bulletin - unitbv
TRANSCRIPT
ISSN 2065-2216
TRANSILVANIA UNIVERSITY OF BRAŞOV
BULLETIN
OF THE
TRANSILVANIA UNIVERSITY
OF
BRAŞOV
VOL. 1 (50) – 2008
SERIES VI MEDICAL SCIENCES
Published by
Transilvania University Press
Braşov, Romania
2008
EDITORIAL BOARD
Editor in Chief
Prof. dr. eng. Ion VIŞA
Co-editors
Prof. dr. eng. Elena Helerea
Prof. dr. eng. Anca Duţă
Prof. dr. med Liliana Rogozea
Coordinating Editor series VI
Prof.dr. chem. Gheorghe COMAN
Final Technical Supervision
Mat. Gabriela MAILAT
Roxana CIOBANU
English Language Supervision
Lect. drd. Lucian RADU
Web-site: http://but.unitbv.ro/BU2008/
Adresa: B-dul Eroilor nr. 29, CP 500036, Braşov, România
Telefon: 0268/413000
E-mail: [email protected]
© All rights reserved
SCIENTIFIC COMMITTEE
Assoc. Prof. chem. Mihaela BADEA, Ph.D., Transilvania University of Brasov, Romania
Prof. Salem ABDEL-BADEEH, Ph.D., Ain Shams University, Cairo, Egypt
Prof. Cristina BORZAN, M.D., Ph.D., UMF Iuliu Haţieganu, Cluj-Napoca, Romania
Prof. Sorin BUZINSCHI, M.D., Ph.D., Transilvania University of Brasov, Romania
Dr. Daniel CATALAN, European Center for Disease Prevention and Control
Prof. chem. Gheorghe COMAN, Ph.D., Transilvania University of Brasov, Romania
Prof. Nina CADIZ, Ph.D., University of the Philippines Los Banos
Assoc. Prof. Carmen DOMNARIU, M.D., Ph.D., University Lucian Blaga, Sibiu, Romania
Prof. Alin CUCU, M.D., Ph.D., Transilvania University of Brasov, Romania
Prof. Dan DUMITRASCU, M.D., Ph.D., UMF Iuliu Hatieganu, Cluj-Napoca, Romania
Prof. Leonida GHERASIM, M.D., Ph.D, UMF Carol Davila, Bucharest, Member of
Romanian Academy, Romania
Prof. Ove HELLZEN, Ph.D., Faculty of Health Sciences, Norway
Prof. Kornelia HELEMBAI, Ph.D., University of Szeged, Hungary
Prof. Teodor LEASU, M.D., Ph.D., Transilvania University of Brasov, Member of the
World Academy of Medicine, Romania
Prof. Jean-Louis MARTY, Ph.D., Universite Perpignan, France
Prof. Dan MINEA, M.D., Ph.D., Transilvania University of Brasov, Romania
Prof. Aurel MIRONESCU, M.D., Ph.D., Transilvania University of Brasov, Romania
Prof. Nicolae MIU, M.D., Ph.D., UMF Iuliu Hatieganu, Cluj-Napoca, Romania
Assoc. Prof. Marius MOGA, M.D., Ph.D., Transilvania University of Brasov, Romania
Prof. Ioana MOISIL, Ph.D., University Lucian Blaga, Sibiu, Romania
Prof. Dimitrie NANU, M.D., Ph.D., UMF Carol Davila, Bucharest, Romania
Assoc. Prof. Laurenţiu NEDELCU, M.D., Ph.D., Transilvania University of Brasov, Romania
Prof. Codruta NEMET, M.D., Ph.D., Transilvania University of Brasov, Romania
Prof. Gilvanda NUNEZ, Ph.D., Federal University of Maranhao, Potugalia
Prof. Lazar ONISÂI, M.D., Ph.D., Transilvania University of Brasov, Romania
Assoc. Prof. Candan OZTURK, Ph.D., Dokuz Eylul University, Turkey
Prof. farm. Honorius POPESCU, Ph.D., UMF Iuliu Haţieganu, Cluj-Napoca, Member of
the “Academie Internationale d’Histoire de la Pharmacie”, Romania
Assoc. Prof. Mariusz PUSZCZEWICZ, M.D., Ph.D., Poznan University of Medical
Science, Poland
Prof. Mariana RADOI., M.D., Ph.D., Transilvania University of Brasov, Romania
Assoc. Prof. Patrizia RESTANI, M.D., Ph.D., State University of Milan, Italy
Prof. Ilia REUBEN, M.D., Ph.D., Ben Gurion University of the Negev, Israel
Prof. Liliana ROGOZEA, M.D., Ph.D., Transilvania University of Brasov, Romania
Prof. Iosif SAMOTA, M.D., Ph.D., Transilvania University of Brasov, Romania
Prof. Erich SORATIN, M.D., Ph.D., Medical University Graz, Austria
CONTENT
Fleancu, A., Sechel, G, Onisâi, L.L.,
Bold, C.L., Fleancu, C., Banuta, I.A.
Grecu, A. : Imagistic Study upon Urinary Malformative Pathology ....................... 1
Sechel, G., Fleancu, A., Ţurcanu, M., Diaconu, S.: Anatomic and Imagistic
Correlations In Bronchial Tree Segmentation ......................................................... 9
Onisâi, L.L., Scârneciu, I., Greavu, M., Peri, G.: The Anterolateral Abdominal
Wall - Vascularisation Development during Morphogenesis ................................ 17
Badea, M., Munteanu, M., Lazoriec, L., Coman, G., Restani, P.: Competitive
Elisa for Aflatoxins and Ochratoxins Detection ..................................................... 21
Nunes, G.S., Badea, M., Medel, M.-L., Noguer, T., Marty, J.-L.: Ultrasensitive
Biosensors for the Detection of Insecticide Residues in Fruit Juices ..................... 29
Restani, P., Caruso, D., Giavarini, F., Moro, E., Persico, A., Uberti, F.,
Ballabio, C., Colombo, M. L., Badea, M.: Analytical Monitoring as a Tool to
Detect Illegal Substances in Foods and Food Supplements .................................. 37
Idomir, M., Nemet, C., Pascu, A., Moleavin, I.: Imipenem Resistance among
Gram Negative Bacilli ............................................................................................ 43
Neculoiu, D., Moleavin, I., Anghel, M., Cristea, A.: Non-Organ Specific
Autoantibodies and the Response to the Therapy in Chronic Hepatitis C............. 47
Agache, I.: Acquired Angioedema in Systemic Lupus Erythematosus ............................ 55 Ifteni, G., Rus, H., Rădoi, M., Pamfil, G.: The Relationship between the Risk
Profile of Arterial Hypertension and the Features of Metabolic
Syndrome-Study on 129 Patients ........................................................................... 61
Scârneciu, C., Nedelcu, I., Scârneciu, I., Scârneciu, V.: Hyperthyroidism at
debut and the left ventricle mass ............................................................................ 67
Rus, H., Rădoi, M., Ciurea, C., Nan, M., Suta, C., Boda, D.: Effect of
Treatement with Omega-3 Fattyacids and Atorvastatin in Patients with
Combined Dyslipidemia.......................................................................................... 75
Bobescu, E., Rădoi, M., Galajda, Z., Datcu, G.: In Patients with Non-St Acute
Coronary Syndrome Diabetes Mellitus and Metabolic Syndrome have an
Important Impact on Prognosis, Left Ventricular Systolic Function,
Inflammatory Syndrome and Oxidative stress ....................................................... 81
Hussain, S., Afzal, N., Kohen, I., Manu, P. : C Reactive Protein and Clozapine-
Induced Fever ........................................................................................................ 89
Man, M. A., Alexandrescu, D., Pop, M., Râjnoveanu, R., Goron, M., Arghir, O.:
Smoking-Risk Factor for Metastasis in Breast Cancer........................................... 93
Falup-Pecurariu, O., Răşină, A., Falup-Pecurariu, C.: Antibiotic Susceptibility
Changes of Staphylococcus Aureus a Retrospective Study ....................................... 99
Burtea, V., Moşoiu, C.: Stigmatization of People with Schizophrenia in Clinical
Settings.................................................................................................................. 107
Ifteni, P., Burtea, V.: The Major Depressive Disorder with Mtabolic Syndrome -
Study on 90 Patients ........................................................................................... 111
Moşoiu, C., Burtea, V.: Positive and Negative Syndrome Scale Clustering of
Schizophrenia ....................................................................................................... 115

II Bulletin of the Transilvania University of Braşov � Vol. 1 (50)� Series VI
Falup-Pecurariu, C., Postelnicu, A., Pamfil, G., Monescu, V.,
Falup-Pecurariu, O., Alexandru, R.: Hemodynamics of the Posterior Cerebral
Artery .................................................................................................................. 119
Buzescu, M.: Comparative Study on the Efficacy of Different Protection
Methods In Chronic Acoustic Trauma .................................................................. 127
Mişarcă, C., Cucu, A., Durach, L.: Enteral Nutrition in the Treatment of Severe
Acute Pancreatitis ................................................................................................ 133
Scârneciu, I., Lupu, S., Onisâi, L.L., Scârneciu, C., Lupu, A.M., Scârneciu, V. D.:
Extracorporeal Shockwave Lithotripsy (ESWL) as a Mean of Treatment
in Urinary Lithiasis.............................................................................................. 139
Fanea, R., Voroneanu, M., Oros, C.: The Patient- Risk Marker for
Medical Emergencies in the Dental and Oral Surgery Office ............................. 145
Comşa, F.: Ultrastructural Changes in a Case of Recurrence after Varicose
Veins Surgery ....................................................................................................... 151
Alexandrescu, D.: Integrated Positron-Emission Tomography and the Staging
of Nodular Non-Small-Cell Lung Cancer ........................................................... 157
Baum, E.: Significance of Embryonic Stem Cells in Regenerative Medicine ................ 163
Bălescu, A., Leaşu, F., Rogozea, L., Chefneux, E.:
Health Promotion and
Elaboration of a Preventive Strategy for Brasov County .................................... 169
Cersosimo, G.: Drugs and Medicine in Youth Culture .................................................. 175
Rogozea, L., Bălescu, A., Domaradzki, J., Wierzejska, E., Baritz, M., Cristea, L.:
Dilemmas and Factors Involved in Promoting Men’s Health in Brasov
County .................................................................................................................. 195
Fătu-Tutoveanu, A.: A Decadent Age - 1900. Freud and Cocaine................................. 203
Authors Index.................................................................................................................. 211
IMAGISTIC STUDY UPON URINARY
MALFORMATIVE PATHOLOGY
A. FLEANCU
1 G. SECHEL
1 L.L. ONISÂI
1
C.L. BOLD1 C. FLEANCU
1 I.A. BANUTA
1
A. GRECU1
Abstract: The present paper has the purpose of realizing an incidence
study of reno-ureteral malformations. It is based on imagistic data obtained
from patients who want in cause services for any type of pathology.
Therefore, a bond with afferent simptomathology was made. It has come to
the conclusion that the majority of urinary malformations are mute form
clinical point of view and only a small percentage of these generate hydro-
nephrosis, urinal infections or a modification of biological parameters
Key words: renal malformation, urography, ecography, computer-
tomography
1 Transilvania University of Brasov, Faculty of Medicine
1. Aim of the Study
The paper aims at analysing the
frequency of reno-ureteral malformations
and of their different types, by correlating
data obtained through dissection and
imagistic methods. The study tries to
research the connections with possible
associated pathologies. [4]
2. Method and Material
Using cases from „Rapid Diagnostic
Polyclinic - Medis” from Brasov (patients
that had abdominal examination in the
period January 2007- December 2007),
144 cases of reno-ureteral malformations
were analysed using: ecography,
urography and computer-tomography. The
study was completed by dissecting 36 adult
bodies belonging to the laboratories of the
Medicine Faculty of Brasov.
3. Results
1. The total number of imagistic
investigated cases was 7200.
2. 4 of 36 cases examined by dissection
were found with renal malformations:
horseshoe kidney, ectopic kidney (2
cases) and big renal pelvis.
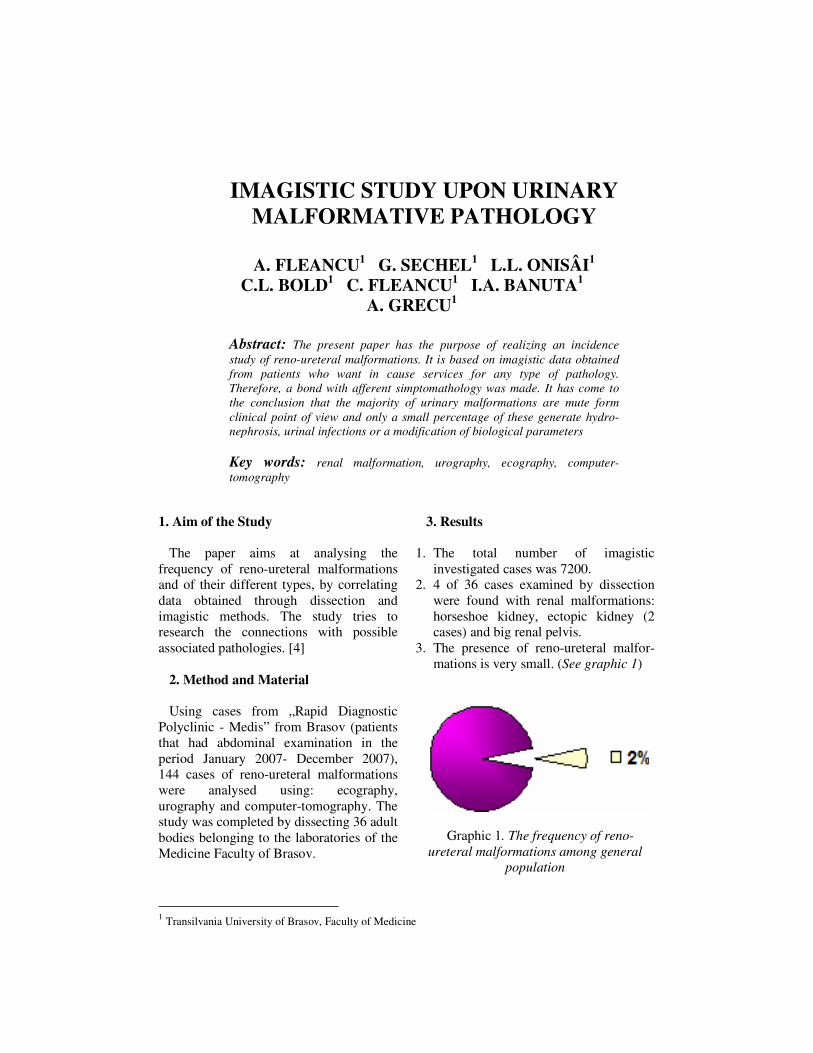
3. The presence of reno-ureteral malfor-
mations is very small. (See graphic 1)
Graphic 1. The frequency of reno-
ureteral malformations among general
population
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
2
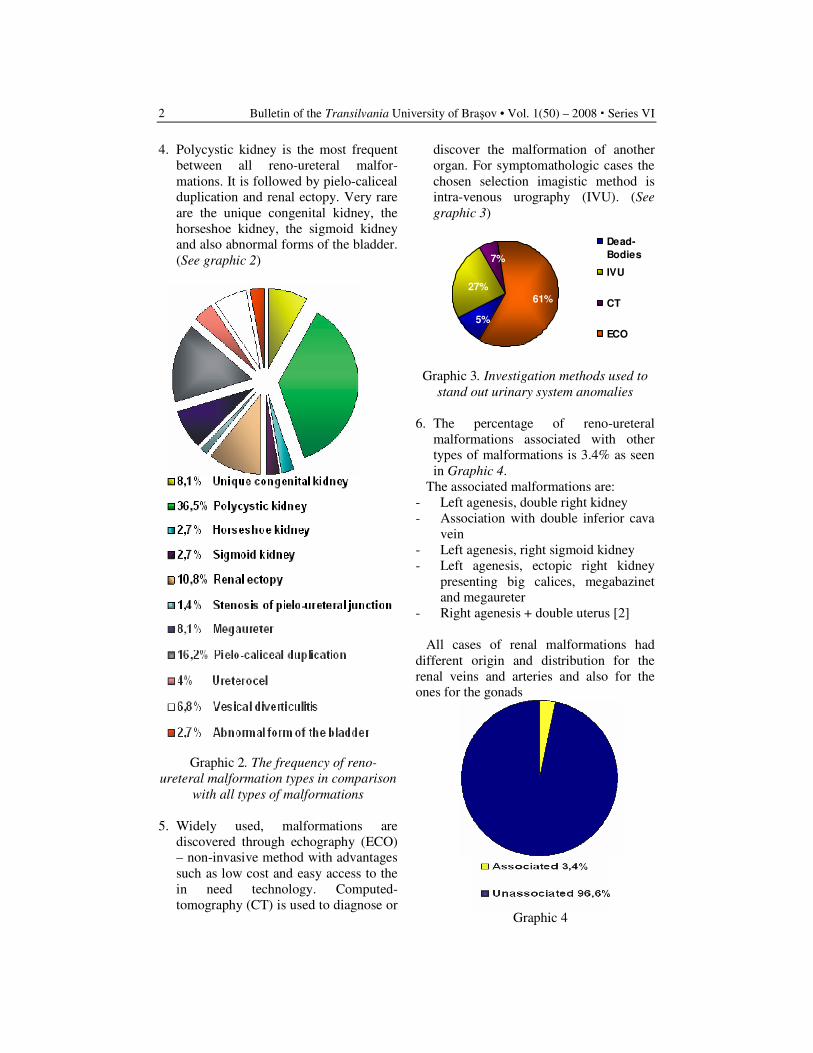
4. Polycystic kidney is the most frequent
between all reno-ureteral malfor-
mations. It is followed by pielo-caliceal
duplication and renal ectopy. Very rare
are the unique congenital kidney, the
horseshoe kidney, the sigmoid kidney
and also abnormal forms of the bladder.
(See graphic 2)
Graphic 2. The frequency of reno-
ureteral malformation types in comparison
with all types of malformations
5. Widely used, malformations are
discovered through echography (ECO)
– non-invasive method with advantages
such as low cost and easy access to the
in need technology. Computed-
tomography (CT) is used to diagnose or
discover the malformation of another
organ. For symptomathologic cases the
chosen selection imagistic method is
intra-venous urography (IVU). (See
graphic 3)
Dead-
Bodies
IVU
CT
ECO
7%
27%
5%
61%
Graphic 3. Investigation methods used to
stand out urinary system anomalies
6. The percentage of reno-ureteral
malformations associated with other
types of malformations is 3.4% as seen
in Graphic 4.
The associated malformations are:
- Left agenesis, double right kidney
- Association with double inferior cava
vein
- Left agenesis, right sigmoid kidney
- Left agenesis, ectopic right kidney
presenting big calices, megabazinet
and megaureter
- Right agenesis + double uterus [2]
All cases of renal malformations had
different origin and distribution for the
renal veins and arteries and also for the
ones for the gonads
Graphic 4
Imagistic Study upon Urinary Malformative Pathology 3
4. Cases
I. Renal malformations of form
A. Polycystic Kidney
Fig.1. Multiple cystic injuries on the
right kidney - echographic section
B. Parapielic Cysts
Fig. 2. Parapielic cysts on left kidney –
echographic section
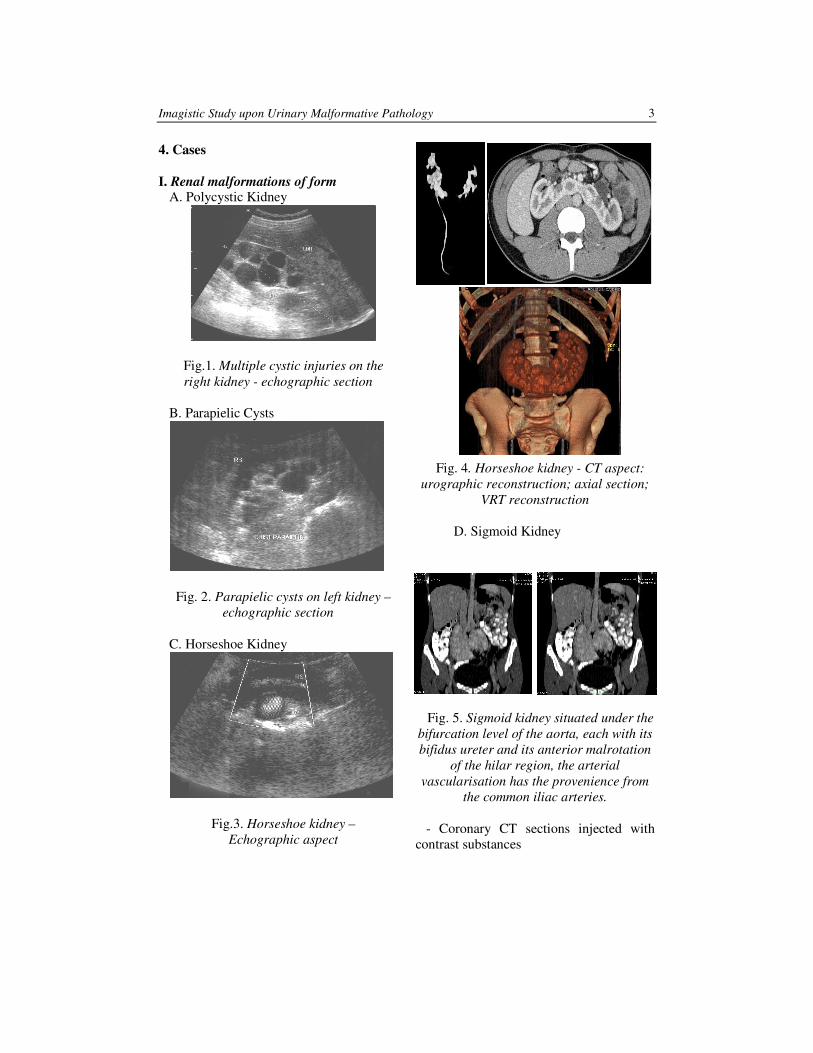
C. Horseshoe Kidney
Fig.3. Horseshoe kidney –
Echographic aspect
Fig. 4. Horseshoe kidney - CT aspect:
urographic reconstruction; axial section;
VRT reconstruction
D. Sigmoid Kidney
Fig. 5. Sigmoid kidney situated under the
bifurcation level of the aorta, each with its
bifidus ureter and its anterior malrotation
of the hilar region, the arterial
vascularisation has the provenience from
the common iliac arteries.
- Coronary CT sections injected with
contrast substances
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
4
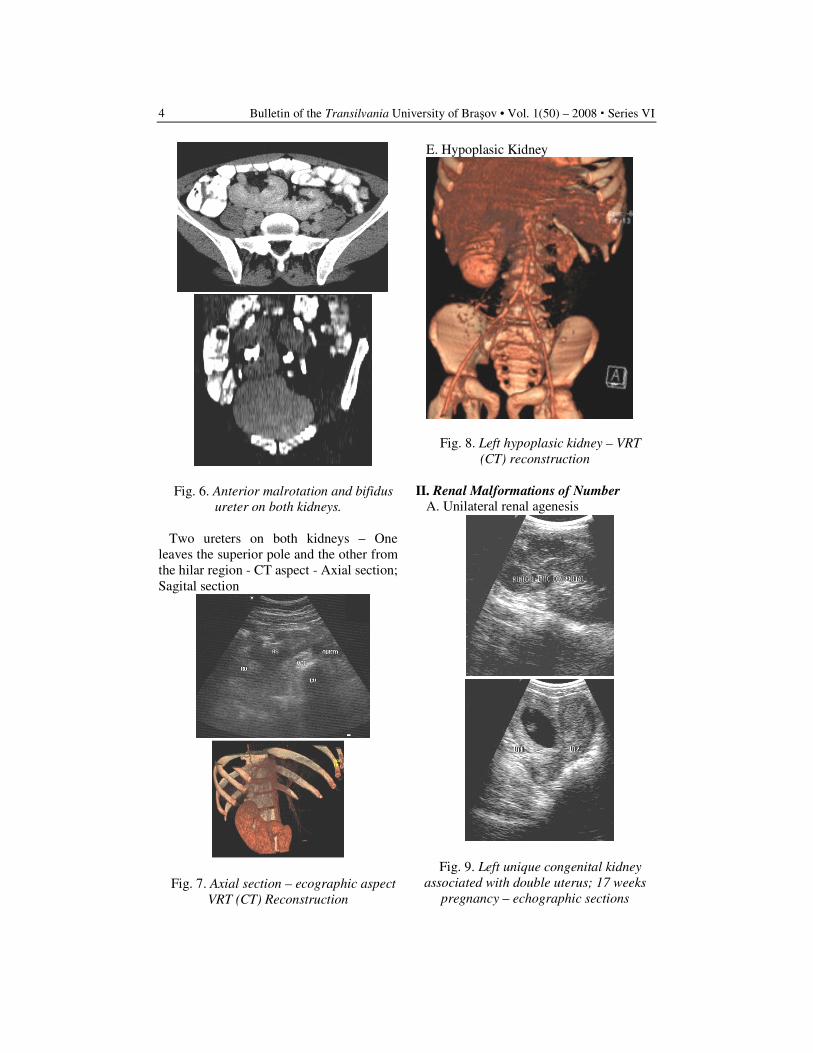
Fig. 6. Anterior malrotation and bifidus
ureter on both kidneys.
Two ureters on both kidneys – One
leaves the superior pole and the other from
the hilar region - CT aspect - Axial section;
Sagital section
Fig. 7. Axial section – ecographic aspect
VRT (CT) Reconstruction
E. Hypoplasic Kidney
Fig. 8. Left hypoplasic kidney – VRT
(CT) reconstruction
II. Renal Malformations of Number
A. Unilateral renal agenesis
Fig. 9. Left unique congenital kidney
associated with double uterus; 17 weeks
pregnancy – echographic sections
Imagistic Study upon Urinary Malformative Pathology 5
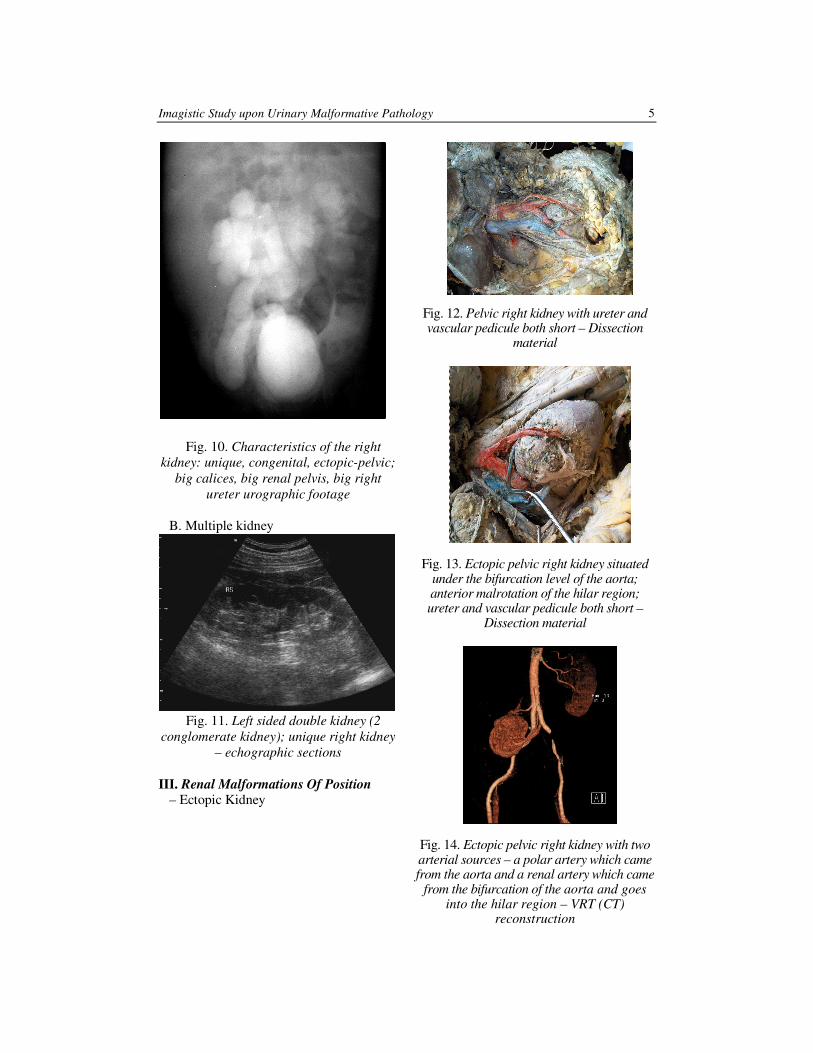
Fig. 10. Characteristics of the right
kidney: unique, congenital, ectopic-pelvic;
big calices, big renal pelvis, big right
ureter urographic footage
B. Multiple kidney
Fig. 11. Left sided double kidney (2
conglomerate kidney); unique right kidney
– echographic sections
III. Renal Malformations Of Position
– Ectopic Kidney
Fig. 12. Pelvic right kidney with ureter and
vascular pedicule both short – Dissection
material
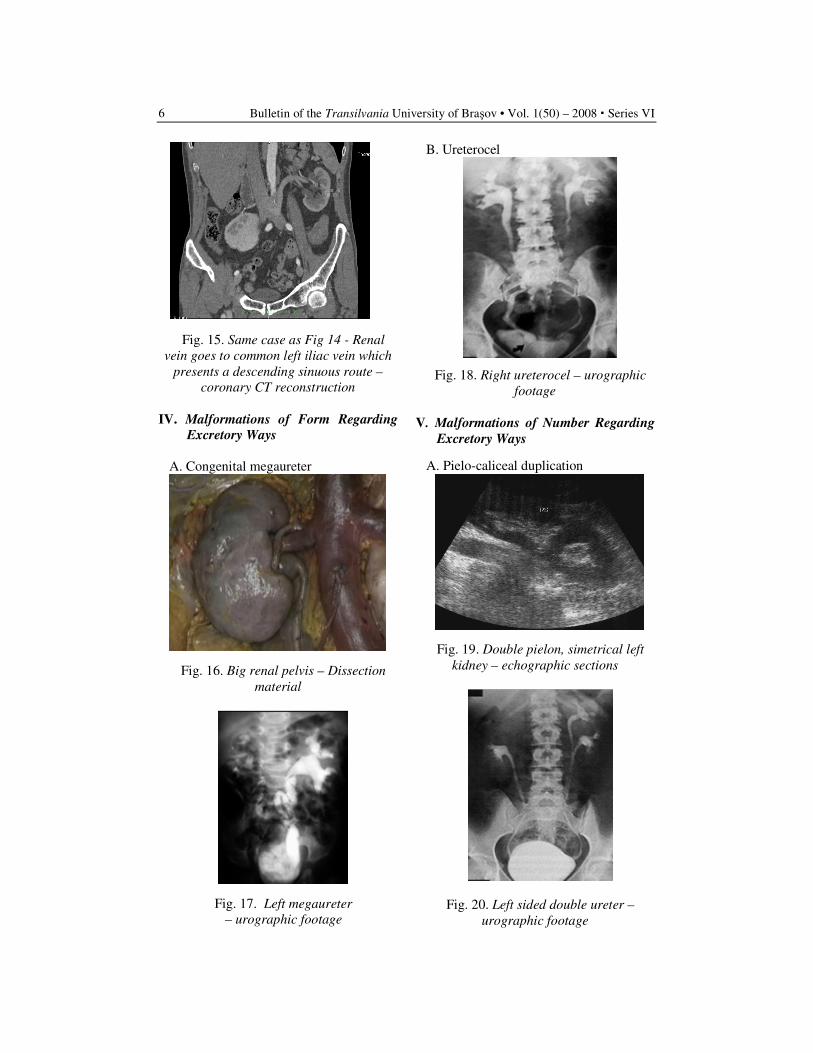
Fig. 13. Ectopic pelvic right kidney situated
under the bifurcation level of the aorta;
anterior malrotation of the hilar region;
ureter and vascular pedicule both short –
Dissection material
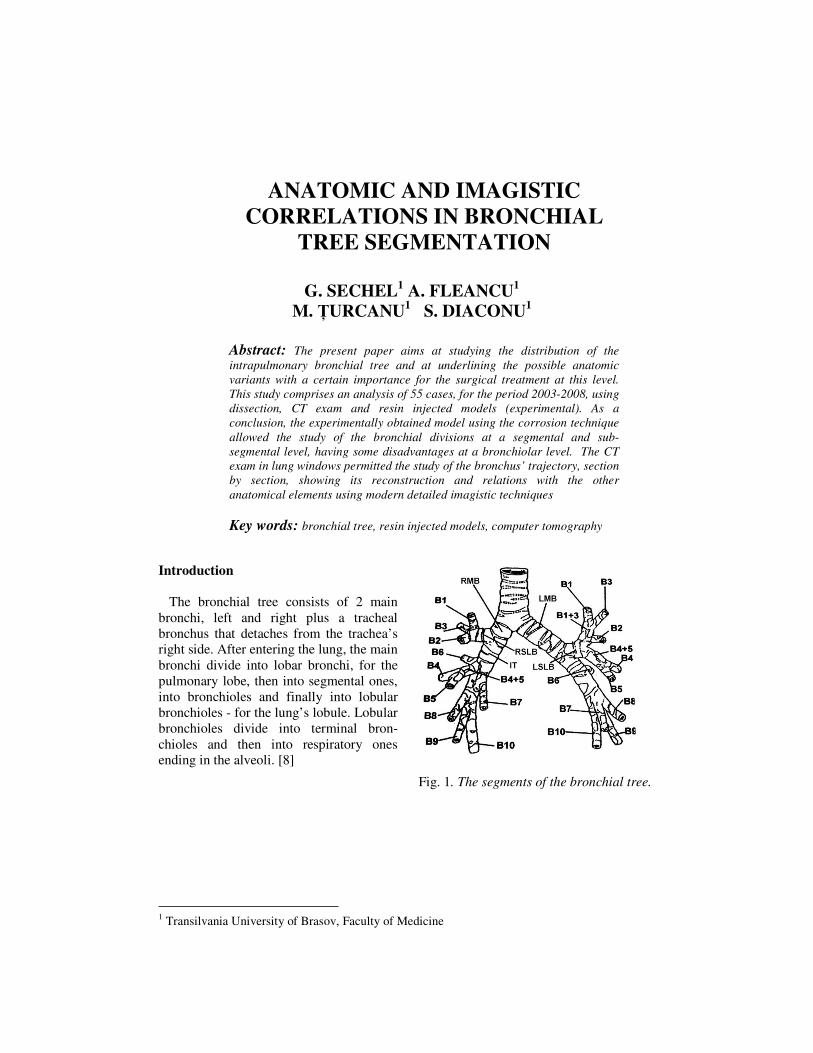
Fig. 14. Ectopic pelvic right kidney with two
arterial sources – a polar artery which came
from the aorta and a renal artery which came
from the bifurcation of the aorta and goes
into the hilar region – VRT (CT)
reconstruction
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
6
Fig. 15. Same case as Fig 14 - Renal
vein goes to common left iliac vein which
presents a descending sinuous route –
coronary CT reconstruction
IV. Malformations of Form Regarding
Excretory Ways
A. Congenital megaureter
Fig. 16. Big renal pelvis – Dissection
material
Fig. 17. Left megaureter
– urographic footage
B. Ureterocel
Fig. 18. Right ureterocel – urographic
footage
V. Malformations of Number Regarding
Excretory Ways
A. Pielo-caliceal duplication
Fig. 19. Double pielon, simetrical left
kidney – echographic sections
Fig. 20. Left sided double ureter –
urographic footage

Imagistic Study upon Urinary Malformative Pathology 7
VI. Malformations of Position Regarding
Excretory Ways
– Vesical Diverticulitis
Fig. 21. Large bladder diverticuli that
are not evacuated during micturition; thick
vesical mucous membrane
Fig. 22. Right posterior-lateral big
diverticuli; Left posterior-lateral small
diverticuli – pelvic CT axial section
5. Conclusions
1. Reno-ureteral malformations have a
2% presence among general population
and a 6% presence among all malfo–
rmations.
2. Polycystic kidney is the most frequent
between all reno-ureteral malforma–
tions. It is followed by pielo-caliceal
duplication and renal ectopy. Very rare
are the unique congenital kidney, the
horseshoe kidney, the sigmoid kidney
and also abnormal forms of the. [1]
3. The most popular imagistic method is
echography because it is very
accessible and non-invasive but it
brings poor information about the
relationships, the vascularization and
specially keeping the functionality of
the malformed segment.
4. Urography is very specific in finding
malformative cases due to its
simptomathology. It gives informations
about functions but not about
relationships and vascularization.
5. Complete morphological and function–
nal data are given by Computed
Tomography 2D and 3D
reconstructions by meanings like
injecting contrast substances. [3]
6. Most of the malformations are disco-
vered at a late stage and by chance, as
they are well tolerated (pielo-caliceal
duplication, the horseshoe kidney or
the unique congenital kidney); the
malformations discovered at an earlier
stage are those that generate hydro-
nefrosis (the syndrome of pielo-
ureteral junction), urinal infections or
modification of biological parameters
(the polycystic kidney).
Sometimes, the malformation is discovered
by investigating a suspicion of an
abdominal-pelvine tumour (the horseshoe
kidney or the ectopic kidney)
References
1. Belsare, S.M., Chimmalgi, M., Vidya
S.A. & Sant S.M.: Ectopic kidney and
associated anomalies: A Case Report
2. Fernandez Rodriguez, A., Arrabal
Martin, M., Mijan Ortiz, J.L., Palao
Yago, F., Zuliaga Gomez, A.:
Renoureteral malformation and
lithiasis

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
8
3. Lee, J.K.T., Sagel, S.S., Stanley, Jay,
R.J., Heiken, P.: Computed Body
Tomography with MRI correlation,
Vol. 2. 2006.
4. Tidy, C.: Congenital Urogenital
Malformation
5. Torra, R.: Polycystic Kidney Disease
ANATOMIC AND IMAGISTIC
CORRELATIONS IN BRONCHIAL
TREE SEGMENTATION
G. SECHEL
1 A. FLEANCU
1
M. ŢURCANU1 S. DIACONU
1
Abstract: The present paper aims at studying the distribution of the
intrapulmonary bronchial tree and at underlining the possible anatomic
variants with a certain importance for the surgical treatment at this level.
This study comprises an analysis of 55 cases, for the period 2003-2008, using
dissection, CT exam and resin injected models (experimental). As a
conclusion, the experimentally obtained model using the corrosion technique
allowed the study of the bronchial divisions at a segmental and sub-
segmental level, having some disadvantages at a bronchiolar level. The CT
exam in lung windows permitted the study of the bronchus’ trajectory, section
by section, showing its reconstruction and relations with the other
anatomical elements using modern detailed imagistic techniques
Key words: bronchial tree, resin injected models, computer tomography
1 Transilvania University of Brasov, Faculty of Medicine
Introduction
The bronchial tree consists of 2 main
bronchi, left and right plus a tracheal
bronchus that detaches from the trachea’s
right side. After entering the lung, the main
bronchi divide into lobar bronchi, for the
pulmonary lobe, then into segmental ones,
into bronchioles and finally into lobular
bronchioles - for the lung’s lobule. Lobular
bronchioles divide into terminal bron-
chioles and then into respiratory ones
ending in the alveoli. [8]
Fig. 1. The segments of the bronchial tree.

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
10
Bronchial nomenclature Table 1
A comprehensive bronchial nomen-
clature is given in Figure 1 and Table 1. [6] The right main bronchus (BPD) is divided
itself into right superior lobar bronchus (BLSD) and intermediary trunk (IT). BLSD has a horizontal trajectory (1-2 cm) then divides into 3 segmental branches: B1, B2, B3. The intermediary trunk has a vertical trajectory about 3cm, from BLSD’s origin to intermediary lobar bronchus’ origin (BLM). On the posterior and internal side of the hilum, the pulmonary parenchyma frames the inter-azygo-esophageal recess, delimitated on the interior by the azygos vein and the esophagus. The intermediary lobar bronchus (BLM) detaches from the anterior lateral side of IT, and it is separated at the origin from the inferior lobar bronchus by a small triangular tissue. After 1-2 cm, it is divided into segmental bronchi, B4 (external) and B5
(internal). Nelson’s bronchus (B6) is generally located superior to BLM. [7]
For the left lung, the segmental bronchi B1 and B3 can be seen like 2 round hypo-densities or like a common trunk (B1+3). They are separated from the left main bronchus (BPS) by the left pulmonary artery. [4]
BLSS is situated lower than BLSD; it detaches from the exterior and anterior side of the main left bronchus and its origin corresponds to the middle part of the IT from the right hilum. BLSS is also divided into B1+3. B2 has a horizontal trajectory and it is located to the anterior. The lingular bronchus (B4+5) appears on the distal side of the superior lobar bronchus and has an oblique trajectory, almost parallel to B2. BLIS is generally divided into 2 trunks: B7+8 and B9+10. [3, 5]
Table 2
The normal findings and the most common bronchial variants in the studied patients
Anatomic and Imagistic Correlations in Bronchial Tree Segmentation 11
Material and Method
For this study there were analyzed 55
cases and 5 animals during 5 years using
these 3 methods within the framework of
the Quick Diagnosis Clinic and the
anatomy laboratories (fig. 2,3):
1. The dissection method on 8%
formolised human bodies;
2. The corrosion technique
For the experimental part of this
study, there have been used the
bronchial trees taken over from 5
pigs and 1 cow. The method
consists of the injection with
pigmented resin (treated with other
substances in order to modify the
fluidity and the viscosity) as well
as in the corrosion with caustic
soda. The modifications of the
fluidity or the main material’s
compounds (even changing the
pigment) implied the extension of
the experiments, from 1 lot to 3,
better results being noticed.
3. Computer tomography thoracal
exam on 35 cases, in order to
investigate various diseases.
Were used:
• CT thoracic exam, spiral acquisi–
tion on a CT Somatom Emotion 6
device. Technique: KV: 130;
Effective mAs: 70; Slice
collimation: 2.0 mm; Increment:
2.5 mm; Kernel B41s (B70s –
parenchyma window)
• MPR in various plans and other
special reconstructions emphasize
the ramifications of the broncho-
pulmonary tree
• also MINIP and VRT recon–
structions.
Fig. 2. The aspect of the bronchial tree;
the dissection method
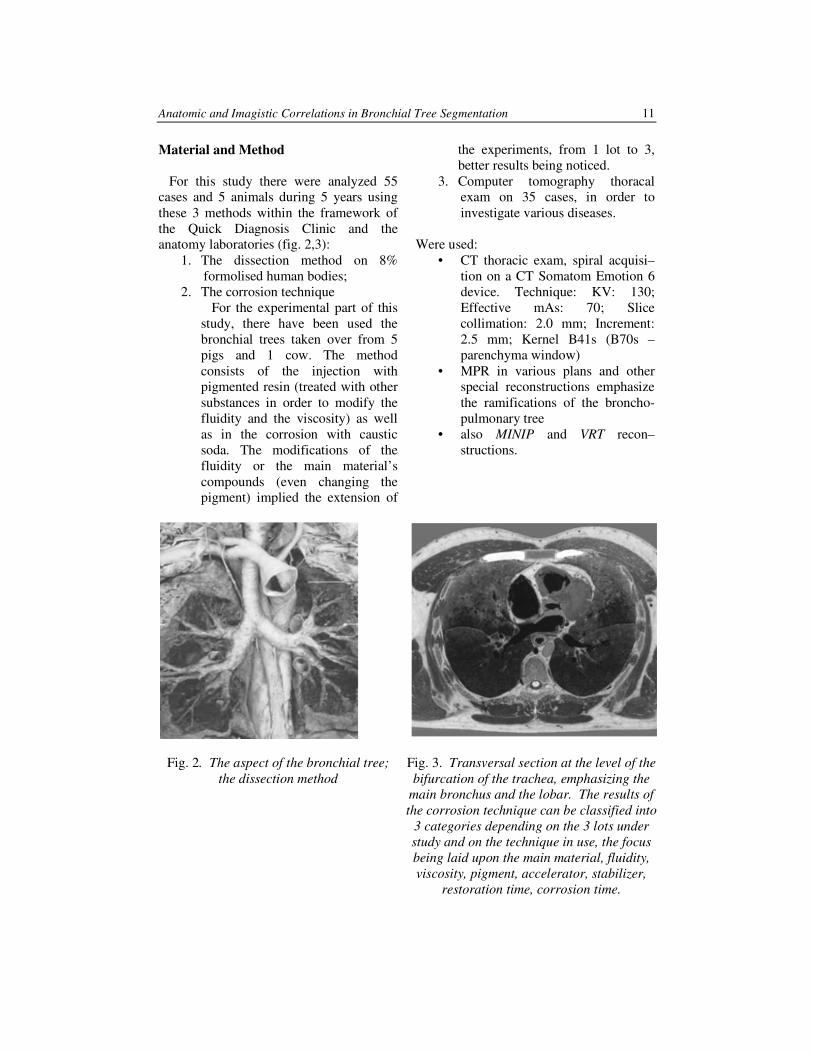
Fig. 3. Transversal section at the level of the
bifurcation of the trachea, emphasizing the
main bronchus and the lobar. The results of
the corrosion technique can be classified into
3 categories depending on the 3 lots under
study and on the technique in use, the focus
being laid upon the main material, fluidity,
viscosity, pigment, accelerator, stabilizer,
restoration time, corrosion time.
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
12
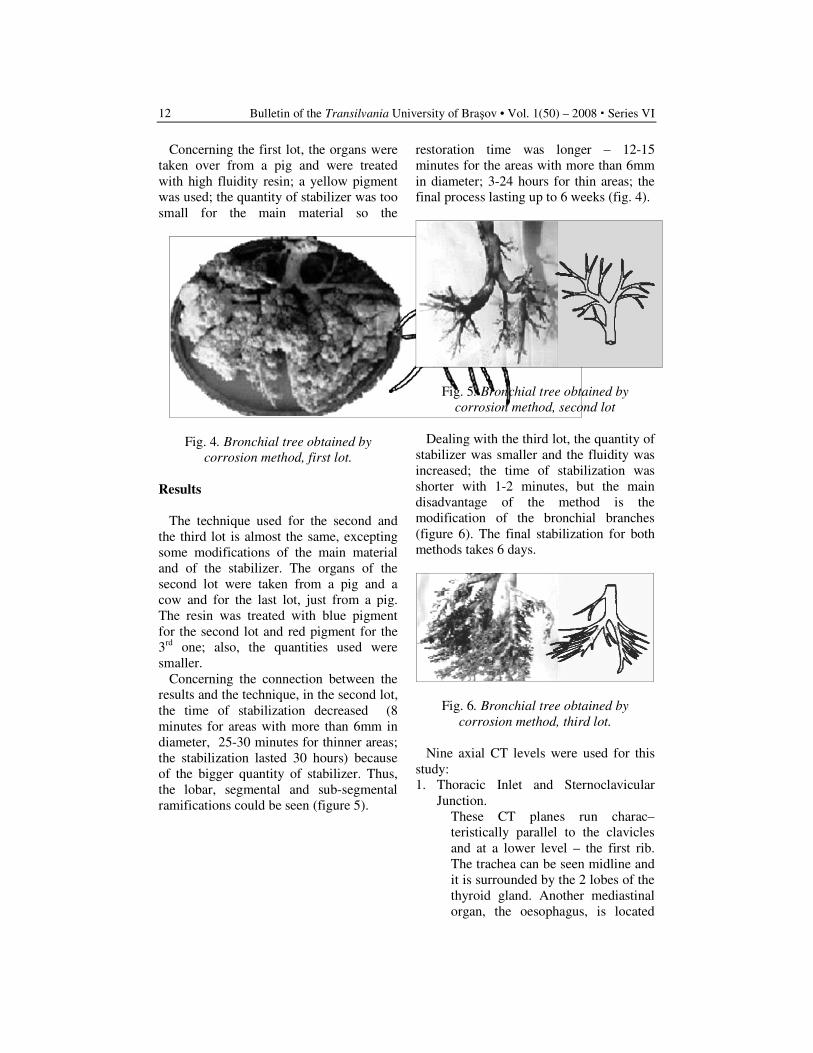
Concerning the first lot, the organs were
taken over from a pig and were treated
with high fluidity resin; a yellow pigment
was used; the quantity of stabilizer was too
small for the main material so the
restoration time was longer – 12-15
minutes for the areas with more than 6mm
in diameter; 3-24 hours for thin areas; the
final process lasting up to 6 weeks (fig. 4).
Fig. 4. Bronchial tree obtained by
corrosion method, first lot.
Results
The technique used for the second and
the third lot is almost the same, excepting
some modifications of the main material
and of the stabilizer. The organs of the
second lot were taken from a pig and a
cow and for the last lot, just from a pig.
The resin was treated with blue pigment
for the second lot and red pigment for the
3rd
one; also, the quantities used were
smaller.
Concerning the connection between the
results and the technique, in the second lot,
the time of stabilization decreased (8
minutes for areas with more than 6mm in
diameter, 25-30 minutes for thinner areas;
the stabilization lasted 30 hours) because
of the bigger quantity of stabilizer. Thus,
the lobar, segmental and sub-segmental
ramifications could be seen (figure 5).
Fig. 5. Bronchial tree obtained by
corrosion method, second lot
Dealing with the third lot, the quantity of
stabilizer was smaller and the fluidity was
increased; the time of stabilization was
shorter with 1-2 minutes, but the main
disadvantage of the method is the
modification of the bronchial branches
(figure 6). The final stabilization for both
methods takes 6 days.
Fig. 6. Bronchial tree obtained by
corrosion method, third lot.
Nine axial CT levels were used for this
study:
1. Thoracic Inlet and Sternoclavicular
Junction.
These CT planes run charac–
teristically parallel to the clavicles
and at a lower level – the first rib.
The trachea can be seen midline and
it is surrounded by the 2 lobes of the
thyroid gland. Another mediastinal
organ, the oesophagus, is located
Anatomic and Imagistic Correlations in Bronchial Tree Segmentation 13
posterior to the trachea, slightly on
the left of the midline. Anterior and
lateral to the trachea, the mediastinal
vessels can be noticed: the three major
branches of the aortic arch (the
brachiocephalic, left common carotid,
left subclavian arteries) and the two
brachioceplaic veins, located posterior
to the clavicular heads. [2]
2. Crossing Left Brachiocephalic Vein
At this level, the junction between
the manubrium and body of the
sternum can be seen. The two
brachiocephalic veins are situated
anterior to the trachea. The left
brachiocephalic vein is longer and
joins the superior vein cava.
3. Aortic Arch
The anterior portion of the arch is
situated anterior to the trachea and
comes into medial contact with the
superior vena cava. The middle part
of the arch is located on the left side
of the trachea and the posterior
portion – at the junction of the aortic
arch and the descending aorta is
lateral to the oesophagus.
4. Aortopulmonary Window
This region contains the distal
trachea, mediastinal fat (beneath the
arch medial to the descending aorta
and above the left pulmonary artery)
and some lymph nodes.
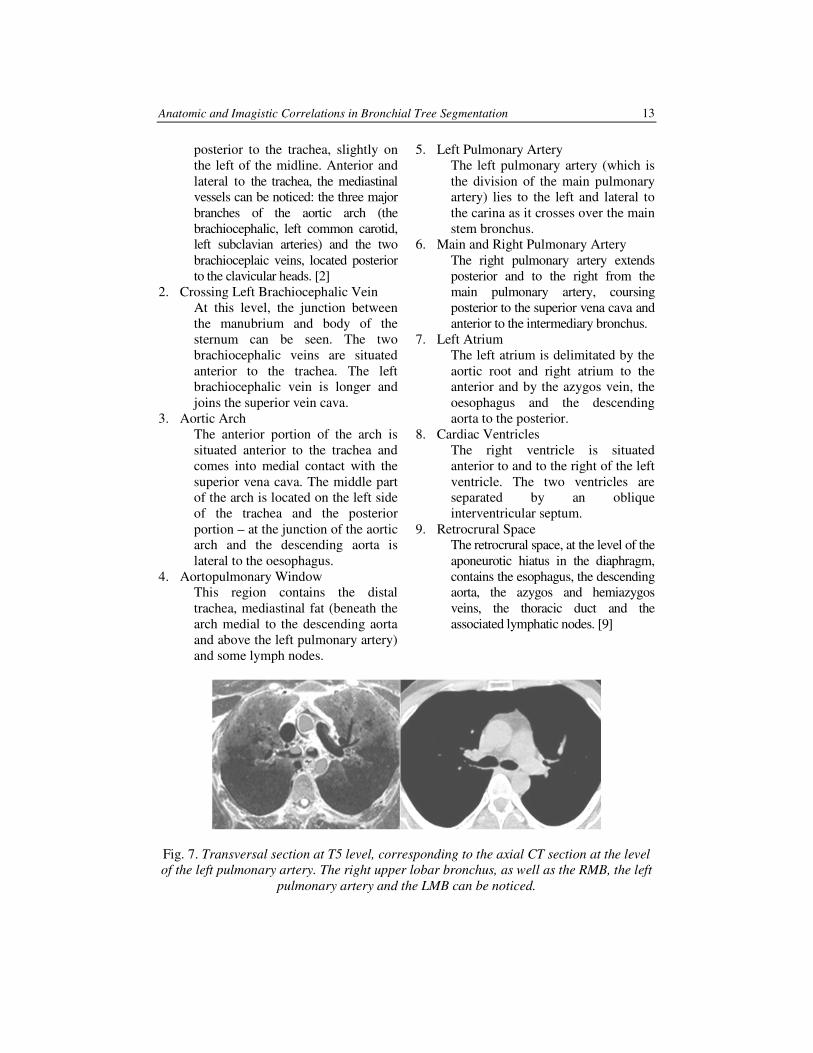
5. Left Pulmonary Artery
The left pulmonary artery (which is
the division of the main pulmonary
artery) lies to the left and lateral to
the carina as it crosses over the main
stem bronchus.
6. Main and Right Pulmonary Artery
The right pulmonary artery extends
posterior and to the right from the
main pulmonary artery, coursing
posterior to the superior vena cava and
anterior to the intermediary bronchus.
7. Left Atrium
The left atrium is delimitated by the
aortic root and right atrium to the
anterior and by the azygos vein, the
oesophagus and the descending
aorta to the posterior.
8. Cardiac Ventricles
The right ventricle is situated
anterior to and to the right of the left
ventricle. The two ventricles are
separated by an oblique
interventricular septum.
9. Retrocrural Space
The retrocrural space, at the level of the
aponeurotic hiatus in the diaphragm,
contains the esophagus, the descending
aorta, the azygos and hemiazygos
veins, the thoracic duct and the
associated lymphatic nodes. [9]
Fig. 7. Transversal section at T5 level, corresponding to the axial CT section at the level
of the left pulmonary artery. The right upper lobar bronchus, as well as the RMB, the left
pulmonary artery and the LMB can be noticed.
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
14
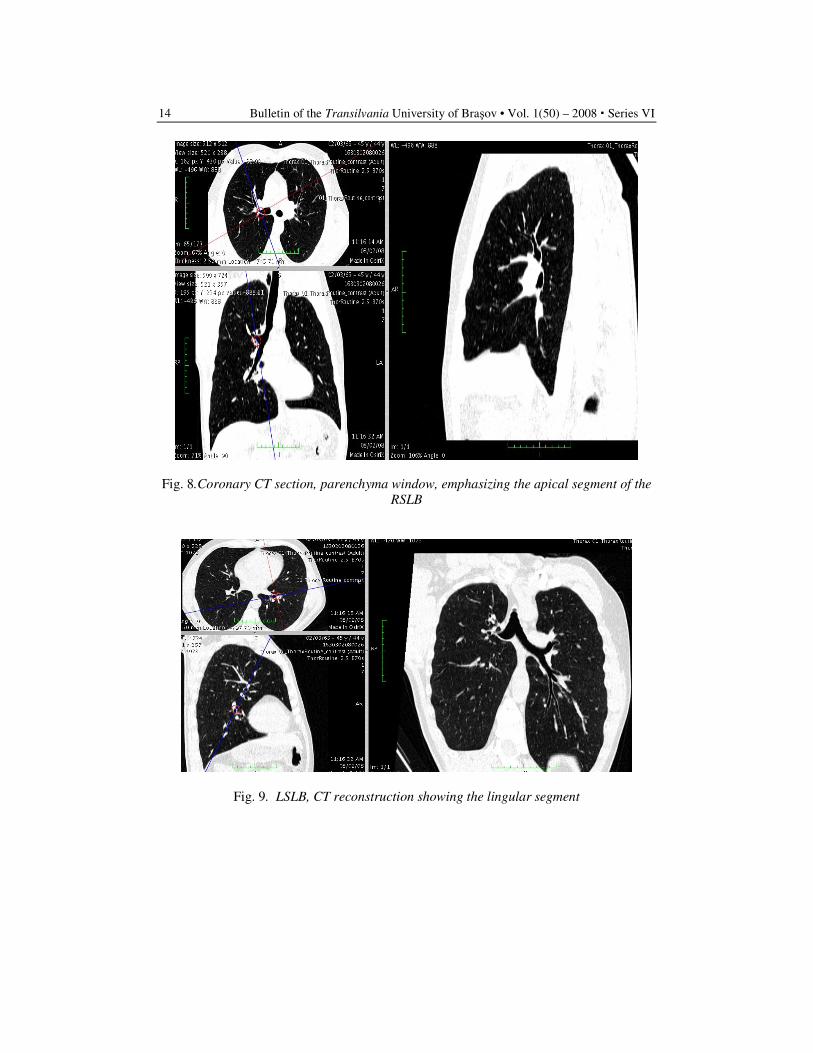
Fig. 8.Coronary CT section, parenchyma window, emphasizing the apical segment of the
RSLB
Fig. 9. LSLB, CT reconstruction showing the lingular segment
Anatomic and Imagistic Correlations in Bronchial Tree Segmentation 15
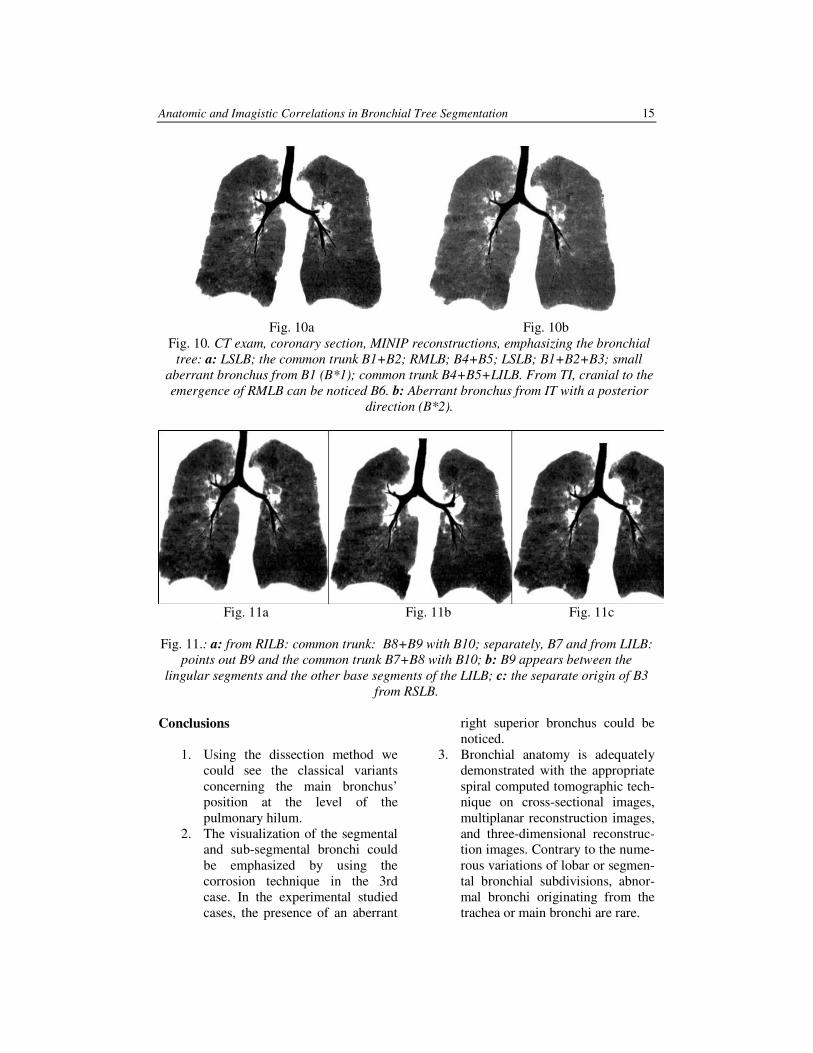
Fig. 10a Fig. 10b
Fig. 10. CT exam, coronary section, MINIP reconstructions, emphasizing the bronchial
tree: a: LSLB; the common trunk B1+B2; RMLB; B4+B5; LSLB; B1+B2+B3; small
aberrant bronchus from B1 (B*1); common trunk B4+B5+LILB. From TI, cranial to the
emergence of RMLB can be noticed B6. b: Aberrant bronchus from IT with a posterior
direction (B*2).
Fig. 11a Fig. 11b Fig. 11c
Fig. 11.: a: from RILB: common trunk: B8+B9 with B10; separately, B7 and from LILB:
points out B9 and the common trunk B7+B8 with B10; b: B9 appears between the
lingular segments and the other base segments of the LILB; c: the separate origin of B3
from RSLB.
Conclusions
1. Using the dissection method we
could see the classical variants
concerning the main bronchus’
position at the level of the
pulmonary hilum.
2. The visualization of the segmental
and sub-segmental bronchi could
be emphasized by using the
corrosion technique in the 3rd
case. In the experimental studied
cases, the presence of an aberrant
right superior bronchus could be
noticed.
3. Bronchial anatomy is adequately
demonstrated with the appropriate
spiral computed tomographic tech-
nique on cross-sectional images,
multiplanar reconstruction images,
and three-dimensional reconstruc-
tion images. Contrary to the nume-
rous variations of lobar or segmen-
tal bronchial subdivisions, abnor-
mal bronchi originating from the
trachea or main bronchi are rare.
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
16
4. The most common variants are:
- for BLSD: bifurcation B1+B2, B3,
followed by the trifurcation B1, B2,
B3
- for BLSS: in all the cases –
bifurcation in B4+B5 and
separately, B1, B2, B3
- for BLID: separately B6, B7;
bifurcation B8+B9, B10 and also
the variant: B9+B10, B8
- for BLIS: separately B6;
trifurcation B7+B8, B9, B10
References
1. Berrocal, T., Madrid, C., Novo, S.,
Gutierrez, J., Arjonilla, A. and
Gomez-Leon, N.: Congenital
Anomalies of the Tracheobronchial
Tree, Lung, and Mediastinum:
Embryology, Radiology, and
Pathology. In: RadioGraphics, January
1, 2004; 24(1): e17.
2. Gamsu, G.: Computed tomography of
the body. In: Moss A.A., Gamsu G.,
Genant H.K., Saunders Edit, 1983;
271 – 320.
3. Ghaye, B., Szapiro, D., Fanchamps,
J.-M., Dondelinger, R.F.: Congenital
Bronchial Abnormalities Revisited. In:
RG, Vol 21, Nr 1; Jan-Feb 2001;
105 – 118.
4. Jardin, M., Remy, J.: Segmental
bronchovascular anatomy of the lower
lobes: CT analysis. In: A.J.R., 1986;
147, 457 – 468.
5. Mastora, I., Ioan-Mihalcea, A.,
Lupescu, L., Georgescu, S.A.:
Anatomia tomodensitometrica a
hilurilor pulmonare; Imagistica
medicală, vol 2; 1998; 40 – 46.
6. Osborne, D., Vock, P., Godwin, D.J.
et al.: CT identification of pulmonary
segments: 50 normal subjects. In:
A.J.R., 1984; 142, 47 – 52.
7. Read, R., St. Cyr, J., Marek, J.,
Whitman, G., Hopeman, A.: Bronchial
anomaly of the right upper lobe. In:
Ann Thorac Surg 1990; 50:980–981.
8. Remy, J., Remy-Jardin, M., Artaud,
D., Fribourg, M.: Multiplanar and
three-dimensional reconstruction
techniques in CT: impact on chest
diseases. In: Eur Radiol 1998;
8:335–351.
9. Sagel, S.S.: Computed Body Tomo–
graphy with MRI Correlation, vol I.,
cap. Lung. 2006; 421 – 555.
THE ANTEROLATERAL ABDOMINAL
WALL - VASCULARISATION
DEVELOPMENT DURING
MORPHOGENESIS
L.L. ONISÂI
1 I. SCARNECIU
2
M. GREAVU3 G. PERI
4
Abstract: The present paper aims to do an objective research over the
ontogenesis process of the vascularisation of the antero-lateral abdominal wall
and, using the results obtained, to verify the validity of the theories formulated
until now; it also aims to elaborate a theory regarding the process, if the analyzed
elements allow it. To fulfil the objectives of this study, we have used dissections,
video images through transillumination, photographic pictures and histological
studies. We have carried out a microscopic study that aims to minutely observe the
processes that happen in dynamic time from early ages on. We have also run a
macroscopic study through the inspection of the vessels at the level of the antero-
lateral abdominal wall.
Key words: somatic, transilumination, plasmodiums.
1 Transilvania University of Brasov, Department of Anatomy, Faculty of Medicine Brasov 2Transilvania University of Brasov, Faculty of Medicine Brasov, Urology Clinic, Clinic Emergency County
Hospital Brasov, 3 Transilvania University of Brasov 4 Department of Anatomy, Faculty of Medicine Palermo
1. Materials and Method
This study was carried out on a number
of 15 subjects: 9 adult embryos and foetus
and 6 human adult corpses. The
macroscopic study involved the inspection
of the antero-lateral abdominal wall,
supplemented by the dissection, the
parietal and umbilical morphometry and
the study by transillumination. The
microscopic study consisted in the
prelevation of parts of the embryos, foetus
and adults studied macroscopically. The
research team carried out Hemalum Eosin
Sofran colouring, the Van Gusson method
and silver impregnation. We also used the
method using the lemon juice and gold
chloride according to Roschin. Moreover,
for the observation of the vessels of the
right abdominal muscle, we used for the
compounds, the method of China ink
injection, clarification, followed by
transillumination and photography.
2. Results
At the same time with the swing of the
cephalic and caudal folds, followed by the
closure of the embryonic body, the parietal
vascular and nervous elements in the
ventral wall are differentiated. They are
well individualized starting with the
seventh week, so that by the occurrence of
the fascicular structures of the right
Bulletin of the Transilvania University of Braşov • Vol. 15(50) - 2008 � Series VI
18
abdominal muscle, the vessels and the
nerves appear in the conjunctive
intrafascicular tissue.
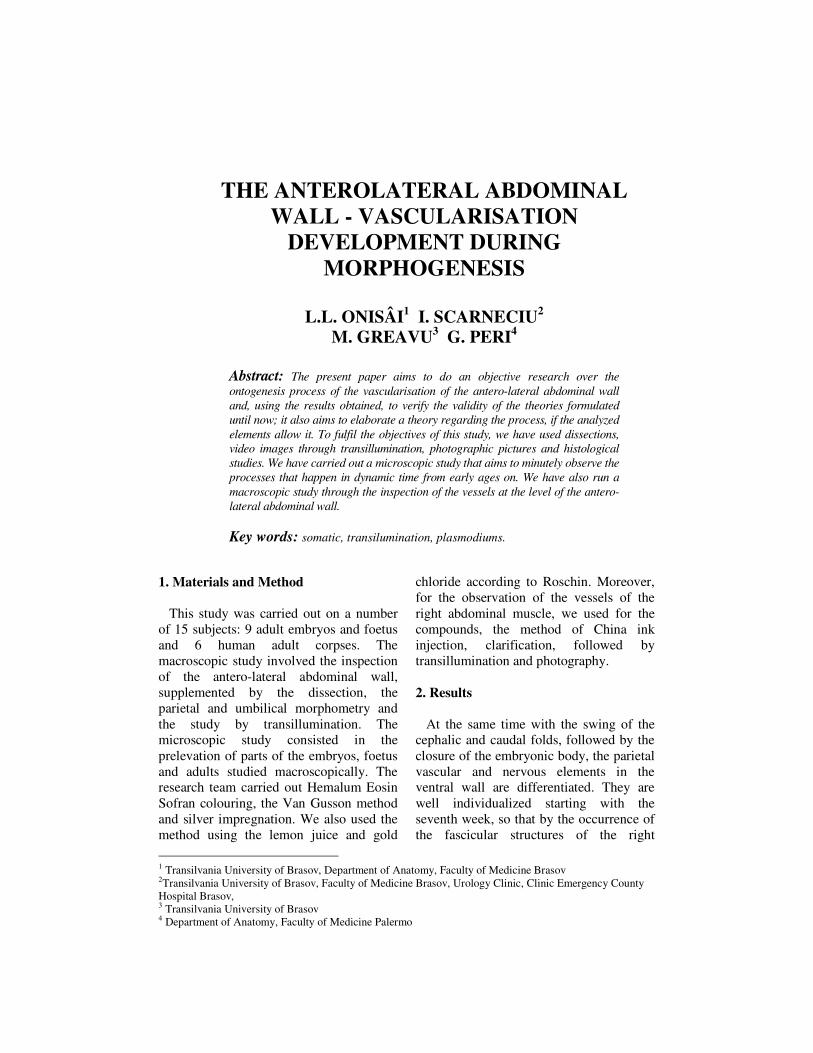
Fig. 1. Blood vessels in formation 18 mm
embryo (week 7), case 11, objective 40x, VG
colouring; in parasagital superumbilical
section. We can see the subcutaneous zone of
the anterolateral abdominal wall where, in
parallel with muscular differentiation, in a
major area as compared to the fascie
exoabdominale, blood vessels appear, the
lumen of which contains red blood corpuscles.
The differentiation of the vessels of the
right abdominal muscle is done in parallel
with the transformation of the myoblasts
into plasmodiums in the weeks 8-14. By
the dissection of the thoracic-abdominal
wall at the foetus of 30-34 weeks, the
presence of the intern thoracic arteries is
highlighted; these arteries are trifurcated at
the end, each one in a medial branch, a
median branch and a lateral one.
Fig. 2. 87 mm foetus (week 12), case 38, in
sagital superumbilical section (all along the
muscle), HE colouring, objective 10x. There
are vessels and nerves which belong to the
muscle, in conjunctive tissue between the
fascicles of the right abdominal muscle.
The first two final branches of the intern
thoracic artery take part to the
vascularization of the right abdominal
muscle. The higher epigastric artery
engages between the right abdominal
muscle, located at the anterior side, and the
posterior strip of its sheath located at the
posterior side, having a path nearly
identical to that of the preperitoneal
arteries located between the peritoneum
and the posterior face of the sheath of the
right abdominal muscle.
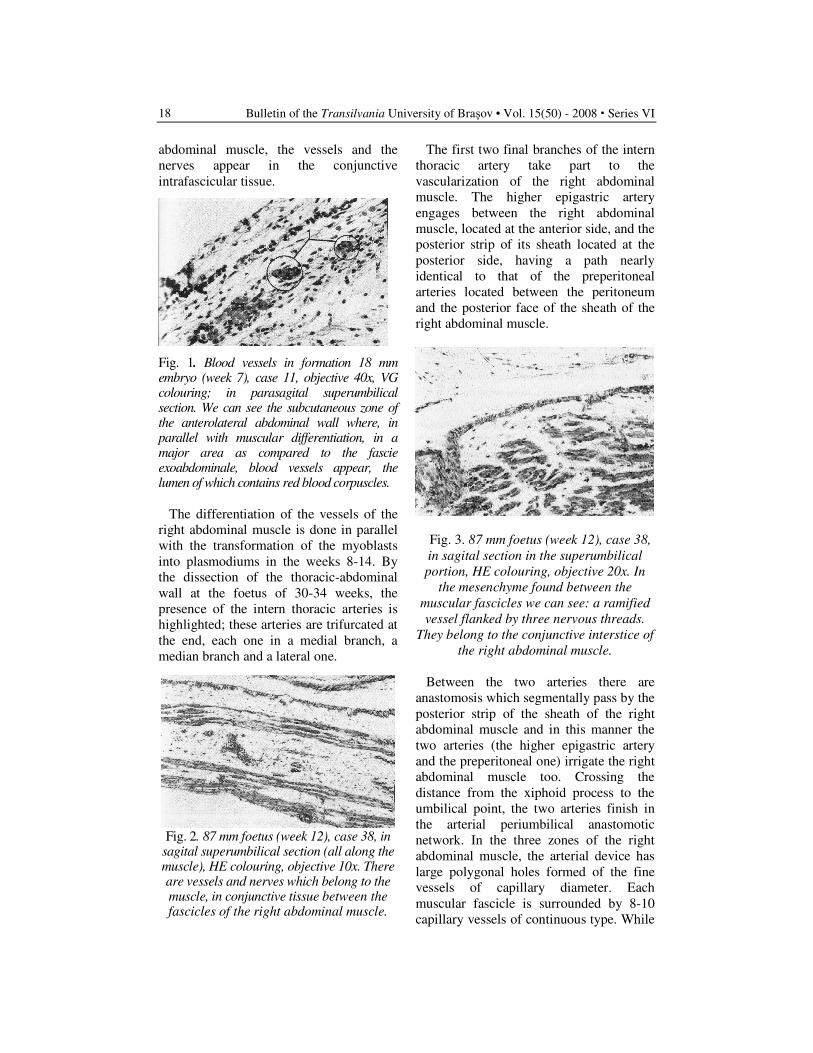
Fig. 3. 87 mm foetus (week 12), case 38,
in sagital section in the superumbilical
portion, HE colouring, objective 20x. In
the mesenchyme found between the
muscular fascicles we can see: a ramified
vessel flanked by three nervous threads.
They belong to the conjunctive interstice of
the right abdominal muscle.
Between the two arteries there are
anastomosis which segmentally pass by the
posterior strip of the sheath of the right
abdominal muscle and in this manner the
two arteries (the higher epigastric artery
and the preperitoneal one) irrigate the right
abdominal muscle too. Crossing the
distance from the xiphoid process to the
umbilical point, the two arteries finish in
the arterial periumbilical anastomotic
network. In the three zones of the right
abdominal muscle, the arterial device has
large polygonal holes formed of the fine
vessels of capillary diameter. Each
muscular fascicle is surrounded by 8-10
capillary vessels of continuous type. While
The Anterolateral Abdominal Wall - Vascularisation Development during Morphogenesis 19
aging, the vascular holes which are formed
between muscle fibers rarefy.
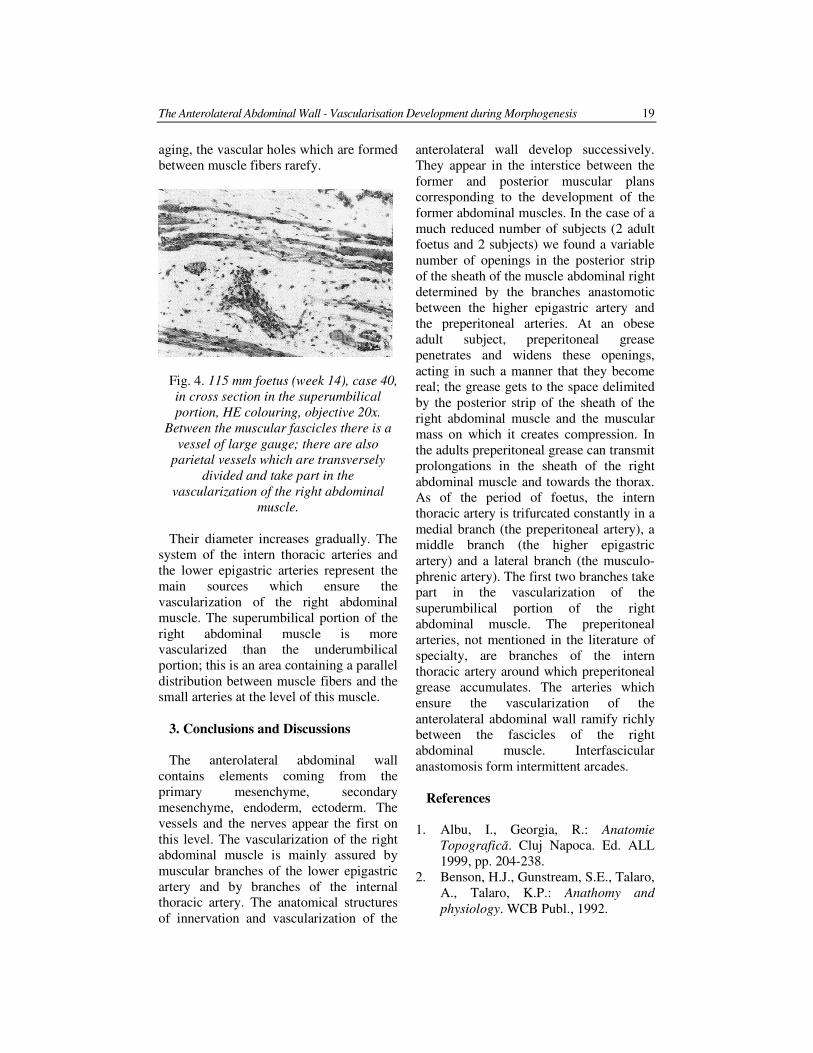
Fig. 4. 115 mm foetus (week 14), case 40,
in cross section in the superumbilical
portion, HE colouring, objective 20x.
Between the muscular fascicles there is a
vessel of large gauge; there are also
parietal vessels which are transversely
divided and take part in the
vascularization of the right abdominal
muscle.
Their diameter increases gradually. The
system of the intern thoracic arteries and
the lower epigastric arteries represent the
main sources which ensure the
vascularization of the right abdominal
muscle. The superumbilical portion of the
right abdominal muscle is more
vascularized than the underumbilical
portion; this is an area containing a parallel
distribution between muscle fibers and the
small arteries at the level of this muscle.
3. Conclusions and Discussions
The anterolateral abdominal wall
contains elements coming from the
primary mesenchyme, secondary
mesenchyme, endoderm, ectoderm. The
vessels and the nerves appear the first on
this level. The vascularization of the right
abdominal muscle is mainly assured by
muscular branches of the lower epigastric
artery and by branches of the internal
thoracic artery. The anatomical structures
of innervation and vascularization of the
anterolateral wall develop successively.
They appear in the interstice between the
former and posterior muscular plans
corresponding to the development of the
former abdominal muscles. In the case of a
much reduced number of subjects (2 adult
foetus and 2 subjects) we found a variable
number of openings in the posterior strip
of the sheath of the muscle abdominal right
determined by the branches anastomotic
between the higher epigastric artery and
the preperitoneal arteries. At an obese
adult subject, preperitoneal grease
penetrates and widens these openings,
acting in such a manner that they become
real; the grease gets to the space delimited
by the posterior strip of the sheath of the
right abdominal muscle and the muscular
mass on which it creates compression. In
the adults preperitoneal grease can transmit
prolongations in the sheath of the right
abdominal muscle and towards the thorax.
As of the period of foetus, the intern
thoracic artery is trifurcated constantly in a
medial branch (the preperitoneal artery), a
middle branch (the higher epigastric
artery) and a lateral branch (the musculo-
phrenic artery). The first two branches take
part in the vascularization of the
superumbilical portion of the right
abdominal muscle. The preperitoneal
arteries, not mentioned in the literature of
specialty, are branches of the intern
thoracic artery around which preperitoneal
grease accumulates. The arteries which
ensure the vascularization of the
anterolateral abdominal wall ramify richly
between the fascicles of the right
abdominal muscle. Interfascicular
anastomosis form intermittent arcades.
References
1. Albu, I., Georgia, R.: Anatomie
Topografică. Cluj Napoca. Ed. ALL
1999, pp. 204-238.
2. Benson, H.J., Gunstream, S.E., Talaro,
A., Talaro, K.P.: Anathomy and
physiology. WCB Publ., 1992.
Bulletin of the Transilvania University of Braşov • Vol. 15(50) - 2008 � Series VI
20
3. Chiriac, M., Zamfir, M., Antohe, D.:
Anatomia trunchiului, Vol. 1. Iaşi. Ed.
Universitară Iasi, 1999, pp. 334-346.
4. Dietrich, K., Felberbaum, R.: Der
Gynäkologe; Die europäische
Gesellschaft für humane Repro-
duktionsmedizin und Embryologie
(ESHRE); Springer Berlin /
Heidelberg; 2002, pp. 444-446.
5. Garcia-Martinez, V., Schoenwolf,
G.C.: Positional Control of Mesoderm
Movement and Fate during Avian
Gastrulation and Neurulation. In:
Acta.Anat., 1992, pp. 249-256.
6. Oligny, L.L.: Pediatric and
Developmental Pathology; Human
Molecular Embryogenesis: An
Overview. Springer New York; 2001,
pp. 324-343.
7. Onisai, L.L.: Anatomia peretilor
trunchiului. Braşov. Ed. Univ.
Transilvania, Brasov, 1997, pp. 104-
116, 142-158, 170-172.
8. Onisai, L.L.: The development of
rectus abdominis muscles. In:
Romanian J. of Anat., vol 1; nr. 2-3,
1999, pp. 67-70.
9. Ordahl, C.P.: Myogenic Lineages
within the developing somite. In:
Development, 1993, pp. 341-353.
10. Williams, P.L.: Gray’s Anatomy, 38 th
New York. Ed. Churchill Livingstone,
1995.
1Transilvania University of Brasov, Faculty of Medicine, Romania
2University of Milan, Dept. of Pharmacological Sciences, Italy
COMPETITIVE ELISA FOR AFLATOXINS
AND OCHRATOXINS DETECTION
M. BADEA1 M. MUNTEANU
1 L. LAZORIEC
1
G. COMAN1 P. RESTANI
2
Abstract. Mycotoxins have attracted worldwide attention because of their
impact on humans and animals health.
The most frequent toxigenic fungi in Europe are Aspergillus, Penicillium and
Fusarium species. They produce aflatoxin B1 transformed into aflatoxin M1
found in the milk, as well as Ochratoxins and Zearalenone. These mycotoxins
are under continuous survey in Europe, but the regulatory aspects still need
to be set up and/or harmonised at European level.
Direct competitive ELISA was used for aflatoxin M1 and ochratoxin A
detection from reference and real samples (milk, coffee). Calibration curves
were plotted and limits of quantification were calculated. A recovery degree
of 98.66% was obtained for spiked sample (coffee).
Key words: aflatoxins, ochratoxins, ELISA, milk, coffee
1. Introduction
Humans and animals are continuously
exposed to different amounts of
exogenously chemicals that have been
shown to have carcinogenic or mutagenic
properties in experimental systems (cells
models, lab animal studies). Exposure can
occur when these agents are present in
different media (food, air or water), and
also endogenously when they are products
of metabolism or pathophysiologic states
such as inflammation [3, 20].
Aflatoxins belong to a large group of
mycotoxins, toxic metabolites that
contaminate food and feed commodities
during growth of certain spoilage molds. In
addition to causing acute toxicity,
aflatoxins are also liver carcinogens in
experimental animals and extensive quality
control measures are necessary to
minimize levels in human foods.
Aflatoxin-contaminated feed was
discovered to be a liver carcinogen in rats
even before the active agent was isolated
and characterized.
Bioassays in various species fish [5],
birds [19], rodents [13] and sub-human
primates eventually revealed that AFB1 is
a liver carcinogen in all animals tested.
Aflatoxin M1 is produced as a metabolite
of aflatoxin B1. It is secreted with the milk
after the feeding of aflatoxin B1 content
feedstuffs to lactating cows. As aflatoxin
M1 is relatively stable towards the
pasteurizing process, not only a
comprehensive routine check of the raw
materials to be processed is required, but
also of the final products.
Ochratoxigenic fungi are natural
contaminants of cereal and the produced
toxins are harmful to humans and animals.
Ochratoxin A (OTA) is among the most
important mycotoxins, and the

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 � Series VI
22
International Agency for Research on
Cancer (IARC) classifies it as possibly
carcinogenic to humans (group 2B) [12].
Ochratoxins induce a caspase-
dependent mitochondrial apoptotic
pathway. The mitochondrial alterations
include: loss of the mitochondrial
transmembrane potential, PTPC opening,
and cytochrome c (but not AIF) release.
OTA is a potent nephrotoxin and renal
carcinogen. However, the pathological
lesions observed in kidneys of rats treated
with OTA appear be rather different from
the clinical and pathological characteristics
of endemic nephropathy. Moreover, in-
creasing evidence suggests that OTA does
not bind to DNA but induces tumors by an
epigenetic, threshold mechanism [11].
The common mycotoxin ochratoxin-A
(OTA) accumulates in brain, causes
oxidative stress, and elicits a DNA repair
response that varies across brain regions
and neuronal populations [17].
2. Analytical Procedures for Mycotoxins
Detection
The fact that mycotoxins are usually
present in agricultural commodities and
products as minor constituents in
concentrations ranging from (sub) µg—
mg/kg, means that the possibilities to
determine mycotoxins are limited to
certain trace analytical methods.
Food processes (sorting, trimming,
cleaning, milling, brewing, cooking,
baking, frying, roasting, canning, flaking,
alkaline cooking, and extrusion) have
variable effects on mycotoxins, with those
that utilize the highest temperatures having
greatest effects. In general the processes
reduce mycotoxin concentrations
significantly, but do not eliminate them
completely [4].
Therefore, the development of methods
for toxic contaminants analysis has been
constantly in demand. In the last ten years,
among the techniques applied in the
detection, analysis and characterization of
mycotoxins, chromatography has so far
been widely accepted because there always
seems to be a need to separate some
primary and secondary fungal metabolites.
Information on the techniques and
methodologies and techniques are
presented in specialty literature [1, 2, 10].
HPLC replace in many laboratories TLC
techniques because of their ability to
analyze a wide variety of compounds,
including compounds that are easily
degraded by heat, light or air, the ease of
adaptation to confirmatory procedures, the
automation, The recent improvement in
instrumentation, including the develop-
ment of increasingly sensitive fluorescence
and electrochemical detectors and short,
high-resolution, reversed-phase columns
[7, 16].
Both normal and reverse-phases HPLC
using fluorescence detection have been
already become the most accepted methods
for the determination of aflatoxins and
ochratoxins due to its several advantages
over other analytical methods [8, 9].
Pieto Simon and colab. investigated two
indirect competitive enzyme-linked immu-
nosorbent assay (ELISA) strategies for the
development of OTA electrochemical
immunosensors based on different OTA
immobilisation procedures [14].
Immunosensors based on avidin/biotin-
OTA showed enhanced performance
characteristics compared to those based on
the adsorption of bovine serum albumin
(BSA)-OTA conjugate. Performance of
polyclonal and monoclonal antibodies
against OTA was compared, showing at
least one-order of magnitude lower IC(50)
values when working with MAb. Alkaline
phosphatase and horseradish peroxidase
were used as labels for secondary
antibodies. The methods were evaluated
and optimized as useful screening tools to
assess OTA levels in wine.
Membrane-based immunoassay has been
developed by Saha and colab. [15] for
simultaneous estimation of aflatoxin B1
(AFB1) and ochratoxin A (OTA) in chili

Competitive Elisa for Aflatoxins and Ochratoxins Detection 23
samples. The method uses a low cost test
device consisting of a membrane with
immobilized anti-AFB1 and anti-OTA
antibodies and a filter paper attached to a
polyethylene card below the membrane.
The AFB1 and OTA values obtained for
spiked and naturally contaminated chili
samples by the simultaneous method were
in good correlation with those measured by
individual ELISA. The combined estima-
tion of both the mycotoxins is more
economical in respect of time, work and
materials than two separate assays.
3. Materials and Methods
Competitive enzyme immunoassay
RIDASCREEN® FAST Ochratoxin A (R-
Biopharm AG, Darmstadt, Germany) was
used for the quantitative analysis of
ochratoxin A in standard and real samples
(coffee kept on humidified medium). For
real sample was used 5 g ground coffee
into a suitable container and was added
12,5mL boiled water. The sample had been
shaking vigorously for three minutes, then
was filtered through Whatman paper. It
was diluted 1 mL filtrate with 1mL
distilled water, and from this mixture, was
used 50 µL per well in the test. Because it
was estimated a lower level of ochratoxin
A in coffee samples, there were prepared
also spiking samples: it was added 5 µL
solution standard 4 (20 ppb OTA) to coffee
sample and after were made the extraction
in boiled water and similar steps indicated
by kit.
The amount of aflatoxin M1 in reference
and real (cow milk) samples was
determined by ELISA test using
Ridascreen Aflatoxin M1 kit (R-Biopharm
AG, Darmstadt, Germany). For real
samples, cow milk was centrifugated for
degreasing: 10 min (10oC). After centri-
fugation, there was removed upper cream
layer completely by aspirating through a
Pasteur pipette. Use the defatted super-
natant directly in the test for aflatoxin M1
detection (50 µL per well). The same
procedure was used also for spiked milk
sample with known concentration of
aflatoxin M1 (8 µL solution standard 5).
4. Results and Discussions
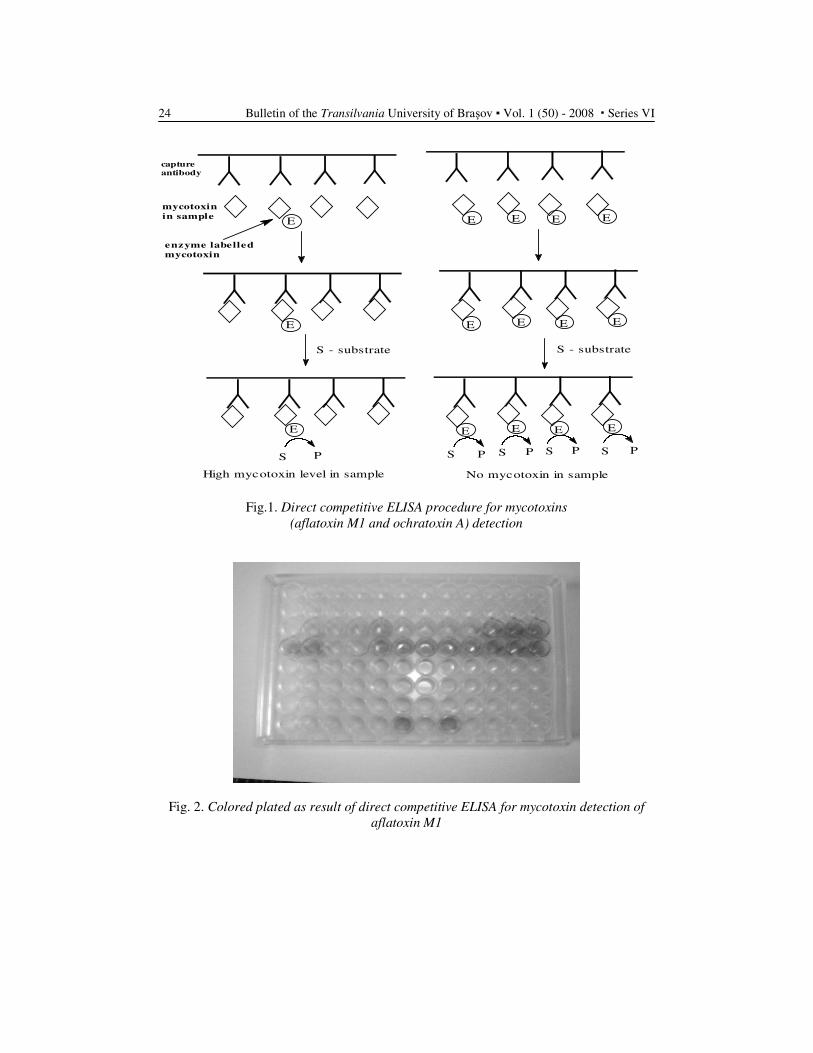
Antibodies are coated on to the wells of
the ELISA plate (Fig.1.). The test sample
(standards and real samples) and enzyme-
labelled mycotoxins (aflatoxin M1 or
ochratoxin A) are added to the wells. If no
toxin is present in the sample, the enzyme
labelled toxin will bind to the capture
antibody coated to the wells. If mycotoxin
is present in the sample, it will compete
with the labelled toxin for binding to the
antibody. During washing procedures any
unbound labelled enzyme will be washed
away.
The intensity of obtained product of the
enzymatic reaction (after substrate was
added) is proportional to the amount of
mycotoxin-enzyme bound to the well; i.e.,
the colour intensity decreases with increa-
sing concentrations of the mycotoxin in the
sample (Fig.2.).
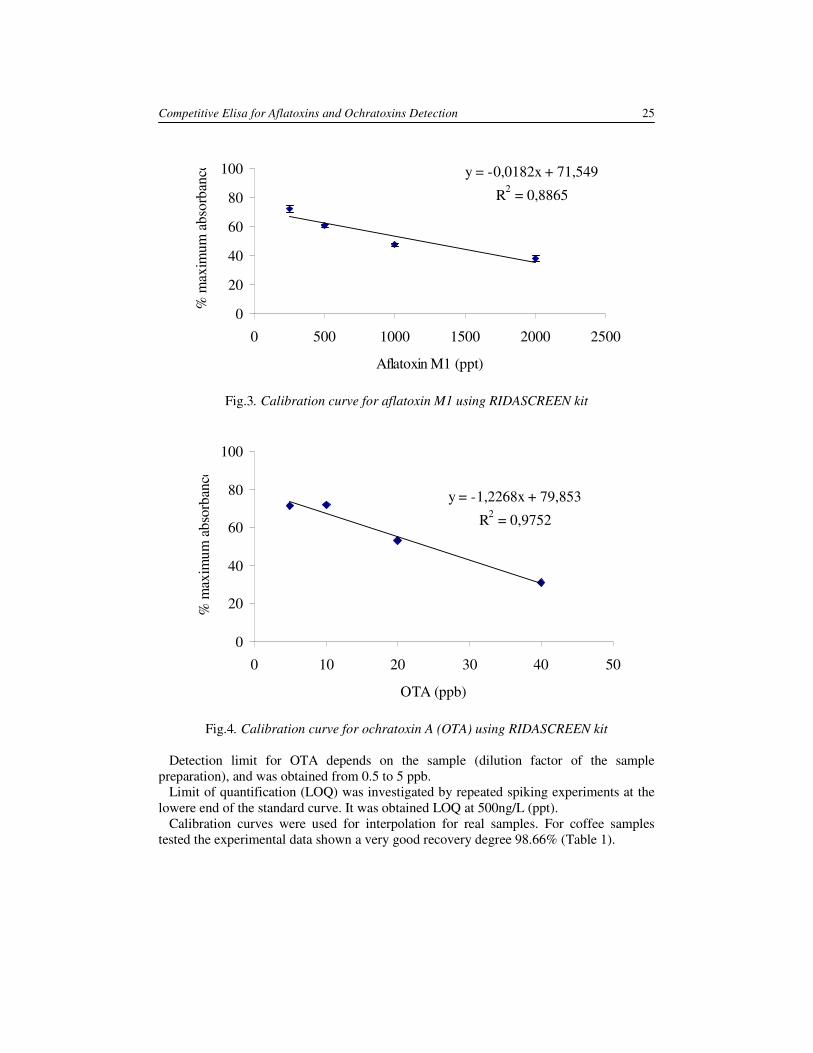
Calibration curves were plotted using the
standards from kit for both methods (Fig.3,
Fig.4.). Linearizations were made for mean
of the obtained values. Data were plotted
using standard deviation correction. Each
StDev values were lower than 8% for all
detections.
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 � Series VI
24
E E E EE
S - substrate S - substrate
E
E E E E E
E E E E
S P S P P P PS S S
High mycotoxin level in sample No mycotoxin in sample
capture
antibody
mycotoxin
in sample
enzyme labelled
mycotoxin
Fig.1. Direct competitive ELISA procedure for mycotoxins
(aflatoxin M1 and ochratoxin A) detection
Fig. 2. Colored plated as result of direct competitive ELISA for mycotoxin detection of
aflatoxin M1
Competitive Elisa for Aflatoxins and Ochratoxins Detection 25
y = -0,0182x + 71,549
R2 = 0,8865
0
20
40
60
80
100
0 500 1000 1500 2000 2500
Aflatoxin M1 (ppt)
% m
axim
um
ab
sorb
ance
Fig.3. Calibration curve for aflatoxin M1 using RIDASCREEN kit
y = -1,2268x + 79,853
R2 = 0,9752
0
20
40
60
80
100
0 10 20 30 40 50
OTA (ppb)
% m
axim
um
ab
sorb
ance
Fig.4. Calibration curve for ochratoxin A (OTA) using RIDASCREEN kit
Detection limit for OTA depends on the sample (dilution factor of the sample
preparation), and was obtained from 0.5 to 5 ppb.
Limit of quantification (LOQ) was investigated by repeated spiking experiments at the
lowere end of the standard curve. It was obtained LOQ at 500ng/L (ppt).
Calibration curves were used for interpolation for real samples. For coffee samples
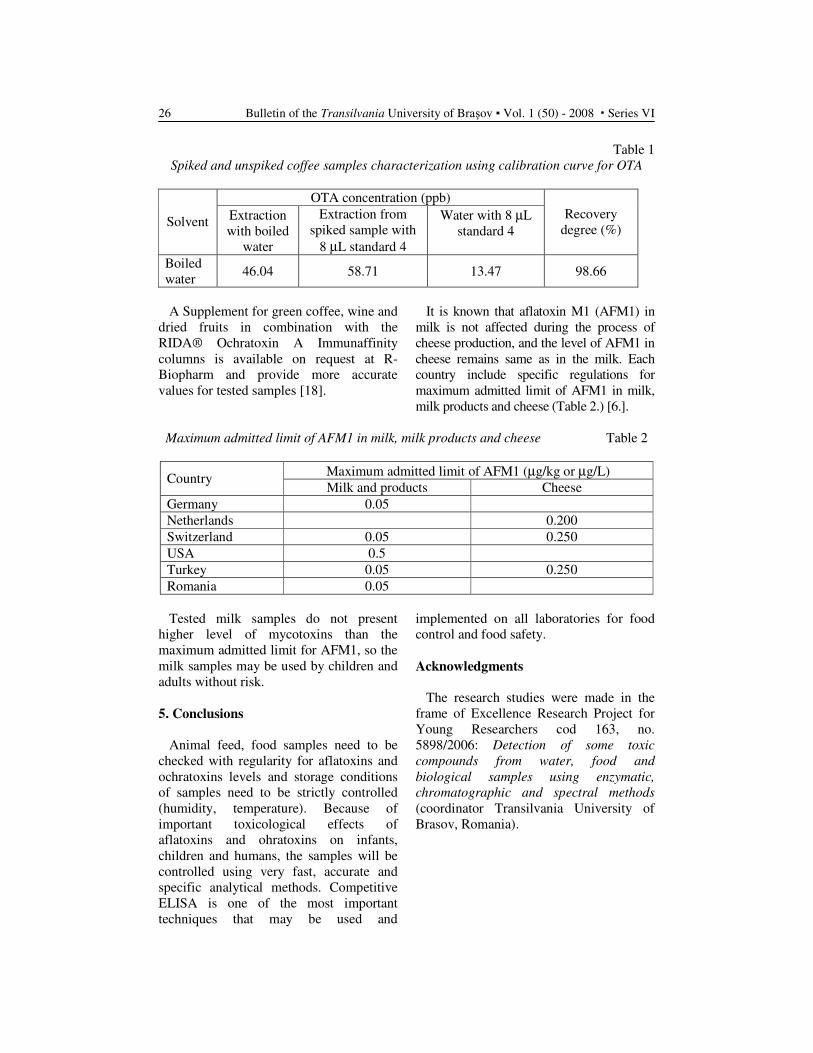
tested the experimental data shown a very good recovery degree 98.66% (Table 1).
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 � Series VI
26
Table 1
Spiked and unspiked coffee samples characterization using calibration curve for OTA
OTA concentration (ppb)
Solvent Extraction
with boiled
water
Extraction from
spiked sample with
8 µL standard 4
Water with 8 µL
standard 4
Recovery
degree (%)
Boiled
water 46.04 58.71 13.47 98.66
A Supplement for green coffee, wine and
dried fruits in combination with the
RIDA® Ochratoxin A Immunaffinity
columns is available on request at R-
Biopharm and provide more accurate
values for tested samples [18].
It is known that aflatoxin M1 (AFM1) in
milk is not affected during the process of
cheese production, and the level of AFM1 in
cheese remains same as in the milk. Each
country include specific regulations for
maximum admitted limit of AFM1 in milk,
milk products and cheese (Table 2.) [6.].
Maximum admitted limit of AFM1 in milk, milk products and cheese Table 2
Maximum admitted limit of AFM1 (µg/kg or µg/L) Country
Milk and products Cheese
Germany 0.05
Netherlands 0.200
Switzerland 0.05 0.250
USA 0.5
Turkey 0.05 0.250
Romania 0.05
Tested milk samples do not present
higher level of mycotoxins than the
maximum admitted limit for AFM1, so the
milk samples may be used by children and
adults without risk.
5. Conclusions
Animal feed, food samples need to be
checked with regularity for aflatoxins and
ochratoxins levels and storage conditions
of samples need to be strictly controlled
(humidity, temperature). Because of
important toxicological effects of
aflatoxins and ohratoxins on infants,
children and humans, the samples will be
controlled using very fast, accurate and
specific analytical methods. Competitive
ELISA is one of the most important
techniques that may be used and
implemented on all laboratories for food
control and food safety.
Acknowledgments
The research studies were made in the
frame of Excellence Research Project for
Young Researchers cod 163, no.
5898/2006: Detection of some toxic
compounds from water, food and
biological samples using enzymatic,
chromatographic and spectral methods
(coordinator Transilvania University of
Brasov, Romania).
Competitive Elisa for Aflatoxins and Ochratoxins Detection 27
References
1. Betina, V.: Thin-layer chromatogra–
phy of mycotoxins. Chromatogr.,
334(3) (1985) 211-276.
2. Betina, V.: Chromatographic methods
as tools in the field of mycotoxins. In:
J Chromatogr. 477(2) (1989) 187-233.
3. Boermans, H.J., Leung, M.C.:
Mycotoxins and the pet food industry:
toxicological evidence and risk
assessment. In: Int J Food Microbiol.
20;119(1-2) (2007) 95-102.
4. Bullerman, L.B., Bianchini, A.:
Stability of mycotoxins during food
processing. In: Int J Food Microbiol.,
119(1-2) (2007) 140-146.
5. Carlson, D.B., Williams, D.E.,
Spitsbergen, J.M., Ross, P.F., Bacon,
C.W., Meredith, F.I., Riley, R.T.:
Fumonisin B1 promotes aflatoxin B1
and N-methyl-N'-nitro-nitrosogua–
nidine-initiated liver tumors in
rainbow trout. In: Toxicol Appl
Pharmacol., 172(1) (2001)
29-36.
6. Creppy, E. E.: Update of survey,
regulation and toxic effects of
mycotoxins in Europe. In: Toxicol.
Letters 127 (2002) 19-28.
7. Holcomb, M., Wilson, D.M.,
Trucksess, M.W., Thompson Jr., H.C.:
Determination of aflatoxins in food
products by chromatography. In: J.
Chromatogr. 624 (1992) 341.
8. Howell, M.V., Taylor, P.W.: Deter–
mination of aflatoxins, ochratoxin a,
and zearalenone in mixed feeds, with
detection by thin layer chromatography
or high performance liquid
chromatography. In: J Assoc Off
Anal Chem., 64(6): (1981) 1356-1363.
9. Jaimez, J., Fente, C.A., Vazquez, B.I.,
Franco, C.M., Cepeda, A., Mahuzier,
G., Prognon, P.: Application of the
assay of aflatoxins by liquid
chromatography with fluorescence
detection in food analysis. In: J
Chromatogr A., 882(1-2) (2000) 1-10.
10. Lin, L., Zhang, J., Wang, P., Wang,
Y., Chen, J.: Thin-layer chroma–
tography of mycotoxins and comparison
with other chromatographic methods.
In: Journal of Chromatography A, 815
(1998): 3–20.
11. Mally, A, Hard, G.C., Dekant, W.:
Ochratoxin A as a potential etiologic
factor in endemic nephropathy:
lessons from toxicity studies in rats.
In: Food Chem Toxicol. 45(11) (2007)
2254-2260.
12. Marin-Kuan, M, Cavin, C., Delatour,
T., Schilter, B.: Ochratoxin A
carcinogenicity involves a complex
network of epigenetic mechanisms. In:
Toxicon., 1;52(2) (2008) 195-202
13. Miranda, D.D., Arçari, D.P., Ladeira,
M.S., Calori-Domingues, M.A.,
Romero, A.C., Salvadori, D.M., Gloria,
E.M., Pedrazzoli, J. Jr, Ribeiro, M.L.:
Analysis of DNA damage induced by
aflatoxin B1 in Dunkin-Hartley guinea
pigs. In: Mycopathologia.163(5),
(2007), 275-80.
14. Prieto-Simón, B., Campàs, M., Marty,
J.L., Noguer, T.: Novel highly-
performing immunosensor-based
strategy for ochratoxin A detection in
wine samples, Biosens Bioelectron.
23(7) (2008) 995-1002.
15. Saha, D., Acharya, D., Roy, D.,
Shrestha, D., Dhar, T.K.:
Simultaneous enzyme immunoassay
for the screening of aflatoxin B1 and
ochratoxin A in chili samples. In: Anal
Chim Acta. 584(2): (2007) 343-349.
16. Santos, E.A., Vargas, E.A.: Immuno–
affinity column clean-up and thin
layer chromatography for
determination of ochratoxin A in
green coffee. In: Food Addit Contam.
19(5) (2002) 447-458.
17. Sava, V., Velasquez, A., Song, S.,
Sanchez-Ramos, J.: Adult hippocam–
pal neural stem/progenitor cells in
vitro are vulnerable to the mycotoxin
ochratoxin-A. Toxicol Sci. 98(1)
(2007) 187-197.
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 � Series VI
28
18. Sibanda, L., De Saeger, S., Van
Peteghem, C.: Development of a
portable field immunoassay for the
detection of aflatoxin M1 in milk. In:
Int J Food Microbiol., 48(3) (1999)
203-209.
19. Tessari, E.N., Oliveira, C.A., Cardoso,
A.L., Ledoux, D.R., Rottinghaus,
G.E.: Effects of aflatoxin B1 and
fumonisin B1 on body weight,
antibody titres and histology of broiler
chicks. In: Br Poult Sci. 47(3) (2006)
357-64.
20. Wogan, G. N., Hecht, S. S., Felton, J.
S., Conney, A. H., Loeb, L. A.:
Environmental and chemical
carcinogenesis. Seminars in Cancer
Biology 14 (2004) 473–486.
1 Universidade Federal do Maranhão, Brazil 2
Transilvania University of Brasov, Romania. 3 Unversité de Perpignan via Domitia, France
ULTRASENSITIVE BIOSENSORS FOR THE
DETECTION OF INSECTICIDE RESIDUES
IN FRUIT JUICES
G. S. NUNES
1 M. BADEA
2 M.-L. MEDEL
3
T. NOGUER3 J.-L. MARTY
3
Abstract: A highly sensitive and rapid fruit juice-screening test based on
disposable screen-printed TCNQ-modified biosensor was developed, which is
suitable for monitoring anticholinesterase pesticides. The biosensor analysis
was based on direct measurement of enzyme inhibition in pH-adjusted
samples. It could detect levels of carbofuran, carbaryl and chlorpyrifos oxon
of 0.2, 0.9 and 1.1 µg.L-1, respectively, and thus clearly fulfills the demands
of both Brazilian and EU regulation.
To evaluate the biosensor efficiency, recovery rates were determined and
were on average 93.9% (RSD from 5.9 to 18.5%) in untreated fruit juices.
The proposed AChE-biosensor has shown enough sensitivity and
reproducibility to be used as a complementary technique to the
chromatographic ones in food pesticide monitoring.
Key words: TCNQ-modified biosensor; AChE-inhibitor pesticides; fruit
juices
1. Introduction
According to the necessity of
substituting the standard methods
utilized in quantitative and qualitative
analysis, large studies were required in
recent years, in order to develop faster,
easier, and less expensive techniques,
with similar or lower detection limits.
Traditional methods for carbamate deter-
mination in foods are based on gas chro-
matography (GC) or high-performance li-
quid chromatography (HPLC); this last
analytical technique normally employing the
highly sensitive fluorescence detection [7,
12]. Organophosphates are normally
analyzed by gas chromatography with a
nitrogen-phosphorous selective detector [17].
Hyphenated chromatographic methods,
such as GC and/or HPLC combined with
mass spectrometry (MS) have been also
used to detect and to confirm residues of
carbamate and organophosphorate insecti–
cides in food samples [3, 5, 9].

