catheterization technique for laser photoablation of atrioventricular conduction from the aortic...
TRANSCRIPT
Catheterization Technique for LaserPhotoahlation of Atrioventricular Conductionfrom the Aortic Root in Dogs
LASZLO LITTMANN, ROBERT H. SVENSON, CHI HUI CHUANG,PAL KEMPLER, ROBERT SPLINTER, JAN R. TUNTELDER. andGEORGE P. TATSIS
From the Laser and Applied Technologies Laboratory, Carolinas Heart Institute, Charlotte,North Carolina
LITTMANN, L., ET AL.: Catheterization Technique for Laser Photoahlation of Atrioventricular Conductionfrom the Aortic Root in Dogs. A simpJe catheterization technique for producing suppression or block ofatrioventricular {AVj conduction in dogs by neodymium.-YAG (Nd:YAG] laser photocoaguJation from theaortic root is described. In 14 canines, electrode catheters were percutaneously advanced to the high rightatrium, to the His bundJe area at the tricuspid valve (right His fRHJ], and the noncoronary cusp of theaortic valve {left His [LH]). A 400 (xm optical fiber was fed into the lumen of the LH catheter. Continuouswave Nd-.YAG lasing at k = 1,064 nm at 15-20 watts was performed at the site of the largest recordedLH deflection, opposite ta the RH catheter, until complete AV block fCAVB, group I, eight dogs) orpersistent A-H prolongation (AHPr, group 11, four dogs) occurred; in two animaJs, laser photoabiationwas unsuccess/ui. CAVB and AHPr were achieved in < 140 seconds of Jasing. Mean losing time was 51± 41 seconds, total energy delivered, 776 ± 601 J. There were no complications. Dogs were followed forup to 120 days. In group I, 6/6 dogs followed/or at least I week continued to have CAVB (three AV nodal,five infra-His). In group II, 1/4 dog progressed to infra-His CAVB; 3/4 had depressed AV nodal function.AV block was not reversed by isoproterenol. Aortic root angiograms revealed intact valve function in all.Histology showed various degrees of damage and repair of AV functional tissue. There were no valvularperforations. Transcatheter Nd.YAG laser photocoagulation of the AV junction from the aortic root is afast, simple, and safe method for creating AV conduction block in dogs. (PACE, Vol. 16, March, Part I1993}
heart block, atrioventricular junction, atrioventricular node. His bundle, catheter ahlation, laser photoco-agulation
IntroductionExperimental production of atrioventricular
(AV) block is frequently required for the study ofatrial and ventricular automaticity and hemody-
^ Several intraoperative and catheteriza-
Supported by a grant from Ihe Hungarian Academy of Sciences,OTKA I/3-10B1.
Presented in part at the 64th Scientific Session of the AmericanHeart Association, Novemher 1991, Anaheim, California.
Address for reprints: Laszlo Littmann, M.D,. Laser and AppliedTechnologies Laboratory, Carolinas Heart Institute, P.O. Box32861, Charlotte, NC 28232. Fax: (704) 355-7217.
Received April 16, 1992; revision (uly 22, 1992: accepted Octo-ber 1, 1992,
tion techniques have been designed to createchronic AV block in dogs.^'^ Open chest proce-dures^"^ are time consuming, costly, and cancause unnecessary discomfort to the experimentalanimal. Transcatheter direct current electric shockablation produces significant barotrauma, and it isfrequently associated with malignant arrhythmiasand structural damage,''*" Laser thermal ablationhas several advantages over D/C shock ablation. Itis a highly directional technique, the laser lightcan be easily transferred through a flexible fi-heroptic, and the delivered energy can be gradedto the desired effect.^ Intraoperative'" and trans-catheter argon laser ablation of AV conduction^^is technically feasible, but can cause significant
PACE, Vol, 16 March, Part I 1993 401
LITTMANN, ET AL.
