clinical features of htlv-i associated uveitis
TRANSCRIPT

BritishJournal ofOphthalmology 1993; 77: 274-279
Clinical features ofHTLV-I associated uveitis
Kumiko Nakao, Norio Ohba
AbstractThe prevalence of human T ceil lymphomavirus type 1 (HTLV-I) was studied amongpatients with endogenous uveitis. Twelve(15.8%) of 76 uveitis patients with knownaetiology or clinical entity were seropositive,the prevalence being comparable with that inthe general population of the southwesternarea of Japan where HTLV-I is highlyendemic. In the comparison, 32 (41-0%) of 78patients with aetiology or entity undefineduveitis were seropositive for HTLV-I, whichindicated a signifcantly higher seroprevalencethan controls matched for sex and age. The 32cases of clinical entity undefined, HTLV-Ipositive uveitis were characterised by acutegranulomatous or non-granulomatous uvealreactions which were accompanied by vitreousopacities and retinal vasculitis. The uvealinflammatory and retinal vascular changesresponded weli to topical and/or systemiccorticosteroids and resolved in a few weeks inthe majority of cases with favourable visualoutcome. The disease affected one or botheyes, and eight cases (25%) showed recurrencewithin a year. The general condition of thepatients remained well otherwise during afoliow up study (mean follow up time 15*4months), except for three cases with a possibleassociation of hyperthyroidism. These find-ings provide additional information favouringan association between HTLV-I and isolateduveitis, a new disease entity which should betermed HTLV-I-associated uveitis.(BrJ Ophthalmol 1993; 77: 274-279)
Department ofOphthalmology,Kagoshima UniversityFaculty ofMedicine,Kagoshima, JapanK NakaoN OhbaCorrespondence to:Kumiko Nakao, MD,Department ofOphthalnmology, KagoshimaUniversity Faculty ofMedicine, Sakuragaoka8-35-1, Kagoshima-shi, 890,Japan.Accepted for publication27 October 1992
Human T cell lymphoma virus type 1 (HTLV-I), a retrovirus distinct from human immuno-deficiency virus (HIV), has been shown to causeat least two systemic diseases. One is a haemato-logical malignancy adult T cell leukaemia/lymphoma in which HTLV-I proviral DNA isintegrated in the proliferating T lymphocytes. 2
Ocular manifestations of the haematologicaldisease include intraocular infiltration of malig-nant T lymphocytes, intraocular opportunisticinfection, such as cytomegalovirus retinitis, andadnexal lymphoma.35 The other disease is achronic progressive neurological disease calledHTLV-I-associated myelopathy6 or tropicalspastic paraparesis.7 Ocular manifestations oftheneurological disease include retinal vasculitis,retinochoroidal degenerative changes, anduveitis.-'2Our previous study showed a significantly
higher prevalence of HTLV-I infection in aseries of uveitis patients whose aetiology orclinical entity was undefined. It suggested an
association between HTLV-I and isolateduveitis, and we proposed the name of 'HTLV-I-associated uveitis (HAU)' for this clinical
entity.'3 However, it has remained to be estab-lished whether HTLV-1 is the causative agent ofuveitis in these patients and whether such uveitisis predictive of the development of HTLV-I-associated haematological or neurologicaldisease.'4 We have enlarged the study of uveitispatients to answer these questions and we reportthe results here.
Materials and methodsWe studied a consecutive series of 154 patientswith endogenous uveitis. There were 75 malesand 79 females, and ranged in age from 12 to 87years (mean 47-0 years, median 48 5 years).These patients were referred to the uveitisservice of Kagoshima University Hospital,which is located in the southwestern area ofJapan, between May 1987 and December 1991.Some patients were included who had had initialdisease before 1987. The patients were followedup during the study period. Examination con-sisted of full physical and ophthalmic history,applanation tonometry, slit-lamp biomicroscopywith a three-mirror contact lens, and binocularophthalmoscopy. Fluorescein fundus angio-gram, electroretinogram, perimetry, and ocularultrasonogram were obtained in selectedpatients. Neurological, endocrinological, andradiological examinations were performed whenindicated. Laboratory studies included chestx ray, assay of serum angiotensin convertingenzyme, and a battery of immunoserologicaltests. HLA typing was performed in selectedpatients. Infection with HTLV-I was assessedfor serum antibodies against HTLV-I using themethod of particle agglutination. An agglutina-tion reaction in patient's serum when dilutedmore than 16 times was regarded as seropositive.The enzyme immunoassay was also carried outon all materials to confirm the accuracy ofdetection of the HTLV-I antibodies.
