chapter 39 antiparasitic agents
TRANSCRIPT
Chapter 39 Antiparasitic Agents
Thomas L. Lemke
Drugs covered in this chapter: Drug treatment of amebiasis, giardiasis, trichomoniasis
l Diloxanide furoate
l Metronidazole
l Nitazoxanide
l Tinidazole
Treatment of pneumocystis
l Atovaquone
l Penamidine isethionate
l Sulfamethoxazole– trimethoprim
l Tr imetrexate glucuronate
Treatment of trypanosomiasis
l Benznidazole
l Ef lorni thine
l Melarsoprol
l Niturt imox
l Pentamidine isethionate
l Suramin sodium
Treatment of leishmaniasis
l Sodium stibogluconate
Antimalarials
l Atovaquone–proguanil
l Chloroquine
l Halofantr ine
l Mefloquine
l Pyr imethamine
l Quinine
Anthelmintics
l Albendazole
l Diethylcarbamazine
Page 1 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

l Ivermectin
l Mebendazole
l Oxamniquine
l Praziquantel
l Pyrantel pamoate
l Thiabendazole
Scabicides and pediculocides
l Crotamiton
l Lindane
l Permethrin
l Pyrethrin
General Considerations An introduct ion to the topic of parasit ic d iseases usually emphasizes two points. First , parasit ic infections affect huge numbers of individuals. It is estimated that well over 1 bi l l ion people are infected wor ldwide. Second, the majori ty of these parasit ic infect ions are found in developing nat ions, in which the cost of health care is the dominant factor that determines whether the pat ient is (or is not) t reated. The incidence of some parasit ic d iseases may exceed 80% of the populat ion. The high cost of drug discovery and the low incidence of many of the parasit ic infections in aff luent Western countr ies have combined to reduce the incent ive for both the study of the diseases and the development of ef fective therapy. This may be changing, however, because of global travel, improved communicat ions, and growth of the developing countries, leading to an increased demand for more effect ive treatments.
The diseases associated with parasitic infect ions represent a large and diverse number of conditions, some common and some relat ively unheard of by the general populat ion. Included under the ti t le of parasitic infect ions are the numerous types of protozoal infect ions: amebiasis, giardiasis, babesiosis, Chagas' disease, leishmaniasis, malar ia, sleeping sickness, toxoplasmosis, t richomoniasis, and pneumocystosis (also considered to be a fungal infect ion). Helminth infections (worms) also are considered to be parasit ic infect ions and may be caused by any of three classes of helminths: nematodes, cestodes, and trematodes. Insect infect ions, such as scabies, l ice (pediculosis) , and chiggers, a lso are considered to be parasitic infect ions.
Protozoal Diseases
Amebiasis Amebiasis is a disease of the large intest ine caused by Entamoeba histolytica. The disease occurs mainly in the tropics, but i t a lso is seen in temperate cl imates. Amebiasis may be carried without signif icant symptoms or may lead to severe, l i fe-threatening dysentery. The organism exists in one of two forms, the moti le trophozoite form or the dormant cyst form. The trophozoite form is found in the intest ine or wall of the colon and may be expel led from the body with the stools. The cyst form is encased by a chit inous wall that protects the organism from the environment, including chlorine used in water puri f icat ion; thus, the organism may be transmit ted through contaminated water and foods. I t is the cyst form that is responsible for transmission of the disease. The cyst is spread by direct person-to -person contact and is commonly associated with l iving condit ions in which poor personal hygiene, poor sanitat ion, poverty, and ignorance exist . The hosts may be rendered suscept ible to infect ion by preexist ing condit ions, such as protein malnutri t ion, pregnancy, HIV infect ion, or h igh carbohydrate intake. Under these conditions, the organism is capable of invading body tissue. The protozoal invasion is not well understood. but it does appear to involve the processes indicated in Table 39.1. Symptoms may range from intermit tent
Page 2 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

diarrhea (foul-smell ing loose/watery stools) to tenderness and enlargement of the l iver (with the extraintest inal form) to acute amoebic dysentery. Many pat ients may exper ience no symptoms, and the organism remains in the bowels as a commensal organism.
Clinical Signif icance Parasit ic infections affect more than half the wor ld's populat ion and are responsible for signif icant health complicat ions, especial ly in underdeveloped areas. Drug therapy for parasit ic infect ions is quite challenging to pract i t ioners for multip le reasons. Many practi t ioners lack experience with these agents and are unfamil iar with the toxici ties and monitoring parameters associated with these drugs. Certain agents are available in only a l imited number of countries, and opinions regarding safety and efficacy vary great ly among pract i t ioners. Understanding the medicinal chemistry, pharmacodynamics, and pharmacokinet ics of these agents is of utmost importance.
Despite ef forts of vaccine development, drug therapy remains the most effect ive means to control parasit ic infect ions. L imited introduction of new ant iparasitic agents and drug shortages make the treatment of parasitic infestat ions chal lenging. Understanding which drugs work at d if ferent parts of the li fe cycle of the parasite also must be taken into considerat ion. Furthermore, the use of many antiparasit ic agents are associated with toxicit ies, including precipitat ing severe inf lammatory react ions, which may then be treated with anti -inf lammatory agents and other supportive measures.
P.1085
Laura Gerard Pharm.D. BCPS Clinical Assistant Professor, Department of Cl inical Science & Administrat ion, University of Houston
College of Pharmacy.
Giardiasis Giardiasis is a disease that shows considerable similari ty to amebiasis. I t is caused by Giardia lamblia , an organism that may be found in the duodenum and jejunum. The organism exists in a motile trophozoite form and an infectious cyst form. The cyst form can be deposited in water (l ives up to 2 months), and the contaminated water may then be ingested by the human. The trophozoite, i f expel led from the gastrointest inal (GI) t ract, normally wil l not survive. Giardia lamblia is the single most common cause of waterborne diarrhea in the United States. Giardiasis is a common disease among campers who drink water from contaminated streams. I t also may be spread between family members, chi ldren in day care centers, and dogs and their masters. The organism can attach to the mucosal wall v ia a ventral sucking disk, and similar to amebiasis, the patient may be asymptomatic or develop watery diarrhea, abdominal cramps, distention and flatulence, anorexia, nausea, and vomit ing. Usually, the condit ion is self limiting in 1 to 4 weeks.
Page 3 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

Trichomoniasis Trichomoniasis is a protozoal infect ion caused by Trichomonas vaginal is , which exists only in a trophozoite form. The organs most commonly involved in the infect ion include the vagina, urethra, and prostate; thus, the disease is considered to be a venereal infect ion. The condit ion is transmit ted by sexual contact, and i t is est imated that t r ichomoniasis affects 180 mil l ion individuals wor ldwide. Infect ions in the male may be asymptomatic, whereas in the female, the symptoms may consist of vaginit is, profuse and foul-smell ing discharge, burning and soreness on ur ination; and vulvar i tching. Diagnosis is based on microscopic ident i fication of the organism in flu ids from the vagina, prostate, or urethra.
Pneumocystis The organism responsible for pneumocyst is (pneumocystosis) in humans is Pneumocyst is carin ii . I t has the morphologic characteristics of a protozoan ( i.e., lack of ergosterol in its cel l membrane), but i ts rRNA and mitochondr ia l DNA pattern resembles that of fungi. Acute pneumocyst is rarely str ikes healthy individuals, although the organism is harbored in a wide variety of animals and most humans without any apparent adverse effect. Pneumocyst is carin ii becomes act ive only in those individuals who have a ser ious impairment of their immune systems. Thus, the organism is considered to be an opportunistic pathogen. More recent ly, th is disease has appeared in patients with AIDS, 80% of whom ult imately contract P. car ini i pneumonia (PCP), as one of the main causes of death. The disease also occurs in those receiving immunosuppressive drugs to prevent reject ion fo llowing organ transplantation or for the treatment of malignant disease. Addit ional ly, pneumocystis is seen in malnour ished infants whose immunologic systems are impaired. The disease is thought to be transmit ted via an airborne route. The disease is character ized by a severe pneumonia caused by rapid mult ip lication of the organisms, almost exclusively in lung tissue, with the organism l in ing the walls of the alveoli and gradually f i l ling the alveolar spaces. Untreated, the acute form of the disease general ly is fatal. Even pat ients who recover from pneumocystosis are at risk of recurrent episodes. Pat ients with AIDS exper ience a recurrence rate of approximately 50%.
Organisms that Commonly Cause Vaginitis Vaginit is also may be caused by Haemophilus vaginalis (bacteria) or Candida albicans (fungus), which are treated di fferently from the protozoal infect ion.
Extrapulmonary pneumocystosis— that is, pneumocystosis outside of the lungs—also is known to exist and may be more common than present ly recognized. This infect ion may be complicated by the presence of coinfectious organisms. Fortunately, drug therapy ut i lized for t reatment of the pulmonary infect ion is benef icia l for the extrapulmonary condit ion, although intravenous ( IV) administration of the drugs may be necessary.
Tritryps Three protozoan pathogens that belong to the family Trypanosomatidae, the order Kinetoplast ida, and the genus Trypanosoma are Leishmania major , which is responsible for le ishmaniasis; Trypanosoma brucei , which is responsible for African trypanosomiasis (Afr ican sleeping sickness); and Trypanosoma cruzi , which is responsible organism for Chagas' d isease. Referred to as the “tr it ryps,” these eukaryot ic organisms share characteristic subcel lu lar structures of a kinetoplast and glycosomes, are unicel lular mot i le protozoa, are transmit ted by various insect vectors, and infect mammalian hosts. The genomes of t ri t ryps have recently been reported (1,2,3). Together, they infect hundreds of mil l ions of people annually.
Table 39.1. Entamoeba Histolytidavasion of Host
P.1086
Page 4 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

Trypanosomiasis (4) There are two dist inct forms of t rypanosomiasis: Chagas' d isease, and African sleeping sickness.
Chagas' disease Chagas' d isease, also known as American trypanosomiasis, is caused by the parasitic protozoa Trypanosoma cruzi and is found only in the Americas, primar i ly in Brazi l but a lso in the southern United States. The protozoa l ives in mammals and is spread by the bloodsucking insect known as the reduvi id bug, assassin bug, or kissing bug. The insect becomes infected by drawing blood from an infected mammal and releasing the protozoa with discharged feces. The pathogen then enters the new host through breaks in the skin. Inf lammatory lesions are seen at the site of entry. The disease also may be spread through transfusion with contaminated blood. Signs of in i tia l infection may include malaise, fever, anorexia, and skin edema at the site where the protozoa entered the host. The disease ultimately may invade the heart, where after decades of infect ion with chronic Chagas' d isease, the pat ient may exper ience an infection-associated heart at tack. I t is estimated that 5% of the Salvadorian and Nicaraguan immigrants to the United States may have chronic Chagas' disease.
African trypanosomiasis Afr ican trypanosomiasis, or sleeping sickness, is caused by several subspecies of Trypanosoma brucei (T. brucei rhodesiense [east African sleeping sickness] and T. brucei gambiense [west Afr ican sleeping sickness]) . In this case, the infected animal is bit ten by the bloodsucking tsetse f ly, which in turn transmits the protozoa via inoculation dur ing a subsequent bite of a human. The protozoa, ini t ial ly present in the gut of the vector. appears in the salivary gland for inoculat ion during the subsequent bit ing of a human. I t is est imated that some 50 mil l ion people are at r isk of African sleeping sickness, with 300,000 to 500,000 cases occurr ing in sub-Saharan Africa each year. The infect ion progresses through two stages. Stage I may present as fever and high temperatures lasting several days; hematologic and immunologic changes occur during this stage. Stage II occurs after the organism enters the central nervous system (CNS) and may involve symptoms suggesting the disease name—daytime somnolence, loss of spontaneity, halting speech, list less gaze, and extrapyramidal signs (e.g., tremors and choreiform movements). A breakdown of neurological funct ion leading to coma and death may occur. Death may occur with in weeks if untreated (T. brucei rhodesiense) or only after several years (T. brucei gambiense ).
It should be noted that the sole source of energy for the trypanosomal organism is glycolysis, which in turn may account for the hypoglycemia seen in the host. In addit ion, the migrat ion of the organism into the CNS may be associated with the organism's search for a rich source of avai lable glucose.
Leishmaniasis Leishmaniasis is a disease caused by a number of protozoa in the genus Leishmania . The protozoa may be harbored in diseased rodents, canines, and var ious other mammals and transmit ted from the infected mammal to man by bites from female sandf lies of the genus Phlehotomus and then appears in one of four major cl inical syndromes: visceral leishmaniasis, cutaneous le ishmaniasis, mucocutaneous leishmaniasis, or dif fuse cutaneous leishmaniasis. The sandfly, the vector involved in spreading the disease, breeds in warm, humid climates; thus, the disease is more common in the tropics. As many as 12 mil l ion individuals, worldwide are infected by th is organism.
The visceral le ishmaniasis, a lso known as kala azar (black fever), is caused by Leishmania donovani . This form of the disease is systemic and is characterized in pat ients by fever, typical ly nocturnal, d iarrhea, cough, and enlarged l iver and spleen. The skin of the patient may become darkened. Without t reatment, death may occur in 20 months and is commonly associated with diarrhea, superinfect ions, or GI hemorrhage. Visceral le ishmaniasis is most commonly found in India and Sudan.
Both cutaneous and monocutaneous leishmaniasis are character ized by single or mult ip le local ized lesions. These slow-healing and, possibly, painful u lcers can lead to secondary bacteria l infect ions. The Old World cutaneous le ishmaniasis is caused by Leishmania topica, which is found most commonly in children and
P.1087
Page 5 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

young adults in regions bordering the Mediterranean, the Middle East, Southern Russia, and India. Leishmania major is endemic to desert areas in Africa, the Middle East, and Russia, whereas Leishmania aethiopica is found in the Kenyan highlands and Ethiopia. The New World disease caused by Leishmania peruviana, Leishmania brazil iensis , and Leishmania panamensis is found in South and Central Amer ica, whereas Leishmania mexicana may be endemic to southcentral Texas. The incubation per iod for cutaneous le ishmaniasis ranges from a few weeks to several months. The slow-healing lesions may be seen on the skin in var ious regions of the body depending on the specif ic strain of organism. Usually, these conditions exhibit spontaneous heal ing, but this also may occur over an extended per iod of t ime (1–2 years) .
Malaria Malar ia is t ransmitted by the infected female Anopheles mosquito. The specif ic protozoan organisms causing malar ia are from the genus Plasmodium. Only 4 of approximately 100 species cause malaria in humans. The remaining species affect birds, monkeys, l ivestock, rodents, and repti les. The four species that affect humans are Plasmodium falciparum, Plasmodium vivax, Plasmodium malar iae , and Plasmodium ovale. Concurrent infect ions by more than one of these species are seen in endemical ly af fected regions of the wor ld. Such mult iple infect ions further complicate pat ient management and the choice of t reatment regimens.
Malar ia af fects as many as 500 mil lion humans global ly and causes more than 2 mill ion deaths annually. It is est imated that a th ird of these fatal i ties occur in chi ldren younger than 5 years. Although this disease is found primar i ly in the tropics and subtropics, i t has been observed far beyond these boundaries.
Malar ia has essent ial ly been eradicated in most temperate-zone countr ies. However, more than 1,000 cases of malar ia were documented recent ly in U.S. ci t izens returning from travel abroad. Today, malaria is found in most countr ies of Afr ica, Central and South America, and Southeast Asia. It is reported to be on the increase in Afghanistan, Bangladesh, Brazil , Burma, Cambodia, Colombia, China, I ran, India, Indonesia, Mexico, the Phil ippines, Thai land, and V ietnam. Infect ion from plasmodia can cause anemia, pulmonary edema, renal fa i lure, jaundice, shock, cerebral malaria, and if not t reated in a timely manner, even death.
Types of Malaria Malar ia l infect ions are known according to the species of the parasite involved.
Plasmodium falciparum Infect ion with Plasmodium falciparum has an incubat ion period (t ime from mosquito bite to cl inical symptoms) of 1 to 3 weeks (average, 12 days). The P. falciparum l i fe cycle in humans begins with the bite of an infected female mosquito. The parasites in the sporozoite stage enter the circulatory system, through which they can reach the liver in approximately 1 hour. These organisms grow and multip ly 30,000- to 40,000-fold by asexual division with in l iver cel ls in 5 to 7 days. Then, as merozoites, they leave the l iver to reenter the blood stream and invade the erythrocytes, or red blood cel ls (RBCs), where they continue to grow and mult ip ly fur ther for 1 to 3 days. Specific receptors on the surface of the erythrocytes serve as binding sites for the merozoite. These infected RBCs rupture, releasing merozoites in intervals of approximately 48 hours. Chemicals released by the ruptured cel l in turn cause act ivat ion and release of addit ional substances associated with the pat ient 's symptoms. The cl inical symptoms include chi l ls, fever, sweating, headaches, fat igue, anorexia, nausea, vomiting, and diarrhea. Some of the released merozoites are sequestered in vita l organs (brain and heart) , where they continue to grow. Recurrence of the cl inical symptoms on alternate days leads to the terminology of ter tian malaria. The P. falciparum parasite also can cause RBCs to clump and adhere to the wall of blood vessels. Such a phenomenon has been known to cause part ial obstruct ion and, sometimes, restrict ion of the blood f low to vita l organs l ike the brain, liver, and kidneys. Reinfect ion of RBCs can occur, al lowing further mult ipl icat ion and remanifestat ion of the malaria symptoms. Some merozoites develop into male and female sexual forms, cal led gametocytes, which can then be acquired by the female mosquito af ter b iting the infected human. Gametocytes mature in the mosquito 's stomach to form zygotes. Growth of the zygotes leads to the formation of oocysts (spherical structures located on the outside wall of the stomach). Sporozoites develop from the oocysts, are released into the body cavity of the mosquito, and migrate to the sal ivary gland of the insect, f rom which they can be transmit ted to another human fol lowing a mosquito bite. The l i fe cycle of the malar ia parasites is shown in
Page 6 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
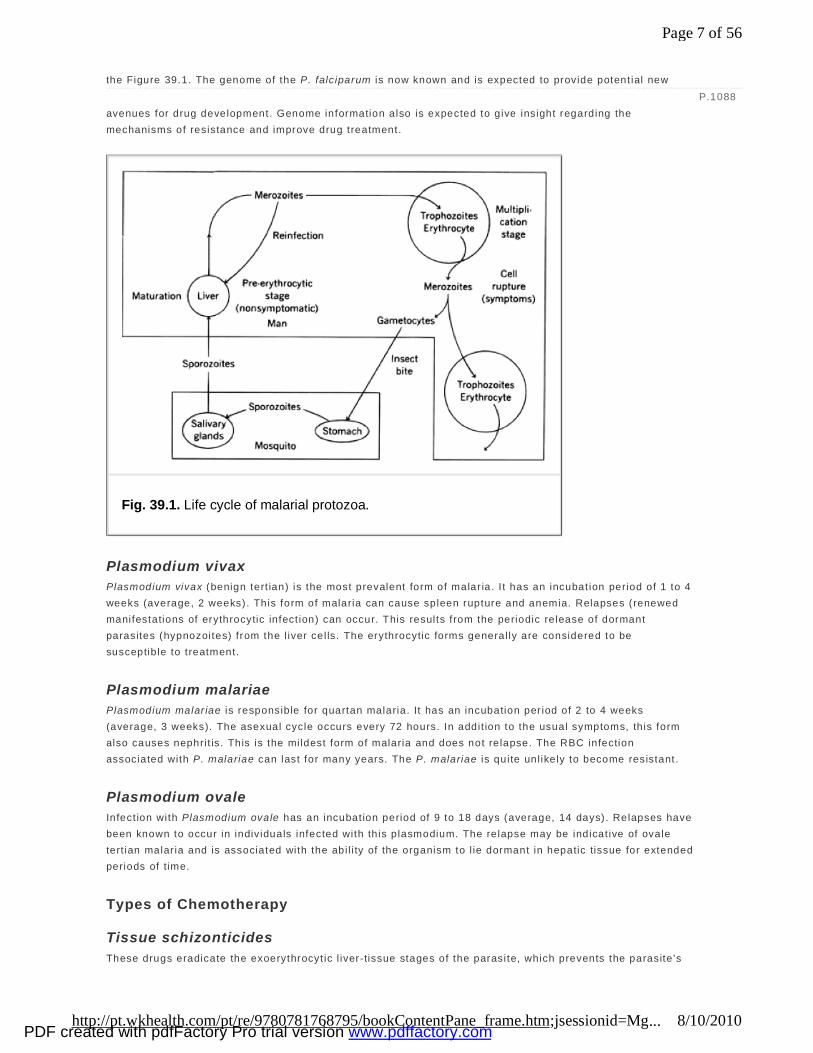
the Figure 39.1. The genome of the P. falciparum is now known and is expected to provide potent ial new avenues for drug development. Genome information also is expected to give insight regarding the mechanisms of resistance and improve drug treatment.
Plasmodium vivax Plasmodium vivax (benign tert ian) is the most prevalent form of malar ia. I t has an incubat ion period of 1 to 4 weeks (average, 2 weeks). This form of malaria can cause spleen rupture and anemia. Relapses (renewed manifestations of erythrocytic infect ion) can occur. This results f rom the periodic release of dormant parasites (hypnozoites) f rom the l iver cel ls. The erythrocytic forms general ly are considered to be susceptib le to treatment.
Plasmodium malariae Plasmodium malar iae is responsible for quartan malaria. It has an incubation per iod of 2 to 4 weeks (average, 3 weeks). The asexual cycle occurs every 72 hours. In addit ion to the usual symptoms, th is form also causes nephrit is. This is the mildest form of malaria and does not re lapse. The RBC infection associated with P. malariae can last for many years. The P. malariae is quite unl ikely to become resistant.
Plasmodium ovale Infect ion with Plasmodium ovale has an incubat ion period of 9 to 18 days (average, 14 days) . Relapses have been known to occur in individuals infected with th is plasmodium. The relapse may be indicat ive of ovale tert ian malar ia and is associated with the abi l i ty of the organism to l ie dormant in hepatic tissue for extended periods of time.
Types of Chemotherapy
Tissue schizonticides These drugs eradicate the exoerythrocyt ic l iver-tissue stages of the parasite, which prevents the parasite 's
P.1088
Fig. 39.1. Life cycle of malarial protozoa.
Page 7 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
entry into the blood. Drugs of this type are useful for prophylaxis. Some t issue schizonticides can act on the long- lived t issue form (hypnozoites of P. vivax and P. ovale ) and, thus, can prevent relapses.
Blood schizonticides These drugs destroy the erythrocytic stages of parasites and can cure cases of falciparum malaria or suppress relapses. This is the easiest phase to treat, because drug del ivery into the blood stream can be accomplished rapidly.
Gametocytocides Agents of th is type ki l l the sexual forms of the plasmodia (gametocytes) , which are transmittable to the Anopheles mosquito, thereby preventing transmission of the disease.
Sporontocides (sporozooiticides) These drugs act against sporozoites and are capable of kil l ing these organisms as soon as they enter the bloodstream following a mosquito bite.
It should be noted that antimalaria ls may operate against more than one form of the organism and may be effect ive against one species of p lasmodium but lack eff icacy against others. In addit ion, ant imalar ial drugs may be classif ied according to their structural types.
General Approaches to Protozoal Therapy
Amebiasis and Giardiasis The most appropriate approach for treatment of th is type of protozoal infection is through prevent ion. Because the infection usual ly occurs by consumption of contaminated dr inking water and food, avoidance is the key to prevention. Drinking bott led water , or boi l ing or disinfect ing the water , wi l l reduce the risk. Improvement in personal hygiene and general sanitat ion also are benef icia l.
Trypanosomiasis, Leishmaniasis, and Malaria For these diseases that are spread by insect vectors, the use of insect icides, protective clothing, and insect repel lents can great ly reduce the incidence of the disease. Unfortunately, many of these protozoal infect ions also can infect other hosts beside humans; thus, even the most successful insect ir radiat ion methods cannot destroy al l the reservoirs of the protozoa. The use of insect repel lents and protect ive clothing may be useful for visi tors to regions with endemic infect ions, but these procedures may prove to be ineffect ive for those liv ing in the area. For such individuals, early detection and drug therapy is the method of t reatment.
