day hospital treatment for anorexia nervosa: a 12-month follow-up study
TRANSCRIPT

RESEARCH ARTICLE
Day Hospital Treatment for Anorexia Nervosa: A 12-Month Follow-upStudy†
Giovanni Abbate-Daga1*, Enrica Marzola1, Carlotta De-Bacco1, Sara Buzzichelli1, Annalisa Brustolin1,Stefania Campisi1, Federico Amianto1, Giuseppe Migliaretti2 & Secondo Fassino1
1Eating Disorders Center, Department of Neuroscience, University of Turin, Turin, Italy2Department of Clinical and Biological Sciences, University of Turin, Turin, Italy
Abstract
Day hospitals (DHs) represent a treatment option for anorexia nervosa (AN), a mental disorder that is difficult to treat and has noevidence-based treatments available. We aimed to determine the effectiveness of a DH treatment that was specifically focused on theemotions of severe AN patients. Body mass index and eating psychopathology were the primary outcome measures.
Fifty-six adult patients with AN were assessed upon admission, at the end of treatment (EOT) and at a 12-month follow-up evaluation(T18) using Eating Disorders Inventory-2, Beck Depression Inventory, Hamilton Rating Scale for Anxiety and Brief Social Phobia Scale.All participants received a multidisciplinary treatment programme that focused on psychodynamic psychotherapy.
Seventy-eight per cent of participants reported positive outcomes at EOT and 68% at T18. Moreover, 82.1% and 65.4% of long-standingpatients showed positive outcomes at EOT and T18, respectively. All measures of psychopathology were significantly improved at EOT andwere maintained at follow-up.
Our DH was effective at treating severe AN patients; however, further investigations of the processes of change are warranted. Copyright© 2015 John Wiley & Sons, Ltd and Eating Disorders Association.
Keywords
anorexia nervosa; eating disorders; day hospital; outcome
*Correspondence
Prof. Giovanni Abbate-Daga, Eating Disorder Center, Department of Neuroscience, University of Turin, Via Cherasco 15, 10126, Turin, Italy. Tel: +39 011 6335196;
Fax: +39 011 6335749.
Email: [email protected]†The work was carried out at the Eating Disorders Centre of the University of Turin, via Cherasco 11, 10126, Turin, Italy.
Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/erv.2369
Introduction
Anorexia nervosa (AN) is a severe psychiatric disorder that ischaracterized by self-imposed starvation and aberrant patternsof feeding behaviour (American Psychiatric Association, 2013).Over the past few decades, day hospitals (DHs) have become anincreasingly relevant therapeutic approach to AN; to date, theyare a recommended treatment for AN (Yager et al., 2012).Because partially hospitalized patients return to their homes atnight and during weekends, this intervention is peculiar inseveral respects (Abbate-Daga et al., 2009). First, DHs allowpatients to maintain their social relationships by avoiding theisolation that inpatient hospitalizations frequently entail,especially when they are lengthy, as is often the case in AN. Forthis reason, patients’ daily exposure to their family and peerscan represent both a source of support and a fruitful opportunityto therapeutically work on environment-related maintainingfactors. Second, patients are provided with real-world feedbackon a daily basis regarding those new skills and strategies that weredeveloped during treatment. Finally, DHs are indicated forpatients whose severity cannot be managed on an outpatient basisbut when an inpatient setting is not strictly necessary.
Eur. Eat. Disorders Rev. (2015)© 2015 John Wiley & Sons, Ltd and Eating Disorders Association.
Currently, DHs are disseminated worldwide and their effectivenesshas been established with regards to outcomes and cost-effectiveness(for reviews see Abbate-Daga et al., 2009; Hepburn & Wilson,2014). However, a wide variety of health care systems, treatmentapproaches and outcome definitions are used across studies,making it difficult to garner solid evidence about this intensiveintervention. Additionally, research on the effectiveness of DHsin AN is scarce and follow-up data are generally lacking.
Furthermore, there is a dearth of effective treatments for AN,particularly for adult patients; substantial evidence shows thatapproximately 20% of affected individuals will develop chronicAN and that approximately 5% will eventually die from thisdisorder (Arcelus, Mitchell, Wales, & Nielsen, 2011). An enduringcourse of AN represents not only a negative prognostic factor(Le Grange et al., 2014) but also a daunting challenge for clinicians(Strober, 2010) as chronic patients often present with greatresistance to treatments (Abbate-Daga, Amianto, Delsedime,De-Bacco, & Fassino, 2013).
Ambivalence towards recovery is a relevant aspect of AN(Abbate-Daga et al., 2013) because it is frequently involved inhindering the patient’s engagement in the therapeutic process.Biological (e.g. the scarring effects of emaciation; Kaye, Fudge,

Day Hospital Treatment for Anorexia Nervosa G. Abbate-Daga et al.
& Paulus, 2009) and psychological (e.g. ‘adaptive’ functioning ofthe disorder; Schmidt & Treasure, 2006) underpinnings may alsobe implicated in the pathophysiology of this phenomenon.Furthermore, difficulties in emotional regulation have been theo-rized to play a role in the development and maintenance of AN(Racine & Wildes, 2013); specific treatments have recently startedto address these components (Abbate-Daga et al., 2012; Wildes &Marcus, 2011) alongside mainstream psychodynamic approaches(Zipfel et al., 2014).
A few lines of research have recently started to focus on treat-ment strategies for patients who have developed a long-standing,non-responding disorder (e.g. cognitive-behavioural therapy;Touyz et al., 2013), whose needs may be very peculiar (Bamford& Mountford, 2012; Hay, Touyz, & Sud, 2012). Althoughfrequently needed, long-standing patients tend to refuse inpatienthospitalizations; therefore, DHs may be a more feasible andacceptable therapeutic alternative. Additionally, no criteria existregarding the staging of AN, making it complicated to developtailored interventions; however, several authors have suggested thata history of illness of 7 years or greater is an acceptable ‘threshold’for defining an enduring or long-standing eating disorder (Maguireet al., 2008; Touyz et al., 2013).
Given the paucity in the medical literature regarding partial hos-pitalization for patients affected by AN, we utilized a 12-month out-come study to determine the effectiveness of a DH programme witha specific psychodynamic focus on emotions and interpersonalfunctioning (Abbate-Daga et al., 2012). Body mass index (BMI)and eating psychopathology were the primary outcomes of ourstudy, and psychological functioning (i.e. depression, anxiety) wasconsidered as secondary outcome. Additionally, prompted by thelack of data on severe and long-standing patients, our secondaryaim was to examine several outcome measures of a subsample ofAN patients who had a history of illness of at least 7 years (Maguireet al., 2008). Notwithstanding the severity of our sample, weexpected that the DH treatment would be effective at improvingthe aforementioned clinical and psychopathology parameters andalso indicate promising results at follow-up.
Methods
The day hospital of Turin
Background
The DH for Eating Disorders of the San Giovanni BattistaHospital of the University of Turin in Italy opened in 2006 as a sec-ondary care facility within the context of a stepped-care continuumof interventions (i.e. inpatient, outpatient and day patientservices). Overall, the DH programme is grounded in a thoroughreview of the scientific literature as well as international guidelines;accordingly, it relies also on a multidisciplinary approach.
The conceptual framework of our DH is psychodynamically andemotionally focused; the improvement of socio-relational skillsalso represents a specific core of this intervention (Abbate-Dagaet al., 2009, 2012). Psychodynamic psychotherapy has been shownto be as effective as cognitive behavioural therapy and superior totreatment as usual in a recent randomized clinical trial (RCT;Zipfel et al., 2014) that examined the treatment of AN outpatients.Treatment is delivered according to the following multi-phasic
Eur.
design: Phase 1 encompasses refeeding and promoting the aware-ness of both emotions and meaning of illness; Phase 2 involvesthe normalization of eating behaviours as well as emotionalcoping; and Phase 3 consists of working on the core beliefs thatcontribute to the maintenance of the disorder, as well as relapseprevention, and the improvement of socio-relational skills(Gramaglia et al., 2011).
