quality indicators for colonoscopy
TRANSCRIPT

Quality indicators for colonoscopyDouglas K. Rex, MD, John L. Petrini, MD, Todd H. Baron, MD, Amitabh Chak, MD, Jonathan Cohen, MD,Stephen E. Deal, MD, Brenda Hoffman, MD, Brian C. Jacobson, MD, MPH, Klaus Mergener, MD, PhD,Bret T. Petersen, MD, Michael A. Safdi, MD, Douglas O. Faigel, MD, ASGE Co-Chair,Irving M. Pike, MD, ACG Co-Chair
ASGE/ACG Taskforce on Quality in Endoscopy
Colonoscopy is widely used for the diagnosis and treat-ment of colonic disorders. Properly performed, colonos-copy is generally safe, accurate, and well tolerated bymost patients. Visualization of the mucosa of the entirelarge intestine and distal terminal ileum is usually possibleat colonoscopy. In patients with chronic diarrhea, biopsyspecimens can help diagnose the underlying condition.Polyps can be identified and removed during colonoscopy,thereby reducing the risk of colon cancer. Colonoscopy isthe preferred method to evaluate the colon in most adultpatients with bowel symptoms, iron deficiency anemia,abnormal radiographic studies of the colon, positive colo-rectal cancer screening tests, postpolypectomy and post-cancer resection surveillance, surveillance in inflammatorybowel disease, and in those with suspected masses.
The use of colonoscopy has become accepted as themost effective method of screening the colon for neopla-sia in patients over the age of 50 years and in younger pa-tients at increased risk.1 The effectiveness of colonoscopyin reducing colon cancer incidence depends on adequatevisualization of the entire colon, diligence in examiningthe mucosa, and patient acceptance of the procedure.Preparation quality affects the ability to perform a com-plete examination, the duration the procedure, and theneed to cancel or reschedule procedures.2,3 Ineffectivepreparation is a major contributor to costs.4 Longer with-drawal times have been demonstrated to improve polypdetection rates,5-7 and conversely, rapid withdrawal maymiss lesions and reduce the effectiveness of colon cancerprevention by colonoscopy. The miss rates of colonoscopyfor large (R1 cm) adenomas may be higher than previ-ously thought.8,9 Thus, careful examinations are necessaryto optimize the effectiveness of recommended intervalsbetween screening and surveillance examinations. Finally,technical expertise will help prevent complications thatcan offset any cost-benefit ratio gained by removing neo-plastic lesions.
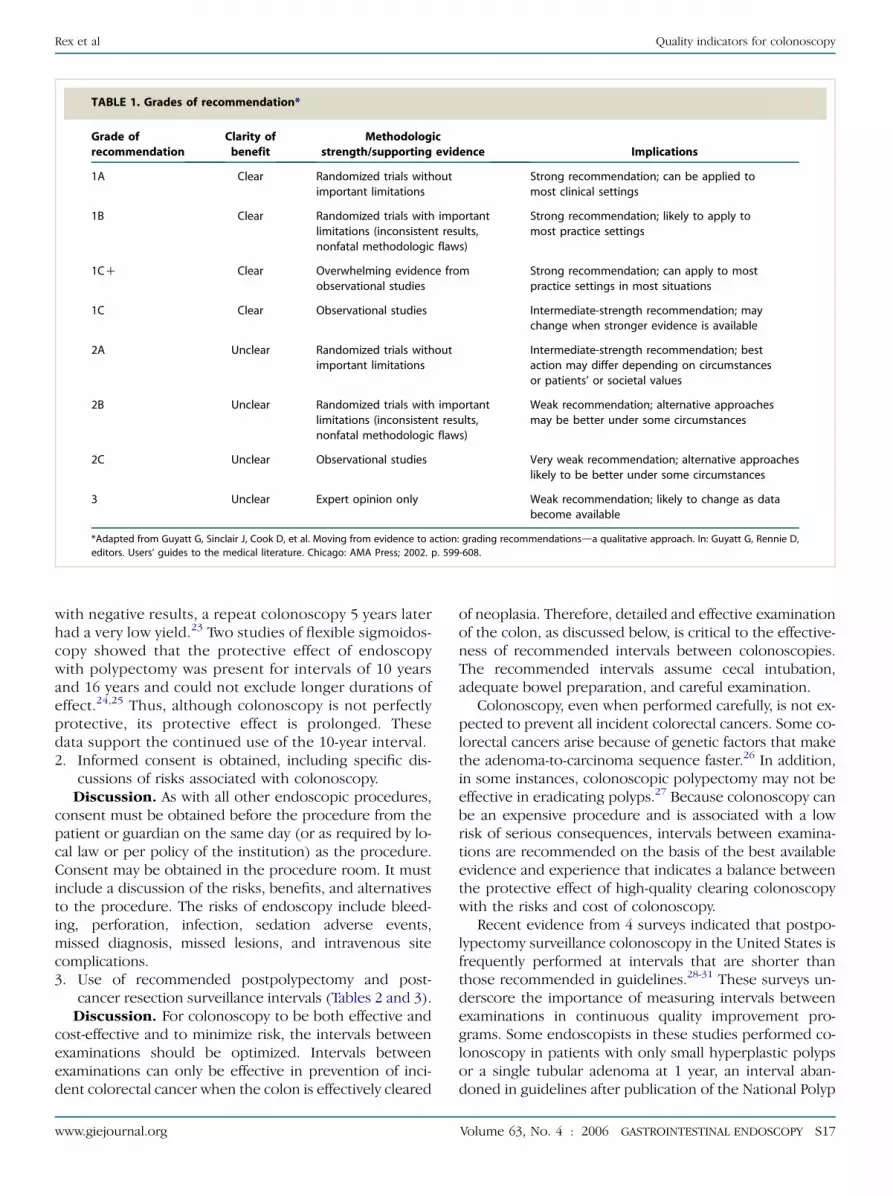
The following quality indicators have been selected toestablish competence in performing colonoscopy andhelp define areas for continuous quality improvement.The levels of evidence supporting these quality indicatorswere graded according to Table 1.
Copyright ª 2006 by the American Society for Gastrointestinal Endoscopy
and the American College of Gastroenterology
0016-5107/$32.00
doi:10.1016/j.gie.2006.02.021
S16 GASTROINTESTINAL ENDOSCOPY Volume 63, No. 4 : 2006
PREPROCEDURE
The preprocedure period encompasses the time fromfirst contact by the patient until administration of sedationor instrument insertion. The aspects of patient care ad-dressed in prior documents apply here as well, includingtimely scheduling, patient preparation, identification,history and physical examination, appropriate choice ofsedation and analgesia, evaluation of bleeding risk, etc. Be-cause many examinations are currently being performedfor colon cancer screening and are elective, care mustbe taken to be certain that all potential risks have beenreduced to as low as practically achievable.
The American Society for Gastrointestinal Endoscopy(ASGE)10 and the U.S. Multi-Society Task Force on ColonCancer have published appropriate indications for colonos-copy11 (Tables 2 and 3).
Specific quality indicators1. Appropriate indication. The ASGE and the U.S. Multi-
Society Task Force on Colon Cancer have published ap-propriate indications for colonoscopy (Tables 2 and 3).An indication should be documented for each proce-dure, and when it is a nonstandard indication it shouldbe justified in the documentation.
Discussion. The ASGE in 2000 published a list of ac-cepted indications for endoscopic procedures.10 This listwas determined by a review of published literature and ex-pert consensus. Studies have shown that when esophago-gastroduodenoscopy and colonoscopy are done forappropriate reasons significantly more clinically relevantdiagnoses are made.12-14 In these studies, which dividedindications into appropriate, uncertain, and inappropriate,and looked at high-volume European centers, 21% to 39%were classified as inappropriate. It is likely that this canbe improved to less than a 20% inappropriate rate.15
The European Panel of Appropriateness of Gastrointesti-nal Endoscopy (EPAGE) Internet guideline is a useful de-cision support tool for determining the appropriatenessof colonoscopy.15 The goal is to minimize as much as pos-sible the number of inappropriate procedures.16-19
In the average-risk population, colonoscopic screen-ing is recommended in all current guidelines at 10-yearintervals.20-22 Direct observational data to support thisinterval are lacking. However, in a cohort of average-risk persons who underwent an initial colonoscopy
www.giejournal.org
Rex et al Quality indicators for colonoscopy
TABLE 1. Grades of recommendation*
Grade of
recommendation
Clarity of
benefit
Methodologic
strength/supporting evidence Implications
1A Clear Randomized trials without
important limitations
Strong recommendation; can be applied to
most clinical settings
1B Clear Randomized trials with important
limitations (inconsistent results,
nonfatal methodologic flaws)
Strong recommendation; likely to apply to
most practice settings
1CC Clear Overwhelming evidence from
observational studies
Strong recommendation; can apply to most
practice settings in most situations
1C Clear Observational studies Intermediate-strength recommendation; may
change when stronger evidence is available
2A Unclear Randomized trials without
important limitations
Intermediate-strength recommendation; best
action may differ depending on circumstances
or patients’ or societal values
2B Unclear Randomized trials with important
limitations (inconsistent results,
nonfatal methodologic flaws)
Weak recommendation; alternative approaches
may be better under some circumstances
2C Unclear Observational studies Very weak recommendation; alternative approaches
likely to be better under some circumstances
3 Unclear Expert opinion only Weak recommendation; likely to change as data
become available
*Adapted from Guyatt G, Sinclair J, Cook D, et al. Moving from evidence to action: grading recommendationsda qualitative approach. In: Guyatt G, Rennie D,
editors. Users’ guides to the medical literature. Chicago: AMA Press; 2002. p. 599-608.
