adult congenital heart disease - nhs networks
TRANSCRIPT
ADULTCONGENITAL
HEART DISEASERESOURCE FILE
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
SPONSORED BY
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
FUNDED BY
PAGE 3
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
1Contents
Useful Contacts 5
Referral guidelines 6
ConditionsDevelopment of Congenital Heart Operations 7
Congenital Heart Disease 8
Atrial Septal Defect 9
Ventricular Septal Defect 11
Atrioventricular Septal Defect 13
Coarctation of the Aorta 14
Valve disease in Congenital Heart Patients 16
Ebstein’s Anomaly 18
Tetralogy of Fallot 20
Transposition of the Great Arteries (TGA) 22
Congenitally Corrected Transposition of the Great Arteries (CCTGA) 24
Fontan Circulation 25
Eisenmenger’s Syndrome 27
Chromosomal AbnormalitiesDiGeorge Syndrome 29
Noonan Syndrome 30
Turner Syndrome 31
Trisomy 21/Downs Syndrome 32
EmergenciesManaging Emergencies 33
Lifestyle/OtherCyanosis 35
Pregnancy and effects on the heart 36
Pregnancy risks 37
Endocarditis 38
Transition to adult services 39
Palliative CarePalliative Care 40
PAGE 4
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
2Increasing your knowledge
This education folder has been developed to provide you with information relating to adults with congenital heart disease, conditions and related information.
We hope you will find it a useful resource to increase your knowledge.
Produced by the ACHD link nurses, Specialist Nurses based in the Specialist Congenital Cardiac centre at Leeds and other hospitals within the Yorkshire Humber Network
Information collated by Jo Quirk, Lead Nurse, August 2019.
Updated by Hannah Swift, ACHD Nurse Specialist, August 2021.
PAGE 5
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Cardiac Nurse Specialists
Jo Birkett (Team Leader) [email protected]
Hannah Swift: [email protected]
Angela Leeper: [email protected]
Sarah Gardner: [email protected]
Group email: [email protected] Telephone: 0113 3928154
If you have any questions or comments regarding the resource file, please contact us. If you need advice about a patient we are happy to be contacted. If you would like to arrange teaching sessions in your place of work we would be happy to do this.
Sarah Hibbert Specialist physiotherapist [email protected]
Clinical psychologists for the Network [email protected]
Useful websites
www.leedscongenitalhearts.com contains lots of useful information about the unit, facilities, services & congenital heart conditions.
www.networks.nhs.uk/nhs-networks/yorkshire-and-humber-congenital-cardiac-network contains guidelines and presentations about different subjects presented by the clinical team at study sessions.
Local charity & support groups
Children’s Heart Surgery Fund www.chsf.org - an active Facebook group for patients and families in the Network.
The Somerville Foundation www.thesforg - a national support group for ACHD patients.
Link Nurses
Each clinical area have identified a link nurse for congenital heart disease, who will assist in improving communication with the specialist team, and update you on upcoming study days or learning opportunities. If you don’t know who yours is please ASK!
3Useful contact details & resources
PAGE 6
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Urgent referrals of any ACHD patient:
In normal working hours: should be discussed with the ACHD cardiologist of the week, who can be contacted;
via the secretarial team on 0113 3925748
via the ACHD specialist nurses on 0113 3928154
via Coronary Care Unit at Leeds on 0113 3927420
Out of hours: should be initially discussed with the on call cardiology SpR via CCU at Leeds General Infirmary: 0113 3927420.
Routine referrals:
Patients with a new diagnosis of congenital heart disease made in adult life. All patients with a new diagnosis of a congenital heart defect should be referred for assessment by an ACHD cardiologist.
Patients with a previously known diagnosis of congenital heart disease. Adult patients with known congenital heart disease who are not under active follow up in ACHD services should be seen at least once by an expert in ACHD for a new baseline assessment. Improvements in imaging quality means that a significant proportion of patients treated or diagnosed in childhood before around 2000 may have significant additional pathology which is currently undiagnosed. These patients should therefore be referred for re-assessment.
Routine referrals by letter to:
ACHD Cardiologist E Floor, Jubilee Wing, Leeds General Infirmary
Leeds LS1 3EX
Tel: 0113 3925748
To reduce delays new referrals are made via the Level 1 centre in Leeds, where the referral will be triaged to be seen either in Leeds or one of the Level 3 centres dependent upon urgency and complexity.
4Referral guidelines & contacts
PAGE 7
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
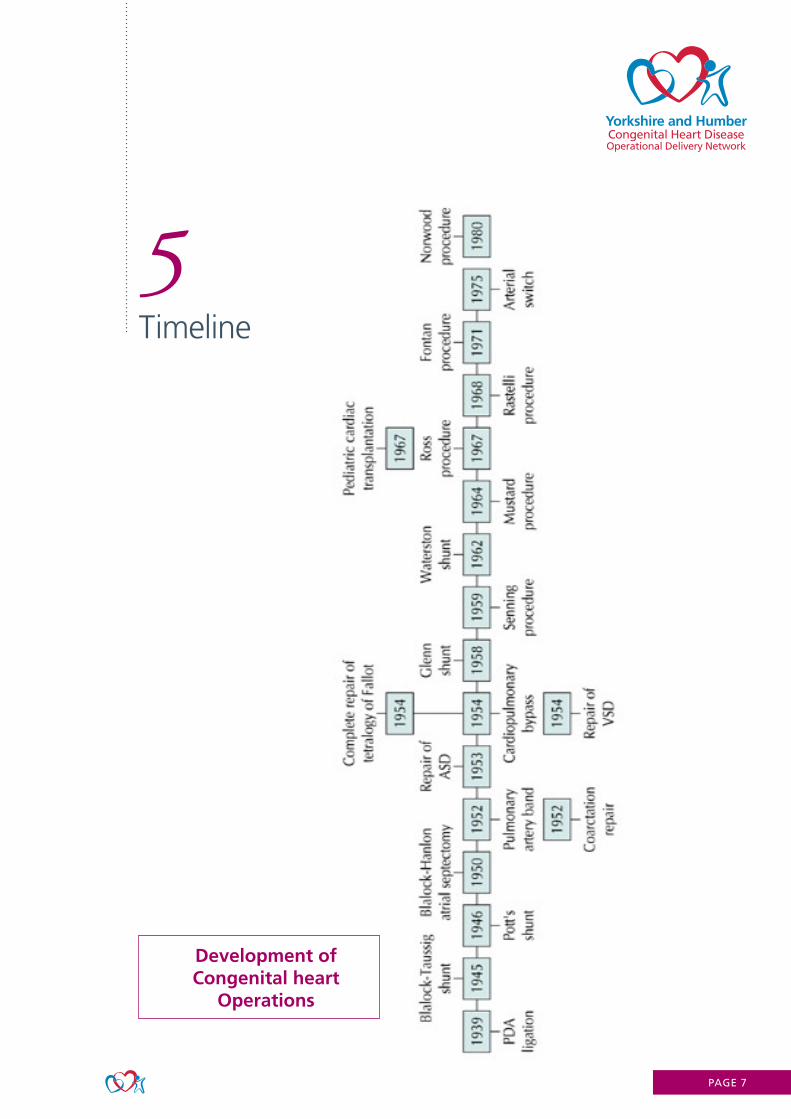
5Timeline
Development of Congenital heart
Operations
PAGE 8
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
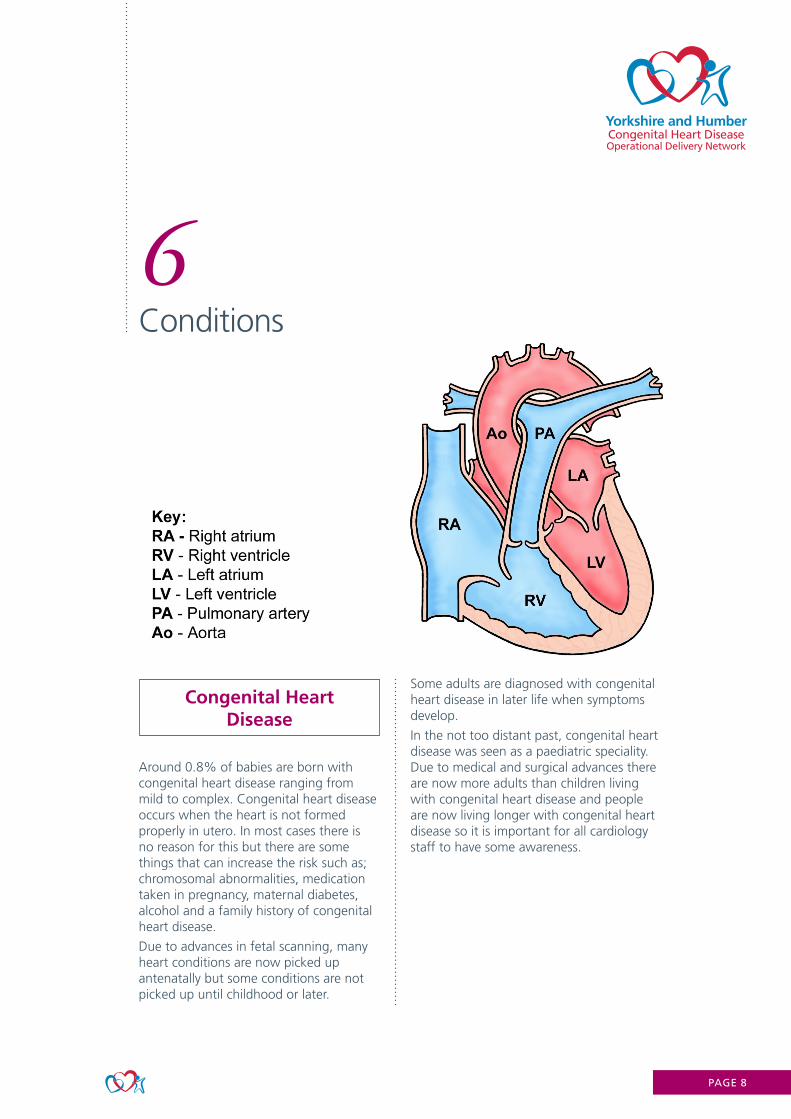
Congenital Heart Disease
Around 0.8% of babies are born with congenital heart disease ranging from mild to complex. Congenital heart disease occurs when the heart is not formed properly in utero. In most cases there is no reason for this but there are some things that can increase the risk such as; chromosomal abnormalities, medication taken in pregnancy, maternal diabetes, alcohol and a family history of congenital heart disease.
