colonoscopy completion rates. potential improvement and financial savings for the nhs
TRANSCRIPT

Colonoscopy completion rates.
Potential improvement and financial savings for the NHS
Authors A Hussain1,2 1General surgery department, Princess Royal University Hospital. Farnborough common, Orpington, Greater London, BR6 8ND 2Honorary Senior Lecturer, King’s College Medical School, London Corresponding Author Mr. A Hussain, [email protected] The Online Journal of Clinical Audits. 2013; Vol 5(4).
Published November 2013 To subscribe to The Online Journal of Clinical Audits go to: http://www.clinicalaudits.com/index.php/ojca/user/register Article submission and authors instructions: http://www.clinicalaudits.com/index.php/ojca/about/submissions
ISSN 2042-4779 ClinicalAudits.com
Abstract Aims – The aim of this study is to explore the completion rate, the complications ,the reasons for incomplete colonoscopy and what can be done to improve the quality of the service and its impact on the total cost at a secondary referral centre within NHS , UK. Methods – This was a clinical audit conducted to study the completion rate and complications of colonoscopy during January 2011-January 2012 for the 15 endoscopists at our hospital. The data of patients who developed complications were further studied. Causes of incomplete colonoscopy were identified. Some of the required changes were fulfilled. Re-auditing was then performed for a further study period of February-August 2012. Results – 3538 patients underwent a colonoscopy procedure during the aforementioned one-year period for a variety of reasons, including a two-weeks referral. A complete colonoscopy was achieved in 3068 patients (86.7%) and failed in 470 patients (13.3%). Several reasons for an incomplete colonoscopy were identified: poor bowel preparation (29.36%), patient discomfort (21.27%), loopy colon (16.8%), pathology encountered (12.21%), narrow lumen (9%) and instrument failure (0.63%) . A further 1932 patients were studied during the next 6 months in order to compare the completion and complication rate after instilling some changes. After adjustment , the completion rate was 91.03%. In the re-auditing period the completion rate was 90.2% and after adjustment, increased to 94.13%, which is within the BSG guidelines. Conclusions – With 29% of failed colonoscopies being due to poor bowel preparation, there is a definite role for improving the efficiency of pre-procedural organisation. By instigating such changes at a national level, a greater financial impact would be achieved. Introduction Colonoscopy is a common procedure for different indications; the most important being colorectal cancer, diverticulosis, and inflammatory bowel disease. Colonoscopy can be therapeutic i.e. to remove polyps and early cancer [1].A Minimum caecal intubation rate (CIR) greater than 90% was endorsed by the American Society for Gastrointestinal Endoscopy (ASGE) and the Joint Advisory Group (JAG) UK [2]. The British Society of Gastroenterologists BSG guidelines have suggested a similar rate (www.bsg.org.uk). The UK national colonoscopy audit in 2011 showed CIR of 92.3% compared to 76.9 % in 2004[3]. Although this was representing a dramatic improvement, an endoscopists aim should be a 100% completion and 0% complication rates, which is beyond reach in the vast majority of units. Reasons for this include: a narrow colon, an obstructing growth, patient discomfort, poor bowel preparation, development of complications and instrument failure. Incomplete colonoscopy by definition is the inadequate examination of the colonic mucosa (360 degree visualization) in addition to the failure of ceacal intubation. With approximately 4.3% of neoplasia missed by an incomplete colonoscopy [4], every effort should be made to visualize the whole mucosa . Aims
1.What is the current completion rate of colonoscopy

ISSN 2042-4779 ClinicalAudits.com
2.Why it is incomplete in other patients 3.What can be done to improve the completion rate 4.What is incidence of complications (perforation, bleeding, other complications) 5.What can be done to reduce or prevent these complications
Audit Standards
1.The BSG & JAG criteria are accepting 90% as minimum completion rate. (2011) 2.Multi-Society Task Force on Colorectal Cancer and Cancer Care Ontario Colonoscopy standards of a 95% completion rate, but adjusted for poor bowel preparation and structural lesions. Methods Colonoscopy completion and complication rates were the primary end points of this audit. The secondary end points were the completion rates for medical and surgical endoscopists in addition to the causes of incomplete colonoscopies Inclusion criteria: all consecutive colonoscopies which were performed by the 5 experienced medical and 10 experienced surgical endoscopists for a variety of indications during January 2011-January 2012 at the endoscopy unit of the Princess Royal University Hospital ( table1). Exclusion criteria: all colonoscopies, which were performed by medical and surgical trainees. The completion and complication rates were calculated for every endoscopist and cumulative data were produced for medical and surgical teams. The causes of an
incomplete colonoscopy were further analyzed and a percentage for each cause was calculated. The data was compared to the national guidelines. The figures were short to match the nationally accepted threshold (before adjustment) and several factors were identified to improve the primary and secondary end points. A Further two assessments were conducted during February-May 2012 and February–August 2012 to evaluate the effect of the changes. Final outcomes were finally compared to national figures (Table 1-5,Figures1-2).
