diagnosis of growth hormone deficiency in adults
TRANSCRIPT
Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/13898101
TheDiagnosisofGrowthHormoneDeficiencyinAdults1
ArticleinJournalofClinicalEndocrinology&Metabolism·November1997
DOI:10.1210/jcem.82.10.4288-1·Source:PubMed
CITATIONS
9
READS
21
5authors,including:
MarianneAndersen
OdenseUniversityHospital
171PUBLICATIONS2,643CITATIONS
SEEPROFILE
GianlucaAimaretti
AmedeoAvogadroUniversityofEasternPiedmont
219PUBLICATIONS5,498CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyGianlucaAimarettion04December2016.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinblueareaddedtotheoriginaldocument
andarelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.
LETTERS TO THE EDITORThe Diagnosis of Growth Hormone Deficiency in
Adultsa
To the editor:
We were most interested to read the recommendation for using theinsulin tolerance test (ITT) for diagnosing growth hormone deficiency(GHD) (1), and we would like to comment on the choice of this testand of the recommended GH cut-off limit of 3 mg/L. The evaluationor introduction of a GH-stimulation test requires the definition of areference interval for healthy adults, taking into consideration thepossible influences of sex, age, obesity, and substitution therapy. Thecurrent choice of method for diagnosing GHD in adults is clearlyarbitrary. In earlier studies of the clinical effect of GH therapy onpatients suffering from GHD, very low stimulated GH-levels wereused as inclusion criteria (2– 6). In addition, it was, at that time,impossible to base the cut-off limits for GH on scientific data, as noreference interval had been published for stimulated GH-responsesto GH-stimulation tests. It has been suggested recently that the cri-terion for the diagnosis of GHD in adults should be a peak GH-response to the ITT of less than 3 mg/L (1). This limit was based onthe further reduction of reported cut-off limit of 5 mg/L in normalsubjects (7) to “allow for the influences of age and adiposity” (1).Hoffmann et al. (7) chose age, sex, and body mass index (BMI)-matched controls, as these parameters have been considered to beimportant to the peak GH-responses to the ITT. However, the match-ing of control subjects does not imply that these results can be au-tomatically extrapolated to healthy adults, as the controls includedobese and elderly individuals. It should be noted that the mean BMIfor this group of individuals was 25.1 kg/m2 (min-max: 15.6 –38.9),and that obesity in otherwise healthy adults has been associated withmarkedly impaired GH-responses to the ITT (8, 9). Furthermore,although the mean age of this group was 47.3 yr (min-max: 17–78),the peak GH-responses of the most elderly subjects to the ITT werenot significantly lower than those of the rest of the group (7). The useof the lowest peak GH-response obtained from a control group thatincludes aged and obese subjects risks reducing the sensitivity of theITT in normal-weight patients with suspected GHD.
The marked discrepancies among GH-assays did not become appar-ent until after monoclonal assays came into widespread use. This is notsurprising, as different monoclonal antibodies would be expected torecognize different GH forms in a disparate manner (10), and problemscaused by incorrect calibration and the use of inappropriate mass unitshave been recorded (11). Nevertheless, the relationship between the twoassays that have been studied (i.e. the polyclonal Pharmacia assay andthe monoclonal Dissociation-Enhanced Lanthanide Fluoro-Immuno-As-say (DELFIA) assay) is reasonably constant, and it is, in fact, possible touse a conversion factor to compare the results of the two assays. Theconversion factor for converting RIA (Pharmacia AB, Uppsala, Sweden)to DELFIA (Wallac, Turku, Finland) is: DELFIA 5 RIA 3 0.63. Theconversion factor proved to be constant throughout the concentrationrange, and the distribution around the mean accorded with the analyt-ical imprecision of the two methods (Andersen et al. to be published).
Although more than 15 different GH-stimulation tests are available,opinion is divided concerning which test is to be used for specific patientgroups. Moreover, many of the tests are unreliable.
The effect of the combination of pyridostigmine (PD) and growthhormone-releasing hormone (GHRH) on peak GH-levels has beenstudied by teams including Ghigo et al. (12), Arvat et al. (13), andAndersen et al. (14). The effect produced is based on direct GHRHstimulation of the pituitary gland and PD-inhibition of somastostatin(15–19). 120 mg PD is administered orally 60 min before the injection
of GHRH (1 mg/kg, time 0) as an iv bolus. Serum samples for themeasurement of GH-levels are then taken at 0, 20, 30, 45, 60, and 90min. The reference interval for the peak GH responses to the PD-GHRH test was established in 40 healthy adults (14), all of whom were22–58 yr of age and within 10% of ideal body weight. The GH re-sponses were Log-Gaussian distributed and were unaffected by fac-tors such as age, sex, and the use of oral contraceptives. The 95%reference interval was 42– 422 mU/L. Please note that the RIA (Phar-macia AB, Uppsala, Sweden) was used in this study. The 2.5 per-centile (21.96 sd) of 42 mU/L was used as the cut-off limit for thebiological GH responses to the PD-GHRH test for adults aged 22–58yr, and the 90% Cl for this percentile ranged from 31–56 mU/L. Usingthe established cut-off limit of 42 mU/L for the PD-GHRH test (14),and the conventional cut-off limit of 20 mU/L for the ITT (20), a highlevel of agreement between the two tests, 44/47 (94%), was found(14). This is a particularly convincing result, especially consideringthe characteristics of the patients examined. In contrast to the resultsof the study carried out by Andersen et al. (14), most studies usingGH stimulation tests included only patients who were consideredGH-deficient (7, 12). The ITT may not be the best tool for the diagnosisof GHD in adults. Hoeck et al. (21) have questioned the reproduc-ibility of the ITT in normal adults. A reference interval for the ITT willbe difficult to establish, and it may prove impossible to evaluate thepossible influences of sex, age, body composition, and cortisol levelson ITT-stimulated GH levels, as patients find the ITT unpleasant.Furthermore, the ITT is potentially hazardous (22). In contrast to this,no severe side effects and only minor, transitory complaints wererecorded in over 400 PD-GHRH tests carried out in Milan andOdense. Of those tested, approximately 10% suffered gastrointestinaldiscomfort, with 1/10 of these experiencing diarrhea and nausea, andthe remainder experiencing heartburn and meteorism. Approxi-mately 10% of those tested displayed tics, and the injection of GHRHcaused flushing lasting 30 seconds in approximately 50% of the sub-jects. Obesity in otherwise healthy adults has been associated withmarkedly impaired GH-responses to the ITT (8, 9), to the PD-GHRHtest (23–26), and to the arginine-GHRH test (27). However, to estab-lish reference intervals for this group of patients it is essential to studythe impact of over-weight on peak GH-responses.
Elderly subjects also pose new diagnostic problems. Ghigo et al.found the PD-GHRH test to be a very reliable tool for the biologicalmeasurement of GHD in 20 – 40-yr-olds (12), but normal adults aged40 – 65 yr were not included in this study. Some subjects from the 651age group who were considered normal still displayed low GH-responses to the PD-GHRH test (12). The combination of arginine andGHRH produced high GH-responses in the 651 age group, and evenin 80-yr-olds. Because of its effectiveness in even very elderly sub-jects, Ghigo et al. preferred the combination of arginine and GHRHfor elderly patients with suspected GHD (12). It must be rememberedthat basal GH and insulin-like growth factor (IGF)-I levels are re-duced in normal, elderly individuals (28, 29), and that GH-levels insome normal individuals will almost certainly be low at a relativelyyoung age. Early somatopause thus makes the diagnosis of GHD inpatients over the age of 65 a discussion of the general attitude toward“the diagnosis GHD” in healthy old people. This is an area whichmerits thorough investigation.
Among the many tests available for the diagnosis of GHD in adults,a particularly strong case can be made for choosing the PD-GHRH test,as it is easy to perform, safe, potent, reproducible, and reliable (14).Furthermore, the cut-off limit of 42 mU/L (90% Cl 31–56 mU/L) hasalready been established for this test (14). The arginine-GHRH test mightalso be considered as a diagnostic test (12).
GHD-evaluation should be a part of the total evaluation procedurefor patients with suspected hypothalamic and/or pituitary diseases.
In conclusion: 1) Important information can be gathered from theclinical characteristics of the patients. Insufficiency of ACTH will implydiminished peak GH-responses to the ITT in approximately 91% (30) to
a Received May 1, 1997. Address correspondence to: MarianneAndersen, Department of Endocrinology, Odense University Hospital,Odense C, Denmark DK-5000.
