psychosis risk society
TRANSCRIPT
324
CHAPTER FOUR: PSYCHOSIS RISK SOCIETY
“Sometimes, in order to see the light, you have to risk the dark.” – Dr. Iris Hineman95
“[Calumny] and flattery have so prospered with some men, as to have given them the power of making you believe, that in things of little consequence, as for instance, opthalmies, and fevers, and intestine complaints, the gods condescend to act as your advisers, and sometimes even your physicians; but that in matters wherein the interest of the state, and your own individual security are concerned, these same gods [fail to provide] council... A wise man will not wait till the earth sends forth vapor, or the atmosphere is infected, if evil comes from above; but he will perceive such things are at hand, not so soon as the gods, yet sooner than the generality of men. The gods see what is to come, men what is come, and wise men what is coming.” – Apollonius of Tyanna96
“You have to believe in fate—science can compel you to. What then grows out of this belief in your case—cowardice, resignation, or frankness and magnanimity—bears witness to the soil upon which that seedcorn has been scattered but not, however, to the seedcorn itself—for out of this anything and everything can grow.” – Friedrich Nietzsche97
“With rare exceptions... the natural sciences are content to study, to investigate, to establish facts. But in our attempts to cope with ambiguity and uncertainty, we create facts... If this is acceptable, then we must not be judged by the ordinary criteria of science, pure or applied. We are engaged in a different sort of undertaking—a permanent experiment with risk taking, a prolonged and loving engagement with uncertainty on behalf of the mentally disabled. It is a proud and desirable calling. And, if we can contain ourselves comfortably within its constraints, the world will continue to reward our efforts.” – John Spiegel98
***
This chapter examines the category of disease as a rhetorical object. It
explores the ways in which defining some state of affairs as a disease or
illness—what I will call a medicalization controversy—motivates action. I
examine the rhetorical maneuvers of interlocutors engaged in a
medicalization controversy, and highlight some problems with the
95 Dr. Iris Hineman is the (fictional) lead researcher of the ‘PreCrime’ technology in the film Minority Report (Spielberg, 2002).96 As relayed by Flavius Philostratos (1809, pp. 434, 450).97 Friedrich Nietzsche (1986, sec. II:363).98 John Spiegel, discussing the role of risk in psychiatry as a field of practice in his presidential address at the 128th annual meeting of the American Psychiatric Association (Spiegel, 1975, p. 697, emphasis in original).
325
evaluations of the argumentation. According to a general deliberative
practice, benefits are weighed against known risks – but what happens when
the benefits are characterized as the management of known risks associated
with inaction, and the particularly dispositive risks of action are important
precisely because they are unknown?
The main controversy under review in this chapter concerns the
proposal to formalize a diagnosis of 'psychosis risk syndrome.' Though the
proposed diagnosis has been incredibly controversial, the idea of diagnosis a
risk syndrome for schizophrenia has been embraced by the mental health
profession, and over 100 clinics devoted to the cause have been set up over
the last decade (Kecmanović, 2011). As a syndrome, it is characterized by a
constellation of signs and symptoms that by their clustering together
suggests a medically relevant morbid unity, an underlying disease process
that can be called by name, with a prognosis that can be speculated on, and,
in an ideal world, that will respond to a specific indicated treatment. As a
risk syndrome, the underlying disease process is not necessarily present, but
its future presence is anticipated on account of the premonitory signs and
symptoms that constitute the syndrome. The very heated public battle over
including psychosis risk syndrome in DSM5 ended in somewhat of a draw, as
the Task Force did include the putative condition (as 'attenuated psychosis
syndrome'), but in a special section for 'conditions for further study,' with the
326
explicit disclaimer that the “proposed criteria sets are not intended for
clinical use” (American Psychiatric Association, 2013, p. 783).99
I argue that psychosis has always been about risk, and that
schizophrenia is the quintessential psychosis risk syndrome. The diagnosis
of psychosis risk syndrome is an expected development of the schizophrenia
construct that matches with the contemporary societal orientations toward
risk. Further, I suggest that the final consensus about psychosis risk
reflected in DSM5 represents a temporary ceasefire between warring forces,
pausing to consider the possibility that a greater threat exists to the integrity
of psychiatric science. In order to unfold this position I will consider classical
views, indicate the configurations of world risk society, and then show how
the DSM5 becomes a contested space in which this issue is fought in terms of
the inevitability and unpredictability of risk. These moves are divided into
four major sections.
1. Risk in Antiquity and Early Modernity. In order to understand
the controversy about institutionalizing psychosis risk syndrome in DSM5,
we need to investigate how cultural resources were drawn forward from the
99 Though it has been rebranded 'attenuated psychosis syndrome' in DSM5 (Table 1), that name is rather uncommon in the scientific literature and popular press, owing to its recent creation. A plurality of the literature refers to the diagnosis as 'psychosis risk syndrome,' including official sources during the DSM5 early development phase. Consequently, I (except when noted) stick to 'psychosis risk syndrome' when referring to the diagnosis. The other neames that are used in the literature to describe this proposed diagnostic category include 'at risk mental state,' 'risk syndrome for psychosis,' 'ultra high risk state,' and the 'prodromal phase' of schizophrenia.
327
time where fate and commonsense informed judgment to those where risk
was understood as potential opportunity, lurking danger and, later,
calculated probability. In late modern epistemic efforts, risk no longer
measures actual dangers, but sets the parameters of likelihood for
populations. The classic and modern points of view entered into the DSM5
controversy through the distinct interpretations of risk that psychosis risk
syndrome simultaneously signified.
2. Psychiatric Rhetoric in a Risk Society. Preoccupation with risk
is pervasive across our late modern society, which Ulrich Beck (1992b) has
called a risk society. Sociologists use this term to describe a “society
increasingly preoccupied with the future (and also with safety), which
generates the notion of risk” (Giddens, 1999, p. 3). Our society is a risk
society not because there are more risks than there used to be (though there
are), or because the risks we face are of greater magnitude than in former
times and in some cases are existential (though this is the case as well);
rather, risk society is so called because risk as both a logic and an object of
knowledge has become a significant organizing principle of all major
institutions (Beck, 1992a, 1992b, 1999, 2000; Beck, Giddens, & Lash, 1994;
Danisch, 2010; Douglas, 1992; Giddens, 1991, 1999; Keränen, 2008, 2011;
Lash, 2000; Luhmann, 1996, 2005; A. Scott, 2000; Van Loon, 2002). Hence, a
study of risk society may be grounded in any significant modern institution
328
(Ericson & Haggerty, 1997). This study of risk society visàvis psychiatry
(and more specifically psychiatric diagnostic controversy) examines “how
forms of rationality inscribe themselves in practices or systems of practices,
and what role they play within them, because... 'practices' don't exist without
a certain regime of rationality” (Foucault, 1991, p. 79). That is, I examine
how risk, as a kind of rationality (or really a cluster of rationalities developed
historically and reproduced discursively), has inscribed itself in the
diagnostic and nosological practices of psychiatry and in the argument
practices of those engaged in controversies concerning those practices. This
section examines a series of related diagnostic controversies (e.g., sluggish
schizophrenia, pedohebephilic disorder, coercive paraphilia) that lurk in the
shadows of psychosis risk.
3. Early Intervention Research. This section examines the
development of early intervention strategies to prevent psychosis. These
efforts occurred concurrently in different nosological frameworks. To a
greater or lesser degree, the various research programs shared three
presuppositions: First, it is possible to identify susceptible individuals
sufficiently early to allow time for intervention; second, it is possible to
develop interventions that in some cases can prevent psychosis from
developing; and third, there is an urgent need for such techniques because of
the irreversible damage that occurs during a first psychotic episode. The
329
section begins with an exploration of Freud's views on the importance of early
diagnosis. It then turns to various twentiethcentury nosological moves
designed to better classify the prognosis of psychotic disorders. It then
examines the development of early intervention research programs, and
concludes with the research of Patrick McGorry, a key figure in the DSM5
controversy.
4. Psychosis Risk Syndrome and DSM5. This section introduces
the argumentative landscape of the controversy, identifying its essential
arguments, stasis points, topoi, and tropes, and the ways in which the
rhetorical agency of the key opinion leaders in the dispute is constrained and
enabled. Special attention is paid to how rhetors appeal to different
conceptions of risk. These arguments about risk, particularly those that
compare one risk to another, enabled novel articulations of psychiatric
illness. However, representations of risk did not flow smoothly and
consistently through the public and technical spheres. The accumulated
concepts of risk and ideas about preventive medicine recirculate in the
discourses of psychosis risk. On one hand, the notion of a psychosis prodrome
in individual patients gives a neurobiological form to a hybridization of fate
and danger. On the other, classical phronesis combines with late modern
Bayesian risk factors in a clinical population. Participants in the controversy
weigh the benefits of these interpretations with the costs, which they also
330
articulate in the language of risk. Some of these risks are known dangers
(stigmatization, medication sideeffects), while some are unknown risks about
what the diagnosis will become once it moves from the marketplace of ideas
to the marketplace.
Risk in Antiquity and Early Modernity
In this section, I trace the historical development of risk as an object of
knowledge and as a regime of rationality. I begin by examining notions of
risk or risklike concepts in antiquity and early modernity, following and
updating the traditional account given by Luhmann (2005) and Beck (1992b),
paying special attention to the rhetorical implications of risk. I then turn to
the ways in which these historical antecedents were transformed into the
contemporary object of knowledge and subject of deliberation we understand
as risk, focusing on the ways in which the concept coevolved with the
institution of psychiatry visàvis the diagnostic entity of schizophrenia. In
the process, I discuss the historically controversial diagnosis of 'sluggish
schizophrenia,' and the DSM5 controversies surrounding pedohebephilia,
coercive paraphilia, and parental alienation syndrome. Finally, I turn to the
specific question of preventive psychiatry and the efforts to develop and
legitimize early interventions in psychosis, an idea that slowly evolved into
the notion of psychosis risk syndrome. I situate the controversy over
psychosis risk syndrome that played out over the last halfdecade in the
331
larger context of developments and debates in the field stretching back into
the 1980s and before, and I explain the key arguments and their implications
in light of the larger issues of risk society and the rhetorical evolution of
psychosis discussed in the previous chapter.
The history of the concept of risk is closely intertwined with the history
of modernity, yet has only recently appeared as an object of social scientific
inquiry. The development of risk as an object of knowledge serving as a
motivator and product of human action is necessarily intertwined with the
cluster of historical and sociological configurations that have characterized
modernity, e.g., industrialization; secularization; capitalism; the nationstate;
and the emergence, development, and rationalization of institutions that
effect “the regularised control of social relations across indefinite timespace
distances” (Giddens, 1991, p. 16). In this section, I shall examine the pre
modern understanding of risk and contrast it with its modern conception, so
as to highlight the aspects of risk that are distinctive features of modernity.
This analysis will clarify the extent to which the diagnosis of schizophrenia
bears the signature of modernity. Building on the arguments and themes
developed in Chapter 2 and Chapter 3, I contend that the development of
psychosis risk syndrome, and the surrounding controversy, is an artifact of
the development of risk as an object of knowledge that occurred as early
modernity gave way to its more reflexive second stage.
332
Risk and Unknown Fate
In an important early study of the sociology of risk, Luhmann
(1993/2005) argues that while humanity has always been concerned about
the uncertain nature of the future, premodern societies tended to
understand the future in terms of fate, over which their control was limited
to divination rituals and practices of piety:
Older civilizations had…no need for a word covering what we now
understand by the term risk… For the most part…one trusted in
divinatory practices, which—although unable to provide reliable
security—nevertheless ensured that a personal decision did not arouse
the ire of the gods or of other awesome powers, but was safeguarded by
contact with the mysterious forces of fate. In many respects the
semantic complex of sin (conduct contravening religious instruction)
also represents a functional equivalent, inasmuch as it can serve to
explain how misfortune comes about. (Luhmann, 2005, p. 8)
Though risk as it is understood in modernity is novel, Giddens (1991) argues
that alternative conceptual variants have been a constant feature of history
and have always been of central importance in human society:
[There] is no nonmodern culture which does not in some sense
incorporate, as a central part of its philosophy, the notions of fate and
destiny. The world is not seen as a directionless swirl of events, in
333
which the only ordering agents are natural laws and human beings,
but as having intrinsic form which relates individual life to cosmic
happenings. (p. 109)
In ancient Greek mythology, even the gods were subject to the Moirai
( ),Μοῖραι the Fates, whose name derived from the word moira (μ ),οῖρα
meaning a portion of the whole—the Fates were literally 'apportioners' of the
goods and dangers of life (Grimal, 1996; E. Hamilton, 1940; Harper, 2013).
At the same time, individuals could make decisions that would affect their
destiny, but that destiny would unfold by necessity according to an unknown
but preordained script. Every person was driven toward his fate and
inevitable death by Moros ( ),Μορος the spirit of doom, and the root of the
word 'morose' (Lawson, 1994).
Risk as Dangerous Opportunity
There were two words in ancient Greek that conveyed something akin
to the modern idea of risk: kindynos ( ),κίνδυνος a noun meaning danger,
risk, hazard, or venture, and peiraō ( )πειράω , a verb meaning to attempt,
endeavor, or try one’s fortune. Though the etymology of κίνδυνος is unclear,
the prefix kin often indicates motion or action (as in the English words
kinetic and cinema), and the root dyn usually means power or force or ability
(as in the English words dynamic and dynamite). In practice, the word had a
dual meaning, with a sense both of danger and of opportunity. Consider the
334
discussion between Glaucon and Socrates in Book V of the Republic,
concerning whether children should be brought to war:
Socrates: …Every animal fights better in the presence of its young.
Glaucon: That’s so. But, Socrates, there’s a considerable danger
[κίνδυνος] that in a defeat—and such things are likely to happen in a
war—they’ll lose their children’s lives as well as their own, making it
impossible for the rest of the city to recover.
Socrates: What you say is true. But do you think that the first thing
we should provide for is the avoidance of all danger [κινδυνεῦσαι]?
Glaucon: Not at all.
Socrates: Well, then, if people will probably have to face some danger
[κινδυνευτέον], shouldn’t it be the sort that will make them better if
they come through it successfully?
Glaucon: Obviously.
Socrates: And do you think that whether or not men who are going to
be warriors observe warfare when they’re still boys makes such a small
difference that it isn’t worth the danger [κινδύνου] of having them do
it?100 (Plato, 1997d, sec. V.467b–c)
100 [467b] S: . G: . , , μπαρόντων ὧν ἂν τέκῃ ἔστιν οὕτω κίνδυνος δέ ὦ Σώκρατες οὐ σ ικρὸς , μ , σφαλεῖσιν οἷα δὴ ἐν πολέ ῳ φιλεῖ πρὸς ἑαυτοῖς παῖδας ἀπολέσαντας ποιῆσαι καὶ τὴν
. S: , , . μ ἄλλην πόλιν ἀδύνατον ἀναλαβεῖν ἀληθῆ ἦν δ ἐγώ λέγεις ἀλλὰ σὺ πρῶτον ὲν μ ; G: μ . S: ; ἡγῇ παρασκευαστέον τὸ ή ποτε κινδυνεῦσαι οὐδα ῶς τί δ εἴ που
, ; G: . [467c] S: κινδυνευτέον οὐκ ἐν ᾧ βελτίους ἔσονται κατορθοῦντες δῆλον δή ἀλλὰμ μ μ σ ικρὸν οἴει διαφέρειν καὶ οὐκ ἄξιον κινδύνου θεωρεῖν ἢ ὴ τὰ περὶ τὸν πόλε ον
μ μ ;παῖδας τοὺς ἄνδρας πολε ικοὺς ἐσο ένους
335
In this passage, it is clear that the outcomes of the risk were not as important
as the experience of taking the risk. The future is not predictable, but it will
unfold by necessity as it is so fated. Risk is understood as a kind of action
antithetical to the avoidance of danger.
Likewise, in the Phaedo, Socrates, imprisoned and soon to be executed,
explains to his followers why he did not attempt to escape, arguing that while
suicide is not morally permissible (because no one owns their own body, as it
is the property of the gods), the opportunity to die by someone else's hand is a
risk worth taking. Here Socrates provides the first technical explanation of
his theory of the Forms, after which he sums up his position thusly:
Because of the things we have enunciated, Simmias, one must make
every effort to share in virtue and wisdom in one’s life, for the reward
is beautiful and the hope is great. No sensible man would insist that
these things are as I have described them, but I think it is fitting for a
man to risk [κινδυνεῦσαι] the belief—for the risk [κίνδυνος] is a
noble one—that this, or something like this, is true about our souls and
their dwelling places, since the soul is evidently immortal, and a man
should repeat this to himself as if it were an incantation, which is why
I have been prolonging my tale… Now you, Simmias, Cebes and the
rest of you, Socrates continued, will each take that tragic journey at
some other time, but my fated day calls me now, as a tragic character
336
might say, and it is about time for me to have my bath, for I think it
better to have it before I drink the poison and save the women the
trouble of washing the corpse.101 (Plato, 1977, sec. 114c–115a)
Even though Socrates’s fate has already been set, his decision to drink the
poison and end his life is a manifestation of his risky belief in the immortality
of his soul. Taking this sort of risk was often signified by the verb πειράω,
probably related etymologically to the Latin word perīculum, meaning
danger, risk; trial, attempt, or test, and both words are likely related to the
English words peril and experiment (Lombroso, 2006; Skeat, 2013;
Traupman, 1966).
Risk and Fortune
Another ancient view of risk, fortune, united the ideas of risk as an
unknown fate and as a dangerous opportunity. With the future largely in the
hands of the goddess Fortuna (in Roman antiquity), the ‘unpredictable’
chance element of events was projected externally, so that human decision
making was largely a matter of prūdentia:
101 [114c] ἀλλὰ τούτων δὴ ἕνεκα χρὴ ὧν μ ,διεληλύθα εν ὦ μμ ,Σι ία πᾶν ποιεῖν ὥστε ἀρετῆς καὶ φρονήσεως ἐν τῷ βίῳ μ :ετασχεῖν καλὸν γὰρ τὸ ἆθλον καὶ ἡ ἐλπὶς μ .εγάλη [114d] τὸ μὲν οὖν ταῦτα διισχυρίσασθαι οὕτως ἔχειν ὡς ἐγὼ ,διελήλυθα οὐ πρέπει νοῦν ἔχοντι :ἀνδρί ὅτι μέντοι ἢ ταῦτ᾽ ἐστὶν ἢ τοιαῦτ᾽ ἄττα περὶ τὰς ψυχὰς μἡ ῶν καὶ τὰς ,οἰκήσεις ἐπείπερ ἀθάνατόν γε ἡ ψυχὴ φαίνεται ,οὖσα τοῦτο καὶ πρέπειν μοι δοκεῖ καὶ ἄξιον κινδυνεῦσαι μοἰο ένῳ οὕτως ἔχειν—καλὸς γὰρ ὁ κίνδυνος—καὶ χρὴ τὰ τοιαῦτα ὥσπερ ἐπᾴδειν ,ἑαυτῷ διὸ δὴ ἔγωγε καὶ πάλαι μηκύνω τὸν μ ...ῦθον [115a]
μὑ εῖς μὲν ,οὖν ,ἔφη ὦ μμΣι ία τε καὶ Κέβης καὶ οἱ ,ἄλλοι εἰς αὖθις ἔν τινι χρόνῳ ἕκαστοι :πορεύσεσθε μἐ ὲ δὲ νῦν ἤδη ,καλεῖ φαίη ἂν ἀνὴρ ,τραγικός ἡ μ μ ,εἱ αρ ένη καὶ σχεδόν τί
μοι ὥρα τραπέσθαι πρὸς τὸ :λουτρόν δοκεῖ γὰρ δὴ βέλτιον εἶναι μλουσά ενον πιεῖν τὸ μφάρ ακον καὶ μὴ μπράγ ατα ταῖς γυναιξὶ παρέχειν νεκρὸν .λούειν
337
An increasing risk awareness apparently became neutralized by
attributing possible future successes and damages to an external
source… [which] explained, albeit in a metaphorical way, the
unpredictability of events and the unforeseeable choice between good
and bad outcomes. External attribution protected the decision maker
from responsibility in the field of future contingencies. Prudence was
viewed as the capacity of humans (as distinct from animals) to choose
between reasonable expectations, contingent on the actions of other
people. So prudence, not risk, was the term for the capability to cope
with temporal and social contingencies. (Luhmann, 1996, p. 3)
The approach to risk called for practical wisdom, using prudence (phronēsis,
φρόνησις) and selfcontrol (sōphrosynē, ; literally, 'healthyσωφροσύνη
mindedness')102 in the ‘right way’ (eukairos, εὔκαιρος), and the apprehension
of kairos (καιρός), i.e., the supreme moment of opportunity in a situation, a
concept of particular importance to rhetoricians. Thus, with the two concepts
of prudence and Fortune, it was possible to attribute responsibility for the
outcome of uncertain events either internally or externally, respectively.
102 The word is notoriously difficult to translate; Plato σωφροσύνη (1997a) wrote an entire dialogue in which Socrates and Plato's uncle Charmides (one of the notorious Thirty Tyrants) attempt to figure out the exact meaning of the word; Socrates in the end thinks it is something closer to 'selfknowledge' or 'selfpossession' than to 'moderation' or 'temperance,' but the issue is never fully resolved. It was one of the four cardinal Greek virtues, along with prudence (phronēsis, ), righteousness (φρόνησις dikaiosunē, ), and piety δικαιοσύνη(eusebia, – the root εὐσέβεια seb refers to a frightful danger, because the original sense of piety was fear of the gods), all of which were important topics of rhetoric during the Second Sophistic (Winter, 1997).
338
One rhetorician in particular who embraced these concepts was the
sophist Isocrates. In the Panathenaicus, Isocrates advanced a populist
approach to practical wisdom:
[Those] who excel in arts [tas technas, τὰς ]τέχνας , in sciences [tas
epistēmas, τὰς μ ]ἐπιστή ας , and in specialized abilities [dynameis,
μδυνά εις]…[for the most part] do not manage their own affairs well,
are intolerable at private gatherings, have contempt for the opinions of
their fellow citizens, and are filled with many other serious faults…
Whom then do I call educated, since I exclude those in the arts…and
sciences…and [specialties]? …[Those] who manage well the daily
affairs of their lives and can form an accurate judgment [doxan,
δόξαν] about a situation [kairōn, καιρῶν] and in most cases can figure
out [stochazesthai, στοχάζεσθαι] what is the best course of action [tou
sympherontos, τοῦ μσυ φέροντος]… [as well as] those who are not
corrupted by their good fortune, do not abandon their true selves, or
become arrogant, but on the contrary, remain in the ranks of those
with good sense and do not rejoice more in the successes that come to
them by chance than in those that come through their own nature and
good sense [phronimous, μ ]φρονί ους .103 (Isocrates, 2004b, sec. 29–32)
103 In this passage I have replaced the transliterated Greek words in parentheses back to their original form, in a few cases correcting errors in the rendering of the word (e.g., doxan for doxa, technas for techne, etc.) in the (otherwise acceptable) translated text.
339
There is a clear ethical dimension in one’s relationship with kismet, a sense
that the prudent man who exercises good sense in the face of uncertainty is
also a man of virtue. This is even more explicit in Nicocles, in which
Isocrates suggests that moral vice is inherently dangerous:
Understand that the unjust acquisition of property will not make you
rich but will put you at risk [κίνδυνον]. Do not think that taking is a
profit, and losing is a penalty. Neither of these always has the same
effect, but whichever of these should occur at the right moment
[καιρός] and with virtue benefits those who do it. (Isocrates, 2000,
sec. 50)
Similarly, in Archidamus, Isocrates connects this ethical component with
pragmatism, contending that neither “war or peace is entirely bad or good,
but how each one turns out must always depend on how someone makes use
of the situation [pragmata, μπράγ ατα] and the opportunities [kairoi, καιρόι]
it presents” (Isocrates, 2004a, sec. 50). In all these cases, the human
decisionmaking element is understood in relation to the externalized and
uncontrollable whims of fate:
[Choosing] the propitious moment was entrusted to intuition, but was
also subject to rational decision making. Neither too early nor too late,
now or never – this pattern of thinking was applied in an effort to cope
with risk situations. And Fortuna had to help, but could also refuse or
340
only pretend to do so. She appeared only in close association with
Virtus, aiding and encouraging the diligent. Closely related thereto we
find warnings against carelessness and foolhardiness, against a
demonstrative use of courage and force incommensurate with the
situation. (Luhmann, 2005, p. 150)
For the most part, the outcomes of dangerous and unpredictable situations
was a matter of good fortune or bad fortune—the only thing that human
actors had complete control over was the ethicality of their responses,
understood in very practical terms.
Risk as the Management of Uncertainty
In a world of uncertainty, the ancient art of risk management was
rhetoric. This view can be seen in the thought of Philo of Alexandria, a
Hellenistic Jewish philosopher who engaged in many debates with the
sophists of his day, and who serves as our best firstcentury CE witness to
the emerging Second Sophistic period (Winter, 1997). Philo developed an
Isocratean view of rhetoric, prudence, and wisdom, in what I might playfully
call a protoFreudian direction. In his commentary on the Patriarch Joseph
(one of the twelve sons of Jacob/Israel, whose story, involving the
interpretation of several dreams, features prominently in the Book of
Genesis), Philo describes the art of rhetoric as being akin to the
interpretation of the dreams of the awake:
341
And men awake too, who, as far as the uncertain character of their
comprehension goes, are in no respect different from people asleep,
deceiving themselves, think themselves competent to contemplate the
nature of things with reasoning powers which cannot err... Since, then,
life is full of all this irregularity, and confusion, and indistinctness, it
is necessary... [to] approach the science of the interpretation of dreams,
so as to understand the dreams and visions which appear by day,
...being guided by probable conjectures and rational probabilities, and
in this way [the rhetor] must explain each separate one, and show that
such and such a thing is honourable, another disgraceful, that this is
good or that is bad; that this thing is just, that thing is on the contrary
unjust; and so on in the same way with respect to prudence, and
courage, and piety, and holiness, and expediency, and usefulness; and
in like manner of the opposite things, with respect to what was not
useful nor reasonable, what was ignoble, impious, unholy, inexpedient,
pernicious, and selfish. (Philo, 1993, pp. 446–447)
Though psychoanalytic approaches (particularly those of a Lacanian flavor)
to rhetorical studies have become popular recently (Lundberg, 2012), Philo
seems to have anticipated this development 2000 years in advance. The
management of uncertainty through the pursuit of rational probabilities is a
notion at the heart of the concept of risk as it emerged at the beginning of
342
modernity.
The modern term ‘risk’ appeared as a neologism at some point during
the transition from the Middle Ages to the early modern period. The Oxford
English Dictionary (“Risk,” 2012) provides a couple of possible etymological
histories of the English word ‘risk.’ Though noting that this theory is poorly
supported by documentary evidence, the OED suggests that the postclassical
Latin noun resicum, risicum, riscus may be derived from the classical Latin
verb for cutting (resecō, resecāre, resectum) suggesting a meaning of rock,
crag, or reef, drawing a connection to the thirteenthcentury Spanish noun el
risco, which means ‘the reef, the shallows, the cliff, the rock.’ Luhmann
suggests that in “the Middle Ages the term risicum was used in highly
specific contexts, above all sea trade and its ensuing legal problems in cases
of losses or damages” (Luhmann, 1996, p. 3). Reefs certainly posed a serious
hazard to the seafaring, and Luhmann notes that “maritime insurance is an
early instance of planned risk control” (1993/2005, p. 9).
