technique was utilized to select sample (n = 48).
A structured knowledge questionnaire was prepared with 34 items on
knowledge regarding renal calculi and its management. The validation of the tool was
done by thirteen experts. Pretesting and reliability (Spearman’s Brown Prophecy
Formula) was established prior to the pilot study. After pilot study, main study was
conducted; data was collected from forty eight renal calculi patients. The data obtained
were analyzed in terms of the objectives and hypotheses using descriptive and
inferential statistics.
71
DEMOGRAPHIC DATA
Majority of the sample (33.34%) belonged to age group 21 – 35 years.
Most of the sample (79.17%) were male.
Maximum number of the sample (27.08%) was having Primary School Education.
Most of the sample (83.33%) were married.
Majority of the sample (25%) were doing business.
Greater percentage of sample (25%) had family income of Rs 1501 – 3000.
Most of the sample (68.75%) belonged to Hindu background.
Most of the sample (85.42%) takes Non-vegetarian.
Most of the sample (87.5%) had no history of previous hospital admission.
Out of 12.5% of sample with history of previous hospital admission, 4.17% sample
admitted for one time, 6.25% for two times and 2.08% for three times admitted to
the hospital before.
Most of the sample (91.67%) had no family history of renal calculi.
Most of the sample (91.67%) reported that they came to know about their disease
when doctor told them while consultation.
Most of the sample (68.75%) did not have the habit of smoking, chewing betal
leaves and taking alcohol.
72
MAJOR FINDINGS OF THE STUDY
Knowledge of renal calculi patients regarding renal calculi and its management.
Most of the renal calculi patients (89.58%) had average knowledge,
while the remaining (10.42%) had good knowledge.
Comparison between pre-test and post-test knowledge scores.
There was a significant difference between pre-test and post-test
knowledge scores ( t(47) =32.81, P<0.05; Tabled value = 2.02 ). Hence, it is inferred
that post-test knowledge scores was higher than the pre-test knowledge scores. This
showed that planned teaching programme was effective.
Areawise comparison of pre-test and post-test knowledge scores.
For the pretest, subjects had attained knowledge scores in the areas of
Anatomy and physiology of urinary system (64.17%), causes of urinary stone
(42.80%), clinical features of urinary stone (65.97%), management of urinary stone
(90.97%) and prevention and recurrence of urinary stone (49.48%). But after the
administration of planned teaching programme, the level of knowledge of the subjects
improved in each area such as Anatomy and physiology of urinary system (87.92%),
causes of urinary stone (69.64%), clinical features of urinary stone (88.89%),
management of urinary stone (97.92%) and prevention and recurrence of urinary stone
(82.68%).
73
Association between the pre-test knowledge with selected demographic variables.
There was significant association between pre-test knowledge scores and
age ( χ2(2) = 17.28, p<0.05; Tabled value = 5.99 ).
There was no significant association between pre-test knowledge score
and the selected variable gender ( χ2(1) = 0.07, P>0.05; Tabled value = 3.84 ).
There was no significant association between pre-test knowledge score
and the selected variable per capita income of the family ( χ2(1) = 0.89, P>0.05; Tabled
value = 3.84 ).
There was no significant association between pre-test knowledge score
and the selected variable dietary pattern ( χ2(1) = 0.03, P>0.05; Tabled value = 3.84 ).
SUMMARY OF THE CHAPTER
This chapter dealt with the discussions on the results obtained,
conclusions, implications for various nursing field of nursing practice, nursing
education, nursing research and nursing administration, limitations of the findings,
future suggestions, recommendations and a brief description of the study and the major
findings.
74
9. BLBLIOGRAPHY
1. Martini A .should dietary calcium and protein be restricted in patients with
Nephrolithiasis? Nutrition Reviews 2000 Apr;5(58):111-6.
2. Prendiville, Black LN, Frager, Buxton A. The effect of vegetables and the animal
protein diet on calcium urate, and oxalate excretion. British Journal of Urology
1992;54:590-593.
3. Crais. The incidence of urinary calcium. British Journal of hospital medicine
2005 Jan 12;2:1021-1029.
4. Blangy s, Folinais D, sibert A, Delmas V, Moulonguet A. effect of changes in
epidemiological factor on the composition and racial distribution of renal calculi.
British Journal of Urology 1989 Nov;60(5):387-92
5. Churchill DN, Morgen J, Got MH. Tea drinking – A risk factor for urolithiasis.
Urological research 1989;12:55
6. Naya Y, Ito MM, Yamaguchi K. Association of dietary fatty acids with Urinary
oxalate excretion in calcium oxalate stone- formers in their fourth decade. British
Journal of Urology International 2002 Jun;89:842-846.
7. Tiselius HG. Epidemiology and medical management of stone disease. British
Journal of Urology International 2003 May;91:758-760.
8. Griffith DP. Urease stone. Urology research 1990 Sep;7(3):215-21.
9. Allen LR, Sonja L. Effects of 5 different diets on Urinary Risk Factors for calcium
oxalate Kidney Stone formation : Evidence of different renal handling mechanisms
in different race groups. The Jourenal of urology 2003sep;168:931-6.
10. Polit DF, Hungler BP. Nursing research: Principles and methods. 3rd ed.
Philadelphia: J.B Lippincott Company;1993. p. 74.
75
11. Asper R. Epidemiological and socioeconomical aspects of urolithiasis. Urological
research 1988 Nov;12:1-5.
12. Vahlensieck W, Hirth R, Bach, Hesse. Epidemiological determinations with 377
recurreent stone formers. Urological research 1989;12:58.
13. Schneider HJ. Epidemiology of urolithiasis. Urolithiasis: etiology,
diagnosis,spiinger-verlag 1990;11:138-79.
14. Kodama H, Ohno Y. Analytical epidemiology of urolithiasis. Hinyokika Kiyo
1991;35(6):935-945.
15. Rose GA, Westbury EJ. The influence of calcium content of water, intake of
vegetables and fruit anf of other food factors upon the incidence of renal calculi.
Urological research 1993 Aug 8;3(2):61-6.
16. Jegar P. Pathogenesis of the renal calculi. Press-medicine 1994;23(25):115-120.
17. Hesse A, Seiner R. Current aspects of epidemiology and nutrition in urinary stone
disease. World journal of urology 1997 May;15:165-171.
18. Borghi L, Meschi T, Schianchi, Briganti A, Guerra A, Allegri F. Urine volume:
stone risk factor and preventive measure. Nephron 1999;81:131-7.
19. Tiselius HG, Larsson L. Studies on urine composition in patients with calcium
oxalate stone disease. Urological research 1988;12:63.
20. Hoskin DH, Wilson RR, Smith. The urinary excretion of citrate in normal persons
and patients with calcium urolithiasis. Urological research 1988 Mar;12:26.
21. Fassen VA. The effect of calcium restricted diet of urolithiasis patients with
absorptive hypercalciuria type II on risk factors for kidney stone and the
osteopenia. Urological research 1998 Apr;26:65-69.
76
22. Preminger GM. The metabolic evaluation of patients with recurrent nephrolithiasis:
A review of comprehensive and simplified approach. The journal of urology
1989;141:760-2.
23. Morton U, Rose R, Jerry W. Biochemical evaluation of calcium stone patients:
How soon it can be done afterstone surgery/passage. Urology 1990;34(5):410-4.
24. Peater ML, Sofijanka S. Drinking water quality and urolithiasis. Urological
research 1988;12:27.
25. Fellstrome BD, Calrlstome. Dietary history and dietary records in renal stone
patients and control. Urological research 1988;12:58.
26. Laminski, Meyers, Kruger, Morgolius. Hyperoxaluria in patients with recurrent
calcium oxalate calculi: dietary and other risk factors. British Journal Urology
1991 Nov;68(5):454-8.
27. Andras T. High excretion of uric acid combined with high excretion of calcium
links kidney stone disease. Nephrology Dialysis Transplantation 2002 Feb;
17(2):23-27.
28. Oliver, Beverley, Gargaret. Effect of Ascorbic Acid and consumption on urinary
stone risk factor. The journal of urology 2003 Aug;170:397-400.
29. Polit DF, Beck. Nursing research: Principles and methods. 3rd. Philadelphia: J.B
Lippincott Company; 2004.
30. Burns N, Grove SK. Understanding Nursing Research. 2nd ed. India: Harcourt
(India) Private Limited; 2002. p. 41,56.
31. Polit DF AND Hungler BP. Nursing research: Principles and methods. 3rd
ed. Philadelphia: J.B Lippincott Company; 2001.
77
32. Kerlinger FN. Foundation of behavioural research. New york: Holt International
Edition; 1973. p. 134.
33. Talbot LA. Principlea ans Practice of Nursing Research. Philadelphia: A times
Mirror Company; 1995. p. 232.
34. Roberts CA, Burke SO. A Quantitative and Qualitative Approach. Boston: Jones
and Baredt Publishers; 1989.
35. Treece K, Treece JW. Elements of research in nursing. St. lous: C.V Mosby;1962.
36. Ramachandra L. health Education – A New Approach. New Delhi: Vikas
Publishing House; 1999.
37. Cockerham WC. Medical sociology. 6th ed. London: Prentice hall International
Ltd; 1995.
38. Fox DJ. Fundamentals of nursing. 2nd ed. Newyork: Appleton Century Crafts;
1979.
39. Gopalan C, Rama S, Balasubramaniam. Nutritive values of Indian foods.
Hyderabad: National institute of nutrition; 1973.
40. Kothari CR. Research Methodology, Methods and Techniques. 2nd ed. New Delhi:
Wishwa Prakasha; 2002.
41. Nieswiadomy RM. Nursing Research. 4th ed. New Jersy: Prentice Hall; 2002.
42. Valesieck EW. Nutrition history of recurrent calcium oxalate stone formers pre and
post diet. Urinary stone. New york: Churchill Livingston; 1984. p. 41-6.
43. Guigan FJ. Experimental psychology. New Delhi: Prentice Hall of India; 1969.
44. Patwarden VN. Nutrition in India. Indian journal of medical science 1954;4:113-5.
45. Suchman EA. Evaluative research. New york: Russell sage foundation; 1967. p.
75.
78
46. Reen V. Idiopathic urinary bladder stones of childhood. American Journal of
Surgery 977;50:18-22.
47. Anita FP. Clinical dietetics and nutrition. 2nd ed. Delhi: Oxford University:1973.
48. Bailey, Love. Short Practice of Surgery. New York: International Students
Edition; 2000. p. 1143-56.
49. Atri SC. Handbook of Surgery. Patna: Scientific Book Company; 2001. p. 106-16.
50. Aronson MD, Rose B. Diagnosis and acute management of suspected
nephrolithiasis. UpToDate, 2002 May 28.
51. Brenner, Rector. The Kidney. 6th ed. W. B. Saunders Company, Copyright ©
2000.
52. Eisendrath, Rolnick. Childhood disorders and diseases. 4th ed. vol I, Philadelphia:
WB Saunders, 1978.
53. Erkonen, William E. Radiology 101: The basics and fundamentals if imaging.
Pliladelphia: Lippincott-Raven, 1998.
54. Tulasi TV. The effectiveness of Instructional Module on Self Care Practices of
Renal Transplant Patients. The Indian journal of Nursing and Midwifery
1999;2(1):21-6.
55. Garret HG. Statistics in psychology and education. Bombay: Vaklis, Feffer and
Simons Ltd; 1981.
56. Minnie. Effectiveness of planned teaching programme about home care of patients
with chronic renal failure patients and their attendants, in a selected hospital in
Udupi district, Manipal. Unpublished Master of Nursing Thesis, MAHE. Manipal;
1999.
79
57. John R. A study to evaluate a planned diet counseling programme on prevention of
recurrence of renal calculi in terms of knowledge, dietary practices, and selected
biochemical components in serum and urine of patients with renal calculi, in a
selected hospital in Udupi district. Unpublished Master of Nursing Thesis, MAHE.
Manipal; 2000.
58. Thankachan A. A study to determine the effectiveness of planned teaching
programme on prevention of anemia among adolescents girls in selected colleges at
Moodbidri. Unpublished Master of Nursing Thesis. Rajiv Gandhi University of
Health Sciences, Bangalore; 2004.
80
1a Letter seeking permission to do pretesting and reliability of the research tool
From Ms. Ch. Babita Devi II Year M.Sc Nursing Alva’s College of Nursing Moodbidri – 574227. To Dr. Krishna Mohan Prabhu Managing Director Prabhu General Hospital Moodbidri – 574227. Through the Research Advisor. Respected Sir, Subject: Permission to do pretesting and reliability of the research tool among the patients with renal calculi in Prabhu General Hospital. In partial fulfillment of M.Sc. Nursing degree, I have to undertake a research in the clinical speciality Medical Surgical Nursing. The topic selected for the study is “A study to evaluate the effectiveness of planned teaching programme on renal calculi and its management among renal calculi patients in selected hospitals in Mangalore taluk.” May I request you to kindly permit me to do pretesting and reliability of the research tool among the above mentioned patients in your hospital. Kindly do the needful for the above mentioned matter. Thanking you with anticipation. Place: Yours sincerely, Date: ( Ch. Babita Devi )

81

82

83
2a Letter seeking permission to conduct pilot study
From Ms. Ch. Babita Devi II Year M.Sc Nursing Alva’s College of Nursing Moodbidri – 574227. To Dr. Harish Nayak Medical Superintendent Alva’s Health Centre Moodbidri – 574227. Through the Research Advisor. Respected Sir, Subject: Permission to conduct pilot study among the patients with renal calculi in Alva’s Health Centre. In partial fulfillment of M.Sc. Nursing degree, I have to undertake a research in the clinical speciality Medical Surgical Nursing. The topic selected for the study is “A study to evaluate the effectiveness of planned teaching programme on renal calculi and its management among renal calculi patients in selected hospitals in Mangalore taluk.” May I request you to kindly permit me to conduct pilot study among the above mentioned patients in your hospital. Kindly do the needful for the above mentioned matter. Thanking you with anticipation. Place: Yours sincerely, Date: ( Ch. Babita Devi )
84
85
86
3a Letter seeking permission to conduct research study
From Ms. Ch. Babita Devi II Year M.Sc Nursing Alva’s College of Nursing Moodbidri – 574227. To Dr. Prasanth Marla Medical Director A. J Hospital and Research Centre Mangalore – 575004. Through the Research Advisor. Respected Sir, Subject: Permission to conduct research study among the patients with renal calculi in your esteemed hospital. In partial fulfillment of M.Sc. Nursing degree, I have to undertake a research in the clinical speciality Medical Surgical Nursing. The topic selected for the study is “A study to evaluate the effectiveness of planned teaching programme on renal calculi and its management among renal calculi patients in selected hospitals in Mangalore taluk.” May I request you to kindly permit me to conduct pilot study among the above mentioned patients in your hospital. Kindly do the needful for the above mentioned matter. Thanking you with anticipation. Place: Yours sincerely, Date: ( Ch. Babita Devi )
87
88
89
90
4 REQUISITION FOR CONTENT VALIDATION OF THE TOOL
From, Ch. Babita Devi I Yr. M.Sc Nursing Student Alva’s College Of Nursing, Moodbidri - 574227 To, --------------------------------- --------------------------------- --------------------------------- Respected Sir/Madam, Subject: Requisition for content validation of the tool I, Ms. Ch. Babita Devi, I Yr. M. Sc Nursing student of Medical – Surgical Nursing speciality at Alva’s College Of Nursing, Moodbidri kindly request you to give consent to validate my tool on “A study to evaluate the effectiveness of planned teaching programmed on renal calculi and its management among renal calculi patients in selected hospitals in mangalore taluk.” I would be highly obliged if you kindly give your acceptance and valuable suggestions. A self addressed envelope and acceptance form are enclosed herewith for your perusal. Thanking you with anticipation. Date: Yours faithfully,

91
5 ACCEPTANCE FORM FOR TOOL VALIDATION
NAME: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ DESIGNATION: _ _ _ _ _ _ _ _ _ _ _ _ NAME OF THE COLLEGE / HOSPITAL: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ STATEMENT OF THE ACCEPTANCE: I give my acceptance / non – acceptance to validate the tool on “A study to evaluate the effectiveness of planned teaching programmed on renal calculi and its management among renal calculi patients in selected hospitals in mangalore taluk.” Date: ( Signature )
92
6 CONTENT VALIDATION CERTIFICATE
I hereby certify that I have validated the tool of Ms. Ch. Babita Devi, I Yr. M.Sc Nursing student who is undertaking the study “A study to evaluate the effectiveness of planned teaching programmed on renal calculi and its management among renal calculi patients in selected hospitals in Mangalore taluk.” Signature of the Expert Date: Place: Designation and Address

93
7a Criteria Checklist For Background Variables
Instructions Kindly review the items in the background variables for the patients with renal calculi and give your suggestions regarding appropriateness of the content. There are three response columns namely strongly agree, agree, and disagree. Kindly place a tick mark (√) against specific column. If there are any suggestions or comments please mention in the remarks column.
Items
Strongly agree Agree Disagree Remarks
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16

94
7b Criteria checklist for validation of the tools
Instructions Kindly review the items in the structured knowledge questionnaire regarding renal calculi and its management and give your suggestions regarding accuracy, relevance and appropriate of the content. There are four response columns namely strongly agree, agree, disagree and strongly disagree. Kindly place a tick mark (√) against specific column. If there are any suggestions or comments please mention in the remarks column. Criteria checklist for structured knowledge questionnaire
Items
Strongly agree
Agree Disagree
Strongly disagree
Remarks
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
95
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
96
7c CRITERIA CHECKLIST FOR EVALUATION OF PLANNED TEACHING
PROGRAMME ON RENAL CALCULI AND ITS MANAGEMENT Dear sir / Madam, Please go through the criteria listed below, which has been formulated for evaluating and validating the planned teaching programme for renal calculi and its management. There are four responses columns in checklist. COLUMN I ( Meets criteria ) Please place a tick mark (√) against this column if you think the contents and specific criteria have congruence / consistency. COLUMN II ( Partially meets criteria ) Please place a tick mark (√) against this column if you think the content is satisfactory. COLUMN III ( Does not meet criteria ) Please place a tick mark (√) against this column if you think the content is not relevant to the criteria. REMARK COLUMN When responses are made in column COLUMN I, COLUMN II, COLUMN III, the evaluator comments are required in this column

97
COLUMN
SL NO.
CONTENT CRITERIA
I
II
III
REMARKS
1 a b
Formulation of objectives Comprehensive enough for renal calculi patient’s knowledge regarding renal calculi and its management. Objectives are in terms of learners behavioural outcome
II a b c
Selection and organization of the content. Content provides adequate information. Content is according to the level of understanding of renal calculi patients Logical sequence.
III
Language used is simple and clear.
IV
Feasibility
V
Practicability

98
8a Letter seeking consent for participation in the study
Dear participant, I am Ms. Ch. Babita Devi, final year M.Sc. Nursing student of Alva’s College of Nursing, Moodbidri. I intent to do a study to determine the effectiveness of planned teaching programme on renal calculi and management among renal calculi patients in a selected hospital in Mangalore taluk. Therefore I request you to respond to the questions in the questionnaire without any hesitation and to co-operate whole heartedly in the study. I assure you that the information given by you will be kept confidential and used only for the purpose of this study. Your participant will helped me to complete my study and contribute to the field of health. Thanking you. Yours faithfully, Place: Ms. Ch. Babita Devi Date:

99
8b Consent Form
I am voluntarily willing to participate in the study conducted by Ms. Ch. Babita Devi, entitled as “A study to determine the effectiveness of planned teaching programme on renal calculi and its management among renal calculi patients in a selected hospital in Mangalore taluk”, and to co-operate in providing information. I am informed that the information will be kept confidential and used only for the above mentioned study. Signature of the investigator Signature of the participant
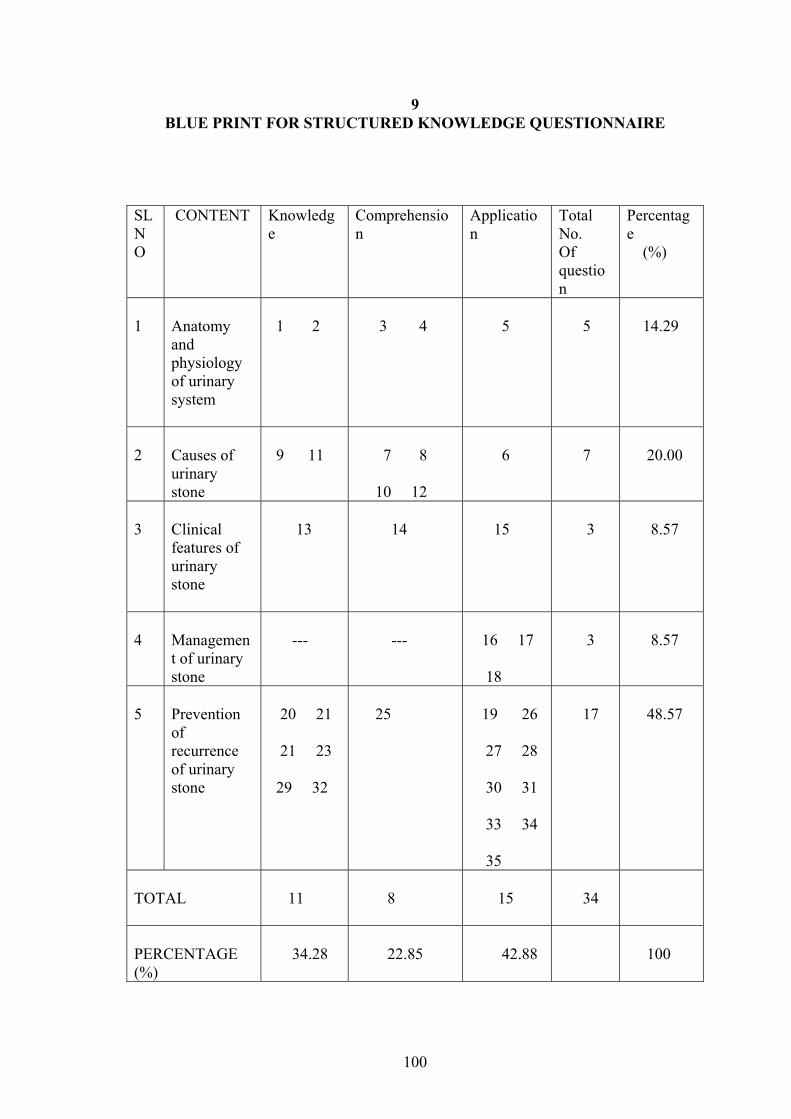
100
9 BLUE PRINT FOR STRUCTURED KNOWLEDGE QUESTIONNAIRE
SL NO
CONTENT Knowledge
Comprehension
Application
Total No. Of question
Percentage (%)
1
Anatomy and physiology of urinary system
1 2
3 4
5
5
14.29
2
Causes of urinary stone
9 11
7 8
10 12
6
7
20.00
3
Clinical features of urinary stone
13
14
15
3
8.57
4
Management of urinary stone
---
---
16 17
18
3
8.57
5
Prevention of recurrence of urinary stone
20 21
21 23
29 32
25
19 26
27 28
30 31
33 34
35
17
48.57
TOTAL
11
8
15
34
PERCENTAGE (%)
34.28
22.85
42.88
100
101
10(1a)
TOOL – 1
DEMOGRAPHIC DATA INSTRUCTION: The interviewee are asked to fill the space provided below or place a tick ( ) mark against the correct response of the following : 1. Name : ………………………….. 2. Age :
a) 21 – 35 years ( ) b) 36 – 50 years ( ) c) 51 – 65 years ( ) c) above 66 years ( )
3. Sex Male ( ) Female ( ) 4. Address : …………………………….. 5. Hospital Number : …………. 6. Educational Background
a) Uneducated ( ) b) Primary school Education ( )
c) High School Education ( ) d) Pre degree ( ) e) Graduate ( ) f) Post – graduate ( ) g) Others ( )
102
7. Marital Status
a) Married ( ) b) Unmarried ( ) c) Widow / Widower ( )
d) Divorced ( ) 8. Occupational Status
a) Coolie ( )
b) Agriculture ( ) c) Beedi worker ( ) d) House wife ( )
e) Business ( ) f) Any others ( )
9. Per capita income in Rupees
a) 1 - 1500 ( ) b) 1501 – 3000 ( )
c) 3001 – 4500 ( ) d) > 4501 ( )
10. Religion
a) Hindu ( ) b) Muslim ( )
c) Christian ( ) d) Others ( Specify) ( ) 11. In which of the following group do you belong to?
a) Vegetarian ( )

103
b) Non-vegetarian ( ) 12. Have you been admitted to the hospital for allopathic treatment for any other problem in the past? Yes ( ) No ( ) 13. If yes, how many times you have been admitted to the hospital so far?
a) One time ( ) b) Two times ( )
c) Three times ( ) d) If more, specify ( )
14. Did any of your family members have the similar type of disease? Yes ( ) No ( ) 15. What is the source of health information on your disease condition?
a) Doctor ( ) b) Nurse ( )
c) Relatives ( ) d) Friends ( )
e) Mass media ( ) f) Any other, specify ( )
16. Do you have any following habit? a) Smoking ( ) b) Betal leaves ( ) c) Alcohol ( ) d) All the above ( ) e) None of the above ( )
104
10(1b)
»£À߯ÉAiÀÄ ««zsÀvÉ ¸ÀÆZÀ£ÉUÀ¼ÀÄ : C¨sÀåyðUÀ¼ÀÄ ¸ÀjºÉÆAzÀĪÀ GvÀÛgÀªÀ£ÀÄß PɼÀUÉ ¸ÀÆa¹zÀ ¸ÁÜ£ÀzÀ°è vÀÄA©j CxÀªÁ ¸Àj aºÉßAiÀÄ£ÀÄß UÀÄgÀÄw¹. 1 ºÉ¸ÀgÀÄ: …………………. 2 ¥ÁæAiÀÄ
J) 21 - 35 ªÀµÀð ( ) ©) 36 - 50 ªÀµÀð ( ) ¹) 51 – 65 ªÀµÀð ( ) r) 65 QÌAvÀ ªÉÄîàlÄÖ ( )
3 °AUÀ
ºÉtÄÚ ( ) UÀAqÀÄ ( )
4 «¼Á¸À:- 5 D¸ÀàvÉæAiÀÄ £ÀA§æ :- 6 «zsÁåºÀðvÉ
J) C£ÀPÀëgÀvÉ ( ) ©) ¥ÁæxÀ«ÄPÀ «zsÁå¨sÁå¸À ( ) ¹) ¥ËæqÀ±Á¯Á «zsÁå¨sÁå¸À ( ) r) ¦ærVæ ( ) E) UÁædÄAiÉÄmï ( ) J¥sï) ¥ÉÇøïÖ UÁædĪÉmï ( ) f) EvÀgÀ ( )
7. ªÉʪÁ»PÀ ¹ÜwUÀw J) ªÀÄzÀĪÉAiÀiÁVzÉAiÉÄà ( ) ©) ªÀÄzÀĪÉ0iÀiÁV®è ( )
105
E) «zsÀªÉ ( ) r) «ZÉíÃzÀ£É ( ) 8. GzÉÆåÃUÀ J) PÀÆ° ( ) ©) ªÀåªÀ¸ÁaiÀÄ ( )
¹) ©Ãr PÁ«ÄðP ( )
r) ªÀÄ£ÉaiÉÆqÀw ( )
E) ªÁå¥ÁgÀ ( )
J¥sï) EvÀgÀ ( ) 9. ªÀiÁ¹PÀ DzÁAiÀÄ
J) 1 - 1500 gÀÆ ( ) ©) 1501 - 3000 gÀÆ ( ) ¹) 3001 – 4500 gÀÆ ( ) r) 4500 gÀÄ ªÉÄîàlÄÖ ( )
10. eÁw
J) »AzÀÆ ( )
©) ªÀÄĹèªÀiï ( ) ¹) Qæ²Ñ0iÀÄ£ï ( ) r) EvÀgÀ ( ) 11. AiÀiÁªÀ UÀÄ0¦UÉ ¸ÉÃjzÀªÀgÀÄ
J) ¸À¸ÀåºÁj ( )
©) ªÀiÁA¸ÁºÁj ( ) 12. ¤ÃªÀÅ F ªÉÆzÀ®Ä aQvÉìAiÀÄ£ÀÄß ¥ÀqÉ¢¢ÝÃgÁ?
106
J) ºËzÀÄ ( ) ©) E®è ( )
13. aQvÉìAiÀÄ£ÀÄß ¥ÀqÉ¢zÀÝ°è JµÀÄÖ ¸À® ¥ÀqÉ¢¢ÝÃgÁ ?
J) M0zÀÄ ¸À® ( )
©) JgÀqÀÄ ¸À® ( ) ¹) ªÀÄÆgÀÄ ¸À® ( ) r) ºÉZÀÄÑ ( ) 14. ¤ªÀÄä PÀÄlÄA§zÀ°è EvÀgÀgÀÄ F ªÁå¢AiÀÄ£ÀÄß ºÉÆA¢gÀĪÀgÉÃ
ºÉÆA¢gÀĪÀgÉà ? J) ºËzÀÄ ( ) ©) E®è ( ) 15. AiÀiÁgÁzÀgÀÆ EzÀgÀ §UÉÎ ªÀiÁ»w PÉÆnÖzÁÝgÁ ?
J) qÁPÀÖgï ( )
©) £À¸ïð ( )
¹) ¸À0§0¢üPÀgÀÄ ( ) r) UɼÉaiÀÄgÀÄ ( )
E) ªÀiÁzsÀåªÀÄ ( )
J¥sï) EvÀgÀ ( ) 16. ¤ªÀÄUÉ F PɼÀV£À C¨sÁå¸ÀUÀ½ªÉAiÉÄà ?
J) ºÉÆUÉ §wÛ ( )
©) ªÀiÁzÀPÀ zÀæªÀå ( )
¹) J¯É CrPÉ ( )
r) ªÉÄð£ÀªÉ®èªÀÅ ( )
E) ªÉÄð£À AiÀiÁªÀÅzÀÆ E®è ( )
10(2a) TOOL – 2

107
STRUCTURED KNOWLEDGE QUESTIONNAIRE
INSTRUCTIONS: Here is a list of questions in relation to Urinary stone and its management. Please read the questions carefully and select the correct answer from the responses given. 1. Which of the following organ is responsible for the formation and elimination of urine?
a) Lung ( ) b) Kidney ( ) c) Liver ( )
2. What is the main function of Kidney?
a) Digestion of food ( ) b) Stores waste products ( ) c) Remove the waste products from the body ( )
3. What is the capacity of urinary bladder?
a) 201 – 300 ml ( ) b) 301 – 400 ml ( ) c) 401 – 500 ml ( )
4. Which of the following substance form the urinary stone?
a) Vitamins ( ) b) Minerals ( ) c) Blood clot ( )
5. How does hot climate contribute to stone formation?
a) Due to increase absorption of solutes during high temperature ( ) b) Due to excessive sweating leading to thick blood concentration ( )
c) Due to loss of appetite during hot season ( )
6. Which of the following liquid foods helps in urinary stone formation? a) Coconut water ( )