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 � Series VI
30
Because of the numerous problems
involved with traditional analytical
methods, such as the large time involved in
classical sample preparation, it is necessary
to develop fastest, easier, more sensitive,
cost-effective and environmentally cleaner
analytical techniques.
Analysis using the biosensor technology
is part of a research area that offers the
advantages of miniaturization, easy sample
manipulation, and the possibility of in-situ
determination which further diminishes the
errors resulted from sample processing
operations, with simple and low-cost
instrumentation, fast response times,
minimum sample pretreatment, and high
sample throughput. Biosensors are devices
consisting of biological active protein
species immobilized on the surface of
physical transducers [15].
Despite all advantages of biosensors, only
a few works employing this analytical tool
for the anticholinesterase pesticides in food
samples have been reported [1, 8, 10, 14].
This work employs an amperometric
biosensor for the detection of AChE
inhibitors in commercial fruit juices by
exploiting their capacity to inhibit AChE
enzymes. Different inhibition assays
utilizing natural fruit juices for performing
the electrochemical measurement with
buffered or solvent-extracted samples were
tested. To evaluate assays efficiencies,
fruit juices samples were spiked with some
AChE inhibitors and the matrix effects
were also evaluated.
2. Materials and Methods
2.1. Reagents, samples and other materials
The inhibitor standards [N-methyl–
carbamates (NMCs): carbofuran and
carbaryl; organophosphates (OPs):
chlorpyrifos and chlorpyrifos-oxon] used
in this work varied in purity from 96 to
99.9%. Carbofuran and carbaryl were
provided by Sigma-Aldrich (Seelze,
Germany). Chlorpyrifos and chlorpyrifos
oxon were supplied by Chem Service
(West Chester, PA). Stock solutions were
prepared by dissolution of the active
principles with a sufficient volume of
grade HPLC-methanol (Merck, Augsburg,
Germany), followed by dilution with
distilled water to 10-2
mol.L-1
con-
centration. Working solutions were kept at
4oC for a maximum of one week. Table 1
presents some general chemical and
toxicological information on these
compounds.
Acetylcholinesterase enzyme from
electric eel (ee), specific activity of 8000
AU.mg-1
, acetylthiocholine chloride
(ATChCl) substrate, 5,5’dithio (2-nitro–
benzoic acid) (DTNB) and polyethylene
glycol 600 (PEG) were purchased from
Sigma Chemicals Co (St Louis, MO).
AChE stock and working solutions were
prepared by dissolution of the enzyme in
NaCl 0.9 % (w/v) solution and storing in a
freezer for a maximum of two months.
Substrate solutions were prepared by
dilution with phosphate buffer solution
containing 0.1 mol.L-1
KCl (PBS), pH 7.5.
PBST solutions were prepared by dilution
of Tween 20 (Aldrich Chem. Co,
Steinheim, Germany) in already prepared
PBS up to 1.0% (v/v) final content.
Hydroxyethyl-cellulose (HEC) and
pyridine-2-aldoxime methochloride (2-
PAM) were obtained from Sigma-Aldrich
Co (Steinheim, Germany). Photocrosslin-
kable poly(vinyl alcohol) bearing styryl-
pyridinium groups (SPP-S-13-bio-PVA-
SbQ of betaine form and polymerization
degree of 1700) was obtained from Toyo
Gosei Co (Chiba, Japan). All other
reagents were analytical grade.
Printing pastes (Electrodag PF-410,
423SS, 6037SS) were purchased from
Acheson (Plymouth, UK) and the mediator
TCNQ from Aldrich Co (Steinheim,
Germany). Graphite T15 was supplied by
Lonza A. G. (Basel, Switzerland). The
surface area of both reference and working
electrode was 0.17 cm2. The screen-printed
electrodes containing TCNQ as mediator

Ultrasensitive Biosensors for the Detection of Insecticide Residues in Fruit Juices 31
used in this study were prepared according
to procedures previously described [2, 9].
2.2. Electrochemicals measurements
The screen-printed electrode was
immersed in a beaker containing 5 mL of
PBS pH 7.5 under constant magnetic
stirring. The pesticide determination was
carried out in a three-step procedure. The
electrode response was first measured in
PBS, and then ATChCl was added,
corresponding to the current before the
inhibition, I0. The electrode was carefully
washed with PBS, and then incubated for
10 min with pesticide solutions at known
concentrations or with spiked fruit juice
untreated/treated samples. After incu-
bation, the cleaning procedure started by
washing the biosensor with 5 mL PBS
containing 1% Tween 20 (PBST) by
continuous agitation during 10 min
followed by washing with PBS. The
second value, corresponding to I, was
reported as the current intensity after
inhibition. Inhibition results were
determined using the following formula:
I(%) = (1 – Io/I) 100 and then related to the
inhibitor concentration present in the
pesticide solutions or spiked juice samples
[11]. Fig. 1 details the sample treatment
and inhibition procedure. Reactivation of
inhibited AChE was performed with
pyridine 2-aldoxime methiodime (2-PAM,
Aldrich Chem. Co, Steinheim, Germany),
according to previously described
procedures [4, 11].
2.3. Reproducibility studies
To establish the reproducibility of the
biosensors, 20 different electrodes
belonging to the same set and fabricated in
the same day were tested by performing
the enzymatic reaction with ATCh
substrate and then recording the current
value, in nA. To evaluate the operational
stability of each electrode, the response of
the biosensor was measured five times by
injecting the same amount of substrate,
resulting in a total of 100 electrochemical
measurements. The response for each
biosensor, represented by the average
current (n = 5) was recorded in a quality
control chart.
2.4. Samples treatments and recovery studies
In order to verify the efficiency of the
inhibition assays in fruit juices, some
samples were spiked with different levels
of AChE inhibitors, depending on the
enzyme sensitivity. The biosensors were
then incubated for 10 min with the samples
under constant stirring. After each
incubation step the biosensor was carefully
washed by immersing it in PBST during 10
min under stirring and then washed well
with PBS. The recoveries were calculated
by comparison between the inhibitions
obtained in the spiked with those of the
solution containing identical pesticide
concentration. Several samples were
analyzed directly with the biosensor
without previous sample treatments; only a
simple adjustment of the pH to ~ 7.5 was
performed. Some samples were treated by
PBS- and organic solvent extraction in
order to decrease the matrix effect. During
solvent extraction, one off-line solid-phase
extraction (SPE) step was needed. For this
purpose, 3 mL Bakerbond SPETM
columns (J. T. Baker, Deventer, Holland)
packed with 500 mg plus polar octadecyl
silica (C18) were used. SPE cartridges
were preconditioned with 10 mL methanol
and after the sample elution; the final
residue was recovered with 500 µL
methanol before dilution with 5 mL PBS.
For the reproducibility study, a control
chart was constructed with the 20
measurements. A conventional statistical
program was used to compare the recovery
averages at 95% significance level
according to the Student’s t test [6].
Limits of detection were calculated with
basis of 10 % enzyme inhibition caused by
pesticide solutions [9].
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 � Series VI
32
Limits of quantification (LOQ) were
determined through inhibition assays
performed with spiked untreated and
treated samples (n = 3). For each tested
method, two blanks were carried out.
3. Results and Discussions
3.1. Biosensor response and stability
The AChE-biosensor was based on the
enzymatic inhibition by carbamates and
organophosphates pesticides and it has
been previously optimized in order to
achieve the highest sensitivity and the
shortest analysis time. When AChE is
immobilized on the working electrode
surface, its interaction with the substrate
produces an electroactive specie. In this
strategy, acetylthiocholine (ATCh) can
substitute the original substrate of AChE
[2]. Thus, ATCh is hydrolyzed in the same
manner as the original substrate, producing
thiocoline and the corresponding
carboxylic acid (acetic acid, in this case).
The electrons generated during this
electrochemical reaction are collected and
the final current is a quantitative measure
of the enzyme activity.
According to Fig. 2, it can be seen that
current intensities obtained during reaction
between enzyme and substrate have not
exceeded the (upper and lower) warning
and action lines established according to a
statistical method described by Vandeginst
and Quadt [16]. The relative standard
deviation was 5.5 %.
3.2. Biosensor sensitivity for the selected
insecticides
The biosensor sensitivity could be
evaluated by performing the enzyme
inhibition with different pesticide
concentrations. In this work, each
experimental point was the average of five
measurements. The inhibition assays
showed a high level of intra-laboratory
reproducibility with an average relative
standard deviation of 8.6 %.
From the complexity of the mechanisms
and kinetics of AChE inhibition the
calibration curves (inhibitor concentration
versus relative inhibition) will not have a
linear correlation for some pesticides,
mainly the carbamates that usually
promote a reversible inhibition (Table 2).
Acceptable linear correlations were
obtained for the pesticides: carbofuran,
chlorpyrifos and chlorpyrifos oxon,
whereas that carbaryl gave a nonlinear
polynomial regression. In some cases,
nonlinear regression models are preferable
in order to improve the relative inhibition
versus concentration correlation and at the
same time to increase the concentration
working range of the calibration diagrams.
Chemical and toxicological information of the selected inhibitors Table 1
Usual Name Water
solubility
(mg.L-1
) a
LD50
(in rats)
(mg.Kg-1
) a
Inhibition constant (Ki) related to
AChE (ee)
(M-1
.min-1
) b
Carbaryl 40 400 - 650 5.5x104
Carbofuran 320 5 - 13 2.5x106
Chlorpyrifos 2 135 - 163 4.5x104
Chlorpyrifos oxon 3 45-60 1.6x105
a Sources: US National Library of Medicine [13];
b Ki values for carbaryl and carbofuran were previously determined; for chlorpyrifos and chlorpyrifos
oxon compounds, Ki values were spectrophotometrically determined in this work.
AChE (ee): commercial acetylcholinesterase extracted from electric eel.
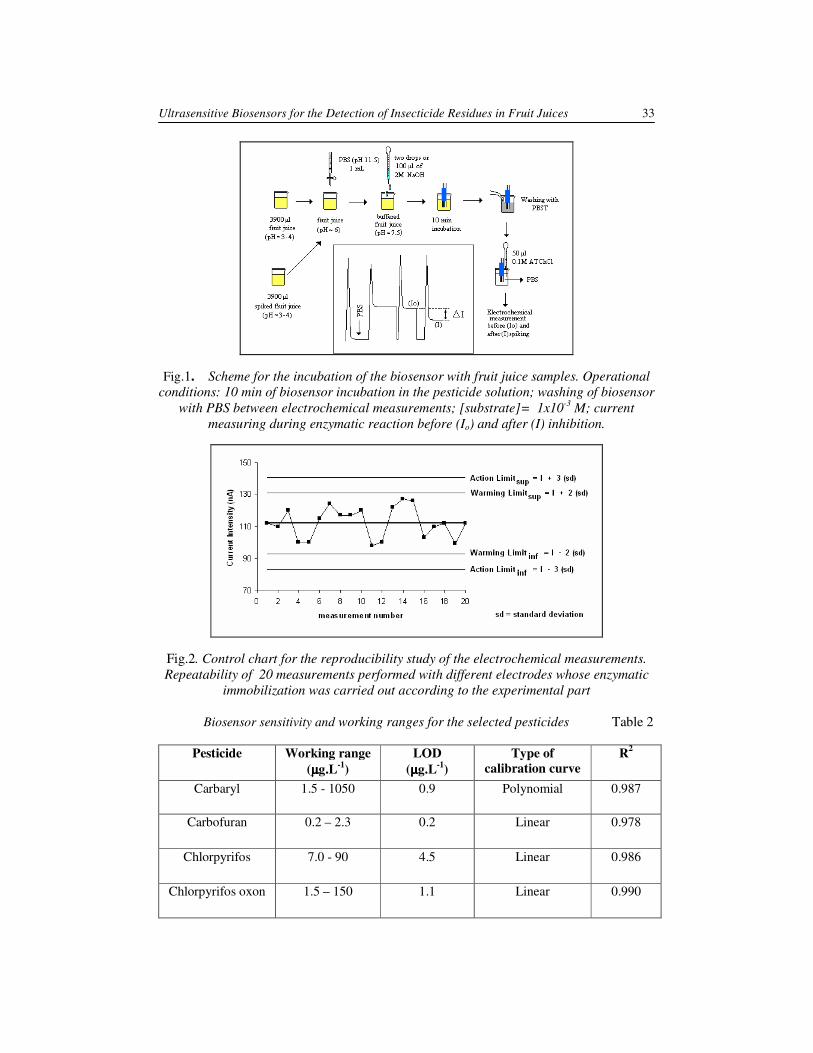
Ultrasensitive Biosensors for the Detection of Insecticide Residues in Fruit Juices 33
Fig.1. Scheme for the incubation of the biosensor with fruit juice samples. Operational
conditions: 10 min of biosensor incubation in the pesticide solution; washing of biosensor
with PBS between electrochemical measurements; [substrate]= 1x10-3
M; current
measuring during enzymatic reaction before (Io) and after (I) inhibition.
Fig.2. Control chart for the reproducibility study of the electrochemical measurements.
Repeatability of 20 measurements performed with different electrodes whose enzymatic
immobilization was carried out according to the experimental part
Biosensor sensitivity and working ranges for the selected pesticides Table 2
Pesticide Working range
(µµµµg.L-1
)
LOD
(µµµµg.L-1
)
Type of
calibration curve
R2
Carbaryl 1.5 - 1050 0.9
Polynomial 0.987
Carbofuran 0.2 – 2.3 0.2 Linear 0.978
Chlorpyrifos 7.0 - 90
4.5 Linear 0.986
Chlorpyrifos oxon 1.5 – 150 1.1 Linear 0.990

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 � Series VI
34
The sensitivities for the selected
pesticides proved to be adequate with
statistically different (p < 0.05) limits of
detection (LOD) values. More suitable
LODs were determined for three
pesticides: carbofuran, carbaryl and
chlorpyrifos oxon, 0.2, 0.9 and 1.1 µg.L-1
,
respectively. Among the studied pesticides
carbofuran is the strongest inhibitor for the
AChE (from electric eel) enzyme as is
confirmed by the higher inhibition
constant, Ki (Table 1). For chlorpyrifos a
higher LOD value (4.5µg.L-1
) was
obtained; it has presented the weaker
inhibition capacity. The concentration
values of working ranges, which are in the
range between 0.2 and 1,050 µg.L-1
depending on the insecticide, are thus
sufficient for the control of maximum
allowed residues in food, according to the
Brazilian and EU regulations [18, 19].
In this work, carbofuran has shown to be
a great AChE inhibitor when the biosensor
contained an enzymatic charge equivalent
to a relative activity of 1 AU/electrode.
Recoveries for the selected pesticides
using the optimized AChE-biosensor are
calculated. For most cases, the higher
pesticide concentration zones give better
accuracy (higher recoveries) and good
reproducibility (lower RDS %). Relative
standard deviations (RSD) varied from 5.9
to 18.5 % (from 5.9 to 14.8 %, from 6.5 to
12.6 %, from 7.4 to 18.4 %, and from 7.6
to 14.3 %, respectively, for orange, apple,
grape and pineapple juices). It is
convenient to mention that lower
reproducibility was also observed for
higher pesticide concentrations during
calibration curve construction.
In this work, a value lower than 10 %
inhibition was considered as the limit of
statistically confidence level for the LOD
calculation (Table 2) because inhibitions
found in lower concentrations lead to
higher errors in the current intensity
recorder, in some cases coinciding with the
apparatus noise depending on the
potentiostat sensitivity.
5. Conclusions
In this study, the use of cholinesterase-
based biosensors for the detection of some
carbamate and organophosphorus
pesticides was evaluated. The previously
developed ChE-biosensor based on a
screen printed electrochemical system was
chosen as biosensor. As a biorecognition
element, AChE from electric eel was used.
This enzyme was more sensitive to the
carbofuran pesticide, followed by
chlorpyrifos oxon (a metabolite product of
chlorpyrifos). Good inhibition results were
also obtained with carbaryl and the
detection of these pesticides can be
achieved in fruit samples without any
complicated pretreatment.
The use of amperometric biosensors to
detect and quantify carbamate and
organophosphorus pesticides is still novel
because it still requires several approaches
in order to improve the selectivity and to
reduce or eliminate numerous problems
before the biosensor can be applied for
routine analysis. These problems include
the skills required for the biosensor
construction, limited dynamic ranges in
some cases in trace levels, and the need for
frequent calibration. In order to apply the
AChE-biosensor in screening works and to
use it as a complementary analytical tool,
the necessity to construct portable devices
is evident.
Acknowledgments
Gilvanda S. Nunes would like to thank
CNPq (Conselho Nacional de
Desenvolvimento Científico-Tecnológico,
Brazil) and CAPES (Coordenação de
Aperfeiçoamento de Pessoal de Nível
Superior, Brazil) for the fellowship and
financial support, respectively. Mihaela
Badea would like to thank UEFISCSU for
the support with 5898/2006 and 1469/2006
CEEX research grants.
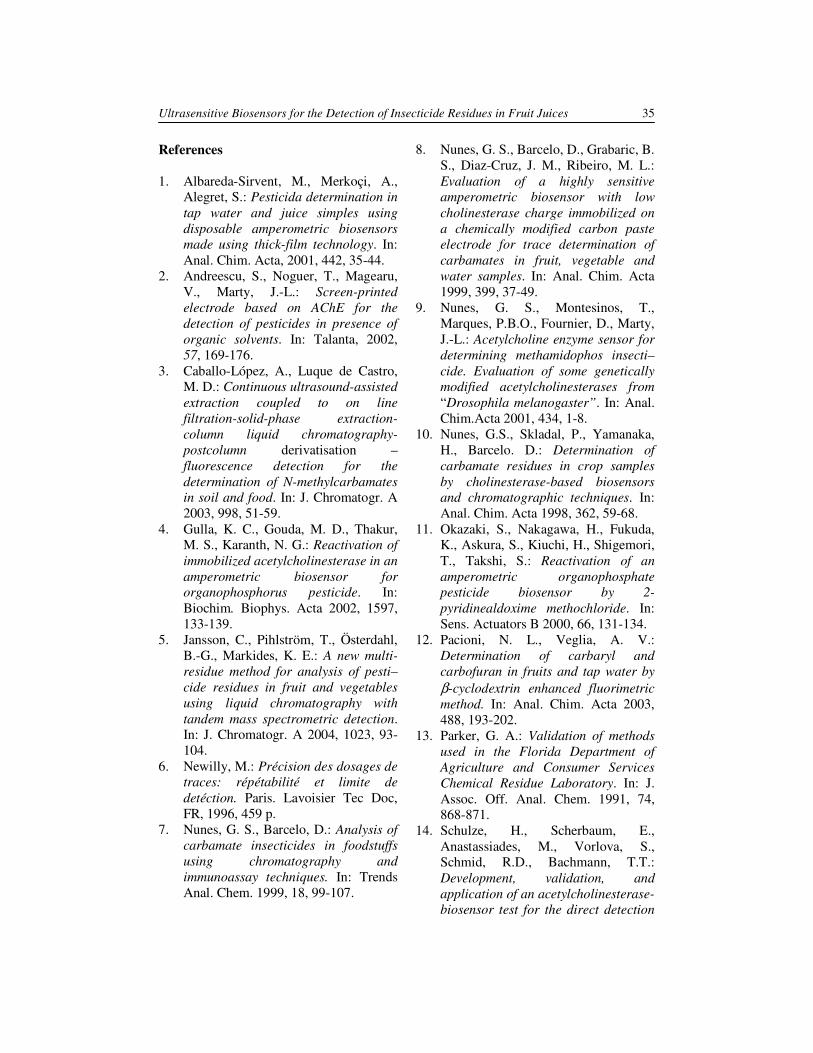
Ultrasensitive Biosensors for the Detection of Insecticide Residues in Fruit Juices 35
References
1. Albareda-Sirvent, M., Merkoçi, A.,
Alegret, S.: Pesticida determination in
tap water and juice simples using
disposable amperometric biosensors
made using thick-film technology. In:
Anal. Chim. Acta, 2001, 442, 35-44.
2. Andreescu, S., Noguer, T., Magearu,
V., Marty, J.-L.: Screen-printed
electrode based on AChE for the
detection of pesticides in presence of
organic solvents. In: Talanta, 2002,
57, 169-176.
3. Caballo-López, A., Luque de Castro,
M. D.: Continuous ultrasound-assisted
extraction coupled to on line
filtration-solid-phase extraction-
column liquid chromatography-
postcolumn derivatisation –
fluorescence detection for the
determination of N-methylcarbamates
in soil and food. In: J. Chromatogr. A
2003, 998, 51-59.
4. Gulla, K. C., Gouda, M. D., Thakur,
M. S., Karanth, N. G.: Reactivation of
immobilized acetylcholinesterase in an
amperometric biosensor for
organophosphorus pesticide. In:
Biochim. Biophys. Acta 2002, 1597,
133-139.
5. Jansson, C., Pihlström, T., Österdahl,
B.-G., Markides, K. E.: A new multi-
residue method for analysis of pesti–
cide residues in fruit and vegetables
using liquid chromatography with
tandem mass spectrometric detection.
In: J. Chromatogr. A 2004, 1023, 93-
104.
6. Newilly, M.: Précision des dosages de
traces: répétabilité et limite de
detéction. Paris. Lavoisier Tec Doc,
FR, 1996, 459 p.
7. Nunes, G. S., Barcelo, D.: Analysis of
carbamate insecticides in foodstuffs
using chromatography and
immunoassay techniques. In: Trends
Anal. Chem. 1999, 18, 99-107.
8. Nunes, G. S., Barcelo, D., Grabaric, B.
S., Diaz-Cruz, J. M., Ribeiro, M. L.:
Evaluation of a highly sensitive
amperometric biosensor with low
cholinesterase charge immobilized on
a chemically modified carbon paste
electrode for trace determination of
carbamates in fruit, vegetable and
water samples. In: Anal. Chim. Acta
1999, 399, 37-49.
9. Nunes, G. S., Montesinos, T.,
Marques, P.B.O., Fournier, D., Marty,
J.-L.: Acetylcholine enzyme sensor for
determining methamidophos insecti–
cide. Evaluation of some genetically
modified acetylcholinesterases from
“Drosophila melanogaster”. In: Anal.
Chim.Acta 2001, 434, 1-8.
10. Nunes, G.S., Skladal, P., Yamanaka,
H., Barcelo. D.: Determination of
carbamate residues in crop samples
by cholinesterase-based biosensors
and chromatographic techniques. In:
Anal. Chim. Acta 1998, 362, 59-68.
11. Okazaki, S., Nakagawa, H., Fukuda,
K., Askura, S., Kiuchi, H., Shigemori,
T., Takshi, S.: Reactivation of an
amperometric organophosphate
pesticide biosensor by 2-
pyridinealdoxime methochloride. In:
Sens. Actuators B 2000, 66, 131-134.
12. Pacioni, N. L., Veglia, A. V.:
Determination of carbaryl and
carbofuran in fruits and tap water by
β-cyclodextrin enhanced fluorimetric
method. In: Anal. Chim. Acta 2003,
488, 193-202.
13. Parker, G. A.: Validation of methods
used in the Florida Department of
Agriculture and Consumer Services
Chemical Residue Laboratory. In: J.
Assoc. Off. Anal. Chem. 1991, 74,
868-871.
14. Schulze, H., Scherbaum, E.,
Anastassiades, M., Vorlova, S.,
Schmid, R.D., Bachmann, T.T.:
Development, validation, and
application of an acetylcholinesterase-
biosensor test for the direct detection
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 � Series VI
36
of insecticide residues in infant food.
In: Biosens. Bioelectron. 2002, 17,
1095-1105. 15. Turner, A.P.F., Karube, I., Wilson,
G.S.: Biosensors: fundamentals and
applications. Oxford. Oxford
University Press, 1987, 770 p.
16. Vandeginst, B.G.M., Quadt, J.F.A.:
Statistical quality control. In: Analusis
1994, 22, M 30-34.
17. AOAC. Association Official
Analytical Chemistry. Methods 970.52
and 968.24. In: Helrich, K. Ed.
Official Methods of Analysis of
AOAC. 15th Ed. Arlington, VA, 1990
18. Brasil. International Life Sciences
Institute of Brazil - ILSE, Relação de
substâncias para uso fitossanitário e
domissanitário:Portarias doMinistério
da Agricultura, São Paulo, SP, 1995.
19. EC, European Communities. Council
Directives 76/895/EEC, 86/362/EEC,
86/363/EEC and 90/642/EEC.
Maximum levels for pesticide residues
in and on cereals, foodstuffs of animal
origin and certain products of plant
origin, including fruits and vegetables.
Commission Directive 2000/24/EC,
April, 28, 2000.

ANALYTICAL MONITORING AS A TOOL
TO DETECT ILLEGAL SUBSTANCES IN
FOODS AND FOOD SUPPLEMENTS
P. RESTANI
1 D. CARUSO1 F. GIAVARINI
1
E. MORO1 A. PERSICO
1 F. UBERTI
1
C. BALLABIO1 M. L. COLOMBO
2 M. BADEA
3
Abstract: From time immemorial, foods have been used to provide an
unsuspected vehicle of poisons. More recently, new criminal approaches use
foods and food supplements which contain illicit substances having
pharmacological effects, facilitating the international transport of drugs,
drug-pushing and the consumption of banned ingredients. Specially targeted
is the world of sport, where athletes often believe they cannot succeed
without taking performance-enhancing drugs. The misuse of substances
having pharmacological activity has become so widespread in sport that the
health of many athletes is compromised. This paper illustrates the use of
analysis of sports supplements as part of a broad system of monitoring the
availability of banned products. Specifically, the illegal inclusion of
ephedrine in a food supplement consisting largely of herbal ingredients has
been demonstrated using HPLC separation followed by mass spectrometry
Key words: food supplements, criminal activity, poisoning, food
contamination, herbal supplements, doping.
1 Dept. of Pharmacological Sciences, University of Milan, Italy. 2 Dept. of Drug Science and Technology, University of Turin, Italy. 3 3Dept. of Fundamental and Prophylactic Disciplines, Transilvania University of Brasov, Romania.
1. Introduction
Foods play a critical role in the health of
human beings and are often an important
part of social, religious and cultural
activity. Several expressions illustrate the
importance of foods in daily life, the most
famous being “We are what we eat”. Most
traditions have a particular, easily recog-
nizable cuisine, which is sometimes the
focus of epidemiological studies (Medit-
erranean diet, vegetarian diet, etc.).
More recently, foods have been
identified as a means of decreasing crime
and violence, since healthy food can
reduce aggressive behaviour. “We are what
we eat” has become “we do what we eat”.
Thus, subjects on a vegetarian diet are
often considered less aggressive than
omnivorous ones. On the other hand, foods
can pose a risk to human health if they
contain unusual or unsuspected ingre-
dients. Numerous cases of accidental food
poisoning have been described in the
scientific and popular literature, in
particular the ingestion of poisonous
mushrooms or plants harvested by inexpert
collectors [2, 3, 6].
Since ancient times, food and water have
been used as tools for homicide, both

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
38
because victims usually have confidence in
their meals and because detecting the fatal
agent can be difficult. Traditional poisons
such as salts of arsenic have often been
used in murder [4], but more recent
investigations have hypothesized poiso-
nous plants as the causative agent or
identified them analytically [8].
The most recent criminal approach
involving foods is to use them to mask
illicit substances, facilitating their transport
across borders and wide distribution. Food
supplements play an important role here, in
particular those containing herbal ingre-
dients. The use of food supplements has
increased enormously in recent years since
consumers believe that natural products are
good or right for the body, whereas some-
thing of synthetic or industrial origin is bad
or wrong. The use of food supplements
containing herbal ingredients has become
common among athletes even when the
scientific rationale is non-existent.
The uncontrolled use of food supple-
ments can represent a health risk,
particularly when the herbal ingredients
have known pharmacological properties.
Herbal ingredients are often undetectable
by the usual anti-doping tests [1], which
make those with stimulant properties
particularly attractive to those seeking
performance enhancement without penalty.
The main hazards in the use of herbal
supplements include: effects due to the
specific pharmacological properties (agita-
tion, insomnia, tachycardia); the risk of
exceeding the appropriate dose to obtain a
pronounced enhancing effect; the risk of
allergy and intolerances – several products
specifically developed for sport activities
actually contain proteins from animal and
vegetable sources that are listed as major
allergens; and finally, the possible pre-
sence of banned ingredients (hormones,
etc) that have been added to enhance the
desired effects [1].
Food supplements containing plants with
known stimulant substances must be
regarded as potential health hazards. The
best-known case is that regarding dietary
supplements containing Ephedra deriva-
tives. Substantial evidence of harm emer-
ged in 2003, when a major study reported
more than 16,000 adverse events asso-
ciated with the use of ephedra-containing
dietary supplements, including heart
palpitations, tremors and insomnia. The
study also found little evidence of the
claimed efficacy of Ephedra in boosting
physical activities and weight loss. In 2004
the FDA banned sales of dietary supple-
ments containing ephedrine alkaloids
(Ephedra species) [11] because such
supplements presented an unreasonable
risk of illness or injury for the consumers
[5], and in the USA the sale of products
containing Ephedra alkaloids is now
considered criminal unless they have been
medically prescribed [10]. Ephedrine is
banned as an ingredient of food or food
supplement in the European Union; in Italy
ephedra alkaloids are banned by the anti-
doping national legislation [9].
This international ban, based as it is on
data illustrating adverse effects of Ephedra
alkaloids, stimulated a series of activities
to monitor food supplements present on the
market and developed for sport. There are
thousands of products on the market
containing herbal ingredients. The quality
control of these products is often
unsatisfactory and their market is wide and
complex, with modern ways of distribution
including athletes’ training centers and
direct delivery from purchase on the
Internet.
As part of the monitoring activity in
Italy, we have received several different
food supplements obtained in “alternative”
markets (away from the usual commercial
outlets) to be analyzed, with the aim of
detecting ingredients included in the list of
doping substances. Amongst the products
received, we describe a food supplement
containing herbal ingredients amongst
which the presence of ephedrine was
suspected and then demonstrated.
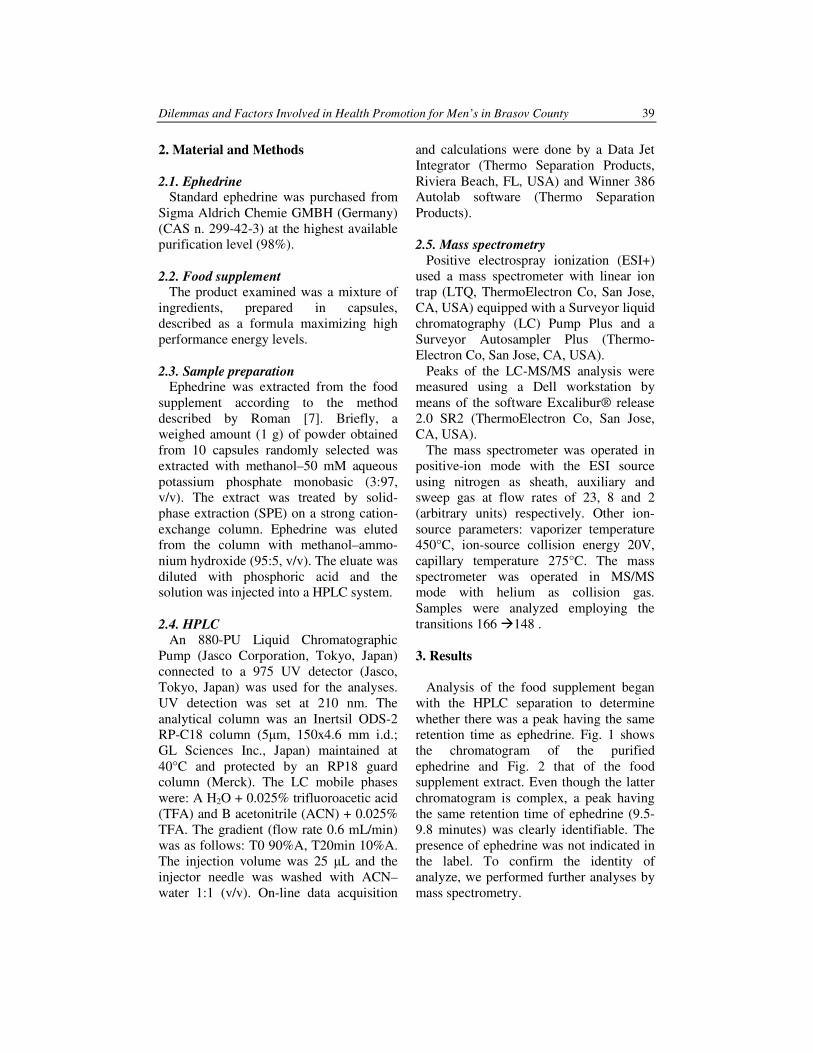
Dilemmas and Factors Involved in Health Promotion for Men’s in Brasov County 39
2. Material and Methods
2.1. Ephedrine
Standard ephedrine was purchased from
Sigma Aldrich Chemie GMBH (Germany)
(CAS n. 299-42-3) at the highest available
purification level (98%).
2.2. Food supplement
The product examined was a mixture of
ingredients, prepared in capsules,
described as a formula maximizing high
performance energy levels.
2.3. Sample preparation
Ephedrine was extracted from the food
supplement according to the method
described by Roman [7]. Briefly, a
weighed amount (1 g) of powder obtained
from 10 capsules randomly selected was
extracted with methanol–50 mM aqueous
potassium phosphate monobasic (3:97,
v/v). The extract was treated by solid-
phase extraction (SPE) on a strong cation-
exchange column. Ephedrine was eluted
from the column with methanol–ammo-
nium hydroxide (95:5, v/v). The eluate was
diluted with phosphoric acid and the
solution was injected into a HPLC system.
2.4. HPLC
An 880-PU Liquid Chromatographic
Pump (Jasco Corporation, Tokyo, Japan)
connected to a 975 UV detector (Jasco,
Tokyo, Japan) was used for the analyses.
UV detection was set at 210 nm. The
analytical column was an Inertsil ODS-2
RP-C18 column (5µm, 150x4.6 mm i.d.;
GL Sciences Inc., Japan) maintained at
40°C and protected by an RP18 guard
column (Merck). The LC mobile phases
were: A H2O + 0.025% trifluoroacetic acid
(TFA) and B acetonitrile (ACN) + 0.025%
TFA. The gradient (flow rate 0.6 mL/min)
was as follows: T0 90%A, T20min 10%A.
The injection volume was 25 µL and the
injector needle was washed with ACN–
water 1:1 (v/v). On-line data acquisition
and calculations were done by a Data Jet
Integrator (Thermo Separation Products,
Riviera Beach, FL, USA) and Winner 386
Autolab software (Thermo Separation
Products).
2.5. Mass spectrometry
Positive electrospray ionization (ESI+)
used a mass spectrometer with linear ion
trap (LTQ, ThermoElectron Co, San Jose,
CA, USA) equipped with a Surveyor liquid
chromatography (LC) Pump Plus and a
Surveyor Autosampler Plus (Thermo-
Electron Co, San Jose, CA, USA).
Peaks of the LC-MS/MS analysis were
measured using a Dell workstation by
means of the software Excalibur® release
2.0 SR2 (ThermoElectron Co, San Jose,
CA, USA).
The mass spectrometer was operated in
positive-ion mode with the ESI source
using nitrogen as sheath, auxiliary and
sweep gas at flow rates of 23, 8 and 2
(arbitrary units) respectively. Other ion-
source parameters: vaporizer temperature
450°C, ion-source collision energy 20V,
capillary temperature 275°C. The mass
spectrometer was operated in MS/MS
mode with helium as collision gas.
Samples were analyzed employing the
transitions 166 �148 .
3. Results
Analysis of the food supplement began
with the HPLC separation to determine
whether there was a peak having the same
retention time as ephedrine. Fig. 1 shows
the chromatogram of the purified
ephedrine and Fig. 2 that of the food
supplement extract. Even though the latter
chromatogram is complex, a peak having
the same retention time of ephedrine (9.5-
9.8 minutes) was clearly identifiable. The
presence of ephedrine was not indicated in
the label. To confirm the identity of
analyze, we performed further analyses by
mass spectrometry.
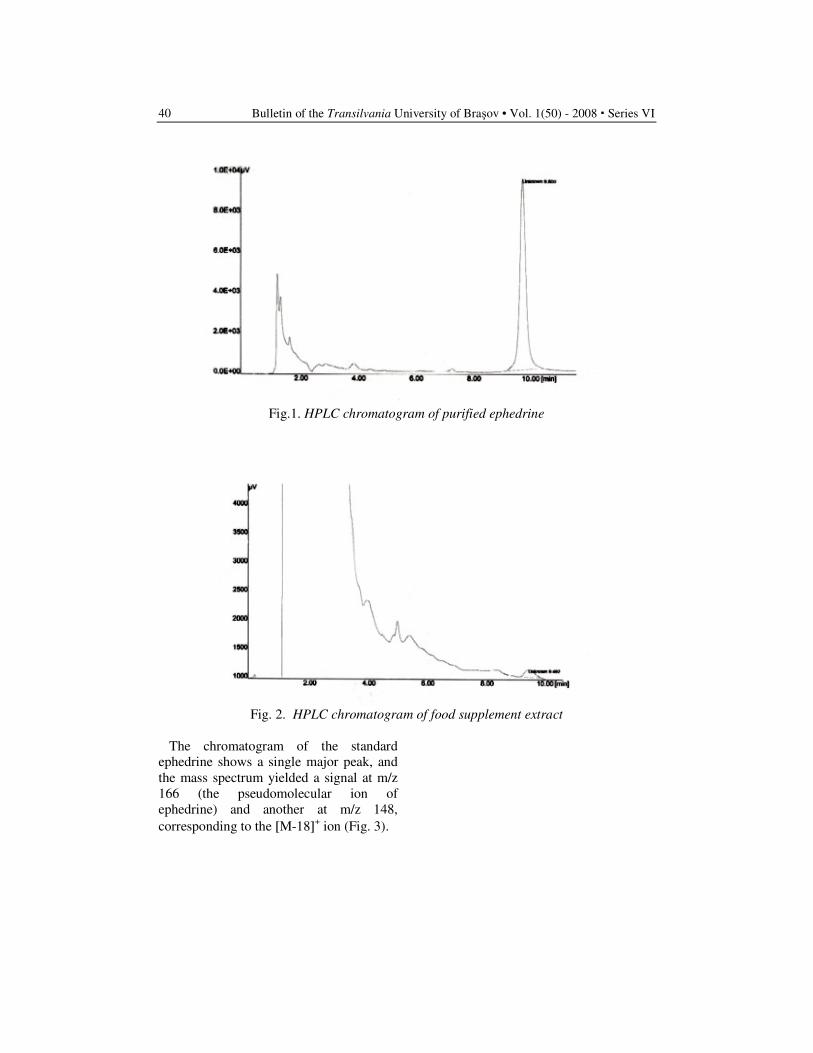
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
40
Fig.1. HPLC chromatogram of purified ephedrine
Fig. 2. HPLC chromatogram of food supplement extract
The chromatogram of the standard
ephedrine shows a single major peak, and
the mass spectrum yielded a signal at m/z
166 (the pseudomolecular ion of
ephedrine) and another at m/z 148,
corresponding to the [M-18]+ ion (Fig. 3).
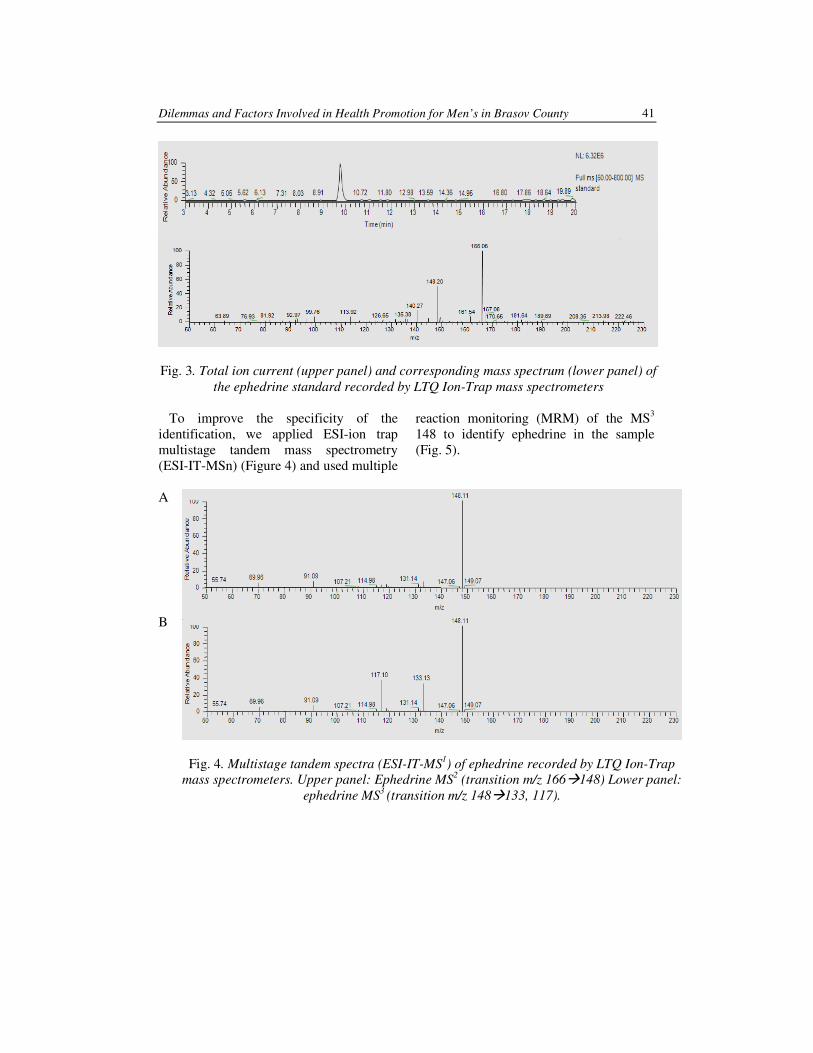
Dilemmas and Factors Involved in Health Promotion for Men’s in Brasov County 41
Fig. 3. Total ion current (upper panel) and corresponding mass spectrum (lower panel) of
the ephedrine standard recorded by LTQ Ion-Trap mass spectrometers
To improve the specificity of the
identification, we applied ESI-ion trap
multistage tandem mass spectrometry
(ESI-IT-MSn) (Figure 4) and used multiple
reaction monitoring (MRM) of the MS3
148 to identify ephedrine in the sample
(Fig. 5).
A
B
Fig. 4. Multistage tandem spectra (ESI-IT-MS1) of ephedrine recorded by LTQ Ion-Trap
mass spectrometers. Upper panel: Ephedrine MS2 (transition m/z 166�148) Lower panel:
ephedrine MS3 (transition m/z 148�133, 117).
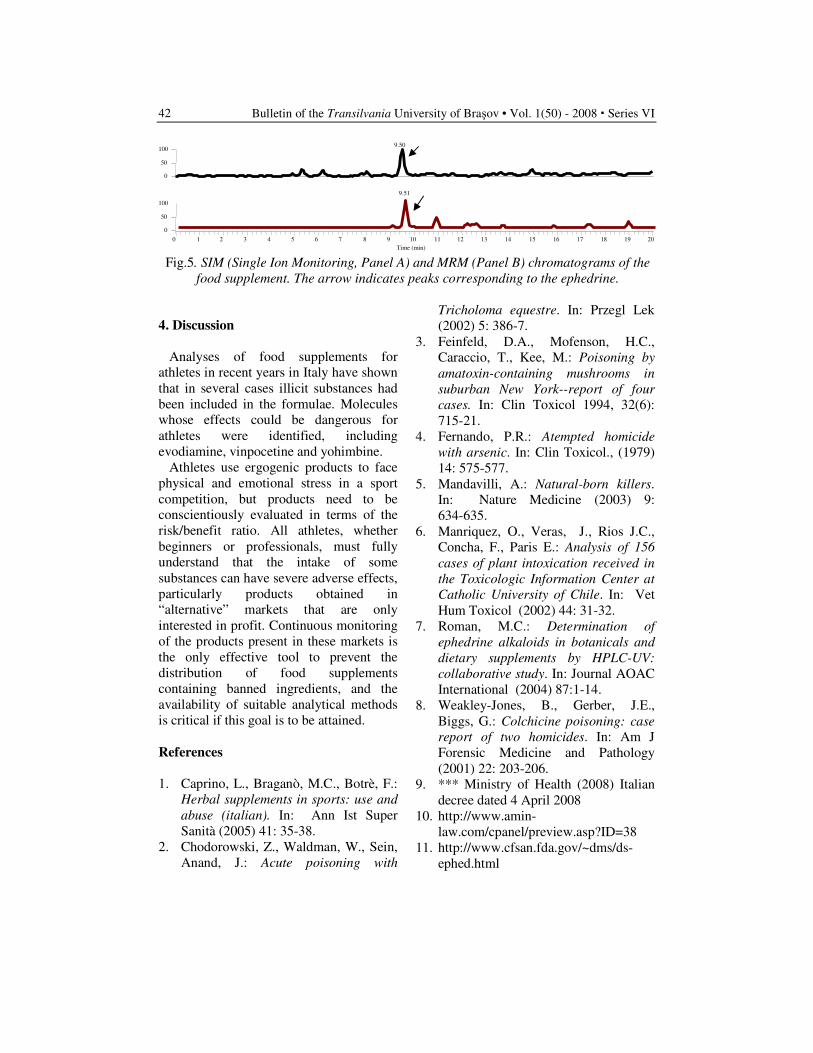
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
42
Fig.5. SIM (Single Ion Monitoring, Panel A) and MRM (Panel B) chromatograms of the
food supplement. The arrow indicates peaks corresponding to the ephedrine.
4. Discussion
Analyses of food supplements for
athletes in recent years in Italy have shown
that in several cases illicit substances had
been included in the formulae. Molecules
whose effects could be dangerous for
athletes were identified, including
evodiamine, vinpocetine and yohimbine.
Athletes use ergogenic products to face
physical and emotional stress in a sport
competition, but products need to be
conscientiously evaluated in terms of the
risk/benefit ratio. All athletes, whether
beginners or professionals, must fully
understand that the intake of some
substances can have severe adverse effects,
particularly products obtained in
“alternative” markets that are only
interested in profit. Continuous monitoring
of the products present in these markets is
the only effective tool to prevent the
distribution of food supplements
containing banned ingredients, and the
availability of suitable analytical methods
is critical if this goal is to be attained.
References
1. Caprino, L., Braganò, M.C., Botrè, F.:
Herbal supplements in sports: use and
abuse (italian). In: Ann Ist Super
Sanità (2005) 41: 35-38.
2. Chodorowski, Z., Waldman, W., Sein,
Anand, J.: Acute poisoning with
Tricholoma equestre. In: Przegl Lek
(2002) 5: 386-7.
3. Feinfeld, D.A., Mofenson, H.C.,
Caraccio, T., Kee, M.: Poisoning by
amatoxin-containing mushrooms in
suburban New York--report of four
cases. In: Clin Toxicol 1994, 32(6):
715-21.
4. Fernando, P.R.: Atempted homicide
with arsenic. In: Clin Toxicol., (1979)
14: 575-577.
5. Mandavilli, A.: Natural-born killers.
In: Nature Medicine (2003) 9:
634-635.
6. Manriquez, O., Veras, J., Rios J.C.,
Concha, F., Paris E.: Analysis of 156
cases of plant intoxication received in
the Toxicologic Information Center at
Catholic University of Chile. In: Vet
Hum Toxicol (2002) 44: 31-32.
7. Roman, M.C.: Determination of
ephedrine alkaloids in botanicals and
dietary supplements by HPLC-UV:
collaborative study. In: Journal AOAC
International (2004) 87:1-14.
8. Weakley-Jones, B., Gerber, J.E.,
Biggs, G.: Colchicine poisoning: case
report of two homicides. In: Am J
Forensic Medicine and Pathology
(2001) 22: 203-206.
9. *** Ministry of Health (2008) Italian
decree dated 4 April 2008
10. http://www.amin-
law.com/cpanel/preview.asp?ID=38
11. http://www.cfsan.fda.gov/~dms/ds-
ephed.html
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Time (min)
0 50
100
0 50
100
9.50
9.51

IMIPENEM RESISTANCE AMONG GRAM
NEGATIVE BACILLI
M. IDOMIR
1 C. NEMET
1
A. PASCU1 I. MOLEAVIN
1
Abstract: Gram negative bacilli are bacteria frequently implicated in human
pathology. The aim of our study has consisted in the detection of Gram negative
strains resistant to imipenem. The obtained frequency of resistant strains was
0.2% for Escherichia coli, 1.4% for Proteus spp., 3.9% for Enterobacter spp. and
22.5% for Pseudomonas aeruginosa. The obtained results have demonstrated
that imipenem remains an important solution for the therapy of infections
produced by multidrug resistant Gram negative bacilli but the selection of
resistant strains represents a threat that needs to be in the attention of the
practitioners.
Key words: imipenem, carbapenems, Gram negative bacilli.
1 Transilvania University of Braşov, Faculty of Medicine.
1. Introduction
Gram negative bacilli are bacteria that are
frequently implicated in human pathology,
in nosocomial and communitary infections.
In present, these pathogenic microorganisms
represent a significant cause of morbidity and
mortality. [1]
The hospital environment favorises the
selection of some multidrug resistant strains
due to the exposure to a wide range of anti-
microbial agents.
Different mechanisms are implicated in the
installation of the resistance to antimicrobial
substances among Gram negative bacilli like
enzyme production (cephalosporinases and
β - lactamases), variability of the antibiotic
target and modification of outer membrane
permeability. [1,7]
Many β - lactams are strong β - lactamases
inducers and they are also rapidly inactivated
by these enzymes. [7]
Carbapenems and β - lactam β - lactamase
inhibitor combinations are often used in the
therapy of the infections produced by Gram
negative bacilii. These antibiotics are strong
β-lactamases inducers too, but have a more
stable β-lactam ring that resists usually to
the action of these enzymes. [7]
The resistance to carbapenems of the germs
belonging to the Enterobacteriaceae family
is rare but is considered to be an emerging
clinical threat. This aspect has been observed
especially at Enterobacter spp. and Serratia
spp. but also at Proteus spp., Salmonella
enterica, Klebsiella pneumoniae, Citrobacter
freundii. [1,2] In the case of Escherichia coli
spp., the resistance to carbapenems, especially
to imipenem, is very rare. [4,5]
Recent studies have ilustrated that the main
mechanisms of resistance to imipenem for
E. coli are the hiperproduction of AmpC
β - lactamases and the loss of porins and for
Enterobacter, the production of chromosomal
cephalosporinases and the decrease of porin
synthesis in outer membrane.[1,5]
Metallo β-lactamases are very important
too. In the last decade, they were detected
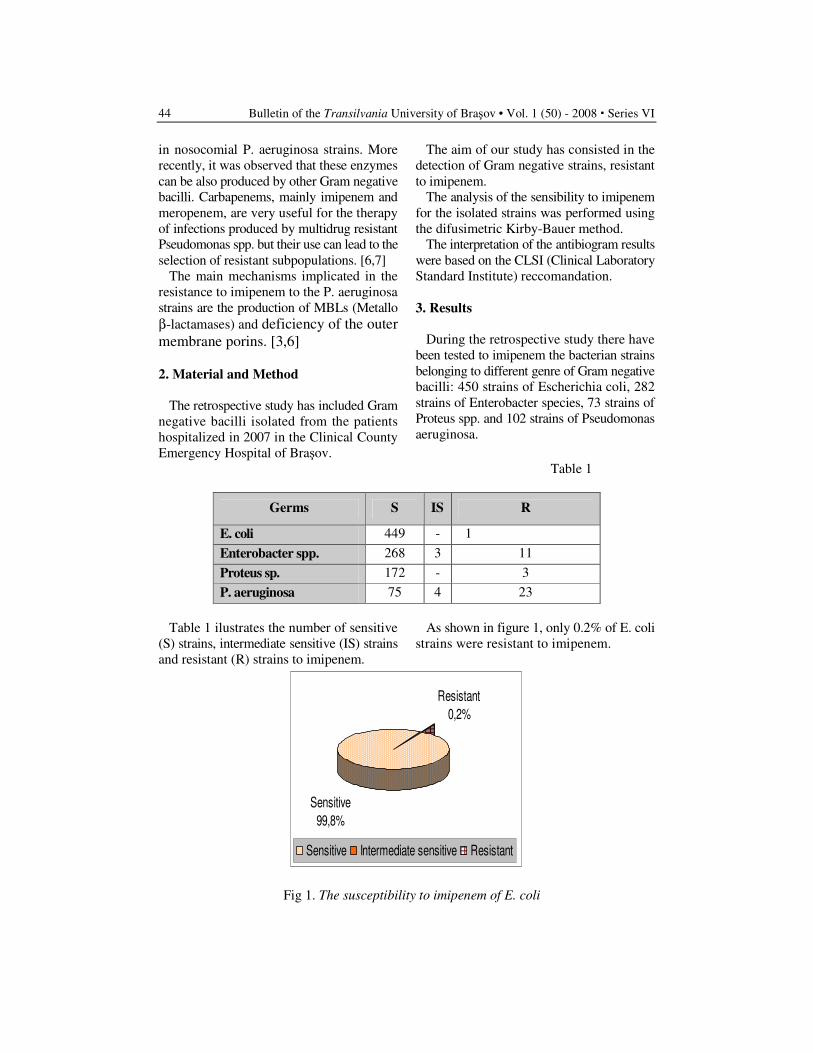
Bulletin of the Transilvania University of Braşov • Vol. 1 (50) - 2008 � Series VI
44
in nosocomial P. aeruginosa strains. More
recently, it was observed that these enzymes
can be also produced by other Gram negative
bacilli. Carbapenems, mainly imipenem and
meropenem, are very useful for the therapy
of infections produced by multidrug resistant
Pseudomonas spp. but their use can lead to the
selection of resistant subpopulations. [6,7]
The main mechanisms implicated in the
resistance to imipenem to the P. aeruginosa
strains are the production of MBLs (Metallo
β-lactamases) and deficiency of the outer
membrane porins. [3,6]
2. Material and Method
The retrospective study has included Gram
negative bacilli isolated from the patients
hospitalized in 2007 in the Clinical County
Emergency Hospital of Braşov.
The aim of our study has consisted in the
detection of Gram negative strains, resistant
to imipenem.
The analysis of the sensibility to imipenem
for the isolated strains was performed using
the difusimetric Kirby-Bauer method.
The interpretation of the antibiogram results
were based on the CLSI (Clinical Laboratory
Standard Institute) reccomandation.
3. Results
During the retrospective study there have
been tested to imipenem the bacterian strains
belonging to different genre of Gram negative
bacilli: 450 strains of Escherichia coli, 282
strains of Enterobacter species, 73 strains of
Proteus spp. and 102 strains of Pseudomonas
aeruginosa.
Table 1
Germs S IS R
E. coli 449 - 1
Enterobacter spp. 268 3 11
Proteus sp. 172 - 3
P. aeruginosa 75 4 23
Table 1 ilustrates the number of sensitive
(S) strains, intermediate sensitive (IS) strains
and resistant (R) strains to imipenem.
As shown in figure 1, only 0.2% of E. coli
strains were resistant to imipenem.
Sensitive
99,8%
Resistant
0,2%
Sensitive Intermediate sensitive Resistant
Fig 1. The susceptibility to imipenem of E. coli
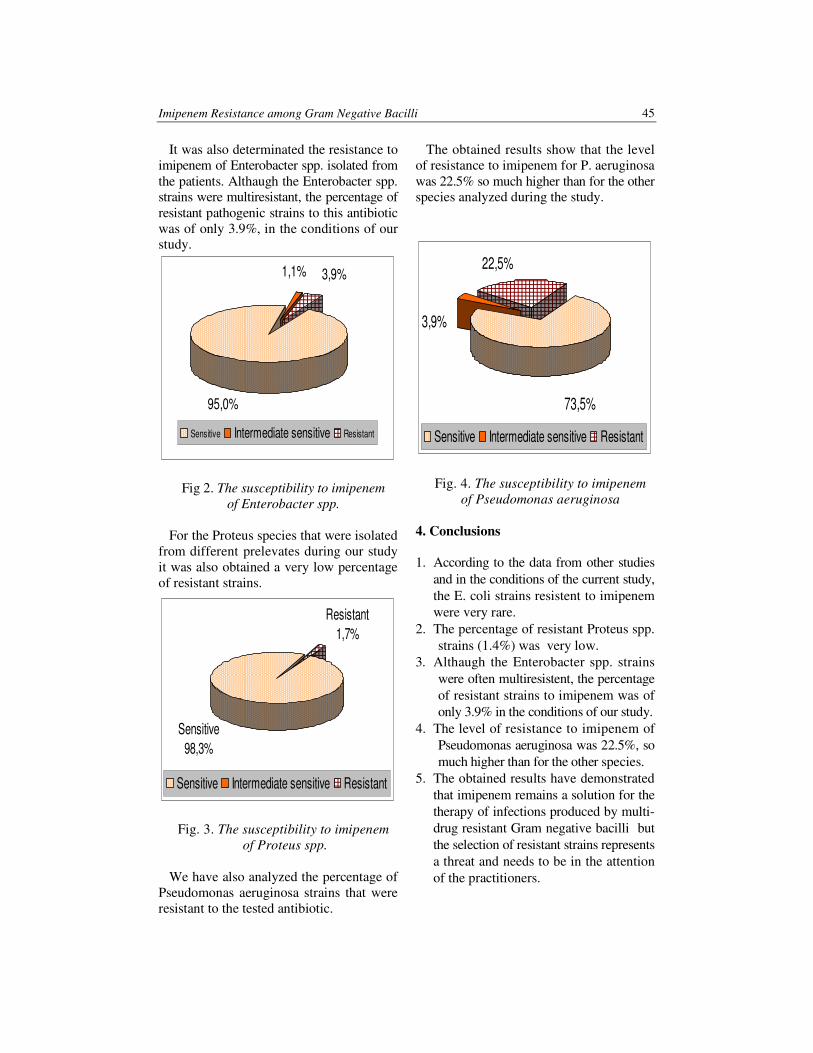
Imipenem Resistance among Gram Negative Bacilli
45
It was also determinated the resistance to
imipenem of Enterobacter spp. isolated from
the patients. Althaugh the Enterobacter spp.
strains were multiresistant, the percentage of
resistant pathogenic strains to this antibiotic
was of only 3.9%, in the conditions of our
study.
95,0%
1,1% 3,9%
Sensitive Intermediate sensitive Resistant
Fig 2. The susceptibility to imipenem
of Enterobacter spp.
For the Proteus species that were isolated
from different prelevates during our study
it was also obtained a very low percentage
of resistant strains.
Resistant
1,7%
Sensitive
98,3%
Sensitive Intermediate sensitive Resistant
Fig. 3. The susceptibility to imipenem
of Proteus spp.
We have also analyzed the percentage of
Pseudomonas aeruginosa strains that were
resistant to the tested antibiotic.
The obtained results show that the level
of resistance to imipenem for P. aeruginosa
was 22.5% so much higher than for the other
species analyzed during the study.
73,5%
3,9%
22,5%
Sensitive Intermediate sensitive Resistant
Fig. 4. The susceptibility to imipenem
of Pseudomonas aeruginosa
4. Conclusions
1. According to the data from other studies
and in the conditions of the current study,
the E. coli strains resistent to imipenem
were very rare.
2. The percentage of resistant Proteus spp.
strains (1.4%) was very low.
3. Althaugh the Enterobacter spp. strains
were often multiresistent, the percentage
of resistant strains to imipenem was of
only 3.9% in the conditions of our study.
4. The level of resistance to imipenem of
Pseudomonas aeruginosa was 22.5%, so
much higher than for the other species.
5. The obtained results have demonstrated
that imipenem remains a solution for the
therapy of infections produced by multi-
drug resistant Gram negative bacilli but
the selection of resistant strains represents
a threat and needs to be in the attention
of the practitioners.

Bulletin of the Transilvania University of Braşov • Vol. 1 (50) - 2008 � Series VI
46
References
1. Bornet, C., Davin-Regli, A., Bosi, C.,
Pages, J-M., et al: Imipenem resistance
of Enterobacter aerogenes mediated by
outer membrane permeability. In: Journal
of Clinical Microbiology, vol. 38, no.
3, 2000, p. 1048-1052.
2. Hae Kyung, L., Park, Y.-J., Kim, J.-Y.,
Chang, E. et al: Prevalence of decreased
susceptibility to carbapenems among
Serratia marcescens, Enterobacter cloacae,
and Citrobacter freundii and investigation
of carbapenemases. In: Diagnostic Micro-
biology and Infectious Disease, vol. 52,
no. 4, 2005, p. 331-336.
3. Mendiratta, D., Vijayshri, D., Narang,
P.: Metallo-[beta]-lactamase producing
Pseudomonas aeruginosa in a hospital
from a rural area. In: Indian Journal of
Medical Research, vol. 121, 2005,
p. 701 -703.
4. Oteo, J., Delgado-Iribarren, A., Vega,
D., Bautista, V., et al: Emergence of
imipenem resistance in clinical E. coli
during therapy. In: International Journal
of Antimicrobial Agents, volume 32, issue
6, p. 534-537.
5. Pavez, M., Neves, P., Dropa, M., Matte,
M.-H., et al: Emergence of carbapenem-
resistant Escherichia coli producing CMY
-2-type AmpC beta-lactamase in Brazil,
In: Journal of Medical Microbiology,
57 (12), 2008, p. 1590-1592.
6. Pournaras, S., Ikonomidis, A., Marko-
giannakis, A., et al: Characterization
of clinical isolates of Pseudomonas
aeruginosa heterogeneously resistant to
carbapenems. In: Journal of Medical
Microbiology, vol. 56, 2007, p. 66-70.
7. Zhanel, G.G., Wiebe, R., Dilay, L., et al:
Comparative review of the carbapenems,
In: Drugs, 67(7), 2007, p. 1027-1052.
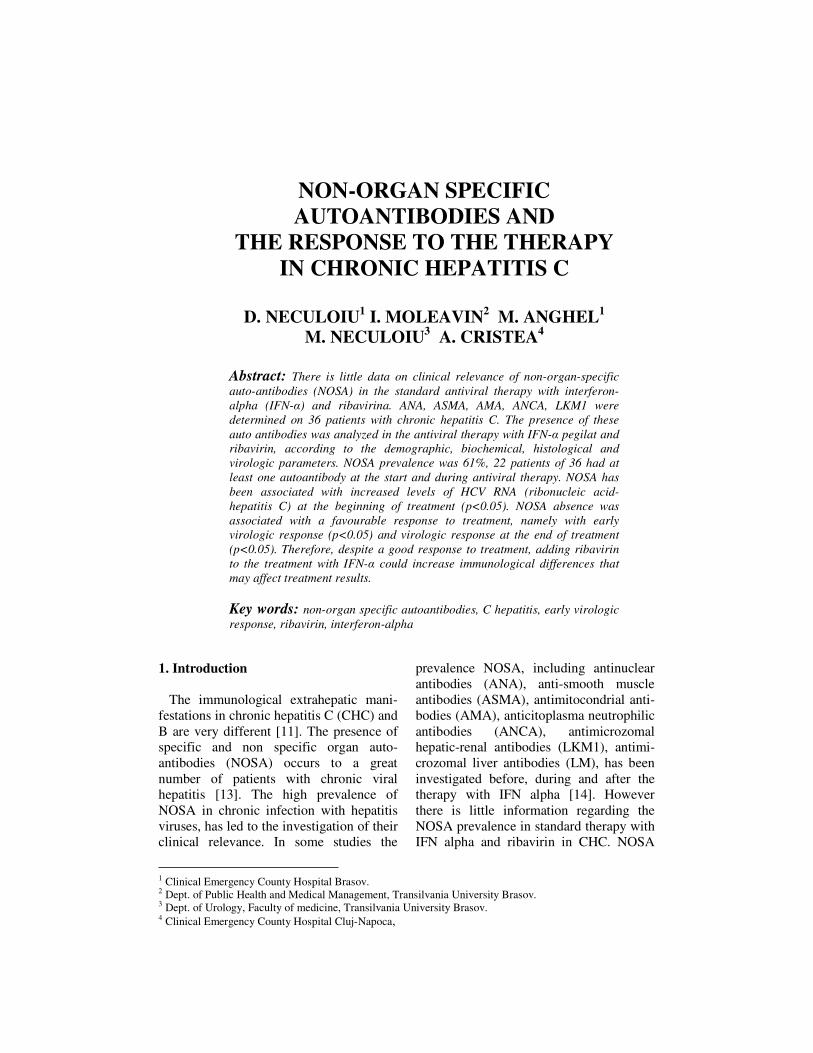
NON-ORGAN SPECIFIC
AUTOANTIBODIES AND
THE RESPONSE TO THE THERAPY
IN CHRONIC HEPATITIS C
D. NECULOIU
1 I. MOLEAVIN
2 M. ANGHEL
1
M. NECULOIU3 A. CRISTEA
4
Abstract: There is little data on clinical relevance of non-organ-specific
auto-antibodies (NOSA) in the standard antiviral therapy with interferon-
alpha (IFN-α) and ribavirina. ANA, ASMA, AMA, ANCA, LKM1 were
determined on 36 patients with chronic hepatitis C. The presence of these
auto antibodies was analyzed in the antiviral therapy with IFN-α pegilat and
ribavirin, according to the demographic, biochemical, histological and
virologic parameters. NOSA prevalence was 61%, 22 patients of 36 had at
least one autoantibody at the start and during antiviral therapy. NOSA has
been associated with increased levels of HCV RNA (ribonucleic acid-
hepatitis C) at the beginning of treatment (p<0.05). NOSA absence was
associated with a favourable response to treatment, namely with early
virologic response (p<0.05) and virologic response at the end of treatment
(p<0.05). Therefore, despite a good response to treatment, adding ribavirin
to the treatment with IFN-α could increase immunological differences that
may affect treatment results.
Key words: non-organ specific autoantibodies, C hepatitis, early virologic
response, ribavirin, interferon-alpha
1 Clinical Emergency County Hospital Brasov. 2 Dept. of Public Health and Medical Management, Transilvania University Brasov. 3 Dept. of Urology, Faculty of medicine, Transilvania University Brasov. 4 Clinical Emergency County Hospital Cluj-Napoca,
1. Introduction
The immunological extrahepatic mani-
festations in chronic hepatitis C (CHC) and
B are very different [11]. The presence of
specific and non specific organ auto-
antibodies (NOSA) occurs to a great
number of patients with chronic viral
hepatitis [13]. The high prevalence of
NOSA in chronic infection with hepatitis
viruses, has led to the investigation of their
clinical relevance. In some studies the
prevalence NOSA, including antinuclear
antibodies (ANA), anti-smooth muscle
antibodies (ASMA), antimitocondrial anti-
bodies (AMA), anticitoplasma neutrophilic
antibodies (ANCA), antimicrozomal
hepatic-renal antibodies (LKM1), antimi-
crozomal liver antibodies (LM), has been
investigated before, during and after the
therapy with IFN alpha [14]. However
there is little information regarding the
NOSA prevalence in standard therapy with
IFN alpha and ribavirin in CHC. NOSA

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
48
prevalence should also be investigated in
standard therapy, being known the immu-
no-modulatory function of ribavirin [9].
In recent years the combination between
RBV and IFN-alpha has increased to 40%,
the rate of biochemical and virologic res-
ponse of the patients with chronic viral
hepatitis C [17]. The effective treatment with
ribavirin in CHC appears to be correlated
with both its immunomodulatory and anti-
inflammatory effects [2]. In particular it
seems that RBV modulates the balance
between subsets of Th1 and Th2
lymphocytes in specific immune response by
activating the type 1 cytokine [19]. However,
RBV may increase the non-viral immune
response and can trigger autoimmune
phenomena to the predisposed patients. [4].
Previous analyses on the influence of
NOSA on hepatitis C virus clearance
during the IFN-alpha monotherapy are
contradictory; some studies have shown a
decreased response to the treatment for the
NOSA positive patients, other analyses
could not demonstrate any influence on
therapy [18].
In contrast there are few studies that
have investigated NOSA relevance and
biochemical and virological response of
the patients treated with IFN-alpha pegilat
and RBV [21]. This combination repre-
sents the standard therapy in the treatment
of CHC, and has proven to be superior to
the interferon monotherapy [15].
In this study we have determined the
NOSA prevalence in patients with chronic
viral hepatitis C and analyzed the
relationship between the NOSA presence
and biochemical and histological activity of
liver, and the impact of these auto antibodies
efficiency on the antiviral therapy which
combines IFN-alpha with RBV.
2. Material and Method
Patients. The patients were tested
retrospectively, 36 patients with CHC. The
demographic and clinic parameter are
show in Tabel 1. In this study, all patients
were treated during a period of 12 months
with standard doses of Pegasis
(180µg/week) and RBV in variable doses
1000-1200mg/day, depending on body
weight.
All patients were positive for anti-VHC
and ARN HVC and were diagnosed with
CHC. The laboratory parameters included
parameters of haematology, coagulation,
biochemistry. Average daily consumption
of alcohol was less than 40 grams. HBs
and HIV tests were negative.
All patients were tested according to the
score system for autoimmune hepatitis
diagnosis. Using this algorithm, none of
the investigated patients obtained more
than 10 points, excluding any association
of an autoimmune hepatitis [1].
Clinical data of the patients Table 1
Age, years 46,22±7,6
Sex (Male/Female) 20/16
Naive/Retreated 20/16
HCV RNA level
(<800.000/>800.000UI/ml)
18/18
NOSA (+/-) 22/14
Hisological activity index 7,69±1,39
Virological response at the end of
the treatment (+/-)
18/18
Auto-antibodies testing. ANA, SMA,
AMA, LKM1, LM were determined by
indirect imunofluorescence on the sections
of liver to cryostat, kidneys and stomachs
of rat: initial serum dilution was 1:80 for
ANA 1: 40 for the other auto antibodies.
ANCA were tested by indirect imuno-
fluorescence on human polymorpho-
nuclears. Standard protocols for testing
were used for the tested antibodies [20].
For each patient NOSA was determined
before the start of the antiviral treatment,
and two serum samples were collected: one
after three months from the beginning of
the treatment and another at the end of it.
Virus testing.Virological tests to detect
anti-HCV antibodies were realized with
ELISA kits of third generation (HCV AB
ETI-K, Sorin Biomedica), and the viral
Non-Organ Specific Autoantibodies and the Response to the Therapy in Chronic Hepatitis C 49
load was done by the RT-PCR method,
quantitative method with HCV Monitor kits
version 2.0, the Cobas Amplicor (Roche)
analyzer. HCV RNA level was tested at the
beginning of treatment (HCV RNA start),
then after 3 months from the beginning of
treatment (HCV RNA 3 months) for
determining early virologic response (EVR)
and at the end of the treatment (VR-end).
Hepatic Histology. All patients were
subjected to liver biopsy and histological
parameters were classified according to the
Knodell score, actualized version proposed
by Ishak and collaborators [12].
Hepatic fibrosis was appreciated by the old
Knodell system: 0 absence of fibrosis, 1 portal
fibrosis; 3 fibrosis in bridges; 4 cirrhosis.
Statistical analysis. In the case of
qualitative variables the Fisher test was
used, and in the case of correlation studies
between a qualitative variable and a
quantitative one the Student test was used,
and the threshold for statistical
significance was set to 0.05.
3. Results
The prevalence of auto antibodies in this
study was the following: 22 patients of 36
had at least one autoantibody (ANA, SMA,
LKM, ANCA) at the start of the treatment
and during it at a titter greater than 1:80 for
ANA, and 1:40 for other auto antibodies
(Table 2). ANA was the most common
auto antibody (38.8%) followed by the
SMA (22.8%). AMA has not been
detected, and ANCA, LM and LKM were
found in a smaller number of cases.
Table 2
The prevalence of NOSA at the patients
with chronic hepatitis C.
n (%)
ANA 14 (38.8)
AMA 0
LKM 4 (11.1)
LM 1 (2.7)
SMA 8 (22.2)
ANCA 2 (5.5)
NOSA 22 (61.1)
Subsequently the patients were divided
into two groups: one group consists of
patients with NOSA negative and the second
group with NOSA positive (Table 3).
Table 3
The comparison of demographic, biochemical, histological and virological parameters
at NOSA positive and NOSA negative patients.
NOSA-Negativ p-value NOSA-
Pozitive
Sex(Male/Female) 6/8 0.221 14/8
Age, years 44.85±6.06 0.205 48.72±10.09
Naiv/retreted 10/4 0.126 10/12
ASAT 0 75.5729.7 0.737 72.09±30.34
ALAT 0 46,56±17,23 0.221 86.09±20.37
ASAT 3 43±20,28 0.482 49.09±27.62
ALAT 3 54.42±36,07 0.425 46.54±22.73
HCV-RNA viremia level (high/low) 10/4 0.004 5/17
EVR(+/-) 7/7 0.05 18/4
VR-end(+/-) 6/8 0.021 18/4
Hisological activity index 8±1.56 0.406 7.63±1.32
Knodel IV(1/3) 4/10 0.311 10/12
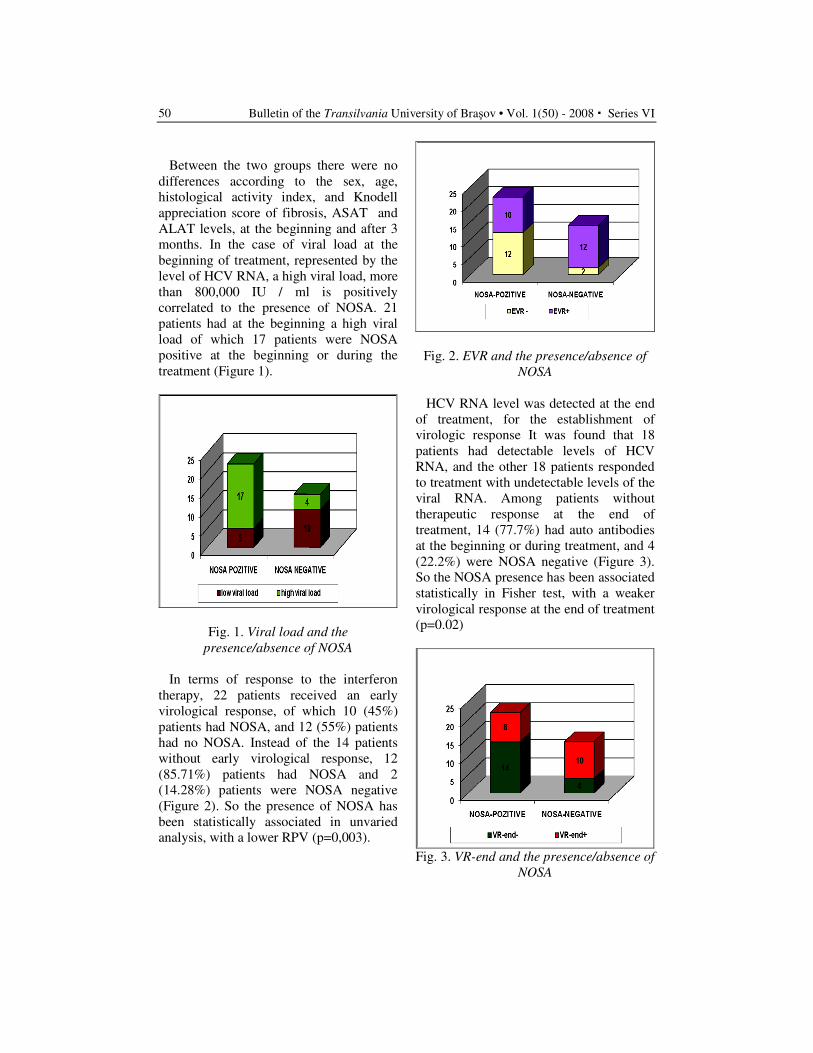
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
50
Between the two groups there were no
differences according to the sex, age,
histological activity index, and Knodell
appreciation score of fibrosis, ASAT and
ALAT levels, at the beginning and after 3
months. In the case of viral load at the
beginning of treatment, represented by the
level of HCV RNA, a high viral load, more
than 800,000 IU / ml is positively
correlated to the presence of NOSA. 21
patients had at the beginning a high viral
load of which 17 patients were NOSA
positive at the beginning or during the
treatment (Figure 1).
Fig. 1. Viral load and the
presence/absence of NOSA
In terms of response to the interferon
therapy, 22 patients received an early
virological response, of which 10 (45%)
patients had NOSA, and 12 (55%) patients
had no NOSA. Instead of the 14 patients
without early virological response, 12
(85.71%) patients had NOSA and 2
(14.28%) patients were NOSA negative
(Figure 2). So the presence of NOSA has
been statistically associated in unvaried
analysis, with a lower RPV (p=0,003).
Fig. 2. EVR and the presence/absence of
NOSA
HCV RNA level was detected at the end
of treatment, for the establishment of
virologic response It was found that 18
patients had detectable levels of HCV
RNA, and the other 18 patients responded
to treatment with undetectable levels of the
viral RNA. Among patients without
therapeutic response at the end of
treatment, 14 (77.7%) had auto antibodies
at the beginning or during treatment, and 4
(22.2%) were NOSA negative (Figure 3).
So the NOSA presence has been associated
statistically in Fisher test, with a weaker
virological response at the end of treatment
(p=0.02)
Fig. 3. VR-end and the presence/absence of
NOSA
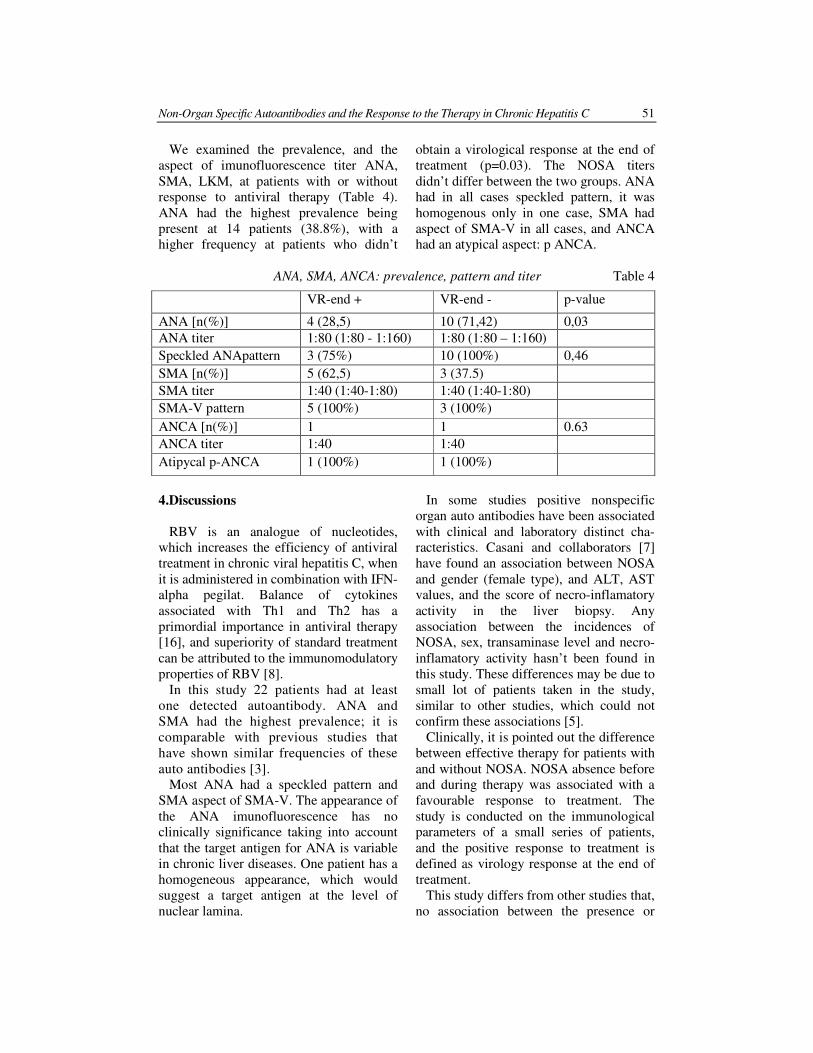
Non-Organ Specific Autoantibodies and the Response to the Therapy in Chronic Hepatitis C 51
We examined the prevalence, and the
aspect of imunofluorescence titer ANA,
SMA, LKM, at patients with or without
response to antiviral therapy (Table 4).
ANA had the highest prevalence being
present at 14 patients (38.8%), with a
higher frequency at patients who didn’t
obtain a virological response at the end of
treatment (p=0.03). The NOSA titers
didn’t differ between the two groups. ANA
had in all cases speckled pattern, it was
homogenous only in one case, SMA had
aspect of SMA-V in all cases, and ANCA
had an atypical aspect: p ANCA.
ANA, SMA, ANCA: prevalence, pattern and titer Table 4
4.Discussions
RBV is an analogue of nucleotides,
which increases the efficiency of antiviral
treatment in chronic viral hepatitis C, when
it is administered in combination with IFN-
alpha pegilat. Balance of cytokines
associated with Th1 and Th2 has a
primordial importance in antiviral therapy
[16], and superiority of standard treatment
can be attributed to the immunomodulatory
properties of RBV [8].
In this study 22 patients had at least
one detected autoantibody. ANA and
SMA had the highest prevalence; it is
comparable with previous studies that
have shown similar frequencies of these
auto antibodies [3].
Most ANA had a speckled pattern and
SMA aspect of SMA-V. The appearance of
the ANA imunofluorescence has no
clinically significance taking into account
that the target antigen for ANA is variable
in chronic liver diseases. One patient has a
homogeneous appearance, which would
suggest a target antigen at the level of
nuclear lamina.
In some studies positive nonspecific
organ auto antibodies have been associated
with clinical and laboratory distinct cha-
racteristics. Casani and collaborators [7]
have found an association between NOSA
and gender (female type), and ALT, AST
values, and the score of necro-inflamatory
activity in the liver biopsy. Any
association between the incidences of
NOSA, sex, transaminase level and necro-
inflamatory activity hasn’t been found in
this study. These differences may be due to
small lot of patients taken in the study,
similar to other studies, which could not
confirm these associations [5].
Clinically, it is pointed out the difference
between effective therapy for patients with
and without NOSA. NOSA absence before
and during therapy was associated with a
favourable response to treatment. The
study is conducted on the immunological
parameters of a small series of patients,
and the positive response to treatment is
defined as virology response at the end of
treatment.
This study differs from other studies that,
no association between the presence or
VR-end + VR-end - p-value
ANA [n(%)] 4 (28,5) 10 (71,42) 0,03
ANA titer 1:80 (1:80 - 1:160) 1:80 (1:80 – 1:160)
Speckled ANApattern 3 (75%) 10 (100%) 0,46
SMA [n(%)] 5 (62,5) 3 (37.5)
SMA titer 1:40 (1:40-1:80) 1:40 (1:40-1:80)
SMA-V pattern 5 (100%) 3 (100%)
ANCA [n(%)] 1 1 0.63
ANCA titer 1:40 1:40
Atipycal p-ANCA 1 (100%) 1 (100%)

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
52
absence of NOSA and effective antiviral
therapy have found. [10] However,
previous studies assumed interferon
monotherapy, and in two other studies,
which include a larger number of patients,
a weaker response to treatment in the case
of auto antibodies presence was
demonstrated [6].
Regarding the results published so far,
these auto antibodies can be interpreted as
markers for activation of nonspecific
lymphocytes in their response to the
infection with hepatitis C virus. This could
be associated with a decreasing of the
specific immune response and a failure in
eliminating the virus and its persistence in
the body.
This assumption could be supported by
the fact that patients with NOSA have a
higher viral load compared with patients
without auto antibodies. RBV has
immunomodulatory distinct properties, and
can modulate the immune response
balance and the specific and non specific
antiviral response of individual patients.
Therefore, despite a general benefit of
ribavirin, association of this immuno-
modulator to the therapy with interferon
could reveal individual differences of the
immune balance, Th1 versus Th2, which
were not evident in studies that have
investigated only interferon monotherapy.
A recent study has shown that adding
ribavirin to interferon therapy, does not
alter the aspect of thyroid auto antibodies,
but grows the risk of hypothyroidism [6].
It is stressed that the safety and efficacy
of therapy, is missing to patients with
hepatitis C and autoimmune abnormalities.
Thus it is compulsory to take into account
the negative potential of the autoimmune
reaction at patients with CHC and NOSA
positive during the therapy with interferon.
To confirm these suppositions studies are
necessary to be done on a larger number of
patients.
These observations are related to the
immunopathologic discrimination between
CHC, autoimmune hepatitis and auto-
immune syndrome overlap-hepatitis C
[18]. In this study we have involved the
revised score system for the diagnosis of
autoimmune hepatitis to exclude a hepatic
autoimmune predominant disease. More-
over, only one patient had low SMA titter
without any SMA-V aspect, one patient
had homogenous ANA and no patient had
LKM 1 antibody, which are usually
associated with autoimmune hepatitis.
5. Conclusions
We have proved the negative
relationship between the effectiveness of
antiviral combined therapy with interferon-
alpha and ribavirin for chronic viral
hepatitis C and the presence of nonspecific
organ antibodies. However studies on a
larger number of patients are necessary
before making decisions regarding
treatment. Future studies should include
the measurement of other immune
parameters: markers of activation of
lymphocytes and cytokines, and genetic
studies to elucidate physiopathological
associations between the presence of auto
antibodies and the reducing of the
effectiveness of treatment with antiviral
interferon-alpha and ribavirin.
References
1. Alvarez, F., Berg, P.A., Bianchi, F.B.,
Bianchi, L., Burroughs, A.K. et al.:
International Autoimmune Hepatitis
Group Report: review of criteria for
diagnosis of autoimmune hepatitis. In:
J Hepatol 1999, 31:929-938.
2. Beragamini, A., Bolacchi, F.,
Cepparulo, M., Demin, F., Uccella, I.,
Bongiovanni, B. et al.: Treatment with
ribavirin and interferon-a reduces
interferon-g expression in patients
with chronic hepatitis C. In: Clinical
Experimental Immunology 2001,
123:459–464.
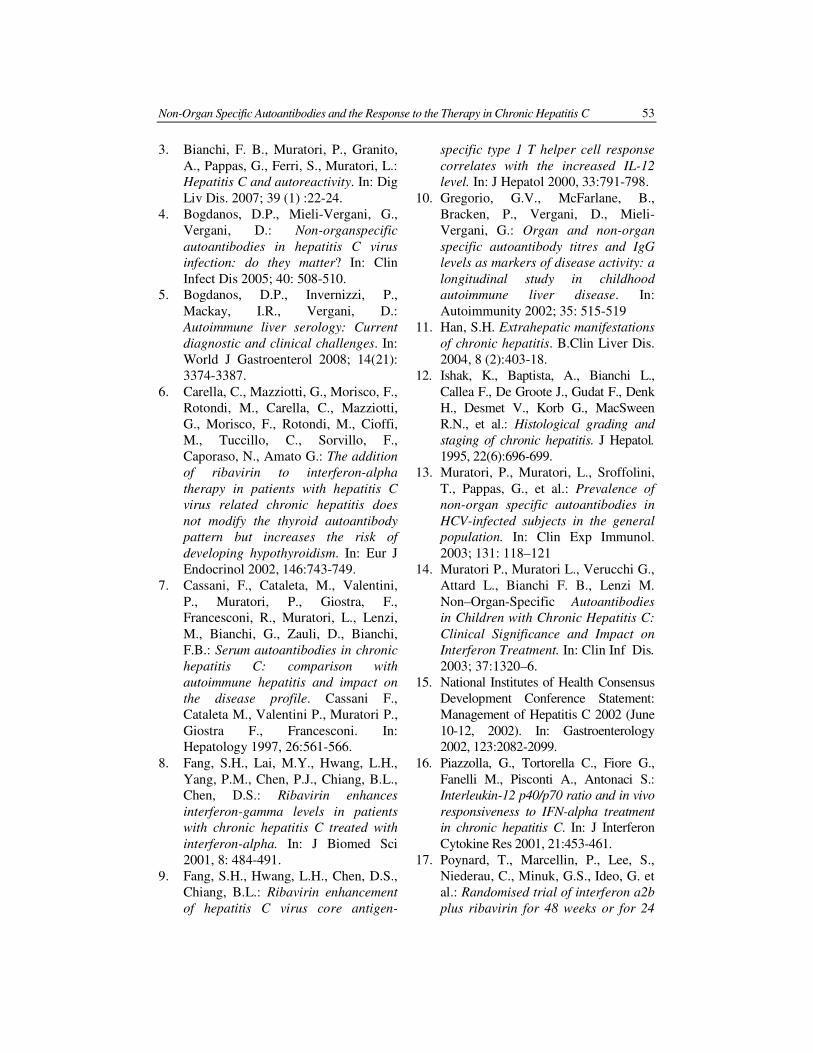
Non-Organ Specific Autoantibodies and the Response to the Therapy in Chronic Hepatitis C 53
3. Bianchi, F. B., Muratori, P., Granito,
A., Pappas, G., Ferri, S., Muratori, L.:
Hepatitis C and autoreactivity. In: Dig
Liv Dis. 2007; 39 (1) :22-24.
4. Bogdanos, D.P., Mieli-Vergani, G.,
Vergani, D.: Non-organspecific
autoantibodies in hepatitis C virus
infection: do they matter? In: Clin
Infect Dis 2005; 40: 508-510.
5. Bogdanos, D.P., Invernizzi, P.,
Mackay, I.R., Vergani, D.:
Autoimmune liver serology: Current
diagnostic and clinical challenges. In:
World J Gastroenterol 2008; 14(21):
3374-3387.
6. Carella, C., Mazziotti, G., Morisco, F.,
Rotondi, M., Carella, C., Mazziotti,
G., Morisco, F., Rotondi, M., Cioffi,
M., Tuccillo, C., Sorvillo, F.,
Caporaso, N., Amato G.: The addition
of ribavirin to interferon-alpha
therapy in patients with hepatitis C
virus related chronic hepatitis does
not modify the thyroid autoantibody
pattern but increases the risk of
developing hypothyroidism. In: Eur J
Endocrinol 2002, 146:743-749.
7. Cassani, F., Cataleta, M., Valentini,
P., Muratori, P., Giostra, F.,
Francesconi, R., Muratori, L., Lenzi,
M., Bianchi, G., Zauli, D., Bianchi,
F.B.: Serum autoantibodies in chronic
hepatitis C: comparison with
autoimmune hepatitis and impact on
the disease profile. Cassani F.,
Cataleta M., Valentini P., Muratori P.,
Giostra F., Francesconi. In:
Hepatology 1997, 26:561-566.
8. Fang, S.H., Lai, M.Y., Hwang, L.H.,
Yang, P.M., Chen, P.J., Chiang, B.L.,
Chen, D.S.: Ribavirin enhances
interferon-gamma levels in patients
with chronic hepatitis C treated with
interferon-alpha. In: J Biomed Sci
2001, 8: 484-491.
9. Fang, S.H., Hwang, L.H., Chen, D.S.,
Chiang, B.L.: Ribavirin enhancement
of hepatitis C virus core antigen-
specific type 1 T helper cell response
correlates with the increased IL-12
level. In: J Hepatol 2000, 33:791-798.
10. Gregorio, G.V., McFarlane, B.,
Bracken, P., Vergani, D., Mieli-
Vergani, G.: Organ and non-organ
specific autoantibody titres and IgG
levels as markers of disease activity: a
longitudinal study in childhood
autoimmune liver disease. In:
Autoimmunity 2002; 35: 515-519
11. Han, S.H. Extrahepatic manifestations
of chronic hepatitis. B.Clin Liver Dis.
2004, 8 (2):403-18.
12. Ishak, K., Baptista, A., Bianchi L.,
Callea F., De Groote J., Gudat F., Denk
H., Desmet V., Korb G., MacSween
R.N., et al.: Histological grading and
staging of chronic hepatitis. J Hepatol.
1995, 22(6):696-699.
13. Muratori, P., Muratori, L., Sroffolini,
T., Pappas, G., et al.: Prevalence of
non-organ specific autoantibodies in
HCV-infected subjects in the general
population. In: Clin Exp Immunol.
2003; 131: 118–121
14. Muratori P., Muratori L., Verucchi G.,
Attard L., Bianchi F. B., Lenzi M.
Non–Organ-Specific Autoantibodies
in Children with Chronic Hepatitis C:
Clinical Significance and Impact on
Interferon Treatment. In: Clin Inf Dis.
2003; 37:1320–6.
15. National Institutes of Health Consensus
Development Conference Statement:
Management of Hepatitis C 2002 (June
10-12, 2002). In: Gastroenterology
2002, 123:2082-2099.
16. Piazzolla, G., Tortorella C., Fiore G.,
Fanelli M., Pisconti A., Antonaci S.:
Interleukin-12 p40/p70 ratio and in vivo
responsiveness to IFN-alpha treatment
in chronic hepatitis C. In: J Interferon
Cytokine Res 2001, 21:453-461.
17. Poynard, T., Marcellin, P., Lee, S.,
Niederau, C., Minuk, G.S., Ideo, G. et
al.: Randomised trial of interferon a2b
plus ribavirin for 48 weeks or for 24

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
54
weeks versus interferon a2b plus
placebo for 48 weeks for treatment of
chronic infection with hepatitis C virus.
In: Lancet 1998, 352:1426–1432.
18. Selmi, C., Mackay, I.R., Gershwin,
M.E.: The immunological milieu of the
liver. In: Semin Liver Dis 2007; 27:
129-139.
19. Tam, R.C., Pai, B., Bard, J., Lim, C.,
Averett, D.R., Phan, U.T. et al.:
Ribavirin polarizes human T cell
responses toward a type 1 cytokine
profile. In: Journal of Hepatology
1999, 30: 376–382.
20. Vergani, D., Alvarez, F., Bianchi,
F.B., Cancado, E.L., Mackay, I.R.,
Manns, M.P., Nishioka, M., Penner, E.
Liver autoimmune serology: a
consensus statement from the
committee for autoimmune serology of
the International Autoimmune
Hepatitis Group. In: J Hepatol 2004;
41: 677-6.
21. Wasmuth, H.E., Stolte, C., Geier, A.,
Dietrich, C.G., Gartung, C., Lorenze,
J., Matern, S., Lammert, F.: The
presence of non-organ-specific auto-
antibodies is associated with a
negative response to combination
therapy with interferon and ribavirin
for chronic hepatitis C. In: BMC
Infect Dis. 2004, 13:41-42.