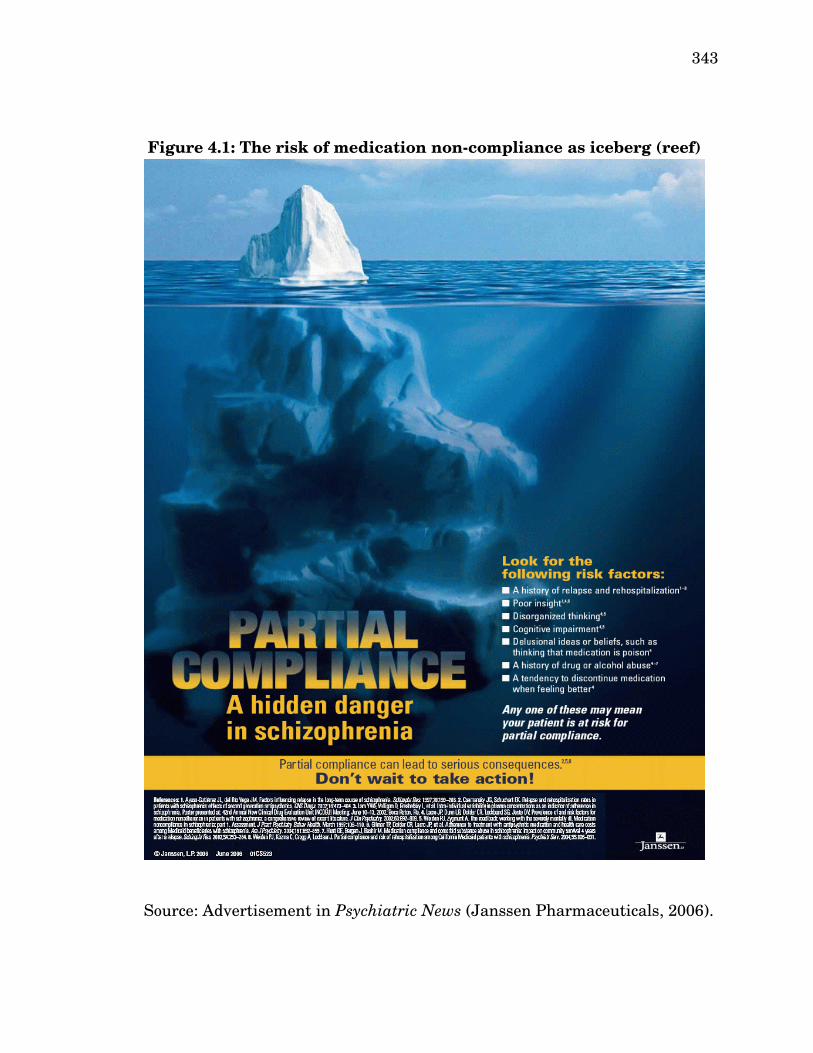
The enduring association of risk with the reef can be seen in Figure
4.1, an advertisement by Janssen Pharmaceuticals appearing in Psychiatric
News that warns of the “serious consequences” posed by the “hidden danger”
of “partial compliance” to antipsychotic medication in schizophrenia.
343
Figure 4.1: The risk of medication noncompliance as iceberg (reef)
Source: Advertisement in Psychiatric News (Janssen Pharmaceuticals, 2006).
344
A list of risk factors for this behavior are provided, including “delusional
ideas or beliefs, such as thinking the medication is poison” and “a tendency to
discontinue medication when feeling better.” This specific kind of risk
representation is discussed in at length later in this chapter.
Slowly, from the beginning of the sixteenth century, the use of the
term risk diffused into other contexts like politics and religion, as in Pascal’s
wager (Reith, 1999). In one of the earliest works of modern political
philosophy, Machiavelli argued that “it may be true that fortune is the ruler
of half our actions, but... she allows the other half or a little less to be
governed by us” (Machiavelli, 1903, p. 99). The significance of the neologism
for Luhmann is that it marks a change in thought, a new discursive or
rhetorical motive that was unfulfilled by existing words: “we may assume
that a new term comes into use to indicate a problem situation that cannot be
expressed precisely enough with the vocabulary available” (Luhmann, 2005,
p. 10).
Though an understanding of risk is a central component of the
configuration of knowledge that characterizes a period of human history, the
ancient world was not quite as monolithic in its approach to risk as the
sociologists of risk make it out to be (e.g., Eidinow, 2007; Luhmann, 2005). In
the history of medicine, there are frequently efforts to read the present into
the past, especially in psychiatry—the differences between the modern ideas
345
of bipolar disorder and major depressive disorder and the ancient notions of
melancholia and mania are much larger than they are often portrayed
(Healy, 1997, 2008). With risk, the opposite phenomenon exists: Rather than
emphasize a supposed continuity with the past, the stress is on the putative
uniqueness of the present. Neither approach is, strictly speaking, incorrect,
insofar as one is interested in accurately representing some historical set of
facts. These kinds of comparisons between some present object of knowledge
and its historical counterpart, in which one’s central purpose is to represent
the past as especially similar or dissimilar to the present, are less about
establishing historical truths than about cultivating an attitude about the
object in its current form.
With respect to our selfunderstanding of risk in late modernity, the
characterization of its historical antecedents as radically different from its
present form enacts a basic feature of modern risk, which
reverses the relationship of past, present, and future. The past loses
its power to determine the present. Its place as the cause of present
day experience and action is taken by the future, that is to say,
something nonexistent, constructed and fictitious. (Beck, 1999, p. 137)
With respect to early intervention for psychosis, we will see the temporal
inversion of modernity manifest in several ways. One of these is the belief,
constantly expressed over a fiftyyear period, that preventive research has
346
about a fifteenyear history. Another is the confused conceptual slippage
between a prodrome (in which present symptoms help establish the probable
existence of a disease process initiated in the past) and a risk syndrome (in
which present symptoms establish the probable existence of a disease state
that will emerge in the future). I shall discuss these issues in depth shortly.
Though there is certainly some basis in fact for the argument that risk
as an object of knowledge has fundamentally changed over time, some
aspects that we tend to regard as novel are traceable to a premodern era.
The closest example from Greek antiquity of the modern concept of risk can
be found in Xenophon’s last work, Ways and Means, written about 50 years
after Plato penned his final dialogue. Xenophon—like Plato, a student of
Socrates—was writing in the context of a Greek (specifically Athenian) fiscal
crisis. In Ways and Means, Xenophon outlines his plan to restore prosperity
to the citystate. In Book IV, Xenophon discusses the possibility of managing
the risks entailed in digging new silver mines:
[27]…It is as possible now to open new veins as in former times. Nor
can one say with any certainty whether the ore is more plentiful in the
area already under work or in the unexplored tracts. [28] Then why, it
may be asked, are fewer new cuttings made nowadays than formerly?
Simply because those interested in the mines are poorer. For
operations have only lately been resumed, and a man who makes a
347
new cutting incurs a serious risk [κίνδυνος δὲ μέγας]. If he strikes
good stuff he makes a fortune; but if he is [29] disappointed, he loses
[ἀπόλλυσιν]104 the money he has spent. Therefore people nowadays
are very chary of taking such a risk [κίνδυνον].105 [30] However, I
think I can meet this difficulty too, and suggest a plan that will make
the opening of new cuttings a perfectly safe undertaking. The
Athenians, of course, are divided into ten tribes. Now assume that the
state were to offer each tribe an equal number of slaves, and that when
new cuttings were made, the tribes were to pool their luck
[ μκοινωσά εναι τὴν τύχην].106 [31] The result would be that if one
tribe found silver, the discovery would be profitable to all; and if two,
three, four, or half the tribes found, the profits from these works would
obviously be greater. Nothing that has happened in the past makes it
probable [ἐοικός] that all would fail to find. [32] Of course, private
individuals also are able to combine on this principle and pool their
fortunes [ μκοινου ένους τὴν τύχην] in order to diminish the risk
104 ἀπόλλυσιν is the third person singular indicative active voice of μἀπόλλυ ι, which means ‘to destroy/ruin/lose utterly.’105 An alternate translation of this sentence reads: “This consideration chiefly has discouraged the adventurers from trying so dangerous an experiment” (Xenophon, 1855, p. 687).106 μΚοινωσά εναι is the middle voice aorist participle of κοινόω, which in the active voice infinitive means ‘to make common’ or ‘to communicate.’ In the middle voice, it means ‘to communicate one to another,’ ‘to put into communication with one another,’ or, when paired with a noun in the accusative case as in this passage, ‘to take part or share in.’ This is the only extant instance of μκοινωσά εναι that I could find in the Perseus digital database of classical texts (Crane & Department of the Classics, Tufts University, 2013).
348
[κινδυνεύειν]. Nevertheless there is no reason to fear [φοβεῖσθε] that
a public company formed on this plan will conflict with the interests of
private persons, or be hampered by them.107 (Xenophon, 1925, sec.
4.27–32)
Here, we have an understanding of risk that is caused by human action—
indeed, human action undertaken in order to remedy the damage caused by a
previous collective human endeavor, the (second) Peloponnesian War. The
risk is somewhat catastrophic, though only primarily catastrophic to the poor
individuals who dig but fail to find silver, the indirect effect is to perpetuate
the poor economic conditions from which all Athenians were suffering. It is
also manageable through good governance, and understood as a function of
probability (though the word translated as probable, ἐοικός, means
something closer to ‘seeming’ than the modern concept of probability, which
had yet to be created). The final argument almost seems to anticipate an
107 [27] καὶ μὴν μκαινοτο εῖν γε οὐδὲν ἧττον ἔξεστι νῦν ἢ .πρότερον οὐ τοίνυν οὐδ᾽ εἰπεῖν ἂν ἔχοι εἰδὼς οὐδεὶς πότερον ἐν τοῖς μ μκατατετ η ένοις πλείων ἀργυρῖτις ἢ ἐν τοῖς μἀτ ήτοις .ἐστί [28] τί ,δῆτα φαίη ἄν ,τις οὐ καὶ ,νῦν ὥσπερ μ ,ἔ προσθεν πολλοὶ
μ ;καινοτο οῦσιν ὅτι πενέστεροι μὲν νῦν εἰσιν οἱ περὶ τὰ μ :έταλλα νεωστὶ γὰρ πάλιν :κατασκευάζονται κίνδυνος δὲ μέγας τῷ μ :καινοτο οῦντι [29] ὁ μὲν γὰρ εὑρὼν ἀγαθὴν
ἐργασίαν πλούσιος ,γίγνεται ὁ δὲ μὴ εὑρὼν πάντα ἀπόλλυσιν ὅσα ἂν .δαπανήσῃ εἰς τοῦτον οὖν τὸν κίνδυνον οὐ μάλα πως ἐθέλουσιν οἱ νῦν .ἰέναι [30] ἐγὼ μέντοι ἔχειν μοι δοκῶ καὶ περὶ τούτου μσυ βουλεῦσαι ὡς ἂν ἀσφαλέστατα μ .καινοτο οῖτο εἰσὶ μὲν γὰρ δήπου Ἀθηναίων δέκα :φυλαί εἰ δ᾽ ἡ πόλις δοίη ἑκάστῃ αὐτῶν ἴσα ,ἀνδράποδα αἱ δὲ
μκοινωσά εναι τὴν τύχην μ ,καινοτο οῖεν οὕτως ,ἄν εἰ μία ,εὕροι [31] πάσαις ἂν λυσιτελὲς ,ἀποδείξειεν εἰ δὲ δύο ἢ τρεῖς ἢ τέτταρες ἢ αἱ μἡ ίσειαι ,εὕροιεν δῆλον ὅτι ἔτι λυσιτελέστερα ἂν τὰ ἔργα ταῦτα .γίγνοιτο τό γε μὴν πάσας ἀποτυχεῖν οὐδενὶ τῶν παρεληλυθότων .ἐοικός [32] οἷόν τε δὴ οὕτως καὶ ἰδιώτας μσυνιστα ένους καὶ
μκοινου ένους τὴν τύχην ἀσφαλέστερον .κινδυνεύειν μηδὲ μέντοι τοῦτο ,φοβεῖσθε ὡς ἢ τὸ μδη όσιον οὕτω μκατασκευαζό ενον παραλυπήσει τοὺς ἰδιώτας ἢ οἱ ἰδιῶται τὸ
μ :δη όσιον
349
objection that a modern day Tea Partier might put forth. This is, as far as I
can tell, the closest the ancient world gets to a modern idea of risk.
Still, even if this example were representative (to the contrary, it
seems to be uniquely ahead of its time), the place and function of risk in the
social lifeworld, in everyday discourse and in more formalized deliberative or
forensic rhetorical contexts, has developed quite a bit over time. Though
noting the importance of kairos for recent events in world history—
Chernobyl, German reunification, Austria’s 1914 ultimatum to Serbia—
Luhmann contends that kairos is no longer the focal point of the relationship
between risk and society:
The assumption that choosing the propitious moment averts risk
nowadays nevertheless lost all justification… [Any] attempt to decide
rationally takes time, and thus entails the risk of letting favorable
opportunities go by or of missing the last chance to prevent inevitable
developments. No one believes any longer that time itself designates
favorable points in time. And when the spouse of an American
president seeks astrological advice, this is noted with astonishment
and displeasure by all. The choice of a propitious moment for a risk
decision has itself become a risky decision. (Luhmann, 2005, p. 151)
This change stems from a more totalizing conception of risk as the concept
transitioned from a predicate of human action to an object of human action.

350
A risk is not something that one decides to experience or not, but rather
something that must be managed. The management (or mismanagement) of
risk occurs through both action and inaction. Risk cannot be eliminated
through caution, for “the cautious man, when it is time to act suddenly, does
not know how to do so and is consequently ruined; for if one could change
one's nature with time and circumstances, fortune would never change”
(Machiavelli, 1903, p. 101).108 This presaged the late modern view that both
action and inaction entail risks, and moreover risks are largely the
consequence of prior human decisions.
In the early stages of modernity, it was assumed that with greater
knowledge concerning the mastery of nature, humans could precisely control
the future. The human subject, as selfidentical and selfcertain, was
grounded in a sort of personal confidence, and as rational and sovereign,
could project that confidence into the future by acting deliberately after
careful study (René Descartes, 1997). The world of early modernity had no
room for chance (Hacking, 1975).
Though determinism as fate was rejected by Machiavelli as a
constraint on human agency, in the early nineteenth century this radical
108 Using a bizarrely misogynistic metaphor, Machiavelli argues that instead of facing the goddess of fortune with caution, one should rape her (because that's how women want to be treated): “I certainly think that it is better to be impetuous than cautious, for fortune is a woman, and it is necessary, if you wish to master her, to conquer her by force; and it can be seen that she lets herself be overcome by these rather than by those who proceed coldly. And therefore, like a woman, she is a friend to the young, because they are less cautious, fiercer, and master her with greater audacity” (p. 102).
351
denial of chance developed into a return of an extreme form of determinism,
posited as a fundamental feature of the universe:
All events, even those which on account of their insignificance do not
seem to follow the great laws of nature, are a result of it just as
necessarily as the revolutions of the sun. In ignorance of the ties
which unite such events to the entire system of the universe, they have
been made to depend upon final causes or upon hazard, according as
they occur and are repeated with regularity, or appear without regard
to order; but these imaginary causes have gradually receded with the
widening bounds of knowledge and disappear entirely before sound
philosophy, which sees in them only the expression of our ignorance of
the true causes... We ought then to regard the present state of the
universe as the effect of its anterior state and as the cause of the one
which is to follow. Given for one instant an intelligence which could
comprehend all the forces by which nature is animated and the
respective situation of the beings who compose it—an intelligence
sufficiently vast to submit these data to analysis—it would embrace in
the same formula the movements of the greatest bodies of the universe
and those of the lightest atom; for it, nothing would be uncertain and
the future, as the past, would be present to its eyes. (Laplace,
352
1814/1902, pp. 3–4)109
This intelligence, which came to be known as Laplace's Demon, was based on
the assumption in classical mechanics that all particles have a defined
position and velocity. Though humanity could never achieve the omniscience
of Laplace's Demon, uncertainty could be minimized and calculated precisely
through the emerging discipline of mathematics known as probability
(Crombie, 1994; Daston, 1988; Gigerenzer et al., 1989; Hacking, 1975, 1990;
Hald, 2005; Krüger, Daston, & Heidelberger, 1990; Prior, Glasner, &
McNally, 2000). Omniscient but not immortal, Laplace's Demon was led to
its doom by the developments of thermodynamics in the nineteenth century
and quantum mechanics in the twentieth century (Ulanowicz, 1986).
With Werner Heisenberg's famous uncertainty principle, uncertainty
moved from the realm of epistemology to ontology, as imprecision
(ungenauigkeit) was built into the very fabric of the universe. In this, the
science of probability was strengthened, as what was once merely calculated
ignorance joined what medieval philosophers had called the praedicamenta,
i.e., Aristotle's categories of being. This transition produced some conceptual
109 Though quite possibly apocryphal, there is an often cited exchange between PierreSimon Laplace and Napoleon in which the latter asked about the Laplace's failure to mention God in his most recent book on astronomy. Laplace had no more need for God than he did for chance, and accordingly is said to have bluntly replied: “Je n'avais pas besoin de cette hypothèselà” (“I had no need for that hypothesis there”). Napoleon, rather amused by this line, relayed it to the Italian astronomer JosephLouis Lagrange, who replied “Ah! c'est une belle hypothèse; ça explique beaucoup de choses!” (“Ah! [But] it is a beautiful hypothesis that explains so many things!”) (Ball, 1888, p. 388). The same could be said, perhaps, for chance in the physical sciences and for risk in the social sciences.
353
confusion that is a source of miscommunication in the debate about psychosis
risk syndrome. Is the diagnosis epistemic, a prediction of future pathology,
or is it metaphysical, a pathological state characterized by its potential to
progress to psychosis? I shall take up this question shortly; for now, it is
enough to observe that the answer depends on the extent to which the events
of the future are thought to be preordained.
Psychiatric Rhetoric in a Risk Society
With this background, I now turn to risk in late modernity, and the
rhetorical climate in which the concepts of dementia praecox, schizophrenia,
and psychosis emerged and developed. The concept of dementia praecox was
born during the nineteenth century within a risk climate that was focused on
degeneracy. It then developed into schizophrenia during the epoch of mental
hygiene and eugenics, and adopted its modern form during the era of
preventive medicine. The rhetoric of risk during these periods profoundly
influenced the development of the concept.
The grandiosity of early modern science was radical, but its expression
was an echo of antiquity, which gave way as modernity matured. The idea of
“providential reason,” according to which increasing human knowledge
enhances and safeguards the human experience,
carries residues of conceptions of fate deriving from premodern eras.
Notions of fate may of course have a sombre cast, but they always

354
imply that a course of events is in some way preordained... To accept
risk as risk, an orientation which is more or less forced on us by the
abstract systems of modernity, is to acknowledge that no aspects of our
activities follow a predestined course, and all are open to contingent
happenings. In this sense it is quite accurate to characterise
modernity, as Ulrich Beck does, as a 'risk society,' a phrase which
refers to more than just the fact that modern social life introduces new
forms of danger which humanity has to face. Living in the 'risk society'
means living with a calculative attitude to the open possibilities of
action, positive and negative, with which, as individuals and globally,
we are confronted in a continuous way in our contemporary social
existence. (Giddens, 1991, p. 28)
The emergence of this late modern risk society is closely tied to developments
in the practice of medicine (especially psychiatry), and the shifting meaning
over the last 150 years of risk, from dangerous predisposition within an
individual subject to a probabilistic risk factor within a population. The
concept of 'risk' in classical psychiatry referred to “the danger embodied in
the mentally ill person capable of violent and unpredictable action,” a danger
that implies “at once the affirmation of a quality immanent to the subject (he
or she is dangerous), and a mere probability, a quantum of uncertainty, given
that the proof of danger can only be provided for after the fact” (Castel, 1991,
355
p. 283).
Risks of Modernity: Degeneracy and the Rise of Hygiene
The concept of predisposition that emerged in the late eighteenth
century referred to “an inherited taint or flaw that would, in the right (or
wrong) circumstances, manifest itself in illness or pathology,” and became
especially popular in the psychiatric imaginary by the midnineteenth
century, when “all manner of problems of social pathology and danger
became understood in terms of degeneracy” (N. S. Rose, 2007, pp. 18–19). A
predisposition to insanity was a latent material dangerousness subsisting in
the body, and during the first half of the nineteenth century, preventive
psychiatry entailed such drastic measures as confinement and/or sterilization
on the grounds of public safety, for “all insane persons, even those who
appear calm, carry a threat, but one whose realization still remains a matter
of chance” (Castel, 1991, p. 283).
Eventually facing practical limitations on their ability to confine the
dangerous, during the second half of the nineteenth century, psychiatrists
shifted their preventive efforts toward the promotion of 'mental hygiene,'
defined as
...the art of preserving the mind against all incidents and influences
calculated to deteriorate its qualities, impair its energies, or derange
its movements. The management of the bodily powers in regard to
356
exercise, rest, food, clothing and climate, the laws of breeding, the
government of the passions, the sympathy with current emotions and
opinions, the discipline of the intellect—all these come within the
province of mental hygiene. (Rossi, 1962, p. 78)
The physician who coined the phrase 'mental hygiene,' William Sweetser,
invoked the theological notions of predestination and sin to explain the
emerging understanding of the heritability of mental illness:
Can we, therefore, escape the conclusion that we may be physically
predisposed, I had almost said predestined, to happiness or misery?
Such, in fact, is implied in the familiar expressions of happy and
unhappy constitution or temperament. As, moreover, these vicious
constitutions are oftentimes inherited, and must, probably, in the first
instance, have grown out of infringements of the organic laws, it
becomes a literal truth, that the sins of the parents may be visited on
their unoffending children, even to remote generations. (Sweetser,
1850, p. 120 my emphasis)
By this sort of rhetoric, moral degeneracy was converted into a biological
phenomenon, though the understanding of heritability was not quite
Darwinian. Bénédict Morel, a prominent French psychiatrist who trained
under JeanPierre Falret (Esquirol's successor) as chief resident at the
Salpêtrière Hospital and who in 1857 penned a Treatise on the physical,
357
intellectual, and moral degeneracy of the human race,110 claimed that
degeneracy was caused by things like poor nutrition, chronic diseases like
tuberculosis or goiter, the consumption of intoxicants such as absinthe or
tobacco, and masturbation along with other sexually deviant behaviors
(Dowbiggin, 1991; Morel, 1860). Furthermore, he contended that this
degeneracy becomes amplified in families as it was passed down through
multiple generations, so that, for example, alcoholic parents might produce
epileptic children, neurasthenic or hysterical grandchildren, and criminally
insane or congenitally idiotic (and probably sterile) greatgrandchildren
(Dowbiggin, 2004).
Morel was the first to argue that mental disorders should be classified
by (presumed) etiological rather than phenomenological factors, and proposed
that many of the separate disorders identified by Pinel and Esquirol be
grouped together into a single nosological category he called hereditary
madness (Dowbiggin, 2004). Morel believed that hereditary madness was one
aspect of the larger phenomenon of degeneracy, which was also manifested in
physical deformities (a point which he established in part by describing the
“facial stigmata” of children who most likely were born with what would later
come to be known as Down Syndrome) (Carlson, 2001, p. 41). As I mentioned
in the previous chapter, Morel coined the term démence précoce—which
110Traité des dégénérescences physiques, intellectuelles, et morales de l'espèce humaine: Et des causes qui produisent ces variétés maladives.
358
became Kraepelin's dementia praecox and then Bleuler's schizophrenia—to
describe the state he believed was “in many cases, the catastrophic end of
hereditary madness.” He continues:
A sudden immobilization of all the faculties, a precocious dementia
[démence précoce], indicates that the young patient has reached the
end of the intellectual life at his disposal. He is at that point referred
to as imbecile or idiot. These sad representatives of degeneration in
humanity constitute the fourth class of our hereditary madness.111
(Morel, 1860, p. 566; my translation, emphasis in the original)
Although it is unclear whether Morel's understanding of degeneration was
the source or result, the association of social, physical, and mental
degeneracy reflected imagery in the nineteenth century popular imaginary.
What was the source of this degeneration that could be found in
abundance everywhere one looked? In the popular imaginary, degeneracy
was sometimes understood geographically as related to urbanization. The
process of moving into cities from villages was thought to in some manner
damage “the constitution of the immigrants, the weakly offspring they gave
birth to, and the further deterioration of those offspring as they were afflicted
by all manner of pathologies” (N. S. Rose, 2007, p. 19). This easily lent itself 111 “...dans bien des cas, la funeste terminaison de la folie héréditaire. Une immobilisation soudaine de toutes les facultés, une démence précoce, indiquent que le jeune sujet a atteint le terme de la vie intellectuelle dont il peut disposer. Il est alors désigné sous le nom d'imbécile, d'idiot. Ces tristes représentants des dégénérescences dans l'humanité forment la quatrième classe de nos folies héréditaires.”
359
to popular negative representations of social classes. Honoré de Balzac, for
example, described lower class politically radical Parisians in 1835 as “a
people fearful to behold, gaunt, yellow, tawny... men whose twisted and
contorted faces give out at every pore the instinct, the desire, the poisons
with which their brains are pregnant; ...its cadaverous physiognomy... has
but two ages—youth and decay” (Balzac, 2010, para. 1). The Parisian
bourgeoisie did not fare much better in Balzac's account, in which his
description of their occupational psychosis bears a striking resemblance to
Morel's clinical description of the arrested development of démence précoce:
They appear to be skeptics and are in reality simpletons; they swamp
their wits in interminable arguments. Almost all conveniently adopt
social, literary, or political prejudices, to do away with the need of
having opinions... Having started early to become men of note, they
turn into mediocrities, and crawl over the high places of the world. So,
too, their faces present the harsh pallor, the deceitful coloring, those
dull, tarnished eyes, and garrulous, sensual mouths, in which the
observer recognizes the symptoms of the degeneracy of the thought and
its rotation in the circle of a special idea which destroys the creative
faculties of the brain. (Balzac, 2010, para. 10; my emphasis)
With scientists and publics expressing concerns about an epidemic of
degeneracy getting ever worse with each generation and potentially
360
threatening the national stock, the eugenics movement was not far off, and
“the idea of degeneracy would be central to the biopolitics of the first half of
the twentieth century” (N. S. Rose, 2007, p. 19). Given that the concepts of
psychosis and schizophrenia were developing during this period, they were
profoundly affected by concerns for managing the risk of degeneracy.
