context-aware based quality of life telemonitoring
TRANSCRIPT
Metadata of the chapter that will be visualized inSpringerLink
Book Title Distributed Systems and Applications of Information Filtering and RetrievalSeries Title 7092
Chapter Title Context-Aware Based Quality of Life Telemonitoring
Copyright Year 2014
Copyright HolderName Springer-Verlag Berlin Heidelberg
Corresponding Author Family Name VargiuParticle
Given Name EloisaSuffix
Division
Organization Barcelona Digital Technology Center
Address Barcelona, Spain
Email [email protected]
Author Family Name FernándezParticle
Given Name Juan ManuelSuffix
Division
Organization Barcelona Digital Technology Center
Address Barcelona, Spain
Email [email protected]
Author Family Name MirallesParticle
Given Name FelipSuffix
Division
Organization Barcelona Digital Technology Center
Address Barcelona, Spain
Email [email protected]
Abstract Telemonitoring Quality of Life of individuals is the base for current and future telemedicine andteleassistance solutions which will become paramount in the sustainability and effectiveness of healthcaresystems. In the framework of the BackHome European R&D project, which aims to provide atelemonitoring and home support system using Brain Computer Interfaces and other assistive technologiesto improve autonomy and quality of life of disabled people, we propose a methodology to assess andtelemonitor quality of life of individuals based on the awareness of user context. This methodology holds ageneric approach to be applied to other eHealth use cases and is based on the acquisition, fusion andprocessing of heterogeneous data coming from sensors, devices, and user interaction, and the knowledgeinferred from the correlation of this processed data and the input coming from our proposed questionnairesmapped to standard taxonomies. The proposed methodology is very ambitious and although we arepresenting preliminary validation, it will have to be formally validated and enhanced with the study ofrepresentative user data which will be acquired within BackHome and other related projects.

UN
CO
RR
EC
TE
D P
RO
OF
Chapter 1Context-Aware Based Quality of LifeTelemonitoring
Eloisa Vargiu, Juan Manuel Fernández and Felip Miralles
Abstract Telemonitoring Quality of Life of individuals is the base for current and1
future telemedicine and teleassistance solutions which will become paramount in2
the sustainability and effectiveness of healthcare systems. In the framework of the3
BackHome European R&D project, which aims to provide a telemonitoring and home4
support system using Brain Computer Interfaces and other assistive technologies to5
improve autonomy and quality of life of disabled people, we propose a methodology6
to assess and telemonitor quality of life of individuals based on the awareness of user7
context. This methodology holds a generic approach to be applied to other eHealth8
use cases and is based on the acquisition, fusion and processing of heterogeneous9
data coming from sensors, devices, and user interaction, and the knowledge inferred10
from the correlation of this processed data and the input coming from our proposed11
questionnaires mapped to standard taxonomies. The proposed methodology is very12
ambitious and although we are presenting preliminary validation, it will have to be13
formally validated and enhanced with the study of representative user data which14
will be acquired within BackHome and other related projects.15
1 Introduction16
The demographic trend of our ageing society is partly due to the amazing progress17
of medicine in the last decades, which has increased life expectancy and improved18
quality of life, specially to people living in developed countries.19 AQ1
E. Vargiu (B) · J. Manuel Fernández · F. MirallesBarcelona Digital Technology Center, Barcelona, Spaine-mail: [email protected]
J. Manuel Fernándeze-mail: [email protected]
F. Mirallese-mail: [email protected]
C. Lai et al. (eds.), Distributed Systems and Applications of Information Filtering, 1and Retrieval, Studies in Computational Intelligence 515,DOI: 10.1007/978-3-642-40621-8_1, © Springer-Verlag Berlin Heidelberg 2014
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f

UN
CO
RR
EC
TE
D P
RO
OF
2 E. Vargiu et al.
However, this demographic shift comes along with an important stress to our20
healthcare systems, which nowadays face sustainability problems.21AQ2
Design of solutions which take advantage of new Information and Communica-22
tion Technologies (ICT) provide efficiency, efficacy and cost-effectiveness to care23
practice. Telemedicine solutions allow treating chronic patients living at home, pre-24
venting and predicting exacerbations and decrease costly hospitalizations. Telereha-25
bilitation solutions enable following continuous interventions which may improve26
health conditions without the need for the patient to physically move to specialized27
facilities. Teleassistance solutions facilitate improving autonomy, safety and social28
participation of people with special needs, namely the elderly and in particular the29
disabled, through home support technologies which postpone socio-sanitary services30
and associated costs.31AQ3
One key common feature of all those novel eHealth solutions is telemonitoring,32
which makes possible to remotely assess health status and quality of life of individu-33
als. By acquiring heterogeneous data coming from sensors (physiological, biometric,34
environmental; non invasive, adaptive and transparent to user) and data coming from35
other sources (e.g., interaction of the user with digital services) to become aware36
of user context; by inferring user behaviour and detecting anomalies from this data;37
and by providing elaborated and smart knowledge to clinicians, therapists, carers,38
families, and the patients themselves, we will be able to foster preventive, predictive39
and personalized care actions, decisions and support.40AQ4
In the context of an assistive environment that provides home support to people41
with disabilities, in this chapter we propose a generic methodology to telemonitor42
quality of life of individuals with a holistic bio-psycho-social approach, which intends43
to become the base for current and future telemedicine and teleassistance solutions.44
The chapter is organized as follows, Sect. 2 resumes main related work concerning45
quality of life assessment, context-aware user profiling, and telemonitoring and home46
support. In Sect. 3, we summarize the objective of the project in which the proposed47
methodology is studied. Section 4 presents and discusses the proposed methodology48
together with preliminary experimental results. Section 5 ends the chapter with some49
conclusions.50
2 Background51
In this chapter, we are interested in presenting a general methodology to telemonitor52
quality of life through a context-aware solution. To give a view of all the related53
issues, in this section, we focus on relevant work on quality of life assessment,54
context-aware user profiling, and telemonitoring and home support.55
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 3
2.1 Quality of Life Assessment56
2.1.1 Definitions57
QoL (sometimes refereed to as Health-Related QoL or HRQoL) is defined by the58
subjective experiences or preferences expressed by an individual, or members of a59
particular group of persons, in relation to specified aspects of health status that are60
meaningful, in definable ways, for that individual or group [50]. According to [19],61
QoL is a state of well-being defined by two components: (i) the ability to perform62
everyday activities, which reflects physical, psychological and social well-being,63
and patient satisfaction with levels of functioning, and (ii) the control of disease64
and treatment symptoms. Also, as Lerer [26] suggests, e-health consumers are now65
empowered by an increased ability to obtain health information via the Internet, with66
the main objective to maintain the highest possible level of QoL.67
The World Health Organization (WHO) defines QoL as the individuals’ percep-68
tion on their position in life within the cultural context and the value system in69
which the individuals live and with respect to their goals, expectations, norms and70
worries [58]. It is a multidimensional and complex concept that includes personal71
aspects, like health, autonomy, independence, satisfaction with life and environmen-72
tal aspects such as support networks and social services, among others. The World73
Health Organization Quality of Life (WHOQOL) project [48] has the aim to develop74
an international, cross-cultural QoL-assessment instrument based on this definition.75
The WHOQOL instrument was collaboratively developed in a number of centers76
worldwide, and has been widely field-tested.77
Patrick et al. [41] define QoL as the value assigned to life duration based on78
the perception of physical, psychological, and social limitations. According to their79
view, QoL is related to the reduction in opportunities due to diseases, their sequel,80
treatment, and to health policies. Naughton et al. [37] define QoL as the subjective81
perception, influenced by the current health status, of the ability to realize activities82
important for the person.83
QoL could also be considered as a dynamic and changing concept that includes84
continuous interactions between the person and the environment. Accordingly, QoL85
in ill people is related to the interaction among the disease, the patients’ character,86
the change in their life, the received social support, as well as the period of life in87
which the disease appears.88
Healthcare organizations use several tools to acquire QoL-related information.89
These tools make use of specific terms, which are sometimes ambiguous: descriptor,90
grade, item, index, indicator, parameter, questionnaire, scale, score, and test. The91
terminology used in this chapter is part of an ontology (and encoded in OWL 2 [22])92
and is defined as follows [9]:93
• Indicator: a (subjective or objective) parameter, category, or descriptor used to94
measure or compare activities and participation, body functions, body structures,95
