casualized employment and turnover intention: home care workers in ontario, canada
TRANSCRIPT

Health Policy 91 (2009) 258–268
Contents lists available at ScienceDirect
Health Policy
journa l homepage: www.e lsev ier .com/ locate /hea l thpol
Casualized employment and turnover intention: Home care workers inOntario, Canada
Isik U. Zeytinoglua,∗, Margaret Dentonb, Sharon Davies1, Jennifer Millen Plenderleithc
a Human Resources and Management Area, DeGroote School of Business, McMaster University, Hamilton, ON L8N 3Z5, Canadab McMaster Centre for Gerontological Studies, Department of Health Aging and Society and Department of Sociology,McMaster University, Hamilton, ON L8N 3Z5, Canadac McMaster Centre for Gerontological Studies, McMaster University, Hamilton, ON L8N 3Z5, Canada
a r t i c l e i n f o
Keywords:Casualized employmentPerceived insecurityHome care workersTurnover intention
a b s t r a c t
The purpose of this paper is to examine the associations between casualized employmentand turnover intention in home care. Casualized employment refers to employment con-ditions of non-permanent contracts, part-time or casual hours, involuntary hours, on-callwork, split shifts, pay per visit, and hourly pay with variable hours. Casualized employmentalso refers to perceived employment insecurity and labour market insecurity. Data are froma survey of 991 visiting nurses, therapists and home support workers in a medium-sized cityin Ontario, Canada. Results show that, controlling for many other factors, casual hours and
perceived employment insecurity and labour market insecurity are positively and on-callwork is negatively associated with home care workers’ turnover intention. Non-permanentcontract, part-time hours, involuntary hours, split shifts, and non-salaried pay are featuresof the market-modelled home care work environment and therefore may not be associatedwith turnover intention. Results provide evidence on the effects of casualized employmentstrategies on home care workers’ turnover intention.1. Introduction
The health care sector is one of the largest employ-ing sectors in Canada. Despite the use of technology inmost aspects of care, the sector is dependent on a largenumber of workers at varying levels of skills. Within the
health care sector, home care has grown significantly inthe last 25 years in Canada. The demographics of an ageingpopulation combined with the trend of early hospital dis-charges, shortage of beds in long-term care institutions and∗ Corresponding author. Tel.: +1 905 525 9140x23957;fax: +1 905 521 8995.
E-mail address: [email protected] (I.U. Zeytinoglu).URL: http://www.business.mcmaster.ca/hrlr/profs/zeytino/
zeytinoglu.html (I.U. Zeytinoglu).1 Previously with McMaster Centre for Gerontological Studies, McMas-
ter University, Hamilton, ON L8N 3Z5, Canada.
0168-8510/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.healthpol.2008.12.004
© 2008 Elsevier Ireland Ltd. All rights reserved.
preference of older adults to age-in-place contribute to anincreased demand for home care services for all ages [1,2].With the health sector restructuring in the 1990s, casual-ized employment became a common feature in the sector[3], which includes home care [4].
The purpose of this paper is to examine the associationsbetween casualized employment and turnover intentionin home care. Casualized employment refers to employ-ment conditions of non-permanent contracts, part-time orcasual hours, involuntary hours, on-call work, split shifts,pay per visit, and hourly pay with variable hours. Casu-alized employment also refers to perceived employmentinsecurity and labour market insecurity. Data come from
our survey of 991 visiting workers in 11 home care agenciesin a medium-sized city in Ontario, Canada.The topic of this paper is timely and important formanagers and policy makers. Staff shortages and reten-tion problems in home care are well known in Canada

ealth Pol
[caaaeitite
2
lppctegiaC4ttavmmpfPCCfa[
tiapswt
io[gdpa[rwsc
I.U. Zeytinoglu et al. / H
1,2,5,6] and the workforce and work environment issuesontinue to be the priority concern for health care man-gers and policy makers [7–9]. Similarly in Europe [10–13]nd in the U.S. [14] labour supply-demand imbalancesre creating challenges for decision-makers. Casualizedmployment is also gaining importance globally since its being prescribed by the international financial institu-ions as flexibility in health care for industrialized andndustrializing countries [15]. Our findings contribute tohe knowledge on the topic and assist all stakehold-rs.
. Background to the study
In the 1990s, rising costs and reduced federal fundinged to health system restructuring in Ontario and otherrovinces in Canada [3]. Hospital beds were closed andatients were discharged quicker and with more acuteare needs. These patients became the priority clients ofhe home care system; clients with ongoing needs wereither dropped from the system or had their care hoursreatly reduced [16]. With the health system restructur-ng, the home care sector went through dramatic changess well [4,17]. The existing Home Care and Placemento-ordination Programs in Ontario were replaced with3 Community Care Access Centres (CCACs), whose func-ion is to choose service providers through a processermed ‘managed competition’. Since then, these have beenmalgamated into 14 CCACs. Delivery of home care ser-ice changed from a ‘non-competitive’ system of sharedarket by not-for-profit home care organizations to aarket-modelled ‘competitive’ system where both for-
rofit and not-for-profit organizations compete in a requestor proposal process to secure contracts to deliver services.roposals are evaluated and contracts are rendered by theCACs. These contracts last a specified period of 1–4 years.ase managers employed by these agencies are responsible
or determining eligibility of clients for services, planningprogram of care and ensuring that services are delivered
18,19].In the labour-intensive service work of home care,
he move to a market-modelled system has led toncreased casualization of work, employment insecuritynd a decrease in pay and benefits [19,18]. Nurses, thera-ists, and personal support workers who once worked inecure organizations are left wondering every few yearshether they will have a job in the market-modelled sys-
em [4,17].Research shows that in a case study city in Ontario dur-
ng the first 5 years of the restructuring, more than halff nurses and home support workers left their employers4]. For those who stayed in their jobs, workers identified areater emphasis on the business side of providing care andiscussed decreased co-worker and organizational sup-ort, staff shortages, work intensification, fewer resourcesnd greater job insecurity as concerns in their workplaces
4]. For those who were employed in the system prior toestructuring and who experienced the restructuring, thereas decreased level of job satisfaction and greater propen-ity to leave [18]. These issues provided impetus to theurrent study.
icy 91 (2009) 258–268 259
3. Theory and factors associated with turnoverintention
The theory on turnover shows that turnover inten-tion is the best predictor of whether an employee willleave the organization [20–24]. This paper is based ondata from workers still employed in their workplaces, andthus, we refer to turnover intention. The theory predictsthat a number of factors from people’s work environmentsand personal lives affect their turnover intention [22–25].Empirical testing of the turnover intention theory showsthat employment conditions such as heavy workload, lackof support from organizational leaders and co-workers, andpoor working conditions are some of the factors affectingturnover intention [26,27]. Studies on Canadian home careworkers show the same factors contributing to turnover[19,2,4] and turnover intention [17].