structural damage to the AV junction area includ-ing crater formation, perforations, and septal de-fect. In contrast to argon, neodymium:YAG (Nd:YAG) laser ablation has the advantage of produc-ing bulk tissue photocoagulation with sharp,clearly defined edges. At properly chosen powerdensities, there is no tissue vaporization."'^ Inprevious studies we have shown that intraopera-tive Nd;YAG laser photoablation of atrial,^^ ven-tricular^-^^ and AV junctional tissues^^ results ingraded depths of tissue coagulation with preserva-tion of structural integrity. The procedures werewell tolerated, and were not associated with signif-icant complications.^•^^"'•' A similar transcathetertechnique, however, is confounded by certaintechnical constraints including the need for spa-cial stability of the catheter during the cardiaccycle, a close fiber-tissue contact, and a perpendic-ular orientation of the fiber tip to the endocardialsurface. From a conventional right heart approach,these difficulties might be hard to overcome. So-phisticated catheter systems that included endos-copy^^ or mirrors and a side window^^ have beendevised for experimental laser ablation of AVjunction from the tricuspid valve area. Because ofthe close proximity of the noncoronary cusp of theaortic root to the His bundle,^^-^^ and because ofits advantageous configuration for the wedging ofa catheter tip, we hypothesized that transcatheterNd;YAG laser coagulation of AV junction might bemore simply and conveniently performed from theaortic root than from the right heart. The followingreport summarizes our experience with this tech-nique.
Materials and Methods
Instrumentation
All interventions performed in this study con-formed with the appropriate institutional guide-lines and the position of the American Heart Asso-ciation on Research Animal Use. Fourteen healthymongrel dogs of both sexes weighing 18-38 kgwere included in the study. Animals were anes-thetized by intravenous pentobarbital sodium, 25mg/kg body weight, and were ventilated by a vol-ume-controlled respirator (Servo, Siemens Elema,Solna, Sweden). Under sterile conditions, two 6French quadripolar electrode catheters were intro-
duced with the Seldinger technique through femo-ral veins and were advanced under fluoroscopiccontrol to the high right atrium and His bundlearea for pacing and recording local bipolar elec-trograms. An 8 French bipolar electrode catheterwith a lumen ("Zucker catheter" USCI Bard, Div.G R Bard, Billerica, MA, USA) was introducedwith the Seidinger technique through a femoralartery, and was advanced to the noncoronary cuspof the aortic root, opposite to the right-sided Hisbundle catbeter, to record bipolar and unipolarHis bundle electrograms. The His catheters weremanipulated to record the largest His bundle po-tentials. Positioning of the His bundle catheterstook < 5 minutes. Surface electrocardiographicleads II and III, bipolar and unipolar His bundleelectrograms were simultaneously displayed on amultichannel oscilloscope and were recorded byan ink-jet recorder (Siemens Mingograf [SiemensElemal) at paper speeds of 100 and 250 mm/sec.Band pass filters of 0.15-30 Hz, 50-1,000 Hz, and0.15-1,000 Hz were used for surface electrocardi-ograms, bipolar, and unipolar intracardiac eiec-trograms, respectively.
Laser Photocoagulation
A bare tip optical fiber with 400 .̂m outer di-ameter was fed into the lumen of the Zucker cathe-ter; the tip of the laser fiher extended 0.5-1 mmfrom the tip of the electrode catheter. Lasing wasperformed using a continuous wave Nd:YAG laser(MediLas II, MBB-Medizintechnik, Mnnich, Ger-many) at the 1,064 nm wavelength with emittedpower set at 15-20 watts. Two- to 5-second burstsof laser energy were consecutively applied untilcomplete AV block (GAVB; group I, eight dogs) orpersistent prolongation of AV nodal conductiontime (A-H prolongation, group II, four dogs) oc-curred.
Electrophysiological Testing
His bundle electrograms were continuouslyrecorded throughout the procedure; 12-lead elec-trocardiograms were recorded before and after ab-lation, The critical atrial cycle lengths resulting inAV nodal Wenckebach periodicity ("Wenckebachcycle lengths") were estimated by incrementalatrial pacing before the procedure and, in the ab-sence of complete heart block, after ablation.