As previously outlined (Abbate-Daga et al., 2009, 2012), this 5-dayDH programme is located away from the inpatient unit and it isoffered between Monday and Friday from 8:30 am to 3:30pm. Amaximum of 12 patients are enrolled in the programme, and theduration of treatment is 6months. The overall structure of the DHis focused on the group setting to facilitate the treatment of botheating psychopathology and psychological functioning and topromote the mobilization of each patient’s resources with respect tosocial interactions and relational skills.
Over the last few years, the development of an integrated DHservice has become increasingly pertinent to the growing numberof patients with severe and enduring AN who are seeking treatmentat the Program for Eating Disorders of our Institution. The DH rep-resents a clinical response to all of those patients who are severelyemaciated but whose medical condition does not require acutemedical stabilization. Additionally, some medical interventions(e.g. EKG, intravenous refeeding, the treatment of electrolyteabnormalities, etc.) are provided in this context of care. Hence,those patients who have been recently discharged from the inpatientservice are frequently stepped-down to partial hospitalization. Inaddition, outpatients who show a deteriorated clinical condition(e.g. an increase in bingeing–purging episodes, rapid weight loss,disruption of social relational functioning, etc.) and refuse inpatienthospitalization will also be offered partial hospitalization. Therefore,a large proportion of partially hospitalized patients consists ofsevere, emaciated and long-standing individuals. It is also worth-while to note that, according to the Italian public health system,all patients have direct access to the Center for Eating Disorders, ifindicated by their primary care physician, without exceptions andregardless of their socioeconomic or insurance status.
Intake, exclusion and inclusion criteria
The intake process is managed by the clinical director, anexperienced psychiatrist, who conducts preliminary interviewswith all candidates. Patients’ diagnoses are then confirmed by asecond psychiatrist using structured interviews. Inclusion criteriaare as follows: (a) a diagnosis of AN, bulimia nervosa (BN) orEating Disorder Not Otherwise Specified (EDNOS) and (b) ageof 16 or over. Exclusion criteria are as follows: (a) acute medicalrisk requiring inpatient hospitalization; (b) BMI <13.5; (c) activesubstance abuse or dependence; (d) psychosis or bipolar disorder;(e) obesity or Binge Eating Disorder; and (f) suicide risk. Patients’ability to engage in group interventions, their motivation for change(i.e. the contemplation phase as defined by Prochaska andDiClemente (1983) is required), their psychosocial functioningand their family dynamics are also carefully evaluated.
Patient contract and clinical management
After the initial interview, all patients are required to carefullyread a standardized contract that outlines behavioural rules(e.g. the management of supervised meals and toilet breaks) of
Eat. Disorders Rev. (2015)© 2015 John Wiley & Sons, Ltd and Eating Disorders Association.
G. Abbate-Daga et al. Day Hospital Treatment for Anorexia Nervosa
everyday life at the DH. Later in the treatment, all patients are alsoprovided with individualized contracts that are designed to engagethem in treatment planning and clearly identify the clinical goals(e.g. BMI and eating psychopathology) and consequences ofeither progress or failure. According to the NICE Guidelines(2004), this intervention is highly multidisciplinary and includepsychiatrists, clinical psychologists, a registered dietician, oneinternal medicine physician and several psychiatric nurses.
Psychodynamic psychotherapy
This DH relies on psychodynamic psychotherapy according to astandardized model that has been previously described (Abbate-Daga et al., 2009; Fassino, Amianto, & Ferrero, 2008). All patientsundergo weekly 45-minute individual sessions and daily 1-hourgroup sessions of psychodynamic psychotherapy. The groups arecomposed of a maximum of 12 individuals and are conducted bytwo experienced psychiatrists who have extensive psychodynamictraining and expertise. The group setting plays a role in mobilizingthe resources required to enhance skills that are necessary to achievea more adaptive social functioning with both family and peers.
Dietetic management and meals
The dietician conducts weekly sessions with all patients toprovide nutritional counselling and intake planning on a qualita-tive and quantitative basis for both weekdays and weekends.Patients are randomly weighed on a weekly basis to avoid mislead-ing results and potential confounders (e.g. fluid shifts duringrefeeding; for a review see Marzola, Nasser, Hashim, Shih, & Kaye,2013); furthermore, they are generally weighed in the morning,after voiding, wearing only their underwear. During the hours ofthe DH programme, patients receive three structured meals(half-morning snack, lunch and mid-afternoon snack); ifindicated, breakfast may also be provided. Psychiatric nurses andthe dietician supervise all meals; however, they do not eat withthe patients. As agreed upon by the behavioural contract, a boosteris provided if patients do not complete their meals.
Behavioural techniques
The clinical psychologist, the dietician and a nurse conduct aweekly behavioural group therapy session that is specifically aimedat providing patients with management skills for their disorder.Patients are asked to complete a daily eating diary that they willdiscuss during this group session; furthermore, they are encour-aged to share their difficulties during meals with other participantsand identify the potential triggers for their eating symptoms. Goalsand strategies for the weekend are also discussed.
Parent counselling
The clinical team offers monthly parent counselling interven-tions to complete the following two tasks: (1) to collect informa-tion and feedback on patients’ behaviours and difficulties whileat home and (2) to provide parents with the necessary tools tosupport and encourage patients’ motivation and compliance withtreatments. Patients’ significant others are also involved on anindividual basis.
Eur. Eat. Disorders Rev. (2015)© 2015 John Wiley & Sons, Ltd and Eating Disorders Association.
Staff meetings and supervision
In addition to daily communications, weekly all-staff meetingsare conducted to update the team about each patient’s clinical sit-uation and share relevant topics that emerge in group or individualsettings. All clinical staff members undergo biweekly psychody-namic supervision sessions provided by an experienced psychiatristto avoid burnout, empower the clinical team and improve theoverall effectiveness of the multidisciplinary treatment.
Participants and measures
Participants
In this study, we enrolled 56 adult patients with AN who wereconsecutively admitted to the DH of the Eating DisordersProgram at the San Giovanni Battista Hospital of the Universityof Turin in Turin, Italy from September 2009 to August 2012.Partially hospitalized patients who were diagnosed with BN(N=8) were excluded from this study. All participants met thediagnostic criteria of the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I; First, Spitzer, Gibbon, & Williams,1997) for both subtypes of AN (restricting, AN-R; andbingeing–purging, AN-BP). AN patients who had a BMI of 17.5or above (stepped-down after inpatient hospitalization) withpersistent eating psychopathology were considered to be eitherpartially (BMI ≤17.5 and ≤18.5) or fully (BMI ≥18.5) weight-restored (AN-WR) patients. All patients had amenorrhea andunderwent the same DH treatment described earlier.
Assessment and measures
Using a naturalistic design, we assessed changes in weight andoverall psychological functioning at baseline (T0), at the end oftreatment (EOT) and at a 12-month follow-up evaluation (T18).All of the clinician-administered assessments performed duringthis study were conducted by researchers who were not involvedin the patients’ clinical management. After obtaining writteninformed consent in accordance with the Ethical Committee ofthe Department of Neuroscience at the University of Turin, allparticipants were assessed using self-report questionnaires at allof the time-points (see succeeding sections). In addition, patients’BMIs were measured and all patients were interviewed in-personby a psychiatrist.
Eating psychopathology
The Eating Disorders Inventory-2 (EDI-2; Garner, 1991) is apsychometrically robust (Thiel & Paul, 2006) self-report measureof disordered eating attitudes, behaviours and personality traitscommon to individuals who are diagnosed with an eating disor-der. Eleven subscales evaluate the symptoms and psychologicalcorrelates of eating disorders; high scores reflect more severepathology.
Depressive and anxious symptomatology
The Beck Depression Inventory (Beck, Ward, Mendelson,Mock, & Erbaugh, 1961) is a self-report questionnaire with goodpsychometric properties (Beck, Steer, & Garbin, 1988) that is usedto evaluate the severity of depressive symptoms. Each answer onthe questionnaire is rated from 0 to 3; in patients who have beenclinically diagnosed with depression, scores from 0 to 4 represent

Day Hospital Treatment for Anorexia Nervosa G. Abbate-Daga et al.
minimal depressive symptoms, scores from 5 to 7 indicate milddepression, scores from 8 to 15 indicate moderate depression andscores from 16 to 39 indicate severe depression.
