chapter 1 introduction - research une
TRANSCRIPT
CHAPTER 1
INTRODUCTION
1.0 Purpose of this Study
Myocardial infarction is a major public health problem in Australia in terms of both
mortality and morbidity (Tonkin, 1988; Worcester, 1986). A number of controllable risk
factors contribute to coronary atherosclerosis such as smoking, high cholesterol and poor
dietary habits, excess alcohol, less exercise and increased stress. The modification of
these lifestyle factors is a major aim of cardiac rehabilitation in an attempt to attenuate
atherosclerotic changes and prevent further infarction. Therefore, the standard cardiac
rehabilitation program consists of providing patients with written information about diet,
quitting smoking, exercise and stress. Some programs also include video tapes providing
relevant health information. Physicians and nurses also reinforce the need to change
behaviour and provide additional advice as necessary. Unfortunately, despite these
efforts, compliance with desirable lifestyle change is often poor (Mayou, 1981;
Oldenburg, Perkins & Andrews, 1985; Worcester, 1986).
Explanations for this failure to comply with recommended health behaviour in the face of
a life threatening condition can be found in the health psychology literature where a
number of psychological models and theories based on Social Learning Theory and Value
Expectancy Theory have been shown to explain compliance. The models and theories
selected for investigation in this study were the Health Belief Model (Rosenstock, 1966;
Janz & Becker, 1984), self-efficacy and outcome expectation (Bandura, 1977a, 1986),
and Multidimensional Health Locus of Control (Wallston, Maides & Wallston, 1976;
Wallston, Wallston & DeVellis, 1978). Psychological distress and psychological ill health
are common among patients experiencing myocardial infarction and were included for
investigation as predictors that might also affect compliance with recommended health
behaviour.
The principal aim of this study was to determine the extent to which self-efficacy,
perceived health threat, cardiac health locus of control, psychological health and the
degree of psychological distress, at the time of hospitalisation, in men experiencing a
myocardial infarction would predict self-reported compliance with recommended health
behaviour over a 6 month period following discharge from hospital.
An additional aim of the study was to explore the relationship between the predictors to
investigate recent claims about how the various models might be integrated. Rosenstock
(1988) and Rosenstock, Strecher and Becker (1988) have argued that there is some
similarity between the models and that health behaviour might be best explained by a
combination of variables from the models rather than by the individual variables.
Finally, the stability of efficacy expectations, health threat beliefs, multidimensional
health locus of control beliefs, psychological health and psychological distress over the 6
month period was also investigated.
The rest of this chapter will examine in detail the theoretical basis for the present study
and supporting research. It begins by looking at the issue of cardiovascular disease as a
public health issue then moves on to the theoretical foundations of Social Learning
Theory and Value Expectancy Theory. Each model is then considered in detail and the
variables derived from the theories are described.
2.0 Cardiovascular Disease
Atherosclerotic heart disease and its sequelae, cardiac ischaemia and myocardial
infarction, are major public health issues in the industrialised world. Approximately 50%
of Australians die from cardiovascular disease, many prematurely (Tonkin, 1988).
Coronary atherosclerosis is hardening and narrowing of the principal arteries supplying
blood to the heart muscle. The process begins with the deposition of fats on the surface of
the arterial lumen. These roughened areas then provide a medium for the formation of
fibrous plaque consisting of smooth muscle cells, collagen, calcium, platelets, cellular
debris and lipids (Blumenthal & Emery, 1988). The plaque grows in size over time
eventually blocking off all or most of the artery. In some cases a clot may form to further
accelerate the process.
When narrowing prevents sufficient blood flow to supply the oxygen needs of the
myocardium on demand, angina pectoris may result. Complete obstruction causes
myocardial infarction which involves necrosis of cardiac muscle tissue. Infarction may
result in death or severe damage to the heart if not treated quickly and effectively.
2.1 Risk Factors for Coronary Atherosclerosis
It is generally acknowledged that the development of coronary atherosclerosis involves a
complex amalgam of multiple causative factors (Jenkins, 1988; Razin, 1982). These
consist of genetic predisposition, smoking, hypertension, hypercholesteraemia and
hyperlipidaemia. Other significant secondary factors that may play a role are stress,
moderate to heavy alcohol consumption, lack of exercise and certain personality
characteristics. Some of these causative factors may be controlled by changes in
behaviour, as described below.
Smoking is a major preventable risk factor for ischaemic heart disease contributing to
atherosclerotic changes, constriction of the coronary arteries, increased blood carbon
dioxide levels, decreased oxygen carrying capacity of the blood and increased potential
for clotting. Men who smoke more than 20 cigarettes a day have two to three times the
risk of experiencing a major cardiac episode, including sudden cardiac death, than those
who do not smoke (Jenkins, 1988). Importantly, cardiac risk decreases by about 50%
about 1 year after cessation of smoking and approximates the risk of a non-smoker after
about 10 years (Tonkin, 1988). Following a myocardial infarction or the development of
other signs of coronary atherosclerosis, such as angina pectoris, the need to quit smoking
is even more acute.
Poor dietary habits, which are also controllable, may contribute to hypercholesterolaemia
and hyperlipidaemia. These are major components in the formation of atherosclerosis by
increasing intake of fats and cholesterol. Raised low density lipoproteins, which carry
cholesterol, have been shown in a number of studies, including the Multiple Risk Factor
Intervention Trial (Stamler, Wentworth & Neaton, 1986), to be associated with cardiac
mortality. In fact, a 1% reduction in serum cholesterol lowers the risk of fatal coronary
artery disease by about 2% (The Lipid Research Clinics Program, 1984).
There is still some debate about the direct effect of stress on coronary risk. A recent report
by the National Heart Foundation of Australia (Stress Working Party, 1988) has stated
that '...there is good evidence that stress and its psychological consequences do affect
several conventional coronary risk factors' (p. 514). Stress, for example, is thought to
increase cholesterol and circulating fat through activation of hormones secreted by the
adrenal cortex. A number of studies have demonstrated that acute stress raises total blood
cholesterol levels between 8% and 65% (Stress Working Party, 1988). Thus, increased
stress may be an important mediating factor in the development of plaques. Sympathetic
activity resulting from stress also increases blood pressure which is a major contributing
factor in heart disease.
While there is some controversy about the protective nature of aerobic exercise in the
development of ischaemic heart disease and mortality, there is evidence that regular
aerobic exercise may assist in reducing weight, blood lipids, smoking, blood pressure
and the negative effects of stress and hostility (Jenkins, 1988; Siegal, Grady, Browner &
Hulley, 1988). Exercise may act to increase high density lipoproteins which appear to
have a protective capacity. Much of the effect of exercise, however, on coronary risk
factors may be indirect. For example, people who exercise are more likely to be health
conscious and therefore smoke less, watch what they eat and keep their weight down.
Not least of all, smoking and obesity make exercise difficult. Exercise also appears to
help in 'working off stress.
Moderate to heavy alcohol consumption is associated with cardiomyopathy, obesity,
hypertension, hypercholesteraemia and electrical disturbance of the cardiac muscle, all of
which predispose to the development of cardiac disease and morbidity (Ponh, 1990).
2.2 Modification of Risk Factors
Some of the risk factors for the development of heart disease and myocardial infarction,
namely smoking, hypercholesteraemia and hyperlipidaemia, exercise, stress and alcohol
consumption are directly or indirectly modifiable by alteration in behaviour associated
with lifestyle (Blumenthal & Emery, 1988; King & Remenyi, 1986; Pomeroy, 1987;
Siegal et al, 1988; Tonkin, 1988).
Risk factor modification following myocardial infarction is a central concern in
rehabilitation of these patients as a means to attenuating the disease process. Attempts to
change behaviour usually start in the coronary care unit and most cardiac rehabilitation
programs include structured patient education. This consists of written material, video
tapes and counselling from nurses and physicians (Jeffery, 1988; Murray, 1989).

However, there is evidence that compliance with required behaviour change is relatively
poor and that many return to their previous lifestyle within 12 months (Oldenburg,
Perkins & Andrews, 1985). Havik and Maeland (1988) found that in a group of 230
smokers who had experienced a myocardial infarction, 40.6% had resumed smoking after
6 months and 49.4% after 3 to 5 years. Similarly, compliance with recommended diet
(Jeffery, 1988; Sackett & Haynes, 1976) and exercise (Mayou, 1981) has been shown to
be poor.
More complex interventions, other than education, that involve counselling and
behavioural techniques have been shown to be more successful in improving compliance
and knowledge (Baile & Engel, 1978). Unfortunately, as a recent review of cardiac
rehabilitation in Australia has shown (Worcester, 1986), such interventions are rare.
Short staffing in hospitals as a result of the dwindling health dollar and a general lack of
recognition of the importance of psychological treatment compared to physical care may
account for this failure to intervene. In addition, hospital stay is generally limited to 8 to
11 days in uncomplicated cases, which is not enough time in which to provide effective
behavioural intervention.
If patients at risk of not changing their behaviour could be identified early in the acute
period following infarction then further reinforcement of the need for compliance and
behavioural interventions could be undertaken. It is for this reason that this study
attempted to predict self-reported compliance by using variables derived from Self-
efficacy Theory, the Health Belief Model, Locus of Control Theory, and measures of
psychological health and psychological distress. These theories and variables are
described in detail below in subsequent sections.
2 . 3 Summary
Myocardial infarction is a major health problem in Australia for which a number of risk
factors have been identified. Some of these factors, namely, smoking, diet, exercise,
stress and alcohol consumption are associated with the person's lifestyle. Rehabilitation
following infarction includes helping patients change their health behaviour and modify
these risk factors. Unfortunately, despite the severity of this disease, compliance with
recommended health behaviour is often poor.
This study was designed to predict self-reported compliance with recommended health
behaviour following myocardial infarction using a number of theories and models derived
from the health psychology literature. In the first instance, the focus of the study
promised to have utility beyond heuristic purposes by investigating behaviour change
likely to affect the outcome from a life threatening condition. Secondly, the study
provided an opportunity to further investigate a number of psychological models and
theories that attempt to explain health behaviour. It is to these theories and models, and
the variables that are derived from them, that the discussion now turns.
3.0 Theories of Health Behaviour
Rosenstock, Strecher and Becker (1988) have suggested that a number of recently
developed models may be applied to our understanding of health behaviour. These
models are derived from cognitive-behavioural theory.
Following on from the seminal work of Lewin (1935) and Tolman (1932), who
emphasised the role of cognition in the determination of behaviour, cognitive-
behavioural theory has given rise to two other important theories: Social Cognitive
Theory (Bandura, 1977a, 1986) and Value Expectancy Theory (Becker & Maiman,
1975; Rosenstock, 1966; Rosenstock, Strecher & Becker, 1988).
3.1 Bandura's Social Learning/Cognitive Theory
One of the major cognitive-behavioural theories, developed by Bandura, was termed
Social Learning Theory (Bandura, 1969, 1977a) but has more recently been renamed
Social Cognitive Theory (Bandura, 1986), presumably due to its emphasis on the role
of cognitive factors in the determination of behaviour.
Social Cognitive Theory attempts to draw together the principles of classical
conditioning, applied behavioural analysis and cognitive theory into one theoretical
framework (Wilson & O'Leary, 1980). In what Bandura (1977a, 1986) has termed
'triadic reciprocity', psychological functioning can be described in terms of the mutual
interaction of behaviour, cognitive factors and environmental influences.
Bandura (1986) has suggested that the degree of influence of each of these three
components on psychological functioning will vary according to the individual, the
particular activity and the circumstances. Similarly, reciprocity between the
components does not occur simultaneously, instead the interaction creates influences
over variable periods of time.
The strength of this model is that it enables a broader analysis of behaviour compared
to applied behaviour analysis which tends to emphasise environmental influences to
the exclusion of other factors. Social Cognitive Theory sees people as being able to
exert influence on what they do rather than, as suggested by Skinner (1971), simply
'being acted upon' by the world. People, then, are agents of their own behaviour in
this cognitive view.
Bandura (1977a, 1986) has described a number of cognitive processes, called
capabilities, that are hypothesised to play a role in determining behaviour. These are:
symbolism, which transforms experiences into an internal code to guide future action;
forethought, that enables anticipation of the consequences of behaviour; vicarious
learning or modelling (Bandura and Walters, 1963); self-regulation, which involves
the regulation of behaviour by the use of internal standards; and self-reflection, which
enables people to consider their experiences and to reflect on their own thoughts.
For Bandura (1986), the most important type of self-referent thought has to do with
people's judgements about their capabilities to deal with certain experiences. This
concept is called self-efficacy (Bandura, 1977a, 1986) and is central to Bandura's
theory. Perceptions of personal efficacy strongly influence what people choose to do,
how much effort they will put into a certain activity, how long they will persist in the
face of difficulties and the degree of anxiety associated with approaching the activity.