environment factors, processes, and results (e.g., dressing).96
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
4 E. Vargiu et al.
• Index: a combination of indicators, questionnaires and possibly other indexes. The97
function representing this combination gives as summarizing result a score (e.g.,98
Barthel index).99
• Item: a single question or concept (e.g., Mobility).100
• Questionnaire (or instrument or test): a set of questions (or items) answered using101
a scale (e.g., EQ-5D).102
• Scale: a mapping between some ordered (qualitative or quantitative) values (or103
grades) and their description. These values are used to answer questionnaires (e.g.,104
I have no problems in walking about, I have some problems in walking about, I105
am confined to bed).106
2.1.2 Questionnaires for Assessment of Quality of Life107
Several questionnaires have been proposed and adopted to assess QoL. Let us sum-108
marize here the most widely adopted:109
• The WHOQOL-BREF questionnaire [35] comprises 26 items, which measure the110
following broad domains: physical health, psychological health, social relation-111
ships, and environment.112
• The EQ-5D-5L questionnaire [51] was developed by the EuroQol Group in order113
to provide a generic measure of health status. Applicable to a wide range of health114
conditions and treatments, it provides a simple descriptive profile and a single115
value for health status that can be used in the clinical and economic evaluation of116
healthcare as well as in population health surveys.117
• The RAND-36 questionnaire [21] is comprised of 36 items that assess eight health118
concepts: physical functioning, role limitations caused by physical health prob-119
lems, role limitations caused by emotional problems, social functioning, emotional120
well-being, energy/fatigue, pain, and general health perceptions.121
• The Short Form (36) Health Survey (SF-36v2) [57] is a questionnaire about patient122
health status and is commonly used in health economics in the quality-adjusted123
life year calculation to determine the cost-effectiveness of a health treatment. The124
SF-36 and RAND-36 include the same set of items, however the scoring of general125
health and pain is different [44].126
• The Barthel questionnaire [40] is used to measure performance in Activities of127
Daily Living (ADLs). It uses ten variables describing ADLs and mobility. The128
higher the score derived from this questionnaire, the greater the likelihood of129
being able to live at home with independence following discharge from hospital.130
2.1.3 Existing Standardization Efforts131
Several standard terminologies and classifications exist, which can be used for an132
interoperable representation of QoL. Some examples are: the Systematized Nomen-133
clature of Medicine Clinical Terms (SNOMED CT); the Unified Medical Language134
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 5
System (UMLS); the International Classification of Diseases version 10 (ICD-135
10); and the International Classification of Functioning, disability and health (ICF)136
defined by the WHO. In addition to terminologies and classifications, information137
models such as the virtual Medical Record (vMR) contribute to solve interoperability138
problems in the electronic exchange of QoL information.139
Several questionnaires are used to evaluate functioning, disability and health. The140
ICF classifies these concepts, specifies their range of values, and can be used to solve141
interoperability problems among health institutions that employ different measuring142
questionnaires. To this aim, questionnaire items can be encoded to ICF concepts143
following the standardization methodology proposed by [10]. Difficulties in mapping144
clinical questionnaires to standard terminologies and ontologies in the rehabilitation145
domain (e.g., data from questionnaires having a finer granularity than ICF categories)146
have been addressed in [9] and [49]. ICF core sets are subsets of the ICF that have147
been created according to specific pathologies or rehabilitation processes. Core sets148
are useful because, in daily practice, clinicians and other professionals can use only149
a fraction of the about 1400 categories found in the ICF.150
2.2 Context-Awareness151
From the first time that the term context-aware computing was introduce by Schilit152
et al. in 1994 [47] several definitions of context have been proposed. Among others,153
let us consider the definition by Dey [14]: “Context is any information that can be154
used to characterize the situation of an entity. An entity is a person, place, or object155
that is considered relevant to the interaction between a user and an application,156
including the user and applications themselves”.157
This definition simplifies the concept of the information related to an interaction;158
avoiding the inclusion of information about other elements that can be at the scenario,159
without influencing the interaction between the user and the application. Following160
this definition, any information related to the involved elements can be used to char-161
acterize the context. In so doing, the context is the conjunction of specific data only162
related to the entities involved in the interaction.163
In order to complement this definition, we follow the classification proposed by164
Zimmerman et al. [59]. This classification takes into account five different cate-165
gories the information of the context, namely “five fundamental categories for con-166
text information”: “Individuality Context”, “Location Context”, “Activity Context”,167
“Relations context” and “Time Context”.168
The “Individuality Context” describes the state of the entity itself, offering the169
information that can be observed about it. This category divides the entities in four170
different types:171
• Natural Entity Context: it contains the entities which appear without the human172
intervention. Include living and inert entities (e.g., atmosphere, water and plants).173
• Human Entity Context: it refers to all the characteristics of human beings (e.g.,174
user’s preferences about language, input device and colour schemes).175
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
6 E. Vargiu et al.
• Artificial Entity Context: as opposite of the Natural Entity Context, it includes all176
the elements developed or built by humans (e.g., buildings, ambient sensors and177
smart home devices).178
• Group Entity Context: it is a collection of entities that share common characteristics179
or have some relation (e.g., a group of people with the same disorder, as “Aquired180
Brain Injury”, or a group of relatives, as “My Family”).181
The “Location Context” includes the information related to the position of the182
entity. It involves the global or relative position among entities, independently from183
the technique used to positioning them. For instance, user’s home can be used as184
spatial information or a coordinated system can be used. Moreover, this information185
can be related to a non-physical position like IP address which is a position a smart186
home device connected to computer network.187
“Activity Context” covers the activities where the entity is, was and will be,188
involved and can be described, for instance, as tasks, aims, and actions.189
The “Relations Context” describes the relations among different entities of a190
context-aware system, such as human beings or things. This information can be191
classified into three kinds of relations: “Social Relations”, “Functional Relations”,192
and “Compositional Relations”.193
Finally, the last category is “Time Context”. In fact, usually the features of the194
context can be evaluated or have variations from one temporal point to other, it means195
that they have a temporal dimension which should be considered as a key information196
for the context [20].197
Other definitions and approaches have been proposed in the literature. In the198
application proposed by Bhattacharyya [4], the following categories have been con-199
sidered:200
• “User information”, which contains knowledge on habits, emotional state, and201
physiological conditions. This category matches with the “Human Entity Context”202
proposed in [59].203
• “Users activities”, which includes spontaneous activity, engaged tasks, or idle204
state. It is quite similar to the “Activity Context”.205
• “Location”, which includes global and relative position, directly matches with206
“Location Context”.207
• “Physical conditions”, which contains light, pressure, heart rate, and temperature.208
It also corresponds to the “Human Entity Context”.209
Summarizing, this approach does not take into account the “Relation Context” infor-210
mation and does not explicitly include the “Time Context”.211
In [6], authors stress the difference between context model and user model by the212
way of obtaining the data. On the one hand, they state that the user model is related to213
data acquired thought the interactions of the user with the application. On the other214
side, the context model is obtained mainly from sensors. Especially this last issue is215
in contradiction from our view. In fact, we consider the context as a complete set of216
information that can come from sensors as well as from interactions and/or relations217
with other entities involved in the same context-aware system.218
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 7
2.3 Telemonitoring and Home Support219
A simple definition of telemonitoring is the one provided by the Institute of Medicine220
in U.S. [27]: “the remote monitoring of patients including the use of audio, video,221
and other telecommunications and electronic information processing technologies222
to monitor patient status at a distance”.223
As reported in [30], telemonitoring systems have been successful adopted in car-224
diovascular, hematologic, respiratory, neurologic, metabolic, and urologic activities225
[28]. In fact, some of the more common things that telemonitoring devices keep226
track of include blood pressure, heart rate, weight, blood glucose, and hemoglobin.227
Telemonitoring is capable of providing information about any vital signs, as long as228
the patient has the necessary monitoring equipment at her/his location. In principle, a229
patient could have several monitoring devices at home. Clinical-care patients’ phys-230
iologic data can be accessed remotely through the Internet and handled computers231
[46]. Depending on the severity of the patient’s condition, the health care provider232
may check these statistics on a daily or weekly basis to determine the best course of233
treatment.234
In addition to objective technological monitoring, most telemonitoring systems235
include subjective questioning regarding the patient’s health and comfort [28]. This236
questioning can take place automatically over the phone, or telemonitoring software237
can help keep the patient in touch with the health care provider. The health care238
provider can then make decisions about the patient’s treatment based on a combina-239
tion of subjective and objective information similar to what would be revealed during240
an on-site appointment.241
Home sensor technology may create a new opportunity to reduce costs by helping242
people stay healthy and in their homes longer as they age. An interest has therefore243
emerged in using home sensors for health promotion [24]. One way to do this is244
by Telemonitoring and Home Support Systems (TMHSSs). TMHSSs are aimed at245
remotely monitoring patients who are not located in the same place of the health246
care provider. Those supports allow patients to be maintained in their home [12].247
Better follow-up of patients is a convenient way for patients to avoid travel and to248
perform some of the more basic work of healthcare for themselves, thus reducing249
the corresponding overall costs [2, 56].250
Summarizing, a TMHSS allows:251
• To improve the quality of clinical services, by facilitating the access to them,252
helping to break geographical barriers.253
• To keep the objective in the assistance centred in the patient, facilitating the com-254
munication between different clinical levels.255
• To extend the therapeutic processes beyond the hospital, like patient’s home.256
• A saving for unnecessary costs and a better costs/benefits ratio.257
In the literature, several TMHSSs have been proposed. Among others, let us258
recall here the works proposed in [7, 11], and [31]. The system proposed in [7]259
provides users personalized health care services through ambient intelligence. That260