The idea of degeneracy is depressing, of course, but the discourses in
which it is advanced are not exclusively pessimistic. There are rhetorical
motives at work, as always. Within a traditionalist/conservative ideological
milieu, the whole world is plunging into madness:
One must take into account the deep psychic anxiety, the
extraordinary prevalence of neurosis, which make our age unique. The
typical modern has the look of the hunted. He senses that we have lost
our grip upon reality. This, in turn, produces disintegration, and
disintegration leaves impossible that kind of reasonable prediction by
which men [sic], in eras of sanity, are able to order their lives. And the
fear accompanying it unlooses the great disorganizing force of hatred,
so that states are threatened and wars ensue. (Weaver, 1948, p. 16)
The proposed solution often “depends upon recovery of the 'ceremony of
innocence,' of that clearness of vision and knowledge of form which enable us
to sense what is alien or destructive, which does not comport with our moral
ambition” (p. 11). The situation is no more pleasant from the left. In a
361
speech published in the Pravda on May 24, 1959, Soviet Premier Nikita
Khrushchev argued:
Can there be diseases, nervous disorders among certain people in a
Communist society? Evidently yes. If that is so, then there will also be
offenses, which are characteristic of people with abnormal minds. Of
those who might start calling for opposition to Communism on this
basis, we can say that clearly their mental state is not normal. (cited in
Tomov, Voren, Keukens, & Puras, 2007, p. 402)
As we will see very soon, this line of thinking in the Soviet Union did not end
well. In either case, there is a solution that will root out and eliminate all
those terrible defilers of our fair society, but we must have the ability to
detect the aliens and traitors in our midst, and the 'moral clarity,' as some
(almost always ironically) say, to be utterly ruthless in our treatment of
them. In this, a restoration of the moral order that has been defiled by
progressives/reactionaries (depending on one's persuasion), there is hope.
The pattern involved is that of “descentascent,” which “reflects a recurrent
rhythm of life and, for humans, a form of consciousness, a form in which
human experience is often symbolized and made meaningful. Put differently,
the descentascent pattern is akin to an archetypal metaphor” (Lake, 1984, p.
426).
In the previous three chapters, I examined the development of the
362
concepts of psychosis and neurosis within the context of the discourses of
medical science. The cyclic inversion of meaning, with ‘(actual) neurosis’
taking on the meaning formerly signified by ‘psychosis,’ followed by inversion
again, testifies to the fluidity of these concepts at this stage and the tensions
between rhetorical continuity and discontinuity. The discourses of hygiene
and degeneracy also influenced the longitudinal course of these signifiers, as
can be seen in Freud's writings. With science, there is always a hope that any
degeneration can be halted or reversed, and this feeling out of terminology
was in part a rhetorical contest over which group of patients constituted the
lost causes, or, worse, the intrinsically dangerous.
At first, Freud's primary concern was in preventing the 'actual
neuroses' (by which he means psychoses, as opposed to the psychoneuroses).
This entailed, of course, stopping the dangerous practices of masturbation
and coitus interruptus, which he believed wrecked their havoc by physically
degenerating the onanists' nerves:
[Actual] neuroses [i.e., psychoses] are entirely preventable as well as
entirely incurable. The physician’s task is wholly shifted on to
prophylaxis. The first part of this task, the prevention of the sexual
noxa of the first period, coincides with prophylaxis against syphilis and
gonorrhea, since they are the noxae which threaten anyone who gives
up masturbation. The only alternative would be free sexual
363
intercourse between young men and respectable girls; but this could
only be adopted if there were innocuous methods of preventing
conception. (Freud, 1893b, p. 60)
Here it would appear that the widespread availability of oral contraceptives
was one of the greatest psychiatric advances of the 20th century. With respect
to the ‘actual neuroses,’ we see in this remark a particular kind of medical
appeal that appears when a diseaseobject is both preventable and difficult to
treat, and which we will see again and again once the era of preventive
medicine truly begins. Importantly, Freud considers these phenomena
serious social problems, pathologies of an entire class or population, rather
than of individuals:
In the absence of such a solution [i.e., innocuous contraception], society
appears doomed to fall a victim to incurable neuroses, which reduce
the enjoyment of life to a minimum, destroy the marriage relation and
bring hereditary ruin on the whole coming generation. The lower
strata of society know nothing of Malthusianism, but they are in full
pursuit, and in the course of things will reach the same point and fall
victim to the same fatality. (Freud, 1893b, p. 60, my emphasis)
The sense of determinism in this fatalistic rhetoric is pronounced, and the
notion of Lamarckian inheritance is fairly typical of the discourses of
degeneracy. The association between preventive medicine, populations, and
364
quasiapocalyptic language is a key cluster that will appear again and again.
The “hygienist” and eugenics movements were both biopolitical
projects concerned with regulating risks posed to populations by dangerous
degeneracy within individuals (Donzelot, 1979, p. 55). The brutal totalitarian
regimes that emerged in the twentieth century developed programs of
political oppression that united the politics of death with the politics of life.
To these, one might also add philanthropy, which also “sought a prophylactic
mode of action, endeavoring to promote certain kinds of moral conduct by
coupling the provision of financial aid with conditions as to the future
conduct of recipients,” thereby stemming the tide of degeneracy (N. S. Rose,
1989, p. 129). What these all have in common is the idea that a hidden
element can lie within an individual body, and be passed down from parent to
child, that could pose a danger to society and that should be managed
through a process of classification, identification, and some form of coercion –
in short, biopolitically.
Risk and Latent Danger
In his original formulation of the disorder, drawing upon the ideas of
Morel, Bleuler (1911a) described a variant of schizophrenia that was hidden
and latent in its development, which he believed was the most frequent form
of schizophrenia:
There is also a latent schizophrenia, and I am convinced that this is
365
the most frequent form, although admittedly these people hardly ever
come for treatment... In this form, we can see in nuce all the symptoms
and all the combinations of symptoms which are present in the
manifest types of the disease. Irritable, odd, moody, withdrawn,
exaggeratedly punctual people arouse, among other things, the
suspicion of being schizophrenic. Often one discovers a concealed
catatonic or paranoid symptom and exacerbations occurring in later
life demonstrate that every form of this disease may take a latent
course. (p. 239)
For some (e.g., Gaupp, 1938), this was understood as a kind of psychotic
disorder with a lengthy prodromal phase, in which the patient is remarkably
lucid all the while an insidious endogenous pathology developed that could, at
any moment, activate. The course of schizophrenia was understood as a
degenerating (splitting) mind, but the seeds of this degeneration were
thought to be latent in these cases. Bleuler's pathological concept of 'latent
schizophrenia' developed under several names: 'abortive schizophrenia'
(Mayer, 1951), 'ambulatory schizophrenia' (Zilboorg, 1941), 'borderline
schizophrenia' (Knight, 1954), 'chronic incipient schizophrenia' (Mace, Koff,
Chelnek, & Garfield, 1949), 'pseudoneurotic schizophrenia' (Hoch & Polatin,
1949), 'pseudopsychopathic schizophrenia' (Hoch, 1950), and, with a hint of
mockery, 'salon schizophrenia,' which stands in contrast “to the honestto
366
goodness state hospital” form of the illness (Bellak, 1955, p. 63).112
Writing thirteen years later, Bleuler seems ambivalent about whether
latent schizophrenia constituted a disease entity, placing the word disease in
scarequotes (possibly to distinguish between the putative disease entity and
its observable expression) and noting that the characteristics of latent
schizophrenia (i.e., that it is frequently basically asymptomatic) were such
that they enabled the affected patients to masquerade as “normal”
individuals:
Latent schizophrenias are very common under all conditions so that
the “disease” schizophrenia has to be a much more extensive term than
the pronounced psychosis of the same name. This is important for
studies of heredity. At what stage of anomaly any one should be
designated as only a “schizoid” psychopathic, or as a schizophrenic
mentally diseased, cannot at all be decided as yet. At all events, the
name latent schizophrenia will always make one think of a morbid
psychopathic state, in which the schizoid peculiarities are within
normal limits. (Bleuler, 1924, p. 437)
The emphasis on heredity here, as well as the idea of a premorbid state, turn
out to be rather prescient with respect to psychosis risk syndrome.
112 Bellak goes on to comment that he does “not mean to question the existence or validity of 'salon schizophrenics.' Rather, I wish to determine the difference between them and those people who were always more or less vegetative. (Undoubtedly, many originally brilliant schizophrenics may reach a terminal stage of deterioration resembling the patients who always manifested an extremely low level of functioning)” (p. 63).
367
DSMII contained a diagnosis of “schizophrenia, latent type,” for
“patients having clear symptoms of schizophrenia but no history of a
psychotic schizophrenic episode. Disorders sometimes designated as
incipient, prepsychotic, pseudoneurotic, pseudopsychopathic, or borderline
schizophrenia are categorized here” (American Psychiatric Association, 1968,
p. 34). This category was not included in DSMIII.
In these different developing pathways of the original concept of latent
schizophrenia, we can see the roots of several later diagnostic categories. The
'schizoid peculiarities' to which Bleuler referred in his description of latent
schizophrenia came to characterize schizoid personality disorder, which is
predicated of individuals who are extreme loners with no desire for social
activities, friendships, or sexual partners, and who are indifferent to praise or
blame (Magnavita, 1990; Shedler & Westen, 2004). Similarly, 'borderline
schizophrenia' eventually became borderline personality disorder, which is
characterized by unregulated affect, cognition, and behavior, unstable
interpersonal relationships (with patterns of idealization and devaluation),
and extreme sensitivity to abandonment, whether real or perceived (Brask,
1959; National Institute of Mental Health, 2014).
As borderline schizophrenia was initially conceived, it was closest to
what is now known as schizotypal personality disorder, “a pattern of acute
discomfort in close relationships, cognitive or perceptual disturbances, and
368
eccentricities of behavior” (American Psychiatric Association, 2013, p. 645).
The term schizotype was coined in 1953 by Sandor Rado:
For psychodynamic purposes I shall abbreviate the term schizophrenic
phenotype to schizotype. Can we diagnose the patient's inherited
predisposition before he develops an open psychosis or even if he never
develops an open psychosis? In other words, are we prepared to view
him as a schizotype from birth to death, or only during his open
psychosis? ...[When] we subject these gross manifestations of the open
psychosis to minute psychodynamic analysis, we discover an
underlying ensemble of psychodynamic traits which... is demonstrable
in the patient during his whole life. This finding will define him as a
schizotype from birth to death, and will allow us to view his life history
as a sequence of schizotypal changes. (Rado, 1953, p. 410)
Though clearly the meaning of schizotypal has drifted somewhat, its
relationship to psychosis risk has been constant and will be discussed below.
Medicalization and Criminalization
While western psychiatry generally sought to distance Bleuler's latent
schizophrenia from the more visible and acute variety, as can be seen in the
development of these personality disorder concepts, the course of latent
schizophrenia in the Soviet Union took a rather insidious turn.
369
Sluggish Schizophrenia
Though remarkably absent from the contemporary debate about
psychosis risk syndrome and the risks posed by this diagnosis, a diagnosis of
Russian providence known as 'sluggish schizophrenia' provides another view
of schizophrenia as a (political) risk syndrome (Smulevich, 1989; Wilkinson,
1986). Six years after Bleuler converted dementia praecox into
schizophrenia, the Bolsheviks dismantled the provisional government in
Petrograd and launched the Russian Civil War. Russian psychiatrists were
one of the earliest professional groups that threw their support behind the
Bolsheviks, and consequently, several psychiatrists managed to acquire
prominent positions in the new government at the conclusion of the war in
1922 (Lavretsky, 1998).
These psychiatrists were the progenitors of what came to be known as
the 'Moscow School' of psychiatry, which exerted immense influence on the
field in the Soviet world (psychiatrists with heterodox 'antiPavlovian' views
risked being sent to the Gulag) and became close partners with the governing
state regime (J. V. Brown, 1994; Popov & Lichko, 1991). At a pivotal
moment, psychiatrists conducting research in neuropsychiatry were ironically
labeled 'antimaterialist' and reactionary, were made to confess and had their
laboratories shut down, and in some cases were tortured after the infamous
October 1951 'Joint Session' (or 'Pavlovian Session') of the Academy of
370
Medical Sciences of the USSR and the AllUnion Neurologic and Psychiatric
Association (Windholz, 1997). The older generation of psychiatrists having
been liquidated, the inquisitors of the Joint Session, chief among them
Andrei Snezhnevsky, took control of the Moscow School.
The nosological approach of the Moscow School was to combine
dimensional and categorical diagnostic entities into a unitary framework, not
unlike the approach taken by DSM5, though for entirely different reasons
(Snezhnevsky, 1968). Central to the nosology was Snezhnevsky's concept of
'sluggish schizophrenia,' a diagnostic entity that “lends itself more than
conveniently to a view of dissent as a kind of illness” (Bloch & Reddaway,
1985, p. 160). Sluggish schizophrenia was characterized by a very slowly
progressing course, although the prognosis was just as bad as the more rapid
'malignant' form of the disease (Lavretsky, 1998). In a way, this was the
logical culmination of Kraepelin's decision to define dementia praecox based
on its course over time; Kendell (1975) politely noted that “Russian
psychiatrists appear to be influenced more by the course of the illness and
less by its actual symptomatology... which has some bearing on recent
political controversies” (p. 80). Comments like Kendell's led Szasz to
complain that “the concepts and methods of the Russian psychiatric
gangsters who perpetrate [abuses] are legitimized and supported by their
colleagues in the West” (Szasz, 1976, p. 101). Despite the Soviet rejection of
371
genetics as capitalist biology under Lysenko, Snezhnevsky advanced the
thesis that schizophrenia was a “biological disorder with a genetic etiology,”
which provided support for the hospitalization of dissidents and their family
members (A. A. Stone, 2002, p. 110).
The political nature of the diagnosis of sluggish schizophrenia was
readily apparent from its signs and symptoms, and it fit in well with state
propaganda. Many believed that sluggish schizophrenia was invented on the
orders of the KGB, although many Soviet psychiatrists apparently lacked
insight into its political character when they made their diagnoses:
[According] to Snezhnevsky and his colleagues, patients with this
diagnosis were able to function almost normally in the social sense.
Their symptoms could resemble those of a neurosis or could take on a
paranoid quality. The patient with paranoid symptoms retained some
insight in his condition but overvalued his own importance and might
exhibit grandiose ideas of reforming society. Thus, symptoms of
sluggish schizophrenia could be “reform delusions,” “struggle for the
truth,” and “perseverance.” While most experts agree that the core
group of psychiatrists who developed this concept did so on the orders
of the party and the Soviet secret service KGB... and knew very well
what they were doing, for many Soviet psychiatrists this seemed a very
logical explanation because they could not explain to themselves
372
otherwise why somebody would be willing to give up his career, family,
and happiness for an idea or conviction that was so different from what
most people believed or forced themselves to believe. (Voren, 2010, pp.
33–34)
These “reform delusions” were diagnosed whenever a patient “develops a new
principle of human knowledge, drafts an academy of human happiness, and
many other projects for the benefit of mankind” (Styazhkin, 1991, p. 122).
Snezhnevsky's emphasis on the “negative axis” of psychotic symptoms
is an important theoretical innovation (although the idea of negative
symptoms preceded him) that has been embraced in the West and is featured
prominently in the DSM. For Snezhnevsky, this axis, which included
“conflict with authorities, poor social adaptation, and pessimism,” was
developed to justify a diagnosis made in the absence of the more dramatic
positive symptoms of frank psychosis (Ougrin, Gluzman, & Dratcu, 2006, p.
458). The distinction between negative and positive psychotic symptoms is
grounded in a humoral way of thinking, as symptoms
that suggest a surplus or exaggeration of normal functioning, such as
delusions, hallucinations, and ideas of reference, are usually referred
to as positive symptoms, and those that refer to interpersonal and
motivational deficits are often referred to as negative symptoms.
(Millon, Millon, Meagher, Grossman, & Ramnath, 2012, p. 404)
373
Modern psychiatrists increasingly focus on the socalled negative symptoms,
like catatonia, flattened affect, asociality, alogia (highly restricted or absent
speech), anhedonia (lack of the ability to feel pleasure), and avolition (lack of
motivation), as antipsychotic medications (especially the older typical anti
psychotics) tend to be more effective against the positive symptoms while
leaving the negative symptoms insufficiently treated in many cases; the
newer atypical class of antipsychotics as a whole tends to perform better on
these symptoms (R. J. Leo & Regno, 2000). For those who show only positive
psychotic symptoms, Hacking (1998) has argued that the diagnosis of
multiple personality disorder has taken the role formerly taken by
schizophrenia before the idea of the importance of the negative axis of
symptoms became taken for granted. Schizophreniform disorder 'with good
prognostic features,' which will be discussed shortly, also represents
schizophrenia (in an early stage) without negative psychotic symptoms (the
absence of which is an indicator of a good prognosis). In any event, it seems
clear that the diagnosis of sluggish schizophrenia was a brazen political
abuse of psychiatry (and it must be noted that it is still in use in Russia today
and in some Latin American countries formerly within the Soviet sphere of
influence).
But it is also clear that the concept in its historical arc of development
(beginning as dementia praecox) was well suited to this sort of expansive
374
interpretation. Further, it reveals a certain kind of risk – social
dangerousness – that was thought (and is thought) to inhere in individuals
who at some later point might manifest clear symptoms of psychosis. To
some extent, the problem relates to a more general nosological issue:
[The] emotive use of language so sways the intellect that phrases
suggesting the 'real' existence of diseases as single objects of
perceptions lead doctors to think as if these diseases were to be kept
away by barbedwire entanglements, or 'stamped out' by physical
agencies ruthlessly employed. (Crookshank, 1923, p. 345)
This seems especially true with risk syndromes that signify possibly
dangerous individuals; morbid descriptors like 'insidious' and 'latent' make it
easy to not just reify but personify an abstraction, and then draw moral
inferences about the person to whom the diagnosis applies.
This was not uniquely a Russian phenomenon. Jonathan Metzl shows
how similar concerns were used in the United States, especially during the
deinstitutionalization period, with a nonetoosubtle racial animus:
Many [individuals who were involuntarily committed] were sent to
Ionia [State Hospital, in Michigan] after convictions for crimes that
ranged from homicide to armed robbery to property destruction during
periods of civil unrest, such as the Detroit riots of 1968... [Ward] notes
emphasized how hallucinations and delusions rendered these men as
375
threats not only to other patients, but to the authority represented by
clinicians, ward attendants, and society itself. “Paranoid against his
doctors and the police.” Or, “would be a danger to society were he not
in an institution.” Ionia held these men using littleknown loopholes in
deinstitutionalization amendments that stipulated that the hospital
would continue to receive or contain patients... who posed
“dangerousness to the community” even after most other patients were
set free. The word NEGRO appeared on the upper right corner of the
face page in eight out of every ten of these charts. And schizophrenia,
paranoid type was overwhelmingly the most common diagnosis applied
to these men, these institutionalized black bodies that
deinstitutionalization left behind. (Metzl, 2009, p. 14, emphasis in the
original)
This resonates with contemporary concerns, frequently given voice after
school shootings and similar tragedies involving firearms, about the dangers
of failing to restrain in advance those who show signs of mental illness.
Further, the association between people with schizophrenia and acts of
political violence or sabotage can be seen in advertisements for formulations
of antipsychotic medication that have been designed to be difficult for
patients to resist them. In an advertisement for an injectable formulation of
chlorpromazine (Thorazine), noncompliant patients are depicted as
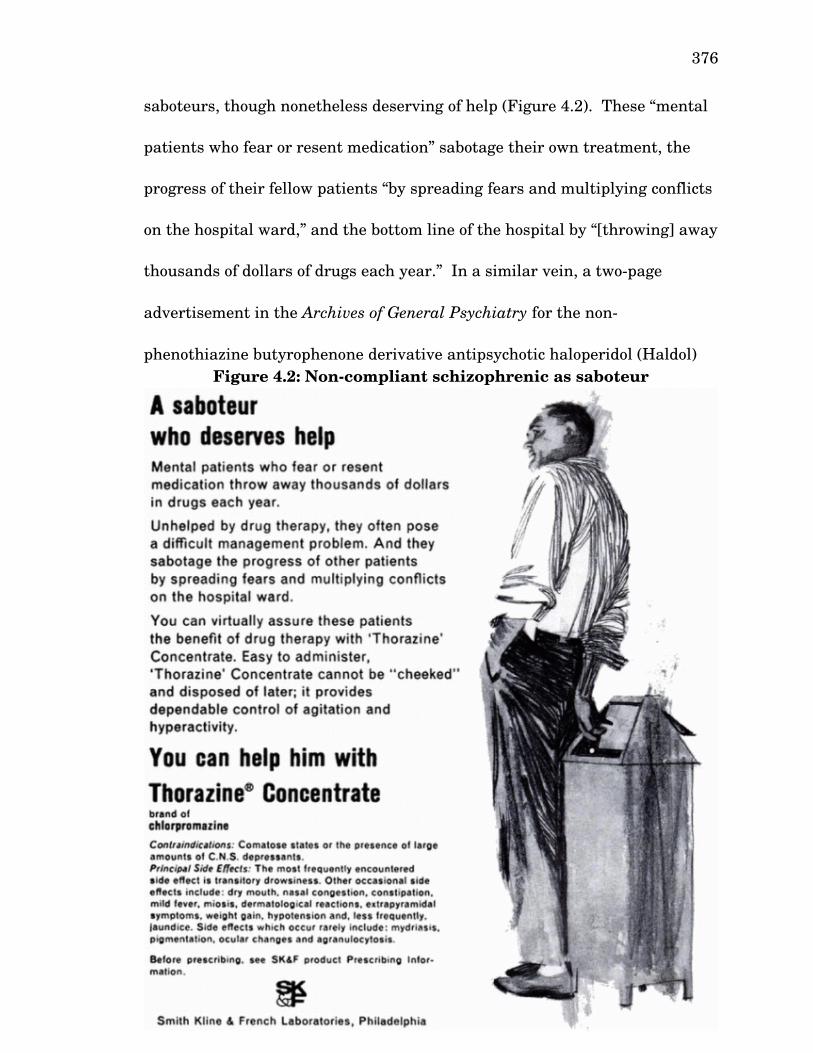
376
saboteurs, though nonetheless deserving of help (Figure 4.2). These “mental
patients who fear or resent medication” sabotage their own treatment, the
progress of their fellow patients “by spreading fears and multiplying conflicts
on the hospital ward,” and the bottom line of the hospital by “[throwing] away
thousands of dollars of drugs each year.” In a similar vein, a twopage
advertisement in the Archives of General Psychiatry for the non
phenothiazine butyrophenone derivative antipsychotic haloperidol (Haldol)
features a drawing of a threatening looking character on the left page with
the caption “Assaultive and belligerent?” On the right page, the reader is
told that “Cooperation often begins with Haldol,” which “acts promptly to
control aggressive, assaultive behavior” (Figure 4.3). Another advertisement
for Haldol, formulated as a “tasteless and undetectable” but “potent” liquid
that can be added surreptitiously to a patient's food, features a similar
message: that the drug can be used to “gain patient cooperation” while
“reducing the disruption of ward life often associated with coercive modes of
administration” (Figure 4.4). These messages all have in common the idea
that a patient with psychosis is physically dangerous and presents the ever
lurking, hidden risk of noncompliance, all problems that can be dealt with
pharmacologically.
Figure 4.2: Noncompliant schizophrenic as saboteur

377
Source: Advertisement in Hospital & Community Psychiatry (Smith, Kline, &
French Laboratories, 1965).
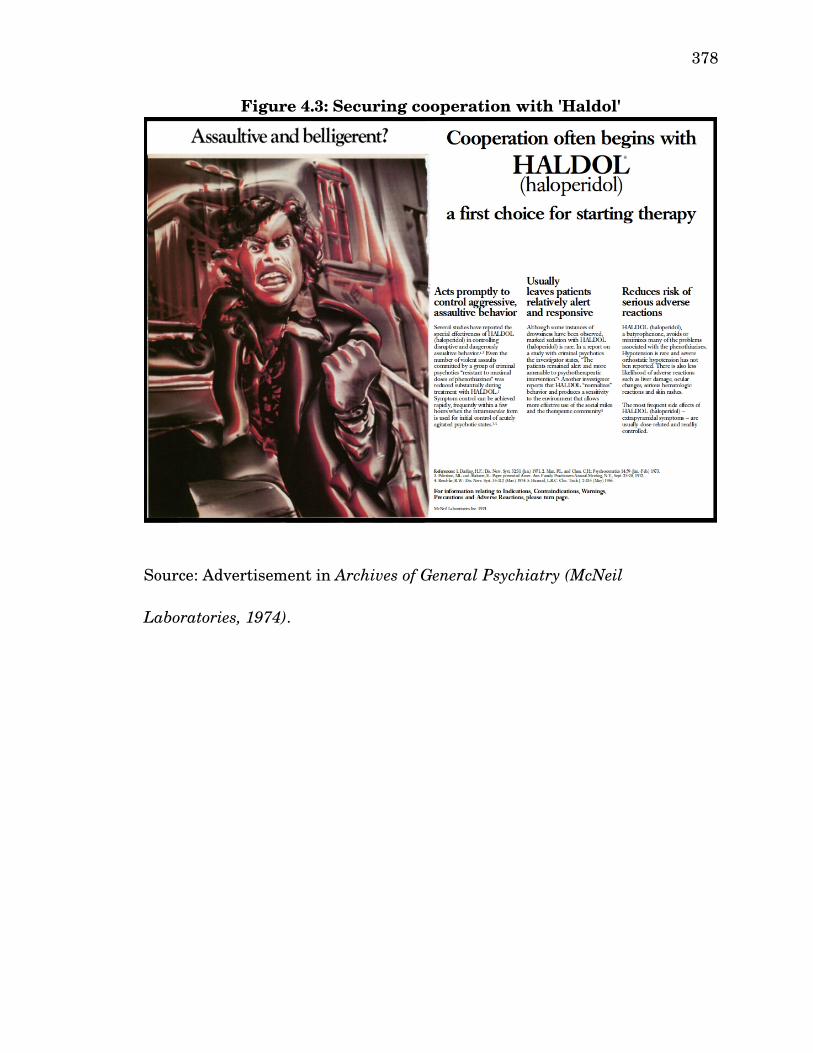
378
Source: Advertisement in Archives of General Psychiatry (McNeil
Laboratories, 1974).
Figure 4.3: Securing cooperation with 'Haldol'
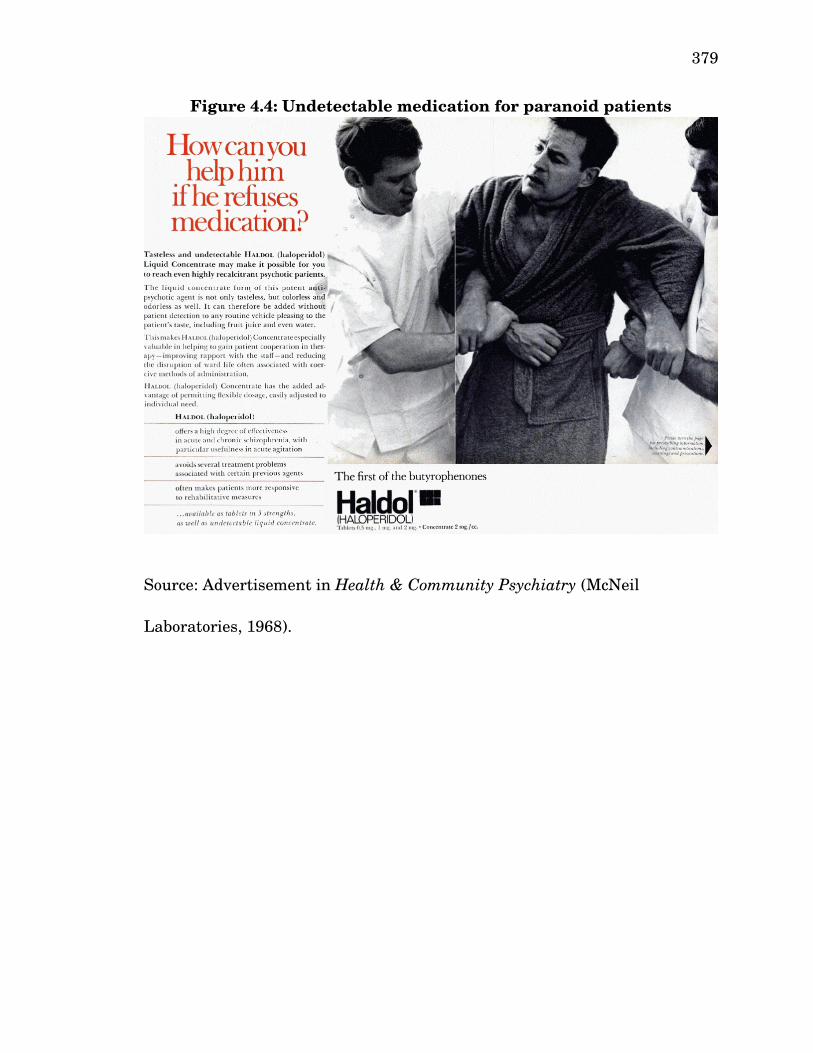
379
Source: Advertisement in Health & Community Psychiatry (McNeil
Laboratories, 1968).
