consistencia interna y validez de la versión española del cuestionario de calidad de vida...
TRANSCRIPT
Validation of a Quality of Life Questionnaire for Bronchiectasis:psychometric analyses of the Spanish QOL-B-V3.0
Casilda Olveira • Gabriel Olveira • Francisco Espildora •
Rosa-Maria Giron • Gerard Munoz •
Alexandra L. Quittner • Miguel-Angel Martinez-Garcia
Accepted: 10 October 2013 / Published online: 19 October 2013
� Springer Science+Business Media Dordrecht 2013
Abstract
Purpose Bronchiectasis is a chronic disease, leading to
worsening of health-related quality of life. This study
evaluated the psychometric properties of a new patient-
reported outcome for non-cystic fibrosis bronchiectasis, the
Quality of Life Questionnaire Bronchiectasis, translated
into Spanish (QOL-B-Sp-V3.0).
Methods This prospective study recruited clinically stable
patients with non-cystic fibrosis bronchiectasis at 4 Spanish
centers. Health status was assessed with multiple indicators
(dyspnea, exacerbations, bronchorrhea, etc.), microbiological,
radiological, spirometric, and anthropometric parameters plus
St-George Respiratory Questionnaire (SGRQ). Psychometric
analyses included internal consistency, test–retest reliability,
convergent validity, predictive validity, and responsivity to
change.
Results The 207 stable patients (mean age 57.2 years) had a
Bhalla score of 11.53 ± 7.39 and FEV1% of 68.3 ± 22.2 %.
One hundred and sixty-one stable patients repeated the test
2 weeks later, and 80 patients who had an exacerbation within
6 months of the assessment also repeated it. Internal consis-
tency was high across all scales (Cronbach’s alpha [0.70).
Thirty-six of 37 items correlated more strongly with their
assigned scale than a competing scale. Test–retest coefficients
were strong (intraclass correlations r = 0.68–0.88). All scales,
except Treatment Burden, discriminated significantly between
patients with mild, moderate, and severe disease according to
FEV1% and other respiratory parameters. Strong convergence
was found between the QOL-B-Sp-V3.0 and SGRQ. Signifi-
cant correlations were found between QOL-B-Sp-V3.0 and
This study is included in the PII of Bronchiectasis of SEPAR (Spanish
Society of Pulmonology and Thoracic Surgery).
Montserrat Vendrell (Universitary Hospital Dr Josep Trueta, Gerona,
Spain) and Nuria Porras (Endocrinology and Nutrition Service, Carlos
Haya University Hospital, Malaga, Spain) also participated in this
study.
C. Olveira (&) � F. Espildora
Pneumology Service, Hospital Regional Universitario de
Malaga. IBIMA (Instituto de Investigacion Biomedica de
Malaga), Universidad de Malaga, Avenida Carlos Haya,
29010 Malaga, Spain
e-mail: [email protected]
F. Espildora
e-mail: [email protected]
G. Olveira
Endocrinology and Nutrition Service, Hospital Regional
Universitario de Malaga. IBIMA (Instituto de Investigacion
Biomedica de Malaga), Universidad de Malaga, Malaga, Spain
e-mail: [email protected]
G. Olveira
CIBERDEM, CIBER of Diabetes and Associated Metabolic
Diseases (Instituto de Salud Carlos III), Madrid, Spain
R.-M. Giron
Pneumology Service, La Princesa Hospital, Madrid, Spain
e-mail: [email protected]
G. Munoz
Pneumology Service, Idibgi, Hospital Universitari Dr Josep
Trueta, Gerona, Spain
e-mail: [email protected]
A. L. Quittner
Department of Psychology, University of Miami,
Coral Gables, FL, USA
e-mail: [email protected]
M.-A. Martinez-Garcia
Pneumology Service, Polytechnic and University La Fe Hospital,
Valencia, Spain
e-mail: [email protected]
123
Qual Life Res (2014) 23:1279–1292
DOI 10.1007/s11136-013-0560-0
various clinical, spirometric, radiological, and anthropometric
variables. Significant differences were found on all QOL-B-Sp-
V3.0 scales, except emotional functioning, between the base-
line responses and onset of an exacerbation; robust sensitivity
to change was observed on the Respiratory Symptoms scale.
Conclusions The QOL-B-Sp-V3.0 questionnaire demon-
strated strong reliability and validity. Scores were repro-
ducible after 2 weeks, and it discriminated between
patients who varied in severity and was responsive to
changes related to exacerbation.
Keywords Bronchiectasis � Health-related quality
of life � Patient-reported outcome � Forced spirometry
volume in the first second
Abbreviations
BQ Bronchiectasis
BMI Body mass index
CDRQ Chronic Respiratory Disease Questionnaire
CF Cystic fibrosis
CFQ-R Cystic Fibrosis Questionnaire Revised
FEV1 Forced spirometry volume in the first second
HI Haemophilus influenzae
HRCT High-resolution computed tomography
HRQOL Health-related quality of life
LCQ Leicester Cough Questionnaire
MID Minimal important difference score
MRC Medical Research Council
PA Pseudomonas aeruginosa
PRO Patient-reported outcome
QOL-B-Sp Quality of Life Questionnaire for patients
with Bronchiectasis. Spanish version
SEPAR Spanish Society of Pulmonology and Thoracic
Surgery
SGRQ St. George Respiratory Questionnaire
Introduction
Bronchiectasis (BQ) is a heterogeneous disease resulting
from different causes, but managed in similar ways. It is
chronic and leads to pulmonary exacerbations, loss of lung
function, and worsening of health-related quality of life
(HRQOL) [1, 2]. Care should be supervised by specialized
units, at least in cases of chronic infection, recurrent
exacerbations, or bronchiectasis with an etiology suscep-
tible to specific therapy [1, 2]. Although pulmonary and
nutritional outcomes are regularly monitored [1, 2], they
are not strongly predictive of how patients function or feel
in their daily lives [3–6]. The patient-reported outcome
(PRO) is a direct measure of how a patient functions, feels,
or survives in relation to his/her chronic illness [3, 5–10].
PROs are used to assess the patient’s perception of severity
[3, 5–10] and may be used as primary or secondary out-
come measures in drug registration trials [7, 11].
Several studies have found that patients with bronchiec-
tasis report worse HRQOL than the general population,
particularly patients with poor lung function, more frequent
exacerbations, bronchorrhea, chronic infection with Pseu-
domonas aeruginosa (PA) [3, 9, 10, 12–14], and symptoms
of depression and anxiety [4]. The St. George Respiratory
Questionnaire (SGRQ) is the most widely used PRO for
bronchiectasis, but is not specific for this disorder and has
certain limitations, such as its length and variable recall [8–
10, 15, 16]. In addition, other PROs used in bronchiectasis,
such as the Leicester Cough Questionnaire [17] (LCQ) and
the Chronic Respiratory Disease Questionnaire (CDRQ)
[18], are not designed specifically for this condition. Neither
the LCQ nor the CDRQ includes a comprehensive list of
respiratory symptoms, and the CRDQ requires an inter-
viewer for administration. Finally, none of these PROs fol-
lowed the instrument development guidelines published by
the Food and Drug Administration [7]. Thus, there is a clear
need for a disease-specific PRO for bronchiectasis.
The purpose of the current study was to evaluate the
psychometric properties of a new PRO for non-cystic fibrosis
(CF) bronchiectasis (QOL-B) that includes assessment of
respiratory symptoms and other domains of HRQOL. The
QOL-B was developed in accordance with the FDA guide-
lines [7], beginning with a physician consensus panel, open-
ended patient interviews, and cognitive testing, with several
revisions made in response to patient data and feedback [19–
21]. Strong evidence of internal consistency, test–retest reli-
ability, and convergent validity was found for the QOL-B in
the USA [20]. This version has been translated into Spanish
for use among Spanish speakers in the USA [2010, Quittner,
Cruz, Kimberg, Marciel, and Barker QOL-B, Version 3.0.
‘‘Appendix’’], and our group has adapted it, with slight
adaptations without changing the sense of the questions, to
make it more suitable for Spain (QOL-B-Spain-V3.0). The
transcultural validation of a HRQOL questionnaire that
already exists in one language has the advantage of obviating
the lengthy and tedious process of designing a new ques-
tionnaire. The aim of the present study was to validate this
questionnaire in Spanish patients with non-CF bronchiectasis.
Patients and methods
This prospective, multicenter sequential study included
patients aged 16 and older who met the diagnostic criteria
for bronchiectasis [1, 2] and attended a specific bronchi-
ectasis unit at one of the four Spanish university hospitals
for routine monitoring and treatment, over a recruitment
period of 8 months. In all cases, bronchiectasis was diag-
nosed by high-resolution computed tomography (HRCT) of
1280 Qual Life Res (2014) 23:1279–1292
123

the chest, with the use of a 1–1.5-mm window every
10 mm and acquisition times of 1 s during full inspiration,
following the criteria of Naidich et al. [22]. All patients had
undergone a full etiological study following the diagnostic
algorithm for bronchiectasis of the Spanish Society of
Pulmonology and Thoracic Surgery (SEPAR) [1]. A full
clinical history, from diagnosis to study participation, was
recorded following the SEPAR protocol [1]. At each visit
(every 2–3 months), demographic and clinical variables
were collected prospectively. Patients performed spirome-
try were weighed and measured, and a sputum sample was
collected and cultured for the usual bronchiectasis patho-
gens [1, 2]. The questionnaires were completed after a
clinical examination to confirm that the patients were in a
stable phase and before completing the clinical measures
(including spirometry) and the various elective medical
procedures in order not to bias responses. If at this time
they had a respiratory exacerbation or a recent hospital
admission, their participation was postponed for at least
60 days, until any acute illness was resolved. Patients were
excluded if they had CF [23], if they had difficulty
understanding the questionnaire, or if they refused to par-
ticipate or sign the consent form.