ISSN 2042-4779 ClinicalAudits.com
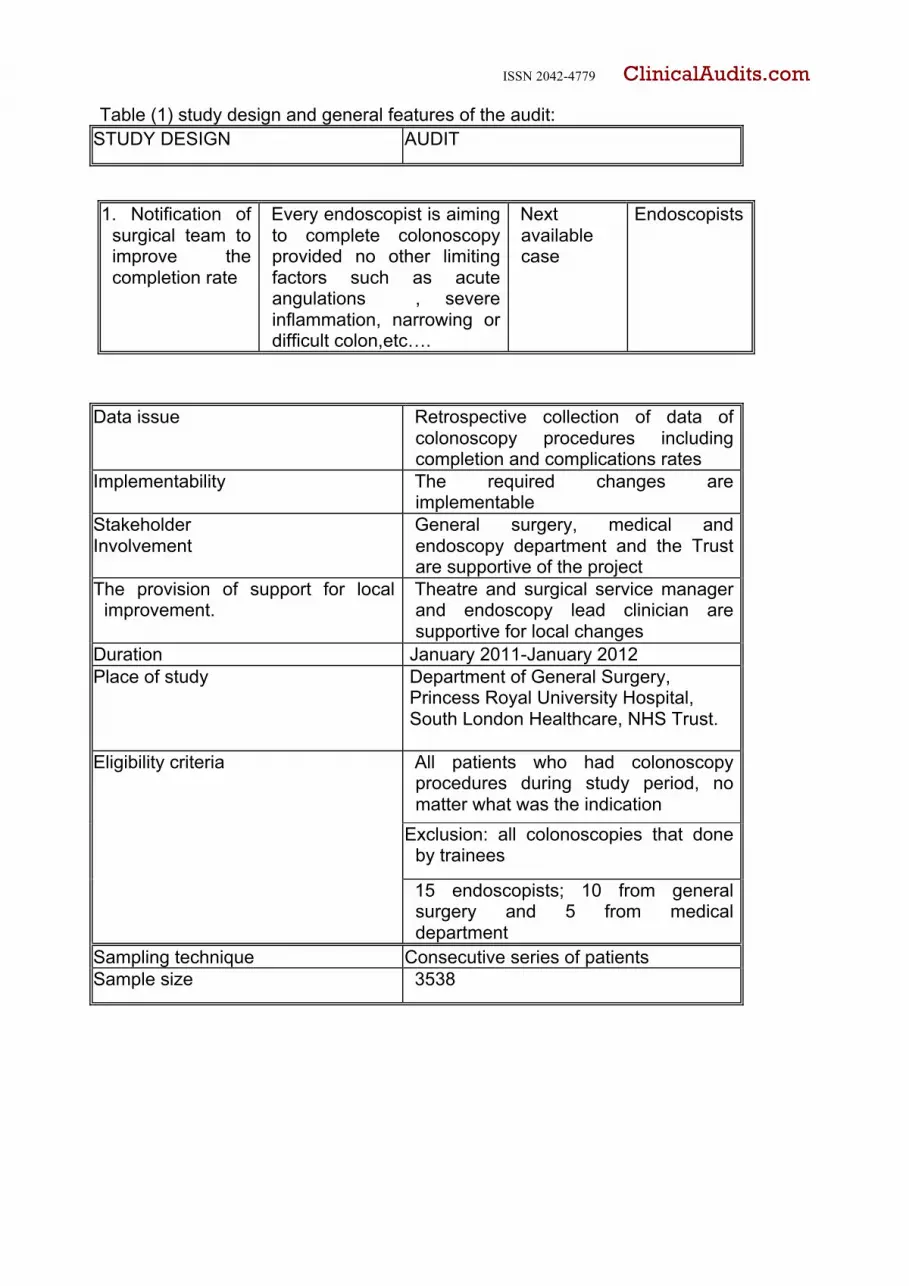
Table (1) study design and general features of the audit: STUDY DESIGN AUDIT
Data issue Retrospective collection of data of colonoscopy procedures including completion and complications rates
Implementability The required changes are implementable
Stakeholder Involvement
General surgery, medical and endoscopy department and the Trust are supportive of the project
The provision of support for local improvement.
Theatre and surgical service manager and endoscopy lead clinician are supportive for local changes
Duration January 2011-January 2012 Place of study Department of General Surgery,
Princess Royal University Hospital, South London Healthcare, NHS Trust.
Eligibility criteria