Figure 4.4: Undetectable medication for paranoid patients
380
Schizophrenia has always been a risk syndrome. Controlling the
hidden threats posed by the afflicted, and identifying in them in the early
stages of the illness (or predicting its later appearance, depending on what
view of the illness one takes, a topic I shall turn to in the next major section),
has always been a project of risk management, or to be more precise, danger
management. However, the development of effective antipsychotic
medications, deinstitutionalization, and changes in public opinion have
limited the extent to which psychosis is used to legitimate coercive political
abuses. Why was it necessary in the first place? After all, a state could just
criminalize certain threatening political activities. Even in thoroughly
repressive systems, some evidence and formal process of prosecution is
required before a citizen is deprived of ordinary liberties, or else a
legitimation crisis becomes very likely. The diagnosis of 'sluggish
schizophrenia' permitted the state to incarcerate future criminals before they
committed any crime, by denying the sanity of those guilty of 'precrime.'
Their incarceration did not need to be legitimized by a formal judicial
process. In modernity, citizens have rights on the basis of their rationality,
and the insane are by definition not rational. Our methods of crime control—
incentives, disincentives, deterrence, education, etc.—all presuppose rational
actors. Disconnected from reality, the psychotic are dangerous and society
needs to be protected from such individuals.
381
Even though the diagnosis of schizophrenia (or a related psychotic
disorder) is no longer, for the most part, used in this fashion, there is another
area, however, in which psychiatric diagnosis is being used, with some
controversy, to deny civil liberties traditionally afforded to all citizens: sexual
crimes. These kinds of crimes are considered so evil, so abnormally deviant,
so unthinkable for a normal, rational citizen, that all criminals who commit
one of these crimes are forever held under suspicion, even after their 'debt to
society' has been paid. People who have been found guilty of rape are more
likely than the average citizen to commit another act of rape; prudence
demands that we take steps to control this controllable risk. Hence, sex
offender registries and the strange paradoxes of sexual crime control, e.g.,
children who 'sext' one another are being prosecuted for distributing child
pornography (Lee, Crofts, Salter, Milivojevic, & McGovern, 2013), and in
some cases one can receive a larger penalty for passively viewing child
pornography than for actually raping a child (Crary, 2012; Jauregui, 2014).
In this section, I shall discuss two proposed disorders that would have
medicalized sexual crime in different ways—pedohebephilic disorder and
coercive paraphilia—as well as a third proposed disorder, parental alienation
syndrome, that illustrates the risks associated with developing diagnoses for
the courtroom. All three diagnoses were ultimately rejected for inclusion in
DSM5.
382
Pedohebephilic Disorder
As Metzl's (2009) research shows, it is easy for certain social categories
that are associated with systematic prejudice, like race, to pervert the
operation of putatively objective judgment producing institutions. One of the
successes of the civil rights movement was the enactment of reforms that
somewhat standardized the prison sentences given for felonies, so that
someone who formerly would have received an especially light or heavy
sentence would now receive one closer to the average. One consequence of
this diminished discretionary power of judges in assigning punishments is
that criminals who for whatever reason seemed more likely to reoffend were
given shorter prison sentences. The solution to this problem came in the
form of a shift from 'needfortreatment' to 'dangerousness' criteria as the
standard for civil commitment (Testa & West, 2010). This led to the creation
of the “sexually violent predator” (SVP)113 as a juridical object of knowledge,
an individual who could be made to undergo chemical castration or else be
forcibly 'treated' for his114 sexual perversions in a mental hospital after the
term of his prison sentence was complete (Frances, 2013, p. 165). Civil
commitment of SVPs is a form of preventive detention.
113 Another term used in some jurisdictions is 'sexually dangerous person.'114 SVPs almost always are male. Even though a survey of victims by the Bureau of Justice Statistics reported that females were responsible for 6% of sexual assaults committed by individuals and involved in 40% of sexual assaults committed by groups, they represent less than .02% of offenders given the SVP classification (D’Orazio, Arkowitz, Adams, & Maram, 2009).
383
A diagnosis of pedophilia, indicating a sexual preference or compulsion
for prepubescent children, is one of the ways one could qualify for such
treatment (Aviv, 2013). The failed proposal either to include the diagnosis of
'hebephilia'—Glueck's (1955) name for sexual attraction toward teenagers—
or to expand pedophilic disorder into a broader 'pedohebephilic disorder,' first
so named by Freund, Seeley, Marshall, and Glinfort (1972), would have
widened this category dramatically. This proposal by the Paraphilias
Subworkgroup was rejected by the APA Board of Trustees for reasons that
remain confidential. The leading argument against treating hebephilia as a
paraphilia, according to Frances, is that it is actually 'normal' for adults
(men) to feel sexually attracted to pubescent115 children:
Numerous studies have proven the obvious—such attraction is
common and completely within the range of normal male lust... The
advertising industry, wise to the fact that many adults remain
sexually attracted to adolescents, cynically exploits their interest by
displaying younglooking models in provocative clothing and poses.
The assertion that sexual urges stimulated by sexy teenagers denote
mental disorder violates common sense, experience, and evidence from
research. It is not a crime or a mental disorder to lust after the newly
pubescent; it is human nature. But it is a very serious crime in our
115 More specifically, children developmentally in Tanner Stage 2 and Tanner Stage 3, generally aged 1114 (Tanner, 1978).
384
society to act on these impulses, one that deserves a long prison term.
(Frances, 2013, pp. 201–202)
One source of possible ambiguity in the debate over hebephilia is that the
category of disorders in question concerns disordered appetites/desires,
rather than disordered conduct.
Along these lines, after reminding his audience of the historical uses of
the category of paraphilic disorders to control deviant and taboo 'perversions,'
Wakefield (2011) sharply criticized the proposal, calling it the “most flawed
and blatantly overpathologizing paraphilia proposal,” and suggested that the
proposed diagnosis “violates the basic constraint that disorder judgments
should not be determined by social disapproval. This is a case where crime
and disorder are being hopelessly confused” (p 206). In response to this kind
of criticism, Ray Blanchard, the chief proponent, argued that if pedophilia is
a mental disorder, it must follow that hebephilia is a mental disorder for the
same reasons; any criticism of hebephilia along the lines offered by Wakefield
or Frances should equally provide reason to exclude pedophilia. Attempts to
distinguish between pedophilia and hebephilia on the basis of fecundity
would imply that homosexuality is paraphilic, Blanchard contended.
Blanchard acknowledged that the diagnosis would have serious
reliability problems, but did not find this to be a very compelling argument:
But so what? Should there exist no diagnosis for men who say they are
385
most attracted to pubescents, who have committed repeated sexual
offenses against pubescents, and who respond most strongly to
laboratory stimuli depicting pubescents just because there are other
men who produce less consistent findings?116 (Blanchard, 2009b, p. 332)
Furthermore, Blanchard argued that his critics missed the entire point:
Hebephilia would apply only to men who exclusively feel attraction for
adolescents; that is, an adult who is attracted to teenagers as well as adults
would not be regarded as a hebephile. While Blanchard is correct that his
opponents do not address this, he never explains why it is actually relevant.
Further, Blanchard relies on an alternative understanding of pedophilia than
used by the DSM since DSMIIIR, which defined pedophilia in absolute
rather than relative terms, as in the DSM5 image of a pedophile as an adult
who has “recurrent, intense sexually arousing fantasies, sexual urges, or
behaviors involving sexual activity with a prepubescent child or children,”
regardless of whether they do or do not have equal or greater feelings of
attraction to adults (American Psychiatric Association, 2013, p. 697).
Perhaps fittingly, his passiveaggressive and argumentative tone is
reminiscent of the manner in which adolescents argue with their parents,
and is rather striking for scientific discourse. For example, he remarks that
the validity of his position “should be obvious to anyone who has read our
116 His critics would have no problem answering this rhetorical question with an emphatic 'no.'
386
article” and comments that it was “ironic” that his opponents cited a
particular finding “when our laboratory was one of the first to report this,”
almost as if to declare ownership of the fact in question, the interpretation of
which was not even in dispute (Blanchard, 2009, p. 332).117
Coercive Paraphilia
The proposed diagnosis 'paraphilic coercive disorder' or 'coercive
paraphilia' would have applied to anyone who has “sought sexual stimulation
from forcing sex on three or more nonconsenting persons on separate
occasions” (American Psychiatric Association, 2010f). This was not a new
idea: In 1985 the DSMIIIR Workgroup proposed the diagnosis of 'paraphilic
rapism,' “which was extensively criticized at the time” (Fuller, Fuller, &
Blashfield, 1990; Krueger & Kaplan, 2012, p. 251). As explained in DSM5, a
paraphilia is sexual desire that is sufficiently deviant that it can almost be
thought of as a kind of arousal psychosis:
The term paraphilia denotes any intense and persistent sexual
interest other than sexual interest in genital stimulation or
preparatory fondling with phenotypically normal, physically mature,
117 Ray Blanchard was a member of the DSM5 Sexual and Gender Identity Disorders Work Group and chair of the Paraphilias Subworkgroup, and while the Board of Trustees of the APA voted not to accept the Subworkgroup's recommendations in favor of adopting Blanchard's view of hebephilia, he did succeed in his efforts to change the definition of a paraphilia adopted in the final manuscript so that it contrasts with what is 'phenotypically normal.' The approach in DSMIV defined paraphilia by concatenation, enumerating a variety of paraphilic fantasies, urges, or behaviors; in contrast, the DSM5 approach, which had been strongly advocated by Blanchard, defines paraphilia by exclusion, i.e., in terms of what it is not (Blanchard, 2009a).
387
consenting human partners... [The] term paraphilia may be defined as
any sexual interest greater than or equal to normophilic sexual
interests. (American Psychiatric Association, 2013, p. 685, emphasis in
the original)
Provoking reactions that range from outrage to humor, coercive paraphilia
remains highly controversial, and most of the discussion about its inclusion
focused on the question of its status as a medical problem. Debate about this
diagnostic category is not so much about whether a coercive sexual
orientation is 'disordered' but, rather, whether it is to be defined as a medical
disorder, i.e., an illness, or as a legal disorder, i.e., a crime. On this point,
Lombroso reminds us that “the distinction between crime and madness is
something constructed not by nature but by society” (2006, pp. 83–84).
That the diagnosis seems designed as a risk management tool struck
critics as too risky, in two opposing ways. On the one hand, there are
concerns about the possible use by defense attorneys presenting an insanity
or diminished capacity defense (Slovenko, 2011). In criticizing the disorder,
Frances noted that the “construct 'paraphilic coercion' has already
contributed significantly to a grave misuse of psychiatry by the legal system
in the handling of sexually violent predators,” and urged the DSM5 Task
Force to withstand the urge to “medicalize undesirable sexual behavior and
thereby provide a psychiatric excuse helpful to those who are attempting to
388
evade personal responsibility” (Frances, 2010a, pp. 3–4). On the other hand,
critics alleged that coercive paraphilia was an “[invented] diagnosis for [the]
civil commitment of rapists” (Zander, 2008, p. 459). The critics maintained
that this should occur “only if the offender's dangerousness is caused by a
mental disorder and is not a manifestation of simple criminality... Being
dangerous is not enough, since released criminals are also potentially
dangerous” (Frances & First, 2011, p. 555).
It appears that Frances was just as (if not more) concerned with this
danger. In Saving Normal, he argued that “we lose constitutional stability
whenever we allow civil rights to be violated, even for those people we most
detest” (Frances, 2013, p. 203). So as to prevent any ambiguity, Frances and
First (who headed the DSMIV Paraphilia Workgroup) stated their opposition
unequivocally:
The evaluators, prosecutors, public defenders, judges, and juries must
all recognize that the act of being a rapist is almost always an aspect of
simple criminality and that rapists should receive longer prison
sentences, not psychiatric hospitalizations. (pp. 558559)
At the 2010 annual conference of the American Academy of Psychiatry and
the Law (AAPL), a group of forensic psychiatrists voted against endorsing
'paraphilic coercive disorder' by a vote of 31 to 2, citing “the dearth of
scientific reliability or validity... [and] the potential for misuse by partisan
389
advocates in the forensic arena, especially in civil commitment proceedings”
(Franklin, 2011, p. 137).
This potential is not theoretical. Even though the DSMIV Paraphilia
Workgroup “definitively rejected the claim that rape should be considered a
mental disorder,” and, moreover, the entire section on paraphilia in DSMIV
was written “before the issue of SVP [sexually violent predator] commitment
arose and was written with clinicians, not forensic proceedings, in mind,”
Frances and First claim that “a misreading of the poorly worded paraphilia
section allowed evaluators to form just the opposite impression,” namely, that
rapists should be given the DSMIV diagnosis of 'paraphilia, not otherwise
specified (NOS)' (Frances & First, 2011, p. 556). As he often does when
criticizing fellow psychiatrists, Frances concedes that his opponents are “well
meaning and honorable,” but argues that even “the best intended misuse of
psychiatric diagnosis to curb risks to society is not worth the cost,” reminding
his audience that “mental health professionals in other countries have been
turned into statesponsored tools in the oppression of political dissidents” (p.
560).
Despite this ethotic concession of good faith, the criticism employs a
tragic frame in which SVP evaluators, who are either acting “naively or
purposefully,” have hubristically exceeded the appropriate limits of
psychiatry (p. 559). Burke suggests that, in tragedy, hubris is the “basic sin...
390
[surrounded] with the connotations of crime,” in “conflict with established
values.” Yet at the same time, “tragedy deals sympathetically with crime,” so
that “we are made to feel that [the criminal's] offense is our offense,” and
ultimately the target of criticism is “admonished... to 'resign' himself to a
sense of his limitations” (Burke, 1984a, p. 39, emphasis in the original).
Critics of coercive paraphilia did not limit themselves to the tragic
frame. In some cases, critics took to open mockery in the public sphere.
While these criticisms sometimes retained the tragic character of the
criticisms presented in expert forums, the turn to the public opens up space
for the comedic frame. Both tragedy and comedy warn “against the dangers
of pride,” but in comedy, the
emphasis shifts from crime to stupidity... The audience... chastened by
dramatic irony... is admonished to remember that when intelligence
means wisdom (in contrast with the modern tendency to look upon
intelligence as merely a coefficient of power for heightening our ability
to get things, be they good things or bad), it requires fear, resignation,
[and] the sense of limits. (Burke, 1984a, pp. 41–42, emphasis in
original).
In other words, comedy is an especially useful frame when one is urging the
exercise of practical wisdom over against expert expressions of technical
rationality. Burke suggests that comedy used in this way “must develop
391
logical forensic causality to its highest point,” which entails “completing the
process of internal organization whereby each event is deduced
'syllogistically' from the premises of the informing situation” (p. 42).
For example, at the 2010 AAPL conference, Karen Franklin, a forensic
psychologist, argued that if coercive paraphilia is a medical disorder, then
apparent outbreaks should be treatable in the same manner as other
contagious medical disorders:
A shocking news story out of Australia makes me think that if Coercive
Paraphilic Disorder exists, it must be contagious. Not just contagious,
but virulently contagious in certain allmale environments. Of the 198
students at St Paul's College at the University of Sydney, a large
proportion were apparently infected with a highly contagious form of
the virus. If Paraphilic Coercive Disorder makes it into the next
Diagnostic and Statistical Manual of Mental Disorders, St. Paul's will
be Ground Zero for the epidemic. According to an article in today's
Sydney Morning Herald, men at the elite, allmale college proudly set
up a prorape Facebook group called “Define Statutory” that promoted
sexual aggression against women. But the elite students did not stop
with words. They fostered an alcoholfueled climate in which rapes
were common, most sexual assaults went unreported, and women
students felt so unsafe that they quit school, the story reports.
392
Reporter Ruth Pollard documented a series of rapes and sexual
assaults, including one incident in which about 30 drunk, naked men
broke into a college and surrounded a young woman, touching and
taunting her. The good news is that, if it's a contagious illness, there
could be an immunization like the one for the H1N1 virus. So, while
the DSM developers are frenetically118 creating new diagnoses, let's not
forget to work on finding some cures, too. (Franklin, 2009, para. 1–5)
While the tone is mocking, the frame is one of acceptance of psychiatry, which
is mistaken rather than evil. Through the comic corrective Franklin gently
reminds psychiatrists that diagnosis is not for its own sake, and that, if they
are going to concern themselves with rapists as a patient class, then they
should be thinking about how to 'cure' them.
Coercive paraphilia did not make it into DSM5, though the definition
of paraphilia (quoted above) explicitly includes a reference to nonconsensual
sexual acts, and a diagnosis that did make it, frotteuristic disorder, is
characterized by “recurrent and intense sexual arousal from touching or
rubbing against a nonconsenting person, as manifested by fantasies, urges, or
behaviors,” which seems to contain coercive paraphilia within an even larger
discrete disease entity concept, since it is difficult to conceive of a scenario in
which one could commit rape without touching or rubbing the victim
118 In these kinds of criticisms, it is almost a pro forma requirement to make a pun in which the production of the DSM is a display of madness.
393
(American Psychiatric Association, 2013, p. 691). As with coercive paraphilic
disorder, a diagnosis of frotteuristic disorder is warranted after three
instances: “'recurrent' touching or rubbing against a nonconsenting
individual... may, as a general rule, be interpreted as three or more victims
on separate occasions” (American Psychiatric Association, 2013, p. 692).
In case this were not enough, two catchall categories were included:
other specified paraphilic disorder and, even more ambiguous, unspecified
paraphilic disorder, for “situations in which the clinician chooses not to
specify the reason” (American Psychiatric Association, 2013, p. 705). The
chapter on paraphilic disorders explicitly cautions that the “listed disorders
to not exhaust the list of possible paraphilic disorders... The diagnoses of the
other specified and unspecified paraphilic disorders are therefore
indispensable and will be required in many cases” (American Psychiatric
Association, 2013, p. 685, my emphasis). This is all despite the fact that
Frances' criticisms of coercive paraphilia appear in the context of criticizing
the “inartful” wording of the DSMIV diagnosis of paraphilia NOS, which was
written at a time when “we were not aware of the consequential problems
that would later arise from the fact that the section lacked the clarity and
precision necessary for legal purposes,” and yet was duplicated in DSM5
(Frances & First, 2011, p. 556). Presumably, it would be possible to diagnose
both coercive paraphilia and hebephilia (provided one does not agree with
394
Frances' contention that hebephilia is normophilic) indirectly with either of
the catchall paraphilic disorder categories.
What is one to conclude from this? It appears that DSM5 was
stripped of this diagnosis by name, while the chapter on paraphilic disorders
was written in such a way that a trained (or just careful) reader would see
that it was still there. Black (1992) suggests that “attitudes toward secrecy
and disclosure are manifested not alone as articulated commitments, but also
as rhetorical forms... [as] commonplaces with uncommon powers of
implication and entailment” (pp. 5253). Giving a disorder a distinct, unique,
and officially named status certainly enhances its visibility—to critics, to
attorneys, to pharmaceutical executives. Keeping the disorder but depriving
it of its name is a way to manage and restrain the risks associated with the
surplus of meaning that overflows from powerful words. This aligns with
Burke's account of the premodern concept of “word magic,” which “has its
origins, paradoxically, not in a naïve belief in the power of words, but in
man's first systematic distrust of words” and which “began with the sense of
the ineffable” (Burke, 1969a, p. 304).
Providing the disorder with its name, a mantra to be recited by
nefarious individuals eager to harness its power, was judged to be too
dangerous; the elimination of coercive paraphilia from the official list should
be thought of as desanctification. Burke notes that “the need to 'desanctify'
395
the world is essentially but an appreciation of the fact that all things possess
power... [and] the rights of desanctification are designed to mitigate the
intensity of these powers” (p. 304). Yet the disorder was not removed, but
only hidden to those on the outside in the parables of the other specified
paraphilic disorder and the unspecific disorder, seemingly “so that they may
be ever seeing but never perceiving, and ever hearing but never
understanding” (Mark 4:12, New International Version). When the text says,
as quoted above, that these two diagnoses “are therefore indispensable and
will be required in many cases,” one could imagine as the next line, “Whoever
has ears to hear, let them hear” (American Psychiatric Association, 2013, p.
685; Mark 4:9, New International Version).
The explicit rationale for listing the eight disorders is that they are
“relatively common” forms of paraphilia, and that “some of them entail
actions for their satisfaction that, because of their noxiousness or potential
harm to others, are classed as criminal offenses” (p. 685). The subtext seems
to be that the lawyers of the world can have at these eight, but the others are
for the true believers endowed with the (dia)gnosis of 'clinical judgment,' and
proper faith in the institution of psychiatry, just as Clement of Alexandria,
writing at the beginning of the third century of the common era, argues in
Book I of his Stromateis:
Nor is the word, given for investigation, to be committed to those who
396
have been reared in the arts of all kinds of words, and in the power of
inflated attempts at proof; whose minds are already preoccupied, and
have not been previously emptied. But whoever chooses to banquet on
faith, is steadfast for the reception of the divine words, having acquired
already faith as a power of judging, according to reason. Hence ensues
to him persuasion in abundance... But secret things are entrusted to
speech, not to writing, as is the case with God... And we profess not to
explain secret things sufficiently – far from it... Some things I
purposely omit, in the exercise of a wise selection, afraid to write what
I guarded against speaking: not grudging – for that were wrong – but
fearing for my readers, lest they should stumble by taking them in a
wrong sense; and, as the proverb says, we should be found “reaching a
sword to a child.” (Clement of Alexandria, 2012, pp. 12–14, Bk. I, ch. 1)
Esoteric knowledge should be trusted least of all in the hands of those who
are trained advocates but who have no genuine understanding and no
orienting faith. Clement is concerned about the risks associated with the
written disclosure of secret knowledge. The Platonic distinction between
speech and writing here is important. In a written text, which is forced to
speak for itself as it were, the writer of esoteric truths must anticipate how
the uninitiated might interpret the text in a dangerous way.
This accords with the argument made by Frances and First against
397
even including the disorder in an appendix (or what became section III of
DSM5). They suggested that, in DSMIV, including rejected diagnoses in the
appendix
seemed like a benignly obscure way to encourage future research. If
paraphilic coercive disorder were like the average rejected DSM
suggestion, it would similarly make sense to park it in the appendix...
This might facilitate the work of researchers and also provide some
guidance to clinicians in assessing the rare rapist who does have a
paraphilic pattern of sexual arousal... Including paraphilic coercive
disorder in the DSM5 appendix and suggesting it as a possible
example of the proposed other specified paraphilic disorder category
would confer an undeserved backdoor legal legitimacy on a disavowed
psychiatric construct... We did not include any reference to paraphilic
coercive disorder in DSMIV, and it should not find its way in any
form, however humble and unofficial, into DSM5. (Frances & First,
2011, pp. 559–560, my emphasis)
By this reasoning, even including the disorder in an appendix would be akin
to 'reaching a sword to a child.'
Perhaps due to the alleged misuse of paraphilia NOS, the first section
of DSM5 ends with a 'Cautionary Statement for Forensic Use of DSM5,'
which argues that in “most situations, the clinical diagnosis of a DSM5
398
mental disorder... does not imply that an individual with such a condition
meets legal criteria for the presence of a mental disorder or a specified legal
standard (e.g., for competence, criminal responsibility, or disability),” and
accordingly the use “of DSM5 to assess for the presence of a mental disorder
by nonclinical, nonmedical, or otherwise insufficiently trained individuals is
not advised” (American Psychiatric Association, 2013, p. 25). This draws a
very careful line, as it does not say that DSM5 cannot be used for forensic
purposes, but rather that the text can be interpreted only by the authorized
priestly caste of experts. The text acquires a certain degree of scientific
eloquence through its ability to balance
withholding and disbursing to the point that they beget mystery.
Enough is disclosed to license the authenticity of the rhetor, but that
same disclosure signals its own fractionality, leaving the audience
aware that what it has come to know is not all there is to be known.
(Black, 1992, p. 95)
Mental health professionals may act as expert witnesses and offer testimony
in support of the judicial relevance of a DSM5 diagnosis, but the rhetorical
force of this testimony should not be unfairly boosted by the authority of the
DSM itself.
Parental Alienation Syndrome
One other extremely controversial disorder, also proposed by rejected,
399
raises similar concerns. Parental Alienation Syndrome (PAS) would have
applied to a child who engages in a “campaign of denigration” against one of
his or her parents with “no justification,” and is at best able to offer only
“weak, frivolous, or absurd rationalizations” for the vilification, which occurs
in the complete “absence of guilt [regarding his or her] cruelty to and/or
exploitation of the alienated parent” (Gardner, 2001, p. 10). Formulated in
this way, PAS is conceived as a kind of psychosis. Like coercive paraphilia,
this diagnosis is much more relevant in the courtroom than in the clinic.
Accordingly, rhetorical concerns are even more relevant than scientific
concerns, although in general it seems that diagnoses that appear to serve
only a forensic purpose tend to have scant scientific backing (after all, justice
and the good tend to resist hypothesis testing). In the case of PAS, supposing
the described phenomena actually occurs, a diagnosis of delusional disorder is
available, so the inclusion of PAS would work primarily to legitimize the idea
that such kinds of delusions are so common that they deserve special
recognition.