with negative results, a repeat colonoscopy 5 years laterhad a very low yield.23 Two studies of flexible sigmoidos-copy showed that the protective effect of endoscopywith polypectomy was present for intervals of 10 yearsand 16 years and could not exclude longer durations ofeffect.24,25 Thus, although colonoscopy is not perfectlyprotective, its protective effect is prolonged. Thesedata support the continued use of the 10-year interval.2. Informed consent is obtained, including specific dis-
cussions of risks associated with colonoscopy.Discussion. As with all other endoscopic procedures,
consent must be obtained before the procedure from thepatient or guardian on the same day (or as required by lo-cal law or per policy of the institution) as the procedure.Consent may be obtained in the procedure room. It mustinclude a discussion of the risks, benefits, and alternativesto the procedure. The risks of endoscopy include bleed-ing, perforation, infection, sedation adverse events,missed diagnosis, missed lesions, and intravenous sitecomplications.3. Use of recommended postpolypectomy and post-
cancer resection surveillance intervals (Tables 2 and 3).Discussion. For colonoscopy to be both effective and
cost-effective and to minimize risk, the intervals betweenexaminations should be optimized. Intervals betweenexaminations can only be effective in prevention of inci-dent colorectal cancer when the colon is effectively cleared
www.giejournal.org
of neoplasia. Therefore, detailed and effective examinationof the colon, as discussed below, is critical to the effective-ness of recommended intervals between colonoscopies.The recommended intervals assume cecal intubation,adequate bowel preparation, and careful examination.
Colonoscopy, even when performed carefully, is not ex-pected to prevent all incident colorectal cancers. Some co-lorectal cancers arise because of genetic factors that makethe adenoma-to-carcinoma sequence faster.26 In addition,in some instances, colonoscopic polypectomy may not beeffective in eradicating polyps.27 Because colonoscopy canbe an expensive procedure and is associated with a lowrisk of serious consequences, intervals between examina-tions are recommended on the basis of the best availableevidence and experience that indicates a balance betweenthe protective effect of high-quality clearing colonoscopywith the risks and cost of colonoscopy.
Recent evidence from 4 surveys indicated that postpo-lypectomy surveillance colonoscopy in the United States isfrequently performed at intervals that are shorter thanthose recommended in guidelines.28-31 These surveys un-derscore the importance of measuring intervals betweenexaminations in continuous quality improvement pro-grams. Some endoscopists in these studies performed co-lonoscopy in patients with only small hyperplastic polypsor a single tubular adenoma at 1 year, an interval aban-doned in guidelines after publication of the National Polyp
Volume 63, No. 4 : 2006 GASTROINTESTINAL ENDOSCOPY S17

Quality indicators for colonoscopy Rex et al
S18
TABLE 2. Colonoscopy indications*
A. Evaluation on barium enema or other imaging study of an abnormality that is likely to be
clinically significant, such as a filling defect or stricture
B. Evaluation of unexplained gastrointestinal bleeding
1. Hematochezia
2. Melena after an upper gastrointestinal source has been excluded
3. Presence of fecal occult blood
C. Unexplained iron deficiency anemia
D. Screening and surveillance for colonic neoplasia
1. Screening of asymptomatic, average-risk patients for colonic neoplasia
2. Examination to evaluate the entire colon for synchronous cancer or neoplastic polyps in
a patient with treatable cancer or neoplastic polyp
3. Colonoscopy to remove synchronous neoplastic lesions at or around time of curative
resection of cancer followed by colonoscopy at 3 years and 3-5 years thereafter to detect
metachronous cancer
4. After adequate clearance of neoplastic polyp(s) survey at 3- to 5-year intervals
5. Patients with significant family history
a. Hereditary nonpolyposis colorectal cancer: colonoscopy every 2 years beginning at the
earlier of age 25 years or 5 years younger than the earliest age of diagnosis of
colorectal cancer. Annual colonoscopy should begin at age 40 years.
b. Sporadic colorectal cancer before age 60 years: colonoscopy every 5 years beginning
at age 10 years earlier than the affected relative or every 3 years if adenoma is found
6. In patients with ulcerative or Crohn’s pancolitis 8 or more years’ duration or left-sided
colitis 15 or more years’ duration every 1-2 years with systematic biopsies to detect
dysplasia
E. Chronic inflammatory bowel disease of the colon if more precise diagnosis or
determination of the extent of activity of disease will influence immediate management
F. Clinically significant diarrhea of unexplained origin
G. Intraoperative identification of a lesion not apparent at surgery (eg, polypectomy site,
location of a bleeding site)
H. Treatment of bleeding from such lesions as vascular malformation, ulceration, neoplasia,
and polypectomy site (eg, electrocoagulation, heater probe, laser or injection therapy)
I. Foreign body removal
J. Excision of colonic polyp
K. Decompression of acute nontoxic megacolon or sigmoid volvulus
L. Balloon dilation of stenotic lesions (eg, anastomotic strictures)
M. Palliative treatment of stenosing or bleeding neoplasms (eg, laser, electrocoagulation,
stenting)
N. Marking a neoplasm for localization
*ASGE. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc 2000;52:831-7.
Study randomized trial in 1993.32 Surgeons were morelikely than gastroenterologists to use short intervals.28
These data underscore the need for endoscopic leadersto promote continuous quality improvement among allspecialties practicing colonoscopy in a given community.
GASTROINTESTINAL ENDOSCOPY Volume 63, No. 4 : 2006
Diminutive hyperplastic polyps, when found only in therectosigmoid colon, can be considered normal. The pres-ence of small distal hyperplastic polyps only should notalter the recommended interval for surveillance.Appropriate intervals in patients with large hyperplastic
www.giejournal.org

Rex et al Quality indicators for colonoscopy
www.giejo
TABLE 3. Indications for colonoscopy and appropriate intervals*
Indication Interval*
Bleeding
Positive FOBT NR
Hematochezia NR
Iron deficiency anemia NR
Melena with negative
esophagogastroduodenoscopy
NR
Screening
Average risk 10 y (begin at age 50 y)
Single FDR with cancer (or adenomas) at age R60 y 10 y (begin at age 40 y)
R2 FDRs with cancer (or adenomas) or 1 FDR
diagnosed at age !60 y
5 y (begin at age 40 y or 10 y
younger, whichever is earlier)
Prior endometrial or ovarian cancer diagnosed
at age !50 y
5 y
HNPCC (begin age 20-25 y) 1-2 y
Abdominal pain, altered bowel habity
Positive sigmoidoscopy (large polyp or polyp of
!1 cm shown to be an adenoma)z
Postadenoma resection
1-2 tubular adenomas of !1 cm 5-10 y
3-10 adenomas or adenoma with villous features,
R1 cm or with HGD
3 y
O10 adenomas !3 y
Sessile adenoma of R2 cm, removed piecemealx 2-6 m
Postcancer resection Clear colon, then in 1 y, then
3 y, then 5 y
Ulcerative colitis, Crohn’s colitis surveillance after 8 y of
pancolitis or 15 y of left-sided colitis
2-3 y until 20 y after onset of
symptoms, then 1 y
FOBT, Fecal occult blood test; NR, interval not recommended; FDR, first-degree relative; HNPCC, hereditary
nonpolyposis colorectal cancer; HGD, high-grade dysplasia.