Empirical testing of turnover theory shows thatturnover decision and the intention to leave can also beaffected by a number of individual characteristics such asoccupation, education, age, tenure, membership in a union,and income [20,22,25]. Those in occupations that are indemand, higher educated, younger workers, those withlower workplace tenure, and those with low earnings aremore inclined to leave their workplaces [25,24,28]. Posi-tive effects of unions on work conditions are well knownand research in home care [1,2] has established that unionsplay a role in addressing the working conditions of work-ers. The theoretical relationship between job satisfactionand turnover intention is also well established in the litera-ture [21,24,29,30], and there is empirical research showingjob satisfaction as a major factor affecting an individual’sdecision to stay or leave the organization [25,31]. The con-ceptual framework of the study is presented in Fig. 1.
In this study we go beyond these well-known fac-tors and focus on the changing work environment and itspossible association with turnover intention (see Fig. 1).For changing work environments we focus on casualizedemployment and perceived insecurity. Although casualizedemployment can equate flexibility for employers and someworkers, at the same time, it can equate insecurity for manyother workers [32].
There can be many forms of casualized employment andin this study we focus on non-permanent contracts, part-time or casual hours, involuntary hours, on-call work, splitshifts, pay per visit, and hourly pay with variable hours. Inthe home care sector non-permanent contracts are com-mon. Some work part-time hours with regularity in thehours assigned and others work casual hours where thereis no regularity in hours worked. Casualized employmentalso refers to employment conditions where employeeswork only available hours offered by employers, i.e. work-ing involuntary hours. On-call work is another form ofcasualized employment where workers are expected to beavailable and ready to work when called but are not guaran-teed hours of work or a schedule. On-call workers in home
care are generally not paid for the hours spent waiting forthe employer to call them to work. Casualized employmentcan also be in the form of working split shifts where workis split into few-hour shifts. In practice this means work-ers are employed, for example, in the early morning and in
260 I.U. Zeytinoglu et al. / Health Policy 91 (2009) 258–268
rkers’ ca
Fig. 1. The conceptual model of home care wothe evening for a few hours in each period in which theirservices are needed. Another form of casualized employ-ment is achieved through pay structures. In home care workthis can be pay per visit or hourly pay with variable hours.While both types of pay are casualized forms of pay sincethey pay only for the time spent with the client, and nei-ther include pay for break-time or lunch-time, the lattertype, i.e. hourly pay with variable hours, provides no pre-dictability in income due to no guarantee of hours worked.The literature on changing work environments shows thatalmost all of these forms of casualized employment are cre-ated by employers for their flexibility interests [32,33]. Inthis study we cover all of these different forms of casualizedemployment types.
Empirical research on casualized employment showsthat while the employment status of temporary workor part-time work is not associated with job satisfactionworkers’ perception of the job insecurity affects their jobsatisfaction [34]. Research on home care workers in Canadasuggests that workers understand that work is availableas long as they are willing to change workplaces, workin casual, insecure jobs, work shifts, accept flexible payschemes and be flexible to keep their jobs [19,4,18,35].
Workers indicate that these are negative aspects of theirjobs [6] affecting their job satisfaction and turnover deci-sion [18].Casualized employment affects workers’ feelings andcan result in perceived employment insecurity and labour
sualized employment and turnover intention.
market insecurity [36,37]. We refer to the broader terminol-ogy of employment insecurity in this study rather than thecommonly used job insecurity terminology. There are noclear definitions of perceived insecurity [38] and researchshows that when asked, most workers refer to a broad con-cept of insecurity [36]. Employment insecurity refers to thesituation where the employer can arbitrarily dismiss or lay-off workers or where regulations on hiring and firing arerelaxed and such actions do not impose costs on employ-ers [33]. It also includes situations where the workplaceenvironment is unregulated and the ability to continue towork is at risk. Employment insecurity also refers to thesituation where the employer can shift workers from onejob to another, or alter or reduce the content of the job atwill.
Labour market insecurity is different than employmentinsecurity. The former refers to the sectoral- or regional-level insecurity while the latter refers to the employmentsituation within the worker’s workplace. Labour marketinsecurity can be defined as workers’ perceptions of laboursurpluses in the sector where, if unemployed, the chancesof securing employment are low [33].
In terms of empirical research, Sverke et al.s’ [28]
meta-analysis shows that there is a substantial negativecorrelation between job insecurity and job satisfaction anda moderate positive correlation between job insecurity andturnover intention. A recent European study shows that jobinsecurity is associated with decreased job satisfaction and
ealth Pol
ic[it
(oWaidcaoBecee
4
4
t(Oftoou
wtaArcarcwetnspstwrd
4
qw
I.U. Zeytinoglu et al. / H
ncreased turnover intention, and that the effect of job inse-urity on turnover intention is mediated by job satisfaction39]. Empirical research on the home health care sectorn Canada shows job insecurity as an important factor inurnover intention [1,2,6,17] and turnover [18].
As presented in the conceptual framework of this studyFig. 1), we test the association of casualized employmentn home care workers’ intention to leave their workplaces.ork schedule and pay satisfaction are tested as the medi-
ting factors in the proposed relationship between thendependent factors of casualized employment and theependent factor of turnover intention. Physical and psy-hosocial work factors and individual characteristics thatre well established in the empirical testing of the the-ry on turnover intention are included as control variables.ased on the theory and empirical literature reviewed, wexpect that casualized employment will be positively asso-iated with home care workers’ turnover intention. We alsoxpect job satisfaction to mediate the effects of casualizedmployment turnover intention.
. Methodology
.1. Research design, sample and data collection process
The paper uses a quantitative research design usinghe survey method. The sample consists of all workersN = 1949) in home care organizations in a mid-sized city inntario. The sample is exhaustive in that all organizations
rom both non-profit and for-profit that received contractso perform home care services as well as the contractingrganization are included in the study. The 11 employingrganizations and 7 union locals representing workers innionized organizations are partners in this study.
A self-administered questionnaire was mailed out to allorkers in 2002. Those who had not returned their ques-
ionnaires by a selected date were mailed a reminder cardnd later a second letter and copy of the questionnaire.
total of 1311 home care workers responded (responseate of 67%). In this paper the focus is on visiting homeare workers (N = 991) since their employment conditionsre more prone to casualized employment and insecu-ity than office staff consisting of managers, supervisors,ase managers, and office support staff. Visiting home careorkers include nurses, therapists and home support work-
rs who assist sick, elderly, or persons with disabilities inheir home environment. Visiting nurses include registeredurses and registered practical nurses. They perform tasksuch as dressings and intravenous therapy. Visiting thera-ists include occupational therapists, physiotherapists, andocial workers. Home support workers assist clients withhe activities of daily living. For example they help clientsith personal health care such as bathing and meal prepa-
ation and they clean only as part of their health supportuties.
.2. Instrument and measures
The instrument of this study is a self-completionuestionnaire on health and work life of home careorkers [40]. For scales adopted from other studies, i.e.
icy 91 (2009) 258–268 261
turnover intention, workload, organizational and peer sup-port scales, confirmatory factor analysis with “varimax”rotation are run. For the ‘employment insecurity’ scalewe developed, exploratory factor analysis with “varimax”rotation (see below). Cronbach’s alphas were calculatedto measure reliability of the scale items for all thescales used within this study. Alphas were found to beacceptable ranging from .81 to .92 for all scales (seeTable 1).
