cad in questions/answers
TRANSCRIPT

R
CR
Ba
b
a
ARA
KCB
dH
0d
European Journal of Radiology 69 (2009) 24–33
Contents lists available at ScienceDirect
European Journal of Radiology
journa l homepage: www.e lsev ier .com/ locate /e j rad
eview
AD in questions/answerseview of the literature
runo Boyera,∗, Corinne Balleyguierb, Olivier Granata, Christian Pharaboza
Cabinet de Radiologie, 6, place d’Italie, 75013 Paris, FranceService de Radiodiagnostic, Institut Gustave Roussy, 94805 Villejuif, France
r t i c l e i n f o
rticle history:eceived 23 July 2008
a b s t r a c t
Generalization of breast screening programs requires an efficient double reading of the mammograms,
ccepted 28 July 2008
eywords:AD mammographyreast screening programs
which allows reduction of false-negative rate, but might be difficult to organize. CAD (Computed AssistedDiagnosis) is dramatically improving and is able to detect suspicious mammographic lesions, either sus-picious microcalcifications, masses or architectural distorsions. CAD mammography might complete orsubstitute to “human” double reading. The aim of this review is to describe major CAD systems commer-cially available, working of CAD and to present principal results of CAD mammography. Specially, placeof CAD within breast screening program, according to the results of recent prospective studies will be
Double readingBreast cancer discussed.
© 2008 Elsevier Ireland Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241.1. Which are the CAD systems commercially available? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 251.2. Which are the marks applied by CAD? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 251.3. Can CAD replace the reader?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 251.4. Which are performances of CAD? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
1.4.1. CAD and reproductibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 251.4.2. Global performances of CAD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 251.4.3. Performances of CAD in function of abnormalities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
1.5. CAD’s performances in false negatives screening mammograms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281.6. Can the CAD be a disadvantage to the radiologist? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281.7. Can CAD help reader in screening? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
1.7.1. Does CAD improve the performances of the first reader? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 311.7.2. Is the association of the first reader + CAD better than double reading? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
1.7.3. Does CAD increase the performances of the second reader? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32. . . . .
. . . . .
. . . . .
Mammography has proven to be the most effective tool foretecting breast cancer in its earliest and most treatable stage [1].owever, there are some limits to this exploration, due to breast’s
∗ Corresponding author.E-mail address: [email protected] (B. Boyer).
scoomab(3i
720-048X/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2008.07.042
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
tructure (high density) and also because mammography is diffi-ult to interpret: as a consequence, mistakes (due to fatigue, lackf attention, failure in detection or interpretation) lead to variationf results between readers but also for a same reader. There are asany missed lesions when they have not been seen (reading errors)
s when they have not been correctly juged (abnormalities detected
1.8. What could be the place of CAD in screening? . . . . . . . . . . . . . . . .2. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1. Introduction
ut reader decides not to recall the patient for further evaluationdecision errors) [2]. The rate of missed cancers varies from 16 to1% [3]. To reduce this rate, double reading of mammographies wasntroduced during screening programs. This double reading allows
B. Boyer et al. / European Journal of Radiology 69 (2009) 24–33 25
marke
tebaib
ai
dd
1
a
-
-
-----
“
1
pofcvann
1
aao
1
1
daid
1
td
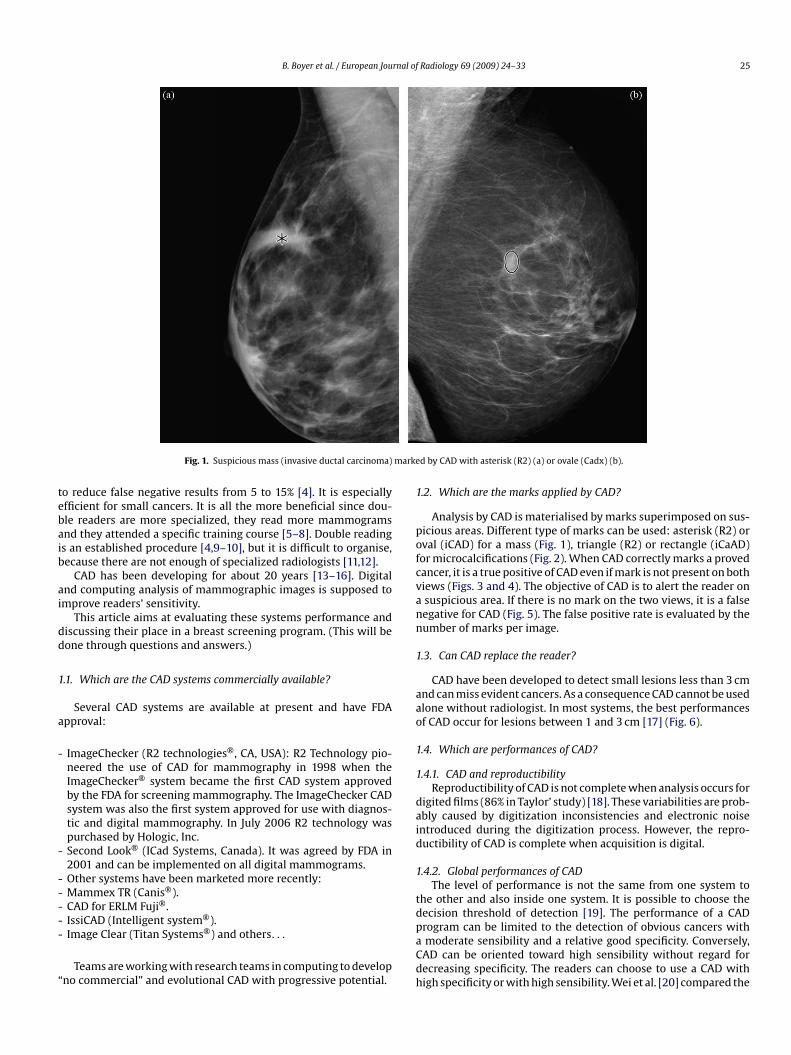
Fig. 1. Suspicious mass (invasive ductal carcinoma)
o reduce false negative results from 5 to 15% [4]. It is especiallyfficient for small cancers. It is all the more beneficial since dou-le readers are more specialized, they read more mammogramsnd they attended a specific training course [5–8]. Double readings an established procedure [4,9–10], but it is difficult to organise,ecause there are not enough of specialized radiologists [11,12].