108
b) Weak tea ( ) c) Pepsi ( ) 7. Who are the people more prone to form urinary stone?
a) People with sedentary lifestyle ( ) b) People who work in the direct sun almost everyday ( )
c) People who work in factory ( )
8. Why do you need to drink excess amount of water when you consume excess green leaf vegetables? a) Water helps in digestion ( ) b) Water helps in absorption of minerals ( ) c) Water helps in the excretion of excess minerals ( ) 9. Which of the following minerals is rich in green leafy vegetables?
a) Calcium ( ) b) Phosphate ( ) c) Uric acid ( )
10. How does deficiency of Vitamin A result in urinary stone development?
a) By causing the smoothness of urinary pathway wall ( ) b) By causing the roughness of the urinary pathway wall ( )
c) By causing absorption of minerals from the contents of urinary pathway ( )
11. Which of the following disease predispose to the formation of urinary stone?
a) Hypertension ( ) b) Hepatitis ( ) c) Hyperparathyroidism ( )
12. What will happen if there is infection of the urinary tract?
a) Obstruction in the urinary pathway ( )

109
b) Erosion of the urinary wall ( )
c) Excessive secretion of urine ( )
13. Which of the following is the warning sign for urinary stone?
a) Sudden, sharp, severe pain in flank ( ) b) Gradual, mild pain in abdomen ( ) c) Severe, fluctuating pain pelvic region ( )
14. Which of the following signs and symptoms is not seen in urinary stone?
a) Excessive urine output ( ) b) Difficulty in passing urine ( ) c) Feeling of fullness of urinary bladder ( )
15. Which of the following condition is indicated by presence of fever, chills, shivering and vomiting?
a) Disease causing micro-organisms in the urinary pathway ( ) b) Increase concentration of urine ( )
c) Mass in the urinary pathway ( )
16. What measure you will take when you suspect stone in the urinary pathway?
a) Take self medication ( ) b) Rely on friends / relatives ( )
c) Seek medical care ( ) 17. Within what time you will seek medical help after the onset of pain?
a) Immediately after the pain ( ) b) After the second attack of pain ( )
c) After one week of onset of pain ( ) 18. When do we need the operation in case of urinary stone?
a) Presence of blood in the urine ( )
110
b) Presence of pus in the urine ( ) c) Presence of large stone in the urinary pathway ( )
19. What is the means to prevent recurrence of urinary stone?
a) Drinking little water ( ) b) Drinking liberal water ( ) c) Eating little food ( )
20. How much water should be taken daily by the patient with urinary stone approximately?
a) 1000 – 2000 ml ( ) b) 2001 – 3000 ml ( ) c) 3001 – 4000 ml ( )
21. Which of the following is contained in excess amount in fruit juices?
a) Sodium ( ) b) Potassium ( ) c) Calcium ( )
22. Which of the following is rich in raw vegetables?
a) Carbohydrate ( ) b) Fats ( ) c) Fiber ( )
23. Which of the following fruit is rich in calcium?
a) Guava ( ) b) Apple ( ) c) Lime ( )
24. Which of the following food items helps in the excretion of urinary stone?
a) Black pepper ( )

111
b) Tamarind ( ) c) Jaggery ( )
25. Which of the following measure should be taken to prevent urinary stone formation for the patients who are bed ridden?
a) Reducing food intake ( ) b) Reducing fluid intake ( )
c) Changed position frequently ( ) 26. Why do you need to avoid animal protein if you are diagnosed as having urinary stone?
a) Accumulation of minerals in the urinary pathway ( ) b) Increase production of urine ( ) c) Causes stagnation of urine ( )
27. What will happen if we consume excess salt in our food?
a) Increase body weight ( ) b) Increases the calcium absorption ( ) c) Decreases blood pressure ( )
28. Which of the following is the richest source of calcium?
a) Potato ( ) b) Tomato ( ) c) Cabbage ( )
29. Which of the following drinks will you avoid if you are diagnosed to have calcium stone?
a) Watermelon ( ) b) Barley water ( ) c) Milk ( )
112
30. What is the problem if you consume foods rich in sugar?
a) Decreases the production of urine ( ) b) Increases the concentration of urine ( ) c) Obstruct the flow of urine ( )
31. Which of the following types of fish is rich in calcium?
a) Small fish with bone ( ) b) Big fleshy fish ( ) c) Medium size fish ( )
32. Why do you need to avoid eating betel leaves with lime?
a) It increases the chances of dental caries. ( ) b) It increases the calcium content of the body ( ) c) It increases the chances of mouth ulcer ( )
33. Why should a person with urinary stone need to avoid drinking alcohol?
a) Alcohol causes excessive excretion of urine ( ) b) Alcohol decreases the excretion of minerals. ( ) c) Alcohol may deposit minerals in urinary pathway. ( )
34. Which one of the following should you need to drink more if you had taken the foodstuff that are supposed to restrict?
a) Commercial drinks ( ) b) Clear water ( ) c) Tea ( )
10(2b) gÀZÀ£ÁvÀäPÀ ¥Àæ±ÉßUÀ¼ÀÄ
113
¸ÀÆZÀ£ÉUÀ¼ÀÄ : F PɼÀV£À ¥Àæ±ÉßUÀ¼ÀÄ ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ½UÉ ¸ÀA§AzsÀ ¥ÀlÖªÀÅ ¥Àæ±ÉßUÀ¼À£ÀÄ ¸ÀjAiÀiÁV N¢ ¸ÀjAiÀÄÄvÀÛgÀªÀ£ÀÄß Dj¹j. 1. ªÀÄÆvÀæ GvÀàwÛAiÀÄ°è ªÀÄvÀÄÛ «¸Àdð£ÉAiÀÄ°è AiÀiÁªÀ CAUÀ
¥ÀæªÀÄÄR ¥ÁvÀæ ªÀ»¸ÀÄvÀÛzÉ ? J) ±Áé¸ÀPÉÆñÀ ( ) ©) ªÀÄÆvÀæ¦AqÀ ( ) ¹) AiÀÄPÀÈvï ( )
2. ªÀÄÆvÀæPÉÆñÀzÀ PÁAiÀÄðªÉãÀÄ ?
J) ¤ÃgÀ£ÀÄß »ÃgÀĪÀÅzÀÄ. ( ) ©) ¨ÉÃqÀªÁzÀ DºÁgÀzÀ ¸ÀAUÀæºÀuÉ ( )
¹) ¨ÉÃqÀªÁzÀªÀ£ÀÄß zÉúÀ¢AzÀ ºÉÆgÀºÁPÀĪÀÅzÀÄ ( ) 3. ªÀÄÆvÀæPÉÆñÀzÀ ¸ÁªÀÄxÀåðªÉµÀÄÖ ?
J) 200 - 300 «Ä° °Ãlgï ( ) ©) 301 – 400 «Ä° °Ãlgï ( ) ¹) 401 – 500 «Ä° °Ãlgï ( )
4. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®Äè AiÀiÁªÀÅzÀjAzÀ DUÀÄvÀÛzÉ ? J) fêÀ¸ÀvÀé ( ) ©) R¤eÁA±À ( ) ¹) ºÉ¥ÀÅöàUÀnÖzÀ Gàpàû ( ) 5. ©¹ ªÁvÁªÀgÀtªÀÅ ªÀÄÆvÀæPÉÆñÉÆÃvÀáwÛAiÀÄ°è
¥ÁvÀæªÀ»¸ÀÄvÀÛzÉ ? J) ©¹ ªÁvÁªÀgÀªÀÅ ºÉaÑ£À zÀæªÀªÀ£ÀÄß »ÃgÀÄvÀÛzÉ. ( ) ©) C¢üPÀ ¸ÉéÃzÀ GvÀàwÛ¬ÄAzÀ ªÀÄÆvÀæzÀ ¥ÀæªÀiÁt PÀrªÉÄAiÀiÁzÀAvÉ DUÀĪÀÅzÀÄ. ( ) ¹) ¨ÉùUÉ PÁ®zÀ°è PÀrªÉÄ ºÀ¹ªÀÅ DUÀĪÀÅzÀÄ. ( )
6. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®Äè GvÀàwÛAiÀÄ°è AiÀiÁªÀ zÀæªÀ ¥ÀzÁxÀð ¥ÀæzsÁ£À ¥ÁvÀæ ªÀ»¸ÀÄvÀÛzÉ.
J) J½îÃgÀÄ ( ) ©) ZÀºÁ ( )
114
¹) ¥É¦ìà ( ) 7. AiÀiÁjUÉ ªÀÄÆvÀæPÉÆñÀzÀ PÀ°è£À vÉÆAzÀgÉUÉ M¼ÀUÁUÀÄvÁÛgÉ ? J) DgÁªÀÄzÀ fêÀ£À ( ) ©) ©¹®°è PÉ®¸À ªÀiÁqÀĪÀªÀgÀÄ ( ) ¹) PÁSÁð£ÉAiÀÄ°è PÉ®¸À ªÀiÁqÀĪÀªÀgÀÄ. ( ) 8. ºÀ¹gÀÄ vÀgÀPÁjUÀ¼À£ÀÄß w£ÀÄߪÁUÀ AiÀiÁPÉ ¤ÃgÀÄ eÁ¹Û PÀÄrAiÀĨÉÃPÀÄ ? J) fÃtðªÁUÀÄ«PÉAiÀÄ°è ¤ÃgÀÄ ¥ÀæªÀÄÄR ¥ÁvÀæªÀ»¸ÀÄvÀÛzÉ. ( ) ©) R¤eÁA±ÀªÀ£ÀÄß ¥ÀZÀ£À ªÀiÁqÀÄvÀÛzÉ. ( ) ¹) ¥ÀZÀ£ÀªÁzÀ R¤eÁA±À «¸Àdð£É. ( ) 9. ºÀ¹gÀÄ vÀgÀPÁjAiÀÄ°è AiÀiÁªÀ CA±À«zÉ ? J) PÁå°ìAiÀÄA ( ) ©) ¥Á¸ÉáÃmï ( ) ¹) AiÀÄÆjPï DªÀÄè ( ) 10. ªÀÄÆvÀæzÀ PÀ°è£À ¨É¼ÀªÀtÂUÉAiÀÄ°è «l«Ä£ï-J ºÉÃUÉ ¥ÁvÀæªÀ»¸ÀÄvÀÛzÉ? J) ªÀÄÆvÀæzÀ zÁj vÀÄA¨Á vɼÀĪÁzÀÝjAzÀ. ( ) ©) ªÀÄÆvÀæPÉÆñÀzÀ ªÀiÁUÀðzÀ°è drvÀ¢AzÀ ( ) ¹) ªÀÄÆvÀæ£Á¼ÀzÀ°è R¤eÁA±ÀUÀ¼À »ÃgÀÄ«PÉ. ( ) 11. ªÀÄÆvÀæzÀ PÀ°è£À GvÀàwÛAiÀÄ°è AiÀiÁªÀ gÉÆÃUÀªÀÅ ¥ÀæªÀÄÄR ¥ÁvÀæªÀ»¸ÀÄvÀÛzÉ? J) gÀPÀÛzÉÆvÀÛqÀ ( ) ©) ºÉ¥ÀmÉÊn¸ï ( ) ¹) ¥ÁågÁxÉÊgÁ«Äqï£À C¢üPÀ ( ) 12. ªÀÄÆvÀæ£Á¼ÀzÀ ¸ÉÆÃAQ¤AzÀ DUÀĪÀ ¥ÀjuÁªÀĪÉãÀÄ ?
J) ªÀÄÆvÀ櫸Àdð£ÉAiÀÄ°è vÀqÉ GAmÁUÀĪÀÅzÀÄ. ( ) ©) ªÀÄÆvÀæ£Á¼ÀzÀ UÉÆÃqÉAiÀÄ£ÀÄß UÁAiÀÄUÉƽ¸ÀĪÀÅzÀÄ. ( ) ¹) C¢üPÀ ªÀÄÆvÀæ GvÀàwÛ G0lĪÀiÁqÀĪÀÅzÀÄ. ( )
115
13. ªÀÄÆvÀæPÉÆñÀzÀ PÀ°è£À GvÀàwÛAiÀÄ ¸ÀÆZÀ£É
J) Cwà ²ÃWÀæzÀ°è GAmÁUÀĪÀ UÀA©üÃgÀ ºÉÆmÉÖ£ÉÆêÀÅ ( ) ©) ¤zsÁ£ÀªÁV DUÀĪÀ ºÉÆmÉÖ £ÉÆêÀÅ ( ) ¹) ºÉZÀÄÑ-PÀrªÉÄAiiÁUÀĪÀ ¥Á±Àéð£ÉÆêÀÅ. ( )
14. PɼÀV£ÀªÀÅUÀ¼À°è ªÀÄÆvÀæPÉÆñÀzÀ PÀ°è£À GvÀàwÛAiÀÄ ®PÀëtUÀ¼À°è PÀAqÀÄ §gÀĪÀÅ¢®è
J) C¢üPÀ ªÀÄÆvÀæ «¸Àdð£É ( ) ©) ªÀÄÆvÀæ «¸Àdð£ÉAiÀÄ vÉÆAzÀgÉ. ( ) ¹) ªÀÄÆvÀæPÉÆñÀ vÀÄA©zÀAvÉ ¨sÁ¸ÀªÁUÀĪÀÅzÀÄ. ( )
15. ZÀ½dégÀ, ªÁ0w, EzÀÄ AiÀiÁªÀ gÉÆÃUÀzÀ°è PÀAqÀÄ §gÀÄvÀÛzÉ.
J) ¸ÀÆPÀë÷ä fëUÀ¼À ªÀÄÆvÀæ£Á¼ÀzÀ°è ¥ÀæªÉñÀ . ( ) ©) PÀrªÉÄ ¥ÀæªÀiÁtzÀ zÀ¥Àà ªÀÄÄvÀæ ( ) ¹) ªÀÄÆvÀæ£Á¼ÀzÀ°è UÀqÉØ. ( )
16. ªÀÄÆvÀæPÉÆñÀzÀ°è PÀ®Äè GvÀàwÛAiÀiÁzÁUÀ ¤ÃªÀÅ
vÉUÉzÀÄPÉƼÀÄîªÀ ªÀÄÄAeÁUÀævÉ K£ÀÄ ? J) ªÀÄ£É ªÀÄzÀÄÝ ( ) ©) §AzsÀÄUÀ¼À ¸À®ºÉ ( ) ¹) ªÉÊzÀågÀ ¸À®ºÉ ( )
17. AiÀiÁªÀ ¸À0zÀ¨sÀðzÀ°è ¤ÃªÀÅ ªÉÊzÀågÀ ¸À®ºÉ ¥ÀqÉAiÀÄÄwÛÃj ?
J) £ÉÆêÀÅ G0mÁzÀ vÀPÀët ( ) ©) £À0vÀgÀ £ÉÆêÀÅ PÀAqÀÄ §AzÁUÀ ( ) ¹) £ÉÆêÀÅ PÀAqÀÄ §AzÀÄ M0zÀÄ ªÁgÀzÀ £À0vÀgÀ. ( )
18. AiÀiÁªÀ ¸À0zÀ¨sÀðzÀ°è £ÀªÀÄUÉ ±À¸ÀÛç aQvÉìAiÀÄ CªÀ±ÀåPÀvÉ
EzÉ? J) ªÀÄÆvÀæzÀ°è gÀPÀÛ PÀt ( ) ©) ªÀÄÆvÀæzÀ°è GAmÁUÀĪÀ QêÀÅ ( ) ¹) ¸Àé®à ¥ÀæªÀiÁtzÀ DºÁgÀ. ( )
19. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®Äè G0mÁUÀzÀ ºÁUÉ ªÀ»¸ÀĪÀ
ªÀÄÄAeÁUÀævÉ ?
J) ¸Àé®à ¥ÀæªÀiÁtzÀ ¤ÃgÀÄ PÀÄrAiÀÄÄ«PÉ. ( )
116
©) zÉÆqÀØ ¥ÀæªÀiÁtzÀ ¤ÃgÀÄ PÀÄrAiÀÄÄ«PÉ. ( ) ¹) ¸Àé®à ¥ÀæªÀiÁtzÀ DºÁgÀ. ( )
20. ªÀÄÆvÀæPÉÆñÀzÀ vÉÆAzÀgÉUÉ M¼ÀUÁzÀªÀgÀÄ
PÀÄrAiÀĨÉÃPÁzÀ ¤Ãj£À ¥ÀæªÀiÁtªÉµÀÄÖ ? J) 1000 - 2000 JA J¯ï. ( ) ©) 2000 – 3000 JA J¯ï. ( ) ¹) 3000 – 4000 JA J¯ï. ( )
21. ºÀtÂÚ£À gÀ¸ÀzÀ°è eÁ¹Û EgÀĪÀ CA±ÀUÀ¼ÀÄ J) ¸ÉÆÃrAiÀÄA ( ) ©) ¥ÉÇmÁ¹AiÀÄ0 ( ) ¹) PÁå°ìAiÀÄA ( )
22. ºÀ¹vÀgÀPÁjAiÀÄ°ègÀĪÀ CA±ÀUÀ¼ÀÄ
J) PÁ¨ÉÆÃðºÉÊqÉæmïì ( ) ©) PÉÆ©â£À CA±À ( ) ¹) £ÁgÀÄ’ ( )
23. AiÀiÁªÀ ºÀtÂÚ£À°è PÁå°ìAiÀÄA C0±À eÁ¹Û EzÉ ?
J) ºÉÃgÀ¼É ( ) ©) ¸ÉÃ§Ä ( ) ¹) °A¨É ( )
24. AiÀiÁªÀ DºÁgÀzÀ°è ºÉZÀÄÑ AiÀÄÆjPï DªÀÄè«zÉ. J) ªÉÆmÉÖ ( ) ©) ¹» ¨Éæqï ( ) ¹) gÁV ( )
25. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®è£ÀÄß «¸Àfð¸ÀĪÀ°è AiÀiÁªÀ DºÁgÀ ¸ÀºÁ0iÀÄ ªÀiÁqÀÄvÀÛzÉ. J) PÁ¼ÀÄ ªÉÄt¸ÀÄ ( ) ©) ºÀÄt¸É ( ) ¹) ¨É®è ( )
26. C¸Àé¸ÀÜ¢AzÀ ºÁ¹UÉ »rzÀ gÉÆÃVUÉ ªÀÄÆvÀæPÉÆñÀzÀ PÀ¯ÁèUÀzÀAvÉ ªÀ»¸ÀĪÀ ªÀÄÄ£ÉßZÀÑjPÉ ? J) PÀrªÉÄ DºÁgÀ ¸ÉêÀ£É. ( ) ©) PÀrªÉÄ zÀæªÀ ¥ÀzÁxÀð ¸ÉêÀ£É. ( ) ¹) ªÀÄ®VzÀ ¹Üw §zÀ¯ÁªÀuÉ. ( )
27. ¸À¸ÁgÀd£ÀPÀ DºÁgÀ ¥ÀzÁxÀðªÀ£ÀÄß AiÀiÁPÉ vÀåf¸À¨ÉÃPÀÄ ? J) ªÀÄÆvÀæ£Á¼ÀzÀ°è R¤eÁA±À ¸À0ZÀAiÀĪÁUÀÄvÀÛzÉ. ( ) ©) ªÀÄÆvÉÆæÃvÀáwÛ eÁ¹ÛAiÀiÁUÀÄ«PÉ. ( ) ¹) ªÀÄÆvÀæzÀ ¹ÜgÀvÉ ( )
28. C¢üPÀ G¦à£À G¥ÀAiÉÆÃUÀ¢AzÀ G0mÁUÀĪÀ vÉÆAzÀgÉ. J) zÉúÀzÀ vÀÆPÀ eÁ¹ÛAiÀiÁUÀÄ«PÉ. ( ) ©) PÁå°ì÷ìAiÀÄ0 »ÃgÀÄ«PÉ ( ) ¹) gÀPÀÛzÀ MvÀÛqÀ PÀrªÉÄAiÀiÁUÀÄ«PÉ. ( )
117
29. AiÀiÁªÀ vÀgÀPÁjAiÀÄ°è PÁå°ìAiÀÄA CA±À«zÉ.
J) §mÁmÉ ( ) ©) mÉƪÉÄmÉÆà ( ) ¹) UÉÆøÀÄ ªÀÄmÉÖ ( )
30. PÁå°ìAiÀÄA PÀ®Äè EzÁÝUÀ AiÀiÁªÀ ¥Á¤Ã0iÀĪÀ£ÀÄß ¤ÃªÀÅ
vÉUÉzÀÄPÉƼÀÄîªÀÅ¢®è. J) PÀ®èAUÀr ºÀtÄÚ ( ) ©) ¨Á°ðAiÀÄ ¤ÃgÀÄ, ( ) ¹) ºÁ®Ä ( )
31. vÀÄA§ ¸ÀPÀÌgÉ EgÀĪÀ DºÁgÀ vÉUÉzÀÄPÉÆ0qÀgÉ DUÀĪÀ
vÉÆAzÀgÉ K£É ? J) ªÀÄÆvÀæzÀ PÀrªÉÄ GvÀàwÛ¬ÄazÀ ( ) ©) ªÀÄÆvÀæzÀ ¸ÀAZÀAiÀÄ ºÉZÀÄѪÀåzÀjAzÀ ( ) ¹) ªÀÄÆvÀæzÀ GvÁàzÀ£É vÀqÉMqÀÄتÀÅzÀjAzÀ ( )
32. AiÀiÁªÀ «zÀzÀ «Ää£À°è ºÉZÀÆÑ PÁå°ìAiÀÄA
zÉÆgÉAiÀÄÄvÀÛzÉ J) ªÀÄÆ¼É EgÀĪÀ ¸ÀtÚ «ÄãÀÄ. ( ) ©) ºÉZÀÄÑ ªÀiÁA¸À EgÀĪÀ «ÄãÀÄ. ( ) ¹) ¸ÁªÀiÁ£Àå jÃwAiÀÄ «ÄãÀÄ. ( )
33. J¯É CrPÉAiÉÆA¢UÉ ¸ÀÄtÚ w£ÀÄߪÀÅzÀ£ÀÄß AiÀiÁPÉ vÀqÉAiÀĨÉÃPÀÄ J) EzÀÄ ºÀ°è£À vÀÆvÀÄ (vÉÆAzÀgÉ)AiÀÄ£ÀÄß ºÉaѸÀÄvÀÛzÉ. ( ) ©) zÉúÀzÀ PÁå°ìAiÀÄ£À C0±À eÁ¹ÛAiÀiÁUÀÄvÀÛzÉ. ( ) ¹) ¨Á¬Ä ºÀÄtÂÚ£À ¸ÀªÀĸÉå eÁ¹ÛAiÀiÁUÀÄvÀÛzÉ. ( )
118
24. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®Äè EgÀĪÀªÀgÀÄ ªÀÄzsÀå¥Á£À vÉUÉzÀÄPÉƼÀî¨ÁgÀzÀÄ AiÀiÁPÉ ? J) ªÀÄzÀå¥Á£À ªÀÄÆvÀæªÀ£ÀÄß eÁ¹Û ªÀiÁqÀÄvÀÛzÉ. ( ) ©) R¤eÁ0±À ºÉgÀ¸ÀƸÀÄ«PÉ PÀrªÉÄ ªÀiÁqÀÄvÀÛzÉ. ( ) ¹) R¤eÁ0±À ªÀÄÆvÀæPÉÆñÀUÀ¼À°è ±ÉÃRj¸ÀÄvÀÛzÉ. ( )
34. ¤µÉâ¸ÀzÀ DºÁgÀªÀ£ÀÄß vÉUÉzÀÄPÉÆAqÁUÀ AiÀiÁªÀ
jÃwAiÀÄ ¥Á¤Ã0iÀÄ vÉUÉzÀÄPÉƼÀî¨ÉÃPÀÄ ? J) vÀA¥ÀÅ ¥Á¤ÃAiÀÄ ( ) ©) ±ÀÄzÀÝ ¤ÃgÀÄ ( ) ¹) ZÀºÁ ( )
ANSWER KEY
1. (b) 2 (c) 3 (b)
4 (b) 5 (b) 6 (c)
7 (b) 8 (c) 9 (a)
10 (b) 11 (c) 12 (a)
13 (a) 14 (a) 15 (a)
16 (c) 17 (a) 18 (c)
19 (b) 20 (c) 21 (b)
22 (c) 23 (c) 24 (b)
25 (c) 26 (a) 27 (b)
28 (b) 29 (c) 30 (b)
31 (a) 32 (b) 33 (c)

119
34 (b) Arbitrary Classification Total score - 34 Good - 0-11 Average - 12-23 Poor - 24-34
120
CONTENT OF TEACHING OUTLINE
1. TOPIC : Planned teaching programme on Renal calculi and its management
2. GROUP : Patients with Renal calculi
3. PLACE : Selected hospitals in Mangalore Taluk, KARNATAKA.
4. DURATION : 1 hour
5. METHOD OF TEACHING : Lecture cum discussion and demonstration
6. TEACHING AIDS : Charts, booklet on Planned teaching programme on Renal calculi and its management
7. CENTRAL OBJECTIVES : On completion of the education programme, the patients with renal calculi will acquire knowledge on renal calculi and its management, and will be able to change their dietary practices.
8. SPECIFIC OBJECTIVES : On completion of the sessions, the client will
list the organs involved in the formation and excretion of urine.
explain the meaning of urinary stone
explain the causes for the development of urinary stone
explain the problem caused by urinary stone explain the methods of confirming the presence of urinary stone
121
list the types of urinary stone
manage the problem without surgery
list the indication for surgery in urinary stone
explain the measures to prevent the recurrence of urinary stone
list some of the foods rich in calcium, uric acid, phosphorus and oxalate Time Objectives Content Teaching
Activity Learning Activity
A V Aids
I INTRODUCTION Urinary system is one of the important system which has the role of

122
4 min 3 min
on completion of this session the participant will be able to contribute in the discussion on recurrence of urinary stone. list the structures involved in the formation and excretion of urine.
excreting waste material from the body. This function may be impaired by many reasons. Important one among them is the presence of stone in the urinary system, which is referred to as urinary stone or renal calculi. Let us see how the disease presents. Mr. John, 40 years came to the hospital with the complaints of severe, agonizing pain passing from loin to groin, vomiting and profuse sweating. He was diagnosed to have urinary stone. Ultrasonography report showed that the stone was large enough and needed to remove only by surgical method. When asked about his disease, he said that he had attacks for three times before. The pain relieved by taking pain killers as per the advice given by his relative. This time the pain was so severe that the pain killer did not help to relieve pain. So he came to the hospital. And he is in need of surgery which might not be required if had sought medical help in time. There are so many such conditions of Mr. John among us that signify the importance of planned teaching programme regarding renal calculi and its management in order to minimize the further progression of stone thereby reducing further complications and morbidity. II THE STRUCTURES INVOLVED IN THE FORMATION AND EXCRETION OF THE URINE. The structures involved in the formation and excretion of the urine are Kidney, Ureter, Bladder and Urethra. Whatever we eat and drinks gets mixed with the enzymes present in the mouth, stomach and small intestine, and get broken down into very small pieces. Some of these small particles get mixed with blood. Blood also gets mixed with oxygen present in the air we breathe. This blood gets circulated throughout our body and supplies food and oxygen to all the body parts for their proper functioning. Thus the kidneys also get their share of blood. Kidneys retain the substance which are useful and the substances which are waste products and harmful for the body are removed along with extra water. III WHAT DO YOU MEAN BY URINARY STONE? Urinary stone is a hard stone like substance which is formed by deposition of certain chemical substances in the structures involved in formation and excretion of
Narration and discussion on urinary stone Lecture cum discussion
Listening and participating in the discussion Listening and asking questions
Charts