ACQUIRED ANGIOEDEMA IN SYSTEMIC
LUPUS ERYTHEMATOSUS
Ioana AGACHE
1
Abstract: Angioedema due to acquired C1-inhibitor (C1-INH) deficiency
(also referred to as acquired angioedema) is a rare, life-threatening disease
with poorly defined aetiology, therapy, and prognosis. The article reports on
acquired angioedema in 8 patients with systemic lupus erythematosus (SLE)
representing 16.66% of the total 48 SLE monitored in our clinic. Sex ratio
was 1/7, medium age 45.5±12.61 years. In 7 cases angioedema preceded the
diagnosis of SLE with 13.28 ±7.8 months, one case developed angioedema 15
years after SLE diagnosis. At the time of acquired angioedema diagnosis the
medium C1-INH concentrations were 0.094±0.039 g/L and C4 was
decreased in all cases, medium values 14.42± 4.83 mg/dl. Angioedema
localization was at face/eyelids in 5(62.5%) cases, larynx in 3(37.5%) cases
and 2(25%) cases had severe abdominal pain. 3(37.5%) patients also
associated pruritic erythematous rash. Compared with the SLE patients not
having angioedema, in the acquired angioedema group there was increased
incidence of systemic symptoms, immune cytopenias, kidney involvement,
antiRo and anti Sm antibodies. Patients evolved with a medium of
angioedema attacks of 6.87/year until SLE was diagnosed; after treatment
for SLE was started the frequency decreased to 2.28 attacks/year and entered
into angioedema complete remission after 11.5 months. C1-INH concentra-
tion reached normal values after 12± 2.16 months in all 7 cases where
angioedema preceded SLE diagnosis and remained low in the SLE patient
developing angioedema after SLE was diagnosed. Acquired angioedema
responded best to SLE treatment with hydroxyclorochine or
immunosuppressant
Key words: angioedema, systemic lupus erythematosus
1 Dept. of Immunology-Allergology, Faculty of Medicine, Transylvania University Brasov
1. Background
Angioedema due to an acquired
deficiency in the inhibitor of the first
component of human complement (CI-
INH) is a rare syndrome that is usually
identified as acquired angioedema (AAE).
Compared to hereditary angioedema
(HAE), angioedema due to acquired C1-
inhibitor deficiency is very rare and less is
known in terms of aetiology, evolution and
treatment. Like HAE it can be a life-
threatening disease.
Acquired angioedema is frequently
associated with lymphoproliferative disea-
ses ranging from monoclonal gammo-
pathies of uncertain significance (MGUS)
to non-Hodgkin's lymphoma (NHL) and/or
anti-C1-INH inactivating autoantibodies in
patients with autoimmune disease or
neoplasm [5, 6, 10]. The coexistence of
true B cell malignancy, non-malignant B
cell proliferation and pathogenic auto-

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
56
immune responses suggests that AAE
patients are all affected by altered B cell
proliferation control although their clinical
evolution may vary.
The main pathogenetic mechanisms of
acquired angioedema are represented by
the excessive production of autoantibodies
anti C1INH and/or increased complement
activation with increased consumption of
C1INH [3, 4, 6]. The reduction in C1-INH
leads to activation of the classical comple-
ment pathway and complement consum-
ption, as well as activation of the contact
system leading to the generation of the
vasoactive peptide bradykinin, increased
vascular permeability, and angioedema.
Clinical manifestations in angioedema
due to acquired C1-INH deficiency are
similar to HAE (subcutaneous, non-pruritic
swelling, involvement of the upper
respiratory tract, and abdominal pain due
to partial obstruction of the gastrointestinal
tract), except that laryngeal attacks are
more frequent, thus increasing the potential
life-threatening character of the disease
[12]. Unlike those with HAE, AAE
patients have no family history of
angioedema and are characterised by the
late onset of symptoms and various
responses to treatment due to the
hypercatabolism of C1-INH. Adults or
elderly patients are most commonly
affected [4, 6].
Diagnostic hallmarks for acquired angio-
edema are low plasma C1INH, low C4,
low C1q and normal C3. Low plasma C1q
is the most important feature of acquired
angioedema [13]. Type I AAE is charac-
terised by accelerated catabolism of C1-
INH and type II AAE characterised by the
presence of autoantibodies to C1-INH.
Less is known on the long-term treat-
ment of AAE compared to HAE. The key
to successful management of AAE is the
control of underlying disease. Recent data
showed that AAE in Sjogren syndrome
responds to rituximab [12].
Aim of the study: Incidence and
prognosis of acquired angioedema in patients
with systemic lupus erythematosus (SLE).
Study design: Study group included 48
SLE patients monitored in the Clinical
Immunology Department of Brasov
County Hospital between 2003 and 2007,
mean age 46.10± 14.30 years, 91.67%
females, and mean SLE duration 6.99±5.41
years.
SLE patients were retrospectively
evaluated for:
• incidence of acquired angioedema
• temporal relation between AAE and
SLE diagnosis
• clinical manifestations of acquired
angioedema
• demographic, clinical and immu-
nologic features of SLE in patients
with acquired angioedema compared
to SLE patients with no angioedema
• evolution of AAE under SLE treat-
ment: number of attacks, C1INH
plasma concentration after 1 year of
SLE treatment and C4 plasma concen-
tration after 6 months of SLE
treatment
• evolution of SLE in patients
associating acquired angioedema
Diagnosis of acquired angioedema was
made combining clinical manifestations with
the presence of low plasma C1INH, low
plasma C4 and normal plasma C3 and by
exclusion of monoclonal gammopathies or B
cell lymphoproliferative diseases and of
other known triggers of angioedema (ACE
inhibitors, analgesics and non steroidal anti-
inflammatory drugs). None of the patients
had a family history of angioedema.
SLE was diagnosed according to ARA
criteria and SLE remission according to
ACR criteria.
Plasma C1INH was determined in
collaboration with Pasteur Institute using a
third generation ELISA method (normal
values 0.15-0.35 g/L), C3 and C4
concentrations were determined using an
Acquired Angioedema in Systemic Lupus Erythematosus 57
immune turbidimetric method (normal C 4
values 20-40 mg/dl, normal C3 values 90-
120 mg/dl).
Data were analysed using Chi test
(Statistica 7). Data are presented as median
(range) values unless otherwise stated.
2. Results
8 (16.66%) SLE patients had recurrent
angioedema with no obvious triggers, sex
ratio 1/7 and medium age 45.5±12.61 years
(minimum 24, maximum 65 years). Mean
plasma C1INH concentration at the
diagnosis of acquired angioedema was
0.094±0.039 g/L (normal values 0.15-0.35
g/L) and mean plasma C4 concentration
was 14.42± 4.83 mg/dl (normal values 20-
40 mg/dl).
AAE preceded the diagnosis of SLE in 7
cases with 13.28 ±7.8 months (minimum 6,
maximum 24 months) and 1 case develop-
ped angioedema 15 years after SLE
diagnosis.
Angioedema was localized at face/
eyelids in 5 (62.5%) cases, 3 (37.5%) cases
had laryngeal oedema and 2(25%) cases
had severe abdominal pain. 3 (37.5%)
cases also associated erythematous rash.
The criteria used to diagnose SLE in the
above described patients with acquired
angioedema are presented in table 1.
Table 1: SLE diagnosis in patients with acquired angioedema
Case 1 Butterfly rash, photosensitivity, oral mucosa erosions, non-erosive arthritis,
pericarditis, proteinuria, autoimmune haemolytic anaemia, ANA and anti Sm
antibodies
Case 2 Butterfly rash, photosensitivity, pleurisy, autoimmune thrombocytopenia, ANA and
anti Ro antibodies
Case 3 Butterfly rash, photosensitivity, oral mucosa erosions, non-erosive arthritis, pleurisy,
proteinuria, autoimmune haemolytic anaemia, ANA and anti double stranded DNA
antibodies
Case 4 Photosensitivity, oral mucosa erosions, autoimmune thrombocytopenia, ANA and anti
Sm antibodies
Case 5 Photosensitivity, non-erosive arthritis, proteinuria, ANA and anti Sm antibodies
Case 6 Butterfly rash, photosensitivity, oral mucosa erosions, ANA and anti double stranded
DNA antibodies
Case 7 Photosensitivity, oral mucosa erosions, pleuro-pericarditis, ANA and anti Sm
antibodies
Case 8 Butterfly rash, discoid rash, photosensitivity, oral mucosa erosions, non-erosive
arthritis, pericarditis, proteinuria, autoimmune haemolytic anaemia, ANA and anti Sm
antibodies
Abbreviations: ANA = antinuclear antibodies
There were no significant differences for
age, mean disease duration or sex ratio
between SLE patients with or without
acquired angioedema (table 2).
Immune cytopenias, kidney involvement
and systemic symptoms were more
frequently encountered in SLE patients
with AAE compared to SLE patients with
no angioedema: 6(75%) vs. 13(32.5%)
(p<0.05) for systemic symptoms; 6(75%)
vs. 14(35%) (p<0.05) for immune
cytopenias; 6(75%) vs. 11(27.5%)
(p<0.05) for kidney involvement (table 2).
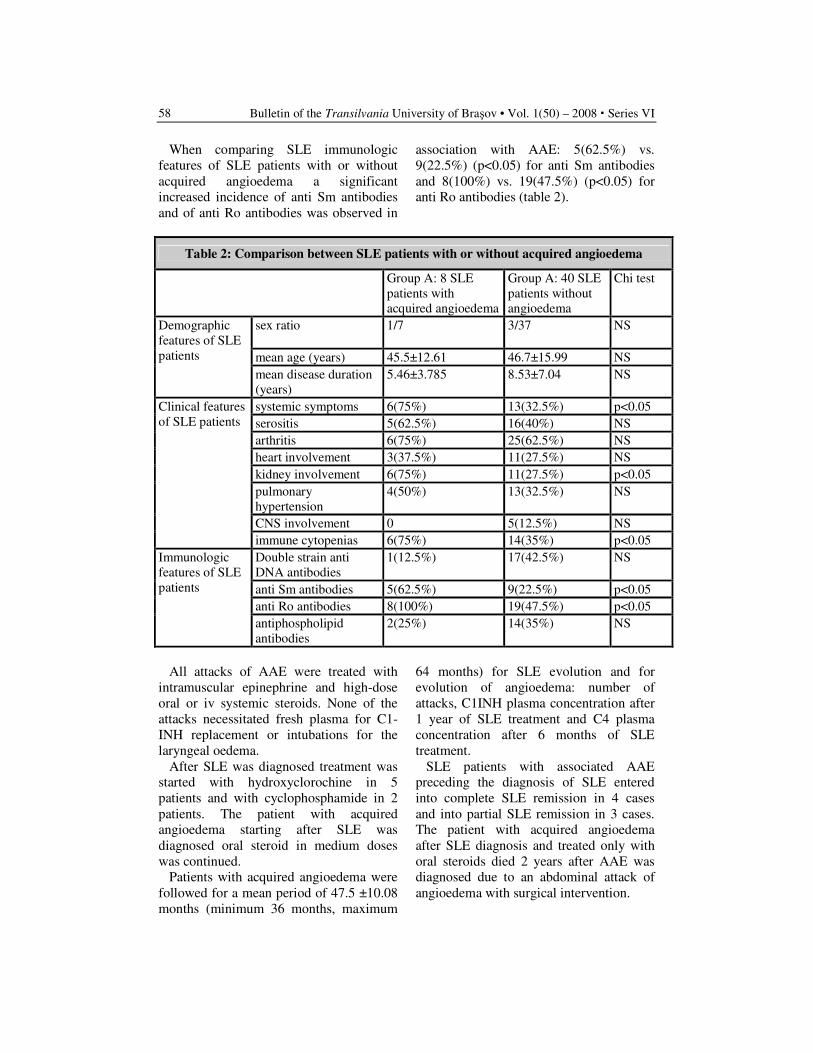
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
58
When comparing SLE immunologic
features of SLE patients with or without
acquired angioedema a significant
increased incidence of anti Sm antibodies
and of anti Ro antibodies was observed in
association with AAE: 5(62.5%) vs.
9(22.5%) (p<0.05) for anti Sm antibodies
and 8(100%) vs. 19(47.5%) (p<0.05) for
anti Ro antibodies (table 2).
Table 2: Comparison between SLE patients with or without acquired angioedema
Group A: 8 SLE
patients with
acquired angioedema
Group A: 40 SLE
patients without
angioedema
Chi test
sex ratio
1/7 3/37 NS
mean age (years) 45.5±12.61 46.7±15.99 NS
Demographic
features of SLE
patients
mean disease duration
(years)
5.46±3.785 8.53±7.04 NS
systemic symptoms 6(75%) 13(32.5%) p<0.05
serositis 5(62.5%) 16(40%) NS
arthritis 6(75%) 25(62.5%) NS
heart involvement 3(37.5%) 11(27.5%) NS
kidney involvement 6(75%) 11(27.5%) p<0.05
pulmonary
hypertension
4(50%) 13(32.5%) NS
CNS involvement 0 5(12.5%) NS
Clinical features
of SLE patients
immune cytopenias 6(75%) 14(35%) p<0.05
Double strain anti
DNA antibodies
1(12.5%) 17(42.5%) NS
anti Sm antibodies 5(62.5%) 9(22.5%) p<0.05
anti Ro antibodies 8(100%) 19(47.5%) p<0.05
Immunologic
features of SLE
patients
antiphospholipid
antibodies
2(25%) 14(35%) NS
All attacks of AAE were treated with
intramuscular epinephrine and high-dose
oral or iv systemic steroids. None of the
attacks necessitated fresh plasma for C1-
INH replacement or intubations for the
laryngeal oedema.
After SLE was diagnosed treatment was
started with hydroxyclorochine in 5
patients and with cyclophosphamide in 2
patients. The patient with acquired
angioedema starting after SLE was
diagnosed oral steroid in medium doses
was continued.
Patients with acquired angioedema were
followed for a mean period of 47.5 ±10.08
months (minimum 36 months, maximum
64 months) for SLE evolution and for
evolution of angioedema: number of
attacks, C1INH plasma concentration after
1 year of SLE treatment and C4 plasma
concentration after 6 months of SLE
treatment.
SLE patients with associated AAE
preceding the diagnosis of SLE entered
into complete SLE remission in 4 cases
and into partial SLE remission in 3 cases.
The patient with acquired angioedema
after SLE diagnosis and treated only with
oral steroids died 2 years after AAE was
diagnosed due to an abdominal attack of
angioedema with surgical intervention.

Acquired Angioedema in Systemic Lupus Erythematosus 59
Patients evolved with a medium of
angioedema attacks of 6.87/year until SLE
was diagnosed. After treatment for SLE
was started the frequency decreased to
2.28 attacks/year and angioedema entered
into complete remission after 11.5 months
in all the 7 cases were angioedema pre-
ceded SLE diagnosis. The patient with
acquired angioedema starting after SLE
was diagnosed continued to experience
frequent and severe angioedema attacks.
C1-INH concentration reached normal
values (mean values 0.24±0.05 g/L,
minimum 0.19 g/L, maximum 0.34 g/L)
after 12± 2.16 months in all the 7 cases
with acquired angioedema preceding SLE
and remained low in the SLE patient
developing AAE after SLE diagnosis,
despite steroids used to treat SLE. C4
increased after SLE treatment was started
from 14.42 ± 4.83 mg/dL to 25.24 ± 8.6
mg/dL (normal C4 values 20-40 mg.dL)
after 7.28± 2.92 months in all 7 cases were
angioedema preceded SLE diagnosis. The
patient with AAE starting after SLE was
diagnosed and treated only with medium
doses oral steroids continued to have low
C4 concentrations.
3. Discussion
The incidence of AAE in SLE patients in
this study (16.66%) is higher compared to
other reports from literature (4%) [7]. This
may be due to the fact that 7 patients out of
8 were first diagnosed with AAE and
afterwards observed for SLE development.
Other studies included patients with
already diagnosed SLE and observed the
incidence of AAE during SLE evolution.
Due to the fact that antibodies against
C1-INH were not measured the differential
diagnosis between type I AAE character-
rised by accelerated catabolism of C1-INH
and type II AAE characterised by the
presence of autoantibodies to C1-INH
could not be done. However, from the
clinical standpoint this distinction is not
always useful and the incidence of
autoantibodies to C1-INH in SLE seems
very low, compared to the functional
deficit of C1-INH which seems to be the
main mechanism of angioedema in SLE [1,
7, 9]. A study of eight SLE patients with
persistently low levels of C4 antigen
showed a normal level of C1-INH antigen
but an abnormal profile of C1-INH
function in seven including dysfunctional
inhibition of C1r and/or C1s and increased
functional levels against C1s [8].
This article reports on 8 patients with
SLE and acquired angioedema and
pinpoints the evolution of acquired
angioedema preceding SLE full
development with several years,
concordant with other case reports in
literature [11]. Thus, all patients with this
rare condition and no obvious cause (B cell
lymphoma or monoclonal gammopathy)
should be followed for SLE development.
SLE patients associating acquired angio-
edema have a peculiar profile with increased
incidence of immune cytopenias, kidney
involvement and systemic symptoms,
normal C3 concentration and anti Ro and
anti Sm antibodies. In these SLE patients
development of antibodies anti C1INH
should be actively seek and treatment with
drugs with potential induction of angioedema
(ACE inhibitors, analgesics, NSAIDS) at
least cautioned.
In the present study there were no life-
threatening events due to angioedema,
except the death due the abdominal attack
of angioedema with surgical intervention.
This is in contrast with other reports
highlighting the severity of AAE in SLE
patients [9, 11]. There were no obvious
triggers of AAE attacks in contrast with
other reports showing infections as main
triggers [11]. As in other observations the
frequency of the attacks was closely
correlated with SLE activity.
In a previous report high dose steroids in
conjunction with immunosupressants were
needed to control AAE in an SLE patient
[11]. In our study acquired angioedema
responded best to SLE treatment with

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
60
hydroxyclorochine or immunosuppressant
and did not respond to respond to medium
doses oral steroids.
References
1. Cicardi, M, Bisiani, G, Cugno, M,
Spath, P, Agostini, A.: Autoimmune C1
inhibitor deficiency: report of eight
patients. In: Am J Med 1993; 95:
169-175.
2. Cicardi, M, Zingale, L.C., Pappalardo,
E., Folcione, A., Agostoni, A.:
Autoantibodies and lympho-
proliferative diseases in acquired C1-
inhibitor deficiencies. In: Medicine
(Baltimore) 2003; 82:274-81.
3. Cheng, W.Y., Smith, W.B., Russell,
W.J.: Acute upper airway obstruction
from acquired angioedema. In: Emerg
Med Australas. 2007; 19 :65-7.
4. Cugno, M., Castelli, R., Cicardi, M.:
Angioedema due to acquired C1-
inhibitor deficiency: A bridging condi-
tion between autoimmunity and lym-
phoproliferation. In: Autoimmun Rev.
2008; 8:156-9.
5. Greaves, M., Lawlor, F.: Angioedema:
manifestations and management. In: J
Am Acad Dermatol 1991; 25:155-61.
6. Jazwinska, E.C., Gatenby, P.A.,
Dunckley, H., Serjeantson, S.W.: C1
inhibitor functional deficiency in
systemic lupus erythematosus (SLE). In:
Clin Exp Immunol 1993; 93: 968 – 973.
7. Lahiri, M., Lim, A.Y.: Angioedema
and systemic lupus erythematosus--a
complementary association? In: Ann
Acad Med Singapore. 2007;36:142-5.
8. Malbran, A, Hammer, C.H., Frank,
M.M., Fries, L.F.: Acquired
angioedema: observations on the
mechanism of action of autoantibodies
directed against C1 esterase inhibitor.
In: J Allergy Clin Immunol 1988; 81:
1199-204.
9. Markovic, S.N., Inwards, D.J., Frigas,
E.A., Phyliky, R.P.: Acquired C1
esterase inhibitor deficiency. In: Ann
Intern Med 2000;132:144-50.
10. Nzeako, U.C., Frigas, E., Tremaine,
W.J.: Hereditary angioedema: a
broad review for clinicians. In: Arch
Intern Med 2001;161:2417-29.
11. Odi-Ros, J., Paredes, J., Detarsio, G.,
Vilardell, M.: Autoantibodies to C1
inhibitor in patients with lupus
disease. In: J Rheumatol 1997; 24:
1856 ± 1858.
12. Sánchez-Cano, D., Callejas-Rubio,
J.L., Lara-Jiménez, M.A., López-
Trascasa, M., Circadi, M., Ortego-
Centeno, N.: Successful use of
rituximab in acquired C1 inhibitor
deficiency secondary to Sjogren's
syndrome. In: Lupus. 2008; 17: 228-9.
13. Thong, B.Y.H., Thumboo, J., Howe,
H.S., Feng, P.H.: Life-threatening
angioedema in systemic lupus
erythematosus. In: Lupus 2001; 10;
304-308.
THE RELATIONSHIP BETWEEN THE RISK
PROFILE OF ARTERIAL HYPERTENSION
AND THE FEATURES OF METABOLIC
SYNDROME-STUDY ON 129 PATIENTS
G. IFTENI
1 H. RUS
1
M. RADOI1 G. PAMFIL
2
Abstract: The objective of study was to assess the severe evolution of
arterial hypertension evaluated by ambulatory blood pressure monitoring in
middle aged hypertensive patients with metabolic syndrome and its
relationship with anthropometric and biochemical parameters and with the
presence of type 2 diabetes mellitus.
Methods: 129 hypertensive patients diagnosed with metabolic syndrome (MetS)
according to the Adult Treatment Panel (ATP) III criteria were evaluated by
ambulatory blood pressure monitoring (ABPM) parameters: 24-hour variability
(diurnal index), heart rate, pulse pressure; anthropometric parameters: body
mass index, waist circumference and laboratory data: serum levels of
triglycerides, cholesterol, LDL-cholesterol, HDL-cholesterol, uric acid. Statistical
analysis including two-taliled Student test-t for comparison of means between two
groups and multivariate logistic regression analysis was performed to identify
independent predictors for the evolution with diurnal index lower than 10% (non-
dipper status).
Results: the non-dipper status was present in 76% of the hypertensive patients
with MetS, significantly frequent in patients with type 2 diabetes mellitus
(p=0.0033). The „non-dipper” status was associated with increased mean values
of waist circumference (121.17 cm versus 115.29 cm, p=0.0245), body mass index
(32.19 kg/m² versus 28.65 kg/m², p=0.0003), duration of diabetes mellitus (2.89
years versus 1.45 years, p=0.0338), heart rate (75.86 beats/min versus 71.13
beats/min, p=0.0467) and triglycerides (266.11mg/dL versus 220.87 mg/dL, p=
0.0078). Independent risk predictors for nondipping status were body mass index
and triglyceride levels (p<0.0001).
Conclusion: In hypertensive patients with MetS the risc for „non-dipper” status is
in relation with increasing of waist circumference, body mass index, heart rate,
triglycerides and with the presence and duration of type 2 diabetes mellitus.
Key words: arterial hypertension, metabolic syndrom.
1 Transilvania University of Brasov, Dep of Internal Medicina. 2 Medical College, Brasov.
1. Background
The National Cholesterol Education
Program (NCEP)-Adult Treatment Panel
(ATP) III [16] considered obesity as
epidemic and the association with
cardiovascular risk as the characteristic of
the metabolic syndrome. The ATP III
criteria for the diagnosis of metabolic
syndrome are based on the categorial

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
62
presence of at least 3 of the following 5
criteria: abdominal obesity (waist
circumference >102 cm in men, and >88 in
women), arterial hypertension (history of
hypertension, systolic blood pressure ≥130
mmHg, and diastolic blood pressure ≥85
mmHg), impaired fasting glucose (fasting
blood glucose level >110 mg/dL), impared
glucose tolerance or type 2diabetes mellitus,
hypertriglyceridemia (>150 mg/dL), low
high-density lioprotein-cholesterol (HDL-C).
Large scales of clinical trials reveald that
hypertension is a classical risk factor for
cardiovascular diseases. The close
relationship of hypertension with glucose
intolerance and diabets melitus type 2 was
observed in epidemiological trials. Further
more, the sub-group of hypertensive subjects
with the lack of nocturnal decline in blood
pressure was reffered as ”non-dipping
pattern” and has been associated with a
greater extent of target organ damages [1,2].
Despite the high frecquency of the „non-
dipping” pattern in diabetes mellitus [12]
and its close relationship with insuline
resistance [4], the association of „non-
dipping” pattern with metabolic syndrome
failed to be proven by some authors [3].
2. Objectives
The present study aimed to examine the
relationship between the risk profile of
arterial hypertension assesed by ambulatory
blood pressure monitoring and the defining
features of metabolic syndrome using the
ATP III criteria for diagnosis.
3. Methods
The study population included 129
patients diagnosed with arterial
hypertension and metabolic syndrome.
Metabolic syndrome was evaluated
according to NCEP-ATP III criteria.
Patients agreed to participate to the study
procedures. Patients with one of the
following conditions such as secondary
hypertension, congestive heart failure,
previous myocardial infarction, cardiac
valve disease, chronic renal failure and any
condition preventing technically adequate
ABPM (atrial fibrillation, other arrhythmias)
were excluded from the study. The patients
were evaluated by detailed questionnaire and
physical examination. The questionnaire
provided information about cardiovascular
risk factors such as smoking and diabetes
mellitus and about past medical history
regarding hypertension duration and its
medical treatment. ABPM was carried out on
the non dominant arm using Schiller BR-102
plus device after validation of its readings.
Recordings were analyzed to obtain 24 hour
daytime and nighttime averages of systolic
blood pressure (SBP), diastolic blood
pressure (DBP), mean arterial blood pressure
(MABP), the degree of day-night decrease in
SBP and DBP, pulse pressure (PP), mean
heart rate (HR). Nocturnal “non-dipping”
refers to a 10% or lesser magnitude reduction
(diurnal index) in average SBP and/or DBP
during the night compared with daytime SBP
average values. Statistical analysis was
carried out using Statistical 6 programs.
Comparison of parametric values between
two groups was performed by means of two-
tailed Student`S t-test. Multivariate logistic
regression analysis was used to identify
independent predictors for the development
of “non-dipping” status. A value of p<0.05
was considered statistically significant.
4. Results
The study population consists of 66 women
(51.2%) with mean age of 55.4 years, and
63 men (48.8%) with mean age of 50.6 years.
Diabetes mellitus was diagnosed in
65 patients (50.4). The study population was
divided in two groups according to the values
of diurnal index (DI). Group 1 included
98 patients (76%) with „non-dipper” status
(DI ≤10%) and group 2, 31 patients (24%)
with „dipper” status (DI >10%).
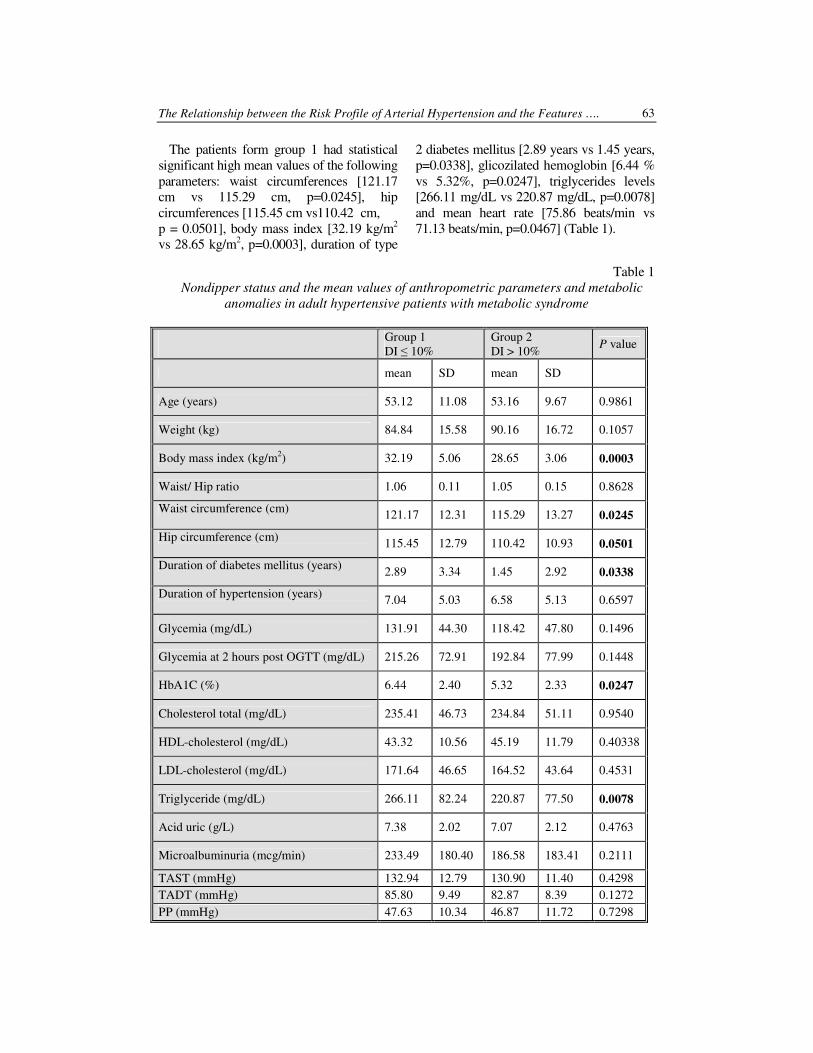
The Relationship between the Risk Profile of Arterial Hypertension and the Features …. 63
The patients form group 1 had statistical
significant high mean values of the following
parameters: waist circumferences [121.17
cm vs 115.29 cm, p=0.0245], hip
circumferences [115.45 cm vs110.42 cm,
p = 0.0501], body mass index [32.19 kg/m2
vs 28.65 kg/m2, p=0.0003], duration of type
2 diabetes mellitus [2.89 years vs 1.45 years,
p=0.0338], glicozilated hemoglobin [6.44 %
vs 5.32%, p=0.0247], triglycerides levels
[266.11 mg/dL vs 220.87 mg/dL, p=0.0078]
and mean heart rate [75.86 beats/min vs
71.13 beats/min, p=0.0467] (Table 1).
Table 1
Nondipper status and the mean values of anthropometric parameters and metabolic
anomalies in adult hypertensive patients with metabolic syndrome
Group 1
DI ≤ 10%
Group 2
DI > 10% P value
mean SD mean SD
Age (years) 53.12 11.08 53.16 9.67 0.9861
Weight (kg) 84.84 15.58 90.16 16.72 0.1057
Body mass index (kg/m2) 32.19 5.06 28.65 3.06 0.0003
Waist/ Hip ratio 1.06 0.11 1.05 0.15 0.8628
Waist circumference (cm) 121.17 12.31 115.29 13.27 0.0245
Hip circumference (cm) 115.45 12.79 110.42 10.93 0.0501
Duration of diabetes mellitus (years) 2.89 3.34 1.45 2.92 0.0338
Duration of hypertension (years) 7.04 5.03 6.58 5.13 0.6597
Glycemia (mg/dL) 131.91 44.30 118.42 47.80 0.1496
Glycemia at 2 hours post OGTT (mg/dL) 215.26 72.91 192.84 77.99 0.1448
HbA1C (%) 6.44 2.40 5.32 2.33 0.0247
Cholesterol total (mg/dL) 235.41 46.73 234.84 51.11 0.9540
HDL-cholesterol (mg/dL) 43.32 10.56 45.19 11.79 0.40338
LDL-cholesterol (mg/dL) 171.64 46.65 164.52 43.64 0.4531
Triglyceride (mg/dL) 266.11 82.24 220.87 77.50 0.0078
Acid uric (g/L) 7.38 2.02 7.07 2.12 0.4763
Microalbuminuria (mcg/min) 233.49 180.40 186.58 183.41 0.2111
TAST (mmHg) 132.94 12.79 130.90 11.40 0.4298
TADT (mmHg) 85.80 9.49 82.87 8.39 0.1272
PP (mmHg) 47.63 10.34 46.87 11.72 0.7298
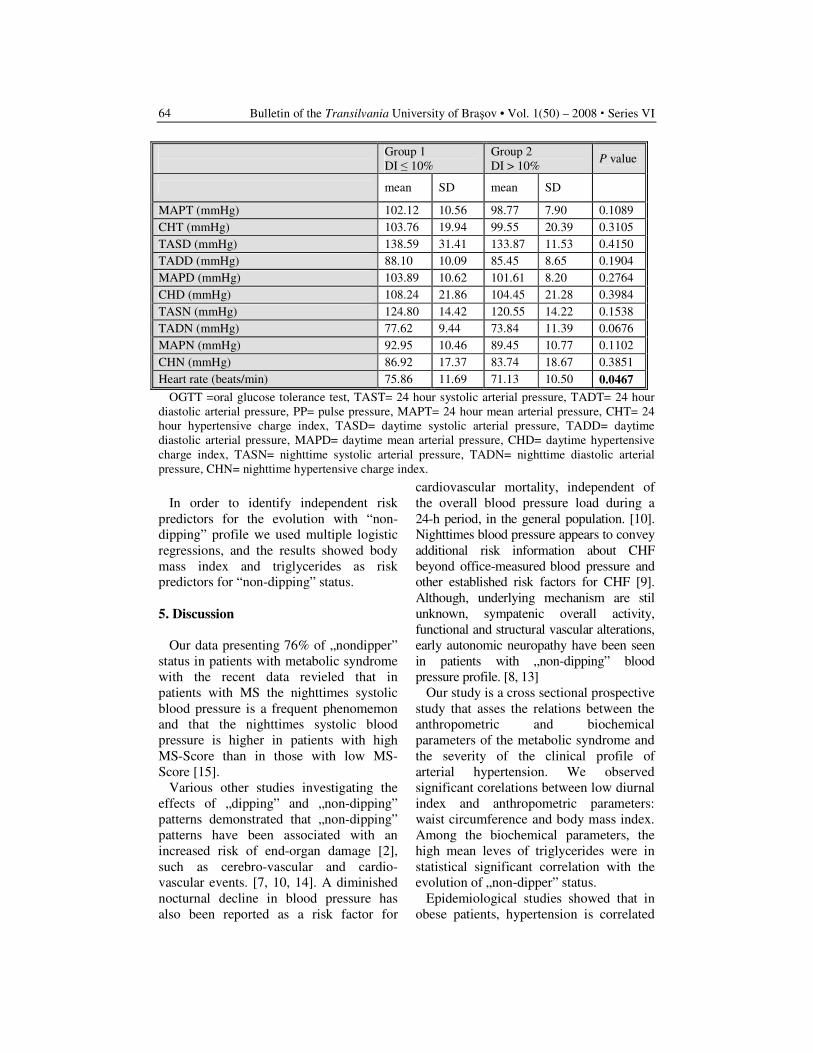
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
64
Group 1
DI ≤ 10%
Group 2
DI > 10% P value
mean SD mean SD
MAPT (mmHg) 102.12 10.56 98.77 7.90 0.1089
CHT (mmHg) 103.76 19.94 99.55 20.39 0.3105
TASD (mmHg) 138.59 31.41 133.87 11.53 0.4150
TADD (mmHg) 88.10 10.09 85.45 8.65 0.1904
MAPD (mmHg) 103.89 10.62 101.61 8.20 0.2764
CHD (mmHg) 108.24 21.86 104.45 21.28 0.3984
TASN (mmHg) 124.80 14.42 120.55 14.22 0.1538
TADN (mmHg) 77.62 9.44 73.84 11.39 0.0676
MAPN (mmHg) 92.95 10.46 89.45 10.77 0.1102
CHN (mmHg) 86.92 17.37 83.74 18.67 0.3851
Heart rate (beats/min) 75.86 11.69 71.13 10.50 0.0467
OGTT =oral glucose tolerance test, TAST= 24 hour systolic arterial pressure, TADT= 24 hour
diastolic arterial pressure, PP= pulse pressure, MAPT= 24 hour mean arterial pressure, CHT= 24
hour hypertensive charge index, TASD= daytime systolic arterial pressure, TADD= daytime
diastolic arterial pressure, MAPD= daytime mean arterial pressure, CHD= daytime hypertensive
charge index, TASN= nighttime systolic arterial pressure, TADN= nighttime diastolic arterial
pressure, CHN= nighttime hypertensive charge index.
In order to identify independent risk
predictors for the evolution with “non-
dipping” profile we used multiple logistic
regressions, and the results showed body
mass index and triglycerides as risk
predictors for “non-dipping” status.
5. Discussion
Our data presenting 76% of „nondipper”
status in patients with metabolic syndrome
with the recent data revieled that in
patients with MS the nighttimes systolic
blood pressure is a frequent phenomemon
and that the nighttimes systolic blood
pressure is higher in patients with high
MS-Score than in those with low MS-
Score [15].
Various other studies investigating the
effects of „dipping” and „non-dipping”
patterns demonstrated that „non-dipping”
patterns have been associated with an
increased risk of end-organ damage [2],
such as cerebro-vascular and cardio-
vascular events. [7, 10, 14]. A diminished
nocturnal decline in blood pressure has
also been reported as a risk factor for
cardiovascular mortality, independent of
the overall blood pressure load during a
24-h period, in the general population. [10].
Nighttimes blood pressure appears to convey
additional risk information about CHF
beyond office-measured blood pressure and
other established risk factors for CHF [9].
Although, underlying mechanism are stil
unknown, sympatenic overall activity,
functional and structural vascular alterations,
early autonomic neuropathy have been seen
in patients with „non-dipping” blood
pressure profile. [8, 13]
Our study is a cross sectional prospective
study that asses the relations between the
anthropometric and biochemical
parameters of the metabolic syndrome and
the severity of the clinical profile of
arterial hypertension. We observed
significant corelations between low diurnal
index and anthropometric parameters:
waist circumference and body mass index.
Among the biochemical parameters, the
high mean leves of triglycerides were in
statistical significant correlation with the
evolution of „non-dipper” status.
Epidemiological studies showed that in
obese patients, hypertension is correlated

The Relationship between the Risk Profile of Arterial Hypertension and the Features …. 65
with high body mass index. In the
Framingham study, 70% of the new cases
of hypertension were related to the excess
of adipose tissue [6] and 78% of cases of
hypertension in men and 65% in women
were attributed to obesity. Other popula-
tional studies showed that arterial pressure
measured at office is closely related with
body mass index and waist/hip ratio [5].
Kotsis et al observed that 55% of patients
with normal weight had „dipper” profile in
contrast to 35% of the obese patients. In
the group of patients with normal blood
pressure after blood pressure measuring at
the office or using ABPM, the „dipper”
status was found in 60% of the
underweight patients, 58.6% of normal
weight subjects, 30.6% of overweight and
28% of the obese patients. In the
hypertensive group the „dipper” status was
found in 50.8% of the underweight
patients, 38.5% of normal weight, 30.5%
of overweight and 27.3% of the obese
patients [11].
Conclusions
In hypertensive patients with metabolic
syndrome the risk of „nondipper” status is
in relationship with increased waist
circumference, body mass index, heart
rate, triglycerides and with the presence
and duration of type 2 diabetes mellitus.
References
1. Bianchi, S., Bigazzi, R., Baldari, G.,
Sgherri, G., Campese, V.M.: Diurnal
variation of blood pressure and
microalbuminuria in essential
hypertension. In: Am J Hypertens
1994; 7: 23-29.
2. Cuspidi, C., Meani, S., Fussi, V.,
Severgnini, B., Valerio, C., Catini, E.,
Leonetti, G., Magrini, F., Zanchetti,
A.: Metabolic synddrome and target
organ damage in untreated essentila
hypertensives. In: J Hypertens
2004a;22:1991-1998.
3. Cuspidi, C., Meani, S., Fussi, V.,
Severgnini, B., Valerio, C., Catini, E.,
Sala, C., Magnaghi, F., Zanchetti, A.:
Is the nocturnal fall in blood pressure
reduced in essential hypertensive
patients with metabolic syndrome? In:
Blood Press. 2004c; 13: 230-235.
4. Della Mea, P., Luia, M., Bandolin, V.,
Guzzon, S., Sonino, N., Vettor, R.,
Fallo, F.: Adiponectin, insulin
resistance and left ventricular
structure in dipper and nondipper
essential hypertensives patients. In:
Am J Hypertens 2005; 18: 30-35.
5. Doll, S., Paccaud, F., Bovet, P.,
Burnier, M., Wietlisbach, V. Body
mass index, abdominal adiposity and
blood pressure: consistency of their
association across developing and
developed countries. In: Int J Obes
Relat Metab Disord. 2002; 26: 48-57.
6. Garrison, R.J., Kannel, W.B., Stokes,
J., Castelli, W.P.: Incidence and
precursors of hypertension in young
adults: the Framingham Offspring
Study. In: Prev Med 1978; 16: 235-
251.
7. Higashi, Y., Nakagawa, K., Kimura,
M., Noma, K., Hara, K., Sasaki, S.,
Goto, C., Oshima, T., Chayama, K.,
Yoshizumi, M.: Circadian variation of
blood pressure and endotelial function
in patients with essential hypertension
a comparison of dippers and non-
dippers. In: J Am. Coll. Cardiol. 2002;
40: 2039-2043.
8. Hommel, E., Mathiesen, E.R., Giese,
J., Niesen, M.D., Schutten, H.,
Parving, H.H.: On the pathogenesis of
arterial blood pressure elevation early
in the course of diabetic nephropathy.
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
66
In: Scand J Clin Lab Invest 1989; 49:
537-544.
9. Ingelsson, E., Björklund-Bodegård,
K., Lind, L., Ärnlöv, J., Sundström, J.:
Diurnal Blood Pressure Pattern and
Risk of Congestive Heart Failure. In:
JAMA. 2006; 295: 2859-2866.
10. Kario, K., Pickering T.G., Matsuo T.,
Hoshide S., Schwartz J.E., Shimada K.
Stroke prognosis and abnormal
nocturnal blood pressure falls in older
hypertensives. Hypertension 2001; 38:
852-857.
11. Kotsis, V., Stabouli, S., Bouldin, M.,
Low, A., Toumanidis, S., Zakopoulos,
N.: Impact of obesity on 24-Hour
Ambulatory Blood Pressure and
Hypertension. In: Hypertension 2005;
45: 602-607.
12. Perk, G., Meckler, J., Ben Ishay, D.,
Bursztyn, M.: Non dipping in diabetic
patients: insights from the siesta. In: J
Hum Hypertens 2002; 16: 435-438.
13. Sherwood, A., Steffen, P.R.,
Blumenthal, J.A., Kuhn, C.,
Hinderliter, A.L.: Night time blood
pressure dipping the role of the
sympatetic nervous sistem. In: Am J
Hypertens 2002; 15 :111-118.
14. Staessen, J.A., Thijs, L., Fagard, R.,
O’Brian, E.T., Clement, D., de Leeuw,
P.W., Mancia, G., Nachev, G.,
Palatini, P., Tuomilehto J., Webster,
J.: Predicting cardiovascular risk
using conventional vs ambulatory
blood pressure in older patients with
systolic hypertension. In: JAMA 1999;
282: 539-546.
15. Tartan, Z., Uyarel, H., Kasikcioglu,
H., Alper, A.T., Ozay, B., Bilsel, T.,
Gul, M., Recep, Ozturk, R., Cam, N.:
Metabolic Syndrome as a Predictor of
Non-Dipping Hypertension. In: The
Tohoku Journal of Experimental
Medicine 2006; 210 (1):57-66.
16. *** NCEP. Expert panel on detection,
evaluation and treatment of high
blood pressure in adults. Executive
summary of the third report of the
National Cholesterol Education
Program (NCEP) expert panel on
detection and evaluation and
treatment of high blood cholesterol in
adults (Adult Treatment Panel III). In:
JAMA 2001;285:2486-2497.

HYPERTHYROIDISM AT DEBUT AND
THE LEFT VENTRICLE MASS
C. SCARNECIU
1 L. NEDELCU
1
I. SCARNECIU2 V. SCARNECIU
3
Abstract: It’s a well known fact that thyroidian hormones stimulate by
direct nuclear action the production of proteins in general, which can lead to
cardiac hypertrophy. We have performed a prospective study on 72
hyperthyroidian patients with ages between 18 and 49 years, newly
diagnosed, without cardiovascular problems of other nature. These patients
were ecocardigraphicaly evaluated at admission and after receiving the
euthyroidism results, these were compared to a control lot formed out of 25
persons. Through 2D ecography a dimension increase in the left ventricle
was observed in all hyperthyroidian patients, on 66% reaching sizes that
define hypertrophy. The increasing of the left ventricle was symmetric,
affecting the septum as well as the ventricular walls. The increasing
procentage was about 25% on average being correlated with the level of
thyroidian hormones and not the disease duration or the type of affliction.
The left ventricular mass grows early in thyreotoxicosis, proportional with
the level of thyroidian hormones and not the type of disease, this being at
least partially reversible when reaching euthyroidism
Key words: thyreotoxicosis, hypertrophy, reversible, left ventricle.
1 Transilvania University of Brasov, Faculty of Medicine, Dep of Internal Medicine. 2 Transilvania University of Brasov, Faculty of Medicine, Dep of Urology. 3 Transilvania University of Brasov, Faculty of Medicine.
Introduction
It’s a well known fact that thyrodidian
hormones through direct nuclear action
stimulate the production of proteins in
general, leading to cardiac hypertrophy.
Through ecographic study we wanted to
highlight if the effect appears early and
what its scale is. Also we wanted to verify
if the effect is reversible when reaching
euthyroidism.
Material and Method
We have performed a study on newly
diagnosed patients with clinical manifested
hyperthyroidism, admitted throughout a
period of 3.5 years at the Endocrinology
Clinic, part of the Emergency County
Hospital Brasov which were selected in
order that they would not present any
cardiovascular affliction of any other
origin or hypekinethical syndrome, with
ages between 18 and 49 (36.7 years
average) and with a 3.39 month period
until the diagnostic was presented and a
free fraction average value of the
thyritoxin(FT4) of 58,76pmol/l.
The 72 hyperthyroidian patients newly
diagnosed have formed the H lot which
was biochemical and ecographical
evaluated at admission and after a period
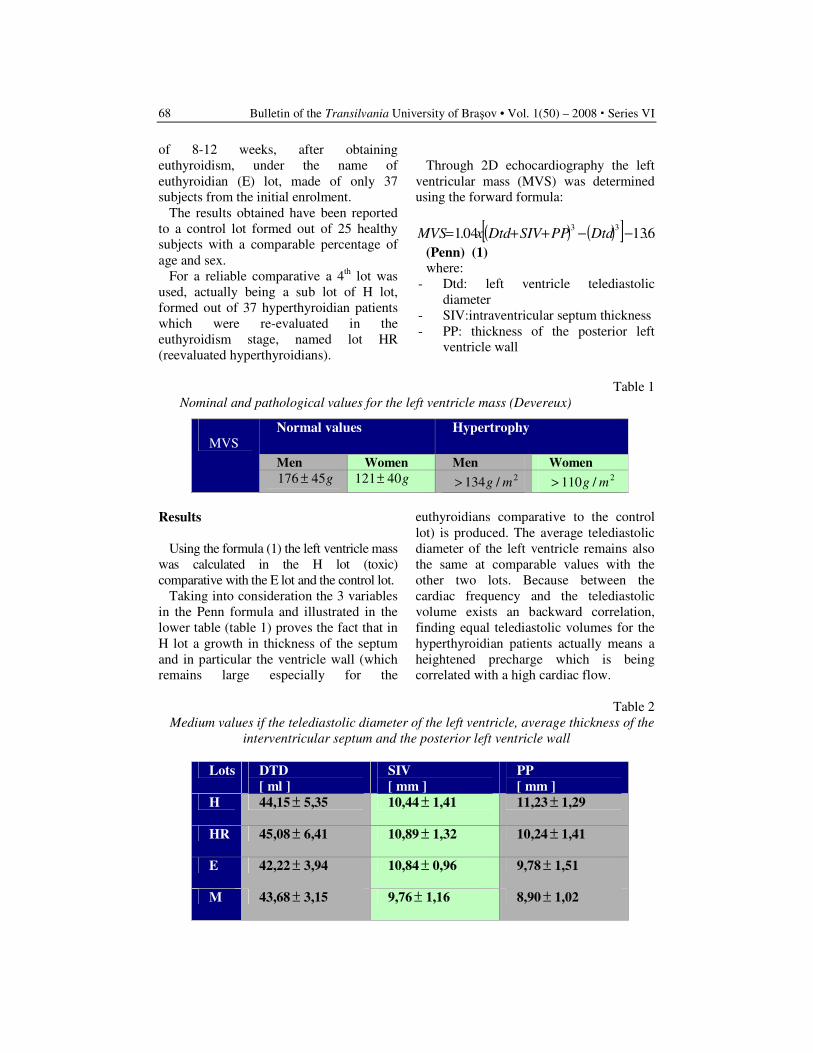
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
68
of 8-12 weeks, after obtaining
euthyroidism, under the name of
euthyroidian (E) lot, made of only 37
subjects from the initial enrolment.
The results obtained have been reported
to a control lot formed out of 25 healthy
subjects with a comparable percentage of
age and sex.
For a reliable comparative a 4th lot was
used, actually being a sub lot of H lot,
formed out of 37 hyperthyroidian patients
which were re-evaluated in the
euthyroidism stage, named lot HR
(reevaluated hyperthyroidians).
Through 2D echocardiography the left
ventricular mass (MVS) was determined
using the forward formula:
( ) ( )[ ] 6.1304.133
−−++= DtdPPSIVDtdxMVS
(Penn) (1)
where:
- Dtd: left ventricle telediastolic
diameter
- SIV:intraventricular septum thickness
- PP: thickness of the posterior left
ventricle wall
Table 1
Nominal and pathological values for the left ventricle mass (Devereux)
Normal values Hypertrophy
Men Women Men Women
MVS
g45176 ± g40121± 2/134 mg>
2/110 mg>
Results
Using the formula (1) the left ventricle mass
was calculated in the H lot (toxic)
comparative with the E lot and the control lot.
Taking into consideration the 3 variables
in the Penn formula and illustrated in the
lower table (table 1) proves the fact that in
H lot a growth in thickness of the septum
and in particular the ventricle wall (which
remains large especially for the
euthyroidians comparative to the control
lot) is produced. The average telediastolic
diameter of the left ventricle remains also
the same at comparable values with the
other two lots. Because between the
cardiac frequency and the telediastolic
volume exists an backward correlation,
finding equal telediastolic volumes for the
hyperthyroidian patients actually means a
heightened precharge which is being
correlated with a high cardiac flow.
Table 2
Medium values if the telediastolic diameter of the left ventricle, average thickness of the
interventricular septum and the posterior left ventricle wall
Lots DTD
[ ml ]
SIV
[ mm ]
PP
[ mm ]
H 44,15 ± 5,35 10,44 ± 1,41 11,23 ± 1,29
HR 45,08 ± 6,41 10,89 ± 1,32 10,24 ± 1,41
E 42,22 ± 3,94 10,84 ± 0,96 9,78 ± 1,51
M 43,68 ± 3,15 9,76 ± 1,16 8,90 ± 1,02
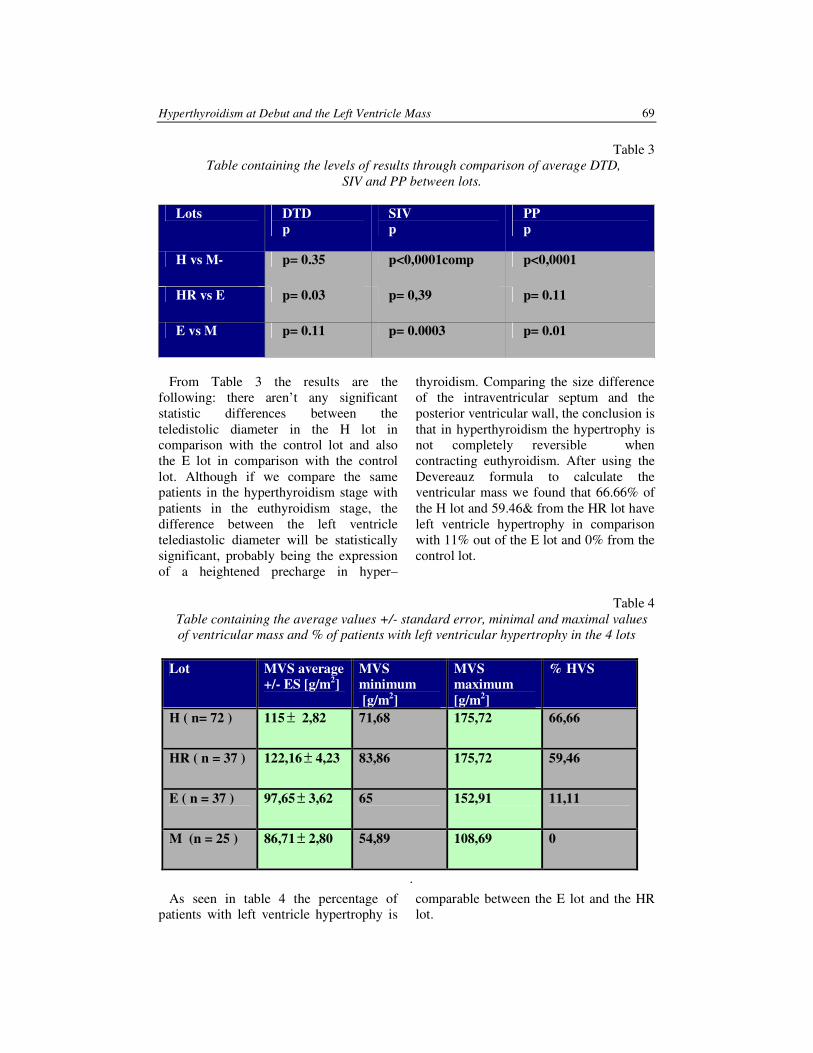
Hyperthyroidism at Debut and the Left Ventricle Mass 69
Table 3
Table containing the levels of results through comparison of average DTD,
SIV and PP between lots.
Lots DTD
p
SIV
p
PP
p
H vs M- p= 0.35 p<0,0001comp p<0,0001
HR vs E p= 0.03 p= 0,39 p= 0.11
E vs M p= 0.11 p= 0.0003 p= 0.01
From Table 3 the results are the
following: there aren’t any significant
statistic differences between the
teledistolic diameter in the H lot in
comparison with the control lot and also
the E lot in comparison with the control
lot. Although if we compare the same
patients in the hyperthyroidism stage with
patients in the euthyroidism stage, the
difference between the left ventricle
telediastolic diameter will be statistically
significant, probably being the expression
of a heightened precharge in hyper–
thyroidism. Comparing the size difference
of the intraventricular septum and the
posterior ventricular wall, the conclusion is
that in hyperthyroidism the hypertrophy is
not completely reversible when
contracting euthyroidism. After using the
Devereauz formula to calculate the
ventricular mass we found that 66.66% of
the H lot and 59.46& from the HR lot have
left ventricle hypertrophy in comparison
with 11% out of the E lot and 0% from the
control lot.
Table 4
Table containing the average values +/- standard error, minimal and maximal values
of ventricular mass and % of patients with left ventricular hypertrophy in the 4 lots
Lot MVS average
+/- ES [g/m2]
MVS
minimum
[g/m2]
MVS
maximum
[g/m2]
% HVS
H ( n= 72 ) 115 ± 2,82 71,68 175,72 66,66
HR ( n = 37 ) 122,16 ± 4,23 83,86 175,72 59,46
E ( n = 37 ) 97,65 ± 3,62 65 152,91 11,11
M (n = 25 ) 86,71 ± 2,80 54,89 108,69 0
.
As seen in table 4 the percentage of
patients with left ventricle hypertrophy is
comparable between the E lot and the HR
lot.
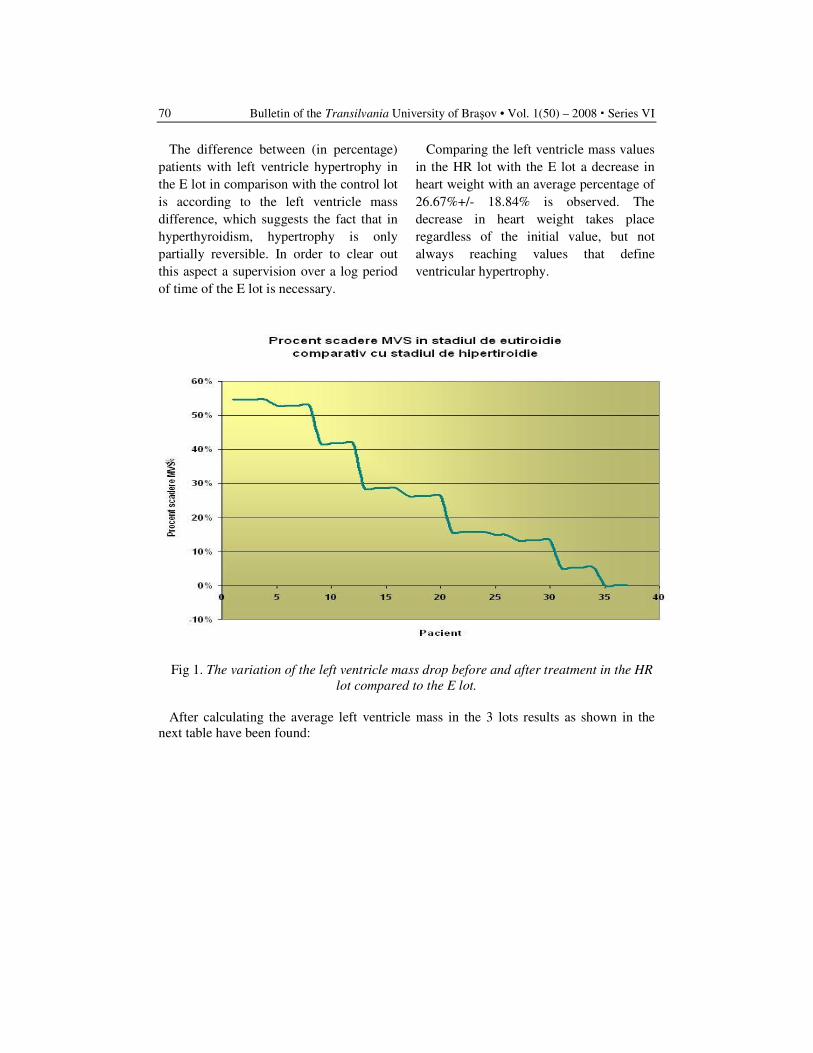
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
70
The difference between (in percentage)
patients with left ventricle hypertrophy in
the E lot in comparison with the control lot
is according to the left ventricle mass
difference, which suggests the fact that in
hyperthyroidism, hypertrophy is only
partially reversible. In order to clear out
this aspect a supervision over a log period
of time of the E lot is necessary.
Comparing the left ventricle mass values
in the HR lot with the E lot a decrease in
heart weight with an average percentage of
26.67%+/- 18.84% is observed. The
decrease in heart weight takes place
regardless of the initial value, but not
always reaching values that define
ventricular hypertrophy.
Fig 1. The variation of the left ventricle mass drop before and after treatment in the HR
lot compared to the E lot.
After calculating the average left ventricle mass in the 3 lots results as shown in the
next table have been found:
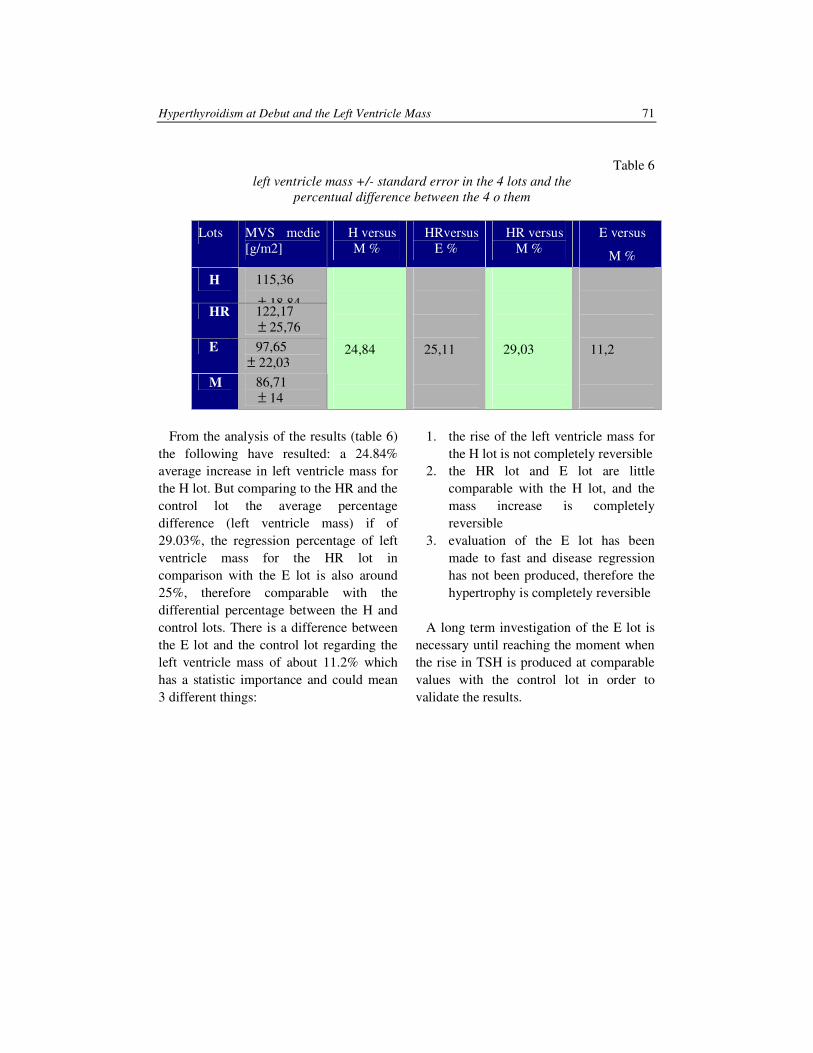
Hyperthyroidism at Debut and the Left Ventricle Mass 71
Table 6
left ventricle mass +/- standard error in the 4 lots and the
percentual difference between the 4 o them
Lots MVS medie
[g/m2]
H versus
M %
HRversus
E %
HR versus
M %
E versus
M %
H 115,36
± 18,84 HR 122,17
± 25,76
E 97,65
± 22,03
M 86,71
± 14
24,84
25,11
29,03
11,2
From the analysis of the results (table 6)
the following have resulted: a 24.84%
average increase in left ventricle mass for
the H lot. But comparing to the HR and the
control lot the average percentage
difference (left ventricle mass) if of
29.03%, the regression percentage of left
ventricle mass for the HR lot in
comparison with the E lot is also around
25%, therefore comparable with the
differential percentage between the H and
control lots. There is a difference between
the E lot and the control lot regarding the
left ventricle mass of about 11.2% which
has a statistic importance and could mean
3 different things:
1. the rise of the left ventricle mass for
the H lot is not completely reversible
2. the HR lot and E lot are little
comparable with the H lot, and the
mass increase is completely
reversible
3. evaluation of the E lot has been
made to fast and disease regression
has not been produced, therefore the
hypertrophy is completely reversible
A long term investigation of the E lot is
necessary until reaching the moment when
the rise in TSH is produced at comparable
values with the control lot in order to
validate the results.
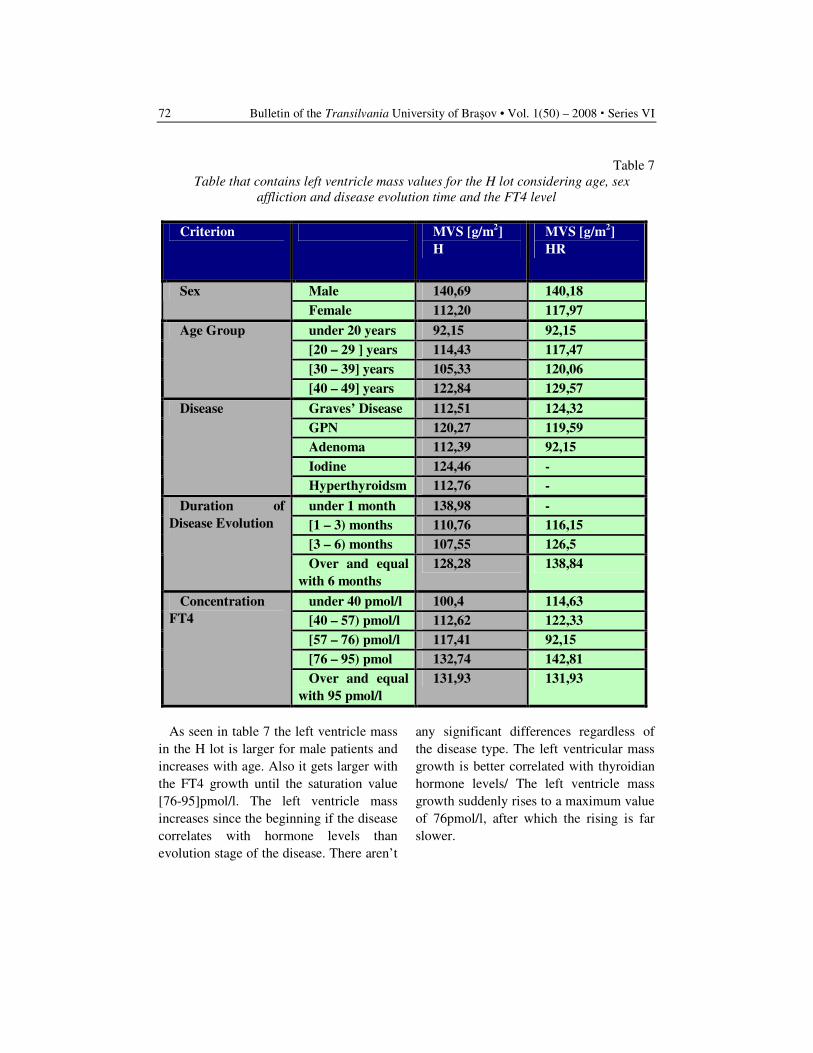
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
72
Table 7
Table that contains left ventricle mass values for the H lot considering age, sex
affliction and disease evolution time and the FT4 level
Criterion MVS [g/m2]
H
MVS [g/m2]
HR
Male 140,69 140,18 Sex
Female 112,20 117,97
under 20 years 92,15 92,15
[20 – 29 ] years 114,43 117,47
[30 – 39] years 105,33 120,06
Age Group
[40 – 49] years 122,84 129,57
Graves’ Disease 112,51 124,32
GPN 120,27 119,59
Adenoma 112,39 92,15
Iodine 124,46 -
Disease
Hyperthyroidsm 112,76 -
under 1 month 138,98 -
[1 – 3) months 110,76 116,15
[3 – 6) months 107,55 126,5
Duration of
Disease Evolution
Over and equal
with 6 months
128,28 138,84
under 40 pmol/l 100,4 114,63
[40 – 57) pmol/l 112,62 122,33
[57 – 76) pmol/l 117,41 92,15
[76 – 95) pmol 132,74 142,81
Concentration
FT4
Over and equal
with 95 pmol/l
131,93 131,93
As seen in table 7 the left ventricle mass
in the H lot is larger for male patients and
increases with age. Also it gets larger with
the FT4 growth until the saturation value
[76-95]pmol/l. The left ventricle mass
increases since the beginning if the disease
correlates with hormone levels than
evolution stage of the disease. There aren’t
any significant differences regardless of
the disease type. The left ventricular mass
growth is better correlated with thyroidian
hormone levels/ The left ventricle mass
growth suddenly rises to a maximum value
of 76pmol/l, after which the rising is far
slower.
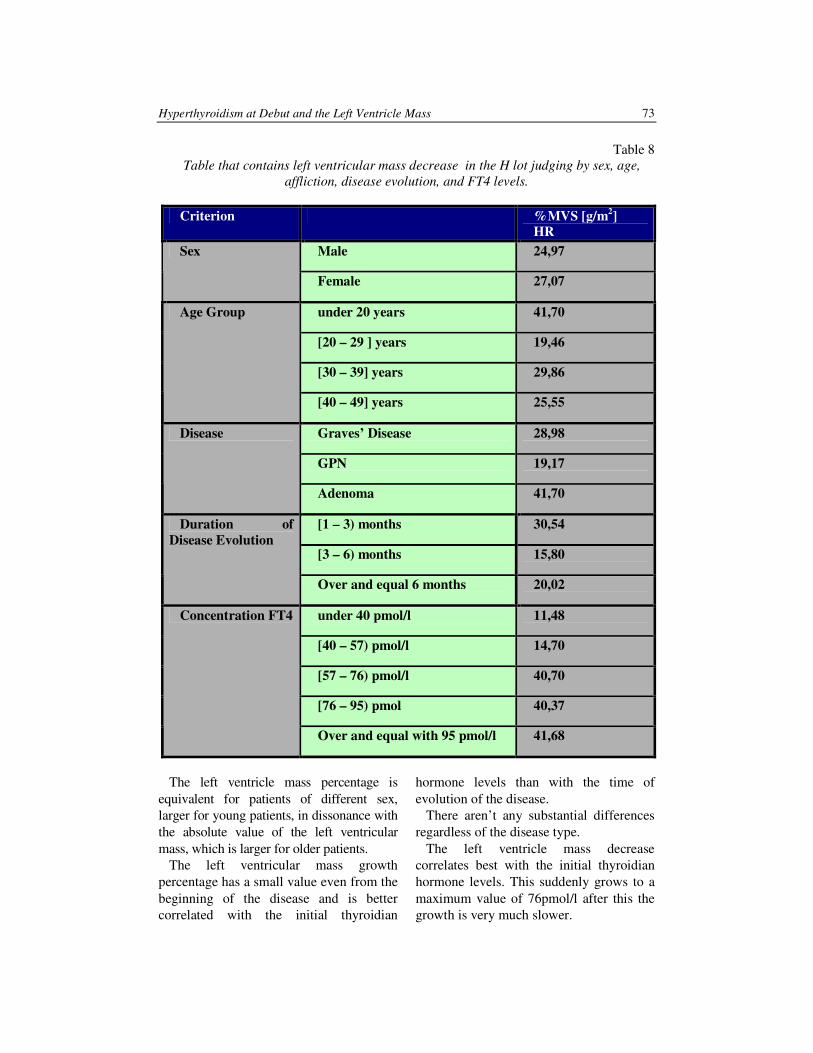
Hyperthyroidism at Debut and the Left Ventricle Mass 73
Table 8
Table that contains left ventricular mass decrease in the H lot judging by sex, age,
affliction, disease evolution, and FT4 levels.
Criterion %MVS [g/m2]
HR
Male 24,97 Sex
Female 27,07
under 20 years 41,70
[20 – 29 ] years 19,46
[30 – 39] years 29,86
Age Group
[40 – 49] years 25,55
Graves’ Disease 28,98
GPN 19,17
Disease
Adenoma 41,70
[1 – 3) months 30,54
[3 – 6) months 15,80
Duration of
Disease Evolution
Over and equal 6 months 20,02
under 40 pmol/l 11,48
[40 – 57) pmol/l 14,70
[57 – 76) pmol/l 40,70
[76 – 95) pmol 40,37
Concentration FT4
Over and equal with 95 pmol/l 41,68
The left ventricle mass percentage is
equivalent for patients of different sex,
larger for young patients, in dissonance with
the absolute value of the left ventricular
mass, which is larger for older patients.
The left ventricular mass growth
percentage has a small value even from the
beginning of the disease and is better
correlated with the initial thyroidian
hormone levels than with the time of
evolution of the disease.
There aren’t any substantial differences
regardless of the disease type.
The left ventricle mass decrease
correlates best with the initial thyroidian
hormone levels. This suddenly grows to a
maximum value of 76pmol/l after this the
growth is very much slower.

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
74
The left ventricle mass growth in the H
lot is positively correlated with the FT4
levels (r=0.74), with the heart frequency at
the moment of examination (r = 0.49) and
negative, although the correlation is weak
(r=0.29) with TSH levels.
Conclusions
In conclusion the left ventricular mass in
the H lot grows early, regardless of the
initial heart weight. 66% of all tyrotoxic
patients reach values that define
hypertrophy.
Growth was symmetrical, afflicting the
septum as well as the ventricular walls.
Growth percentage was an average of 25%
correlating with thyroidian hormone levels
(r=0.74) therefore correlating with
tyreotoxicosis also and not with the disease
type.
The effect is reversible, at least partially
when contracting euthyroidism.
References
1. Biondi, B., Palmieri, E. A., Gaetano,
L., Deradino Fazio: Effects of
Thyroid Hormone on Cardiac
Function: The Relative Importance
of Heart Rate, Loading Conditions,
and Myocardial Contractility in the
Regulation of Cardiac Performance
in Human Hyperthyroidism, 2002,
In: The Journal of Clinical
Endocrinology & Metabolism 87(3):
968-974.
2. Braunwald – Heard disease – A Text
Book of cardiovascular medicine –
VI –Edition WB Saunders Comp.,
2005.
3. Gherasim, L. şi colaboratorii:
Medicina Internă. Bolile
cardiovasculare şi metabolice. Vol
I+II, Ed. Medicală, 2004.
4. Kahaly G.: The Thyroid and the
Heart. Thyroid International 4,
1998:2-21.
5. Klein, I., Levery, G.S.: The
cardiovascular system in
thyrotoxicosis. In: Braverman LE,
Utinger RD, eds. The thyroid, 8th
ed.
Philadelphia. Lippincott-Raven,
2001.
6. Scarneciu, C. C.: Afectarea cardio–
vasculara in tirotoxicoz. Ed.
Universitatii Transilvania, Brasov,
2007.
7. Scarneciu, C. C., Scarneciu, I., Rus,
H.: Evaluarea ecocardiografica a
functiei diastolice a ventriculului
stang in hipertiroidism la debut. In:
Medicina interna, Vol. V, nr.6, 2007.
8. Scarneciu, C. C., Scarneciu, I.,
Nedelcu, L., Rus, H.: Tireotoxicoza
la debut şsi funcţia sistolică a
ventriculului stâng. Medicina
interna, Vol. V, nr. 4, 2008.
9. Toft, A.D., Boon, N.A.: Thyroid
disease and the heart. In: Heart
2000, 84: 445-460.
EFFECT OF TREATEMENT WITH
OMEGA-3 FATTYACIDS AND
ATORVASTATIN IN PATIENTS WITH
COMBINED DYSLIPIDEMIA
H. RUS
1 M. RĂDOI
1 C. CIUREA
1
M. NAN1 C. SUTA
2 D. BODA
3
Abstract:
Objective: Treatment with omega-3 free fatty acids determine a significant
reduction of the serum level of tryglicerides, reduce the risk of coronary
artery disease-related death, nonfatal cardiac events, and suppress the
cardiac arrhythmias. We evaluate the effectiveness of omega-3 free fatty
acids added to atorvastatin in patients with combined dyslipidemia.
Material and method: We evaluate 40 patients, 20 males (50%), age between
35 and 55 years old, nonsmokers, nonhypertensive, and with no diagnosed
coronary artery disease, randomized in Group A (20p.) treated 8 weeks with
atorvastatin 20mg/day and Group B (20p.) Treated free fatty acids 3Gr/day
last 4 weeks added to atorvastatin 20mg/day 8 weeks.
Statistical analysis pair t-Student test.
Results: Adding omega-3 fatty acids 3gr/day to the treatment with
atorvastatin significantly reduce the plasmatic level of total cholesterol(
280mg/dl vs 256mg/dl, p < 0,003), tryglicerides (180 vs 170 mg/dl, p <0,01),
and nonHDL Cholesterol (-4% Vs 1,5%, P <0,004).
Conclusions: combining the atorvastatin treatment with omega-3 free fatty
acids in patients with combined dyslipidemia, causes an important decrease
of plasma tryglicerides, and in a lesser degree LDL and total cholesterol.
Key words: omega-3 fattyacids, atorvastatin, dyslipidemia.
1 Transilvania University of Brasov, Internal Medicine Dept., Faculty of Medicine. 2 Research Assistant, Heart Institute “N. Stancioiu” , Cluj-Napoca. 3 Research Assistant, University “Carol Davilla”, Bucharest.
Due to the growing incidence of
cardiovascular pathology the decrease of
the lipids serum level represents a main
element in the strategy of decrease of
cardiovascular risk In this frame the LDL
cholesterol is the main therapeutic target of
the European Guides of modern treatment
in dyslipidemias. Decreasing the level of
LDL associates an decreased risk of
cardiovascular morbimortalitaty.
In the case combined dyslipidemias the
problem is more complex by reason of
having new targets: decrease of the
plasmatic level of tryglicerides (TG), and
growth of HDL cholesterol [1].
Atorvastatin, as a member of statin class,
represents at this moment a basic element
of the therapeutic arsenal used to the
reduce LDL cholesterol.

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 ▪ Series VI
76
The other classes of drugs besides
statines, are being used generally added to
a statin in the sight of improving the lipidic
parameters [3].
Therapeutic target for LDL of 100 mg/dl
to the patients with high risks, respectively
70 mg/dl to ones with very high risk is
hard to touch, as showed Neptune clinical
trial, realized with one drug just for 27%
from patients. The therapeutic current
arsenal associates to statines drugs
different classes.
Fibrates reduces TG up to 50%, and raise
HDL with as far as 15%, but with the
exception of fenofibrate brought high risk
of myopathia and rabdomyolisis.
Niacine reduces LDL Col (10-20%),
raise HDL (up to 40%), and diminishes TG
(30%), but is hard to tolerated due to the
adverse reactions binded of the
disengagement from prostaglandine: flush,
diarrhea, hypotension.
Cholelstiramina and her modern
derivates, reduce LDL cholesterol with 10-
25%, but frequently associates distur-
bances of intestinal transits.
The acids omega 3, biochemical basic
component of the fishy oil, reduces
significantly the plasmatic level of TG,
effect depending on dose, reduces the
cardiovascular deadly risk post myocardial
infarct, reduce the risk of nonfatal cardiac
events, and reduce the degree of malignity
of cardiac arrhythmias. Just in utilization
as the alimentary supplements, signi-
ficantly reduce the level TG and LDL Col
and raise HDL cholesterol.
They do not increase glicemia, and are
not associated with rabdomyolisis or the
hepatic affectation [4].
The partnership of acids omega 3 with
statines was evaluated also in another trial.
Thus the association of pravastatin 40mg
day with fish oil 6gr day for 12 weeks
produce reduce of VLDL and IDL with as
far as 35%.
As far as we know there was no trial that
evaluates the effects on lipid profile of
combining atorvastatine with omega-3 free
fatty acids [6].
Objective
Impact of the treatment with acids
omega-3 fatty acids added atorvastatine,
versus atorvastatine alone, from the view
of improvement the lipidic profile, in
patients with combined dyslipidemia.
Materials and Method
We evaluate 40 patients, 20 men (50%),
age contained between 35 and 55 years,
non-smokers, with no history of
hypertension, valvular disease or coronary
artery disease.
The patients were randomized on 2 arms:
group A and B which contained each 20
patients. The 2 groups of patients are
homogeneous to evaluated criteria: age, sex:
glycaemia, plasmatic levels of lipids, index
of corporal mass (IMC), arterial blood
pressure as systolic (TAS), respectively
diastolic (TAD) blood pressure.
General characteristic of the two groups of patients Table 1
Parameter Group A Group B
Age 35-45 38-48, p<0,5
Glycaemia a jeune mg/dl 98 101, p<0,3
Total cholesterol mg/dl 245 250,p<0,25
HDL Col mg/dl 44 46,p<0,3
TG mg/dl 288 266,p<0,26
TAS mm Hg 128 118,p<0,22
TAD mm Hg 76 80,p<0,08
BMI 27,5 27, p<0,04

Effect of Treatment with Omega-3 Fattyacids and Atorvastatin … 77
Patients from both lots received the
treatments with atorvastatin 20 mg/day for
4 weeks thereto treated differently.
Group A- continued the treatment with
atorvastatin 20mg day but associate acids
omega3 in dose of 3 gr/day (3x1 dragee-
Omacor, in order to assured a standard of
purity.
The group B was treated on whole period
of pursuits, 2 month, with atorvastatin
20mg day.
The evaluation of the patients is realized
to enlistment and to ultimate 2 months.
Analyze statistics: Analyzes between the
two groups through T-Student.
Results.
The treatment with atorvastatin 20 mg
day for 4 weeks to the patients with mixt
dyslipidemia causes a significant decrease
of the plasmatic level of cholesterol the
total (280 vs 256mg/dl, p < 0,003).
Combining the treatment with omega-3
fatty acids with atorvastatin increase the
variation of the cholesterol plasmatic level
(-9.1 Vs 6.65%, P <0,04).
The level of LDL cholesterol is reduced
statistically significant in both groups. At
the end of the study there was no
statistically significant difference between
the two groups. (-2.7 vs 2.6%, p<0,2). In
relation with LDL level adding omega-3
fatty acids to atorvastatin does not have an
additional effect.
Treatment with atorvastatin significantly
reduces triglycerides plasmatic level (180
vs 170 mg/dl, p<0.01). At the group of
patients treated with omega-3 that decrease
it is more important than in the group
treated only with atorvastatin (-4.7vs 1.6%,
p<0,002).
HDL cholesterol plasmatic level,
following the 2 month of treatment with
atorvastatin, is increased. That increment is
more important in the group of patients
treated with omega 3 free fatty acids (3.6
vs 1.5%, p<0,012).
If we consider non HDL cholesterol as a
marker of therapeutic efficiency, treatment
with omega-3 free fatty acids added to
atorvastatin produce an increase of
statines’s plasmatic level in comparison
with the treatment with atorvastatin (3.5 vs
1.6, p<0,004).
Reduction of the plasmatic level of non
HDL cholesterol is more important in the
group treated with omega-3 fatty acids (-4
vs 1.5%, p<0,004).
The fraction total cholesterol /HDL is
more reduced, at the end of the study in
patients with combined treatment (-1.3 vs
0,9,p<0,01).
Conclusions:
Combining the atorvastatin treatment
with omega-3 free fatty acids in patients
with combined dyslipidemia, causes an
important decrease of plasma triglycerides,
and in a lesser degree LDL and total
cholesterol.
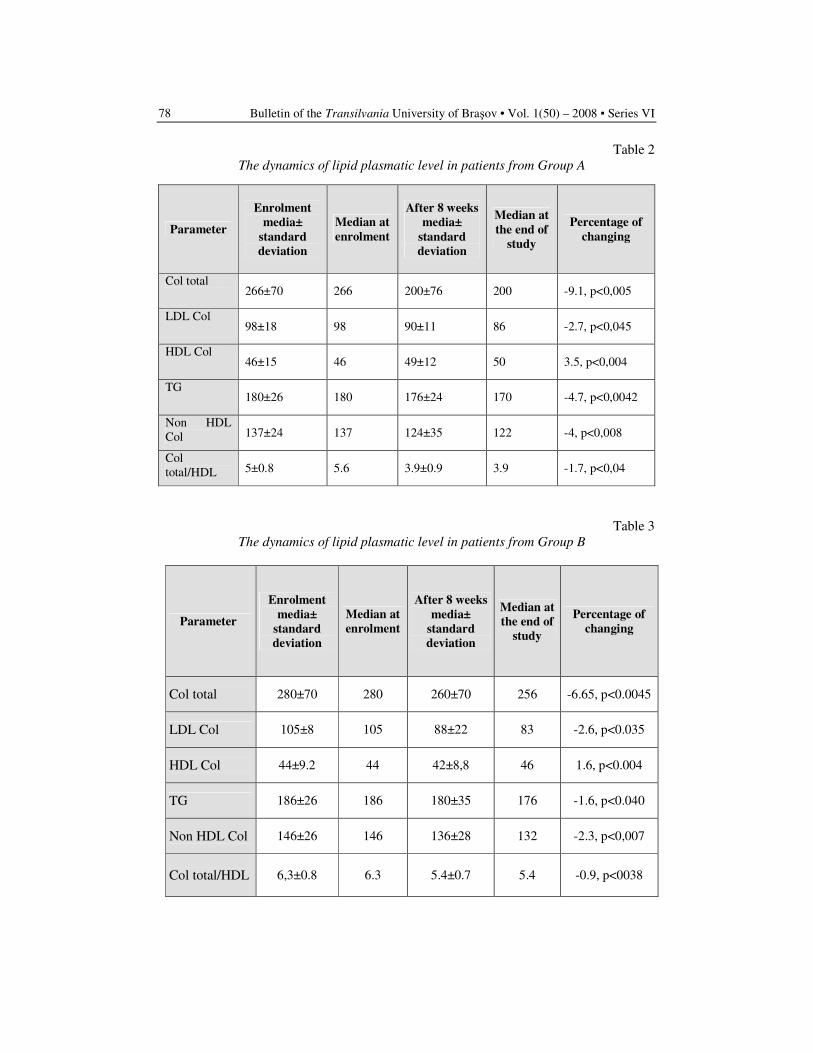
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 ▪ Series VI
78
Table 2
The dynamics of lipid plasmatic level in patients from Group A
Parameter
Enrolment
media±
standard
deviation
Median at
enrolment
After 8 weeks
media±
standard
deviation
Median at
the end of
study
Percentage of
changing
Col total 266±70 266 200±76 200 -9.1, p<0,005
LDL Col 98±18 98 90±11 86 -2.7, p<0,045
HDL Col 46±15 46 49±12 50 3.5, p<0,004
TG 180±26 180 176±24 170 -4.7, p<0,0042
Non HDL
Col 137±24 137 124±35 122 -4, p<0,008
Col
total/HDL 5±0.8 5.6 3.9±0.9 3.9 -1.7, p<0,04
Table 3
The dynamics of lipid plasmatic level in patients from Group B
Parameter
Enrolment
media±
standard
deviation
Median at
enrolment
After 8 weeks
media±
standard
deviation
Median at
the end of
study
Percentage of
changing
Col total 280±70 280 260±70 256 -6.65, p<0.0045
LDL Col 105±8 105 88±22 83 -2.6, p<0.035
HDL Col 44±9.2 44 42±8,8 46 1.6, p<0.004
TG 186±26 186 180±35 176 -1.6, p<0.040
Non HDL Col 146±26 146 136±28 132 -2.3, p<0,007
Col total/HDL 6,3±0.8 6.3 5.4±0.7 5.4 -0.9, p<0038

Effect of Treatment with Omega-3 Fattyacids and Atorvastatin … 79
Conclusions
Association of omega3 free fatty acids to
atorvastatin, in patients with combined
dyslidemia, produce an important
favorable change in the lipid plasmatic
level. The main change is important
reducing of triglycerides in patients treated
with the combined treatment. That aspect
of variation in relation with the combined
treatment show a lesser dynamics for LDL
and total cholesterol
Discussions
Reduction of the cardiovascular risk
represents a main issue when we judge the
medical treatment in patients with
dyslipidemias. Association of multiple
drugs in order to change lipid levels,
according to the recent guidelines,
represent a therapeutic target [3].
If as for now the target lipid plasmatic
levels refer mostly on LDL, in patients
with hypertrigliceridemia reducing non
HDL cholesterol is an indication.
In that context adding omega-3 free fatty
acids in high dose (3gr) induce an
important change of lipid profile with TG
and non HDL reduction, and increase of
HDL.
The dosage of atorvastatin used was in
relation with some other trials.
References
1. Ballantyne, C.M., Bertolami, M.,
Hernandez Garcia, H.R., Nul, D.,
Stein, E.A., Theroux, P., Weiss, R.,
Cain, V.A. and Raichlen, J.S.:
Achieving LDL cholesterol, non-HDL
cholesterol, and apolipoprotein B
target levels in high-risk patients:
Measuring Effective Reductions in
Cholesterol Using Rosuvastatin
Therapy (MERCURY) II, In: Am
Heart J 151 (2006), pp. 975–979.
2. Expert Panel on Detection Evaluation
and Treatment of High Blood
Cholesterol in Adults, Third report of
the National Cholesterol Education
Program (NCEP) Expert Panel on
Detection, Evaluation, and Treatment
of High Blood Cholesterol in Adults
(Adult Treatment Panel III) final
report, Circulation 106 (2002), pp.
3143–3421.
3. Grundy, S.M., Cleeman, J.I., Merz
C.N., Brewer Jr., H.B., Clark, L.T.,
Hunninghake, D.B., Pasternak, R.C.,
Smith Jr., S.C. and Stone, N.J.:
Implications of recent clinical trials
for the National Cholesterol
Education Program Adult Treatment
Panel III guidelines. In: Circulation
110 (2004), pp. 227–239.
4. Jacobson, T.A.: The safety of
aggressive statin therapy: how much
can low-density lipoprotein
cholesterol be lowered? In: Mayo
Clin Proc 81 (2006), pp. 1225–1231.
5. McKenney, J.M., Jones, P.H.,
Adamczyk, M.A., Cain, V.A.,
Bryzinski, B.S. and Blasetto, J.W.:
Comparison of the efficacy of
rosuvastatin versus atorvastatin,
simvastatin, and pravastatin in
achieving lipid goals: results from the
STELLAR trial. In: Curr Med Res
Opin 19 (2003), pp. 689–698.
6. Pearson, T.A., Laurora, I., Chu, H. and
Kafonek, S.: The Lipid Treatment
Assessment Project (L-TAP): a
multicenter survey to evaluate the
percentages of dyslipidemic patients
receiving lipid-lowering therapy and
achieving low-density lipoprotein

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 ▪ Series VI
80
cholesterol goals. In: Arch Intern Med
160 (2000), pp. 459–467.
7. Wiviott, S.D., Cannon, C.P., Morrow,
D.A., Ray, K.K., Pfeffer, M.A. and
Braunwald, E.: Can low-density
lipoprotein be too low? The safety and
efficacy of achieving very low low-
density lipoprotein with intensive
statin therapy: a PROVE IT-TIMI 22
substudy. In: J Am Coll Cardiol 46
(2005), pp. 1411–1416.