The Hamilton Rating Scale for Anxiety (HAM-A) is a clinician-administered scale measuring anxiety severity (Hamilton, 1959).Scores can range from 0 to 56, where 0–7 suggests no or minimalsymptoms, 8–14 indicates mild anxiety, 15–23 indicates moderateanxiety, and ≥24 indicates severe anxiety). HAM-A has showngood reliability, validity and sensitivity to change in previousstudies (Maier, Buller, Philipp, & Heuser, 1988).
The Brief Social Phobia Scale (Davidson et al., 1997) is aclinician-rated measure of social phobia symptoms that showsgood psychometric properties (Davidson et al., 1997); it con-sists of 11 items, of which seven evaluate commonly feared oravoided situations and four evaluate additional items relatedto autonomic distress.
Outcomes
At the EOT, the outcome was considered good, intermediate orpoor according to the following criteria: (1) Good: remissioncriteria, as proposed by Kordy et al. (2002), including a BMI>17.5, the absence of bingeing–purging episodes and normalscores on EDI-2 subscales 1–3 (drive for thinness, bulimia andbody dissatisfaction); (2) Intermediate: an increase in BMI with-out achieving a BMI >17.5, bingeing–purging episodes ≤1/week,scores on EDI-2 subscales 1–3 that are within 1 SD of the norm;and (3) Poor: the absence of improvement in either BMI orbingeing–purging symptoms and scores on EDI-2 subscales 1–3that are outside of the statistical norm.
At the T18, the outcome was considered good, intermediateor poor according to the following criteria: (1) Good: recoveryand remission, as proposed by Kordy et al. (2002), whererecovery is defined as a BMI >19, the absence of bingeing–purging episodes and normal scores on EDI-2 subscales 1–3(drive for thinness, bulimia and body dissatisfaction), and re-mission is defined as a BMI >17.5, the absence of bingeing–purging episodes and normal scores on EDI-2 subscales 1–3;(2) Intermediate: BMI is increased compared with the EOTbut is still <17.5, bingeing–purging episodes ≤1/week andscores on EDI-2 subscales 1–3 that are within 1 SD of thenorm; and (3) Poor: failure to either maintain or improveBMI, bingeing–purging symptoms and scores on EDI-2 sub-scales 1–3 that are outside of the statistical norm.
Eating psychopathology was assessed using both the EDI-2 andthe SCID-I.
Statistical analysis
Our sample size estimation was based on the EDI-2 globalscore variation between T0 and T18. Assuming a standard devia-tion of 50 and an effect (μ2�μ1) of 20 units, a total of 51 patientswere required to achieve a power of 80% with a two-sided alphaerror of 0.05.
A lost-case analysis was performed to ascertain whether thosewho dropped out of the study differed from participants whocompleted the study. Baseline continuous and categorical vari-ables were examined using the Mann–Whitney–Wilcoxon testand the Fisher’s exact test, respectively.
Eur.
Quantitative measures were described using means, standarddeviations (SD) and relative 95% confidence intervals (95% CI).Changes between different time-points were analysed usingan analysis of variance (ANOVA) for repeated measure models;to analyse the differences between time-points, a specific post-hoc analysis was performed using Student’s t-test for paired dataand was properly adjusted for the multiple significance levels ofcomparisons. The effect size of all of our findings was measuredusing the partial eta squared (ηP
2) calculation. According toCohen’s study (1988), the effect size can be interpreted as beingsmall (ηP
2 = 0.01–0.06), moderate (ηP2 = 0.06–0.14) or large
(ηP2> 0.14).Repeated measures ANOVA models were also performed to
compare changes over time during the period from T0 to T18within AN diagnostic groups. The most relevant results are pre-sented in the text.
All statistical analyses were performed using STATA statisticalsoftware (StataCorp. Statistical Software: Release 7.0. CollegeStation, TX: Stata Corporation. 2001).
Results
Baseline assessments
Clinical features of the sample
All of our patients were Caucasian women. With regard todiagnostic subtypes, 34 were AN-R and 22 were AN-BP. In thelatter group, the mean number of weekly bingeing episodes atbaseline was 4.86 (SD=4.91) and the mean number of weeklypurging episodes was 9.5 (SD= 14.91). The number of restored-weight patients was 12 (N= 3 AN-R and N=9 AN-BP, Fisher’sexact test p=0.007).
The mean age of the sample was 25.03 years (SD= 5.75), themean age at onset was 17.33 years (SD= 3.34) and the mean dura-tion of illness was 7.8 years (SD= 5.34, range: 0.8–24). The meanbaseline BMI of the entire sample was 16.31 (SD= 2.66); however,the mean baseline BMI dropped to 15.37 (SD= 0.25) if theweight-restored patients were excluded from the analysis.
Thirty-one patients (55%) had a long-standing duration ofillness (7 or more years, as defined by Maguire et al., 2008). Themean BMI of this subsample, excluding weight-restored patients,was 15.03 (SD= 1.74), the mean age of onset was 16.87 years(SD=3.5), the mean age was 28.41 years (SD= 4.8) and the meanduration of illness was 11.66 years (SD= 3.9).
Most participants had comorbid Axis I (N=47, 83.9%) andAxis II (N=38, 67.9%) disorders; in particular, 27 (48.2%)individuals had an anxiety disorder and 43 (76.8%) individualshad a depressive disorder (Table 1). Moreover, the majority ofpatients had failed previous treatments (N=42, 75%) such as res-idential (N=5, 11.9%), outpatient (N= 16, 38.1%) and combined(N=21, 50%) treatments. Six patients (10.7%) were not on anypsychiatric medications, 17 (30.4%) received monotherapy and33 (58.9%) received multiple medications. Thirty-nine patients(69.6%) were on selective serotonin reuptake inhibitors (SSRIs)and 10 (17%) patients were on an atypical antipsychotic inaddition to the SSRI. Finally, the majority of the sample had beenhospitalized during the prior year (N= 40, 71.4%). For furtherdetails, see Table 1.
Eat. Disorders Rev. (2015)© 2015 John Wiley & Sons, Ltd and Eating Disorders Association.