The study was approved by the Malaga Northeast Ethics
and Research Committee, and all the participants provided
written informed consent.
Clinical and demographic variables
Data were gathered on demographic (age, sex), anthropo-
metric (body mass index—BMI), clinical, and etiological
aspects of bronchiectasis. The degree of dyspnea was
recorded using the Medical Research Council (MRC) scale
[24] and the comorbidity, with the Charlson index [25].
Spirometry was also performed, with the forced expiratory
volume in 1 s (FEV1) expressed in absolute terms (mL) and
as a percentage, using a reference population [26]. Struc-
tural damage was assessed with HRCT using the Bhalla
scoring system (lower values indicate worse damage) at
baseline or during the previous 12 months [27]. Assess-
ment of the mean amount of sputum produced daily (in
milliliters) was evaluated by instructing the patients to
collect sputum during the 3 days prior to the visit in three-
graded sterile containers (one per day), marking the amount
reached each day on the container. Instructions were given
to ensure that sputum was collected correctly, with low
percentages of saliva recorded [12]. We analyzed chronic
colonization by microorganisms, considering their
appearance in sputum (at least 3 positive), regardless of
their persistence at the time of the study [1]. Pulmonary
exacerbations were assessed prospectively using the
SEPAR criteria [1]. A mild–moderate exacerbation was
defined as the acute development and persistence of
changes in sputum characteristics (increased volume,
thicker consistency, greater purulence, or hemoptysis), and/
or increased breathlessness unrelated to other causes, with
or without other symptoms, and if they could be treated
with oral antibiotics. An exacerbation was considered to be
severe if intravenous antibiotics were necessary and there
were tachypnea, acute respiratory failure, exacerbated
chronic respiratory failure, a significant decline in oxygen
saturation or respiratory function, hypercapnia, fever of
more than 38 �C, hemodynamic instability, and/or
impaired cognitive function [1]. The number of exacerba-
tions and hemoptysis (whatever amount) in the year prior
to the evaluation was also included in the analyses.
Questionnaires
QOL-B-Spain-V3.0
This is a disease-specific questionnaire for patients with
bronchiectasis. It is a self-report measure consisting of 37
questions and takes about 10 min to complete. The scores
are standardized across 8 scales, ranging from 0 to 100, with
higher scores indicating better health-related quality of life.
Strong evidence of internal consistency, test–retest reli-
ability, and convergent validity was found for the QOL-B in
the USA [19–21]. The Spanish version for Hispanic patients
in the USA [2010, Quittner, Cruz, Kimberg, Marciel, and
Barker QOL-B, Version 3.0. ‘‘Appendix’’] was adapted by
us for use in Spain. This adaptation was initially adminis-
tered to 20 patients to ensure complete understanding of all
the items, after which slight changes in the Spanish were
made without changing the sense of the questions.
The SGRQ is a self-report health status measure, yield-
ing three domain scores (symptoms, activity, and impact)
and a total score. Scores range from 0 to 100, with higher
scores representing worse health status [8]. The Spanish
version has been validated for use in patients with bron-
chiectasis and been shown to be a valid instrument for
analyzing health-related quality of life [9, 10].
Data analysis
Data were analyzed with SPSS version 12 (SPSS-Inc,
Chicago, IL). Quantitative variables were expressed as
means ± standard deviations, with 95 % confidence inter-
vals. Qualitative variables were compared using chi-square
tests, with Fisher’s exact test where necessary. The nor-
mality of distributions was verified using the Kolmogorov–
Smirnov test. For all variables, significance was set at
p \ 0.05 for two tails.
Qual Life Res (2014) 23:1279–1292 1281
123

Validation design
The following psychometric tests were conducted to evalu-
ate the reliability and validity of the Spanish QOL-B-Spain-
V3.0:
Reliability
Reliability measures were of two types: 1. Internal con-
sistency was evaluated using Cronbach’s alpha calculated
for each scale and 2. Test–retest reliability (reproducibil-
ity): the QOL-B-Spain-V3.0 was administered twice to a
subset of patients during stable visits, separated by a two-
week interval; intraclass correlation coefficients quantified
reproducibility of scores over 2 weeks.
Construct validity
Item-scale convergent and discriminant validity were
examined by comparing the item-scale correlation. Con-
vergent validity was supported if an item correlated
(r C 0.4) with the scale it was hypothesized to belong to.
Discriminant validity was supported whenever a correla-
tion between an item and its hypothesized scale was higher
than its correlation with the other components.
Criterion validity
Convergent validity: Spearman’s correlation coefficients were
calculated for each QOL-B scale with the SGRQ domains
and with demographic and health indicators, including age,
FEV1 % predicted, number of exacerbations in the previous
year, bronchiectasis severity as measured by the Bhalla score,
daily bronchorrhea, dyspnea, Charlson morbidity index, and
BMI. Discriminant (divergent) validity: to evaluate whether
the QOL-B-Spain-V3.0 discriminates between patients who
differ in disease severity based on lung function [26, 28]
(FEV1% predicted), presence of hemoptysis during the past
year, colonization by pathogens, and Bhalla scores (dichot-
omized based on the median of the sample- 13-). To compare
scores between these groups, a Mann–Whitney nonparamet-
ric test or Student’s t test was used, depending on the nor-
mality of scores. To compare scores across three or more
groups, we used an ANOVA or Kruskal–Wallis test.
Responsiveness (sensitivity to change)
In a subset of patients who experienced an exacerbation
within 6 months of the baseline visit, comparisons of their
scores prior to initiating treatment for the exacerbation
were evaluated using the Student’s t test for paired data or
Wilcoxon test, depending on normality. Effect sizes from
baseline to exacerbation were also calculated as the
difference between the two means of each scale (baseline
and exacerbation) divided by the pooled standard deviation
for those means. Effect size was interpreted as trivial
(\0.2), small (0.2–0.5), moderate (0.5–0.8), and large
([0.8) following the guidelines proposed by Cohen [29].
To determine the minimal important difference score
(MID) on the Respiratory Symptoms scale, which repre-
sents the smallest change a patient can detect, two distri-
bution-based methods were used: (1) � SD of the change on
the Respiratory Symptoms scale (exacerbation score minus
baseline score) and (2) one standard error of the mean
(SEM) for the Respiratory Symptoms scale, calculated as
SEM ¼ SDffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi
1� að Þp
[SD = SD of mean baseline QOL-B
Spain V3.0 respiratory score; a = scale reliability] [30].
Results
A total of 218 patients were approached for the study and
207 agreed to participate. Of the 11 patients who were
excluded, 3 had problems understanding the questionnaires
and 8 declined participation.
The mean age of the participants was 57.2 years (range
17–86) and 62.8 % were women. The mean Bhalla score was
11.53 (SD 7.39), and the mean FEV1% was 68.3 ± 22.2 %
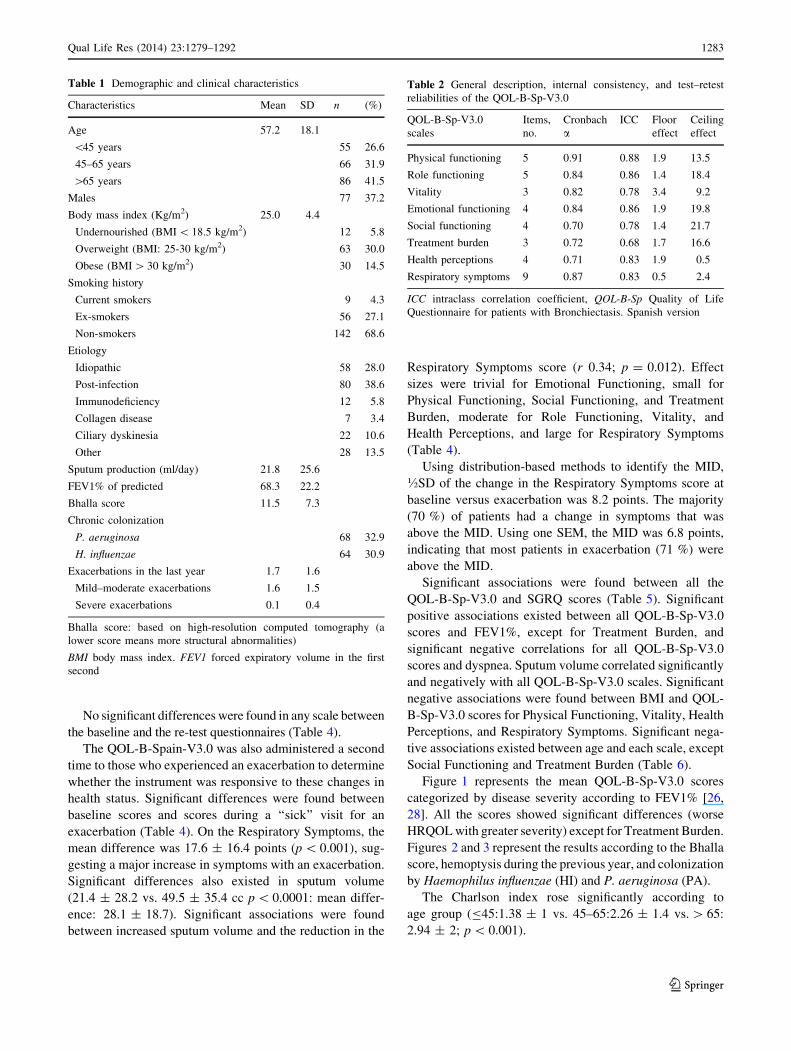
(range 15–123 %). Table 1 summarizes the clinical, spiro-
metric, microbiological, radiological, and anthropometric
characteristics of the sample.