123
2 min 14 min
explain the meaning of urinary stone explain the cause for the development of urinary stone.
urine. These chemical substances are mainly calcium, uric acid and phosphorus. These are also known as minerals. IV CAUSES OF DEVELOPMENT OF URINARY STONE a) Fluid intake
This include water and other liquid food stuffs our body need about 2 – 3 liters of water/fluid intake per day and lost nearly the same amount in the form of urine, sweat, feces and through breaths. If we do not drink adequate water to compensate the loss, our urine becomes thick with minerals like calcium, oxalate and phosphorus. Deposition of these minerals in urine may lead to formation of stones. b) Food Habits
The food stuff which we eat daily contains all the nutrients including minerals. For example, Green leafy vegetables are the rich sources of calcium and oxalates. Likewise, milk and milk products are the rich source of calcium and phosphates. And such foodstuff is very good for health and we need to eat in plenty. At the same time we should also drink more amount of water so that more amounts of oxalate and calcium will be excreted from our body. If we do not drink adequate amount of water, the calcium or the oxalate or the phosphate will get deposited and give rise to stone formation. Similarly, if we eat food stuff which are rich in uric acid or magnesium or cystine without drinking adequate water, it will cause formation of urinary stones. Other habits include alcohol, chewing betal leaves, smoking. c) Climate
During hot weather, we sweat profusely and pass less urine. We know that the metabolic waste products from the body are excreted through urine. When we pass less urine, these waste products are retained in the urine, that is why urine becomes thick and look dark in color and it has a very strong smell. In addition, we expose ourselves to the sun, so more vitamin D is formed in our body. This vitamin D helps to absorb more calcium from the food we eat and send it to the blood stream. Therefore calcium level increases in our blood and contribute formation of calcium stone.
Questioning what is urinary stone? Lecturing, discussion, questioning Lecturing, discussing, questioning List the causes of development
Answering Listening Answering Listening Taking part in the discussion Answering
Charts
124
d) Occupation People who have to work in the direct sun almost everyday for a long time have more chance of getting urinary stone. Because they sweat too much and generally pass concentrated urine. Such people are coolie workers, farmers etc. e) Vitamin A
Cement is necessary for the construction of a smooth wall. Solid dirt cannot attach easily on a smooth wall. Similarly, if the wall of our urinary pathway is smooth, these minerals cannot get deposited easily on it and form the stone. Vitamin A, which is richly found in yellow foods like carrot, helps to maintain the smoothness of the urinary pathway wall. Hence, if our daily food is lacking in vitamin A, the smooth wall of the urinary pathway becomes rough, the minerals gets deposited on it and cause stone formation. f) Hyperparathyroidism Our bones are made up of mainly calcium. In patient with hyperparathyroidism, much of calcium is removed from the bones, which gets absorbed in the blood and from blood it goes to the kidney. The excess amount of calcium gets deposited in the urinary pathway and helps in the formation of urinary stone. g) Infection of the urinary tract Some disease causing micro-organisms (which cannot be seen by our naked eye) can get into the urinary pathway through blood. They can also enter directly from outside if out private parts are not cleaned properly. Also when there is an obstruction in the pathway of urine flow, the micro-organisms can grow in the stagnated urine causing infections. Such infections may lead to the formation of urinary stone. h) Prolonged illness and restricted movement i) Prolonged illness, particularly when a patient is immobilized, as in the case of paralysis (weakness) of hands and/or legs or treatment of features, the small calcium particles get loosened from the bones and deposited in the urinary pathway walls. If the condition continues for a long period of time, gradually
of urinary stone
125
the calcium stones are formed in our urinary pathway. ii) Dependency (position of the kidney): urine cannot come out freely increasing stagnation of urine leading to stone formation. Some urine always retained in the renal pelvis in supine position. i) Drugs Certain drugs which we take to relieve stomach pain like antacid also cause urinary calcium (stone). Other common drugs are Diamox, vitamin D, high dose of aspirin, laxatives etc. j) Congenital malformations and stasis Any defect by birth in any of the organs involved in urine formation and excretion (may be in renal pelvis; ureter or bladder), stasis due to stricture (narrowing) or prostatic enlargement, may predispose to the formation of urinary stone. k) Hereditary Urinary stones are found to occur among blood relatives. It can transfer from one generation to other, like parents to children. But the chances of recurrence of urinary stone is more in males than females. V Signs and symptoms of urinary stone a) Sometimes there may be no symptom i.e silent type.
b) Sharp, severe pain: there will be a sudden, sharp severe pain in the mid lateral abdomen, flanks or groin which radiates toward genitalia and thigh. It is the natural warning signal for going for a medical check up. c) Fever, chills, shivering and vomiting shows that there are disease-causing micro-organisms in the urinary pathway d) Pain in the flanks even on mild touch e) Frequent loose stools f) Feeling of vomiting or vomiting g) Decreased amount of urine h) Difficulty in passing urine i) Presence of blood in the urine j) Feeling of fullness in the urinary bladder k) Increased frequency of urination
126
4 min 3 min 3 min
explain the problems caused by urinary stone. explain the methods of confirming the presence of urinary stone. list the types of urinary
l) Cold moist skin m) Guarding and rigidity of the back and abdominal muscles during severe attack of pain VI How will you confirm the presence of urinary stone You need to collect urine in a small pot and check for the presence of any hard sand like particles and the presence of blood. If blood is present in urine you need to seek immediate medical help in any clinic/hospital where the urine will be sent for laboratory test to confirm the presence of stone. There are some other tests which may be done to confirm the presence of urinary stone. They are blood tests, special X – rays, ultrasonography, etc. VII Types of urinary stone Depending on the minerals that form stone, there are different types of stone. They are calcium, oxalate, phosphorus or mixed stones which contains little of all these minerals. Stones which are made up of calcium is known as calcium stones; stones which are made up of oxalate is known as oxalate stones and stones which are made up of phosphorus is known as phosphorus stones. Other types are uric acid which are common for the people who consume red meat and also in patients with gout (a disease condition due to deposition of large amount of uric acid in the cartilage and joints), cystine, xanthine and struvite stones. VIII How to mange when stone is present in urinary pathway If the size of the stone is small (< 0.5 cm in diameter) to pass through the urinary pathway, you need to drink large amount of water or infuse large amount of fluids into the veins. This will help to remove stone from the urinary pathway. IX When do we need an operation When
• the stone is too large to pass with urine • the stone is formed because of chronic infections • the stone is causing persistent pain and severe vomiting • the signs and symptoms are not relieved only with medicine
Lecture cum
Listening
Charts
127
2 min 3 min 8 min
stone. explain the management without surgery list the indications for surgery in urinary stone explain the measures to prevent the recurrence of urinary stone
X Prevention of recurrence of urinary stones There are many things that we need to consider to prevent the recurrence of urinary stone. Here we shall talk about some common activities which we should do and some which we should not do for the prevention of recurrence of urinary stone. DO’S
• Increase the fluid intake At least 3 – 4 liters of water per day (15 – 16 glass of water, 1 glass = 200 ml water). Plain water, coconut water, barley water, sherbet, weak tea, fruit juice can be taken to dilute the urine. Diluted urine prevents the concentration of the solids in it and thus prevents the stone formation. A heavy manual worker in a hot humid climate should drink more fluids than a sedentary office worker in a cooler climate, to compensate for the fluid loss through perspiration.
Remember clear water is better than artificial sweetened drinks e.g. Pepsi, cola etc.
Increase the intake of fruit juice, because fruit juice help in the breaking down of the stone into small pieces and thus gets excreted easily with the urine
Eat plenty of fruits and raw vegetables, which are rich in fiber. The fiber causes break down of the minerals and facilitates its elimination from the blood.
Add more tamarind in your food it helps in the excretion of urinary stone. Seek prompt and proper treatment for any type of discomfort in excretion of
urine. For example, burning sensation and pain while passing urine. For the patients who are bed ridden position should be changed frequently
and body and private parts should be cleaned thoroughly several times a day.
DON’TS Avoid excessive consumption of strong tea and coffee because the mineral oxalate is present in more quantity in it.
discussion Lecturing Lecture cum discussion Asking questions
And taking part in the discussion Listening and taking part in discussion Answering the questions and asking doubts
charts
128
Cut down the animal protein (e.g. Milk, Egg, Meat, etc). Because proteins will increase the amount of calcium, oxalate, minerals in our blood and excess minerals will get accumulated in the urinary pathway and cause formation of urinary stone.
Do not include more than one of the following items in your daily meals. o Egg – 1 o Meat – One portion ( 25 grams) o Fish – One portion ( 25 grams) o Milk – 200 ml o Cheese – 20 grams
Avoid too much of refined food e.g. white sugar. Cut down sugar in the drinks because white sugar increases the
concentration of the urine. Avoid sweets, chocolates, soft drinks, tinned fruits, sweet cakes, and
biscuits as these contains high amount of white sugar. Avoid drinking alcohol because alcohol increases the excretion of the uric
acid, calcium and phosphate in urine which may get deposited and form urinary stone
Avoid eating pan (betel leaves) with lime because it increases the calcium consumption and calcium amount in the body. Lime contains high amount of calcium.
Avoid adding extra salt to your food because salt increases the calcium absorption from the blood and there by increases the chance of development of urinary stone.
Avoid smoking. If not possible try to reduce the number of cigarettes and increase the internal between two smokes, because it increases the elimination of more minerals.
Avoid spending more time under direct sun. If unavoidable and you sweat more, drink plenty of water (10 – 15 glass of water daily). Use sun shade like hats while working under the direct sun.
Avoid stressful situations do relaxation, yoga, meditation, etc.
Lecture / discussion Lecture / discussion Lecture cum discussion Asking discussion
listening Taking part in discussion Taking part in discussion And Asking doubts
Charts
129
4 min
list some of the foods rich in calcium,
XI Foods to be restricted i) FOR PATIENTS WHO HAVE CALCIUM STONES The patients with calcium stones should restrict the intake of calcium. The following are some of the food stuffs rich in calcium, increase the amount of water intake if you are taking these foods. a) VEGETABLES: Green leafy vegetables (beans, spinach, carrot leaves, agathy, pumpkin leaves), potatoes, cauliflower, soya beans. The spinach is having more amount of calcium than oxalate and phosphorus. b) CEREALS: Ragi is one of the richest source of calcium. c) FRUITS: Dried fruits (grapes), nuts, peanuts. The citrus fruits like lime and lemon are richest source of calcium. d) FOODE CONTAINING FLOURS: Bread. Oat meal. e) BEVERAGES: Tea, Cocoa, Pepsi, Cola, Bear, Milkshakes, Ice creams, Milk and milk products (butter, ghee, cheese, milk powder etc.) f) FISH: Small fishes with bones and dried fishes. g) OTHERS: Ragi, excess salt, cake, pickle, cheese, egg yolk. h) VITAMIN D RICH FOODS: Fish liver oil (cod liver oil, shark liver oil), fatty fish, egg (hen). i) CHEWING BETAL LEAVES J) HARD WATER (water which does not make lather)
ii) FOR PATIENTS WHO HAVE URIC ACID STONES The patients having uric acid stones should restrict the foods rich in uric acid. The following are some of the foods rich in uric acid, you have to drink extra amount of water if you consume the following foods. a) VEGETABLES: Beans (dried, baked, green), Fenu green leaves. b) CEREALS: Bengal gram, black gram, green gram, horse gram, lentils whole, peas dry, red gram. c) NUTS: Groundnut, mustard seed. d) OTHERS: Sweet breads is one of the commonest source of uric acid. e) ALL TYPES OF MEAT f) ALL TYPES OF FISH
130
4 min 4 min
list some of the foods rich in uric acid list some of the foods rich in phosphorus
iii) FOR PATIENTS WHO HAVE PHOSPHATE STONES Patients who diagnosed to have phosphate stone should restrict the intake of excess amount of phosphorus. The following are some foods rich in phosphorus, you have to drink extra amount of water if you consume the following foods. a) VEGETABLES: Green leafy vegetables (carrot leaves, amaranth, agathi), Carrot, Potato, Cauliflower, beans. b) FRUITS: Banana, Custard apple. c) Whole cereals: Bagra, Maize, Oat meal, Little millet, Wheat flour> d) PULSES: Beans, Lentils, Peas, Bengal gram dhal, Soya bean. e) NUTS AND OIL SEEDS f) FISH: Small g) MEAT: Beef, Liver. h) EGG: Hen i) MILK AND MILK PRODUCTS j) FOODS CONTAINING FLOURS: Sweet breads. iv) FOR PATIENTS WHO HAVE OXALATE STONES Patients who diagnosed to have oxalate stone should restrict the intake of excess amount of oxalate. The following are some foods phosphorus. You have to drink extra amount of water if you consume the following foods. a) VEGETABLES: Spinach, tomato b) FRUITS: Chickoo, strawberries c) BEVERAGES: Cocoa, Tea, Chocolates d) NUTS: Cashew nuts, groundnuts e) MEAT: Beef
SUMMARY Teaching points
• Meaning of urinary stone
Demonstration
Taking part in discussion Taking part in discussion
Real models
131
2 min
list some of the foods rich in oxalate
• Causes of urinary stone • Signs and symptoms • Diagnostic tests • Management and indications for surgery • Measures to prevent the recurrence of urinary stone.
EVALUATION QUESTIONS
1. What are the structures involved in the formation and excretion of urine? 2. What is the function of kidney? 3. What do you mean by urinary stone? 4. List the causes of urinary stone. 5. What are the problems that develop due to urinary stone? 6. How will you confirm the presence of urinary stone? 7. What are the types of urinary stone? 8. What is the management of urinary stone? 9. When does a person need surgery for urinary stone? 10. Why do you need to take large amount of fluid for prevention of urinary
stone? 11. How does hot weather increases the chances of the urinary stone? 12. How does hyperparathyroidism lead to urinary stone? 13. Mention some of the foods rich in - calcium, uric acid, phosphorus and
oxalate. CONCLUSION Today we have discuss about urinary stone and its management and how few changes in our daily food practice can help in prevention of recurrence of urinary stone.
Demonstration Demonstration Demonstration
Taking part in discussion Taking part in discussion Taking part in discussion
Real Models Real Models Real models
132
11b ¨sÉÆÃzsÀ£Á ¥Àj«r
1. «µÀAiÀÄ : ªÀÄÆvÀæ PÉÆñÀzÀ PÀ®ÄèUÀ¼ÀÄ ªÀÄvÀÄÛ CzÀgÀ PÁAiÀÄð¤ªÀðºÀuÉAiÀÄ §UÉÎ ºÀ«ÄäPÉƼÀî¨ÉÃPÁzÀ PÀ°PÁ PÁAiÀÄðPÀæªÀÄ. 2. UÀÄA¥ÀÅ : ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼À£ÀÄß ºÉÆA¢gÀĪÀ gÉÆÃUÀUÀ¼ÀÄ. 3. ¸ÀܼÀ : ªÀÄAUÀ¼ÀÆgÀÄ vÁ®ÆQ¤AzÀ Dj¹zÀ D¸ÀàvÉæUÀ¼ÀÄ. 4. PÁ¯ÁªÀ¢ü : M0zÀÄ UÀAmÉ 5. PÀ°PÁ «zsÁ£À : G¥À£Áå¸ÀzÀ eÉÆvÉUÉ ZÀZÉð ªÀÄvÀÄÛ ¥ÀæªÀiÁtÂÃPÀgÀt 6. PÀ°PÁ ªÀiÁzsÀåªÀÄUÀ¼ÀÄ : £ÀPÉëUÀ¼ÀÄ, ¥ÀŸÀÛPÀUÀ¼ÀÄ, ¸ÉàöÊqÀÄUÀ¼ÀÄ ªÀÄvÀÄÛ «ÃrAiÉÆà PÁå¸ÉmïUÀ¼À
ªÀÄÆ®PÀ ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼À §UÉÎ ªÀÄvÀÄÛ CzÀgÀ PÁAiÀÄð¤ªÀðºÀuÉ §UÉÎ PÀ°PÁ PÁAiÀÄðPÀæªÀĪÀ£ÀÄß ºÀ«Ää PÉƼÀÄîªÀÅzÀÄ.
7. ªÀÄÄRå UÀÄtUÀ¼ÀÄ : PÁAiÀÄðPÀæªÀÄzÀ ªÀÄÄPÁÛAiÀÄzÀ ºÀ0vÀzÀ°è ªÀÄÆvÀæPÉÆñÀzÀ PÀ®è£ÀÄß ºÉÆA¢gÀĪÀ gÉÆÃVAiÀÄÄ ªÀÄÆvÀæPÉÆñÀzÀ PÀ°è£À ¨É¼ÀªÀtÂUÉ ªÀÄvÀÄÛ CzÀgÀ PÁAiÀÄð¤ªÀðºÀuÉAiÀÄ §UÉÎ w¼ÀĪÀ½PÉAiÀÄ£ÀÄß ¥ÀqÉAiÀÄĪÀÅzÀgÀ eÉÆvÉUÉ CªÀgÀÄ vÀªÀÄä ¢£À¤vÀåzÀ DºÁgÀzÀ°è §zÀ¯ÁªÀuÉAiÀÄ£ÀÄß ªÀiÁrPÉƼÀÄî®Ä ±ÀPÀågÀ£ÁßV¸ÀĪÀÅzÀÄ F PÀ°PÁ PÁAiÀÄðPÀæªÀÄzÀ ªÀÄÆRå UÀÄjAiÀiÁVzÉ
133
8. ¤²ÑvÀ UÀÄjUÀ¼ÀÄ : vÀgÀUÀw ªÀÄÄVAiÀÄĪÀ ªÉüÉUÉ gÉÆÃVAiÀÄÄ ªÀÄÆvÀæPÉÆñÀzÀ°è ªÀÄÆvÀæzÀ GvÁàzÀ£É ªÀÄvÀÄÛ «¸Àdð£É0iÀÄ°è ¨sÁVAiÀiÁUÀĪÀ
CAUÀªÀ£ÀÄß ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ. ªÀÄÆvÀæ PÉÆñÀzÀ PÀ®ÄèUÀ¼À CxÀðªÀ£ÀÄß «ªÀj¸ÀĪÀÅzÀÄ. ªÀÄÆvÀæ PÉÆñÀzÀ PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉUÉ PÁgÀtªÀ£ÀÄß UÀÄgÀÄw¸ÀĪÀÅzÀÄ. ªÀÄÆvÀæ PÉÆñÀzÀ PÀ®ÄèUÀ½AzÀÄAmÁUÀĪÀ vÉÆAzÀgÉUÀ¼À£ÀÄß «ªÀj¸ÀĪÀÅzÀÄ. ªÀÄÆvÀæPÉÆñÀzÀ°è PÀ®ÄèUÀ½ªÉ JA§ÄzÀ£ÀÄß zÀÈrüÃPÀj¸ÀĪÀ «zsÁ£ÀUÀ¼À£ÀÄß «ªÀj¸ÀĪÀÅzÀÄ ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼À «zsÀUÀ¼À£ÀÄß ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ ±À¸ÀÛaQvÉì gÀ»vÀ vÉÆAzÀgÉAiÀÄ£ÀÄß ¸Àj¥Àr¸ÀĪÀÅzÀÄ. ªÀÄÆvÀæPÉÆñÀzÀ PÀ°è£À ±À¸ÀûçaQvÉìAiÀÄ CUÀvÀåvÉAiÀÄ ¸ÀÆZÀ£Á ¥ÀnÖ. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼ÀÄ ¥ÀÅ£ÀgÁªÀvÀð£ÉAiÀiÁUÀzÀAvÉ ªÀ»¸ÀĪÀ ªÀÄÄ£ÉßZÀÑjPÉ. DºÁgÀzÀ°è PÁå°ìAiÀÄA, ¥sÁ¸ÉáÃmï, AiÀÄÆjPï Då¹qï ªÀÄvÀÄÛ DPÀì¯ÉÃmï ºÉZÁÑVgÀĪÀ DºÁgÀ
ªÀ¸ÀÄÛUÀ¼À ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ.
134
¸ÀªÀÄAiÀÄ £Á®ÄÌ ¤«ÄµÀ UÀ¼ÀÄ ªÀÄÆgÀÄ
UÀÄjUÀ¼ÀÄ vÀgÀUÀw ªÀÄÄVAiÀÄĪÀ ªÉüÉUÉ PÁAiÀÄð PÀæªÀÄzÀ°è ¨sÁUÀªÀ»¹zÀªÀgÀÄ ªÀÄÆvÀæ PÉÆñÀzÀ PÀ®ÄèUÀ¼À ¥ÀÅ£ÀgÁªÀ vÀð£É §UÉÎ ZÀað¸À®Ä ¸ÀªÀÄxÀðgÁVgÀÄvÁÛgÉ.
¥Àj«r ¥ÀjZÀAiÀÄ : ªÀÄÆvÀæ «¸Àdð£ÁAUÀ ªÀÇåºÀªÀÅ M0zÀÄ ªÀÄÄRå ªÀåªÀ¸ÉÜAiÀiÁVzÀÄÝ, CzÀÄ ¨ÉÃqÀªÁzÀ vÁådå ªÀ¸ÀÄÛUÀ¼À£ÀÄß zÉúÀ¢AzÀ ºÉÆgÀ ºÁPÀĪÀ°è ªÀÄÄRå ¥ÁvÀæªÀ»¸ÀÄvÀÛzÉ. EzÀgÀ PÁAiÀÄ𠤪ÀðºÀuÉAiÀÄÄ ¨ÉÃgÉ ¨ÉÃgÉ PÁgÀtUÀ½AzÀ KgÀÄ¥ÉÃgÁUÀÄvÀÛzÉ. CªÀÅUÀ¼À°è ªÀÄÄRåªÁzÀÄzÉAzÀgÉ E0zÀÄ ªÀÄÆvÀæPÉÆñÀzÀ°è PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉ CzÀ£ÀÄß ªÀÄÆvÀæ PÉÆñÀzÀ PÀ®ÄèUÀ¼É0zÀÄ PÀgÉAiÀÄÄvÁÛgÉ. FUÀ £ÁªÀÅ F ªÀÄÆvÀæPÉÆñÀzÀ PÀ®Äè ºÉÃUÉ GvÀàwÛ DUÀÄvÀÛzÉ J0zÀÄ w½AiÉÆÃt. £À®ªÀvÀÄÛ ªÀµÀð ¥ÁæAiÀÄzÀ eÁ£ï JA§ªÀgÀÄ ¸ÉÆAl ªÀÄvÀÄÛ vÉÆqɸÀ0zÀÄ«£À°è AiÀiÁvÀ£ÁªÀÄAiÀÄ £ÉÆêÀÅ, ªÁ0wªÀiÁqÀĪÀÅzÀÄ ºÁUÀÆ CwzsÁgÁ¼ÀªÁzÀ ¨ÉªÀj¤AzÀ §¼À®ÄwÛgÀĪÀÅzÁV D¸ÀàvÉæUÉ §A¢zÀÝgÀÄ. CªÀjUÉ ªÀÄÆvÀæPÉÆñÀzÀ°è PÀ®ÄèUÀ½ªÉ J0zÀÄ gÉÆÃUÀ ¤tðAiÀÄ ªÀiÁqÀ¯Á¬ÄvÀÄ. C¯ÁÖç¸ÉÆãÉÆÃUÀæ¦ ªÀgÀ¢AiÀÄ ¥ÀæPÁgÀ Qrß PÀ®Äè vÀÄA¨Á zÉÆqÀØzÁVzÀÄÝ CzÀ£ÀÄß ±À¸ÀÛçaQvÉÛAiÀÄ ªÀÄÆ®PÀ ºÉÆgÀvÉUÉAiÀħºÀÄzÀÄ J0zÀÄ eÁ£ïUÉ ºÉýzÁUÀ, eÁ£ï F gÉÆÃUÀªÀÅ EzÀQÌAvÀ ªÉÆzÀ®Ä ªÀÄÆgÀÄ ¸À® DPÀæªÀÄt ªÀiÁrzÉ J0zÀgÀÄ. £ÉÆêÀŤªÁgÀPÀ ªÀiÁvÉæAiÀÄ£ÀÄß vÉUÉzÀÄPÉÆAqÁUÀ ªÀiÁvÀæ £ÉÆêÀÅ PÀrªÉÄAiÀiÁUÀÄvÀÛzÉ J0zÀÄ CªÀgÀ ¸ÀA§A¢üPÀgÀÄ ºÉýzÀgÀÄ. DzÀgÉ FUÀ £ÉÆêÀÅ ¤ªÁgÀPÀ ªÀiÁvÉæ vÉUÉzÀÄPÉÆAqÀgÀÄ £ÉÆêÀÅ PÀrªÉÄAiÀiÁUÀzÉ EgÀĪÀzÀjAzÀ D¸ÀàvÉæUÉ §A¢zÀÝgÀÄ, ªÀÄvÀÄÛ CªÀjUÉ ±À¸ÀÛç
PÀ°PÁ ZÀlĪÀ nPÉUÀ¼ÀÄ «ªÀj¸ÀÄ«PÉ ªÀÄvÀÄÛ ªÀÄÆvÀæ PÉÆñÀzÀ PÀ°è£À §UÉÎ ZÀað¸ÀĪÀÅzÀÄ G¥À£Áå¸À ªÀÄvÀÄÛ
PÀ°AiÀÄĪÀ ZÀlĪÀnPÉ PÉüÀĪÀÅzÀÄ ªÀÄvÀÄÛ ZÀZÉðAiÀÄ°è ¨sÁUÀªÀ»¸ÀÄ ªÀÅzÀÄ
DrAiÉÆà «ÃrAiÉÆà ªÀiÁzsÀåªÀÄ £ÀPÉëUÀ¼ÀÄ
135
¤«ÄµÀ UÀ¼ÀÄ ºÀ¢£Á ®ÄÌ ¤«ÄµÀ UÀ¼ÀÄ
ªÀÄÆvÀæzÀ vÀAiÀiÁj ªÀÄvÀÄÛ «¸Àdð£É0iÀÄ°è ¨sÁVAiÀiÁVgÀĪÀ C0UÀUÀ¼À£ÀÄß ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼À CxÀðªÀ£ÀÄß «ªÀj¸ÀĪÀÅizÀÄ Qrß PÀ®ÄèUÀ¼À GvÀàwÛUÉ PÁgÀtUÀ¼À£ÀÄß «ªÀj¸ÀĪÀÅz
aPÉvÉì CUÀvÀåªÁV ¨ÉÃPÀÄ. KPÉAzÀgÉ CªÀgÀÄ ¸ÀjAiÀiÁzÀ ¸ÀªÀÄAiÀÄzÀ°è aQvÉìAiÀÄ£ÀÄß ¥ÀqÉ¢zÀÝgÉ F ±À¸ÀÛçaQvÉìAiÀÄ CªÀ±ÀåPÀvÉ EgÀÄwÛgÀ°®è. F QrßPÀ®ÄèUÀ¼ÀÄ ªÀÄvÀÄÛ CzÀgÀ PÁAiÀÄð¤ªÀðºÀuÉ §UÉÎ w½zÀÄPÉƼÀî®Ä ºÁUÀÆ ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼ÀÄ ¥ÀÅ£ÀgÁªÀvÀð£ÉAiÀiÁUÀzÀ0vÉ ºÁUÀÆ D §UÉÎ ªÀÄÄAzÉ vÀ¯ÉzÉÆgÀ§ºÀÄzÁzÀ vÉÆAzÀgÉUÀ¼ÀÄ ªÀÄvÀÄÛ VüÀ£ÀÄß PÀrªÉĪÀiÁqÀĪÀÅzÀgÀ §UÉÎ w½zÀÄPÉƼÀî®Ä eÁ£ïgÀAvÀ C£ÉÃPÀgÀÄ £ÀªÉÆäqÀ¤zÁÝgÉ. 2. ªÀÄÆvÀæzÀ vÀAiÀiÁj ªÀÄvÀÄÛ «¸Àdð£É0iÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀ CAUÀzÀ gÀZÀ£É :- ªÀÄÆvÀæzÀ GvÁàzÀ£É ªÀÄvÀÄÛ «¸Àdð£É0iÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀ C0UÀUÀ¼É0zÀgÉ ªÀÄÆvÀæd£ÀPÁAUÀ (Qrß), ªÀÄÆvÀæ£Á¼À, ªÀÄÆvÀæPÉÆñÀ (AiÀÄÆj£Àj ¨ÁèqÀgï) ªÀÄvÀÄÛ AiÀÄÆgÉvÀæ¢AzÀ ªÀÄÆvÀæªÀ£ÀÄß ºÉÆgÀºÁPÀĪÀ CAUÀ. £ÁªÀÅ w£ÀÄߪÀ ªÀÄvÀÄÛ PÀÄrAiÀÄĪÀ AiÀiÁªÀÅzÉà DºÁgÀ ªÀ¸ÀÄÛUÀ¼ÀÄ ¨Á¬Ä, doÀgÀ, ¸ÀtÚPÀgÀĽ£À°ègÀĪÀ QtéUÀ¼À ¸ÀºÁ0iÀÄ¢AzÀ ¸ÀtÚ ¸ÀtÚ ZÀÆgÀÄUÀ¼ÁV ¥ÀjªÀwð¸ÀĪÀÅzÀÄ F ¸ÀtÚ DºÁgÀzÀ PÀtUÀ¼ÀÄ gÀPÀÛzÀ eÉÆvÉ ¨ÉgÉvÀÄ £ÀªÀÄä zÉúÀzÀ J¯Áè ¨sÁUÀUÀ½UÉ ¥ÀjZÀ°¸ÀÄvÀÛzÉ. »ÃUÉ gÀPÀÛªÀÅ DºÁgÀ ªÀÄvÀÄÛ DªÀÄèd£ÀPÀªÀ£ÀÄß zÉúÀzÀ J¯Áè ¨sÁUÀUÀ½UÉ PÉÆAqÉÆAiÀÄÄÝ zÉúÀªÀÅ ¸ÀjAiÀiÁzÀ jÃwAiÀÄ°è PÉ®¸À ªÀiÁqÀÄvÀÛzÉ. QrßAiÀÄÄ PÀÆqÀ gÀPÀÛzÀ ¥Á®£ÀÄß ¥ÀqÉAiÀÄÄvÀÛzÉ. QrßAiÀÄÄ zÉúÀPÉÌ CUÀvÀåªÁzÀ ªÀ¸ÀÄÛUÀ¼À£ÀÄß Ej¹PÉÆAqÀÄ C£ÀUÀvÀå vÁdå ªÀ¸ÀÄÛUÀ¼À£ÀÄß zÉúÀ¢AzÀ ¨ÉÃqÀªÁzÀ ¤Ãj£À ªÀÄÆ®PÀ «¸Àfð¸ÀÄvÀÛzÉ. 3. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼É0zÀgÉãÀÄ ? ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼Ài UÀnÖAiÀiÁzÀ PÀ°è£ÀAwzÀÄÝ CzÀÄ ªÀÄÆvÀæ GvÁࢸÀĪÀ ªÀÄvÀÄÛ
ZÀað¸ÀĪÀÅzÀÄ. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼É0zÀgÉãÀÄ J0zÀÄ ¥Àæ²ß¸ÀĪÀÅzÀÄ. G¥À£Áå¸À, ZÀað¸ÀĪÀÅzÀÄ ¥Àæ²ß¸ÀĪÀÅzÀÄ.
PÉüÀĪÀÅzÀÄ ªÀÄvÀÄÛ ¥Àæ²ß¸ÀĪÀÅzÀÄ. GvÀÛj¸ÀĪÀÅzÀÄ. PÉüÀĪÀÅzÀÄ GvÀÛj¸ÀĪÀÅzÀÄ
£ÀPÉëUÀ¼ÀÄ.