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
8 E. Vargiu et al.
system is responsible of collecting relevant information about the environment. An261
enhancement of the monitoring capabilities is achieved by adding portable mea-262
surement devices worn by the user thus vital data is also collected out of the house.263
Corchado et al. [11] propose a TMHSS aimed at improving healthcare and assistance264
to dependent people at their homes. That system is based on a SOA model for integrat-265
ing heterogeneous wearable sensor networks into ambient intelligence systems. The266
adopted model provides a flexible distribution of resources and facilitates the inclu-267
sion of new functionalities in highly dynamic environments. Sensor networks provide268
an infrastructure capable of supporting the distributed communication needed in the269
dependency scenario, increasing mobility, flexibility, and efficiency, since resources270
can be accessed regardless their physical location. Biomedical sensors allow the sys-271
tem to acquire continuously data about the vital signs of the patient. Mitchell et al.272
[31] propose ContextProvider, a framework that offers a unified, query-able inter-273
face to contextual data on the device. In particular, it offers interactive user feedback,274
self-adaptive sensor polling, and minimal reliance on third-party infrastructure. It275
also allows for rapid development of new context and bio-aware applications.276
As for BNCI users, some work has been presented to provide smart home control277
[15, 17, 23, 52]. To our best knowledge, telemonitoring has not been integrated yet278
with BNCI systems apart as a way to allow remote communication between therapists279
and users [32].280
3 The BackHome Project281
BackHome1 is an EU project concerning physical and social autonomy of people282
with disabilities, by using mainly Brain/Neural Computer Interface (BNCI) and inte-283
grating other assistive technologies as well.284
“BNCI” includes two types of technologies: EEG based Brain Computer Interface285
(BCI) for command and control and affective computing based on EEG activity and286
other physiological signals. BCIs are devices that allow for communication and287
control via thought alone [29, 39, 42]. The term “BNCI” is broader than BCI, since288
BNCIs include systems that sense indirect measures of brain activity, and may not289
provide real-time feedback [5, 33, 43].290
BackHome is partly based on the outcomes coming from BrainAble,2 an EU291
project aimed at offering an ICT-based human-computer-interaction composed of292
BNCI system combined with affective computing, virtual environments and the pos-293
sibility to control heterogeneous devices like smart home environments and social294
networks [38]. BackHome advances BrainAble in supporting the transition from295
institutional care to home post rehabilitation and discharge [13].296
BackHome aims to study the transition from the hospital to the home, focusing on297
how people use BNCIs in both settings. Moreover, it is aimed to learn how different298
1 www.Backhome-FP7.eu2 www.brainable.org
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f

UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 9
BNCIs and other assistive technologies work together and can help clinicians, dis-299
abled people, and their families in the transition from the hospital to the home. The300
final goal of BackHome is to reduce the cost and hassle of the transition from the301
hospital to the home by developing improved products. To produce applied results,302
BackHome will provide: new and better integrated practical electrodes; friendlier303
and more flexible BNCI software; and better telemonitoring and home support tools.304
Among the overall provided functionalities, in this chapter, we are mainly concerned305
with how to provide telemonitoring and home support to improve users QoL.306
3.1 A Reference Scenario307
To better illustrate the objectives of the overall project and the urgent need for the308
approach presented in this chapter, let us illustrate a reference scenario.3309
Paul is a 60 years old man depressed about his recent stroke. Although Paul does310
not want to try new technologies, Dr. Jones suggests him to try to use a BNCI system311
at home, because he heard good things about the new BackHome system. Thus,312
Dr. Jones asks to Amanda a nurse with over 10 years experience helping people in313
managing care environments and tools to work with Jonas. At the beginning, she says314
that she does not want to. In fact, in the past, she had a bad experience mounting315
the cap, getting a new connection, and dealing with all the hassles of getting a316
BNCI to work. Dr. Jones asks her to try again and Amanda visits Pauls home. The317
first day, Amanda shows to Paul how to use the BackHome system and how it is318
easy to perform different tasks. The second day, Paul decides to try it and, thanks319
to the friendly support tools, Amanda is easily able to find all the solutions to the320
encountered troubles. In the next days, through the telemonitoring stations located321
at the hospital and at Pauls home, respectively, Dr. Jones is able to continuously322
verify the status of Paul and to suggest him new and personalized exercises to his323
rehabilitation therapy. In few weeks, Paul becomes more motivated, performs the324
rehabilitation exercises daily, joins a chess club, and starts to talk online to friends.325
Through BackHome system, Dr. Jones notes the progresses in Pauls daily activities326
and in his mood, and the corresponding general improved quality of life. Thus, he327
decides to assign other nurses to introduce BackHome to further patients.328
3.2 The BackHome Platform329
Before illustrating the proposed methodology to assess QoL through context aware-330
ness, let us introduce the BackHome platform, its main modules and the provided331