Drug Therapy for Protozoal Infections
Treatment of Amebiasis, Giardiasis, and Trichomoniasis
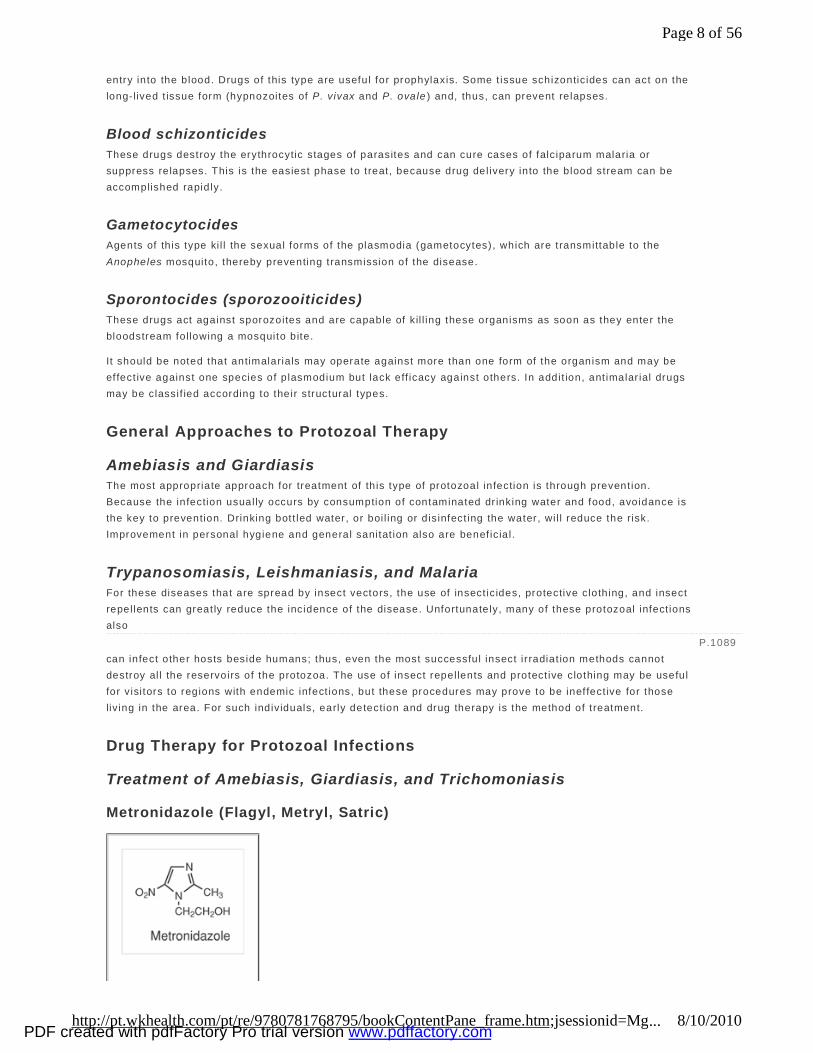
Metronidazole (Flagyl, Metryl, Satric)
P.1089
Page 8 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Metronidazole was init ial ly introduced for the treatment of vaginal infect ions caused by Trichomonas vaginal is but has since been shown to be effective for treatment of amebiasis, g iardiasis, and anaerobic bacteria l infect ions, including Clostr idium diff ic ile .
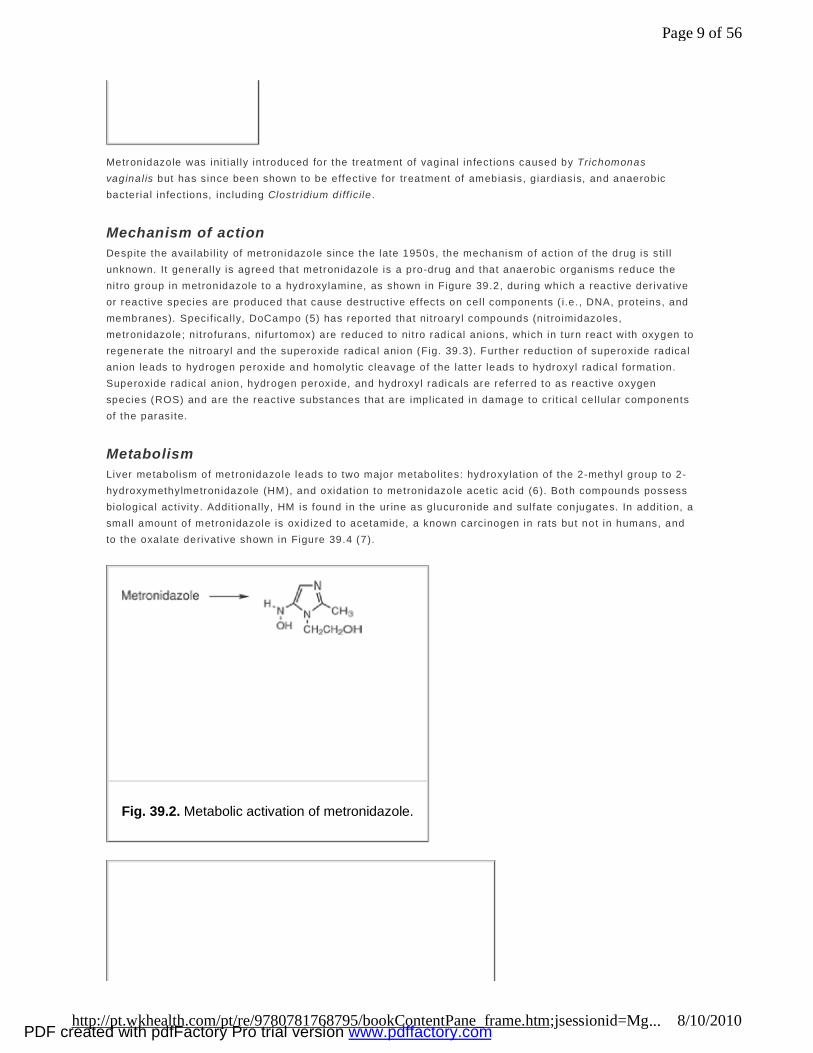
Mechanism of action Despite the avai labi l i ty of metronidazole since the late 1950s, the mechanism of action of the drug is sti l l unknown. It general ly is agreed that metronidazole is a pro-drug and that anaerobic organisms reduce the nit ro group in metronidazole to a hydroxylamine, as shown in Figure 39.2, during which a reactive der ivat ive or reactive species are produced that cause destruct ive effects on cel l components ( i .e. , DNA, proteins, and membranes). Specif ical ly, DoCampo (5) has reported that nit roaryl compounds (nit ro imidazoles, metronidazole; n it rofurans, nifur tomox) are reduced to nit ro radical anions, which in turn react with oxygen to regenerate the nit roaryl and the superoxide radical anion (Fig. 39.3). Further reduction of superoxide radical anion leads to hydrogen peroxide and homolyt ic cleavage of the lat ter leads to hydroxyl radical formation. Superoxide radical anion, hydrogen peroxide, and hydroxyl radicals are referred to as reactive oxygen species (ROS) and are the reactive substances that are implicated in damage to cri t ical cel lular components of the parasite.
Metabolism Liver metabol ism of metronidazole leads to two major metabol ites: hydroxylat ion of the 2-methyl group to 2-hydroxymethylmetronidazole (HM), and oxidat ion to metronidazole acet ic acid (6). Both compounds possess biological act ivi ty. Addit ional ly, HM is found in the ur ine as glucuronide and sulfate conjugates. In addit ion, a small amount of metronidazole is oxidized to acetamide, a known carcinogen in rats but not in humans, and to the oxalate derivat ive shown in Figure 39.4 (7).
Fig. 39.2. Metabolic activation of metronidazole.
Page 9 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Pharmacokinetics (6) Metronidazole is avai lable in a var iety of dosage forms, including IV, oral, rectal, and vaginal suppositor ies. The bioavai labi l i ty of metronidazole is nearly 100% when administered orally but is signif icant ly less when administered via the rectal route (67–82%) or the vaginal route (19–56%). The drug is not bound to plasma protein. Distribut ion of the drug is fa ir ly uniform through out the body, including mother's milk.
Therapeutic application Metronidazole is considered to be the drug of choice for t reatment for the protozoal infect ions amebiasis (intestinal and extraintest inal), g iardiasis, and tr ichomoniasis (8). I t is the drug of choice for t reatment of the Gram-posit ive baci l l i Clostr idium diff ic ile and in combination is an alternative therapy for Helicobacter pylori infect ions (9). The common side effects exhibited with metronidazole include abdominal d istress, a metal l ic taste, and a disulfi ram-like effect i f taken with alcohol. The drug is reported to be carcinogenic in mice, possibly related to the metaboli te acetamide, and as a result should not be used during the first t rimester of pregnancy.
Tinidazole (Tindamax)
Fig. 39.3. Formation of ROS from nitroaryl compounds.
Fig. 39.4. Metabolism of metronidazole.
P.1090
Page 10 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Tinidazole has recent ly been approved by the U.S. Food and Drug Administration (FDA) for the treatment of amebiasis, g iardiasis, and trichomoniasis. I t a lso appears to be highly ef fect ive against Helicobacter pylori infect ions, a lthough i t is not approved for this use. The drug is rapidly and completely absorbed fol lowing oral administrat ion and can be administered with food to reduce GI disturbance. Tinidazole has a mechanism of act ion that paral lels that of metronidazole as well as a similar metabol ic pathway leading to hydroxylat ion at the 2-methyl group catalyzed by CYP3A4. Basical ly, t inidazole appears to mimic the act ions of metronidazole, a lthough there are reports that i t is ef fect ive against some protozoa which are resistant to metronidazole.
Nitazoxanide (Alinia)
Nitazoxanide (NTZ) has been approved as an orphan drug for the treatment of d iarrhea in chi ldren (age, 1–11 years) and is associated with giardiasis, but i t a lso is approved for d iarrhea caused by crytospor id iosis in patients with AIDS. Crytospor idiosis is a protozoal infection caused by Cryptosporid ium parvum . The condit ion is uncommon in healthy individuals but can be l i fe- threatening in immunosuppressed patients and those with HIV infect ions.
Mechanism of action (10) Nitazoxanide is a pro-drug that is metabol ical ly converted into the deactylated drug tizoxanide (TIZ) (Fig. 39.5). The TIZ then undergoes a four-electron reduction of the 5-nitro group giving var ious short-lived intermediates, which may include the hydroxylamine derivat ive. It is these reduced products that represent the active form of NTZ. Whereas these intermediates would suggest that NTZ has the same mechanism of act ion as metronidazole, th is does not appear to be the case. Nitazoxanide is thought to inhibit the enzyme pyruvate:ferredoxin oxidoreductase in Trichomonas vaginal is, Entamoeba histolyt ica, and Clostr idium perf ingens . The results of th is inhibition is disrupt ion of the bioenerget ics of these organisms. Unlike metronidazole and t inidazole, which fragment DNA and are suspected mutagenic agents, NTZ and TIZ do not cause DNA fragmentat ion and are not considered to be mutagenic. This might be associated with the higher redox potent ia l found for NTZ, a nit rothiazole, in compar ison with very low redox potent ia l found for the
Page 11 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
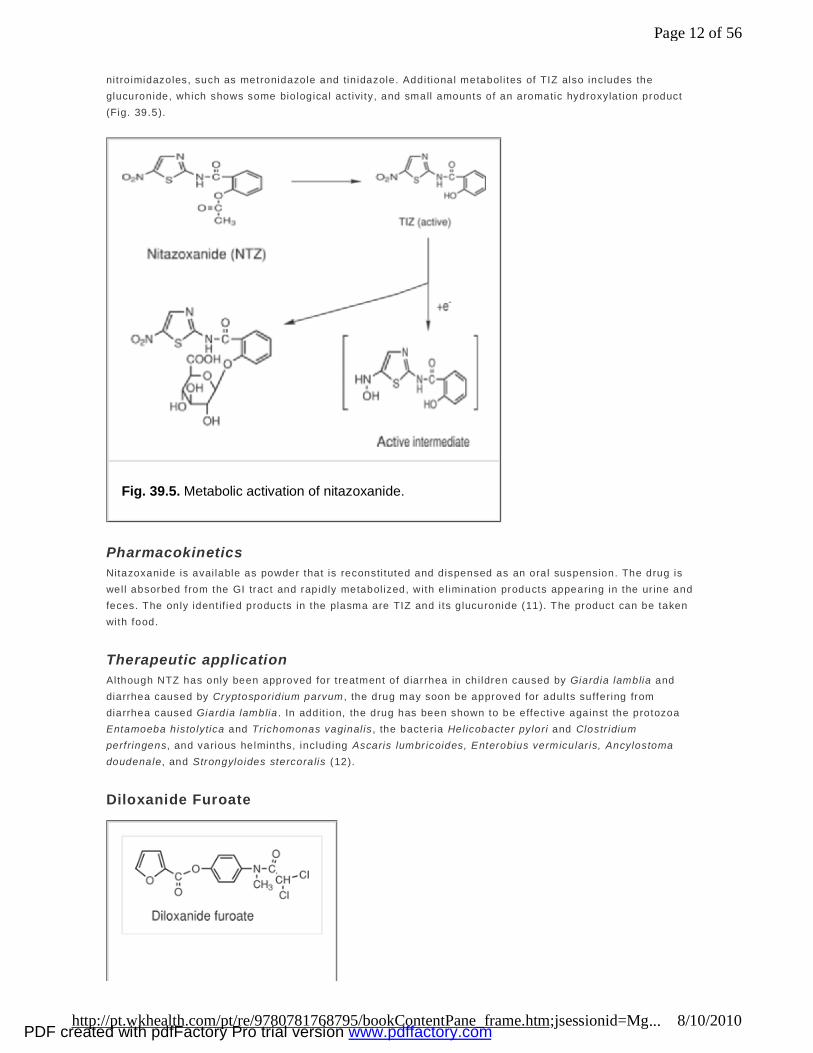
nitro imidazoles, such as metronidazole and tin idazole. Additional metabol i tes of TIZ also includes the glucuronide, which shows some biological act ivi ty, and small amounts of an aromatic hydroxylat ion product (Fig. 39.5).
Pharmacokinetics Nitazoxanide is avai lable as powder that is reconsti tuted and dispensed as an oral suspension. The drug is well absorbed from the GI tract and rapidly metabol ized, with el iminat ion products appearing in the ur ine and feces. The only ident if ied products in the plasma are TIZ and i ts glucuronide (11). The product can be taken with food.
Therapeutic application Although NTZ has only been approved for t reatment of d iarrhea in chi ldren caused by Giardia lamblia and diarrhea caused by Cryptosporid ium parvum , the drug may soon be approved for adults suffering from diarrhea caused Giardia lamblia . In addit ion, the drug has been shown to be effective against the protozoa Entamoeba histolytica and Trichomonas vaginal is , the bacteria Helicobacter pylori and Clostr idium perfringens, and various helminths, including Ascaris lumbr icoides, Enterobius vermicular is, Ancylostoma doudenale, and Strongyloides stercoralis (12).
Diloxanide Furoate
Fig. 39.5. Metabolic activation of nitazoxanide.
Page 12 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
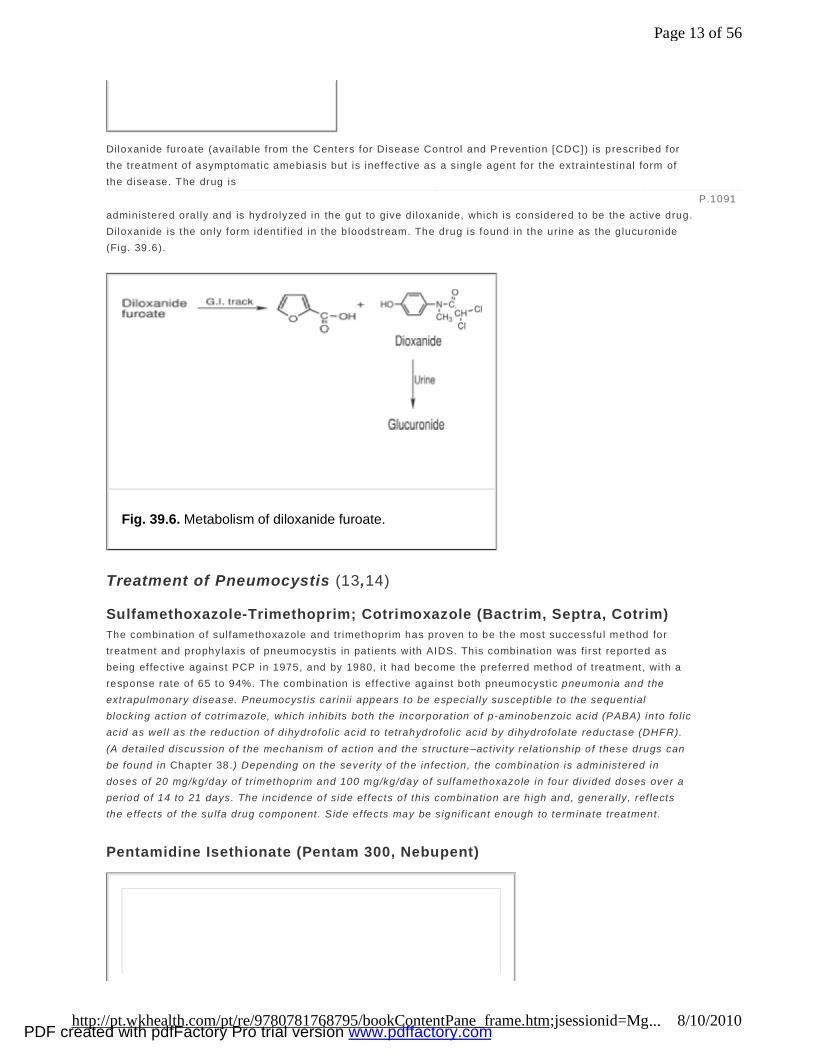
Diloxanide furoate (avai lable from the Centers for Disease Control and Prevention [CDC]) is prescr ibed for the treatment of asymptomatic amebiasis but is ineffective as a single agent for the extraintest inal form of the disease. The drug is administered oral ly and is hydrolyzed in the gut to give di loxanide, which is considered to be the active drug. Di loxanide is the only form identi f ied in the bloodstream. The drug is found in the urine as the glucuronide (Fig. 39.6).
Treatment of Pneumocystis (13,14)
Sulfamethoxazole-Trimethoprim; Cotrimoxazole (Bactrim, Septra, Cotrim) The combination of sulfamethoxazole and trimethoprim has proven to be the most successful method for treatment and prophylaxis of pneumocystis in pat ients with AIDS. This combinat ion was first reported as being effect ive against PCP in 1975, and by 1980, i t had become the preferred method of t reatment, with a response rate of 65 to 94%. The combinat ion is ef fect ive against both pneumocystic pneumonia and the extrapulmonary disease. Pneumocyst is carin ii appears to be especial ly susceptib le to the sequent ial blocking act ion of cotrimazole, which inhibits both the incorporat ion of p-aminobenzoic acid (PABA) into fo l ic acid as well as the reduct ion of d ihydrofol ic acid to tetrahydrofol ic acid by dihydrofolate reductase (DHFR). (A detai led discussion of the mechanism of action and the structure–act ivi ty relationship of these drugs can be found in Chapter 38 .) Depending on the sever ity of the infect ion, the combinat ion is administered in doses of 20 mg/kg/day of t rimethoprim and 100 mg/kg/day of sulfamethoxazole in four divided doses over a period of 14 to 21 days. The incidence of side effects of th is combination are high and, generally, ref lects the effects of the sulfa drug component. S ide effects may be signif icant enough to terminate treatment.
Pentamidine Isethionate (Pentam 300, Nebupent)
P.1091
Fig. 39.6. Metabolism of diloxanide furoate.
Page 13 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Orphan Drug Product Dapsone plus trimethoprim also has been uti lized for the treatment of pneumocystis, wi th effect iveness nearly equal to that of cotrimazole.
Pentamidine is avai lable as the water-soluble isethionate salt, which is used both IV and as an aerosol. The drug can be used via the intramuscular route, but significant complications have been reported and. therefore, this route of administrat ion is not recommended. The drug has fungicidal and ant iprotozoal act iv i ty, but today, i t is used primar ily for t reatment of PCP.
Mechanism of action The mechanism of act ion of pentamidine is not known with certainty, but strong evidence supports var ious mechanisms of act ion for pentamidine. Pentamidine select ively binds to the DNA in trypanosoma parasite (see below). Pentamidine has also been shown to inhibit topoisomerase in Pneumocyst is carin ii , which leads to double-strand cleavage of DNA in trypanosoma (12,13,14 ). I t has been suggested that pentamidine's mechanism of action may be dif ferent in different organisms and, therefore, that the act ions reported for trypanosoma may not carry over to pneumocyst is.
Pharmacokinetics Pentamidine must be administered IV and, af ter mult iple in ject ions dai ly or on alternate days, accumulates in body t issue. Plasma concentrations were measured up to 8 months fo l lowing a single, 2-hour IV infusion. The accumulat ion aids in treatment as well as in prophylaxis. The drug shows poor penetrat ion of the CNS.
Therapeutic application Pentamidine is used as a second- line agent either by itself or in combinat ion for the treatment and prophylaxis of PCP. For prophylaxis, the aerosol form of the drug is indicated and has minimum toxicity. The limitat ion of pentamidine— that is, the need for IV administrat ion—may be associated with the potent ial for severe toxici ty, which includes breathlessness, tachycardia, d izziness, headache, and vomit ing. These symptoms may occur in as many as 50% of the pat ients. These effects are thought to be associated with a too rapid IV administrat ion, resulting in the release of histamine.
Atovaquone (Mepron)
Page 14 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

Atovaquone, a chemical with structural similar ity to the ubiquinone metaboli tes, was in itia l ly synthesized and invest igated as an ant imalaria l, a use for which i t has recent ly gained acceptance when used in combinat ion therapy with other ant imalar ial agents. Today, its usefulness is pr imari ly d irected toward the treatment of PCP.
Mechanism of action Atovaquone is thought to produce its ant iparasit ic action by virtue of i ts abi l i ty to inhibit the mitochondria l respiratory chain. More specif ical ly, atovaquone is a ubiquinone reductase inhibitor, inhibit ing at the cytochrome bc1 complex (15). This act ion leads to a col lapse of the mitochondria l membrane
potentia l. The compound shows stereospecif ic inhibition, with the trans isomer being more act ive than the cis isomer.
Pharmacokinetics Atovaquone is poor ly absorbed from the GI tract because of i ts poor water solubi l i ty and high fat solubi l ity, but the absorpt ion can be signif icantly increased if taken with a fat-rich meal. The drug is highly bound to plasma protein (94%) and does not enter the CNS in signif icant quant i ties. I t is not significant ly metabol ized in humans and is exclusively el iminated in feces via the bi le.
Therapeutic applications With as many as 70% of pat ients with AIDS developing pneumocyst is and, of these, near ly 60% of the patients on cotrimoxazole developing ser ious side effects to th is combination, atovaquone is an important alternat ive drug (16). Atovaquone also has been reported to be effect ive for the treatment of toxoplasmosis caused by Toxoplasma gondii , al though i t has not been approved for th is use.
Trimetrexate Glucuronate (Neutrexin)
Trimetrexate (TMQ) has been approved for the treatment of Pneumocyst is carin ii in patients with AIDS and also exhibits ant iprotozoal act iv i ty against Trypanosoma cruzi . The drug is avai lable as a single- ingredient medication, but i t can be administered along with fo l in ic acid in much the same way that methotrexate is administered with calcium leucovorin in cancer chemotherapy. Tr imetrexate is a derivative of methotrexate.
Mechanism of action Trimetrexate is considered to be a nonclassical folate antagonist, whereas methotrexate, the structural ly similar analogue of TMQ, is a classical fo late antagonist . The dif ference between these two drugs is that methotrexate, with i ts polar glutamate side chain, is t ransported into the cel l v ia a carrier-mediated transport
P.1092
Page 15 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
system, whereas TMQ, without the glutamate moiety, is absorbed by the cel l v ia a passive diffusion. Once in the cell , TMQ inhibits DHFR. Trimetrexate binds to Pneumocyst is carin ii DHFR 1,500 t imes more strongly than tr imethopr im and somewhat more strongly than methotrexate. It also has been reported that TMQ readi ly enters the P. car ini i cell because of the l ipophi l ic nature of th is drug (17 ). Methotrexate and leucovorin are not able to enter the cel l , however, because the cel l membrane of P. car ini i does not possess the transporter protein (17).
Therapeutic application Trimetrexate, when combined with the cytoprotective agent leucovor in, is more effect ive and better to lerated than pentamidine in the treatment of PCP (18). Because the first- and second-line agents are successful in only 50 to 75% of these cases, and because adverse react ions severely l imit the use of some of the older agents, TMQ may offer some advantages in treatment. Tr imetrexate is administered by IV infusion over 60 to 90 minutes and should be combined with the cytoprotect ive drug leucovorin. The leucovor in protects against bone marrow suppression and against renal and hepat ic dysfunct ion. Leucovorin administrat ion should continue for 72 hours after the last dose of TMQ. Addit ionally, TMQ has been reported to be effect ive in the treatment of Chagas' d isease.
Treatment of Trypanosomiasis (19)
Suramin Sodium (Available from the CDC)
Introduced into therapy for the treatment of ear ly t rypanosomiasis in the 1920s, suramin, a bis-hexasulfonatednaphthylurea, is st i l l considered to be the drug of choice for t reatment of non-CNS-associated Afr ican trypanosomiasis.
Mechanism of action The mechanism of act ion of suramin is unproven, but the drug is known to have a high aff ini ty for binding to a number of cri t ical enzymes in the pathogen. Among the enzymes to which suramin has been shown to bind are several dehydrogenases and kinases. As a result of binding, suramin has been shown to be an inhibitor of DHFR, a crucial enzyme in folate metabol ism, and thymidine kinase. In addition, suramin is an inhibitor of glycolyt ic enzymes in Trypanosoma brucei , with binding constants much lower than those seen in mammalian cel ls. Inhibit ion of g lycolysis would be expected to block energy sources of the pathogen, leading to lysis. Whether one or more of these inhibitor act ions represent the toxic act ion of suramin on the pathogen
Page 16 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
remains unproven.