136
À Qrß PÀ®ÄèUÀ½AzÀ GAmÁUÀĪÀ vÉÆAzÀgÉAiÀ£ÀÄß «ªÀj¸ÀĪÀÅzÀÄ.
«¸Àdð£ÁAUÀzÀ°è gÁ¸ÁAiÀĤPÀ ªÀ¸ÀÄÛUÀ¼ÀÄ ±ÉÃRgÀuÉAiÀiÁzÁUÀ GAmÁUÀÄvÀÛzÉ. F gÁ¸ÁAiÀĤPÀ ªÀ¸ÀÄÛUÀ¼É0zÀgÉ PÁå°ìAiÀÄA, AiÀÄÆjPï Då¹qï ªÀÄvÀÄÛ ¥sÁ¸ÉÆáÃgÀ¸ï EªÀÅUÀ¼À£ÀÄß R¤eÁ0±ÀUÀ¼É0zÀÆ PÉgÉAiÀÄÄvÁÛgÉ. 4. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉUÉ PÁgÀtUÀ¼ÀÄ J) zÀæªÀ ¥ÀzÁxÀðUÀ¼À ¸ÉêÀ£É: EzÀÄ ¤ÃgÀÄ ªÀÄvÀÄÛ zÀæªÀ¨sÀjvÀ DºÁgÀ ªÀ¸ÀÄÛUÀ¼À£ÀÄß M¼ÀUÉÆArzÀÄÝ £ÀªÀÄä zÉúÀPÉÌ ¢£ÀPÉÌ JgÀqÀjAzÀ ªÀÄÆgÀÄ °Ãl£ÀðµÀÄÖ ¤ÃgÀÄ/zÀæªÀ ¥ÀzÁxÀð ¨ÉÃPÁUÀÄvÀÛzÉ. ªÀÄvÀÄÛ CµÉÖà ¥ÀæªÀiÁtzÀ ¤ÃgÀÄ ªÀÄÆvÀæ, ¨ÉªÀgÀÄ ªÀÄ®zÀgÀÆ¥ÀzÀ°è ªÀÄvÀÄÛ G¹gÁlzÀ ªÀÄÆ®PÀ ºÉÆgÀºÉÆÃUÀÄvÀÛzÉ. ºÉÆgÀºÉÆÃzÀ ¤Ãj£À PÉÆgÀvÉAiÀÄ£ÀÄß ¸ÀjzÀÆV¸À®Ä ¸ÀjAiÀiÁzÀ ¥ÀæªÀiÁtzÀ°è ¤ÃgÀ£ÀÄß vÉUÉzÀÄPÉƼÀî¢zÀÝgÉ £ÀªÀÄä ªÀÄÆvÀæªÀÅ PÁå°ìAiÀÄA, DPÀì¯ÉÃmï ªÀÄvÀÄÛ ¥sÁ¸ÉÆáÃgÀ¸ï R¤eÁA±ÀUÀ¼À eÉÆvÉ ¸ÉÃj ªÀÄvÀÄÛ F R¤eÁA±ÀUÀ¼ÀÄ ªÀÄÆvÀæzÀ°è ±ÉÃRgÀuÉAiÀiÁV ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼ÀÄAmÁUÀÄvÀÛzÉ. ©) DºÁgÀ (¥ÀzÀÞw) PÀæªÀÄ : £ÁªÀÅ ¢£Á®Æ vÉUÉzÀÄPÉƼÀÄîªÀ DºÁgÀzÀ°è ¥ÉǵÀPÁ0±ÀUÀ½zÀÄÝ R¤eÁA±ÀUÀ½AzÀ PÀÆÃrgÀÄvÀÛzÉ. GzÁgÀuÉ : ºÀ¹gÀÄ J¯É vÀgÀPÁjUÀ¼À°è ºÉaÑ£À PÁå°ìAiÀÄA ªÀÄvÀÄÛ DPÉì¯ÉÃmïUÀ½gÀÄvÀÛzÉ. CzÀgÀAvÉ ºÁ®Ä ºÁUÀÆ ºÁ°¤AzÀ vÀAiÀiÁj¹zÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼ÀÄ PÁå°ìAiÀÄA ªÀÄvÀÄÛ ¥sÁ¸ÉáÃl£ÀÄß ºÉÆA¢zÀÄÝ DgÉÆÃUÀåPÉÌ GvÀÛªÀÄ DºÁgÀªÁVgÀĪÀÅzÀjAzÀ £ÁªÀÅ ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è vÉUÉzÀÄPÉƼÀî¨ÉÃPÀÄ. ºÁUÀÆ ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è ¤ÃgÀ£ÀÄß PÀÄrAiÀÄĪÀÅzÀjAzÀ ºÉaÑ£À PÁå°ìAiÀÄA ªÀÄvÀÄÛ DPÀì¯ÉÃl£ÀÄß zÉúÀ¢AzÀ ºÉÆgÀºÁPÀ§ºÀÄzÀÄ. M0zÀÄ ªÉÃ¼É £ÁªÀÅ ¸ÁPÀµÀÄÖ ¤ÃgÀÄ PÀÄrAiÀÄ¢zÀÝgÉ PÁå°ìAiÀÄA,
G¥À£Áå¸À, ZÀZÉðAiÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀÅzÀÄ. GvÀÛj¸ÀĪÀÅzÀÄ. Qrß PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉUÉ PÁgÀtUÀ¼À£ÀÄß ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ.
PÉüÀĪÀÅzÀÄ ZÀað¸ÀĪÀÅzÀÄ ¥Àæ²ß¸ÀĪÀÅzÀÄ
137
DPÀì¯ÉÃmï CxÀªÁ ¥sÁ¸ÉáÃmïUÀ¼ÀÄ ±ÉÃRgÀuÉAiÀiÁV PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉUÉ PÁgÀtªÁUÀÄvÀÛzÉ. EzÀgÉAvÉ AiÀÄÆjPï Då¹qï, ªÉÄUÉßùAiÀÄA CxÀªÁ ¹¹Ö£ï eÁ¹Û EgÀĪÀ DºÁgÀ ªÀ¸ÀÄÛUÀ¼À eÉÆvÉUÉ ºÉaÑ£À ¤ÃgÀÄ PÀÄrAiÀÄ¢zÀÝgÉ Qrß PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉAiÀiÁUÀÄvÀÛzÉ. EvÀgÀ DºÁgÀ PÀæªÀÄUÀ¼ÁzÀ ªÀÄzÀå¥Á£À, ¹UÀgÉÃlÄ J¼ÉAiÀÄĪÀÅzÀÄ, J¯ÉCrPÉ w£ÀÄߪÀÅzÀjAzÀ®Æ Qrß PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉ ¸ÁzsÀåªÁUÀÄvÀÛzÉ. ¹) ºÀªÁªÀiÁ£À : ¨ÉùUÉ PÁ®zÀ°è £ÀªÀÄUÉ CwAiÀiÁV ¨ÉªÀgÀĪÀÅzÀjAzÀ PÀrªÉÄ ªÀÄÆvÀæ «¸Àdð¸À ®àqÀÄvÀÛzÉ. ªÀÄÆvÀæzÀ ªÀÄÆ®PÀ zÉúÀPÉÌ ¨ÉÃqÀªÁzÀ vÁdå ªÀ¸ÀÄÛUÀ¼ÀÄ zÉúÀ¢AzÀ «¸Àfð¸À®àqÀÄvÀÛzÉ. £ÁªÀÅ PÀrªÉÄ ªÀÄÆvÀæ «¸Àfð¸ÀÄwÛzÀÝ°è F ¨ÉÃqÀªÁqÀ PÀ®ä±ÀUÀ¼ÀÄ ªÀÄÆvÀæzÀ°è G½zÀÄPÉÆAqÀÄ ªÀÄÆvÀæzÀ §tÚ §zÀ¯ÁªÀuÉAiÀiÁUÀĪÀÅzÀgÀ eÉÆvÉUÉ vÀÄA¨Á UÀqÀ¸ÀÄ ªÁ¸À£É¬Ä0zÀ PÀÆrgÀÄvÀÛzÉ. eÉÆvÉUÉ £ÁªÀÅ ©¹°UÉ ªÉÄÊAiÉÆqÀÄتÀÅzÀjAzÀ r fêÀ¸ÀvÀéªÀÅ £ÀªÀÄä zÉúÀzÀ°è eÁ¹ÛAiÀiÁV, F r fêÀ¸ÀvÀéªÀÅ DºÁgÀzÀ°è ºÉaÑ£À PÁå°ìAiÀÄA£ÀÄß »Ãj, gÀPÀÛzÀ eÉÆvÉ ¥ÀjZÀ®£ÉAiÀiÁUÀĪÀÅzÀjAzÀ PÁå°ìAiÀÄA ¥ÀæªÀiÁt gÀPÀÛzÀ°è eÁ¹Û0iÀiÁV PÁå°ìAiÀÄA PÀ®ÄèUÀ¼À GvÀàwÛUÉ PÁgÀtªÁUÀÄvÀÛzÉ. r) GzÉÆåÃUÀ : ¸ÀÆAiÀÄð£À ©¹°UÉ eÁ¹Û ¸ÀªÀÄAiÀÄ ªÉÄÊAiÉÆrØ PÉ®¸À ªÀiÁqÀĪÀªÀgÀ°è F Qrß PÀ®ÄèUÀ¼ÀÄ GvÀàwÛAiÀiÁUÀĪÀ ¸ÀA¨sÀªÀ ºÉZÁÑVgÀÄvÀÛzÉ. KPÉAzÀgÉ EªÀgÀÄ eÁ¹Û ¨ÉªÉgÀÄvÁÛgÉ ªÀÄvÀÄÛ PÀrªÉÄ ¥ÀæªÀiÁtzÀ ªÀÄÆvÀæªÀ£ÀÄß «¸Àfð¸ÀÄvÁÛgÉ. CªÀgÉAzÀgÉ PÀÆ° PÉ®¸ÀzÀªÀgÀÄ, gÉÊvÀgÀÄ ªÉÆzÀ¯ÁzÀªÀgÀÄ. E) fêÀ¸ÀvÀé J : UÉÆÃqÉUÀ½UÉ £ÀAiÀĪÁzÀ ªÉÄïÉäöÊ §gÀ®Ä ¹ªÉÄAmï£À CUÀvÀå«zÉ. PÉÆ¼É vÀÄA©zÀ UÀnÖ ªÀ¸ÀÄÛUÀ¼ÀÄ
138
£Á®ÄÌ ¤«ÄµÀ UÀ¼ÀÄ
£ÀAiÀĪÁzÀ UÉÆÃqÉUÀ½UÉ ¸ÀÄ®¨sÀªÁV CAnPÉÆArgÀĪÀÅ¢®è ºÁUÉAiÉÄà £ÀªÀÄä ªÀÄÆvÀæ «¸Àdð£ÁAUÀ ªÀÇåºÀzÀ UÉÆÃqÉUÀ¼ÀÄ ªÀÄÈzÀĪÁVzÀÝgÉ F R¤eÁA±ÀUÀ¼ÀÄ ¸ÀÄ®¨sÀªÁV ±ÉÃRgÀuÉAiÀiÁUÀĪÀÅ¢®è ªÀÄvÀÄÛ Qrß PÀ®ÄèUÀ¼ÀÄ0mÁUÀÄvÀÛzÉ. fêÀ¸ÀvÀé J ºÀ¼À¢ vÉUÉzÀÄPÉƼÀÄîªÀ DºÁgÀzÀ°è EgÀÄvÀÛzÉ. fêÀ¸ÀvÀé J E®è¢zÀÝ°è ªÀÄÆvÀæ «¸Àdð£ÁAUÀ ªÀÇåªÀzÀ UÉÆÃqÉUÀ¼ÀÄ MgÀmÁV R¤eÁA±ÀUÀ¼ÀÄ F UÉÆÃqÉUÀ¼À°è ±ÉÃRgÀuÉAiÀiÁV Qrß PÀ®ÄèUÀ¼À GvÀàwÛUÉ PÁgÀtªÁUÀÄvÀÛzÉ. J¥sï) CvÀÄåvÀÌöȵÀÖ ¥ÁgÁxÉÊgÉÊr¸ÀªÀiï : £ÀªÀÄä ªÀÄƼÉ/J®Ä§ÄUÀ¼ÀÄ ªÀÄÄRåªÁV PÁå°ìAiÀÄA¤AzÀ ªÀiÁqÀ®ànÖªÉ. CvÀÄåvÀÌöȵÀÖ ¥ÁgÁxÉÊgÉÊr¸ÀA EgÀĪÀ gÉÆÃVAiÀÄ°è ºÉaÑ£À PÁå°ìAiÀÄA J®Ä©¤0zÀ ºÉÆgÀºÁPÀ®àqÀÄvÀÛzÉ. CzÀ£ÀÄß gÀPÀÛªÀÅ »ÃjPÉÆAqÀÄ gÀPÀÛ¢AzÀ QrßAiÀÄ£ÀÄß ¸ÉÃgÀÄvÀÛzÉ. »ÃUÉ ºÉaÑ£À ¥ÀæªÀiÁtzÀ PÁå°ìAiÀÄA ªÀÄÆvÀæ «¸Àdð£ÁAUÀ ªÀÇåºÀzÀ ºÁ¢AiÀÄ°è ±ÉÃRj¸À®àqÀÄvÀÛzÉ ªÀÄvÀÄÛ Qrß PÀ®ÄèUÀ¼ÀÄ GvÀàwÛAiÀiÁUÀÄvÀÛzÉ. f) ªÀÄÆvÀæ «¸Àdð£ÁAUÀ ªÀÇåºÀPÉÌ ¸ÉÆÃAPÀÄ vÀUÀ®Ä«PÉ : PÉ®ªÀÅ gÉÆÃUÀPÁgÀPÀ ¸ÀÆPÁë÷ätÄ fëUÀ¼ÀÄ (§jPÀtÂÚUÉ PÁtzÀÄÝ) ªÀÄÆvÀæ «¸Àdð£ÁAUÀ ªÀÇåºÀzÀ ºÁ¢UÉ gÀPÀÛzÀ ªÀÄÆ®PÀ §gÀÄvÀÛzÉ KPÉAzÀgÉ ºÉÆgÀV£À «¸Àdð£ÁAUÀ ªÀÇåºÀzÀ ¨sÁUÀªÀ£ÀÄß ¸ÀjAiÀiÁV ±ÀÄaUÉƽ¸À¢zÀÝgÉ ªÀÄvÀÄÛ K£ÁzÀgÀÆ vÉÆAzÀgÉUÀ½zÀÝgÉ F ¸ÀÆPÁë÷ätÄUÀ¼ÀÄ ºÉÆgÀV¤AzÀ £ÉÃgÀªÁV £ÀªÀÄä zÉúÀªÀ£ÀÄß ¥ÀæªÉò¹, ªÀÄvÀÄÛ zÉúÀzÀ°è ªÀÈ¢Þ0iÀiÁV «¸Àdð£ÁAUÀPÉÌ ¸ÉÆÃAPÀÄ vÀUÀ®ÄªÀ0vÉ ªÀiÁqÀÄvÀÛzÉ. F ¸ÉÆÃAQ¤AzÁV ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼ÀÄ GAmÁUÀÄvÀÛzÉ.
G¥À£Áå¸ÀzÀ
£ÀPÉëUÀ¼ÀÄ
139
ªÀÄÆgÀÄ ¤«ÄµÀUÀ
¼ÀÄ
£Á®ÄÌ ¤«ÄµÀ UÀ¼ÀÄ JgÀqÀÄ ¤«ÄµÀ UÀ¼ÀÄ
Qrß PÀ®ÄèUÀ½ªÉ JA§ÄzÀ£ÀÄß zÀÈrüÃPÀj¸ÀĪÀ «zsÁ£ÀUÀ¼À£ÀÄß «ªÀj ¸ÀĪÀÅzÀÄ. Qrß PÀ®ÄèUÀ¼À «zsÀUÀ¼À£ÀÄß ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ ±À¸ÀÛçaQvÉì gÀ»vÀ PÁAiÀÄð
JZï) ¢ÃWÀðPÁ¬Ä¯É ªÀÄvÀÄÛ ¤§ðA¢üvÀ ZÀ®£ÀªÀ®£À : ¢ÃWÀð PÁ®zÀ PÁ¬Ä¯É¬Ä0zÁV, gÉÆÃVAiÀÄÄ ¤±ÀPÀÛ£ÁV C0zÀgÉ ¥ÀPÀëªÁvÀªÁzÁUÀ PÉÊAiÀÄ/PÁ°£À CxÀªÁ £ÁªÀÅ £ÀqÉzÀÄPÉƼÀîªÀ ®PÀëtUÀ½AzÀ ¸ÀtÚ ¸ÀtÚ PÁå°ìAiÀÄA PÀtUÀ¼ÀÄ ªÀÄƼɬÄ0zÀ ¨ÉÃ¥ÀðlÄÖ ªÀÄÆvÀæd£ÀPÁAUÀzÀ ºÁ¢AiÀÄ UÉÆÃqÉUÀ¼À°è ±ÉÃRgÀuÉAiÀiÁUÀÄvÀÛzÉ. EzÀÄ vÀÄ0¨Á ¸ÀªÀÄAiÀÄzÀªÀgÉUÉ ªÀÄÄAzÀĪÀjzÀgÉ PÁå°ìAiÀÄA PÀ®ÄèUÀ¼ÀÄAmÁUÀÄvÀÛzÉ. ¢ÃWÀðPÁ® ªÀÄ®VzÀ¯Éè EgÀĪÀ gÉÆÃVUÀ¼À°è ªÀÄÆvÀæ ºÉÆgÀ¨ÁgÀzÉ EgÀÄvÀÛzÉ. ¢ÃWÀðPÁ® ªÀÄÆvÀæ zÉúÀzÀ¯Éèà ±ÉÃRgÀuÉAiÀiÁVgÀĪÀÅzÀjAzÀ Qrß PÀ®ÄèUÀ¼ÁV GvÀàwÛAiÀiÁUÀÄvÀÛªÉ. L) e˵À¢üUÀ¼ÀÄ :- ºÉÆmÉÖ £ÉÆêÀÅ PÀrªÉÄ ªÀiÁqÀ®Ä vÉUÉzÀÄPÉƼÀÄîªÀ Då0mÁ¹qï£À0vÀ PÉ®ªÀÅ £ÉÆêÀÅ ¤ªÁgÀPÀ ªÀiÁvÉæUÀ¼ÀÄ UÀĽUÉUÀ¯ÁzÀ qÉʪÀiÁPïì, r-fêÀ¸ÀvÀé ºÁUÀÆ MªÉÄä¯É ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è vÉUÉzÀÄPÉƼÀÄîªÀ D¹àj£ï, CzÀgÀ0vÉ C¸ÀqÉØvÀ£À ªÀÄÄAvÁzÀĪÀÅ Qrß PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉUÉ PÁgÀtªÁUÀÄvÀÛªÉ. eÉ) ºÀÄnÖ¤AzÀ¯Éà §gÀĪÀ PÉ®ªÀÅ £ÀÆå£ÀåvÉUÀ¼ÀÄ/ vÉÆqÀPÀÄUÀ¼ÀÄ : ºÀÄnÖ¤AzÀ¯Éà ªÀÄÆvÀæzÀ GvÁàzÀ£É ªÀÄvÀÄÛ «¸Àdð£ÁAUÀzÀ°è K£ÁzÀgÀÆ PÉÆgÀvɬÄzÀÝgÉ (C0zÀgÉ ªÀÄÆvÀæPÉÆñÀzÀ ¥ÀPÉ̮ħÄ, ªÀÄÆvÀæ£Á¼À CxÀªÁ ªÀÄÆvÀæPÉÆñÀ) «¸Àdð£ÁAUÀ ªÀÇåºÀzÀ ¨sÁUÀUÀ¼ÀÄ ¸ÀAPÀÄavÀªÁUÀĪÀÅzÀjAzÀ CxÀªÁ «PÀ¹¸ÀĪÀÅzÀjAzÀ ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉUÉ PÁgÀtªÁUÀÄvÀÛzÉ. PÉ) ªÀA±À¥ÁgÀA¥ÀAiÀÄð : gÀPÀÛ ¸ÀA§A¢üUÀ¼À°è ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼ÀÄAmÁUÀĪÀ ¸ÁzsÀåvÉ ºÉZÀÄÑ. CzÀÄ M0zÀÄ vÀ¯ÉªÀiÁj¤AzÀ E£ÉÆßßAzÀÄ vÀ¯ÉªÀiÁjUÉ
eÉÆvÉUÉ ZÀað¸ÀĪÀÅzÀÄ G¥À£Áå¸À
PÉüÀĪÀÅzÀÄ ªÀÄvÀÄÛ ZÀZÉðAiÀÄ°è ¥Á¯ÉÆÎüÀÄîªÀÅzÀÄ.
£ÀPÉëUÀ¼ÀÄ
140
£Á®ÄÌ ¤«ÄµÀ UÀ¼ÀÄ JAlÄ ¤«ÄµÀ UÀ¼ÀÄ
¤ªÀðºÀuÉAiÀÄ£ÀÄß «ªÀj ¸ÀĪÀÅzÀÄ. ªÀÄÆvÀæPÉÆñÀzÀ ±À¸ÀÛç aQvÉì ¨ÉÃPÉ£ÀÄߪÀ ¸ÀÆZÀ£ÉUÀ¼À£ÀÄß ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ Qrß PÀ®ÄèUÀ¼ÀÄ ¥ÀÅ£ÀgÁªÀvÀð£ÉAiÀiÁUÀzÀ0vÉ vÀqÉUÀlÄÖªÀ «zsÁ£ÀUÀ¼À£ÀÄß «ªÀj ¸ÀĪÀÅzÀÄ.
§gÀ§ºÀÄzÀÄ C0zÀgÉ vÀAzÉvÁ¬Ä¬Ä0zÀ ªÀÄPÀ̽UÉ, DzÀgÉ ºÉAUÀ¸ÀjVAvÀ UÀAqÀ¸ÀjUÉ F Qrß PÀ®ÄèUÀ¼ÀÄ G0mÁUÀĪÀ ¸ÁzsÀåvÉ ºÉZÀÄÑ. 5. QrßPÀ®ÄèUÀ¼À aºÉß ªÀÄvÀÄÛ ®PÀëtUÀ¼ÀÄ J) wÃPÀë÷Ú, vÁ¼À¯ÁgÀzÀ £ÉÆêÀÅ : ªÀÄzsÀå ºÉÆmÉÖAiÀÄ CqÀØ ªÀÄUÀÄΰ£À°è, vÉÆqɸÀAzÀÄUÀ¼À°è vÀqÉAiÀįÁgÀzÀAvÀºÀ £ÉÆëzÀÄÝ CzÀÄ d£À£Á0UÀ ªÀÄvÀÄÛ vÉÆqÉAiÀÄ ¨sÁUÀUÀ¼ÁZÉ ºÀgÀqÀÄvÀÛzÉ EzÀÄ aQvÉìUÉ ºÉÆÃUÀ¨ÉÃPÁzÀ ¸Áé¨sÁ«PÀ JZÀÑjPÉAiÀÄ ¸ÀAPÉÃvÀªÁVgÀÄvÀÛzÉ. PÉ®ªÀÅ ¸À0zÀ¨sÀðUÀ¼À°è AiÀiÁªÀÅzÉà £ÉÆêÀÅ CxÀªÁ ®PÀëtUÀ¼ÀÄ PÁt¸ÀzÉà EgÀ§ºÀÄzÀÄ. F ¹ÜwAiÀÄ£ÀÄß ¸ÁʯÉ0mï mÉÊ¥ï (±Á0vÀ ¹Üw) J£ÀߧºÀÄzÀÄ. ©) dégÀ, ZÀ½, £ÀqÀUÀĪÀÅzÀÄ ªÀÄvÀÄÛ ªÁ0wªÀiÁqÀĪÀÅzÀj0zÀ ªÀÄÆvÀæ «¸Àdð£ÁAUÀ ªÀÇåºÀzÀ ªÀiÁUÀðzÀ°è gÉÆÃUÀ vÀgÀĪÀ ¸ÀÆPÁë÷äUÀ¼ÀÄ EªÉ J0zÀÄ w½AiÀÄÄvÀÛzÉ. ¹) vÉÆqɸÀ0zÀÄUÀ¼À ªÀÄzsÀåzÀ°è ªÀÄÄnÖzÀgÀÆ £ÉÆëgÀÄvÀÛzÉ. r) ¥ÀzÉà ¥ÀzÉà ªÀÄ®«¸Àfð¸ÀĪÀÅzÀÄ. E) ªÁ0w §0zÀ0vÀ¤¸ÀĪÀÅzÀÄ. J¥sóï) ªÀÄÆvÀæzÀ ¥ÀæªÀiÁt PÀrªÉÄAiÀiÁUÀĪÀÅzÀÄ. f) ªÀÄÆvÀæ «¸Àfð¸ÀĪÀÅzÉà PÀµÀÖ C¤¸ÀĪÀÅzÀÄ. JZï) ªÀÄÆvÀæzÀ°è gÀPÀÛ EgÀÄ«PÉ. L) ªÀÄÆvÀæPÉÆñÀ vÀÄ0©zÀAvÉ EgÀĪÀ ¨sÁªÀ£É. eÉ) ¥ÀzÉà ¥ÀzÉà ªÀÄÆvÀæ eÁ¹Û0iÀiÁzÀAvÀ¤¸ÀĪÀÅzÀÄ. PÉ) vÀA¥ÁzÀ ªÀÄvÀÄÛ vÉêÀ¨sÀjvÀ ZÀªÀÄð. J¯ï) £ÉÆêÀÅ PÁt¹PÉƼÀÄîªÀ ¸À0zÀ¨sÀðzÀ°è ¨É£ÀÄß ªÀÄvÀÄÛ ºÉÆmÉÖAiÀÄ ¸ÁßAiÀÄÄUÀ¼ÀÄ vÀÄA¨Á PÀptªÁUÀÄvÀÛªÉ. 6) Qrß PÀ®ÄèUÀ½ªÉ J0zÀÄ ¤ÃªÀÅ ºÉÃUÉ zÀÈrüÃPÀj¸ÀÄ«j ?
G¥À£Áå¸ÀzÀ eÉÆvÉUÉ ZÀað¸ÀĪÀÅzÀÄ G¥À£Áå¸ÀzÀ eÉÆvÉUÉ ZÀað¸ÀĪÀÅzÀÄ G¥À£Áå¸À ZÀZÉð¸ÀĪÀÅzÀÄ
PÉüÀĪÀÅzÀÄ ªÀÄvÀÄÛ ZÀZÉðAiÀÄ°è ¨sÁUÀªÀ»¸ÀÄzÀÄ. ¥Àæ±ÉßUÉ GvÀÛj¸ÀĪÀÅzÀÄ ªÀÄvÀÄÛ ¸ÀA±ÀAiÀÄUÀ¼À£ÀÄß PÉüÀĪÀÅzÀÄ