Two weeks after the baseline visit, the QOL-B-Spain-
V3.0 was administered a second time to 161 participants
who were stable. In addition, to estimate the MID, 80
patients who experienced an exacerbation (all mild or
moderate) within 6 months of the baseline visit also com-
pleted the QOL-B-Sp-V3.0, prior to starting treatment.
The QOL-B-Sp-V3.0 showed strong internal consistency,
as demonstrated by the strong Cronbach’s alpha coefficients
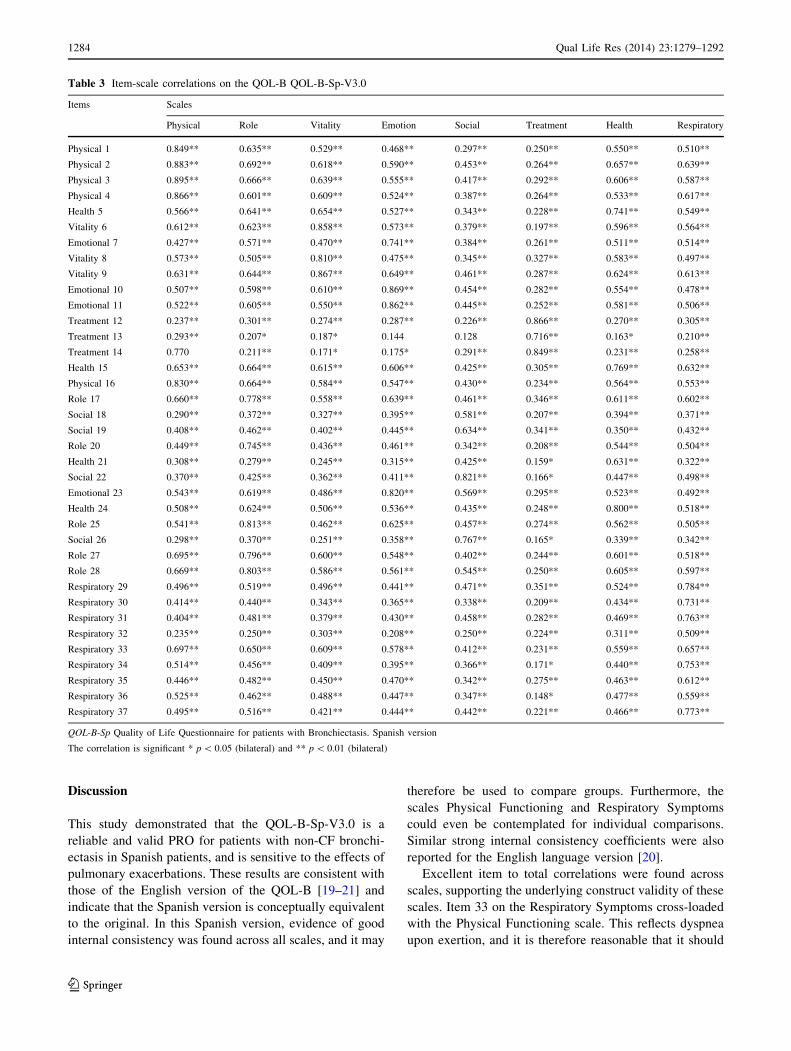
(C0.70) on each scale (Table 2). Item to total correlations
supported the content validity of the scales. Significant
associations (r [ 0.40) were found between all items and
their assigned versus competing scales (Table 3), except for
Respiratory item 33 (Have you had shortness of breath with
greater activity?), which correlated r = 0.66 on the Respi-
ratory Symptoms scale and r = 0.70 with Physical Func-
tioning. Floor effects were observed in \4 % and ceiling
effects in\15 % of respondents on four of the eight scales.
Test–retest reliability was also very strong, with a majority of
ICCs above 0.70 for the scales, except Treatment Burden
(0.68) (Table 2).
Few gender differences were found in scores on the QOL-
B-Sp-V3.0: Emotional Functioning (women: 67.6 ± 25.5;
men: 76.4 ± 24.5; p \ 0.05) and Treatment Burden (women:
63.6 ± 24.2; men: 72.3 ± 23.7; p \ 0.05).
1282 Qual Life Res (2014) 23:1279–1292
123
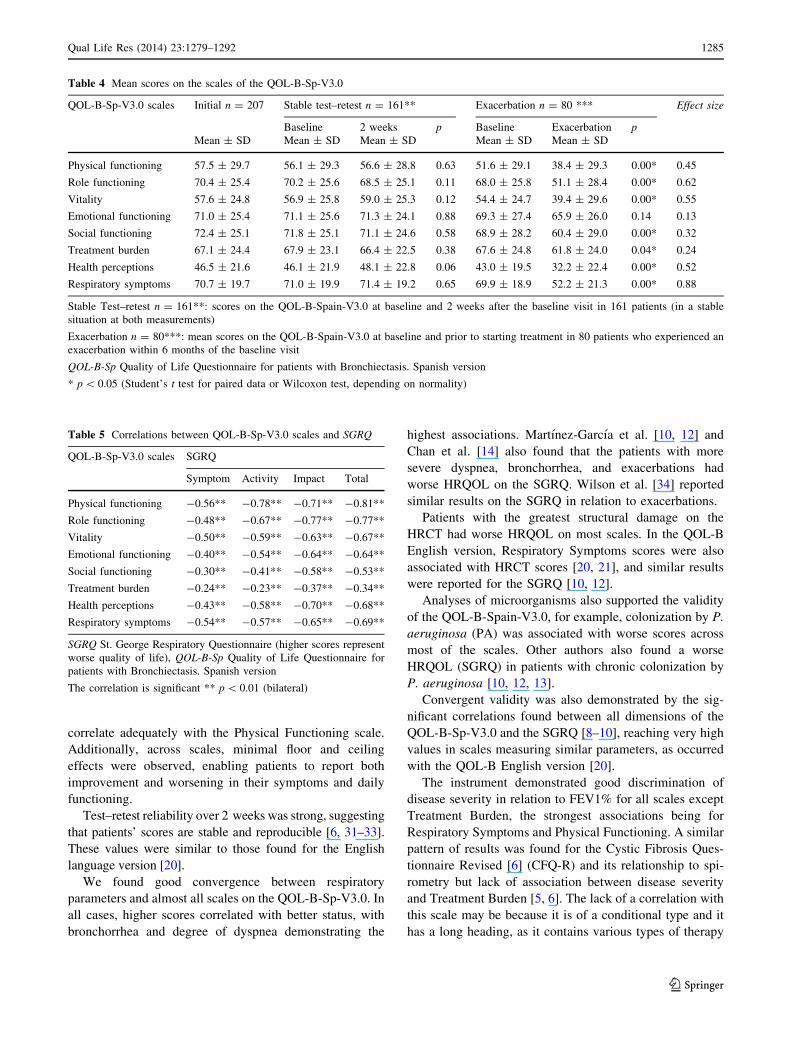
No significant differences were found in any scale between
the baseline and the re-test questionnaires (Table 4).
The QOL-B-Spain-V3.0 was also administered a second
time to those who experienced an exacerbation to determine
whether the instrument was responsive to these changes in
health status. Significant differences were found between
baseline scores and scores during a ‘‘sick’’ visit for an
exacerbation (Table 4). On the Respiratory Symptoms, the
mean difference was 17.6 ± 16.4 points (p \ 0.001), sug-
gesting a major increase in symptoms with an exacerbation.
Significant differences also existed in sputum volume
(21.4 ± 28.2 vs. 49.5 ± 35.4 cc p \ 0.0001: mean differ-
ence: 28.1 ± 18.7). Significant associations were found
between increased sputum volume and the reduction in the
Respiratory Symptoms score (r 0.34; p = 0.012). Effect
sizes were trivial for Emotional Functioning, small for
Physical Functioning, Social Functioning, and Treatment
Burden, moderate for Role Functioning, Vitality, and
Health Perceptions, and large for Respiratory Symptoms
(Table 4).
Using distribution-based methods to identify the MID,
�SD of the change in the Respiratory Symptoms score at
baseline versus exacerbation was 8.2 points. The majority
(70 %) of patients had a change in symptoms that was
above the MID. Using one SEM, the MID was 6.8 points,
indicating that most patients in exacerbation (71 %) were
above the MID.
Significant associations were found between all the
QOL-B-Sp-V3.0 and SGRQ scores (Table 5). Significant
positive associations existed between all QOL-B-Sp-V3.0
scores and FEV1%, except for Treatment Burden, and
significant negative correlations for all QOL-B-Sp-V3.0
scores and dyspnea. Sputum volume correlated significantly
and negatively with all QOL-B-Sp-V3.0 scales. Significant
negative associations were found between BMI and QOL-
B-Sp-V3.0 scores for Physical Functioning, Vitality, Health
Perceptions, and Respiratory Symptoms. Significant nega-
tive associations existed between age and each scale, except
Social Functioning and Treatment Burden (Table 6).