All patients who had colonoscopy procedures during study period, no matter what was the indication
Exclusion: all colonoscopies that done by trainees
15 endoscopists; 10 from general surgery and 5 from medical department
Sampling technique Consecutive series of patients Sample size 3538
1. Notification of surgical team to improve the completion rate
Every endoscopist is aiming to complete colonoscopy provided no other limiting factors such as acute angulations , severe inflammation, narrowing or difficult colon,etc….
Next available case
Endoscopists

ISSN 2042-4779 ClinicalAudits.com
Table (2) identification of changes and making improvements (Achieved, partially achieved, Not achieved)
Table (3) Key Results after re-audit: KEY RESULTS NUMBER/ % Completion 1588(90.2) Failed procedure 172(9.8) Perforation 1 (0.032) Bleeding 2(0.064) Cardio-
respiratory 0
Others 0 Mortality 0
2.Improve skills Attend colonoscopy courses
6 months Endoscopists
3.Bowel preparation
1.Patients: should follow the instructions of the endoscopy unit 2.Endoscopists:once bowel preparation is judged poor by finding solid faeces in the lower colon, the procedure should be abandoned and not considered as failure 3.Bowel preparation medication: to change to other medication or use maximum dose
Next available list
Endoscopists
4.Narrow lumen Use small size scope such as paediatric scope
Next available list
Endoscopists
5.Patient discomfort
1.Optimize the sedation 2.Predict low threshold pain patients and book them for GA list
Next available list
Endoscopists
ISSN 2042-4779 ClinicalAudits.com