0021-972X/97/$03.00/0 Vol. 82, No. 10Journal of Clinical Endocrinology and Metabolism Printed in U.S.A.Copyright © 1997 by The Endocrine Society
3513
100% (14) of patients. However, it should be noted that Toogood et al.(30) reported that 28% of patients suffered from only GHD and not frominsufficiency of any other pituitary hormones. Therefore, GHD does notnecessarily imply deficiency of other pituitary hormones; 2) A subnor-mal total IGF-I value essentially confirms the diagnosis, whereas IGF-llevels within the normal range do not preclude GHD (7, 14); 3) Werecommend using the PD-GHRH test to diagnose GHD and would liketo stress that in normal subjects aged 22–58 yr, the PD-GHRH-stimulatedGH-responses were not significantly affected by factors such as age, sex,or the use of oral contraceptives (14).
However, the influence of body composition still remains to be eval-uated, and it is still necessary to clarify the state of somatotrophs inhealthy elderly people.
Marianne Andersen and Jørgen Hangaard,Claus HagenOdense University HospitalOdense C, Denmark DK-5000
Gianluca Aimaretti and Ezio GhigoUniversity of Turin10126 Turin, Italy
References
1. Thorner MO, Bengtsson BA, Ho KY, et al. 1995 The diagnosis of growthhormone deficiency (GHD) in adults (letter). J Clin Endocrinol Metab.80:3097–3098.
2. Jørgensen JOL, Thuesen L, Ingemann-Hansen T, et al. 1989 Beneficial effectsof growth hormone treatment in GH-deficient adults. Lancet. 3:1221–1225.
3. Salomon F, Cuneo RC, Hesp R, Sonksen PH. 1989 The effects of treatmentwith recombinant human growth hormone on body composition and metab-olism in adults with growth hormone deficiency. N Engl J Med. 321:1797–1803.
4. Mårdh G, Lundin K, Borg G, Jonsson B, Lindeberg A. 1994 Growth hormonereplacement therapy in adult hypopituitary patients with growth hormonedeficiency: Combined data from 12 European placebo-controlled clinical trials.Endocrinol Metab. 1 [Suppl A]:43–49.
5. Whitehead HM, Boreham C, McIlrath EM, et al. 1992 Growth hormonetreatment of adults with growth hormone deficiency: results of a 13-monthplacebo controlled cross-over study. Clin Endocrinol (Oxf). 36:45–52.
6. Whitehead HM, Aiken B, Lewis S, Sheridan B, Hadden DR. 1991 Physio-logical growth hormone secretion in adult growth hormone deficiency: com-parison with normal controls. Clin Endocrinol (Oxf). 34:371–376.
7. Hoffman DM, O’Sullivan AJ, Baxter RC, Ho KK. 1994 Diagnosis of growth-hormone deficiency in adults. Lancet. 343:1064–1068.
8. Rasmussen MH, Hvidberg A, Juul A. 1995 Massive weight loss restores24-hour growth hormone release profiles and serum insulin-like growth fac-tor-l levels in obese subjects. J Clin Endocrinol Metab. 80:1407–1415.
9. Cordido F, Dieguez C, Casanueva FF. 1990 Effect of central cholinergic neu-rotransmission enhancement by pyridostigmine on the growth hormone se-cretion elicited by clonidine, arginine, or hypoglycemia in normal and obesesubjects. J Clin Endocrinol Metab. 70:1361–1370.
10. Baumann G. 1990 Growth hormone binding proteins and various forms ofgrowth hormone: implications for measurements. Acta Paediatr Scand Suppl.370:72–80.
11. Seth J, Ellis AR, Sturgeon CM. 1995 UKNEQUAS for peptide hormones andrelated substances. 19–22 (Abstract).
12. Ghigo E, Aimaretti G, Gianotti L, Bellone J, Arvat E, Camanni F. 1996 Newapproach to the diagnosis of growth hormone deficiency in adults. Eur JEndocrinol. 134:352–356.
13. Arvat E, Cappa M, Casanueva FF. 1993 Pyridostigmine potentiates growthhormone (GH)-releasing hormone-induced GH release in both men andwomen. J Clin Endocrinol Metab. 76:374–377.
14. Andersen M, Hansen TB, Støving RK. 1996 The pyridostigmine-growth-hormone-releasing-hormone test in adults. The reference interval and a com-parison with the insulin tolerance test. Endocrino Metab. 3:197–206.
15. Richardson SB, Hollander CS, D’Eletto RD, Greenleaf PW, Than C. 1980Acetylcholine inhibits the release of somatostatin from rat hypothalamus invitro. 107:1837.
16. Locatelli V, Torsello A, Redaelli M, Ghigo E, Massara F, Muller EE. 1986Cholinergic agonist and antagonist drugs modulate the growth hormone re-sponse to growth hormone-releasing hormone in the rat: evidence for medi-ation by somatostatin. J Endocrinol. 111:271–278.
17. Torsello A, Panzeri G, Cermenati P, et al. 1988 Involvement of the soma-tostatin and cholinergic systems in the mechanism of growth hormoneautofeedback regulation in the rat. J Endocrinol. 117:273–281.
18. Wehrenberg WB, Wiviott SD, Voltz DM, Giustina A. 1992 Pyridostigmine-mediated growth hormone release: evidence for somatostatin involvement.Endocrinology. 130:1445–1450.
19. Casanueva FF, Villanueva L, Dieguez C, et al. 1986 Atropine blockade of
growth hormone (GH)-releasing hormone-induced GH secretion in man is notexerted at pituitary level. J Clin Endocrinol Metab. 62:186–191.
20. Wass JAH, Besser GM. 1989 Tests of pituitary function. In: DeGroot LJ, ed.Endocrinology Philadelphia: W.B. Saunders; 492–502.
21. Hoeck HC, Vestergaard P, Jakobsen PE, Laurberg P. 1995 Test of growthhormone secretion in adults: poor reproducibility of the insulin tolerance test.Eur J Endocrinol. 133:305–312.
22. Shah A, Stanhope R, Matthew D. 1992 Hazards of pharmacological tests ofgrowth hormone secretion in childhood. Brit Med J. 304:173–174.
23. De Marinis L, Mancini A, Zuppi P, et al. 1992 Influence of pyridostigmineon growth hormone (GH) response to GH-releasing hormone pre- andpostprandially in normal and obese subjects. J Clin Endocrinol Metab.74:1253–1257.
24. Cordido F, Casanueva FF, Dieguez C. 1989 Cholinergic receptor activation bypyridostigmine restores growth hormone (GH) responsiveness to GH-releas-ing hormone administration in obese subjects: evidence for hypothalamicsomatostatinergic participation in the blunted GH release of obesity. J ClinEndocrinol Metab. 68:290–293.
25. Ghigo E, Mazza E, Corrias A. 1989 Effect of cholinergic enhancement bypyridostigmine on growth hormone secretion in obese adults and children.Metabolism. 38:631–633.
26. Castro RC, Vieira JG, Chacra AR, Besser GM, Grossman AB, Lengyel AM.1990 Pyridostigmine enhances, but does not normalise, the GH response toGH-releasing hormone in obese subjects. Acta Endocrinol (Copenh).122:385–390.
27. Maccario M, Valetto MR, Savio P, et al. 1997 Maximal secretory capacity ofsomatotrope cells in obesity: comparison with GH deficiency. Int J Obesity.21:27–32.
28. Iranmanesh A, Lizarraide G, Veldhuis JD. 1991 Age and relative adiposity arespecific negative determinants of the frequency and amplitude of growthhormone (GH) secretory bursts and the half-life of endogenous GH in healthymen. J Clin Endocrinol Metab. 73:1081–1088.
29. Ghigo E, Goffi S, Nicolosi M, et al. 1990 Growth hormone (GH) responsive-ness to combined administration of arginine and GH-releasing hormone doesnot vary with age in man. J Clin Endocrinol Metab. 71:1481–1485.
30. Toogood AA, Beardwell CG, Shalet SM. 1994 The severity of growth hormonedeficiency in adults with pituitary disease is related to the degree of hypop-ituitarism. Clin Endocrinol (Oxf). 41:511–516.
Not Only Growth Hormone (GH)-Deficient Men AreMore Responsive to GH Than Womenb
To the editor:
We read with great interest the report of Burman et al. (1), whichshowed that the reduction in body fat percentage and abdominal fatmass after 9 months of rhGH replacement therapy was significantlylarger in GH-deficient men than in women. Furthermore the reportsuggested that the change in body fat distribution resulting from re-placement therapy differed between GH-deficient men and women. Theconcomitant increase in fat-free mass did not differ significantly betweenmen and women. These results support our previous findings of genderdifferences during GH replacement in adult hypopituitary patients (2,3). However, one has to be aware of the distinct differences in bodycomposition and fat distribution between males and females in bothnormal and hypopituitary adults. After adjusting for these baselinedifferences the gender-specific difference in change of body compositionduring GH-replacement therapy was clearly attenuated (2). Concerningthe effect of GH on bone metabolism, a 2-yr GH-replacement studydemonstrated that markers reflecting bone resorption and bone forma-tion increased more in men than in women, but total body mineraldensity increased more in women (3), reflecting the fact that estrogen,in contrast to GH, attenuates bone remodeling. Regarding the genderdifferences during GH-replacement a confounding factor may be that,in all previous trials, including the one by Dr. Burman and colleagues,GH was administered according to body weight or body surface area,neglecting that healthy fertile women secrete more GH than young men(4). This may have led to relative underdosing in women and overdosingin men.