CAD has been developing for about 20 years [13–16]. Digitalnd computing analysis of mammographic images is supposed tomprove readers’ sensitivity.
This article aims at evaluating these systems performance andiscussing their place in a breast screening program. (This will beone through questions and answers.)
.1. Which are the CAD systems commercially available?
Several CAD systems are available at present and have FDApproval:
ImageChecker (R2 technologies®, CA, USA): R2 Technology pio-neered the use of CAD for mammography in 1998 when theImageChecker® system became the first CAD system approvedby the FDA for screening mammography. The ImageChecker CADsystem was also the first system approved for use with diagnos-tic and digital mammography. In July 2006 R2 technology waspurchased by Hologic, Inc.Second Look® (ICad Systems, Canada). It was agreed by FDA in2001 and can be implemented on all digital mammograms.Other systems have been marketed more recently:Mammex TR (Canis®).CAD for ERLM Fuji®.IssiCAD (Intelligent system®).
Image Clear (Titan Systems®) and others. . .Teams are working with research teams in computing to developno commercial” and evolutional CAD with progressive potential.
paCdh
d by CAD with asterisk (R2) (a) or ovale (Cadx) (b).
.2. Which are the marks applied by CAD?
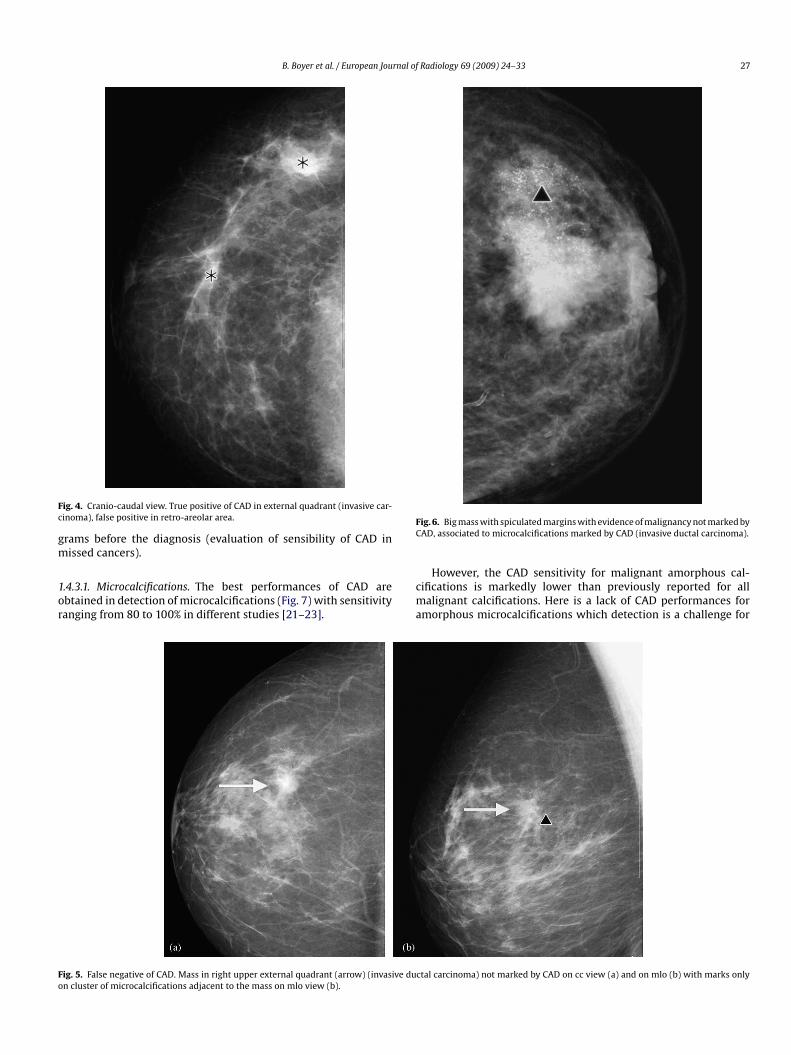
Analysis by CAD is materialised by marks superimposed on sus-icious areas. Different type of marks can be used: asterisk (R2) orval (iCAD) for a mass (Fig. 1), triangle (R2) or rectangle (iCaAD)or microcalcifications (Fig. 2). When CAD correctly marks a provedancer, it is a true positive of CAD even if mark is not present on bothiews (Figs. 3 and 4). The objective of CAD is to alert the reader onsuspicious area. If there is no mark on the two views, it is a falseegative for CAD (Fig. 5). The false positive rate is evaluated by theumber of marks per image.
.3. Can CAD replace the reader?
CAD have been developed to detect small lesions less than 3 cmnd can miss evident cancers. As a consequence CAD cannot be usedlone without radiologist. In most systems, the best performancesf CAD occur for lesions between 1 and 3 cm [17] (Fig. 6).
.4. Which are performances of CAD?
.4.1. CAD and reproductibilityReproductibility of CAD is not complete when analysis occurs for
igited films (86% in Taylor’ study) [18]. These variabilities are prob-bly caused by digitization inconsistencies and electronic noisentroduced during the digitization process. However, the repro-uctibility of CAD is complete when acquisition is digital.