One psychiatrist who opposed PAS's inclusion in DSM5 is Paul Fink,
a past president of the APA. His criticism of PAS's scientific basis was
explicitly framed as a rhetorical matter:
[Many] of the controversies [about what to include in DSM5] are and
will be political with proponents on each side of the issue. All of us love
400
rhetoric that seems reasonable to the reader. One such area is parental
alienation syndrome (PAS). I am personally involved in opposing the
inclusion of this bit of junk science invented by a psychiatrist in the
1980s, the late Dr. Richard A. Gardner. All of his books and most of his
papers were published by his own publishing company. He protected
child sexual abusers in court and was very abusive to the mothers of
the children caught up in custody hearings. Many children and
mothers have been hurt by this man's beliefs, but over 15 years, he
developed many converts to his beliefs, including judges, lawyers,
guardians at litem, and psychologists who liked the neat packaging of
his ideas. In recent years, the ball has been picked up by "father's
rights" groups who don't like to be interfered with when they are
sexually abusing their children. This group has petitioned the DSM
task force to include PAS in the publication. This is a good example of
the political activity into which DSM is drawn. The task force members
want to be fair to all parties, so we are now involved in putting together
data around this issue to disprove it to the DSM task force. (Fink, 2010,
para. 29–34, my emphasis)
By combining science and rhetoric, emotion and reason, morality and
medicine, personal character and public credibility, this criticism is
representative of many DSM5related arguments. The legitimacy of a
401
particular forensic tactic (i.e., expert witness impeachment) is now a medical
question. Dr. Gardner is described as an effective rhetor who has managed to
persuade legal authorities to accept his “junk science” by means of the “neat
packaging of his ideas.” According to this depiction, Gardner has engaged in
a form of sophistry that Plato compared to pastry baking, which he defined as
the flattery that wears the mask of medicine... [It is] a mischievous,
deceptive, disgraceful... thing... that perpetrates deception by means of
shaping and coloring, smoothing out and dressing up... [What] pastry
making is to medicine, oratory is to justice. (Plato, 1997b, sec. 469b–
469c)
The diagnosis is not problematic merely because it is 'incorrect' or 'invalid,'
but because it is risky. The risks posed by this diagnosis derive from the way
it functions rhetorically, which Fink undermined by marshaling scientific
data that he believed “disprove” its medical validity. Fink viewed the DSM5
debate as an opportunity to challenge the validity claims implied in
Gardner's discourse before those claims could become unquestionable.
Risk (Factors) and Susceptibility
The next stage of the conceptual development of risk in late modernity
turned from risks (dangers) hiding inside individuals to risks hiding inside
populations, a move that was joined by the rise of advanced liberalism,
according to which the biopolitics of risk entail
402
a variety of strategies that try to identify, treat, manage, or administer
those individuals, groups, or localities where risk is seen to be high...
Risk here denotes a family of ways of thinking and acting that involve
calculations about probable futures in the present followed by
interventions in the present in order to control that potential future.
(N. S. Rose, 2007, p. 70)
Recognizing the costs and inefficiencies inherent in a diseasecontainment
model, the dominant paradigm in medicine began to shift toward health
promoting/illnesspreventing strategies and techniques. In his landmark
essay “From dangerousness to risk,” Robert Castel contends that the
fundamental characteristic of the new strategies of biopolitical risk
management utilized in advanced industrial societies (more or less
corresponding with Rose's concept of advanced liberalism) is that they
“dissolve the notion of a subject or a concrete individual, and put in its place a
combinatory of factors, the factors of risk” (Castel, 1991, p. 281, emphasis in
the original). These strategies also emphasize prevention, which is consonant
with a set of neoliberal values that place “a premium on individual
responsibility for one's own health and wellbeing” (Grob & Horwitz, 2010, p.
106).
Along with this came the modern notion of preventive psychiatry,
which Castel argues was a solution to the moral and technical difficulties
403
involved in attempting to confine or sterilize anyone who might contain a
kernel of dangerousness. The transition to preventive psychiatry was
something that Morel gestured toward by focusing on frequencies and other
objective measures of risk in populations, but was unable to fully realize
because “he did not have at his disposal the specific techniques... with which
to instrumentalize” the requirement to “act directly on the conditions liable to
produce risk,” which also had been the principal failing of the eugenics
movement (Castel, 1991, pp. 285–286). The transition required that “the
notion of risk is made autonomous from that of danger. A risk does not arise
from the presence of particular precise danger embodied in a concrete
individual or group,” but rather the “effect of a combination of abstract
factors which render more or less probable the occurrence of undesirable
modes of behavior” (p. 287, emphasis in the original).
With this conceptual shift in place, the new biopolitics of risk were
ushered in with the rise of population data and increasingly sophisticated
methods of statistical analysis, which drove new ways of thinking about the
measurement and management of mortality, morbidity, and risk (Hacking,
1975, 1982). Writing two years after its publication, which in large part was
driven by concern over reliability (Kirk & Kutchins, 1992; Kutchins & Kirk,
1997), Hacking argued that the categories in DSMIII “are as responsible to
the need to count uniformly as they are to any interest in 'correct' diagnosis...
404
the fetishism for counting... brings with it the need for easily applied
categories in terms of which to count” (Hacking, 1982, pp. 293–294).
Accordingly, the DSM serves as a biopolitical apparatus that enables
individuals to be assigned to risk pools based on factors identified by
probabilistic and epidemiological knowledge, which constitutes “a new mode
of surveillance: that of systematic predetection... in effect [promoting]
suspicion to the dignified scientific rank of a calculus of probabilities” (Castel,
1991, p. 288).
With this “conception of prevention,” underpinned by “a grandiose
technocratic rationalizing dream of absolute control of the accidental,
understood as the irruption of the unpredictable,” very little falls outside the
circumference of its gaze (Castel, 1991, pp. 288–289). The scope of the
surveillance suggests that everyone, despite being “existentially healthy, [is]
actually asymptomatically or presymptomatically ill. Technologies of life not
only seek to reveal these individual pathologies, but intervene upon them,” a
consequence of which is that “new forms of life” are emerging around the idea
of risk as susceptibility (N. S. Rose, 2007, p. 19). The danger in this approach
is that it fosters a set of institutional logics that are constantly generating
risks to manage without “a trace of reflection on the social and human cost of
this new witchhunt... [e.g.,] the iatrogenic aspects of prevention” (Castel,
1991, p. 289, emphasis in the original).
405
Risk Production and Risk Society
One very important change that has coincided with 'reflexive
modernization' or the emergence of a second modernity is the emergence of
risk production as the dominating logic of the systems world. In the first
stage of modernity, the mystifications of religion and privilege were
dismantled by the likes of Marx and Nietzsche. In the second stage, “the
same is happening to the understanding of science and technology in the
classical industrial society, as well as to the modes of existence in work,
leisure, the family, and sexuality” (Beck, 1992b, p. 10). Beck argues that the
productive forces of industrialization “have lost their innocence in the
reflexivity of modernization processes. The gain in power from techno
economic 'progress' is being increasingly overshadowed by the production of
risks” (pp. 1213). In the first stage, the logic of wealth production was a
driving force in urbanization; the degeneracy that seemed (in the popular
imaginary) to result was “legitimated as [a] 'latent side [effect]'” (p. 13).
Urbanization brought pollution, stress, dislocation of families and
alteration of their structure, nutritional changes, socioeconomic conditions
that produced an increase in nonreproductive sexual activities and the
spread of sexually transmitted diseases (including, importantly, syphilis,
responsible for the 'general paresis of the insane'), etc., all of which received
blame (in some cases fairly, in others unfairly) for the apparent epidemic of
406
degeneracy and associated mental illness. Our efforts to manage these
hazards and 'side effects' of modernization give rise to secondorder risks,
with each intervention encompassing an increasingly wider scope. In the
beginning, social risks seem to live inside individual human beings. The
latent danger in these individuals can be medicalized and regulated through
strict coercive measures, some of which are more acceptable to those tasked
with enforcing them if they can be conceived as noncoercive, as in the second
Haldol advertisement (Figure 4.3, supra). This was somewhat more of an
issue in totalitarian regimes, in which classical ideas about the role of
sovereign authority continued to hold sway, modernized only insofar as they
were revised to incorporate novel methods of disciplining subjects, than in
liberal societies in which “governmentality,” that is, a focus on “maximizing
the forces of the population collectively and individually,” was the field within
which “the thematics of sovereignty, of discipline and of biopower [were] all
relocated” (N. S. Rose, 1999, p. 23).
During the twentieth century, following the impulse first expressed (as
far as I can tell) by Xenophon, “security against risk was socialized” (N. S.
Rose, 1999, p. 158). The old virtue of prudentia to which the individual was
exhorted, for the sake of providing for his own and his family's needs, at a
certain point came to involve the prudent move of contracting private
insurance policies, which in turn were made compulsory and nationalized.
407
As the insured expand to include institutions and corporations, the social
insurance perversely contributes to a 'too big to fail' kind of moral hazard, a
new risk that we created as a direct consequence of our efforts to manage an
old risk.
As our knowledge expanded and expands, so too does our uncertainty,
which can now be quantified and experienced with an unprecedented level of
precision, thanks to recently developed theories of probability and methods of
statistical analysis. There is risk in acting and in not acting; risks in
managing prior risks (or choosing not to); risks that we can predict in
advance and risks that we cannot foresee (except insofar as we can predict
that there might be unintended consequences about which we can only
guess). As we realize things are more complicated than we thought,
impersonal risk factors lying in measurable populations rise to our attention,
and the prevailing imperative is to prevent problems before they start, if
possible, rather than treating them after they have come to fruition. This led
to preventive psychiatry. But as with each preceding stage in the process of
reflexive modernization, this maneuver will create entirely new risks, and
the controversies that result will turn ultimately on stasis points relating to
the salience, predictability, and importance of old risks compared with the
new.
408
Early Intervention Research
With the advent of preventive medicine, and in particular preventive
psychiatry, we now have sufficient context to discuss the idea of early
interventions in schizophrenia, from which the controversy about psychosis
risk syndrome directly descends. This idea has a much longer history than is
evident in the contemporary controversy.
Freud's Views on Early Diagnosis
We have seen already that Freud was keenly interested in identifying
schizophrenia as early as possible, but this was not in the interest of
treatment. The kind of damage to the nervous system that he believed
precipitated psychosis was preventable (a simple matter of stopping
adolescent male masturbation) but once symptoms were observable, it was
already too late, if in fact the cause was schizophrenia and not a more
treatable ailment like hysteria or obsessional neurosis. Writing 20 years
later, Freud displayed a different kind of concern for risk that he tied with
diagnosis and which thoroughly inverts the modern understanding:
Often enough, when one sees a neurosis with hysterical or obsessional
symptoms, which is not excessively marked and has not been in
existence for long—just the type of case, that is, that one would regard
as suitable for treatment—one has to reckon with the possibility that it
may be a preliminary stage of what is known as dementia praecox
409
(‘schizophrenia,’ in Bleuler’s terminology; ‘paraphrenia,’ as I have
proposed to call it), and that sooner or later it will show a wellmarked
picture of that affection. I do not agree that it is always possible to
make the distinction so easily. I am aware that there are psychiatrists
who hesitate less often in their differential diagnosis, but I have
become convinced that just as often they make mistakes. To make a
mistake, moreover, is of far greater moment for the psychoanalyst
than it is for the clinical psychiatrist, as he is called. For the latter is
not attempting to do anything that will be of use, whichever kind of
case it may be. He merely runs the risk of making a theoretical
mistake, and his diagnosis is of no more than academic interest.
Where the psychoanalyst is concerned, however, if the case is
unfavorable he has committed a practical error; he has been
responsible for a wasted expenditure and has discredited his method of
treatment. He cannot fulfill his promise of cure if the patient is
suffering not from hysteria or obsessional neurosis, but from
paraphrenia, and he therefore has particularly strong motives for
avoiding mistakes in diagnosis. In an experimental treatment of a few
weeks he will often observe suspicious signs which may determine him
not to pursue the attempt any further. Unfortunately I cannot assert
that an attempt of this kind always enables us to arrive at a certain
410
decision; it is only one wise precaution the more (Freud, 1913a, pp.
364–365)
Here, the disorienting suggestion that psychoanalysis is the only psychiatric
treatment that works (or that carries possible side effects) reminds us that
this is a prepharmacological era.119 In contrast to the recent trend in
psychiatry, his motivation was to avoid an early intervention, for
schizophrenia was hopeless and attempting to treat it could only discredit
psychoanalysis. Hence the early diagnosis of schizophrenia was about
reducing risk to the profession rather than to the patient.
It is clear that already by this point, practitioners of psychoanalysis
and their more biologicallyinclined colleagues had already started to draw
interdisciplinary battle lines, reflecting perhaps the “narcissism of minor
differences” (Freud, 1989, p. 72).120 Risk and diagnosis are caught up
together, though not in the same fashion as in psychosis risk syndrome, but
119 By prepharmacological, I am referring to the time before modern pharmacological treatments, i.e., (major and minor) tranquilizers, mood stabilizers, and antidepressants. The discovery of an effective treatment for acute psychosis in chlorpromazine (Thorazine) fundamentally changed psychiatry, but certainly did not introduce the use of pharmaceutical treatments in psychiatry (Healy, 2004b). In the late nineteenth century, alienists made extensive use of sedatives, including camphor, chloroform, chloral hydrate, ether, hemlock, hyoscine, hyoscyamine, hypnal (which could refer to a wide variety of substances, most often phenazone), marijuana, morphine, paraldehyde, and potassium bromide (and other bromide salts, the hypnotic properties of which provide the basis for the metaphor of bromide as verbal sedative), along with many more, detailed in Daniel Tuke’s (1892) Dictionary of Psychological Medicine (Reynolds, 1894; Ringer & Sainsbury, 1892). As Noll observed, the “pharmacological treatment of insanity was not an innovation of the late twentieth century by any means” (2011, p. 32).120 Freud uses this phrase in his explanation of the “phenomenon that it is precisely communities with adjoining territories, and related to each other in other ways as well, who are engaged in constant feuds and in ridiculing each other” (p. 72).
411
Freud does understand a certain kind of untreatable/incurable psychosis to
exist that follows a standard declining course.
Complicating the problem of differential diagnosis is that Freud’s
division of the psychoneuroses is dimensional, while Bleuler's schizophrenia
was very much part of a categorical nosological structure. The adoption of a
categorical nosology tends to provoke controversies about 'subthreshold'
disorders:
The controversy surrounding subthreshold disorders exemplifies the
way in which classification of mental disorders influences the
definition of the discipline of psychiatry. The existence of subthreshold
disorders is a byproduct of the use of operational criteria that define
categories of mental disorders on the basis of a consensus rather than
evidence... [Problems] related to subthreshold disorders are close to
problems related to states that show some similarity to mental
disorders but are considered different from them and therefore should
not receive psychiatric treatment, such as grief reactions as well as
excessive religious zeal and related behavior (e.g., selfflagellation and
even crucifixion). (Sartorius, 2011, pp. 64–65)
Given that Freud's psychodynamic nosology is noncategorical, however, a
subthreshold disorder, if the concept is meaningful at all, is apparently more
of an opportunity than a problem.
412
Diagnostic AntiFatalism: Schizophreniform Disorder
Schizophrenia has always signified a fatalistic course, even before it
was called schizophrenia. This semiotic identity has been rather immune to
falsification. Sometimes psychiatrists observe cases that seem like
schizophrenia, but resolve in less than half a year. This is a phenomenon (or
set of similar phenomena) now known as schizophreniform disorder, the
characteristic symptoms of [which] are identical to those of
schizophrenia... Schizophreniform disorder is distinguished by its
difference in duration: the total duration of the illness, including
prodromal, active, and residual phases, is at least 1 month but less
than 6 months. (American Psychiatric Association, 2013, p. 97)
Shorter still is brief psychotic disorder, which resolves in less than a month
(p. 94). It may seem odd to have a diagnostic category that has its own
resolution as its distinguishing clinical sign (since this sign cannot be
observed until after the expertise of a physician is no longer required), but in
practice it is diagnosed provisionally until the symptoms have lasted six
months, at which point the diagnosis is changed to schizophrenia: “the
diagnosis should be noted as 'schizophreniform disorder (provisional)' because
it is uncertain if the individual will recover from the disturbance within the
6month period” (p. 97). In other words, the diagnosis itself is a category
designed for targeting potentially schizophrenic individuals for early
413
intervention. Apparently the diagnosis is accurate (i.e., a patient given the
diagnosis in fact recovers within six months) about onethird of the time,
while the “majority of the remaining twothirds of individuals will eventually
receive a diagnosis of schizophrenia or schizoaffective disorder” (p. 98).121
Schizophreniform disorder was first so called by Gabriel Langfeldt,
who wanted to distinguish those whose apparent psychotic states were
precipitated by a stressful life event from those who exhibit psychosis without
any apparent exogenous cause (Langfeldt, 1939). This is the same distinction
as Freud made using slightly different terms, and the core idea seems to be
that etiologically endogenous illness must have a strictly biological
pathogenesis, while etiologically exogenous illness must have a strictly
psychological pathogenesis, and so the latter was treatable (with
psychoanalysis) while the former was not, a view that changed sharply with
the discovery of the antipsychotic properties of the phenothiazine compound
chlorpromazine (Thorazine) in the 1950s (Healy, 2004b).
This distinction repeated with depression (distinguishing 'endogenous
depression' from 'reactive depression,' where the word reactive refers to a
neurotic reaction of the kind described by Freud), and was rather obscure
121 Schizoaffective disorder is similar to schizophrenia except that the psychotic symptoms are very often (though occasionally not) accompanied by the symptoms of a mood disorder. If the psychotic symptoms are always accompanied by the symptoms of an affective disorder, then the proper diagnosis is either 'depressive disorder with psychotic features' or 'bipolar disorder with psychotic features' (American Psychiatric Association, 2013, pp. 105–110). The meaningfulness of such distinctions has been questioned, but is generally upheld (Maier et al., 1992, 1993; Taylor, 1992).
414
until the discovery of the first tricyclic antidepressant imipramine (Tofranil)
by Kuhn (1958), who indicated it was an effective treatment for endogenous
depression (Healy, 1997). For the most part, DSMIII eliminated diagnostic
terms that implied an etiological theory (though see the discussion of
conversion disorder in Chapter 3), and the current consensus is that mental
illnesses previously thought to be 'endogenous' are usually precipitated by
stressors, and conversely, mental illnesses preceded by stressors usually have
a biological pathogenesis of some sort (Keller, Neale, & Kendler, 2007;
Kendler & Gardner, 2010; Kendler & Halberstadt, 2013). Furthermore, most
of the states that Langfeldt identified as schizophreniform disorder would
now be diagnosed as mood disorders (P. J. Cowen et al., 2012). But the name
schizophreniform disorder remains, along with the basic idea of trying to
distinguish, in cases of recent first psychosis states, those with a good
prognosis from those with a bad prognosis.122
Early Intervention for Psychosis
Frequently in recent discussions about psychosis risk syndrome in the
context of DSM5, it is asserted that research programs aimed at identifying
individuals at high risk of developing psychosis began in the late 1990s. For
example:
122 Though not sufficient to make twoway predictions with any reasonable degree of confidence, it is apparent that the absence of symptoms from the negative axis, as well as good eye contact when being interviewed, are “good prognostic features” (American Psychiatric Association, 2013, p. 97; Troisi, Pasini, Bersani, Mauro, & Ciani, 1991).
415
For the past 15 years, wellintentioned research efforts have sought to
identify individuals at highest risk to develop a psychotic disorder
(usually based on the presence of transient or attenuated positive
symptoms) and to develop effective early interventions for adolescents
and young adults at risk. (Pierre, 2013, p. 115)
Defenders of these efforts seem to use this 'fact' to emphasize the cutting
edge nature of this research; detractors similarly use the assertion to
emphasize the novelty of the idea, which they contend is wellintentioned but
“not ready for prime time” (Frances, 2010d, para. 14). The suggested
chronology, however, is not precisely accurate.123
More than 75 years ago, researchers were aware that it may be
possible to diagnose schizophrenia early, and concerned themselves with
questions about diagnostic criteria and early intervention strategies.
Cameron suggested that
antedating the clinically recognizable symptoms there is a group of
behavior changes which we refer to as nonspecific... These non
specific symptoms persist for periods ranging from weeks to years
before the onset of the specific schizophrenic symptoms and were
123 I say 'not precisely' because it is accurate to say that this research has been in progress for the past 15 years, but it is inaccurate to imply that these efforts began only 15 years ago; the true number is more than double that. Interestingly, at nearly every period of time going back to the mid 1950s, when researchers indicated the length of time research into some form of psychosis risk had been going on, the length invariably was between 15 and 20 years. I can only speculate as to the causes of this observed trend.
416
described in 83 of our 100 cases... We have tried to see in what
environment the patient is during these early stages and how the
various people around him during this time—his relatives and friends,
his employer and his physician—react to his growing abnormality.
Finally we have considered the development of certain social trends—
the growing acceptance of routing health examinations and the
increasing utilization of general hospitals for psychiatric treatment—
which may be of immense importance in the satisfactory detection and
treatment of early schizophrenia. (D. E. Cameron, 1938, pp. 568–569,
577)
Two decades later, a study was announced in Detroit in which researchers
test[ed] and interview[ed] a group of normal children... From these
tests and interviews, we shall predict which of these children will
become schizophrenic... If our predictions prove to be supported, we are
then in a position to do research which is aimed at the prevention of
schizophrenia. (Mednick, 1960, p. 69)
Twenty years later, in May of 1980, the same year that saw publication of
DSMIII, the National Institute of Mental Health (NIMH) sponsored a
conference at the University of California, Los Angeles, entitled: “Preventive
intervention in schizophrenia: Are we ready?” (Goldstein, 1981, p. i). This
followed the establishment in 1979 of an 'Office of Prevention.' Herbert
417
Pardes, then director of NIMH, in the foreword to the proceedings from this
conference, seemed to answer in the affirmative (in contrast to most of the
papers given):
For more than three decades, the National Institute of Mental Health
has conducted and supported a broad spectrum of research programs
to add to our knowledge and understanding of schizophrenia. A major
focus of this work has involved diagnostic issues... Research
emphases... have been directed toward... studies of individuals and
populations hypothesized to be at high risk for the disorder... While
the core mystery of schizophrenia continues to challenge researchers
and clinicians, the incremental advances... constitute impressive
overall progress As information accumulates, so does the possibility
that we can intervene earlier and more effectively, aiming at
prevention of the premonitory signs of the disorder rather than at
signs which indicate the disorder has taken hold. (Pardes, 1981, p. iii)
Notice that Pierre and Pardes, writing thirtytwo years apart, employ very
similar language. Also significant in this passage is the oracular rhetoric –
the 'core mystery' of psychosis is still intact, but our seers are divining the
'premonitory signs' of the disorder. Similarly, Cowen argues that like “moths
attracted to a flame, our relentless quest has been to solve the riddle of
profound psychological disorder... [Recent] 'advances' notwithstanding, the
418
mysteries of extreme disorder are still not unraveled” (E. L. Cowen, 1981, p.
180). This kind of gnostic (or should I say prognostic) and esoteric mystery
tradition language is less common in recent discussions on the topic.
A variety of perspectives are expressed in the papers given at this
conference, and many of them can be read as epideictic praise of and
exhortation to primary prevention. Primary prevention was defined in the
following way:
(1) Identify something worth preventing, and develop reliable methods
to differentiate victims from nonvictims; (2) Through epidemiological
and laboratory studies, locate its most probable cause(s); (3) Mount
and evaluate programs to circumvent those causes... That model has
well served society's efforts to stamp out oncebaffling, devastating
disorders, such as smallpox, malaria, diphtheria, typhoid fever, and
polio... Indeed, the very successes of the model have sustained it, won
it recognition and plaudits, and helped to extend it to new domains in
which, unfortunately, it may be less applicable. (E. L. Cowen, 1981, pp.
178–179)
One author suggests that there “are probably few issues of greater scientific,
social, and humanitarian importance” (Holzman, 1981, p. 19). Samuel Keith
emphasized the exigence of the research by describing the “individual,
familial, and clinical despair” that this “heartbreaking condition” brings
419
about: Even thirty years after the discovery of the antipsychotic properties of
chlorpromazine, there “is no term in all of mental illness that elicits more
fear, pessimism, or therapeutic nihilism than chronic schizophrenia” (Keith,
1981, p. 306). Michael Goldstein, the first director of the thenrecently
christened NIMH Office of Prevention, notes that primary prevention is of
particular importance for schizophrenia because “a schizophrenic episode is
so disorganizing and recovery so arduous and unpredictable” (Goldstein,
1981, p. v).
Warnings and admonitions on the subject were also offered. Asarnow
and Asarnow (1981) remind their audience about the failures of the Mental
Hygiene movement, emphasizing the “importance of deriving our attempts at
preventive intervention for schizophrenia from the best available research
evidence concerning the nature of the central deficits in schizophrenia” (p.
91). One participant bemoaned the emphasis on biology at the expense of
communication, arguing:
The studies of communication in families has [sic] revealed that there
appear to be certain simple, fundamental properties of transactions
which, when they proceed well across time, promote human growth
and wellbeing. When these communication properties go astray, the
cost is high. (Singer, 1981, p. 173)
Another participant warned that the DSM criteria pose a fundamental
420
barrier to effective primary prevention research, and antiprophetically
suggested that “the identification of the psychiatrist and things psychiatric
with the DSM approach may be loosening” (Cromwell, 1981, pp. 119–120).
Keith suggested that “we are probably doing ourselves a disservice by
confining to schizophrenia the impact of the past 20 years of research in high
risk,” because the true object of preventive efforts ought to have been on the
psychosocial and institutional barriers that frustrate the efforts of chronically
mentally ill patients to become “fully functioning members of society” (Keith,
1981, pp. 305–306). He also noted a logical problem with the overall primary
prevention research program:
[The] more closely an individual behavioral item is related to
diagnosable schizophrenia, the more risk we run of creating a
tautology. Those people who have “symptoms” of incipient or
impending schizophrenia can be predicted to have a very high risk
indeed of developing the disorder. The challenge to prevention
programs will be in developing specific interventions to correct for
maladaptive behavior patterns before the fullfledged disorder becomes
manifest and to obviate the necessity for secondary prevention. (p. 307)
Finally, he admonished his colleagues to remember that “if our interventions
are powerful enough to create something good, then they are powerful
enough, if used inappropriately, to create something bad” (p. 309).
421
With the exception of this last, brief point, none of the papers dwell on
the issues of the unnecessary stigmatizing and medicating of 'false positive'
individuals raised by current critics of psychosis risk syndrome. Perhaps this
was related to the fact that virtually all proposed interventions were psycho
social in nature, with the exception of a single paper (Friedhoff, 1981) that
discussed injecting high doses of haloperidol into pregnant rats and then
dissecting and measuring the brains of the newborn rats a week after they
were born (but even in this paper the objective was theoretical and the author
did not suggest or even gesture toward the idea that pharmaceutical
intervention was appropriate for humans).
At this point, it is important to note that specific intervention
strategies were still in their infancy, and the focus almost entirely placed on
thinking about how to identify people for targeted interventions. Preventive
intervention strategies can be subdivided into three categories: universal
interventions that target the general population (e.g., seat belts, general
vaccinations, sanitation, etc.); selective interventions that target a subgroup
at risk (e.g., mammograms for women with family history of breast cancer);
and indicated interventions that target individuals who can be identified on
the basis of some specific manifest sign(s) or symptom(s) that can be
measured on an individual basis and suggest the very early stages of a
disorder or illness (Gordon, 1983). The line between the latter two categories
422
is blurry, but a key dividing line is that those in the 'selective' category are
for asymptomatic patients, while those in the 'indicated' category have
“minimal but detectable signs or symptoms foreshadowing mental disorder,
or biological markers indicating predisposition for a mental disorder”
(Mrazek & Haggerty, 1994, p. 8). This suggests that it is necessary to
carefully articulate what is meant when it is suggested that someone is 'at
risk' for a disorder.
Theoretical Perspective of Patrick McGorry
One individual in particular seems to be close to the center of much of
the development of research into psychosis risk during the last two decades,
prolifically publishing on the subject and frequently named as its chief
exponent: the Australian psychiatrist Patrick McGorry. Before beginning his
work on early interventions, McGorry published an article in which he
challenged the “dominant neoKraepelinian paradigm” and instead offered a
model of psychosis called the “loose linkage model” (McGorry, 1991, p. 43).