IN PATIENTS WITH NON-ST ACUTE
CORONARY SYNDROME DIABETES
MELLITUS AND METABOLIC SYNDROME
HAVE AN IMPORTANT IMPACT ON
PROGNOSIS, LEFT VENTRICULAR
SYSTOLIC FUNCTION, INFLAMMATORY
SYNDROME AND OXIDATIVE STRESS
E. BOBESCU
1,2 M. RĂDOI
1,2 Z. GALAJDA
3 G. DATCU
4
Abstract: Aims: To evaluate oxidative stress, inflammatory syndrome, left
ventricular systolic function and prognosis in patients with non ST acute
coronary syndrome and metabolic syndrome or diabetes mellitus. Methods:
172 patients (pts) with non ST acute coronary syndrome (ACS) were included
in a prospective study for a period of 3 years and were divided in three
groups in relation with association of metabolic syndrome (MS) or diabetes
mellitus (DM). Results: In non ST ACS patients, presence of metabolic
syndrome or diabetes mellitus were associated with significant higher
incidence of inflammatory syndrome (p< 0.05) and oxidative stress (p< 0.05)
at 1 and 6 months and with a significant increased incidence of left ventricle
systolic dysfunction (p< 0.05) at 1,2 and 3 years. Incidence of cardiovascular
death, acute myocardial infarction and unstable angina with readmission, at
1.2 and 3 years were significantly higher (p< 0.05) in comparison with ACS
nonMS nonDM group. It was no significant differences between non ST
acute coronary syndrome with metabolic syndrome and with diabetes
mellitus groups at 1.2 and 3 years of follow up. Conclusions: In non ST acute
coronary syndrome patients, presence of metabolic syndrome or diabetes
mellitus were associated with a significant higher incidence of inflammatory
syndrome, oxidative stress at 1 and 6 months and a significant higher
incidence of low ejection fraction, unstable angina with readmission, acute
myocardial infarction and cardiovascular death at 1.2 and 3 years of follow
up.
Key words: acute coronary syndrome, metabolic syndrome, diabetes
mellitus, inflammatory syndrome, oxidative stress, prognosis.
1 Transilvania” University - Faculty of Medicine. 2 Clinic County Emergency Hospital- Clinic of Cardiology, Brasov, Romania. 3 Institute of Cardiology, Cardiac Surgery Center, Medical and Health Science Center, University of
Debrecen, Hungary. 4 University of Medicine and Pharmacy ”Gr.T.Popa Iasi, Romania.
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) – 2008 ▪ Series VI 82
Background In patients with diabetes mellitus, 75%
of deaths are represented by cardiovascular deaths. Cardiovascular risk is 3-5 folds higher in diabetic’s patients and 3 folds higher in metabolic syndrome. Incidence of metabolic syndrome in patients with acute coronary syndrome is 29-46%, with increased incidence of heart failure, and worse long-term mortality compared to those without metabolic syndrome. The main causes of this burden of disease in diabetes mellitus and metabolic syndrome are high LDL cholesterol, low HDL cholesterol serum values, prothrombotic status - high plasminogen activator inhibitor-1 (PAI-1) and fibrinogen, endothelial dysfunction, high leucocytes adhesively to endothelium and mycroalbu-minuria [1, 2, 4, 5, 12, 19, 21, 24, 25].
Methods
172 patients (pts) with non ST ACS were included in a prospective study for a period of 3 years and were divided in three groups in relation with association of MS or DM.
Clinic evaluation, electrocardiography and echocardiography were performed initial and at 1, 6 months, 1, 2 and 3 years. Biologic markers were determinate initial, at 1 and 6 months. C-reactive protein serum level (Immune-turbidimetry method) and fibrinogen plasma level (Turbidimetry method) were determinate as markers of inflammatory syndrome. Anti ox-LDL antibody titers (ELISA technique INOVA kit manufacturer) and total antioxidant status (TAS) serum level (ABTS
® Method-
RANDOX kits) were measured for oxidative stress evaluation. Left ventricular ejection fraction was measured by 2-D Echocardiography, volume/ dimension Simpson’s method [5-9, 11, 14, 16, 31].
Groups of study
ACS non SM non DM - 37 patients with acute non ST coronary syndrome without metabolic syndrome and diabetes mellitus; ACS MS - 79 patients with acute non ST coronary syndrome and metabolic syndrome and diabetes mellitus; ACS DM – 59 patients with acute non ST coronary syndrome and diabetes mellitus (Figure 1).
A C S
MS
7 6 p
(4 4 .2 % )
A C S n o n S M
n o n D M
3 7 p
(2 1 .5 % )
A C S
D M
5 9 p
(3 4 .3 % )
Fig. 1. Groups of study
Statistical Analysis
Comparison between groups was
performed using Chi-squared test and multiple regression analysis. A value of p < 0.05 was considered statistically significant.
Results and discussions
Baseline characteristics of patients were
represented by additional markers, old and new factors with role in cardiovascular risk evaluation and optimal standard medical
therapy in accordance with ESC and ACC/AHA guideline update for the management of patients’ non ST-segment elevation acute coronary syndrome
[3, 5-7,
10]. It was no significant differences in baseline characteristics between study groups.
Inflammatory syndrome
The incidence of high serum level C-
reactive protein (CRP>5 mg/l) was significantly higher at 1 month in ACS MS
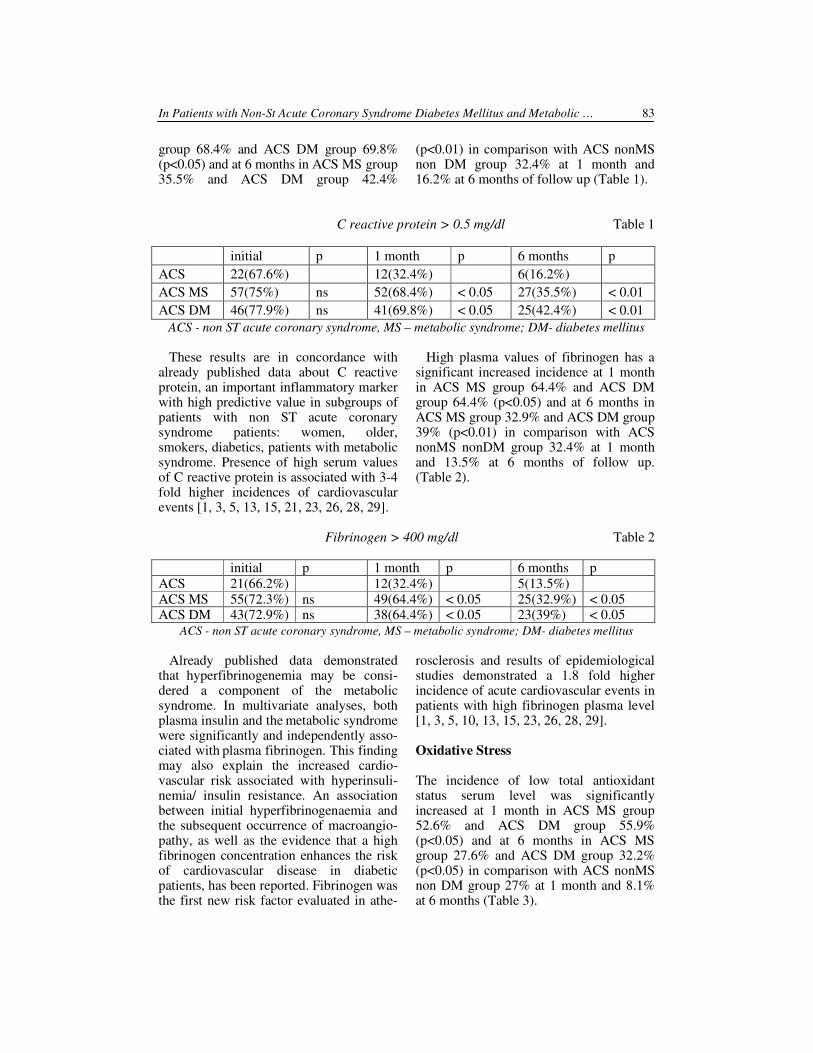
In Patients with Non-St Acute Coronary Syndrome Diabetes Mellitus and Metabolic … 83
group 68.4% and ACS DM group 69.8% (p<0.05) and at 6 months in ACS MS group 35.5% and ACS DM group 42.4%
(p<0.01) in comparison with ACS nonMS non DM group 32.4% at 1 month and 16.2% at 6 months of follow up (Table 1).
C reactive protein > 0.5 mg/dl Table 1
initial p 1 month p 6 months p
ACS 22(67.6%) 12(32.4%) 6(16.2%)
ACS MS 57(75%) ns 52(68.4%) < 0.05 27(35.5%) < 0.01
ACS DM 46(77.9%) ns 41(69.8%) < 0.05 25(42.4%) < 0.01
ACS - non ST acute coronary syndrome, MS – metabolic syndrome; DM- diabetes mellitus
These results are in concordance with already published data about C reactive protein, an important inflammatory marker with high predictive value in subgroups of patients with non ST acute coronary syndrome patients: women, older, smokers, diabetics, patients with metabolic syndrome. Presence of high serum values of C reactive protein is associated with 3-4 fold higher incidences of cardiovascular events [1, 3, 5, 13, 15, 21, 23, 26, 28, 29].
High plasma values of fibrinogen has a significant increased incidence at 1 month in ACS MS group 64.4% and ACS DM group 64.4% (p<0.05) and at 6 months in ACS MS group 32.9% and ACS DM group 39% (p<0.01) in comparison with ACS nonMS nonDM group 32.4% at 1 month and 13.5% at 6 months of follow up. (Table 2).
Fibrinogen > 400 mg/dl Table 2
initial p 1 month p 6 months p
ACS 21(66.2%) 12(32.4%) 5(13.5%)
ACS MS 55(72.3%) ns 49(64.4%) < 0.05 25(32.9%) < 0.05 ACS DM 43(72.9%) ns 38(64.4%) < 0.05 23(39%) < 0.05
ACS - non ST acute coronary syndrome, MS – metabolic syndrome; DM- diabetes mellitus
Already published data demonstrated that
hyperfibrinogenemia may be consi-
dered a component of the metabolic
syndrome. In multivariate analyses, both plasma insulin and the
metabolic syndrome
were significantly and independently asso-ciated with
plasma fibrinogen. This finding
may also explain the increased cardio-vascular risk
associated with hyperinsuli-
nemia/ insulin resistance. An association between initial hyperfibrinogenaemia and the subsequent occurrence of macroangio-pathy, as well as the evidence that a high fibrinogen concentration enhances the risk of cardiovascular disease in diabetic patients, has been reported. Fibrinogen was the first new risk factor evaluated in athe-
rosclerosis and results of epidemiological studies demonstrated a 1.8 fold higher incidence of acute cardiovascular events in patients with high fibrinogen plasma level [1, 3, 5, 10, 13, 15, 23, 26, 28, 29].
Oxidative Stress
The incidence of low total antioxidant status serum level was significantly increased at 1 month in ACS MS group 52.6% and ACS DM group 55.9% (p<0.05) and at 6 months in ACS MS group 27.6% and ACS DM group 32.2% (p<0.05) in comparison with ACS nonMS non DM group 27% at 1 month and 8.1% at 6 months (Table 3).
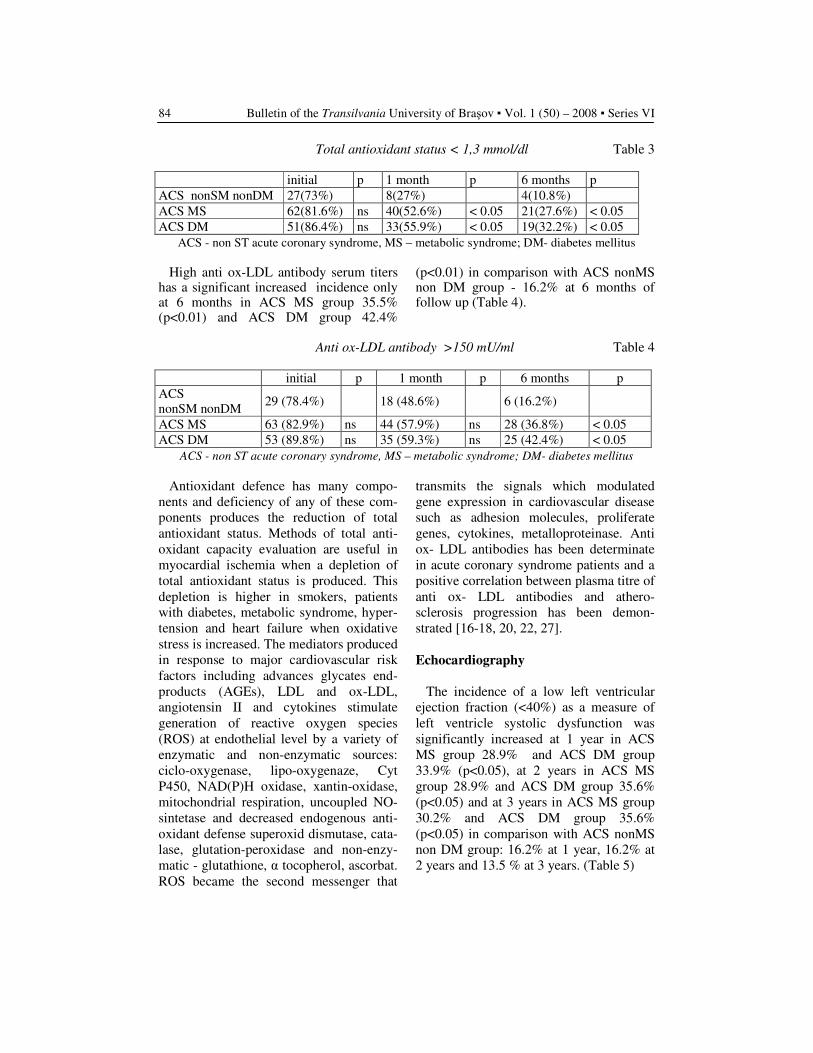
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) – 2008 ▪ Series VI 84
Total antioxidant status < 1,3 mmol/dl Table 3
initial p 1 month p 6 months p
ACS nonSM nonDM 27(73%) 8(27%) 4(10.8%)
ACS MS 62(81.6%) ns 40(52.6%) < 0.05 21(27.6%) < 0.05
ACS DM 51(86.4%) ns 33(55.9%) < 0.05 19(32.2%) < 0.05
ACS - non ST acute coronary syndrome, MS – metabolic syndrome; DM- diabetes mellitus
High anti ox-LDL antibody serum titers has a significant increased incidence only at 6 months in ACS MS group 35.5% (p<0.01) and ACS DM group 42.4%
(p<0.01) in comparison with ACS nonMS non DM group - 16.2% at 6 months of follow up (Table 4).
Anti ox-LDL antibody >150 mU/ml Table 4
initial p 1 month p 6 months p
ACS
nonSM nonDM 29 (78.4%) 18 (48.6%) 6 (16.2%)
ACS MS 63 (82.9%) ns 44 (57.9%) ns 28 (36.8%) < 0.05
ACS DM 53 (89.8%) ns 35 (59.3%) ns 25 (42.4%) < 0.05
ACS - non ST acute coronary syndrome, MS – metabolic syndrome; DM- diabetes mellitus
Antioxidant defence has many compo-
nents and deficiency of any of these com-
ponents produces the reduction of total
antioxidant status. Methods of total anti-
oxidant capacity evaluation are useful in
myocardial ischemia when a depletion of
total antioxidant status is produced. This
depletion is higher in smokers, patients
with diabetes, metabolic syndrome, hyper-
tension and heart failure when oxidative
stress is increased. The mediators produced
in response to major cardiovascular risk
factors including advances glycates end-
products (AGEs), LDL and ox-LDL,
angiotensin II and cytokines stimulate
generation of reactive oxygen species
(ROS) at endothelial level by a variety of
enzymatic and non-enzymatic sources:
ciclo-oxygenase, lipo-oxygenaze, Cyt
P450, NAD(P)H oxidase, xantin-oxidase,
mitochondrial respiration, uncoupled NO-
sintetase and decreased endogenous anti-
oxidant defense superoxid dismutase, cata-
lase, glutation-peroxidase and non-enzy-
matic - glutathione, α tocopherol, ascorbat.
ROS became the second messenger that
transmits the signals which modulated
gene expression in cardiovascular disease
such as adhesion molecules, proliferate
genes, cytokines, metalloproteinase. Anti
ox- LDL antibodies has been determinate
in acute coronary syndrome patients and a
positive correlation between plasma titre of
anti ox- LDL antibodies and athero-
sclerosis progression has been demon-
strated [16-18, 20, 22, 27].
Echocardiography
The incidence of a low left ventricular
ejection fraction (<40%) as a measure of
left ventricle systolic dysfunction was
significantly increased at 1 year in ACS
MS group 28.9% and ACS DM group
33.9% (p<0.05), at 2 years in ACS MS
group 28.9% and ACS DM group 35.6%
(p<0.05) and at 3 years in ACS MS group
30.2% and ACS DM group 35.6%
(p<0.05) in comparison with ACS nonMS
non DM group: 16.2% at 1 year, 16.2% at
2 years and 13.5 % at 3 years. (Table 5)

In Patients with Non-St Acute Coronary Syndrome Diabetes Mellitus and Metabolic … 85
Left ventricular ejection fraction < 40%: Table 5
1 month 6 months 1 year 2 years 3 years
ACS nonSM, nonDM
9(24.3%) 7(18.9%) 6(16.2%) 6(16.2%) 5(13.5%)
ACS MS 17(22.3%) 19(25%) 22(28.9%) p<0.05
22(28.9%) p<0.05
23(30.2%) p<0.05
ACS DM 14(23.7%) 17(28.8%) 20(33.9%) p<0.05
21(35.6%) p<0.05
22(37.3%) p<0.05
ACS - non ST acute coronary syndrome, MS – metabolic syndrome; DM- diabetes mellitus
Already published data demonstrated that
evaluation of ejection fraction with bidi-mensional echocardiography is correlated with angiographic determination of left ventricle function and a low ejection fraction is associated with increased incidence of cardiovascular death. [18, 20, 24, 25]
Major acute Cardiovascular Events
(MACE)
The incidence of MACE was significantly higher in patients with non ST
acute coronary syndrome patients and metabolic syndrome or diabetes mellitus.
Cardiovascular mortality was significantly increased at 1 year in ACS MS group 13.2% and ACS DM group 18.6% (p<0.05), at 2 years in ACS MS group 17.1% and ACS DM group 23.7% (p<0.05) and at 3 years in ACS MS group 18.4% and ACS DM group 23.7% (p<0.05) in comparison with ACS nonMS non DM group: 5.4% at 1 year, 5.4% at 2 years and 5.4 % at 3 years of follow up. (Table 6)
Cardiovascular death Table 6
ACS - non ST acute coronary syndrome, MS – metabolic syndrome; DM- diabetes mellitus
A significant increased incidence of
acute myocardial infarction was observed at 1 year in ACS MS group 15.8% and ACS DM group 18.6% (p<0.05), at 2 years in ACS MS group 19.7% and ACS DM group 25.4% (p<0.05) and at 3 years in
ACS MS group 23.7% and ACS DM group 28.8% (p<0.05) in comparison with ACS nonMS non DM group: 2.7% at 1 year, 5.4% at 2 years and 5.4 % at 3 years of follow up. (Table 7)
Acute myocardial infarction Table 7
ACS - non ST acute coronary syndrome, MS – metabolic syndrome; DM- diabetes mellitus
1 month 6 months 1 year 2 years 3 years
ACS
nonSM nonDM 0 1(2.7%) 2(5.4%) 2(5.4%) 2(5.4%)
ACS MS 4(5.3%) 8(10.5%) 10(13.2%)
p<0.05
13(17.1%)
p<0.05
14(18.4%)
p<0.05
ACS DM 4(6.8%) 7(11.8%) 11(18.6%)
p<0.05
14(23.7%)
p<0.05
14(23.7%)
p<0.05
1 month 6 months 1 year 2 years 3 years
ACS nonSM nonDM
1(2.7%) 1(2.7%) 1(2.7%) 2(5.4%) 2(5.4%)
ACS MS 5(6.6%) 9(11.8%) 12(15.8% p<0.05
15(19.7%) p<0.05
18(23.7%) p<0.025
ACS DM 5(8.5%) 8(13.5%) 11(18.6%) p<0.05
15(25.4%) p<0.05
17(28.8%) p<0.025
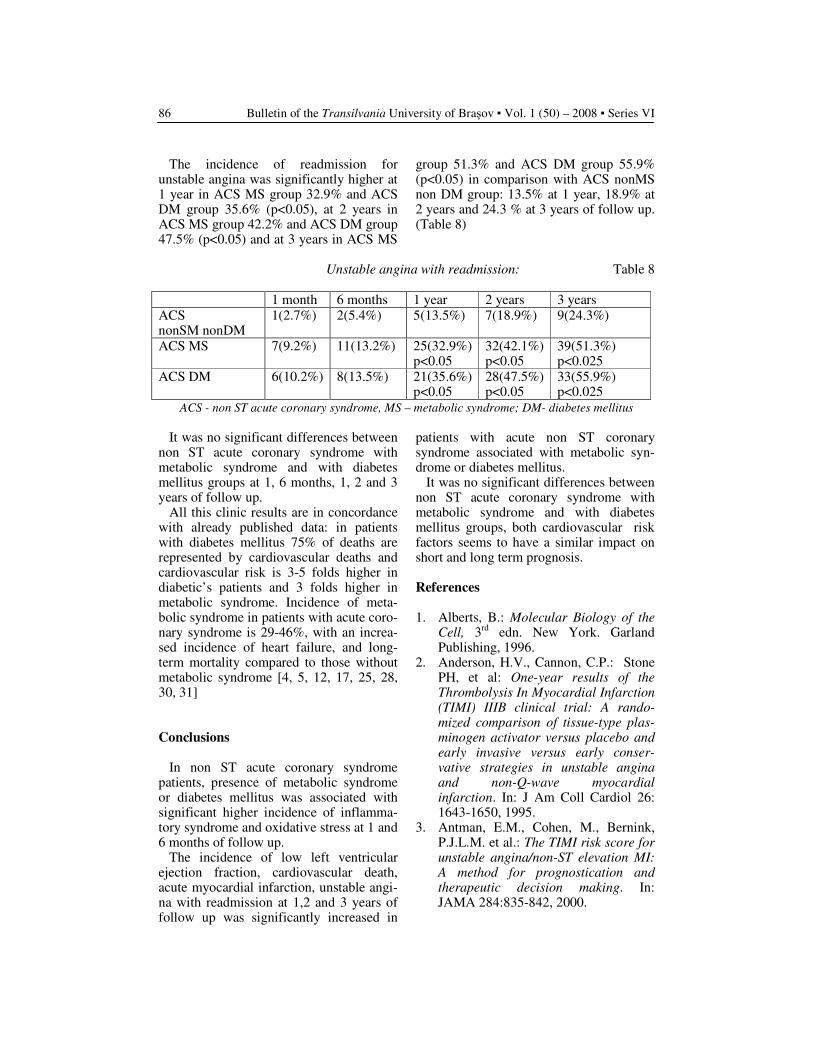
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) – 2008 ▪ Series VI 86
The incidence of readmission for unstable angina was significantly higher at 1 year in ACS MS group 32.9% and ACS DM group 35.6% (p<0.05), at 2 years in ACS MS group 42.2% and ACS DM group 47.5% (p<0.05) and at 3 years in ACS MS
group 51.3% and ACS DM group 55.9% (p<0.05) in comparison with ACS nonMS non DM group: 13.5% at 1 year, 18.9% at 2 years and 24.3 % at 3 years of follow up. (Table 8)
Unstable angina with readmission: Table 8
1 month 6 months 1 year 2 years 3 years
ACS nonSM nonDM
1(2.7%) 2(5.4%) 5(13.5%) 7(18.9%) 9(24.3%)
ACS MS 7(9.2%) 11(13.2%) 25(32.9%) p<0.05
32(42.1%) p<0.05
39(51.3%) p<0.025
ACS DM 6(10.2%) 8(13.5%) 21(35.6%) p<0.05
28(47.5%) p<0.05
33(55.9%) p<0.025
ACS - non ST acute coronary syndrome, MS – metabolic syndrome; DM- diabetes mellitus
It was no significant differences between
non ST acute coronary syndrome with metabolic syndrome and with diabetes mellitus groups at 1, 6 months, 1, 2 and 3 years of follow up.
All this clinic results are in concordance with already published data: in patients with diabetes mellitus 75% of deaths are represented by cardiovascular deaths and cardiovascular risk is 3-5 folds higher in diabetic’s patients and 3 folds higher in metabolic syndrome. Incidence of meta-bolic syndrome in patients with acute coro-nary syndrome is 29-46%, with an increa-sed incidence of heart failure, and long-term mortality compared to those without metabolic syndrome [4, 5, 12, 17, 25, 28, 30, 31]
Conclusions In non ST acute coronary syndrome
patients, presence of metabolic syndrome or diabetes mellitus was associated with significant higher incidence of inflamma-tory syndrome and oxidative stress at 1 and 6 months of follow up.
The incidence of low left ventricular ejection fraction, cardiovascular death, acute myocardial infarction, unstable angi-na with readmission at 1,2 and 3 years of follow up was significantly increased in
patients with acute non ST coronary syndrome associated with metabolic syn-drome or diabetes mellitus.
It was no significant differences between non ST acute coronary syndrome with metabolic syndrome and with diabetes mellitus groups, both cardiovascular risk factors seems to have a similar impact on short and long term prognosis.
References
1. Alberts, B.: Molecular Biology of the
Cell, 3rd
edn. New York. Garland Publishing, 1996.
2. Anderson, H.V., Cannon, C.P.: Stone PH, et al: One-year results of the
Thrombolysis In Myocardial Infarction
(TIMI) IIIB clinical trial: A rando-
mized comparison of tissue-type plas-
minogen activator versus placebo and
early invasive versus early conser-
vative strategies in unstable angina
and non-Q-wave myocardial
infarction. In: J Am Coll Cardiol 26: 1643-1650, 1995.
3. Antman, E.M., Cohen, M., Bernink, P.J.L.M. et al.: The TIMI risk score for
unstable angina/non-ST elevation MI:
A method for prognostication and
therapeutic decision making. In: JAMA 284:835-842, 2000.
In Patients with Non-St Acute Coronary Syndrome Diabetes Mellitus and Metabolic … 87
4. Assman, G., Schulte, H., von Eckardstein, A. et al.: High-density
lipoprotein cholesterol as a predictor
of coronary heart disease risk. The
PROCAM experience and pathophy-
siological implications for reverse
cholesterol transport. In: Atherosclerosis 124: S11-S20. 1996.
5. Braunwald, E., Antman, E.M., Califf, R.M. et al.: ACC AHA guideline update for the management of patients
with unstable angina and non-ST-
segment elevation, myocardial
infarction - 2002: summary article: a report of the American College of Cardiology, American Heart Asso-ciation, Task Force on Practice Guide-lines (Committee on the Management of Patients with Unstable Angina). Circulation 2002; 106: 1893-1900.
6. Braunwald, E., Antman, E.M., Beasley, J.W. et al.: ACC/ AHA
guidelines for the management of
patients with unstable angina/non-ST
segment elevation myocardial
infarction: A report of the American
College of Car- diology/American
Heart Association Task Force on
Practice Guidelines (Committee on the Management of Unstable Angina and Non-ST Segment Elevation Myocardial Infarction). In: J Am CoIl Cardiol 36:970-1062, 2000.
7. Braunwald, E.: Application of current
guidelines to the management of unsta-
ble angina and non-ST-elevation myo-
cardial infarction. In: Circulation 2003; 108: 28111-28137.
8. Buja, L.M., Willerson, J.T.: Role of
inflammation in coronary plaque
disruption. In: Circulation. 1994; 89: 503-505.
9. Cheitlin, M.D., Alpert, J.S., Amstrong, W.F., et al.: ACC/AHA guidelines for
the clinical application of Echocardio-
graphy: Executive summary. A report
of the American College of Cardio-
logy/ American Heart Association
Task Force on practice guidelines
(Committee on Clinical Application of
Echocardiography); Developed in
collaboration with the American
Society of Echocardiography. In: J Am CoIl Cardiol 29:862-879, 1997.
10. Ernst, E., Resch, K.L.: Fibrinogen as a
cardiovascular risk factor: A meta-
nalysis and review of the literature. In: Ann Intern Med 118:956-963, 1993.
11. Fisman, E.Z., Tenenbaum, A.: Cardio-
vascular Diabetology: Clinical, Meta-
bolic and Inflammatory Facets. In: Adv Cardiol. Basel, Karger, 2008, vol 45, pp. 114-126.
12. Fuster, V., Badimon, L., Badimon, J.J. et al.: The pathogenesis of coronary
artery disease and the acute coronary
syndromes. In: N EngI J Med. 1992; 326: 242-250,310-318.
13. Fuster, V., Lewis, A.: Mechanisms
leading to myocardial infarction:
insights from studies of vascular
biology. In: Circulation. 1994; 90: 2126-2146. Conner Memorial Lecture.
14. Goldberg, R.J., Currie, K., White, K. et al.: Six-month outcomes in a
multinational registry of patients
hospitalized with an acute coronary
syndrome (The Global Registry of Acute Coronary Events [GRACE]). In: Am J Cardiol 2004; 93: 288-293.
15. Granger, C.B., Goldberg, R.J., Dabbous, O. et al.: The Global
Registry of Acute Registry of Acute
Coronary Events Investigators.
Predictors of hospital mortality in the
global registry of acute coronary
events. In: Arch Intern Med 2003; 163:2345-2353.
16. Halliwell, B.: Antioxidant character-
rization. Methodology and mechanism. In: Biochem. Pharmacol, (2005) 49, 1341.
17. Hasdai, D., Behar, S., Wallentin, L. et al.: A prospective survey of the
characterristics, treatments and
outcomes of patients with acute
coronary syndromes in Europe and the
Mediterranean basin. The Euro Heart
Survey of Acute Coronary Syndromes (Euro Heart Survey ACS). In: Eur Heart J2002; 23: 1190-1201.
18. Hochman, J.S., Tamis, J.E., Thompson, T.D. et al.: Sex, clinical
presentation. and outcome in patients
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) – 2008 ▪ Series VI 88
with acute coronary syndromes.
Global Use of Strategies to Open
Occluded Coronary Arteries in Acute
Coronary Syndromes IIb Investigators. In: N Engl J Med 341:226-232, 1999.
19. Hyde, T.A., French, J.K., Wong, C.K. et al.: Four-year survival of patients
with acute coronary syndromes without ST-segment elevation and
prognostic significance of 0.5-mm ST-
segment depression. In: Am J Cardiol 1999; 84: 379-85.
20. Iayes, R.L.I., Beshansky, J.R., D' Agostino, R.B. et al.: Do patients
coronary risk factor reports predict
acute cardiac ischemia in the
emergency department? A multicenter
study. In: J Clin Epidemiol 1992; 45:621-6.
21. International Task Force for Preven-tion of Coronary Heart Disease. Su-mmary of the Expert Panel Meeting: Cholesterol- lowering with statins- are they all the same? New Orleans March 7 2004
22. Jaber, W.A., Prior, D.L., Marso, S.P. et al.: CHF on presentation is associated
with markedly worse outcomes among
patients with acute coronary syndro-
mes: PURSUIT trial findings (abstract). In: Circulation 100 (Suppl. I): I-433, 1999.
23. Koenig, W., Sund, M., Froelich, M. et al.: C-reactive protein, a sensitive
marker of inflammation, predicts
future risk of coronary heart disease in
initially healthy middle-aged men:
Results from the MONICA (Monitoring
Trends and Determinants in Cardio-
vascular Disease) Augsberg Cohort Study, 1984 to 1992. In: Circulation 99:237-242, 1999.
24. Lakka, H.M., Laaksonen, D.E., Timo, A. et al: The Metabolic Syndrome and
Total and Cardiovascular Disease
Mortality in Middle-aged Men. In: JAMA. 2002; 288: 2709-2716.
25. Manson, I.E., Coldjtz, G.A., Stampfer M.I., et al.: A prospective study of
obesity and risk of coronary heart
disease in women. In: N Engl J Med 322: 882-889, 1990.
26. Morrow, D.A., Rifai, N., Antman, E.M., et al.: C-reactive protein is a
potent predictor of mortality
independently of and in combination
with troponin T in acute coronary
syndromes: a TIMI II A sub- study.
Thrombolysis in Myocardial
Infarction. In: J Am CoIl Cardiol 1998; 31: 1460-5.
27. Ridker, P.M., Buring I.E., Shih, I. et al: Prospective study of C-reactive
protein and the risk of future
cardiovascular events among
apparently healthy women. In: Circulation 98: 731-733, 1998.
28. Ridker, P.M., Hennekens, C.H., Buring, I.E. et al.: C-reactive protein
and other markers of inflammation in
the prediction of cardiovascular
disease in women. In: N Engl I Med 342:836-843, 2000.
29. Ridker, P.M., Rifai, N., Clearfield, M. et al.: The Air Force/Texas Coronary
Atherosclerosis Prevention Study
Investigators. Measurement of C-
reactive protein for the targeting of
statin therapy in the primary preven-
tion of acute coronary events. In: N Engl J Med. 2001; 344: 1959-1965.
30. Roivairien, M., Viik-Kajander, M., Palosuo, T. et al: Infections,
inflammation, and the risk of
coronary heart disease. In: Circulation 101:252-257, 2000.
31. Rosengren, A., Wedel, H., Wilhelmsen, L.: Body weight and
weight gain during adult life in men
in relation to coronary heart disease
and mortality. A prospective
population study. In: Eur Heart J 20:269-271 1999.
C REACTIVE PROTEIN AND CLOZAPINE-
INDUCED FEVER
S. HUSSAIN
1 N. AFZAL
1
I. KOHEN1 P.MANU
Abstract: We report a case of recurrent clozapine-induced fever which was
associated with a rise in C reactive protein (CRP). The patient was a 73-
year-old man with Lewy Body dementia who was admitted for psychosis. He
was treated with clozapine and developed a benign fever that was associated
with a rise in CRP. The CRP initially normalized off clozapine. However,
after the patient was rechallenged with clozapine, the CRP became elevated
with a subsequent recurrence of fever. We postulate that the elevation in CRP
and the subsequent fever was caused by the effects of clozapine on the
cytokine system via interleukin- 6 and tumour necrosis factor-alpha resulting
in an inflammatory response with an acute phase reaction.
Key words: clozapine, immunomodulatory, C reactive.
1 The Zucker Hillside Hospital, Glen Oaks and Albert Einstein College of Medicine, Bronx, New York.
1. Introduction
Clozapine-related fever is a common
adverse reaction that is usually benign but
can be challenging to assess and diagnose.
[16] The differential diagnosis must
include other dangerous conditions inclu-
ding agranulocytosis and neuroleptic
malignant syndrome (NMS). [9]
We describe a case of an elderly patient
who developed clozapine fever two weeks
after beginning treatment with clozapine.
We will discuss the relationship between
clozapine fever and C reactive protein
(CRP). We propose that an increase in
CRP in the absence of evidence for
infectious or inflammatory causes may be
used to predict recurrence of clozapine
fever and be a useful tool in its
management.
2. Case Report
Mr. H is a 73 year old male with a
diagnosis of Lewy Body dementia (LBD)
who was admitted to a geriatric inpatient
psychiatric unit after presenting with
depressive symptoms with suicidal idea-
tion and a plan to kill himself. He also had
worsening psychotic symptoms in the form
of command auditory hallucinations telling
him to kill himself. His medications at
home included quetiapine 100 mg at
bedtime and donepezil 10 mg daily. On
admission, the patient was afebrile with a
normal complete blood count (CBC) and
no findings of infection on a urinalysis or a
chest x-ray.
In the psychiatric hospital, quetiapine
was titrated up to 300 mg at bedtime over
two weeks for persistent psychotic
symptoms. However, the patient did not
improve and continued to report
derogatory voices telling him to hurt self.

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 ▪ Series VI
90
As such, clozapine was started at a 12.5
mg dose at bedtime while the quetiapine
was tapered off. The clozapine dose was
titrated up to 75mg at bedtime over the
next 15 days, while the quetiapine dose
was reduced to 50 mg at bedtime. On the
15th day on clozapine, the patient deve-
loped a fever with a maximum temperature
(Tmax) of 101.1 F. All other vital signs
were stable. He appeared lethargic and
complained of abdominal pain and
tenderness. The patient did not have
rigidity on exam. He was transferred to a
medical hospital and had an extensive
workup for the fever including a chest x-
ray, urinalysis, abdominal x-ray, compu-
terized tomography scan (CT scan) of his
brain and abdomen and pelvis, and blood
work including complete metabolic panel
(CMP) and CBC. The only abnormal
finding was an elevated white blood count
at 12.3 x 10 3 /uL with an absolute
neutrophil count (ANC) of 8.8. His
creatinine phosphokinase (CPK) was
normal at 74. His electrocardiogram and
cardiac enzymes were normal as well. The
quetiapine and clozapine were discon-
tinued and the fever resolved in two days.
The patient was readmitted to the
psychiatric hospital. He was afebrile with a
WBC of 12.6 x 10 3 /uL and an ANC of
8.9. His CRP was slightly elevated at 3.96
mg/dL (normal range of 0-0.49 mg/dL) on
readmission to the psychiatric unit (2 days
off clozapine). The CRP was rechecked
again a week later (off clozapine) and was
trending down at 0.60 mg/dL with a
normal WBC of 9.16 x 10 3 /uL. Two days
later, a repeat CRP was within normal
limits at 0.30 mg/dL. The patient continued
to be afebrile.
The patient remained psychotic with
command auditory hallucinations to kill
himself. Ten days after being transferred
back to the psychiatric hospital, he was
restarted on clozapine 12.5 mg at bedtime.
After three days, the clozapine dose was
raised to 25 mg at bedtime. His CRP after
three days at this dose was elevated at 4.36
mg/dL with a WBC of 12.8 x 10 3 /uL.
The patient was afebrile and asympto-
matic. However, two days later, the patient
again became febrile with a Tmax of
101.7F and was transferred to the medical
hospital. Again, the patient did not have
rigidity on exam. At that time, he had a
medical workup with a CT head, chest x-
ray, urinalysis and blood work which did
not reveal any abnormalities except for an
elevated WBC. The clozapine was stopped
and his fever resolved within two days
without any other interventions. No repeat
CRP was done. The patient was started on
lorazepam 0.5 mg twice a day and was
discharged to a skilled nursing facility
from the medical hospital.
3. Discussion
Clozapine became available in 1990 as
an atypical antipsychotic medication with a
low risk of extrapyramidal symptoms.
Common side effects include weight gain,
hyperglycemia, hyperlipidemia, hyper-
triglyceridemia, tachycardia, sedation,
hypersalivation, hypotension, and
constipation. Rare complications include
agranulocytosis (absolute neutrophil count
<0.5 x 10 3 /uL), cardiovascular or
respiratory arrest, myocarditis, and
seizures. [9]
A common adverse effect of clozapine is
a mild to high-grade fever that is usually
benign. The reported rate of clozapine
fever in the literature varies from 0.5-55%.
[16] The fever lasts 2.5 days on average
and generally resolves between days 8 and
16 of treatment even if clozapine is
continued. The fever typically occurs
within the first month of therapy.
Typically, clozapine fever is not correlated
with clozapine dose. [6, 11, 15] At one
year follow-up, clozapine-induced fever
has not been linked to neutropenia or
agranulocytosis. [15] Some case reports
have shown that patients with clozapine
fever may have mild leukocytosis, but

C Reactive Protein and Clozapine-Induced Fever 91
rarely manifest other physical signs
indicating an infection. [16]
The differential diagnosis of clozapine
fever must include more serious and
potentially fatal conditions including
neuroleptic malignant syndrome (NMS)
and agranulocytosis. [11] The prevalence
of agranulocytosis in patients on clozapine
is 0.38-1.3%. [16] Agranulocytosis may
predispose patients to neutropenic sepsis
which has a mortality rate of 3-4%. [4]
NMS is typically diagnosed based on
clinical signs including severe muscular
rigidity (classic “lead pipe” rigidity),
hyperthermia (temp >38 degrees Celsius),
autonomic instability and changes in
consciousness. [1] Onset varies from 1 day
to 30 days from starting an antipsychotic.
Most cases occur within the first week. [2]
NMS has a mortality rate of up to 10% if
not diagnosed and treated promptly. [14]
There are also reports of an “atypical”
presentation of NMS that may be caused
by clozapine and other atypical antipsy-
chotics (such as aripiprazole and or
olanzapine). This form of NMS commonly
presents with tachycardia, mental status
changes, and diaphoresis. It is less likely to
be associated with extrapyramidal
symptoms or a rapid rise in CPK. [7]
The mechanism of clozapine fever is still
not clearly understood. One theory
involves the immunomodulating effects of
clozapine. [6, 10] Interleukin- 6 (IL-6) and
tumor necrosis factor alpha (TNF-alpha)
are cytokines released by monocytes and
tissue macrophages that mediate the
primary host response during infla-
mmation, infection, and fever. [8] They are
not detectable in healthy humans. [5]
These cytokines stimulate the acute phase
reaction and lead to a systemic reaction
including fever, elevated erythrocyte sedi-
mentation rate (ESR), increased secretion
of glucocorticoids, and activation of
complement and clotting cascades. They
also increase production of CRP. Several
studies have reported that patients with
schizophrenia have increased activation of
monocytes and T cells as well as baseline
increases in serum IL-6 levels. [3, 13]
One in vivo study evaluated the effects
of clozapine on rectal temperatures, blood
cell counts, and cytokine and soluble
cytokine receptor plasma levels during six
weeks of clozapine treatment in 27 patients
with schizophrenia. The study revealed
significant increases in TNF-alpha and
soluble interleukin-2 receptor (sIL-2R)
after six weeks of treatment. IL-6 and
leukocyte counts only transiently increased
at week two but did not differ from
baseline after six weeks. [9] The twelve
patients who developed fever had
pronounced increases in TNF-alpha and
sIL-2R at week two. They also showed an
increase in plasma IL-6 levels and
granulocyte counts at two weeks. In
addition, the patients’ fevers subsided
without any interventions even when
clozapine was continued. [12
4. Conclusion
Clozapine fever is generally benign but
can be difficult to assess and manage. This
case report may provide a tool for
monitoring and possibly predicting
clozapine fever. Further research is needed
to evaluate whether the data can be
generalized to patients with schizophrenia
and other psychotic disorders. In addition,
future studies are needed to determine
whether an increase in CRP may predict
the emergence or recurrence of clozapine
fever.
References
1. American Psychiatric Association:
Diagnostic and Statistical Manual of
Mental Disorders, 4th ed. Washington,
DC, American Psychiatric Association,
1994.
2. Caroff, S.N., Mann, S.C.: Neuroleptic
malignant syndrome. In : Psycho-
pharmacol Bull 1998; 24: 25-9.
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 ▪ Series VI
92
3. Ganguli, R., Yang, Z., Shurin, G.:
Serum interleukin-6 concentration in
schizophrenia: elevation associated
with duration of illness. In: Psychiatry
Res 1994; 51: 1-10.
4. Gerson, S.L.: G-CSF and the mana-
gement of clozapine induced agra-
nulocytosis. In: J Clin Psychiatry 1994;
55: 139-42.
5. Gudewill, S., Pollmacher, T., Vedder,
H.: Nocturnal plasma levels of cyto-
kines in healthy men. In: Eur Arch
Psychiatry Clin Neurosci 1992; 242:
53-6.
6. Jeong, S.H., Ahn, Y.M., Koo, Y.J.:
The characteristics of clozapine-
induced fever. In: Schizophr Res 2002;
56: 191-3.
7. Karagianis, J.I., Phillips, L.S., Hogan,
K.P., et al.: Clozapine-associated
neuroleptic malignant syndrome: Two
new cases and a review of the
literature. In: Ann Pharmacother 1999;
33: 623-30. DOI 10.1345/aph.1K141.
8. Kluger, M.J.: Fever: role of pyogens
and cryogens. In: Physiol Rev 1991;
71: 93-117.
9. Lowe, C.M., Grube, R.R., Scated,
A.C.: Characterization and clinical
management of clozapine-induced
fever. In: Ann Pharmacother 2007; 41:
1700-4. DOI 10.1345/aph.1K126
10. Maes, M., Bosmans E., Kenis G., et
al.: In vivo immunomodulatory effects
of clozapine in schizophrenia. In:
Schizophr Res 1997; 26: 221-5.
11. Nittenson, N.C., Kando, J.C.,
Frakenburg, F.R., et al.: Fever
associated with clozapine admi-
nistration. In: Am J Psychiatry 1195;
152: 1102.
12. Pollmacher, T., Hinze-Selch, D.,
Mullington, J.: Effects of clozapine on
plasma cytokines and soluble cytokine
receptor levels. In: J Clin Psycho-
pharmacol 1996; 16: 403-9.
13. Smith, R.S.: A comprehensive macro-
phage-T-lymphocyte theory of
schizophrenia. In: Med Hypotheses
1992; 39: 248-57.
14. Strawn, J.R., Keck, P.E., Caroff, S.N.:
Neuroleptic Malignant Syndrome. In:
Am J Psychiatry 2007; 164: 870-6.
15. Tham, J.C., Dickson, R.A.: Clozapine-
induced fevers and 1-year disconti-
nuation rate. In: J Clin Psychiatry
2002; 63: 880-4.
16. Young, C.R., Bowers, M.B., Mazure,
C.M.: Management of the adverse
effects of clozapine. In: Schizophr Bull
1998; 24; 381-90.

1 UMF Iuliu Hatieganu Cluj Napoca. 2 „Transylvania” University Brasov. 3 Pneumology Hospital Baia Mare. 4 Ovidius University Constanţa.
SMOKING-RISK FACTOR FOR
METASTASIS IN BREAST CANCER
M. A. MAN
1 D. ALEXANDRESCU
2
M. POP1 R. RÂJNOVEANU
1
M. GORON3 O. ARGHIR
4
Abstract: Breast cancer is one of the most frequent neoplasia in women.
The discovery of metastasis risk factors can influence the evolution of the
disease. Environmental factors, especially smoking, play a very important
role in the evolution of many neoplasms. We evaluated the status of smokers
of patients with metastases against the witness batch, patients with breast
cancer without metastases. We compared the age arithmetical mean of
patients who smoked to that of patients who did not smoke (p = 0, 00029) and
we observed there is a significant difference between the age means of
smokers and that of non smokers. Our study results suggest that smoking,
represented a risk factor, significantly influences the apparition of metastases
(p = 0, 001044). Systemic effects of smoking may play a role in influencing
the course of breast cancer and other cancers
Keyword: metastasis, smoking, breast cancer
1. Introduction
Breast cancer is one of the most frequent
neoplasia in women (27% of the total types
of breast cancer). It represents the second
cause of death in the USA after pulmonary
cancer [2, 4]. Of the total patients suffering
from breast cancer, 10% already have
metastases and 50% will develop
metastases in time. Approximately 60% to
70% of the women who die of breast
cancer present pulmonary determination
upon autopsy. In 21% of cases the lung is
the sole metastases focus [7]. Patients with
metastases are not curable by conventional
therapy. Despite the inability to treat
recurrence and metastasized cancer, the
early discovery of metastases and
application of a palliative treatment
improves the quality of life and increases
the survival rate. The discovery of
metastasis risk factors can influence the
evolution of the disease.
The purpose of the study is that of
discovering metastasizing environment
related risk factors, mostly smoking.
2. Materials and Methods
We conducted a survey during January
2000 and December 2005 on 120 patients
admitted with the Cluj-Napoca Oncology
Institute, “Leon Daniello” Pneumology
Clinical Hospital, the Department of
Oncology and Radiotherapy of the Cluj County Hospital.
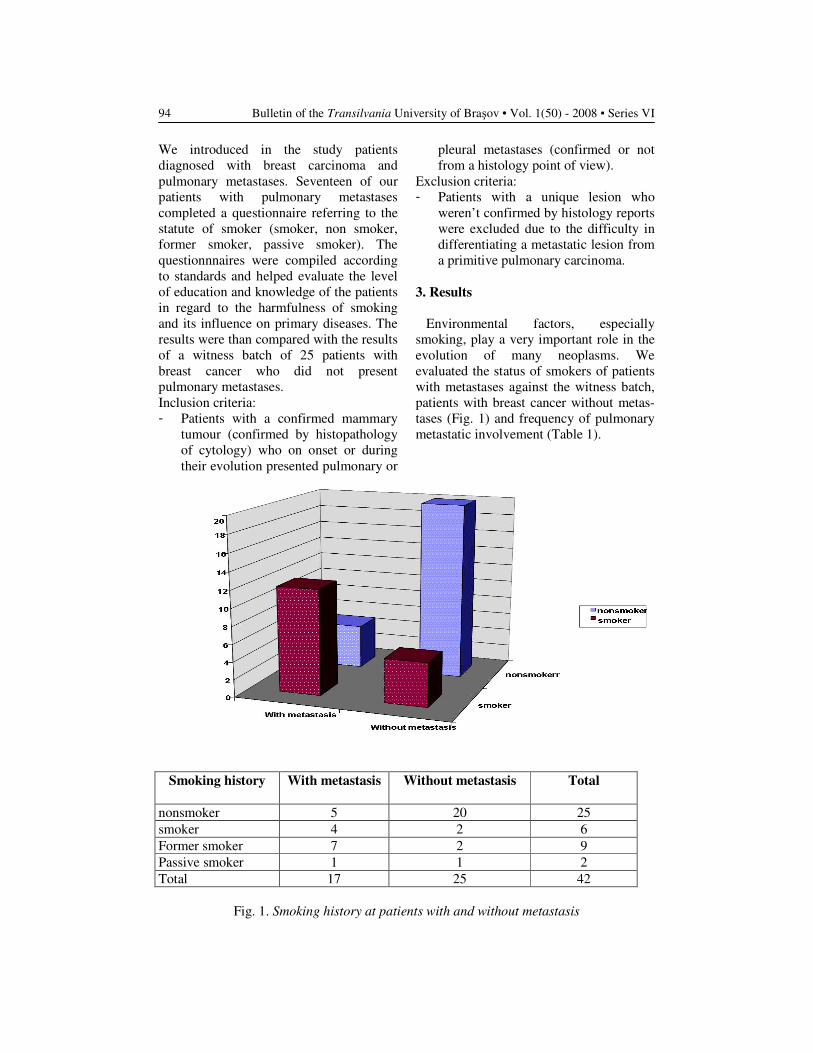
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 ▪ Series VI
94
We introduced in the study patients
diagnosed with breast carcinoma and
pulmonary metastases. Seventeen of our
patients with pulmonary metastases
completed a questionnaire referring to the
statute of smoker (smoker, non smoker,
former smoker, passive smoker). The
questionnnaires were compiled according
to standards and helped evaluate the level
of education and knowledge of the patients
in regard to the harmfulness of smoking
and its influence on primary diseases. The
results were than compared with the results
of a witness batch of 25 patients with
breast cancer who did not present
pulmonary metastases.
Inclusion criteria:
- Patients with a confirmed mammary
tumour (confirmed by histopathology
of cytology) who on onset or during
their evolution presented pulmonary or
pleural metastases (confirmed or not
from a histology point of view).
Exclusion criteria:
- Patients with a unique lesion who
weren’t confirmed by histology reports
were excluded due to the difficulty in
differentiating a metastatic lesion from
a primitive pulmonary carcinoma.
3. Results
Environmental factors, especially
smoking, play a very important role in the
evolution of many neoplasms. We
evaluated the status of smokers of patients
with metastases against the witness batch,
patients with breast cancer without metas-
tases (Fig. 1) and frequency of pulmonary
metastatic involvement (Table 1).
Smoking history
With metastasis
Without metastasis
Total
nonsmoker 5 20 25
smoker 4 2 6
Former smoker 7 2 9
Passive smoker 1 1 2
Total 17 25 42
Fig. 1. Smoking history at patients with and without metastasis
Smoking – Risk Factor for Metastasis in Breast Cancer
95
Frequency of Pulmonary Metastatic Involvement Table 1
Type of Invol-
vement
Parenchymal
nodules
Pleural effusion Lymphangitic
carcinomatosis
No patients (17) 10 8 2
The average onset age was 22, 42857
years and the average yearly number of
cigarette packets was 67, 08333. Smoking
significantly influences the apparition of
metastases (p = 0,001044).
We compared the age arithmetical mean
of patients with metastases to that of
patients without metastases and we
obtained p = 0,3 so we concluded there is
no significant difference between the age
mean of patients with metastases and that
of patients without metastases (Table 2).
Mean age of patients with and without metastasis Table 2
No
patients
Mean age
Standard
Deviation
P
with
metastastasis 17 50,29 7,86 Age
without
metastasis 25 53,32 10,01
0,30
We also compared the age arithmetical
mean of patients who smoked to that of
patients who did not smoke (p = 0, 00029)
and we observed there is a significant
difference between the age means of
smokers and that of non smokers (Table 3).
Breast cancer and its complications are
more easily triggered for smokers than for
non smokers.
Mean age of patients smokers/nonsmokers Table 3
No.patients
Mean age
Standard
Deviation
P
Nonsmokers 27 55,70 8,71 Age
smokers 15 45,60 6,16 0,00029
For persons who had breast cancer but
no metastases we compared the age
arithmetical mean of smokers and non
smokers (p = 0,015) and we noticed a
significant difference between the age
mean of smoking patients and non

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 ▪ Series VI
96
smoking patients among those without
metastases. Cancer is more rapidly
triggered among smokers than among non
smokers.
For patients who have metastases we
compared the age arithmetic mean of
smoking persons who smoke and persons
who do not smoke (p = 0,0064) and we
concluded that there is an important
difference between the age means of
persons who smoke and those who do not
smoke among those who have metastases.
Metastases of breast cancer appear faster
among smokers than among non smokers.
The results of the statistical analysis
emphasized that smoking is a risk factor
for the apparition of pulmonary metastases.
Smoking is considered the most
important negative prognosis factor of all
other environmental factors [8]. Our
comparative survey indicates that smoking
represents a risk factors for metastasizing
as it significantly influences the apparition
of metastases (p = 0,001044).
Recent studies reported that smoking
increases the risk of breast carcinoma only
if smoking begun at an early age or before
the first pregnancy when the epithelial
tissue is more susceptible to the aggression
of the environment. Other studies report
smoking as a risk factor for breast
carcinoma only in the case of very young
women or women with a family history of
breast carcinoma [3].
Several epidemiology surveys have
indicated that smoking increases the death
rate of breast carcinoma patients compared
with non smokers suffering from the same
affection in conditions where smoking is
not associated with the increase of breast
cancer incidence. This suggests that
smoking can influence in an unfavourable
manner the biology and natural history of
breast cancer. Many clinical studies have
associated smoking with an increase of
metastases in lung, breast and bladder
neoplasia [9].
Smoking produces numerous effects at a
pulmonary and systemic level, effects that
might contribute in the increase of
attraction towards metastasizing of the
breast carcinoma and other types of cancer.
Two epidemiology surveys have
demonstrated the association between
smoking and pulmonary metastases among
women with breast carcinoma. Smoking
was associated with the unfavourable
evolution of other tumours, which suggests
the possibility of side effects of smoking
on the biology of cancer.
The specific mechanism that uses smoke
exposure as a way to produce pulmonary
metastases is not completely known.
Smoking can produce systemic effects that
include the increase of vascular and
epithelial permeability, changes at the level
of local immunity, modifications of anti
tumour defence system, status of
coagulation, platelets’ stickiness, and
increase in the adhesion of molecules. In
addition, exposure to smoking affects the
metastatic potential of tumour cells by
influencing the effects of the signal’s
transduction. In his study, Murin has not
found any differentiation between the
statute of active smoker, passive smoker or
former smoker [6].
Nistrosamine 4 (Methyl nidrosamino) - 1
- (3 - piridy) – 1 – butanane (NNH) was
identified as the most potent carcinogen
from the cigarette smoke. It mimics the
increase factors that stimulate
phosphorilate and µ and n – calpain
activation (family of protease cysteins
implicated in proteolysis which next to
metallo-proteins dissolves the basal
membrane of blood vessels favouring
invasion, increases access to blood of
lymph vessels for dissemination [10].
Nicotine also induces c-SRC activation
also known as Ci protein kinase (which
induces µ and n-calpains phosphorilate)
[10].
The role of smoking was emphasized on
the increase adherence of tumor
proliferation and extravasations. Subse-
quent, smoking no longer affects the rate

Smoking – Risk Factor for Metastasis in Breast Cancer
97
of increase of metastases after these have
already developed [6].
The results of the study revealed that
38% of the patients who smoked had
pulmonary metastases compared to 29% of
patients who never smoked. Of the patients
who smoked accidentally at the moment of
diagnosis of breast carcinoma, 24, 1% of
them developed pulmonary metastases
compared to 15, 3% of those who never
smoked (p = 0,06) [5].
Harry and collaborators report the
existence of metastasized axillaries gan-
glions more frequent with smokers than
with non smoker. He claims the presence
of larger metastases and records the asso-
ciation smoking – unfavourable prognosis
factors in other neoplasia (myeloid
leukemia, prostate carcinoma, melanoma,
and also the endometriosis of the uterine
cervix, bladder, and colon) either by
stimulation of malignant cells or by the
inhibition of the host’s defence system [1].
Conclusion
1. A number of clinical and pathologic
factors, such as tumour size, nodal
involvement, and degree of tumour
differentiation,
are predictors of
disease course.
2. Much of the apparent heterogeneity
in the risk of disease progression,
and in the
sites of disease
progression, remains unexplained.
3. An effect of smoking on the
development of
metastasis disease
from breast cancer provides an
intriguing and biologically plausible
explanation for the higher rate of
fatal breast cancer among smokers.
4. Systemic effects of smoking may
play a role in adversely influencing
the course of other cancers. 5. The effect of
smoking on the natural
history of breast cancer and other
non-pulmonary malignancies
warrants further investigation.
References
1. Daniell, H. W.: Breast Cancer in
Smokers. In: Chest; 2003; 123:1771-
1772.
2. De Vito, V.: Principles of Molecular
Cell Biology of Cancer. In: Cancer
Metastasis 1998, Lippincott,
Philadelphia, p.134-148.
3. Hanajina, N, Hirose, K., Tajina, K.,
Rohan, T., Kalle, E.: Alchool, Tabacco
and Brest Cancer Colaborative
reanalysis of Individual Data From 53
Epidemiological Studies Including
58.515 Women With Brest Cancer and
95.067 Women without the disease.
In: British Journal of Cancer; 2002;
1.234-1.245.
4. Moosa, A. R., Stephen, C., Schimpff,
M., Robson, M.C.: Comprehensive
Textbook of Oncology. Baltimore,
Maryland USA. Williams & Wilkins,
1986, 855-863.
5. Murin, S., Inciardi, J.: Cigarette
Smoking And The Risk Of Pulmonary
metastasis from Breast Cancer. In:
Chest 2001, 119, 1.635-1.640.
6. Murin, S., Pinkerton, K.E., Hubbardi,
N., Erickson, K.: The effect of Cigarette
Smoke Exposure on Pulmonary
Metastatic Disease in a Murine model
of metastatic breast Cancer. In: Chest;
125; 2004; 1467-1471.
7. Naunov, G. N, Mac Donald, I.C,
Weinneiste, N., Kerkvliet Nadkarni,
K.V., Wison, S.M, Maris, V.L.,
Groam, A.C, Chambers, A.F.:
Persistence of solitary mamary
carcinom cells in a secondary site: a
posible contribution to dormancy. In:
Cancer Research 62, 2002, 2162-2168.
8. Reynolds, P., Hurleg, S., Goldberg,
D., Andan-Cutrer, H., Bernstein, H.,
Deaper, D.: Active Smoking, House
Hold Passive Smoking and Breast
Cancer: Evidence From The
California Teachers Study, Journal of
The National Cancer Institute 96,
2004.

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 ▪ Series VI
98
9. Xu, L., Deng, X. M.: Tobaco –
specific Nitrosamine 4 –
(Methylnitrasamino)-1-(3-pyrydil)-1-
butanane induces Phosphorylation of
micro- and n-Calpain in Association
with increased Secretion, Cell
Migration and Invasion, Journal
Biology chemically; vol279; 51; dec
2004, 53683-53690.
10. Xu, L., Ming Deng, X.: Protein
Kinase Ci promotes Nicotine-Induced
Migration and Invasion of Cancer
Cells via Phosphorylation of micro-
and n- Calpains. In: Journal Biology
Chemicaly; vol.281; 7; Feb. 2006;
4457-4466.
ANTIBIOTIC SUSCEPTIBILITY
CHANGES OF
STAPHYLOCOCCUS AUREUS
A RETROSPECTIVE STUDY
O. FALUP-PECURARIU
1 A. RĂŞINĂ2
C. FALUP-PECURARIU3
Abstract: Antibiotherapy resistance is an emerging health care issue due to
the extended usage of antibiotics.
The aim of the study was to determine the changes in antibiotherapy
resistance of Staphylococcus aureus over a 5 years period between 2003 to
2007. Patients and method: retrospective study over a 5 years period that
analyzed the resistance trends of Staphylococcus aureus in the cultures of
newborns, that were taken at the Newborn Department of the Children’
Hospital of the Transilvania University. Results: 116 strains were studied,
strains from skin lesions, umbilical secretion, blood culture, eye secretion,
nasal and pharyngeal swab. From these 94 were resistant to penicillin,
74.1% sensible to meticillin, 9.48% resistant to gentamicin, 72% sensible to
ciprofloxacin and 72% sensible to clindamicin. Conclusions: there was in
our study a slight predominance of boys. We observe a constant trend
towards metcillin resistance. Most of the meticillin resistant strains were
isolated from skin lesions. Still active antibiotics are clindamicin, gentamicin
and rifampicin
Key words: Staphylococcus aureurs, newborn, antibiotic resistance
1 Transilvania University of Brasov, Dept. of Pediatrics 2 Children’s Hospital Braşov 3 Transilvania University of Brasov, Dept. of Neurology, Transilvania University of Braşov
Introduction
Staphylococcus aureus causes 96000
diseases each year causing around 16000
deaths per year. It is still one of the major
pathogen determining sepsis, endocarditis,
arthritis, osteomielitis and soft tissues
infections. It is one of the most aggressive
nosocomial agents [2]. It comprises about
27 different species of Staphylococcus,
which are divided due to their ability to
secrete an enzyme called coagulase: in
coagulase negative and positive staphy-
lococcus. A complex of factors and
interactions between the host, the
environment and the bug itself determines
the transmission of the pathogen.
Throughout the world, there are over 2
billion healthy carriers and 53 million
carriers of MRSA [12]. Shortly after
penicillin became available Staphy-
lococcus developed strains resistant to beta
lactamase [13]. During the years 1999-
2002 in Europe 53264 strains of
Staphylococcus, where cultured from
which 5-20% was MRSA. Romania had 83
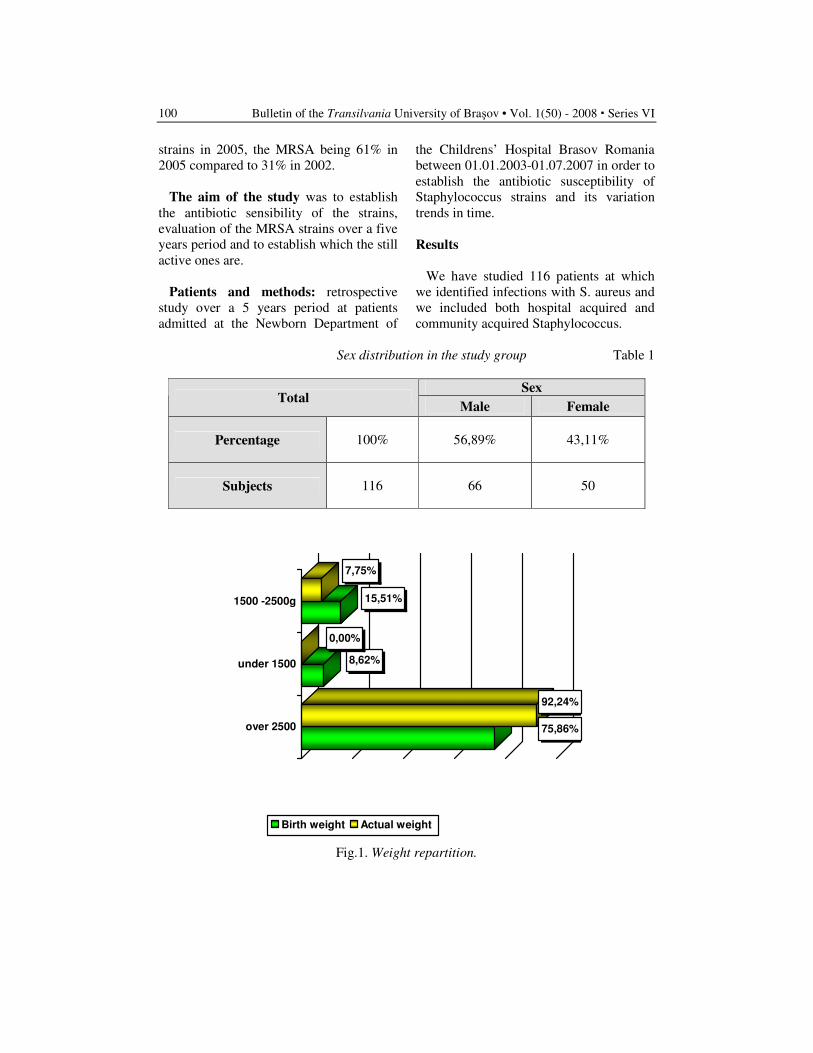
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
100
strains in 2005, the MRSA being 61% in
2005 compared to 31% in 2002.
The aim of the study was to establish
the antibiotic sensibility of the strains,
evaluation of the MRSA strains over a five
years period and to establish which the still
active ones are.
Patients and methods: retrospective
study over a 5 years period at patients
admitted at the Newborn Department of
the Childrens’ Hospital Brasov Romania
between 01.01.2003-01.07.2007 in order to
establish the antibiotic susceptibility of
Staphylococcus strains and its variation
trends in time.
Results
We have studied 116 patients at which
we identified infections with S. aureus and
we included both hospital acquired and
community acquired Staphylococcus.
Sex distribution in the study group Table 1
Sex Total
Male Female
Percentage 100% 56,89% 43,11%
Subjects 116 66 50
75,86%
92,24%
8,62%
0,00%
15,51%
7,75%
over 2500
under 1500
1500 -2500g
Birth weight Actual weight
Fig.1. Weight repartition.
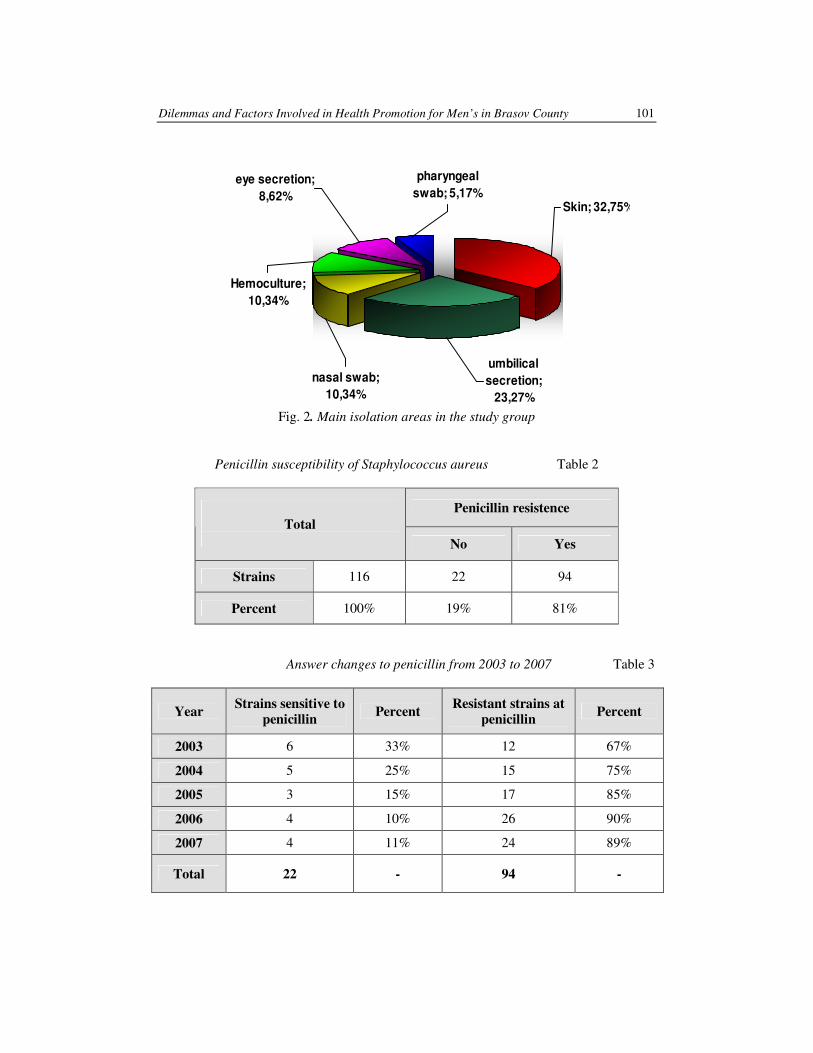
Dilemmas and Factors Involved in Health Promotion for Men’s in Brasov County 101
umbilical
secretion;
23,27%
nasal swab;
10,34%
Hemoculture;
10,34%
eye secretion;
8,62%
pharyngeal
swab; 5,17%
Skin; 32,75%
Fig. 2. Main isolation areas in the study group
Penicillin susceptibility of Staphylococcus aureus Table 2
Penicillin resistence
Total
No Yes
Strains 116 22 94
Percent 100% 19% 81%
Answer changes to penicillin from 2003 to 2007 Table 3
Year Strains sensitive to
penicillin Percent
Resistant strains at
penicillin Percent
2003 6 33% 12 67%
2004 5 25% 15 75%
2005 3 15% 17 85%
2006 4 10% 26 90%
2007 4 11% 24 89%
Total 22 - 94 -
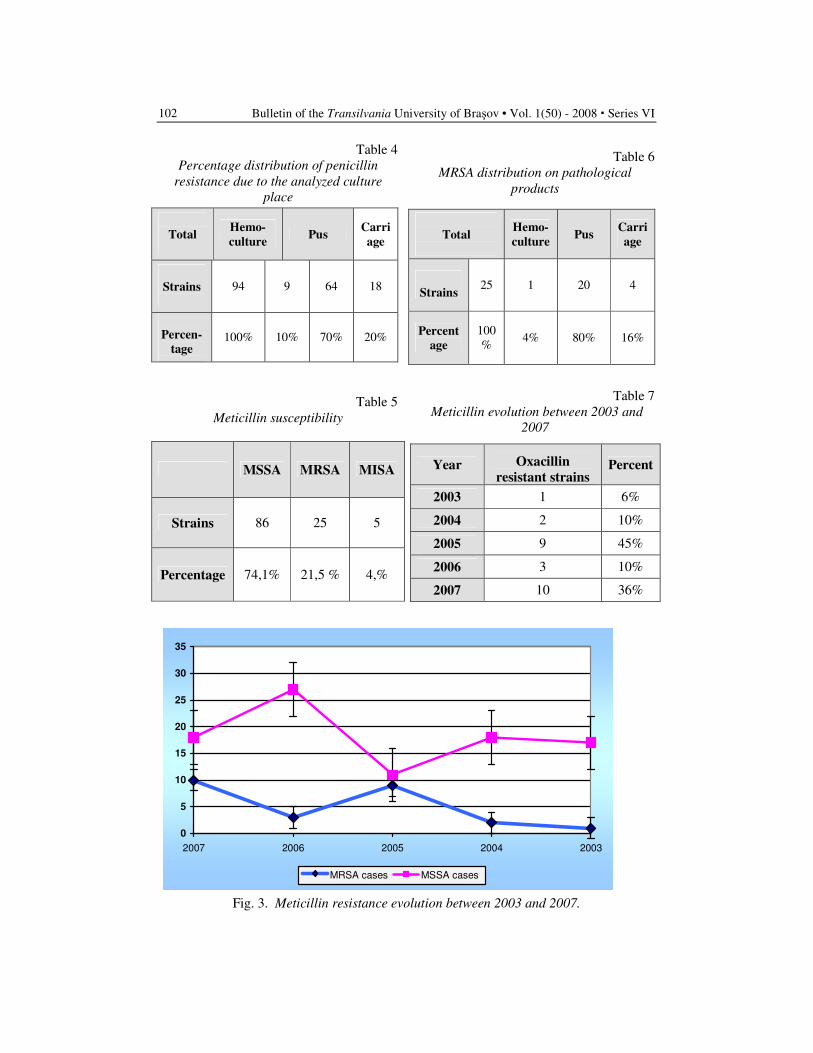
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
102
Table 4
Percentage distribution of penicillin
resistance due to the analyzed culture
place
Total
Hemo-
culture Pus
Carri
age
Strains
94 9 64 18
Percen-
tage
100% 10% 70% 20%
Table 5
Meticillin susceptibility
MSSA MRSA MISA
Strains 86 25 5
Percentage 74,1% 21,5 % 4,%
Table 6
MRSA distribution on pathological
products
Total
Hemo-
culture Pus
Carri
age
Strains 25 1 20 4
Percent
age
100
% 4% 80% 16%
Table 7
Meticillin evolution between 2003 and
2007
Year
Oxacillin
resistant strains Percent
2003 1 6%
2004 2 10%
2005 9 45%
2006 3 10%
2007 10 36%
0
5
10
15
20
25
30
35
2007 2006 2005 2004 2003
MRSA cases MSSA cases
Fig. 3. Meticillin resistance evolution between 2003 and 2007.
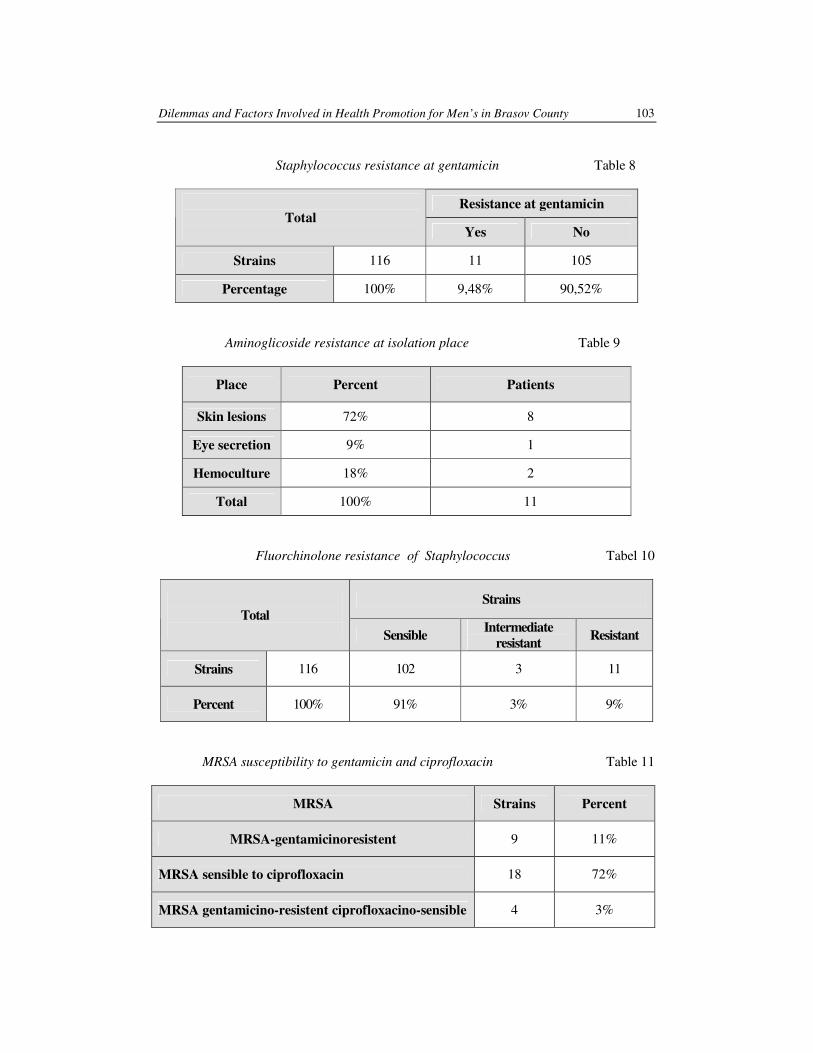
Dilemmas and Factors Involved in Health Promotion for Men’s in Brasov County 103
Staphylococcus resistance at gentamicin Table 8
Resistance at gentamicin
Total
Yes No
Strains 116 11 105
Percentage 100% 9,48% 90,52%
Aminoglicoside resistance at isolation place Table 9
Place Percent Patients
Skin lesions 72% 8
Eye secretion 9% 1
Hemoculture 18% 2
Total 100% 11
Fluorchinolone resistance of Staphylococcus Tabel 10
Strains
Total
Sensible Intermediate
resistant Resistant
Strains 116 102 3 11
Percent 100% 91% 3% 9%
MRSA susceptibility to gentamicin and ciprofloxacin Table 11
MRSA Strains Percent
MRSA-gentamicinoresistent 9 11%
MRSA sensible to ciprofloxacin 18 72%
MRSA gentamicino-resistent ciprofloxacino-sensible 4 3%
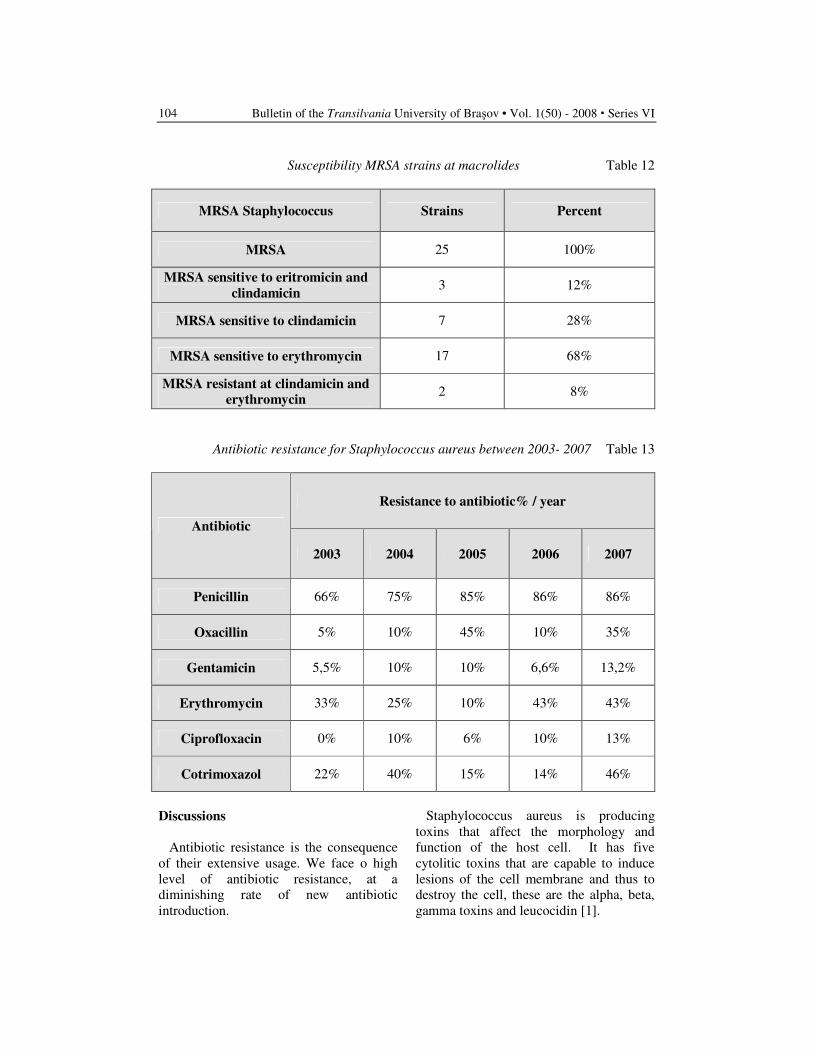
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
104
Susceptibility MRSA strains at macrolides Table 12
MRSA Staphylococcus Strains Percent
MRSA 25 100%
MRSA sensitive to eritromicin and
clindamicin 3 12%
MRSA sensitive to clindamicin 7 28%
MRSA sensitive to erythromycin 17 68%
MRSA resistant at clindamicin and
erythromycin 2 8%
Antibiotic resistance for Staphylococcus aureus between 2003- 2007 Table 13
Resistance to antibiotic% / year
Antibiotic
2003 2004 2005 2006 2007
Penicillin 66% 75% 85% 86% 86%
Oxacillin 5% 10% 45% 10% 35%
Gentamicin 5,5% 10% 10% 6,6% 13,2%
Erythromycin 33% 25% 10% 43% 43%
Ciprofloxacin 0% 10% 6% 10% 13%
Cotrimoxazol 22% 40% 15% 14% 46%
Discussions
Antibiotic resistance is the consequence
of their extensive usage. We face o high
level of antibiotic resistance, at a
diminishing rate of new antibiotic
introduction.
Staphylococcus aureus is producing
toxins that affect the morphology and
function of the host cell. It has five
cytolitic toxins that are capable to induce
lesions of the cell membrane and thus to
destroy the cell, these are the alpha, beta,
gamma toxins and leucocidin [1].

Dilemmas and Factors Involved in Health Promotion for Men’s in Brasov County 105
Among the studied strains 94 were
penicillin resistant representing 81% a rate
which is comparable with other countries
Sweden 86%, France 87% [14]. The
majority of MRSA were from skin lesions
[4]. Our strains were sensitive to
clindamicin and erythromycin.
Other authors reported the MRSA
Staphylococcus would be resistant also to
clindamicin and eitromicin [6].
Our data are still comparable with the
data coming from a study from Bogota
were the MRSA was 26% from which
3.2% being multiresistant [3]. From the
studied strains, three strains were resistant
to vancomicin. Recently similar strains
were reported in different countries, among
which, cited are the U.S.A, France, Spain,
Italy, Germany [8, 9, 11]. These strains are
named VISA with intermediate resistance
to vancomicin or GISA with intermediate
resistance to glicopeptides. All the VISA
described strains were MRSA.
Also from the studied strains, 11 were
resistant to gentamicin and 11 to
ciprofloxacin [5].
The resistance to gentamicin is mediated
through inactivating enzymes aminozid
acetiltransferase that causes resistance to
all aminoglicosides’, aminozid nucleotidil
transferase that causes resistance at
amikacin and tobramicin among other
antibiotics, aminozid phopfotransferase
that causes resistance also at amikacin and
isepamicin.
The action mechanism is modifying the
action target, ribosomal 50S encoded by
the ermA genes but also by the ermB ermC
and there are two described mechanisms
for these: constitutive and inducible one.
The resistance mechanisms towards
fluoroquinolones is modification of AND
girase and topoisomerase IV due to
mutation at gene gyrA and parC, efflux
pumps, diminished penetration of bacterial
wall [10]. In addition, there are described
inactivating enzymes and active efflux.
Antibiotic resistance is the consequence
of their extensive usage. Among the
studied strains 94 were penicillin resistant
representing 81% a rate which is
comparable with other countries Sweden
86%, France 87% (14). The majority of
MRSA were from skin lesions [7].
The limits of our study were a short
period of time only 5 years, relative small
number of strains 116, including criteria
were quiet strict only strains from the
newborn department and culture
Staphylococcus positive.
Conclusions
1. In the study group there was a slight
predominance of male.
2. We are facing a slight but constant
increase of meticcilllin resistance.
3. Most of the isolated MRSA are from
skin lesions.
4. Three of the studied strains have an
intermediate resistance at
vancomicin.
5. Still active antibiotics are
aminoglicoside, clindamicin and
rifampicin.
References
1. Ayliffe, G.: The progressive
intercontinental spread of methicillin-
resistant Staphylococcus aureus. In:
Clinical Infectious Diseases 1997; 24
Suppl 1: S74-9.
2. Celebi, S., Hacimustafaoglu, M.,
Ozdemir, O., Ozakin, C.: Mosocomial
Gram-positive bacterial infections in
children: results of a 7 year study. In:
Pediatr Int 2007, 49(6): 875-882.
3. Cortes, J.A., Andrés Gómez, C.,
Cuervo, S.I., Leal, A.L.: Community-
acquired methicillin-resistant Sta–
phylococcus aureus in Bogotá,
Colombia. In: Rev. Salud pública, 9, 3
Bogotá jul./sep. 2007.
4. Frank, A.L., Marcinak, J.F., Mangat,
P.D., Schreckenberger, P.C.: Comm-
unity- acquired and clindamycin-
susceptible methicillin-resistant Sta-
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
106
phylococcus aureus in children. In: Pe-
diatric Infect Dis J. 1999; 18: 993-
1000.
5. Gregory, J., Moran, M. D.,
Kirshnadasan. A.: MRSA infections
among patients in the emergency
departament. In: New Engl J Med
2006; 355:666-74.
6. Hand, W.L., King-Thompson, N.L.,
Steinberg, T.H.: Interactions of anti-
biotic and phagocytes. In: J
Antimicrob Chemother. 1983; 12
(suppl C):1-11.
7. Herold, B.C., Immergluck, L.C.,
Maranan, M.C. et al.: Community
acquiered meticillin resistant
Staphylococcus aureus in children
with no predisposing factor. In:
JAMA.1998; 279: 593-598. 8. Howden, B.P., Ward, P.B., Charles,
P.G., Korman, T.K., Fuller, A., du
Cros, P., Grbasch, E.A., Roberts, S.A.,
Robson, J., Read K., Bak, N., Hurley,
J., Johnson, P.D., Morris, A.J., Mayall,
B.C., Grayson, M.L.: Treatment
outcomes of serious infections caused
by methicillin-resistant Staphylococcus
aureus with reduced vancomycin
susceptibility. In: Clin Infect Dis 2004;
38:521-528.
9. Kantzanou, M., Tassios, P.T., Tseleni-
Kotsovili, A., Legakis, N.J., Vatopoulos,
A.C.: Reduced susceptibility to
vancomycin of nosocomial isolates of
methicillin-resistant Staphylococcus
aureus. In: J Antimicrob Chemother
1999; 43:729-31.
10. Lowy, F.D.: Staphylococcus aureus
infections. In: New Engl J Med. 1998;
339: 520-32.
11. Marchese, A., Balistreri, G., Tonoli,
E., Debbia, E.A., Schito, G.C.: Hetero-
geneous vancomycin resistance in
methicillin-resistant Staphylococcus
aureus strains isolated in a large
Italian hospital. In: J. Microbiol 2000;
38:866-869.
12. NNIS System - National Nosocomial
Infections Surveillance (NNIS) System
Report, data summary from January
1992 through June 2003, issued
August 2003. In: Am J Infect Control,
2003, 31: 481-498.
13. Santos, F., Mankarious, L.A., Eavey,
R.D.: Methicillin-resistant Staphylo-
coccus aureus: pediatric otitis. In:
Arch Otolaryngol Head Neck Surg.
2000; 126:1383-1385.
14. Van der Mee-Marquet, Epinette, C.,
Loyau, J. et al. : S.: aureus strains
isolated from bloodstream infections
changed significantly in 2006. In: J
Clin Microb, 2007; 851-857.
STIGMATIZATION OF PEOPLE WITH
SCHIZOPHRENIA IN CLINICAL
SETTINGS
V. BURTEA
1 C. MOŞOIU
1
Abstract: The stigmatizing of, and discrimination against, people with
mental disorders is as old as humanity. It is also known that stigma and
discrimination negatively affect the treatment and recovery of people with
mental illness. The main target of the study is to begin to collect robust data
about stigma in schizophrenia in order to make possible to carry out specific
programmes against it. Our study intended to measure the stigma of people
with schizophrenia using the Stigma Experiences Scale -Consumer Version,
hospitalized in Psychiatric and Neurologic Hospital Brasov between 1 iulie
2007-1 July 2008, in order to see how this problem is managed in clinical
settings. Conclusions of the study reflected the opinion of the respondents:
they think that they were been harassed because of mental illness, they
considered that they rights were been denied and that stigma affected
negatively their quality of life
Key words: Stigmatization, patients with schizophrenia.
1 Transilvania University of Brasov, Dep of Psychiatry.
Introduction
Stigma is not a static concept, but a
social construction that is linked to values
placed on social identities, a process
consisting of two fundamental compo-
nents: the recognition of the differentiating
“mama” and the subsequent devaluation of
the bearer [1]. Thus, stigma could be
conceived of as a relational construct that
is based on attributes, which may change
with time and from one culture to another.
Stigma develops within a social matrix of
relationships and interactions so that new
conditions could become stigmatizing and
conditions that may be stigmatizing at one
time or within a given culture could come
to be accepted later so that their bearers
stop being stigmatized. Furthermore,
stigma can be understood within a three-
dimensional axis involving perspective,
identity and reactions. Stigma is different,
whether it be perceived by the person who
does the stigmatizing (perceiver) or by the
person who is being stigmatized
(target).cultural perceptions of mental
illness consider it as posing a tangible
threat to the health of society because it
engenders two kinds of fear: the fear of
potential immediate physical threat of
attack and fear that we may all share in
losing our own sanity [3].
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
108
Methods
We assess the stigmatization of people
with schizophrenia the Stigma Experiences
Scale-Consumer Version with 10 items: as
in table A.
The Stigma Experiences Scale-
Consumer Version
Scale item:
1. Do you think that people think less
of you if they know you have a
mental illness?
2. Do you think that the average
person is afraid of someone with a
serious mental illness?
3. Have you ever been teased, bullied
or harassed because you have a
mental illness?
4. Have you felt that you have been
treated unfairly or that your rights
have been denied because you have
a mental illness?
5. Have your experiences with stigma
affected your recovery?
6. Have your experiences with stigma
caused you to think less about
yourself or your abilities?
7. Have your experiences with stigma
affected your ability to make or
keep friends?
8. Have your experiences with stigma
affected your ability to interact with
your family?
9. Have your experiences with stigma
affected your satisfaction or quality
of life?
10. Do you avoid situations that may be
stigmatizing to you?
The first two items refer to expectation
of stigma and are scored on a 5-point
Likert-type scale using the response
categories of never, rarely, some times,
often and always. These responses were
recoded into a binary variable, with 1
reflecting a high expectation of stigma
(often and always), and zero reflecting no
or low expectation (never, rarely, and
sometimes).
The remaining eight items used three
response categories: no, unsure and yes.
These were also recoded into binary
categories reflecting the presence (yes) or
absence (no and unsure) of each
experience.
We assess 32 patients with schizophrenia
according with DSM-IV criteria
hospitalized in. the period 1 July 2007-1
July 2008 in the Psychiatric and
Neurological Hospital Brasov. Region of
residence, age, gender, were recorded. All
the respondents were in pension. More
detailed information on the development
and testing of this scale is published by
Stuart, Milov and Koller [4].
Statistical Methods
The responses recorded on the 5 point
scales were converted into scores as
follows: scores 1 and 2 were coded as
negative, scores 4 and 5 were coded as
positive, and those who were unsure or
could not answer the question were
assigned to the central code 3. An overall
opinion score was obtained by summing
the scores of all items. The resulting score
varies from 10-34
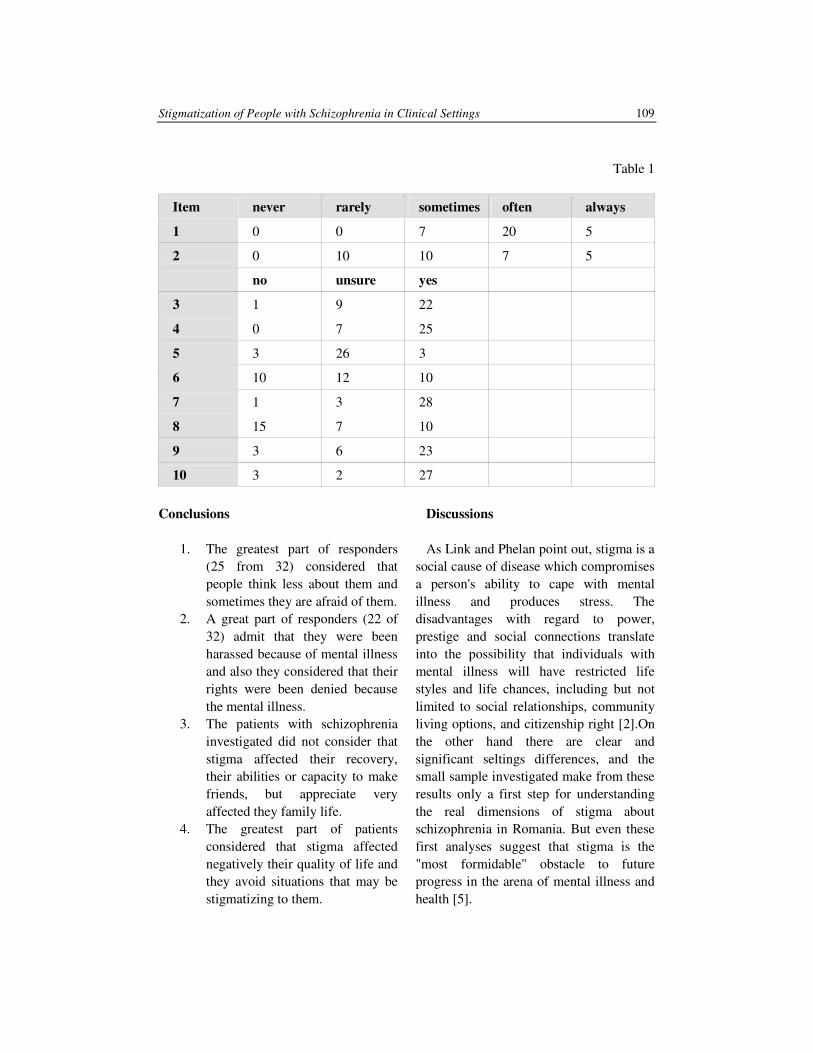
Stigmatization of People with Schizophrenia in Clinical Settings 109
Table 1
Item never rarely sometimes often always
1 0 0 7 20 5
2 0 10 10 7 5
no unsure yes
3 1 9 22
4 0 7 25
5 3 26 3
6 10 12 10
7 1 3 28
8 15 7 10
9 3 6 23
10 3 2 27
Conclusions
1. The greatest part of responders
(25 from 32) considered that
people think less about them and
sometimes they are afraid of them.
2. A great part of responders (22 of
32) admit that they were been
harassed because of mental illness
and also they considered that their
rights were been denied because
the mental illness.
3. The patients with schizophrenia
investigated did not consider that
stigma affected their recovery,
their abilities or capacity to make
friends, but appreciate very
affected they family life.
4. The greatest part of patients
considered that stigma affected
negatively their quality of life and
they avoid situations that may be
stigmatizing to them.
Discussions
As Link and Phelan point out, stigma is a
social cause of disease which compromises
a person's ability to cape with mental
illness and produces stress. The
disadvantages with regard to power,
prestige and social connections translate
into the possibility that individuals with
mental illness will have restricted life
styles and life chances, including but not
limited to social relationships, community
living options, and citizenship right [2].On
the other hand there are clear and
significant seltings differences, and the
small sample investigated make from these
results only a first step for understanding
the real dimensions of stigma about
schizophrenia in Romania. But even these
first analyses suggest that stigma is the
"most formidable" obstacle to future
progress in the arena of mental illness and
health [5].