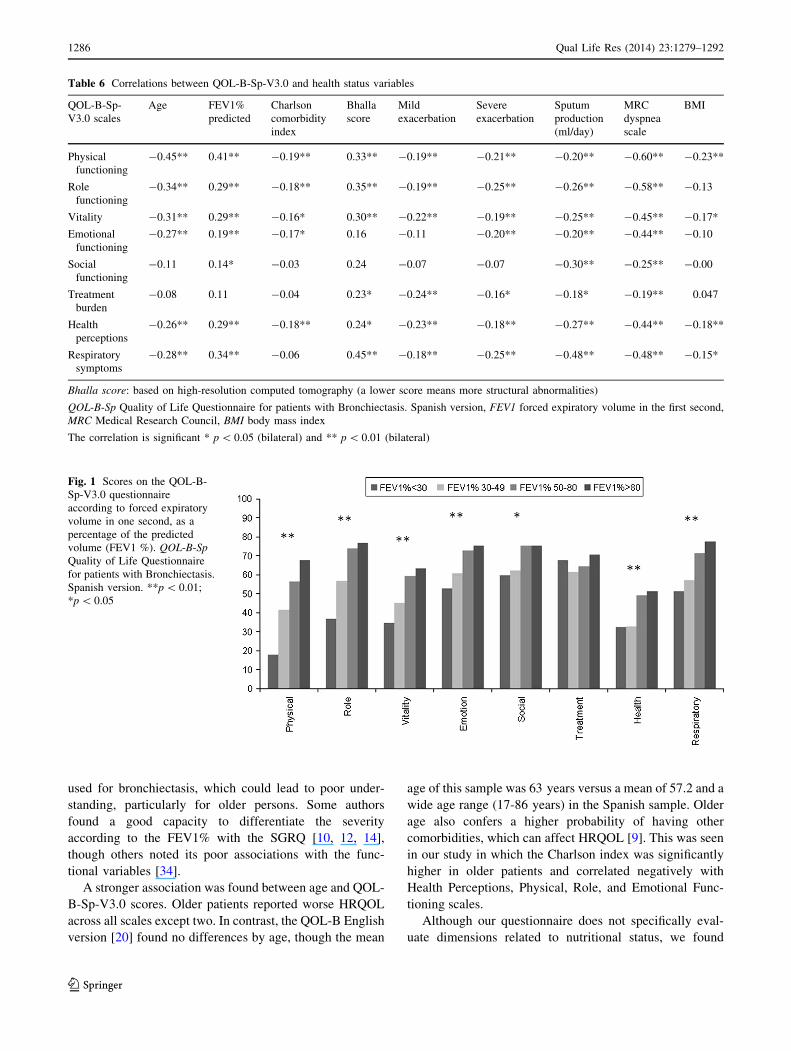
Figure 1 represents the mean QOL-B-Sp-V3.0 scores
categorized by disease severity according to FEV1% [26,
28]. All the scores showed significant differences (worse
HRQOL with greater severity) except for Treatment Burden.
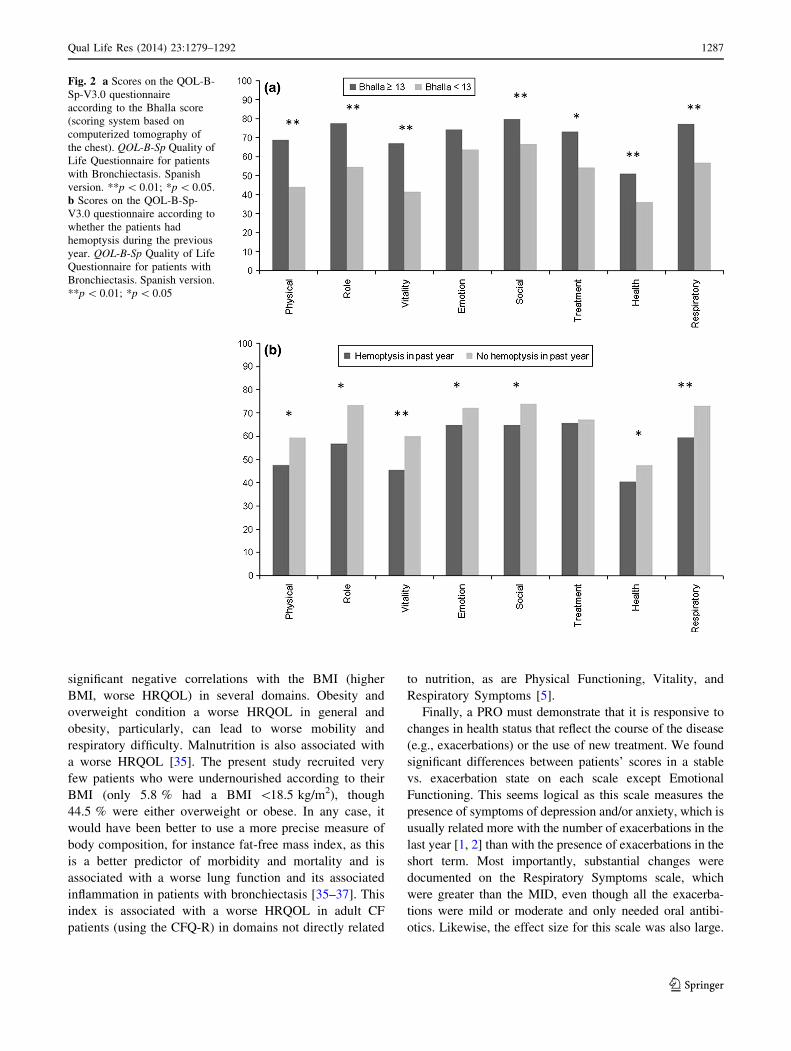
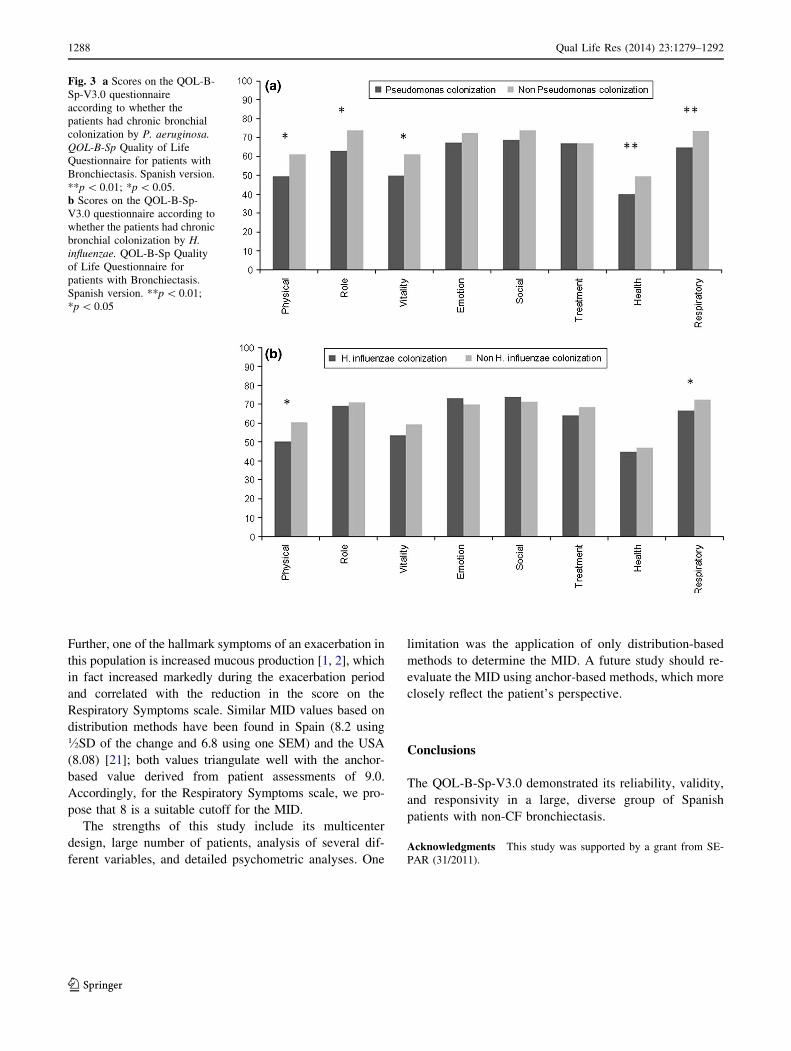
Figures 2 and 3 represent the results according to the Bhalla
score, hemoptysis during the previous year, and colonization
by Haemophilus influenzae (HI) and P. aeruginosa (PA).
The Charlson index rose significantly according to
age group (B45:1.38 ± 1 vs. 45–65:2.26 ± 1.4 vs. [ 65:
2.94 ± 2; p \ 0.001).
Table 1 Demographic and clinical characteristics
Characteristics Mean SD n (%)
Age 57.2 18.1
\45 years 55 26.6
45–65 years 66 31.9
[65 years 86 41.5
Males 77 37.2
Body mass index (Kg/m2) 25.0 4.4
Undernourished (BMI \ 18.5 kg/m2) 12 5.8
Overweight (BMI: 25-30 kg/m2) 63 30.0
Obese (BMI [ 30 kg/m2) 30 14.5
Smoking history
Current smokers 9 4.3
Ex-smokers 56 27.1
Non-smokers 142 68.6
Etiology
Idiopathic 58 28.0
Post-infection 80 38.6
Immunodeficiency 12 5.8
Collagen disease 7 3.4
Ciliary dyskinesia 22 10.6
Other 28 13.5
Sputum production (ml/day) 21.8 25.6
FEV1% of predicted 68.3 22.2
Bhalla score 11.5 7.3
Chronic colonization
P. aeruginosa 68 32.9
H. influenzae 64 30.9
Exacerbations in the last year 1.7 1.6
Mild–moderate exacerbations 1.6 1.5
Severe exacerbations 0.1 0.4
Bhalla score: based on high-resolution computed tomography (a
lower score means more structural abnormalities)
BMI body mass index. FEV1 forced expiratory volume in the first
second
Table 2 General description, internal consistency, and test–retest
reliabilities of the QOL-B-Sp-V3.0
QOL-B-Sp-V3.0
scales
Items,
no.