The question can be raised whether the apparent gender-specificbody composition response to GH is limited to a GH status varying fromdeficiency towards adequate substitution. In a previous study, using
b Received June 11, 1997. Address correspondence to: Robert-J.M.Brummer, MD PhD, Department of Internal Medicine, University Hos-pital Maastricht, P.O. Box 5800, NL-6202 AZ Maastricht, The Nether-lands. E-mail: [email protected].
3514 LETTERS TO THE EDITOR JCE & M • 1997Vol 82 • No 10

multiscan computed tomography (CT), we have shown that in patientswith acromegaly the subcutaneous adipose tissue volume increased 53%in males and only 20% in females, 1 yr after transspheniodal adenectomy(5). The decrease in muscle and skin volume did not significantly differbetween both sexes. In contrast to the dual energy x-ray absorptiometry(DXA) method used by Burman and colleagues (1), the multiscan CTtechnique specifically enables the determination of the visceral adiposetissue volume, which is important with respect to insulin resistance andlipoprotein concentrations (6). In acromegaly the visceral adipose tissuevolume increased 84% in males compared with 25% in females afteradenectomy, and we provided evidence that the adipose tissue distri-bution in acromegalic men changed significantly (P , 0.005) after ther-apy, while this was not the case in women (5). Hence, we would like toconclude that GH has more pronounced effects on abdominal/visceraladipose tissue in men than in women, varying from GH-deficiencytowards acromegaly, but that the large baseline differences in bodycomposition between men and women should be considered in theevaluation of gender-specific responses to GH.
Robert-J.M. BrummerUniversity Hospital MaatrichtMaastricht, The Netherlands
Gudmundur JohannssonBengt-Åke BengtssonResearch Center for Endocrinology and MetabolismSahlgrenska University HospitalGoteborg, Sweden
References
1. Burman P, Johansson AG, Siegbahn A, Vessby B, Karlsson FA. 1997 Growthhormone (GH)-deficient men are more responsive to GH replacement therapythan women. J Clin Endocrinol Metab. 82:550–555.
2. Johannsson G, Bjarnason R, Bramnert M, et al. 1996 The individual respon-siveness to growth hormone (GH) treatment in GH-deficient adults is depen-dent on the level of GH binding protein, body mass index, age and gender.J Clin Endocrinol Metab. 81:1575–1581.
3. Johannsson G, Rosen T, Bosaeus I, Sjostrom L, Bengtsson B-Å. 1996 Twoyears of growth hormone (GH) treatment increases bone mineral content anddensity in hypopituitary patients with adult-onset GH deficiency. J Clin En-docrinol Metab. 81:2865–2873.
4. Ho KKY, Evans WS, Blizzard RM, et al. 1987 Effects of sex and age on the24-hour profile of growth hormone secretion in man. Importance of endoge-nous estradiol concentrations. J Clin Endocrinol Metab. 64:51–58.
5. Brummer R-JM, Lonn L, Kvist H, Grangård, Bengtsson B-Å, Sjostrom L. 1993Adipose tissue and muscle volume determination by computed tomographyin acromegaly, before and 1 year after adenectomy. Eur J Clin Invest.23:199–205.
6. Pouliot MC, Despres JP, Nadeau A, et al. 1992 Visceral adiposity in men,associations with glucose intolerance, plasma insulin, and lipoprotein levels.Diabetes. 41:826–834.
GH-Deficient Men Are More Responsive to GHReplacement Therapy Than Women—Author’s
Responsec
To the editor:
We fully agree with Brummer et al. in the preceding letter, whosuggest that gender differences in response to GH, as shown in our studyof patients with growth hormone deficiency (GHD) (1), are probably notrestricted to GHD, but will also be observed in patients with growthhormone excess. In our view, it is likely that a different sensitivity to GH,in normal as well as pathological conditions, will mirror the knownsexual dimorphism in GH secretion (2).
The study of patients with acromegaly by Brummer et al. (3) showingchanges in body composition, particularly marked increases in abdom-inal/visceral adipose tissue following adenomectomy, is of great inter-est. After neurosurgery, the men seemed to gain more fat than thewomen, but as reported in the paper, the difference between the sevenfemale and the eight male patients was not significant. Possibly, the
comparison was hampered by the fact that two of the women were notcured by the treatment, reflected by the nearly twice as high IGF-I levelsin the women compared with the men.
Adipose tissue is highly responsive to GH, and pronounced re-ductions in the fat mass after treatment with GH was found in earlystudies of patients with GHD (4, 5). To observe a gender differencewe believe it is necessary to study men and women with similarseverity of GHD. Further, we think that the administration of an equaldose of GH to men and women made it possible to discover thegender difference in GH responsiveness (1). In our study, the residualspontaneous GH secretion during the night and the peak GH re-sponse to two stimulation tests, insulin-induced hypoglycemia, andafter iv injection of GHRH were similar in the men and the women.The results by Johannsson et al. (6), showing no gender difference inbody composition, albeit a higher IGF-I level and a more pronouncedgain in total body water in men than in women after 12 months of GH,might reflect a heterogeneity among the GHD patients. For instance,GH secretory status was investigated by either of four different meth-ods (insulin-induced hypoglycemia, glucagon-, clonidine-, or argin-ine-stimulation) known to give discordant results in healthy subjects.No data on the test results in the men and women were provided. Inaddition, 20 out of the 68 patients were selected because of a lowserum IGF-I, which might have skewed the distribution of the pa-tients in terms of GH secretory status.
We, as Brummer et al. consider that the gender difference in GH re-sponsiveness should have implications for the recommended replacementdose of GH. Recently, in healthy women compared with healthy men themean 24-h GH secretion was reported to be about two times higher (7). Thegender difference in GH secretion seems even more pronounced in youngadults (Eden-Engstrom et al, submitted). Currently, in our hospital the dailydose of GH (mean, range) in GHD adults, based on clinical outcome anda serum IGF-I within the normal age-adjusted reference range, is 1.8 (0.5-3.5)IU in women and 1.0 (0.4-2.0) IU in men.
Pia Burman, Anna G. Johansson, Britt Eden-Engstrom, andF. Anders Karlsson
University HospitalS-751 85 Uppsala, Sweden
References
1. Burman P, Johansson AG, Siegbahn A, Vessby B, Karlsson FA. 1997 Growthhormone (GH)-deficient men are more responsive to GH replacement therapythan women. J Clin Endocrinol Metab. 82:550–555.
2. Jansson J-O, Eden S, Isaksson O. 1985 Sexual dimorphism in the control ofgrowth hormone secretion. Endocr Rev. 6:128–149.
3. Brummer R-JM, Lonn L, Kvist H, Grangård U, Bengtsson B-Å, Sjostrom L.Adipose tissue and muscle volume determination by computed tomographyin acromegaly, before and 1 year after adenomectomy. 1993 Eur J Clin Invest.23:199–205.
4. Salomon F, Cuneo RC, Hesp R, Sonksen PH. 1989 The effects of treatmentwith recombinant human growth hormone on body composition and me-tabolism in adults with growth hormone deficiency. N Engl J Med.321:1797–1803.
5. Jorgensen JOL, Pedersen SA, Thuessen L, et al. 1989 Beneficial effects ofgrowth hormone treatment in GH-deficient adults. Lancet. 1:1221–1225.
6. Johannsson G, Bjarnason R, Bramnert M, et al. 1996 The individual respon-siveness to growth hormone (GH) treatment in GH-deficient adults is depen-dent on the level of GH-binding protein, body mass index, age, and gender.J Clin Endocrinol Metab. 81:1575–1581.
7. Veldhuis JD. 1996 Gender differences in secretory activity of human soma-totropic (growth hormone) axis. Eur J Endocrinol. 134:287–295.