Another type of self-referent thought described by Bandura (1977a, 1986) is outcome
expectancy. This is the extent to which people believe that a certain behaviour will
achieve a particular outcome. Self-efficacy and outcome expectancy are two of the
independent variables investigated in this study and are described in greater detail in
Section Four.
In summary, Bandura's (1986) Social Cognitive Theory provides a modern,
psychologically interesting and potentially useful framework for understanding human
behaviour. Two concepts derived from Social Cognitive Theory, self-efficacy and
outcome expectation, have been used extensively in research investigating health
behaviour and health behaviour change.
7
3.2 Value-Expectancy Theory
The second cognitive-behavioural theory to be considered here which also takes into
account cognitive factors is Value Expectancy Theory. Models derived from this
theoretical position emphasise both the motivational role of a person's expectancy of
success that a behaviour will attain a particular goal and the value of that goal
(Broome, 1989).
Like Social Cognitive Theory, Value Expectancy Theory arose from the work of Kurt
Lewin in social psychology (Becker & Maiman, 1975; Rosenstock, 1966;
Rosenstock, Strecher & Becker, 1988). Lewin's principal concept from Field Theory
was the interdependent relationship between the person and his or her environment
which proposed that it is the person's interpretation of the environment that guides
behaviour rather than just the environment itself.
Value Expectancy Theory attempts to describe behaviour under conditions of
uncertainty (Becker & Maiman, 1975). Thus, 'Behaviour is predicted from the value
of an outcome to an individual, and from the individual's expectation that a given
action will result in that outcome' (Becker & Maiman, 1975, p. 11). A person will be
motivated to act if there is a state of readiness and if some benefit for the effort can be
expected. According to this theory, compliance with recommended health behaviour
depends on a readiness to comply due to a belief that a threat actually exists, the belief
that compliance is in fact feasible and that a particular health behaviour or treatment
will indeed lead to beneficial results.
Rotter's (1954) Social Learning Theory and the Health Belief Model are two
important examples of Value-Expectancy models which have been used extensively as
a means to understanding health behaviour.
Rotter's social learning approach is an attempt to integrate stimulus-response theories
and cognitive theories into a coherent account of behaviour (Rotter, 1975; Rotter,
Chance & Phares, 1972) in a similar way to Bandura's theorising. Thus, behaviour is
predicted by the interaction of the person's values, expectancies and psychological
situation. Rotter's theory states that behaviour is a function of the expectancy that the
behaviour will lead to a particular reinforcement in that situation and the value of the
reinforcement to the individual (Rotter, 1954).
8
Expectancies in this formulation have a particular emphasis on reinforcement value
where reinforcement strengthens an expectancy that a particular behaviour will be
followed by a reinforcement in the future (Rotter, 1966). One general expectancy that
stems from this theory and that was used in the present study is Health Locus of
Control.
The Health Belief Model (Becker, 1974; Rosenstock, 1966, 1974) emphasises the
relative role of perceived gains and losses in determining the motivation to carry out a
particular health related behaviour. The model was developed by a group of public
health investigators in the United States during the 1950's, hence its specific
application to health related behaviour.
The model is based on the Lewinian (1935) concept of the life space in which there
are negatively valued, positively valued and neutral regions. According to this model,
disease represents a negative region from which the person is motivated to move away
and health represents a region towards which the individual is pulled. As Rosenstock
(1974, p. 330) put it, behaviour depends on being pulled by positive forces and
repelled by negative forces.
A number of dimensions are derived from this theoretical base and represent the
individual's beliefs about disease or health problems and about the effect of likely
health-related action. These dimensions are beliefs about susceptibility to, and beliefs
about, severity of an illness or health problem, perceived benefits of taking a
particular course of health action and the value of an outcome minus the barriers to
taking action (Becker, 1974).
The Health Belief Model and the research conducted with it are described in more
detail below in Section Five.
While both Social Cognitive Theory and Value Expectancy Theory are derived from
similar theoretical assumptions about the role of cognitive factors in the determination
of behaviour, there is competition between them with respect to explaining health
behaviour. As will be shown below, very few studies into health behaviour have
investigated variables from both models at the same time. This may explain why only
a relatively small amount of the variance in health behaviour is explained in these
studies.
9
Somewhat better predictions of behaviour may be obtained by measuring the
contribution of self-efficacy, outcome expectancy, health locus of control and
variables derived from the Health Belief Model in explaining the behaviour in question
(Rosenstock, 1988). Unlike other research in this area, the present study combined
variables derived from Social Cognitive Theory and Value Expectancy Theory in an
attempt to explain health behaviour following a myocardial infarction.
3.3 Summary
A number of psychological theories and models have been developed that may be
applied to the understanding of health behaviour. Some of the theories and models
used in this study are based on Cognitive-behavioural Theory which combines
stimulus-response and cognitive explanations of human behaviour into one
framework. Cognitive-behavioural Theory has resulted in the development of two
additional theories, Social Cognitive Theory and Value Expectancy Theory, from
which many of the models, theories and variables used in this study were derived.
This study attempted to investigate the extent to which variables obtained from Social
Cognitive Theory and Value Expectancy Theory might explain health behaviour,
while previous research has tended to emphasise one theory in isolation from the
other.
4.0 Self-Efficacy
4.1 Expectancies
As described above, one aspect of Social Cognitive Theory that has created considerable
interest in the analysis of behaviour change has been that of the role of self- referent
thought as a mediator between knowledge and action (Bandura, 1986). In this model,
perceived self-efficacy and outcome expectation are seen as the major determinants in the
prediction of behaviour. In this section self-efficacy and outcome expectation are
outlined, and their potential role in the prediction of health behaviour is described in
relation to research in the area.
Self-efficacy has been defined as a judgement of one's ability to successfully organise
and execute courses of action required to attain particular outcomes or performances
(Bandura, 1977b, 1986). A high degree of self-efficacy about performing a behaviour to
achieve some desired outcome refers to a person's judgement that he or she is very
confident of performing that behaviour. Conversely, low self-efficacy is a judgement of a
low confidence of success.
Application of self-efficacy theory to health behaviour would mean that people's ability to
engage in health behaviours that contribute to the prevention of myocardial infarction,
such as cessation of smoking, for example, might be affected by perceptions of self-
efficacy for these behaviours.
Self-efficacy can be measured in terms of magnitude or level, strength and generality
(Bandura, 1977a). Self-efficacy magnitude is a measure of the level of performance
people believe they are capable of achieving. Thus, in foundation research that tested self-
efficacy theory with subjects suffering from snake phobia, Bandura, Adams and Beyer
(1977) presented their subjects with a hierarchical list of 29 increasingly threatening
behaviours involving interaction with a boa constrictor. These behaviours ranged from
subjects approaching the snake in a glass case to them actually allowing the serpent to
crawl on their laps. The level of self-efficacy was taken as the most threatening behaviour
from the list that the subject thought they would be able to perform.
Self-efficacy strength is a measure of confidence about successfully performing a
particular behaviour. The subjects in the above mentioned experiment (Bandura, Adams
& Beyer, 1977) were asked to indicate on a 10-point scale, for those approach behaviours
they believed they could perform, the degree of their confidence that they would be
successful at performing them. The scale consisted of 10-point intervals ranging from 0
to 100 indicating high uncertainty through to complete certainty.
Generality of self-efficacy refers to the extent to which a self-efficacy belief can be
generalised beyond a specific behaviour or treatment situation (Bandura, 1977a). Some
experiences may create a sense of personal mastery for a number of actions whereas
others may not be generalised at all. Bandura and Adams (1982) obtained a measure of
generality in a snake phobia experiment by asking subjects to rate the level and strength of
their perceived ability to cope with other snakes. Self-efficacy measures were also
obtained for being able to approach other animals.
According to Bandura (1977a, 1977b, 1986) one's self-efficacy beliefs may be obtained
from four principal sources. These are, in order of influence on self-efficacy:
performance accomplishments; vicarious experience; verbal persuasion; and emotional
arousal.
The most powerful source of self-efficacy information is actually performing and being
successful in a particular task or behaviour since this involves personal mastery
(Bandura, 1977b). Conversely, failures and avoidance will decrease self-efficacy.
The next most influential means by which self-efficacy information is obtained is through
vicarious experiences or modelling. Like behaviour in general, beliefs are not learned
only from actual performance. Perceptions of self-efficacy can also be obtained from live
and symbolic modelling (Bandura, 1977a, 1986). Seeing other people perform
behaviours increases perceptions of the observer that they too can perform the behaviour.
Verbal persuasion is the third source of self-efficacy information and is probably the most
often used means used to help people change their behaviour, particularly health
behaviour. Like modelling, verbal persuasion also increases the likelihood that the person
will sustain effort and persist in the face of difficulties (Bandura, 1977a, 1986).
The final means by which self-efficacy information may be obtained is through feedback
obtained by one's level of emotional arousal (Bandura, 1977b, 1986). Anxiety is usually
interpreted by a person as a sign that the situation is difficult, taxing or likely to result in
some negative experience. Thus, the higher the anxiety, the greater the likelihood that
self-efficacy for dealing with the situation will be low.
Bandura (1983, 1986) argues that there is a contingent relationship between self-efficacy
and outcome expectancies based on the straightforward notion that people come to learn
that performance affects outcome. Despite this relationship between self-efficacy and
outcome expectancy (Bandura, 1983, 1986), the two concepts can be clearly
distinguished.
Perceived outcome expectancy refers to a judgement that a given behaviour will lead to
certain desired outcomes (Bandura, 1977b, 1986). Outcomes are the consequences of
behaviour and may be in the form of intrinsic satisfaction, reduction of threat, an extrinsic
reward, or achieving something one desires.
Thus, performance of a particular behaviour is dependent upon the beliefs (rather than
actual abilities or real outcomes) of individuals as to their self-efficacy and their outcome
expectancy. However, self-efficacy represents for Bandura (1977a, 1977b, 1982, 1986)
the central cognitive mechanism through which behaviour change is mediated. He
believes that expected outcomes add little to the prediction of behaviour (Bandura, 1983,
1986). In fact, Bandura (1978) argues that in the absence of strong self-efficacy beliefs,
outcome expectancies, skills and motivation are incapable of producing successful
behaviour change.
A major criticism of self-efficacy theory stems from Bandura's assertion that self-efficacy
is the chief determinant of behaviour (1977a, 1984, 1986). In discussing the application
of Self-efficacy Theory to health behaviour, Rosenstock (1988) suggests that self-
efficacy is but one factor in the determination of health behaviour. Rosenstock argues that
perceptions of health threat seriousness, the degree of perceived susceptibility to a health
threat, barriers to carrying out recommended courses of health behaviour and perceived
benefits of that behaviour also contribute to health behaviour. These beliefs are all
variables derived from the Health Belief Model which is described in Section Five below.
Rosenstock argues that these variables also consistently predict health behaviour and that
self-efficacy is a potential barrier to health behaviour change and only one small
component of the whole model.
Lee (1989), Eysenck (1978) and Skinner (1987) have claimed that self-efficacy cannot be
evoked to explain behaviour because it is more of a metaphor and descriptor of behaviour
rather than having explanatory power.
Despite these criticisms there is a growing body of research to support the role of self-
efficacy as a determinant of behaviour. Some of this research is described below and
provides a basis for the investigation of self-efficacy in the present study.
4.2 Research into Self-Efficacy
Judgements of one's ability to cope, ability to use available skills, or effectiveness in
particular situations, will affect one's choice of activities, the effort that will be given to
that activity and persistence of effort when confronted with difficulties (Bandura, 1986).
Several lines of evidence have been obtained to support this hypothesis starting with the
analysis of fearful and avoidant behaviour by Bandura and his colleagues. Some of this
foundation research has been mentioned above and will be detailed below.
As suggested earlier, support for self-efficacy theory has also been used extensively in
research investigating health behaviour and health behaviour change. This research will
also be examined.
4.2.1. Foundation Research
The early support for self-efficacy theory was obtained in the analysis and treatment of
fearful and avoidance behaviour (e.g., Bandura, 1982; Bandura & Adams, 1977;
Bandura, Adams & Beyer, 1977; Biran & Wilson, 1981) where self-efficacy has been
used widely as a model in the investigation of behaviour change initiation and
maintenance.
Bandura, Adams and Beyer (1977) investigated the relationship between self-efficacy and
approach behaviour among a group of 33 severely snake phobics. The degree of
approach by each subject to a boa constrictor was measured. Level of fear when
approaching the snake and self-efficacy strength for approach behaviours they thought
they might be able to perform on a scale of 10 (low confidence) to 100 (high confidence)
with the boa constrictor and with snakes in general were obtained. Subjects were then
randomly assigned to one of three treatment conditions consisting of participant
modelling, vicarious modelling and no-treatment control.