Results
PREVALENCE OF SERUM ANTIBODIES AGAINSTHTLV-ITable 1 shows HTLV-I seroprevalence inpatients with uveitis, grouped by age intospecific and non-specific. uveitis depending onwhether the aetiology or clinical entity wasdefined. HTLV-I seroprevalence in the generalpopulation of the southwestern area of Japan,and published elsewhere,'3 is also shown forreference.Of a total of 154 patients with endogenous
uveitis, 76 patients, 35 males and 41 femalesranging in age from 12 to 78 years (mean 450,median 47-5) could be defined for aetiology orspecific clinical entities including toxoplasmicretinochoroiditis, Behcet's disease, Harada's
274
group.bmj.com on August 15, 2016 - Published by http://bjo.bmj.com/Downloaded from
Clinicalfeatures ofHTLV-I associated uveitis
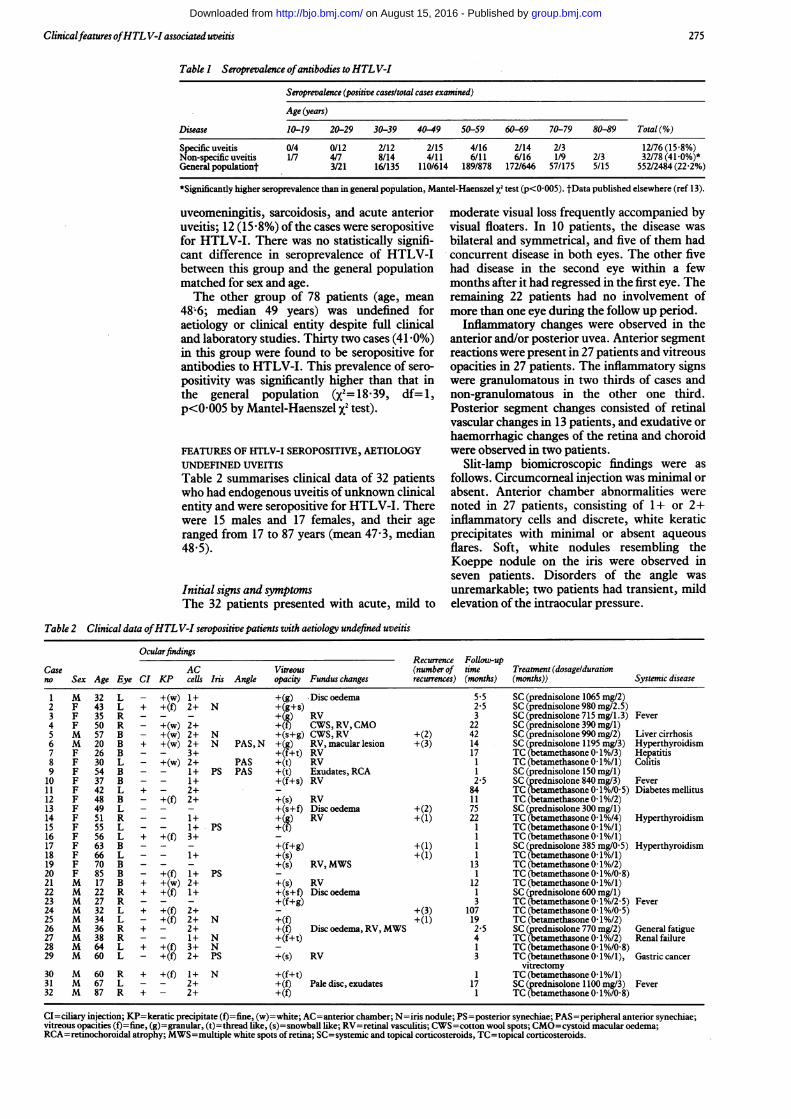
Tabk I Seroprevalence ofantibodies toHTLV-I
Seroprevalence (positive cases/total cases examined)
Age (years)
Disease 10-19 20-29 30-39 40-49 50-59 60-69 70-79 80-89 Total (%)
Specific uveitis 0/4 0/12 2/12 2/15 4/16 2/14 2/3 12/76 (15-8%)Non-specific uveitis 1/7 4/7 8/14 4/11 6/11 6/16 1/9 2/3 32/78 (41-0%)*General populationt 3/21 16/135 110/614 189/878 172/646 57/175 5/15 552/2484(22 2%)
*Significantly higher seroprevalence than in general population, Mantel-Haenszel XI test (p<0 005). tData published elsewhere (ref 13).
uveomeningitis, sarcoidosis, and acute anterioruveitis; 12 (15-8%) of the cases were seropositivefor HTLV-I. There was no statistically signifi-cant difference in seroprevalence of HTLV-Ibetween this group and the general populationmatched for sex and age.The other group of 78 patients (age, mean
48;6; median 49 years) was undefined foraetiology or clinical entity despite full clinicaland laboratory studies. Thirty two cases (41-0%)in this group were found to be seropositive forantibodies to HTLV-I. This prevalence of sero-
positivity was significantly higher than that inthe general population (X2=18-39, df= 1,
p<0-005 by Mantel-Haenszel X2 test).
FEATURES OF HTLV-I SEROPOSITIVE, AETIOLOGY
UNDEFINED UVEITIS
Table 2 summarises clinical data of 32 patientswho had endogenous uveitis of unknown clinicalentity and were seropositive for HTLV-I. Therewere 15 males and 17 females, and their ageranged from 17 to 87 years (mean 47-3, median48-5).
Initial signs and symptomsThe 32 patients presented with acute, mild to
moderate visual loss frequently accompanied byvisual floaters. In 10 patients, the disease was
bilateral and symmetrical, and five of them hadconcurrent disease in both eyes. The other fivehad disease in the second eye within a fewmonths after it had regressed in the first eye. Theremaining 22 patients had no involvement ofmore than one eye during the follow up period.