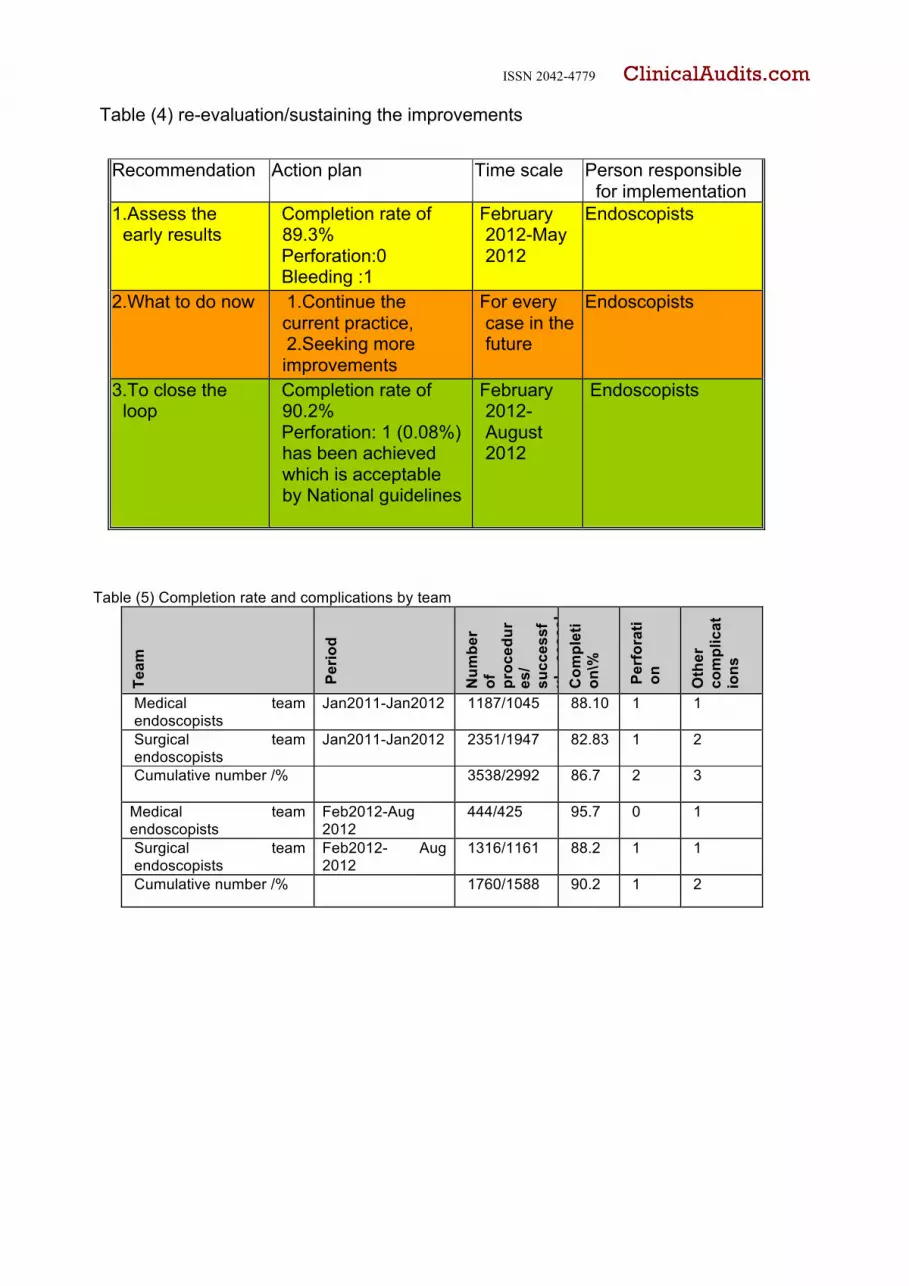
Table (4) re-evaluation/sustaining the improvements
Table (5) Completion rate and complications by team
Team
Per
iod
Num
ber
of
proc
edur
es/
succ
essf
ul
ceac
al
intu
batio
n Com
plet
ion
\%
R
ate
Perf
orat
ion
Oth
er
com
plic
atio
ns
Medical team endoscopists
Jan2011-Jan2012 1187/1045
88.10
1
1
Surgical team endoscopists
Jan2011-Jan2012
2351/1947 82.83 1 2
Cumulative number /%
3538/2992 86.7 2 3
Medical team endoscopists
Feb2012-Aug 2012
444/425 95.7 0 1
Surgical team endoscopists
Feb2012- Aug 2012
1316/1161 88.2 1 1
Cumulative number /% 1760/1588 90.2 1 2
Recommendation Action plan Time scale Person responsible for implementation
1.Assess the early results
Completion rate of 89.3%
Perforation:0 Bleeding :1
February 2012-May 2012
Endoscopists