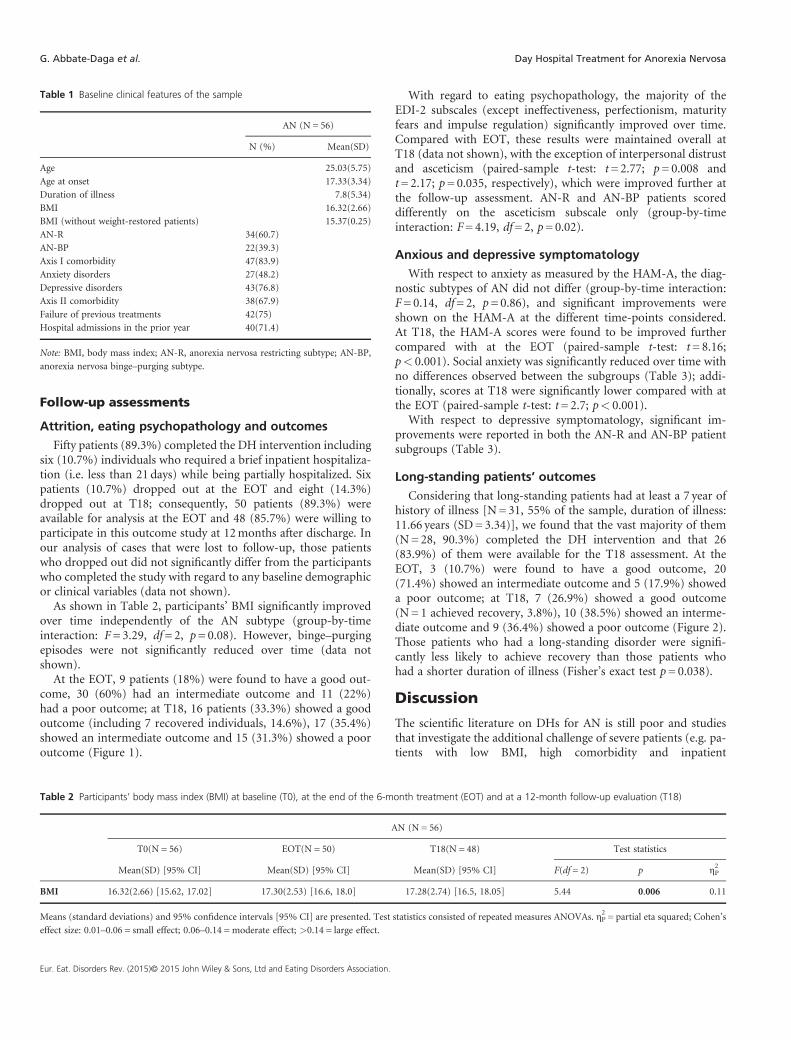
Table 1 Baseline clinical features of the sample
AN (N = 56)
N (%) Mean(SD)
Age 25.03(5.75)
Age at onset 17.33(3.34)
Duration of illness 7.8(5.34)
BMI 16.32(2.66)
BMI (without weight-restored patients) 15.37(0.25)
AN-R 34(60.7)
AN-BP 22(39.3)
Axis I comorbidity 47(83.9)
Anxiety disorders 27(48.2)
Depressive disorders 43(76.8)
Axis II comorbidity 38(67.9)
Failure of previous treatments 42(75)
Hospital admissions in the prior year 40(71.4)
Note: BMI, body mass index; AN-R, anorexia nervosa restricting subtype; AN-BP,
anorexia nervosa binge–purging subtype.
G. Abbate-Daga et al. Day Hospital Treatment for Anorexia Nervosa
Follow-up assessments
Attrition, eating psychopathology and outcomes
Fifty patients (89.3%) completed the DH intervention includingsix (10.7%) individuals who required a brief inpatient hospitaliza-tion (i.e. less than 21 days) while being partially hospitalized. Sixpatients (10.7%) dropped out at the EOT and eight (14.3%)dropped out at T18; consequently, 50 patients (89.3%) wereavailable for analysis at the EOT and 48 (85.7%) were willing toparticipate in this outcome study at 12months after discharge. Inour analysis of cases that were lost to follow-up, those patientswho dropped out did not significantly differ from the participantswho completed the study with regard to any baseline demographicor clinical variables (data not shown).
As shown in Table 2, participants’ BMI significantly improvedover time independently of the AN subtype (group-by-timeinteraction: F=3.29, df=2, p=0.08). However, binge–purgingepisodes were not significantly reduced over time (data notshown).
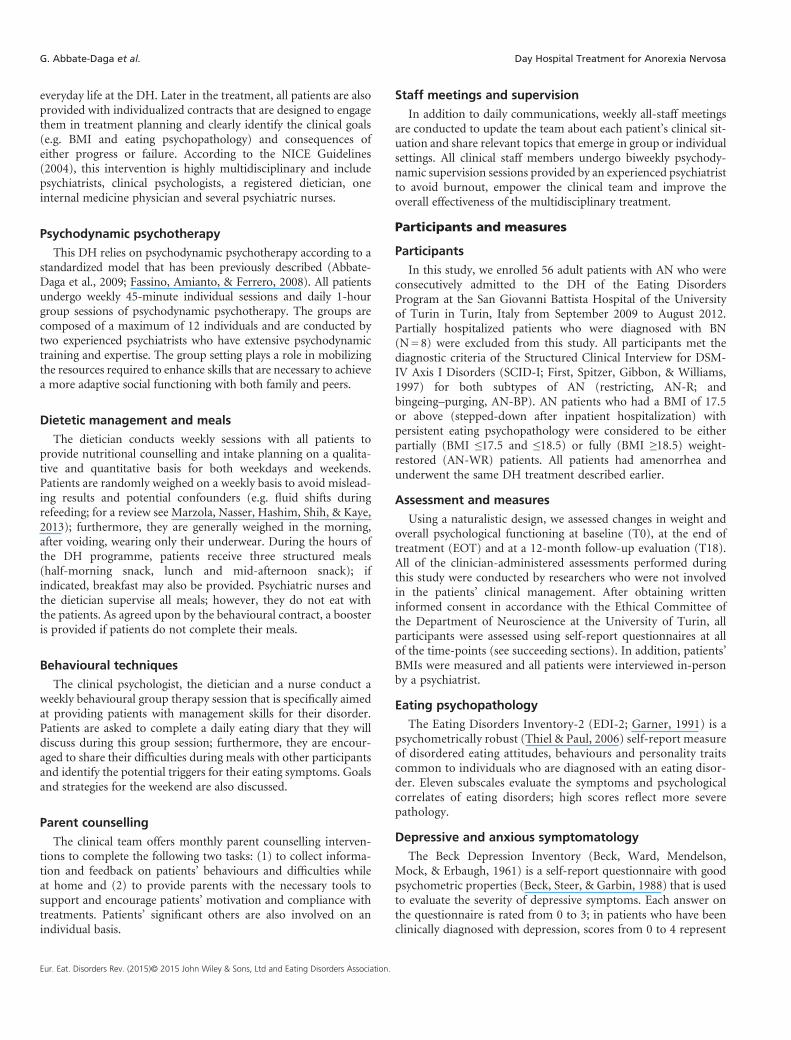
At the EOT, 9 patients (18%) were found to have a good out-come, 30 (60%) had an intermediate outcome and 11 (22%)had a poor outcome; at T18, 16 patients (33.3%) showed a goodoutcome (including 7 recovered individuals, 14.6%), 17 (35.4%)showed an intermediate outcome and 15 (31.3%) showed a pooroutcome (Figure 1).
Table 2 Participants’ body mass index (BMI) at baseline (T0), at the end of the 6-m
T0(N = 56) EOT(N = 50)
Mean(SD) [95% CI] Mean(SD) [95% CI]
BMI 16.32(2.66) [15.62, 17.02] 17.30(2.53) [16.6, 18.0]
Means (standard deviations) and 95% confidence intervals [95% CI] are presented. Test
effect size: 0.01–0.06 = small effect; 0.06–0.14 =moderate effect; >0.14 = large effect.
Eur. Eat. Disorders Rev. (2015)© 2015 John Wiley & Sons, Ltd and Eating Disorders Association.
With regard to eating psychopathology, the majority of theEDI-2 subscales (except ineffectiveness, perfectionism, maturityfears and impulse regulation) significantly improved over time.Compared with EOT, these results were maintained overall atT18 (data not shown), with the exception of interpersonal distrustand asceticism (paired-sample t-test: t=2.77; p=0.008 andt=2.17; p=0.035, respectively), which were improved further atthe follow-up assessment. AN-R and AN-BP patients scoreddifferently on the asceticism subscale only (group-by-timeinteraction: F=4.19, df=2, p=0.02).
Anxious and depressive symptomatology
With respect to anxiety as measured by the HAM-A, the diag-nostic subtypes of AN did not differ (group-by-time interaction:F=0.14, df=2, p=0.86), and significant improvements wereshown on the HAM-A at the different time-points considered.At T18, the HAM-A scores were found to be improved furthercompared with at the EOT (paired-sample t-test: t=8.16;p< 0.001). Social anxiety was significantly reduced over time withno differences observed between the subgroups (Table 3); addi-tionally, scores at T18 were significantly lower compared with atthe EOT (paired-sample t-test: t=2.7; p< 0.001).
With respect to depressive symptomatology, significant im-provements were reported in both the AN-R and AN-BP patientsubgroups (Table 3).