Following treatment, the participant modelling and the vicarious modelling groups
showed an increase in self-efficacy level, self-efficacy strength and approach behaviour
with the snake. Participant modelling was found to be the best procedure in increasing
self-efficacy followed by vicarious modelling. The congruence between self-efficacy and
actual performance was 89% for the participant modelling group and 86% for the
vicarious modelling group.
Higher levels of self-efficacy level and strength at the completion of treatment were
associated with higher levels of approach behaviour and personal efficacy with respect to
approaching the snakes. Self-efficacy level, but not self-efficacy strength, was associated
with lower levels of anticipatory fear.
Bandura, Reese and Adams (1982) more directly tested the effect of self-efficacy on
behaviour by creating pre-determined levels of self-efficacy in individuals and then testing
behavioural and arousal effects.
Severely snake phobic subjects were tested for their level of behavioural avoidance, fear
arousal and self-efficacy judgements with respect to 18 approach behaviours involving a
boa constrictor. Those who could handle the snake with a gloved hand were considered
insufficiently phobic for the experiment. Subjects were then randomly assigned to low,
medium or high efficacy-induction conditions. Participant modelling was used to raise the
level of approach behaviour of subjects to the level of the group to which they were
assigned. Self-efficacy level and strength were associated with higher levels of approach
behaviour and lower levels of fear arousal.
Bandura, Taylor, Williams, Mefford and Barchas (1985) demonstrated additional
support, but with a small sample of 10, for the mediating effect of self-efficacy on arousal
due to environmental events in a study involving women with severe arachnaphobia. The
women were allocated to one of three groups on the basis of having a low, medium or
high self-efficacy for approach behaviours involving a Wolf spider.
Self-efficacy was assessed in the usual way with subjects being presented with a list of
18 hierarchical approach behaviours involving the spider such as watching it in a plastic
bowl, handling the spider with gloves, allowing the spider to crawl on the arm, and so
forth. Subjects were asked to indicate which of the behaviours they felt they would be
able to perform (self-efficacy level). They then indicated, on a 100-point scale with 10-
point intervals, how confident they were that they could perform the behaviours.
The women were then asked to engage in three of the performance tasks with the spider.
Blood catecholamine levels were monitored as a measure of autonomic arousal.
Epinephrine and norepinephrine levels were found to be differentially related to self-
efficacy. During interaction with the spider high perception of self-efficacy for a
behaviour resulted in low levels of these catecholamines and moderate self-efficacy led to
an increase in plasma catecholamine levels. Interestingly, when subjects decided not to
perform behaviours for which they had an extremely low level of self-efficacy their level
of catecholamines dropped, presumably because the need to cope with an anxiety
provoking situation was removed.
There is some support from these studies that high self-efficacy results in lowered arousal
and vice versa. It seems likely that people with a high degree of confidence that they can
successfully perform a particular task or behaviour will feel better able to cope with, and
hence feel less anxiety about, the behaviour than those with less confidence.
This notion is in concert with recent evidence suggesting that a person's perception of
control over a threat rather than actual ability to deal with the stressor is an important
determinant of the level of stress experienced (Lazarus, 1982; Lazarus & Folkman,
1988). While actual ability to control the threat may be low, a perception that one can
cope with an aversive event will result in little stress compared to a perception that one is
helpless. Self-efficacy, then, is one cognitive mechanism whereby the person's perceived
ability or inability to deal with threatening situations will affect the level of stress
(Bandura, 1986).
Myocardial infarction, the focus of this study, is a frightening event. Thus, it could be
expected that levels of anxiety felt by these people might be affected by their level and
strength of self-efficacy.
Since these important foundation studies, self-efficacy has been applied in a wide variety
of contexts including health behaviour, to which this discussion now turns.
4.2.2 Research in Health Behaviour and Self-efficacy
A number of studies have investigated the relationship between self-efficacy and some of
the health behaviours that were the focus of this study (Chambliss & Murray, 1979;
Colletti, Supnick & Payne, 1985; Condiotte & Lichtenstein, 1981; Devins & Edwards,
1988; DiClemente, 1981; DiClemente, Prochaska & Gilbertini, 1985; Garcia, Godding &
Glasgow, 1989; Chambliss & Murray, 1979; Ewalt, Taylor, Reese & DeBusk, 1983;
Jeffrey, Bjornson-Benson, Rosenthal, Lindquits, Kurth & Johnson, 1984; Prochaska,
Crimi, Lapsanski, Martel & Reid, 1982; Schmitz & Doerfler, 1990; Strecher, Becker,
Kirscht, Eraker & Graham-Tomasi, 1985). These studies provide support for the role of
self-efficacy in predicting smoking, dietary behaviour, exercise, relaxation and alcohol
consumption following myocardial infarction.
Studies investigating the role of self-efficacy in smoking behaviour, cessation and relapse
have provided consistent evidence that self-efficacy measures for smoking behaviour
predicts future abstinence. Furthermore, self-efficacy has predicted relapse following
intention to quit and enhancement of self-efficacy has contributed to success at quitting
(Strecher, DeVellis, Becker, & Rosenstock, 1986).

Devins and Edwards (1988) evaluated the role of self-efficacy, among other social
cognitive variables, in predicting changes in smoking behaviour. Subjects were presented
with a list of common stop-smoking techniques, that is, relaxation, engaging in alternate
activity, avoiding smokers and smoking situations, thinking of the negative effects of
smoking, buying fewer cigarettes, rewarding oneself with incentives and attending a
workshop. Outcome expectancy was measured by asking subjects to rate, on a 9-point
scale, their perceptions of the effectiveness of each technique in helping people give up
smoking. Similarly, self-efficacy strength was measured by asking subjects to indicate,
on a 9-point scale, how confident they were of performing each technique. The authors
found that higher self-efficacy for a particular technique was associated with low smoking
behaviour 1 month and 3 months later. A combination of high outcome expectancy and
high self-efficacy also predicted smoking behaviour.
Self-efficacy has been show to be related to relapse in attempts to stop smoking in a
number of other studies. Condiotte and Lichtenstein (1981) measured self-efficacy
strength, level and generality for resisting the urge to smoke in 48 common situations.
Seventy eight subjects enrolled in two quit smoking programs responded to each item
with a confidence score of between 10 (low confidence) and 100 (high confidence) using
a 10-point scale. Higher levels of self-efficacy were associated with continued abstinence
during treatment and abstinence for longer periods after treatment. There was also a high
degree of congruence between the clusters of situations in which subjects reported low
self-efficacy and in which they reported having eventually relapsed.
More recently, Garcia, Schmitz and Doerfler (1990), using a questionnaire developed by
Condiotte and Lichtenstein (1981), demonstrated a significant but small correlation
between self-efficacy for resisting smoking and the number of cigarettes smoked in a 4
week quit smoking program. Self-efficacy measured before the quit date was not
significantly correlated with resisting the urge to smoke in the first 2 weeks of the quit
smoking program. However, self-efficacy taken 2 weeks into the program did correlate
with the percentage of high risk situations in which subjects managed to resist the urge to
smoke in the final 2 weeks of the program. It appears that self-efficacy may well have
changed by becoming more realistic as the program progressed.
With respect to cardiac rehabilitation, the topic of this research, Ewart et al (1983)
examined the relationship between self-efficacy and exercise performance in subjects
recovering from uncomplicated myocardial infarction. Subjects were asked to indicate on
a 100-point scale, ranging from 10 (uncertain) to 100 (complete certainty), their self-
efficacy judgements for walking, running distances ranging from 1 block to 5 miles,
climbing stairs from a few steps to 4 flights, engaging in sexual intercourse for 1 to 20
minutes, lifting objects from 10 to 75 pounds and overall ability to tolerate physical
activity. Those with higher self-efficacy for these tasks performed better on the treadmill
test than those with lower self-efficacy. Higher self-efficacy also predicted increased
tolerance for sexual intercourse, lifting and general exertion at home as recorded on an
activity log and by heart rate monitoring.
Self-efficacy research with respect to dietary behaviour has largely been confined to
weight loss. Weinberg, Hughes, Critilli, England and Jackson (1984) asked subjects
involved in a weight reduction program to estimate their self-efficacy strength for success
in losing weight. Subjects were then split into high and low self-efficacy groups on the
basis of this pre-treatment questionnaire. They were also given a number of psychological
tests designed to give the impression of a psychological evaluation. On the basis of these
tests, subjects were given bogus but convincing feedback about their self-efficacy. Thus,
some subjects were given high self-efficacy feedback and some low self-efficacy
feedback no matter what their self-efficacy was prior to the weight reduction program.
Those given high self-efficacy feedback lost more weight than those given low self-
efficacy feedback.
Few studies have investigated the relationship between self-efficacy and alcohol
consumption. In a study primarily designed to investigate the effect of assertiveness on
the treatment outcome of 145 female alcoholics, Rist and Watzl (1983) also assessed self-
efficacy for resisting the urge to drink alcohol. These subjects were involved in a social
skills training program and were asked to rate, on a 10-point scale, the extent to which
they would be able to resist the urge to drink alcohol in certain social situations. Ignoring
those subjects who failed to remain abstemious during actual treatment, greater
perceptions of ability to resist the urge to drink alcohol in social situations predicted
treatment success 3 months later.
In summary, studies involving the self-efficacy construct have consistently demonstrated
self-efficacy to be a significant predictor of health behaviour. High levels of confidence in
the ability to perform a prescribed or desired health behaviour seem to predict greater
compliance with, and success in, achieving the behaviour. Stronger support for the
explanatory power of self-efficacy is found in studies in which self-efficacy has been
manipulated.
In many of the studies described above, the researchers attempted to test the hypotheses
about the predictive ability of self-efficacy by correlating the self-efficacy measures with
the measures of behaviours under investigation. A look at the statistical results of the
studies shows that the correlations between self-efficacy and health behaviour are
significant but often low. These results mean that though self-efficacy is a significant
predictor of health behaviour, it accounts for only a small percentage of variance in health
behaviour. It appears from the result of the studies on self-efficacy and health behaviour
that, for a stronger prediction of health behaviour, variables other than self-efficacy
should be taken into account. The present study investigated the ability of variables
derived from the Health Belief Model, Health Locus of Control variables and
psychological distress variables, in addition to the variables derived from Self-efficacy
Theory, to predict health behaviour.
An additional predictor of health behaviour derived from Self-efficacy Theory is outcome
expectation which was mentioned as a part of Bandura's (1977a) early theorising and is
conceptually related to self-efficacy. It is towards this construct that the discussion now
turns.
4.3 Outcome expectancy
Outcome expectancy, within the context of Bandura's (1977a) theory, has not received as
much attention as self-efficacy. Most studies involving self-efficacy do not include
outcome expectancy as a predictor measure of behaviour (Strecher et al, 1986). The
reason for this lack of attention may rest with Bandura's (1986) more recent contention
that outcome expectancy is so dependent on self-efficacy expectations that it adds little to
the prediction of behaviour. However, where it has been included the findings about the
relationship between outcome expectancy and behaviour have been mixed (Bandura,
1986).
For example, Devins and Edwards (1988) in a study on smoking cessation among
subjects with Chronic Obstructive Airways Disease, described in the previous section,
measured outcome expectancies for stop-smoking techniques. Subjects were asked to rate
the extent to which they believed certain quit smoking techniques would help them stop
smoking. Outcome expectation for each quit smoking technique was measured on a 9-
point scale ranging from 'not at all effective' to 'very effective'. An average outcome
expectancy score was calculated. Outcome efficacy was not a significant predictor of the
number of cigarettes smoked.
However, Stanley and Maddux (1986) found more positive results in investigating the
effects of self-efficacy, outcome expectation and outcome value on the intention of
subjects (195 male and female undergraduate psychology students) to engage in an
exercise program. The study involved the manipulation of high or low levels of self-
efficacy, outcome expectancy and outcome value by way of persuasive written
communication in a 2 x 2 x 2 factorial design. In order to manipulate outcome expectation
bogus research was used to indicate the benefits or otherwise of exercise on health and
well-being. Outcome value was manipulated by information related to the value placed on
such a program by society. High or low levels of self-efficacy expectation were created
by providing subjects with bogus research that indicated the ability or inability of students
in other studies to complete exercise programs of this sort. Manipulation checks showed
that the communications had affected the independent variables in the desired direction.
Subjects were then asked to indicate their intention of engaging in the exercise program
and were given the opportunity to actually sign up for an orientation to the program as a
measure of their motivation.
Both outcome expectancy and self-efficacy were significantly related to intention to
exercise. A hierarchical regression analysis revealed that outcome expectancy was the best
predictor of intention to exercise, accounting for 26% of the variance. Self-efficacy
accounted for an additional 17% of the explained variance.
It must be emphasised that intention to exercise, rather than actual exercise behaviour,
was used by Stanley and Maddux (1986). A much more robust test of the effectiveness of
outcome expectancy would be to compare the effects of outcome expectation on actual
future behaviour as tested by Devins and Edwards (1988), for example.
