cerebrospinal fluid and plasma monoamine metabolites and their relation to psychosis implications...
TRANSCRIPT

Cerebrospinal Fluid andPlasma Monoamine Metabolites andTheir Relation to PsychosisImplications for Regional Brain Dysfunction in SchizophreniaDavid Pickar, MD; Alan Breier, MD; John K. Hsiao, MD; Allen R. Doran, MD; Owen M. Wolkowitz, MD;Carlos N. Pato, MD; P. Eric Konicki, MD; William Z. Potter, MD, PhD
\s=b\The relationship between central (cerebrospinal fluid [CSF])and peripheral (plasma) monoaminergic metabolites and psy-chotic symptoms was examined in 22 drug-free schizophrenicinpatients. The CSF homovanillic acid levels did not differ signifi-cantly between patients and normal controls (n = 33). The CSFhomovanillic acid levels, however, were negatively correlatedwith ratings of psychosis and positive symptoms, and the CSFhomovanillic acid and 5-hydroxyindoleacetic acid levels corre-lated negatively with individual deficit symptoms. Stepwise andhierarchical multiple-regression analysis revealed that amongmonoaminergic measures, only the CSF and plasma homovanil-lic acid levels contributed significantly to the total Brief Psychiat-ric Rating Scale and positive symptom variance with negativeand positive partial correlations, respectively. Levels of CSF 3\x=req-\methoxy-4-hydroxyphenylglycol, but not of CSF norepinephrine,were significantly elevated in the schizophrenic patients com-
pared with controls, and plasma 3-methoxy-4-hydroxyphenyl-glycol levels were positively correlated with negative symptoms.We discuss the potential implications of these findings for amodel of dopaminergic dysfunction in schizophrenia involvingdistinct cortical and subcortical contributions.
(Arch Gen Psychiatry. 1990;47:641-648)
The sensitive determination of amine metabolites in cere-
brospinal fluid (CSF) as a means for assessing brainneurotransmitter activity represented a significant méthodo¬logie advance for schizophrenia research. The expectation,however, that these methods would support the hypothesizedoveractivity of dopamine systems was never borne out. Infact, although a clearly defined dopamine abnormality has yetto be identified, there may be better support for diminishedCSF dopamine metabolite levels than for their increase inschizophrenic patients (C. A. Kaufman, MD, unpublisheddata, 1990). "4 Nevertheless, consistent evidence linking theantipsychotic effects of neuroleptic drugs with effects oncentral nervous system (CNS) dopamine systems continuesto implicate dopaminergic dysfunction in schizophrenia.15,16
The delineation of the structure and function of CNS dopa¬minergic systems, in conjunction with recent clinical data, hashelped to renew speculation regarding the nature of dopa¬mine dysfunction in schizophrenia. Functional brain-imagingstudies, for example, have, with remarkable consistency,demonstrated diminished activity of the prefrontal cortex inpatients with schizophrenia.17"20 Because of the possible role ofdopamine innervation for prefrontal cortex-mediated beha¬viors,21 deficient mesocortical dopamine activity in schizo¬phrenia has been suggested.22"25 Relevant to this hypothesisare the unique properties ofmesocortical neurons,26 includingevidence from animal experiments that lesioning of the meso¬cortical dopamine system increases functional output of thesubcortical nigrostriatal and mesolimbic systems.27 Thus, asdiscussed by Weinberger,22 diminished mesocortical activitycould be coupled with increased subcortical dopaminergicactivity, resulting in a "bidirectional" dopamine model ofpsychosis.
The effects of a negative feedback relationship betweencortical and subcortical dopamine systems on CSF dopaminemetabolite levels are likely to be complex. For instance, while
Accepted for publication December 7,1989.From the Section on Clinical Studies, Clinical Neuroscience Branch, Nation-
al Institute of Mental Health, Bethesda, Md. Dr Breier is now with theMaryland Psychiatric Research Center, Baltimore. Dr Hsiao is now with theSection on Analytic Biochemistry, Laboratory of Clinical Science, NationalInstitute of Mental Health, Bethesda, Md. Dr Doran is now with the Depart-ment of Psychiatry, University of California-Davis, Sacramento. DrWolkowitz is now with the Langley-Porter Psychiatric Institute and Universi-ty ofCalifornia, San Francisco. Dr Pato is now with the Schizophrenia ResearchBranch, Division of Clinical Research, National Institute of Mental Health,Rockville, Md.
Reprint requests to Section on Clinical Studies, Clinical NeuroscienceBranch, National Institute of Mental Health, National Institutes of Health,Bldg 10, Room 4N212, 9000 Rockville Pike, Bethesda, MD 20892 (Dr Pickar).
Downloaded From: http://archpsyc.jamanetwork.com/ by a Department of Veterans Affairs User on 08/11/2016
CSF homovanillic acid (HVA), the principal metabolite ofdopamine in humans, traditionally has been thought to reflectsubcortical, principally nigrostriatal, activity,28,29 other dataare compatible with the notion that CSF HVA may, undercertain conditions, be influenced by cortical system activity aswell.30"38 Thus, from this perspective, alterations in metaboliteproduction by one brain region might be "offset" by changes inanother. Further complexities arise from the fact that CSFmetabolites represent an integrated measure determined notonly by neuronal activity in brain but also by physiologicparameters, such as egress rates and spinal cord metabolism.
In contrast to CSF, plasma HVA measurements in schizo¬phrenia have yielded a more consistent pattern of clinicalfindings. The use of plasma HVA determinations as a markerfor CNS processes is based largely on animal experiments inwhich plasma HVA has been shown to change in parallel withbrain HVA in response to pharmacologie probes3"2 and on thenotion that some HVA circulating in plasma owes its origin tothe CNS.43 The lack of invasiveness of plasma collection,coupled with reports of correlations between plasma HVAlevels and psychotic symptoms4"7 and/or treatment re¬
sponse46,48'55 in schizophrenic patients, support its applicationto clinical research. However, unlike CSF in which HVA isderived from dopaminergic metabolism in the CNS, the likelyorigin of the majority of plasma HVA is the peripheral ner¬vous system.39 Thus, the CNS "signal" that drives correla¬tions between plasma HVA and clinical symptoms is unlikelyto be based simply on transfer of brain-produced HVA to thegeneral circulation.
In the present study, we investigated the relationshipsbetween central and peripheral monoaminergic measures andpsychosis. We compared CSF monoaminergic measures inpatients with schizophrenia with normal controls and exam¬ined, in some detail, in schizophrenic patients the relation¬ships between psychosis ratings and CSF and plasma mono¬
aminergic measures. The specific question was whethercentral and peripheral monoaminergic measures provide in¬dependent information regarding symptoms or if their rela¬tionships to symptoms overlap with one another. We ap¬proached this problem through the use of hierarchical andstepwise multiple regression, with symptom ratings as thedependent variables and the various CSF and plasma mono-amine metabolite levels as predictor variables.
PATIENTS AND METHODSProcedures
Twenty-two psychiatric inpatients who met DSM-Hf* criteria forschizophrenia on the basis of a structured interview, medical recordreview, and consensus agreement among three research psychia¬trists were studied, along with 33 inpatient normal controls who werewithout a history of psychiatric disorder. The patients were relative¬ly young (mean± SD age, 27.8±8.3 years) and had chronic illnesses(mean ± SD duration of illness, 9.7 ± 10.2 years) with an early onset ofillness (mean ± SD age at onset, 18.1 ±4.1) and histories of multiplehospitalizations (mean ± SD number of hospitalizations, 6.4 ±8.4).All subjects granted written informed consent before participation inthis study. Patients and controls were free from significant medicalillness and followed a low-monoamine, alcohol-free, and caffeine-restricted diet for at least 2 weeks before study. (All lumbar punc¬tures [LPs] were performed between the years of 1983 and 1986;inclusive, and biochemical assays were carried out within 6 months ofthe LP. The CSF data from 15 of the 22 patients and 21 of the 33controls were previously used in a study that reported the relation¬ship between a structural brain abnormality and CSF metabolitelevels32; neither CSF group means nor their relation to symptomswere previously reported.)
The procedures for LP were identical for patients and controls. Allsubjects fasted and remained at bed rest after midnight; the LP was
performed with subjects in the lateral decubitus position between8:30 and 9:30 AM. The first 12 mL of CSF was collected as a pool and
placed on ice at the bedside, subsequently aliquoted, and then frozenat -80°C until the time of assay. Cerebrospinal fluid was assayed forlevels of the dopamine metabolite, HVA, norepinephrine (NE) and itsmetabolite 3-methoxy-4-hydroxy-phenylglycol (MHPG), and the se¬rotonin metabolite 5-hydroxyindoleacetic acid (5-HIAA) by high-pressure liquid chromatography with electrochemical detection.57The precision of the high-pressure liquid Chromatographie methodwith electrochemical detection is high, with intra-assay and interas-say coefficients ofvariation ranging from 2% to 6% and less than 15%,respectively, in the concentration ranges of the metabolites encoun¬tered in human lumbar CSF.