402 March, Part I 1993 PACE, Vol. 16
LASER ABLATION OF AV CONDUCTION
Follow-Up
Two animals were sacrificed immediatelyafter laser photoabiation. Twelve dogs were keptfor 7-120days;sixof these, three from each group,were followed for over 3 months. Before sacrific-ing, each animal was retested by 12-lead electro-cardiography, His bundle recording from the tri-cuspid area, and incremental atrial pacing. In ani-mals that developed and maintained chronic
CAVB, the effects of isoproterenol infusion (4 fig/min for 5 minutes) on AV conduction was alsotested. Aortic root angiograms were performed todetect possihle perforation/leakage of the aorticvalve.
Histology
The conduction system was examined in all14 animals. Hearts were removed, and the aortic
-A9
N
BE'RH
BE-LH
UE-LH
^ A
*
*
H
HV
— -
^ '
A
A
A
H
••"vA "^•^'^Hy \
BEFORE LASING
400 400 3B0 3B0 370 300
BERHH
BE-LH
UEIXV*' •
' ^ « . M . N .
HIS BUNDLE /CCELERATION
DURING LASING; HIS BUNDLE /CCELERAOON
la ttlmfrt
aOO 500 S80
A/NOCALBLDCK
IMMEDIATELY AFTER LASING:* NODAL BLDCK
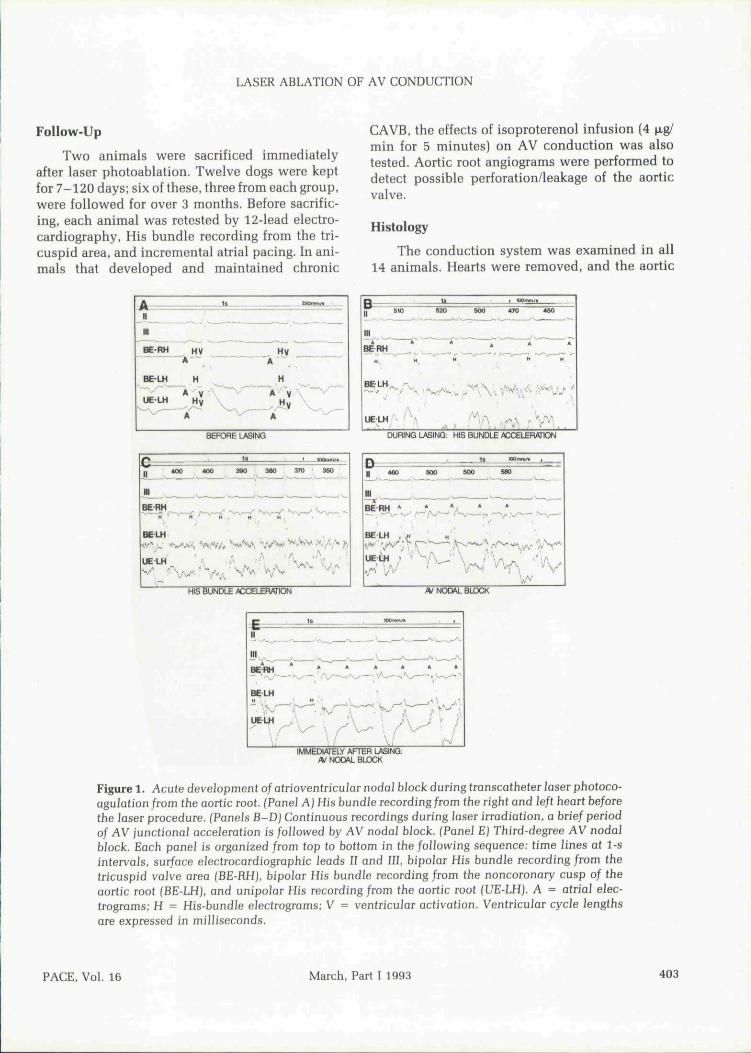
Figure 1. Acute development of atrioventricular nodaJ block during transcatheter laser photoco-agulation from the aortic root. (Panel A) His bundle recording/rom the right and left heart beforethe laser procedure. fPaneJs B-D) Continuous recordings during laser irradiation, a brief periodof AV junctionai acceleration is followed by AV nodal block. fPanel E) Third-degree AV nodalblock. Each panel is organized from top to bottom in the following sequence: time lines at 1-sintervals, surface electrocardiographic leads II and III, bipolar His bundle recording from thetricuspid valve area (BE-RHJ, bipolar His bundle recording from the noncoronary cusp of theaortic root (BE-LH), and unipolar His recording from the aortic root (UE-LH). A ^ atrial elec-trograms; H - His-bundle eJectrograms; V ^ ventricular activation. Ventricular cycle lengthsare expressed in milliseconds.