141
PÁå°ìAiÀÄA eÁ¹Û EgÀĪÀ DºÁgÀUÀ¼À £ÀÄß ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ. AiÀÄÆjPï Då¹qï eÁ¹Û EgÀĪÀ DºÁ gÀ ¥ÀzÁxÀðUÀ¼À ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ. ¥Á¸ï¥ÉÇÃgÀ¸ï eÁ¹Û EgÀĪÀ PÉ®ªÀÅ DºÁgÀ
¤ÃªÀÅ M0zÀÄ ¸ÀtÚ ªÀÄqÀPÉAiÀÄ°è ªÀÄÆvÀæªÀ£ÀÄß ¸ÀAUÀ滸À¨ÉÃPÁUÀÄvÀÛzÉ. ªÀÄvÀÄÛ CzÀgÀ°è UÀnÖ ªÀÄgÀ½£À0vÀ PÀtUÀ¼ÀÄ ºÁUÀÆ gÀPÀÛ EzÉAiÉÄà J0zÀÄ PÀAqÀÄ»rAiÀĨÉÃPÀÄ. J0zÀÄ gÀPÀÛ ªÀÄÆvÀæzÀ°èzÀÝgÉ vÀPÀët ªÉÊzÀåQÃAiÀÄ £ÉgÀªÀÅ ¨ÉÃPÁzÀ°è AiÀiÁªÀÅzÉà D¸ÀàvÉæUÉ PÉÆAqÉÆAiÀÄÄÝ C°è0zÀ ªÀÄÆvÀæªÀ£ÀÄß ¥ÀæAiÉÆÃUÁ®AiÀÄPÉÌ PÀ¼ÀÄ»¸ÀĪÀÅzÀgÀ ªÀÄÆ®PÀ ¥ÀjÃPÉëUÉƼÀ¥Àr¹ Qrß PÀ®ÄèUÀ½ªÉAiÉÆà J0zÀÄ zÀÈrüÃPÀj¸À¯ÁUÀÄvÀÛzÉ. ªÀÄÆvÀæªÀ£ÀÄß EvÀgÀ C£ÉÃPÀ jÃwAiÀÄ ¥ÀjÃPÉëUÉƼÀ¥Àr¸ÀĪÀÅzÀjAzÀ QrßPÀ®ÄèUÀ½ªÉ J0zÀÄ zÀÈrüÃPÀj¸À§ºÀÄzÀÄ CªÉ0zÀgÉ; gÀPÀÛzÀ ¥ÀjÃPÉë, «±ÉõÀ PÀë-QgÀt ¥ÀjÃPÉë C¯ÁÖç¸ÉÆãÉÆÃUÀæ¦ü ªÉÆzÀ¯ÁzÀĪÀÅ. 7.) Qrß PÀ®ÄèUÀ¼À «zsÀUÀ¼ÀÄ R¤eÁ0±ÀUÀ¼À£ÀÄß CªÀ®0©¹ GAmÁUÀĪÀ Qrß PÀ®ÄèUÀ¼ÀÄ: C£ÉÃPÀ «zsÀzÀ Qrß PÀ®ÄèUÀ½ªÉ. CªÀÅUÀ¼É0zÀgÉ, PÁå°ìAiÀÄA, DPÀì¯ÉÃmï, ¥sÁ¸ÉÆáÃgÀ¸ï CxÀªÁ «Ä±Àæ PÀ®ÄèUÀ¼ÀÄ C0zÀgÉ PÁå°ìAiÀÄA, DPÀì¯ÉÃmï, ¥sÁ¸ÉÆáÃgÀ¸ï R¤eÁ0±ÀUÀ¼À£ÉÆß¼ÀUÉÆArgÀĪÀ PÀ®ÄèUÀ¼ÀÄ PÉ®ªÀÅ PÀ®ÄèUÀ¼ÀÄ PÁå°ìAiÀÄA¤0zÀ ªÀiÁqÀ®ànÖgÀĪÀÅzÀjAzÀ PÁå°ìAiÀÄA PÀ®ÄèUÀ¼É0zÀÄ DPÀì¯ÉÃmïUÀ½0zÀÄ0mÁzÀ PÀ®ÄèUÀ¼À£ÀÄß DPÀì¯ÉÃmï PÀ®ÄèUÀ¼É0zÀÆ, ¥sÁ¸ÉÆáÃgÀ¸ï¤AzÀÄAmÁzÀ PÀ®ÄèUÀ¼À£ÀÄß ¥Á¸ÉÆáÃgÀ¸ï PÀ®ÄèUÀ¼É0zÀÆ PÀgÉAiÀÄÄvÁÛgÉ. EvÀgÀ «zsÀUÀ¼É0zÀgÉ AiÀÄÆjPï Då¹qï PÀ®ÄèUÀ¼Ài.. ¸ÁªÀiÁ£ÀåªÁV ªÀiÁA¸ÁºÁjUÀ¼À°è ªÀÄvÀÄÛ ªÀÄÈzÀĪÁzÀ J®Ä§Ä, ¸ÀAzÀÄUÀ¼À°è AiÀÄÆjPï Då¹qï vÀÄA©gÀĪÀ0vÀºÀ gÉÆÃVUÀ¼À°è ¹¹Ö£ï PÀ®ÄèUÀ¼ÀÄ, ¸ÀÄÖçªÉÊmï PÀ®ÄèUÀ¼ÀÄ ªÀÄvÀÄÛ PÁìA¯É£ï PÀ®ÄèUÀ¼ÀÄ. 8) ªÀÄÆvÀæ «¸Àdð£Á ªÀÇåºÀzÀ ºÁ¢AiÀÄ°è PÀ®ÄèUÀ½gÀĪÀ ¸À0zÀ¨sÀðzÀ°è ºÉÃUÉ PÁAiÀÄð¤ªÀð»¸À¨ÉÃPÀÄ?
¥ÀæªÀiÁtÂPÀgÀt
PÉüÀĪÀÅzÀÄ ZÀZÉðAiÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀÅzÀÄ.
¤dªÁzÀ DPÀÈwUÀ¼ÀÄ
142
£Á®ÄÌ ¤«ÄµÀ UÀ¼ÀÄ
¥ÀzÁxÀð UÀ¼À ¥ÀnÖ ªÀiÁqÀĪÀÅzÀÄ.
ªÀÄÆvÀæ «¸Àdð£Á ºÁ¢AiÀÄ°è QrßPÀ®ÄèUÀ¼ÀÄ §0zÀÄ LzÀÄ ¸É0n «ÄÃlgïV0vÀ PÀrªÉÄ EzÀÝ°è, £ÁªÀÅ ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è ¤ÃgÀ£ÀÄß PÀÄrAiÀĨÉÃPÀÄ. CxÀªÁ ºÉaÑ£À zÀæªÀ ¥ÀzÁxÀðUÀ¼À£ÀÄß gÀPÀÛ£Á¼ÀUÀ¼À ªÀÄÆ®PÀ PÉÆr¸ÀĪÀÅzÀjAzÀ ªÀÄÆvÀæ «¸Àdð£Á ªÀÇåºÀzÀ ºÁ¢AiÀÄ°è£À PÀ®ÄèUÀ¼À£ÀÄß vÉUÉzÀĺÁPÀ§ºÀÄzÀÄ. 9) ±À¸ÀÛç aQvÉì £ÀªÀÄUÉ AiÀiÁªÁUÀ ¨ÉÃPÁUÀÄvÀÛzÉ ? AiÀiÁªÁUÀ ±À¸ÀÛç aQvÉì ¨ÉÃPÉAzÀgÉ [ PÀ®Äè zÉÆqÀØzÁVzÀÄÝ ªÀÄÆvÀæ «¸Àfð¸À®Ä PÀµÀÖªÁzÁUÀ [ F PÀ®ÄèUÀ¼ÀÄ ¢ÃWÀðPÁ®zÀ £ÉÆëUÉ ªÀÄvÀÄÛ ªÁ0wUÉ
PÁgÀtªÁzÁUÀ. [ PÀ®ÄèUÀ¼À aºÉß ªÀÄvÀÄÛ ®PÀëtUÀ¼ÀÄ PÉêÀ®
e˵À¢üUÀ½AzÀ PÀrªÉÄAiÀiÁUÀ¢zÁÝUÀ. 9. Qrß PÀ®ÄèUÀ¼À ¥ÀÅ£ÀgÁªÀvÀð£ÉAiÀiÁUÀzÀ0vÉ vÀqÉUÀlÄÖªÀÅzÀÄ. Qrß PÀ®ÄèUÀ¼ÀÄ ¥ÀÅ£ÀgÁªÀvÀð£ÉAiÀiÁUÀzÀ0vÉ vÀqÉUÀlÄÖ®Ä C£ÉÃPÀ «zsÁ£ÀUÀ¼À£ÀÄß £ÁªÀÅ UÀªÀÄ£ÀzÀ°èlÄÖPÉƼÀî¨ÉÃPÀÄ. E°è£ÁªÀÅ QrßPÀ®ÄèUÀ¼ÀÄ ¥ÀÅ£ÀgÁªÀvÀð£ÉAiÀiÁUÀzÀ0vÉ vÀqÉUÀlÖ®Ä ªÀÄvÀÄÛ C£ÀĸÀj¸À¨ÉÃPÁzÀ PÉ®ªÀÅ ¸ÁªÀiÁ£Àå ZÀlĪÀnPÉUÀ¼À §UÉÎ w½AiÉÆÃt. ªÀiÁqÀ¨ÉÃPÁzÀÄÝ ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è zÀæªÀ¥ÀzÁxÀðUÀ¼À£ÀÄß vÉUÉzÀÄPÉƼÀÄîªÀÅzÀÄ ¢£ÀPÉÌ ªÀÄÆgÀjAzÀ £Á®ÄÌ °Ãlgï£ÀµÀÄÖ ¤ÃgÀ£ÀÄß (ºÀ¢£ÉêzÀjAzÀ- ºÀ¢£ÁgÀÄ ¯ÉÆÃlzÀµÀÄÖ ¤ÃgÀÄ, M0zÀÄ ¯ÉÆÃl ¤ÃgÀÄ C0zÀgÉ E£ÀÆßgÀÄ «Ä° °Ãlgï ¤ÃgÀÄ) PÉêÀ® ¤ÃgÀÄ, ¹Ã0iÀiÁ¼ÀzÀ ¤ÃgÀÄ, ¨Á°ðAiÀÄ
¥ÀæªÀiÁtÂPÀgÀt ¥ÀæªÀiÁtÂP
ZÀZÉðAiÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀÅzÀÄ
¸ÀºÀdªÁ zÀ DPÀÈw UÀ¼ÀÄ. ¸ÀºÀdªÁ zÀ DPÀÈw UÀ¼ÀÄ.
143
£Á®ÄÌ ¤«ÄµÀ UÀ¼À
¤ÃgÀÄ, ±ÀgÀ§vï (¥Á£ÀPÀ),zÀħð®ªÁzÀ ºÀtÂÚ£À gÀ¸ÀªÀ£ÀÄß vÉUÉzÀÄPÉÆAqÀgÉ ¤ÃgÁ0±À ªÀÄÆvÀæzÀ°è eÁ¹ÛAiÀiÁUÀÄvÀÛzÉ. ªÀÄvÀÄÛ UÀnÖ ªÀ¸ÀÄÛUÀ¼ÀÄ ªÀÄÆvÀæzÀ°è ºÉZÁÑUÀzÀAvÉ vÀqÉAiÀÄĪÀÅzÀ®èzÉ PÀ®ÄèUÀ¼ÀÄ0mÁUÀzÀ0vÉ vÀqÉAiÀÄÄvÀÛzÉ.
©¹°£À°è ºÉZÀÄÑ ºÉÆvÀÄÛªÉÄÊAiÉÆrØ ºÉZÀÄÑ ¨sÁgÀ JvÀÄÛªÀ PÉ®¸À ªÀiÁqÀĪÀªÀgÀÄ, ºÉZÁÑV PÀZÉÃjUÀ¼À°è PÀĽvÉà PÉ®¸À ªÀiÁqÀĪÀªÀjAzÀ ºÉaÑ£À ¥ÀæªÀiÁtzÀ zÀæªÀ ¥ÀzÁxÀðUÀ¼Á£ÀÄß ¨ÉªÀj£À ªÀÄÄ®PÀ PɼÉzÀÄPÉƼÀÄîªÀ ¤Ãj£ÀA±ÀªÀ£ÀÄß ¸ÀjzÀÆV¸À¨ÉÃPÀÄ. [ PÀÈvÀPÀ vÀA¥ÀÅ ¥Á¤ÃAiÀÄUÀ¼ÁzÀ ¥É¦ì, PÉÆïÁ
ªÉÆzÀ¯ÁzÀªÀÅUÀ¼À£ÀÄß PÀÄrAiÀÄĪÀÅzÀQÌAvÀ ±ÀÄzÀÞ ¤ÃgÀ£ÀÄß PÀÄrAiÀÄĪÀÅzÉ M¼ÉîAiÀÄzÉAzÀÄ £É£À¦lÄÖPÉƼÀî¨ÉÃPÀÄ.
[ ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è ºÀtÂÚ£À gÀ¸ÀªÀ£ÀÄß PÀÄrAiÀÄĪÀÅzÀjAzÀ zÉÆqÀØ UÁvÀæzÀ PÀ®ÄèUÀ¼À£ÀÄß ¸ÀtÚ ¸ÀtÚ ZÀÆgÀÄUÀ¼ÁV ªÀiÁqÀĪÀÅzÀ®èzÉ ªÀÄvÀÄÛ ¸ÀÄ®¨sÀªÁV ªÀÄÆvÀæzÀ eÉÆvÉUÉ «¸Àfð¸À®àqÀĪÀ0vÉ ªÀiÁqÀÄvÀÛzÉ. ºÀtÄÚUÀ¼À£ÀÄß ªÀÄvÀÄÛ ºÀ¹ vÀgÀPÁjUÀ¼À£ÀÄß ºÉZÁÑV w£ÀߨÉÃPÀÄ. CªÀÅUÀ¼ÀÄ ºÉaÑ£À £Áj£ÀA±ÀªÀ£ÀÄß ºÉÆA¢gÀÄvÀÛªÉ. £Áj£ÀA±ÀUÀ¼À£ÀÄß ºÉÆ0¢gÀĪÀ ºÀ¹gÀÄ vÀgÀPÁjUÀ¼ÀÄ zÉÆqÀØ zÉÆqÀØ R¤eÁ0±ÀUÀ¼À£ÀÄß ¸ÀtÚ ¸ÀtÚ ZÀÆgÀÄUÀ¼ÁV ªÀiÁr gÀPÀÛ¢AzÀ ºÉÆgÀºÉÆÃUÀĪÀ0vÉ ªÀiÁqÀÄvÀÛzÉ.
[ DºÁgÀzÀ°è ºÉZÁÑV ºÀĽUÀ¼À£ÀÄß ¸ÉÃj¸ÀĪÀÅzÀjAzÀ Qrß PÀ®Äè ¸ÀÄ®¨sÀªÁV «¸Àdð£ÉAiÀiÁUÀ®Ä ¸ÀºÁ0iÀĪÁUÀÄvÀÛzÉ.
[ Që¥ÀæªÁzÀ ªÀÄvÀÄÛ ¸ÀjAiÀiÁzÀ aQvÉìAiÀÄ£ÀÄß vÉUÉzÀÄPÉƼÀî¨ÉÃPÀÄ. ªÀÄÆvÀæ «¸Àfð¸ÀĪÁUÀ AiÀiÁªÀÅzÉ jÃwAiÀÄ vÉÆAzÀgÉ PÁt¹zÁUÀ CxÀªÁ PÀµÀÖ
ÀgÀt ¥ÀæªÀiÁtÂPÀgÀt
ZÀZÉðAiÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀÅzÀÄ. ZÀZÉðAiÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀÅzÀÄ
¸ÀºÀdªÁ zÀ DPÀÈw UÀ¼ÀÄ.
144
Ä £Á®ÄÌ ¤«ÄµÀUÀ¼ÀÄ
C¤¹zÁUÀ GzÁºÀgÀuÉUÉ: GjzÀAvÉ C¤¸ÀĪÀÅzÀÄ, ªÀÄvÀÄÛ ªÀÄÆvÀæ «¸Àfð¸ÀĪÁUÀ £ÉÆêÁzÀ C£ÀĨsÀªÀ.
[ «±Áæ0w ¹ÜwAiÀÄ°è ªÀÄ®VzÀ¯Éè EgÀĪÀ gÉÆÃVUÀ¼ÀÄ DUÁUÀ ªÀÄUÀ먀 §zÀ¯Á¬Ä¸ÀÄwÛgÀ¨ÉÃPÀÄ.
[ ¨ÉúÀ ªÀÄvÀÄÛ UÉÆÃ¥Àå C0UÀUÀ¼À£ÀÄß C£ÉÃPÀ ¸À® ¸ÀjAiÀiÁV ±ÀÄaUÉƽ¸ÀÄwÛgÀ¨ÉÃPÀÄ.
ªÀiÁqÀ¨ÁgÀzÀÄÝ [ PÀ¥ÀÅöà ZÀºÁ ªÀÄvÀÄÛ PÁ¦üAiÀÄ£ÀÄß ºÉZÁÑV
vÉUÉzÀÄPÉƼÀÄîwÛzÀÝgÉPÀrªÉÄUÉƽ¸À¨ÉÃPÀÄ. KPÉAzÀgÉ DPÀì¯ÉÃmï ¥ÀæªÀiÁt eÁ¹ÛAiÀiÁVgÀÄvÀÛzÉ.
[ ªÀÄzÀå¥Á£À PÀrªÉÄ ªÀiÁqÀ¨ÉÃPÀÄ KPÉAzÀgÉ PÁå°ìAiÀÄA ¥sÁ¸ÉáÃmï, AiÀÄÆjPï Då¹qï ºÁUÀÆ ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è ºÉÆgÀºÉÆÃUÀĪÀ0vÉ ªÀiÁqÀĪÀÅzÀ®èzÉ F T¤eÁ0±ÀUÀ¼ÀÄ «¸Àdð£Á0UÀ ªÀÇåºÀzÀ ºÁ¢AiÀÄ°è ±ÉÃRgÀuÉAiÀiÁV QrßPÀ®ÄèUÀ¼ÀÄ0mÁUÀÄvÀÛzÉ.
[ ¸ÀÄtÚ ¨ÉgɹzÀ J¯É CrPÉAiÀÄ£ÀÄß w£ÀߨÁgÀzÀÄ AiÀiÁPÉAzÀgÉ EzÀÄ zÉúÀzÀ°è PÁå°ìAiÀÄA ¥ÀæªÀiÁtªÀ£ÀÄß ºÉaѸÀÄvÀÛzÉ. ¸ÀÄtÚªÀÅ ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è PÁå°ìAiÀÄA£ÀÄß ºÉÆA¢gÀÄvÀÛzÉ.
[ £ÀªÀÄä÷ DºÁgÀzÀ°è ºÉaÑ£À G¥Àà£ÀÄß ¸ÉÃj¸À¨ÁgÀzÀÄ KPÉAzÀgÉ G¥ÀÅöà PÁå°ìAiÀÄA ¥ÀæªÀiÁtªÀ£ÀÄß ºÉaѸÀÄvÀÛzÉ. G¥ÀÅöà gÀPÀÛzÀ°è ºÉaÑ£À PÁå°ìAiÀÄA£ÀÄß »ÃjPÉÆAqÀÄ Qrß PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉAiÀÄ ªÀÄlÖªÀ£ÀÄß ºÉaѸÀÄvÀÛzÉ.
[ zsÀƪÀÄ¥Á£À¢AzÀ zÀÆgÀ«gÀ¨ÉÃPÀÄ. CzÀÄ ¸ÁzsÀåªÁUÀ¢zÀÝgÉ ¸ÁzsÀåªÁzÀµÀÄÖ ªÀÄnÖUÉ zsÀƪÀÄ¥Á£À (¹UÀgÉÃlÄ) vÀÄA¨Á ¸À® J¼ÉAiÀÄĪÀÅzÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀ¨ÉÃPÀÄ ªÀÄvÀÄÛ MªÉÄä J¼ÉzÀ £À0vÀgÀ E£ÉÆߪÉÄä J¼ÉAiÀĨÉÃPÁzÀgÉ ¸ÀªÀÄAiÀÄzÀ C0vÀgÀªÀ£ÀÄß EqÀ¨ÉÃPÀÄ . KPÉAzÀgÉ EzÀÄ vÀÄA¨Á R¤eÁA±ÀUÀ¼ÀÄ «¸Àfð¸À®àqÀĪÀÅzÀ£ÀÄß ºÉaѸÀÄvÀÛzÉ.
[ ‘¸ÀÆAiÀÄð£À ©¹°UÉ eÁ¹Û ºÉÆvÀÄÛ £ÉÃgÁªÁV
ZÀZÉðAiÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀÅzÀÄ

145
ªÉÄÊAiÉÆqÀبÁgÀzÀÄ. CzÀÄ ¸ÁzsÀåªÁUÀ¢zÀÝgÉ ªÀÄvÀÄÛ ¤ªÀÄUÉ eÁ¹Û ¨ÉªÀgÀĪÀÅzÀjAzÀ eÁ¹Û ¤ÃgÀ£ÀÄß PÀÄrAiÀĨÉÃPÀÄ (ºÀvÀÛjAzÀ ºÀ¢£ÉÊzÀÄ ¯ÉÆÃl ¢£ÀPÉÌ) ªÀÄvÀÄÛ ©¹°UÉ ªÉÄÊAiÉÆqÀÄتÀªÀgÀÄ mÉÆæAiÀÄ£ÀÄß §¼À¸À¨ÉÃPÀÄ.
[ ¥Àj±ÀæªÀÄ/ PÀµÀÖzÀ ¸À0zÀ¨sÀðzÀ°è DAiÀiÁ¸ÀªÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀ®Ä «±ÁæAwAiÀÄ£ÀÄß vÉUÉzÀÄPÉƼÀÄîªÀÅzÀÄ, AiÉÆÃUÀ ªÀÄvÀÄÛ zsÁå£À ªÉÆzÀ¯ÁzÀªÀ£ÀÄß ªÀiÁqÀ¨ÉÃPÀÄ.
10) »vÀ«ÄvÀªÁzÀ (¤§ðA¢üvÀ) DºÁgÀ 1. PÁå°ìAiÀÄA PÀ®ÄèUÀ½gÀĪÀ gÉÆÃVUÀ½UÉ: PÁå°ìAiÀÄA
PÀ®ÄèUÀ½gÀĪÀ gÉÆÃVUÀ¼ÀÄ PÁå°ìAiÀÄA ¨sÀjvÀ DºÁgÀ ªÀ¸ÀÄÛUÀ¼À£ÀÄß ¸Éë¸ÀĪÀÅzÀjAzÀ ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è ¤ÃgÀ£ÀÄ PÀÄrAiÀĨÉÃPÀÄ.
J) vÀgÀPÁjUÀ¼ÀÄ: ºÀ¹gÀÄ (¸ÉÆ¥ÀÅöàvÀgÀPÁjUÀ¼ÁzÀ ©Ã£ïì, ¹à£ÁPï, PÁågÉmï( ªÀÄÆ®AV), J¯ÉUÀ¼ÀÄ, CUÀw, PÀÄA§¼ÀPÁ¬ÄaiÀÄ J¯ÉUÀ¼ÀÄ) §mÁmÉ, (UÉt¸ÀÄUÀ¼ÀÄ) ºÀƪÀÅPÉÆøÀÄ, ¸ÉÆÃAiÀĩãïì, ¹Ö£ÁPïUÀ¼À°è PÁå°ìAiÀÄA, DPÀì¯ÉÃmï ªÀÄvÀÄÛ ¥sÁ¸ÉÆáÃgÀ¸ïVAvÀ eÁ¹Û0iÀiÁVgÀÄvÀÛzÉ. ©) zsÁ£ÀåUÀ¼ÀÄ: gÁVAiÀÄ°è ºÉaÑ£À ¥ÀæªÀiÁtzÀ PÁå°ìAiÀÄA EgÀÄvÀÛzÉ. ¹) ºÀtÄÚUÀ¼ÀÄ: MtV¹zÀ ºÀtÄÚUÀ¼ÀÄ (zÁæQë, ©ÃdUÀ¼ÀÄ, PÁ¼ÀÄUÀ¼ÀÄ, ¤A¨É eÁwAiÀÄ ºÀtÄÚUÀ¼ÁzÀ ªÀÄĸÀA© ªÉÆzÀ¯ÁzÀªÀÅUÀ¼ÀÄ PÁå°ìAiÀÄ0£À DPÀgÀUÀ¼ÀÄ. r) »nÖ¤AzÀ vÀAiÀiÁj¹zÀ DºÁgÀ ªÀ¸ÀÄÛUÀ¼ÀÄ: ¨Éæqï, vÉÆÃPÉUÉÆâü¬Ä0zÀ vÀAiÀiÁj¹zÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼ÀÄ. E) vÀA¥ÀÅ ¥Á¤ÃAiÀÄUÀ¼ÀÄ: ZÁ, PÉÆÃPÁ PÉÆïÁ, ¥É¦ì, ©AiÀÄgï, ºÁ°¤AzÀ vÀAiÀiÁj¹zÀ zÀæªÀ ¥ÀzÁxÀðUÀ¼ÀÄ, L¸ïQæÃA, ºÁ®Ä ªÀÄvÀÄÛ ºÁ°£À GvÁàzÀ£É( ¨ÉuÉÚ, vÀÄ¥Àà, VtÄÚ, ºÁ°£À ºÀÄr ªÉÆzÀ¯ÁzÀĪÀÅ) J¥ï) «ÄãÀÄ: ªÀÄƼɸÀ»vÀ ¸ÀtÚ «ÄäUÀ¼ÀÄ ªÀÄvÀÄÛ MtV¹zÀ
146
«ÄãÀÄUÀ¼ÀÄ. f) EvÀgÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼ÀÄ: gÁV, ºÉaÑ£À G¥ÀÅöà, PÉÃPï, G¦à£À PÁ¬Ä, VtÄÚ, ªÉÆmÉÖAiÀÄ ºÀ¼À¢¨sÁUÀ, ºï) r. fêÀ¸ÀvÀé ºÉZÁÑVgÀĪÀ DºÁgÀUÀ¼ÀÄ: zÉÆqÀØ zÉÆqÀØ «ÄãÀÄUÀ¼À AiÀÄPÀÈvï¤AzÀ(°ªÀgï) vÀAiÀiÁj¹zÀ JuÉÚ(PÁqï °ªÀgï JuÉÚ ±ÁPïð «Ää£À AiÀÄPÀÈwÛ¤0zÀ vÁAiÀiÁj¹zÀ JuÉÚ) PÉƧâ£ÀÄß ºÉÆ0¢zÀ «ÄãÀÄUÀ¼ÀÄ, PÉÆýªÉÆmÉÖ. L) J¯É CrPÉ dVAiÀÄĪÀÅzÀÄ. eÉ) UÀqÀ¸ÀÄ ¤ÃgÀÄ (CxÀªÁ ¸Á§Æ¤£ÉÆA¢UÉ £ÉÆgÉAiÀÄ£ÀÄß PÉÆqÀzÀ ¤ÃgÀÄ) 2) AiÀÄÆjPï Då¹qï PÀ®ÄèUÀ½gÀĪÀ gÉÆÃVUÀ½UÉ AiÀÄÆjPï DªÀÄèzÀ PÀ®ÄèUÀ½AzÀ §¼À®ÄwÛgÀĪÀ gÉÆÃVUÀ¼ÀÄ AiÀÄÆjPï DªÀÄè eÁ¹Û EgÀĪÀ DºÁgÀªÀ£ÀÄß PÀrªÉÄUÉƽ¸À¨ÉÃPÀÄ. PɼÀV£ÀªÀÅUÀ¼À°è PÉ®ªÀÅ, AiÀÄÆjPï DA® eÁ¹Û EgÀĪÀ DºÁgÀªÀ£ÀÄß ºÉaÑ£À ¥ÀæªÀiÁtzÀ°èvÉUÉzÀÄPÉÆAzÀgÉ eÁ¹Û ¤ÃgÀ£ÀÄß PÀÄrAiÀĨÉÃPÀÄ. J) vÀgÀPÁjUÀ¼ÀÄ: ©Ã¸ïì( MtV¹zÀ ¨ÉìĹzÀ ºÀ¹) PÉ®ªÀÅ ºÀ¹gÀÄ J¯É vÀgÀPÁjUÀ¼ÀÄ. ©) zsÁ£ÀåUÀ¼ÀÄ : PÀqÀ¯ÉÃPÁ¬Ä G¢Ý£ÀPÁ¼ÀÄ, ºÉ¸ÀgÀÄPÁ¼ÀÄ, ºÀÄgÀĽPÁ¼ÀÄ vÉÆUÀj, §mÁt PÁ¼ÀÄ PÉA¥ÀÅ PÁ¼ÀÄUÀ¼ÀÄ. ¹) ©ÃdUÀ¼ÀÄ: £É¯ÉPÀqÀ¯É, ¸Á¹ªÉ PÁ¼ÀÄ. r) EvÀgÀ: ¹» ¨Éæqï, AiÀÄÄjPÁªÀÄèªÀ£ÀÄß ºÉÆA¢gÀĪÀ ¸ÁªÀiÁ£Àå DPÁgÀUÀ¼À°è M0zÁVzÉ. E) J¯Áè «zsÀzÀ ªÀiÁA¸ÀUÀ¼ÀÄ. J¥sóï) J¯Áè «zsÀzÀ «ÄãÀÄUÀ¼ÀÄ. 3. ¥Á¸ï¥ÉÇÃgÀ¸ï PÀ®ÄèUÀ¼À£ÀÄß ºÉÆA¢gÀĪÀ gÉÆÃVUÀ½UÉ. ¥Á¸ï¥ÉÇÃgÀ¸ï PÀ®ÄèUÀ½ªÉ JAzÀÄ ¤tðAiÀÄ ªÀiÁrzÀ gÉÆÃVUÀ¼ÀÄ ¥Á¸ï¥ÉÇÃgÀ¸ï eÁ¹Û EgÀĪÀ DºÁgÀªÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀ¨ÉÃPÀÄ. PɼÀV£À PÀ®ªÀÅ DºÁgÀzÀ°è ¥Á¸ï¥ÉÇÃgÀ¸ï eÁ¹Û
147
EgÀĪÀÅ zÀjAzÀ CAvÀºÀ DºÁgÀªÀ£ÀÄß vÉUÉzÀÄPÉÆAqÀgÉ eÁ¹Û ¤ÃgÀ£ÀÄß vÉUÉzÀÄPÉƼÀî¨ÉÃPÁUÀÄvÀÛzÉ. CªÀÅUÀ¼ÉAzÀgÉ. J) vÀgÀPÁjUÀ¼ÀÄ:- ºÀ¹gÀÄ J¯É vÀgÀPÁjUÀ¼ÀÄ(ªÀÄÄ®AV J¯ÉUÀ¼ÀÄ, CrPÉ ºÀƪÀÅUÀ¼ÀÄ, CUÀw) ªÀÄÆ®AV, §mÁmÉ, ºÀÆPÉÆøÀÄ, ©Ã£ïì ©) ºÀtÄÚUÀ¼ÀÄ : ¨Á¼ÉºÀtÄÚ, ¸ÉçĺÀtÄÚ ªÉÆzÀ¯ÁzÀªÀÅ. ¹) Erà zÀªÀ¸À zsÁ£ÀåUÀ¼ÀÄ : ¨ÁUÀæ eÉÆüÀ, vÉÆÃPÉ UÉÆâü »nÖ¤AzÀ vÀAiÀiÁj¹zÀ DºÁgÀ, gÁV, CxÀªÁ zsÁ£Àå UÉÆâü »lÄÖ. r) PÁ¼ÀÄUÀ¼ÀÄ: ©Ã£ïì, CªÀgÉPÁ¼ÀÄ, §mÁtÂ, vÉÆUÀj¨ÉüÉ, ¸ÉÆÃAiÀĩãïì , E) PÁ¬ÄUÀ¼ÀÄ ªÀÄvÀÄÛ JuÉÚ ©ÃdUÀ¼ÀÄ J¥ï) ¸ÀtÚ. «ÄãÀÄ f) ªÀiÁA¸À : zÀ£ÀzÀ AiÀÄPÀÄævÀÄÛ JZï) ªÉÆmÉÖ, PÉÆýzÀÄÝ. L) ºÁ®Ä ªÀÄvÀÄÛ ºÁ°£À GvÁàzÀ£ÉUÀ¼ÀÄ eÉ) »nÖ¤AzÀ vÀAiÀiÁj¹zÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼ÀÄ ¹»¨Éæqï. 4) DPÀì¯ÉÃmï PÀ®ÄèUÀ¼À£ÀÄß ºÉÆA¢gÀĪÀ gÉÆÃVUÀ½UÉ DPÀì¯ÉÃmï PÀ®ÄèUÀ½gÀĪÀ gÉÆÃVUÀ¼ÉAzÀÄ ¥ÀvÉÛAiÀiÁzÀªÀgÀÄ DPÀì¯ÉÃmï eÁ¹Û EgÀĪÀ DºÁgÀªÀ£ÀÄß vÉUÉzÀÄPÉƼÀÄîªÀÅzÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀ¨ÉÃPÀÄ. PɼÀV£ÀªÀÅUÀ¼À°è PÉ®ªÀÅ, DPÀì¯ÉÃmï£ÀÄß ºÉÆA¢gÀĪÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼À£ÀÄß vÉUÉzÀÄPÉÆAqÀ°è ºÉaÑ£À ¥ÀæªÀiÁtzÀ ¤ÃgÀ£ÀÄß PÀÄrAiÀĨÉÃPÀÄ. J) vÀgÀPÁjUÀ¼ÀÄ: ¹à£ÁPï, vÉÆêÉÄvÉÆà ©) ºÀtÄÚUÀ¼ÀÄ: ¸À¥ÉÇÃmÁ, ¸ÁÖÀæ§j ºÀtÄÚUÀ¼ÀÄ ¹) ¥Á¤ÃAiÀÄUÀ¼ÀÄ: PÉÆïÁ ZÀºÁ, ZÁPÉÆïÉÃmïUÀ¼ÀÄ r) PÁ¬ÄUÀ¼ÀÄ : UÉÃgÀÄ ©Ãd, £É®UÀqÀ¯É E) ªÀiÁA¸À: zÀ£ÀzÀ ªÀiÁA¸À. ¸ÁgÁ0±À

148
¨sÉÆÃzÀ£À CA±ÀUÀ¼ÀÄ. Qrß PÀ®ÄèUÀ¼À CxÀð Qrß PÀ®ÄèUÀ½UÉ PÁgÀtUÀ¼ÀÄ aºÉß ªÀÄvÀÄÛ ®PÀëtUÀ¼ÀÄ gÉÆÃUÀ ¤uÁðAiÀÄPÀ ¥ÀjÃPÉë ±À¸ÀÛ aQvÉìUÉ ¨ÉPÁzÀ PÁAiÀÄ𠤪ÀðºÀuÉ ªÀÄvÀÄÛ
«ªÀgÀuÉUÀ¼ÀÄ Qrß PÀ®ÄèUÀ¼ÀÄ ¥ÀÅ£ÀgÁªÀvÀð£É0iÀiÁUÀzÀAvÉ
vÀqÉUÀlÄÖªÀ «zsÁ£À. ¥Àæ±ÉßUÀ¼ÀÄ 1. ªÀÄÆvÀæ vÀAiÀiÁj ªÀÄvÀÄÛ «¸Àdð£Á PÁAiÀÄðzÀ°è
¨sÁVAiÀiÁUÀĪÀ CAUÀUÀ¼ÁªÀŪÀÅ? 2. QrßAiÀÄ PÉ®¸ÀªÉãÀÄ? 3. Qrß PÀ®ÄèUÀ¼É0zÀgÉãÀÄ ? 4. Qrß PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉUÉ PÁgÀtUÀ¼À£ÀÄß ¥ÀnÖ
ªÀiÁr. 5. Qrß PÀ®ÄèUÀ½AzÀÄAmÁUÀĪÀ ¸ÀªÀĸÉåUÀ¼ÉãÀÄ ? 6. Qßrß PÀ®ÄèUÀ½ªÉ J0zÀÄ ºÉÃUÉ zÀÈrüÃPÀj¸ÀÄ«j ? 7. Qrß PÀ®ÄèUÀ¼À «zsÀUÀ¼ÁªÀŪÀÅ? 8. Qrß PÀ®ÄèUÀ¼À §UÉÎ ºÉÃUÉ PÁAiÀÄð¤ªÀð»¸À¨ÉÃPÀÄ? 9. Qrß PÀ®ÄèUÀ¼À£ÀÄß ºÉÆA¢gÀĪÀ gÉÆÃVUÉ ±À¸ÀÛçaQvÉì
AiÀiÁªÁUÀ CUÀvÀå«zÉ? 10. Qrß PÀ®ÄèUÀ¼À£ÀÄßvÀqÉUÀlÖ®Ä ¤ÃªÀÅ AiÀiÁPÉ ºÉaÑ£À
¥ÀæªÀiÁtzÀ ¤ÃgÀ£ÀÄß vÉUÉzÀÄPÉƼÀî¨ÉÃPÀÄ? 11. ©¹ vÁ¥ÀªÀiÁ£ÀzÀ°è Qrß PÀ®ÄèUÀ¼ÀÄAmÁUÀĪÀ ¸ÀA¨sÀªÀ
eÁ¹Û ºÉÃUÉ? 12. CvÀÄåvÀÌöȵÀÖ xÉÊgÉÊr¸ÀA EgÀĪÀªÀgÀ°è Qrß
PÀ®ÄèUÀ¼ÀÄ ºÉÃUÉ GAmÁUÀÄvÀÛzÉ? 13. PÁå°ìAiÀÄA, AiÀÄÆjPï Då¹qï DPÀì¯ÉÃmï ªÀÄvÀÄÛ ¥sÁ¸ÉÆágÀ¸ï
eÁ¹Û EgÀĪÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼À£ÀÄß ºÉ¸Àj¹.
149
G¥À¸ÀAºÁgÀ(wÃ¥ÀÅð, ¤tðAiÀÄ) E0zÀÄ £ÁªÀÅ Qrß PÀ®ÄèUÀ¼ÀÄ ªÀÄvÀÄÛ CzÀgÀ PÁAiÀÄð¤ªÀðºÀuÉ ºÁUÀÆ £ÁªÀÅ vÉUÉzÀÄPÉƼÀÄîªÀ DºÁgÀzÀ°è ¸Àé®à §zÀ¯ÁªÀuÉAiÀÄ£ÀÄß ªÀiÁqÀĪÀÅzÀj0zÀ £ÀªÀÄUÉ Qrß PÀ®ÄèUÀ¼À ¥ÀÅ£ÀgÁªÀvÀð£ÉAiÀiÁUÀzÀAvÉ vÀqÉUÀlÄÖªÀ°è ¸ÀºÀPÁjAiÀiÁUÀ§ºÀÄzÀÄ JA§ÄzÀgÀ §UÉÎ ZÀað¹zÉÝêÉ.