Pseudoacromegaly and Hyperinsulinemia: APossibility of Premature Atherosclerosis?d
To the editor:
In a recent article, Kumar et al. (1) presented a case with an unusualcombination of severe insulin resistance, diabetes mellitus, hypertri-glyceridemia, and pseudoacromegaly.
c Received July 10, 1997. Address correspondence to: Pia Burman,M.D., Ph.D., Department of Medicine, Uppsala University Hospital,Uppsala, Sweden S-751 85.
d Received April 11, 1997. Address correspondence to: Hiroyuki Ko-shiyama, M.D., Division of Endocrinology and Metabolism, Departmentof Internal Medicine, Hyogo Prefectural Amagasaki Hospital, Ama-gasaki, Hyogo 660, Japan.
LETTERS TO THE EDITOR 3515

We here describe a similar case of 17-yr-old Japanese female stu-dent. A possibility that she might have acromegaly had been sug-gested by several endocrinologists since the age of 12 yr. She wasmuscular with large hands and feet, and her face showed features ofacromegaly with a protrusion of brows and mandible. She had mod-erate hirsutism and axillary acanthosis nigricans. Her menstrual pe-riod was regular. She was tall (174 cm) as a Japanese teen-age girl andweighed 77 kg. Her GH levels were within normal range in severalmeasurements (0.2–1.1 ng/mL). Serum IGF-I level was also normal(402 ng/mL). The fasting glucose levels were normal (102 mg/dL),but fasting insulin levels were high (48 –325 mU/mL). Both antiinsulinand antiinsulin receptor antibodies were negative. Other hormonelevels were normal. A 75 g oral glucose test showed normal responseof glucose and marginal increase in GH (up to 2.3 ng/mL). GHshowed paradoxical response to TRH test (peak 29.8 ng/mL), but notto LHRH test. Serum cholesterol and triglyceride levels were normal.Magnetic resonance imaging study did not show any abnormal find-ing of the pituitary gland. She often complained of abdominal musclecramps, which is reported to be a common prominent feature of thisdisorder (1, 2). The intimal and medial complex thickness (IMT) of thecommon catorid artery, which was measured with B-mode ultra-sound technique, was markedly high (0.900 mmol/L) considering herage (mean sd of Japanese normal subjects of 10 –19 yr: 0.444[0.057]mmol/L) (3).
There is increasing evidence that hyperinsulinemia may be causallyrelated to atherosclerosis (4). We have recently found that IMT is pos-itively associated with endogenous insulin levels in subjects with non-insulin-dependent diabetes mellitus (5). Unopposed mitogenic and an-abolic actions of hyperinsulinemia is viewed as the main manifestationof pseudoacromegaly, although the primary defect remains unknown (1,2). It is therefore conceivable that the increases in IMT in the present caseis attributable to hyperinsulinemia. Further studies are required to in-vestigate whether premature atherosclerosis might be another commonfeature of this unique disorder.
Yasutomo Fukunaga, Jun Minamikawa,Daisuke Inoue, Hiroyuki KoshiyamaHyogo Prefectural Amagasaki HospitalAmagasaki, Hyogo 660, Japan
Ichiro FujisawaKishiwada City Hospital,Kishiwada, Osaka 596, Japan
References
1. Kumar S, Durrington PN, O’Rahilly S, et al. 1996 Severe insulin resistance,diabetes mellitus, hypertriglyceridemia, and pseudoacromegaly. J Clin Endo-crinol Metab. 81:3465–3468.
2. Flier JS, Moller DE, Moses AC, et al. 1993 Insulin-mediated pseudoacro-megaly: clinical and biochemical characterization of a syndrome of selectiveinsulin resistance. J Clin Endocrinol Metab. 76:1533–1541.
3. Yamasaki Y, Kawamori R, Matsushima H, et al. 1994 Atherosclerosis incarotid artery of young IDDM patients monitored by ultrasound high-reso-lution B-mode imaging. Diabetes. 43:634–639.
4. Stout RW. 1996 Hyperinsulinemia and atherosclerosis. Diabetes. 45:S45–S46.5. Minamikawa J, Fukunaga Y, Inoue D, Koshiyama H, Nakao K. The rela-
tionship between carotid arterial wall thickness and endogenous insulin levelin non-insulin-dependent diabetes mellitus [Abstract]. 79th Annual Meeting ofThe Endocrine Society 1997:474.
Pseudoacromegaly and Hyperinsulinemia: APossibility of Premature Atherosclerosis?—Author’s
Responsee
To the editor:
The patient described by Fukunaga et al. in the preceding letter hasfeatures in common with the one reported by us (1, 2). In our patient,however, the serum nonesterified fatty acid (NEFA) levels were grosslyelevated, and this appeared to be the cause of the insulin resistance andthus the hyperinsulinemia. NEFA levels are not reported by Fukunaga
et al. Our patient was also diabetic, but this may simply have been afunction of the penetrance of the condition and her greater age. Sup-pression of circulating NEFA levels with a long-acting nicotinic acidanalogue reversed the diabetes (1), and readers may be interested toknow, that, since this medication was discontinued, we have success-fully kept her diabetes at bay with fenofibrate, one of the fibric acidderivatives that also cause some suppression of NEFA (3). It is temptingto speculate that the ultrasound findings in the patient of Fukunaga andcolleagues might be a consequence of persistently elevated circulatingNEFA (4).
P.N. DurringtonManchester Royal InfirmaryManchester M13 9WL, United Kingdom
References
1. Kumar S, Durrington PN, Laing T, Bhatnagar D. 1994 Suppression of non-esterified fatty acids to treat type A insulin resistance syndrome. Lancet.343:1073–1074.
2. Kumar S, Durrington PN, O’Rahilly S, et al. 1996 Severe insulin resistance,diabetes mellitus, hypertriglyceridemia, and pseudoacromegaly. J Clin EndMetab. 81:3465–3468.
3. Kissebah AH, Adams PW, Harrigan P, Wynn V. 1974 The mechanism of actionof clofibrate and tetranicotinoylfructose (Bradilan) on the kinetics of plasmafree fatty acid and triglyceride transport in type IV and type V hypertriglyc-eridemia. Eur J Clin Invest. 4:163–174.
4. Hennig B, Shasby DM, Spector AA. 1985 Exposure to fatty acid increases lowdensity lipoprotein transfer across cultured endothelial monolayers. Circ Res.57:776–780.
1,25 Dihydroxyvitamin D and Cancerf
To the editor:
Mawer et al. (1) recently reported in JCEM that serum 1,25-(OH)2Dconcentration decreases in patients with progressive breast cancer. Tothe various hypothetical mechanisms discussed by the authors, Iwould like to add the possibility that 1,25-(OH)2D becomes bound toimmunoregulatory cells resulting in reduced blood levels of the hor-mone. In 1989, we reported two patients, with different, acute andsevere immune challenges, who had undetectable 1,25-(OH)2D. Onewas a patient with acute tuberculosis (TB) and the other had a recentdiagnosis of multiple myeloma (2). Both patients had normal serumionized calcium and 25 hydroxyvitamin D. After successful clinicalresponse to chemotherapy (isoniazid 1 rifampin in the first andmelphalan 1 prednisone in the second), serum 1,25 Vitamin D roseto 76 and 99 pg/mL, respectively (normal range 20 –76). No vitaminD supplementation was given to the patients. Because both patientshad normal renal function, we proposed that the undetectable levelsof 1,25-(OH)2D observed before treatment suggested that the hor-mone was avidly bound to the abundant immuno-regulatory and/orcancer cells (3, 4). More recently, reduced serum 1,25-(OH)2D wasobserved in patients with AIDS and disseminated mycobacteriumavium complex infection (5).
The elevation of 1,25-(OH)2D observed in our patients after treatmentcould have reflected either a decreased demand or overproduction of thehormone by TB granuloma (6) or by immunoregulatory cells (7). Al-though 1,25-(OH)2D has immunoregulatory effects in vitro (8, 9), thereis a paucity of clinical reports supporting this role. However, the avail-able information appears to indicate a possible important role of 1,25-(OH)2D in severe immune challenges.
Dr. Mawer et al. (1) were reluctant to recommend normalization of1,25-(OH)2D levels in breast cancer patients by the administration of thehormone because of the potential side effects of hypercalcemia andhypercalciuria. It is noteworthy, however, that the patient with multiplemyeloma had hypercalciuria (463 mg/24 h) before treatment, at the sametime that 1,25-(OH)2D was undetectable. Following treatment, while the1,25-(OH)2D was 99 pg/mL, the 24 h urine Ca excretion fell to 163 mg.This suggests that cautious administration of 1,25-(OH)2D, maintainingthe serum levels of the hormone within the normal range, would not
e Received May 14, 1997. Address correspondence to: P.N.Durrington, M.D., Department of Medicine, Manchester Royal Infir-mary, Oxford Road, Manchester, M13 9WL United Kingdom.
f Received February 5, 1997. Address correspondence to: GenaroM. A. Palmieri, Department of Medicine, The University of Tennessee atMemphis, 956 Court Avenue, Room E336, Memphis, Tennessee 38163.