Inflammatory changes were observed in theanterior and/or posterior uvea. Anterior segmentreactions were present in 27 patients and vitreousopacities in 27 patients. The inflammatory signswere granulomatous in two thirds of cases andnon-granulomatous in the other one third.Posterior segment changes consisted of retinalvascular changes in 13 patients, and exudative or
haemorrhagic changes of the retina and choroidwere observed in two patients.
Slit-lamp biomicroscopic findings were as
follows. Circumcorneal injection was minimal or
absent. Anterior chamber abnormalities were
noted in 27 patients, consisting of 1 + or 2+inflammatory cells and discrete, white keraticprecipitates with minimal or absent aqueousflares. Soft, white nodules resembling theKoeppe nodule on the iris were observed inseven patients. Disorders of the angle was
unremarkable; two patients had transient, mildelevation of the intraocular pressure.
Table 2 Clinical data ofHTLV-I seropositive patients with aetiology undefined uveitis
OcularfindingsRecurrence Follow-up
Case AC Vitreous (number of time Treatment (dosageldurationno Sex Age Eye CI KP cells Iris Angle opacity Fundus changes recurrences) (months) (months)) Systemic disease
1 M 32 L - +(w) 1+ +(g) Disc oedema 5 5 SC (prednisolone 1065 mg/2)2 F 43 L + +(f) 2+ N +(g+s) 2-5 SC (prednisolone 980 mg/2.5)3 F 35 R - - - +(g) RV 3 SC (prednisolone 715 mg/1.3) Fever4 F 50 R - +(w) 2+ +(f) CWS, RV,CMO 22 SC (prednisolone 390 mg/1)5 M 57 B - +(w) 2+ N +(s+g) CWS, RV +(2) 42 SC (prednisolone 990 mg/2) Liver cirrhosis6 M 20 B + +(w) 2+ N PAS, N +(g) RV, macular lesion +(3) 14 SC (prednisolone 1195 mg/3) Hyperthyroidism7 F 26 B - - 3+ +(f+t) RV 17 TC(betamethasone0-1%/3) Hepatitis8 F 30 L - +(w) 2+ PAS +(t) RV 1 TC(betamethasone0 1%/1) Colitis9 F 54 B - - 1+ PS PAS +(t) Exudates, RCA 1 SC (prednisolone 150 mg/i)10 F 37 B - - 1+ +(f+s) RV 2-5 SC (prednisolone 840 mg/3) Fever11 F 42 L + - 2+ 84 TC (betamethasone 0-1%/O-5) Diabetes mellitus12 F 48 B - +(f) 2+ +(s) RV 11 TC (betamethasone 0-1%/2)13 F 49 L - - - +(s+f) Disc oedema +(2) 75 SC (prednisolone 300 mg/1)14 F 51 R - - 1+ +(g) RV +(1) 22 TC (betamethasone 0-1%/4) Hyperthyroidism15 F 55 L - - 1+ PS +(f) 1 TC (betamethasone0 1%/1)16 F 56 L + +(f) 3+ 1 TC (betamethasone0 1%/1)17 F 63 B - - - +(f+g) +(1) 1 SC (prednisolone 385 mg/0 5) Hyperthyroidism18 F 66 L - - 1+ +(s) +(1) 1 TC(betamethasone 0l%/1)19 F 70 B - - - +(s) RV,MWS 13 TC (betamethasone 0-1%/2)20 F 85 B - +(f) 1+ PS - 1 TC (betamethasone 0-1%/0-8)21 M 17 B + +(w) 2+ +(s) RV 12 TC(betamethasone0 1%/1)22 M 22 R + +(f) 1+ +(s+f) Disc oedema 1 SC (prednisolone 600 mg/i)23 M 27 R - - - +(f+g) 3 TC (betamethasone 0-1%/2-5) Fever24 M 32 L + +(f) 2+ +(3) 107 TC (betamethasone 0-1%/O-5)25 M 34 L - +(f) 2+ N +(f) +(1) 19 TC (betamethasone 0-1%/2)26 M 36 R + - 2+ +(f) Disc oedema, RV, MWS 2-5 SC (prednisolone 770 mg/2) General fatigue27 M 38 R - - 1+ N +(f+t) 4 TC(betamethasone0-1%/2) Renalfailure28 M 64 L + +(f) 3+ N - 1 TC (betamethasone 0-1%/0-8)29 M 60 L - +(f) 2+ PS +(s) RV 3 TC(betamethasone0d %/1), Gastriccancer
vitrectomy30 M 60 R + +(f) 1+ N +(f+t) 1 TC(betamethasone0 1%/1)31 M 67 L - - 2+ +(f) Pale disc, exudates 17 SC (prednisolone 1100 mg/3) Fever32 M 87 R + - 2+ +(f) 1 TC(betamethasone0-1%/0-8)
CI=ciliary injection; KP=keratic precipitate (f)=fine, (w)=white; AC=anterior chamber; N=iris nodule; PS=posterior synechiae; PAS=peripheral anterior synechiae;vitreous opacities (f)=fine, (g)=granular, (t)=thread like, (s)=snowball like; RV=retinal vasculitis; CWS=cotton wool spots; CMO=cystoid macular oedema;RCA=retinochoroidal atrophy; MWS=multiple white spots of retina; SC=systemic and topical corticosteroids, TC=topical corticosteroids.