150

151

152
INFORMATONAL BOOKLET
ON
URINARY STONE
CONTENTS
I. Structured involved in the formation and excretion of urine II. Description about urinary stone 1. What do you mean by urinary stone? 2. What are the causes of urinary stone? 3. How can we identify the presence of urinary stone? 4. How will we confirm the presence of urinary stone? 5. Types of urinary stone? 6. Management / treatment of urinary stone? III. FOODS TO BE RESTRICTED
144
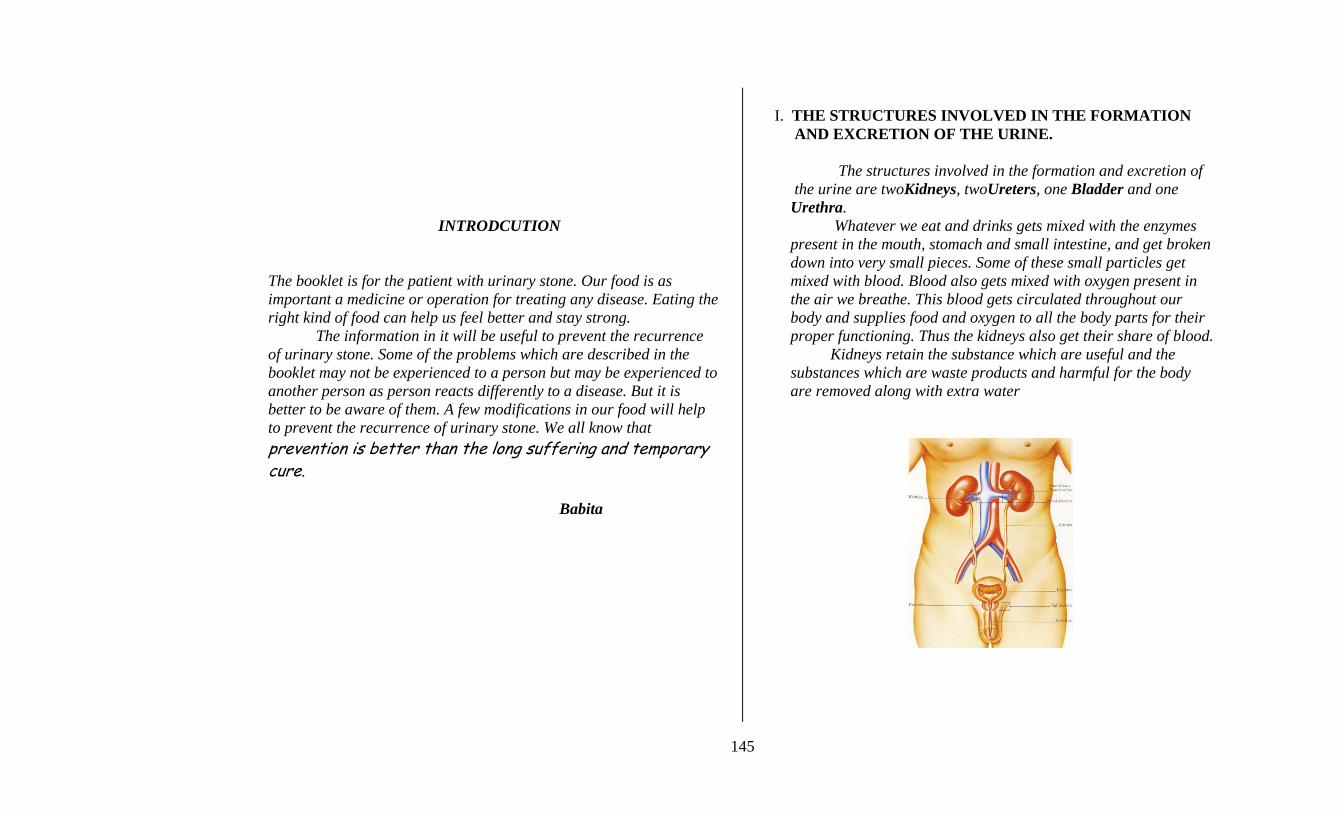
INTRODCUTION The booklet is for the patient with urinary stone. Our food is as important a medicine or operation for treating any disease. Eating the right kind of food can help us feel better and stay strong. The information in it will be useful to prevent the recurrence of urinary stone. Some of the problems which are described in the booklet may not be experienced to a person but may be experienced to another person as person reacts differently to a disease. But it is better to be aware of them. A few modifications in our food will help to prevent the recurrence of urinary stone. We all know that prevention is better than the long suffering and temporary cure. Babita
I. THE STRUCTURES INVOLVED IN THE FORMATION AND EXCRETION OF THE URINE. The structures involved in the formation and excretion of the urine are twoKidneys, twoUreters, one Bladder and one Urethra. Whatever we eat and drinks gets mixed with the enzymes present in the mouth, stomach and small intestine, and get broken down into very small pieces. Some of these small particles get mixed with blood. Blood also gets mixed with oxygen present in the air we breathe. This blood gets circulated throughout our body and supplies food and oxygen to all the body parts for their proper functioning. Thus the kidneys also get their share of blood. Kidneys retain the substance which are useful and the substances which are waste products and harmful for the body are removed along with extra water
145
II. DESCRIPTION ABOUT URINARY STONE 1. What do you mean by urinary stone? Urinary stone is a hard stone like substance which is formed by deposition of certain chemical substances in the structures involved in formation and excretion of urine. These chemical substances are mainly calcium, oxalate, uric acid and phosphorus. These are also known as minerals.
2. What are the causes of urinary stone?
LIQUIDS: Inadequate intake of water, inadequate intake of Vit A containing foods. DIETARY HABITS: More salt, excessive green leafy vegetables, excessive animal protein Eg. Egg, meat, fish etc.
OCCUPATION: More among people who work directly under sunlight. Eg. Coolie worker, Traffic police etc.
CLIMATE: More in summer season due to excessive sweating.
RARE CONDITION:
* Hereditary * Diseases of the parathyroid gland, Cushing’s disease, Paget’s disease, sarcoidosis etc * Growth and multiplication of the disease causing micro- organisms in the urinary pathway. * Prolonged illness and restricted movement * Certain drugs such as antacid, diamox, vitamin D, high dose of aspirin, laxatives etc. * Birth defects in the structure of urinary organs.
146
3. How we can identify the presence of urinary stone?
# SHARP, SEVERE RADIATING PAIN in the flanks # PAIN IN THE FLANKS EVEN WITH MILD TOUCH # FEELING OF VOMITING AND / VOMITING
#FEVER, CHILLS, VOMITING AND SHIVERING - shows growth of disease causing micro-organisms in the urinary pathway
# URINARY PROBLEMS Decreased urinary output Burning sensation while passing urine Difficulty in passing urine Presence of blood in the urine Increased frequency of urination Feeling of fullness of bladder Frequent loose stools
4. How we will confirm the presence of urinary stone?
The presence of urinary stone can be confirmed by special X-ray, Ultra sound and other blood and urine studies. 5. Types of urinary stone?
a. STONE RICH IN CALCIUM b. STONE RICH IN OXALATE c. STONE RICH IN PHOSPHORUS d. STONE RICH IN URIC ACID e. MIXED STONE. f. CYSTINE STONE g. STRUVITE STONE h. XANTHINE STONE
6. Management / Treatment of urinary stone? DIETARY CHANGES: To prevent further stone formation CRUSHING OF STONE: which get eliminated through urine OPERATION: to remove stone from the urinary pathway
III. FOOD RELATED FACTORS IN URINARY STONE Diet plays an important role in recurrence of urinary stone
and one can prevent the risk through appropriate changes in the dietary practices.
147
DO’S • DRINK MORE WATER [15-16 glasses of water daily,
1 glass = 200ml]
• EAT PLENTY OF FRESH FRUITS /FRUIT JUICE, RAW VEGETABLES RICH IN FIBER DAILY
• ADD MORE TAMARIND IN YOUR FOOD • SEEK PROMPT MEDICAL TREATMENT FOR ANY
DISCOMFORT IN PASSING URINE • CHANGES THE POSITION OF THE BED RIDDEN
PATIENTS EVERY SECOND HOURLY.
DONT’S • DO NOT EAT EXCESS AMOUNT OF ANIMAL PROTEIN
• AVOID TOO MUCH OF REFINED FOOD
• REDUCE SUGAR IN DRINKS • AVOID SWEETS, CHOCOLATES, SOFT DRINKS, TINNED
FRUITS, SWEET BREAD, CAKES AND BISCUITS.
• AVOID SWEETENED WATER LIKE PEPSI, COLA ETC.
• AVOID EXCESS AMOUNT OF TEA AND COFFEE.
148
• STOP THE FOLLOWING
o Smoking
o Drinking alcohol
o Eating pan o Adding extra salt to your food o Spending too much time under the sun o Stressful situation which causes anger, frustration,
worry, etc III. FOODS TO BE RESTRICTED 1. FOR PATIENTS WHO HAVE CALCIUM STONES The patients with calcium stones should restrict the intake of calcium. The following are some of the food stuffs rich in calcium. Increase the amount of water intake if you are taking these foods.
a. VEGETABLES: Green leafy vegetables (spinach, carrot leaves, agathy, pumpkin leaves), cauliflower, soya beans. The colacassia is having amount of calcium than uric acid and phosphorus.
b. CEREALS: Ragi is one of the riches source of calcium c. FRUITS: Dried fruits (grapes), nut, peanuts. The citrus fruits
like lime and lemon are riches sources of calcium. d. BEVERAGES: Tea, Coffee, Cola, Bear, Milk shake, Milk
products. e. FOODS CONTAINING FLOURS: Bread, Oat meal. f. MEAT: Beef, Mutton. g. OTHER: Jaggery, excess salt, cake, pickle, cheese. h. VITAMIN D RICH FOODS: Fish liver oil, fatty fish. i. CHEWING BEETLES LEAVES. j. HARD WATER.
2. FOR PATIENT WHO HAVE URIC ACID STONES. The patients who have uric acid stone restrict the following foods rich in uric acid. The following are some of the foods rich in uric acid. You have to drink extra amount of water if you consumed the following foods. a. VEGETABLES: Beans (dried, baked, green) Fenu greek leaves. b. CEREALS: Bengal gram, green gram, black gram, horse gram, lentils whole, red gram. c. NUTS: Gingelly seed, ground nut, peas, dry gram. d. OTHERS: Sweet bread is one of the riches sources of uric acid. e. ALL MEAT AND FISH. 3. PATIENTS WHO HAVE PHOSPHORUS STONE Patients who diagnose to have phosphate stone should restrict the intake of excess amount of phosphorus. The following are some foods rich in phosphorus, you have to drink extra amount of water if you consumed the following foods.
a. VEGETABLES: Green leafy vegetables, (carrot leaves, agathy, amaranth), carrot, potato, cauliflower, beans.
b. FRUITS: Banana. c. WHOLE CEREALS: Bajra, maize, oat meal, little millet,
wheat flour.
149
d. PULSES: Beans, lentils, peas, soyabeans. e. NUTS AND OIL SEEDS f. MEAT & FISH g. EGG – Hen h. MILK AND MILK PRODUCTS i. FOODS CONTAINING FLOUR.
4 FOR PATIENTS WHO HAVE OXALATE STONES
Patients who diagnosed to have oxalate stone should restrict the intake of excess amount of oxalate. The following are some foods rich in oxalate. You have to drink extra amount of water if you consume the following foods.
a) VEGETABLES: Spinach, tomato b) FRUITS: Chickoo, strawberries c) BEVERAGES: Cocoa, tea, chocolates d) NUTS: Cashew nuts, groundnuts e) MEAT: Beef
150
QgÀÄ ¥ÀjZÀ0iÀÄ
ªÀÄÆvÀæPÉÆñÀ PÀ®ÄèUÀ¼À
¥Àj«r
ªÀÄÆvÀæzÀ vÀAiÀiÁj ªÀÄvÀÄÛ «¸Àdð£É0iÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀ CAUÀzÀ gÀZÀ£É :-
ªÀÄÆvÀæ PÉÆñÀ PÀ®ÄèUÀ¼À «ªÀgÀuÉ.
1. ªÀÄÆvÀæzÀ PÀ®Äè J0zÀgÉãÀÄ? 2. ªÀÄÆvÀæPÉÆñÀzÀ°è PÀ®ÄèUÀ¼ÁUÀ®Ä PÁgÀtUÀ¼ÉãÀÄ ? 3. ªÀÄÆvÀæPÉÆñÀzÀ°è PÀ®ÄèUÀ½ªÉ J0zÀÄ ºÉÃUÉ UÀÄgÀÄw¸ÀÄ«j ? 4. Qrß PÀ®ÄèUÀ½ªÉ J0zÀÄ ¤ÃªÀÅ ºÉÃUÉ zÀÈrüÃPÀj¸ÀÄ«j ? 5. Qrß PÀ®ÄèUÀ¼À «zsÀUÀ¼ÀÄ? 6. Qrß PÀ®ÄèUÀ¼À aQvÉì / ¤ªÀðºÀuÉ ?
»vÀ«ÄvÀªÁzÀ DºÁgÀ.
151

¥ÀjZÀ0iÀÄ
F ¥ÀŸÀÛPÀªÀÅ ªÀÄÆvÀæPÉÆñÀzÀ°ègÀĪÀ gÉÆÃVUÀ½UÉ :
£ÀªÀÄä DºÁgÀ 0iÀiÁªÀÅzÉà M0zÀÄ
PÁ¬Ä¯ÉUÉ CUÀvÀåªÁzÀ ªÀÄzÀÄÝ CxÀªÁ
aQvÉì0iÀiÁVzÉ. ¸Àj0iÀiÁzÀ DºÁgÀ ¸ÉêÀ£É £ÀªÀÄä
zÉúÀªÀ£ÀÄß GvÀÛªÀÄ ¹Üw0iÀÄ°èqÀÄvÀÛzÉ.
EzÀgÀ°è Qrß PÀ®ÄèUÀ¼À ¥ÀÅ£ÀgÁªÀvÀð£É
vÀqÉUÀlÄÖ §UÉÎ ªÀiÁ»w EzÉ. F ¥ÀŸÀÛPÀzÀ°è
PÉÆnÖgÀĪÀ PÉ®ªÀÅ gÉÆÃUÀ ®PÀëtUÀ¼À£ÀÄß
PÉ®ªÀÅ gÉÆÃVUÀ¼ÀÄ C£ÀĨsÀ«¹gÀ§ºÀÄzÀÄ.
KPÉ0zÀgÉ EzÀgÀ ®PÀëtUÀ¼À d£Àj0zÀ d£ÀjUÉ
«©ü£ÀߪÁVgÀÄvÀÛzÉ. DzÀgÉ EzÀgÀ §UÉÎ
w½zÀÄPÉƼÀÄîªÀÅzÀÄ M¼Éî0iÀÄzÀÄ.
DºÁgÀzÀ°è£À §zÀ¯ÁªÀuɬÄ0zÀ
ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼ÀÄ
¥ÀÅ£ÀgÁªÀvÀð£É0iÀiÁUÀzÀ0vÉ
vÀqÉUÀlÖ§ºÀÄzÀÄ. £ÀªÀÄUÉ w½¢gÀĪÀ0vÉ
¢ÃWÀðPÁ® C£ÁgÉÆÃUÀå ºÁUÀÆ vÁvÁÌ°PÀ
UÀÄt¥Àr¸ÀÄ«PɬÄ0zÀ vÀqÉUÀlÄÖ«PÉ
M¼Éî0iÀÄzÀÄ.
§©vÀ
ªÀÄÆvÀæzÀ vÀAiÀiÁj ªÀÄvÀÄÛ «¸Àdð£É0iÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀ CAUÀzÀ gÀZÀ£É :- ªÀÄÆvÀæzÀ GvÁàzÀ£É ªÀÄvÀÄÛ «¸Àdð£É0iÀÄ°è ¨sÁUÀªÀ»¸ÀĪÀ C0UÀUÀ¼É0zÀgÉ ªÀÄÆvÀæd£ÀPÁAUÀ (Qrß), ªÀÄÆvÀæ£Á¼À, ªÀÄÆvÀæPÉÆñÀ (AiÀÄÆj£Àj ¨ÁèqÀgï) ªÀÄvÀÄÛ AiÀÄÆgÉvÀæ¢AzÀ ªÀÄÆvÀæªÀ£ÀÄß ºÉÆgÀºÁPÀĪÀ CAUÀ. £ÁªÀÅ w£ÀÄߪÀ ªÀÄvÀÄÛ PÀÄrAiÀÄĪÀ AiÀiÁªÀÅzÉà DºÁgÀ ªÀ¸ÀÄÛUÀ¼ÀÄ ¨Á¬Ä, doÀgÀ, ¸ÀtÚPÀgÀĽ£À°ègÀĪÀ QtéUÀ¼À ¸ÀºÁ0iÀÄ¢AzÀ ¸ÀtÚ ¸ÀtÚ ZÀÆgÀÄUÀ¼ÁV ¥ÀjªÀwð¸ÀĪÀÅzÀÄ F ¸ÀtÚ DºÁgÀzÀ PÀtUÀ¼ÀÄ gÀPÀÛzÀ eÉÆvÉ ¨ÉgÉvÀÄ £ÀªÀÄä zÉúÀzÀ J¯Áè ¨sÁUÀUÀ½UÉ ¥ÀjZÀ°¸ÀÄvÀÛzÉ. »ÃUÉ gÀPÀÛªÀÅ DºÁgÀ ªÀÄvÀÄÛ DªÀÄèd£ÀPÀªÀ£ÀÄß zÉúÀzÀ J¯Áè ¨sÁUÀUÀ½UÉ PÉÆAqÉÆAiÀÄÄÝ zÉúÀªÀÅ ¸ÀjAiÀiÁzÀ jÃwAiÀÄ°è PÉ®¸À
152
ªÀiÁqÀÄvÀÛzÉ. QrßAiÀÄÄ PÀÆqÀ gÀPÀÛzÀ ¥Á®£ÀÄß ¥ÀqÉAiÀÄÄvÀÛzÉ. QrßAiÀÄÄ zÉúÀPÉÌ CUÀvÀåªÁzÀ ªÀ¸ÀÄÛUÀ¼À£ÀÄß Ej¹PÉÆAqÀÄ C£ÀUÀvÀå vÁdå ªÀ¸ÀÄÛUÀ¼À£ÀÄß zÉúÀ¢AzÀ ¨ÉÃqÀªÁzÀ ¤Ãj£À ªÀÄÆ®PÀ «¸Àfð¸ÀÄvÀÛzÉ.
II. ªÀÄÆvÀæ PÉÆñÀ PÀ®ÄèUÀ¼À «ªÀgÀuÉ. 1. ªÀÄÆvÀæzÀ PÀ®Äè J0zÀgÉãÀÄ? ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼À UÀnÖAiÀiÁzÀ PÀ°è£ÀAwzÀÄÝ CzÀÄ ªÀÄÆvÀæ GvÁࢸÀĪÀ ªÀÄvÀÄÛ «¸Àìdð£ÁAUÀzÀ°è gÁ¸ÁAiÀĤPÀ ªÀ¸ÀÄÛUÀ¼ÀÄ ±ÉÃRgÀuÉAiÀiÁzÁUÀ GAmÁUÀÄvÀÛzÉ. F gÁ¸ÁAiÀĤPÀ ªÀ¸ÀÄÛUÀ¼É0zÀgÉ PÁå°ìAiÀÄA, AiÀÄÆjPï Då¹qï ªÀÄvÀÄÛ
¥sÁ¸ÉÆáÃgÀ¸ï EªÀÅUÀ¼À£ÀÄß R¤eÁ0±ÀUÀ¼É0zÀÆ PÉgÉAiÀÄÄvÁÛgÉ.
2. ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼À ¨É¼ÀªÀtÂUÉUÉ PÁgÀtUÀ¼ÀÄ
zÀæªÀ ¥ÀzÁxÀðUÀ¼À ¸ÉêÀ£É: ¤ÃgÀÄ ªÀÄvÀÄÛ zÀæªÀgÀ»vÀ DºÁgÀ ªÀÄvÀÄÛ fêÀ¸ÀvÀé J PÉÆgÀvÉ EzÀÝ DºÁgÀ. DºÁgÀzÀ ¥ÀzÀÝw: C¢üPÀ G¥ÀÅöà, ºÉaÑ£À ºÀ¹gÀÄ vÀgÀPÁj ¸ÉêÀ£É ºÁUÀÆ ºÉaÑ£À D¤ªÀÄ¯ï ¥ÉÇæÃnãï GzÁ: ªÉÆmÉÖ, ªÀiÁ0¸À, «ÄãÀÄ, EvÁå¢.
GzÉÆåÃUÀ: ¸ÀÆ0iÀÄð£À ©¹°UÉ ªÉÄÊ0iÉÆrØ PÉ®¸À ªÀiÁqÀĪÀªÀgÀ°è. GzÁ: PÀÆ° PÉ®¸À, mÁæ¦üPï ¥ÉÇðøï, EvÁå¢.
153
ºÀªÁªÀiÁ£À : ¨ÉùUÉ PÁ®zÀ°è ºÉZÁÑV ¨ÉªÀgÀĪÀÅzÀj0zÀ
«gÁ¼À ¹Üw • ªÀ0±À¥ÁgÀ0¥À0iÀÄð • ¥ÁgÀvÉÊgÉÆÃåqï PÁ¬Ä¯ÉUÀ¼ÀÄ: PÀIJ0Uïì
PÁ¬Ä¯ï, ¥ÁUÉmïì PÁ¬Ä¯ï, ¸ÁgïPÉÆìÄqÉÆù¸ï. • ªÀÄÆvÀ櫸Àdð£Á0UÀ ªÀÇåºÀzÀ°è PÁ¬Ä¯ÉUÉ
PÁgÀtªÁzÀ ¸ÀÆPÀë÷äfëUÀ¼ÀÄ ¨É¼É0iÀÄÄzÀÄ. • ¢ÃWÀðPÁ® PÁ¬Ä¯É ºÁUÀÆ ZÀ®£É0iÀÄ°è vÀqÉ. • PÉ®ªÀÅ e˵À¢üUÀ¼ÁzÀ Då0mÁ¹qï, qÉʪÀiÁPïì, r-
fêÀ¸ÀvÀ÷é, ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è D¹àj£ï, ¯ÁåPïìnêïì
• ªÀÄÆvÀæ PÉÆñÀ d£Á0UÀzÀ°è ºÀÄnÖ¤0zÀ §0zÀ £ÀÆå£ÀvÉ.
3. ªÀÄÆvÀæPÉÆñÀzÀ°è PÀ®ÄèUÀ½ªÉ J0zÀÄ ºÉÃUÉ UÀÄgÀÄw¸ÀÄ«j ?
wÃPÀë÷Ú, vÁ¼À¯ÁgÀzÀ £ÉÆêÀÅ ªÀÄzsÀå ºÉÆmÉÖAiÀÄ CqÀØ ªÀÄUÀÄΰ£À°è, vÉÆzɸÀAzÀÄUÀ¼À°è vÀqÉAiÀįÁgÀzÀAvÀºÀ £ÉÆêÀÅ.
vÉÆqɸÀ0zÀÄUÀ¼À ªÀÄzsÀåzÀ°è ªÀÄÄnÖzÀgÀÆ £ÉÆëgÀÄvÀÛzÉ.
ªÁ0w §0zÀ0vÀ¤¸ÀĪÀÅzÀÄ.
dégÀ, ZÀ½, £ÀqÀUÀĪÀÅzÀÄ ªÀÄvÀÄÛ ªÁ0wªÀiÁqÀĪÀÅzÀj0zÀ ªÀÄÆvÀæ «¸Àdð£ÁAUÀ ªÀÇåºÀzÀ ªÀiÁUÀðzÀ°è gÉÆÃUÀ vÀgÀĪÀ ¸ÀÆPÁë÷äUÀ¼ÀÄ EªÉ J0zÀÄ w½AiÀÄÄvÀÛzÉ.
154
ªÀÄÆvÀæ «¸Àdð£É0iÀÄ°è vÉÆ0zÀgÉUÀ¼ÀÄ
ªÀÄÆvÀæzÀ ¥ÀæªÀiÁt PÀrªÉÄAiÀiÁUÀĪÀÅzÀÄ.
ªÀÄÆvÀæ «¸Àfð¸ÀĪÀÅzÉà PÀµÀÖ C¤¸ÀĪÀÅzÀÄ. ªÀÄÆvÀæzÀ°è gÀPÀÛ EgÀÄ«PÉ. ªÀÄÆvÀæPÉÆñÀzÀ vÀÄ0©zÀAvÉ EgÀĪÀ ¨sÁªÀ£É. ¥ÀzÉà ¥ÀzÉà ªÀÄÆvÀæ eÁ¹Û0iÀiÁzÀAvÀ¤¸ÀĪÀÅzÀÄ. ¥ÀzÉà ¥ÀzÉà ªÀÄ®«¸Àfð¸ÀĪÀÅzÀÄ.
4. Qrß PÀ®ÄèUÀ½ªÉ J0zÀÄ ¤ÃªÀÅ ºÉÃUÉ zÀÈrüÃPÀj¸ÀÄ«j ? ªÀÄÆvÀæªÀ£ÀÄß EvÀgÀ C£ÉÃPÀ jÃwAiÀÄ ¥ÀjÃPÉëUÉƼÀ¥Àr¸ÀĪÀÅzÀjAzÀ QrßPÀ®ÄèUÀ½ªÉ J0zÀÄ zÀÈrüÃPÀj¸À§ºÀÄzÀÄ CªÉ0zÀgÉ; gÀPÀÛzÀ ¥ÀjÃPÉë, «±ÉõÀ PÀë-QgÀt ¥ÀjÃPÉë C¯ÁÖç¸ÉÆãÉÆÃUÀæ¦ü ªÉÆzÀ¯ÁzÀĪÀÅ.
5 Qrß PÀ®ÄèUÀ¼À «zsÀUÀ¼ÀÄ
a. PÁå°ìAiÀÄA PÀ®ÄèUÀ¼ÀÄ b. DPÀì¯ÉÃmï PÀ®ÄèUÀ¼ÀÄ c. ¥sÁ¸ÉÆáÃgÀ¸ï PÀ®ÄèUÀ¼ÀÄ d. AiÀÄÆjPï Då¹qï PÀ®ÄèUÀ¼ÀÄ e. ¹¹Ö£ï PÀ®ÄèUÀ¼ÀÄ f. ¸ÀÄÖçªÉÊmï PÀ®ÄèUÀ¼ÀÄ
g. eÉ£ïn£ï PÀ®Äè
6. Qrß PÀ®ÄèUÀ¼À aQvÉì / ¤ªÀðºÀuÉ ? - DºÁgÀ §zÀ¯ÁªÀuÉ: ªÀÄÆvÀæPÉÆñÀzÀ PÀ®ÄèUÀ¼À£ÀÄß vÀqÉUÀlÖ®Ä
- PÀ®ÄèUÀ¼À£ÀÄß ¥ÀÅr ªÀiÁqÀĪÀÅzÀÄ: EªÀÅ ªÀÄÆvÀæzÀ ªÀÄÆ®PÀ «¸Àdð£É0iÀiÁUÀÄvÀÛzÉ.
- ±À¸ÀÛç aQvÉì: ªÀÄÆvÀæ d£Á0UÀ¢0zÀ PÀ®ÄèUÀ¼À£ÀÄß vÉUÉzÀÄ ºÁPÀ®Ä.
III. DºÁgÀ ¥ÀzÀÝw0iÀÄÄ Qrß PÀ®ÄèUÀ¼ÀÄ ¥ÀÅ£ÁgÁªÀvÀð£É.
DºÁgÀ ¥ÀzÀÝw0iÀÄÄ Qrß PÀ®ÄèUÀ¼ÀÄ ¥ÀÅ£ÁgÁªÀvÀð£É0iÀÄ°è M0zÀÄ ªÀÄÄRåªÁzÀ
¥ÁvÀæªÀ»¸ÀÄvÀÛzÉ. F C¥Á0iÀĪÀ£ÀÄß vÀqÉUÀlÖ®Ä DºÁgÀ ¥ÀzÀÝw0iÀÄ°è ¨ÉÃPÁzÀ §zÀ¯ÁªÀuÉ ªÀiÁqÀ¨ÉÃPÀÄ.
ªÀiÁqÀ¨ÉÃPÁzÀÄÝ eÁ¹Û ¥ÀæªÀiÁtzÀ°è ¤ÃgÀÄ ¸ÉêÀ£É [15-¯ÉÆÃl ¢£ÀPÉÌ 1 ¯ÉÆÃl = 200ml]
• ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è ºÀtÂÚ£À gÀ¸ÀªÀ£ÀÄß
PÀÄrAiÀÄĪÀÅzÀi , £Áj£ÀA±ÀUÀ¼À£ÀÄß ºÉÆ0¢gÀĪÀ ºÀ¹gÀÄ vÀgÀPÁjUÀ¼À£ÀÄß w£ÀߨÉÃPÀÄ
155