PACE, Vol. 16 March, Part I 1993 403
LITTMANN, ET AL.
root and tricuspid valve areas were visually in-spected. The aortic, mitral, and tricuspid valveswere microscopically studied. A block containingthe approaches to the AV node, the AV node, thepenetrating part of the His bundle, and the branch-ing and bifurcating portions of the His bundlewere taken and sectioned at 5-20 \xm thickness.Every 20th section was retained and stained withMasson's Trichrome or Masson's Trichrome andhematoxylin-eosin alternately. A mean of 140 ±55 sections were examined from each heart.
Statistical Methods
Data were expressed as mean values ± stan-dard deviation. Student's paired t-test was used tocompare electrophysiological measurements be-fore and after photoablation.
Results
Acute Effects of Lasing
Eight dogs developed CAVB (group I) at5.1-60 seconds of laser photocoagulation. In eachcase, lasing at the appropriate site resulted in AV
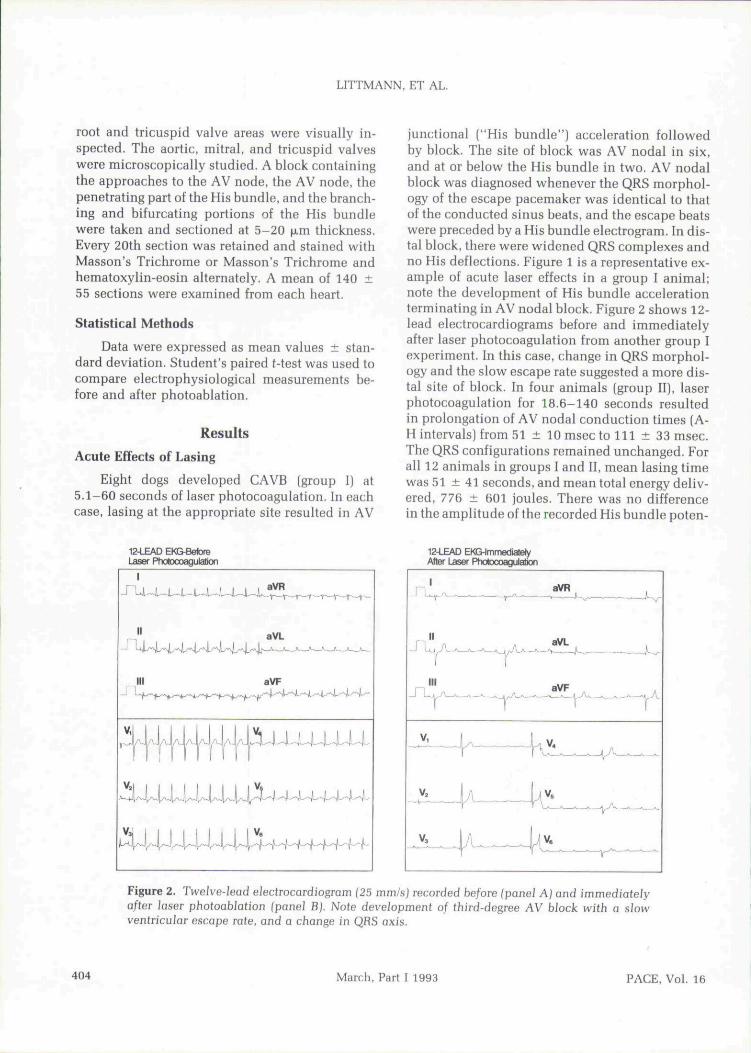
junctional ("His bundle") acceleration followedby block. The site of block was AV nodal in six,and at or below the His bundle in two. AV nodalblock was diagnosed whenever the QRS morphol-ogy of the escape pacemaker was identical to thatof the conducted sinus beats, and the escape beatswere preceded by a His bundle electrogram. In dis-tal block, there were widened QRS complexes andno His deflections. Figure 1 is a representative ex-ample of acute laser effects in a group I animal;note the development of His bundle accelerationterminating in AV nodal block. Figure 2 shows 12-lead electrocardiograms before and immediatelyafter laser photocoagulation from another group Iexperiment. In this case, change in QRS morphol-ogy and the