Blood was collected in the patients by venipuncture three timesduring the week of the LP (although not on the day of the LP)between 7 and 8:30 AM under restricted activity conditions andfasting from the previous midnight. Plasma, obtained within 30 min¬utes of collection by centrifüging whole blood (800g, 10 minutes), wasstored at -20°C until assay. Plasma HVA58 and MHPG59 were as¬
sayed by high-pressure liquid chromatography with electrochemicaldetection. The sensitivity of the HVA assay was 0.5 pmol/mL with anintra-assay variability of 2.2% and an interassay variability of 6.3%.The sensitivity of the assay for MHPG was 2.0 pmol/mL with an intra-assay variability of 7.5% and interassay variability of 8.8%. Plasma-free HVA was determined on each of the three samples takenthroughout the course of a week; plasma-free MHPG was assayed ontwo samples per week. The average of the three weekly HVA and twoweekly MHPG values was used in the data analysis.
All patients were eligible for a treatment protocol and, therefore,were treated with coded capsules so that rating physicians and pa¬tients were blind to the treatment condition. As part of the generalward procedure, patients received placebo capsules for at least 15days before venipuncture and LPs: range, 15 to 58 drug-free days;mean ± SD, 26.3±0.7 drug-free days. Physicians rated the patientsat the completion of the week of the LP and venipunctures by usingthe Brief Psychiatric Rating Scale (BPRS) (24 items),60 includingsubscales for depression-anxiety, paranoia-suspicion, positive symp¬toms, and negative symptoms. The patients were highly symptom¬atic at the time of the LP, displaying prominent positive and negativesymptoms. The means ± SD of total, positive, and negative symptomBPRS scores were 72.6 ±17.4, 14.6 ±4.7, and 13.0 ±3.8, respective¬ly, reflecting a severity of illness comparable with other patientgroups that we have studied in the past.
Statistical AnalysisThe CSF measures from patients and controls were compared by
using a two-way analysis of variance with diagnosis and sex asgrouping factors. Relationships between individual monoaminergicmeasures and clinical variables were examined by using PearsonProduct-Moment Correlation Coefficients or Spearman's rank-ordercorrelation coefficients, as indicated in the text. To examine therelationships between psychosis ratings and central and peripheralmonoaminergic measures, hierarchical or stepwise multiple-regres¬sion analysis was performed with total BPRS, positive symptom, andnegative symptom ratings as dependent variables and monoaminer¬gic measures as independent predictor variables.
Some further explanation of this data analytic approach may behelpful. While bivariate regressions/correlations are informative,they do not take into account intercorrelations between predictorvariables. Thus, two variables may each correlate significantly withpsychosis ratings, but if the two predictor variables correlate withone another, their individual correlations with psychosis will not beindependent (ie, correlations between the predictor variables couldaccount for some or all of the correlation between each predictorvariable and psychosis). The usual approach to this problem isthrough the use of multiple-regression/correlation analysis: the si¬multaneous examination of the relationship between an entire set ofpredictor variables and some dependent variable. Multiple-regres¬sion/correlation analysis yields an Ä2, which is the amount of varianceshared between the predictor variables and the dependent variable.Shared variance is literally that proportion of the variability of thedependent variable that can be accounted for or predicted by the setof independent variables.
A limitation of the above is that the individual partial correlationsobtained from a multiple-regression/correlation analysis are not agood means for apportioning this shared variance.61 The only way to
Downloaded From: http://archpsyc.jamanetwork.com/ by a Department of Veterans Affairs User on 08/11/2016
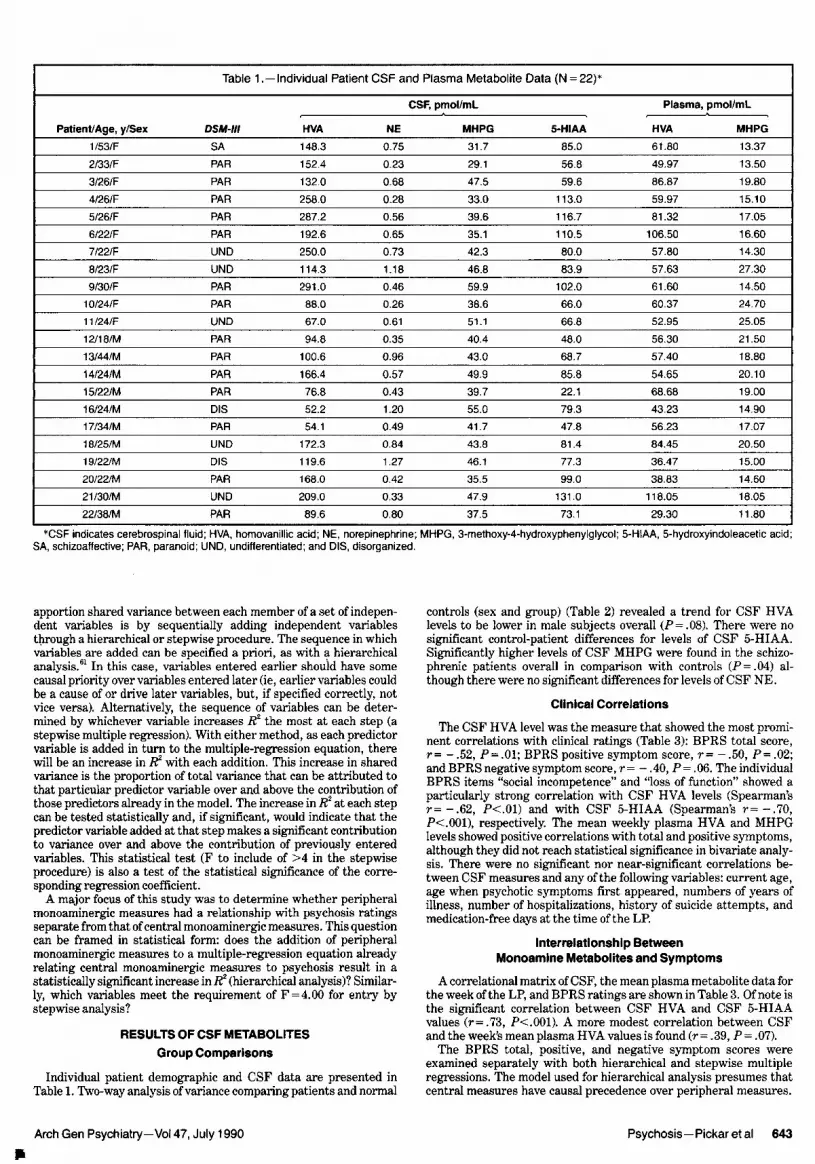
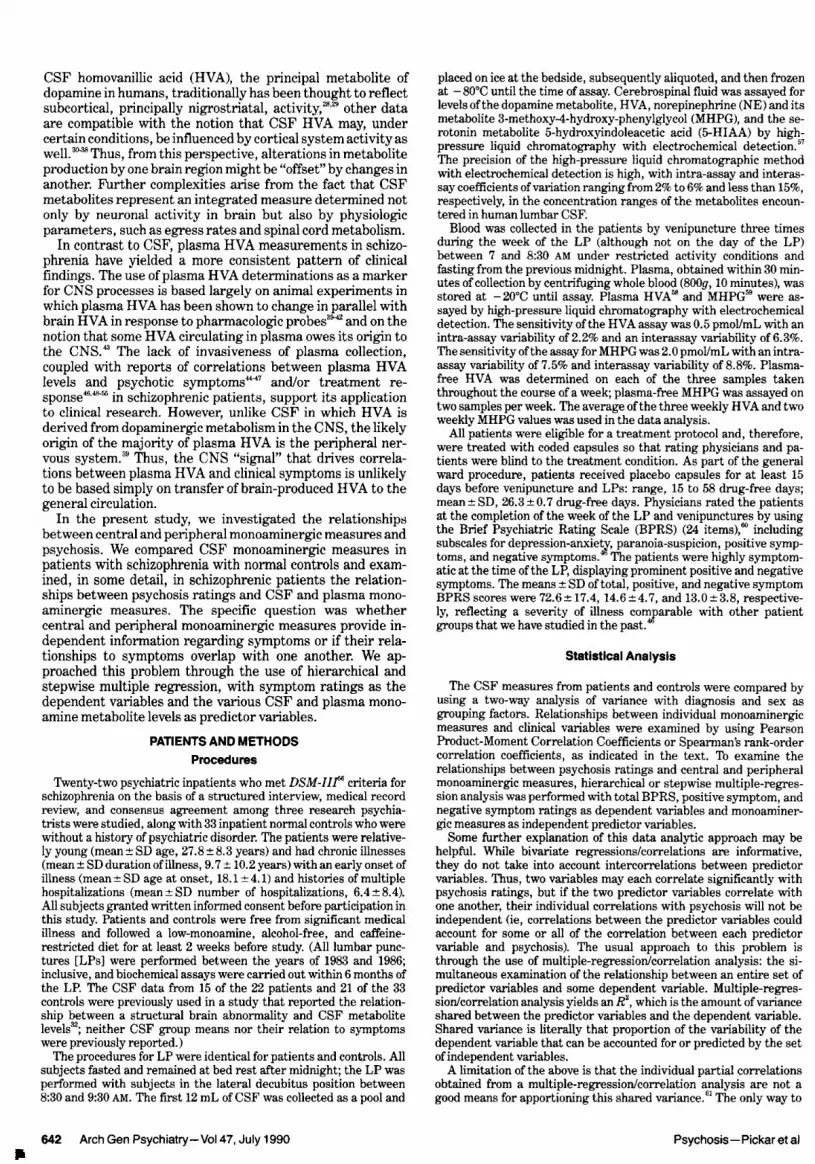
Table 1 .-Individual Patient CSF and Plasma Metabolite Data (N = 22)*
Patient/Age, y/Sex
CSF, pmol/mLDSM-III HVA NE MHPG 5-HIAA
Plasma, pmol/mLHVA MHPG
1/53/F SA 148.3 0.75 31.7 85.0 61.80 13.372/33/F PAR 152.4 0.23 29.1 56.8 49.97 13.503/26/F PAR 132.0 0.68 47.5 59.6 86.87 19.804/26/F PAR 258.0 0.28 33.0 113.0 59.97 15.105/26/F PAR 287.2 0.56 39.6 116.7 81.32 17.056/22/F PAR 192.6 0.65 35.1 110.5 106.50 16.607/22/F UND 250.0 0.73 42.3 80.0 57.80 14.308/23/F UND 114.3 1.18 46.8 83.9 57.63 27.309/30/F PAR 291.0 0.46 59.9 102.0 61.60 14.50