Long-standing patients’ outcomes
Considering that long-standing patients had at least a 7 year ofhistory of illness [N=31, 55% of the sample, duration of illness:11.66 years (SD= 3.34)], we found that the vast majority of them(N=28, 90.3%) completed the DH intervention and that 26(83.9%) of them were available for the T18 assessment. At theEOT, 3 (10.7%) were found to have a good outcome, 20(71.4%) showed an intermediate outcome and 5 (17.9%) showeda poor outcome; at T18, 7 (26.9%) showed a good outcome(N=1 achieved recovery, 3.8%), 10 (38.5%) showed an interme-diate outcome and 9 (36.4%) showed a poor outcome (Figure 2).Those patients who had a long-standing disorder were signifi-cantly less likely to achieve recovery than those patients whohad a shorter duration of illness (Fisher’s exact test p=0.038).
Discussion
The scientific literature on DHs for AN is still poor and studiesthat investigate the additional challenge of severe patients (e.g. pa-tients with low BMI, high comorbidity and inpatient
onth treatment (EOT) and at a 12-month follow-up evaluation (T18)
AN (N = 56)
T18(N = 48) Test statistics
Mean(SD) [95% CI] F(df = 2) p ηP2
17.28(2.74) [16.5, 18.05] 5.44 0.006 0.11
statistics consisted of repeated measures ANOVAs. ηP2= partial eta squared; Cohen’s
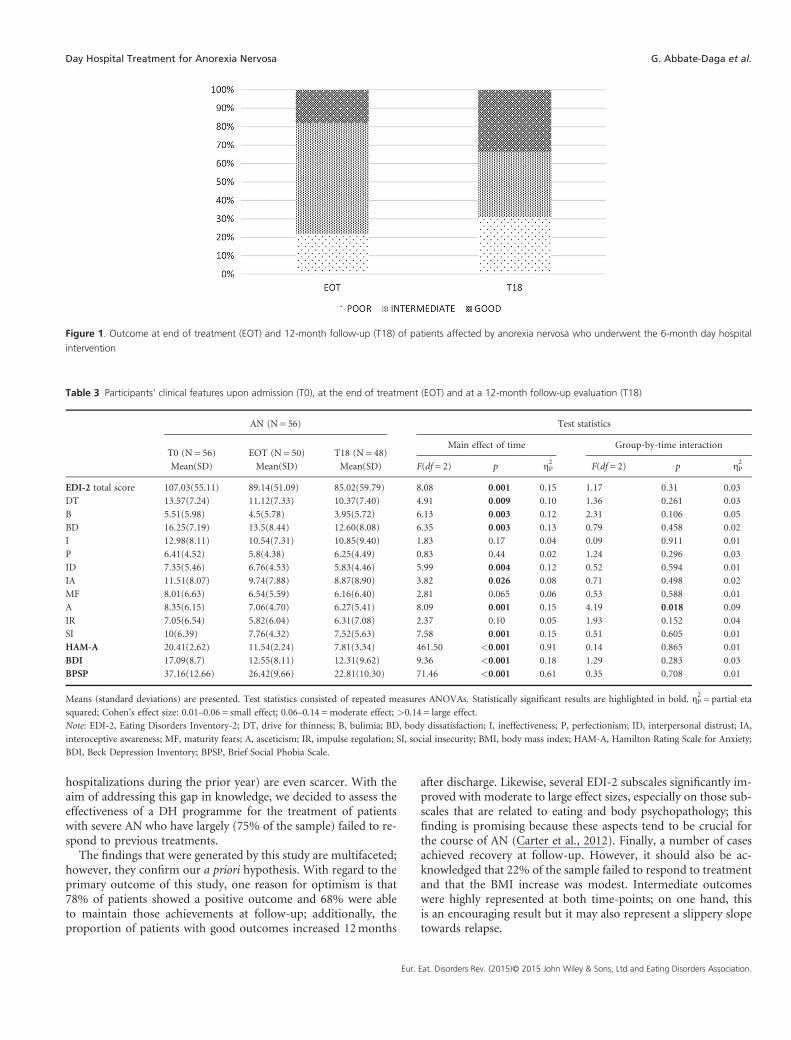
Figure 1. Outcome at end of treatment (EOT) and 12-month follow-up (T18) of patients affected by anorexia nervosa who underwent the 6-month day hospital
intervention
Table 3 Participants’ clinical features upon admission (T0), at the end of treatment (EOT) and at a 12-month follow-up evaluation (T18)
AN (N = 56) Test statistics
T0 (N = 56) EOT (N = 50) T18 (N = 48)Main effect of time Group-by-time interaction
Mean(SD) Mean(SD) Mean(SD) F(df = 2) p ηP2
F(df = 2) p ηP2
EDI-2 total score 107.03(55.11) 89.14(51.09) 85.02(59.79) 8.08 0.001 0.15 1.17 0.31 0.03
DT 13.57(7.24) 11.12(7.33) 10.37(7.40) 4.91 0.009 0.10 1.36 0.261 0.03
B 5.51(5.98) 4.5(5.78) 3.95(5.72) 6.13 0.003 0.12 2.31 0.106 0.05
BD 16.25(7.19) 13.5(8.44) 12.60(8.08) 6.35 0.003 0.13 0.79 0.458 0.02
I 12.98(8.11) 10.54(7.31) 10.85(9.40) 1.83 0.17 0.04 0.09 0.911 0.01
P 6.41(4.52) 5.8(4.38) 6.25(4.49) 0.83 0.44 0.02 1.24 0.296 0.03
ID 7.35(5.46) 6.76(4.53) 5.83(4.46) 5.99 0.004 0.12 0.52 0.594 0.01
IA 11.51(8.07) 9.74(7.88) 8.87(8.90) 3.82 0.026 0.08 0.71 0.498 0.02
MF 8.01(6.63) 6.54(5.59) 6.16(6.40) 2.81 0.065 0.06 0.53 0.588 0.01
A 8.35(6.15) 7.06(4.70) 6.27(5.41) 8.09 0.001 0.15 4.19 0.018 0.09
IR 7.05(6.54) 5.82(6.04) 6.31(7.08) 2.37 0.10 0.05 1.93 0.152 0.04
SI 10(6.39) 7.76(4.32) 7.52(5.63) 7.58 0.001 0.15 0.51 0.605 0.01
HAM-A 20.41(2.62) 11.54(2.24) 7.81(3.34) 461.50 <0.001 0.91 0.14 0.865 0.01
BDI 17.09(8.7) 12.55(8.11) 12.31(9.62) 9.36 <0.001 0.18 1.29 0.283 0.03
BPSP 37.16(12.66) 26.42(9.66) 22.81(10.30) 71.46 <0.001 0.61 0.35 0.708 0.01
Means (standard deviations) are presented. Test statistics consisted of repeated measures ANOVAs. Statistically significant results are highlighted in bold. ηP2= partial eta
squared; Cohen’s effect size: 0.01–0.06 = small effect; 0.06–0.14 =moderate effect; >0.14 = large effect.
Note: EDI-2, Eating Disorders Inventory-2; DT, drive for thinness; B, bulimia; BD, body dissatisfaction; I, ineffectiveness; P, perfectionism; ID, interpersonal distrust; IA,
interoceptive awareness; MF, maturity fears; A, asceticism; IR, impulse regulation; SI, social insecurity; BMI, body mass index; HAM-A, Hamilton Rating Scale for Anxiety;
BDI, Beck Depression Inventory; BPSP, Brief Social Phobia Scale.
Day Hospital Treatment for Anorexia Nervosa G. Abbate-Daga et al.
hospitalizations during the prior year) are even scarcer. With theaim of addressing this gap in knowledge, we decided to assess theeffectiveness of a DH programme for the treatment of patientswith severe AN who have largely (75% of the sample) failed to re-spond to previous treatments.
The findings that were generated by this study are multifaceted;however, they confirm our a priori hypothesis. With regard to theprimary outcome of this study, one reason for optimism is that78% of patients showed a positive outcome and 68% were ableto maintain those achievements at follow-up; additionally, theproportion of patients with good outcomes increased 12months
Eur.
after discharge. Likewise, several EDI-2 subscales significantly im-proved with moderate to large effect sizes, especially on those sub-scales that are related to eating and body psychopathology; thisfinding is promising because these aspects tend to be crucial forthe course of AN (Carter et al., 2012). Finally, a number of casesachieved recovery at follow-up. However, it should also be ac-knowledged that 22% of the sample failed to respond to treatmentand that the BMI increase was modest. Intermediate outcomeswere highly represented at both time-points; on one hand, thisis an encouraging result but it may also represent a slippery slopetowards relapse.