functionalities.332
3 Names have been changed for privacy reasons.
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
10 E. Vargiu et al.
B&
WIN
PRIN
T
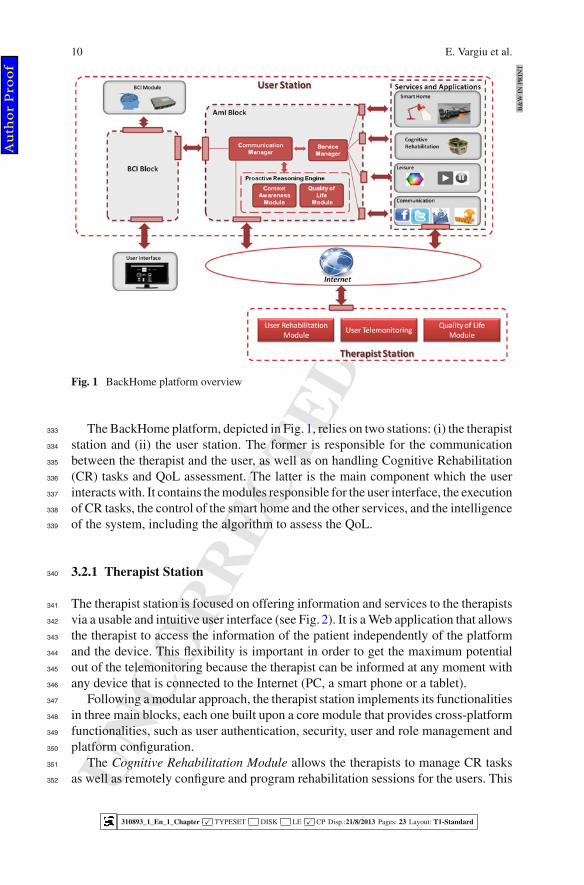
Fig. 1 BackHome platform overview
The BackHome platform, depicted in Fig. 1, relies on two stations: (i) the therapist333
station and (ii) the user station. The former is responsible for the communication334
between the therapist and the user, as well as on handling Cognitive Rehabilitation335
(CR) tasks and QoL assessment. The latter is the main component which the user336
interacts with. It contains the modules responsible for the user interface, the execution337
of CR tasks, the control of the smart home and the other services, and the intelligence338
of the system, including the algorithm to assess the QoL.339
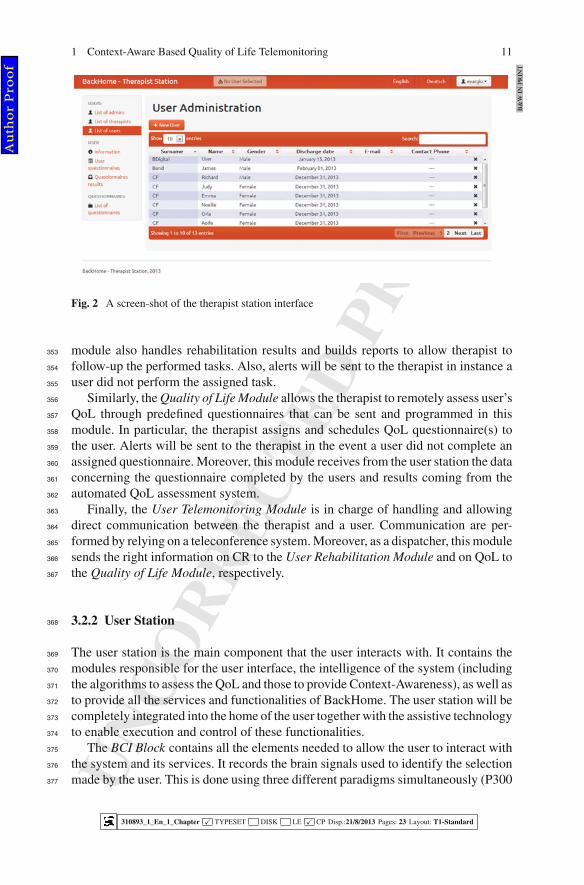
3.2.1 Therapist Station340
The therapist station is focused on offering information and services to the therapists341
via a usable and intuitive user interface (see Fig. 2). It is a Web application that allows342
the therapist to access the information of the patient independently of the platform343
and the device. This flexibility is important in order to get the maximum potential344
out of the telemonitoring because the therapist can be informed at any moment with345
any device that is connected to the Internet (PC, a smart phone or a tablet).346
Following a modular approach, the therapist station implements its functionalities347
in three main blocks, each one built upon a core module that provides cross-platform348
functionalities, such as user authentication, security, user and role management and349
platform configuration.350
The Cognitive Rehabilitation Module allows the therapists to manage CR tasks351
as well as remotely configure and program rehabilitation sessions for the users. This352
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 11
B&
WIN
PRIN
T
Fig. 2 A screen-shot of the therapist station interface
module also handles rehabilitation results and builds reports to allow therapist to353
follow-up the performed tasks. Also, alerts will be sent to the therapist in instance a354
user did not perform the assigned task.355
Similarly, the Quality of Life Module allows the therapist to remotely assess user’s356
QoL through predefined questionnaires that can be sent and programmed in this357
module. In particular, the therapist assigns and schedules QoL questionnaire(s) to358
the user. Alerts will be sent to the therapist in the event a user did not complete an359
assigned questionnaire. Moreover, this module receives from the user station the data360
concerning the questionnaire completed by the users and results coming from the361
automated QoL assessment system.362
Finally, the User Telemonitoring Module is in charge of handling and allowing363
direct communication between the therapist and a user. Communication are per-364
formed by relying on a teleconference system. Moreover, as a dispatcher, this module365
sends the right information on CR to the User Rehabilitation Module and on QoL to366
the Quality of Life Module, respectively.367
3.2.2 User Station368
The user station is the main component that the user interacts with. It contains the369
modules responsible for the user interface, the intelligence of the system (including370
the algorithms to assess the QoL and those to provide Context-Awareness), as well as371
to provide all the services and functionalities of BackHome. The user station will be372
completely integrated into the home of the user together with the assistive technology373
to enable execution and control of these functionalities.374
The BCI Block contains all the elements needed to allow the user to interact with375
the system and its services. It records the brain signals used to identify the selection376
made by the user. This is done using three different paradigms simultaneously (P300377
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
12 E. Vargiu et al.
[25], SSVEP [33] and SMR/MI [45]). At the same time the BCI block assesses378
the user’s fatigue state, which is used to switch the BackHome prototype into a379
stand-by mode in case the user is not attending or sleeping. A dedicated fusion380
process will ensure that only selections are conveyed to the attached applications381
and services. The corresponding output is then converted into their corresponding382
application and service commands. Subsequently, these will be transmitted to the383
different applications, services and BackHome systems using a dedicated network384
protocol.385
The AmI Block includes the elements for communicating with the BCI Block, the386
different services of the platform and the therapist station. This module also includes387
all the intelligence of the system devoted to process all the information from the user388
habits, the ambient, and the social interaction with the aim of helping the user to389
get the maximum potential of the system. The Communication Manager is the key390
module of the AmI Block. It implements the different interfaces interconnecting the391
AmI Block with the Therapist Station and the BCI Block. It also is the responsible to392
communicate the user’s action to the Service Manager, which is responsible for the393
execution of the actions by the smart home devices. This module implements several394
interfaces to connect all the devices and services supported by the platform. The395
Proactive Reasoning Engine constantly processes the actions of the user, the changes396
in the environment, and the services. It is aimed at understanding the context, detect397
habits, and predict situations that can help the user to better interact with the system398
and get more comfortable with it. In other words, it is in charge of processing data399
by relying on machine learning techniques aimed at learning from the user and the400
environment and adapting accordingly. The processed data will be used to change401
the context (by the Context Awareness Module) and/or to assess user’s QoL (by the402
Quality of Life Module).403
The User Station provides several services and applications:404
• Smart Home. The user can interact and control home devices, such as light, TV,405
and air conditioning. Moreover, environmental sensors allows the user to interact406
with the environment.407
• Cognitive Rehabilitation. It is the service that allows the interactions with the AmI408
Block to perform CR tasks.409
• Leisure. Through the BackHome platform, the user is able to interact with a suitable410
multimedia player. Moreover, s/he can use Brain Painting [34] to draw.411
• Communication. Through a suitable browser, the user can navigate the Internet412
and handling emails. Moreover, s/he can communicate and exchange information413
with the most popular social networks (i.e., Twitter and Facebook).414
4 Context-Aware Quality of Life Assessment415
As already said, this chapter aims to propose a general methodology to assess QoL416
by relying on context-aware techniques. The proposed methodology is currently417
adopted in the BackHome project. Nothing prevents to adopt it in a more general way418
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 13
in presence of persons to be remotely monitored or in case of disorder preventions.419
In fact, typically beneficiary will be older people or chronic patients.420
The underlying idea of the proposed methodology comes from a previous work421
[53]. To our best knowledge it is the first attempt to adopt context-aware techniques422
to assess QoL.423
4.1 The Proposed Telemonitoring System424
To monitor the QoL of disabled people, we propose a sensor-based Telemonitoring425
and Home Support System (TMHSS) aimed at helping the user to be more indepen-426
dent by providing smart home control. It also increases the eInclusion thanks to the427
possibility to perform Web browsing, use e-mail services, as well as interact with the428
most popular social networks.429
The sensor-based TMHSS is able to monitor the evolution of the user’s daily life430
activity at home, once discharged from the hospital [55], providing QoL automated431
assessment based on information gathering and data mining techniques [54]. Specif-432
ically, wearable sensors allow to monitor fatigue, spasticity, stress, and further user’s433
conditions. Environmental sensors are used to monitor—for instance—temperature434
and humidity, as well as the movements (motion sensors) and the physical position435
of the user (location sensors). Smart home devices enable physical autonomy of the436
user and help her/him carry out daily life activities. From the social perspective,437
an Internet-connected device allows the user to communicate with remote thera-438
pists, careers, relatives, and friends through Skype, email, or social networks (i.e.,439
Facebook and Twitter).440
The proposed sensor-based system acquires personalized information through441
data coming from: (i) a BNCI system4 that allows monitoring ElectroEncephalo-442
Gram (EEG), ElectroOculoGram (EOG), and ElectroMyoGram (EMG) signals; (ii)443
wearable, physiological, and biometric sensors, such as ElectroCardioGram (ECG)444
sensor, heart-rate sensor, respiration-rate sensor, Galvanic Skin Response (GSR)445
sensor, EMG switches, and inertial sensors (e.g., accelerometer, gyrocompass, and446
magnetometer); (iii) environmental sensors (i.e. gas, smoke, luminosity, humidity,447
and temperature sensors); (iv) smart home devices (e.g., home lights and TV); and448
(v) devices that allow interaction activities (i.e., a desktop PC).449
4.2 Quality of Life450
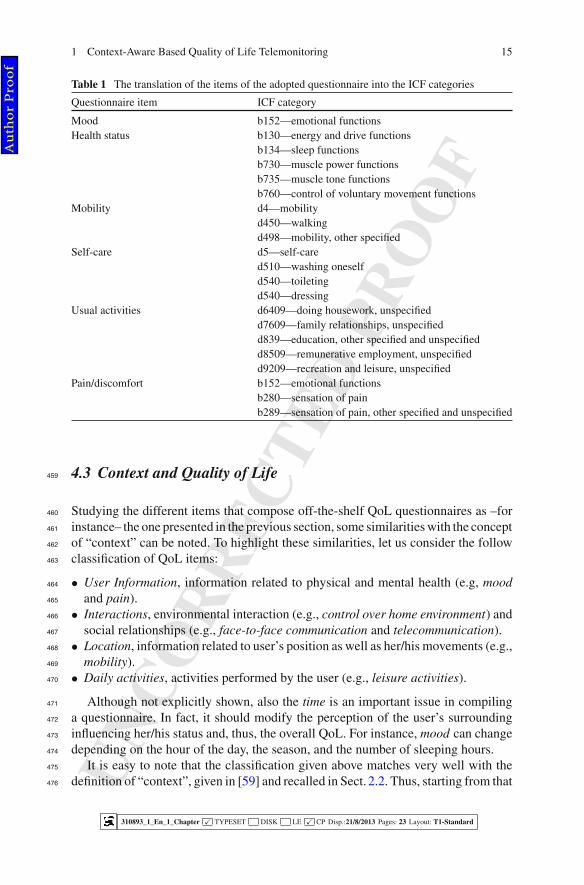
Starting from the standard questionnaires found in the literature, we propose a new451
Visual Analogue Scale (VAS) QoL questionnaire (see Fig. 3). The proposed ques-452
tionnaire is based on the standard EQ-5D-5L questionnaire, is designed to assess453