10/24/F PAR 88.0 0.26 38.6 66.0 60.37 24.7011/24/F UND 67.0 0.61 51.1 66.8 52.95 25.05
12/18/M PAR 94.8 0.35 40.4 48.0 56.30 21.50
13/44/M PAR 100.6 0.96 43.0 68.7 57.40 188014/24/M PAR 1É 0.57 49.9 85.8 54.65 20.1015/22/M PAR 76.8 0.43 39.7 22.1 68.68 19 0016/24/M DIS 52.2 1.20 55.0 79.3 43.23 14.9017/34/M PAR 54.1 0.49 41.7 47.8 56.23 17.0718/25/M UND 172.3 0.84 43.8 81.4 84.45 20.5019/22/M DIS 119.6 1.27 46.1 77.3 36.47 15.00
20/22/M PAR 168.0 0.42 35.5 99.0 38.83 14.60
21/30/M UND 209.0 0.33 47.9 131.0 118.05 18.0522/38/M PAR 89.6 0.80 37.5 73.1 29.30 11.80
*CSF indicates cerebrospinal fluid; HVA, homovanillic acid; NE, norepinephrine; MHPG, 3-methoxy-4-hydroxyphenylglycol; 5-HIAA, 5-hydroxyindoleacetic acid;SA, schizoaffective; PAR, paranoid; UND, undifferentiated; and DIS, disorganized.
apportion shared variance between each member of a set of indepen¬dent variables is by sequentially adding independent variablesthrough a hierarchical or stepwise procedure. The sequence in whichvariables are added can be specified a priori, as with a hierarchicalanalysis.61 In this case, variables entered earlier should have somecausal priority over variables entered later (ie, earlier variables couldbe a cause of or drive later variables, but, if specified correctly, notvice versa). Alternatively, the sequence of variables can be deter¬mined by whichever variable increases Ä2 the most at each step (astepwise multiple regression). With either method, as each predictorvariable is added in turn to the multiple-regression equation, therewill be an increase in Ä2 with each addition. This increase in sharedvariance is the proportion of total variance that can be attributed tothat particular predictor variable over and above the contribution ofthose predictors already in the model. The increase in Ä2 at each stepcan be tested statistically and, if significant, would indicate that thepredictor variable added at that step makes a significant contributionto variance over and above the contribution of previously enteredvariables. This statistical test (F to include of >4 in the stepwiseprocedure) is also a test of the statistical significance of the corre¬sponding regression coefficient.
A major focus of this study was to determine whether peripheralmonoaminergic measures had a relationship with psychosis ratingsseparate from that ofcentral monoaminergic measures. This questioncan be framed in statistical form: does the addition of peripheralmonoaminergic measures to a multiple-regression equation alreadyrelating central monoaminergic measures to psychosis result in astatistically significant increase in Rl (hierarchical analysis)? Similar¬ly, which variables meet the requirement of F = 4.00 for entry bystepwise analysis?
RESULTS OF CSF METABOLITESGroup Comparisons
Individual patient demographic and CSF data are presented inTable 1. Two-way analysis of variance comparing patients and normal
controls (sex and group) (Table 2) revealed a trend for CSF HVAlevels to be lower in male subjects overall (P=.08). There were no
significant control-patient differences for levels of CSF 5-HIAA.Significantly higher levels of CSF MHPG were found in the schizo¬phrenic patients overall in comparison with controls (P=.04) al¬though there were no significant differences for levels of CSF NE.
Clinical Correlations
The CSF HVA level was the measure that showed the most promi¬nent correlations with clinical ratings (Table 3): BPRS total score,r= -.52, P=.01; BPRS positive symptom score, r= -.50, P=.02;and BPRS negative symptom score, r= -.40, P = .06. The individualBPRS items "social incompetence" and "loss of function" showed aparticularly strong correlation with CSF HVA levels (Spearman'sr=-.62, P<.01) and with CSF 5-HIAA (Spearman's r=-.70,P<.001), respectively. The mean weekly plasma HVA and MHPGlevels showed positive correlations with total and positive symptoms,although they did not reach statistical significance in bivariate analy¬sis. There were no significant nor near-significant correlations be¬tween CSF measures and any of the following variables: current age,age when psychotic symptoms first appeared, numbers of years ofillness, number of hospitalizations, history of suicide attempts, andmedication-free days at the time of the LP.
Interrelationship BetweenMonoamine Metabolites and Symptoms
A correlational matrix of CSF, the mean plasma metabolite data forthe week of the LP, and BPRS ratings are shown in Table 3. Of note isthe significant correlation between CSF HVA and CSF 5-HIAAvalues (r=.73, P<.001). A more modest correlation between CSFand the week's mean plasma HVA values is found (r= .39, = .07).