.4.2. Global performances of CADThe level of performance is not the same from one system to
he other and also inside one system. It is possible to choose theecision threshold of detection [19]. The performance of a CAD
rogram can be limited to the detection of obvious cancers withmoderate sensibility and a relative good specificity. Conversely,AD can be oriented toward high sensibility without regard forecreasing specificity. The readers can choose to use a CAD withigh specificity or with high sensibility. Wei et al. [20] compared the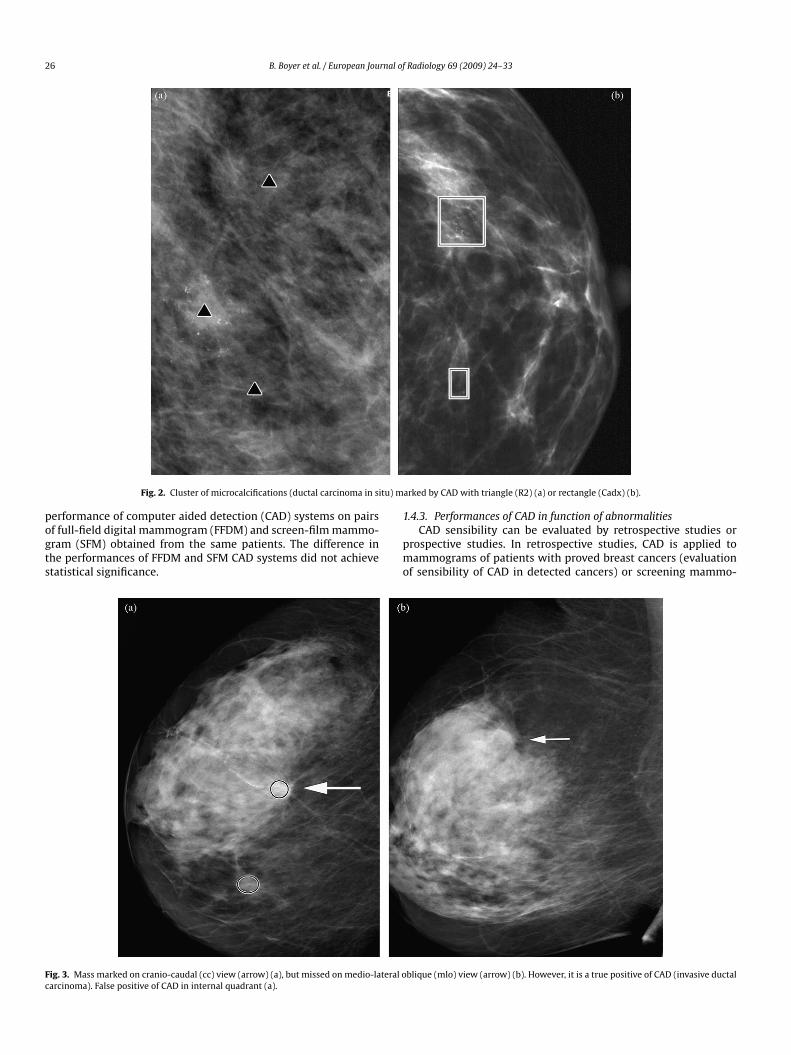
26 B. Boyer et al. / European Journal of Radiology 69 (2009) 24–33
tu) m
pogts
Fc
Fig. 2. Cluster of microcalcifications (ductal carcinoma in si
erformance of computer aided detection (CAD) systems on pairsf full-field digital mammogram (FFDM) and screen-film mammo-ram (SFM) obtained from the same patients. The difference inhe performances of FFDM and SFM CAD systems did not achievetatistical significance.
1
pmo
ig. 3. Mass marked on cranio-caudal (cc) view (arrow) (a), but missed on medio-lateral oarcinoma). False positive of CAD in internal quadrant (a).
arked by CAD with triangle (R2) (a) or rectangle (Cadx) (b).
.4.3. Performances of CAD in function of abnormalitiesCAD sensibility can be evaluated by retrospective studies or
rospective studies. In retrospective studies, CAD is applied toammograms of patients with proved breast cancers (evaluation
f sensibility of CAD in detected cancers) or screening mammo-
blique (mlo) view (arrow) (b). However, it is a true positive of CAD (invasive ductal
B. Boyer et al. / European Journal of Radiology 69 (2009) 24–33 27
Fc
gm
1or
FC
Fo
ig. 4. Cranio-caudal view. True positive of CAD in external quadrant (invasive car-inoma), false positive in retro-areolar area.
rams before the diagnosis (evaluation of sensibility of CAD inissed cancers).
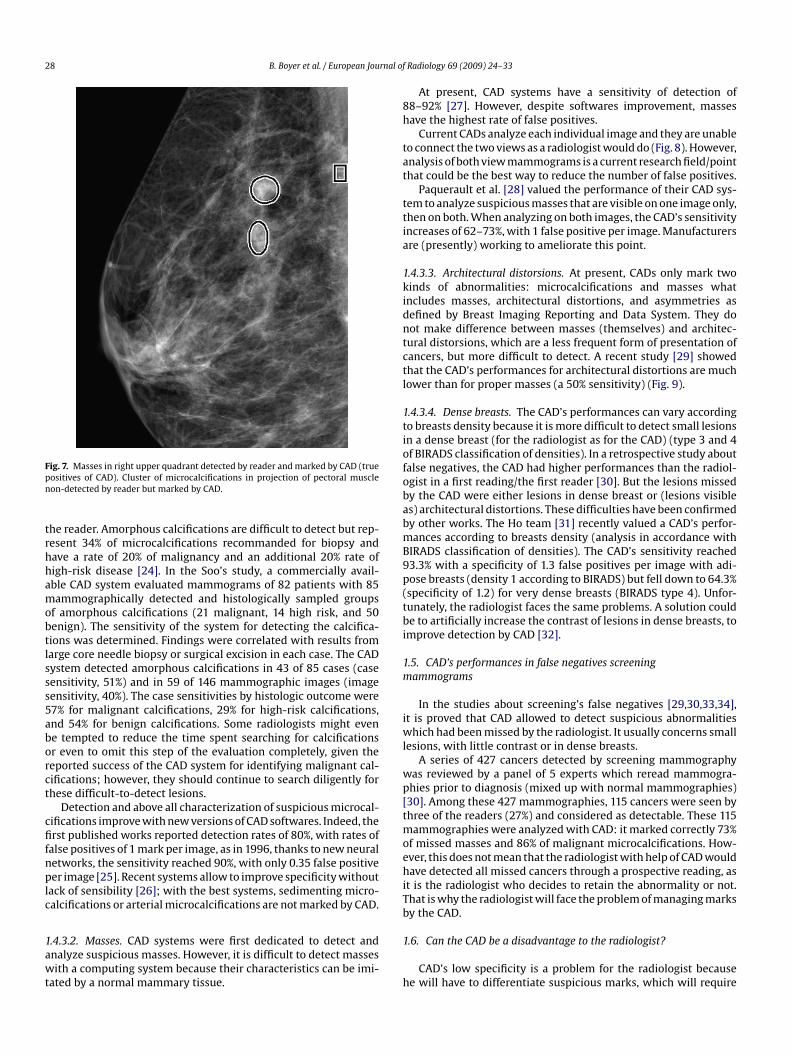
.4.3.1. Microcalcifications. The best performances of CAD arebtained in detection of microcalcifications (Fig. 7) with sensitivityanging from 80 to 100% in different studies [21–23].
cma
ig. 5. False negative of CAD. Mass in right upper external quadrant (arrow) (invasive dun cluster of microcalcifications adjacent to the mass on mlo view (b).
ig. 6. Big mass with spiculated margins with evidence of malignancy not marked byAD, associated to microcalcifications marked by CAD (invasive ductal carcinoma).