slow escape rate suggested a more dis-tal site of block. In four animals (group II), laserphotocoagulation for 18.6-140 seconds resultedin prolongation of AV nodal conduction times (A-H intervals) from 51 ± 10 msec to 111 ± 33 msec.The QRS configurations remained unchanged. Forall 12 animals in groups I and II, mean lasing timewas 51 ± 41 seconds, and mean total energy deliv-ered, 776 ± 601 joules. There was no differencein the amplitude of the recorded His bundle poten-
12-4_EAD EM3-BelbreLaser Photocoagulation
I
-i LJt—IU-JU^JU-JU—i—lU-J
II
III
VJ j 1 1 1 j 1 1
aVL
aVF
—^—»—"—'—
1 ' IJJ
12-LEAD EH&lmmediatelyAftBT Laser Photacoagulation
Figure 2. Twelve-lead electrocardiogram (25 mni/s) recorded be/ore (panel AJ and immediatelyafter laser photoabJation (panel B). Note development of tbird-degree AV block witb a slowventricular escape rate, and a change in QRS axis.
404 March, Part I 1993 PACE, Vol. 16
LASER ABLATION OF AV CONDUCTION
COMPLETE AV BLOCK
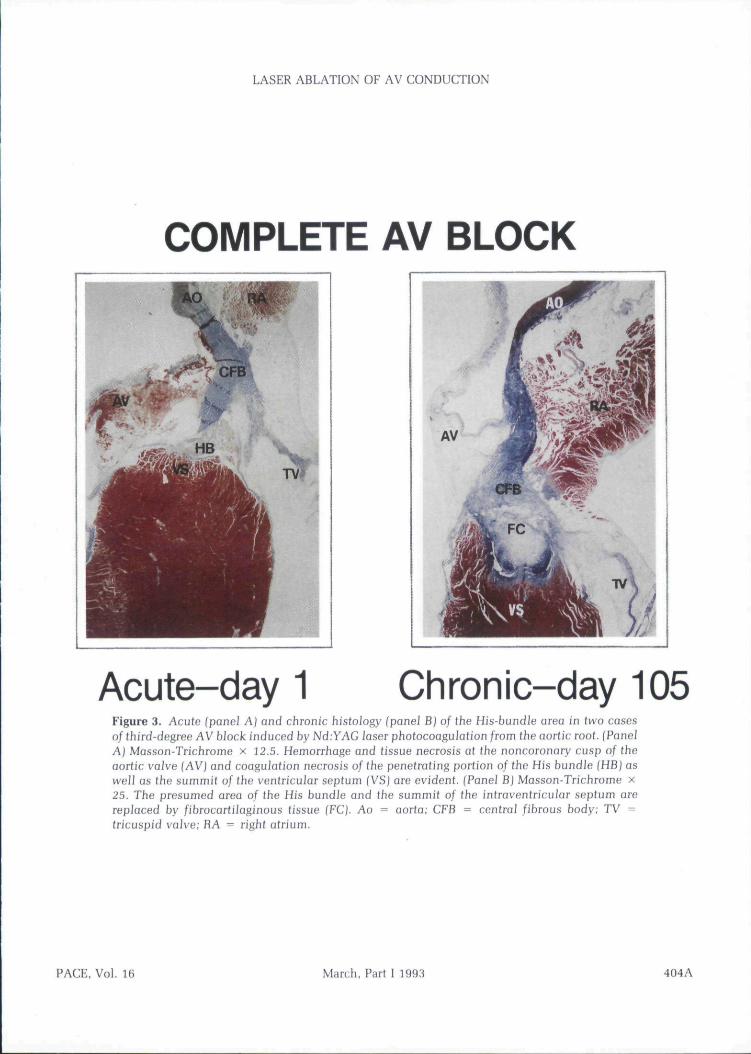
Acute-day 1 Chronic-day 105Figure 3. Acate (panel AJ and cbronic bistology (panel BJ of ihe His-bundle area in two casesof Ihird-degree AV block induced by Nd.YAG laser photocoagulation from tbe aortic root. (PanelA) Masson-Trichrome x 12.5. Hemorrhage and (issue necrosis at tbe noncoronary cusp of theaortic vaive (AV) and coaguiafion necrosis of tbe penetrating portion of the His bundle (HBJ aswell as tbe summit of tbe ventricular septum (VSJ are evident. (Panel BJ Masson-Trichrome x25. Tbe presumed area of the His bundle and tbe summit of tbe intravenlricular septum arereplaced by fibrocartilaginoas tissue fFCJ. Ao ^ aorta; CFB = central fibrous body; TV =tricuspid volve; RA = right afrium.