*From: Rex DK, Bond JH, Winawer S, et al. Quality in the technical performance of colonoscopy and the
continuous quality improvement process for colonoscopy: recommendations of the U.S. Multi-Society Task
Force on Colorectal Cancer. Am J Gastroenterol 2002;97:1296-308. Updated based on guideline revisions in
press. Used with permission.
yIf colonoscopy has negative results and symptoms are stable, repeat examination should be done
according to screening recommendations.
zSee postadenoma resection recommendation.
xThe goal is to reexamine the site for residual polyp; repeating a flexible sigmoidoscopy is adequate for
a distal polyp.
polyps located in the proximal colon, or in patients whohave many hyperplastic polyps (30 or more) are not yetestablished, but close follow-up may be appropriate.33,34
Patients who have evidence of colonic bleeding that oc-curs after a colonoscopy with negative results may needrepeat examinations at intervals shorter than those recom-mended in Tables 2 and 3. However, the use of fecal occultblood testing for the first 5 years after a colonoscopy isdiscouraged because the positive predictive value of
urnal.org
guaiac-based fecal occult blood testing during that intervalis extremely low.35 Additional study of fecal immunochem-ical testing for blood in this setting as an adjunct to colo-noscopy is warranted.36
4. The use of recommended ulcerative colitis andCrohn’s colitis surveillance.
Discussion. In ulcerative colitis and Crohn’s colitis,surveillance refers to interval examinations of patientswith long-standing disease who have undergone an initial
Volume 63, No. 4 : 2006 GASTROINTESTINAL ENDOSCOPY S19

Quality indicators for colonoscopy Rex et al
examination in which dysplasia is not detected. The termis also used when patients who are asymptomatic are pro-spectively entered into interval colonoscopy programs onthe basis of their duration of disease. Surveillance doesnot refer to diagnostic examinations or examinations inpreviously diagnosed patients to assess symptoms. Bothulcerative colitis and Crohn’s colitis of long duration areassociated with an increased risk of colorectal cancer.37,38
There are no randomized trials to support the effective-ness of surveillance colonoscopy in ulcerative colitis orCrohn’s colitis, but case control studies in ulcerative colitissuggest a survival benefit for patients who participate insurveillance.39,40 Surveys of practitioners in the UnitedStates41 and the United Kingdom42 demonstrate thatmany practitioners are not familiar with surveillance rec-ommendations, have a poor understanding of dysplasia,and make inappropriate recommendations in responseto findings of dysplasia.41,42
Patients should be encouraged to undergo surveillancecolonoscopy, and surveillance has emerged as a standardof medical care in the United States. The onset of diseaseis timed to the onset of symptoms for the purpose of tim-ing the initiation of surveillance in both ulcerative colitisand Crohn’s colitis. Because the yield of ulcerative colitisin surveillance for cancer and severe dysplasia is relativelylow,43,44 it is important to not overuse surveillance colonos-copy during the first 20 years because overuse is notcost-effective.45 Shorter intervals between examinationsare indicated for patients with long-duration diseaseand may be initiated earlier in the course of disease inpatients with established risk modifiers, such as a familyhistory of colorectal cancer or a personal history of pri-mary sclerosing cholangitis.46,47 Persons with primarysclerosing cholangitis who are discovered to have asymp-tomatic ulcerative colitis should begin surveillance at thetime ulcerative colitis is diagnosed.5. Preparation: in every case the procedure note should
document the quality of preparation.Discussion. In each colonoscopy, the colonoscopist
should document the quality of the bowel preparation.In clinical trials of bowel preparation, terms used to com-monly characterize bowel preparation include ‘‘excellent,’’‘‘good,’’ ‘‘fair,’’ and ‘‘poor.’’ In clinical practice, theseterms do not have standardized definitions. In clinical tri-als on the effectiveness of various laxative regimens forbowel preparation, excellent is typically defined as no orminimal solid stool and only small amounts of clear fluidrequiring suctioning. ‘‘Good’’ is typically no or minimalsolid stool with large amounts of clear fluid requiring suc-tioning. ‘‘Fair’’ refers to collections of semisolid debristhat are cleared with difficulty. ‘‘Poor’’ refers to solid orsemisolid debris that cannot be effectively cleared. Theseterms can be interpreted as having more to do withretained intraluminal contents that often can be removedby suctioning rather than the quality of inspection allowedafter suctionable material has been fully removed;
S20 GASTROINTESTINAL ENDOSCOPY Volume 63, No. 4 : 2006
however, these terms are probably reasonable guides tothe appropriate use of bowel descriptors.
Poor bowel preparation is a major impediment to the ef-fectiveness of colonoscopy. Poor preparation prolongs cecalintubation time and withdrawal time and reduces detectionof both small2 and large2,3 polyps. In every colonoscopicpractice, some colonoscopies must be repeated at intervalsshorter than those recommended in Table 3 because of in-adequate preparation. The task force recommends that theprocedure be considered adequate if it allows (within thetechnical limitations of the procedure) detection of polyps5 mm or larger.11 The economic burden of repeatingexaminations because of inadequate bowel preparation issubstantial.4 No thresholds are recommended by the com-mittee for the percentage of examinations that are repeatedfor poor preparation because the percentage of patients re-quiring repeat examination may depend mostly on patientpopulation characteristics.4 However, measurement of indi-vidual practitioners’ percentage of examinations requiringrepeat because of preparation is recommended. Individualendoscopists may compare their percentages to otherswithin the same practice or to other endoscopists practicingin the same hospital. This can allow identification of outlierswithin that hospital for whom corrective measures shouldbe taken.
Preprocedure research questionsd What are the most effective methods to disseminate
guidelines and educate physicians on quality recom-mendations?
d Why do physicians fail to follow recommended guide-lines for screening and surveillance intervals? Do theyknow the guidelines? Are they concerned about missedlesions?
d Which hyperplastic polyps in the proximal colon areclinically important? What are cost-effective intervalsfor follow-up after removal of large hyperplastic polyps?
d What is the current understanding among clinicians ofsurveillance guidelines for ulcerative colitis and Crohn’scolitis?
d Can patients with ulcerative colitis be triaged on thebasis of endoscopic findings into low- and high-riskgroups for surveillance intervals?
d What method would allow same-day bowel preparationin the endoscopy unit in patients with poor prepara-tion? Would this prevent patients with poor preparationfrom being lost to follow-up?
d What bowel preparation is the best combination ofsafety, effectiveness, and tolerability?
INTRAPROCEDURE
Quality evaluation of the colon consists of intubation ofthe entire colon and a detailed mucosal inspection. Cecalintubation improves sensitivity and reduces costs by
www.giejournal.org

Rex et al Quality indicators for colonoscopy
eliminating the need for radiographic procedures or re-peat colonoscopy to complete examination. Careful muco-sal inspection is essential to effective colorectal cancerprevention and reduction of cancer mortality. The detec-tion of neoplastic lesions is the primary goal of most colo-noscopic examinations.
Cost-benefit analyses of colonoscopy for the detectionof neoplastic lesions are well within acceptable rates (ap-proximately $20,000 per year of life saved).20-22 However,complications, repeat procedures, and inappropriate sur-gical intervention for endoscopically removable polypscan significantly reduce this benefit. It is incumbent on en-doscopists to evaluate their practices and seek to makeimprovements wherever possible to reduce the costs asso-ciated with neoplasia detection.6. Cecal intubation rates: visualization of the cecum by
notation of landmarks and photodocumentation oflandmarks should be documented in every procedure.
Discussion. In the United States, colonoscopy is gen-erally undertaken with the intent to intubate the cecum.Cecal intubation is defined as passage of the colonoscopetip to a point proximal to the ileocecal valve so that theentire cecal caput, including the medial wall of the cecumbetween the ileocecal valve and appendiceal orifice, is vis-ible. The need for cecal intubation is based on the persis-tent finding that a substantial fraction of colorectalneoplasms are located in the proximal colon, includingthe cecum.48 Techniques of cecal intubation are discussedelsewhere.49 Cecal intubation should be documented bynaming the identified cecal landmarks. Most important,these include the appendiceal orifice and the ileocecalvalve. In cases where there is uncertainty as to whetherthe cecum has been entered, visualization of the lips ofthe ileocecal valve (ie, the orifice) or intubation of the ter-minal ileum will be needed. Experienced colonoscopistscan verify cecal intubation in real time in 100% of cases,50
because there is no other portion of the gastrointestinaltract with a similar appearance. It can be helpful to docu-ment other landmarks, such as the cecal sling fold or intu-bation of the terminal ileum.
Photography of the cecum is also recommended. Stillphotography of the cecum may not be convincing in allcases because of variations in cecal anatomy.50 Thus, theileocecal valve may not be notched or may not have alipomatous appearance; however, still photography is con-vincing in a substantial majority of cases, and its use allowsverification of cecal intubation rates of individual endo-scopists in the continuous quality improvement program.The best photographs of the cecum to prove intubationare of the appendiceal orifice, taken from a distance suffi-ciently far away that the cecal strap fold is visible aroundthe appendix, and a photograph of the cecum takenfrom distal to the ileocecal valve.50 Photographs of the ter-minal ileum are sometimes convincing if they show villi,circular valvulae connivente, and lymphoid hyperplasia,but they are less likely to be effective compared with the
www.giejournal.org
above-mentioned photographs.50 Videotaping of the ce-cum is not necessary in clinical practice because its feasi-bility remains low at this time; however, the appearanceof the cecum is unmistakable in real time and videotapingof the cecum can be a very effective way of documentingcecal intubation for an examiner whose rates of cecal intu-bation require verification.50
Effective colonoscopists should be able to intubate thececum in R90% of all cases51 and in R95% of cases whenthe indication is screening in a healthy adult.52-61 All colonos-copy studies done for screening have reported cecalintubation rates of 97% or higher.52-61 Cases in which proce-dures are aborted because of poor preparation or severe co-litis need not be counted in determining cecal intubationrates. It is also not necessary to count cases in which the ini-tial intent of the procedure is colonoscopic treatment ofa benign or malignant stricture or a large polyp (providedthat complete colonic imaging by some method has beenpreviously performed). All other colonoscopies, includingthose in which a previously unknown benign or malignantstricture is encountered, should be counted.7. Detection of adenomas in asymptomatic individuals
(screening).Discussion. Among healthy asymptomatic patients un-
dergoing screening colonoscopy, adenomas should be de-tected in R25% of men and R15% women more than 50years old. Measuring adenoma detection rates of individ-ual colonoscopists is a priority in the quality improvementprocess for colonoscopy for multiple reasons. First, thefundamental goal of colonoscopy for most indications isdetection of neoplastic lesions in the colon. Second,although early studies in the 1990s indicated that colonos-copy and polypectomy prevented 76% to 90% of incidentcancers and provided an even higher level of mortality re-duction,62-64 recent studies of adenoma cohorts havedemonstrated incident cancer rates after clearing colonos-copy that are substantially higher than those identified inthe earlier studies65-67 and suggest that colonoscopy mayprovide a lower protection level against incident cancers.Analysis of individual cases in one of these trials suggestedthat at least a portion of the incident cancers were relatedto missed lesions.27 Third, recent data from two U.S. prac-tice groups, one in private practice6 and one in acade-mia,68 have indicated large disparities between practicinggastroenterologists in their rates of detection of bothsmall and large adenomas. Thus, suboptimal performanceof colonoscopy by some practitioners, as evidenced by var-iable performance, may be a fundamental obstacle to colo-noscopy’s ability to provide near-complete protectionagainst incident colorectal cancers.