4 Currently, the EEG-P300-2D, a standard P300 control paradigm.
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f

UN
CO
RR
EC
TE
D P
RO
OF
14 E. Vargiu et al.
B&
WIN
PRIN
T
Fig. 3 BackHome questionnaire
the key QoL features of an individual, which correspond with the main features454
that BackHome aims to monitor. In other words, we consider the user’s QoL as the455
conjunction of the following items: Mood, Health Status, Mobility, Self-care, Usual456
Activities, and Pain/Discomfort. According to [18], Table 1 shows the translation of457
the selected questionnaire into the ICF categories.458
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 15
Table 1 The translation of the items of the adopted questionnaire into the ICF categories
Questionnaire item ICF category
Mood b152—emotional functionsHealth status b130—energy and drive functions
b134—sleep functionsb730—muscle power functionsb735—muscle tone functionsb760—control of voluntary movement functions
Mobility d4—mobilityd450—walkingd498—mobility, other specified
Self-care d5—self-cared510—washing oneselfd540—toiletingd540—dressing
Usual activities d6409—doing housework, unspecifiedd7609—family relationships, unspecifiedd839—education, other specified and unspecifiedd8509—remunerative employment, unspecifiedd9209—recreation and leisure, unspecified
Pain/discomfort b152—emotional functionsb280—sensation of painb289—sensation of pain, other specified and unspecified
4.3 Context and Quality of Life459
Studying the different items that compose off-the-shelf QoL questionnaires as –for460
instance– the one presented in the previous section, some similarities with the concept461
of “context” can be noted. To highlight these similarities, let us consider the follow462
classification of QoL items:463
• User Information, information related to physical and mental health (e.g, mood464
and pain).465
• Interactions, environmental interaction (e.g., control over home environment) and466
social relationships (e.g., face-to-face communication and telecommunication).467
• Location, information related to user’s position as well as her/his movements (e.g.,468
mobility).469
• Daily activities, activities performed by the user (e.g., leisure activities).470
Although not explicitly shown, also the time is an important issue in compiling471
a questionnaire. In fact, it should modify the perception of the user’s surrounding472
influencing her/his status and, thus, the overall QoL. For instance, mood can change473
depending on the hour of the day, the season, and the number of sleeping hours.474
It is easy to note that the classification given above matches very well with the475
definition of “context”, given in [59] and recalled in Sect. 2.2. Thus, starting from that476
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
16 E. Vargiu et al.
definition, let us classify the QoL items according to the “five fundamental categories477
for context information”:478
• Individuality, it describes the state of the entity. In QoL, being the entity the479
individual, Individuality corresponds to the User Information category.480
• Relations, it describes the relations among different entities of a context-aware481
system. In QoL, it can be viewed as relations among entities (e.g., users), as well482
as “external” entities (e.g., caregivers and relatives). In a more broad view, it483
could also consider interaction with the environment. In other words, Relations484
corresponds to the Interactions category of the previous classification.485
• Location, it describes the position of an entity. In QoL, it is translated into the486
position of the individual and her/his ability in moving around.487
• Activity, it describes the activity corresponding to an entity in a context-aware488
scenario. In QoL, it covers all the daily life activities performed by the individual.489
Thus, it corresponds to the Daily Activities category.490
• Time, it describes the temporal dimension of the gathered information and it is491
really important in the classification of context [20]. In the case of QoL, “time”492
not only affects the context status of the individual’s surrounding, it also influences493
her/his physical status (e.g., the same fatigue value associated to daily activities494
has a different impact depending on the time in which it is gathered). As already495
said, Time does not have a direct correspondence with the QoL items. On the other496
hand, it can be considered as a “transversal” category that affects all the others.497
The correspondence between context and QoL assessment allows us to study how498
to automatically assess QoL by relying on context-aware techniques. In fact, those499
techniques have been proposed and used for recognizing activities and behavioural500
patterns [3, 36] or monitoring diet and exercise [16]. Similarly, we claim that context-501
aware techniques can be adopted to automatically assess QoL of individuals.502
Keeping in mind the above classifications, we can identify all the sensors involved503
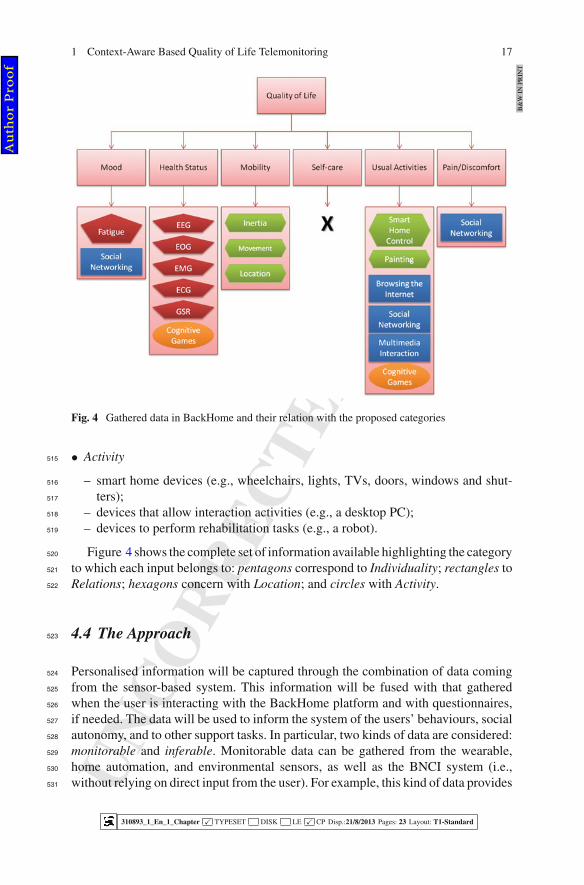
in the process of gathering data to assess QoL:504
• Individuality505
– the BNCI system, which allows monitoring EEG, EOG, and EMG signals;506
– wearable, physiological, and biometric sensors, such as ECG sensor, heart-rate507
sensor, respiration-rate sensor, GSR sensor, EMG switches, and inertial sensors508
(e.g., accelerometer, gyrocompass, and magnetometer).509
• Relations510
– social networking (i.e., through Facebook and Twitter)511
– communications to the therapists (i.e., through the telemedicine platform).512
• Location513
– environmental sensors (e.g., temperature and humidity sensors);514
– inertial, location, and motion sensors.