FACE, Vol. 16 March, Part I 1993 404A

LASER ABLATION OF AV CONDUCTION
tials at the lasing site between experimentalgroups I (0.15 ± 0.04 mV] and II (0.14 ± 0.04mV). The ratio of the amplitude of the local bipolaratrial and ventricular electrograms was also simi-lar in the two groups. In two experimental ani-mals, repeated photocoagulation from several sitesfailed to produce AV junctional acceleration, A-Hprolongation, or AV block. Premature ventricularcontractions or ventricular tachycardia were notseen during and for about 30 minutes after the in-tervention in any case, and each animal [exceptfor the two that were acutely sacrificed) recovereduneventfully.
Chronic Electrophysiological Effects
Dogs were kept for 7-120 days following laserphotocoagulation. CAVB persisted in each group Ianimal. Interestingly, however, in three of six dogsthat initially had AV nodal block, the site of block[or the escape pacemaker) shifted to a more distalarea as evidenced by a change of QRS morphologyon the escape beats. During tbe final restudy, wewere unable to record His bundle activity eitherfrom the right or the left heart in any of the dogs,including those that maintained a supraventricu-lar morphology to the escape rhythm. Isoprotere-nol infusion at 4 ^ig/min for 5 minutes failed toreverse the CAVB. In group II, one of four animalsprogressed to CAVB; the other three continued tohave prolonged AV nodal conduction. The AVnodal Wenckebach cycle lengths in these tbree an-imals increased from 150 ± 8 msec before the laserprocedure to 180 ± 8 msec at the chronic restudy[P < 0.05).
Angiography
Biplane aortic root angiograms failed to revealaortic regurgitation in the experimental animals.