Pharmacokinetics Suramin sodium is a water-soluble compound that is poor ly absorbed via oral administration and must be administered IV in multip le in ject ions. Because of i t highly ionic nature, suramin wil l not cross the blood-brain barrier and, therefore, is ineffect ive for the treatment of t rypanosomal infections that reach the CNS. In addition, suramin is t ight ly bound to serum albumin. Despite this binding, the drug is preferent ia lly absorbed by trypanosomes through a receptor-mediated endocytosis of serum protein. Because the drug remains in the bloodstream for an extended period of time, suramin has value as a prophylact ic drug.
Therapeutic application Seramin sodium is effective against east African trypanosomiasis, but i t has l imited value against west Afr ican trypanosomiasis. As indicated, because the drug wil l not enter the CNS, the drug is only useful for the treatment of ear ly stages of the disease. The drug exhibits a wide variety of side effects, which can be severe in debi l i tated individuals, and include nausea, vomit ing, and fat igue.
Pentamidine, Isethionate (Pentam 300, Nebupent) First introduced as a therapy for t rypanosomiasis in 1937, pentamidine is now used in a variety of protozoal and fungal infect ions and, as such, f inds use in the treatment of trypanosomiasis, le ishmaniasis, and pneumocystis (PCP). The drug is pr imari ly used for t reatment of PCP. When used for t rypanosomiasis, pentamidine is only ef fective against Trypanosoma brucei rhodesiense (east African sleeping sickness) and, even then, only during the early stage of the disease,. because the drug does not readi ly cross the blood-brain barrier.
Mechanism of action As indicated above, several b iochemical act ions have been reported for pentamidine. The drug has been shown to bind to DNA through hydrogen-bonding of the amidine proton and AT-rich regions of DNA. More specif ical ly, pentamidine binds to the N-3 of adenine, spans four to five base pairs, and binds to a second adenine to form interstrand cross-bonding (20). In addit ion to and, possibly, separate from this action, pentamidine appears to be a potent inhibitor of type I I topoisomerase of mitochondr ia DNA (kinetoplast DNA) of the trypanosoma parasite (21). The mitochondrial DNA is a cycl ic DNA. This inhibit ion leads to double -stand breaks in the DNA and l inearization of the DNA. The relationship between binding to specific regions of the DNA and inhibition of topoisomerase is unclear.
In the case of Trypanosoma brucei , resistant strains are common. It is thought that resistance develops through an inabi l i ty of the drug to reach the mitochondrial DNA (22). Transport into the mitochondr ia is a carr ier-mediated process, with the absence of carrier in the resistant strains.
Eflornithine (Ornidyl)
P.1093
Page 17 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Metcalf et a l. (23) reported the synthesis of ef lornith ine (dif luoromethyl ornith ine [DFMO]) in 1978. Their interest arose from the desire to prepare ornith ine decarboxylase (ODC) inhibitors as tools for studying the role of polyamines as regulators of growth processes. Ornithine decarboxylase catalyzes the conversion of ornithine to putrescine (1,4-diaminobutane), which in turn leads to the formation of the polyamines, spermine, and spermidine. I t was not unt i l 1980 that Bacchi et a l. (24) demonstrated the potent ia l of DFMO in the treatment of t rypanosomiasis.
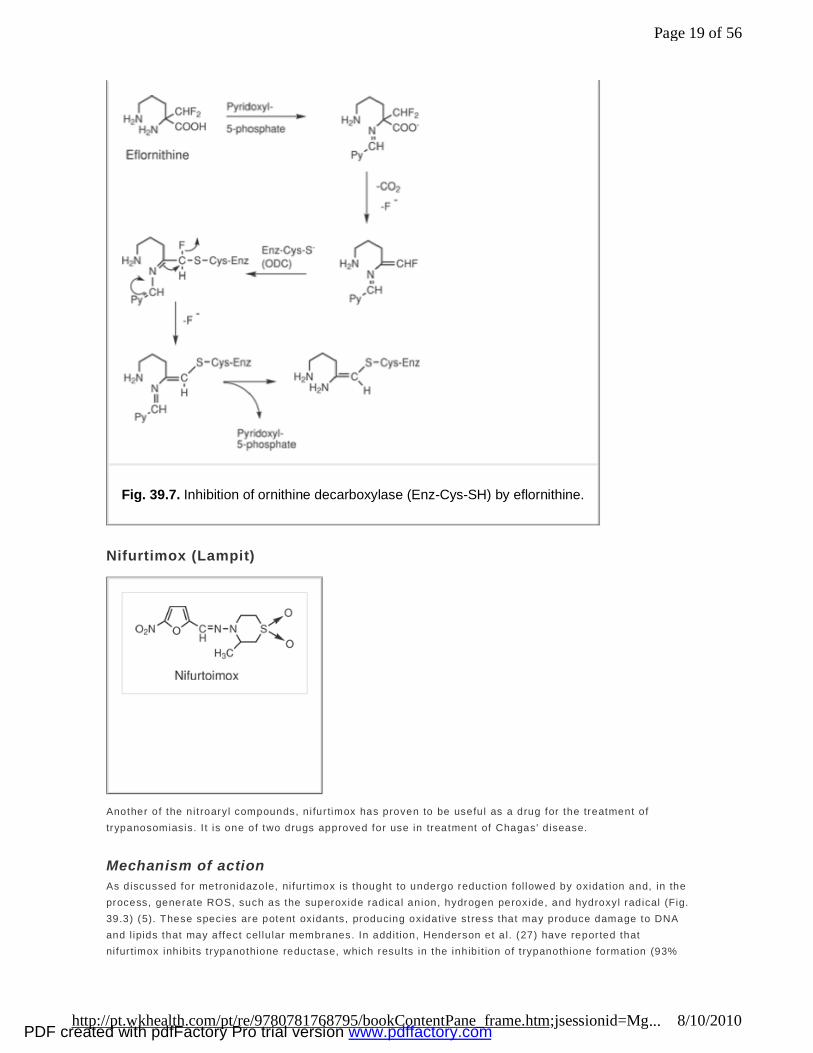
Mechanism of action Dif luoromethyl ornith ine is a suicide inhibitor of ODC, a pyridoxal phosphate–dependent enzyme, as shown in Figure 39.7. Evidence suggests that cysteine -360 in ODC is the site of eflornith ine alkylat ion (25). Alkylation of ODC blocks the synthesis of putrescine, the rate-determining step in the synthesis of polyamines. Mammalian ODC also may be inhibited, but because the turnover of ODC is so rapid in mammals, ef lornithine does not produce serious side effects.
Pharmacokinetics Eflornith ine may be administered either IV or oral ly. Administrat ion IV requires large doses and frequent dosing, whereas poor oral absorpt ion and rapid excret ion because of the zwit ter ionic nature of the drug (an amino acid) has l imited that route of administrat ion. The drug does not bind to plasma protein and enters the CNS readily, most l ikely via an amino acid transport system. As a result, the drug can be used for both early and late stages of t rypanosomiasis.
Therapeutic application Eflornith ine is indicated for the treatment of west African trypanosomiasis caused by Trypanosoma brucei gambiense but has proven to be ineffective against east African trypanosomiasis. The cause of th is ineffect iveness remains a mystery, a lthough evidence suggests that in the resistant organism, endogenous ornithine plus increased act iv i ty of S-adenosylmethionine decarboxylase al lows suffic ient synthesis of spermidine and spermine to support cel l d ivision, thus bypassing the need for organism-synthesized ornith ine (26). Side effects reported for ef lornithine consist of anemia, d iarrhea, and leukopenia.
P.1094
Page 18 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Nifurtimox (Lampit)
Another of the nit roaryl compounds, nifur timox has proven to be useful as a drug for the treatment of trypanosomiasis. I t is one of two drugs approved for use in treatment of Chagas' d isease.
Mechanism of action As discussed for metronidazole, nifur t imox is thought to undergo reduct ion fol lowed by oxidat ion and, in the process, generate ROS, such as the superoxide radical anion, hydrogen peroxide, and hydroxyl radical (Fig. 39.3) (5). These species are potent oxidants, producing oxidative stress that may produce damage to DNA and l ipids that may affect cel lu lar membranes. In addition, Henderson et a l. (27) have reported that nifur timox inhibits t rypanothione reductase, which results in the inhibit ion of t rypanothione formation (93%
Fig. 39.7. Inhibition of ornithine decarboxylase (Enz-Cys-SH) by eflornithine.
Page 19 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

inhibit ion). Trypanothione is a cri t ical protect ive enzyme found uniquely in trypanosomal parasites.
Therapeutic application Nifurt imox is the drug of choice for the treatment of acute Chagas' disease. The drug is not ef fective for the chronic stages of the disease. In the acute stage, the drug has an 80% cure rate. Side effects of the drug include hypersensit ivi ty react ions, GI complications (nausea and vomit ing) , myalgia, and weakness.
Benznidazole (Rochagan)
Benznidazole is the second of the drugs approved for t reatment of Chagas' d isease. Like nifurt imox, i t is ef fect ive against the circulating form of Trypanosoma cruzi dur ing the acute phase of the disease, but also like nifur timox, i t is ineffective during the chronic stage of the disease.
Mechanism of action Studies suggest that benznidazole does not catalyze the formation of ROS and, therefore, has a mechanism of act ion different from that of nifurt imox. It has been proposed that benznidazole undergoes an one-electron transfer to the nit ro group, which in turn dismutates to give back the nit ro imidazole and a nit rosoimidazole (28). The lat ter product may then undergo an electrophil ic addit ion to trypanothione, which leads to depletion of t rypanothione, an essentia l enzyme system in the Trypanosoma cruzi (Fig. 39.8).
Benznidazole is not avai lable in the United States but is avai lable in South American countries. It is administered oral ly in a tablet form.
Fig. 39.8. Proposed mechanism of action of benznidazole.
Page 20 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Melarsoprol (Available from the CDC)
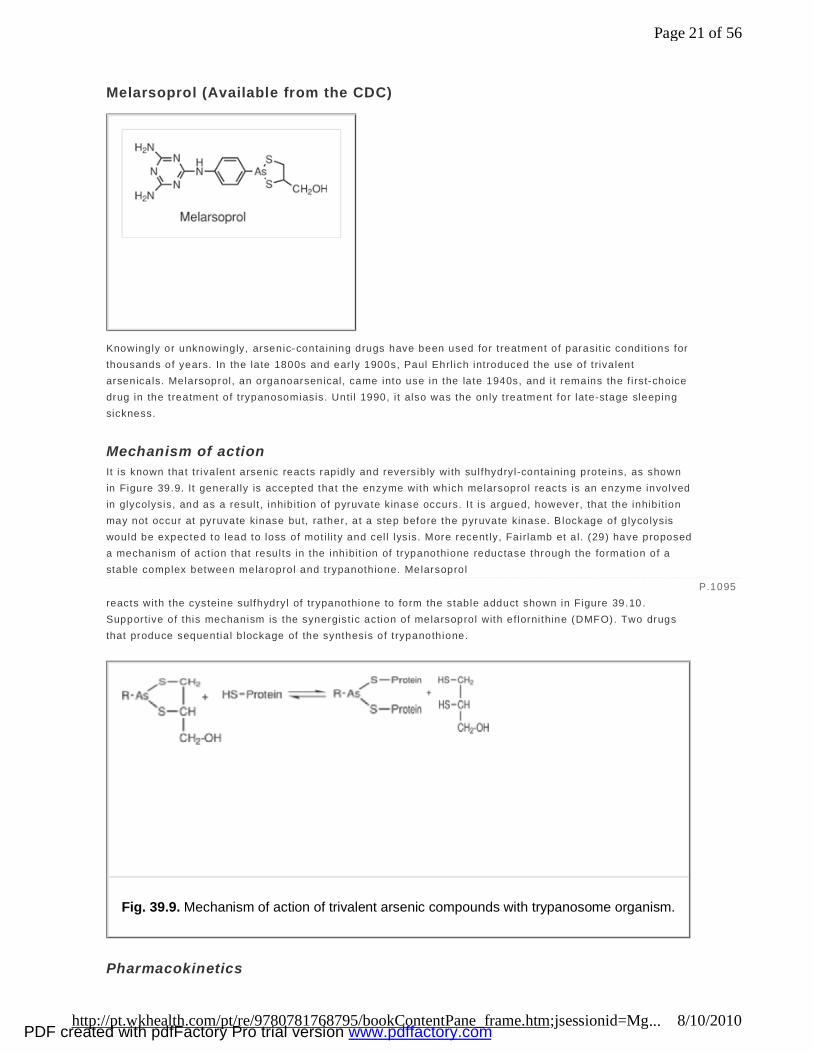
Knowingly or unknowingly, arsenic-containing drugs have been used for t reatment of parasit ic conditions for thousands of years. In the late 1800s and ear ly 1900s, Paul Ehrl ich introduced the use of t rivalent arsenicals. Melarsoprol, an organoarsenical, came into use in the late 1940s, and i t remains the f irst-choice drug in the treatment of t rypanosomiasis. Unti l 1990, i t also was the only treatment for late-stage sleeping sickness.
Mechanism of action It is known that t rivalent arsenic reacts rapidly and reversibly with sulfhydryl-containing proteins, as shown in Figure 39.9. It general ly is accepted that the enzyme with which melarsoprol reacts is an enzyme involved in glycolysis, and as a result , inhibition of pyruvate kinase occurs. I t is argued, however, that the inhibition may not occur at pyruvate kinase but, rather, at a step before the pyruvate kinase. B lockage of g lycolysis would be expected to lead to loss of mot i li ty and cel l lysis. More recent ly, Fairlamb et a l. (29) have proposed a mechanism of act ion that results in the inhibit ion of trypanothione reductase through the formation of a stable complex between melaroprol and trypanothione. Melarsoprol reacts with the cysteine sulfhydryl of trypanothione to form the stable adduct shown in Figure 39.10 . Supportive of this mechanism is the synergist ic action of melarsoprol with ef lornithine (DMFO). Two drugs that produce sequentia l b lockage of the synthesis of t rypanothione.
Pharmacokinetics
P.1095
Fig. 39.9. Mechanism of action of trivalent arsenic compounds with trypanosome organism.
Page 21 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

Melarsoprol is administered IV in mult ip le doses and mult ip le sessions. Its major metabol ite in humans is the lipophi lic melarsen oxide, which can penetrate into the CNS. This metabol i te apparent ly is responsible for the protein-binding character ist ic for melarsoprol.
Therapeutic application Melarsoprol is the drug of choice for the treatment of late-stage meningoencephalit ic t rypanosomiasis caused by the west and east Afr ican strains of the disease. Because the drug has the potentia l for ser ious nervous system toxici t ies (e.g., convulsions, acute cerebral edema, and coma), the drug usual ly is administered in a hospital sett ing with supervision. An addit ional problem with melarsoprol is the development of resistance by the parasite.
Treatment of Leishmaniasis
Sodium Stibogluconate (Pentostam, Available from the CDC)
Leishmaniasis was first described in the medical l iterature by Deishman and Donovan in 1903, and short ly af ter that, the use of ant imony-based drugs were introduced as therapeutic agents to treat the condit ion (30 ). Although the structure of sodium st ibogluconate is commonly drawn as shown, the actual compound probably is much more complex. The drug is a water-soluble preparat ion that is administered IM or IV. Pentavalent antimony compounds are thought to inhibit b ioenerget ic processes in the pathogen, with catabol ism of glucose and inhibit ion of glycolyt ic enzymes being the primary sites of act ion (glucose catabol ism is inhibited by 86–94%). This in turn results in inhibit ion of adenosine tr iphosphate (ATP)/guanosine triphosphate formation. Sodium sibogluconate is the drug of choice for the treatment of most forms of le ishmaniasis (or
Fig. 39.10. Structure of melarsoprol trypanothione complex.
Page 22 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
meglumine ant imonate, another pentavalent ant imony agent). The recommended dose is 20 mg antimony/kg/day, not to exceed 850 mg ant imony/day. A number of other drugs have been reported to be effect ive in the treatment of le ishmaniasis, and these include pentamidine, amphoter icin B, paromomycin, alkylphosphocholine analogues, r ifampicin, and ketoconazole (31 ,32 ).
Treatment of Malaria
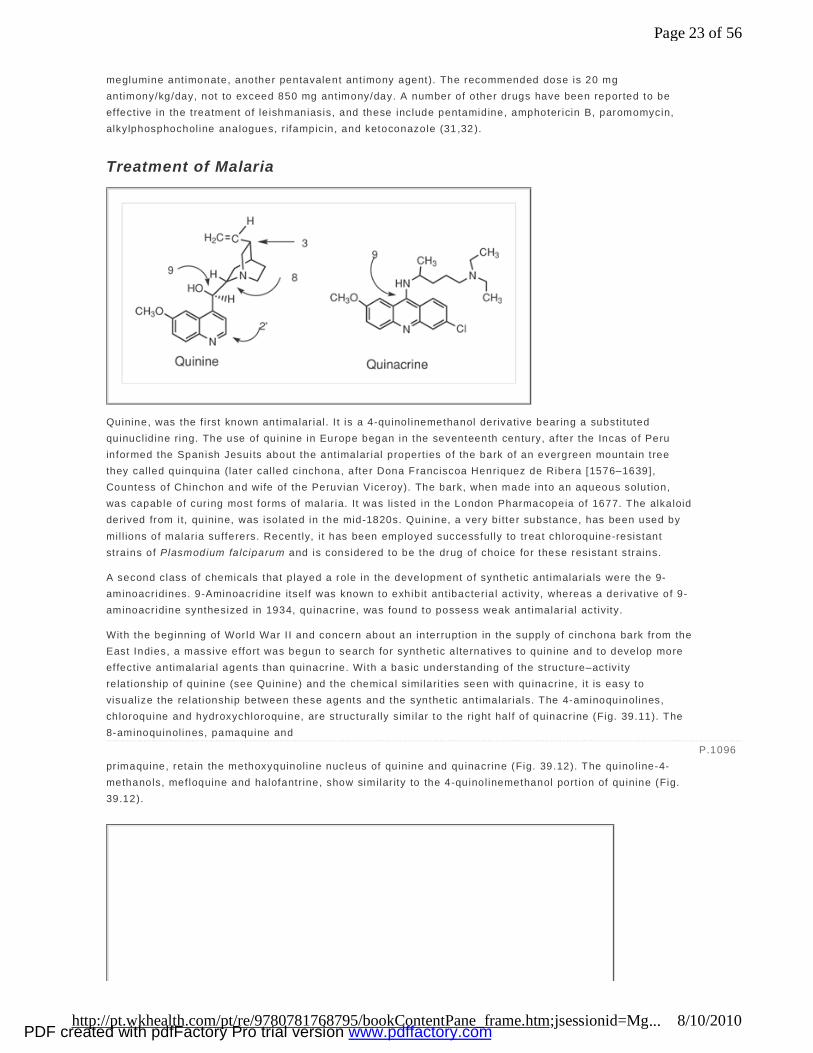
Quinine, was the f irst known ant imalar ial. I t is a 4-quinol inemethanol derivative bear ing a substi tuted quinucl id ine ring. The use of quinine in Europe began in the seventeenth century, af ter the Incas of Peru informed the Spanish Jesuits about the ant imalar ial propert ies of the bark of an evergreen mountain tree they cal led quinquina (later cal led cinchona, after Dona Franciscoa Henriquez de Ribera [1576–1639], Countess of Chinchon and wife of the Peruvian Viceroy). The bark, when made into an aqueous solut ion, was capable of cur ing most forms of malar ia. It was listed in the London Pharmacopeia of 1677. The alkaloid derived from it, quinine, was isolated in the mid-1820s. Quinine, a very bitter substance, has been used by mil l ions of malaria sufferers. Recent ly, i t has been employed successful ly to treat chloroquine-resistant strains of Plasmodium falciparum and is considered to be the drug of choice for these resistant strains.
A second class of chemicals that p layed a role in the development of synthet ic ant imalaria ls were the 9-aminoacr idines. 9-Aminoacrid ine itself was known to exhibit ant ibacteria l activ i ty, whereas a derivat ive of 9-aminoacr idine synthesized in 1934, quinacrine, was found to possess weak ant imalar ial act iv ity.
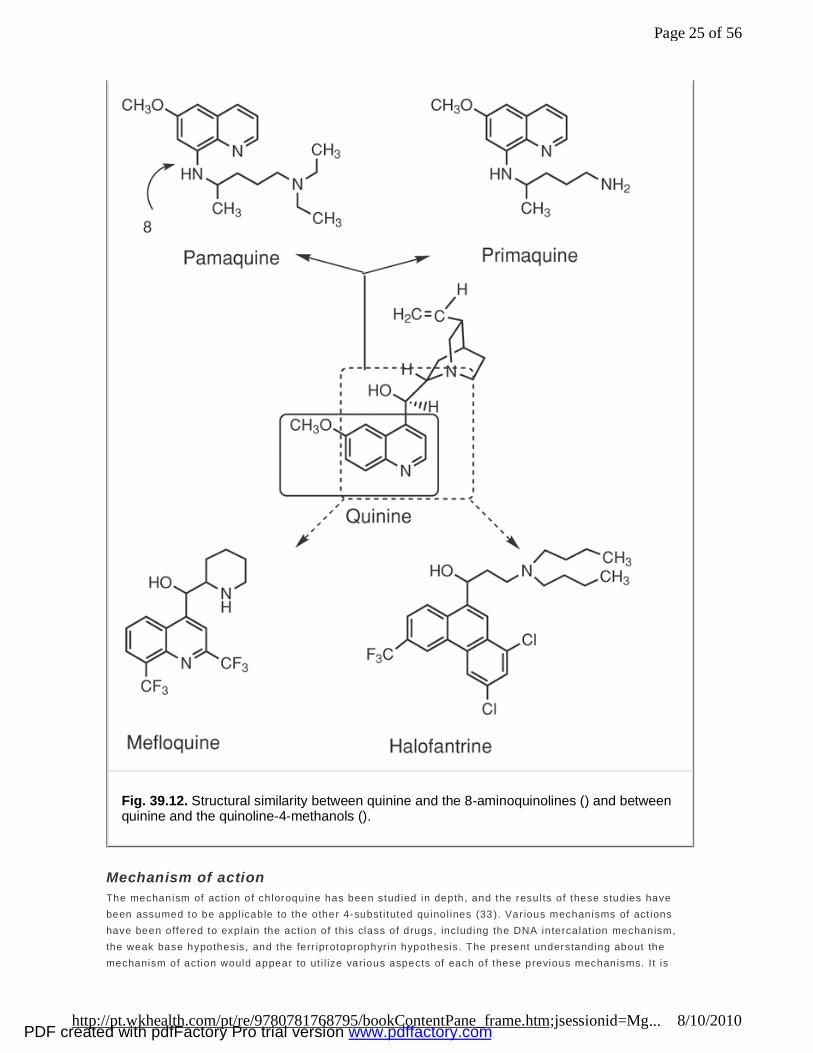
With the beginning of Wor ld War I I and concern about an interrupt ion in the supply of cinchona bark from the East Indies, a massive effort was begun to search for synthet ic alternatives to quinine and to develop more effect ive antimalaria l agents than quinacr ine. With a basic understanding of the structure–act ivi ty re lat ionship of quinine (see Quinine) and the chemical similari t ies seen with quinacrine, i t is easy to visual ize the relat ionship between these agents and the synthet ic ant imalar ials. The 4-aminoquinol ines, chloroquine and hydroxychloroquine, are structurally similar to the right half of quinacr ine (Fig. 39.11). The 8-aminoquinol ines, pamaquine and pr imaquine, retain the methoxyquinol ine nucleus of quinine and quinacrine (Fig. 39.12). The quinol ine-4-methanols, mef loquine and halofantrine, show similar ity to the 4-quinol inemethanol port ion of quinine (Fig. 39.12).
P.1096
Page 23 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
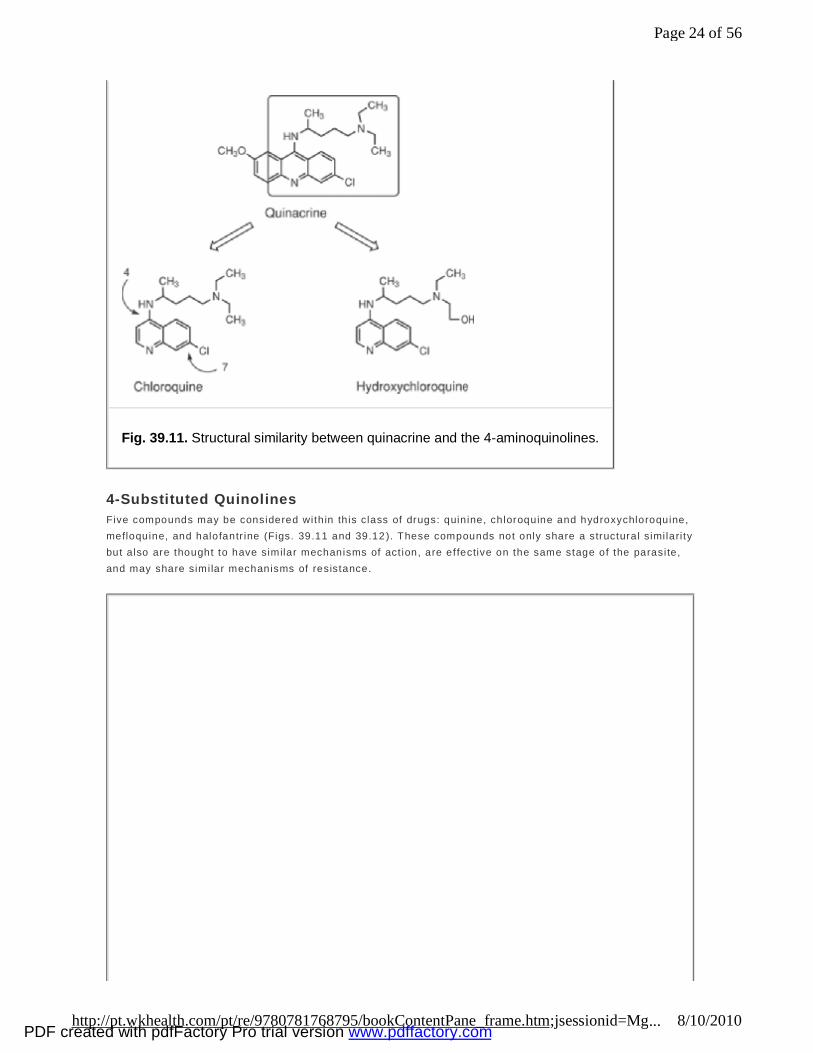
4-Substituted Quinolines Five compounds may be considered with in th is class of drugs: quinine, chloroquine and hydroxychloroquine, mefloquine, and halofantr ine (Figs. 39.11 and 39.12 ). These compounds not only share a structural similari ty but a lso are thought to have similar mechanisms of act ion, are effective on the same stage of the parasite, and may share similar mechanisms of resistance.