3516 LETTERS TO THE EDITOR JCE & M • 1997Vol 82 • No 10

necessarily result in serious complications and could have a potentiallybeneficial effect in progressive breast cancer.
Genaro M. A. PalmieriUniversity of Tennessee at MemphisMemphis, Tennessee 38163
References
1. Mawer EB, Walls J, Howell A, Davies M, Ratcliffe WA, Bundred NJ. 1997Serum 1,25-dihydroxyvitamin D may be related inversely to disease activityin breast cancer patients with bone metastases. J Clin Endocrinol Metab.82:118–122.
2. Stack KM, Palmieri GMA. 1989 1,25 dihydroxyvitamin D in severe immunechallenges. Immunol Lett. 23:77.
3. Eisman JA, Sher E, Suva LJ, Frampton RJ, McLean FL. 1984 1a25-dihy-droxyvitamin D3 specifically induces its own metabolism in a human cancercell line. Endocrinology. 114:1225–1231.
4. Provvedini DM, Deftos LJ, Manolagas SC. 1986 1,25 Dihydroxyvitamin D3promotes in vitro morphologic and enzymatic changes in normal human mono-cytes consistent with their differentiation into macrophages. Bone. 7:23–28.
5. Haug CJ, Aukrust P, Liem E, Muller F, Espevik T, Frøland SS. 1996 Dis-seminated Mycobacterium avium complex infection in AIDS: Immunopatho-genic significance of an activated tumor necrosis factor system and depressedserum levels of 1,25 dihydroxyvitamin D. J Infect Dis. 173:259–262.
6. Epstein S, Stern PH, Bell NH, Dowdeswell I, Turner RT. 1984 Evidence forabnormal regulation of circulating 1a25-dihydroxyvitamin D in patients withpulmonary tuberculosis and normal calcium metabolism. Calcif Tissue Int.36:541–544.
7. Adams JS, Sharma OP, Gacad MA, Singer FR. 1983 Metabolism of 25-hy-droxyvitamin D3 by cultured pulmonary alveolar macrophages in sarcoidosis.J Clin Invest. 72:1856–1860.
8. Tsoukas CD, Provvedini DM, Manolagas SC. 1984 1,25 DihydroxyvitaminD3: a novel immunoregulatory hormone. Science. 224:1438–1440.
9. Manolagas SC, Provvedini DM, Tsoukas CD. 1985 Interactions of 1,25-Di-hydroxyvitamin D3 and the immune system. Mol Cell Endocrinol. 43:113–122.
1,25 Dihydroxyvitamin D and Cancer—Author’sResponseg
To the editor:
Dr. Palmieri (in his letter above) suggests that the serum 1,25-dihy-droxyvitamin D [1,25-(OH)2D] concentration may be lowered by binding(presumably via vitamin D receptors) to immunoregulatory or cancer cellswhen these are present in large numbers. This is an interesting hypothesisand worthy of testing. It might be predicted, however, that if such bindingwere to occur, the result would be similar to that seen when the serumvitamin D binding protein is increased. In these cases, the total 1,25-(OH)2Dincreases because the reduced unbound fraction, which is the physiolog-ically important moiety, is sensed by the kidney to be low, and the renal1a-hydroxylase is stimulated to produce more 1,25-(OH)2D, thus restoringthe free concentration and increasing the total (1).
This was not the picture we saw in breast cancer patients (2), nor isit what Palmieri saw in patients with severe immune challenges (3) inwhom 1,25-(OH)2D was low, suggesting that renal synthesis of 1,25-(OH)2D in these cases was in fact suppressed, either by a raised renal cellcalcium level or by a hypothetical inhibitor present in the cancer cells.
In cases like Dr. Palmieri’s patient with multiple myeloma, the hy-percalciuria might have arisen from increased bone turnover, and theconsequent suppression of the 1a-hydroxylase could be seen as a mech-anism to prevent or delay the onset of hypercalcemia.
We are still of the opinion that administration of 1,25-(OH)2D insuch cases may precipitate hypercalcemia, although concurrent par-enteral administration of an antiresorptive agent such as bisphos-phonate might prevent this complication, especially if coupled witha low calcium diet. We have shown that, in cases of vitamin Dpoisoning where 1,25-(OH)2D levels are supranormal, intravenouspamidronate can restore normocalcemia without suppressing 1,25-(OH)2D (4). This indicates that bisphosphonate treatment might in-deed allow normal serum 1,25-(OH)2D to be restored by 1,25-(OH)2D
treatment, without hypercalcemia, thus permitting a trial of the hor-mone’s antiproliferative properties.
E. Barbara MawerDepartment of MedicineManchester Royal InfirmaryManchester M13 9WL, United Kingdom
References
1. Bouillon R, Van Assche FA, Van Baelen H, Heyns W, De Moor P. 1981Influence of the vitamin D-binding protein on the serum concentration of1,25-dihydroxyvitamin D3. J Clin Invest. 67:589–596.
2. Mawer EB, Walls J, Howell A, Davies M, Ratcliffe WA, Bundred NJ. 1997Serum 1,25-dihydroxyvitamin D may be related to disease activity in breastcancer patients with bone metastases. J Clin Endocrinol Metab. 82:118–122.
3. Stack KM, Palmieri GMA. 1989 1,25-Dihydroxyvitamin D in severe immunechallenges. Immunol Lett. 23:77.
4. Selby PS, Davies M, Marks JS, Mawer EB. 1995 Vitamin D intoxication causeshypercalcaemia by increased bone resorption, which responds to pamidronate.Clin Endocrinol (Oxf). 43:531–536.
Spontaneous Complete Remission of PrimaryPigmented Adrenocortical Diseaseh
To the editor:
We read with great interest the illustrative case reported by Sarliset al. (1), recently published in JCEM, about a patient with primarypigmented nodular adrenocortical disease (PPNAD), who wastreated by unilateral adrenalectomy. Although his daily urinary freecortisol (UFC) rate normalized and the major clinical manifestationsof Cushing’s Syndrome (CS) subsided, loss of a circadian cortisolrhythm persisted after surgery. Twenty-seven years later, the patientpresented again with short stature, severe osteopenia, skeletal de-formities, and myopathy. In the extensive series published by Carneyand Young (2), subtotal adrenalectomy was performed in 17 patients.Among these patients, 6 were considered successfully treated. How-ever, they only showed remission of the clinical features of CS despitethe persistence of autonomous adrenocortical function observed inthose patients who were tested. This case showed that adrenal au-tonomous hyperfunction, despite the lack of biochemical hypercor-tisolism may lead to significant morbidity over the course of severalyears.
We have a patient who, at 12 yr of age, had hypercortisolismassociated with unilateral adrenocortical uptake of 131I iodomethyl-norcholesterol. The initial diagnosis was ACTH-independent CS byadenoma. Subsequent surgical exploration was performed. At thetime of operation, the adrenal glands appeared normal. The surgeon,guided by the scintigraphic image, performed a unilateral adrena-lectomy on the right side. Histologic study of surgical material re-vealed PPNAD. One year later, CS disappeared, and the patientshowed increasing energy and muscular strength, weight loss, andincreased height velocity. UFC rate and basal plasma cortisol werewithin normal ranges, but loss of diurnal rythmicity (plasma cortisol8 h 5 10 mg/dL, 20 h 5 9.7 mg/dL) and suppressed basal ACTH levels(8 h # 5 pg/mL) were present. This case was previously published(3). The patient and his parents refused a new adrenalectomy becausehe felt well. The hormonal pattern described remained during 4 yr.Five years after unilateral adrenalectomy, diurnal rythmicity (plasmacortisol 8 h 5 15.4 mg/dL, 20 h 5 7.7 mg/dL) was spontaneouslyrecovered, associated with serum basal ACTH (8 h 5 26.5 pg/mL)within normal range. The patient remained free of clinical features ofCS. His final height is in accordance with his midparental height, andbone densitometry revealed normal bone density. Thus our patienthas had a complete remission of PPNAD.
The possibility that stimulating antibodies play a role in the patho-genesis of PPNAD was suggested by Wulffraat et al. (4), who reportedthat immunoglobulins prepared from serum of patients with PPNADstimulated adrenal DNA synthesis in vitro. Such stimulation of theadrenal cortex would be analogous to the stimulation of thyroid tissueby thyroid stimulating immunoglobulin in Graves’ disease. In Graves’
g Received July 25, 1997. Address correspondence to: E. BarbaraMawer, University Department of Medicine, The Royal Infirmary, Ox-ford Road, Manchester, M13 9WL, United Kingdom.
h Received June 18, 1997. Address correspondence to: Dr. Ricardo V.Garcia-Mayor, P.O. Box 1691, 36201 Vigo, Spain.