• DºÁgÀzÀ°è ºÉZÁÑV ºÀĽUÀ¼À£ÀÄß
¸ÉÃj¸ÀĪÀÅzÀi • ªÀÄÆvÀæ «¸Àfð¸ÀĪÁUÀ AiÀiÁªÀÅzÉ jÃwAiÀÄ
vÉÆAzÀgÉ PÁt¹zÁUÀ Që¥ÀæªÁzÀ ªÀÄvÀÄÛ ¸ÀjAiÀiÁzÀ aQvÉìAiÀÄ£ÀÄß vÉUÉzÀÄPÉƼÀî¨ÉÃPÀÄ.
• «±Áæ0w ¹ÜwAiÀÄ°è ªÀÄ®VzÀ¯Éè EgÀĪÀ gÉÆÃVUÀ¼ÀÄ DUÁUÀ ªÀÄUÀ먀 §zÀ¯Á¬Ä¸ÀÄwÛgÀ¨ÉÃPÀÄ. ªÀiÁqÀ¨ÁgÀzÀÄÝ
• C¢üPÀ D¤ªÀÄ¯ï ¥ÉÇæÃnãï vÉUÉzÀÄPÉƼÀî¨ÉÃr.
• j¥ÉÊ£ïØ DºÁgÀªÀ£ÀÄß PÀrªÉÄ ¸Éë¹.
• ¸ÀPÀÌgÉ ¥ÀzÁxÀðªÀ£ÀÄß zÀæªÀ ¥ÀzÁxÀðzÀ°è PÀrªÉÄ ªÀiÁr. • ¹»w0r,ZÉÆÃPÉÆïÉÃmï,¸ÁÖ¥sï ræìPïì, PÉÃPï, ©¹Ìmïì, ¹»
¨ÉæqïUÀ¼À£ÀÄß vÀ¦à¹.
• vÀ0¥ÀÅö ¥Á¤Ã0iÀÄUÀ¼ÁzÀ ¥É¦ì, PÉÆïÁUÀ¼À£ÀÄß
vÀ¦à¹. • ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è ZÁ, PÁ¦üUÀ¼À£ÀÄß ¸Éë¸À¨ÉÃr.
• PÀ¥ÀÅöà ZÀºÁ ªÀÄvÀÄÛ PÁ¦üAiÀÄ£ÀÄß
PÀrªÉÄUÉƽ¸À¨ÉÃPÀÄ
• vÀqÉUÀnÖ¹.
o zsÀƪÀÄ¥Á£À
156
o ªÀÄzÀå¥Á£À
• ¸ÀÄtÚ ¨ÉgɹzÀ J¯É CrPÉAiÀÄ£ÀÄß w£Àßi ªÀÅzÀi • C¢üPÀ G¥ÀÅöà • C¢üPÀ ¸ÀªÀÄAiÀÄ ¸ÀÆ0iÀÄð£À ©¹°UÉ ªÉÄÊ0iÉÆrØ
PÉ®¸À ªÀiÁqÀĪÀÅzÀi • ¸ÀégÁWÀvÀ ¥Àj¹ÜwUÀ¼ÀzÀ ¹lÄÖ, D±Á¨sÀ0UÀ a0vÉ EvÁå¢.
»vÀ«ÄvÀªÁzÀ (¤§ðA¢üvÀ) DºÁgÀ 1. PÁå°ìAiÀÄA PÀ®ÄèUÀ½gÀĪÀ gÉÆÃVUÀ½UÉ:
PÁå°ìAiÀÄA PÀ®ÄèUÀ½gÀĪÀ gÉÆÃVUÀ¼ÀÄ PÁå°ìAiÀÄA ¨sÀjvÀ DºÁgÀ ªÀ¸ÀÄÛUÀ¼À£ÀÄß ¸Éë¸ÀĪÀÅzÀjAzÀ ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è ¤ÃgÀ£ÀÄß PÀÄrAiÀĨÉÃPÀÄ.
J) vÀgÀPÁjUÀ¼ÀÄ: ºÀ¹gÀÄ (¸ÉÆ¥ÀÅöàvÀgÀPÁjUÀ¼ÁzÀ ©Ã£ïì, ¹à£ÁPï, PÁågÉmï( ªÀÄÆ®AV), J¯ÉUÀ¼ÀÄ, CUÀw, PÀÄA§¼ÀPÁ¬ÄaiÀÄ J¯ÉUÀ¼ÀÄ) §mÁmÉ, (UÉt¸ÀÄUÀ¼ÀÄ) ºÀƪÀÅPÉÆøÀÄ, ¸ÉÆÃAiÀĩãïì, ¹Ö£ÁPïUÀ¼À°è PÁå°ìAiÀÄA, DPÀì¯ÉÃmï ªÀÄvÀÄÛ ¥sÁ¸ÉÆáÃgÀ¸ïVAvÀ eÁ¹Û0iÀiÁVgÀÄvÀÛzÉ. ©) zsÁ£ÀåUÀ¼ÀÄ: gÁVAiÀÄ°è ºÉaÑ£À ¥ÀæªÀiÁtzÀ PÁå°ìAiÀÄA EgÀÄvÀÛzÉ. ¹) ºÀtÄÚUÀ¼ÀÄ: MtV¹zÀ ºÀtÄÚUÀ¼ÀÄ (zÁæQë, ©ÃdUÀ¼ÀÄ, PÁ¼ÀÄUÀ¼ÀÄ, ¤A¨É eÁwAiÀÄ ºÀtÄÚUÀ¼ÁzÀ ªÀÄĸÀA© ªÉÆzÀ¯ÁzÀªÀÅUÀ¼ÀÄ PÁå°ìAiÀÄ0£À DPÀgÀUÀ¼ÀÄ. r) »nÖ¤AzÀ vÀAiÀiÁj¹zÀ DºÁgÀ ªÀ¸ÀÄÛUÀ¼ÀÄ: ¨Éæqï, vÉÆÃPÉUÉÆâü¬Ä0zÀ vÀAiÀiÁj¹zÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼ÀÄ. E) vÀA¥ÀÅ ¥Á¤ÃAiÀÄUÀ¼ÀÄ: ZÁ, PÉÆÃPÁ, ¥É¦ì, PÉÆïÁ, ©AiÀÄgï, ºÁ°¤AzÀÄ vÀAiÀiÁj¹zÀ zÀæªÀ ¥ÀzÁxÀðUÀ¼ÀÄ,
L¸ïQæÃA, ºÁ®Ä ªÀÄvÀÄÛ ºÁ°£À GvÁàzÀ£É( ¨ÉuÉÚ, vÀÄ¥Àà, VtÄÚ, ºÁ°£À ºÀÄr ªÉÆzÀ¯ÁzÀĪÀÅ) J¥ï) «ÄãÀÄ: ªÀÄƼɸÀ»vÀ ¸ÀtÚ «ÄäUÀ¼ÀÄ ªÀÄvÀÄÛ MtV¹zÀ «ÄãÀÄUÀ¼ÀÄ. f) EvÀgÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼ÀÄ: gÁV, ºÉaÑ£À G¥ÀÅöà, PÉÃPï, G¦à£À PÁ¬Ä, VtÄÚ, ªÉÆmÉÖAiÀÄ ºÀ¼À¢¨sÁUÀ, ºï) r. fêÀ¸ÀvÀé ºÉZÁÑVgÀĪÀ DºÁvÀUÀ¼ÀÄ: zÉÆqÀØ zÉÆqÀØ «ÄäUÀ¼À AiÀÄPÀÈvï¤AzÀ(°ªÀgï) vÀAiÀiÁj¹zÀ JuÉÚ(PÁqï °ªÀgï JuÉÚ ±ÁPïð «Ää£À AiÀÄPÀÈwÛ¤0zÀ vÁAiÀiÁj¹zÀ JuÉÚ) PÉƧâ£ÀÄß ºÉÆ0¢zÀ «ÄãÀÄUÀ¼ÀÄ PÉÆýªÉÆmÉÖ. L) J¯É CrPÉ dVAiÀÄĪÀÅzÀÄ. eÉ) UÀqÀ¸ÀÄ ¤ÃgÀÄ (CxÀªÁ ¸Á§Æ¤£ÉÆA¢UÉ £ÉÆgÉAiÀÄ£ÀÄß PÉÆqÀzÀ ¤ÃgÀÄ) 2) AiÀÄÆjPï DªÀÄèzÀ PÀ®ÄèUÀ½gÀĪÀ gÉÆÃVUÀ½UÉ AiÀÄÆjPï DªÀÄèzÀ PÀ®ÄèUÀ½AzÀ §¼À®ÄwÛgÀĪÀ gÉÆÃVUÀ¼ÀÄ AiÀÄÆjPï DªÀÄè eÁ¹Û EgÀĪÀ DºÁgÀªÀ£ÀÄß PÀrªÉÄUÉƽ¸À¨ÉÃPÀÄ. PɼÀV£ÀªÀÅUÀ¼À°è PÉ®ªÀÅ, AiÀÄÆjPï DA® eÁ¹Û EgÀĪÀ DºÁgÀªÀ£ÀÄß ºÉaÑ£À ¥ÀæªÀiÁtzÀ°èvÉUÉzÀÄPÉÆAzÀgÉ eÁ¹Û ¤ÃgÀ£ÀÄß PÀÄrAiÀĨÉÃPÀÄ. J) vÀgÀPÁjUÀ¼ÀÄ: ©Ã¸ïì( MtV¹zÀ ¨ÉìĹzÀ ºÀ¹) PÉ®ªÀÅ ºÀ¹gÀÄ J¯É vÀgÀPÁjUÀ¼ÀÄ. ©) zsÁ£ÀåUÀ¼ÀÄ : PÀqÀ¯ÉÃPÁ¬Ä G¢Ý£ÀPÁ¼ÀÄ, ºÉ¸ÀgÀÄPÁ¼ÀÄ, ºÀÄgÀĽPÁ¼ÀÄ vÉÆUÀj, §mÁt PÁ¼ÀÄ PÉA¥ÀÅ PÁ¼ÀÄUÀ¼ÀÄ. ¹) ©ÃdUÀ¼ÀÄ: £É¯ÉPÀqÀ¯É, ¸Á¹ªÉ PÁ¼ÀÄ. r) EvÀgÀ: ¹» ¨Éæqï, AiÀÄÄjPÁªÀÄèªÀ£ÀÄß ºÉÆA¢gÀĪÀ ¸ÁªÀiÁ£Àå DPÁgÀUÀ¼À°è M0zÁVzÉ. E) J¯Áè «zsÀzÀ ªÀiÁA¸ÀUÀ¼ÀÄ. J¥sóï) J¯Áè «zsÀzÀ «ÄãÀÄUÀ¼ÀÄ. 3. ¥Á¸ï¥ÉÇÃgÀ¸ï PÀ®ÄèUÀ¼À£ÀÄß ºÉÆA¢gÀĪÀ gÉÆÃVUÀ½UÉ.
157
¥Á¸ï¥ÉÇÃgÀ¸ï PÀ®ÄèUÀ½ªÉ JazÀÄ gÉÆÃUÀ ¤tðAiÀÄ ªÀiÁrzÀ gÉÆÃVUÀ¼ÀÄ ¥Á¸ï¥ÉÇÃgÀ¸ï eÁ¹Û EgÀĪÀ DºÁgÀªÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀ¨ÉÃPÀÄ. PɼÀV£À PÀ®ªÀÅ DºÁgÀzÀ°è ¥Á¸ï¥ÉÇÃgÀ¸ï eÁ¹Û EgÀĪÀåzÀjAzÀ CavÀºÀ DºÁgÀªÀ£ÀÄß vÉUÉzÀÄPÉÆAqÀgÉ eÁ¹Û ¤ÃgÀ£ÀÄß vÉUÉzÀÄPÉƼÀî¨ÉÃPÁUÀÄvÀÛzÉ. CªÀÅUÀ¼ÉAzÀgÉ. J) vÀgÀPÁjUÀ¼ÀÄ:- ºÀ¹gÀÄ J¯É vÀgÀPÁjUÀ¼ÀÄ(ªÀÄÄ®AV J¯ÉUÀ¼ÀÄ) CrPÉ ºÀƪÀÅUÀ¼ÀÄ, CUÀw) ªÀÄÆ®AV, §mÁmÉ, ºÀÆPÉÆøÀÄ, ©Ã£ïì ©) ºÀtÄÚUÀ¼ÀÄ : ¨Á¼ÉºÀtÄÚ, ¸ÉçĺÀtÄÚ ªÉÆzÀ¯ÁzÀªÀÅ. ¹) Erà zÀªÀ¸À zsÁ£ÀåUÀ¼ÀÄ : ¨ÁUÀæ eÉÆüÀ, vÉÆÃPÉ UÉÆâü »nÖ¤AzÀ vÀAiÀiÁj¹zÀ DºÁgÀ, gÁV, CxÀªÁ zsÁ£Àå UÉÆâü »lÄÖ. r) PÁ¼ÀÄUÀ¼ÀÄ: ©Ã£ïì, CªÀgÉPÁ¼ÀÄ, §mÁtÂ, vÉÆUÀj¨ÉüÉ, ¸ÉÆÃAiÀĩãï, E) PÁ¬ÄUÀ¼ÀÄ ªÀÄvÀÄÛ JuÉÚ ©ÃdUÀ¼ÀÄ J¥ï) «ÄãÀÄ ¸ÀtÚ. f) ªÀiÁA¸À : zÀ£ÀzÀ AiÀÄPÀÄævÀÄÛ JZï) ªÉÆmÉÖ, PÉÆýzÀÄÝ. L) ºÁ®Ä ªÀÄvÀÄÛ ºÁ°£À GvÁàzÀ£ÉUÀ¼ÀÄ eÉ) »nÖ¤AzÀ vÀAiÀiÁj¹zÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼ÀÄ ¹»¨Éæqï. 4) DPÀì¯ÉÃmï PÀ®ÄèUÀ¼À£ÀÄß ºÉÆA¢gÀĪÀ gÉÆÃVUÀ½UÉ DPÀì¯ÉÃmï PÀ®ÄèUÀ½gÀĪÀ gÉÆÃVUÀ¼ÉAzÀÄ ¥ÀvÉÛAiÀiÁzÀªÀgÀÄ DPÀì¯ÉÃmï eÁ¹Û EgÀĪÀ DºÁgÀªÀ£ÀÄß vÉUÉzÀÄPÉƼÀÄîªÀÅzÀ£ÀÄß PÀrªÉÄ ªÀiÁqÀ¨ÉÃPÀÄ. PɼÀV£ÀªÀÅUÀ¼À°è PÉ®ªÀÅ, DPÀì¯ÉÃmï£ÀÄß ºÉÆA¢gÀĪÀ DºÁgÀ ¥ÀzÁxÀðUÀ¼À£ÀÄß vÉUÉzÀÄPÉÆAqÀ°è ºÉaÑ£À ¥ÀæªÀiÁtzÀ ¤ÃgÀ£ÀÄß PÀÄrAiÀĨÉÃPÀÄ. J) vÀgÀPÁjUÀ¼ÀÄ: ¹à£ÁPï, vÉÆêÉÄvÉÆà ©) ºÀtÄÚUÀ¼ÀÄ: ¸À¥ÉÇÃmÁ, ¸Áå§j ºÀtÄÚUÀ¼ÀÄ ¹) ¥Á¤ÃAiÀÄUÀ¼ÀÄ: PÉÆïÁ ZÀºÁ, ZÁPÉÆïÉÃmïUÀ¼ÀÄ
r) PÁ¬ÄUÀ¼ÀÄ : UÉÃgÀÄ ©Ãd, £É®UÀqÀ¯É E) ªÀiÁA¸À: zÀ£ÀzÀ ªÀiÁA¸À.
158
159
158
13
Lists of experts of content validity 1. Prof. B.V Kathyayani
Principal and HOD of Medical Surgical Department Dr. M.V Shetty Institute of Health Sciences, Mangalore 2. Sr. Anndrose HOD of Medical Surgical Department Fr. Muller’s College of Nursing, Mangalore 3. Mini Sacharias
Assistant Professor College of Nursing, Kottayam
4. Theresa Leonelda Mindonea
Assistant Professor Laxmi Memorial College of Nursing, Mangalore 5. Elsa Sanatombi Devi
Lecturer Manipal College of Nursing, MAHE Manipal 6. Dr. Jitendra Singh
Consultant Urologist Shija Hospital and Research Institute
Imphal, Manipur
7. Dr. S. P Shenoy Senior Consultant Urologist
A.J Hospital and Research Centre, Mangalore 8. Dr. Sinam Rajendra Singh
Associate Professor Department of Urology Regional Institute of Medical Sciences, Imphal, Manipur
9. Dr. Harish Nayak
Surgeon, Alva’s Health Centre Moodbidri, Mangalore
159
10. Dr. Y. Achouba Singh Surgeon, Raj Polyclinics, Royal Hospital Imphal, Manipur 11. Dr. Sadananda Naik
Medicine, Alva’s Health Centre Moodbidri, Mangalore
12. Dr. Sheetal Kumar General Medicine Community Health Centre Belthangady
13. Mrs. Archana Prabhat Lecturer, Department of Food, Nutrition and Dietatics Alva’s College of BFND Moodbidri, Mangalore
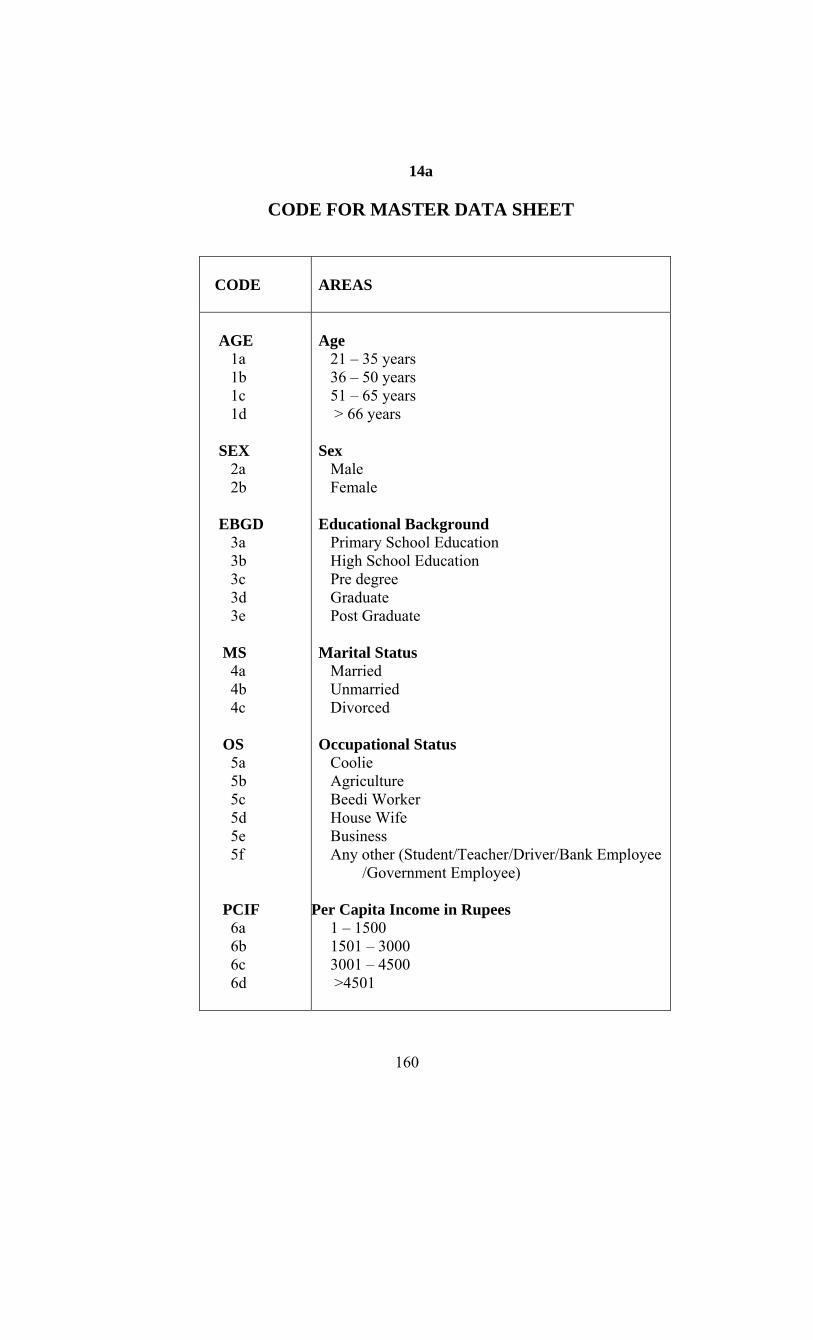
160
14a
CODE FOR MASTER DATA SHEET
CODE
AREAS
AGE 1a 1b 1c 1d SEX 2a 2b EBGD 3a 3b 3c 3d 3e MS 4a 4b 4c OS 5a 5b 5c 5d 5e 5f PCIF 6a 6b 6c 6d
Age 21 – 35 years 36 – 50 years 51 – 65 years > 66 years Sex Male Female Educational Background Primary School Education High School Education Pre degree Graduate Post Graduate Marital Status Married Unmarried Divorced Occupational Status Coolie Agriculture Beedi Worker House Wife Business Any other (Student/Teacher/Driver/Bank Employee /Government Employee)
Per Capita Income in Rupees 1 – 1500 1501 – 3000 3001 – 4500 >4501
161
RGN 7a 7b 7c DP 8a 8b PHA 9a 9b NPHA 10a 10b 10c FHRC 11a 11b SHI 12a 12b 12c 12d HBT 13a 13b 13c 13d K1 – K3 KI K2 K3 TKNOW
Religion Hindu Muslim Christian Dietary Pattern Vegetarian Non-vegetarian Previous hospital Admission Yes No Number of Previous Hospital Admission One time Two times Three times Any Family History of Renal Calculi Yes No Sources of health information on the disease condition Doctor Relatives Friends Any other Habit(s) Smoking Betal leaves chewing Alcohol None of the above Content areas of Knowledge Questionnaire 0 – 11 12 – 23 24 – 34 Total Knowledge Questionnaire
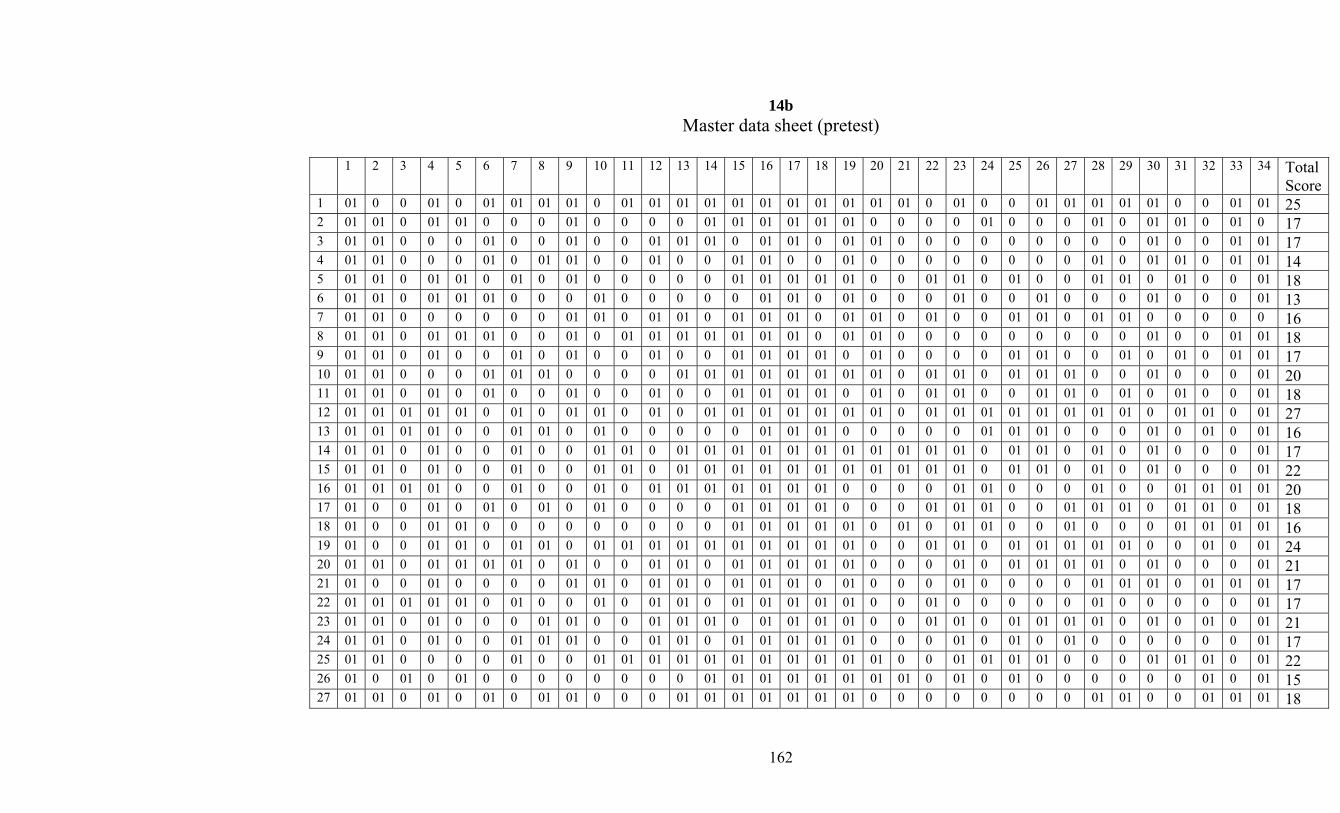
162
14b Master data sheet (pretest)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 Total
Score1 01 0 0 01 0 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 0 01 0 0 01 01 01 01 01 0 0 01 01 25 2 01 01 0 01 01 0 0 0 01 0 0 0 0 01 01 01 01 01 01 0 0 0 0 01 0 0 0 01 0 01 01 0 01 0 17 3 01 01 0 0 0 01 0 0 01 0 0 01 01 01 0 01 01 0 01 01 0 0 0 0 0 0 0 0 0 01 0 0 01 01 17 4 01 01 0 0 0 01 0 01 01 0 0 01 0 0 01 01 0 0 01 0 0 0 0 0 0 0 0 01 0 01 01 0 01 01 14 5 01 01 0 01 01 0 01 0 01 0 0 0 0 0 01 01 01 01 01 0 0 01 01 0 01 0 0 01 01 0 01 0 0 01 18 6 01 01 0 01 01 01 0 0 0 01 0 0 0 0 0 01 01 0 01 0 0 0 01 0 0 01 0 0 0 01 0 0 0 01 13 7 01 01 0 0 0 0 0 0 01 01 0 01 01 0 01 01 01 0 01 01 0 01 0 0 01 01 0 01 01 0 0 0 0 0 16 8 01 01 0 01 01 01 0 0 01 0 01 01 01 01 01 01 01 0 01 01 0 0 0 0 0 0 0 0 0 01 0 0 01 01 18 9 01 01 0 01 0 0 01 0 01 0 0 01 0 0 01 01 01 01 0 01 0 0 0 0 01 01 0 0 01 0 01 0 01 01 17 10 01 01 0 0 0 01 01 01 0 0 0 0 01 01 01 01 01 01 01 01 0 01 01 0 01 01 01 0 0 01 0 0 0 01 20 11 01 01 0 01 0 01 0 0 01 0 0 01 0 0 01 01 01 01 0 01 0 01 01 0 0 01 01 0 01 0 01 0 0 01 18 12 01 01 01 01 01 0 01 0 01 01 0 01 0 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 0 01 01 0 01 27 13 01 01 01 01 0 0 01 01 0 01 0 0 0 0 0 01 01 01 0 0 0 0 0 01 01 01 0 0 0 01 0 01 0 01 16 14 01 01 0 01 0 0 01 0 0 01 01 0 01 01 01 01 01 01 01 01 01 01 01 0 01 01 0 01 0 01 0 0 0 01 17 15 01 01 0 01 0 0 01 0 0 01 01 0 01 01 01 01 01 01 01 01 01 01 01 0 01 01 0 01 0 01 0 0 0 01 22 16 01 01 01 01 0 0 01 0 0 01 0 01 01 01 01 01 01 01 0 0 0 0 01 01 0 0 0 01 0 0 01 01 01 01 20 17 01 0 0 01 0 01 0 01 0 01 0 0 0 0 01 01 01 01 0 0 0 01 01 01 0 0 01 01 01 0 01 01 0 01 18 18 01 0 0 01 01 0 0 0 0 0 0 0 0 0 01 01 01 01 01 0 01 0 01 01 0 0 01 0 0 0 01 01 01 01 16 19 01 0 0 01 01 0 01 01 0 01 01 01 01 01 01 01 01 01 01 0 0 01 01 0 01 01 01 01 01 0 0 01 0 01 24 20 01 01 0 01 01 01 01 0 01 0 0 01 01 0 01 01 01 01 01 0 0 0 01 0 01 01 01 01 0 01 0 0 0 01 21 21 01 0 0 01 0 0 0 0 01 01 0 01 01 0 01 01 01 0 01 0 0 0 01 0 0 0 0 01 01 01 0 01 01 01 17 22 01 01 01 01 01 0 01 0 0 01 0 01 01 0 01 01 01 01 01 0 0 01 0 0 0 0 0 01 0 0 0 0 0 01 17 23 01 01 0 01 0 0 0 01 01 0 0 01 01 01 0 01 01 01 01 0 0 01 01 0 01 01 01 01 0 01 0 01 0 01 21 24 01 01 0 01 0 0 01 01 01 0 0 01 01 0 01 01 01 01 01 0 0 0 01 0 01 0 01 0 0 0 0 0 0 01 17 25 01 01 0 0 0 0 01 0 0 01 01 01 01 01 01 01 01 01 01 01 0 0 01 01 01 01 0 0 0 01 01 01 0 01 22 26 01 0 01 0 01 0 0 0 0 0 0 0 0 01 01 01 01 01 01 01 01 0 01 0 01 0 0 0 0 0 0 01 0 01 15 27 01 01 0 01 0 01 0 01 01 0 0 0 01 01 01 01 01 01 01 0 0 0 0 0 0 0 0 01 01 0 0 01 01 01 18
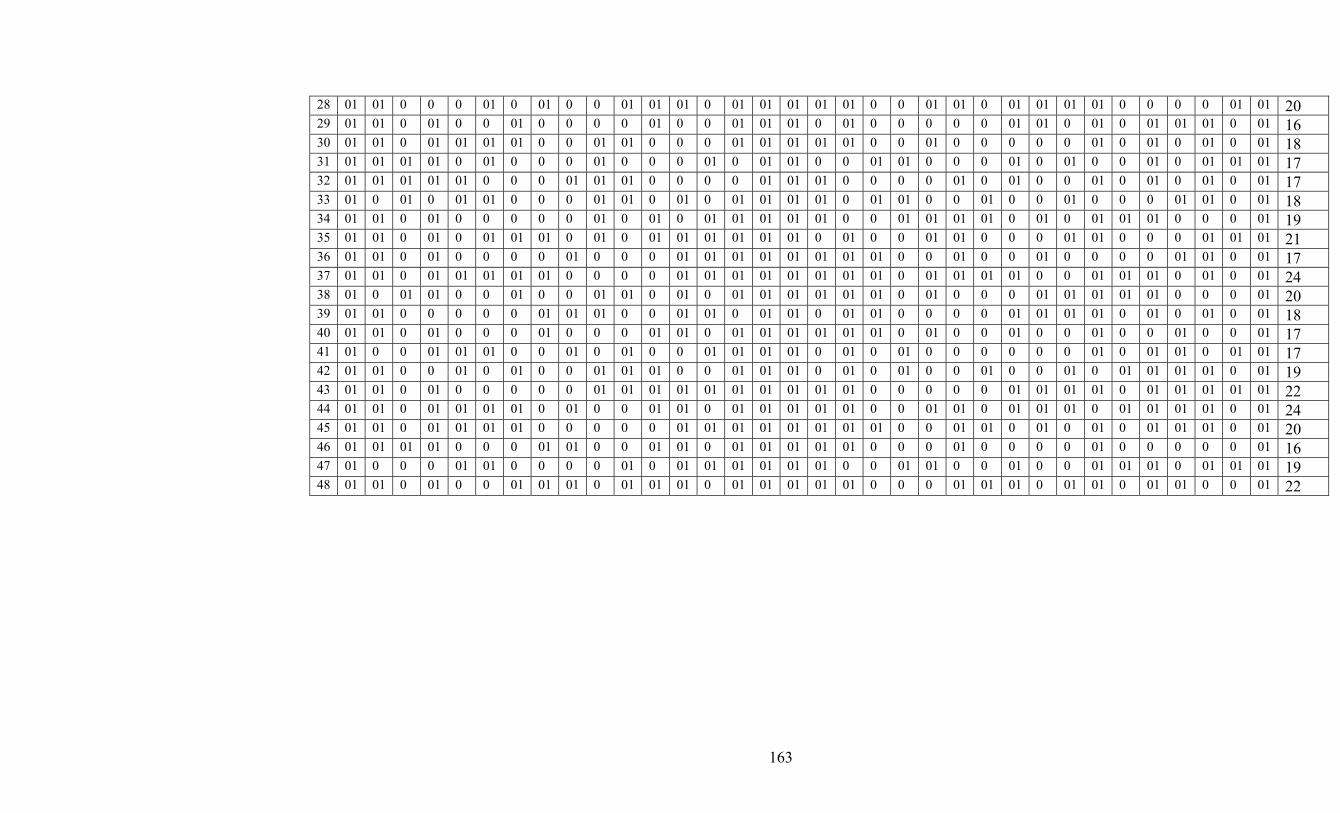
163
28 01 01 0 0 0 01 0 01 0 0 01 01 01 0 01 01 01 01 01 0 0 01 01 0 01 01 01 01 0 0 0 0 01 01 20 29 01 01 0 01 0 0 01 0 0 0 0 01 0 0 01 01 01 0 01 0 0 0 0 0 01 01 0 01 0 01 01 01 0 01 16 30 01 01 0 01 01 01 01 0 0 01 01 0 0 0 01 01 01 01 01 0 0 01 0 0 0 0 0 01 0 01 0 01 0 01 18 31 01 01 01 01 0 01 0 0 0 01 0 0 0 01 0 01 01 0 0 01 01 0 0 0 01 0 01 0 0 01 0 01 01 01 17 32 01 01 01 01 01 0 0 0 01 01 01 0 0 0 0 01 01 01 0 0 0 0 01 0 01 0 0 01 0 01 0 01 0 01 17 33 01 0 01 0 01 01 0 0 0 01 01 0 01 0 01 01 01 01 0 01 01 0 0 01 0 0 01 0 0 0 01 01 0 01 18 34 01 01 0 01 0 0 0 0 0 01 0 01 0 01 01 01 01 01 0 0 01 01 01 01 0 01 0 01 01 01 0 0 0 01 19 35 01 01 0 01 0 01 01 01 0 01 0 01 01 01 01 01 01 0 01 0 0 01 01 0 0 0 01 01 0 0 0 01 01 01 21 36 01 01 0 01 0 0 0 0 01 0 0 0 01 01 01 01 01 01 01 01 0 0 01 0 0 01 0 0 0 0 01 01 0 01 17 37 01 01 0 01 01 01 01 01 0 0 0 0 01 01 01 01 01 01 01 01 0 01 01 01 01 0 0 01 01 01 0 01 0 01 24 38 01 0 01 01 0 0 01 0 0 01 01 0 01 0 01 01 01 01 01 01 0 01 0 0 0 01 01 01 01 01 0 0 0 01 20 39 01 01 0 0 0 0 0 01 01 01 0 0 01 01 0 01 01 0 01 01 0 0 0 0 01 01 01 01 0 01 0 01 0 01 18 40 01 01 0 01 0 0 0 01 0 0 0 01 01 0 01 01 01 01 01 01 0 01 0 0 01 0 0 01 0 0 01 0 0 01 17 41 01 0 0 01 01 01 0 0 01 0 01 0 0 01 01 01 01 0 01 0 01 0 0 0 0 0 0 01 0 01 01 0 01 01 17 42 01 01 0 0 01 0 01 0 0 01 01 01 0 0 01 01 01 0 01 0 01 0 0 01 0 0 01 0 01 01 01 01 0 01 19 43 01 01 0 01 0 0 0 0 0 01 01 01 01 01 01 01 01 01 01 0 0 0 0 0 01 01 01 01 0 01 01 01 01 01 22 44 01 01 0 01 01 01 01 0 01 0 0 01 01 0 01 01 01 01 01 0 0 01 01 0 01 01 01 0 01 01 01 01 0 01 24 45 01 01 0 01 01 01 01 0 0 0 0 0 01 01 01 01 01 01 01 01 0 0 01 01 0 01 0 01 0 01 01 01 0 01 20 46 01 01 01 01 0 0 0 01 01 0 0 01 01 0 01 01 01 01 01 0 0 0 01 0 0 0 0 01 0 0 0 0 0 01 16 47 01 0 0 0 01 01 0 0 0 0 01 0 01 01 01 01 01 01 0 0 01 01 0 0 01 0 0 01 01 01 0 01 01 01 19 48 01 01 0 01 0 0 01 01 01 0 01 01 01 0 01 01 01 01 01 0 0 0 01 01 01 0 01 01 0 01 01 0 0 01 22
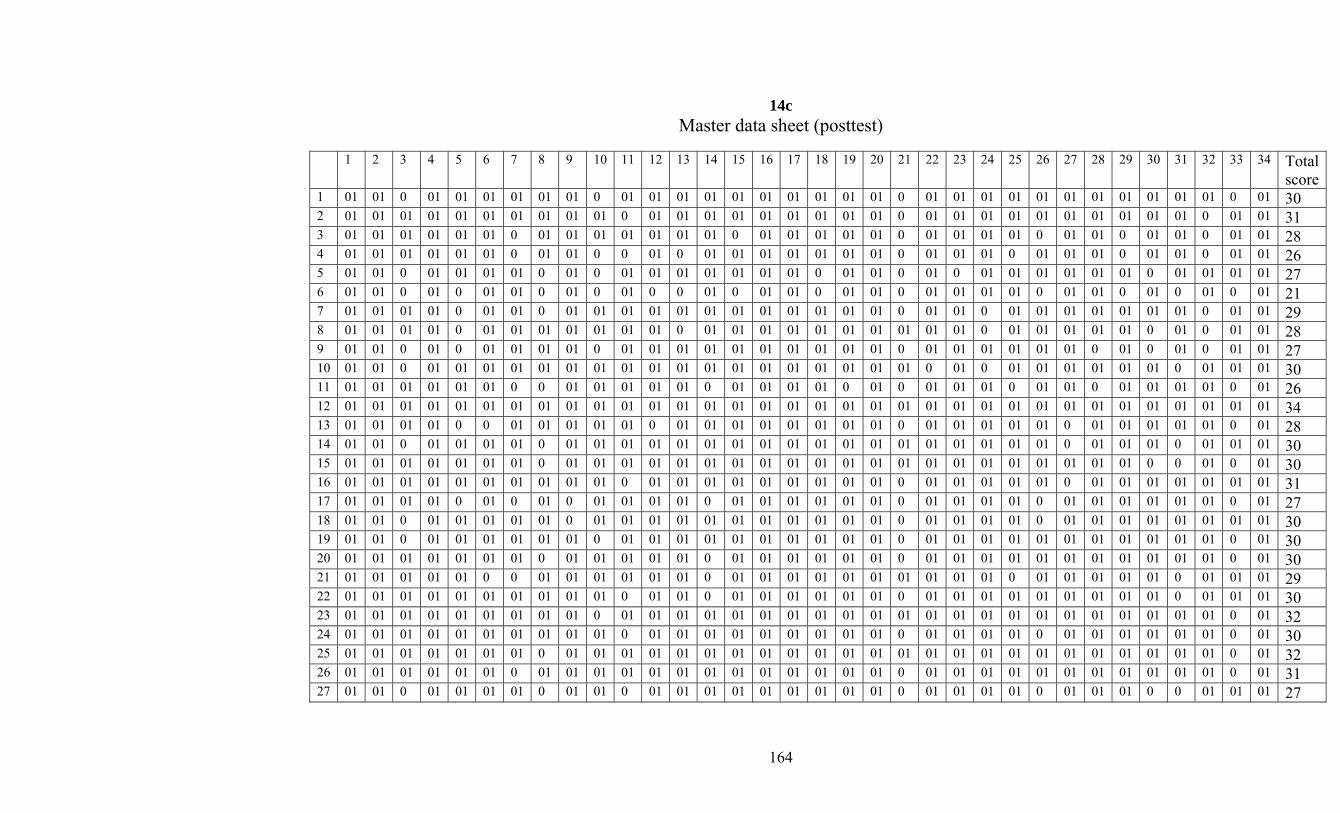
164
14c Master data sheet (posttest)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 Total
score 1 01 01 0 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 0 01 30 2 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 0 01 01 31 3 01 01 01 01 01 01 0 01 01 01 01 01 01 01 0 01 01 01 01 01 0 01 01 01 01 0 01 01 0 01 01 0 01 01 28 4 01 01 01 01 01 01 0 01 01 0 0 01 0 01 01 01 01 01 01 01 0 01 01 01 0 01 01 01 0 01 01 0 01 01 26 5 01 01 0 01 01 01 01 0 01 0 01 01 01 01 01 01 01 0 01 01 0 01 0 01 01 01 01 01 01 0 01 01 01 01 27 6 01 01 0 01 0 01 01 0 01 0 01 0 0 01 0 01 01 0 01 01 0 01 01 01 01 0 01 01 0 01 0 01 0 01 21 7 01 01 01 01 0 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 0 01 01 0 01 01 01 01 01 01 01 0 01 01 29 8 01 01 01 01 0 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 0 01 0 01 01 28 9 01 01 0 01 0 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 0 01 0 01 0 01 01 27 10 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 0 01 01 01 01 01 01 0 01 01 01 30 11 01 01 01 01 01 01 0 0 01 01 01 01 01 0 01 01 01 01 0 01 0 01 01 01 0 01 01 0 01 01 01 01 0 01 26 12 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 34 13 01 01 01 01 0 0 01 01 01 01 01 0 01 01 01 01 01 01 01 01 0 01 01 01 01 01 0 01 01 01 01 01 0 01 28 14 01 01 0 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 01 01 0 01 01 01 30 15 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 0 0 01 0 01 30 16 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 0 01 01 01 01 01 01 01 31 17 01 01 01 01 0 01 0 01 0 01 01 01 01 0 01 01 01 01 01 01 0 01 01 01 01 0 01 01 01 01 01 01 0 01 27 18 01 01 0 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 0 01 01 01 01 01 01 01 01 30 19 01 01 0 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 0 01 30 20 01 01 01 01 01 01 01 0 01 01 01 01 01 0 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 0 01 30 21 01 01 01 01 01 0 0 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 0 01 01 01 29 22 01 01 01 01 01 01 01 01 01 01 0 01 01 0 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 0 01 01 01 30 23 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 32 24 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 0 01 01 01 01 0 01 01 01 01 01 01 0 01 30 25 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 32 26 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 0 01 31 27 01 01 0 01 01 01 01 0 01 01 0 01 01 01 01 01 01 01 01 01 0 01 01 01 01 0 01 01 01 0 0 01 01 01 27
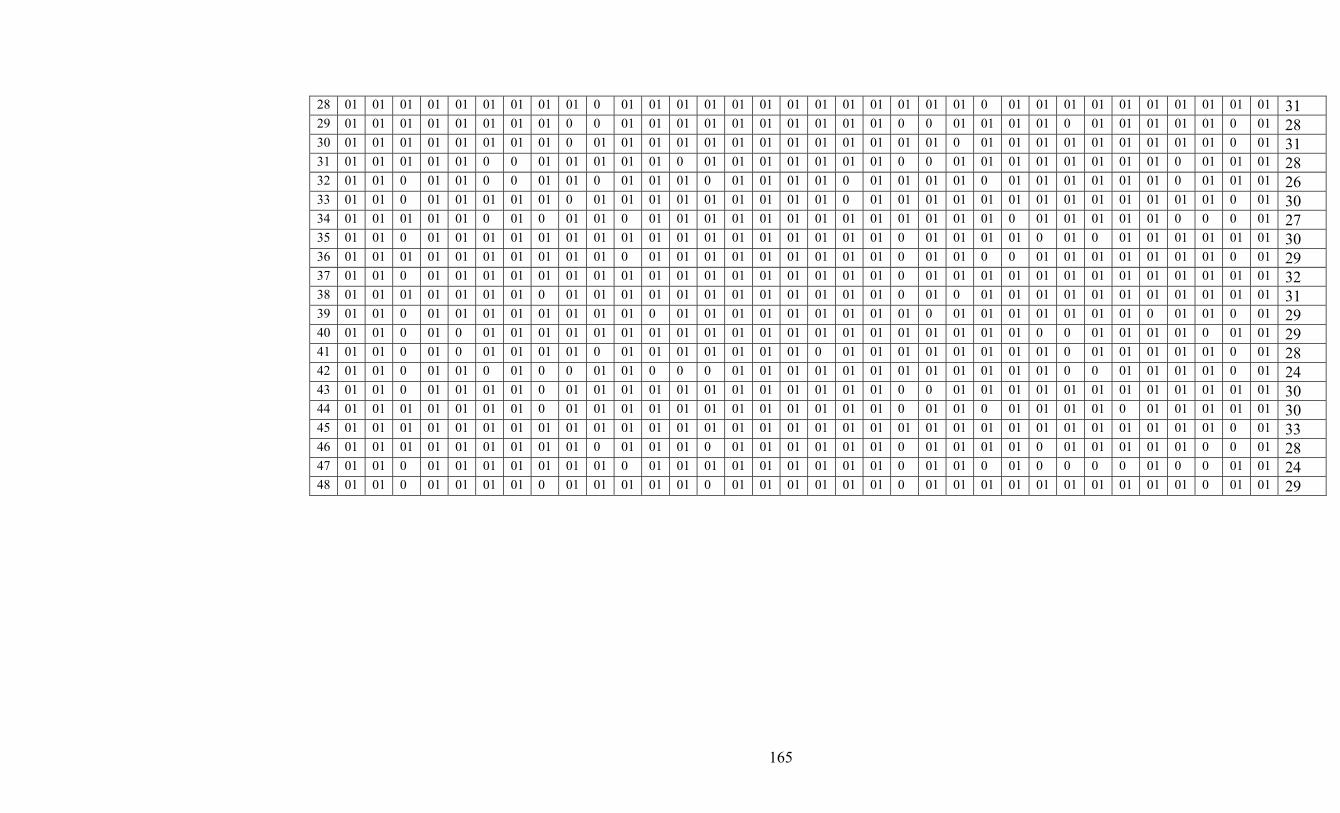
165
28 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 31 29 01 01 01 01 01 01 01 01 0 0 01 01 01 01 01 01 01 01 01 01 0 0 01 01 01 01 0 01 01 01 01 01 0 01 28 30 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 0 01 31 31 01 01 01 01 01 0 0 01 01 01 01 01 0 01 01 01 01 01 01 01 0 0 01 01 01 01 01 01 01 01 0 01 01 01 28 32 01 01 0 01 01 0 0 01 01 0 01 01 01 0 01 01 01 01 0 01 01 01 01 0 01 01 01 01 01 01 0 01 01 01 26 33 01 01 0 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 30 34 01 01 01 01 01 0 01 0 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 0 0 0 01 27 35 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 0 01 0 01 01 01 01 01 01 30 36 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 0 01 01 0 0 01 01 01 01 01 01 01 0 01 29 37 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 32 38 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 0 01 0 01 01 01 01 01 01 01 01 01 01 01 31 39 01 01 0 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 0 01 01 0 01 29 40 01 01 0 01 0 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 0 0 01 01 01 01 0 01 01 29 41 01 01 0 01 0 01 01 01 01 0 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 0 01 01 01 01 01 0 01 28 42 01 01 0 01 01 0 01 0 0 01 01 0 0 0 01 01 01 01 01 01 01 01 01 01 01 01 0 0 01 01 01 01 0 01 24 43 01 01 0 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 0 0 01 01 01 01 01 01 01 01 01 01 01 01 30 44 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 01 01 0 01 01 0 01 01 01 01 0 01 01 01 01 01 30 45 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 01 0 01 33 46 01 01 01 01 01 01 01 01 01 0 01 01 01 0 01 01 01 01 01 01 0 01 01 01 01 0 01 01 01 01 01 0 0 01 28 47 01 01 0 01 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 0 01 01 0 01 0 0 0 0 01 0 0 01 01 24 48 01 01 0 01 01 01 01 0 01 01 01 01 01 0 01 01 01 01 01 01 0 01 01 01 01 01 01 01 01 01 01 0 01 01 29
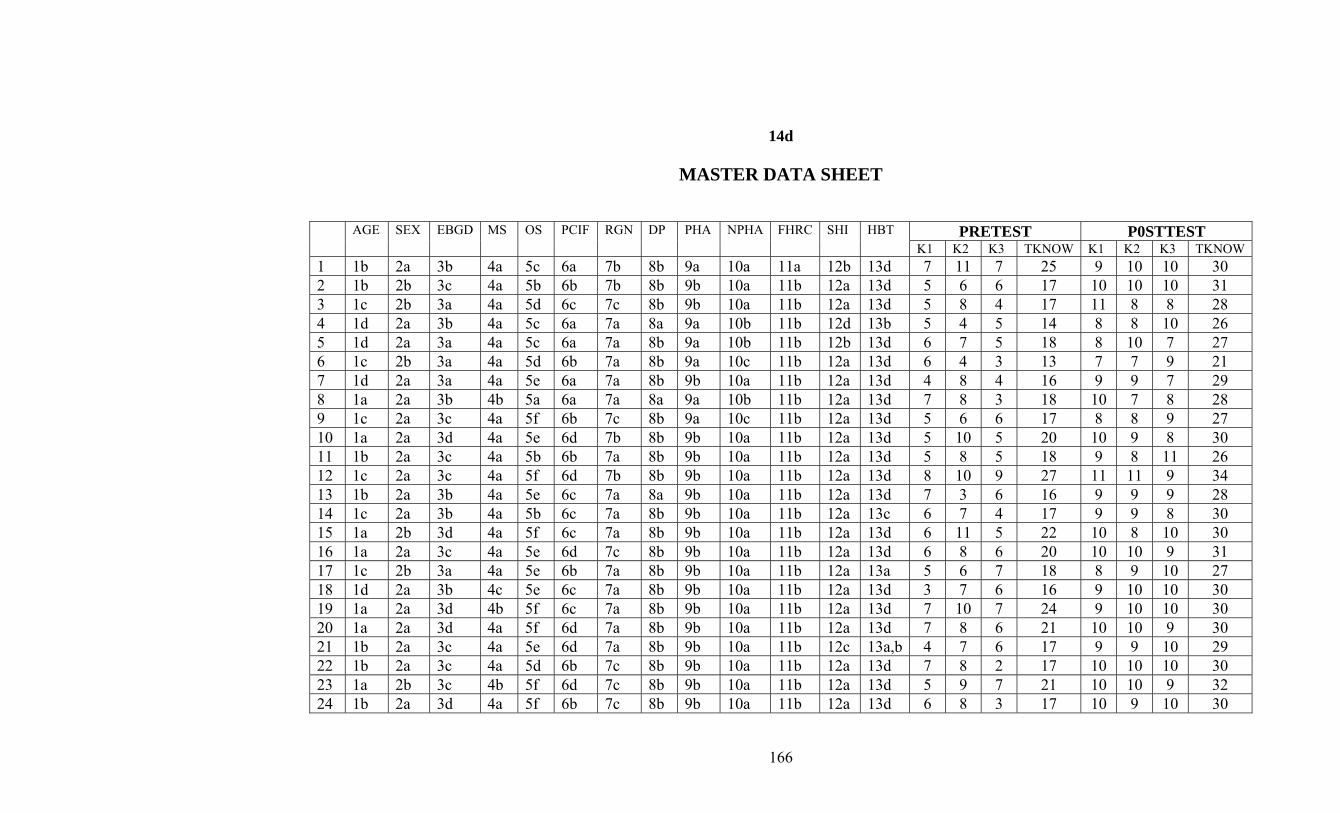
166
14d
MASTER DATA SHEET
PRETEST P0STTEST AGE SEX EBGD MS OS PCIF RGN DP PHA NPHA FHRC SHI HBT K1 K2 K3 TKNOW K1 K2 K3 TKNOW
1 1b 2a 3b 4a 5c 6a 7b 8b 9a 10a 11a 12b 13d 7 11 7 25 9 10 10 30 2 1b 2b 3c 4a 5b 6b 7b 8b 9b 10a 11b 12a 13d 5 6 6 17 10 10 10 31 3 1c 2b 3a 4a 5d 6c 7c 8b 9b 10a 11b 12a 13d 5 8 4 17 11 8 8 28 4 1d 2a 3b 4a 5c 6a 7a 8a 9a 10b 11b 12d 13b 5 4 5 14 8 8 10 26 5 1d 2a 3a 4a 5c 6a 7a 8b 9a 10b 11b 12b 13d 6 7 5 18 8 10 7 27 6 1c 2b 3a 4a 5d 6b 7a 8b 9a 10c 11b 12a 13d 6 4 3 13 7 7 9 21 7 1d 2a 3a 4a 5e 6a 7a 8b 9b 10a 11b 12a 13d 4 8 4 16 9 9 7 29 8 1a 2a 3b 4b 5a 6a 7a 8a 9a 10b 11b 12a 13d 7 8 3 18 10 7 8 28 9 1c 2a 3c 4a 5f 6b 7c 8b 9a 10c 11b 12a 13d 5 6 6 17 8 8 9 27 10 1a 2a 3d 4a 5e 6d 7b 8b 9b 10a 11b 12a 13d 5 10 5 20 10 9 8 30 11 1b 2a 3c 4a 5b 6b 7a 8b 9b 10a 11b 12a 13d 5 8 5 18 9 8 11 26 12 1c 2a 3c 4a 5f 6d 7b 8b 9b 10a 11b 12a 13d 8 10 9 27 11 11 9 34 13 1b 2a 3b 4a 5e 6c 7a 8a 9b 10a 11b 12a 13d 7 3 6 16 9 9 9 28 14 1c 2a 3b 4a 5b 6c 7a 8b 9b 10a 11b 12a 13c 6 7 4 17 9 9 8 30 15 1a 2b 3d 4a 5f 6c 7a 8b 9b 10a 11b 12a 13d 6 11 5 22 10 8 10 30 16 1a 2a 3c 4a 5e 6d 7c 8b 9b 10a 11b 12a 13d 6 8 6 20 10 10 9 31 17 1c 2b 3a 4a 5e 6b 7a 8b 9b 10a 11b 12a 13a 5 6 7 18 8 9 10 27 18 1d 2a 3b 4c 5e 6c 7a 8b 9b 10a 11b 12a 13d 3 7 6 16 9 10 10 30 19 1a 2a 3d 4b 5f 6c 7a 8b 9b 10a 11b 12a 13d 7 10 7 24 9 10 10 30 20 1a 2a 3d 4a 5f 6d 7a 8b 9b 10a 11b 12a 13d 7 8 6 21 10 10 9 30 21 1b 2a 3c 4a 5e 6d 7a 8b 9b 10a 11b 12c 13a,b 4 7 6 17 9 9 10 29 22 1b 2a 3c 4a 5d 6b 7c 8b 9b 10a 11b 12a 13d 7 8 2 17 10 10 10 30 23 1a 2b 3c 4b 5f 6d 7c 8b 9b 10a 11b 12a 13d 5 9 7 21 10 10 9 32 24 1b 2a 3d 4a 5f 6b 7c 8b 9b 10a 11b 12a 13d 6 8 3 17 10 9 10 30