Eat. Disorders Rev. (2015)© 2015 John Wiley & Sons, Ltd and Eating Disorders Association.
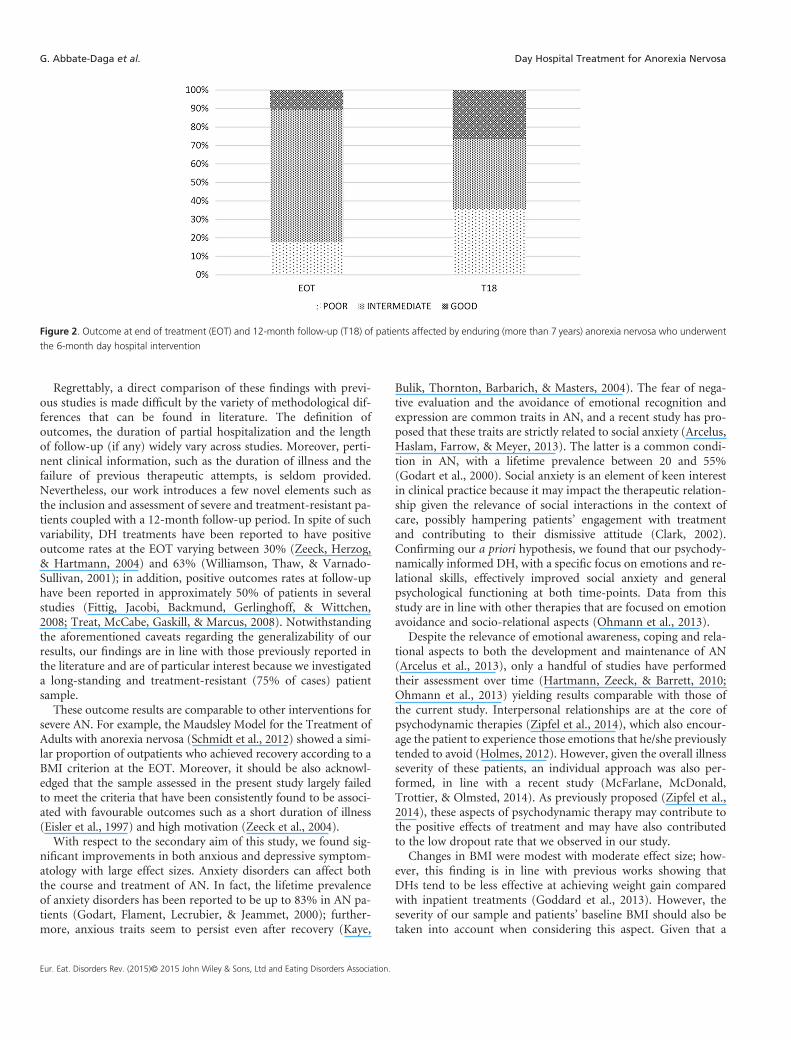
Figure 2. Outcome at end of treatment (EOT) and 12-month follow-up (T18) of patients affected by enduring (more than 7 years) anorexia nervosa who underwent
the 6-month day hospital intervention
G. Abbate-Daga et al. Day Hospital Treatment for Anorexia Nervosa
Regrettably, a direct comparison of these findings with previ-ous studies is made difficult by the variety of methodological dif-ferences that can be found in literature. The definition ofoutcomes, the duration of partial hospitalization and the lengthof follow-up (if any) widely vary across studies. Moreover, perti-nent clinical information, such as the duration of illness and thefailure of previous therapeutic attempts, is seldom provided.Nevertheless, our work introduces a few novel elements such asthe inclusion and assessment of severe and treatment-resistant pa-tients coupled with a 12-month follow-up period. In spite of suchvariability, DH treatments have been reported to have positiveoutcome rates at the EOT varying between 30% (Zeeck, Herzog,& Hartmann, 2004) and 63% (Williamson, Thaw, & Varnado-Sullivan, 2001); in addition, positive outcomes rates at follow-uphave been reported in approximately 50% of patients in severalstudies (Fittig, Jacobi, Backmund, Gerlinghoff, & Wittchen,2008; Treat, McCabe, Gaskill, & Marcus, 2008). Notwithstandingthe aforementioned caveats regarding the generalizability of ourresults, our findings are in line with those previously reported inthe literature and are of particular interest because we investigateda long-standing and treatment-resistant (75% of cases) patientsample.
These outcome results are comparable to other interventions forsevere AN. For example, the Maudsley Model for the Treatment ofAdults with anorexia nervosa (Schmidt et al., 2012) showed a simi-lar proportion of outpatients who achieved recovery according to aBMI criterion at the EOT. Moreover, it should be also acknowl-edged that the sample assessed in the present study largely failedto meet the criteria that have been consistently found to be associ-ated with favourable outcomes such as a short duration of illness(Eisler et al., 1997) and high motivation (Zeeck et al., 2004).
With respect to the secondary aim of this study, we found sig-nificant improvements in both anxious and depressive symptom-atology with large effect sizes. Anxiety disorders can affect boththe course and treatment of AN. In fact, the lifetime prevalenceof anxiety disorders has been reported to be up to 83% in AN pa-tients (Godart, Flament, Lecrubier, & Jeammet, 2000); further-more, anxious traits seem to persist even after recovery (Kaye,
Eur. Eat. Disorders Rev. (2015)© 2015 John Wiley & Sons, Ltd and Eating Disorders Association.
Bulik, Thornton, Barbarich, & Masters, 2004). The fear of nega-tive evaluation and the avoidance of emotional recognition andexpression are common traits in AN, and a recent study has pro-posed that these traits are strictly related to social anxiety (Arcelus,Haslam, Farrow, & Meyer, 2013). The latter is a common condi-tion in AN, with a lifetime prevalence between 20 and 55%(Godart et al., 2000). Social anxiety is an element of keen interestin clinical practice because it may impact the therapeutic relation-ship given the relevance of social interactions in the context ofcare, possibly hampering patients’ engagement with treatmentand contributing to their dismissive attitude (Clark, 2002).Confirming our a priori hypothesis, we found that our psychody-namically informed DH, with a specific focus on emotions and re-lational skills, effectively improved social anxiety and generalpsychological functioning at both time-points. Data from thisstudy are in line with other therapies that are focused on emotionavoidance and socio-relational aspects (Ohmann et al., 2013).
Despite the relevance of emotional awareness, coping and rela-tional aspects to both the development and maintenance of AN(Arcelus et al., 2013), only a handful of studies have performedtheir assessment over time (Hartmann, Zeeck, & Barrett, 2010;Ohmann et al., 2013) yielding results comparable with those ofthe current study. Interpersonal relationships are at the core ofpsychodynamic therapies (Zipfel et al., 2014), which also encour-age the patient to experience those emotions that he/she previouslytended to avoid (Holmes, 2012). However, given the overall illnessseverity of these patients, an individual approach was also per-formed, in line with a recent study (McFarlane, McDonald,Trottier, & Olmsted, 2014). As previously proposed (Zipfel et al.,2014), these aspects of psychodynamic therapy may contribute tothe positive effects of treatment and may have also contributedto the low dropout rate that we observed in our study.
Changes in BMI were modest with moderate effect size; how-ever, this finding is in line with previous works showing thatDHs tend to be less effective at achieving weight gain comparedwith inpatient treatments (Goddard et al., 2013). However, theseverity of our sample and patients’ baseline BMI should also betaken into account when considering this aspect. Given that a

Day Hospital Treatment for Anorexia Nervosa G. Abbate-Daga et al.