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
110
References
1. Davidio, J.F., Major, B and Crocker,
J.: Stigma: Introduction and
overview. In T.F. Heatherton, R.E.
Kleck, MR. Hebl and J.G Hull. The
social Psychology of Stigma. New
York: Guilford Press, 2000.
2. Failer, J.L.: Who Qualifies for Rights
Homelessness, Mental Illness, and
Civil Commitment. Ithaca, NY:
Cornell University Press, 2002.
3. Link, B.G., Phelan, J.C.:
Conceptualizing stigma. In: Annual
Review of Sociology 27, (2001)
363-385.
4. Stuart, H, Milev, R., and Koller, M.:
The inventory of stigmatizing
experiences: its development and
reliability. In: Word Psychiatry 4 S1,
(2005) : 35-39.
5. US Department of Health and Human
Services (1999) Mental Health: A
Report of the Surgeon General.
Rockville, MD: US. Department of
Health and Human Servicies,
Substance Abuse and Mental Services
Administration, Center for Mental
Health, National Institute of Mental
Health.

THE MAJOR DEPRESSIVE DISORDER
WITH METABOLIC SYNDROME - STUDY
ON 90 PATIENTS
P. IFTENI
1 V. BURTEA
1
Abstract: Patients with severe depression have elevated rates of
cardiovascular disease (CVD) and diabetes compared with the general
population, but little is known about the prevalence of the metabolic
syndrome that predisposes patients with depression to metabolic syndrome.
Key words: depressive disorder, metabolic syndrome.
1 Transilvania University of Brasov, Faculty of Medicine.
1. Background
Major depressive disorder is the most
prevalent psychiatric illness in the United
States, affecting more than 12% of men and
more than 21% of women in their lifetime
[3]. Previous studies indicate that prevalence
of major depression has increased during the
past century, although these trends may, in
part, be explained by methodological
problems [6]. Depression has been
associated with a variety of diseases;
specifically it has been implicated in the
development of cardiovascular disease
(CVD) and all-cause mortality [2, 5].
However, little is understood about
mechanisms that may account for poor
health outcomes associated with depression.
Previous reports have speculated that
depression may be linked to adverse health
outcomes through an association with the
metabolic syndrome [1, 2, 4].
2. Objectives
Previous reports have suggested that
depression may lead to the development of
cardiovascular disease through its
association with the metabolic syndrome;
however, little is known about the
relationship between depression and the
metabolic syndrome. The aim of this study
was to establish an association between
depression and the development of
metabolic syndrome.
3. Methods
Our study included 90 participants, aged
18 to 65 years, hospitalized in Psychiatry
and Neurology Hospital Brasov. The
interview on the lifetime prevalence of a
major depressive episode (MDE) was
based on criteria specified in the
Diagnostic and Statistical Manual of
Mental Disorders, Forth Edition, Revised
(DSM-IV-TR) [9]. The Diagnostic
Interview Schedule also yielded
information about number of episodes, age
of first episode, and the presence of a
current episode. The severity of depression
was evaluated using HAM-21 (Hamilton
Depression Scale), GAF (Global
Assessment of Functioning), CGI (Clinical
Global Impression), number of episodes
and the time between episodes.
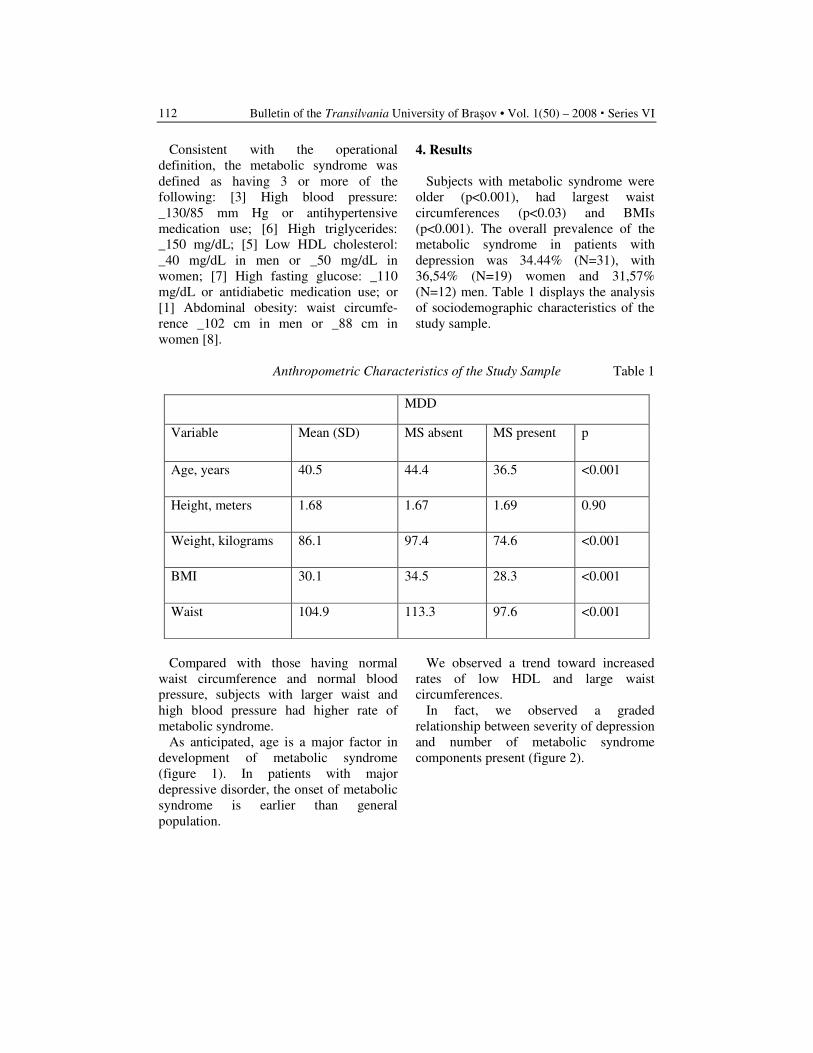
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
112
Consistent with the operational
definition, the metabolic syndrome was
defined as having 3 or more of the
following: [3] High blood pressure:
_130/85 mm Hg or antihypertensive
medication use; [6] High triglycerides:
_150 mg/dL; [5] Low HDL cholesterol:
_40 mg/dL in men or _50 mg/dL in
women; [7] High fasting glucose: _110
mg/dL or antidiabetic medication use; or
[1] Abdominal obesity: waist circumfe-
rence _102 cm in men or _88 cm in
women [8].
4. Results
Subjects with metabolic syndrome were
older (p<0.001), had largest waist
circumferences (p<0.03) and BMIs
(p<0.001). The overall prevalence of the
metabolic syndrome in patients with
depression was 34.44% (N=31), with
36,54% (N=19) women and 31,57%
(N=12) men. Table 1 displays the analysis
of sociodemographic characteristics of the
study sample.
Anthropometric Characteristics of the Study Sample Table 1
MDD
Variable Mean (SD) MS absent MS present p
Age, years 40.5 44.4 36.5 <0.001
Height, meters 1.68 1.67 1.69 0.90
Weight, kilograms 86.1 97.4 74.6 <0.001
BMI 30.1 34.5 28.3 <0.001
Waist 104.9 113.3 97.6 <0.001
Compared with those having normal
waist circumference and normal blood
pressure, subjects with larger waist and
high blood pressure had higher rate of
metabolic syndrome.
As anticipated, age is a major factor in
development of metabolic syndrome
(figure 1). In patients with major
depressive disorder, the onset of metabolic
syndrome is earlier than general
population.
We observed a trend toward increased
rates of low HDL and large waist
circumferences.
In fact, we observed a graded
relationship between severity of depression
and number of metabolic syndrome
components present (figure 2).
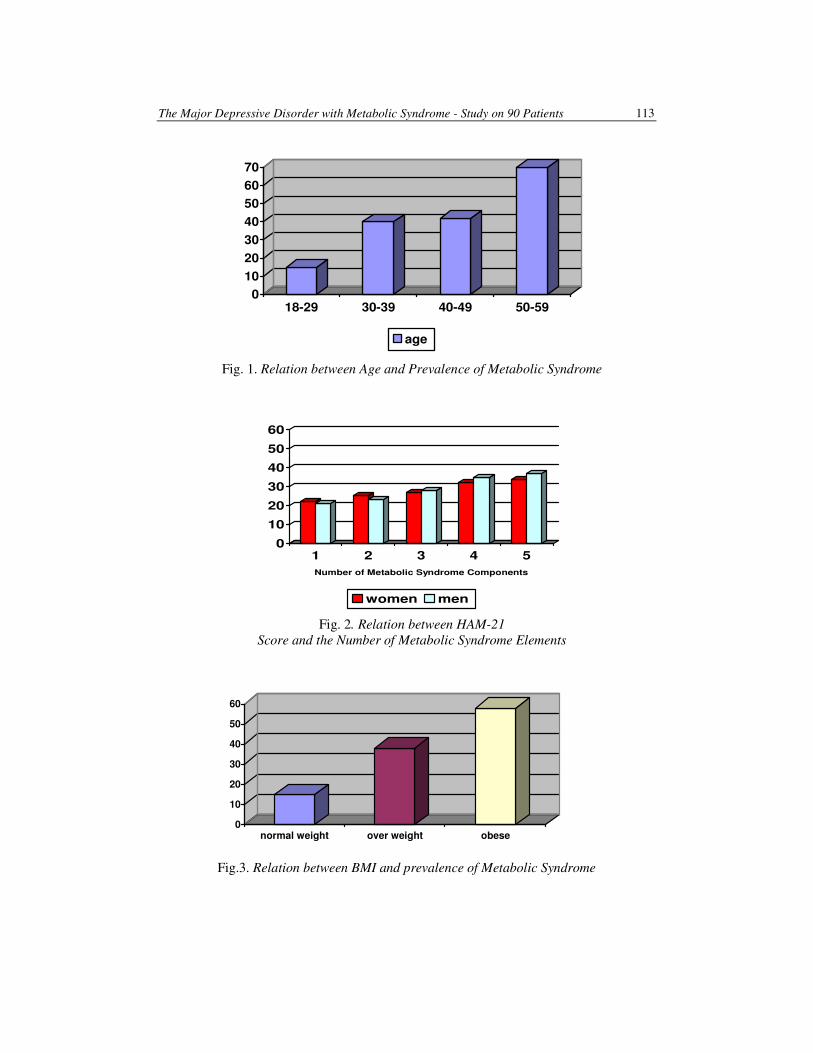
The Major Depressive Disorder with Metabolic Syndrome - Study on 90 Patients 113
0
10
20
30
40
50
60
70
18-29 30-39 40-49 50-59
age
Fig. 1. Relation between Age and Prevalence of Metabolic Syndrome
0
10
20
30
40
50
60
1 2 3 4 5
Number of Metabolic Syndrome Components
women men
Fig. 2. Relation between HAM-21
Score and the Number of Metabolic Syndrome Elements
0
10
20
30
40
50
60
normal weight over weight obese
Fig.3. Relation between BMI and prevalence of Metabolic Syndrome

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
114
Conclusions
This is the first study in Romania who
tried to examine the relationship between
depression and the metabolic syndrome, as
defined by the ATP III guidelines, in a
representative sample of patients, during a
period of four years. The results presented
here demonstrate that patients with major
depressive disorder were more than twice
as likely to have the metabolic syndrome
compared with those with no history of
depression.
Specifically, depression appeared to be
most closely associated with high blood
pressure and large waist circumferences.
The co-morbidity of depression and the
metabolic syndrome, in terms of severity
of depression, demonstrate that the
elements of metabolic syndrome aggravate
depression through increased CGI score
and decreased GAF score. The relapses
were more frequently in patients with
depression and metabolic syndrome and
the periods between episodes were
significantly shorter.
References
1. Bjorntorp, P.: Stress and
cardiovascular disease. In: Acta
Physiol Scand Suppl 1997; 640: 144-8.
2. Chrousos, G.P.: The role of stress and
the hypothalamic-pituitary-adrenal
axis in the pathogenesis of the meta-
bolic syndrome: neuro-endocrine and
target tissue-related causes. In: Int J
Obes 2000; 24: S50–5.
3. Kessler, R.C., McGonagle, K.A.,
Zhao, S., Nelson, C.B., Hughes, M.,
Eshleman, S., Wittchen, H., Kendler,
K.S.: Lifetime and 12-month
prevalence of DSMIII–R psychiatric
disorders in the United States: results
from the National Comorbidity Study.
In: Arch Gen Psychiatry 1994; 51:
8–19.
4. Kinder, L.S., Kamarck, T.W., Baum,
A., Orchard, T.J.: Depressive
symptomatology and coronary heart
disease in Type I diabetes mellitus: a
study of possible mechanisms. In:
Health Psychol 2002; 21: 542–52.
5. Musselman, D.L., Evans, D.L.,
Nemeroff, C.B.: The relationship of
depression to cardiovascular disease.
In: Arch Gen Psychiatry 1998; 55:
580–92.
6. Simon, G.E., VonKorff, M.:
Reevaluation of secular trends in
depression rates. In: Am J Epidemiol
1992; 135: 1411–22.
7. Wulsin, L.R., Vaillant, G.E., Wells,
V.E.: A systematic review of the
mortality of depression. In: Psychosom
Med 1999; 61: 6–17.
8. *** Centers for Disease Control and
Prevention. The Third National Health
and Nutrition Examination Survey
(NHANES III 1988–94) Reference
Manuals and Reports. Bethesda, MD:
National Center for Health Statistics,
1996.
9. *** Diagnostic and statistical manual of
mental disorders, 3rd ed. revised.
Washington, DC: American
Psychiatric Association, 1987.

POSITIVE AND NEGATIVE SYNDROME
SCALE CLUSTERING OF
SCHIZOPHRENIA
C. MOŞOIU
1 V. BURTEA
1
Abstract: Clustering deals with finding a structure in a collection of unlabeled
data with the aid of unsupervised learning. The aim of the study was to investigate
evidence of a more complex structure of schizophrenia. Analysis with hierarchical
clustering was applied to a sample of schizophrenic patients who had been scored
on the Positive and Negative Syndrome Scale.
Key words: schizophrenia, clustering, evaluation scale.
1 Transilvania University of Brasov, Dep Fundam. and Prophylactic Disciplines.
1. Introduction
The aim of this article is to investigate
the subtypes of schizophrenia with the aid
of a method of cluster analysis that was
applied to the Positive and Negative
Syndrome Scale (PANSS).
Clustering can be considered the most
important unsupervised learning method and
it deals with finding a structure in a
collection of unlabeled data. Loose definition
of clustering is the process of organizing
objects into groups whose members are
similar. A cluster is a collection of objects
which are “similar” between them and are
“dissimilar” to the objects belonging to other
clusters. The similarity criterion is distance:
two or more objects belong to the same
cluster if they are “close” according to a
given distance (e.g.geometrical distance) in
distance-based clustering.
Another kind of clustering is conceptual
clustering which means that objects belong
to the same cluster if this one defines a
concept common to all objects. In other
words, objects are grouped according to
their fit to descriptive concepts, not
according to simple similarity measures.
2. Material and Methods
The aim of the study was to investigate
evidence of a more complex structure of
schizophrenia than the relatively simple
negative-positive symptoms concept [2, 3, 5,
6]. For this purpose, hierarchical duster
analysis was applied to a sample of patients
who had been scored on the Positive and
Negative Syndrome Scale (PANSS) [4]. This
particular instrument was chosen because of
its known validity and its widespread use and
because it includes negative, positive, and
general psychopathology items (such as
depression and anxiety).
A total of 38 patients were included.
(mean age = 38.7 years, mean duration
of illness = 12,8 years, 43% males). The
patients used in this investigation
belonged to a cohort of schizophrenia
patients at the Braşov psychiatric unit.
The patients were rated as having
schizophrenia according to diagnostic
criteria defined by DSM IV- TR [1].
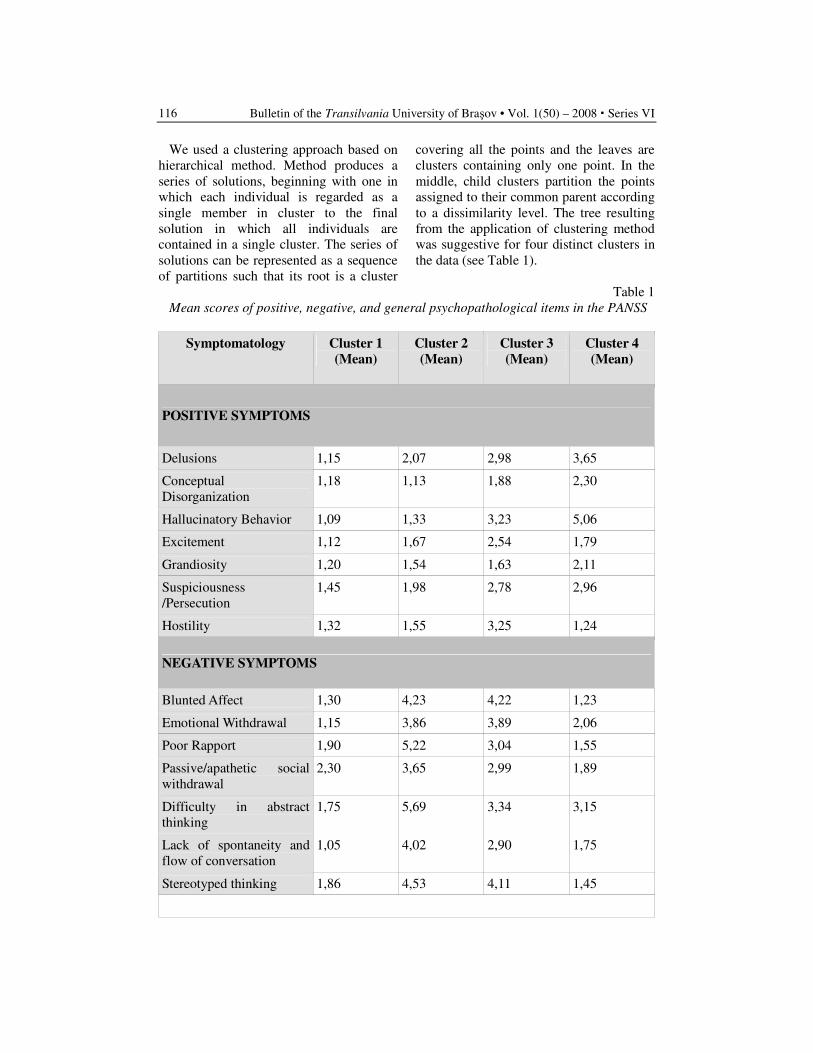
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
116
We used a clustering approach based on
hierarchical method. Method produces a
series of solutions, beginning with one in
which each individual is regarded as a
single member in cluster to the final
solution in which all individuals are
contained in a single cluster. The series of
solutions can be represented as a sequence
of partitions such that its root is a cluster
covering all the points and the leaves are
clusters containing only one point. In the
middle, child clusters partition the points
assigned to their common parent according
to a dissimilarity level. The tree resulting
from the application of clustering method
was suggestive for four distinct clusters in
the data (see Table 1).
Table 1
Mean scores of positive, negative, and general psychopathological items in the PANSS
Symptomatology Cluster 1
(Mean)
Cluster 2
(Mean)
Cluster 3
(Mean)
Cluster 4
(Mean)
POSITIVE SYMPTOMS
Delusions 1,15 2,07 2,98 3,65
Conceptual
Disorganization
1,18 1,13 1,88 2,30
Hallucinatory Behavior 1,09 1,33 3,23 5,06
Excitement 1,12 1,67 2,54 1,79
Grandiosity 1,20 1,54 1,63 2,11
Suspiciousness
/Persecution
1,45 1,98 2,78 2,96
Hostility 1,32 1,55 3,25 1,24
NEGATIVE SYMPTOMS
Blunted Affect 1,30 4,23 4,22 1,23
Emotional Withdrawal 1,15 3,86 3,89 2,06
Poor Rapport 1,90 5,22 3,04 1,55
Passive/apathetic social
withdrawal
2,30 3,65 2,99 1,89
Difficulty in abstract
thinking
1,75 5,69 3,34 3,15
Lack of spontaneity and
flow of conversation
1,05 4,02 2,90 1,75
Stereotyped thinking 1,86 4,53 4,11 1,45
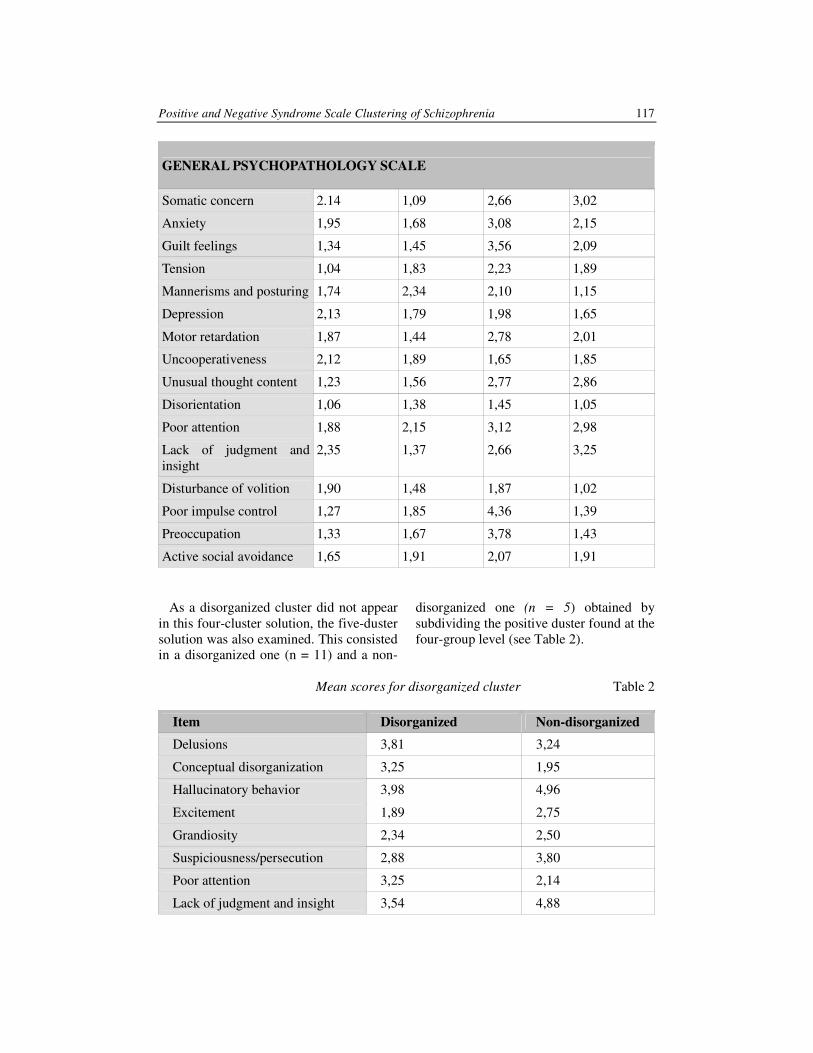
Positive and Negative Syndrome Scale Clustering of Schizophrenia 117
GENERAL PSYCHOPATHOLOGY SCALE
Somatic concern 2.14 1,09 2,66 3,02
Anxiety 1,95 1,68 3,08 2,15
Guilt feelings 1,34 1,45 3,56 2,09
Tension 1,04 1,83 2,23 1,89
Mannerisms and posturing 1,74 2,34 2,10 1,15
Depression 2,13 1,79 1,98 1,65
Motor retardation 1,87 1,44 2,78 2,01
Uncooperativeness 2,12 1,89 1,65 1,85
Unusual thought content 1,23 1,56 2,77 2,86
Disorientation 1,06 1,38 1,45 1,05
Poor attention 1,88 2,15 3,12 2,98
Lack of judgment and
insight
2,35 1,37 2,66 3,25
Disturbance of volition 1,90 1,48 1,87 1,02
Poor impulse control 1,27 1,85 4,36 1,39
Preoccupation 1,33 1,67 3,78 1,43
Active social avoidance 1,65 1,91 2,07 1,91
As a disorganized cluster did not appear
in this four-cluster solution, the five-duster
solution was also examined. This consisted
in a disorganized one (n = 11) and a non-
disorganized one (n = 5) obtained by
subdividing the positive duster found at the
four-group level (see Table 2).
Mean scores for disorganized cluster Table 2
Item Disorganized Non-disorganized
Delusions 3,81 3,24
Conceptual disorganization 3,25 1,95
Hallucinatory behavior 3,98 4,96
Excitement 1,89 2,75
Grandiosity 2,34 2,50
Suspiciousness/persecution 2,88 3,80
Poor attention 3,25 2,14
Lack of judgment and insight 3,54 4,88

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
118
3. Conclusions
The first cluster (n = 5) had low scores
on all the negative, positive, and general
psychopathological items of the PANSS
and contains patients characterized by a
mild symptomatology.
The second cluster (n = 7) contains
patients having high scores on negative
items and on some general items
(mannerisms and posturing, depression,
motor retardation, poor attention, lack of
judgment and insight) and low scores on
positive.
The third duster (n = 11) is a mixed one
because of high scores on the positive,
negative, and general psychopathological
items.
The fourth duster (n = 15) contains
patients that were higher on positive items
and some general psychopathological
items (somatic concerns, anxiety, tension,
unusual thought content, poor attention).
Conceptual disorganization, excitement,
grandiosity, and poor attention were
significantly more severe in the
disorganized than in the non-disorganized
cluster. Also delusions, hallucinatory
behaviour, suspiciousness/ persecution,
and lack of judgment and insight were
more severe in the non-disorganized
cluster.
4. Discussion
Data gathered from this small sample of
schizophrenic patients identify four or five
clusters of symptoms instead of
positive/negative concepts. Further studies
based on larger samples need to be
performed in order to improve validity
and reliability of clustering method and
maybe to discover latent variables on the
sample.
References
1. American Psychiatric Association.
DSM-IV-TR: Diagnostic and
Statistical Manual of Mental
Disorders. 4th ed., revised.
Washington, DC: The Association,
2002.
2. Blanchard, J.J., Horan, W.P., Collins
L.M.: Examining the latent structure
of negative symptoms: is there a
distinct subtype of negative symptom
schizophrenia? In: Schizophr Res.
2005; 77: 151–165.
3. Gottesman, I.I., Gould, T.D.: The
endophenotype concept in psychiatry:
etymology and strategic intentions. In:
Am J Psychiatry. 2003; 160: 636–645.
4. Kay, S.R., Fiszbein, A., Opler, L.A.:
The Positive and Negative Syndrome
Scale (PANSS) for schizophrenia. In:
Schizophrenia Bulletin, 13(2): 261-
276, 1987.
5. Kendell, R., Jablensky, A.:
Distinguishing between the validity
and the utility of psychiatric
diagnoses. In: Am J Psychiatry.
2003;160:4–12
6. Lindenmayer, J.P., Brown, E., Baker,
R.W., et al.: An excitement subscale of
the positive and negative syndrome
scale. In: Schizophr Res. 2004; 68:
331–337.
HEMODYNAMICS OF THE POSTERIOR
CEREBRAL ARTERY
C. FALUP-PECURARIU
1 A. POSTELNICU
2
G. PAMFIL3 V. MONESCU
4
O. FALUP-PECURARIU5 R. ALEXANDRU
6
Abstract: Willis Circle is a key element during cerebral autoregulation.
There are mathematical models which evaluate its global hemodynamics or
part of them. The aim of this study is to evaluate flow rates and pressures of
the posterior cerebral artery in 1D Willis Circle model with variables
geometries. Based on 1D model we varied lengths and diameters of each
component artery and developed 3D models. We used lengths and diameters
and by using Statistic 7 software, we developed colour-coded graphs. We
obtained colour spectrums together with legends. We elaborated flow rates
based on lengths and diameters for each component artery of Willis Circle.
Variation trend of flow rates for segment P1 of PCA obtained by spine
method demonstrated that biggest flow rates were obtained for minimal
lengths and maximal diameters. The smallest flow rates were obtained for
smallest diameters independent by length.
Key words: Willis Circle, posterior cerebral artery, hemodynamics,
mathematical model.
1 Dept. of Neurology, Transilvania University of Braşov 2 Dept. of Thermotechnics and Fluid Mechanics, Transilvania University of Braşov 3 Dept. of Automathics, Transilvania University of Braşov 4 Dept. of Mathematics, Transilvania University of Braşov 5 Dept. of Pediatrics, Transilvania University of Braşov 6 Student, Faculty of Medicine, Transilvania University of Braşov
1. Introduction
Willis Circle was described for the first
time by Johann Wepfer (1620-1695).
Thomas Willis (1621-1675) described this
completely, so this circle takes his names.
Afterwards many authors have studied its
morphology and its variants: Vicq D’Azir,
Duret, de Vriese, Alpers (cit. by Alpers
and Berry (1963) [3], Lazorthes and
Goauze (1968) [9], Lazorthes et al. (1976)
[10], Lazorthes et al. (1979) [11],
Lazorthes et al. [12], Batujeff 1889, Mori
1893, Cavatorti 1908, Busse 1921,
Mitterwalkner 1955, Decker and Hipp
1958, Servida and Mortillaro 1963,
Cavallotti 1980 (cit. by Padget (1948)
[14]).
2. Anatomy
Posterior cerebral artery (PCA) born
from bifurcation of basilar artery at ponto-
mesencephalic sulk (Bracard et al. [6],
Arseni and Popoviciu [4]). Branches with
cortical destination are born constantly at
P1 and P2 segments.
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
120
Banias-Palaghiţă (1999) [5] published
mean lengths of 6.46 mm for posterior
cerebral artery. Branches P1 of PCA have
greater values in the right. At women the
mean length was 6.8 mm and for men 6.5
mm. Posterior cerebral artery had mean
value of 11.6 mm with a mean value of
12.1 mm in the right and 11,83 mm in the
left. At women mean value was 11.92 mm
and at men 11.34 mm [5].
The aim of this study is to evaluate flow
rates and pressures at posterior cerebral
artery in 1D Willis Circle model with
variables geometries.
Material and Method
Based on 1D model we developed 3D
models. We used lengths and diameters
and by using Statistic 7 software we
developed colour coded graphs. We
obtained colour spectrums together with
legends. We elaborated flow rates based on
lengths and diameters for each component
artery of Willis Circle. In the followings
we will present data regarding posterior
cerebral artery (PCA).
Graphic 1. Distribution of variations of lengths, diameters
and flow rates at right PCA segment P1
In this case the most of the points were at
diameter of 3 mm and respectively 3.5
mm. For lengths most of the points were at
15, 20 and 25 mm.
Most of combinations of points were at
minimal lengths (15 mm) and maximal
diameter (3 and 3,5 mm), followed by
diameters of 20 and 3 mm, respectively 20
and 3.5 mm, 25 and 3 mm, respectively 20
and 35 mm, 25 and 3 mm, 25 and 3,5 mm.
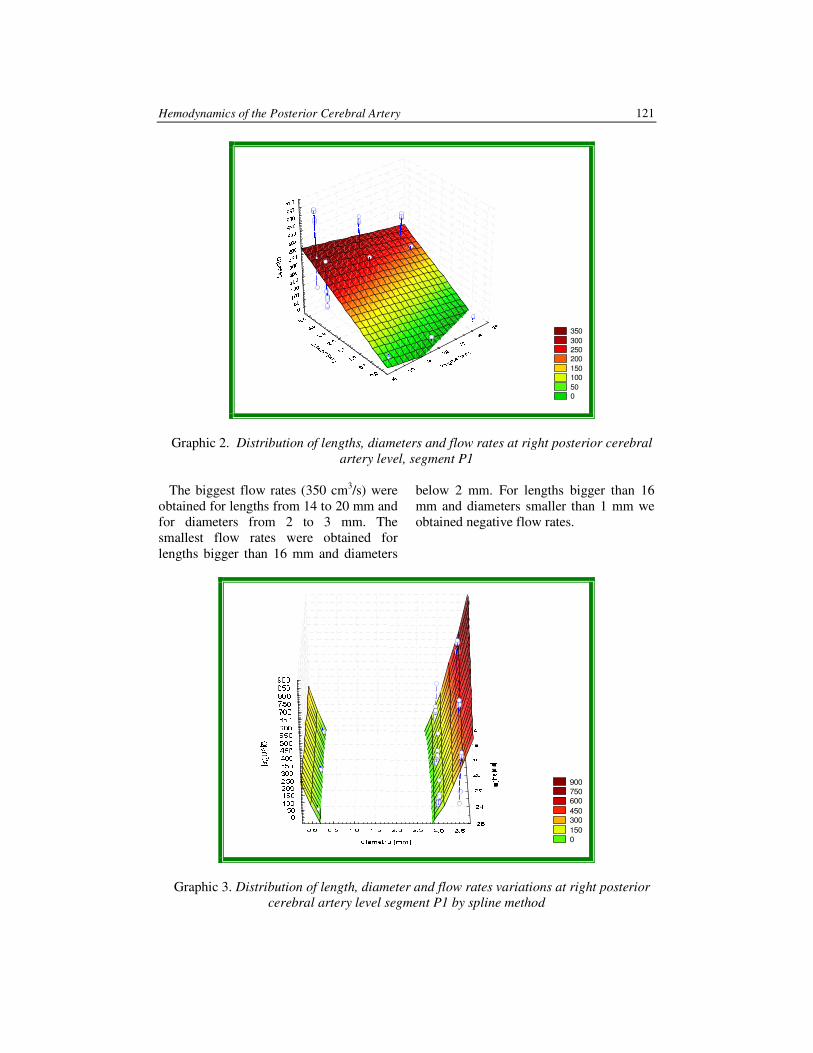
Hemodynamics of the Posterior Cerebral Artery 121
350
300 250 200
150 100
50 0
Graphic 2. Distribution of lengths, diameters and flow rates at right posterior cerebral
artery level, segment P1
The biggest flow rates (350 cm3/s) were
obtained for lengths from 14 to 20 mm and
for diameters from 2 to 3 mm. The
smallest flow rates were obtained for
lengths bigger than 16 mm and diameters
below 2 mm. For lengths bigger than 16
mm and diameters smaller than 1 mm we
obtained negative flow rates.
900 750 600
450 300
150 0
Graphic 3. Distribution of length, diameter and flow rates variations at right posterior
cerebral artery level segment P1 by spline method
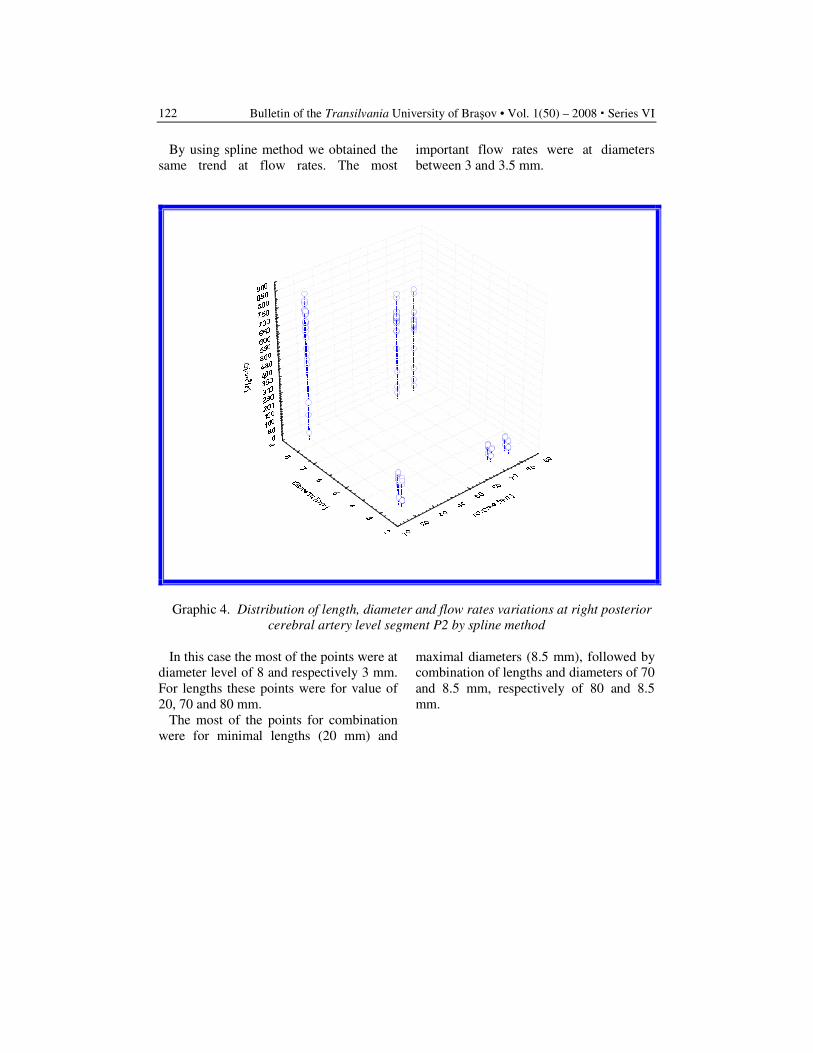
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
122
By using spline method we obtained the
same trend at flow rates. The most
important flow rates were at diameters
between 3 and 3.5 mm.
Graphic 4. Distribution of length, diameter and flow rates variations at right posterior
cerebral artery level segment P2 by spline method
In this case the most of the points were at
diameter level of 8 and respectively 3 mm.
For lengths these points were for value of
20, 70 and 80 mm.
The most of the points for combination
were for minimal lengths (20 mm) and
maximal diameters (8.5 mm), followed by
combination of lengths and diameters of 70
and 8.5 mm, respectively of 80 and 8.5
mm.
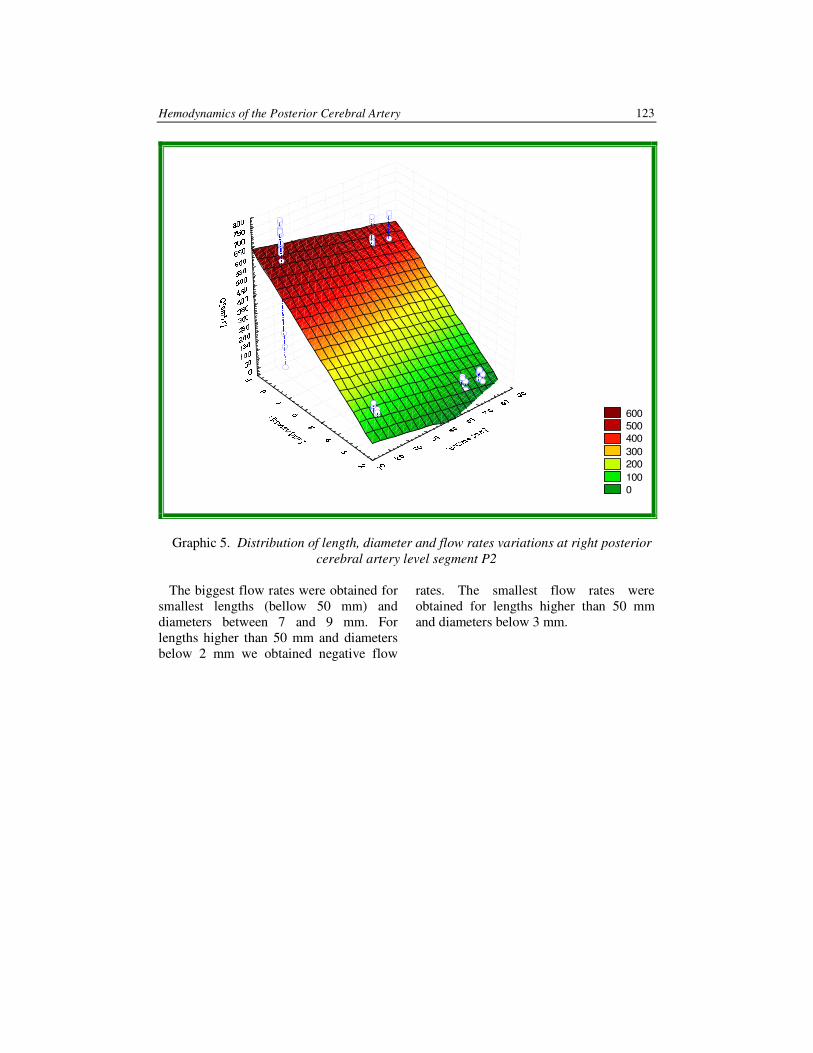
Hemodynamics of the Posterior Cerebral Artery 123
600 500 400
300 200
100 0
Graphic 5. Distribution of length, diameter and flow rates variations at right posterior
cerebral artery level segment P2
The biggest flow rates were obtained for
smallest lengths (bellow 50 mm) and
diameters between 7 and 9 mm. For
lengths higher than 50 mm and diameters
below 2 mm we obtained negative flow
rates. The smallest flow rates were
obtained for lengths higher than 50 mm
and diameters below 3 mm.
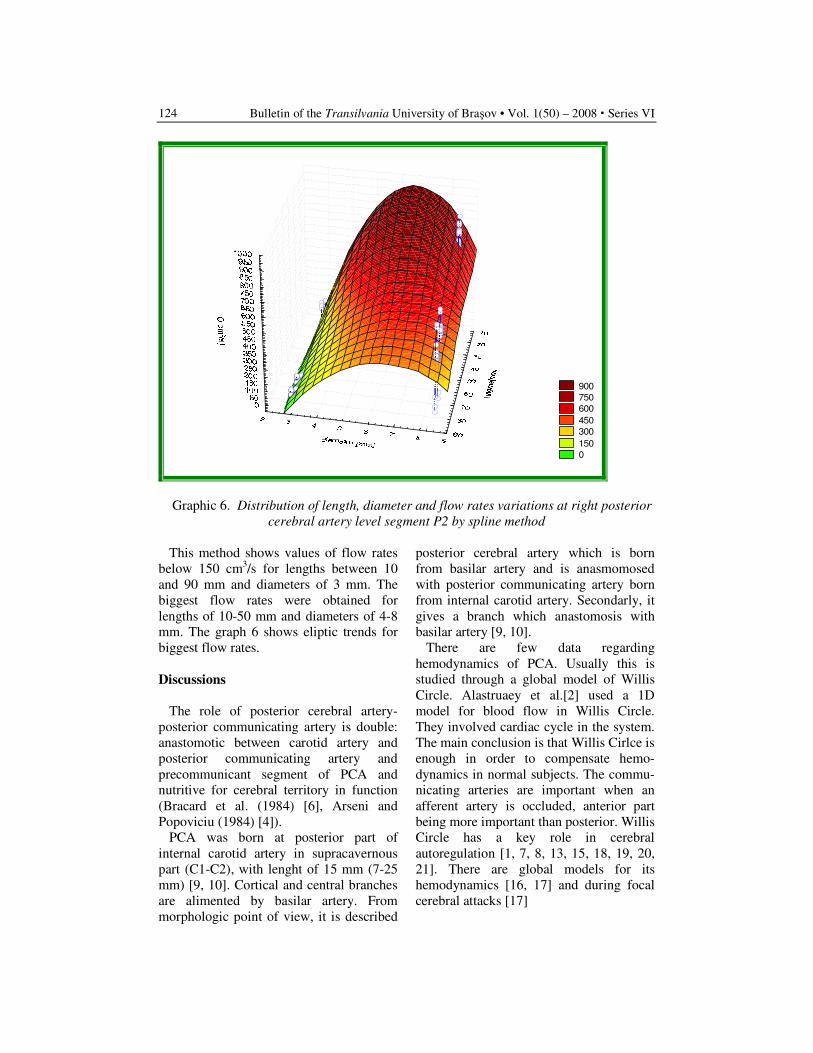
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
124
900 750 600
450 300
150 0
Graphic 6. Distribution of length, diameter and flow rates variations at right posterior
cerebral artery level segment P2 by spline method
This method shows values of flow rates
below 150 cm3/s for lengths between 10
and 90 mm and diameters of 3 mm. The
biggest flow rates were obtained for
lengths of 10-50 mm and diameters of 4-8
mm. The graph 6 shows eliptic trends for
biggest flow rates.
Discussions
The role of posterior cerebral artery-
posterior communicating artery is double:
anastomotic between carotid artery and
posterior communicating artery and
precommunicant segment of PCA and
nutritive for cerebral territory in function
(Bracard et al. (1984) [6], Arseni and
Popoviciu (1984) [4]).
PCA was born at posterior part of
internal carotid artery in supracavernous
part (C1-C2), with lenght of 15 mm (7-25
mm) [9, 10]. Cortical and central branches
are alimented by basilar artery. From
morphologic point of view, it is described
posterior cerebral artery which is born
from basilar artery and is anasmomosed
with posterior communicating artery born
from internal carotid artery. Secondarly, it
gives a branch which anastomosis with
basilar artery [9, 10].
There are few data regarding
hemodynamics of PCA. Usually this is
studied through a global model of Willis
Circle. Alastruaey et al.[2] used a 1D
model for blood flow in Willis Circle.
They involved cardiac cycle in the system.
The main conclusion is that Willis Cirlce is
enough in order to compensate hemo-
dynamics in normal subjects. The commu-
nicating arteries are important when an
afferent artery is occluded, anterior part
being more important than posterior. Willis
Circle has a key role in cerebral
autoregulation [1, 7, 8, 13, 15, 18, 19, 20,
21]. There are global models for its
hemodynamics [16, 17] and during focal
cerebral attacks [17]
Hemodynamics of the Posterior Cerebral Artery 125
Conclusions
1. Variation trend of flow rates for
segment P1 of PCA obtained by spine
method demonstrated that biggest
flow rates (bigger than 600 cm3/s)
were obtained for minimal lenghts
and maximal diameters.
2. The smallest flow rates were obtained
for smallest diameters (below 3 mm)
independent by lenght.
References
1. Aaslid, R., Newell D.W., Stooss R.,
Sorteberg, W., Lindegaard, K.F.:
Assessment of cerebral autoregulation
dynamics from simultaneous arterial
and venous transcranial Doppler
recordings in humans. In: Stroke.
1991; 22: 1148-1154.
2. Alastruey, J., Parker, K.H., Peiró, J.,
Byrd, S.M., Sherwin, S.J.: Modelling
the circle of Willis to assess the effects
of anatomical variations and
occlusions on cerebral flows. In: J
Biomech. 2007; 40(8): 1794-805.
3. Alpers, B.J., Berry, R.G.: Circle of
Willis in cerebral vascular disorders.
In: Arch Neurol. 1963; 8: 398-402.
4. Arseni, C., Popoviciu, L.: Bolile
vasculare ale creierului şi măduvei
spinării, partea I-a. Ed. Academiei
RSR, 1984.
5. Banias-Palaghita, L.: Morfologia
normală şi aspecte particulare ale
Poligonului Willis la om. Târgu-
Mureş. 1999. Teză de doctorat.
Conducător ştiinţific Prof. Dr. Ion
Pascu.
6. Bracard, S., Roland, J., Picard, L.:
Variations des arteres de l’encephal,
Livre 1, Tome 2. Paris. Ed.Masson,
Paris 1984.
7. Giulioni, M., Ursino, M.: Impact of
cerebral perfusion pressure and
autoregulation on intracranial
dynamics: a modeling study. In:
Neurosurgery. 1996; 39: 1005-14.
8. Irikura, K., Morii, S., Miyasaka, Y.,
Yamada, M., Tokiwa, K., Yada, K.:
Impaired autoregulation in an
experimental model of chronic
cerebral hypoperfusion in rats. In:
Stroke. 1996; 27: 1399-404.
9. Lazorthes, G., Gouaze A.: Les voies
anastomotiques de supleance de la
vascularization arterielle de l’axe
cerebro-medullaire. In : C.R. Ass.
Anat. 1968; 139:103-222.
10. Lazorthes, G., Gouaze, A., Salamon,
G.: Vascularisation et circulation de
l’encephale. Tome premier. Anatomie
descriptive et fonctionelle. Paris.
Masson Ed., 1976.
11. Lazorthes, G., Gouaze, A., Santini,
J.J., Salamon, G.: Le cercle arteriel de
cerveau. In : Anatomia Clinica. 1979;
1:241-258.
12. Lazorthes, G., Gouaze, A., Santini,
J.J., Salamon, G.: The arterial circle
of the brain (circulus arteriosus
cerebri). In: Anatomia Clinica 1.
1979; 241-257.
13. Newell D.W., Aaslid R., Lam A.,
Mayberg T.S., Winn H.R.:
Comparison of flow and velocity
during dynamic autoregulation testing
in humans, Stroke. 1994; 25:793-7.
14. Padget, D.H.: The development of
cranial arteries in human body. In:
Cont Embryol Carneg Instit. 1948;
32:105-261.
15. Paulson, O.B., Olesen, J., Christensen,
M.S.: Restoration of autoregulation of
cerebral blood flow by hypocapnia.
In: Neurology, 1972; 22:286-93.
16. Pascu, I.: A computerized model of the
Circle of Willis. Note I: simulation of
the autoregulation of cerebral blood
flow. In: Revista Medicala 1989; 5-8.
17. Skinhoj, E., Hoedt-Rasmussen, K.,
Paulson, O.B., Lassen, N.A.: Regional
cerebral blood flow and its
autoregulation in patients with
transient focal cerebral ischemic
attacks. In: Neurology. 1970; 20:
485-93.
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
126
18. Strandgaard, S.: Autoregulation of
cerebral blood flow in hypertensive
patients. The modifying influence of
prolonged antihypertensive treatment
on the tolerance to acute, drug-
induced hypotension. In: Circulation.
1976; 53:720-727.
19. Strandgaard, S., Olesen, J., Skinhoj,
Lassen, N.A.: Autoregulation of brain
circulation in severe hypertension. In:
Br Med J. 1973; 1:507-510.
20. Vavilala, M.S., Lee, L.A., Lee M.,
Graham, A., Visco, E., Lam, A.M.:
Cerebral autoregulation in children
during sevoflurane anaesthesia. In:
Br J Anaesth. 2003; 90:636-41.
21. White, R.P., Markus, H.S.: Impaired
dynamic cerebral autoregulation in
carotid artery stenosis. Stroke. 1997;
28:1340-4.
COMPARATIVE STUDY ON THE
EFFICACY OF DIFFERENT PROTECTION
METHODS IN CHRONIC ACOUSTIC
TRAUMA
Mădălina BUZESCU
1
Abstract: This study aims at evaluating the medical and economic efficacy
of the main known protective methods in order to prevent hearing loss due to
chronic acoustic trauma. The study subjects work in various noisy
environments and have different professions, requiring various education
levels and hearing capabilities. These conditions lead to various possibilities
and acceptability for the hearing protection. The study subjects’ hearing
levels were evaluated by pure tone audiometry, after testing the noise levels
with the help of a sonodosimeter. The protection methods used and analyzed
were mechanic protection devices and two kinds of antioxidant therapy – a
combination of vitamins A, C and E with Selenium and alpha-lipoic acid, in a
6 month therapy. The data were computed using a suitable statistic software.
The results showed a reduced acceptability for the mechanical protection
devices in the industrial environment, a very high efficiency of the
antioxidant therapy with alpha-lipoic acid and a lower level of protection
with vitamins and Selenium. The conclusions of the study underline the
importance of implementing educational programs in order to provide a
more extended use of the protection devices in the industrial noisy
environments and the efficacy of the antioxidant preventive therapy for the
professionals whose hearing is essential in order to accomplish their work
Key words: acoustic trauma, antioxidant, alpha-lipoic acid.
1 Transilvania University of Brasov, Faculty of Medicine.
1. Introduction
Acoustic trauma is defined as an
alteration of the hearing caused by
exposure of the cochlea to excessive
acoustic pressure.
Noise is an acoustic perception of
various type and intensity, having an
unpleasant character, capable to lead to
reactions or changes of the organism and
especially of the hearing.
The measuring unit used for the sound
intensity is the decibel (dB). The decibel
scale is a logarithmic scale where 0 dB
approximates the hearing level at medium
frequencies in young adults with
discomfort level at 85-95 dB and pain level
between 120 and 140 dB.
The harmful level is the sound level that,
reached or surpassed, requires the use of a
method to prevent the risk of hearing loss by
acoustic trauma. The usual criteria establish
an average of 8 hours daily in an average
noise of 85 dB, value from which there is
required the implementation of an acoustic
prevention program [2].

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
128
The sound level determination is made
with the help of a sonodosimeter,
instrument that measures the noise level on
a specified interval, which deposits the
measured values and computes the sound
as a relation between the noise level and
duration, describing the results as dose,
temporal average and other parameters
such as maximal level or sound level
exposure.
The impact of noise on the cochlea
depends, besides intensity, on other sound
characters, especially its variability.
The effects of noise on human organism
are primarily auditory, leading to cellular
alterations in the cochlea. Recent
researches claims that, the molecular
support of deafness through acoustic
trauma is the elevation of the level of
reactive oxygen species with important
role in the death of cochlear hair cells, by
necrosis as well as by apoptosis. These
new discoveries are the basis for new
protection strategies with antioxidant drugs
[7].
Besides the effects on hearing, noise
exposure also leads to sleep, cardio-
vascular, respiratory, metabolic, beha-
vioural and hormonal disorders. These
effects lead us to consider noise as a stress
factor.
The most simple and widely known
protection, the insulating devices, suitable
especially in industrial environments, do
not meet as much success as they should,
due to various reasons. Other, more recent,
protection methods, use internal use of
antioxidants, to avoid extensive destruction
of cochlear hearing cells by high pressure
noise levels.
Cochlear noise aggression reduction can
also be reached by limitation of workers’
exposure to noise, changing of their
program and location and projects for
technical improvement leading to a more
silent function of the equipments [6].
2. Material and Methods
The study represents a clinical, statistic,
prospective, longitudinal research, exten-
ded on a 5-year period of time, from
October 1999 to October 2004.
4225 subjects working in potentially
noisy environments were routinely tested
with a screening audiometer by pure tone
audiometry, resulting 730 subjects with
hearing loss of over 20 dB at least one ear.
Of these 730 patients, after a diagnostic,
standard hearing evaluation with a clinic
audiometer, in a silent testing room, 512
patients were diagnosed with hearing
losses of various degrees. These were
included in the study after verifying their
professional noise exposure with the help
of a sonodosimeter Norsonic NOR 116.
In the industrial environment, where the
use of insulating hearing protection devices
is suitable, the effective use of these devices
was researched, as well as their efficacy in
the prevention of acoustic trauma. Other
directions of research in these subjects were
the motivations of refusal of these devices.
There were also gathered three groups of
subjects for the study of antioxidant therapy
(group A, treated with alpha-lipoic acid,
group B, treated with vitamins A, C, E and
Selenium and group C, control, with
placebo).
Another study group was formed by
musicians working in symphonic or
modern musical environments, as well as
by people exposed to leisure acoustic
trauma. These subjects can not benefit
from hearing insulating devices, so only
the efficacy of antioxidant therapy was
searched among them, by completing the
three groups of study (A, B and C)
previously described for the workers.
The hearing tests were made at more
than 24 hours after noise exposure, at the
beginning of the therapy, as well as at its
finish, the main parameter used in the
statistical analysis being the hearing
threshold at 4000 Hz, where the typical
“V” for acoustic trauma appears.
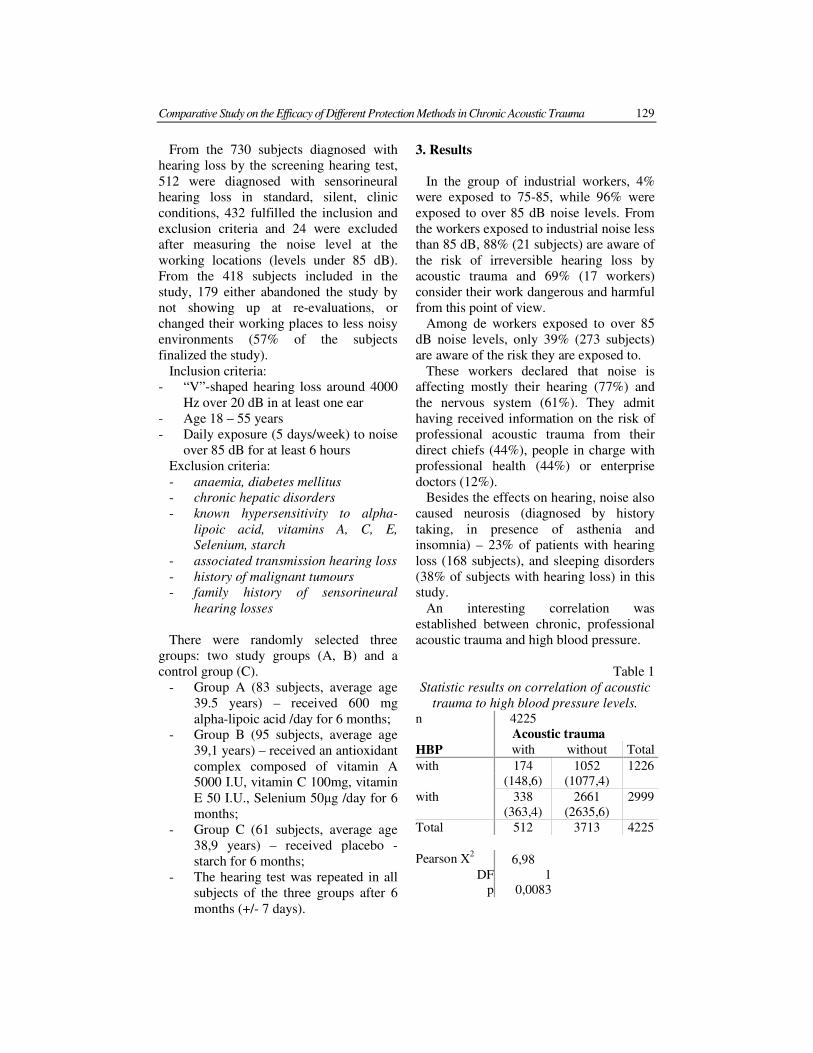
Comparative Study on the Efficacy of Different Protection Methods in Chronic Acoustic Trauma 129
From the 730 subjects diagnosed with
hearing loss by the screening hearing test,
512 were diagnosed with sensorineural
hearing loss in standard, silent, clinic
conditions, 432 fulfilled the inclusion and
exclusion criteria and 24 were excluded
after measuring the noise level at the
working locations (levels under 85 dB).
From the 418 subjects included in the
study, 179 either abandoned the study by
not showing up at re-evaluations, or
changed their working places to less noisy
environments (57% of the subjects
finalized the study).
Inclusion criteria:
- “V”-shaped hearing loss around 4000
Hz over 20 dB in at least one ear
- Age 18 – 55 years
- Daily exposure (5 days/week) to noise
over 85 dB for at least 6 hours
Exclusion criteria:
- anaemia, diabetes mellitus
- chronic hepatic disorders
- known hypersensitivity to alpha-
lipoic acid, vitamins A, C, E,
Selenium, starch
- associated transmission hearing loss
- history of malignant tumours
- family history of sensorineural
hearing losses
There were randomly selected three
groups: two study groups (A, B) and a
control group (C).
- Group A (83 subjects, average age
39.5 years) – received 600 mg
alpha-lipoic acid /day for 6 months;
- Group B (95 subjects, average age
39,1 years) – received an antioxidant
complex composed of vitamin A
5000 I.U, vitamin C 100mg, vitamin
E 50 I.U., Selenium 50µg /day for 6
months;
- Group C (61 subjects, average age
38,9 years) – received placebo -
starch for 6 months;
- The hearing test was repeated in all
subjects of the three groups after 6
months (+/- 7 days).
3. Results
In the group of industrial workers, 4%
were exposed to 75-85, while 96% were
exposed to over 85 dB noise levels. From
the workers exposed to industrial noise less
than 85 dB, 88% (21 subjects) are aware of
the risk of irreversible hearing loss by
acoustic trauma and 69% (17 workers)
consider their work dangerous and harmful
from this point of view.
Among de workers exposed to over 85
dB noise levels, only 39% (273 subjects)
are aware of the risk they are exposed to.
These workers declared that noise is
affecting mostly their hearing (77%) and
the nervous system (61%). They admit
having received information on the risk of
professional acoustic trauma from their
direct chiefs (44%), people in charge with
professional health (44%) or enterprise
doctors (12%).
Besides the effects on hearing, noise also
caused neurosis (diagnosed by history
taking, in presence of asthenia and
insomnia) – 23% of patients with hearing
loss (168 subjects), and sleeping disorders
(38% of subjects with hearing loss) in this
study.
An interesting correlation was
established between chronic, professional
acoustic trauma and high blood pressure.
Table 1
Statistic results on correlation of acoustic
trauma to high blood pressure levels.
n 4225
Acoustic trauma
HBP with without Total
with 174 1052 1226
(148,6) (1077,4)
with 338 2661 2999
(363,4) (2635,6)
Total 512 3713 4225
Pearson X2 6,98
DF 1
p 0,0083

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
130
The Pearson’s statistic test shows a
statistically significant correlation between
acoustic trauma and high blood pressure.
Wearing hearing protection devices is
admitted only by 21% (861) of the
subjects. Those who do not use these
devices motivate that the employers did
not offer them this devices (55% - 2255
subjects), that these devices affect the
communication with their colleagues (14%
- 574 subjects), ear discomfort or pain (6%
- 246 subjects) or other reasons (5%).
The average hearing threshold at 4 kHz
among the workers who systematically
used hearing protection devices was 18,2
dB, compared to the 24,3 dB average
hearing threshold of those who never do
that. This comparison was made between
selected groups of the two categories, in
order to have comparable average ages (31
years). The statistic significant difference
of 6,1 dB (p<0,01) proves the very high
efficacy of hearing insulating protective
devices in noisy industrial environment.
However, these devices, with their actual
use, seem to have a slight impact on the
workers’ hearing conservation.
The voluntary, leisure exposure to
phonic pollution was explored in subjects
without professional noise exposure.
From the 108 subjects who admitted to
attend at least twice a week discotheques
or listen at least 2 hours a day loud music
in headphones, 11 subjects (10%) showed
hearing losses of at least 20 dB in at least
one ear at 4 kHz (average hearing loss –
24,5 dB). The average age of this group
was 23.7 years and 80% of the, (86
subjects) never thought of the risk of
hearing loss. From the 11 subjects with
hearing loss at 4 kHz, only 2 people (18%)
had noticed having a hearing problem.
These subjects also had among the highest
hearing losses in the group (30 respectively
40 dB at 4 kHz).
Before applying the statistical t-test
(Student) to establish the significance of
the outcomes, the normality of the
distribution of the collected data was
statistically evaluated (Shapiro-Wilk test),
to assure the results’ reliability.
A synthesis of statistical outcomes in the
study on antioxidant therapy for prevention
of chronic acoustic trauma is presented in
the table below:
Table 2
Synthesis of statistical results on
antioxidant therapy in chronic acoustic
trauma
Gr. A
(n=83)
Gr. B
(n=95)
Gr. C
(n=61)
Average age 39,5 39,1 38,9
Average initial
hearing
threshold (dB)
22,5 17,9 18,4
Average final
hearing
threshold (dB)
20 16,8 19,1
Difference (dB) 2,5 0,4 - 0,7
p < 0,01 0,0110 0,0031
4. Discussions
A major factor influencing the efficacy
of acoustic trauma preventive methods is
the awareness of the subjects exposed to
noise regarding this risk [3]. The outcomes
of this study show a strange distribution of
awareness on this risk, workers in louder
working places being less informed and
caring for their hearing than those working
in less noise. An explanation for this would
be that very noisy industrial environments
(especially in heavy industry) are usually
populated with less educated and qualified
workers. Usually, people study hard to
accomplish as high educational levels as
possible, in order to avoid such stressing,
noisy working places.
The major stress caused by high noise
levels also explains the statistically
significant correlation between acoustic
trauma and high blood pressure levels.
In spite of their good protecting
properties, the insulating hearing
protection devices do not seem to offer the

Comparative Study on the Efficacy of Different Protection Methods in Chronic Acoustic Trauma 131
ideal solution in the industrial field,
because of their insufficient use by
workers.
A recent study of the University in Sao
Paolo, Brazil, systematically analyzed the
programs that promote the use of hearing
protection devices, considering that
hearing loss due to acoustic trauma can
only be prevented by reducing exposure to
noise. The conclusion of this evaluation is
that firmer educational interventions are
necessary to increase the frequency of
using hearing protection devices among
workers exposed to loud noise [4].
Similar to the present study, another
research, carried out in Australia, indicated
a reduced awareness on the risk of acoustic
trauma and, by consequence, a minimal
self-protective behaviour [5].
The key factors that hinder the progress
in promoting hearing loss prevention
methods arise from the numerous variables
implied. These variables are even harder to
control because they include behavioural
factors such as the attitude regarding noise
and if noise is a secondary consequence or
a product of the professional activity.
Acoustic trauma caused by leisure noise,
especially music, is only responsible for
0.2% of hearing losses, but this percent
drastically increases if we consider only
the age group 18 to 25 (53%), showing that
leisure musical acoustic trauma is
increasing, especially by listening music in
headphones and discotheques, situations
where the noise level often surpasses 100
dB. As painful noise level is around 120-
140 dB, the harmful level of 90 dB is often
surpassed and the harmful effects of noise,
underestimated.
The results of the study on antioxidant
therapy efficacy in protection against
acoustic trauma showed a statistical
significant hearing improvement in 6
months by therapy with alpha-lipoic acid, a
stationary evolution of hearing in people
exposed to noise treated with the ACESe
complex and a statistically significant
hearing loss in the control group of
subjects exposed to loud noise and
receiving placebo for 6 months.
The use of mechanic insulating hearing
protection devices is the safest, for long
periods of time tested method to prevent
acoustic trauma, so intensive promotion
programs to spread their use should be a
priority for all noisy industrial fields’
employers.
Comparing the three methods described
above (mechanic hearing protection
devices, alpha-lipoic acid therapy and
vitamins ACE + Selenium therapy) only
regarding the hearing level outcomes
would recommend alpha-lipoic acid as the
best method for protection. However,
economic reasons would surely limit its
wide use among all those who work in
noisy environments. Moreover, the limited
awareness on acoustic trauma of industrial
workers makes it hard to expect that these
would be more compliant to swallowing
daily a tablet of alpha-lipoic acid.
Outcomes of the vitamins ACE and
Selenium therapy study are similar to the
protection offered by daily, systematically
use of hearing protective devices. The cost
of this therapy being about four times
lower than the one with alpha-lipoic acid,
these results suggest that it is a good
protective alternative for workers who are
aware of the acoustic trauma risk but do
not accept mechanic protection devices for
different reasons.
Hearing protection methods in musical
professions usually exclude the use of
insulating protection devices, antioxidant
therapy showing here its most important
benefits [1]. The choice of antioxidant
therapy in this professional group should
consider, besides individual hyper-
sensitivities to any of the components, the
individual susceptibility to hearing loss or
other possible systemic benefits of the
antioxidant therapies.

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
132
5. Conclusions
Acoustic trauma in noisy industrial
environments should be reduced by
implementing intensive educational
programs to increase awareness of hearing
loss risk and systematically use of efficient
hearing protection devices. Employers
should also be convinced to provide
efficient and comfortable hearing
protection devices.
For professionals who can not use such
devices, the use of acoustic trauma
preventive antioxidant therapy might be a
good alternative that should be evaluated
in other wider, double-blind controlled
studies.
References
1. Buzescu, M.: Actual aspects in the
non-prosthetic therapy of
sensorineural hearing loss. In:
Revista Română de ORL 2007; 29(2):
pp. 122-7.
2. Calogero, B., Giannini, P., Marciano,
E.: Recent advances in hearing
screening. In: Adv Otorhinolaryngol
1987; 37: pp.60-78.
3. Crandell, C., Mills, T.L., Gauthier, R.:
Knowledge, behaviours, and attitudes
about hearing loss and hearing
protection among racial/ethnically
diverse young adults. In: J Natl Med
Assoc. 2004 Feb; 96(2): pp. 176-86.
4. Daniel, E.: Noise and Hearing Loss: a
review. In: J Sch Health. 2007; 77(5):
pp. 225-31.
5. Dineen, R., Reid, J., Livy, P.: Knock
out noise injury. Noise Effects. 7th In:
International Congress on Noise as a
Public Health Problem. Sydney,
Australia: pp. 135-138, 1998.
6. El Dib, R.P., Atallah, A.N., Andriolo,
R.B., Soares, B.G., Verbeek, J.: A
systematic review of the interventions
to promote the wearing of hearing
protection. In: Sao Paulo Med J. 2007
Nov 1; 125(6): pp. 362-9.
7. Fetoni, A.R., Ferraresi, A., Greca, C.,
Rizzo, D., Sergi, B., Tringali, G.,
Piacentin, R., Troiani, D.: Antioxidant
protection against acoustic trauma by
co-administration of idebenone and
vitamin E. In: Neuroreport. 2008,
19(3): pp. 277-81.

ENTERAL NUTRITION IN THE
TREATMENT OF SEVERE ACUTE
PANCREATITIS
C. MIŞARCĂ1
A. CUCU1 L. DURACH
1
Abstract: Development, septic complication, and accentuated catabolism
in patients with AP were the reasons that motivated our study.
Material and method: We study prospectively and retrospectively 186 cases
of severe AP in patients operated between 1998 and 2005 in Surgery Clinic
(I-III) of Brasov County Hospital.
Results: Within the group of 186 patients in 72 the treatment of choice was
laparostomy in association to antibiotics and in 54 cases enteral nutrition
through jejunostomy was added. The cases taken into study were divided in
two groups - group A: 32 patients with enteral feeding by jejunostomy and
group B: 18 patients without enteral feeding. The evaluation was performed
by clinical and paraclinical methods. On feeding jejunostomy (Witzel type)
was first administrated normal saline solution (20ml/h) and then Survimed
after minimum 24 h, starting with 20-25ml/h reaching 100ml/h. Antibiotic
therapy - imipenem or quinolone were used. Conclusions: enteral nutrition
ensure rehabilitation of intestinal physiology, prevents bacterial
translocation, it is cost effective and improves life quality.
Key words: acute pancreatitis, enteral feeding, feeding jejunostomy
1 Transilvania University of Brasov, Chirurgical Dep, Faculty of Medicine, Brasov County Clinical
Emergency Hospital
1. Introduction
Acute Pancreatitis represents the
anatomo-clinical expression of the acute
pancreatic and peripancreatic auto
digestion [1]. The main features of Acute
Pancreatitis are: severe ness, asynchronism
in evolution and outset of complication and
hyper catabolism (inflammatory stress,
edema, sepsis).
The clinical classification of Acute
Pancreatitis (Atlanta 1992) consists of two
aspects:
• Mild – minimal organ and system
dysfunction, completely reversible
• Severe – systemic complications, pan-
creatic and peripancreatic collections
For a long time, oral feeding was seen as
harmful in Acute Pancreatitis, by the fact it
would stimulate the exocrine secretion of
the pancreas and thus its autodigestion. On
the other hand, in patients with protracted
evolutions and complications of necrotic
Acute Pancreatitis, nutritional deficits
occur.
Approximately 80% of patients with
Acute Pancreatitis have mild-to-moderate
forms of the disease, with mortality rate of
1%. Such patients require only the usual
treatment, without special nutritional
support and return to normal diet by day 3
-7 [6] (table 1).
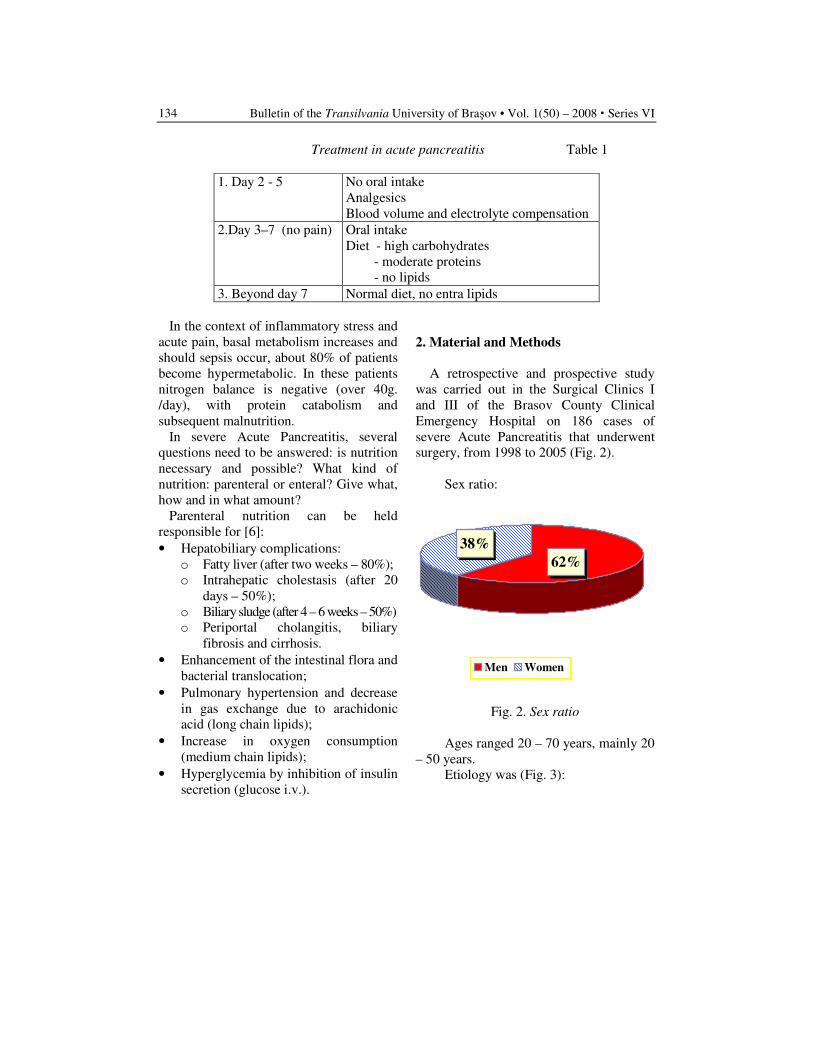
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
134
Treatment in acute pancreatitis Table 1
1. Day 2 - 5 No oral intake
Analgesics
Blood volume and electrolyte compensation
2.Day 3–7 (no pain) Oral intake
Diet - high carbohydrates
- moderate proteins
- no lipids
3. Beyond day 7 Normal diet, no entra lipids
In the context of inflammatory stress and
acute pain, basal metabolism increases and
should sepsis occur, about 80% of patients
become hypermetabolic. In these patients
nitrogen balance is negative (over 40g.
/day), with protein catabolism and
subsequent malnutrition.
In severe Acute Pancreatitis, several
questions need to be answered: is nutrition
necessary and possible? What kind of
nutrition: parenteral or enteral? Give what,
how and in what amount?
Parenteral nutrition can be held
responsible for [6]:
• Hepatobiliary complications:
o Fatty liver (after two weeks – 80%);
o Intrahepatic cholestasis (after 20
days – 50%);
o Biliary sludge (after 4 – 6 weeks – 50%)
o Periportal cholangitis, biliary
fibrosis and cirrhosis.
• Enhancement of the intestinal flora and
bacterial translocation;
• Pulmonary hypertension and decrease
in gas exchange due to arachidonic
acid (long chain lipids);
• Increase in oxygen consumption
(medium chain lipids);
• Hyperglycemia by inhibition of insulin
secretion (glucose i.v.).
2. Material and Methods
A retrospective and prospective study
was carried out in the Surgical Clinics I
and III of the Brasov County Clinical
Emergency Hospital on 186 cases of
severe Acute Pancreatitis that underwent
surgery, from 1998 to 2005 (Fig. 2).
Sex ratio:
38%
62%
Men Women
Fig. 2. Sex ratio
Ages ranged 20 – 70 years, mainly 20
– 50 years.
Etiology was (Fig. 3):
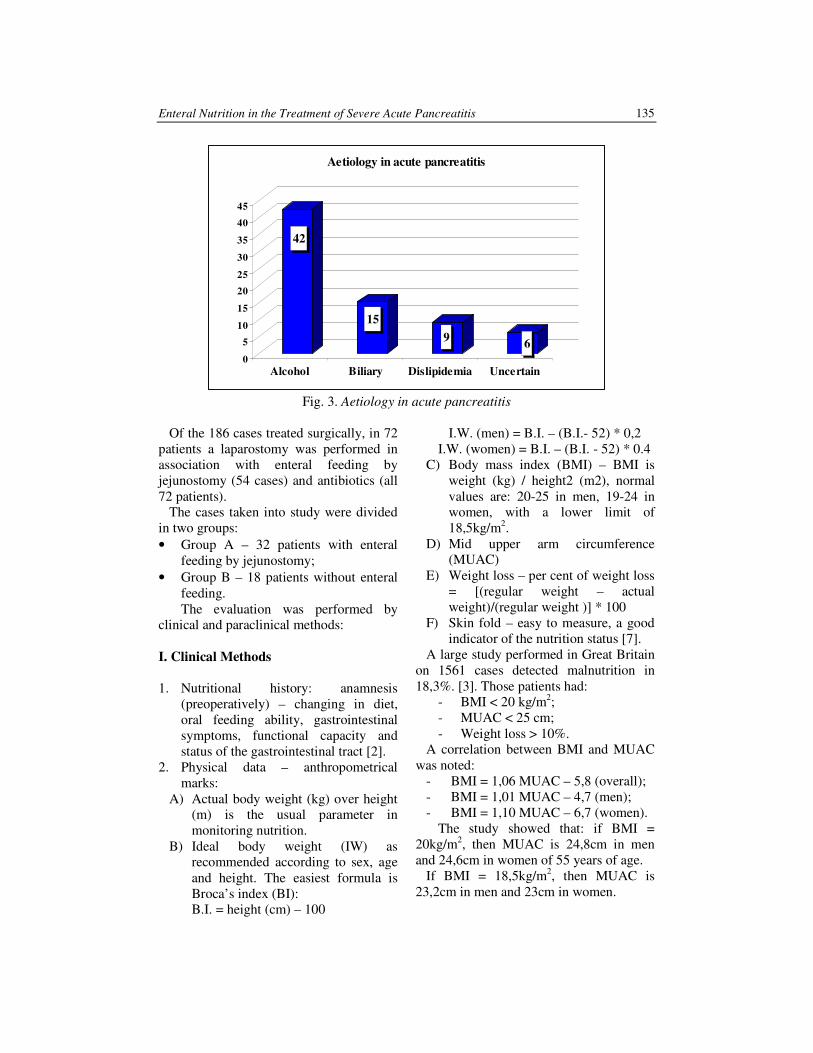
Enteral Nutrition in the Treatment of Severe Acute Pancreatitis 135
42
15
96
0
5
10
15
20
25
30
35
40
45
Alcohol Biliary Dislipidemia Uncertain
Aetiology in acute pancreatitis
Fig. 3. Aetiology in acute pancreatitis
Of the 186 cases treated surgically, in 72
patients a laparostomy was performed in
association with enteral feeding by
jejunostomy (54 cases) and antibiotics (all
72 patients).
The cases taken into study were divided
in two groups:
• Group A – 32 patients with enteral
feeding by jejunostomy;
• Group B – 18 patients without enteral
feeding.
The evaluation was performed by
clinical and paraclinical methods:
I. Clinical Methods
1. Nutritional history: anamnesis
(preoperatively) – changing in diet,
oral feeding ability, gastrointestinal
symptoms, functional capacity and
status of the gastrointestinal tract [2].
2. Physical data – anthropometrical
marks:
A) Actual body weight (kg) over height
(m) is the usual parameter in
monitoring nutrition.
B) Ideal body weight (IW) as
recommended according to sex, age
and height. The easiest formula is
Broca’s index (BI):
B.I. = height (cm) – 100
I.W. (men) = B.I. – (B.I.- 52) * 0,2
I.W. (women) = B.I. – (B.I. - 52) * 0.4
C) Body mass index (BMI) – BMI is
weight (kg) / height2 (m2), normal
values are: 20-25 in men, 19-24 in
women, with a lower limit of
18,5kg/m2.
D) Mid upper arm circumference
(MUAC)
E) Weight loss – per cent of weight loss
= [(regular weight – actual
weight)/(regular weight )] * 100
F) Skin fold – easy to measure, a good
indicator of the nutrition status [7].
A large study performed in Great Britain
on 1561 cases detected malnutrition in
18,3%. [3]. Those patients had:
- BMI < 20 kg/m2;
- MUAC < 25 cm;
- Weight loss > 10%.
A correlation between BMI and MUAC
was noted:
- BMI = 1,06 MUAC – 5,8 (overall);
- BMI = 1,01 MUAC – 4,7 (men);
- BMI = 1,10 MUAC – 6,7 (women).
The study showed that: if BMI =
20kg/m2, then MUAC is 24,8cm in men
and 24,6cm in women of 55 years of age.
If BMI = 18,5kg/m2, then MUAC is
23,2cm in men and 23cm in women.
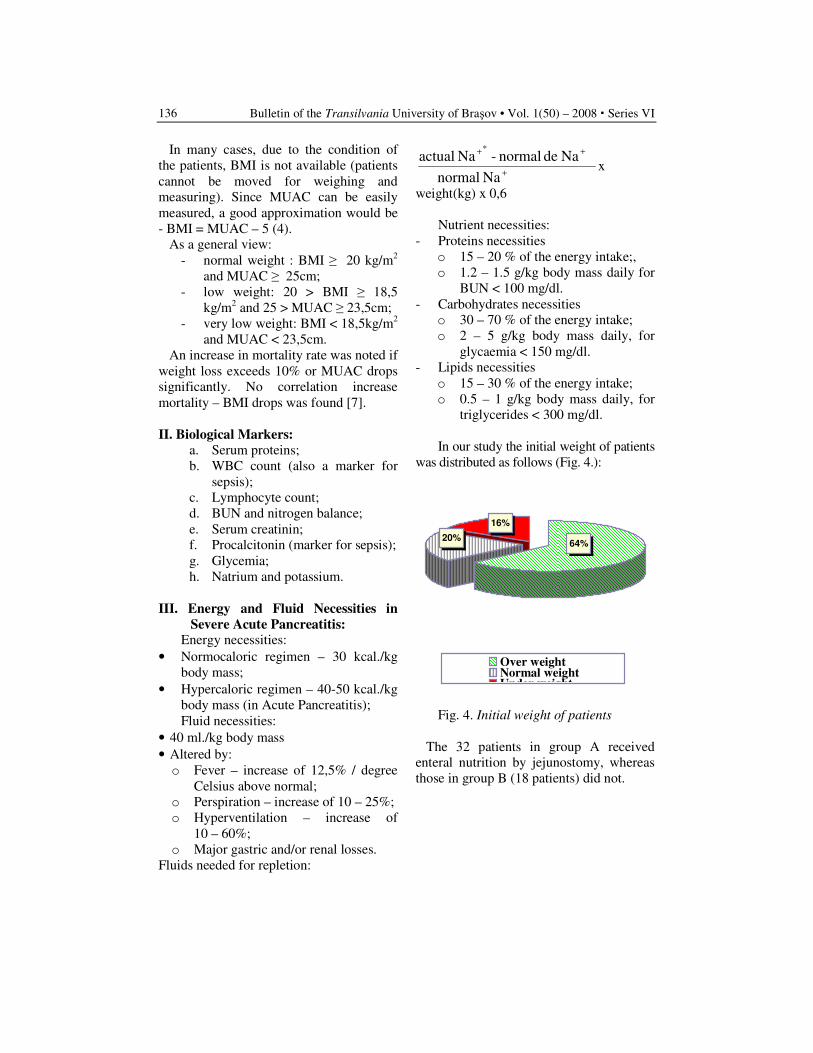
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
136
In many cases, due to the condition of
the patients, BMI is not available (patients
cannot be moved for weighing and
measuring). Since MUAC can be easily
measured, a good approximation would be
- BMI = MUAC – 5 (4).
As a general view:
- normal weight : BMI ≥ 20 kg/m2
and MUAC ≥ 25cm;
- low weight: 20 > BMI ≥ 18,5
kg/m2 and 25 > MUAC ≥ 23,5cm;
- very low weight: BMI < 18,5kg/m2
and MUAC < 23,5cm.
An increase in mortality rate was noted if
weight loss exceeds 10% or MUAC drops
significantly. No correlation increase
mortality – BMI drops was found [7].
II. Biological Markers:
a. Serum proteins;
b. WBC count (also a marker for
sepsis);
c. Lymphocyte count;
d. BUN and nitrogen balance;
e. Serum creatinin;
f. Procalcitonin (marker for sepsis);
g. Glycemia;
h. Natrium and potassium.
III. Energy and Fluid Necessities in
Severe Acute Pancreatitis: Energy necessities:
• Normocaloric regimen – 30 kcal./kg
body mass;
• Hypercaloric regimen – 40-50 kcal./kg
body mass (in Acute Pancreatitis);
Fluid necessities:
• 40 ml./kg body mass
• Altered by:
o Fever – increase of 12,5% / degree
Celsius above normal;
o Perspiration – increase of 10 – 25%;
o Hyperventilation – increase of
10 – 60%;
o Major gastric and/or renal losses.
Fluids needed for repletion:
Na normal
Na de normal - Na actual*
+
++
x
weight(kg) x 0,6
Nutrient necessities:
- Proteins necessities
o 15 – 20 % of the energy intake;,
o 1.2 – 1.5 g/kg body mass daily for
BUN < 100 mg/dl.
- Carbohydrates necessities
o 30 – 70 % of the energy intake;
o 2 – 5 g/kg body mass daily, for
glycaemia < 150 mg/dl.
- Lipids necessities
o 15 – 30 % of the energy intake;
o 0.5 – 1 g/kg body mass daily, for
triglycerides < 300 mg/dl.
In our study the initial weight of patients
was distributed as follows (Fig. 4.):
Fig. 4. Initial weight of patients
The 32 patients in group A received
enteral nutrition by jejunostomy, whereas
those in group B (18 patients) did not.
16%
20%64%
Over weightNormal weightUnder weight
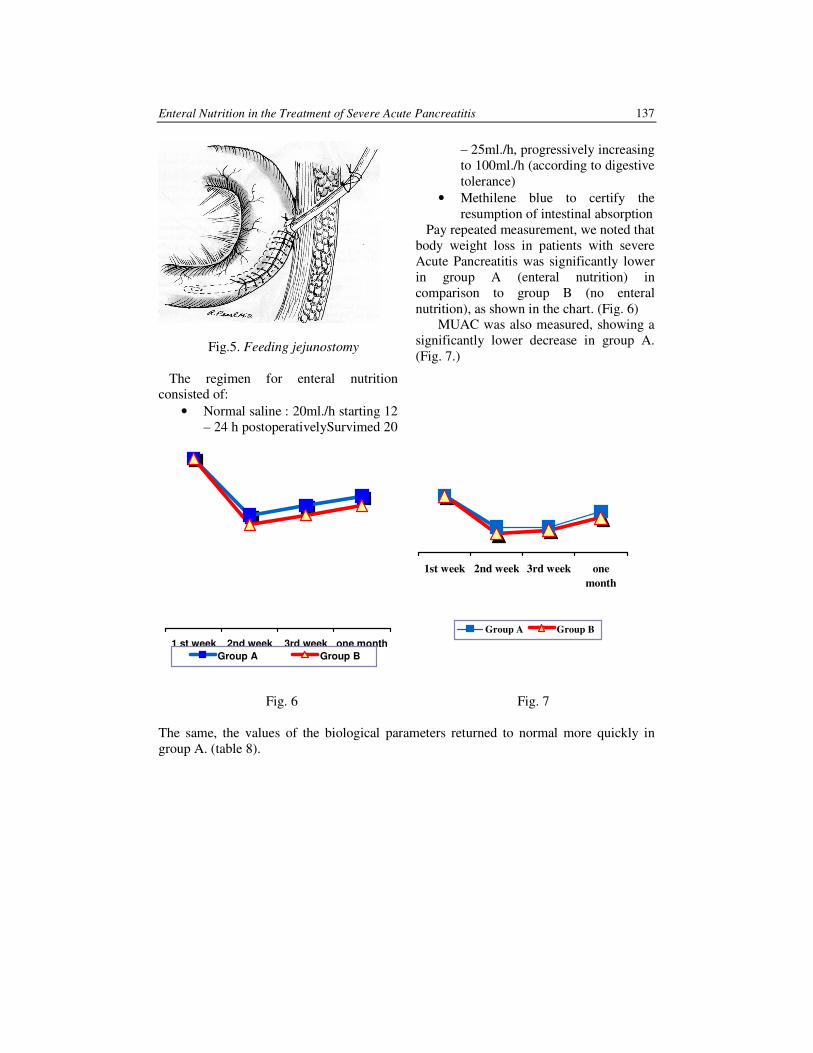
Enteral Nutrition in the Treatment of Severe Acute Pancreatitis 137
Fig.5. Feeding jejunostomy
The regimen for enteral nutrition
consisted of:
• Normal saline : 20ml./h starting 12
– 24 h postoperativelySurvimed 20
– 25ml./h, progressively increasing
to 100ml./h (according to digestive
tolerance)
• Methilene blue to certify the
resumption of intestinal absorption
Pay repeated measurement, we noted that
body weight loss in patients with severe
Acute Pancreatitis was significantly lower
in group A (enteral nutrition) in
comparison to group B (no enteral
nutrition), as shown in the chart. (Fig. 6)
MUAC was also measured, showing a
significantly lower decrease in group A.
(Fig. 7.)
1st week 2nd week 3rd week one
month
Group A Group B
Fig. 6 Fig. 7
The same, the values of the biological parameters returned to normal more quickly in
group A. (table 8).
1 st week 2nd week 3rd week one month
Group A Group B
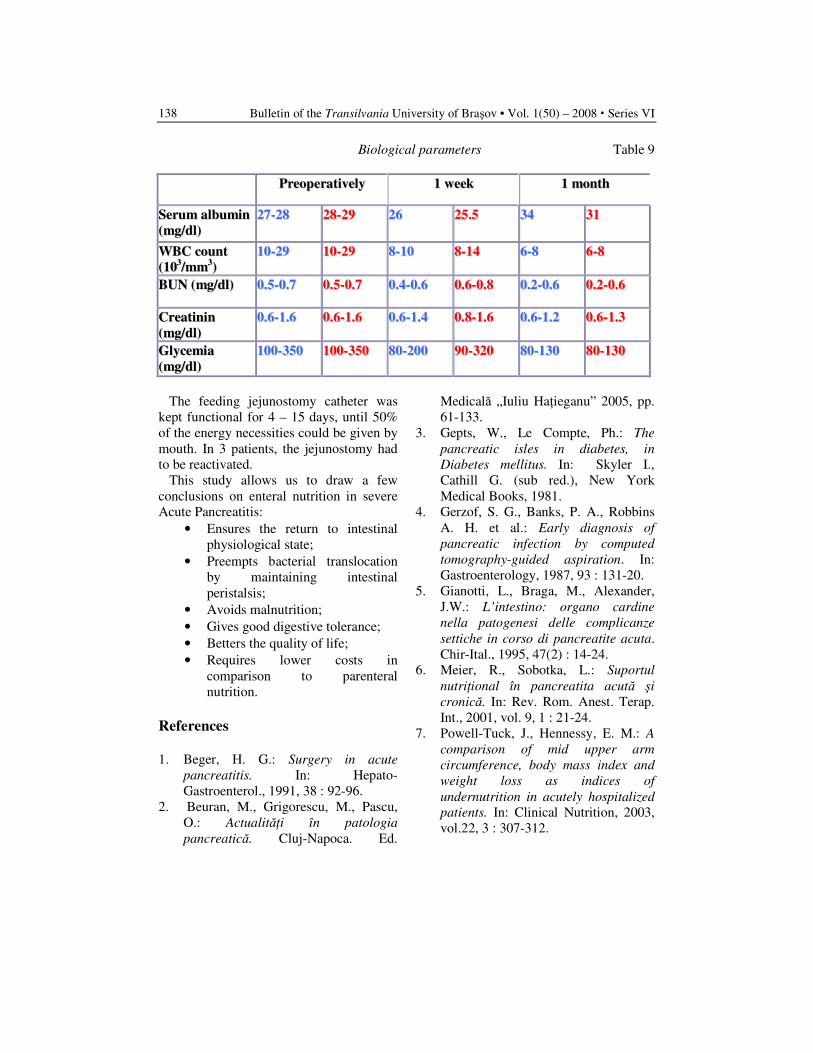
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
138
Biological parameters Table 9
PPrreeooppeerraattiivveellyy 11 wweeeekk 11 mmoonntthh
SSeerruumm aallbbuummiinn
((mmgg//ddll))
2277--2288 2288--2299 2266 2255..55 3344 3311
WWBBCC ccoouunntt
((110033//mmmm
33))
1100--2299 1100--2299 88--1100 88--1144 66--88 66--88
BBUUNN ((mmgg//ddll)) 00..55--00..77 00..55--00..77 00..44--00..66 00..66--00..88 00..22--00..66 00..22--00..66
CCrreeaattiinniinn
((mmgg//ddll))
00..66--11..66 00..66--11..66 00..66--11..44 00..88--11..66 00..66--11..22 00..66--11..33
GGllyycceemmiiaa
((mmgg//ddll))
110000--335500 110000--335500 8800--220000 9900--332200 8800--113300 8800--113300
The feeding jejunostomy catheter was
kept functional for 4 – 15 days, until 50%
of the energy necessities could be given by
mouth. In 3 patients, the jejunostomy had
to be reactivated.
This study allows us to draw a few
conclusions on enteral nutrition in severe
Acute Pancreatitis:
• Ensures the return to intestinal
physiological state;
• Preempts bacterial translocation
by maintaining intestinal
peristalsis;
• Avoids malnutrition;
• Gives good digestive tolerance;
• Betters the quality of life;
• Requires lower costs in
comparison to parenteral
nutrition.
References
1. Beger, H. G.: Surgery in acute
pancreatitis. In: Hepato-
Gastroenterol., 1991, 38 : 92-96.
2. Beuran, M., Grigorescu, M., Pascu,
O.: Actualităţi în patologia
pancreatică. Cluj-Napoca. Ed.
Medicală „Iuliu Haţieganu” 2005, pp.
61-133.
3. Gepts, W., Le Compte, Ph.: The
pancreatic isles in diabetes, in
Diabetes mellitus. In: Skyler I.,
Cathill G. (sub red.), New York
Medical Books, 1981.
4. Gerzof, S. G., Banks, P. A., Robbins
A. H. et al.: Early diagnosis of
pancreatic infection by computed
tomography-guided aspiration. In:
Gastroenterology, 1987, 93 : 131-20.
5. Gianotti, L., Braga, M., Alexander,
J.W.: L’intestino: organo cardine
nella patogenesi delle complicanze
settiche in corso di pancreatite acuta.
Chir-Ital., 1995, 47(2) : 14-24.
6. Meier, R., Sobotka, L.: Suportul
nutriţional în pancreatita acută şi
cronică. In: Rev. Rom. Anest. Terap.
Int., 2001, vol. 9, 1 : 21-24.
7. Powell-Tuck, J., Hennessy, E. M.: A
comparison of mid upper arm
circumference, body mass index and
weight loss as indices of
undernutrition in acutely hospitalized
patients. In: Clinical Nutrition, 2003,
vol.22, 3 : 307-312.
EXTRACORPOREAL SHOCKWAVE
LITHOTRIPSY (ESWL) AS A MEAN OF
TREATMENT IN URINARY LITHIASIS
I. SCÂRNECIU
1 S. LUPU
2 L. L. ONISÂI
3
C. C. SCÂRNECIU4 A. M. LUPU
5
V. D. SCÂRNECIU6
Abstract: In the present, Extracorporeal Shockwave Lithotripsy (ESWL)
represent the mean modality to treat urinary lithiasis, covering 80-90% from
treatment indications. Lithotripsy machines become more performant and
benefit of two methods to localize stones: ultrasonographic and fluoroscopic.
There are still more controversies about the results of using different types of
machines
Key words: renal lithiasis, ESW
1 Transilvania University of Brasov, Faculty of Medicine Brasov, Urology Clinic, Clinic Emergency County
Hospital Brasov. 2 Urology Clinic, Clinic Emergency County Hospital Brasov. 3 Transilvania University of Brasov, Department of Anatomy, Faculty of Medicine Brasov. 4 Transilvania University of Brasov, Department of Internal Medicine. 5 Radiology and Medical Imagistics Department, Clinic Emergency County Hospital Brasov. 6 Transilvania University of Brasov, Faculty of Medicine Brasov.
1. Introduction
Extracorporeal Shockwave Lithotripsy
(or ESWL) was described and used for the
first time in 1980, as research result made
by a German company specialized in the
manufacture of supersonic planes. Under
the effect of the shockwave generated
outside the organism, urinary stones are
disintegrated in small fragments which can
subsequently be eliminated naturally.
Extracorporeal Shockwave Lithotripsy
Devices can generate shockwave using
electrohydraulic, piezoelectric or
electromagnetic systems, and the stone
locating is made through echographic or
radiographic guiding. The two imagistic
guiding systems have both advantages and
disadvantages: echographic guiding system
is non-radiating and can be used in
locating and visualization of radio-opaque
stones or radio-transparent renal stones;
radiographic guiding system (florroscopic)
is radiating and can be used in locating and
visualization of radio-opaque stones both
renal and uretheral. State of the art,
Extracorporeal Shockwave Lithotripsy
Devices is equipped with dual-localization
systems, this way, covering a large palette
of imagistic guiding possibilities. [1, 2, 3]
From the moment they are emitted,
shockwaves spread through tissues with a
inessential energy dispersal, even though at
the urinary stone level cavitations (by the
cavitations „bubbles”) and erosion
phenomenon occur or force elements
directly performed by the shockwave.
These phenomenon lead to the calculus

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
140
disintegration and are formed at a solid-
liquid level (large density difference).
Phenomenon exercised by the cavitations
„bubbles” produced at the solid-liquid
level represent the most important aspect
in all researches made in order to increase
Extracorporeal Shockwave Lithotripsy
Device efficiency. [1, 2, 3, 4, 5]
ESWL represents a modern approach to
non-invasiv treatment of stones under 12-
20 mm, which covers about 90% of
treatment reference for urinary lithiasis
disease. [1, 2, 3, 7, 8]
The purpose of the study is to evaluate
the efficiency of ESWL in the treatment of
renal stones, but also complications that
may occur and most important the
restrictions of this modern treatment
method, as seen from the experience of the
Urology Clinic, Brasov.
Materials and Method
During the period May 2005 –
November 2008, 412 patients have been
treated by using ESWL at the Urology
Clinic, part of the Emergency County
Hospital in Brasov.
The investigation protocol was standard,
recommended by both The European and
the Romanian Association of Urology, and
it has contained the clinical examination,
usual laboratory investigation (including
urine exam and uroculture), abdominal
echography, reno-vesical radiography,
intravenous urography and in selected
cases retrograde pyelography.
The number of male patients treated with
ESWL was of 195 patients, and the female
patients count was 217. Renal stones were
bilateral in 32 cases, 183 patients in the
right kidney and 197 patients in the left
kidney.
Basinet stones were most frequently
encountered (119 cases), those located in
the middle caliceal group being present in
97 cases, a number of 73 cases calculus
were encountered in the upper caliceal
group and the lower caliceal group had an
incidence of 82 cases. Multiple lythiasis
was encountered in 47 cases.
Imagisticaly speaking, radio-opaque
stones were present in 261 cases and radio-
transparent stones in 151 cases.
The calculus scale treated with ESWL
ranged between 7 and 24 mm (193 cases
under 10 mm, 211 between 10 and 20 mm
and 8 cases above 20 mm).
All procedures were made by using a
Piezolith 2003 (Richard Wolf)
Extracorporeal Shockwave Lithotripsy
Device with echographic guiding.
Extracorporeal Shockwave Lithotripsy
sessions required analgesic treatment for
241 patients (58.5% of all cases),
consisting of injectable administration
before the session of Algocalmin, Piafen or
Fortral, combined or not with a systemic
anti-inflamator.
After the Extracorporeal Shockwave
Lithotripsy, all patients have received
antibiotic, analgesic, antispastic and anti-
inflammatory treatment.
Patients were observed for a period of 3
months, being re-evaluated by echography
or reno-vesical radiography and in some
cases by i.v. urography or chemical
analysis of eliminated calculus.
2. Results
Each session of Extracorporeal
Shockwave Lithotripsy usually lasts
between 30 and 50 (including the time
necessary for positioning the patient on the
Extracorporeal Shockwave Lithotripsy
table). A longer period was needed for
non-cooperant patients, with very thin
patients (positioning them on the table is
more difficult), patients with severe
alteration to their spinal cord (congenital or
degenerative) or patients with a low
threshold of sensibility. Then number of
administrated to each patient was between
1000 and 3000 at frequencies between 60
and 120 per minute (2500 impulses each
session).