The evolution of evidence regarding missed lesionsduring colonoscopy is as follows. First, tandem colonos-copy studies in the mid 1990s demonstrated miss ratesduring colonoscopy for adenomas R1 cm of 0% to 6%,12% to 13% for adenomas 6 to 9 mm in size, and 15% to27% for adenomas %5 mm in size.69,70 A tandem study
Volume 63, No. 4 : 2006 GASTROINTESTINAL ENDOSCOPY S21

Quality indicators for colonoscopy Rex et al
that used flexible sigmoidoscopy confirmed these find-ings.71 Subsequently, citing the obvious defect of studiesusing colonoscopy as its own gold standard,8,9 centers ofexcellence in computed tomography (CT)–colonographymeasured miss rates of conventional colonoscopy of ade-nomas R1 cm in size of 12%8 and 17%.9 In these studies,conventional colonoscopy comparisons used the tech-nique of ‘‘segmental unblinding.’’72 CT-colonographythus far is not usable as a method of measuring miss ratesfor conventional colonoscopy for adenomas !1 cm in sizebecause the sensitivity of CT-colonography is fallingmore precipitously for polyps !1 cm than is that of con-ventional colonoscopy; however, the results of these CT-colonography studies8,9 indicate that miss rates calculatedby tandem endoscopic studies probably substantially un-derestimate the miss rates of colonoscopy and sigmoidos-copy for polyps of all sizes. In addition, miss rates ofcolonoscopy for colorectal cancer have also been identi-fied in two large studies as 5%73 and 4%.74
Studies demonstrating variable sensitivity among endo-scopists constitute the evidence indicating suboptimalperformance as an important factor in the failure ofcolonoscopy to identify and prevent colorectal cancers.With regard to cancer detection, one study demonstratedmiss rates of 3% for gastroenterologists versus 13% fornongastroenterologists; however, miss rates for cancerwere 5% for one group of gastroenterologists comparedwith 1% for all other gastroenterologists studied.73 In a re-cent study in Canada, higher miss rates for cancer were as-sociated with lesions in the right colon and were higherwhen colonoscopy was performed by internists or familyphysicians and when colonoscopy was performed in anoffice setting.75
With regard to variable detection of adenomas, a largetandem colonoscopy study involving 26 colonoscopistsdemonstrated a range of miss rates from 17% to 48%.69
A comparison of withdrawal techniques between the twoexaminers in this study at the extremes of adenoma detec-tion showed that higher sensitivity was associated withlonger examinations, superior examination of mucosaproximal to folds and flexures, better colonic distention,and better cleaning of debris and fluid from the colon.5
A flexible sigmoidoscopy screening study involving 12 en-doscopists in the United Kingdom demonstrated a rangeof detection of adenomas from 21 per 100 examinationsto 11 per 100 examinations.76 A private practice group of12 gastroenterologists in the United States performingscreening colonoscopy in adults aged 50 years and olderdescribed a range of adenoma detection from O100 ade-nomas per 100 colonoscopies for the highest performer to!10% this rate for the lowest performer.6 Detection ofsmall adenomas correlated with detection of large adeno-mas. Persons who spent longer than 6 minutes of with-drawal time had a detection rate of adenomas R1 cm of6.6% compared with 3% for persons who averaged lessthan 6 minutes of withdrawal time. A group of 9 academic
S22 GASTROINTESTINAL ENDOSCOPY Volume 63, No. 4 : 2006
gastroenterologists in the United States were shown tohave detection rates of adenomas during colonoscopy inpersons aged 50 years and older that ranged from 86 ad-enomas per 100 colonoscopies to 21 adenomas per 100colonoscopies, and a range of prevalences of adenomasR1 cm of 5.5% to 1.5%.68
There is a strong interaction between the quality withwhich the colon is cleared of neoplasia and the effective-ness of recommended intervals for surveillance. Thus,suboptimal performers with low detection rates for largeadenomas and for multiple adenomas have recentlybeen demonstrated.6,68 These individuals will recommendthat fewer persons undergo surveillance colonoscopy at 3years, rather than at 5-year intervals, on the basis of largeadenomas or the presence of 3 or more adenomas, al-though these same colonoscopists have been less effec-tive at clearing the colon of neoplasia. Recommendedintervals for surveillance and screening can only have ad-equate effectiveness when the current disparities betweenexaminers in clearing the colon of neoplasia areimproved.
The principal demographic features that predict adeno-mas at colonoscopy are age and sex and, to a lesser extent,family history of colorectal neoplasia. The indication forthe procedure is not a strong predictor of the presenceof adenomas.43 Screening colonoscopy studies in theUnited States have identified adenomas in 25% to 40%of patients more than 50 years old.52-61 The best estab-lished neoplasia-related quality indicator is the actualprevalence of adenomas detected. Prevalence rates ofadenomas in colonoscopy screening studies have beenconsistently over 25% in men and 15% in women morethan 50 years old.52-61 Although detection of overall num-bers of adenomas per colonoscopy could prove to be theideal measure of adenoma detection, there are currentlyinsufficient data to establish acceptable compliance ratesfor this threshold. Overall adenoma prevalence rates cor-relate with detection rates of large adenomas,6,68 are eas-ier to measure and have better established thresholds foracceptable compliance rates. Individuals who reach theprimary goals for prevalence rates of adenomas are likelyto have a satisfactory withdrawal technique. For these ex-aminers, secondary measures, such as the time taken forwithdrawal (see below), are of less importance.8. Withdrawal times: studies have demonstrated in-
creased detection of significant neoplastic lesionsin colonoscopic examinations where the withdrawaltime is 6 minutes or more. Mean withdrawal timeshould be R6 minutes in colonoscopies with normalresults performed in patients with intact colons.
Discussion. In instances of low detection rates of ad-enomas, measurement of withdrawal time is appropriateas a quality indicator. To measure withdrawal time, thetime at which the cecum is reached and the time at whichthe scope is withdrawn from the anus must be noted.Some electronic report-generating systems allow the
www.giejournal.org

Rex et al Quality indicators for colonoscopy
time to be noted electronically when cecal photographsare taken. On the basis of the mean withdrawal times ofan examiner with very low miss rates5 and previously citedevidence that the detection rate of large adenomas wasgreater for examiners who took longer than 6 minutesfor withdrawal during screening colonoscopy,6 it is recom-mended that the withdrawal phase of colonoscopy in pa-tients without previous surgical resection should last atleast 6 minutes on average. Application of this standardto an individual case is not appropriate because colons dif-fer in length and in some instances a very well preparedcolon of relatively short length and with nonprominenthaustral markings can be carefully examined in less than6 minutes. Further, recent evidence suggests that colono-scopes with a wide angle of view allow quicker examina-tion without increasing miss rates for polyps.77
9. Biopsy specimens should be obtained from the colonin patients with chronic diarrhea.
Discussion. Patients with microscopic colitis (collage-nous and lymphocytic colitis) may have normal-appearingmucosa at colonoscopy. The diagnosis requires biopsy ofotherwise unremarkable-appearing colon. All patients un-dergoing colonoscopy for the evaluation of chronic diar-rhea should have biopsy specimens obtained. Theoptimal number and location of biopsy specimens is notestablished. Inclusion of samples from the proximal colonimproves the sensitivity for collagenous colitis.78,79
10. Number and distribution of biopsy samples in ulcera-tive colitis and Crohn’s colitis surveillance. Goal: 4per 10-cm section of involved colon or approximately32 biopsy specimens in cases of panulcerative colitis.