Due to advances in fetal scanning, many heart conditions are now picked up antenatally but some conditions are not picked up until childhood or later.
Some adults are diagnosed with congenital heart disease in later life when symptoms develop.
In the not too distant past, congenital heart disease was seen as a paediatric speciality. Due to medical and surgical advances there are now more adults than children living with congenital heart disease and people are now living longer with congenital heart disease so it is important for all cardiology staff to have some awareness.
PAGE 9
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
Atrial Septal Defect
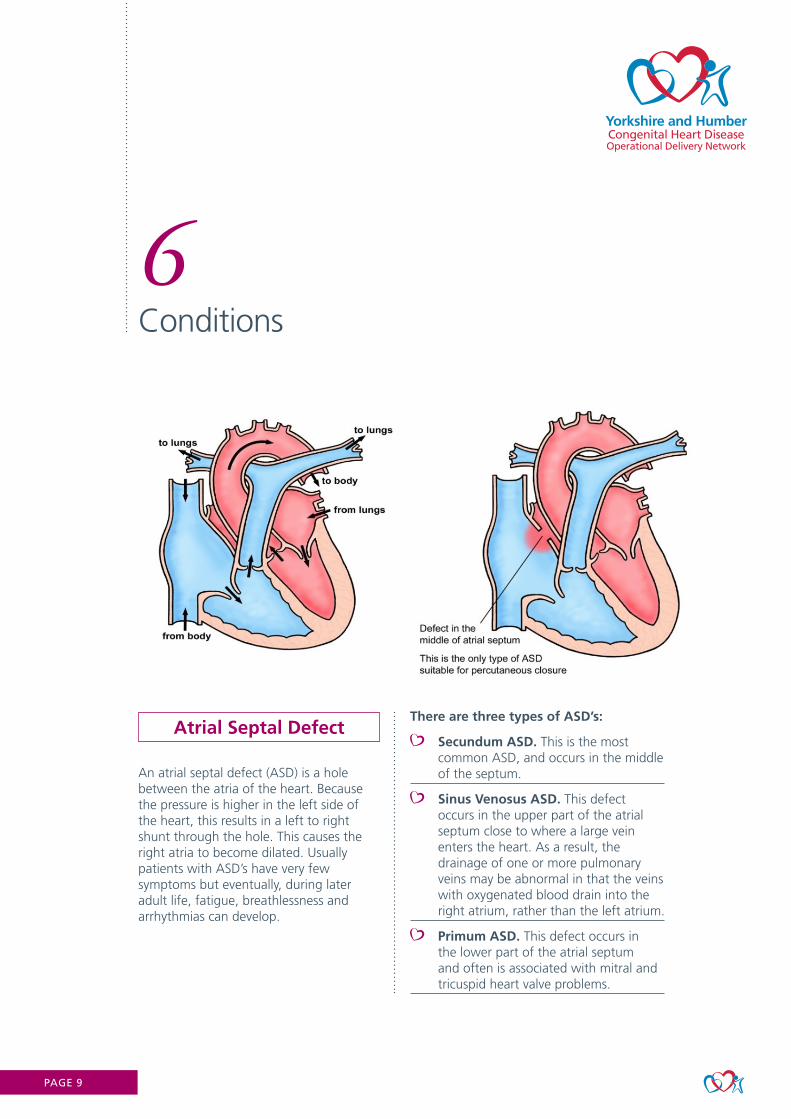
An atrial septal defect (ASD) is a hole between the atria of the heart. Because the pressure is higher in the left side of the heart, this results in a left to right shunt through the hole. This causes the right atria to become dilated. Usually patients with ASD’s have very few symptoms but eventually, during later adult life, fatigue, breathlessness and arrhythmias can develop.
There are three types of ASD’s:
Secundum ASD. This is the most common ASD, and occurs in the middle of the septum.
Sinus Venosus ASD. This defect occurs in the upper part of the atrial septum close to where a large vein enters the heart. As a result, the drainage of one or more pulmonary veins may be abnormal in that the veins with oxygenated blood drain into the right atrium, rather than the left atrium.
Primum ASD. This defect occurs in the lower part of the atrial septum and often is associated with mitral and tricuspid heart valve problems.
PAGE 10
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Closing the defect
We would generally recommend closure of all but the smallest of ASD’s, unless other problems are present that would make this unwise (for example pulmonary hypertension, which can occur in some patients with ASD’s).
Surgical closure
Surgical closure involves the surgeon stitching the hole closed or covering it with a patch, usually from the patient’s own pericardium or a Dacron patch.
Pericardial effusion can occur a few weeks after surgical closure of ASD.
Recovery from heart surgery takes 6-12 weeks.
Interventional closure
Keyhole treatment is not suitable for all ASD’s depending on the position of the hole. The most commonly used device is called the “Amplatzer” device. All devices fold into a thin tube (catheter) which is inserted into a vein in the groin under general anaesthetic. The device is then unfolded into the hole and released. The device stays in the heart and eventually becomes covered by the patient’s own tissue during the healing process.
Following keyhole treatment we advise treatment with aspirin for 6 months after closure.
This procedure only needs 1 night in hospital and recovery should not take longer than 1 week.
No restrictions to physical activity are required.
Following repair, the right heart may remodel back to near normal but this is not always the case.
Most people will remain well and lead a completely normal life after ASD closure.
The later the ASD is repaired, the more likelihood there is of the patient developing atrial arrhythmias due to right heart stretch.
Key points
PAGE 11
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
Ventricular Septal Defect
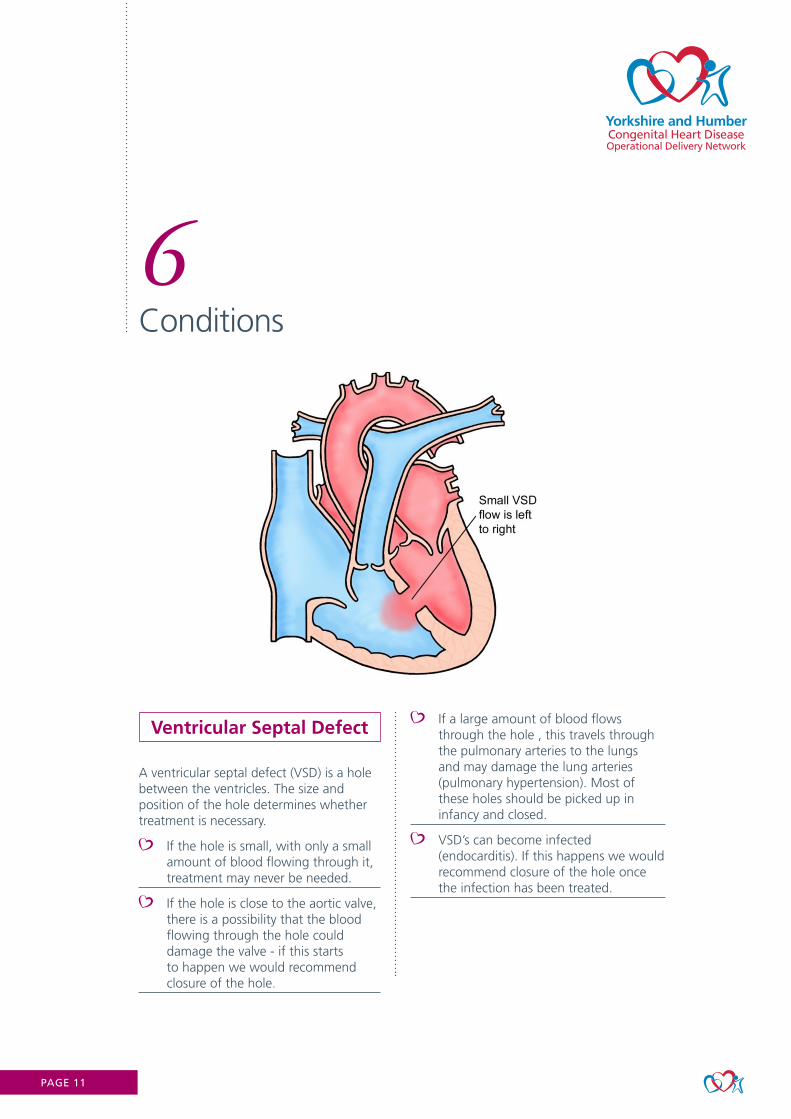
A ventricular septal defect (VSD) is a hole between the ventricles. The size and position of the hole determines whether treatment is necessary.
If the hole is small, with only a small amount of blood flowing through it, treatment may never be needed.
If the hole is close to the aortic valve, there is a possibility that the blood flowing through the hole could damage the valve - if this starts to happen we would recommend closure of the hole.
If a large amount of blood flows through the hole , this travels through the pulmonary arteries to the lungs and may damage the lung arteries (pulmonary hypertension). Most of these holes should be picked up in infancy and closed.
VSD’s can become infected (endocarditis). If this happens we would recommend closure of the hole once the infection has been treated.

PAGE 12
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Surgical closure
Surgical closure involves the surgeon stitching the hole closed or covering it with a patch, usually from the patient’s own pericardium or a Dacron patch.