BMI of 19 and below has been shown to be a negative predictorfor DH treatments (Howard, Evans, Quintero-Howard, Bowers,& Andersen, 1999), the improvement that we report at the EOTand its maintenance at follow-up is valuable. In fact, for manypatients, the achievement of complete weight restoration over aperiod of a few months is beyond the realm of possibility (Strober,2010; Touyz et al., 2013). Nonetheless, this finding should notpreclude therapists from engaging these patients in treatmentand setting shared and safe goals (Bamford & Mountford, 2012)that are carefully matched to patients’ readiness to change (Touyz,Thornton, Rieger, George, & Beumont, 2003). Moreover, those‘in action programmes’ (Prochaska & DiClemente, 1983) thatare strictly focused on weight restoration may not be helpful forlong-standing patients, who are largely represented in our studysample. Because these patients are often characterized by a pre-contemplative stage of change or several previous treatmentfailures, some complementary therapeutic tools should be consid-ered closely. For example, the therapeutic alliance and the under-standing of both the adaptive function and burden of the illness(e.g. quality of life, social isolation) could represent a usefultherapeutic armamentarium. Such theoretical principles haveguided our work at the University of Turin and are in line withother renowned treatment centres (e.g. the Program of theUniversity of Sydney) with respect to focusing on patients’readiness to change the duration of their treatment (Touyzet al., 2003).
In line with previous literature (Eisler et al., 1997; Le Grangeet al., 2014), data from this study showed that long-standingpatients are less likely to achieve recovery. This finding shouldpave the way towards the development of early interventionsand tailored therapies for those who have an enduring illness(Hay et al., 2012). In the latter case, dynamic psychotherapy thatfocuses on emotive and relational aspects could represent asuitable treatment option; however, future studies will need toclarify its effectiveness.
Eur.
Finally, the impact of pharmacological treatments on the over-all outcome cannot be evaluated in this study. Our patients re-ceived different types of medications and this fact hampersdefinitive conclusions. Nonetheless, pharmacological therapiesare reported to be of limited effectiveness in AN (Walsh et al.,2006). Furthermore, medications were not modified during theDH treatment so a negligible effect of medications could be hy-pothesized given that the vast majority of patients failed previoustherapeutic attempts.
This study has several strengths such as its naturalistic designthat assumes a high external validity and the involvement of pa-tients who were particularly challenging to treat in everyday clin-ical practice. However, some limitations should be acknowledged.The sample size of our study was relatively small, the DH treat-ment lacked effectiveness in a number of cases and a longerfollow-up is likely warranted. It is also worth acknowledging thatour DH programme was only minimally effective in reducingbinge–purging episodes. Although cognitive approaches havebeen shown to be more effective in treating these episodes(Poulsen et al., 2014), more studies are needed to fill this gap inknowledge as it pertains to clinical practice. Finally, given thewell-known difficulties with conducting RCTs in AN patients(Halmi, 2008), there was no control group in our study.
In conclusion, our DH intervention provided support to theeffectiveness of a psychodynamic approach to individuals whoare affected by severe or long-standing AN, as hypothesized. Thedynamic interventions and the therapeutic challenge ofsocialization that were provided by the DH could enhance theseaspects. Further research is needed not only to confirm these re-sults but also to generate new ideas on how to stage this disorderand determine appropriate goals for long-standing patients.
Acknowledgements
None.
REFERENCES
Abbate-Daga, G., Amianto, F., Delsedime, N., De-Bacco, C., &
Fassino, S. (2013). Resistance to treatment and change in
anorexia nervosa [corrected]: A clinical overview. BMC Psychiatry,
13, 294.
Abbate-Daga, G., Gramaglia, C., Preda, S., Comba, E., Brustolin, A.,
& Fassino, S. (2009). Day hospital programmes for eating disor-
ders: A review of the similarities, differences and goals. Eating
and Weight Disorders, 14, e31–e41.
Abbate-Daga, G., Marzola, E., Gramaglia, C., Brustolin, A., Campisi,
S., De-Bacco, C., et al. (2012). Emotions in eating disorders:
Changes of anger control after an emotion-focused day hospital
treatment. European Eating Disorders Review, 20, 496–501.
American Psychiatric Association (2013). Diagnostic and Statistical
Manual of Mental Disorders: DSM-5 (5th ed.). Arlington, VA:
American Psychiatric Association.
Arcelus, J., Haslam, M., Farrow, C., & Meyer, C. (2013). The role of
interpersonal functioning in the maintenance of eating psycho-
pathology: A systematic review and testable model. Clinical
Psychology Review, 33, 156–167.
Arcelus, J., Mitchell, A. J., Wales, J., & Nielsen, S. (2011). Mortality
rates in patients with anorexia nervosa and other eating
disorders. A meta-analysis of 36 studies. Archives of General
Psychiatry, 68, 724–731.
Bamford, B. H., & Mountford, V. A. (2012). Cognitive behavioural
therapy for individuals with longstanding anorexia nervosa:
Adaptations, clinician survival and system issues. European
Eating Disorders Review, 20, 49–59.
Beck, A., Steer, R., & Garbin, M. (1988). Psychometric properties of
the beck depression inventory: Twenty-five years of evaluation.
Clinical Psychology Review, 1, 77–100.
Beck, A., Ward, C., Mendelson, M., Mock, J., & Erbaugh, J. (1961).
An inventory for measuring depression. Archives of General
Psychiatry, 4, 561–571.
Carter, J. C., Mercer-Lynn, K. B., Norwood, S. J., Bewell-Weiss, C. V.,
Crosby, R. D., Woodside, D. B., et al. (2012). A prospective study of
predictors of relapse in anorexia nervosa: Implications for relapse pre-
vention. Psychiatry Research, 200, 518–523.
Clark, D. M. (2002). A cognitive perspective on social phobia. In
Crozier, R., & Alden, L. E. (Eds.), International handbook of
social anxiety. Chichester: John Wiley.
Cohen, J. W. (1988). Statistical power analysis for the behavioral
sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum Associates.
Davidson, J. R., Miner, C. M., De Veaugh-Geiss, J., Tupler, L. A.,
Colket, J. T., & Potts, N. L. (1997). The Brief Social Phobia
Eat. Disorders Rev. (2015)© 20
Scale: A psychometric evaluation. Psychological Medicine, 27,
161–166.
Eisler, I., Dare, C., Russell, G. F., Szmukler, G., le Grange, D., &
Dodge, E. (1997). Family and individual therapy in anorexia
nervosa. A 5-year follow-up. Archives of General Psychiatry, 54,
1025–1030.
Fassino, S., Amianto, F., & Ferrero, A. (2008). Brief Adlerian psycho-
dynamic psychotherapy: Theoretical issues and process indica-
tors. Panminerva Medica, 50, 165–175.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1997).
Structured Clinical Interview for DSM IV Axis I Disorders
(SCID-I), clinician version, administration booklet. Washington,
DC: American Psychiatric Publishing.
Fittig, E., Jacobi, C., Backmund, H., Gerlinghoff, M., & Wittchen, H. U.
(2008). Effectiveness of day hospital treatment for anorexia
nervosa and bulimia nervosa. European Eating Disorders Review,
16, 341–351.
Garner, D. M. (1991). Eating Disorder Inventory 2: Professional
manual. Odessa: Psychological Assessment Resources.
Godart, N. T., Flament, M. F., Lecrubier, Y., & Jeammet, P. (2000).
Anxiety disorders in anorexia nervosa and bulimia nervosa:
Co-morbidity and chronology of appearance. European Psychiatry,
15, 38–45.
15 John Wiley & Sons, Ltd and Eating Disorders Association.

G. Abbate-Daga et al. Day Hospital Treatment for Anorexia Nervosa
Goddard, E., Hibbs, R., Raenker, S., Salerno, L., Arcelus, J.,
Boughton, N., et al. (2013). A multi-centre cohort study of short
term outcomes of hospital treatment for anorexia nervosa in the
UK. BMC Psychiatry, 13, 287.