The BPRS total, positive, and negative symptom scores wereexamined separately with both hierarchical and stepwise multipleregressions. The model used for hierarchical analysis presumes thatcentral measures have causal precedence over peripheral measures.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Department of Veterans Affairs User on 08/11/2016
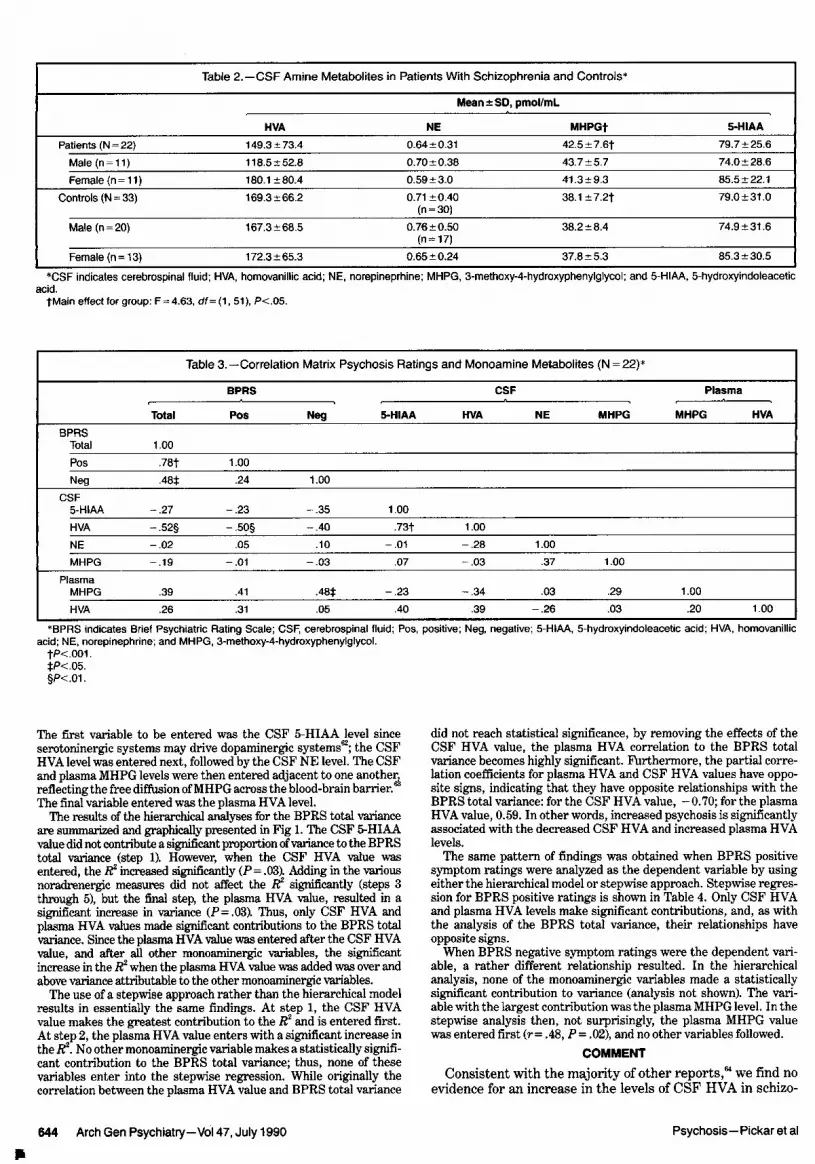
Table 2.—CSF Amine Metabolites in Patients With Schizophrenia and Controls*
Mean±SD, pmol/mL
HVA NE MHPGt 5-HIAAPatients (N = 22) 149.3 ±73.4 0.64 ±0.31 42.5±7.6f 79.7 ±25.6
Male(n = 11) 118.5 + 52.8 0.70 ±0.38 43.7 ±5.7 74.0 ±28.6
Female (n = 11) 180.1 ±80.4 0.59 ±3.0 41.3 + 9.3 85.5 ±22.1
Controls (N = 33) 169.3±66.2 0.71 ±0.40(n = 30)
38.1±7.2t 79.0 ±31.0
Male (n = 20) 167.3 ±68.5 0.76 ±0.50(n = 17)
38.2 ±8.4 74.9 ±31.6
Female (n = 13) 172.3 ±65.3 0.65 ±0.24 37.8 ±5.3 85.3 ±30.5
*CSF indicates cerebrospinal fluid; HVA, homovanillic acid; NE, norepineprhine; MHPG, 3-methoxy-4-hydroxyphenylglycol; and 5-HIAA, 5-hydroxyindoleaceticacid.
tMain effect for group: F = 4.63, df=(1, 51), P<.05.
Table 3.—Correlation Matrix Psychosis Ratings and Monoamine Metabolites (N = 22)*
Total
BPRS CSF
Pos Neg 5-HIAA HVA NE MHPG
Plasma
MHPG HVABPRS
Total 1.00Pos 78t 1.00
Neg .48i. .24 1.00CSF
5-HIAA .27 .23 .35 1.00HVA 52§ 50§ .40 73t 1.00NE -.02 .05 .10 .01 .28 1.00
MHPG .19 -.01 -.03 .07 .03 .37 1.00Plasma
MHPG .39 .48t .23 -.34 .03 .29 1.00
HVA .26 .31 .05 .40 .39 .26 .03 .20 1.00
*BPRS indicates Brief Psychiatric Rating Scale; CSF, cerebrospinal fluid; Pos, positive; Neg, negative; 5-HIAA, 5-hydroxylndoleacetic acid; HVA, homovanillicacid; NE, norepinephrine; and MHPG, 3-methoxy-4-hydroxyphenylglycol.
fP<.001. <05.§P<.01.
The first variable to be entered was the CSF 5-HIAA level sinceserotoninergic systems may drive dopaminergic systems62; the CSFHVA level was entered next, followed by the CSF NE level. The CSFand plasma MHPG levels were then entered adjacent to one another,reflecting the free diffusion ofMHPG across the blood-brain barrier.The final variable entered was the plasma HVA level.
The results of the hierarchical analyses for the BPRS total varianceare summarized and graphically presented in Fig 1. The CSF 5-HIAAvalue did not contribute a significant proportion ofvariance to the BPRStotal variance (step 1). However, when the CSF HVA value was
entered, the R2 increased significantly (P = .03). Adding in the variousnoradrenergic measures did not affect the R2 significantly (steps 3through 5), but the final step, the plasma HVA value, resulted in a
significant increase in variance (P = .03). Thus, only CSF HVA andplasma HVA values made significant contributions to the BPRS totalvariance. Since the plasma HVA value was entered after the CSF HVAvalue, and after all other monoaminergic variables, the significantincrease in the R2 when the plasma HVA value was added was over andabove variance attributable to the other monoaminergic variables.
The use ofa stepwise approach rather than the hierarchical modelresults in essentially the same findings. At step 1, the CSF HVAvalue makes the greatest contribution to the R and is entered first.At step 2, the plasma HVA value enters with a significant increase inthe R2. No other monoaminergic variable makes a statistically signifi¬cant contribution to the BPRS total variance; thus, none of thesevariables enter into the stepwise regression. While originally thecorrelation between the plasma HVA value and BPRS total variance
did not reach statistical significance, by removing the effects of theCSF HVA value, the plasma HVA correlation to the BPRS totalvariance becomes highly significant. Furthermore, the partial corre¬lation coefficients for plasma HVA and CSF HVA values have oppo¬site signs, indicating that they have opposite relationships with theBPRS total variance: for the CSF HVA value,
-
0.70; for the plasmaHVA value, 0.59. In other words, increased psychosis is significantlyassociated with the decreased CSF HVA and increased plasma HVAlevels.
The same pattern of findings was obtained when BPRS positivesymptom ratings were analyzed as the dependent variable by usingeither the hierarchical model or stepwise approach. Stepwise regres¬sion for BPRS positive ratings is shown in Table 4. Only CSF HVAand plasma HVA levels make significant contributions, and, as withthe analysis of the BPRS total variance, their relationships haveopposite signs.
When BPRS negative symptom ratings were the dependent vari¬able, a rather different relationship resulted. In the hierarchicalanalysis, none of the monoaminergic variables made a statisticallysignificant contribution to variance (analysis not shown). The vari¬able with the largest contribution was the plasma MHPG level. In thestepwise analysis then, not surprisingly, the plasma MHPG valuewas entered first (r = .48, = .02), and no other variables followed.
COMMENTConsistent with the majority of other reports,64 we find no
evidence for an increase in the levels of CSF HVA in schizo-
Downloaded From: http://archpsyc.jamanetwork.com/ by a Department of Veterans Affairs User on 08/11/2016

Fig 1.—Total variance pie graphs represent total variance in BriefPsychiatric Rating Scale total scores at each step of the hierarchicalmultiple-regression analysis. Each wedge indicates that portion ofvariance explained by a particular monoamine metabolite; asteriskedand crosshatched wedges, statistically significant increases in vari¬ance; ft2, proportion of total variance explained at each step in thehierarchical multiple-regression analysis; AR2, the increase in vari¬ance from the previous step attributable to the inclusion of anothermonoamine metabolite in the hierarchical multiple-regression analy¬sis; f, df, and values, the statistical significance of the increase invariance ( 2) at each step of the analysis; CSF, cerebrospinal fluid;5-HIAA, 5-hydroxyindoleacetic acid; HVA, homovanillic acid; NE, nor-epinephrine; MHPG, 3-methoxy-4-hydroxyphenylglycol; and NS, notsignificant. The final regression equation (after step 6) is as follows:
Brief Psychiatric Rating Scale Total = 0.11 (CSF 5-HIAA)-
0.18 (CSF HVA)-
0.74 (CSF NE)-
0.63 (CSF MHPG)+ 0.59 (Plasma MHPG) + 39 (Plasma HVA) + 83.91
phrenic patients compared with normal subjects. The solesignificant difference from controls, increased CSF MHPGlevels, may be related to enhanced peripheral noradrenergicactivity.63 Interestingly, we found no group differences inCSF NE levels in contrast to other studies8,13,65,66 that did notinclude measures of MHPG in CSF. The most compellingfinding in this study, however, is that only CSF and plasmaHVA levels have significant relationships to psychosis and to
Table 4.—Stepwise Multiple Regression for BPRS-PositiveSymptom Score*
Variable Step 0 Step 11 Step 2fCSF
HVA -.50 -.504 -70ÍNE .05 -.11 -.01MHPG -.02 -.03 -.085-HIAA -.23 .22 .13
PlasmaHVA§ .31 .63 ,63tMHPG§ .41 .29 .07
Multiple R...