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 17
B&
WIN
PRIN
T
Fig. 4 Gathered data in BackHome and their relation with the proposed categories
• Activity515
– smart home devices (e.g., wheelchairs, lights, TVs, doors, windows and shut-516
ters);517
– devices that allow interaction activities (e.g., a desktop PC);518
– devices to perform rehabilitation tasks (e.g., a robot).519
Figure 4 shows the complete set of information available highlighting the category520
to which each input belongs to: pentagons correspond to Individuality; rectangles to521
Relations; hexagons concern with Location; and circles with Activity.522
4.4 The Approach523
Personalised information will be captured through the combination of data coming524
from the sensor-based system. This information will be fused with that gathered525
when the user is interacting with the BackHome platform and with questionnaires,526
if needed. The data will be used to inform the system of the users’ behaviours, social527
autonomy, and to other support tasks. In particular, two kinds of data are considered:528
monitorable and inferable. Monitorable data can be gathered from the wearable,529
home automation, and environmental sensors, as well as the BNCI system (i.e.,530
without relying on direct input from the user). For example, this kind of data provides531
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
18 E. Vargiu et al.
the answer to the item on “Mobility” (Today, my ability to move about was...). On532
the other hand, all data inferred by analysing data retrieved by the system (e.g., by533
considering activities performed by the user while interacting with a social network)534
belong to the latter category. This kind of data allows, for instance, answering the535
item on “Mood” (Today, my overall mood was...).536
Let us note that this does not imply that monitorable and inferable data are neces-537
sarily monitored or inferred. In particular, in BackHome we decided to not monitor538
nor infer some data (such as, those related to Self-care and sleeping activities), due539
to privacy issues. Moreover, users can decide to switch off the monitoring of any540
descriptor.541
In the following, we briefly describe how each monitored data can be gathered to542
assess the items of the given questionnaire.543
Monitorable data544
Health Status: Through the adoption of wearable, physiological, and biometric545
sensors, the system is able to monitor improvement and/or worsening of the health546
status of the user.547
Mobility: Through the adoption of environmental location sensors, the system is548
able to know the position of the user, time after time. It is worth pointing out that,549
in BackHome, users are typically on a wheelchair, thus the walking activity is not of550
interest here. To detect the position of the wheelchair and its movements, RFID tags551
could be embedded into the wheelchair together with following sensors.552
Usual Activities: Being human-computer-interaction made through a BNCI sys-553
tem, it is possible to monitor all the activities performed by the user on the PC and554
while interacting with smart home control and communication devices. In other555
words, the system is able, through the BNCI system, to know which action is556
performed, such as home environment interactions, face-to-face communications,557
telecommunications, and leisure activities. Moreover, the activities performed on558
further devices that allow some kind of interaction and stimulation activities (e.g.,559
devices to game, hear music, perform painting activities and/or further leisure activ-560
ities) will be stored to further studies on the user’s interaction and leisure activities.561
Inferable data562
Mood: Changes observed in habits of daily life activities can be studied to assess563
the mood. The degree of overall satisfaction can be also inferred by analysing data on564
fatigue, spasticity, stress, and further users conditions retrieved by the BNCI system565
and the other wearable sensors. Moreover, analogously to pain and discomfort, anx-566
iety and depression can be inferred by the system by adopting suitable text mining567
algorithms on the performed social activities.568
Usual Activities: The user can interact with her/his family and friends through the569
support of a communication system (e.g., Skype) or social network (e.g., Facebook570
and Twitter). Thus, suitable text mining algorithms can be adopted to infer the family571
and friend relationships.572
Pain/Discomfort: Text mining algorithms, applied to social networking and com-573
munication activities, will be adopted to assess the degree of pain or discomfort. Of574
course, privacy and technological considerations will be taken into account to define575
the scope of those analyses.576
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 19
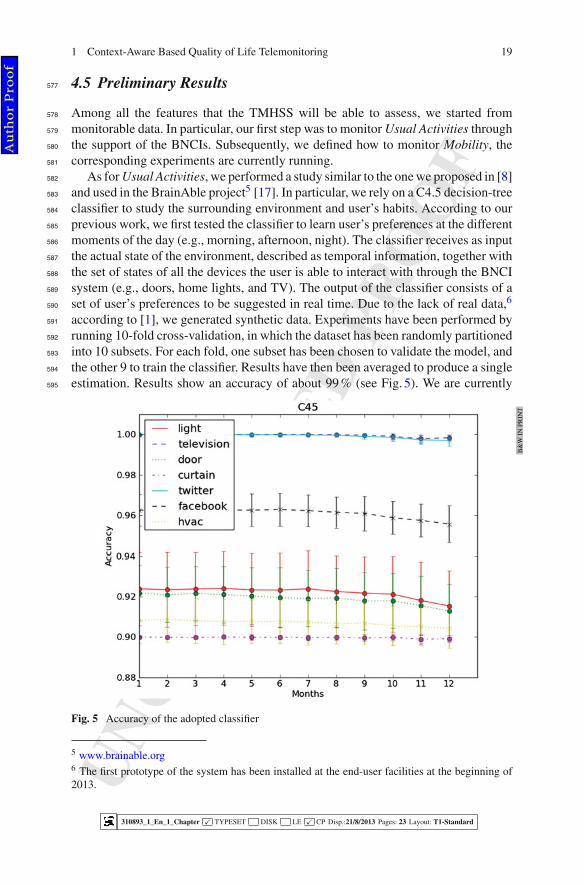
4.5 Preliminary Results577
Among all the features that the TMHSS will be able to assess, we started from578
monitorable data. In particular, our first step was to monitor Usual Activities through579
the support of the BNCIs. Subsequently, we defined how to monitor Mobility, the580
corresponding experiments are currently running.581
As for Usual Activities, we performed a study similar to the one we proposed in [8]582
and used in the BrainAble project5 [17]. In particular, we rely on a C4.5 decision-tree583
classifier to study the surrounding environment and user’s habits. According to our584
previous work, we first tested the classifier to learn user’s preferences at the different585
moments of the day (e.g., morning, afternoon, night). The classifier receives as input586
the actual state of the environment, described as temporal information, together with587
the set of states of all the devices the user is able to interact with through the BNCI588
system (e.g., doors, home lights, and TV). The output of the classifier consists of a589
set of user’s preferences to be suggested in real time. Due to the lack of real data,6590
according to [1], we generated synthetic data. Experiments have been performed by591
running 10-fold cross-validation, in which the dataset has been randomly partitioned592
into 10 subsets. For each fold, one subset has been chosen to validate the model, and593
the other 9 to train the classifier. Results have then been averaged to produce a single594
estimation. Results show an accuracy of about 99 % (see Fig. 5). We are currently595
B&
WIN
PRIN
T
Fig. 5 Accuracy of the adopted classifier
5 www.brainable.org6 The first prototype of the system has been installed at the end-user facilities at the beginning of2013.