Cronbach
aICC Floor
effect
Ceiling
effect
Physical functioning 5 0.91 0.88 1.9 13.5
Role functioning 5 0.84 0.86 1.4 18.4
Vitality 3 0.82 0.78 3.4 9.2
Emotional functioning 4 0.84 0.86 1.9 19.8
Social functioning 4 0.70 0.78 1.4 21.7
Treatment burden 3 0.72 0.68 1.7 16.6
Health perceptions 4 0.71 0.83 1.9 0.5
Respiratory symptoms 9 0.87 0.83 0.5 2.4
ICC intraclass correlation coefficient, QOL-B-Sp Quality of Life
Questionnaire for patients with Bronchiectasis. Spanish version
Qual Life Res (2014) 23:1279–1292 1283
123
Discussion
This study demonstrated that the QOL-B-Sp-V3.0 is a
reliable and valid PRO for patients with non-CF bronchi-
ectasis in Spanish patients, and is sensitive to the effects of
pulmonary exacerbations. These results are consistent with
those of the English version of the QOL-B [19–21] and
indicate that the Spanish version is conceptually equivalent
to the original. In this Spanish version, evidence of good
internal consistency was found across all scales, and it may
therefore be used to compare groups. Furthermore, the
scales Physical Functioning and Respiratory Symptoms
could even be contemplated for individual comparisons.
Similar strong internal consistency coefficients were also
reported for the English language version [20].
Excellent item to total correlations were found across
scales, supporting the underlying construct validity of these
scales. Item 33 on the Respiratory Symptoms cross-loaded
with the Physical Functioning scale. This reflects dyspnea
upon exertion, and it is therefore reasonable that it should
Table 3 Item-scale correlations on the QOL-B QOL-B-Sp-V3.0
Items Scales
Physical Role Vitality Emotion Social Treatment Health Respiratory
Physical 1 0.849** 0.635** 0.529** 0.468** 0.297** 0.250** 0.550** 0.510**
Physical 2 0.883** 0.692** 0.618** 0.590** 0.453** 0.264** 0.657** 0.639**
Physical 3 0.895** 0.666** 0.639** 0.555** 0.417** 0.292** 0.606** 0.587**
Physical 4 0.866** 0.601** 0.609** 0.524** 0.387** 0.264** 0.533** 0.617**
Health 5 0.566** 0.641** 0.654** 0.527** 0.343** 0.228** 0.741** 0.549**
Vitality 6 0.612** 0.623** 0.858** 0.573** 0.379** 0.197** 0.596** 0.564**
Emotional 7 0.427** 0.571** 0.470** 0.741** 0.384** 0.261** 0.511** 0.514**
Vitality 8 0.573** 0.505** 0.810** 0.475** 0.345** 0.327** 0.583** 0.497**
Vitality 9 0.631** 0.644** 0.867** 0.649** 0.461** 0.287** 0.624** 0.613**
Emotional 10 0.507** 0.598** 0.610** 0.869** 0.454** 0.282** 0.554** 0.478**
Emotional 11 0.522** 0.605** 0.550** 0.862** 0.445** 0.252** 0.581** 0.506**
Treatment 12 0.237** 0.301** 0.274** 0.287** 0.226** 0.866** 0.270** 0.305**
Treatment 13 0.293** 0.207* 0.187* 0.144 0.128 0.716** 0.163* 0.210**
Treatment 14 0.770 0.211** 0.171* 0.175* 0.291** 0.849** 0.231** 0.258**
Health 15 0.653** 0.664** 0.615** 0.606** 0.425** 0.305** 0.769** 0.632**
Physical 16 0.830** 0.664** 0.584** 0.547** 0.430** 0.234** 0.564** 0.553**
Role 17 0.660** 0.778** 0.558** 0.639** 0.461** 0.346** 0.611** 0.602**
Social 18 0.290** 0.372** 0.327** 0.395** 0.581** 0.207** 0.394** 0.371**
Social 19 0.408** 0.462** 0.402** 0.445** 0.634** 0.341** 0.350** 0.432**
Role 20 0.449** 0.745** 0.436** 0.461** 0.342** 0.208** 0.544** 0.504**
Health 21 0.308** 0.279** 0.245** 0.315** 0.425** 0.159* 0.631** 0.322**
Social 22 0.370** 0.425** 0.362** 0.411** 0.821** 0.166* 0.447** 0.498**
Emotional 23 0.543** 0.619** 0.486** 0.820** 0.569** 0.295** 0.523** 0.492**
Health 24 0.508** 0.624** 0.506** 0.536** 0.435** 0.248** 0.800** 0.518**
Role 25 0.541** 0.813** 0.462** 0.625** 0.457** 0.274** 0.562** 0.505**
Social 26 0.298** 0.370** 0.251** 0.358** 0.767** 0.165* 0.339** 0.342**
Role 27 0.695** 0.796** 0.600** 0.548** 0.402** 0.244** 0.601** 0.518**
Role 28 0.669** 0.803** 0.586** 0.561** 0.545** 0.250** 0.605** 0.597**
Respiratory 29 0.496** 0.519** 0.496** 0.441** 0.471** 0.351** 0.524** 0.784**
Respiratory 30 0.414** 0.440** 0.343** 0.365** 0.338** 0.209** 0.434** 0.731**
Respiratory 31 0.404** 0.481** 0.379** 0.430** 0.458** 0.282** 0.469** 0.763**
Respiratory 32 0.235** 0.250** 0.303** 0.208** 0.250** 0.224** 0.311** 0.509**
Respiratory 33 0.697** 0.650** 0.609** 0.578** 0.412** 0.231** 0.559** 0.657**
Respiratory 34 0.514** 0.456** 0.409** 0.395** 0.366** 0.171* 0.440** 0.753**
Respiratory 35 0.446** 0.482** 0.450** 0.470** 0.342** 0.275** 0.463** 0.612**
Respiratory 36 0.525** 0.462** 0.488** 0.447** 0.347** 0.148* 0.477** 0.559**
Respiratory 37 0.495** 0.516** 0.421** 0.444** 0.442** 0.221** 0.466** 0.773**
QOL-B-Sp Quality of Life Questionnaire for patients with Bronchiectasis. Spanish version
The correlation is significant * p \ 0.05 (bilateral) and ** p \ 0.01 (bilateral)
1284 Qual Life Res (2014) 23:1279–1292
123
correlate adequately with the Physical Functioning scale.
Additionally, across scales, minimal floor and ceiling
effects were observed, enabling patients to report both
improvement and worsening in their symptoms and daily
functioning.
Test–retest reliability over 2 weeks was strong, suggesting
that patients’ scores are stable and reproducible [6, 31–33].
These values were similar to those found for the English
language version [20].
We found good convergence between respiratory
parameters and almost all scales on the QOL-B-Sp-V3.0. In
all cases, higher scores correlated with better status, with
bronchorrhea and degree of dyspnea demonstrating the
highest associations. Martınez-Garcıa et al. [10, 12] and
Chan et al. [14] also found that the patients with more
severe dyspnea, bronchorrhea, and exacerbations had
worse HRQOL on the SGRQ. Wilson et al. [34] reported
similar results on the SGRQ in relation to exacerbations.
Patients with the greatest structural damage on the
HRCT had worse HRQOL on most scales. In the QOL-B
English version, Respiratory Symptoms scores were also
associated with HRCT scores [20, 21], and similar results
were reported for the SGRQ [10, 12].
Analyses of microorganisms also supported the validity
of the QOL-B-Spain-V3.0, for example, colonization by P.
aeruginosa (PA) was associated with worse scores across
most of the scales. Other authors also found a worse
HRQOL (SGRQ) in patients with chronic colonization by
P. aeruginosa [10, 12, 13].
Convergent validity was also demonstrated by the sig-
nificant correlations found between all dimensions of the
QOL-B-Sp-V3.0 and the SGRQ [8–10], reaching very high
values in scales measuring similar parameters, as occurred
with the QOL-B English version [20].
The instrument demonstrated good discrimination of
disease severity in relation to FEV1% for all scales except
Treatment Burden, the strongest associations being for
Respiratory Symptoms and Physical Functioning. A similar
pattern of results was found for the Cystic Fibrosis Ques-
tionnaire Revised [6] (CFQ-R) and its relationship to spi-
rometry but lack of association between disease severity
and Treatment Burden [5, 6]. The lack of a correlation with
this scale may be because it is of a conditional type and it
has a long heading, as it contains various types of therapy
Table 4 Mean scores on the scales of the QOL-B-Sp-V3.0
QOL-B-Sp-V3.0 scales Initial n = 207 Stable test–retest n = 161** Exacerbation n = 80 *** Effect size
Baseline 2 weeks p Baseline Exacerbation p
Mean ± SD Mean ± SD Mean ± SD Mean ± SD Mean ± SD
Physical functioning 57.5 ± 29.7 56.1 ± 29.3 56.6 ± 28.8 0.63 51.6 ± 29.1 38.4 ± 29.3 0.00* 0.45
Role functioning 70.4 ± 25.4 70.2 ± 25.6 68.5 ± 25.1 0.11 68.0 ± 25.8 51.1 ± 28.4 0.00* 0.62
Vitality 57.6 ± 24.8 56.9 ± 25.8 59.0 ± 25.3 0.12 54.4 ± 24.7 39.4 ± 29.6 0.00* 0.55
Emotional functioning 71.0 ± 25.4 71.1 ± 25.6 71.3 ± 24.1 0.88 69.3 ± 27.4 65.9 ± 26.0 0.14 0.13
Social functioning 72.4 ± 25.1 71.8 ± 25.1 71.1 ± 24.6 0.58 68.9 ± 28.2 60.4 ± 29.0 0.00* 0.32
Treatment burden 67.1 ± 24.4 67.9 ± 23.1 66.4 ± 22.5 0.38 67.6 ± 24.8 61.8 ± 24.0 0.04* 0.24
Health perceptions 46.5 ± 21.6 46.1 ± 21.9 48.1 ± 22.8 0.06 43.0 ± 19.5 32.2 ± 22.4 0.00* 0.52
Respiratory symptoms 70.7 ± 19.7 71.0 ± 19.9 71.4 ± 19.2 0.65 69.9 ± 18.9 52.2 ± 21.3 0.00* 0.88
Stable Test–retest n = 161**: scores on the QOL-B-Spain-V3.0 at baseline and 2 weeks after the baseline visit in 161 patients (in a stable
situation at both measurements)
Exacerbation n = 80***: mean scores on the QOL-B-Spain-V3.0 at baseline and prior to starting treatment in 80 patients who experienced an
exacerbation within 6 months of the baseline visit
QOL-B-Sp Quality of Life Questionnaire for patients with Bronchiectasis. Spanish version
* p \ 0.05 (Student’s t test for paired data or Wilcoxon test, depending on normality)
Table 5 Correlations between QOL-B-Sp-V3.0 scales and SGRQ
QOL-B-Sp-V3.0 scales SGRQ
Symptom Activity Impact Total
Physical functioning -0.56** -0.78** -0.71** -0.81**
Role functioning -0.48** -0.67** -0.77** -0.77**
Vitality -0.50** -0.59** -0.63** -0.67**
Emotional functioning -0.40** -0.54** -0.64** -0.64**
Social functioning -0.30** -0.41** -0.58** -0.53**
Treatment burden -0.24** -0.23** -0.37** -0.34**
Health perceptions -0.43** -0.58** -0.70** -0.68**
Respiratory symptoms -0.54** -0.57** -0.65** -0.69**
SGRQ St. George Respiratory Questionnaire (higher scores represent
worse quality of life), QOL-B-Sp Quality of Life Questionnaire for
patients with Bronchiectasis. Spanish version
The correlation is significant ** p \ 0.01 (bilateral)
Qual Life Res (2014) 23:1279–1292 1285
123
used for bronchiectasis, which could lead to poor under-
standing, particularly for older persons. Some authors
found a good capacity to differentiate the severity
according to the FEV1% with the SGRQ [10, 12, 14],
though others noted its poor associations with the func-
tional variables [34].