Interventional closure
It is possible for some VSDs to be closed using a keyhole device like with an ASD but this is not as common as it is still a fairly new approach with the first carried out in 2013.
Some VSDs spontaneously close on their own in childhood.
If left untreated, medium to large VSDs can cause Eisenmenger’s syndrome because of the excess pulmonary blood flow.
VSDs may be picked up in infancy due to a heart murmur. Or babies may be breathless.
Key points
PAGE 13
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
Atrioventricular Septal Defect
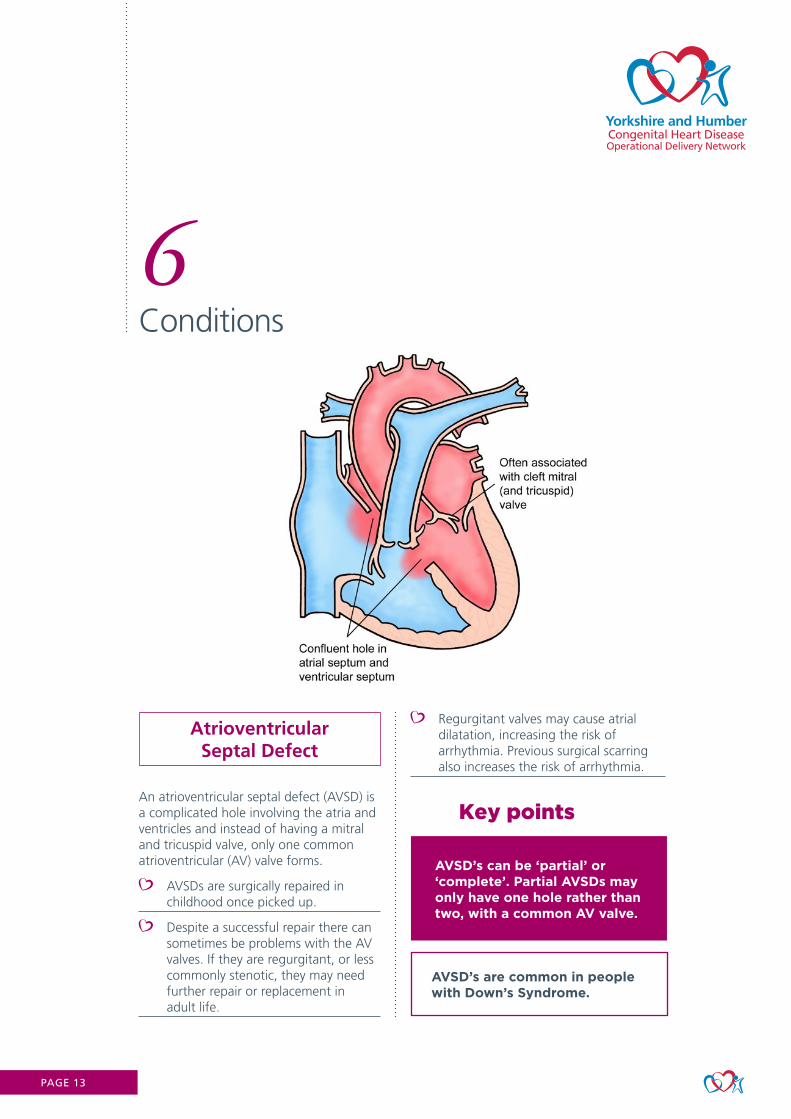
An atrioventricular septal defect (AVSD) is a complicated hole involving the atria and ventricles and instead of having a mitral and tricuspid valve, only one common atrioventricular (AV) valve forms.
AVSDs are surgically repaired in childhood once picked up.
Despite a successful repair there can sometimes be problems with the AV valves. If they are regurgitant, or less commonly stenotic, they may need further repair or replacement in adult life.
Regurgitant valves may cause atrial dilatation, increasing the risk of arrhythmia. Previous surgical scarring also increases the risk of arrhythmia.
AVSD’s are common in people with Down’s Syndrome.
AVSD’s can be ‘partial’ or ‘complete’. Partial AVSDs may only have one hole rather than two, with a common AV valve.
Key points
PAGE 14
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
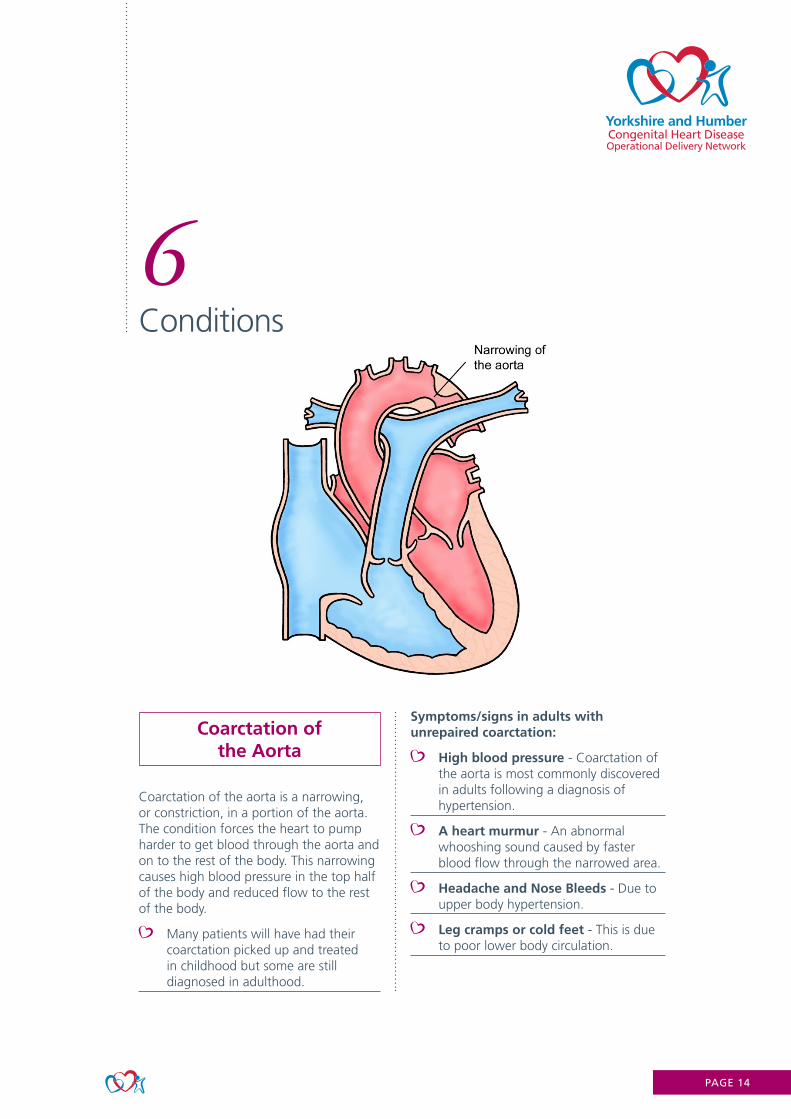
Coarctation of the Aorta
Coarctation of the aorta is a narrowing, or constriction, in a portion of the aorta. The condition forces the heart to pump harder to get blood through the aorta and on to the rest of the body. This narrowing causes high blood pressure in the top half of the body and reduced flow to the rest of the body.
Many patients will have had their coarctation picked up and treated in childhood but some are still diagnosed in adulthood.
Symptoms/signs in adults with unrepaired coarctation:
High blood pressure - Coarctation of the aorta is most commonly discovered in adults following a diagnosis of hypertension.
A heart murmur - An abnormal whooshing sound caused by faster blood flow through the narrowed area.
Headache and Nose Bleeds - Due to upper body hypertension.
Leg cramps or cold feet - This is due to poor lower body circulation.
PAGE 15
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Management
If diagnosed as a child - surgery via a thoracotomy is usually the preferred choice. There are different types of surgery including end to end anastomosis, subclavian flap repair, patch repair or interposition graft repair.
If diagnosed as an adult, or if further treatment is needed following an initial surgical repair - balloon angioplasty, often with stenting, is the preferred option.
Although repairing aortic coarctation improves blood pressure, many people still need to take blood pressure medication, even after successful surgery or stenting. Good blood pressure control is essential to avoid early coronary artery disease.
Patients will have regular follow up including cardiac MRI to monitor for re-coarctation or weakening of the repair site.
Some people need repeat procedures.
Between 5-8% of people with congenital heart disease have coarctation of the aorta.
Coarctation of the aorta can occur on its own or with other defects such as bicuspid aortic valves.
Men are almost twice more likely to have an aortic coarctation than women.
Blood pressure should be checked on the RIGHT ARM ONLY!! It is likely to be falsely low in the left .
Key points
PAGE 16
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
Valve disease in Congenital Heart
Patients
Valves can be stenotic or regurgitant or both (mixed disease). Valve disease can be mild, moderate or severe. Depending on which valve is affected and the severity of the problem deems what treatment is necessary (if any). We would usually only intervene if valve disease is severe or if the patient is having symptoms that reflect their valve disease. Younger patients often manage well with severe valve disease for many years but regular follow up is essential. Intervention is usually offered before a patient becomes symptomatic but decision about timing of treatment is important.
Aortic Valve
The valves of the heart have 3 leaflets which allow blood to flow through them. Around 2% of people have 2 leaflets (bicuspid aortic valve). For some people this isn’t an issue and their heart continues to function well. However some people need intervention if the valve deteriorates with time.
Mitral Valve
Some people with mitral valve disease may have something called a ‘parachute’ mitral valve.
Tricuspid Valve
Tricuspid valves may be “Ebstenoid” and displaced into the right atrium or may be in the correct position but abnormal.
Pulmonary Valve
Isolated pulmonary valve disease is often asymptomatic and people will probably never need treatment for mild to moderate cases. Pulmonary valve disease alongside conditions such as Tetralogy of Fallot may require repeat pulmonary valve replacements over a lifetime.