LETTERS TO THE EDITOR 3517
disease, spontaneous remission of the disease has been described (5). Asimilar mechanism could explain our patient’s outcome.
The present case suggests the following considerations: 1) it sup-ports the view that an autoimmune mechanism may be involved inPPNAD; 2) some but rare cases of PPNAD may have complete re-mission of the disease, at least temporarily; and 3) some cases ofPPNAD treated with unilateral adrenalectomy and which have pre-sented with clinical remission of CS associated with normal UFCrates, must be carefully followed for some time before completion oftotal adrenalectomy.
Ricardo V. Garcia-Mayor, Luisa F. Perez Mendez,Concepcion Paramo, and Reyes Luna Cano
Hospital Xeral-Cies de VigoVigo, Spain
References
1. Sarlis NJ, Chrousos GP, Doppman JL, Carney JA, Stratakis CA. 1997 Primarypigmented nodular adrenocortical disease: reevaluation of a patient with Car-ney complex 27 years after unilateral adrenalectomy. J Clin Endocrinol Metab.82:1274–1278.
2. Carney JA, Young WFJ. 1992 Primary pigmented nodular adrenocortical dis-ease and its associated conditions. Endocrinologist. 2:6–21.
3. Garcia-Mayor RV, Perez Mendez LF, Paramo C, Andrade A, Guitian R,Butron M. 1993 Primary adrenocortical nodular dysplasia presented as ad-renal adenoma by functional scintigraphy. Clin Nucl Med. 18:220–222.
4. Wulffraat NM, Drehage HA, Wiersinga WM, Van Der Gaag RD, Jeucken P,Mol JA. 1988 Immunoglobulins of patients with Cushing’s Syndrome due topigmented adrenocortical micronodular dysplasia stimulated in vitro steroi-dogenesis. J Clin Endocrinol Metab. 66:301–307.
5. Burman KD, Baker JR. 1985 Immune mechanism in Graves’ disease. EndocrRev. 6:183–232.
Thyroglobulin-Like Immunoreactivity WithinGoitrous Thyroid Stroma after Iodine Overloadi
To the editor:Recently, using Secondary Ion Mass Spectrometry (SIMS), we showed
the presence of high amounts of bound 127I (iodine) in thyroid stromaof multinodular goiters inhabiting a region of goiter endemicity, espe-cially after absorption of high doses of Lugol’s solution (2% potassiumiodide solution) (1).
We tried to identify the iodinated molecules present in these stroma,using immunohistochemical techniques.
The eight patients previously described (1) were included in this
study. One did not receive any treatment, two received L-thyroxine(L-T4) (100 mg/day), three received Lugol’s solution (3.8 mg iodine perday), and the last two patients received Lugol’s and L-T4 (3.8 mg iodineand 100 mg per day) during a six-month period of treatment.
All were euthyroid, and had a large multinodular goiter before treat-ment. Their nodules were cold on scintigraphy. After the six-monthtreatment period, their serum thyroglobulin concentrations dropped,and all subjects underwent subthyroidectomy.
Fragments of nodules were immersed in a Bouin solution for a periodof three days. The fixed tissues were dehydrated in alcohol, cleared intoluen, and embedded in parrafin. Sections with a thickness of 3 mmwere processed for immunoperoxidase techniques.
For facilities, we gathered the patient who did not received treatmentand the two patients receiving L-T4, in a control group, as we did for theSIMS study.
The following rabbit primary antibodies were used: antiperoxidase(CIS International, Paris, France)(4,000 U/mL), antialbumin (1:50), an-tithyroxine (Immunotech, Marseille, France)(1:1), antitriiodothyronin(1:1) (Netria, London, England), and antithyroglobulin (CIS Interna-tional)(3,100 U/mL).
The following monoclonal primary antibodies were used: anti-thyroglobulin (CIS International)(1:1), antiIgG (Dako, Copenhagen,Denmark)(1:50).
The indirect method was performed on rehydrated sections. Theywere incubated overnight at 4 C with primary antisera diluted in Tris-HCl-NaCl buffer. After washing, the sections were incubated for 1 h atroom tempature with a peroxidase labeled antirabbit or antimouse an-tiserum (Dako; 1:100). Revelation was performed for a few minutes ina freshly prepared diaminobenzidine and hydrogen peroxide (0.03%)solution. The sections were examined in a Leitz microscope. (Ernst LeitzGMBH, Wetzlar, Germany).
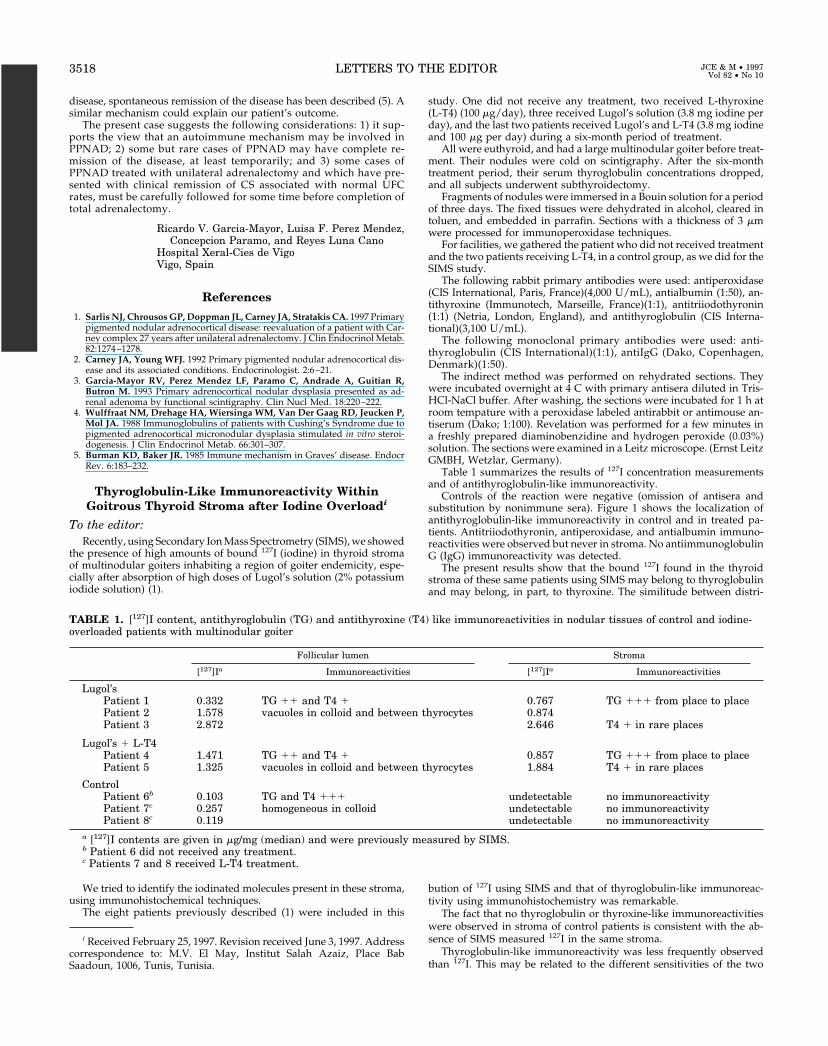
Table 1 summarizes the results of 127I concentration measurementsand of antithyroglobulin-like immunoreactivity.