275
group.bmj.com on August 15, 2016 - Published by http://bjo.bmj.com/Downloaded from
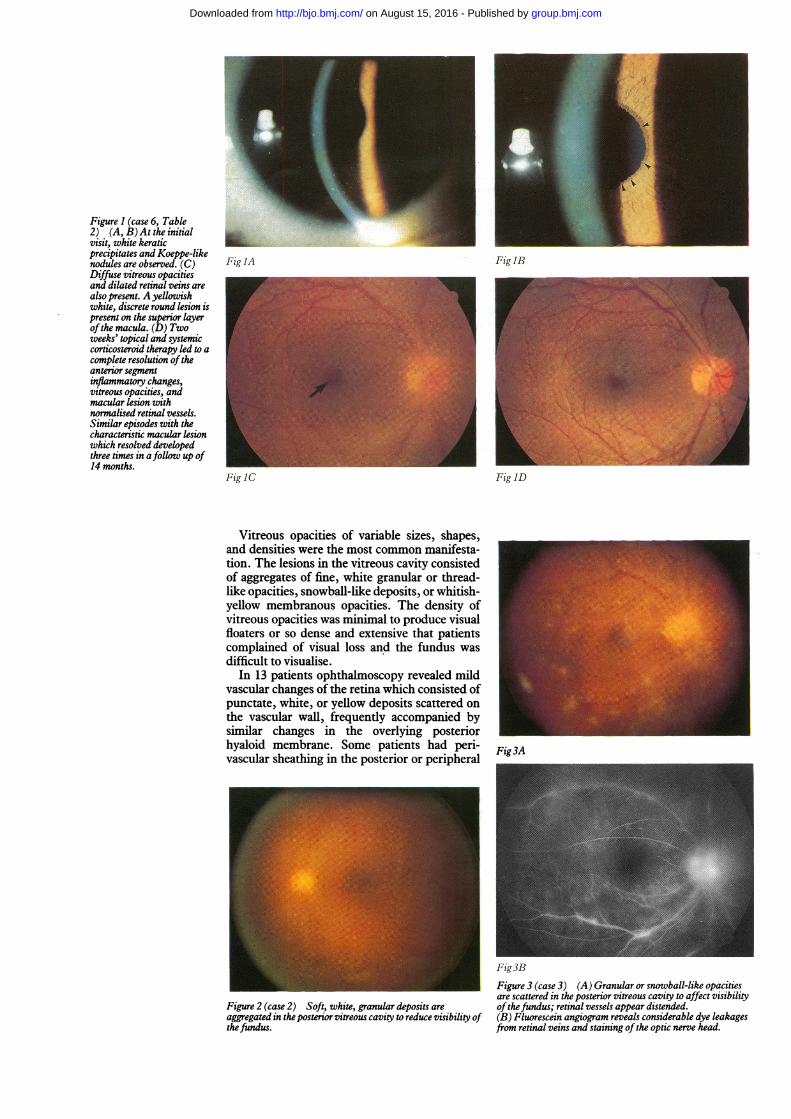
Figure I (case 6, Table2) (A, B) At the initialvisit, white keraticprecipitates and Koeppe-likenodules are observed. (C) Fig IADiffuse vitreous opacitiesand dilated retinal veins arealso present. A yellowishwhite, discrete round lesion ispresent on the superior layerofthe macula. (D) Twoweeks' topical and systemiccorticosteroid therapy led to acomplete resolution oftheanterior segmentinflammatory changes,vitreous opacitties, andmacular lesion withnormalised retinal vessels.Similar episodes with thecharacteristic macular lesionwhich resolved developedthree times in afollow up of14 months.
Fig IC
Vitreous opacities of variable sizes, shapes,and densities were the most common manifesta-tion. The lesions in the vitreous cavity consistedof aggregates of fine, white granular or thread-like opacities, snowball-like deposits, or whitish-yellow membranous opacities. The density ofvitreous opacities was minimal to produce visualfloaters or so dense and extensive that patientscomplained of visual loss and the fundus wasdifficult to visualise.
In 13 patients ophthalmoscopy revealed mildvascular changes of the retina which consisted ofpunctate, white, or yellow deposits scattered onthe vascular wall, frequently accompanied bysimilar changes in the overlying posteriorhyaloid membrane. Some patients had peri-vascular sheathing in the posterior or peripheral
Figure 2 (case 2) Soft, white, granular deposits areaggregated in the posterior vitreous cavity to reduce visibility ofthefundus.
Fig3R
Figure 3 (case 3) (A) Granular or snowball-like opacitiesare scattered in the posterior vitreous cavity to affect visibilityofthefundus; retinal vessels appear distended.(B) Fluorescein angiogram reveals considerable dye leakagesfrom retinal veins and staining ofthe optic nerve head.