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
20 E. Vargiu et al.
setting up a new classifier instance able also to recognise the performed activities596
(instead of suggesting ones) to monitor the overall user’s behaviour and its trend.597
As for Mobility, through the adoption of inertial, location, and motion sensors,598
the system is able to know the position of the user, time after time. All information599
about location, performed movements, covered distance, visited rooms, time spent600
on the bed (and thus on the wheelchair) are used as classification features to build a601
multi-class k-NN. The considered classes concern the user’s satisfaction in her/his602
mobility ability (from “Very Bad” to “Very Good”) and the training set is built directly603
asking users to assess their level of satisfaction. Once the system has been trained,604
we are able to infer user’s satisfaction, to study the behaviour trend, and to assess605
the improvement/worsening of the user’s QoL. Results will be evaluated in term of606
classical information theory measures, i.e., precision, recall, and F1.607
5 Conclusions608
A methodology to telemonitor quality of life based on the awareness of user context609
(fusion and processing of heterogeneous data coming from sensors, services and user610
interaction) has been proposed.611
This methodology has been devised in the framework of a particular application,612
the BackHome project and BackHome platform. Nonetheless, it holds a generic613
approach, able to be adapted to other telemedicine and teleassistance applications.614
The problem we are tackling here is very ambitious. In order to properly validate615
and enhance this methodology we will need to get big and varied amounts of data,616
from an extensive sample of users, within a wide range of conditions and environ-617
ments, along representative periods of time. This work will be continued during the618
duration of the BackHome project and others projects to come.619
Acknowledgments The research leading to these results has received funding from the European620
Community’s, Seventh Framework Programme FP7/2007-2013, BackHome project grant agree-621
ment n. 288566.622
References623
1. Armac, I., Retkowitz, D.: Simulation of smart environments. In: Pervasive Services, IEEE624
International Conference on, pp. 322–331 (2007)625
2. Artinian, N.: Effects of home telemonitoring and community-based monitoring on blood pres-626
sure control in urban African Americans: a pilot study. Heart Lung 30, 191–199 (2001)627
3. Barger, T.S., Brown, D.E., Alwan, M.: Health-status monitoring through analysis of behavioral628
patterns. IEEE Trans. Syst. Man Cybern. Part A Syst. Hum. 35(1), 22–27 (2005)629
4. Bhattacharyya, S.: Context aware health care application. Int. J. Adv. Technol. 2(3), 461–470630
(2011)631
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 21
5. Birbaumer, N., Ghanayim, N., Hinterberger, T., Iversen, I., Kotchoubey, B., Kubler, A., Perel-632
mouter, J., Taub, E., Flor, H.: A spelling device for the paralysed. Nature 398(6725), 297–298633
(1999)634
6. Byun, H.E., Cheverst, K.: Exploiting user models and context-awareness to support personal635
daily activities. In: Workshop in UM2001 on User Modeling for Context-Aware Applications636
(2001)637
7. Carneiro, D., Costa, R., Novais, P., Machado, J., Neves, J.: Simulating and monitoring ambient638
assisted living. In: Proceeding of ESM (2008)639
8. Casale, P., Fernández, J.M., Rafael, X., Torrellas, S., Ratsgoo, M., Miralles, F.: Enhanching640
user experience with brain neural computer interfaces in smart home environments. In: 8th641
IEEE International Conference of Intelligent, Environments 2012, INTENV12 (2012)642
9. Ceccaroni, L., Subirats, L.: Interoperable knowledge representation in clinical decision support643
systems for rehabilitation. Int. J. Appl. Comput. Math. 11(2), 303–316 (2012)644
10. Cieza, A., Geyh, S., Chatterji, S., Kostanjsek, N., Üstün, B., Stucki, G.: Icf linking rules: an645
update based on lessons learned. Rehabil. Med. 37, 212–218 (2005)646
11. Corchado, J., Bajo, J., Tapia, D., Abraham, A.: Using heterogeneous wireless sensor networks647
in a telemonitoring system for healthcare. IEEE Trans. Inf. Technol. Biomed. 14(2), 234–240648
(2010)649
12. Cordisco, M., Benjaminovitz, A., Hammond, K., Mancini, D.: Use of telemonitoring to decrease650
the rate of hospitalization in patients with severe congestive heart failure. Am. J. Cardiol. 84(7),651
860–862 (1999)652
13. Daly, J., Armstrong, E., Miralles, F., Vargiu, E., Müller-Putz, G., Hintermller, C., Guger, C.,653
Kuebler, A., Martin, S.: Backhome: Brain-neural-computer interfaces on track to home. In:654
RAatE 2012—Recent Advances in Assistive Technology and Engineering (2012)655
14. Dey, A.K.: Understanding and using context. Pers. Ubiquitous Comput. 5(1), 4–7 (2001)656
15. Edlinger, G., Holzner, C., Guger, C.: A hybrid brain-computer interface for smart home con-657
trol. In: Proceedings of the 14th International Conference on Human-Computer Interaction:658
Interaction Techniques and Environments—Volume Part II, HCII’11, pp. 417–425. Springer,659
Berlin (2011)660
16. Farringdon, J., Nashold, S.: Continuous body monitoring. In: Ambient Intelligence for Scien-661
tific Discovery, pp. 202–223. Springer, Berlin (2005)662
17. Fernández, J.M., Dauwalder, S., Torrellas, S., Faller, J., Scherer, R., Omedas, P., Verschure,663
P., Espinosa, A., Guger, C., Carmichael, C., Costa, U., Opisso, E., Tormos, J., Miralles, F.:664
Connecting the disabled to their physical and social world: The BrainAble experience. In: TOBI665
Workshop IV Practical Brain-Computer Interfaces for End-Users: Progress and Challenges666
(2013)667
18. Geyh, S., Cieza, A., Kollerits, B., Grimby, G., Stucki, G.: Content comparison of health-related668
quality of life measures used in stroke based on the international classification of functioning,669
disability and health (icf): a systematic review. Qual. Life Res. 16(5), 833–851 (2007)670
19. Gotay, C., Moore, T.: Assessing quality of life in head and neck cancer. Qual. Life Res. 1, 5–17671
(1992)672
20. Gross, T., Specht, M.: Awareness in context-aware information systems. In: Mensch and Com-673
puter 2001, pp. 173–182. Springer, New York (2001)674
21. Hays, R., Morales, L., RAND Health, P., RAND, C.: The RAND-36 Measure of Health-related675
Quality of Life. RAND Health reprint. RAND (2001)676
22. Hitzler, P., Krötzsch, M., Parsia, B., Patel-Schneider, P.F., Rudolph, S. (eds.): OWL 2 Web677
Ontology Language: Primer. W3C Recommendation (2009)678
23. Holzner, C., Schaffelhofer, S., Guger, C., Groenegress, C., Edlinger, G., Slater, M.: Using a679
p300 brain-computer interface for smart home control. In: World Congress (2009)680
24. Intille, S.S., Kaushik, P., Rockinson, R.: Deploying Context-Aware Health Technology at681
Home: Human-Centric Challenges. In: Human-Centric Interfaces for Ambient Intelligence682
(2009)683
25. Jin, J., Allison, B.Z., Sellers, E.W., Brunner, C., Horki, P., Wang, X., Neuper, C.: Optimized684
stimulus presentation patterns for an event-related potential eeg-based brain-computer inter-685
face. Med. Biol. Eng. Comput. 49(2), 181–191 (2011)686
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f