The dependent variable of turnover intention is Lyons’ [41]three-item propensity to leave scale. The questions include,‘if I were completely free to choose, I would prefer to con-tinue working at this agency; I would like to stay at thisagency for a long time; and if I had to quit work for a while,I would be likely to return to this agency’. The responsesare coded on a five point Likert scale from “1 = strongly dis-agree” to “5 = strongly agree” and the scale is developedby summing the scores of the three items. All items arereversed in creating the scale with possible scores rangefrom 3 to 15; higher scores indicate higher turnover inten-tion. Descriptive statistics for this scale can be found inTable 1.
The independent variable is casualized employment.Casualized employment is measured as whether theemployment contract is permanent (=1) or not (=0), work isfull-time, part-time or casual hours (each coded as 1 = yes,0 = otherwise), involuntary hours (1 = if involuntary, 0 = ifprefer to work these hours), on call work (Likert scale of1 = none of the time to 5 = all of the time), work split shifts(Likert scale of 1 = none of the time to 5 = all of the time),and salaried (paid the same amount each week, biweeklyor monthly), pay per visit, or hourly pay with variable hours(each coded as 1 = yes, 0 = otherwise).
Casualized employment is also measured as employ-ment insecurity and labour market insecurity. The measureof employment insecurity is developed based on the jobinsecurity scale of Cameron et al. [42] and items includedfrom the qualitative study of Denton et al. [43]. Theemployment insecurity measure is a summative variableconsisting of six items: ‘I am presently safe from dismissalat this agency’ (reversed in coding), ‘I feel I am likely tobe laid off at this agency’; ‘I am worried about my futurewith this agency’; ‘I feel uneasy about the security in mypresent job’; ‘I am worried about my job security’; ‘I amconcerned about losing my job due to overall changes inthe long-term care sector’. Responses are coded on a Lik-ert scale of 1 = strongly disagree to 5 = strongly agree. Weuse exploratory factor analysis (principal components fac-tor analysis) with “varimax” rotation method to identifyitems composing the scale. There are a few other items inCameron et al. scale [42] (worded positively or negatively)but they are not included since they did not contribute tothe scale or, in our view, are not related to perceived inse-curity. The employment insecurity scale is composed bysumming the six items.
Labour market insecurity is the second measure of inse-
curities in casualized employment. This is a single itemmeasure worded as ‘If I lose my job here I will likely findanother job in my profession’ (coded on a Likert scaleof 1 = strongly disagree to 5 = strongly agree, and reversecoded).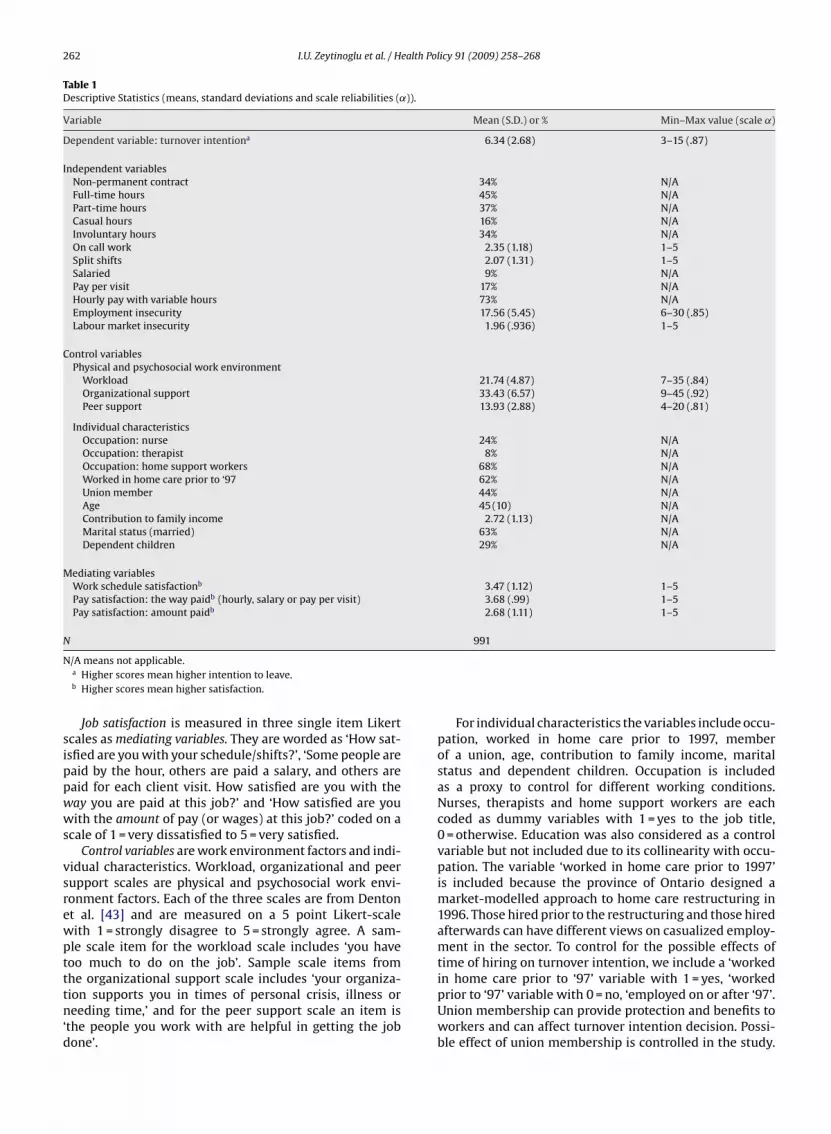
262 I.U. Zeytinoglu et al. / Health Policy 91 (2009) 258–268
Table 1Descriptive Statistics (means, standard deviations and scale reliabilities (˛)).
Variable Mean (S.D.) or % Min–Max value (scale ˛)
Dependent variable: turnover intentiona 6.34 (2.68) 3–15 (.87)
Independent variablesNon-permanent contract 34% N/AFull-time hours 45% N/APart-time hours 37% N/ACasual hours 16% N/AInvoluntary hours 34% N/AOn call work 2.35 (1.18) 1–5Split shifts 2.07 (1.31) 1–5Salaried 9% N/APay per visit 17% N/AHourly pay with variable hours 73% N/AEmployment insecurity 17.56 (5.45) 6–30 (.85)Labour market insecurity 1.96 (.936) 1–5
Control variablesPhysical and psychosocial work environment
Workload 21.74 (4.87) 7–35 (.84)Organizational support 33.43 (6.57) 9–45 (.92)Peer support 13.93 (2.88) 4–20 (.81)
Individual characteristicsOccupation: nurse 24% N/AOccupation: therapist 8% N/AOccupation: home support workers 68% N/AWorked in home care prior to ‘97 62% N/AUnion member 44% N/AAge 45 (10) N/AContribution to family income 2.72 (1.13) N/AMarital status (married) 63% N/ADependent children 29% N/A
Mediating variablesWork schedule satisfactionb 3.47 (1.12) 1–5Pay satisfaction: the way paidb (hourly, salary or pay per visit) 3.68 (.99) 1–5Pay satisfaction: amount paidb 2.68 (1.11) 1–5
N 991
N/A means not applicable.a Higher scores mean higher intention to leave.b Higher scores mean higher satisfaction.