Fig IB
Fig ID
Fig3A
group.bmj.com on August 15, 2016 - Published by http://bjo.bmj.com/Downloaded from
Clinicalfeatures ofHTLV-I associated uveitis
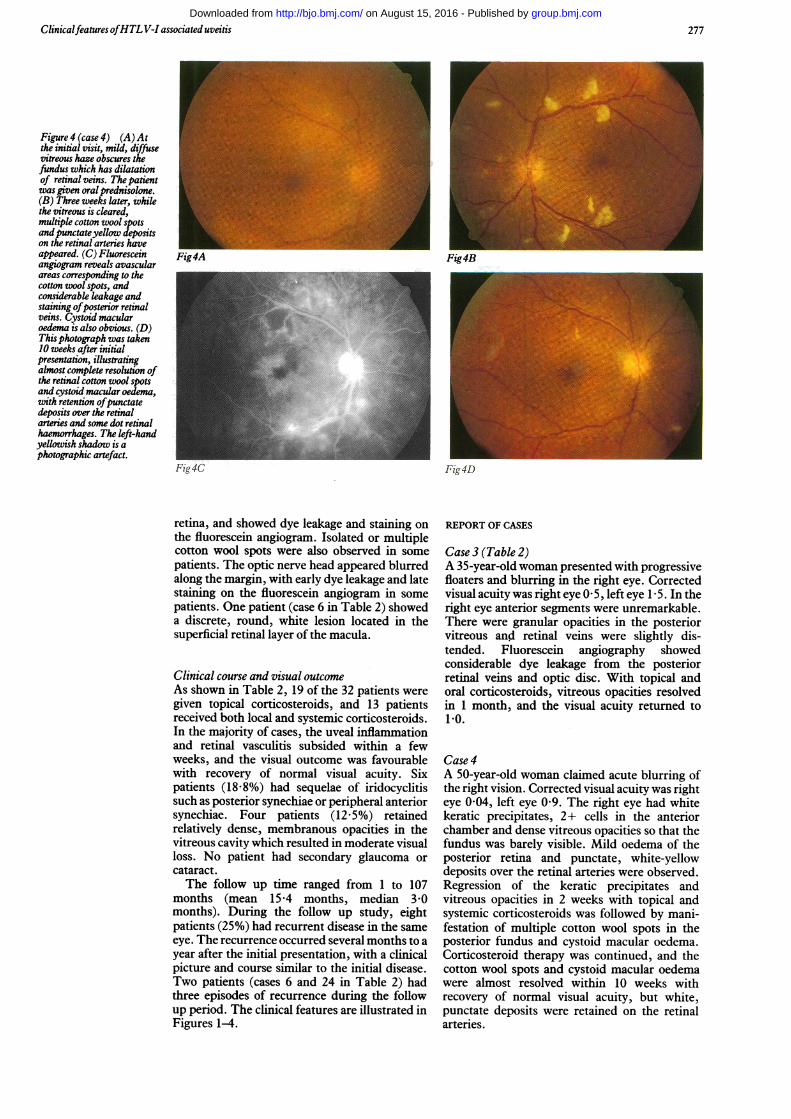
Figure 4 (case 4) (A) Atthe initial visit, mild, diffusevitreous haze obscures thefundus which has dilatationof retinal veins. The patientwas given oral prednisolone.(B) Three weeks later, whilethe vitreous is cleared,multiple cotton wool spotsand punctateyellow depositson the retinal arteries haveappeared. (C) Fluoresceinangiogram reveals avascularareas corresponding to thecotton wool spots, andconsiderable leakage andstaining ofposterior retinalveins. Cystoid macularoedema is also obvious. (D)This photograph was taken10 weeks after initialpresentation, illustratingalmost complete resolution ofthe retinal cotton wool spotsand cystoid macular oedema,with retention ofpunctatedeposits over the retinalarteries and some dot retinalhaemorrhages. The left-handyellowish shadow is aphotographic artefact.
Fig4A Fig4B
Fig4D
retina, and showed dye leakage and staining onthe fluorescein angiogram. Isolated or multiplecotton wool spots were also observed in somepatients. The optic nerve head appeared blurredalong the margin, with early dye leakage and latestaining on the fluorescein angiogram in somepatients. One patient (case 6 in Table 2) showeda discrete, round, white lesion located in thesuperficial retinal layer of the macula.
Clinical course and visual outcomeAs shown in Table 2, 19 of the 32 patients weregiven topical corticosteroids, and 13 patientsreceived both local and systemic corticosteroids.In the majority of cases, the uveal inflammationand retinal vasculitis subsided within a fewweeks, and the visual outcome was favourablewith recovery of normal visual acuity. Sixpatients (18-8%) had sequelae of iridocyclitissuch as posterior synechiae or peripheral anteriorsynechiae. Four patients (12-5%) retainedrelatively dense, membranous opacities in thevitreous cavity which resulted in moderate visualloss. No patient had secondary glaucoma orcataract.The follow up time ranged from 1 to 107
months (mean 15-4 months, median 3-0months). During the follow up study, eightpatients (25%) had recurrent disease in the sameeye. The recurrence occurred several months to ayear after the initial presentation, with a clinicalpicture and course similar to the initial disease.Two patients (cases 6 and 24 in Table 2) hadthree episodes of recurrence during the followup period. The clinical features are illustrated inFigures 1-4.