A stronger association was found between age and QOL-
B-Sp-V3.0 scores. Older patients reported worse HRQOL
across all scales except two. In contrast, the QOL-B English
version [20] found no differences by age, though the mean
age of this sample was 63 years versus a mean of 57.2 and a
wide age range (17-86 years) in the Spanish sample. Older
age also confers a higher probability of having other
comorbidities, which can affect HRQOL [9]. This was seen
in our study in which the Charlson index was significantly
higher in older patients and correlated negatively with
Health Perceptions, Physical, Role, and Emotional Func-
tioning scales.
Although our questionnaire does not specifically eval-
uate dimensions related to nutritional status, we found
Table 6 Correlations between QOL-B-Sp-V3.0 and health status variables
QOL-B-Sp-
V3.0 scales
Age FEV1%
predicted
Charlson
comorbidity
index
Bhalla
score
Mild
exacerbation
Severe
exacerbation
Sputum
production
(ml/day)
MRC
dyspnea
scale
BMI
Physical
functioning
-0.45** 0.41** -0.19** 0.33** -0.19** -0.21** -0.20** -0.60** -0.23**
Role
functioning
-0.34** 0.29** -0.18** 0.35** -0.19** -0.25** -0.26** -0.58** -0.13
Vitality -0.31** 0.29** -0.16* 0.30** -0.22** -0.19** -0.25** -0.45** -0.17*
Emotional
functioning
-0.27** 0.19** -0.17* 0.16 -0.11 -0.20** -0.20** -0.44** -0.10
Social
functioning
-0.11 0.14* -0.03 0.24 -0.07 -0.07 -0.30** -0.25** -0.00
Treatment
burden
-0.08 0.11 -0.04 0.23* -0.24** -0.16* -0.18* -0.19** 0.047
Health
perceptions
-0.26** 0.29** -0.18** 0.24* -0.23** -0.18** -0.27** -0.44** -0.18**
Respiratory
symptoms
-0.28** 0.34** -0.06 0.45** -0.18** -0.25** -0.48** -0.48** -0.15*
Bhalla score: based on high-resolution computed tomography (a lower score means more structural abnormalities)
QOL-B-Sp Quality of Life Questionnaire for patients with Bronchiectasis. Spanish version, FEV1 forced expiratory volume in the first second,
MRC Medical Research Council, BMI body mass index
The correlation is significant * p \ 0.05 (bilateral) and ** p \ 0.01 (bilateral)
Fig. 1 Scores on the QOL-B-
Sp-V3.0 questionnaire
according to forced expiratory
volume in one second, as a
percentage of the predicted
volume (FEV1 %). QOL-B-Sp
Quality of Life Questionnaire
for patients with Bronchiectasis.
Spanish version. **p \ 0.01;
*p \ 0.05
1286 Qual Life Res (2014) 23:1279–1292
123
significant negative correlations with the BMI (higher
BMI, worse HRQOL) in several domains. Obesity and
overweight condition a worse HRQOL in general and
obesity, particularly, can lead to worse mobility and
respiratory difficulty. Malnutrition is also associated with
a worse HRQOL [35]. The present study recruited very
few patients who were undernourished according to their
BMI (only 5.8 % had a BMI \18.5 kg/m2), though
44.5 % were either overweight or obese. In any case, it
would have been better to use a more precise measure of
body composition, for instance fat-free mass index, as this
is a better predictor of morbidity and mortality and is
associated with a worse lung function and its associated
inflammation in patients with bronchiectasis [35–37]. This
index is associated with a worse HRQOL in adult CF
patients (using the CFQ-R) in domains not directly related
to nutrition, as are Physical Functioning, Vitality, and
Respiratory Symptoms [5].
Finally, a PRO must demonstrate that it is responsive to
changes in health status that reflect the course of the disease
(e.g., exacerbations) or the use of new treatment. We found
significant differences between patients’ scores in a stable
vs. exacerbation state on each scale except Emotional
Functioning. This seems logical as this scale measures the
presence of symptoms of depression and/or anxiety, which is
usually related more with the number of exacerbations in the
last year [1, 2] than with the presence of exacerbations in the
short term. Most importantly, substantial changes were
documented on the Respiratory Symptoms scale, which
were greater than the MID, even though all the exacerba-
tions were mild or moderate and only needed oral antibi-
otics. Likewise, the effect size for this scale was also large.
Fig. 2 a Scores on the QOL-B-
Sp-V3.0 questionnaire
according to the Bhalla score
(scoring system based on
computerized tomography of
the chest). QOL-B-Sp Quality of
Life Questionnaire for patients
with Bronchiectasis. Spanish
version. **p \ 0.01; *p \ 0.05.
b Scores on the QOL-B-Sp-
V3.0 questionnaire according to
whether the patients had
hemoptysis during the previous
year. QOL-B-Sp Quality of Life
Questionnaire for patients with
Bronchiectasis. Spanish version.
**p \ 0.01; *p \ 0.05
Qual Life Res (2014) 23:1279–1292 1287
123
Further, one of the hallmark symptoms of an exacerbation in
this population is increased mucous production [1, 2], which
in fact increased markedly during the exacerbation period
and correlated with the reduction in the score on the
Respiratory Symptoms scale. Similar MID values based on
distribution methods have been found in Spain (8.2 using
�SD of the change and 6.8 using one SEM) and the USA
(8.08) [21]; both values triangulate well with the anchor-
based value derived from patient assessments of 9.0.
Accordingly, for the Respiratory Symptoms scale, we pro-
pose that 8 is a suitable cutoff for the MID.
The strengths of this study include its multicenter
design, large number of patients, analysis of several dif-
ferent variables, and detailed psychometric analyses. One
limitation was the application of only distribution-based
methods to determine the MID. A future study should re-
evaluate the MID using anchor-based methods, which more
closely reflect the patient’s perspective.
Conclusions
The QOL-B-Sp-V3.0 demonstrated its reliability, validity,
and responsivity in a large, diverse group of Spanish
patients with non-CF bronchiectasis.
Acknowledgments This study was supported by a grant from SE-
PAR (31/2011).
Fig. 3 a Scores on the QOL-B-
Sp-V3.0 questionnaire
according to whether the
patients had chronic bronchial
colonization by P. aeruginosa.
QOL-B-Sp Quality of Life
Questionnaire for patients with
Bronchiectasis. Spanish version.
**p \ 0.01; *p \ 0.05.
b Scores on the QOL-B-Sp-
V3.0 questionnaire according to
whether the patients had chronic
bronchial colonization by H.
influenzae. QOL-B-Sp Quality
of Life Questionnaire for
patients with Bronchiectasis.