However, the CAD sensitivity for malignant amorphous cal-ifications is markedly lower than previously reported for allalignant calcifications. Here is a lack of CAD performances for
morphous microcalcifications which detection is a challenge for
ctal carcinoma) not marked by CAD on cc view (a) and on mlo (b) with marks only
28 B. Boyer et al. / European Journal of
Fpn
trhhamobtlsss5aborct
cfifnplc
1awt
8h
tat
ttia
1kidntctl
1tiofobabmB9p(tbi
1m
iwl
wp[tmoehiTb
ig. 7. Masses in right upper quadrant detected by reader and marked by CAD (trueositives of CAD). Cluster of microcalcifications in projection of pectoral muscleon-detected by reader but marked by CAD.
he reader. Amorphous calcifications are difficult to detect but rep-esent 34% of microcalcifications recommanded for biopsy andave a rate of 20% of malignancy and an additional 20% rate ofigh-risk disease [24]. In the Soo’s study, a commercially avail-ble CAD system evaluated mammograms of 82 patients with 85ammographically detected and histologically sampled groups
f amorphous calcifications (21 malignant, 14 high risk, and 50enign). The sensitivity of the system for detecting the calcifica-ions was determined. Findings were correlated with results fromarge core needle biopsy or surgical excision in each case. The CADystem detected amorphous calcifications in 43 of 85 cases (caseensitivity, 51%) and in 59 of 146 mammographic images (imageensitivity, 40%). The case sensitivities by histologic outcome were7% for malignant calcifications, 29% for high-risk calcifications,nd 54% for benign calcifications. Some radiologists might evene tempted to reduce the time spent searching for calcificationsr even to omit this step of the evaluation completely, given theeported success of the CAD system for identifying malignant cal-ifications; however, they should continue to search diligently forhese difficult-to-detect lesions.
Detection and above all characterization of suspicious microcal-ifications improve with new versions of CAD softwares. Indeed, therst published works reported detection rates of 80%, with rates of
alse positives of 1 mark per image, as in 1996, thanks to new neuraletworks, the sensitivity reached 90%, with only 0.35 false positiveer image [25]. Recent systems allow to improve specificity without
ack of sensibility [26]; with the best systems, sedimenting micro-alcifications or arterial microcalcifications are not marked by CAD.
.4.3.2. Masses. CAD systems were first dedicated to detect andnalyze suspicious masses. However, it is difficult to detect massesith a computing system because their characteristics can be imi-
ated by a normal mammary tissue.
1
h
Radiology 69 (2009) 24–33
At present, CAD systems have a sensitivity of detection of8–92% [27]. However, despite softwares improvement, massesave the highest rate of false positives.
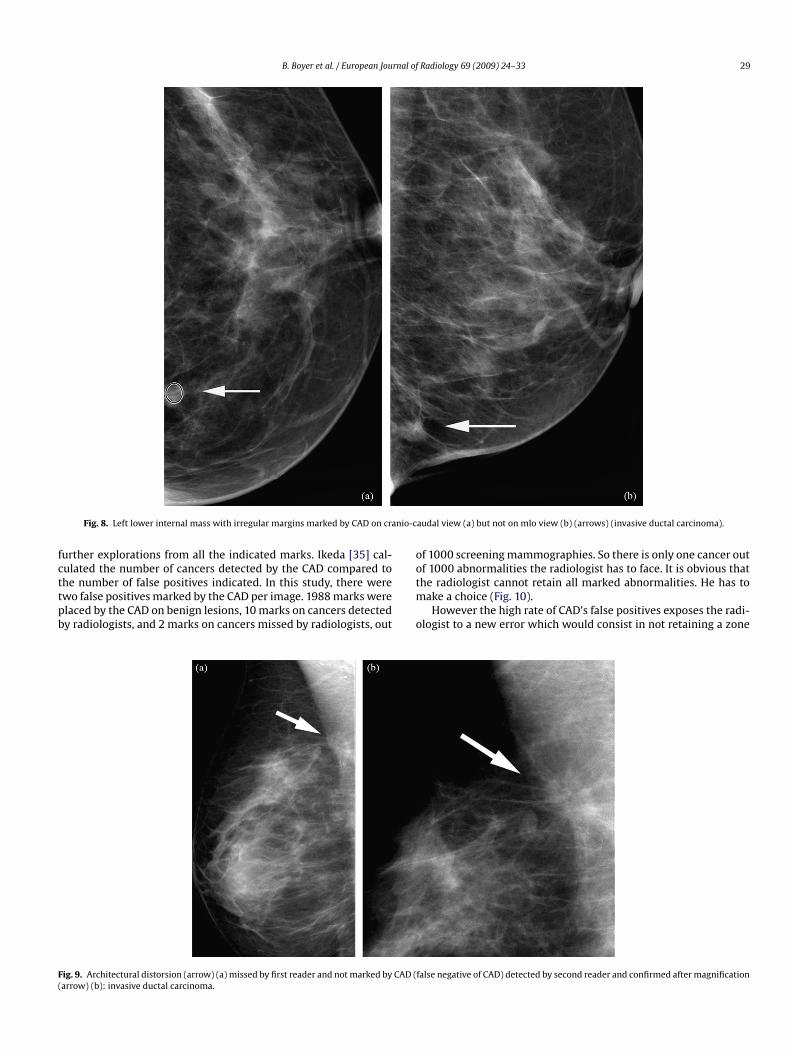
Current CADs analyze each individual image and they are unableo connect the two views as a radiologist would do (Fig. 8). However,nalysis of both view mammograms is a current research field/pointhat could be the best way to reduce the number of false positives.
Paquerault et al. [28] valued the performance of their CAD sys-em to analyze suspicious masses that are visible on one image only,hen on both. When analyzing on both images, the CAD’s sensitivityncreases of 62–73%, with 1 false positive per image. Manufacturersre (presently) working to ameliorate this point.
.4.3.3. Architectural distorsions. At present, CADs only mark twoinds of abnormalities: microcalcifications and masses whatncludes masses, architectural distortions, and asymmetries asefined by Breast Imaging Reporting and Data System. They doot make difference between masses (themselves) and architec-ural distorsions, which are a less frequent form of presentation ofancers, but more difficult to detect. A recent study [29] showedhat the CAD’s performances for architectural distortions are muchower than for proper masses (a 50% sensitivity) (Fig. 9).