McGorry complained about the failure of researchers working within the
constraints of the current model to elucidate the etiology or pathogenesis of
schizophrenia:
With each passing year, it becomes more of a paradox that, despite
exponential growth in knowledge in the neurosciences, the
pathogenesis of this group of disorders remains obscure. Nevertheless,
423
the expectation that a breakthrough is imminent has been with us for
some time and continues to build. The rise of biotechnology certainly
holds out the promise that, if such technology could be appropriately
deployed, it would merely be a matter of time before the psychoses
would be forced to yield up their secrets; yet there is a growing sense
that it is perhaps no longer the crudeness of the research techniques
which is causing the delay. (McGorry, 1991, pp. 43–44, my emphasis)
The esoteric rhetoric recalls that of Cowen (1981) a decade before, and the
emphasis on the sense of discontinuity between the crude or primitive past
and the advanced scientific present can also be seen in the ways in which
antipsychotics were marketed in the first three decades after their discovery,
as we saw in Chapter 3.
McGorry argues that the key assumptions of the neoKraepelinian
framework are problematic. One assumption in particular stands out: that
“clinical boundaries can be drawn reflecting specific underlying disorders of
pathophysiology, and it is assumed that we already have an accurate idea of
the location of these 'joints' at which nature should be carved” (McGorry,
1991, p. 45). This observation recalls a metaphor in Plato's Phaedrus, in
which Socrates discusses the use of rhetoric to account for the different kinds
of madness systematically, noting that the key task is to “cut up each kind
according to its species along its natural joints, and to try not to splinter each
424
part, as a bad butcher might do... [Our speeches] placed all mental
derangements into one common kind” (Plato, 1997c, sec. 265e).124 The neo
Kraepelinian model identifies the location of these 'natural joints' by looking
at clusters of symptoms, which works rhetorically to persuade psychiatrists
implicitly that there is a “close linkage of symptomatology with underlying
disease process” (McGorry, 1991, p. 45). This process is implicit because, as I
discussed in Chapter 1, DSMIII explicitly disclaimed any connection
between diagnostic categories and aetiopathological knowledge.
This belief guided research into vulnerability factors, as the search
tried to find biological phenomena that varied more between (neo
Kraepelinian defined) groups than within groups. McGorry suggests that
this belief was reinforced by a story about the historical discovery of the
etiology of neurosyphlis which he regards as mythical and factually wrong.
He further subtly suggests that the neoKraepelinian nosological approach to
schizophrenia is itself schizophrenic, “displaying the 'splitting' tendency in
classification... [which] has been termed 'splitomania'” (p. 46). To return to
the Platonic metaphor, McGorry would see this 'splitomania' as missing the
'natural joints' and producing many 'splinters.' McGorry notes that “despite
supportive research findings... [a dimensional model] has failed to displace
124 μ , μ τὸ πάλιν κατ᾽ εἴδη δύνασθαι διατέ νειν κατ᾽ ἄρθρα ᾗ πέφυκεν καὶ ὴ ἐπιχειρεῖν μ μ , μ μ : καταγνύναι έρος ηδέν κακοῦ αγείρου τρόπῳ χρώ ενον ἀλλ᾽ ὥσπερ ἄρτι τὼ λόγω
μ ...τὸ ὲν ἄφρον τῆς διανοίας ἕν τι κοινῇ εἶδος ἐλαβέτην
425
the categorical approach in the psychoses” (p. 47). He discusses several
possible reasons, and then suggests that a hybrid categorical/dimensional
model is needed. His “loose linkage model” is based on previous theoretical
work by Jaspers (1963) and Brockington and Meltzer (1983). It posits that,
due to the complex relationship between the manifest symptoms of psychosis
and the underlying pathophysiology, “a close or constant linkage between
symptom patterns and changes at the anatomical or physiological level is
unlikely” (McGorry, 1991, p. 48). Finally, he predicted a very poor prognosis
for the concept of schizophrenia: “its days as a candidate for disease entity
status and diagnostic term are numbered, and its demise is merely a matter
of time” (p. 53).
Shortly after this theoretical work, McGorry initiated a vast research
program into secondary prevention of schizophrenia and other psychotic
disorders at his new clinic, the Early Psychosis Prevention and Intervention
Centre (EPPIC), informed by the prodrome interpretation of psychosis risk
(Lincoln & McGorry, 1995; McGorry, 1992, 1993, 1994, 1995). He argued for
a phaseoriented classification of psychosis rather than a prognosisbased
classification, arguing that the latter is worse than useless because
iatrogenic effects of applying a diagnosis which connotes in the mind of
the clinician, the relatives and the sufferer a prospect of prolonged
pervasive disorder, disability and even inevitable deterioration... can
426
be appreciated by any clinician who has witnessed the impact of this
unnecessarily threatening diagnostic process on patients and families.
(McGorry, 1995, p. 556)
The phaseoriented classification is still coursebased to some extent, but
emphasizes the dimension of staging, and can allow biological research to
focus on the stage of 'early psychosis' and help to identify the
psychopathological mechanisms at work during the 'critical period' that
determines whether a patient is going to have prolonged psychosis or not.
Shortly after this study, McGorry began working with Alison Yung on
elucidating the nature and clinical features of the prodromal phase (Yung et
al., 1996; Yung, Phillips, & McGorry, 2004; Yung & McGorry, 1996a, 1997).
The two would continue to work together on this problem for the next two
decades. Two key research questions concerned how to define the beginning
of illness (the onset of the prodromal phase), which requires an analysis of
the difference between 'abnormality' and 'normality,' and how to define the
point at which the prodrome ends and the “definitive disorder” begins (the
onset of frank psychosis) (Yung, Phillips, & McGorry, 2004, p. 12). They
defined eight categories of prodromal symptoms: neurotic symptoms (anger,
anxiety, irritability, restlessness); moodrelated symptoms (anhedonia,
depression, guilt, mood swings, suicidal ideation); volitional symptoms
(apathy, boredom, fatigue); cognitive symptoms (attentional/concentration
427
problems, daydreaming, neurocognitive deficits, preoccupations, reduced
abstraction, thoughtblocking); physical symptoms (appetite problems, sleep
disturbances, somatic complaints, weight loss); attenuated/subthreshold
psychotic symptoms (changes in affect, changes in motility, changes in sense
of self or others or the world, perceptual disturbances, suspiciousness); other
symptoms (dissociative phenomena, interpersonal sensitivity, obsessive
compulsive phenomena); and behavioral changes (aggressive or disruptive
behavior, deterioration in rolefunctioning, impulsivity, odd behavior, social
withdrawal) (Klosterkötter, Ebel, SchultzeLutter, & Steinmeyer, 1996, p.
149; Yung & McGorry, 1996a; Yung, Phillips, & McGorry, 2004, p. 21).
McGorry and his colleagues investigated an array of different
interventions, focusing predominantly on cognitivebehavior therapy (CBT),
omega3 fatty acid supplements (generally from fish oil), and, “in those who
fail to respond to initial intervention with gentler therapies,” pharmacological
therapy involving “broadspectrum antipsychotics with minimal side effects,
[which] ...may still have a place in delaying or preventing psychosis onset,”
especially risperidone (Larson, Walker, & Compton, 2010; McGorry et al.,
2009, p. 1210; Stafford, Jackson, MayoWilson, Morrison, & Kendall, 2013;
van der Gaag et al., 2012; Yung, Phillips, & McGorry, 2004). Other, less
commonly used interventions include glycine treatment (Woods et al., 2013),
family therapy (Bird et al., 2010), psychoeducation (Hauser & Juckel, 2012;
428
McFarlane, Lynch, & Melton, 2012), and skills training (Kecmanović, 2011;
F. Singh, DeJoseph, & Cadenhead, 2014). Some of these proposals are
obviously more controversial than others, and it is sometimes difficult to
determine what enters into the 'clinical judgment' used to decide which
intervention is most appropriate. Nevertheless, McGorry and his colleagues
did not use or endorse antipsychotic interventions unless they were
warranted by the presence of some specific symptom or complaint for which
antipsychotic medication would be indicated, keeping in mind also that
everyone included in any of their studies was helpseeking to begin with (T.
Jones, 2011; McGorry, 2011; McGorry et al., 2009).
Psychosis Risk Syndrome and DSM5
In 2009, the Psychotic Disorders Work Group recommended the
diagnosis of ‘psychosis risk syndrome’ for inclusion in DSM5. This set off a
firestorm of controversy. Before the disorder was proposed for inclusion, the
hypothetical diagnostic category was largely uncontroversial: Research still
needed to be done, but just about everyone who was concerned enough to
publish on the subject seemed to be in favor of the idea of early interventions,
simply because the overriding sentiment across various nosological
paradigms was that disability accumulates as psychotic disorders progress,
creating a ceiling on the quality of the eventual recovery. In other words, it is
generally conceded by virtually all controversy partners that in the
429
progression of psychotic disorders, the earlier one is treated, the better
chance they have a meaningful recovery, while, when a psychotic disorder
progresses long enough without treatment, they will reach a point where
recovery probably is impossible. The proposal to include psychosis risk
syndrome as an official diagnostic entity in DSM5, however, changed
everything, perhaps provoking more controversy than any other proposed
diagnosis. This is in spite of the fact that there is a consensus about the key
technical aspects of the controversy, i.e., how accurately we can predict future
psychosis and how effectively we can prevent psychosis through intervention.
Psychosis Risk Syndrome Formalized
As conceptualized by the Psychotic Disorders Work Group, psychosis
risk syndrome is “a condition with recent onset of modest, psychoticlike
symptoms and clinically relevant distress and disability” (American
Psychiatric Association, 2012c, para. 2). A patient so diagnosed is not frankly
psychotic: Though some psychotic symptoms may be present in milder form,
they would be recognized as such because the patient's capacity for reality
testing would be relatively intact (Paris, 2013b).
The official DSM5 diagnostic features of this “not officially recognized”
disorder lend themselves to two parallel readings due to inherently
ambiguous linguistic choices. On one hand, one could see the description of a
very disturbed individual whose connection with reality becomes increasingly
430
tenuous by the day; on the other hand, one could just as plausibly read the
description as the typical weirdness of “midtolate adolescence or early
adulthood,” the syndrome's usual age of onset. The patient, and/or his or her
family and friends, have noticed “changes in experiences and behaviors...
suggesting a change in mental state.” These changes can take a few forms.
Regardless of the specific symptoms experienced, the patient “maintains
reasonable insight into the psychoticlike experiences and generally
appreciates that altered perceptions are not real” (American Psychiatric
Association, 2013, pp. 784–786).
The first general category of psychoticlike symptoms that the patient
may have are “attenuated delusions,” which differ from true delusions (fixed
beliefs that are maintained in spite of overwhelming evidence to the contrary)
in that “reality testing and perspective can be elicited with nonconfirming
evidence.” For example, the patient may have a “propensity for viewing the
world as hostile and dangerous,” or might “[harbor] notions of being gifted,
influential, or special,” perhaps resulting in “unrealistic plans and
investments,” though the individual can be made to express skepticism about
these attenuated delusions with “persistent questioning.” Second, the patient
might have “attenuated hallucinations,” possibly seeing some phantom
movement or false shadow in his or her peripheral vision, or perhaps hearing
some faint murmuring or rumbling, which the patient regards as “unusual or
431
puzzling,” but which is not experienced with the full force of normal
perceptions and is not believed to be real (American Psychiatric Association,
2013, pp. 783–784).
The third psychoticlike symptom variant is an attenuated version of
the “disorganized communication” of psychosis. The 'disconnection from
reality' involved in this symptom differs from that in the first two, as they
constitute a disconnection from objective reality, while disorganized
communication constitutes a disconnection from intersubjective reality. In
acute schizophrenia, disorganized communication may manifest as catatonic
nonresponsiveness, or grossly illogical or incomprehensible speech that is
completely disconnected from attempts at conversation. For example,
Kraepelin (1917) described a patient who
when asked where he is, responds with “You want to know that too; I
tell you who is being measured and is measured and shall be
measured. I know all that, and could tell you, but I do not want to.”
When asked his name, he screams, “What is your name? What does he
shut? He shuts his eyes. What does he hear? He does not understand;
he understands not. How? Who? Where? When? …How can you be
so impudent? I'm coming! I'll show you! You don't turn whore for me...
How they attend, they do attend,” and so on. At the end he scolds in
quite inarticulate sounds... He speaks in an affected way, now babbling
432
like a child, now lisping and stammering, sings suddenly in the middle
of what he is saying, and grimaces.” (pp. 77–78)
In contrast, a patient suffering from the attenuated “psychosislike” variant
of this symptom might use speech that is “vague,” “metaphorical,” “muddled,”
“off track,” or “meandering;” although clearly understandable, in “severe”
cases “the individual fails to get to the point without external guidance” or
may have trouble coming up with the right word, “especially when the
individual is under pressure, but reorienting questions quickly return
structure and organization to the conversation.”
Psychosis Risk Syndrome as Representative Anecdote
For many critics, psychosis risk syndrome was an exemplar case of all
the excesses of DSM5. Expressing a level of vehemence fairly typical of the
polemics on either side of the controversy, Allen Frances sharply denounced
the proposal, even while acknowledging his interlocutors' good intentions:
1) The “risk syndrome” would misidentify many (somewhere between
39) kids for every one correctly identified; and 2) the treatment most
likely to be offered has no proven efficacy, but can have extremely
dangerous complications. This is clearly the prescription for an
iatrogenic public health disaster. The goal of early identification and
proactive treatment in psychiatry is laudable—but elusive and not
currently attainable. Prevention requires having a happy combination
433
of accurate identification and effective and safe treatment. Instead, we
now have the opposite dangerous combination: wildly inaccurate
identification with a likely ineffective but definitely risky treatment.
(Frances, 2010c, para. 9–10; my emphasis)
I contend that the firestorm surrounding this proposed disorder was due in
part to the wide range of contested issues that are entangled in the debate
about its risks and benefits. I conceptualize the disorder as a Burkean
representative anecdote, a case exemplifying a terministic screen in which a
special vocabulary is united with a motivational calculus “supple and
complex enough to be representative of the subject matter it is designed to
calculate. It must have scope. Yet it must also possess simplicity, in that it
is broadly a reduction of the subject matter” (Burke, 1969a, p. 60). Psychosis
risk syndrome entails all or nearly all of the concepts and assumptions
involved in the dominant view of psychosis in contemporary psychiatry, the
approach to risk management in preventive psychiatry, and as can be seen in
McGorry's corpus, the latent conflicts and unresolved ambiguities embedded
in the epistemic compromise on which DSM rests.
Terministic Screen, Interpellation, and Stigma
The terministic screen metaphor is visual in nature, referring to
optical filters that can be applied to photographs. Such filters make it
possible to modify images so that they represent reality as conceived by the
434
photographer. Filters accomplish this by selecting some aspects of the
captured image (e.g., color balance, contrast, etc.) to be featured and other
aspects are excluded:
I have particularly in mind some photographs I once saw. They were
different photographs of the same objects, the difference being that
they were made with different color filters. Here something so
“factual” as a photograph revealed notable distinctions in texture, and
even in form, depending upon which color filter was used for the
documentary description of the event being recorded. (Burke, 1969a, p.
45, emphasis in the original)
Following Burke's metaphor, the relevant 'photographs' of adolescents being
evaluated for psychosis risk syndrome come in the form of case reports in
which biographical narratives are organized into 'symptoms' of the syndrome,
each of which is reduced to a numerical score representing the degree to
which the psychotic symptom is attenuated. Each symptom is conceived as a
continuous quantifiable continuum from 'normal' to 'psychotic' (the actual
scales used vary by clinic). Any quirky or unusual characteristic of the
'patient' is thus seen only as an attenuated expression of psychosis. If a
teenager views herself as especially creative or gifted, a psychiatrist looking
through the lens of attenuated psychosis sees very mild grandiosity (a subset
of delusional thoughts; a psychotic patient with delusions of grandeur, for
435
example, might selfidentify as Jesus). Hence, the process of revealing a risk
factor involves the corresponding concealing of nonmedicalized
interpretations of the 'patient's' personality traits, beliefs, and subjective
experiences.
A diagnosis of psychosis risk is not simply a passive label that only
functions to indicate a clinical judgment about the probability that a
particular pathological course will present in the patient so diagnosed.
Following Althusser (1994), I contend that the act of psychiatric diagnosis is
a “ritual of ideological recognition…[that] hails or interpellates concrete
individuals as concrete subjects” (p. 130). Correspondingly, the DSM
functions as an ‘ideological state apparatus,’ a relatively autonomous
superstructural edifice that controls and regulates the working knowledge
necessary to navigate the concrete and material network of mental health
institutions. A diagnosis designates the subject identity that constitutes a
patient’s selfrepresentation for all social relationships and connected
practices within this network. By accepting a diagnosis, patients produce
imaginary accounts of their relationship to the real world, and the image of
those accounts makes up the currently dominant biopolitical ideology.
This has long been the case, and it certainly is not limited to the
domain of mental health. Furthermore, it is not necessarily a negative trend
in world history. As we will see in Chapter 4, a reified diagnosis can be
436
alienating while simultaneously serving as a basis for solidarity formation.
Furthermore, most individuals who will receive a DSM5 diagnosis at some
point are suffering, and the diagnosis opens new opportunities for relief.
Nevertheless, the diagnosis of a risk syndrome extends the totalizing reach of
this ideological formation, for good or ill. There is a nonzero probability that
any given person is in the early, presymptomatic phase of some mental
illness. This is all the truer given the trend toward viewing the symptoms of
mental illness as falling on a relatively smooth continuum between normalcy
and insanity.
For Althusser, the act of interpellation by its very nature is never
recognized by the individual as a process of transformation by which they
receive their subject position. Instead, individuals misrecognize the event as
a confirmation of their “alwaysalready” status as subjects (Althusser, 1994,
p. 130). Upon receiving the initial diagnosis, the patient did not just become
‘depressed’ or ‘bipolar’ in her mind; that’s how she’s always been, and now she
has a name for it, a way to make sense of it and to relate to others. This new
identity and set of terms with which one can finally put into words the
heretofore ineffable psychic distress that led to the diagnosis are the
discursive mechanisms by which the misrecognition of interpellation occurs.
From the “evidentness of the subject” proceeds the “evidentness of meaning,”
which is further confirmed by the institutional checking of identity that
437
occurs every time the patientsubject fills a prescription, makes an
appointment, or makes a health insurance claim (Pêcheux, 2012, p. 147,
emphasis in the original). The diagnosis of psychosis risk syndrome, then,
has the potential to transform the selfconcepts of patients according to
autobiographical narratives governed by the terministic screen of attenuated
psychosis.
Risks of Psychosis Risk Syndrome
The magnitude of the potential impacts on either side of the
controversy is high. All parties involved concede that all courses of action
will both help and harm, though they disagree on the ratios. These
differences are not quantitative, but qualitative. On one hand, with a three
year ‘false positive’ rate of 68%, treatment options that include the atypical
antipsychotic drugs aripiprazole (Abilify), olanzapine (Zyprexa), and
risperidone (Risperdal), and children as the target population, the diagnosis
is depicted as a recipe for drugging all the children not already on
psychostimulants for ADHD with major tranquilizers, with the full
knowledge that the vast majority of children treated would not have become
psychotic if left untreated. On the other hand, given that a diagnosis of
schizophrenia very often means a life of partial or full disability, early
interventions have been shown to be very effective in preventing psychosis,
and no patient can (currently) receive the diagnosis without first being help
438
seeking, critics of the diagnosis are depicted as paranoid, vaguely Szaszian
opponents of medical progress. Both sides concede that there is a great deal
of uncertainty about how the diagnosis would be deployed by nonspecialist
clinicians and research departments of pharmaceutical corporations. Which
risk is the biggest?
False Positives and the Rhetorical Ontology of Risk
The issue of socalled false positives has been at the forefront of the
controversy. The predictive validity of the selection criteria for diagnosing an
ARMS or a psychosis prodrome has been one of the chief concerns of early
intervention researchers (Cannon, Cornblatt, & McGorry, 2007; Yung, Fusar
Poli, & Nelson, 2012; Yung, Nelson, Thompson, & Wood, 2010; Yung, Phillips,
& McGorry, 2004). A fairly consistent finding that, with the best criteria that
have been developed, about onethird of those identified will transition to
frank psychosis within two years, although one longitudinal study
determined that after eight years more than 50% of the identified individuals
had received a psychotic disorder diagnosis (Chuma & Mahadun, 2011;
Frances, 2010c; Kecmanović, 2011; Thompson, Nelson, & Yung, 2011; Yung &
Nelson, 2011; Yung, Phillips, & McGorry, 2004). Yung and McGorry also
conceded that “the onset of psychosis is arbitrarily defined and does not differ
qualitatively from subthreshold psychosis,” raising a fundamental epistemic
problem (Yung & McGorry, 2007, p. s1). Indeed, Parnas (2005) suggests that
439
this is “not only a psychometric problem, but a theoretical issue intimately
associated with the conceptual validity of schizophrenia, that is what we take
schizophrenia to be in the first place” (p. s112).
It gets worse. It turns out that as time went on, the 'false positive' rate
of every clinic seemed to get worse, as they became more wellknown and
were referred more marginal cases (Yung et al., 2003). This points to the fact
that these clinics are all highly specialized and run by psychiatrists whose
careers have been devoted to psychosis risk. We know what happens when
those psychiatrists try to predict psychosis. What would happen if regular
psychiatrists, or worse, primary care physicians, were to try to apply the
same criteria? This gets at a basic distinction between risk and uncertainty.
For contemporary theorists, risk entails the quantification of probabilities,
while with uncertainty, “We know that we do not know, but that is almost all
that we know” (Callon et al., 2009, p. 21). Yet amidst the uncertainty, there
is calculation. If there is a problem in specialized clinics, then, a fortiori,
regular psychiatrists and general practitioners should be even less accurate
(bracketing off the question of what the pharmaceutical industry will do to
change the way the category is put into practice). Even the most ardent
proponents of early interventions concede that the risk is substantial
(McGorry, 2011). Frances suggests that “the false positive rate would jump...
to about 90 percent in general practice. This means that as many as an
440
astounding nine in ten individuals identified as 'risk syndrome' would not
really be at risk for developing psychosis” (Frances, 2010c, para. 4). This
would expose a potentially large population to risks that “include
unnecessary fear of illness, restriction of life goals, use of medication and
their sideeffects” (Warner, 2005, p. s104).
But whether an individual case of nontransition to frank psychosis
within a set time period should be regarded as a 'false positive' depends on
the rhetorical ontology of the 'at risk state.' The issue rests on what Prelli
calls an 'interpretivedefinitional' stasis point – that is, “What does construct
y mean?” (Prelli, 1989, p. 146). One frequent topic of discussion at the UCLA
conference over thirty years ago was this metaphysical question: what exactly
is meant when an individual is said to be 'at risk' or 'at high risk' of
developing a psychotic disorder? I contend that there are essentially three
basic interpretations of psychosis risk, and an additional interpretation that
is a permutation of two: (1) a confluence of risk factors that are neither
necessary nor sufficient for psychosis but increase the probability that an
individual will later meet the diagnostic criteria for a psychotic disorder; (2)
vulnerability, a trait that makes an individual particularly susceptible to
developing a psychotic disorder; (3) a prodrome or prodromal phase that
precedes psychosis in those destined (barring an intervention of some sort) to
become psychotic; and (4) a combination of the prodrome and risk factors

441
interpretations, which treats the phenomenology of the prodrome as a state
risk factor (an 'at risk mental state') for developing a psychotic disorder in the
future (Table 1).
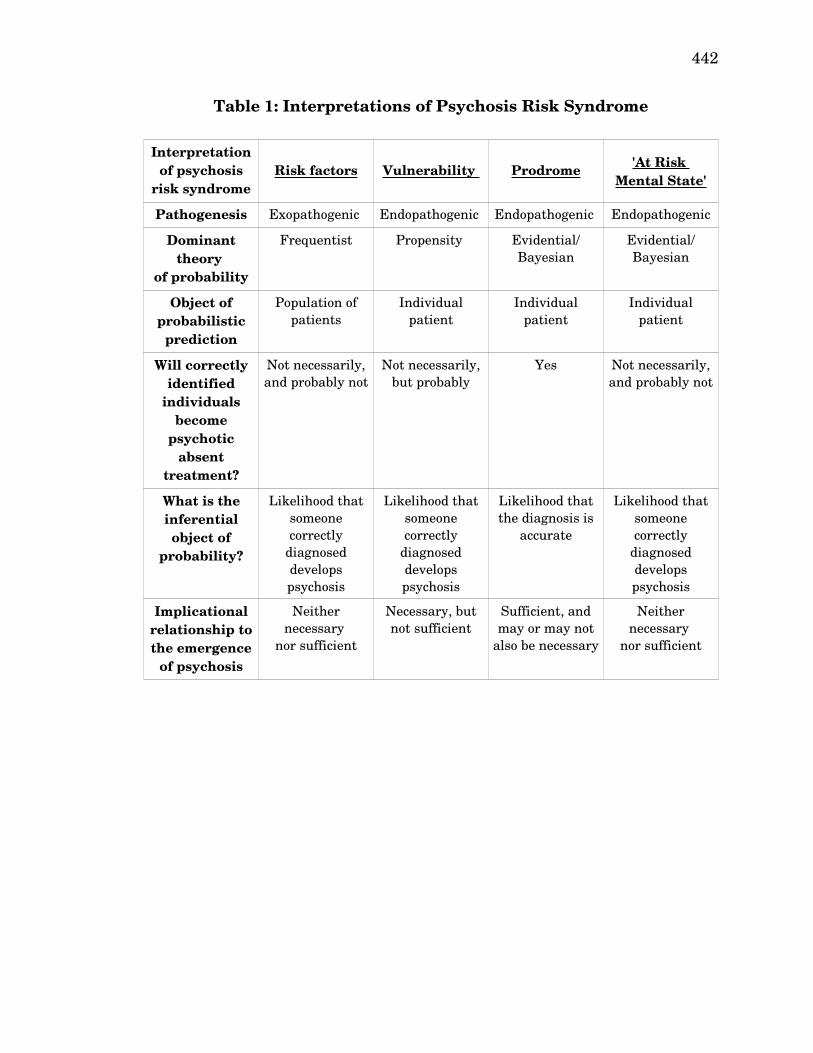
442
Table 1: Interpretations of Psychosis Risk Syndrome
Interpretation of psychosis
risk syndromeRisk factors Vulnerability Prodrome
'At Risk Mental State'
Pathogenesis Exopathogenic Endopathogenic Endopathogenic Endopathogenic
Dominant theory
of probability
Frequentist Propensity Evidential/Bayesian
Evidential/Bayesian
Object of probabilistic
prediction
Population of patients
Individual patient
Individual patient
Individual patient
Will correctly identified
individuals become
psychotic absent
treatment?
Not necessarily, and probably not
Not necessarily, but probably
Yes Not necessarily, and probably not
What is the inferential object of
probability?
Likelihood that someone correctly
diagnosed develops psychosis
Likelihood that someone correctly
diagnosed develops psychosis
Likelihood that the diagnosis is
accurate
Likelihood that someone correctly
diagnosed develops psychosis
Implicational relationship to the emergence
of psychosis
Neither necessary
nor sufficient
Necessary, but not sufficient
Sufficient, and may or may not
also be necessary
Neither necessary
nor sufficient
443
I shall provide examples of each of these interpretations, discuss their
presence in the recent debate surrounding DSM5, and explain why the
failure of the majority of interlocutors to carefully define their terms or
acknowledge the existence of alternative interpretations made much of their
debate incoherent.