Spanish version. **p \ 0.01;
*p \ 0.05
1288 Qual Life Res (2014) 23:1279–1292
123
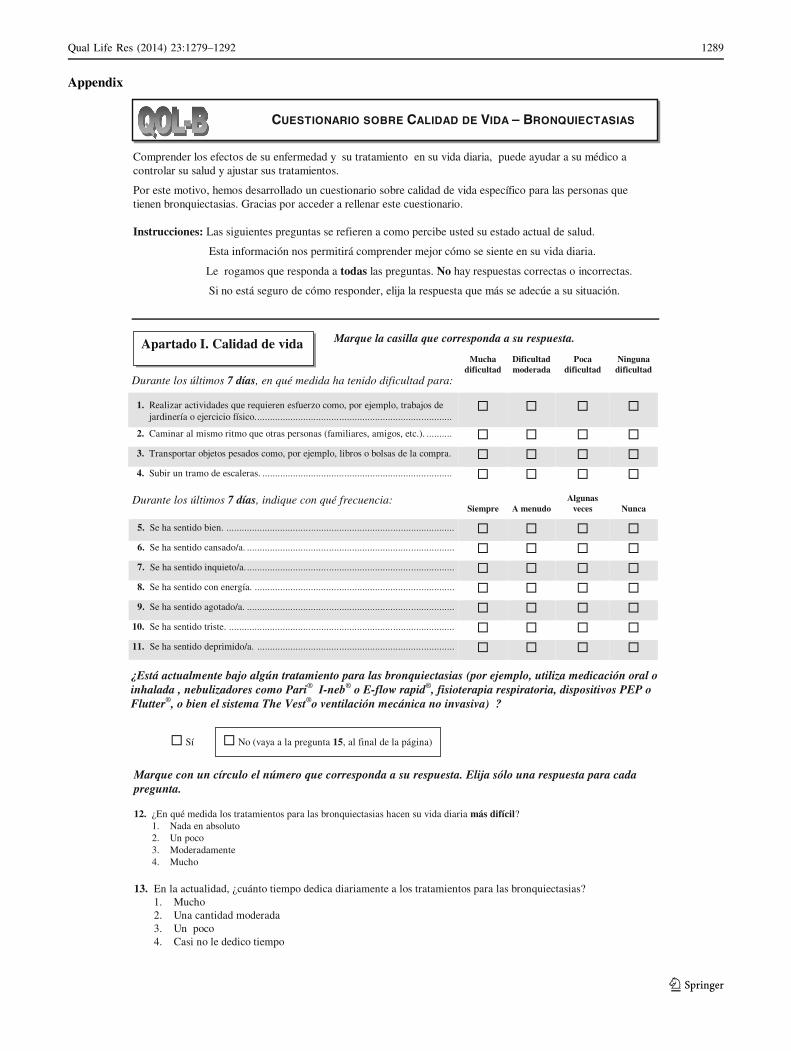
CUESTIONARIO SOBRE CALIDAD DE VIDA – BRONQUIECTASIAS
Comprender los efectos de su enfermedad y su tratamiento en su vida diaria, puede ayudar a su médico a controlar su salud y ajustar sus tratamientos.
Por este motivo, hemos desarrollado un cuestionario sobre calidad de vida específico para las personas que tienen bronquiectasias. Gracias por acceder a rellenar este cuestionario.
Instrucciones: Las siguientes preguntas se refieren a como percibe usted su estado actual de salud.
Esta información nos permitirá comprender mejor cómo se siente en su vida diaria.
Le rogamos que responda a todas las preguntas. No hay respuestas correctas o incorrectas.
Si no está seguro de cómo responder, elija la respuesta que más se adecúe a su situación.
Durante los últimos 7 días, en qué medida ha tenido dificultad para:
Mucha dificultad
Dificultad moderada
Poca dificultad
Ninguna dificultad
1. Realizar actividades que requieren esfuerzo como, por ejemplo, trabajos de jardinería o ejercicio físico.
2. Caminar al mismo ritmo que otras personas (familiares, amigos, etc.).
3. Transportar objetos pesados como, por ejemplo, libros o bolsas de la compra.
4. Subir un tramo de escaleras.
Durante los últimos 7 días, indique con qué frecuencia:Siempre A menudo
Algunas veces Nunca
5. Se ha sentido bien.
6. Se ha sentido cansado/a.
7. Se ha sentido inquieto/a.
8. Se ha sentido con energía.
9. Se ha sentido agotado/a.
10. Se ha sentido triste.
11. Se ha sentido deprimido/a.
Apartado I. Calidad de vida Marque la casilla que corresponda a su respuesta.
¿Está actualmente bajo algún tratamiento para las bronquiectasias (por ejemplo, utiliza medicación oral o inhalada , nebulizadores como Pari® I-neb® o E-flow rapid®, fisioterapia respiratoria, dispositivos PEP o Flutter®, o bien el sistema The Vest®o ventilación mecánica no invasiva) ?
Sí No (vaya a la pregunta 15, al final de la página)
Marque con un círculo el número que corresponda a su respuesta. Elija sólo una respuesta para cada pregunta.
12. ¿En qué medida los tratamientos para las bronquiectasias hacen su vida diaria más difícil?1. Nada en absoluto2. Un poco3. Moderadamente4. Mucho
13. En la actualidad, ¿cuánto tiempo dedica diariamente a los tratamientos para las bronquiectasias?1. Mucho2. Una cantidad moderada 3. Un poco 4. Casi no le dedico tiempo
Appendix
Qual Life Res (2014) 23:1279–1292 1289
123
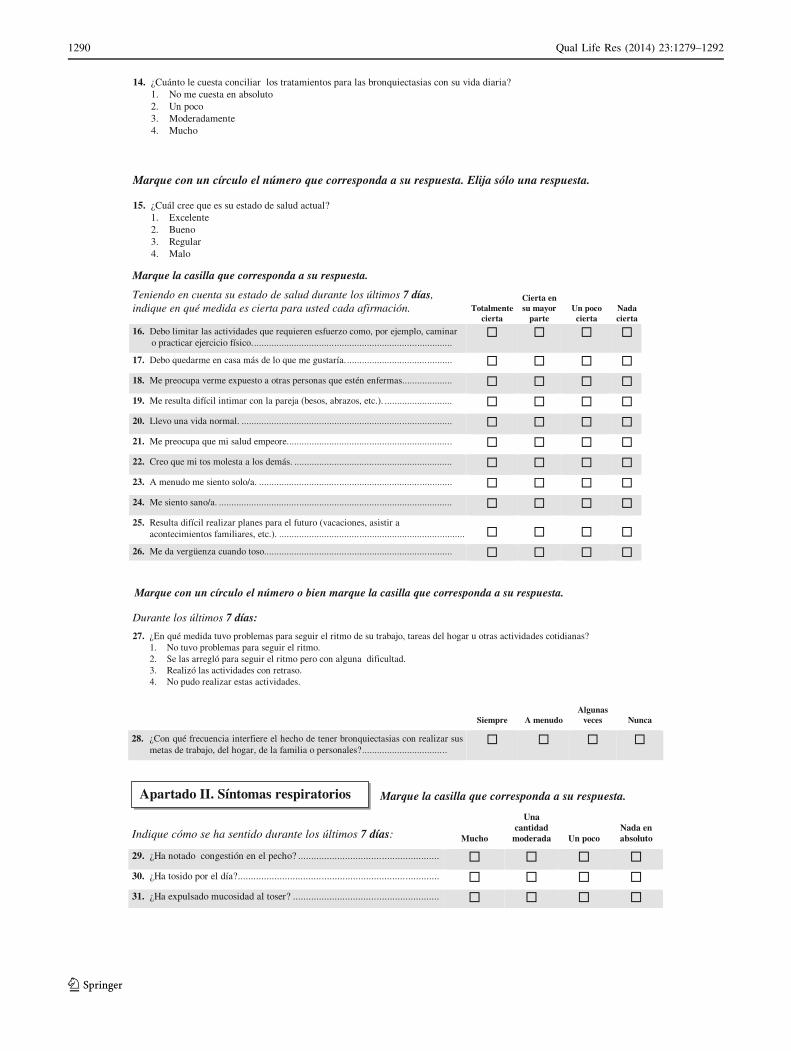
Marque la casilla que corresponda a su respuesta.
Teniendo en cuenta su estado de salud durante los últimos 7 días, indique en qué medida es cierta para usted cada afirmación. Totalmente
cierta
Cierta en su mayor
parteUn poco
ciertaNada cierta
16. Debo limitar las actividades que requieren esfuerzo como, por ejemplo, caminar o practicar ejercicio físico.
17. Debo quedarme en casa más de lo que me gustaría.
18. Me preocupa verme expuesto a otras personas que estén enfermas.
19. Me resulta difícil intimar con la pareja (besos, abrazos, etc.).
20. Llevo una vida normal.
21. Me preocupa que mi salud empeore.
22. Creo que mi tos molesta a los demás.
23. A menudo me siento solo/a.
24. Me siento sano/a.
25. Resulta difícil realizar planes para el futuro (vacaciones, asistir a acontecimientos familiares, etc.).
26. Me da vergüenza cuando toso.
Durante los últimos 7 días:
27. ¿En qué medida tuvo problemas para seguir el ritmo de su trabajo, tareas del hogar u otras actividades cotidianas?1. No tuvo problemas para seguir el ritmo.2. Se las arregló para seguir el ritmo pero con alguna dificultad.3. Realizó las actividades con retraso.4. No pudo realizar estas actividades.
Siempre A menudoAlgunas
veces Nunca
28. ¿Con qué frecuencia interfiere el hecho de tener bronquiectasias con realizar sus metas de trabajo, del hogar, de la familia o personales?
Marque con un círculo el número o bien marque la casilla que corresponda a su respuesta.
14. ¿Cuánto le cuesta conciliar los tratamientos para las bronquiectasias con su vida diaria?1. No me cuesta en absoluto2. Un poco3. Moderadamente4. Mucho
Marque con un círculo el número que corresponda a su respuesta. Elija sólo una respuesta.
15. ¿Cuál cree que es su estado de salud actual?1. Excelente2. Bueno3. Regular4. Malo
Indique cómo se ha sentido durante los últimos 7 días: Mucho
Una cantidad
moderada Un pocoNada en absoluto
29. ¿Ha notado congestión en el pecho?
30. ¿Ha tosido por el día?
31. ¿Ha expulsado mucosidad al toser?
Apartado II. Síntomas respiratorios Marque la casilla que corresponda a su respuesta.
1290 Qual Life Res (2014) 23:1279–1292
123

References
1. Vendrell, M., de Gracia, J., Olveira, C., et al. (2008). Diagnosis
and treatment of bronchiectasis. Recommendations of The
Spanish Society of Pulmonology and Thoracic Surgery (SEPAR).
Archivos de Bronconeumologia, 44, 629–640.
2. Pasteur, M. C., Bilton, D., Hill, A. T., & On behalf of the British
Thoracic Society Bronchiectasis (non-CF) Guidelines Group.
(2010). British Thoracic Society for non-CF bronchiectasis.
Thorax, 65, i1–i58.