Endocarditis
People with heart valve issues are at higher risk of developing endocarditis. Bacteria can settle on abnormal valves which can lead to degeneration of the valve further. Endocarditis can sometimes go undetected for many weeks. People with valve disease (or any congenital heart disease), with unexplained pyrexia/night sweats/elevated CRP should be investigated for endocarditis.
PAGE 17
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Surgical treatments for valve disease include:
Tissue Valves
Long term anticoagulation not required.
Reoperation is likely to be required (usually last on average 10 years).
No restrictions needed in terms of exercise and activity.
Tissue valve may be more suitable for women of childbearing age due to the risks of mechanical valves, warfarin and pregnancy.
Mechanical Valves
Advantage of mechanical heart valve is its durability.
Patients must take warfarin.
Refrain from contact sports (rugby) and caution with high risk activities (skiing, mountain bikes).
Pregnancy in patients with mechanical valves is classed as high risk.
Higher maternal complication rate (require close monitoring in pregnancy).
Risk of thrombus and emboli if anticoagulation discontinued or poor compliance.
Mechanical valves not suitable for the right side of heart due to lower pressures increasing risk of thrombus.
Percutaneous Valves
Percutaneous valves are increasingly being used in congenital heart disease. Most commonly in pulmonary valve procedures and less commonly in tricuspid valves. Percutaneous aortic valves (TAVI) are not routinely offered due to surgical options currently having better outcomes in our patient group.
Warfarin in pregnancy- Warfarin is teratogenic, particularly between 6 and 12 weeks gestation and can lead to ‘fetal warfarin syndrome’. Heparin is considered safer for the fetus as it does not cross the placenta. However, due to the difficulty in ensuring adequate anticoagulation, for the mother it may be less safe.Women must have very tight control of whatever anticoagulation they take and must attend regular blood tests and medical reviews.
Key points
Ross Operation
The Ross operation is sometimes used for aortic valve disease. It involves moving the patients own pulmonary valve into the aortic valve position and using a homograft to replace the pulmonary valve. This means the patient now has 2 valves that have been operated on but if often works well for many years and avoids the need for warfarin.
Pregnancy
A large number of female congenital patients with valvular heart disease will be of childbearing age. Counselling pre-pregnancy, extensive guidance and close obstetric monitoring from a specialised multidisciplinary team is of particular importance in those with certain valve disease or those with a mechanical valve.
PAGE 18
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
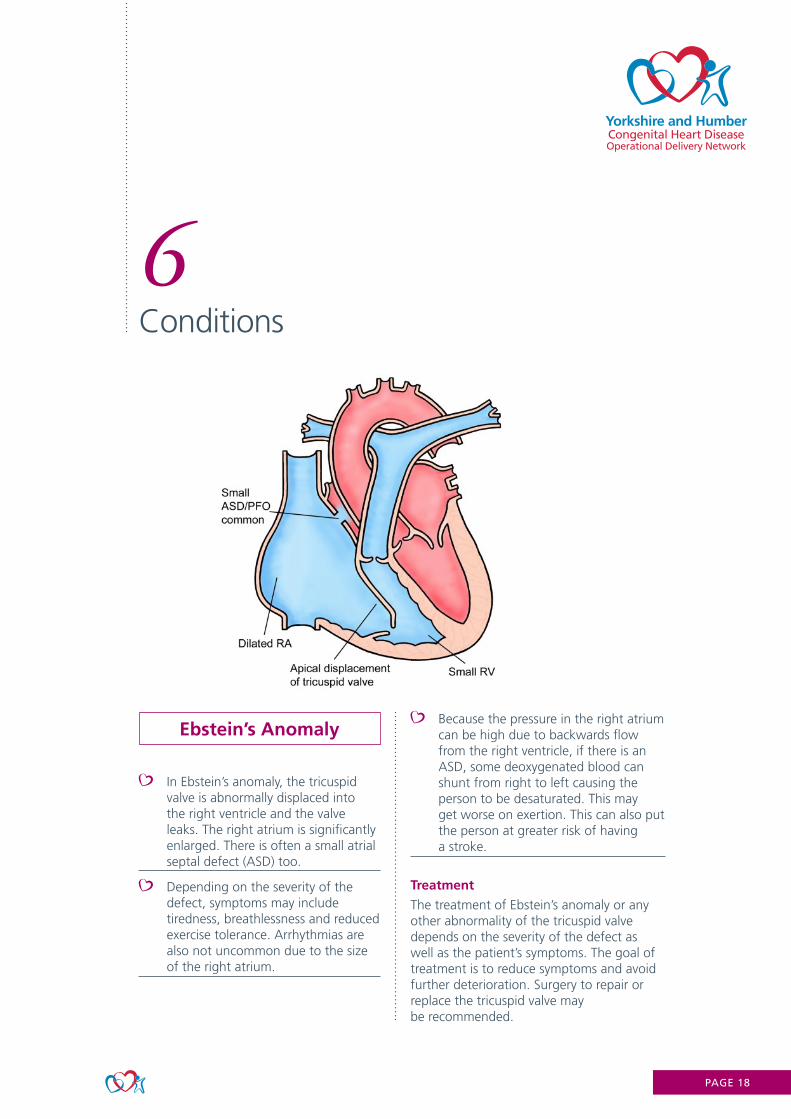
Ebstein’s Anomaly
In Ebstein’s anomaly, the tricuspid valve is abnormally displaced into the right ventricle and the valve leaks. The right atrium is significantly enlarged. There is often a small atrial septal defect (ASD) too.
Depending on the severity of the defect, symptoms may include tiredness, breathlessness and reduced exercise tolerance. Arrhythmias are also not uncommon due to the size of the right atrium.
Because the pressure in the right atrium can be high due to backwards flow from the right ventricle, if there is an ASD, some deoxygenated blood can shunt from right to left causing the person to be desaturated. This may get worse on exertion. This can also put the person at greater risk of having a stroke.
Treatment
The treatment of Ebstein’s anomaly or any other abnormality of the tricuspid valve depends on the severity of the defect as well as the patient’s symptoms. The goal of treatment is to reduce symptoms and avoid further deterioration. Surgery to repair or replace the tricuspid valve may be recommended.
PAGE 19
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Surgical Options
Repair
If the tricuspid valve is leaking the surgeon may repair the valve by separating tethered valve leaflets, closing holes in the leaflets and by reshaping the valve leaflets so that they can make contact with each other and prevent backward flow.
The surgeon may reduce the size of the valve opening to allow the existing valve leaflets to come together to work properly. A ring may be placed around the valve to support it. This is referred to as an annuloplasty.
Another surgical approach is called the ‘Cone procedure’. This involves the surgeon separating the leaflets of the tricuspid valve from the heart muscle. The leaflets are then rotated and reattached creating a cone from the existing valve leaflets.
Replacement
Tricuspid valve replacement is less common and surgeons prefer to repair the heart valve rather than replace it when possible. If the valve cannot be repaired, the surgeon will replace the valve by removing the existing valve and inserting a tissue valve. Mechanical valves have a high risk of thrombosis on the right side of the heart, even with warfarin so are not routinely used.
Patients can suffer with palpitations and troublesome atrial arrhythmias. Some patients may require a pacemaker at the time of surgery due to the valve being situated close to the AV node.
It is useful to take a baseline oxygen saturation reading at rest and then monitor the patient’s saturations when they are walking around to see if they become desaturated.
Patients with poor ventricular function may not benefit from tricuspid valve surgery and could be deemed as too high risk. This is because the ventricle might not cope with the valve working effectively. In such cases, patients may be considered for cardiac transplant.
Key points
PAGE 20
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
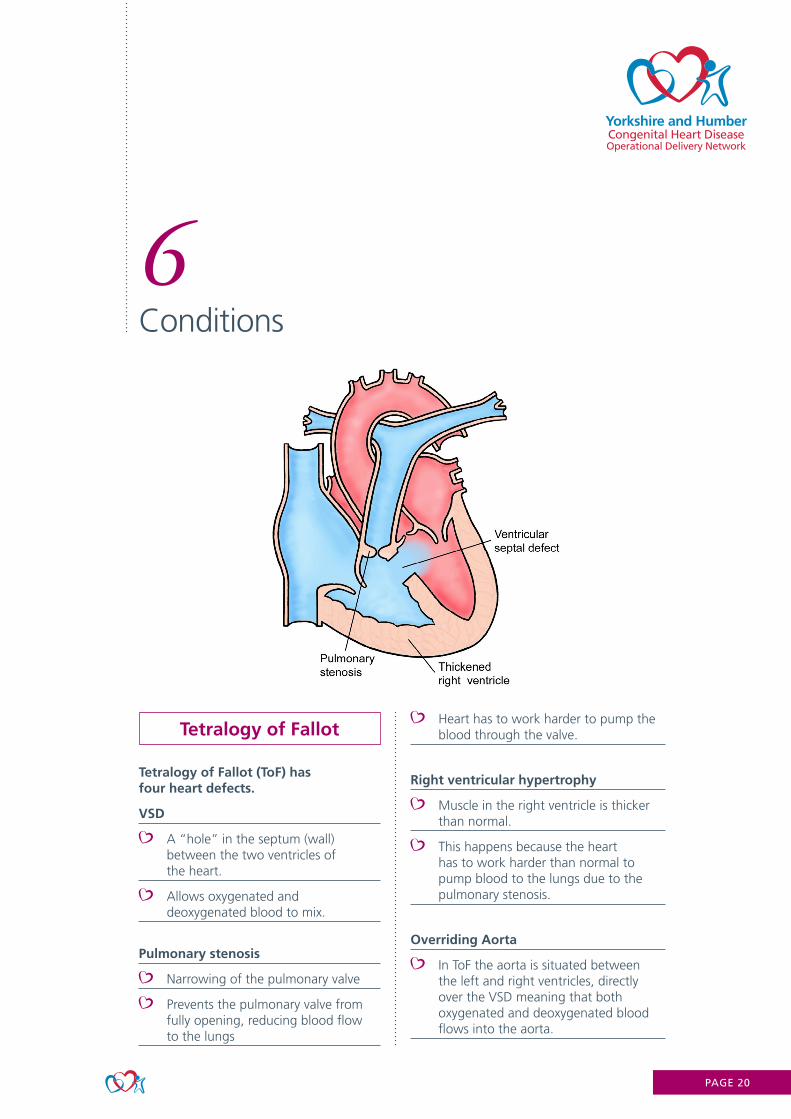
Tetralogy of Fallot
Tetralogy of Fallot (ToF) has four heart defects.