(1) Risk Factors Interpretation
Arnold Friedhoff introduces the issue and explains its importance,
mentioning as popular an interpretation grounded in frequentist probability:
Before addressing the issues of risk measurement and modification, it
is necessary to have a precise understanding of the word, “risk.”
“Highrisk group” generally is taken to mean a group in which some
members will eventually develop the condition in question, while
others will not. Thus, preventive intervention or risk modification
carried out with members of a highrisk group will invariably be
applied to some individuals who would not have developed the
condition in the first place, inasmuch as those actually at risk may not
be distinguishable from those potentially at risk until sometime after
the preventive intervention has been carried out. (Friedhoff, 1981, p.
39)
As basic and as reasonable as this seems, such a discussion is remarkably
underdiscussed in the current debate, even when the meaning left
444
ambiguous directly bares on the arguments being made, as I will show
shortly.
Certainly, if one's definition of an atrisk state implies that pathology
is already present, then primary prevention is no longer possible, and efforts
directed toward the identified population are in fact “secondary prevention,”
i.e., preventing already present but unrecognized pathology from becoming
worse, or “tertiary prevention,” to slow down the progress of a disease that
has already very clearly initiated (Fish, 1981, p. 226). Holzman argues that
the “risk factors” interpretation
refers to statistical probabilities that some groups of people will become
affected by a particular disorder. Thus, being a child of a schizophrenic
parent puts that child in a group with a larger statistical risk than the
general population runs, although that child may not be at all
vulnerable because he or she may not have the specific—but as yet
unknown—structural underpinning that predisposes to schizophrenia.
Risk factors are neither necessary nor sufficient conditions for the
occurrence of a disease... They... are not intrinsically characteristic of
the person at risk. (Holzman, 1981, p. 20, my emphasis)
An example of a risk factor, which Holzman calls “exopathogenic,” is cigarette
smoking, which dramatically increases the risk that one will develop lung
cancer (p. 20).
445
With this interpretation, one can make a diagnosis while remaining
fairly agnostic about the actual mechanisms involved. As that follows the
general ideology of DSMIII, it could be taken as a default position in the post
DSMIII era, though it is not used consistently or unambiguously by the vast
majority of participants in the controversy. Further, this interpretation is
grounded in a frequentist theory of probability, according to which the
probability of an event is conceived of as the likely frequency of that event's
occurrence were the situation repeated an arbitrarily large number of times.
This is wellsuited to describe the probability of events that are specific to
individuals in a population, because each individual within the population
provides a unique trial, and the overall frequency of the event in the
population can be measured directly (Venn, 1888). If nrf is the total number
of people in a population defined by a set of risk factors, and npd is the
number of those individuals that developed a psychotic disorder within a
given time limit (two years is usually used), then the probability P(pd) of an
individual with the specified risk factors will develop a psychotic disorder can
be approximated according to this equation:
P ( pd )=n pdnrf
Frequentist inferences are only approximations in the short run or for single
individuals, but provided that one is interested in populations rather than
446
individual subjects, one can take a direct measurement. Since the risk factor
interpretation gives approximate estimates for individuals, an individual who
is diagnosed as having a relevant risk factor who does not end up with a
psychotic disorder is not a 'false positive' unless the criteria were incorrectly
measured.
(2) Vulnerability Interpretation
Friedhoff suggested a second interpretation, one he embraced in his
research, that more clearly embraces the notion of susceptibility:
Another way in which the notion of biological risk is often used is that
an individual carries a marker that is associated with vulnerability to
a condition or with the condition itself. The implication is that a
person so affected will get the disorder associated with the marker or is
more vulnerable to that disorder. (Friedhoff, 1981, p. 40)
This vulnerability interpretation was also distinguished from the risk factors
interpretation by Holzman, who stressed the troubles that can arise from
carelessnessdriven ambiguity, especially “when the disease processes
involved are poorly understood,” while articulating the meaning of
'vulnerability' more precisely:
[The] terms “vulnerability” and “risk factors” ...are not synonymous,
and using them interchangeably can lead to confusion among
conceptual and empirical issues. Vulnerability refers to a perceivable,
447
palpable, or measurable variation in structure or function that
represents a predisposition to a specific disease process... All of these
[vulnerability] traits are identifiable prior to the onset of the disease
and place the person possessing such traits in a position of being
susceptible to the specific disorders, given certain known or as yet
unknown environmental conditions. These traits, moreover, are not
intrinsically the disease. They represent a necessary but not sufficient
condition for the disease to develop. (Holzman, 1981, pp. 19–20, my
emphasis)
An example of a vulnerability trait, which Holzman calls “endopathogenic,” is
a genetic mutation that prevents an individual from being able to
manufacture the enzyme phenylalanine hydroxylase (PAH), which would
make one vulnerable to phenylketonuria (PKU). One (humoral)
endopathogen that Holzman believes might be relevant to psychosis, studied
by Freud (1937) and Pavlov (1927), is temperament.
Holzman is explicit that vulnerability is distinct from the disease itself.
This is not mere metaphysical posturing – in the example of genetic
susceptibility to PKU, the process by which one is susceptible and the process
by which the disease itself proceeds are arguably distinguishable if not
clearly distinct. Classical PKU is caused by a mutation in a gene located on
the twelfth chromosome that is responsible for the enzyme PAH (Filiano,
448
2006). The enzyme PAH converts an amino acid called phenylalanine into
another amino acid called tyrosine, which is necessary for the synthesis of
certain neurotransmitters called catecholamines (dopamine, norepinephrine,
and epinephrine). A small amount of the phenylalanine will be metabolized
through alternate pathways, but all the unconverted phenylalanine will
compete with other large neutral amino acids for transport across the blood
brain barrier (Pietz et al., 1999). The combination of insufficient tyrosine and
excess phenylalanine in the brain contribute to frontal lobe dysfunction,
which can produce severe intellectual impairments (Janke & KleinTasman,
2012; Michals & Matalon, 1985).
The question is whether the essence of the disease entity PKU is the
genetic mutation or is the processes by which intellectual impairments occur
that are caused by the genetic mutation. If the genetic mutation is identified
in a newborn, a combination of diet and medication will allow for normal
brain development; in untreated adults, the damage is beyond repair
(MacLeod & Ney, 2010). Is that intervention a way of preventing the disease
in someone who is vulnerable, or is it a way of treating the disease in
someone who is afflicted by it? This is not a question that is answerable by
science. Rather, it is an artifact of the human communication processes that
are enlisted to produce a nosological terministic screen.
The vulnerability interpretation dominated the discussion at the
449
UCLA conference on preventive intervention in schizophrenia, but has
essentially disappeared from the discussion, except insofar as individual risk
factors or hypothetical prodromal mechanisms are elaborated in terms of
susceptibility—but the etiological nihilism of DSMIII has led to a repression
of this mode of argumentative reasoning.
(3) Prodrome or Prodromal Phase Interpretation
If one is inclined to view the genetic mutation as an integral
component of the disease entity, then its detection in asymptomatic newborns
allows for an early diagnosis, and barring that, early developmental
problems, along with seizures, certain skin problems, and other symptoms
could be thought of as a prodromal phase of PKU.
This is the language that is used by many who are involved in the
psychosis risk controversy and who understand the diagnosis to apply to
patients in the earliest stage of schizophrenia or a related psychotic disorder,
called the ‘prodromal phase’ or ‘prodrome,’ from the Greek pródromos
( μ ), meaning ‘forerunner’ πρόδρο ος (Fava, Grandi, Canestrari, & Molnar,
1990; Fava & Kellner, 1991; Jackson, Cavanagh, & Scott, 2003; Yung &
McGorry, 1996b). The word prodrome is used in migraine sufferers to
describe the constellation of signs and symptoms—mood changes; irritability;
thirst; yawning; an 'aura' of flickering light, or hallucinations, or partial
vision loss—that precede the onset of a migraine headache (Kelman, 2004).
450
Like John the Baptist, whom Christians call the Prodromos ( μ ), Πρόδρο ος
the migraine prodrome in a sense testifies concerning the headache, that
through these symptoms, the migraineur might believe he or she is about to
suffer a migraine; the prodrome itself is not the headache, but comes as a
witness to the headache which is to follow.125 Prodromal symptoms are
described as “premonitory,” which is to say that they are like an oracle that
gives a warning in advance of some set of events which are fated to occur
(Kelman, 2004, p. 865).
If the cause of schizophrenia was something like a mutation to a
specific known gene (as with PKU), this might not make much of a difference.
The etiology of psychotic disorders is unfortunately still unknown, and while
some aspects of its pathophysiology are understood (some sort of excess of
dopamine and/or deficiency in glutamate, as discussed in Chapter 2), even
those are debated. Most people agree that there are usually some early signs
and symptoms that precede the onset of frank psychosis, but those signs and
symptoms are notably nonspecific and heterogeneous – the same symptoms
precede lots of other mental disorders or sometimes no disorder at all. Kline
indicated that “hysterical and and neurasthenic symptoms are the
commonest precursors, but we cannot assume that the 'neurasthenia'
developed into schizophrenia, but rather that in the beginning stages of
125 John 1:78. It is also worth noting that the eleventh century monk Psellos ('the stammerer') called rhetoric the pródromos of philosophical conversion (Kaldellis, 1999).
451
schizophrenia, neurasthenic symptoms dominated the picture” (Kline, 1966,
p. 28). In this we can see an intentional commitment to the prodromal
interpretation rather than the vulnerability or risk factor interpretation.
There are two implications of the prodrome interpretation. First, the
individual is symptomatic during the prodromal phase, which is possible but
not necessarily true of the vulnerability interpretation (if, for example, the
vulnerability factor was a specific gene that infants could be screened for);
second, the individual “will develop a fullblown illness following the
prodrome” (Yung, Phillips, & McGorry, 2004, p. 6). This rests on an
evidential (or Bayesian) theory of probability, according to which
probabilities reflect the degree of certainty one has that a given outcome will
occur based on the state of the evidence (Erickson & Smith, 1988). That is
because any probability measurement is an estimation of how confident the
diagnostician is that the symptoms he or she is observing in a given patient
are in fact manifestations of a prodrome. Individuals diagnosed as prodromal
who do not develop a psychotic disorder are 'false positives,' and we can say
the diagnosis was objectively incorrect.
(4) 'At Risk Mental State' (ARMS) Interpretation
For this reason, it is only possible to diagnosis a prodrome
retrospectively. This fact was emphasized by Yung, Phillips, and McGorry
(2004), who argue:
452
This issue is more than just semantics. The danger of labelling a
syndrome prospectively as a schizophrenia 'prodrome' (or of labelling
an individual crosssectionally as 'prodromal') tends to reify the
syndrome as a disorder or disease, with its own natural history and
prognosis (eventual transition to frank psychosis). Instead, the
syndrome, which seems like, or could be, a prodrome should be thought
of, not as a disease entity, but as a state risk factor for fullblown
psychosis. That is, the presence of the syndrome implies that the
affected person is at that time more likely to develop psychosis in the
near future than someone without the syndrome. However, if the
symptoms resolve then the danger of increased risk remits as well. In
an attempt to deal with these issues we have coined a new term, the 'at
risk mental state.' (Yung, Phillips, & McGorry, 2004, p. 25)
This approach is not limited to retrogressive analysis, which can tell you a lot
about the people who eventually developed frank psychosis, but nothing
about the people who seemed identical to the first group except that the
never developed frank psychosis. Instead, this interpretation suggests that
researchers should examine 'enriched samples' via a 'closein strategy' that
include people who are positive for multiple distinct risk factors (Bell, 1992;
Häfner et al., 1994; Poulton et al., 2000). Sometimes individuals so identified
are considered to be at 'ultra high risk' (UHR) (Yung et al., 2012, 2010; Yung,
453
Phillips, Yuen, & McGorry, 2004). This permuted interpretation was the one
adopted by those conducting research on early interventions in psychosis risk
over the last two decades, though their interlocutors at various points adopt
different interpretations or no clear interpretation.
Several ideas of risk are combined in this interpretation. To be 'at' risk
implies that risk is a location that one can occupy. That it is conferred on
individuals implies that risk is a status, as it is often explicitly described. It
is also common to see risk in this context described as a possession, i.e., that
someone has increased risk. It is also common to see risk treated as an
attribute or quality, i.e., that someone is a 'high risk patient.' This all
suggests that risk is a term that can operate on multiple discursive
modalities at once. This flexibility can sometimes be a weakness in that it
increases the discursive space for misunderstanding and miscommunication.
Stephan Heckers (2009) suggests that the prodrome interpretation,
which he links with Bleuler's concept of latent schizophrenia, and the risk
factors interpretation are not actually compatible:
The period of subthreshold psychosis before the first episode of a
psychotic disorder is often referred to as the prodrome. The prodrome
is, by definition, the nascent stage of a disorder (hence the term latent
schizophrenia). In contrast, a risk syndrome is not necessarily linked
to a disorder. The value of a risk syndrome increases with the
454
accuracy in predicting future outcomes (e.g., metabolic syndrome
leading to diabetes or cardiovascular disease; mild cognitive
impairment leading to dementia), but the conversion to disease is, by
definition, less than 100%. In short, a prodrome is part and parcel of
the disorder, [while] a risk syndrome is not. (Heckers, 2009, p. 849)
Because of the ambiguity involved in combining two basic interpretations,
and because debates often center around core issues like false positives (or
'false false positives,' in which “a true vulnerability exists though it has not
yet been fully expressed”) and specific statistical measures, this permuted
interpretation tends to promote muddled debates with essential concepts
poorly defined or never even considered (Yung, Phillips, & McGorry, 2004, p.
30). If the disorder is a risk syndrome, then the rate of transition to frank
psychosis really has nothing to do with the 'false positive' rate, but if the
disorder is a prodrome, it has everything to do with it.
Brief Excursus on Melancholia
Further muddling the issue is that the risk factors interpretation and
the prodrome interpretation are individually grounded in distinct nosological
assumptions, one reflecting the paradigm of DSMIII and DSMIV while the
other reflecting some of the ideas behind DSM5, which is another reason
why this diagnostic controversy is synecdochic for the larger set of
controversies surrounding DSM5. As I discussed in the Chapter 1, DSMIII
455
came with a revolution of etiological nihilism designed to desanctify the
psychodynamic theories of the past. The unstated goal of course was not to
remain agnostic with respect to the underlying disease processes, but to move
toward a biological model. DSM5 was supposed to do that, although it
largely did not abandon the etiological nihilism of the previous two editions.
One example that illustrates the problem is 'melancholia.'
In 2010, a list of seventeen eminent mental health professionals,
including Robert Spitzer (DSMIII chair), Max Fink, David Healy, Edward
Shorter, Gordon Parker, and Michael Taylor – a collection that includes
psychiatrists, psychoanalysts, psychopharmacologists, historians, and critics
of the pharmaceutical industry – wrote an article in the American Journal of
Psychiatry advancing the case for DSM5 to include an independent diagnosis
of melancholia,
a syndrome with a long history and distinctly specific
psychopathological features... [which] possesses a distinctive biological
homogeneity in clinical experience and laboratory test markers, and...
is differentially responsive to specific treatment interventions. It
therefore deserves recognition as a separate identifiable mood disorder.
(Parker et al., 2010, p. 745)
The advocates of melancholia combined diagnostic data, treatment data, and
historical analysis to make an extremely convincing case that melancholia is
456
an entirely distinct form of depression, and that there are in fact “two
separate depressions” (Shorter, 2007, p. 5).
This is exactly the kind of diagnosis that fit the DSM5 ideology. As
Greenberg observed:
Distinctive signs, symptoms, lab studies, course, and outcome—if
melancholia wasn’t the Holy Grail, it was at least a sip from the
chalice of science, one disorder that could go beyond appearances. You
would think that the committee would at least have been eager to
consider it as a partial remedy for ongoing concerns about the
profession’s lack of scientific rigor. (Greenberg, 2013b, para. 8)
Melancholia is a specific subtype of depression that can be identified with
biological tests – it measurably disrupts the sleep architecture of the patient
and causes hypercortisolism (i.e., excessive blood levels of cortisol), which can
be identified with a dexamethasone suppression test (DST). All of this
testing has a purpose, because unlike other variants of depression, it
responds best to the older, seldom prescribed tricyclic antidepressants as well
as electroconvulsive therapy (ECT) (Parker et al., 2010).
These apparent strengths were actually weaknesses, as William
Coryell, one of the members of the DSM5 Mood Disorders Work Group,
wrote in a private correspondence to Max Fink: “I agree there is more data to
support using DST for melancholia than for using any other measure for any
457
other diagnosis,” but it would be “very hard to sell since it would be... the only
biological test for any diagnosis being considered” (cited in Greenberg, 2013a,
p. 337). The diagnosis did not even make it into the draft proposals, which is
to say that it was not even considered. Greenberg argues that the reason is
clear:
[A] test for melancholia would make the lack of biological measures
elsewhere in the DSM that much more glaring. It was a success that
would only highlight the APA's failures... Offered a key to one of the
cells of its epistemic prison, the APA had decided that the cost of
freedom was too high. (pp. 337338)
As one blogger and professional scientist commented about the affair:
“Psychiatry finally encounters science—and rejects it” (Couch, 2013, para. 1).
What does this have to do with psychosis risk syndrome? It provides a
glimpse of a scientific field caught in between two paradigms, grasping hold
of each with one hand and falling through the middle. The confused
interpretation of psychosis risk syndrome as both a risk syndrome and a
prodrome is symptomatic of this problem – on the one hand, committed to
etiological nihilism, on the other hand reaching for biological etiology,
pathogenesis, tests, and treatments. And the failure of most of the most
vocal participants in the controversy to even bother to clarify the
interpretation of psychosis risk as they saw it is betrays an argument
458
community in chaos.
Changes in the DSM5 Draft Revisions
In August of 2010, following the first round of public comments on the
manuscript, the work group renamed the proposed diagnosis ‘attenuated
psychotic symptoms syndrome,’ and in April of 2012, following the second
round of public comments, the work group again renamed the proposed
diagnosis ‘attenuated psychosis syndrome’ and recommended it be included
in Section III of DSM5 along with other “conditions that require further
research” (American Psychiatric Association, 2012a). The final version of the
proposed criteria set for the condition of attenuated psychosis syndrome,
which appears in Table 3 (Table 2 shows the changes between each draft that
appeared on dsm5.org), is a mildly revised form of the April 2012 draft
(American Psychiatric Association, 2013, pp. 783–786).
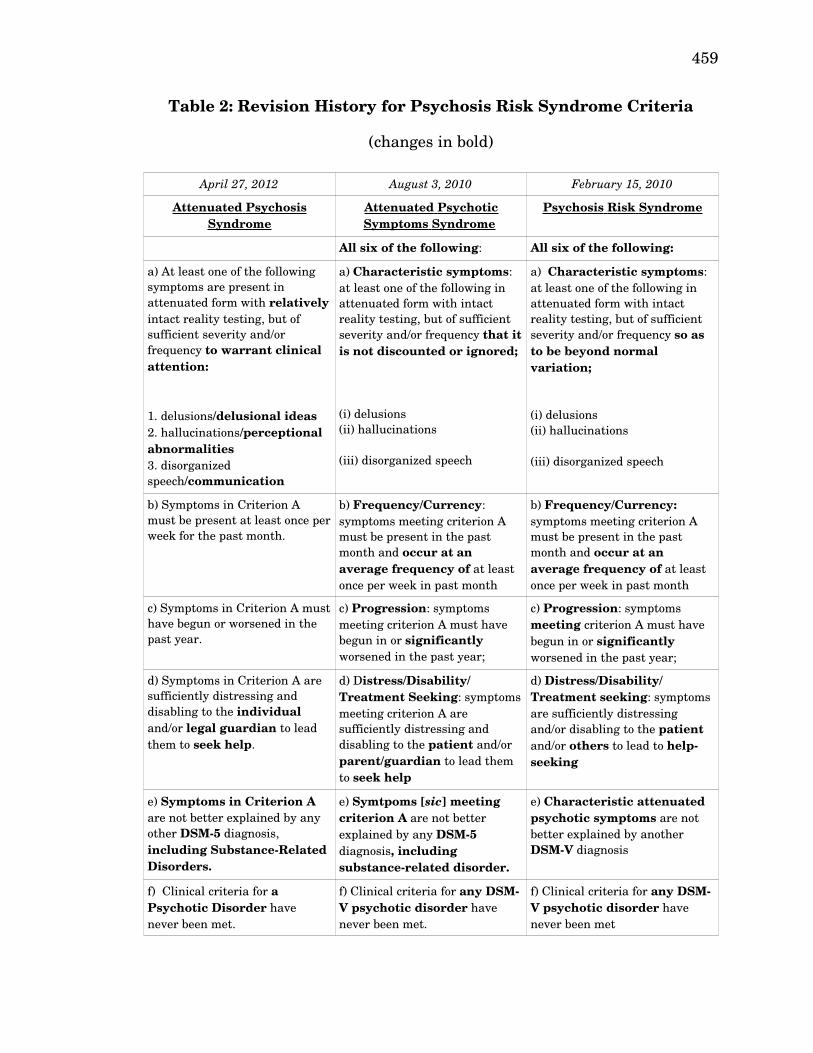
459
Table 2: Revision History for Psychosis Risk Syndrome Criteria
(changes in bold)
April 27, 2012 August 3, 2010 February 15, 2010
Attenuated Psychosis Syndrome
Attenuated Psychotic Symptoms Syndrome
Psychosis Risk Syndrome
All six of the following: All six of the following:
a) At least one of the following symptoms are present in attenuated form with relatively intact reality testing, but of sufficient severity and/or frequency to warrant clinical attention:
1. delusions/delusional ideas2. hallucinations/perceptional abnormalities3. disorganized speech/communication
a) Characteristic symptoms: at least one of the following in attenuated form with intact reality testing, but of sufficient severity and/or frequency that it is not discounted or ignored;
(i) delusions(ii) hallucinations
(iii) disorganized speech
a) Characteristic symptoms: at least one of the following in attenuated form with intact reality testing, but of sufficient severity and/or frequency so as to be beyond normal variation;
(i) delusions(ii) hallucinations
(iii) disorganized speech
b) Symptoms in Criterion A must be present at least once per week for the past month.
b) Frequency/Currency: symptoms meeting criterion A must be present in the past month and occur at an average frequency of at least once per week in past month
b) Frequency/Currency: symptoms meeting criterion A must be present in the past month and occur at an average frequency of at least once per week in past month
c) Symptoms in Criterion A must have begun or worsened in the past year.
c) Progression: symptoms meeting criterion A must have begun in or significantly worsened in the past year;
c) Progression: symptoms meeting criterion A must have begun in or significantly worsened in the past year;
d) Symptoms in Criterion A are sufficiently distressing and disabling to the individual and/or legal guardian to lead them to seek help.
d) Distress/Disability/ Treatment Seeking: symptoms meeting criterion A are sufficiently distressing and disabling to the patient and/or parent/guardian to lead them to seek help
d) Distress/Disability/ Treatment seeking: symptoms are sufficiently distressing and/or disabling to the patient and/or others to lead to helpseeking
e) Symptoms in Criterion A are not better explained by any other DSM5 diagnosis, including SubstanceRelated Disorders.
e) Symtpoms [sic] meeting criterion A are not better explained by any DSM5 diagnosis, including substancerelated disorder.
e) Characteristic attenuated psychotic symptoms are not better explained by another DSMV diagnosis
f) Clinical criteria for a Psychotic Disorder have never been met.
f) Clinical criteria for any DSMV psychotic disorder have never been met.
f) Clinical criteria for any DSMV psychotic disorder have never been met
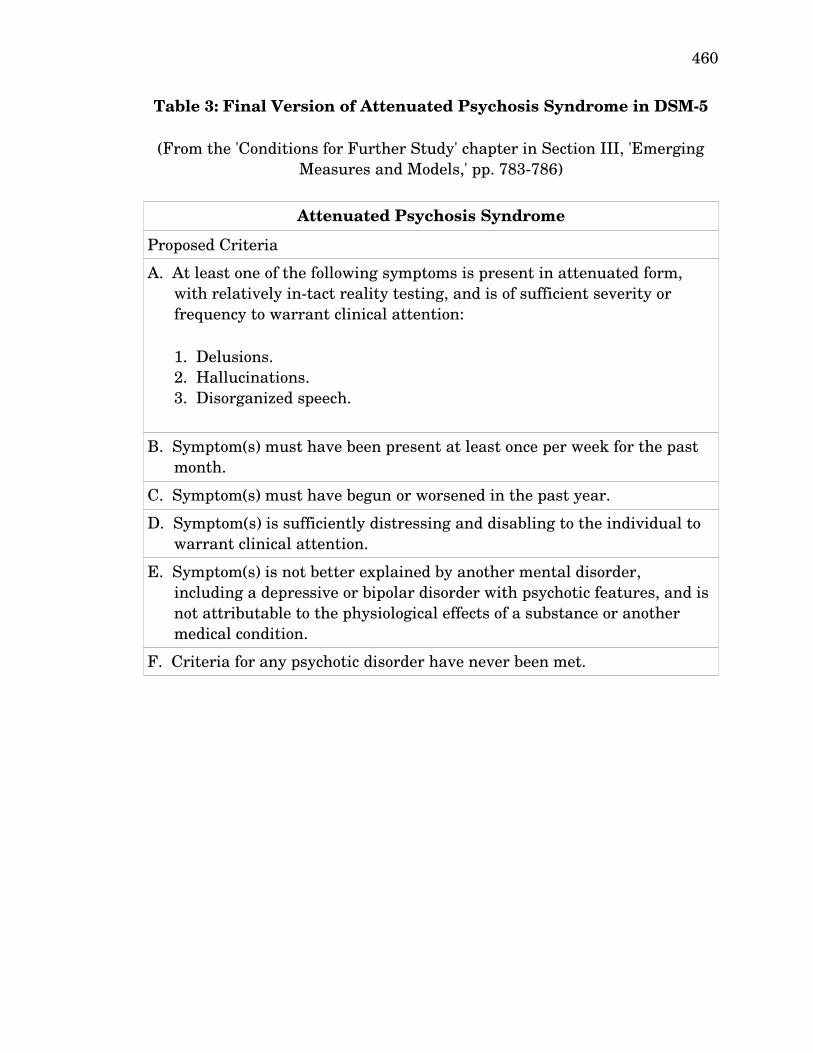
460
Table 3: Final Version of Attenuated Psychosis Syndrome in DSM5
(From the 'Conditions for Further Study' chapter in Section III, 'Emerging Measures and Models,' pp. 783786)
Attenuated Psychosis Syndrome
Proposed Criteria
A. At least one of the following symptoms is present in attenuated form, with relatively intact reality testing, and is of sufficient severity or frequency to warrant clinical attention:
1. Delusions. 2. Hallucinations. 3. Disorganized speech.
B. Symptom(s) must have been present at least once per week for the past month.
C. Symptom(s) must have begun or worsened in the past year.
D. Symptom(s) is sufficiently distressing and disabling to the individual to warrant clinical attention.
E. Symptom(s) is not better explained by another mental disorder, including a depressive or bipolar disorder with psychotic features, and is not attributable to the physiological effects of a substance or another medical condition.