REPORT OF CASES
Case 3 (Table 2)A 35-year-old woman presented with progressivefloaters and blurring in the right eye. Correctedvisual acuity was right eye 0 5, left eye 15. In theright eye anterior segments were unremarkable.There were granular opacities in the posteriorvitreous and retinal veins were slightly dis-tended. Fluorescein angiography showedconsiderable dye leakage from the posteriorretinal veins and optic disc. With topical andoral corticosteroids, vitreous opacities resolvedin 1 month, and the visual acuity returned to1*0.
Case 4A 50-year-old woman claimed acute blurring ofthe right vision. Corrected visual acuity was righteye 0 04, left eye 0 9. The right eye had whitekeratic precipitates, 2+ cells in the anteriorchamber and dense vitreous opacities so that thefundus was barely visible. Mild oedema of theposterior retina and punctate, white-yellowdeposits over the retinal arteries were observed.Regression of the keratic precipitates andvitreous opacities in 2 weeks with topical andsystemic corticosteroids was followed by mani-festation of multiple cotton wool spots in theposterior fundus and cystoid macular oedema.Corticosteroid therapy was continued, and thecotton wool spots and cystoid macular oedemawere almost resolved within 10 weeks withrecovery of normal visual acuity, but white,punctate deposits were retained on the retinalarteries.
277group.bmj.com on August 15, 2016 - Published by http://bjo.bmj.com/Downloaded from
Nakao, Ohba
13 0
121.
11
10o
91c
040
4)
._I-
I
c
8
7
6
5
4
3
2
:_*
Ato___
__.
*000
0
0
0
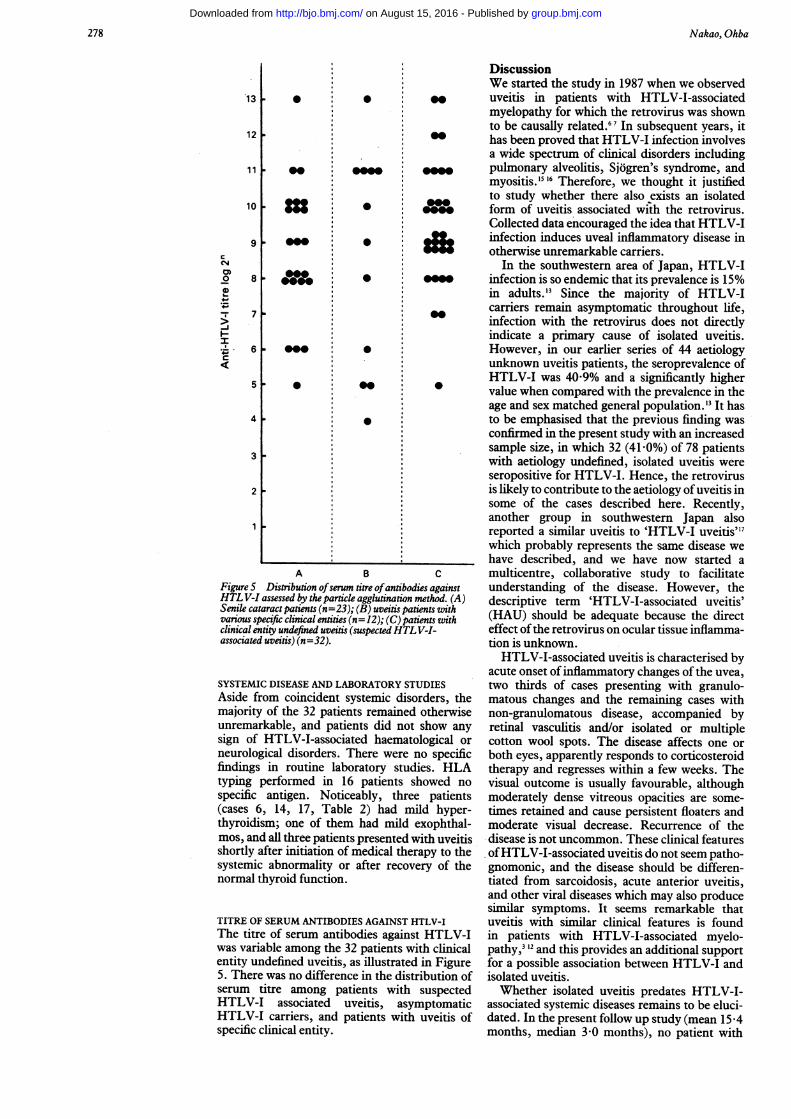
A BFigure S Distribution ofserum titre ofantibodHTL V-I assessed by the particle agglutination nSenile cataract patients (n=23); (B) uveitis pativarious specific clinical entities (n= 12); (C) paticlinical entity undefined uveitis (suspectedHTLassociated uveitis) (n=32).
SYSTEMIC DISEASE AND LABORATORY STIAside from coincident systemic disomajority of the 32 patients remainedunremarkable, and patients did notsign of HTLV-I-associated haematoneurological disorders. There were r
findings in routine laboratory studityping performed in 16 patients sJspecific antigen. Noticeably, three(cases 6, 14, 17, Table 2) had mithyroidism; one of them had mild emos, and all three patients presented wshortly after initiation of medical thersystemic abnormality or after recovcnormal thyroid function.