Fig. 39.11. Structural similarity between quinacrine and the 4-aminoquinolines.
Page 24 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Mechanism of action The mechanism of act ion of chloroquine has been studied in depth, and the results of these studies have been assumed to be appl icable to the other 4-subst i tuted quinol ines (33 ). Var ious mechanisms of act ions have been offered to explain the action of this class of drugs, including the DNA intercalat ion mechanism, the weak base hypothesis, and the ferr iprotoprophyr in hypothesis. The present understanding about the mechanism of action would appear to ut i l ize various aspects of each of these previous mechanisms. I t is
Fig. 39.12. Structural similarity between quinine and the 8-aminoquinolines () and between quinine and the quinoline-4-methanols ().
Page 25 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
known that hemoglobin is transported into the food vacuoles of the plasmodium, where digest ion of the hemoglobin supplies the organism with a source of amino acids. One of the products of th is digestion is f ree heme, a substance toxic to the plasmodium cel ls, which in the plasmodium vacuole is polymerized to hemozoin. I t has been demonstrated that the quinol ines bind to hemozoin through a drug–heme complex in which the aromatic quinol ine r ing π-bonds to the porphyrin nucleus (34). This drug–heme complex caps the growing hemozoin polymer, thus blocking further extension of the polymer. The result of th is complexation is that newly formed, free toxic heme is now present, which leads to the death of the plasmodium. The accumulat ion of the 4-subst i tuted quinol ines in the acidic food vacuoles (pH 4.8–5.2) is based on the fact that these drugs are weak bases, as indicated by their pKa values. The extracel lu lar flu id of the parasite is
at pH 7.4, and as a result , the weak base will move toward the more acidic pH of the vacuoles, reaching concentrat ions hundreds of t imes those in the plasma. Additional ly, the binding of the quinol ine to the heme draws addit ional quanti t ies into the vacuole.
Mechanism of resistance A l imit ing factor for most of the antimalaria l drugs is the development of resistant strains of p lasmodium. I t should be noted that resistance dif fers from region to region, and in some cases, a resistant strain may develop to a part icular drug without that drug ever having been introduced to the region (possible cross-resistance). The development of resistance is thought to be a spontaneous gene mutat ion. Several mechanisms of resistance appear to be operating. One of these mechanisms is based on the Plasmodium falciparium chloroquine-resistance transporter (pfrcrt) mechanism, which is suff icient and necessary to impart resistance (35). A gene encodes for a transmembrane transporter protein found in the membrane of the food vacuole. Multip le mutat ions with in a specif ic region th is gene result in reduced accumulation of chloroquine, resulting from the increased eff lux of the drug. Addit ional t ransporter proteins also may be involved in resistance. Rapid metabolism of the ant imalar ials by resistant strains of plasmodium also might be considered to play a signif icant role in the development of resistance. I t has been shown that cytochrome P450 act ivi ty paral le ls increased resistance to specif ic drugs.
Therapeutic application The 4-subst i tuted quinol ines are referred to as rapidly act ing blood schizonticides, with act iv i ty against plasmodium in the erythrocytic stage. Chloroquine is the drug of choice, but unfortunately, the incidence of chloroquine-resistance infections are extremely common today. The spread of chloroquine resistance has reached almost al l malarious areas of the world. In addition, mult idrug-resistant and cross-resistant strains of p lasmodium are now common. The drug of choice for the treatment of malar ia caused by Plasmodium falciparum, P lasmodium ovale, P lasmodium vivax, and Plasmodium malar iae in regions infected by chloroquine-resistant P. falciparum is quinine, in combination with tradit ional ant ibiotics, mef loquine, or various other combinat ions as alternat ive treatment agents (Table 39.2). Of interest is the observation that af ter years of nonuse of chloroquine, a reemergence of chloroquine-sensit ive parasites has been found.
The 4-subst i tuted quinol ines, depending on the specif ic drug in question, also may be used for prophylaxis of malar ia. Two types of prophylaxis are possible: causal prophylaxis, and suppressive prophylaxis. The former prevents the establ ishment of hepat ic forms of the parasite, whereas the lat ter eradicates the erythrocyt ic parasites but has no effect on the hepat ic forms. Several of the 4-subst i tuted quinol ines are effect ive suppressive prophylact ics.
P.1097
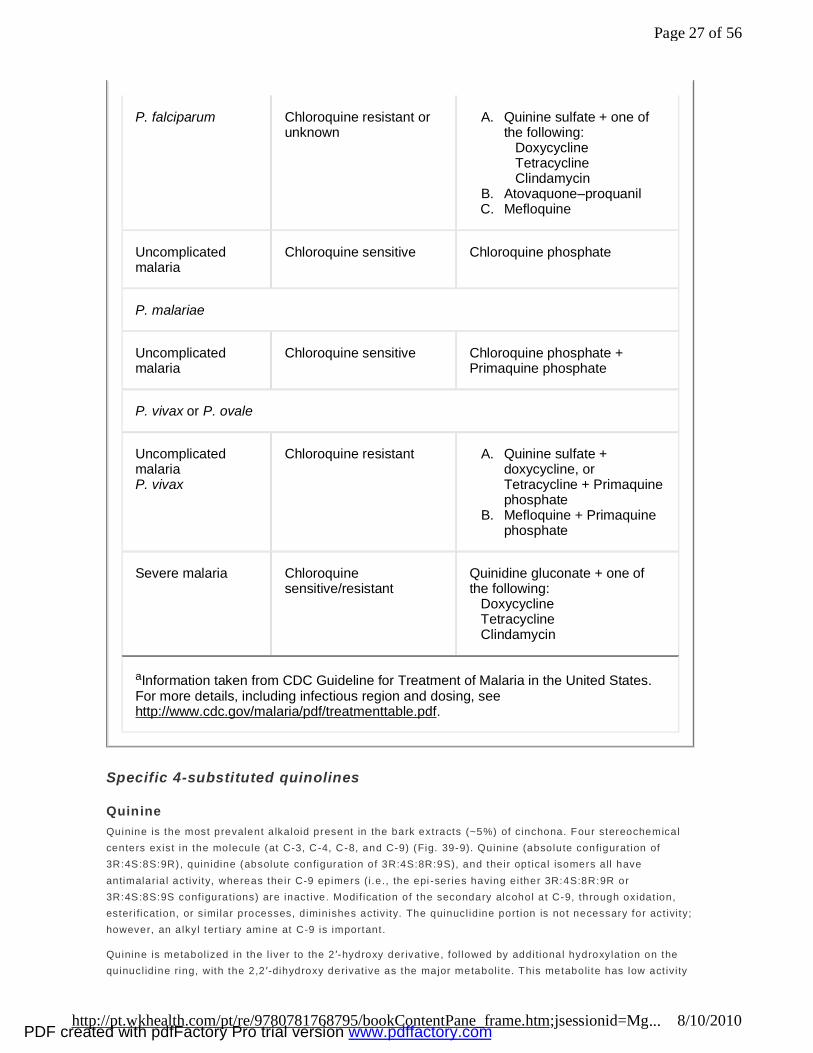
Table 39.2. Guidelines for Treatment of Malaria in the United Statesa
Clinical Diagnosis Sensitivity Drug Recommendation
Uncomplicated malaria
Chloroquine sensitive Chloroquine phosphate
Page 26 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Specific 4-substituted quinolines
Quinine Quinine is the most prevalent a lkaloid present in the bark extracts (~5%) of cinchona. Four stereochemical centers exist in the molecule (at C-3, C-4, C-8, and C-9) (Fig. 39-9). Quinine (absolute configurat ion of 3R:4S:8S:9R), quinidine (absolute configuration of 3R:4S:8R:9S), and their opt ical isomers all have antimalaria l activ i ty, whereas their C-9 epimers (i .e., the epi -series having either 3R:4S:8R:9R or 3R:4S:8S:9S conf igurat ions) are inact ive. Modif icat ion of the secondary alcohol at C-9, through oxidat ion, ester i ficat ion, or similar processes, diminishes activ i ty. The quinucl id ine port ion is not necessary for act ivi ty; however, an alkyl ter tiary amine at C-9 is important.
Quinine is metabol ized in the l iver to the 2 ′-hydroxy der ivat ive, fol lowed by additional hydroxylation on the quinucl id ine ring, with the 2,2 ′-dihydroxy derivat ive as the major metabol i te. This metaboli te has low act iv i ty
P. falciparum Chloroquine resistant or unknown
A. Quinine sulfate + one of the following: Doxycycline Tetracycline Clindamycin
B. Atovaquone–proquanil C. Mefloquine
Uncomplicated malaria
Chloroquine sensitive Chloroquine phosphate
P. malariae
Uncomplicated malaria
Chloroquine sensitive Chloroquine phosphate + Primaquine phosphate
P. vivax or P. ovale
Uncomplicated malaria P. vivax
Chloroquine resistant A. Quinine sulfate + doxycycline, or Tetracycline + Primaquine phosphate
B. Mefloquine + Primaquine phosphate
Severe malaria Chloroquine sensitive/resistant
Quinidine gluconate + one of the following: Doxycycline Tetracycline Clindamycin
aInformation taken from CDC Guideline for Treatment of Malaria in the United States. For more details, including infectious region and dosing, see http://www.cdc.gov/malaria/pdf/treatmenttable.pdf.
Page 27 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
and is rapidly excreted. The metabol iz ing enzyme of quinine is CYP3A4. With the increased use of quinine and i ts use in combination with other drugs, the potentia l for drug interact ions based on the many known substrates for CYP3A4 (see Chapter 10) is of concern (36 ).
A quinine overdose causes tinnitus and visual d isturbances; these side effects disappear on discont inuation of the drug. Quinine also can cause premature contract ions during the late stages of pregnancy. Although quinine is suitable for parenteral administration, th is route is considered to be hazardous because of i ts abi li ty to cause hemolysis. Quinidine, the (+)- isomer of quinine, has been shown to be more effective in combating the disease, but it has undesirable cardiac side effects.
Chloroquine (Aralen) Chloroquine is the most effect ive of the hundreds of 4-aminoquinol ines synthesized and tested during World War I I as potentia l ant imalaria ls. Structure–act ivi ty relationships demonstrated that the chloro at the 8-posit ion increased act ivi ty, whereas alkylat ion at C-3 and C-8 diminished act iv i ty. The replacement of one of its N-ethyl groups with an hydroxyethyl produced hydroxychloroquine, a compound with reduced toxici ty that is rarely used today except in cases of rheumatoid ar thr it is.
Chloroquine is commonly administered as the racemic mixture, because l i tt le is gained by using the individual isomers. The drug is well absorbed from the GI tract and distributed to many t issues, where it is tight ly bound and slowly el iminated. The drug is metabol ized by N-dealkylat ion by CYP2D6 and CYP3A4 isoforms. I t has been reported that the level of metabol ism correlates closely with the degree of resistance. The suggest ion has been made to coadminister chloroquine with CYP2D6 and CYP3A4 inhibitors to potentate act iv i ty and reduce resistance. Although this may be possible, i t is not commonly pract iced.
Chloroquine is an excel lent suppressive agent for treat ing acute attacks of malaria caused by Plasmodium vivax and Plasmodium ovale . The drug also is effect ive for cure and as a suppressive prophylact ic for the treatment of Plasmodium malar iae and suscept ible Plasmodium falciparum.
Chloroquine general ly is a safe drug, with toxicity occurring at h igh doses of medication i f the drug is administered too rapidly via parenteral routes. With oral administration, the side effects pr imari ly are GI ef fects, mild headache, visual d isturbances, and urt icaria.
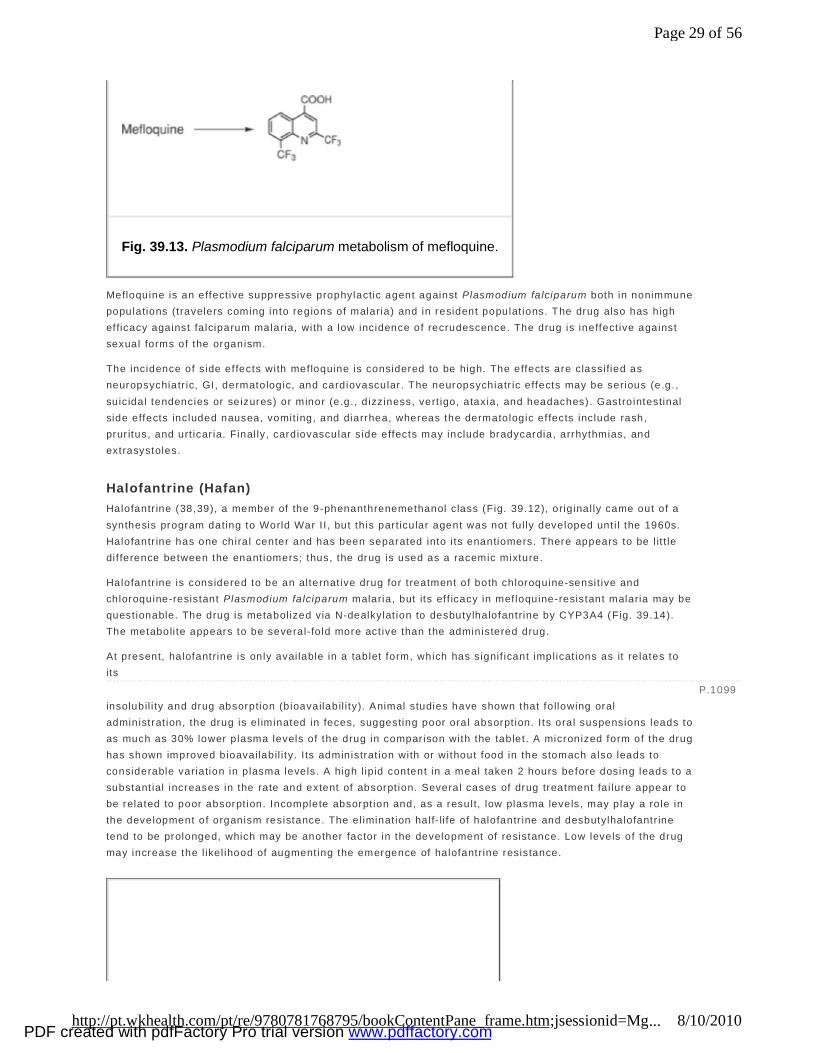
Mefloquine (Lariam) (37) Mefloquine, which was synthesized with the intent of blocking the site of metabol ism in quinine with the chemical ly stable CF3 group, exists as four opt ical isomers of nearly equal act iv i ty. The drug is act ive
against chloroquine-resistant strains of plasmodium, yet cross-resistance is not uncommon. Metabol ism is ci ted as the possible mechanism of resistance. Mefloquine is slowly metabol ized through CYP3A4 oxidat ion to i ts major inact ive metabol i te, carboxymefloquine (Fig. 39.13 ). Most of the parent drug is excreted unchanged into the urine. I ts coadministrat ion with CYP3A4 inhibitors (e.g., ketoconazole) has increased the area under the curve for mef loquine by inhibit ing i ts metabol ism to carboxymefloquine.
Mefloquine is only avai lable in an oral dosage form, which is well absorbed. The presence of food in the GI tract af fects the pharmacokinet ic properties of the drug, usual ly enhancing absorption. The l ipophi l ic nature of the drug accounts for the extensive t issue binding and low clearance of total drug, although the drug does not accumulate after prolonged administrat ion. The drug has a high aff ini ty for erythrocyte membranes.
Additional Therapeutic Indications for Chloroquine Chloroquine also is prescribed for treatment of rheumatoid arthrit is, discoid lupus erythematosus, and photosensi tivity diseases.
P.1098
Page 28 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Mefloquine is an effect ive suppressive prophylactic agent against Plasmodium falciparum both in nonimmune populations (travelers coming into regions of malaria) and in resident populat ions. The drug also has high efficacy against fa lciparum malaria, with a low incidence of recrudescence. The drug is ineffect ive against sexual forms of the organism.
The incidence of side effects with mefloquine is considered to be high. The effects are classified as neuropsychiatr ic, GI, dermatologic, and cardiovascular . The neuropsychiatr ic effects may be serious (e.g., suicidal tendencies or seizures) or minor (e.g., d izziness, vert igo, ataxia, and headaches). Gastrointestinal side effects included nausea, vomit ing, and diarrhea, whereas the dermatologic ef fects include rash, prur itus, and urt icar ia. Final ly, cardiovascular side effects may include bradycardia, arrhythmias, and extrasystoles.
Halofantrine (Hafan) Halofantr ine (38,39), a member of the 9-phenanthrenemethanol class (Fig. 39.12), orig inal ly came out of a synthesis program dating to World War I I , but th is par ticular agent was not fu l ly developed unt i l the 1960s. Halofantr ine has one chiral center and has been separated into i ts enantiomers. There appears to be l it t le dif ference between the enant iomers; thus, the drug is used as a racemic mixture.
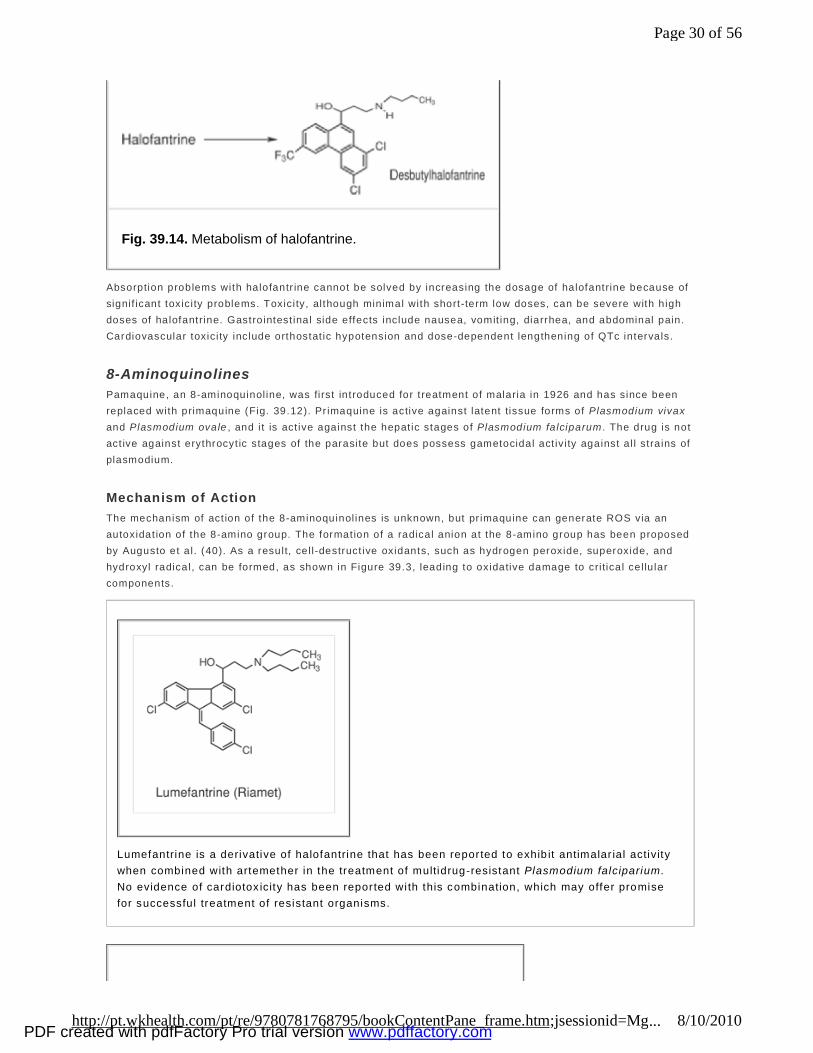
Halofantr ine is considered to be an alternat ive drug for t reatment of both chloroquine-sensit ive and chloroquine-resistant Plasmodium falciparum malaria, but its ef f icacy in mefloquine-resistant malaria may be quest ionable. The drug is metabol ized via N-dealkylat ion to desbutylhalofantrine by CYP3A4 (Fig. 39.14). The metaboli te appears to be several-fo ld more act ive than the administered drug.
At present, halofantrine is only avai lable in a tablet form, which has signif icant implicat ions as it re lates to its insolubil i ty and drug absorption (bioavailabil i ty). Animal studies have shown that fo llowing oral administrat ion, the drug is el iminated in feces, suggesting poor oral absorpt ion. I ts oral suspensions leads to as much as 30% lower plasma levels of the drug in compar ison with the tablet . A micronized form of the drug has shown improved bioavailabil i ty. I ts administrat ion with or without food in the stomach also leads to considerable variation in plasma levels. A high l ip id content in a meal taken 2 hours before dosing leads to a substant ial increases in the rate and extent of absorpt ion. Several cases of drug treatment fa i lure appear to be related to poor absorpt ion. Incomplete absorpt ion and, as a result, low plasma levels, may play a role in the development of organism resistance. The el iminat ion half- li fe of halofantr ine and desbutylhalofantr ine tend to be prolonged, which may be another factor in the development of resistance. Low levels of the drug may increase the l ikel ihood of augmenting the emergence of halofantrine resistance.
Fig. 39.13. Plasmodium falciparum metabolism of mefloquine.
P.1099
Page 29 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Absorption problems with halofantr ine cannot be solved by increasing the dosage of halofantrine because of signif icant toxici ty problems. Toxicity, although minimal with short-term low doses, can be severe with high doses of halofantrine. Gastrointest inal side effects include nausea, vomit ing, diarrhea, and abdominal pain. Cardiovascular toxici ty include orthostat ic hypotension and dose-dependent lengthening of QTc intervals.
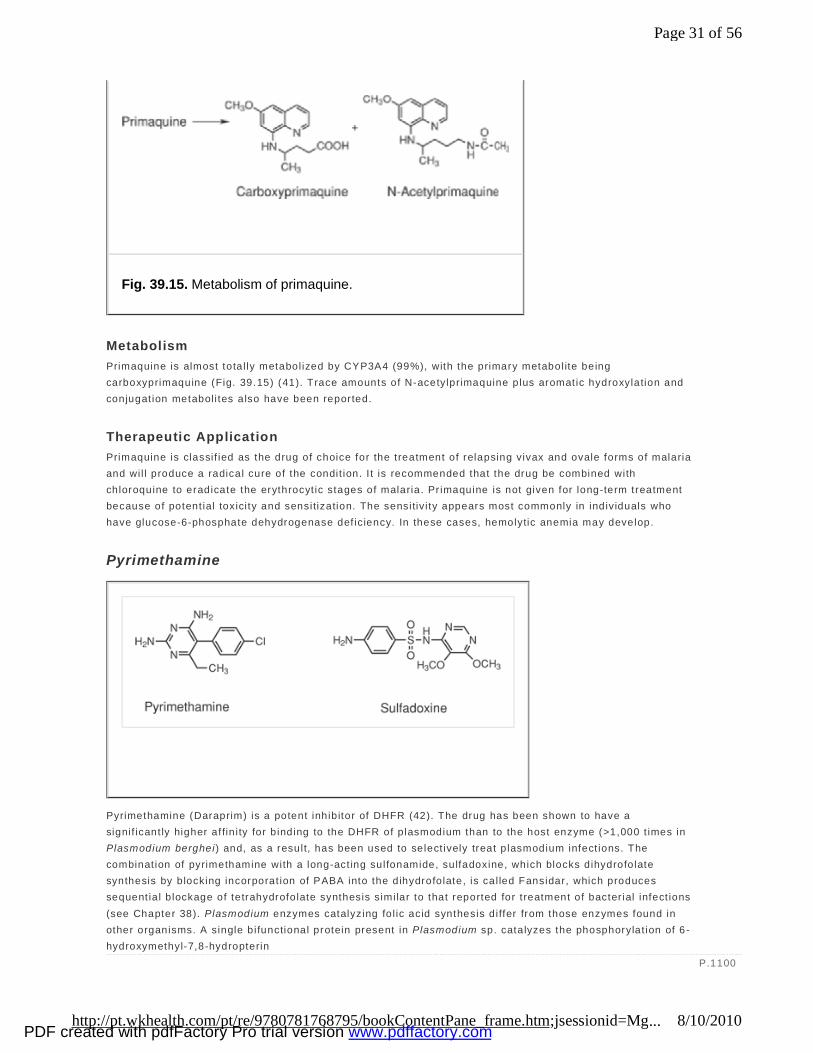
8-Aminoquinolines Pamaquine, an 8-aminoquinol ine, was first introduced for t reatment of malaria in 1926 and has since been replaced with primaquine (Fig. 39.12). Pr imaquine is active against latent tissue forms of Plasmodium vivax and Plasmodium ovale , and i t is act ive against the hepat ic stages of Plasmodium falciparum . The drug is not act ive against erythrocyt ic stages of the parasite but does possess gametocidal act iv i ty against a l l stra ins of plasmodium.