VSD
A “hole” in the septum (wall) between the two ventricles of the heart.
Allows oxygenated and deoxygenated blood to mix.
Pulmonary stenosis
Narrowing of the pulmonary valve
Prevents the pulmonary valve from fully opening, reducing blood flow to the lungs
Heart has to work harder to pump the blood through the valve.
Right ventricular hypertrophy
Muscle in the right ventricle is thicker than normal.
This happens because the heart has to work harder than normal to pump blood to the lungs due to the pulmonary stenosis.
Overriding Aorta
In ToF the aorta is situated between the left and right ventricles, directly over the VSD meaning that both oxygenated and deoxygenated blood flows into the aorta.
PAGE 21
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Management
Most patients with ToF will have had a full “repair” as a child to stretch open the pulmonary valve (valvotomy) and close the VSD, ensuring the aorta comes from the left ventricle.
The repair usually leaves the person with a regurgitant pulmonary valve.
Adults with ToF often need a pulmonary valve replacement at some point - this can be done surgically or percutaneously (if the patient’s anatomy is suitable).
Biological or homograft valves are used which do degenerate (average 10 years).
Percutaneous valves are becoming more common with minimal recovery time and so far with good outcomes.
Percutaneous ‘valve in valve’ procedures are possible to avoid open heart surgery.
People with Tetralogy of Fallot are at higher risk of atrial and ventricular arrhythmias due to scar tissue. Sometimes an ICD may be needed but this is becoming less common with improving surgical techniques.
Women with repaired ToF should tolerate pregnancy very well. There is a slight inheritability risk - around 3-5% compared with 1% of the general population.
Key points
PAGE 22
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
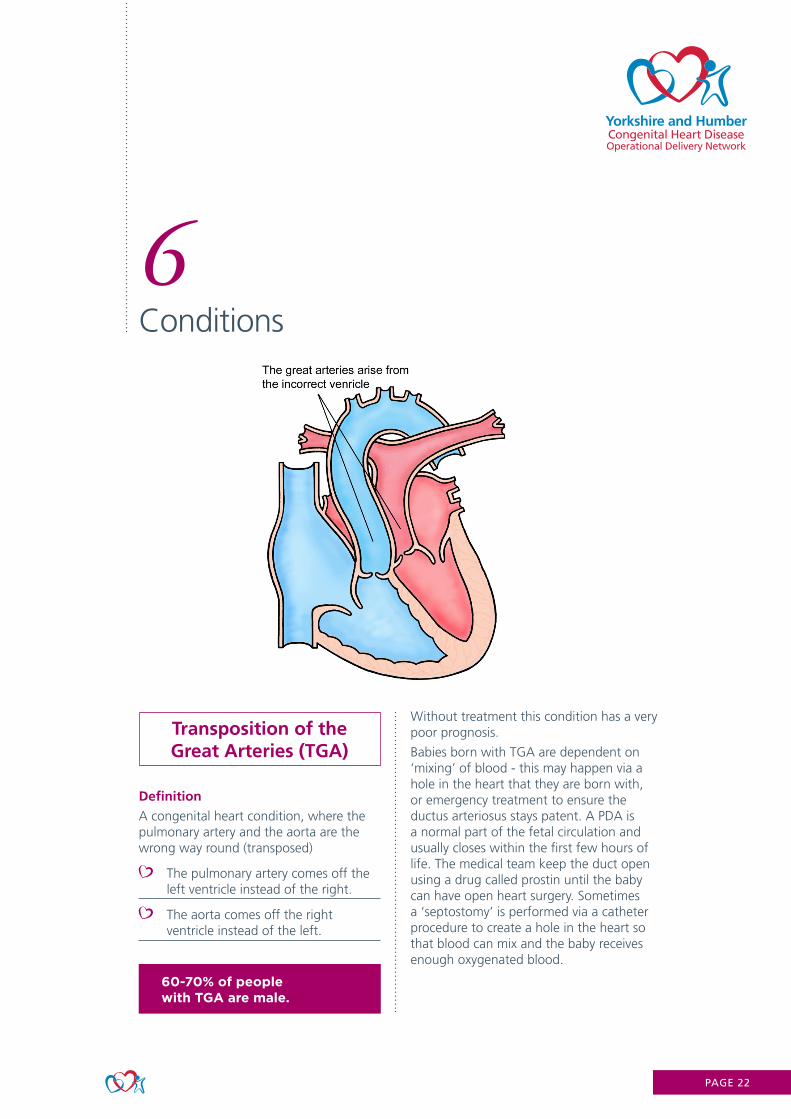
Transposition of the Great Arteries (TGA)
Definition
A congenital heart condition, where the pulmonary artery and the aorta are the wrong way round (transposed)
The pulmonary artery comes off the left ventricle instead of the right.
The aorta comes off the right ventricle instead of the left.
Without treatment this condition has a very poor prognosis.
Babies born with TGA are dependent on ‘mixing’ of blood - this may happen via a hole in the heart that they are born with, or emergency treatment to ensure the ductus arteriosus stays patent. A PDA is a normal part of the fetal circulation and usually closes within the first few hours of life. The medical team keep the duct open using a drug called prostin until the baby can have open heart surgery. Sometimes a ‘septostomy’ is performed via a catheter procedure to create a hole in the heart so that blood can mix and the baby receives enough oxygenated blood.
60-70% of people with TGA are male.

PAGE 23
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
The MUSTARD or the SENNING procedure, also known as an atrial switch, was performed in the 1960’s to early 1990’s for patients with TGA. Surgical baffles in the atria re-direct blood but the right ventricle remains the systemic ventricle.
Long-term complications following a Mustard/Senning procedure
Poor ventricular function (as the right ventricle is acting as the systemic ventricle and is naturally weaker which can lead to heart failure).
Arrhythmia - Bradycardia due to scar tissue often leading to pacemaker. Ventricular/atrial tachycardia that can be poorly tolerated if reduced ventricular function.
Stenosis or leaks around the surgical baffles - this may require intervention in the catheter lab or further surgery.
Likely to have a reduced exercise tolerance. May be desaturated if there are baffle leaks.
May be a cardiac transplant candidate.
This operation is no longer routinely performed.
The ARTERIAL SWITCH was developed in the 1990’s.
Generally this operation has much better outcomes for patients although the heart is never completely normal.
The great arteries are switched around so the left ventricle is now the systemic ventricle as it should be.
The coronary arteries have to be translocated.
Potential long-term complications following Arterial Switch operation
The pulmonary arteries may may be narrower than normal as they have been stretched into position.
The aortic root and ascending aorta can be dilated due to the surgical techniques used.
The aortic valve may become regurgitant if the aortic root is dilated
There is a potential for the coronary arteries which have been translocated to be susceptible to narrowing.
Although so far, only a small percentage have experienced the above problems, it is too soon to tell how common it may be in later life so people are kept under life-long follow up although for straightforward repairs this may only be every 2-3 years.
PAGE 24
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
Congenitally Corrected Transposition of the Great
Arteries (CCTGA)
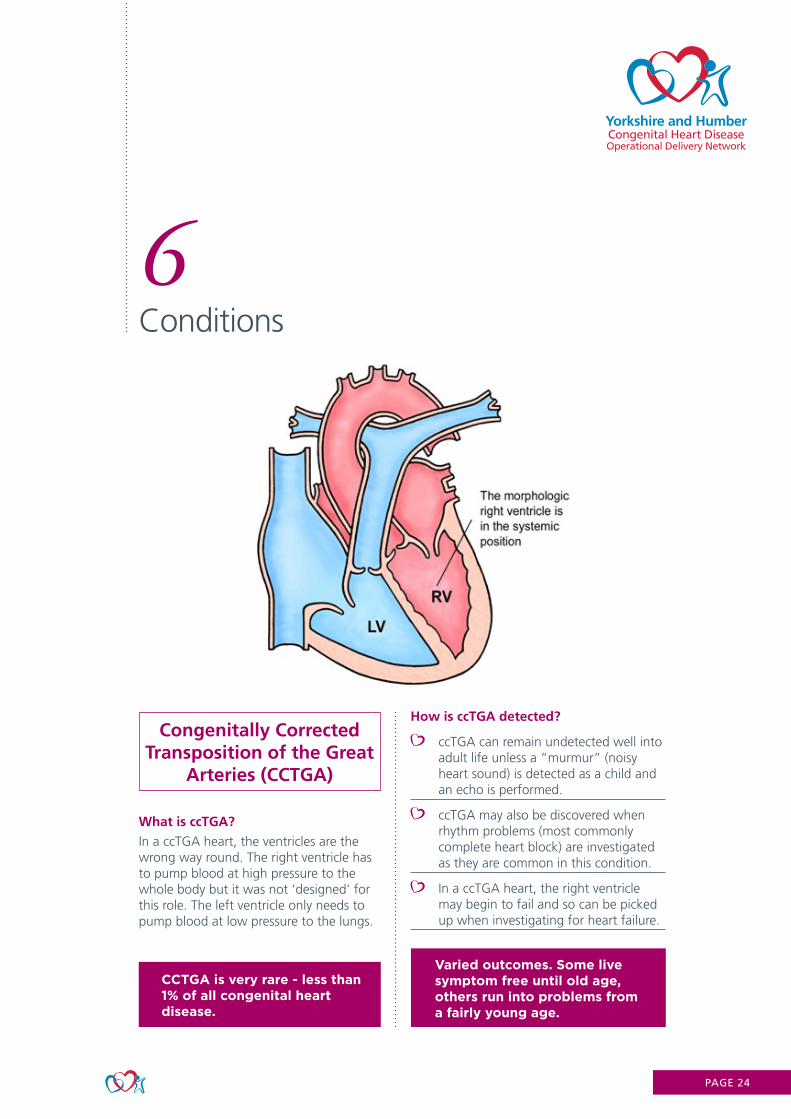
What is ccTGA?