Pathology
In the two unsuccessful cases, acute necrosisand hemorrhage were seen in the right coronarycusp rather than the noncoronary cusp of the aor-tic valve suggesting an inappropriate site of laserphotoabiation. In the successful cases, there werevarying degrees of damage and repair of AV junc-tional tissues, corresponding to the timing of thehistologic study relative to that of lasing, and alsoto whether complete or incomplete AV block hadbeen achieved. Figure 3A is an example of an
acutely harvested case following development ofcomplete AV block. There is hemorrhage and tis-sue necrosis at the base of the noncoronary cuspof the aortic valve, and coagulation necrosis of thepenetrating portion of the His bundle and the sum-mit and left ventricular aspect of tbe interventricu-lar septum. By day 8, repair by granulation tissuewas under way. At 3 months, repair of damagedtissue was histologically complete, and the pre-sumed area of the His bundle at the summit of theintraventricular septum, together with damagedadjoining areas, was replaced by cartilage and con-nective tissue [Fig. 3B]. In some cases with a moreproximal AV nodal block, connective tissue trans-formation was seen at the region of the compactAV node. In cases of chronic incomplete AV block,strands of surviving fibers of the His bundle wereseen embedded in adiposofibrous tissue.
Discussion
This study shows tbat transcatheter Nd:YAGlaser photocoagulation of the AV junction from theaortic root is a fast and safe method for achievingexperimental ablation/modification of AV con-duction. With our simple tecbnique, the exact siteand degree of block is not precisely predictable.Damage can occur to either the AV node or the Hisbundle. Once achieved, CAVB is permanent, andit is not reversed by isoproterenol infusion. Histo-logic repair of the aortic root structures is com-plete; aortic regurgitation does not occur.
The main advantages of this approach for cre-ating experimental AV block are its safety and sim-plicity. Sterile intraoperative procedures forchronic AV block models are costly, time consum-ing, and may be associated with morbidity andprolonged recovery of the experimental animal.Transcatheter direct current electrical shock abla-tion and transcatheter argon laser vaporizationmay cause significant structural damage.^''•^^ Ra-diofrequency ablation of the AV node is more be-nign and should probably be the procedure of firstchoice. Radiofrequency ablation, however, is notinvariably successful for creating experimentalAV block.^^ Nd:YAG laser photoabiation from theaortic root is an encouraging alternative techniquefor AV ablation/modification. With improvementin the guiding technology involving some steer-ability at the tip of the electrode catbeter, an evenmore precise delivery of laser energy might be an-
PACE, Vol. 16 March, Part I 1993 405
LITTMANN, ET AL.
ticipated with more predictable areas of damage,and a 100% success rate.
It is intriguing to speculate whether Nd:YAGlaser photocoagulation from the aortic root mightbecome a clinically useful tool of catheter ablationof AV conduction. Right beart approaches may bemore advantageous because access is through avein rather than an artery, and energy transmis-sion does not have to occur through a valvularstructure. Radiofrequency ablation from the rightheart has a high clinical success rate, and is associ-ated with low morbidity.^^ In a minority of pa-References
1. Starzl TE, GaertnerRA, Baker RR. Acute completeheart block in dogs. Circulation 1955; 12:82-89.
2. Guzman SV, DeLeon AC. West IW. et al. Cardiaceffects of isoproterenol, norepinephrine and epi-nephrine in complete A-V heart hlock during ex-perimental acidosis and hyperkalemia. Circ Res1959; 7:666-672.
3. Pruett JK, Woods EF. Technique for experimentalcomplete heart block. ) Appl Physiol 1967; 22:830-831.
4. Starzl TE, Gaertner RA. Chronic heart hlock indogs. A method for producing experimental heartfailure. Circulation 1955; 12:259-270.
5. Day TK, Muir WW. A technique for productionof complete atrioventricular block in dogs. Am JPhysiol 1991; 261:H1312-H1316.
6. Randall OS. Westerhof N. Van den Bos GC. et al.Production of chronic heart block in closed-chestdogs; An improved technique. Am } Physiol 1981;241:H279-H282.
7. Lerman BB, Weiss ]L, Bukley BH. et al. Myocardialinjury and induction of arrhythmia by direct cur-rent shock delivered via endocardia! catheters indogs. Circulation 1984; 69:1006-1012.