Mechanism of Action The mechanism of act ion of the 8-aminoquinol ines is unknown, but pr imaquine can generate ROS via an autoxidat ion of the 8-amino group. The formation of a radical anion at the 8-amino group has been proposed by Augusto et a l. (40). As a result, cel l-destruct ive oxidants, such as hydrogen peroxide, superoxide, and hydroxyl radical, can be formed, as shown in Figure 39.3, leading to oxidative damage to cri tical cel lu lar components.
Lumefantrine is a derivative of halofantrine that has been repor ted to exhib it antimalar ial activity when combined with artemether in the treatment of multidrug-resistant Plasmodium falciparium. No evidence of cardiotox icity has been repor ted wi th this combination, which may offer promise for successful treatment of resistant organisms.
Fig. 39.14. Metabolism of halofantrine.
Page 30 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
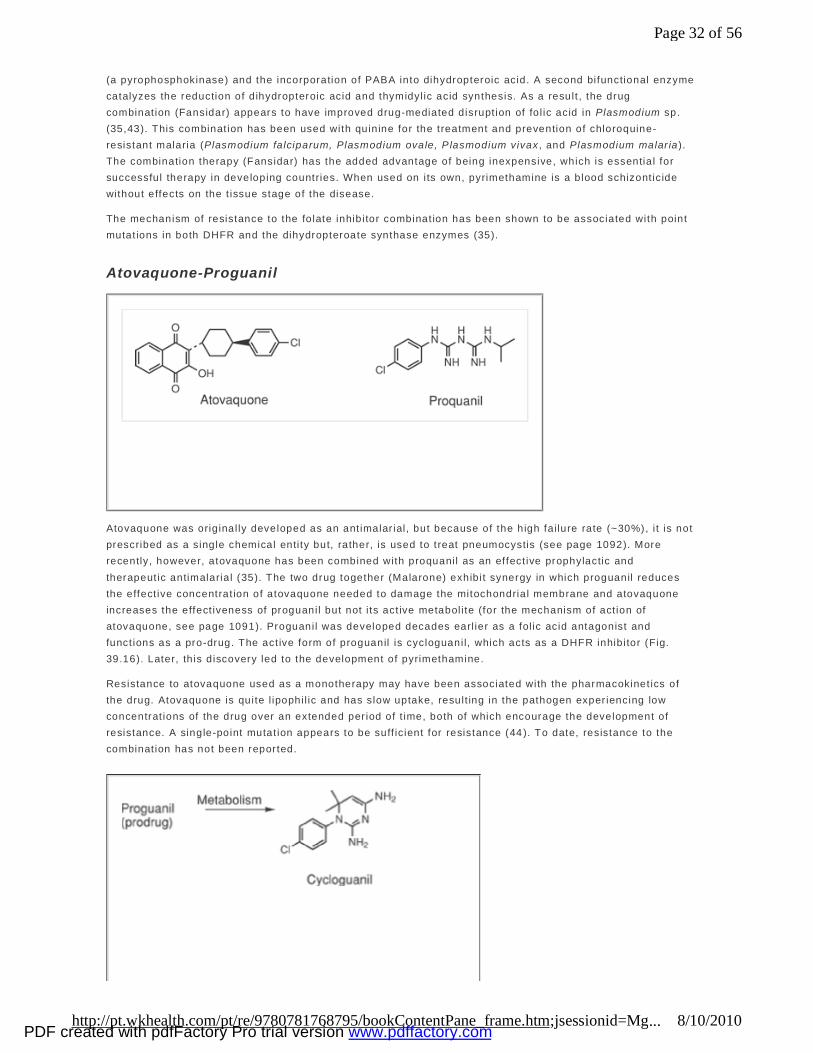
Metabolism Primaquine is almost total ly metabol ized by CYP3A4 (99%), with the primary metabol ite being carboxyprimaquine (Fig. 39.15) (41). Trace amounts of N-acetylprimaquine plus aromatic hydroxylation and conjugat ion metabol i tes also have been reported.
Therapeutic Application Primaquine is classif ied as the drug of choice for the treatment of relapsing vivax and ovale forms of malaria and wil l produce a radical cure of the condit ion. I t is recommended that the drug be combined with chloroquine to eradicate the erythrocyt ic stages of malaria. Pr imaquine is not given for long-term treatment because of potent ial toxici ty and sensitization. The sensitiv i ty appears most commonly in individuals who have glucose-6-phosphate dehydrogenase def iciency. In these cases, hemolytic anemia may develop.
Pyrimethamine
Pyrimethamine (Daraprim) is a potent inhibitor of DHFR (42). The drug has been shown to have a signif icant ly higher af fin i ty for b inding to the DHFR of plasmodium than to the host enzyme (>1,000 t imes in Plasmodium berghei) and, as a result, has been used to select ively treat p lasmodium infect ions. The combinat ion of pyrimethamine with a long-act ing sulfonamide, sulfadoxine, which blocks dihydrofolate synthesis by blocking incorporat ion of PABA into the dihydrofolate, is cal led Fansidar, which produces sequent ia l b lockage of tetrahydrofolate synthesis similar to that reported for t reatment of bacter ial infect ions (see Chapter 38). Plasmodium enzymes catalyzing fo l ic acid synthesis differ from those enzymes found in other organisms. A single bifunctional protein present in Plasmodium sp. catalyzes the phosphorylat ion of 6 -hydroxymethyl-7,8-hydropterin
Fig. 39.15. Metabolism of primaquine.
P.1100
Page 31 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
(a pyrophosphokinase) and the incorporation of PABA into dihydropteroic acid. A second bifunctional enzyme catalyzes the reduction of d ihydropteroic acid and thymidyl ic acid synthesis. As a result , the drug combinat ion (Fansidar) appears to have improved drug-mediated disrupt ion of fo l ic acid in Plasmodium sp. (35,43). This combinat ion has been used with quinine for the treatment and prevention of chloroquine-resistant malaria (Plasmodium falciparum, Plasmodium ovale, P lasmodium vivax , and Plasmodium malar ia ). The combination therapy (Fansidar) has the added advantage of being inexpensive, which is essentia l for successful therapy in developing countries. When used on i ts own, pyrimethamine is a blood schizont icide without effects on the t issue stage of the disease.
The mechanism of resistance to the fo late inhibitor combinat ion has been shown to be associated with point mutat ions in both DHFR and the dihydropteroate synthase enzymes (35).
Atovaquone-Proguanil
Atovaquone was orig inal ly developed as an ant imalar ial, but because of the high fa ilure rate (~30%), i t is not prescribed as a single chemical enti ty but, rather, is used to treat pneumocystis (see page 1092). More recently, however, atovaquone has been combined with proquanil as an effect ive prophylactic and therapeut ic antimalaria l (35). The two drug together (Malarone) exhibit synergy in which proguanil reduces the effect ive concentrat ion of atovaquone needed to damage the mitochondria l membrane and atovaquone increases the effect iveness of proguanil but not i ts act ive metabol i te (for the mechanism of act ion of atovaquone, see page 1091). Proguanil was developed decades earl ier as a fol ic acid antagonist and funct ions as a pro-drug. The act ive form of proguanil is cycloguanil, which acts as a DHFR inhibitor (Fig. 39.16). Later, th is discovery led to the development of pyrimethamine.
Resistance to atovaquone used as a monotherapy may have been associated with the pharmacokinet ics of the drug. Atovaquone is quite l ipophi l ic and has slow uptake, result ing in the pathogen exper iencing low concentrat ions of the drug over an extended per iod of t ime, both of which encourage the development of resistance. A single-point mutat ion appears to be suff ic ient for resistance (44 ). To date, resistance to the combinat ion has not been reported.
Page 32 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
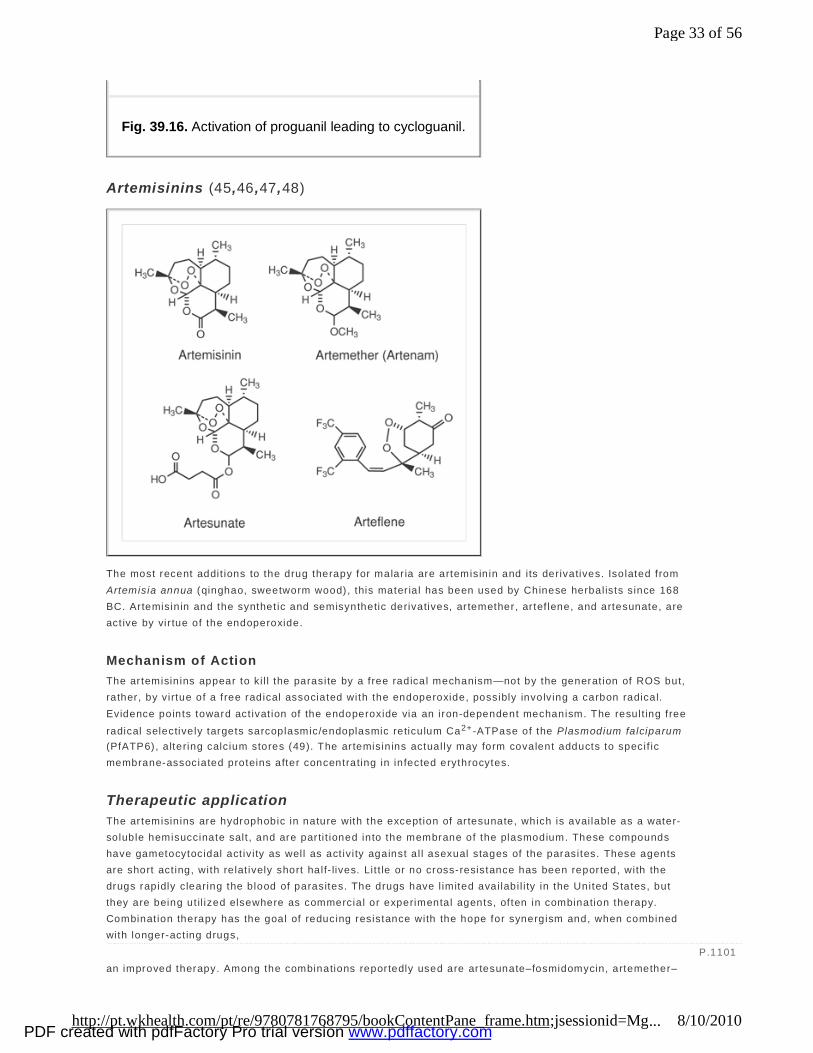
Artemisinins (45,46 ,47,48)
The most recent addit ions to the drug therapy for malar ia are artemisinin and i ts derivatives. Isolated from Artemisia annua (qinghao, sweetworm wood), this mater ia l has been used by Chinese herbal ists since 168 BC. Artemisinin and the synthet ic and semisynthetic derivatives, ar temether, ar tef lene, and artesunate, are act ive by vir tue of the endoperoxide.
Mechanism of Action The ar temisinins appear to ki l l the parasite by a free radical mechanism—not by the generat ion of ROS but, rather, by virtue of a free radical associated with the endoperoxide, possibly involving a carbon radical. Evidence points toward act ivat ion of the endoperoxide via an iron-dependent mechanism. The result ing free
radical selectively targets sarcoplasmic/endoplasmic reticulum Ca2+ -ATPase of the Plasmodium falciparum (PfATP6), a ltering calcium stores (49). The ar temisinins actual ly may form covalent adducts to specif ic membrane-associated proteins after concentrating in infected erythrocytes.
Therapeutic application The ar temisinins are hydrophobic in nature with the except ion of ar tesunate, which is avai lable as a water-soluble hemisuccinate salt , and are parti t ioned into the membrane of the plasmodium. These compounds have gametocytocidal act iv i ty as well as act iv i ty against a l l asexual stages of the parasites. These agents are short act ing, with relat ively short half- lives. Lit t le or no cross-resistance has been reported, with the drugs rapidly clearing the blood of parasites. The drugs have l imited avai labi l i ty in the United States, but they are being ut il ized elsewhere as commercial or experimental agents, of ten in combination therapy. Combinat ion therapy has the goal of reducing resistance with the hope for synergism and, when combined with longer-act ing drugs, an improved therapy. Among the combinations reportedly used are ar tesunate–fosmidomycin, artemether–
Fig. 39.16. Activation of proguanil leading to cycloguanil.
P.1101
Page 33 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

lumefantrine (Coartem), amodiaquine–artesunate, chloroquine–artemisinin, and artesunate–sulfadoxine–pyrimethamine (50). These combinations are referred to as ar temisinin -based combinat ion therapy (ACT). These ACTs have been reported to show cure rates of greater than 90%. The fixed-dose combination Coartem has been used in more than 10 mil l ion treatments, with signif icant increases being forecast.
Helminth Infections Helminthiasis, or worm infestat ion, is one of the most prevalent diseases—and one of the most serious publ ic health problems— in the world. Many worms are parasitic in humans and cause serious complicat ions. Hundreds of mil l ions ( if not b i l l ions) of human infections by helminths exist wor ldwide, and with increased wor ld travel and immigrat ion from developing countries, one might expect to see this pattern of infection continue. I t is est imated that one-fourth of the world populat ion may be infected. I t is interest ing to note that helminths dif fer f rom many other parasites in that these organisms multip ly outside of the def init ive host and have the unique abi l i ty to evade host immune defenses for reasons that are not fu l ly understood. As a result , helminth infect ions tend to be chronic, possibly lasting for the ent ire l i fet ime of the host (for a discussion of the uniqueness of helminth infect ions, see Maizels et al. in Suggested Readings). Helminths that infect human hosts are divided into two categories, or phyla: P latyhelminths ( f latworms), and Aschelminths or nematodes (roundworms). The flatworms include the classes Cestode (tapeworms) and Trematode ( f lukes or schistosomes). The nematode class includes helminths common to the United States: roundworm, hookworm, pinworm, and whipworm. These worms are cyl indrical in shape, with signif icant variations in size, proport ion, and structure.
Nematode Infections
Ancylostomiasis or Hookworm Infection The two most widespread types of hookworm in humans are the American hookworm (Necator americanus) and the “Old Wor ld ” hookworm (Ancylostoma doudenale ). The li fe cycles of both are similar. The larvae are found in the soi l and are transmit ted either by penetrat ing the skin or being ingested orally. The circulatory system transports the larvae via the respiratory tree to the digestive tract, where they mature and l ive for 9 to 15 years i f lef t untreated. These worms feed on intest inal tissue and blood. Infestat ions cause pulmonary lesions, skin react ions, intestinal u lcerat ion, and anemia. The worms are most prevalent in regions of the wor ld with temperatures of 23 to 33°C, abundant rainfal l , and well-drained, sandy soi l .
Enterobiasis or Pinworm Infection (Enterobius Vermicularis) These worms are widespread in temperate zones and are a common infestat ion of households and insti tutions. The pinworm l ives in the lumen of the GI tract, at taching i tself by the mouth to the mucosa of the cecum. Mature worms reach 10 mm in size. The female migrates to the rectum, usually at night, to deposit her eggs. This event is noted by the symptom of perianal pruri tus. The eggs infect f ingers and contaminate nightclothes and bed l inen, where they remain infect ive for up to three weeks. Eggs resist drying and can be inhaled with household dust to cont inue the li fe cycle. Detect ion of the worm in the per ianal region can be accomplished by means of a cel lophane tape swabbed in the per ianal region in the evening. The worms may be visible with the naked eye. The eggs can be col lected in a similar manner but can only be seen under a microscope.
Ascariasis or Roundworm Infections (Ascaris lumbricoides) These roundworms are common in developing countr ies, with the adult roundworm reaching 25 to 30 cm in length and lodging in the small intest ine. Some infect ions are without symptoms, but abdominal discomfort and pain are common with heavy infestat ion. Roundworm eggs are released into the soi l , where they incubate and remain viable for up to 6 years. When the egg is ingested, the larvae are released in the small intest ine, penetrate the intest inal wal ls, and are carried via the blood to the lungs. The pulmonary phase of the disease lasts approximately 10 days, with the larvae passing through the bronchioles, bronchi, and trachea before being swallowed and returning to the small intestine. Some patients have reported adult worms exit ing the esophagus through the oral cavity, and it is not unusual for live ascar is to be expelled with a bowel movement. Poor or lacking sanitary faci l i ties expose the populat ion to infestation through
Page 34 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

contaminated foods and beverages.
Trichuriasis or Whipworm Infections (Trichuris trichiura) Infect ions by this parasite are caused by swallowing eggs from contaminated foods and beverages. The eggs are passed with the feces from an infected individual. These eggs may live in the soil for many years. The ingested eggs hatch in the small intestine, and the larvae embed in the intest inal wal l . The worms then migrate to the large intest ine, where they mature. Adult worms, which reach approximately 5 cm in length, thread their bodies into the epithel ium of the colon. They feed on tissue flu ids and blood. Infect ions from this worm cause symptoms of irr i tat ion and inf lammation of the colonic mucosa, abdominal pain, d iarrhea, and distention. Infect ions can last 5 or more years if not t reated. Whipworm infect ions are commonly seen in individuals returning from visi ts to the subtropics and are more common in rural areas of the southeastern United States.
Trichinosis or Trichina Infection (Trichinella spiralis) Trichinel la spiral is produces an infection that may be both intest inal and systemic. The worm is found in muscle meat, where the organism exists as an encysted larvae. Tradit ional ly, the worm has been associated with domestic pork that feeds on untreated garbage. More recently, outbreaks have occurred in individuals eat ing infected game, such as wild boar, bear, or walrus. Trichinosis infections are more l ikely to occur af ter consumption of homemade pork or wi ld-game sausages. After ingest ion, the larvae are released from the cyst form and then migrate into the intestinal mucosa. After maturat ion and reproduction, the newly released larvae penetrate the mucosal l in ing and are distr ibuted throughout the body, where they enter skeletal muscle. During the adult intest inal stage, diarrhea, abdominal pain, and nausea are the most common symptom, whereas the muscular form of the disease has symptoms that may include muscle pain and tenderness, edema, conjunctivi t is, and weakness.
Filariasis The term “fi lar iasis ” denotes infect ions with any of the Fi lar ioidea, although i t is commonly used to refer to lymphatic-dwelling f i lar iae, such as Wucherer ia bancroft i , Brugia malayi , and Brugia timor i. Other f ilaria l infect ions include Loa loa and Onchocerca volvulus. The lat ter two are known as the eyeworm and the river bl indness worm, respectively. E lephantiasis is the most common disease associated with fi lariasis. These parasites vary in length from 6 cm for brugia to 50 cm for onchocerca. The incubat ion periods also vary from 2 months for brugia to 12 months for bancroft ian fi laria. I t is estimated that 400 mil l ion persons are infected with human f i laria l parasites. Depending on the specif ic organism, various intermediate hosts are involved in spreading the infect ion. Mosquitoes are involved with the spread of Wucherer ia bancroft i , Brugia malayi , and Brugia timor i , whereas the female blackf ly spreads r iver bl indness. The larvae released by the female f i lar ia are referred to as microf i lar iae and commonly may be found in the lymphat ics.
Cestode and Trematode Infections
Cysticercosis or Tapeworm Infection Helminths of th is class that are of concern as potent ia l parasites in humans include:
n Beef tapeworm (Taenia saginata ). This worm is found worldwide and infects people who eat undercooked beef. The worm reaches a length of more than 5 m, and it contains approximately 100 segments/m. Each of these segments contains its own reproduct ive organs.
n Pork tapeworm (Taenia solium ). Pork tapeworms sometimes are cal led bladder worms and occasional ly are found in uncooked pork. The worm attaches i tself to the intest inal wal l of the human host. The adult worm reaches 5 m in length and, i f untreated, survives in the host for many years.
n Dwarf tapeworm (Hymenolepis nana ). This infect ion is t ransmit ted direct ly f rom one human to
P.1102
Page 35 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
another without an intermediate host. Hymenolepis nana reaches only 3 to 4 cm in length. I t is found in temperate zones, and children are most f requent ly infected.
n Fish tapeworm (Diphyllobothrium latum ). The fish tapeworm reaches a length of 10 m and contains approximately 400 segments/m. These tapeworms attach themselves to the intest inal wal l and rob the host of nutrients. They especial ly absorb vitamin B12 and fol ic acid. Deplet ion of these cr i tical nutr ients, especial ly vi tamin B12 , can lead to pernicious anemia. Tapeworm eggs are passed in the
patient's feces, and contaminat ion of food and drink may result in t ransmission of the infection.
Schistosomiasis or Blood Flukes Three pr imary trematode species cause schistosomiasis in humans: Schistosoma hematobium, Schistosoma mansoni , and Schistosoma japonicum. Infections result f rom the penetrat ion of normal skin by l iv ing ( free-swimming) cercaria ( the name given to the infectious stage of the parasite) with the aid of secreted enzymes. The cercar ia develop to preadult forms in the lungs and skin. Then, these parasites travel in pairs via the bloodstream and invade various tissues. The adult worm reaches approximately 2 cm in length. The female deposits her eggs near the capi llary beds, where granulomas form. Some of the eggs wil l move into the lumen of the intest ines, b ladder, or ureters and are released into the environmental surrounding, where the parasite wi l l seek out the intermediate snai l vector . Asexual reproduct ion occurs in the snai l . After a period of t ime, the cercaria are again released from the snai l to continue the cycle. The pat ients might exper ience headache, fatigue, fever, and GI disturbances during the early stages of the disease. Hepatic fibrosis and ascites occur dur ing later stages. Untreated patients can harbor as many as 100 pairs of worms. Untreated worms can l ive 5 to 10 years with in the host. It is est imated that as many as 200 mil l ion persons wor ldwide are infected with schistosomes. Depending on the species of schistosome, the disease is found in parts of South America, the Car ibbean Islands, Africa, and the Middle East.
Drug Therapy for Helminth Infections (51) Helminths represent a biological ly d iverse group of parasit ic organisms dif fering in size, l ife cycle, si te of infect ion (local and systemic), and susceptib i li ty to chemotherapy. With such var iat ion in infect ious organisms, i t is not surpr ising that the drugs used to control helminth infect ions also represent a varied group of chemical classes. As indicated in Table 39.3, the drugs may have fair ly narrow spectra of act ivi ty (pyrantel pamoate) or a broad spectra of activ i ty (benzimidazoles) .
Benzimidazoles The benzimidazoles (Table 39.4) are a broad-spectrum group of drugs discovered in the 1960s with act ivi ty against GI helminths. Several thousand benzimidazoles have been synthesized and screened for anthelmintic act iv i ty, with albendazole, mebendazole, and thiabendazole represent ing the benzimidazole marketed today. The development and chemistry of this class of agents has been reviewed by Townsend and Wise (52).
P.1103
Page 36 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
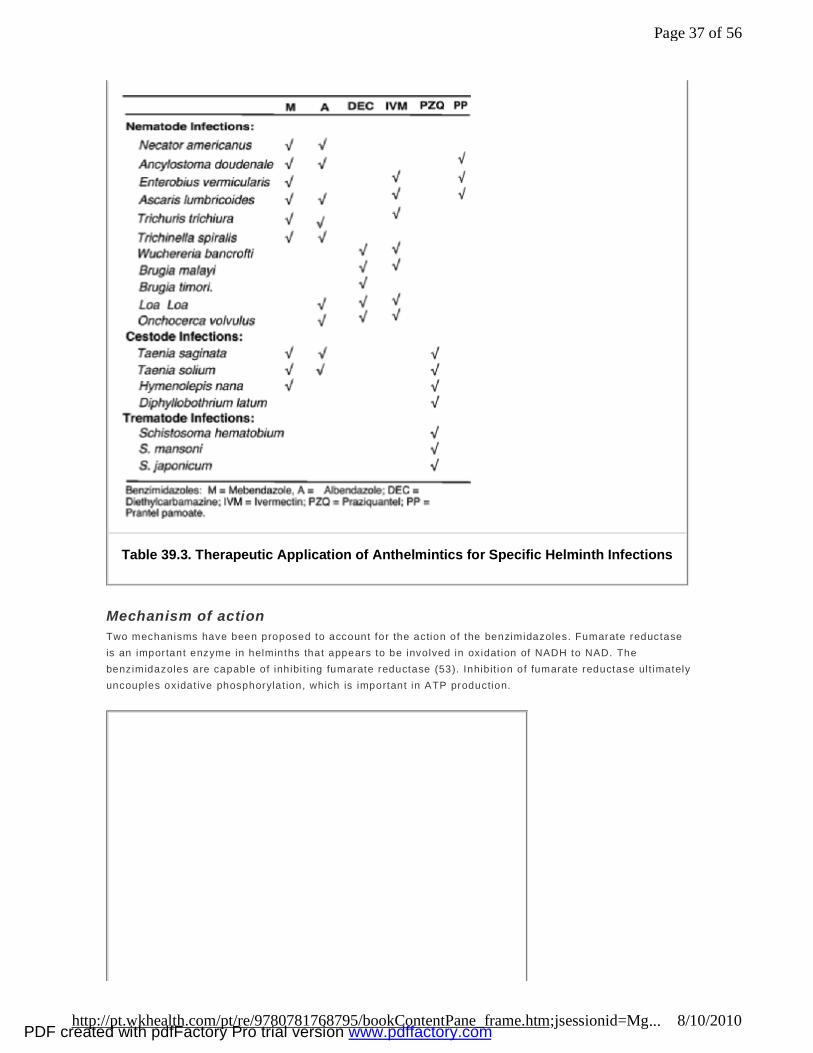
Mechanism of action Two mechanisms have been proposed to account for the action of the benzimidazoles. Fumarate reductase is an important enzyme in helminths that appears to be involved in oxidat ion of NADH to NAD. The benzimidazoles are capable of inhibit ing fumarate reductase (53). Inhibit ion of fumarate reductase ult imately uncouples oxidat ive phosphorylat ion, which is important in ATP production.