Extracorporeal Shockwave Lithotripsy (ESWL) as a Mean of Treatment in Urinary Lithiasis 141
Total disintegration and elimination of
renal stones has been achieved in 93% of
the cases (384 patients). Between 1 and 9
sessions were needed to totally fragment
the calculus. In the great majority of
situations (334 patients) 1 or 2 sessions
have assured the „stone-free” status. 298
patients (72.3%) have eliminated
fragments in the first 24 hours since the
session.
For 24 of all patients assembling of an
ureteral stent was needed, after the renal
push-back of some lobar ureteral calculus
(16 patients), even in case of higher
dimension calculi (aprox. 20mm) when the
use of ESWL could cause the popup of
some high dimension fragments which
uretheral passage would be difficult if not
impossible (8 patients).
Also, Extracorporeal Shockwave
Lithotripsy has been timed in some cases
or urinary infection or cases that presented
us this febrile episode during the
internment (13 patients). In these cases
patients received antibiotherapy and have
been re-evaluated by 2 criteria:
aproximatively 3 weeks of afebrile
condition and sterile urine culture.
Not more than 2 sessions of ESWL were
made in one internment (1 day break). In
all situations patients were re-evaluated at
30 days after ESWL.
The chemical composition of the renal
calculi has an exquisite influence on the
rate of success when using ESWL.
Extracorporeal Shockwave Lithotripsy of
stones made of uric acid were
accompanied by a 30 day rate of success of
95%, and in case of calcium oxalate calculi
the rate of success was of 82% for
dehydrate, also 31% for monohydrate
calculi.
The number of cases that required more
than 2 sessions was 78, especially when
dealing with monohydrate calcium oxalate
with a scale pf over 15 mm.
Uric acid calculi and dehydrate oxalate
have disintegrated into small fragments
with a more easy elimination.
During the procedure 25 patients have
presented with vomiting sensation (anti-
emetic treatment has been administrated),
in 7 cases session halt was necessary
because of patients experiencing vomiting.
Minimal tegumentary lesions were
highlighted in 71 of all cases at the spot of
shockwave penetration, which
spontaneously disappeared in a maximum
period of 24 hours after the procedure.
Haematuria was minimal after each
procedure (considered normal) and has not
caused therapeutically problems, being
present for more than 24 hours.
In 31 patients the evolution has been
complicated by some of the fragments
hitting different segments of the urether
(steinstrasse), 21 of these complications
evolved favourably, with spontaneous
elimination of fragments within a period of
3 days (helped by diuretics, antispastic
medication, antiinflamatory and in some
cases alfa-blockers). 10 of the patients
required uretheroscopy with ballistic
intracorporeal lithotripsy and/or fragment
extraction.
Fig. 1. Renovesical radiography: radio-
opaque image in right renal area (stone)
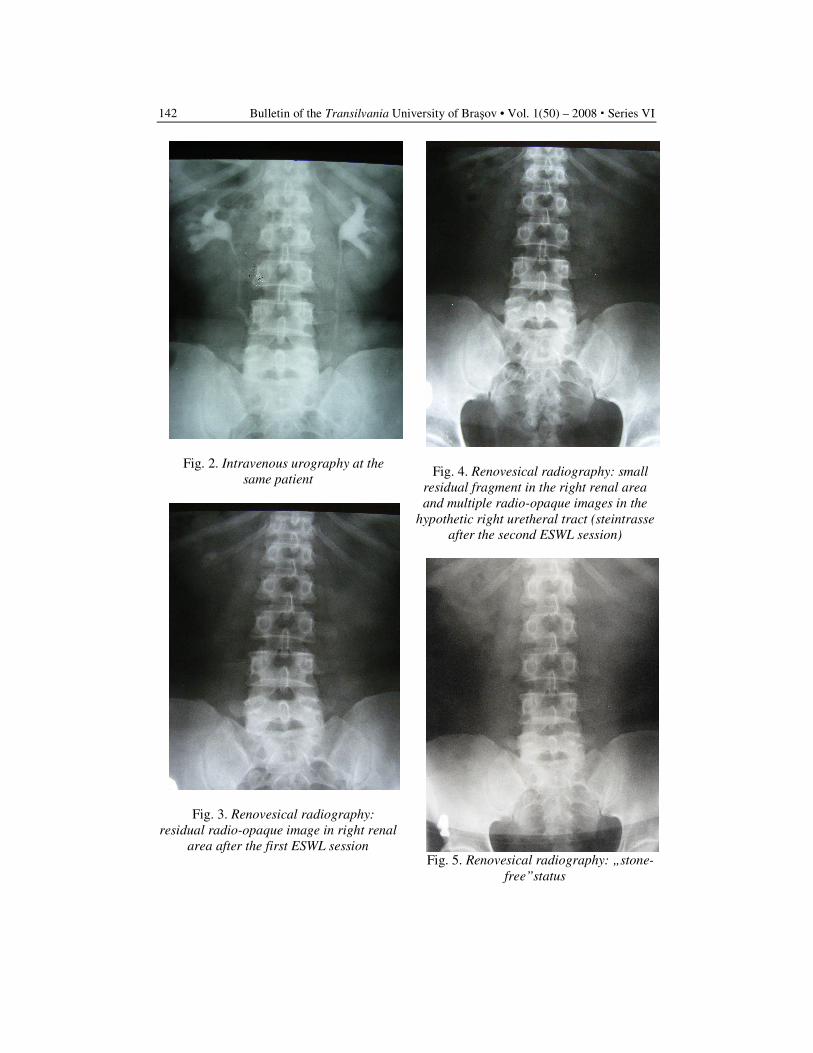
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
142
Fig. 2. Intravenous urography at the
same patient
Fig. 3. Renovesical radiography:
residual radio-opaque image in right renal
area after the first ESWL session
Fig. 4. Renovesical radiography: small
residual fragment in the right renal area
and multiple radio-opaque images in the
hypothetic right uretheral tract (steintrasse
after the second ESWL session)
Fig. 5. Renovesical radiography: „stone-
free”status
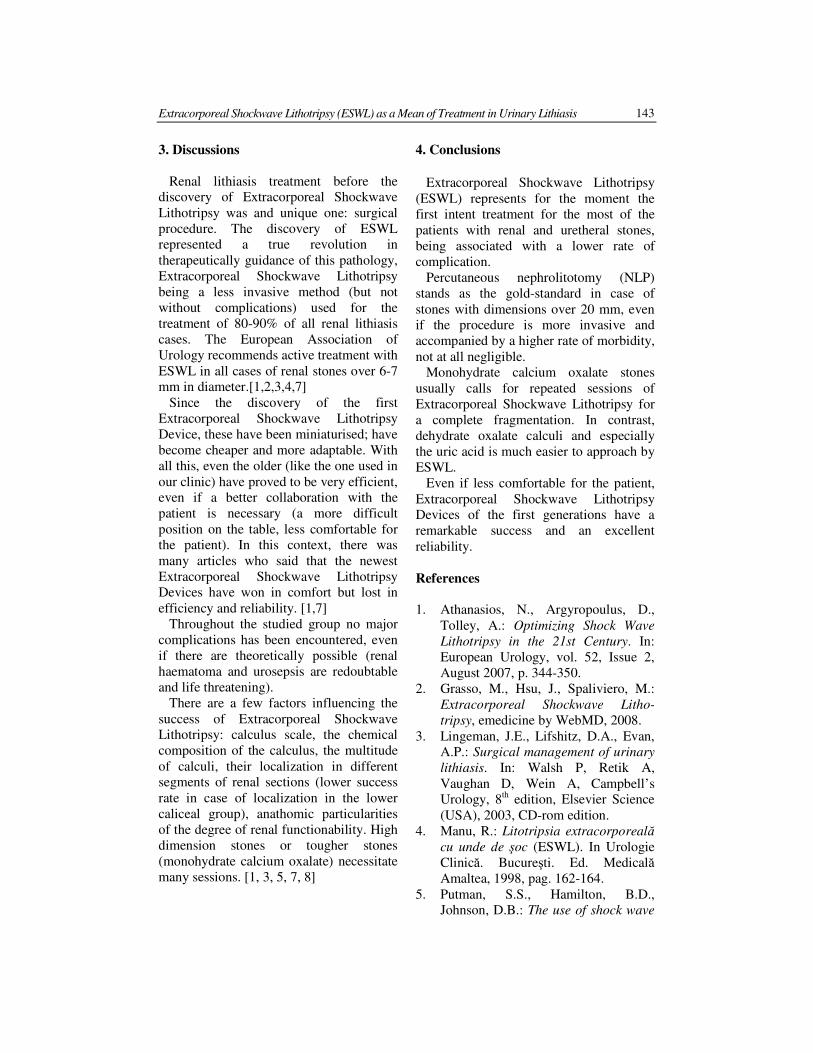
Extracorporeal Shockwave Lithotripsy (ESWL) as a Mean of Treatment in Urinary Lithiasis 143
3. Discussions
Renal lithiasis treatment before the
discovery of Extracorporeal Shockwave
Lithotripsy was and unique one: surgical
procedure. The discovery of ESWL
represented a true revolution in
therapeutically guidance of this pathology,
Extracorporeal Shockwave Lithotripsy
being a less invasive method (but not
without complications) used for the
treatment of 80-90% of all renal lithiasis
cases. The European Association of
Urology recommends active treatment with
ESWL in all cases of renal stones over 6-7
mm in diameter.[1,2,3,4,7]
Since the discovery of the first
Extracorporeal Shockwave Lithotripsy
Device, these have been miniaturised; have
become cheaper and more adaptable. With
all this, even the older (like the one used in
our clinic) have proved to be very efficient,
even if a better collaboration with the
patient is necessary (a more difficult
position on the table, less comfortable for
the patient). In this context, there was
many articles who said that the newest
Extracorporeal Shockwave Lithotripsy
Devices have won in comfort but lost in
efficiency and reliability. [1,7]
Throughout the studied group no major
complications has been encountered, even
if there are theoretically possible (renal
haematoma and urosepsis are redoubtable
and life threatening).
There are a few factors influencing the
success of Extracorporeal Shockwave
Lithotripsy: calculus scale, the chemical
composition of the calculus, the multitude
of calculi, their localization in different
segments of renal sections (lower success
rate in case of localization in the lower
caliceal group), anathomic particularities
of the degree of renal functionability. High
dimension stones or tougher stones
(monohydrate calcium oxalate) necessitate
many sessions. [1, 3, 5, 7, 8]
4. Conclusions
Extracorporeal Shockwave Lithotripsy
(ESWL) represents for the moment the
first intent treatment for the most of the
patients with renal and uretheral stones,
being associated with a lower rate of
complication.
Percutaneous nephrolitotomy (NLP)
stands as the gold-standard in case of
stones with dimensions over 20 mm, even
if the procedure is more invasive and
accompanied by a higher rate of morbidity,
not at all negligible.
Monohydrate calcium oxalate stones
usually calls for repeated sessions of
Extracorporeal Shockwave Lithotripsy for
a complete fragmentation. In contrast,
dehydrate oxalate calculi and especially
the uric acid is much easier to approach by
ESWL.
Even if less comfortable for the patient,
Extracorporeal Shockwave Lithotripsy
Devices of the first generations have a
remarkable success and an excellent
reliability.
References
1. Athanasios, N., Argyropoulus, D.,
Tolley, A.: Optimizing Shock Wave
Lithotripsy in the 21st Century. In:
European Urology, vol. 52, Issue 2,
August 2007, p. 344-350.
2. Grasso, M., Hsu, J., Spaliviero, M.:
Extracorporeal Shockwave Litho-
tripsy, emedicine by WebMD, 2008.
3. Lingeman, J.E., Lifshitz, D.A., Evan,
A.P.: Surgical management of urinary
lithiasis. In: Walsh P, Retik A,
Vaughan D, Wein A, Campbell’s
Urology, 8th edition, Elsevier Science
(USA), 2003, CD-rom edition.
4. Manu, R.: Litotripsia extracorporeală
cu unde de şoc (ESWL). In Urologie
Clinică. Bucureşti. Ed. Medicală
Amaltea, 1998, pag. 162-164.
5. Putman, S.S., Hamilton, B.D.,
Johnson, D.B.: The use of shock wave
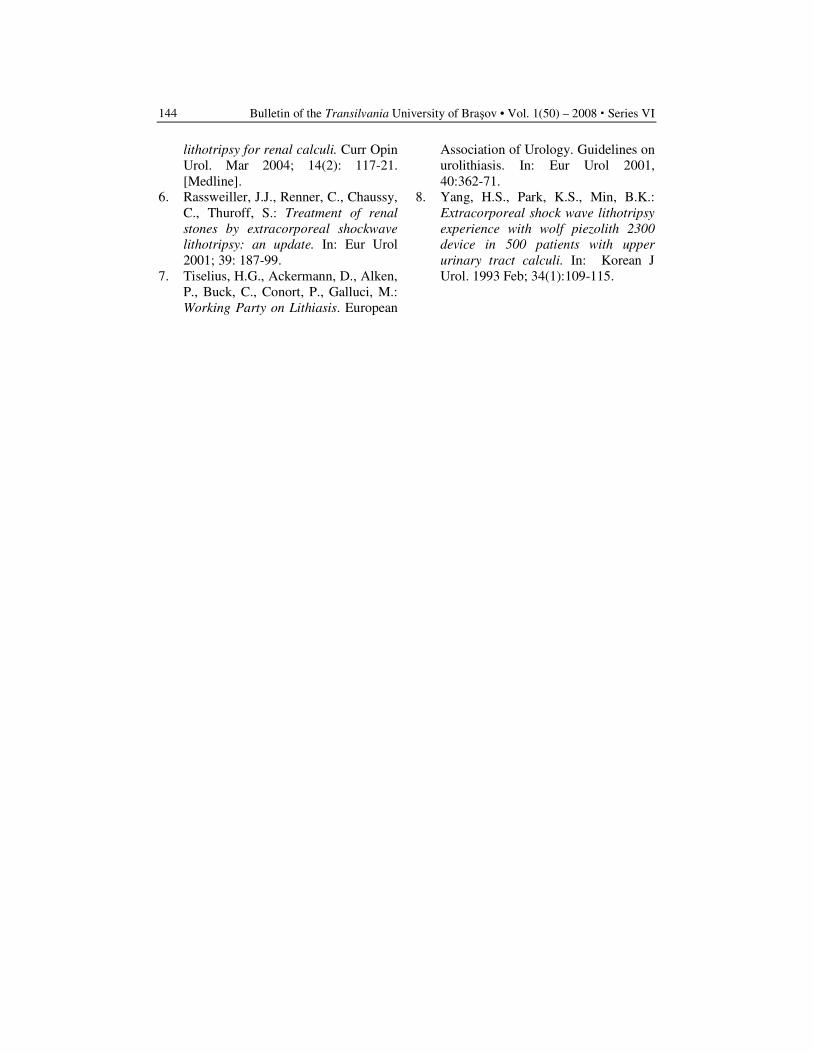
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
144
lithotripsy for renal calculi. Curr Opin
Urol. Mar 2004; 14(2): 117-21.
[Medline].
6. Rassweiller, J.J., Renner, C., Chaussy,
C., Thuroff, S.: Treatment of renal
stones by extracorporeal shockwave
lithotripsy: an update. In: Eur Urol
2001; 39: 187-99.
7. Tiselius, H.G., Ackermann, D., Alken,
P., Buck, C., Conort, P., Galluci, M.:
Working Party on Lithiasis. European
Association of Urology. Guidelines on
urolithiasis. In: Eur Urol 2001,
40:362-71.
8. Yang, H.S., Park, K.S., Min, B.K.:
Extracorporeal shock wave lithotripsy
experience with wolf piezolith 2300
device in 500 patients with upper
urinary tract calculi. In: Korean J
Urol. 1993 Feb; 34(1):109-115.
1Apollonia Dental Medicine Faculty , Petre Andrei University Iaşi
2Dental Medicine Faculty , U.M.F. „Gr. T. Popa” Iaşi
THE PATIENT- RISK MARKER FOR
MEDICAL EMERGENCIES IN THE
DENTAL AND ORAL SURGERY OFFICE
R. FANEA
1 M. VORONEANU
2 C. OROS
2
Abstract: Systemic vision on the case is clinically essential to
understanding the particulars involved in the patient, allowing the detection
of potential factors which could cause emergency dental office.
Therapeutic attitude must be individualized for each case, linking data
obtained through the clinical case history and paraclinical exams, in order to
obtain favorable results. Interdisciplinary approach allows the patient's
knowledge of systemic pathology associated with the medication followed
and particularities that dental treatment involved. Main sources in medical
emergencies in dental office are lacunars evaluations of the patients
constants, spontaneously neuro - psychical reactions or a lack of special
training of the medical staff. Our study was performed on 1680 patients. The
level of installed medical emergencies was 3, 85% distributed as come : 38%
vaso-vagal sincopa ,35% cardio-vascular emergencies, 11% alergic
emergencies, 9% neurologic emergencies,7% other emergencies .
Key words: medical emergencies in dental office, patient systemic risk,
dental fear
1. Introduction
Health care in dentistry and surgery
dentoalveolar, involving two apparently
different aspects: a technically well-
defined, the strict specialist and one less
area that includes the virtually all the
particulars that the patient is presented to
the dental office [7]. Whatever the precise
technique would be dental and physician's
skill if not taken into account the specific
conditions of each patient, medical service
may not be up to a higher level, the final
outcome may be compromised by the
appearance of complications with high
medical risk. Preoperatory stage is
absolutely necessary to know the patient,
anesthetic risk assessment [1]. Many
doctors are concerned about the idea of not
losing too much time in discussion with
patients and to move as quickly as the
dental care itself.
Many accidents that occur in dental
offices are attributable to just a superficial
examination incomplete, messy. Patient
exam limited to oral cavity is totally
inadequate, causing the wrong conclusions,
often generating accidents and serious
complications [2, 3]. Patients to be
subjected to an oral surgical intervention
have more or less a combination of general
potential problems, known or unknown.
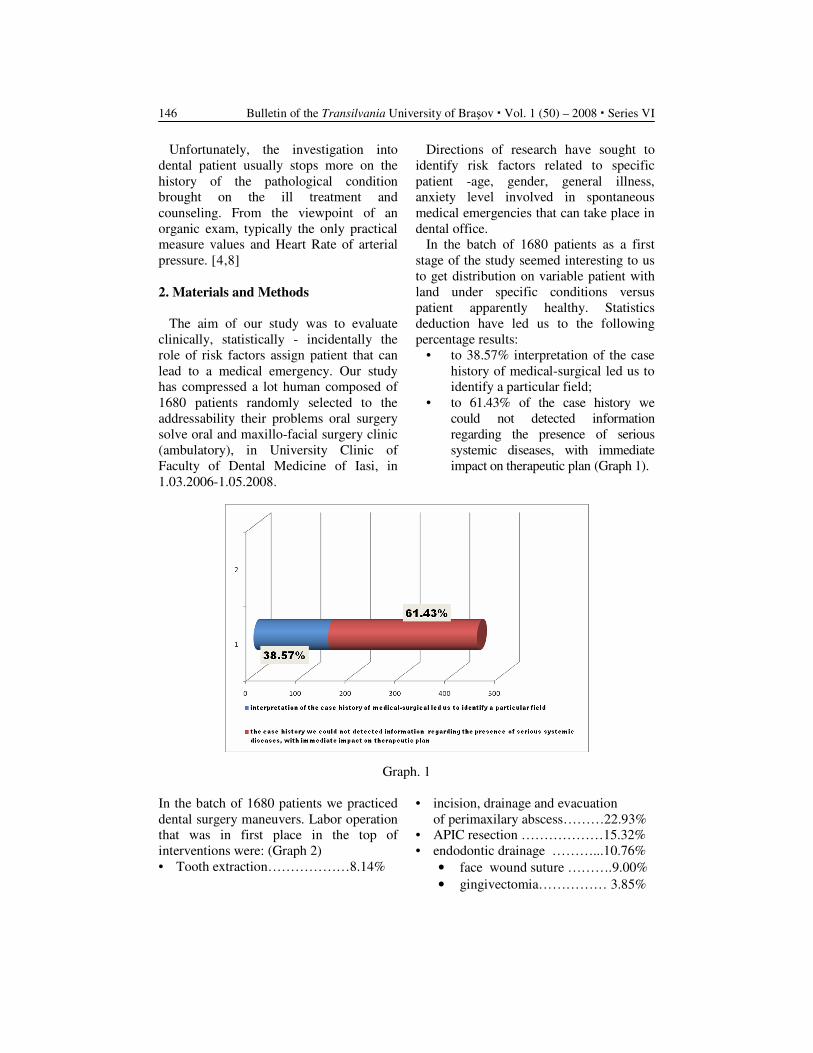
Bulletin of the Transilvania University of Braşov � Vol. 1 (50) – 2008 � Series VI 146
Unfortunately, the investigation into
dental patient usually stops more on the
history of the pathological condition
brought on the ill treatment and
counseling. From the viewpoint of an
organic exam, typically the only practical
measure values and Heart Rate of arterial
pressure. [4,8]
2. Materials and Methods
The aim of our study was to evaluate
clinically, statistically - incidentally the
role of risk factors assign patient that can
lead to a medical emergency. Our study
has compressed a lot human composed of
1680 patients randomly selected to the
addressability their problems oral surgery
solve oral and maxillo-facial surgery clinic
(ambulatory), in University Clinic of
Faculty of Dental Medicine of Iasi, in
1.03.2006-1.05.2008.
Directions of research have sought to
identify risk factors related to specific
patient -age, gender, general illness,
anxiety level involved in spontaneous
medical emergencies that can take place in
dental office.
In the batch of 1680 patients as a first
stage of the study seemed interesting to us
to get distribution on variable patient with
land under specific conditions versus
patient apparently healthy. Statistics
deduction have led us to the following
percentage results:
• to 38.57% interpretation of the case
history of medical-surgical led us to
identify a particular field;
• to 61.43% of the case history we
could not detected information
regarding the presence of serious
systemic diseases, with immediate
impact on therapeutic plan (Graph 1).
Graph. 1
In the batch of 1680 patients we practiced
dental surgery maneuvers. Labor operation
that was in first place in the top of
interventions were: (Graph 2)
• Tooth extraction………………8.14%
• incision, drainage and evacuation
of perimaxilary abscess………22.93%
• APIC resection ………………15.32%
• endodontic drainage ………...10.76%
• face wound suture ……….9.00%
• gingivectomia…………… 3.85%
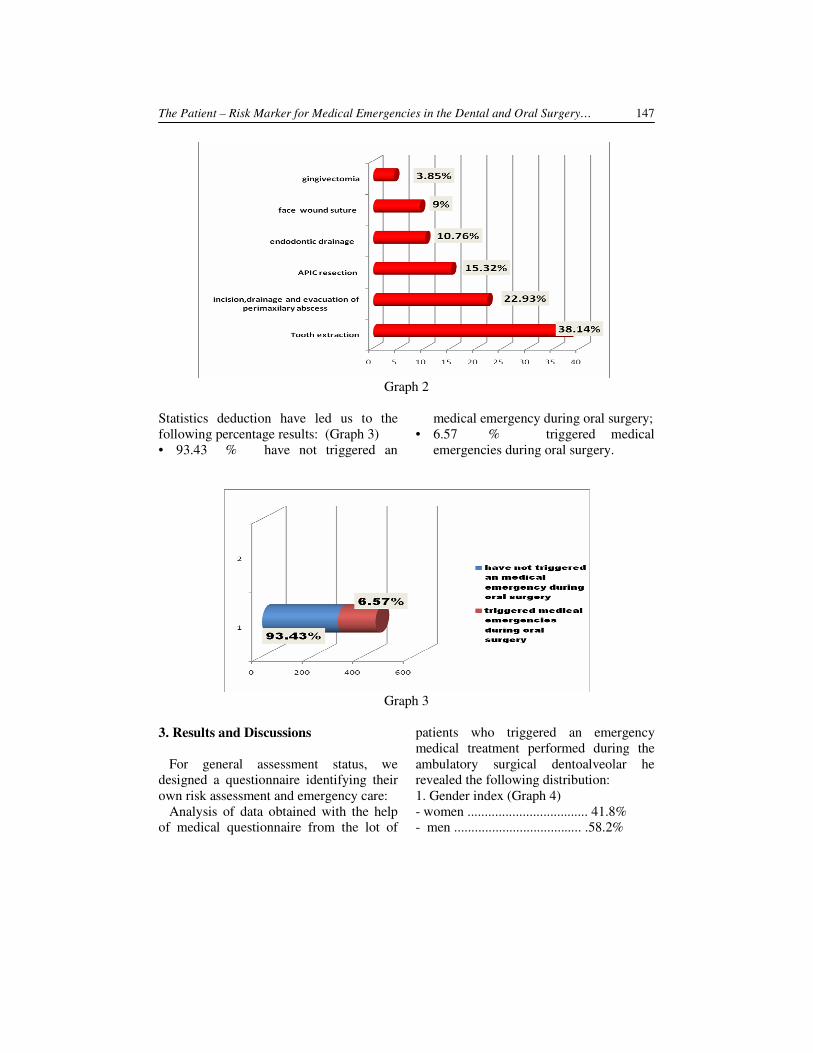
The Patient – Risk Marker for Medical Emergencies in the Dental and Oral Surgery… 147
Graph 2
Statistics deduction have led us to the
following percentage results: (Graph 3)
• 93.43 % have not triggered an
medical emergency during oral surgery;
• 6.57 % triggered medical
emergencies during oral surgery.
Graph 3
3. Results and Discussions
For general assessment status, we
designed a questionnaire identifying their
own risk assessment and emergency care:
Analysis of data obtained with the help
of medical questionnaire from the lot of
patients who triggered an emergency
medical treatment performed during the
ambulatory surgical dentoalveolar he
revealed the following distribution:
1. Gender index (Graph 4)
- women ................................... 41.8%
- men ..................................... .58.2%
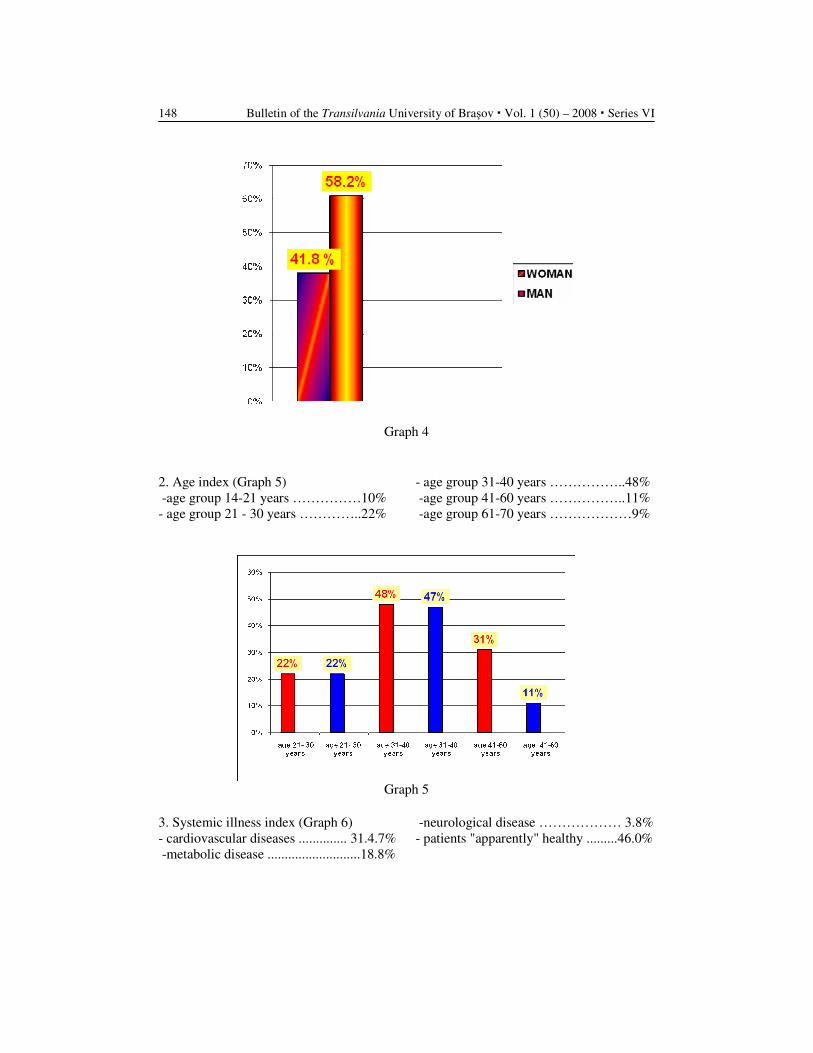
Bulletin of the Transilvania University of Braşov � Vol. 1 (50) – 2008 � Series VI 148
Graph 4
2. Age index (Graph 5)
-age group 14-21 years ……………10%
- age group 21 - 30 years …………..22%
- age group 31-40 years ……………..48%
-age group 41-60 years ……………..11%
-age group 61-70 years ………………9%
Graph 5
3. Systemic illness index (Graph 6)
- cardiovascular diseases .............. 31.4.7%
-metabolic disease ...........................18.8%
-neurological disease ……………… 3.8%
- patients "apparently" healthy .........46.0%
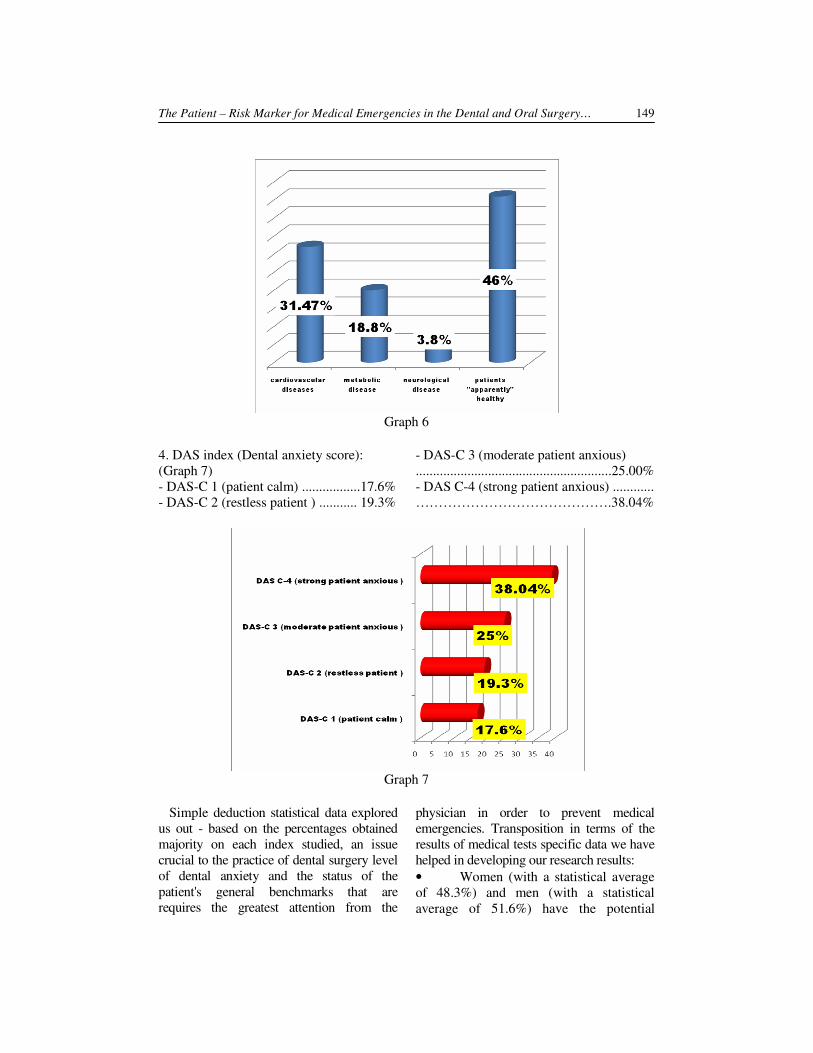
The Patient – Risk Marker for Medical Emergencies in the Dental and Oral Surgery… 149
Graph 6
4. DAS index (Dental anxiety score):
(Graph 7)
- DAS-C 1 (patient calm) .................17.6%
- DAS-C 2 (restless patient ) ........... 19.3%
- DAS-C 3 (moderate patient anxious)
.........................................................25.00%
- DAS C-4 (strong patient anxious) ............
…………………………………….38.04%
Graph 7
Simple deduction statistical data explored
us out - based on the percentages obtained
majority on each index studied, an issue
crucial to the practice of dental surgery level
of dental anxiety and the status of the
patient's general benchmarks that are
requires the greatest attention from the
physician in order to prevent medical
emergencies. Transposition in terms of the
results of medical tests specific data we have
helped in developing our research results:
• Women (with a statistical average
of 48.3%) and men (with a statistical
average of 51.6%) have the potential

Bulletin of the Transilvania University of Braşov � Vol. 1 (50) – 2008 � Series VI 150
trigger an emergency medical men are
more often involved in triggering an
unforeseen medical event during dental or
dentoalveolar surgery.
• During dental or surgical
maneuvers, installing a medical emergency
is influenced by patient age, patients younger
21 - 30 years (with an average percentage of
22%), 31-40 years (with an average of 47
percentage 5%) were more likely to launch
an unforeseen medical event.
• During dental or dentoalveolar
surgery installing an emergency medical
field is influenced by the patient. Although
the largest is owned by patients "apparently
healthy" (with a statistical average of 51%)
patients had pre-existing general showed a
certain tendency to launch an unforeseen
medical event: cardiovascular diseases (with
a statistical average of 23. 35%), metabolic
diseases (with a statistical average of 17. 9%),
pulmonary disease (with a statistical average
of 11.7%) and neurological disorders (with a
statistical average of 3. 8%).
• During dental or dentoalveolar
surgery, installing a medical emergency is
strongly influenced by the level of anxiety
of the patient. Thus our research showed
that 38% of patients, who have triggered
medical emergencies, are part of the
category of patients with strong anxiety,
responsive (DAS C-4). Is closely patients
and moderate anxious DAS C-3 (with a
statistical average of 32.1%), followed by
patients slightly uneasy DAS C-2 (with a
statistical average of 25%) and finally
patients calm DAS-C 1 (with a statistical
average of 23.26%).
Conclusions
During dental treatment to patients with
general illness and patient apparently
healthy- fear, pain triggers compensatory
vegetative and humoral mechanisms,
leading to the amendment primarily to
cardio-vascular parameters. Medical
emergencies although not a right and a
notable frequency in the practice of
dentistry, they are not exceptions,
therefore, identify risk factors puzzle in
which the patient is the central piece, is the
first essential step.
References
1. Academy Report: Periodontal
management of patients with
cardiovascular diseases. In: J.
Periodont., 73: 954-968, 2002.
2. ACC/ AHA: Guideline update for the
management of patients with unstable
angina and non-ST-segment elevation
myocardial infarction. Summary
article: a report of the American
College of Cardiology American
Heart Association task force on
practice guidelines (Committee on the
Management of Patients With
Unstable Angina). In: J. Amer. Coll.
Cardiolog. 40: 1366-1374, 2002.
3. AHA Guideline: Evidence Based
Guidelines for Cardiovascular
Disease Prevention in women. In: J.
Circulation, 109: 672-693, 2004.
4. American Dental Association:
Council on Community Health,
Hospital Institution and Medical
Affairs. Patients with cardiovascular
disease. In: Oral Health Care
Guidelines,1-13, 1990.
5. American Heart Association: Heart
Disease and Stroke Statistics. Update,
Dallas, 2004.
6. Balan, H., Iordache, N.: Urgenţe
medico-chirurgicale. (curs pentru
stud. an V, Facultatea de Medicină
Dentară, U.M.F. “Carol Davila”).
Bucureşti. Ed. Medicală, 2005.
7. Jowett, N.I., Cabot, L.B.: Patients
with cardiac disease: considerations
for the dental practitioner. In: Brit.
Dent. J. , 189: 297-302, 2002.
8. Voroneanu, M., Bucur, A, Vicol, C.,
Dinescu, N.N.: Actualităţi privind riscul
urgenţelor medicale în cabinetul de
medicină dentară. Iaşi. Ed. PIM, 2007.
ULTRASTRUCTURAL CHANGES IN A
CASE OF RECURRENCE AFTER
VARICOSE VEINS SURGERY
Florin COMŞA
1
Abstract: Heredity plays an important role in varicose veins disease. The
weak wall theory with secondary valvulare incompetence has been proposed
as the most likely cause for primary varicose vein disease. Ultrastructural
wall changes in varicose veins have been deeply studied. We present a case
of varicose vein recurrence in which we have been searching for histological
changes using light and electron microscopy in comparison with those found
in primary varicose vein disease
Key words: Varicose veins recurrence, smooth muscle cells, electron
microscope
1 Diagnostic and Treatment Center „Dr. Victor Babeş”, Bucharest.
1. Introduction
In the varicose veins disease, the
heredity is an important key element [3, 6,
7]. More than a half of the affected persons
have positive family records for the
varicose veins disease, which suggests a
genetically inherited bad quality of the
veins wall. The parietal theory with
secondary valvulare insufficiency has been
referred to as the most likely cause of
primary varicose veins disease, offering an
explanation why the varicose veins
dilatations are often located under a
competent valve [2].
In the last decade, the clinical and
experimental studies revealed a deficiency
of the vein wall as a cause of varicose
veins disease. Varicose veins dilatation at
the level of the inferior lower limbs can
occur even in the absence of valvulare
incompetence. Moreover, when a vein is
subject to high pressures (which is for
example the case in the insufficiency of a
perforating vein or when the vein is used
as a graft in an arterial by-pass) the wall
hypertrophies itself in a first stage and
afterwards distends uniformly or non-
uniformly. The alternation of the
apparently normal segments with those
much dilated ones noticed at the level of
varicose veins has nothing to do with the
disposing of the valve or its functionality,
most of the dilated varicose veins segments
being located immediately under the
valves which appear competent on Doppler
examination.
2. Case Report
We present the case of Ms. EL, a 36
years old patient, which was hospitalized
at „Dr. Victor Babeş” Diagnosis and
Treatment Center on the date of November
5th, 2007. The reason for hospitalization
was the recurrence and development of
dilatation of the superficial venous net-
work at the level of the right pelvic limb.
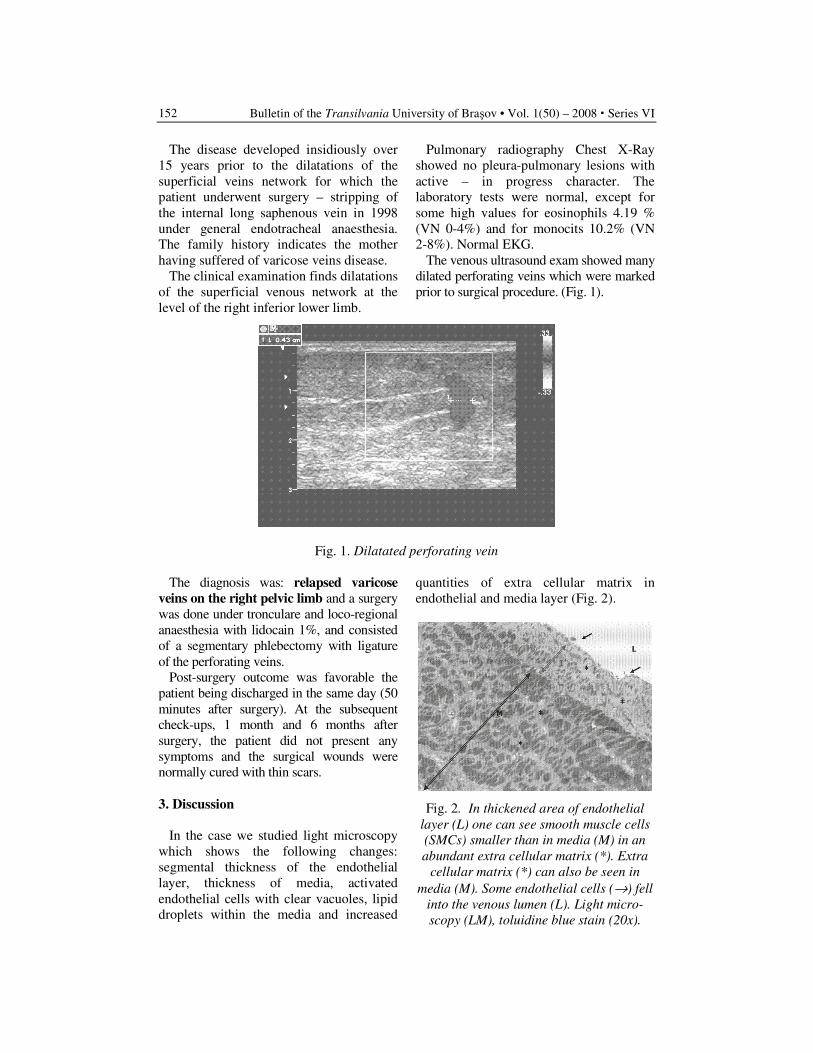
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
152
The disease developed insidiously over
15 years prior to the dilatations of the
superficial veins network for which the
patient underwent surgery – stripping of
the internal long saphenous vein in 1998
under general endotracheal anaesthesia.
The family history indicates the mother
having suffered of varicose veins disease.
The clinical examination finds dilatations
of the superficial venous network at the
level of the right inferior lower limb.
Pulmonary radiography Chest X-Ray
showed no pleura-pulmonary lesions with
active – in progress character. The
laboratory tests were normal, except for
some high values for eosinophils 4.19 %
(VN 0-4%) and for monocits 10.2% (VN
2-8%). Normal EKG.
The venous ultrasound exam showed many
dilated perforating veins which were marked
prior to surgical procedure. (Fig. 1).
Fig. 1. Dilatated perforating vein
The diagnosis was: relapsed varicose
veins on the right pelvic limb and a surgery
was done under tronculare and loco-regional
anaesthesia with lidocain 1%, and consisted
of a segmentary phlebectomy with ligature
of the perforating veins.
Post-surgery outcome was favorable the
patient being discharged in the same day (50
minutes after surgery). At the subsequent
check-ups, 1 month and 6 months after
surgery, the patient did not present any
symptoms and the surgical wounds were
normally cured with thin scars.
3. Discussion
In the case we studied light microscopy
which shows the following changes:
segmental thickness of the endothelial
layer, thickness of media, activated
endothelial cells with clear vacuoles, lipid
droplets within the media and increased
quantities of extra cellular matrix in
endothelial and media layer (Fig. 2).
Fig. 2. In thickened area of endothelial
layer (L) one can see smooth muscle cells
(SMCs) smaller than in media (M) in an
abundant extra cellular matrix (*). Extra
cellular matrix (*) can also be seen in
media (M). Some endothelial cells (→) fell
into the venous lumen (L). Light micro-
scopy (LM), toluidine blue stain (20x).
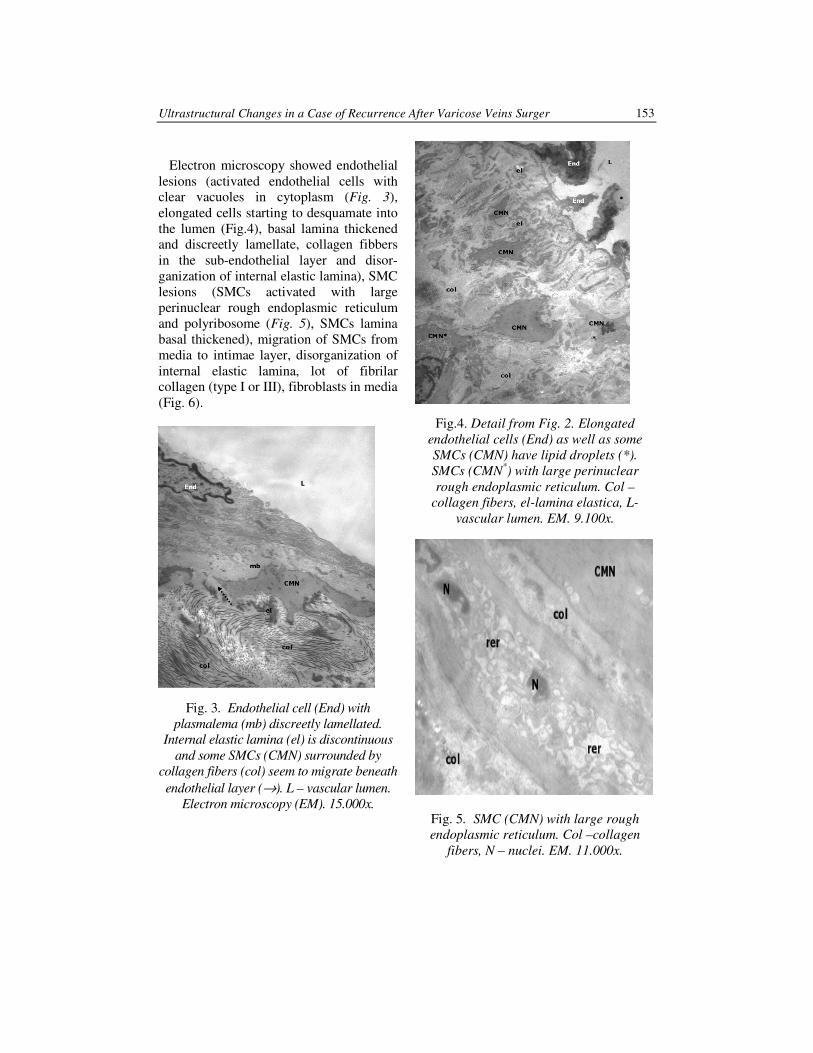
Ultrastructural Changes in a Case of Recurrence After Varicose Veins Surger 153
Electron microscopy showed endothelial
lesions (activated endothelial cells with
clear vacuoles in cytoplasm (Fig. 3),
elongated cells starting to desquamate into
the lumen (Fig.4), basal lamina thickened
and discreetly lamellate, collagen fibbers
in the sub-endothelial layer and disor-
ganization of internal elastic lamina), SMC
lesions (SMCs activated with large
perinuclear rough endoplasmic reticulum
and polyribosome (Fig. 5), SMCs lamina
basal thickened), migration of SMCs from
media to intimae layer, disorganization of
internal elastic lamina, lot of fibrilar
collagen (type I or III), fibroblasts in media
(Fig. 6).
Fig. 3. Endothelial cell (End) with
plasmalema (mb) discreetly lamellated.
Internal elastic lamina (el) is discontinuous
and some SMCs (CMN) surrounded by
collagen fibers (col) seem to migrate beneath
endothelial layer (→). L – vascular lumen.
Electron microscopy (EM). 15.000x.
Fig.4. Detail from Fig. 2. Elongated
endothelial cells (End) as well as some
SMCs (CMN) have lipid droplets (*).
SMCs (CMN*) with large perinuclear
rough endoplasmic reticulum. Col –
collagen fibers, el-lamina elastica, L-
vascular lumen. EM. 9.100x.
Fig. 5. SMC (CMN) with large rough
endoplasmic reticulum. Col –collagen
fibers, N – nuclei. EM. 11.000x.
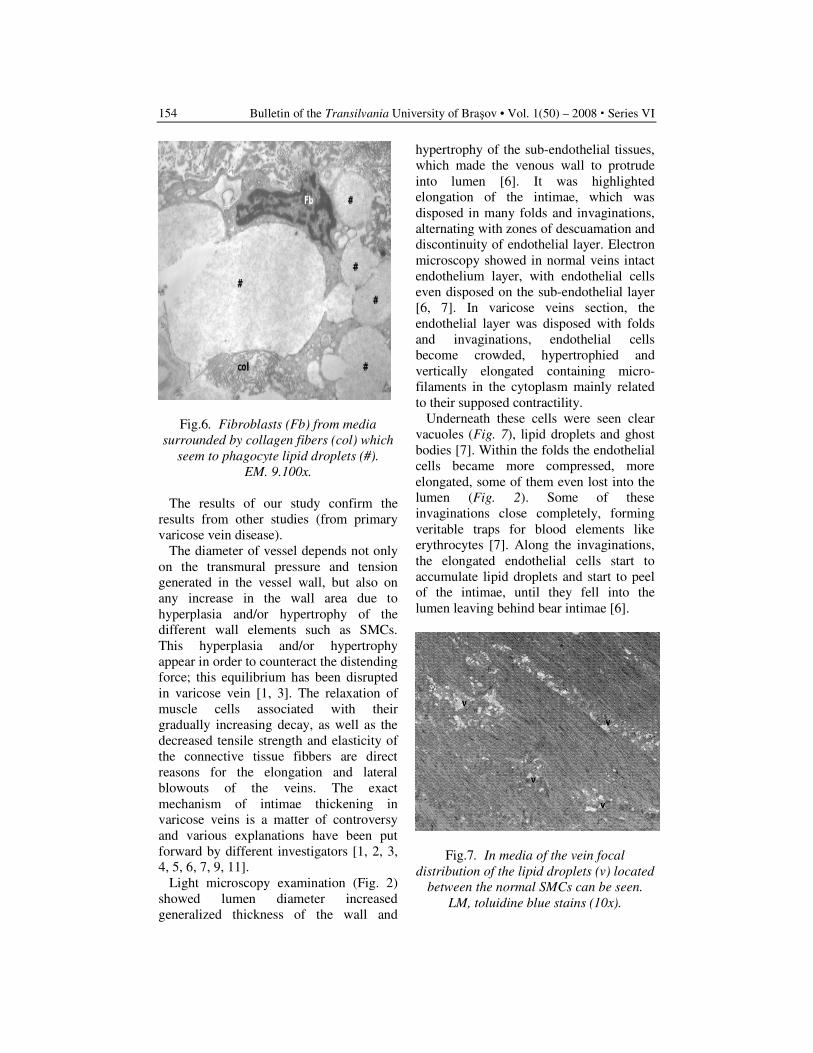
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
154
Fig.6. Fibroblasts (Fb) from media
surrounded by collagen fibers (col) which
seem to phagocyte lipid droplets (#).
EM. 9.100x.
The results of our study confirm the
results from other studies (from primary
varicose vein disease).
The diameter of vessel depends not only
on the transmural pressure and tension
generated in the vessel wall, but also on
any increase in the wall area due to
hyperplasia and/or hypertrophy of the
different wall elements such as SMCs.
This hyperplasia and/or hypertrophy
appear in order to counteract the distending
force; this equilibrium has been disrupted
in varicose vein [1, 3]. The relaxation of
muscle cells associated with their
gradually increasing decay, as well as the
decreased tensile strength and elasticity of
the connective tissue fibbers are direct
reasons for the elongation and lateral
blowouts of the veins. The exact
mechanism of intimae thickening in
varicose veins is a matter of controversy
and various explanations have been put
forward by different investigators [1, 2, 3,
4, 5, 6, 7, 9, 11].
Light microscopy examination (Fig. 2)
showed lumen diameter increased
generalized thickness of the wall and
hypertrophy of the sub-endothelial tissues,
which made the venous wall to protrude
into lumen [6]. It was highlighted
elongation of the intimae, which was
disposed in many folds and invaginations,
alternating with zones of descuamation and
discontinuity of endothelial layer. Electron
microscopy showed in normal veins intact
endothelium layer, with endothelial cells
even disposed on the sub-endothelial layer
[6, 7]. In varicose veins section, the
endothelial layer was disposed with folds
and invaginations, endothelial cells
become crowded, hypertrophied and
vertically elongated containing micro-
filaments in the cytoplasm mainly related
to their supposed contractility.
Underneath these cells were seen clear
vacuoles (Fig. 7), lipid droplets and ghost
bodies [7]. Within the folds the endothelial
cells became more compressed, more
elongated, some of them even lost into the
lumen (Fig. 2). Some of these
invaginations close completely, forming
veritable traps for blood elements like
erythrocytes [7]. Along the invaginations,
the elongated endothelial cells start to
accumulate lipid droplets and start to peel
of the intimae, until they fell into the
lumen leaving behind bear intimae [6].
Fig.7. In media of the vein focal
distribution of the lipid droplets (v) located
between the normal SMCs can be seen.
LM, toluidine blue stains (10x).

Ultrastructural Changes in a Case of Recurrence After Varicose Veins Surger 155
In sections of the distal calf varicosities,
break down of the intimal surface and loss
of the endothelial cells exposed the basal
lamina and the subintimal tissues to the
lumen (Fig. 5). This let blood components,
like platelets, erythrocytes and lipid
droplets, to stick to the bare intimae and
migrate through the wall and lay within the
wall [6, 7]. When SMCs come into close
contact with monocytes, their capacity for
collagen phagocytosis, decomposition and
disintegration is increased. This might
explain the process of clinical superficial
thrombophlebitis, which sometimes
complicates cases of varicose veins. The
rational surgical approach would therefore
be, as proposed by Venturi et al. [1], to
remove the whole long saphenous vein,
rather than removing only the varices.
Electron microscopy examination of
varicose vein sections showed in tunica
intimae and media wide separation of the
SMCs by an increased amount of extra-
cellular matrix and variable bands of
collagen fibbers. These changes were
present in both the medial and intimal
SMCs. SMCs were abnormal in shape and
lost their regular fusiform appearance, with
extension of plasmalemal projections,
some of which separated completely from
the cell surface [6, 7] forming ghost
bodies. With the loss of their cellular
integrity, some SMCs split into fiber-like
material, possibly collagen fibers, small
fragments that are widely scattered in the
extracellular space. Another ability of
SMCs is to phagocytose not only collagen
and elastic fibers (Fig. 7), but also other
damaged SMCs [6].
The only logic treatment is the surgical
one consisting of segmentary phlebectomy
with ligature of the incompetent
perforating veins.
The recurrence of varicose vein can lead
to skin alterations, superficial thrombo-
phlebitis and venous ulcer. Natural evo-
lution of this disease is severe and inva-
lidating in case it is untreated or treated
conventional. Ligature of the incompetent
perforating veins and segmentary phleb-
ectomy is therefore the elective treatment.
Each treatment must be personalized
accordingly to the disease stage.
The peculiarity of this case is the period
from initial surgical procedure and
recurrence of varicose vein.
Conclusion
Among paraclinical examinations, the
venous ultrasound exam has a great value,
allowing an accurate assessment of the
condition of the superficial and deep
venous system and of the perforating veins
as well as of the anatomic situation of
every specific case.
The surgical procedure must follow to
the ligature of the incompetent perforating
veins as much as possible and remove the
varicose veins packs in order to suppress
the deep venous reflux because of the risk
of local complications, among which
venous ulcer is the most dreadful.
Regular clinical exams during the whole
lifetime of the patients suffering from
varicose veins are totally justified as
proven by the 9 years recurrence in the
above presented case.
Electronic microscopy indicates the same
type of changes in varicose veins disease
and in its recurrence.
References
1. Amould, T., Michiels, C., Janssens, D.,
Berma, N. and Remacle, J.: Effect of
Ginkor Fort on Hypoxia-induced
neutrophils adherence to human
saphenous vein endothelium. In: J.
Cardiovasc. Pharmacol. 1998, 31:
456–463.
2. Coleridge-Smith, P.D.: The micro-
circulation in venous hypertension. In:
Vasc. Med. 1997, 2: 203–213.
3. Janssens, D., Michiels, C., Guillaume,
G., Cuisinier, B., Lonagie, Y. and
Remacle, J.: Increase in circulating
endothelial cells in patients with

Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
156
primary chronic venous insufficiency:
protective effect of Ginkor Forte in a
randomized double-blind, placebo-
controlled trial. In: J. Cardiovasc.
Pharmacol. 1999, 33: 7–11.
4. Khan, A.A., Eid, R.A. and Hamdi, A.:
Structural changes in the tunica intima
of varicose veins: A histopathological
and ultrastructural study. In: Pathol.
2000, 32: 253–257.
5. Lengyel, L. and Acsady, G.Y.:
Histomorphological and patho–
biochemical changes of varicose veins:
a possible explanation of the
development of varicosis. In: Acta
Morphol. Hungar. 1990, 38: 259– 267.
6. Mahmoud, A.W. and Refaat, A.E.
Smooth Muscle Changes in Varicose
Veins: An Ultrastructural Study. In: J.
Smooth Muscle Res. 2001, 37 (5, 6):
123–135.
7. Mahmoud, A.W. and Refaat, A.E.
Intimal Changes in Varicose Veins: an
Ultrastructural Study. In: J. Smooth
Muscle Res. 2002, 38 (3): 63–74.
8. Obitsu, T.: Histopathological studies
of the valves of varicose veins. In:
Phlebol. 1990, 5: 245–254.
9. Psaila, J.V. and Melhuish, J.: Visco–
elastic properties and collagen content
of the long saphenous vein in normal
and varicose veins. Br. J. Surg. 1989,
76: 37–40.
10. Travers, J.P., Brookes, C.E., Evans, J.,
Baker, D.M., Kent, C., Makin, G.S.
and Mayhew, T.M.: Assessment of
wall structure and composition of
varicose veins with reference to
collagen, elastin and smooth muscle
content. In: Eur. J. Vasc. Endovasc.
Surg. 1996, 11: 230–237.
11. Venturi, M., Bonavina, L., Annoni, F.,
Colombo, L., Butera, C., Peracchia, A.
and Mussini, E.: Biochemical assay of
coragen and elastin in the normal and
varicose vein wan. In: J. Surg. Res.
1996, 60: 245–248.
INTEGRATED POSITRON-EMISSION
TOMOGRAPHY AND THE STAGING OF
NODULAR NON-SMALL-CELL LUNG
CANCER
Dana ALEXANDRESCU
1
Abstract: We compared the diagnostic accuracy of integrated positron-
emission tomography and computed tomography (PET-CT) with that of CT
alone, that of PET alone and that of conventional visual correlation of PET
and CT in determining the stage of disease in non-small-cell lung cancer,
less than 3 cm
Key words: Integrated positron-emission tomography, stadialisation of
disease in non-small-cell lung cancer.
1 Transilvania University of Brasov, Faculty of Medicine.
1. Introduction
Computed tomography (CT) has an
important role in the initial determination
of the stage of disease in lung cancer. CT
provides excellent morphologic infor-
mation on the extent of disease but has
limited ability to differentiate between
benign and malignant lesions in an organ
or in lymph nodes. Whole-body positron-
emission tomography (PET) with
fludeoxyglucose F18 ([18 F]fluoro-2-
deoxy-D-glucose) has a higher rate of
detection of mediastinal lymph-node
metastases as well as of extrathoracic
metastases [4, 6, 8, 10, 12, 14]. It has also
proved effective in the management of
non-small-cell lung cancer [4, 6, 11, 13].
Since commercial PET scanners provide
nominal spatial resolution of 4.5 to 6 mm
in the center of the axial field of view,
even lesions that are less than 1 cm in
diameter can be detected on the basis of an
increased uptake of fludeoxyglucose F 18.
However, fludeoxyglucose F 18 is also
taken up by muscles and inflammatory
processes. Furthermore, PET provides
imprecise information on the exact
location of focal abnormalities. Thus, even
if the results of PET and CT are visually
correlated, the precise location of lesions is
sometimes difficult to determine. Recently,
integrated PET-CT scanners have been
introduced [1]. Initial results in oncology
have been encouraging. Therefore, we
prospectively compared the accuracy of
integrated PET-CT with that of other
imaging methods in staging nodular non-
small-cell lung cancer.
Materials and Methods
46 patients with proven or suspected
non-small-cell lung cancer were enrolled
in the study at the Universitary Hospital
Luzern. All performed PET-CT scan at the
University Hospital of Zürich, Switzerland,
a teaching and tertiary care hospital and a
major referral site for patients with cancer.

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
158
Thoracic surgeons from Cantonal
Hospital Luzern at the facility have been
using PET routinely preoperative
assessment of disease stage since 1996. All
patients underwent conventional staging
based on a review of the medical history,
physical findings and results of blood tests,
bronchoscopy and contrast-enhanced CT
of the chest and upper abdomen and all
also underwent integrated whole-body
PET-CT.
All patients were referred for surgery
between July 2002 - December 2005 in
Thoracic Surgical Department of the
Universitary Hospital Luzern and were
included in the study after giving written
informed consent in accordance with the
regulations of the institutional review
board. Seven patients were excluded from
further study because histologic analysis
revealed in 3 cases benign tumors and in 4
cases metastases of oral cavity and
pharynx carcinoma, large intestine carci-
noma, breast carcinoma and melanoma.
Thus, 39 patients (28 men and 11 women)
with a mean age of 61.59 (range, 38 and
78) remained in the study. Histologic
analysis revealed adenocarcinoma in 5
patients, squamous-cell carcinoma in 9
patients, large-cell carcinoma in one case
and tipic carcinoma in one patient.
Patients received an intravenous
injection of 350 to 400 MBq of fludeo-
xyglucose F 18 and then rested for appro-
ximately 50 minutes before undergoing
imaging. Image acquisition was performed
with use of an integrated PET-CT device
(Discovery LS, GE Medical Systems)
consisting of an Advance NXi PET
scanner and a four-slice Light Speed Plus
CT scanner. The axes of both systems were
mechanically aligned so that shifting the
examination table by 60 cm moved the
patient from the CT into the PET gantry.
The resulting PET and CT images were
coregistered on hardware.
An unenhanced CT image was obtained
from the patient’s head to the pelvic floor
with use of a standardized protocol
involving 140kV, 80 mA, a tube-rotation
time of 0.5 second per rotation, a pich of 6,
and a section thickness of 5 mm, which
was matched to the section thickness of the
PET images. Immediately after CT, PET
was performed that covered the identical
axial field of view. The acquisition time
for PET was 4 minutes per table position
and 24 minutes in all. Patients were
instructed to hold their breath in normal
expiration for 22 seconds during the
acquisition of the CT images and to
breathe shallowly during the acquisition of
the PET images. PET-image data sets were
reconstructed iteratively with segmented
correction for attenuation with use of the
CT data. Corregistered images were
displayed by means of eNTEGRA
software (GE Medical Systems) [2, 7, 9].
Lung resections were performed with
mediastinal lymph-node dissection, which
consisted of dissection of all nodes at
stations 2 through 4 and 7 through 9 on the
right side and of stations 4 through 9 on
the left side, according to the mapping
system of the American Thoracic Society.
The images were prospectively analyzed
by a nuclear-radiology physician and a
thoracic surgeon (both with more than 10
years of medical experience) and assigned
a TNM stage. After reviewing the CT
images for each patient, the reviewers
assessed attenuation-corrected PET
images. Thus, the reviewers interpreted the
PET images with the knowledge of the CT
findings and visually correlated the PET
and CT images. This approach was chosen
because it represents the standard practice
of combined reading of PET and CT
images. On the basis of their visual
correlation, the reviewers again assigned a
TNM stage. When a clear differentiation
between different tumor stages was not
possible, both stages were noted and the
findings were deemed equivocal. They
analyzed also the attenuation-corrected
PET images, co-rregistered PET-CT
images and assigned a TNM stage. Finally,
TNM stages based on the various imaging
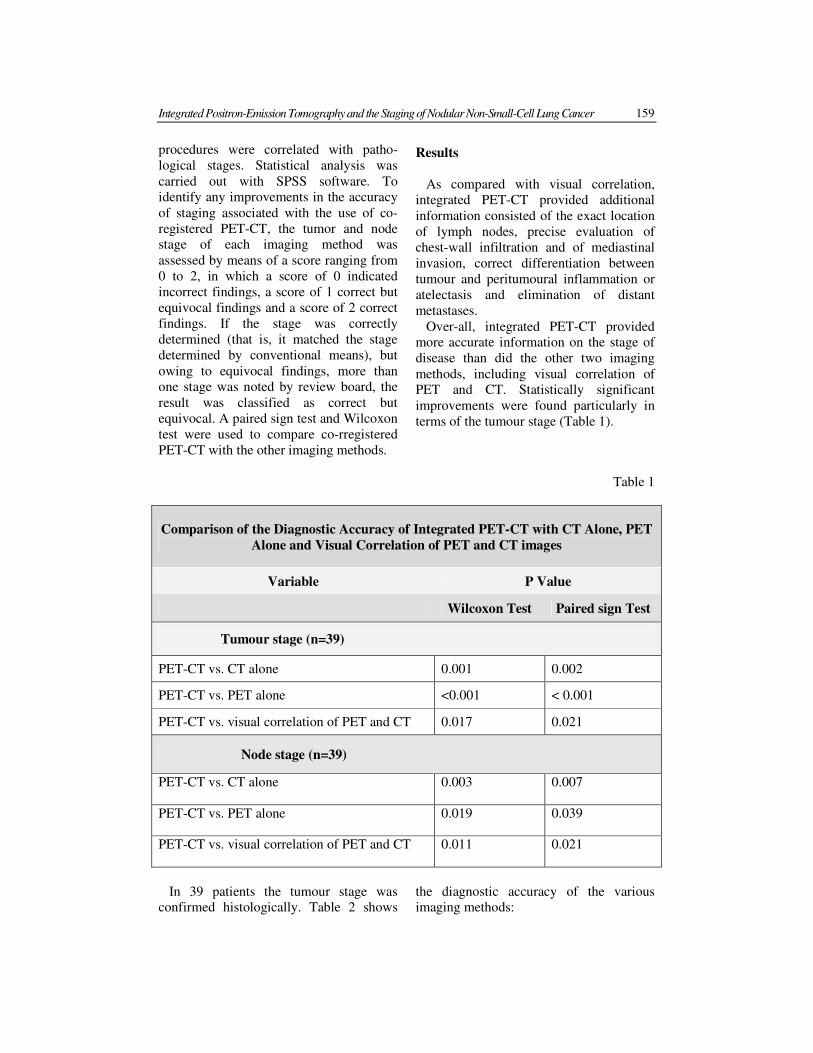
Integrated Positron-Emission Tomography and the Staging of Nodular Non-Small-Cell Lung Cancer 159
procedures were correlated with patho-
logical stages. Statistical analysis was
carried out with SPSS software. To
identify any improvements in the accuracy
of staging associated with the use of co-
registered PET-CT, the tumor and node
stage of each imaging method was
assessed by means of a score ranging from
0 to 2, in which a score of 0 indicated
incorrect findings, a score of 1 correct but
equivocal findings and a score of 2 correct
findings. If the stage was correctly
determined (that is, it matched the stage
determined by conventional means), but
owing to equivocal findings, more than
one stage was noted by review board, the
result was classified as correct but
equivocal. A paired sign test and Wilcoxon
test were used to compare co-rregistered
PET-CT with the other imaging methods.
Results
As compared with visual correlation,
integrated PET-CT provided additional
information consisted of the exact location
of lymph nodes, precise evaluation of
chest-wall infiltration and of mediastinal
invasion, correct differentiation between
tumour and peritumoural inflammation or
atelectasis and elimination of distant
metastases.
Over-all, integrated PET-CT provided
more accurate information on the stage of
disease than did the other two imaging
methods, including visual correlation of
PET and CT. Statistically significant
improvements were found particularly in
terms of the tumour stage (Table 1).
Table 1
Comparison of the Diagnostic Accuracy of Integrated PET-CT with CT Alone, PET
Alone and Visual Correlation of PET and CT images
Variable P Value
Wilcoxon Test Paired sign Test
Tumour stage (n=39)
PET-CT vs. CT alone 0.001 0.002
PET-CT vs. PET alone <0.001 < 0.001
PET-CT vs. visual correlation of PET and CT 0.017 0.021
Node stage (n=39)
PET-CT vs. CT alone 0.003 0.007
PET-CT vs. PET alone 0.019 0.039
PET-CT vs. visual correlation of PET and CT 0.011 0.021
In 39 patients the tumour stage was
confirmed histologically. Table 2 shows
the diagnostic accuracy of the various
imaging methods:
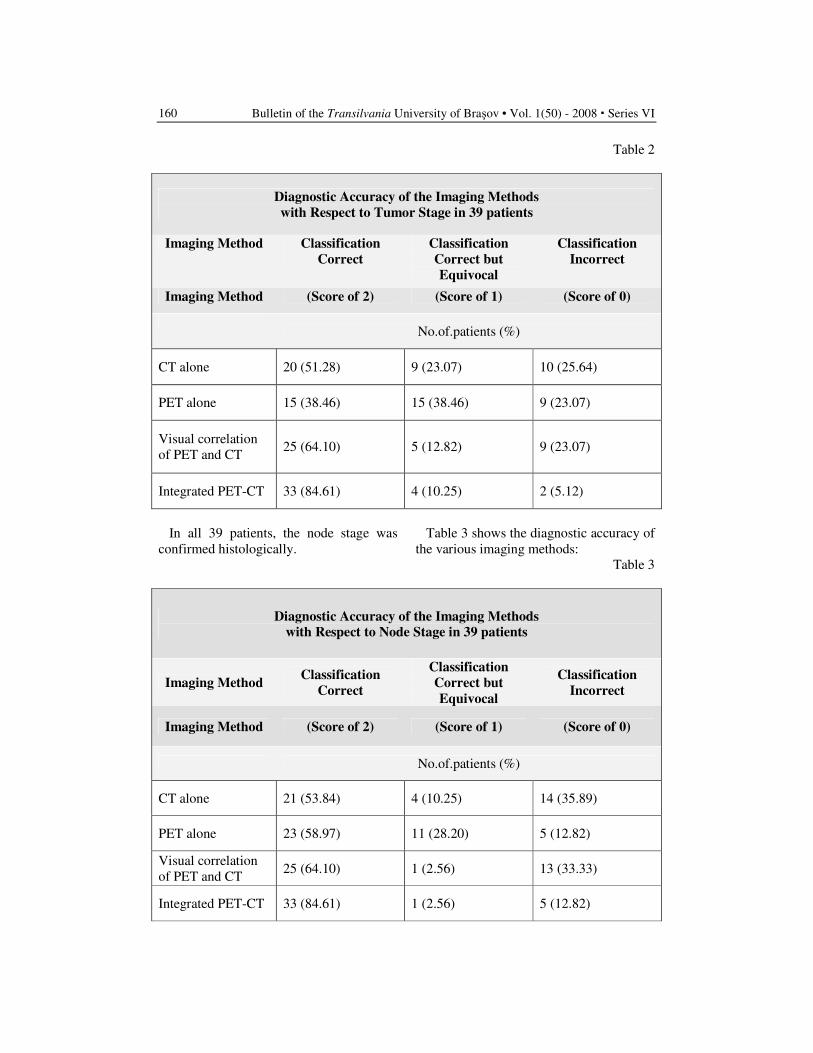
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
160
Table 2
Diagnostic Accuracy of the Imaging Methods
with Respect to Tumor Stage in 39 patients
Imaging Method Classification
Correct
Classification
Correct but
Equivocal
Classification
Incorrect
Imaging Method (Score of 2) (Score of 1) (Score of 0)
No.of.patients (%)
CT alone 20 (51.28) 9 (23.07) 10 (25.64)
PET alone 15 (38.46) 15 (38.46) 9 (23.07)
Visual correlation
of PET and CT 25 (64.10) 5 (12.82) 9 (23.07)
Integrated PET-CT 33 (84.61) 4 (10.25) 2 (5.12)
In all 39 patients, the node stage was
confirmed histologically.
Table 3 shows the diagnostic accuracy of
the various imaging methods:
Table 3
Diagnostic Accuracy of the Imaging Methods
with Respect to Node Stage in 39 patients
Imaging Method Classification
Correct
Classification
Correct but
Equivocal
Classification
Incorrect
Imaging Method (Score of 2) (Score of 1) (Score of 0)
No.of.patients (%)
CT alone 21 (53.84) 4 (10.25) 14 (35.89)
PET alone 23 (58.97) 11 (28.20) 5 (12.82)
Visual correlation
of PET and CT 25 (64.10) 1 (2.56) 13 (33.33)
Integrated PET-CT 33 (84.61) 1 (2.56) 5 (12.82)
Integrated Positron-Emission Tomography and the Staging of Nodular Non-Small-Cell Lung Cancer 161
Conclusion
1. The results suggest that integrated
PET-CT is superior to PET alone, CT
alone, or visual correlation of PET
with CT in determining the stage of
disease in non-small-cell lung cancer.
2. The anatomical correlation of the
radionuclide uptake made possible a
more precise delineation of the
location of the primary tumour.
3. With integrated PET-CT were found
significant improvements in tumour
staging, improved the diagnosis of
chest-wall infiltration and mediastinal
invasion by the tumour.
References
1. Beyer, T., Townsend, D.W., Brun, T,
et al.: A combined PET/CT scanner for
clinical oncology. In: J Nucl Med
2000; 41: 1369-79.
2. Camara, O., Colliot, O., Delso, G.,
Bloch, I.: Apport de contraintes
anatomique au recalage non lineaire
d’image TDM et TEP dans les regions
thoracique et abdominales, n
Reconnaissance des Formes et
Intelligence Artificielle RFIA 2004.
Toulouse. France, 2004; 97-806 .
3. Dietlein, M., Weber, K., Gandjour, A.,
et al.: Cost-effectiveness of FDG-PET
for the management of potentially
operable non-s mall cell lung cancer:
priority for a PET-based strategy after
nodal-negative CT results. In: Eur J
Nucl Med 2000; 27: 1598-609.
4. Dwamena, B.A., Sonnad S.S.,
Angobaldo J.O., Wahl R.L..
Metastases from non-small cell lung
cancer: mediastinal staging in the
1990s-meta-analytic comparison of
PET and CT. Radiology 1999; 213:
530-6.
5. Gupta, N.C., Graeber, G.M., Rogers,
J.S. II, Bishop, H.A.: Comparative
efficacy of positron emission
tomography with FDG computed
tomographic scanning in preoperative
staging of non-small cell lung cancer.
In: Ann Surg 1999; 229: 286-91.
6. Kalff, V., Hicks, R.J., MacManus
M.P., et al.: Clinical impact of (18)F
fluorodeoxyglucose positron emission
tomography in patients with non-
small-cell lung cancer: a prospective
study. In: J Clin Oncol 2001; 19:.111-8
7. Lardinois, D., Werder W., Hany T. F.,
Kamel E.M., Korom, S., Seifert, B.,
Schulthess G. K. von, Steinert, H. C.:
Staging of non-small-cell lung cancer
with integrated positron-emission
tomography and computed
tomography. In : N. Engl J Med 2003,
348: 2500-7.
8. Marom, E.M., McAdams, H.P.,
Erasmus, J.J., et al.: Staging non-small
cell lung cancer with whole-body PET.
In: Radiology 1999; 212: 803-9.
9. Nagel, C.C.A., Bosmans, G., Dekker,
A.L.A.J., Öllers, M.C., De Ruysscher,
D.K.M., Lambin, P., Minken, A.W.H.,
Lang, N., Schäfers, K.P.: Phased
attenuation correction in respiration
correlated CT/PET. In: Med Phys
2006, 33: 1840-1847.
10. Pieterman, R.M., van Putten, J.W.G.,
Meuzelaar, J.J., et al.: Preoperative
staging of non-small-cell lung cancer
with positron-emission tomography.
In: N Engl J Med 2000; 343: 254-61.
11. Seltzer, M.A., Yap, C.S., Silverman,
D.H., et al.: The impact of PET on the
management of lung cancer: the
referring physician’s perspective. In: J
Nucl Med 2002; 43: 752-6.

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
162
12. Steinert, H.C., Hauser M., Allemann
F., et al.: Non-small cell lung cancer:
nodal staging with FDG PET versus
CT with correlative lymph node
mapping and sampling. In: Radiology
1997, 202: 441-6.
13. van Tinteren, H., Hoekstra, O.S., Smit,
E.F., et al.: Effectiveness of positron
emission tomography in the
preoperative assessment of patients
with suspected non-small-cell lung
cancer_the PLUS multicenter
randomised trial. In: Lancet 2002,
359: 1388-93.
14. Weder, W., Schmid, R.A., Bruchhas,
H., Hillinger, S., von Schulthess, G.K.,
Steinert, H.C.: Detection of extra-
thoracic metastases by positron
emission tomography in lung cancer.
In: Ann Thorac Surg 1998; 66: 886-92.

1Poznan University of Medical Sciences
SIGNIFICANCE OF EMBRYONIC STEM
CELLS IN REGENERATIVE
MEDICINE
Ewa BAUM
1
Abstract: The turn of 21
st century is a period of rapid progress in the field
of biological sciences. Scientific discoveries constitute the foundation for the
development of new medical technologies that are used in the treatment of
various conditions. An example of this is the use of stem cells in organ
transplantation. Stem cells, which are present not only in the bodies of
foetuses, but also in adult people, are used for repairing damaged tissue and
organs. The development of techniques for isolating, breeding and
reimplanting stem cells makes it possible to use them for these purposes.
However, using stem cells in organ transplants, especially embryonic stem
cells, is also the source of ethical dilemmas that result from the fact that
biological material is transferred from a donor to a recipient. Experts believe
that the future of stem cells in organ transplantation depends not only on the
advancement of biology, but also, to an equal extent, on the solving of the
ethical considerations associated with this type of therapy. Finally questions
of both essential and ethical significance of the embryonic stem cells in
regenerative medicine are also the result of progress in medical sciences.
Keyword: Ethics, embryonic steam, transplant
The term regenerative medicine
encompasses a field of medicine aiming at
the recreation of damaged human cells and
organs. One of the pioneers in this field,
Professor Ioannis V. Yannas, claims that if
any part of a human body is damaged, the
whole effort of the organism is targeted at
the healing process and at limiting the
systemic reactions at the expense of the
damaged organ which atrophies [25]. Such
a reaction is determined by the human
body’s restricted capacity to regenerate.
Hence, for many years, scientists looked
for ways to overcome this weakness and
this was one of the reasons for the
development of transplantation science, i.e.
the science of organ grafting. Progress in
this field depended not only on the
surgeons’ efficiency of surgeons, but also
on the knowledge of immunology which
was necessary to stop the rejection of
grafted organs. The first transplantation
attempt was a kidney transplant on a pair
of twins in 1954, followed by
transplantations of the liver (1963), the
pancreas (1966) and the heart (1967) [8].
The ensuing transplantation, performed in
1968, was that of bone marrow and the
significance of this procedure proved
extremely important. Contrary to the
previous transplantations which included
mature, fully morphologically and
functionally developed organs, the
transplantation of bone marrow introduced
into the host organism undifferentiated
elementary marrow cells which are then
transformed, in the host organism, into
differentiated blood cells [8].