While there is marginal support for outcome expectation as a predictor of health behaviour
it has received little attention despite being an important component of Bandura's (1977a)
original model. There is also some evidence that there may be a relationship between self-
efficacy and outcome expectation that warrants further investigation. Devins and Edwards
(1988), for example, found a large correlation between self-efficacy and outcome
expectation in their research on smoking cessation.
It was decided, in the present study, to further investigate the role of outcome
expectation, in relation to self-efficacy, in predicting health behaviour. More specifically,
the extent to which beliefs about smoking less, eating a low fat diet, exercising more,
drinking less alcohol and relaxing more might help prevent future heart attacks would
affect a person's compliance with performing these behaviours following a heart attack,
was measured.
4 . 6 Summary
According to Bandura's (1977a, 1986) Social Cognitive Theory, behaviour is determined
by judgements about how successful one will be in executing the behaviour (self-
efficacy) and by judgements about the likely outcomes of the behaviour (outcome
expectation).
Self-efficacy judgements have consistently been shown to predict behaviour in a number
of contexts including health-related behaviour. Outcome expectation has not been shown
to be a good predictor of behaviour in the few studies in which it has been investigated
and it is often excluded from studies investigating self-efficacy. In the present study, both
self-efficacy and outcome expectation with respect to health behaviour following
myocardial infarction were measured to shed further light on the predictive power of each
construct and the relationship between them.
The amount of variance in health behaviour explained by these two variables is often quite
small, however, and suggests that self-efficacy and outcome expectation should be
included in the Health Belief Model (Rosenstock, Strecher and Becker, 1988). This
model is now described in detail.
5.0 The Health Belief Model
The Health Belief Model was developed in the 1950's as a means of explaining the failure
of disease prevention programs in the United States (Kirscht, 1974) rather than out of
mainstream psychological research. However, as described in Section Three of this
chapter, the model has theoretical underpinnings based in Value Expectancy Theory but
with specific reference to health-related behaviour. Value Expectancy Theory posits that
the potential performance of a particular health behaviour will depend on the value of
being healthy and the expectancy that the behaviour will in fact achieve that health state.
From a motivational point of view, Kirscht (1988) suggests that the model represents the
beliefs that will result in a state of readiness to act in the face of a threat.
This section will describe the specific components of the model and review the research
relating specifically to changing health habits, the focus of this study.
5.1 The Components of the Model
The Health Belief Model (Becker & Maiman, 1975; Janz & Becker, 1984; Rosenstock,
1974) consists of a number of components that affect a person's goal directed health
behaviour. These components are as follows:
Susceptibility
Susceptibility refers to the subjective perception by the individual of the actual risk of
contracting a condition or susceptibility to illness in general (Janz & Becker, 1984).
Seriousness or Severity
Health related behaviour is also determined by how serious an illness or potential health
threat is perceived by the person (Janz & Becker, 1984).
Benefits minus Barriers
It is hypothesised in the model that the perceived benefits minus the perceived costs of or
barriers to engaging in a particular health behaviour will affect motivation to proceed.
Benefits have been compared to outcome expectations as described in Social Cognitive
Theory (Rosenstock, Strecher & Becker, 1988). Barriers to health behaviour such as
exercising or attending quit-smoking classes, for example, consist of the time
commitment, inconvenience and financial cost.
Cues to Action
Previous experiences and knowledge are also considered important by providing cues to a
preferred path of action. Cues may be derived from internal bodily states or from external
sources such as the media or health professionals, for example.
Thus, according to Rosenstock (1974):
• the belief that one is susceptible to an illness and the belief that the consequences of the
illness are severe leads to a drive to act,
• an evaluation of perceived benefits minus perceived barriers provides a path of action,
and
• other cues to action are found in information provided by the media, advice from
people such as health care professionals, reading and real life experiences.
Thus, measures derived from the Health Belief Model were obtained from participants in
this study to determine their effect on engaging in health related behaviour following a
myocardial infarction.
Finally, the beliefs and understanding a person has about his or her actual health
behaviour and desired health behaviour leaves considerable room for conflict within the
individual. For example, a person might believe that he or she is at considerable risk of
developing heart disease due to smoking but feels unable to stop the habit because
smoking meets some special need. This state of affairs is likely to result in distress. The
relationship between distress and variables from the Health Belief Model was also
investigated in this study.
5.2 Measures of Health Beliefs
Health belief components are measured using questionnaires which vary from long, fairly
complex questionnaires (e.g., Becker, Maiman, Kirscht, Haefner & Drachman, 1977;
Wessfeld, Kirscht & Brock, 1990) to single questions representing each variable of the
model related to a particular health behaviour (e.g., Rundall & Wheeler, 1979; Beck &
Lund, 1882). Studies also vary as to the number of components investigated and often
ignore the interaction between the various components of the model.
Items relating to health beliefs are invariably put in a Likert format using 4-point to 10-
point scales and may refer to specific health behaviours or diseases (e.g., heart attacks,
cancer or influenza) or more general states of concern, susceptibility or seriousness.
Typically, items ask questions such as 'How likely is it that you will have a heart attack
(or some other disease) in the future?' or 'How concerned are you about getting cancer in
the future?'. Alternatively, questions involve statements such as, 'Diabetes can be a
serious disease if you don't control it', to which the subject responds with a degree of
agreement or disagreement (Given, Given, Gallin & Condon, 1983).
Janz and Becker (1984), in their comprehensive review of research with the Health Belief
Model between 1974 and 1984, reported a wide variety of 'self-made' health belief
questionnaires varying greatly in sophistication. They have argued, however, that '...it is
a testament to the robustness of the model that the dimensions remain predictive despite
these different measures' (1984, p. 45).
Two studies provide evidence that questions of this type actually measure the components
of the Health Belief Model. Weissfeld, Kirscht and Brock (1990) undertook a factor
analysis of a list of 32 questionnaire items from previous health belief research in an
investigation of health beliefs with respect to high blood pressure. The responses to 2802
interviews revealed six factors. These were: general health concern, general health threat,
belief in personal susceptibility to cardiovascular diseases, belief about severity of certain
cardiovascular diseases, beliefs about the medical benefits of treatment and beliefs about
what one can do personally about one's health (self-help benefits).
Jette, Cummings, Brock, Phelps and Naessens (1981) investigated the structure and
reliability of health belief indices. A questionnaire was constructed using 31 items from a
number of previous studies that measured specific and general health beliefs. These
beliefs were: susceptibility to, and severity of, specific illnesses such as heart attacks, flu,
dental cavities and a cold; general threat to health; concern about health matters; barriers to
taking prescribed medications; health locus of control; trust in physicians; and health
status.
The responses from two independent samples were factor analysed and eight factors were
identified. These were; general health threat, perceived barriers to taking medication,
perceived severity, perceived susceptibility, health locus of control, trust in physicians,
concern about health and perceived health status. The factor loadings and measures of
item reliability provided considerable support for the reliability of items used commonly
in health belief research and also for the independence of health belief components.
However, the absence of a standardised questionnaire for measuring the components of
the health belief model and the variety of items that are used can be seen as a limiting
factor in health belief research. Nonetheless, there appears to be considerable support for
the predictive value of the various components of the Health Belief Model.
5.3 Research with the Health Belief Model
A large number of studies have investigated the role of variables from the Health Belief
Model in determining health behaviour. Very few of these studies have involved health
behaviour and coronary artery disease, the focus of this study. However, compliance
with recommended health action, smoking and dietary behaviour, all components of this
study, have been investigated and lend support to the use of components of the Health
Belief Model in predicting health behaviour following myocardial infarction.
In a relatively recent review of 29 studies conducted over a 10 year period from 1974 to
1984, Janz and Becker (1984) concluded that there was considerable empirical support
for all the components of the Health Belief Model.
The research reviewed by Janz and Becker (1984) covered a wide range of preventive
health behaviours including inoculation (Aho, 1979; Cummings, Jette and Brock, 1979;
Rundall & Wheeler, 1979; Larsen, Bergman & Heidrich, 1982), screening behaviours
(Becker, Drachman & Kirscht, 1972; Hallal, 1982; King, 1982 ) and risk factor
behaviour (Aho, 1977; Becker et al, 1977; Langlie, 1977) as well as compliance with
medical advice such as diet and medication regimens (Hartman & Becker, 1978; Kirscht
& Rosenstock, 1977).
Unfortunately, most of the research reviewed was retrospective. Limits to generalisability
of these studies, other than the fact that they were retrospective, include small sample
sizes, low response rates and sometimes unclear explanations of how the dependent and
independent variables were measured.
However, 12 of the studies reviewed by Janz and Becker (1984) were prospective and
offer more convincing support for the Health Belief Model. One early prospective and
well constructed study was conducted by the Becker and Maiman team in which they
investigated dietary compliance (Becker et al, 1977). The study attempted to determine the
relationship between weight loss, as a measure of treatment compliance, in a group of
obese children and the health beliefs of their mothers or carers. Since the mothers or
carers spent a great deal of time with their children, it was argued that the mothers' or
carers' health beliefs would have a significant effect on the children's weight.
Perceptions about concern for the child's health, perceived susceptibility to illness,
perception of the severity of illness and feelings about of the child being overweight were
obtained by way of a structured interview. The mother's or carer's concern about the
child's health and beliefs about the susceptibility of the child to illness were predictive of
weight loss after 2 months. Beliefs in the severity of general illnesses and obesity were
also predictive of weight loss. Unfortunately, the correlations between these health beliefs
and weight loss, although significant, ranged from .21 to .31. Like much of the research
with the Health Belief Model, these correlations were very small and left a large
proportion of the variance in health behaviour unexplained.
Similarly, a more recent study by Contento and Murphy (1990) attempted to differentiate
between people who had made desirable dietary changes lasting for at least 12 months
and those who had not. Those who had made dietary changes in that period believed
themselves to be more susceptible to disease, perceived greater benefits from dietary
change and had greater overall health concern than those who had not. While a
discriminant function analysis demonstrated that perceived benefits to dietary change and
susceptibility to illness were predictive of dietary change, the coefficients were relatively
low suggesting that other factors influenced dietary change in this study as well as health
beliefs; a finding similar to many other studies. The investigation suffered from being
retrospective and from using only a convenience sample.
In an unpublished but prospective study reported by Kirscht (1988), Kirscht, Janz and
Becker investigated the relationship of health beliefs to smoking cessation among 250
patients who were attending an internal medicine clinic. Intention to quit smoking was the
best predictor of cessation at a 6 month follow-up. However, intention to quit was
predicted by beliefs about the reduction in susceptibility to health problems and perceived
susceptibility to health problems if smoking continued. Unfortunately, statistical data
were not reported by Kirscht so it is difficult to evaluate the efficacy of the findings.
With respect to heart disease, Aho (1977) investigated the health beliefs of 187 wives of
men who had suffered a myocardial infarction, in relation to their preventive health
orientation. The study of wives' health beliefs was considered important because the
author assumed that their health beliefs would influence their husbands' health behaviour.
The women were placed in a high, medium or low preventive orientation group,
depending on their response to an interview. A significant proportion of women in the
high preventive orientation group believed that their husbands were likely to suffer a heart
attack in the future.
The severity of having heart disease, as measured by a question about how normal a life
one might lead with a heart condition, was related to a high preventive health orientation
on the part of the wives. Twice as many women in the low preventative health orientation
group viewed heart disease as likely to interfere with a normal life as in the high
orientation group. However, measuring severity of heart disease with a question about
the chances of leading a normal life may be too indirect a measure. Beliefs about the
effectiveness of treatment for heart disease were significantly related to a high preventive
health orientation. Unfortunately preventive health orientation is rather a weak measure in
Aho's (1977) study. Better measures would have been specific health behaviours such as
smoking and dietary behaviour, for example.
Other studies in areas unrelated to the health behaviours investigated in the present study
but which measure compliance with recommended courses of health action have
demonstrated that components of the Health Belief Model may play a role in determining
health behaviour.
For example, Carter, Beach, Inui, Kirscht and Prodzinski (1986) recommended to 874
patients with chronic illnesses that they have vaccinations the following year against
influenza. They found that beliefs about susceptibility to influenza accounted for some
25% of the variance in actual compliance 12 months later.
In a study not reviewed by Janz and Becker (1984), Wurtele, Roberts and Leeper (1982)
enrolled 553 people in a tuberculosis (TB) detection drive. The study investigated the
effect of health beliefs on compliance with an instruction to return to have a skin test
checked 48 hours after the initial test. Beliefs about the severity of TB, susceptibility to
TB, barriers to returning and outcome efficacy predicted return for the test.
Champion (1988), in another prospective study, found that susceptibility, seriousness,
barriers and health motivation accounted for 61% of the variance in predicting proficiency
in breast self-examination among 380 women. Beck and Lund (1982) manipulated
perceptions of seriousness and susceptibility to peridontal disease. Subjects with higher
levels of perceived seriousness flossed more frequently, in accordance with advice, than
those with lower levels. However, the correlation, while significant, was only .35.