UN
CO
RR
EC
TE
D P
RO
OF
22 E. Vargiu et al.
26. Lerer, L.: The healthcare 2020 platform: The e-health consumer. Ph.D. thesis, INSEAD (2000)687
27. Marilyn J. Field Editor; Committee on Evaluating Clinical Applications of Telemedicine,688
I.o.M.: Telemedicine: A Guide to Assessing Telecommunications for Health Care. The National689
Academies Press, Washington (1996)690
28. Martn-Lesende, I., Orruño, E., Cairo, C., Bilbao, A., Asua, J., Romo, M., Vergara, I., Bayn,691
J., Abad, R., Reviriego, E., Larrañaga, J.: Assessment of a primary care-based telemonitoring692
intervention for home care patients with heart failure and chronic lung disease. The TELBIL693
study. BMC Health Serv. Res. 11(56), (2011)694
29. Mason, S.G., Bashashati, A., Fatourechi, M., Navarro, K.F., Birch, G.E.: A comprehensive695
survey of brain interface technology designs. Ann. Biomed. Eng. 35, 137–169 (2007)696
30. Meystre, S.: The current state of telemonitoring: a comment on the literature. Telemed. J. E697
Health 11(1), 63–69 (2005)698
31. Mitchell, M., Meyers, C., Wang, A., Tyson, G.: Contextprovider: context awareness for med-699
ical monitoring applications. In: Conference Proceeding IEEE Engineering in Medicine and700
Bioliogy Society (2011)701
32. Müller, G., Neuper, C., Pfurtscheller, G.: Implementation of a telemonitoring system for the702
control of an EEG-based brain-computer interface. IEEE Trans. Neural Syst. Rehabil. Eng.703
11(1), 54–59 (2003)704
33. Müller-Putz, G.R., Pfurtscheller, G.: Control of an electrical prosthesis with an ssvep-based705
bci. IEEE Trans. Biomed. Eng. 55(1), 361–364 (2008)706
34. Münssinger, J., Halder, S., Kleih, S., Furdea, A., Raco, V., Hösle, A., Kübler, A.: Brain painting:707
first evaluation of a new braincomputer interface application with als-patients and healthy708
volunteers. Front Neurosci. 4, 182. doi: 10.3389/fnins.2010.00182 (2010)709
35. Murphy, B., Herrman, H., Hawthorne, G., Pinzone, T., Evert, H.: Australian WHOQoL instru-710
ments: user’s manual and interpretation guide. Australian WHOQoL Field Study Centre. Mel-711
bourne, Australia (2000)712
36. Nambu, M., Nakajima, K., Noshiro, M., Tamura, T.: An algorithm for the automatic detection713
of health conditions. Eng. Med. Biol. Mag. IEEE 24(4), 38–42 (2005)714
37. Naughton, M., Shumaker, S., Anderson, R., Czajkowski, S.: Psychological aspects of healthre-715
lated quality of life measurement: tests and scales. Qual. Life Pharmaco Econ. Clin. Trials 15,716
117–131 (1996)717
38. Navarro, A., Ceccaroni, L., Velickovski, F., Torrellas, S., Miralles, F., Allison, B., Scherer, R.,718
Faller, J.: Context-awareness as an enhancement of brain-computer interfaces. In: III Interna-719
tional Workshop on Ambient Assisted Living IWAAL 2011 (2011)720
39. Neuper, C., Pfurtscheller, G.: Neurofeedback Training for BCI Control Brain-Computer Inter-721
faces. The Frontiers Collection, Chap. 4, pp. 65–78. Springer, Berlin (2010)722
40. O’Sullivan, S., Schmitz, T.: Physical Rehabilitation. Information and Interdisciplinary Subjects723
Series. F.A. Davis, G— Reference (2007)724
41. Patrick, D., Erickson, P.: Health Status and Health Policy: Quality of Life in Health Care725
Evaluation and Resource Allocation. No. p. 314 in Health Status and Health Policy: Quality of726
Life in Health Care Evaluation and Resource Allocation. Oxford University Press, New York727
(1993).http://books.google.es/books?id=IjgQAQAAMAAJ728
42. Pfurtscheller, G., Allison, B.Z., Brunner, C., Bauernfeind, G., Solis-Escalante, T., Scherer, R.,729
Zander, T.O., Mueller-Putz, G., Neuper, C., Birbaumer, N.: The hybrid BCI. Frontiers Neurosci.730
4 (2010)731
43. Pfurtscheller, G., Müller-Putz, G.R., Scherer, R., Neuper, C.: Rehabilitation with brain-732
computer interface systems. IEEE Comput. 41(10), 58–65 (2008)733
44. Rand, C., Health Sciences, P., Hays, R., Sherbourne, C., Mazel, R.: RAND 36-item Health734
Survey 1.0: RAND Health Sciences Program. RAND reprints. RAND (1992)http://books.735
google.es/books?id=FUkKHAAACAAJ736
45. Sannelli, C., Dickhaus, T., Halder, S., Hammer, E.M., Müller, K.R., Blankertz, B.: On optimal737
channel configurations for smr-based brain-computer interfaces. Brain topogr. 23(2), 186–193738
(2010)739
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f

UN
CO
RR
EC
TE
D P
RO
OF
1 Context-Aware Based Quality of Life Telemonitoring 23
46. Barro, S., Castro, D., Fernndez-Delgado, M., Fraga, S., Lama, M., Rodrguez, J.M., Vila, J.A.:740
Intelligent telemonitoring of critical-care patients. IEEE Eng. Med. Biol. Mag. 18, 80–88 (1999)741
47. Schilit, B., Adams, N., Want, R.: Context-aware computing applications. In: Mobile Computing742
Systems and Applications, 1994. WMCSA 1994. First Workshop on, pp. 85–90. IEEE (1994)743
48. Skevington, S.M., Lotfy, M., O’Connell, K.A., WHOQOL Group: The World Health Organiza-744
tion’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the745
international field trial. A report from the WHOQOL group. Qual. Life Res. Int. J. Qual. Life A.746
Treat. Care Rehabil. 13(2), 299–310 (2004). http://view.ncbi.nlm.nih.gov/pubmed/15085902747
49. Subirats, L., Ceccaroni, L., Miralles, F.: Knowledge representation for prognosis of health748
status in rehabilitation. Future Internet 4(3), 762–775 (2012)749
50. Sutherland, H., Till, J.: Quality of life assessments and levels of decision making: differentiating750
objectives. Qual. Life Res. 2(4), 297–303 (1993). http://www.biomedsearch.com/nih/Quality-751
life-assessments-levels-decision/8220364.html752
51. The Euroqol Group: Euroqol a facility for the measurement of health-related quality of life.753
Health Policy 16, 199–208 (1990)754
52. Tonin, L., Leeb, R., Tavella, M., Perdikis, S., Millán, J.: A bci-driven telepresence robot. Int.755
J. Bioelectromagn. 13(3), 125–126 (2011)756
53. Vargiu, E., Ceccaroni, L., Subirats, L., Martin, S., Miralles, F.: User profiling of people with757
disabilities - a proposal to pervasively assess quality of life. In: 5th International Conference758
on Agents and Artificial Intelligence (2013)759
54. Vargiu, E., Fernández, J.M., Torrellas, S., Dauwalder, S., Solà, M., Miralles, F.: A sensor-760
based telemonitoring and home support system to improve quality of life through bnci. In:761
12th European AAATE Conference (2013)762
55. Vargiu, E., Miralles, F., Martin, S., Markey, D.: BackHome: Assisting and telemonitoring people763
with disabilities. In: RAatE 2012—Recent Advances in Assistive Technology and Engineering764
(2012)765
56. Vincent, J., Cavitt, D., Karpawich, P.: Diagnostic and cost effectiveness of telemonitoring the766
pediatric pacemaker patient. Pediatr. Cardiol. 18(2), 86–90 (1997)767
57. Ware, J., Kosinski, M., Dewey, J.: How to Score Version 2 of the SF-36 Health Survey: Standars768
and Acute Forms. QualityMetric (2001)769
58. WHO: Global Age-Friendly Cities: A Guide. Nonserial Publication. World Health Organization770
(2007). http://books.google.es/books?id=4uWtQy6rGywC771
59. Zimmermann, A., Lorenz, A., Oppermann, R.: An operational definition of context. In: Mod-772
eling and using context, pp. 558–571. Springer, Berlin (2007)773
310893_1_En_1_Chapter � TYPESET DISK LE � CP Disp.:21/8/2013 Pages: 23 Layout: T1-Standard
Au
tho
r P
roo
f
UN
CO
RR
EC
TE
D P
RO
OF
Author Queries
Chapter 1
Query Refs. Details Required Author’s response
AQ1 As keywords are mandatory for this chapter, please provide 3-6keywords.
AQ2 Please confirm the corresponding author is correctly identified andamend if necessary.
AQ3 Please provide page range for Ref. [28, 42].
AQ4 Please provide editor group and for Refs. [16, 20, 59].
Au
tho
r P
roo
f
MARKED PROOF
Please correct and return this set
Instruction to printer
Leave unchanged under matter to remain
through single character, rule or underline
New matter followed by
or
or
or
or
or
or
or
or
or
and/or
and/or
e.g.
e.g.
under character
over character
new character
new characters
through all characters to be deleted
through letter or
through characters
under matter to be changed
under matter to be changed
under matter to be changed
under matter to be changed
under matter to be changed
Encircle matter to be changed
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
linking characters
through character or
where required
between characters or
words affected
through character or
where required
or
indicated in the margin
Delete
Substitute character or
substitute part of one or
more word(s)Change to italics
Change to capitals
Change to small capitals
Change to bold type
Change to bold italic
Change to lower case
Change italic to upright type
Change bold to non-bold type
Insert ‘superior’ character
Insert ‘inferior’ character
Insert full stop
Insert comma
Insert single quotation marks
Insert double quotation marks
Insert hyphen
Start new paragraph
No new paragraph
Transpose
Close up
Insert or substitute space
between characters or words
Reduce space betweencharacters or words
Insert in text the matter
Textual mark Marginal mark
Please use the proof correction marks shown below for all alterations and corrections. If you
in dark ink and are made well within the page margins.
wish to return your proof by fax you should ensure that all amendments are written clearly