.50 .74
.02 .0006*BPRS indicates Brief Psychiatrie Rating Scale; HVA, homovanillic acid;
NE, norepinephrine; MHPG, 3-methoxy-4-hydroxyphenylglycol; and 5-HIAA,5-hydroxyindoleacetic acid.
fPartial correlation.^Indicates variables entered.§Mean weekly levels.
positive symptoms. Greater symptoms are associated withlower levels of CSF HVA and with higher levels of plasmaHVA.
The negative correlations between CSF HVA and psychot¬ic symptoms are, in general, compatible with some earlystudies that employed fluorometric assay techniques and pro-benecid administration to prevent efflux of acid metabolitesfrom CSF. Bowers3 reported that patients who displayedschneiderian symptoms tended to have low levels of CSFHVA following the administration of probenecid to preventefflux ofacid metabolites from CSF. In subsequent investiga¬tions, Bowers4 reported that schizophrenic patients with poorprognoses—a group similar to the patients with DSM-III-diagnosed chronic illnesses in our study—had significantlylower levels of CSF HVA than those with better prognoses.Post et al5 found significant negative correlations betweenpost-probenecid CSF HVA levels and the number of first-rank schneiderian symptoms in a group of patients withschizophrenia who had generally good prognoses. These au¬thors also found in schizophrenic, but not in manic patients,that CSF HVA levels were significantly lower during a stabi¬lized recovery period than during a period of acute psychosis.Moreover, the lowest levels were found in the schizophrenicpatients with greater chronic illnesses. Recently, Lindstrom14reported significantly lower levels of CSF HVA in 40 patientswith acute schizophrenia (including 21 patients who had neverreceived neuroleptic treatment) in comparison with 21 normalcontrols and found CSF HVA levels to be negatively correlat¬ed with the negative symptoms "lassitude" and "slowness ofmovement."
In contrast to the CSF HVA level, we found the plasmaHVA level to be positively correlated with psychosis andpositive symptom ratings, a finding consistent with thatfound in previous studies,4"7 although somewhat less robustthan we had previously reported.46 This difference may berelated to the fact that the plasma HVA levels in the currentstudy were collected following a shorter drug-free periodnecessitated by correspondence to the LP. Unfortunately,plasma measures were not available from control subjects;thus, the issue of whether plasma HVA levels are elevated inpatients with schizophrenia49 could not be addressed. In arecent investigation of daily plasma HVA rhythms, however,Doran et al67 observed a trend for elevated plasma HVA levelsduring the day but not during the evening or night hours inpatients with schizophrenia compared with normal subjects,and they found that fluphenazine treatment significantly re-
Downloaded From: http://archpsyc.jamanetwork.com/ by a Department of Veterans Affairs User on 08/11/2016
dueed levels across the 24-hour period. Davidson and Davis47reported significantly lower plasma HVA levels in schizo¬phrenic patients compared with controls over a multiple sam¬ple night study; nevertheless, they observed positive correla¬tions between plasma HVA and psychotic symptoms. Thus,like CSF HVA value, the plasma HVA correlation with symp¬toms does not necessarily imply differences from controls inmetabolite levels.
Our finding that negative symptoms were best correlatedwith plasma MHPG levels may be consistent with the reportof Ko et al68 in which individual change in plasma MHPG levelsin drug-free patients with schizophrenia across periods of lowand high psychosis was correlated with a change in the totalBPRS score. Recently, van Kämmen et al69 observed elevatedCSF MHPG and NE levels in patients with schizophrenia whorelapsed following drug discontinuation, further suggestingnoradrenergic relationships to psychotic processes. In a pre¬vious study46 and in the recent report by Muscettola et al,70plasma HVA levels were correlated positively with negative,as well as with positive, symptoms, although in both cases
plasma MHPG levels were not available for analysis. Theapparent relationship among sympathetic nervous systemactivity, arousal, and negative symptoms, however, may sug¬gest further prospective study.
The possibility that the frontal cortical dopaminergic sys¬tem may contribute significantly to HVA levels in CSF couldhave important implications in interpreting the negative cor¬relations between CSF HVA and symptoms found in thisstudy. Most of the evidence that the mesocortical dopaminer¬gic system contributes to the CSF HVA value comes fromclinical studies. Lower levels of CSF HVA have been found inpatients with computed tomographic evidence, suggestingcortical2930 and/or prefrontal cortical atrophy,31 as well as withenlargement ofcerebral ventricles.29,32'36 In a study that linkedCSF neurotransmitter levels to regional brain function, Ber-man et al18 observed that CSF HVA levels were significantlycorrelated with regional cerebral blood flow of the prefrontalcortex during the prefrontal cortex-mediated WisconsinCard Sort test36 but not during a nonspecific number-match¬ing task. Stanley et al37 reported, in a human postmortemstudy, that CSF HVA levels were significantly correlatedwith HVA levels in the frontal cortex but not with HVA levelsin the caudate. Similar findings were reported by EIsworth etal38 in a primate postmortem study in which CSF levels ofHVA were significantly correlated with the prefrontal HVAlevel but not with HVA levels in the cingulate cortex nor inthe caudate. It is also relevant to consider that noradrenergic,as well as dopaminergic, nerve endings may provide a sourceofprefrontal HVA.71,72 In any case, it seems likely that relativecontributions of cortical and subcortical sources of dopamineto CSF HVA levels are not static but depend as well on statevariables, such as stress73,74 and drug treatment.16
The CSF 5-HIAA levels were significantly correlated withthe CSF HVA levels in our subjects, a relationship that hasbeen well documented and may reflect a functional interactionbetween CNS dopaminergic and serotoninergic systems.62 Itis not surprising, therefore, that 5-HIAA showed an overlapwith some HVA relationships to symptoms. Hsiao et al75 havereported significantly lower CSF HVA-5-HIAA correlationcoefficients in depressed patients who were poor respondersto antidepressant treatment in comparison with good re¬
sponders. The implications of CSF HVA-5-HIAA relation¬ships in schizophrenic patients, including the effect of neuro-
leptic treatment, is discussed in detail in a separate report(J.K.H., A.R.D., W.Z.P, D.P., and J. J. Bartko, PhD, un¬
published data, 1990).In humans, the best support for the use of the plasma HVA
level as a CNS "marker" is its consistent correlation with