2.What to do now 1.Continue the current practice,
2.Seeking more improvements
For every case in the future
Endoscopists
3.To close the loop
Completion rate of 90.2%
Perforation: 1 (0.08%) has been achieved which is acceptable by National guidelines
February 2012-August 2012
Endoscopists
ISSN 2042-4779 ClinicalAudits.com
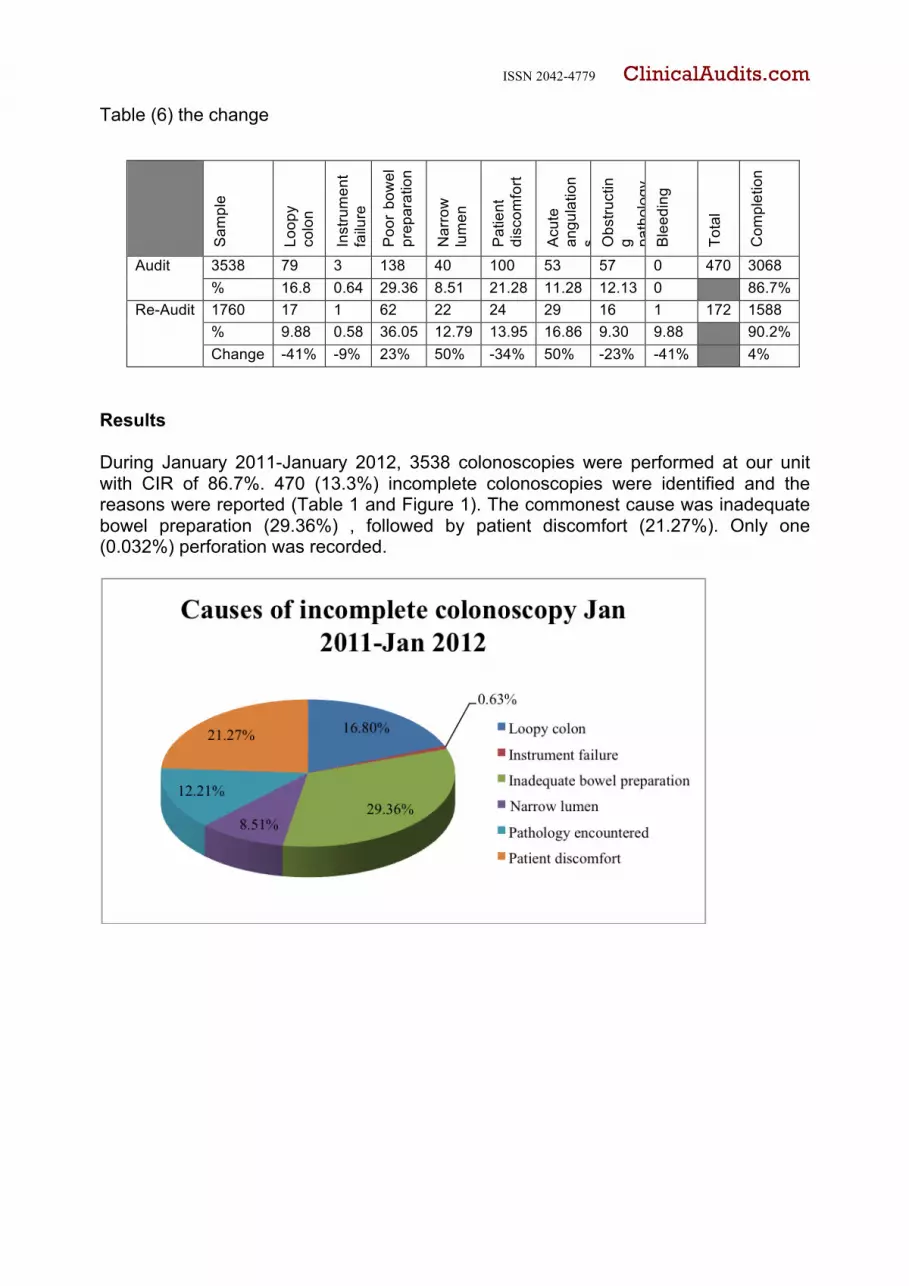
Table (6) the change
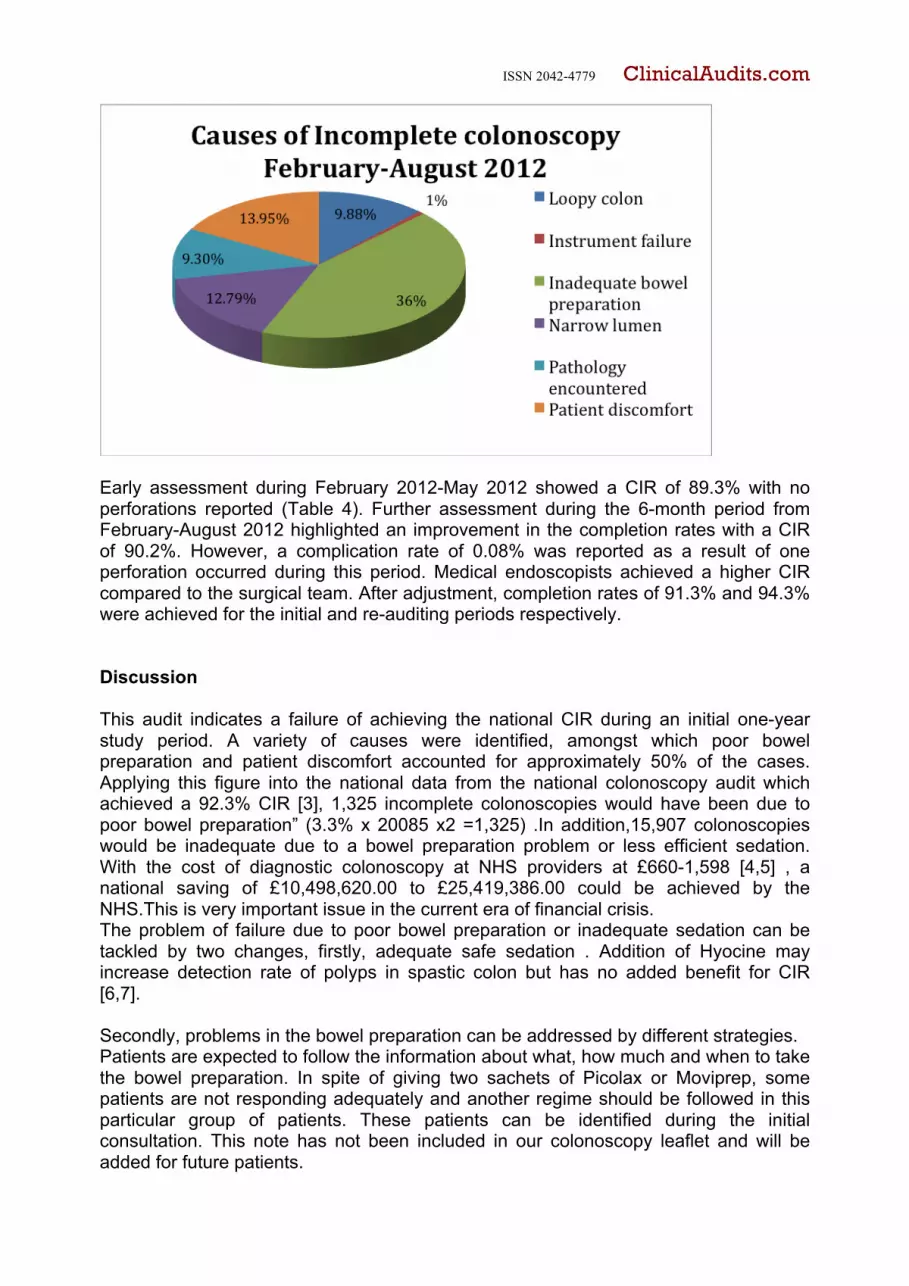
Results During January 2011-January 2012, 3538 colonoscopies were performed at our unit with CIR of 86.7%. 470 (13.3%) incomplete colonoscopies were identified and the reasons were reported (Table 1 and Figure 1). The commonest cause was inadequate bowel preparation (29.36%) , followed by patient discomfort (21.27%). Only one (0.032%) perforation was recorded.