Job satisfaction is measured in three single item Likertscales as mediating variables. They are worded as ‘How sat-isfied are you with your schedule/shifts?’, ‘Some people arepaid by the hour, others are paid a salary, and others arepaid for each client visit. How satisfied are you with theway you are paid at this job?’ and ‘How satisfied are youwith the amount of pay (or wages) at this job?’ coded on ascale of 1 = very dissatisfied to 5 = very satisfied.
Control variables are work environment factors and indi-vidual characteristics. Workload, organizational and peersupport scales are physical and psychosocial work envi-ronment factors. Each of the three scales are from Dentonet al. [43] and are measured on a 5 point Likert-scalewith 1 = strongly disagree to 5 = strongly agree. A sam-ple scale item for the workload scale includes ‘you havetoo much to do on the job’. Sample scale items from
the organizational support scale includes ‘your organiza-tion supports you in times of personal crisis, illness orneeding time,’ and for the peer support scale an item is‘the people you work with are helpful in getting the jobdone’.For individual characteristics the variables include occu-pation, worked in home care prior to 1997, memberof a union, age, contribution to family income, maritalstatus and dependent children. Occupation is includedas a proxy to control for different working conditions.Nurses, therapists and home support workers are eachcoded as dummy variables with 1 = yes to the job title,0 = otherwise. Education was also considered as a controlvariable but not included due to its collinearity with occu-pation. The variable ‘worked in home care prior to 1997’is included because the province of Ontario designed amarket-modelled approach to home care restructuring in1996. Those hired prior to the restructuring and those hiredafterwards can have different views on casualized employ-ment in the sector. To control for the possible effects oftime of hiring on turnover intention, we include a ‘worked
in home care prior to ‘97’ variable with 1 = yes, ‘workedprior to ‘97’ variable with 0 = no, ‘employed on or after ‘97’.Union membership can provide protection and benefits toworkers and can affect turnover intention decision. Possi-ble effect of union membership is controlled in the study.
ealth Pol
Tceiwy1fayctmot
4
Liomvfcts5ts
ptsviwstfiaiv
5
5r
(cttdvt1st
I.U. Zeytinoglu et al. / H
his variable is coded as 1 = member, 0 = not. Older workersan be more inclined to stay and those whose employmentarnings contribute greatly to family income will be lessnterested in turnover intention. To control for these effects,
e include age and income variables. Age is measured byears and contribution to family income is measured as= 1–25% to 4 = 76–100%. Tenure in the job is considered
or the study but not included due to its collinearity withge. Marital status and having dependent children (childrenounger that 13 years of age in household) are included toontrol for their possible associations with turnover inten-ion. Marital status is coded as 1 = married/common law
arriage, and 0 = otherwise (divorced, separated, widowedr never married). Those with dependent children youngerhan 13 at home are coded as 1, others are coded as 0.
.3. Analysis
Descriptive statistics, bivariate regression and Ordinaryeast Square (OLS) regression are conducted. The equalnterval assumption is used for Likert scale measurementf the dependent variable. To maintain our sample sizeissing cases in the analyses were coded to the mean for
ariables on that scale. They are coded to the value of “0”or dichotomous variables. In all variables, missing valuesomprise less than 5% of the responses and thus codinghe mean is at the acceptable level for statistical analy-is, except two variables. On-call work and split-shifts have.6% and 5.3% missing, respectively, and missing values inhese variables are coded as “0 = does not work on-call orplit-shift”.
In the OLS regression for satisfaction variables, inde-endent and control variables are entered together. In theurnover intention analysis, the mediating variables of jobatisfaction are included in Step 2. Adjusted R2 is pro-ided to show the variance explained by factors includedn each model. Testing for mediation effects are conducted
ith each job satisfaction variable (though not included forpace restrictions). We conducted tests for mediation usinghe three-stage regression analysis of Baron and Kenny [44],rst regressing each mediator on the independent vari-bles, second regressing the dependent variable on thendependent variables, and third regressing the dependentariable on both mediator and independent variables.
. Results
.1. Work and demographic characteristics of surveyespondents
The mean value for turnover intention is 6.34S.D. = 2.68) (see Table 1). About 1 in 10 visiting homeare workers report turnover intention. Findings showhat 59% of workers are satisfied or very satisfied withheir work schedule, while 20% are neither satisfied norissatisfied, leaving 21% of the workers dissatisfied or
ery dissatisfied. Similar findings are found for satisfac-ion with the way they were paid with 70% being satisfied,6% neither satisfied or dissatisfied and 14% being dis-atisfied. Findings are quite opposite when it comes tohe amount they are paid with only 29% being satisfied,icy 91 (2009) 258–268 263
21% neither satisfied or dissatisfied and 49% dissatis-fied.
In terms of casualized employment variables, as shownin Table 1, 34% have non-permanent contracts, and, while45% have full-time hours of employment, more than halfhave part-time or casual hours of employment (37% and16%, respectively). More than a third report working invol-untary hours. Twelve percent work on-call and 14% worksplit shifts all or most of the time. While employers seemto have flexibility in pay, workers have little income secu-rity in these jobs: only 9% are salaried with the otherseither being paid per visit (17%) or hourly paid with variablehours (73%). There is a moderately high level of perceivedemployment insecurity among visiting home health careworkers (M = 17.56, S.D. = 5.45). The labour market insecu-rity variable shows that only 7% of visiting home health careworkers feel that if they lose their job they will not be ableto find another job in their profession.
In terms of demographic characteristics of workers,starting with occupational distribution, 68% of the respon-dents are home support workers, 24% are nurses, and 8%are therapists. Almost half of the workers are members of aunion (44.4%). The majority of home health care workers inthis study are female (94%), which is also characteristic ofthe industry. Workers’ ages range from 20 to 72 years withthe average age at 45 years. Most respondents are marriedor living with a partner (63%) with the remainder beingwidowed, divorced, separated or never married. Close toa third have dependent children. These statistics are pre-sented in Table 1. The occupation, gender, age and maritalstatus characteristics of the sample closely resemble themost recent profile of the home health care workforce inCanada [1,2].
5.2. Bivariate and OLS regression results for jobsatisfaction
Since job satisfaction is examined as a mediating vari-able, we first focus on the associations of casualizationvariables significantly related to the three job satisfac-tion variables. Bivariate regression coefficients, presentedin Table 2, column 2, shows that having a permanent con-tract, working full-time or casual hours and being a salariedworker are positively, and involuntary hours, on call work,split shifts, hourly pay with variable hours and employmentinsecurity are negatively associated with satisfaction withwork schedule. The other variables, i.e. part-time hours, payper visit and labour market insecurity, are not related towork schedule satisfaction.