Cortical
Subcortical
PeripheralNervous System
CPIasma\_HVA_J
Determinants of CSF and Plasma HVA
lHVAJV (-)
I Psychosis J
/Plasma^*fl','^ ( + )V_HVA J
Correlations Between Plasma and CSF HVA and Psychosis
Cortical
Subcortical
A 'Bidirectional' Model of Psychosis
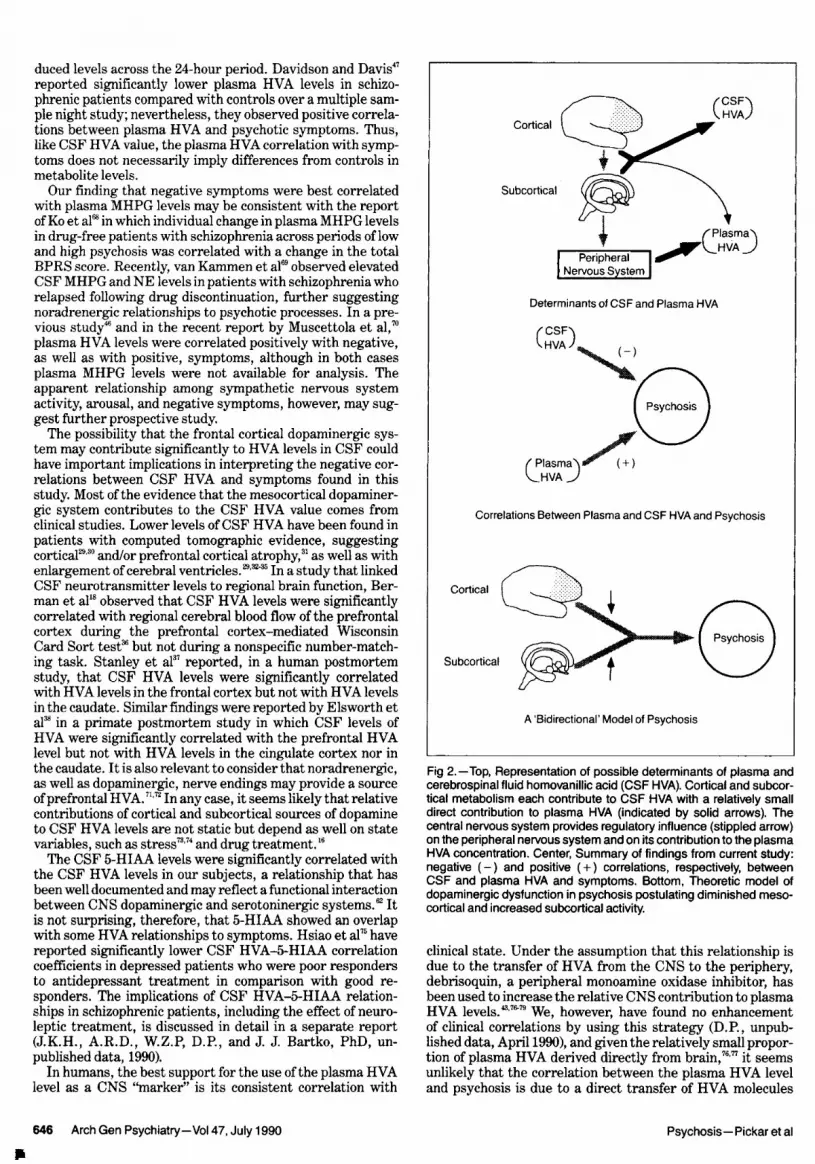
Fig 2.—Top, Representation of possible determinants of plasma andcerebrospinal fluid homovanillic acid (CSF HVA). Cortical and subcor¬tical metabolism each contribute to CSF HVA with a relatively smalldirect contribution to plasma HVA (indicated by solid arrows). Thecentral nervous system provides regulatory influence (stippled arrow)on the peripheral nervous system and on its contribution to the plasmaHVA concentration. Center, Summary of findings from current study:negative (-) and positive ( + ) correlations, respectively, betweenCSF and plasma HVA and symptoms. Bottom, Theoretic model ofdopaminergic dysfunction in psychosis postulating diminished meso¬cortical and increased subcortical activity.
clinical state. Under the assumption that this relationship isdue to the transfer of HVA from the CNS to the periphery,debrisoquin, a peripheral monoamine oxidase inhibitor, hasbeen used to increase the relative CNS contribution to plasmaHVA levels.43,76"79 We, however, have found no enhancementof clinical correlations by using this strategy (D.P., unpub¬lished data, April 1990), and given the relatively small propor¬tion of plasma HVA derived directly from brain,76,77 it seems
unlikely that the correlation between the plasma HVA leveland psychosis is due to a direct transfer of HVA molecules
Downloaded From: http://archpsyc.jamanetwork.com/ by a Department of Veterans Affairs User on 08/11/2016

from the CNS to the periphery. At the same time, it isprobably overly simplistic to view CSF HVA as a purelycentral and plasma HVA as a purely peripheral measure. Asdemonstrated in this study, for example, plasma HVA makesa contribution to psychosis variance above and beyond thatmade by CSF HVA, although the biologic determinants un¬derlying the positive correlation between plasma HVA andpsychosis remain obscure. Plasma HVA originates primarilyfrom the peripheral sympathetic nervous system39 and a num¬ber of brain-stem and hypothalamic centers, including nora¬drenergic, serotoninergic, and dopaminergic nuclei, whichhave been implicated in the control of sympathetic nervous
system outflow.80"82 The plasma HVA level presumably re¬flects, in part, activity of these subcortical neurons, althoughit is not known whether these nuclei directly pertain to patho-physiologic mechanisms that underlie psychosis. At the same
time, plasma HVA levels are unlikely to be simply a reflectionof peripheral catecholamine turnover,83,84 and other determi¬nants (for instance, renal clearance85) may be important aswell. Furthermore, CSF metabolite levels themselves maybe influenced by "peripheral" factors, such as body position(vertical vs horizontal) or even transfer of peripheral HVA tothe CSF. In the present study, free plasma MHPG, anothermeasure of sympathetic nervous system turnover, did notsignificantly contribute to total BPRS or positive symptomvariance, while plasma HVA did contribute significantly toboth.
In light of these issues, how might our findings relate to the
pathophysiology of schizophrenia? One theoretic approach isillustrated in Fig 2. As diagrammed in the top panel, CSFHVA originates from both cortical and subcortical sources,while plasma HVA is largely derived from peripheral metabo¬lism with only a small direct contribution from the CNS.Subcortical monoaminergic neurons, however, can influenceplasma HVA levels by modulating peripheral nervous systemactivity. In the center panel of Fig 2, the principal findingsthat relate metabolites to symptoms from the present studyare summarized. The CSF HVA correlates negatively withpsychosis, while plasma HVA correlates positively, with eachmaking significant contributions to total variance. Finally, inthe bottom panel ofFig 2, a "bidirectional" dopamine model ofpsychosis16,22 is summarized: decreased frontal cortical releaseand/or metabolism of dopamine is coupled with increasedsubcortical activity, resulting in psychotic symptoms. Whilethe lower two panels of the figure provide some interestingparallels, we would caution against overinterpreting thesesimilarities, given the almost certain interaction of otherneurotransmitter systems and the need for more direct vali¬dation with methods that are better suited to assessing specif¬ic regional brain function.86
The authors gratefully acknowledge the editorial assistance of MarjorieOrnsteen and Andrea Hobbs and the suggestions of Daniel R. Weinberger,MD. The nursing staff of the 4-East Research Ward provided expert clinicalcare of the patients in this study. Mark Stipetic and the National Institute ofMental Health Central Laboratory, Bethesda, Md, provided critical assaysupport for this project.
References
1. Persson T, Roos B-E. Acid metabolites from monoamines in cerebrospinalfluid of chronic schizophrenics. Br J Psychiatry. 1969;115:95-98.
2. Rimon R, Roos B-E, Rakkolainen V, Alanen Y. The content of 5-HIAAand HVA in the CSF of patients with acute schizophrenia. J Psychosom Res.1971;15:375-378.
3. Bowers MB Jr. 5-Hydroxyindoleacetic acid (5HIAA) and homovanillicacid (HVA) following probenecid in acute psychotic patients treated withphenothiazines. Psychopharmacology (Berlin). 1973;28:309-318.
4. Bowers MB Jr. Central dopamine turnover in schizophrenic syndromes.Arch Gen Psychiatry. 1974;31:50-54.
5. Post RM, Fink E, Carpenter WT Jr, Goodwin FK. Cerebrospinal fluidamine metabolites in acute schizophrenia. Arch Gen Psychiatry. 1975;32:1063\x=req-\1069.
6. van Praag HM, Korf J. Neuroleptics, catecholamines, and psychoses: a
study oftheir interrelations. Am JPsychiatry. 1975;132:593-597.7. Berger PA, Faull KM, Kilkowski J, Anderson PJ, Kraemer H, Davis KL,
BarchasJD. CSF monoamine metabolites in depression and schizophrenia. AmJ Psychiatry. 1980;137:174-180.
8. Gomes UCR, Shanley BC, Potgieter L, Roux JT. Noradrenergic overac-
tivity in chronic schizophrenia: evidence based on cerebrospinal fluid noradren-aline and cyclic nucleotide concentrations. Br J Psychiatry. 1980;137:346-351.
9. Gattaz WF, Waldmeier P, Beckmann H. CSF monoamine metabolites inschizophrenic patients. Acta Psychiatr Scand. 1982;66:350-360.
10. Gattaz WF, Riederer P, Reynolds GP, Gattaz D, Beckmann H. Dopa-mine and noradrenalin in the cerebrospinal fluid of schizophrenic patients.Psychiatry Res. 1983;8:243-250.
11. Nyback H, Berggren B-M, Hindmarsh T, Sedvall G, Wiesel F-A. Cere-broventricular size and cerebrospinal fluid monoamine metabolites in schizo-phrenic patients and healthy volunteers. Psychiatry Res. 1983;9:301-308.