In a study of smoking behaviour, Weinberger, Greene, Mamlin and Jerin (1981)
compared the health beliefs of heavy, moderate, and ex-smokers. Severity of the health
effects of smoking was measured by asking respondents why people should quit
smoking. Responses were coded as 'no reason', 'vague reasons' or 'clearly identified
specific health consequences of smoking'. Subjects were also asked to rate their
susceptibility to ill effects on their own health as a result of smoking and the likelihood of
their experiencing health problems as a result of smoking in the future.
Discriminant analysis produced two functions. The first function discriminated ex-
smokers from the other groups. Ex-smokers were more likely to cite reasons why people
should quit smoking and to perceive the complications smoking can create to their health.
The second function identified that moderate smokers were able to state acute
complications associated with smoking but did not feel susceptible to these diseases.
5 . 4 Summary
There has been a considerable amount of research with the Health Belief Model with a
wide variety of health behaviours. These studies have shown health belief variables to
predict compliance with recommended health behaviour and generally support the model.
However, the research also suggests that the Health Belief Model may need further
development. Many of the studies suffer from the problem of being retrospective. In
addition, the correlation coefficients between health beliefs and health behaviour are often
very low leaving a large proportion of variance unexplained, thereby suggesting that the
model needs further refinement in identifying other factors that play a role in health related
behaviour.
There is sufficient support for the inclusion of variables from the Health Belief Model,
particularly those that measure perceptions of health threat seriousness and susceptibility,
to include them in this study with other potential predictors.
Therefore, understanding the role of health beliefs in determining the likelihood of self-
reported health behaviour change following myocardial infarction was seen as being of
considerable utility in this study. As suggested previously, compliance with health
behaviour change such as modifying diet, cessation of smoking, relaxing more, limiting
alcohol and increasing exercise is an essential component of rehabilitation and prevention
of further infarction.
In particular, a person's health beliefs at the time of acute recovery were seen as potential
predictors of the likelihood of self-reported compliance with recommended health
behaviour in this study. It was thought that if health beliefs did in fact predict compliance,
then counselling could be directed towards modifying inappropriate beliefs during
rehabilitation.
The discussion now turns to the role of locus of control beliefs in predicting health
behaviour.
6.0 Locus of Control
6.1 Generalised Locus of Control
As described earlier, Rotter's (1954, 1966) Social Learning Theory emphasises the
interaction of expectancies or reinforcement, need value, experience and outcomes in the
prediction of behaviour. The generalisation of expectancies enables people to hypothesise
about expectancy of reinforcement in novel situations based on previous experiences.
Clearly the emphasis on generalised expectancy of reinforcement increases as the
individual's specific experience in the situation decreases (Rotter, 1966, 1975).
There are two kinds of generalised expectancies in Rotter's theory. One involves
expectancies for a particular kind of reinforcement and the other is a problem solving
expectancy. Problem solving expectancy refers to situations which involve different types
of reinforcements and where the person has to find ways to achieve outcomes in the face
of intervening factors. Generalised expectancies for a particular reinforcement and
problem solving represent a personality characteristic that enables a broad prediction of
behaviour.
One type of generalised expectancy is internal-external locus of control of reinforcement.
Locus of control of reinforcement is defined as the '...degree to which individuals
perceive events in their lives as being a consequence of their own actions, and thereby
controllable (internal control), or as being unrelated to their own behaviour, and therefore
beyond personal control (external control)' (Lefcourt, 1976, p. 145).
Individuals with a strong internal locus of control of reinforcement attribute rewards (the
achievement of desired outcomes) as resulting from their own actions. Conversely,
people with external locus of control of reinforcement believe that desired outcomes are
the result of fate, luck, chance or other forces beyond personal control.
One of the important variables that needs to be taken into consideration when evaluating
the effect of locus of control is the value of the reinforcement to the person (Rotter,
1975). Clearly, if a person does not value a particular outcome then motivation to behave
purposefully will be reduced, irrespective of locus of control.
According to Rotter, Chance and Phares (1972) a person with an internal locus of control
of reinforcement is likely to behave differently to a person with external locus of control
in four principal ways. Firstly, the person with an internal orientation will be more open
to seeking out and using information from the environment. Secondly, 'internals' will be
more likely to do things to influence environmental conditions to obtain benefit. Thirdly,
'internals' will place greater value on skill and personal ability. Lastly, 'internals' are
more resistant to attempts to influence them. More recently, studies have revealed that
'internals' have greater achievement motivation (Findlay & Cooper, 1983) and cope
better with stresses and difficulties (Lefcourt, 1982; Wolk & Bloom, 1977).
Originally, locus of control was measured as a unidimensional construct with Rotter's I-E
Scale (Rotter, 1966) being the most notable and widely used tool. Levenson (1973)
factor analysed Rotter's I-E Scale and found two other dimensions in addition to
internality-externality. These were the influence of powerful others and the influence of
chance or fate. People with high powerful others locus of control believe that what
happens to them results from the influence of significant people. People with a high
chance locus of control believe that they are the victims of fate or chance.
On the basis of this finding Levenson (1973) developed a multidimensional locus of
control scale consisting of three Liken scales, each consisting of eight items, which she
called Internality, Powerful Others and Chance. The Powerful Others and Chance scales
were positively (r = .59) correlated whereas neither was correlated with internality.
Since the development of general and multidimensional locus of control scales, the
construct has been more specifically applied to health behaviour.
6.2 Health Locus of Control
6.2.1. Measures of Health Locus of Control
It is not surprising that the concept of locus of control should be specifically applied to
health and illness behaviour. Strickland's (1978) review of a number of early studies
demonstrated a positive relationship between internal control of reinforcement and
physical health. As Strickland (1978) pointed out, one would expect that 'internals'
would seek out health knowledge, be more receptive to health messages and be more
active in health related behaviour than 'externals'.
However, Wallston, Maides and Wallston (1976) and Wallston and Wallston (1978) in
their reviews stated that Strickland failed to mention a number of negative findings that
showed no relationship between health behaviour and locus of control, These authors
also suggested that there are a number unpublished studies that also show no
relationship. Lau (1988) has stated that this is highly likely since the Wallston research
group have acted as a clearing house for locus of control research in health and had
access to considerable unpublished research.
Nonetheless, Wallston, Maides and Wallston (1976) claimed that expectancies for
specific situations are more likely to determine behaviour than generalised expectancies
Thus, they argued that a specific health locus of control scale would provide a more
sensitive measure of health related behaviour than a general locus of control scale.
The first real attempt to develop a health specific locus of control scale was undertaken by
Wallston, Maides and Wallston (1976). Rather than using a forced choice format, as in
previous scales such as Rotter's I-E Scale, they used a 6-point Likert scale ranging from
strongly disagree to strongly agree. The scale was designed to provide a single health
internality-externality score.
Following Levenson's (1974) contention that locus of control is a multidimensional
construct, Wallston, Wallston and DeVellis (1978) developed the Multidimensional
Health Locus of Control Scale (MHLCS). As described above, this consisted of three
constructs; internality, powerful others and chance health locus of control. People with a
high powerful others health locus of control believe that their health results from what
others such as doctors or nurses do for them. People with high chance health locus of
control beliefs attribute their health or ill health to fate or chance.
The MHLCS was developed using the original 11 items from the Health Locus of
Control scale (Wallston, Maides & Wallston, 1976) to which were added more
internality-externality items, as well as powerful others and chance items, to a total of 81.
A questionnaire containing these items, a desirability scale and two health status items
was distributed to 282 people waiting at an airport. These people were asked to mail the
completed questionnaires back to the authors. Eventually 115 questionnaires were
returned and analysed.
Item analysis was conducted on the internal, powerful others and chance items. Six pairs
of items were chosen for each group on the basis of closeness to the midpoint, wide
distribution of response alternatives on the item, significant correlation between the scale
and the scale minus the item itself, low correlation with the item and the social desirability
factor, and item wording. The pairs were used to construct two alternative scales, A and
B, each with 18 items equally divided into internal, powerful others and chance
constructs. There was a high degree of equivalency between the A and B scales.
For the combined scale (A & B), there was a small non-significant correlation between
powerful others and internality, a significant negative correlation between internality and
chance, and a positive but non-significant correlation between powerful others and
chance.
There have been mixed findings, since this original study, regarding the relationship
between the three constructs and the internal validity of the scale in unhealthy
populations.
Hartke and Kunce (1982) subjected all 18 items on Form A to factor analysis using a
sample of 86 medical patients and confirmed the independence of the three subscales.
Similarly, Russell and Ludenia (1983) demonstrated the factorial validity and
independence of both versions of the scale on an alcoholic population of 10. Hase and
Douglas (1987), in a small sample of 30 patients who had experienced myocardial
infarction, found that powerful others was independent of internality and chance.
Internality was found to be negatively correlated with chance.
Conversely, with a population of British university students, O'Looney and Barrett
(1983) found only two factors in a male sample of 70 and three factors in a female sample
of 77. The factors in the male sample consisted of the internality and chance subscales
together as the first factor, and the powerful others subscale as the second factor.
Umlauf and Frank (1986) investigated the scale with a sample of 107 rehabilitation
patients and were able to replicate only internality in their factor analysis. Cooper and
Fraboni (1988) demonstrated the distinctiveness of internality in the scale in a healthy
population of 82 staff in a psychiatric hospital. However, powerful others and chance did
not appear as independent factors.
It would appear that different populations yield somewhat different results in terms of the
relationship between the subscales. It is possible that specific health concerns in specific
circumstances are not adequately measured by a general health locus of control scale. It is
interesting to note that many of the studies utilising health locus of control scales with
patient populations have demonstrated significant relationships with respect to health
behaviour while research with non-patient populations has not (Wallston & Wallston,
1981). Wallston and Wallston (1981) have also suggested that the use of highly specific
health locus of control scales should be encouraged.
Thus, a specific scale to measure cardiac health locus of control beliefs was developed for
use in the present study. This scale was derived by taking Form A of the MHLCS and
substituting reference to 'health' or 'illness' with the more specific problem of 'heart
attack'. Subjects indicated on a 6-point scale, the extent to which they agreed or disagreed
with 18 statements relating to their health locus of control beliefs with respect to heart
attacks. A low score indicated strong disagreement and a high score indicated strong
agreement.
The complete questionnaire, the Multidimensional Cardiac Health Locus of Control Scale
(MCHLCS is provided in the Appendix to this thesis (Appendix A8) and consists of three
subscales, Internality, Powerful Others and Chance, each being composed of six
randomly distributed items. Thus, each subscale has a range of between 6 and 36.
To provide a measure of validity for the MCHLCS a sample of 28 male surgical patients
completed both the MHLCS and MCHLCS on subsequent days. The correlations
between the three subscales, internality, powerful others and chance on the two
questionnaires were .89, .83 and .78 respectively, lending support for the MCHLCS as a
measure of Cardiac Health Locus of Control.
6.2.2 Research With Health Locus of Control and Health Behaviour
As stated previously, early reviews (Strickland, 1978; Wallston & Wallston, 1981, 1982)
have demonstrated mixed findings regarding the role of locus of control in the
determination of health behaviour. The reasons for this may be the poorly refined
measurement of the construct and the lack of a specific health locus of control measure,
the use of different instruments and a failure to measure locus of control in the context of
health value (Wallston & Wallston, 1981).
According to Rotter (1975) the value of the reinforcement to the person is an important
variable affecting locus of control judgements. Clearly, if a person does not value a
particular outcome then motivation to behave purposefully will be reduced irrespective of
locus of control.
Rotter (1975) provided a very good example of how value interacts with locus of control.
A person with a general internal orientation may not belong to a protest group because he
or she does not believe in the objectives of the group and therefore does not act.
Conversely, an external may belong to the same group for any number of reasons such as
liking the other members, a desire to upset other people or simply for something to do.
There has been some research investigating the role of Health Locus of Control and the
health behaviours investigated in this study.
A number of recent studies have demonstrated a relationship between health locus of
control and health related behaviour. However, as Speake, Cowan and Pellet (1989)
showed in a study investigating the health behaviour of a large sample of elderly people,
the correlations are sometimes very small. Internal locus of control was significantly
correlated with positive exercise behaviour, low stress, nutrition, health responsiveness
and self-actualisation but the correlations were very low and ranged from .12 to .2.
Houts and Warland (1989) investigated the relationship between internal health locus of
control and dietary behaviour in a sample of 458 subjects (414 women and 44 men) who
prepared food for their household. Consistent with the notion of using specific locus of
control scales, Houts and Warland (1989) adapted five items from the Internal subscale
of the Health Locus of Control Scale (Wallston & Wallston, 1981) and related them to
eating behaviour.