Table 39.3. Therapeutic Application of Anthelmintics for Specific Helminth Infections
Page 37 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
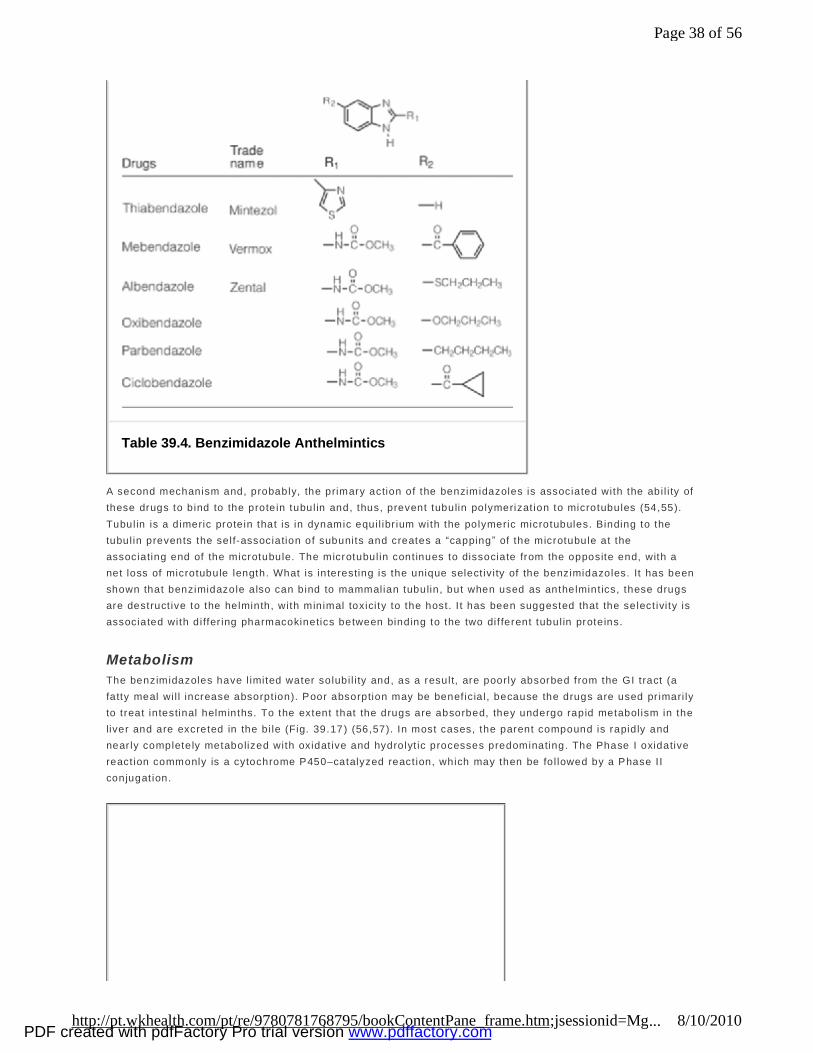
A second mechanism and, probably, the primary action of the benzimidazoles is associated with the abi l i ty of these drugs to bind to the protein tubul in and, thus, prevent tubulin polymerizat ion to microtubules (54,55). Tubulin is a dimeric protein that is in dynamic equi l ibr ium with the polymeric microtubules. Binding to the tubul in prevents the self-association of subunits and creates a “capping ” of the microtubule at the associating end of the microtubule. The microtubul in cont inues to dissociate from the opposite end, with a net loss of microtubule length. What is interesting is the unique select iv i ty of the benzimidazoles. It has been shown that benzimidazole also can bind to mammalian tubulin, but when used as anthelmint ics, these drugs are destruct ive to the helminth, with minimal toxici ty to the host. I t has been suggested that the select ivi ty is associated with differ ing pharmacokinetics between binding to the two dif ferent tubul in proteins.
Metabolism The benzimidazoles have l imited water solubi l i ty and, as a result, are poorly absorbed from the GI tract (a fatty meal wi l l increase absorpt ion). Poor absorption may be benef icia l, because the drugs are used pr imari ly to treat intestinal helminths. To the extent that the drugs are absorbed, they undergo rapid metabol ism in the liver and are excreted in the bi le (Fig. 39.17 ) (56,57). In most cases, the parent compound is rapidly and near ly completely metabolized with oxidat ive and hydrolyt ic processes predominating. The Phase I oxidative react ion commonly is a cytochrome P450–catalyzed react ion, which may then be fol lowed by a Phase I I conjugat ion.
Table 39.4. Benzimidazole Anthelmintics
Page 38 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
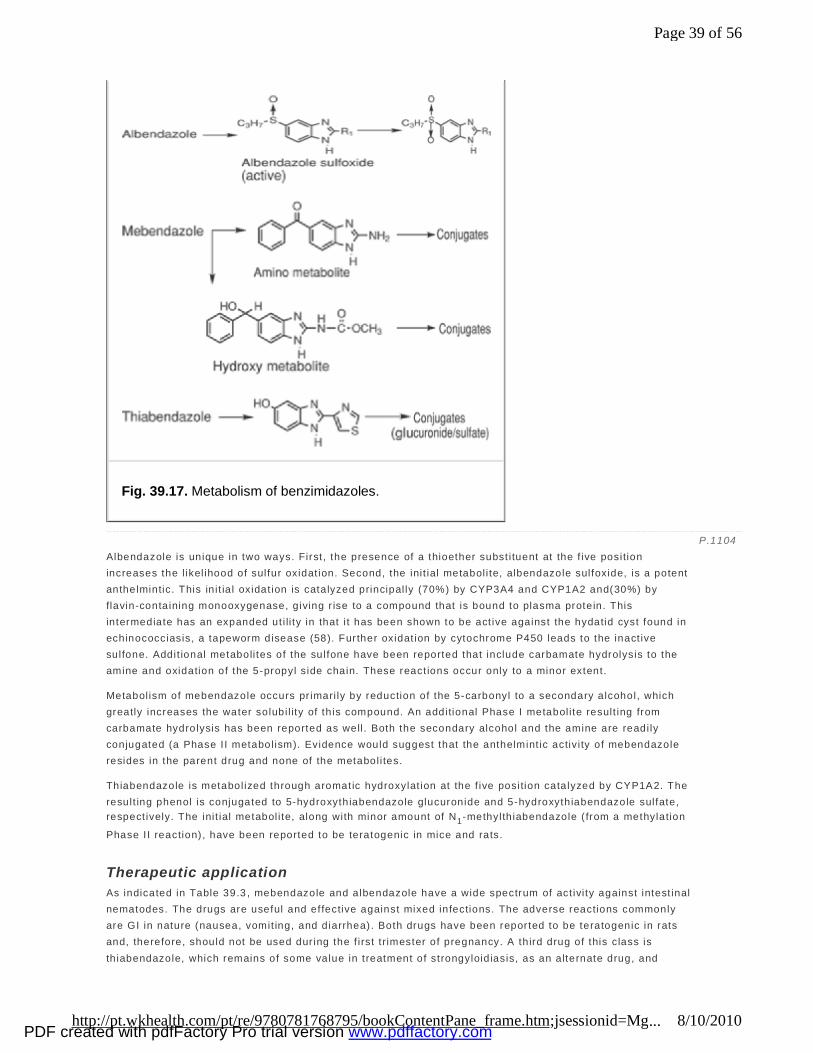
Albendazole is unique in two ways. First , the presence of a thioether subst i tuent at the f ive position increases the l ikel ihood of sulfur oxidat ion. Second, the init ial metabol i te, albendazole sulfoxide, is a potent anthelmintic. This in i t ia l oxidat ion is catalyzed principal ly (70%) by CYP3A4 and CYP1A2 and(30%) by flavin-containing monooxygenase, giving r ise to a compound that is bound to plasma protein. This intermediate has an expanded ut i li ty in that i t has been shown to be act ive against the hydatid cyst found in echinococciasis, a tapeworm disease (58). Further oxidat ion by cytochrome P450 leads to the inact ive sulfone. Addit ional metaboli tes of the sulfone have been reported that include carbamate hydrolysis to the amine and oxidation of the 5-propyl side chain. These react ions occur only to a minor extent.
Metabol ism of mebendazole occurs pr imari ly by reduction of the 5-carbonyl to a secondary alcohol, which greatly increases the water solubi l ity of th is compound. An additional Phase I metabol i te result ing from carbamate hydrolysis has been reported as well . Both the secondary alcohol and the amine are readi ly conjugated (a Phase I I metabol ism). Evidence would suggest that the anthelmint ic activ i ty of mebendazole resides in the parent drug and none of the metabol i tes.
Thiabendazole is metabol ized through aromatic hydroxylat ion at the f ive position catalyzed by CYP1A2. The result ing phenol is conjugated to 5-hydroxythiabendazole glucuronide and 5-hydroxythiabendazole sulfate, respect ively. The init ial metabol i te, along with minor amount of N1-methylth iabendazole ( from a methylation
Phase I I reaction) , have been reported to be teratogenic in mice and rats.
Therapeutic application As indicated in Table 39.3 , mebendazole and albendazole have a wide spectrum of act ivi ty against intest inal nematodes. The drugs are useful and effective against mixed infections. The adverse reactions commonly are GI in nature (nausea, vomit ing, and diarrhea). Both drugs have been reported to be teratogenic in rats and, therefore, should not be used dur ing the f irst t rimester of pregnancy. A th ird drug of this class is th iabendazole, which remains of some value in treatment of strongyloidiasis, as an alternate drug, and
Fig. 39.17. Metabolism of benzimidazoles.
P.1104
Page 39 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
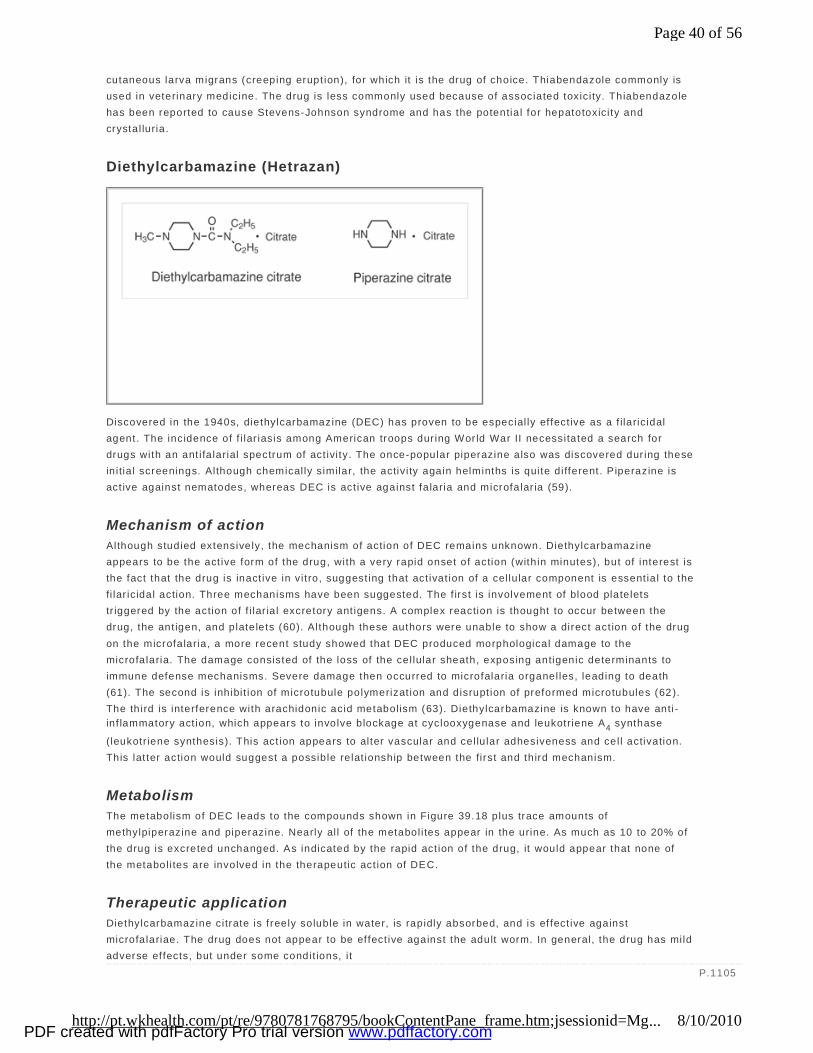
cutaneous larva migrans (creeping erupt ion), for which it is the drug of choice. Thiabendazole commonly is used in veterinary medicine. The drug is less commonly used because of associated toxici ty. Thiabendazole has been reported to cause Stevens-Johnson syndrome and has the potentia l for hepatotoxici ty and crystal luria.
Diethylcarbamazine (Hetrazan)
Discovered in the 1940s, diethylcarbamazine (DEC) has proven to be especial ly ef fect ive as a f ilaric idal agent. The incidence of f i lar iasis among American troops dur ing Wor ld War II necessitated a search for drugs with an ant i fa larial spectrum of act ivi ty. The once-popular piperazine also was discovered dur ing these in itia l screenings. Although chemical ly similar, the activ i ty again helminths is quite different. P iperazine is act ive against nematodes, whereas DEC is act ive against fa laria and microfalar ia (59).
Mechanism of action Although studied extensively, the mechanism of action of DEC remains unknown. Diethylcarbamazine appears to be the act ive form of the drug, with a very rapid onset of action (with in minutes), but of interest is the fact that the drug is inact ive in vi t ro, suggest ing that act ivat ion of a cel lu lar component is essent ia l to the fi lar ic idal action. Three mechanisms have been suggested. The f irst is involvement of blood platelets tr iggered by the action of f i lar ia l excretory ant igens. A complex reaction is thought to occur between the drug, the ant igen, and platelets (60). Although these authors were unable to show a direct act ion of the drug on the microfalaria, a more recent study showed that DEC produced morphological damage to the microfalaria. The damage consisted of the loss of the cel lular sheath, exposing antigenic determinants to immune defense mechanisms. Severe damage then occurred to microfalaria organelles, leading to death (61). The second is inhibit ion of microtubule polymerizat ion and disrupt ion of preformed microtubules (62 ). The third is interference with arachidonic acid metabolism (63). Diethylcarbamazine is known to have anti -inf lammatory act ion, which appears to involve blockage at cyclooxygenase and leukotriene A4 synthase
(leukotr iene synthesis). This act ion appears to alter vascular and cel lu lar adhesiveness and cel l activation. This lat ter action would suggest a possible relat ionship between the first and third mechanism.
Metabolism The metabolism of DEC leads to the compounds shown in Figure 39.18 plus trace amounts of methylpiperazine and piperazine. Nearly al l of the metabol i tes appear in the urine. As much as 10 to 20% of the drug is excreted unchanged. As indicated by the rapid act ion of the drug, it would appear that none of the metabol i tes are involved in the therapeutic act ion of DEC.
Therapeutic application Diethylcarbamazine citrate is f reely soluble in water, is rapidly absorbed, and is ef fect ive against microfalariae. The drug does not appear to be effect ive against the adult worm. In general, the drug has mild adverse effects, but under some condit ions, i t
P.1105
Page 40 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
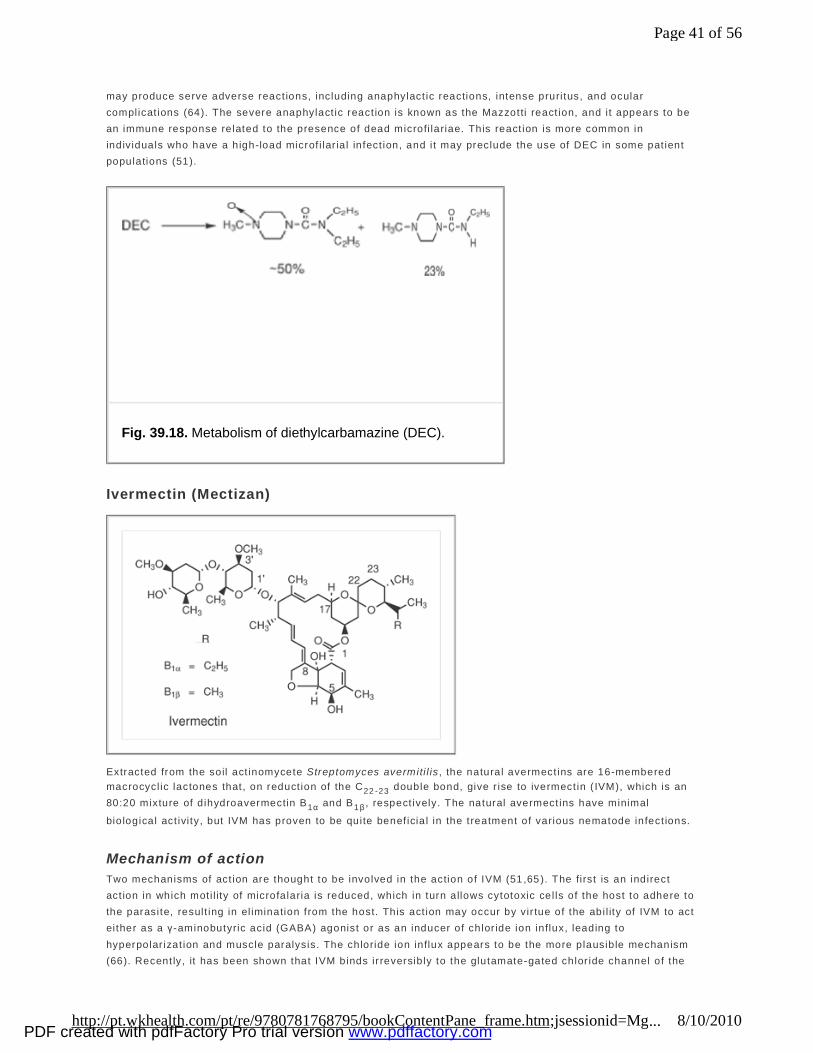
may produce serve adverse react ions, including anaphylact ic reactions, intense pruri tus, and ocular complicat ions (64). The severe anaphylact ic react ion is known as the Mazzotti react ion, and i t appears to be an immune response related to the presence of dead microfi lariae. This react ion is more common in individuals who have a high-load microf i lar ia l infect ion, and i t may preclude the use of DEC in some pat ient populations (51).
Ivermectin (Mectizan)
Extracted from the soil act inomycete Streptomyces avermiti l is , the natural avermect ins are 16-membered macrocycl ic lactones that, on reduct ion of the C22 -23 double bond, give r ise to ivermect in ( IVM), which is an 80:20 mixture of d ihydroavermectin B1α and B1β , respect ively. The natural avermect ins have minimal
bio logical act ivi ty, but IVM has proven to be quite benef icia l in the treatment of various nematode infect ions.
Mechanism of action Two mechanisms of act ion are thought to be involved in the action of IVM (51 ,65 ). The first is an indirect act ion in which moti l ity of microfalaria is reduced, which in turn allows cytotoxic cel ls of the host to adhere to the parasite, result ing in el imination from the host. This act ion may occur by vir tue of the abi l ity of IVM to act either as a γ-aminobutyric acid (GABA) agonist or as an inducer of chlor ide ion influx, leading to hyperpolar izat ion and muscle paralysis. The chloride ion influx appears to be the more plausible mechanism (66). Recent ly, it has been shown that IVM binds ir reversibly to the glutamate-gated chlor ide channel of the
Fig. 39.18. Metabolism of diethylcarbamazine (DEC).
Page 41 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
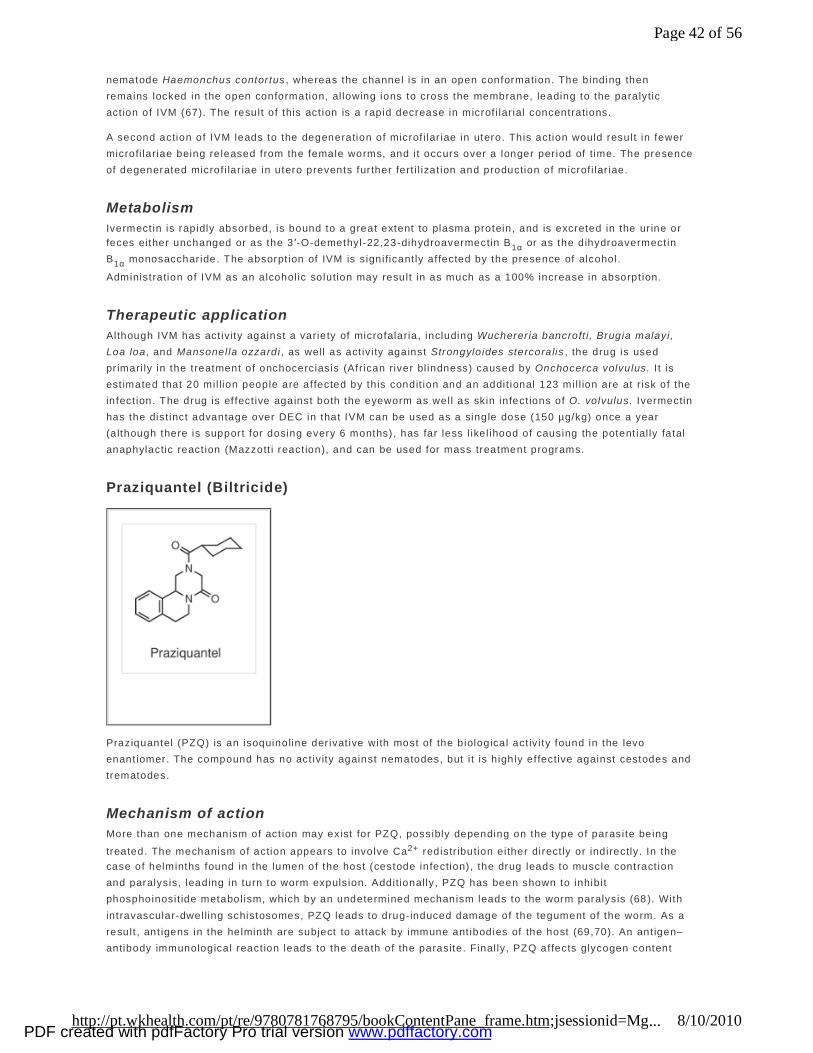
nematode Haemonchus contor tus , whereas the channel is in an open conformation. The binding then remains locked in the open conformation, al lowing ions to cross the membrane, leading to the paralytic act ion of IVM (67). The result of this act ion is a rapid decrease in microf i lar ial concentrations.
A second action of IVM leads to the degeneration of microf i lar iae in utero. This action would result in fewer microfi lariae being released from the female worms, and i t occurs over a longer per iod of time. The presence of degenerated microf i lar iae in utero prevents fur ther fert i l izat ion and production of microf i lar iae.
Metabolism Ivermect in is rapidly absorbed, is bound to a great extent to plasma protein, and is excreted in the ur ine or feces either unchanged or as the 3 ′-O-demethyl-22,23-dihydroavermectin B1α or as the dihydroavermect in B1α monosacchar ide. The absorpt ion of IVM is significant ly af fected by the presence of alcohol.
Administration of IVM as an alcohol ic solution may result in as much as a 100% increase in absorpt ion.
Therapeutic application Although IVM has act iv ity against a variety of microfalaria, including Wucherer ia bancroft i , Brugia malayi, Loa loa, and Mansonella ozzardi , as well as act iv i ty against Strongyloides stercoralis , the drug is used pr imari ly in the treatment of onchocerciasis (African river bl indness) caused by Onchocerca volvulus. I t is est imated that 20 mil lion people are affected by th is condit ion and an addit ional 123 mil l ion are at risk of the infect ion. The drug is ef fect ive against both the eyeworm as well as skin infect ions of O. volvulus. Ivermectin has the dist inct advantage over DEC in that IVM can be used as a single dose (150 µg/kg) once a year (although there is support for dosing every 6 months) , has far less l ikel ihood of causing the potent ial ly fatal anaphylactic react ion (Mazzott i react ion), and can be used for mass treatment programs.