Similarly, focusing on satisfaction with the way theyare paid as hourly, salaried and pay per client visit, col-umn 4 illustrates that those in involuntary hours, on-callwork, split-shifts, pay per visit, and perceiving employmentinsecurity report lower level of pay satisfaction whereassalaried workers report higher pay satisfaction. Other casu-alization variables are not associated with pay satisfaction.
The last group of bivariate regressions examine the asso-ciations between casualization variables and satisfactionwith the amount paid. As presented in Table 2, column6, working on a permanent contract, full-time hours, splitshifts and employment insecurity are related to lower pay

264
I.U.Zeytinoglu
etal./H
ealthPolicy
91(2009)
258–268
Table 2Factors associated with visiting home health care workers’ work schedule and pay satisfaction (bivariate and OLS regressions).
Column 1 Column 2 Column 3 Column 4 Column 5 Column 6 Column 7
Work schedule satisfaction Pay satisfaction: the way paid (hourly, salary or pay per visit) Pay satisfaction: amount paid
Bivariate regressioncoefficients, B (S.E.)
OLS regression,B (S.E.)
Bivariate regressioncoefficients, B (S.E.)
OLS regression,B (S.E.)
Bivariate regressioncoefficients, B (S.E.)
OLS regression,B (S.E.)
Constant 3.948 (.368) 4.521 (.352)*** 3.372 (.404)***
Independent variablesPermanent contract .177 (.075)* −.084 (.080) −.074 (.066) −.073 (.077) −.146 (.074)* −.127 (.088)Full-time hours .220 (.071)** Reference −.095 (.063) Reference −.148 (.071)* ReferencePart-time hours −.003 (.074) −.122 (.074) .083 (.065) .031 (.071) .096 (.073) .002 (.081)Casual hours .332 (.097)*** −.262 (.110)* .063 (.087) .047 (.106) .120 (.097) .068 (.121)Involuntary hours −.954 (.069)*** −.674 (.069)*** −.369 (.066)*** −.143 (.066)* −.136 (.075) .024 (.076)On call work −.164 (.031)*** −.056 (.028)* −.076 (.027)** −.018 (.027) −.035 (.031) .010 (.031)Split shifts −.227 (.027)*** −.139 (.025)*** −.106 (.024)*** −.048 (.024)* −.131 (.027)*** −.113 (.028)Salaried .452 (.122) *** Reference .581 (.107)*** Reference .071 (.121) ReferencePay per visit −.051 (.095) −.263 (.122)* −.506 (.083)*** −.855 (.117)*** .074 (.094) −.086 (.134)Hourly pay with variable hours −.196 (.080)* −.164 (.110) .100 (.071) −.312 (.106)** −.085 (.079) .016 (.121)Employment insecurity −.050 (.006)*** −.031 (.006)*** −.037 (.006)*** −.025 (.006)*** −.043 (.006)*** −.035 (.007)***
Labour market insecurity −.044 (.038) −.013 (.033) −.034 (.034) −.012 (.031) −.009 (.038) .016 (.036)
Control variablesWork environment
Workload −.034 (.007)*** −.017 (.007)** −.039 (.006)*** −.028 (.006)*** −.043 (.007)*** −.026 (.007)***
Organizational support .054 (.005)*** .029 (.005)*** .031 (.005)*** .015 (.005)** .037 (.005)*** .020 (.006)***
Peer support .108 (.012) .044 (.012)*** .078 (.011)*** .036 (.012)** .055 (.012)*** .023 (.014)
Individual characteristicsOccupation: nurse .058 (.083) −.077 (.082) .269 (.073)*** .243 (.079)** −.241 (.082)** −.119 (.090)Occupation: therapist .605 (.126)*** .265 (.133)* .259 (.113)* .376 (.128)** .864 (.123)*** .864 (.146)***
Occupation: home support worker −.263 (.076)*** Reference −.315 (.067)*** Reference −.107 (.075) ReferenceWorked in home care prior to 97 .072 (.073) −.034 (.068) .058 (.065) .032 (.065)Union member −.090 (.071) −.003 (.071) −.118 (.063) −.004 (.068) −.204 (.071)** .122 (.078)Age .005 (.003) −.000 (.003) .003 (.003) −.003 (.003) −.005 (.003) −.005 (.004)Contribution to family income −.034 (.032) −.022 (.031) −.026 (.029) .006 (.029) −.068 (.032)* −.060 (.034)Marital status −.180 (.074)* −.045 (.071) −.170 (.065)** −.116 (.068) −.0421 (.073) .063 (.078)Dependent children −.063 (.079) −.039 (.073) −.093 (.070) −.121 (.070) −.021 (.078) −.055 (.080)
Adj. R2 .308 .190 .149N 991 991 991 991 991 991
* p < .05.** p < .01.
*** p < .001.

ealth Pol
svtcs
mwTawcicciw
TF
V
C
I
C
M
AN
I.U. Zeytinoglu et al. / H
atisfaction (the amount paid). The other casualizationariables are not associated with this type of pay satisfac-ion. We do not discuss the bivariate regressions for theontrol variables due to space limitations, but they are pre-ented in Table 2.
Turning to OLS regression results, and focusing on theodel including both control and independent variables,e start with work schedule satisfaction, presented in
able 2, column 3. It is clear that many of the casu-lized employment variables are associated with lowerork schedule satisfaction. Controlling for other factors,
ompared to working full-time hours, casual hours, andnvoluntary hours, on call work and split shifts are asso-
iated with lower work schedule satisfaction. Similarly,ompared to salaried work, pay per visit and employmentnsecurity are significantly and negatively associated withork schedule satisfaction. Other variables are not associ-
able 3actors associated with visiting home health care workers’ turnover intention (bi
ariables Bivariate regressioncoefficients, B (S.E.)
onstant
ndependent variablesPermanent contract −.601 (.179)***
Full-time hours −.560 (.170)***
Part-time hours .076 (.176)Casual hours .874 (.233)***
Involuntary hours .729 (.180)***
On call work −.100 (.074)Split shifts −.066 (.067)Salaried −1.111 (.291)***
Pay per visit −.213 (.228)Hourly pay with variable hours .671 (.190)***
Employment insecurity .020 (.016)Labour market insecurity .436 (.090)***
ontrol variablesWork environmentHeavy workload .017 (.017)Organizational support −.166 (.012)***
Peer support −.305 (.028)***
Individual characteristicsOccupation
Nurse −.188 (.200)Therapist −1.202 (.303)***
Home support worker .583 (.181)***
Worked in home care prior to ‘97 −.532 (.174)**
Union member −.177 (.171)Age −.043 (.008)***
Contribution to family income −.053 (.077)Marital status .260 (.177)Dependent children .446 (.188)*
ediating variables:Work schedule satisfaction −.505 (.075)***
Pay satisfaction: the way paid −.672 (.083)***
Pay satisfaction: amount paid −.529 (.075)***
dj. R2 change in R2
* p < .05.** p < .01.