Gramaglia, C., Abbate-Daga, G., Amianto, F., Brustolin, A., Campisi,
S., De-Bacco, C., et al. (2011). Cinematherapy in the day hospital
treatment of patients with eating disorders. Case study and
clinical considerations. Art Psychotherapy, 38, 261–266.
Halmi, K. A. (2008). The perplexities of conducting randomized,
double-blind, placebo-controlled treatment trials in anorexia
nervosa patients. The American Journal of Psychiatry, 165,
1227–1228.
Hamilton, M. (1959). The assessment of anxiety states by rating.
British Journal of Medical Psychology, 32, 50–55.
Hartmann, A., Zeeck, A., & Barrett, M. S. (2010). Interpersonal
problems in eating disorders. International Journal of Eating
Disorders, 43, 619–627.
Hay, P. J., Touyz, S., & Sud, R. (2012). Treatment for severe and en-
during anorexia nervosa: A review. The Australian and New
Zealand Journal of Psychiatry, 46, 1136–1144.
Hepburn, Z., &Wilson, K. (2014). Effectiveness of adult day treatment
for eating disorders. Mental Health Review Journal, 19, 131–144.
Holmes, J. (2012). Psychodynamic psychiatry’s green shoots. British
Journal of Psychiatry, 200, 439–441.
Howard, W. T., Evans, K. K., Quintero-Howard, C. V., Bowers, W.
A., & Andersen, A. E. (1999). Predictors of success or failure of
transition to day hospital treatment for inpatients with anorexia
nervosa. The American Journal of Psychiatry, 156, 1697–1702.
Kaye, W. H., Bulik, C. M., Thornton, L., Barbarich, N., & Masters, K.
(2004). Comorbidity of anxiety disorders with anorexia and
bulimia nervosa. The American Journal of Psychiatry, 161,
2215–2221.
Kaye, W. H., Fudge, J. L., & Paulus, M. (2009). New insights into
symptoms and neurocircuit function of anorexia nervosa. Nature
Review Neuroscience, 10, 573–584.
Kordy, H., Krämer, B., Palmer, R. L., Papezova, H., Pellet, J., Richard,
M., et al. (2002). Remission, recovery, relapse, and recurrence in
eating disorders: Conceptualization and illustration of a valida-
tion strategy. Journal of Clinical Psychology, 58, 833–846.
Le Grange, D., Fitzsimmons-Craft, E. E., Crosby, R. D., Hay, P.,
Lacey, H., Bamford, B., et al. (2014). Predictors and moderators
of outcome for severe and enduring anorexia nervosa. Behaviour
Research and Therapy, 56, 91–98.
Eur. Eat. Disorders Rev. (2015)© 2015 John Wiley & Sons, Ltd a
Maguire, S., Le Grange, D., Surgenor, L., Marks, P., Lacey, H., &
Touyz, S. (2008). Staging anorexia nervosa: Conceptualizing ill-
ness severity. Early Intervention in Psychiatry, 2, 3–10.
Maier, W., Buller, R., Philipp, M., & Heuser, I. (1988). The Hamilton
Anxiety Scale: Reliability, validity and sensitivity to change in
anxiety and depressive disorders. Journal of Affective Disorders,
14, 61–68.
Marzola, E., Nasser, J. A., Hashim, S. A., Shih, P. A., & Kaye, W. H.
(2013). Nutritional rehabilitation in anorexia nervosa: Review of
the literature and implications for treatment. BMC Psychiatry,
13, 290.
McFarlane, T., MacDonald, D. E., Trottier, K., & Olmsted, M. P.
(2014). The effectiveness of an individualized form of day hospi-
tal treatment. Eating Disorders, 20, 1–15.
National Institute for Health and Care Excellence (2004). Core inter-
ventions in the treatment and management of anorexia nervosa,
bulimia nervosa and related eating disorders (Clinical Guideline
9). London: National Collaborating Centre for Medical Health.
Ohmann, S., Popow, C., Wurzer, M., Karwautz, A., Sackl-Pammer,
P., & Schuch, B. (2013). Emotional aspects of anorexia nervosa:
Results of prospective naturalistic cognitive behavioral group
therapy. Neuropsychiatrie, 27, 119–128.
Poulsen, S., Lunn, S., Daniel, S. I., Folke, S., Mathiesen, B. B.,
Katznelson, H., et al. (2014). A randomized controlled trial of
psychoanalytic psychotherapy or cognitive-behavioral therapy
for bulimia nervosa. The American Journal of Psychiatry, 171,
109–116.
Prochaska, J. O., & DiClemente, C. C. (1983). Stages and processes
of self-change of smoking: Toward an integrative model of
change. Journal of Consulting and Clinical Psychology, 51,
390–395.
Racine, S. E., & Wildes, J. E. (2013). Emotion dysregulation and
symptoms of anorexia nervosa: The unique roles of lack of emo-
tional awareness and impulse control difficulties when upset.
International Journal of Eating Disorders, 46, 713–720.
Schmidt, U., Oldershaw, A., Jichi, F., Sternheim, L., Startup, H.,
McIntosh, V., et al. (2012). Out-patient psychological therapies
for adults with anorexia nervosa: Randomised controlled trial.
British Journal of Psychiatry, 201, 392–399.
Schmidt, U., & Treasure, J. (2006). Anorexia nervosa: Valued and
visible. A cognitive-interpersonal maintenance model and its im-
plications for research and practice. British Journal of Clinical
Psychology, 45, 343–366.
nd Eating Disorders Association.
Strober, M. (2010). The chronically ill patient with anorexia nervosa:
Development, phenomenology and therapeutic considerations.
In Grilo, C. M., & Mitchell, J. E. (Eds.), The treatment of eating
disorders: A clinical handbook (ed., pp. 225 – 238). New York:
Guilford.
Thiel, A., & Paul, T. (2006). Test-retest reliability of the Eating Dis-
order Inventory 2. Journal of Psychosomatic Research, 61,
567–569.
Touyz, S., Le Grange, D., Lacey, H., Hay, P., Smith, R., Maguire, S.,
et al. (2013). Treating severe and enduring anorexia nervosa: A
randomized controlled trial. Psychological Medicine, 43,
2501–2511.
Touyz, S., Thornton, C., Rieger, E., George, L., & Beumont, P.
(2003). The incorporation of the stage of change model in the
day hospital treatment of patients with anorexia nervosa.
European Child and Adolescent Psychiatry, 12, 65–71.
Treat, T. A., McCabe, E. B., Gaskill, J. A., & Marcus, M. D. (2008).
Treatment of anorexia nervosa in a specialty care continuum.
International Journal of Eating Disorders, 41, 564–572.
Walsh, B. T., Kaplan, A. S., Attia, E., Olmsted, M., Parides, M.,
Carter, J. C., et al. (2006). Fluoxetine after weight restoration in
anorexia nervosa: A randomized controlled trial. JAMA, 14,
2605–2612.
Wildes, J. E., & Marcus, M. D. (2011). Development of emotion
acceptance behavior therapy for anorexia nervosa: A case series.
International Journal of Eating Disorders, 44, 421–427.
Williamson, D. A., Thaw, J. M., & Varnado-Sullivan, P. J. (2001).
Cost-effectiveness analysis of a hospital-based cognitive-
behavioral treatment program for eating disorders. Behavior
Therapy, 32, 459–477.
Yager, J., Devlin, M. J., Halmi, K. A., Herzog, D. B., Mitchell, J. E.,
Powers, P., et al. (2012). Guideline watch (August 2012): Practice
guideline for the treatment of patients with eating disorders 3rd
ed.. American Psychiatric Association online publication http://
psychiatryonline.org.
Zeeck, A., Herzog, T., & Hartmann, A. (2004). Day clinic or inpa-
tient care for severe bulimia nervosa? European Eating Disorders
Review, 12, 79–86.
Zipfel, S., Wild, B., Groß, G., Friederich, H. C., Teufel, M.,
Schellberg, D., et al. (2014). Focal psychodynamic therapy, cog-
nitive behaviour therapy, and optimised treatment as usual in
outpatients with anorexia nervosa (ANTOP study): Randomised
controlled trial. Lancet, 383, 127–137.