In a ccTGA heart, the ventricles are the wrong way round. The right ventricle has to pump blood at high pressure to the whole body but it was not ‘designed’ for this role. The left ventricle only needs to pump blood at low pressure to the lungs.
How is ccTGA detected?
ccTGA can remain undetected well into adult life unless a “murmur” (noisy heart sound) is detected as a child and an echo is performed.
ccTGA may also be discovered when rhythm problems (most commonly complete heart block) are investigated as they are common in this condition.
In a ccTGA heart, the right ventricle may begin to fail and so can be picked up when investigating for heart failure.
CCTGA is very rare - less than 1% of all congenital heart disease.
Varied outcomes. Some live symptom free until old age, others run into problems from a fairly young age.
PAGE 25
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
Fontan Circulation
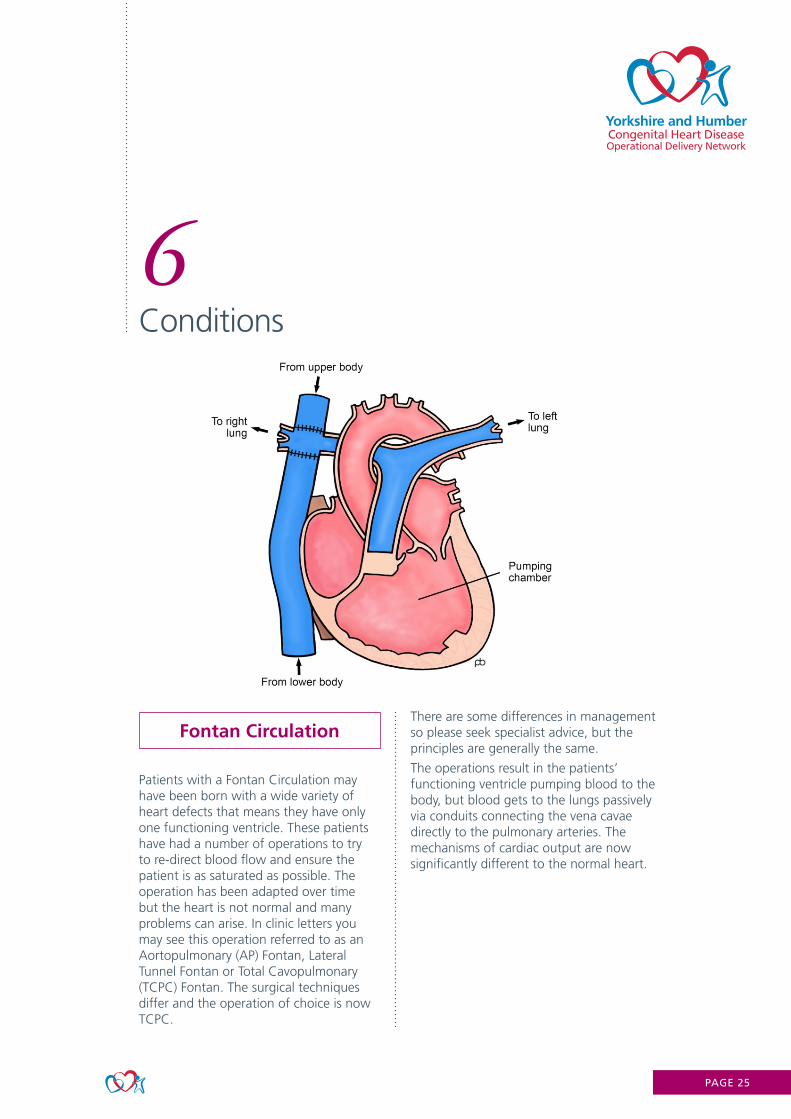
Patients with a Fontan Circulation may have been born with a wide variety of heart defects that means they have only one functioning ventricle. These patients have had a number of operations to try to re-direct blood flow and ensure the patient is as saturated as possible. The operation has been adapted over time but the heart is not normal and many problems can arise. In clinic letters you may see this operation referred to as an Aortopulmonary (AP) Fontan, Lateral Tunnel Fontan or Total Cavopulmonary (TCPC) Fontan. The surgical techniques differ and the operation of choice is now TCPC.
There are some differences in management so please seek specialist advice, but the principles are generally the same.
The operations result in the patients’ functioning ventricle pumping blood to the body, but blood gets to the lungs passively via conduits connecting the vena cavae directly to the pulmonary arteries. The mechanisms of cardiac output are now significantly different to the normal heart.
PAGE 26
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Complications
Issues are related to increased venous pressure, venous congestion and chronic low cardiac output.
Ventricular dysfunction or “Failing Fontan”. This may happen sooner if the systemic ventricle is the right ventricle rather than the left.
Conduction disturbances requiring pacemaker.
Arrhythmia - atrial arrhythmias are common and are often poorly tolerated as they further reduce cardiac output - must be treated promptly.
Venous congestion causing liver problems.
Lymphatic dysfunction - protein losing enteropathy.
Pulmonary hypertension.
High risk for general anaesthesia (must be a cardiac anaesthetist with congenital experience).
Thrombosis - patients should be on anticoagulation.
Desaturation - almost all Fontan patients will have some level of desaturation but this will vary from patient to patient.
Progressive decline in exercise tolerance.
Heart transplant may be an option for some.
Patients with a Fontan circulation should avoid being dehydrated and should pay particular attention to this if unwell.
Women are able to become pregnant and carry babies to term but pregnancy is high risk. Miscarriage and premature delivery are common.
As with all CHD, ask the patient what their normal saturations are. Or look back through their clinic letters if available.
Key points
PAGE 27
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
6Conditions
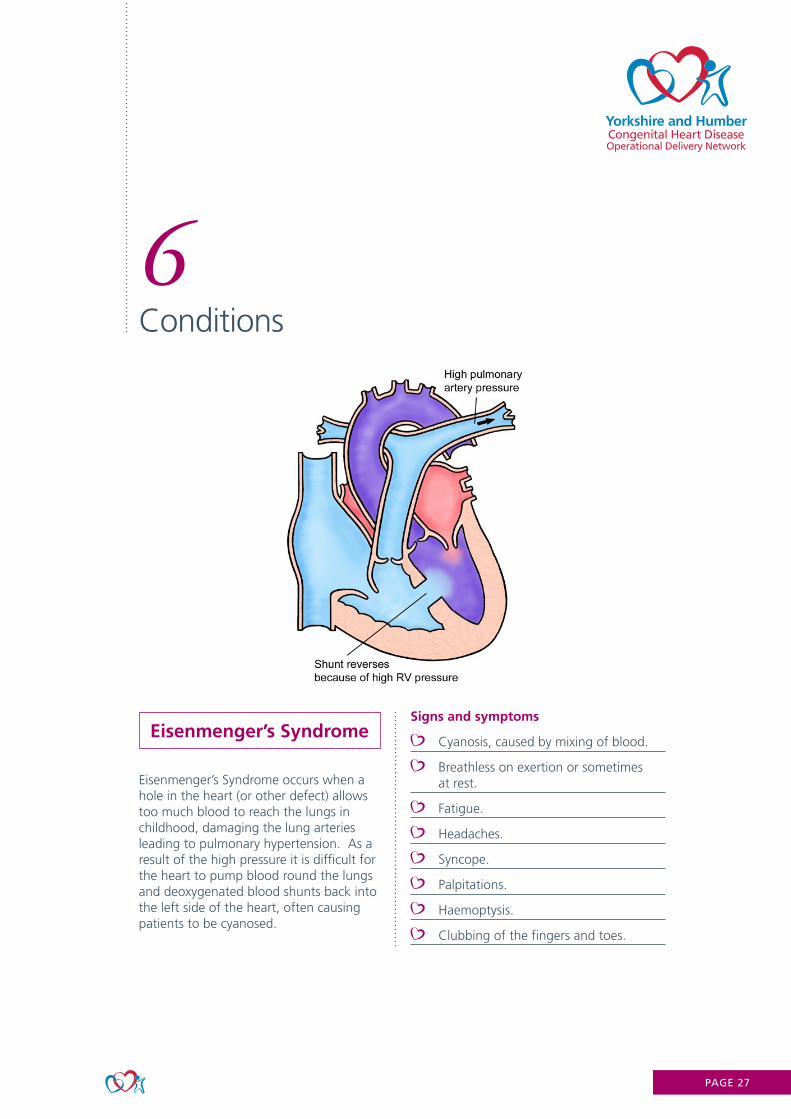
Eisenmenger’s Syndrome
Eisenmenger’s Syndrome occurs when a hole in the heart (or other defect) allows too much blood to reach the lungs in childhood, damaging the lung arteries leading to pulmonary hypertension. As a result of the high pressure it is difficult for the heart to pump blood round the lungs and deoxygenated blood shunts back into the left side of the heart, often causing patients to be cyanosed.
Signs and symptoms
Cyanosis, caused by mixing of blood.
Breathless on exertion or sometimes at rest.
Fatigue.
Headaches.
Syncope.
Palpitations.
Haemoptysis.
Clubbing of the fingers and toes.