Discussion. Systematic biopsy of the colon and termi-nal ileum can assist in establishing the extent of ulcerativecolitis and Crohn’s disease and in differentiating ulcera-tive colitis from Crohn’s disease. During surveillance, a sys-tematic biopsy protocol is needed to maximize thesensitivity of surveillance for dysplasia.80 The recommen-ded protocol includes biopsies in all 4 quadrants fromeach 10 cm of the colon. This typically results in 28 to32 biopsy samples as a minimum. The procedure reportin ulcerative colitis surveillance examinations shouldnote the number and locations of specimens from flatmucosa and the location and endoscopic appearance ofany mass or suspicious polypoid lesions that were sam-pled or removed.
Recent studies have reported that patients with endo-scopically abnormal colons (eg, endoscopic scarring,pseudopolyp formation, or cobblestoning) are at in-creased risk for development of cancer compared withthose with colons that are endoscopically normal.81
Thus, patients with endoscopically normal colons mightbe triaged to longer intervals of surveillance than thosewith scarred or endoscopically abnormal colons.81 Recentstudies have reported that panchromoscopy of the colonand targeted biopsies results in a higher yield of dysplasiathan systematic 4-quadrant biopsies in non-dye-sprayed
www.giejournal.org
colons.82,83 This intriguing observation deserves addi-tional consideration and evaluation.11. Mucosally based pedunculated polyps and sessile
polyps !2 cm in size should not be sent for surgicalresection without an attempt at endoscopic resectionor documentation of endoscopic inaccessibility.
Discussion. Colonoscopists should be able to performbiopsy and routine polypectomy. Consistent referral ofsmall ‘‘routine’’ colorectal polyps identified during diagnos-tic colonoscopy for repeat colonoscopy and polypectomyby others is unacceptable. On the other hand, referral oftechnically difficult polyps to more experienced endoscop-ists for endoscopic resection is encouraged (see below).
Patients with sessile polyps !2 cm in size should sel-dom be referred for surgical resection because thesepolyps are readily resectable in most cases by competentcolonoscopists. Consistent referral of sessile polyps!2 cm in size for surgical resection is inappropriate. Insome cases, these polyps may be difficult to access orproperly position for polypectomy, and referral toa more experienced endoscopist may be appropriate.
Certainly endoscopists should not attempt removal ofpolyps they consider beyond their skill or comfort level,and they should feel comfortable in referring such polypsto other endoscopists for a second opinion (eg, review ofphotographs) or endoscopic resection. Many sessilepolyps O2 cm in size are also removable endoscopically,depending on their location within the colon, their size,and the ability to access them endoscopically. Essentiallyall mucosally based pedunculated polyps can be removedendoscopically. All polyps referred for surgical resectionshould be photographed to document the need for sur-gical resection in the continuous quality improvementprocess. Review of photographs by a second, moreexperienced endoscopist can be useful to ensure theappropriateness of surgical referral. When surgical referralis pursued, correlation of photographs and endoscopicand pathologic measurements of polyp size should beundertaken to confirm the appropriateness of surgicalreferral.
Intraprocedure research questionsd Can electronic report generating systems automate
collection of intraprocedural quality indicator data?d What technical improvements could improve the ease,
speed, and safety of colonoscopy?d Can physicians already in practice with low cecal intuba-
tion rates improve? What are effective measures andteaching methods that produce improvement?
d Can physicians with low adenoma detection ratesimprove? What is needed to produce improvement(ie, Is slowing down enough? Is additional trainingneeded?)
d What are the key elements of examination by endoscop-ists with high adenoma detection rates? How can these
Volume 63, No. 4 : 2006 GASTROINTESTINAL ENDOSCOPY S23

Quality indicators for colonoscopy Rex et al
elements be taught to other colonoscopists? Can suchinformation improve suboptimal performance?
d What technical improvements in colonoscopy canreduce variation between endoscopists in adenomadetection rates (eg, chromoendoscopy? autofluores-cence? narrow-band imaging?)?
d What is the optimal duration of the withdrawal phasewith white-light colonoscopy (ie, at what durationdoes detection of clinically significant neoplasmsplateau?)?
d What technical advances would allow reliable and effi-cient detection of flat dysplastic tissue without chromo-scopy or other practices that reduce efficiency?
d How is dysplasia in flat mucosa, dysplasia associatedlesion or mass (DALM), and sporadic adenoma man-aged in community practice?
d What is the degree of adherence to recommended bi-opsy protocols for irritable bowel disease in communitypractice?
d How are large (O2 cm) colon polyps managed in com-munity practice, and does this management differamong colonoscopists in different specialties (eg, gas-troenterologists vs surgeons)?
d What is the success rate of endoscopic resection oflarge sessile polyps (O2 cm) in community practice?
d What is the optimal biopsy protocol for detection of mi-croscopic colitis?
POSTPROCEDURE
The aspects of postprocedure care that have been dis-cussed in previous sections also apply here. A completeand accurate report, describing the procedure and find-ings, must be completed immediately after the procedure.The report should include photo documentation of ab-normalities and identification of any biopsy specimens ob-tained. Expectations for follow-up care and determinationof who will provide the follow-up should be specified.
The postprocedure interval also provides an opportu-nity to determine the safety of the procedure asperformed by any given endoscopist. Although some com-plications are discovered immediately, each practitionershould establish a system to contact patients after a periodof time to determine whether any delayed complicationshave occurred. Methods to report and evaluate thesecomplications should be in place so that systematic errorscan be discovered and corrected.12. Incidence of perforation by procedure type (all indi-
cations vs screening) is measured.Discussion. Perforation is the most serious complica-
tion in the short term during or after colonoscopy. About5% of colonoscopic perforations are fatal.84-86 The rates ofcolonoscopic perforation vary widely in the medical litera-ture. One study from an established endoscopic center re-ported an overall perforation rate of 1 in 500 in the
S24 GASTROINTESTINAL ENDOSCOPY Volume 63, No. 4 : 2006
1990s.87 A population-based study of Medicare patients re-ported an overall risk of perforation of 1 in 500 but a riskof less than 1 in 1,000 screening patients.88 A review ofscreening colonoscopy studies revealed no perforationsin the first 6,000 reported cases.11 Expected perforationrates in screening patients are lower because the patientsare generally healthy and tend not to have associatedcolonic conditions that have been associated with per-foration, including pseudoobstruction, ischemia, severecolitis, radiation-induced changes, stricture formation,bulky colorectal cancers, more severe forms of diverticulardisease, and chronic corticosteroid therapy.
Considering all the available data, perforation ratesgreater than 1 in 500 overall or greater than 1 in 1,000in screening patients should raise concerns as to whetherinappropriate practices are the cause of the perforations.
Perforations are of two general types. Diagnostic perfo-rations occur as a result of insertion of the colonoscope.They are most commonly mechanical and caused by rup-ture of the side of the instrument through the rectosig-moid region. They typically result in large rents in thecolon that may be recognized during the procedure. Me-chanical perforations can also result from barotraumas.89
Barotrauma perforations are the result of pneumatic pres-sures in the cecum that exceed its bursting pressure. Theyare most likely to occur when the colonoscope has passedeither a stricture or severe diverticular disease and the pa-tient has an ileocecal valve that is competent to air. Baro-trauma perforations can probably be avoided in mostcases by judicious use of air during insufflation, particu-larly after passing strictures, perhaps by insufflation of car-bon dioxide rather than air, and by ensuring that the airpump and the light source will not continue to insufflateair when intraluminal pressures exceed the burstingpressure of the colon.89 Mechanical perforations canalso occur during attempts to pass benign or malignantstrictures.
Perforations may also result from polypectomy. In virtu-ally every case, they are the result of the electrocauteryburn. The risk of perforation is greatest with large polypsin the proximal colon. Submucosal saline solution injec-tion polypectomy is now frequently used by gastroenterol-ogists,90 although no standardized guidelines regardingthe size and location of polyps that require submucosalsaline solution injection have been developed. In experi-mental models, injection reduces the chance of electro-cautery damage to the muscularis propria,91 but norandomized controlled clinical trial has been performedthat demonstrates reduction of risk of perforation or post-polypectomy syndrome by injection. Therefore, colono-scopists should be familiar with and comfortable withthe technique of submucosal saline solution injection,but clinical judgment is necessary in determining whichpolyps should undergo submucosal injection.