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
164
We can accept that the bone marrow
transplantation was a pioneering albeit
unconscious example of using stems cells
in medicine.
Concurrently to the development of
transplantation science, significant
progress was made in in vitro cell growth
techniques. This launched a new field of
regenerative medicine referred to as tissue
engineering, a term introduced by
Professor Yuan-Cheng B. Fung of the
University of California, San Diego, USA
[8]. Attempts were made to concurrently
and jointly grow, in in vitro conditions,
living tissue which could be transplanted
into living organisms. This was how the
so-called ‘artificial biological skin’
developed. It was approved for clinical
practice in the USA in 1988. Different
variations of this product appeared in the
following years. An alternative approach
included the creation of substrates that
consisted of biologic connective tissue
components, e.g. glycosaminoglycans and
collagen, which, after being implanted in
an organism, became a base for the growth
of autologous cells from the host’s skin.
This was introduced to clinical practice in
2002 under the name Integra®. The initial
success in the field of tissue engineering
gave an impulse for further research
concerning other tissue and organs. One of
the most spectacular projects, due to the
expectations of millions of diabetic
patients, was the research (launched in the
1970’s) on the growing of pancreas cells
that could be implanted to provide a source
of insulin for the host organism [2]. The
turn of the millennium was a time of great
optimism about the possibility of growing
new organs in vitro. In the year 2000, the
Time magazine pronounced tissue
engineering the most attractive field of
science that, in the subsequent years, was
to provide innovative solutions in the
treatment of numerous diseases. Such
hopes were very high and many people
optimistically assumed that, in the near
future, it would be possible to grow organs
in vitro and to implant them in human
bodies to replace damaged tissue or organs
[10]. However, contrary to these
expectations and despite the funding
involved in the experimental and clinical
studies, the remote therapeutic effects were
not satisfying. Some of the skin
preparations were degraded in the
recipients’ bodies initiating the process of
connective tissue hyperplasia and
cicatrisation, whilst the attempts of
growing pancreas cells that were meant to
be a source of insulin in living organisms
came to nothing [12]. Consequently,
discouraged by the lack of anticipated
clinical effects, the private investors who
had provided 90 percent of the funding for
research on tissue engineering withdrew
from these operations. The lack of funding
stopped further studies whilst scientist
came to understand that it was not possible
to fully imitate the conditions that occurred
in a living organism (with multiple mutual
effects of various cell types) in the
relatively simple in vitro system.
As the hopes related to tissue
engineering declined some new biological
discoveries were made that directly or
indirectly provided new potential for the
advancement of regenerative medicine. In
1996, the sheep Dolly was cloned in
Scotland [22] and this was followed by the
first new reports about the isolation of
human embryonic stem cells [20, 17]. At
the start of the 21st century, stem cells
became the new hope of regenerative
medicine.
Stem Cells, Definitions
During the development of a human
organism, initiated with the formation of
the zygote as a result of the fertilisation of
an ovum with a sperm, a rapid growth of
the number of cells occurs accompanied by
their differentiation towards tissue or
organs. In the early stages of development
cells are featured by the capacity to
differentiate towards any type of tissue,
Significance of Embryonic Stem Cells in Regenerative Medicine
165
however, as the cells begin to specialise
this capacity is gradually lost. These cells
are called stem cells and their basic
characteristics include:
� An unlimited cell division capacity
� The ability to differentiate into other
specialised cells
Stem cells are divided into the following
types, according to the source which they
originate from:
A. Embryonic stem cells which occur
during embryogenesis displaying the
features of totipotent and pluripotent
cells,
B. Foetal stem cells obtained from
foetal tissue and blood displaying
the features of multipotent stem
cells,
C. Umbilical cord blood stem cells
displaying the features of
multipotent stem cells,
D. Adult stem cells displaying the
features of multipotent and
unipotent stem cells.
Embryonic Stem Cells
Embryonic stem cells are relatively easy
to multiply in vitro, whilst the high activity
of the telomerase enzyme stops them from
ageing, making them similar to neoplastic
cells [13]. They can differentiate into all
types of somatic cells. This feature makes
them suitable for the recreation of all types
of tissue, but also leads to potential threats:
embryonic stem cells may differentiate in
the body in the desired direction, e.g.
transform into liver cells, whilst also being
capable of transforming into intermixed
cells of various tissues causing organ
function disorders. The implantation of
embryonic stem cells in mice may lead to
the formation of teratoma, a tumour
containing various types of cells and tissue
deprived of their proper structure and
function [16]. Another potential threat is
the formation of neoplastic cell lines from
stem cells, which becomes a potential
hazard to the recipient’s health and life.
The presence of stem cells that initiate the
formation of neoplastic tissue has been
described in relation to tumours occurring
in the haematopoietic system [3], the
central nervous system [18] and the
mammary gland [11]. The lack of
neoplastic stem cell elimination during
cancer therapy can be one of the causes of
tumour recurrence [6].
Many discoveries which brought closer
the possibility of using embryonic stem
cells in therapy were made at the end of
the 20th century. Embryonic stem cells
were isolated firstly from mice [14] and
then from humans [20], to enable the
development of in vitro growth methods. It
is now possible to provide growth
conditions that initiate the differentiation
of human stem cells towards more
specialised cells [20]. A haploid ovum has
even been grown from stem cells
originating from mice [4].
However, creating a method of isolating,
growing and differentiating stem cells in
vitro is only the first step confirming their
usefulness in regenerative medicine. An
important factor which requires further
assessment is their survival and
functioning within the host. Methods of
differentiating human embryonic stem
cells towards specialised cells are already
available [1], but the potential to test their
properties after reimplantation in a living
human organism is limited due to ethical
concerns. A viable option is to observe
experiments with animals and cautiously
apply the results of these to the conditions
of a human organism. It seems that the
initial results of experimental stem cell
research with animals are promising. A
brief description of selected results is given
below:
• The implantation of cardiomyocytes
from differentiated stem cells to
dystrophic mice results in the
integration of these cells in the
animals’ cardiac muscle and the taking
up of the contractile function. The
presence of these functionally efficient
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
166
cells in the cardiac muscle was
confirmed throughout the whole
observation period, i.e. seven weeks,
and no neoplastic transformation
features were recorded. According to
the authors, it is possible to preserve
the contractile capacity of cardio-
myocytes in in vitro cultures for at
least eleven months [9].
• Min et al. proved on an experimental
model of cardionecrosis in a rat that
the implantation of embryonic stem
cells to the damaged myocardium led
to an improvement in its contractile
properties [15].
• Embryonic stem cells of monkeys
which were differentiated in an in vitro
culture into endothelium cells and
implanted under the animals’ skin
initiated the formation of new blood
vessels and stimulated the growth of
the remaining endothelial cells [7].
• Embryonic stem cells of mice which
were differentiated in an in vitro
culture became capable of producing
insulin. The implantation of these cells
in mice with experimentally triggered
diabetes led to the normalisation of
glucose levels and body weight [19].
• Embryonic stem cells of mice which
were differentiated in an in vitro
culture into hepatocytes were
implemented in mice with acute
hepatic damage following poisoning
with carbon tetrachloride. The cells
were integrated into the structure of
the hepatic parenchyma and undertook
the metabolic functions that are typical
for this organ [24].
The current advancement of modern
biology techniques enables the therapeutic
cloning of embryonic stem cells containing
genetic material from the donor. Despite
the fact that this still carries a biological
risk and, what is more, is associated with
ethical concerns, the results of these
research projects may be used in less
controversial circumstances in the future.
The procedure involves the implanting of a
nucleus from an adult patient’s cell into an
enucleated ovum followed by
embryogenesis stimulation. A thus created
embryo has stem cells that are
immunologically and genetically identical
to the adult donor. Such embryos can be
used to repair damaged tissue or organs in
the donor [23]. The study results which are
currently available confirm the effecti-
veness of this method in relation to human
cells whose genetic material was used to
grow pluripotent cells divided in in vitro
cultures (over 70 passages). These did not
exhibit changes in the karyotype and
displayed the capacity to differentiate
towards specialised cells [5]. The
advantage of this technique is the possi-
bility of growing autologous pluripotent
stem cells whilst reducing the risk of the
donor’s immunologic reaction to the graft.
The recent progress of research on stem
cells and their application in regenerative
medicine raises great hopes. It is,
nevertheless, necessary to remember the
expectations and disappointments related
to regenerative medicine so far [8, 10]. The
usage of stem cells in this field of medicine
has its ethical concerns [21] in addition to
important biological limitations. The
quantity of biological issues related to
using stem cells in medicine is tantamount
to the extent of hope generated by the
advancement of biological sciences.
However, the final and indisputable factor
that verifies the potential of using new
therapeutic methods in medicine is their
compliance with the generally accepted
ethical principles.
References
1. Amit, M., Carpenter, M.K., Inokuma,
M.S. i wsp.: Clonally derived human
embryonic stem cell lines maintain
pluripotency and prolferative potential
for prolonged periods of culture. In:
Dev. Biol. 2000: 227: 271-278.
Significance of Embryonic Stem Cells in Regenerative Medicine
167
2. Chick, W.L., Like, A.A., Lauris, V. i
wsp.: A hybrid artificial pancreas. In:
Trans. Am. Soc. Artif. Organs 1975:
21: 8-15.
3. Dick, J.E.: Acute myeloid leukemia
stem cells. In: Ann N Y Acad. Sci.
2005: 1044: 1-5.
4. Hubner, K., Fuhrmann, G.,
Christenson, L.K. i wsp. Derivation of
oocytes from mouse embryonic stem
cells. In: Science 2003: 300: 1251-
1256.
5. Hwang, W.S., Ryu, Y.J., Park, J.H., i
wsp.: Evidence of a pluripotent human
embryonic stem cell line derived from
a cloned blastocyst. In: Science 2004:
303: 1669-1674.
6. Jordan, C.T., Guzman, M.L., Noble,
M.: Cancer Stem Cells. In: N. Engl. J.
Med. 2006: 355: 1253-1261.
7. Kaufman, D.S., Lewis, R.L., Hanson,
E.T. i wsp. Functional endothelial
cells derived from rhesus monkey
embryonic stem cells. In: Blood 2003:
103: 1325-1332.
8. Kemp, P.: History of regenerative
medicine: looking backwards to move
forwards. In: Regenerative Medicine
2006: 1: 653-669
9. Klug, M.G., Soonpaa, M.H., Koh,
G.Y. i wsp. Genetically selected
cardiomyocytes from differentiating
embryonic stem cells for stable
intracardiac grafts. In: J. Clin. Invest.
1996: 98: 216-224.
10. Kratz, G., Huss, F.: Tissue engineering
– body parts from the Petri dish.
Scand. In: J. Surg. 2003: 92: 241-247.
11. Li, Y., Rosen, J.M.: Stem/progenitor
cells in mouse mammary gland
development and breast cancer. In: J.
Mammary Gland. Biol. Neoplasia
2005: 10: 17-24.
12. Lysaght, M.J., Hazlehurst, A.L.: Tissue
engineering: the end of the beginning.
In: Tissue Eng. 2004: 10: 309-320.
13. Mantell, L.L., Greider, C.W.:
Telomerase activity in germline and
embryonic cells of Xenopus. In:
EMBO J. 1994: 13: 3211-3217
14. Martin, G.R.: Isolation of a pluripotent
cell line from early mouse embryos
cultured in medium conditioned by
teratocarcinoma stem cells. In: Proc.
Natl Acad. Sci USA 1981: 78: 7634-
7638.
15. Min, J.Y., Yang, Y., Converso, K.L. i
wsp. Transplantation of embryonic
stem cells improves cardiac function in
postinfarcted rats. J. Appl. Physiol.
2002: 92: 288 – 296.
16. Morange, M.: What history tells us VII.
Twenty-five years ago: the production
of mouse embryonic stem cells. In: J.
Biosci. 2006: 31: 537-541.
17. Shamblott, M.J., Axelman, J., Wang,
S. i wsp.: Derivation of pluripotent
stem cells from cultured human
primordial stem cells. In:
Proc. Natl. Acad. Sc i. USA 1998:
95: 13726-13731.
18. Singh, S.K., Clarke, I.D., Terasaki, M.
i wsp.: Identification of a cancer stem
cell in human brain tumors. In: Cancer
Res. 2003: 63: 5821-5828.
19. Soria, B., Roche, E., Berna, G., i wsp.:
Insulin- secreting cells derived from
embryonic stem cells normalize
glycemia in streptozocin-induced
diabetic mice. In: Diabetes 2000:
49: 157-162.
20. Thomson, J.A., Itskovitz-Eldor, J.:
Embryonic stem cell lines derived from
human blastocytes. In: Science 1998:
282: 1145-1147.
21. Weissman, I.L.: Stem cells- scientific,
medical and political issues. In: N.
Engl. J. Med. 2002: 346: 1576-1579.
22. Wilmut, I, Schnieke, A.E., McWhir, J.,
i wsp.: Viable offspring derived from
fetal and adult mammalian cells. In:
Nature 1997: 385: 810-813.
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
168
23. Wobus, A.M., Boheler, K.R.:
Embryonic stem cells: prospects for
developmental biology and cell
therapy. In: Physiol. Rev. 2005: 85:
635-678.
24. Yamamaoto, H., Quinn, G, Asari, A., i
wsp.: Differentiation of embryonic
stem cells into hepatocytes: biological
functions and therapeutic application.
In: Hepatology 2003: 37: 983-993.
25. Yannas, I.V.: Regenerative Medicine.
Springer NY, USA, 2005.
1 „Transilvania” University of Brasov. 2 The Public Health Authority Brasov.
HEALTH PROMOTION AND
ELABORATION OF A
PREVENTIVE STRATEGY FOR
BRASOV COUNTY
A. BĂLESCU
1 F. LEAŞU
1
L. ROGOZEA1 E. CHEFNEUX
2
Abstract: The Romanian population is characterized both by a pronounce
ageing and the existence of risk factors which make the population growth to
be negative. It also has been found that not only social and economic factors
can have an influence on health in childhood, but also education can be very
effective for affecting mother’s and child’s health.
Key word: Infant mortality, health promotion, strategy.
1. European Context
Many European governments consider
health promotion an efficient method to
reduce health care costs. The role and the
importance of promoting health are well
known from Avicenna who said that:
“Medicine is the art of preserving health
and likely to cure the disease”. In our days,
organizing health systems is mostly a
matter of financing and than a matter of
preventing health.
In the last years there was a concern of
the decision factors regarding the increase
of health care costs. As a result, they start
to evaluate the health system and to create
new professionals trained to evaluate this
system.
The worldwide infant mortality rate is
68‰ in 2007, according to UNICEF. [8].
But UNICEF noted in a press release that
the improvements have been felt
worldwide. In industrialized countries,
there is now an average of just six deaths
for every 1,000 births. In Africa, the
continent with the worst rates, Eritrea,
Ethiopia, Malawi, Mozambique and Niger
have slashed their death rates.
In 2006 the infant mortality was for the
first time fewer than 10 millions death,
compared to almost 13 millions in 1990.
[8]
On the entire planet, the infant mortality
is reduced with 27% between 1990 (93
death at 1.000 children which were born
alive) and 2007 (68 for 1000). This
decrease is not an enough to reach the
standards required by the Organization of
United Nations, a 67% decrease of infant
mortality until 2015.
The international conference from Alma
Ata, in 12th September 1978, emphasized
the need of an urgent action, in order to
protect and promote health in every state
of the world. After 30 years, the numbers
of infant mortality are still showing a
serious contrast between poor and rich
countries. [6]
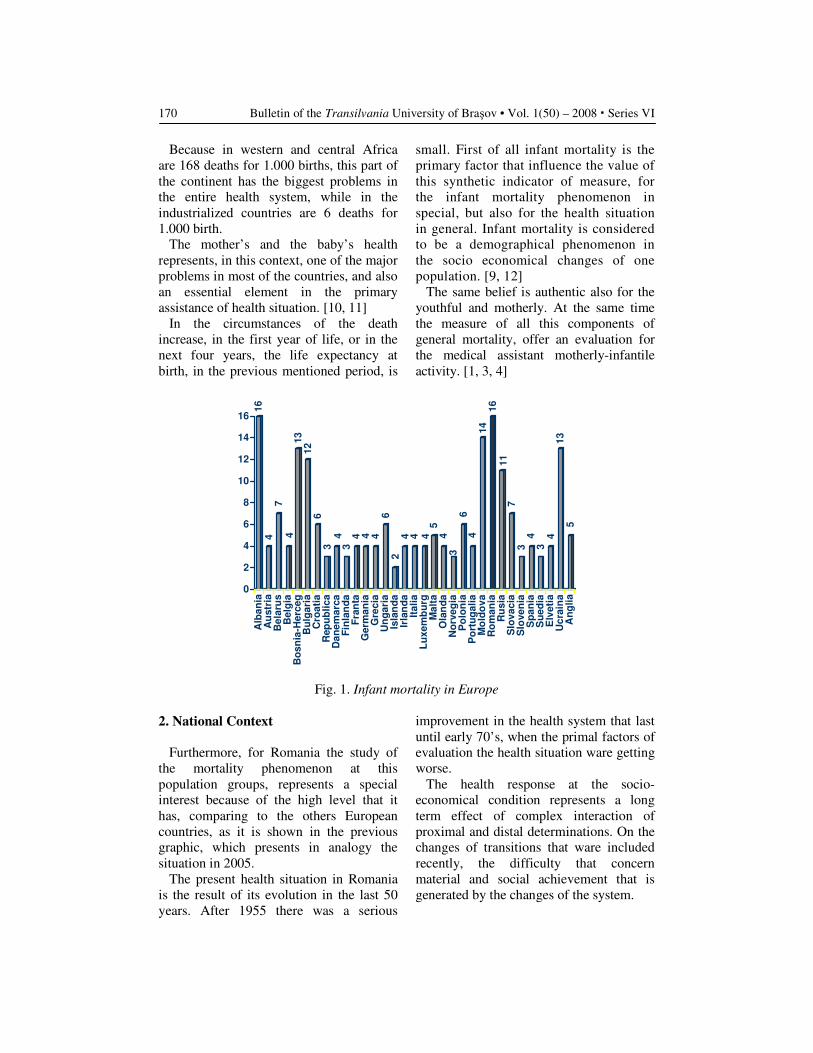
Bulletin of the Transilvania University of Braşov • Vol. 1(50) – 2008 � Series VI
170
Because in western and central Africa
are 168 deaths for 1.000 births, this part of
the continent has the biggest problems in
the entire health system, while in the
industrialized countries are 6 deaths for
1.000 birth.
The mother’s and the baby’s health
represents, in this context, one of the major
problems in most of the countries, and also
an essential element in the primary
assistance of health situation. [10, 11]
In the circumstances of the death
increase, in the first year of life, or in the
next four years, the life expectancy at
birth, in the previous mentioned period, is
small. First of all infant mortality is the
primary factor that influence the value of
this synthetic indicator of measure, for
the infant mortality phenomenon in
special, but also for the health situation
in general. Infant mortality is considered
to be a demographical phenomenon in
the socio economical changes of one
population. [9, 12]
The same belief is authentic also for the
youthful and motherly. At the same time
the measure of all this components of
general mortality, offer an evaluation for
the medical assistant motherly-infantile
activity. [1, 3, 4]
16
4
7
413
12
6
3
43
4 4 4
6
2
4 4 45
4
3
64
14
16
11
7
34
3
413
5
0
2
4
6
8
10
12
14
16
Alb
an
ia
Au
str
ia
Bela
rus
Belg
ia
Bo
sn
ia-H
erc
eg
Bu
lgaria
Cro
ati
a
Rep
ub
lica
Dan
em
arca
Fin
lan
da
Fran
taG
erm
an
ia
Gre
cia
Un
garia
Isla
nd
a
Irla
nd
a
Italia
Lu
xem
bu
rg
Malt
a
Ola
nd
a
No
rveg
ia
Po
lon
ia
Po
rtu
galia
Mo
ldo
va
Ro
man
ia
Ru
sia
Slo
vacia
Slo
ven
ia
Sp
an
iaS
ued
ia
Elv
eti
a
Ucra
ina
An
glia
Fig. 1. Infant mortality in Europe
2. National Context
Furthermore, for Romania the study of
the mortality phenomenon at this
population groups, represents a special
interest because of the high level that it
has, comparing to the others European
countries, as it is shown in the previous
graphic, which presents in analogy the
situation in 2005.
The present health situation in Romania
is the result of its evolution in the last 50
years. After 1955 there was a serious
improvement in the health system that last
until early 70’s, when the primal factors of
evaluation the health situation ware getting
worse.
The health response at the socio-
economical condition represents a long
term effect of complex interaction of
proximal and distal determinations. On the
changes of transitions that ware included
recently, the difficulty that concern
material and social achievement that is
generated by the changes of the system.
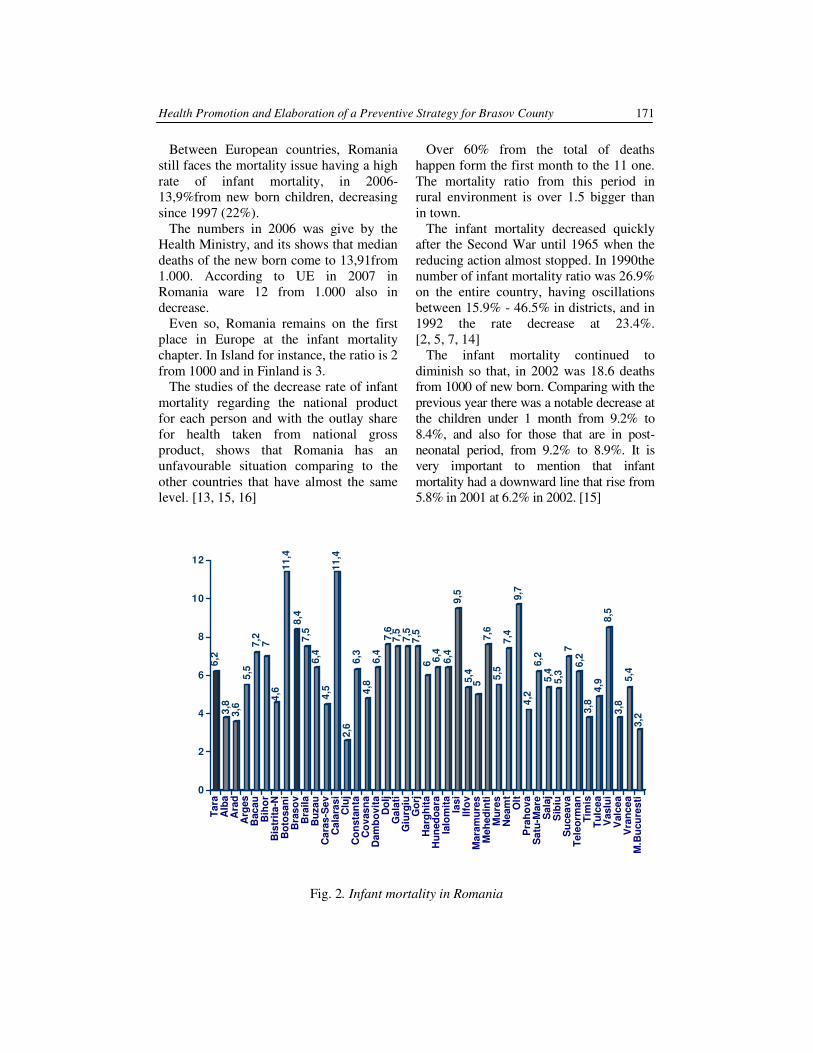
Health Promotion and Elaboration of a Preventive Strategy for Brasov County
171
Between European countries, Romania
still faces the mortality issue having a high
rate of infant mortality, in 2006-
13,9%from new born children, decreasing
since 1997 (22%).
The numbers in 2006 was give by the
Health Ministry, and its shows that median
deaths of the new born come to 13,91from
1.000. According to UE in 2007 in
Romania ware 12 from 1.000 also in
decrease.
Even so, Romania remains on the first
place in Europe at the infant mortality
chapter. In Island for instance, the ratio is 2
from 1000 and in Finland is 3.
The studies of the decrease rate of infant
mortality regarding the national product
for each person and with the outlay share
for health taken from national gross
product, shows that Romania has an
unfavourable situation comparing to the
other countries that have almost the same
level. [13, 15, 16]
Over 60% from the total of deaths
happen form the first month to the 11 one.
The mortality ratio from this period in
rural environment is over 1.5 bigger than
in town.
The infant mortality decreased quickly
after the Second War until 1965 when the
reducing action almost stopped. In 1990the
number of infant mortality ratio was 26.9%
on the entire country, having oscillations
between 15.9% - 46.5% in districts, and in
1992 the rate decrease at 23.4%.
[2, 5, 7, 14]
The infant mortality continued to
diminish so that, in 2002 was 18.6 deaths
from 1000 of new born. Comparing with the
previous year there was a notable decrease at
the children under 1 month from 9.2% to
8.4%, and also for those that are in post-
neonatal period, from 9.2% to 8.9%. It is
very important to mention that infant
mortality had a downward line that rise from
5.8% in 2001 at 6.2% in 2002. [15]
6,2
3,8
3,6
5,5
7,2
74
,6
11
,4
8,4
7,5
6,4
4,5
11
,4
2,6
6,3
4,8
6,4
7,6
7,5
7,5
7,5
66,4
6,4
9,5
5,4
5
7,6
5,5
7,4
9,7
4,2
6,2
5,4
5,3
7
6,2
3,8
4,9
8,5
3,8
5,4
3,2
0
2
4
6
8
10
12
Ta
ra
Alb
a
Ara
d
Arg
es
Bac
au
Bih
or
Bis
trit
a-N
Bo
tos
an
i
Bras
ov
Bra
ila
Bu
za
u
Ca
ras
-Se
v
Ca
lara
si
Clu
j
Co
ns
tan
ta
Co
vas
na
Da
mb
ov
ita
Do
lj
Ga
lati
Giu
rg
iu
Go
rj
Ha
rgh
ita
Hu
ned
oa
ra
Ialo
mit
a
Ias
i
Ilfo
v
Mara
mu
res
Me
he
din
ti
Mu
re
s
Ne
am
t
Olt
Pra
ho
va
Sa
tu-M
are
Sa
laj
Sib
iu
Su
ce
av
a
Te
leo
rm
an
Tim
is
Tu
lce
a
Vas
lui
Valc
ea
Vra
nc
ea
M.B
ucu
res
ti
Fig. 2. Infant mortality in Romania
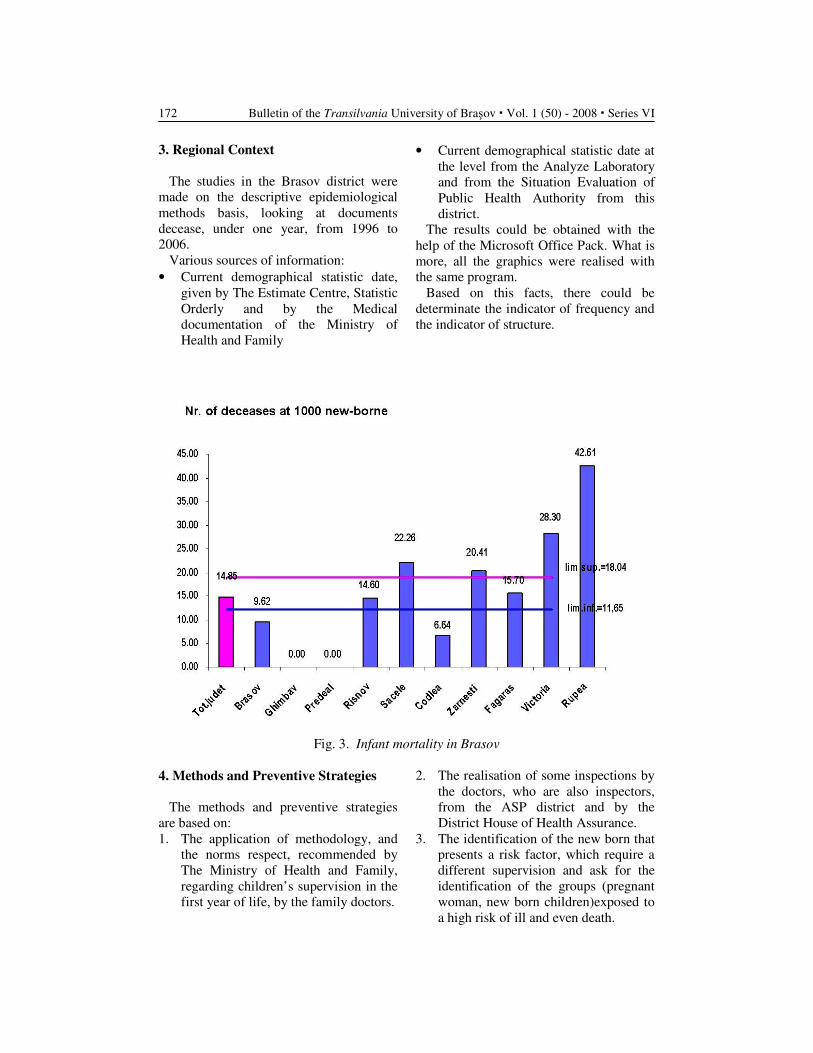
Bulletin of the Transilvania University of Braşov � Vol. 1 (50) - 2008 � Series VI
172
3. Regional Context
The studies in the Brasov district were
made on the descriptive epidemiological
methods basis, looking at documents
decease, under one year, from 1996 to
2006.
Various sources of information:
• Current demographical statistic date,
given by The Estimate Centre, Statistic
Orderly and by the Medical
documentation of the Ministry of
Health and Family
• Current demographical statistic date at
the level from the Analyze Laboratory
and from the Situation Evaluation of
Public Health Authority from this
district.
The results could be obtained with the
help of the Microsoft Office Pack. What is
more, all the graphics were realised with
the same program.
Based on this facts, there could be
determinate the indicator of frequency and
the indicator of structure.
Fig. 3. Infant mortality in Brasov
4. Methods and Preventive Strategies
The methods and preventive strategies
are based on:
1. The application of methodology, and
the norms respect, recommended by
The Ministry of Health and Family,
regarding children’s supervision in the
first year of life, by the family doctors.
2. The realisation of some inspections by
the doctors, who are also inspectors,
from the ASP district and by the
District House of Health Assurance.
3. The identification of the new born that
presents a risk factor, which require a
different supervision and ask for the
identification of the groups (pregnant
woman, new born children)exposed to
a high risk of ill and even death.
Health Promotion and Elaboration of a Preventive Strategy for Brasov County
173
4. The available resource assignment
based on the general thesis: “to assure
for everybody the best services, but to
offer a special treatment for those who
really need it.”
In the health domain motherly-infant, the
general objectives of the strategy are:
1. The transaction of a practical method
of evaluation for the risks on which
the persons (mother and children) are
liable at.
2. The launching of some local strategy
of intervention, taking in consideration
the risks and the existent resources.
3. The examination of the efficiency of
those strategies.
The organization of some lectures about
taking care of the pregnancy and of the
baby between 0-1 year, for the family
doctors, with the help of District Medical
College, and with the support Public
Health Direction, and also some lectures
for those that have a smaller level of
education.
In this context is imposed
• The development of the neonatology
services in every hospital from the
district.
• The insurance with at least a member
in every local area.
• The elaboration and the
implementation of the education
programs for health addressed to
women between 15 and 35 years.
Conclusions
• The infant mortality in Romania holds
itself at a high level comparing to the
European countries, with U.E. and
even with the previous socialist
countries: Romania is on the last level
along Ukraine, Bulgaria, Moldova and
Russian Federation.
• Looking back at the results of the
studies, in Brasov the infant mortality
rate kept itself under national
standards, until 2006 when this level
was crossed.
• The post-neonatal mortality (28 days at
least) in Brasov (8.4/1000) cross in
2006 the national level and also the
level of some other district such as
Cluj (2.3/1000) and of some towns that
are localized in the same geographical
area: Sibiu (5.3/1000) and Covasna
(4.8/1000).
• For the number of the new born deaths
is to blame prenatal causes and of
course congenital malformations, the
evolution bend after death month looks
as a “J” and not as an “U”, as it should.
• The program development in order to
promote health is a necessity, that should
be well organised in order to benefit by
the entire infrastructure of ASP.
• It is obvious that today, because of the
improper undernormed, the health
system is obligated to manage by their
self so that they found a solution based
on voluntaries. Moreover is found to
be important a discipline such as
Health Promoting and The Primal
Assistance of Health Scale that should
involve future practitioner in health at
the primal preventive objective.
• The same that is in the OMS
documents:” Promoting reproducing
health and maternal one”- The United
National Elements for the population
that struggled for the implement of this
program of planning volunteers. As a
result the woman that live in a country
which is in course of development
have at less than three children
comparing to six in the 60’ period
creating a delay on the rise population
in entire globe. In 1969 just 20% from
the couples ware practising familial
planning, but now this is made by 61%
from couples. In this context is
required that maternal health
promotion to incline more and more
for the development of life conditions
of mothers and of the new birth
children, in order to improve programs
of reducing the motherly-infant
mortality.
Bulletin of the Transilvania University of Braşov � Vol. 1 (50) - 2008 � Series VI
174
References
1. Beaglehole, R., Bonita, R., Kjellström,
T.: Bazele Epidemiologie. Bucureşti.
Ed. “ALL Educational”, 1997.
2. Bocşan, I.S. sub. red. : Asistenţa primară
a stării de sănătate: aplicaţii în
epidemiologie şi statistică. Ed. Presa
Universitară Clujeană, 1996.
3. Dabis, F., Drucker J. : Epidemiologie
d’Intervention. Paris. Arnette, 1992.
4. Dever, A.: Epidemiology in health
services management. ASPEN
publication, 1984.
5. Enăchescu, D., Marcu, M. Gr.:
Sănătate Publică şi Management
Sanitar. Ed. ALL, Bucureşti, 1995.
6. Forster, D.R., Jozan, P.: Health in
Eastern Europe. The Lancet, feb. 24,
1990.
7. Geormăneanu, M., Muntean, I.:
Pediatria, vol. I şi II. Bucureşti. Ed.
Medicală, 1995.
8. Global child mortality rates continue
to drop, UNICEF reports
9. Kontula, O.: Reproductive health
behaviour of young Europeans. Vol.2:
The role of education and information,
in Population Studies No. 45. Council
of Europe Publishing. Council of
Europe. Strasbourg 2004. in press
10. Kontula, O.: Trends in Teenage Sexual
Behaviour, Pregnancies, Sexually
Transmitted Infections and HIV
infections in Europe. In ‘Reproductive
health behaviour of young Europeans.’
Vol.1. Population Studies No. 42.
Council of Europe Publishing. Council
of Europe. Strasbourg 2003. pp. 77-
137.
11. Last, M.J.: A Dictionary of Epidemiology.
Oxford University Press, 1993.
12. Lavoie, A. : Les Problèmes de Sante
Prioritaires – une perspective
epidemiologique. Ottawa. Agence
D’Arc Inc., 1987.
13. Marcu, A.: Epidemiologia utilizată în
studiul mortalităţii infantile. Bucureşti,
1992.
14. Marcu, A. (coord.) : Metode utilizate în
monitorizarea stării de sănătate.
Bucureşti. Ed. Institutului de Sănătate
Publică, 2002.
15. Marcu, M. Gr., Mincă, D. G.: Sănătate
Publică şi Management Sanitar.
Bucureşti. Ed. Universitară “Carol
Davila”, 2003.
16. Zarcovici, G., Enăchescu, D.:
Probleme privind politicile de sănătate
în ţările Europei Centrale şi de
Răsărit. Bucureşti. Ed. InfoMedica,
1989.

1 University of Salerno, Italy.
DRUGS AND MEDICINE IN THE CONTEXT
OF YOUTH CULTURE
Giuseppina CERSOSIMO
1
Abstract: The study is interested in a specific social category (youth) in
relation to an important factor influencing health and well being
(medicine/drugs). As the dimension of health is a key element in the analysis
of individual life courses, this research is carried out of two considerations
(the health dimension/the importance of the body to young people and the
factors that contribute to the medicalization of young people’s lives (such as
prescription drugs). Field research (such as the one carried on in the
University of Salerno and presented in the present study) reveals that, as
shown by the reality under examination, there is a desire to resolve internal
problems typical of the younger generation through the application of
externally introduced elements (pharmaceutical products). The conclusions
of the field research regard the fact that for young people drugs are a means
of maintaining constant the rhythms and activities relative to and in parallel
with existential frequencies and patterns. Another conclusion is that it is
possible to understand how the perception of young people on both health
and illness is dependent upon a series of social configurations in which they
are involved and which contribute to forming the identity structure of
individual young people.
Keywords: youth, drug, medicine, field research, pharmaceutics
1. Reasons for the Research
In the generational continuum the term
“young” has acquired numerous socio-
historical connotations but it has almost
always been viewed by society in general
as a synonym of differentiation and/or
contestation, establishing a “condition”
and a privileged image of change. A
specific focus on the young people of
southern Italy has occasionally been
undertaken, but only in part, and without
sufficient care to the differences present in
this part of the country and to the
heterogeneities that have been, and
continue to be, an essential part of its
modernisation. The processes by which
youth identities are built up are often
founded on and, at the same time,
determine a central role for young people
as consumers and yet a minor role as they
are effectively relegated to the margins of
society.
The causes of this confinement process
can be sought by investigating the ways in
which the social, political and cultural
establishment builds up young people in
the contemporary context as necessary and
integrated social subjects, on the one hand,
and yet places them in a marginal,
generalised and undifferentiated condition
on the other.

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
176
This type of circumstances gives rise to a
non-predetermined process of entry,
presence, exit and absence from social
roles that has clearly contradictory effects
on the personality and that, obviously,
makes the subjects’ extrinsication
objectively precarious, partial and often
temporary. In terms of existential
condition, in Italy and, more specifically,
in Southern Italy, this accentuates
situations of anxiety, tensions, a painfully
long wait for employment and, at the same
time, it exalts collective dimensions, the
need for self-representation of the
individual and symbolic manifestations. It
must also be remembered that, in a society
of symbols, health also becomes a
consumer product, a symbol of potential
and social status and, hence, a projection
of the idea of health as social prestige
(transferred first and foremost into the
representation of the body). This prestige
is achieved through the sometimes
relentless pursuit of what is considered
individual wellbeing, with the result that it
may give rise to stress and malaise.
The number of people enrolled at gyms
for physical fitness does not only indicate
awareness in the achievement of
wellbeing: control over one’s own body is
not merely a personal factor, it must be
flaunted and this ostentation encapsulates
the contradictions of the modern
conception of the body, its use and its
language (Rella, 2000; Sassatelli, 2000).
With regard to these premises, in the
research sphere there emerges the issue of
conducting a series of investigations in
southern Italy that can truly capture the
structural processes present in this part of
the country as well as the effects of
territorial dimensions on single individuals
at the intersection of urban and community
realities, in the perspective of establishing
a relationship with the dynamics of
everyday life and with the processes and
problems of individual (and collective) life
courses, within the historical context of the
relationship between the establishment and
young people.
The numerous research studies carried
out in Italy on the youth issue have
investigated different areas of the
problematic dimension of young people,
from unemployment and the various
processes of education, both in and out of
school, to forms of refusal (or self-
segregation) of communication,
dimensions of aggregation and the
resulting dynamics that give rise to life
processes, forms of solitude that end up in
mental illness and, finally, to the failure of
any attempt of interaction, which
culminates in suicide (1). However, the
research carried out on the condition of
young people seems to have left several
central (and extensive) existential areas
unexplored, for instance concerning problem
issues such as maternity, love, running away
from home, unexpected events, sudden life
changes, health, the urban condition and so
on. There thus emerges a clear contradiction
between the considerable research that has
addressed the “youth condition” over the
years and the number of issues that have been
neglected, not to mention the specific areas of
southern Italy which, in the majority of cases
are not even taken into consideration (2).
These premises may therefore contribute
to clarifying the reasons why, in agreement
with the observations now being made
along the lines of existing research, this
investigation needs to be carried out on
young people, prescription drugs, health
and medicine. This research is carried out
with two considerations in mind: on the
one hand, the health dimension and the
importance of the body to young people;
and, on the other, the factors that
contribute (prescription drugs) to the
medicalization of young people’s lives.

Drugs and Medicine in the Context of Youth Culture
177
The dimension of health is a key element
in the analysis of individual life courses, of
well-being and malaise, of citizenship
rights, and of the system of social, gender
and generational inequalities.
The race to improve performance
sometimes turns well-being and malaise
into the two sides of the same coin, first in
a diachronic and then in a synchronic
perspective. Our research is intended to
pinpoint, by means of a quantitative and
qualitative methodology, when, where and
why young people request both medical
and pharmacological help in order to
improve their relationships. This
perception stems from a structured and
consolidated awareness of a me/self, that is
to say of how a person feels they are
perceived by “significant” others [29].
The body contributes to the emergence
of these dynamics. We may then assert that
one of the motivations pushing young
people to take excessive care of their own
body is that a body language shared [by the
other] legitimates the role of one’s own
look to the point of considering it as the
matrix of a “status or non status” of health
that has been called the “body idiom”, a
conventional reasoning that plays a symbolic
and normative role [40]. The body idiom, a
performer without a voice, conveys a non-
verbal communication that allows spectators
to capture an important image of the
individual’s outer balance, through his
capacity to send images while concealing
any state of anxiety, depression or other.
Medicalization of the everyday life of the
young people involves a process by which
nonmedical problems become defined and
treated as medical problems, usually in
terms of illness and disorders [13]. In other
words, medicalization can be described as
the extension of medical categories in
everyday life.
Recently, The Lancet (369/2007) has
dedicated ample space to the issue of
medicalization. Here, McLellan states the
question clearly: “Once upon a time,
plenty of children were unruly, some
adults were shy, and bald men wore hats.
Now all of these descriptions might be
attributed to diseases - entities with names,
diagnostic criteria, and an increasing array
of therapeutic options” (2007: 627).
Therefore the Lancet raised this issue by
publishing a number of papers that tried to
shed a new light on some crucial aspects of
the medicalization process by looking at it
from a new perspective. While in the past,
according to the early definition given by
[21] the term medicalization meant a
process promoted mainly by the doctor,
today many promoting agents have come
to the fore. Jonathan Metzl and Rebecca
Herzig (2007) identify some of them, such
as the patients and the practice of “direct-
to-consumer advertising”, and the
pharmaceutical companies with their
economic policies.
Other authors think that while “young
people, who were once considered as the
passive victims of medicalization, now play
an active role, especially in the decision-
making process. The key factor seems to be
the influence of medicine upon the ethical
attitude of young individuals, the
relationship with ourselves, our judgment
about the kind of person we wish to
become and the kind of life we wish to
lead” [34].
In the U.S., for instance, with the
liberalisation of Direct-To-Consumer
(DTC) advertising, the physician-patient
relationship has undergone significant
changes. Hollon (2005) states that patient
requests for prescription drugs consistently
affect the prescription attitudes of
physicians. About 40% of appointments in
which the discussion involves DTC
advertised drugs end up with that drug
being prescribed. Then, through a
metanalysis of a great deal of research,

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
178
Hollon demonstrates that almost 80% of
physicians are convinced that DTC ads
encourage people to look for treatments
they do not really need (2005: 2031).
All this can be attributed to the fact that
nowadays young people are increasingly
"demanding", nor can we deny that there is
a different health culture today. Health is
not only “lack of pathology”, but also
“enhancement”; furthermore, an enlarged
“health literacy” [23] pushes the patients to
become consumers who look after their
wellbeing (Ingrosso 2007).
In this context, it would be worthwhile to
focus on the Drugs National Agency’s
report of a steady growth in prescriptions
of anxiolytic and antidepressive drugs in
Italy over the last few years. Most of these
treatments are prescribed by general
practitioners, who have to face a huge
demand for medicalization from younger
people as a result of difficulties in the
socio-relational sphere. A set of symptoms
is increasingly becoming a “disorder” and
in today’s society we are witnessing a
growing medicalization, not only of what
is pathological, but also of what can be
“improved” (the cases of Viagra and
cosmetic surgery are emblematic).
In mass media communication health
turns into a fashion, a consumer product, a
look. There is an increase in fitness
practices that promote a “well-shaped”
body and mind able to yield a high
performance level that is fit for the society
of the perfectible and which therefore
requires flexible procedures at work and in
present-day social life. The consumption of
new substances, with a greater or lesser
doping effect is increasing to meet the
demands for efficiency, visibility or
compensation for fears of inadequacy and
isolation [8]. Because of the mocking
paradox of mass society, in which the
relational dimension of “being there”
rather than “being” haunts the present time
of everybody and the process of “staying
with” seems more important than
“staying”, solitude, exorcised in a thousand
ways, materializes again as a companion
escorting individuals, above all younger
people, on their social pathway [9].
Thus normality, in contemporary society,
seems to take a violent and de-structuring
semantic twist: from an expression aimed
at recognizing a status of “good health”, of
“being like” to a concept of hedonistic
perfectibility and implementation.
This article, based on research conducted
amongst young people living in the
southern regions of Italy, discusses the
largely under-researched theme of the
association between pharmaceutical use,
health and young people.
Field research reveals that, as shown by
the reality under examination, there is a
desire to resolve internal problems typical
of the younger generation through the
application of externally introduced
elements (pharmaceutical products).
In adolescence, assumption of
pharmaceuticals is seen as an answer to
problems of insecurity or, in some cases,
identity. Drugs are also seen as a means of
resolving difficulties relative to the process
of transition, to contradictions and to
situations typical of the younger generation
such as anxiety problems, mortality, future
prospects and to the inevitable upheavals
arising from a confusion of subjectivity.
For young people, prescription drugs seem
to represent what Valéry says art
represented for the author. He identified
the original motivation for artistic creation
in that aesthetic need that belongs solely to
the “author”, who initially displays
indifference towards a possible
“audience”. At first there is the anxiety
(spleen) of a man who feels horror for the
void – in our case, the time and space of
uncertainty experienced by the youth
population – which is both a void of space

Drugs and Medicine in the Context of Youth Culture
179
and time. The restlessness characterising
sensibility can indeed be related to the
sense of “instability” that the subject
experiences when faced by empty space
and waiting. In short, the need to fill up an
empty gap in time or to fill an empty space
is a natural need because it is innate to man
(Valéry, 1935). Zygmunt Bauman recalls
the complex mechanisms underlying the
construction of uncertainty and insecurity:
if our society tends to reassure the public
dimension of subjects but attacks them in
their every private niche, what is
manifested in terms of the subject’s
potential crisis, i.e. the erosion of
confidence in his/her body and lifestyle
certainly assumes a “striking” nature for
the individual, especially if it is a young
person (Bauman, 2000).
Therefore, in young people, there is an
increasing need to distance themselves
from times and spaces that can suspend (or
suggest that they are unable to follow and
control) the frenetic rhythms of everyday
life. The anxiety of contemporary reality,
the uncertainties of the existential process,
the question marks looming over one’s
own future (not actually expressed but
present on the individual level, often
unsaid but not necessarily unlived or
unperceived), the crises within one’s
symbolic universes [2], the discontinuities
in relational processes, the crisis of an
increasingly rarefied and unsatisfactory
relationship with the historic reference
institutions of socialisation are all elements
that exert a dynamic effect also in the
creation and maintenance of the ability to
control one’s own body, subjectivity,
individuality and inherent differences. The
latter become guaranteed by prescription
drugs, the means by which the individual
may not be obliged to interrupt the dynamics
of their own existential frequency but remain
able to keep up with it.
For young people, drugs are a means of
maintaining constant the rhythms and
activities relative to and in parallel with
existential frequencies and patterns.
Young people seem to have accepted the
idea that, in a physical and cultural
colonisation process, the pharmacological
world is invading all walks of life. The
self-proclaimed objective is to help
individuals to constantly improve their
daily abilities by reducing difficulties,
ensuring certitude and the capacity to
exteriorise.
The research also demonstrates that
some habits of youth regarding the use of
pharmaceutical products (drugs) are the
products of a social construction
originating in the primary social group -
the family - which then become
fashionable within peer group structures.
2. Premiss and Methodology
Judging from this research, in a process
of physical and cultural colonisation,
pharmacology is invading every aspect of
the life (and body). The self-proclaimed
objective is to help individuals (at both a
physical and psychological level) to
constantly improve their capacity in the
course of daily life by reducing difficulties,
ensuring certitude and facilitating a greater
degree of exteriority.
These considerations have led to the
decision to investigate what may be, or
could be, the reaction of young people and
the generation preceding towards the
assumption of pharmaceuticals.
Moreover, when a subject abandons,
delegates and places trust in
pharmacological and medicinal treatment,
health protection becomes an act of faith,
independent of the effect which the
pharmacy has upon the organism.
It is therefore important to understand
the trust, or lack of it, towards individual

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
180
organisms and also the kind of relationship
which exists between the assumption of
pharmaceuticals and the various levels of
information and disinformation. Starting
from this hypothesis, field research was
carried on a sample base of 550 students
from the University of Salerno. In order to
obtain a balanced cross-section, the
samples were taken from faculties and
degree courses in Mathematics, Pharmacy,
Engineering, Economics, Law, Sociology
and the Communication Sciences. Only
511 young people answered the
questionnaire: 49% male, 51% female, one
third attending science faculties, and two
thirds attending humanistic ones. The
sampling procedure employed the two-
phase cluster technique. The first phase
sampled the Faculties present at the
University of Salerno, while the second
phase selected the lessons timetabled for
the period of the investigation (according
to the degree courses, the sample included
all the courses from the first to the final
year so that its composition was
representative of the university student
population in terms of age and course
attended).
The origin of the sample is
heterogeneous: 56% come from Campania
while the remaining 44% are from other
Italian regions (Basilicata (21%), Puglia
(10%) and Calabria (13%).
Principally, research was aimed at the
relationship which students have with the
use or abuse of pharmaceuticals and the
relative degree of information or
disinformation regarding their use. In
particular, the investigation was geared
towards analysing and understanding: a)
how the daily discomforts encountered by
young people are faced and overcome - or
kept in check - by the use of
pharmacological substances; b) the social
importance which drugs assume in the
various existential life-patterns of young
people; c) to evaluate the varying extent to
which factors relating to social context and
cultural roots have an influence – and to
what measure - on behaviour patterns.
3. Drug Indoctrination
Young people appear to want to resolve
internal problems and conditions typical of
youth by resorting to external remedies to
their problems and to their condition:
pharmaceuticals. Indeed, the majority of
the sample admitted to the occasional use
of pharmaceuticals (40.3%); 32.1% stated
that recourse was “hardly ever”, whereas
4.3% maintained “never”. 16% of the
sample accounted for “fairly regular use”
and 7% classed themselves as “frequent
users”. However reassuring on the surface,
these statistics do not conform to answers
posed by a check question to which only
3.1% failed to reply and 0.4% attested that
they never used pharmaceuticals at all. The
vast majority of the remainder of the
sample is distributed amongst a percentage
of assumption of various pharmacological
compounds whenever symptoms –
however minor or trivial – present
themselves.
Drugs are legitimised by a reassuring
importance which is both expressed and
perceived: “drugs have an essential role;
above all, they validate the ability to
intervene on the part of a doctor – ‘I am
prescribing this, therefore I know what you
have’ would appear to be the comment of the
doctor making out a prescription and
avoiding further examination or referring the
patient to a specialist or hospital - an
alternative which could be interpreted as a
sign of incompetence” (Dupuy/Karsenty
1974).
Beginning with this encouraging
legitimisation, drugs become the mediator
between the potential subjects who
consume them or are likely to (at this

Drugs and Medicine in the Context of Youth Culture
181
stage, it is no longer important whether
they are prescribed by a doctor or on the
suggestion of a chemist or family and
friends) and the progressive scientific
society.
From this research it is also possible to
evaluate the real success of
pharmaceuticals.
The investigation illustrates how drugs
are perceived by young people and how
that perception contributes towards a
guarantee of the success of officially
recognised medicines and, alternatively,
how they can enrich and improve the
quality of life.
One of the first results of the sample is
the almost unanimous recognition of the
role which drugs have acquired in
guaranteeing the state of health of the
individual, data which evidences the
widely held conviction, amongst the
young, of the scientific foundations on
which social progress is based.
Moreover, such data becomes even more
convincing when confronted with figures
of 19.7% and 26.4% of the university
student sample, all of whom maintain that
drugs are not yet fully capable of
guaranteeing an improved state of health.
This poll result underlines the desire and
trust that young people place in future
advances in the field of scientific and
pharmacological research which are geared
towards the improvement of the actual
governance of well-being. The
expectations, therefore, given to the role of
pharmacy are clear: to guarantee continuity
to the existential life pattern of the
individual. In particular when one
considers that only 6% of the sample do
not trust drugs or are simply incapable of
assuming a personal position over the
question.
A perspective which seems to remain
unchanged even when young people are
asked in which alternative they place most
faith: in official medicine, in homeopathy
(3) or otherwise. Here again, with the
impossibility of alternative medicine
asserting itself to the same degree, the
sample places unequivocal trust in official
medicine.
When the influence of socio-
demographic variables are considered in
relation to the subject gender, it becomes
evident that belief in pharmacological
discovery is analogous for both males and
females. However, when the relative
erudition of the parents is taken into
consideration, different data is forthcoming
– indeed, in parallel with the elevation of
family scholarship, there is a
corresponding increase of trust in official
medicine and pharmaceutical remedies.
The argument discussed so far is
confirmed by the section of the
questionnaire devoted to the level of
compliance (assumption of
pharmaceuticals and degree of therapeutic
efficacy) and also illustrates to what extent
individual subjects are prepared to delegate
or abandon themselves to pharmaceuticals
- or to place their unreserved trust in them
- in order to improve their psycho-physical
potential. This was so much so that when a
sample was taken from senior secondary
school students, 80.8% echoed agreement
with 79.9% of the university student
sample affirming that the effect which
pharmaceuticals had upon the organism
was “fairly good”.
Furthermore, when the 13.6% of the first
sample and the 15.7% of the control
sample are taken into consideration and
which state that the physical effects of
pharmaceuticals are “sufficient”, it can be
added that 95% of the sample base of
young people examined demonstrate that
pharmaceuticals have an increasing
tendency to co-exist in the existential
pattern of the subject. Moreover, drugs are
assuming an increasingly reassuring

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
182
characteristic within the individual lives of
young people.
It is then, perhaps, no accident that in
another section of the questionnaire 97%
of the sample – 9.7 students out of 10 –
state that they have taken and are taking
pharmacological substances.
This same percentage is also confirmed
by the answers to a control question which
underlines how drugs – from anti-anxiety
to anti-inflammatory – are assumed
conscientiously and appropriately for
several symptoms. Young people, when
affected by certain maladies, are no longer
prepared to wait for a natural
counterbalancing reaction from the body
itself but prefer to accelerate the process
with chemical products.
In an attempt to explain the relationship
between the trust invested in drugs and the
effect that any pharmaceutical product may
have on the organism, the following
question was posed: “Before taking any
kind of drug, do you read the
accompanying instructions?” (while
conscious that, despite the advice given in
the legal decree no. 44 - 18.02.97, such
instructions are still a long way short of
offering clear warnings and explanations
over an arc of three hundred and sixty
degrees).
70.6% of the sample read the
accompanying instructions, 10.4% do not
bother, whereas 18.6% were inconstant. As
regards the majority (70%) the comment
made was: young people who read the
accompanying instructions (nick-named
“little liar”) already have good reason to
be wary of the side-effects which even the
most mundane substances can provoke.
However, this would appear to be short-
sighted, it is impossible to guarantee that
all the possible undesirable side-effects, as
documented in the “instructions for use”,
have been previously identified and
confronted (4). This is a possible answer as
to why drugs are increasingly successful
between and with young people:
paradoxically, it is as though a vague
understanding of the nature of a drug is
also its certificate of guarantee for use.
Besides which, at this point we are
facing that which Luhmann defined as the
negative aspects and/or the “malfunction”
of modernity. In other words, society finds
itself having to confront consequences
determined through its own structural
selection, such as ecological problems in
the modern world and increasing tension
fuelled by the attempts to maintain the
actual level of social well-being.
It is, then, precisely this tension created
through the maintenance of well-being
which could provide an answer, in
Luhmannian terms, to the taking of
pharmaceuticals on the part of young
people at risk. The risk that a young person
makes in taking pharmacy without first
referring to the “instructions for use” or,
alternatively, when conscious of the likely
side-effects, is determined by an appraisal
of the potential damage which, in itself,
derives from a decision taken by the self-
same person (Luhmann, 1993).
The motivations referring to those of
sample quote who declare to not reading
the accompanying instructions (56.9%) are
particularly interesting: those who do not
read the instructions say it is because they
have prior knowledge, whereas the residual
37.2% argue that the instructions are
difficult to understand and that it is better
not to bother (always remembering that the
subjects are at a university level, which
provokes reflection upon the greater part of
the population who, under completely
different circumstances, must be unable to
read or understand the indications
anyway).
In this instance, we are confronted by the
category at dangerous discussed by
Luhmann, in other words, the potential

Drugs and Medicine in the Context of Youth Culture
183
damage to which the individual is
unaware, inasmuch that the obscure
terminology adopted to describe the
pharmacy does not permit the person who
is about to take the medicine to understand
the implications of doing so.
Moreover, the last consideration with
reference to the sample raises a bi-lateral
observation: a) could this contribute to
successful economic returns for
pharmacological multi-nationals?; b) could
the success of pharmaceuticals amongst
young people be part of a generalised and
voluntary disinformation strategy
concerning potential pharmacy users?
This type of behaviour could indeed be
common to other processes in which young
individuals decide to assume certain
substances: they are aware that
assimilation will, in any case, modify the
condition of their body. Nevertheless, the
knowledge of the final result of the
process, however approximate, is
sufficiently satisfying to annul any
information regarding the internal bodily
process leading to the final result. Thus, it
is the end result which is decisive;
regardless of any harmful side-effects, the
determining factor is the modification.
4. Pharmaceuticals in General and
Alternative Therapy
Interesting research data comes out of
21% of the sample who have prior
knowledge of pharmaceuticals in general,
data which is subsequently confirmed by a
later question to which 22% of the sample
attribute therapeutic properties and effects
to commercial medicines already marketed
by well-known pharmaceutical companies.
The data relative to the information
which young people have of
pharmaceuticals in general underlines
concepts and signals which public opinion
has been indicating for some time. Signals
systemised in the understanding and belief
of the individual - not at an “emotive” but
rather at a “rational” and “conceptual”
level – in certain therapeutic schemes
which are no longer simply tied to well-
known pharmaceuticals (and which have
become part of a way of life) but to
pharmaceuticals in general (5) as is also
the case with therapeutic treatments related
to alternative medicine.
Trusting in this form of therapy is
dependant upon whatever kind of
familiarity and information the young
person may possess – together with the
existing relationships, discussed
previously, such as doctor/patient or with
other important socialising elements. This
would explain why 17.4% of the sample
believe in unofficial forms of medicine and
why, out of this 17.4%, 14.1% claim to
have greater faith in homeopathic
medicine. Indeed, the function of
homeopathic medicine would seem to
vindicate that therapeutic mandate which,
in the words of Thomas Sandoz is “a
profane rite of exorcism”. To follow, to
recognise and to trust in this practice has
the effect of rationalising some of the
procedures of improvement, both of the
cure and of the therapy of the actual state
of well-being or indisposition. This could
occur through a decomposition of the
function of the vindication of homeopathy
in “four projects” (Sandoz, 2001).
In the first place, homeopathy introduces
the possibility of contrasting medical
impotence by seeking auxiliary solutions
outside of the parameters of the biomedical
verdict (or medical practitioner), thereby
overcoming the innate passivity of the
subject towards illness.
Secondly, homeopathy encourages the
fight against the mounting uncertainty
which afflicts people suffering from illness
(regarding the origins, the prognosis, etc.)

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
184
by directly including and involving them in
a cultured dialogue of explanation.
Furthermore, homeopathy overcomes
that silence which can often follow the
pronouncements of experts, maintaining
intact latent resources in the subject which
official medicine has a tendency to nullify.
Finally – the fourth and last project –
homeopathy endorses opposition to the
modern movement towards the
medicalization of society and opposes
scientific reasoning and materialism which
is perceived as “the power of dominating
forces” (Sandoz, cit.)
Thus, whilst not “justifying
assimilation” of homeopathic therapy over
that of official medicine, the myth of the
therapeutic potential of homeopathy may
be attributable to the power of its
credibility, a factor which exercised a
distinct fascination over part of the
research sample. Young people exorcise
uncertainty – to which, in terms of health
care rights, official medicine is still
incapable of responding – by resorting to
alternative medicines and medicaments
which facilitate (or are said to facilitate)
aggregation in the dramatically decisive
moments of their existence.
5. From the Recognition of Professional
Status to the Recognition of Social
Status
In order to isolate and verify some of the
answers previously given by the sample, in
the fifth section individuals were asked to
indicate in which subject – family doctor,
specialist, chemist, friends/family – they
invested most trust when looking for
advice or a pharmacological prescription.
Replies indicate that, of the four subjects,
in terms of trust, social and professional
recognition and the expedience of
prescriptions, specialists were adjudicated
most competent (49.7%). This figure was
followed by general practitioners
(37.2%), friends/family (5.7%) and,
lastly, chemists (3,7%).
Turning to various exponents of the
structural-functionalist school, such as
Talcott Parsons or William Goode, it could
be said that such a high level of
recognition of the professional status of
medical practitioners - greater even than
that given to specialists - has taken shape
in the wake of the organisational reform of
labour within industrial and urban society
(1968; 1969). A development which has
privileged the division of functions and
tasks and produced a consequent demand
for qualified or specialised services outside
of the family environment.
All of which, however, has led to an
ulterior consequence: the ever-increasing
fragmentation of medical knowledge, a
phenomenon which has had an inevitable
effect upon the ability to prescribe any
required pharmacy. Moreover, in the midst
of this fragmentation process, although a
deeper bodily understanding has evolved,
it is often difficult to grasp that what is
being lost is the link between states of
illness not attributable to a specific part of
the body but rather to the body in its
entirety. Thus, the importance given to
medicine and pharmacy is a consequence
of the values attached to health, life and
death. According to these authors the
progress of knowledge and preparation has
induced a need: recourse to medicine in
order to legitimise professional status.
However, the symbolic
commutationalists and theoreticians of the
Chicago school – in particular, E. Freidson
(1970) – refute both concepts: inasmuch
that the rise in status of the medical
profession automatically depends on the
new division of labour and, that it stems,
fundamentally, from the progression of
knowledge.

Drugs and Medicine in the Context of Youth Culture
185
The medical profession, in this respect,
gains professional status through those
who, averaging out a multiplicity of
considerations, manage to persuade
themselves of the unsubstitutional nature –
in terms of character and service - of their
competence and their ability. (in other
words, a professionality which, rather than
being achieved, is recognised by others).
Knowledge certainly contributes to the
definition of professionalism but it is not
easy to establish that precise moment in
which such recognition legitimises and
confirms the privileges of professional
status (Parsons, 1968).
Moreover, this research verifies that
young people’s trust is placed – as they
themselves confirm in one of the replies to
the questionnaire – in those representatives
of official health care with whom they deal
directly in daily life. Trust in medicines
prescribed by specialist practitioners,
greater than that invested in the
representatives previously mentioned,
would not appear to be different as regards
the type, whereas the level of trust given to
such professional figures increases in
correspondence to the educational quotient
of the family and, in consequence to
parental professionalism and the nature of
their work.
The research also opens the possibility of
analysing the way in which a prescription -
or the recommendation by a specialist of a
particular medicine and its subsequent
acquisition - results in a dual-recognition:
on one side, that of professional status and,
on the other, that of social status within the
family.
6. The Perception of Young People
towards Change
What also becomes evident from the
questionnaire is the perception among
young people that medicines have changed
in substance and role. It is in the
transformation of the role (and objectives)
of medicines that the “personal data bank”
of any subject “needing” medicine is being
modified and filters back, through the
various generations, to young people and
children.
Today, medicines are no longer merely
therapeutic, no longer is there recourse to
pills when a state of illness is diagnosed
(indeed, not long ago, pharmacy was only
resorted to after immunity mechanisms
were found to be insufficient) but rather,
for many, medicine has become a means of
prevention, both in short and long-term
circumstances.
The sample would appear to be
conscious of this process which has seen
conceptions of pharmaceutical use move
from care, treatment and cure of illness
through to a preventative means of
forestalling it. As regards this data, it
perhaps worth reflecting that many young
people, approximately 66% of the sample,
turn to pharmacy at the first sign of a
possible attack of influenza or similar
discomfort.
This fact must also lead us to reflect on
how these continually ambivalent young
people are at the same time subjects of
transformation and objects of
subordination with respect to consumer
processes: it contributes to temporarily
assigning them with citizenship and to
structuring their identity, and as such it
must be recognised, albeit tacitly. The
ironic paradox is that, in this case, unlike
in clothing fashion, tastes in music or any
other area of commercialised leisure time,
this is a consumption that acts directly on
them personally, on their body and on their
identity. Therefore, prescription drugs have
today become a consumer product for
young people, through which to assert,
construct and project an individual and a
collective identity – on this issue,

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
186
advertising never presents us examples of
isolated subjects coming into contact with
a substance, but we are always shown this
practice being manifested within a group
of people bound together by friendship,
affection, etc.. In many cases among
campus students, therefore, prescription
drugs assume the role of a “fashion” with
the characteristics described by Simmel:
«fashion is imitation of a given model and
thus satisfies the need for a social
approach, it leads the individual along the
road everyone follows, from a universal
model which reduces the behaviour of the
individual to a mere example. But
nevertheless, fashion satisfies a need for
difference, the tendency towards
differentiation, variation and
distinguishing oneself from the others»
(Simmel, 1905, pp. 30-1). It must not be
forgotten that the prescription drug at the
centre of attention (like all the others) will
have different effects on the individual
bodies and on the individual identities
(and, in spite of everything, this is the very
expectation of the individuals): hence,
analogous performance for different and
differentiated results. A consideration
which has repercussions in a subsequent
observation which reveals how the sample
cross-section under examination are
influenced and socialised towards
pharmacy.
Evidently, pharmaceutical use plays a
constituent role in the existential life
pattern of any individual. From the outset,
there is a consecration of the positive
nature of pharmacy which, subsequently,
has inevitable repercussions on initial
impressions: the first use of pharmacy is
that administered by parents to their
children. Clearly, this introduces an
element which both anticipates and
reinforces, beyond all other reasoning, the
socialisation of the substance: how could
our parents have possibly given us harmful
substances? And, given that for every child
parents “know all”, children assume that
they must be far better informed about
such substances than they could ever be.
It is, therefore, during the process of
cognitive and cultural differentiation
between child and parent that individuals
begin to acquire an awareness and,
contemporarily, ask questions about
pharmacy.
It would appear that the greater part of
the sample under examination have grown
up with the idea (probably due to the
argument previously outlined) that
medicine is good for them. Only a minor
number of the young people interviewed
introduced a different evaluation, arguing
that, in the meantime on their part, they
had converted to alternative therapy in the
conviction that such cures are not harmful.
Despite differences of faculty or degree
course, the sample group, with absolutely
no variation, continue to grow up under the
belief that for whatever anxiety, ache or
indisposition it can be easily overcome
with the aid of medicine: “for every health
problem or illness there is a suitable
pharmaceutical remedy”. An awareness
which, as testified by the sample, derives
from the principal agents of socialisation.
Fragmentary information such as that
relative to the theme health/illness (the
index of individual and social patterns
followed by young people) should perhaps
also be introduced; such information
derives in 40.1% of cases from television
and, in 20.4%, from parents.
Besides the mass-communication
influence of television on young people
regarding information relative to health
and illness, 4.3% of the sample also
nominates the radio and 11% specialised
publications. As regards this last assertion,
it would seem likely that the word
“specialised” covers an ample range: that
is to say, not merely those specialised

Drugs and Medicine in the Context of Youth Culture
187
journals and periodicals which have
proliferated over the last ten years or so
and which specifically deal with health and
illness, but rather the inserts, notebooks or
weekly supplements which have become
standard to every daily newspaper and the
weekly and fortnightly publications which
come out at both a national and local level.
Despite the well-known fact that Italians
read little (particularly daily newspapers),
it is also true that in the case of health (and
pharmacy), a veritable communication
network exists from which, it would
appear, it has become extremely difficult
to escape. In consequence, for certain
themes - such as those relative to the
physical aspect - they become, in a real
sense, communal mass movements;
whereas, for many other medical
questions, particularly those of an
“intimate” nature, reflections either do not
exist or, alternatively, fail to become
interlocutory - an observation which is
particularly apposite when such questions
are directed at precisely those subjects who
have – and ought to assume - the
responsibility of replying.
Moreover, considering the statistics of
those who advise young people when not
visiting a medical practitioner (and who,
notwithstanding, take medicine for
physical or psycho-physical disturbance),
57.3% are parents, 5.9% are family
members, 4.1% are relatives, 4.9% are
friends and 17.8% take advice from a
chemist. Only 2.4% state that they do not
assume medicines unless it is on the advice
of a doctor. To this data other sources of
information can also be taken into account,
all of which, nevertheless, are constituent
elements in a pattern of socialisation.
Above all, an attempt was made to
corroborate the role and the effects of the
information or disinformation supplied to
young people by secondary agents of
socialisation.
At the end of 1999, the specialised
journal “Sanità. Il Sole 24 Ore” published
an article saying: “The fight for
promotional exposure together with
research into synergic relations with
sales personnel has resulted in a series of
heterogeneous initiatives. Some of them a
little embarrassing. A promotional
campaign, launched in 1998 by a
multinational operating in the
pharmaceutical sector, created a
promotional tie-up between one of the best
known headache pills and a compact disc
of relaxing melodies. Chemists were
expected to pull out the promo from under
the counter each time they sold a packet of
the pills.”
This advertising spot was transmitted
many times a day on both radio and
television, despite the fact that WHO
(World Health Organisation - the
international health agency of ONU)
recommends that the role of the mass-
communications media, due to its
enormous influence upon public opinion
and perception, should be: “…to control
the authenticity and importance of every
fact relating to pharmaceutical products…
avoid becoming the spokesmen for
promotional campaigns in favour of the
pharmaceutical industry…” (WHO, 1983).
Information broadcast by the mass media
– television, radio, newspapers, magazines
and specialist journals – is disciplined
under the legislative decree n. 541, 30
December 1992. This decree prohibits the
media from transmitting messages
contrived to persuade their audience to buy
products which proclaim to be uniquely
capable of improving a state of health or,
indeed, to allude that failure to assume
such products could lead to deterioration.
The decree also prohibits the marketing of
medicinal products which encourage the
belief that the guarantee of relief and
fitness is determined by natural products.

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
188
26.1% of the sample admitted to taking
pharmaceutical products without a medical
prescription. The principal agents of
socialisation influencing the choice of
pharmacy to be taken – as underlined by
WHO – were, in order of importance,
television, radio, specialised journals and
internet. For young people, then, such
mediums are suggestive and seductive.
Statistics which take on far greater
validity when confronted with the 30.3%
of the sample who admit to receiving
information relative to health and illness
through the communication channels listed
previously, either to avoid choosing
medicines autonomously or having to visit
a doctor for minor aliments.
Seductive propaganda has the effect of
inducing individuals to associate a series of
natural properties - in other words, rendering
them harmless – to certain products.
The success of pharmacology, of official
medicine and even that of alternative
medicine, is largely determined by the
influence of the mass media. The
underlying message communicated is that
of a fascinating ideal designed to overcome
any form of subjective analysis - as for
example when facing a statement of
propaganda such as: “better a tried and
tested traditional remedy which has no
harmful side-effects on the body”. A
slogan which is then linked to the image of
a slim and beautiful woman visually
eulogising the product at hand.
In other words, audio-visual
communication designed to neutralise
rational responses towards the assumption
of a therapeutically orientated product.
How many of the young people
interviewed are conscious of the
“provenance” of products within the field
of alternative medicine? How many of
them are aware that bio-therapy/herbalist
and homeopathic remedies are, in any case,
laboratory derivatives? Are they equally
alive to the idea that the herbal extractions
from which such palliatives are “made”
are cultivated and chemically treated:
manure, fertilizers, insecticides – chemical
additives essential for the optimisation of
the process of cultivation and industrial
production of “medicinal” herbs?
The effects, the therapeutic properties of
herbs – which, once upon a time, grew
spontaneously and naturally – are today
largely the end-products of chemical or
bio-chemical cultivation; whatever
substances administered, herbal-based cure
is the most traditional form of pharmacy
associated to official medicine. In modern
society, these so-called biological-
derivatives – widely considered to be both
therapeutic and non-toxic – are also the
end-products of a laboratory-produced
chemical process (6).
Clearly, commercial media is primarily
interested in constructing messages which
emphasise the beneficial effects of
pharmaceutical products and conceal any
undesirable side effects; whilst, at the same
time, ignoring an equally interesting and
opportune occasion to inform individuals
of the correct usage and circumstances
under which the product is consumed.
Apart from the media, the other principal
socialising agent which has an influence
over the use of medicines and medical
information, is the family. Much research
demonstrates that, as regards the
assumption of pharmacy, the level of
education and relative medical knowledge
of the mother determines differential
behaviour on the part of the children.
In the book “To grow up well and better:
one reply to the most frequent questions of
mothers” (AA.VV., 2000) it is made
evident how much this relationship is
dependant upon a continual flow of
information regarding those medicines
utilised for curing their own children, from
aspirins to anti-histamines.

Drugs and Medicine in the Context of Youth Culture
189
In the opinion of the authors, the most
interesting aspect of the research is to have
been able to evince that, in terms of the
information and health education
requirements of Italian mothers, no
differences are imposed by geographical
and cultural variables (always
remembering that the survey deals with an
indeterminate sample covering mothers
residing in totally opposed cultural and
geographical realities such as Milan and
Matera). The research clarifies why the
socio-demographic variables taken into
consideration during the predisposition of
the questionnaire – such as educational
qualifications and place of birth – do not
influence the way in which young people
are informed about, or socialised towards,
the use of pharmacy as a means of
regularising their state of health.
At this point, it becomes clear (given that
57.3% of the sample state that
pharmaceuticals are taken on the advice of
the parent and, in particular, the mother)
that, in the case of medicines, the principal
factor of influence over young people is
also the most powerful agent of primary
socialisation. This data, relative to the
influence emanating from the previously
defined primary socialisation agent, is
confirmed by 5.9% who state that
pharmacy is taken on family advice; by
4.1% who receive advice from relatives
and a further 4.9% who follow the
indications of friends.
Moreover, in this investigative section of
the questionnaire we can observe that not
only do the young people in our sample
advise their friends on the drugs to take, on
the basis of their previous experience, but,
at the same time, they themselves receive
advice from parents, neighbours, family
members or friends when they do not turn
to their doctor, while only 2.3% claim not
to take drugs unless prescribed or
recommended by their doctor. There seems
to emerge another consideration of that
fashion that «gives the individual the
certainty that he is not alone in this action
and proceeds on the basis of previous
experience as if on a solid platform that
alleviates the activity of the moment from
the difficulty of sustaining oneself»
(Simmel, cit., p. 30).
Socialisation of drugs, which for young
people is the product of peer group
influence, explains the widespread social
recognition which is attributed to one
medicine rather than another. For example,
it could be supposed that the limited
success of generic medicines amongst the
sample group, as previously stated, is
probably due to their fledgeling
appearance on the generic pharmaceutical
(7) market and a limited notoriety within
family peer group structures. Moreover, in
the absence of customary recognition and
use of the product, young people ignore it
(at least, for the moment).
However, as time passes and new
pharmaceutical products claim more
attention and greater acceptance amongst
the primary socialisation agents, the same
process of the usage of generics (which at
present can be seen to operate with well-
known multinational pharmaceutical
products) will also become the rule.
Indeed, it is hardly casual that young
people refuse to assume “new” drugs – in
the face of advice from doctors, nurses,
medical orderlies and/or a chemists – even
when the motive for their use (and the
substitution of well-known alternatives) is
justified by a potentially superior
therapeutic effect coupled with minor
collateral consequences (8).
Pharmaceuticals have been invested,
through advertising and peer-group habits,
with a whole range of precise
connotations. Above all, on the part of
consumers, they have become consumer
products; chemical composition,

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
190
therapeutic efficacy and undesirable side-
effects have become secondary
considerations: “Any pharmaceutical
carries more importance as a label than as
a medicine” (Bert, 1977).
7. Interim Conclusions for the Base of
Further Research
An extension of this research would
entail taking into consideration a
constructivist approach which consented –
as regards youth health themes,
environment and the inherent self-
awareness of the subjects themselves – to
understand how perception towards certain
interrogatives (such as conceptions of
illness and well-being from both a personal
and general perspective) are individually
constructed in parallel with the assembly
of information and experience.
Regarding any consideration of the
possible understanding that young Salerno
students may have towards the subject of
health naturally depends upon the
importance that each individual attributes
to the argument - not forgetting those
factors which can influence the
construction (or non-construction) of that
importance (social-demographic variables:
age; sex; the provenance of both student
and family; schooling, etc.) – in other
words, precisely that importance motivated
both from within the subject and from
individual external experience (Luhmann,
1971). Nevertheless, it can be safely
assumed that any young person will have
acquired a rudimental understanding of
pharmaceuticals, not only as regards their
potential efficacy relative to health and
illness but also in terms of subjective
analysis and active response to such
themes.
And, whereas the field of medicine often
encounters transitory difficulties
determined by the massive growth in
technological and pharmacological
innovation, it is also true that, despite
everything, medicine as a discipline enjoys
notable recognition on the part of young
people. This is confirmed, for example, by
those young people who, often
ingenuously, undergo cures, therapy and
even cosmetic surgery in order to resolve
inter-personal and existential relationships.
Young people now seem to be aware of
these dynamics and have established a
fatalistic attitude of yielding,
relinquishment, refuge and delegation to
discovery and scientific research and to
those who hold this knowledge and
represent for them one of the few
certainties for the improvement of their
future. Baudrillard certainly springs to
mind in this connection: «it is with
generalised individual somatisation, with
the body becoming an object of prestige
and salvation (…) that the medical class
establishes itself in the position of social
super-privilege it currently occupies »
(Baudrillard, 1976, p. 199).
In order to interpret the new ways of
appealing to young people - through the
schematics of perception, understanding
and information of health within an
individual context and of those instruments
and techniques which govern or re-educate
these aspects - the starting point is
undoubtedly the theory of Norbert Elias.
Moreover, it is only by following a
progressive approach over an extended
period that transformation can be
satisfactorily identified. Indeed, to
successfully reveal the mutation of interest
of young people in matters of health - from
initial curiosity through to conversion -
matched with gradual improvements in
well-being, the minimum research period
required would be twenty years. Long-term
analysis of this nature could identify the
various phases and figures of influence
through, for example, an analysis of the

Drugs and Medicine in the Context of Youth Culture
191
internal mechanics of groups of teachers,
of parents and of those institutions
principally concerned with the health and
welfare of young people.
Through the employment of a process of
semantic destructuralisation, what also
needs to be considered is that, in an
attempt to come to grips with the crisis
within modern medicine, analysis would
appear to be orientated towards
understanding in terms of “Canons and
Procedures” (“Rules and Regulations”) -
Cavicchi, 2000 - rather than attempting to
reduce the crisis to a single scientific
paradigm.
Khun himself asserted that scientific
change was a product of rupture and
conflict, inasmuch that the employment of
canons and procedures as a solution to
crisis clearly indicates how some difficult
moments can be overcome through
different interpretations and theories.
At which point new semantic categories
– set up to overcome the impasse in which
the medical-scientific community finds
itself languishing – step into play.
Interpreting the crisis from the
etymological point of view of choice,
shows how (through changes in the criteria
used by the social-medical-health
community for communicating matters of
health, diagnosis and the construction of a
supportive reference base for operative
medical opinion) the institutions charged
with the promotion and distribution - in
terms of prevention and information - of
“public health” amongst young people can
be influenced into varying their
procedures.
It is not, however, simply a question of
isolating the interdependent factors and the
interaction between those subjects who
modify the existing situation in order to
create a new one, but rather the whole
range of factors – reinforced through
reciprocal inter-reaction – which ensure
the modification and restructuring of this
cognitive process relative to the theme of
health. As a result, it is possible to
understand how the perception that young
people have of both health and illness is
dependent upon a series of social
configurations in which they are involved
and which contribute to forming the
identity structure of individual young
people. On the basis of this premise, albeit
brief, any network of collaboration
installed between institutions, public or
private, whose objective is that of creating
a policy aimed at the younger generation
and geared towards the promotion of
culture, the environment, the safeguard of
rights, working conditions, self-realisation
and the pursuit of personal interests, needs
to give priority to both the theme of youth
and health and the consequences and
effects upon the individual, upon
individual identities and the inter-personal
relationships established with and within
society.
Notes
(1) The problem of suicide, which is
obviously related to the strength of the
social bond, is rooted in the history of
society and, at the same time, of the
sociological tradition, albeit in the
awareness of the different dynamics
attributed throughout the ages to the
choice to end one’s own existence. From
Durkheim’s work on the relationship
between the differing degree of social
interaction and suicide « A society is
highly integrated when its individuals are
kept dependent on it » (Durkheim, 1897).
(2) Think of the utterly insignificant number
on the youth issue in southern Italy
conducted by Cavalli (1990), Leccardi
(1994), Trigilia (1995), Giannotti (1996),
Merico and Rauty (1999), Rauty (1999)
and Siebert (1999).
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
192
(3) Homeopathic medicine falls into the
category of alternative medicine.
Originating in the late XVIII Century,
this therapeutic approach was first given
credibility through the work of doctor
Samuel Christian Hahnermann. The most
sensational discovery was that the effect
of therapy was inversely proportional to
its quantity. For the homeopath, as
opposed to orthodox colleagues,
diagnosis and therapy concerns the entire
body, referred to as the “unitary
organism”. In the majority of cases,
medications and other elements used in
homeopathic medicine are individually
prepared using biological raw materials
of natural vegetable or animal origin. The
homeopathic term for these medications
is “tintura madre” (“mother tincture”).
(4) When references are made to values not
taken into consideration within the
territory, this is principally an allusion to
the historical importance of popular
medicine in Southern Italy and of its
particular role relative to the poorest and
least literate of the social community
(though not exclusively so) and, in
particular, to those lacking the necessary
resources to undergo or resort to
traditional methods of treatment. This has
given rise to a practical relationship
between traditional pharmaceuticals
incorporating natural products (above all,
herbs) linked to those organisational
structures and individuals invested with
the specific task of propagating its
validity and function: the process of
modernisation, which would appear to be
in a permanent state of evolution, has
given itself the task of accelerating this
process towards the eventual “triumph”
of official medicine (in all of its aspects).
In reference to popular medicine, see,
amongst others: Marino, 1991; and,
Seppilli, 1989.
(5) “Quite good” is not a possible reply to
the questionnaire itself but rather a
convenient expression adopted by the
author to indicate the approximate
percentage of replies ranging from
“discreet” to “very high”.
(6) By definition, alternative medicine
expresses an optional – or, indeed, in
opposition – to official medicine: Its
success is rooted in the inability of
scientific medicine – evidence-based
medicine – to adequately respond to
matters of health as well as the diagnosis
of illness. For debate, see Cavicchi
(2000)
(7) The term generic pharmaceuticals
(medicines?) describes those medicines
which have the same active principles
and chemical composition as well-known
brand names (following years of
successful marketing on the part of the
pharmaceutical companies). A typical
example might be: Aulin = well-known
pharmaceutical; Nimesulide = generic
pharmaceutical.
(8) In the documentation of all
pharmacological research, it is stated that
collateral effects are those resulting from
research upon human organisms; to
which end, a sample group of patients
volunteers to assume, experiment, test
and reveal any positive or negative side-
effects of the medicine.
(9) In Europe, such remedies are associated
to the culture of pre-industrial society
and, as opposed to knowledge of
primitive cultures, are “a product of the
re-elaboration of popular and past
traditions on the part of the general
populace” (Velimirovic, 1982). In
consequence, two distinct and opposed
definitions of medicine or traditional
remedies emerge: on the one hand, an
almost parallel confluence between
traditional and alternative medicine and,
on the other, the romantic idea of a
popular medicine with its own origins but
with no foundations and quite separate
from evidence-based medicine.

Drugs and Medicine in the Context of Youth Culture
193
References
1. Bauman, Z.: In Search of Politics.
Milano. Feltrinelli, 2000.
2. Berger, P. e Luckmann, P.: The social
construction of reality : a treatise in
the sociology of knowledge, NY,
Garden City, 1967 [tr.it., La realtà
come costruzione sociale, Il Mulino,
Bologna, 1969].
3. Berlinguer, G.: Medicina e politica.
Bari. De Donato, 1973.
4. Berlinguer, G.: Il corpo come merce e
come valore. In Rodotà S., “Questioni
di bioetica”, Roma-Bari.Laterza, 1997.
5. Bert, G.: Il farmaco come segno e
come mediazione. Milano. Feltrinelli,
1977.
6. Cavalli, A. (a cura di): I giovani del
mezzogiorno. Bologna. il Mulino,
1990.
7. Cavicchi, I.: La medicina della scelta.
Torino. Bollati Boringhieri, 2000.
8. Cersosimo, G.: La coesistenza di
benessere e malessere. In: L’odore
della Bellezza. Wellness e Fitness (a
cura di) D. Scafoglio. Salerno. Marlin
Editore, 2007.
9. Cersosimo, G., Rauty, R.: Riflessioni
sul controllo sociale: dalla normalità
della devianza alla normalità della
malattia. Keiron , n. 5, 2001, pp. 128-
139.
10. Ciacci, M., Gualandi, V. (a cura di):
La costruzione sociale della devianza.
Bologna. Il Mulino, 1977.
11. Clarke, A. E., Mamo, L., Shim, J. K.,
Fishman, J.R., Fosket, J. R.:
Technoscience and the New
Biomedicalization: Western Roots,
Global Rhizomes. In: Sciences
sociales et santé 18, 2000, 2, 11–42.
12. Conrad, P.: Medicalization, Etiology
and Hyperactivity: A Reply to Whalen
and Henker. In: Social Problems 1977,
24:596-98.
13. Conrad, P.: The medicalization of
Society: On the Transformation of
Human Conditions into Treatable
Disorders. Baltimore. Jhons Hopkins
University Press, 2007.
14. Conrad, P., Schneider, J. V.: Deviance
and Medicalization: From Badness to
Sickness. St. Louis: Mosby, 1980.
15. Dupuy, J.P., Karsenty, S. : L’invasion
pharmaceutique, Paris. Seuil, 1974.
16. Duster, T.: Medicalisation of race.
Lancet, 2007, 369:702-04
17. Giannotti, G. et al.: Anziani e giovani
nel Salento. Un contributo per le
politiche e le attività sociali educative
del territorio, Lecce.Piero Manni,
1996.
18. Goffman, E.: Asylums: Essays on the
Social Situation of Mental Patients
and Other Inmates. Torino. Einaudi,
1968.
19. Goffman, E.: Stigma. Bari. Laterza,
1970.
20. Goode, W.J.: The teorical limits of
professionalization, In: A. Etzioni (a
cura di), The Semi-Professions and
Their Organization: Teachers, Nurses,
Social Workers. New York. The Fre
Press, 1969.
21. Illich, I.: Limits to Medicine. Medical
Nemesis: The expropriation of Health.
London. Calder & Boyars, 1975.
22. Jennings, D.: The Confusion between
Disease and Illness in Clinical
Medicine. In: Can. Med. Ass. J., 1986,
135, 865-870.
23. Kickbush, I, Maag, D.: Lo sviluppo
della Health Literacy nelle moderne
società della salute, in Ingrosso M. (a
cura di) (2007), op.cit.
24. Leccardi, C.: Crescere nel
Mezzogiorno. Giovani e adulti in una
comunità calabrese degli anni
novanta. Rubbettino, Soveria
Mannelli, 1994.
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
194
25. Luhmann, N.: Sozale Systeme:
Grundrisz einer allgemeinen Theorie.
Frankfurt am Main. Suhrkamp, 1988
[tr. it., Sistemi sociali. Fondamenti di
una teoria generale, il Mulino,
Bologna, 1990].
26. Luhmann, N. : Soziologie des Risikos.
Berlin-New-York, 1993 [tr. it.,
Sociologia del Rischio, Mondadori,
Milano, 1996].
27. Luhmann N., «Tautology and Paradox
in the Self- Descripition of Modern
Society», Sociological Theory, 6,
1988, p. 36.
28. MCLellan, F.: Medicalisation: a
medical nemesis. Lancet , 2007,
369:627-8.
29. Mead, G.H.: Mind, Self and Society.
The University Chicago Press, 1932.
30. Merico, M., Rauty, R.: Giovani a
Montoro Inferiore tra modernità e
tradizione. Forino. Phorograf, 1999.
31. Metzl, J.M., Herzig, R.M.:
Medicalisation in the 21st century:
introduction. Lancet, 2007, 369:697-8.
32. Parsons, T.: Profession. In:
International Encyclopedia of the
Social Sciences, 1968, p. 536.
33. Rauty R. (a cura di), 1999, Una
tranquilla estraneità. Caratteri della
condizione giovanile ad Avellino,
Tipografia Grappone, Mercogliano.
34. Rose, N.: Beyond medicalisation.
Lancet, 2007, 369:700-702.
35. Sandoz T. (2001), «L’homéopathie
comme rituel de conjuration»,
Medicina e Storia. Rivista di Medicina
e Storia della Sanità, 1, pp. 73-98.
36. Seppilli, T.: Medicine e magie.
Milano. Electa, 1989.
37. Siebert, R.: Cenerentola non abita più
qui. Uno sguardo di donna sulla
realtà meridionale. Torino.
Rosemberg & Sellier, 1999.
38. Trigilia C. (a cura. di), 1995, Cultura e
sviluppo. L’associazionismo nel
Mezzogiorno, Meridiana Libri, Roma.
39. Velimirovic, B., Velimirovic, H.:
Therapeutischer Pluralismus?. In:
Curare, vol. 5, 1, 1982.
40. Williams, S. J., Bendelow, G.: The
Lived Body. Sociological Themes,
Embodied Issues. London & New
York. Routledge, 1998.
41. World Health Organization: Self-help
and Health in Europe. Ginevra. Who-
Oms, 1983.

1 University of Salerno, Italy.
DRUGS AND MEDICINE IN THE CONTEXT
OF YOUTH CULTURE
Giuseppina CERSOSIMO
1
Abstract: The study is interested in a specific social category (youth) in
relation to an important factor influencing health and well being
(medicine/drugs). As the dimension of health is a key element in the analysis
of individual life courses, this research is carried out of two considerations
(the health dimension/the importance of the body to young people and the
factors that contribute to the medicalization of young people’s lives (such as
prescription drugs). Field research (such as the one carried on in the
University of Salerno and presented in the present study) reveals that, as
shown by the reality under examination, there is a desire to resolve internal
problems typical of the younger generation through the application of
externally introduced elements (pharmaceutical products). The conclusions
of the field research regard the fact that for young people drugs are a means
of maintaining constant the rhythms and activities relative to and in parallel
with existential frequencies and patterns. Another conclusion is that it is
possible to understand how the perception of young people on both health
and illness is dependent upon a series of social configurations in which they
are involved and which contribute to forming the identity structure of
individual young people.
Keywords: youth, drug, medicine, field research, pharmaceutics
1. Reasons for the Research
In the generational continuum the term
“young” has acquired numerous socio-
historical connotations but it has almost
always been viewed by society in general
as a synonym of differentiation and/or
contestation, establishing a “condition”
and a privileged image of change. A
specific focus on the young people of
southern Italy has occasionally been
undertaken, but only in part, and without
sufficient care to the differences present in
this part of the country and to the
heterogeneities that have been, and
continue to be, an essential part of its
modernisation. The processes by which
youth identities are built up are often
founded on and, at the same time,
determine a central role for young people
as consumers and yet a minor role as they
are effectively relegated to the margins of
society.
The causes of this confinement process
can be sought by investigating the ways in
which the social, political and cultural
establishment builds up young people in
the contemporary context as necessary and
integrated social subjects, on the one hand,
and yet places them in a marginal,
generalised and undifferentiated condition
on the other.

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
176
This type of circumstances gives rise to a
non-predetermined process of entry,
presence, exit and absence from social
roles that has clearly contradictory effects
on the personality and that, obviously,
makes the subjects’ extrinsication
objectively precarious, partial and often
temporary. In terms of existential
condition, in Italy and, more specifically,
in Southern Italy, this accentuates
situations of anxiety, tensions, a painfully
long wait for employment and, at the same
time, it exalts collective dimensions, the
need for self-representation of the
individual and symbolic manifestations. It
must also be remembered that, in a society
of symbols, health also becomes a
consumer product, a symbol of potential
and social status and, hence, a projection
of the idea of health as social prestige
(transferred first and foremost into the
representation of the body). This prestige
is achieved through the sometimes
relentless pursuit of what is considered
individual wellbeing, with the result that it
may give rise to stress and malaise.
The number of people enrolled at gyms
for physical fitness does not only indicate
awareness in the achievement of
wellbeing: control over one’s own body is
not merely a personal factor, it must be
flaunted and this ostentation encapsulates
the contradictions of the modern
conception of the body, its use and its
language (Rella, 2000; Sassatelli, 2000).
With regard to these premises, in the
research sphere there emerges the issue of
conducting a series of investigations in
southern Italy that can truly capture the
structural processes present in this part of
the country as well as the effects of
territorial dimensions on single individuals
at the intersection of urban and community
realities, in the perspective of establishing
a relationship with the dynamics of
everyday life and with the processes and
problems of individual (and collective) life
courses, within the historical context of the
relationship between the establishment and
young people.
The numerous research studies carried
out in Italy on the youth issue have
investigated different areas of the
problematic dimension of young people,
from unemployment and the various
processes of education, both in and out of
school, to forms of refusal (or self-
segregation) of communication,
dimensions of aggregation and the
resulting dynamics that give rise to life
processes, forms of solitude that end up in
mental illness and, finally, to the failure of
any attempt of interaction, which
culminates in suicide (1). However, the
research carried out on the condition of
young people seems to have left several
central (and extensive) existential areas
unexplored, for instance concerning problem
issues such as maternity, love, running away
from home, unexpected events, sudden life
changes, health, the urban condition and so
on. There thus emerges a clear contradiction
between the considerable research that has
addressed the “youth condition” over the
years and the number of issues that have been
neglected, not to mention the specific areas of
southern Italy which, in the majority of cases
are not even taken into consideration (2).
These premises may therefore contribute
to clarifying the reasons why, in agreement
with the observations now being made
along the lines of existing research, this
investigation needs to be carried out on
young people, prescription drugs, health
and medicine. This research is carried out
with two considerations in mind: on the
one hand, the health dimension and the
importance of the body to young people;
and, on the other, the factors that
contribute (prescription drugs) to the
medicalization of young people’s lives.

Drugs and Medicine in the Context of Youth Culture
177
The dimension of health is a key element
in the analysis of individual life courses, of
well-being and malaise, of citizenship
rights, and of the system of social, gender
and generational inequalities.
The race to improve performance
sometimes turns well-being and malaise
into the two sides of the same coin, first in
a diachronic and then in a synchronic
perspective. Our research is intended to
pinpoint, by means of a quantitative and
qualitative methodology, when, where and
why young people request both medical
and pharmacological help in order to
improve their relationships. This
perception stems from a structured and
consolidated awareness of a me/self, that is
to say of how a person feels they are
perceived by “significant” others [29].
The body contributes to the emergence
of these dynamics. We may then assert that
one of the motivations pushing young
people to take excessive care of their own
body is that a body language shared [by the
other] legitimates the role of one’s own
look to the point of considering it as the
matrix of a “status or non status” of health
that has been called the “body idiom”, a
conventional reasoning that plays a symbolic
and normative role [40]. The body idiom, a
performer without a voice, conveys a non-
verbal communication that allows spectators
to capture an important image of the
individual’s outer balance, through his
capacity to send images while concealing
any state of anxiety, depression or other.
Medicalization of the everyday life of the
young people involves a process by which
nonmedical problems become defined and
treated as medical problems, usually in
terms of illness and disorders [13]. In other
words, medicalization can be described as
the extension of medical categories in
everyday life.
Recently, The Lancet (369/2007) has
dedicated ample space to the issue of
medicalization. Here, McLellan states the
question clearly: “Once upon a time,
plenty of children were unruly, some
adults were shy, and bald men wore hats.
Now all of these descriptions might be
attributed to diseases - entities with names,
diagnostic criteria, and an increasing array
of therapeutic options” [28: 627].
Therefore the Lancet raised this issue by
publishing a number of papers that tried to
shed a new light on some crucial aspects of
the medicalization process by looking at it
from a new perspective. While in the past,
according to the early definition given by
[21] the term medicalization meant a
process promoted mainly by the doctor,
today many promoting agents have come
to the fore. Jonathan Metzl and Rebecca
Herzig [31] identify some of them, such as
the patients and the practice of “direct-to-
consumer advertising”, and the
pharmaceutical companies with their
economic policies.
Other authors think that while “young
people, who were once considered as the
passive victims of medicalization, now play
an active role, especially in the decision-
making process. The key factor seems to be
the influence of medicine upon the ethical
attitude of young individuals, the
relationship with ourselves, our judgment
about the kind of person we wish to
become and the kind of life we wish to
lead” [34].
In the U.S., for instance, with the
liberalisation of Direct-To-Consumer
(DTC) advertising, the physician-patient
relationship has undergone significant
changes. Hollon (2005) states that patient
requests for prescription drugs consistently
affect the prescription attitudes of
physicians. About 40% of appointments in
which the discussion involves DTC
advertised drugs end up with that drug
being prescribed. Then, through a
metanalysis of a great deal of research,

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
178
Hollon demonstrates that almost 80% of
physicians are convinced that DTC ads
encourage people to look for treatments
they do not really need (2005: 2031).
All this can be attributed to the fact that
nowadays young people are increasingly
"demanding", nor can we deny that there is
a different health culture today. Health is
not only “lack of pathology”, but also
“enhancement”; furthermore, an enlarged
“health literacy” [23] pushes the patients to
become consumers who look after their
wellbeing (Ingrosso 2007).
In this context, it would be worthwhile to
focus on the Drugs National Agency’s
report of a steady growth in prescriptions
of anxiolytic and antidepressive drugs in
Italy over the last few years. Most of these
treatments are prescribed by general
practitioners, who have to face a huge
demand for medicalization from younger
people as a result of difficulties in the
socio-relational sphere. A set of symptoms
is increasingly becoming a “disorder” and
in today’s society we are witnessing a
growing medicalization, not only of what
is pathological, but also of what can be
“improved” (the cases of Viagra and
cosmetic surgery are emblematic).
In mass media communication health
turns into a fashion, a consumer product, a
look. There is an increase in fitness
practices that promote a “well-shaped”
body and mind able to yield a high
performance level that is fit for the society
of the perfectible and which therefore
requires flexible procedures at work and in
present-day social life. The consumption of
new substances, with a greater or lesser
doping effect is increasing to meet the
demands for efficiency, visibility or
compensation for fears of inadequacy and
isolation [8]. Because of the mocking
paradox of mass society, in which the
relational dimension of “being there”
rather than “being” haunts the present time
of everybody and the process of “staying
with” seems more important than
“staying”, solitude, exorcised in a thousand
ways, materializes again as a companion
escorting individuals, above all younger
people, on their social pathway [9].
Thus normality, in contemporary society,
seems to take a violent and de-structuring
semantic twist: from an expression aimed
at recognizing a status of “good health”, of
“being like” to a concept of hedonistic
perfectibility and implementation.
This article, based on research conducted
amongst young people living in the
southern regions of Italy, discusses the
largely under-researched theme of the
association between pharmaceutical use,
health and young people.
Field research reveals that, as shown by
the reality under examination, there is a
desire to resolve internal problems typical
of the younger generation through the
application of externally introduced
elements (pharmaceutical products).
In adolescence, assumption of
pharmaceuticals is seen as an answer to
problems of insecurity or, in some cases,
identity. Drugs are also seen as a means of
resolving difficulties relative to the process
of transition, to contradictions and to
situations typical of the younger generation
such as anxiety problems, mortality, future
prospects and to the inevitable upheavals
arising from a confusion of subjectivity.
For young people, prescription drugs seem
to represent what Valéry says art
represented for the author. He identified
the original motivation for artistic creation
in that aesthetic need that belongs solely to
the “author”, who initially displays
indifference towards a possible
“audience”. At first there is the anxiety
(spleen) of a man who feels horror for the
void – in our case, the time and space of
uncertainty experienced by the youth
population – which is both a void of space

Drugs and Medicine in the Context of Youth Culture
179
and time. The restlessness characterising
sensibility can indeed be related to the
sense of “instability” that the subject
experiences when faced by empty space
and waiting. In short, the need to fill up an
empty gap in time or to fill an empty space
is a natural need because it is innate to man
(Valéry, 1935). Zygmunt Bauman recalls
the complex mechanisms underlying the
construction of uncertainty and insecurity:
if our society tends to reassure the public
dimension of subjects but attacks them in
their every private niche, what is
manifested in terms of the subject’s
potential crisis, i.e. the erosion of
confidence in his/her body and lifestyle
certainly assumes a “striking” nature for
the individual, especially if it is a young
person [1].
Therefore, in young people, there is an
increasing need to distance themselves
from times and spaces that can suspend (or
suggest that they are unable to follow and
control) the frenetic rhythms of everyday
life. The anxiety of contemporary reality,
the uncertainties of the existential process,
the question marks looming over one’s
own future (not actually expressed but
present on the individual level, often
unsaid but not necessarily unlived or
unperceived), the crises within one’s
symbolic universes [2], the discontinuities
in relational processes, the crisis of an
increasingly rarefied and unsatisfactory
relationship with the historic reference
institutions of socialisation are all elements
that exert a dynamic effect also in the
creation and maintenance of the ability to
control one’s own body, subjectivity,
individuality and inherent differences. The
latter become guaranteed by prescription
drugs, the means by which the individual
may not be obliged to interrupt the dynamics
of their own existential frequency but remain
able to keep up with it.
For young people, drugs are a means of
maintaining constant the rhythms and
activities relative to and in parallel with
existential frequencies and patterns.
Young people seem to have accepted the
idea that, in a physical and cultural
colonisation process, the pharmacological
world is invading all walks of life. The
self-proclaimed objective is to help
individuals to constantly improve their
daily abilities by reducing difficulties,
ensuring certitude and the capacity to
exteriorise.
The research also demonstrates that
some habits of youth regarding the use of
pharmaceutical products (drugs) are the
products of a social construction
originating in the primary social group -
the family - which then become
fashionable within peer group structures.
2. Premiss and Methodology
Judging from this research, in a process
of physical and cultural colonisation,
pharmacology is invading every aspect of
the life (and body). The self-proclaimed
objective is to help individuals (at both a
physical and psychological level) to
constantly improve their capacity in the
course of daily life by reducing difficulties,
ensuring certitude and facilitating a greater
degree of exteriority.
These considerations have led to the
decision to investigate what may be, or
could be, the reaction of young people and
the generation preceding towards the
assumption of pharmaceuticals.
Moreover, when a subject abandons,
delegates and places trust in
pharmacological and medicinal treatment,
health protection becomes an act of faith,
independent of the effect which the
pharmacy has upon the organism.
It is therefore important to understand
the trust, or lack of it, towards individual

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
180
organisms and also the kind of relationship
which exists between the assumption of
pharmaceuticals and the various levels of
information and disinformation. Starting
from this hypothesis, field research was
carried on a sample base of 550 students
from the University of Salerno. In order to
obtain a balanced cross-section, the
samples were taken from faculties and
degree courses in Mathematics, Pharmacy,
Engineering, Economics, Law, Sociology
and the Communication Sciences. Only 511
young people answered the questionnaire:
49% male, 51% female, one third attending
science faculties, and two thirds attending
humanistic ones. The sampling procedure
employed the two-phase cluster technique.
The first phase sampled the Faculties present
at the University of Salerno, while the
second phase selected the lessons timetabled
for the period of the investigation (according
to the degree courses, the sample included all
the courses from the first to the final year so
that its composition was representative of the
university student population in terms of age
and course attended).
The origin of the sample is
heterogeneous: 56% come from Campania
while the remaining 44% are from other
Italian regions (Basilicata (21%), Puglia
(10%) and Calabria (13%).
Principally, research was aimed at the
relationship which students have with the
use or abuse of pharmaceuticals and the
relative degree of information or
disinformation regarding their use. In
particular, the investigation was geared
towards analysing and understanding: a)
how the daily discomforts encountered by
young people are faced and overcome - or
kept in check - by the use of
pharmacological substances; b) the social
importance which drugs assume in the
various existential life-patterns of young
people; c) to evaluate the varying extent to
which factors relating to social context and
cultural roots have an influence – and to
what measure - on behaviour patterns.
3. Drug Indoctrination
Young people appear to want to resolve
internal problems and conditions typical of
youth by resorting to external remedies to
their problems and to their condition:
pharmaceuticals. Indeed, the majority of
the sample admitted to the occasional use
of pharmaceuticals (40.3%); 32.1% stated
that recourse was “hardly ever”, whereas
4.3% maintained “never”. 16% of the
sample accounted for “fairly regular use”
and 7% classed themselves as “frequent
users”. However reassuring on the surface,
these statistics do not conform to answers
posed by a check question to which only
3.1% failed to reply and 0.4% attested that
they never used pharmaceuticals at all. The
vast majority of the remainder of the
sample is distributed amongst a percentage
of assumption of various pharmacological
compounds whenever symptoms –
however minor or trivial – present
themselves.
Drugs are legitimised by a reassuring
importance which is both expressed and
perceived: “drugs have an essential role;
above all, they validate the ability to
intervene on the part of a doctor – ‘I am
prescribing this, therefore I know what you
have’ would appear to be the comment of the
doctor making out a prescription and
avoiding further examination or referring the
patient to a specialist or hospital - an
alternative which could be interpreted as a
sign of incompetence” [15].
Beginning with this encouraging
legitimisation, drugs become the mediator
between the potential subjects who
consume them or are likely to (at this
stage, it is no longer important whether
they are prescribed by a doctor or on the
suggestion of a chemist or family and

Drugs and Medicine in the Context of Youth Culture
181
friends) and the progressive scientific
society.
From this research it is also possible to
evaluate the real success of
pharmaceuticals.
The investigation illustrates how drugs
are perceived by young people and how
that perception contributes towards a
guarantee of the success of officially
recognised medicines and, alternatively,
how they can enrich and improve the
quality of life.
One of the first results of the sample is
the almost unanimous recognition of the
role which drugs have acquired in
guaranteeing the state of health of the
individual, data which evidences the
widely held conviction, amongst the
young, of the scientific foundations on
which social progress is based.
Moreover, such data becomes even more
convincing when confronted with figures
of 19.7% and 26.4% of the university
student sample, all of whom maintain that
drugs are not yet fully capable of
guaranteeing an improved state of health.
This poll result underlines the desire and
trust that young people place in future
advances in the field of scientific and
pharmacological research which are geared
towards the improvement of the actual
governance of well-being. The
expectations, therefore, given to the role of
pharmacy are clear: to guarantee continuity
to the existential life pattern of the
individual. In particular when one
considers that only 6% of the sample do
not trust drugs or are simply incapable of
assuming a personal position over the
question.
A perspective which seems to remain
unchanged even when young people are
asked in which alternative they place most
faith: in official medicine, in homeopathy
(3) or otherwise. Here again, with the
impossibility of alternative medicine
asserting itself to the same degree, the
sample places unequivocal trust in official
medicine.
When the influence of socio-
demographic variables are considered in
relation to the subject gender, it becomes
evident that belief in pharmacological
discovery is analogous for both males and
females. However, when the relative
erudition of the parents is taken into
consideration, different data is forthcoming
– indeed, in parallel with the elevation of
family scholarship, there is a
corresponding increase of trust in official
medicine and pharmaceutical remedies.
The argument discussed so far is
confirmed by the section of the
questionnaire devoted to the level of
compliance (assumption of
pharmaceuticals and degree of therapeutic
efficacy) and also illustrates to what extent
individual subjects are prepared to delegate
or abandon themselves to pharmaceuticals
- or to place their unreserved trust in them
- in order to improve their psycho-physical
potential. This was so much so that when a
sample was taken from senior secondary
school students, 80.8% echoed agreement
with 79.9% of the university student
sample affirming that the effect which
pharmaceuticals had upon the organism
was “fairly good”.
Furthermore, when the 13.6% of the first
sample and the 15.7% of the control
sample are taken into consideration and
which state that the physical effects of
pharmaceuticals are “sufficient”, it can be
added that 95% of the sample base of
young people examined demonstrate that
pharmaceuticals have an increasing
tendency to co-exist in the existential
pattern of the subject. Moreover, drugs are
assuming an increasingly reassuring
characteristic within the individual lives of
young people.