12. Gerner RH, Fairbanks L, Anderson GM, Young JG, Scheinin M, Lin-noila M, Hare TA, Shaywitz BA, Cohen DJ. CSF neurochemistry in depressed,manic, and schizophrenic patients compared with that ofnormal controls. Am JPsychiatry.1984;141:1533-1540.
13. Kemali D, Maj M, Iorio G, Marciano F, Nolfe G, Galderisi S, Salvati A.Relationship between CSF noradrenaline levels, C-EEG indicators of activa-tion and psychosis ratings in drug-free schizophrenic patients. Acta PsychiatrScand. 1985;71:19-24.
14. Lindstrom LH. Low HVA and normal 5-HIAA CSF levels in drug-freeschizophrenic patients compared to healthy volunteers: correlations to symp-tomatology and family history. Psychiatry Res. 1985;14:265-273.
15. Carlsson A. The current status of the dopamine hypothesis of schizo-phrenia. Neuropsychopharmacology. 1988;1:179-186.
16. Pickar D. Perspectives on a time-dependent model ofneuroleptic action.Schizophr Bull. 1988;14:255-268.
17. Weinberger DR, Berman KF, Zec RF. Physiological dysfunction ofdorsolateral prefrontal cortex in schizophrenia, I: regional cerebral blood flow(rCBF) evidence. Arch Gen Psychiatry. 1986;43:114-125.
18. Berman KF, Zec RF, Weinberger DR. Physiological dysfunction ofdorsolateral prefrontal cortex in schizophrenia, II: role of medication, atten-tion, and mental effort. Arch Gen Psychiatry. 1986;43:126-143.
19. Weinberger DR, Berman KF, Illowsky BP. Physiological dysfunction ofdorsolateral prefrontal cortex in schizophrenia, III: a new cohort and evidencefor a monoaminergic mechanism. Arch Gen Psychiatry. 1988;45:609-615.
20. Cohen RM, Semple WE, Gross M, Nordahl TE, DeLisi LE, HolcombHH, Morhisa JM, Pickar D. Dysfunction in a prefrontal substrate of sustainedattention in schizophrenia. Life Sci. 1987;40:2031-2039.
21. Brozoski TJ, Brown RM, Rosvold HE, Goldman PS. Cognitive deficitcaused by regional depletion of dopamine in prefrontal cortex of rhesus mon-
key. Science. 1979;205:929-932.22. Weinberger DR. Implications of normal brain development for the
pathogenesis of schizophrenia. Arch Gen Psychiatry. 1987;44:660-669.23. Weinberger DR, Berman KF. Speculation on the meaning of cerebral
metabolic hypofrontality in schizophrenia. Schizophr Bull. 1988;14:157-168.24. Weinberger DR, Berman KF, Chase TN. Mesocortical dopaminergic
function and human cognition. Ann NY Acad Sci. 1988;537:330-338.25. Goldberg TE, Weinberger DR. Probing prefrontal function in schizo-
phrenia with neuropsychological paradigms. Schizophr Bull. 1988;14:179-183.26. Bannon MJ, Roth RH. Pharmacology ofmesocortical dopamine neurons.
Pharmacol Rev. 1983;35:53-68.27. Pycock CJ, Kerwin RW, Carter CJ. Effect of lesion of cortical dopamine
terminals on subcortical dopamine in rats. Nature. 1980;286:74-77.28. Wood JH. Sites oforigin and cerebrospinal fluid concentration gradients.
In: Wood JH, ed. Neurobiology of Cerebrospinal Fluid. New York, NY:Plenum Press; 1980:53-62.
29. Chase TN. Neurochemical alterations in Parkinson's disease. In: WoodJH, ed. Neurobiology ofCerebrospinal Fluid. New York, NY: Plenum Press;1980:207-218.
30. van Kammen DP, Mann LS, Sternberg DE, Scheinin M, Ninan PT,Marder SR, van Kammen WB, Rieder RO, Linnoila M. Dopamine-B-hydroxy-lase activity and homovanillic acid in spinal fluid of schizophrenics with brainatrophy. Science. 1983;220:947-977.
31. van Kammen DP, van Kammen WB, Mann LS, Sepala T, Linnoila M.Dopamine metabolism in the cerebrospinal fluid of drug-free schizophrenicpatients with and without cortical atrophy. Arch Gen Psychiatry. 1986;43:978\x=req-\983.
32. Doran AR, Boronow J, Weinberger DR, Wolkowitz OM, Breier A,Pickar D. Structural brain pathology in schizophrenia revisited: prefrontalcortex pathology is inversely correlated with cerebrospinal fluid levels ofhomovanillic acid. Neuropsychopharmacology. 1987;1:25-32.
33. Nyback H, Wiesel F-A, Berggren B-M, Hindmarsh T. Computed tomog-raphy of the brain in patients with acute psychosis and in healthy volunteers.Acta Psychiatr Scand. 1982;65:403-413.
34. Nyback H, Berggren B-M, Hindmarsh T, Sedvall G, Wiesel F-A. Cere-broventricular size and cerebrospinal fluid monoamine metabolites in schizo-
Downloaded From: http://archpsyc.jamanetwork.com/ by a Department of Veterans Affairs User on 08/11/2016

phrenic patients and healthy volunteers. Psychiatry Res. 1983;9:301-308.35. Jennings WS Jr, Schulz SC, Narasimhachari N, Hamer RM, Friedel RO.
Brain ventricular size and CSF monoamine metabolites in an adolescent inpa-tient population. Psychiatry Res. 1985;16:87-94.
36. Houston JP, Maas JW, Bowden CL, Conteras SA, McIntyre KL, JavorsMA. Cerebrospinal fluid HVA, central brain atrophy, and clinical state inschizophrenia. Psychiatry Res. 1986;19:207-214.
37. Stanley M, Traskman-Bendz L, Dorovini-Zis K. Correlations betweenaminergic metabolites simultaneously obtained from human CSF and brain.Life Sci. 1985;37:1279-1286.
38. Elsworth JD, Leahy DJ, Roth RH, Redmond DE Jr. Homovanillic acidconcentrations in brain, CSF and plasma as indicators of central dopaminefunction in primates. J Neural Transm. 1987;68:51-62.
39. Bacopoulos NG, Hattox SE, Roth RH. 3-4-Dihydroxyphenylacetic acidand homovanillic acid in rat plasma: possible indicators of central dopaminergicactivity. Eur J Pharmacol. 1979;56:225-236.
40. Kendler KS, Davis KL. Acute and chronic effects ofneuroleptic drugs on
plasma and brain homovanillic acid in the rat. Psychiatry Res. 1984;13:51-58.41. Sternberg DE, Heninger G, Roth RH. Plasma homovanillic acid as an
index of brain dopaminergic metabolism: enhancement with debrisoquin. LifeSci. 1983;32:2447-2452.
42. Labarca R, Thomas JW, Koulu K, Kim YS, Janowsky A, Wilkinson L,Linnoila M, Paul SM, Pickar D. A central 6-hydroxydopamine lesion preventsfluphenazine-induced increase in plasma homovanillic acid. Brain Res Bull.1988;20:567-571.
43. Pickar D, Breier A, Kelsoe J. Plasma homovanillic acid as an index ofcentral dopaminergic activity: studies in schizophrenic patients. Ann NY AcadSci. 1988;537:339-346.
44. Bowers MB, Heninger GR, Sternberg D, Meltzer HY. Clinical processesand central dopaminergic activity in psychotic disorders. Commun Psycho-pharmacol. 1980;4:177-188.
45. Davis KL, Davidson M, Mohs RC, Kendler KS, Davis BM, Johns CA,DeNigris Y, Horvath TH. Plasma homovanillic acid concentration and theseverity ofschizophrenic illness. Science. 1985;227:1601-1602.
46. Pickar D, Labarca R, Doran AR, Wolkowitz OM, Roy A, Breier A,Linnoila M, Paul SM. Longitudinal measurement of plasma homovanillic acid inschizophrenic patients: correlation with psychosis and response to neuroleptictreatment. Arch Gen Psychiatry. 1986;43:669-676.
47. Davidson M, Davis KL. A comparison of plasma homovanillic acid con-centration in schizophrenic patients and normal controls. Arch Gen Psychiatry.1988;45:561-563.
48. Bowers MB JR, Swigar ME, Jatlow PI, Goicoecha N. Plasma catechol-amine metabolites and early response to haloperidol. J Clin Psychiatry.1984;6:248-251.
49. Pickar D, Labarca R, Linnoila M, Roy A, Hommer D, Everett D, PaulSM. Neuroleptic-induced decrease in plasma homovanillic acid and antipsy-chotic activity in schizophrenic patients. Science. 1984;225:954-957.