.4.3.4. Dense breasts. The CAD’s performances can vary accordingo breasts density because it is more difficult to detect small lesionsn a dense breast (for the radiologist as for the CAD) (type 3 and 4f BIRADS classification of densities). In a retrospective study aboutalse negatives, the CAD had higher performances than the radiol-gist in a first reading/the first reader [30]. But the lesions missedy the CAD were either lesions in dense breast or (lesions visibles) architectural distortions. These difficulties have been confirmedy other works. The Ho team [31] recently valued a CAD’s perfor-ances according to breasts density (analysis in accordance with
IRADS classification of densities). The CAD’s sensitivity reached3.3% with a specificity of 1.3 false positives per image with adi-ose breasts (density 1 according to BIRADS) but fell down to 64.3%specificity of 1.2) for very dense breasts (BIRADS type 4). Unfor-unately, the radiologist faces the same problems. A solution coulde to artificially increase the contrast of lesions in dense breasts, to
mprove detection by CAD [32].
.5. CAD’s performances in false negatives screeningammograms
In the studies about screening’s false negatives [29,30,33,34],t is proved that CAD allowed to detect suspicious abnormalities
hich had been missed by the radiologist. It usually concerns smallesions, with little contrast or in dense breasts.
A series of 427 cancers detected by screening mammographyas reviewed by a panel of 5 experts which reread mammogra-hies prior to diagnosis (mixed up with normal mammographies)30]. Among these 427 mammographies, 115 cancers were seen byhree of the readers (27%) and considered as detectable. These 115
ammographies were analyzed with CAD: it marked correctly 73%f missed masses and 86% of malignant microcalcifications. How-ver, this does not mean that the radiologist with help of CAD wouldave detected all missed cancers through a prospective reading, as
t is the radiologist who decides to retain the abnormality or not.hat is why the radiologist will face the problem of managing marksy the CAD.
.6. Can the CAD be a disadvantage to the radiologist?
CAD’s low specificity is a problem for the radiologist becausee will have to differentiate suspicious marks, which will require
B. Boyer et al. / European Journal of Radiology 69 (2009) 24–33 29
nio-c
fcttpb
oo
F(
Fig. 8. Left lower internal mass with irregular margins marked by CAD on cra
urther explorations from all the indicated marks. Ikeda [35] cal-ulated the number of cancers detected by the CAD compared to
he number of false positives indicated. In this study, there werewo false positives marked by the CAD per image. 1988 marks werelaced by the CAD on benign lesions, 10 marks on cancers detectedy radiologists, and 2 marks on cancers missed by radiologists, outtm
o
ig. 9. Architectural distorsion (arrow) (a) missed by first reader and not marked by CAD (arrow) (b): invasive ductal carcinoma.
audal view (a) but not on mlo view (b) (arrows) (invasive ductal carcinoma).
f 1000 screening mammographies. So there is only one cancer outf 1000 abnormalities the radiologist has to face. It is obvious that
he radiologist cannot retain all marked abnormalities. He has toake a choice (Fig. 10).However the high rate of CAD’s false positives exposes the radi-
logist to a new error which would consist in not retaining a zone
false negative of CAD) detected by second reader and confirmed after magnification
30 B. Boyer et al. / European Journal of Radiology 69 (2009) 24–33
F by CAi e posi
mbtBrcbir
crpab
Fb
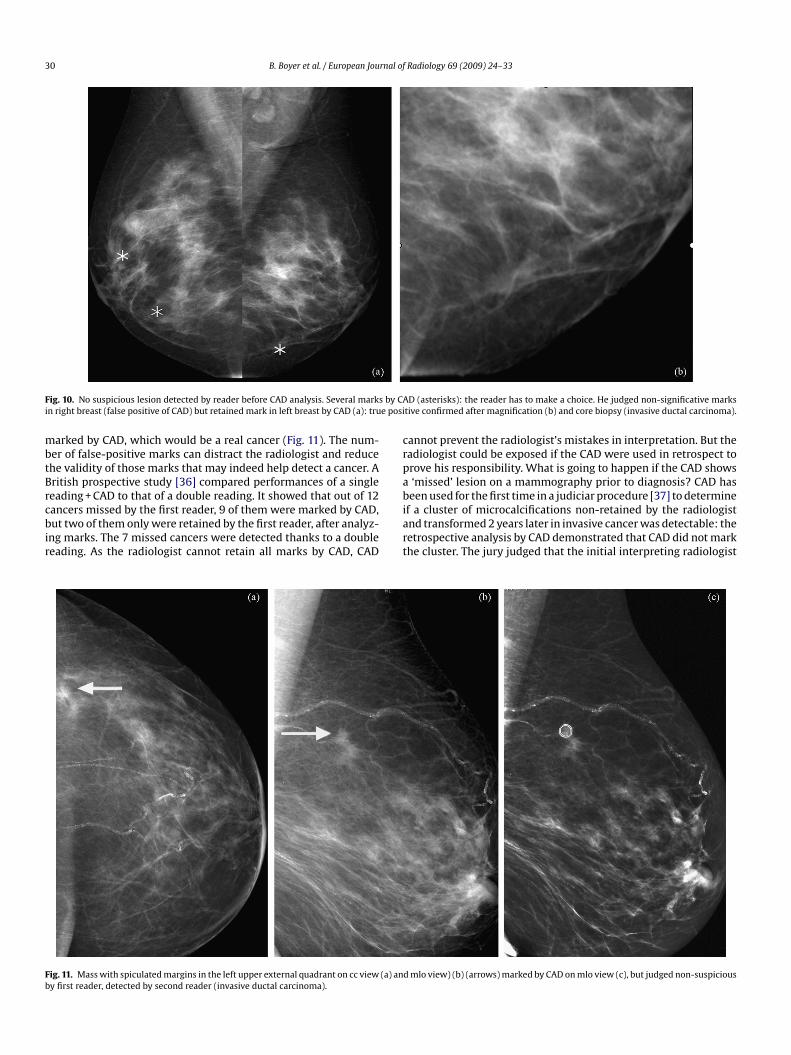
ig. 10. No suspicious lesion detected by reader before CAD analysis. Several marksn right breast (false positive of CAD) but retained mark in left breast by CAD (a): tru
arked by CAD, which would be a real cancer (Fig. 11). The num-er of false-positive marks can distract the radiologist and reducehe validity of those marks that may indeed help detect a cancer. Aritish prospective study [36] compared performances of a singleeading + CAD to that of a double reading. It showed that out of 12
ancers missed by the first reader, 9 of them were marked by CAD,ut two of them only were retained by the first reader, after analyz-ng marks. The 7 missed cancers were detected thanks to a doubleeading. As the radiologist cannot retain all marks by CAD, CAD
iart
ig. 11. Mass with spiculated margins in the left upper external quadrant on cc view (a) any first reader, detected by second reader (invasive ductal carcinoma).