*** p < .001.
icy 91 (2009) 258–268 265
ated with this type of satisfaction. The model explains 31%of the variance in work schedule satisfaction.
Table 2, column 5 presents regression coefficients forpay satisfaction. Of the independent variables, those ininvoluntary hours, split shifts, paid per visit, and perceiveemployment insecurity are the ones reporting lower sat-isfaction with the way paid. Those paid hourly but withvariable hours are reporting higher satisfaction with theway paid. Other independent variables are not significantlyassociated with this type of satisfaction. With all variablesincluded, the model explains 19% of the variance in satis-faction with the way paid.
Next we examine the association between independent
variables and satisfaction with the amount paid while con-trolling for all other factors in the model (Table 2, column7). Split shifts and employment insecurity are the onlytwo independent variables associated with decreased payvariate and OLS regressions).
Step 1: independent andcontrol variables, B (S.E.)
Step 2: mediatorsincluded, B (S.E.)
13.638 (.918)*** 16.337 (1.012)***
−.049 (.200) −.115 (.196)Reference Reference.158 (.185) .165 (.181).526 (.275) .553 (.270)*
.214 (.173) .146 (.177)−.245 (.071)*** −.250 (.070)***
−.015 (.063) −.070 (.063)Reference Reference.142 (.304) −.186 (.306).300 (.275) .192 (.271)−.013 (.016) −.033 (.016)*
.399 (.082)*** .399 (.080)***
.008 (.017) −.010 (.017)−.140 (.014)*** −.128 (.014)***
−.105 (.031)*** −.084 (.030)**
−.617 (.205)** −.572 (.202)**
−.891 (.332)** −.495 (.331)Reference Reference−.191 (.169) −.192 (.165)−.136 (.178) −.101 (.174)−.038 (.008)*** −.040 (.008)***
.068 (.077) .051 (.075)
.133 (.177) .110 (.174)
.104 (.182) .045 (.179)
−.037 (.080)−.342 (.086)***
−.298 (.075)***
.251 .282 .033991 991

ealth Pol
266 I.U. Zeytinoglu et al. / Hsatisfaction (the amount paid). The model, including allvariables, explains 15% of the variance in satisfaction withthe amount paid.
5.3. Bivariate and OLS regression results for turnoverintention
In Table 3, bivariate regression coefficients show theassociation between casualized employment, control vari-ables and turnover intention. Permanent contract, workingfull-time hours and salaried pay are significantly and neg-atively associated with turnover intention. Casual hours,involuntary hours, hourly pay with variable hours, labourmarket insecurity and employment insecurity are associ-ated with increased intention to leave though the level ofsignificance is = .053 for the latter variable. However, part-time hours, working on call or split shifts are not related toturnover intention.
Turning to multivariate analysis, as presented in Table 3,step 1, the associations between control variables andturnover intention are generally in line with establishedknowledge in prior research. For independent variables ashypothesized, casual hours as compared to full-time hoursand labour market insecurity are significantly and posi-tively associated with turnover intention. Contrary to ourexpectations, other casualized employment variables arenot associated with turnover intention and those workingon call have less intention to leave.
In step 2, satisfaction variables are included in theanalysis to show the additional effect of job satisfactionvariables on turnover intention. Controlling for all othervariables in the model, results show that pay satisfaction,i.e. hourly, salary or per visit, and satisfaction with theamount paid are both significantly and negatively associ-ated with turnover intention. Work schedule satisfaction,however, is not related to intention to leave. The expectedrelationships between casual hours as compared to full-time hours, on call work, and labour market insecurity withturnover intention continue in step 2. In addition, employ-ment insecurity becomes weakly significant but, contraryto expectations, negative. The full model with all vari-ables included explains 28% of turnover intention of visitinghome health care workers with job satisfaction contribut-ing to the 3% of the variance.
Contrary to our expectations, job satisfaction variablesdo not mediate the associations of casualized employ-ment on turnover intention. For mediation testing separateregressions are run with each job satisfaction variableincluded in the analysis. Results show that none of the casu-alized employment variables’ association with turnoverintention is mediated through job satisfaction. Tables forthis analysis are not provided due to space restrictions butare available from the first author.
6. Discussion and policy implications
Results of this study show that many of the casu-alized employment variables included in this study arerelated to home care workers’ decreased job satisfactionand increased turnover intention. In particular, those work-ing casual hours, involuntary hours, on-call, split shifts, and
icy 91 (2009) 258–268
being paid per visit are also the ones less satisfied withtheir work schedules. For pay satisfaction, focusing on theway paid, i.e. hourly, salary or per visit pay, those workinginvoluntary hours, split shifts, in paid per visit contracts areless satisfied with the way they are paid. Those workingsplit shifts are less satisfied with their hourly rate. How-ever, those working on an hourly basis with variable hoursare more satisfied with the way they are paid. It is possi-ble that some of these workers with variable hours have asecond job and are satisfied because they have control overwhere and when they work. Indeed, a further analysis ofthis issue showed that among our respondents 22% have asecond job in home care and more than three-quarters ofthose working on an hourly basis with variable hours haveone or more second jobs in home care.
Similar to the literature [28], our study shows thatemployment insecurity is associated with decreased jobsatisfaction. Casualized employment in the home caresector is an outcome of health system reforms in the1990s [3] which affected work environments, manage-ment of human resources, union-management relations,and employee attitudes. Short-term consequences of thesereforms are job dissatisfaction, which in the long-term canresult in increased turnover intention.
Consistent with the literature [25,31], our results indi-cate that decreased pay satisfaction is associated withturnover intention. We suggest that dissatisfaction withpay should be addressed in policy for possible retentionof workers in the home care field. Other studies show thatwage discrepancy between home care workers and hospitaland institutional health care workers is contributing to thewidespread labour market shortage in the home care field[17,18]. In Ontario, it is well known that hospital workers arepaid significantly more than home care workers. This is aserious injustice considering that hospitals are dischargingpatients “quicker and sicker” and in turn, home care clientshave more complex and acute care needs. Under these cir-cumstances, one has to question the incentive for workersto stay in home care sector if they can find better payingemployment in hospitals and institutions.
Our results show those employed in casual hours arealso the ones intending to leave their workplaces. Asexpected in casual type of employment, workers have ahigher tendency to leave their jobs when they can find bet-ter jobs. The new job can be full-time employment in homecare or even a few part-time jobs pieced together creatingfull-time hours in hospitals and long-term care institutions,but it is clear that casual workers do not intend to stay withtheir organizations. It is also possible that casual workersopt for this kind of employment because they do not wantfull-time employment in home care field [45].