F. Criteria for any psychotic disorder have never been met.
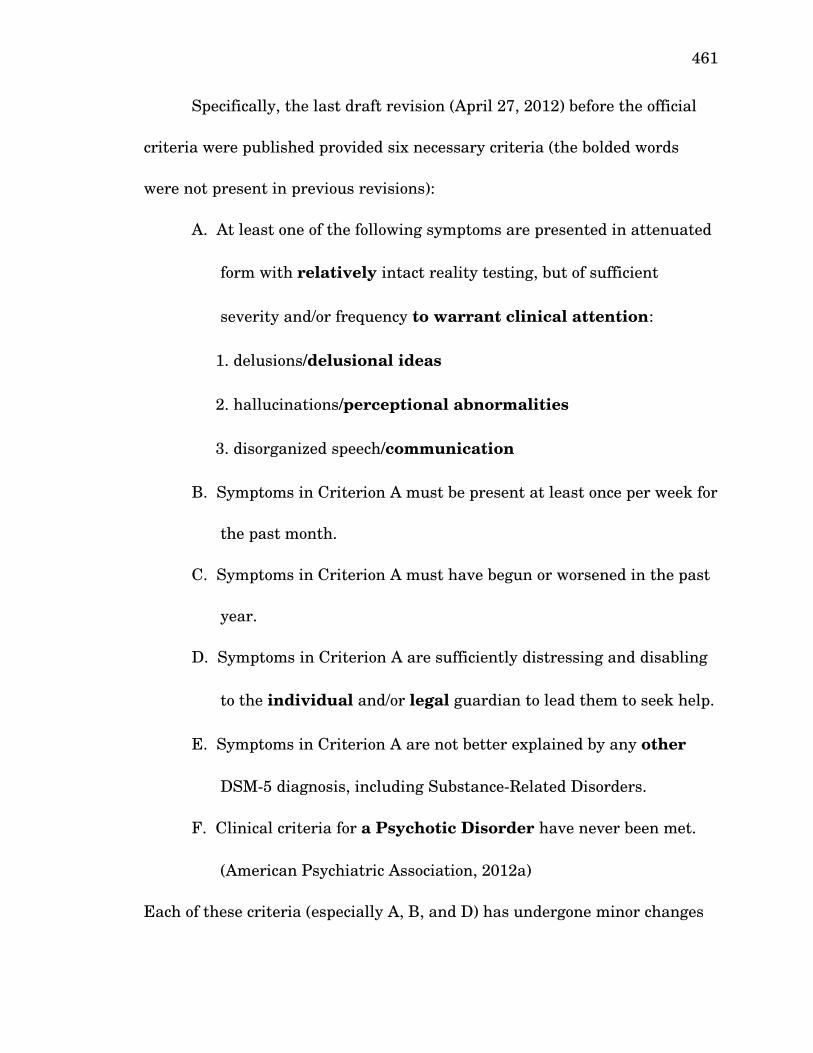
461
Specifically, the last draft revision (April 27, 2012) before the official
criteria were published provided six necessary criteria (the bolded words
were not present in previous revisions):
A. At least one of the following symptoms are presented in attenuated
form with relatively intact reality testing, but of sufficient
severity and/or frequency to warrant clinical attention:
1. delusions/delusional ideas
2. hallucinations/perceptional abnormalities
3. disorganized speech/communication
B. Symptoms in Criterion A must be present at least once per week for
the past month.
C. Symptoms in Criterion A must have begun or worsened in the past
year.
D. Symptoms in Criterion A are sufficiently distressing and disabling
to the individual and/or legal guardian to lead them to seek help.
E. Symptoms in Criterion A are not better explained by any other
DSM5 diagnosis, including SubstanceRelated Disorders.
F. Clinical criteria for a Psychotic Disorder have never been met.
(American Psychiatric Association, 2012a)
Each of these criteria (especially A, B, and D) has undergone minor changes
462
in wording over the course of the revisions. In the August 2010 version,
when the disorder was called ‘Attenuated Psychotic Symptoms Syndrome,’
Criterion A did not contain the word “relatively,” but did contain the words
“…that it is not discounted or ignored” instead of “…to warrant clinical
attention” (American Psychiatric Association, 2010h). This was also a change
from the initial February 2010 version, when the disorder was called
‘Psychosis Risk Syndrome,’ in which Criterion A instead ended with the
words “…so as to be beyond normal variation” (American Psychiatric
Association, 2010g). In both earlier versions, the three subpoints of
Criterion A were simply ‘delusions,’ ‘hallucinations,’ and ‘disorganized
speech.’ The first four criteria were also all named: ‘a) Characteristic
symptoms,’ ‘b) Frequency/Currency,’ ‘c) Progression,’ and ‘d)
Distress/Disability/Treatment Seeking.’ In both earlier versions, Criterion B
contained the words “at an average frequency of” immediately before the
words “at least once per week,” and both contained the word “significantly”
before “worsened” in Criterion C. Criterion D was worded differently in the
August 2010 version: “Distress/Disability/Treatment Seeking: symptoms
meeting criterion A are sufficiently distressing and disabling to the patient
and/or guardian to lead them to seek help” (American Psychiatric
Association, 2010h). Before that, it read “Distress/Disability/Treatment
Seeking: symptoms are sufficiently distressing and/or disabling to the patient
463
and/or others to lead to help seeking” (American Psychiatric Association,
2010g). In the original version, Criterion E was worded differently and did
not mention SubstanceRelated Disorders: “Characteristic attenuated
psychotic symptoms are not better explained by another DSMV diagnosis.”
Finally, Criterion F in both previous versions specified “any DSMV psychotic
disorder” instead of “a Psychotic Disorder.” See Table 2 for a sidebyside
comparison of the different drafts of the proposed revision.
These changes reflect rhetorical interests rather than scientific ones.
Though they appear mostly trivial, so did all the handwringing concerning
the term 'neurosis' in DSMIII that the Assembly of Delegates of the APA
hashed out in a meeting, much of which
was taken up with disputes over the placement of words, the use of
modifiers, the capitalization of entries... Each adjustment, each
attempt at fine tuning, carried with it symbolic importance to those
engaged in a process that was at once political and scientific. (Bayer &
Spitzer, 1985, p. 193)
In other words, every subtle change is undoubtedly the deliberate result of a
consensusforming process, the details of which are secret. The name of the
‘condition’ (the noun introduced in the final revision) changed, we are told,
because a “review of the data” revealed that it would be
premature to recommend a new category based primarily on future
464
risk (i.e., “Psychosis Risk Syndrome”) and not on current clinical need.
We recognized that a majority of individuals with this condition did
not go on to develop a psychotic disorder and that most individuals
with this condition had additional relevant clinical needs other than
risk of conversion to psychosis. Consequently, a condition that
described current clinical need (“Attenuated Psychosis Syndrome”) was
considered instead. (American Psychiatric Association, 2012a,
emphasis in original)
This explanation is dubious because the most significant change to the
diagnosis was the name of the condition. It points to an unresolved identity
crisis from which this diagnosis suffers. The only conceivable rationale for
this change in name is the concern raised by critics about the socalled 'false
positives.' The APA in its rationale for the disorder was careful not to
articulate which interpretation of risk syndrome it accepted, but the issue
lurked in the background, though not as a matter of science. By
manipulating the name of the disorder, more confusion regarding the terms
of the debate could be manufactured. If the name change indicates any
substantive difference, it is that the diagnosis went from being a ‘risk
syndrome’ – that is, a constellation of risk factors – to a mental disorder (or
‘condition,’ as they say) in its own right.
The text of the proposed diagnostic criteria was further altered
465
between the April 2012 draft and the final version appearing in Table 3. The
final 's' in 'symptoms' was given parentheses, i.e., 'symptom(s)', emphasizing
that the patient might only have a single category of attenuated psychotic
symptoms. The secondary descriptors of these categories in criterion A
('delusional ideas' after 'delusions,' 'perceptual abnormalities' after
'hallucinations,' and 'communication' after 'disorganized speech') that had
been added to the April draft were dropped. Also in criterion A, a subtle
change was made to the conjunction following the phrase 'relatively intact
reality testing.' Those words were followed by “but of sufficient severity...” in
the draft version, and “and is of sufficient severity...” in the final version.
This has the effect of militating against the notion that attenuated psychotic
symptoms in a patient with insight are inherently insufficiently severe.
Criterion E was modified to clarify that an individual who did not have a
“Substance Related Disorder,” but nevertheless was under the influence of a
drug capable of inducing psychosis, so that the observed attenuated psychotic
symptoms could be attributed to the “physiological effects” of the drug, should
not be given the diagnosis.
More significantly, Criterion D was modified from requiring that the
symptoms be “sufficiently distressing and disabling to the individual and/or
legal guardian to lead them to seek help” to instead requiring that they be
“sufficiently distressing and disabling to the individual to warrant clinical
466
attention.” There are two significant changes here. First, removing the
“and/or legal guardian...” clause helps mollify concerns that the proposed
diagnosis will be used to classify individuals against their will or on the basis
of a recommendation from an annoyed teacher or frustrated parent. The
second change works somewhat in the opposite direction, modifying the
criterion so that it is no longer sufficient to be helpseeking—one's symptoms
must actually “warrant clinical attention.” This would perhaps exclude the
socalled 'worried well' that might be suffering from what used to be called
hypochondriasis, now “Illness Anxiety Disorder” (American Psychiatric
Association, 2013, p. 315). But it would also include the nonhelp seeking
who perhaps ought to be helpseeking in the judgment of the diagnosing
clinician. That change seems, in my judgment, counterproductive, as the
emphasis on careseeking patients provides a strong answer to concerns
about overdiagnosis, as it ensures that the diagnosis would only be applied
to people who, at a minimum, already were seeking a diagnosis. It also
suggests the final redactor curiously was more concerned about the problem
of 'false negatives' than 'false positives.'
Controversy During DSM5 Revision Process
What difference does it make if there are many false positives or few?
After all, the issue of false positives is never even raised with other risk
syndromes like high blood pressure or high cholesterol. People who are
467
prescribed a statin126 who don't have a heart attack are not regarded as 'false
positives,' nor are people who smoke tobacco but live to be 100. Apparently,
the equation changes when the intervention entails the possibility of
medicating nonpsychotic children with antipsychotic medication.
As I stated earlier, McGorry and his colleagues used a variety of
interventions including antipsychotic medication, but they found that CBT
and essential fatty acid supplementation were equally effective at preventing
psychosis, and could reduce the rate of transition from onethird to
approximately 10% (McGorry, Killackey, & Yung, 2008). This suggests that
if 100 patients are diagnosed, 20 of the could be prevented from developing a
psychotic disorder, at the cost of unnecessarily treating about 70 of them
(although the assumption that at least some of those 70 would not
nevertheless benefit from the intervention is not necessarily sound).
Several other research groups in recent years have found similar
results. Research groups in Copenhagen, Denmark, and at the Institute of
Psychiatry in London have established a similar program for early diagnosis
and intervention, also using atypical antipsychotics, fatty acid
supplementation, and cognitive therapy. Results were equivocal for those
receiving treatment for firstepisode psychosis (Gafoor et al., 2010). There is
some evidence that in these cases, early intervention is associated with a
126 The world's top selling medicine in 2010 was a statin, branded 'Lipitor,' which provided Pfizer with $13.3 billion in revenue that year (R. Cooper, 2011).
468
positive outcome, but the meaning of this finding is obscure because patients
“suffering from a psychosis of recent onset, however, are more likely to
experience a spontaneous remission of illness, and this may readily explain
the observed association” (Warner, 2005, p. s104). A metaanalysis of 66
studies found that they could significantly reduce the rate of a second
psychotic episode, but that it was necessary to treat 8 patients to prevent one
relapse (AlvarezJiménez, Parker, Hetrick, McGorry, & Gleeson, 2011). A
Scandinavian study, 'Treatment and Intervention in Psychosis' (TIPS), has
experienced success treating psychosis (not prepsychosis) early, finding that
early treatment “not only facilitates recovery, it also affects the core
neurobiological deficit process that characterises the early course of the
disorder” (S. P. Singh, 2010, pp. 343–344).
In the face of all the arguments about predictive validity, coupled with
the arguments about the unknown risk associated with unleashing the
diagnosis on general practitioners, school nurses, teachers, etc., especially
given the ability of the pharmaceutical industry to run directtoconsumer
advertising in the United States, McGorry had a sudden change of heart in
2011 about the desirability of formally including the diagnosis in DSM5,
saying “I think it's a valid point to be concerned about the harms particularly
in places like America... I think probably I have given a bit more weight to
that argument now” (cited in Corderoy, 2012, para. 4). This was after he
469
completed a long series of exchanges with his critics, one of whom praised
him for “engaging in constructive, robust, debate” and having the courage to
“restate his new position unambiguously in the mainstream media” (Whitely,
2011, 2012, para. 3–4).
McGorry and his colleagues understood that their views were
controversial, and that, to an certain extent, reaching consensus would
require more than just data:
In psychiatric as well as other reform processes, logic and scientific
evidence are necessary but insufficient. Rhetoric, marketing, effective
networking, altruistic promotion of a vital public health issue,
economic arguments and a confluence of common interests have fuelled
the momentum and are vital for real reform to take root. This is public
policy analysis complementing evidencebased medicine. Given the
history of psychiatry where some of these factors have driven reform in
the absence of evidence, this naturally makes some people nervous, but
without these factors operating we will not only fail to translate the
most strongly evidencebased practices... but our systems of care will
fail to evolve and will again become paralysed... Evidence is the
language of reform but there are other elements in communication.
There is also rhetoric, prosody, persuasion and at the heart of things, a
chorus of voices reflecting the human experience of illness and
470
recovery. (McGorry, Nordentoft, & Simonsen, 2005, pp. s2–s3)
This kind of frank acknowledgement of the importance of rhetoric in scientific
deliberation is insightful, but nevertheless (or, perhaps, as a result), it
arouses the suspicions of scientists. Rhetoric, Weaver (1970a) notes, arouses
“skepticism and suspicion… [It] is no exaggeration to say that eloquence
itself has fallen into disfavor… [and] there emerges a conviction that man
should dispense with persuasive speech and limit himself to mere
communication” (pp. 161162). One unfortunate artifact of the
Enlightenment is that 'science' has claimed ownership over 'facts,' and
equated the nonscientific with the nonfactual (Weaver, 1970b). Further, in
light of the great propaganda campaigns of the twentieth century, the
classical view, defended by Aristotle, Isocrates, Cicero, Quintilian, and
others, that, ceteris paribus, rhetoric prefers the good, even if it is sometimes
enlisted by evil, seems entirely foreign to many in the scientific community
(Crowley & Hawhee, 2004).
Allen Frances gave voice to this kind of suspicion of rhetoric. Though
delighted that McGorry had changed his mind, having been persuaded by the
arguments he and others had been making, Frances remained wary of
McGorry. Frances expressed concern about McGorry's recognition as
Australian 'man of the year' in 2010, suggesting that “a dark cloud surrounds
the silver lining of having one psychiatrist in a position of almost unopposed
471
influence,” and arguing that McGorry has
developed the messianic blind spot that is so common in visionary
prophets. His zeal has made him an unreliable evaluator of scientific
evidence, allowing him to defend absolutely indefensible positions with
the convincing, but inaccurate, force of a true believer. A review of
Professor McGorry’s public statements shows his willingness to ignore
any evidence contrary to his belief, to change stated views back and
forth when he regards this to be necessary or convenient, and to
unfairly attack those who point out the fallacies and inconsistencies in
his comments. His are the skills of a prophet and rainmaker, not those
of a policy maker or a program developer or a sober reviewer of
scientific evidence. (Frances, 2011c, para. 3)
Such a reaction suggests that changing one's mind after engaging in a public
deliberative process, with an open mind and a willingness to be convinced, is
a fundamentally radical act in late modern culture. The paranoia about the
risks of rhetoric is so strong that, even after successfully persuading him,
Frances remained suspicious of the rhetorical skill of his past interlocutor. It
strikes me as rather ironic that Frances criticized McGorry for wielding great
influence as a psychiatrist with pseudocelebrity status. Still, although
McGorry did change his mind about the desirability of DSM5 reification of
psychosis risk syndrome, he and Frances still fundamentally disagree about
472
the value of early interventions in psychosis given the current state of
knowledge, so there is a point to Frances' protests.
Frances is not alone in criticizing the dangers of rhetoric in the context
of psychosis risk. Amos (2013) suggests that “early intervention rhetoric
distorts public policy” (p. 317). Amos is not especially worried about the
undue influence of rhetorical factors in the scientific debate among experts.
Instead, his primary concern lies with the nonexpert audience that is in a
position to make funding decisions for research projects:
[The] best antidote for the expert reader is to read the references and
draw their own conclusions... [The] funding of mental health services is
heavily influenced by expert opinion. Robust debate and critical
analysis is the only way to ensure that nonexpert decisionmakers can
place their trust in the advice they receive regarding allocation of
resources to competing mental health programmes. If their peers do
not identify flaws and insist upon high standards from EI proponents,
the nonexpert bodies who rely upon their advice will continue to make
crucial decisions on grounds that can be questioned” (p.320)
He accuses early intervention researchers, especially McGorry and Yung, of
having a “tendency to selectively report and liberally interpret results” (p.
318), and of taking his efforts to point out their methodological errors and
distortions as personal attacks rather than as demands for better
473
justification of their claims:
Despite being accused of personal incivility and an unstated agenda, in
a spirit of scientific detachment I have given detailed examples of
selective analysis and report which is likely to misrepresent the
evidence regarding early intervention in psychosis. I call for similarly
detached responses. (p. 320)
It is clear that by 'rhetoric,' Amos is grouping all sorts of argumentation
outside the norms of dispassionate scientific discourse. Like Frances'
polemic, Amos shows how these debates can get very personal.
For his part, McGorry attributed his differences with Frances to the
larger differences in health care between Australia and the United States:
A fundamental difference between the USA and Australia is that
mental health professionals conceive of mental ill health and mental
illness in a much more biopsychosocial and holistic manner. Both
conceptually and through our universal system of health financing we
respect and provide a much stronger level of psychosocial input to
patients. We do not equate treatment with the prescription of
medication. We do not permit direct marketing of pharmaceutical
products to the public... Operating within such a different healthcare
system, it is perhaps understandable that Dr. Frances might struggle
to grasp that the real impact of the youth mental health reforms in
474
Australia will be to make psychosocial interventions available to young
people with mental ill health to a much greater extent, as both an
alternative and complement to medication. A measurable outcome will
be less reliance on medication for those accessing care. (McGorry,
2011, para. 8–9)
What this reveals is that the problem of managing risks is always multisided
–the risks of the intervention itself (in terms of stigma and unnecessary
treatment) are joined with the even less predictable risks posed by the
pharmaceutical industry and the model of health care in the United States.
One of the claimed benefits of intervening, at least in Australia, is not merely
to prevent psychosis, but to protect children from future pharmaceutical
interventions that are inherently more risky and, as they would come later,
less efficacious than the nonpharmaceutical interventions McGorry
supports.
Even if the terms of the debate were not so distorted by clashing
worldviews and notions of disorder and probability, McGorry notes that
Evidence will never be conclusive and the perfect truly is the enemy of
the good. The real question is where does the onus of proof lie? Given
the serious and often irreversible personal and social damage wrought
by untreated serious mental illness, surely we can assume that late
intervention is not a practice we wish to support. (para. 16)
475
The late modern regime of risk rationality inverts classic ideas of
presumption and burden of proof, and McGorry skillfully flips the accusation
of risky recklessness back on Frances:
The notion that early diagnosis and treatment should be an optional
extra is in any case quite bizarre. Reckless even, given that the lives
and futures of young people are at stake. Why do we never see
oncologists arguing about the relative value of palliative care and early
diagnosis, or insisting that we must have perfect palliative care
services before we tackle early intervention? Perhaps it is partly due to
the historical neglect of mental health care and our own ambivalence
about what we have to offer patients. These are stigmarelated issues
we must confront. (para. 19)
Even the issue of stigma is redeployed in reverse. McGorry is not merely a
skilled rhetor, he is in tune with the radical reversals that are afforded by the
topos of contemporary risk.
The questions of evidence and burden of proof raise an important
question: Why is there not better evidence at this point? Researchers had
'brain wave' data that they believed would prove promising 75 years ago (D.
E. Cameron, 1938). Particularly if the 'prodrome' interpretation is accurate,
one would think that with all the neuroimaging techniques that have been
developed over the last decade and discussed in Chapter 3, there would be
476
some credible evidence that not only helps us identify people at risk of
psychosis earlier and with better accuracy, but would also shed some light on
the organic nature of psychotic disorders. Rose and AbiRached (2013) argue:
Despite the penetrating gaze of neuroscience, which has opened up the
brain to vision in so many ways... psychiatric classification remains
superficial. The neuromolecular vision seems incapable of grounding
the clinical work of psychiatry in the way that has become routine in
other areas of medicine... [Although] the [DSM] criteria have
summoned up an image of a mental disorder in thought—a specific
genetic sequence or set of sequences linked to anomalies in the
neurotransmitter system or other aspects of neurobiology causally
related to a particular array of cognitive, affective, volitional, or
behavioral dysfunctions—this assemblage has proved impossible to
summon up in reality, despite the expenditure of millions of dollars
and thousands of personhours. (p. 138)
Perhaps the reaction against psychodynamic nosology, and the concomitant
downgrading of trauma, works against these efforts. None of the major
research programs in psychosis risk consider trauma among their principal
criteria. In the drive to overcome mindbody dualism, perhaps the advocates
of a neuropsychiatric biomedical nosology have recreated it by not realizing
that, if the mind is material, then our ability to observe psychic phenomena
477
in all their rich complexity represents another untapped technique to look at
the brain. Further, if the theory of the prodrome is incorrect—that is, if any
observed abnormalities in prepsychotic patients are signs of susceptibility
that can be conceptually distinguished from premorbid processes, then
perhaps that error places a hard epistemic limit on their research efforts.
Finally, it strikes me as odd that there has not been more research
that attempts to collect some evidence that would be relevant in the debate
about what would happen were a diagnosis of psychosis risk utilized by non
experts. One study examined whether general practitioners could be trained
to improve early detection and intervention rates, finding modest support
(Power et al., 2007). But this does not really test the question of how non
experts who do not receive training would use the categories. Nor has there
been any discussion of possible strategies to mitigate this sort of risk (aside
from not including psychosis risk syndrome in DSM5). In other areas of
medicine, there is an awareness that certain treatments require special
expertise to avoid pitfalls. For example, while any physician in the United
States can prescribe the opiate buprenorphine offlabel, a special waiver from
the DEA is required to prescribe it to addicts using it as replacement therapy
(Cunningham, Kunins, Roose, Elam, & Sohler, 2007). The uncertainty
associated with permitting nonspecialists to use the diagnosis by non
specialists could be managed through a similar scheme, though that would
478
also limit the potential benefits. Alternatively, a systematic populationlevel
primary/second prevention program could involve nonspecialists in screening
but not in implementing pharmaceutical interventions without some other
verification step. These ideas may be flawed, but my point is that the
controversy seems to be missing this category of harmmitigation proposals
designed to be responsive to the arguments of the other side.
Conclusion
Having explored the controversy surrounding the diagnosis of
psychosis risk syndrome, placing it in the wider context of the discourses of
risk in advanced liberalism, I can draw two overarching conclusions. First,
building upon the discussion in Chapter 3, I contend that the modern history
of psychosis, broadly, or schizophrenia in particular, can be understood as
synechdochic of the modern history of risk. In the previous chapter, I argued
that schizophrenia as a diagnostic category enacts the rhetorical
discontinuity that characterizes the Kraepelinian nosology, a splitting of the
mind on the one hand and a splitting of insanity into discrete disease entities
on the other. Schizophrenia has, since the time it was first formalized as
dementia praecox, been defined not so much by currently extant signs and
symptoms but by its characteristic progressively deteriorating course.
Much like an asset bubble, it cannot be diagnosed with certainty until
some time has passed—schizophreniform disorder, as we have seen, is
479
diagnosed when the signs of schizophrenia clear up after a short period of
time (Lin, 1988; Troisi, Pasini, Bersani, Mauro, & Ciani, 1991). The diagnosis
of schizophrenia is fundamentally concerned with a probable future course of
events. Further, psychosis represents a danger to society to such a degree
that psychotic individuals were confined involuntarily to asylums before the
discovery of effective neuroleptic medication made outpatient management a
realistic option. The evolution of our conceptualizations of psychosis and
schizophrenia track the transformation of the early modern concern with
managing dangerousness into the late modern preoccupation with regulating
risk. When dangerousness was seen as a degenerate property potentially
living inside the individual subject, the concepts of 'latent schizophrenia' and
'sluggish schizophrenia' came on the scene. As the larger risk focus
transitioned to populations and risk factors, the idea of a psychosis risk
syndrome and early interventions on a population deemed to be at ultrahigh
risk came to fore. These transitions were not clean, and so much of what
bubbled up into controversy was the vestige of competing fragmented regimes
of risk rationality, animated by the anxieties of the larger risk society as it
was undergoing the reflexive transformations wrought by advanced
liberalism.
The second conclusion I would like to highlight from this analysis is
that contested representations of risk, and of the relative importance of
480
different risks, are the sites in which advocates of competing models of
madness—and competing institutional logics that govern psychiatry—engage
in battle. Clinicians, journalists, patients, regulators, scientists, and
members of the general public each have a distinct understanding of risk that
flows from their social location, a situation that at its best can lead to
confusion and miscommunication, and at its worst can be deliberately and
instrumentally exploited through a program of systematically distorted
communication.
Technical systems operate according to their own unique instrumental
logics, imperatives, and levels of tolerance for uncertainty and risk, and the
discourses that circulate throughout can become systematically distorted
through the exploitation of deficient integration between systems (Habermas,
1987). When the effects of this process become publicly salient in the “life
historical background of violated interests and threatened identities,” a
public controversy can arise that may provoke legitimation crises for the
institutions involved at the intersection of the relevant technical systems
(Habermas, 1996, p. 351). We must understand the controversy about
psychosis risk syndrome in this context, that is, as a potential legitimation
crisis that relates the institution of psychiatry to the larger risk society in
which it is embedded.
A common feature of risk legitimation crises – that is, problems that
481
derive from anxieties about the unknown effects of legitimating an
instrument that makes authoritative judgments about the unknown – is that
there is ambiguity about whether the 'risk problem' at the heart of the crisis
is primarily a technical problem or a practical problem. With respect to
psychosis risk syndrome, should the risk problem best be understood as a
technical problem, concerned with to what extent we can identify pre
psychotic patients, or as a practical problem, concerned with to what extent
we should attempt to manage risk with this sort of intervention. We have
seen that in the case of coercive paraphilia, this question gets tackled
through the combined use of tragic frames in the scientific literature and
comedic frames in literature directed toward a public audience.
Contemporary psychiatry is plagued by a new Oedipal complex – but
not as Freud imagined (except insofar as it wants to kill its psychodynamic
father while embracing his dimensional spouse). In Sophocles' classic
tragedy, Oedipus does kill his father and sleep with his mother, but the
reason he does so is not his unconscious desire. Rather, his actions resulted
from an attempt to avoid a Delphic prophecy that (correctly) identified them
as part of his destiny, fated from the beginning. The controversy about
including psychosis risk syndrome in DSM5 speaks to a profound anxiety
about predicting fate, on one hand, and the risks entailed in attempting to
thwart fate, on the other. This is the Oedipus complex that plagues

482
psychiatry today.