Praziquantel (Biltricide)
Praziquantel (PZQ) is an isoquinoline der ivat ive with most of the biological act iv i ty found in the levo enant iomer. The compound has no act iv ity against nematodes, but i t is h ighly ef fective against cestodes and trematodes.
Mechanism of action More than one mechanism of act ion may exist for PZQ, possibly depending on the type of parasite being
treated. The mechanism of action appears to involve Ca2+ redistr ibution either direct ly or indirectly. In the case of helminths found in the lumen of the host (cestode infection) , the drug leads to muscle contract ion and paralysis, leading in turn to worm expulsion. Additional ly, PZQ has been shown to inhibit phosphoinosit ide metabol ism, which by an undetermined mechanism leads to the worm paralysis (68 ). With intravascular-dwelling schistosomes, PZQ leads to drug-induced damage of the tegument of the worm. As a result , ant igens in the helminth are subject to at tack by immune ant ibodies of the host (69,70). An ant igen–antibody immunological react ion leads to the death of the parasite. Final ly, PZQ affects glycogen content
Page 42 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
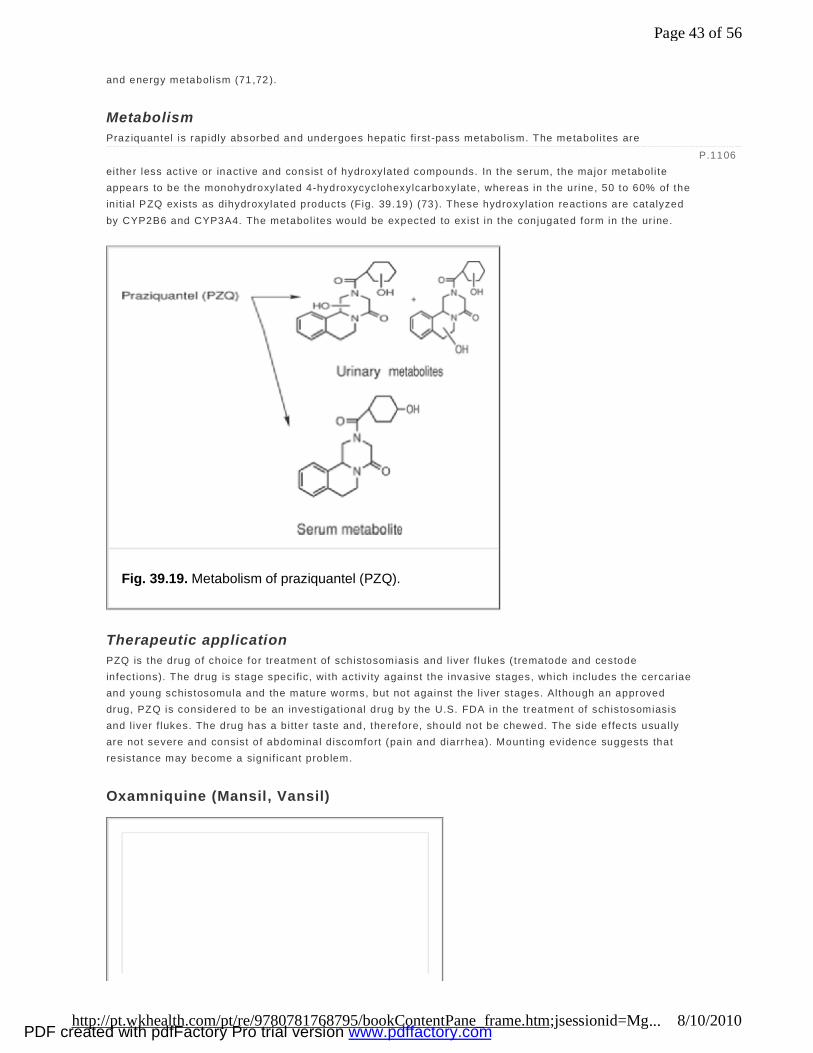
and energy metabol ism (71 ,72 ).
Metabolism Praziquantel is rapidly absorbed and undergoes hepatic fi rst-pass metabol ism. The metaboli tes are either less act ive or inact ive and consist of hydroxylated compounds. In the serum, the major metabol i te appears to be the monohydroxylated 4-hydroxycyclohexylcarboxylate, whereas in the urine, 50 to 60% of the in itia l PZQ exists as dihydroxylated products (Fig. 39.19 ) (73 ). These hydroxylat ion react ions are catalyzed by CYP2B6 and CYP3A4. The metabol i tes would be expected to exist in the conjugated form in the ur ine.
Therapeutic application PZQ is the drug of choice for treatment of schistosomiasis and l iver f lukes ( trematode and cestode infect ions). The drug is stage specific, with activ i ty against the invasive stages, which includes the cercar iae and young schistosomula and the mature worms, but not against the l iver stages. Although an approved drug, PZQ is considered to be an invest igat ional drug by the U.S. FDA in the treatment of schistosomiasis and l iver f lukes. The drug has a bitter taste and, therefore, should not be chewed. The side effects usual ly are not severe and consist of abdominal d iscomfort (pain and diarrhea). Mounting evidence suggests that resistance may become a signif icant problem.
Oxamniquine (Mansil, Vansil)
P.1106
Fig. 39.19. Metabolism of praziquantel (PZQ).
Page 43 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
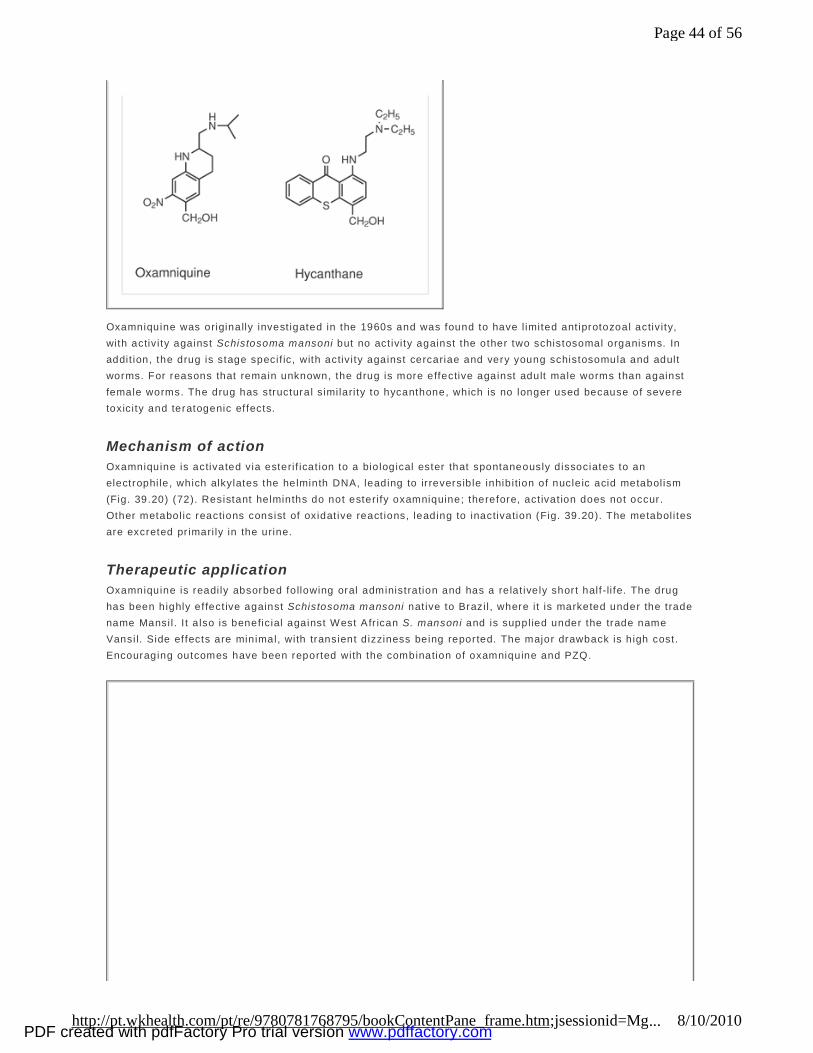
Oxamniquine was originally invest igated in the 1960s and was found to have l imited ant iprotozoal activ i ty, with activ i ty against Schistosoma mansoni but no act ivi ty against the other two schistosomal organisms. In addit ion, the drug is stage specif ic, with activ i ty against cercariae and very young schistosomula and adult worms. For reasons that remain unknown, the drug is more effective against adult male worms than against female worms. The drug has structural similari ty to hycanthone, which is no longer used because of severe toxici ty and teratogenic ef fects.
Mechanism of action Oxamniquine is activated via esteri f icat ion to a biological ester that spontaneously dissociates to an electrophi le, which alkylates the helminth DNA, leading to ir reversible inhibition of nucleic acid metabol ism (Fig. 39.20) (72). Resistant helminths do not esteri fy oxamniquine; therefore, act ivat ion does not occur. Other metabol ic reactions consist of oxidat ive react ions, leading to inactivation (Fig. 39.20). The metabol i tes are excreted pr imari ly in the urine.
Therapeutic application Oxamniquine is readi ly absorbed following oral administration and has a relat ively short half-li fe. The drug has been highly ef fect ive against Schistosoma mansoni nat ive to Brazi l , where i t is marketed under the trade name Mansi l . I t a lso is beneficial against West Afr ican S. mansoni and is suppl ied under the trade name Vansi l. Side effects are minimal, with transient d izziness being reported. The major drawback is high cost. Encouraging outcomes have been reported with the combination of oxamniquine and PZQ.
Page 44 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
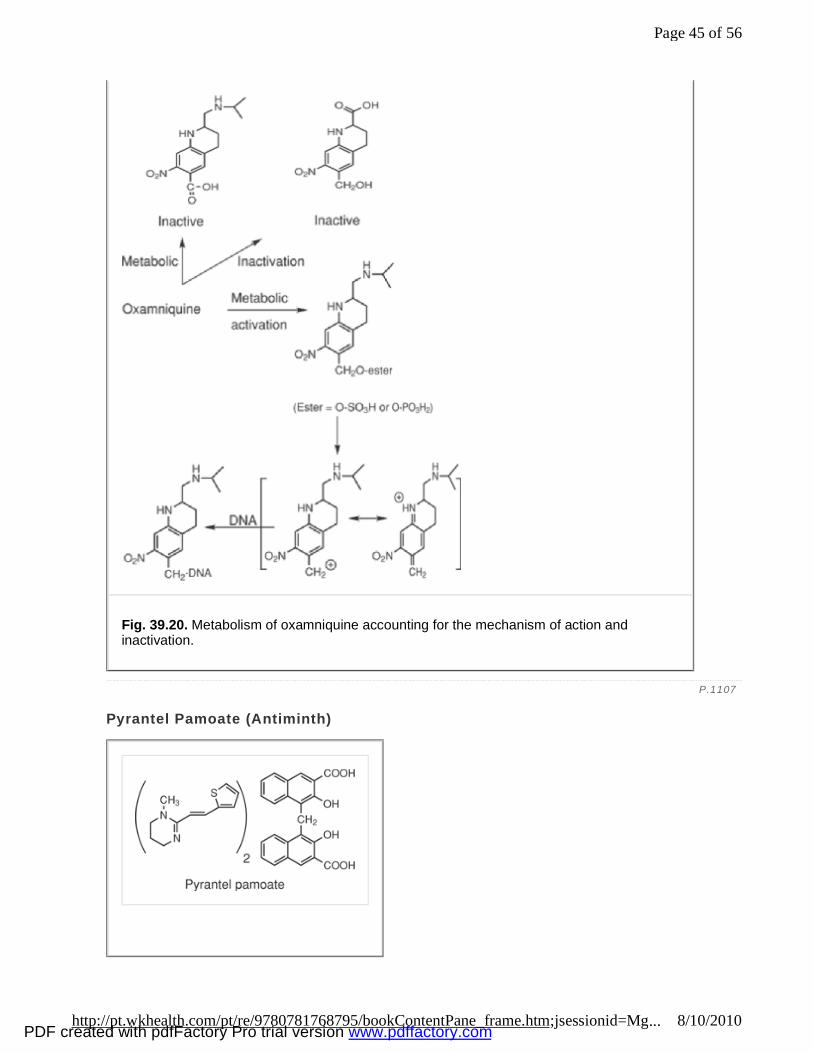
Pyrantel Pamoate (Antiminth)
Fig. 39.20. Metabolism of oxamniquine accounting for the mechanism of action and inactivation.
P.1107
Page 45 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

Pyrantel was f irst reported for i ts anthelmint ic act iv ity in 1966 (74 ). Although i t has act ivi ty against most intest inal roundworm infect ions, i t has not been approved by the U.S. FDA for several of these infestat ions. It is considered to be the drug of choice in the treatment of p inworms. The drug is used as the pamoate salt , which is quite insoluble and, as a result, is not readi ly absorbed. This property improves the usefulness of the drug for t reatment of intest inal helminths. In addition to i ts value in treating enterobiasis, the drug is ef fect ive for hookworm and roundworm (ascariasis) infect ions. Pyrantel acts as a depolar izing neuromuscular blocking agent that act ivates nicot inic receptors and inhibits chol inesterase, ult imately leading to worm paralysis.
Ectoparasitic Infections Two parasit ic organisms that cause common topical infect ions are Sarcoptes scabiei , which is responsible for scabies, and Pediculus humanus , which is responsible for l ice infections.
Scabies Scabies, commonly referred to as the “seven year i tch,” is a condition caused by Sarcoptes scabiei , or the itch mite. The condit ion commonly is spread by direct, person-to-person contact, a lthough the organism is capable of l iving for 2 to 3 days in clothing, bedding, or house dust. Sharing of clothing is a common means whereby the condit ion spreads. The organism burrows into the epidermis, usual ly in the fo lds of the skin of the f ingers, the elbows, female breast, penis, scrotum, and buttocks. The female parasite lays eggs in the skin, which then hatch and mature to adults. The i tch mite can l ive for 30 to 60 days. The infect ions are most common in children, but they also may be found in adults in inst i tut ional sett ings. The primary symptom of severe i tching may foster secondary infect ions at the site of scratching. Because of the potent ia l for spread to other members of a family, i t is common to treat a l l members of the family. This wi l l prevent reinfection from a second family member after successful therapy of the f irst family member.
Lice Pediculosis or lice is caused by any of the parasites Pediculus humanus capit is , the head louse; Pediculus humanus corporis , the body louse; or Phthir ius pubis , the crab louse (found in the genita l area). L ice are bloodsucking insects that l ive for 30 to 40 days on the body of the host. The organisms reproduce, and the female lays her eggs, the nits, which become attached to hair . The nits are white in color and hatch in 8 to 10 days. For the parasite to l ive, it must feed on blood, which i t sucks through punctures in the skin. A hypersensit iv i ty react ion occurs at these puncture sites, which then leads to pruri tus, host scratching, and possible secondary infect ion. In addit ion to the scalp and skin, the eyebrows, eyel ids, and beard may become sites of infect ion. The transfer of infect ion can occur through person-to-person contact and from infected clothing, on which the organism can survive for up to 1 week. The shar ing of clothing is a common means for the spread of body l ice. Head l ice are quite common among chi ldren in grade school, whereas crab l ice are common among individuals who are sexually act ive. Treatment of family members is recommended, and clothing and bed linen should be removed and washed in very hot water.
Drug Therapy for Scabies and Pediculosis
Lindane (Kwell)
Page 46 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com

Chlorinat ion and reduct ion of benzene leads to a mixture of hexachlorocyclohexanes. The insect icidal act iv i ty resides pr imari ly in the γ-isomer of hexachlorocyclohexane (γ-benzene hexachlor ide). The compound is thought to produce i ts insecticidal act ion by vir tue of a CNS st imulatory act ion that occurs by blockage of GABA. The compound is readi ly absorbed through the chitinous exoskeleton of the parasite. Unfortunately, lindane also is readi ly absorbed through intact human skin, especial ly the scalp, and has the potentia l for systemic neurotoxici ty in the host. Infants and chi ldren and, possibly, the elder ly are most prone to the neurotoxic effects of the drug. Because the l indane is quite l ipophi l ic and, is applied to the scalp as a shampoo, i t may be absorbed where upon i t can readi ly enter the CNS of the pat ient producing signs of neurotoxici ty (convulsions, d izziness, clumsiness, and unsteadiness).
The drug is avai lable in a lot ion and a shampoo and is recommended for the treatment of both pediculosis and scabies. When using the lot ion topical ly, i t should be appl ied to dry skin, cover ing the ent ire surface and being lef t in place for 8 hours. The l indane then should be removed by washing thoroughly. I f the shampoo is used for Pediculosis capitis , the hair should be cleaned of oi l and dried before appl icat ion of the l indane shampoo. The shampoo is then worked into the hair and scalp, being appl ied in such a way as to prevent other par ts of the body from coming into contact with the drug. After approximately 4 minutes, the drug is removed by washing with water , and the hair is dr ied and then combed with a f ine-toothed comb to remove nits.
Pyrethrum and Pyrethroids The natural ly occurring pyrethrums have been used as insecticides since the 1800s. These compounds are extracted from the flower ing port ion of the Chrysanthemum plant. The f lowers produced in Kenya have, on average, 1.3% pyrethrins. These pyrethrum extracts are a major agricultural product for that country.
Chemistry The Chrysanthemum extract is a mixture of ester consist ing of the acids chrysanthemic and pyrethric and the alcohols pyrethrolone and cinerolone (Fig. 39.21). The esters are prone to hydrolysis and oxidat ion and, as a result , should be stored in the cold and protected from l ight. Because of the high cost, l imited avai labi l ity, and rapid degradat ion, synthet ic derivat ives have been invest igated. The result has been the preparat ion of pyrethroids, the synthetic derivatives of pyrethrins. The compound used therapeut ical ly is permethrin, which exists as a 60:40 mixture of trans:cis isomers.
Mechanism of action (75 ,76 ,77,78) The pyrethrins and pyrethroids (permethrin) are nerve membrane sodium channel toxins that do not af fect potassium channels. The compounds bind to specif ic sodium channel proteins and slow the rate of inact ivat ion of the sodium current e lic i ted by membrane depolarization and, as a result , prolong the open time of the sodium channel. At low concentrations, the pyrethroids produce repet i t ive act ion potentia ls and neuron fir ing; at h igh concentrat ions, the nerve membrane is depolar ized completely and excitat ion blocked.
The receptor interact ion of the pyrethrums with the sodium channel complex is stereospecific and dependent on the stereochemistry of the carboxyl ic acid. In the case of the pyrethroids, the most active isomers are the 1R,3-cis- and 1R,3-trans-cyclopropanecarboxylates. The 1S-cis - and - trans- isomers are inact ive and actual ly are antagonists to the act ion of the 1R-isomers.
P.1108
Page 47 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
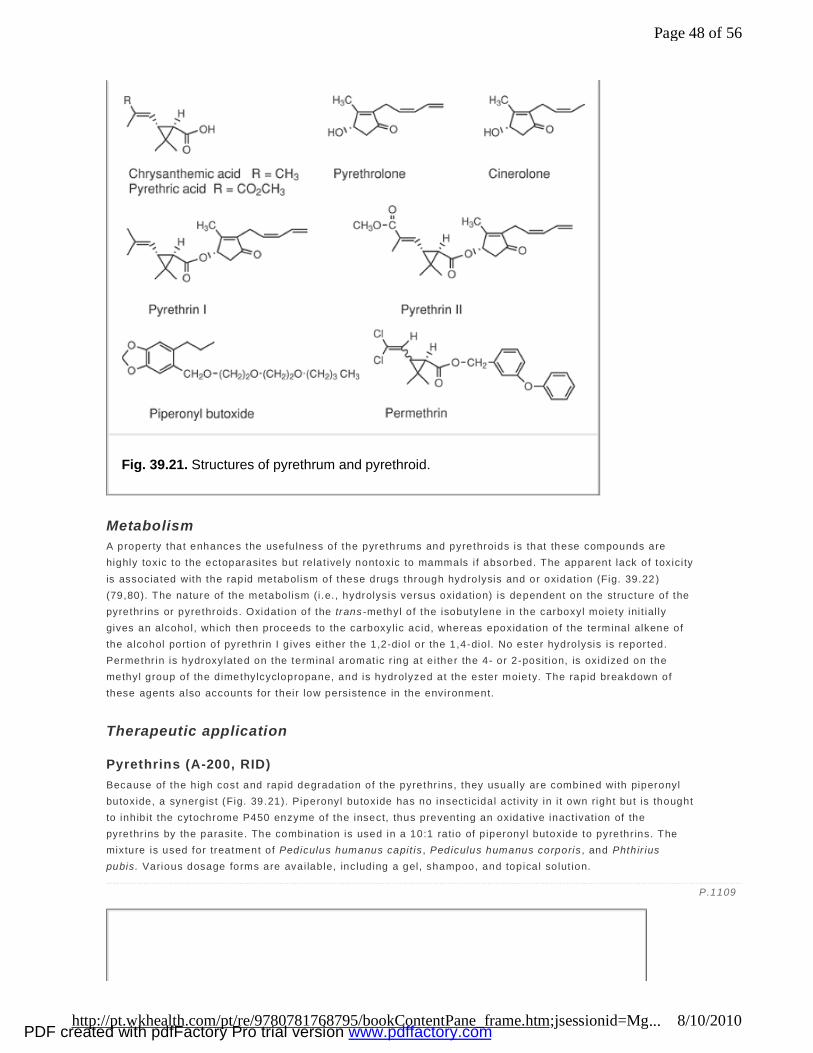
Metabolism A property that enhances the usefulness of the pyrethrums and pyrethroids is that these compounds are highly toxic to the ectoparasites but re lat ively nontoxic to mammals i f absorbed. The apparent lack of toxici ty is associated with the rapid metabol ism of these drugs through hydrolysis and or oxidation (Fig. 39.22 ) (79,80). The nature of the metabol ism (i .e. , hydrolysis versus oxidation) is dependent on the structure of the pyrethr ins or pyrethroids. Oxidation of the trans -methyl of the isobutylene in the carboxyl moiety ini t ial ly gives an alcohol, which then proceeds to the carboxyl ic acid, whereas epoxidation of the terminal alkene of the alcohol port ion of pyrethrin I g ives either the 1,2-diol or the 1,4-diol. No ester hydrolysis is reported. Permethr in is hydroxylated on the terminal aromatic r ing at e ither the 4- or 2-posit ion, is oxidized on the methyl group of the dimethylcyclopropane, and is hydrolyzed at the ester moiety. The rapid breakdown of these agents also accounts for their low persistence in the environment.
Therapeutic application
Pyrethrins (A-200, RID) Because of the high cost and rapid degradation of the pyrethr ins, they usual ly are combined with piperonyl butoxide, a synergist (Fig. 39.21). Piperonyl butoxide has no insect icidal act iv i ty in i t own right but is thought to inhibit the cytochrome P450 enzyme of the insect, thus prevent ing an oxidative inact ivat ion of the pyrethr ins by the parasite. The combinat ion is used in a 10:1 ratio of p iperonyl butoxide to pyrethr ins. The mixture is used for treatment of Pediculus humanus capit is , Pediculus humanus corporis , and Phthir ius pubis. Various dosage forms are avai lable, including a gel, shampoo, and topical solut ion.
Fig. 39.21. Structures of pyrethrum and pyrethroid.
P.1109
Page 48 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
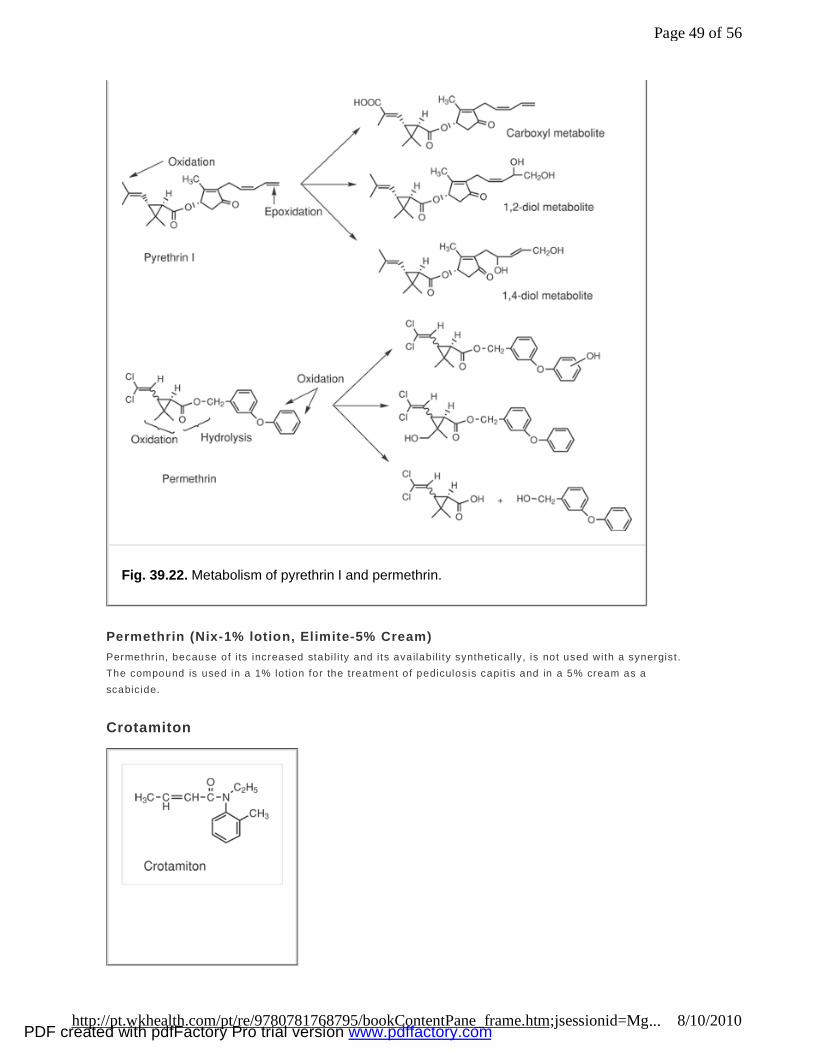
Permethrin (Nix-1% lotion, Elimite-5% Cream) Permethr in, because of i ts increased stabi l i ty and i ts availabil i ty synthet ical ly, is not used with a synergist . The compound is used in a 1% lotion for the treatment of pediculosis capit is and in a 5% cream as a scabicide.