As shown, work on call is negatively associated withturnover intention. This may be because of a shift by manyhome care organizations, after restructuring, to an elect-to-work model of care for those who work on-call. In thismodel workers may decide, without penalty, whether or
not to work when requested [6]. This change provideschoice to workers and is viewed positively by some workers[6].Literature suggests that job (employment) insecurityis positively associated with turnover intention [28,39],

ealth Pol
yewmrs
imfiimw
FA(ttrcceeiihlt
fmacranjoihcCwowciachuabf
slots
I.U. Zeytinoglu et al. / H
et unexpectedly, with mixed results we conclude thatmployment insecurity is positively but weakly associatedith turnover intention. Employment insecurity within thearket-modelled home care is a feature of the work envi-
onment for all visiting workers and may therefore not betrongly related to intention to leave.
Literature also indicates that turnover intention is highn the home care sector where workers experience labour
arket insecurity [1,2,6,17]. Similar to the literature, wend that when controlling for many work, workplace and
ndividual factors, employees who are perceiving labourarket insecurity are the ones intending to leave theirorkplace.
It is important to note several limitations of our study.irst, it is a survey of workers in a single location in Ontario.lthough conducting the study focusing on a single location
but including all home health care workers in that loca-ion) allows us to examine the issues in-depth, we cautionhe readers in generalizing from our results. Though theesults reflecting the respondents’ views are valid, and theharacteristics of the sample closely resemble home healthare workers in Canada [1,2] they cannot be entirely gen-ralized to all home health care workers in Ontario andlsewhere. We suggest further studies on the topic, anddeally, a national-level analysis of these issues for general-zations. Second, although the response rate to our study isigh, we recognize that it is possible that those with higher
evels of interest in the topic are more likely to respond tohis survey, and thus may bias the results.
In light of our findings that casualized employment is aeature of the market-modelled home care work environ-
ent and employment and labour market insecurity aressociated with turnover intentions, we recommend somehanges to the current home care system to contribute toetention of workers in the sector. This can involve the cre-tion of a more stable workforce that includes a greaterumber of full-time, permanent jobs. This can benefit not
ust the workers, but the clients as well. It is well known thatne of the most positive and rewarding aspects of workingn home care is the personal contact and relationships thatome care workers form with their clients [43]. Turnoveran affect patient outcomes including the quality of care.lients and workers alike prefer to have continuity of care,hich results from having the same home care worker(s)
ver time. Continuity of care is nearly impossible to sustainithin the current market-modelled ‘competitive’ home
are system that relies on different organizations compet-ng for contracts to deliver home care every few years. Inddition, as our results show, supportive workplaces ando-workers are additional factors that can contribute toome care workers job satisfaction and retention. Partic-larly co-worker support through the team model of carend informal opportunities to meet with co-workers mighte making the job less isolating and contributing to satis-action and retention.
The shift to market-modelled ‘competitive’ home care
ystem in Ontario resulted in an increasingly casualizedabour force. This has direct consequences for workers. Asur study shows workers are more likely to consider leavingheir jobs if they work casual hours. The market-modelledystem is also a contributing factor in the shortage of homeicy 91 (2009) 258–268 267
care workers in the province of Ontario. Indeed, a study inthis region showed that the restructuring in home care (theshift to market-modelled system) resulted in many homecare workers leaving the field altogether [4,17]. The Ontariohome care worker shortage is a growing problem and pol-icy efforts are crucial to retain home care workers in thefield.
Recent attention has been called to these home careissues in the city in where this study took place. The case inHamilton, Ontario serves to highlight the impact of restruc-turing on turnover in the home care field. In December2007, when two organizations that provided 80% of thehome care within the Hamilton area were not providedwith contracts, there was a massive mobilization in thecommunity. The loss of contract would have resulted in joblosses for many workers in these organizations, and mov-ing to other workplaces where there might be a mismatchbetween their and the new employer’s care philosophy. Yet,in the current market-modelled system they were expectedto just shift to another agency where they would loseseniority, benefits and pension plans. As a result, many saidthey would leave the field altogether [46]. When clients,workers and citizens protested with media campaigns anda mass protest rally in January of 2008, the Minister ofHealth in Ontario made the decision to stop the awardingof new contracts for home care in the Hamilton area pend-ing their view of market-modelled competitive system. Thetwo agencies were told to continue delivering home careservices for the foreseeable future [47]. This case showsthat when confronted with all stakeholders, the govern-ment has the ability to make positive changes to a systemthat is currently in crisis.
The effects of the casualization on workers’ job sat-isfaction and retention in home care are just emergingin the literature. This paper contributes to fill thesegaps and provides evidence to government, managementand unions who seek solutions to their mutual issuesof concern—decreasing turnover, increasing employeeengagement, and creating a satisfied workforce. We antic-ipate that the results of this study can inform policydecisions that can provide good quality work environ-ments.
References
[1] Canadian Home Care Human Resources Study. Canadian Home CareHuman Resources Study. Synthesis report; 2003a. http://www.cacc-acssc.com/english/pdf/homecareresources/.
[2] Canadian Home Care Human Resources Study. Canadian Home CareHuman Resources Study. Technical report; 2003b. http://www.cacc-acssc.com/english/pdf/homecareresources/.
[3] Wetzel K. The Canadian context. In Wetzel K with contributions fromBach S, Bray M, White N, editors. Labour relations and health reform.Hampshire, UK: Palgrave Macmillan; 2005. p. 86–90.
[4] Denton M, Zeytinoglu IU, Davies S, Hunter D. The impact of imple-menting managed competition on home care workers’ turnoverdecisions. Healthcare Policy 2006;1:106–23.
[5] Abelson J, Tedford, Gold S, Woodward C, O’Connor D, HutchisonB. Managing under managed community care: the experiences ofclients, providers and manages in Ontario’s competitive home care
sector. Health Policy 2004;68:359–72.[6] Caplan Report. Realizing the potential of home care competing forexcellence by rewarding results. Toronto, ON: Ontario Ministry ofHealth and Long-Term Care; 2005.
[7] CHSRF (Canadian Health Services Research Foundation). Lis-tening for directions III: a national consultation on health

ealth Pol
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
268 I.U. Zeytinoglu et al. / H
service and policy issues; 2007 [Accessed in November 2007]http://chsrf.ca/other documents/listening/index e.php.
[8] Health Council of Canada. Modernizing the management of healthhuman resources in Canada: identifying areas for accelerated change;2005 [Accessed in April 2006] http://www.healthcouncilcanada.ca.
[9] Dault M, Lomas J, Barer M, on behalf of the Listening fir Directions IIpartners. Listening for directions II: national consultation on healthservices policy issues for 2004–2007, final report. Canadian HealthServices Research Foundation and Institute for Health Services andPolicy Research, CIHR; 2004. http://www.chsrf.ca [downloaded inFebruary 2006].
10] Munday B. The future for employment in social care in Europe. Con-ference report. European Foundation; 2006. http://www.eurofound.europa.eu/publications/htmlfiles/ef05125.htm.
[11] Saltman RB, Dubois HFW, Chawla M. The impact of aging onlong-term care in Europe and some potential policy responses. Inter-national Journal of Health Services 2006;36(4):719–46.