D (asterisks): the reader has to make a choice. He judged non-significative markstive confirmed after magnification (b) and core biopsy (invasive ductal carcinoma).
annot prevent the radiologist’s mistakes in interpretation. But theadiologist could be exposed if the CAD were used in retrospect torove his responsibility. What is going to happen if the CAD shows‘missed’ lesion on a mammography prior to diagnosis? CAD haseen used for the first time in a judiciar procedure [37] to determine
f a cluster of microcalcifications non-retained by the radiologistnd transformed 2 years later in invasive cancer was detectable: theetrospective analysis by CAD demonstrated that CAD did not markhe cluster. The jury judged that the initial interpreting radiologist
d mlo view) (b) (arrows) marked by CAD on mlo view (c), but judged non-suspicious
rnal of
cdchr
1
trn
1
pCccat(iidap
gtdcw
aratFl(dyDt1toptCc
1d
rhsahb
Fcb
B. Boyer et al. / European Jou
omported with the standard of care and rended an unanimous ver-ict for the defendant. What would happen if CAD had marked theluster? So it is important to keep in mind that CAD’s marks canave value only when diagnosis is made, and not for an analysis inetrospect.
.7. Can CAD help reader in screening?
Prospective studies are needed to evaluate the benefice of rou-ine use of CAD but they are difficult to organize because theyequire a great number of mammographies to be statistically sig-ificant.
.7.1. Does CAD improve the performances of the first reader?In Freer’s series [38], 12 860 analogic screening mammogra-
hies were analyzed by reader, without CAD first, with CAD then.AD allowed to detect 19.5% of additional cancers (9 cases). 8ases were carcinomes in situ regarding as clusters of microcal-ifications; the ninth one was a carcinome infiltrant regarding asmass. 9 cancers regarding as masses which had been seen by
he reader were not detected by CAD. In this study, the recall ratebecause of the analysis by CAD at a later time) was not muchncreased, changing from 6.5% without to 7.7% with CAD. In a sim-lar study, Morton et al. [39] reported a 7.62% increase in canceretection, with eight additional cancers (three invasive carcinomand five ductal carcinoma in situ) identified from the total of 18 096atients.
Two studies have compared detection rate of a panel of radiolo-
ist before and after implementation of CAD in their institution. Inhe first study, Cupples et al. [40] reported a 16.1% increase in canceretection rate, with a 164% increase in the detection rate of invasiveancers 1.0 cm or smaller in size and a 8.1% increase in recall rateith the use of CAD. In the second study, Gur et al. [41] reported noC
phc
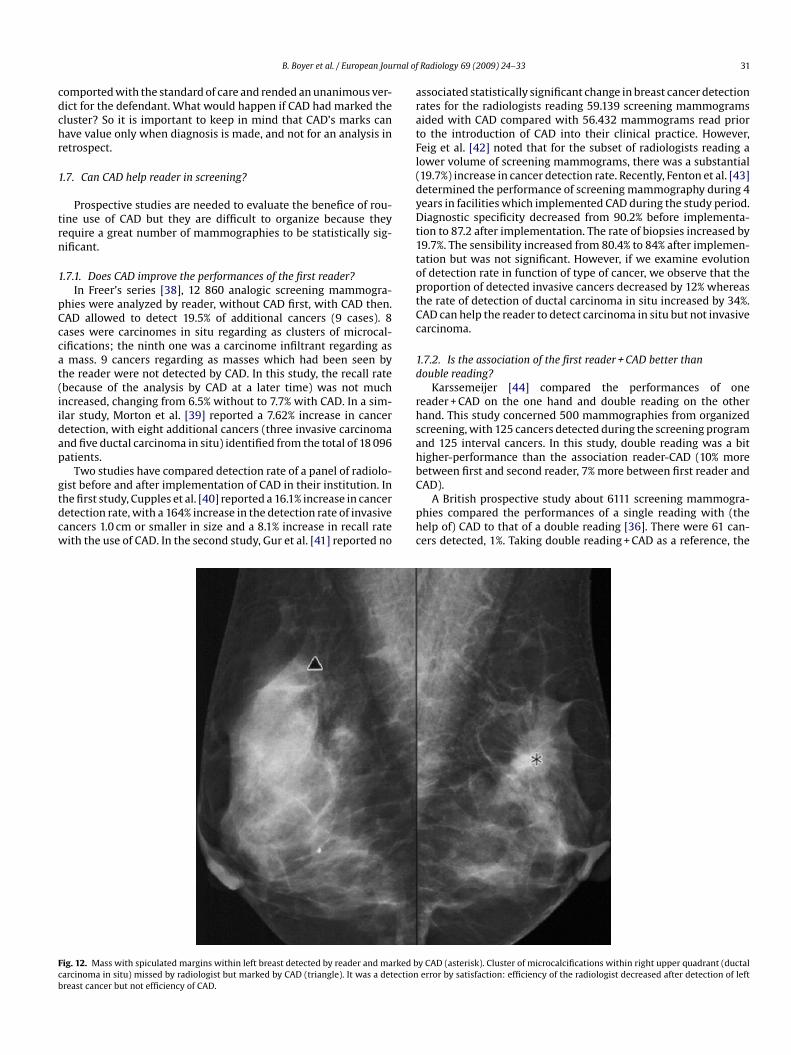
ig. 12. Mass with spiculated margins within left breast detected by reader and marked barcinoma in situ) missed by radiologist but marked by CAD (triangle). It was a detectionreast cancer but not efficiency of CAD.