PAGE 28
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
Complications
If patients are cyanosed, their blood becomes thicker than normal (polycythaemia). This can lead to headaches and loss of concentration, pains in arms and legs and pins and needles. Venesection is not recommended as this can lead to iron deficiency.
With polycythaemia, the body produces more red blood cells but they are of poorer quality and this may lead to low blood iron levels. It is important to monitor iron stores and not just haemoglobin.
The right ventricle becomes hypertrophied (thickened) as it struggles to pump blood to the lungs, this can lead to right sided heart failure.
People are more likely to suffer with gout (painful, swollen and red joints) and gallstones.
Brain abscesses are rare but can occur in people with Eisenmenger’s. This is due to the right to left shunting - if bacteria are in the blood stream they can reach the brain.
Treatments
The treatments are aimed at lowering the blood pressure in the lungs by relaxing the small arteries, this should improve the oxygen levels in the blood and patients may feel like they have more energy.
Phosphodiesterase type 5 (PDE5) inhibitors (tablets) sildenafil or tadalafil.
Endothelin receptor antagonists (ERA) (tablets) ambrisentan, bosentan or macitentan.
Prostanoids (inhaled or delivered into the bloodstream): epoprostenol (intravenous), iloprost (nebulised).
Closing the hole (or other defect) would be dangerous as the pressure would get even higher.
If a patient requires a non-cardiac operation they need to be discussed with a cardiologist or congenital anaesthetist as the heart may not cope well with an anaesthetic. Decisions will need to be made carefully.
The body tries to make more red blood cells to try and carry more oxygen. Patients will have a high Hb (polycythaemia) but this is normal for them.
Pregnancy in patients with Eisenmenger’s is usually fatal. Effective contraception is vital and progestogen-only preparations are recommended.
Key points
PAGE 29
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
7Chromosomal abnormalities
10% of patients with congenital heart disease have a known learning disability related to a syndrome.
The following pages will look at some of the main syndromes associated with congenital heart disease.
DiGeorge Syndrome
22q11 deletion - a small part of chromosome 22 is missing.
It is very variable - from mild to severe.
It is a “multi-system” disorder.
People with ‘mild’ DiGeorge syndrome may not have been diagnosed.
Associated problems
Learning disabilities,
Speech and hearing problems,
Mouth problems including a cleft lip or palate,
Facial dysmorphia,
Hormone problems (hypothyroid, hypocalcaemia),
Bone, muscle and joint problems,
Short stature,
Immunodeficiency.
70% of people with DiGeorge syndrome have congenital heart disease.
Associated cardiac problems include;
Truncus Arteriosus
Tetralogy of Fallot
Pulmonary atresia
If one parent has DiGeorge syndrome there is a 50% chance of passing it onto their child.
People with DiGeorge and congenital heart disease will be at an even greater risk of endocarditis due to their immunodeficiency.
Adults with DiGeorge are at greater risk of developing mental health problems such as schizophrenia, depression and bipolar disorder.
People with DiGeorge may need input from many medical specialities as well as social care input and educational support.
PAGE 30
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
7Chromosomal abnormalities
Noonan Syndrome
Noonan syndrome is caused by a fault in one of several genes and can be inherited from one of the child’s parents. The faulty gene prevents normal development in various parts of the body.
Associated problems
A characteristic facial appearance.
Developmental delay.
Short stature.
Congenital heart disease.
A broad or webbed neck.
Minor eye problems.
Associated cardiac problems
Pulmonary valve stenosis is the most common.
Hypertrophic cardiomyopathy (thickening of the heart muscle).
Septal defects.
What are the treatments?
There is currently no single treatment for Noonan syndrome, but it is often possible to successfully manage many aspects of the condition. Some heart defects may require surgical intervention. Growth hormone medication may also be used to help prevent restricted growth. Children may need treatment and support to help manage the various problems. However, they will usually need much less care as they get older, as the condition tends to cause fewer problems in adulthood.
PAGE 31
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
7Chromosomal abnormalities
Turner Syndrome
A syndrome affecting only females.
Affects around 1 in 2000 females.
Females usually have XX chromosomes.
Females with Turner syndrome have one missing or incomplete X chromosome.
Most have underdeveloped ovaries resulting in infertility.
May not be diagnosed until girls fail to show developments associated with puberty.
Associated problems
Most are shorter than average - growth hormones required as a child.
Hearing loss.
High blood pressure.
Hypothyroid.
Increased risk of diabetes.
Increased risk of osteoporosis.
Treatment with female hormones is required.
Low self-esteem/depression.
Cardiac defects associated with Turner Syndrome:
Coarctation of the aorta.
Bicuspid aortic valve.
Aortic dilatation.
Surgery/intervention may be needed to treat these:
Coarctation stents.
Aortic valve/root replacements.
Surgery is higher risk due to people with Turner syndrome having poor aortic tissue quality. They are more at risk of haemorrhage around the time of surgery/intervention.
Women treated with oestrogen will need to stop this around the time of surgery due to the increased risk of thrombus.
More than 8 out of 10 females with Turner syndrome have difficulty understanding spatial relationships and numeracy. This can make learning to drive difficult.
PAGE 32
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
7Chromosomal abnormalities
Trisomy 21 / Downs Syndrome
A genetic disorder caused by the presence of either a whole or a part third copy of chromosome 21.
Associated problems
Developmental delay
Increased risk of epilepsy
Hearing and vision disorders
Stunted growth
Endocrine e.g. hypothyroid
Dementia in later life
Associated cardiac problems
Atrioventricular septal defect is the most common
VSD
PDA
Mental Capacity ActAs with all learning disabilities it is essential to know about capacity.People must be presumed to have capacity and we must do all we can to help a person make their own decisions.
If a person is deemed not to have capacity, then all decisions must be in the person’s best interests and the relevant paperwork must be completed.
There are a number of patients with Downs Syndrome with Eisenmenger’s syndrome - this is because in the past, surgery wasn’t routinely offered to people with Downs Syndrome but this is certainly not the case today.
PAGE 33
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
8Emergencies
Managing Emergencies
Initial treatment (the same as any other unwell patient)
Treat arrhythmias with haemodynamic compromise with immediate cardioversion
Treat acute breathlessness with oxygen and diuretics if evidence of pulmonary oedema
Treat acute pain with analgesia
Treat acute haemorrhage with volume replacement
When to be concerned
Patients with a Fontan circulation Ensure adequate hydration to maintain filling pressures
Patients with previously repaired congenital heart defects presenting with palpitations and syncope
Haemoptysis or haematemesis in a previous coarctation repair Low threshold for CT Aorta
Pregnant patients with underlying ACHD
Patients with a mechanical valve presenting with breathlessness or chest pain
Clinical Presentations
Tachyarrhythmia
Intra-atrial re-entry tachycardia are the most common
Young AV nodes may allow very fast ventricular response rates leading to syncope
If poor systemic ventricular function they are unlikely to tolerate arrhythmia
In some patients, the ventricular rate may be surprisingly slow, but still poorly tolerated (e.g. 100bpm) so try and compare to an old ECG
Occurs more commonly in:
Tetralogy of Fallot
Following any atrial surgery
Transposition of the great arteries with a Mustard or Senning procedure
Patients with a Fontan circulation
Ebstein’s anomaly
Management:
Early DCCV is preferred management
IV amiodarone can slow the intrinsic atrial rate leading to 1:1 conduction
Atrial over drive pacing can be successful
Avoid Flecainide
If cardioverting a Fontan patient, ensure they are given IV fluids to maintain filling pressures while NBM
PAGE 34
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
8Emergencies
Chest Pain
Common in ACHD patients - often musculoskeletal due to previous surgeries
Assess as for any patient with chest pain
In Eisenmenger patients, chest pain may represent RV angina
In previous coarctation repair consider aortic dissection
Mechanical Valves
Have a high index of suspicion for valve thrombosis if:
Pregnant
On the oral contraceptive pill
More common in the mitral position
In atrial fibrillation
Poor compliance with Warfarin
Should have urgent inpatient echocardiogram
Cerebral Abscesses
Increased suspicion if:
Cyanotic heart disease (unrepaired)
New neurological symptoms
Symptoms can often be vague
Things to remember
Collect as much information as possible from the patient and clinic letters
In cyanotic patients, target oxygen saturation is usually the patient’s usual saturation
In cyanotic patients, the haemoglobin is often raised. So don’t be reassured by a normal haemoglobin in a patient presenting with an acute bleed
In patients with a right to left shunt, any IV access needs to have an air filter attached
If possible avoid positive pressure ventilation in a patient with a Fontan circulation - make sure the anaesthetist understands the physiology
If following a review/advice from your on-site registrar or consultant further advice is needed, please contact the on-call cardiology registrar at the LGI. They can then contact the ACHD consultant on call if required.
PAGE 35
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
9Lifestyle/Other
Cyanosis
Many congenital heart conditions cause cyanosis. This can be seen as a blue tinge to the skin and lips. It is also often associated with an unusual shape to the ends of the finger tips (called ‘clubbing’). Cyanosis is caused by either the mixing of oxygenated and deoxygenated blood via a hole or holes in the heart, or due to lack of blood supply going to the lungs.
The effects of low oxygen levels in the blood (cyanosis)
Symptoms vary depending on how cyanosed a person is, but some patients have the following symptoms:
Breathlessness, especially when walking
Being unable to walk long distances
Tiredness
Having low oxygen levels in the blood stimulates the body to produce more red blood cells in an attempt to carry more oxygen around the body. This leads to an increase in the red blood cell count (this is called ‘polycythaemia’) it and can make the blood a little more sticky than usual. Having a high red blood cell count can lead to the following problems.
Headache
Blood shot eyes
Gout (pain in the joints)
It also makes the body more sensitive to certain types of drugs, particularly anti-inflammatory drugs such as ibuprofen or diclofenac. These drugs should be avoided if possible. Patients with polycythaemia are at greater risk of thrombotic events but are not usually suitable for anticoagulation as they have a higher risk of bleeding.