8. Lee BL Gottdiener JS. Fletcher RD, et al. Transcath-eter ablation: Comparison between laser photoah-lation and electrode shock ablation in the dog. Cir-culation 1985; 71;579-586.
9. Svenson RH, Littmann L, Splinter R. et al. Applica-tion of lasers for arrhythmia ablation. In DP Zipes,J Jalife [eds.]; Cardiac Electrophysiology, From Cellto Bedside. Philadelphia, PA. W.B. Saunders,1990, pp. 986-997.
10. Curtis AB, Abela GS, Griffin JC, et al. Transvascu-lar argon laser ablation of atrioventricular conduc-tion in dogs: Feasibility and morphological results.PACE 1989; 12:347-357.
11. Narula OS, Bharati S, Chan MC, et al. Microtran-section of the His bundle with laser radiationthrough a pervenous catheter: Correlation of histo-logic and electrophysiologic data. Am J Cardiol1984; 54:186-192.
12. Svenson RH, Littmann L, Gallagher JJ. et al. Lasermodification of the myocardium for the treatment
tients, however, right-sided direct current and ra-diofrequency ablation remain unsuccessful.^""^^Further long-term experimental efficacy/safetystudies with a more advanced steerable catheterare needed to clarify whether Nd:YAC lasing fromthe aortic root has a clinical role for creating AVblock in cases where other modes of ablation havefailed.
Acknowledgment; The authors wish to acknowledge theexpert assistance of Michelle Thompson, BS, Kathy Dezern,RVMT, Keyna C. Winkler, and Steve Carico.
of cardiac arrhythmias: Background, current re-sults, and future possibilities. In GS Abela [ed.):Lasers in Cardiovascular Medicine and Surgery:Fundamentals and Techniques, Boston, MA,Kluwer Academic, 1990, pp, 327-346.
13. Littmann L, Svenson RH, Gallagher JJ, et al. Modifi-cation of sinus node function hy epicardial laserirradiation in dogs. Circulation 1990; 81;350-359.
14. Littmann L, Svenson RH, Tomcsanyi I. et al, Modi-fication of atrioventricular node transmissionproperties by intraoperative neodymium-YAGlaser photocoagulation in dogs. J Am Coll Cardioi1991; 17:797-804.
15. Ohelienius V, Knepa A, Ambartzumian R, et al.Transvenous ablation of the atrioventricular con-duction system by laser irradiation under endo-scopic control. Lasers Surg Med 1985; 5:469-474.
16. Mansour M, Curtis AB, Abela CS. et al. Modifica-tion of A-V conduction using a percutaneous com-bined laser-electrode catheter, [abstract]} Am CollCardiol 1990; 15:102A,
17. Lev M. The conduction system. In SE Gould [ed.];Pathology of the Heart and Blood Vessels. 3rd Edi-tion. Springfield, IL. Charles C. Thomas, 1968, pp.180-220.
18. Huang SK, Bharati S, Graham AR. et al. Closedchest catheter desiccation of the atrioventricularjunction using radiofrequency energy—a newmethod of catheter ablation. J Am Coll Cardiol1987; 9;349-358.
19. Jackman WM, Wang X. Friday KJ, et al. Catheterablation of atrioventricular junction using radio-frequency current in 17 patients: Comparison ofstandard and large-tip catheter electrodes. Circula-tion 1991; 83;1562-1576.
20. Sousa }, El-Atassi R, Rosenheck S, et al. Radiofre-quency catheter ablation of the atrioventricularjunction from the left ventricle. Circulation 1991;84;567-571.
21. Huang SKS, Chenarides JC, Cuenoud H, et al.Long-term follow-up of radiofrequency catheterablation of the atrioventricular node for supraven-tricular tachyarrhythmias. (abstract) J Am Coll Gar-diol 1990; 15;19A,
406 March, Part I 1993 PACE. Vol. 16