TITRE OF SERUM ANTIBODIES AGAINST HThe titre of serum antibodies againstwas variable among the 32 patients wientity undefined uveitis, as illustrated5. There was no difference in the distrserum titre among patients withHTLV-I associated uveitis, asyrHTLV-I carriers, and patients withspecific clinical entity.
DiscussionWe started the study in 1987 when we observeduveitis in patients with HTLV-I-associatedmyelopathy for which the retrovirus was shownto be causally related.67 In subsequent years, ithas been proved that HTLV-I infection involvesa wide spectrum of clinical disorders includingpulmonary alveolitis, Sjogren's syndrome, andmyositis.'516 Therefore, we thought it justifiedto study whether there also exists an isolated
a0" form of uveitis associated with the retrovirus.Collected data encouraged the idea that HTLV-I
ff, infection induces uveal inflammatory disease inotherwise unremarkable carriers.
In the southwestern area of Japan, HTLV-Iinfection is so endemic that its prevalence is 15%in adults.'3 Since the majority of HTLV-Icarriers remain asymptomatic throughout life,infection with the retrovirus does not directlyindicate a primary cause of isolated uveitis.However, in our earlier series of 44 aetiologyunknown uveitis patients, the seroprevalence ofHTLV-I was 40 9% and a significantly highervalue when compared with the prevalence in theage and sex matched general population.'3 It hasto be emphasised that the previous finding wasconfirmed in the present study with an increasedsample size, in which 32 (41-0%) of 78 patientswith aetiology undefined, isolated uveitis wereseropositive for HTLV-I. Hence, the retrovirusis likely to contribute to the aetiology ofuveitis insome of the cases described here. Recently,another group in southwestern Japan alsoreported a similar uveitis to 'HTLV-I uveitis"7which probably represents the same disease wehave described, and we have now started a
c multicentre, collaborative study to facilitate'ies against understanding of the disease. However, thenethod. (A) descriptive term 'HTLV-I-associated uveitis'ients with (HAU) should be adequate because the directv-i- effect ofthe retrovirus on ocular tissue inflamma-
tion is unknown.HTLV-I-associated uveitis is characterised by
acute onset ofinflammatory changes of the uvea,UDIES two thirds of cases presenting with granulo-brders, the matous changes and the remaining cases withotherwise non-granulomatous disease, accompanied byshow any retinal vasculitis and/or isolated or multiplelogical or cotton wool spots. The disease affects one orio specific both eyes, apparently responds to corticosteroidies. HLA therapy and regresses within a few weeks. Thehowed no visual outcome is usually favourable, although
patients moderately dense vitreous opacities are some-id hyper- times retained and cause persistent floaters and.xophthal- moderate visual decrease. Recurrence of thevith uveitis disease is not uncommon. These clinical featuresapy to the ofHTLV-I-associated uveitis do not seem patho-Ery of the gnomonic, and the disease should be differen-
tiated from sarcoidosis, acute anterior uveitis,and other viral diseases which may also producesimilar symptoms. It seems remarkable that
[TLV-I uveitis with similar clinical features is foundt HTLV-I in patients with HTLV-I-associated myelo-ith clinical pathy,3' 12 and this provides an additional supportLin Figure for a possible association between HTLV-I andribution of isolated uveitis.suspected Whether isolated uveitis predates HTLV-I-nptomatic associated systemic diseases remains to be eluci-uveitis of dated. In the present follow up study (mean 15 4
months, median 3-0 months), no patient with
278
group.bmj.com on August 15, 2016 - Published by http://bjo.bmj.com/Downloaded from
Clinicalfeatures ofHTL V-I associated uveitis
isolated uveitis developed haematological or
neurological disease. Aside from coincidentsystemic diseases in adults, it is noticeable thatmild hyperthyroidism was found in threepatients. A total of nine cases of associationbetween uveitis and hyperthyroidism is des-cribed in the literature. It is interesting that oneof the cases was infected with HTLV-I'8 andthat, although the remaining cases were notexamined for HTLV-I, they were residents ofthe southwestern area ofJapan where HTLV-I isendemic. 1920The pathomechanism of HTLV-I-associated
uveitis is not clear. Our previous assessment ofaqueous antibodies to HTLV-I did not provideany evidence for intraocular proliferation of theretrovirus.'2 Response to corticosteroids and therecurrent nature of the disease suggest an
undefined immune mechanism similar to thatproposed for HTLV-I-associated myelopathyand other HTLV-I-related disease com-
plexes615 16; there was no specific HLA antigen inthe present series of HTLV-I-associated uveitis,and the serum titre ofHTLV-I-associated uveitiswas comparable with that of asymptomaticcarriers.HTLV-I is widespread in the world, with
endemic areas in Japan, the Caribbean, CentralAfrica, and South America. Many patients withHTLV-I-associated myelopathy or adult T cellleukaemia/lymphoma are found not only in theseendemic areas but also among immigrants inEurope and North America. This study indicatesthat assessment for HTLV-I infection would beworthwhile in those patients whose uveitisremains undefined for aetiology or clinicalentity. Further studies are needed to support ourview that HTLV-I is a causative agent of isolateduveitis.