Eating habits were measured by nine questions using a 3-point Likert scale. A high score
reflected the avoidance of cholesterol, salt, sugar and calories, and the eating of
vegetables and fruit. The value of food preparation was also measured and subjects were
grouped according to a positive or a negative value orientation. 'Internals' demonstrated
more nutritious eating habits than 'externals'. However, internal health locus of control
contributed to only 13% of the variance in nutritious food behaviour.
Some research, involving locus of control as a variable, has been conducted with patients
recovering from myocardial infarction. Cromwell, Butterfield, Brayfield and Curry
(1977) investigated, in part, how patients coped with the life threatening experience of a
myocardial infarction. Using Rotter's I-E scale, subjects were classified as having either
an internal or an external locus of control.
'Externals' were found to be more depressed and had significantly higher temperatures,
had poorer physiological outcome on three measures (sedimentation rates, serum
glutamic oxaloacetic transaminase and lactate dehydrogenase) and spent more days in the
coronary care unit than 'internals'. In general, 'externals' had a poorer prognostic rating.
It was found that 'internals' participated more in their own self care than 'externals' and
experienced a better outcome over a 12 week period. Unfortunately, no measure of health
value of these subjects was obtained by Cromwell et al (1977).
In a study investigating return to work following myocardial infarction, Smith and
O'Rourke (1988) included Rotter's I-E scale as a measure of locus of control.
'Internality' was not significantly related to early return to work. However, the study
failed to use a specific health locus of control scale nor was any measure of health value
taken.
Havik and Maeland (1988) investigated the smoking behaviour of 230 people who had
experienced a myocardial infarction. Smoking cessation is an important goal for patients
following an infarction and Havik and Maeland (1988) attempted to determine the reasons
for continuation of smoking in approximately half of all these patients. Among the
independent variables, an 11 item shortened version of the Health Locus of Control Scale
(Wallston, Wallston, Kaplan & Maides, 1976) was administered. Other variables
included cardiac health knowledge, psychological adjustment, severity of infarct, anxiety
and depression. It was found that high internal health locus of control beliefs tended to
delay relapse in smoking habits. However, it was not related to long term quitting.
Finally, some studies have shown internal health locus of control to change as a result of
illness or treatment (e.g., Bloom, 1979; Nicholson, 1980). Hase and Douglas (1987)
investigated the effect of teaching relaxation to patients recovering from uncomplicated
myocardial infarction on a number of recovery and psychological variables. Three of
these variables were internality, powerful others and chance as measured in the MHLC
Scale (Wallston, Wallston & Maides, 1978). It was found that compared with a non-
treatment control group, the relaxation group maintained their internal health locus of
control beliefs. The control group, however, become significantly more 'external' during
hospitalisation.
The present study investigated the stability of cardiac health locus of control beliefs as
well as their role in predicting self-reports of health behaviour following myocardial
infarction
6.4 Summary
There have been mixed findings about the role of internal health locus of control as a
predictor of the health behaviours investigated in this study, including recovery from
myocardial infarction.
The reasons for this inconsistency may have been the failure of many studies to consider
the value placed on health by subjects and that many have used general locus of control
scales rather than more specific scales to measure locus of control related to health
behaviour. However, locus of control has been shown to play a role in health-related
behaviour and may, in conjunction with other variables, add to the understanding of
health behaviour following myocardial infarction.
In the present study, both health value and cardiac health locus of control were used as
predictor variables for self-reported health behaviour.
The discussion now turns to the relationship between psychological distress and
psychological health, on the one hand, and health variables related to myocardial
infarction, on the other.
7.0 Psychological Distress and Psychological Health
In this study psychological distress specifically refers to self-reports of distress of
subjects with respect to their thoughts and to recent life events. Psychological health
refers to more general feelings of psychological well being.
Psychological distress and psychological health were of interest in this study for three
reasons. The first was that people who suffer from myocardial infarction experience
considerable distress and psychological morbidity both early and late in rehabilitation.
The second reason was that higher levels of distress and poorer psychological health have
been associated with lower compliance with health-related behaviour. Thirdly, both self-
efficacy and locus of control have been shown to predict psychological distress and
psychological health.
7.1 Psychological Distress and Psychological Health Following
Myocardial Infarction
There is evidence that a high proportion of patients recovering from myocardial infarction
experience emotional distress while in hospital (e.g., Byrne & Whyte, 1978; Byrne,
Whyte & Butler, 1981; Cay, Vetter, Phillip & Dugard, 1972; Dellipiani et al, 1976;
Hackett, Cassem & Wishnie, 1968; Hase & Douglas, 1987; Wynn, 1967).
In a review of a number of studies, Razin (1982) concluded that long lasting emotional
turmoil and occupational problems exist for perhaps 25% of these patients. Wiklund,
Same, Vedin and Wilhelmson (1984) found that 2 months after myocardial infarction and
1 year later, patients demonstrated emotional distress, a high number of self-reported
symptoms, avoidance behaviour, over-protection, pessimism and diminished sexual
activity. Moreover, depression, low morale and psychological distress have been shown
to be significant predictors of mortality (Mumford, Schlesinger & Glass, 1982).
Byrne and Whyte (1978) identified eight dimensions of illness behaviour following
myocardial infarction. These were somatic concern, a history of worry or stressful life
events, affective disruption, subjective tension, inability to express emotion, a recognition
of the seriousness of the illness, affirmation of the sick role and confidence in medical
care.
In an extension of the Byrne and Whyte (1978) study, Byrne, Whyte and Butler (1981)
prospectively examined the relationship of these dimensions of illness behaviour to a
number of outcomes over an 8 month period. Patients who identified areas of significant
stress in their lives and who attributed their initial infarction to stress experienced a higher
level of mortality and morbidity.
Subjects who adopted what Byrne, Whyte and Butler described as a 'sick role' were less
likely to return to work in the 8 month period than those who did not accept such a role.
The authors described the sick role as similar to cardiac neurosis, in which the person
expresses a high degree of self-preoccupation, particularly with cardiac symptoms, which
leads to a sense of invalidism. Interestingly, the study failed to show a significant
relationship between affective disruption and outcome although there was a small
association between subjective tension and putting off return to work. However, the
questionnaire used by Byrne, Whyte and Butler consisted of only two or three questions
measuring each of the eight dimensions and may not have been sufficiently sensitive to
measure changes in distress.
There is also some evidence that greater psychological distress and poorer psychological
health are associated with less compliance with recommended health behaviour.
Oldenburg, Perkins and Andrews (1985) compared the effects of counselling and
education on psychological function and lifestyle factors in 46 subjects following
myocardial infarction. The treatment groups showed less psychological dysfunction and
better adherence to healthy lifestyle factors than a control group. Lifestyle factors included
number of cigarettes smoked, alcohol consumption and frequency of vigorous physical
activity. Psychological dysfunction was measured by the General Health Questionnaire
(Goldberg, 1972), the Spielberger State Anxiety Scale (Spielberger, Gorsuch & Lushene,
1970) and the Attitudes Towards Illness Scale (Haynes, Levine, Scotch, Feinleib &
Kannel, 1978).
However, these authors failed to correlate psychological dysfunction and lifestyle, so the
relationship between the two remains unclear. It would be interesting to know if
psychological distress predicted healthy lifestyle behaviour independent of treatment. The
present study attempted to address this issue in relation to smoking, exercise, diet,
alcohol consumption and relaxation.
Compliance with smoking cessation and exercise behaviour has been associated with
increased distress. Havik and Maeland (1988), for example, investigated changes in
smoking behaviour among 230 patients following a myocardial infarction. Among other
variables, they measured anxiety and depression using a semantic differential
questionnaire. Short term quitters reported a decrease in anxiety and depression compared
to relapsers and non-quitters while early relapsers reported an increase in anxiety and
depression.
Prosser, Carson and Phillips (1985) examined the exercise behaviour of patients
following myocardial infarction. Of the 215 patients studied only 14 were exercising
vigorously as recommended in a cardiac rehabilitation program 6 to 9 years later. The
authors of this study suggested that anxiety may have been a cause of this failure to
comply.
There have been demonstrated relationships between measures of psychological distress,
and self-efficacy and locus of control. According to Bandura (1986), Lazarus (1982), and
Folkman and Lazarus (1984), anxiety (distress) arises from the perception that one will
not be able to cope with an aversive event. Thus, people with low self-efficacy for
performing a particular behaviour in an aversive situation will experience more anxiety
than people with high levels of self-efficacy.
A review of the research with the Health Belief Model has shown that psychological
distress does not appear to be normally measured in relation to health beliefs. One might
expect that high levels of health concern, beliefs about susceptibility to illness and beliefs
about the seriousness of illness might lead to high levels of distress. In turn, this distress
may immobilise people rather than lead them to change their behaviour and could account
for some of the unexplained variance in studies employing the Health Belief Model.
A number of studies have demonstrated a relationship between internal-external locus of
control and distress (e.g., Crisson & Keefe, 1988; Wolk & Bloom, 1977). Donham,
Ludenia, Sands and Holtzer (1983) found that external locus of control was related to
depression, anger and anxiety in a sample of medical inpatients. As described in Section
Six, Cromwell et al (1977) investigated the responses of myocardial infarction patients to
procedures conducted while they were patients in the coronary care unit. They found that
patients with internal locus of control experienced less depression compared to those with
an external locus of control orientation. Physiologically, 'externals' had worse prognostic
ratings, as measured by cardiac enzymes, than 'internals'.
The present study aimed to further investigate:
• the effect of psychological distress and psychological health on self-reported health
behaviour following myocardial infarction; and
• the relationship between psychological distress and psychological health, and self-
efficacy, outcome expectation, health beliefs and cardiac health locus of control.
7.2 Measures of Psychological Distress and Psychological Health
The General Health Questionnaire (Goldberg, 1972) was chosen to measure
psychological health and the Thoughts and Real Life Experiences Scale (Dua, 1987,
1990) was chosen to measure psychological distress in this study.
7.3.1 The General Health Questionnaire
Goldberg's (1972) General Health Questionnaire (GHQ) was constructed by carefully
examining symptoms, personality traits and adjustment identified by normal people and
by psychiatrists. Items were developed as questions with a 4-point Liken scale asking
respondents to indicate whether they experienced feelings or behaviours 'less than usual',
'no more than usual', 'rather more than usual' or 'much more than usual'. The GHQ 28,
used in the present study, is detailed in Appendix A9.
In constructing the questionnaire 140 items were calibrated using three psychiatric
groups; a severely ill group, a mildly ill group and a normal group. Forty seven items
were eliminated because they were not endorsed by the appropriate group. The remaining
93 items were subjected to a principal components analysis which revealed five
meaningful factors after varimax rotation (Goldberg, 1972).
Since a questionnaire consisting of 93 items was considered too long, these items were
reduced to 60 items and the questionnaire was called the GHQ-60 (Goldberg & Williams,
1988). The questionnaire has been subjected to intense investigation and has been found
to be a reliable and valid instrument (Goldberg & Williams, 1988). Goldberg and
colleagues have developed 30-item, 28-item and 12-item versions of the GHQ. The 28-
item version (GHQ-28) was developed by Goldberg and Hillier (1979) and was used in
the present study. A principal components analysis revealed four factors: somatic
symptoms, anxiety/insomnia, social dysfunction and severe depression.
All the versions of the GHQ have proved to be reliable and valid. However, since the
GHQ-28 was used in the present study because of its frequent use by researchers it is
worth noting that Goldberg and Williams (1988) reported 12 studies showing the GHQ-
28 to be a valid instrument for the assessment of the general psychological health of the
individual.
The GHQ has been used in some studies investigating myocardial infarction. Mayou,
MacMahon, Sleight and Florencio (1981) used the GHQ to measure the mental state of a
sample of patients entering a rehabilitation program after a myocardial infarction. The
questionnaire identified people to be suffering from significant distress 18 months later.
Oldenberg, Perkins and Andrews (1985) used the 12 item GHQ in their study, which has
been described previously, in which they compared the effects of education and
counselling on psychological functioning, life-style and use of health care resources
following myocardial infarction. The GHQ was included with a number of other scales to
measure psychological functioning and was found to be a good measure of psychological
dysfunction.
Finally, Philip (1987) noted that a number of different scales have been used to measure
psychological distress after myocardial infarction. Three measures of distress, the GHQ,
a psychiatric interview and the IPAT anxiety scale, were compared. The GHQ was found
to be a reasonably sensitive but very specific predictor of psychiatric illness among
myocardial infarction patients.
In summary, the GHQ is a valid measure of psychological health able to identify common
symptoms described by patients having experienced myocardial infarction such as
anxiety, depression and somatic symptoms.
7.3.2 The Thoughts and Real Life Experiences Scale
The Thoughts and Real Life Experiences scale (THARL scale) has recently been
developed (Dua, 1990) as a predictive measure of psychological distress.
It was developed in response to beliefs about the proposed inter-relationship between
cognitions, affect and behaviours posited by cognitive-behaviour therapists (Dua, 1990).