167
25 1a 2a 3d 4b 5f 6d 7c 8b 9b 10a 11b 12a 13d 5 10 7 22 10 10 10 32 26 1b 2b 3a 4a 5a 6a 7b 8b 9b 10a 11b 12a 13a,c 3 9 3 15 10 10 8 31 27 1b 2b 3a 4a 5d 6b 7b 8b 9b 10a 11b 12a 13d 6 7 5 18 8 8 10 27 28 1b 2a 3d 4a 5f 6d 7a 8b 9b 10a 11b 12a 13d 5 9 6 20 9 10 9 31 29 1c 2a 3a 4a 5b 6b 7a 8a 9b 10a 11b 12a 13a,c 4 5 7 16 9 9 10 28 30 1b 2a 3b 4a 5d 6c 7a 8b 9a 10a 11b 12a 13d 8 6 4 18 10 10 10 31 31 1c 2a 3a 4a 5b 6b 7a 8b 9a 10a 11b 12a 13c 6 5 6 17 9 10 9 28 32 1c 2a 3a 4a 5b 6b 7b 8b 9b 10a 11b 12a 13a 7 5 5 17 7 9 10 26 33 1c 2a 3a 4a 5b 6b 7a 8a 9b 10a 11b 12a 13c 6 6 5 18 10 10 7 30 34 1a 2a 3b 4a 5b 6b 7b 8b 9b 10a 11b 12a 13d 4 9 6 19 8 7 9 27 35 1a 2a 3d 4a 5f 6c 7a 8b 9b 10a 11b 12a 13d 7 9 5 21 10 11 8 30 36 1c 2a 3b 4a 5b 6b 7a 8b 9b 10a 11b 12a 13c 4 9 4 17 10 11 11 29 37 1b 2a 3c 4a 5f 6c 7a 8b 9b 10a 11b 12a 13d 7 10 7 24 10 11 11 32 38 1b 2a 3b 4a 5d 6c 7a 8a 9b 10a 11b 12a 13d 6 8 6 20 10 10 9 31 39 1a 2a 3d 4a 5f 6d 7c 8b 9b 10a 11b 12a 13c 5 6 7 18 10 10 8 29 40 1a 2b 3c 4b 5f 6b 7b 8b 9b 10a 11b 12a 13c 4 9 4 17 9 12 9 29 41 1b 2b 3a 4a 5d 6a 7a 8b 9b 10a 11b 12a 13c 6 6 5 17 7 12 8 28 42 1c 2a 3b 4a 5f 6b 7a 8b 9b 10a 11b 12a 13a 6 6 7 19 7 11 11 24 43 1c 2a 3c 4a 5d 6c 7a 8b 9b 10a 11b 12a 13a,b 5 8 9 22 9 10 9 30 44 1a 2a 3c 4a 5f 6d 7a 8b 9b 10a 11b 12a 13d 7 9 8 24 10 11 10 30 45 1a 2b 3c 4a 5d 6c 7a 8b 9b 10a 11b 12a 13d 6 7 7 20 11 12 10 33 46 1b 2a 3b 4a 5e 6b 7a 8b 9b 10a 11b 12b 13a 6 8 2 16 10 10 8 28 47 1c 2a 3a 4a 5a 6a 7a 8b 9b 10a 11b 12a 13a,c 4 18 7 19 9 11 4 24 48 1a 2b 3c 4b 5f 6d 7a 8b 9b 10a 11b 12a 13d 7 8 7 22 9 10 10 29

168
15
STATISTICAL FORMULAE USED FOR ANALYSIS AND INTERPRETATION
1. Formula 1: Karl Pearson’s Co-efficient of Correlation Σ XY γ = ___________________________
_________________ √ Σ X² x Σ Y² __ __ where X = x – x and Y = y - y
2. Formula 2: Spearman’s Brown Prophecy Formula 2r = ___________ 1 + r 3. Formula 3: Paired ‘t’ test ___________ √ Σ (d – d )2 SD (d) = ____________________ n - 1 SD(d) SE (d) = _________ ___ √ n _ d tcal = _________ SE (d)
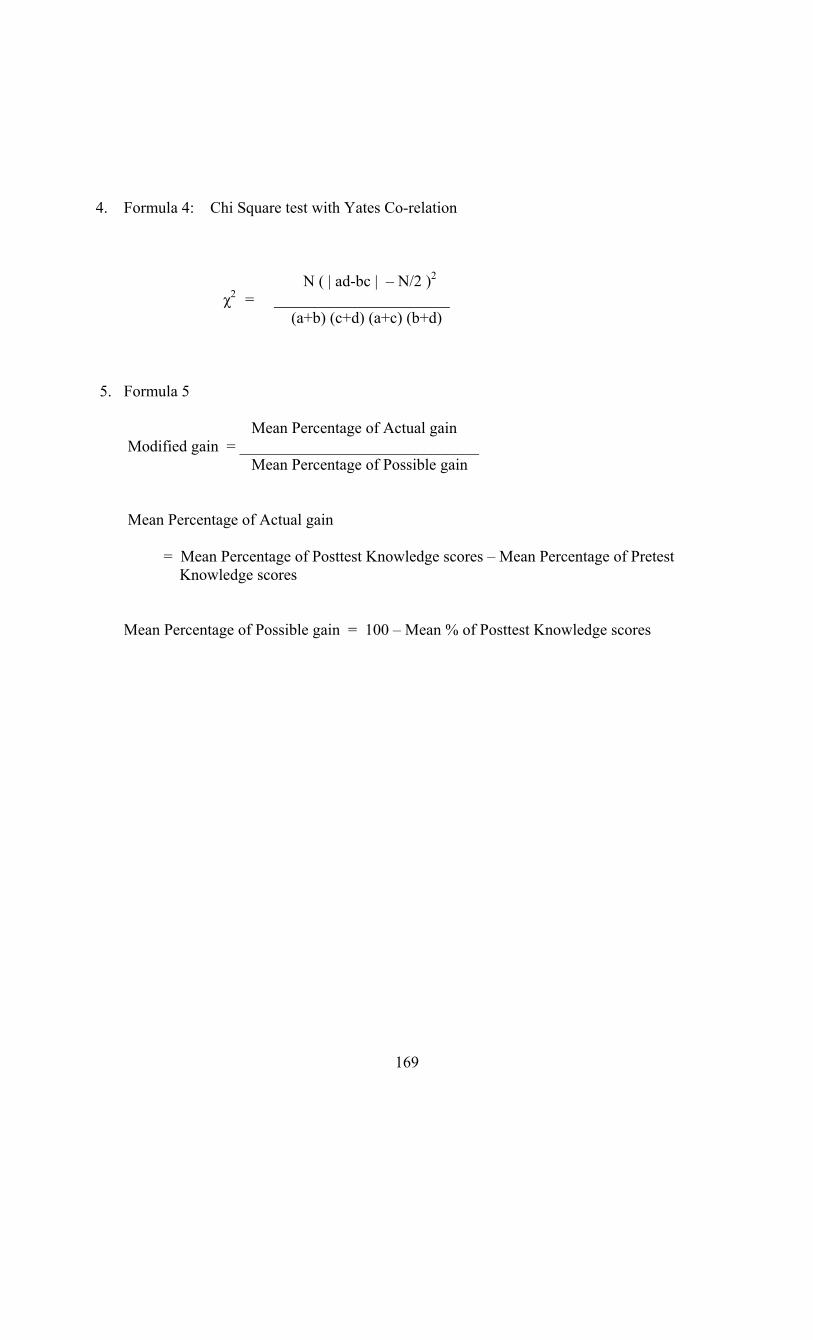
169
4. Formula 4: Chi Square test with Yates Co-relation N ( | ad-bc | – N/2 )2 χ2 = ______________________ (a+b) (c+d) (a+c) (b+d) 5. Formula 5 Mean Percentage of Actual gain Modified gain = ______________________________ Mean Percentage of Possible gain Mean Percentage of Actual gain = Mean Percentage of Posttest Knowledge scores – Mean Percentage of Pretest Knowledge scores Mean Percentage of Possible gain = 100 – Mean % of Posttest Knowledge scores