3. O’Leary, C. J., Wilson, C. B., Hansell, D. M., Cole, P. J., Wilson, R.,
& Jones, P. W. (2002). Relationship between psychological well-
being and lung health status in patients with bronchiectasis. Respi-
ratory Medicine, 96, 686–692.
4. Olveira, C., Olveira, G., Gaspar, I., et al. (2013). Depression and
anxiety symptoms in bronchiectasis: associations with health-
related quality of life. Quality of Life Research, 22, 597–605.
5. Olveira, G., Olveira, C., Gaspar, I., et al. (2010). Validation of the
Spanish version of the revised cystic fibrosis quality of life
questionnaire in adolescents and adults (CFQR 14 ? Spain).
Archivos de Bronconeumologia, 46, 165–175.
6. Quittner, A. L., Buu, A., Messer, M. A., Modi, A. C., & Watrous, M.
(2005). Development and validation of The Cystic Fibrosis Ques-
tionnaire in the United States: A health-related quality-of-life mea-
sure for cystic fibrosis. Chest Journal, 128, 2347–2354.
7. US Food and Drug Administration. (2009). Guidance for industry
patient-reported outcome measures: Use in medial product develop-
ment to support label ing claims. Retrieved April 13, 2011. http://
www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatory
Information/Guidances/UCM193282.pdf.
8. Jones, P. W., Quirk, F. H., Baveystock, C. M., & Littlejohns, P.
(1992). A self-complete measure of health status for chronic
airflow limitation: The St. George’s Respiratory Questionnaire.
American Journal of Respiratory and Critical Care Medicine,
145, 1321–1327.
9. Padilla, A., Olveira, G., Olveira, C., et al. (2007). Validity and
reliability of the St George’s Respiratory Questionnaire in adults
with cystic fibrosis. Archivos de Bronconeumologia, 43, 205–211.
10. Martınez-Garcıa, M. A., Perpina Tordera, M., Roman Sanchez, P.,
& Soler Cataluna, J. J. (2005). Internal consistency and validity of
the Spanish version of the St. George’s respiratory questionnaire
for use in patients with clinically stable bronchiectasis. Archivos
de Bronconeumologia, 41, 110–117.
11. Retsch-Bogart, G. Z., Quittner, A. L., Gibson, R. L., et al. (2009).
Efficacy and safety of inhaled aztreonam lysine for airway
pseudomonas in cystic fibrosis. Chest Journal, 135, 1223–1232.
12. Martınez-Garcıa, M. A., Perpina-Tordera, M., Roman-Sanchez, P., &
Soler-Cataluna, J. J. (2005). Quality-of-life determinants in patients
with clinically stable bronchiectasis. Chest Journal, 128, 739–745.
13. Wilson, C. B., Jones, P. W., O’Leary, C. J., Hansell, D. M., Cole,
P. J., & Wilson, R. (1997). Effect of sputum bacteriology on the
quality of life of patients with bronchiectasis. European Respi-
ratory Journal, 10, 1754–1760.
14. Chan, S. L., Chan-Yeung, M. M., Ooi, G. C., et al. (2002).
Validation of the Hong Kong Chinese version of the St. George
Respiratory Questionnaire in patients with bronchiectasis. Chest
Journal, 122, 2030–2037.
15. Jones, P. W. (2002). Interpreting thresholds for a clinically sig-
nificant change in health status in asthma and COPD. European
Respiratory Journal, 19, 398–404.
16. Martınez-Garcıa, M. A., Soler-Cataluna, J. J., Catalan-Serra, P.,
Roman-Sanchez, P., & Tordera, M. P. (2012). Clinical efficacy
and safety of budesonide formoterol in non-cystic fibrosis BQ.
Chest Journal, 141, 461–468.
17. Murray, M. P., Turnbull, K., Mac Quarrie, S., Pentland, J. L., &
Hill, A. T. (2009). Validation of the Leicester Cough Question-
naire in non-cystic fibrosis bronchiectasis. European Respiratory
Journal, 34, 125–131.
18. Reda, A. A., Kotz, D., Kocks, J. W., Wesseling, G., & Van
Schayck, C. P. (2010). Reliability and validity of the clinical
COPD questionnaire and chronic respiratory questionnaire.
Respiratory Medicine, 104, 1675–1682.
19. Quittner, A. L., Cruz, I., Marciel, K. K., Ilowite, J., Gotfried, M. H., &
Barker, A. (2009). A new PRO for non-CF bronchiectasis: Associ-
ations between the QOL-B and health outcomes. [Abstract]. Euro-
pean Respiratory Journal, 34(Suppl. 53), 1010.
20. Quittner, A. L., Salathe, M., Gotfried, M., et al. (2010). National
validation of a patient-reported outcome measure for bronchiec-
tasis: Psychometric results on the QOL-B.[Abst.] American
Journal of Respiratory Critical Care Medicine A5793. www.
atsjournals.org Online Abstracts Issue.
21. Quittner, A. L. (2012). Development of a disease-specific PRO
for non-CF bronchiectasis: The QOL-B FDA Workshop 2012.
22. Naidich, D. P., McCauley, D. I., Khouri, N. F., Stitik, F. P., &
Siegelman, S. S. (1982). Computed tomography of bronchiecta-
sis. Journal of Computer Assisted Tomography, 6, 437–444.
32. Sus esputos han sido mayoritariamente: Transparentes Entre transparentes y amarillos
Entre amarillentos y verdes Entre parduzcos y marrones oscuros
Verdes con trazas de sangre No lo sé.
Cantidad de esputo total en un día estando agudizado (MAL): cc
Con qué frecuencia durante los últimos 7 días:Siempre A menudo
Algunas veces Nunca
33. ¿Le ha faltado la respiración al realizar una mayor actividad como, por ejemplo, tareas del hogar o de jardinería?
34. ¿Ha experimentado silbidos (pitos)?
35. ¿Ha experimentado dolor en el pecho?
36. ¿Le ha faltado la respiración mientras hablaba?
37. ¿La tos le ha despertado durante la noche?
Le rogamos que compruebe que ha respondido a todas las preguntas.
Qual Life Res (2014) 23:1279–1292 1291
123
23. Rosenstein, B. J., & Cutting, G. R. (1998). The diagnosis of cystic
fibrosis: a consensus statement. Cystic Fibrosis Foundation
Consensus Panel. Journal of Pediatrics, 132, 589–595.
24. Medical Research Council. (1982). Committee on research into
chronic bronchitis: Instruction for use on the questionnaire on
respiratory symptoms. In S. M. Brooks (Ed.), Surveillance for
respiratory hazards (Vol. 8, pp. 12–16). ATS News. Devon: WJ
Holman 1966.
25. Charlson, M. E., Pompei, P., Ales, K. L., & MacKenzie, C. R.
(1987). A new method of classifying prognostic comorbidity in
longitudinal studies: Development and validation. Journal of
Chronic Disease, 40, 373–383.
26. Roca, J., Sanchis, J., Agustı Vidal, A., et al. (1986). Spirometric
reference values for a Mediterranean population. Bulletin Euro-
peen de Physiopathologie Respiratoire, 22, 217–224.
27. Bhalla, M., Turcios, N., Aponte, V., et al. (1991). Cystic fibrosis:
Scoring system with thin-section CT. Radiology, 179, 783–788.
28. Snider, G. L., Kory, R. C., & Lyons, H. A. (1967). Grading of
pulmonary function impairment by means of pulmonary function
test. Diseases of the Chest, 52, 270–271.
29. Cohen, J. (1988). Statistical power analysis for the behavioral
sciences (2nd ed.). Hillsdale, NJ: Erlbaum Associates.
30. Quittner, A. L., Avani Modi, A. C., Wainwright, C., Otto, K.,
Kirihara, J., & Montgomery, B. (2009). Determination of the
minimal clinically important difference scores for the Cystic
Fibrosis Questionnaire-revised respiratory symptom scale in two
populations of patients with cystic fibrosis and chronic Pseudo-
monas aeruginosa airway infection. Chest Journal, 135,
1610–1618.
31. Quittner, A. L., Sawicki, G. S., Mc Mulen, A., et al. (2012).
Psychometric evaluation of the Cystic Fibrosis Questionnaire-
revised in a national US simple. Quality of Life Research, 21,
1279–1290.
32. Schmidt, A., Wenninger, K., Niemann, N., Wahn, U., & Staab, D.
(2009). Health-related quality of life in children with cystic
fibrosis: Validation of the German CFQ-R. Health and Quality of
Life Outcomes, 7, 97.
33. Bregnballe, V., Thastum, M., Lund, L., Hansen, C. R., Preissler,
T., & Schiøtz, P. O. (2008). Validation of the Danish version of the
revised cystic fibrosis quality of life questionnaire in adolescents
and adults (CFQ-R14?). Journal of Cystic Fibrosis, 7, 531–536.
34. Wilson, C. B., Jones, P. W., O’Leary, C. J., Cole, P. J., & Wilson, R.
(1997). Validation of the St George’s Respiratory Questionnaire in
bronchiectasis. American Journal of Respiratory and Critical Care
Medicine, 156, 536–541.
35. Olveira, G., Olveira, C., Gaspar, I., et al. (2011). Malnutrition and
inflammation in patients with bronchiectasis. Clinical Nutrition,
6(suppl 1), 150–151.
36. Olveira, G., Olveira, C., Gaspar, I., et al. (2012). Fat-free mass
depletion and inflammation in patients with bronchiectasis.
Journal of the Academy of Nutrition and Dietetics, 112,
1999–2006.
37. Olveira, G., Olveira, C., Dorado, A., et al. (2013). Cellular and
plasma oxidative stress biomarkers are raised in adults with
bronchiectasis. Clinical Nutrition, 32, 112–117.
1292 Qual Life Res (2014) 23:1279–1292
123