Radiology 69 (2009) 24–33 31
ssociated statistically significant change in breast cancer detectionates for the radiologists reading 59.139 screening mammogramsided with CAD compared with 56.432 mammograms read prioro the introduction of CAD into their clinical practice. However,eig et al. [42] noted that for the subset of radiologists reading aower volume of screening mammograms, there was a substantial19.7%) increase in cancer detection rate. Recently, Fenton et al. [43]etermined the performance of screening mammography during 4ears in facilities which implemented CAD during the study period.iagnostic specificity decreased from 90.2% before implementa-
ion to 87.2 after implementation. The rate of biopsies increased by9.7%. The sensibility increased from 80.4% to 84% after implemen-ation but was not significant. However, if we examine evolutionf detection rate in function of type of cancer, we observe that theroportion of detected invasive cancers decreased by 12% whereashe rate of detection of ductal carcinoma in situ increased by 34%.AD can help the reader to detect carcinoma in situ but not invasivearcinoma.
.7.2. Is the association of the first reader + CAD better thanouble reading?
Karssemeijer [44] compared the performances of oneeader + CAD on the one hand and double reading on the otherand. This study concerned 500 mammographies from organizedcreening, with 125 cancers detected during the screening programnd 125 interval cancers. In this study, double reading was a bitigher-performance than the association reader-CAD (10% moreetween first and second reader, 7% more between first reader and
AD).A British prospective study about 6111 screening mammogra-hies compared the performances of a single reading with (theelp of) CAD to that of a double reading [36]. There were 61 can-ers detected, 1%. Taking double reading + CAD as a reference, the
y CAD (asterisk). Cluster of microcalcifications within right upper quadrant (ductalerror by satisfaction: efficiency of the radiologist decreased after detection of left

3 rnal of
sCCstDt
tfr
bam
1
daaae
1
g[cpwra
utsho
2
fcttsiii
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
2 B. Boyer et al. / European Jou
ensitivity of the first reader alone was of 60.2%. The sensitivity ofAD alone/only was of 84%. The increase of sensitivity thanks toAD was limited to 1.3% because 7 cancers out of 9 which had beeneen by the first reader but marked by CAD were not retained byhe first reader, whereas they were detected with double reading.ouble reading increased the rate of cancers of 8.2% compared to
he first reader: this allowed to obtain a 98.4% sensitivity.The recall rate was of 6.1% without CAD, and increased of 5.8%
hanks to CAD. We can conclude that using CAD does not preventrom interpretation errors, since the reader can reject marks put oneal cancers which would be detected by other readers (Fig. 11).
Therefore, double reading is much better than the associationetween one reader and CAD. These results were obtained withnalogical mammographies; they have to be confirmed on digitalammographies.
.7.3. Does CAD increase the performances of the second reader?In a retrospective study analyzing mammographies prior to
iagnosis of 318 cancers, Destounis [45] shows that the false neg-tive rate decreases from 31% after a double reading to 19% afternalysis by the CAD. But he calculates this drop in false negativebout the CAD’s analysis only; it does not evaluate the CAD’s influ-nce on readers.
.8. What could be the place of CAD in screening?
We know that double reading organized during screening pro-rams allows to reduce the number of false negative of 5–15%5,10,11]. Considering the CADs’ high sensitivity for detecting suspi-ious mammographies, we can wonder if a CAD used in a screeningrogram could permit to eliminate false negative(s). Which stageould be the best to involve it? We have seen that it cannot possibly
eplace the first reader; it cannot replace the second reader either,s double reading is superior to the association of one reader + CAD.
In the present state of its performances, the CAD can only besed in addition to readers. As a result of its low specificity, it layshe reader open to rejecting a mark corresponding to a real cancer:o it does not always overcome interpretation errors. On the otherand, it is more efficient for detection errors (notably for clustersf microcalcifications) (Fig. 12) than for decision errors.
. Conclusion
CAD detection rate is low for architectural distorsions, increasesor masses and reaches nearly 100% for microcalcifications. CADan help readers to decrease errors of detection of cancers, notablyhose that manifested as microcalcifications. However, false posi-ive rate is too high with 1000 benign marks for one cancer. This lowpecificity does not allow CAD to replace second reader in screen-ng and further developments are necessary. Cad’s implementationn screening will be envisaged only in case of digital acquisition formmediate use.
eferences
[1] Beam CA, Sullivan DC, Layde PM. Effect of human variability on independentdouble reading in screening mammography. Acad Radiol 1996;3:891–7.
[2] Boyer B, Hauret L, Bellaiche R, Graf C, Bourcier B, Fichet G. Retrospectivelydetectable carcinomas: review of the literature. J Radiol 2004;85:2071–8.
[3] Bird RE, Wallace TW, Yankaskas BC. Analysis of cancers missed at screeningmammography. Radiology 1992;184:613–7.
[4] Hall FM. Opinions about mammographic double reading. Am J Roentgenol
1997;168:846.[5] Homer MJ. Mammography training in diagnostic radiology residency programs.Radiology 1980;135:529–31.
[6] Jackson VP, Bresch JA, Bassett LW, Dershaw DD, Jessop NW. Status ofmammography education and knowledge of radiology residents. Radiology1996;201:773–6.
[
[
Radiology 69 (2009) 24–33
[7] Laming D, Warren R. Improving the detection of cancer in the screening ofmammograms. J Med Screen 2000;7:24–30.
[8] Pisano ED, McLelland R, Clark RL, Dicke K, Muller K. A formal curriculum inbreast imaging for radiology residents. Invest Radiol 1993;28:762–6.
[9] Ciatto S, Del Turco MR, Morrone D, et al. Independent double reading of screen-ing mammograms. J Med Screen 1995;2:99–101.
10] Thurfjell EL, Lernevall KA, Taube AA. Benefit of independent double read-ing in a population-based mammography screening program. Radiology1994;191:241–4.
11] Bassett LW, Cassady CI, Gold RH. Present status of residency training in mam-mography. AJR Am J Roentgenol 1991;156:59–62.
12] Nodine CF, Kundel HL, Mello-Thoms C, et al. How experience and training influ-ence mammography expertise. Acad Radiol 1999;6:575–85.
13] Doi K, Giger ML, Nishikawa RM, Schmidt RA. Computer-aided diagnosis ofbreast cancer on mammograms. Breast Cancer 1997;4:228–33.
14] Giger ML, Doi K, MacMahon H, et al. An “intelligent” workstation for computer-aided diagnosis. Radiographics 1993;13:647–56.