Read previous clinic letters or ask the patient what their normal oxygen saturations are.Oxygen is not required unless needed for a different reason such as a chest infection or for symptomatic relief.
A ‘normal’ Hb for a cyanotic patient may not be normal for them. Please check previous Hb or ask patient if they know what’s normal for them.Iron studies may be needed and treatment may be needed if patient is anaemic. E.g. patient’s normal Hb is 200 but on admission it is 150. Although this is ‘normal’ it is not normal for the patient so may need treating.
Patients with cyanosis are likely to need an IV filter to prevent paradoxical emboli entering the systemic circulation. If in doubt, use one and it can always be removed if not needed.
PAGE 36
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
9Lifestyle/Other
Pregnancy and effects on the heart
Blood volume
Increases from week 6 to 20 gestation by on average 50%
Blood pressure
Systemic vascular resistance reduces from week 5 with a corresponding reduction in BP, until mid-pregnancy
Increase from 32 weeks and normalises before term
Hormones
Relaxin levels - may mediate systemic vasodilatation
Relaxin also stimulates drinking and vasopressin release which can lead to water retention
Clotting
Prothrombotic state – risk of systemic emboli
Relevant if there are intra-cardiac shunts or mechanical heart valves
Overall
The heart needs to be able to substantially increase cardiac output
Cardiac disease may mean this is not readily achieved
It needs to cope with a significant volume load, especially around delivery
There are also specific problems for women with aortopathy or cyanosis
Normal pregnancy symptoms
Fatigue and exertional breathlessness
Oedema in up to 80%
Symptoms may be worse with congenital heart disease
Risk assessment
Pre-pregnancy counselling
Individualised risk assessment
Drugs (Medications that need urgent assessment to consider stopping or alternatives: Warfarin, ACEi/ARB, Digoxin, Amiodarone, Spironolactone)
Risk scores are used to calculate which women are more at risk
Need to consider the risk to baby as well as the woman when counselling in clinic
Summary
The risk associated with pregnancy depends on the underlying type and severity of heart disease (See next page)
Management is coordinated through the multidisciplinary cardiac/obstetric clinics based at Leeds General Infirmary, Sheffield & Hull
PAGE 37
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
9Lifestyle/Other
Pregnancy risks
Low Risk
Mild mitral/aortic regurgitation
Mild aortic stenosis
Mild/moderate pulmonary stenosis / regurgitation
Restrictive VSD (unrepaired)
Repaired ASD/VSD
Isolated Patent Ductus Arteriosus (without pulmonary hypertension)
Repaired total anomalous pulmonary venous drainage
Bicuspid aortic valve; no aortopathy
Moderate Risk
Moderate aortic /mitral regurgitation
Severe Pulmonary regurgitation
Mild mitral stenosis
Moderate aortic stenosis (Pre-preg peak gradient <50mmHg)
Unrepaired ASD
Repaired Tetralogy of Fallot
TGA repair: Good quality/function arterial switch
High Risk
Severe aortic or mitral regurgitation
Severe pulmonary stenosis
Moderate or severe aortic stenosis
Moderate or severe mitral stenosis
Coarctation of aorta, native, operated or intervened on TGA repair: Mustard/Senning, Arterial Switch (not good function/quality)
Congenitally corrected TGA
Fontan circulation
Cyanotic heart disease without pulmonary hypertension
Bicuspid aortic valve (BAV) with aortopathy or Turner’s syndrome with maximum aortic root/ascending aorta diameter <45mm
Very High Risk
BAV with aortopathy or Turner’s syndrome with max aortic root/ascending aorta diameter ≥45mm
Marfan’s syndrome or other CTD* with dilated aortic root
Pulmonary arterial hypertension
Severe systemic ventricular impairment
Mechanical (metal) valve
*includes Ehlers-Danlos Type 4, Loeys-Dietz, Familial Thoracic Aortic Aneurysm and Dissection syndrome or high suspicion of unidentified cause.
PAGE 38
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
9Lifestyle/Other
Endocarditis
Endocarditis is an infection that affects the inner lining of the heart (endocardium), including the heart valves.
Patients often report weeks-months of feeling generally unwell with no obvious cause. Night sweats, breathlessness, palpitations, fever, fatigue, joint and muscle pain. Sometimes a rash is present or splinter haemorrhages in the finger nails. Primary care may have prescribed antibiotics with no resolve in symptoms.
Clinical history.
Check bloods including CRP and blood cultures.
ECHO.
CHD patients are more at risk because bacteria likes to settle on abnormal areas of the heart and previous surgical sites/prosthetic material.
Twice as many men are affected than women.
Treatment includes 4-6 weeks in hospital on IV antibiotics may be required.Surgery may be required to remove infection/replace valves etc.
Prevention is better than cureHealth education with the patient is important:Good oral hygiene and visiting the dentist every 6-12 months (one of the main sources of bacteraemia is through the mouth).Avoid procedures that can lead to skin infections e.g. Tattoos and piercings.Treat infections appropriately.
PAGE 39
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
9Lifestyle/Other
Transition to adult services
There are now more adults than children living with congenital heart disease.
Caring for young people
People age 11-25 should be treated as ‘young people’, not children or adults.
Life may be different to somebody of the same age with a ‘normal’ heart.
Life expectancy may also be reduced depending on which condition/lesion they have).
Living with a chronic illness can impact on the whole family. The patient may have less independence and rely on family members for information and support. The needs of the family need to be considered and extra support may be required.
Patients may be used to the environment on paediatric wards so it can be a shock being admitted to an adult ward.
It may be helpful to let a parent or relative visit more than normally is permitted, especially for those with learning disabilities.
Compliance can be an issue - the young person often just wants to be ‘normal’. May want to go out and drink alcohol whilst taking warfarin for example. Be understanding of their wishes but guide to make the right choices.
Some careers may be off limits e.g. army, jobs that involve standing for long periods. Education/careers may have to be put on hold because of health/surgery.
16 and 17 year olds can consent to or refuse their own treatment if they have capacity to do so.
It is recently thought that the neurodevelopment of some people with congenital heart disease may have been affected by a lack of oxygen in early life causing higher incidences of developmental delays, behavioural concerns or conditions such as autism and ADHD but more research is needed in this area.
PAGE 40
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
10Palliative Care
Palliative Care
Palliative care for ACHD patients can often be challenging for clinical teams due to the fact patients are often young and often unpredictable in terms of prognosis.
There are a number of different types of conditions that lead to the need for palliative care, but it is generally those patients who have complex congenital heart conditions or those that have had palliative procedures that eventually lead to heart failure such as patients with/following:
Mustard/Senning procedure
Fontan procedure
Eisenmenger’s syndrome
Single ventricle with palliated shunts
This information provides you with some of the processes and contacts that may help when nursing patients with complex congenital heart disease.
INPATIENT CARE at Leeds General Infirmary
Palliative care for ACHD patients is provided jointly by the ACHD specialist team and inpatient Palliative care team based at Leeds Teaching Hospital Trust.
Referrals to the Palliative care team are taken via telephone, and patients seen within 24-48 hours.
Palliative care guidelines for all staff working on the clinical areas can access the palliative care guidelines on the intranet
http://lthweb.leedsth.nhs.uk/sites/palliative-care
Team approach
A Consultant Cardiologist is on call for 7 days for all inpatient care, therefore providing continuity of care for patient requiring palliative/end of life treatment. The Cardiac Nurse Specialist is involved in the inpatient ward round.
Documentation
Leeds Teaching Hospitals Trust launched the ReSPECT form in 2018 which is the first Trust in the UK to have a digitally generated form. ReSPECT is a national initiative, transitioning from regional DNACPR/LOTA forms to shared decision-making between individuals and clinicians, completing ReSPECT forms. These forms, once completed are printed and given to patients prior to discharge.
http://lthweb.leedsth.nhs.uk/sites/resuscitation-services/respect/respect
PAGE 41
Yorkshire and HumberCongenital Heart DiseaseOperational Delivery Network
10Palliative Care
A shared electronic database (PPM+) allows ALL professionals to document conversations with families, to ensure good communication between all services.
Bereavement
If a patient dies in the hospital, the Bereavement office staff assists families with practical arrangements and advice. They provide details of support organisations including national and local charities that families can access such as Cruse Bereavement Care, Charlie’s Angel Centre.
The hospices within the Network provide bereavement support and referrals are made via the Specialist Nurses or the GP to local services
https://www.hospiceuk.org/about-hospice-care/find-a-hospice
Follow-up. If a patient dies in hospital at Leeds, a card is sent to the family by the Specialist Nurse within a week of death. A letter is sent by the named cardiologist to the family 6 weeks after the patient has died, inviting them to meet with the team if they have any questions or require any further support
OUTPATIENT PALLIATIVE CARE
Patients with complex congenital heart disease are allocated to a named consultant clinic to provide continuity of care, and information giving over the years. These clinics are attended by the cardiac nurse specialists who provide
additional support. The pulmonary hypertension service is run by Dr Oliver & Jo Birkett, with joint working with the pulmonary hypertension team based at Sheffield.
Community heart failure nurses are a valuable resource for patients in heart failure who require monitoring and advising regarding symptoms. Shared care with both specialists assists in keeping patients out of hospital.
Hospice care is introduced early, by referring patients to the outpatient services as appropriate, to encourage relationships with the hospice staff and provide support locally. This model has enabled patients at the end of life to feel comfortable in accessing inpatient care if they choose to die in the local hospice.
To find a local hospice for the patient https://www.hospiceuk.org/about-hospice-care/find-a-hospice
Bereavement/Local care. If a patient dies at home or in a local hospital and the cause of death is related to their congenital condition please contact the Specialist Nurse ([email protected]) who will contact the family. A letter is also sent by the named cardiologist to the family 6 weeks after the patient has died, inviting them to meet with the team if they have any questions or require any further support.