50. Chang W-H, Chen T-Y, Lee C-F, Hung J-C, Hu W-H, Yeh E-K. Plasmahomovanillic acid levels and subtyping of schizophrenia. Psychiatry Res.1988;23:239-244.
51. Davila R, Manero E, Zumarraga M, Andia I, Schweitzer JW, FriedhoffAJ. Plasma homovanillic acid as a predictor of response to neuroleptics. ArchGen Psychiatry. 1988;45:564-567.
52. Wolkowitz OM, Breier A, Doran A, Kelsoe J, Lucas P, Paul SM, PickarD. Alprazolam augmentation of the antipsychotic effects of fluphenazine inschizophrenic patients. Arch Gen Psychiatry. 1988;45:664-671.
53. Pickar D, Wolkowitz OM, Doran AR, Labarca R, Roy A, Breier A,Narang PK. Clinical and biochemical effects of verapamil administration toschizophrenic patients. Arch Gen Psychiatry. 1987;44:113-118.
54. Golden RN, Rudorfer MV, Sherer MA, Linnoila M, Potter WZ. Bupro-pion in depression, I: biochemical effects and clinical response. Arch GenPsychiatry. 1988;45:139-143.
55. Sharma R, Javaid JI, Jamicak P, Faull K, Comaty J, Davis JM. Plasmaand CSF HVA before and after pharmacological treatment. Psychiatry Res.1989;28:97-104.
56. American Psychiatric Association, Committee on Nomenclature andStatistics. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed.Washington, DC: American Psychiatric Association; 1980.
57. Scheinin M, Chang WH, Kirk KL, Linnoila M. Simultaneous determina-tion of 3-methoxy-4-hydroxyphenylglycol, 5-hydroxyindoleacetic acid, and ho-movanillic acid in cerebrospinal fluid with high-performance liquid chromatog-raphy using electrochemical detection. Anal Biochem. 1983;131:246-253.
58. Chang WH, Scheinin M, Burns RS, Linnoila M. Rapid and simpledetermination of homovanillic acid in plasma using high performance liquidchromatography with electrochemical detection. Acta Pharmacol Toxicol.1983;53:275-279.
59. Scheinin M, Chang WH, Jimerson DC, Linnoila M. Measurement of 3\x=req-\methoxy-4-hydroxyphenylglycol in human plasma with high performance liq-uid chromatography using electrochemical detection. Anal Biochem.
1983;132:165-170.60. Overall JE, Gorham DE. The Brief Psychiatric Rating Scale. Psychol
Rep. 1961;10:799-812.61. Cohen J, Cohen P. Applied Multiple-Regression Correlation Analysis
for the Behavioral Sciences. Hillsdale, NJ: Erlbaum; 1983.62. Agren H, Mefford IN, Rudorfer MV, Linnoila M, Potter WZ. Interact-
ing neurotransmitter systems: a non-experimental approach to the 5-HIAA-HVA correlation in human CSF. J Psychiatr Res. 1986;20:175-193.
63. Kopin IJ, Gordon EK, Jimerson DC, Polinsky RJ. Relation betweenplasma and cerebrospinal fluid levels of 3-methoxy-4-hydroxyphenylglycol.Science. 1983;219:73-75.
64. Widerlov E. A critical appraisal ofCSF monoamine metabolite studies inschizophrenia. Ann NY Acad Sci. 1988;537:309-323.
65. Lake CR, Sternberg DE, van Kammen DP, Ballenger JC, Ziegler MG,Post RM, Kopin IJ, Bunney WE. Schizophrenia: elevated cerebrospinal fluidnorepinephrine. Science. 1980;207:331-333.
66. Sternberg DE, van Kammen DP, Lake CR, Ballenger JC, Marder SR,Bunney WE. The effect of pimozide on CSF norepinephrine in schizophrenia.Am J Psychiatry. 1981;138:1945-1951.
67. Doran AR, Labarca R, Wolkowitz OM, Roy A, Douillet P, Pickar D.Circadian variation of plasma HVA levels is attenuated by fluphenazine inpatients with schizophrenia. Arch Gen Psychiatry. In press.
68. Ko GN, Jimerson DC, Wyatt RJ, Bigelow LB. Plasma 3-methoxy-4-\x=req-\hydroxy-phenylglycol changes associated with clinical state and schizophrenicsubtype. Arch Gen Psychiatry. 1988;45:842-846.
69. van Kammen DP, Peters J, van Kammen WB, Nugent A, Goetz KL, YaoJ, Linnoila M. CSF norepinephrine in schizophrenia is elevated prior to relapseafter haloperidol withdrawal. Biol Psychiatry. 1989;26:176-188.
70. Muscettola G, Barbato G, de Bartolomeis A, Monteleone P, Pickar D.Plasma HVA, tardive dyskinesia and psychosis symptoms in long-term drug-free inpatients with schizophrenia.
71. Kopin IJ. Catecholamine metabolism: basic aspects and clinical signifi-cance. Pharmacol Rev. 1985;37:333-364.
72. Sheinin H. Enhanced noradrenergic neuronal activity increases homo-vanillic acid levels in cerebrospinal fluid. JNeurochem. 1986;43:665-667.
73. Thierry AM, Tassin JP, Blanc G, Glowinski J. Selective activation of themesocortical DA system by stress. Nature. 1976;263:242-244.
74. Breier A, Wolkowitz OM, Doran AR, Beller S, Pickar D. Neurobiologi-cal effects of lumbar puncture stress in psychiatric patients and healthy volun-teers. Psychiatry Res. 1988;2:187-194.
75. Hsiao JK, Angren H, Bartko JJ, Rudorfer MV, Linnoila M, Potter WZ.Monoamine neurotransmitter interactions and the prediction ofantidepressantresponse. Arch Gen Psychiatry. 1987;44:1078-1083.
76. Kopin IJ, Bankiewicz KS, Harvey-White J. Assessment of brain dopa-mine metabolism from plasma HVA and MHPG during debrisoquin treatment:validation in monkeys treated with MPTP. Neuropsychopharmacology.1988;1:119-125.
77. Swann AC, Maas JW, Hattox SE, Landia H. Catecholamine metabolitesin human plasma as indices of brain function: effects of debrisoquin. Life Sci.1980;27:1857-1862.
78. Maas JW, Conteras SA, Seleski E, Bowden CL. Dopamine metabolismand disposition in schizophrenic patients. Arch Gen Psychiatry. 1988;45:553\x=req-\559.
79. Davidson M, Losonczy MF, Mohs RC, Lesser JC, Powchik P, Freed LB,Davis BM, Mykytyn V, Davis KL. Effects of debrisoquin and haloperidol on
plasma homovanillic acid concentrations in schizophrenic patients. Neuropsy-chopharmacology. 1987;1:17-23.
80. Alexander N, Ross-Cisneros F, Kogosov E, De Cuir M, Haun CK,Nagatsu T. Nigrostriatal and cardiovascular systems interactions. In: Naka-mura K, ed. Brain and Blood Pressure Control. New York, NY: ElsevierScience Publishing Co Inc; 1986:61-66.
81. Smith OA, Devito JL. Central neural integration for the control ofautonomic responses associated with emotion. Annu Rev Neurosci. 1984;7:43\x=req-\65.
82. Umeda T, Hamasaki S, Naomi S, Inoue J, Miura F, Ohno M, Iwaoka T,Sato T. Evidence for reduced central dopaminergic activity in salt-sensitiveessential hypertension. In: Nakamura K, ed. Brain and Blood Pressure Con-trol. New York, NY: Elsevier Publishing Co Inc; 1986:353-358.
83. Sowers JR, Vlachakis N. Circadian variation in plasma dopamine levelsin man. J Endocrinol Invest. 1984;7:341-345.
84. Woolf PD, Akowriah S, Lee L, Kelly M, Feibel J. Evaluation of dopa-mine responses to stress in man. J Clin Endocrinol Metab. 1983;56:246.
85. Potter WZ, HsiaoJK, Goldman SM. Effects of renalclearance on plasmaconcentrations of homovanillic acid. Arch Gen Psychiatry. 1989;46:558-562.
86. Pickar D, Litman RE, Konicki PE, Wolkowitz OM, Breier A. Neuro-chemical and neural mechanisms of positive and negative symptoms in schizo-phrenia. In: Andreasen NC, ed. Modern Problems of Pharmacopsychiatry:Positive and Negative Symptoms and Syndromes. In press.
Downloaded From: http://archpsyc.jamanetwork.com/ by a Department of Veterans Affairs User on 08/11/2016