These therapists (e.g., Ellis, 1977; Meichenbaum, 1977) have argued that negative or
maladaptive thoughts produce negative feelings which in turn lead to maladaptive
behaviour. Positive thoughts, on the other hand, result in positive feelings and adaptive
behaviour. Our day-to-day experiences can also result in positive or negative feelings.
The complete scale, (see Appendix 10) consists of four subscales; Thought-related
Distress; Thought-related relaxation; Real-life related Distress; and Real-life related
Relaxation. In completing the scale, respondents are asked to indicate the degree of
distress due to thoughts, the degree of contentment due to thoughts, the degree of distress
due to real-life experiences and the degree of contentment due to real-life experiences for
14 items.
Respondents are asked to report their degree of distress and contentment on a scale of 0
(not at all) to 100 (extremely high) in a number of categories. A score of 5-15 indicates
very little distress, 25-35 , a little distress, 45-55, distress to some extent, 65-75, much
dristess and 85-95, very much distress. A total score or an average score may be obtained
for each subscale. An average score allows for items indicated by respondents as 'not
applicable' by obtaining a total score and dividing by the number of items actually rated
by the subject.
A number of studies by Dua and colleagues have demonstrated the reliability and validity
of the subscales of the THARL Scale (e.g., Dua, 1990; Dua & Price, 1992). These
studies showed that the more the reported negative affect or distress the more the anxiety,
stress and depression experienced by subjects and the lower the psychological health of
subjects.
7 . 4 Summary
Following myocardial infarction people experience a considerable degree of distress and
this may well affect their ability to comply with recommended health behaviour. Some
studies have also indicated that there is a relationship between psychological distress, and
self-efficacy and locus of control. These findings suggested that measures of
psychological distress and psychological health should be included in this study as
predictors of health behaviour.
Two scales were chosen to measure psychological health and psychological distress in
this study. The General Health Questionnaire (Goldberg, 1977) is a valid and reliable
measure of psychological health considered suitable for this study because it measures
feelings often experienced by patients following myocardial infarction such as anxiety,
depression and somatic symptoms. The Thought and Real-life Experiences Scale (Dua,
1990) has been shown to be a valid and reliable measure of psychological distress.
The next section attempts to draw together the ideas expressed in the discussion so far
and details the rationale, aims, design, and hypotheses of the present study.
8.0 The Present Study
8.1 Rationale and Aims
As indicated in the discussion so far, one of the principal aims of rehabilitation following
myocardial infarction is the modification of lifestyle factors that contribute to the disease
process. These lifestyle factors are cigarette smoking, high fat and cholesterol diet,
inadequate exercise, excessive alcohol intake and stress. All patients, following
infarction, are given advice and counselling about necessary lifestyle changes from
physicians, nurses and through National Heart Foundation literature while they are in
hospital. Unfortunately, compliance with this advice is often poor which leads to an
increased risk of further infarction for these patients in the future.
The research discussed in the previous sections shows that self-efficacy, outcome
expectation, factors constituting the Health Belief Model and health locus of control
predict health behaviours which may be important for the maintenance of good health
following myocardial infarction. In addition, the discussion on psychological distress and
psychological health indicates that, following myocardial infarction, patients are
psychologically distressed and tend to have low emotional or psychological health. The
high distress and the low emotional health experienced by these patients may also affect
compliance with health behaviour.
One aim of the present study was to investigate seperately the effects of self-efficacy,
outcome expectancy, health threat, cardiac health locus of control, psychological distress
as a result of real-life experiences and thoughts, and general psychological health at the
time of hospitalisation, on compliance with recommended health behaviours following
myocardial infarction 3 and 6 months later.
It is also likely that self-efficacy, outcome expectancy, components of the Health Belief
Model, cardiac health locus of control, psychological distress and psychological health
may be measuring common elements of behaviour. Thus, a second aim of this study was
to investigate the relationship between these variables measured while patients having
experienced a myocardial infarction were hospitalised.
The final aim of the study was to determine the stability of self-efficacy, outcome
expectancy, health threat, cardiac health locus of control, psychological distress as a
result of real-life experiences and thoughts, and general psychological health over a 6
month period.
8.2 Design of the Study
A sample of patients who had been admitted to the coronary care unit of a metropolitan
hospital suffering from an uncomplicated myocardial infarction was obtained.
Approximately 5 days after admission and after transfer from the coronary care unit,
subjects completed a questionnaire asking them to report their health behaviour prior to
their infarction in relation to smoking, diet, exercise, relaxation and alcohol consumption.
Subjects were also asked to determine the level and strength of self-efficacy for
achieving, within 6 months, recommended health behaviour in the same five categories.
Outcome expectations for the health behaviours were also obtained along with current
health threat beliefs, health value, cardiac health locus of control beliefs, psychological
health and psychological distress. Additional demographic data and a measure of severity
of infarction were also obtained.
Approximately 3 months and 6 months later, the subjects were asked to complete similar
questionnaires measuring their current health behaviour, self-efficacy, outcome
expectation, health threat beliefs, health value, cardiac health locus of control,
psychological distress and psychological health. Correlational, principal components
factor analysis and forward regression analyses were then performed to determine the
prediction of health behaviour and the relationships between the independent variables.
Repeated measures multiple analysis of variance was used to determine the stability of the
independent variables over the 6 month period.
8.3 Hypotheses
A number of hypotheses are described below that were developed to investigate the aims
of this study.
1) Perceptions of self-efficacy level and self-efficacy strength have consistently been
shown to predict health behaviour. In comparison, the role of outcome expectancy is
unclear since it is often not included in studies investigating Self-efficacy Theory, but
there is some evidence to support outcome expectancy as a predictor of behaviour.
Therefore, it was hypothesised that high self-efficacy level, self-efficacy strength and
outcome expectancy, at the time of hospitalisation, would predict self-reported
compliance with recommended courses of health action 3 months and 6 months after
experiencing a myocardial infarction.
2) The Health Belief Model has been used in a variety of contexts to predict health
behaviour. Three measures from the Health Belief Model that have been extensively
researched and that were considered here were health threat seriousness, the likelihood of
further health threat and concern about the particular health threat.
It was hypothesised that high levels of concern about having a myocardial infarction, a
strong belief in the likelihood of having another infarction in the future and a strong belief
in the seriousness of a myocardial infarction, at the time of hospitalisation, would predict
self-reported compliance with recommended courses of health action 3 months and 6
months after experiencing a myocardial infarction.
3) With respect to health locus of control, it is best measured as a multidimensional
construct, should be as specific as possible and needs to be considered with regard to
health value. Therefore, a Multidimensional Cardiac Health Locus of Control Scale
derived from the Multidimensional Health Locus of Control Scale was developed for use
in this study and the health value of subjects was also measured.
It was hypothesised that for subjects who place a high value on health, high levels of
internal cardiac health locus of control, and low levels of powerful others cardiac health
locus of control and low levels of chance cardiac health locus of control, at the time of
hospitalisation, would predict self-reported compliance with recommended courses of
health action 3 months and 6 months after experiencing a myocardial infarction.
4) The recovery period following myocardial infarction has been associated with high
levels of psychological distress and low levels of psychological health.
It was hypothesised that better psychological health and less distress as a result of real-life
experiences and thoughts, at the time of hospitalisation, would predict self-reported
compliance with recommended courses of health action 3 months and 6 months after
experiencing a myocardial infarction.
5) The introduction to this study sought to establish that there is a theoretical and
empirical relationship between the models and the variables derived from them.
Rosenstock (1988) has argued that despite this relationship self-efficacy has been largely
ignored in research with the Health Belief Model. He suggests that modifying behaviour
associated with long term habits such as smoking and drinking, for example, is a problem
that may well be better understood by incorporating self-efficacy into the Health Belief
Model.
However, Rosenstock (1988) also claims that self-efficacy theorists and researchers
(Bandura in particular) have staked too much on self-efficacy in attempting to explain
behaviour change and compliance. Rosenstock argues that self-efficacy is but one
dimension and health behaviour is more adequately explained by the interaction of a
number of factors, particularly those found in the Health Belief Model. Furthermore he
warns that self-efficacy, developed out of the need to understand snake phobias, should
not become a 'snake oil - a patent medicine to cure all ills' (Rosenstock, 1988, p. 180).
It can be seen from the above that there is competition about the relative contribution the
different variables make to health behaviour change and a question about the relationship
between the variables themselves. This study attempted to shed further light on this issue
and on the possible relationship between these concepts in the context of a life threatening
health problem.
It was hypothesised that self-efficacy level, self-efficacy strength, outcome expectancy,
concern about having a myocardial infarction, belief in the likelihood of having another
myocardial infarction, belief in the seriousness of having a myocardial infarction, and
internal, cardiac health locus of control would be positively correlated with each other.
Chance and powerful others cardiac health locus of control would be negatively correlated
with the above mentioned variables. It was further expected that these variables would be
negatively correlated with psychological health and distress as a result of real-life
experiences and thoughts.
As described above, a major issue of interest in this study was the relationship between
variables derived from the social learning models and the value expectancy models as to
their ability to predict health behaviour. Therefore, it was decided to determine how all the
independent variables interacted in predicting self-reported compliance with recommended
health behaviour 3 months and 6 months after experiencing a myocardial infarction.
6) This study sought to investigate the stability of self-efficacy, outcome expectation,
health threat beliefs, cardiac health locus of control beliefs, psychological distress and
psychological health.
It was hypothesised that self-efficacy level, self-efficacy strength, outcome expectancy,
concern about having a myocardial infarction, belief in the likelihood of having another
myocardial infarction, beliefs in the seriousness of having a myocardial infarction,
internal cardiac health locus of control, powerful others cardiac health locus of control,
chance cardiac health locus of control, psychological health, and distress as a result of
real-life experiences and thoughts would remain stable over a 6 month period.
The study method will now be described in detail.
CHAPTER 2
METHOD
1.0 Subjects
The subjects for this study were selected, over a 7 month period, from those patients
admitted to the coronary care unit of a major metropolitan public teaching hospital with a
diagnosis of acute myocardial infarction . This diagnosis was made by the unit medical
team on the presence of at least two of the following criteria: a clinical history of
infarction, elevated cardiac enzymes and appropriate electrocardiograph changes.
All male patients admitted during this period under the age of 70 years were considered
for inclusion in the study. Subsequently, those considered by the medical staff to have
severe physical complications such as advanced cardiac failure, renal failure, pulmonary
disease, diabetes and debilitating arthritis, for example, were also excluded.
It was determined that those over 70 were more likely to have other health problems that
might interfere with lifestyle changes. The severely ill were excluded on humanitarian
grounds as well as the fact that a debilitating condition would affect attitudes and the
ability to achieve the lifestyle changes in question. Females were also excluded as an
additional measure to obtain as homogeneous sample as possible since their numbers
were expected to be relatively small considering the short time frame of the study.
Thus, 71 male subjects met the selection criteria. However, not all of these participants
completed all the requirements of the study.
Two subjects refused to participate in the study. One had difficulties in understanding the
questionnaires due to a poor command of the English language. Two subjects declined to
participate further because of other commitments when they were asked to complete the
questionnaires 3 months after hospitalisation and one other could not be located, having
changed address.
Two subjects were eliminated from the study, one after 3 months and the other after 4
months due to their undergoing coronary artery by-pass surgery as a result of persistent
angina pectoris.
Sixty three men completed all requirements of the study. Their average age was 48.8 yrs
with a range of 33 yrs to 68 yrs. Thirty nine of these men were married, 19 single, 4
widowed and 1 was divorced.
2.0 Questionnaires
After indicating their consent on the form shown in Appendix Al, subjects completed the
questionnaires described below and which are provided in full in Appendix A of this
document.
2.1 Subject Information.
Name, address and telephone number were obtained from subjects to enable further
contact to be made after 3 and 6 months. Demographic information that might have had a
bearing on the findings of the study, namely age, marital status and occupation were also
obtained (Appendix A2).
Additional information was obtained from the subjects' medical files.
The Prognostic Index (Norris, Caughey & Mercer, 1970) is a measure of the severity of
infarction and was determined by the admitting doctor in the Coronary Care Unit and is
routinely noted in the subject's medical file. A higher Prognostic Index indicates a greater
degree of heart failure at the time of infarction and is correlated with a poorer outcome.
This measure was recovered from the medical notes to provide a check that the severity of
the infarct did not independently influence compliance with health behaviour.
Evidence of complications, as determined by each subject's doctor, was carefully noted
since severe cardiac failure, or other severe organ involvement, was cause for exclusion
from the study as described above.
2.2 Pre-heart Attack Health Behaviours Questionnaire
This questionnaire (Appendix A3), completed at the time of hospitalisation, asked
respondents to choose, with a tick, one of five behaviours from each of five health
behaviour categories which best represented their health behaviour prior to their
myocardial infarction.