Sam
ple
Loop
y co
lon
Inst
rum
ent
failu
re
Poo
r bo
wel
pr
epar
atio
n
Nar
row
lu
men
Pat
ient
di
scom
fort
Acu
te
angu
latio
ns O
bstru
ctin
g path
olog
y B
leed
ing
Tota
l
Com
plet
ion
Audit 3538 79 3 138 40 100 53 57 0 470 3068 % 16.8 0.64 29.36 8.51 21.28 11.28 12.13 0 86.7%
Re-Audit 1760 17 1 62 22 24 29 16 1 172 1588 % 9.88 0.58 36.05 12.79 13.95 16.86 9.30 9.88 90.2% Change -41% -9% 23% 50% -34% 50% -23% -41% 4%
ISSN 2042-4779 ClinicalAudits.com
Early assessment during February 2012-May 2012 showed a CIR of 89.3% with no perforations reported (Table 4). Further assessment during the 6-month period from February-August 2012 highlighted an improvement in the completion rates with a CIR of 90.2%. However, a complication rate of 0.08% was reported as a result of one perforation occurred during this period. Medical endoscopists achieved a higher CIR compared to the surgical team. After adjustment, completion rates of 91.3% and 94.3% were achieved for the initial and re-auditing periods respectively. Discussion This audit indicates a failure of achieving the national CIR during an initial one-year study period. A variety of causes were identified, amongst which poor bowel preparation and patient discomfort accounted for approximately 50% of the cases. Applying this figure into the national data from the national colonoscopy audit which achieved a 92.3% CIR [3], 1,325 incomplete colonoscopies would have been due to poor bowel preparation” (3.3% x 20085 x2 =1,325) .In addition,15,907 colonoscopies would be inadequate due to a bowel preparation problem or less efficient sedation. With the cost of diagnostic colonoscopy at NHS providers at £660-1,598 [4,5] , a national saving of £10,498,620.00 to £25,419,386.00 could be achieved by the NHS.This is very important issue in the current era of financial crisis. The problem of failure due to poor bowel preparation or inadequate sedation can be tackled by two changes, firstly, adequate safe sedation . Addition of Hyocine may increase detection rate of polyps in spastic colon but has no added benefit for CIR [6,7]. Secondly, problems in the bowel preparation can be addressed by different strategies. Patients are expected to follow the information about what, how much and when to take the bowel preparation. In spite of giving two sachets of Picolax or Moviprep, some patients are not responding adequately and another regime should be followed in this particular group of patients. These patients can be identified during the initial consultation. This note has not been included in our colonoscopy leaflet and will be added for future patients.