This study was supported by grants-in-aid for scientific research(No 03771230, 03454417) from the Ministry of Education, Scienceand Culture of Japan.
1 Hinuma Y, Nagata K, Hanaoka M, Matsumoto T, KinoshitaK, Shirakawa S, et al. Adult T-cell leukemia: antigen in an
ATL cell line and detection of antibodies to the antigen inhuman sera. Proc Natl Acad Sci USA 1981; 78: 6476-80.
2 Yoshida M, Miyoshi I, Hinuma Y. Isolation and characteriza-tion of retrovirus from cell lines of human adult T-cellleukemia and its implication in the disease. Proc Natl AcadSci USA 1982; 79: 2031-5.
3 Ohba N, Matsumoto M, Sameshima M, Kabayama Y, NakaoK, Unoki K, et al. Ocular manifestations in patients withhuman T-lymphotropic virus type I.jpnJ Ophthalmol 1989;33: 1-12.
4 Okubo A, Nakao K, Uemura A. A case of adult T-celllymphoma in human T-cell lymphoma with intraocularinfiltration. J Eye (in Japanese) 1990; 7: 107-10.
5 Lauer SA, Fischer J, Jones J, Gartner S, Dutcher J, Hoxie JA.Orbital T-cell lymphoma in human T-cell leukemia virustype I infection. Ophthalmology 1988; 95: 110-5.
6 Osame M, Matsumoto M, Usuku K, Izumo S, Ijichi N,Amitani H, et al. Chronic progressive myelopathy associatedwith elevated antibodies to human T-lymphotropic virustype 1 and adult T-cell leukemialike cells. Ann Neurol 1987;21: 117-22.
7 Gessain A, Barin F, Vernant JC, Gout 0, Maurs L, CalenderA, et al. Antibodies to human T-lymphotropic virus type-Iin patients with tropical spastic paraparesis. Lancet 1985; ii:407-10.
8 Nakao K, Uemura A, Hirashima S, Unoki K. Cotton-woolspots on the retina in patients infected with human T-lymphotropic virus type 1 (HTLV-I). Folia Ophthalmoljpn1989; 40:2051-7.
9 Sasaki K, Morooka A, Inomata H, Akamine T, Osame M.Retinal vasculitis in human T-lymphotropic virus type 1associated myelopathy. BrJ Ophthalmol 1989; 73: 812-5.
10 Hayasaka S, Takatori Y, Noda S, Setogawa T, Hayashi H.Retinal vasculitis in a mother and her son with humanT-lymphotropic virus type 1 associated myelopathy.BrJ Ophthalmol 1991; 75: 566-7.
11 Nakao K, Ohba N, Isashiki M, Isashiki Y, Unoki K, OsameM. Pigmentary retinal degeneration in patients with HTLV-I-associated myelopathy. Jpn J Ophthalmol 1989; 33: 383-91.
12 Nakao K, Ohba N, Matsumoto M. Noninfectious anterioruveitis in patients with human T-lymphotropic virus type 1.JpnJ Ophthalmol 1989; 33: 472-81.
13 Nakao K, Matsumoto M, Ohba N. Seroprevalence of anti-bodies to HTLV-I in patients with ocular disorders. Br _JOphthalmol 1991; 75: 76-8.
14 Spalton DJ, Nicholson F. HTLV-I infection in humandisease. BrJ Ophthalmol 1991; 75: 174-5.
15 Vernant JC, Buisson G, Magdeleine J, DeThore J, JouannelleA, Neisson-Vernant C, et al. T-lymphocytic alveolitis,tropical spastic paraparesis, and Sjogren's syndrome. Lancet1988;i: 177.
16 Morgan OS, Rodgers-Johnson P, Mora C, Char G. HTLV-Iand polymyositis in Jamaica. Lancet 1989; ii: 1184-7.
17 Mochizuki M, Watanabe T, Yamaguchi K, Takatsuki K,Yoshimura K, Shirao M, et al. HTLV-I uveitis: a distinctclinical entity caused by HTLV-I. Jpn J Cancer Res 1992;83:236-9.
18 Yamamoto S, Kakisu Y. Severe uveitis developed in a case ofdysthyroid ophthalmopathy [in Japanese]. Ganka RinshoIhoh (Clin Rev Ophthalmol) 1991; 85: 335-8.
19 Mizoguchi T, Sato T, Dake Y, Amemiya T. Hyperthyroidismand uveitis [in Japanese]. Rinshoganka (Jpn J ClinOphthalmol) 1990; 44: 908-9.
20 Shimada E, Yamanaka H, Hirayama Y, Mizoguchi T,Amemiya T. Uveitis in three patients with hyperthyroidism[in Japanese]. Folia OphthalmolJpn 1991; 42: 1755-60.
279
group.bmj.com on August 15, 2016 - Published by http://bjo.bmj.com/Downloaded from
Clinical features of HTLV-I associated uveitis.
K Nakao and N Ohba
doi: 10.1136/bjo.77.5.2741993 77: 274-279 Br J Ophthalmol
http://bjo.bmj.com/content/77/5/274Updated information and services can be found at:
These include:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on August 15, 2016 - Published by http://bjo.bmj.com/Downloaded from