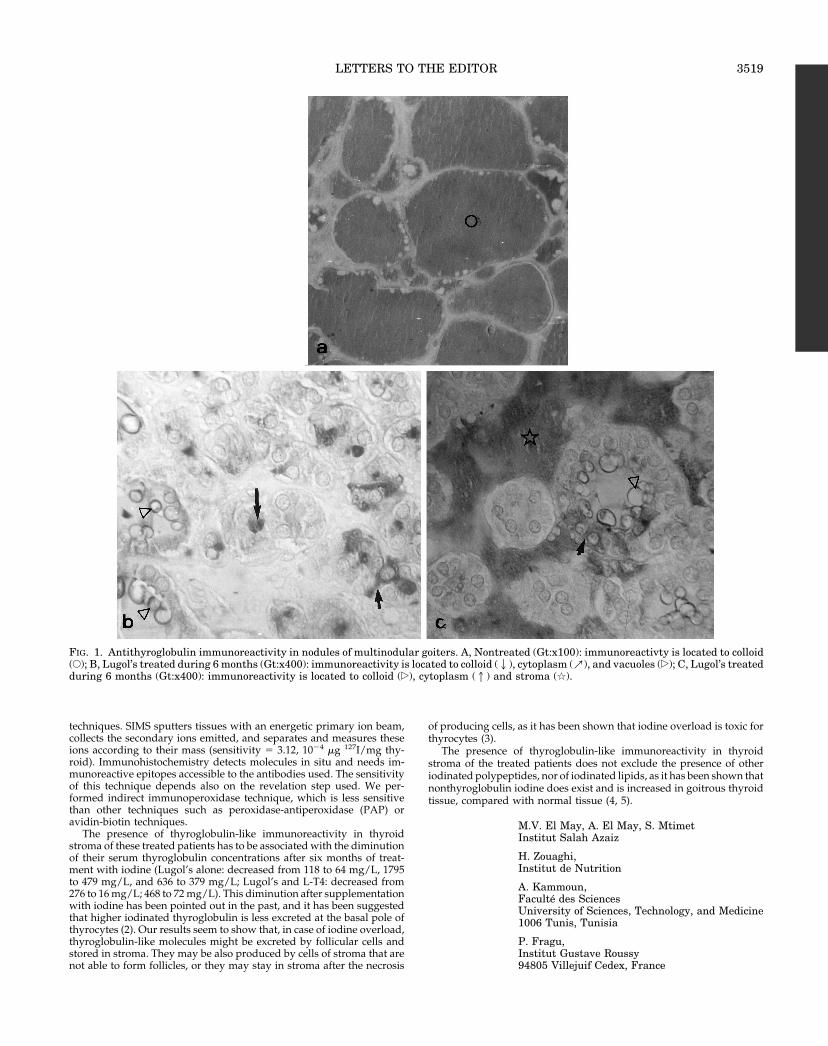
Controls of the reaction were negative (omission of antisera andsubstitution by nonimmune sera). Figure 1 shows the localization ofantithyroglobulin-like immunoreactivity in control and in treated pa-tients. Antitriiodothyronin, antiperoxidase, and antialbumin immuno-reactivities were observed but never in stroma. No antiimmunoglobulinG (IgG) immunoreactivity was detected.
The present results show that the bound 127I found in the thyroidstroma of these same patients using SIMS may belong to thyroglobulinand may belong, in part, to thyroxine. The similitude between distri-
bution of 127I using SIMS and that of thyroglobulin-like immunoreac-tivity using immunohistochemistry was remarkable.
The fact that no thyroglobulin or thyroxine-like immunoreactivitieswere observed in stroma of control patients is consistent with the ab-sence of SIMS measured 127I in the same stroma.
Thyroglobulin-like immunoreactivity was less frequently observedthan 127I. This may be related to the different sensitivities of the two
i Received February 25, 1997. Revision received June 3, 1997. Addresscorrespondence to: M.V. El May, Institut Salah Azaiz, Place BabSaadoun, 1006, Tunis, Tunisia.
TABLE 1. [127]I content, antithyroglobulin (TG) and antithyroxine (T4) like immunoreactivities in nodular tissues of control and iodine-overloaded patients with multinodular goiter
Follicular lumen Stroma
[127]Ia Immunoreactivities [127]Ia Immunoreactivities
Lugol’sPatient 1 0.332 TG 11 and T4 1 0.767 TG 111 from place to placePatient 2 1.578 vacuoles in colloid and between thyrocytes 0.874Patient 3 2.872 2.646 T4 1 in rare places
Lugol’s 1 L-T4Patient 4 1.471 TG 11 and T4 1 0.857 TG 111 from place to placePatient 5 1.325 vacuoles in colloid and between thyrocytes 1.884 T4 1 in rare places
ControlPatient 6b 0.103 TG and T4 111 undetectable no immunoreactivityPatient 7c 0.257 homogeneous in colloid undetectable no immunoreactivityPatient 8c 0.119 undetectable no immunoreactivity
a [127]I contents are given in mg/mg (median) and were previously measured by SIMS.b Patient 6 did not received any treatment.c Patients 7 and 8 received L-T4 treatment.
3518 LETTERS TO THE EDITOR JCE & M • 1997Vol 82 • No 10
techniques. SIMS sputters tissues with an energetic primary ion beam,collects the secondary ions emitted, and separates and measures theseions according to their mass (sensitivity 5 3.12, 1024 mg 127I/mg thy-roid). Immunohistochemistry detects molecules in situ and needs im-munoreactive epitopes accessible to the antibodies used. The sensitivityof this technique depends also on the revelation step used. We per-formed indirect immunoperoxidase technique, which is less sensitivethan other techniques such as peroxidase-antiperoxidase (PAP) oravidin-biotin techniques.
The presence of thyroglobulin-like immunoreactivity in thyroidstroma of these treated patients has to be associated with the diminutionof their serum thyroglobulin concentrations after six months of treat-ment with iodine (Lugol’s alone: decreased from 118 to 64 mg/L, 1795to 479 mg/L, and 636 to 379 mg/L; Lugol’s and L-T4: decreased from276 to 16 mg/L; 468 to 72 mg/L). This diminution after supplementationwith iodine has been pointed out in the past, and it has been suggestedthat higher iodinated thyroglobulin is less excreted at the basal pole ofthyrocytes (2). Our results seem to show that, in case of iodine overload,thyroglobulin-like molecules might be excreted by follicular cells andstored in stroma. They may be also produced by cells of stroma that arenot able to form follicles, or they may stay in stroma after the necrosis
of producing cells, as it has been shown that iodine overload is toxic forthyrocytes (3).
The presence of thyroglobulin-like immunoreactivity in thyroidstroma of the treated patients does not exclude the presence of otheriodinated polypeptides, nor of iodinated lipids, as it has been shown thatnonthyroglobulin iodine does exist and is increased in goitrous thyroidtissue, compared with normal tissue (4, 5).
M.V. El May, A. El May, S. MtimetInstitut Salah Azaiz
H. Zouaghi,Institut de Nutrition
A. Kammoun,Faculte des SciencesUniversity of Sciences, Technology, and Medicine1006 Tunis, Tunisia
P. Fragu,Institut Gustave Roussy94805 Villejuif Cedex, France
FIG. 1. Antithyroglobulin immunoreactivity in nodules of multinodular goiters. A, Nontreated (Gt:x100): immunoreactivty is located to colloid(E); B, Lugol’s treated during 6 months (Gt:x400): immunoreactivity is located to colloid (2), cytoplasm (m), and vacuoles (�); C, Lugol’s treatedduring 6 months (Gt:x400): immunoreactivity is located to colloid (�), cytoplasm (1) and stroma (q).
LETTERS TO THE EDITOR 3519

References
1. El May MV, Jeusset J, El May A, Mtimet S, Fragu P. 1996 Evidence of iodinestorage within thyroid stroma after iodine treatment: imaging by SecondaryIon Mass Spectrometry Microscopy in goitrous tissue. J Clin Endocrinol Metab.81:2370–2375.
2. Othaki S, Moriya S, Suzuki H, Horinchi Y. 1967 Nonhormonal iodine escapefrom the normal and abnormal thyroid gland. J Clin Endocrinol Metab.27:728–733.
3. Many MC, Mestdagh C, Van Den Hove MF, Denef JF. 1992 In Vitro studyof acute toxic effects of high iodide doses in human thyroid follicles. Endo-crinology. 131:621–630.
4. Lemansky P, Popp GM, Tietz J, Herzog V. 1994 Identification of iodinatedproteins in cultured thyrocytes and their possible significance for thyroidhormone formation. Endocrinology. 135:1566–1575.
5. Aechimann S, Buergi U, Wagner HE, Kaempf J, Lauber K, Studer H. 1994Low intrathyroidal iodine concentration in non-endemic human goitres: aconsequence rather than a cause of autonomous goitre growth. J Endocrinol.140:155–164.
What Should Be Considered A Low Dose in theACTH Stimulation Test? j
To the editor:
In their paper, Shankar et al. (1) claim that they found no im-provement in the sensitivity of the low dose ACTH test for theevaluation of the HPA axis. However, they use the term “low doseACTH test” wrongly.
The dose of ACTH in the low dose test was defined previously asbeing 1.0 mg for adults (2–4), or 0.5 mg/1.73 m2 for children (5, 6). Thesewere the doses proven to increase sensitivity. Tordjman et al. (3) haveshown that 5.0 mg (which equals 0.06–1.0 mg/kg) is too high a dose forthis purpose. The dose the authors use in the current study is muchhigher, equaling about 15 mg for adults and about 10.0 mg/1.73 m2 forchildren. All that this paper shows is that such a dose does not increasethe sensitivity of the ACTH test, which is not surprising, knowing thateven lower doses do not.