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
182
It is then, perhaps, no accident that in
another section of the questionnaire 97%
of the sample – 9.7 students out of 10 –
state that they have taken and are taking
pharmacological substances.
This same percentage is also confirmed
by the answers to a control question which
underlines how drugs – from anti-anxiety
to anti-inflammatory – are assumed
conscientiously and appropriately for
several symptoms. Young people, when
affected by certain maladies, are no longer
prepared to wait for a natural
counterbalancing reaction from the body
itself but prefer to accelerate the process
with chemical products.
In an attempt to explain the relationship
between the trust invested in drugs and the
effect that any pharmaceutical product may
have on the organism, the following
question was posed: “Before taking any
kind of drug, do you read the
accompanying instructions?” (while
conscious that, despite the advice given in
the legal decree no. 44 - 18.02.97, such
instructions are still a long way short of
offering clear warnings and explanations
over an arc of three hundred and sixty
degrees).
70.6% of the sample read the
accompanying instructions, 10.4% do not
bother, whereas 18.6% were inconstant. As
regards the majority (70%) the comment
made was: young people who read the
accompanying instructions (nick-named
“little liar”) already have good reason to
be wary of the side-effects which even the
most mundane substances can provoke.
However, this would appear to be short-
sighted, it is impossible to guarantee that
all the possible undesirable side-effects, as
documented in the “instructions for use”,
have been previously identified and
confronted (4). This is a possible answer as
to why drugs are increasingly successful
between and with young people:
paradoxically, it is as though a vague
understanding of the nature of a drug is
also its certificate of guarantee for use.
Besides which, at this point we are
facing that which Luhmann defined as the
negative aspects and/or the “malfunction”
of modernity. In other words, society finds
itself having to confront consequences
determined through its own structural
selection, such as ecological problems in
the modern world and increasing tension
fuelled by the attempts to maintain the
actual level of social well-being.
It is, then, precisely this tension created
through the maintenance of well-being
which could provide an answer, in
Luhmannian terms, to the taking of
pharmaceuticals on the part of young
people at risk. The risk that a young person
makes in taking pharmacy without first
referring to the “instructions for use” or,
alternatively, when conscious of the likely
side-effects, is determined by an appraisal
of the potential damage which, in itself,
derives from a decision taken by the self-
same person [26].
The motivations referring to those of
sample quote who declare to not reading
the accompanying instructions (56.9%) are
particularly interesting: those who do not
read the instructions say it is because they
have prior knowledge, whereas the residual
37.2% argue that the instructions are
difficult to understand and that it is better
not to bother (always remembering that the
subjects are at a university level, which
provokes reflection upon the greater part of
the population who, under completely
different circumstances, must be unable to
read or understand the indications
anyway).
In this instance, we are confronted by the
category at dangerous discussed by
Luhmann, in other words, the potential
damage to which the individual is
unaware, inasmuch that the obscure

Drugs and Medicine in the Context of Youth Culture
183
terminology adopted to describe the
pharmacy does not permit the person who
is about to take the medicine to understand
the implications of doing so.
Moreover, the last consideration with
reference to the sample raises a bi-lateral
observation: a) could this contribute to
successful economic returns for
pharmacological multi-nationals?; b) could
the success of pharmaceuticals amongst
young people be part of a generalised and
voluntary disinformation strategy
concerning potential pharmacy users?
This type of behaviour could indeed be
common to other processes in which young
individuals decide to assume certain
substances: they are aware that
assimilation will, in any case, modify the
condition of their body. Nevertheless, the
knowledge of the final result of the
process, however approximate, is
sufficiently satisfying to annul any
information regarding the internal bodily
process leading to the final result. Thus, it
is the end result which is decisive;
regardless of any harmful side-effects, the
determining factor is the modification.
4. Pharmaceuticals in General and
Alternative Therapy
Interesting research data comes out of
21% of the sample who have prior
knowledge of pharmaceuticals in general,
data which is subsequently confirmed by a
later question to which 22% of the sample
attribute therapeutic properties and effects
to commercial medicines already marketed
by well-known pharmaceutical companies.
The data relative to the information
which young people have of
pharmaceuticals in general underlines
concepts and signals which public opinion
has been indicating for some time. Signals
systemised in the understanding and belief
of the individual - not at an “emotive” but
rather at a “rational” and “conceptual”
level – in certain therapeutic schemes
which are no longer simply tied to well-
known pharmaceuticals (and which have
become part of a way of life) but to
pharmaceuticals in general (5) as is also
the case with therapeutic treatments related
to alternative medicine.
Trusting in this form of therapy is
dependant upon whatever kind of
familiarity and information the young
person may possess – together with the
existing relationships, discussed
previously, such as doctor/patient or with
other important socialising elements. This
would explain why 17.4% of the sample
believe in unofficial forms of medicine and
why, out of this 17.4%, 14.1% claim to
have greater faith in homeopathic
medicine. Indeed, the function of
homeopathic medicine would seem to
vindicate that therapeutic mandate which,
in the words of Thomas Sandoz is “a
profane rite of exorcism”. To follow, to
recognise and to trust in this practice has
the effect of rationalising some of the
procedures of improvement, both of the
cure and of the therapy of the actual state
of well-being or indisposition. This could
occur through a decomposition of the
function of the vindication of homeopathy
in “four projects” [35].
In the first place, homeopathy introduces
the possibility of contrasting medical
impotence by seeking auxiliary solutions
outside of the parameters of the biomedical
verdict (or medical practitioner), thereby
overcoming the innate passivity of the
subject towards illness.
Secondly, homeopathy encourages the
fight against the mounting uncertainty
which afflicts people suffering from illness
(regarding the origins, the prognosis, etc.)
by directly including and involving them in
a cultured dialogue of explanation.

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
184
Furthermore, homeopathy overcomes
that silence which can often follow the
pronouncements of experts, maintaining
intact latent resources in the subject which
official medicine has a tendency to nullify.
Finally – the fourth and last project –
homeopathy endorses opposition to the
modern movement towards the
medicalization of society and opposes
scientific reasoning and materialism which
is perceived as “the power of dominating
forces” [35].
Thus, whilst not “justifying
assimilation” of homeopathic therapy over
that of official medicine, the myth of the
therapeutic potential of homeopathy may
be attributable to the power of its
credibility, a factor which exercised a
distinct fascination over part of the
research sample. Young people exorcise
uncertainty – to which, in terms of health
care rights, official medicine is still
incapable of responding – by resorting to
alternative medicines and medicaments
which facilitate (or are said to facilitate)
aggregation in the dramatically decisive
moments of their existence.
5. From the Recognition of Professional
Status to the Recognition of Social
Status
In order to isolate and verify some of the
answers previously given by the sample, in
the fifth section individuals were asked to
indicate in which subject – family doctor,
specialist, chemist, friends/family – they
invested most trust when looking for
advice or a pharmacological prescription.
Replies indicate that, of the four subjects,
in terms of trust, social and professional
recognition and the expedience of
prescriptions, specialists were adjudicated
most competent (49.7%). This figure was
followed by general practitioners
(37.2%), friends/family (5.7%) and,
lastly, chemists (3,7%).
Turning to various exponents of the
structural-functionalist school, such as
Talcott Parsons [32] or William Goode
[20], it could be said that such a high level
of recognition of the professional status of
medical practitioners - greater even than
that given to specialists - has taken shape
in the wake of the organisational reform of
labour within industrial and urban society.
A development which has privileged the
division of functions and tasks and
produced a consequent demand for
qualified or specialised services outside of
the family environment.
All of which, however, has led to an
ulterior consequence: the ever-increasing
fragmentation of medical knowledge, a
phenomenon which has had an inevitable
effect upon the ability to prescribe any
required pharmacy. Moreover, in the midst
of this fragmentation process, although a
deeper bodily understanding has evolved,
it is often difficult to grasp that what is
being lost is the link between states of
illness not attributable to a specific part of
the body but rather to the body in its
entirety. Thus, the importance given to
medicine and pharmacy is a consequence
of the values attached to health, life and
death. According to these authors the
progress of knowledge and preparation has
induced a need: recourse to medicine in
order to legitimise professional status.
However, the symbolic commutational–
ists and theoreticians of the Chicago school
– in particular, E. Freidson (1970) – refute
both concepts: inasmuch that the rise in
status of the medical profession
automatically depends on the new division
of labour and, that it stems, fundamentally,
from the progression of knowledge.
The medical profession, in this respect,
gains professional status through those
who, averaging out a multiplicity of

Drugs and Medicine in the Context of Youth Culture
185
considerations, manage to persuade
themselves of the unsubstitutional nature –
in terms of character and service - of their
competence and their ability. (in other
words, a professionality which, rather than
being achieved, is recognised by others).
Knowledge certainly contributes to the
definition of professionalism but it is not
easy to establish that precise moment in
which such recognition legitimises and
confirms the privileges of professional
status [32].
Moreover, this research verifies that
young people’s trust is placed – as they
themselves confirm in one of the replies to
the questionnaire – in those representatives
of official health care with whom they deal
directly in daily life. Trust in medicines
prescribed by specialist practitioners,
greater than that invested in the
representatives previously mentioned,
would not appear to be different as regards
the type, whereas the level of trust given to
such professional figures increases in
correspondence to the educational quotient
of the family and, in consequence to
parental professionalism and the nature of
their work.
The research also opens the possibility of
analysing the way in which a prescription -
or the recommendation by a specialist of a
particular medicine and its subsequent
acquisition - results in a dual-recognition:
on one side, that of professional status and,
on the other, that of social status within the
family.
6. The Perception of Young People
towards Change
What also becomes evident from the
questionnaire is the perception among
young people that medicines have changed
in substance and role. It is in the
transformation of the role (and objectives)
of medicines that the “personal data bank”
of any subject “needing” medicine is being
modified and filters back, through the
various generations, to young people and
children.
Today, medicines are no longer merely
therapeutic, no longer is there recourse to
pills when a state of illness is diagnosed
(indeed, not long ago, pharmacy was only
resorted to after immunity mechanisms
were found to be insufficient) but rather,
for many, medicine has become a means of
prevention, both in short and long-term
circumstances.
The sample would appear to be
conscious of this process which has seen
conceptions of pharmaceutical use move
from care, treatment and cure of illness
through to a preventative means of
forestalling it. As regards this data, it
perhaps worth reflecting that many young
people, approximately 66% of the sample,
turn to pharmacy at the first sign of a
possible attack of influenza or similar
discomfort.
This fact must also lead us to reflect on
how these continually ambivalent young
people are at the same time subjects of
transformation and objects of
subordination with respect to consumer
processes: it contributes to temporarily
assigning them with citizenship and to
structuring their identity, and as such it
must be recognised, albeit tacitly. The
ironic paradox is that, in this case, unlike
in clothing fashion, tastes in music or any
other area of commercialised leisure time,
this is a consumption that acts directly on
them personally, on their body and on their
identity. Therefore, prescription drugs have
today become a consumer product for
young people, through which to assert,
construct and project an individual and a
collective identity – on this issue,
advertising never presents us examples of
isolated subjects coming into contact with
a substance, but we are always shown this

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
186
practice being manifested within a group
of people bound together by friendship,
affection, etc.. In many cases among
campus students, therefore, prescription
drugs assume the role of a “fashion” with
the characteristics described by Simmel:
«fashion is imitation of a given model and
thus satisfies the need for a social
approach, it leads the individual along the
road everyone follows, from a universal
model which reduces the behaviour of the
individual to a mere example. But
nevertheless, fashion satisfies a need for
difference, the tendency towards
differentiation, variation and distinguish–
ing oneself from the others» (Simmel, 1905,
pp. 30-1). It must not be forgotten that the
prescription drug at the centre of attention
(like all the others) will have different
effects on the individual bodies and on the
individual identities (and, in spite of
everything, this is the very expectation of
the individuals): hence, analogous
performance for different and differentiated
results. A consideration which has
repercussions in a subsequent observation
which reveals how the sample cross-section
under examination are influenced and
socialised towards pharmacy.
Evidently, pharmaceutical use plays a
constituent role in the existential life
pattern of any individual. From the outset,
there is a consecration of the positive
nature of pharmacy which, subsequently,
has inevitable repercussions on initial
impressions: the first use of pharmacy is
that administered by parents to their
children. Clearly, this introduces an
element which both anticipates and
reinforces, beyond all other reasoning, the
socialisation of the substance: how could
our parents have possibly given us harmful
substances? And, given that for every child
parents “know all”, children assume that
they must be far better informed about
such substances than they could ever be.
It is, therefore, during the process of
cognitive and cultural differentiation
between child and parent that individuals
begin to acquire an awareness and,
contemporarily, ask questions about
pharmacy.
It would appear that the greater part of
the sample under examination have grown
up with the idea (probably due to the
argument previously outlined) that
medicine is good for them. Only a minor
number of the young people interviewed
introduced a different evaluation, arguing
that, in the meantime on their part, they
had converted to alternative therapy in the
conviction that such cures are not harmful.
Despite differences of faculty or degree
course, the sample group, with absolutely
no variation, continue to grow up under the
belief that for whatever anxiety, ache or
indisposition it can be easily overcome
with the aid of medicine: “for every health
problem or illness there is a suitable
pharmaceutical remedy”. An awareness
which, as testified by the sample, derives
from the principal agents of socialisation.
Fragmentary information such as that
relative to the theme health/illness (the
index of individual and social patterns
followed by young people) should perhaps
also be introduced; such information
derives in 40.1% of cases from television
and, in 20.4%, from parents.
Besides the mass-communication
influence of television on young people
regarding information relative to health
and illness, 4.3% of the sample also
nominates the radio and 11% specialised
publications. As regards this last assertion,
it would seem likely that the word
“specialised” covers an ample range: that
is to say, not merely those specialised
journals and periodicals which have
proliferated over the last ten years or so
and which specifically deal with health and
illness, but rather the inserts, notebooks or

Drugs and Medicine in the Context of Youth Culture
187
weekly supplements which have become
standard to every daily newspaper and the
weekly and fortnightly publications which
come out at both a national and local level.
Despite the well-known fact that Italians
read little (particularly daily newspapers),
it is also true that in the case of health (and
pharmacy), a veritable communication
network exists from which, it would
appear, it has become extremely difficult
to escape. In consequence, for certain
themes - such as those relative to the
physical aspect - they become, in a real
sense, communal mass movements;
whereas, for many other medical
questions, particularly those of an
“intimate” nature, reflections either do not
exist or, alternatively, fail to become
interlocutory - an observation which is
particularly apposite when such questions
are directed at precisely those subjects who
have – and ought to assume - the
responsibility of replying.
Moreover, considering the statistics of
those who advise young people when not
visiting a medical practitioner (and who,
notwithstanding, take medicine for
physical or psycho-physical disturbance),
57.3% are parents, 5.9% are family
members, 4.1% are relatives, 4.9% are
friends and 17.8% take advice from a
chemist. Only 2.4% state that they do not
assume medicines unless it is on the advice
of a doctor. To this data other sources of
information can also be taken into account,
all of which, nevertheless, are constituent
elements in a pattern of socialisation.
Above all, an attempt was made to
corroborate the role and the effects of the
information or disinformation supplied to
young people by secondary agents of
socialisation.
At the end of 1999, the specialised
journal “Sanità. Il Sole 24 Ore” published
an article saying: “The fight for
promotional exposure together with
research into synergic relations with
sales personnel has resulted in a series of
heterogeneous initiatives. Some of them a
little embarrassing. A promotional
campaign, launched in 1998 by a
multinational operating in the
pharmaceutical sector, created a
promotional tie-up between one of the best
known headache pills and a compact disc
of relaxing melodies. Chemists were
expected to pull out the promo from under
the counter each time they sold a packet of
the pills.”
This advertising spot was transmitted
many times a day on both radio and
television, despite the fact that WHO
(World Health Organisation - the
international health agency of ONU)
recommends that the role of the mass-
communications media, due to its
enormous influence upon public opinion
and perception, should be: “…to control
the authenticity and importance of every
fact relating to pharmaceutical products…
avoid becoming the spokesmen for
promotional campaigns in favour of the
pharmaceutical industry…” [41].
Information broadcast by the mass media
– television, radio, newspapers, magazines
and specialist journals – is disciplined
under the legislative decree n. 541, 30
December 1992. This decree prohibits the
media from transmitting messages
contrived to persuade their audience to buy
products which proclaim to be uniquely
capable of improving a state of health or,
indeed, to allude that failure to assume
such products could lead to deterioration.
The decree also prohibits the marketing of
medicinal products which encourage the
belief that the guarantee of relief and
fitness is determined by natural products.
26.1% of the sample admitted to taking
pharmaceutical products without a medical
prescription. The principal agents of
socialisation influencing the choice of

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
188
pharmacy to be taken – as underlined by
WHO – were, in order of importance,
television, radio, specialised journals and
internet. For young people, then, such
mediums are suggestive and seductive.
Statistics which take on far greater
validity when confronted with the 30.3%
of the sample who admit to receiving
information relative to health and illness
through the communication channels listed
previously, either to avoid choosing
medicines autonomously or having to visit
a doctor for minor aliments.
Seductive propaganda has the effect of
inducing individuals to associate a series of
natural properties - in other words, rendering
them harmless – to certain products.
The success of pharmacology, of official
medicine and even that of alternative
medicine, is largely determined by the
influence of the mass media. The
underlying message communicated is that
of a fascinating ideal designed to overcome
any form of subjective analysis - as for
example when facing a statement of
propaganda such as: “better a tried and
tested traditional remedy which has no
harmful side-effects on the body”. A
slogan which is then linked to the image of
a slim and beautiful woman visually
eulogising the product at hand.
In other words, audio-visual
communication designed to neutralise
rational responses towards the assumption
of a therapeutically orientated product.
How many of the young people
interviewed are conscious of the
“provenance” of products within the field
of alternative medicine? How many of
them are aware that bio-therapy/herbalist
and homeopathic remedies are, in any case,
laboratory derivatives? Are they equally
alive to the idea that the herbal extractions
from which such palliatives are “made”
are cultivated and chemically treated:
manure, fertilizers, insecticides – chemical
additives essential for the optimisation of
the process of cultivation and industrial
production of “medicinal” herbs?
The effects, the therapeutic properties of
herbs – which, once upon a time, grew
spontaneously and naturally – are today
largely the end-products of chemical or
bio-chemical cultivation; whatever
substances administered, herbal-based cure
is the most traditional form of pharmacy
associated to official medicine. In modern
society, these so-called biological-
derivatives – widely considered to be both
therapeutic and non-toxic – are also the
end-products of a laboratory-produced
chemical process (6).
Clearly, commercial media is primarily
interested in constructing messages which
emphasise the beneficial effects of
pharmaceutical products and conceal any
undesirable side effects; whilst, at the same
time, ignoring an equally interesting and
opportune occasion to inform individuals
of the correct usage and circumstances
under which the product is consumed.
Apart from the media, the other principal
socialising agent which has an influence
over the use of medicines and medical
information, is the family. Much research
demonstrates that, as regards the
assumption of pharmacy, the level of
education and relative medical knowledge
of the mother determines differential
behaviour on the part of the children.
In the book “To grow up well and better:
one reply to the most frequent questions of
mothers” (AA.VV., 2000) it is made
evident how much this relationship is
dependant upon a continual flow of
information regarding those medicines
utilised for curing their own children, from
aspirins to anti-histamines.
In the opinion of the authors, the most
interesting aspect of the research is to have
been able to evince that, in terms of the
information and health education

Drugs and Medicine in the Context of Youth Culture
189
requirements of Italian mothers, no
differences are imposed by geographical
and cultural variables (always remember–
ing that the survey deals with an
indeterminate sample covering mothers
residing in totally opposed cultural and
geographical realities such as Milan and
Matera). The research clarifies why the
socio-demographic variables taken into
consideration during the predisposition of
the questionnaire – such as educational
qualifications and place of birth – do not
influence the way in which young people
are informed about, or socialised towards,
the use of pharmacy as a means of
regularising their state of health.
At this point, it becomes clear (given that
57.3% of the sample state that
pharmaceuticals are taken on the advice of
the parent and, in particular, the mother)
that, in the case of medicines, the principal
factor of influence over young people is
also the most powerful agent of primary
socialisation. This data, relative to the
influence emanating from the previously
defined primary socialisation agent, is
confirmed by 5.9% who state that
pharmacy is taken on family advice; by
4.1% who receive advice from relatives
and a further 4.9% who follow the
indications of friends.
Moreover, in this investigative section of
the questionnaire we can observe that not
only do the young people in our sample
advise their friends on the drugs to take, on
the basis of their previous experience, but,
at the same time, they themselves receive
advice from parents, neighbours, family
members or friends when they do not turn
to their doctor, while only 2.3% claim not
to take drugs unless prescribed or
recommended by their doctor. There seems
to emerge another consideration of that
fashion that «gives the individual the
certainty that he is not alone in this action
and proceeds on the basis of previous
experience as if on a solid platform that
alleviates the activity of the moment from
the difficulty of sustaining oneself»
(Simmel, cit., p. 30).
Socialisation of drugs, which for young
people is the product of peer group
influence, explains the widespread social
recognition which is attributed to one
medicine rather than another. For example,
it could be supposed that the limited
success of generic medicines amongst the
sample group, as previously stated, is
probably due to their fledgeling
appearance on the generic pharmaceutical
(7) market and a limited notoriety within
family peer group structures. Moreover, in
the absence of customary recognition and
use of the product, young people ignore it
(at least, for the moment).
However, as time passes and new
pharmaceutical products claim more
attention and greater acceptance amongst
the primary socialisation agents, the same
process of the usage of generics (which at
present can be seen to operate with well-
known multinational pharmaceutical
products) will also become the rule.
Indeed, it is hardly casual that young
people refuse to assume “new” drugs – in
the face of advice from doctors, nurses,
medical orderlies and/or a chemists – even
when the motive for their use (and the
substitution of well-known alternatives) is
justified by a potentially superior
therapeutic effect coupled with minor
collateral consequences (8).
Pharmaceuticals have been invested,
through advertising and peer-group habits,
with a whole range of precise
connotations. Above all, on the part of
consumers, they have become consumer
products; chemical composition,
therapeutic efficacy and undesirable side-
effects have become secondary
considerations: “Any pharmaceutical
carries more importance as a label than as
a medicine” [5].

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
190
7. Interim Conclusions for the Base of
Further Research
An extension of this research would
entail taking into consideration a
constructivist approach which consented –
as regards youth health themes,
environment and the inherent self-
awareness of the subjects themselves – to
understand how perception towards certain
interrogatives (such as conceptions of
illness and well-being from both a personal
and general perspective) are individually
constructed in parallel with the assembly
of information and experience.
Regarding any consideration of the
possible understanding that young Salerno
students may have towards the subject of
health naturally depends upon the
importance that each individual attributes
to the argument - not forgetting those
factors which can influence the
construction (or non-construction) of that
importance (social-demographic variables:
age; sex; the provenance of both student
and family; schooling, etc.) – in other
words, precisely that importance motivated
both from within the subject and from
individual external experience (Luhmann,
1971). Nevertheless, it can be safely
assumed that any young person will have
acquired a rudimental understanding of
pharmaceuticals, not only as regards their
potential efficacy relative to health and
illness but also in terms of subjective
analysis and active response to such
themes.
And, whereas the field of medicine often
encounters transitory difficulties
determined by the massive growth in
technological and pharmacological
innovation, it is also true that, despite
everything, medicine as a discipline enjoys
notable recognition on the part of young
people. This is confirmed, for example, by
those young people who, often
ingenuously, undergo cures, therapy and
even cosmetic surgery in order to resolve
inter-personal and existential relationships.
Young people now seem to be aware of
these dynamics and have established a
fatalistic attitude of yielding,
relinquishment, refuge and delegation to
discovery and scientific research and to
those who hold this knowledge and
represent for them one of the few
certainties for the improvement of their
future. Baudrillard (1976) certainly springs
to mind in this connection: «it is with
generalised individual somatisation, with
the body becoming an object of prestige
and salvation (…) that the medical class
establishes itself in the position of social
super-privilege it currently occupies »
In order to interpret the new ways of
appealing to young people - through the
schematics of perception, understanding
and information of health within an
individual context and of those instruments
and techniques which govern or re-educate
these aspects - the starting point is
undoubtedly the theory of Norbert Elias.
Moreover, it is only by following a
progressive approach over an extended
period that transformation can be
satisfactorily identified. Indeed, to
successfully reveal the mutation of interest
of young people in matters of health - from
initial curiosity through to conversion -
matched with gradual improvements in
well-being, the minimum research period
required would be twenty years. Long-term
analysis of this nature could identify the
various phases and figures of influence
through, for example, an analysis of the
internal mechanics of groups of teachers,
of parents and of those institutions
principally concerned with the health and
welfare of young people.
Through the employment of a process of
semantic destructuralisation, what also
needs to be considered is that, in an

Drugs and Medicine in the Context of Youth Culture
191
attempt to come to grips with the crisis
within modern medicine, analysis would
appear to be orientated towards
understanding in terms of “Canons and
Procedures” (“Rules and Regulations”) –
[7] - rather than attempting to reduce the
crisis to a single scientific paradigm.
Khun himself asserted that scientific
change was a product of rupture and
conflict, inasmuch that the employment of
canons and procedures as a solution to
crisis clearly indicates how some difficult
moments can be overcome through
different interpretations and theories.
At which point new semantic categories
– set up to overcome the impasse in which
the medical-scientific community finds
itself languishing – step into play.
Interpreting the crisis from the
etymological point of view of choice,
shows how (through changes in the criteria
used by the social-medical-health
community for communicating matters of
health, diagnosis and the construction of a
supportive reference base for operative
medical opinion) the institutions charged
with the promotion and distribution - in
terms of prevention and information - of
“public health” amongst young people can
be influenced into varying their
procedures.
It is not, however, simply a question of
isolating the interdependent factors and the
interaction between those subjects who
modify the existing situation in order to
create a new one, but rather the whole
range of factors – reinforced through
reciprocal inter-reaction – which ensure
the modification and restructuring of this
cognitive process relative to the theme of
health. As a result, it is possible to
understand how the perception that young
people have of both health and illness is
dependent upon a series of social
configurations in which they are involved
and which contribute to forming the
identity structure of individual young
people. On the basis of this premise, albeit
brief, any network of collaboration
installed between institutions, public or
private, whose objective is that of creating
a policy aimed at the younger generation
and geared towards the promotion of
culture, the environment, the safeguard of
rights, working conditions, self-realisation
and the pursuit of personal interests, needs
to give priority to both the theme of youth
and health and the consequences and
effects upon the individual, upon
individual identities and the inter-personal
relationships established with and within
society.
Notes
(1) The problem of suicide, which is
obviously related to the strength of the
social bond, is rooted in the history of
society and, at the same time, of the
sociological tradition, albeit in the
awareness of the different dynamics
attributed throughout the ages to the
choice to end one’s own existence. From
Durkheim’s work on the relationship
between the differing degree of social
interaction and suicide « A society is
highly integrated when its individuals are
kept dependent on it » (Durkheim, 1897).
(2) Think of the utterly insignificant number
on the youth issue in southern Italy
conducted by [6], [24], [38], [17], [30]
[33] and [37].
(3) Homeopathic medicine falls into the
category of alternative medicine.
Originating in the late XVIII Century,
this therapeutic approach was first given
credibility through the work of doctor
Samuel Christian Hahnermann. The most
sensational discovery was that the effect
of therapy was inversely proportional to
its quantity. For the homeopath, as
opposed to orthodox colleagues,
diagnosis and therapy concerns the entire

Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
192
body, referred to as the “unitary
organism”. In the majority of cases,
medications and other elements used in
homeopathic medicine are individually
prepared using biological raw materials
of natural vegetable or animal origin. The
homeopathic term for these medications
is “tintura madre” (“mother tincture”).
(4) When references are made to values not
taken into consideration within the
territory, this is principally an allusion to
the historical importance of popular
medicine in Southern Italy and of its
particular role relative to the poorest and
least literate of the social community
(though not exclusively so) and, in
particular, to those lacking the necessary
resources to undergo or resort to
traditional methods of treatment. This has
given rise to a practical relationship
between traditional pharmaceuticals
incorporating natural products (above all,
herbs) linked to those organisational
structures and individuals invested with
the specific task of propagating its
validity and function: the process of
modernisation, which would appear to be
in a permanent state of evolution, has
given itself the task of accelerating this
process towards the eventual “triumph”
of official medicine (in all of its aspects).
In reference to popular medicine, see,
amongst others [36].
(5) “Quite good” is not a possible reply to
the questionnaire itself but rather a
convenient expression adopted by the
author to indicate the approximate
percentage of replies ranging from
“discreet” to “very high”.
(6) By definition, alternative medicine
expresses an optional – or, indeed, in
opposition – to official medicine: Its
success is rooted in the inability of
scientific medicine – evidence-based
medicine – to adequately respond to
matters of health as well as the diagnosis
of illness. For debate, see [7].
(7) The term generic pharmaceuticals
(medicines?) describes those medicines
which have the same active principles
and chemical composition as well-known
brand names (following years of
successful marketing on the part of the
pharmaceutical companies). A typical
example might be: Aulin = well-known
pharmaceutical; Nimesulide = generic
pharmaceutical.
(8) In the documentation of all
pharmacological research, it is stated that
collateral effects are those resulting from
research upon human organisms; to
which end, a sample group of patients
volunteers to assume, experiment, test
and reveal any positive or negative side-
effects of the medicine.
(9) In Europe, such remedies are associated
to the culture of pre-industrial society
and, as opposed to knowledge of
primitive cultures, are “a product of the
re-elaboration of popular and past
traditions on the part of the general
populace” [39]. In consequence, two
distinct and opposed definitions of
medicine or traditional remedies emerge:
on the one hand, an almost parallel
confluence between traditional and
alternative medicine and, on the other, the
romantic idea of a popular medicine with
its own origins but with no foundations
and quite separate from evidence-based
medicine.
References
1. Bauman, Z.: In Search of Politics.
Milano. Feltrinelli, 2000.
2. Berger, P. e Luckmann, P.: The social
construction of reality : a treatise in
the sociology of knowledge, NY,
Garden City, 1967 [tr.it., La realtà
come costruzione sociale, Il Mulino,
Bologna, 1969].
3. Berlinguer, G.: Medicina e politica.
Bari. De Donato, 1973.
Drugs and Medicine in the Context of Youth Culture
193
4. Berlinguer, G.: Il corpo come merce e
come valore. In Rodotà S., “Questioni
di bioetica”, Roma-Bari.Laterza, 1997.
5. Bert, G.: Il farmaco come segno e
come mediazione. Milano. Feltrinelli,
1977.
6. Cavalli, A. (a cura di): I giovani del
mezzogiorno. Bologna. Il Mulino,
1990.
7. Cavicchi, I.: La medicina della scelta.
Torino. Bollati Boringhieri, 2000.
8. Cersosimo, G.: La coesistenza di
benessere e malessere. In: L’odore
della Bellezza. Wellness e Fitness (a
cura di) D. Scafoglio. Salerno. Marlin
Editore, 2007.
9. Cersosimo, G., Rauty, R.: Riflessioni
sul controllo sociale: dalla normalità
della devianza alla normalità della
malattia. Keiron, n. 5, 2001, pp.
128-139.
10. Ciacci, M., Gualandi, V. (a cura di):
La costruzione sociale della devianza.
Bologna. Il Mulino, 1977.
11. Clarke, A. E., Mamo, L., Shim, J. K.,
Fishman, J.R., Fosket, J. R.:
Technoscience and the New
Biomedicalization: Western Roots,
Global Rhizomes. In: Sciences
sociales et santé 18, 2000, 2, 11–42.
12. Conrad, P.: Medicalization, Etiology
and Hyperactivity: A Reply to Whalen
and Henker. In: Social Problems 1977,
24:596-98.
13. Conrad, P.: The medicalization of
Society: On the Transformation of
Human Conditions into Treatable
Disorders. Baltimore. Jhons Hopkins
University Press, 2007.
14. Conrad, P., Schneider, J. V.: Deviance
and Medicalization: From Badness to
Sickness. St. Louis: Mosby, 1980.
15. Dupuy, J.P., Karsenty, S. : L’invasion
pharmaceutique, Paris. Seuil, 1974.
16. Duster, T.: Medicalisation of race.
Lancet, 2007, 369:702-04
17. Giannotti, G. et al.: Anziani e giovani
nel Salento. Un contributo per le
politiche e le attività sociali educative
del territorio, Lecce.Piero Manni,
1996.
18. Goffman, E.: Asylums: Essays on the
Social Situation of Mental Patients
and Other Inmates. Torino. Einaudi,
1968.
19. Goffman, E.: Stigma. Bari. Laterza,
1970.
20. Goode, W.J.: The teorical limits of
professionalization, In: A. Etzioni (a
cura di), The Semi-Professions and
Their Organization: Teachers, Nurses,
Social Workers. New York. The Fre
Press, 1969.
21. Illich, I.: Limits to Medicine. Medical
Nemesis: The expropriation of Health.
London. Calder & Boyars, 1975.
22. Jennings, D.: The Confusion between
Disease and Illness in Clinical
Medicine. In: Can. Med. Ass. J., 1986,
135, 865-870.
23. Kickbush, I, Maag, D.: Lo sviluppo
della Health Literacy nelle moderne
società della salute, in Ingrosso M. (a
cura di) (2007), op.cit.
24. Leccardi, C.: Crescere nel
Mezzogiorno. Giovani e adulti in una
comunità calabrese degli anni
novanta. Rubbettino, Soveria
Mannelli, 1994.
25. Luhmann, N.: Sozale Systeme:
Grundrisz einer allgemeinen Theorie.
Frankfurt am Main. Suhrkamp, 1988
[tr. it., Sistemi sociali. Fondamenti di
una teoria generale. Il Mulino,
Bologna, 1990].
26. Luhmann, N. : Soziologie des Risikos.
Berlin-New-York, 1993 [tr. it.,
Sociologia del Rischio, Mondadori,
Milano, 1996].
27. Luhmann, N.: Tautology and Paradox
in the Self- Descripition of Modern
Society. In: Sociological Theory, 6,
1988, p. 36.
Bulletin of the Transilvania University of Braşov ▪ Vol. 1 (50) - 2008 ▪ Series VI
194
28. MCLellan, F.: Medicalisation: a
medical nemesis. In: Lancet, 2007,
369:627-8.
29. Mead, G.H.: Mind, Self and Society.
The University Chicago Press, 1932.
30. Merico, M., Rauty, R.: Giovani a
Montoro Inferiore tra modernità e
tradizione. Forino. Phorograf, 1999.
31. Metzl, J.M., Herzig, R.M.:
Medicalisation in the 21st century:
introduction. Lancet, 2007, 369:697-8.
32. Parsons, T.: Profession. In:
International Encyclopedia of the
Social Sciences, 1968, p. 536.
33. Rauty, R. (a cura di): Una tranquilla
estraneità. Caratteri della condizione
giovanile ad Avellino. Mercogliano.
Tipografia Grappone, 1999.
34. Rose, N.: Beyond medicalisation. In:
Lancet, 2007, 369:700-702.
35. Sandoz, T.: L’homéopathie comme
rituel de conjuration. In: Medicina e
Storia. Rivista di Medicina e Storia
della Sanità, 1, 2001, pp. 73-98.
36. Seppilli, T.: Medicine e magie.
Milano. Electa, 1989.
37. Siebert, R.: Cenerentola non abita più
qui. Uno sguardo di donna sulla
realtà meridionale. Torino.
Rosemberg & Sellier, 1999.
38. Trigilia, C. (a cura. di): Cultura e
sviluppo. L’associazionismo nel
Mezzogiorno. Roma. Meridiana Libri,
1995.
39. Velimirovic, B., Velimirovic, H.:
Therapeutischer Pluralismus? In:
Curare, vol. 5, 1, 1982.
40. Williams, S. J., Bendelow, G.: The
Lived Body. Sociological Themes,
Embodied Issues. London & New
York. Routledge, 1998.
41. World Health Organization: Self-help
and Health in Europe. Ginevra. Who-
Oms, 1983.

DILEMMAS AND FACTORS INVOLVED IN
PROMOTING MEN’S HEALTH
IN BRASOV COUNTY
L. ROGOZEA
1 A. BĂLESCU
1
J. DOMARADZKI2 E. WIERZEJSKA
3
M. BARITZ4 L. CRISTEA
4
Abstract: This study of the gender profiles of the health care populations in
Brasov County fills a gap in the research literature by presenting the
relationship existing between morbidity and gender data. There are also used
the experiences developed in 2 universities - Transilvania University of
Brasov and Poznan University of Medical Science, in understanding the
importance of health promotion for different kind of people and there are
compared these data with the data from Poland, especially in the field of
human behaviour and in the health promotion topics.
Key words: morbidity, gender, health promotion.
1 Transilvania University of Brasov, Dep Fundam. and Prophylactic Disciplines. 2 Poznan University of Medical Sciences, Chair of Social Sciences. 3 Poznan University of Medical Sciences, Chair of Preventive Medicine. 4 Transilvania University of Brasov.
1. General Context
Men's health is poor compared to
women's, according to a range of
measures, and varies according to ethnicity
and to the socio-economic class. [6]
For a good understanding of the gender-
based approach in health promotion, it is
important to know the local context and the
correlation with the other data from another
county, including from another country.
In the second half of the 20th century the
number of human beings increased by 3.5
billion, which is over 140%. This growth
was over one billion higher than the number
of people at the beginning of that period. [2]
In the year 2000, the United Nations
Organization estimated that the number of
people has increased dramatically, as it has
reached 6 billion 56,7 millions.
It is estimated that the number of the
elderly will still grow from 600 millions in
the year 2000 to 2 billions in the year
2050. [1]
Another important change is the
increased number of the so called “old-
old” (age 75 years and beyond) in relation
to the so called “young-old” (those
between 65 – official WHO’s age for the
beginning of the old age – and 74 years of
age).
In that context, we mention that in
Romania the ratio between female and man
is: 1.05 and the structure is: urban: rural
53.4 : 46.6 and life expectancy is: 67 for
males and 75 for females, which means
that the health promotion programme must
be focused on male life style.
Developing a health promotion
programme needs to identify the risk
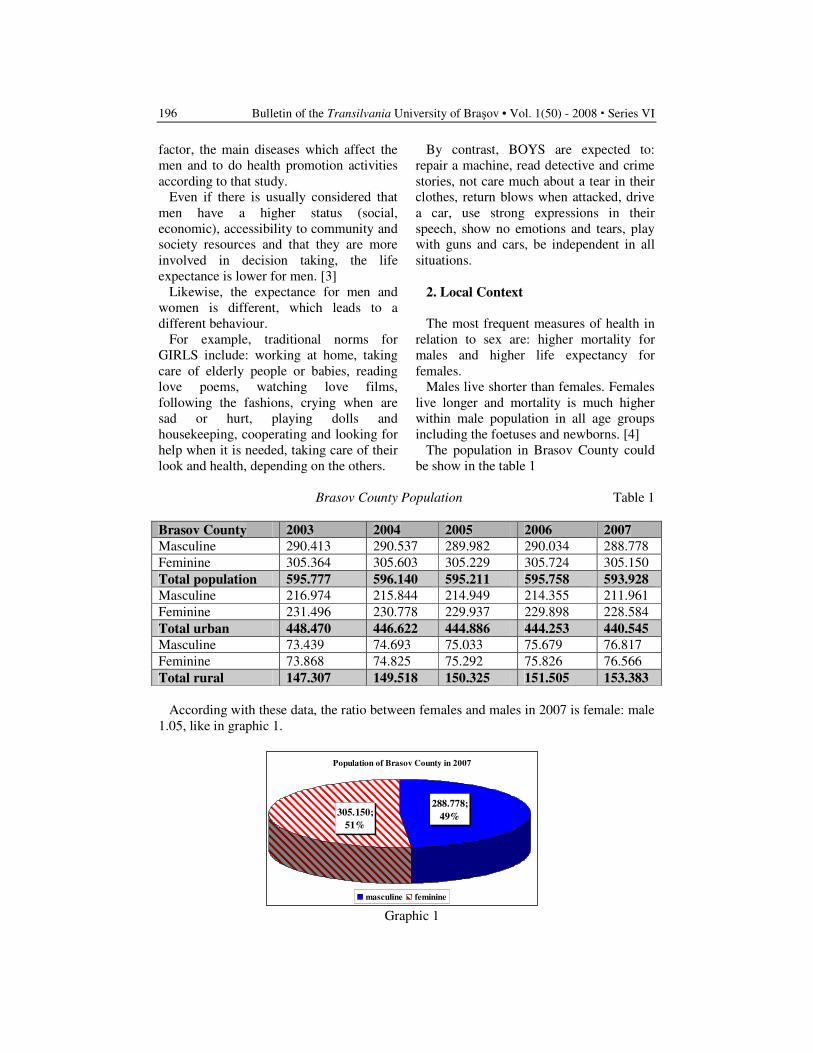
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
196
factor, the main diseases which affect the
men and to do health promotion activities
according to that study.
Even if there is usually considered that
men have a higher status (social,
economic), accessibility to community and
society resources and that they are more
involved in decision taking, the life
expectance is lower for men. [3]
Likewise, the expectance for men and
women is different, which leads to a
different behaviour.
For example, traditional norms for
GIRLS include: working at home, taking
care of elderly people or babies, reading
love poems, watching love films,
following the fashions, crying when are
sad or hurt, playing dolls and
housekeeping, cooperating and looking for
help when it is needed, taking care of their
look and health, depending on the others.
By contrast, BOYS are expected to:
repair a machine, read detective and crime
stories, not care much about a tear in their
clothes, return blows when attacked, drive
a car, use strong expressions in their
speech, show no emotions and tears, play
with guns and cars, be independent in all
situations.
2. Local Context
The most frequent measures of health in
relation to sex are: higher mortality for
males and higher life expectancy for
females.
Males live shorter than females. Females
live longer and mortality is much higher
within male population in all age groups
including the foetuses and newborns. [4]
The population in Brasov County could
be show in the table 1
Brasov County Population Table 1
Brasov County 2003 2004 2005 2006 2007
Masculine 290.413 290.537 289.982 290.034 288.778
Feminine 305.364 305.603 305.229 305.724 305.150
Total population 595.777 596.140 595.211 595.758 593.928
Masculine 216.974 215.844 214.949 214.355 211.961
Feminine 231.496 230.778 229.937 229.898 228.584
Total urban 448.470 446.622 444.886 444.253 440.545
Masculine 73.439 74.693 75.033 75.679 76.817
Feminine 73.868 74.825 75.292 75.826 76.566
Total rural 147.307 149.518 150.325 151.505 153.383
According with these data, the ratio between females and males in 2007 is female: male
1.05, like in graphic 1.
Population of Brasov County in 2007
288.778;
49%305.150;
51%
masculine feminine
Graphic 1
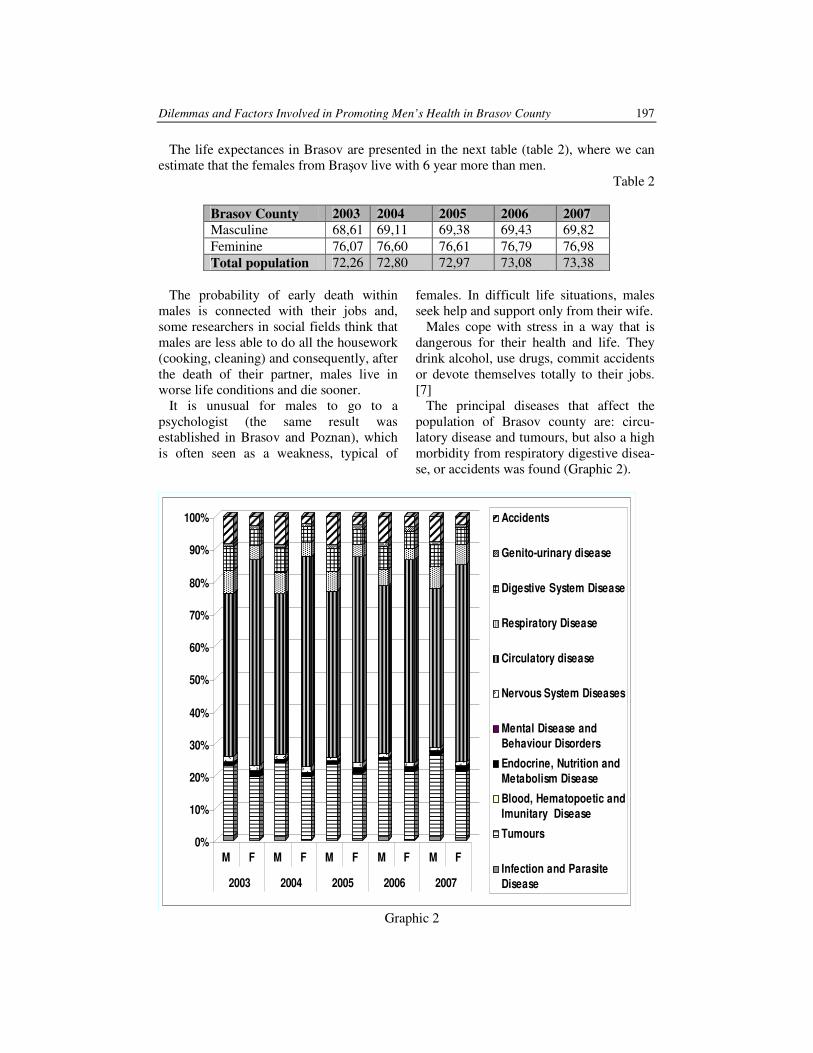
Dilemmas and Factors Involved in Promoting Men’s Health in Brasov County 197
The life expectances in Brasov are presented in the next table (table 2), where we can
estimate that the females from Braşov live with 6 year more than men.
Table 2
Brasov County 2003 2004 2005 2006 2007
Masculine 68,61 69,11 69,38 69,43 69,82
Feminine 76,07 76,60 76,61 76,79 76,98
Total population 72,26 72,80 72,97 73,08 73,38
The probability of early death within
males is connected with their jobs and,
some researchers in social fields think that
males are less able to do all the housework
(cooking, cleaning) and consequently, after
the death of their partner, males live in
worse life conditions and die sooner.
It is unusual for males to go to a
psychologist (the same result was
established in Brasov and Poznan), which
is often seen as a weakness, typical of
females. In difficult life situations, males
seek help and support only from their wife.
Males cope with stress in a way that is
dangerous for their health and life. They
drink alcohol, use drugs, commit accidents
or devote themselves totally to their jobs.
[7]
The principal diseases that affect the
population of Brasov county are: circu-
latory disease and tumours, but also a high
morbidity from respiratory digestive disea-
se, or accidents was found (Graphic 2).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
M F M F M F M F M F
2003 2004 2005 2006 2007
Accidents
Genito-urinary disease
Digestive System Disease
Respiratory Disease
Circulatory disease
Nervous System Diseases
Mental Disease and
Behaviour Disorders
Endocrine, Nutrition and
Metabolism Disease
Blood, Hematopoetic and
Imunitary Disease
Tumours
Infection and Parasite
Disease
Graphic 2
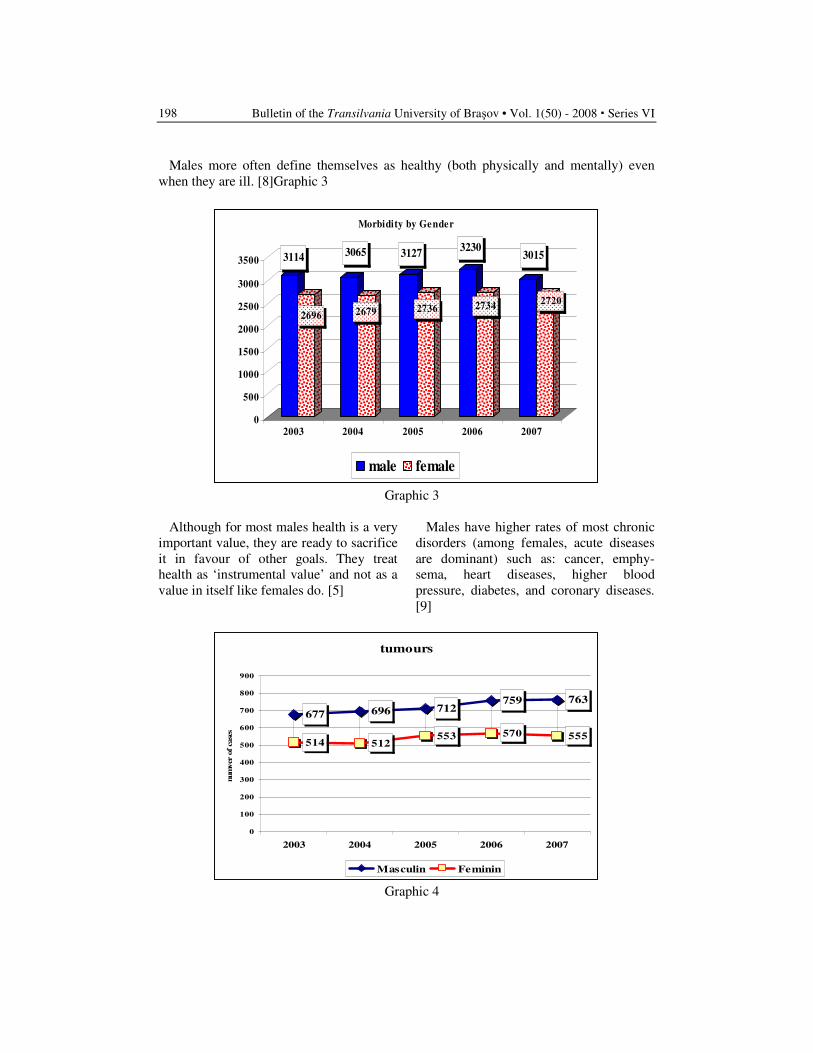
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
198
Males more often define themselves as healthy (both physically and mentally) even
when they are ill. [8]Graphic 3
3114
2696
3065
2679
3127
2736
3230
2734
3015
2720
0
500
1000
1500
2000
2500
3000
3500
2003 2004 2005 2006 2007
Morbidity by Gender
male female
Graphic 3
Although for most males health is a very
important value, they are ready to sacrifice
it in favour of other goals. They treat
health as ‘instrumental value’ and not as a
value in itself like females do. [5]
Males have higher rates of most chronic
disorders (among females, acute diseases
are dominant) such as: cancer, emphy-
sema, heart diseases, higher blood
pressure, diabetes, and coronary diseases.
[9]
tumours
677 696 712759 763
514 512553 570 555
0
100
200
300
400
500
600
700
800
900
2003 2004 2005 2006 2007
num
ver o
f case
s
Masculin Feminin
Graphic 4
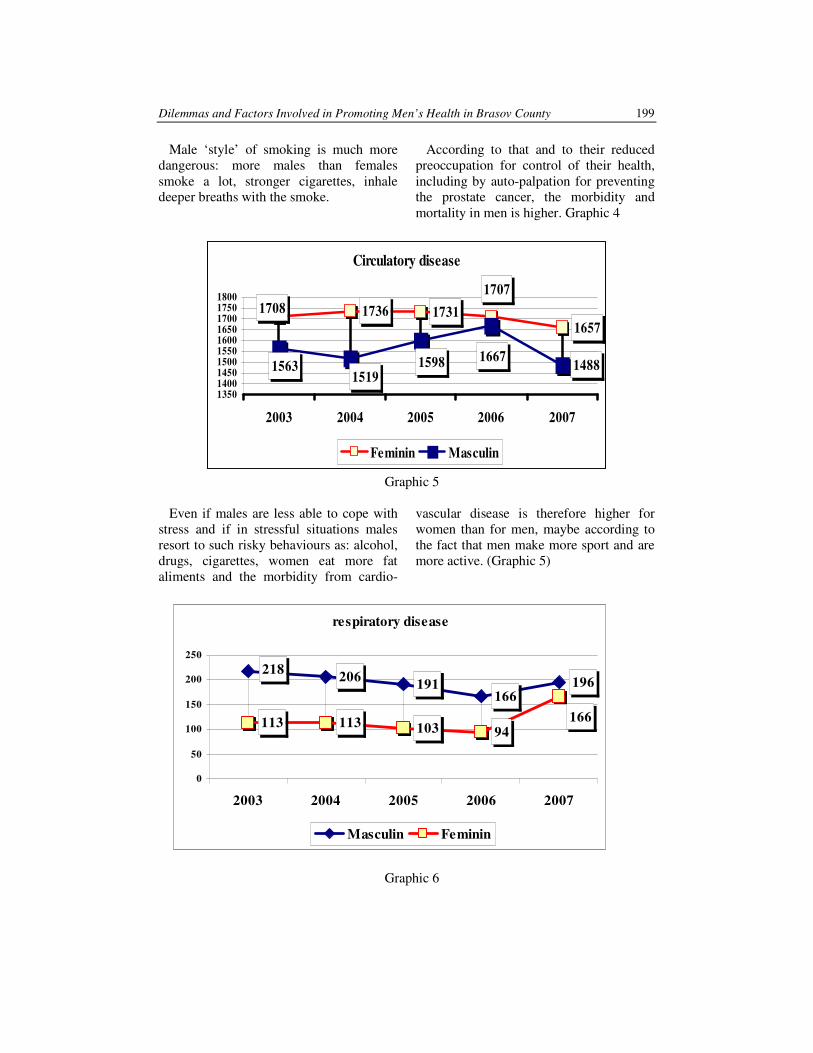
Dilemmas and Factors Involved in Promoting Men’s Health in Brasov County 199
Male ‘style’ of smoking is much more
dangerous: more males than females
smoke a lot, stronger cigarettes, inhale
deeper breaths with the smoke.
According to that and to their reduced
preoccupation for control of their health,
including by auto-palpation for preventing
the prostate cancer, the morbidity and
mortality in men is higher. Graphic 4
Circulatory disease
1736 17311657
1488
1707
1708
166715981519
1563
1350140014501500155016001650170017501800
2003 2004 2005 2006 2007
Feminin Masculin
Graphic 5
Even if males are less able to cope with
stress and if in stressful situations males
resort to such risky behaviours as: alcohol,
drugs, cigarettes, women eat more fat
aliments and the morbidity from cardio-
vascular disease is therefore higher for
women than for men, maybe according to
the fact that men make more sport and are
more active. (Graphic 5)
respiratory disease
206191
166196
113 113 103 94
218
166
0
50
100
150
200
250
2003 2004 2005 2006 2007
Masculin Feminin
Graphic 6
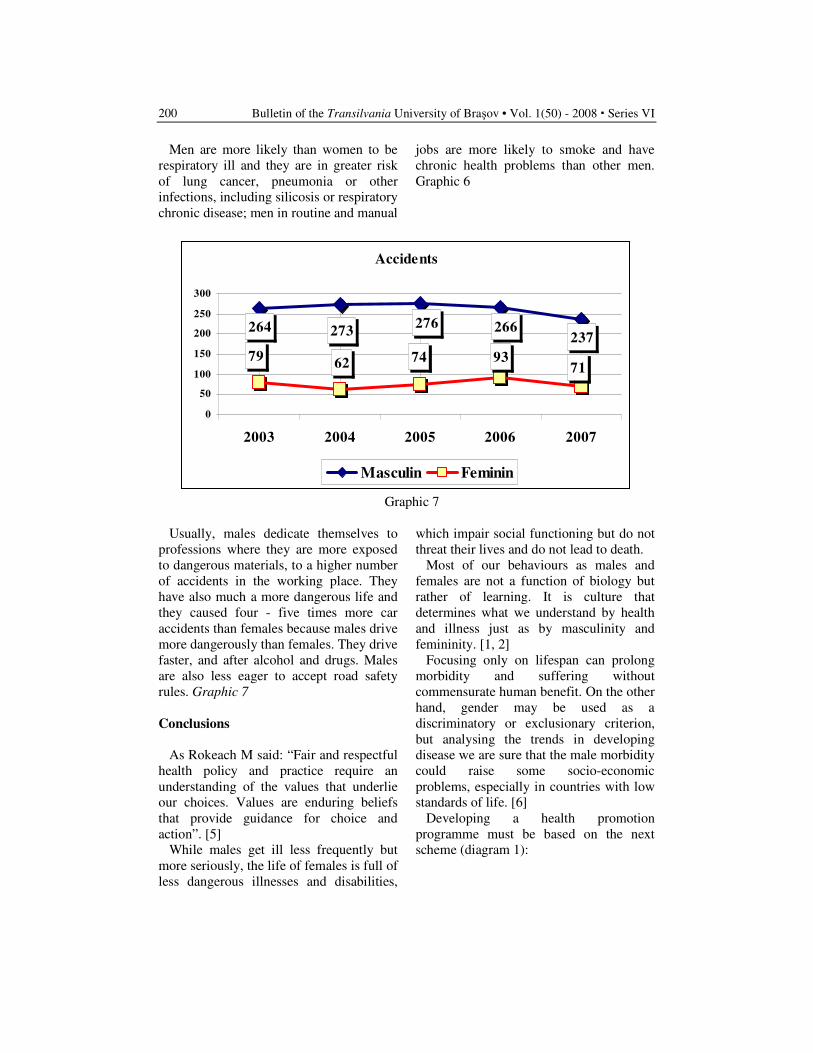
Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
200
Men are more likely than women to be
respiratory ill and they are in greater risk
of lung cancer, pneumonia or other
infections, including silicosis or respiratory
chronic disease; men in routine and manual
jobs are more likely to smoke and have
chronic health problems than other men.
Graphic 6
Accidents
237266276
273264
71937462
79
0
50
100
150
200
250
300
2003 2004 2005 2006 2007
Masculin Feminin
Graphic 7
Usually, males dedicate themselves to
professions where they are more exposed
to dangerous materials, to a higher number
of accidents in the working place. They
have also much a more dangerous life and
they caused four - five times more car
accidents than females because males drive
more dangerously than females. They drive
faster, and after alcohol and drugs. Males
are also less eager to accept road safety
rules. Graphic 7
Conclusions
As Rokeach M said: “Fair and respectful
health policy and practice require an
understanding of the values that underlie
our choices. Values are enduring beliefs
that provide guidance for choice and
action”. [5]
While males get ill less frequently but
more seriously, the life of females is full of
less dangerous illnesses and disabilities,
which impair social functioning but do not
threat their lives and do not lead to death.
Most of our behaviours as males and
females are not a function of biology but
rather of learning. It is culture that
determines what we understand by health
and illness just as by masculinity and
femininity. [1, 2]
Focusing only on lifespan can prolong
morbidity and suffering without
commensurate human benefit. On the other
hand, gender may be used as a
discriminatory or exclusionary criterion,
but analysing the trends in developing
disease we are sure that the male morbidity
could raise some socio-economic
problems, especially in countries with low
standards of life. [6]
Developing a health promotion
programme must be based on the next
scheme (diagram 1):
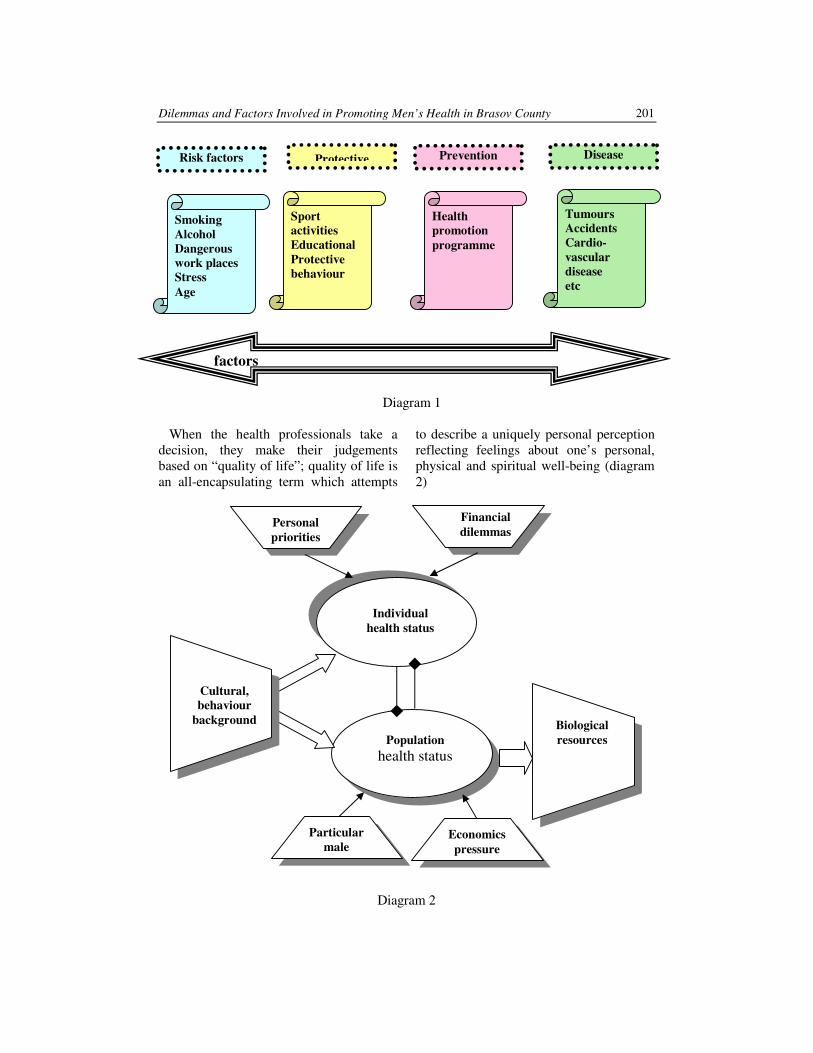
Dilemmas and Factors Involved in Promoting Men’s Health in Brasov County 201
Risk factors Disease Prevention Protective
Smoking
Alcohol
Dangerous
work places
Stress
Age
Sport
activities
Educational
Protective
behaviour
Health
promotion
programme
Tumours
Accidents
Cardio-
vascular
disease
etc
factors
Diagram 1
When the health professionals take a
decision, they make their judgements
based on “quality of life”; quality of life is
an all-encapsulating term which attempts
to describe a uniquely personal perception
reflecting feelings about one’s personal,
physical and spiritual well-being (diagram
2)
Diagram 2
Individual
health status
Population
health status
Economics
pressure
Particular
male
problems
Financial
dilemmas Personal
priorities
Biological
resources
Cultural,
behaviour
background

Bulletin of the Transilvania University of Braşov • Vol. 1(50) - 2008 � Series VI
202
References
1. Keene, J., Li X.: Age and gender
differences in health service
utilization. In: Journal of Public
Health, VoI. 27, No. 1, pp. 74–79,
Advance Access Publication 6 January
2005.
2. Leishman, J: Around the world with
men's health and women's health
organisations. In: J Men's Health Gend
2005, 2:133-134.
3. Men's Health Forum Scotland: Razing
men's health awareness. [http://www.
mhfs.org.uk/mhfs/index.php]
4. Meryn, S., Jadad, A.R: The future of
men and their health. Are men in
danger of extinction? In: Brit Med J
2001, 323:1013-1014.
5. Rokeach, M.: The nature of human
values. New York. The Free Press,
Collier MacMillan; 1973.
6. Taylor, R. J., Smith, B. H., van
Teijlingen, E. R: Health and illness in
the community. Oxford: Oxford
University Press, 2003.
7. Thom, B.: Smoking, drinking and drug
use: a privilege and a burden. In: J R
Soc Health 2004, 5:207-209.
8. Vasianovich, A., van Teijlingen, E. R,
Reid, G., Scott, N. W.: Key health
promotion factors among male
members of staff at a higher
educational institution: A cross-
sectional postal survey. In: BMC
Public Health 2008,
8:58doi:10.1186/1471-2458-8-58.
9. Wyllie, A, Casswell, S.: Gender focus
of target groups for alcohol health
promotion strategies in New Zealand.
Health Promotion International, Vol.
12, 141-149, Oxford University Press.
1 Research Assistant (Human Sciences), Transilvania University, Brasov. 2Theodor Aschenbrandt, "Die physiologische Wirkung und die Bedeutung des Cocains," Deutsche
medizinische Wochenschrift (December 12, 1883) în vol. Ernest Jones, The Life and Work of Sigmund Freud,
Volume I (1856-1900) (New York: Basic Books, 1953), p. 80. 3 In 1883, Freud was 27 years-old 4 Ernest Jones, Life and Work of Sigmund Freud, 1, 81
A DECADENT AGE - 1900.
FREUD AND COCAINE
Andrada FĂTU-TUTOVEANU
1
Abstract. In 1883-1884, Sigmund Freud was a young neurologist in search
for a brilliant medical discovery to launch his scientific career. After
studying some American papers on the subject, but also the results Dr.
Theodor Aschenbrandt had obtained on German ground, Freud has become
interested in cocaine. A less familiar drug at the time (in comparison with the
opiates), cocaine would prove impressive effects - during experiments – on
fatigue, pain and many other medical problems. Freud was both interested
in the substance as a cure for different diseases and as an intellectual
stimulant (as he could notice trying the drug himself). As Freud becomes
involved at various levels (at scientific, clinical, personal level and so on),
the study analysis the stages of his interest in cocaine, also the part he has
played in the scientific research regarding cocaine and last but not least, his
relation with the ‘decadent’ world around the year 1900.
Key words: cocaine, Sigmund Freud, 19th
century, panacea, opium,
medicine, hallucinogens
In 1883, Dr. Theodor Aschenbrandt
obtained a dose of pure cocaine from the
Merck Company of pharmaceutics and
gave it, with positive results (subsequently
published) to the Bavarian soldiers during
the fall manoeuvres.2 Freud was at the
time3 a young neurologist, confronted
himself with neurotic symptoms due to
exhaustion/ chronic fatigue and financial
problems. Cocaine seemed to be a solution
to all his problems, providing him with the
energy and high spirits for his intellectual
work, but also promising to be an
extremely important discovery in his
research career: “If it goes well [Freud had
already tried cocaine himself and also
prescribed it to two patients] I will write an
essay on it and I expect it will win its place
in therapeutics by the side of morphium
and superior to it. I have other hopes and
intentions regarding it. I take very small
doses of it regularly against depression
and against indigestion, and with the most
brilliant success.... In short it is only now
that I feel I am a doctor, since I have
helped one patient and hope to help more.
If things go on in this way we need have
no concern about being able to come
together and to stay in Vienna.”4

Bulletin of the Transilvania University of Braşov � Vol. 1 (50) - 2008 � Series VI
204
His enthusiasm and also the conviction
in the positive, even spectacular effects of
cocaine (which seemed to embody the
medical ideal of the 19th century, a
scientific panaceum universalis) made
Freud share the “magic” medicine with his
group of friends, his fiancée, his sisters,
colleagues and patients, which seems
particularly dangerous if regarded from the
point of view of subsequent medical
discoveries5. Freud’s letters on cocaine
continue in the same enthusiastic voice,
nourished by the observations provided by
his own experiences: In my last severe
depression I took coca again and a small
dose lifted me to the heights in a wonderful
fashion. I am just now busy collecting the
literature for a song of praise to this
magical substance.”6 At the 21
st of April
1884, Freud expresses in a letter towards
Martha his interest for a promising
therapeutic project, having acquired the
product for the purpose of some
experiments on heart and neurological
diseases. Also, on the 18th of July, he ends
his first paper7 (Über Coca
8), on the plant
of coca and cocaine (the derivative of the
former), which would be published a
month later. As a researcher, he was
interested in the common simulative
qualities of these substances, with effects
in the treatment of neurasthenia and also
providing the energy for a continuous good
rhythm in the intellectual work, free from
any sensation of hunger or thirst. The
article combines scientific methodology
(historical account, scientific description of
the plant of coca, chemical formula,
clinical observations and so on) with
subjective accents, suggesting personal
5 “looked at from the vantage point of our present
knowledge, he was rapidly becoming a public
menace.", Ernest Jones, on
http://www.druglibrary.org/schaffer/library/studies/c
u/CU35.html 6 Ernest Jones, Life and Work of Sigmund Freud, 1,
84 7 Cocaine, the alkaloid produced from leafs of coca 8 Sigmund Freud, ‘Über Coca’, Centralblatt für die
ges. Therapie, 2, pp. 289–314, 1884
involvement and unrestrained enthusiasm.9
It is most obvious that so far all the
premises were supporting Freud’s
professional ambitions regarding the
discovery of the Cure, the absolute
remedy. It is a common concern to the 19th
century scientists, an idea belonging to the
ambivalent area between medicine/ science
and magic, still present while science itself
was building its separate identity. The
magical/religious implications from the
letters are also to be found in the article
Über Coca (1884), even beyond the choice
of terms from this semantic area. Freud
makes references to saga from the
Peruvian mythology, where the plant of
coca is mentioned as a gift from the gods
offered to men in order to ‘satisfy the
hungry, fortify the weary, and make the
unfortunate forget their sorrows”10
. The
clinical observations of Freud’s own
symptoms refer to the action of cocaine
over depression and the restoration of high
spirits of a person in perfect health, also to
the increased work capacity (both physical
and mental) and finally, to the absence of
any sensation of addiction recorded in the
absence of the drogue, which was a
particular aspect in Freud’s own case.
Even more, one of the main causes of the
generalized use of cocaine at the end of the
19th century was the opinion (based upon
Bentley’s 1878 idea11
and afterwards,
among others, upon Freud’s studies on the
9In statements such as 'the most gorgeous
excitement', and administering an 'offering' of it
rather than a 'dose' , see also
http://www.druglibrary.org/schaffer/library/studies/c
u/CU35.html 10 “the mythical saga of how Manco Capac, the
Royal Son of the Sun-God, had sent it as 'a gift from
the gods to satisfy the hungry, fortify the weary, and
make the unfortunate forget their sorrows.' " Ernest
Jones, în
http://www.druglibrary.org/schaffer/library/studies/c
u/CU35.html 11 Dr .Jaffe (1965),
http://www.druglibrary.org/schaffer/library/studies/c
u/CU35.html
www.psikeba.com.ar/articulos/RAcocaina.htm

A Decadent Age – 1900. Freud and Cocaine
205
subject) regarding the capacity of cocaine
to cure morphine addiction.
Some of these observations were
confirmed by the subsequent research
(such as the effects of euphoria,
diminished sensations of hunger, pain or
tiredness and even increase of mental
capacity12
. This recognition was visible not
only at the scientific level, but also in
representations such as the early Coca-
Cola advertisements, which focused
precisely these qualities of the drink, as it
had contained coca until the beginning of
the 20th century. Still, there is more than
one element suggesting Freud’s later
acknowledgement of what cocaine actually
meant in its negative aspects (its strongly
addictive characteristics, the lethal danger,
its psycho-pathological implications and so
on), recognition equivalent to a powerful
deception towards this chemical solution
for all pains and especially for nervous
diseases. After an obvious descent in his
enthusiastic attitude (as in a 1887 study,
actually his last on the subject), next to a
diminishing use of the substance, from
1925 an even more radical cleavage takes
place, as cocaine is now referred to by the
use of the term allotrion (which in the
medical language of the time was
designating, in a pejorative manner, an
object which was foreign from the
scientific field)13
.
Some of those who have research
Freud’s biography go even further, by
admitting that the disenchantment and
mistrust regarding pharmaceutical
solutions (originated, as it seems, in the
“cocaine episode”) are the source of his
option for an alternative psychotherapy,
the psychoanalysis. More than that, it
seems that the latter emerges “historically
precisely in the moment when the medical
12 V. Denis Richard, La coca et la cocaïne, Presses
Universitaires de France, Paris 1994, p. 28 13 V. Rosa Aksenchuk, Freud y la cocaína:
¿experimentos con uno mismo?, în
www.psikeba.com.ar/articulos/RAcocaina.htm
practice meets its limits.”14
Among these,
Pierre Eyguesier15
regards this cocaine
“moment” as a gate to the psychoanalytical
stage, equally important as the self-
analysis16
, while the abandonment of the
substance, others say, overlaps the
discovery in the relation to dependence
between hysterical episodes and language
facts, which have eventually led to therapy
through words17
.
Analysing the historical moment of the
late 19th century, the moment cocaine is
obtained and gains field in the medical
conscience, one important aspect observed
is that at the time the prohibition and
opprobrium (which are nowadays related
to the notion of drug) were not present, as
they appeared as the effect of certain
historical and medical experiences and
moved towards the field of legislation and
sociologically involved campaigns18
. In
the 1880s, Vienna records an increasing
interest for the effects cocaine has in
achieving anaesthesia. “Sigmund Freud,
having discovered these researches and
noticing that many American doctors were
already using the product, convinces an
ophthalmologist friend of his, Königstein,
to try it; the latter would obtain miraculous
results”19
. From now on, many successful
interventions and not only ophthalmologic
ones, take place. The new discovery
becomes the subject of many discussions
and articles and “the medical environment
is literally enflamed towards the
miraculous alkaloid to the point that its
price becomes exorbitant”20
.
14 Ibid. 15Pierre Eyguesier, Comment Freud devint drogman.
Etude sur coca et la cocaine a la Belle Epoque,
Nevarin Editeur, Diffusion Seuil, Paris, 1983 16 Rosa Aksenchuk, op.cit., în
www.psikeba.com.ar/articulos/RAcocaina.htm 17 Ibid 18 Roland Jaccard, Freud, Presses Universitaires de
France, Paris, 1996, p. 31 19 Denis Richard, p. 13 20 Ibid.

Bulletin of the Transilvania University of Braşov � Vol. 1 (50) - 2008 � Series VI
206
Freud was interested in the studies
American researchers had made (and those
of surgeon Hammons, particularly) and
was interested himself in it clinically
“verifying the observations of the
Americans and developing new indications
on the product and searching, under this
pretext, the means to better understand the
origins of mental pathologies: from a
certain point of view, cocaine was one of
the cornerstones of the reflection on
psychoanalysis. On the 30th of April 1884
he would use the alkaloid upon himself”21
.
Soon he starts taking it regularly, as he was
convinced of the qualities cocaine
possessed22
and particularly enthusiastic
about its antidepressant and stimulation
effects, hoping that from all these points of
view cocaine would “launch” his career.
One of the ardent problems of the moment,
morphine addiction (stimulated mainly by
the generalized use in hospitals and
especially during crisis moments such as
wars, as doctors needed its powerful effect
on pain and initially ignored its addictive
character) seemed to submit to cocaine
treatment. Of course, it was another form
of addiction replacing the older one, but
this aspect became obvious only later. In
this context, Freud recommends the
magical treatment to one of his friends, Dr.
Ernst von Fleischl-Marxow (who was
addicted to morphine, due to a painful
nervous disease), but the results are tragic,
as the latter dies eventually from a cocaine
overdose. Subsequently, Freud would
recognize, as well as Lewin23
, the negative
effects of the medicine becoming more and
more aware of the side effects cocaine
implied.
21 Freud et la cocaïne, in Denis Richard, op.cit., p. 15 22Psycho-stimulation characteristics. Freud’s
prescriptions :
”physical and mental stimulation, indigestion, ;
indigestie; caşexie22; morfinism şi alcoolosm [s.n.];
astm; impotenţă; anestezie locală; sângerări nazale.
Aceste indicaţii vor dispărea la începutul secolului
XX, cu excepţia celei de anestezic.”, Denis Richard,
op.cit., p. 14 23 See above
There are some stages of his research, the
first study being Über Coca (1884) where
“Freud proves to be a brilliant
pharmacologist, by pertinently observing that
the treatment of various mental diseases by
chemical substances could prove possible.
Despite the failure Morselli and Buccola had
registered in the use of the alkaloid24
for the
treatment of severe nervous breakdowns, he
[Freud] underlined that because of «the
efficiency of coca25
in the cases of mental
and physical frailness research should be
continued». He also asserts that cocaine could
exert an antidepressant action especially in the
benign and neurasthenic cases”26
.
A second study, from 1885, Contribution
to the Knowledge of the Effect of Cocaine,
brought to the fore positive conclusions
and being followed by some others (all
these, proofs of his constant interest on the
subject) and also by his lecture in 1885,
Freud to the Viennese Psychiatric Society.
In 1887, his last article from what was later
called “the Cocaine papers”, Cocaine-
mania and Cocaine-phobia, besides his
response to the attacks some of his
colleagues had laid upon his previous
work, one can perceive also a certain
reticence of the author himself (such as
that referring to cocaine injections) and
some shifts on some older ideas. Despite
these changes in his scientific perspective
and although he significantly had
developed no addiction whatsoever, Freud
continued using the drug until 1895, with
some discontinuities. His personal interest
is still related to continuous research but
also to the stimulant benefits he was
recording in his program of intense work.
A loss of interest occurs gradually, as he
becomes more and more aware of the
complex dangers cocaine involves (after
the Fleischl episode27
, of cocaine-maniac
24 Cocaine 25 Here, the plant 26 Denis Richard, p. 16 27 Fleischl consuma după un an un gram de cocaină
pe zi, adică de dou-zeci de ori mai mult decât lua
Freud însuşi, însă mult mai sporadic, v. Edward M.

A Decadent Age – 1900. Freud and Cocaine
207
psychosis, then death, he would warn
Martha, to whom he was sending it
regularly): addiction, tolerance28
, which
was leading to a continuous growth of the
dose etc. Another factor, influencing this
decrease, is the constant criticism rising
from different directions. The chemist
Erlenmeyer29
, the first to criticize the
method (1885) describes, for instance, the
acute intoxication with cocaine, almost
simultaneously with Freud’s positive
theory. In De la quête de la morphine
(1887), the former speaks of “a third
plague of human kind” after alcohol and
morphine (his area refers especially to the
19th century main addictions). He also
demonstrates that there was confusion (in
the treatment of morphine addiction by
cocaine) between morphine withdrawal
symptoms and the psychotic episodes
produced by overdoses of cocaine.30
In
1886, a friend of Freud’s, Obersteiner, who
had initially promoted the use of cocaine,
changes his mind and becomes a critic of
it, after experimenting some nervous
disorders similar to delirium tremens. An
important critic is Louis Lewin, the author
of a famous toxicological classification in
the volume Phantastica and author of
various studies31
on the consequences of
cocaine use32
.
Brecher, The Consumers Union Report on Licit and
Illicit Drugs. 35. Cocaine,
http://www.druglibrary.org/schaffer/library/studies/c
u/CU35.html 28
Drug tolerance occurs when a subject's reaction to
a psychoactive drug (such as a painkiller or
intoxicant) decreases so that larger doses are
required to achieve the same effect. Drug tolerance
can involve both psychological drug tolerance and
physiological factors,
http://en.wikipedia.org/wiki/Drug_tolerance 29 Richard August Carl Emil Erlenmeyer (28 June
1825 – 22 January 1909), German chemist 30 Denis Richard, op.cit., p. 20 31 „Über Morphium-Intoxication," in "Deutsche
Zeitschrift für Praktische Medizin," 1874, No. 26;
"Experimentelle Untersuchungen über die
Wirkungen des Aconitin auf das Herz," in
"Centralblatt für die Medizinische Wissenschaft,"
1875, No. 25; "Über die Verwerthung des Alkohols
in Fieberhaften Krankheiten," in "Deutsches Archiv
In its first stage (the last decades of the
19th century), cocaine belongs mostly to
the medical environment, the consumers
being mainly doctors, pharmacists or
morphine-addicted patients, while the fin
de siècle/ turn of the century period (circa
1900) is the moment when it extends to all
social classes, as an individualized
attraction. Edward M. Brecher asserts that
Fleischl's experience was not “unique;
subsequent observations were to reveal
that repeated use of large doses of cocaine
produces a characteristic paranoid
psychosis in all or almost all users, and
that the tendency to overuse is widespread.
A peculiar characteristic of this psychosis
is ‘fornication’– hallucinations that of, or
insects, or (as in Fleischl's case) snakes,
are crawling along the skin or under it”33
.
Despite all these, as we have already
mentioned Freud himself does not
experience any “tolerance” or addiction,
continuously taking very small doses34
,
without feeling any withdrawal symptoms
whenever he interrupts the habit. Ernest
Jones, psychoanalyst and biographer, tries
to offer an explanation for this unexpected
für Klinische Medizin," 1876; "Über Maximale
Dosen der Arzneimittel," in "Transactions of the
International Medical Congress," ninth session,
Washington, 1887; "Über Allgemeine
Hautvergiftung Durch Petroleum," in Virchow's
"Archiv," cxii., 1888; "Über Anhalonium Lewinii
und Andere Cacteen," in "Archiv für Experimentelle
Pathologie und Pharmakologie," 1894; "Die
Behandlung der Lepra," in "Deutsche Medizinische
Wochenschrift," 1898; "Die Untersuchungen von
Blutflecken," ib. 1899; "Die Vergiftungen in
Betrieben," ib. 1890 (also translated by Pannier in
"Bulletin Général de Thérapeutique," 1902); "Über
die Behandlung der Lepra," ib. 1900. "Die
Nebenwirkungen der Arzneimittellehre," Berlin,
1881, 2d ed. 1893 (translated into Russian);
"Lehrbuch der Toxicologie," Vienna, 1885, 2d ed.
1897 (translated into French by Pouchet, Paris,
1902); "Über Piper Methysticum (Kawa Kawa),"
Berlin, 1886; "Über Areca Catechu, Chavica Detle,
und das Betelkauen," Stuttgart, 1889. 32 Denis Richard, p. 21 33 Edward M. Brecher, op.cit., în
http://www.druglibrary.org/schaffer/library/studies/c
u/CU35.html 34 30-50 miligrams of injectable product

Bulletin of the Transilvania University of Braşov � Vol. 1 (50) - 2008 � Series VI
208
absence of reaction through the criteria of
“addictive personality", as a factor for the
establishment of an addiction (still, the
author observes that in the case of cigars,
the addiction did exist)35
. Actually, Freud
himself was writing in 1887 that no
chemical product establishes addiction
entirely by itself, a psychic or emotional
predisposition being actually involved.
Some other explanations, of a
pharmaceutical nature, also suggest that on
one hand, there could be some biochemical
differences between individuals in what
concerns addictions and on the other hand
that quantity and frequency of use could
also prove decisive (in Freud’s particular
case – which functions somehow as an
exception - there are small doses, taken
from time to time, without the need to
increase the amount).
Until 1890 the psychosis and addiction
related to cocaine had become already a
medical certainty, fact which does not imply
a lessening in its popularity, especially in the
absence of a legal prohibition or even
involvement for the two following decades.
In the USA, cocaine was being used as an
ingredient for Coca-Cola, for tonic drinks or
very popular medicines in the treatment of
catarrh36
, which involved nasal aspiration of
the substance, procedure which seems to be
at the origin of this type of use of the
substance. The new (American) philosophy
surrounding this substance was focused on
the idea of high spirits and wellbeing, in
opposition to pessimism or melancholy, this
mal de siècle of the 19th century: “don’t lose
your time, be happy! If you feel pessimistic
or depressed ask for cocaine!” was one of the
formulas promoting the substance at the
end of the 19th century.
35 See Ernest Jones, The Cocaine Episode in Life
and Work of Sigmund Freud, Volume I (1856-1900)
(New York: Basic Books, 1953) 36“catarrh: inflammation of a mucous membrane in
humans or animals; especially : one chronically
affecting the human nose and air passages”,
http://medical.merriam-webster.com/medical/catarrh
As we have already mentioned Freud
admits at a certain moment that both these
side effects cocaine use involve (addiction,
physical disorder/ paranoia) as well as its
therapeutic failure (it had proved unable,
as well as psychoanalysis, to cure
morphine addiction). Yet, his scientific
observations (often experienced by
himself) represent a rigorous and important
part of turn of the century research on the
subject. In 1899 (though post-dated as
1900 by the publisher), The Interpretation
of Dreams (Die Traumdeutung)37
was
published, symbolizing a fundamental
switch of perspective, Freud having
discovered a solution beyond the “infernal
chemistry” of drugs, by going inside the
secret mechanisms of psychic and
language representations. Michael Pollak
observes that to use dreams as a basis for a
scientific paper meant a legitimate a
manner of writing and conceiving life,
already used by many writers, writing
becoming a space of self-reflection38
. With
a passion for archaeology and Greek and
Roman Antiquity39
, Freud develops, under
the inspiration of the former, a system
which investigates the inaccessible areas of
the mind (as he believed - William M.
Johnston asserts –at least until 1914 in a
level of invisible order under the chaos of
emotions and that bringing the hidden
conflicts to the light would disperse
them40
). From the Antiquity, Freud takes
37 „Freud considera Interpretarea viselor atât cea
mai semnificativă lucrare ştiinţifică a lui, piatra de
temelie a intregii sale creaţii, cât şi lucrarea care i-a
adus echilibrul pe plan individual, o sursă a forţei de
a ţine din nou piept unei existente agitate”, Carl E.
Schorske, op.cit., p. 175 38 Michael Pollak, op.cit., p. 124 sqq. 39 William M. Johnston, op.cit., p. 262: „ca în multe
case vieneze, sala de aşteptare a lui Freud avea pe
jos covoare orientale groase, iar pe pereţi
reproduceri după Lecţia de anatomie a lui
Rembrandt şi Coşmarul lui Johann Heinrich Füssli.
În biroul său se aflau nişte vitrine pline cu obiecte de
artă provenind din Grecia antică şi Egipt şi câteva
basoreliefuri egiptene în mărime naturală [...] Freud
venera Antichitatea greco-romană [266] 40 William M. Johnston, p. 265

A Decadent Age – 1900. Freud and Cocaine
209
over some essential structural patterns and
symbols, in a system which would
influence essentially the next century, as
William M. Johnston observes41
.
There is one more perspective describing
Freud’s relations to the cultural key-
moment of 1900 – less obvious - and that
is what Charles Bernheimer called
“Freud’s decadence”. This is affiliated
with the theories of the moment, on
decadence and the way in which a society
obsessed by degeneration can affect the
study of mental pathologies. Bernheimer
observed that, despite his biographers
having noticed Freud’s despise for Max
Nordau when the two meet in Paris in
1886, “Freud’s diagnosis of fin de siècle
decadence is not at all different from
Nordau’s”42
. In his study, ‘Civilized’
Sexual Morality and Modern Nervous
Illness, 1908, “Freud starts out by citing
just the sort of medico-psychiatric
authorities that Nordau repeatedly invokes
to give his cultural analysis the stamp of
scientific validity”43
, one of the quoted
studies, that of Wilhelm Erb44
, having
focused on the same influence of modern
literature and life on the growing number
of patients suffering from nervous
diseases. Yet, Freud considers that the
main factor of this expansion is sexuality,
more precisely the “’harmful suppression
of the sexualized life of civilized people’
by their own morality”45
and the
encouragement, by transforming this into a
taboo, of a constant feeling of guilt,
maintained mainly in the subconscious and
less motivated objectively (“the price we
pay for our advance in civilization is a loss
of happiness through the heightening of the
sense of guilt”46
, Freud writes). Although
the conclusion would be that of a mutual
41 Ibid., p. 417 42 Charles Bernheimer, Decadent Subjects, The John
Hopkins University Press, 2002, p. 163 43 Ibid. 44 Über die wachsende Nervosität unserer Zeit, 1893 45 See Charles Bernheimer, pp. 163-164 46 Ibid., p. 168
exclusion between civilization and sexual
health (having psychological implications),
he suggests the idea that a normal sexual
behaviour is useful to civilization, as the
concept of normality is related to that of
repression. One more concept comes to mind
in this context, that of “perversion”,
obsession of the fin de siècle “decadent”
society. It stands in relation to neurosis (both
considered as forms of deviance), as the
latter is understood as a perverse complex of
tendencies, impulses in a state of repression.
Civilization, Freud observes, implies a series
of restrictions stronger than the ability to
tolerate, as it places satisfaction in the field
of prohibition: “normalcy is being
constructed as a ‘modern nervous illness’.
Deviation from the norm is the norm.”47
Despite the context of successful theories of
degeneration at the turn of the century, an
essential observation Freud makes is that at
the basis of inheriting, transmission of
“perversion” from an individual to another
there is no biological determinism or
hereditary degeneration, but a psychological
and conduct transfer of the maternal
dissatisfaction from mother to child.
“Decadence sets in when individuals begin
to put their own pleasures first.”48
, as
becomes obvious that in order to assume
what society forbids and sanctions and
“break” the limit. There has to exist an
excess of constraint and despair or a moment
of crisis, allowing this excessive outburst. Later, Freud moves the centre of debate
from the socio-historical to the psychoanalytical area, speaking about normality as a utopia: “a normal ego…is, like normality in general, an ideal fiction. Every normal person, in fact, is normal on the average”
49. Neurosis seems to be more
of social illness, at a larger scale, than an individual problem. “Decadence is resolutely antiteleological and antimetaphisical, yet it cannot do without the illusion of a telos, the mirage of truth.
47 See Charles Bernheimer 48Bernheimer, p.167 49 Ibid., p. 166
Bulletin of the Transilvania University of Braşov � Vol. 1 (50) - 2008 � Series VI
210
[…] Freud has little sympathy with the decadent traits that he diagnoses in contemporary civilization. Perverse sexualities, regressive fixations, nervous exhaustion, impotence – Freud finds none of the creative potential in such negative states that decadent writers extol. […]Yet Freud’s antidecadence, like Nietzsche’s
has a decadent dimension: the place of judgment is not immune to contamination from below”
50 and a proof in this respect is
precisely his episode of fascination for the “magical” substance of the fin de siècle
medicine, cocaine.
References
1. Aksenchuk, R.: Freud y la cocaína:
¿experimentos con uno mismo?, from www.psikeba.com.ar/articulos/RAcocaina.htmwww.psikeba.com.ar/articulos/RAcocaina.htm
2. Bachmann, C., Coppel, A.: Le dragon
domestique. Deux siècles de relations
étranges entre occident et la drogue. Paris. Edition Albin Michel, 1989.
3. Bernheimer, Charles: Decadent
Subjects. Baltimore. The John Hopkins University Press, 2002.
4. Brecher, E. M.: and the Editors of Consumer Reports Magazine, The
Consumers Union Report on Licit and
Illicit Drugs. 35. Cocaine, 1972. from http://www.druglibrary.org/schaffer/library/studies/cu/CU35.html
5. de Liedekerke, A.: La Belle époque de
l'opium, [suivi d'une] Anthologie littéraire de la drogue de Charles Baudelaire à Jean Cocteau. avant-propos de Patrick Waldberg. Paris. Éditions de la Différence, 1984.
6. Eyguesier, P.: Comment Freud devint
drogman. Etude sur coca et la cocaine
a la Belle Epoque. Paris. Nevarin Editeur, Diffusion Seuil, 1983.
7. Freud, S.: Introducere în
psihanaliza: prelegeri de
psihanaliza: psihopatologia vieţii cotidiene. Traducere, studiu introductiv si note: Leonard Gavriliu.
50 See Charles Bernheimer
Bucureşti. E. D. P. 1980. 8. Greenslade, W.: Degeneration,
Culture and the Novel. 1880-1940. Cambridge. Cambridge University Press, 1994.
9. http://dexonline.ro/http://en.wikipedia.org 10. http://fr.wikipedia.org/ 11. http://fr.wikipedia.org/wiki/Exposition
s_universelles_de_Paris#Exposition_universelle_de_1900
12. http://www.observator.mednet.md/droguri/consum/
13. http://www.webwritingthatworks.com/ 14. Jaccard, R.: Freud. Paris. Presses
Universitaires de France, 1996. 15. Johnston, W. M.: Spiritul Vienei. O
istorie intelectuala si sociala 1848-
1938, Traducere de Magda Teodorescu. Iaşi. Editura Polirom, 2000, [1972].
16. Jones, E.: The Life and Work of
Sigmund Freud, Volume I. New York. Basic Books, 1953.
17. Le Rider, J. : Jurnale intime vieneze, Traducere din limba franceză şi prefaţă de Magda Jeanrenaud. Iaşi. Editura Polirom, 2001, [2000].
18. Milner, M. (ed.): Littérature et
pathologie. Vincennes. Presses Universitaires Vincennes, 1989.
19. Milner, M.: L'imaginaire des drogues: de Thomas de Quincey à Henry Michaux. Paris. Gallimard, 2000.
20. Pichot, P.: Un siècle de psychiatrie.
Paris. Synthélabo, 1996. 21. Porter, R. (ed.): Drugs and Narcotics
in History. Cambridge. Cambridge University Press, 1996.
22. Richard, D.: La coca et la cocaïne. Paris. Presses Universitaires de France, 1994.
23. Schorske, C. E. : Viena fin de siècle.
Politică şi cultură, Traducere de Claudia Ioana Doroholschi şi Ioana Ploeşteanu. Iaşi. Ed. Polirom,1998 [1961].
24. Sfez, L.(ed.) : L’utopie de la santé
parfaite, Presses Universitaires de France, Paris, 2001.
25. Vidal, B.: Histoire de la chimie, Presses universitaires de France, Paris, 1985.
26. Yvorel, J.-J.: Les Poisons de l’esprit.
Drogues et drogués au XIXe siècle. Paris. Quai Voltaire, 1992.
AUTHORS INDEX
A
Afzal, N. 89
Agache, I. 55
Alexandrescu, D. 93, 157
Alexandru, R. 119
Anghel, M. 47
Arghir, O. 93
B
Badea, M. 21, 29, 37
Ballabio, C. 37
Banuta, I.A. 1
Baritz, M. 195
Baum, E. 163
Bălescu, A. 169, 195
Bobescu, E. 81
Boda, D. 75
Bold, C.L. 1
Burtea, V. 107, 111, 115
Buzescu, M. 127
C
Caruso, D. 37
Cersosimo, G. 175
Chefneux, E. 169
Ciurea, C. 75
Colombo, M. L. 37
Coman, G. 21
Comşa, F. 151
Cristea, A. 47
Cristea, L. 195 Cucu, A. 133
D
Datcu, G. 81
Diaconu, S. 9
Domaradzki, J. 195
Durach, L. 133
F
Falup-Pecurariu, C. 99, 119
Falup-Pecurariu, O. 99, 119
Fanea, R. 145
Fătu-Tutoveanu, A. 203
Fleancu, A. 1, 9
Fleancu, C. 1
G
Galajda, Z. 81
Giavarini, F. 37
Goron, M. 93
Greavu, M. 17
Grecu, A. 1
H
Hussain, S. 89
I
Idomir, M. 43
Ifteni, G. 61
Ifteni, P. 111
K
Kohen, I. 89
L
Lazoriec, L. 21
Leaşu, F. 169
Lupu, A.M. 139
Lupu, S. 139
M
Man, M. A. 93
Manu, P. 89
Marty, J.-L 29
Medel, M.-L. 29
Mişarcă, C. 133
Moleavin, I. 43, 47
Monescu, V. 119
Moro, E. 37
Moşoiu, C. 107, 115
Munteanu, M. 21
Bulletin of the Transilvania University of Braşov � Vol. 1 (50) � Series VI 212
N
Nan, M. 75
Neculoiu, D. 47
Nedelcu, I. 67
Nemet, C. 43
Noguer, T. 29
Nunes, G.S. 29
O
Onisâi, L.L. 1, 17, 139
Oros, C. 145
P
Pamfil, G. 61, 119
Pascu, A. 43
Peri, G. 17
Persico, A. 37
Pop, M. 93
Postelnicu, A. 119
R
Râjnoveanu, R. 93
Rădoi, M. 61, 75, 81
Răşină, A. 99
Restani, P. 21, 37
Rogozea, L. 169, 195
Rus, H. 61, 75
S
Scârneciu, C. 67, 139
Scârneciu, I. 17, 67, 139
Scârneciu, V. 67
Scârneciu, V. D. 139
Sechel, G. 1, 9
Suta, C. 75
T
Ţurcanu, M. 9
U
Uberti, F. 37
V
Voroneanu, M. 145
W
Wierzejska, E. 195