Anecdotal reports have suggested an increased risk ofcomplications associated with the use of hot biopsy
www.giejournal.org

Rex et al Quality indicators for colonoscopy
TABLE 4. Summary of proposed quality indicators for colonoscopy*
Quality indicator
Grade of
recommendation
1. Appropriate indication 1CC
2. Informed consent is obtained, including specific discussion of risks associated with colonoscopy 3
3. Use of recommended postpolypectomy and postcancer resection surveillance intervals 1A
4. Use of recommended ulcerative colitis/Crohn’s disease surveillance intervals 2C
5. Documentation in the procedure note of the quality of the preparation 2C
6. Cecal intubation rates (visualization of the cecum by notation of landmarks and photo documentation of
landmarks should be present in every procedure)
1C
7. Detection of adenomas in asymptomatic individuals (screening) 1C
8. Withdrawal time: mean withdrawal time should be R6 minutes in colonoscopies with normal results
performed in patients with intact anatomy
2C
9. Biopsy specimens obtained in patients with chronic diarrhea 2C
10. Number and distribution of biopsy samples in ulcerative colitis and Crohn’s colitis surveillance. Goal:
4 per 10-cm section of involved colon or approximately 32 specimens per case of pancolitis
1C
11. Mucosally based pedunculated polyps and sessile polyps !2 cm in size should be endoscopically
resected or documentation of unresectabiltiy obtained
3
12. Incidence of perforation by procedure type (all indications vs screening) is measured 2C
13. Incidence of postpolypectomy bleeding is measured 2C
14. Postpolypectomy bleeding managed nonoperatively 1C
*This list of potential quality indicators was meant to be a comprehensive listing of measurable end points. It is not the intention of the task force that all end
points be measured in every practice setting. In most cases, validation may be required before a given end point may be universally adopted.
forceps,92 and forceps removal of small polyps reduces thechance of complete removal.93 Cold snaring is attractivefor the removal of small polyps because it effectivelyremoves small polyps and has been associated with ex-ceedingly low risks of complications.94-96 Cold snaring of-ten results in immediate bleeding that is of no clinicalsignificance and allows effective retrieval of polyps.96
13. Incidence of postpolypectomy bleeding is measured.Discussion. Bleeding is the most common complica-
tion of polypectomy.84-86,97,98 Bleeding can be either imme-diate (during the procedure) or delayed. In general, the useof blended or cutting current is associated with an increasedrisk of immediate bleeding, whereas pure low-power coag-ulation is associated with a greater risk of delayed bleed-ing.99,100 In clinical practice, the use of pure low-powercoagulation or blended current is common, and the useof pure cutting current for polypectomy is rare.90
Endoscopic series suggests that the overall risk for post-polypectomy bleeding should be less than 1%.84-86,97,98
Overall, bleeding rates for polypectomy that exceed thisrate should prompt review by experts from within or out-side the institution regarding whether polypectomypractices are appropriate. In general, the risk of bleedingincreases with the size of the polyps and with a moreproximal colonic location. For polyps larger than 2 cm,
www.giejournal.org
particularly in the proximal colon, bleeding rates mayexceed 10%.97,98,101,102
Inclusion of epinephrine in submucosal injection fluidhas been shown to reduce the risk of immediate bleed-ing103,104 but not delayed bleeding. Because the overallrisk of immediate bleeding with pure low-power coagula-tion current is low and immediate bleeding can generallybe treated successfully by experienced endoscopists, thereis no mandate to include epinephrine in injection fluid.Many experts prefer pretreatment of pedunculated polypswith thick stalks by epinephrine injection or placement ofdetachable snares. Two trials have demonstrated benefitfrom the use of detachable snares.104,105 However, theclinical benefit may be marginally significant, and there-fore the use of detachable snares in clinical practice forpedunculated polyps is not mandated.14. Postpolypectomy bleeding should be managed non-
operatively. In the presence of continuous bleeding,repeat colon examination and endoscopic treatmentof polypectomy sites results in successful hemostasis.
Discussion. In general, O90% of postpolypectomybleeding can be managed nonoperatively. Immediate post-polypectomy bleeding can generally be treated effectivelyby endoscopic means and should seldom require opera-tive treatment. After transection, immediate bleeding
Volume 63, No. 4 : 2006 GASTROINTESTINAL ENDOSCOPY S25

Quality indicators for colonoscopy Rex et al
from the stalk of the pedunculated polyp can be treatedby regrasping the stalk and holding it for 10 to 15 minutes.This causes spasm in the bleeding artery. Immediatebleeding can also be treated by application of clips106 orby injection of epinephrine, followed by application ofmultipolar cautery.107
Delayed bleeding frequently stops spontaneously.107
In-hospital observation may be appropriate if the patienthas comorbidities or lives far from the treating physician.Repeat colonoscopy in patients who have stopped bleedingis optional and should be performed at the discretion of thecolonoscopist. Patients seen for delayed bleeding who arecontinuing to pass bright red blood are usually having an ar-terial hemorrhage. Prompt repeat colonoscopy, which maybe performed without bowel preparation,107 is warranted.Treatment can be either by application of clips106 or byinjection in combination with multipolar cautery.107 Multi-polar cautery is generally applied at low power, withoutforceful tamponade (especially in the proximal colon),and continued until there is subjective cessation of bleed-ing. Findings in the base of the bleeding polypectomy sitecan include an actively bleeding visible vessel, a non-bleeding visible vessel, an apparent clot without bleeding,or an apparent clot with bleeding. Rebleeding seldom oc-curs after postpolypectomy bleeding has either stoppedspontaneously or from endoscopic therapy.
Postprocedure research questionsd What are the causes of colonoscopic perforations in
population-based studies? How many perforations areavoidable by improved training, altered technique, ornew or improved techniques?
d Do perforation rates vary in clinical practice by specialtyor by extent of training or duration of experience?
d Can efficient methods for endoscopic removal of largesessile polyps be developed that substantially reduce oreliminate the risk of bleeding or perforation?
d Does cold resection definitely reduce small polypec-tomy complications?
d Does submucosal injection definitely reduce large ses-sile polyp perforation rates?
CONCLUSION
Reduction in variation of quality has emerged as an im-portant priority for colonoscopy practice. The continuousquality improvement process should be instituted and em-braced in all colonoscopy practices. This article summarizescurrent evidence and expert consensus on quality indictorsto be used in this process (Table 4). The task force hasattempted to create a comprehensive list of potential qualityindicators. We recognize that not every indicator will beapplicable to every practice setting. Facilities should selectthe subset most appropriate to their individual needs.
S26 GASTROINTESTINAL ENDOSCOPY Volume 63, No. 4 : 2006
REFERENCES
1. Rex DK, Johnson DA, Lieberman DA, et al. Colorectal cancer preven-
tion 2000: screening recommendations of the American College of
Gastroenterology. Am J Gastroenterol 2000;95:868-77.
2. Harewood GC, Sharma VK, de Garmo P. Impact of colonoscopy prep-
aration quality on detection of suspected colonic neoplasia. Gastro-
intest Endosc 2003;58:76-9.
3. Froelich F, Wietlisbach V, Gonvers JJ, et al. Impact of colonic cleans-
ing on quality and diagnostic yield of colonoscopy: the European
Panel of Appropriateness of Gastrointestinal Endoscopy European
Multicenter Study. Gastrointest Endosc 2005;61:378-84.
4. Rex DK, Imperiale TF, Latinovich DR, et al. Impact of bowel prepara-
tion on efficiency and cost of colonoscopy. Am J Gastroenterol
2002;97:1696-700.
5. Rex DK. Colonoscopic withdrawal technique is associated with ade-
noma miss rates. Gastrointest Endosc 2000;51:33-6.
6. Barclay R, Vicari JJ, Johanson JF, et al. Variation in adenoma detection
rates and colonoscopic withdrawal times during screening colono-
scopy [abstract]. Gastrointest Endosc 2005;61:AB107.
7. Sanchez W, Harewood GC, Petersen BT. Evaluation of polyp detection
in relation to procedure time of screening or surveillance colono-
scopy. Am J Gastroenterol 2004;99:1941-5.
8. Pickhardt PJ, Nugent PA, Mysliwiec PA, et al. Location of adenomas
missed by optical colonoscopy. Ann Intern Med 2004;141:352-9.
9. Van Gelder RE, Nio CY, Florie J, et al. Computed tomographic colo-
nography compared with colonoscopy in patients at increased risk
for colorectal cancer. Gastroenterology 2004;127:41-8.
10. Minoli G, Meucci G, Bortoli A, et al. The ASGE guidelines for the ap-
propriate use of colonoscopy in an open access system. Gastrointest
Endosc 2000;52:39-44.
11. Rex D, Bond J, Winawer S, et al. Quality in the technical performance
of colonoscopy and the continuous quality improvement process for
colonoscopy: Recommendations of the U.S. Multi-Society Task Force
on Colorectal Cancer. Am J Gastroenterol 2002;97:1296-308.
12. Balaguer F, Llach J, Castells A, et al. The European panel on the ap-
propriateness of gastrointestinal endoscopy guidelines colonoscopy
in an open-access endoscopy unit: a prospective study. Aliment
Pharmacol Ther 2005;21:609-13.
13. Vader JP, Pache I, Froehlich F, et al. Overuse and underuse of colono-
scopy in a European primary care setting. Gastrointest Endosc
2000;52:593-9.
14. de Bosset V, Froehlich F, Rey JP, et al. Do explicit appropriateness cri-
teria enhance the diagnostic yield of colonoscopy? Endoscopy
2002;34:360-8.
15. Terraz O, Wietlisbach V, Jeannot JG, et al. The EPAGE internet guide-
line as a decision support tool for determining the appropriateness
of colonoscopy. Digestion 2005;71:72-7.
16. Morini S, Hassan C, Meucci G, et al. Diagnostic yield of open access
colonoscopy according to appropriateness. Gastrointest Endosc
2001;54:175-9.
17. Bersani G, Rossi A, Ricci G, et al. Do ASGE guidelines for the appro-
priate use of colonoscopy enhance the probability of finding relevant
pathologies in an open access service? Dig Liver Dis 2005;37:609-14.