15] Doi K, MacMahon H, Katsuragawa S, Nishikawa RM, Jiang Y. Computer-aideddiagnosis in radiology: potential and pitfalls. Eur J Radiol 1999;31:97–109.
16] Feig SA. Breast cancer screening: potential role of computer-aided detection(CAD). Technol Cancer Res Treat 2002;1:127–31.
17] Malich A, Sauner D, Marx C, et al. Influence of breast lesion size and histo-logic findings on tumor detection rate of a computer-aided detection system.Radiology 2003;228:851–6.
18] Taylor CG, Champness J, Reddy M, Taylor P, Potts HW, Given-Wilson R. Repro-ductibility of prompts in computer-aided detection (CAD) of breast cancer. ClinRadiol 2003;58:733–8.
19] Helvie MA, Hadjiiski L, Makariou E, et al. Sensitivity of noncommercialcomputer-aided detection system for mammographic breast cancer detection:pilot clinical trial. Radiology 2004, 2311030429.
20] Wei J, Hadjiiski LM, Sahiner B, et al. Computer-aided detection systems forbreast masses: comparison of performances on full-field digital mammo-grams and digitized screen-film mammograms. Acad Radiol 2007;14(6):659–66.
21] Brem RF, Hoffmeister JW, Zisman G, DeSimio MP, Rogers MK. A computer-aided detection system for the evaluation of breast cancer by mammographicappearance and lesion size. Am J Roentgenol 2005;184:893–6.
22] Yang SK, Moon WK, Cho N, et al. Screening mammography-detected cancers:sensitivity of a computer-aided detection system applied to full-field digitalmammograms. Radiology 2007;244:104–11.
23] Gavrielides MA, Lo JY, Vargas-Voracek R, Floyd Jr CE. Segmentation of suspi-cious clustered microcalcifications in mammograms. Med Phys 2000;27:13–22.
24] Soo MS, Rosen EL, Xia JQ, Ghate S, Baker JA. Computer-aided detection of amor-phous calcifications. Am J Roentgenol 2005;184:887–92.
25] Chan HP, Lo SC, Sahiner B, Lam KL, Helvie MA. Computer-aided detection ofmammographic calcifications: pattern recognition with an artificial neural net-work. Med Phys 1996;23:1325–36.
26] Brem RF, Schoonjans JM. Radiologist detection of microcalcifications withand without computer-aided detection: a comparative study. Clin Radiol2001;56:150–4.
27] Li L, Clark RA, Thomas JA. Computer-aided diagnosis of masses with full-fielddigital mammography. Acad Radiol 2002;9:4–12.
28] Paquerault S, Petrick N, Chan HP, Sahiner B, Helvie MA. Improvement of com-puterized mass detection on mammograms: fusion of two-view information.Med Phys 2002;29:238–47.
29] Baker JA, Rosen EL, Lo JY, Gimenez EI, Walsh R, Soo MS. Computer-aided detec-tion (CAD) in screening mammography: sensitivity of commercial CAD systemsfor detecting architectural distortion. Am J Roentgenol 2003;181:1083–8.
30] Birdwell RL, Ikeda DM, O’Shaughnessy KF, Sickles EA. Mammographiccharacteristics of 115 missed cancers later detected with screening mam-mography and the potential utility of computer-aided detection. Radiology2001;219:192–202.
31] Ho WT, Lam PW. Clinical performance of computer-assisted detection (CAD)system in detecting carcinoma in breasts of different densities. Clin Radiol2003;58:133–6.
32] Nunes FL, Schiabel H, Benatti RH. Contrast enhancement in dense breast imagesusing the modulation transfer function. Med Phys 2002;29:2925–36.
33] Lepori D, De Landtsheer JP, Piguet JC, De Geer G, Schnyder PYM. Utilisationd’un système d’aide à la détection par ordinateur dans un programme dedépistage. Analyse rétrospective des mammographies de 49 cancers. Le Sein2002;12:295–303.
34] Seradour B, Heid P, Pagliuchi C, et al. Apport d’un système d’aide à la détectionassistée par ordinateur dans le cadre d’un programme de dépistage. Le Sein2001;11:13–6.
35] Ikeda DM, Birdwell RL, KF OS, Sickles EA, Brenner RJ. Computer-aided detectionoutput on 172 subtle findings on normal mammograms previously obtained inwomen with breast cancer detected at follow-up screening mammography.Radiology 2004.
36] Khoo LA, Taylor P, Given-Wilson RM. Computer-aided detection in the UnitedKingdom National Breast Screening Programme: prospective study. Radiology2005;237:444–9.
37] Brenner RJ, Ulissey MJ, Wilt RM. Computer-aided detection as evidence inthe courtroom: potential implications of an appellate court’s ruling. Am JRoentgenol 2006;186:48–51.

rnal of
[
[
[
[
[
[
[versus independent double reading of masses on mammograms. Radiology2003;227:192–200.
B. Boyer et al. / European Jou
38] Freer TW, Ulissey MJ. Screening mammography with computer-aided detec-tion: prospective study of 12 860 patients in a community breast center.Radiology 2001;220:781–6.
39] Morton MJ, Whaley DH, Brandt KR, Amrami KK. Screening mammograms: inter-pretation with computer-aided detection—prospective evaluation. Radiology2006;239:375–83.
40] Cupples TE, Cunningham JE, Reynolds JC. Impact of computer-aided detec-tion in a regional screening mammography program. Am J Roentgenol
2005;185:944–50.41] Gur D, Sumkin JH, Rockette HE, et al. Changes in breast cancer detection andmammography recall rates after the introduction of a computer-aided detec-tion system. J Natl Cancer Inst 2004;96:185–90.
42] Feig SA, Sickles EA, Evans WP, Linver MN. Re: changes in breast cancer detec-tion and mammography recall rates after the introduction of a computer-aided
[
Radiology 69 (2009) 24–33 33
detection system [letter]. J Natl Cancer Inst 2004;96:1260–1, author reply1261.
43] Fenton JJ, Taplin SH, Carney PA, et al. Influence of computer-aideddetection on performance of screening mammography. N Engl J Med2007;356(14):1399–409.
44] Karssemeijer N, Otten JDM, Verbeek ALM, et al. Computer-aided detection
45] Destounis SV, DiNitto P, Logan-Young W, Bonaccio E, Zuley ML, Willison KM.Can computer-aided detection with double reading of screening mammo-grams help decrease the false-negative rate? Initial experience. Radiology2004;232:578–84.