Crotamiton
Fig. 39.22. Metabolism of pyrethrin I and permethrin.
Page 49 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
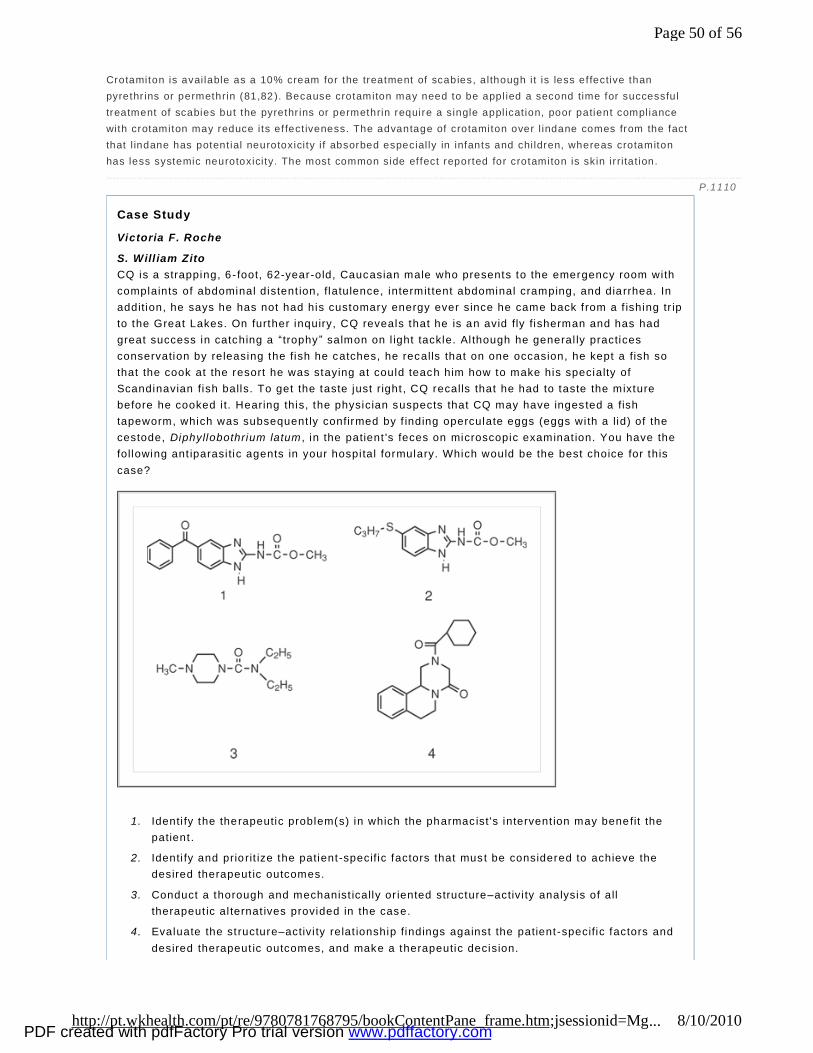
Crotamiton is avai lable as a 10% cream for the treatment of scabies, a lthough i t is less effective than pyrethr ins or permethrin (81,82 ). Because crotamiton may need to be appl ied a second time for successful treatment of scabies but the pyrethr ins or permethrin require a single appl icat ion, poor patient compliance with crotamiton may reduce i ts ef fect iveness. The advantage of crotamiton over l indane comes from the fact that l indane has potent ial neurotoxici ty i f absorbed especial ly in infants and chi ldren, whereas crotamiton has less systemic neurotoxici ty. The most common side effect reported for crotamiton is skin ir ri tat ion.
Case Study
Victoria F. Roche
S. Will iam Zito CQ is a strapping, 6 - foot, 62-year-old, Caucasian male who presents to the emergency room with complaints of abdominal distent ion, flatulence, intermit tent abdominal cramping, and dia rrhea. In addition, he says he has not had his customary energy ever since he came back f rom a f ishing tr ip to the Great Lakes. On further inquiry, CQ reveals that he is an avid fly fisherman and has had great success in catching a “trophy ” salmon on l ight tackle. Al though he general ly practices conservation by releasing the fish he catches, he recalls that on one occasion, he kept a fish so that the cook at the resort he was staying at could teach him how to make his specialty of Scandinavian fish balls. To get the taste just right , CQ recalls that he had to taste the mixture before he cooked i t. Hearing this, the physician suspects that CQ may have ingested a fish tapeworm, which was subsequent ly confirmed by f inding operculate eggs (eggs wi th a lid) of the cestode, Diphyllobothrium latum , in the patient 's feces on microscopic examinat ion. You have the following ant iparasi tic agents in your hospi tal formulary. Which would be the best choice for this case?
1. Identi fy the therapeutic problem(s) in which the pharmac ist's intervent ion may benefit the patient .
2. Identi fy and prio rit ize the patient-specific factors that must be considered to achieve the desired therapeut ic outcomes.
3. Conduct a thorough and mechanist ically or iented structure–activi ty analysis of all therapeut ic al ternat ives provided in the case.
4. Evaluate the st ructure–activi ty relat ionship findings against the patient-specific factors and desired therapeut ic outcomes, and make a therapeutic decision.
P.1110
Page 50 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
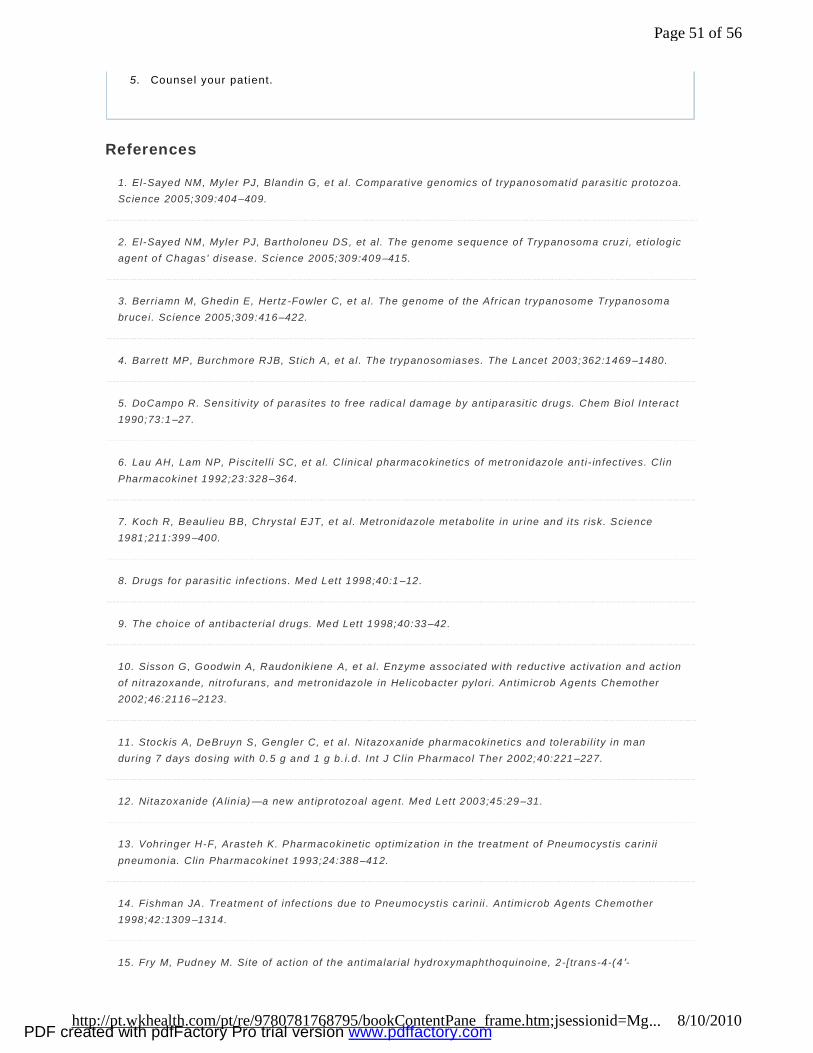
5. Counsel your patient.
References
1. El-Sayed NM, Myler PJ, Blandin G, et a l. Comparative genomics of t rypanosomatid parasit ic protozoa. Science 2005;309:404–409.
2. El-Sayed NM, Myler PJ, Bartholoneu DS, et al. The genome sequence of Trypanosoma cruzi, et io logic agent of Chagas' d isease. Science 2005;309:409–415.
3. Berriamn M, Ghedin E, Hertz -Fowler C, et a l. The genome of the Afr ican trypanosome Trypanosoma brucei. Science 2005;309:416–422.
4. Barrett MP, Burchmore RJB, St ich A, et a l. The trypanosomiases. The Lancet 2003;362:1469–1480.
5. DoCampo R. Sensitiv i ty of parasites to free radical damage by antiparasit ic drugs. Chem Biol Interact 1990;73:1–27.
6. Lau AH, Lam NP, P iscitel l i SC, et a l. Cl in ical pharmacokinetics of metronidazole ant i- infect ives. Cl in Pharmacokinet 1992;23:328–364.
7. Koch R, Beaulieu BB, Chrystal EJT, et a l. Metronidazole metabol i te in ur ine and i ts r isk. Science 1981;211:399–400.
8. Drugs for parasit ic infections. Med Lett 1998;40:1–12.
9. The choice of ant ibacteria l drugs. Med Lett 1998;40:33–42.
10. Sisson G, Goodwin A, Raudonikiene A, et a l. Enzyme associated with reduct ive act ivat ion and act ion of n it razoxande, nit rofurans, and metronidazole in Helicobacter pylori . Antimicrob Agents Chemother 2002;46:2116–2123.
11. Stockis A, DeBruyn S, Gengler C, et a l. Nitazoxanide pharmacokinet ics and tolerabi l i ty in man during 7 days dosing with 0.5 g and 1 g b. i.d. Int J Cl in Pharmacol Ther 2002;40:221–227.
12. Nitazoxanide (A lin ia)—a new ant iprotozoal agent. Med Lett 2003;45:29–31.
13. Vohringer H-F, Arasteh K. Pharmacokinetic opt imizat ion in the treatment of Pneumocyst is carin ii pneumonia. Clin Pharmacokinet 1993;24:388–412.
14. Fishman JA. Treatment of infect ions due to Pneumocyst is carin ii . Antimicrob Agents Chemother 1998;42:1309–1314.
15. Fry M, Pudney M. Site of act ion of the ant imalar ial hydroxymaphthoquinoine, 2-[ trans-4-(4 ′-
Page 51 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
chlorophenyl)cyclohexyl]-3-hydroxy -1,4-naphthoquinone (566C80). Biochem Pharmacol 1992;43:1545–1553.
16. Hughes WT, Gray VL, Gutter idge WE, et a l. Eff icacy of a hydroxynaphthoquinone, 566C80, in exper imental Pneumocyst is carin i i pneumonit is. J Ant imicrob Chemother 1990;34:225–228.
17. Al legra CJ, Kovacs JA, Drake JC, et al. Act iv i ty of ant ifo lates against Pneumocyst is carin ii dihydrofolate reductase and indent i fication of a potent new agent. J Exp Med 1987;165:926–931.
18. Koda RT, Dube' MP, Li WY, et a l. Pharmacokinet ics of t rimetrexate and dapsone in AIDS pat ients with Pneumocyst is carin ii pneumonia. J Cl in Pharmacol 1999;39:268–274.
19. Wang CC. Molecular mechanisms and therapeut ic approaches to the treatment of Afric ian trypanosomiasis. Annu Rev Pharmacol Toxicol 1995;35:93–127.
20. Edwards KJ, Jenkins T, Neidle S. Crystal structure of a pentamidine–oligonucleot ide complex: implications for DNA-binding propert ies. Biochemistry 1992;31:7104–7109.
21. Shapiro T, Englund PT. Selective cleavage of kinetoplast DNA minicircles promoted by anti t rypanosomal drugs. Proc Natl Acad Sci U S A 1990;87:950–954.
22. Dykstra CC, Tidwell RR. Inhibit ion of topoisomerase from Pneumocyst is carin ii by aromatic dicat ionic molecules. J Protozool 1991;38:78S–81S.
23. Metcalf BW, Bey P, Danzin C, et al. Catalyt ic irreversible inhibit ion of mammalian ornith ine decarboxylase (E.C. 4.1.1.17) by substrate and product analogues. J Am Chem Soc 1978;100:2551–2553.
24. Bacchi CJ, Nathan HC, Hutner SH, et a l. Polyamine metabol ism: a potent ial therapeutic target in trypanosomes. Science 1980;210:332–334.
25. Poulin R, Lu L, Ackermann B, et al. Mechanism of the ir reversible inact ivat ion of mouse ornithine decarboxylase by α-dif luoromethylornith ine. J Biol Chem 1992;267:150–158.
26. Bacchi CJ, Garofalo J, Ciminel li M, et al. Resistance to DL-α-dif luoromethylornith ine by cl in ical isolates of Trypanosoma brucei rhodeniense : role of S-adenosylmethionine. Biochem Pharmacol 1993;46:471–481.
27. Henderson GB, Ulr ich P, Fairlamb AH, et a l. “Subversive ” substrates for the enzyme trypanothione disulf ide reductase. Alternat ive approach to chemotherapy of Chagas' d isease. Proc Nat l Acad Sci U S A 1988;85:5374–5378.
28. Maya JD, Bol lo S, Nunez-Vergara LJ, et a l. Trypanosoma cruzi: effect and mode of act ion of nit ro imidazole and nitrofuran der ivat ives. Biochem Pharmacol 2003;65:999–1006.
P.1111
Page 52 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
29. Fair lamb AH, Henderson GB, Cerami A. Trypanothione is the pr imary target for arsenical drugs against African trypanosomes. Proc Nat l Acad Sci U S A 1989;86:2607–2611.
30. Berman JD. Chemotherapy for le ishmaniasis: b iochemical mechanisms, cl in ical eff icacy, and future strategies. Rev Infect Dis 1988;10:560–586.
31. Cook GC. Leishmaniasis: some recent developments in chemotherapy. J Ant imicrob Chemother 1993;31:327–330.
32. Singh S, Sivakumar R. Challenges and new discoveries in the treatment of leishmaniasis. J Infect Chemother 2004;10:307–331.
33. Ward SA. Mechanisms of chloroquine resistance in malaria l chemotherapy. Trends Pharmacol Sci 1988;9:241–246.
34. Sul l ivan DJ Jr, Gluzman IY, Russel l DG, et al. On the molecular mechanism of chloroquine's antimalaria l action. Proc Nat l Acad Sci U S A 1996;93: 11865–11869.
35. Arav-Boger R, Shapiro TA. Molecular mechanisms of resistance in antimalaria l chemotherapy: the unmet chal lenge. Annu Rev Pharmacol Toxicol 2005;45:565–585.
36. Zhao X -J, Ishizaki T. Metabol ic interactions of selected ant imalarial and nonantimalaria l drugs with the major pathway (3-hydroxylation) of quinine in human l iver microsomes. Br J Cl in Pharmacol 1997;44:505–511.
37. Palmer KJ, Holl iday SM, Brogden RN. Mefloquine: a review of i ts ant imalar ia l act iv i ty, pharmacokinet ic properties, and therapeut ic ef ficacy. Drugs 1993; 45:430–475.
38. Bryson HM, Goa KL. Halofantrine: a review of i ts ant imalarial act iv i ty, pharmacokinet ic properties, and therapeut ic potent ial. Drugs 1992;43:236–258.
39. Karbwang J, Bangchang KN. Clin ical pharmacokinetics of halofantrine. Clin Pharmacokinet 1994;27:104–119.
40. Augusto O, Schr ieber J, Mason RP. Direct ESR detect ion of a free radical intermediate drug in the peroxidase-catalyzed oxidat ion of the ant imalarial drug primaquine. Biochem Pharmacol 1988;37:2791–2797.
41. Mihaly GW, Ward SA, Edwards G, et a l. Pharmacokinet ics of primaquine in man: ident i ficat ion of the carboxyl ic acid der ivat ive as a major plasma metaboli te. Br J Cl in Pharmacol 1984;17:441–446.
42. Ferone R, Burchal l JJ, Hitchings GH. Plasmodium berghei d ihydrofolate reductase isolation, propert ies, and inhibit ion by ant ifo lates. Mol Pharmacol 1969;5:49–59.
43. Trig l ia T, Cowman AF. Primary structure and expression of the dihydropteroate synthetase gene of
Page 53 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Plasmodium falciparum. Proc Nat l Acad Sci U S A 1994;91:7149–7153.
44. Oll iaro P. Mode of act ion and mechanisms of resistance for ant imalaria l drugs. Pharmacol Ther 2001;89:207–219.
45. Cumming JN, Ploypradith P, Posner GH. Ant imalar ial act iv ity of artemisinin (Qinghaosu) and related tr ioxanes: mechanism(s) of action. Adv Pharmacol 1997;37:253–297.
46. Meshnick SR, Taylor TE, Kamchonwongpaisan S. Artemisinin and the ant imalar ial endoperoxides: from herbal remedy to targeted chemotherapy. Microbiol Rev 1996;60:301–315.
47. Posner GH, Cumming JN, Woo S-H, et al. Oral ly act ive ant imalaria l 3-subst i tuted tr ioxanes: new synthetic methodology and biological evaluat ion. J Med Chem 1998;41:940–951.
48. Cumming JN, Wang D, Shapiro TA, et al. Design, synthesis, der ivat izat ion, and structure–act ivi ty re lat ionships of simpli fied, tetracycl ic, 1,2,4-tr ioxane alcohol analogues of the antimalaria l artemisinin. J Med Chem 1998;41:952–964.
49. Eckstein -Ludwig, Webb RJ, van Goethem DK, et a l. Ar temisinins target the SERCA of Plasmodium falciparum. Nature 2003;424:957–961.
50. Rosenthal PJ. Antimalaria l drug discovery: o ld and new approaches. J Exp Biol 2003;206:3735–3744.
51. de S ilva N, Guyatt H, Bundy D. Anthelmint ics: a comparat ive review of their clin ical pharmacology. Drugs 1997;53:769–786.
52. Townsend LB, Wise DS. The synthesis and chemistry of certain anthelmintic benzimidazoles. Parasitol Today 1990;6:107–112.
53. Prichard RK. Mode of action of the anthelmintic th iabendazole in Haemonchus contor tus . Nature 1970;228:684–685.
54. Friedman PA, Platzer EG. Interact ion of anthelmintic benzimidazoles and benzimidazole derivatives with bovine brain tubul in. Biochim Biophys Acta 1978;544:605–614.
55. Lacey E. Mode of action of benzimidazoles. Parasitol Today 1990;6:112–115.
56. Braithwaite PA, Roberts MS, Al lan RJ, et a l. Cl inical pharmacokinet ics of h igh -dose mebendazole in patients treated for hydatid disease. Eur J Cl in Pharmacol 1982;22:161–169.
57. Gottschal l DW, Theodor ides EJ, Wang R. The metabol ism of benzimidazole anthelmint ics. Parasito l Today 1990;6:115–124.
58. Marr iner SE, Morr is DL, Dickson B, et a l. Pharmacokinetics of a lbendazole in man. Eur J Cl in
Page 54 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Pharmacol 1986;30:705–708.
59. Hawking F. Diethylcarbamazine and new compounds for the treatment of fi lariasis. Adv Pharmacol Chemother 1979;16:129–194.
60. Cesbron J -Y, Capron A, Vargaft ig BB, et al. Platelets mediate the act ion of diethylcarbamazine on microfi lariae. Nature 1987;325:533–536.
61. Florencio MS, Peixoto CA. The effect of diethylcarbamazine on the ultrastructure of microfi lariae of Wucherer ia bancroft i . Parasito logy 2003;126: 551–554.
62. Fujimaki Y, Ehara M, Kimura E, et al. Diethylcarbamazine, anti f i lar ial drug, inhibits microtubule polymerizat ion and disrupts preformed microtubules. Biochem Pharmacol 1990;39:851–856.
63. Maizels RM, Denham DA. Diethylcarbamazine (DEC): immunopharmacological interact ions of an anti f i lar ial drug. Parasitol 1992;105:S49–S60.
64. Mackenzie CD. Diethylcarbamazine: a review of i ts act ion in onchocerciasis, lymphat ic f i lar iasis, and inflammation. Trop Disease Bull 1985;82:R1–R37.
65. Goa KL, McTavish D, Cl issold SP. Ivermect in: a review of i ts ant i fi larial act iv i ty, pharmacokinet ic propert ies and cl inical eff icacy in onchocerciasis. Drugs 1991;42:640–658.
66. Ottesen EA, Campbell WC. Ivermect in in human medicine. J Ant imicrob Chemother 1994;34:195–203.
67. Forrester SG, Beech RN, Prichard RK. Agonist enhancement of macrocycl ic lactone act iv i ty at a glutamate-gated chlor ide channel subunit f rom Haemonchus contor tus. Biochem Pharmacol 2004;67:1019–1024.
68. Wiest PM, Li Y, Olds GR, et al. Inhibition of phosphoinosit ide turnover by praziquantel in Schistosoma mansoni. J Parasito l 1992;78:753–755.
69. Xiao S -H, Catto BA, Webster LT Jr. Effects of praziquantel on different developmental stages of Schistosoma mansoni in vi t ro and in vivo. J Infect Dis 1985;151:1130–1137.
70. Fallon PG, Cooper RO, Probert AJ, et al. Immune-dependent chemotherapy of schistosomiasis. Parasitology 1992;105:S41–S48.
71. Utzinger J, Keiser J, Shuhua X, et al. Combinat ion chemotherapy of schistosomiasis in laboratory studies and clin ical tr ials. Ant imicrob Agents Chemother 2003;47:1487–1495.
72. Ciol i D, Pica-Mattoccia L, Archer S. Ant ischistosomal drugs: past, present … and future? Pharmacol Ther 1995;68:35–85.
73. Buhring KU, Diekmann HW, Muller H, et a l. Metabol ism of praziquantel in man. Eur J Drug Metab
Page 55 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com
Pharmacokinet 1978;3:179–190.
74. Aust in WC, Courtney WC, Danilewicz W, et a l. Pyrantal tar trate, a new anthelmint ic ef fective against infect ions of domestic animals. Nature 1966; 212:1273–1274.
75. Narahashi T. Nerve membrane ionic channels as the primary target of pyrethroids. Neurotoxicology 1985;6:3–22.
76. Vi jverberg HPM, de Weil le JR. The interact ion of pyrethroids with voltage -dependent Na channels. Neurotoxicology 1985;6:23–34.
77. Grammon DW, Sanders G. Pyrethroid– receptor interactions: stereospecif ic b inding and effects on sodium channels in mouse brain preparat ions. Neurotoxicology 1985;6:35–46.
78. Lombet A, Mourre C, Lazdunski M. Interact ion of insect icides of the pyrethroid family with specif ic binding sites on the voltage-dependent sodium channel f rom mammalian brain. Brain Res 1988;459:44–53.
79. Soderund DM. Metabol ic considerat ion in pyrethroid design. Xenobiotica 1992;22:1185–1194.
80. Ruzo LO, Casida JE. Metabol ism and toxicology of pyrethroids with dihalovinyl substi tuents. Environ Health Perspect 1977;21:285–292.
81. Tapl in D, Meinkin TL, Joaquin BA, et al. Comparison of cr i tamiton 10% cream (Eurax) and permethrin 5% cream (El imite) for the treatment of scabies in chi ldren. Pediatr Dermatol 1990;7:67–73.
82. Amer M, El -Ghariband I . Permethrin versus crotamiton and l indane in the treatment of scabies. Int J Dermatol 1992;31:357–358.
Suggested Readings
Freeman CD, K lutman EE, Lamp KC. Metronidazole: a therapeut ic review and update. Drugs 1997;54:679–708.
Maizels RM, Bundy DAP, Selkirk ME, et al. Immunological modulat ion and evasion by helminth parasites in human populat ions Nature 1993;365:797–805.
Wilson JD, Braunwald E, Isselbacher KJ, et a l. , eds. Harr ison's Pr inciples of Internal Medicine. 12th Ed. New York: McGraw-Hil l , 1991:772.
Page 56 of 56
8/10/2010http://pt.wkhealth.com/pt/re/9780781768795/bookContentPane_frame.htm;jsessionid=Mg...PDF created with pdfFactory Pro trial version www.pdffactory.com