However, the term “low dose ACTH test” should not have been usedin this study, as readers might wrongly think that their low dose ACTHtest is similar to the one used in the past and proven to increasesensitivity.
We have also a comment regarding the study design. We find thatboth ACTH tests (high dose and so called low dose) should not havebeen done on the same day, and definitely not in the order they were.The correct way should be either to perform tests in random order, aswe did (2), or start with the lower dose, as the higher one might primethe adrenal gland, rather than deplete it. Actually, the fact that onepatient did not respond to the huge dose of 250 mg but responded to thelower ACTH later in the same day suggests that this is really the case.However, considering the too large ACTH dose used as a low dose, thispoint is minor in the current study.
Gabriel DicksteinBnai Zion Medical CenterHaifa, 31048, Israel
References
1. Shankar RR, Jakacki RI, Haider A, et al. 1997 Testing the hypothalamic-pituitary-adrenal axis in survivors of childhood brain and skull-based tumors.J Clin Endocrinol Metab. 82:1995–1998.
2. Dickstein G, Shechner C, Nicholson WF, et al. 1991 Adrenocorticotropinstimulation test: effects of basal cortisol level, time of day, and suggested newsensitive low dose test. J Clin Endocrinol Metab. 72:772–778.
3. Tordjman K, Jaffe A, Grazas N, Apter C, Stern N. 1995 The role of the lowdose (1 mg) adrenocorticotropin test in the evaluation of patients with pituitarydiseases. J Clin Endocrinol Metab. 80:1301–1305.
4. Rasmuson S, Olsson T, Hagg E. 1996 A low dose ACTH test to assess thefunction of the hypothalamic-pituitary-adrenal axis. Clin Endocrinol.44:151–156.
5. Crowley S, Hindmarsh PC, Holownia P, Honour JW, Brook CGD. 1991 The
use of low doses of ACTH in the investigation of adrenal function in man. JEndocrinol. 130:475–479.
6. Brodie J, Soferman R, Kivity S, et al. 1995 Low dose adrenocorticotropin testreveals impaired adrenal function in patients taking inhaled corticosteroids.J Clin Endocrinol Metab. 80:1243–1246.
What Should Be Considered a Low Dose in the ACTHStimulation Test?—Author’s Responsek
To the editor:
Thank you very much for the opportunity to respond to Dr.Dickstein’s letter. Our study was designed several years before the“low dose ACTH test” Dickstein and others published (1). Our studydesign was based on the work of Graybeal and Fang (2). The “lowdose” of ACTH we used is approximately 15–20 times higher than thedose recommended by Dickstein and colleagues. We agree with Dr.Dickstein that a lower dose of ACTH, such as the one he and hiscolleagues recommend (1.0 mg for adults or 0.5 mg/1.73 m2 for chil-dren) might have improved the sensitivity of ACTH testing in oursubjects. In fact, we address this possibility in our Discussion on p.1997.
We regret not having referenced Dr. Dickstein’s pivotal 1991 pa-per. The term “low dose ACTH test” was used to permit distinctionbetween the two tests that we investigated. We agree with Dr. Dick-stein that this shows that “such a dose does not increase the sensitivityof the ACTH.” Our data also suggest that an alternative approach toimproving the sensitivity of ACTH testing might be to increase thelower limits of the “normal cortisol” response to ACTH testing to 688nmol/L (25 mg/dL).
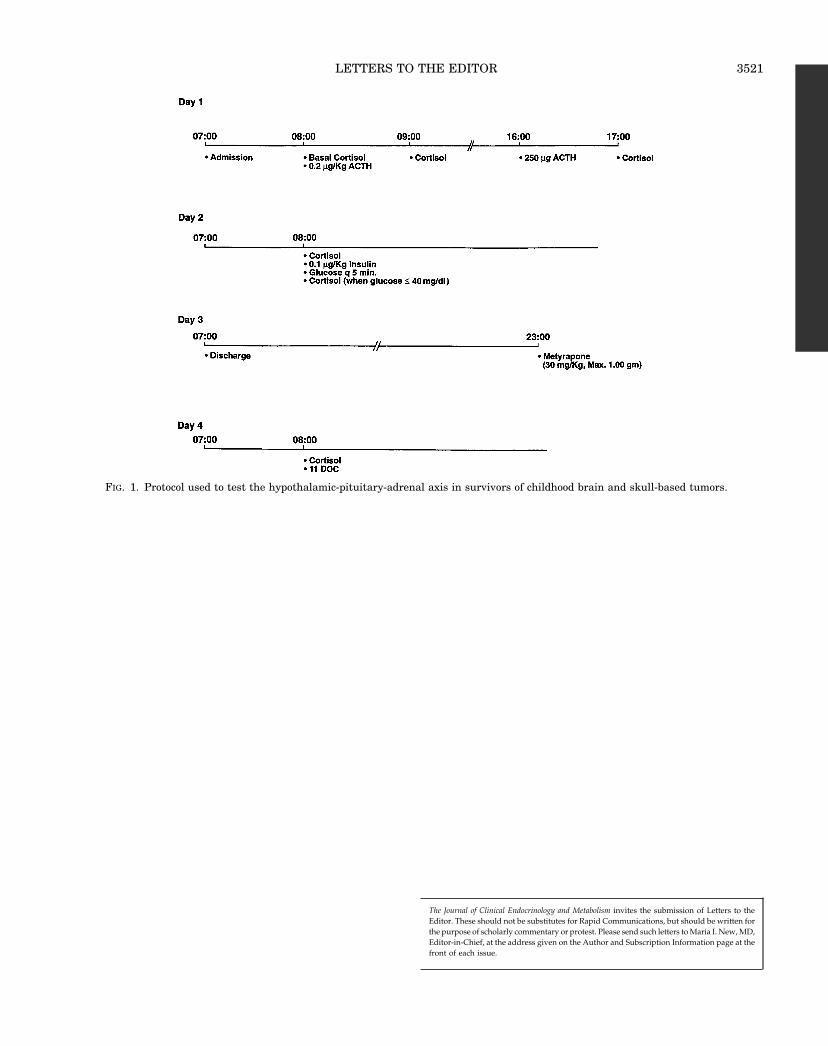
Dr. Dickstein’s comments regarding the order of ACTH testing arelegitimate. His comments led us to identify an error that was made inthe Discussion section of the manuscript. In fact, in our study, the lowerdose of ACTH was administered in the morning and not in the afternoon(see Fig. 1). In an attempt to minimize the amount of time children werehospitalized in our GCRC, we performed both tests on the same day.However, we agree that a better study design would have been torandomize the order of the two tests.
We appreciate Dr. Dickstein’s comments. His major concern aboutour use of the term “low dose test” raises an additional issue. Whendoes a test or procedure graduate from being investigational to beingthe accepted norm? When does a term that has a generic ring to it (i.e.low dose test) become a specific test (1.0 mg for adults or 0.5 mg/1.73m2 for children)? What criteria should be met before a test entersclinical practice as a specific test? We hope that discussions of suchissues will result in further research to improve diagnosis and man-agement of often subtle clinical problems such as adrenalinsufficiency.
Ravi ShankarRegina JakackiAnar HaiderMelissa LeeOra Hirsch PescovitzIndiana University School of MedicineIndianapolis, IN 46202
References
1. Dickstein G, Schechner C, Nicholson WF, et al. 1991 Adrenocorticotropinstimulation test: effects of basal cortisol level, time of day, and suggested newsensitive low dose test. J Clin Endocrinol Metab. 72:772–778.
2. Graybeal ML, Fang VS. 1985 Physiological dosing of exogenous ACTH. ActaEndocrinol (Copenh). 108:401–406.
j Received June 19, 1997. Address correspondence to: Gabriel Dick-stein, Division of Endocrinology, Oregon Health Sciences UniversityL607, 3181 SW Sam Jackson Park Road, Portland, Oregon 97201-3098.
k Received July 10, 1997. Address correspondence to: Ora Pescovitz,Department of Pediatric Physiology/Biochemistry James WhitcombRiley Hospital for Children, 702 Barnhill Drive, Room A5984, Indian-apolis, Indiana 46202-5225.
3520 LETTERS TO THE EDITOR JCE & M • 1997Vol 82 • No 10
The Journal of Clinical Endocrinology and Metabolism invites the submission of Letters to theEditor. These should not be substitutes for Rapid Communications, but should be written forthe purpose of scholarly commentary or protest. Please send such letters to Maria I. New, MD,Editor-in-Chief, at the address given on the Author and Subscription Information page at thefront of each issue.
FIG. 1. Protocol used to test the hypothalamic-pituitary-adrenal axis in survivors of childhood brain and skull-based tumors.
LETTERS TO THE EDITOR 3521