18. Baron TH, Kimery BD, Sorbi D, et al. Strategies to address increased
demand for colonoscopy: guidelines in an open endoscopy practice.
Clin Gastroenterol Hepatol 2004;2:178-82.
19. MacKenzie S, Norrie J, Vella M, et al. Randomized clinical trial compar-
ing consultant-led or open access investigation for large bowel
symptoms. Br J Surg 2003;90:941-7.
20. Winawer S, Fletcher R, Rex D, et al. Gastrointestinal Consortium P,
colorectal cancer screening and surveillance: clinical guidelines and
rationaledupdate based on new evidence. Gastroenterology
2003;124:544-60.
21. U.S. Preventive Services Task Force. Screening for colorectal cancer:
recommendation and rationale. Ann Intern Med 2002;137:129-31.
www.giejournal.org

Rex et al Quality indicators for colonoscopy
22. Smith R, Cokkinides V, von Eschenbach AC, et al. American Cancer
Society guidelines for the early detection of cancer. Cancer J Clin
2002;52:8-22.
23. Rex DK, Cummings OW, Helper DJ, et al. 5-year incidence of adeno-
mas after negative colonoscopy in asymptomatic average-risk per-
sons [see comment]. Gastroenterology 1996;111:1178-81.
24. Selby JV, Friedman GD, Quesenberry CP Jr, et al. A case-control study
of screening sigmoidoscopy and mortality from colorectal cancer.
N Engl J Med 1992;326:653-7.
25. Newcomb PA, Storer BE, Morimoto LM, et al. Long-term efficacy of
sigmoidoscopy in the reduction of colorectal cancer incidence.
J Natl Cancer Inst 2003;95:622-5.
26. Jarvinen HJ, Aarnio M, Mustonen H, et al. Controlled 15-year trial on
screening for colorectal cancer in families with hereditary nonpoly-
posis colorectal cancer. Gastroenterology 2000;118:829-34.
27. Pabby A, Schoen RE, Weissfeld JL, et al. Analysis of colorectal cancer
occurrence during surveillance colonoscopy in the dietary Polyp
Prevention Trial. Gastrointest Endosc 2005;61:385-91.
28. Mysliwiec PA, Brown ML, Klabunde CN, et al. Are physicians doing
too much colonoscopy? A national survey of colorectal surveillance
after polypectomy. Ann Intern Med 2004;141:264-71.
29. Saini S, Nayak R, Bernard L, et al. Knowledge of colorectal polyp
surveillance guidelines and current practices: results of a national
survey [abstract]. Gastroenterology 2005;128:A97.
30. Burke C, Issa M, Chruch J. A nationwide survey of post-polypectomy
surveillance colonoscopy: too many too soon! [abstract]. Gastroen-
terology 2005;128:A566.
31. Boolchand V, Singh J, Olds G, et al. Colonoscopy surveillance after
polypectomy: a national survey study of primary care physicians.
Am J Gastroenterol 2005;100(Suppl):S384-5.
32. Winawer S, Zauber A, Ho M, et al. Randomized comparison of surveil-
lance intervals after colonoscopic removal of newly diagnosed ade-
nomatous polyps. N Engl J Med 1993;328:901-6.
33. Jass JR. Hyperplastic polyps and colorectal cancer: is there a link? Clin
Gastroenterol Hepatol 2004;2:1-8.
34. Higuchi T, Sugihara K, Jass JR. Demographic and pathological charac-
teristics of serrated polyps of colorectum. Histopathology 2005;47:
32-40.
35. Finkelstein S, Bini EJ. Annual fecal occult blood testing can be safely
suspended for up to 5 years after a negative colonoscopy in asymp-
tomatic average-risk patients [abstract]. Gastrointest Endosc 2005;61:
AB250.
36. Bampton PA, Sandford JJ, Cole SR, et al. Interval faecal occult blood
testing in a colonoscopy based screening programme detects addi-
tional pathology. Gut 2005;54:803-6.
37. Katzka I, Brody RS, Morris E, et al. Assessment of colorectal cancer risk
in patients with ulcerative colitis: experience from a private practice.
Gastroenterology 1983;85:22-9.
38. Friedman S, Rubin PH, Bodian C, et al. Screening and surveillance colo-
noscopy in chronic Crohn’s colitis. Gastroenterology 2001;120:820-6.
39. Connell WR, Talbot IC, Harpaz N, et al. Clinicopathological character-
istics of colorectal carcinoma complicating ulcerative colitis. Gut
1994;35:1419-23.
40. Karlen P, Kornfeld D, Brostrom O, et al. Is colonoscopic surveillance
reducing colorectal cancer mortality in ulcerative colitis? A popula-
tion based case control study. Gut 1998;42:711-4.
41. Bernstein CN, Weinstein WM, Levine DS, et al. Physicians’ perceptions
of dysplasia and approaches to surveillance colonoscopy in ulcera-
tive colitis. Am J Gastroenterol 1995;90:2106-14.
42. Eaden JA, Ward BA, Mayberry JF. How gastroenterologists screen
for colonic cancer in ulcerative colitis: an analysis of performance.
Gastrointest Endosc 2000;51:123-8.
43. Rex DK. Colonoscopy: a review of its yield for cancers and adenomas
by indication. Am J Gastroenterol 1995;90:353-65.
44. Lynch DA, Lobo AJ, Sobala GM, et al. Failure of colonoscopic surveil-
lance in ulcerative colitis. Gut 1993;34:1075-80.
www.giejournal.org
45. Provenzale D, Onken J. Surveillance issues in inflammatory bowel
disease: ulcerative colitis. J Clin Gastroenterol 2001;32:99-105.
46. Askling J, Dickman PW, Karlen P, et al. Family history as a risk factor
for colorectal cancer in inflammatory bowel disease. Gastroenterol-
ogy 2001;120:1356-62.
47. Marchesa P, Lashner BA, Lavery IC, et al. The risk of cancer and
dysplasia among ulcerative colitis patients with primary sclerosing
cholangitis. Am J Gastroenterol 1997;92:1285-8.
48. Rabeneck L, Souchek J, El-Serag HB. Survival of colorectal cancer
patients hospitalized in the Veterans Affairs Health Care System.
Am J Gastroenterol 2003;98:1186-92.
49. Williams C. Insertion technique. In: Waye J, Rex D, Williams C, editors.
Colonoscopy: principles and practice. Oxford: Blackwell Publishing;
2003. p. 318-38.
50. Rex DK. Still photography versus videotaping for documentation of
cecal intubation: a prospective study. Gastrointest Endosc 2000;51:
451-9.
51. Marshall JB, Barthel JS. The frequency of total colonoscopy and terminal
ileal intubation in the 1990s. Gastrointest Endosc 1993;39:518-20.
52. Johnson DA, Gurney MS, Volpe RJ, et al. A prospective study of the
prevalence of colonic neoplasms in asymptomatic patients with an
age-related risk. Am J Gastroenterol 1990;85:969-74.
53. Foutch PG, Mai H, Pardy K, et al. Flexible sigmoidoscopy may be in-
effective for secondary prevention of colorectal cancer in asymptom-
atic, average-risk men. Dig Dis Sci 1991;36:924-8.
54. Lieberman DA, Smith FW. Screening for colon malignancy with colo-
noscopy. Am J Gastroenterol 1991;86:946-51.
55. Rogge JD, Elmore MF, Mahoney SJ, et al. Low-cost, office-based,
screening colonoscopy. Am J Gastroenterol 1994;89:1775-80.
56. Rex D, Sledge G, Harper P, et al. Colonic neoplasia in asymptomatic
persons with negative fecal occult blood tests: influence of age, gen-
der, and family history. Am J Gastrenterol 1993;88:825-31.
57. Kadakia S, Wrobleski C, Kadakia A, et al. Prevelance of proximal
colonic polyps in average-risk asymptomatic patients with negative
fecal occult blood tests and flexible sigmoidoscopy. Gastrointest
Endosc 1996;44:112-7.
58. Lieberman DA, Weiss DG, Bond JH, et al. Use of colonoscopy to
screen asymptomatic adults for colorectal cancer: Veterans Affairs
Cooperative Study Group 380. N Engl J Med 2000;343:162-8.
59. Imperiale T, Wagner D, Lin C, et al. Risk of advanced proximal neo-
plasms in asymptomatic adults according to the distal colorectal
findings. N Engl J Med 2000;343:169-74.
60. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. Fecal DNA versus fecal
occult blood for colorectal-cancer screening in an average-risk pop-
ulation. N Engl J Med 2004;351:2704-14.
61. Schoenfeld P, Cash B, Flood A, et al. Colonoscopic screening of average-
risk women for colorectal neoplasia. N Engl J Med 2005;352:2061-8.
62. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer
by colonoscopic polypectomy: the National Polyp Study Workgroup.
N Engl J Med 1993;329:1977-81.
63. Citarda F, Tomaselli G, Capocaccia R, et al. Efficacy in standard clinical
practice of colonoscopic polypectomy in reducing colorectal cancer
incidence. Gut 2001;48:812-5.