ISSN 2042-4779 ClinicalAudits.com
The second point is to use the appropriate type of bowel preparation; At the beginning of 2010, our unit changed the bowel preparation from Picolax to Moviprep.The BSG guidelines on bowel preparation (www.bsg.org.uk) mention 5 types of bowel preparations with no preference over the other. It is clearly pointed out that no bowel preparation is suitable for every patients “, in particularly patients with chronic kidney disease (www.bsg.org.uk).The bowel preparation can be tailored to the patient according to his/her comorbidities, the current clinical state of bowel pathology and the kidney function. Finally the endoscopist can make a prompt decision as to when to stop the procedure when the rectum and sigmoid are seen to be filled with solid faeces. Although it’s worth trying to pass solid faeces in the lower rectum, attempting to pass the faeces and to wash the loaded colon may waste time, thus causing the subsequent cancellation of patients awaiting the procedure .In addition, patients are at risk of severe complications and missing serious pathology due to inadequate vision. The other finding from this study is that medical endoscopists are achieving better completion rates than surgeons without adjustment being made for other variables. Although gastroenterologists are achieving better completion rates and efficacy compared to other endoscopists [8], a US study showed equal completion rates of surgeons, gastroenterologists, and colorectal surgeons [9]. Conclusions The national figures for colonoscopy completion and complication rates can be achieved by increasing the endoscopist’s experience, improving the adequacy of the analgesia and sedation, thus improving patient comfort and by insuring adequate bowel preparation. Poor bowel preparation has been proven to be an important factor in the outcome of an incomplete colonoscopy. By addressing this factor alone, large financial savings are expected to be achieved for the NHS when it is considered at a national level. Recommendations 1.Every endoscopist has to put more determination to complete colonoscopy provided no other limiting factors such as acute angulation, severe inflammation, narrowing or difficult colon. 2. Attend colonoscopy courses. 3.Patients: should be following the instrcutions by endoscopy unit. Once bowel prep is judged poor by finding faeces in the lower colon, the procedure should be abandoned and not considered as failure. Suitable type and dose and timing of bowel preparation medication. 4. Use small size scope such as paediatric scope when encounter difficult and narrow colon. This can be predicted from history and clinical assessment before the procedure. 5. Optimize the sedation and predict low threshold pain patients .There will be some patients that are not able to tolerate colonoscopy under sedation .It is worth trying with sedation, if failed then they need general anaesthesia .

ISSN 2042-4779 ClinicalAudits.com
References 1.Hon SS, Ng SS, Chiu PW, Chan FK, Ng EK, Li JC, Lee JF, Leung KL.Endoscopic submucosal dissection versus local excision for early rectal neoplasms: a comparative study.Surg Endosc. 2011;25:3923-7 2.Leyden JE, Doherty GA, Hanley A, McNamara DA, Shields C, Leader M, Murray FE, Patchett SE, Harewood GC.Quality of colonoscopy performance among gastroenterology and surgical trainees: a need for common training standards for all trainees?Endoscopy. 2011;43:935-40. 3.Gavin DR, Valori RM, Anderson JT, Donnelly MT, Williams JG, Swarbrick ET.The national colonoscopy audit: a nationwide assessment of the quality and safety of colonoscopy in the UK.Gut. 2012: 1. doi:10.1136 /gutjnl-2011-30181848 4.Mehran A, Jaffe P, Efron J, Vernava A, Liberman MA.Colonoscopy: why are general surgeons being excluded?Surg Endosc. 2003 ;17:1971-3. 5.http://www.shef.ac.uk/polopoly_fs/1.43375!/file/HEDS-DP-08-11.pdf .Date of access 28/11/2012
6.Lee JM, Cheon JH, Park JJ, Moon CM, Kim ES, Kim TI, Kim WH.Effects of Hyosine N-butyl bromide on the detection of polyps during colonoscopy. Hepatogastroenterology. 2010 ;57:90-4. 7.Yoong KY, Perkin D, Portal J, Strickland I, Heymann T.Intravenous hyoscine as a premedication for colonoscopy: a randomized double-blind controlled trial.Endoscopy. 2004 ;36:720-2. 8.Provenzale D, Ofman J, Gralnek I, Rabeneck L, Koff R, McCrory D. Gastroenterologist specialist care and care provided by generalists--an evaluation of effectiveness and efficiency.Am J Gastroenterol. 2003;98:21-8. 9.Mehran A, Jaffe P, Efron J, Vernava A, Liberman MA.Colonoscopy: why are general surgeons being excluded?Surg Endosc. 2003 ;17:1971-3.
Acknowledgement: Thanks to Miss K Baple for checking the language of this manuscript