12] Martineau T, Willetts A. The health workforce: managing the crisisethical recruitment of health professionals: Wil codes of prac-tice protect developing country health systems? Health Policy2006;75:358–67.
13] Breedveld EJ, Meijboom BR, de Roo A. Labour supply in the homecare industry: a case study in a Dutch region. Health Policy2006;76:144–55.
14] Eaton, Susan C. Eldercare in the United States: inadequate,inequitable, but not a lost cause. Feminist Economics 2005;11(2):37–51.
15] Waitzin H, Jasso-Aguilar R, Iriart C. Privatization of health services inless developed countries: an empirical response to the proposals ofthe World Bank and Wharton School. International Journal of HealthServices 2007;37(2):205–27.
16] Baranek P, Deber R, Williams P. Almost Home: reforming home andcommunity care in Ontario. Buffalo, NY: University of Toronto Press;2004.
[17] Denton M, Zeytinoglu IU, Davies S, Hunter D. Where have all the homecare workers gone? In: Beach C, editor. Health services restructur-ing: new evidence and new directions. John Deutsch Institute for theStudy of Economic Policy. Kingston, ON: McGill-Queen’s Press; 2007.p. 245–68.
[18] Denton M, Zeytinoglu IU, Kusch K, Davies S. Market-modelled homecare: impact of job satisfaction and propensity to leave. CanadianPublic Policy-Analyse De Politiques XXXIII Supplement 2007:S81–99.
19] Aronson J, Denton M, Zeytinoglu I, Davies S. Market-modeled homecare in Ontario. Canadian Journal of Public Policy 2004;30:111–25.
20] Hom P, Griffeth RW. Structural equations modeling test of a turnovertheory: cross-sectional and longitudinal analyses. Journal of AppliedPsychology 1991;76(3):350–66.
21] Hom PW, Kinicki AJ. Toward a greater understanding of how dissatis-faction drives employee turnover. Academy of Management Journal1991;44(5):976–87.
22] Griffeth RW, Hom PW, Gaertner S. A meta-analysis of antecedentsand correlates of employee turnover: update, moderator tests, andresearch implications for the millennium. Journal of Management2000;26:463–88.
23] Lee TW, Holtom BS, McDaniel LS, Hill JW. The unfolding model ofvoluntary turnover: a replication and extension. Academy of Man-agement Journal 1999;42(4):450–62.
24] Steel R. Turnover theory at the empirical interface: problem of fit andfunction. Academy of Management Review 2002;27(3):346–60.
25] Arthur D. Employee recruitment and retention handbook. New York:AMACOM Books; 2001.
26] Bloom JR, Alexander JA, Nuchols BA. The effect of social organizationof work on the voluntary turnover rate of hospital nurses in the UnitedStates. Social Science and Medicine 1992;43(12):1413–92.
27] Mitchell TR, Holtom BC, Lee TW, Erez M. Why people stay: using jobembeddedness to predict voluntary turnover. Academy of Manage-ment Journal 2001;44(6):1102–21.
[
icy 91 (2009) 258–268
28] Sverke M, Hellgren J, Näswall K. No security: a meta-analysis andreview of job insecurity and its consequences. Journal of OccupationalHealth Psychology 2002;7(3):242–64.
29] Mobley WH. Intermediate linkages in the relationship between jobsatisfaction and employee turnover. Journal of Applied Psychology1977;62:237–40.
30] Mobley WH, Griffeth RW, Hand HH, Meglino BM. Review and con-ceptual analysis of employee turnover process. Psychological Bulletin1977;86:493–522.
31] Lawler III, Edward E. Motivating and satisfying excellent individu-als. In: Management skills: a Jossey-Bass reader. San Francisco, CA:Jossey-Bass; 2005. p. 423–49.
32] Zeytinoglu IU. Flexible work arrangements: an overview of devel-opments in Canada. In: Zeytinoglu IU, editor. Changing workrelationships in industrialized economies. Amsterdam, The Nether-lands: John Benjamin; 1999. p. 41–58.
33] Standing G. Globalization, labour flexibility and insecurity: theera of market regulation. European Journal of Industrial Relations1997;3:7–37.
34] De Witte H, Näswall K. ‘Objective’ vs ‘subjective’ job insecurity: con-sequences of temporary work for job satisfaction and organizationalcommitment in four European countries. Economic and IndustrialDemocracy 2003;24:149–88.
35] Parent K, Anderson M, Gleberzon W, Cutler J. CARP’s report card onhome care in Canada. Mimeo; 2001. http://www.fifty-plus.net.
36] Burchell B. The prevalence and redistribution of job insecurity andwork intensification. In: Burchell B, Lapido D, Wilkinson F, editors. Jobinsecurity and work intensification. London, UK: Routledge; 2002. p.61–76.
37] de Ruyter A, Burgess J. Growing labour insecurity in Australiaand the UK in the midst of job growth: beware the Anglo-Saxon model. European Journal of Industrial Relations 2003;9:223–44.
38] Saloniemi A, Virtanen P. A flexible future? Dimensions of job inse-curity and future expectations. Paper presented at Flexible WorkPatterns Study Group Meeting, IIRA 14th World Congress in Lima,Peru, 11–14 September 2006.
39] Chirulombolo A, Hellgren J. Individual and organizational conse-quences of job insecurity: a European Study. Economic and IndustrialDemocracy 2003;24:217–40.
40] Denton M, Zeytinoglu IU, Davies S. Health and worklife question-naire, with Dr. M. Denton as the PI of the organizational change andhealth and well-being of home care workers research project fundedby WSIB; 2002.
[41] Lyons TF. Propensity to leave scale of 1971. In: Cook JD, Hepworth SJ,Wall TD, Warr PB, editors. Experience of work: a compendium andreview of 249 measures and their use. New York: Academic Press;1981.
42] Cameron S, Horsburgh M, Armstrong-Stassen M. Effects of downsiz-ing on RNs and RNAs in community hospitals. Hamilton, ON: NursingEffectiveness, Utilization and Outcomes Research Unit; 1994.
43] Denton M, Zeytinoglu IU, Davies S. Organizational change and thehealth and well-being of home care workers. Hamilton, ON: Socialand Economic Dimensions of an Aging Population Research Program;2003.
44] Kenny DA, Kashy DA, Bolger N. Data analysis in social psychology.In: Gilbert DT, Fiske ST, Lindzey G, editors. The handbook of socialpsychology. Boston, MA: McGraw-Hill; 1998. p. 223–65.
45] Korczyk S. Long-term workers in five countries: issues and options.Washington, DC: AARP Public Policy Institute; 2004.
46] Reilly E. VON shut out of home health care: failure to win new
contract means 88 nurses will be jobless come March 31. Hamil-ton, Ontario: The Hamilton Spectator; 2008, http://www.thespec.com/articles/295708.47] Nolan D. Minister kills nursing care bid process. Hamilton,Ontario: The Hamilton Spectator; 2008, http://www.thespec.com/articles/313640.