64. Thiis-Evensen E, Hoff G, Sauar J, et al. Population-based surveillance
by colonoscopy: effect on the incidence of colorectal cancer: Tele-
mark Polyp Study I Scand. J Gastroenterol 1999;34:414-20.
65. Schatzkin A, Lanza E, Corle D, et al. The Polyp Prevention Trial Study
Group: lack of effect of a low-fat, high-fiber diet on the recurrence of
colorectal adenomas. N Engl J Med 2000;342:1149-55.
66. Alberts DS, Martinez ME, Roe DJ, et al. Lack of effect of a high-fiber
cereal supplement on the recurrence of colorectal adenomas:
Phoenix Colon Cancer Prevention Physicians’ Network. N Engl J
Med 2000;342:1156-62.
67. Robertson DJ, Greenberg ER, Beach M, et al. Colorectal cancer in pa-
tients under close colonoscopic surveillance. Gastroenterology
2005;129:34-41.
Volume 63, No. 4 : 2006 GASTROINTESTINAL ENDOSCOPY S27

Quality indicators for colonoscopy Rex et al
68. Chen S, Rex DK. Endoscopist is comparable to age and gender as
predictor of adenomas at colonoscopy. Am J Gastroenterol
2005;100(Suppl):S393.
69. Rex D, Cutler CS, Lemmel GT, et al. Colonoscopic miss rates of ade-
nomas determined by back-to-back colonoscopies. Gastroenterology
1997;112:24-8.
70. Hixson LJ, Fennerty MB, Sampliner RE, et al. Prospective study of the
frequency and size distribution of polyps missed by colonoscopy.
J Natl Cancer Inst 1990;82:1769-72.
71. Schoenfeld P, Lipscomb S, Crook J, et al. Accuracy of polyp detec-
tion by gastroenterologists and nurse endoscopists during flexible
sigmoidoscopy: a randomized trial. Gastroenterology 1999;117:
312-8.
72. Winawer SJ, Stewart ET, Zauber AG, et al. A comparison of colonoscopy
and double-contrast barium enema for surveillance after polypectomy:
National Polyp Study Work Group. N Engl J Med 2000;342:1766-72.
73. Rex DK, Rahmani EY, Haseman JH, et al. Relative sensitivity of colono-
scopy and barium enema for detection of colorectal cancer in clinical
practice. Gastroenterology 1997;112:17-23.
74. Bressler B, Paszat LF, Vinden C, et al. Colonoscopic miss rates for
right-sided colon cancer: a population-based analysis. Gastroenterol-
ogy 2004;127:452-6.
75. Bressler B, Paszat L, Rothwell D, et al. Predictors of missed colorectal
cancer during colonoscopy: a population-based analysis [abstract].
Gastrointest Endosc 2005;61:AB24.
76. Atkin W, Rogers P, Cardwell C, et al. Wide variation in adenoma de-
tection rates at screening flexible sigmoidoscopy. Gastroenterology
2004;126:1247-56.
77. Deenadayalu VP, Chadalawada V, Rex DK. 170 degrees wide-angle
colonoscope: effect on efficiency and miss rates. Am J Gastroenterol
2004;99:2138-42.
78. Yusoff IF, Ormonde DG, Hoffman NE. Routine colonic mucosal biopsy
and ileoscopy increases diagnostic yield in patients undergoing colo-
noscopy for diarrhea. J Gastroenterol Hepatol 2002;17:276-80.
79. Zins BJ, Tremaine WJ, Carpenter HA. Collagenous colitis: mucosal biop-
sies and association with fecal leukocytes. Mayo Clin Proc 1995;70:430-3.
80. Rubin CE, Haggitt RC, Burmer GC, et al. DNA aneuploidy in colonic
biopsies predicts future development of dysplasia in ulcerative
colitis. Gastroenterology 1992;103:1611-20.
81. Rutter M, Saunders BP, Wilkinson KH, et al. Cancer surveillance in
longstanding ulcerative colitis: endoscopic appearances help predict
cancer risk. Gut 2004;53:1813-6.
82. Kiesslich R, Fritsch J, Holtmann M, et al. Methylene blue–aided
chromoendoscopy for the detection of intraepithelial neoplasia and
colon cancer in ulcerative colitis. Gastroenterology 2003;124:880-8.
83. Rutter MD, Saunders BP, Schofield G, et al. Pancolonic indigo carmine
dye spraying for the detection of dysplasia in ulcerative colitis. Gut
2004;53:256-60.
84. Fruhmorgen P, Demling L. Complications of diagnostic and thera-
peutic colonoscopy in the Federal-Republic-of-Germany: results of
an inquiry. Endoscopy 1979;11:146-50.
85. Nivatvongs S. Complications in colonoscopic polypectomydan experi-
ence with 1555 polypectomies. Dis Colon Rectum 1986;29:825-30.
86. Silvis SE, Nebel O, Rogers G, et al. Endoscopic complications: results
of the 1974 American Society for Gastrointestinal Endoscopy Survey.
JAMA 1976;235:928-30.
87. Anderson ML, Pasha TM, Leighton JA. Endoscopic perforation of
the colon: lessons from a 10-year study. Am J Gastroenterol 2000;95:
3418-22.
S28 GASTROINTESTINAL ENDOSCOPY Volume 63, No. 4 : 2006
88. Gatto NM, Frucht H, Sundararajan V, et al. Risk of perforation after
colonoscopy and sigmoidoscopy: a population-based study. J Natl
Cancer Inst 2003;95:230-6.
89. Woltjen JA. A retrospective analysis of cecal barotrauma caused by
colonoscope air flow and pressure. Gastrointest Endosc 2005;61:37-45.
90. Singh N, Harrison M, Rex DK. A survey of colonoscopic polypectomy
practices among clinical gastroenterologists. Gastrointest Endosc
2004;99:414-8.
91. Norton ID, Wang LN, Levine SA, et al. Efficacy of submucosal saline
injection in the limitation of colonic thermal injury by electrosurgical
devices [abstract]. Gastrointest Endosc 2000;51:AB131.
92. Weston AP, Campbell DR. Diminutive colonic polyps: histopathology,
spatial distribution, concomitant significant lesions, and treatment
complications. Am J Gastroenterol 1995;90:24-8.
93. Peluso F, Goldner F. Follow-up of hot biopsy forceps treatment of
diminutive colonic polyps. Gastrointest Endosc 1991;37:604-6.
94. Tappero G, Gaia E, De Giuli P, et al. Cold snare excision of small
colorectal polyps. Gastrointest Endosc 1992;38:310-3.
95. Waye J. New methods of polypectomy. Gastrointest Endosc Clin
North Am 1997;7:413-22.
96. Deenadayalu VP, Rex DK. Colon polyp retrieval after cold snaring.
Gastrointest Endosc 2005;62:253-6.
97. Zubarik R, Fleischer DE, Mastropietro C, et al. Prospective analysis of
complications 30 days after outpatient colonoscopy. Gastrointest
Endosc 1999;50:322-8.
98. Sorbi D, Norton I, Conio M, et al. Postpolypectomy lower GI bleeding:
descriptive analysis. Gastrointest Endosc 2000;51:690-6.
99. Van Gossum A, Cozzoli A, Adler M, et al. Colonoscopic snare polypec-
tomy: analysis of 1485 resections comparing two types of current.
Gastrointest Endosc 1992;38:472-5.
100. Parra-Blanco A, Kaminaga N, Kojima T, et al. Colonoscopic polypec-
tomy with cutting current: is it safe? Gastrointest Endosc 2000;51:
676-81.
101. Waye J. Saline injection colonoscopic polypectomy. Am J Gastroen-
terol 1994;89:305-6.
102. Hurlstone DP, Sanders DS, Cross SS, et al. Colonoscopic resection
of lateral spreading tumours: a prospective analysis of endoscopic
mucosal resection. Gut 2004;53:1334-9.
103. Hsieh YH, Lin HJ, Tseng GY, et al. Is submucosal epinephrine injection
necessary before polypectomy? A prospective, comparative study.
Hepatogastroenterology 2001;48:1379-82.
104. Di Giorgio P, De Luca L, Calcagno G, et al. Detachable snare versus
epinephrine injection in the prevention of postpolypectomy
bleeding: a randomized and controlled study. Endoscopy 2004;36:
860-3.
105. Iishi H, Tatsuta M, Narahara H, et al. Endoscopic resection of large pe-
dunculated colorectal polyps using a detachable snare. Gastrointest
Endosc 1996;44:594-7.
106. Binmoeller KF, Thonke F, Soehendra N. Endoscopic hemoclip treat-
ment for gastrointestinal bleeding. Endoscopy 1993;25:167-70.
107. Rex DK, Lewis BS, Waye JD. Colonoscopy and endoscopic therapy for
delayed post-polypectomy hemorrhage. Gastrointest Endosc 1992;
38:127-9.
Disclosure: This paper was not subject to the peer review process of GIE.
Reprint requests: ASGE Communications Department, 1520 Kensington
Road, Suite 202, Oak Brook, IL 60523. E-mail: [email protected].
www.giejournal.org