The five health behaviour categories were smoking, diet, exercise, alcohol consumption
and relaxation. Each category consisted of five behaviours organised in a graded
hierarchical fashion with the most positive health behaviour at the top, scoring 5, and the
least positive at the bottom, scoring 1. A mean pre-heart attack health behaviour score
was calculated for the total scale.
These same categories and hierarchies were used for all other questionnaires in this study
relating to health behaviour such as the Current Health Behaviour Questionnaire, the Self-
efficacy Questionnaire and the Outcome Expectancy Questionnaire.
2.3 Self-efficacy Questionnaire
This questionnaire (Appendix A4) consisted of the same five health categories and the
same five behaviours organised hierarchically, as used in the Pre-heart Attack Health
Behaviour Questionnaire described above. However, in completing this questionnaire,
the respondents were asked to indicate that behaviour they expected to achieve in 6
months time (self-efficacy level) for each of the health categories.
Subjects were also asked to indicate, on a scale of 0 to 100, for the chosen behaviour in
each category, their degree of confidence (self-efficacy strength) that they would achieve
that behaviour in 6 months time. A low score indicated low self-efficacy strength (low
confidence of success) and a high score high self-efficacy strength (high confidence of
success).
The five behavioural levels in each of the categories were scored from 5 down to 1 in
order of health 'desirability'. Thus, giving up smoking was given a score of 5, smoking
less than 5 cigarettes per day a score of 4, and so on. The scores for the performance
level chosen by the subject in each of the 5 categories were summed and divided by 5 to
provide a mean health behaviour self-efficacy level score. The range of possible scores
was therefore between 1 and 5. The self-efficacy strength scores were also summed
across all five health categories and divided by five to compute a mean health behaviour
self-efficacy strength score.
This questionnaire was completed by subjects at the time of hospitalisation, then 3
months and 6 months later. On each occasion subjects were asked to indicate their self-
efficacy beliefs for achieving the health behaviours in 6 months time.
2.4. Outcome Expectancy Questionnaire
The same five health categories and levels of behaviour as for the self-efficacy
questionnaire were presented to measure outcome expectancy (Appendix A5). For each
category, subjects were asked to indicate, for the same level chosen by them in the Self-
efficacy Questionnaire, the degree, on a scale of 0 to 100, to which they believed that
achieving that behaviour would actually help in preventing a future heart attack. A high
score indicated a strong belief that the behaviour would be effective (high outcome
expectancy strength) and a low score to the contrary (low outcome expectancy strength).
The outcome expectancy strength scores were summed across the five categories and
divided by five to provide a mean health behaviour outcome expectancy strength score.
2.5 Health Threat Beliefs Questionnaire
As described in the introduction, the Health Belief Model consists of a number of
components. Three of these components, which are most widely used in investigations
with the Health Belief Model, were chosen for inclusion in this study. They were
perceptions of: how serious subjects thought having a heart attack was, how concerned
they were about having a heart attack and how likely they thought it was that they would
have a heart attack in the future. Together these three components measured a perception
of health threat.
This questionnaire (Appendix A6) consisted of three questions, one measuring the
subjects' perceptions of the seriousness of having a heart attack, another measuring
concern about having a heart attack and the third measuring beliefs about the likelihood of
having a future heart attack. Subjects were asked to circle, for each question, their
response on a 4-point Liken scale.
2.6 Multidimensional Cardiac Health Locus of Control
2.6.1. Health Value
As described in Chapter 1, both Rotter (1975) and Wallston and Wallston (1981) have
said that locus of control is only meaningful if the value of the reinforcement to the
individual is taken into account. Therefore, prior to measuring cardiac health locus of
control, a measure of the subjects' health value was obtained to differentiate between
those subjects with a positive and those with a negative health value orientation
(Appendix A7).
In accordance with previous research with health locus of control (Wallston, Maides &
Wallston, 1976; Wallston, Wallston & DeVellis, 1978), subjects were asked to place in
order of importance the 10 potentially valued states indicated in the questionnaire, one of
which was 'Good Health'. It was decided that, consistent with the original research
conducted by the Wallston group (Wallston, Maides & Wallston, 1976; Wallston,
Wallston & DeVellis, 1978), those subjects who placed 'Good Health' in the top half of
their list were classified as having a positive health value. Conversely, those relegating
'Good Health' to the bottom half were classified as having a negative health value.
Subjects could then be placed in one of four groups: high health value and high cardiac
health locus of control; high health value and low cardiac health locus of control; low
health value and high cardiac health locus of control; and low health value and low
cardiac health locus of control.
2.6.2 The Multidimensional Health Locus of Control Scale
The Multidimensional Cardiac Health Locus of Control Scale (Appendix A8) was adapted
from the Multidimensional Health Locus of Control Scale (Wallston & Wallston, 1979),
as described in detail in the introduction. The scale consists of three, 6-item subscales
measuring internal, powerful others and chance cardiac health locus of control. Items
belonging to each of the three subscales are indicated on the questionnaire in Appendix
A8. Respondents were asked to indicate on a scale of 1 (strongly disagree) to 6 (strongly
agree) the extent to which they agreed or disagreed with each of 18 statements relating to
cardiac health locus of control.
The sum of ratings for the 'internal' questions provided the internal cardiac health locus
of control score, the sum of ratings for the 'powerful others' questions provided the
powerful others cardiac health locus of control score and the sum of the 'chance'
questions provided the chance cardiac health locus of control score. A high score
indicated high internal, powerful others and chance beliefs.
Health value and cardiac health locus of control were measured at the time of
hospitalisation, and 3 months and 6 months later.
2.7 Psychological Distress and Psychological Health
As described in Chapter 1, the General Health Questionnaire (Goldberg, 1972) and the
Thoughts and Real-Life Experiences scale (Dua, 1990) are valuable measures of
psychological health and psychological distress. The GHQ-28 (Appendix A9) was used
because it offered a valid and reliable shorter (only 28 items) alternative to the 60 item
version. The shorter scale was preferred to minimise effort on the part of subjects
obviously susceptible to the cardiovascular effects of stress. A single score of
psychological distress was obtained by combining scores on each of the four, seven-item
sub-scales. Each item was scored from 1 to 4 on a Likert scale with a range of 28 to 112
for the whole questionnaire. A high score indicated poorer psychological health.
The two distress scales (Appendix A 10) were used from the Thoughts and Real-life
Experiences Scale (THARL Scale: Dua, 1990). Average scores for each of the two scales
were obtained by summing the scores for all items and then dividing by the total number
of items to which subjects responded. Average scores were computed since there were a
number of items which subjects would be likely to judge to be 'not applicable' to them.
Measures of psychological health, and distress as a result of real-life experiences and
thoughts were obtained at the time of hospitalisation, and 3 months and 6 months later.
2.8 Current Health Behaviour Questionnaire
The Current Health Behaviour Questionnaire (Appendix Al 1) was presented to subjects 3
months and 6 months after discharge from hospital. Subjects were asked to indicate their
current health behaviour in relation to the same five categories used in the Pre-Heart
Attack Health Behaviours Questionnaire.
3.0 Procedure
Following selection, as described above, prospective subjects were approached between
3 days and 5 days after being diagnosed as having had an uncomplicated myocardial
infarction and were still inpatients in either the coronary care unit or in a general ward of
the public teaching hospital chosen for this study. Permission involve patients in the
study was obtained from the physician in charge.
Initial contact with prospective subjects was by the researcher who introduced himself
and asked each man to '...help in a research project aimed at finding out more about how
people recover from heart attacks'. It was explained that they would be required to
complete fairly lengthy questionnaires on three occasions, that complete confidentiality
was assured and that they could decide to 'drop out' from the study at any time with no
prejudice. Subjects were also reassured that neither their treatment nor rehabilitation
would be altered in any way to that normally provided by their participation or non-
participation in the study.
Subjects were asked to give their written consent to be included in the study. The consent
form (Appendix A1) was cleared by the Ethics Committee of the University of New
England.
Once consent was obtained, the subject completed the Pre-Heart Attack Health
Behaviours Questionnaire, Self-efficacy Questionnaire, Outcome Expectancy
Questionnaire, Health Threat Beliefs Questionnaire, Health Value Questionnaire,
Multidimensional Cardiac Health Locus of Control Scale, GHQ, and the distressing
thoughts and real-life experiences parts of the THARL Scale.
The questionnaires were completed by the subject with the researcher present who was
able to answer any queries as they arose. Subjects were then reminded that further
questionnaires would be posted to them in 3 months and 6 months time and that they
would be contacted by telephone to discuss any problems with completing them.
Information about the subject's age, marital status, occupation and Prothrombin Index
was obtained from medical records.
Approximately 3 months and 6 months later, all the above questionnaires, with the
exception of the Pre Heart Attack Questionnaire, were sent with a stamp addressed
envelope to the subjects with a brief letter requesting their ongoing participation. Subjects
were also contacted by telephone to facilitate questionnaire return and deal with any
difficulties.
The schedule of questionnaires answered by the subjects on each of the three occasions is
shown in Table 1 below.
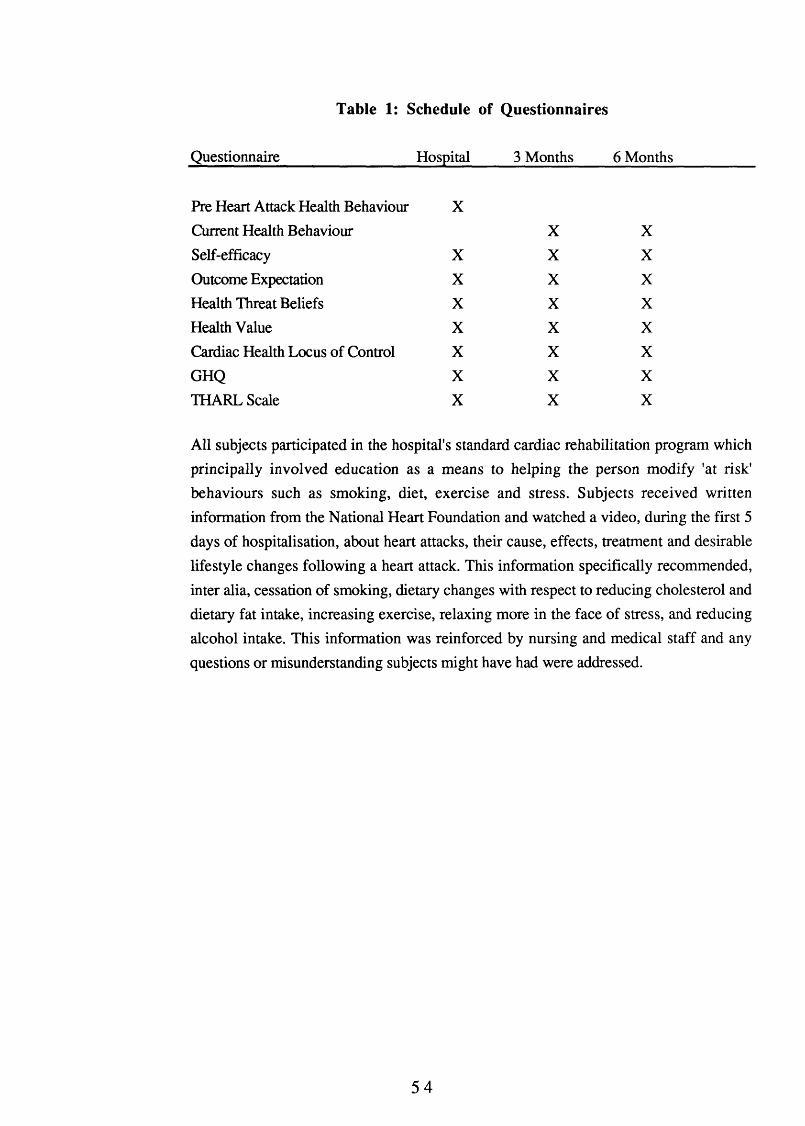
Table 1: Schedule of Questionnaires
Questionnaire Hospital 3 Months 6 Months
Pre Heart Attack Health Behaviour X
Current Health Behaviour X X
Self-efficacy X X X
Outcome Expectation X X X
Health Threat Beliefs X X X
Health Value X X X
Cardiac Health Locus of Control X X X
GHQ X X X
THARL Scale X X X
All subjects participated in the hospital's standard cardiac rehabilitation program which
principally involved education as a means to helping the person modify 'at risk'
behaviours such as smoking, diet, exercise and stress. Subjects received written
information from the National Heart Foundation and watched a video, during the first 5
days of hospitalisation, about heart attacks, their cause, effects, treatment and desirable
lifestyle changes following a heart attack. This information specifically recommended,
inter alia, cessation of smoking, dietary changes with respect to reducing cholesterol and
dietary fat intake, increasing exercise, relaxing more in the face of stress, and reducing
alcohol intake. This information was reinforced by nursing and medical staff and any
questions or misunderstanding subjects might have had were addressed.